User login
177Lu-Dotatate for advanced midgut neuroendocrine tumors
177Lu-Dotatate, a radionuclide related to octreotide, reduced the risk of disease progression or death by 79% in a phase III trial involving 229 adults with advanced, progressive midgut neuroendocrine tumors, investigators reported in the New England Journal of Medicine.
“The response rate of 18% in the 177Lu-Dotatate group (as compared with 3% in the control group) is also notable, given that response rates above 5% have not been observed in large randomized clinical trials of other systemic therapies in this patient population,” said Jonathan R. Strosberg, MD, of the Moffitt Cancer Center, Tampa, and his associates.

All the study participants had metastatic disease that progressed despite first-line treatment using octreotide LAR; 80% had also undergone surgical resection, and nearly half had received some other form of systemic therapy before entering this study. The primary tumor site was the ileum in most patients, and most also had metastases in the liver, the lymph nodes, or both, “typically in the mesentery or retroperitoneum.”
The primary efficacy endpoint – the estimated rate of progression-free survival at month 20 – was 65.2% in the intervention group, compared with 10.8% in the control group. This represents a 79% lower risk of disease progression or death with 177Lu-Dotatate. An interim analysis of overall survival (an endpoint that cannot be determined definitively until more time has passed) showed a 60% lower risk of death in the intervention group than in the control group. Treatment response rates were 18% and 3%, respectively, Dr. Strosberg and his associates reported (New Engl J Med. 2017 Jan 12. doi:10.1056/NEJMoa1607427).
177Lu-Dotatate was administered together with a renal-protection agent, and there has been no evidence of renal toxic effects to date. Rates of low-grade hematologic toxicities were low. The most common adverse effects were nausea and vomiting, which were largely attributed to the renal-protection agent, as well as fatigue, asthenia, abdominal pain, and diarrhea. Adverse events leading to premature withdrawal from the trial developed in more of the control group (9%) than of the intervention group (6%).
177Lu-Dotatate, a radionuclide related to octreotide, reduced the risk of disease progression or death by 79% in a phase III trial involving 229 adults with advanced, progressive midgut neuroendocrine tumors, investigators reported in the New England Journal of Medicine.
“The response rate of 18% in the 177Lu-Dotatate group (as compared with 3% in the control group) is also notable, given that response rates above 5% have not been observed in large randomized clinical trials of other systemic therapies in this patient population,” said Jonathan R. Strosberg, MD, of the Moffitt Cancer Center, Tampa, and his associates.
All the study participants had metastatic disease that progressed despite first-line treatment using octreotide LAR; 80% had also undergone surgical resection, and nearly half had received some other form of systemic therapy before entering this study. The primary tumor site was the ileum in most patients, and most also had metastases in the liver, the lymph nodes, or both, “typically in the mesentery or retroperitoneum.”
The primary efficacy endpoint – the estimated rate of progression-free survival at month 20 – was 65.2% in the intervention group, compared with 10.8% in the control group. This represents a 79% lower risk of disease progression or death with 177Lu-Dotatate. An interim analysis of overall survival (an endpoint that cannot be determined definitively until more time has passed) showed a 60% lower risk of death in the intervention group than in the control group. Treatment response rates were 18% and 3%, respectively, Dr. Strosberg and his associates reported (New Engl J Med. 2017 Jan 12. doi:10.1056/NEJMoa1607427).
177Lu-Dotatate was administered together with a renal-protection agent, and there has been no evidence of renal toxic effects to date. Rates of low-grade hematologic toxicities were low. The most common adverse effects were nausea and vomiting, which were largely attributed to the renal-protection agent, as well as fatigue, asthenia, abdominal pain, and diarrhea. Adverse events leading to premature withdrawal from the trial developed in more of the control group (9%) than of the intervention group (6%).
177Lu-Dotatate, a radionuclide related to octreotide, reduced the risk of disease progression or death by 79% in a phase III trial involving 229 adults with advanced, progressive midgut neuroendocrine tumors, investigators reported in the New England Journal of Medicine.
“The response rate of 18% in the 177Lu-Dotatate group (as compared with 3% in the control group) is also notable, given that response rates above 5% have not been observed in large randomized clinical trials of other systemic therapies in this patient population,” said Jonathan R. Strosberg, MD, of the Moffitt Cancer Center, Tampa, and his associates.
All the study participants had metastatic disease that progressed despite first-line treatment using octreotide LAR; 80% had also undergone surgical resection, and nearly half had received some other form of systemic therapy before entering this study. The primary tumor site was the ileum in most patients, and most also had metastases in the liver, the lymph nodes, or both, “typically in the mesentery or retroperitoneum.”
The primary efficacy endpoint – the estimated rate of progression-free survival at month 20 – was 65.2% in the intervention group, compared with 10.8% in the control group. This represents a 79% lower risk of disease progression or death with 177Lu-Dotatate. An interim analysis of overall survival (an endpoint that cannot be determined definitively until more time has passed) showed a 60% lower risk of death in the intervention group than in the control group. Treatment response rates were 18% and 3%, respectively, Dr. Strosberg and his associates reported (New Engl J Med. 2017 Jan 12. doi:10.1056/NEJMoa1607427).
177Lu-Dotatate was administered together with a renal-protection agent, and there has been no evidence of renal toxic effects to date. Rates of low-grade hematologic toxicities were low. The most common adverse effects were nausea and vomiting, which were largely attributed to the renal-protection agent, as well as fatigue, asthenia, abdominal pain, and diarrhea. Adverse events leading to premature withdrawal from the trial developed in more of the control group (9%) than of the intervention group (6%).
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: 177Lu-Dotatate cuts the risk of disease progression or death by 79% in patients with advanced progressive midgut neuroendocrine tumors.
Major finding: The primary efficacy endpoint – the estimated rate of progression-free survival at month 20 – was 65.2% in the intervention group, compared with 10.8% in the control group.
Data source: An international, open-label phase III randomized clinical trial involving 229 adults followed for a median of 14 months.
Disclosures: This study was sponsored by Advanced Accelerator Applications. Dr. Strosberg reported having no relevant financial disclosures; his associates reported ties to numerous industry sources.
Ibrutinib continues to wow in CLL/SLL
SAN DIEGO – More than 90% of the first patients with previously untreated chronic lymphocytic leukemia who received ibrutinib in an early study are alive and without disease progression 5 years later, investigators reported.
Among 31 treatment-naive patients with chronic lymphocytic leukemia/small lymphocytic leukemia (CLL/SLL) who were started on the Bruton’s tyrosine kinase inhibitor ibrutinib (Imbruvica) in the phase Ib/II PCYC-1102/1103 study, the 5-year progression-free survival (PFS) rate was 92%, with the median PFS not reached. Estimated 5-year overall survival (OS) among these patients was also 92%, with the median not reached, Susan O’Brien, MD, of the University of California, Irvine, reported at the annual meeting of the American Society of Hematology.
The 5-year PFS rate for patients with relapsed/refractory disease who had received a median of four prior lines of therapy before starting on single-agent ibrutinib was 43%, with a median PFS of 52 months. In this group, the overall survival (OS) rate was 57%, with the median not reached.
“At 5 years of follow-up, there are very durable responses in treatment-naive and relapsed refractory patients. You saw that, in the treatment-naive group, there is, in fact, only one patient who has progressed so far,” Dr. O’Brien said.
In a separate study, investigators from the phase III RESONATE-2 trial reported updated safety and efficacy data showing that in first-line therapy for patients aged 65 years and older with CLL/SLL with active disease, ibrutinib was associated with significantly better PFS at 24 months, compared with chlorambucil.
In this study by Dr. O’Brien and colleagues, 31 patients with previously untreated CLL/SLL and 101 patients with relapsed/refractory disease (progression or no objective response within 24 months of starting on chemoimmunotherapy) were treated with oral ibrutinib once daily at doses of 420 mg or 840 mg until disease progression or unacceptable toxicity.
After 5 years of follow-up, 20 of the 31 treatment-naive patients (65%) and 30 of the 101 relapsed/refractory patients (30%) remained on ibrutinib therapy. The primary reasons for discontinuation among relapsed/refractory patients included progressive disease in 33%, adverse events in 21%, and investigator decision in 11%.
Best response rates in treatment-naive patients were 87% (29% complete response, 55% partial response, 3% partial response-L) and 89% in relapsed/refractory patients (10%, 76%, and 3%, respectively).
An analysis of survival by IGHV (immunoglobulin heavy chain variable) mutational status in patients with relapsed/refractory disease showed a 53% 5-year PFS rate among patients with mutated IGHV and a median PFS of 63 months, compared with 38% and 43 months for patients with unmutated IGHV. Respective 5-year overall survival rates were 66% (median OS, 63 months) and 55% (median not reached).
In an analysis of survival outcomes by chromosomal abnormalities detected by FISH (fluorescent in situ hybridization) among patients with relapsed/refractory disease, median PFS and OS rates were highest among patients with the 13q deletion, at 91% for both PFS and OS, compared with 80% for each in patients with trisomy 12, 33% and 61% for patients with deletion 11q, and 19% and 32% for patients with deletion 17p. In patients with no chromosomal abnormalities, the 5-year PFS rate was 66% (median not reached), and the 5-year OS rate was 83% (median not reached).
Among patients with complex karyotype, 90% of whom had relapsed refractory disease, the 5-year PFS rate was 36% (median 33 months), and the OS rate was 46% (median 57 months). In contrast, respective PFS and OS rates for patients without complex karyotype were 69% and 84%, with the median not reached in either survival category.
In multivariate analysis, only deletion 17p was identified as a significant predictor of PFS and OS.
Grade 3 or greater treatment-emergent adverse events occurred mostly frequently in the first year of therapy and declined thereafter. The most common grade 3 or greater events were hypertension, (26% of all patients), pneumonia (22%), neutropenia (17%), and atrial fibrillation (9%).
Paul M. Barr, MD, of the University of Rochester presented updated data from RESONATE-2, comparing ibrutinib with chlorambucil in patients 65 and older with newly diagnosed, active CLL/SLL.
At a median follow-up of 29 months, the rates of 2-year PFS were 89% for patients treated with ibrutinib (median PFS not reached) vs. 34% for chlorambucil (median PFS 15 months). This translated into a hazard ratio for ibrutinib of 0.121 (P less than .0001). The benefit of ibrutinib occurred without regard to IGHV status, and ibrutinib continues to demonstrate an OS benefit over chlorambucil with longer follow-up and crossover. Overall survival at 24 months was 95% for patients treated with ibrutinib (included 55 patients who were crossed over from chlorambucil) vs. 84% for patients treated with chlorambucil only.
“The depth of the responses has improved over time, now with 18% of patients achieving a CR with ibrutinib, and lastly, ibrutinib remains tolerable in this elderly population, with 79% of patients that are continuing on therapy,” Dr. Barr said.
Both studies were funded by Pharmacyclics. Dr. Barr and Dr. O’Brien disclosed serving as consultants to the company, and Dr. O’Brien further disclosed honoraria and research funding from Pharmacyclics.
SAN DIEGO – More than 90% of the first patients with previously untreated chronic lymphocytic leukemia who received ibrutinib in an early study are alive and without disease progression 5 years later, investigators reported.
Among 31 treatment-naive patients with chronic lymphocytic leukemia/small lymphocytic leukemia (CLL/SLL) who were started on the Bruton’s tyrosine kinase inhibitor ibrutinib (Imbruvica) in the phase Ib/II PCYC-1102/1103 study, the 5-year progression-free survival (PFS) rate was 92%, with the median PFS not reached. Estimated 5-year overall survival (OS) among these patients was also 92%, with the median not reached, Susan O’Brien, MD, of the University of California, Irvine, reported at the annual meeting of the American Society of Hematology.
The 5-year PFS rate for patients with relapsed/refractory disease who had received a median of four prior lines of therapy before starting on single-agent ibrutinib was 43%, with a median PFS of 52 months. In this group, the overall survival (OS) rate was 57%, with the median not reached.
“At 5 years of follow-up, there are very durable responses in treatment-naive and relapsed refractory patients. You saw that, in the treatment-naive group, there is, in fact, only one patient who has progressed so far,” Dr. O’Brien said.
In a separate study, investigators from the phase III RESONATE-2 trial reported updated safety and efficacy data showing that in first-line therapy for patients aged 65 years and older with CLL/SLL with active disease, ibrutinib was associated with significantly better PFS at 24 months, compared with chlorambucil.
In this study by Dr. O’Brien and colleagues, 31 patients with previously untreated CLL/SLL and 101 patients with relapsed/refractory disease (progression or no objective response within 24 months of starting on chemoimmunotherapy) were treated with oral ibrutinib once daily at doses of 420 mg or 840 mg until disease progression or unacceptable toxicity.
After 5 years of follow-up, 20 of the 31 treatment-naive patients (65%) and 30 of the 101 relapsed/refractory patients (30%) remained on ibrutinib therapy. The primary reasons for discontinuation among relapsed/refractory patients included progressive disease in 33%, adverse events in 21%, and investigator decision in 11%.
Best response rates in treatment-naive patients were 87% (29% complete response, 55% partial response, 3% partial response-L) and 89% in relapsed/refractory patients (10%, 76%, and 3%, respectively).
An analysis of survival by IGHV (immunoglobulin heavy chain variable) mutational status in patients with relapsed/refractory disease showed a 53% 5-year PFS rate among patients with mutated IGHV and a median PFS of 63 months, compared with 38% and 43 months for patients with unmutated IGHV. Respective 5-year overall survival rates were 66% (median OS, 63 months) and 55% (median not reached).
In an analysis of survival outcomes by chromosomal abnormalities detected by FISH (fluorescent in situ hybridization) among patients with relapsed/refractory disease, median PFS and OS rates were highest among patients with the 13q deletion, at 91% for both PFS and OS, compared with 80% for each in patients with trisomy 12, 33% and 61% for patients with deletion 11q, and 19% and 32% for patients with deletion 17p. In patients with no chromosomal abnormalities, the 5-year PFS rate was 66% (median not reached), and the 5-year OS rate was 83% (median not reached).
Among patients with complex karyotype, 90% of whom had relapsed refractory disease, the 5-year PFS rate was 36% (median 33 months), and the OS rate was 46% (median 57 months). In contrast, respective PFS and OS rates for patients without complex karyotype were 69% and 84%, with the median not reached in either survival category.
In multivariate analysis, only deletion 17p was identified as a significant predictor of PFS and OS.
Grade 3 or greater treatment-emergent adverse events occurred mostly frequently in the first year of therapy and declined thereafter. The most common grade 3 or greater events were hypertension, (26% of all patients), pneumonia (22%), neutropenia (17%), and atrial fibrillation (9%).
Paul M. Barr, MD, of the University of Rochester presented updated data from RESONATE-2, comparing ibrutinib with chlorambucil in patients 65 and older with newly diagnosed, active CLL/SLL.
At a median follow-up of 29 months, the rates of 2-year PFS were 89% for patients treated with ibrutinib (median PFS not reached) vs. 34% for chlorambucil (median PFS 15 months). This translated into a hazard ratio for ibrutinib of 0.121 (P less than .0001). The benefit of ibrutinib occurred without regard to IGHV status, and ibrutinib continues to demonstrate an OS benefit over chlorambucil with longer follow-up and crossover. Overall survival at 24 months was 95% for patients treated with ibrutinib (included 55 patients who were crossed over from chlorambucil) vs. 84% for patients treated with chlorambucil only.
“The depth of the responses has improved over time, now with 18% of patients achieving a CR with ibrutinib, and lastly, ibrutinib remains tolerable in this elderly population, with 79% of patients that are continuing on therapy,” Dr. Barr said.
Both studies were funded by Pharmacyclics. Dr. Barr and Dr. O’Brien disclosed serving as consultants to the company, and Dr. O’Brien further disclosed honoraria and research funding from Pharmacyclics.
SAN DIEGO – More than 90% of the first patients with previously untreated chronic lymphocytic leukemia who received ibrutinib in an early study are alive and without disease progression 5 years later, investigators reported.
Among 31 treatment-naive patients with chronic lymphocytic leukemia/small lymphocytic leukemia (CLL/SLL) who were started on the Bruton’s tyrosine kinase inhibitor ibrutinib (Imbruvica) in the phase Ib/II PCYC-1102/1103 study, the 5-year progression-free survival (PFS) rate was 92%, with the median PFS not reached. Estimated 5-year overall survival (OS) among these patients was also 92%, with the median not reached, Susan O’Brien, MD, of the University of California, Irvine, reported at the annual meeting of the American Society of Hematology.
