User login
Cost equilibrium in Canada: Inpatient and outpatient treatment of herpes zoster
Rates of herpes zoster infections have increased substantially since the late 1990s in Canada. This, combined with rising per-episode medical costs and constant per-episode drug costs has led to increased total outpatient costs. But this has been offset by a dramatic drop in hospitalization rates and costs, according to a study published by BMC Infectious Diseases.
“A number of recent studies have looked at the burden of HZ-PHN [herpes zoster–postherpetic neuralgia] in a variety of health care systems, including Belgium, France, Germany, Greece, Italy, Spain, the United Kingdom, and Israel. However, little recent Canadian data have been published,” wrote Kevin J. Friesen, MD, and his associates at the University of Manitoba, Winnipeg, explaining that the goal of this study was to “establish the current burden of HZ and PHN in the setting of a universal health care system, and to look at long-term trends in their treatment costs.”

From 1997-1998 through 2013-2014, there were a total of 73,886 HZ incidents. In the final year alone, incidents numbered 5,746, which represents a 49.5% increase over 1997-1998. From the first year through 2009-2010, age-adjusted rates increased at a rate of 4.7 episodes per 1,000 person-years, but after that point, that rate increased to 5.7 episodes per 1,000 person-years, and continued that way through 2013-2014 (BMC Infect Dis. 2017. doi: 10.1186/s12879-017-2185-3).
Over the same 15-year time period, costs for drugs increased from an average of $89.77 to $127.34 per incident (P less than .03). Total medical costs increased from $57.98 to $78.84 per incident (P less than .00001).
However, the total annual cost of treating HZ and PHN dipped, particularly in 2011-2012, when it was $1,997,183, compared with $2,095,633 in the first year. Hospitalization rates also declined, going from 3.1% in 1997-1998 to 1.36% in 2011-2012 and bringing mean per-episode cost for the hospital down from $397 to $195.
“The combination of these trends in per-episode costs arising from medical care and drug treatment were multiplied by the increase in the annual incidence of HZ, causing total outpatient costs to increase,” the authors explained. “However, this increase was offset by the dramatic drop in rates of hospitalization and the resulting decrease in hospital costs.”
The study was funded by a grant from Merck Canada. Dr. Friesen and his coauthors did not report any relevant financial disclosures.
Rates of herpes zoster infections have increased substantially since the late 1990s in Canada. This, combined with rising per-episode medical costs and constant per-episode drug costs has led to increased total outpatient costs. But this has been offset by a dramatic drop in hospitalization rates and costs, according to a study published by BMC Infectious Diseases.
“A number of recent studies have looked at the burden of HZ-PHN [herpes zoster–postherpetic neuralgia] in a variety of health care systems, including Belgium, France, Germany, Greece, Italy, Spain, the United Kingdom, and Israel. However, little recent Canadian data have been published,” wrote Kevin J. Friesen, MD, and his associates at the University of Manitoba, Winnipeg, explaining that the goal of this study was to “establish the current burden of HZ and PHN in the setting of a universal health care system, and to look at long-term trends in their treatment costs.”
From 1997-1998 through 2013-2014, there were a total of 73,886 HZ incidents. In the final year alone, incidents numbered 5,746, which represents a 49.5% increase over 1997-1998. From the first year through 2009-2010, age-adjusted rates increased at a rate of 4.7 episodes per 1,000 person-years, but after that point, that rate increased to 5.7 episodes per 1,000 person-years, and continued that way through 2013-2014 (BMC Infect Dis. 2017. doi: 10.1186/s12879-017-2185-3).
Over the same 15-year time period, costs for drugs increased from an average of $89.77 to $127.34 per incident (P less than .03). Total medical costs increased from $57.98 to $78.84 per incident (P less than .00001).
However, the total annual cost of treating HZ and PHN dipped, particularly in 2011-2012, when it was $1,997,183, compared with $2,095,633 in the first year. Hospitalization rates also declined, going from 3.1% in 1997-1998 to 1.36% in 2011-2012 and bringing mean per-episode cost for the hospital down from $397 to $195.
“The combination of these trends in per-episode costs arising from medical care and drug treatment were multiplied by the increase in the annual incidence of HZ, causing total outpatient costs to increase,” the authors explained. “However, this increase was offset by the dramatic drop in rates of hospitalization and the resulting decrease in hospital costs.”
The study was funded by a grant from Merck Canada. Dr. Friesen and his coauthors did not report any relevant financial disclosures.
Rates of herpes zoster infections have increased substantially since the late 1990s in Canada. This, combined with rising per-episode medical costs and constant per-episode drug costs has led to increased total outpatient costs. But this has been offset by a dramatic drop in hospitalization rates and costs, according to a study published by BMC Infectious Diseases.
“A number of recent studies have looked at the burden of HZ-PHN [herpes zoster–postherpetic neuralgia] in a variety of health care systems, including Belgium, France, Germany, Greece, Italy, Spain, the United Kingdom, and Israel. However, little recent Canadian data have been published,” wrote Kevin J. Friesen, MD, and his associates at the University of Manitoba, Winnipeg, explaining that the goal of this study was to “establish the current burden of HZ and PHN in the setting of a universal health care system, and to look at long-term trends in their treatment costs.”
From 1997-1998 through 2013-2014, there were a total of 73,886 HZ incidents. In the final year alone, incidents numbered 5,746, which represents a 49.5% increase over 1997-1998. From the first year through 2009-2010, age-adjusted rates increased at a rate of 4.7 episodes per 1,000 person-years, but after that point, that rate increased to 5.7 episodes per 1,000 person-years, and continued that way through 2013-2014 (BMC Infect Dis. 2017. doi: 10.1186/s12879-017-2185-3).
Over the same 15-year time period, costs for drugs increased from an average of $89.77 to $127.34 per incident (P less than .03). Total medical costs increased from $57.98 to $78.84 per incident (P less than .00001).
However, the total annual cost of treating HZ and PHN dipped, particularly in 2011-2012, when it was $1,997,183, compared with $2,095,633 in the first year. Hospitalization rates also declined, going from 3.1% in 1997-1998 to 1.36% in 2011-2012 and bringing mean per-episode cost for the hospital down from $397 to $195.
“The combination of these trends in per-episode costs arising from medical care and drug treatment were multiplied by the increase in the annual incidence of HZ, causing total outpatient costs to increase,” the authors explained. “However, this increase was offset by the dramatic drop in rates of hospitalization and the resulting decrease in hospital costs.”
The study was funded by a grant from Merck Canada. Dr. Friesen and his coauthors did not report any relevant financial disclosures.
FROM BMC INFECTIOUS DISEASES
Key clinical point: Increasing herpes zoster rates combined with rising per-episode medical costs and constant per-episode drug costs has led to increased total outpatient costs. But this has been offset by a dramatic drop in hospitalization rates and costs.
Major finding: Incidence of herpes zoster between 1997-1998 and 2013-2014 increased by 49.5% in Canada.
Data source: Observational cohort study of data from the Manitoba Centre for Health Policy between April 1, 1997 and March 31, 2014.
Disclosures: Funded via grant from Merck Canada. Authors reported no relevant financial disclosures.
MedPAC leaning toward hybrid for paying for Part B drugs
WASHINGTON – The Medicare Payment Advisory Commission is putting the finishing touches on a recommendation for a hybrid approach to reforming how Medicare pays doctors for drugs administered in the office.
If adopted by the Centers for Medicare & Medicaid Services, MedPAC’s recommendations first would refine the current system which pays physicians for Medicare Part B drugs based on the average sales price (ASP), then eventually would allow physicians to either remain in the improved ASP system or switch to a drug value program (DVP), a revamped version of the failed Competitive Acquisition Program.
Under the potential MedPAC recommendations, new drugs – those that do not have an ASP – would be paid at wholesale acquisition cost plus 3%, which MedPAC staff said is more in line the standard ASP plus 6%.
To help stem the impact of pricing increases, the proposal calls on manufacturers to provide additional rebates when ASP growth exceeds inflation. This approach is commonly used by states collecting Medicaid drug rebates.
Finally, the proposal would consolidate billing codes to help foster competition. The plan would combine billing codes for a brand name drug and all associated generics, as well as combining biosimilars with their reference biologic products. Commission staff highlighted two cases where combining codes for a biologic/biosimilar would have an impact: Medicare’s payment rate for the biosimilar filgrastim-sndz (Zarxio) declined by 20% during the first 6 quarters on the market while the reference product (Neupogen) remained static. Further, first quarter of pricing data on the biosimilar infliximab-dyyb (Inflectra) is 22% greater than the reference product (Remicade).
MedPAC is likely to recommend that, as those changes go into effect, CMS develop the DVP, which would be voluntary beginning in 2022. In parallel with the launch of DVP, MedPAC is likely to recommend that CMS reduce the add-on percentage in the ASP program, as a stick to drive DVP participation.
Under the DVP, physicians would contract with one of a number of vendors that would negotiate prices for physicians and offer opportunities for shared savings.
Physicians would buy their drugs at the vendor-negotiated price from a network of wholesalers and distributors. Vendors would have additional negotiation tools such as formularies, step therapy, and prior authorization, and a price cap of 100% of ASP. Medicare would pay physicians at the DVP rate without any add-ons, but physicians would continue to receive fees for administrative services under the physician fee schedule or the outpatient prospective payment system.
The recommendations received general support from the MedPAC commissioners, but some of the finer details were met with concerns.
One was the possible impact of the ongoing budget sequestration, which lowers total payments from the government by 2%.
“I think the possibility that the sequester will still be in effect really casts a pall over proposals like [wholesale acquisition cost plus 3%], and we just have to think about what wording we’re going to use,” Commissioner Paul Ginsburg, PhD, of the Brookings Institution, said. “We realize that if a sequester is still in effect, we might have to make a temporary change.”
Another aspect of the DVP that raised questions was an arbitration process that would allow prices to be challenged for sole-source products.
Commissioner Amy Bricker, vice president of supply chain strategy at Express Scripts, said she was “not in favor of the arbitration,” questioning its administrative burden, cost, and turn-around time for decisions. She added that rather than arbitration, “I would like to see us provide incentives to manufacturers to bring competition to the market versus trying to create a system that doesn’t exist today for us to go to court.”
Regarding the DVP, Commissioner Jack Hoadley, PhD, research professor at Georgetown University, Washington, said that he is “not convinced that this process is going to work,” but acknowledged the MedPAC staff’s work in developing it. “It does feel like it’s worth putting out there and trying to see if it happens or trying to set it up to happen.”
MedPAC Vice Chairman Jon Christianson, PhD, of the University of Minnesota, Minneapolis, concurred. “I think we should go ahead and continue to explore that, but maybe temper our enthusiasm a little bit,” questioning how effective multiple groups would be in negotiating separately for Medicare drug pricing.
Commissioner William Hall, MD, of the University of Rochester, N.Y., also questioned the effect on patients. “Do any of these manipulations really have a direct correlation to quality of care for the patient population that is most affected by Part B?” he asked.
MedPAC staff will take the commissioners’ comments on these options and refine them for the upcoming March 2-3 meeting and will present the final recommendations to the commissioners to vote on in April for inclusion in the June report to Congress.
WASHINGTON – The Medicare Payment Advisory Commission is putting the finishing touches on a recommendation for a hybrid approach to reforming how Medicare pays doctors for drugs administered in the office.
If adopted by the Centers for Medicare & Medicaid Services, MedPAC’s recommendations first would refine the current system which pays physicians for Medicare Part B drugs based on the average sales price (ASP), then eventually would allow physicians to either remain in the improved ASP system or switch to a drug value program (DVP), a revamped version of the failed Competitive Acquisition Program.
Under the potential MedPAC recommendations, new drugs – those that do not have an ASP – would be paid at wholesale acquisition cost plus 3%, which MedPAC staff said is more in line the standard ASP plus 6%.
To help stem the impact of pricing increases, the proposal calls on manufacturers to provide additional rebates when ASP growth exceeds inflation. This approach is commonly used by states collecting Medicaid drug rebates.
Finally, the proposal would consolidate billing codes to help foster competition. The plan would combine billing codes for a brand name drug and all associated generics, as well as combining biosimilars with their reference biologic products. Commission staff highlighted two cases where combining codes for a biologic/biosimilar would have an impact: Medicare’s payment rate for the biosimilar filgrastim-sndz (Zarxio) declined by 20% during the first 6 quarters on the market while the reference product (Neupogen) remained static. Further, first quarter of pricing data on the biosimilar infliximab-dyyb (Inflectra) is 22% greater than the reference product (Remicade).
MedPAC is likely to recommend that, as those changes go into effect, CMS develop the DVP, which would be voluntary beginning in 2022. In parallel with the launch of DVP, MedPAC is likely to recommend that CMS reduce the add-on percentage in the ASP program, as a stick to drive DVP participation.
Under the DVP, physicians would contract with one of a number of vendors that would negotiate prices for physicians and offer opportunities for shared savings.
Physicians would buy their drugs at the vendor-negotiated price from a network of wholesalers and distributors. Vendors would have additional negotiation tools such as formularies, step therapy, and prior authorization, and a price cap of 100% of ASP. Medicare would pay physicians at the DVP rate without any add-ons, but physicians would continue to receive fees for administrative services under the physician fee schedule or the outpatient prospective payment system.
The recommendations received general support from the MedPAC commissioners, but some of the finer details were met with concerns.
One was the possible impact of the ongoing budget sequestration, which lowers total payments from the government by 2%.
