User login
Trump travel policy may affect medical meetings
President Trump’s revised executive order blocking travelers from six Muslim-majority countries from entering the United States could land a damaging blow to global cooperation in scientific research and could impede assemblies of the world’s top medical experts.
The March 6 executive order bars citizens of Iran, Libya, Somalia, Sudan, Syria, and Yemen from obtaining visas for 90 days and blocks refugees from those countries from entering the United States for 120 days. The measure, which takes effect March 16, supersedes President Trump’s original Jan. 27 travel ban. The new order exempts citizens of the six countries who are legal permanent U.S. residents or who have current visas.
The policy could have detrimental effects on future collaboration between U.S. and international scientists and may ultimately endanger the health and well-being of patients, said International Antiviral Society–U.S.A. executive director and president Donna M. Jacobsen, regarding the original travel ban.
There is “serious reason for concern” that the policy will dissuade scientists and researchers “from traveling to the [United States] in the future overall and sharing their work with colleagues here,” she said.
Thousands of academics from around the world, including physicians, researchers, and professors, have vowed to boycott U.S.-based conferences in light of the Trump administration policy. A Google Docs petition started shortly after the original ban was announced garnered more than 5,000 signatures by professionals acting in solidarity with those affected by the travel restrictions. The academicians who signed the petition said they would not attend international conferences in the United States until those restricted from participating could rejoin their colleagues and freely share their ideas.
The new executive order comes nearly 2 months after President Trump’s original travel ban caused nationwide protests and led to a series of legal challenges. The states of Washington and Minnesota, which sued President Trump over his original ban, argued that such a ban harms the teaching and research missions of their universities and prevents students and faculty from traveling for research and academic collaboration. In addition, the executive order restricts universities from hiring attractive candidates from countries affected by the ban, state officials said. A federal court temporarily blocked the original travel ban on Feb. 3, a decision upheld by the 9th U.S. Circuit Court of Appeals on Feb. 9. The circuit judges said the plaintiffs were likely to succeed in their arguments and that the president had demonstrated no evidence that his executive order advances national security.
The new executive order excludes Iraq and also removes language that had indefinitely banned Syrian refugees. In a March 6 memorandum, the White House said the purpose of the ban is to prevent “foreign nationals who may aid, support, or commit violent, criminal, or terrorist acts,” while the administration enhances the screening and vetting protocols and procedures for granting visas and admission to the United States.
“This nation cannot delay the immediate implementation of additional heightened screening and vetting protocols and procedures for issuing visas to ensure that we strengthen the safety and security of our country,” the memo states.
[email protected]
On Twitter @legal_med
February 7, 2017
The Honorable John F. Kelly
Secretary
U.S. Department of Homeland Security
Washington, DC 20528
Dear Secretary Kelly:
The undersigned organizations are greatly concerned that the executive order signed by President Trump on January 27, 2017 will result in discrimination against foreign-born persons from certain predominantly Muslim countries. We are particularly concerned that by restricting entry of physicians and medical students from seven designated Muslim majority countries, the order will undermine medical education and result in patients losing access to their doctors. We are also greatly concerned that the 120 day ban on accepting refugees, and the indefinite ban on Syrian refugees, will contribute to an ongoing public health crisis for those affected, needlessly subjecting them to violence, injury, illness, deprivation and even death. While we are pleased that the courts have temporarily halted implementation of the executive order, the underlying issues of concern about the harm caused by the executive order remain.
The restrictions in the executive order will hinder the free exchange of information and travel among medical students, residents and physicians around the world and result in Americans having poorer access to care. In 2016, 3,769 non-U.S. citizen international medical graduates (IMGs) obtained first-year residency positions. More than half of internal medicine residency positions were filled by IMGs. Approximately 25% of the nation’s physicians are IMGs and provide a disproportionate share of the care to Americans in underserved communities that have a shortage of U.S. born and trained physicians. They also add necessary diversity and cultural competency to our healthcare workforce. If the executive order prevents IMGs from being able to come to the U.S. this could potentially affect the care for thousands of patients.
Our organizations are also especially concerned about refugees with dire medical conditions who had been approved for visas to enter the U.S. but since the executive order, have been unable to enter the country to receive much needed medical care.
While we urge that the executive order be rescinded and replaced with non-discriminatory policies that support families, public health, and medical education, and are pleased that the courts have temporarily halted implementation, there are steps that DHS can take immediately to selectively ease travel restrictions that impact medical education, access to health care services, and public health for individuals who otherwise meet the criteria for immigration, including those from the seven countries identified in the executive order. Specifically, we urge the Department of Homeland Security to:
1. Reinstate the Visa Interview Waiver Program. Suspension of the program “risks creating substantial backlogs in the processing of new and renewal visas for trainees from any foreign
country — delays that create substantial problems for residency programs with trainees on visas and that could interfere with the residency match process this year.”
2. Remove restrictions on entering the U.S. for physicians from the seven designated countries who have been approved for J-1 or H-1B visas and students from those countries with F-1 visas who have been accepted to U.S. medical schools.
3. Develop and implement a plan to allow physicians from the seven designated countries to obtain travel visas to travel to the U.S. for medical conferences and other medical and research-related engagements.
4. Make it a priority to implement a process to admit refugees, without further delay, who had already been vetted and approved for entry prior to the executive order and who are in need of urgent medical care. We note that even with such revisions, the executive order will still inappropriately bar immigrants and refugees based on discriminatory criteria (religion and country of origin) including family members of physicians and medical students in the U.S.
Our organizations are committed to non-discrimination against physicians, medical students and others in immigration policies and offer our assistance in developing policies that support access to health care services, public health, and medical education while balancing the nation’s security needs. Until or unless the executive order is completely rescinded or permanently blocked, it is essential that DHS move forward to ensure that restrictions on physicians and medical students are not reimposed, and that priority is given to refugees with medical conditions needing treatment.
Sincerely,
Alliance for Academic Internal Medicine
American College of Chest Physicians
American College of Physicians
American Society for Gastrointestinal Endoscopy
American Society of Hematology
American Society of Nephrology
American Thoracic Society
Infectious Diseases Society of America
Renal Physicians Association
Society for Adolescent Health and Medicine
Society of Critical Care Medicine
Society of General Internal Medicine
February 7, 2017
The Honorable John F. Kelly
Secretary
U.S. Department of Homeland Security
Washington, DC 20528
Dear Secretary Kelly:
The undersigned organizations are greatly concerned that the executive order signed by President Trump on January 27, 2017 will result in discrimination against foreign-born persons from certain predominantly Muslim countries. We are particularly concerned that by restricting entry of physicians and medical students from seven designated Muslim majority countries, the order will undermine medical education and result in patients losing access to their doctors. We are also greatly concerned that the 120 day ban on accepting refugees, and the indefinite ban on Syrian refugees, will contribute to an ongoing public health crisis for those affected, needlessly subjecting them to violence, injury, illness, deprivation and even death. While we are pleased that the courts have temporarily halted implementation of the executive order, the underlying issues of concern about the harm caused by the executive order remain.
The restrictions in the executive order will hinder the free exchange of information and travel among medical students, residents and physicians around the world and result in Americans having poorer access to care. In 2016, 3,769 non-U.S. citizen international medical graduates (IMGs) obtained first-year residency positions. More than half of internal medicine residency positions were filled by IMGs. Approximately 25% of the nation’s physicians are IMGs and provide a disproportionate share of the care to Americans in underserved communities that have a shortage of U.S. born and trained physicians. They also add necessary diversity and cultural competency to our healthcare workforce. If the executive order prevents IMGs from being able to come to the U.S. this could potentially affect the care for thousands of patients.
Our organizations are also especially concerned about refugees with dire medical conditions who had been approved for visas to enter the U.S. but since the executive order, have been unable to enter the country to receive much needed medical care.
While we urge that the executive order be rescinded and replaced with non-discriminatory policies that support families, public health, and medical education, and are pleased that the courts have temporarily halted implementation, there are steps that DHS can take immediately to selectively ease travel restrictions that impact medical education, access to health care services, and public health for individuals who otherwise meet the criteria for immigration, including those from the seven countries identified in the executive order. Specifically, we urge the Department of Homeland Security to:
1. Reinstate the Visa Interview Waiver Program. Suspension of the program “risks creating substantial backlogs in the processing of new and renewal visas for trainees from any foreign
country — delays that create substantial problems for residency programs with trainees on visas and that could interfere with the residency match process this year.”
2. Remove restrictions on entering the U.S. for physicians from the seven designated countries who have been approved for J-1 or H-1B visas and students from those countries with F-1 visas who have been accepted to U.S. medical schools.
3. Develop and implement a plan to allow physicians from the seven designated countries to obtain travel visas to travel to the U.S. for medical conferences and other medical and research-related engagements.
4. Make it a priority to implement a process to admit refugees, without further delay, who had already been vetted and approved for entry prior to the executive order and who are in need of urgent medical care. We note that even with such revisions, the executive order will still inappropriately bar immigrants and refugees based on discriminatory criteria (religion and country of origin) including family members of physicians and medical students in the U.S.
Our organizations are committed to non-discrimination against physicians, medical students and others in immigration policies and offer our assistance in developing policies that support access to health care services, public health, and medical education while balancing the nation’s security needs. Until or unless the executive order is completely rescinded or permanently blocked, it is essential that DHS move forward to ensure that restrictions on physicians and medical students are not reimposed, and that priority is given to refugees with medical conditions needing treatment.
Sincerely,
Alliance for Academic Internal Medicine
American College of Chest Physicians
American College of Physicians
American Society for Gastrointestinal Endoscopy
American Society of Hematology
American Society of Nephrology
American Thoracic Society
Infectious Diseases Society of America
Renal Physicians Association
Society for Adolescent Health and Medicine
Society of Critical Care Medicine
Society of General Internal Medicine
February 7, 2017
The Honorable John F. Kelly
Secretary
U.S. Department of Homeland Security
Washington, DC 20528
Dear Secretary Kelly:
The undersigned organizations are greatly concerned that the executive order signed by President Trump on January 27, 2017 will result in discrimination against foreign-born persons from certain predominantly Muslim countries. We are particularly concerned that by restricting entry of physicians and medical students from seven designated Muslim majority countries, the order will undermine medical education and result in patients losing access to their doctors. We are also greatly concerned that the 120 day ban on accepting refugees, and the indefinite ban on Syrian refugees, will contribute to an ongoing public health crisis for those affected, needlessly subjecting them to violence, injury, illness, deprivation and even death. While we are pleased that the courts have temporarily halted implementation of the executive order, the underlying issues of concern about the harm caused by the executive order remain.
The restrictions in the executive order will hinder the free exchange of information and travel among medical students, residents and physicians around the world and result in Americans having poorer access to care. In 2016, 3,769 non-U.S. citizen international medical graduates (IMGs) obtained first-year residency positions. More than half of internal medicine residency positions were filled by IMGs. Approximately 25% of the nation’s physicians are IMGs and provide a disproportionate share of the care to Americans in underserved communities that have a shortage of U.S. born and trained physicians. They also add necessary diversity and cultural competency to our healthcare workforce. If the executive order prevents IMGs from being able to come to the U.S. this could potentially affect the care for thousands of patients.
Our organizations are also especially concerned about refugees with dire medical conditions who had been approved for visas to enter the U.S. but since the executive order, have been unable to enter the country to receive much needed medical care.
While we urge that the executive order be rescinded and replaced with non-discriminatory policies that support families, public health, and medical education, and are pleased that the courts have temporarily halted implementation, there are steps that DHS can take immediately to selectively ease travel restrictions that impact medical education, access to health care services, and public health for individuals who otherwise meet the criteria for immigration, including those from the seven countries identified in the executive order. Specifically, we urge the Department of Homeland Security to:
1. Reinstate the Visa Interview Waiver Program. Suspension of the program “risks creating substantial backlogs in the processing of new and renewal visas for trainees from any foreign
country — delays that create substantial problems for residency programs with trainees on visas and that could interfere with the residency match process this year.”
2. Remove restrictions on entering the U.S. for physicians from the seven designated countries who have been approved for J-1 or H-1B visas and students from those countries with F-1 visas who have been accepted to U.S. medical schools.
3. Develop and implement a plan to allow physicians from the seven designated countries to obtain travel visas to travel to the U.S. for medical conferences and other medical and research-related engagements.
4. Make it a priority to implement a process to admit refugees, without further delay, who had already been vetted and approved for entry prior to the executive order and who are in need of urgent medical care. We note that even with such revisions, the executive order will still inappropriately bar immigrants and refugees based on discriminatory criteria (religion and country of origin) including family members of physicians and medical students in the U.S.
Our organizations are committed to non-discrimination against physicians, medical students and others in immigration policies and offer our assistance in developing policies that support access to health care services, public health, and medical education while balancing the nation’s security needs. Until or unless the executive order is completely rescinded or permanently blocked, it is essential that DHS move forward to ensure that restrictions on physicians and medical students are not reimposed, and that priority is given to refugees with medical conditions needing treatment.
Sincerely,
Alliance for Academic Internal Medicine
American College of Chest Physicians
American College of Physicians
American Society for Gastrointestinal Endoscopy
American Society of Hematology
American Society of Nephrology
American Thoracic Society
Infectious Diseases Society of America
Renal Physicians Association
Society for Adolescent Health and Medicine
Society of Critical Care Medicine
Society of General Internal Medicine
President Trump’s revised executive order blocking travelers from six Muslim-majority countries from entering the United States could land a damaging blow to global cooperation in scientific research and could impede assemblies of the world’s top medical experts.
The March 6 executive order bars citizens of Iran, Libya, Somalia, Sudan, Syria, and Yemen from obtaining visas for 90 days and blocks refugees from those countries from entering the United States for 120 days. The measure, which takes effect March 16, supersedes President Trump’s original Jan. 27 travel ban. The new order exempts citizens of the six countries who are legal permanent U.S. residents or who have current visas.
The policy could have detrimental effects on future collaboration between U.S. and international scientists and may ultimately endanger the health and well-being of patients, said International Antiviral Society–U.S.A. executive director and president Donna M. Jacobsen, regarding the original travel ban.
There is “serious reason for concern” that the policy will dissuade scientists and researchers “from traveling to the [United States] in the future overall and sharing their work with colleagues here,” she said.