The 5-year PFS rate for patients with relapsed/refractory disease who had received a median of four prior lines of therapy before starting on single-agent ibrutinib was 43%, with a median PFS of 52 months. In this group, the overall survival (OS) rate was 57%, with the median not reached.
“At 5 years of follow-up, there are very durable responses in treatment-naive and relapsed refractory patients. You saw that, in the treatment-naive group, there is, in fact, only one patient who has progressed so far,” Dr. O’Brien said.
In a separate study, investigators from the phase III RESONATE-2 trial reported updated safety and efficacy data showing that in first-line therapy for patients aged 65 years and older with CLL/SLL with active disease, ibrutinib was associated with significantly better PFS at 24 months, compared with chlorambucil.
In this study by Dr. O’Brien and colleagues, 31 patients with previously untreated CLL/SLL and 101 patients with relapsed/refractory disease (progression or no objective response within 24 months of starting on chemoimmunotherapy) were treated with oral ibrutinib once daily at doses of 420 mg or 840 mg until disease progression or unacceptable toxicity.
After 5 years of follow-up, 20 of the 31 treatment-naive patients (65%) and 30 of the 101 relapsed/refractory patients (30%) remained on ibrutinib therapy. The primary reasons for discontinuation among relapsed/refractory patients included progressive disease in 33%, adverse events in 21%, and investigator decision in 11%.
Best response rates in treatment-naive patients were 87% (29% complete response, 55% partial response, 3% partial response-L) and 89% in relapsed/refractory patients (10%, 76%, and 3%, respectively).
An analysis of survival by IGHV (immunoglobulin heavy chain variable) mutational status in patients with relapsed/refractory disease showed a 53% 5-year PFS rate among patients with mutated IGHV and a median PFS of 63 months, compared with 38% and 43 months for patients with unmutated IGHV. Respective 5-year overall survival rates were 66% (median OS, 63 months) and 55% (median not reached).
In an analysis of survival outcomes by chromosomal abnormalities detected by FISH (fluorescent in situ hybridization) among patients with relapsed/refractory disease, median PFS and OS rates were highest among patients with the 13q deletion, at 91% for both PFS and OS, compared with 80% for each in patients with trisomy 12, 33% and 61% for patients with deletion 11q, and 19% and 32% for patients with deletion 17p. In patients with no chromosomal abnormalities, the 5-year PFS rate was 66% (median not reached), and the 5-year OS rate was 83% (median not reached).
Among patients with complex karyotype, 90% of whom had relapsed refractory disease, the 5-year PFS rate was 36% (median 33 months), and the OS rate was 46% (median 57 months). In contrast, respective PFS and OS rates for patients without complex karyotype were 69% and 84%, with the median not reached in either survival category.
In multivariate analysis, only deletion 17p was identified as a significant predictor of PFS and OS.
Grade 3 or greater treatment-emergent adverse events occurred mostly frequently in the first year of therapy and declined thereafter. The most common grade 3 or greater events were hypertension, (26% of all patients), pneumonia (22%), neutropenia (17%), and atrial fibrillation (9%).
Paul M. Barr, MD, of the University of Rochester presented updated data from RESONATE-2, comparing ibrutinib with chlorambucil in patients 65 and older with newly diagnosed, active CLL/SLL.
At a median follow-up of 29 months, the rates of 2-year PFS were 89% for patients treated with ibrutinib (median PFS not reached) vs. 34% for chlorambucil (median PFS 15 months). This translated into a hazard ratio for ibrutinib of 0.121 (P less than .0001). The benefit of ibrutinib occurred without regard to IGHV status, and ibrutinib continues to demonstrate an OS benefit over chlorambucil with longer follow-up and crossover. Overall survival at 24 months was 95% for patients treated with ibrutinib (included 55 patients who were crossed over from chlorambucil) vs. 84% for patients treated with chlorambucil only.
“The depth of the responses has improved over time, now with 18% of patients achieving a CR with ibrutinib, and lastly, ibrutinib remains tolerable in this elderly population, with 79% of patients that are continuing on therapy,” Dr. Barr said.
Both studies were funded by Pharmacyclics. Dr. Barr and Dr. O’Brien disclosed serving as consultants to the company, and Dr. O’Brien further disclosed honoraria and research funding from Pharmacyclics.
AT ASH 2016
Key clinical point: Long-term follow-up of two studies shows a progression-free and overall survival advantage with ibrutinib in chronic lymphocytic leukemia/small lymphocytic leukemia.
Major finding: 5-year PFS and OS rates were 92% for treatment-naive patients with CLL/SLL treated with ibrutinib.
Data source: Phase Ib/II study and randomized phase III study of ibrutinib for treatment-naive and relapsed/refractory CLL/SLL.
Disclosures: Both studies were funded by Pharmacyclics. Dr. Barr and Dr. O’Brien disclosed serving as consultants to the company; Dr. O’Brien disclosed honoraria and research funding from the company.
Perfect attendance
A few years ago I audited a college course on leadership taught by Angus King (I-ME), former governor and now independent Senator from Maine. He emphasized that an important characteristic of effective leaders is that they show up for work. They are there, present, on the scene. Attempting to lead in absentia is seldom successful. Knowledge gathered firsthand can be critical when it’s decision-making time. And the connectedness fostered by the leader’s physical presence can bolster morale in a crisis.
Being a parent is more complex than simply being a leader, but showing up is just as important to being a good parent as it is to being an effective leader. Most parents already believe that “being there” is important, and feel guilty when they have obligations that prevent them from maintaining a perfect attendance record.

Common sense also may suggest to parents that their presence is less important as their children get older. Certainly, the behavior of most teenagers would suggest that adolescents couldn’t care less whether their parents were at home or vacationing in the Bahamas. However, this is one of those situations where appearances may be deceiving. The author of an opinion piece in the New York Times presents some compelling evidence that in fact, adolescents place a higher value on their parents’ presence than the common stereotype of teenage behavior would suggest (”What Do Teenagers Want? Potted Plants Parents,” By Lisa Damour, Dec. 14, 2016).
Citing her own experience as a psychologist in private practice in Ohio and several recent studies from the psychology literature, the author observes that “sheer proximity confers a benefit [to the adolescent’s psychological health] over and above feeling of closeness or connectedness between parent and child.” At present there is no explanation for this benefit of just being there for your teenage child. But it may be that a parental presence, even if it is silent, provides a stable base and comfort zone that the adolescent can return to as he or she tests the ability to function independently in the world outside of the family.
I suspect that most of you have observed this counter-intuitive phenomenon in which teenagers who give every outward appearance of wanting nothing to do with their parents actually would like to have at least one parent be at home. They just don’t want to be hovered over. Ninety-nine percent of the time the parent will receive no positive feedback for just being there like a “potted plant” to use Ms. Damour’s analogy.
The problem is how to get this message to parents early enough in their parenting trajectory that they can adjust work schedules and priorities to be home with their adolescents. It was not unusual for new parents to ask for my thoughts as they were considering various day care and work schedule options for their infants. If I thought they were really going to take my advice seriously I would add, “You know you should also be thinking ahead when she is a teen. She won’t ask, but she probably would like it if you were home in the afternoon when she gets home from school.”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.” Email him at [email protected].
A few years ago I audited a college course on leadership taught by Angus King (I-ME), former governor and now independent Senator from Maine. He emphasized that an important characteristic of effective leaders is that they show up for work. They are there, present, on the scene. Attempting to lead in absentia is seldom successful. Knowledge gathered firsthand can be critical when it’s decision-making time. And the connectedness fostered by the leader’s physical presence can bolster morale in a crisis.
Being a parent is more complex than simply being a leader, but showing up is just as important to being a good parent as it is to being an effective leader. Most parents already believe that “being there” is important, and feel guilty when they have obligations that prevent them from maintaining a perfect attendance record.
Common sense also may suggest to parents that their presence is less important as their children get older. Certainly, the behavior of most teenagers would suggest that adolescents couldn’t care less whether their parents were at home or vacationing in the Bahamas. However, this is one of those situations where appearances may be deceiving. The author of an opinion piece in the New York Times presents some compelling evidence that in fact, adolescents place a higher value on their parents’ presence than the common stereotype of teenage behavior would suggest (”What Do Teenagers Want? Potted Plants Parents,” By Lisa Damour, Dec. 14, 2016).
Citing her own experience as a psychologist in private practice in Ohio and several recent studies from the psychology literature, the author observes that “sheer proximity confers a benefit [to the adolescent’s psychological health] over and above feeling of closeness or connectedness between parent and child.” At present there is no explanation for this benefit of just being there for your teenage child. But it may be that a parental presence, even if it is silent, provides a stable base and comfort zone that the adolescent can return to as he or she tests the ability to function independently in the world outside of the family.
I suspect that most of you have observed this counter-intuitive phenomenon in which teenagers who give every outward appearance of wanting nothing to do with their parents actually would like to have at least one parent be at home. They just don’t want to be hovered over. Ninety-nine percent of the time the parent will receive no positive feedback for just being there like a “potted plant” to use Ms. Damour’s analogy.
The problem is how to get this message to parents early enough in their parenting trajectory that they can adjust work schedules and priorities to be home with their adolescents. It was not unusual for new parents to ask for my thoughts as they were considering various day care and work schedule options for their infants. If I thought they were really going to take my advice seriously I would add, “You know you should also be thinking ahead when she is a teen. She won’t ask, but she probably would like it if you were home in the afternoon when she gets home from school.”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.” Email him at [email protected].
A few years ago I audited a college course on leadership taught by Angus King (I-ME), former governor and now independent Senator from Maine. He emphasized that an important characteristic of effective leaders is that they show up for work. They are there, present, on the scene. Attempting to lead in absentia is seldom successful. Knowledge gathered firsthand can be critical when it’s decision-making time. And the connectedness fostered by the leader’s physical presence can bolster morale in a crisis.
Being a parent is more complex than simply being a leader, but showing up is just as important to being a good parent as it is to being an effective leader. Most parents already believe that “being there” is important, and feel guilty when they have obligations that prevent them from maintaining a perfect attendance record.
Common sense also may suggest to parents that their presence is less important as their children get older. Certainly, the behavior of most teenagers would suggest that adolescents couldn’t care less whether their parents were at home or vacationing in the Bahamas. However, this is one of those situations where appearances may be deceiving. The author of an opinion piece in the New York Times presents some compelling evidence that in fact, adolescents place a higher value on their parents’ presence than the common stereotype of teenage behavior would suggest (”What Do Teenagers Want? Potted Plants Parents,” By Lisa Damour, Dec. 14, 2016).
Citing her own experience as a psychologist in private practice in Ohio and several recent studies from the psychology literature, the author observes that “sheer proximity confers a benefit [to the adolescent’s psychological health] over and above feeling of closeness or connectedness between parent and child.” At present there is no explanation for this benefit of just being there for your teenage child. But it may be that a parental presence, even if it is silent, provides a stable base and comfort zone that the adolescent can return to as he or she tests the ability to function independently in the world outside of the family.
I suspect that most of you have observed this counter-intuitive phenomenon in which teenagers who give every outward appearance of wanting nothing to do with their parents actually would like to have at least one parent be at home. They just don’t want to be hovered over. Ninety-nine percent of the time the parent will receive no positive feedback for just being there like a “potted plant” to use Ms. Damour’s analogy.
The problem is how to get this message to parents early enough in their parenting trajectory that they can adjust work schedules and priorities to be home with their adolescents. It was not unusual for new parents to ask for my thoughts as they were considering various day care and work schedule options for their infants. If I thought they were really going to take my advice seriously I would add, “You know you should also be thinking ahead when she is a teen. She won’t ask, but she probably would like it if you were home in the afternoon when she gets home from school.”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.” Email him at [email protected].
HIV research update: Late December 2016
A great volume of HIV and AIDS research enters the medical literature every month. It’s difficult to monitor everything, so here’s a quick look at some notable news items and journal articles published over the past few weeks.
Liver stiffness is very accurate for predicting liver-related events in HIV-infected patients with chronic hepatitis C infection, according to a Spanish study.
A study in the journal AIDS found that HIV/HCV coinfection is associated with a greater homeostasis model assessment of insulin resistance, even after controlling for demographic, lifestyle, and metabolic factors. The authors said sCD163, a marker of monocyte/macrophage activation which appears independent of intestinal epithelial damage and inflammation, partly explains this association.
Liver stiffness (LS) identifies HIV/HCV-coinfected patients with compensated cirrhosis with a very low risk of portal hypertensive gastrointestinal bleeding, according to a recent study, and as a result upper gastrointestinal endoscopy may be safely spared in patients with LS less than 21 kPa.
A study in HIV Medicine found that MicroRNA-155 levels in the peripheral blood of HIV-1–infected patients are increased and associated with T-cell activation, and therefore miR-155 is a potential biomarker of the immune response following HIV-1 infection.
A study in AIDS Care found no major differences between rural and urban South Carolina residents at the various stages of engagement in HIV care, using the HIV continuum of care model.
Investigators said identification of a cytokine signature specific for the preseroconversion stage of primary HIV infection may help to understand the earliest HIV pathogenic events and identify new potential targets for immunotherapy aimed at modulating the cytokine response to HIV infection.
Intimate partner violence is linked to less HIV testing uptake among high-risk, HIV-negative women in Atlanta, according to researchers at Emory University.
In HIV-positive women with sequential pregnancies, the second pregnancy was characterized by a significant improvement in several outcomes, a recent study found, suggesting that women with HIV infection who desire multiple children may proceed safely and confidently with subsequent pregnancies.
An estimated 29% of HIV care providers had not adopted recommendations to initiate antiretroviral therapy regardless of patient CD4 count, barring contraindications or barriers to treatment, according to a study in JAIDS. The leading reasons for deferring ART included patient refusal and adherence concerns.
Baseline vitamin D deficiency decreased the effectiveness of rosuvastatin in HIV-positive adults, according to a recent study, and researchers said vitamin D supplementation may be warranted for deficient patients initiating statin therapy.
A European study found HIV/HCV–coinfected patients with a favorable virologic response to PEG-interferon + ribavirin treatment had reduced risk of all-cause and liver-related death, while there was no difference in risk of non–liver-related death when comparing responders and nonresponders.
Unlike the prevalences in the general U.S. population, there was no difference in smoking prevalence for female versus male persons living with HIV (both greater than 50%) indicating that HIV infection status was associated with a greater relative increase in smoking for women than men, according to results of a recent study.
[email protected]
On Twitter @richpizzi
A great volume of HIV and AIDS research enters the medical literature every month. It’s difficult to monitor everything, so here’s a quick look at some notable news items and journal articles published over the past few weeks.
Liver stiffness is very accurate for predicting liver-related events in HIV-infected patients with chronic hepatitis C infection, according to a Spanish study.
A study in the journal AIDS found that HIV/HCV coinfection is associated with a greater homeostasis model assessment of insulin resistance, even after controlling for demographic, lifestyle, and metabolic factors. The authors said sCD163, a marker of monocyte/macrophage activation which appears independent of intestinal epithelial damage and inflammation, partly explains this association.
Liver stiffness (LS) identifies HIV/HCV-coinfected patients with compensated cirrhosis with a very low risk of portal hypertensive gastrointestinal bleeding, according to a recent study, and as a result upper gastrointestinal endoscopy may be safely spared in patients with LS less than 21 kPa.
A study in HIV Medicine found that MicroRNA-155 levels in the peripheral blood of HIV-1–infected patients are increased and associated with T-cell activation, and therefore miR-155 is a potential biomarker of the immune response following HIV-1 infection.
A study in AIDS Care found no major differences between rural and urban South Carolina residents at the various stages of engagement in HIV care, using the HIV continuum of care model.
Investigators said identification of a cytokine signature specific for the preseroconversion stage of primary HIV infection may help to understand the earliest HIV pathogenic events and identify new potential targets for immunotherapy aimed at modulating the cytokine response to HIV infection.
Intimate partner violence is linked to less HIV testing uptake among high-risk, HIV-negative women in Atlanta, according to researchers at Emory University.
In HIV-positive women with sequential pregnancies, the second pregnancy was characterized by a significant improvement in several outcomes, a recent study found, suggesting that women with HIV infection who desire multiple children may proceed safely and confidently with subsequent pregnancies.