“I think the possibility that the sequester will still be in effect really casts a pall over proposals like [wholesale acquisition cost plus 3%], and we just have to think about what wording we’re going to use,” Commissioner Paul Ginsburg, PhD, of the Brookings Institution, said. “We realize that if a sequester is still in effect, we might have to make a temporary change.”
Another aspect of the DVP that raised questions was an arbitration process that would allow prices to be challenged for sole-source products.
Commissioner Amy Bricker, vice president of supply chain strategy at Express Scripts, said she was “not in favor of the arbitration,” questioning its administrative burden, cost, and turn-around time for decisions. She added that rather than arbitration, “I would like to see us provide incentives to manufacturers to bring competition to the market versus trying to create a system that doesn’t exist today for us to go to court.”
Regarding the DVP, Commissioner Jack Hoadley, PhD, research professor at Georgetown University, Washington, said that he is “not convinced that this process is going to work,” but acknowledged the MedPAC staff’s work in developing it. “It does feel like it’s worth putting out there and trying to see if it happens or trying to set it up to happen.”
MedPAC Vice Chairman Jon Christianson, PhD, of the University of Minnesota, Minneapolis, concurred. “I think we should go ahead and continue to explore that, but maybe temper our enthusiasm a little bit,” questioning how effective multiple groups would be in negotiating separately for Medicare drug pricing.
Commissioner William Hall, MD, of the University of Rochester, N.Y., also questioned the effect on patients. “Do any of these manipulations really have a direct correlation to quality of care for the patient population that is most affected by Part B?” he asked.
MedPAC staff will take the commissioners’ comments on these options and refine them for the upcoming March 2-3 meeting and will present the final recommendations to the commissioners to vote on in April for inclusion in the June report to Congress.
WASHINGTON – The Medicare Payment Advisory Commission is putting the finishing touches on a recommendation for a hybrid approach to reforming how Medicare pays doctors for drugs administered in the office.
If adopted by the Centers for Medicare & Medicaid Services, MedPAC’s recommendations first would refine the current system which pays physicians for Medicare Part B drugs based on the average sales price (ASP), then eventually would allow physicians to either remain in the improved ASP system or switch to a drug value program (DVP), a revamped version of the failed Competitive Acquisition Program.
Under the potential MedPAC recommendations, new drugs – those that do not have an ASP – would be paid at wholesale acquisition cost plus 3%, which MedPAC staff said is more in line the standard ASP plus 6%.
To help stem the impact of pricing increases, the proposal calls on manufacturers to provide additional rebates when ASP growth exceeds inflation. This approach is commonly used by states collecting Medicaid drug rebates.
Finally, the proposal would consolidate billing codes to help foster competition. The plan would combine billing codes for a brand name drug and all associated generics, as well as combining biosimilars with their reference biologic products. Commission staff highlighted two cases where combining codes for a biologic/biosimilar would have an impact: Medicare’s payment rate for the biosimilar filgrastim-sndz (Zarxio) declined by 20% during the first 6 quarters on the market while the reference product (Neupogen) remained static. Further, first quarter of pricing data on the biosimilar infliximab-dyyb (Inflectra) is 22% greater than the reference product (Remicade).
MedPAC is likely to recommend that, as those changes go into effect, CMS develop the DVP, which would be voluntary beginning in 2022. In parallel with the launch of DVP, MedPAC is likely to recommend that CMS reduce the add-on percentage in the ASP program, as a stick to drive DVP participation.
Under the DVP, physicians would contract with one of a number of vendors that would negotiate prices for physicians and offer opportunities for shared savings.
Physicians would buy their drugs at the vendor-negotiated price from a network of wholesalers and distributors. Vendors would have additional negotiation tools such as formularies, step therapy, and prior authorization, and a price cap of 100% of ASP. Medicare would pay physicians at the DVP rate without any add-ons, but physicians would continue to receive fees for administrative services under the physician fee schedule or the outpatient prospective payment system.
The recommendations received general support from the MedPAC commissioners, but some of the finer details were met with concerns.
One was the possible impact of the ongoing budget sequestration, which lowers total payments from the government by 2%.
“I think the possibility that the sequester will still be in effect really casts a pall over proposals like [wholesale acquisition cost plus 3%], and we just have to think about what wording we’re going to use,” Commissioner Paul Ginsburg, PhD, of the Brookings Institution, said. “We realize that if a sequester is still in effect, we might have to make a temporary change.”
Another aspect of the DVP that raised questions was an arbitration process that would allow prices to be challenged for sole-source products.
Commissioner Amy Bricker, vice president of supply chain strategy at Express Scripts, said she was “not in favor of the arbitration,” questioning its administrative burden, cost, and turn-around time for decisions. She added that rather than arbitration, “I would like to see us provide incentives to manufacturers to bring competition to the market versus trying to create a system that doesn’t exist today for us to go to court.”
Regarding the DVP, Commissioner Jack Hoadley, PhD, research professor at Georgetown University, Washington, said that he is “not convinced that this process is going to work,” but acknowledged the MedPAC staff’s work in developing it. “It does feel like it’s worth putting out there and trying to see if it happens or trying to set it up to happen.”
MedPAC Vice Chairman Jon Christianson, PhD, of the University of Minnesota, Minneapolis, concurred. “I think we should go ahead and continue to explore that, but maybe temper our enthusiasm a little bit,” questioning how effective multiple groups would be in negotiating separately for Medicare drug pricing.
Commissioner William Hall, MD, of the University of Rochester, N.Y., also questioned the effect on patients. “Do any of these manipulations really have a direct correlation to quality of care for the patient population that is most affected by Part B?” he asked.
MedPAC staff will take the commissioners’ comments on these options and refine them for the upcoming March 2-3 meeting and will present the final recommendations to the commissioners to vote on in April for inclusion in the June report to Congress.
AT A MEDPAC MEETING
Antibiotic use may hamper checkpoint inhibitors for mRCC
Antibiotics may hamper the effectiveness of immune checkpoint inhibitors for patients with metastatic renal cell carcinoma, according to a small, retrospective study. Using antibiotics within 1 month of starting a checkpoint inhibitor was associated with significantly shorter progression-free survival, as well as a trend toward shorter overall survival, in a study of 80 patients with metastatic renal cell carcinoma.
Although the mechanism remains unknown, the prevailing theory is that antibiotics adversely alter the composition of the gut microbiome, and in so doing, slash the ability of beneficial bacteria to boost efficacy of immune checkpoint blockade.
“The data I presented today are just preliminary. But the results are really important because there is a kind of connection between the microbiome, antibiotics, and immune checkpoint blockade,” Lisa Derosa, MD, of Paris-Sud University, Villejuif, France, said during a press briefing prior to the 2017 genitourinary cancers symposium sponsored by the American Society of Clinical Oncology, ASTRO, and the Society of Urologic Oncology.
Dr. Derosa and her colleagues retrospectively assessed 80 people with metastatic renal cell carcinoma enrolled in prospective trials at Gustave Roussy Cancer Institute. The patients were treated with the PD1/PD-L1 inhibitors alone or in combination. The researchers compared survival of 16 patients who also received broad-spectrum antibiotic therapy within 1 month of their first dose of immunotherapy with 64 others who did not receive antibiotics.
Progression-free survival was significantly shorter for patients in the antibiotic group, 2.3 months versus 8.1 months for the nonantibiotic group (P less than .001) on Kaplan-Meier curves. The statistical significance persisted even after the researchers controlled for age, gender, International Metastatic Renal-Cell Carcinoma Database Consortium (IMDC) risk classification, tumor burden, and PPI use in a multivariate analysis. Similarly, the objective response rate to checkpoint inhibition therapy was significantly lower among patients in the antibiotic group (P less than .002).
“There was no significant difference, however, between these groups in overall survival,” Dr. Derosa said.
Despite the findings, Dr. Derosa said it’s too soon to say antibiotics are contraindicated in this patient population. “It may be important to pay attention to these antibiotics in patients treated with immune response inhibitors, but the data are still preliminary.”
“I would propose this data is very intriguing, but it was retrospectively generated, so I consider it hypothesis-generating,” said Sumanta Pal, MD, of City of Hope Medical Center in Duarte, Calif., and moderator of the press briefing. “One has to consider the fact that antibiotics are used under circumstances of medical necessity. I wouldn’t forgo treatment of any active infection … I would use as medically necessary.”
Beta-lactamases and fluoroquinolones comprised the majority of antibiotics in the study. The majority, 67 patients, received immune monotherapy with single-agent PD-1 or PD-L1 inhibitors. Another 10 patients received a combination of a PD-1 inhibitor and a CTLA-4 inhibitor, and 3 were treated with a PD-L1 inhibitor and bevacizumab.
“This is the first analysis evaluating impact of antibiotics on outcome of advanced renal carcinoma patients treated in the era of immune checkpoint blockade,” Dr. Derosa said. “We have a lot of work to do.” She and her colleagues plan to continue enrolling patients in the study. They also plan to evaluate whether alteration of the microbiome composition does play a role in diminishing the effectiveness of immunotherapy, and if so, which types of bacteria are the most likely culprits.
Antibiotics may hamper the effectiveness of immune checkpoint inhibitors for patients with metastatic renal cell carcinoma, according to a small, retrospective study. Using antibiotics within 1 month of starting a checkpoint inhibitor was associated with significantly shorter progression-free survival, as well as a trend toward shorter overall survival, in a study of 80 patients with metastatic renal cell carcinoma.
Although the mechanism remains unknown, the prevailing theory is that antibiotics adversely alter the composition of the gut microbiome, and in so doing, slash the ability of beneficial bacteria to boost efficacy of immune checkpoint blockade.
“The data I presented today are just preliminary. But the results are really important because there is a kind of connection between the microbiome, antibiotics, and immune checkpoint blockade,” Lisa Derosa, MD, of Paris-Sud University, Villejuif, France, said during a press briefing prior to the 2017 genitourinary cancers symposium sponsored by the American Society of Clinical Oncology, ASTRO, and the Society of Urologic Oncology.
Dr. Derosa and her colleagues retrospectively assessed 80 people with metastatic renal cell carcinoma enrolled in prospective trials at Gustave Roussy Cancer Institute. The patients were treated with the PD1/PD-L1 inhibitors alone or in combination. The researchers compared survival of 16 patients who also received broad-spectrum antibiotic therapy within 1 month of their first dose of immunotherapy with 64 others who did not receive antibiotics.
Progression-free survival was significantly shorter for patients in the antibiotic group, 2.3 months versus 8.1 months for the nonantibiotic group (P less than .001) on Kaplan-Meier curves. The statistical significance persisted even after the researchers controlled for age, gender, International Metastatic Renal-Cell Carcinoma Database Consortium (IMDC) risk classification, tumor burden, and PPI use in a multivariate analysis. Similarly, the objective response rate to checkpoint inhibition therapy was significantly lower among patients in the antibiotic group (P less than .002).
“There was no significant difference, however, between these groups in overall survival,” Dr. Derosa said.
Despite the findings, Dr. Derosa said it’s too soon to say antibiotics are contraindicated in this patient population. “It may be important to pay attention to these antibiotics in patients treated with immune response inhibitors, but the data are still preliminary.”
“I would propose this data is very intriguing, but it was retrospectively generated, so I consider it hypothesis-generating,” said Sumanta Pal, MD, of City of Hope Medical Center in Duarte, Calif., and moderator of the press briefing. “One has to consider the fact that antibiotics are used under circumstances of medical necessity. I wouldn’t forgo treatment of any active infection … I would use as medically necessary.”
Beta-lactamases and fluoroquinolones comprised the majority of antibiotics in the study. The majority, 67 patients, received immune monotherapy with single-agent PD-1 or PD-L1 inhibitors. Another 10 patients received a combination of a PD-1 inhibitor and a CTLA-4 inhibitor, and 3 were treated with a PD-L1 inhibitor and bevacizumab.
“This is the first analysis evaluating impact of antibiotics on outcome of advanced renal carcinoma patients treated in the era of immune checkpoint blockade,” Dr. Derosa said. “We have a lot of work to do.” She and her colleagues plan to continue enrolling patients in the study. They also plan to evaluate whether alteration of the microbiome composition does play a role in diminishing the effectiveness of immunotherapy, and if so, which types of bacteria are the most likely culprits.
Antibiotics may hamper the effectiveness of immune checkpoint inhibitors for patients with metastatic renal cell carcinoma, according to a small, retrospective study. Using antibiotics within 1 month of starting a checkpoint inhibitor was associated with significantly shorter progression-free survival, as well as a trend toward shorter overall survival, in a study of 80 patients with metastatic renal cell carcinoma.
Although the mechanism remains unknown, the prevailing theory is that antibiotics adversely alter the composition of the gut microbiome, and in so doing, slash the ability of beneficial bacteria to boost efficacy of immune checkpoint blockade.
“The data I presented today are just preliminary. But the results are really important because there is a kind of connection between the microbiome, antibiotics, and immune checkpoint blockade,” Lisa Derosa, MD, of Paris-Sud University, Villejuif, France, said during a press briefing prior to the 2017 genitourinary cancers symposium sponsored by the American Society of Clinical Oncology, ASTRO, and the Society of Urologic Oncology.
Dr. Derosa and her colleagues retrospectively assessed 80 people with metastatic renal cell carcinoma enrolled in prospective trials at Gustave Roussy Cancer Institute. The patients were treated with the PD1/PD-L1 inhibitors alone or in combination. The researchers compared survival of 16 patients who also received broad-spectrum antibiotic therapy within 1 month of their first dose of immunotherapy with 64 others who did not receive antibiotics.
