User login
Lightweight mesh reduces erosion risk after sacrocolpopexy
SAN ANTONIO – Compared with heavier mesh types, ultralightweight polypropylene (Restorelle Y) did not increase the risk of mesh erosion after sacrocolpopexy in a retrospective, case-control study.
Delayed–absorbable monofilament polydioxanone suture (PDS) also decreased the risk, compared with nonabsorbable braided suture (Ethibond Excel) for vaginal mesh attachment.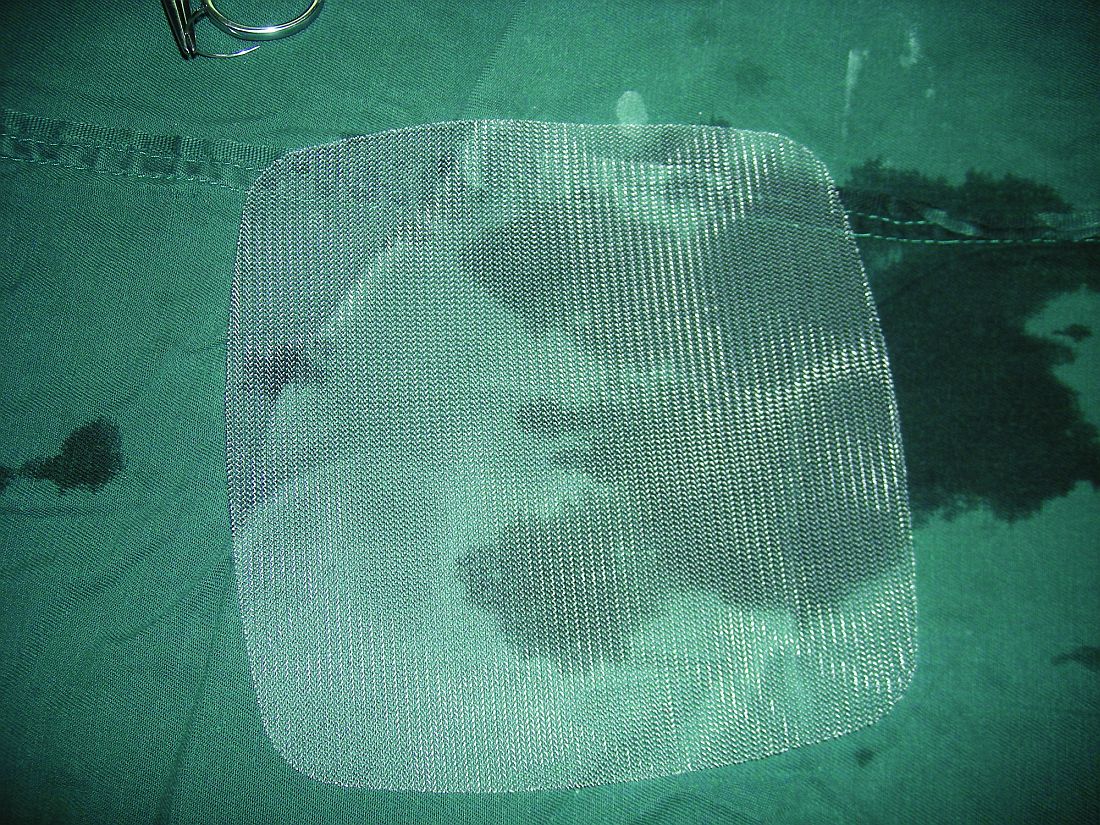
The odds ratio for the ultralightweight polypropylene mesh exposure, versus heavier mesh, was not statistically significant (odds ratio, 2.18; 95% confidence interval, 0.33-14.57), which led to the main study conclusion.
“Mesh choice and suture selection [are] important independent predictors of” erosion, she said at the annual scientific meeting of the Society of Gynecologic Surgeons. “Based on this study, surgeons should consider use of [PDS over nonabsorbable braided suture] to reduce the risk of mesh exposure when using ultralightweight mesh.”
The team also found that prior surgery for incontinence, as well as immediate postoperative complications, which likely impede healing, increase erosion risk. The findings are useful in counseling patients and perhaps guiding follow-up, at least early on. Most of the 133 erosions in the study – out of 1,247 sacrocolpopexies performed at the university from 2003 to2013 – occurred in the first year, usually in the first 3 months.
The 133 women with erosions were randomly matched with 261 women who did not have erosions after sacrocolpopexy. The erosion rate hovered around 9.5% for most years. They shot up to 19% in 2006, the first year of robot-assisted sacrocolpopexies and fell to about 6% in 2011, 4% in 2012, and 2% in 2013, when surgeons started using the ultralightweight mesh.
“Our study also confirmed several known risk factors,” Dr. Durst said, including smoking, stage IV prolapse, nonabsorbable braided suture, and heavyweight polypropylene mesh.
On multivariate regression, prior surgery for incontinence (OR, 2.87; 95% CI, 1.19-6.96), porcine acellular collagen matrix with soft polypropylene mesh (Pelvicol with soft Prolene, OR, 4.95; 95% CI, 1.70-14.42), other polypropylene mesh (OR, 6.73; 95% CI, 1.12-40.63); braided suture for vaginal mesh attachment (OR, 4.52; 95% CI, 1.53-13.37), and immediate perioperative complications (OR, 1.04; 95% CI, 1.58-8.43) all remained independent risk factors for mesh exposure, as did duration of follow-up (OR, 1.04; 95% CI, 1.03-1.06).
There was no industry funding for the study, and the investigators reported having no financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
SAN ANTONIO – Compared with heavier mesh types, ultralightweight polypropylene (Restorelle Y) did not increase the risk of mesh erosion after sacrocolpopexy in a retrospective, case-control study.
Delayed–absorbable monofilament polydioxanone suture (PDS) also decreased the risk, compared with nonabsorbable braided suture (Ethibond Excel) for vaginal mesh attachment.
The odds ratio for the ultralightweight polypropylene mesh exposure, versus heavier mesh, was not statistically significant (odds ratio, 2.18; 95% confidence interval, 0.33-14.57), which led to the main study conclusion.
“Mesh choice and suture selection [are] important independent predictors of” erosion, she said at the annual scientific meeting of the Society of Gynecologic Surgeons. “Based on this study, surgeons should consider use of [PDS over nonabsorbable braided suture] to reduce the risk of mesh exposure when using ultralightweight mesh.”
The team also found that prior surgery for incontinence, as well as immediate postoperative complications, which likely impede healing, increase erosion risk. The findings are useful in counseling patients and perhaps guiding follow-up, at least early on. Most of the 133 erosions in the study – out of 1,247 sacrocolpopexies performed at the university from 2003 to2013 – occurred in the first year, usually in the first 3 months.
The 133 women with erosions were randomly matched with 261 women who did not have erosions after sacrocolpopexy. The erosion rate hovered around 9.5% for most years. They shot up to 19% in 2006, the first year of robot-assisted sacrocolpopexies and fell to about 6% in 2011, 4% in 2012, and 2% in 2013, when surgeons started using the ultralightweight mesh.
“Our study also confirmed several known risk factors,” Dr. Durst said, including smoking, stage IV prolapse, nonabsorbable braided suture, and heavyweight polypropylene mesh.
On multivariate regression, prior surgery for incontinence (OR, 2.87; 95% CI, 1.19-6.96), porcine acellular collagen matrix with soft polypropylene mesh (Pelvicol with soft Prolene, OR, 4.95; 95% CI, 1.70-14.42), other polypropylene mesh (OR, 6.73; 95% CI, 1.12-40.63); braided suture for vaginal mesh attachment (OR, 4.52; 95% CI, 1.53-13.37), and immediate perioperative complications (OR, 1.04; 95% CI, 1.58-8.43) all remained independent risk factors for mesh exposure, as did duration of follow-up (OR, 1.04; 95% CI, 1.03-1.06).
There was no industry funding for the study, and the investigators reported having no financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
SAN ANTONIO – Compared with heavier mesh types, ultralightweight polypropylene (Restorelle Y) did not increase the risk of mesh erosion after sacrocolpopexy in a retrospective, case-control study.
Delayed–absorbable monofilament polydioxanone suture (PDS) also decreased the risk, compared with nonabsorbable braided suture (Ethibond Excel) for vaginal mesh attachment.
The odds ratio for the ultralightweight polypropylene mesh exposure, versus heavier mesh, was not statistically significant (odds ratio, 2.18; 95% confidence interval, 0.33-14.57), which led to the main study conclusion.
“Mesh choice and suture selection [are] important independent predictors of” erosion, she said at the annual scientific meeting of the Society of Gynecologic Surgeons. “Based on this study, surgeons should consider use of [PDS over nonabsorbable braided suture] to reduce the risk of mesh exposure when using ultralightweight mesh.”
The team also found that prior surgery for incontinence, as well as immediate postoperative complications, which likely impede healing, increase erosion risk. The findings are useful in counseling patients and perhaps guiding follow-up, at least early on. Most of the 133 erosions in the study – out of 1,247 sacrocolpopexies performed at the university from 2003 to2013 – occurred in the first year, usually in the first 3 months.
The 133 women with erosions were randomly matched with 261 women who did not have erosions after sacrocolpopexy. The erosion rate hovered around 9.5% for most years. They shot up to 19% in 2006, the first year of robot-assisted sacrocolpopexies and fell to about 6% in 2011, 4% in 2012, and 2% in 2013, when surgeons started using the ultralightweight mesh.
“Our study also confirmed several known risk factors,” Dr. Durst said, including smoking, stage IV prolapse, nonabsorbable braided suture, and heavyweight polypropylene mesh.
On multivariate regression, prior surgery for incontinence (OR, 2.87; 95% CI, 1.19-6.96), porcine acellular collagen matrix with soft polypropylene mesh (Pelvicol with soft Prolene, OR, 4.95; 95% CI, 1.70-14.42), other polypropylene mesh (OR, 6.73; 95% CI, 1.12-40.63); braided suture for vaginal mesh attachment (OR, 4.52; 95% CI, 1.53-13.37), and immediate perioperative complications (OR, 1.04; 95% CI, 1.58-8.43) all remained independent risk factors for mesh exposure, as did duration of follow-up (OR, 1.04; 95% CI, 1.03-1.06).
There was no industry funding for the study, and the investigators reported having no financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
AT SGS 2017
Key clinical point:
Major finding: The odds ratio for ultralightweight polypropylene (Restorelle Y) exposure, versus heavier polypropylene mesh, was not statistically significant (OR, 2.18; 95% CI, 0.33-14.57).
Data source: A single-center study matching 133 erosion cases to 261 controls.
Disclosures: There was no industry funding of the study, and the investigators reported no financial disclosures.
Decision tool helps patients compare SAVR, TAVR
WASHINGTON – A decision-assistance tool will soon be available that is designed to help intermediate-risk patients with severe aortic stenosis and their physicians better compare each patient’s expected outcome from surgical or transcatheter valve replacement based on each patient’s individual clinical and demographic features.
The decision tool will be available as both a web-based calculator and a downloadable app. It is derived from the outcomes of 4,732 patients who underwent surgical aortic valve replacement (SAVR) during 2011-2013 and who were included in the registry maintained by the Society of Thoracic Surgeons (STS), as well as an equal number of closely matched patients who underwent transcatheter aortic valve replacement (TAVR) during 2014-2015 and entered in the Transcatheter Valve (TVT) registry run by STS and the American College of Cardiology. Tool development also used longer-term outcomes data collected through Medicare.

After receiving patient-specific data, the decision tool estimates the patient’s short-term and 1-year predicted risks for death and stroke and likelihood of being discharged home, as well as the predicted number of days the patient would remain alive and out of the hospital during the first postprocedural year, J. Matthew Brennan, MD, said at the annual meeting of the American College of Cardiology.
Cardiologists and cardiac surgeons “are desperately looking for something like this” because, currently, the only option is to estimate a patient’s risk after SAVR or TAVR using tools developed only from patients who underwent one of these procedures. The new tool gives clinicians and patients a way to compare the two options for an individual patient in a way that “minimizes the biases,” said Dr. Brennan, an interventional cardiologist at Duke University in Durham, N.C., and principal investigator for development of the website and the tool.

Dr. Brennan and his associates developed the decision assistance tool with funding from the Patient-Center Outcomes Research Institute, and it will be available online at no cost at valveadvice.org. The website was already up and running when Dr. Brennan announced the tool during the meeting, and it currently has patient-centered information about aortic valve disease and the options available for treating it. He expects the decision tool to be posted on the site by April or May.
The data he and his associates used to create the decision tool came from a total of more than 197,000 SAVR patients entered into the STS SAVR database during 2011-2013 and more than 25,000 TAVR patients enrolled in the TVT registry during 2014-2015. They used propensity score matching to identify 4,732 matched patients from each group. The patients averaged 81-82 years old, nearly half were women, and their average STS risk score was 5.5-5.8, which meant that patients fell in an intermediate-risk range by this criterion. Just over three-quarters of the TAVR patients had their procedure done via a transfemoral route.
The analysis showed that, overall, 1-year mortality and stroke rates following each type of procedure were not significantly different, and several subgroup analyses failed to identify any type of patient who fell outside this overall pattern. The TAVR patients had a stroke rate that continued to rise during 12-month follow-up, compared with a much flatter pattern among the SAVR patients. While this did not result in an excess stroke rate, the pattern over time suggested that TAVR patients may not have received optimal anticoagulant treatment during the year following their procedure, Dr. Brennan said. The number of months that patients were alive and not hospitalized was also very similar in the SAVR and TAVR groups.
While the 1-year outcomes were very similar, the periprocedural outcomes showed several statistically significant differences. In-hospital mortality was significantly higher in the SAVR patients at 5%, compared with 3% in the TAVR patients. The SAVR patients also were significantly more likely to develop a need for dialysis and a need for red cells and to have a doubled duration in their ICU stay and in their postprocedural length of hospitalization, compared with TAVR patients. On the other hand, TAVR patients were significantly more likely to need a new pacemaker while hospitalized and had a 10 times higher rate of major vascular complications. The stroke rates were very similar in both arms, Dr. Brennan reported.
According to Dr. Brennan, the most striking difference in hospital outcomes was the discharge destination for patients: 70% of TAVR patients went home after their procedural hospitalization, compared with 41% of the SAVR patients. Discharges home following periprocedural hospitalization were “substantially higher” with TAVR, he said.
Another notable feature of these data was how they contrasted with the 1-year outcomes reported from the German Aortic Valve Registry at the American Heart Association Scientific Sessions in November 2016. In the German registry, 1-year mortality after propensity-score adjustment was about 11% among SAVR patients and about 14% among TAVR patients treated with a transfemoral approach, a statistically significant difference, reported Nicolas Werner, MD, of the Ludwigshafen (Germany) Clinic.
“I think the reason we see a difference in the German data is they weren’t able to remove from their analysis the really high-risk patients” who preferentially underwent TAVR, suggested Dr. Brennan. “We had the ability to match patients who had equipoise for undergoing SAVR or TAVR. That’s why our results are more consistent with the findings from the TAVR clinical trials.”
“One of the most important findings from [Dr. Brennan’s] study is [that] it makes the German Registry results look like the outliers rather than the results from the TAVR clinical trials,” commented Howard C. Hermann, MD, professor of cardiovascular disease and director of the cardiac catheterization laboratories at the University of Pennsylvania in Philadelphia.
The data analysis and development of the valveadvice.org website and decision tool received no commercial support. Dr. Brennan had no disclosures. Dr. Hermann has received honoraria and research support from Edwards Pharmaceuticals, research support from Medtronic, and honoraria and research support from several other companies.
[email protected]
On Twitter @mitchelzoler
WASHINGTON – A decision-assistance tool will soon be available that is designed to help intermediate-risk patients with severe aortic stenosis and their physicians better compare each patient’s expected outcome from surgical or transcatheter valve replacement based on each patient’s individual clinical and demographic features.