Thousands of academics from around the world, including physicians, researchers, and professors, have vowed to boycott U.S.-based conferences in light of the Trump administration policy. A Google Docs petition started shortly after the original ban was announced garnered more than 5,000 signatures by professionals acting in solidarity with those affected by the travel restrictions. The academicians who signed the petition said they would not attend international conferences in the United States until those restricted from participating could rejoin their colleagues and freely share their ideas.
The new executive order comes nearly 2 months after President Trump’s original travel ban caused nationwide protests and led to a series of legal challenges. The states of Washington and Minnesota, which sued President Trump over his original ban, argued that such a ban harms the teaching and research missions of their universities and prevents students and faculty from traveling for research and academic collaboration. In addition, the executive order restricts universities from hiring attractive candidates from countries affected by the ban, state officials said. A federal court temporarily blocked the original travel ban on Feb. 3, a decision upheld by the 9th U.S. Circuit Court of Appeals on Feb. 9. The circuit judges said the plaintiffs were likely to succeed in their arguments and that the president had demonstrated no evidence that his executive order advances national security.
The new executive order excludes Iraq and also removes language that had indefinitely banned Syrian refugees. In a March 6 memorandum, the White House said the purpose of the ban is to prevent “foreign nationals who may aid, support, or commit violent, criminal, or terrorist acts,” while the administration enhances the screening and vetting protocols and procedures for granting visas and admission to the United States.
“This nation cannot delay the immediate implementation of additional heightened screening and vetting protocols and procedures for issuing visas to ensure that we strengthen the safety and security of our country,” the memo states.
[email protected]
On Twitter @legal_med
President Trump’s revised executive order blocking travelers from six Muslim-majority countries from entering the United States could land a damaging blow to global cooperation in scientific research and could impede assemblies of the world’s top medical experts.
The March 6 executive order bars citizens of Iran, Libya, Somalia, Sudan, Syria, and Yemen from obtaining visas for 90 days and blocks refugees from those countries from entering the United States for 120 days. The measure, which takes effect March 16, supersedes President Trump’s original Jan. 27 travel ban. The new order exempts citizens of the six countries who are legal permanent U.S. residents or who have current visas.
The policy could have detrimental effects on future collaboration between U.S. and international scientists and may ultimately endanger the health and well-being of patients, said International Antiviral Society–U.S.A. executive director and president Donna M. Jacobsen, regarding the original travel ban.
There is “serious reason for concern” that the policy will dissuade scientists and researchers “from traveling to the [United States] in the future overall and sharing their work with colleagues here,” she said.
Thousands of academics from around the world, including physicians, researchers, and professors, have vowed to boycott U.S.-based conferences in light of the Trump administration policy. A Google Docs petition started shortly after the original ban was announced garnered more than 5,000 signatures by professionals acting in solidarity with those affected by the travel restrictions. The academicians who signed the petition said they would not attend international conferences in the United States until those restricted from participating could rejoin their colleagues and freely share their ideas.
The new executive order comes nearly 2 months after President Trump’s original travel ban caused nationwide protests and led to a series of legal challenges. The states of Washington and Minnesota, which sued President Trump over his original ban, argued that such a ban harms the teaching and research missions of their universities and prevents students and faculty from traveling for research and academic collaboration. In addition, the executive order restricts universities from hiring attractive candidates from countries affected by the ban, state officials said. A federal court temporarily blocked the original travel ban on Feb. 3, a decision upheld by the 9th U.S. Circuit Court of Appeals on Feb. 9. The circuit judges said the plaintiffs were likely to succeed in their arguments and that the president had demonstrated no evidence that his executive order advances national security.
The new executive order excludes Iraq and also removes language that had indefinitely banned Syrian refugees. In a March 6 memorandum, the White House said the purpose of the ban is to prevent “foreign nationals who may aid, support, or commit violent, criminal, or terrorist acts,” while the administration enhances the screening and vetting protocols and procedures for granting visas and admission to the United States.
“This nation cannot delay the immediate implementation of additional heightened screening and vetting protocols and procedures for issuing visas to ensure that we strengthen the safety and security of our country,” the memo states.
[email protected]
On Twitter @legal_med
Methotrexate use justified for early RA, disease prevention
Efforts to delay or prevent rheumatoid arthritis (RA) in individuals at high risk for the disease received a boost from the findings of a subgroup analysis of an older Dutch prevention trial involving methotrexate that were published recently in Arthritis & Rheumatology.
However, while the 22-patient subgroup analysis of the 2007 trial, called PROMPT (Probable RA: Methotrexate Versus Placebo Treatment), showed that 1 year of methotrexate prevented the development of rheumatoid arthritis in significantly more individuals at high risk for the disease than did placebo, hindsight has shown that most of these high-risk individuals actually had RA at baseline as defined by the 2010 American College or Rheumatology/European League Against Rheumatism classification criteria.

Even though the “landscape of RA has changed since this study was conceived, enrolled, and performed,” Dr. Sparks noted that the study provides evidence that today’s “standard of care really works” by making use of data that are unobtainable today.
“Nowadays, we wouldn’t be able to do a placebo-controlled trial in early RA because those patients need to be treated, but at the time, it was perfectly fine, based on the treatment landscape, to put these patients in a [placebo-controlled] trial,” he said in an interview.
“It also demonstrates that you really need to find high-risk individuals, because, if you recruit people who are never going to develop RA, you’re just diluting your effect, and you’re not going to find the difference in the groups based on that diluted effect when there could be a true effect in that special subgroup,” he added.
Senior study author Annette van der Helm-van Mil, MD, PhD, and her colleagues at Leiden (the Netherlands) University Medical Center performed the reanalysis after the initial finding that methotrexate had no preventative effect may have been falsely negative because the study included patients with a low risk of progressing to RA (Arthritis Rheumatol. 2017 Feb 19. doi: 10.1002/art.40062).

In the reanalysis, the investigators defined 22 out of the trial’s 110 participants as high risk based on their score of 8 or higher on the Leiden prediction rule at baseline. Of those 22, 18 also fulfilled the 2010 classification criteria for RA.
This “definition of high risk [in the trial] very much coincided with the new classification criteria and reinforces the standard of care that patients with new diagnosed RA should be treated with DMARDs [disease-modifying antirheumatic drugs] front line,” Dr. Sparks said.
The Leiden prediction rule score is based on ACPA statuses, as well as age, sex, distribution of involved joints, number of swollen and tender joints, severity of morning stiffness, C-reactive protein level, and rheumatoid factor. In previous studies of patients with undifferentiated arthritis, a score of 8 or higher with the prediction rule had a positive predictive value of 84% in patients with undifferentiated arthritis, according to the investigators.
Based on a primary outcome of fulfilling the 1987 classification criteria for RA after 5 years of follow-up, the investigators found that 6 of 11 (55%) in the methotrexate arm developed RA, compared with all 11 patients in the placebo arm (P = .011). “A 1-year course of methotrexate was associated with an absolute risk reduction of 45% on RA development, resulting in a number needed to treat of 2.2 (95% [confidence interval], 1.3-6.2),” the authors wrote.
Furthermore, the time to the development of RA based on the 1987 criteria was longer with methotrexate than with placebo (median of 22.5 months vs. 3 months; P less than .001).
Drug-free remission was also achieved by 4 of 11 (36%) patients taking methotrexate, compared with none of the patients taking placebo (P = .027).
The beneficial effects of methotrexate were seen in ACPA-positive and ACPA-negative high-risk patients but not in patients without a high risk of RA.
For the patients who did not fulfill the 2010 RA criteria at baseline, only one of four of those in the placebo arm did go on to develop RA based on 1987 criteria, whereas only one of three who received methotrexate did.
Overall, the reanalysis of PROMPT trial data illustrates how “noninformative inclusions can blur highly relevant study outcomes, such as prevention of RA,” the study authors concluded.
“As trials are now being conducted to evaluate the efficacy of treatment initiated in the phase of arthralgia, the development of adequate risk prediction models are of importance in order to prevent false-negative study results in the future,” they added.
The PROMPT trial was supported by the Dutch Arthritis Foundation and the Netherlands Organisation for Scientific Research.
Small numbers not withstanding, the findings of this reanalysis of the PROMPT trial are exciting, and they address the importance of identifying the right individuals to include in any type of prevention study in RA.
Given the temporal limits of clinical trials, inclusion criteria will need to incorporate both the likelihood of an important outcome and the timing of that outcome – right individuals, right time, right drug/intervention.

It is hoped that investigators will be able to demonstrate conclusively that preventive interventions work for rheumatic disease once these issues are addressed.
Kevin D. Deane, MD, PhD, and his coauthors are with the division of rheumatology at the University of Colorado, Denver, and made these remarks in an editorial accompanying the PROMPT trial reanalysis (Arthritis Rheumatol. 2017 Feb 19. doi: 10.1002/art.40061).
Small numbers not withstanding, the findings of this reanalysis of the PROMPT trial are exciting, and they address the importance of identifying the right individuals to include in any type of prevention study in RA.
Given the temporal limits of clinical trials, inclusion criteria will need to incorporate both the likelihood of an important outcome and the timing of that outcome – right individuals, right time, right drug/intervention.
It is hoped that investigators will be able to demonstrate conclusively that preventive interventions work for rheumatic disease once these issues are addressed.
Kevin D. Deane, MD, PhD, and his coauthors are with the division of rheumatology at the University of Colorado, Denver, and made these remarks in an editorial accompanying the PROMPT trial reanalysis (Arthritis Rheumatol. 2017 Feb 19. doi: 10.1002/art.40061).
Small numbers not withstanding, the findings of this reanalysis of the PROMPT trial are exciting, and they address the importance of identifying the right individuals to include in any type of prevention study in RA.
Given the temporal limits of clinical trials, inclusion criteria will need to incorporate both the likelihood of an important outcome and the timing of that outcome – right individuals, right time, right drug/intervention.
It is hoped that investigators will be able to demonstrate conclusively that preventive interventions work for rheumatic disease once these issues are addressed.
Kevin D. Deane, MD, PhD, and his coauthors are with the division of rheumatology at the University of Colorado, Denver, and made these remarks in an editorial accompanying the PROMPT trial reanalysis (Arthritis Rheumatol. 2017 Feb 19. doi: 10.1002/art.40061).
Efforts to delay or prevent rheumatoid arthritis (RA) in individuals at high risk for the disease received a boost from the findings of a subgroup analysis of an older Dutch prevention trial involving methotrexate that were published recently in Arthritis & Rheumatology.
However, while the 22-patient subgroup analysis of the 2007 trial, called PROMPT (Probable RA: Methotrexate Versus Placebo Treatment), showed that 1 year of methotrexate prevented the development of rheumatoid arthritis in significantly more individuals at high risk for the disease than did placebo, hindsight has shown that most of these high-risk individuals actually had RA at baseline as defined by the 2010 American College or Rheumatology/European League Against Rheumatism classification criteria.
Even though the “landscape of RA has changed since this study was conceived, enrolled, and performed,” Dr. Sparks noted that the study provides evidence that today’s “standard of care really works” by making use of data that are unobtainable today.
“Nowadays, we wouldn’t be able to do a placebo-controlled trial in early RA because those patients need to be treated, but at the time, it was perfectly fine, based on the treatment landscape, to put these patients in a [placebo-controlled] trial,” he said in an interview.
“It also demonstrates that you really need to find high-risk individuals, because, if you recruit people who are never going to develop RA, you’re just diluting your effect, and you’re not going to find the difference in the groups based on that diluted effect when there could be a true effect in that special subgroup,” he added.
Senior study author Annette van der Helm-van Mil, MD, PhD, and her colleagues at Leiden (the Netherlands) University Medical Center performed the reanalysis after the initial finding that methotrexate had no preventative effect may have been falsely negative because the study included patients with a low risk of progressing to RA (Arthritis Rheumatol. 2017 Feb 19. doi: 10.1002/art.40062).
In the reanalysis, the investigators defined 22 out of the trial’s 110 participants as high risk based on their score of 8 or higher on the Leiden prediction rule at baseline. Of those 22, 18 also fulfilled the 2010 classification criteria for RA.
This “definition of high risk [in the trial] very much coincided with the new classification criteria and reinforces the standard of care that patients with new diagnosed RA should be treated with DMARDs [disease-modifying antirheumatic drugs] front line,” Dr. Sparks said.
The Leiden prediction rule score is based on ACPA statuses, as well as age, sex, distribution of involved joints, number of swollen and tender joints, severity of morning stiffness, C-reactive protein level, and rheumatoid factor. In previous studies of patients with undifferentiated arthritis, a score of 8 or higher with the prediction rule had a positive predictive value of 84% in patients with undifferentiated arthritis, according to the investigators.
Based on a primary outcome of fulfilling the 1987 classification criteria for RA after 5 years of follow-up, the investigators found that 6 of 11 (55%) in the methotrexate arm developed RA, compared with all 11 patients in the placebo arm (P = .011). “A 1-year course of methotrexate was associated with an absolute risk reduction of 45% on RA development, resulting in a number needed to treat of 2.2 (95% [confidence interval], 1.3-6.2),” the authors wrote.
Furthermore, the time to the development of RA based on the 1987 criteria was longer with methotrexate than with placebo (median of 22.5 months vs. 3 months; P less than .001).
Drug-free remission was also achieved by 4 of 11 (36%) patients taking methotrexate, compared with none of the patients taking placebo (P = .027).
The beneficial effects of methotrexate were seen in ACPA-positive and ACPA-negative high-risk patients but not in patients without a high risk of RA.
For the patients who did not fulfill the 2010 RA criteria at baseline, only one of four of those in the placebo arm did go on to develop RA based on 1987 criteria, whereas only one of three who received methotrexate did.
Overall, the reanalysis of PROMPT trial data illustrates how “noninformative inclusions can blur highly relevant study outcomes, such as prevention of RA,” the study authors concluded.
“As trials are now being conducted to evaluate the efficacy of treatment initiated in the phase of arthralgia, the development of adequate risk prediction models are of importance in order to prevent false-negative study results in the future,” they added.
The PROMPT trial was supported by the Dutch Arthritis Foundation and the Netherlands Organisation for Scientific Research.
Efforts to delay or prevent rheumatoid arthritis (RA) in individuals at high risk for the disease received a boost from the findings of a subgroup analysis of an older Dutch prevention trial involving methotrexate that were published recently in Arthritis & Rheumatology.
However, while the 22-patient subgroup analysis of the 2007 trial, called PROMPT (Probable RA: Methotrexate Versus Placebo Treatment), showed that 1 year of methotrexate prevented the development of rheumatoid arthritis in significantly more individuals at high risk for the disease than did placebo, hindsight has shown that most of these high-risk individuals actually had RA at baseline as defined by the 2010 American College or Rheumatology/European League Against Rheumatism classification criteria.