Progression-free survival was significantly shorter for patients in the antibiotic group, 2.3 months versus 8.1 months for the nonantibiotic group (P less than .001) on Kaplan-Meier curves. The statistical significance persisted even after the researchers controlled for age, gender, International Metastatic Renal-Cell Carcinoma Database Consortium (IMDC) risk classification, tumor burden, and PPI use in a multivariate analysis. Similarly, the objective response rate to checkpoint inhibition therapy was significantly lower among patients in the antibiotic group (P less than .002).
“There was no significant difference, however, between these groups in overall survival,” Dr. Derosa said.
Despite the findings, Dr. Derosa said it’s too soon to say antibiotics are contraindicated in this patient population. “It may be important to pay attention to these antibiotics in patients treated with immune response inhibitors, but the data are still preliminary.”
“I would propose this data is very intriguing, but it was retrospectively generated, so I consider it hypothesis-generating,” said Sumanta Pal, MD, of City of Hope Medical Center in Duarte, Calif., and moderator of the press briefing. “One has to consider the fact that antibiotics are used under circumstances of medical necessity. I wouldn’t forgo treatment of any active infection … I would use as medically necessary.”
Beta-lactamases and fluoroquinolones comprised the majority of antibiotics in the study. The majority, 67 patients, received immune monotherapy with single-agent PD-1 or PD-L1 inhibitors. Another 10 patients received a combination of a PD-1 inhibitor and a CTLA-4 inhibitor, and 3 were treated with a PD-L1 inhibitor and bevacizumab.
“This is the first analysis evaluating impact of antibiotics on outcome of advanced renal carcinoma patients treated in the era of immune checkpoint blockade,” Dr. Derosa said. “We have a lot of work to do.” She and her colleagues plan to continue enrolling patients in the study. They also plan to evaluate whether alteration of the microbiome composition does play a role in diminishing the effectiveness of immunotherapy, and if so, which types of bacteria are the most likely culprits.
FROM THE GENITOURINARY CANCERS SYMPOSIUM
Key clinical point: The effectiveness of immune checkpoint inhibitors for patients with metastatic renal cell carcinoma may be hampered by antibiotic use.
Major finding: Patients treated with antibiotics had significantly shorter progression-free survival, 2.3 months versus 8.1 months (P less than.001).
Data source: Retrospective study of 80 patients treated with immune checkpoint inhibitors.
Disclosures: The study was supported by grants from the Philanthropia Foundation. Dr. Derosa had no relevant financial disclosures.
Circulating tumor DNA could guide therapy for advanced prostate cancer
ORLANDO – New research indicates that genetic changes over time in circulating cell-free tumor DNA of patients with advanced prostate cancer could help clinicians detect emerging treatment resistance and adjust treatment regimens accordingly. Also, specific genetic changes were associated with worse outcomes, suggesting a role in prognosis for these “liquid biopsies.”
In addition, the genetic changes detected in the 10-mL blood samples were similar to those seen in traditional tissue biopsies, indicating a noninvasive strategy could be a viable alternative in the future.

In contrast, circulating tumor DNA testing is noninvasive and not confounded by sampling bias of the biopsy, Dr. Sonpavde said during a press briefing prior to the 2017 genitourinary cancers symposium sponsored by the American Society of Clinical Oncology, ASTRO, and the Society of Urologic Oncology.
Dr. Sonpavde and his colleagues analyzed blood samples from 514 people with metastatic castration-resistant prostate cancer. They used a commercially available test to assess the cell-free, circulating tumor DNA (ctDNA) for 73 cancer-related, potentially actionable genes.
An overwhelming majority of patients, 94%, had at least one genetic change. “The most important takeaway is that ctDNA is frequently seen in patients with metastatic castration-resistant prostate cancer,” Dr. Sonpavde said. “So it looks rather promising for studying this tumor with ctDNA assays.”
“Circulating tumor DNA offers a simple and convenient way to assess an individual patient’s tumor DNA composition, and often, it can reveal new mutations clinicians like me can use to personalize therapy,” said Sumanta Pal, MD, of City of Hope Medical Center in Duarte, Calif. and moderator of the press briefing.
A likely target will be the androgen receptor (AR) gene, which was found in 22% of patients in the study. Other common recurrent somatic mutations occurred in TP53, APC, NF1, EGFR, CTNNB1, ARID1A, BRCA1, BRCA2, and PIK3CA genes, affecting from 36% to 5% of patients. The AR gene was also one of the most commonly amplified genes in the study, with an increase in copy numbers observed in 30% of patients. Increased cancer gene copies can spur an overabundance of proteins that drive cancer growth.
Alterations and outcomes
Investigators also performed a subanalysis of 163 patients for whom they had clinical values and outcome information. “What we found was something interesting,” Dr. Sonpavde said. “A higher number of overall ctDNA gene alterations and AR alterations appeared associated with poor clinical outcomes.”
For example, a higher number of any alterations of the genes on the panel was associated with a shorter time to failure (hazard ratio, 1.05; P = .026). In addition, AR gene changes were associated with a trend for shorter time to failure (HR, 1.42; P = .053) and survival (HR, 2.51), although the survival difference in this instance was not statistically significant (P = 0.09). The investigators also report that treatment-naive patients were less likely to develop AR gene changes, compared with previously treated patient (37% versus 56%; P = .028).
Changes over time could be prognostic
Of the group of patients with outcomes information, 63 underwent serial blood testing. “What we found in this subset is that the evolution of alterations in AR was the most frequent new alteration found,” again underlining its importance as a therapeutic target, Dr. Sonpavde said. Another important implication of emerging mutations is development of treatment resistance and a need to switch individual patients to a more effective treatment.
“New mutations in AR protein are important … because AR is the most common target of hormone therapies for prostate cancer,” Dr. Pal said. “This suggests that developing new agents that target this protein more effectively is certainly a good direction for future research.”
Guiding new treatment targets
An estimated 161,360 men in the United States will be diagnosed with prostate cancer in 2017 and close to 27,000 will die from the disease, according to American Cancer Society Facts & Figures 2017. Although no treatments are yet Food and Drug Administration–approved to treat prostate cancer based on specific genetic mutations, several therapies are in development. Results from the study could be used to identify novel molecular targets for future therapy, the authors said, provided a prospective, controlled trial confirms that treatment guidance based on the blood test in the study improves patient outcomes.
“In terms of next steps, it would be interesting to look at patients given therapy based on the alterations found, which would help us develop tailored and more efficient medicine,” Dr. Sonpavde said.
Dr. Sonpavde is a consultant/advisor for Bayer, Genetech, Sanofi, Merck, Novartis, Pfizer, Argos Therapeutics and Agensys; a member of the speakers’ bureau for Clinical Care Options/NCCN; receives honoraria from UpToDate; and receives institutional research funding from Onyx, Bayer, and Boehringer Ingelheim. Dr. Pal had no relevant financial disclosures.
ORLANDO – New research indicates that genetic changes over time in circulating cell-free tumor DNA of patients with advanced prostate cancer could help clinicians detect emerging treatment resistance and adjust treatment regimens accordingly. Also, specific genetic changes were associated with worse outcomes, suggesting a role in prognosis for these “liquid biopsies.”
In addition, the genetic changes detected in the 10-mL blood samples were similar to those seen in traditional tissue biopsies, indicating a noninvasive strategy could be a viable alternative in the future.
In contrast, circulating tumor DNA testing is noninvasive and not confounded by sampling bias of the biopsy, Dr. Sonpavde said during a press briefing prior to the 2017 genitourinary cancers symposium sponsored by the American Society of Clinical Oncology, ASTRO, and the Society of Urologic Oncology.
Dr. Sonpavde and his colleagues analyzed blood samples from 514 people with metastatic castration-resistant prostate cancer. They used a commercially available test to assess the cell-free, circulating tumor DNA (ctDNA) for 73 cancer-related, potentially actionable genes.
An overwhelming majority of patients, 94%, had at least one genetic change. “The most important takeaway is that ctDNA is frequently seen in patients with metastatic castration-resistant prostate cancer,” Dr. Sonpavde said. “So it looks rather promising for studying this tumor with ctDNA assays.”
“Circulating tumor DNA offers a simple and convenient way to assess an individual patient’s tumor DNA composition, and often, it can reveal new mutations clinicians like me can use to personalize therapy,” said Sumanta Pal, MD, of City of Hope Medical Center in Duarte, Calif. and moderator of the press briefing.
A likely target will be the androgen receptor (AR) gene, which was found in 22% of patients in the study. Other common recurrent somatic mutations occurred in TP53, APC, NF1, EGFR, CTNNB1, ARID1A, BRCA1, BRCA2, and PIK3CA genes, affecting from 36% to 5% of patients. The AR gene was also one of the most commonly amplified genes in the study, with an increase in copy numbers observed in 30% of patients. Increased cancer gene copies can spur an overabundance of proteins that drive cancer growth.
Alterations and outcomes
Investigators also performed a subanalysis of 163 patients for whom they had clinical values and outcome information. “What we found was something interesting,” Dr. Sonpavde said. “A higher number of overall ctDNA gene alterations and AR alterations appeared associated with poor clinical outcomes.”
For example, a higher number of any alterations of the genes on the panel was associated with a shorter time to failure (hazard ratio, 1.05; P = .026). In addition, AR gene changes were associated with a trend for shorter time to failure (HR, 1.42; P = .053) and survival (HR, 2.51), although the survival difference in this instance was not statistically significant (P = 0.09). The investigators also report that treatment-naive patients were less likely to develop AR gene changes, compared with previously treated patient (37% versus 56%; P = .028).
Changes over time could be prognostic
Of the group of patients with outcomes information, 63 underwent serial blood testing. “What we found in this subset is that the evolution of alterations in AR was the most frequent new alteration found,” again underlining its importance as a therapeutic target, Dr. Sonpavde said. Another important implication of emerging mutations is development of treatment resistance and a need to switch individual patients to a more effective treatment.
“New mutations in AR protein are important … because AR is the most common target of hormone therapies for prostate cancer,” Dr. Pal said. “This suggests that developing new agents that target this protein more effectively is certainly a good direction for future research.”
Guiding new treatment targets
An estimated 161,360 men in the United States will be diagnosed with prostate cancer in 2017 and close to 27,000 will die from the disease, according to American Cancer Society Facts & Figures 2017. Although no treatments are yet Food and Drug Administration–approved to treat prostate cancer based on specific genetic mutations, several therapies are in development. Results from the study could be used to identify novel molecular targets for future therapy, the authors said, provided a prospective, controlled trial confirms that treatment guidance based on the blood test in the study improves patient outcomes.
“In terms of next steps, it would be interesting to look at patients given therapy based on the alterations found, which would help us develop tailored and more efficient medicine,” Dr. Sonpavde said.
Dr. Sonpavde is a consultant/advisor for Bayer, Genetech, Sanofi, Merck, Novartis, Pfizer, Argos Therapeutics and Agensys; a member of the speakers’ bureau for Clinical Care Options/NCCN; receives honoraria from UpToDate; and receives institutional research funding from Onyx, Bayer, and Boehringer Ingelheim. Dr. Pal had no relevant financial disclosures.
ORLANDO – New research indicates that genetic changes over time in circulating cell-free tumor DNA of patients with advanced prostate cancer could help clinicians detect emerging treatment resistance and adjust treatment regimens accordingly. Also, specific genetic changes were associated with worse outcomes, suggesting a role in prognosis for these “liquid biopsies.”
In addition, the genetic changes detected in the 10-mL blood samples were similar to those seen in traditional tissue biopsies, indicating a noninvasive strategy could be a viable alternative in the future.
In contrast, circulating tumor DNA testing is noninvasive and not confounded by sampling bias of the biopsy, Dr. Sonpavde said during a press briefing prior to the 2017 genitourinary cancers symposium sponsored by the American Society of Clinical Oncology, ASTRO, and the Society of Urologic Oncology.
Dr. Sonpavde and his colleagues analyzed blood samples from 514 people with metastatic castration-resistant prostate cancer. They used a commercially available test to assess the cell-free, circulating tumor DNA (ctDNA) for 73 cancer-related, potentially actionable genes.
An overwhelming majority of patients, 94%, had at least one genetic change. “The most important takeaway is that ctDNA is frequently seen in patients with metastatic castration-resistant prostate cancer,” Dr. Sonpavde said. “So it looks rather promising for studying this tumor with ctDNA assays.”
“Circulating tumor DNA offers a simple and convenient way to assess an individual patient’s tumor DNA composition, and often, it can reveal new mutations clinicians like me can use to personalize therapy,” said Sumanta Pal, MD, of City of Hope Medical Center in Duarte, Calif. and moderator of the press briefing.
A likely target will be the androgen receptor (AR) gene, which was found in 22% of patients in the study. Other common recurrent somatic mutations occurred in TP53, APC, NF1, EGFR, CTNNB1, ARID1A, BRCA1, BRCA2, and PIK3CA genes, affecting from 36% to 5% of patients. The AR gene was also one of the most commonly amplified genes in the study, with an increase in copy numbers observed in 30% of patients. Increased cancer gene copies can spur an overabundance of proteins that drive cancer growth.
