User login
CDC: Greater activity limitations accompany rising arthritis prevalence
The number of adults with arthritis in the United States continues to rise, with the number projected to climb as high as 78 million by the year 2040. Some of the keys to stemming this rising tide are exercise, along with greater knowledge of how to manage symptoms, according to a new report from the Centers for Disease Control and Prevention.
“Arthritis is at an all-time high: more than 54 million people report a diagnosis of it, and alarmingly, more people with arthritis are suffering from it,” said Anne Schuchat, MD, acting director of the CDC, during a conference call regarding the agency’s latest Vital Signs report (MMWR Morb Mortal Wkly Rep. 2017 Mar 7. doi: org/10.15585/mmwr.mm6609e1). “Among adults with arthritis, the percentage whose lives are particularly limited has increased by about 20% since 2002, from about 36% in 2002 to 43% in 2015. We’re seeing this increase independent of aging of the population.”

“Physical activity can be the antidote for many people [and] can actually decrease pain and improve function by almost 40%,” Dr. Schuchat explained. “Right now, one in three adults with arthritis report being inactive [because of] pain or fear of pain or not knowing what exercise is safe for their joints.”
This inactivity can lead to arthritis patients developing other serious chronic conditions, such as heart disease, diabetes and obesity – conditions that all require physical activity in order to properly manage them. Arthritis alone puts an extraordinary financial burden on the domestic health care industry, as direct medical costs associated with the condition total roughly $81 billion per year, according to the CDC. Additionally, about half of all adults with heart disease or diabetes, and about one-third of obese adults, also have arthritis.
In addition to engaging in regular physical activity, the Vital Signs report also recommends that arthritis patients attend disease management education programs, which are available regionally but often go underutilized, largely due to lack of awareness about them or trepidation regarding how effective the programs really are. To combat this, the CDC is calling on health care providers to help them educate patients about these classes and spread the word about the steps that can be taken to manage arthritis. In 2017, the CDC is funding arthritis programs in 12 states (California, Kansas, Kentucky, Michigan, Missouri, Montana, New York, Oregon, Pennsylvania, Rhode Island, South Carolina, and Utah) to disseminate arthritis-appropriate evidence-based physical activity and self-management education interventions.
“Men or women with arthritis can reduce their symptoms by 10%-20% by participating in disease management education programs to acquire skills to better manage their symptoms. Right now, these programs are only reaching about 1 in 10 people with arthritis, but the classes are available in many community settings,” Dr. Schuchat said. “We know that adults with arthritis are significantly more likely to attend a disease management education program when a health care provider recommends it to them.”
When seeing patients with arthritis, Dr. Schuchat advised health care providers to recommend routine physical activity, such as walking, biking, swimming, and physical activity programs offered by local parks and recreation centers, as well as weight loss, in order to ease joint pain. The American College of Rheumatology and other professional organizations provide guidelines for discussing treatment options with patients. Providing treatment or additional services for depression or anxiety, which occur in about one-third of adult arthritis patients, may help individuals to better manage their arthritis symptoms.
The agency’s report derives from its analysis of 2013-2015 data from the National Health Interview Survey, which comprised a nationally representative sample of about 36,000 in-person interviews. The survey classifies individuals with physician-diagnosed arthritis as those who answered “yes” to the question “Have you ever been told by a doctor or other health professional that you have some form of arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia?”
The number of adults with arthritis in the United States continues to rise, with the number projected to climb as high as 78 million by the year 2040. Some of the keys to stemming this rising tide are exercise, along with greater knowledge of how to manage symptoms, according to a new report from the Centers for Disease Control and Prevention.
“Arthritis is at an all-time high: more than 54 million people report a diagnosis of it, and alarmingly, more people with arthritis are suffering from it,” said Anne Schuchat, MD, acting director of the CDC, during a conference call regarding the agency’s latest Vital Signs report (MMWR Morb Mortal Wkly Rep. 2017 Mar 7. doi: org/10.15585/mmwr.mm6609e1). “Among adults with arthritis, the percentage whose lives are particularly limited has increased by about 20% since 2002, from about 36% in 2002 to 43% in 2015. We’re seeing this increase independent of aging of the population.”
“Physical activity can be the antidote for many people [and] can actually decrease pain and improve function by almost 40%,” Dr. Schuchat explained. “Right now, one in three adults with arthritis report being inactive [because of] pain or fear of pain or not knowing what exercise is safe for their joints.”
This inactivity can lead to arthritis patients developing other serious chronic conditions, such as heart disease, diabetes and obesity – conditions that all require physical activity in order to properly manage them. Arthritis alone puts an extraordinary financial burden on the domestic health care industry, as direct medical costs associated with the condition total roughly $81 billion per year, according to the CDC. Additionally, about half of all adults with heart disease or diabetes, and about one-third of obese adults, also have arthritis.
In addition to engaging in regular physical activity, the Vital Signs report also recommends that arthritis patients attend disease management education programs, which are available regionally but often go underutilized, largely due to lack of awareness about them or trepidation regarding how effective the programs really are. To combat this, the CDC is calling on health care providers to help them educate patients about these classes and spread the word about the steps that can be taken to manage arthritis. In 2017, the CDC is funding arthritis programs in 12 states (California, Kansas, Kentucky, Michigan, Missouri, Montana, New York, Oregon, Pennsylvania, Rhode Island, South Carolina, and Utah) to disseminate arthritis-appropriate evidence-based physical activity and self-management education interventions.
“Men or women with arthritis can reduce their symptoms by 10%-20% by participating in disease management education programs to acquire skills to better manage their symptoms. Right now, these programs are only reaching about 1 in 10 people with arthritis, but the classes are available in many community settings,” Dr. Schuchat said. “We know that adults with arthritis are significantly more likely to attend a disease management education program when a health care provider recommends it to them.”
When seeing patients with arthritis, Dr. Schuchat advised health care providers to recommend routine physical activity, such as walking, biking, swimming, and physical activity programs offered by local parks and recreation centers, as well as weight loss, in order to ease joint pain. The American College of Rheumatology and other professional organizations provide guidelines for discussing treatment options with patients. Providing treatment or additional services for depression or anxiety, which occur in about one-third of adult arthritis patients, may help individuals to better manage their arthritis symptoms.
The agency’s report derives from its analysis of 2013-2015 data from the National Health Interview Survey, which comprised a nationally representative sample of about 36,000 in-person interviews. The survey classifies individuals with physician-diagnosed arthritis as those who answered “yes” to the question “Have you ever been told by a doctor or other health professional that you have some form of arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia?”
The number of adults with arthritis in the United States continues to rise, with the number projected to climb as high as 78 million by the year 2040. Some of the keys to stemming this rising tide are exercise, along with greater knowledge of how to manage symptoms, according to a new report from the Centers for Disease Control and Prevention.
“Arthritis is at an all-time high: more than 54 million people report a diagnosis of it, and alarmingly, more people with arthritis are suffering from it,” said Anne Schuchat, MD, acting director of the CDC, during a conference call regarding the agency’s latest Vital Signs report (MMWR Morb Mortal Wkly Rep. 2017 Mar 7. doi: org/10.15585/mmwr.mm6609e1). “Among adults with arthritis, the percentage whose lives are particularly limited has increased by about 20% since 2002, from about 36% in 2002 to 43% in 2015. We’re seeing this increase independent of aging of the population.”
“Physical activity can be the antidote for many people [and] can actually decrease pain and improve function by almost 40%,” Dr. Schuchat explained. “Right now, one in three adults with arthritis report being inactive [because of] pain or fear of pain or not knowing what exercise is safe for their joints.”
This inactivity can lead to arthritis patients developing other serious chronic conditions, such as heart disease, diabetes and obesity – conditions that all require physical activity in order to properly manage them. Arthritis alone puts an extraordinary financial burden on the domestic health care industry, as direct medical costs associated with the condition total roughly $81 billion per year, according to the CDC. Additionally, about half of all adults with heart disease or diabetes, and about one-third of obese adults, also have arthritis.
In addition to engaging in regular physical activity, the Vital Signs report also recommends that arthritis patients attend disease management education programs, which are available regionally but often go underutilized, largely due to lack of awareness about them or trepidation regarding how effective the programs really are. To combat this, the CDC is calling on health care providers to help them educate patients about these classes and spread the word about the steps that can be taken to manage arthritis. In 2017, the CDC is funding arthritis programs in 12 states (California, Kansas, Kentucky, Michigan, Missouri, Montana, New York, Oregon, Pennsylvania, Rhode Island, South Carolina, and Utah) to disseminate arthritis-appropriate evidence-based physical activity and self-management education interventions.
“Men or women with arthritis can reduce their symptoms by 10%-20% by participating in disease management education programs to acquire skills to better manage their symptoms. Right now, these programs are only reaching about 1 in 10 people with arthritis, but the classes are available in many community settings,” Dr. Schuchat said. “We know that adults with arthritis are significantly more likely to attend a disease management education program when a health care provider recommends it to them.”
When seeing patients with arthritis, Dr. Schuchat advised health care providers to recommend routine physical activity, such as walking, biking, swimming, and physical activity programs offered by local parks and recreation centers, as well as weight loss, in order to ease joint pain. The American College of Rheumatology and other professional organizations provide guidelines for discussing treatment options with patients. Providing treatment or additional services for depression or anxiety, which occur in about one-third of adult arthritis patients, may help individuals to better manage their arthritis symptoms.
The agency’s report derives from its analysis of 2013-2015 data from the National Health Interview Survey, which comprised a nationally representative sample of about 36,000 in-person interviews. The survey classifies individuals with physician-diagnosed arthritis as those who answered “yes” to the question “Have you ever been told by a doctor or other health professional that you have some form of arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia?”
FROM MMWR
Key clinical point:
Major finding: About 24 million American adults report being significantly limited due to their arthritis.
Data source: 2013-2015 data from the National Health Interview Survey.
Disclosures: No disclosures were reported.
Depression and deep brain stimulation: ‘Furor therapeuticus redux’
Looking back after a long and distinguished career, Leon Eisenberg, MD, invoked the term “furor therapeuticus” to describe overzealous treatment by doctors who became frustrated with therapeutic limitations or motivated by professional enthusiasm.1
With this in mind, Dr. Eisenberg criticized expansive marketing and prescribing of psychotropic drugs in an editorial published exactly 10 years ago. He might also have questioned the current interest in deep brain stimulation (DBS) as a treatment for depression and a growing list of behavioral disorders. Initial studies of DBS in depression were promising, but recent setbacks have brought research to a scientific and ethical crossroads that compels broader discussion.