Even though the “landscape of RA has changed since this study was conceived, enrolled, and performed,” Dr. Sparks noted that the study provides evidence that today’s “standard of care really works” by making use of data that are unobtainable today.
“Nowadays, we wouldn’t be able to do a placebo-controlled trial in early RA because those patients need to be treated, but at the time, it was perfectly fine, based on the treatment landscape, to put these patients in a [placebo-controlled] trial,” he said in an interview.
“It also demonstrates that you really need to find high-risk individuals, because, if you recruit people who are never going to develop RA, you’re just diluting your effect, and you’re not going to find the difference in the groups based on that diluted effect when there could be a true effect in that special subgroup,” he added.
Senior study author Annette van der Helm-van Mil, MD, PhD, and her colleagues at Leiden (the Netherlands) University Medical Center performed the reanalysis after the initial finding that methotrexate had no preventative effect may have been falsely negative because the study included patients with a low risk of progressing to RA (Arthritis Rheumatol. 2017 Feb 19. doi: 10.1002/art.40062).
In the reanalysis, the investigators defined 22 out of the trial’s 110 participants as high risk based on their score of 8 or higher on the Leiden prediction rule at baseline. Of those 22, 18 also fulfilled the 2010 classification criteria for RA.
This “definition of high risk [in the trial] very much coincided with the new classification criteria and reinforces the standard of care that patients with new diagnosed RA should be treated with DMARDs [disease-modifying antirheumatic drugs] front line,” Dr. Sparks said.
The Leiden prediction rule score is based on ACPA statuses, as well as age, sex, distribution of involved joints, number of swollen and tender joints, severity of morning stiffness, C-reactive protein level, and rheumatoid factor. In previous studies of patients with undifferentiated arthritis, a score of 8 or higher with the prediction rule had a positive predictive value of 84% in patients with undifferentiated arthritis, according to the investigators.
Based on a primary outcome of fulfilling the 1987 classification criteria for RA after 5 years of follow-up, the investigators found that 6 of 11 (55%) in the methotrexate arm developed RA, compared with all 11 patients in the placebo arm (P = .011). “A 1-year course of methotrexate was associated with an absolute risk reduction of 45% on RA development, resulting in a number needed to treat of 2.2 (95% [confidence interval], 1.3-6.2),” the authors wrote.
Furthermore, the time to the development of RA based on the 1987 criteria was longer with methotrexate than with placebo (median of 22.5 months vs. 3 months; P less than .001).
Drug-free remission was also achieved by 4 of 11 (36%) patients taking methotrexate, compared with none of the patients taking placebo (P = .027).
The beneficial effects of methotrexate were seen in ACPA-positive and ACPA-negative high-risk patients but not in patients without a high risk of RA.
For the patients who did not fulfill the 2010 RA criteria at baseline, only one of four of those in the placebo arm did go on to develop RA based on 1987 criteria, whereas only one of three who received methotrexate did.
Overall, the reanalysis of PROMPT trial data illustrates how “noninformative inclusions can blur highly relevant study outcomes, such as prevention of RA,” the study authors concluded.
“As trials are now being conducted to evaluate the efficacy of treatment initiated in the phase of arthralgia, the development of adequate risk prediction models are of importance in order to prevent false-negative study results in the future,” they added.
The PROMPT trial was supported by the Dutch Arthritis Foundation and the Netherlands Organisation for Scientific Research.
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point:
Main finding: In people deemed to be at high risk for RA, a 1-year course of methotrexate was associated with an absolute risk reduction of 45% of RA development, resulting in a number needed to treat of 2.2 (95% CI, 1.3-6.2).
Data source: A reanalysis of the PROMPT trial involving 110 patients with undifferentiated arthritis randomized to a 1-year course of methotrexate or placebo.
Disclosures: The PROMPT trial was supported by the Dutch Arthritis Foundation and the Netherlands Organisation for Scientific Research.
Cutaneous Manifestations of Tick-Borne Diseases


GOP health plan clears first hurdle as opposition lines up
The Republican plan to replace the Affordable Care Act cleared the first legislative hurdle when two house committees passed language that would repeal revenue provisions of the Affordable Care Act and lay the foundation for replacing the health care reform law.
The House Ways and Means Committee–approved legislation would eliminate the individual mandate in favor of allowing insurance companies to penalize individuals by up to 30% of premiums for lapses in coverage and would repeal taxes on high-cost health plans (Cadillac tax), over-the-counter and prescription medications, health savings accounts, tanning, investment, and on health insurers.
The language passed with a party-line vote March 9 with 23 Republicans voting for and 16 Democrats voting against after nearly 18 hours of debate and amendments.
The House Energy and Commerce Committee, after 27 hours of debate that started March 8, also passed its language along party lines with 31 Republicans voting for and 23 Democrats voting against. Their bill would end Medicaid expansion and reset the program’s funding to a per capita allotment based on population indicators, along with block grants, to provide states more flexibility to better manage its population.
A key concern raised in both committee debates was the brief window between the public unveiling of the legislation and the committees’ efforts, especially the lack of financial impact analysis or “score” from the Congressional Budget Office. Democrats efforts in both committees to hold action for a CBO score were voted down on across party lines.
In both committees, Democrats introduced a wide range of amendments, including guarantees there would be no impact from the reduction of Medicaid expansion and on funding to support coverage for mental health, women, children, seniors, and veterans, all of which were voted down. Ways and Means members also offered an amendment to require President Trump to release his income tax filings.
Rep. Frank Pallone (D-N.J.), lead Democrat in the Energy and Commerce Committee, voiced his colleagues’ objections to the bill and the process.
The bill “would rip health care away from millions of Americans, raise costs for working families and seniors, and lead to the rationing of care for 76 million Americans who receive Medicaid. … This has not been a transparent process. We did not go through regular order. The bill was posted less than 2 days before markup. No hearings were held, and we don’t have a CBO score,” Rep. Pallone said during committee debate.
A CBO score of the budget and coverage impacts of the Republican health care proposal could come as early as March 13.
The pace of action in the House even drew criticism from some in the GOP. Sen. Tom Cotton (R-Ark.) took to Twitter with a stern warning to the House.
“House health-care bill can’t pass w/o major changes,” Sen. Cotton tweeted. “To my friends in House: pause, start over. Get it right, don’t get it fast.”
He followed up with two more tweets: “GOP shouldn’t act like Dems did in O’care. No excuse to release bill Mon night, start voting Wed. With no budget estimate!” He added: “What matters in long run is better, more affordable health care for Americans, NOT house leaders’ arbitrary legislative calendar.”
Four Republican senators – Rob Portman (Ohio), Shelley Moore Capito (W.Va.), Cory Gardner (Colo.), and Lisa Murkowski (Alaska) – also expressed concerns regarding how Medicaid will be changed under the repeal/replace effort and vowed not to support any plan “that does not include stability for Medicaid expansion populations or flexibility for states.”
Republicans hold a slim 52-seat majority in the Senate and need only 50 votes to pass any legislation that uses the budget reconciliation process. If those four senators voted with Democrats, who are expected to vote as a party against the repeal effort, the current House Republican legislation would not clear the Senate.
Physicians’ groups also have voiced their opposition. American Medical Association President Andrew Gurman, MD, said in a statement that it is “not legislation we can support. The replacement bill, as written, would reverse the coverage gains of the ACA, causing many Americans to lose the health coverage they have come to depend on.” He added that the proposed changes to Medicaid “would limit states’ ability to respond to changes in service demands and threaten coverage for people with low incomes.”
Likewise, a joint statement issued by the American Academy of Family Physicians, American Academy of Pediatricians, American College of Physicians, American Congress of Obstetricians and Gynecologists and the American Osteopathic Association, expressed concern that the proposal “will likely result in less access to coverage and higher costs for millions of patients.”
The Republican plan to replace the Affordable Care Act cleared the first legislative hurdle when two house committees passed language that would repeal revenue provisions of the Affordable Care Act and lay the foundation for replacing the health care reform law.
The House Ways and Means Committee–approved legislation would eliminate the individual mandate in favor of allowing insurance companies to penalize individuals by up to 30% of premiums for lapses in coverage and would repeal taxes on high-cost health plans (Cadillac tax), over-the-counter and prescription medications, health savings accounts, tanning, investment, and on health insurers.
The language passed with a party-line vote March 9 with 23 Republicans voting for and 16 Democrats voting against after nearly 18 hours of debate and amendments.
The House Energy and Commerce Committee, after 27 hours of debate that started March 8, also passed its language along party lines with 31 Republicans voting for and 23 Democrats voting against. Their bill would end Medicaid expansion and reset the program’s funding to a per capita allotment based on population indicators, along with block grants, to provide states more flexibility to better manage its population.
A key concern raised in both committee debates was the brief window between the public unveiling of the legislation and the committees’ efforts, especially the lack of financial impact analysis or “score” from the Congressional Budget Office. Democrats efforts in both committees to hold action for a CBO score were voted down on across party lines.
In both committees, Democrats introduced a wide range of amendments, including guarantees there would be no impact from the reduction of Medicaid expansion and on funding to support coverage for mental health, women, children, seniors, and veterans, all of which were voted down. Ways and Means members also offered an amendment to require President Trump to release his income tax filings.
Rep. Frank Pallone (D-N.J.), lead Democrat in the Energy and Commerce Committee, voiced his colleagues’ objections to the bill and the process.
The bill “would rip health care away from millions of Americans, raise costs for working families and seniors, and lead to the rationing of care for 76 million Americans who receive Medicaid. … This has not been a transparent process. We did not go through regular order. The bill was posted less than 2 days before markup. No hearings were held, and we don’t have a CBO score,” Rep. Pallone said during committee debate.
A CBO score of the budget and coverage impacts of the Republican health care proposal could come as early as March 13.
The pace of action in the House even drew criticism from some in the GOP. Sen. Tom Cotton (R-Ark.) took to Twitter with a stern warning to the House.
“House health-care bill can’t pass w/o major changes,” Sen. Cotton tweeted. “To my friends in House: pause, start over. Get it right, don’t get it fast.”
He followed up with two more tweets: “GOP shouldn’t act like Dems did in O’care. No excuse to release bill Mon night, start voting Wed. With no budget estimate!” He added: “What matters in long run is better, more affordable health care for Americans, NOT house leaders’ arbitrary legislative calendar.”
Four Republican senators – Rob Portman (Ohio), Shelley Moore Capito (W.Va.), Cory Gardner (Colo.), and Lisa Murkowski (Alaska) – also expressed concerns regarding how Medicaid will be changed under the repeal/replace effort and vowed not to support any plan “that does not include stability for Medicaid expansion populations or flexibility for states.”
Republicans hold a slim 52-seat majority in the Senate and need only 50 votes to pass any legislation that uses the budget reconciliation process. If those four senators voted with Democrats, who are expected to vote as a party against the repeal effort, the current House Republican legislation would not clear the Senate.
Physicians’ groups also have voiced their opposition. American Medical Association President Andrew Gurman, MD, said in a statement that it is “not legislation we can support. The replacement bill, as written, would reverse the coverage gains of the ACA, causing many Americans to lose the health coverage they have come to depend on.” He added that the proposed changes to Medicaid “would limit states’ ability to respond to changes in service demands and threaten coverage for people with low incomes.”
Likewise, a joint statement issued by the American Academy of Family Physicians, American Academy of Pediatricians, American College of Physicians, American Congress of Obstetricians and Gynecologists and the American Osteopathic Association, expressed concern that the proposal “will likely result in less access to coverage and higher costs for millions of patients.”
The Republican plan to replace the Affordable Care Act cleared the first legislative hurdle when two house committees passed language that would repeal revenue provisions of the Affordable Care Act and lay the foundation for replacing the health care reform law.
The House Ways and Means Committee–approved legislation would eliminate the individual mandate in favor of allowing insurance companies to penalize individuals by up to 30% of premiums for lapses in coverage and would repeal taxes on high-cost health plans (Cadillac tax), over-the-counter and prescription medications, health savings accounts, tanning, investment, and on health insurers.
The language passed with a party-line vote March 9 with 23 Republicans voting for and 16 Democrats voting against after nearly 18 hours of debate and amendments.
The House Energy and Commerce Committee, after 27 hours of debate that started March 8, also passed its language along party lines with 31 Republicans voting for and 23 Democrats voting against. Their bill would end Medicaid expansion and reset the program’s funding to a per capita allotment based on population indicators, along with block grants, to provide states more flexibility to better manage its population.
A key concern raised in both committee debates was the brief window between the public unveiling of the legislation and the committees’ efforts, especially the lack of financial impact analysis or “score” from the Congressional Budget Office. Democrats efforts in both committees to hold action for a CBO score were voted down on across party lines.
In both committees, Democrats introduced a wide range of amendments, including guarantees there would be no impact from the reduction of Medicaid expansion and on funding to support coverage for mental health, women, children, seniors, and veterans, all of which were voted down. Ways and Means members also offered an amendment to require President Trump to release his income tax filings.
Rep. Frank Pallone (D-N.J.), lead Democrat in the Energy and Commerce Committee, voiced his colleagues’ objections to the bill and the process.
The bill “would rip health care away from millions of Americans, raise costs for working families and seniors, and lead to the rationing of care for 76 million Americans who receive Medicaid. … This has not been a transparent process. We did not go through regular order. The bill was posted less than 2 days before markup. No hearings were held, and we don’t have a CBO score,” Rep. Pallone said during committee debate.
A CBO score of the budget and coverage impacts of the Republican health care proposal could come as early as March 13.
The pace of action in the House even drew criticism from some in the GOP. Sen. Tom Cotton (R-Ark.) took to Twitter with a stern warning to the House.
“House health-care bill can’t pass w/o major changes,” Sen. Cotton tweeted. “To my friends in House: pause, start over. Get it right, don’t get it fast.”
He followed up with two more tweets: “GOP shouldn’t act like Dems did in O’care. No excuse to release bill Mon night, start voting Wed. With no budget estimate!” He added: “What matters in long run is better, more affordable health care for Americans, NOT house leaders’ arbitrary legislative calendar.”
Four Republican senators – Rob Portman (Ohio), Shelley Moore Capito (W.Va.), Cory Gardner (Colo.), and Lisa Murkowski (Alaska) – also expressed concerns regarding how Medicaid will be changed under the repeal/replace effort and vowed not to support any plan “that does not include stability for Medicaid expansion populations or flexibility for states.”