The decision tool will be available as both a web-based calculator and a downloadable app. It is derived from the outcomes of 4,732 patients who underwent surgical aortic valve replacement (SAVR) during 2011-2013 and who were included in the registry maintained by the Society of Thoracic Surgeons (STS), as well as an equal number of closely matched patients who underwent transcatheter aortic valve replacement (TAVR) during 2014-2015 and entered in the Transcatheter Valve (TVT) registry run by STS and the American College of Cardiology. Tool development also used longer-term outcomes data collected through Medicare.
After receiving patient-specific data, the decision tool estimates the patient’s short-term and 1-year predicted risks for death and stroke and likelihood of being discharged home, as well as the predicted number of days the patient would remain alive and out of the hospital during the first postprocedural year, J. Matthew Brennan, MD, said at the annual meeting of the American College of Cardiology.
Cardiologists and cardiac surgeons “are desperately looking for something like this” because, currently, the only option is to estimate a patient’s risk after SAVR or TAVR using tools developed only from patients who underwent one of these procedures. The new tool gives clinicians and patients a way to compare the two options for an individual patient in a way that “minimizes the biases,” said Dr. Brennan, an interventional cardiologist at Duke University in Durham, N.C., and principal investigator for development of the website and the tool.
Dr. Brennan and his associates developed the decision assistance tool with funding from the Patient-Center Outcomes Research Institute, and it will be available online at no cost at valveadvice.org. The website was already up and running when Dr. Brennan announced the tool during the meeting, and it currently has patient-centered information about aortic valve disease and the options available for treating it. He expects the decision tool to be posted on the site by April or May.
The data he and his associates used to create the decision tool came from a total of more than 197,000 SAVR patients entered into the STS SAVR database during 2011-2013 and more than 25,000 TAVR patients enrolled in the TVT registry during 2014-2015. They used propensity score matching to identify 4,732 matched patients from each group. The patients averaged 81-82 years old, nearly half were women, and their average STS risk score was 5.5-5.8, which meant that patients fell in an intermediate-risk range by this criterion. Just over three-quarters of the TAVR patients had their procedure done via a transfemoral route.
The analysis showed that, overall, 1-year mortality and stroke rates following each type of procedure were not significantly different, and several subgroup analyses failed to identify any type of patient who fell outside this overall pattern. The TAVR patients had a stroke rate that continued to rise during 12-month follow-up, compared with a much flatter pattern among the SAVR patients. While this did not result in an excess stroke rate, the pattern over time suggested that TAVR patients may not have received optimal anticoagulant treatment during the year following their procedure, Dr. Brennan said. The number of months that patients were alive and not hospitalized was also very similar in the SAVR and TAVR groups.
While the 1-year outcomes were very similar, the periprocedural outcomes showed several statistically significant differences. In-hospital mortality was significantly higher in the SAVR patients at 5%, compared with 3% in the TAVR patients. The SAVR patients also were significantly more likely to develop a need for dialysis and a need for red cells and to have a doubled duration in their ICU stay and in their postprocedural length of hospitalization, compared with TAVR patients. On the other hand, TAVR patients were significantly more likely to need a new pacemaker while hospitalized and had a 10 times higher rate of major vascular complications. The stroke rates were very similar in both arms, Dr. Brennan reported.
According to Dr. Brennan, the most striking difference in hospital outcomes was the discharge destination for patients: 70% of TAVR patients went home after their procedural hospitalization, compared with 41% of the SAVR patients. Discharges home following periprocedural hospitalization were “substantially higher” with TAVR, he said.
Another notable feature of these data was how they contrasted with the 1-year outcomes reported from the German Aortic Valve Registry at the American Heart Association Scientific Sessions in November 2016. In the German registry, 1-year mortality after propensity-score adjustment was about 11% among SAVR patients and about 14% among TAVR patients treated with a transfemoral approach, a statistically significant difference, reported Nicolas Werner, MD, of the Ludwigshafen (Germany) Clinic.
“I think the reason we see a difference in the German data is they weren’t able to remove from their analysis the really high-risk patients” who preferentially underwent TAVR, suggested Dr. Brennan. “We had the ability to match patients who had equipoise for undergoing SAVR or TAVR. That’s why our results are more consistent with the findings from the TAVR clinical trials.”
“One of the most important findings from [Dr. Brennan’s] study is [that] it makes the German Registry results look like the outliers rather than the results from the TAVR clinical trials,” commented Howard C. Hermann, MD, professor of cardiovascular disease and director of the cardiac catheterization laboratories at the University of Pennsylvania in Philadelphia.
The data analysis and development of the valveadvice.org website and decision tool received no commercial support. Dr. Brennan had no disclosures. Dr. Hermann has received honoraria and research support from Edwards Pharmaceuticals, research support from Medtronic, and honoraria and research support from several other companies.
[email protected]
On Twitter @mitchelzoler
WASHINGTON – A decision-assistance tool will soon be available that is designed to help intermediate-risk patients with severe aortic stenosis and their physicians better compare each patient’s expected outcome from surgical or transcatheter valve replacement based on each patient’s individual clinical and demographic features.
The decision tool will be available as both a web-based calculator and a downloadable app. It is derived from the outcomes of 4,732 patients who underwent surgical aortic valve replacement (SAVR) during 2011-2013 and who were included in the registry maintained by the Society of Thoracic Surgeons (STS), as well as an equal number of closely matched patients who underwent transcatheter aortic valve replacement (TAVR) during 2014-2015 and entered in the Transcatheter Valve (TVT) registry run by STS and the American College of Cardiology. Tool development also used longer-term outcomes data collected through Medicare.
After receiving patient-specific data, the decision tool estimates the patient’s short-term and 1-year predicted risks for death and stroke and likelihood of being discharged home, as well as the predicted number of days the patient would remain alive and out of the hospital during the first postprocedural year, J. Matthew Brennan, MD, said at the annual meeting of the American College of Cardiology.
Cardiologists and cardiac surgeons “are desperately looking for something like this” because, currently, the only option is to estimate a patient’s risk after SAVR or TAVR using tools developed only from patients who underwent one of these procedures. The new tool gives clinicians and patients a way to compare the two options for an individual patient in a way that “minimizes the biases,” said Dr. Brennan, an interventional cardiologist at Duke University in Durham, N.C., and principal investigator for development of the website and the tool.
Dr. Brennan and his associates developed the decision assistance tool with funding from the Patient-Center Outcomes Research Institute, and it will be available online at no cost at valveadvice.org. The website was already up and running when Dr. Brennan announced the tool during the meeting, and it currently has patient-centered information about aortic valve disease and the options available for treating it. He expects the decision tool to be posted on the site by April or May.
The data he and his associates used to create the decision tool came from a total of more than 197,000 SAVR patients entered into the STS SAVR database during 2011-2013 and more than 25,000 TAVR patients enrolled in the TVT registry during 2014-2015. They used propensity score matching to identify 4,732 matched patients from each group. The patients averaged 81-82 years old, nearly half were women, and their average STS risk score was 5.5-5.8, which meant that patients fell in an intermediate-risk range by this criterion. Just over three-quarters of the TAVR patients had their procedure done via a transfemoral route.
The analysis showed that, overall, 1-year mortality and stroke rates following each type of procedure were not significantly different, and several subgroup analyses failed to identify any type of patient who fell outside this overall pattern. The TAVR patients had a stroke rate that continued to rise during 12-month follow-up, compared with a much flatter pattern among the SAVR patients. While this did not result in an excess stroke rate, the pattern over time suggested that TAVR patients may not have received optimal anticoagulant treatment during the year following their procedure, Dr. Brennan said. The number of months that patients were alive and not hospitalized was also very similar in the SAVR and TAVR groups.
While the 1-year outcomes were very similar, the periprocedural outcomes showed several statistically significant differences. In-hospital mortality was significantly higher in the SAVR patients at 5%, compared with 3% in the TAVR patients. The SAVR patients also were significantly more likely to develop a need for dialysis and a need for red cells and to have a doubled duration in their ICU stay and in their postprocedural length of hospitalization, compared with TAVR patients. On the other hand, TAVR patients were significantly more likely to need a new pacemaker while hospitalized and had a 10 times higher rate of major vascular complications. The stroke rates were very similar in both arms, Dr. Brennan reported.
According to Dr. Brennan, the most striking difference in hospital outcomes was the discharge destination for patients: 70% of TAVR patients went home after their procedural hospitalization, compared with 41% of the SAVR patients. Discharges home following periprocedural hospitalization were “substantially higher” with TAVR, he said.
Another notable feature of these data was how they contrasted with the 1-year outcomes reported from the German Aortic Valve Registry at the American Heart Association Scientific Sessions in November 2016. In the German registry, 1-year mortality after propensity-score adjustment was about 11% among SAVR patients and about 14% among TAVR patients treated with a transfemoral approach, a statistically significant difference, reported Nicolas Werner, MD, of the Ludwigshafen (Germany) Clinic.
“I think the reason we see a difference in the German data is they weren’t able to remove from their analysis the really high-risk patients” who preferentially underwent TAVR, suggested Dr. Brennan. “We had the ability to match patients who had equipoise for undergoing SAVR or TAVR. That’s why our results are more consistent with the findings from the TAVR clinical trials.”
“One of the most important findings from [Dr. Brennan’s] study is [that] it makes the German Registry results look like the outliers rather than the results from the TAVR clinical trials,” commented Howard C. Hermann, MD, professor of cardiovascular disease and director of the cardiac catheterization laboratories at the University of Pennsylvania in Philadelphia.
The data analysis and development of the valveadvice.org website and decision tool received no commercial support. Dr. Brennan had no disclosures. Dr. Hermann has received honoraria and research support from Edwards Pharmaceuticals, research support from Medtronic, and honoraria and research support from several other companies.
[email protected]
On Twitter @mitchelzoler
AT ACC 17
Key clinical point:
Major finding: In matched U.S. patients, TAVR led to 29% more patients being discharged home following their procedures, compared with SAVR.
Data source: Records for 9,464 U.S. patients who underwent TAVR or SAVR during 2011-2015.
Disclosures: Data analysis and development of the valveadvice.org website and decision tool received no commercial support. Dr. Brennan had no disclosures. Dr. Hermann has received honoraria and research support from Edwards Pharmaceuticals, research support from Medtronic, and honoraria and research support from several other companies.
BUN increase tracks with upper GI bleeding outcomes
In patients with acute nonvariceal upper GI bleeding (UGIB), increased blood urea nitrogen (BUN) levels at 24 hours were associated with worse outcomes. The marker, already proven useful in acute pancreatitis, could help physicians determine a patient’s prognosis.
Existing measures of UGIB risk are effective, but only about 30% of physicians ever calculate risk scores when evaluating UGIB patients, perhaps because they require measurements at multiple time points. “We personally think the reason for this is the busyness of clinical practices, especially the acute nature of upper GI bleeding. It’s often hard to step back to calculate a score that has multiple variables,” said study author Navin Kumar, MD, a fellow in gastroenterology at Brigham and Women’s Hospital, Boston.
The study was published in Gastrointestinal Endoscopy (2017. doi: 10.1016/j.gie.2017.03.1533).
Like acute pancreatitis, upper GI bleeding requires resuscitation management, which suggested that BUN levels might be a useful marker in this condition as well. To find out, the researchers analyzed data from 357 patients who were treated at the Brigham and Women’s Hospital emergency department and ultimately hospitalized for UGIB during 2004-2014.
The researchers analyzed BUN levels measured at admission and at the time closest to 24 hours after hospitalization, which ranged from 6 hours to 48 hours.
Thirty-seven patients (10%) experienced an increase in BUN level, while all the rest had levels that stayed steady or decreased. Those patients with BUN increases had a lower mean Glasgow-Blatchford score (7.8 vs. 9.6; P =.010), but there was no difference in AIMS65 scores.
Patients with BUN increases had greater odds of the composite outcome, which included inpatient death from any cause, inpatient rebleeding, a need for surgical or radiologic intervention, and/or a need for endoscopic reintervention during hospitalization (22% vs. 9%; P =.014). Inpatient mortality was higher in the increased BUN group (8% vs. 1%; P =.004).
Overall, BUN increase at 24 hours was associated with an odds ratio of 2.75 for the composite outcome (95% confidence interval, 1.13-6.70; P = .026).
A potential limitation to using the BUN is that it could just be catching patients with underlying renal disease. But when researchers adjusted for this, the odds ratio for increased BUN remained significant (OR, 3.00; P =.021).
“The nice part of the study is that it’s so easy to interpret and apply in a clinical setting. You just need two data points: BUN at presentation and at 24 hours. If the BUN level has risen, you need to have a higher degree of suspicion for the prognosis of those patients,” said Dr. Kumar.
The downside to BUN is that it doesn’t provide information for the first 24 hours. For that reason, BUN shouldn’t replace measures like the Glasgow-Blatchford score and the AIMS65 score. “But it’s very helpful to use this change in BUN score to get a sense of where the patient is trending. If it’s rising, there’s a higher risk of worse outcomes, and this could influence decisions about whether the patient should be in the ICU or the medical ward,” said Dr. Kumar.
In patients with acute nonvariceal upper GI bleeding (UGIB), increased blood urea nitrogen (BUN) levels at 24 hours were associated with worse outcomes. The marker, already proven useful in acute pancreatitis, could help physicians determine a patient’s prognosis.
Existing measures of UGIB risk are effective, but only about 30% of physicians ever calculate risk scores when evaluating UGIB patients, perhaps because they require measurements at multiple time points. “We personally think the reason for this is the busyness of clinical practices, especially the acute nature of upper GI bleeding. It’s often hard to step back to calculate a score that has multiple variables,” said study author Navin Kumar, MD, a fellow in gastroenterology at Brigham and Women’s Hospital, Boston.
The study was published in Gastrointestinal Endoscopy (2017. doi: 10.1016/j.gie.2017.03.1533).
Like acute pancreatitis, upper GI bleeding requires resuscitation management, which suggested that BUN levels might be a useful marker in this condition as well. To find out, the researchers analyzed data from 357 patients who were treated at the Brigham and Women’s Hospital emergency department and ultimately hospitalized for UGIB during 2004-2014.
The researchers analyzed BUN levels measured at admission and at the time closest to 24 hours after hospitalization, which ranged from 6 hours to 48 hours.
Thirty-seven patients (10%) experienced an increase in BUN level, while all the rest had levels that stayed steady or decreased. Those patients with BUN increases had a lower mean Glasgow-Blatchford score (7.8 vs. 9.6; P =.010), but there was no difference in AIMS65 scores.
Patients with BUN increases had greater odds of the composite outcome, which included inpatient death from any cause, inpatient rebleeding, a need for surgical or radiologic intervention, and/or a need for endoscopic reintervention during hospitalization (22% vs. 9%; P =.014). Inpatient mortality was higher in the increased BUN group (8% vs. 1%; P =.004).
Overall, BUN increase at 24 hours was associated with an odds ratio of 2.75 for the composite outcome (95% confidence interval, 1.13-6.70; P = .026).
A potential limitation to using the BUN is that it could just be catching patients with underlying renal disease. But when researchers adjusted for this, the odds ratio for increased BUN remained significant (OR, 3.00; P =.021).
“The nice part of the study is that it’s so easy to interpret and apply in a clinical setting. You just need two data points: BUN at presentation and at 24 hours. If the BUN level has risen, you need to have a higher degree of suspicion for the prognosis of those patients,” said Dr. Kumar.
The downside to BUN is that it doesn’t provide information for the first 24 hours. For that reason, BUN shouldn’t replace measures like the Glasgow-Blatchford score and the AIMS65 score. “But it’s very helpful to use this change in BUN score to get a sense of where the patient is trending. If it’s rising, there’s a higher risk of worse outcomes, and this could influence decisions about whether the patient should be in the ICU or the medical ward,” said Dr. Kumar.
In patients with acute nonvariceal upper GI bleeding (UGIB), increased blood urea nitrogen (BUN) levels at 24 hours were associated with worse outcomes. The marker, already proven useful in acute pancreatitis, could help physicians determine a patient’s prognosis.
Existing measures of UGIB risk are effective, but only about 30% of physicians ever calculate risk scores when evaluating UGIB patients, perhaps because they require measurements at multiple time points. “We personally think the reason for this is the busyness of clinical practices, especially the acute nature of upper GI bleeding. It’s often hard to step back to calculate a score that has multiple variables,” said study author Navin Kumar, MD, a fellow in gastroenterology at Brigham and Women’s Hospital, Boston.