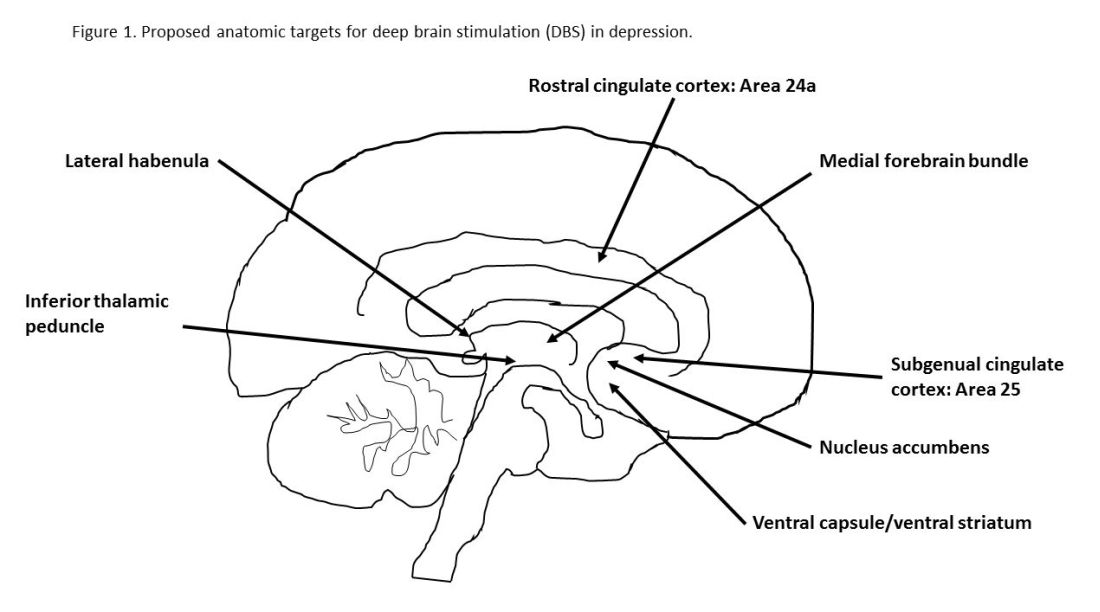
Besides uncertainties over the right targets to stimulate, identification of the right candidates for DBS treatment can be difficult. Trials of DBS recruited highly selected depressed subjects with no consensus on symptoms or biomarkers that could be used to predict who might respond. Doctors still rely on clinical symptoms to distinguish patients with melancholic depression, who respond to medications or electroconvulsive therapy and might also respond to DBS, from patients with depressed mood because of psychosocial problems, who respond to psychotherapy or social interventions.
Evidence on the efficacy and safety of DBS in depression is mixed. Initial open trials were promising, with dramatic and sustained recovery in some patients, but they were limited by small numbers of subjects and a lack of randomized controls and standardized methods.4,5
DBS is not without serious side effects, and substantial maintenance costs are not always covered by insurance. So, two recent industry trials were eagerly anticipated but showed no significant differences between active and sham stimulations in depression.6,7 These disappointing results prompted soul-searching among investigators, who presented ingenious ideas for correcting shortcomings that could be tested in future trials but also raised doubts as to the prospects of DBS in depression.4,5
Given that DBS devices already are marketed for neurological disorders, regulation of practice is crucial to prevent off-label misuse in behavioral disorders.8 Federal agencies enforce rules governing DBS devices but rely on investigators and local review boards in research and on voluntary postmarketing reports by individual practitioners to monitor compliance and safety. Unscrupulous commercial interests could expand the market for these devices, as demonstrated by the proliferation of psychotropic drug prescribing decried by Dr. Eisenberg. DBS also must be restricted to specialized teams and medical centers to prevent inappropriate implantation by poorly trained providers.
Because behavioral disorders exact an enormous toll on patients, families, and society, better access to effective care and the search for better treatments must remain public health priorities.
Transformative, breakthrough discoveries in brain research will undoubtedly lead to improvements in treatment, including surgical devices in some cases, but, DBS is at risk of being exaggerated and oversold. Adverse consequences of misuse could provoke a public backlash that would have a chilling effect on vital brain research.
One possible way to prevent this is the risk evaluation and mitigation strategy established by the Food and Drug Administration to manage high-risk pharmaceuticals. The FDA mandates that certain high-risk drugs can be prescribed only if doctors are certified and only if patients are enrolled in a national registry where eligibility, course, and outcome are monitored. A similar mechanism should apply to high-risk surgical devices when used for behavioral disorders.9,10
People with behavioral disorders deserve the right to volunteer for experimental programs that offer hope of recovery for themselves and future generations, but they also deserve to be treated with the utmost scientific rigor and protection that society can provide.
Dr. Caroff is emeritus professor of psychiatry at the University of Pennsylvania, Philadelphia. He has received research grant funding from Sunovion Pharmaceuticals and serves as a consultant to Neurocrine Biosciences and TEVA.
References
1. Am J Psychiatry. 2007;164(4):552-5
2. Curr Behav Neurosci Rep. 2014;1(2):55-63
3. J Affect Disord. 2014;156:1-7
4. JAMA Psychiatry. 2016;739(5):439-40
5. Biol Psychiatry. 2016;79(4):e9-10
6. Stereotact Funct Neurosurg. 2015;93:366-9
7. Neurotherapeutics. 2014;11(3):475-84
8. J Neurol Neurosurg Psychiatry. 2014;85(9):1003-8
9. Brain Stimul. 2012;5(4):653-5
10. Fed Reg. 1977 May 23;42(99):26318-32
Looking back after a long and distinguished career, Leon Eisenberg, MD, invoked the term “furor therapeuticus” to describe overzealous treatment by doctors who became frustrated with therapeutic limitations or motivated by professional enthusiasm.1
With this in mind, Dr. Eisenberg criticized expansive marketing and prescribing of psychotropic drugs in an editorial published exactly 10 years ago. He might also have questioned the current interest in deep brain stimulation (DBS) as a treatment for depression and a growing list of behavioral disorders. Initial studies of DBS in depression were promising, but recent setbacks have brought research to a scientific and ethical crossroads that compels broader discussion.
Besides uncertainties over the right targets to stimulate, identification of the right candidates for DBS treatment can be difficult. Trials of DBS recruited highly selected depressed subjects with no consensus on symptoms or biomarkers that could be used to predict who might respond. Doctors still rely on clinical symptoms to distinguish patients with melancholic depression, who respond to medications or electroconvulsive therapy and might also respond to DBS, from patients with depressed mood because of psychosocial problems, who respond to psychotherapy or social interventions.
Evidence on the efficacy and safety of DBS in depression is mixed. Initial open trials were promising, with dramatic and sustained recovery in some patients, but they were limited by small numbers of subjects and a lack of randomized controls and standardized methods.4,5
DBS is not without serious side effects, and substantial maintenance costs are not always covered by insurance. So, two recent industry trials were eagerly anticipated but showed no significant differences between active and sham stimulations in depression.6,7 These disappointing results prompted soul-searching among investigators, who presented ingenious ideas for correcting shortcomings that could be tested in future trials but also raised doubts as to the prospects of DBS in depression.4,5
Given that DBS devices already are marketed for neurological disorders, regulation of practice is crucial to prevent off-label misuse in behavioral disorders.8 Federal agencies enforce rules governing DBS devices but rely on investigators and local review boards in research and on voluntary postmarketing reports by individual practitioners to monitor compliance and safety. Unscrupulous commercial interests could expand the market for these devices, as demonstrated by the proliferation of psychotropic drug prescribing decried by Dr. Eisenberg. DBS also must be restricted to specialized teams and medical centers to prevent inappropriate implantation by poorly trained providers.
Because behavioral disorders exact an enormous toll on patients, families, and society, better access to effective care and the search for better treatments must remain public health priorities.
Transformative, breakthrough discoveries in brain research will undoubtedly lead to improvements in treatment, including surgical devices in some cases, but, DBS is at risk of being exaggerated and oversold. Adverse consequences of misuse could provoke a public backlash that would have a chilling effect on vital brain research.
One possible way to prevent this is the risk evaluation and mitigation strategy established by the Food and Drug Administration to manage high-risk pharmaceuticals. The FDA mandates that certain high-risk drugs can be prescribed only if doctors are certified and only if patients are enrolled in a national registry where eligibility, course, and outcome are monitored. A similar mechanism should apply to high-risk surgical devices when used for behavioral disorders.9,10
People with behavioral disorders deserve the right to volunteer for experimental programs that offer hope of recovery for themselves and future generations, but they also deserve to be treated with the utmost scientific rigor and protection that society can provide.
Dr. Caroff is emeritus professor of psychiatry at the University of Pennsylvania, Philadelphia. He has received research grant funding from Sunovion Pharmaceuticals and serves as a consultant to Neurocrine Biosciences and TEVA.
References
1. Am J Psychiatry. 2007;164(4):552-5
2. Curr Behav Neurosci Rep. 2014;1(2):55-63
3. J Affect Disord. 2014;156:1-7
4. JAMA Psychiatry. 2016;739(5):439-40
5. Biol Psychiatry. 2016;79(4):e9-10
6. Stereotact Funct Neurosurg. 2015;93:366-9
7. Neurotherapeutics. 2014;11(3):475-84
8. J Neurol Neurosurg Psychiatry. 2014;85(9):1003-8
9. Brain Stimul. 2012;5(4):653-5
10. Fed Reg. 1977 May 23;42(99):26318-32
Looking back after a long and distinguished career, Leon Eisenberg, MD, invoked the term “furor therapeuticus” to describe overzealous treatment by doctors who became frustrated with therapeutic limitations or motivated by professional enthusiasm.1
With this in mind, Dr. Eisenberg criticized expansive marketing and prescribing of psychotropic drugs in an editorial published exactly 10 years ago. He might also have questioned the current interest in deep brain stimulation (DBS) as a treatment for depression and a growing list of behavioral disorders. Initial studies of DBS in depression were promising, but recent setbacks have brought research to a scientific and ethical crossroads that compels broader discussion.
Besides uncertainties over the right targets to stimulate, identification of the right candidates for DBS treatment can be difficult. Trials of DBS recruited highly selected depressed subjects with no consensus on symptoms or biomarkers that could be used to predict who might respond. Doctors still rely on clinical symptoms to distinguish patients with melancholic depression, who respond to medications or electroconvulsive therapy and might also respond to DBS, from patients with depressed mood because of psychosocial problems, who respond to psychotherapy or social interventions.
Evidence on the efficacy and safety of DBS in depression is mixed. Initial open trials were promising, with dramatic and sustained recovery in some patients, but they were limited by small numbers of subjects and a lack of randomized controls and standardized methods.4,5
DBS is not without serious side effects, and substantial maintenance costs are not always covered by insurance. So, two recent industry trials were eagerly anticipated but showed no significant differences between active and sham stimulations in depression.6,7 These disappointing results prompted soul-searching among investigators, who presented ingenious ideas for correcting shortcomings that could be tested in future trials but also raised doubts as to the prospects of DBS in depression.4,5
Given that DBS devices already are marketed for neurological disorders, regulation of practice is crucial to prevent off-label misuse in behavioral disorders.8 Federal agencies enforce rules governing DBS devices but rely on investigators and local review boards in research and on voluntary postmarketing reports by individual practitioners to monitor compliance and safety. Unscrupulous commercial interests could expand the market for these devices, as demonstrated by the proliferation of psychotropic drug prescribing decried by Dr. Eisenberg. DBS also must be restricted to specialized teams and medical centers to prevent inappropriate implantation by poorly trained providers.
Because behavioral disorders exact an enormous toll on patients, families, and society, better access to effective care and the search for better treatments must remain public health priorities.
Transformative, breakthrough discoveries in brain research will undoubtedly lead to improvements in treatment, including surgical devices in some cases, but, DBS is at risk of being exaggerated and oversold. Adverse consequences of misuse could provoke a public backlash that would have a chilling effect on vital brain research.
One possible way to prevent this is the risk evaluation and mitigation strategy established by the Food and Drug Administration to manage high-risk pharmaceuticals. The FDA mandates that certain high-risk drugs can be prescribed only if doctors are certified and only if patients are enrolled in a national registry where eligibility, course, and outcome are monitored. A similar mechanism should apply to high-risk surgical devices when used for behavioral disorders.9,10
People with behavioral disorders deserve the right to volunteer for experimental programs that offer hope of recovery for themselves and future generations, but they also deserve to be treated with the utmost scientific rigor and protection that society can provide.