Republicans hold a slim 52-seat majority in the Senate and need only 50 votes to pass any legislation that uses the budget reconciliation process. If those four senators voted with Democrats, who are expected to vote as a party against the repeal effort, the current House Republican legislation would not clear the Senate.
Physicians’ groups also have voiced their opposition. American Medical Association President Andrew Gurman, MD, said in a statement that it is “not legislation we can support. The replacement bill, as written, would reverse the coverage gains of the ACA, causing many Americans to lose the health coverage they have come to depend on.” He added that the proposed changes to Medicaid “would limit states’ ability to respond to changes in service demands and threaten coverage for people with low incomes.”
Likewise, a joint statement issued by the American Academy of Family Physicians, American Academy of Pediatricians, American College of Physicians, American Congress of Obstetricians and Gynecologists and the American Osteopathic Association, expressed concern that the proposal “will likely result in less access to coverage and higher costs for millions of patients.”
Everything We Say & Do: What PFACs reveal about patient experience
Editor’s note: “Everything We Say and Do” is an informational series developed by the Society of Hospital Medicine’s Patient Experience Committee to provide readers with thoughtful and actionable tactics that have great potential to positively impact patients’ experience of care.
Patient and Family Advisory Councils (PFACs) provide a tool for understanding the patient perspective and are utilized nationwide. These councils, typically consisting of former and current patients and/or their family members, meet on a regular basis to advise provider communities on a wide range of care-related matters. At my institution, Beth Israel Deaconess Medical Center, our PFAC has weighed in on a wide range of issues, such as how to conduct effective nursing rounds and the best methods for supporting patients with disabilities.
Most recently, we have utilized an innovative approach to both understanding the patient experience and capitalizing on the expertise of our PFAC members. Modeled after a program developed at the Dartmouth-Hitchcock Medical Center, we have trained members of our PFAC to interview inpatients at the bedside about their experience. Time-sensitive information is immediately reported back to the nurse manager, who responds with real-time solutions. Oftentimes, problems can be easily resolved using the right communication, or just providing the “listening ear” of someone to whom the patient relates.

In addition, the information is aggregated to provide us with a broad-based perspective of the patient experience at BIDMC. For example, we found that our patients often discuss issues with volunteers that they have not addressed with providers, suggesting they may at times feel more comfortable disclosing concerns to people outside of their medical team.
The Society of Hospital Medicine (SHM) also recognizes the central role of the patient’s voice in quality medical care. Through the work of its Patient Experience Committee, SHM has convened a nationwide “virtual” PFAC consisting of leaders of PFACs from medical facilities across the country. Members of the SHM PFAC share questions posed by SHM’s committees with their constituents, and the responses are reported back to the Patient Experience Committee.
What lessons have we learned from the SHM PFAC? Make no assumptions. While some of us have been patients ourselves and all of us interact with patients, our ability to understand the patient perspective is blurred by the lenses of medical training, system constraints, and the pressures of the challenging work that we do.
It is often impossible to predict the response when you question a patient about his or her experience. For example, the first question we asked SHM’s nationwide PFAC was: “What is one thing that a hospitalist could do to improve the patient experience?” The most common response we received was: “What is a hospitalist?” These responses suggest that we (hospitalists) need to redirect our efforts in a way that we had not anticipated, with a focus on clarifying who we are and what we do.
Other, more predictable themes emerged as well. Our patients want consistency and continuity throughout their hospitalization. They value a good bedside manner and want us to engage in sensitivity training. They ask us to work on minimizing errors and ensuring accountability both during hospitalization as well as pre- and post hospitalization.
Ultimately we hope that the SHM PFAC will be utilized by all of SHM’s committees, allowing for the patient experience to be a common thread woven through all SHM initiatives.
Amber Moore, MD, MPH, is a hospitalist at Beth Israel Deaconess Medical Center, and instructor of medicine, Harvard Medical School.
Editor’s note: “Everything We Say and Do” is an informational series developed by the Society of Hospital Medicine’s Patient Experience Committee to provide readers with thoughtful and actionable tactics that have great potential to positively impact patients’ experience of care.
Patient and Family Advisory Councils (PFACs) provide a tool for understanding the patient perspective and are utilized nationwide. These councils, typically consisting of former and current patients and/or their family members, meet on a regular basis to advise provider communities on a wide range of care-related matters. At my institution, Beth Israel Deaconess Medical Center, our PFAC has weighed in on a wide range of issues, such as how to conduct effective nursing rounds and the best methods for supporting patients with disabilities.
Most recently, we have utilized an innovative approach to both understanding the patient experience and capitalizing on the expertise of our PFAC members. Modeled after a program developed at the Dartmouth-Hitchcock Medical Center, we have trained members of our PFAC to interview inpatients at the bedside about their experience. Time-sensitive information is immediately reported back to the nurse manager, who responds with real-time solutions. Oftentimes, problems can be easily resolved using the right communication, or just providing the “listening ear” of someone to whom the patient relates.
In addition, the information is aggregated to provide us with a broad-based perspective of the patient experience at BIDMC. For example, we found that our patients often discuss issues with volunteers that they have not addressed with providers, suggesting they may at times feel more comfortable disclosing concerns to people outside of their medical team.
The Society of Hospital Medicine (SHM) also recognizes the central role of the patient’s voice in quality medical care. Through the work of its Patient Experience Committee, SHM has convened a nationwide “virtual” PFAC consisting of leaders of PFACs from medical facilities across the country. Members of the SHM PFAC share questions posed by SHM’s committees with their constituents, and the responses are reported back to the Patient Experience Committee.
What lessons have we learned from the SHM PFAC? Make no assumptions. While some of us have been patients ourselves and all of us interact with patients, our ability to understand the patient perspective is blurred by the lenses of medical training, system constraints, and the pressures of the challenging work that we do.
It is often impossible to predict the response when you question a patient about his or her experience. For example, the first question we asked SHM’s nationwide PFAC was: “What is one thing that a hospitalist could do to improve the patient experience?” The most common response we received was: “What is a hospitalist?” These responses suggest that we (hospitalists) need to redirect our efforts in a way that we had not anticipated, with a focus on clarifying who we are and what we do.
Other, more predictable themes emerged as well. Our patients want consistency and continuity throughout their hospitalization. They value a good bedside manner and want us to engage in sensitivity training. They ask us to work on minimizing errors and ensuring accountability both during hospitalization as well as pre- and post hospitalization.
Ultimately we hope that the SHM PFAC will be utilized by all of SHM’s committees, allowing for the patient experience to be a common thread woven through all SHM initiatives.
Amber Moore, MD, MPH, is a hospitalist at Beth Israel Deaconess Medical Center, and instructor of medicine, Harvard Medical School.
Editor’s note: “Everything We Say and Do” is an informational series developed by the Society of Hospital Medicine’s Patient Experience Committee to provide readers with thoughtful and actionable tactics that have great potential to positively impact patients’ experience of care.
Patient and Family Advisory Councils (PFACs) provide a tool for understanding the patient perspective and are utilized nationwide. These councils, typically consisting of former and current patients and/or their family members, meet on a regular basis to advise provider communities on a wide range of care-related matters. At my institution, Beth Israel Deaconess Medical Center, our PFAC has weighed in on a wide range of issues, such as how to conduct effective nursing rounds and the best methods for supporting patients with disabilities.
Most recently, we have utilized an innovative approach to both understanding the patient experience and capitalizing on the expertise of our PFAC members. Modeled after a program developed at the Dartmouth-Hitchcock Medical Center, we have trained members of our PFAC to interview inpatients at the bedside about their experience. Time-sensitive information is immediately reported back to the nurse manager, who responds with real-time solutions. Oftentimes, problems can be easily resolved using the right communication, or just providing the “listening ear” of someone to whom the patient relates.
In addition, the information is aggregated to provide us with a broad-based perspective of the patient experience at BIDMC. For example, we found that our patients often discuss issues with volunteers that they have not addressed with providers, suggesting they may at times feel more comfortable disclosing concerns to people outside of their medical team.
The Society of Hospital Medicine (SHM) also recognizes the central role of the patient’s voice in quality medical care. Through the work of its Patient Experience Committee, SHM has convened a nationwide “virtual” PFAC consisting of leaders of PFACs from medical facilities across the country. Members of the SHM PFAC share questions posed by SHM’s committees with their constituents, and the responses are reported back to the Patient Experience Committee.
What lessons have we learned from the SHM PFAC? Make no assumptions. While some of us have been patients ourselves and all of us interact with patients, our ability to understand the patient perspective is blurred by the lenses of medical training, system constraints, and the pressures of the challenging work that we do.
It is often impossible to predict the response when you question a patient about his or her experience. For example, the first question we asked SHM’s nationwide PFAC was: “What is one thing that a hospitalist could do to improve the patient experience?” The most common response we received was: “What is a hospitalist?” These responses suggest that we (hospitalists) need to redirect our efforts in a way that we had not anticipated, with a focus on clarifying who we are and what we do.
Other, more predictable themes emerged as well. Our patients want consistency and continuity throughout their hospitalization. They value a good bedside manner and want us to engage in sensitivity training. They ask us to work on minimizing errors and ensuring accountability both during hospitalization as well as pre- and post hospitalization.
Ultimately we hope that the SHM PFAC will be utilized by all of SHM’s committees, allowing for the patient experience to be a common thread woven through all SHM initiatives.
Amber Moore, MD, MPH, is a hospitalist at Beth Israel Deaconess Medical Center, and instructor of medicine, Harvard Medical School.
The beginning of the end
No matter on which side of the aisle you sit, and even if you’d prefer to just sit in your car and check Instagram, the results of the November election were likely a surprise. Speculation abounds by pundits and so-called experts as to what a Trump presidency means for health care in this country. The shape and scope of health care initiatives that a Trump administration will attempt to advance in place of the Affordable Care Act (ACA), which has likely met its demise, is unknown at the time of this writing. How Trump’s new initiatives fare in Congress and then get translated into practical changes in health care delivery and financing is even more muddled.

The U.S. medical community has remained largely silent, which is wise given the lack of evidence that would support any rational prediction, but perhaps it’s easier to pronounce judgment from across the pond. The Lancet recently reported the comment of Sophie Harman, PhD, a political scientist at Queen Mary University in London, who told an audience at the London School of Hygiene & Tropical Medicine to “ignore the dead cat in the room.”1 I spent 6 months of my residency in the United Kingdom, and this phrase never came up in my travels across the wards, streets, and pubs of the mother country. Apparently, the “dead cat strategy” is a legislative maneuver to distract attention from a party’s political shortcomings by raising a ruckus about a salacious or social hot-button topic. In this case, the dead cat may just be the carcass of Obamacare, exuding the fetor of millions of people losing their health insurance.
The BMJ, another respected U.K. journal, offered the pronouncement by Don Berwick, MD, former administrator of the Centers for Medicare & Medicaid Services, that Trump’s election would be “disastrous” for U.S. health care, but not much else.2
Out-of-pocket health care expenses for patients and families insured under Medicaid and its ACA-mandated expansion decreased to, on average, less than $500 per year; however, 19 states, all with Republican governors, blocked the Medicaid expansion.5 This denied more than 2.5 million people Medicaid coverage in these states; the overwhelming majority of these people remained uninsured. Uninsured people incur significant out-of-pocket costs when they do require health care, and have worse outcomes.6,7 The end of ACA throws Medicaid expansion in any state, with its protections to limit out-of-pocket expenses, into doubt.
Before the ACA expanded Medicaid coverage, patients faced significant wait times and travel costs associated with the low numbers of providers accepting Medicaid’s low reimbursement rate.8 These numbers had begun to improve after the ACA increased primary care physicians’ Medicaid reimbursements to Medicare rates in 2013 and 2014, but only a limited number of states will continue the increases after the end of federal subsidies.
For people who purchased plans on the ACA’s marketplace, out-of-pocket exposure is capped in 2017 at no more than $7,150 for an individual plan and $14,300 for a family plan before marketplace subsidies. Even those who qualified for cost-sharing deductions, with incomes between 100% and 250% of the federal poverty level, had out-of-pocket caps that varied widely depending on plan and state. For example, in 2016 at the $17,000 annual income level, out-of-pocket caps could range from $500 to $2,250.9
Clinician concern
On a provider level, incentives to reduce readmissions and limit health care–associated harm events mandated by the ACA may soon evaporate, throwing into question many quality metrics pursued by health systems. In response, will health system administrators abandon efforts to reduce readmissions and hospital-acquired conditions (HACs)? Or will health systems, despite the lack of a Medicare penalty “stick,” move forward with efforts to reduce readmissions and HACs? There’s no question of what would benefit the pocketbooks of our patients the most – every hospitalization results in significant direct out-of-pocket costs, not to mention lost productivity and income.10
It seems unlikely that a Republican-led government will pursue efforts to decrease out-of-pocket expenses. More likely, new proposals will aim to provide tax benefits to encourage use of health savings accounts (HSAs), continuing the shift of health care to employees.11 HSAs benefit employers, who pay less for the health care costs of employees, but are associated with worsened adherence to recommended treatments for patients.8,12
A 2016 study analyzed health care policies considered by Trump, including the following:
- Full repeal of the ACA.
- Repeal of the ACA plus tax deductions of health insurance premiums.
- Repeal of the ACA plus block grants to states for Medicaid and Children’s Health Insurance Program (CHIP).
- Repeal plus promotion of selling health insurance across state lines.
Not surprisingly, all four scenarios resulted in significant increases in out-of-pocket expenses for those in individual insurance plans.13
Although at the time of writing, the “replace” segment of “repeal-and-replace” is not known, Mr. Trump’s nominee for Secretary of Health and Human Services (HHS), Rep. Tom Price (R-Ga.), has given a hint of what he would champion based on his prior legislative proposals. Along with his support of increasing accessibility of armor-piercing bullets, reduced regulations on cigars, and opposition to expanding the State Children’s Health Insurance Program, he proposed H.R. 2300, “Empower Patients First Act.” This would eliminate the ACA’s Medicaid expansion and replace it with flat tax credits based on age, not income, which turns out to offer greater subsidies relative to income for those with higher incomes. A 30-year-old would, on average, face a premium bill of $2,532, along with a potential out-of-pocket liability of $7,000, with only a $1,200 credit to cover this from Mr. Price’s plan.14
In sum
So what’s a conscientious advocate for the physical and financial health of patients to do? Beyond political action, hospitalists need to keep abreast of the effect of changes in health care policy on their patients, as unpleasant as it may be. Do you know what the copays and out-of-pocket costs are for your patient’s (or your own) health care? Knowing how your recommendations for treatment and follow-up affect your patient’s pocketbook will not only help protect their finances, but will also protect their health, as people are less likely to be compliant with treatment if it involves out-of-pocket costs.
