User login
Familial and sporadic ankylosing spondylitis differ in small ways
While differences do exist between familial and sporadic ankylosing spondylitis, key similarities suggest that the two conditions can be treated the same way, according to a new study presented at the annual meeting of the Canadian Rheumatology Association.
“AS [ankylosing spondylitis] patients with a family history of AS are not very different from patients without any family history,” Nigil Haroon, MD, of the University Health Network in Toronto, explained in an interview. “They have similar disease activity as measured by markers of inflammation [and] similar disease severity as assessed by radiographic scoring for spinal damage.”
Dr. Haroon, along with his coinvestigators – including Bruce Sheng, MD,of the same institution, who presented the study at the meeting – prospectively followed AS patients satisfying the New York criteria for a period of 15 years, collecting data on 888 eligible subjects who were eventually included in the study. Of the subjects included, 74% were male, the average age was 45.6 years (standard deviation, 13.7 years), and average disease duration was 15 years (SD, 11.5 years).

The investigators found some similarities between the 177 (20%) patients with familial AS who had at least one first- or second-generation relative with the disease and the 711 with sporadic AS. Anti–tumor necrosis factor (anti-TNF) treatment failed in 23.1% of familial AS patients and 23.6% of sporadic disease patients based on the lack of a “sustained clinical effect” for more than 1 year. There were also no differences found between the groups in clinical and radiographic severity of disease.
However, patients with familial AS did record earlier onset of disease (22.5 years vs. 24.3 years; P = .016), longer disease duration (17.4 years vs. 14.3 years; P = .003), and higher HLA-B27 positivity (90% vs. 65%; P less than .001), along with higher rates of uveitis, psoriatic arthritis, and inflammatory bowel disease.
“Some of the findings are expected, including the higher prevalence of HLA-B27 due to gene sharing in the family. ... The higher B27 sharing may also affect the uveitis prevalence as well in familial AS,” Dr. Haroon explained. “The similar radiographic progression rates and treatment responses are interesting findings.”
In terms of the ramifications of these findings, Dr. Haroon stated that clinicians should reevaluate how they prescribe drugs to their AS patients.
“The high likelihood of uveitis in familial AS patients – 43% versus 29% – may affect the choice of treatment as all drugs are not equally effective in uveitis,” he said. “As the family history of extra-articular manifestations is high in familial AS, it remains to be seen if a lower threshold for investigating symptoms suggestive of IBD/uveitis will decrease delays in diagnosis of these conditions in individuals with a family history of AS.”
Moving forward from here, Dr. Haroon called for family studies, especially those including families with multiple individuals affected with AS, as these can help identify genetic risk factors that may be contribute to the development of AS.
“There is paucity of data on familial AS,” Dr. Haroon said. “The strength of this study is the large dataset.”
The study was funded by the Canadian Rheumatology Association’s Summer Research Program, which supported Dr. Sheng. Dr. Sheng and Dr. Haroon did not report any other relevant financial disclosures.
While differences do exist between familial and sporadic ankylosing spondylitis, key similarities suggest that the two conditions can be treated the same way, according to a new study presented at the annual meeting of the Canadian Rheumatology Association.
“AS [ankylosing spondylitis] patients with a family history of AS are not very different from patients without any family history,” Nigil Haroon, MD, of the University Health Network in Toronto, explained in an interview. “They have similar disease activity as measured by markers of inflammation [and] similar disease severity as assessed by radiographic scoring for spinal damage.”
Dr. Haroon, along with his coinvestigators – including Bruce Sheng, MD,of the same institution, who presented the study at the meeting – prospectively followed AS patients satisfying the New York criteria for a period of 15 years, collecting data on 888 eligible subjects who were eventually included in the study. Of the subjects included, 74% were male, the average age was 45.6 years (standard deviation, 13.7 years), and average disease duration was 15 years (SD, 11.5 years).
The investigators found some similarities between the 177 (20%) patients with familial AS who had at least one first- or second-generation relative with the disease and the 711 with sporadic AS. Anti–tumor necrosis factor (anti-TNF) treatment failed in 23.1% of familial AS patients and 23.6% of sporadic disease patients based on the lack of a “sustained clinical effect” for more than 1 year. There were also no differences found between the groups in clinical and radiographic severity of disease.
However, patients with familial AS did record earlier onset of disease (22.5 years vs. 24.3 years; P = .016), longer disease duration (17.4 years vs. 14.3 years; P = .003), and higher HLA-B27 positivity (90% vs. 65%; P less than .001), along with higher rates of uveitis, psoriatic arthritis, and inflammatory bowel disease.
“Some of the findings are expected, including the higher prevalence of HLA-B27 due to gene sharing in the family. ... The higher B27 sharing may also affect the uveitis prevalence as well in familial AS,” Dr. Haroon explained. “The similar radiographic progression rates and treatment responses are interesting findings.”
In terms of the ramifications of these findings, Dr. Haroon stated that clinicians should reevaluate how they prescribe drugs to their AS patients.
“The high likelihood of uveitis in familial AS patients – 43% versus 29% – may affect the choice of treatment as all drugs are not equally effective in uveitis,” he said. “As the family history of extra-articular manifestations is high in familial AS, it remains to be seen if a lower threshold for investigating symptoms suggestive of IBD/uveitis will decrease delays in diagnosis of these conditions in individuals with a family history of AS.”
Moving forward from here, Dr. Haroon called for family studies, especially those including families with multiple individuals affected with AS, as these can help identify genetic risk factors that may be contribute to the development of AS.
“There is paucity of data on familial AS,” Dr. Haroon said. “The strength of this study is the large dataset.”
The study was funded by the Canadian Rheumatology Association’s Summer Research Program, which supported Dr. Sheng. Dr. Sheng and Dr. Haroon did not report any other relevant financial disclosures.
While differences do exist between familial and sporadic ankylosing spondylitis, key similarities suggest that the two conditions can be treated the same way, according to a new study presented at the annual meeting of the Canadian Rheumatology Association.
“AS [ankylosing spondylitis] patients with a family history of AS are not very different from patients without any family history,” Nigil Haroon, MD, of the University Health Network in Toronto, explained in an interview. “They have similar disease activity as measured by markers of inflammation [and] similar disease severity as assessed by radiographic scoring for spinal damage.”
Dr. Haroon, along with his coinvestigators – including Bruce Sheng, MD,of the same institution, who presented the study at the meeting – prospectively followed AS patients satisfying the New York criteria for a period of 15 years, collecting data on 888 eligible subjects who were eventually included in the study. Of the subjects included, 74% were male, the average age was 45.6 years (standard deviation, 13.7 years), and average disease duration was 15 years (SD, 11.5 years).
The investigators found some similarities between the 177 (20%) patients with familial AS who had at least one first- or second-generation relative with the disease and the 711 with sporadic AS. Anti–tumor necrosis factor (anti-TNF) treatment failed in 23.1% of familial AS patients and 23.6% of sporadic disease patients based on the lack of a “sustained clinical effect” for more than 1 year. There were also no differences found between the groups in clinical and radiographic severity of disease.
However, patients with familial AS did record earlier onset of disease (22.5 years vs. 24.3 years; P = .016), longer disease duration (17.4 years vs. 14.3 years; P = .003), and higher HLA-B27 positivity (90% vs. 65%; P less than .001), along with higher rates of uveitis, psoriatic arthritis, and inflammatory bowel disease.
“Some of the findings are expected, including the higher prevalence of HLA-B27 due to gene sharing in the family. ... The higher B27 sharing may also affect the uveitis prevalence as well in familial AS,” Dr. Haroon explained. “The similar radiographic progression rates and treatment responses are interesting findings.”
In terms of the ramifications of these findings, Dr. Haroon stated that clinicians should reevaluate how they prescribe drugs to their AS patients.
“The high likelihood of uveitis in familial AS patients – 43% versus 29% – may affect the choice of treatment as all drugs are not equally effective in uveitis,” he said. “As the family history of extra-articular manifestations is high in familial AS, it remains to be seen if a lower threshold for investigating symptoms suggestive of IBD/uveitis will decrease delays in diagnosis of these conditions in individuals with a family history of AS.”
Moving forward from here, Dr. Haroon called for family studies, especially those including families with multiple individuals affected with AS, as these can help identify genetic risk factors that may be contribute to the development of AS.
“There is paucity of data on familial AS,” Dr. Haroon said. “The strength of this study is the large dataset.”
The study was funded by the Canadian Rheumatology Association’s Summer Research Program, which supported Dr. Sheng. Dr. Sheng and Dr. Haroon did not report any other relevant financial disclosures.
FROM THE CRA SCIENTIFIC CONFERENCE
Key clinical point:
Major finding: Anti-TNF treatment failed in 23.1% of familial AS patients and 23.6% of sporadic disease patients based on the lack of a “sustained clinical effect” for more than 1 year.
Data source: Prospective cohort study of 888 patients with AS over 15 years.
Disclosures: Funded by the Canadian Rheumatology Association’s Summer Research Program. No other relevant disclosures were reported.
Strategies for preventing and detecting false-negatives in urine drug screens
Urine drug screening (UDS) is an important tool in emergency settings and substance abuse or pain management clinics. According to the 2015 National Survey on Drug Use and Health, 9.2% of individuals age ≥12 used an illicit drug other than marijuana within the previous year.1
There are 2 types of UDS: gas chromatography–mass spectroscopy (GC-MS) and enzymatic immunoassay (EIA). A GC-MS uses a 2-step mechanisms to detect chemical compounds. First the GC separate the illicit substance into molecules, which is then introduced to the MS, which then separates compounds depending on their mass and charge using magnetic fields.2,3 Although GC-MS is a more definitive means to confirm the presence of a specific drug, it rarely is used in clinical settings because it is expensive and time-consuming.
EIA is an anti-drug antibody added to the patient’s urine that causes a positive indicator reaction that can be measured.2,3 It is a rapid, accurate, and cost-effective way of detecting illicit substances.4 However, there are limitations to EIAs used in most hospital laboratories.
Limitations of EIAs
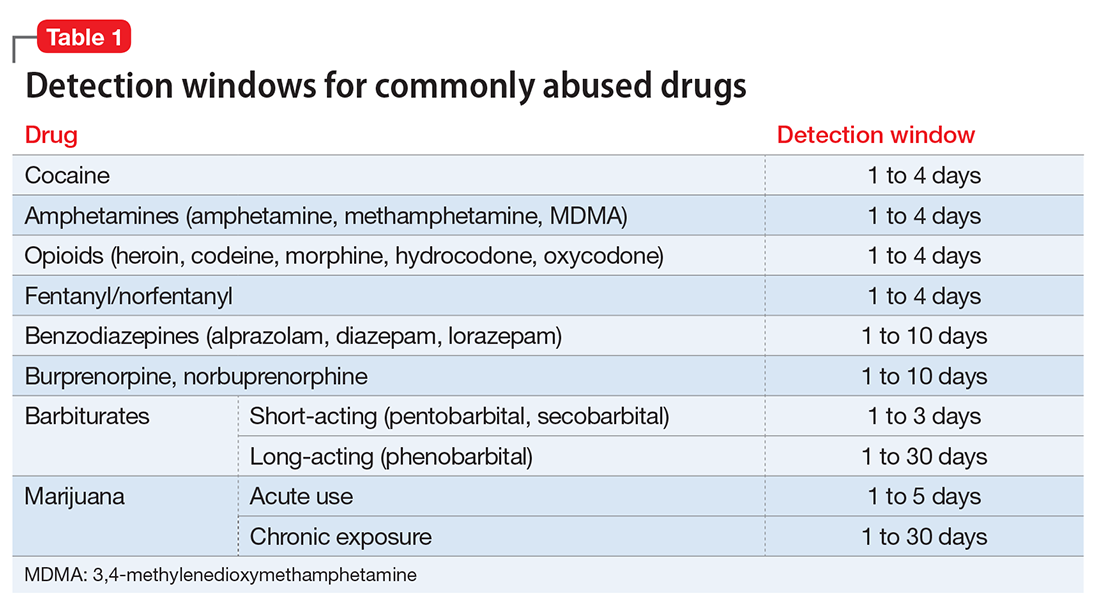
Timing. Results of the drug screen depend on the time and frequency of drug use (Table 1).5
Sensitivity. The immunoassay methods used vary in their ability to detect substances and depend on the test’s sensitivity; however, most of these versions have high sensitivity for detecting many illicit substances.4
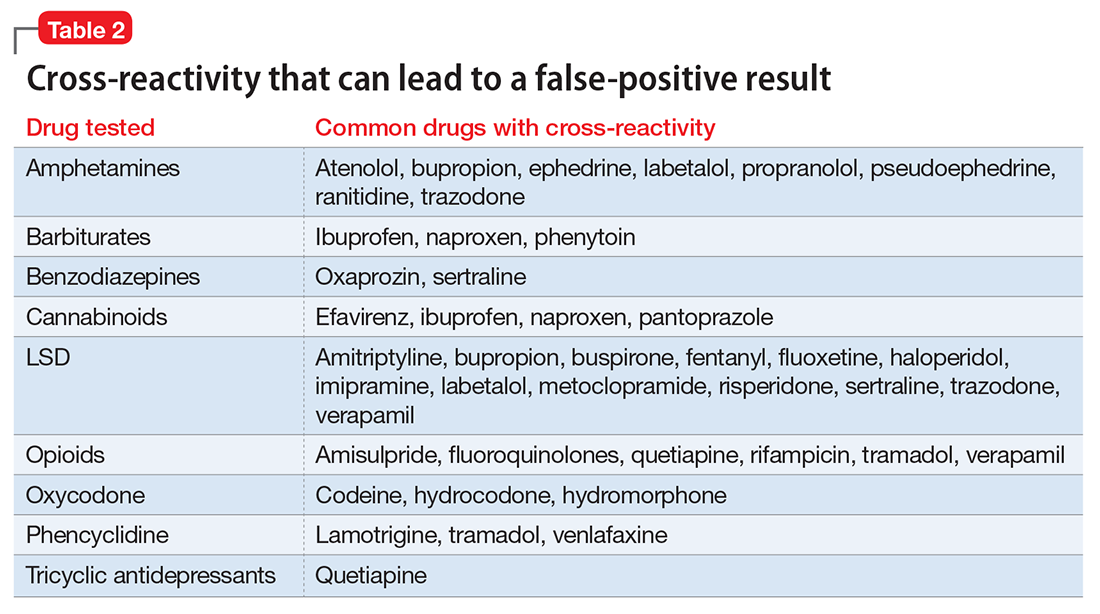
Specificity and cross-reactivity. Unfortunately, many drugs, such as opioids, amphetamines, and commonly prescribed medications, exhibit cross-reactivity that can produce false-positive results (Table 2).5,6
Synthetic cannabinoids, such as “spice” and cathinones, also known as “bath salts,” cannot be detected with standard UDS. However, some newer EIA kits can detect synthetic cannabinoids but do not detect newer designer drugs.7 Detection of specific cathinones by EIA is not yet available.7
Preventing false-negatives
Substance abusing individuals could try to avoid detection of illicit drug use by using the following techniques:
- In vivo methods, such as drinking a large amount of water or using herbal products, can lead to false-negative results because of dilution.8
- In vitro adulterants are substances added to urine samples after urination to avoid drug detection. Active ingredients include glutaraldehyde (Clean-X), sodium or potassium nitrate (Klear, Whizzies), pyridinium chlorochromate (Urine Luck), andj (Stealth).9
- Other methods used to avoid drug detection include substituting a urine sample with someone else’s clean urine or adding household products, such as bleach, vinegar, or pipe cleaner.