Dr. Caroff is emeritus professor of psychiatry at the University of Pennsylvania, Philadelphia. He has received research grant funding from Sunovion Pharmaceuticals and serves as a consultant to Neurocrine Biosciences and TEVA.
References
1. Am J Psychiatry. 2007;164(4):552-5
2. Curr Behav Neurosci Rep. 2014;1(2):55-63
3. J Affect Disord. 2014;156:1-7
4. JAMA Psychiatry. 2016;739(5):439-40
5. Biol Psychiatry. 2016;79(4):e9-10
6. Stereotact Funct Neurosurg. 2015;93:366-9
7. Neurotherapeutics. 2014;11(3):475-84
8. J Neurol Neurosurg Psychiatry. 2014;85(9):1003-8
9. Brain Stimul. 2012;5(4):653-5
10. Fed Reg. 1977 May 23;42(99):26318-32
Small study: Watchful waiting better for pediatric IBS
Children with irritable bowel syndrome (IBS) may recover more successfully with reassurance than with medication, according to a study from Federico II University in Naples, Italy.
Of 83 children in this single-center observational study, 30 of the 48 children (62.8%) who reported symptom resolution were not put on medication, according to Eleonora Giannetti, MD, and her colleagues (J Pediatr. 2017 Jan 18. doi: 10.1016/j.jpeds.2016.12.036).
Researchers assessed children using a symptom survey, having patients and their parents report “how often days off school or interruption of daily activities because of IBS were needed,” as well as a scale of disruption ranging from 0 to 4.
A total of 47 children received verbal reassurance only, with no medication, while 9 received polyethylene glycol, 24 received probiotics, and 3 received trimebutine (not available in the United States), according to Dr. Giannetti.
Dr. Giannetti and her colleagues argued the data showed not only a positive correlation between decreased symptoms and lack of pharmaceutical intervention, but a negative impact of medication on children with IBS.
“Despite larger interventional studies being needed, our results also seem to suggest that traditionally prescribed medications, particularly probiotics and [polyethlene glycol], poorly affect the progression of IBS symptoms,” Dr. Giannetti wrote. “There was even a trend toward worse outcome of patients receiving probiotics.”
Limitations included a small sample size and medication not being randomly allocated.
Researchers said they also were limited by a short time frame, which, in regards to the “recurrent nature” of IBS, makes it difficult for researchers to know if and when IBS is completely resolved.
[email protected]
On Twitter @EAZtweets
Children with irritable bowel syndrome (IBS) may recover more successfully with reassurance than with medication, according to a study from Federico II University in Naples, Italy.
Of 83 children in this single-center observational study, 30 of the 48 children (62.8%) who reported symptom resolution were not put on medication, according to Eleonora Giannetti, MD, and her colleagues (J Pediatr. 2017 Jan 18. doi: 10.1016/j.jpeds.2016.12.036).
Researchers assessed children using a symptom survey, having patients and their parents report “how often days off school or interruption of daily activities because of IBS were needed,” as well as a scale of disruption ranging from 0 to 4.
A total of 47 children received verbal reassurance only, with no medication, while 9 received polyethylene glycol, 24 received probiotics, and 3 received trimebutine (not available in the United States), according to Dr. Giannetti.
Dr. Giannetti and her colleagues argued the data showed not only a positive correlation between decreased symptoms and lack of pharmaceutical intervention, but a negative impact of medication on children with IBS.
“Despite larger interventional studies being needed, our results also seem to suggest that traditionally prescribed medications, particularly probiotics and [polyethlene glycol], poorly affect the progression of IBS symptoms,” Dr. Giannetti wrote. “There was even a trend toward worse outcome of patients receiving probiotics.”
Limitations included a small sample size and medication not being randomly allocated.
Researchers said they also were limited by a short time frame, which, in regards to the “recurrent nature” of IBS, makes it difficult for researchers to know if and when IBS is completely resolved.
[email protected]
On Twitter @EAZtweets
Children with irritable bowel syndrome (IBS) may recover more successfully with reassurance than with medication, according to a study from Federico II University in Naples, Italy.
Of 83 children in this single-center observational study, 30 of the 48 children (62.8%) who reported symptom resolution were not put on medication, according to Eleonora Giannetti, MD, and her colleagues (J Pediatr. 2017 Jan 18. doi: 10.1016/j.jpeds.2016.12.036).
Researchers assessed children using a symptom survey, having patients and their parents report “how often days off school or interruption of daily activities because of IBS were needed,” as well as a scale of disruption ranging from 0 to 4.
A total of 47 children received verbal reassurance only, with no medication, while 9 received polyethylene glycol, 24 received probiotics, and 3 received trimebutine (not available in the United States), according to Dr. Giannetti.
Dr. Giannetti and her colleagues argued the data showed not only a positive correlation between decreased symptoms and lack of pharmaceutical intervention, but a negative impact of medication on children with IBS.
“Despite larger interventional studies being needed, our results also seem to suggest that traditionally prescribed medications, particularly probiotics and [polyethlene glycol], poorly affect the progression of IBS symptoms,” Dr. Giannetti wrote. “There was even a trend toward worse outcome of patients receiving probiotics.”
Limitations included a small sample size and medication not being randomly allocated.
Researchers said they also were limited by a short time frame, which, in regards to the “recurrent nature” of IBS, makes it difficult for researchers to know if and when IBS is completely resolved.
[email protected]
On Twitter @EAZtweets
FROM THE JOURNAL OF PEDIATRICS
Key clinical point:
Major finding: Thirty of 48 children who reported IBS symptom resolution received no medical intervention; 18 were treated with one of three drugs.
Data Source: An observational, single-center study of 83 children.
Disclosures: The investigators reported no relevant conflicts of interest.
Vulvovaginal disorders: When should you biopsy a suspicious lesion?
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Also from PAGS 2016:
- Dr. Tommaso Falcone offers Top 3 things I learned at the PAGS 2016 symposium
- Visit PAGS
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Also from PAGS 2016:
- Dr. Tommaso Falcone offers Top 3 things I learned at the PAGS 2016 symposium
- Visit PAGS
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Also from PAGS 2016:
- Dr. Tommaso Falcone offers Top 3 things I learned at the PAGS 2016 symposium
- Visit PAGS
Biosimilars: No big dollar savings, but are clinically ‘dead on’
SNOWMASS, COLO. – If you thought biosimilars would bring sharply reduced pricing compared with their parent agents, with resultant greater patient access to highly effective therapies for rheumatic diseases ... think again.
“The promise to our patients of biosimilars – greater access to treatments – is something I think we’re just not going to see, at least not here in the U.S.,” Michael E. Weinblatt, MD, declared at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
In contrast, the safety and efficacy of the biosimilars, as well as their interchangeability with their reference products, appear to be as hoped for. At the 2016 annual meeting of the American College of Rheumatology, Dr. Weinblatt presented the week 24 results of a phase III, randomized trial involving rheumatoid arthritis patients on background methotrexate plus either adalimumab (Humira) or its biosimilar SB5.
“Essentially, they’re dead on in clinical response, they’re dead on in antibody levels, and they’re dead on in toxicity. And, you can put any of the biosimilars up there and the results are the same. If they get approved, this is what you’re going to see,” the rheumatologist said.
Also at the 2016 ACR annual meeting, he noted, Danish investigators presented reassuring 1-year follow-up data on 802 Danes with inflammatory rheumatic diseases who switched from infliximab (Remicade) to its biosimilar Remsima. Disease activity and flare rates in the year following the switch were similar to those in the year before. The 1-year rate of adherence to Remsima was 84%, similar to the historical 86% 1-year rate with infliximab.
“So, I’m pretty comfortable with the biosimilars,” Dr. Weinblatt continued.
He observed that, of all the systemic rheumatic diseases, the greatest progress has occurred in the treatment of rheumatoid arthritis.
“We have made great advances in the treatment of this disease, unlike many of our other diseases. Methotrexate and combination therapies with small molecules and biologics has dramatically changed the course of the disease,” he noted. “The greatest challenge we have now as rheumatologists is access barriers for our patients.”
Dr. Weinblatt reported receiving research grants from half a dozen companies and serving as a consultant to more than two dozen.
SNOWMASS, COLO. – If you thought biosimilars would bring sharply reduced pricing compared with their parent agents, with resultant greater patient access to highly effective therapies for rheumatic diseases ... think again.
“The promise to our patients of biosimilars – greater access to treatments – is something I think we’re just not going to see, at least not here in the U.S.,” Michael E. Weinblatt, MD, declared at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
In contrast, the safety and efficacy of the biosimilars, as well as their interchangeability with their reference products, appear to be as hoped for. At the 2016 annual meeting of the American College of Rheumatology, Dr. Weinblatt presented the week 24 results of a phase III, randomized trial involving rheumatoid arthritis patients on background methotrexate plus either adalimumab (Humira) or its biosimilar SB5.
“Essentially, they’re dead on in clinical response, they’re dead on in antibody levels, and they’re dead on in toxicity. And, you can put any of the biosimilars up there and the results are the same. If they get approved, this is what you’re going to see,” the rheumatologist said.
Also at the 2016 ACR annual meeting, he noted, Danish investigators presented reassuring 1-year follow-up data on 802 Danes with inflammatory rheumatic diseases who switched from infliximab (Remicade) to its biosimilar Remsima. Disease activity and flare rates in the year following the switch were similar to those in the year before. The 1-year rate of adherence to Remsima was 84%, similar to the historical 86% 1-year rate with infliximab.
“So, I’m pretty comfortable with the biosimilars,” Dr. Weinblatt continued.
He observed that, of all the systemic rheumatic diseases, the greatest progress has occurred in the treatment of rheumatoid arthritis.
“We have made great advances in the treatment of this disease, unlike many of our other diseases. Methotrexate and combination therapies with small molecules and biologics has dramatically changed the course of the disease,” he noted. “The greatest challenge we have now as rheumatologists is access barriers for our patients.”
Dr. Weinblatt reported receiving research grants from half a dozen companies and serving as a consultant to more than two dozen.
SNOWMASS, COLO. – If you thought biosimilars would bring sharply reduced pricing compared with their parent agents, with resultant greater patient access to highly effective therapies for rheumatic diseases ... think again.
“The promise to our patients of biosimilars – greater access to treatments – is something I think we’re just not going to see, at least not here in the U.S.,” Michael E. Weinblatt, MD, declared at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
In contrast, the safety and efficacy of the biosimilars, as well as their interchangeability with their reference products, appear to be as hoped for. At the 2016 annual meeting of the American College of Rheumatology, Dr. Weinblatt presented the week 24 results of a phase III, randomized trial involving rheumatoid arthritis patients on background methotrexate plus either adalimumab (Humira) or its biosimilar SB5.
“Essentially, they’re dead on in clinical response, they’re dead on in antibody levels, and they’re dead on in toxicity. And, you can put any of the biosimilars up there and the results are the same. If they get approved, this is what you’re going to see,” the rheumatologist said.
Also at the 2016 ACR annual meeting, he noted, Danish investigators presented reassuring 1-year follow-up data on 802 Danes with inflammatory rheumatic diseases who switched from infliximab (Remicade) to its biosimilar Remsima. Disease activity and flare rates in the year following the switch were similar to those in the year before. The 1-year rate of adherence to Remsima was 84%, similar to the historical 86% 1-year rate with infliximab.
“So, I’m pretty comfortable with the biosimilars,” Dr. Weinblatt continued.
He observed that, of all the systemic rheumatic diseases, the greatest progress has occurred in the treatment of rheumatoid arthritis.