And easy as it would be to simply tune out the partisan rancor, stay engaged as a citizen, if for nothing else, the benefit of your patients.
Dr. Chang is pediatric editor of The Hospitalist. He is associate clinical professor of pediatrics at the University of Massachusetts, Worcester, and chief of pediatric hospital medicine at Baystate Children's Hospital, Springfield, Mass. Send comments and questions to [email protected].
References
1. Horton R. Offline: Looking forward to Donald Trump. The Lancet. 2016;388[10061]:2726.
2. Page L. What Donald Trump would do with the US healthcare system. BMJ. 2016;353:i2996.
3. Uberoi N, Finegold, K. and Gee, E. Health Insurance Coverage and the Affordable Care Act, 2010-2016. Department of Health and Human Services, ASPE Issue Brief, 2016 March 3.
4. Claxton G, Rae M, Long M, Damico A, Whitmore H, Foster G. Health Benefits In 2016: Family Premiums Rose Modestly, And Offer Rates Remained Stable. Health Aff (Millwood). 2016 Sep. doi: 10.1377/hlthaff.2016.0951.
5. Ku L, Broaddus M. Public and private health insurance: stacking up the costs. Health Aff (Millwood). 2008;27:w318-327.
6. Waters H, Steinhardt L, Oliver TR, Burton A, Milner S. The costs of non-insurance in Maryland. J Health Care Poor Underserved. 2007 Feb;18[1]:139-51.
7. Cheung MR. Lack of health insurance increases all cause and all cancer mortality in adults: an analysis of National Health and Nutrition Examination Survey (NHANES III) data. Asian Pac J Cancer Prev. 2013;14[4]:2259-63.
8. Gillis JZ, Yazdany J, Trupin L, et al. Medicaid and access to care among persons with systemic lupus erythematosus. Arthritis Rheum. 2007;57[4]:601-7.
9. Collins SR, Gunja M, Beutel S. How Will the Affordable Care Act’s Cost-Sharing Reductions Affect Consumers’ Out-of-Pocket Costs in 2016? Issue Brief (Commonw Fund) 2016;6:1-17.
10. Leader S, Yang H, DeVincenzo J, Jacobson P, Marcin JP, Murray DL. Time and out-of-pocket costs associated with respiratory syncytial virus hospitalization of infants. Value Health. 2003;6[2]:100-6.
11. Antos J CJ. The House Republicans’ Health Plan. Bethesda, MD: Health Affairs Blog, Project HOPE; 2016 June 22.
12. Fronstin P, Roebuck MC. Health care spending after adopting a full-replacement, high-deductible health plan with a health savings account: a five-year study. EBRI Issue Brief 2013 July:3-15.
13. Saltzman E EC. Donald Trump’s Health Care Reform Proposals: Anticipated Effects on Insurance Coverage, Out-of-Pocket Costs, and the Federal Deficit. The Commonwealth Fund September 2016.
14. Glied SA, Frank RG. Care for the Vulnerable vs. Cash for the Powerful – Trump’s Pick for HHS. N Engl J Med. 2017;376:103-5.
No matter on which side of the aisle you sit, and even if you’d prefer to just sit in your car and check Instagram, the results of the November election were likely a surprise. Speculation abounds by pundits and so-called experts as to what a Trump presidency means for health care in this country. The shape and scope of health care initiatives that a Trump administration will attempt to advance in place of the Affordable Care Act (ACA), which has likely met its demise, is unknown at the time of this writing. How Trump’s new initiatives fare in Congress and then get translated into practical changes in health care delivery and financing is even more muddled.
The U.S. medical community has remained largely silent, which is wise given the lack of evidence that would support any rational prediction, but perhaps it’s easier to pronounce judgment from across the pond. The Lancet recently reported the comment of Sophie Harman, PhD, a political scientist at Queen Mary University in London, who told an audience at the London School of Hygiene & Tropical Medicine to “ignore the dead cat in the room.”1 I spent 6 months of my residency in the United Kingdom, and this phrase never came up in my travels across the wards, streets, and pubs of the mother country. Apparently, the “dead cat strategy” is a legislative maneuver to distract attention from a party’s political shortcomings by raising a ruckus about a salacious or social hot-button topic. In this case, the dead cat may just be the carcass of Obamacare, exuding the fetor of millions of people losing their health insurance.
The BMJ, another respected U.K. journal, offered the pronouncement by Don Berwick, MD, former administrator of the Centers for Medicare & Medicaid Services, that Trump’s election would be “disastrous” for U.S. health care, but not much else.2
Out-of-pocket health care expenses for patients and families insured under Medicaid and its ACA-mandated expansion decreased to, on average, less than $500 per year; however, 19 states, all with Republican governors, blocked the Medicaid expansion.5 This denied more than 2.5 million people Medicaid coverage in these states; the overwhelming majority of these people remained uninsured. Uninsured people incur significant out-of-pocket costs when they do require health care, and have worse outcomes.6,7 The end of ACA throws Medicaid expansion in any state, with its protections to limit out-of-pocket expenses, into doubt.
Before the ACA expanded Medicaid coverage, patients faced significant wait times and travel costs associated with the low numbers of providers accepting Medicaid’s low reimbursement rate.8 These numbers had begun to improve after the ACA increased primary care physicians’ Medicaid reimbursements to Medicare rates in 2013 and 2014, but only a limited number of states will continue the increases after the end of federal subsidies.
For people who purchased plans on the ACA’s marketplace, out-of-pocket exposure is capped in 2017 at no more than $7,150 for an individual plan and $14,300 for a family plan before marketplace subsidies. Even those who qualified for cost-sharing deductions, with incomes between 100% and 250% of the federal poverty level, had out-of-pocket caps that varied widely depending on plan and state. For example, in 2016 at the $17,000 annual income level, out-of-pocket caps could range from $500 to $2,250.9
Clinician concern
On a provider level, incentives to reduce readmissions and limit health care–associated harm events mandated by the ACA may soon evaporate, throwing into question many quality metrics pursued by health systems. In response, will health system administrators abandon efforts to reduce readmissions and hospital-acquired conditions (HACs)? Or will health systems, despite the lack of a Medicare penalty “stick,” move forward with efforts to reduce readmissions and HACs? There’s no question of what would benefit the pocketbooks of our patients the most – every hospitalization results in significant direct out-of-pocket costs, not to mention lost productivity and income.10
It seems unlikely that a Republican-led government will pursue efforts to decrease out-of-pocket expenses. More likely, new proposals will aim to provide tax benefits to encourage use of health savings accounts (HSAs), continuing the shift of health care to employees.11 HSAs benefit employers, who pay less for the health care costs of employees, but are associated with worsened adherence to recommended treatments for patients.8,12
A 2016 study analyzed health care policies considered by Trump, including the following:
- Full repeal of the ACA.
- Repeal of the ACA plus tax deductions of health insurance premiums.
- Repeal of the ACA plus block grants to states for Medicaid and Children’s Health Insurance Program (CHIP).
- Repeal plus promotion of selling health insurance across state lines.
Not surprisingly, all four scenarios resulted in significant increases in out-of-pocket expenses for those in individual insurance plans.13
Although at the time of writing, the “replace” segment of “repeal-and-replace” is not known, Mr. Trump’s nominee for Secretary of Health and Human Services (HHS), Rep. Tom Price (R-Ga.), has given a hint of what he would champion based on his prior legislative proposals. Along with his support of increasing accessibility of armor-piercing bullets, reduced regulations on cigars, and opposition to expanding the State Children’s Health Insurance Program, he proposed H.R. 2300, “Empower Patients First Act.” This would eliminate the ACA’s Medicaid expansion and replace it with flat tax credits based on age, not income, which turns out to offer greater subsidies relative to income for those with higher incomes. A 30-year-old would, on average, face a premium bill of $2,532, along with a potential out-of-pocket liability of $7,000, with only a $1,200 credit to cover this from Mr. Price’s plan.14
In sum
So what’s a conscientious advocate for the physical and financial health of patients to do? Beyond political action, hospitalists need to keep abreast of the effect of changes in health care policy on their patients, as unpleasant as it may be. Do you know what the copays and out-of-pocket costs are for your patient’s (or your own) health care? Knowing how your recommendations for treatment and follow-up affect your patient’s pocketbook will not only help protect their finances, but will also protect their health, as people are less likely to be compliant with treatment if it involves out-of-pocket costs.
And easy as it would be to simply tune out the partisan rancor, stay engaged as a citizen, if for nothing else, the benefit of your patients.
Dr. Chang is pediatric editor of The Hospitalist. He is associate clinical professor of pediatrics at the University of Massachusetts, Worcester, and chief of pediatric hospital medicine at Baystate Children's Hospital, Springfield, Mass. Send comments and questions to [email protected].
References
1. Horton R. Offline: Looking forward to Donald Trump. The Lancet. 2016;388[10061]:2726.
2. Page L. What Donald Trump would do with the US healthcare system. BMJ. 2016;353:i2996.
3. Uberoi N, Finegold, K. and Gee, E. Health Insurance Coverage and the Affordable Care Act, 2010-2016. Department of Health and Human Services, ASPE Issue Brief, 2016 March 3.
4. Claxton G, Rae M, Long M, Damico A, Whitmore H, Foster G. Health Benefits In 2016: Family Premiums Rose Modestly, And Offer Rates Remained Stable. Health Aff (Millwood). 2016 Sep. doi: 10.1377/hlthaff.2016.0951.
5. Ku L, Broaddus M. Public and private health insurance: stacking up the costs. Health Aff (Millwood). 2008;27:w318-327.
6. Waters H, Steinhardt L, Oliver TR, Burton A, Milner S. The costs of non-insurance in Maryland. J Health Care Poor Underserved. 2007 Feb;18[1]:139-51.
7. Cheung MR. Lack of health insurance increases all cause and all cancer mortality in adults: an analysis of National Health and Nutrition Examination Survey (NHANES III) data. Asian Pac J Cancer Prev. 2013;14[4]:2259-63.
8. Gillis JZ, Yazdany J, Trupin L, et al. Medicaid and access to care among persons with systemic lupus erythematosus. Arthritis Rheum. 2007;57[4]:601-7.
9. Collins SR, Gunja M, Beutel S. How Will the Affordable Care Act’s Cost-Sharing Reductions Affect Consumers’ Out-of-Pocket Costs in 2016? Issue Brief (Commonw Fund) 2016;6:1-17.
10. Leader S, Yang H, DeVincenzo J, Jacobson P, Marcin JP, Murray DL. Time and out-of-pocket costs associated with respiratory syncytial virus hospitalization of infants. Value Health. 2003;6[2]:100-6.
11. Antos J CJ. The House Republicans’ Health Plan. Bethesda, MD: Health Affairs Blog, Project HOPE; 2016 June 22.
12. Fronstin P, Roebuck MC. Health care spending after adopting a full-replacement, high-deductible health plan with a health savings account: a five-year study. EBRI Issue Brief 2013 July:3-15.
13. Saltzman E EC. Donald Trump’s Health Care Reform Proposals: Anticipated Effects on Insurance Coverage, Out-of-Pocket Costs, and the Federal Deficit. The Commonwealth Fund September 2016.
14. Glied SA, Frank RG. Care for the Vulnerable vs. Cash for the Powerful – Trump’s Pick for HHS. N Engl J Med. 2017;376:103-5.
No matter on which side of the aisle you sit, and even if you’d prefer to just sit in your car and check Instagram, the results of the November election were likely a surprise. Speculation abounds by pundits and so-called experts as to what a Trump presidency means for health care in this country. The shape and scope of health care initiatives that a Trump administration will attempt to advance in place of the Affordable Care Act (ACA), which has likely met its demise, is unknown at the time of this writing. How Trump’s new initiatives fare in Congress and then get translated into practical changes in health care delivery and financing is even more muddled.
The U.S. medical community has remained largely silent, which is wise given the lack of evidence that would support any rational prediction, but perhaps it’s easier to pronounce judgment from across the pond. The Lancet recently reported the comment of Sophie Harman, PhD, a political scientist at Queen Mary University in London, who told an audience at the London School of Hygiene & Tropical Medicine to “ignore the dead cat in the room.”1 I spent 6 months of my residency in the United Kingdom, and this phrase never came up in my travels across the wards, streets, and pubs of the mother country. Apparently, the “dead cat strategy” is a legislative maneuver to distract attention from a party’s political shortcomings by raising a ruckus about a salacious or social hot-button topic. In this case, the dead cat may just be the carcass of Obamacare, exuding the fetor of millions of people losing their health insurance.
The BMJ, another respected U.K. journal, offered the pronouncement by Don Berwick, MD, former administrator of the Centers for Medicare & Medicaid Services, that Trump’s election would be “disastrous” for U.S. health care, but not much else.2
Out-of-pocket health care expenses for patients and families insured under Medicaid and its ACA-mandated expansion decreased to, on average, less than $500 per year; however, 19 states, all with Republican governors, blocked the Medicaid expansion.5 This denied more than 2.5 million people Medicaid coverage in these states; the overwhelming majority of these people remained uninsured. Uninsured people incur significant out-of-pocket costs when they do require health care, and have worse outcomes.6,7 The end of ACA throws Medicaid expansion in any state, with its protections to limit out-of-pocket expenses, into doubt.
Before the ACA expanded Medicaid coverage, patients faced significant wait times and travel costs associated with the low numbers of providers accepting Medicaid’s low reimbursement rate.8 These numbers had begun to improve after the ACA increased primary care physicians’ Medicaid reimbursements to Medicare rates in 2013 and 2014, but only a limited number of states will continue the increases after the end of federal subsidies.
