User login
Hearing Loss in People With Good Hearing
About 1 in 4 American adults who say they have good or excellent hearing has hearing damage. According to a Vital Signs report, much of the damage is due to everyday loud sounds, such as leaf blowers, concerts, even portable devices. The rumble of a washing machine approaches the 85 decibels at which extended exposure can cause hearing damage. Sixty seconds of listening to a nearby siren (120 dB) also can cause hearing damage.
CDC researchers analyzed > 3,500 hearing tests conducted on adult participants in the 2012 National Health and Nutrition Examination Survey. Of those participants, 20% who reported no job-related noise exposure nonetheless had hearing damage in a pattern usually caused by noise.
People may delay reporting hearing loss because they don’t know or won’t admit they have a problem, the CDC says. Only 46% of adults who reported having trouble hearing saw a health care provider (HCP) for their hearing in the past 5 years. But chronic noise exposure has been associated with worsening heart disease, increased blood pressure, and other adverse health effects.
The CDC suggests HCPs ask patients (even those as young as 20) about their hearing. For instance, they can ask, “Do you find it difficult to follow a conversation if there is background noise?” and “Can you usually hear and understand what someone says in a normal tone of voice when you can’t see that person’s face?”
At routine health care visits, the CDC suggests HCPs explain to patients how noise exposure can permanently damage hearing. They also suggest recommending earplugs or noise-canceling headphones. About 70% of people exposed to loud noise never or seldom wear hearing protection, CDC says. The CDC suggests advising patients to turn down the volume when watching TV, listening to music, and using earbuds or headphones, as well as asking whether patients are taking medicines that increase the risk of hearing damage. If patients show or report hearing problems, the CDC suggests HCPs examine their hearing or refer them to a hearing specialist.
About 1 in 4 American adults who say they have good or excellent hearing has hearing damage. According to a Vital Signs report, much of the damage is due to everyday loud sounds, such as leaf blowers, concerts, even portable devices. The rumble of a washing machine approaches the 85 decibels at which extended exposure can cause hearing damage. Sixty seconds of listening to a nearby siren (120 dB) also can cause hearing damage.
CDC researchers analyzed > 3,500 hearing tests conducted on adult participants in the 2012 National Health and Nutrition Examination Survey. Of those participants, 20% who reported no job-related noise exposure nonetheless had hearing damage in a pattern usually caused by noise.
People may delay reporting hearing loss because they don’t know or won’t admit they have a problem, the CDC says. Only 46% of adults who reported having trouble hearing saw a health care provider (HCP) for their hearing in the past 5 years. But chronic noise exposure has been associated with worsening heart disease, increased blood pressure, and other adverse health effects.
The CDC suggests HCPs ask patients (even those as young as 20) about their hearing. For instance, they can ask, “Do you find it difficult to follow a conversation if there is background noise?” and “Can you usually hear and understand what someone says in a normal tone of voice when you can’t see that person’s face?”
At routine health care visits, the CDC suggests HCPs explain to patients how noise exposure can permanently damage hearing. They also suggest recommending earplugs or noise-canceling headphones. About 70% of people exposed to loud noise never or seldom wear hearing protection, CDC says. The CDC suggests advising patients to turn down the volume when watching TV, listening to music, and using earbuds or headphones, as well as asking whether patients are taking medicines that increase the risk of hearing damage. If patients show or report hearing problems, the CDC suggests HCPs examine their hearing or refer them to a hearing specialist.
About 1 in 4 American adults who say they have good or excellent hearing has hearing damage. According to a Vital Signs report, much of the damage is due to everyday loud sounds, such as leaf blowers, concerts, even portable devices. The rumble of a washing machine approaches the 85 decibels at which extended exposure can cause hearing damage. Sixty seconds of listening to a nearby siren (120 dB) also can cause hearing damage.
CDC researchers analyzed > 3,500 hearing tests conducted on adult participants in the 2012 National Health and Nutrition Examination Survey. Of those participants, 20% who reported no job-related noise exposure nonetheless had hearing damage in a pattern usually caused by noise.
People may delay reporting hearing loss because they don’t know or won’t admit they have a problem, the CDC says. Only 46% of adults who reported having trouble hearing saw a health care provider (HCP) for their hearing in the past 5 years. But chronic noise exposure has been associated with worsening heart disease, increased blood pressure, and other adverse health effects.
The CDC suggests HCPs ask patients (even those as young as 20) about their hearing. For instance, they can ask, “Do you find it difficult to follow a conversation if there is background noise?” and “Can you usually hear and understand what someone says in a normal tone of voice when you can’t see that person’s face?”
At routine health care visits, the CDC suggests HCPs explain to patients how noise exposure can permanently damage hearing. They also suggest recommending earplugs or noise-canceling headphones. About 70% of people exposed to loud noise never or seldom wear hearing protection, CDC says. The CDC suggests advising patients to turn down the volume when watching TV, listening to music, and using earbuds or headphones, as well as asking whether patients are taking medicines that increase the risk of hearing damage. If patients show or report hearing problems, the CDC suggests HCPs examine their hearing or refer them to a hearing specialist.
Long-term safety, efficacy of hemophilia B therapy

Interim results from the B-YOND trial suggest prophylactic treatment with a recombinant factor IX Fc fusion protein (rFIXFc) can provide long-term safety and efficacy, according to researchers.
B-YOND is an extension study for adults and adolescents who completed the B-LONG study and children who completed the Kids B-LONG study.
In both trials, researchers tested rFIXFc in patients with hemophilia B.
The median duration of rFIXFc treatment has surpassed 3 years for the adults and adolescents enrolled in B-YOND and exceeded 1.5 years for children in this trial.
Researchers said the median annualized bleeding rates (ABRs) have been low in these patients, and none of the patients have developed inhibitors.
“The interim data from B-YOND confirm the safety profile of [rFIXFc] and show that adult, adolescent, and pediatric subjects maintained low annual bleed rates with prophylactic dosing of [rFIXFc] every 1 to 2 weeks,” said principal investigator John Pasi, MD, PhD, of Barts and the London School of Medicine and Dentistry in London, UK.
“These results come from the longest-term study of an extended half-life therapy for hemophilia B and provide physicians across the globe with important insights and information about the treatment of hemophilia B.”
The results were published in Thrombosis and Haemostasis.
The research was sponsored by Bioverativ Therapeutics Inc., the company developing rFIXFc (also known as eftrenonacog alfa and by the brand name Alprolix) in collaboration with Sobi. rFIXFc is approved to treat hemophilia B in the US, European Union, and other countries.
Treatment
B-YOND has enrolled 116 patients with hemophilia B who completed B-LONG (n=93) or Kids B-LONG (n=23). The patients were placed in 1 of 4 treatment groups (but could change at any point):
- Weekly prophylaxis—20 to 100 IU/kg every 7 days (50 adults/adolescents, 19 children)
- Individualized prophylaxis—100 IU/kg every 8 to 16 days (30 adults/adolescents, 5 children)
- Modified prophylaxis, which was defined as further dosing personalization to optimize prophylaxis (13 adults/adolescents, 1 child)
- Episodic treatment, which was available only to adults and adolescents (n=15).
In the weekly prophylaxis group, the median dosing interval was 7.0 days for adults, adolescents, and children. The average weekly prophylactic dose was 49.5 IU/kg in adults/adolescents, 64.4 IU/kg in kids younger than 6, and 63.1 IU/kg in kids ages 6 to 11.
In the individualized prophylaxis group, the median dosing interval was 13.7 days for adults and adolescents and 10.0 days in pediatric patients (ages 6 to 11 only). The average weekly prophylactic dose was 50.2 IU/kg in adults/adolescents, and 66.6 IU/kg in kids ages 6 to 11.
In the modified prophylaxis group, the median dosing interval was 6.9 days for adults and adolescents and 4.1 days in the single pediatric patient (who was older than 6). The average weekly prophylactic dose was 61.7 IU/kg in adults/adolescents and 157.9 IU/kg in the pediatric patient.
From the start of B-LONG to the B-YOND interim data cut, adults/adolescents had a median of 39.5 months of cumulative rFIXFc treatment and a median of 162 cumulative exposure days.
From the start of Kids B-LONG to the data cut, pediatric patients had a median of 21.9 months of cumulative rFIXFc treatment and a median of 94 cumulative exposure days.
ABRs
As of the interim data cut, the overall median ABR was 2.3 for adults/adolescents in both the weekly and individualized prophylaxis groups.
The median ABR was 2.4 for adults/adolescents in the modified prophylaxis group and 11.3 for those receiving on-demand treatment.
Among children under age 6 (n=9), the median ABR in the weekly prophylaxis group was 0. (None of the younger children had individualized or modified prophylaxis.)
For children ages 6 to 11, the median ABR was 2.7 in the weekly prophylaxis group (n=10) and 2.4 in the individualized prophylaxis group (n=5). The patient in the modified prophylaxis group had an ABR of 3.1.
Safety
The researchers said rFIXFc was well-tolerated, and the adverse events (AEs) reported were typical of the population studied.
AEs were reported in 75.9% of patients. The most common were headache (n=14, 12.1%) and common cold (n=13, 11.2%), and the majority of AEs were considered unrelated to rFIXFc.
Three adult/adolescent patients experienced AEs during B-YOND that were considered treatment-related, including noncardiac chest pain, hematuria, and obstructive uropathy. All 3 events resolved.
One patient experienced breath odor during B-LONG that was considered treatment-related. And 1 patient reported decreased appetite during Kids B-LONG that was considered treatment-related. Neither of these events resolved.
There were 39 serious AEs in 23 patients (19.8%). All but 1 of these events were considered unrelated to rFIXFc.
The treatment-related serious AE was renal colic in a patient originally enrolled in the B-LONG study. The patient had a medical history of previous clot colic. The event resolved and did not lead to study discontinuation.
There have been no reports of serious allergic reactions or anaphylaxis associated with rFIXFc, no vascular thrombotic events, and no deaths. ![]()
Interim results from the B-YOND trial suggest prophylactic treatment with a recombinant factor IX Fc fusion protein (rFIXFc) can provide long-term safety and efficacy, according to researchers.
B-YOND is an extension study for adults and adolescents who completed the B-LONG study and children who completed the Kids B-LONG study.
In both trials, researchers tested rFIXFc in patients with hemophilia B.
The median duration of rFIXFc treatment has surpassed 3 years for the adults and adolescents enrolled in B-YOND and exceeded 1.5 years for children in this trial.
Researchers said the median annualized bleeding rates (ABRs) have been low in these patients, and none of the patients have developed inhibitors.