An estimated 29% of HIV care providers had not adopted recommendations to initiate antiretroviral therapy regardless of patient CD4 count, barring contraindications or barriers to treatment, according to a study in JAIDS. The leading reasons for deferring ART included patient refusal and adherence concerns.
Baseline vitamin D deficiency decreased the effectiveness of rosuvastatin in HIV-positive adults, according to a recent study, and researchers said vitamin D supplementation may be warranted for deficient patients initiating statin therapy.
A European study found HIV/HCV–coinfected patients with a favorable virologic response to PEG-interferon + ribavirin treatment had reduced risk of all-cause and liver-related death, while there was no difference in risk of non–liver-related death when comparing responders and nonresponders.
Unlike the prevalences in the general U.S. population, there was no difference in smoking prevalence for female versus male persons living with HIV (both greater than 50%) indicating that HIV infection status was associated with a greater relative increase in smoking for women than men, according to results of a recent study.
[email protected]
On Twitter @richpizzi
A great volume of HIV and AIDS research enters the medical literature every month. It’s difficult to monitor everything, so here’s a quick look at some notable news items and journal articles published over the past few weeks.
Liver stiffness is very accurate for predicting liver-related events in HIV-infected patients with chronic hepatitis C infection, according to a Spanish study.
A study in the journal AIDS found that HIV/HCV coinfection is associated with a greater homeostasis model assessment of insulin resistance, even after controlling for demographic, lifestyle, and metabolic factors. The authors said sCD163, a marker of monocyte/macrophage activation which appears independent of intestinal epithelial damage and inflammation, partly explains this association.
Liver stiffness (LS) identifies HIV/HCV-coinfected patients with compensated cirrhosis with a very low risk of portal hypertensive gastrointestinal bleeding, according to a recent study, and as a result upper gastrointestinal endoscopy may be safely spared in patients with LS less than 21 kPa.
A study in HIV Medicine found that MicroRNA-155 levels in the peripheral blood of HIV-1–infected patients are increased and associated with T-cell activation, and therefore miR-155 is a potential biomarker of the immune response following HIV-1 infection.
A study in AIDS Care found no major differences between rural and urban South Carolina residents at the various stages of engagement in HIV care, using the HIV continuum of care model.
Investigators said identification of a cytokine signature specific for the preseroconversion stage of primary HIV infection may help to understand the earliest HIV pathogenic events and identify new potential targets for immunotherapy aimed at modulating the cytokine response to HIV infection.
Intimate partner violence is linked to less HIV testing uptake among high-risk, HIV-negative women in Atlanta, according to researchers at Emory University.
In HIV-positive women with sequential pregnancies, the second pregnancy was characterized by a significant improvement in several outcomes, a recent study found, suggesting that women with HIV infection who desire multiple children may proceed safely and confidently with subsequent pregnancies.
An estimated 29% of HIV care providers had not adopted recommendations to initiate antiretroviral therapy regardless of patient CD4 count, barring contraindications or barriers to treatment, according to a study in JAIDS. The leading reasons for deferring ART included patient refusal and adherence concerns.
Baseline vitamin D deficiency decreased the effectiveness of rosuvastatin in HIV-positive adults, according to a recent study, and researchers said vitamin D supplementation may be warranted for deficient patients initiating statin therapy.
A European study found HIV/HCV–coinfected patients with a favorable virologic response to PEG-interferon + ribavirin treatment had reduced risk of all-cause and liver-related death, while there was no difference in risk of non–liver-related death when comparing responders and nonresponders.
Unlike the prevalences in the general U.S. population, there was no difference in smoking prevalence for female versus male persons living with HIV (both greater than 50%) indicating that HIV infection status was associated with a greater relative increase in smoking for women than men, according to results of a recent study.
[email protected]
On Twitter @richpizzi
Wheat in skin care
Gluten-free food products have inundated the marketplace in recent years as the food industry has responded to greater awareness of celiac sprue disease and wheat sensitivity. Gluten is the primary form of wheat protein.
Wheat is a versatile and globally popular member of the Poaceae or Gramineae family known as grasses; it is of the Triticum species with Triticum aestivum and Triticum vulgare being particularly pervasive.1 In traditional Iranian medicine, the topical application of wheat germ oil has been used to treat psoriasis.2

Moisturization
In 2008, N. Akhtar and Y. Yazan investigated the effects of a stable emulsion containing two ingredients included to exert anti-aging effects: vitamin C and wheat protein. The antioxidant vitamin C was entrapped in the inner aqueous phase of the water-in-oil-in-water emulsion while wheat protein was incorporated in the oily phase. The investigators prepared and applied stable emulsions to the cheeks of 11 volunteers over 4 weeks, finding that the formulation increased skin moisture.7
Melanoma and wheat supplementation
Demidov et al. reported in 2008 on a randomized, pilot, phase II clinical trial to assess the impact of the adjuvant use of a fermented wheat germ extract nutraceutical (Avemar) in high-risk cutaneous melanoma patients. Investigators compared the efficacy of dacarbazine-based adjuvant chemotherapy on survival parameters of melanoma patients to that of the identical treatment supplemented with a 1-year administration of fermented wheat germ extract nutraceutical (FWGE), which is generally recognized as safe. They reported that after a 7-year follow-up, significant differences favoring the nutraceutical group were observed in progression-free and overall survival. Including nutraceutical as an adjuvant treatment for such patients was recommended by the authors.8
Telekes et al. noted that nutraceutical is registered as a special nutriment for cancer patients in Hungary that has exhibited potent anticancer activity on cell lines and immunomodulatory activity in vivo.9 In 2005, Boros et al. reported that orally administered FWGE suppressed metastatic tumor dissemination and proliferation during and after chemotherapy, surgery, or radiation, with benefits seen in some human cancers and cultured cells as well as some autoimmune disorders and in chemical carcinogenesis prevention.10
Hypersensitivity and allergic reactions
The risks of sensitization to topical wheat proteins are thought to be higher in patients with atopic dermatitis, who have an impaired skin barrier.1 Indeed, Codreanu et al. have suggested that topical products containing food proteins of known allergenicity (including wheat) are contraindicated for neonates and infants with atopic dermatitis.11
In 2015, Bonciolini et al. studied 17 patients (13 females and 4 males, median age 36 years) with nonceliac gluten sensitivity presenting with nonspecific skin lesions. The eczema-, psoriasis-, or dermatitis herpetiformis-like lesions on the extensor surfaces of the upper and lower limbs, especially, were confirmed histologically, but immunopathological evaluations revealed pervasive C3 deposits along the dermoepidermal junction in a microgranular/granular pattern (82%). Notably, all of the patients improved markedly after initiating a gluten-free diet.12
In 2014, Fukutomi et al. conducted a case-control study of Japanese women aged 20-54 years (157 cases) who self-reported wheat allergy to ascertain the epidemiologic relationship between food allergy to wheat after exposure to facial soaps containing hydrolyzed wheat protein. There were 449 age-matched controls without wheat allergy. Participants answered a Web-based questionnaire about their use of skin and hair care products. The investigators found that current use of the facial soap Cha no Shizuku (Drop of Tea), which contains hydrolyzed wheat protein, was significantly linked to a greater risk of wheat allergy, with use of the soap more frequent in consumers whose wheat allergy had newly emerged (11% vs. 6% in controls).13
Cha no Shizuku had earlier been implicated in provoking hundreds of cases of allergic reactions between 2009 and June 2013. R. Teshima noted that the soap contains acid-hydrolyzed wheat protein produced from gluten after partial hydrolysis with hydrogen chloride at 95 ° C for 40 minutes.14
It is worth noting that case reports of allergic reactions to facial soap containing hydrolyzed wheat protein continue to appear. Iseki et al. described in 2014 a 38-year-old woman who experienced irregular headaches, sleepiness, and an episode of facial rash eruption after daily use for about 1 year of a facial soap with hydrolyzed wheat proteins (Glupearl 19s, which is also used in Cha no Shizuku). The investigators added that the patient’s serum contained wheat-specific IgE antibodies. Symptoms disappeared after the patient abstained from wheat.15
In 2012, Tammaro studied cutaneous hypersensitivity to gluten in 14 female patients (aged 12-60 years) with celiac disease who presented with eczema on the face, neck, and arms, after topical application of gluten-containing emollient cream, bath or face powder, or contact with foods containing wheat and durum. Five of the patients tested positive for wheat and durum wheat, while none of the 14 control patients tested positive. Improvement in cutaneous lesions, with no relapses during a 6-month follow-up, resulted when these patients used gluten-free cream and bath powder, and wore gloves before handling wheat-containing food.16
In 2011, Celakovská et al. studied the impact of wheat allergy in 179 adults with atopic eczema (128 females, 51 males; average age 26 years), using open exposure and double-blind, placebo-controlled food challenge tests, as well as specific serum IgE, skin prick, and atopy patch tests. The double-blind, placebo-controlled food challenge test showed that the course of atopic eczema was exacerbated by wheat allergy in eight patients (4.5%). A positive trend revealing that the course of atopic eczema was impacted by wheat allergy emerged during follow-up (at 3, 6, 9, and 12 months).17
Contact urticaria also has been reported to have been induced by hydrolyzed wheat proteins in cosmetics and is notable for the potential to precede food allergies.2,3 A wide variety of protein hydrolysates found in hair products have been associated with inducing contact urticaria, particularly in patients with atopic dermatitis.4
In 2006, Laurière et al. studied nine female patients without common wheat allergy who presented with contact urticaria to cosmetics containing hydrolyzed wheat proteins; six also had experienced generalized urticaria or anaphylaxis in response to foods containing such wheat proteins. Analyses revealed the importance of hydrolysis in augmenting the allergenicity of wheat proteins through contact or consumption.18 Immediate contact urticaria in reaction to hydrolyzed wheat protein in topical products also has been reported in a child.19
Conclusion
Can the presence of wheat hydrolysates in personal care products adversely affect a patient with celiac sprue or wheat sensitivity? The short answer appears to be “yes.” Given the use of hydrolyzed wheat protein in various skin care products, it is important that consumers who have celiac disease or sensitivity to wheat be advised to avoid skin care formulations with such active ingredients. On the positive side of the wheat ledger, there are some indications (albeit in very limited research) that the plant protein may impart beneficial health effects. Much more research is necessary to delineate the full impact of wheat on skin health.
I thank my dermatologist colleague Sharon E. Jacob, MD, at the University of Miami, for suggesting this topic.
References
1. Dermatitis. 2013 Nov-Dec;24(6):291-5.
2. Iran J Med Sci. 2016 May;41(3 Suppl):S54.
3. Contact Dermatitis. 2007 Feb;56(2):119-20.
4. Ann Dermatol Venereol. 2010 Apr;137(4):281-4.
5. Allergy. 1998 Nov;53(11):1078-82.
6. J Drugs Dermatol. 2013 Sep;12(9 Suppl):s133-6.
7. Pak J Pharm Sci. 2008 Jan;21(1):45-50.
8. Cancer Biother Radiopharm. 2008 Aug;23(4):477-82.
9. Nutr Cancer. 2009;61(6):891-9.
10. Ann N Y Acad Sci. 2005 Jun;1051:529-42.
11. Eur Ann Allergy Clin Immunol. 2006 Apr;38(4):126-30.
12. Nutrients. 2015 Sep 15;7(9):7798-805.
13. Allergy. 2014 Oct;69(10):1405-11.
14. Yakugaku Zasshi. 2014;134(1):33-8.
15. Intern Med. 2014;53(2):151-4.
16. Dermatitis. 2012 Sep-Oct;23(5):220-1.
17. Acta Medica (Hradec Kralove). 2011;54(4):157-62.
18. Contact Dermatitis. 2006 May;54(5):283-9.
19. Contact Dermatitis. 2013 Jun;68(6):379-80.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever. Dr. Baumann also developed and owns the Baumann Skin Type Solution skin typing systems and related products.
Gluten-free food products have inundated the marketplace in recent years as the food industry has responded to greater awareness of celiac sprue disease and wheat sensitivity. Gluten is the primary form of wheat protein.
Wheat is a versatile and globally popular member of the Poaceae or Gramineae family known as grasses; it is of the Triticum species with Triticum aestivum and Triticum vulgare being particularly pervasive.1 In traditional Iranian medicine, the topical application of wheat germ oil has been used to treat psoriasis.2
Moisturization
In 2008, N. Akhtar and Y. Yazan investigated the effects of a stable emulsion containing two ingredients included to exert anti-aging effects: vitamin C and wheat protein. The antioxidant vitamin C was entrapped in the inner aqueous phase of the water-in-oil-in-water emulsion while wheat protein was incorporated in the oily phase. The investigators prepared and applied stable emulsions to the cheeks of 11 volunteers over 4 weeks, finding that the formulation increased skin moisture.7
Melanoma and wheat supplementation
Demidov et al. reported in 2008 on a randomized, pilot, phase II clinical trial to assess the impact of the adjuvant use of a fermented wheat germ extract nutraceutical (Avemar) in high-risk cutaneous melanoma patients. Investigators compared the efficacy of dacarbazine-based adjuvant chemotherapy on survival parameters of melanoma patients to that of the identical treatment supplemented with a 1-year administration of fermented wheat germ extract nutraceutical (FWGE), which is generally recognized as safe. They reported that after a 7-year follow-up, significant differences favoring the nutraceutical group were observed in progression-free and overall survival. Including nutraceutical as an adjuvant treatment for such patients was recommended by the authors.8
Telekes et al. noted that nutraceutical is registered as a special nutriment for cancer patients in Hungary that has exhibited potent anticancer activity on cell lines and immunomodulatory activity in vivo.9 In 2005, Boros et al. reported that orally administered FWGE suppressed metastatic tumor dissemination and proliferation during and after chemotherapy, surgery, or radiation, with benefits seen in some human cancers and cultured cells as well as some autoimmune disorders and in chemical carcinogenesis prevention.10
Hypersensitivity and allergic reactions
The risks of sensitization to topical wheat proteins are thought to be higher in patients with atopic dermatitis, who have an impaired skin barrier.1 Indeed, Codreanu et al. have suggested that topical products containing food proteins of known allergenicity (including wheat) are contraindicated for neonates and infants with atopic dermatitis.11
In 2015, Bonciolini et al. studied 17 patients (13 females and 4 males, median age 36 years) with nonceliac gluten sensitivity presenting with nonspecific skin lesions. The eczema-, psoriasis-, or dermatitis herpetiformis-like lesions on the extensor surfaces of the upper and lower limbs, especially, were confirmed histologically, but immunopathological evaluations revealed pervasive C3 deposits along the dermoepidermal junction in a microgranular/granular pattern (82%). Notably, all of the patients improved markedly after initiating a gluten-free diet.12
In 2014, Fukutomi et al. conducted a case-control study of Japanese women aged 20-54 years (157 cases) who self-reported wheat allergy to ascertain the epidemiologic relationship between food allergy to wheat after exposure to facial soaps containing hydrolyzed wheat protein. There were 449 age-matched controls without wheat allergy. Participants answered a Web-based questionnaire about their use of skin and hair care products. The investigators found that current use of the facial soap Cha no Shizuku (Drop of Tea), which contains hydrolyzed wheat protein, was significantly linked to a greater risk of wheat allergy, with use of the soap more frequent in consumers whose wheat allergy had newly emerged (11% vs. 6% in controls).13
Cha no Shizuku had earlier been implicated in provoking hundreds of cases of allergic reactions between 2009 and June 2013. R. Teshima noted that the soap contains acid-hydrolyzed wheat protein produced from gluten after partial hydrolysis with hydrogen chloride at 95 ° C for 40 minutes.14
It is worth noting that case reports of allergic reactions to facial soap containing hydrolyzed wheat protein continue to appear. Iseki et al. described in 2014 a 38-year-old woman who experienced irregular headaches, sleepiness, and an episode of facial rash eruption after daily use for about 1 year of a facial soap with hydrolyzed wheat proteins (Glupearl 19s, which is also used in Cha no Shizuku). The investigators added that the patient’s serum contained wheat-specific IgE antibodies. Symptoms disappeared after the patient abstained from wheat.15
In 2012, Tammaro studied cutaneous hypersensitivity to gluten in 14 female patients (aged 12-60 years) with celiac disease who presented with eczema on the face, neck, and arms, after topical application of gluten-containing emollient cream, bath or face powder, or contact with foods containing wheat and durum. Five of the patients tested positive for wheat and durum wheat, while none of the 14 control patients tested positive. Improvement in cutaneous lesions, with no relapses during a 6-month follow-up, resulted when these patients used gluten-free cream and bath powder, and wore gloves before handling wheat-containing food.16
In 2011, Celakovská et al. studied the impact of wheat allergy in 179 adults with atopic eczema (128 females, 51 males; average age 26 years), using open exposure and double-blind, placebo-controlled food challenge tests, as well as specific serum IgE, skin prick, and atopy patch tests. The double-blind, placebo-controlled food challenge test showed that the course of atopic eczema was exacerbated by wheat allergy in eight patients (4.5%). A positive trend revealing that the course of atopic eczema was impacted by wheat allergy emerged during follow-up (at 3, 6, 9, and 12 months).17
Contact urticaria also has been reported to have been induced by hydrolyzed wheat proteins in cosmetics and is notable for the potential to precede food allergies.2,3 A wide variety of protein hydrolysates found in hair products have been associated with inducing contact urticaria, particularly in patients with atopic dermatitis.4
In 2006, Laurière et al. studied nine female patients without common wheat allergy who presented with contact urticaria to cosmetics containing hydrolyzed wheat proteins; six also had experienced generalized urticaria or anaphylaxis in response to foods containing such wheat proteins. Analyses revealed the importance of hydrolysis in augmenting the allergenicity of wheat proteins through contact or consumption.18 Immediate contact urticaria in reaction to hydrolyzed wheat protein in topical products also has been reported in a child.19
Conclusion
Can the presence of wheat hydrolysates in personal care products adversely affect a patient with celiac sprue or wheat sensitivity? The short answer appears to be “yes.” Given the use of hydrolyzed wheat protein in various skin care products, it is important that consumers who have celiac disease or sensitivity to wheat be advised to avoid skin care formulations with such active ingredients. On the positive side of the wheat ledger, there are some indications (albeit in very limited research) that the plant protein may impart beneficial health effects. Much more research is necessary to delineate the full impact of wheat on skin health.