“We have made great advances in the treatment of this disease, unlike many of our other diseases. Methotrexate and combination therapies with small molecules and biologics has dramatically changed the course of the disease,” he noted. “The greatest challenge we have now as rheumatologists is access barriers for our patients.”
Dr. Weinblatt reported receiving research grants from half a dozen companies and serving as a consultant to more than two dozen.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM
How Can Neurologists Diagnose and Manage Sport-Related Concussion?
RIVIERA BEACH, FL—If a neurologist is at a sporting event during which a player sustains a head injury, audience members or officials may look to him or her for guidance, according to an overview delivered at the 44th Annual Meeting of the Southern Clinical Neurological Society. Understanding how to diagnose and manage concussion may be a vital skill for neurologists, regardless of specialty.
What Is Concussion?

Loss of consciousness previously was considered necessary for a diagnosis of concussion. Later, it was taken as a marker of serious injury. Neither of these principles is accepted any longer. Data indicate that at least 90% of concussions are not associated with loss of consciousness, and studies have not shown that loss of consciousness portends a worse prognosis or protracted recovery from the injury, said Dr. Kosa.
The pathophysiology of concussion is not certain. The current proposal is that concussion entails disruption of neuronal cell membranes resulting from disruption of normal ion channels (eg, calcium, potassium, and sodium), leading to a loss of normal neuronal homeostasis. This situation can cause a cascade of events, including mitochondrial dysfunction that causes neuronal energy failure, loss of normal glucose metabolism, activation of NMDA receptors from increased levels of glutamate, production of lactic acid, and generation of free radicals, all of which damage the neurons and supporting cells. Most cells survive the concussive injury, but can be functionally compromised. Severe injuries can lead to neuronal cell death.
What Are the Possible Sequelae of Concussion?
Concussion increases the risk of second impact syndrome, which can occur if the patient sustains another injury at between 24 hours and 10 days after a concussion. Research on second impact syndrome is limited, but the syndrome is understood to entail rapid and massive brain edema that leads to brain herniation and likely death or severe disability. The syndrome occurs within minutes of the second impact and is thought to be enabled by the period of vulnerability that follows an initial concussion. The syndrome occurs mostly in young patients, but has been described in boxers. For this reason, neurologists should be especially cautious when deciding whether to let a child with concussion return to play, said Dr. Kosa. The Centers for Disease Control and Prevention (CDC) estimate that second impact syndrome causes four to six deaths in patients under age 18 annually.
Concussion may be accompanied by traumatic brain injury (TBI). In 2010, the CDC reported 2.5 million hospital encounters related to TBI. Among these encounters, 87% of patients were treated in the emergency department and released, 11% were hospitalized and discharged, and 2% died. The highest incidence of TBI is in young children, and causes include sports accidents, bicycle accidents, skateboard accidents, vehicular accidents, and falls. The CDC estimates that between 3.2 million and 5.3 million people in the United States have permanent TBI-related disability, which results in great economic, physical, and emotional burdens.
Patients with repeated mild TBI may be at risk of chronic traumatic encephalopathy (CTE). This disorder has been described in football players, veterans, and boxers. Symptoms develop later in the patient’s life, and four stages have been described. The first stage includes headaches, inattention, and poor concentration. Stage two consists of significant mood disturbance with depression, along with explosive bouts of anger and short-term memory impairment. The third stage includes further cognitive or memory impairment that manifests as prominent executive dysfunction, where reasoning and organization or planning are most affected. In stage four, the patient has dementia; the cognitive and memory impairment has progressed to the point where the patient depends on others for activities of daily living.
McKee et al observed that CTE was associated with cerebral atrophy, mammillary body atrophy, dilation of the lateral ventricles, fenestrations of the septum pellucidum, and tau deposition. Researchers and clinicians, however, have not arrived at a consensus about the pathologic and clinical criteria for CTE. Furthermore, Cantu et al stated that it is not yet possible to determine the causality or risk factors of CTE with certainty. The hypothesis that repeated concussion or subconcussive impacts leads to the development of CTE has not been scientifically proven to date, they added.
What Should Be Done on the Field?
If a player at a sporting event sustains a head injury, he or she should be removed from play immediately and not allowed to return to the game. If he or she has not directly observed the injury, the neurologist should get information about it from witnesses. The neurologist should perform a focused physical examination, searching for evidence of decreased level of consciousness, confusion, focal weakness or incoordination, visual disturbance, cervical spine injury, or facial fractures. The Sport Concussion Assessment Tool (SCAT) can assist the clinician in concussion evaluation and treatment in a standardized and methodical way to determine whether and when a player can safely return to play.
A patient with an abnormal examination may need to be transferred to the local emergency department for further testing. CT imaging should not be performed automatically, because it may expose the patient to radiation unnecessarily. Two sets of criteria offer guidance about CT imaging. The New Orleans criteria state that a patient should undergo CT if he or she has a headache, has vomited, is older than 60, had been using alcohol or other drugs, had a seizure, has visible trauma above the clavicle, or has a short-term memory deficit. The Canadian CT Head Rule lists similar criteria, including a Glasgow Coma Scale score at two hours of less than 15, any sign of a basal skull fracture, and amnesia for events that took place 30 minutes before the injury.
Anticoagulants increase the risk of immediate or delayed hemorrhage after head injury. If a patient has intracranial hemorrhage on CT and has been using anticoagulants, the clinician should rapidly reverse the anticoagulant effect with the appropriate agent. A repeat head CT 24 hours later should be considered in those thought to be at high risk for intracranial hemorrhage and whose initial CT imaging is negative for bleed. “Err on the side of admitting these patients, at least for observation,” said Dr. Kosa. Before the patient is discharged from the emergency room, he or she should receive education about postconcussion symptoms that should prompt another visit to the emergency department. Educational materials are available on the CDC’s website.
When Can a Patient Return to Play?
The consensus statement on concussion in sport adopted at the Third International Conference on Concussion in Sport includes guidelines for graduated return to play. At first, the patient should undergo symptom-limited physical and cognitive rest until he or she recovers. Next, the patient may start light aerobic exercise such as walking, swimming, or cycling. The goal is to increase heart rate, but the patient should reduce activity if symptoms occur. Then, the patient may engage in sport-specific exercise. If recovery proceeds well, the patient may begin noncontact training drills and, later, full contact practice. Only when the patient has full confidence and coaching or training staff has assessed his or her functional skills can the athlete return to play.
What Concussion Research Is Under Way?
Investigations currently under way aim to improve understanding of concussion, as well as to aid diagnosis and treatment. Researchers are looking for a reliable biomarker of concussion that can be detected with an easy, cost-effective, and preferably noninvasive test. Saliva, tears, urine, blood, and CSF are among the candidate samples being studied. CSF is the most reliable fluid to test because of its proximity to the brain and its low susceptibility to extracerebral confounders, but it is the most invasive option. Groups are examining potential serum biomarkers such as S100b, neuron-specific enolase, myelin basic protein, glial fibrillary acidic protein, and cleaved tau.
In addition, McKee and colleagues are working to define clear pathologic criteria defining the various stages of CTE. They also are seeking a way of distinguishing CTE from Alzheimer’s disease, amyotrophic lateral sclerosis, and other neurodegenerative diseases in postmortem brain tissue. The group’s ultimate goal is to identify features that may assist in the diagnosis of CTE in living people using advanced neuroimaging.
—Erik Greb
Suggested Reading
Giza CC, Kutcher JS, Ashwal S, et al. Summary of evidence-based guideline update: evaluation and management of concussion in sports: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80(24):2250-2257.
McCrory P, Meeuwisse W, Johnston K, et al. Consensus statement on concussion in sport--the 3rd International Conference on concussion in sport, held in Zurich, November 2008. J Clin Neurosci. 2009;16(6):755-763.
Omalu BI, Hamilton RL, Kamboh MI, et al. Chronic traumatic encephalopathy (CTE) in a National Football League Player: Case report and emerging medicolegal practice questions. J Forensic Nurs. 2010;6(1):40-46.
RIVIERA BEACH, FL—If a neurologist is at a sporting event during which a player sustains a head injury, audience members or officials may look to him or her for guidance, according to an overview delivered at the 44th Annual Meeting of the Southern Clinical Neurological Society. Understanding how to diagnose and manage concussion may be a vital skill for neurologists, regardless of specialty.
What Is Concussion?
Loss of consciousness previously was considered necessary for a diagnosis of concussion. Later, it was taken as a marker of serious injury. Neither of these principles is accepted any longer. Data indicate that at least 90% of concussions are not associated with loss of consciousness, and studies have not shown that loss of consciousness portends a worse prognosis or protracted recovery from the injury, said Dr. Kosa.
The pathophysiology of concussion is not certain. The current proposal is that concussion entails disruption of neuronal cell membranes resulting from disruption of normal ion channels (eg, calcium, potassium, and sodium), leading to a loss of normal neuronal homeostasis. This situation can cause a cascade of events, including mitochondrial dysfunction that causes neuronal energy failure, loss of normal glucose metabolism, activation of NMDA receptors from increased levels of glutamate, production of lactic acid, and generation of free radicals, all of which damage the neurons and supporting cells. Most cells survive the concussive injury, but can be functionally compromised. Severe injuries can lead to neuronal cell death.
What Are the Possible Sequelae of Concussion?
Concussion increases the risk of second impact syndrome, which can occur if the patient sustains another injury at between 24 hours and 10 days after a concussion. Research on second impact syndrome is limited, but the syndrome is understood to entail rapid and massive brain edema that leads to brain herniation and likely death or severe disability. The syndrome occurs within minutes of the second impact and is thought to be enabled by the period of vulnerability that follows an initial concussion. The syndrome occurs mostly in young patients, but has been described in boxers. For this reason, neurologists should be especially cautious when deciding whether to let a child with concussion return to play, said Dr. Kosa. The Centers for Disease Control and Prevention (CDC) estimate that second impact syndrome causes four to six deaths in patients under age 18 annually.
Concussion may be accompanied by traumatic brain injury (TBI). In 2010, the CDC reported 2.5 million hospital encounters related to TBI. Among these encounters, 87% of patients were treated in the emergency department and released, 11% were hospitalized and discharged, and 2% died. The highest incidence of TBI is in young children, and causes include sports accidents, bicycle accidents, skateboard accidents, vehicular accidents, and falls. The CDC estimates that between 3.2 million and 5.3 million people in the United States have permanent TBI-related disability, which results in great economic, physical, and emotional burdens.
Patients with repeated mild TBI may be at risk of chronic traumatic encephalopathy (CTE). This disorder has been described in football players, veterans, and boxers. Symptoms develop later in the patient’s life, and four stages have been described. The first stage includes headaches, inattention, and poor concentration. Stage two consists of significant mood disturbance with depression, along with explosive bouts of anger and short-term memory impairment. The third stage includes further cognitive or memory impairment that manifests as prominent executive dysfunction, where reasoning and organization or planning are most affected. In stage four, the patient has dementia; the cognitive and memory impairment has progressed to the point where the patient depends on others for activities of daily living.
McKee et al observed that CTE was associated with cerebral atrophy, mammillary body atrophy, dilation of the lateral ventricles, fenestrations of the septum pellucidum, and tau deposition. Researchers and clinicians, however, have not arrived at a consensus about the pathologic and clinical criteria for CTE. Furthermore, Cantu et al stated that it is not yet possible to determine the causality or risk factors of CTE with certainty. The hypothesis that repeated concussion or subconcussive impacts leads to the development of CTE has not been scientifically proven to date, they added.
What Should Be Done on the Field?