“The interim data from B-YOND confirm the safety profile of [rFIXFc] and show that adult, adolescent, and pediatric subjects maintained low annual bleed rates with prophylactic dosing of [rFIXFc] every 1 to 2 weeks,” said principal investigator John Pasi, MD, PhD, of Barts and the London School of Medicine and Dentistry in London, UK.
“These results come from the longest-term study of an extended half-life therapy for hemophilia B and provide physicians across the globe with important insights and information about the treatment of hemophilia B.”
The results were published in Thrombosis and Haemostasis.
The research was sponsored by Bioverativ Therapeutics Inc., the company developing rFIXFc (also known as eftrenonacog alfa and by the brand name Alprolix) in collaboration with Sobi. rFIXFc is approved to treat hemophilia B in the US, European Union, and other countries.
Treatment
B-YOND has enrolled 116 patients with hemophilia B who completed B-LONG (n=93) or Kids B-LONG (n=23). The patients were placed in 1 of 4 treatment groups (but could change at any point):
- Weekly prophylaxis—20 to 100 IU/kg every 7 days (50 adults/adolescents, 19 children)
- Individualized prophylaxis—100 IU/kg every 8 to 16 days (30 adults/adolescents, 5 children)
- Modified prophylaxis, which was defined as further dosing personalization to optimize prophylaxis (13 adults/adolescents, 1 child)
- Episodic treatment, which was available only to adults and adolescents (n=15).
In the weekly prophylaxis group, the median dosing interval was 7.0 days for adults, adolescents, and children. The average weekly prophylactic dose was 49.5 IU/kg in adults/adolescents, 64.4 IU/kg in kids younger than 6, and 63.1 IU/kg in kids ages 6 to 11.
In the individualized prophylaxis group, the median dosing interval was 13.7 days for adults and adolescents and 10.0 days in pediatric patients (ages 6 to 11 only). The average weekly prophylactic dose was 50.2 IU/kg in adults/adolescents, and 66.6 IU/kg in kids ages 6 to 11.
In the modified prophylaxis group, the median dosing interval was 6.9 days for adults and adolescents and 4.1 days in the single pediatric patient (who was older than 6). The average weekly prophylactic dose was 61.7 IU/kg in adults/adolescents and 157.9 IU/kg in the pediatric patient.
From the start of B-LONG to the B-YOND interim data cut, adults/adolescents had a median of 39.5 months of cumulative rFIXFc treatment and a median of 162 cumulative exposure days.
From the start of Kids B-LONG to the data cut, pediatric patients had a median of 21.9 months of cumulative rFIXFc treatment and a median of 94 cumulative exposure days.
ABRs
As of the interim data cut, the overall median ABR was 2.3 for adults/adolescents in both the weekly and individualized prophylaxis groups.
The median ABR was 2.4 for adults/adolescents in the modified prophylaxis group and 11.3 for those receiving on-demand treatment.
Among children under age 6 (n=9), the median ABR in the weekly prophylaxis group was 0. (None of the younger children had individualized or modified prophylaxis.)
For children ages 6 to 11, the median ABR was 2.7 in the weekly prophylaxis group (n=10) and 2.4 in the individualized prophylaxis group (n=5). The patient in the modified prophylaxis group had an ABR of 3.1.
Safety
The researchers said rFIXFc was well-tolerated, and the adverse events (AEs) reported were typical of the population studied.
AEs were reported in 75.9% of patients. The most common were headache (n=14, 12.1%) and common cold (n=13, 11.2%), and the majority of AEs were considered unrelated to rFIXFc.
Three adult/adolescent patients experienced AEs during B-YOND that were considered treatment-related, including noncardiac chest pain, hematuria, and obstructive uropathy. All 3 events resolved.
One patient experienced breath odor during B-LONG that was considered treatment-related. And 1 patient reported decreased appetite during Kids B-LONG that was considered treatment-related. Neither of these events resolved.
There were 39 serious AEs in 23 patients (19.8%). All but 1 of these events were considered unrelated to rFIXFc.
The treatment-related serious AE was renal colic in a patient originally enrolled in the B-LONG study. The patient had a medical history of previous clot colic. The event resolved and did not lead to study discontinuation.
There have been no reports of serious allergic reactions or anaphylaxis associated with rFIXFc, no vascular thrombotic events, and no deaths. ![]()
Interim results from the B-YOND trial suggest prophylactic treatment with a recombinant factor IX Fc fusion protein (rFIXFc) can provide long-term safety and efficacy, according to researchers.
B-YOND is an extension study for adults and adolescents who completed the B-LONG study and children who completed the Kids B-LONG study.
In both trials, researchers tested rFIXFc in patients with hemophilia B.
The median duration of rFIXFc treatment has surpassed 3 years for the adults and adolescents enrolled in B-YOND and exceeded 1.5 years for children in this trial.
Researchers said the median annualized bleeding rates (ABRs) have been low in these patients, and none of the patients have developed inhibitors.
“The interim data from B-YOND confirm the safety profile of [rFIXFc] and show that adult, adolescent, and pediatric subjects maintained low annual bleed rates with prophylactic dosing of [rFIXFc] every 1 to 2 weeks,” said principal investigator John Pasi, MD, PhD, of Barts and the London School of Medicine and Dentistry in London, UK.
“These results come from the longest-term study of an extended half-life therapy for hemophilia B and provide physicians across the globe with important insights and information about the treatment of hemophilia B.”
The results were published in Thrombosis and Haemostasis.
The research was sponsored by Bioverativ Therapeutics Inc., the company developing rFIXFc (also known as eftrenonacog alfa and by the brand name Alprolix) in collaboration with Sobi. rFIXFc is approved to treat hemophilia B in the US, European Union, and other countries.
Treatment
B-YOND has enrolled 116 patients with hemophilia B who completed B-LONG (n=93) or Kids B-LONG (n=23). The patients were placed in 1 of 4 treatment groups (but could change at any point):
- Weekly prophylaxis—20 to 100 IU/kg every 7 days (50 adults/adolescents, 19 children)
- Individualized prophylaxis—100 IU/kg every 8 to 16 days (30 adults/adolescents, 5 children)
- Modified prophylaxis, which was defined as further dosing personalization to optimize prophylaxis (13 adults/adolescents, 1 child)
- Episodic treatment, which was available only to adults and adolescents (n=15).
In the weekly prophylaxis group, the median dosing interval was 7.0 days for adults, adolescents, and children. The average weekly prophylactic dose was 49.5 IU/kg in adults/adolescents, 64.4 IU/kg in kids younger than 6, and 63.1 IU/kg in kids ages 6 to 11.
In the individualized prophylaxis group, the median dosing interval was 13.7 days for adults and adolescents and 10.0 days in pediatric patients (ages 6 to 11 only). The average weekly prophylactic dose was 50.2 IU/kg in adults/adolescents, and 66.6 IU/kg in kids ages 6 to 11.
In the modified prophylaxis group, the median dosing interval was 6.9 days for adults and adolescents and 4.1 days in the single pediatric patient (who was older than 6). The average weekly prophylactic dose was 61.7 IU/kg in adults/adolescents and 157.9 IU/kg in the pediatric patient.
From the start of B-LONG to the B-YOND interim data cut, adults/adolescents had a median of 39.5 months of cumulative rFIXFc treatment and a median of 162 cumulative exposure days.
From the start of Kids B-LONG to the data cut, pediatric patients had a median of 21.9 months of cumulative rFIXFc treatment and a median of 94 cumulative exposure days.
ABRs
As of the interim data cut, the overall median ABR was 2.3 for adults/adolescents in both the weekly and individualized prophylaxis groups.
The median ABR was 2.4 for adults/adolescents in the modified prophylaxis group and 11.3 for those receiving on-demand treatment.
Among children under age 6 (n=9), the median ABR in the weekly prophylaxis group was 0. (None of the younger children had individualized or modified prophylaxis.)
For children ages 6 to 11, the median ABR was 2.7 in the weekly prophylaxis group (n=10) and 2.4 in the individualized prophylaxis group (n=5). The patient in the modified prophylaxis group had an ABR of 3.1.
Safety
The researchers said rFIXFc was well-tolerated, and the adverse events (AEs) reported were typical of the population studied.
AEs were reported in 75.9% of patients. The most common were headache (n=14, 12.1%) and common cold (n=13, 11.2%), and the majority of AEs were considered unrelated to rFIXFc.
Three adult/adolescent patients experienced AEs during B-YOND that were considered treatment-related, including noncardiac chest pain, hematuria, and obstructive uropathy. All 3 events resolved.
One patient experienced breath odor during B-LONG that was considered treatment-related. And 1 patient reported decreased appetite during Kids B-LONG that was considered treatment-related. Neither of these events resolved.
There were 39 serious AEs in 23 patients (19.8%). All but 1 of these events were considered unrelated to rFIXFc.
The treatment-related serious AE was renal colic in a patient originally enrolled in the B-LONG study. The patient had a medical history of previous clot colic. The event resolved and did not lead to study discontinuation.
There have been no reports of serious allergic reactions or anaphylaxis associated with rFIXFc, no vascular thrombotic events, and no deaths. ![]()
Group reports rejuvenation of aging HSCs
Preclinical research suggests osteopontin, a protein made by osteoblasts, plays a role in hematopoietic stem cell (HSC) aging.
Experiments in mice revealed that, with age, there is a reduction in the expression of osteopontin in the bone marrow stroma.
A lack of osteopontin induced young HSCs to “act” older, while treating older HSCs with recombinant osteopontin restored youthful properties.
Hartmut Geiger, PhD, of the University of Ulm in Germany, and his colleagues reported these findings in EMBO.
“We show that the place where HSCs form in the bone marrow loses osteopontin upon aging, but if you give back the missing protein to the blood-forming cells, they suddenly rejuvenate and act younger,” Dr Geiger said.
“Our study points to exciting, novel ways to have a better immune system and possibly less blood cancer upon aging by therapeutically targeting the place where blood stem cells form.”
The researchers conducted a number of experiments to test the formation and vitality of cells in and near the bone marrow microenvironment.
The team looked at the formation of endosteum stroma cells in aging mice and monitored levels of osteopontin and other proteins linked to distinct cells in the bone marrow during the aging process.
The researchers said they observed reduced production of osteoblasts and other stroma cells in the endosteum of older mice. They also saw decreased osteopontin levels in the bone marrow of older animals, which was associated with reduced vigor and function of HSCs.
The team followed up these experiments by transplanting bone marrow cells from older mice (19 to 21 months) into young mice (8 to 10 weeks).
The researchers also transplanted aged HSCs from older mice into younger mice, and the team treated aged HSCs with a recombinant form of the osteopontin protein.