Alterations and outcomes
Investigators also performed a subanalysis of 163 patients for whom they had clinical values and outcome information. “What we found was something interesting,” Dr. Sonpavde said. “A higher number of overall ctDNA gene alterations and AR alterations appeared associated with poor clinical outcomes.”
For example, a higher number of any alterations of the genes on the panel was associated with a shorter time to failure (hazard ratio, 1.05; P = .026). In addition, AR gene changes were associated with a trend for shorter time to failure (HR, 1.42; P = .053) and survival (HR, 2.51), although the survival difference in this instance was not statistically significant (P = 0.09). The investigators also report that treatment-naive patients were less likely to develop AR gene changes, compared with previously treated patient (37% versus 56%; P = .028).
Changes over time could be prognostic
Of the group of patients with outcomes information, 63 underwent serial blood testing. “What we found in this subset is that the evolution of alterations in AR was the most frequent new alteration found,” again underlining its importance as a therapeutic target, Dr. Sonpavde said. Another important implication of emerging mutations is development of treatment resistance and a need to switch individual patients to a more effective treatment.
“New mutations in AR protein are important … because AR is the most common target of hormone therapies for prostate cancer,” Dr. Pal said. “This suggests that developing new agents that target this protein more effectively is certainly a good direction for future research.”
Guiding new treatment targets
An estimated 161,360 men in the United States will be diagnosed with prostate cancer in 2017 and close to 27,000 will die from the disease, according to American Cancer Society Facts & Figures 2017. Although no treatments are yet Food and Drug Administration–approved to treat prostate cancer based on specific genetic mutations, several therapies are in development. Results from the study could be used to identify novel molecular targets for future therapy, the authors said, provided a prospective, controlled trial confirms that treatment guidance based on the blood test in the study improves patient outcomes.
“In terms of next steps, it would be interesting to look at patients given therapy based on the alterations found, which would help us develop tailored and more efficient medicine,” Dr. Sonpavde said.
Dr. Sonpavde is a consultant/advisor for Bayer, Genetech, Sanofi, Merck, Novartis, Pfizer, Argos Therapeutics and Agensys; a member of the speakers’ bureau for Clinical Care Options/NCCN; receives honoraria from UpToDate; and receives institutional research funding from Onyx, Bayer, and Boehringer Ingelheim. Dr. Pal had no relevant financial disclosures.
FROM THE GENITOURINARY CANCERS SYMPOSIUM
Key clinical point: A majority of patients with metastatic castration-resistant prostate cancer have detectable tumor DNA in their blood.
Major finding: 94% of 514 patients had one or more cancer-associated genetic alterations in their blood samples.
Data source: Retrospective study of 514 patients diagnosed with metastatic castration-resistant prostate cancer.
Disclosures: Dr. Sonpavde is a consultant/advisor for Bayer, Genetech, Sanofi, Merck, Novartis, Pfizer, Argos Therapeutics and Agensys; a member of the speakers’ bureau for Clinical Care Options/NCCN; receives honoraria from UpToDate; and receives institutional research funding from Onyx, Bayer, and Boehringer Ingelheim. Dr. Pal had no relevant financial disclosures.
Comorbid mental illness linked to worse surgical outcomes
LAS VEGAS – A comorbid mental illness may predispose surgical patients to poor outcomes, increasing the risk of postoperative complications, a prolonged length of stay, and – in some cases – even in-hospital mortality.
The link between mental illness and physical response to surgery is not well elucidated, and is likely an extremely complicated one, Elizabeth Bailey, MD, said at the Association for Academic Surgery/Society of University Surgeons Academic Surgical Congress.

Dr. Bailey said there is an extreme paucity of data on the relationship between mental illness and surgical outcomes. To investigate it, she examined 580,000 patient records contained in the National Inpatient Sample.
The cases spanned 2009-2011 and represented the four most common surgical procedures in the United States: cholecystectomy, appendectomy, adhesion excision/lysis, and colorectal resection.
She compared surgical outcomes among patients without a DSM-IV diagnosis and those with one of the five most common: mood disorder, anxiety, impulse control, schizophrenia, and substance abuse disorder.
The study’s primary outcomes were length of hospital stay, in-hospital mortality, and postoperative complications. Her analysis controlled for age, gender, race, admission status, operative approach, non–mental health comorbidities, insurance, and income.
Of the 580,000 in the study group 7% (39,000) had at least one of the mental health comorbidities. Mood disorder was the most common (59%), followed by substance abuse (24%), schizophrenia (13%), anxiety disorder (12%), and impulse control disorder (5%).
There were a number of significant baseline differences between those with a mental diagnosis and those without. Those with a DSM-IV diagnosis were younger (52 vs. 54 years), more often women (61% vs. 57%), and white (78% vs. 69%). They more often had additional physical comorbidities (80% vs. 68%). They were more likely to be admitted through the emergency room (74% vs. 71%), to have nonlaparoscopic surgery (60% vs 63%), to be on public insurance (53% vs. 43%), and to be in the lowest income quartile (28% vs. 25%).
Surgical outcomes were almost universally significantly worse among these patients. They were 41% more likely to experience a prolonged length of stay and 18% more likely to experience a complication. These included wound disruption, ileus, and small bowel obstruction. They faced a 24% increased risk for needing total parenteral nutrition; a 29% increased risk of abdominal pain; an 18% increased risk of percutaneous abdominal drainage; and a 15% increased risk of needing another operation in the same admission.
Dr. Bailey also broke down overall risks by DSM-IV diagnosis.
• Patients with a mood disorder were 35% more likely to have a prolonged length of stay and 13% more likely to have a surgical complication.
• Patients with an anxiety disorder were 16% more likely to have a prolonged length of stay and 10% more likely to have a complication.
• Patients with schizophrenia were 77% more likely to have a prolonged length of stay, 3% more likely to die, and 28% more likely to have a complication.
• Patients with substance abuse were 70% more likely to have a prolonged length of stay, 6% more likely to die, and 39% more likely to have a complication.
Interestingly, Dr. Bailey said, the risk of in-hospital death was 16% lower in patients with a mood disorder, 59% lower in those with an anxiety disorder, and 77% lower in those with an impulse control disorder.
She stressed that the National Inpatient Sample provides a limited look into a patient’s hospital experience. The study can’t assess how long patients were sick before they came to the hospital, their medications or medication adherence, or how well they managed their mental and physical comorbidities.
“While we lacked the means to delve into potential clinical mediators, look at unplanned readmissions, or the use of inpatient psychiatric consults, we can clearly see the association with worse surgical outcomes,” Dr. Bailey said. “Recognizing this is the first step in learning how to optimize care for this frequently marginalized population.”
She had no financial disclosures.
[email protected]
On Twitter @Alz_Gal
LAS VEGAS – A comorbid mental illness may predispose surgical patients to poor outcomes, increasing the risk of postoperative complications, a prolonged length of stay, and – in some cases – even in-hospital mortality.
The link between mental illness and physical response to surgery is not well elucidated, and is likely an extremely complicated one, Elizabeth Bailey, MD, said at the Association for Academic Surgery/Society of University Surgeons Academic Surgical Congress.
Dr. Bailey said there is an extreme paucity of data on the relationship between mental illness and surgical outcomes. To investigate it, she examined 580,000 patient records contained in the National Inpatient Sample.
The cases spanned 2009-2011 and represented the four most common surgical procedures in the United States: cholecystectomy, appendectomy, adhesion excision/lysis, and colorectal resection.
She compared surgical outcomes among patients without a DSM-IV diagnosis and those with one of the five most common: mood disorder, anxiety, impulse control, schizophrenia, and substance abuse disorder.
The study’s primary outcomes were length of hospital stay, in-hospital mortality, and postoperative complications. Her analysis controlled for age, gender, race, admission status, operative approach, non–mental health comorbidities, insurance, and income.
Of the 580,000 in the study group 7% (39,000) had at least one of the mental health comorbidities. Mood disorder was the most common (59%), followed by substance abuse (24%), schizophrenia (13%), anxiety disorder (12%), and impulse control disorder (5%).
There were a number of significant baseline differences between those with a mental diagnosis and those without. Those with a DSM-IV diagnosis were younger (52 vs. 54 years), more often women (61% vs. 57%), and white (78% vs. 69%). They more often had additional physical comorbidities (80% vs. 68%). They were more likely to be admitted through the emergency room (74% vs. 71%), to have nonlaparoscopic surgery (60% vs 63%), to be on public insurance (53% vs. 43%), and to be in the lowest income quartile (28% vs. 25%).
Surgical outcomes were almost universally significantly worse among these patients. They were 41% more likely to experience a prolonged length of stay and 18% more likely to experience a complication. These included wound disruption, ileus, and small bowel obstruction. They faced a 24% increased risk for needing total parenteral nutrition; a 29% increased risk of abdominal pain; an 18% increased risk of percutaneous abdominal drainage; and a 15% increased risk of needing another operation in the same admission.
Dr. Bailey also broke down overall risks by DSM-IV diagnosis.
• Patients with a mood disorder were 35% more likely to have a prolonged length of stay and 13% more likely to have a surgical complication.
• Patients with an anxiety disorder were 16% more likely to have a prolonged length of stay and 10% more likely to have a complication.
• Patients with schizophrenia were 77% more likely to have a prolonged length of stay, 3% more likely to die, and 28% more likely to have a complication.
• Patients with substance abuse were 70% more likely to have a prolonged length of stay, 6% more likely to die, and 39% more likely to have a complication.
Interestingly, Dr. Bailey said, the risk of in-hospital death was 16% lower in patients with a mood disorder, 59% lower in those with an anxiety disorder, and 77% lower in those with an impulse control disorder.
She stressed that the National Inpatient Sample provides a limited look into a patient’s hospital experience. The study can’t assess how long patients were sick before they came to the hospital, their medications or medication adherence, or how well they managed their mental and physical comorbidities.
“While we lacked the means to delve into potential clinical mediators, look at unplanned readmissions, or the use of inpatient psychiatric consults, we can clearly see the association with worse surgical outcomes,” Dr. Bailey said. “Recognizing this is the first step in learning how to optimize care for this frequently marginalized population.”
She had no financial disclosures.
[email protected]
On Twitter @Alz_Gal
LAS VEGAS – A comorbid mental illness may predispose surgical patients to poor outcomes, increasing the risk of postoperative complications, a prolonged length of stay, and – in some cases – even in-hospital mortality.
The link between mental illness and physical response to surgery is not well elucidated, and is likely an extremely complicated one, Elizabeth Bailey, MD, said at the Association for Academic Surgery/Society of University Surgeons Academic Surgical Congress.
Dr. Bailey said there is an extreme paucity of data on the relationship between mental illness and surgical outcomes. To investigate it, she examined 580,000 patient records contained in the National Inpatient Sample.
The cases spanned 2009-2011 and represented the four most common surgical procedures in the United States: cholecystectomy, appendectomy, adhesion excision/lysis, and colorectal resection.
She compared surgical outcomes among patients without a DSM-IV diagnosis and those with one of the five most common: mood disorder, anxiety, impulse control, schizophrenia, and substance abuse disorder.
The study’s primary outcomes were length of hospital stay, in-hospital mortality, and postoperative complications. Her analysis controlled for age, gender, race, admission status, operative approach, non–mental health comorbidities, insurance, and income.
Of the 580,000 in the study group 7% (39,000) had at least one of the mental health comorbidities. Mood disorder was the most common (59%), followed by substance abuse (24%), schizophrenia (13%), anxiety disorder (12%), and impulse control disorder (5%).
There were a number of significant baseline differences between those with a mental diagnosis and those without. Those with a DSM-IV diagnosis were younger (52 vs. 54 years), more often women (61% vs. 57%), and white (78% vs. 69%). They more often had additional physical comorbidities (80% vs. 68%). They were more likely to be admitted through the emergency room (74% vs. 71%), to have nonlaparoscopic surgery (60% vs 63%), to be on public insurance (53% vs. 43%), and to be in the lowest income quartile (28% vs. 25%).
Surgical outcomes were almost universally significantly worse among these patients. They were 41% more likely to experience a prolonged length of stay and 18% more likely to experience a complication. These included wound disruption, ileus, and small bowel obstruction. They faced a 24% increased risk for needing total parenteral nutrition; a 29% increased risk of abdominal pain; an 18% increased risk of percutaneous abdominal drainage; and a 15% increased risk of needing another operation in the same admission.
Dr. Bailey also broke down overall risks by DSM-IV diagnosis.
• Patients with a mood disorder were 35% more likely to have a prolonged length of stay and 13% more likely to have a surgical complication.
• Patients with an anxiety disorder were 16% more likely to have a prolonged length of stay and 10% more likely to have a complication.
• Patients with schizophrenia were 77% more likely to have a prolonged length of stay, 3% more likely to die, and 28% more likely to have a complication.
• Patients with substance abuse were 70% more likely to have a prolonged length of stay, 6% more likely to die, and 39% more likely to have a complication.
Interestingly, Dr. Bailey said, the risk of in-hospital death was 16% lower in patients with a mood disorder, 59% lower in those with an anxiety disorder, and 77% lower in those with an impulse control disorder.
She stressed that the National Inpatient Sample provides a limited look into a patient’s hospital experience. The study can’t assess how long patients were sick before they came to the hospital, their medications or medication adherence, or how well they managed their mental and physical comorbidities.
“While we lacked the means to delve into potential clinical mediators, look at unplanned readmissions, or the use of inpatient psychiatric consults, we can clearly see the association with worse surgical outcomes,” Dr. Bailey said. “Recognizing this is the first step in learning how to optimize care for this frequently marginalized population.”