If a player at a sporting event sustains a head injury, he or she should be removed from play immediately and not allowed to return to the game. If he or she has not directly observed the injury, the neurologist should get information about it from witnesses. The neurologist should perform a focused physical examination, searching for evidence of decreased level of consciousness, confusion, focal weakness or incoordination, visual disturbance, cervical spine injury, or facial fractures. The Sport Concussion Assessment Tool (SCAT) can assist the clinician in concussion evaluation and treatment in a standardized and methodical way to determine whether and when a player can safely return to play.
A patient with an abnormal examination may need to be transferred to the local emergency department for further testing. CT imaging should not be performed automatically, because it may expose the patient to radiation unnecessarily. Two sets of criteria offer guidance about CT imaging. The New Orleans criteria state that a patient should undergo CT if he or she has a headache, has vomited, is older than 60, had been using alcohol or other drugs, had a seizure, has visible trauma above the clavicle, or has a short-term memory deficit. The Canadian CT Head Rule lists similar criteria, including a Glasgow Coma Scale score at two hours of less than 15, any sign of a basal skull fracture, and amnesia for events that took place 30 minutes before the injury.
Anticoagulants increase the risk of immediate or delayed hemorrhage after head injury. If a patient has intracranial hemorrhage on CT and has been using anticoagulants, the clinician should rapidly reverse the anticoagulant effect with the appropriate agent. A repeat head CT 24 hours later should be considered in those thought to be at high risk for intracranial hemorrhage and whose initial CT imaging is negative for bleed. “Err on the side of admitting these patients, at least for observation,” said Dr. Kosa. Before the patient is discharged from the emergency room, he or she should receive education about postconcussion symptoms that should prompt another visit to the emergency department. Educational materials are available on the CDC’s website.
When Can a Patient Return to Play?
The consensus statement on concussion in sport adopted at the Third International Conference on Concussion in Sport includes guidelines for graduated return to play. At first, the patient should undergo symptom-limited physical and cognitive rest until he or she recovers. Next, the patient may start light aerobic exercise such as walking, swimming, or cycling. The goal is to increase heart rate, but the patient should reduce activity if symptoms occur. Then, the patient may engage in sport-specific exercise. If recovery proceeds well, the patient may begin noncontact training drills and, later, full contact practice. Only when the patient has full confidence and coaching or training staff has assessed his or her functional skills can the athlete return to play.
What Concussion Research Is Under Way?
Investigations currently under way aim to improve understanding of concussion, as well as to aid diagnosis and treatment. Researchers are looking for a reliable biomarker of concussion that can be detected with an easy, cost-effective, and preferably noninvasive test. Saliva, tears, urine, blood, and CSF are among the candidate samples being studied. CSF is the most reliable fluid to test because of its proximity to the brain and its low susceptibility to extracerebral confounders, but it is the most invasive option. Groups are examining potential serum biomarkers such as S100b, neuron-specific enolase, myelin basic protein, glial fibrillary acidic protein, and cleaved tau.
In addition, McKee and colleagues are working to define clear pathologic criteria defining the various stages of CTE. They also are seeking a way of distinguishing CTE from Alzheimer’s disease, amyotrophic lateral sclerosis, and other neurodegenerative diseases in postmortem brain tissue. The group’s ultimate goal is to identify features that may assist in the diagnosis of CTE in living people using advanced neuroimaging.
—Erik Greb
Suggested Reading
Giza CC, Kutcher JS, Ashwal S, et al. Summary of evidence-based guideline update: evaluation and management of concussion in sports: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80(24):2250-2257.
McCrory P, Meeuwisse W, Johnston K, et al. Consensus statement on concussion in sport--the 3rd International Conference on concussion in sport, held in Zurich, November 2008. J Clin Neurosci. 2009;16(6):755-763.
Omalu BI, Hamilton RL, Kamboh MI, et al. Chronic traumatic encephalopathy (CTE) in a National Football League Player: Case report and emerging medicolegal practice questions. J Forensic Nurs. 2010;6(1):40-46.
RIVIERA BEACH, FL—If a neurologist is at a sporting event during which a player sustains a head injury, audience members or officials may look to him or her for guidance, according to an overview delivered at the 44th Annual Meeting of the Southern Clinical Neurological Society. Understanding how to diagnose and manage concussion may be a vital skill for neurologists, regardless of specialty.
What Is Concussion?
Loss of consciousness previously was considered necessary for a diagnosis of concussion. Later, it was taken as a marker of serious injury. Neither of these principles is accepted any longer. Data indicate that at least 90% of concussions are not associated with loss of consciousness, and studies have not shown that loss of consciousness portends a worse prognosis or protracted recovery from the injury, said Dr. Kosa.
The pathophysiology of concussion is not certain. The current proposal is that concussion entails disruption of neuronal cell membranes resulting from disruption of normal ion channels (eg, calcium, potassium, and sodium), leading to a loss of normal neuronal homeostasis. This situation can cause a cascade of events, including mitochondrial dysfunction that causes neuronal energy failure, loss of normal glucose metabolism, activation of NMDA receptors from increased levels of glutamate, production of lactic acid, and generation of free radicals, all of which damage the neurons and supporting cells. Most cells survive the concussive injury, but can be functionally compromised. Severe injuries can lead to neuronal cell death.
What Are the Possible Sequelae of Concussion?
Concussion increases the risk of second impact syndrome, which can occur if the patient sustains another injury at between 24 hours and 10 days after a concussion. Research on second impact syndrome is limited, but the syndrome is understood to entail rapid and massive brain edema that leads to brain herniation and likely death or severe disability. The syndrome occurs within minutes of the second impact and is thought to be enabled by the period of vulnerability that follows an initial concussion. The syndrome occurs mostly in young patients, but has been described in boxers. For this reason, neurologists should be especially cautious when deciding whether to let a child with concussion return to play, said Dr. Kosa. The Centers for Disease Control and Prevention (CDC) estimate that second impact syndrome causes four to six deaths in patients under age 18 annually.
Concussion may be accompanied by traumatic brain injury (TBI). In 2010, the CDC reported 2.5 million hospital encounters related to TBI. Among these encounters, 87% of patients were treated in the emergency department and released, 11% were hospitalized and discharged, and 2% died. The highest incidence of TBI is in young children, and causes include sports accidents, bicycle accidents, skateboard accidents, vehicular accidents, and falls. The CDC estimates that between 3.2 million and 5.3 million people in the United States have permanent TBI-related disability, which results in great economic, physical, and emotional burdens.
Patients with repeated mild TBI may be at risk of chronic traumatic encephalopathy (CTE). This disorder has been described in football players, veterans, and boxers. Symptoms develop later in the patient’s life, and four stages have been described. The first stage includes headaches, inattention, and poor concentration. Stage two consists of significant mood disturbance with depression, along with explosive bouts of anger and short-term memory impairment. The third stage includes further cognitive or memory impairment that manifests as prominent executive dysfunction, where reasoning and organization or planning are most affected. In stage four, the patient has dementia; the cognitive and memory impairment has progressed to the point where the patient depends on others for activities of daily living.
McKee et al observed that CTE was associated with cerebral atrophy, mammillary body atrophy, dilation of the lateral ventricles, fenestrations of the septum pellucidum, and tau deposition. Researchers and clinicians, however, have not arrived at a consensus about the pathologic and clinical criteria for CTE. Furthermore, Cantu et al stated that it is not yet possible to determine the causality or risk factors of CTE with certainty. The hypothesis that repeated concussion or subconcussive impacts leads to the development of CTE has not been scientifically proven to date, they added.
What Should Be Done on the Field?
If a player at a sporting event sustains a head injury, he or she should be removed from play immediately and not allowed to return to the game. If he or she has not directly observed the injury, the neurologist should get information about it from witnesses. The neurologist should perform a focused physical examination, searching for evidence of decreased level of consciousness, confusion, focal weakness or incoordination, visual disturbance, cervical spine injury, or facial fractures. The Sport Concussion Assessment Tool (SCAT) can assist the clinician in concussion evaluation and treatment in a standardized and methodical way to determine whether and when a player can safely return to play.
A patient with an abnormal examination may need to be transferred to the local emergency department for further testing. CT imaging should not be performed automatically, because it may expose the patient to radiation unnecessarily. Two sets of criteria offer guidance about CT imaging. The New Orleans criteria state that a patient should undergo CT if he or she has a headache, has vomited, is older than 60, had been using alcohol or other drugs, had a seizure, has visible trauma above the clavicle, or has a short-term memory deficit. The Canadian CT Head Rule lists similar criteria, including a Glasgow Coma Scale score at two hours of less than 15, any sign of a basal skull fracture, and amnesia for events that took place 30 minutes before the injury.
Anticoagulants increase the risk of immediate or delayed hemorrhage after head injury. If a patient has intracranial hemorrhage on CT and has been using anticoagulants, the clinician should rapidly reverse the anticoagulant effect with the appropriate agent. A repeat head CT 24 hours later should be considered in those thought to be at high risk for intracranial hemorrhage and whose initial CT imaging is negative for bleed. “Err on the side of admitting these patients, at least for observation,” said Dr. Kosa. Before the patient is discharged from the emergency room, he or she should receive education about postconcussion symptoms that should prompt another visit to the emergency department. Educational materials are available on the CDC’s website.
When Can a Patient Return to Play?
The consensus statement on concussion in sport adopted at the Third International Conference on Concussion in Sport includes guidelines for graduated return to play. At first, the patient should undergo symptom-limited physical and cognitive rest until he or she recovers. Next, the patient may start light aerobic exercise such as walking, swimming, or cycling. The goal is to increase heart rate, but the patient should reduce activity if symptoms occur. Then, the patient may engage in sport-specific exercise. If recovery proceeds well, the patient may begin noncontact training drills and, later, full contact practice. Only when the patient has full confidence and coaching or training staff has assessed his or her functional skills can the athlete return to play.
What Concussion Research Is Under Way?
Investigations currently under way aim to improve understanding of concussion, as well as to aid diagnosis and treatment. Researchers are looking for a reliable biomarker of concussion that can be detected with an easy, cost-effective, and preferably noninvasive test. Saliva, tears, urine, blood, and CSF are among the candidate samples being studied. CSF is the most reliable fluid to test because of its proximity to the brain and its low susceptibility to extracerebral confounders, but it is the most invasive option. Groups are examining potential serum biomarkers such as S100b, neuron-specific enolase, myelin basic protein, glial fibrillary acidic protein, and cleaved tau.
In addition, McKee and colleagues are working to define clear pathologic criteria defining the various stages of CTE. They also are seeking a way of distinguishing CTE from Alzheimer’s disease, amyotrophic lateral sclerosis, and other neurodegenerative diseases in postmortem brain tissue. The group’s ultimate goal is to identify features that may assist in the diagnosis of CTE in living people using advanced neuroimaging.
—Erik Greb
Suggested Reading
Giza CC, Kutcher JS, Ashwal S, et al. Summary of evidence-based guideline update: evaluation and management of concussion in sports: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80(24):2250-2257.
McCrory P, Meeuwisse W, Johnston K, et al. Consensus statement on concussion in sport--the 3rd International Conference on concussion in sport, held in Zurich, November 2008. J Clin Neurosci. 2009;16(6):755-763.
Omalu BI, Hamilton RL, Kamboh MI, et al. Chronic traumatic encephalopathy (CTE) in a National Football League Player: Case report and emerging medicolegal practice questions. J Forensic Nurs. 2010;6(1):40-46.