The study was published in Gastrointestinal Endoscopy (2017. doi: 10.1016/j.gie.2017.03.1533).
Like acute pancreatitis, upper GI bleeding requires resuscitation management, which suggested that BUN levels might be a useful marker in this condition as well. To find out, the researchers analyzed data from 357 patients who were treated at the Brigham and Women’s Hospital emergency department and ultimately hospitalized for UGIB during 2004-2014.
The researchers analyzed BUN levels measured at admission and at the time closest to 24 hours after hospitalization, which ranged from 6 hours to 48 hours.
Thirty-seven patients (10%) experienced an increase in BUN level, while all the rest had levels that stayed steady or decreased. Those patients with BUN increases had a lower mean Glasgow-Blatchford score (7.8 vs. 9.6; P =.010), but there was no difference in AIMS65 scores.
Patients with BUN increases had greater odds of the composite outcome, which included inpatient death from any cause, inpatient rebleeding, a need for surgical or radiologic intervention, and/or a need for endoscopic reintervention during hospitalization (22% vs. 9%; P =.014). Inpatient mortality was higher in the increased BUN group (8% vs. 1%; P =.004).
Overall, BUN increase at 24 hours was associated with an odds ratio of 2.75 for the composite outcome (95% confidence interval, 1.13-6.70; P = .026).
A potential limitation to using the BUN is that it could just be catching patients with underlying renal disease. But when researchers adjusted for this, the odds ratio for increased BUN remained significant (OR, 3.00; P =.021).
“The nice part of the study is that it’s so easy to interpret and apply in a clinical setting. You just need two data points: BUN at presentation and at 24 hours. If the BUN level has risen, you need to have a higher degree of suspicion for the prognosis of those patients,” said Dr. Kumar.
The downside to BUN is that it doesn’t provide information for the first 24 hours. For that reason, BUN shouldn’t replace measures like the Glasgow-Blatchford score and the AIMS65 score. “But it’s very helpful to use this change in BUN score to get a sense of where the patient is trending. If it’s rising, there’s a higher risk of worse outcomes, and this could influence decisions about whether the patient should be in the ICU or the medical ward,” said Dr. Kumar.
FROM GASTROINTESTINAL ENDOSCOPY
Key clinical point: BUN could be a useful prognostic marker.
Major finding: BUN increase indicated a threefold increased risk of poor outcomes.
Data source: Retrospective analysis of 357 patients at a single center.
Disclosures: The study did not receive external funding. Dr. Kumar reported having no financial disclosures.
Transanal TME comparable to open, lap approaches to rectal cancer
HOUSTON – Transanal total mesorectal excision can consistently achieve good pathological results for obtaining specimens in rectal cancer, and overcome the shortcomings of the open and laparoscopic approaches to rectal cancer surgery, particularly in the distal part of the rectum where obtaining quality specimens can be technically challenging, researchers at the Hospital Clinic of Barcelona have found.
Reporting at the annual meeting of the Society of American Gastrointestinal and Endoscopic Surgeons, Jacqueline van Laarhoven, MD, PhD, said, “Pathologically, transanal total mesorectal excision [TME] provides good results on integrity of the mesorectum, negative circumferential and distal resection margins, and lymph nodes per specimen.” This study represents the first results of a relatively large, single-institution cohort, Dr. van Laarhoven said.

The study involved 187 patients with mid- or low-rectal cancer who had transanal TME from November 2011 to June 2016. Dr. van Laarhoven explained that obtaining high-quality specimens is an important prognostic factor for determining locoregional recurrence in rectal cancer. The study analyzed results of excised specimens in the mesorectum, circumferential and distal resected margins, and lymph nodes, and compared outcomes with those in two randomized clinical trials of both open and laparoscopic TME – the COLOR II (Lancet Oncol. 2013;14:210-8) and COREAN trials (Lancet Oncol. 2014;15:767-74) – where applicable.
In the Barcelona study population, 63.1% had tumors in the midrectum and 36.9% in the low rectum. Transanal TME yielded complete mesorectal quality in 95.7% of cases, almost-complete quality in 1.6% and incomplete in 1.1%, but comparison with COLOR II and COREAN trials was difficult because of differing inclusion criteria, Dr. van Laarhoven said.
Mean distal margin was 2.1 cm in midrectal cancer with a positive distal resection margin in 3.2%. In low-rectal cancer, the mean distal margin was 1.1 cm with a positive distal resection margin in 7.8%. Dr. van Laarhoven noted the overall circumferential resection margin (CRM) was 8.6% in this study, compared with 8.3% overall for the COREAN trial. As for COLOR II, the overall rate for positive CRM in mid- and low-rectal tumors was around 9%, Dr. van Laarhoven said, but in the open group the positive CRM was 3% in the midrectal excisions and 22% in low-rectal disease.
With regard to lymph nodes, the Barcelona study reported a median of 14 per specimen, with a range of 11 to 18, Dr. van Laarhoven said. However, in nonirradiated patients, the median was 15 per specimen. “This is consistent with the fact that neoadjuvant radiotherapy leads to a decrease in the lymph-node harvest,” she said. “These results are comparable to the COREAN and the COLOR II trials.”
Sixty-two percent of patients received neoadjuvant chemoradiotherapy, 3.2% received radiotherapy only, and 2.1% chemotherapy only.
On preoperative staging, 3.2% had T1 tumors, 20.3% T2, 67.9% T3, and 7.5% T4. The overall positive CRM (less than 1 mm) was 8.6% (including T4 tumors).
Postoperative pathological staging showed complete remission in 16% of patients, pT1 in 6.4%, pT2 in 28.9%, pT3 in 42.8%, pT4 in 2.7%, and pTis in 1.6%.
Dr. van Laarhoven commented, “As the quality of the surgical treatment is a surrogate marker for survival, transanal TME can be regarded as an oncologically safe method to treat patients with rectal cancer.”
Dr. van Laarhoven reported having no financial disclosures.
HOUSTON – Transanal total mesorectal excision can consistently achieve good pathological results for obtaining specimens in rectal cancer, and overcome the shortcomings of the open and laparoscopic approaches to rectal cancer surgery, particularly in the distal part of the rectum where obtaining quality specimens can be technically challenging, researchers at the Hospital Clinic of Barcelona have found.
Reporting at the annual meeting of the Society of American Gastrointestinal and Endoscopic Surgeons, Jacqueline van Laarhoven, MD, PhD, said, “Pathologically, transanal total mesorectal excision [TME] provides good results on integrity of the mesorectum, negative circumferential and distal resection margins, and lymph nodes per specimen.” This study represents the first results of a relatively large, single-institution cohort, Dr. van Laarhoven said.
The study involved 187 patients with mid- or low-rectal cancer who had transanal TME from November 2011 to June 2016. Dr. van Laarhoven explained that obtaining high-quality specimens is an important prognostic factor for determining locoregional recurrence in rectal cancer. The study analyzed results of excised specimens in the mesorectum, circumferential and distal resected margins, and lymph nodes, and compared outcomes with those in two randomized clinical trials of both open and laparoscopic TME – the COLOR II (Lancet Oncol. 2013;14:210-8) and COREAN trials (Lancet Oncol. 2014;15:767-74) – where applicable.
In the Barcelona study population, 63.1% had tumors in the midrectum and 36.9% in the low rectum. Transanal TME yielded complete mesorectal quality in 95.7% of cases, almost-complete quality in 1.6% and incomplete in 1.1%, but comparison with COLOR II and COREAN trials was difficult because of differing inclusion criteria, Dr. van Laarhoven said.
Mean distal margin was 2.1 cm in midrectal cancer with a positive distal resection margin in 3.2%. In low-rectal cancer, the mean distal margin was 1.1 cm with a positive distal resection margin in 7.8%. Dr. van Laarhoven noted the overall circumferential resection margin (CRM) was 8.6% in this study, compared with 8.3% overall for the COREAN trial. As for COLOR II, the overall rate for positive CRM in mid- and low-rectal tumors was around 9%, Dr. van Laarhoven said, but in the open group the positive CRM was 3% in the midrectal excisions and 22% in low-rectal disease.
With regard to lymph nodes, the Barcelona study reported a median of 14 per specimen, with a range of 11 to 18, Dr. van Laarhoven said. However, in nonirradiated patients, the median was 15 per specimen. “This is consistent with the fact that neoadjuvant radiotherapy leads to a decrease in the lymph-node harvest,” she said. “These results are comparable to the COREAN and the COLOR II trials.”
Sixty-two percent of patients received neoadjuvant chemoradiotherapy, 3.2% received radiotherapy only, and 2.1% chemotherapy only.
On preoperative staging, 3.2% had T1 tumors, 20.3% T2, 67.9% T3, and 7.5% T4. The overall positive CRM (less than 1 mm) was 8.6% (including T4 tumors).
Postoperative pathological staging showed complete remission in 16% of patients, pT1 in 6.4%, pT2 in 28.9%, pT3 in 42.8%, pT4 in 2.7%, and pTis in 1.6%.
Dr. van Laarhoven commented, “As the quality of the surgical treatment is a surrogate marker for survival, transanal TME can be regarded as an oncologically safe method to treat patients with rectal cancer.”
Dr. van Laarhoven reported having no financial disclosures.
HOUSTON – Transanal total mesorectal excision can consistently achieve good pathological results for obtaining specimens in rectal cancer, and overcome the shortcomings of the open and laparoscopic approaches to rectal cancer surgery, particularly in the distal part of the rectum where obtaining quality specimens can be technically challenging, researchers at the Hospital Clinic of Barcelona have found.
Reporting at the annual meeting of the Society of American Gastrointestinal and Endoscopic Surgeons, Jacqueline van Laarhoven, MD, PhD, said, “Pathologically, transanal total mesorectal excision [TME] provides good results on integrity of the mesorectum, negative circumferential and distal resection margins, and lymph nodes per specimen.” This study represents the first results of a relatively large, single-institution cohort, Dr. van Laarhoven said.
The study involved 187 patients with mid- or low-rectal cancer who had transanal TME from November 2011 to June 2016. Dr. van Laarhoven explained that obtaining high-quality specimens is an important prognostic factor for determining locoregional recurrence in rectal cancer. The study analyzed results of excised specimens in the mesorectum, circumferential and distal resected margins, and lymph nodes, and compared outcomes with those in two randomized clinical trials of both open and laparoscopic TME – the COLOR II (Lancet Oncol. 2013;14:210-8) and COREAN trials (Lancet Oncol. 2014;15:767-74) – where applicable.
In the Barcelona study population, 63.1% had tumors in the midrectum and 36.9% in the low rectum. Transanal TME yielded complete mesorectal quality in 95.7% of cases, almost-complete quality in 1.6% and incomplete in 1.1%, but comparison with COLOR II and COREAN trials was difficult because of differing inclusion criteria, Dr. van Laarhoven said.
Mean distal margin was 2.1 cm in midrectal cancer with a positive distal resection margin in 3.2%. In low-rectal cancer, the mean distal margin was 1.1 cm with a positive distal resection margin in 7.8%. Dr. van Laarhoven noted the overall circumferential resection margin (CRM) was 8.6% in this study, compared with 8.3% overall for the COREAN trial. As for COLOR II, the overall rate for positive CRM in mid- and low-rectal tumors was around 9%, Dr. van Laarhoven said, but in the open group the positive CRM was 3% in the midrectal excisions and 22% in low-rectal disease.
With regard to lymph nodes, the Barcelona study reported a median of 14 per specimen, with a range of 11 to 18, Dr. van Laarhoven said. However, in nonirradiated patients, the median was 15 per specimen. “This is consistent with the fact that neoadjuvant radiotherapy leads to a decrease in the lymph-node harvest,” she said. “These results are comparable to the COREAN and the COLOR II trials.”
Sixty-two percent of patients received neoadjuvant chemoradiotherapy, 3.2% received radiotherapy only, and 2.1% chemotherapy only.
On preoperative staging, 3.2% had T1 tumors, 20.3% T2, 67.9% T3, and 7.5% T4. The overall positive CRM (less than 1 mm) was 8.6% (including T4 tumors).
Postoperative pathological staging showed complete remission in 16% of patients, pT1 in 6.4%, pT2 in 28.9%, pT3 in 42.8%, pT4 in 2.7%, and pTis in 1.6%.
Dr. van Laarhoven commented, “As the quality of the surgical treatment is a surrogate marker for survival, transanal TME can be regarded as an oncologically safe method to treat patients with rectal cancer.”
Dr. van Laarhoven reported having no financial disclosures.
AT SAGES 2017
Key clinical point: Transanal total mesorectal excision (TME) is a viable alternative to open or laparoscopic TME in cancers of the low and midrectum.
Major finding: Postoperative pathological staging showed complete remission in 16%, with pT1 in 6.4%, pT2 in 28.9%, pT3 in 42.8%, pT4 in 2.7%, and pTis in 1.6%.
Data source: Analysis of 187 patients prospectively enrolled in a standardized database who had transanal TME from November 2011 to June 2016 at a single center.
Disclosures: Dr. van Laarhoven reported having no financial disclosures.
Young patients with first-episode psychosis face far higher mortality risk
Young people in the United States experiencing first-episode psychosis face a mortality risk that is 24 times greater than that of their peers in the general population, a new study shows.
“The hugely elevated mortality observed here underscores that young people experiencing psychosis warrant intensive clinical attention,” wrote Michael Schoenbaum, PhD, senior adviser for mental health services, epidemiology, and economics at the National Institute of Mental Health, and his associates. “In the general population, only individuals over 70 years of age have all-cause 12-month mortality approaching the rates we observed among young psychosis patients here.”
The researchers analyzed data on about 5,000 people aged 16-30 with commercial health insurance coverage who had a new ICD-9 diagnosis of schizophrenia, brief psychotic disorder, or psychotic disorder not otherwise specified, and followed them for 12 months. They limited the sample to people who had continuous insurance coverage over a period of 12 months or greater before their first observed diagnosis of psychosis – which they called the “index diagnosis.”
For the entire psychosis cohort, the 12-month mortality was 2.0% (1,968 per 100,000 people), compared with less than 0.1% in the general population (89 per 100,000). The researchers further found mortality “an order of magnitude higher in those with incident psychosis after age 25, compared with those with an incident diagnosis between ages 16 and 20” (Schizophr Bull. 2017 Apr 7. doi: 10.1093/schbul/sbx009).
Information on the cause of death was not available, but the researchers were able to look at the diagnoses that the decedents had received 12 months before their index psychosis diagnosis. Fifteen of the decedents had been diagnosed with cancer, nine with renal disease (end-stage), and one with cystic fibrosis. When those patients were removed from the mortality cohort, the 12-month mortality stood at 1.5%, a rate they said was 18 times higher than mortality in the general population.
“These findings show the importance of tracking mortality in individuals with mental illness,” Dr. Schoenbaum said in a statement. “Health systems do this in other areas of medicine, such as cancer and cardiology, but not for mental illness. Of course, we also need to learn how these young people are losing their lives.”
The study might not be generalizable because the cohort studied had access to continuous access to health insurance coverage “before and after the index psychosis diagnosis.” Also, the size of the cohort was relatively small. Nevertheless, they said, the findings are consistent with other studies showing that care for those with early psychosis falls short.
“Taken together, these findings provide a strong rationale for initiatives to improve early identification and integrated treatment for psychotic disorders in U.S. treatment settings,” Dr. Schoenbaum and his associates wrote.
The Commonwealth Fund provided support for the study. The researchers reported having no conflicts of interest, and said the views expressed in the study are their own and do not necessarily reflect those of the National Institute of Mental Health, or any other organizations or entities.
[email protected]
On Twitter @ginalhenderson
Young people in the United States experiencing first-episode psychosis face a mortality risk that is 24 times greater than that of their peers in the general population, a new study shows.
“The hugely elevated mortality observed here underscores that young people experiencing psychosis warrant intensive clinical attention,” wrote Michael Schoenbaum, PhD, senior adviser for mental health services, epidemiology, and economics at the National Institute of Mental Health, and his associates. “In the general population, only individuals over 70 years of age have all-cause 12-month mortality approaching the rates we observed among young psychosis patients here.”