Transplantation into the younger animals caused HSCs to behave in a younger, more vital manner, the researchers said. This meant smaller numbers of HSCs with greater potential for forming different blood cells, which included larger populations of B and T cells and decreased production of myeloid cells.
The researchers also saw aged HSCs treated with recombinant osteopontin regain their youthful characteristics and capacity to form different blood cell types. Also observed was diminished signaling of Cdc42, a protein previously shown to cause aging in HSCs.
Osteopontin levels are not only low in the bone marrow niche but also in the blood upon aging. As a follow-up to the current study, the researchers are investigating the possibility of using osteopontin replacement therapy in mice to counter the influence of an aging niche directly in the animals. ![]()
Preclinical research suggests osteopontin, a protein made by osteoblasts, plays a role in hematopoietic stem cell (HSC) aging.
Experiments in mice revealed that, with age, there is a reduction in the expression of osteopontin in the bone marrow stroma.
A lack of osteopontin induced young HSCs to “act” older, while treating older HSCs with recombinant osteopontin restored youthful properties.
Hartmut Geiger, PhD, of the University of Ulm in Germany, and his colleagues reported these findings in EMBO.
“We show that the place where HSCs form in the bone marrow loses osteopontin upon aging, but if you give back the missing protein to the blood-forming cells, they suddenly rejuvenate and act younger,” Dr Geiger said.
“Our study points to exciting, novel ways to have a better immune system and possibly less blood cancer upon aging by therapeutically targeting the place where blood stem cells form.”
The researchers conducted a number of experiments to test the formation and vitality of cells in and near the bone marrow microenvironment.
The team looked at the formation of endosteum stroma cells in aging mice and monitored levels of osteopontin and other proteins linked to distinct cells in the bone marrow during the aging process.
The researchers said they observed reduced production of osteoblasts and other stroma cells in the endosteum of older mice. They also saw decreased osteopontin levels in the bone marrow of older animals, which was associated with reduced vigor and function of HSCs.
The team followed up these experiments by transplanting bone marrow cells from older mice (19 to 21 months) into young mice (8 to 10 weeks).
The researchers also transplanted aged HSCs from older mice into younger mice, and the team treated aged HSCs with a recombinant form of the osteopontin protein.
Transplantation into the younger animals caused HSCs to behave in a younger, more vital manner, the researchers said. This meant smaller numbers of HSCs with greater potential for forming different blood cells, which included larger populations of B and T cells and decreased production of myeloid cells.
The researchers also saw aged HSCs treated with recombinant osteopontin regain their youthful characteristics and capacity to form different blood cell types. Also observed was diminished signaling of Cdc42, a protein previously shown to cause aging in HSCs.
Osteopontin levels are not only low in the bone marrow niche but also in the blood upon aging. As a follow-up to the current study, the researchers are investigating the possibility of using osteopontin replacement therapy in mice to counter the influence of an aging niche directly in the animals. ![]()
Preclinical research suggests osteopontin, a protein made by osteoblasts, plays a role in hematopoietic stem cell (HSC) aging.
Experiments in mice revealed that, with age, there is a reduction in the expression of osteopontin in the bone marrow stroma.
A lack of osteopontin induced young HSCs to “act” older, while treating older HSCs with recombinant osteopontin restored youthful properties.
Hartmut Geiger, PhD, of the University of Ulm in Germany, and his colleagues reported these findings in EMBO.
“We show that the place where HSCs form in the bone marrow loses osteopontin upon aging, but if you give back the missing protein to the blood-forming cells, they suddenly rejuvenate and act younger,” Dr Geiger said.
“Our study points to exciting, novel ways to have a better immune system and possibly less blood cancer upon aging by therapeutically targeting the place where blood stem cells form.”
The researchers conducted a number of experiments to test the formation and vitality of cells in and near the bone marrow microenvironment.
The team looked at the formation of endosteum stroma cells in aging mice and monitored levels of osteopontin and other proteins linked to distinct cells in the bone marrow during the aging process.
The researchers said they observed reduced production of osteoblasts and other stroma cells in the endosteum of older mice. They also saw decreased osteopontin levels in the bone marrow of older animals, which was associated with reduced vigor and function of HSCs.
The team followed up these experiments by transplanting bone marrow cells from older mice (19 to 21 months) into young mice (8 to 10 weeks).
The researchers also transplanted aged HSCs from older mice into younger mice, and the team treated aged HSCs with a recombinant form of the osteopontin protein.
Transplantation into the younger animals caused HSCs to behave in a younger, more vital manner, the researchers said. This meant smaller numbers of HSCs with greater potential for forming different blood cells, which included larger populations of B and T cells and decreased production of myeloid cells.
The researchers also saw aged HSCs treated with recombinant osteopontin regain their youthful characteristics and capacity to form different blood cell types. Also observed was diminished signaling of Cdc42, a protein previously shown to cause aging in HSCs.
Osteopontin levels are not only low in the bone marrow niche but also in the blood upon aging. As a follow-up to the current study, the researchers are investigating the possibility of using osteopontin replacement therapy in mice to counter the influence of an aging niche directly in the animals. ![]()
Cell-free DNA mutational analysis in AITL

SAN FRANCISCO—An exploratory study suggests cell-free DNA from peripheral blood may be a viable alternative to tumor DNA for mutational profiling in angioimmunoblastic T-cell lymphoma (AITL).
Investigators sequenced cell-free DNA and tumor DNA collected from 13 patients with AITL and found that, in 85% of cases, there was concordance between the tumor mutational profile and the cell-free DNA mutational profile.
“The cell-free DNA mutational analysis seems to mirror the mutational analysis of the tumor in the majority of cases,” said Neha Mehta-Shah, MD, of Memorial Sloan Kettering Cancer Center in New York, New York.
“This may be particularly interesting when we don’t have very much tumor DNA available for sequencing, as occurs frequently in this patient population.”
Dr Mehta-Shah presented these findings at the 9th Annual T-cell Lymphoma Forum.
She said the primary objective of this study was to evaluate whether somatic mutation analysis of cell-free DNA for IDH2 correlates with tumor mutational profiling for IDH2.
The secondary objective was to evaluate whether somatic mutational analysis of cell-free DNA mirrors the mutational profile of the tumor.
So Dr Mehta-Shah and her colleagues sequenced various samples from 14 patients with AITL (4 who were newly diagnosed and 10 with relapsed disease).
The investigators compared cell-free DNA obtained from peripheral blood samples with genomic DNA obtained from primary tumor biopsies and with DNA from peripheral blood mononuclear cells (for germline comparison). One of the 14 patients didn’t have tumor tissue available, so 13 patients were included in the analysis.
The team performed targeted next-generation sequencing using Memorial Sloan Kettering Cancer Center’s IMPACT platform, which sequences 410 genes known to be recurrently mutated in cancer.
The investigators observed concordance between the tumor mutational profile and the cell-free DNA profile in 85% of cases (11/13).
Identical alterations in TET2, RHOA, IDH2, DNMT3A, and ROS1 were detected in cell-free DNA from peripheral blood and tumor genomic DNA, with a similar variant allele frequency.
On the other hand, mutational analysis of cell-free DNA obtained from urine samples from 2 of the patients did not correlate with somatic mutations from tumor DNA.
This research also revealed that some samples had multiple mutations in TET2, which are indicative of subclonal populations.
And sequential samples from 2 patients, collected at the start of salvage therapy and at subsequent relapse, showed the disappearance of mutations in RHOA, TET2, and IDH2. This observation has been attributed to clonal evolution and/or changes in overall disease burden. ![]()
SAN FRANCISCO—An exploratory study suggests cell-free DNA from peripheral blood may be a viable alternative to tumor DNA for mutational profiling in angioimmunoblastic T-cell lymphoma (AITL).
Investigators sequenced cell-free DNA and tumor DNA collected from 13 patients with AITL and found that, in 85% of cases, there was concordance between the tumor mutational profile and the cell-free DNA mutational profile.
“The cell-free DNA mutational analysis seems to mirror the mutational analysis of the tumor in the majority of cases,” said Neha Mehta-Shah, MD, of Memorial Sloan Kettering Cancer Center in New York, New York.
“This may be particularly interesting when we don’t have very much tumor DNA available for sequencing, as occurs frequently in this patient population.”
Dr Mehta-Shah presented these findings at the 9th Annual T-cell Lymphoma Forum.
She said the primary objective of this study was to evaluate whether somatic mutation analysis of cell-free DNA for IDH2 correlates with tumor mutational profiling for IDH2.
The secondary objective was to evaluate whether somatic mutational analysis of cell-free DNA mirrors the mutational profile of the tumor.
So Dr Mehta-Shah and her colleagues sequenced various samples from 14 patients with AITL (4 who were newly diagnosed and 10 with relapsed disease).
The investigators compared cell-free DNA obtained from peripheral blood samples with genomic DNA obtained from primary tumor biopsies and with DNA from peripheral blood mononuclear cells (for germline comparison). One of the 14 patients didn’t have tumor tissue available, so 13 patients were included in the analysis.
The team performed targeted next-generation sequencing using Memorial Sloan Kettering Cancer Center’s IMPACT platform, which sequences 410 genes known to be recurrently mutated in cancer.
The investigators observed concordance between the tumor mutational profile and the cell-free DNA profile in 85% of cases (11/13).
Identical alterations in TET2, RHOA, IDH2, DNMT3A, and ROS1 were detected in cell-free DNA from peripheral blood and tumor genomic DNA, with a similar variant allele frequency.
On the other hand, mutational analysis of cell-free DNA obtained from urine samples from 2 of the patients did not correlate with somatic mutations from tumor DNA.
This research also revealed that some samples had multiple mutations in TET2, which are indicative of subclonal populations.
And sequential samples from 2 patients, collected at the start of salvage therapy and at subsequent relapse, showed the disappearance of mutations in RHOA, TET2, and IDH2. This observation has been attributed to clonal evolution and/or changes in overall disease burden. ![]()
SAN FRANCISCO—An exploratory study suggests cell-free DNA from peripheral blood may be a viable alternative to tumor DNA for mutational profiling in angioimmunoblastic T-cell lymphoma (AITL).
Investigators sequenced cell-free DNA and tumor DNA collected from 13 patients with AITL and found that, in 85% of cases, there was concordance between the tumor mutational profile and the cell-free DNA mutational profile.
“The cell-free DNA mutational analysis seems to mirror the mutational analysis of the tumor in the majority of cases,” said Neha Mehta-Shah, MD, of Memorial Sloan Kettering Cancer Center in New York, New York.