Dactylitis signals more severe psoriatic arthritis
SNOWMASS, COLO. – Dactylitis is a common and painful extra-articular manifestation of psoriatic arthritis that takes on added clinical significance because it’s also a marker of greater disease severity, Christopher T. Ritchlin, MD, said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Indeed, psoriatic arthritis (PsA) patients with dactylitis are more likely to have polyarticular disease and radiologic evidence of bony damage, noted Dr. Ritchlin, professor of medicine and chief of the allergy, immunology, and rheumatology division at the University of Rochester (N.Y.).
“We have no idea why this is,” confessed Dr. Ritchlin, who is also director of the Clinical Immunology Research Center at the university.
The differential diagnosis for dactylitis includes psoriatic arthritis, other spondyloarthropathies, sickle cell disease, tuberculosis, sarcoidosis, and pyogenic flexor tenosynovitis, a closed-space infection that is the major issue in the differential. Dr. Ritchlin sees many more cases of dactylitis due to PsA that get misdiagnosed as a flexor tendon sheath infection and inappropriately subjected to surgery and/or intravenous antibiotics than vice versa.
Pyogenic flexor tenosynovitis can be identified using the four Kanavel signs: diffuse swelling of a digit, often with discoloration; intense pain over the whole length of the tendon sheath, but limited to the sheath; the involved digit being held in a semiflexed posture; and exquisite pain upon passive extension of the digit, with the pain being worst at the proximal end.
University of Toronto investigators have demonstrated that, in their large longitudinal database of PsA patients, the prevalence of radiologic damage in participants with acute dactylitis of the hands is twice as great as in PsA patients without dactylitis.
“I’ve been struck over the years by how often I see psoriatic arthritis patients with dactylitic digits who not only have erosions but who actually have a complete fusion or ankylosis of the joint. The point is, when you have a joint with diffuse inflammation, in many patients it’s associated with activation of both osteoclasts and osteoblasts,” according to the rheumatologist.
Enthesitis
Enthesitis, another cardinal extra-articular manifestation of PsA, is defined by inflammation at the sites where tendons, ligaments, and joint capsules attach into bone. The most commonly involved sites are the Achilles tendon and plantar fascia.
“It can also involve a lot of other areas and can lead to misdiagnosis as a result. Many of these patients end up in rheumatologists’ offices with previous diagnoses ranging from fibromyalgia or other chronic pain syndromes to malingering,” Dr. Ritchlin said.
Sites to examine for enthesitis, in addition to the foot and Achilles tendon, include the patellar and quadriceps tendons, iliac crest, greater trochanter, lateral epicondyle, the small joints of the hands, and the supraspinatus tendon.
“We have a registry of several hundred psoriatic arthritis patients, and I’ve been struck by the amount of enthesopathy when we examine these points,” the rheumatologist observed.
Enthesitis is a prominent feature of both early and established PsA. Power Doppler ultrasound is more sensitive than radiographs at identifying it. Italian investigators have shown ultrasound to be useful in the differential diagnosis between early rheumatoid arthritis and early PsA in patients with hand involvement. They assessed 52 clinically involved joints in 26 patients with early PsA and 68 involved joints in 34 early-RA patients. Synovitis was detected in 91% of the joints of the RA patients, compared with only 60% of the PsA patients’ joints.
In contrast, soft tissue edema was present in 42% of the most clinically involved fingers of the early PsA patients, compared with just 3% in those with early RA. Central slip enthesitis was seen in 21% of the clinically involved proximal interphalangeal joints of the PsA patients but in none of those belonging to patients with early RA. Peritendon inflammation of the extensor digitorum tendon was noted in 54% of the joints of the PsA group, compared with less than 3% of the early RA group (Clin Exp Rheumatol. 2016 May-Jun;34[3]:459-65).
“Basically, if you do ultrasound, you see there is significantly more enthesitis in early psoriatic arthritis than early rheumatoid arthritis, which has certainly been our experience as well,” Dr. Ritchlin commented.
Enthesitis is not as simple a disease process as most physicians were taught in training. Dr. Ritchlin credits Dennis McGonagle, MD, of the University of Leeds (England) with introducing the now-accepted concept of a synovio-entheseal complex as being a key player in the expression of PsA (Arthritis Rheum. 2007 Aug;56[8]:2482-91).
“The old idea is that the enthesis inserts onto bone and that’s where the pathology is. But it’s more complicated than that,” Dr. Ritchlin explained.
Dr. McGonagle and his coworkers showed that fibrocartilagenous entheses attach to bone much more deeply than previously recognized, like a tree with deep roots. That makes for lots of intimate contact between bony cells and vascular channels. And key structures are located near the intersection of enthesis and bone, including bursae and synovial membrane. For example, the Achilles tendon synovio-entheseal complex includes sesamoid fibrocartilage, periosteal fibrocartilage, the retrocalcaneal bursa, subchondral bone, and enthesis fibrocartilage, as well as the tendon itself.
Dr. McGonagle and coworkers argued that the pathogenesis of tissue inflammation and damage in PsA involves biomechanical stress, with resultant synovial inflammation accompanied by the release of inflammatory cytokines, which in turn leads to diffuse inflammation in and around the area where the enthesis inserts.
“The purpose of the enthesis is to distribute force away from the area where the tendon inserts into bone. So when biomechanical stress pulls on that tendon, other adjacent areas are also affected. What’s come out from imaging studies is that there’s synovial inflammation, bursitis, and also inflammation in and around the fibrocartilage in areas of enthesitis,” Dr. Ritchlin said.
He reported serving as a consultant to half a dozen pharmaceutical companies.
SNOWMASS, COLO. – Dactylitis is a common and painful extra-articular manifestation of psoriatic arthritis that takes on added clinical significance because it’s also a marker of greater disease severity, Christopher T. Ritchlin, MD, said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Indeed, psoriatic arthritis (PsA) patients with dactylitis are more likely to have polyarticular disease and radiologic evidence of bony damage, noted Dr. Ritchlin, professor of medicine and chief of the allergy, immunology, and rheumatology division at the University of Rochester (N.Y.).
“We have no idea why this is,” confessed Dr. Ritchlin, who is also director of the Clinical Immunology Research Center at the university.
The differential diagnosis for dactylitis includes psoriatic arthritis, other spondyloarthropathies, sickle cell disease, tuberculosis, sarcoidosis, and pyogenic flexor tenosynovitis, a closed-space infection that is the major issue in the differential. Dr. Ritchlin sees many more cases of dactylitis due to PsA that get misdiagnosed as a flexor tendon sheath infection and inappropriately subjected to surgery and/or intravenous antibiotics than vice versa.
Pyogenic flexor tenosynovitis can be identified using the four Kanavel signs: diffuse swelling of a digit, often with discoloration; intense pain over the whole length of the tendon sheath, but limited to the sheath; the involved digit being held in a semiflexed posture; and exquisite pain upon passive extension of the digit, with the pain being worst at the proximal end.
University of Toronto investigators have demonstrated that, in their large longitudinal database of PsA patients, the prevalence of radiologic damage in participants with acute dactylitis of the hands is twice as great as in PsA patients without dactylitis.
“I’ve been struck over the years by how often I see psoriatic arthritis patients with dactylitic digits who not only have erosions but who actually have a complete fusion or ankylosis of the joint. The point is, when you have a joint with diffuse inflammation, in many patients it’s associated with activation of both osteoclasts and osteoblasts,” according to the rheumatologist.
Enthesitis
Enthesitis, another cardinal extra-articular manifestation of PsA, is defined by inflammation at the sites where tendons, ligaments, and joint capsules attach into bone. The most commonly involved sites are the Achilles tendon and plantar fascia.
“It can also involve a lot of other areas and can lead to misdiagnosis as a result. Many of these patients end up in rheumatologists’ offices with previous diagnoses ranging from fibromyalgia or other chronic pain syndromes to malingering,” Dr. Ritchlin said.
Sites to examine for enthesitis, in addition to the foot and Achilles tendon, include the patellar and quadriceps tendons, iliac crest, greater trochanter, lateral epicondyle, the small joints of the hands, and the supraspinatus tendon.
“We have a registry of several hundred psoriatic arthritis patients, and I’ve been struck by the amount of enthesopathy when we examine these points,” the rheumatologist observed.
Enthesitis is a prominent feature of both early and established PsA. Power Doppler ultrasound is more sensitive than radiographs at identifying it. Italian investigators have shown ultrasound to be useful in the differential diagnosis between early rheumatoid arthritis and early PsA in patients with hand involvement. They assessed 52 clinically involved joints in 26 patients with early PsA and 68 involved joints in 34 early-RA patients. Synovitis was detected in 91% of the joints of the RA patients, compared with only 60% of the PsA patients’ joints.
In contrast, soft tissue edema was present in 42% of the most clinically involved fingers of the early PsA patients, compared with just 3% in those with early RA. Central slip enthesitis was seen in 21% of the clinically involved proximal interphalangeal joints of the PsA patients but in none of those belonging to patients with early RA. Peritendon inflammation of the extensor digitorum tendon was noted in 54% of the joints of the PsA group, compared with less than 3% of the early RA group (Clin Exp Rheumatol. 2016 May-Jun;34[3]:459-65).
“Basically, if you do ultrasound, you see there is significantly more enthesitis in early psoriatic arthritis than early rheumatoid arthritis, which has certainly been our experience as well,” Dr. Ritchlin commented.
Enthesitis is not as simple a disease process as most physicians were taught in training. Dr. Ritchlin credits Dennis McGonagle, MD, of the University of Leeds (England) with introducing the now-accepted concept of a synovio-entheseal complex as being a key player in the expression of PsA (Arthritis Rheum. 2007 Aug;56[8]:2482-91).
“The old idea is that the enthesis inserts onto bone and that’s where the pathology is. But it’s more complicated than that,” Dr. Ritchlin explained.
Dr. McGonagle and his coworkers showed that fibrocartilagenous entheses attach to bone much more deeply than previously recognized, like a tree with deep roots. That makes for lots of intimate contact between bony cells and vascular channels. And key structures are located near the intersection of enthesis and bone, including bursae and synovial membrane. For example, the Achilles tendon synovio-entheseal complex includes sesamoid fibrocartilage, periosteal fibrocartilage, the retrocalcaneal bursa, subchondral bone, and enthesis fibrocartilage, as well as the tendon itself.
Dr. McGonagle and coworkers argued that the pathogenesis of tissue inflammation and damage in PsA involves biomechanical stress, with resultant synovial inflammation accompanied by the release of inflammatory cytokines, which in turn leads to diffuse inflammation in and around the area where the enthesis inserts.
“The purpose of the enthesis is to distribute force away from the area where the tendon inserts into bone. So when biomechanical stress pulls on that tendon, other adjacent areas are also affected. What’s come out from imaging studies is that there’s synovial inflammation, bursitis, and also inflammation in and around the fibrocartilage in areas of enthesitis,” Dr. Ritchlin said.
He reported serving as a consultant to half a dozen pharmaceutical companies.
SNOWMASS, COLO. – Dactylitis is a common and painful extra-articular manifestation of psoriatic arthritis that takes on added clinical significance because it’s also a marker of greater disease severity, Christopher T. Ritchlin, MD, said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Indeed, psoriatic arthritis (PsA) patients with dactylitis are more likely to have polyarticular disease and radiologic evidence of bony damage, noted Dr. Ritchlin, professor of medicine and chief of the allergy, immunology, and rheumatology division at the University of Rochester (N.Y.).
“We have no idea why this is,” confessed Dr. Ritchlin, who is also director of the Clinical Immunology Research Center at the university.