She had no financial disclosures.
[email protected]
On Twitter @Alz_Gal
AT THE ACADEMIC SURGICAL CONGRESS
Key clinical point:
Major finding: They were 41% more likely to experience a prolonged length of stay and 18% more likely to experience a complication.
Data source: The database review comprised 580,000 patients.
Disclosures: Dr. Bailey had no financial disclosures.
Scalp cooling reduces hair loss in 50% or more of women in separate studies
Scalp cooling resulted in significant reductions in hair loss in about half of all women who were treated before, during, and after chemotherapy for breast cancer in both the Scalp Cooling Alopecia Prevention (SCALP) randomized clinical trial and in a multicenter prospective cohort study.
However, the effects of the reduced alopecia on quality of life measures were mixed, according to the findings of the studies, which were published online in JAMA.
The findings of the multicenter SCALP trial are from a planned interim analysis of data from 95 women with breast cancer who were undergoing chemotherapy and who were randomized to undergo scalp cooling using the Orbis Paxman Hair Loss Prevention System (OPHLPS), and 47 controls. Successful hair preservation occurred in 50.5% of those in the scalp cooling group, compared with 0% of those in the control group – results which led to early study termination, reported Julie Nangia, MD, of Baylor College of Medicine, Houston, and her colleagues (JAMA 2017 Feb 14. doi: 10.1001/jama.2016.20939).
No serious adverse device-related events occurred in the cooling group, but there also were no significant differences between the groups with respect to changes in quality of life scales from baseline to chemotherapy cycle 4, the investigators found.
Study subjects were women with a mean age of 52.6 years who were receiving anthracycline-based chemotherapy (36%) or taxane-based chemotherapy (64%). Successful hair preservation was defined as grade 0 or 1 based on the Common Terminology Criteria for Adverse Events version 4.1 scale, representing no hair loss or less than 50% hair loss not requiring a wig, respectively. Five women had grade 0 hair loss, and 43 had grade 1 hair loss.
Quality of life was measured using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 (EORTC-QLQ-30), the Hospital Anxiety and Depression Scale (HADS), and a summary scale of the Body Image Scale. Changes in emotional and social functioning as measured using the EORTC-QLQ-30 did not differ between the groups, including among those with and without hair preservation, after four treatment cycles, and HADS anxiety and depression summary scores were normal both at baseline and after four cycles in both groups, regardless of hair preservation.
Patients will be followed for 5 years to assess for safety and overall survival, the investigators noted.
During a presentation of these findings at the San Antonio Breast Cancer Symposium in December, Dr. Nangia noted that the maker of the OPHLPS is seeking Food and Drug Administration clearance based on the findings, and if approved, the system would compete with the DigniCap (Dignitana AB), which has already received Food and Drug Administration clearance.*
The DigniCap was the device evaluated (at the time under an FDA investigational device exemption) in the prospective cohort study also published in JAMA.
In that study, 106 women receiving adjuvant or neoadjuvant chemotherapy for stage 1 or II breast cancer were treated with scalp cooling between August 2013 and October 2014, and, along with 16 control subjects, were followed for a median of 29.5 months. Self-estimated hair loss at 4 weeks after the last chemotherapy dose was 50% or less, based on the Dean scale (score of 0-2) in 67 of 101 evaluable patients in the scalp cooling group, vs. 0 of 16 in the control group, reported Dr. Hope S. Rugo, MD, of the Helen Diller Family Comprehensive Cancer Center, San Francisco, and her colleagues.

Five patients had no hair loss, and 62 had less than 50% hair loss, the investigators said (JAMA. 2017 Feb 14. doi: 10.1001/jama.2016.21038).
Three of five quality of life measures, as assessed using the EORTC-QLQ, were significantly better at 1 month after the end of chemotherapy vs. at baseline in the cooling group, compared with the control group. For example, 27.3% vs. 56.3% of treatment and control subjects, respectively, reported feeling less physically attractive. The results were similar among those with 50% or less hair loss vs. controls, they noted.
Adverse events associated with cooling included mild headache in four patients. Three patients discontinued treatment due to feeling cold.
The mean age of the women was 53 years. None of those in the treatment group received anthracyclines, thus further research is needed to assess scalp cooling outcomes after treatment with anthracycline regimens, the investigators said, noting that additional research is also needed to assess long-term measures of alopecia and adverse effects. Patients will be followed for a total of 5 years.
Taken together, the findings of these two studies suggest that increased use of scalp cooling is warranted, as it has the potential to both reduce a troublesome side effect of chemotherapy and to remove a common concern – and sometimes a deterrent – among women considering chemotherapy, according to Dawn L. Hershman, MD, of the Herbert Irving Comprehensive Cancer Center at Columbia University.

In an editorial, Dr. Hershman noted that adjuvant chemotherapy reduces the 10-year relative risk of death from breast cancer by about 35%, but that “a substantial number of women who are advised to undergo chemotherapy choose not to receive treatment because of concerns about adverse effects.”
About 50% of patients consider hair loss the most traumatic aspect of chemotherapy, and about 8% said they would decline chemotherapy because of concerns about hair loss, she said.
“Therefore an intervention that could reduce the adverse effects of chemotherapy may lead to improvement in the initiation and completion of therapy, in quality of life, and in survival outcomes,” she wrote (JAMA. 2017 Feb 14;317[6]:587-8).
At face value, the “reassuringly similar” findings from these two studies appear to represent a major step forward for improving the quality of life for individuals with cancer, she added, explaining that while the quality of life data suggest a limited effect, they should be interpreted with caution as the overall effects of the patients’ diagnoses, surgery, and treatment may have influenced the patient-reported outcomes, diminishing the likelihood of detecting differences in quality of life associated with lower rates of alopecia.
Further, the unblinded nature of the intervention may also bias patient-reported outcomes results, she said, adding that “better measures may be needed to capture the effect of treatments on outcomes that are meaningful to patients so that important adverse effects are fully captured in comparative clinical trials.”
Although questions about cost and coverage of scalp cooling remain, Dr. Hershman concluded that until chemotherapy is no longer necessary and some of the distressing adverse effects of cancer treatment can be avoided, interventions such as scalp cooling that can reduce or eliminate toxic effects will help ease the distress and may thereby improve outcomes for patients with breast cancer.
In a separate editorial, Howard (Jack) West, MD, of the Swedish Cancer Institute in Seattle, further notes that a “lingering concern” with respect to scalp cooling is “the speculated potential for increased scalp metastases ... owing to poor local circulation of chemotherapy.”
However, this has not been observed in studies to date, he noted (JAMA. 2017 Feb 14. doi: 10.1001/jamaoncol.2017.0051).
“While some may argue that we need long-term data on timing and patterns of recurrence as well as overall survival to ensure that there is no increased risk of scalp metastases or otherwise compromised outcomes for scalp cooling, there is no evidence thus far to suggest this,” he said, concluding that “it is arguable that growing attention on interventions to reduce chemotherapy-induced alopecia are reaching an inflection point that justifies far more widespread adoption.”
The SCALP trial was supported by Paxman Coolers Ltd. Dr. Nangia reported having no disclosures. The study by Dr. Rugo et al. was funded in part by Dignitana AB, the Laszlo Tauber Family Foundation, the Anne Moore Breast Cancer Research Fund, and the Friedman Family Foundation. Dr. Rugo, Dr. Hershman, and Dr. West reported having no disclosures.
*Correction, 4/5/17: An earlier version of this article misstated the device's FDA status.
Scalp cooling resulted in significant reductions in hair loss in about half of all women who were treated before, during, and after chemotherapy for breast cancer in both the Scalp Cooling Alopecia Prevention (SCALP) randomized clinical trial and in a multicenter prospective cohort study.
However, the effects of the reduced alopecia on quality of life measures were mixed, according to the findings of the studies, which were published online in JAMA.
The findings of the multicenter SCALP trial are from a planned interim analysis of data from 95 women with breast cancer who were undergoing chemotherapy and who were randomized to undergo scalp cooling using the Orbis Paxman Hair Loss Prevention System (OPHLPS), and 47 controls. Successful hair preservation occurred in 50.5% of those in the scalp cooling group, compared with 0% of those in the control group – results which led to early study termination, reported Julie Nangia, MD, of Baylor College of Medicine, Houston, and her colleagues (JAMA 2017 Feb 14. doi: 10.1001/jama.2016.20939).
No serious adverse device-related events occurred in the cooling group, but there also were no significant differences between the groups with respect to changes in quality of life scales from baseline to chemotherapy cycle 4, the investigators found.
Study subjects were women with a mean age of 52.6 years who were receiving anthracycline-based chemotherapy (36%) or taxane-based chemotherapy (64%). Successful hair preservation was defined as grade 0 or 1 based on the Common Terminology Criteria for Adverse Events version 4.1 scale, representing no hair loss or less than 50% hair loss not requiring a wig, respectively. Five women had grade 0 hair loss, and 43 had grade 1 hair loss.
Quality of life was measured using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 (EORTC-QLQ-30), the Hospital Anxiety and Depression Scale (HADS), and a summary scale of the Body Image Scale. Changes in emotional and social functioning as measured using the EORTC-QLQ-30 did not differ between the groups, including among those with and without hair preservation, after four treatment cycles, and HADS anxiety and depression summary scores were normal both at baseline and after four cycles in both groups, regardless of hair preservation.
Patients will be followed for 5 years to assess for safety and overall survival, the investigators noted.
During a presentation of these findings at the San Antonio Breast Cancer Symposium in December, Dr. Nangia noted that the maker of the OPHLPS is seeking Food and Drug Administration clearance based on the findings, and if approved, the system would compete with the DigniCap (Dignitana AB), which has already received Food and Drug Administration clearance.*
The DigniCap was the device evaluated (at the time under an FDA investigational device exemption) in the prospective cohort study also published in JAMA.
In that study, 106 women receiving adjuvant or neoadjuvant chemotherapy for stage 1 or II breast cancer were treated with scalp cooling between August 2013 and October 2014, and, along with 16 control subjects, were followed for a median of 29.5 months. Self-estimated hair loss at 4 weeks after the last chemotherapy dose was 50% or less, based on the Dean scale (score of 0-2) in 67 of 101 evaluable patients in the scalp cooling group, vs. 0 of 16 in the control group, reported Dr. Hope S. Rugo, MD, of the Helen Diller Family Comprehensive Cancer Center, San Francisco, and her colleagues.
Five patients had no hair loss, and 62 had less than 50% hair loss, the investigators said (JAMA. 2017 Feb 14. doi: 10.1001/jama.2016.21038).
Three of five quality of life measures, as assessed using the EORTC-QLQ, were significantly better at 1 month after the end of chemotherapy vs. at baseline in the cooling group, compared with the control group. For example, 27.3% vs. 56.3% of treatment and control subjects, respectively, reported feeling less physically attractive. The results were similar among those with 50% or less hair loss vs. controls, they noted.
Adverse events associated with cooling included mild headache in four patients. Three patients discontinued treatment due to feeling cold.
The mean age of the women was 53 years. None of those in the treatment group received anthracyclines, thus further research is needed to assess scalp cooling outcomes after treatment with anthracycline regimens, the investigators said, noting that additional research is also needed to assess long-term measures of alopecia and adverse effects. Patients will be followed for a total of 5 years.
Taken together, the findings of these two studies suggest that increased use of scalp cooling is warranted, as it has the potential to both reduce a troublesome side effect of chemotherapy and to remove a common concern – and sometimes a deterrent – among women considering chemotherapy, according to Dawn L. Hershman, MD, of the Herbert Irving Comprehensive Cancer Center at Columbia University.
In an editorial, Dr. Hershman noted that adjuvant chemotherapy reduces the 10-year relative risk of death from breast cancer by about 35%, but that “a substantial number of women who are advised to undergo chemotherapy choose not to receive treatment because of concerns about adverse effects.”
About 50% of patients consider hair loss the most traumatic aspect of chemotherapy, and about 8% said they would decline chemotherapy because of concerns about hair loss, she said.
“Therefore an intervention that could reduce the adverse effects of chemotherapy may lead to improvement in the initiation and completion of therapy, in quality of life, and in survival outcomes,” she wrote (JAMA. 2017 Feb 14;317[6]:587-8).
At face value, the “reassuringly similar” findings from these two studies appear to represent a major step forward for improving the quality of life for individuals with cancer, she added, explaining that while the quality of life data suggest a limited effect, they should be interpreted with caution as the overall effects of the patients’ diagnoses, surgery, and treatment may have influenced the patient-reported outcomes, diminishing the likelihood of detecting differences in quality of life associated with lower rates of alopecia.
Further, the unblinded nature of the intervention may also bias patient-reported outcomes results, she said, adding that “better measures may be needed to capture the effect of treatments on outcomes that are meaningful to patients so that important adverse effects are fully captured in comparative clinical trials.”
Although questions about cost and coverage of scalp cooling remain, Dr. Hershman concluded that until chemotherapy is no longer necessary and some of the distressing adverse effects of cancer treatment can be avoided, interventions such as scalp cooling that can reduce or eliminate toxic effects will help ease the distress and may thereby improve outcomes for patients with breast cancer.
In a separate editorial, Howard (Jack) West, MD, of the Swedish Cancer Institute in Seattle, further notes that a “lingering concern” with respect to scalp cooling is “the speculated potential for increased scalp metastases ... owing to poor local circulation of chemotherapy.”