You can spot and prevent false-negatives by:
Directly observing the patient, which helps to prevent individuals from adding foreign materials or substituting the urine sample.
Visually inspecting the urine helps identify sample tampering. Adding household adulterants can produce unusually bubbly, cloudy, clear, or dark sample.
On-site analyses and laboratory analyses of samples. Commercially sold kits can detect adulterants by on-site analysis, such as Intect 7 and AdultaCheck 4 test strips.9 Simple on-site methods can help discover tampering, such as measuring the urine’s temperature and using pigmented toilet water. The U.S. Substance Abuse and Mental Health Services Administration recommends validity checks during laboratory analysis for all urine samples, including temperature, creatinine, specific gravity, pH, and tests for oxidizing adulterants.10
Considerations
The results of UDS should not be interpreted as absolute. Knowing the sensitivity and specificity of the UDS that your institution uses and the patient’s current medication regimen is valuable in distinguishing between true results and false-positives. False-positives can strain the relationship between patient and provider, thus compromising care. When EIA is positive and patient denies substance use, confirming the result with GC-MS may be a good clinical practice.3 Ordering a GC-MS test can be helpful in situations requiring greater precision, such as in methadone or pain management clinics, to verify if the patient is taking a prescribed medication properly or to rule out illicit exposures with greater certainty.
Acknowledgment
The authors would like to thank Steven Lippmann, MD, for his mentorship, encouragement, and editorial support.
1. Substance Abuse and Mental Health Services Administration. Results from the National Survey on Drug Use and Health: detailed tables. Prevalence estimates, standard errors, P values, and sample sizes. https://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015.pdf. Published September 8, 2016. Accessed February 7, 2017.
2. Schweitzer BN. An assessment of lateral flow immunoassay testing and gas chromatography mass spectrometry as methods for the detection of five drugs of abuse in forensic bloodstains. https://open.bu.edu/bitstream/handle/2144/19477/Schweitzer_bu_0017N_12357.pdf?sequence=1. Published 2016. Accessed February 7, 2017.
3. Pawlowski J, Ellingrod VL. Urine drug screens: when might a test result be false-positive? Current Psychiatry. 2015;14(10):17,22-24.
4. Tenore PL. Advanced urine toxicology testing. J Addict Dis. 2010;29(4):436-448.
5. AIT Laboratories. Physician’s reference for urine and blood drug testing and interpretation. http://web.archive.org/web/20160312195526/http://aitlabs.com/uploadedfiles/services/pocket_guide_smr086.pdf. Published 2011. Accessed February 7, 2017.
6. Saitman A, Park HD, Fitzgerald RL. False-positive interferences of common urine drug screen immunoassays: a review. J Anal Toxicol. 2014;38(7):387-396.
7. Namera A, Kawamura M, Nakamoto A, et al. Comprehensive review of the detection methods for synthetic cannabinoids and cathinones. Forensic Toxicol. 2015;33(2):175-194.
8. Cone EJ, Lange R, Darwin WD. In vivo adulteration: excess fluid ingestion causes false-negative marijuana and cocaine urine test results. J Anal Toxicol. 1998;22(6):460-473.
9. Jaffee WB, Trucco E, Levy S, et al. Is this urine really negative? A systematic review of tampering methods in urine drug screening and testing. J Subst Abuse Treat. 2007;33(1):33-42.
10. Substance Abuse and Mental Health Services Administration. Mandatory guidelines for federal workplace drug testing programs. Federal Register. 2004;69:19644-19673.
Urine drug screening (UDS) is an important tool in emergency settings and substance abuse or pain management clinics. According to the 2015 National Survey on Drug Use and Health, 9.2% of individuals age ≥12 used an illicit drug other than marijuana within the previous year.1
There are 2 types of UDS: gas chromatography–mass spectroscopy (GC-MS) and enzymatic immunoassay (EIA). A GC-MS uses a 2-step mechanisms to detect chemical compounds. First the GC separate the illicit substance into molecules, which is then introduced to the MS, which then separates compounds depending on their mass and charge using magnetic fields.2,3 Although GC-MS is a more definitive means to confirm the presence of a specific drug, it rarely is used in clinical settings because it is expensive and time-consuming.
EIA is an anti-drug antibody added to the patient’s urine that causes a positive indicator reaction that can be measured.2,3 It is a rapid, accurate, and cost-effective way of detecting illicit substances.4 However, there are limitations to EIAs used in most hospital laboratories.
Limitations of EIAs
Timing. Results of the drug screen depend on the time and frequency of drug use (Table 1).5
Sensitivity. The immunoassay methods used vary in their ability to detect substances and depend on the test’s sensitivity; however, most of these versions have high sensitivity for detecting many illicit substances.4
Specificity and cross-reactivity. Unfortunately, many drugs, such as opioids, amphetamines, and commonly prescribed medications, exhibit cross-reactivity that can produce false-positive results (Table 2).5,6
Synthetic cannabinoids, such as “spice” and cathinones, also known as “bath salts,” cannot be detected with standard UDS. However, some newer EIA kits can detect synthetic cannabinoids but do not detect newer designer drugs.7 Detection of specific cathinones by EIA is not yet available.7
Preventing false-negatives
Substance abusing individuals could try to avoid detection of illicit drug use by using the following techniques:
- In vivo methods, such as drinking a large amount of water or using herbal products, can lead to false-negative results because of dilution.8
- In vitro adulterants are substances added to urine samples after urination to avoid drug detection. Active ingredients include glutaraldehyde (Clean-X), sodium or potassium nitrate (Klear, Whizzies), pyridinium chlorochromate (Urine Luck), andj (Stealth).9
- Other methods used to avoid drug detection include substituting a urine sample with someone else’s clean urine or adding household products, such as bleach, vinegar, or pipe cleaner.
You can spot and prevent false-negatives by:
Directly observing the patient, which helps to prevent individuals from adding foreign materials or substituting the urine sample.
Visually inspecting the urine helps identify sample tampering. Adding household adulterants can produce unusually bubbly, cloudy, clear, or dark sample.
On-site analyses and laboratory analyses of samples. Commercially sold kits can detect adulterants by on-site analysis, such as Intect 7 and AdultaCheck 4 test strips.9 Simple on-site methods can help discover tampering, such as measuring the urine’s temperature and using pigmented toilet water. The U.S. Substance Abuse and Mental Health Services Administration recommends validity checks during laboratory analysis for all urine samples, including temperature, creatinine, specific gravity, pH, and tests for oxidizing adulterants.10
Considerations
The results of UDS should not be interpreted as absolute. Knowing the sensitivity and specificity of the UDS that your institution uses and the patient’s current medication regimen is valuable in distinguishing between true results and false-positives. False-positives can strain the relationship between patient and provider, thus compromising care. When EIA is positive and patient denies substance use, confirming the result with GC-MS may be a good clinical practice.3 Ordering a GC-MS test can be helpful in situations requiring greater precision, such as in methadone or pain management clinics, to verify if the patient is taking a prescribed medication properly or to rule out illicit exposures with greater certainty.
Acknowledgment
The authors would like to thank Steven Lippmann, MD, for his mentorship, encouragement, and editorial support.
Urine drug screening (UDS) is an important tool in emergency settings and substance abuse or pain management clinics. According to the 2015 National Survey on Drug Use and Health, 9.2% of individuals age ≥12 used an illicit drug other than marijuana within the previous year.1
There are 2 types of UDS: gas chromatography–mass spectroscopy (GC-MS) and enzymatic immunoassay (EIA). A GC-MS uses a 2-step mechanisms to detect chemical compounds. First the GC separate the illicit substance into molecules, which is then introduced to the MS, which then separates compounds depending on their mass and charge using magnetic fields.2,3 Although GC-MS is a more definitive means to confirm the presence of a specific drug, it rarely is used in clinical settings because it is expensive and time-consuming.
EIA is an anti-drug antibody added to the patient’s urine that causes a positive indicator reaction that can be measured.2,3 It is a rapid, accurate, and cost-effective way of detecting illicit substances.4 However, there are limitations to EIAs used in most hospital laboratories.
Limitations of EIAs
Timing. Results of the drug screen depend on the time and frequency of drug use (Table 1).5
Sensitivity. The immunoassay methods used vary in their ability to detect substances and depend on the test’s sensitivity; however, most of these versions have high sensitivity for detecting many illicit substances.4
Specificity and cross-reactivity. Unfortunately, many drugs, such as opioids, amphetamines, and commonly prescribed medications, exhibit cross-reactivity that can produce false-positive results (Table 2).5,6
Synthetic cannabinoids, such as “spice” and cathinones, also known as “bath salts,” cannot be detected with standard UDS. However, some newer EIA kits can detect synthetic cannabinoids but do not detect newer designer drugs.7 Detection of specific cathinones by EIA is not yet available.7
Preventing false-negatives
Substance abusing individuals could try to avoid detection of illicit drug use by using the following techniques:
- In vivo methods, such as drinking a large amount of water or using herbal products, can lead to false-negative results because of dilution.8
- In vitro adulterants are substances added to urine samples after urination to avoid drug detection. Active ingredients include glutaraldehyde (Clean-X), sodium or potassium nitrate (Klear, Whizzies), pyridinium chlorochromate (Urine Luck), andj (Stealth).9
- Other methods used to avoid drug detection include substituting a urine sample with someone else’s clean urine or adding household products, such as bleach, vinegar, or pipe cleaner.
You can spot and prevent false-negatives by:
Directly observing the patient, which helps to prevent individuals from adding foreign materials or substituting the urine sample.
Visually inspecting the urine helps identify sample tampering. Adding household adulterants can produce unusually bubbly, cloudy, clear, or dark sample.
On-site analyses and laboratory analyses of samples. Commercially sold kits can detect adulterants by on-site analysis, such as Intect 7 and AdultaCheck 4 test strips.9 Simple on-site methods can help discover tampering, such as measuring the urine’s temperature and using pigmented toilet water. The U.S. Substance Abuse and Mental Health Services Administration recommends validity checks during laboratory analysis for all urine samples, including temperature, creatinine, specific gravity, pH, and tests for oxidizing adulterants.10
Considerations
The results of UDS should not be interpreted as absolute. Knowing the sensitivity and specificity of the UDS that your institution uses and the patient’s current medication regimen is valuable in distinguishing between true results and false-positives. False-positives can strain the relationship between patient and provider, thus compromising care. When EIA is positive and patient denies substance use, confirming the result with GC-MS may be a good clinical practice.3 Ordering a GC-MS test can be helpful in situations requiring greater precision, such as in methadone or pain management clinics, to verify if the patient is taking a prescribed medication properly or to rule out illicit exposures with greater certainty.
Acknowledgment
The authors would like to thank Steven Lippmann, MD, for his mentorship, encouragement, and editorial support.
1. Substance Abuse and Mental Health Services Administration. Results from the National Survey on Drug Use and Health: detailed tables. Prevalence estimates, standard errors, P values, and sample sizes. https://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015.pdf. Published September 8, 2016. Accessed February 7, 2017.
2. Schweitzer BN. An assessment of lateral flow immunoassay testing and gas chromatography mass spectrometry as methods for the detection of five drugs of abuse in forensic bloodstains. https://open.bu.edu/bitstream/handle/2144/19477/Schweitzer_bu_0017N_12357.pdf?sequence=1. Published 2016. Accessed February 7, 2017.
3. Pawlowski J, Ellingrod VL. Urine drug screens: when might a test result be false-positive? Current Psychiatry. 2015;14(10):17,22-24.
4. Tenore PL. Advanced urine toxicology testing. J Addict Dis. 2010;29(4):436-448.
5. AIT Laboratories. Physician’s reference for urine and blood drug testing and interpretation. http://web.archive.org/web/20160312195526/http://aitlabs.com/uploadedfiles/services/pocket_guide_smr086.pdf. Published 2011. Accessed February 7, 2017.
6. Saitman A, Park HD, Fitzgerald RL. False-positive interferences of common urine drug screen immunoassays: a review. J Anal Toxicol. 2014;38(7):387-396.
7. Namera A, Kawamura M, Nakamoto A, et al. Comprehensive review of the detection methods for synthetic cannabinoids and cathinones. Forensic Toxicol. 2015;33(2):175-194.
8. Cone EJ, Lange R, Darwin WD. In vivo adulteration: excess fluid ingestion causes false-negative marijuana and cocaine urine test results. J Anal Toxicol. 1998;22(6):460-473.
9. Jaffee WB, Trucco E, Levy S, et al. Is this urine really negative? A systematic review of tampering methods in urine drug screening and testing. J Subst Abuse Treat. 2007;33(1):33-42.
10. Substance Abuse and Mental Health Services Administration. Mandatory guidelines for federal workplace drug testing programs. Federal Register. 2004;69:19644-19673.
1. Substance Abuse and Mental Health Services Administration. Results from the National Survey on Drug Use and Health: detailed tables. Prevalence estimates, standard errors, P values, and sample sizes. https://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015.pdf. Published September 8, 2016. Accessed February 7, 2017.