The researchers analyzed data on about 5,000 people aged 16-30 with commercial health insurance coverage who had a new ICD-9 diagnosis of schizophrenia, brief psychotic disorder, or psychotic disorder not otherwise specified, and followed them for 12 months. They limited the sample to people who had continuous insurance coverage over a period of 12 months or greater before their first observed diagnosis of psychosis – which they called the “index diagnosis.”
For the entire psychosis cohort, the 12-month mortality was 2.0% (1,968 per 100,000 people), compared with less than 0.1% in the general population (89 per 100,000). The researchers further found mortality “an order of magnitude higher in those with incident psychosis after age 25, compared with those with an incident diagnosis between ages 16 and 20” (Schizophr Bull. 2017 Apr 7. doi: 10.1093/schbul/sbx009).
Information on the cause of death was not available, but the researchers were able to look at the diagnoses that the decedents had received 12 months before their index psychosis diagnosis. Fifteen of the decedents had been diagnosed with cancer, nine with renal disease (end-stage), and one with cystic fibrosis. When those patients were removed from the mortality cohort, the 12-month mortality stood at 1.5%, a rate they said was 18 times higher than mortality in the general population.
“These findings show the importance of tracking mortality in individuals with mental illness,” Dr. Schoenbaum said in a statement. “Health systems do this in other areas of medicine, such as cancer and cardiology, but not for mental illness. Of course, we also need to learn how these young people are losing their lives.”
The study might not be generalizable because the cohort studied had access to continuous access to health insurance coverage “before and after the index psychosis diagnosis.” Also, the size of the cohort was relatively small. Nevertheless, they said, the findings are consistent with other studies showing that care for those with early psychosis falls short.
“Taken together, these findings provide a strong rationale for initiatives to improve early identification and integrated treatment for psychotic disorders in U.S. treatment settings,” Dr. Schoenbaum and his associates wrote.
The Commonwealth Fund provided support for the study. The researchers reported having no conflicts of interest, and said the views expressed in the study are their own and do not necessarily reflect those of the National Institute of Mental Health, or any other organizations or entities.
[email protected]
On Twitter @ginalhenderson
Young people in the United States experiencing first-episode psychosis face a mortality risk that is 24 times greater than that of their peers in the general population, a new study shows.
“The hugely elevated mortality observed here underscores that young people experiencing psychosis warrant intensive clinical attention,” wrote Michael Schoenbaum, PhD, senior adviser for mental health services, epidemiology, and economics at the National Institute of Mental Health, and his associates. “In the general population, only individuals over 70 years of age have all-cause 12-month mortality approaching the rates we observed among young psychosis patients here.”
The researchers analyzed data on about 5,000 people aged 16-30 with commercial health insurance coverage who had a new ICD-9 diagnosis of schizophrenia, brief psychotic disorder, or psychotic disorder not otherwise specified, and followed them for 12 months. They limited the sample to people who had continuous insurance coverage over a period of 12 months or greater before their first observed diagnosis of psychosis – which they called the “index diagnosis.”
For the entire psychosis cohort, the 12-month mortality was 2.0% (1,968 per 100,000 people), compared with less than 0.1% in the general population (89 per 100,000). The researchers further found mortality “an order of magnitude higher in those with incident psychosis after age 25, compared with those with an incident diagnosis between ages 16 and 20” (Schizophr Bull. 2017 Apr 7. doi: 10.1093/schbul/sbx009).
Information on the cause of death was not available, but the researchers were able to look at the diagnoses that the decedents had received 12 months before their index psychosis diagnosis. Fifteen of the decedents had been diagnosed with cancer, nine with renal disease (end-stage), and one with cystic fibrosis. When those patients were removed from the mortality cohort, the 12-month mortality stood at 1.5%, a rate they said was 18 times higher than mortality in the general population.
“These findings show the importance of tracking mortality in individuals with mental illness,” Dr. Schoenbaum said in a statement. “Health systems do this in other areas of medicine, such as cancer and cardiology, but not for mental illness. Of course, we also need to learn how these young people are losing their lives.”
The study might not be generalizable because the cohort studied had access to continuous access to health insurance coverage “before and after the index psychosis diagnosis.” Also, the size of the cohort was relatively small. Nevertheless, they said, the findings are consistent with other studies showing that care for those with early psychosis falls short.
“Taken together, these findings provide a strong rationale for initiatives to improve early identification and integrated treatment for psychotic disorders in U.S. treatment settings,” Dr. Schoenbaum and his associates wrote.
The Commonwealth Fund provided support for the study. The researchers reported having no conflicts of interest, and said the views expressed in the study are their own and do not necessarily reflect those of the National Institute of Mental Health, or any other organizations or entities.
[email protected]
On Twitter @ginalhenderson
FROM SCHIZOPHRENIA BULLETIN
Myelofibrosis therapies moving beyond ruxolitinib
ORLANDO – Ruxolitinib is currently the only drug approved for the treatment of myelofibrosis, but a number of other therapies are in clinical trials and showing promise, according to Ruben A. Mesa, MD.
“Our field ... is rapidly in evolution,” he said at the annual conference of the National Comprehensive Cancer Network, adding that efforts are underway to determine where these drugs might fit in.

Among those being considered specifically for myelofibrosis are pacritinib, momelotinib, PRM-151, and imetelstat, he said.
Pacritinib
This JAK2/FT3 inhibitor reduces splenomegaly and its related symptoms, but may also help patients who have low platelet counts and a worse prognosis. Pacritinib has demonstrated safety in that population, said Dr. Mesa of Mayo Clinic Cancer Center, Phoenix, Ariz.
Concerns about increased mortality related to risk of intracranial hemorrhage and cardiovascular events led the Food and Drug Administration to place a full clinical hold on pacritinib in February 2016. That hold was lifted in January 2017 when data from the randomized, controlled, phase III PERSIST-2 study, as presented at the American Society of Hematology annual meeting in December 2016, showed the risks did not hold up among study patients.
PERSIST-2 compared pacritinib doses of 400 mg once daily and 200 mg twice daily with best alternative therapy, which was ruxolitinib in most patients, Dr. Mesa said. He noted that the study included patients who had marked thrombocytopenia and were allowed prior JAK2 inhibitor exposure.
The 200-mg twice-daily dosing was superior in achieving spleen volume reductions greater than 35%: 22% of patients in the 200-mg dosing group vs. 15% in the 400-mg once-daily dosing group, compared with 3% of those receiving best available therapy. The twice-daily dosing group also experienced greater symptom improvement: Thirty-two percent in the 200-mg twice-daily group vs. 17% in the 400-mg once-daily group achieved at least a 50% reduction in total symptom scale scores, compared with 14% of those receiving best available therapy.
Additional studies of pacritinib will begin enrolling soon, Dr. Mesa said, noting that these studies will look at lower doses in an effort to identify the minimally effective dose with the optimal balance of safety and efficacy.
Momelotinib
Momelotinib, a JAK1/JAK2 inhibitor, was evaluated in two large recently concluded phase III trials (SIMPLIFY-1 and SIMPLIFY-2). SIMPIFY-1 compared momelotinib to ruxolitinib in the front-line setting, and showed momelotinib to be noninferior for reducing splenomegaly.
“However, it was inferior for improvement in the symptom burden,” Dr. Mesa said, noting that while there seemed to be a favorable difference in terms of anemia, the study was structured in such a way that the agent needed to be noninferior for both spleen and symptoms for the anemia response to be evaluable.
SIMPLIFY-2 evaluated momelotinib in patients who had not responded to ruxolitinib. In this second-line setting, momelotinib was not superior to the best alternative therapy, but since the vast majority of the ruxolitinib failure patients remained on ruxolitinib, it is “a bit of a confounded study to assess,” he said.
The top-line data from these studies were issued in a press release from the manufacturer (Gilead) in November 2016, and the complete results are expected to be made public in the near future, at which time more will be known about the next steps for momelotinib, he said.
If approved, pacritinib and momelotinib could ultimately be positioned as a front-line and/or second-line treatment for myelofibrosis, Dr. Mesa predicted.
There has been a goal, in terms of trial design, to see if there is a niche for these drugs in the front-line setting based on blood counts.
“Those recommendations would clearly be very much dependent on the risk, the safety, and the efficacy,” he said.
PRM-151
This antifibrosing agent was shown to be active in early-phase trials – including in stage 1 of an adaptive phase II trial. PRM-151 is currently being evaluated in the fully-accrued ongoing phase II PROMOTE study to determine whether it improves splenomegaly, symptoms, and cytopenia. The primary endpoint of the study is the bone marrow response rate. Study subjects are patients with primary myelofibrosis, post–polycythemia vera myelofibrosis, or post–essential thrombocythemia myelofibrosis, and grade 2-3 fibrosis, said Dr. Mesa, who is the principal investigator for the study.
Imetelstat
This telomerase inhibitor is being evaluated in the randomized, multicenter, phase II IMbark study, designed to assess spleen volume and total symptom score as primary end points. Earlier studies have shown deep responses in patients with myelofibrosis who were treated with imetelstat, Dr. Mesa said.
The IMbark study (NCT02426086) was originally designed to evaluate two dosing regimens administered as a single agent to participants with intermediate-2 or high-risk myelofibrosis who were refractory to or relapsed after JAK inhibitor treatment. Participants received either 9.4 mg/kg or 4.7 mg/kg intravenously every 3 weeks until disease progression, unacceptable toxicity, or study end.
According to information from Geron, which is developing the agent, enrollment of new participants is currently suspended following a planned internal data review, but enrollment “may be resumed after a second internal data review that is planned by the end of the second quarter of 2017.” If resumed, enrollment would be only to the higher-dose treatment arm; patients initially randomized to that arm may continue treatment, and those randomized to the lower-dose arm may see their dose increased at the investigator’s discretion.
If approved, PRM-151 and imetelstat would likely be positioned as second-line treatments for myelofibrosis, Dr. Mesa said, noting that determining which patients would be most likely to benefit from treatment with these agents would require a close look at the evidence from second-line studies.
Combination therapies
In addition to these investigational treatments, nearly 20 different combination treatments involving ruxolitinib plus another agent have been looked at to try to further improve activity. Some improvements in splenomegaly have been seen with combinations including ruxolitinib and either panobinostat (a histone deacytelase inhibitor), LDE225 (a hedgehog signaling pathway inhibitor), and BKM120 (a PI3-kinase inhibitor), he noted.
“For the area of greatest interest – which was to see incremental improvements in thrombocytopenia, anemia, or fibrosis – there have been favorable data, but they have been modest. It’s not quite clear that there is a combination that is ready for prime time, nor is there yet a combination that we have recommended through the treatment guidelines to be utilized for these patients,” he said.
Dr. Mesa has received consulting fees, honoraria, and/or grant/research support from ARIAD Pharmaceuticals; Celgene Corporation, CTI BioPharma, the maker of pacritinib; Galena Biopharma; Gilead, the maker of momelotinib; Incyte, the maker of ruxolitinib; Novartis, the maker of panobinostat and BKM120; and Promedior, the maker of PRM-151.
ORLANDO – Ruxolitinib is currently the only drug approved for the treatment of myelofibrosis, but a number of other therapies are in clinical trials and showing promise, according to Ruben A. Mesa, MD.
“Our field ... is rapidly in evolution,” he said at the annual conference of the National Comprehensive Cancer Network, adding that efforts are underway to determine where these drugs might fit in.
Among those being considered specifically for myelofibrosis are pacritinib, momelotinib, PRM-151, and imetelstat, he said.
Pacritinib
This JAK2/FT3 inhibitor reduces splenomegaly and its related symptoms, but may also help patients who have low platelet counts and a worse prognosis. Pacritinib has demonstrated safety in that population, said Dr. Mesa of Mayo Clinic Cancer Center, Phoenix, Ariz.
Concerns about increased mortality related to risk of intracranial hemorrhage and cardiovascular events led the Food and Drug Administration to place a full clinical hold on pacritinib in February 2016. That hold was lifted in January 2017 when data from the randomized, controlled, phase III PERSIST-2 study, as presented at the American Society of Hematology annual meeting in December 2016, showed the risks did not hold up among study patients.
PERSIST-2 compared pacritinib doses of 400 mg once daily and 200 mg twice daily with best alternative therapy, which was ruxolitinib in most patients, Dr. Mesa said. He noted that the study included patients who had marked thrombocytopenia and were allowed prior JAK2 inhibitor exposure.
The 200-mg twice-daily dosing was superior in achieving spleen volume reductions greater than 35%: 22% of patients in the 200-mg dosing group vs. 15% in the 400-mg once-daily dosing group, compared with 3% of those receiving best available therapy. The twice-daily dosing group also experienced greater symptom improvement: Thirty-two percent in the 200-mg twice-daily group vs. 17% in the 400-mg once-daily group achieved at least a 50% reduction in total symptom scale scores, compared with 14% of those receiving best available therapy.
Additional studies of pacritinib will begin enrolling soon, Dr. Mesa said, noting that these studies will look at lower doses in an effort to identify the minimally effective dose with the optimal balance of safety and efficacy.
Momelotinib
Momelotinib, a JAK1/JAK2 inhibitor, was evaluated in two large recently concluded phase III trials (SIMPLIFY-1 and SIMPLIFY-2). SIMPIFY-1 compared momelotinib to ruxolitinib in the front-line setting, and showed momelotinib to be noninferior for reducing splenomegaly.
“However, it was inferior for improvement in the symptom burden,” Dr. Mesa said, noting that while there seemed to be a favorable difference in terms of anemia, the study was structured in such a way that the agent needed to be noninferior for both spleen and symptoms for the anemia response to be evaluable.
SIMPLIFY-2 evaluated momelotinib in patients who had not responded to ruxolitinib. In this second-line setting, momelotinib was not superior to the best alternative therapy, but since the vast majority of the ruxolitinib failure patients remained on ruxolitinib, it is “a bit of a confounded study to assess,” he said.
The top-line data from these studies were issued in a press release from the manufacturer (Gilead) in November 2016, and the complete results are expected to be made public in the near future, at which time more will be known about the next steps for momelotinib, he said.
If approved, pacritinib and momelotinib could ultimately be positioned as a front-line and/or second-line treatment for myelofibrosis, Dr. Mesa predicted.
There has been a goal, in terms of trial design, to see if there is a niche for these drugs in the front-line setting based on blood counts.
“Those recommendations would clearly be very much dependent on the risk, the safety, and the efficacy,” he said.
PRM-151
This antifibrosing agent was shown to be active in early-phase trials – including in stage 1 of an adaptive phase II trial. PRM-151 is currently being evaluated in the fully-accrued ongoing phase II PROMOTE study to determine whether it improves splenomegaly, symptoms, and cytopenia. The primary endpoint of the study is the bone marrow response rate. Study subjects are patients with primary myelofibrosis, post–polycythemia vera myelofibrosis, or post–essential thrombocythemia myelofibrosis, and grade 2-3 fibrosis, said Dr. Mesa, who is the principal investigator for the study.
Imetelstat
This telomerase inhibitor is being evaluated in the randomized, multicenter, phase II IMbark study, designed to assess spleen volume and total symptom score as primary end points. Earlier studies have shown deep responses in patients with myelofibrosis who were treated with imetelstat, Dr. Mesa said.
The IMbark study (NCT02426086) was originally designed to evaluate two dosing regimens administered as a single agent to participants with intermediate-2 or high-risk myelofibrosis who were refractory to or relapsed after JAK inhibitor treatment. Participants received either 9.4 mg/kg or 4.7 mg/kg intravenously every 3 weeks until disease progression, unacceptable toxicity, or study end.
According to information from Geron, which is developing the agent, enrollment of new participants is currently suspended following a planned internal data review, but enrollment “may be resumed after a second internal data review that is planned by the end of the second quarter of 2017.” If resumed, enrollment would be only to the higher-dose treatment arm; patients initially randomized to that arm may continue treatment, and those randomized to the lower-dose arm may see their dose increased at the investigator’s discretion.
If approved, PRM-151 and imetelstat would likely be positioned as second-line treatments for myelofibrosis, Dr. Mesa said, noting that determining which patients would be most likely to benefit from treatment with these agents would require a close look at the evidence from second-line studies.