However, this has not been observed in studies to date, he noted (JAMA. 2017 Feb 14. doi: 10.1001/jamaoncol.2017.0051).
“While some may argue that we need long-term data on timing and patterns of recurrence as well as overall survival to ensure that there is no increased risk of scalp metastases or otherwise compromised outcomes for scalp cooling, there is no evidence thus far to suggest this,” he said, concluding that “it is arguable that growing attention on interventions to reduce chemotherapy-induced alopecia are reaching an inflection point that justifies far more widespread adoption.”
The SCALP trial was supported by Paxman Coolers Ltd. Dr. Nangia reported having no disclosures. The study by Dr. Rugo et al. was funded in part by Dignitana AB, the Laszlo Tauber Family Foundation, the Anne Moore Breast Cancer Research Fund, and the Friedman Family Foundation. Dr. Rugo, Dr. Hershman, and Dr. West reported having no disclosures.
*Correction, 4/5/17: An earlier version of this article misstated the device's FDA status.
Scalp cooling resulted in significant reductions in hair loss in about half of all women who were treated before, during, and after chemotherapy for breast cancer in both the Scalp Cooling Alopecia Prevention (SCALP) randomized clinical trial and in a multicenter prospective cohort study.
However, the effects of the reduced alopecia on quality of life measures were mixed, according to the findings of the studies, which were published online in JAMA.
The findings of the multicenter SCALP trial are from a planned interim analysis of data from 95 women with breast cancer who were undergoing chemotherapy and who were randomized to undergo scalp cooling using the Orbis Paxman Hair Loss Prevention System (OPHLPS), and 47 controls. Successful hair preservation occurred in 50.5% of those in the scalp cooling group, compared with 0% of those in the control group – results which led to early study termination, reported Julie Nangia, MD, of Baylor College of Medicine, Houston, and her colleagues (JAMA 2017 Feb 14. doi: 10.1001/jama.2016.20939).
No serious adverse device-related events occurred in the cooling group, but there also were no significant differences between the groups with respect to changes in quality of life scales from baseline to chemotherapy cycle 4, the investigators found.
Study subjects were women with a mean age of 52.6 years who were receiving anthracycline-based chemotherapy (36%) or taxane-based chemotherapy (64%). Successful hair preservation was defined as grade 0 or 1 based on the Common Terminology Criteria for Adverse Events version 4.1 scale, representing no hair loss or less than 50% hair loss not requiring a wig, respectively. Five women had grade 0 hair loss, and 43 had grade 1 hair loss.
Quality of life was measured using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 (EORTC-QLQ-30), the Hospital Anxiety and Depression Scale (HADS), and a summary scale of the Body Image Scale. Changes in emotional and social functioning as measured using the EORTC-QLQ-30 did not differ between the groups, including among those with and without hair preservation, after four treatment cycles, and HADS anxiety and depression summary scores were normal both at baseline and after four cycles in both groups, regardless of hair preservation.
Patients will be followed for 5 years to assess for safety and overall survival, the investigators noted.
During a presentation of these findings at the San Antonio Breast Cancer Symposium in December, Dr. Nangia noted that the maker of the OPHLPS is seeking Food and Drug Administration clearance based on the findings, and if approved, the system would compete with the DigniCap (Dignitana AB), which has already received Food and Drug Administration clearance.*
The DigniCap was the device evaluated (at the time under an FDA investigational device exemption) in the prospective cohort study also published in JAMA.
In that study, 106 women receiving adjuvant or neoadjuvant chemotherapy for stage 1 or II breast cancer were treated with scalp cooling between August 2013 and October 2014, and, along with 16 control subjects, were followed for a median of 29.5 months. Self-estimated hair loss at 4 weeks after the last chemotherapy dose was 50% or less, based on the Dean scale (score of 0-2) in 67 of 101 evaluable patients in the scalp cooling group, vs. 0 of 16 in the control group, reported Dr. Hope S. Rugo, MD, of the Helen Diller Family Comprehensive Cancer Center, San Francisco, and her colleagues.
Five patients had no hair loss, and 62 had less than 50% hair loss, the investigators said (JAMA. 2017 Feb 14. doi: 10.1001/jama.2016.21038).
Three of five quality of life measures, as assessed using the EORTC-QLQ, were significantly better at 1 month after the end of chemotherapy vs. at baseline in the cooling group, compared with the control group. For example, 27.3% vs. 56.3% of treatment and control subjects, respectively, reported feeling less physically attractive. The results were similar among those with 50% or less hair loss vs. controls, they noted.
Adverse events associated with cooling included mild headache in four patients. Three patients discontinued treatment due to feeling cold.
The mean age of the women was 53 years. None of those in the treatment group received anthracyclines, thus further research is needed to assess scalp cooling outcomes after treatment with anthracycline regimens, the investigators said, noting that additional research is also needed to assess long-term measures of alopecia and adverse effects. Patients will be followed for a total of 5 years.
Taken together, the findings of these two studies suggest that increased use of scalp cooling is warranted, as it has the potential to both reduce a troublesome side effect of chemotherapy and to remove a common concern – and sometimes a deterrent – among women considering chemotherapy, according to Dawn L. Hershman, MD, of the Herbert Irving Comprehensive Cancer Center at Columbia University.
In an editorial, Dr. Hershman noted that adjuvant chemotherapy reduces the 10-year relative risk of death from breast cancer by about 35%, but that “a substantial number of women who are advised to undergo chemotherapy choose not to receive treatment because of concerns about adverse effects.”
About 50% of patients consider hair loss the most traumatic aspect of chemotherapy, and about 8% said they would decline chemotherapy because of concerns about hair loss, she said.
“Therefore an intervention that could reduce the adverse effects of chemotherapy may lead to improvement in the initiation and completion of therapy, in quality of life, and in survival outcomes,” she wrote (JAMA. 2017 Feb 14;317[6]:587-8).
At face value, the “reassuringly similar” findings from these two studies appear to represent a major step forward for improving the quality of life for individuals with cancer, she added, explaining that while the quality of life data suggest a limited effect, they should be interpreted with caution as the overall effects of the patients’ diagnoses, surgery, and treatment may have influenced the patient-reported outcomes, diminishing the likelihood of detecting differences in quality of life associated with lower rates of alopecia.
Further, the unblinded nature of the intervention may also bias patient-reported outcomes results, she said, adding that “better measures may be needed to capture the effect of treatments on outcomes that are meaningful to patients so that important adverse effects are fully captured in comparative clinical trials.”
Although questions about cost and coverage of scalp cooling remain, Dr. Hershman concluded that until chemotherapy is no longer necessary and some of the distressing adverse effects of cancer treatment can be avoided, interventions such as scalp cooling that can reduce or eliminate toxic effects will help ease the distress and may thereby improve outcomes for patients with breast cancer.
In a separate editorial, Howard (Jack) West, MD, of the Swedish Cancer Institute in Seattle, further notes that a “lingering concern” with respect to scalp cooling is “the speculated potential for increased scalp metastases ... owing to poor local circulation of chemotherapy.”
However, this has not been observed in studies to date, he noted (JAMA. 2017 Feb 14. doi: 10.1001/jamaoncol.2017.0051).
“While some may argue that we need long-term data on timing and patterns of recurrence as well as overall survival to ensure that there is no increased risk of scalp metastases or otherwise compromised outcomes for scalp cooling, there is no evidence thus far to suggest this,” he said, concluding that “it is arguable that growing attention on interventions to reduce chemotherapy-induced alopecia are reaching an inflection point that justifies far more widespread adoption.”
The SCALP trial was supported by Paxman Coolers Ltd. Dr. Nangia reported having no disclosures. The study by Dr. Rugo et al. was funded in part by Dignitana AB, the Laszlo Tauber Family Foundation, the Anne Moore Breast Cancer Research Fund, and the Friedman Family Foundation. Dr. Rugo, Dr. Hershman, and Dr. West reported having no disclosures.
*Correction, 4/5/17: An earlier version of this article misstated the device's FDA status.
FROM JAMA
Key clinical point:
Major finding: About half of the treated women in both studies experienced reduced or no hair loss during chemotherapy.
Data source: A randomized clinical trial involving 142 women, and a prospective cohort study involving 122 women.
Disclosures: The SCALP trial was supported by Paxman Coolers Ltd. Dr. Nangia reported having no disclosures. The study by Dr. Rugo et al. was funded in part by Dignitana AB, the Laszlo Tauber Family Foundation, the Anne Moore Breast Cancer Research Fund, and the Friedman Family Foundation. Dr. Rugo, Dr. Hershman, and Dr. West reported having no disclosures.
Osteoarthritis in hip or knee can increase diabetes risk
Individuals who have osteoarthritis in the hip or knee are significantly more likely to develop diabetes than are people without the condition, according to findings from a population-based cohort study.
The relationship between osteoarthritis (OA) and new-onset diabetes was largely explained by the walking limitations brought on by OA, which was unsurprising to lead author Tetyana Kendzerska, MD, PhD, of the University of Toronto, who presented the study at the annual meeting of the Canadian Rheumatology Association.

But Dr. Kendzerska noted that even though “the World Health Organization has determined that osteoarthritis is the fastest growing chronic disease and the single most common cause of disability in older adults [and] the majority of people with OA have at least one other chronic condition – usually diabetes, high blood pressure, [or] heart disease ... few studies have examined the impact of OA on these other conditions, including on the development of diabetes.”
Dr. Kendzerska and her coauthors used existing data to study a population of 16,362 adults aged 55 or older who did not have diabetes at baseline enrollment during 1996-1998 and were then followed until 2014 for a median period of 13 years. The adults’ median age was 68 years and median body mass index was 25.3 kg/m2; 61% were female. Cox regression modeling was used to quantify any association found between osteoarthritis and diabetes.
A total of 1,637 (10%) had hip osteoarthritis, 2,431 (15%) had knee osteoarthritis, and 3,908 (24%) had some type of walking limitation. Over the course of the follow-up period, 3,539 (22%) developed diabetes. The risk for diabetes was significantly elevated in particular for individuals with two hip or knee joints with OA, where the hazard ratio was 1.25 (95% CI, 1.08-1.44; P = .003) for hips and 1.16 (95% CI, 1.04-1.29; P = .008) for knees, after adjustment for baseline age, sex, income, body mass index, preexisting hypertension and cardiovascular disease, and prior primary care exposure. However, further adjustment to the comparisons for walking limitation attenuated the relationships so that they were no longer statistically significant.
The next steps for research may be to assess the impact of evidence-based osteoarthritis care on mobility and metabolic derangements, she said.
Previous “studies have been limited by a number of methodological limitations, [such as] cross-sectional design or failure to control for other factors that may explain a relationship. Our study has addressed these limitations and thus provides important evidence to suggest that osteoarthritis-related difficulty walking contributes causally to the development of diabetes [but] now we need studies to show if effective treatment of hip and knee osteoarthritis can reduce diabetes risk.”
The Canadian Institutes of Health Research funded the study. Dr. Kendzerska did not report any relevant financial disclosures.
Individuals who have osteoarthritis in the hip or knee are significantly more likely to develop diabetes than are people without the condition, according to findings from a population-based cohort study.
The relationship between osteoarthritis (OA) and new-onset diabetes was largely explained by the walking limitations brought on by OA, which was unsurprising to lead author Tetyana Kendzerska, MD, PhD, of the University of Toronto, who presented the study at the annual meeting of the Canadian Rheumatology Association.
But Dr. Kendzerska noted that even though “the World Health Organization has determined that osteoarthritis is the fastest growing chronic disease and the single most common cause of disability in older adults [and] the majority of people with OA have at least one other chronic condition – usually diabetes, high blood pressure, [or] heart disease ... few studies have examined the impact of OA on these other conditions, including on the development of diabetes.”
Dr. Kendzerska and her coauthors used existing data to study a population of 16,362 adults aged 55 or older who did not have diabetes at baseline enrollment during 1996-1998 and were then followed until 2014 for a median period of 13 years. The adults’ median age was 68 years and median body mass index was 25.3 kg/m2; 61% were female. Cox regression modeling was used to quantify any association found between osteoarthritis and diabetes.
A total of 1,637 (10%) had hip osteoarthritis, 2,431 (15%) had knee osteoarthritis, and 3,908 (24%) had some type of walking limitation. Over the course of the follow-up period, 3,539 (22%) developed diabetes. The risk for diabetes was significantly elevated in particular for individuals with two hip or knee joints with OA, where the hazard ratio was 1.25 (95% CI, 1.08-1.44; P = .003) for hips and 1.16 (95% CI, 1.04-1.29; P = .008) for knees, after adjustment for baseline age, sex, income, body mass index, preexisting hypertension and cardiovascular disease, and prior primary care exposure. However, further adjustment to the comparisons for walking limitation attenuated the relationships so that they were no longer statistically significant.
The next steps for research may be to assess the impact of evidence-based osteoarthritis care on mobility and metabolic derangements, she said.
Previous “studies have been limited by a number of methodological limitations, [such as] cross-sectional design or failure to control for other factors that may explain a relationship. Our study has addressed these limitations and thus provides important evidence to suggest that osteoarthritis-related difficulty walking contributes causally to the development of diabetes [but] now we need studies to show if effective treatment of hip and knee osteoarthritis can reduce diabetes risk.”
The Canadian Institutes of Health Research funded the study. Dr. Kendzerska did not report any relevant financial disclosures.