2. Schweitzer BN. An assessment of lateral flow immunoassay testing and gas chromatography mass spectrometry as methods for the detection of five drugs of abuse in forensic bloodstains. https://open.bu.edu/bitstream/handle/2144/19477/Schweitzer_bu_0017N_12357.pdf?sequence=1. Published 2016. Accessed February 7, 2017.
3. Pawlowski J, Ellingrod VL. Urine drug screens: when might a test result be false-positive? Current Psychiatry. 2015;14(10):17,22-24.
4. Tenore PL. Advanced urine toxicology testing. J Addict Dis. 2010;29(4):436-448.
5. AIT Laboratories. Physician’s reference for urine and blood drug testing and interpretation. http://web.archive.org/web/20160312195526/http://aitlabs.com/uploadedfiles/services/pocket_guide_smr086.pdf. Published 2011. Accessed February 7, 2017.
6. Saitman A, Park HD, Fitzgerald RL. False-positive interferences of common urine drug screen immunoassays: a review. J Anal Toxicol. 2014;38(7):387-396.
7. Namera A, Kawamura M, Nakamoto A, et al. Comprehensive review of the detection methods for synthetic cannabinoids and cathinones. Forensic Toxicol. 2015;33(2):175-194.
8. Cone EJ, Lange R, Darwin WD. In vivo adulteration: excess fluid ingestion causes false-negative marijuana and cocaine urine test results. J Anal Toxicol. 1998;22(6):460-473.
9. Jaffee WB, Trucco E, Levy S, et al. Is this urine really negative? A systematic review of tampering methods in urine drug screening and testing. J Subst Abuse Treat. 2007;33(1):33-42.
10. Substance Abuse and Mental Health Services Administration. Mandatory guidelines for federal workplace drug testing programs. Federal Register. 2004;69:19644-19673.

Doctors, drug reps, and free speech
Question: The First Amendment guarantees the right of free speech, but the U.S. Supreme Court has held that under a strict scrutiny standard, the government may regulate:
A. Obscenity.
B. Fighting words.
C. Professional speech.
D. A and B.
E. A, B, and C.
Answer: D. The First Amendment forbids the government from “abridging the freedom of speech,” which extends to certain nonverbal conduct, such as flag burning. At the same time, the U.S. Supreme Court has also ruled that certain categories of speech such as obscenity and fighting words can be regulated under a strict scrutiny standard. However, it remains unsettled whether and to what extent professional speech – such as in the context of the doctor-patient relationship – may be curtailed.
Two recent cases grapple with this issue of free speech – with rather unexpected results.
The first, overturning a decades-old prohibition of the off-label detailing of drugs, surprisingly was decided against the government. The second challenges a Florida statute censoring the discussion of firearms safety between a doctor and a patient. An early decision, under reconsideration, in fact supported the state’s regulation of physicians’ freedom of speech under the circumstances.

Because the FDA has no jurisdiction over physician conduct, it has no power to regulate the off-label use of an otherwise approved drug, which explains why such off-label prescriptions are widespread, especially in the oncology field.
In U.S. v. Caronia, the defendant, a pharmaceutical sales representative, was criminally prosecuted and found guilty of conspiracy in a New York court for introducing a misbranded drug into interstate commerce.1 Specifically, Alfred Caronia promoted the drug Xyrem for use in a manner not approved by the FDA.
Orphan Medical, now known as Jazz Pharmaceuticals, is the manufacturer of Xyrem, a powerful central nervous system depressant. Xyrem’s active ingredient is gamma-hydroxybutyrate, which has been federally classified as the “date rape drug” for its use in the commission of sexual assaults. The FDA had approved Xyrem for two conditions: to treat narcolepsy patients who experience cataplexy, a condition associated with weak or paralyzed muscles; and to treat those with excessive daytime sleepiness.
Caronia was found to provide off-label detailing of the drug to doctors for unapproved indications such as chronic fatigue, fibromyalgia, restless leg syndrome, and Parkinson’s disease.
Caronia argued that in promoting an FDA-approved drug, albeit for off-label use, he was within his right of free speech under the First Amendment. In overturning his conviction, a three-judge panel of the U.S. Second Circuit Court of Appeals agreed, noting the overly broad FDA regulations and specifically that nothing Caronia did constituted conspiracy to put a false or misleading or deficient label on a drug product.
The court concluded: “The government cannot prosecute pharmaceutical manufacturers and their representatives under the FDCA [Federal Food, Drug, and Cosmetic Act] for speech promoting the lawful, off-label use of an FDA-approved drug.”
In 2011, the U.S. Supreme Court had used a First Amendment argument to invalidate a Vermont law that prohibited the practice of pharmaceutical data mining – purchasing information about prescribers from pharmacies and others.2
Taken together, the FDA now appears resigned to the free speech argument.3 For example, it has decided not to appeal a judge’s ruling that the First Amendment protects Amarin from promoting its fish-oil capsules for unapproved uses. Just recently, the FDA published a draft proposal in tacit acceptance of this new policy position, merely recommending the disclosure of relevant information including limitations and unfavorable or inconsistent findings surrounding the off-label use of a drug.
The next issue concerns professional speech. It is well documented that the presence of a gun in the home increases the risk of death especially by suicide, and this serves as the impetus for the long-established recommendation that physicians discuss firearm safety with their patients.
The medical profession was therefore aghast when Florida enacted its law on “Privacy of Firearm Owners.”4 Codified on June 2, 2011, it provides that a licensed practitioner or facility may not record firearm ownership information in a patient’s medical record, and that unless information is relevant to the patient’s medical care or safety or safety of others, inquiries regarding firearm ownership or possession should not be made. A practitioner is also forbidden from unnecessarily harassing a patient about firearm ownership during an examination.
Violation can result in disciplinary action; the original intent was to make this a third-degree felony with penalties of up to $5 million in fines and 5 years of imprisonment, but the final bill was stripped of criminal penalties.
In July 2015, a panel of three judges of the U.S. 11th Circuit Court of Appeals, in a split 2-1 decision, found that the inquiry, record-keeping, and harassment provisions of the act specifically regulate professional speech, which is subject to an intermediate level of scrutiny. Under this level of scrutiny, the court found that the act was precisely tailored to directly advance the state’s substantial interests in protecting the public and patient privacy rights.
Holding that the act was not so overly broad as to violate the First Amendment, the court ruled that laws regulating speech that occurs in the course of the physician-patient relationship are constitutional if they directly advance a substantial state interest.5
Predictably, several medical societies, including the AMA, have filed briefs arguing that the law is unconstitutional and intrudes on the practice of medicine. Effective medical care is believed to require “unfettered communications” between physicians and their patients. Besides, the law is at odds with the AMA’s longstanding policy that encourages members to inquire into the presence of firearms in households and to promote the use of safety locks on guns in an effort to reduce injuries to children.
On June 21, 2016, the full 11th Circuit Court of Appeals (sitting “en banc”) heard arguments, and the profession eagerly awaits its final opinion.
Meanwhile, commentators have expressed concerns that such laws threaten the sanctity of the physician-patient relationship, which relies on truthful communication to freely counsel patients.
This infringement may be gathering force. Missouri and Montana already have similar gun privacy laws, while other states have required physicians to keep confidential any information regarding chemicals used in fracking, or mandate the provision of various birth-related information prior to a woman’s decision to have an abortion.6
References
1. U.S. v. Caronia, 703 F.3d 149 (2d Cir. 2012).
2. Sorrell v. IMS Health, 131 S. Ct. 2653 (2011).
3. N Engl J Med. 2013 Jan 10;368(2):103-5.
4. Fla. St. 381.026, 456.072, 790.338.
5. Wollschlaeger v. Governor of Florida, 797 F.3d 859 (11th Cir. 2015).
6. N Engl J Med. 2016 Jun 16;374(24):2304-7.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Question: The First Amendment guarantees the right of free speech, but the U.S. Supreme Court has held that under a strict scrutiny standard, the government may regulate:
A. Obscenity.
B. Fighting words.
C. Professional speech.
D. A and B.
E. A, B, and C.
Answer: D. The First Amendment forbids the government from “abridging the freedom of speech,” which extends to certain nonverbal conduct, such as flag burning. At the same time, the U.S. Supreme Court has also ruled that certain categories of speech such as obscenity and fighting words can be regulated under a strict scrutiny standard. However, it remains unsettled whether and to what extent professional speech – such as in the context of the doctor-patient relationship – may be curtailed.
Two recent cases grapple with this issue of free speech – with rather unexpected results.
The first, overturning a decades-old prohibition of the off-label detailing of drugs, surprisingly was decided against the government. The second challenges a Florida statute censoring the discussion of firearms safety between a doctor and a patient. An early decision, under reconsideration, in fact supported the state’s regulation of physicians’ freedom of speech under the circumstances.
Because the FDA has no jurisdiction over physician conduct, it has no power to regulate the off-label use of an otherwise approved drug, which explains why such off-label prescriptions are widespread, especially in the oncology field.
In U.S. v. Caronia, the defendant, a pharmaceutical sales representative, was criminally prosecuted and found guilty of conspiracy in a New York court for introducing a misbranded drug into interstate commerce.1 Specifically, Alfred Caronia promoted the drug Xyrem for use in a manner not approved by the FDA.
Orphan Medical, now known as Jazz Pharmaceuticals, is the manufacturer of Xyrem, a powerful central nervous system depressant. Xyrem’s active ingredient is gamma-hydroxybutyrate, which has been federally classified as the “date rape drug” for its use in the commission of sexual assaults. The FDA had approved Xyrem for two conditions: to treat narcolepsy patients who experience cataplexy, a condition associated with weak or paralyzed muscles; and to treat those with excessive daytime sleepiness.
Caronia was found to provide off-label detailing of the drug to doctors for unapproved indications such as chronic fatigue, fibromyalgia, restless leg syndrome, and Parkinson’s disease.
Caronia argued that in promoting an FDA-approved drug, albeit for off-label use, he was within his right of free speech under the First Amendment. In overturning his conviction, a three-judge panel of the U.S. Second Circuit Court of Appeals agreed, noting the overly broad FDA regulations and specifically that nothing Caronia did constituted conspiracy to put a false or misleading or deficient label on a drug product.
The court concluded: “The government cannot prosecute pharmaceutical manufacturers and their representatives under the FDCA [Federal Food, Drug, and Cosmetic Act] for speech promoting the lawful, off-label use of an FDA-approved drug.”
In 2011, the U.S. Supreme Court had used a First Amendment argument to invalidate a Vermont law that prohibited the practice of pharmaceutical data mining – purchasing information about prescribers from pharmacies and others.2
Taken together, the FDA now appears resigned to the free speech argument.3 For example, it has decided not to appeal a judge’s ruling that the First Amendment protects Amarin from promoting its fish-oil capsules for unapproved uses. Just recently, the FDA published a draft proposal in tacit acceptance of this new policy position, merely recommending the disclosure of relevant information including limitations and unfavorable or inconsistent findings surrounding the off-label use of a drug.
The next issue concerns professional speech. It is well documented that the presence of a gun in the home increases the risk of death especially by suicide, and this serves as the impetus for the long-established recommendation that physicians discuss firearm safety with their patients.
The medical profession was therefore aghast when Florida enacted its law on “Privacy of Firearm Owners.”4 Codified on June 2, 2011, it provides that a licensed practitioner or facility may not record firearm ownership information in a patient’s medical record, and that unless information is relevant to the patient’s medical care or safety or safety of others, inquiries regarding firearm ownership or possession should not be made. A practitioner is also forbidden from unnecessarily harassing a patient about firearm ownership during an examination.
Violation can result in disciplinary action; the original intent was to make this a third-degree felony with penalties of up to $5 million in fines and 5 years of imprisonment, but the final bill was stripped of criminal penalties.
In July 2015, a panel of three judges of the U.S. 11th Circuit Court of Appeals, in a split 2-1 decision, found that the inquiry, record-keeping, and harassment provisions of the act specifically regulate professional speech, which is subject to an intermediate level of scrutiny. Under this level of scrutiny, the court found that the act was precisely tailored to directly advance the state’s substantial interests in protecting the public and patient privacy rights.
Holding that the act was not so overly broad as to violate the First Amendment, the court ruled that laws regulating speech that occurs in the course of the physician-patient relationship are constitutional if they directly advance a substantial state interest.5
Predictably, several medical societies, including the AMA, have filed briefs arguing that the law is unconstitutional and intrudes on the practice of medicine. Effective medical care is believed to require “unfettered communications” between physicians and their patients. Besides, the law is at odds with the AMA’s longstanding policy that encourages members to inquire into the presence of firearms in households and to promote the use of safety locks on guns in an effort to reduce injuries to children.
On June 21, 2016, the full 11th Circuit Court of Appeals (sitting “en banc”) heard arguments, and the profession eagerly awaits its final opinion.
Meanwhile, commentators have expressed concerns that such laws threaten the sanctity of the physician-patient relationship, which relies on truthful communication to freely counsel patients.
This infringement may be gathering force. Missouri and Montana already have similar gun privacy laws, while other states have required physicians to keep confidential any information regarding chemicals used in fracking, or mandate the provision of various birth-related information prior to a woman’s decision to have an abortion.6
References
1. U.S. v. Caronia, 703 F.3d 149 (2d Cir. 2012).
2. Sorrell v. IMS Health, 131 S. Ct. 2653 (2011).
3. N Engl J Med. 2013 Jan 10;368(2):103-5.
4. Fla. St. 381.026, 456.072, 790.338.
5. Wollschlaeger v. Governor of Florida, 797 F.3d 859 (11th Cir. 2015).
6. N Engl J Med. 2016 Jun 16;374(24):2304-7.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Question: The First Amendment guarantees the right of free speech, but the U.S. Supreme Court has held that under a strict scrutiny standard, the government may regulate:
A. Obscenity.
B. Fighting words.
C. Professional speech.
D. A and B.
E. A, B, and C.
Answer: D. The First Amendment forbids the government from “abridging the freedom of speech,” which extends to certain nonverbal conduct, such as flag burning. At the same time, the U.S. Supreme Court has also ruled that certain categories of speech such as obscenity and fighting words can be regulated under a strict scrutiny standard. However, it remains unsettled whether and to what extent professional speech – such as in the context of the doctor-patient relationship – may be curtailed.