For people who purchased plans on the ACA’s marketplace, out-of-pocket exposure is capped in 2017 at no more than $7,150 for an individual plan and $14,300 for a family plan before marketplace subsidies. Even those who qualified for cost-sharing deductions, with incomes between 100% and 250% of the federal poverty level, had out-of-pocket caps that varied widely depending on plan and state. For example, in 2016 at the $17,000 annual income level, out-of-pocket caps could range from $500 to $2,250.9
Clinician concern
On a provider level, incentives to reduce readmissions and limit health care–associated harm events mandated by the ACA may soon evaporate, throwing into question many quality metrics pursued by health systems. In response, will health system administrators abandon efforts to reduce readmissions and hospital-acquired conditions (HACs)? Or will health systems, despite the lack of a Medicare penalty “stick,” move forward with efforts to reduce readmissions and HACs? There’s no question of what would benefit the pocketbooks of our patients the most – every hospitalization results in significant direct out-of-pocket costs, not to mention lost productivity and income.10
It seems unlikely that a Republican-led government will pursue efforts to decrease out-of-pocket expenses. More likely, new proposals will aim to provide tax benefits to encourage use of health savings accounts (HSAs), continuing the shift of health care to employees.11 HSAs benefit employers, who pay less for the health care costs of employees, but are associated with worsened adherence to recommended treatments for patients.8,12
A 2016 study analyzed health care policies considered by Trump, including the following:
- Full repeal of the ACA.
- Repeal of the ACA plus tax deductions of health insurance premiums.
- Repeal of the ACA plus block grants to states for Medicaid and Children’s Health Insurance Program (CHIP).
- Repeal plus promotion of selling health insurance across state lines.
Not surprisingly, all four scenarios resulted in significant increases in out-of-pocket expenses for those in individual insurance plans.13
Although at the time of writing, the “replace” segment of “repeal-and-replace” is not known, Mr. Trump’s nominee for Secretary of Health and Human Services (HHS), Rep. Tom Price (R-Ga.), has given a hint of what he would champion based on his prior legislative proposals. Along with his support of increasing accessibility of armor-piercing bullets, reduced regulations on cigars, and opposition to expanding the State Children’s Health Insurance Program, he proposed H.R. 2300, “Empower Patients First Act.” This would eliminate the ACA’s Medicaid expansion and replace it with flat tax credits based on age, not income, which turns out to offer greater subsidies relative to income for those with higher incomes. A 30-year-old would, on average, face a premium bill of $2,532, along with a potential out-of-pocket liability of $7,000, with only a $1,200 credit to cover this from Mr. Price’s plan.14
In sum
So what’s a conscientious advocate for the physical and financial health of patients to do? Beyond political action, hospitalists need to keep abreast of the effect of changes in health care policy on their patients, as unpleasant as it may be. Do you know what the copays and out-of-pocket costs are for your patient’s (or your own) health care? Knowing how your recommendations for treatment and follow-up affect your patient’s pocketbook will not only help protect their finances, but will also protect their health, as people are less likely to be compliant with treatment if it involves out-of-pocket costs.
And easy as it would be to simply tune out the partisan rancor, stay engaged as a citizen, if for nothing else, the benefit of your patients.
Dr. Chang is pediatric editor of The Hospitalist. He is associate clinical professor of pediatrics at the University of Massachusetts, Worcester, and chief of pediatric hospital medicine at Baystate Children's Hospital, Springfield, Mass. Send comments and questions to [email protected].
References
1. Horton R. Offline: Looking forward to Donald Trump. The Lancet. 2016;388[10061]:2726.
2. Page L. What Donald Trump would do with the US healthcare system. BMJ. 2016;353:i2996.
3. Uberoi N, Finegold, K. and Gee, E. Health Insurance Coverage and the Affordable Care Act, 2010-2016. Department of Health and Human Services, ASPE Issue Brief, 2016 March 3.
4. Claxton G, Rae M, Long M, Damico A, Whitmore H, Foster G. Health Benefits In 2016: Family Premiums Rose Modestly, And Offer Rates Remained Stable. Health Aff (Millwood). 2016 Sep. doi: 10.1377/hlthaff.2016.0951.
5. Ku L, Broaddus M. Public and private health insurance: stacking up the costs. Health Aff (Millwood). 2008;27:w318-327.
6. Waters H, Steinhardt L, Oliver TR, Burton A, Milner S. The costs of non-insurance in Maryland. J Health Care Poor Underserved. 2007 Feb;18[1]:139-51.
7. Cheung MR. Lack of health insurance increases all cause and all cancer mortality in adults: an analysis of National Health and Nutrition Examination Survey (NHANES III) data. Asian Pac J Cancer Prev. 2013;14[4]:2259-63.
8. Gillis JZ, Yazdany J, Trupin L, et al. Medicaid and access to care among persons with systemic lupus erythematosus. Arthritis Rheum. 2007;57[4]:601-7.
9. Collins SR, Gunja M, Beutel S. How Will the Affordable Care Act’s Cost-Sharing Reductions Affect Consumers’ Out-of-Pocket Costs in 2016? Issue Brief (Commonw Fund) 2016;6:1-17.
10. Leader S, Yang H, DeVincenzo J, Jacobson P, Marcin JP, Murray DL. Time and out-of-pocket costs associated with respiratory syncytial virus hospitalization of infants. Value Health. 2003;6[2]:100-6.
11. Antos J CJ. The House Republicans’ Health Plan. Bethesda, MD: Health Affairs Blog, Project HOPE; 2016 June 22.
12. Fronstin P, Roebuck MC. Health care spending after adopting a full-replacement, high-deductible health plan with a health savings account: a five-year study. EBRI Issue Brief 2013 July:3-15.
13. Saltzman E EC. Donald Trump’s Health Care Reform Proposals: Anticipated Effects on Insurance Coverage, Out-of-Pocket Costs, and the Federal Deficit. The Commonwealth Fund September 2016.
14. Glied SA, Frank RG. Care for the Vulnerable vs. Cash for the Powerful – Trump’s Pick for HHS. N Engl J Med. 2017;376:103-5.
Revisiting citizenship bonus and surge capacity
I devoted an entire column to the idea of a citizenship bonus in November 2011. At that time I expressed some ambivalence about its effectiveness. Since then I’ve become disenchanted and think it may do more harm than good.
SHM’s 2016 State of Hospital Medicine (SOHM) Report, based on 2015 data, shows that 46% of Hospital Medicine Groups (HMGs) connect some portion of bonus dollars to a provider’s citizenship.1 This is a relatively new phenomenon in the last 5 years or so. My anecdotal experience is that it isn’t limited to hospitalists; it is pretty common for doctors in any specialty who are employed by a hospital or other large organization.

HMGs vary in their definitions of what constitutes citizenship, but usually include things like committee participation, lectures, grand rounds presentations, community talks, research publications.
Our hospitalist group at my hospital has well-defined criteria that require attendance at more than 75% of meetings as a “light switch” (pays nothing itself, but “turns on” availability to citizenship bonus). Bonus dollars are paid for success in any one of several activities, such as making an in-person visit to two PCP offices or completing a meaningful project related to practice operations or clinical care.
I’ve been a supporter of a citizenship bonus for a long time, but two things have made me ambivalent or even opposed to it. The first is a book by Daniel Pink titled Drive: The Surprising Truth About What Motivates Us. It’s a short and very thought-provoking book summarizing research that suggests the effect of providing external rewards like compensation is to “…extinguish intrinsic motivation, diminish performance, crush creativity, and crowd out good behavior.”
The second reason for my ambivalence is my experience working with a lot of HMGs around the country. Those that have a citizenship bonus don’t seem to realize improved operations, more engaged doctors, or lower turnover, and so on. In fact, my experience is that the bonus tends to do exactly what Pink says – steer individuals and the group as a whole away from what is desired.
I’m not ready to say a citizenship bonus is always a bad idea. But it sure seems like it works out badly for many or most groups.
But if you do have a citizenship bonus, then don’t make the mistake of tying it to very basic expectations of the job, like attending group meetings or completing chart documentation on time. Doing those things should never be seen as a reason for a bonus.
Jeopardy (‘surge’) staffing: Not catching on?
As I write, influenza has swept through our region, and my hospital – like most along the west coast – is experiencing incredibly high volumes. I enter the building through a patient care unit that has been mothballed for several years, but today people from building maintenance were busy getting it ready for patients. The hospital is offering various incentives for patient care staff to work extra shifts to manage this volume surge, and our hospitalists have days with encounters near or at our highest-ever level. So surge capacity is once again on my mind.
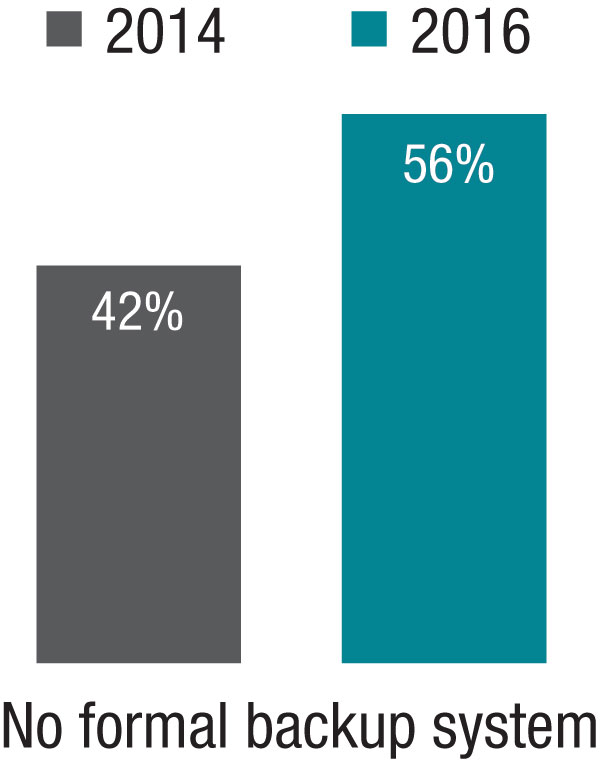
But if every hospitalist in the group went from, say, 156 to 190 shifts annually, the practice might be able to staff every day with an additional provider without adding staff or spending more money. And a doc’s average day would be less busy, which for some people (okay, not very many) would be a worthwhile trade-off. I realize this is a tough sell and to many people it sounds crazy.
The 2014 SOHM showed 42% of HMGs had “no formal backup system,” and this had climbed to 58% in the 2016 Report. I don’t know if jeopardy or surge backup systems are really becoming less common, but it seems pretty clear they aren’t becoming more common. So it’s worth thinking about whether there is a practical way to remove inhibitors of surge capacity.
Dr. Nelson has been a practicing hospitalist since 1988. He is cofounder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Endnotes
1. Note that this is down from 2014, when 64% of groups reported having a citizenship element in their bonus. But I’m skeptical this is a real trend of decreasing popularity and suspect the drop is mostly explained by a much larger portion of respondents in this particular survey coming from hospitalist management companies which I think much less often have a citizenship bonus.
I devoted an entire column to the idea of a citizenship bonus in November 2011. At that time I expressed some ambivalence about its effectiveness. Since then I’ve become disenchanted and think it may do more harm than good.
SHM’s 2016 State of Hospital Medicine (SOHM) Report, based on 2015 data, shows that 46% of Hospital Medicine Groups (HMGs) connect some portion of bonus dollars to a provider’s citizenship.1 This is a relatively new phenomenon in the last 5 years or so. My anecdotal experience is that it isn’t limited to hospitalists; it is pretty common for doctors in any specialty who are employed by a hospital or other large organization.
HMGs vary in their definitions of what constitutes citizenship, but usually include things like committee participation, lectures, grand rounds presentations, community talks, research publications.
Our hospitalist group at my hospital has well-defined criteria that require attendance at more than 75% of meetings as a “light switch” (pays nothing itself, but “turns on” availability to citizenship bonus). Bonus dollars are paid for success in any one of several activities, such as making an in-person visit to two PCP offices or completing a meaningful project related to practice operations or clinical care.
I’ve been a supporter of a citizenship bonus for a long time, but two things have made me ambivalent or even opposed to it. The first is a book by Daniel Pink titled Drive: The Surprising Truth About What Motivates Us. It’s a short and very thought-provoking book summarizing research that suggests the effect of providing external rewards like compensation is to “…extinguish intrinsic motivation, diminish performance, crush creativity, and crowd out good behavior.”
The second reason for my ambivalence is my experience working with a lot of HMGs around the country. Those that have a citizenship bonus don’t seem to realize improved operations, more engaged doctors, or lower turnover, and so on. In fact, my experience is that the bonus tends to do exactly what Pink says – steer individuals and the group as a whole away from what is desired.
I’m not ready to say a citizenship bonus is always a bad idea. But it sure seems like it works out badly for many or most groups.
But if you do have a citizenship bonus, then don’t make the mistake of tying it to very basic expectations of the job, like attending group meetings or completing chart documentation on time. Doing those things should never be seen as a reason for a bonus.
Jeopardy (‘surge’) staffing: Not catching on?
As I write, influenza has swept through our region, and my hospital – like most along the west coast – is experiencing incredibly high volumes. I enter the building through a patient care unit that has been mothballed for several years, but today people from building maintenance were busy getting it ready for patients. The hospital is offering various incentives for patient care staff to work extra shifts to manage this volume surge, and our hospitalists have days with encounters near or at our highest-ever level. So surge capacity is once again on my mind.
But if every hospitalist in the group went from, say, 156 to 190 shifts annually, the practice might be able to staff every day with an additional provider without adding staff or spending more money. And a doc’s average day would be less busy, which for some people (okay, not very many) would be a worthwhile trade-off. I realize this is a tough sell and to many people it sounds crazy.
The 2014 SOHM showed 42% of HMGs had “no formal backup system,” and this had climbed to 58% in the 2016 Report. I don’t know if jeopardy or surge backup systems are really becoming less common, but it seems pretty clear they aren’t becoming more common. So it’s worth thinking about whether there is a practical way to remove inhibitors of surge capacity.
Dr. Nelson has been a practicing hospitalist since 1988. He is cofounder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Endnotes
1. Note that this is down from 2014, when 64% of groups reported having a citizenship element in their bonus. But I’m skeptical this is a real trend of decreasing popularity and suspect the drop is mostly explained by a much larger portion of respondents in this particular survey coming from hospitalist management companies which I think much less often have a citizenship bonus.
I devoted an entire column to the idea of a citizenship bonus in November 2011. At that time I expressed some ambivalence about its effectiveness. Since then I’ve become disenchanted and think it may do more harm than good.
SHM’s 2016 State of Hospital Medicine (SOHM) Report, based on 2015 data, shows that 46% of Hospital Medicine Groups (HMGs) connect some portion of bonus dollars to a provider’s citizenship.1 This is a relatively new phenomenon in the last 5 years or so. My anecdotal experience is that it isn’t limited to hospitalists; it is pretty common for doctors in any specialty who are employed by a hospital or other large organization.