Individuals who have osteoarthritis in the hip or knee are significantly more likely to develop diabetes than are people without the condition, according to findings from a population-based cohort study.
The relationship between osteoarthritis (OA) and new-onset diabetes was largely explained by the walking limitations brought on by OA, which was unsurprising to lead author Tetyana Kendzerska, MD, PhD, of the University of Toronto, who presented the study at the annual meeting of the Canadian Rheumatology Association.
But Dr. Kendzerska noted that even though “the World Health Organization has determined that osteoarthritis is the fastest growing chronic disease and the single most common cause of disability in older adults [and] the majority of people with OA have at least one other chronic condition – usually diabetes, high blood pressure, [or] heart disease ... few studies have examined the impact of OA on these other conditions, including on the development of diabetes.”
Dr. Kendzerska and her coauthors used existing data to study a population of 16,362 adults aged 55 or older who did not have diabetes at baseline enrollment during 1996-1998 and were then followed until 2014 for a median period of 13 years. The adults’ median age was 68 years and median body mass index was 25.3 kg/m2; 61% were female. Cox regression modeling was used to quantify any association found between osteoarthritis and diabetes.
A total of 1,637 (10%) had hip osteoarthritis, 2,431 (15%) had knee osteoarthritis, and 3,908 (24%) had some type of walking limitation. Over the course of the follow-up period, 3,539 (22%) developed diabetes. The risk for diabetes was significantly elevated in particular for individuals with two hip or knee joints with OA, where the hazard ratio was 1.25 (95% CI, 1.08-1.44; P = .003) for hips and 1.16 (95% CI, 1.04-1.29; P = .008) for knees, after adjustment for baseline age, sex, income, body mass index, preexisting hypertension and cardiovascular disease, and prior primary care exposure. However, further adjustment to the comparisons for walking limitation attenuated the relationships so that they were no longer statistically significant.
The next steps for research may be to assess the impact of evidence-based osteoarthritis care on mobility and metabolic derangements, she said.
Previous “studies have been limited by a number of methodological limitations, [such as] cross-sectional design or failure to control for other factors that may explain a relationship. Our study has addressed these limitations and thus provides important evidence to suggest that osteoarthritis-related difficulty walking contributes causally to the development of diabetes [but] now we need studies to show if effective treatment of hip and knee osteoarthritis can reduce diabetes risk.”
The Canadian Institutes of Health Research funded the study. Dr. Kendzerska did not report any relevant financial disclosures.
FROM THE CRA SCIENTIFIC CONFERENCE
Key clinical point:
Major finding: The risk for diabetes was significantly elevated for individuals with two hip or knee joints with OA, where the hazard ratio was 1.25 (95% CI, 1.08-1.44; P = .003) for hips and 1.16 (95% CI, 1.04-1.29; P = .008) for knees.
Data source: Population-based cohort study of 16,362 individuals without diabetes at baseline.
Disclosures: The Canadian Institutes of Health Research funded the study. Dr. Kendzerska did not report any relevant financial disclosures.
Hypertension in SLE pregnancy: Is it lupus flare or preeclampsia?
SNOWMASS, COLO. – No hard and fast test exists that would enable a physician to tell a flare of systemic lupus erythematosus from preeclampsia in a pregnant lupus patient who becomes hypertensive and ill, but there are highly useful clues, Bonnie L. Bermas, MD, said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“There is no perfect way of distinguishing between a lupus flare and preeclampsia. I’ve never walked away from the labor floor and said, ‘This is great – I know this is a lupus flare,’ or ‘I know this is preeclampsia.’ But you make your best guess as to which one it is, and that will inform your management,” explained Dr. Bermas, a rheumatologist and director of the clinical lupus program at Brigham and Women’s Hospital in Boston.

“Why do we care? Because if it’s preeclampsia the mother needs to be delivered immediately for her safety, while if it’s an SLE flare sometimes you can treat it and get the fetus to a more viable age. A 23-week-old baby isn’t at all likely to make it, but a 27-week-old could,” Dr. Bermas said.
The fact that the patient has thrombocytopenia isn’t helpful in making the distinction, since that feature is shared in common by SLE flares and preeclampsia. But the uric acid level is a useful clue.
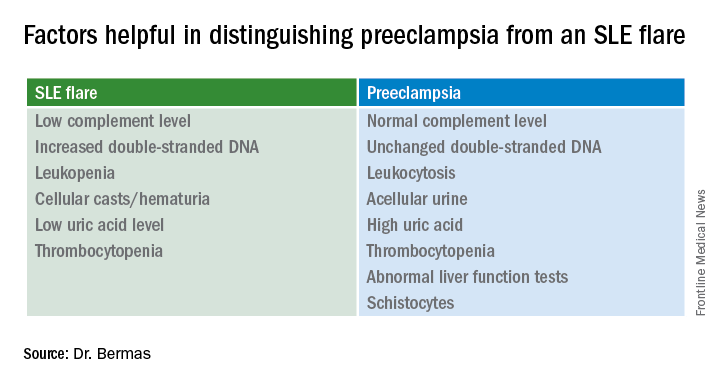
It’s quite possible that much of the current guesswork in predicting preeclampsia and other adverse pregnancy outcomes in lupus patients will give way to reliable risk testing within the next several years. Investigators in the U.S. multicenter prospective PROMISSE (Predictors of Pregnancy Outcome: Biomarkers in APL Syndrome and SLE) study have reported that circulating levels of the angiogenic factors soluble fms-like tyrosine kinase-1 and placental growth factor were abnormal as early as gestational weeks 12-15 in patients who went on to develop preeclampsia or other adverse pregnancy outcomes.
Indeed, monthly testing demonstrated that SLE patients in the top quartile for soluble fms-like tyrosine kinase-1 at weeks 12-15 had an adjusted 17.3-fold greater likelihood of experiencing a severe adverse pregnancy outcome than did those in the lowest quartile. A high level had a positive predictive value of 61% and a negative predictive value of 93% (Am J Obstet Gynecol. 2016 Jan;214[1]:108.e1-14). These findings are being further explored in ongoing studies.
“Hopefully, in another few years we’re going to be able to say early in pregnancy, ‘This person is set up to get preeclampsia.’ Maybe that will lead to better treatment as well,” Dr. Bermas said.
The risk of preeclampsia has been shown to be threefold higher in women with SLE than in the general population of pregnant women in a study of more than 16.7 million admissions for childbirth in the United States during a 4-year period. The SLE patients were also at 2.4-fold increased risk for preterm labor. Their risks of infection, thrombosis, thrombocytopenia, and transfusion were each three- to seven-fold higher as well (Am J Obstet Gynecol. 2008 Aug;199[2]:127.e1-16).
Dr. Bermas reported serving as a consultant to UCB.
SNOWMASS, COLO. – No hard and fast test exists that would enable a physician to tell a flare of systemic lupus erythematosus from preeclampsia in a pregnant lupus patient who becomes hypertensive and ill, but there are highly useful clues, Bonnie L. Bermas, MD, said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“There is no perfect way of distinguishing between a lupus flare and preeclampsia. I’ve never walked away from the labor floor and said, ‘This is great – I know this is a lupus flare,’ or ‘I know this is preeclampsia.’ But you make your best guess as to which one it is, and that will inform your management,” explained Dr. Bermas, a rheumatologist and director of the clinical lupus program at Brigham and Women’s Hospital in Boston.
“Why do we care? Because if it’s preeclampsia the mother needs to be delivered immediately for her safety, while if it’s an SLE flare sometimes you can treat it and get the fetus to a more viable age. A 23-week-old baby isn’t at all likely to make it, but a 27-week-old could,” Dr. Bermas said.
The fact that the patient has thrombocytopenia isn’t helpful in making the distinction, since that feature is shared in common by SLE flares and preeclampsia. But the uric acid level is a useful clue.
It’s quite possible that much of the current guesswork in predicting preeclampsia and other adverse pregnancy outcomes in lupus patients will give way to reliable risk testing within the next several years. Investigators in the U.S. multicenter prospective PROMISSE (Predictors of Pregnancy Outcome: Biomarkers in APL Syndrome and SLE) study have reported that circulating levels of the angiogenic factors soluble fms-like tyrosine kinase-1 and placental growth factor were abnormal as early as gestational weeks 12-15 in patients who went on to develop preeclampsia or other adverse pregnancy outcomes.
Indeed, monthly testing demonstrated that SLE patients in the top quartile for soluble fms-like tyrosine kinase-1 at weeks 12-15 had an adjusted 17.3-fold greater likelihood of experiencing a severe adverse pregnancy outcome than did those in the lowest quartile. A high level had a positive predictive value of 61% and a negative predictive value of 93% (Am J Obstet Gynecol. 2016 Jan;214[1]:108.e1-14). These findings are being further explored in ongoing studies.
“Hopefully, in another few years we’re going to be able to say early in pregnancy, ‘This person is set up to get preeclampsia.’ Maybe that will lead to better treatment as well,” Dr. Bermas said.
The risk of preeclampsia has been shown to be threefold higher in women with SLE than in the general population of pregnant women in a study of more than 16.7 million admissions for childbirth in the United States during a 4-year period. The SLE patients were also at 2.4-fold increased risk for preterm labor. Their risks of infection, thrombosis, thrombocytopenia, and transfusion were each three- to seven-fold higher as well (Am J Obstet Gynecol. 2008 Aug;199[2]:127.e1-16).
Dr. Bermas reported serving as a consultant to UCB.
SNOWMASS, COLO. – No hard and fast test exists that would enable a physician to tell a flare of systemic lupus erythematosus from preeclampsia in a pregnant lupus patient who becomes hypertensive and ill, but there are highly useful clues, Bonnie L. Bermas, MD, said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“There is no perfect way of distinguishing between a lupus flare and preeclampsia. I’ve never walked away from the labor floor and said, ‘This is great – I know this is a lupus flare,’ or ‘I know this is preeclampsia.’ But you make your best guess as to which one it is, and that will inform your management,” explained Dr. Bermas, a rheumatologist and director of the clinical lupus program at Brigham and Women’s Hospital in Boston.
“Why do we care? Because if it’s preeclampsia the mother needs to be delivered immediately for her safety, while if it’s an SLE flare sometimes you can treat it and get the fetus to a more viable age. A 23-week-old baby isn’t at all likely to make it, but a 27-week-old could,” Dr. Bermas said.
The fact that the patient has thrombocytopenia isn’t helpful in making the distinction, since that feature is shared in common by SLE flares and preeclampsia. But the uric acid level is a useful clue.
It’s quite possible that much of the current guesswork in predicting preeclampsia and other adverse pregnancy outcomes in lupus patients will give way to reliable risk testing within the next several years. Investigators in the U.S. multicenter prospective PROMISSE (Predictors of Pregnancy Outcome: Biomarkers in APL Syndrome and SLE) study have reported that circulating levels of the angiogenic factors soluble fms-like tyrosine kinase-1 and placental growth factor were abnormal as early as gestational weeks 12-15 in patients who went on to develop preeclampsia or other adverse pregnancy outcomes.
Indeed, monthly testing demonstrated that SLE patients in the top quartile for soluble fms-like tyrosine kinase-1 at weeks 12-15 had an adjusted 17.3-fold greater likelihood of experiencing a severe adverse pregnancy outcome than did those in the lowest quartile. A high level had a positive predictive value of 61% and a negative predictive value of 93% (Am J Obstet Gynecol. 2016 Jan;214[1]:108.e1-14). These findings are being further explored in ongoing studies.
“Hopefully, in another few years we’re going to be able to say early in pregnancy, ‘This person is set up to get preeclampsia.’ Maybe that will lead to better treatment as well,” Dr. Bermas said.
The risk of preeclampsia has been shown to be threefold higher in women with SLE than in the general population of pregnant women in a study of more than 16.7 million admissions for childbirth in the United States during a 4-year period. The SLE patients were also at 2.4-fold increased risk for preterm labor. Their risks of infection, thrombosis, thrombocytopenia, and transfusion were each three- to seven-fold higher as well (Am J Obstet Gynecol. 2008 Aug;199[2]:127.e1-16).
Dr. Bermas reported serving as a consultant to UCB.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM
Flu activity levels high in 23 states
The number of states at the highest level of flu activity jumped from 7 to 19 during the week ending Feb. 4, 2017, according to the Centers for Disease Control and Prevention.
The 19 states at level 10 on the CDC’s 1-10 scale of influenza-like illness (ILI) activity were largely concentrated in the South and lower Midwest, with another grouping mainly in the Mid-Atlantic. They were joined in the “high” range of ILI activity by four other states: Indiana and Minnesota at level 9 and New Mexico and Virginia at level 8, the CDC reported.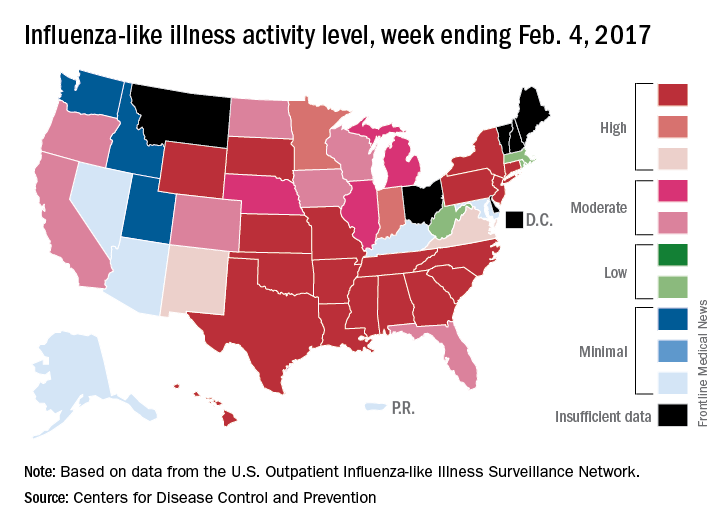
For the 2016-2017 season, 20 flu-related pediatric deaths have been reported: 5 were reported during the week ending Feb. 4, but 4 occurred during the week ending Jan. 28 and 1 occurred during the week ending Jan. 14, according to the CDC.