Combination therapies
In addition to these investigational treatments, nearly 20 different combination treatments involving ruxolitinib plus another agent have been looked at to try to further improve activity. Some improvements in splenomegaly have been seen with combinations including ruxolitinib and either panobinostat (a histone deacytelase inhibitor), LDE225 (a hedgehog signaling pathway inhibitor), and BKM120 (a PI3-kinase inhibitor), he noted.
“For the area of greatest interest – which was to see incremental improvements in thrombocytopenia, anemia, or fibrosis – there have been favorable data, but they have been modest. It’s not quite clear that there is a combination that is ready for prime time, nor is there yet a combination that we have recommended through the treatment guidelines to be utilized for these patients,” he said.
Dr. Mesa has received consulting fees, honoraria, and/or grant/research support from ARIAD Pharmaceuticals; Celgene Corporation, CTI BioPharma, the maker of pacritinib; Galena Biopharma; Gilead, the maker of momelotinib; Incyte, the maker of ruxolitinib; Novartis, the maker of panobinostat and BKM120; and Promedior, the maker of PRM-151.
ORLANDO – Ruxolitinib is currently the only drug approved for the treatment of myelofibrosis, but a number of other therapies are in clinical trials and showing promise, according to Ruben A. Mesa, MD.
“Our field ... is rapidly in evolution,” he said at the annual conference of the National Comprehensive Cancer Network, adding that efforts are underway to determine where these drugs might fit in.
Among those being considered specifically for myelofibrosis are pacritinib, momelotinib, PRM-151, and imetelstat, he said.
Pacritinib
This JAK2/FT3 inhibitor reduces splenomegaly and its related symptoms, but may also help patients who have low platelet counts and a worse prognosis. Pacritinib has demonstrated safety in that population, said Dr. Mesa of Mayo Clinic Cancer Center, Phoenix, Ariz.
Concerns about increased mortality related to risk of intracranial hemorrhage and cardiovascular events led the Food and Drug Administration to place a full clinical hold on pacritinib in February 2016. That hold was lifted in January 2017 when data from the randomized, controlled, phase III PERSIST-2 study, as presented at the American Society of Hematology annual meeting in December 2016, showed the risks did not hold up among study patients.
PERSIST-2 compared pacritinib doses of 400 mg once daily and 200 mg twice daily with best alternative therapy, which was ruxolitinib in most patients, Dr. Mesa said. He noted that the study included patients who had marked thrombocytopenia and were allowed prior JAK2 inhibitor exposure.
The 200-mg twice-daily dosing was superior in achieving spleen volume reductions greater than 35%: 22% of patients in the 200-mg dosing group vs. 15% in the 400-mg once-daily dosing group, compared with 3% of those receiving best available therapy. The twice-daily dosing group also experienced greater symptom improvement: Thirty-two percent in the 200-mg twice-daily group vs. 17% in the 400-mg once-daily group achieved at least a 50% reduction in total symptom scale scores, compared with 14% of those receiving best available therapy.
Additional studies of pacritinib will begin enrolling soon, Dr. Mesa said, noting that these studies will look at lower doses in an effort to identify the minimally effective dose with the optimal balance of safety and efficacy.
Momelotinib
Momelotinib, a JAK1/JAK2 inhibitor, was evaluated in two large recently concluded phase III trials (SIMPLIFY-1 and SIMPLIFY-2). SIMPIFY-1 compared momelotinib to ruxolitinib in the front-line setting, and showed momelotinib to be noninferior for reducing splenomegaly.
“However, it was inferior for improvement in the symptom burden,” Dr. Mesa said, noting that while there seemed to be a favorable difference in terms of anemia, the study was structured in such a way that the agent needed to be noninferior for both spleen and symptoms for the anemia response to be evaluable.
SIMPLIFY-2 evaluated momelotinib in patients who had not responded to ruxolitinib. In this second-line setting, momelotinib was not superior to the best alternative therapy, but since the vast majority of the ruxolitinib failure patients remained on ruxolitinib, it is “a bit of a confounded study to assess,” he said.
The top-line data from these studies were issued in a press release from the manufacturer (Gilead) in November 2016, and the complete results are expected to be made public in the near future, at which time more will be known about the next steps for momelotinib, he said.
If approved, pacritinib and momelotinib could ultimately be positioned as a front-line and/or second-line treatment for myelofibrosis, Dr. Mesa predicted.
There has been a goal, in terms of trial design, to see if there is a niche for these drugs in the front-line setting based on blood counts.
“Those recommendations would clearly be very much dependent on the risk, the safety, and the efficacy,” he said.
PRM-151
This antifibrosing agent was shown to be active in early-phase trials – including in stage 1 of an adaptive phase II trial. PRM-151 is currently being evaluated in the fully-accrued ongoing phase II PROMOTE study to determine whether it improves splenomegaly, symptoms, and cytopenia. The primary endpoint of the study is the bone marrow response rate. Study subjects are patients with primary myelofibrosis, post–polycythemia vera myelofibrosis, or post–essential thrombocythemia myelofibrosis, and grade 2-3 fibrosis, said Dr. Mesa, who is the principal investigator for the study.
Imetelstat
This telomerase inhibitor is being evaluated in the randomized, multicenter, phase II IMbark study, designed to assess spleen volume and total symptom score as primary end points. Earlier studies have shown deep responses in patients with myelofibrosis who were treated with imetelstat, Dr. Mesa said.
The IMbark study (NCT02426086) was originally designed to evaluate two dosing regimens administered as a single agent to participants with intermediate-2 or high-risk myelofibrosis who were refractory to or relapsed after JAK inhibitor treatment. Participants received either 9.4 mg/kg or 4.7 mg/kg intravenously every 3 weeks until disease progression, unacceptable toxicity, or study end.
According to information from Geron, which is developing the agent, enrollment of new participants is currently suspended following a planned internal data review, but enrollment “may be resumed after a second internal data review that is planned by the end of the second quarter of 2017.” If resumed, enrollment would be only to the higher-dose treatment arm; patients initially randomized to that arm may continue treatment, and those randomized to the lower-dose arm may see their dose increased at the investigator’s discretion.
If approved, PRM-151 and imetelstat would likely be positioned as second-line treatments for myelofibrosis, Dr. Mesa said, noting that determining which patients would be most likely to benefit from treatment with these agents would require a close look at the evidence from second-line studies.
Combination therapies
In addition to these investigational treatments, nearly 20 different combination treatments involving ruxolitinib plus another agent have been looked at to try to further improve activity. Some improvements in splenomegaly have been seen with combinations including ruxolitinib and either panobinostat (a histone deacytelase inhibitor), LDE225 (a hedgehog signaling pathway inhibitor), and BKM120 (a PI3-kinase inhibitor), he noted.
“For the area of greatest interest – which was to see incremental improvements in thrombocytopenia, anemia, or fibrosis – there have been favorable data, but they have been modest. It’s not quite clear that there is a combination that is ready for prime time, nor is there yet a combination that we have recommended through the treatment guidelines to be utilized for these patients,” he said.
Dr. Mesa has received consulting fees, honoraria, and/or grant/research support from ARIAD Pharmaceuticals; Celgene Corporation, CTI BioPharma, the maker of pacritinib; Galena Biopharma; Gilead, the maker of momelotinib; Incyte, the maker of ruxolitinib; Novartis, the maker of panobinostat and BKM120; and Promedior, the maker of PRM-151.
EXPERT ANALYSIS AT THE NCCN ANNUAL CONFERENCE
Redness and Painful Ulcerations in the Perineal Area
The Diagnosis: PELVIS Syndrome
Infantile hemangiomas (IHs) are present in up to 10% of infants by 1 year of age and are most commonly located on the face and upper extremities. Less than 10% of IHs develop in the perineum.1 Perineal IHs are benign tumors of the vascular endothelium that present as plaques and commonly are accompanied by painful ulcerations. Ulceration is more common in the diaper area secondary to irritation from urine, stool, and friction.2 Although most IHs are benign isolated findings, facial IHs have been associated with several syndromes including Sturge-Weber and PHACE (posterior fossa brain malformations, hemangiomas, arterial anomalies, cardiac anomalies and coarctation of the aorta, and eye and endocrine abnormalities) syndromes.3 Researchers also have identified an association between lumbosacral IHs and spinal dysraphism (tethered spinal cord).4
A smaller number of studies have investigated congenital anomalies related to perineal IH,1,5 specifically PELVIS syndrome. The acronym PELVIS has been used to describe a syndrome of congenital malformations including perineal hemangioma, external genital malformations, lipomyelomeningocele, vesicorenal abnormalities, imperforate anus, and skin tag.1 An alternative description of similar findings is LUMBAR (lower body hemangioma and other cutaneous defects; urogenital anomalies, ulceration; myelopathy; bony deformities; anorectal malformations, arterial anomalies; and renal anomalies).5 Researchers have suggested that both of these acronyms describe the same syndrome, and it is common for the syndrome to be incomplete.6 One study (N=11) found that perineal hemangiomas are most commonly associated with anal malformations (8 patients), followed by urinary tract abnormalities (7 patients) and malformation of the external genitalia (7 patients). A skin tag was present in 5 patients.1 The pathogenesis of PELVIS syndrome is unknown.
When an infant presents with a perineal hemangioma and physical examination suggests PELVIS syndrome, imaging should be performed to evaluate for other anomalies. Before 4 months of age, ultrasound should be utilized to investigate the presence of reno-genitourinary or spinal malformations. Magnetic resonance imaging is the preferred imaging modality in children older than 4 months.7 Management of PELVIS syndrome requires a multidisciplinary approach and early recognition of the full extent of congenital malformations. Pediatric dermatologists, urologists, endocrinologists, and neonatologists have a role in its diagnosis and treatment.
- Girard C, Bigorre M, Guillot B, et al. PELVIS syndrome. Arch Dermatol. 2006;142:884-888.
- Bruckner AL, Frieden IJ. Hemangiomas of infancy. J Am Acad Dermatol. 2003;48:477-496.
- Frieden IJ, Reese V, Cohen D. PHACE syndrome: the association of posterior fossa brain malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, and eye abnormalities. Arch Dermatol. 1996;132:307-311.
- Albright AL, Gartner JC, Wiener ES. Lumbar cutaneous hemangiomas as indicators of tethered spinal cords. Pediatrics. 1989;83:977-980.
- Iacobas I, Burrows PE, Frieden IJ, et al. LUMBAR: association between cutaneous infantile hemangiomas of the lower body and regional congenital anomalies. J Pediatr. 2010;157:795-801.
- Frade FN, Kadlub V, Soupre S, et al. PELVIS or LUMBAR syndrome: the same entity. two case reports. Arch Pediatr. 2012;19:55-58.
- Berk DR, Bayliss SJ, Merritt DF. Management quandary: extensive perineal infantile hemangioma with associated congenital anomalies: an example of the PELVIS syndrome. J Pediatr Adolesc Gynecol. 2007;20:105-108.
The Diagnosis: PELVIS Syndrome
Infantile hemangiomas (IHs) are present in up to 10% of infants by 1 year of age and are most commonly located on the face and upper extremities. Less than 10% of IHs develop in the perineum.1 Perineal IHs are benign tumors of the vascular endothelium that present as plaques and commonly are accompanied by painful ulcerations. Ulceration is more common in the diaper area secondary to irritation from urine, stool, and friction.2 Although most IHs are benign isolated findings, facial IHs have been associated with several syndromes including Sturge-Weber and PHACE (posterior fossa brain malformations, hemangiomas, arterial anomalies, cardiac anomalies and coarctation of the aorta, and eye and endocrine abnormalities) syndromes.3 Researchers also have identified an association between lumbosacral IHs and spinal dysraphism (tethered spinal cord).4
A smaller number of studies have investigated congenital anomalies related to perineal IH,1,5 specifically PELVIS syndrome. The acronym PELVIS has been used to describe a syndrome of congenital malformations including perineal hemangioma, external genital malformations, lipomyelomeningocele, vesicorenal abnormalities, imperforate anus, and skin tag.1 An alternative description of similar findings is LUMBAR (lower body hemangioma and other cutaneous defects; urogenital anomalies, ulceration; myelopathy; bony deformities; anorectal malformations, arterial anomalies; and renal anomalies).5 Researchers have suggested that both of these acronyms describe the same syndrome, and it is common for the syndrome to be incomplete.6 One study (N=11) found that perineal hemangiomas are most commonly associated with anal malformations (8 patients), followed by urinary tract abnormalities (7 patients) and malformation of the external genitalia (7 patients). A skin tag was present in 5 patients.1 The pathogenesis of PELVIS syndrome is unknown.
When an infant presents with a perineal hemangioma and physical examination suggests PELVIS syndrome, imaging should be performed to evaluate for other anomalies. Before 4 months of age, ultrasound should be utilized to investigate the presence of reno-genitourinary or spinal malformations. Magnetic resonance imaging is the preferred imaging modality in children older than 4 months.7 Management of PELVIS syndrome requires a multidisciplinary approach and early recognition of the full extent of congenital malformations. Pediatric dermatologists, urologists, endocrinologists, and neonatologists have a role in its diagnosis and treatment.
The Diagnosis: PELVIS Syndrome
Infantile hemangiomas (IHs) are present in up to 10% of infants by 1 year of age and are most commonly located on the face and upper extremities. Less than 10% of IHs develop in the perineum.1 Perineal IHs are benign tumors of the vascular endothelium that present as plaques and commonly are accompanied by painful ulcerations. Ulceration is more common in the diaper area secondary to irritation from urine, stool, and friction.2 Although most IHs are benign isolated findings, facial IHs have been associated with several syndromes including Sturge-Weber and PHACE (posterior fossa brain malformations, hemangiomas, arterial anomalies, cardiac anomalies and coarctation of the aorta, and eye and endocrine abnormalities) syndromes.3 Researchers also have identified an association between lumbosacral IHs and spinal dysraphism (tethered spinal cord).4
A smaller number of studies have investigated congenital anomalies related to perineal IH,1,5 specifically PELVIS syndrome. The acronym PELVIS has been used to describe a syndrome of congenital malformations including perineal hemangioma, external genital malformations, lipomyelomeningocele, vesicorenal abnormalities, imperforate anus, and skin tag.1 An alternative description of similar findings is LUMBAR (lower body hemangioma and other cutaneous defects; urogenital anomalies, ulceration; myelopathy; bony deformities; anorectal malformations, arterial anomalies; and renal anomalies).5 Researchers have suggested that both of these acronyms describe the same syndrome, and it is common for the syndrome to be incomplete.6 One study (N=11) found that perineal hemangiomas are most commonly associated with anal malformations (8 patients), followed by urinary tract abnormalities (7 patients) and malformation of the external genitalia (7 patients). A skin tag was present in 5 patients.1 The pathogenesis of PELVIS syndrome is unknown.
When an infant presents with a perineal hemangioma and physical examination suggests PELVIS syndrome, imaging should be performed to evaluate for other anomalies. Before 4 months of age, ultrasound should be utilized to investigate the presence of reno-genitourinary or spinal malformations. Magnetic resonance imaging is the preferred imaging modality in children older than 4 months.7 Management of PELVIS syndrome requires a multidisciplinary approach and early recognition of the full extent of congenital malformations. Pediatric dermatologists, urologists, endocrinologists, and neonatologists have a role in its diagnosis and treatment.
- Girard C, Bigorre M, Guillot B, et al. PELVIS syndrome. Arch Dermatol. 2006;142:884-888.
- Bruckner AL, Frieden IJ. Hemangiomas of infancy. J Am Acad Dermatol. 2003;48:477-496.
- Frieden IJ, Reese V, Cohen D. PHACE syndrome: the association of posterior fossa brain malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, and eye abnormalities. Arch Dermatol. 1996;132:307-311.
- Albright AL, Gartner JC, Wiener ES. Lumbar cutaneous hemangiomas as indicators of tethered spinal cords. Pediatrics. 1989;83:977-980.
- Iacobas I, Burrows PE, Frieden IJ, et al. LUMBAR: association between cutaneous infantile hemangiomas of the lower body and regional congenital anomalies. J Pediatr. 2010;157:795-801.