I thank my dermatologist colleague Sharon E. Jacob, MD, at the University of Miami, for suggesting this topic.
References
1. Dermatitis. 2013 Nov-Dec;24(6):291-5.
2. Iran J Med Sci. 2016 May;41(3 Suppl):S54.
3. Contact Dermatitis. 2007 Feb;56(2):119-20.
4. Ann Dermatol Venereol. 2010 Apr;137(4):281-4.
5. Allergy. 1998 Nov;53(11):1078-82.
6. J Drugs Dermatol. 2013 Sep;12(9 Suppl):s133-6.
7. Pak J Pharm Sci. 2008 Jan;21(1):45-50.
8. Cancer Biother Radiopharm. 2008 Aug;23(4):477-82.
9. Nutr Cancer. 2009;61(6):891-9.
10. Ann N Y Acad Sci. 2005 Jun;1051:529-42.
11. Eur Ann Allergy Clin Immunol. 2006 Apr;38(4):126-30.
12. Nutrients. 2015 Sep 15;7(9):7798-805.
13. Allergy. 2014 Oct;69(10):1405-11.
14. Yakugaku Zasshi. 2014;134(1):33-8.
15. Intern Med. 2014;53(2):151-4.
16. Dermatitis. 2012 Sep-Oct;23(5):220-1.
17. Acta Medica (Hradec Kralove). 2011;54(4):157-62.
18. Contact Dermatitis. 2006 May;54(5):283-9.
19. Contact Dermatitis. 2013 Jun;68(6):379-80.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever. Dr. Baumann also developed and owns the Baumann Skin Type Solution skin typing systems and related products.
Gluten-free food products have inundated the marketplace in recent years as the food industry has responded to greater awareness of celiac sprue disease and wheat sensitivity. Gluten is the primary form of wheat protein.
Wheat is a versatile and globally popular member of the Poaceae or Gramineae family known as grasses; it is of the Triticum species with Triticum aestivum and Triticum vulgare being particularly pervasive.1 In traditional Iranian medicine, the topical application of wheat germ oil has been used to treat psoriasis.2
Moisturization
In 2008, N. Akhtar and Y. Yazan investigated the effects of a stable emulsion containing two ingredients included to exert anti-aging effects: vitamin C and wheat protein. The antioxidant vitamin C was entrapped in the inner aqueous phase of the water-in-oil-in-water emulsion while wheat protein was incorporated in the oily phase. The investigators prepared and applied stable emulsions to the cheeks of 11 volunteers over 4 weeks, finding that the formulation increased skin moisture.7
Melanoma and wheat supplementation
Demidov et al. reported in 2008 on a randomized, pilot, phase II clinical trial to assess the impact of the adjuvant use of a fermented wheat germ extract nutraceutical (Avemar) in high-risk cutaneous melanoma patients. Investigators compared the efficacy of dacarbazine-based adjuvant chemotherapy on survival parameters of melanoma patients to that of the identical treatment supplemented with a 1-year administration of fermented wheat germ extract nutraceutical (FWGE), which is generally recognized as safe. They reported that after a 7-year follow-up, significant differences favoring the nutraceutical group were observed in progression-free and overall survival. Including nutraceutical as an adjuvant treatment for such patients was recommended by the authors.8
Telekes et al. noted that nutraceutical is registered as a special nutriment for cancer patients in Hungary that has exhibited potent anticancer activity on cell lines and immunomodulatory activity in vivo.9 In 2005, Boros et al. reported that orally administered FWGE suppressed metastatic tumor dissemination and proliferation during and after chemotherapy, surgery, or radiation, with benefits seen in some human cancers and cultured cells as well as some autoimmune disorders and in chemical carcinogenesis prevention.10
Hypersensitivity and allergic reactions
The risks of sensitization to topical wheat proteins are thought to be higher in patients with atopic dermatitis, who have an impaired skin barrier.1 Indeed, Codreanu et al. have suggested that topical products containing food proteins of known allergenicity (including wheat) are contraindicated for neonates and infants with atopic dermatitis.11
In 2015, Bonciolini et al. studied 17 patients (13 females and 4 males, median age 36 years) with nonceliac gluten sensitivity presenting with nonspecific skin lesions. The eczema-, psoriasis-, or dermatitis herpetiformis-like lesions on the extensor surfaces of the upper and lower limbs, especially, were confirmed histologically, but immunopathological evaluations revealed pervasive C3 deposits along the dermoepidermal junction in a microgranular/granular pattern (82%). Notably, all of the patients improved markedly after initiating a gluten-free diet.12
In 2014, Fukutomi et al. conducted a case-control study of Japanese women aged 20-54 years (157 cases) who self-reported wheat allergy to ascertain the epidemiologic relationship between food allergy to wheat after exposure to facial soaps containing hydrolyzed wheat protein. There were 449 age-matched controls without wheat allergy. Participants answered a Web-based questionnaire about their use of skin and hair care products. The investigators found that current use of the facial soap Cha no Shizuku (Drop of Tea), which contains hydrolyzed wheat protein, was significantly linked to a greater risk of wheat allergy, with use of the soap more frequent in consumers whose wheat allergy had newly emerged (11% vs. 6% in controls).13
Cha no Shizuku had earlier been implicated in provoking hundreds of cases of allergic reactions between 2009 and June 2013. R. Teshima noted that the soap contains acid-hydrolyzed wheat protein produced from gluten after partial hydrolysis with hydrogen chloride at 95 ° C for 40 minutes.14
It is worth noting that case reports of allergic reactions to facial soap containing hydrolyzed wheat protein continue to appear. Iseki et al. described in 2014 a 38-year-old woman who experienced irregular headaches, sleepiness, and an episode of facial rash eruption after daily use for about 1 year of a facial soap with hydrolyzed wheat proteins (Glupearl 19s, which is also used in Cha no Shizuku). The investigators added that the patient’s serum contained wheat-specific IgE antibodies. Symptoms disappeared after the patient abstained from wheat.15
In 2012, Tammaro studied cutaneous hypersensitivity to gluten in 14 female patients (aged 12-60 years) with celiac disease who presented with eczema on the face, neck, and arms, after topical application of gluten-containing emollient cream, bath or face powder, or contact with foods containing wheat and durum. Five of the patients tested positive for wheat and durum wheat, while none of the 14 control patients tested positive. Improvement in cutaneous lesions, with no relapses during a 6-month follow-up, resulted when these patients used gluten-free cream and bath powder, and wore gloves before handling wheat-containing food.16
In 2011, Celakovská et al. studied the impact of wheat allergy in 179 adults with atopic eczema (128 females, 51 males; average age 26 years), using open exposure and double-blind, placebo-controlled food challenge tests, as well as specific serum IgE, skin prick, and atopy patch tests. The double-blind, placebo-controlled food challenge test showed that the course of atopic eczema was exacerbated by wheat allergy in eight patients (4.5%). A positive trend revealing that the course of atopic eczema was impacted by wheat allergy emerged during follow-up (at 3, 6, 9, and 12 months).17
Contact urticaria also has been reported to have been induced by hydrolyzed wheat proteins in cosmetics and is notable for the potential to precede food allergies.2,3 A wide variety of protein hydrolysates found in hair products have been associated with inducing contact urticaria, particularly in patients with atopic dermatitis.4
In 2006, Laurière et al. studied nine female patients without common wheat allergy who presented with contact urticaria to cosmetics containing hydrolyzed wheat proteins; six also had experienced generalized urticaria or anaphylaxis in response to foods containing such wheat proteins. Analyses revealed the importance of hydrolysis in augmenting the allergenicity of wheat proteins through contact or consumption.18 Immediate contact urticaria in reaction to hydrolyzed wheat protein in topical products also has been reported in a child.19
Conclusion
Can the presence of wheat hydrolysates in personal care products adversely affect a patient with celiac sprue or wheat sensitivity? The short answer appears to be “yes.” Given the use of hydrolyzed wheat protein in various skin care products, it is important that consumers who have celiac disease or sensitivity to wheat be advised to avoid skin care formulations with such active ingredients. On the positive side of the wheat ledger, there are some indications (albeit in very limited research) that the plant protein may impart beneficial health effects. Much more research is necessary to delineate the full impact of wheat on skin health.
I thank my dermatologist colleague Sharon E. Jacob, MD, at the University of Miami, for suggesting this topic.
References
1. Dermatitis. 2013 Nov-Dec;24(6):291-5.
2. Iran J Med Sci. 2016 May;41(3 Suppl):S54.
3. Contact Dermatitis. 2007 Feb;56(2):119-20.
4. Ann Dermatol Venereol. 2010 Apr;137(4):281-4.
5. Allergy. 1998 Nov;53(11):1078-82.
6. J Drugs Dermatol. 2013 Sep;12(9 Suppl):s133-6.
7. Pak J Pharm Sci. 2008 Jan;21(1):45-50.
8. Cancer Biother Radiopharm. 2008 Aug;23(4):477-82.
9. Nutr Cancer. 2009;61(6):891-9.
10. Ann N Y Acad Sci. 2005 Jun;1051:529-42.
11. Eur Ann Allergy Clin Immunol. 2006 Apr;38(4):126-30.
12. Nutrients. 2015 Sep 15;7(9):7798-805.
13. Allergy. 2014 Oct;69(10):1405-11.
14. Yakugaku Zasshi. 2014;134(1):33-8.
15. Intern Med. 2014;53(2):151-4.
16. Dermatitis. 2012 Sep-Oct;23(5):220-1.
17. Acta Medica (Hradec Kralove). 2011;54(4):157-62.
18. Contact Dermatitis. 2006 May;54(5):283-9.
19. Contact Dermatitis. 2013 Jun;68(6):379-80.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever. Dr. Baumann also developed and owns the Baumann Skin Type Solution skin typing systems and related products.

Endocrinologists report little training in transgender care
Although endocrinologists are often the go-to specialists for hormone therapy, more than 80% of those surveyed had no training in how to treat transgender patients, a study showed.
Meanwhile, more than a quarter of endocrinology fellowship directors surveyed said their programs don’t offer education in transgender care.
According to a June 2016 report by the Williams Institute at the University of California, Los Angeles, an estimated 0.58% of adults in the United States identify as transgender, with numbers reaching as high as 2.77% in Washington, D.C., 0.78% in Hawaii, 0.76% in California, and 0.75% in New Mexico and Georgia.
Endocrinologists are especially likely to see transgender patients in order to assist with hormone therapy. Of course, they also see them for general endocrinology needs, said lead study author Caroline Davidge-Pitts, MBBCh, of the Mayo Clinic’s department of endocrinology in Rochester, Minn.
For the current study of transgender care, “we wanted to assess what the current knowledge and practice is among practicing physicians as well as the state of education for our endocrinology fellows,” she said in an interview.
Dr. Davidge-Pitts and her colleagues sent an anonymous Internet survey to 104 endocrinology fellowship program directors (PDs) and 6,992 physician members of the Endocrine Society in the United States. Fifty-four of the program directors responded (51.9%), as did 411 of the clinicians (5.9%) (J Clin Endocrinol Metab. 2017 Jan 10. doi: 10.1210/jc.2016-3007).
The program directors represent 54 programs, of which 35 (72.2%) provide instruction regarding transgender care. All offer instruction about hormone therapy in this context.
Almost 94% of the program directors described education about transgender care as important. Forty-two respondents said challenges to better education regarding transgender care include lack of faculty interest or experience (59.5%), lack of resources for training (47.6%), and lack of money (40.5%).
Of 46 respondents, 91% said online training modules for students would be helpful; 71.7% pointed to modules for professors, and 71.7% mentioned lectures from visiting faculty.
Among clinicians, 79.8% said they had ever treated a transgender patient, and 55% reported treating more than five transgender patients a year. But 80.6% of 382 responders said they’d never had training in the treatment of these patients.
Most of the responding endocrinologists said they felt confident regarding definitions, taking a history, and prescribing hormones, but 42.4% or less felt that way about sex change operations, organ-specific screening guidelines, and psychosocial/legal issues.
Dr. Davidge-Pitts said the study indicates more education in transgender care is needed in fellowship programs: “We envision a more structured approach ... with an introductory curriculum in the first year of fellowship aligned to specific competencies, followed by a more advanced curriculum in the second or third year.”
Overall, “we need to allocate resources to develop online training modules to help our endocrine fellows and practitioners too, to give them the ability to get education in their office,” Dr. Davidge-Pitts said.
As for the clinical setting, the study supports changes to make transgender patients more comfortable, such as gender-neutral restrooms and training for staff about how to treat transgender patients with respect, she said.
Dr. Safer, medical director of the center for transgender medicine and surgery at Boston University and Boston Medical Center, said things have changed since he graduated from medical school in 1990. “I didn’t even hear the word transgender in medical school, residency, or fellowship,” he said, “and I don’t think much changed in the next 10-20 years.”
Now, there’s more focus on treating these patients sensitively, but “they still don’t still teach the underlying medicine, so the physicians are still not equipped with the basic knowledge they need to take care of the patients,” Dr. Safer said.
He suggested that endocrinologists who are interested in learning more about transgender care get in touch with the World Professional Association for Transgender Health at wpath.org.
Although endocrinologists are often the go-to specialists for hormone therapy, more than 80% of those surveyed had no training in how to treat transgender patients, a study showed.
Meanwhile, more than a quarter of endocrinology fellowship directors surveyed said their programs don’t offer education in transgender care.
According to a June 2016 report by the Williams Institute at the University of California, Los Angeles, an estimated 0.58% of adults in the United States identify as transgender, with numbers reaching as high as 2.77% in Washington, D.C., 0.78% in Hawaii, 0.76% in California, and 0.75% in New Mexico and Georgia.
Endocrinologists are especially likely to see transgender patients in order to assist with hormone therapy. Of course, they also see them for general endocrinology needs, said lead study author Caroline Davidge-Pitts, MBBCh, of the Mayo Clinic’s department of endocrinology in Rochester, Minn.
For the current study of transgender care, “we wanted to assess what the current knowledge and practice is among practicing physicians as well as the state of education for our endocrinology fellows,” she said in an interview.
Dr. Davidge-Pitts and her colleagues sent an anonymous Internet survey to 104 endocrinology fellowship program directors (PDs) and 6,992 physician members of the Endocrine Society in the United States. Fifty-four of the program directors responded (51.9%), as did 411 of the clinicians (5.9%) (J Clin Endocrinol Metab. 2017 Jan 10. doi: 10.1210/jc.2016-3007).
The program directors represent 54 programs, of which 35 (72.2%) provide instruction regarding transgender care. All offer instruction about hormone therapy in this context.