“This may be particularly interesting when we don’t have very much tumor DNA available for sequencing, as occurs frequently in this patient population.”
Dr Mehta-Shah presented these findings at the 9th Annual T-cell Lymphoma Forum.
She said the primary objective of this study was to evaluate whether somatic mutation analysis of cell-free DNA for IDH2 correlates with tumor mutational profiling for IDH2.
The secondary objective was to evaluate whether somatic mutational analysis of cell-free DNA mirrors the mutational profile of the tumor.
So Dr Mehta-Shah and her colleagues sequenced various samples from 14 patients with AITL (4 who were newly diagnosed and 10 with relapsed disease).
The investigators compared cell-free DNA obtained from peripheral blood samples with genomic DNA obtained from primary tumor biopsies and with DNA from peripheral blood mononuclear cells (for germline comparison). One of the 14 patients didn’t have tumor tissue available, so 13 patients were included in the analysis.
The team performed targeted next-generation sequencing using Memorial Sloan Kettering Cancer Center’s IMPACT platform, which sequences 410 genes known to be recurrently mutated in cancer.
The investigators observed concordance between the tumor mutational profile and the cell-free DNA profile in 85% of cases (11/13).
Identical alterations in TET2, RHOA, IDH2, DNMT3A, and ROS1 were detected in cell-free DNA from peripheral blood and tumor genomic DNA, with a similar variant allele frequency.
On the other hand, mutational analysis of cell-free DNA obtained from urine samples from 2 of the patients did not correlate with somatic mutations from tumor DNA.
This research also revealed that some samples had multiple mutations in TET2, which are indicative of subclonal populations.
And sequential samples from 2 patients, collected at the start of salvage therapy and at subsequent relapse, showed the disappearance of mutations in RHOA, TET2, and IDH2. This observation has been attributed to clonal evolution and/or changes in overall disease burden. ![]()
MSC product granted fast track designation

The US Food and Drug Administration (FDA) has granted fast track designation to a mesenchymal stem cell (MSC) product, MSC-100-IV, as a treatment for children with steroid-refractory acute graft-vs-host disease (aGVHD).
MSC-100-IV consists of human MSCs derived from donor bone marrow and expanded in culture.
Fast track designation has the potential to shorten the time to FDA approval for MSC-100-IV through priority review, which reduces the FDA review process from 10 months to 6 months.
The designation also allows for a rolling review process, whereby completed sections of the Biologics License Application can be submitted for FDA review as they become available, instead of waiting for all sections to be completed.
In addition, fast track designation provides product developers with opportunities for more frequent meetings and written communications with the FDA.
MSC-100-IV is being developed by Mesoblast Limited in partnership with Mallinckrodt Pharmaceuticals.
Trial results
The application for fast track designation for MSC-100-IV was supported by a trial of 241 pediatric patients with steroid-refractory aGVHD. Results from this trial were presented at the 2016 BMT Tandem Meetings.
Patients initially received 2 million MSCs/kg twice a week for 4 weeks, at least 3 days apart. If they achieved a partial or mixed response (improvement in one organ with deterioration in another) at the day-28 assessment, patients then received 2 million MSCs/kg once a week for 4 weeks.
The patients received a total of 2434 infusions—a median of 11 (range, 1-24)—and had a median treatment duration of 46 days (range, 1-186).
Fifty-seven percent of patients (n=138) had at least 1 serious adverse event. About 5% (n=11) were considered treatment-related, and 1.7% (n=4) led to study discontinuation. There was 1 infusion reaction.
The overall response rate at day 28 was 65%, and the complete response rate was 14%. Responses were observed for all aGVHD grades and did not differ by baseline organ involvement.
Day 100 survival was significantly better in children who achieved a response at day 28—82%, compared to 39% for non-responders (P<0.0001).
In November 2016, Mesoblast reported success in an ongoing, phase 3 registration trial of MSC-100-IV in 60 children with steroid-refractory aGVHD.
The company said the trial was successful in a pre-specified interim futility analysis using the primary endpoint of day-28 overall response. Enrollment in this trial is expected to be complete in mid-2017. ![]()
The US Food and Drug Administration (FDA) has granted fast track designation to a mesenchymal stem cell (MSC) product, MSC-100-IV, as a treatment for children with steroid-refractory acute graft-vs-host disease (aGVHD).
MSC-100-IV consists of human MSCs derived from donor bone marrow and expanded in culture.
Fast track designation has the potential to shorten the time to FDA approval for MSC-100-IV through priority review, which reduces the FDA review process from 10 months to 6 months.
The designation also allows for a rolling review process, whereby completed sections of the Biologics License Application can be submitted for FDA review as they become available, instead of waiting for all sections to be completed.
In addition, fast track designation provides product developers with opportunities for more frequent meetings and written communications with the FDA.
MSC-100-IV is being developed by Mesoblast Limited in partnership with Mallinckrodt Pharmaceuticals.
Trial results
The application for fast track designation for MSC-100-IV was supported by a trial of 241 pediatric patients with steroid-refractory aGVHD. Results from this trial were presented at the 2016 BMT Tandem Meetings.
Patients initially received 2 million MSCs/kg twice a week for 4 weeks, at least 3 days apart. If they achieved a partial or mixed response (improvement in one organ with deterioration in another) at the day-28 assessment, patients then received 2 million MSCs/kg once a week for 4 weeks.
The patients received a total of 2434 infusions—a median of 11 (range, 1-24)—and had a median treatment duration of 46 days (range, 1-186).
Fifty-seven percent of patients (n=138) had at least 1 serious adverse event. About 5% (n=11) were considered treatment-related, and 1.7% (n=4) led to study discontinuation. There was 1 infusion reaction.
The overall response rate at day 28 was 65%, and the complete response rate was 14%. Responses were observed for all aGVHD grades and did not differ by baseline organ involvement.
Day 100 survival was significantly better in children who achieved a response at day 28—82%, compared to 39% for non-responders (P<0.0001).
In November 2016, Mesoblast reported success in an ongoing, phase 3 registration trial of MSC-100-IV in 60 children with steroid-refractory aGVHD.
The company said the trial was successful in a pre-specified interim futility analysis using the primary endpoint of day-28 overall response. Enrollment in this trial is expected to be complete in mid-2017. ![]()
The US Food and Drug Administration (FDA) has granted fast track designation to a mesenchymal stem cell (MSC) product, MSC-100-IV, as a treatment for children with steroid-refractory acute graft-vs-host disease (aGVHD).
MSC-100-IV consists of human MSCs derived from donor bone marrow and expanded in culture.
Fast track designation has the potential to shorten the time to FDA approval for MSC-100-IV through priority review, which reduces the FDA review process from 10 months to 6 months.
The designation also allows for a rolling review process, whereby completed sections of the Biologics License Application can be submitted for FDA review as they become available, instead of waiting for all sections to be completed.
In addition, fast track designation provides product developers with opportunities for more frequent meetings and written communications with the FDA.
MSC-100-IV is being developed by Mesoblast Limited in partnership with Mallinckrodt Pharmaceuticals.
Trial results
The application for fast track designation for MSC-100-IV was supported by a trial of 241 pediatric patients with steroid-refractory aGVHD. Results from this trial were presented at the 2016 BMT Tandem Meetings.
Patients initially received 2 million MSCs/kg twice a week for 4 weeks, at least 3 days apart. If they achieved a partial or mixed response (improvement in one organ with deterioration in another) at the day-28 assessment, patients then received 2 million MSCs/kg once a week for 4 weeks.
The patients received a total of 2434 infusions—a median of 11 (range, 1-24)—and had a median treatment duration of 46 days (range, 1-186).
Fifty-seven percent of patients (n=138) had at least 1 serious adverse event. About 5% (n=11) were considered treatment-related, and 1.7% (n=4) led to study discontinuation. There was 1 infusion reaction.
The overall response rate at day 28 was 65%, and the complete response rate was 14%. Responses were observed for all aGVHD grades and did not differ by baseline organ involvement.
Day 100 survival was significantly better in children who achieved a response at day 28—82%, compared to 39% for non-responders (P<0.0001).
In November 2016, Mesoblast reported success in an ongoing, phase 3 registration trial of MSC-100-IV in 60 children with steroid-refractory aGVHD.
The company said the trial was successful in a pre-specified interim futility analysis using the primary endpoint of day-28 overall response. Enrollment in this trial is expected to be complete in mid-2017. ![]()
Shedding Light on the Problem
A 49-year-old man presents to dermatology for evaluation of an itchy rash that manifested several months ago. Attempts to eradicate or ameliorate it—which have included topical and systemic steroids and oral antibiotics (minocycline)—have had no effect. A biopsy ordered by his primary care provider (PCP) showed nonspecific changes, termed “dermatitis” in the report.
The patient denies any history of atopy, such as seasonal allergies or eczema. His only medical problem is moderate hypertension, for which his PCP prescribed hydrochlorothiazide. He started taking the drug a few weeks before the rash appeared.
He claims to be in good health otherwise, with no weakness or weight loss. He has never smoked.
EXAMINATION
A bright red, blanchable, maculopapular rash is notably confined to the patient’s sun-exposed skin; it sharply spares the areas covered by clothing and the watch on his left wrist. His palms, soles, scalp, and face are also spared. No nail changes are noted.

Otherwise, the patient appears well and is able to rise from a seated position without difficulty. No nodes are palpable in the head or neck, and there is no organomegaly detected on abdominal examination.
What is the diagnosis?
DISCUSSION
Photosensitivity to hydrochlorothiazide was the obvious culprit, so the patient was advised to stop using that product (after consulting his PCP). He’ll remain off the medication for at least two months, then present for follow-up.
There are some potentially troubling items in the differential, particularly dermatomyositis (DM). Patients with DM may exhibit a sunburn-like rash, but they will additionally demonstrate muscle weakness and chronic fatigue. A significant proportion of their complaints are driven by an occult carcinoma (eg, stomach, lung, colon, breast). While it’s doubtful that this patient has DM, his follow-up may include a fresh biopsy, blood work, anteroposterior and lateral chest films, and possibly a colonoscopy.
Another item in the differential is lupus. However, the original biopsy yielded no suggestive findings (eg, interface dermatitis), nor did the patient have any complaints referable to the disease.
This case nicely demonstrates the concept that it is equally important to note which areas are affected by and spared by a skin condition. With that in mind, we can at least establish that sunlight is a major factor in the genesis of this rash. Unfortunately, that still leaves room for conjecture as to the diagnosis.
TAKE-HOME LEARNING POINTS
- Rashes confined to sun-exposed skin can be a symptom of systemic disease, such as lupus or dermatomyositis.