- Frade FN, Kadlub V, Soupre S, et al. PELVIS or LUMBAR syndrome: the same entity. two case reports. Arch Pediatr. 2012;19:55-58.
- Berk DR, Bayliss SJ, Merritt DF. Management quandary: extensive perineal infantile hemangioma with associated congenital anomalies: an example of the PELVIS syndrome. J Pediatr Adolesc Gynecol. 2007;20:105-108.
- Girard C, Bigorre M, Guillot B, et al. PELVIS syndrome. Arch Dermatol. 2006;142:884-888.
- Bruckner AL, Frieden IJ. Hemangiomas of infancy. J Am Acad Dermatol. 2003;48:477-496.
- Frieden IJ, Reese V, Cohen D. PHACE syndrome: the association of posterior fossa brain malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, and eye abnormalities. Arch Dermatol. 1996;132:307-311.
- Albright AL, Gartner JC, Wiener ES. Lumbar cutaneous hemangiomas as indicators of tethered spinal cords. Pediatrics. 1989;83:977-980.
- Iacobas I, Burrows PE, Frieden IJ, et al. LUMBAR: association between cutaneous infantile hemangiomas of the lower body and regional congenital anomalies. J Pediatr. 2010;157:795-801.
- Frade FN, Kadlub V, Soupre S, et al. PELVIS or LUMBAR syndrome: the same entity. two case reports. Arch Pediatr. 2012;19:55-58.
- Berk DR, Bayliss SJ, Merritt DF. Management quandary: extensive perineal infantile hemangioma with associated congenital anomalies: an example of the PELVIS syndrome. J Pediatr Adolesc Gynecol. 2007;20:105-108.

A 7-week-old boy with ambiguous genitalia presented for evaluation of what the parents described as progressively worsening diaper rash. The patient was born at full-term after an uncomplicated gestation via normal spontaneous vaginal delivery. Examination of the external genitalia revealed microphallus with phimosis and a bifid scrotum. Two weeks after birth, the patient developed redness and painful ulcerations in the diaper area. At the time of presentation, the patient had bright red plaques along the suprapubic lines, inguinal creases, and in the perineal region. Physical examination also was notable for tender ulcerations of the inguinal creases and perineum and a perineal skin tag.

Disseminated Superficial Actinic Porokeratosis Treated With Ingenol Mebutate Gel 0.05%
Disseminated superficial actinic porokeratosis (DSAP) is a chronic condition characterized by numerous atrophic papules and patches with a distinctive peripheral keratotic ridge, typically found on sun-exposed areas.1,2 Treatment of DSAP is warranted not only for cosmetic and symptomatic benefits but also to prevent malignant transformation.3,4 Successful treatment of DSAP often is difficult and frequently requires the use of multiple modalities. Ingenol mebutate gel 0.05% is a topical medication primarily used for the treatment of actinic keratosis (AK) by inducing cell death.5 We report a case of DSAP treated effectively with ingenol mebutate gel 0.05%.
Case Report
A 37-year-old woman was referred to the dermatology department for counseling for pseudoxanthoma elasticum (PXE), which had been proven on biopsy by an outside dermatologist 2 years prior. Physical examination revealed yellow papules on the neck that were characteristic of PXE, but no lesions were noted on the arms or legs. The only other cutaneous finding was a soft nodule on the right hip consistent with a lipoma. The patient returned to our institution 6 years later with lesions on both lower legs. She reported that these lesions had been present for 3 years and were exacerbated by sun exposure. On physical examination, multiple scattered, erythematous, annular, scaling papules and plaques were noted on the bilateral legs. A biopsy showed the histopathologic findings of DSAP (Figure 1). The patient had no family history of DSAP or PXE.
To determine the best treatment modality, we treated 4 test areas on both upper and lower legs: one with trichloroacetic acid (TCA), one with cryotherapy, one with imiquimod cream 5%, and one with tretinoin cream 0.1%. The patient returned 4 weeks later and showed modest response to TCA, cryotherapy, and tretinoin cream. Because cryotherapy was determined to be most effective, 20 more lesions were frozen at that visit. Over the next 2 years, the patient was treated with TCA, imiquimod cream 5%, and tretinoin cream 0.1%, but all ultimately proved ineffective for DSAP.
The patient returned 2 years after treatment failure (age 47 years) and was prescribed ingenol mebutate gel 0.05% for 2 days over an area of 25 cm2 on the right lower leg (Figure 2A). She returned for follow-up at days 3, 15, 30, and 60. At day 3, the patient developed an inflammatory response to the medication with moderate erythema and scaling of individual lesions. No vesiculation, pustulation, edema, or ulceration was exhibited (Figure 2B). At day 30, there was a marked reduction in scaling with some postinflammatory erythema (Figure 2C). At day 60, much of the erythema had faded and the scale remained notably reduced (Figure 2D).
Comment
Disseminated superficial actinic porokeratosis is the most common subtype of porokeratosis, a keratinization disorder. There are 6 subtypes of porokeratosis identified in the literature: DSAP, disseminated superficial porokeratosis, classic porokeratosis of Mibelli, porokeratosis plantaris palmaris et disseminata, linear porokeratosis, and punctate porokeratosis.6 Disseminated superficial actinic porokeratosis has a female predominance (1.8:1 ratio)7 and generally appears in the third or fourth decades of life. Clonal proliferations of atypical keratinocytes have been implicated in the etiology of DSAP; however, the exact pathogenesis is unclear. Risk factors for DSAP include genetic susceptibility (eg, autosomal-dominant inheritance pattern), exposure to UV radiation, and drug-related immunosuppression or immunodeficiency.7 Other proposed etiologic risk factors include trauma and infection.8 Clinical diagnosis of DSAP is confirmed by the histological presence of a cornoid lamella (a thin column ofparakeratotic cells), a thinning epidermis, an absent or thinned granular cell layer, and a prominent dermal lymphocytic infiltrate.9,10
Disseminated superficial actinic porokeratosis clinically presents as small atrophic scaly papules and/or patches with raised peripheral ridges symmetrically dispersed on sun-exposed areas of the arms, legs, back, and shoulders. Although these lesions are extensive, they typically spare the mucous membranes, palms, and soles11; only a small percentage of cases report facial lesions,12 which often are asymptomatic but cosmetically bothersome. Additionally, approximately half of patients report symptoms of pruritus and/or stinging,13 thus treatment of DSAP is mainly indicated for symptomatic relief and cosmetic purposes. Malignant degeneration14,15 occurs in approximately 7.5% to 11% of porokeratosis cases,10,16 warranting treatment for preventative measures.
Management of DSAP is dependent on the extent of the disease and the level of concern for malignant transformation. Localized disease can be treated with cryotherapy, CO2 laser, and/or ablative techniques (eg, excision, curettage, dermabrasion) with variable degrees of success but high risk for scarring.1 More extensive disease requires treatment with topical retinoids, topical 5-fluorouracil, imiquimod cream 5%, diclofenac gel 3%, topical vitamin D3 analogues, and photodynamic therapy.1 Several other therapies have been reported in the literature with partial and/or complete success, including systemic retinoids (eg, acitretin), Q-switched ruby laser, Nd:YAG laser, fractional photothermolysis, Grenz rays, pulsed dye laser, fractional photothermolysis, topical corticosteroids, and fluor-hydroxy pulse peel.6 Although there is an extensive array of therapies for DSAP, treatment results are variable with mostly limited success. Successful treatment of DSAP is difficult and often requires the use of multiple modalities.
Ingenol mebutate is the active compound found in the sap of Euphorbia peplus used for the topical treatment of various skin conditions, including AKs.17 Ingenol mebutate gel 0.05% once daily for 2 days has been approved by the US Food and Drug Administration for the topical treatment of AKs. The mechanism of action of ingenol mebutate in AK therapy is not yet fully understood. In vivo and in vitro models have demonstrated both an induction of local lesion cell death and promotion of lesion-specific inflammatory response.18 When used in the treatment of AKs, ingenol mebutate gel 0.05% may cause a mild to moderate localized inflammatory response (eg, erythema, flaking/scaling, crusting, vesiculation/pustulation, erosion/ulceration, edema).
Our case is a rare report of successful treatment of DSAP with ingenol mebutate gel 0.05%. We found that treatment with ingenol mebutate gel 0.05% resulted in clinical improvement of DSAP lesions with minimal discomfort and good cosmetic response. This 2-day regimen is easy to use and patient friendly, improving medication compliance in such a cumbersome disease. We hope this case suggests that ingenol mebutate gel 0.05% could be a useful treatment alternative for DSAP, but future clinical studies should be conducted.
- Martin-Clavijo A, Kanelleas A, Vlachou C, et al. Porokeratoses. In: Lebwohl M, Heymann WR, Berth-Jones J, et al, eds. Treatment of Skin Disease Comprehensive Therapeutic Strategies. 3rd ed. China: Elsevier Limited; 2010:584-586.
- Rouhani P, Fischer M, Meehan S, et al. Disseminated superficial actinic porokeratosis. Dermatology Online J. 2012;18:24.
- Sasson M, Krain AD. Porokeratosis and cutaneous malignancy. a review. Dermatol Surg. 1996;22:339-342.
- Lee HR, Han TY, Son SJ, et al. Squamous cell carcinoma developing within lesions of disseminated superficial actinic porokeratosis. Ann Dermatol. 2011;23:536-538.
- Lebwohl M, Swanson N, Anderson LL, et al. Ingenol mebutate gel for actinic keratosis. N Engl J Med. 2012;366:1010-1019.
- O’Regan GM, Irvine AD. Porokeratosis. In: Goldsmith LA, Katz SI, Gilchrest BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill Professional; 2012:442-446.
- Sertznig P, von Felbert V, Megahed M. Porokeratosis: present concepts. J Eur Acad Dermatol Venereol. 2012;26:404-412.
- Brauer JA, Mandal R, Walters R, et al. Disseminated superficial porokeratosis. Dermatology Online J. 2010;16:20.
- Tallon B. Porokeratosis pathology. DermNet New Zealand website. http://www.dermnet.org.nz/pathology/porokeratosis-path.html. Updated December 2016. Accessed January 12, 2017.
- Skupsky H, Skupsky J, Goldenberg G. Disseminated superficial actinic porokeratosis: a treatment review [published online October 22, 2010]. J Dermatolog Treat. 2012;23:52-56.
- Spencer LV. Porokeratosis. UpToDate web site. https://eresources.library.mssm.edu:3285/contents/porokeratosis?source=search_result&search=porokeratosis&selectedTitle=1~22. Updated September 1, 2016. Accessed April 3, 2017.
- Sawyer R, Picou KA. Facial presentation of disseminated superficial actinic porokeratosis. Ear Nose Throat J. 1989;68:57-59.
- Schwarz T, Seiser A, Gschnait F. Disseminated superficial “actinic” porokeratosis. J Am Acad Dermatol. 1984;11(4, pt 2):724-730.
- Maubec E, Duvillard P, Margulis A, et al. Common skin cancers in porokeratosis. Br J Dermatol. 2005;152:1389-1391.
- Lee HR, Han TY, Son SJ, et al. Squamous cell carcinoma developing within lesions of disseminated superficial actinic porokeratosis [published online November 3, 2011]. Ann Dermatol. 2011;23:536-538.
- Kumari S, Mathur M. Disseminated superficial actinic porokeratosis. Nepal J Dermatol Venereol Leprol. 2010;9:22-24.
- Lebwohl M, Shumack S, Stein Gold L, et al. Long-term follow-up study of ingenol mebutate gel for the treatment of actinic keratosis. JAMA Dermatol. 2013;149:666-670.
- Stahlhut M, Bertelsen M, Hoyer-Hansen M, et al. Ingenol mebutate: induced cell death patterns in normal and cancer epithelial cells. J Drugs Dermatol. 2012;11:1181-1192.
Disseminated superficial actinic porokeratosis (DSAP) is a chronic condition characterized by numerous atrophic papules and patches with a distinctive peripheral keratotic ridge, typically found on sun-exposed areas.1,2 Treatment of DSAP is warranted not only for cosmetic and symptomatic benefits but also to prevent malignant transformation.3,4 Successful treatment of DSAP often is difficult and frequently requires the use of multiple modalities. Ingenol mebutate gel 0.05% is a topical medication primarily used for the treatment of actinic keratosis (AK) by inducing cell death.5 We report a case of DSAP treated effectively with ingenol mebutate gel 0.05%.
Case Report
A 37-year-old woman was referred to the dermatology department for counseling for pseudoxanthoma elasticum (PXE), which had been proven on biopsy by an outside dermatologist 2 years prior. Physical examination revealed yellow papules on the neck that were characteristic of PXE, but no lesions were noted on the arms or legs. The only other cutaneous finding was a soft nodule on the right hip consistent with a lipoma. The patient returned to our institution 6 years later with lesions on both lower legs. She reported that these lesions had been present for 3 years and were exacerbated by sun exposure. On physical examination, multiple scattered, erythematous, annular, scaling papules and plaques were noted on the bilateral legs. A biopsy showed the histopathologic findings of DSAP (Figure 1). The patient had no family history of DSAP or PXE.
To determine the best treatment modality, we treated 4 test areas on both upper and lower legs: one with trichloroacetic acid (TCA), one with cryotherapy, one with imiquimod cream 5%, and one with tretinoin cream 0.1%. The patient returned 4 weeks later and showed modest response to TCA, cryotherapy, and tretinoin cream. Because cryotherapy was determined to be most effective, 20 more lesions were frozen at that visit. Over the next 2 years, the patient was treated with TCA, imiquimod cream 5%, and tretinoin cream 0.1%, but all ultimately proved ineffective for DSAP.
The patient returned 2 years after treatment failure (age 47 years) and was prescribed ingenol mebutate gel 0.05% for 2 days over an area of 25 cm2 on the right lower leg (Figure 2A). She returned for follow-up at days 3, 15, 30, and 60. At day 3, the patient developed an inflammatory response to the medication with moderate erythema and scaling of individual lesions. No vesiculation, pustulation, edema, or ulceration was exhibited (Figure 2B). At day 30, there was a marked reduction in scaling with some postinflammatory erythema (Figure 2C). At day 60, much of the erythema had faded and the scale remained notably reduced (Figure 2D).
Comment
Disseminated superficial actinic porokeratosis is the most common subtype of porokeratosis, a keratinization disorder. There are 6 subtypes of porokeratosis identified in the literature: DSAP, disseminated superficial porokeratosis, classic porokeratosis of Mibelli, porokeratosis plantaris palmaris et disseminata, linear porokeratosis, and punctate porokeratosis.6 Disseminated superficial actinic porokeratosis has a female predominance (1.8:1 ratio)7 and generally appears in the third or fourth decades of life. Clonal proliferations of atypical keratinocytes have been implicated in the etiology of DSAP; however, the exact pathogenesis is unclear. Risk factors for DSAP include genetic susceptibility (eg, autosomal-dominant inheritance pattern), exposure to UV radiation, and drug-related immunosuppression or immunodeficiency.7 Other proposed etiologic risk factors include trauma and infection.8 Clinical diagnosis of DSAP is confirmed by the histological presence of a cornoid lamella (a thin column ofparakeratotic cells), a thinning epidermis, an absent or thinned granular cell layer, and a prominent dermal lymphocytic infiltrate.9,10
Disseminated superficial actinic porokeratosis clinically presents as small atrophic scaly papules and/or patches with raised peripheral ridges symmetrically dispersed on sun-exposed areas of the arms, legs, back, and shoulders. Although these lesions are extensive, they typically spare the mucous membranes, palms, and soles11; only a small percentage of cases report facial lesions,12 which often are asymptomatic but cosmetically bothersome. Additionally, approximately half of patients report symptoms of pruritus and/or stinging,13 thus treatment of DSAP is mainly indicated for symptomatic relief and cosmetic purposes. Malignant degeneration14,15 occurs in approximately 7.5% to 11% of porokeratosis cases,10,16 warranting treatment for preventative measures.