Almost 94% of the program directors described education about transgender care as important. Forty-two respondents said challenges to better education regarding transgender care include lack of faculty interest or experience (59.5%), lack of resources for training (47.6%), and lack of money (40.5%).
Of 46 respondents, 91% said online training modules for students would be helpful; 71.7% pointed to modules for professors, and 71.7% mentioned lectures from visiting faculty.
Among clinicians, 79.8% said they had ever treated a transgender patient, and 55% reported treating more than five transgender patients a year. But 80.6% of 382 responders said they’d never had training in the treatment of these patients.
Most of the responding endocrinologists said they felt confident regarding definitions, taking a history, and prescribing hormones, but 42.4% or less felt that way about sex change operations, organ-specific screening guidelines, and psychosocial/legal issues.
Dr. Davidge-Pitts said the study indicates more education in transgender care is needed in fellowship programs: “We envision a more structured approach ... with an introductory curriculum in the first year of fellowship aligned to specific competencies, followed by a more advanced curriculum in the second or third year.”
Overall, “we need to allocate resources to develop online training modules to help our endocrine fellows and practitioners too, to give them the ability to get education in their office,” Dr. Davidge-Pitts said.
As for the clinical setting, the study supports changes to make transgender patients more comfortable, such as gender-neutral restrooms and training for staff about how to treat transgender patients with respect, she said.
Dr. Safer, medical director of the center for transgender medicine and surgery at Boston University and Boston Medical Center, said things have changed since he graduated from medical school in 1990. “I didn’t even hear the word transgender in medical school, residency, or fellowship,” he said, “and I don’t think much changed in the next 10-20 years.”
Now, there’s more focus on treating these patients sensitively, but “they still don’t still teach the underlying medicine, so the physicians are still not equipped with the basic knowledge they need to take care of the patients,” Dr. Safer said.
He suggested that endocrinologists who are interested in learning more about transgender care get in touch with the World Professional Association for Transgender Health at wpath.org.
Although endocrinologists are often the go-to specialists for hormone therapy, more than 80% of those surveyed had no training in how to treat transgender patients, a study showed.
Meanwhile, more than a quarter of endocrinology fellowship directors surveyed said their programs don’t offer education in transgender care.
According to a June 2016 report by the Williams Institute at the University of California, Los Angeles, an estimated 0.58% of adults in the United States identify as transgender, with numbers reaching as high as 2.77% in Washington, D.C., 0.78% in Hawaii, 0.76% in California, and 0.75% in New Mexico and Georgia.
Endocrinologists are especially likely to see transgender patients in order to assist with hormone therapy. Of course, they also see them for general endocrinology needs, said lead study author Caroline Davidge-Pitts, MBBCh, of the Mayo Clinic’s department of endocrinology in Rochester, Minn.
For the current study of transgender care, “we wanted to assess what the current knowledge and practice is among practicing physicians as well as the state of education for our endocrinology fellows,” she said in an interview.
Dr. Davidge-Pitts and her colleagues sent an anonymous Internet survey to 104 endocrinology fellowship program directors (PDs) and 6,992 physician members of the Endocrine Society in the United States. Fifty-four of the program directors responded (51.9%), as did 411 of the clinicians (5.9%) (J Clin Endocrinol Metab. 2017 Jan 10. doi: 10.1210/jc.2016-3007).
The program directors represent 54 programs, of which 35 (72.2%) provide instruction regarding transgender care. All offer instruction about hormone therapy in this context.
Almost 94% of the program directors described education about transgender care as important. Forty-two respondents said challenges to better education regarding transgender care include lack of faculty interest or experience (59.5%), lack of resources for training (47.6%), and lack of money (40.5%).
Of 46 respondents, 91% said online training modules for students would be helpful; 71.7% pointed to modules for professors, and 71.7% mentioned lectures from visiting faculty.
Among clinicians, 79.8% said they had ever treated a transgender patient, and 55% reported treating more than five transgender patients a year. But 80.6% of 382 responders said they’d never had training in the treatment of these patients.
Most of the responding endocrinologists said they felt confident regarding definitions, taking a history, and prescribing hormones, but 42.4% or less felt that way about sex change operations, organ-specific screening guidelines, and psychosocial/legal issues.
Dr. Davidge-Pitts said the study indicates more education in transgender care is needed in fellowship programs: “We envision a more structured approach ... with an introductory curriculum in the first year of fellowship aligned to specific competencies, followed by a more advanced curriculum in the second or third year.”
Overall, “we need to allocate resources to develop online training modules to help our endocrine fellows and practitioners too, to give them the ability to get education in their office,” Dr. Davidge-Pitts said.
As for the clinical setting, the study supports changes to make transgender patients more comfortable, such as gender-neutral restrooms and training for staff about how to treat transgender patients with respect, she said.
Dr. Safer, medical director of the center for transgender medicine and surgery at Boston University and Boston Medical Center, said things have changed since he graduated from medical school in 1990. “I didn’t even hear the word transgender in medical school, residency, or fellowship,” he said, “and I don’t think much changed in the next 10-20 years.”
Now, there’s more focus on treating these patients sensitively, but “they still don’t still teach the underlying medicine, so the physicians are still not equipped with the basic knowledge they need to take care of the patients,” Dr. Safer said.
He suggested that endocrinologists who are interested in learning more about transgender care get in touch with the World Professional Association for Transgender Health at wpath.org.
FROM THE JOURNAL OF CLINICAL ENDOCRINOLOGY & METABOLISM
Key clinical point:
Major finding: Of endocrinologists surveyed, 80.6% said they’d never received training in transgender care, while 72.2% of fellowship program directors reported offering instruction in how to treat these patients.
Data source: Responses to surveys from 54 endocrinology fellowship program directors and 411 clinical endocrinologists.
Disclosures: The study authors reported no relevant financial disclosures.
Home treatment of PE remains rare
Clinical question: What is the prevalence of outpatient treatment of acute pulmonary embolism (PE)?
Background: PE traditionally is perceived as a serious condition requiring hospitalization. Many studies, however, have shown that outpatient treatment of PE in low-risk, compliant patients is safe. Several scoring systems have been derived to identify patients with PE who are at low risk of adverse events and may be candidates for home treatment.
Setting: Five U.S. EDs.
Synopsis: Among 983 patients diagnosed with acute PE, 237 (24.1%) were unstable and hypoxic. Only a small proportion of patients (1.7%) were eligible for outpatient therapy, and an additional 16.2% of hospitalized patients were discharged early (2 days or less). Novel oral anticoagulants were administered to fewer than one-third of patients.
Bottom line: In the era of novel anticoagulants, the majority of patients with acute PE were hospitalized, and home treatment was infrequently selected for stable low-risk patients.
Citation: Stein PD, Matta F, Hughes PG, et al. Home treatment of pulmonary embolism in the era of novel oral anticoagulants. Am J Med. 2016;129(9):974-977.
Dr. Gummalla is an assistant professor at the University of Miami Miller School of Medicine and a hospitalist at University of Miami Hospital and Jackson Memorial Hospital.
Clinical question: What is the prevalence of outpatient treatment of acute pulmonary embolism (PE)?
Background: PE traditionally is perceived as a serious condition requiring hospitalization. Many studies, however, have shown that outpatient treatment of PE in low-risk, compliant patients is safe. Several scoring systems have been derived to identify patients with PE who are at low risk of adverse events and may be candidates for home treatment.
Setting: Five U.S. EDs.
Synopsis: Among 983 patients diagnosed with acute PE, 237 (24.1%) were unstable and hypoxic. Only a small proportion of patients (1.7%) were eligible for outpatient therapy, and an additional 16.2% of hospitalized patients were discharged early (2 days or less). Novel oral anticoagulants were administered to fewer than one-third of patients.
Bottom line: In the era of novel anticoagulants, the majority of patients with acute PE were hospitalized, and home treatment was infrequently selected for stable low-risk patients.
Citation: Stein PD, Matta F, Hughes PG, et al. Home treatment of pulmonary embolism in the era of novel oral anticoagulants. Am J Med. 2016;129(9):974-977.
Dr. Gummalla is an assistant professor at the University of Miami Miller School of Medicine and a hospitalist at University of Miami Hospital and Jackson Memorial Hospital.
Clinical question: What is the prevalence of outpatient treatment of acute pulmonary embolism (PE)?
Background: PE traditionally is perceived as a serious condition requiring hospitalization. Many studies, however, have shown that outpatient treatment of PE in low-risk, compliant patients is safe. Several scoring systems have been derived to identify patients with PE who are at low risk of adverse events and may be candidates for home treatment.
Setting: Five U.S. EDs.
Synopsis: Among 983 patients diagnosed with acute PE, 237 (24.1%) were unstable and hypoxic. Only a small proportion of patients (1.7%) were eligible for outpatient therapy, and an additional 16.2% of hospitalized patients were discharged early (2 days or less). Novel oral anticoagulants were administered to fewer than one-third of patients.
Bottom line: In the era of novel anticoagulants, the majority of patients with acute PE were hospitalized, and home treatment was infrequently selected for stable low-risk patients.
Citation: Stein PD, Matta F, Hughes PG, et al. Home treatment of pulmonary embolism in the era of novel oral anticoagulants. Am J Med. 2016;129(9):974-977.
Dr. Gummalla is an assistant professor at the University of Miami Miller School of Medicine and a hospitalist at University of Miami Hospital and Jackson Memorial Hospital.
Updated recommendations for managing gout
Clinical question: What are the new treatment options for gout?
Background: The 2006 European League Against Rheumatism (EULAR) guidelines recommend that acute flares of gout be treated as early as possible with either oral colchicine, oral corticosteroids, or intra-articular corticosteroids. Experts recommend starting urate-lowering therapy (ULT) only when certain severe clinical features occur, such as recurrent acute attacks and tophi.
Study design: Systematic review.
Setting: EULAR task force members from 12 European countries.
Synopsis: Since the last guidelines, interleukin-1 blockers (IL-1) were found to play a crucial role in crystal-induced inflammation. IL-1, NSAIDs, and corticosteroids should be considered in patients with frequent flares and contraindications to colchicine.
Unlike in the previous guidelines, ULT should be considered from first presentation of gout; for severe disease, serum uric acid (SUA) levels should be maintained at less than 6 mg/dL and less than 5 mg/dL.
Allopurinol is recommended for first-line ULT, and if the SUA target cannot be reached, it should be switched to another xanthine oxidase inhibitor (febuxostat) or a uricosuric or combined with a uricosuric.
Pegloticase is recommended for refractory gout.
Bottom line: The updated 2016 EULAR guidelines recommend new treatment options for gout and updated indications for ULT.
Citation: Richette P, Doherty M, Pascual E, et al. 2016 updated EULAR evidence-based recommendations for the management of gout [published online ahead of print July 25, 2016]. Ann Rheum Dis. doi: 10.1136/annrheumdis-2016-209707.
Dr. Gummalla is an assistant professor at the University of Miami Miller School of Medicine and a hospitalist at University of Miami Hospital and Jackson Memorial Hospital.
Clinical question: What are the new treatment options for gout?
Background: The 2006 European League Against Rheumatism (EULAR) guidelines recommend that acute flares of gout be treated as early as possible with either oral colchicine, oral corticosteroids, or intra-articular corticosteroids. Experts recommend starting urate-lowering therapy (ULT) only when certain severe clinical features occur, such as recurrent acute attacks and tophi.
Study design: Systematic review.
Setting: EULAR task force members from 12 European countries.
Synopsis: Since the last guidelines, interleukin-1 blockers (IL-1) were found to play a crucial role in crystal-induced inflammation. IL-1, NSAIDs, and corticosteroids should be considered in patients with frequent flares and contraindications to colchicine.
Unlike in the previous guidelines, ULT should be considered from first presentation of gout; for severe disease, serum uric acid (SUA) levels should be maintained at less than 6 mg/dL and less than 5 mg/dL.
Allopurinol is recommended for first-line ULT, and if the SUA target cannot be reached, it should be switched to another xanthine oxidase inhibitor (febuxostat) or a uricosuric or combined with a uricosuric.
Pegloticase is recommended for refractory gout.
Bottom line: The updated 2016 EULAR guidelines recommend new treatment options for gout and updated indications for ULT.
Citation: Richette P, Doherty M, Pascual E, et al. 2016 updated EULAR evidence-based recommendations for the management of gout [published online ahead of print July 25, 2016]. Ann Rheum Dis. doi: 10.1136/annrheumdis-2016-209707.
Dr. Gummalla is an assistant professor at the University of Miami Miller School of Medicine and a hospitalist at University of Miami Hospital and Jackson Memorial Hospital.
Clinical question: What are the new treatment options for gout?
Background: The 2006 European League Against Rheumatism (EULAR) guidelines recommend that acute flares of gout be treated as early as possible with either oral colchicine, oral corticosteroids, or intra-articular corticosteroids. Experts recommend starting urate-lowering therapy (ULT) only when certain severe clinical features occur, such as recurrent acute attacks and tophi.
Study design: Systematic review.
Setting: EULAR task force members from 12 European countries.
Synopsis: Since the last guidelines, interleukin-1 blockers (IL-1) were found to play a crucial role in crystal-induced inflammation. IL-1, NSAIDs, and corticosteroids should be considered in patients with frequent flares and contraindications to colchicine.
Unlike in the previous guidelines, ULT should be considered from first presentation of gout; for severe disease, serum uric acid (SUA) levels should be maintained at less than 6 mg/dL and less than 5 mg/dL.
Allopurinol is recommended for first-line ULT, and if the SUA target cannot be reached, it should be switched to another xanthine oxidase inhibitor (febuxostat) or a uricosuric or combined with a uricosuric.
Pegloticase is recommended for refractory gout.
Bottom line: The updated 2016 EULAR guidelines recommend new treatment options for gout and updated indications for ULT.
Citation: Richette P, Doherty M, Pascual E, et al. 2016 updated EULAR evidence-based recommendations for the management of gout [published online ahead of print July 25, 2016]. Ann Rheum Dis. doi: 10.1136/annrheumdis-2016-209707.
Dr. Gummalla is an assistant professor at the University of Miami Miller School of Medicine and a hospitalist at University of Miami Hospital and Jackson Memorial Hospital.
Diagnosis at a Glance: Partial Hydatidiform Molar Pregnancy
Case
A 26-year-old gravida 3, para 2-0-0-2, aborta 0 whose last menstrual period was 15 weeks 5 days, presented to the ED with complaints of mild vaginal spotting, which she first noted postcoitally the previous day. The patient denied fatigue, lightheadedness, dyspnea, abdominal pain, nausea, or vomiting.
Physical examination revealed a well-appearing patient with normal vital signs. The abdomen was soft and nontender, and the fundus was palpable at the level of the umbilicus. A speculum examination was unremarkable, with normal external genitalia, a closed cervical os, no adnexal masses or tenderness, and no blood in the vaginal vault. Laboratory studies were significant for a serum beta human chorionic gonadotropin (beta-hCG) of 7,442 mIU/mL (reference range for 15 weeks: 12,039-70,971 mIU/mL). The patient was Rh positive with a stable hematocrit.
A bedside ultrasound, performed by an ultrasound-]trained emergency physician (EP), was noted to demonstrate a complex intrauterine mass comprised of several small, rounded anechoic clusters (Figure). 
An obstetric consultation was made and the patient was taken to the operating room the following day for a dilation and curettage (D&C) procedure. She was discharged home the next day without complications. The products of conception were sent to pathology, and confirmed a triploid karyotype and p57 trophoblastic immunopositivity, diagnostic of a partial hydatidiform mole.