- Various drugs—including hydrochlorothiazide, NSAIDs, sulfas, and certain tetracyclines—can also cause photosensitivity reactions.
- Hydrochlorothiazide is one of the more common drugs to cause such a rash, which may take weeks to clear after cessation of use.
- If terminating hydrochlorothiazide doesn’t help, skin biopsy and labs (especially creatine kinase and immunoglobulins) are the next step in determining the problem.
A 49-year-old man presents to dermatology for evaluation of an itchy rash that manifested several months ago. Attempts to eradicate or ameliorate it—which have included topical and systemic steroids and oral antibiotics (minocycline)—have had no effect. A biopsy ordered by his primary care provider (PCP) showed nonspecific changes, termed “dermatitis” in the report.
The patient denies any history of atopy, such as seasonal allergies or eczema. His only medical problem is moderate hypertension, for which his PCP prescribed hydrochlorothiazide. He started taking the drug a few weeks before the rash appeared.
He claims to be in good health otherwise, with no weakness or weight loss. He has never smoked.
EXAMINATION
A bright red, blanchable, maculopapular rash is notably confined to the patient’s sun-exposed skin; it sharply spares the areas covered by clothing and the watch on his left wrist. His palms, soles, scalp, and face are also spared. No nail changes are noted.
Otherwise, the patient appears well and is able to rise from a seated position without difficulty. No nodes are palpable in the head or neck, and there is no organomegaly detected on abdominal examination.
What is the diagnosis?
DISCUSSION
Photosensitivity to hydrochlorothiazide was the obvious culprit, so the patient was advised to stop using that product (after consulting his PCP). He’ll remain off the medication for at least two months, then present for follow-up.
There are some potentially troubling items in the differential, particularly dermatomyositis (DM). Patients with DM may exhibit a sunburn-like rash, but they will additionally demonstrate muscle weakness and chronic fatigue. A significant proportion of their complaints are driven by an occult carcinoma (eg, stomach, lung, colon, breast). While it’s doubtful that this patient has DM, his follow-up may include a fresh biopsy, blood work, anteroposterior and lateral chest films, and possibly a colonoscopy.
Another item in the differential is lupus. However, the original biopsy yielded no suggestive findings (eg, interface dermatitis), nor did the patient have any complaints referable to the disease.
This case nicely demonstrates the concept that it is equally important to note which areas are affected by and spared by a skin condition. With that in mind, we can at least establish that sunlight is a major factor in the genesis of this rash. Unfortunately, that still leaves room for conjecture as to the diagnosis.
TAKE-HOME LEARNING POINTS
- Rashes confined to sun-exposed skin can be a symptom of systemic disease, such as lupus or dermatomyositis.
- Various drugs—including hydrochlorothiazide, NSAIDs, sulfas, and certain tetracyclines—can also cause photosensitivity reactions.
- Hydrochlorothiazide is one of the more common drugs to cause such a rash, which may take weeks to clear after cessation of use.
- If terminating hydrochlorothiazide doesn’t help, skin biopsy and labs (especially creatine kinase and immunoglobulins) are the next step in determining the problem.
A 49-year-old man presents to dermatology for evaluation of an itchy rash that manifested several months ago. Attempts to eradicate or ameliorate it—which have included topical and systemic steroids and oral antibiotics (minocycline)—have had no effect. A biopsy ordered by his primary care provider (PCP) showed nonspecific changes, termed “dermatitis” in the report.
The patient denies any history of atopy, such as seasonal allergies or eczema. His only medical problem is moderate hypertension, for which his PCP prescribed hydrochlorothiazide. He started taking the drug a few weeks before the rash appeared.
He claims to be in good health otherwise, with no weakness or weight loss. He has never smoked.
EXAMINATION
A bright red, blanchable, maculopapular rash is notably confined to the patient’s sun-exposed skin; it sharply spares the areas covered by clothing and the watch on his left wrist. His palms, soles, scalp, and face are also spared. No nail changes are noted.
Otherwise, the patient appears well and is able to rise from a seated position without difficulty. No nodes are palpable in the head or neck, and there is no organomegaly detected on abdominal examination.
What is the diagnosis?
DISCUSSION
Photosensitivity to hydrochlorothiazide was the obvious culprit, so the patient was advised to stop using that product (after consulting his PCP). He’ll remain off the medication for at least two months, then present for follow-up.
There are some potentially troubling items in the differential, particularly dermatomyositis (DM). Patients with DM may exhibit a sunburn-like rash, but they will additionally demonstrate muscle weakness and chronic fatigue. A significant proportion of their complaints are driven by an occult carcinoma (eg, stomach, lung, colon, breast). While it’s doubtful that this patient has DM, his follow-up may include a fresh biopsy, blood work, anteroposterior and lateral chest films, and possibly a colonoscopy.
Another item in the differential is lupus. However, the original biopsy yielded no suggestive findings (eg, interface dermatitis), nor did the patient have any complaints referable to the disease.
This case nicely demonstrates the concept that it is equally important to note which areas are affected by and spared by a skin condition. With that in mind, we can at least establish that sunlight is a major factor in the genesis of this rash. Unfortunately, that still leaves room for conjecture as to the diagnosis.
TAKE-HOME LEARNING POINTS
- Rashes confined to sun-exposed skin can be a symptom of systemic disease, such as lupus or dermatomyositis.
- Various drugs—including hydrochlorothiazide, NSAIDs, sulfas, and certain tetracyclines—can also cause photosensitivity reactions.
- Hydrochlorothiazide is one of the more common drugs to cause such a rash, which may take weeks to clear after cessation of use.
- If terminating hydrochlorothiazide doesn’t help, skin biopsy and labs (especially creatine kinase and immunoglobulins) are the next step in determining the problem.

Rash around belly button
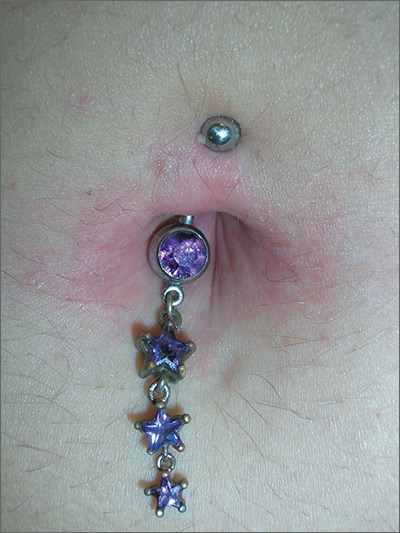
The family physician (FP) recognized that the patient’s new belly ring was the cause of this case of contact dermatitis. The FP suspected that the belly ring contained nickel—a common culprit in cases of allergic contact dermatitis (ACD).
ACD is a delayed-type hypersensitivity reaction that occurs when skin proteins form an antigen complex in reaction to a foreign substance. Upon reexposure of the epidermis to the antigen, the sensitized T cells initiate an inflammatory cascade, leading to the skin changes seen in ACD.
The FP told the patient that patch testing could be used to confirm her allergy, but it required wearing patches on her back for 3 days and involved 3 office visits to complete the testing. He also asked her if she wanted to have her jewelry tested for nickel content.
The patient removed the belly button jewelry and the FP used a nickel testing kit, which showed the jewelry was, in fact, positive for nickel. The patient asked if she could still wear the jewelry if she got medication to treat the allergy, but the FP explained that it was unlikely that the rash would go away completely with a topical cream if the jewelry remained in place. The FP prescribed 0.1% triamcinolone cream to be applied twice daily to the area. He also suggested that she look for a jewelry replacement that was nickel-free.
At a one-month follow-up visit, the patient acknowledged that the FP had been right: While she was able to wear the jewelry for another 2 weeks with decreased erythema and pruritus while using the triamcinolone cream, the rash never went away. The patient switched to a nickel-free belly button ring and her rash cleared completely.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R. Contact dermatitis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:591-596.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The family physician (FP) recognized that the patient’s new belly ring was the cause of this case of contact dermatitis. The FP suspected that the belly ring contained nickel—a common culprit in cases of allergic contact dermatitis (ACD).
ACD is a delayed-type hypersensitivity reaction that occurs when skin proteins form an antigen complex in reaction to a foreign substance. Upon reexposure of the epidermis to the antigen, the sensitized T cells initiate an inflammatory cascade, leading to the skin changes seen in ACD.
The FP told the patient that patch testing could be used to confirm her allergy, but it required wearing patches on her back for 3 days and involved 3 office visits to complete the testing. He also asked her if she wanted to have her jewelry tested for nickel content.
The patient removed the belly button jewelry and the FP used a nickel testing kit, which showed the jewelry was, in fact, positive for nickel. The patient asked if she could still wear the jewelry if she got medication to treat the allergy, but the FP explained that it was unlikely that the rash would go away completely with a topical cream if the jewelry remained in place. The FP prescribed 0.1% triamcinolone cream to be applied twice daily to the area. He also suggested that she look for a jewelry replacement that was nickel-free.
At a one-month follow-up visit, the patient acknowledged that the FP had been right: While she was able to wear the jewelry for another 2 weeks with decreased erythema and pruritus while using the triamcinolone cream, the rash never went away. The patient switched to a nickel-free belly button ring and her rash cleared completely.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R. Contact dermatitis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:591-596.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The family physician (FP) recognized that the patient’s new belly ring was the cause of this case of contact dermatitis. The FP suspected that the belly ring contained nickel—a common culprit in cases of allergic contact dermatitis (ACD).
ACD is a delayed-type hypersensitivity reaction that occurs when skin proteins form an antigen complex in reaction to a foreign substance. Upon reexposure of the epidermis to the antigen, the sensitized T cells initiate an inflammatory cascade, leading to the skin changes seen in ACD.
The FP told the patient that patch testing could be used to confirm her allergy, but it required wearing patches on her back for 3 days and involved 3 office visits to complete the testing. He also asked her if she wanted to have her jewelry tested for nickel content.
The patient removed the belly button jewelry and the FP used a nickel testing kit, which showed the jewelry was, in fact, positive for nickel. The patient asked if she could still wear the jewelry if she got medication to treat the allergy, but the FP explained that it was unlikely that the rash would go away completely with a topical cream if the jewelry remained in place. The FP prescribed 0.1% triamcinolone cream to be applied twice daily to the area. He also suggested that she look for a jewelry replacement that was nickel-free.