Since Oct. 1, 2016, there have been 6,804 laboratory-confirmed flu-related hospitalizations reported in the 13 states – including California, Georgia, New York, and Ohio – of the CDC’s Influenza Hospitalization Surveillance Network, for an overall hospitalization rate of 24.3 per 100,000 population. That rate, however, is “likely to be an underestimate as influenza-related hospitalizations can be missed, either because testing is not performed, or because cases may be attributed to other causes of pneumonia or other common influenza-related complications,” the CDC said.
The number of states at the highest level of flu activity jumped from 7 to 19 during the week ending Feb. 4, 2017, according to the Centers for Disease Control and Prevention.
The 19 states at level 10 on the CDC’s 1-10 scale of influenza-like illness (ILI) activity were largely concentrated in the South and lower Midwest, with another grouping mainly in the Mid-Atlantic. They were joined in the “high” range of ILI activity by four other states: Indiana and Minnesota at level 9 and New Mexico and Virginia at level 8, the CDC reported.
For the 2016-2017 season, 20 flu-related pediatric deaths have been reported: 5 were reported during the week ending Feb. 4, but 4 occurred during the week ending Jan. 28 and 1 occurred during the week ending Jan. 14, according to the CDC.
Since Oct. 1, 2016, there have been 6,804 laboratory-confirmed flu-related hospitalizations reported in the 13 states – including California, Georgia, New York, and Ohio – of the CDC’s Influenza Hospitalization Surveillance Network, for an overall hospitalization rate of 24.3 per 100,000 population. That rate, however, is “likely to be an underestimate as influenza-related hospitalizations can be missed, either because testing is not performed, or because cases may be attributed to other causes of pneumonia or other common influenza-related complications,” the CDC said.
The number of states at the highest level of flu activity jumped from 7 to 19 during the week ending Feb. 4, 2017, according to the Centers for Disease Control and Prevention.
The 19 states at level 10 on the CDC’s 1-10 scale of influenza-like illness (ILI) activity were largely concentrated in the South and lower Midwest, with another grouping mainly in the Mid-Atlantic. They were joined in the “high” range of ILI activity by four other states: Indiana and Minnesota at level 9 and New Mexico and Virginia at level 8, the CDC reported.
For the 2016-2017 season, 20 flu-related pediatric deaths have been reported: 5 were reported during the week ending Feb. 4, but 4 occurred during the week ending Jan. 28 and 1 occurred during the week ending Jan. 14, according to the CDC.
Since Oct. 1, 2016, there have been 6,804 laboratory-confirmed flu-related hospitalizations reported in the 13 states – including California, Georgia, New York, and Ohio – of the CDC’s Influenza Hospitalization Surveillance Network, for an overall hospitalization rate of 24.3 per 100,000 population. That rate, however, is “likely to be an underestimate as influenza-related hospitalizations can be missed, either because testing is not performed, or because cases may be attributed to other causes of pneumonia or other common influenza-related complications,” the CDC said.
Why can’t my patient have that miracle drug?
Modern medicine is truly blessed. Dermatology is no exception. With the development of more precise medications, our patients with severe psoriasis and atopic dermatitis no longer have to suffer in misery and social isolation. There is new hope for patients with metastatic melanoma. I recently watched President Jimmy Carter – a man with melanoma in his brain, certainly dead except for the advent of new drugs that are truly miraculous – release a rehabilitated sea turtle.
What is the drawback to such miracles? Cost! The cost of these medications can be extraordinary (hundreds of thousands of dollars a year); and guess what, everyone wants and needs their insurance plans to foot the bill for them. Biosimilars are not going to solve the cost issue, since biologic drugs are difficult to manufacture and get approved. The biosimilars are pricing in at only 5%-10% less than costs of the original biologic.

Drug costs obviously drive part of the increase in health care premiums. Insurance companies often make drug coverage as difficult as possible, which makes sense from the insurers’ point of view. They require prior authorizations, have restricted formularies, or even insist patients switch biologics in midstream for cost savings or because of manufacturer rebates.
Sometimes a patient has an adverse event, or even dies, because of insurance plan delays. How can this be legal? Isn’t this the practice of medicine? There ought to be a law!
There is a law. Meet the Employee Retirement Income Security Act (ERISA) of 1974 (Meyer JA. ERISA Preemption: Protecting Employer Laboratories of Health Care Reform. Washington, DC: New Directions for Policy; 1995).
ERISA not only protects pensions (and established individual retirement accounts) but also health benefits. ERISA restricts compensation in lawsuits against insurers to the value of the services withheld or delayed and supersedes state laws (State regulation of managed care and the Employee Retirement Income Security Act. Mariner WK, N Engl J Med. 1996 Dec 26;335[26]:1986-90). This minimal payout makes such lawsuits unattractive to law firms. This is why insurers have become so bold in ignoring physician requests for treatment of their patients. The insurers attitude is: “Go ahead, sue me! You won’t get anything!”
Now, as physicians, we are not only patient advocates, but we also must be husbanders of scarce resources. Should we not pursue 100% clearance of that patient with psoriasis? This issue is worth debating, as the medical reimbursement pond gets sucked dry by medication costs.
Still, if you really hate prior authorizations, demented formularies, step therapy, drug denials, and outright stalling of medical care, you should ask Congress to amend ERISA. In writing about Justice Ruth Bader Ginsburg’s concurring Supreme Court opinion in a 2004 case regarding ERISA (Aetna Health Inc. v. Davila 542 U.S. 200), legal expert David S. Senoff said that amending ERISA “may be the only mechanism to provide patients with adequate compensation for damages as a result of coverage decisions by employer-sponsored health plans.” (Senoff DS. An anticipated decision with far-reaching results. Legal Intelligencer. 2004;230:5-7).
Amending ERISA is not going to happen in our current political environment. I’m not even sure I would want it to happen, since it would raise insurance costs even higher, and could make insurance unaffordable for many more people. Still, you and your patients deserve to know the cause of medication denials. Also, I suspect you have no idea how much an insurance executive will twitch (and a liberal member of Congress will smile) when you mention the possibility of amending ERISA. So if you are having a particularly acrimonious argument with an insurance executive about patient drug coverage, pull this nuke out of your arsenal and rap him or her with it.
Dr. Coldiron is past president of the American Academy of Dermatology. He is currently in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at [email protected].
Modern medicine is truly blessed. Dermatology is no exception. With the development of more precise medications, our patients with severe psoriasis and atopic dermatitis no longer have to suffer in misery and social isolation. There is new hope for patients with metastatic melanoma. I recently watched President Jimmy Carter – a man with melanoma in his brain, certainly dead except for the advent of new drugs that are truly miraculous – release a rehabilitated sea turtle.
What is the drawback to such miracles? Cost! The cost of these medications can be extraordinary (hundreds of thousands of dollars a year); and guess what, everyone wants and needs their insurance plans to foot the bill for them. Biosimilars are not going to solve the cost issue, since biologic drugs are difficult to manufacture and get approved. The biosimilars are pricing in at only 5%-10% less than costs of the original biologic.
Drug costs obviously drive part of the increase in health care premiums. Insurance companies often make drug coverage as difficult as possible, which makes sense from the insurers’ point of view. They require prior authorizations, have restricted formularies, or even insist patients switch biologics in midstream for cost savings or because of manufacturer rebates.
Sometimes a patient has an adverse event, or even dies, because of insurance plan delays. How can this be legal? Isn’t this the practice of medicine? There ought to be a law!
There is a law. Meet the Employee Retirement Income Security Act (ERISA) of 1974 (Meyer JA. ERISA Preemption: Protecting Employer Laboratories of Health Care Reform. Washington, DC: New Directions for Policy; 1995).
ERISA not only protects pensions (and established individual retirement accounts) but also health benefits. ERISA restricts compensation in lawsuits against insurers to the value of the services withheld or delayed and supersedes state laws (State regulation of managed care and the Employee Retirement Income Security Act. Mariner WK, N Engl J Med. 1996 Dec 26;335[26]:1986-90). This minimal payout makes such lawsuits unattractive to law firms. This is why insurers have become so bold in ignoring physician requests for treatment of their patients. The insurers attitude is: “Go ahead, sue me! You won’t get anything!”
Now, as physicians, we are not only patient advocates, but we also must be husbanders of scarce resources. Should we not pursue 100% clearance of that patient with psoriasis? This issue is worth debating, as the medical reimbursement pond gets sucked dry by medication costs.
Still, if you really hate prior authorizations, demented formularies, step therapy, drug denials, and outright stalling of medical care, you should ask Congress to amend ERISA. In writing about Justice Ruth Bader Ginsburg’s concurring Supreme Court opinion in a 2004 case regarding ERISA (Aetna Health Inc. v. Davila 542 U.S. 200), legal expert David S. Senoff said that amending ERISA “may be the only mechanism to provide patients with adequate compensation for damages as a result of coverage decisions by employer-sponsored health plans.” (Senoff DS. An anticipated decision with far-reaching results. Legal Intelligencer. 2004;230:5-7).
Amending ERISA is not going to happen in our current political environment. I’m not even sure I would want it to happen, since it would raise insurance costs even higher, and could make insurance unaffordable for many more people. Still, you and your patients deserve to know the cause of medication denials. Also, I suspect you have no idea how much an insurance executive will twitch (and a liberal member of Congress will smile) when you mention the possibility of amending ERISA. So if you are having a particularly acrimonious argument with an insurance executive about patient drug coverage, pull this nuke out of your arsenal and rap him or her with it.
Dr. Coldiron is past president of the American Academy of Dermatology. He is currently in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at [email protected].
Modern medicine is truly blessed. Dermatology is no exception. With the development of more precise medications, our patients with severe psoriasis and atopic dermatitis no longer have to suffer in misery and social isolation. There is new hope for patients with metastatic melanoma. I recently watched President Jimmy Carter – a man with melanoma in his brain, certainly dead except for the advent of new drugs that are truly miraculous – release a rehabilitated sea turtle.
What is the drawback to such miracles? Cost! The cost of these medications can be extraordinary (hundreds of thousands of dollars a year); and guess what, everyone wants and needs their insurance plans to foot the bill for them. Biosimilars are not going to solve the cost issue, since biologic drugs are difficult to manufacture and get approved. The biosimilars are pricing in at only 5%-10% less than costs of the original biologic.
Drug costs obviously drive part of the increase in health care premiums. Insurance companies often make drug coverage as difficult as possible, which makes sense from the insurers’ point of view. They require prior authorizations, have restricted formularies, or even insist patients switch biologics in midstream for cost savings or because of manufacturer rebates.
Sometimes a patient has an adverse event, or even dies, because of insurance plan delays. How can this be legal? Isn’t this the practice of medicine? There ought to be a law!
There is a law. Meet the Employee Retirement Income Security Act (ERISA) of 1974 (Meyer JA. ERISA Preemption: Protecting Employer Laboratories of Health Care Reform. Washington, DC: New Directions for Policy; 1995).
ERISA not only protects pensions (and established individual retirement accounts) but also health benefits. ERISA restricts compensation in lawsuits against insurers to the value of the services withheld or delayed and supersedes state laws (State regulation of managed care and the Employee Retirement Income Security Act. Mariner WK, N Engl J Med. 1996 Dec 26;335[26]:1986-90). This minimal payout makes such lawsuits unattractive to law firms. This is why insurers have become so bold in ignoring physician requests for treatment of their patients. The insurers attitude is: “Go ahead, sue me! You won’t get anything!”
Now, as physicians, we are not only patient advocates, but we also must be husbanders of scarce resources. Should we not pursue 100% clearance of that patient with psoriasis? This issue is worth debating, as the medical reimbursement pond gets sucked dry by medication costs.
Still, if you really hate prior authorizations, demented formularies, step therapy, drug denials, and outright stalling of medical care, you should ask Congress to amend ERISA. In writing about Justice Ruth Bader Ginsburg’s concurring Supreme Court opinion in a 2004 case regarding ERISA (Aetna Health Inc. v. Davila 542 U.S. 200), legal expert David S. Senoff said that amending ERISA “may be the only mechanism to provide patients with adequate compensation for damages as a result of coverage decisions by employer-sponsored health plans.” (Senoff DS. An anticipated decision with far-reaching results. Legal Intelligencer. 2004;230:5-7).
Amending ERISA is not going to happen in our current political environment. I’m not even sure I would want it to happen, since it would raise insurance costs even higher, and could make insurance unaffordable for many more people. Still, you and your patients deserve to know the cause of medication denials. Also, I suspect you have no idea how much an insurance executive will twitch (and a liberal member of Congress will smile) when you mention the possibility of amending ERISA. So if you are having a particularly acrimonious argument with an insurance executive about patient drug coverage, pull this nuke out of your arsenal and rap him or her with it.
Dr. Coldiron is past president of the American Academy of Dermatology. He is currently in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Write to him at [email protected].