Two recent cases grapple with this issue of free speech – with rather unexpected results.
The first, overturning a decades-old prohibition of the off-label detailing of drugs, surprisingly was decided against the government. The second challenges a Florida statute censoring the discussion of firearms safety between a doctor and a patient. An early decision, under reconsideration, in fact supported the state’s regulation of physicians’ freedom of speech under the circumstances.
Because the FDA has no jurisdiction over physician conduct, it has no power to regulate the off-label use of an otherwise approved drug, which explains why such off-label prescriptions are widespread, especially in the oncology field.
In U.S. v. Caronia, the defendant, a pharmaceutical sales representative, was criminally prosecuted and found guilty of conspiracy in a New York court for introducing a misbranded drug into interstate commerce.1 Specifically, Alfred Caronia promoted the drug Xyrem for use in a manner not approved by the FDA.
Orphan Medical, now known as Jazz Pharmaceuticals, is the manufacturer of Xyrem, a powerful central nervous system depressant. Xyrem’s active ingredient is gamma-hydroxybutyrate, which has been federally classified as the “date rape drug” for its use in the commission of sexual assaults. The FDA had approved Xyrem for two conditions: to treat narcolepsy patients who experience cataplexy, a condition associated with weak or paralyzed muscles; and to treat those with excessive daytime sleepiness.
Caronia was found to provide off-label detailing of the drug to doctors for unapproved indications such as chronic fatigue, fibromyalgia, restless leg syndrome, and Parkinson’s disease.
Caronia argued that in promoting an FDA-approved drug, albeit for off-label use, he was within his right of free speech under the First Amendment. In overturning his conviction, a three-judge panel of the U.S. Second Circuit Court of Appeals agreed, noting the overly broad FDA regulations and specifically that nothing Caronia did constituted conspiracy to put a false or misleading or deficient label on a drug product.
The court concluded: “The government cannot prosecute pharmaceutical manufacturers and their representatives under the FDCA [Federal Food, Drug, and Cosmetic Act] for speech promoting the lawful, off-label use of an FDA-approved drug.”
In 2011, the U.S. Supreme Court had used a First Amendment argument to invalidate a Vermont law that prohibited the practice of pharmaceutical data mining – purchasing information about prescribers from pharmacies and others.2
Taken together, the FDA now appears resigned to the free speech argument.3 For example, it has decided not to appeal a judge’s ruling that the First Amendment protects Amarin from promoting its fish-oil capsules for unapproved uses. Just recently, the FDA published a draft proposal in tacit acceptance of this new policy position, merely recommending the disclosure of relevant information including limitations and unfavorable or inconsistent findings surrounding the off-label use of a drug.
The next issue concerns professional speech. It is well documented that the presence of a gun in the home increases the risk of death especially by suicide, and this serves as the impetus for the long-established recommendation that physicians discuss firearm safety with their patients.
The medical profession was therefore aghast when Florida enacted its law on “Privacy of Firearm Owners.”4 Codified on June 2, 2011, it provides that a licensed practitioner or facility may not record firearm ownership information in a patient’s medical record, and that unless information is relevant to the patient’s medical care or safety or safety of others, inquiries regarding firearm ownership or possession should not be made. A practitioner is also forbidden from unnecessarily harassing a patient about firearm ownership during an examination.
Violation can result in disciplinary action; the original intent was to make this a third-degree felony with penalties of up to $5 million in fines and 5 years of imprisonment, but the final bill was stripped of criminal penalties.
In July 2015, a panel of three judges of the U.S. 11th Circuit Court of Appeals, in a split 2-1 decision, found that the inquiry, record-keeping, and harassment provisions of the act specifically regulate professional speech, which is subject to an intermediate level of scrutiny. Under this level of scrutiny, the court found that the act was precisely tailored to directly advance the state’s substantial interests in protecting the public and patient privacy rights.
Holding that the act was not so overly broad as to violate the First Amendment, the court ruled that laws regulating speech that occurs in the course of the physician-patient relationship are constitutional if they directly advance a substantial state interest.5
Predictably, several medical societies, including the AMA, have filed briefs arguing that the law is unconstitutional and intrudes on the practice of medicine. Effective medical care is believed to require “unfettered communications” between physicians and their patients. Besides, the law is at odds with the AMA’s longstanding policy that encourages members to inquire into the presence of firearms in households and to promote the use of safety locks on guns in an effort to reduce injuries to children.
On June 21, 2016, the full 11th Circuit Court of Appeals (sitting “en banc”) heard arguments, and the profession eagerly awaits its final opinion.
Meanwhile, commentators have expressed concerns that such laws threaten the sanctity of the physician-patient relationship, which relies on truthful communication to freely counsel patients.
This infringement may be gathering force. Missouri and Montana already have similar gun privacy laws, while other states have required physicians to keep confidential any information regarding chemicals used in fracking, or mandate the provision of various birth-related information prior to a woman’s decision to have an abortion.6
References
1. U.S. v. Caronia, 703 F.3d 149 (2d Cir. 2012).
2. Sorrell v. IMS Health, 131 S. Ct. 2653 (2011).
3. N Engl J Med. 2013 Jan 10;368(2):103-5.
4. Fla. St. 381.026, 456.072, 790.338.
5. Wollschlaeger v. Governor of Florida, 797 F.3d 859 (11th Cir. 2015).
6. N Engl J Med. 2016 Jun 16;374(24):2304-7.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Senate confirms Price as HHS secretary
The U.S. Senate voted to confirm Rep. Tom Price, MD, as secretary of the Department of Health & Human Services.
The final tally, recorded in the early hours of Feb. 10, was a strict party-line vote, with all 52 Republicans voting in favor of Rep. Price (R-Ga.) and 47 Democrats voting against. One Democrat, Sen. Claire McCaskill of Missouri, did not vote. Only a simple majority is needed to confirm cabinet members to their posts.
The confirmation comes amid ongoing concerns presented by Senate Democrats on Dr. Price’s stock purchases, particularly of Australia-based Innate Immunotherapeutics. Dr. Price was serving as a representative from Georgia at the time of his nomination, and there have been questions of possible ethics violations related to this and other securities purchases.
Democrats also rallied against the policies that Dr. Price advocated for when he was a U.S. House member, including dismantling the Affordable Care Act and pushing for block grants to fund Medicaid. He has also supported policies that would promote more extensive use of health savings accounts linked to high-deductible health plans, and high-risk pools to help ensure that those with pre-existing conditions are able to get insurance coverage without a need for guaranteed issue.
However, Democratic objections were not enough to cause any waver in support from Senate Republicans.
The American Medical Association “looks forward to working with Secretary Price to improve the health of our nation through policies that promote access to high-quality, affordable care, delivery innovation, and reduced regulatory burdens that helps patients and their physicians,” AMA President Andrew Gurman, MD, said in a statement.
The U.S. Senate voted to confirm Rep. Tom Price, MD, as secretary of the Department of Health & Human Services.
The final tally, recorded in the early hours of Feb. 10, was a strict party-line vote, with all 52 Republicans voting in favor of Rep. Price (R-Ga.) and 47 Democrats voting against. One Democrat, Sen. Claire McCaskill of Missouri, did not vote. Only a simple majority is needed to confirm cabinet members to their posts.
The confirmation comes amid ongoing concerns presented by Senate Democrats on Dr. Price’s stock purchases, particularly of Australia-based Innate Immunotherapeutics. Dr. Price was serving as a representative from Georgia at the time of his nomination, and there have been questions of possible ethics violations related to this and other securities purchases.
Democrats also rallied against the policies that Dr. Price advocated for when he was a U.S. House member, including dismantling the Affordable Care Act and pushing for block grants to fund Medicaid. He has also supported policies that would promote more extensive use of health savings accounts linked to high-deductible health plans, and high-risk pools to help ensure that those with pre-existing conditions are able to get insurance coverage without a need for guaranteed issue.
However, Democratic objections were not enough to cause any waver in support from Senate Republicans.
The American Medical Association “looks forward to working with Secretary Price to improve the health of our nation through policies that promote access to high-quality, affordable care, delivery innovation, and reduced regulatory burdens that helps patients and their physicians,” AMA President Andrew Gurman, MD, said in a statement.
The U.S. Senate voted to confirm Rep. Tom Price, MD, as secretary of the Department of Health & Human Services.
The final tally, recorded in the early hours of Feb. 10, was a strict party-line vote, with all 52 Republicans voting in favor of Rep. Price (R-Ga.) and 47 Democrats voting against. One Democrat, Sen. Claire McCaskill of Missouri, did not vote. Only a simple majority is needed to confirm cabinet members to their posts.
The confirmation comes amid ongoing concerns presented by Senate Democrats on Dr. Price’s stock purchases, particularly of Australia-based Innate Immunotherapeutics. Dr. Price was serving as a representative from Georgia at the time of his nomination, and there have been questions of possible ethics violations related to this and other securities purchases.
Democrats also rallied against the policies that Dr. Price advocated for when he was a U.S. House member, including dismantling the Affordable Care Act and pushing for block grants to fund Medicaid. He has also supported policies that would promote more extensive use of health savings accounts linked to high-deductible health plans, and high-risk pools to help ensure that those with pre-existing conditions are able to get insurance coverage without a need for guaranteed issue.
However, Democratic objections were not enough to cause any waver in support from Senate Republicans.
The American Medical Association “looks forward to working with Secretary Price to improve the health of our nation through policies that promote access to high-quality, affordable care, delivery innovation, and reduced regulatory burdens that helps patients and their physicians,” AMA President Andrew Gurman, MD, said in a statement.
Rituximab is dramatically effective in IgG4-related disease
SNOWMASS, COLO. – Glucocorticoids remain the first-line therapy in immunoglobulin G4-related disease, but it’s essential to bear in mind that their long-term efficacy in this immune-mediated fibroinflammatory disease is the exception rather than the rule, John H. Stone, MD, said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Dr. Stone, professor of medicine at Harvard Medical School, Boston, was a coauthor of an international expert consensus statement on the treatment of IgG4-related disease (IgG4-RD) which emphasized that point (Arthritis Rheumatol. 2015 Jul;67[7]:1688-99).
“I typically start with prednisone at 40 mg/day, and there’s a dramatic response in these patients. Then I taper them off after 2-3 months. If 2-3 months doesn’t put them into a long-term sustained remission, it’s time to go to something else,” said Dr. Stone, who also serves as director of clinical rheumatology at Massachusetts General Hospital, Boston.
“Glucocorticoids are rapidly effective, but initial reports were overoptimistic about their long-term efficacy. They don’t cure this disease any more than they cure giant cell arteritis in most of our patients, or ANCA-associated vasculitis. And since patients with IgG4-related disease are often older and may already have disease-induced damage to the pancreas and other organs, the morbidity from steroids in this population is formidable,” the rheumatologist explained.
In his series of 125 patients with biopsy-proven IgG4-RD, 83% responded to steroids initially, but 77% of steroid-treated patients failed to achieve a stable steroid-free remission after treatment discontinuation (Arthritis Rheumatol. 2015 Sep;67[9]:2466-75).
There is no evidence at all to indicate that conventional steroid-sparing drugs such as methotrexate, azathioprine, and mycophenolate mofetil are effective in IgG4-RD, the rheumatologist noted.
So what’s the next move, then, after steroids fail? Dr. Stone was a pioneer in the strikingly successful use of B cell depletion via rituximab (Rituxan) in patients with IgG4-RD. First he and his coinvestigators demonstrated that this off-label use of rituximab led to rapid clinical and histologic improvement (Ann Rheum Dis. 2015 Jun; 74[6]:1171-7), then they showed it also causes levels of circulating plasmablasts, serum IgG4, and biomarkers of fibrosis to plunge, suggesting B cell depletion may halt the destructive process of collagen deposition that characterizes this immune-related disease (Ann Rheum Dis. 2015 Dec;74[12]:2236-43). They have also reported that patients with very elevated baseline serum IgG4 levels are at more than sixfold increased risk of relapse at a median of 244 days from their first rituximab infusion (Rheumatology [Oxford]. 2016 Jun;55[6]:1000-8).
The success with rituximab is just one example of how improved understanding of the pathophysiology of IgG4-RD has opened the door to novel treatments. Dr. Stone is the lead investigator in an ongoing phase II, open-label study in which 15 patients with active IgG4-RD will receive intravenous XmAb5871 every 2 weeks for 6 months to evaluate the effect on the IgG4-RD Responder Index. XmAb5871 is a monoclonal antibody that binds to CD19 and FCgammaRIIb in order to downregulate activated B cells and plasmablasts. It is also being developed for treatment of systemic lupus erythematosus.
Dr. Stone and his coinvestigators are working on a therapeutic approach to IgG4-RD that targets antigen presentation by activated B cells to CD4+ cytotoxic T cells at sites of disease. These CD4+ cytotoxic T cells contain signaling lymphocyte activation molecule F7 (SLAMF7) as a surface marker. Elotuzumab (Empliciti), an immunostimulatory humanized monoclonal antibody targeting SLAMF7, is already on the market for treatment of multiple myeloma, he noted.
Dr. Stone reported receiving IgG4-RD-related research funding from and serving as a consultant to Genentech and Xencor, which is developing XmAb5871.
SNOWMASS, COLO. – Glucocorticoids remain the first-line therapy in immunoglobulin G4-related disease, but it’s essential to bear in mind that their long-term efficacy in this immune-mediated fibroinflammatory disease is the exception rather than the rule, John H. Stone, MD, said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Dr. Stone, professor of medicine at Harvard Medical School, Boston, was a coauthor of an international expert consensus statement on the treatment of IgG4-related disease (IgG4-RD) which emphasized that point (Arthritis Rheumatol. 2015 Jul;67[7]:1688-99).
“I typically start with prednisone at 40 mg/day, and there’s a dramatic response in these patients. Then I taper them off after 2-3 months. If 2-3 months doesn’t put them into a long-term sustained remission, it’s time to go to something else,” said Dr. Stone, who also serves as director of clinical rheumatology at Massachusetts General Hospital, Boston.