At a one-month follow-up visit, the patient acknowledged that the FP had been right: While she was able to wear the jewelry for another 2 weeks with decreased erythema and pruritus while using the triamcinolone cream, the rash never went away. The patient switched to a nickel-free belly button ring and her rash cleared completely.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R. Contact dermatitis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:591-596.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

APA task force urges caution in off-label use of ketamine for mood disorders
A new consensus statement on the use of ketamine as an off-label treatment for mood disorders provides psychiatrists some guidance for patient selection and evaluation, as well as dosing and duration of therapy. The statement was issued against the backdrop of newer studies showing ketamine’s rapid, though not durable, efficacy in treating depression and anxiety disorders.
From start to end, however, the statement urges caution and marks out areas for further study, citing a paucity of data on longer-term efficacy and safety and a literature largely made up of smaller studies.

Dr. Sanacora, professor of psychiatry at Yale University, New Haven, Conn., and his coauthors made clear that “this report is not intended to serve as a standard, guideline, clinical policy, or absolute requirement.” Rather, the document identifies the current state of the field and identifies factors to consider in determining the appropriateness of ketamine therapy.
When a clinician is considering giving ketamine to a patient, a preprocedural evaluation is recommended, both to assess whether ketamine is likely to benefit the patient and to evaluate potential risks. Recommended components include a comprehensive psychiatric diagnostic assessment, paying particular attention to substance use and psychosis history, if any; assessment of baseline symptom severity; history of prior antidepressant treatment; review of systems to assess risk factors; physical examination and laboratory screening that follows accepted guidelines for the anticipated level of sedation, with the recommended addition of a baseline urine toxicology screen; and records review and family corroboration with a particular eye to past substance use.
Finally, the informed consent process should ensure that the patient is aware not only of potential treatment risks, but also of the relatively limited data on the off-label use of ketamine for mood disorders. Thorough written documentation is recommended.
Regarding the appropriate amount of experience and training a clinician should have before administering ketamine, Dr. Sanacora and his coauthors noted that the subanesthetic doses of ketamine that are used to treat mood disorders have been found generally very safe in the limited studies that have been done. Typical peak plasma concentrations will not induce general anesthesia. However, systolic and diastolic blood pressure and heart rate elevations are not uncommon. The statement cites a study that found “blood pressure levels exceeding 180/100 mm Hg or heart rates exceeding 110 beats per minute in approximately 30% of the patients treated.”
Accordingly, the statement recommends that clinicians administering ketamine have Advanced Cardiac Life Support certification and be able to administer Drug Enforcement Administration Schedule III medications. Individual organizations, according to the statement, should follow accepted standards of practice for granting privileges to administer ketamine. A statement developed by the American Society of Anesthesiologists on granting privileges for conscious sedation to nonanesthesia professionals may be used for guidance.
The most-studied dose of ketamine in the treatment of mood disorders is 0.5 mg/kg, administered intravenously over 40 minutes. Though other routes, and lower doses, have been studied, Dr. Sanacora and his colleagues wrote that they consider that “insufficient benefit was provided in those studies to allow any meaningful analysis of any specific dose or route of treatment compared with the standard dose.”
The statement includes a strong recommendation to develop a site-specific–standard operating procedure for the administration of ketamine that incorporates the preprocedural evaluation. In addition, the procedure should assess baseline vital signs, include criteria for acceptable vital signs, and incorporate a “time-out” procedure before initiating ketamine treatment.
Also, standard operating procedures should include continued assessment of respiratory, cardiovascular, and mental status throughout the infusion. Stopping criteria should be clearly defined, as should a plan aimed at managing any cardiovascular or behavioral problems. Discharge procedures should include documentation of vital signs and mental status, ensuring that an adult caregiver can take the patient home, and a thorough review of discharge instructions.
The statement’s section on follow-up and assessments noted: “The existing data surrounding the benefits of repeated infusions of ketamine remain limited.” However, some studies have shown that twice-weekly infusions were as efficacious as infusions given three times a week. In terms of longer-term treatment, the data are sparse, wrote Dr. Sanacora and his coauthors. Some clinics, they said, are giving ketamine two or three times weekly for 2 or 3 weeks, then tapering or adjusting the regimen based on clinical response, but high-quality studies are lacking.” The scarcity of this information is one of the major drawbacks to be considered before initiating ketamine therapy for patients with mood disorders and should be discussed with the patient before beginning treatment,” they wrote.
The known risks of cognitive impairment and cystitis with more chronic high-frequency ketamine use, taken together with the significant potential for abuse, mean that ketamine should be discontinued if more than once-weekly dosing is required after 2 months of treatment. “The goal remains to eventually taper and discontinue treatment until more long-term safety data can be collected,” wrote Dr. Sanacora and his coauthors.
The statement, while acknowledging the hope and excitement that currently surround the use of ketamine for mood disorders, calls for further research that would include a patient registry and coordinated data collection to facilitate answering the many important questions remaining about ketamine’s efficacy and safety.
The report was neither endorsed nor promulgated as policy of the APA. Dr. Sanacora reported multiple relationships with pharmaceutical companies, as did all of his coauthors.
[email protected]
On Twitter @karioakes
A clear need exists for better treatments for the up to one-third of patients with major depression who do not respond to currently available therapies. Ketamine, which can produce rapid antidepressant effects, holds promise for this population and is increasingly being used off-label.
However, clinical guidance is lacking, and the small studies done to date leave many knowledge gaps. Though ketamine is known to be an N-methyl-D-aspartate (NMDA) glutamate receptor antagonist, rodent studies show that its action, or perhaps that of its metabolites, on another glutamate pathway may primarily underlie its antidepressant effects. Also, researchers are trialling adjunctive agents such as clonidine to help mute the undesirable psychomimetic and cardiorespiratory effects of ketamine. As the science rapidly develops, more targeted rapid treatments may become available, an evolution that could fundamentally change many aspects of the practice of psychiatry.
Uncertainty created by the current limitations in knowledge permeates the consensus statement and appropriately so. The authors provide clinical guidance based on what data are available but call for caution and transparency when treating mood disorder patients with ketamine. Gaps in data can be ameliorated by the formation of a patient registry for coordinated data collection and safety monitoring.
Charles F. Zorumski, MD, and Charles R. Conway, MD, are professors of psychiatry at Washington University in St. Louis, where Dr. Zorumski also holds an appointment in the department of neuroscience. Dr. Zorumski reported serving on the scientific advisory board of Sage Therapeutics, which also has funded research conducted by both authors. Dr. Conway reported serving as an unpaid consultant to LivaNova. These remarks were drawn from invited commentary accompanying the consensus statement.
A clear need exists for better treatments for the up to one-third of patients with major depression who do not respond to currently available therapies. Ketamine, which can produce rapid antidepressant effects, holds promise for this population and is increasingly being used off-label.
However, clinical guidance is lacking, and the small studies done to date leave many knowledge gaps. Though ketamine is known to be an N-methyl-D-aspartate (NMDA) glutamate receptor antagonist, rodent studies show that its action, or perhaps that of its metabolites, on another glutamate pathway may primarily underlie its antidepressant effects. Also, researchers are trialling adjunctive agents such as clonidine to help mute the undesirable psychomimetic and cardiorespiratory effects of ketamine. As the science rapidly develops, more targeted rapid treatments may become available, an evolution that could fundamentally change many aspects of the practice of psychiatry.
Uncertainty created by the current limitations in knowledge permeates the consensus statement and appropriately so. The authors provide clinical guidance based on what data are available but call for caution and transparency when treating mood disorder patients with ketamine. Gaps in data can be ameliorated by the formation of a patient registry for coordinated data collection and safety monitoring.
Charles F. Zorumski, MD, and Charles R. Conway, MD, are professors of psychiatry at Washington University in St. Louis, where Dr. Zorumski also holds an appointment in the department of neuroscience. Dr. Zorumski reported serving on the scientific advisory board of Sage Therapeutics, which also has funded research conducted by both authors. Dr. Conway reported serving as an unpaid consultant to LivaNova. These remarks were drawn from invited commentary accompanying the consensus statement.
A clear need exists for better treatments for the up to one-third of patients with major depression who do not respond to currently available therapies. Ketamine, which can produce rapid antidepressant effects, holds promise for this population and is increasingly being used off-label.
However, clinical guidance is lacking, and the small studies done to date leave many knowledge gaps. Though ketamine is known to be an N-methyl-D-aspartate (NMDA) glutamate receptor antagonist, rodent studies show that its action, or perhaps that of its metabolites, on another glutamate pathway may primarily underlie its antidepressant effects. Also, researchers are trialling adjunctive agents such as clonidine to help mute the undesirable psychomimetic and cardiorespiratory effects of ketamine. As the science rapidly develops, more targeted rapid treatments may become available, an evolution that could fundamentally change many aspects of the practice of psychiatry.
Uncertainty created by the current limitations in knowledge permeates the consensus statement and appropriately so. The authors provide clinical guidance based on what data are available but call for caution and transparency when treating mood disorder patients with ketamine. Gaps in data can be ameliorated by the formation of a patient registry for coordinated data collection and safety monitoring.
Charles F. Zorumski, MD, and Charles R. Conway, MD, are professors of psychiatry at Washington University in St. Louis, where Dr. Zorumski also holds an appointment in the department of neuroscience. Dr. Zorumski reported serving on the scientific advisory board of Sage Therapeutics, which also has funded research conducted by both authors. Dr. Conway reported serving as an unpaid consultant to LivaNova. These remarks were drawn from invited commentary accompanying the consensus statement.
A new consensus statement on the use of ketamine as an off-label treatment for mood disorders provides psychiatrists some guidance for patient selection and evaluation, as well as dosing and duration of therapy. The statement was issued against the backdrop of newer studies showing ketamine’s rapid, though not durable, efficacy in treating depression and anxiety disorders.
From start to end, however, the statement urges caution and marks out areas for further study, citing a paucity of data on longer-term efficacy and safety and a literature largely made up of smaller studies.
Dr. Sanacora, professor of psychiatry at Yale University, New Haven, Conn., and his coauthors made clear that “this report is not intended to serve as a standard, guideline, clinical policy, or absolute requirement.” Rather, the document identifies the current state of the field and identifies factors to consider in determining the appropriateness of ketamine therapy.
When a clinician is considering giving ketamine to a patient, a preprocedural evaluation is recommended, both to assess whether ketamine is likely to benefit the patient and to evaluate potential risks. Recommended components include a comprehensive psychiatric diagnostic assessment, paying particular attention to substance use and psychosis history, if any; assessment of baseline symptom severity; history of prior antidepressant treatment; review of systems to assess risk factors; physical examination and laboratory screening that follows accepted guidelines for the anticipated level of sedation, with the recommended addition of a baseline urine toxicology screen; and records review and family corroboration with a particular eye to past substance use.