HMGs vary in their definitions of what constitutes citizenship, but usually include things like committee participation, lectures, grand rounds presentations, community talks, research publications.
Our hospitalist group at my hospital has well-defined criteria that require attendance at more than 75% of meetings as a “light switch” (pays nothing itself, but “turns on” availability to citizenship bonus). Bonus dollars are paid for success in any one of several activities, such as making an in-person visit to two PCP offices or completing a meaningful project related to practice operations or clinical care.
I’ve been a supporter of a citizenship bonus for a long time, but two things have made me ambivalent or even opposed to it. The first is a book by Daniel Pink titled Drive: The Surprising Truth About What Motivates Us. It’s a short and very thought-provoking book summarizing research that suggests the effect of providing external rewards like compensation is to “…extinguish intrinsic motivation, diminish performance, crush creativity, and crowd out good behavior.”
The second reason for my ambivalence is my experience working with a lot of HMGs around the country. Those that have a citizenship bonus don’t seem to realize improved operations, more engaged doctors, or lower turnover, and so on. In fact, my experience is that the bonus tends to do exactly what Pink says – steer individuals and the group as a whole away from what is desired.
I’m not ready to say a citizenship bonus is always a bad idea. But it sure seems like it works out badly for many or most groups.
But if you do have a citizenship bonus, then don’t make the mistake of tying it to very basic expectations of the job, like attending group meetings or completing chart documentation on time. Doing those things should never be seen as a reason for a bonus.
Jeopardy (‘surge’) staffing: Not catching on?
As I write, influenza has swept through our region, and my hospital – like most along the west coast – is experiencing incredibly high volumes. I enter the building through a patient care unit that has been mothballed for several years, but today people from building maintenance were busy getting it ready for patients. The hospital is offering various incentives for patient care staff to work extra shifts to manage this volume surge, and our hospitalists have days with encounters near or at our highest-ever level. So surge capacity is once again on my mind.
But if every hospitalist in the group went from, say, 156 to 190 shifts annually, the practice might be able to staff every day with an additional provider without adding staff or spending more money. And a doc’s average day would be less busy, which for some people (okay, not very many) would be a worthwhile trade-off. I realize this is a tough sell and to many people it sounds crazy.
The 2014 SOHM showed 42% of HMGs had “no formal backup system,” and this had climbed to 58% in the 2016 Report. I don’t know if jeopardy or surge backup systems are really becoming less common, but it seems pretty clear they aren’t becoming more common. So it’s worth thinking about whether there is a practical way to remove inhibitors of surge capacity.
Dr. Nelson has been a practicing hospitalist since 1988. He is cofounder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Endnotes
1. Note that this is down from 2014, when 64% of groups reported having a citizenship element in their bonus. But I’m skeptical this is a real trend of decreasing popularity and suspect the drop is mostly explained by a much larger portion of respondents in this particular survey coming from hospitalist management companies which I think much less often have a citizenship bonus.
Wired to win
In 1929, an industrialist in Philadelphia whose factories had been plagued by vandalism sought to curtail the problem by organizing the boys in the community into athletic teams. Within a few years, his effort became Pop Warner Football. A few years later, a group of parents in Williamsport, Pa., started what was to become Little League Baseball.
Prior to the development of these two programs, kids organized their own games using shared equipment, if any at all. They drew foul lines and cobbled together goals in the bare dirt and the stubbly weeds of vacant lots and backyards. Kids shared equipment with each other. They picked teams in a manner that reflected the sometimes painful reality that some kids were proven winners and others were not. Rules were adjusted to fit the situation. Disagreements were settled without referees, or the game dissolved and a lesson was learned.
From its start in the 1930’s, the model of adult-organized and miniaturized versions of professional sports has spread from baseball and football to almost every team sport, including soccer, hockey, and lacrosse. Children may have been deprived of some self-organizing and negotiating skills, but, when one considers the electronically dominated sedentary alternatives, for the most part, adult-organized team youth sports have been a positive.

Of course, there have been some growing pains because an adult sport that has simply been miniaturized doesn’t necessarily fit well with young minds and bodies that are still developing. In some sports, adult/parent coaches now are required to undergo rigorous training in hopes of making the sport more child appropriate. However, the truth remains that, when teams compete, there are going to be winners and losers.
I recently read a newspaper article that included references to a few recent studies that suggest humans are hard wired to win (Sapolsky, Robert. “The Grim Truth Behind the ‘Winner Effect.’ ”The Wall Street Journal. Feb. 24, 2017). Well, not to win exactly but to be more likely to win again once they have been victorious, a phenomenon known as the “winner effect.”
A mouse that has been allowed to win a fixed fight with another mouse is more likely to win his next fight. Other studies on a variety of species, including humans, have found that winning can elevate testosterone levels and suppress stress-mediating hormones – winning boosts confidence and risk taking. More recent studies on zebra fish have demonstrated that a region of the habenula, a portion of the brain, seems to be critical for controlling these behaviors and chemical mediators.
Of course, the problem is that, when there are winners, there have to be losers. From time to time, the adult organizers have struggled with how to compensate for this unfortunate reality in the structure of their youth sports programs. One response has been to give every participant a trophy. Except when the children are so young that they don’t know which goal is theirs, however, awarding trophies to all is a transparent and foolish charade. The winners know who they are and so do the losers. Skillful and compassionate coaches of both winning and losing teams can cooperate to soften the cutting edge of competition, but it will never disappear. It should be fun to play, but it is always going to be more fun to win.
If there is a solution, it falls on the shoulders of parents, educators, and sometimes pediatricians to help the losers find environments and activities in which their skills and aptitudes will give them the greatest chance of enjoying the benefits of the “winner effect.” Winning isn’t everything, but it feels a lot better than losing. If we can help a child to win once – whether it is on the athletic field or in a classroom – it is more likely he or she will do it again.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
In 1929, an industrialist in Philadelphia whose factories had been plagued by vandalism sought to curtail the problem by organizing the boys in the community into athletic teams. Within a few years, his effort became Pop Warner Football. A few years later, a group of parents in Williamsport, Pa., started what was to become Little League Baseball.
Prior to the development of these two programs, kids organized their own games using shared equipment, if any at all. They drew foul lines and cobbled together goals in the bare dirt and the stubbly weeds of vacant lots and backyards. Kids shared equipment with each other. They picked teams in a manner that reflected the sometimes painful reality that some kids were proven winners and others were not. Rules were adjusted to fit the situation. Disagreements were settled without referees, or the game dissolved and a lesson was learned.
From its start in the 1930’s, the model of adult-organized and miniaturized versions of professional sports has spread from baseball and football to almost every team sport, including soccer, hockey, and lacrosse. Children may have been deprived of some self-organizing and negotiating skills, but, when one considers the electronically dominated sedentary alternatives, for the most part, adult-organized team youth sports have been a positive.
Of course, there have been some growing pains because an adult sport that has simply been miniaturized doesn’t necessarily fit well with young minds and bodies that are still developing. In some sports, adult/parent coaches now are required to undergo rigorous training in hopes of making the sport more child appropriate. However, the truth remains that, when teams compete, there are going to be winners and losers.
I recently read a newspaper article that included references to a few recent studies that suggest humans are hard wired to win (Sapolsky, Robert. “The Grim Truth Behind the ‘Winner Effect.’ ”The Wall Street Journal. Feb. 24, 2017). Well, not to win exactly but to be more likely to win again once they have been victorious, a phenomenon known as the “winner effect.”
A mouse that has been allowed to win a fixed fight with another mouse is more likely to win his next fight. Other studies on a variety of species, including humans, have found that winning can elevate testosterone levels and suppress stress-mediating hormones – winning boosts confidence and risk taking. More recent studies on zebra fish have demonstrated that a region of the habenula, a portion of the brain, seems to be critical for controlling these behaviors and chemical mediators.
Of course, the problem is that, when there are winners, there have to be losers. From time to time, the adult organizers have struggled with how to compensate for this unfortunate reality in the structure of their youth sports programs. One response has been to give every participant a trophy. Except when the children are so young that they don’t know which goal is theirs, however, awarding trophies to all is a transparent and foolish charade. The winners know who they are and so do the losers. Skillful and compassionate coaches of both winning and losing teams can cooperate to soften the cutting edge of competition, but it will never disappear. It should be fun to play, but it is always going to be more fun to win.
If there is a solution, it falls on the shoulders of parents, educators, and sometimes pediatricians to help the losers find environments and activities in which their skills and aptitudes will give them the greatest chance of enjoying the benefits of the “winner effect.” Winning isn’t everything, but it feels a lot better than losing. If we can help a child to win once – whether it is on the athletic field or in a classroom – it is more likely he or she will do it again.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
In 1929, an industrialist in Philadelphia whose factories had been plagued by vandalism sought to curtail the problem by organizing the boys in the community into athletic teams. Within a few years, his effort became Pop Warner Football. A few years later, a group of parents in Williamsport, Pa., started what was to become Little League Baseball.
Prior to the development of these two programs, kids organized their own games using shared equipment, if any at all. They drew foul lines and cobbled together goals in the bare dirt and the stubbly weeds of vacant lots and backyards. Kids shared equipment with each other. They picked teams in a manner that reflected the sometimes painful reality that some kids were proven winners and others were not. Rules were adjusted to fit the situation. Disagreements were settled without referees, or the game dissolved and a lesson was learned.
From its start in the 1930’s, the model of adult-organized and miniaturized versions of professional sports has spread from baseball and football to almost every team sport, including soccer, hockey, and lacrosse. Children may have been deprived of some self-organizing and negotiating skills, but, when one considers the electronically dominated sedentary alternatives, for the most part, adult-organized team youth sports have been a positive.
Of course, there have been some growing pains because an adult sport that has simply been miniaturized doesn’t necessarily fit well with young minds and bodies that are still developing. In some sports, adult/parent coaches now are required to undergo rigorous training in hopes of making the sport more child appropriate. However, the truth remains that, when teams compete, there are going to be winners and losers.
I recently read a newspaper article that included references to a few recent studies that suggest humans are hard wired to win (Sapolsky, Robert. “The Grim Truth Behind the ‘Winner Effect.’ ”The Wall Street Journal. Feb. 24, 2017). Well, not to win exactly but to be more likely to win again once they have been victorious, a phenomenon known as the “winner effect.”
A mouse that has been allowed to win a fixed fight with another mouse is more likely to win his next fight. Other studies on a variety of species, including humans, have found that winning can elevate testosterone levels and suppress stress-mediating hormones – winning boosts confidence and risk taking. More recent studies on zebra fish have demonstrated that a region of the habenula, a portion of the brain, seems to be critical for controlling these behaviors and chemical mediators.
Of course, the problem is that, when there are winners, there have to be losers. From time to time, the adult organizers have struggled with how to compensate for this unfortunate reality in the structure of their youth sports programs. One response has been to give every participant a trophy. Except when the children are so young that they don’t know which goal is theirs, however, awarding trophies to all is a transparent and foolish charade. The winners know who they are and so do the losers. Skillful and compassionate coaches of both winning and losing teams can cooperate to soften the cutting edge of competition, but it will never disappear. It should be fun to play, but it is always going to be more fun to win.
If there is a solution, it falls on the shoulders of parents, educators, and sometimes pediatricians to help the losers find environments and activities in which their skills and aptitudes will give them the greatest chance of enjoying the benefits of the “winner effect.” Winning isn’t everything, but it feels a lot better than losing. If we can help a child to win once – whether it is on the athletic field or in a classroom – it is more likely he or she will do it again.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
New 52-week EASI, pruritus data strengthen case for dupilumab in adult atopic dermatitis
ORLANDO – Treatment with dupilumab was associated with significantly improved measures of disease severity, including in quality of life and pruritus symptoms, at 16 and 52 weeks in adults with moderate to severe atopic dermatitis (AD) in the phase III CHRONOS trial.
In the CHRONOS study of adults with uncontrolled, moderate to severe AD, patients were treated with the investigational biologic dupilumab (Dupixent), an interleukin-4 and interleukin-13 pathway blocker administered in subcutaneous injections, in combination with topical corticosteroids. At 52 weeks, they had achieved significantly improved measures of overall disease severity, compared with those who received corticosteroids alone, according to Andrew Blauvelt, MD, MBA, president of Oregon Medical Research Center, Portland, who presented the new data from the study in a late-breaking clinical session at the annual meeting of the American Academy of Dermatology.

The new 52-week data presented at AAD show that the mean improvement in the EASI score from baseline was 80% in the 300 mg dupilumab every week plus corticosteroid group (group 1) and 78% in the group treated every 2 weeks (group 2), compared with 46% in the placebo plus corticosteroids group (control) (P less than .0001).
The mean improvement in self-reported itch from baseline, as measured by the Pruritus Numerical Rating Scale, was 54% in the first group, 56% in the second group, compared with 27% in controls (P less than .0001).
In the first group, 65% achieved a 4-point or greater improvement in their Patient Oriented Eczema Measure scores, as did 76% of the second group, compared with 26% of controls (P less than .0001).
At least a 4-point improvement over baseline in Dermatology Life Quality Index scores was seen in 63% of group 1, 80% of group 2, and 30% of controls (P less than .0001).
Adverse events across the study were similar, although the treatment groups had higher incidences of injection site reactions: 19% in group 1 and 15% in group 2, compared with 8% in controls. The treatment groups also had higher rates of conjunctivitis: 19% in group 1 and 14% in group 2, compared with 8% in controls.
Dr. Blauvelt said that patients who were “exited from the trial were continued for follow-up” and that rescue therapies such as cyclosporine, and other systemic agents, were also available. The rate of rescue therapy was about 15% in the first two groups, while half of controls needed rescue therapy. “We considered those patients who needed rescue nonresponders,” he noted.
The dropout rate at week 52 was about 15% across the treatment groups, compared with twice that in controls.
“Atopic dermatitis is the new psoriasis. We’re in an exciting area now, and we’ll be seeing more biologic therapies for moderate to severe atopic dermatitis. We have a tremendous need for this,” Dr. Blauvelt commented.
The Food and Drug Administration is expected to make a decision on approval of dupilumab by March 29, 2017. Dupilumab was designated by the FDA as a breakthrough therapy for uncontrolled, moderate to severe AD in 2014.
Dr. Blauvelt disclosed many pharmaceutical industry relationships, including with Regeneron Pharmaceuticals and Sanofi, which are developing dupilumab. (If approved, Regeneron and Sanofi Genzyme, part of Sanofi, will commercialize dupilumab).