Discussion
Hydatidiform moles are a subset of abnormal pregnancies termed gestational trophoblastic disease (GTD). The two greatest risk factors for GTD are previous GTD and extremis of maternal age.1 Patients often present to the ED because of painless heavy vaginal bleeding, hyperemesis gravidarum, symptoms of hyperthyroidism, or preeclampsia before 20 weeks.2 Clinically, these patients present with an enlarged uterus for gestational age and very high beta-hCG levels, often greater than 100,000 mIU/mL.3 The high beta-hCG levels can lead the patient to present with symptoms of hyperthyroidism, such as severe hypertension, given the similar chemical structures of beta-hCG and thyroid-stimulating hormone.4
After a D&C, interval beta-hCG levels need to be obtained to ensure resolution. A patient with beta-hCG levels that do not fall by 10% after 3 weeks, or are still present after 6 months, should be referred to a gynecologic oncologist.5,6 Furthermore, a chest X-ray is strongly suggested, as the lungs are often the first place of metastasis.7
Partial hydatidiform moles are formed by a dispermic fertilization of a normal ovum leading to a triploid pattern, and are clinically distinguished from complete molar pregnancies because affected patients have a uterus that is often small for gestational age.8 Also, while the beta-hCG is also abnormally elevated, the median value is more modest at approximately 50,000 mIU/mL.3
According to the American College of Radiology’s Appropriateness Criteria, ultrasound is the gold standard for evaluating gestational trophoblastic disease. While the classic sonographic appearance of a molar pregnancy is described as a “snowstorm” appearance, advancement in technology more clearly demonstrates a “cluster of grapes” or “honeycomb” appearance.9 On Doppler mode, increased vascularity peripherally can also be detected due to engorgement of the spiral arteries. While partial moles tend to have more focal lesions, the greatest distinguishing factor is the presence of embryonic or fetal tissue, which is not seen in complete moles. However, due to the heterogeneous appearance of the uterus in all GTD, molar pregnancies can sometimes be misinterpreted as missed abortions or clotted blood, so that pathological confirmation is mandatory for all products of conception in the United States and Canada.2,10
Summary
This case is of particular interest because it demonstrates an atypical presentation of a partial hydatidiform mole. While most classic presentations include older patients with heavy vaginal bleeding, a smaller uterus than expected, significantly elevated beta-hCGs, and hyperemesis gravidarum, our patient was relatively young with no history of molar pregnancies in the past, a larger-than-expected uterus, and no vaginal bleeding noted. Laboratory values also indicated a significantly lower-than-expected beta-hCG level. As such, bedside ultrasound findings were unexpected but resulted in the prompt diagnosis, an emergent obstetric consultation, and confirmatory radiology imaging. The ED bedside ultrasound findings did demonstrate the characteristic “cluster of grapes” appearance surrounded by the hyperechoic appearance of the spiral arteries (Figure). An intrauterine yolk sac was also identified by ultrasound, which strongly suggested a partial rather than a complete hydatidiform molar pregnancy.
While hydatidiform pregnancies are relatively rare, EPs should be aware of the clinical and sonographic features of these diseases. This case, particularly given the atypical clinical presentation for a partial molar pregnancy, highlights the importance of ultrasound in pregnancy, and the utility of bedside ultrasound in the evaluation of the etiology of vaginal bleeding in the early pregnant patient that presents to the ED.
1. Ngan H, Bender H, Benedet JL, et al. Gestational trophoblastic neoplasia, FIGO 2000 staging and classification. Int J Gynaecol Obstet. 2003;83 Suppl 1:175-177.
2. Tie W, Tajnert K, Plavsic SK. Ultrasound imaging of gestational trophoblastic disease. Donald School J Ultrasound Obstet Gynecol. 2013;7(1):105-112.
3. Berkowitz RS, Goldstein DP. Current advances in the management of gestational trophoblastic disease. Gynecol Oncol. 2013;128(1):3-5.
4. Cole LA, Butler S. Detection of hCG in trophoblastic disease: The USA hCG reference service experience. J Reprod Med. 2002;47(6):433-444.
5. Lavie I, Rao GG, Castrillon DH, Miller DS, Schorge JO. Duration of human chorionic gonadotropin surveillance for partial hydatidiform moles. Am J Obstet Gynecol. 2005;192(5):1362-1364.
6. Kenny L, Seckl MJ. Treatments for gestational trophoblastic disease. Expert Rev of Obstet Gynecol. 2010;5(2):215-225.
7. Soto-Wright V, Bernstein M, Goldstein DP, Berkowitz RS. The changing clinical presentation of complete molar pregnancy. Obstet Gynecol. 1995;86(5):775-779.
8. Berkowitz RS, Goldstein DP. Clinical practice. Molar pregnancy. N Engl J Med. 2009;360(16):1639-1645. doi: 10.1056/NEJMcp0900696.
9. Kirk E, Papageorghiou AT, Condous G, Bottomley C, Bourne T. The accuracy of first trimester ultrasound in the diagnosis of hydatidiform mole. Ultrasound Obstet Gynecol. 2007;29(1):70-75.
10. Wang Y, Zhao S. Vascular Biology of the Placenta. Chapter 4. Cell Types of the Placenta. San Rafael, CA: Morgan & Claypool Life Sciences; 2010.
Case
A 26-year-old gravida 3, para 2-0-0-2, aborta 0 whose last menstrual period was 15 weeks 5 days, presented to the ED with complaints of mild vaginal spotting, which she first noted postcoitally the previous day. The patient denied fatigue, lightheadedness, dyspnea, abdominal pain, nausea, or vomiting.
Physical examination revealed a well-appearing patient with normal vital signs. The abdomen was soft and nontender, and the fundus was palpable at the level of the umbilicus. A speculum examination was unremarkable, with normal external genitalia, a closed cervical os, no adnexal masses or tenderness, and no blood in the vaginal vault. Laboratory studies were significant for a serum beta human chorionic gonadotropin (beta-hCG) of 7,442 mIU/mL (reference range for 15 weeks: 12,039-70,971 mIU/mL). The patient was Rh positive with a stable hematocrit.
A bedside ultrasound, performed by an ultrasound-]trained emergency physician (EP), was noted to demonstrate a complex intrauterine mass comprised of several small, rounded anechoic clusters (Figure).
An obstetric consultation was made and the patient was taken to the operating room the following day for a dilation and curettage (D&C) procedure. She was discharged home the next day without complications. The products of conception were sent to pathology, and confirmed a triploid karyotype and p57 trophoblastic immunopositivity, diagnostic of a partial hydatidiform mole.
Discussion
Hydatidiform moles are a subset of abnormal pregnancies termed gestational trophoblastic disease (GTD). The two greatest risk factors for GTD are previous GTD and extremis of maternal age.1 Patients often present to the ED because of painless heavy vaginal bleeding, hyperemesis gravidarum, symptoms of hyperthyroidism, or preeclampsia before 20 weeks.2 Clinically, these patients present with an enlarged uterus for gestational age and very high beta-hCG levels, often greater than 100,000 mIU/mL.3 The high beta-hCG levels can lead the patient to present with symptoms of hyperthyroidism, such as severe hypertension, given the similar chemical structures of beta-hCG and thyroid-stimulating hormone.4
After a D&C, interval beta-hCG levels need to be obtained to ensure resolution. A patient with beta-hCG levels that do not fall by 10% after 3 weeks, or are still present after 6 months, should be referred to a gynecologic oncologist.5,6 Furthermore, a chest X-ray is strongly suggested, as the lungs are often the first place of metastasis.7
Partial hydatidiform moles are formed by a dispermic fertilization of a normal ovum leading to a triploid pattern, and are clinically distinguished from complete molar pregnancies because affected patients have a uterus that is often small for gestational age.8 Also, while the beta-hCG is also abnormally elevated, the median value is more modest at approximately 50,000 mIU/mL.3
According to the American College of Radiology’s Appropriateness Criteria, ultrasound is the gold standard for evaluating gestational trophoblastic disease. While the classic sonographic appearance of a molar pregnancy is described as a “snowstorm” appearance, advancement in technology more clearly demonstrates a “cluster of grapes” or “honeycomb” appearance.9 On Doppler mode, increased vascularity peripherally can also be detected due to engorgement of the spiral arteries. While partial moles tend to have more focal lesions, the greatest distinguishing factor is the presence of embryonic or fetal tissue, which is not seen in complete moles. However, due to the heterogeneous appearance of the uterus in all GTD, molar pregnancies can sometimes be misinterpreted as missed abortions or clotted blood, so that pathological confirmation is mandatory for all products of conception in the United States and Canada.2,10
Summary
This case is of particular interest because it demonstrates an atypical presentation of a partial hydatidiform mole. While most classic presentations include older patients with heavy vaginal bleeding, a smaller uterus than expected, significantly elevated beta-hCGs, and hyperemesis gravidarum, our patient was relatively young with no history of molar pregnancies in the past, a larger-than-expected uterus, and no vaginal bleeding noted. Laboratory values also indicated a significantly lower-than-expected beta-hCG level. As such, bedside ultrasound findings were unexpected but resulted in the prompt diagnosis, an emergent obstetric consultation, and confirmatory radiology imaging. The ED bedside ultrasound findings did demonstrate the characteristic “cluster of grapes” appearance surrounded by the hyperechoic appearance of the spiral arteries (Figure). An intrauterine yolk sac was also identified by ultrasound, which strongly suggested a partial rather than a complete hydatidiform molar pregnancy.
While hydatidiform pregnancies are relatively rare, EPs should be aware of the clinical and sonographic features of these diseases. This case, particularly given the atypical clinical presentation for a partial molar pregnancy, highlights the importance of ultrasound in pregnancy, and the utility of bedside ultrasound in the evaluation of the etiology of vaginal bleeding in the early pregnant patient that presents to the ED.
Case
A 26-year-old gravida 3, para 2-0-0-2, aborta 0 whose last menstrual period was 15 weeks 5 days, presented to the ED with complaints of mild vaginal spotting, which she first noted postcoitally the previous day. The patient denied fatigue, lightheadedness, dyspnea, abdominal pain, nausea, or vomiting.
Physical examination revealed a well-appearing patient with normal vital signs. The abdomen was soft and nontender, and the fundus was palpable at the level of the umbilicus. A speculum examination was unremarkable, with normal external genitalia, a closed cervical os, no adnexal masses or tenderness, and no blood in the vaginal vault. Laboratory studies were significant for a serum beta human chorionic gonadotropin (beta-hCG) of 7,442 mIU/mL (reference range for 15 weeks: 12,039-70,971 mIU/mL). The patient was Rh positive with a stable hematocrit.
A bedside ultrasound, performed by an ultrasound-]trained emergency physician (EP), was noted to demonstrate a complex intrauterine mass comprised of several small, rounded anechoic clusters (Figure).
An obstetric consultation was made and the patient was taken to the operating room the following day for a dilation and curettage (D&C) procedure. She was discharged home the next day without complications. The products of conception were sent to pathology, and confirmed a triploid karyotype and p57 trophoblastic immunopositivity, diagnostic of a partial hydatidiform mole.
Discussion
Hydatidiform moles are a subset of abnormal pregnancies termed gestational trophoblastic disease (GTD). The two greatest risk factors for GTD are previous GTD and extremis of maternal age.1 Patients often present to the ED because of painless heavy vaginal bleeding, hyperemesis gravidarum, symptoms of hyperthyroidism, or preeclampsia before 20 weeks.2 Clinically, these patients present with an enlarged uterus for gestational age and very high beta-hCG levels, often greater than 100,000 mIU/mL.3 The high beta-hCG levels can lead the patient to present with symptoms of hyperthyroidism, such as severe hypertension, given the similar chemical structures of beta-hCG and thyroid-stimulating hormone.4
After a D&C, interval beta-hCG levels need to be obtained to ensure resolution. A patient with beta-hCG levels that do not fall by 10% after 3 weeks, or are still present after 6 months, should be referred to a gynecologic oncologist.5,6 Furthermore, a chest X-ray is strongly suggested, as the lungs are often the first place of metastasis.7
Partial hydatidiform moles are formed by a dispermic fertilization of a normal ovum leading to a triploid pattern, and are clinically distinguished from complete molar pregnancies because affected patients have a uterus that is often small for gestational age.8 Also, while the beta-hCG is also abnormally elevated, the median value is more modest at approximately 50,000 mIU/mL.3
According to the American College of Radiology’s Appropriateness Criteria, ultrasound is the gold standard for evaluating gestational trophoblastic disease. While the classic sonographic appearance of a molar pregnancy is described as a “snowstorm” appearance, advancement in technology more clearly demonstrates a “cluster of grapes” or “honeycomb” appearance.9 On Doppler mode, increased vascularity peripherally can also be detected due to engorgement of the spiral arteries. While partial moles tend to have more focal lesions, the greatest distinguishing factor is the presence of embryonic or fetal tissue, which is not seen in complete moles. However, due to the heterogeneous appearance of the uterus in all GTD, molar pregnancies can sometimes be misinterpreted as missed abortions or clotted blood, so that pathological confirmation is mandatory for all products of conception in the United States and Canada.2,10
Summary
This case is of particular interest because it demonstrates an atypical presentation of a partial hydatidiform mole. While most classic presentations include older patients with heavy vaginal bleeding, a smaller uterus than expected, significantly elevated beta-hCGs, and hyperemesis gravidarum, our patient was relatively young with no history of molar pregnancies in the past, a larger-than-expected uterus, and no vaginal bleeding noted. Laboratory values also indicated a significantly lower-than-expected beta-hCG level. As such, bedside ultrasound findings were unexpected but resulted in the prompt diagnosis, an emergent obstetric consultation, and confirmatory radiology imaging. The ED bedside ultrasound findings did demonstrate the characteristic “cluster of grapes” appearance surrounded by the hyperechoic appearance of the spiral arteries (Figure). An intrauterine yolk sac was also identified by ultrasound, which strongly suggested a partial rather than a complete hydatidiform molar pregnancy.
While hydatidiform pregnancies are relatively rare, EPs should be aware of the clinical and sonographic features of these diseases. This case, particularly given the atypical clinical presentation for a partial molar pregnancy, highlights the importance of ultrasound in pregnancy, and the utility of bedside ultrasound in the evaluation of the etiology of vaginal bleeding in the early pregnant patient that presents to the ED.
1. Ngan H, Bender H, Benedet JL, et al. Gestational trophoblastic neoplasia, FIGO 2000 staging and classification. Int J Gynaecol Obstet. 2003;83 Suppl 1:175-177.
2. Tie W, Tajnert K, Plavsic SK. Ultrasound imaging of gestational trophoblastic disease. Donald School J Ultrasound Obstet Gynecol. 2013;7(1):105-112.
3. Berkowitz RS, Goldstein DP. Current advances in the management of gestational trophoblastic disease. Gynecol Oncol. 2013;128(1):3-5.
4. Cole LA, Butler S. Detection of hCG in trophoblastic disease: The USA hCG reference service experience. J Reprod Med. 2002;47(6):433-444.
5. Lavie I, Rao GG, Castrillon DH, Miller DS, Schorge JO. Duration of human chorionic gonadotropin surveillance for partial hydatidiform moles. Am J Obstet Gynecol. 2005;192(5):1362-1364.
6. Kenny L, Seckl MJ. Treatments for gestational trophoblastic disease. Expert Rev of Obstet Gynecol. 2010;5(2):215-225.
7. Soto-Wright V, Bernstein M, Goldstein DP, Berkowitz RS. The changing clinical presentation of complete molar pregnancy. Obstet Gynecol. 1995;86(5):775-779.
8. Berkowitz RS, Goldstein DP. Clinical practice. Molar pregnancy. N Engl J Med. 2009;360(16):1639-1645. doi: 10.1056/NEJMcp0900696.
9. Kirk E, Papageorghiou AT, Condous G, Bottomley C, Bourne T. The accuracy of first trimester ultrasound in the diagnosis of hydatidiform mole. Ultrasound Obstet Gynecol. 2007;29(1):70-75.
10. Wang Y, Zhao S. Vascular Biology of the Placenta. Chapter 4. Cell Types of the Placenta. San Rafael, CA: Morgan & Claypool Life Sciences; 2010.
1. Ngan H, Bender H, Benedet JL, et al. Gestational trophoblastic neoplasia, FIGO 2000 staging and classification. Int J Gynaecol Obstet. 2003;83 Suppl 1:175-177.
2. Tie W, Tajnert K, Plavsic SK. Ultrasound imaging of gestational trophoblastic disease. Donald School J Ultrasound Obstet Gynecol. 2013;7(1):105-112.
3. Berkowitz RS, Goldstein DP. Current advances in the management of gestational trophoblastic disease. Gynecol Oncol. 2013;128(1):3-5.
4. Cole LA, Butler S. Detection of hCG in trophoblastic disease: The USA hCG reference service experience. J Reprod Med. 2002;47(6):433-444.
5. Lavie I, Rao GG, Castrillon DH, Miller DS, Schorge JO. Duration of human chorionic gonadotropin surveillance for partial hydatidiform moles. Am J Obstet Gynecol. 2005;192(5):1362-1364.