Finally, the informed consent process should ensure that the patient is aware not only of potential treatment risks, but also of the relatively limited data on the off-label use of ketamine for mood disorders. Thorough written documentation is recommended.
Regarding the appropriate amount of experience and training a clinician should have before administering ketamine, Dr. Sanacora and his coauthors noted that the subanesthetic doses of ketamine that are used to treat mood disorders have been found generally very safe in the limited studies that have been done. Typical peak plasma concentrations will not induce general anesthesia. However, systolic and diastolic blood pressure and heart rate elevations are not uncommon. The statement cites a study that found “blood pressure levels exceeding 180/100 mm Hg or heart rates exceeding 110 beats per minute in approximately 30% of the patients treated.”
Accordingly, the statement recommends that clinicians administering ketamine have Advanced Cardiac Life Support certification and be able to administer Drug Enforcement Administration Schedule III medications. Individual organizations, according to the statement, should follow accepted standards of practice for granting privileges to administer ketamine. A statement developed by the American Society of Anesthesiologists on granting privileges for conscious sedation to nonanesthesia professionals may be used for guidance.
The most-studied dose of ketamine in the treatment of mood disorders is 0.5 mg/kg, administered intravenously over 40 minutes. Though other routes, and lower doses, have been studied, Dr. Sanacora and his colleagues wrote that they consider that “insufficient benefit was provided in those studies to allow any meaningful analysis of any specific dose or route of treatment compared with the standard dose.”
The statement includes a strong recommendation to develop a site-specific–standard operating procedure for the administration of ketamine that incorporates the preprocedural evaluation. In addition, the procedure should assess baseline vital signs, include criteria for acceptable vital signs, and incorporate a “time-out” procedure before initiating ketamine treatment.
Also, standard operating procedures should include continued assessment of respiratory, cardiovascular, and mental status throughout the infusion. Stopping criteria should be clearly defined, as should a plan aimed at managing any cardiovascular or behavioral problems. Discharge procedures should include documentation of vital signs and mental status, ensuring that an adult caregiver can take the patient home, and a thorough review of discharge instructions.
The statement’s section on follow-up and assessments noted: “The existing data surrounding the benefits of repeated infusions of ketamine remain limited.” However, some studies have shown that twice-weekly infusions were as efficacious as infusions given three times a week. In terms of longer-term treatment, the data are sparse, wrote Dr. Sanacora and his coauthors. Some clinics, they said, are giving ketamine two or three times weekly for 2 or 3 weeks, then tapering or adjusting the regimen based on clinical response, but high-quality studies are lacking.” The scarcity of this information is one of the major drawbacks to be considered before initiating ketamine therapy for patients with mood disorders and should be discussed with the patient before beginning treatment,” they wrote.
The known risks of cognitive impairment and cystitis with more chronic high-frequency ketamine use, taken together with the significant potential for abuse, mean that ketamine should be discontinued if more than once-weekly dosing is required after 2 months of treatment. “The goal remains to eventually taper and discontinue treatment until more long-term safety data can be collected,” wrote Dr. Sanacora and his coauthors.
The statement, while acknowledging the hope and excitement that currently surround the use of ketamine for mood disorders, calls for further research that would include a patient registry and coordinated data collection to facilitate answering the many important questions remaining about ketamine’s efficacy and safety.
The report was neither endorsed nor promulgated as policy of the APA. Dr. Sanacora reported multiple relationships with pharmaceutical companies, as did all of his coauthors.
[email protected]
On Twitter @karioakes
A new consensus statement on the use of ketamine as an off-label treatment for mood disorders provides psychiatrists some guidance for patient selection and evaluation, as well as dosing and duration of therapy. The statement was issued against the backdrop of newer studies showing ketamine’s rapid, though not durable, efficacy in treating depression and anxiety disorders.
From start to end, however, the statement urges caution and marks out areas for further study, citing a paucity of data on longer-term efficacy and safety and a literature largely made up of smaller studies.
Dr. Sanacora, professor of psychiatry at Yale University, New Haven, Conn., and his coauthors made clear that “this report is not intended to serve as a standard, guideline, clinical policy, or absolute requirement.” Rather, the document identifies the current state of the field and identifies factors to consider in determining the appropriateness of ketamine therapy.
When a clinician is considering giving ketamine to a patient, a preprocedural evaluation is recommended, both to assess whether ketamine is likely to benefit the patient and to evaluate potential risks. Recommended components include a comprehensive psychiatric diagnostic assessment, paying particular attention to substance use and psychosis history, if any; assessment of baseline symptom severity; history of prior antidepressant treatment; review of systems to assess risk factors; physical examination and laboratory screening that follows accepted guidelines for the anticipated level of sedation, with the recommended addition of a baseline urine toxicology screen; and records review and family corroboration with a particular eye to past substance use.
Finally, the informed consent process should ensure that the patient is aware not only of potential treatment risks, but also of the relatively limited data on the off-label use of ketamine for mood disorders. Thorough written documentation is recommended.
Regarding the appropriate amount of experience and training a clinician should have before administering ketamine, Dr. Sanacora and his coauthors noted that the subanesthetic doses of ketamine that are used to treat mood disorders have been found generally very safe in the limited studies that have been done. Typical peak plasma concentrations will not induce general anesthesia. However, systolic and diastolic blood pressure and heart rate elevations are not uncommon. The statement cites a study that found “blood pressure levels exceeding 180/100 mm Hg or heart rates exceeding 110 beats per minute in approximately 30% of the patients treated.”
Accordingly, the statement recommends that clinicians administering ketamine have Advanced Cardiac Life Support certification and be able to administer Drug Enforcement Administration Schedule III medications. Individual organizations, according to the statement, should follow accepted standards of practice for granting privileges to administer ketamine. A statement developed by the American Society of Anesthesiologists on granting privileges for conscious sedation to nonanesthesia professionals may be used for guidance.
The most-studied dose of ketamine in the treatment of mood disorders is 0.5 mg/kg, administered intravenously over 40 minutes. Though other routes, and lower doses, have been studied, Dr. Sanacora and his colleagues wrote that they consider that “insufficient benefit was provided in those studies to allow any meaningful analysis of any specific dose or route of treatment compared with the standard dose.”
The statement includes a strong recommendation to develop a site-specific–standard operating procedure for the administration of ketamine that incorporates the preprocedural evaluation. In addition, the procedure should assess baseline vital signs, include criteria for acceptable vital signs, and incorporate a “time-out” procedure before initiating ketamine treatment.
Also, standard operating procedures should include continued assessment of respiratory, cardiovascular, and mental status throughout the infusion. Stopping criteria should be clearly defined, as should a plan aimed at managing any cardiovascular or behavioral problems. Discharge procedures should include documentation of vital signs and mental status, ensuring that an adult caregiver can take the patient home, and a thorough review of discharge instructions.
The statement’s section on follow-up and assessments noted: “The existing data surrounding the benefits of repeated infusions of ketamine remain limited.” However, some studies have shown that twice-weekly infusions were as efficacious as infusions given three times a week. In terms of longer-term treatment, the data are sparse, wrote Dr. Sanacora and his coauthors. Some clinics, they said, are giving ketamine two or three times weekly for 2 or 3 weeks, then tapering or adjusting the regimen based on clinical response, but high-quality studies are lacking.” The scarcity of this information is one of the major drawbacks to be considered before initiating ketamine therapy for patients with mood disorders and should be discussed with the patient before beginning treatment,” they wrote.
The known risks of cognitive impairment and cystitis with more chronic high-frequency ketamine use, taken together with the significant potential for abuse, mean that ketamine should be discontinued if more than once-weekly dosing is required after 2 months of treatment. “The goal remains to eventually taper and discontinue treatment until more long-term safety data can be collected,” wrote Dr. Sanacora and his coauthors.
The statement, while acknowledging the hope and excitement that currently surround the use of ketamine for mood disorders, calls for further research that would include a patient registry and coordinated data collection to facilitate answering the many important questions remaining about ketamine’s efficacy and safety.
The report was neither endorsed nor promulgated as policy of the APA. Dr. Sanacora reported multiple relationships with pharmaceutical companies, as did all of his coauthors.
[email protected]
On Twitter @karioakes
FROM JAMA PSYCHIATRY

CLL boost in PFS came at high cost in side effects
Add-on idelalisib boosted the progression-free survival (PFS) of patients with relapsed and refractory chronic lymphocytic leukemia by over 9 months in a double-blind, placebo-controlled trial of 416 participants. But that improvement came at the price of a 4% absolute increase in treatment-emergent adverse events leading to death.
At a median follow-up of 14 months, the median PFS was 20.8 months in the 207 patients in the idelalisib group and 11.1 months in the 209 patients in the placebo group. However, 11% of patients in the idelalisib group and 7% of those in the placebo group had treatment-related adverse events that resulted in death.
Overall, 68% of those in the idelalisib group, and 44% in the placebo group, had serious adverse events that included febrile neutropenia, pneumonia, and pyrexia. Six deaths resulted from infections in the idelalisib group, and three deaths resulted from infections in the placebo group.
All 416 participants in the international, multicenter study had measurable lymphadenopathy by CT or MRI and progression of chronic lymphocytic leukemia within 36 months of their last therapy. Patients were stratified by high-risk genetic mutations (IGHV, del[17p], or TP53) and refractory versus relapsed disease. Participants were randomly assigned to receive daily idelalisib or placebo, plus a maximum of six cycles of bendamustine and rituximab.
The primary endpoint of PFS was assessed by an independent review committee in the intention-to-treat population.
A 150 mg dose of idelalisib or placebo was given twice daily until disease progressed or drug-related toxicity was intolerable. Bendamustine was given intravenously at 70 mg/m2 on days 1 and 2 for six 28-day cycles. Rituximab was given at 375 mg/m2 on day 1 of cycle 1 and at 500 mg/m2 on day 1 of cycles 2–6.
The trial is ongoing, the researchers reported.
The trial is funded by Gilead Sciences, the maker of idelalisib (Zydelig). Dr. Zelenetz disclosed consulting with multiple drug companies, including Gilead.
[email protected]
On Twitter @maryjodales
Add-on idelalisib boosted the progression-free survival (PFS) of patients with relapsed and refractory chronic lymphocytic leukemia by over 9 months in a double-blind, placebo-controlled trial of 416 participants. But that improvement came at the price of a 4% absolute increase in treatment-emergent adverse events leading to death.
At a median follow-up of 14 months, the median PFS was 20.8 months in the 207 patients in the idelalisib group and 11.1 months in the 209 patients in the placebo group. However, 11% of patients in the idelalisib group and 7% of those in the placebo group had treatment-related adverse events that resulted in death.