“Glucocorticoids are rapidly effective, but initial reports were overoptimistic about their long-term efficacy. They don’t cure this disease any more than they cure giant cell arteritis in most of our patients, or ANCA-associated vasculitis. And since patients with IgG4-related disease are often older and may already have disease-induced damage to the pancreas and other organs, the morbidity from steroids in this population is formidable,” the rheumatologist explained.
In his series of 125 patients with biopsy-proven IgG4-RD, 83% responded to steroids initially, but 77% of steroid-treated patients failed to achieve a stable steroid-free remission after treatment discontinuation (Arthritis Rheumatol. 2015 Sep;67[9]:2466-75).
There is no evidence at all to indicate that conventional steroid-sparing drugs such as methotrexate, azathioprine, and mycophenolate mofetil are effective in IgG4-RD, the rheumatologist noted.
So what’s the next move, then, after steroids fail? Dr. Stone was a pioneer in the strikingly successful use of B cell depletion via rituximab (Rituxan) in patients with IgG4-RD. First he and his coinvestigators demonstrated that this off-label use of rituximab led to rapid clinical and histologic improvement (Ann Rheum Dis. 2015 Jun; 74[6]:1171-7), then they showed it also causes levels of circulating plasmablasts, serum IgG4, and biomarkers of fibrosis to plunge, suggesting B cell depletion may halt the destructive process of collagen deposition that characterizes this immune-related disease (Ann Rheum Dis. 2015 Dec;74[12]:2236-43). They have also reported that patients with very elevated baseline serum IgG4 levels are at more than sixfold increased risk of relapse at a median of 244 days from their first rituximab infusion (Rheumatology [Oxford]. 2016 Jun;55[6]:1000-8).
The success with rituximab is just one example of how improved understanding of the pathophysiology of IgG4-RD has opened the door to novel treatments. Dr. Stone is the lead investigator in an ongoing phase II, open-label study in which 15 patients with active IgG4-RD will receive intravenous XmAb5871 every 2 weeks for 6 months to evaluate the effect on the IgG4-RD Responder Index. XmAb5871 is a monoclonal antibody that binds to CD19 and FCgammaRIIb in order to downregulate activated B cells and plasmablasts. It is also being developed for treatment of systemic lupus erythematosus.
Dr. Stone and his coinvestigators are working on a therapeutic approach to IgG4-RD that targets antigen presentation by activated B cells to CD4+ cytotoxic T cells at sites of disease. These CD4+ cytotoxic T cells contain signaling lymphocyte activation molecule F7 (SLAMF7) as a surface marker. Elotuzumab (Empliciti), an immunostimulatory humanized monoclonal antibody targeting SLAMF7, is already on the market for treatment of multiple myeloma, he noted.
Dr. Stone reported receiving IgG4-RD-related research funding from and serving as a consultant to Genentech and Xencor, which is developing XmAb5871.
SNOWMASS, COLO. – Glucocorticoids remain the first-line therapy in immunoglobulin G4-related disease, but it’s essential to bear in mind that their long-term efficacy in this immune-mediated fibroinflammatory disease is the exception rather than the rule, John H. Stone, MD, said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Dr. Stone, professor of medicine at Harvard Medical School, Boston, was a coauthor of an international expert consensus statement on the treatment of IgG4-related disease (IgG4-RD) which emphasized that point (Arthritis Rheumatol. 2015 Jul;67[7]:1688-99).
“I typically start with prednisone at 40 mg/day, and there’s a dramatic response in these patients. Then I taper them off after 2-3 months. If 2-3 months doesn’t put them into a long-term sustained remission, it’s time to go to something else,” said Dr. Stone, who also serves as director of clinical rheumatology at Massachusetts General Hospital, Boston.
“Glucocorticoids are rapidly effective, but initial reports were overoptimistic about their long-term efficacy. They don’t cure this disease any more than they cure giant cell arteritis in most of our patients, or ANCA-associated vasculitis. And since patients with IgG4-related disease are often older and may already have disease-induced damage to the pancreas and other organs, the morbidity from steroids in this population is formidable,” the rheumatologist explained.
In his series of 125 patients with biopsy-proven IgG4-RD, 83% responded to steroids initially, but 77% of steroid-treated patients failed to achieve a stable steroid-free remission after treatment discontinuation (Arthritis Rheumatol. 2015 Sep;67[9]:2466-75).
There is no evidence at all to indicate that conventional steroid-sparing drugs such as methotrexate, azathioprine, and mycophenolate mofetil are effective in IgG4-RD, the rheumatologist noted.
So what’s the next move, then, after steroids fail? Dr. Stone was a pioneer in the strikingly successful use of B cell depletion via rituximab (Rituxan) in patients with IgG4-RD. First he and his coinvestigators demonstrated that this off-label use of rituximab led to rapid clinical and histologic improvement (Ann Rheum Dis. 2015 Jun; 74[6]:1171-7), then they showed it also causes levels of circulating plasmablasts, serum IgG4, and biomarkers of fibrosis to plunge, suggesting B cell depletion may halt the destructive process of collagen deposition that characterizes this immune-related disease (Ann Rheum Dis. 2015 Dec;74[12]:2236-43). They have also reported that patients with very elevated baseline serum IgG4 levels are at more than sixfold increased risk of relapse at a median of 244 days from their first rituximab infusion (Rheumatology [Oxford]. 2016 Jun;55[6]:1000-8).
The success with rituximab is just one example of how improved understanding of the pathophysiology of IgG4-RD has opened the door to novel treatments. Dr. Stone is the lead investigator in an ongoing phase II, open-label study in which 15 patients with active IgG4-RD will receive intravenous XmAb5871 every 2 weeks for 6 months to evaluate the effect on the IgG4-RD Responder Index. XmAb5871 is a monoclonal antibody that binds to CD19 and FCgammaRIIb in order to downregulate activated B cells and plasmablasts. It is also being developed for treatment of systemic lupus erythematosus.
Dr. Stone and his coinvestigators are working on a therapeutic approach to IgG4-RD that targets antigen presentation by activated B cells to CD4+ cytotoxic T cells at sites of disease. These CD4+ cytotoxic T cells contain signaling lymphocyte activation molecule F7 (SLAMF7) as a surface marker. Elotuzumab (Empliciti), an immunostimulatory humanized monoclonal antibody targeting SLAMF7, is already on the market for treatment of multiple myeloma, he noted.
Dr. Stone reported receiving IgG4-RD-related research funding from and serving as a consultant to Genentech and Xencor, which is developing XmAb5871.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM
Peripheral B cells reflect intestinal damage in celiac disease
B-cell gene expression in the peripheral blood strongly correlates with the extent of gluten-induced damage to the intestinal mucosa in patients with celiac disease, according to a report in Cellular and Molecular Gastroenterology and Hepatology.
If this finding from a single-center cohort study is validated in other patient populations, the B-cell signature may become a useful, minimally invasive tool for diagnosing celiac disease. Eventually, if biomarkers are developed from the peripheral B-cell signature, a simple blood test could be used for monitoring changes in gut inflammation over time as well as treatment response, said Mitchell E. Garber, PhD, of Alvine Pharmaceuticals, San Carlos, Calif., and the department of chemistry at Stanford University, and his associates.
However, it would be “premature but intriguing” to speculate about using this discovery to devise new, B cell–centered treatments for celiac disease, they added.
Noting that an inflammatory, gluten-induced immune response in the gut can be reflected in the peripheral blood, the investigators assessed whether a 6-week gluten challenge would induce damage to the small intestine that would show up in B-cell gene expression detected in blood samples. They assigned 73 patients at a single medical center in Finland to follow their usual gluten-free diets but to ingest an additional 6 g (20 patients), 3 g (26 patients), or 1.5 g (27 patients) of wheat gluten with a meal once per day for the study period.
The study participants (median age, 59 years; range, 23-74 years) underwent small-bowel biopsies obtained from the descending duodenum at baseline and after the gluten challenge. Damage to the intestinal mucosa was assessed by measuring the ratio of the height of the intestinal villi to the depth of the proliferative crypts at the base of the villi (villi height to crypt depth, or Vh:Cd). In celiac disease, gluten blunts the projection of the villi and causes hypertrophy or elongation of the crypts, resulting in flattened mucosa and a Vh:Cd approaching zero.
The study participants showed a wide variation in mucosal damage from the gluten exposure, with some patients showing no change and relatively healthy mucosa, and others showing extensive change and nearly flattened mucosa. The mucosal damage did not differ by gluten dose.
The largest change in Vh:Cd occurred in three patients who transitioned from relatively healthy intestinal mucosa (Vh:Cd 3.1) at baseline to nearly flat mucosa (Vh:Cd 0.2) after gluten exposure.
Patients with undamaged gut mucosa showed a relative increase in B-cell gene expression during the study period, while those who had increasing damage showed a relative decrease in B-cell expression. “The peripheral B cell therefore tracked with oral tolerance across the full spectrum of intestinal damage, from no change to a nearly flat mucosa,” Dr. Garber and his associates said (Cell Molec Gastroenterol Hepatol. 2017. doi: 10.1016/j.jcmgh.2017.01.011).
“The net increase in B-cell gene expression from baseline to 6 weeks in patients with little to no intestinal damage [suggests] that these individuals may have mounted a B-cell immune response to maintain mucosal homeostasis and circumvent inflammation,” they added.
Further study is needed to determine whether peripheral B cells are a marker that indicates tolerance to gluten but doesn’t play a functional role in the inflammatory process, or whether B cells may actually promote immune tolerance, the investigators said.
This study was funded by Alvine Pharmaceuticals, the American Recovery and Reinvestment Act, Tampere (Finland) University Hospital, the Academy of Finland Research Council for Health, and the U.S. National Institutes of Health. Dr. Garber reported ties to Alvine Pharmaceuticals, and his associates reported ties to ImmusanT, Celimmune, and ImmunogenX.
B-cell gene expression in the peripheral blood strongly correlates with the extent of gluten-induced damage to the intestinal mucosa in patients with celiac disease, according to a report in Cellular and Molecular Gastroenterology and Hepatology.
If this finding from a single-center cohort study is validated in other patient populations, the B-cell signature may become a useful, minimally invasive tool for diagnosing celiac disease. Eventually, if biomarkers are developed from the peripheral B-cell signature, a simple blood test could be used for monitoring changes in gut inflammation over time as well as treatment response, said Mitchell E. Garber, PhD, of Alvine Pharmaceuticals, San Carlos, Calif., and the department of chemistry at Stanford University, and his associates.
However, it would be “premature but intriguing” to speculate about using this discovery to devise new, B cell–centered treatments for celiac disease, they added.
Noting that an inflammatory, gluten-induced immune response in the gut can be reflected in the peripheral blood, the investigators assessed whether a 6-week gluten challenge would induce damage to the small intestine that would show up in B-cell gene expression detected in blood samples. They assigned 73 patients at a single medical center in Finland to follow their usual gluten-free diets but to ingest an additional 6 g (20 patients), 3 g (26 patients), or 1.5 g (27 patients) of wheat gluten with a meal once per day for the study period.
The study participants (median age, 59 years; range, 23-74 years) underwent small-bowel biopsies obtained from the descending duodenum at baseline and after the gluten challenge. Damage to the intestinal mucosa was assessed by measuring the ratio of the height of the intestinal villi to the depth of the proliferative crypts at the base of the villi (villi height to crypt depth, or Vh:Cd). In celiac disease, gluten blunts the projection of the villi and causes hypertrophy or elongation of the crypts, resulting in flattened mucosa and a Vh:Cd approaching zero.
The study participants showed a wide variation in mucosal damage from the gluten exposure, with some patients showing no change and relatively healthy mucosa, and others showing extensive change and nearly flattened mucosa. The mucosal damage did not differ by gluten dose.
The largest change in Vh:Cd occurred in three patients who transitioned from relatively healthy intestinal mucosa (Vh:Cd 3.1) at baseline to nearly flat mucosa (Vh:Cd 0.2) after gluten exposure.
Patients with undamaged gut mucosa showed a relative increase in B-cell gene expression during the study period, while those who had increasing damage showed a relative decrease in B-cell expression. “The peripheral B cell therefore tracked with oral tolerance across the full spectrum of intestinal damage, from no change to a nearly flat mucosa,” Dr. Garber and his associates said (Cell Molec Gastroenterol Hepatol. 2017. doi: 10.1016/j.jcmgh.2017.01.011).
“The net increase in B-cell gene expression from baseline to 6 weeks in patients with little to no intestinal damage [suggests] that these individuals may have mounted a B-cell immune response to maintain mucosal homeostasis and circumvent inflammation,” they added.
Further study is needed to determine whether peripheral B cells are a marker that indicates tolerance to gluten but doesn’t play a functional role in the inflammatory process, or whether B cells may actually promote immune tolerance, the investigators said.
This study was funded by Alvine Pharmaceuticals, the American Recovery and Reinvestment Act, Tampere (Finland) University Hospital, the Academy of Finland Research Council for Health, and the U.S. National Institutes of Health. Dr. Garber reported ties to Alvine Pharmaceuticals, and his associates reported ties to ImmusanT, Celimmune, and ImmunogenX.
B-cell gene expression in the peripheral blood strongly correlates with the extent of gluten-induced damage to the intestinal mucosa in patients with celiac disease, according to a report in Cellular and Molecular Gastroenterology and Hepatology.
If this finding from a single-center cohort study is validated in other patient populations, the B-cell signature may become a useful, minimally invasive tool for diagnosing celiac disease. Eventually, if biomarkers are developed from the peripheral B-cell signature, a simple blood test could be used for monitoring changes in gut inflammation over time as well as treatment response, said Mitchell E. Garber, PhD, of Alvine Pharmaceuticals, San Carlos, Calif., and the department of chemistry at Stanford University, and his associates.
However, it would be “premature but intriguing” to speculate about using this discovery to devise new, B cell–centered treatments for celiac disease, they added.
Noting that an inflammatory, gluten-induced immune response in the gut can be reflected in the peripheral blood, the investigators assessed whether a 6-week gluten challenge would induce damage to the small intestine that would show up in B-cell gene expression detected in blood samples. They assigned 73 patients at a single medical center in Finland to follow their usual gluten-free diets but to ingest an additional 6 g (20 patients), 3 g (26 patients), or 1.5 g (27 patients) of wheat gluten with a meal once per day for the study period.