Management of DSAP is dependent on the extent of the disease and the level of concern for malignant transformation. Localized disease can be treated with cryotherapy, CO2 laser, and/or ablative techniques (eg, excision, curettage, dermabrasion) with variable degrees of success but high risk for scarring.1 More extensive disease requires treatment with topical retinoids, topical 5-fluorouracil, imiquimod cream 5%, diclofenac gel 3%, topical vitamin D3 analogues, and photodynamic therapy.1 Several other therapies have been reported in the literature with partial and/or complete success, including systemic retinoids (eg, acitretin), Q-switched ruby laser, Nd:YAG laser, fractional photothermolysis, Grenz rays, pulsed dye laser, fractional photothermolysis, topical corticosteroids, and fluor-hydroxy pulse peel.6 Although there is an extensive array of therapies for DSAP, treatment results are variable with mostly limited success. Successful treatment of DSAP is difficult and often requires the use of multiple modalities.
Ingenol mebutate is the active compound found in the sap of Euphorbia peplus used for the topical treatment of various skin conditions, including AKs.17 Ingenol mebutate gel 0.05% once daily for 2 days has been approved by the US Food and Drug Administration for the topical treatment of AKs. The mechanism of action of ingenol mebutate in AK therapy is not yet fully understood. In vivo and in vitro models have demonstrated both an induction of local lesion cell death and promotion of lesion-specific inflammatory response.18 When used in the treatment of AKs, ingenol mebutate gel 0.05% may cause a mild to moderate localized inflammatory response (eg, erythema, flaking/scaling, crusting, vesiculation/pustulation, erosion/ulceration, edema).
Our case is a rare report of successful treatment of DSAP with ingenol mebutate gel 0.05%. We found that treatment with ingenol mebutate gel 0.05% resulted in clinical improvement of DSAP lesions with minimal discomfort and good cosmetic response. This 2-day regimen is easy to use and patient friendly, improving medication compliance in such a cumbersome disease. We hope this case suggests that ingenol mebutate gel 0.05% could be a useful treatment alternative for DSAP, but future clinical studies should be conducted.
Disseminated superficial actinic porokeratosis (DSAP) is a chronic condition characterized by numerous atrophic papules and patches with a distinctive peripheral keratotic ridge, typically found on sun-exposed areas.1,2 Treatment of DSAP is warranted not only for cosmetic and symptomatic benefits but also to prevent malignant transformation.3,4 Successful treatment of DSAP often is difficult and frequently requires the use of multiple modalities. Ingenol mebutate gel 0.05% is a topical medication primarily used for the treatment of actinic keratosis (AK) by inducing cell death.5 We report a case of DSAP treated effectively with ingenol mebutate gel 0.05%.
Case Report
A 37-year-old woman was referred to the dermatology department for counseling for pseudoxanthoma elasticum (PXE), which had been proven on biopsy by an outside dermatologist 2 years prior. Physical examination revealed yellow papules on the neck that were characteristic of PXE, but no lesions were noted on the arms or legs. The only other cutaneous finding was a soft nodule on the right hip consistent with a lipoma. The patient returned to our institution 6 years later with lesions on both lower legs. She reported that these lesions had been present for 3 years and were exacerbated by sun exposure. On physical examination, multiple scattered, erythematous, annular, scaling papules and plaques were noted on the bilateral legs. A biopsy showed the histopathologic findings of DSAP (Figure 1). The patient had no family history of DSAP or PXE.
To determine the best treatment modality, we treated 4 test areas on both upper and lower legs: one with trichloroacetic acid (TCA), one with cryotherapy, one with imiquimod cream 5%, and one with tretinoin cream 0.1%. The patient returned 4 weeks later and showed modest response to TCA, cryotherapy, and tretinoin cream. Because cryotherapy was determined to be most effective, 20 more lesions were frozen at that visit. Over the next 2 years, the patient was treated with TCA, imiquimod cream 5%, and tretinoin cream 0.1%, but all ultimately proved ineffective for DSAP.
The patient returned 2 years after treatment failure (age 47 years) and was prescribed ingenol mebutate gel 0.05% for 2 days over an area of 25 cm2 on the right lower leg (Figure 2A). She returned for follow-up at days 3, 15, 30, and 60. At day 3, the patient developed an inflammatory response to the medication with moderate erythema and scaling of individual lesions. No vesiculation, pustulation, edema, or ulceration was exhibited (Figure 2B). At day 30, there was a marked reduction in scaling with some postinflammatory erythema (Figure 2C). At day 60, much of the erythema had faded and the scale remained notably reduced (Figure 2D).
Comment
Disseminated superficial actinic porokeratosis is the most common subtype of porokeratosis, a keratinization disorder. There are 6 subtypes of porokeratosis identified in the literature: DSAP, disseminated superficial porokeratosis, classic porokeratosis of Mibelli, porokeratosis plantaris palmaris et disseminata, linear porokeratosis, and punctate porokeratosis.6 Disseminated superficial actinic porokeratosis has a female predominance (1.8:1 ratio)7 and generally appears in the third or fourth decades of life. Clonal proliferations of atypical keratinocytes have been implicated in the etiology of DSAP; however, the exact pathogenesis is unclear. Risk factors for DSAP include genetic susceptibility (eg, autosomal-dominant inheritance pattern), exposure to UV radiation, and drug-related immunosuppression or immunodeficiency.7 Other proposed etiologic risk factors include trauma and infection.8 Clinical diagnosis of DSAP is confirmed by the histological presence of a cornoid lamella (a thin column ofparakeratotic cells), a thinning epidermis, an absent or thinned granular cell layer, and a prominent dermal lymphocytic infiltrate.9,10
Disseminated superficial actinic porokeratosis clinically presents as small atrophic scaly papules and/or patches with raised peripheral ridges symmetrically dispersed on sun-exposed areas of the arms, legs, back, and shoulders. Although these lesions are extensive, they typically spare the mucous membranes, palms, and soles11; only a small percentage of cases report facial lesions,12 which often are asymptomatic but cosmetically bothersome. Additionally, approximately half of patients report symptoms of pruritus and/or stinging,13 thus treatment of DSAP is mainly indicated for symptomatic relief and cosmetic purposes. Malignant degeneration14,15 occurs in approximately 7.5% to 11% of porokeratosis cases,10,16 warranting treatment for preventative measures.
Management of DSAP is dependent on the extent of the disease and the level of concern for malignant transformation. Localized disease can be treated with cryotherapy, CO2 laser, and/or ablative techniques (eg, excision, curettage, dermabrasion) with variable degrees of success but high risk for scarring.1 More extensive disease requires treatment with topical retinoids, topical 5-fluorouracil, imiquimod cream 5%, diclofenac gel 3%, topical vitamin D3 analogues, and photodynamic therapy.1 Several other therapies have been reported in the literature with partial and/or complete success, including systemic retinoids (eg, acitretin), Q-switched ruby laser, Nd:YAG laser, fractional photothermolysis, Grenz rays, pulsed dye laser, fractional photothermolysis, topical corticosteroids, and fluor-hydroxy pulse peel.6 Although there is an extensive array of therapies for DSAP, treatment results are variable with mostly limited success. Successful treatment of DSAP is difficult and often requires the use of multiple modalities.
Ingenol mebutate is the active compound found in the sap of Euphorbia peplus used for the topical treatment of various skin conditions, including AKs.17 Ingenol mebutate gel 0.05% once daily for 2 days has been approved by the US Food and Drug Administration for the topical treatment of AKs. The mechanism of action of ingenol mebutate in AK therapy is not yet fully understood. In vivo and in vitro models have demonstrated both an induction of local lesion cell death and promotion of lesion-specific inflammatory response.18 When used in the treatment of AKs, ingenol mebutate gel 0.05% may cause a mild to moderate localized inflammatory response (eg, erythema, flaking/scaling, crusting, vesiculation/pustulation, erosion/ulceration, edema).
Our case is a rare report of successful treatment of DSAP with ingenol mebutate gel 0.05%. We found that treatment with ingenol mebutate gel 0.05% resulted in clinical improvement of DSAP lesions with minimal discomfort and good cosmetic response. This 2-day regimen is easy to use and patient friendly, improving medication compliance in such a cumbersome disease. We hope this case suggests that ingenol mebutate gel 0.05% could be a useful treatment alternative for DSAP, but future clinical studies should be conducted.
- Martin-Clavijo A, Kanelleas A, Vlachou C, et al. Porokeratoses. In: Lebwohl M, Heymann WR, Berth-Jones J, et al, eds. Treatment of Skin Disease Comprehensive Therapeutic Strategies. 3rd ed. China: Elsevier Limited; 2010:584-586.
- Rouhani P, Fischer M, Meehan S, et al. Disseminated superficial actinic porokeratosis. Dermatology Online J. 2012;18:24.
- Sasson M, Krain AD. Porokeratosis and cutaneous malignancy. a review. Dermatol Surg. 1996;22:339-342.
- Lee HR, Han TY, Son SJ, et al. Squamous cell carcinoma developing within lesions of disseminated superficial actinic porokeratosis. Ann Dermatol. 2011;23:536-538.
- Lebwohl M, Swanson N, Anderson LL, et al. Ingenol mebutate gel for actinic keratosis. N Engl J Med. 2012;366:1010-1019.
- O’Regan GM, Irvine AD. Porokeratosis. In: Goldsmith LA, Katz SI, Gilchrest BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill Professional; 2012:442-446.
- Sertznig P, von Felbert V, Megahed M. Porokeratosis: present concepts. J Eur Acad Dermatol Venereol. 2012;26:404-412.
- Brauer JA, Mandal R, Walters R, et al. Disseminated superficial porokeratosis. Dermatology Online J. 2010;16:20.
- Tallon B. Porokeratosis pathology. DermNet New Zealand website. http://www.dermnet.org.nz/pathology/porokeratosis-path.html. Updated December 2016. Accessed January 12, 2017.
- Skupsky H, Skupsky J, Goldenberg G. Disseminated superficial actinic porokeratosis: a treatment review [published online October 22, 2010]. J Dermatolog Treat. 2012;23:52-56.
- Spencer LV. Porokeratosis. UpToDate web site. https://eresources.library.mssm.edu:3285/contents/porokeratosis?source=search_result&search=porokeratosis&selectedTitle=1~22. Updated September 1, 2016. Accessed April 3, 2017.
- Sawyer R, Picou KA. Facial presentation of disseminated superficial actinic porokeratosis. Ear Nose Throat J. 1989;68:57-59.
- Schwarz T, Seiser A, Gschnait F. Disseminated superficial “actinic” porokeratosis. J Am Acad Dermatol. 1984;11(4, pt 2):724-730.
- Maubec E, Duvillard P, Margulis A, et al. Common skin cancers in porokeratosis. Br J Dermatol. 2005;152:1389-1391.
- Lee HR, Han TY, Son SJ, et al. Squamous cell carcinoma developing within lesions of disseminated superficial actinic porokeratosis [published online November 3, 2011]. Ann Dermatol. 2011;23:536-538.
- Kumari S, Mathur M. Disseminated superficial actinic porokeratosis. Nepal J Dermatol Venereol Leprol. 2010;9:22-24.
- Lebwohl M, Shumack S, Stein Gold L, et al. Long-term follow-up study of ingenol mebutate gel for the treatment of actinic keratosis. JAMA Dermatol. 2013;149:666-670.
- Stahlhut M, Bertelsen M, Hoyer-Hansen M, et al. Ingenol mebutate: induced cell death patterns in normal and cancer epithelial cells. J Drugs Dermatol. 2012;11:1181-1192.
- Martin-Clavijo A, Kanelleas A, Vlachou C, et al. Porokeratoses. In: Lebwohl M, Heymann WR, Berth-Jones J, et al, eds. Treatment of Skin Disease Comprehensive Therapeutic Strategies. 3rd ed. China: Elsevier Limited; 2010:584-586.
- Rouhani P, Fischer M, Meehan S, et al. Disseminated superficial actinic porokeratosis. Dermatology Online J. 2012;18:24.
- Sasson M, Krain AD. Porokeratosis and cutaneous malignancy. a review. Dermatol Surg. 1996;22:339-342.
- Lee HR, Han TY, Son SJ, et al. Squamous cell carcinoma developing within lesions of disseminated superficial actinic porokeratosis. Ann Dermatol. 2011;23:536-538.
- Lebwohl M, Swanson N, Anderson LL, et al. Ingenol mebutate gel for actinic keratosis. N Engl J Med. 2012;366:1010-1019.
- O’Regan GM, Irvine AD. Porokeratosis. In: Goldsmith LA, Katz SI, Gilchrest BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill Professional; 2012:442-446.
- Sertznig P, von Felbert V, Megahed M. Porokeratosis: present concepts. J Eur Acad Dermatol Venereol. 2012;26:404-412.
- Brauer JA, Mandal R, Walters R, et al. Disseminated superficial porokeratosis. Dermatology Online J. 2010;16:20.
- Tallon B. Porokeratosis pathology. DermNet New Zealand website. http://www.dermnet.org.nz/pathology/porokeratosis-path.html. Updated December 2016. Accessed January 12, 2017.
- Skupsky H, Skupsky J, Goldenberg G. Disseminated superficial actinic porokeratosis: a treatment review [published online October 22, 2010]. J Dermatolog Treat. 2012;23:52-56.
- Spencer LV. Porokeratosis. UpToDate web site. https://eresources.library.mssm.edu:3285/contents/porokeratosis?source=search_result&search=porokeratosis&selectedTitle=1~22. Updated September 1, 2016. Accessed April 3, 2017.
- Sawyer R, Picou KA. Facial presentation of disseminated superficial actinic porokeratosis. Ear Nose Throat J. 1989;68:57-59.
- Schwarz T, Seiser A, Gschnait F. Disseminated superficial “actinic” porokeratosis. J Am Acad Dermatol. 1984;11(4, pt 2):724-730.
- Maubec E, Duvillard P, Margulis A, et al. Common skin cancers in porokeratosis. Br J Dermatol. 2005;152:1389-1391.
- Lee HR, Han TY, Son SJ, et al. Squamous cell carcinoma developing within lesions of disseminated superficial actinic porokeratosis [published online November 3, 2011]. Ann Dermatol. 2011;23:536-538.
- Kumari S, Mathur M. Disseminated superficial actinic porokeratosis. Nepal J Dermatol Venereol Leprol. 2010;9:22-24.
- Lebwohl M, Shumack S, Stein Gold L, et al. Long-term follow-up study of ingenol mebutate gel for the treatment of actinic keratosis. JAMA Dermatol. 2013;149:666-670.
- Stahlhut M, Bertelsen M, Hoyer-Hansen M, et al. Ingenol mebutate: induced cell death patterns in normal and cancer epithelial cells. J Drugs Dermatol. 2012;11:1181-1192.
Practice Points
- Disseminated superficial actinic porokeratosis (DSAP) is an uncommon skin condition consisting of multiple annular hyperkeratotic lesions on sun-exposed areas.
- Treatment of DSAP is necessary due to its potential for progression to malignancy.
- Consider ingenol mebutate gel 0.05% for the treatment of DSAP on the arms and legs.

MAGNIFY in relapsed/refractory mantle cell lymphoma
MAGNIFY is a phase IIIB randomized trial actively recruiting patients with relapsed/refractory mantle cell lymphoma, based on studies posted at ClinicalTrials.gov.
MAGNIFY (NCT01996865) is a study of lenalidomide (CC-5013) plus rituximab maintenance therapy, followed by lenalidomide single-agent maintenance therapy, versus rituximab. Sponsored by Celgene, the maker of lenalidomide (Revlimid), the trial’s primary outcome measure is progression-free survival at up to 8 years.
The MAGNIFY trial includes patients with grades 1-3b or transformed follicular lymphoma, marginal zone lymphoma, or mantle cell lymphoma who had received at least one prior therapy and had stage I-IV measurable disease. About 500 patients are planned to enroll in 12 cycles of R2 induction, and slightly more than 300 patients are projected to be randomized after induction to the two maintenance arms. Induction includes oral lenalidomide 20 mg/day, days 1-21 per 28-day cycle; plus intravenous rituximab 375 mg/m2 on days 1, 8, 15, and 22 of cycle 1 and day 1 of cycles 3, 5, 7, 9, and 11 (28-day cycles).