6. Kenny L, Seckl MJ. Treatments for gestational trophoblastic disease. Expert Rev of Obstet Gynecol. 2010;5(2):215-225.
7. Soto-Wright V, Bernstein M, Goldstein DP, Berkowitz RS. The changing clinical presentation of complete molar pregnancy. Obstet Gynecol. 1995;86(5):775-779.
8. Berkowitz RS, Goldstein DP. Clinical practice. Molar pregnancy. N Engl J Med. 2009;360(16):1639-1645. doi: 10.1056/NEJMcp0900696.
9. Kirk E, Papageorghiou AT, Condous G, Bottomley C, Bourne T. The accuracy of first trimester ultrasound in the diagnosis of hydatidiform mole. Ultrasound Obstet Gynecol. 2007;29(1):70-75.
10. Wang Y, Zhao S. Vascular Biology of the Placenta. Chapter 4. Cell Types of the Placenta. San Rafael, CA: Morgan & Claypool Life Sciences; 2010.
Cardiofaciocutaneous Syndrome and the Dermatologist’s Contribution to Diagnosis
To the Editor:
RASopathies, a class of developmental disorders, are caused by mutations in genes that encode protein components of the RAS/mitogen-activated protein kinase (MAPK) pathway. Each syndrome exhibits its phenotypic features; however, because all of them cause dysregulation of the RAS/MAPK pathway, there are numerous overlapping phenotypic features between the syndromes including cardiac defects, cutaneous abnormalities, characteristic facial features, neurocognitive impairment, and increased risk for developing some neoplastic disorders.
Cardiofaciocutaneous (CFC) syndrome is a RASopathy and is a genetic sporadic disease characterized by multiple congenital anomalies associated with mental retardation. It has a complex dermatological phenotype with many cutaneous features that can be helpful to differentiate CFC syndrome from Noonan and Costello syndromes, which also are classified as RASopathies.
A 3-year-old girl presented with skin xerosis and follicular hyperkeratosis of the face, neck, trunk, and limbs (Figure 1). Facial follicular hyperkeratotic papules on an erythematous base were associated with alopecia of the eyebrows (ulerythema ophryogenes). Hair was sparse and curly (Figure 2A). Facial dysmorphic features included a prominent forehead with bitemporal constriction, bilateral ptosis, a broad nasal base, lip contour in a Cupid’s bow, low-set earlobes with creases (Figure 2B), and a short and webbed neck.


Congenital heart disease, hypothyroidism, bilateral hydronephrosis, delayed motor development, and seizures were noted for the first 2 years. Brain computed tomography detected a dilated ventricular system with hydrocephalus. There was no family history of consanguinity.
Pregnancy was complicated by polyhydramnios and preeclampsia. The neonate was delivered at full-term and was readmitted at 6 days of age due to respiratory failure secondary to congenital chylothorax. Cardiac malformation was diagnosed as the ostium secundum atrial septal defect and interventricular and atrioventricular septal defects. Up to this point she was being treated for Turner syndrome.
The RASopathies are a class of human genetic syndromes that are caused by germ line mutations in genes that encode components of the RAS/MAPK pathway.1 There are many syndromes classified as RASopathies (Table).2,3
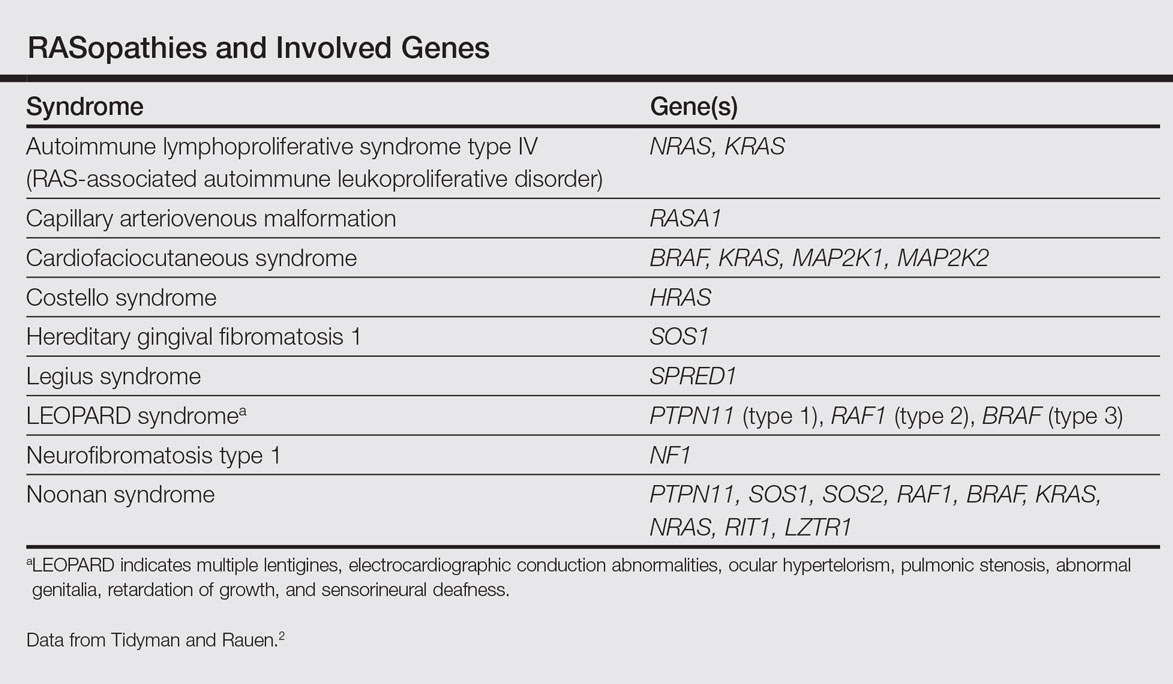
Cardiofaciocutaneous syndrome (Online Mendelian Inheritance in Man [OMIM] 115150) is a genetic disorder first described by Reynolds et al4 and is characterized by several cutaneous abnormalities, cardiac defects, dysmorphic craniofacial features, gastrointestinal dysmotility, and mental retardation. It occurs sporadically and is caused by functional activation of mutations in 4 different genes—BRAF, KRAS, MAP2K1, MAP2K2—of the RAS extracellular signal–regulated kinase molecular cascade that regulates cell differentiation, proliferation, and apoptosis.1
As a RASopathy, CFC syndrome is a member of a family of syndromes with similar phenotypes, which includes mainly Noonan and Costello syndromes. Psychomotor retardation and physical anomalies, the common denominator of all syndromes, may be explained by the effects of the mutations during early development.5,6
In CFC, relative macrocephaly, prominent forehead, bitemporal constriction, absence of eyebrows, palpebral ptosis, broad nasal root, bulbous nasal tip, and small chin commonly are found. The eyes are widely spaced and the palpebral fissures are downward slanting with epicanthic folds.1,4,7
Follicular keratosis of the arms, legs, and face occurs in 80% of cases of CFC and ulerythema ophryogenes with sparse eyebrows in 90% of cases. Sparse, curly, and slow-growing hair is found in 93% of patients. Xerotic scaly skin, hyperkeratosis of the palms and soles, infantile hemangiomas, and multiple melanocytic nevi also may occur.8
Cardiac abnormalities are seen in 75.7% of patients.1 Other features include mental retardation, delayed motor development, and structural abnormalities in the central nervous system, as well as seizures and electroencephalogram abnormalities. Unlike Noonan and Costello syndromes, it is unclear if patients with CFC syndrome are at an increased risk for cancer.1
Noonan syndrome (OMIM #163950) is a disorder characterized by congenital heart defects, short stature, skeletal abnormalities, distinctive facial dysmorphic features, and variable cognitive deficits. Other associated features include cryptorchidism, lymphatic dysplasia, bleeding tendency, and occasional hematologic malignancies during childhood. This syndrome is related to mutations in the PTPN11, SOS1, SOS2, RAF1, BRAF, KRAS, NRAS, RIT1, and LZTR1 genes.2,9-11 The typical ear shape and placement in Noonan syndrome is oval with an overfolded helix that is low set and posteriorly angulated, which is uncommon in CFC syndrome. Noonan syndrome is characterized by an inverted triangular face; hypertelorism; blue or blue-green iris color; webbed neck; limited skin involvement, mainly represented by multiple nevi; and a much milder developmental delay compared to CFC and Costello syndromes.1,11
Costello syndrome (OMIM #218040) is a rare condition comprised of severe postnatal feeding difficulties, mental retardation, coarse facial features, cardiovascular abnormalities (eg, pulmonic stenosis, hypertrophic cardiomyopathy, atrial tachycardia), tumor predisposition, and skin and musculoskeletal abnormalities.12 Costello syndrome is clinically diagnosed. This syndrome shows coarse facies with macrocephaly, downward-slanting palpebral fissures, epicanthal folds, bulbous nose with anteversed nostrils and low nasal bridge, full cheeks, large mouth, thick lips, large tongue, nasal papillomas, cutis laxa, low-set ears, short neck, diffuse skin hyperpigmentation, ulnar deviation of the hands, and nail dystrophy that are not observed in CFC. It is now accepted that the term Costello syndrome should be reserved for patients with HRAS mutation because of the specific risk profile of these patients.12 Remarkably, patients with Costello syndrome are at increased tumor risk (eg, rhabdomyosarcoma, neuroblastoma, bladder carcinoma).2,12
The diagnosis of CFC syndrome is purely clinical. There have been many attempts to delineate the syndrome, but none of the described traits are pathognomonic. In 2002, Kavamura et al7 created the CFC index, a useful diagnostic approach based on 82 clinical characteristics and their frequencies in the CFC population.
Skin abnormalities are helpful manifestations to differentiate CFC syndrome from Noonan and Costello syndromes. Patients with CFC syndrome present with follicular hyperkeratosis and absent eyebrows. Absent eyebrows, narrowed temples, and Cupid’s bow lip are hallmark features of CFC syndrome and are absent in Noonan and Costello syndromes. The presentation of palmoplantar hyperkeratosis also is a differentiating feature; in patients with Costello syndrome, it is found outside the pressure zones, whereas in those with CFC syndrome, it is present mainly in the pressure zones.1 Dermatologists can assist geneticists in the differential diagnosis of these syndromes.
The treatment of disorders with follicular plugging and xerosis is challenging. Emollients with urea, glycolic acid, and lactic acid could improve the appearance of the skin. Treatment with mutated MEK gene inhibitors is under investigation to restore normal development of affected embryos with CFC.2,13 This case and theoretical data show that skin manifestations can be helpful to differentiate CFC syndrome from other RASopathies such as Noonan and Costello syndromes.
- Roberts A, Allanson J, Jadico SK, et al. The cardiofaciocutaneous syndrome. J Med Genet. 2006;43:833-842.
- Tidyman WE, Rauen KA. The RASopathies: developmental syndromes of Ras/MAPK pathway dysregulation. Curr Opin Genet Dev. 2009;19:230-236.
- Stevenson D, Viskochil D, Mao R, et al. Legius syndrome. In: Pagon RA, Bird TD, Dolan CR, et al, eds. GeneReviews. Seattle, WA: University of Washington, Seattle; 1993. http://www.ncbi.nlm.nih.gov/books/NBK47312.
- Reynolds JF, Neri G, Herrmann JP, et al. New multiple congenital anomalies/mental retardation syndrome with cardio-facio-cutaneous involvement—the CFC syndrome. Am J Med Genet. 1986;25:413-427.
- Zenker M, Lehmann K, Schulz AL, et al. Expansion of the genotypic and phenotypic spectrum in patients with KRAS germline mutations. J Med Genet. 2007;44:131-135.
- Rodriguez-Viciana P, Tetsu O, Tidyman WE, et al. Germline mutations in genes within the MAPK pathway cause cardio-facio-cutaneous syndrome. Science. 2006;311:1287-1290.
- Kavamura MI, Peres CA, Alchorne MM, et al. CFC index for the diagnosis of cardiofaciocutaneous syndrome. Am J Med Genet. 2002;112:12-16.
- Siegel DH, McKenzie J, Frieden IJ, et al. Dermatological findings in 61 mutation-positive individuals with cardiofaciocutaneous syndrome. Br J Dermatol. 2011;164:521-529.
- Tartaglia M, Zampino G, Gelb BD. Noonan syndrome: clinical aspects and molecular pathogenesis. Mol Syndromol. 2010;1:2-26.
- Lo FS, Lin JL, Kuo MT, et al. Noonan syndrome caused by germline KRAS mutation in Taiwan: report of two patients and a review of the literature. Eur J Pediatr. 2009;168:919-923.
- Allanson JE, Roberts AE. Noonan syndrome. In: Pagon RA, Bird TD, Dolan CR, et al, eds. GeneReviews. Seattle, WA: University of Washington, Seattle; 1993. http://www.ncbi.nlm.nih.gov/books/NBK1124/.
- Gripp KW, Lin AE. Costello syndrome. In: Pagon RA, Bird TD, Dolan CR, et al, eds. GeneReviews. Seattle, WA: University of Washington, Seattle; 1993. http://www.ncbi.nlm.nih.gov/books/NBK1507/.
- Inoue S, Moriya M, Watanabe Y, et al. New BRAF knockin mice provide a pathogenetic mechanism of developmental defects and a therapeutic approach in cardio-facio-cutaneous syndrome. Hum Mol Genet. 2014;23:6553-6566.
To the Editor:
RASopathies, a class of developmental disorders, are caused by mutations in genes that encode protein components of the RAS/mitogen-activated protein kinase (MAPK) pathway. Each syndrome exhibits its phenotypic features; however, because all of them cause dysregulation of the RAS/MAPK pathway, there are numerous overlapping phenotypic features between the syndromes including cardiac defects, cutaneous abnormalities, characteristic facial features, neurocognitive impairment, and increased risk for developing some neoplastic disorders.
Cardiofaciocutaneous (CFC) syndrome is a RASopathy and is a genetic sporadic disease characterized by multiple congenital anomalies associated with mental retardation. It has a complex dermatological phenotype with many cutaneous features that can be helpful to differentiate CFC syndrome from Noonan and Costello syndromes, which also are classified as RASopathies.
A 3-year-old girl presented with skin xerosis and follicular hyperkeratosis of the face, neck, trunk, and limbs (Figure 1). Facial follicular hyperkeratotic papules on an erythematous base were associated with alopecia of the eyebrows (ulerythema ophryogenes). Hair was sparse and curly (Figure 2A). Facial dysmorphic features included a prominent forehead with bitemporal constriction, bilateral ptosis, a broad nasal base, lip contour in a Cupid’s bow, low-set earlobes with creases (Figure 2B), and a short and webbed neck.
Congenital heart disease, hypothyroidism, bilateral hydronephrosis, delayed motor development, and seizures were noted for the first 2 years. Brain computed tomography detected a dilated ventricular system with hydrocephalus. There was no family history of consanguinity.
Pregnancy was complicated by polyhydramnios and preeclampsia. The neonate was delivered at full-term and was readmitted at 6 days of age due to respiratory failure secondary to congenital chylothorax. Cardiac malformation was diagnosed as the ostium secundum atrial septal defect and interventricular and atrioventricular septal defects. Up to this point she was being treated for Turner syndrome.