The study participants (median age, 59 years; range, 23-74 years) underwent small-bowel biopsies obtained from the descending duodenum at baseline and after the gluten challenge. Damage to the intestinal mucosa was assessed by measuring the ratio of the height of the intestinal villi to the depth of the proliferative crypts at the base of the villi (villi height to crypt depth, or Vh:Cd). In celiac disease, gluten blunts the projection of the villi and causes hypertrophy or elongation of the crypts, resulting in flattened mucosa and a Vh:Cd approaching zero.
The study participants showed a wide variation in mucosal damage from the gluten exposure, with some patients showing no change and relatively healthy mucosa, and others showing extensive change and nearly flattened mucosa. The mucosal damage did not differ by gluten dose.
The largest change in Vh:Cd occurred in three patients who transitioned from relatively healthy intestinal mucosa (Vh:Cd 3.1) at baseline to nearly flat mucosa (Vh:Cd 0.2) after gluten exposure.
Patients with undamaged gut mucosa showed a relative increase in B-cell gene expression during the study period, while those who had increasing damage showed a relative decrease in B-cell expression. “The peripheral B cell therefore tracked with oral tolerance across the full spectrum of intestinal damage, from no change to a nearly flat mucosa,” Dr. Garber and his associates said (Cell Molec Gastroenterol Hepatol. 2017. doi: 10.1016/j.jcmgh.2017.01.011).
“The net increase in B-cell gene expression from baseline to 6 weeks in patients with little to no intestinal damage [suggests] that these individuals may have mounted a B-cell immune response to maintain mucosal homeostasis and circumvent inflammation,” they added.
Further study is needed to determine whether peripheral B cells are a marker that indicates tolerance to gluten but doesn’t play a functional role in the inflammatory process, or whether B cells may actually promote immune tolerance, the investigators said.
This study was funded by Alvine Pharmaceuticals, the American Recovery and Reinvestment Act, Tampere (Finland) University Hospital, the Academy of Finland Research Council for Health, and the U.S. National Institutes of Health. Dr. Garber reported ties to Alvine Pharmaceuticals, and his associates reported ties to ImmusanT, Celimmune, and ImmunogenX.
FROM CELLULAR AND MOLECULAR GASTROENTEROLOGY AND HEPATOLOGY
Key clinical point: B-cell gene expression in peripheral blood strongly correlates with the extent of gluten-induced intestinal damage in patients with celiac disease.
Major finding: Patients with undamaged gut mucosa showed a relative increase in B-cell gene expression during the study period, while those who had increasing damage showed a relative decrease in B-cell expression.
Data source: A single-center cohort study involving 73 adults with celiac disease who underwent a 6-week gluten challenge.
Disclosures: This study was funded by Alvine Pharmaceuticals, the American Recovery and Reinvestment Act, Tampere (Finland) University Hospital, the Academy of Finland Research Council for Health, and the U.S. National Institutes of Health. Dr. Garber reported ties to Alvine Pharmaceuticals, and his associates reported ties to ImmusanT, Celimmune, and ImmunogenX.
Moderate stenosis in coronary arteries grows severe over time
HOUSTON – Most nongrafted, moderately stenosed coronary arteries progress to severe stenosis or occlusion in the long term, results from a large, long-term study have shown.
“Not uncommonly, patients referred for coronary surgery have one or more coronary arteries with only moderate stenosis,” Joseph F. Sabik III, MD, said at the annual meeting of the Society of Thoracic Surgeons.
“There is controversy as to whether arteries with only moderate stenosis should be grafted during coronary surgery, and if it should be grafted, with what conduit?” For example, the Fractional Flow Reserve-Guided PCI versus Medical Therapy in Stable Coronary Disease study, known as FAME, suggests not intervening on moderate stenosis, since stenting non–ischemia-producing lesions led to worse outcomes (N Engl J Med. 2012 Sep 13;367:991-1001). However, Dr. Sabik, who chairs the department of surgery at University Hospitals Cleveland Medical Center, and his associates recently reported that grafting moderately stenosed coronary arteries during surgical revascularization is not harmful and can be beneficial by improving survival if an internal thoracic artery graft is used (J. Thoracic Cardiovasc Surg. 2016 Mar;151[3]:806-11).
In an effort to determine how grafting moderately stenosed coronary arteries influences native-vessel disease progression, and whether grafting may be protective from late ischemia, Dr. Sabik and his associates evaluated the medical records of 55,567 patients who underwent primary isolated coronary artery bypass graft (CABG) surgery at the Cleveland Clinic from 1972 to 2011. Of the 55,567 patients, 1,902 had a single coronary artery with angiographically moderate stenosis (defined as a narrowing of 50%-69%) and results of at least one postoperative angiogram available. Of these moderately stenosed coronary arteries (MSCAs), 488 were not grafted, 385 were internal thoracic artery (ITA)–grafted, and 1,028 were saphenous vein (SV)–grafted. At follow-up angiograms, information about disease progression was available for 488 nongrafted, 371 ITA-grafted, and 957 SV-grafted MSCAs, and patency information was available for 376 ITA and 1,016 SV grafts to these MSCAs. Grafts were considered patent if they were not occluded. Severe occlusion was defined as a narrowing of more than 70%.

The researchers found that at 1, 5, 10, and 15 years, native-vessel disease progressed from moderate to severe stenosis/occlusion in 32%, 52%, 66%, and 72% of nongrafted MSCAs, respectively; in 55%, 73%, 84%, and 87% of ITA-grafted MSCAs, and in 67%, 82%, 90%, and 92% of SV-grafted MSCAs. After Dr. Sabik and his associates adjusted for patient characteristics, disease progression in MSCAs was significantly higher with ITA and SV grafting, compared with nongrafting (odds ratios, 3.6 and 9.9, respectively). At 1, 5, 10, and 15 years, occlusion in grafts to MSCAs was 8%, 9%, 11%, and 15%, respectively, for ITA grafts and 13%, 32%, 46%, and 56% for SV grafts. At these same time points, protection from myocardial ischemia in ITA-grafted vs. nongrafted MSCAs was 29%, 47%, 59%, and 61%.
“Our opinion is you that shouldn’t ignore moderate lesions,” Dr. Sabik, surgeon-in-chief and vice president for surgical operations for the University Hospitals system, said in an interview at the meeting. “Although it may not help that patient over the next short period of time, over their lifespan it will. What works for intervention doesn’t necessarily mean it’s right for bypass surgery. If you have a vessel that’s only moderately stenosed you should at least consider grafting it, because moderate lesions progress over time. Bypassing it helps people live longer when you use an internal thoracic artery graft, because they are likely to remain patent. You always have to individualize the therapy, but the key is to use your grafts in the best way possible.”
Dr. Sabik disclosed that he has received research grants from Medtronic, Abbott Vascular, and Edwards Lifesciences.
HOUSTON – Most nongrafted, moderately stenosed coronary arteries progress to severe stenosis or occlusion in the long term, results from a large, long-term study have shown.
“Not uncommonly, patients referred for coronary surgery have one or more coronary arteries with only moderate stenosis,” Joseph F. Sabik III, MD, said at the annual meeting of the Society of Thoracic Surgeons.
“There is controversy as to whether arteries with only moderate stenosis should be grafted during coronary surgery, and if it should be grafted, with what conduit?” For example, the Fractional Flow Reserve-Guided PCI versus Medical Therapy in Stable Coronary Disease study, known as FAME, suggests not intervening on moderate stenosis, since stenting non–ischemia-producing lesions led to worse outcomes (N Engl J Med. 2012 Sep 13;367:991-1001). However, Dr. Sabik, who chairs the department of surgery at University Hospitals Cleveland Medical Center, and his associates recently reported that grafting moderately stenosed coronary arteries during surgical revascularization is not harmful and can be beneficial by improving survival if an internal thoracic artery graft is used (J. Thoracic Cardiovasc Surg. 2016 Mar;151[3]:806-11).
In an effort to determine how grafting moderately stenosed coronary arteries influences native-vessel disease progression, and whether grafting may be protective from late ischemia, Dr. Sabik and his associates evaluated the medical records of 55,567 patients who underwent primary isolated coronary artery bypass graft (CABG) surgery at the Cleveland Clinic from 1972 to 2011. Of the 55,567 patients, 1,902 had a single coronary artery with angiographically moderate stenosis (defined as a narrowing of 50%-69%) and results of at least one postoperative angiogram available. Of these moderately stenosed coronary arteries (MSCAs), 488 were not grafted, 385 were internal thoracic artery (ITA)–grafted, and 1,028 were saphenous vein (SV)–grafted. At follow-up angiograms, information about disease progression was available for 488 nongrafted, 371 ITA-grafted, and 957 SV-grafted MSCAs, and patency information was available for 376 ITA and 1,016 SV grafts to these MSCAs. Grafts were considered patent if they were not occluded. Severe occlusion was defined as a narrowing of more than 70%.
The researchers found that at 1, 5, 10, and 15 years, native-vessel disease progressed from moderate to severe stenosis/occlusion in 32%, 52%, 66%, and 72% of nongrafted MSCAs, respectively; in 55%, 73%, 84%, and 87% of ITA-grafted MSCAs, and in 67%, 82%, 90%, and 92% of SV-grafted MSCAs. After Dr. Sabik and his associates adjusted for patient characteristics, disease progression in MSCAs was significantly higher with ITA and SV grafting, compared with nongrafting (odds ratios, 3.6 and 9.9, respectively). At 1, 5, 10, and 15 years, occlusion in grafts to MSCAs was 8%, 9%, 11%, and 15%, respectively, for ITA grafts and 13%, 32%, 46%, and 56% for SV grafts. At these same time points, protection from myocardial ischemia in ITA-grafted vs. nongrafted MSCAs was 29%, 47%, 59%, and 61%.
“Our opinion is you that shouldn’t ignore moderate lesions,” Dr. Sabik, surgeon-in-chief and vice president for surgical operations for the University Hospitals system, said in an interview at the meeting. “Although it may not help that patient over the next short period of time, over their lifespan it will. What works for intervention doesn’t necessarily mean it’s right for bypass surgery. If you have a vessel that’s only moderately stenosed you should at least consider grafting it, because moderate lesions progress over time. Bypassing it helps people live longer when you use an internal thoracic artery graft, because they are likely to remain patent. You always have to individualize the therapy, but the key is to use your grafts in the best way possible.”
Dr. Sabik disclosed that he has received research grants from Medtronic, Abbott Vascular, and Edwards Lifesciences.
HOUSTON – Most nongrafted, moderately stenosed coronary arteries progress to severe stenosis or occlusion in the long term, results from a large, long-term study have shown.
“Not uncommonly, patients referred for coronary surgery have one or more coronary arteries with only moderate stenosis,” Joseph F. Sabik III, MD, said at the annual meeting of the Society of Thoracic Surgeons.
“There is controversy as to whether arteries with only moderate stenosis should be grafted during coronary surgery, and if it should be grafted, with what conduit?” For example, the Fractional Flow Reserve-Guided PCI versus Medical Therapy in Stable Coronary Disease study, known as FAME, suggests not intervening on moderate stenosis, since stenting non–ischemia-producing lesions led to worse outcomes (N Engl J Med. 2012 Sep 13;367:991-1001). However, Dr. Sabik, who chairs the department of surgery at University Hospitals Cleveland Medical Center, and his associates recently reported that grafting moderately stenosed coronary arteries during surgical revascularization is not harmful and can be beneficial by improving survival if an internal thoracic artery graft is used (J. Thoracic Cardiovasc Surg. 2016 Mar;151[3]:806-11).
In an effort to determine how grafting moderately stenosed coronary arteries influences native-vessel disease progression, and whether grafting may be protective from late ischemia, Dr. Sabik and his associates evaluated the medical records of 55,567 patients who underwent primary isolated coronary artery bypass graft (CABG) surgery at the Cleveland Clinic from 1972 to 2011. Of the 55,567 patients, 1,902 had a single coronary artery with angiographically moderate stenosis (defined as a narrowing of 50%-69%) and results of at least one postoperative angiogram available. Of these moderately stenosed coronary arteries (MSCAs), 488 were not grafted, 385 were internal thoracic artery (ITA)–grafted, and 1,028 were saphenous vein (SV)–grafted. At follow-up angiograms, information about disease progression was available for 488 nongrafted, 371 ITA-grafted, and 957 SV-grafted MSCAs, and patency information was available for 376 ITA and 1,016 SV grafts to these MSCAs. Grafts were considered patent if they were not occluded. Severe occlusion was defined as a narrowing of more than 70%.
The researchers found that at 1, 5, 10, and 15 years, native-vessel disease progressed from moderate to severe stenosis/occlusion in 32%, 52%, 66%, and 72% of nongrafted MSCAs, respectively; in 55%, 73%, 84%, and 87% of ITA-grafted MSCAs, and in 67%, 82%, 90%, and 92% of SV-grafted MSCAs. After Dr. Sabik and his associates adjusted for patient characteristics, disease progression in MSCAs was significantly higher with ITA and SV grafting, compared with nongrafting (odds ratios, 3.6 and 9.9, respectively). At 1, 5, 10, and 15 years, occlusion in grafts to MSCAs was 8%, 9%, 11%, and 15%, respectively, for ITA grafts and 13%, 32%, 46%, and 56% for SV grafts. At these same time points, protection from myocardial ischemia in ITA-grafted vs. nongrafted MSCAs was 29%, 47%, 59%, and 61%.
“Our opinion is you that shouldn’t ignore moderate lesions,” Dr. Sabik, surgeon-in-chief and vice president for surgical operations for the University Hospitals system, said in an interview at the meeting. “Although it may not help that patient over the next short period of time, over their lifespan it will. What works for intervention doesn’t necessarily mean it’s right for bypass surgery. If you have a vessel that’s only moderately stenosed you should at least consider grafting it, because moderate lesions progress over time. Bypassing it helps people live longer when you use an internal thoracic artery graft, because they are likely to remain patent. You always have to individualize the therapy, but the key is to use your grafts in the best way possible.”
Dr. Sabik disclosed that he has received research grants from Medtronic, Abbott Vascular, and Edwards Lifesciences.
AT THE STS ANNUAL MEETING
Key clinical point:
Major finding: At 15 years, native-vessel disease progressed from moderate to severe stenosis/occlusion in 72% of nongrafted coronary arteries, in 87% of internal thoracic artery–grafted arteries, and in 92% of saphenous vein–grafted moderately stenosed coronary arteries.