The differential diagnosis for dactylitis includes psoriatic arthritis, other spondyloarthropathies, sickle cell disease, tuberculosis, sarcoidosis, and pyogenic flexor tenosynovitis, a closed-space infection that is the major issue in the differential. Dr. Ritchlin sees many more cases of dactylitis due to PsA that get misdiagnosed as a flexor tendon sheath infection and inappropriately subjected to surgery and/or intravenous antibiotics than vice versa.
Pyogenic flexor tenosynovitis can be identified using the four Kanavel signs: diffuse swelling of a digit, often with discoloration; intense pain over the whole length of the tendon sheath, but limited to the sheath; the involved digit being held in a semiflexed posture; and exquisite pain upon passive extension of the digit, with the pain being worst at the proximal end.
University of Toronto investigators have demonstrated that, in their large longitudinal database of PsA patients, the prevalence of radiologic damage in participants with acute dactylitis of the hands is twice as great as in PsA patients without dactylitis.
“I’ve been struck over the years by how often I see psoriatic arthritis patients with dactylitic digits who not only have erosions but who actually have a complete fusion or ankylosis of the joint. The point is, when you have a joint with diffuse inflammation, in many patients it’s associated with activation of both osteoclasts and osteoblasts,” according to the rheumatologist.
Enthesitis
Enthesitis, another cardinal extra-articular manifestation of PsA, is defined by inflammation at the sites where tendons, ligaments, and joint capsules attach into bone. The most commonly involved sites are the Achilles tendon and plantar fascia.
“It can also involve a lot of other areas and can lead to misdiagnosis as a result. Many of these patients end up in rheumatologists’ offices with previous diagnoses ranging from fibromyalgia or other chronic pain syndromes to malingering,” Dr. Ritchlin said.
Sites to examine for enthesitis, in addition to the foot and Achilles tendon, include the patellar and quadriceps tendons, iliac crest, greater trochanter, lateral epicondyle, the small joints of the hands, and the supraspinatus tendon.
“We have a registry of several hundred psoriatic arthritis patients, and I’ve been struck by the amount of enthesopathy when we examine these points,” the rheumatologist observed.
Enthesitis is a prominent feature of both early and established PsA. Power Doppler ultrasound is more sensitive than radiographs at identifying it. Italian investigators have shown ultrasound to be useful in the differential diagnosis between early rheumatoid arthritis and early PsA in patients with hand involvement. They assessed 52 clinically involved joints in 26 patients with early PsA and 68 involved joints in 34 early-RA patients. Synovitis was detected in 91% of the joints of the RA patients, compared with only 60% of the PsA patients’ joints.
In contrast, soft tissue edema was present in 42% of the most clinically involved fingers of the early PsA patients, compared with just 3% in those with early RA. Central slip enthesitis was seen in 21% of the clinically involved proximal interphalangeal joints of the PsA patients but in none of those belonging to patients with early RA. Peritendon inflammation of the extensor digitorum tendon was noted in 54% of the joints of the PsA group, compared with less than 3% of the early RA group (Clin Exp Rheumatol. 2016 May-Jun;34[3]:459-65).
“Basically, if you do ultrasound, you see there is significantly more enthesitis in early psoriatic arthritis than early rheumatoid arthritis, which has certainly been our experience as well,” Dr. Ritchlin commented.
Enthesitis is not as simple a disease process as most physicians were taught in training. Dr. Ritchlin credits Dennis McGonagle, MD, of the University of Leeds (England) with introducing the now-accepted concept of a synovio-entheseal complex as being a key player in the expression of PsA (Arthritis Rheum. 2007 Aug;56[8]:2482-91).
“The old idea is that the enthesis inserts onto bone and that’s where the pathology is. But it’s more complicated than that,” Dr. Ritchlin explained.
Dr. McGonagle and his coworkers showed that fibrocartilagenous entheses attach to bone much more deeply than previously recognized, like a tree with deep roots. That makes for lots of intimate contact between bony cells and vascular channels. And key structures are located near the intersection of enthesis and bone, including bursae and synovial membrane. For example, the Achilles tendon synovio-entheseal complex includes sesamoid fibrocartilage, periosteal fibrocartilage, the retrocalcaneal bursa, subchondral bone, and enthesis fibrocartilage, as well as the tendon itself.
Dr. McGonagle and coworkers argued that the pathogenesis of tissue inflammation and damage in PsA involves biomechanical stress, with resultant synovial inflammation accompanied by the release of inflammatory cytokines, which in turn leads to diffuse inflammation in and around the area where the enthesis inserts.
“The purpose of the enthesis is to distribute force away from the area where the tendon inserts into bone. So when biomechanical stress pulls on that tendon, other adjacent areas are also affected. What’s come out from imaging studies is that there’s synovial inflammation, bursitis, and also inflammation in and around the fibrocartilage in areas of enthesitis,” Dr. Ritchlin said.
He reported serving as a consultant to half a dozen pharmaceutical companies.
Corticosteroids reduce risks in elective extubation
Prophylactic corticosteroids before elective extubation could significantly reduce postextubation stridor and the incidence of reintubation, particularly in patients at high risk of airway obstruction, suggests a systematic review and meta-analysis.
While current guidelines for the management of tracheal extubation call for prophylactic use of corticosteroids in patients with airway compromise, Akira Kuriyama, MD, of Kurashiki Central Hospital in Japan, and coauthors noted that there is an outstanding question as to which patients are most likely to benefit.
Writing in the February 20 online edition of Chest, they reported on an analysis of 11 randomized, controlled trials of prophylactic corticosteroids given before elective extubation, involving 2,472 participants (Chest 2017 Feb 20. doi: 10.1016/j.chest.2017.02.017).
They found that the use of prophylactic corticosteroids was associated with a significant 57% reduction in the incidence of postextubation airway obstruction, laryngeal edema, or stridor, and a 58% reduction in reintubation rates, compared with placebo or no treatment.
A subgroup analysis showed that the benefit in reduction of postextubation airway events was evident only in the six trials that selected patients at high risk of airway obstruction, identified by a cuff-leak test (RR = 0.34), and was not seen in trials with an unselected patient population. Similarly, the reduced incidence of reintubation was evident in trials of high-risk individuals (RR = 0.35) but not in the general patient population.
The authors noted that while the latest systematic reviews had shown that corticosteroids reduce the incidence of postextubation stridor and reintubation, only one review examined the efficacy in high-risk populations and even then, it was a pooled subgroup analysis of only three trials.
“The numbers needed to prevent one episode of postextubation airway events and reintubation in individuals at high risk for postextubation airway obstruction were 5 (95%; CI: 4-7) and 16 (95%; CI: 8-166) respectively,” they wrote, noting that routine administration of corticosteroids before elective extubation is not recommended.
“While the use of prophylactic corticosteroids was associated with few adverse events, it is reasonable to use the cuff-leak test as a screening method, and administer prophylactic steroids only to those who are at risk of developing postextubation obstruction, given our study findings.”
Two of the six trials that identified high-risk individuals used a cuff-leak volume less than 24% of tidal volume during inflation, three used a cuff-leak volume of less than 110 mL, and one used a cuff-leak volume less than 25% of tidal volume.
“This potentially indicates that cuff-leak testing, while applied with varying cut-off values, might be able to select those at similar risk for airway obstruction and underlines the importance of screening for high-risk patients,” the authors said.
Researchers also noted that the longer patients were intubated, the lower the effect size of prophylactic corticosteroids on both postexutubation airway events and reintubation.
“Patients thus tended to benefit from prophylactic corticosteroids to prevent postextubation airway events and subsequent reintubation when the duration of mechanical ventilation was short,” they wrote.
The authors noted that the included trials did differ in terms of populations, corticosteroid protocols, and observation periods. However, they pointed out that the statistical heterogeneity in their primary outcome analysis was due to the risk of postextubation airway obstruction.
No conflicts of interest were declared.
Prophylactic corticosteroids before elective extubation could significantly reduce postextubation stridor and the incidence of reintubation, particularly in patients at high risk of airway obstruction, suggests a systematic review and meta-analysis.
While current guidelines for the management of tracheal extubation call for prophylactic use of corticosteroids in patients with airway compromise, Akira Kuriyama, MD, of Kurashiki Central Hospital in Japan, and coauthors noted that there is an outstanding question as to which patients are most likely to benefit.
Writing in the February 20 online edition of Chest, they reported on an analysis of 11 randomized, controlled trials of prophylactic corticosteroids given before elective extubation, involving 2,472 participants (Chest 2017 Feb 20. doi: 10.1016/j.chest.2017.02.017).
They found that the use of prophylactic corticosteroids was associated with a significant 57% reduction in the incidence of postextubation airway obstruction, laryngeal edema, or stridor, and a 58% reduction in reintubation rates, compared with placebo or no treatment.
A subgroup analysis showed that the benefit in reduction of postextubation airway events was evident only in the six trials that selected patients at high risk of airway obstruction, identified by a cuff-leak test (RR = 0.34), and was not seen in trials with an unselected patient population. Similarly, the reduced incidence of reintubation was evident in trials of high-risk individuals (RR = 0.35) but not in the general patient population.
The authors noted that while the latest systematic reviews had shown that corticosteroids reduce the incidence of postextubation stridor and reintubation, only one review examined the efficacy in high-risk populations and even then, it was a pooled subgroup analysis of only three trials.
“The numbers needed to prevent one episode of postextubation airway events and reintubation in individuals at high risk for postextubation airway obstruction were 5 (95%; CI: 4-7) and 16 (95%; CI: 8-166) respectively,” they wrote, noting that routine administration of corticosteroids before elective extubation is not recommended.
“While the use of prophylactic corticosteroids was associated with few adverse events, it is reasonable to use the cuff-leak test as a screening method, and administer prophylactic steroids only to those who are at risk of developing postextubation obstruction, given our study findings.”
Two of the six trials that identified high-risk individuals used a cuff-leak volume less than 24% of tidal volume during inflation, three used a cuff-leak volume of less than 110 mL, and one used a cuff-leak volume less than 25% of tidal volume.
“This potentially indicates that cuff-leak testing, while applied with varying cut-off values, might be able to select those at similar risk for airway obstruction and underlines the importance of screening for high-risk patients,” the authors said.
Researchers also noted that the longer patients were intubated, the lower the effect size of prophylactic corticosteroids on both postexutubation airway events and reintubation.
“Patients thus tended to benefit from prophylactic corticosteroids to prevent postextubation airway events and subsequent reintubation when the duration of mechanical ventilation was short,” they wrote.
The authors noted that the included trials did differ in terms of populations, corticosteroid protocols, and observation periods. However, they pointed out that the statistical heterogeneity in their primary outcome analysis was due to the risk of postextubation airway obstruction.
No conflicts of interest were declared.
Prophylactic corticosteroids before elective extubation could significantly reduce postextubation stridor and the incidence of reintubation, particularly in patients at high risk of airway obstruction, suggests a systematic review and meta-analysis.
While current guidelines for the management of tracheal extubation call for prophylactic use of corticosteroids in patients with airway compromise, Akira Kuriyama, MD, of Kurashiki Central Hospital in Japan, and coauthors noted that there is an outstanding question as to which patients are most likely to benefit.
Writing in the February 20 online edition of Chest, they reported on an analysis of 11 randomized, controlled trials of prophylactic corticosteroids given before elective extubation, involving 2,472 participants (Chest 2017 Feb 20. doi: 10.1016/j.chest.2017.02.017).
They found that the use of prophylactic corticosteroids was associated with a significant 57% reduction in the incidence of postextubation airway obstruction, laryngeal edema, or stridor, and a 58% reduction in reintubation rates, compared with placebo or no treatment.