The RASopathies are a class of human genetic syndromes that are caused by germ line mutations in genes that encode components of the RAS/MAPK pathway.1 There are many syndromes classified as RASopathies (Table).2,3
Cardiofaciocutaneous syndrome (Online Mendelian Inheritance in Man [OMIM] 115150) is a genetic disorder first described by Reynolds et al4 and is characterized by several cutaneous abnormalities, cardiac defects, dysmorphic craniofacial features, gastrointestinal dysmotility, and mental retardation. It occurs sporadically and is caused by functional activation of mutations in 4 different genes—BRAF, KRAS, MAP2K1, MAP2K2—of the RAS extracellular signal–regulated kinase molecular cascade that regulates cell differentiation, proliferation, and apoptosis.1
As a RASopathy, CFC syndrome is a member of a family of syndromes with similar phenotypes, which includes mainly Noonan and Costello syndromes. Psychomotor retardation and physical anomalies, the common denominator of all syndromes, may be explained by the effects of the mutations during early development.5,6
In CFC, relative macrocephaly, prominent forehead, bitemporal constriction, absence of eyebrows, palpebral ptosis, broad nasal root, bulbous nasal tip, and small chin commonly are found. The eyes are widely spaced and the palpebral fissures are downward slanting with epicanthic folds.1,4,7
Follicular keratosis of the arms, legs, and face occurs in 80% of cases of CFC and ulerythema ophryogenes with sparse eyebrows in 90% of cases. Sparse, curly, and slow-growing hair is found in 93% of patients. Xerotic scaly skin, hyperkeratosis of the palms and soles, infantile hemangiomas, and multiple melanocytic nevi also may occur.8
Cardiac abnormalities are seen in 75.7% of patients.1 Other features include mental retardation, delayed motor development, and structural abnormalities in the central nervous system, as well as seizures and electroencephalogram abnormalities. Unlike Noonan and Costello syndromes, it is unclear if patients with CFC syndrome are at an increased risk for cancer.1
Noonan syndrome (OMIM #163950) is a disorder characterized by congenital heart defects, short stature, skeletal abnormalities, distinctive facial dysmorphic features, and variable cognitive deficits. Other associated features include cryptorchidism, lymphatic dysplasia, bleeding tendency, and occasional hematologic malignancies during childhood. This syndrome is related to mutations in the PTPN11, SOS1, SOS2, RAF1, BRAF, KRAS, NRAS, RIT1, and LZTR1 genes.2,9-11 The typical ear shape and placement in Noonan syndrome is oval with an overfolded helix that is low set and posteriorly angulated, which is uncommon in CFC syndrome. Noonan syndrome is characterized by an inverted triangular face; hypertelorism; blue or blue-green iris color; webbed neck; limited skin involvement, mainly represented by multiple nevi; and a much milder developmental delay compared to CFC and Costello syndromes.1,11
Costello syndrome (OMIM #218040) is a rare condition comprised of severe postnatal feeding difficulties, mental retardation, coarse facial features, cardiovascular abnormalities (eg, pulmonic stenosis, hypertrophic cardiomyopathy, atrial tachycardia), tumor predisposition, and skin and musculoskeletal abnormalities.12 Costello syndrome is clinically diagnosed. This syndrome shows coarse facies with macrocephaly, downward-slanting palpebral fissures, epicanthal folds, bulbous nose with anteversed nostrils and low nasal bridge, full cheeks, large mouth, thick lips, large tongue, nasal papillomas, cutis laxa, low-set ears, short neck, diffuse skin hyperpigmentation, ulnar deviation of the hands, and nail dystrophy that are not observed in CFC. It is now accepted that the term Costello syndrome should be reserved for patients with HRAS mutation because of the specific risk profile of these patients.12 Remarkably, patients with Costello syndrome are at increased tumor risk (eg, rhabdomyosarcoma, neuroblastoma, bladder carcinoma).2,12
The diagnosis of CFC syndrome is purely clinical. There have been many attempts to delineate the syndrome, but none of the described traits are pathognomonic. In 2002, Kavamura et al7 created the CFC index, a useful diagnostic approach based on 82 clinical characteristics and their frequencies in the CFC population.
Skin abnormalities are helpful manifestations to differentiate CFC syndrome from Noonan and Costello syndromes. Patients with CFC syndrome present with follicular hyperkeratosis and absent eyebrows. Absent eyebrows, narrowed temples, and Cupid’s bow lip are hallmark features of CFC syndrome and are absent in Noonan and Costello syndromes. The presentation of palmoplantar hyperkeratosis also is a differentiating feature; in patients with Costello syndrome, it is found outside the pressure zones, whereas in those with CFC syndrome, it is present mainly in the pressure zones.1 Dermatologists can assist geneticists in the differential diagnosis of these syndromes.
The treatment of disorders with follicular plugging and xerosis is challenging. Emollients with urea, glycolic acid, and lactic acid could improve the appearance of the skin. Treatment with mutated MEK gene inhibitors is under investigation to restore normal development of affected embryos with CFC.2,13 This case and theoretical data show that skin manifestations can be helpful to differentiate CFC syndrome from other RASopathies such as Noonan and Costello syndromes.
To the Editor:
RASopathies, a class of developmental disorders, are caused by mutations in genes that encode protein components of the RAS/mitogen-activated protein kinase (MAPK) pathway. Each syndrome exhibits its phenotypic features; however, because all of them cause dysregulation of the RAS/MAPK pathway, there are numerous overlapping phenotypic features between the syndromes including cardiac defects, cutaneous abnormalities, characteristic facial features, neurocognitive impairment, and increased risk for developing some neoplastic disorders.
Cardiofaciocutaneous (CFC) syndrome is a RASopathy and is a genetic sporadic disease characterized by multiple congenital anomalies associated with mental retardation. It has a complex dermatological phenotype with many cutaneous features that can be helpful to differentiate CFC syndrome from Noonan and Costello syndromes, which also are classified as RASopathies.
A 3-year-old girl presented with skin xerosis and follicular hyperkeratosis of the face, neck, trunk, and limbs (Figure 1). Facial follicular hyperkeratotic papules on an erythematous base were associated with alopecia of the eyebrows (ulerythema ophryogenes). Hair was sparse and curly (Figure 2A). Facial dysmorphic features included a prominent forehead with bitemporal constriction, bilateral ptosis, a broad nasal base, lip contour in a Cupid’s bow, low-set earlobes with creases (Figure 2B), and a short and webbed neck.
Congenital heart disease, hypothyroidism, bilateral hydronephrosis, delayed motor development, and seizures were noted for the first 2 years. Brain computed tomography detected a dilated ventricular system with hydrocephalus. There was no family history of consanguinity.
Pregnancy was complicated by polyhydramnios and preeclampsia. The neonate was delivered at full-term and was readmitted at 6 days of age due to respiratory failure secondary to congenital chylothorax. Cardiac malformation was diagnosed as the ostium secundum atrial septal defect and interventricular and atrioventricular septal defects. Up to this point she was being treated for Turner syndrome.
The RASopathies are a class of human genetic syndromes that are caused by germ line mutations in genes that encode components of the RAS/MAPK pathway.1 There are many syndromes classified as RASopathies (Table).2,3
Cardiofaciocutaneous syndrome (Online Mendelian Inheritance in Man [OMIM] 115150) is a genetic disorder first described by Reynolds et al4 and is characterized by several cutaneous abnormalities, cardiac defects, dysmorphic craniofacial features, gastrointestinal dysmotility, and mental retardation. It occurs sporadically and is caused by functional activation of mutations in 4 different genes—BRAF, KRAS, MAP2K1, MAP2K2—of the RAS extracellular signal–regulated kinase molecular cascade that regulates cell differentiation, proliferation, and apoptosis.1
As a RASopathy, CFC syndrome is a member of a family of syndromes with similar phenotypes, which includes mainly Noonan and Costello syndromes. Psychomotor retardation and physical anomalies, the common denominator of all syndromes, may be explained by the effects of the mutations during early development.5,6
In CFC, relative macrocephaly, prominent forehead, bitemporal constriction, absence of eyebrows, palpebral ptosis, broad nasal root, bulbous nasal tip, and small chin commonly are found. The eyes are widely spaced and the palpebral fissures are downward slanting with epicanthic folds.1,4,7
Follicular keratosis of the arms, legs, and face occurs in 80% of cases of CFC and ulerythema ophryogenes with sparse eyebrows in 90% of cases. Sparse, curly, and slow-growing hair is found in 93% of patients. Xerotic scaly skin, hyperkeratosis of the palms and soles, infantile hemangiomas, and multiple melanocytic nevi also may occur.8
Cardiac abnormalities are seen in 75.7% of patients.1 Other features include mental retardation, delayed motor development, and structural abnormalities in the central nervous system, as well as seizures and electroencephalogram abnormalities. Unlike Noonan and Costello syndromes, it is unclear if patients with CFC syndrome are at an increased risk for cancer.1
Noonan syndrome (OMIM #163950) is a disorder characterized by congenital heart defects, short stature, skeletal abnormalities, distinctive facial dysmorphic features, and variable cognitive deficits. Other associated features include cryptorchidism, lymphatic dysplasia, bleeding tendency, and occasional hematologic malignancies during childhood. This syndrome is related to mutations in the PTPN11, SOS1, SOS2, RAF1, BRAF, KRAS, NRAS, RIT1, and LZTR1 genes.2,9-11 The typical ear shape and placement in Noonan syndrome is oval with an overfolded helix that is low set and posteriorly angulated, which is uncommon in CFC syndrome. Noonan syndrome is characterized by an inverted triangular face; hypertelorism; blue or blue-green iris color; webbed neck; limited skin involvement, mainly represented by multiple nevi; and a much milder developmental delay compared to CFC and Costello syndromes.1,11
Costello syndrome (OMIM #218040) is a rare condition comprised of severe postnatal feeding difficulties, mental retardation, coarse facial features, cardiovascular abnormalities (eg, pulmonic stenosis, hypertrophic cardiomyopathy, atrial tachycardia), tumor predisposition, and skin and musculoskeletal abnormalities.12 Costello syndrome is clinically diagnosed. This syndrome shows coarse facies with macrocephaly, downward-slanting palpebral fissures, epicanthal folds, bulbous nose with anteversed nostrils and low nasal bridge, full cheeks, large mouth, thick lips, large tongue, nasal papillomas, cutis laxa, low-set ears, short neck, diffuse skin hyperpigmentation, ulnar deviation of the hands, and nail dystrophy that are not observed in CFC. It is now accepted that the term Costello syndrome should be reserved for patients with HRAS mutation because of the specific risk profile of these patients.12 Remarkably, patients with Costello syndrome are at increased tumor risk (eg, rhabdomyosarcoma, neuroblastoma, bladder carcinoma).2,12
The diagnosis of CFC syndrome is purely clinical. There have been many attempts to delineate the syndrome, but none of the described traits are pathognomonic. In 2002, Kavamura et al7 created the CFC index, a useful diagnostic approach based on 82 clinical characteristics and their frequencies in the CFC population.
Skin abnormalities are helpful manifestations to differentiate CFC syndrome from Noonan and Costello syndromes. Patients with CFC syndrome present with follicular hyperkeratosis and absent eyebrows. Absent eyebrows, narrowed temples, and Cupid’s bow lip are hallmark features of CFC syndrome and are absent in Noonan and Costello syndromes. The presentation of palmoplantar hyperkeratosis also is a differentiating feature; in patients with Costello syndrome, it is found outside the pressure zones, whereas in those with CFC syndrome, it is present mainly in the pressure zones.1 Dermatologists can assist geneticists in the differential diagnosis of these syndromes.
The treatment of disorders with follicular plugging and xerosis is challenging. Emollients with urea, glycolic acid, and lactic acid could improve the appearance of the skin. Treatment with mutated MEK gene inhibitors is under investigation to restore normal development of affected embryos with CFC.2,13 This case and theoretical data show that skin manifestations can be helpful to differentiate CFC syndrome from other RASopathies such as Noonan and Costello syndromes.
- Roberts A, Allanson J, Jadico SK, et al. The cardiofaciocutaneous syndrome. J Med Genet. 2006;43:833-842.
- Tidyman WE, Rauen KA. The RASopathies: developmental syndromes of Ras/MAPK pathway dysregulation. Curr Opin Genet Dev. 2009;19:230-236.
- Stevenson D, Viskochil D, Mao R, et al. Legius syndrome. In: Pagon RA, Bird TD, Dolan CR, et al, eds. GeneReviews. Seattle, WA: University of Washington, Seattle; 1993. http://www.ncbi.nlm.nih.gov/books/NBK47312.
- Reynolds JF, Neri G, Herrmann JP, et al. New multiple congenital anomalies/mental retardation syndrome with cardio-facio-cutaneous involvement—the CFC syndrome. Am J Med Genet. 1986;25:413-427.
- Zenker M, Lehmann K, Schulz AL, et al. Expansion of the genotypic and phenotypic spectrum in patients with KRAS germline mutations. J Med Genet. 2007;44:131-135.
- Rodriguez-Viciana P, Tetsu O, Tidyman WE, et al. Germline mutations in genes within the MAPK pathway cause cardio-facio-cutaneous syndrome. Science. 2006;311:1287-1290.
- Kavamura MI, Peres CA, Alchorne MM, et al. CFC index for the diagnosis of cardiofaciocutaneous syndrome. Am J Med Genet. 2002;112:12-16.
- Siegel DH, McKenzie J, Frieden IJ, et al. Dermatological findings in 61 mutation-positive individuals with cardiofaciocutaneous syndrome. Br J Dermatol. 2011;164:521-529.
- Tartaglia M, Zampino G, Gelb BD. Noonan syndrome: clinical aspects and molecular pathogenesis. Mol Syndromol. 2010;1:2-26.
- Lo FS, Lin JL, Kuo MT, et al. Noonan syndrome caused by germline KRAS mutation in Taiwan: report of two patients and a review of the literature. Eur J Pediatr. 2009;168:919-923.
- Allanson JE, Roberts AE. Noonan syndrome. In: Pagon RA, Bird TD, Dolan CR, et al, eds. GeneReviews. Seattle, WA: University of Washington, Seattle; 1993. http://www.ncbi.nlm.nih.gov/books/NBK1124/.
- Gripp KW, Lin AE. Costello syndrome. In: Pagon RA, Bird TD, Dolan CR, et al, eds. GeneReviews. Seattle, WA: University of Washington, Seattle; 1993. http://www.ncbi.nlm.nih.gov/books/NBK1507/.
- Inoue S, Moriya M, Watanabe Y, et al. New BRAF knockin mice provide a pathogenetic mechanism of developmental defects and a therapeutic approach in cardio-facio-cutaneous syndrome. Hum Mol Genet. 2014;23:6553-6566.
- Roberts A, Allanson J, Jadico SK, et al. The cardiofaciocutaneous syndrome. J Med Genet. 2006;43:833-842.
- Tidyman WE, Rauen KA. The RASopathies: developmental syndromes of Ras/MAPK pathway dysregulation. Curr Opin Genet Dev. 2009;19:230-236.
- Stevenson D, Viskochil D, Mao R, et al. Legius syndrome. In: Pagon RA, Bird TD, Dolan CR, et al, eds. GeneReviews. Seattle, WA: University of Washington, Seattle; 1993. http://www.ncbi.nlm.nih.gov/books/NBK47312.
- Reynolds JF, Neri G, Herrmann JP, et al. New multiple congenital anomalies/mental retardation syndrome with cardio-facio-cutaneous involvement—the CFC syndrome. Am J Med Genet. 1986;25:413-427.
- Zenker M, Lehmann K, Schulz AL, et al. Expansion of the genotypic and phenotypic spectrum in patients with KRAS germline mutations. J Med Genet. 2007;44:131-135.
- Rodriguez-Viciana P, Tetsu O, Tidyman WE, et al. Germline mutations in genes within the MAPK pathway cause cardio-facio-cutaneous syndrome. Science. 2006;311:1287-1290.
- Kavamura MI, Peres CA, Alchorne MM, et al. CFC index for the diagnosis of cardiofaciocutaneous syndrome. Am J Med Genet. 2002;112:12-16.
- Siegel DH, McKenzie J, Frieden IJ, et al. Dermatological findings in 61 mutation-positive individuals with cardiofaciocutaneous syndrome. Br J Dermatol. 2011;164:521-529.
- Tartaglia M, Zampino G, Gelb BD. Noonan syndrome: clinical aspects and molecular pathogenesis. Mol Syndromol. 2010;1:2-26.
- Lo FS, Lin JL, Kuo MT, et al. Noonan syndrome caused by germline KRAS mutation in Taiwan: report of two patients and a review of the literature. Eur J Pediatr. 2009;168:919-923.
- Allanson JE, Roberts AE. Noonan syndrome. In: Pagon RA, Bird TD, Dolan CR, et al, eds. GeneReviews. Seattle, WA: University of Washington, Seattle; 1993. http://www.ncbi.nlm.nih.gov/books/NBK1124/.
- Gripp KW, Lin AE. Costello syndrome. In: Pagon RA, Bird TD, Dolan CR, et al, eds. GeneReviews. Seattle, WA: University of Washington, Seattle; 1993. http://www.ncbi.nlm.nih.gov/books/NBK1507/.
- Inoue S, Moriya M, Watanabe Y, et al. New BRAF knockin mice provide a pathogenetic mechanism of developmental defects and a therapeutic approach in cardio-facio-cutaneous syndrome. Hum Mol Genet. 2014;23:6553-6566.
Practice Points
- RASopathies, a class of developmental disorders, are caused by mutations in genes that encode protein components of the RAS/mitogen-activated protein kinase pathway. Cardiofaciocutaneous (CFC) syndrome is a RASopathy.
- Skin manifestations may help in differentiating CFC syndrome from other RASopathies.