Data source: An analysis of medical records from 55,567 patients who underwent primary isolated CABG at the Cleveland Clinic from 1972 to 2011.
Disclosures: Dr. Sabik disclosed that he has received research grants from Medtronic, Abbott Vascular, and Edwards Lifesciences.
Cabozantinib versus everolimus in advanced RCC with bone mets
AMSTERDAM – Among patients with advanced renal cell carcinoma (RCC) with metastases to bone, cabozantinib (Cabometyx) was associated with better survival compared with everolimus (Afinitor), according to a subanalysis of data from the METEOR trial.
After 2 years of follow-up, median progression-free survival (PFS), overall survival (OS), and objective response rates (ORR) were significantly better for patients with bone metastases who received cabozantinib compared with those who received everolimus, reported Sergio Bracarda, MD, of Presidio Ospedaliero San Donato, Italy, and his colleagues.
“Cabozantinib is a new treatment option for previously-treated patients with advanced RCC with benefits that are maintained in patients with bone metastases,” they wrote in a poster presented at an annual congress sponsored by the European Cancer Organisation.
Previous studies have shown that patients with advanced RCC with bone metastases have generally poor prognosis compared with patients without bone metastases, the authors noted.
As previously reported, the METEOR trial, a randomized phase III study of 658 patients with advanced RCC, showed a significant survival advantage for patients treated with cabozantinib, with a median OS of 21.4 months compared with 16.5 months for patients treated with everolimus, with a hazard ratio (HR) of 0.66 (P = .0003).
In the current sub-analysis, the investigators looked at a subgroup of 142 patients with bone metastases at baseline as seen on CT or MRI. They conducted an exploratory analysis of bone scan response among 162 patients evaluated for bone lesions at baseline by technetium bone scans, and compared the incidence of skeletal-related events (SREs) for 181 patients with a history of SREs, and 477 with no prior SREs. SREs included pathological fractures, spinal cord compression, surgery to bone, and external radiation therapy to bone.
Patients underwent CT or MRI screening every 8 weeks for the first 12 months post randomization, then every 12 weeks thereafter. All patients were screened with technetium bone scans every 18 weeks for the first years, and those patients with bone lesions at baseline were followed with additional scans every 24 weeks.
The authors also looked at serum bone biomarkers, including bone-specific alkaline phosphatase (BSAP), N-terminal propeptide of type 1 collagen (P1NP), and C-terminal cross-linked telopeptides of type I collagen.
The median PFS for patients with bone metastases treated with cabozantinib was 7.4 months, compared with 2.7 months for everolimus (HR 0.33, 95% confidence interval [CI] 0.21-0.51). For patients with both bone and visceral metastasis, median PFS was 5.6 months vs. 1.9 months, respectively (HR 0.26, 95% CI, 0.16-0.43).
Median OS for the cabozantinib group was 20.1 months compared with 12.1 months for everolimus (HR 0.54, 95% CI, 0.34-0.84) for patients with bone metastases alone. For patients with both bone and visceral metastases, median OS was 20.1 months with cabozantinib, and 10.7 months with everolimus (HR 0.45, 95% CI, 0.28-0.72).
The ORR with cabozantinib as rated by an independent radiology committee was 17% for patients with bone metastases alone, and 20% for patients with bone and visceral metastases. In contrast, there were no objective responses seen in patients treated with everolimus.
Bone scan responses, defined as a 30% or greater decrease from baseline in bone scan lesion area, were seen in 18% of patients on cabozantinib vs. 10% with everolimus (significance not shown).
Among patients with a history of SREs, 22% had an SRE on cabozantinib, compared with 31% on everolimus. Respective rates among patients without a prior history of SREs were 27% and 15%. At least one SRE occurred in 12% (cabo) and 14% (eve) of patients, including four (cabo) and eight (eve) cases of spinal cord compression. For patients with a history of SREs at randomization, the incidence of postrandomization SREs was 16% (cabo) and 34% (eve) and included zero (cabo) and five (eve) cases of spinal cord compression. Reductions in the bone markers P1NP and CTx were greater with cabo vs. eve. The most common adverse events in patients with bone metastases were consistent with those observed in the overall study population.
The investigators noted that “the safety profile of cabozantinib in the bone metastases subgroup was consistent with the safety profile in the overall population.”
Dr. Bracarda has served as a consultant to Exelixis, which supported the trial and subanalysis. Two coauthors are employees of the company.
AMSTERDAM – Among patients with advanced renal cell carcinoma (RCC) with metastases to bone, cabozantinib (Cabometyx) was associated with better survival compared with everolimus (Afinitor), according to a subanalysis of data from the METEOR trial.
After 2 years of follow-up, median progression-free survival (PFS), overall survival (OS), and objective response rates (ORR) were significantly better for patients with bone metastases who received cabozantinib compared with those who received everolimus, reported Sergio Bracarda, MD, of Presidio Ospedaliero San Donato, Italy, and his colleagues.
“Cabozantinib is a new treatment option for previously-treated patients with advanced RCC with benefits that are maintained in patients with bone metastases,” they wrote in a poster presented at an annual congress sponsored by the European Cancer Organisation.
Previous studies have shown that patients with advanced RCC with bone metastases have generally poor prognosis compared with patients without bone metastases, the authors noted.
As previously reported, the METEOR trial, a randomized phase III study of 658 patients with advanced RCC, showed a significant survival advantage for patients treated with cabozantinib, with a median OS of 21.4 months compared with 16.5 months for patients treated with everolimus, with a hazard ratio (HR) of 0.66 (P = .0003).
In the current sub-analysis, the investigators looked at a subgroup of 142 patients with bone metastases at baseline as seen on CT or MRI. They conducted an exploratory analysis of bone scan response among 162 patients evaluated for bone lesions at baseline by technetium bone scans, and compared the incidence of skeletal-related events (SREs) for 181 patients with a history of SREs, and 477 with no prior SREs. SREs included pathological fractures, spinal cord compression, surgery to bone, and external radiation therapy to bone.
Patients underwent CT or MRI screening every 8 weeks for the first 12 months post randomization, then every 12 weeks thereafter. All patients were screened with technetium bone scans every 18 weeks for the first years, and those patients with bone lesions at baseline were followed with additional scans every 24 weeks.
The authors also looked at serum bone biomarkers, including bone-specific alkaline phosphatase (BSAP), N-terminal propeptide of type 1 collagen (P1NP), and C-terminal cross-linked telopeptides of type I collagen.
The median PFS for patients with bone metastases treated with cabozantinib was 7.4 months, compared with 2.7 months for everolimus (HR 0.33, 95% confidence interval [CI] 0.21-0.51). For patients with both bone and visceral metastasis, median PFS was 5.6 months vs. 1.9 months, respectively (HR 0.26, 95% CI, 0.16-0.43).
Median OS for the cabozantinib group was 20.1 months compared with 12.1 months for everolimus (HR 0.54, 95% CI, 0.34-0.84) for patients with bone metastases alone. For patients with both bone and visceral metastases, median OS was 20.1 months with cabozantinib, and 10.7 months with everolimus (HR 0.45, 95% CI, 0.28-0.72).
The ORR with cabozantinib as rated by an independent radiology committee was 17% for patients with bone metastases alone, and 20% for patients with bone and visceral metastases. In contrast, there were no objective responses seen in patients treated with everolimus.
Bone scan responses, defined as a 30% or greater decrease from baseline in bone scan lesion area, were seen in 18% of patients on cabozantinib vs. 10% with everolimus (significance not shown).
Among patients with a history of SREs, 22% had an SRE on cabozantinib, compared with 31% on everolimus. Respective rates among patients without a prior history of SREs were 27% and 15%. At least one SRE occurred in 12% (cabo) and 14% (eve) of patients, including four (cabo) and eight (eve) cases of spinal cord compression. For patients with a history of SREs at randomization, the incidence of postrandomization SREs was 16% (cabo) and 34% (eve) and included zero (cabo) and five (eve) cases of spinal cord compression. Reductions in the bone markers P1NP and CTx were greater with cabo vs. eve. The most common adverse events in patients with bone metastases were consistent with those observed in the overall study population.
The investigators noted that “the safety profile of cabozantinib in the bone metastases subgroup was consistent with the safety profile in the overall population.”
Dr. Bracarda has served as a consultant to Exelixis, which supported the trial and subanalysis. Two coauthors are employees of the company.
AMSTERDAM – Among patients with advanced renal cell carcinoma (RCC) with metastases to bone, cabozantinib (Cabometyx) was associated with better survival compared with everolimus (Afinitor), according to a subanalysis of data from the METEOR trial.
After 2 years of follow-up, median progression-free survival (PFS), overall survival (OS), and objective response rates (ORR) were significantly better for patients with bone metastases who received cabozantinib compared with those who received everolimus, reported Sergio Bracarda, MD, of Presidio Ospedaliero San Donato, Italy, and his colleagues.
“Cabozantinib is a new treatment option for previously-treated patients with advanced RCC with benefits that are maintained in patients with bone metastases,” they wrote in a poster presented at an annual congress sponsored by the European Cancer Organisation.
Previous studies have shown that patients with advanced RCC with bone metastases have generally poor prognosis compared with patients without bone metastases, the authors noted.
As previously reported, the METEOR trial, a randomized phase III study of 658 patients with advanced RCC, showed a significant survival advantage for patients treated with cabozantinib, with a median OS of 21.4 months compared with 16.5 months for patients treated with everolimus, with a hazard ratio (HR) of 0.66 (P = .0003).
In the current sub-analysis, the investigators looked at a subgroup of 142 patients with bone metastases at baseline as seen on CT or MRI. They conducted an exploratory analysis of bone scan response among 162 patients evaluated for bone lesions at baseline by technetium bone scans, and compared the incidence of skeletal-related events (SREs) for 181 patients with a history of SREs, and 477 with no prior SREs. SREs included pathological fractures, spinal cord compression, surgery to bone, and external radiation therapy to bone.
Patients underwent CT or MRI screening every 8 weeks for the first 12 months post randomization, then every 12 weeks thereafter. All patients were screened with technetium bone scans every 18 weeks for the first years, and those patients with bone lesions at baseline were followed with additional scans every 24 weeks.
The authors also looked at serum bone biomarkers, including bone-specific alkaline phosphatase (BSAP), N-terminal propeptide of type 1 collagen (P1NP), and C-terminal cross-linked telopeptides of type I collagen.
The median PFS for patients with bone metastases treated with cabozantinib was 7.4 months, compared with 2.7 months for everolimus (HR 0.33, 95% confidence interval [CI] 0.21-0.51). For patients with both bone and visceral metastasis, median PFS was 5.6 months vs. 1.9 months, respectively (HR 0.26, 95% CI, 0.16-0.43).
Median OS for the cabozantinib group was 20.1 months compared with 12.1 months for everolimus (HR 0.54, 95% CI, 0.34-0.84) for patients with bone metastases alone. For patients with both bone and visceral metastases, median OS was 20.1 months with cabozantinib, and 10.7 months with everolimus (HR 0.45, 95% CI, 0.28-0.72).
The ORR with cabozantinib as rated by an independent radiology committee was 17% for patients with bone metastases alone, and 20% for patients with bone and visceral metastases. In contrast, there were no objective responses seen in patients treated with everolimus.
Bone scan responses, defined as a 30% or greater decrease from baseline in bone scan lesion area, were seen in 18% of patients on cabozantinib vs. 10% with everolimus (significance not shown).
Among patients with a history of SREs, 22% had an SRE on cabozantinib, compared with 31% on everolimus. Respective rates among patients without a prior history of SREs were 27% and 15%. At least one SRE occurred in 12% (cabo) and 14% (eve) of patients, including four (cabo) and eight (eve) cases of spinal cord compression. For patients with a history of SREs at randomization, the incidence of postrandomization SREs was 16% (cabo) and 34% (eve) and included zero (cabo) and five (eve) cases of spinal cord compression. Reductions in the bone markers P1NP and CTx were greater with cabo vs. eve. The most common adverse events in patients with bone metastases were consistent with those observed in the overall study population.
The investigators noted that “the safety profile of cabozantinib in the bone metastases subgroup was consistent with the safety profile in the overall population.”
Dr. Bracarda has served as a consultant to Exelixis, which supported the trial and subanalysis. Two coauthors are employees of the company.
AT ECCO2017
Key clinical point: Survival among patients with advanced renal cell carcinoma metastatic to bone was better with cabozantinib than everolimus.
Major finding: Median overall survival for the cabozantinib group was 20.1 months compared with 12.1 months for everolimus.
Data source: Subanalysis of 142 patients with bone metastases in the randomized phase III METEOR trial.
Disclosures: Dr. Bracarda has served as a consultant to Exelixis, which supported the trial and subanalysis. Two coauthors are employees of the company.
Computer predicts remission, relapse in AML

Photo by Darren Baker
Researchers say they have developed the first computer machine-learning model to accurately predict which patients diagnosed with acute
myeloid leukemia (AML) will go into remission after treatment and which will relapse.
“It’s pretty straightforward to teach a computer to recognize AML, once you develop a robust algorithm, and, in previous work, we did it with almost 100% accuracy,” said study author Murat Dundar, PhD of Indiana University-Purdue University Indianapolis.
“What was challenging was to go beyond that work and teach the computer to accurately predict the direction of change in disease progression in AML patients, interpreting new data to predict the unknown: which new AML patients will go into remission and which will relapse.”
Dr Dundar and his colleagues described this work in IEEE Transactions on Biomedical Engineering.
The researchers said they modeled data from multiple flow cytometry samples to identify functionally distinct cell populations and their local realizations. Each sample was characterized by the proportions of recovered cell populations, which were used to predict the direction of change in disease progression for each AML patient.
“As the input, our computational system employs data from flow cytometry, a widely utilized technology that can rapidly provide detailed characteristics of single cells in samples such as blood or bone marrow,” explained study author Bartek Rajwa, PhD, of Purdue University in Lafayette, Indiana.
“Traditionally, the results of flow cytometry analyses are evaluated by highly trained human experts rather than by machine-learning algorithms. But computers are often better at extracting knowledge from complex data than humans are.”