CORRECTION 3/10/17: An earlier version of this article misstated the rates of clear or nearly clear skin.
[email protected]
On Twitter @whitneymcknight
ORLANDO – Treatment with dupilumab was associated with significantly improved measures of disease severity, including in quality of life and pruritus symptoms, at 16 and 52 weeks in adults with moderate to severe atopic dermatitis (AD) in the phase III CHRONOS trial.
In the CHRONOS study of adults with uncontrolled, moderate to severe AD, patients were treated with the investigational biologic dupilumab (Dupixent), an interleukin-4 and interleukin-13 pathway blocker administered in subcutaneous injections, in combination with topical corticosteroids. At 52 weeks, they had achieved significantly improved measures of overall disease severity, compared with those who received corticosteroids alone, according to Andrew Blauvelt, MD, MBA, president of Oregon Medical Research Center, Portland, who presented the new data from the study in a late-breaking clinical session at the annual meeting of the American Academy of Dermatology.
The new 52-week data presented at AAD show that the mean improvement in the EASI score from baseline was 80% in the 300 mg dupilumab every week plus corticosteroid group (group 1) and 78% in the group treated every 2 weeks (group 2), compared with 46% in the placebo plus corticosteroids group (control) (P less than .0001).
The mean improvement in self-reported itch from baseline, as measured by the Pruritus Numerical Rating Scale, was 54% in the first group, 56% in the second group, compared with 27% in controls (P less than .0001).
In the first group, 65% achieved a 4-point or greater improvement in their Patient Oriented Eczema Measure scores, as did 76% of the second group, compared with 26% of controls (P less than .0001).
At least a 4-point improvement over baseline in Dermatology Life Quality Index scores was seen in 63% of group 1, 80% of group 2, and 30% of controls (P less than .0001).
Adverse events across the study were similar, although the treatment groups had higher incidences of injection site reactions: 19% in group 1 and 15% in group 2, compared with 8% in controls. The treatment groups also had higher rates of conjunctivitis: 19% in group 1 and 14% in group 2, compared with 8% in controls.
Dr. Blauvelt said that patients who were “exited from the trial were continued for follow-up” and that rescue therapies such as cyclosporine, and other systemic agents, were also available. The rate of rescue therapy was about 15% in the first two groups, while half of controls needed rescue therapy. “We considered those patients who needed rescue nonresponders,” he noted.
The dropout rate at week 52 was about 15% across the treatment groups, compared with twice that in controls.
“Atopic dermatitis is the new psoriasis. We’re in an exciting area now, and we’ll be seeing more biologic therapies for moderate to severe atopic dermatitis. We have a tremendous need for this,” Dr. Blauvelt commented.
The Food and Drug Administration is expected to make a decision on approval of dupilumab by March 29, 2017. Dupilumab was designated by the FDA as a breakthrough therapy for uncontrolled, moderate to severe AD in 2014.
Dr. Blauvelt disclosed many pharmaceutical industry relationships, including with Regeneron Pharmaceuticals and Sanofi, which are developing dupilumab. (If approved, Regeneron and Sanofi Genzyme, part of Sanofi, will commercialize dupilumab).
CORRECTION 3/10/17: An earlier version of this article misstated the rates of clear or nearly clear skin.
[email protected]
On Twitter @whitneymcknight
ORLANDO – Treatment with dupilumab was associated with significantly improved measures of disease severity, including in quality of life and pruritus symptoms, at 16 and 52 weeks in adults with moderate to severe atopic dermatitis (AD) in the phase III CHRONOS trial.
In the CHRONOS study of adults with uncontrolled, moderate to severe AD, patients were treated with the investigational biologic dupilumab (Dupixent), an interleukin-4 and interleukin-13 pathway blocker administered in subcutaneous injections, in combination with topical corticosteroids. At 52 weeks, they had achieved significantly improved measures of overall disease severity, compared with those who received corticosteroids alone, according to Andrew Blauvelt, MD, MBA, president of Oregon Medical Research Center, Portland, who presented the new data from the study in a late-breaking clinical session at the annual meeting of the American Academy of Dermatology.
The new 52-week data presented at AAD show that the mean improvement in the EASI score from baseline was 80% in the 300 mg dupilumab every week plus corticosteroid group (group 1) and 78% in the group treated every 2 weeks (group 2), compared with 46% in the placebo plus corticosteroids group (control) (P less than .0001).
The mean improvement in self-reported itch from baseline, as measured by the Pruritus Numerical Rating Scale, was 54% in the first group, 56% in the second group, compared with 27% in controls (P less than .0001).
In the first group, 65% achieved a 4-point or greater improvement in their Patient Oriented Eczema Measure scores, as did 76% of the second group, compared with 26% of controls (P less than .0001).
At least a 4-point improvement over baseline in Dermatology Life Quality Index scores was seen in 63% of group 1, 80% of group 2, and 30% of controls (P less than .0001).
Adverse events across the study were similar, although the treatment groups had higher incidences of injection site reactions: 19% in group 1 and 15% in group 2, compared with 8% in controls. The treatment groups also had higher rates of conjunctivitis: 19% in group 1 and 14% in group 2, compared with 8% in controls.
Dr. Blauvelt said that patients who were “exited from the trial were continued for follow-up” and that rescue therapies such as cyclosporine, and other systemic agents, were also available. The rate of rescue therapy was about 15% in the first two groups, while half of controls needed rescue therapy. “We considered those patients who needed rescue nonresponders,” he noted.
The dropout rate at week 52 was about 15% across the treatment groups, compared with twice that in controls.
“Atopic dermatitis is the new psoriasis. We’re in an exciting area now, and we’ll be seeing more biologic therapies for moderate to severe atopic dermatitis. We have a tremendous need for this,” Dr. Blauvelt commented.
The Food and Drug Administration is expected to make a decision on approval of dupilumab by March 29, 2017. Dupilumab was designated by the FDA as a breakthrough therapy for uncontrolled, moderate to severe AD in 2014.
Dr. Blauvelt disclosed many pharmaceutical industry relationships, including with Regeneron Pharmaceuticals and Sanofi, which are developing dupilumab. (If approved, Regeneron and Sanofi Genzyme, part of Sanofi, will commercialize dupilumab).
CORRECTION 3/10/17: An earlier version of this article misstated the rates of clear or nearly clear skin.
[email protected]
On Twitter @whitneymcknight
AT AAD 2017
Key clinical point:
Major finding: At 52 weeks, dupilumab 300 mg administered in a subcutaneous injection once a week or every two weeks plus topical corticosteroids resulted in significantly more clearing compared with topical corticosteroids alone (P less than .0001). Self-reported measures of itch and quality-of-life measures were also higher across treatment groups.
Data source: A phase III trial of 740 adults with moderate to severe AD, randomized to treatment with one of the two regimens or corticosteroids alone.
Disclosures: Dr. Blauvelt disclosed many pharmaceutical industry relationships, including with Regeneron Pharmaceuticals and Sanofi, which are developing dupilumab. (If approved, Regeneron and Sanofi Genzyme, part of Sanofi, will commercialize dupilumab).
Cannabis associated with increased risk of heart failure and stroke
Cannabis use was associated with an increased risk of cerebrovascular accidents and heart failure in a retrospective analysis of the Nationwide Inpatient Sample (NIS).
Aditi Kalla, MD, a cardiology fellow at Einstein Medical Center in Philadelphia, and her colleagues analyzed data from nearly 21 million adult patients aged 18-55 years from the NIS 2009-2010 database. Approximately 1.5% (316,397) were diagnosed as cannabis users.
Cannabis users also were more likely to report cardiac risk factors such as hypertension (19.9% vs. 15.7% of nonusers), tobacco use (47.2% vs. 11.4%), alcohol use (28.1% vs 3.8%), and obesity (7% vs. 6.5%). They were older, on average, with a mean age of 33 years, compared with 26 years, and were likely to be male (60%), Dr. Kalla noted during a press briefing held in advance of the annual meeting of the American College of Cardiology.
Using multivariate regression analysis to adjust for these traditional cardiovascular risk factors, the investigators found cannabis remained an independent predictor for heart failure, with an odds ratio of 1.1 (P less than .01) and cerebrovascular accident, with an OR of 1.24 (P less than .001).
“Even when we corrected for known risks, we still found a higher rate of both stroke and heart failure in these patients,” Dr. Kalla said. “That leads us to believe that there is something else going on besides just obesity or diet-related cardiovascular side effects.”
Dr. Kalla noted that an expert analysis published by the ACC in September 2016 linked cannabinoid receptor type 1 with atherogenesis.
Further research is needed on the topic of cannabis and cardiovascular effects, especially as the legalization of medical and recreational cannabis spreads across the country, Dr. Kalla said. “Decriminalization of cannabis has passed in several states, bringing the total count now up to 28 states, plus the District of Columbia. We now need to be more knowledgeable of the risks and benefits of cannabis, as patients in these states may inquire into the use of it, or even ask us for prescriptions for it.”
While the NIS provided a large and strong data set for this analysis, the number of cannabis users likely was underreported because cannabis was legal in just 14 states at the time, Dr. Kalla noted. The study also was limited by a lack of specific information regarding cannabis intake, method of intake (ingestion or smoking), quantity and frequency of use, and whether use was medical or recreational.
The information collected also excluded whether patients used marijuana for medical or recreational purpose and how it was taken, by smoking or ingestion.
[email protected]
On Twitter @EAZTweets
Cannabis use was associated with an increased risk of cerebrovascular accidents and heart failure in a retrospective analysis of the Nationwide Inpatient Sample (NIS).
Aditi Kalla, MD, a cardiology fellow at Einstein Medical Center in Philadelphia, and her colleagues analyzed data from nearly 21 million adult patients aged 18-55 years from the NIS 2009-2010 database. Approximately 1.5% (316,397) were diagnosed as cannabis users.
Cannabis users also were more likely to report cardiac risk factors such as hypertension (19.9% vs. 15.7% of nonusers), tobacco use (47.2% vs. 11.4%), alcohol use (28.1% vs 3.8%), and obesity (7% vs. 6.5%). They were older, on average, with a mean age of 33 years, compared with 26 years, and were likely to be male (60%), Dr. Kalla noted during a press briefing held in advance of the annual meeting of the American College of Cardiology.
Using multivariate regression analysis to adjust for these traditional cardiovascular risk factors, the investigators found cannabis remained an independent predictor for heart failure, with an odds ratio of 1.1 (P less than .01) and cerebrovascular accident, with an OR of 1.24 (P less than .001).
“Even when we corrected for known risks, we still found a higher rate of both stroke and heart failure in these patients,” Dr. Kalla said. “That leads us to believe that there is something else going on besides just obesity or diet-related cardiovascular side effects.”
Dr. Kalla noted that an expert analysis published by the ACC in September 2016 linked cannabinoid receptor type 1 with atherogenesis.
Further research is needed on the topic of cannabis and cardiovascular effects, especially as the legalization of medical and recreational cannabis spreads across the country, Dr. Kalla said. “Decriminalization of cannabis has passed in several states, bringing the total count now up to 28 states, plus the District of Columbia. We now need to be more knowledgeable of the risks and benefits of cannabis, as patients in these states may inquire into the use of it, or even ask us for prescriptions for it.”
While the NIS provided a large and strong data set for this analysis, the number of cannabis users likely was underreported because cannabis was legal in just 14 states at the time, Dr. Kalla noted. The study also was limited by a lack of specific information regarding cannabis intake, method of intake (ingestion or smoking), quantity and frequency of use, and whether use was medical or recreational.
The information collected also excluded whether patients used marijuana for medical or recreational purpose and how it was taken, by smoking or ingestion.
[email protected]
On Twitter @EAZTweets
Cannabis use was associated with an increased risk of cerebrovascular accidents and heart failure in a retrospective analysis of the Nationwide Inpatient Sample (NIS).
Aditi Kalla, MD, a cardiology fellow at Einstein Medical Center in Philadelphia, and her colleagues analyzed data from nearly 21 million adult patients aged 18-55 years from the NIS 2009-2010 database. Approximately 1.5% (316,397) were diagnosed as cannabis users.
Cannabis users also were more likely to report cardiac risk factors such as hypertension (19.9% vs. 15.7% of nonusers), tobacco use (47.2% vs. 11.4%), alcohol use (28.1% vs 3.8%), and obesity (7% vs. 6.5%). They were older, on average, with a mean age of 33 years, compared with 26 years, and were likely to be male (60%), Dr. Kalla noted during a press briefing held in advance of the annual meeting of the American College of Cardiology.
Using multivariate regression analysis to adjust for these traditional cardiovascular risk factors, the investigators found cannabis remained an independent predictor for heart failure, with an odds ratio of 1.1 (P less than .01) and cerebrovascular accident, with an OR of 1.24 (P less than .001).
“Even when we corrected for known risks, we still found a higher rate of both stroke and heart failure in these patients,” Dr. Kalla said. “That leads us to believe that there is something else going on besides just obesity or diet-related cardiovascular side effects.”
Dr. Kalla noted that an expert analysis published by the ACC in September 2016 linked cannabinoid receptor type 1 with atherogenesis.
Further research is needed on the topic of cannabis and cardiovascular effects, especially as the legalization of medical and recreational cannabis spreads across the country, Dr. Kalla said. “Decriminalization of cannabis has passed in several states, bringing the total count now up to 28 states, plus the District of Columbia. We now need to be more knowledgeable of the risks and benefits of cannabis, as patients in these states may inquire into the use of it, or even ask us for prescriptions for it.”
While the NIS provided a large and strong data set for this analysis, the number of cannabis users likely was underreported because cannabis was legal in just 14 states at the time, Dr. Kalla noted. The study also was limited by a lack of specific information regarding cannabis intake, method of intake (ingestion or smoking), quantity and frequency of use, and whether use was medical or recreational.
The information collected also excluded whether patients used marijuana for medical or recreational purpose and how it was taken, by smoking or ingestion.
[email protected]
On Twitter @EAZTweets
FROM ACC 17
Key clinical point:
Major finding: Cannabis users showed 26% increased risk (OR, 1.24) of stroke and 10% increased risk (OR, 1.1) of heart failure.
Data source: Retrospective study of over 20 million patients’ records aged 18-55 years gathered from the Nationwide Inpatient Sample 2009-2010 database.
Disclosures: Researchers reported no relevant conflicts of interest.