Patients will then be randomized to maintenance lenalidomide 10 mg/day, given on days 1-21 per 28-day cycle for cycles 13-30; plus rituximab 375 mg/m2, given on day 1 of cycles 13, 15, 17, 19, 21, 23, 25, 27, and 29 (R2, Arm A), or rituximab alone (same schedule, Arm B). Patients receiving R2 maintenance after 18 cycles may continue maintenance lenalidomide monotherapy at 10 mg/day, days 1-21 per 28-day cycle, at the discretion of the patient and/or investigator, until disease progression as tolerated.
The primary endpoint is progression-free survival. Secondary endpoints include safety, overall survival, response rates, duration of response, and quality of life. Patients will be followed for at least 5 years after the last patient-initiated induction therapy. Enrollment in MAGNIFY began in March 2014; as of January 2016, 133 patients are enrolled, according to the study page at ClinicalTrials.gov.
MAGNIFY is a phase IIIB randomized trial actively recruiting patients with relapsed/refractory mantle cell lymphoma, based on studies posted at ClinicalTrials.gov.
MAGNIFY (NCT01996865) is a study of lenalidomide (CC-5013) plus rituximab maintenance therapy, followed by lenalidomide single-agent maintenance therapy, versus rituximab. Sponsored by Celgene, the maker of lenalidomide (Revlimid), the trial’s primary outcome measure is progression-free survival at up to 8 years.
The MAGNIFY trial includes patients with grades 1-3b or transformed follicular lymphoma, marginal zone lymphoma, or mantle cell lymphoma who had received at least one prior therapy and had stage I-IV measurable disease. About 500 patients are planned to enroll in 12 cycles of R2 induction, and slightly more than 300 patients are projected to be randomized after induction to the two maintenance arms. Induction includes oral lenalidomide 20 mg/day, days 1-21 per 28-day cycle; plus intravenous rituximab 375 mg/m2 on days 1, 8, 15, and 22 of cycle 1 and day 1 of cycles 3, 5, 7, 9, and 11 (28-day cycles).
Patients will then be randomized to maintenance lenalidomide 10 mg/day, given on days 1-21 per 28-day cycle for cycles 13-30; plus rituximab 375 mg/m2, given on day 1 of cycles 13, 15, 17, 19, 21, 23, 25, 27, and 29 (R2, Arm A), or rituximab alone (same schedule, Arm B). Patients receiving R2 maintenance after 18 cycles may continue maintenance lenalidomide monotherapy at 10 mg/day, days 1-21 per 28-day cycle, at the discretion of the patient and/or investigator, until disease progression as tolerated.
The primary endpoint is progression-free survival. Secondary endpoints include safety, overall survival, response rates, duration of response, and quality of life. Patients will be followed for at least 5 years after the last patient-initiated induction therapy. Enrollment in MAGNIFY began in March 2014; as of January 2016, 133 patients are enrolled, according to the study page at ClinicalTrials.gov.
MAGNIFY is a phase IIIB randomized trial actively recruiting patients with relapsed/refractory mantle cell lymphoma, based on studies posted at ClinicalTrials.gov.
MAGNIFY (NCT01996865) is a study of lenalidomide (CC-5013) plus rituximab maintenance therapy, followed by lenalidomide single-agent maintenance therapy, versus rituximab. Sponsored by Celgene, the maker of lenalidomide (Revlimid), the trial’s primary outcome measure is progression-free survival at up to 8 years.
The MAGNIFY trial includes patients with grades 1-3b or transformed follicular lymphoma, marginal zone lymphoma, or mantle cell lymphoma who had received at least one prior therapy and had stage I-IV measurable disease. About 500 patients are planned to enroll in 12 cycles of R2 induction, and slightly more than 300 patients are projected to be randomized after induction to the two maintenance arms. Induction includes oral lenalidomide 20 mg/day, days 1-21 per 28-day cycle; plus intravenous rituximab 375 mg/m2 on days 1, 8, 15, and 22 of cycle 1 and day 1 of cycles 3, 5, 7, 9, and 11 (28-day cycles).
Patients will then be randomized to maintenance lenalidomide 10 mg/day, given on days 1-21 per 28-day cycle for cycles 13-30; plus rituximab 375 mg/m2, given on day 1 of cycles 13, 15, 17, 19, 21, 23, 25, 27, and 29 (R2, Arm A), or rituximab alone (same schedule, Arm B). Patients receiving R2 maintenance after 18 cycles may continue maintenance lenalidomide monotherapy at 10 mg/day, days 1-21 per 28-day cycle, at the discretion of the patient and/or investigator, until disease progression as tolerated.
The primary endpoint is progression-free survival. Secondary endpoints include safety, overall survival, response rates, duration of response, and quality of life. Patients will be followed for at least 5 years after the last patient-initiated induction therapy. Enrollment in MAGNIFY began in March 2014; as of January 2016, 133 patients are enrolled, according to the study page at ClinicalTrials.gov.
Neoadjuvant chemoradiation may give transplant the edge over resection in biliary cancer
MIAMI BEACH – Survival for patients with hilar cholangiocarcinoma was similar between those who underwent transplantation and those who underwent resection, but neoadjuvant therapy may give transplant strategy the edge, findings of a study and meta-analysis suggest.
“Neoadjuvant chemoradiation therapy is clearly a factor that affects patient survival, and may be the only reason the patients who received transplantation had better overall survival than [did those who had] resection,” Michele Gage, MD, a general surgeon at Johns Hopkins Medicine in Baltimore, said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
“We found survival in the group that received neoadjuvant chemoradiation therapy and transplant had a statistically significantly better outcome compared to a control group of resection,” Dr. Gage said. More importantly, patients who received a transplant without neoadjuvant therapy had a statistically significant worse outcome than patients who got resection alone.”
The investigators noted that patient selection for neoadjuvant therapy might also be a factor contributing to superior overall survival. In a multicenter study of 147 patients undergoing liver transplantation for hilar cholangiocarcinoma, a subgroup of patients who met the selection criteria of the Mayo Clinic protocol but had not undergone neoadjuvant therapy had a 59% 5-year survival rate (PLoS One. 2016:11:e0156127).
Study discussant Maria B. Majella Doyle, MD, a general surgeon at Washington University in St. Louis, agreed that patient selection for transplantation is a likely factor.
Dr. Doyle then asked Dr. Gage how she accounts for the heterogeneity among studies performed over a 20-year period.
“That is why we did subgroup analysis of neoadjuvant versus no neoadjuvant therapy,” Dr. Gage replied.
In the future, an intent-to-treat analysis might be more accurate, Dr. Majella Doyle said, because more patients are placed on a liver transplant list than typically have the procedure.
Dr. Gage noted that 28%-48% of patients started on neoadjuvant therapy in the two studies that offered both neoadjuvant therapy and a transplant in the meta-analysis never made it to transplantation. When they were included, overall survival dropped to approximately 35% in one study and 44% in the other.
In the primary meta-analysis (before the subanalysis looking at neoadjuvant therapy), 398 patients underwent resection and another 200 underwent liver transplantation between 1996 and 2106. Patient demographics were similar between groups, including more men than women, except the average age in the resection group was older, Dr. Gage said.
Overall survival favored the transplant group at each time point: 78% versus 70% with resection at 1 year; 56% versus 42% at 3 years; and 46% versus 29% at 5 years. The odds ratios, respectively, were 1.27, 1.49 and 1.83, but the findings were not statistically significant at a 95% confidence interval.
Margin involvement was 9% in the transplant patients versus 32% in the resection patients, Dr. Gage said. The best chance of cure is R0 resection, but half of patients with hilar cholangiocarcinoma, the most common cancer of the biliary tract, are unresectable, she added.
Six of the nine studies in the meta-analysis reported margin status. Of the 344 patients in these studies, 79% achieved R0 status overall.
“The goal of treatment is R0 resection,” Dr. Gage said in response to a question about when neoadjuvant therapy is warranted. “In the patients who are resectable, I think the correct answer would be to proceed with resection. However, for those patients who are borderline resectable, it would be reasonable to consider neoadjuvant therapy.”
“One of the major things that is undervalued is neoadjuvant therapy allows better patient selection,” said session moderator Eric Jensen, MD, FACS, of University of Minnesota Health in Minneapolis. “When you say an obviously resectable tumor, when you look at the data – we’re wrong 30% of the time. So I’m in favor of neoadjuvant therapy for everybody, but that is just my bias.”
The small number of studies is a limitation of the study, Dr. Gage said. Also, all the studies were nonrandomized and retrospective, and some research spanned many years, which could introduce bias because of changes in practice over time, she added.
Based on their findings, the investigators proposed that future studies explore routine administration of neoadjuvant therapy prior to resection.
Dr. Gage and Dr. Majella Doyle had no relevant financial disclosures.
MIAMI BEACH – Survival for patients with hilar cholangiocarcinoma was similar between those who underwent transplantation and those who underwent resection, but neoadjuvant therapy may give transplant strategy the edge, findings of a study and meta-analysis suggest.
“Neoadjuvant chemoradiation therapy is clearly a factor that affects patient survival, and may be the only reason the patients who received transplantation had better overall survival than [did those who had] resection,” Michele Gage, MD, a general surgeon at Johns Hopkins Medicine in Baltimore, said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
“We found survival in the group that received neoadjuvant chemoradiation therapy and transplant had a statistically significantly better outcome compared to a control group of resection,” Dr. Gage said. More importantly, patients who received a transplant without neoadjuvant therapy had a statistically significant worse outcome than patients who got resection alone.”
The investigators noted that patient selection for neoadjuvant therapy might also be a factor contributing to superior overall survival. In a multicenter study of 147 patients undergoing liver transplantation for hilar cholangiocarcinoma, a subgroup of patients who met the selection criteria of the Mayo Clinic protocol but had not undergone neoadjuvant therapy had a 59% 5-year survival rate (PLoS One. 2016:11:e0156127).
Study discussant Maria B. Majella Doyle, MD, a general surgeon at Washington University in St. Louis, agreed that patient selection for transplantation is a likely factor.
Dr. Doyle then asked Dr. Gage how she accounts for the heterogeneity among studies performed over a 20-year period.
“That is why we did subgroup analysis of neoadjuvant versus no neoadjuvant therapy,” Dr. Gage replied.
In the future, an intent-to-treat analysis might be more accurate, Dr. Majella Doyle said, because more patients are placed on a liver transplant list than typically have the procedure.
Dr. Gage noted that 28%-48% of patients started on neoadjuvant therapy in the two studies that offered both neoadjuvant therapy and a transplant in the meta-analysis never made it to transplantation. When they were included, overall survival dropped to approximately 35% in one study and 44% in the other.
In the primary meta-analysis (before the subanalysis looking at neoadjuvant therapy), 398 patients underwent resection and another 200 underwent liver transplantation between 1996 and 2106. Patient demographics were similar between groups, including more men than women, except the average age in the resection group was older, Dr. Gage said.
Overall survival favored the transplant group at each time point: 78% versus 70% with resection at 1 year; 56% versus 42% at 3 years; and 46% versus 29% at 5 years. The odds ratios, respectively, were 1.27, 1.49 and 1.83, but the findings were not statistically significant at a 95% confidence interval.
Margin involvement was 9% in the transplant patients versus 32% in the resection patients, Dr. Gage said. The best chance of cure is R0 resection, but half of patients with hilar cholangiocarcinoma, the most common cancer of the biliary tract, are unresectable, she added.
Six of the nine studies in the meta-analysis reported margin status. Of the 344 patients in these studies, 79% achieved R0 status overall.
“The goal of treatment is R0 resection,” Dr. Gage said in response to a question about when neoadjuvant therapy is warranted. “In the patients who are resectable, I think the correct answer would be to proceed with resection. However, for those patients who are borderline resectable, it would be reasonable to consider neoadjuvant therapy.”
“One of the major things that is undervalued is neoadjuvant therapy allows better patient selection,” said session moderator Eric Jensen, MD, FACS, of University of Minnesota Health in Minneapolis. “When you say an obviously resectable tumor, when you look at the data – we’re wrong 30% of the time. So I’m in favor of neoadjuvant therapy for everybody, but that is just my bias.”
The small number of studies is a limitation of the study, Dr. Gage said. Also, all the studies were nonrandomized and retrospective, and some research spanned many years, which could introduce bias because of changes in practice over time, she added.
Based on their findings, the investigators proposed that future studies explore routine administration of neoadjuvant therapy prior to resection.
Dr. Gage and Dr. Majella Doyle had no relevant financial disclosures.
MIAMI BEACH – Survival for patients with hilar cholangiocarcinoma was similar between those who underwent transplantation and those who underwent resection, but neoadjuvant therapy may give transplant strategy the edge, findings of a study and meta-analysis suggest.
“Neoadjuvant chemoradiation therapy is clearly a factor that affects patient survival, and may be the only reason the patients who received transplantation had better overall survival than [did those who had] resection,” Michele Gage, MD, a general surgeon at Johns Hopkins Medicine in Baltimore, said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
“We found survival in the group that received neoadjuvant chemoradiation therapy and transplant had a statistically significantly better outcome compared to a control group of resection,” Dr. Gage said. More importantly, patients who received a transplant without neoadjuvant therapy had a statistically significant worse outcome than patients who got resection alone.”
The investigators noted that patient selection for neoadjuvant therapy might also be a factor contributing to superior overall survival. In a multicenter study of 147 patients undergoing liver transplantation for hilar cholangiocarcinoma, a subgroup of patients who met the selection criteria of the Mayo Clinic protocol but had not undergone neoadjuvant therapy had a 59% 5-year survival rate (PLoS One. 2016:11:e0156127).
Study discussant Maria B. Majella Doyle, MD, a general surgeon at Washington University in St. Louis, agreed that patient selection for transplantation is a likely factor.
Dr. Doyle then asked Dr. Gage how she accounts for the heterogeneity among studies performed over a 20-year period.
“That is why we did subgroup analysis of neoadjuvant versus no neoadjuvant therapy,” Dr. Gage replied.
In the future, an intent-to-treat analysis might be more accurate, Dr. Majella Doyle said, because more patients are placed on a liver transplant list than typically have the procedure.
Dr. Gage noted that 28%-48% of patients started on neoadjuvant therapy in the two studies that offered both neoadjuvant therapy and a transplant in the meta-analysis never made it to transplantation. When they were included, overall survival dropped to approximately 35% in one study and 44% in the other.
In the primary meta-analysis (before the subanalysis looking at neoadjuvant therapy), 398 patients underwent resection and another 200 underwent liver transplantation between 1996 and 2106. Patient demographics were similar between groups, including more men than women, except the average age in the resection group was older, Dr. Gage said.
Overall survival favored the transplant group at each time point: 78% versus 70% with resection at 1 year; 56% versus 42% at 3 years; and 46% versus 29% at 5 years. The odds ratios, respectively, were 1.27, 1.49 and 1.83, but the findings were not statistically significant at a 95% confidence interval.
Margin involvement was 9% in the transplant patients versus 32% in the resection patients, Dr. Gage said. The best chance of cure is R0 resection, but half of patients with hilar cholangiocarcinoma, the most common cancer of the biliary tract, are unresectable, she added.
Six of the nine studies in the meta-analysis reported margin status. Of the 344 patients in these studies, 79% achieved R0 status overall.
“The goal of treatment is R0 resection,” Dr. Gage said in response to a question about when neoadjuvant therapy is warranted. “In the patients who are resectable, I think the correct answer would be to proceed with resection. However, for those patients who are borderline resectable, it would be reasonable to consider neoadjuvant therapy.”
“One of the major things that is undervalued is neoadjuvant therapy allows better patient selection,” said session moderator Eric Jensen, MD, FACS, of University of Minnesota Health in Minneapolis. “When you say an obviously resectable tumor, when you look at the data – we’re wrong 30% of the time. So I’m in favor of neoadjuvant therapy for everybody, but that is just my bias.”
The small number of studies is a limitation of the study, Dr. Gage said. Also, all the studies were nonrandomized and retrospective, and some research spanned many years, which could introduce bias because of changes in practice over time, she added.
Based on their findings, the investigators proposed that future studies explore routine administration of neoadjuvant therapy prior to resection.
Dr. Gage and Dr. Majella Doyle had no relevant financial disclosures.
AT AHPBA 2017