The researchers used 200 diseased and non-diseased immunophenotypic panels for training and tested
the computational system with samples collected at multiple time points from 36 additional AML patients.
The system was able to predict remission with 100% accuracy (26 of 26 cases) and relapse with 90% accuracy (9 of 10 cases).
“Machine learning is not about modeling data,” Dr Dundar noted. “It’s about extracting knowledge from the data you have so you can build a powerful, intuitive tool that can make predictions about future data that the computer has not previously seen. The machine is learning, not memorizing, and that’s what we did.” ![]()
Photo by Darren Baker
Researchers say they have developed the first computer machine-learning model to accurately predict which patients diagnosed with acute
myeloid leukemia (AML) will go into remission after treatment and which will relapse.
“It’s pretty straightforward to teach a computer to recognize AML, once you develop a robust algorithm, and, in previous work, we did it with almost 100% accuracy,” said study author Murat Dundar, PhD of Indiana University-Purdue University Indianapolis.
“What was challenging was to go beyond that work and teach the computer to accurately predict the direction of change in disease progression in AML patients, interpreting new data to predict the unknown: which new AML patients will go into remission and which will relapse.”
Dr Dundar and his colleagues described this work in IEEE Transactions on Biomedical Engineering.
The researchers said they modeled data from multiple flow cytometry samples to identify functionally distinct cell populations and their local realizations. Each sample was characterized by the proportions of recovered cell populations, which were used to predict the direction of change in disease progression for each AML patient.
“As the input, our computational system employs data from flow cytometry, a widely utilized technology that can rapidly provide detailed characteristics of single cells in samples such as blood or bone marrow,” explained study author Bartek Rajwa, PhD, of Purdue University in Lafayette, Indiana.
“Traditionally, the results of flow cytometry analyses are evaluated by highly trained human experts rather than by machine-learning algorithms. But computers are often better at extracting knowledge from complex data than humans are.”
The researchers used 200 diseased and non-diseased immunophenotypic panels for training and tested
the computational system with samples collected at multiple time points from 36 additional AML patients.
The system was able to predict remission with 100% accuracy (26 of 26 cases) and relapse with 90% accuracy (9 of 10 cases).
“Machine learning is not about modeling data,” Dr Dundar noted. “It’s about extracting knowledge from the data you have so you can build a powerful, intuitive tool that can make predictions about future data that the computer has not previously seen. The machine is learning, not memorizing, and that’s what we did.” ![]()
Photo by Darren Baker
Researchers say they have developed the first computer machine-learning model to accurately predict which patients diagnosed with acute
myeloid leukemia (AML) will go into remission after treatment and which will relapse.
“It’s pretty straightforward to teach a computer to recognize AML, once you develop a robust algorithm, and, in previous work, we did it with almost 100% accuracy,” said study author Murat Dundar, PhD of Indiana University-Purdue University Indianapolis.
“What was challenging was to go beyond that work and teach the computer to accurately predict the direction of change in disease progression in AML patients, interpreting new data to predict the unknown: which new AML patients will go into remission and which will relapse.”
Dr Dundar and his colleagues described this work in IEEE Transactions on Biomedical Engineering.
The researchers said they modeled data from multiple flow cytometry samples to identify functionally distinct cell populations and their local realizations. Each sample was characterized by the proportions of recovered cell populations, which were used to predict the direction of change in disease progression for each AML patient.
“As the input, our computational system employs data from flow cytometry, a widely utilized technology that can rapidly provide detailed characteristics of single cells in samples such as blood or bone marrow,” explained study author Bartek Rajwa, PhD, of Purdue University in Lafayette, Indiana.
“Traditionally, the results of flow cytometry analyses are evaluated by highly trained human experts rather than by machine-learning algorithms. But computers are often better at extracting knowledge from complex data than humans are.”
The researchers used 200 diseased and non-diseased immunophenotypic panels for training and tested
the computational system with samples collected at multiple time points from 36 additional AML patients.
The system was able to predict remission with 100% accuracy (26 of 26 cases) and relapse with 90% accuracy (9 of 10 cases).
“Machine learning is not about modeling data,” Dr Dundar noted. “It’s about extracting knowledge from the data you have so you can build a powerful, intuitive tool that can make predictions about future data that the computer has not previously seen. The machine is learning, not memorizing, and that’s what we did.” ![]()
Genetic profiling can guide HSCT in MDS, team says

Genetic profiling can be used to determine which patients with myelodysplastic syndrome (MDS) are likely to benefit from allogeneic hematopoietic stem cell transplant (HSCT), according to research published in NEJM.
Targeted sequencing of 129 genes revealed mutations that, after adjustment for clinical variables, were associated with shorter survival and/or relapse after HSCT.
Patients with mutations in TP53, JAK2, and the RAS pathway tended to have worse outcomes after HSCT than patients without such mutations.
“Although donor stem cell transplantation is the only curative therapy for MDS, many patients die after transplantation, largely due to relapse of the disease or complications relating to the transplant itself,” said study author R. Coleman Lindsley, MD, PhD, of Dana-Farber Cancer Institute in Boston, Massachusetts.
“As physicians, one of our major challenges is to be able to predict which patients are most likely to benefit from a transplant. Improving our ability to identify patients who are most likely to have a relapse or to experience life-threatening complications from a transplant could lead to better pre-transplant therapies and strategies for preventing relapse.”
Researchers have long known that specific genetic mutations are closely related to the course MDS takes. With this study, Dr Lindsley and his colleagues sought to discover whether mutations can be used to predict how patients will fare following allogeneic HSCT.
The team analyzed blood samples from 1514 MDS patients, performing targeted sequencing of 129 genes. The genes were selected based on their known or suspected involvement in the pathogenesis of myeloid cancers or bone marrow failure syndromes.
Dr Lindsley and his colleagues then evaluated the association between mutations and HSCT outcomes, including overall survival, relapse, and death without relapse.
After adjusting for significant clinical variables, the researchers found that having mutated TP53 was significantly associated with shorter survival and shorter time to relapse after HSCT (P<0.001 for both comparisons). This was true whether patients received standard conditioning or reduced-intensity conditioning.
In patients age 40 and older who did not have TP53 mutations, mutations in RAS pathway genes (P=0.004) or JAK2 (P=0.001) were significantly associated with shorter survival.
The shorter survival in patients with mutated RAS pathway genes was due to a higher risk of relapse, while the shorter survival in patients with JAK2 mutations was due to a higher risk of death without relapse.
In contrast to TP53 mutations, the adverse effect of RAS mutations on survival and risk of relapse was evident only in patients who received reduced-intensity conditioning (P<0.001). This suggests these patients may benefit from higher intensity conditioning regimens, the researchers said.
This study also yielded insights about the biology of MDS in specific groups of patients.
For example, the researchers found that 4% of MDS patients between the ages of 18 and 40 had mutations associated with Shwachman-Diamond syndrome (in the SBDS gene), but most of them had not previously been diagnosed with the syndrome.
In each case, the patients had acquired a TP53 mutation, suggesting not only how MDS develops in patients with Schwachman-Diamond syndrome but also what underlies their poor prognosis after HSCT.
The researchers also analyzed patients with therapy-related MDS. The team found that TP53 mutations and mutations in PPM1D, a gene that regulates TP53 function, were far more common in these patients than in those with primary MDS (15% and 3%, respectively, P<0.001).
“In deciding whether a stem cell transplant is appropriate for a patient with MDS, it’s always necessary to balance the potential benefit with the risk of complications,” Dr Lindsley noted.
“Our findings offer physicians a guide—based on the genetic profile of the disease and certain clinical factors—to identifying patients for whom a transplant is appropriate, and the intensity of treatment most likely to be effective.” ![]()
Genetic profiling can be used to determine which patients with myelodysplastic syndrome (MDS) are likely to benefit from allogeneic hematopoietic stem cell transplant (HSCT), according to research published in NEJM.
Targeted sequencing of 129 genes revealed mutations that, after adjustment for clinical variables, were associated with shorter survival and/or relapse after HSCT.
Patients with mutations in TP53, JAK2, and the RAS pathway tended to have worse outcomes after HSCT than patients without such mutations.
“Although donor stem cell transplantation is the only curative therapy for MDS, many patients die after transplantation, largely due to relapse of the disease or complications relating to the transplant itself,” said study author R. Coleman Lindsley, MD, PhD, of Dana-Farber Cancer Institute in Boston, Massachusetts.
“As physicians, one of our major challenges is to be able to predict which patients are most likely to benefit from a transplant. Improving our ability to identify patients who are most likely to have a relapse or to experience life-threatening complications from a transplant could lead to better pre-transplant therapies and strategies for preventing relapse.”
Researchers have long known that specific genetic mutations are closely related to the course MDS takes. With this study, Dr Lindsley and his colleagues sought to discover whether mutations can be used to predict how patients will fare following allogeneic HSCT.
The team analyzed blood samples from 1514 MDS patients, performing targeted sequencing of 129 genes. The genes were selected based on their known or suspected involvement in the pathogenesis of myeloid cancers or bone marrow failure syndromes.
Dr Lindsley and his colleagues then evaluated the association between mutations and HSCT outcomes, including overall survival, relapse, and death without relapse.
After adjusting for significant clinical variables, the researchers found that having mutated TP53 was significantly associated with shorter survival and shorter time to relapse after HSCT (P<0.001 for both comparisons). This was true whether patients received standard conditioning or reduced-intensity conditioning.
In patients age 40 and older who did not have TP53 mutations, mutations in RAS pathway genes (P=0.004) or JAK2 (P=0.001) were significantly associated with shorter survival.
The shorter survival in patients with mutated RAS pathway genes was due to a higher risk of relapse, while the shorter survival in patients with JAK2 mutations was due to a higher risk of death without relapse.
In contrast to TP53 mutations, the adverse effect of RAS mutations on survival and risk of relapse was evident only in patients who received reduced-intensity conditioning (P<0.001). This suggests these patients may benefit from higher intensity conditioning regimens, the researchers said.
This study also yielded insights about the biology of MDS in specific groups of patients.
For example, the researchers found that 4% of MDS patients between the ages of 18 and 40 had mutations associated with Shwachman-Diamond syndrome (in the SBDS gene), but most of them had not previously been diagnosed with the syndrome.
In each case, the patients had acquired a TP53 mutation, suggesting not only how MDS develops in patients with Schwachman-Diamond syndrome but also what underlies their poor prognosis after HSCT.
The researchers also analyzed patients with therapy-related MDS. The team found that TP53 mutations and mutations in PPM1D, a gene that regulates TP53 function, were far more common in these patients than in those with primary MDS (15% and 3%, respectively, P<0.001).
“In deciding whether a stem cell transplant is appropriate for a patient with MDS, it’s always necessary to balance the potential benefit with the risk of complications,” Dr Lindsley noted.
“Our findings offer physicians a guide—based on the genetic profile of the disease and certain clinical factors—to identifying patients for whom a transplant is appropriate, and the intensity of treatment most likely to be effective.” ![]()
Genetic profiling can be used to determine which patients with myelodysplastic syndrome (MDS) are likely to benefit from allogeneic hematopoietic stem cell transplant (HSCT), according to research published in NEJM.
Targeted sequencing of 129 genes revealed mutations that, after adjustment for clinical variables, were associated with shorter survival and/or relapse after HSCT.
Patients with mutations in TP53, JAK2, and the RAS pathway tended to have worse outcomes after HSCT than patients without such mutations.
“Although donor stem cell transplantation is the only curative therapy for MDS, many patients die after transplantation, largely due to relapse of the disease or complications relating to the transplant itself,” said study author R. Coleman Lindsley, MD, PhD, of Dana-Farber Cancer Institute in Boston, Massachusetts.
“As physicians, one of our major challenges is to be able to predict which patients are most likely to benefit from a transplant. Improving our ability to identify patients who are most likely to have a relapse or to experience life-threatening complications from a transplant could lead to better pre-transplant therapies and strategies for preventing relapse.”
Researchers have long known that specific genetic mutations are closely related to the course MDS takes. With this study, Dr Lindsley and his colleagues sought to discover whether mutations can be used to predict how patients will fare following allogeneic HSCT.
The team analyzed blood samples from 1514 MDS patients, performing targeted sequencing of 129 genes. The genes were selected based on their known or suspected involvement in the pathogenesis of myeloid cancers or bone marrow failure syndromes.
Dr Lindsley and his colleagues then evaluated the association between mutations and HSCT outcomes, including overall survival, relapse, and death without relapse.
After adjusting for significant clinical variables, the researchers found that having mutated TP53 was significantly associated with shorter survival and shorter time to relapse after HSCT (P<0.001 for both comparisons). This was true whether patients received standard conditioning or reduced-intensity conditioning.
In patients age 40 and older who did not have TP53 mutations, mutations in RAS pathway genes (P=0.004) or JAK2 (P=0.001) were significantly associated with shorter survival.
The shorter survival in patients with mutated RAS pathway genes was due to a higher risk of relapse, while the shorter survival in patients with JAK2 mutations was due to a higher risk of death without relapse.
In contrast to TP53 mutations, the adverse effect of RAS mutations on survival and risk of relapse was evident only in patients who received reduced-intensity conditioning (P<0.001). This suggests these patients may benefit from higher intensity conditioning regimens, the researchers said.
This study also yielded insights about the biology of MDS in specific groups of patients.
For example, the researchers found that 4% of MDS patients between the ages of 18 and 40 had mutations associated with Shwachman-Diamond syndrome (in the SBDS gene), but most of them had not previously been diagnosed with the syndrome.
In each case, the patients had acquired a TP53 mutation, suggesting not only how MDS develops in patients with Schwachman-Diamond syndrome but also what underlies their poor prognosis after HSCT.
The researchers also analyzed patients with therapy-related MDS. The team found that TP53 mutations and mutations in PPM1D, a gene that regulates TP53 function, were far more common in these patients than in those with primary MDS (15% and 3%, respectively, P<0.001).
“In deciding whether a stem cell transplant is appropriate for a patient with MDS, it’s always necessary to balance the potential benefit with the risk of complications,” Dr Lindsley noted.
“Our findings offer physicians a guide—based on the genetic profile of the disease and certain clinical factors—to identifying patients for whom a transplant is appropriate, and the intensity of treatment most likely to be effective.” ![]()