A subgroup analysis showed that the benefit in reduction of postextubation airway events was evident only in the six trials that selected patients at high risk of airway obstruction, identified by a cuff-leak test (RR = 0.34), and was not seen in trials with an unselected patient population. Similarly, the reduced incidence of reintubation was evident in trials of high-risk individuals (RR = 0.35) but not in the general patient population.
The authors noted that while the latest systematic reviews had shown that corticosteroids reduce the incidence of postextubation stridor and reintubation, only one review examined the efficacy in high-risk populations and even then, it was a pooled subgroup analysis of only three trials.
“The numbers needed to prevent one episode of postextubation airway events and reintubation in individuals at high risk for postextubation airway obstruction were 5 (95%; CI: 4-7) and 16 (95%; CI: 8-166) respectively,” they wrote, noting that routine administration of corticosteroids before elective extubation is not recommended.
“While the use of prophylactic corticosteroids was associated with few adverse events, it is reasonable to use the cuff-leak test as a screening method, and administer prophylactic steroids only to those who are at risk of developing postextubation obstruction, given our study findings.”
Two of the six trials that identified high-risk individuals used a cuff-leak volume less than 24% of tidal volume during inflation, three used a cuff-leak volume of less than 110 mL, and one used a cuff-leak volume less than 25% of tidal volume.
“This potentially indicates that cuff-leak testing, while applied with varying cut-off values, might be able to select those at similar risk for airway obstruction and underlines the importance of screening for high-risk patients,” the authors said.
Researchers also noted that the longer patients were intubated, the lower the effect size of prophylactic corticosteroids on both postexutubation airway events and reintubation.
“Patients thus tended to benefit from prophylactic corticosteroids to prevent postextubation airway events and subsequent reintubation when the duration of mechanical ventilation was short,” they wrote.
The authors noted that the included trials did differ in terms of populations, corticosteroid protocols, and observation periods. However, they pointed out that the statistical heterogeneity in their primary outcome analysis was due to the risk of postextubation airway obstruction.
No conflicts of interest were declared.
FROM CHEST
Key clinical point: Prophylactic corticosteroids before elective extubation could significantly reduce postextubation stridor and the incidence of reintubation in high-risk patients.
Major finding: Prophylactic corticosteroids were associated with a 57% reduction in the incidence of postextubation airway events, and a 58% reduction in reintubation rates.
Data source: Systematic review and meta-analysis of 11 randomized controlled trials.
Disclosures: No conflicts of interest were declared.
Ask patients about sexual function at first visit
LAS VEGAS – A brief sexual history should be part of the first patient visit, according to Anita H. Clayton, MD. However, addressing sexual health can prove challenging, especially if the patient is experiencing difficulty in that aspect of life.
“In America, we don’t talk about sex in a serious kind of way,” Dr. Clayton said at an annual psychopharmacology update held by the Nevada Psychiatric Association. “If people are talking about sex they’re either bragging or lying.”

Sexual functioning assessment tools to consider using include the Changes in Sexual Functioning Questionnaire, the Sexual Interest and Desire Inventory for females, and the Decreased Sexual Desire Screener. In premenopausal women, hypoactive sexual desire disorder is a common primary sexual dysfunction. Hypoactive sexual desire disorder is equally common in postmenopausal women, Dr. Clayton said, with the addition of complaints related to vaginal atrophy or genitourinary symptoms of menopause. In men, erectile dysfunction ranks as the most common primary sexual dysfunction. It can occur at any time but tends to increase in frequency at midlife.
Dr. Clayton recommends opening the dialogue with a brief questionnaire or an open-ended question, while maintaining cultural sensitivity, including references to sexual orientation and age. “It can be helpful to define terms,” she added. “I find that people often say, ‘I don’t get aroused anymore,’ but it could possibly mean that they’re not interested in sex anymore. You have to delineate what they’re talking about. Find out if they’re doing the kind of things that previously led them to having a satisfying sexual life. If they’re dissatisfied now, what is the issue? Desire? Arousal?” Taking a ubiquity-style approach to questions also can prove helpful: “Many people with depression experience sexual dysfunction. Do you have any complaints?” Or, “As people get older, sometimes they experience problems in their sexual function or changes in their level of desire. Have you had any such changes?”
The discussion itself might be therapeutic for the patient. “You may find out that what they’re experiencing. It’s not an unusual phenomenon,” said Dr. Clayton, who is a member of the board of directors of the International Society for the Study of Women’s Sexual Health. “For example, if women at midlife are having difficulty with arousal, they might try lubricants. Or, in talking with a younger woman who may not have yet experienced an orgasm, you can tell her it’s not that uncommon and talk about how that can be helped.”
If a sexual problem persists, ask about the nature and duration of the problem and/or changes. Ask about possible stressors and try to rule out any relationship issues or situational problems. “Is the problem generalized or does it occur in all situations? If it’s situational, you probably should work on that first,” said Dr. Clayton, who also has a secondary appointment at the university as professor of clinical obstetrics and gynecology.
Diagnosis of a primary sexual dysfunction is based on clinical presentation, not on testosterone levels or other laboratory values.
Dr. Clayton disclosed having received research grants from several entities, including Forest Research Institute, Janssen, and Takeda Pharmaceuticals. She also has received advisory board fees and/or consulting fees from several companies, including Fabre-Kramer, Takeda, S1 Biopharma, and Sprout Pharmaceuticals, a division of Valeant Pharmaceuticals. Dr. Clayton also has ownership interest in Euthymics Bioscience and S1 Biopharma.
LAS VEGAS – A brief sexual history should be part of the first patient visit, according to Anita H. Clayton, MD. However, addressing sexual health can prove challenging, especially if the patient is experiencing difficulty in that aspect of life.
“In America, we don’t talk about sex in a serious kind of way,” Dr. Clayton said at an annual psychopharmacology update held by the Nevada Psychiatric Association. “If people are talking about sex they’re either bragging or lying.”
Sexual functioning assessment tools to consider using include the Changes in Sexual Functioning Questionnaire, the Sexual Interest and Desire Inventory for females, and the Decreased Sexual Desire Screener. In premenopausal women, hypoactive sexual desire disorder is a common primary sexual dysfunction. Hypoactive sexual desire disorder is equally common in postmenopausal women, Dr. Clayton said, with the addition of complaints related to vaginal atrophy or genitourinary symptoms of menopause. In men, erectile dysfunction ranks as the most common primary sexual dysfunction. It can occur at any time but tends to increase in frequency at midlife.
Dr. Clayton recommends opening the dialogue with a brief questionnaire or an open-ended question, while maintaining cultural sensitivity, including references to sexual orientation and age. “It can be helpful to define terms,” she added. “I find that people often say, ‘I don’t get aroused anymore,’ but it could possibly mean that they’re not interested in sex anymore. You have to delineate what they’re talking about. Find out if they’re doing the kind of things that previously led them to having a satisfying sexual life. If they’re dissatisfied now, what is the issue? Desire? Arousal?” Taking a ubiquity-style approach to questions also can prove helpful: “Many people with depression experience sexual dysfunction. Do you have any complaints?” Or, “As people get older, sometimes they experience problems in their sexual function or changes in their level of desire. Have you had any such changes?”
The discussion itself might be therapeutic for the patient. “You may find out that what they’re experiencing. It’s not an unusual phenomenon,” said Dr. Clayton, who is a member of the board of directors of the International Society for the Study of Women’s Sexual Health. “For example, if women at midlife are having difficulty with arousal, they might try lubricants. Or, in talking with a younger woman who may not have yet experienced an orgasm, you can tell her it’s not that uncommon and talk about how that can be helped.”
If a sexual problem persists, ask about the nature and duration of the problem and/or changes. Ask about possible stressors and try to rule out any relationship issues or situational problems. “Is the problem generalized or does it occur in all situations? If it’s situational, you probably should work on that first,” said Dr. Clayton, who also has a secondary appointment at the university as professor of clinical obstetrics and gynecology.
Diagnosis of a primary sexual dysfunction is based on clinical presentation, not on testosterone levels or other laboratory values.
Dr. Clayton disclosed having received research grants from several entities, including Forest Research Institute, Janssen, and Takeda Pharmaceuticals. She also has received advisory board fees and/or consulting fees from several companies, including Fabre-Kramer, Takeda, S1 Biopharma, and Sprout Pharmaceuticals, a division of Valeant Pharmaceuticals. Dr. Clayton also has ownership interest in Euthymics Bioscience and S1 Biopharma.
LAS VEGAS – A brief sexual history should be part of the first patient visit, according to Anita H. Clayton, MD. However, addressing sexual health can prove challenging, especially if the patient is experiencing difficulty in that aspect of life.
“In America, we don’t talk about sex in a serious kind of way,” Dr. Clayton said at an annual psychopharmacology update held by the Nevada Psychiatric Association. “If people are talking about sex they’re either bragging or lying.”
Sexual functioning assessment tools to consider using include the Changes in Sexual Functioning Questionnaire, the Sexual Interest and Desire Inventory for females, and the Decreased Sexual Desire Screener. In premenopausal women, hypoactive sexual desire disorder is a common primary sexual dysfunction. Hypoactive sexual desire disorder is equally common in postmenopausal women, Dr. Clayton said, with the addition of complaints related to vaginal atrophy or genitourinary symptoms of menopause. In men, erectile dysfunction ranks as the most common primary sexual dysfunction. It can occur at any time but tends to increase in frequency at midlife.
Dr. Clayton recommends opening the dialogue with a brief questionnaire or an open-ended question, while maintaining cultural sensitivity, including references to sexual orientation and age. “It can be helpful to define terms,” she added. “I find that people often say, ‘I don’t get aroused anymore,’ but it could possibly mean that they’re not interested in sex anymore. You have to delineate what they’re talking about. Find out if they’re doing the kind of things that previously led them to having a satisfying sexual life. If they’re dissatisfied now, what is the issue? Desire? Arousal?” Taking a ubiquity-style approach to questions also can prove helpful: “Many people with depression experience sexual dysfunction. Do you have any complaints?” Or, “As people get older, sometimes they experience problems in their sexual function or changes in their level of desire. Have you had any such changes?”
The discussion itself might be therapeutic for the patient. “You may find out that what they’re experiencing. It’s not an unusual phenomenon,” said Dr. Clayton, who is a member of the board of directors of the International Society for the Study of Women’s Sexual Health. “For example, if women at midlife are having difficulty with arousal, they might try lubricants. Or, in talking with a younger woman who may not have yet experienced an orgasm, you can tell her it’s not that uncommon and talk about how that can be helped.”
If a sexual problem persists, ask about the nature and duration of the problem and/or changes. Ask about possible stressors and try to rule out any relationship issues or situational problems. “Is the problem generalized or does it occur in all situations? If it’s situational, you probably should work on that first,” said Dr. Clayton, who also has a secondary appointment at the university as professor of clinical obstetrics and gynecology.
Diagnosis of a primary sexual dysfunction is based on clinical presentation, not on testosterone levels or other laboratory values.
Dr. Clayton disclosed having received research grants from several entities, including Forest Research Institute, Janssen, and Takeda Pharmaceuticals. She also has received advisory board fees and/or consulting fees from several companies, including Fabre-Kramer, Takeda, S1 Biopharma, and Sprout Pharmaceuticals, a division of Valeant Pharmaceuticals. Dr. Clayton also has ownership interest in Euthymics Bioscience and S1 Biopharma.
EXPERT ANALYSIS AT THE NPA PSYCHOPHARMACOLOGY UPDATE