Overall, 68% of those in the idelalisib group, and 44% in the placebo group, had serious adverse events that included febrile neutropenia, pneumonia, and pyrexia. Six deaths resulted from infections in the idelalisib group, and three deaths resulted from infections in the placebo group.
All 416 participants in the international, multicenter study had measurable lymphadenopathy by CT or MRI and progression of chronic lymphocytic leukemia within 36 months of their last therapy. Patients were stratified by high-risk genetic mutations (IGHV, del[17p], or TP53) and refractory versus relapsed disease. Participants were randomly assigned to receive daily idelalisib or placebo, plus a maximum of six cycles of bendamustine and rituximab.
The primary endpoint of PFS was assessed by an independent review committee in the intention-to-treat population.
A 150 mg dose of idelalisib or placebo was given twice daily until disease progressed or drug-related toxicity was intolerable. Bendamustine was given intravenously at 70 mg/m2 on days 1 and 2 for six 28-day cycles. Rituximab was given at 375 mg/m2 on day 1 of cycle 1 and at 500 mg/m2 on day 1 of cycles 2–6.
The trial is ongoing, the researchers reported.
The trial is funded by Gilead Sciences, the maker of idelalisib (Zydelig). Dr. Zelenetz disclosed consulting with multiple drug companies, including Gilead.
[email protected]
On Twitter @maryjodales
Add-on idelalisib boosted the progression-free survival (PFS) of patients with relapsed and refractory chronic lymphocytic leukemia by over 9 months in a double-blind, placebo-controlled trial of 416 participants. But that improvement came at the price of a 4% absolute increase in treatment-emergent adverse events leading to death.
At a median follow-up of 14 months, the median PFS was 20.8 months in the 207 patients in the idelalisib group and 11.1 months in the 209 patients in the placebo group. However, 11% of patients in the idelalisib group and 7% of those in the placebo group had treatment-related adverse events that resulted in death.
Overall, 68% of those in the idelalisib group, and 44% in the placebo group, had serious adverse events that included febrile neutropenia, pneumonia, and pyrexia. Six deaths resulted from infections in the idelalisib group, and three deaths resulted from infections in the placebo group.
All 416 participants in the international, multicenter study had measurable lymphadenopathy by CT or MRI and progression of chronic lymphocytic leukemia within 36 months of their last therapy. Patients were stratified by high-risk genetic mutations (IGHV, del[17p], or TP53) and refractory versus relapsed disease. Participants were randomly assigned to receive daily idelalisib or placebo, plus a maximum of six cycles of bendamustine and rituximab.
The primary endpoint of PFS was assessed by an independent review committee in the intention-to-treat population.
A 150 mg dose of idelalisib or placebo was given twice daily until disease progressed or drug-related toxicity was intolerable. Bendamustine was given intravenously at 70 mg/m2 on days 1 and 2 for six 28-day cycles. Rituximab was given at 375 mg/m2 on day 1 of cycle 1 and at 500 mg/m2 on day 1 of cycles 2–6.
The trial is ongoing, the researchers reported.
The trial is funded by Gilead Sciences, the maker of idelalisib (Zydelig). Dr. Zelenetz disclosed consulting with multiple drug companies, including Gilead.
[email protected]
On Twitter @maryjodales
Key clinical point:
Major finding: Add-on idelalisib boosted the progression-free survival of patients with relapsed and refractory chronic lymphocytic leukemia by over 9 months.
Data source: A double-blind, placebo-controlled trial of 416 participants.
Disclosures: Gilead Sciences, the maker of idelalisib (Zydelig), sponsored the study. Dr. Zelenetz disclosed consulting with multiple drug companies, including Gilead.
In CML, imatinib benefits persist at 10 years
In patients with chronic myeloid leukemia (CML), the safety and benefits of imatinib persisted over the course of 10 years in a follow-up study reported online March 9 in the New England Journal of Medicine.
The initial results of the phase III International Randomized Study of Interferon and ST1571 (IRIS) trial “fundamentally changed CML treatment and led to marked improvements in prognosis for patients” when imatinib was shown more effective than interferon plus cytarabine among newly diagnosed patients in the chronic phase of the disease, said Andreas Hochhaus, MD, of the Klinik für Innere Medizin II, Universitätsklinikum Jena (Germany), and his associates. The researchers are now reporting the final follow-up results after a median of 10.9 years for the 553 patients who had been randomly assigned to receive daily oral imatinib in the IRIS trial.
The high rate of crossover to the imatinib group among IRIS study participants precluded a direct comparison of overall survival between the two study groups at 10 years. However, the estimated overall 10-year survival in the imatinib group alone was 83.3%. “A total of 260 patients (47.0%) were alive and still receiving study treatment at 10 years, 96 patients (17.4%) were alive and not receiving study treatment, 86 known deaths (15.6% of patients) had occurred, and 11 patients (20.1%) had unknown survival status,” Dr. Hochhaus and his associates reported (N Engl J Med. 2017 Mar 9. doi: 10.1056/NEJMoa1609324).
Approximately 9% of those in the imatinib group had a serious adverse event during follow-up, including 4 patients (0.7%) in whom the event was considered to be related to the drug. Most occurred during the first year of treatment and declined over time. No new safety signals were observed after the 5-year follow-up.
“These results highlight the safety and efficacy of imatinib therapy, with a clear improvement over the outcomes that were expected n patients who received a diagnosis of CML before the introduction of tyrosine kinase inhibitor therapy, when interferon alfa and hematopoietic stem-cell transplantation were the standard therapies,” the investigators said.
Second-generation tyrosine kinase inhibitors have been developed since the IRIS trial was begun, and “it remains to be seen whether they will have similarly favorable long-term safety. Given the long-term safety and efficacy results with imatinib and the increasing availability of generic imatinib, comparative analyses evaluating the available tyrosine kinase inhibitors for first-line therapy are likely to be forthcoming,” they noted.
In patients with chronic myeloid leukemia (CML), the safety and benefits of imatinib persisted over the course of 10 years in a follow-up study reported online March 9 in the New England Journal of Medicine.
The initial results of the phase III International Randomized Study of Interferon and ST1571 (IRIS) trial “fundamentally changed CML treatment and led to marked improvements in prognosis for patients” when imatinib was shown more effective than interferon plus cytarabine among newly diagnosed patients in the chronic phase of the disease, said Andreas Hochhaus, MD, of the Klinik für Innere Medizin II, Universitätsklinikum Jena (Germany), and his associates. The researchers are now reporting the final follow-up results after a median of 10.9 years for the 553 patients who had been randomly assigned to receive daily oral imatinib in the IRIS trial.
The high rate of crossover to the imatinib group among IRIS study participants precluded a direct comparison of overall survival between the two study groups at 10 years. However, the estimated overall 10-year survival in the imatinib group alone was 83.3%. “A total of 260 patients (47.0%) were alive and still receiving study treatment at 10 years, 96 patients (17.4%) were alive and not receiving study treatment, 86 known deaths (15.6% of patients) had occurred, and 11 patients (20.1%) had unknown survival status,” Dr. Hochhaus and his associates reported (N Engl J Med. 2017 Mar 9. doi: 10.1056/NEJMoa1609324).
Approximately 9% of those in the imatinib group had a serious adverse event during follow-up, including 4 patients (0.7%) in whom the event was considered to be related to the drug. Most occurred during the first year of treatment and declined over time. No new safety signals were observed after the 5-year follow-up.
“These results highlight the safety and efficacy of imatinib therapy, with a clear improvement over the outcomes that were expected n patients who received a diagnosis of CML before the introduction of tyrosine kinase inhibitor therapy, when interferon alfa and hematopoietic stem-cell transplantation were the standard therapies,” the investigators said.
Second-generation tyrosine kinase inhibitors have been developed since the IRIS trial was begun, and “it remains to be seen whether they will have similarly favorable long-term safety. Given the long-term safety and efficacy results with imatinib and the increasing availability of generic imatinib, comparative analyses evaluating the available tyrosine kinase inhibitors for first-line therapy are likely to be forthcoming,” they noted.
In patients with chronic myeloid leukemia (CML), the safety and benefits of imatinib persisted over the course of 10 years in a follow-up study reported online March 9 in the New England Journal of Medicine.
The initial results of the phase III International Randomized Study of Interferon and ST1571 (IRIS) trial “fundamentally changed CML treatment and led to marked improvements in prognosis for patients” when imatinib was shown more effective than interferon plus cytarabine among newly diagnosed patients in the chronic phase of the disease, said Andreas Hochhaus, MD, of the Klinik für Innere Medizin II, Universitätsklinikum Jena (Germany), and his associates. The researchers are now reporting the final follow-up results after a median of 10.9 years for the 553 patients who had been randomly assigned to receive daily oral imatinib in the IRIS trial.
The high rate of crossover to the imatinib group among IRIS study participants precluded a direct comparison of overall survival between the two study groups at 10 years. However, the estimated overall 10-year survival in the imatinib group alone was 83.3%. “A total of 260 patients (47.0%) were alive and still receiving study treatment at 10 years, 96 patients (17.4%) were alive and not receiving study treatment, 86 known deaths (15.6% of patients) had occurred, and 11 patients (20.1%) had unknown survival status,” Dr. Hochhaus and his associates reported (N Engl J Med. 2017 Mar 9. doi: 10.1056/NEJMoa1609324).
Approximately 9% of those in the imatinib group had a serious adverse event during follow-up, including 4 patients (0.7%) in whom the event was considered to be related to the drug. Most occurred during the first year of treatment and declined over time. No new safety signals were observed after the 5-year follow-up.
“These results highlight the safety and efficacy of imatinib therapy, with a clear improvement over the outcomes that were expected n patients who received a diagnosis of CML before the introduction of tyrosine kinase inhibitor therapy, when interferon alfa and hematopoietic stem-cell transplantation were the standard therapies,” the investigators said.
Second-generation tyrosine kinase inhibitors have been developed since the IRIS trial was begun, and “it remains to be seen whether they will have similarly favorable long-term safety. Given the long-term safety and efficacy results with imatinib and the increasing availability of generic imatinib, comparative analyses evaluating the available tyrosine kinase inhibitors for first-line therapy are likely to be forthcoming,” they noted.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Imatinib’s benefits in chronic myeloid leukemia and its safety profile persisted over the long term in a 10-year follow-up study.
Major finding: The estimated overall 10-year survival was 83.3%, and no new safety signals were observed after 5-year follow-up.
Data source: Extended follow-up of an open-label international randomized trial involving 553 adults with CML.
Disclosures: This study was funded by Novartis. Dr. Hochhaus reported ties to Novartis and other drug companies.