User login
MicroRNAs linked to treatment response in lupus nephritis
MELBOURNE – Researchers have identified six microRNAs that may indicate a better likelihood of response to cyclophosphamide in patients with lupus nephritis, according to a study presented at an international conference on systemic lupus erythematosus.
“MicroRNA has been shown to be important in systemic lupus in several studies, and they’ve identified several microRNA that have been shown to affect the outcome measures in patients,” said Sarfaraz Hasni, MD, director of the Lupus Clinical Research Program at the National Institute of Arthritis and Musculoskeletal and Skin Diseases in Bethesda, Md., who presented a poster on the study at the meeting.

The aim of this study, involving 71 patients with lupus nephritis, was to look for microRNAs associated with treatment response to cyclophosphamide.
The first stage of the study involved isolating microRNAs from kidney biopsies taken from a first cohort of 17 responders and 15 nonresponders.
Responders were patients who, after 2 years of intravenous cyclophosphamide, showed no active urinary sediments, less than five red blood cells or white blood cells in urine, and proteinuria below 1 g/24 hours.
After analyzing 300-400 microRNAs in these biopsies, the investigators identified 6 that were significantly upregulated in association with treatment outcome in both the first cohort as well as a second validation cohort of 22 responders and 17 nonresponders.
When the researchers looked at the most likely genetic targets of these microRNAs, they identified genes associated with G2/M DNA damage checkpoint regulation, which points to a link with cyclophosphamide efficacy, as well as associations with immunological disease and renal inflammation.
Dr. Hasni said that previous studies of microRNA had looked in the peripheral blood but suggested this may not necessarily reflect what was happening in the kidney.
The next step for researchers is to see if upregulation of these microRNAs is predictive of treatment response.
“If you are giving cyclophosphamide for 2 years, it comes with a high risk of side effects, especially in young women because there is potential for premature ovarian failure,” Dr. Hasni said in an interview. “If we can predict that this patient is not going to respond to cyclophosphamide or will not have a good outcome, we can use alternative therapy, or perhaps use more aggressive or a combination therapy approach rather than keep doing the same thing and 2 years later find out the patient is not going to respond.”
The researchers are also keen to investigate whether these same microRNAs can be isolated from serum or urine, which would reduce the need for kidney biopsy.
“The testing for microRNA is not that hard – it’s the biopsy and extracting the tissue from the biopsy... that’s obviously cumbersome and can only be done in a research setting.”
No conflicts of interest were declared.
MELBOURNE – Researchers have identified six microRNAs that may indicate a better likelihood of response to cyclophosphamide in patients with lupus nephritis, according to a study presented at an international conference on systemic lupus erythematosus.
“MicroRNA has been shown to be important in systemic lupus in several studies, and they’ve identified several microRNA that have been shown to affect the outcome measures in patients,” said Sarfaraz Hasni, MD, director of the Lupus Clinical Research Program at the National Institute of Arthritis and Musculoskeletal and Skin Diseases in Bethesda, Md., who presented a poster on the study at the meeting.
The aim of this study, involving 71 patients with lupus nephritis, was to look for microRNAs associated with treatment response to cyclophosphamide.
The first stage of the study involved isolating microRNAs from kidney biopsies taken from a first cohort of 17 responders and 15 nonresponders.
Responders were patients who, after 2 years of intravenous cyclophosphamide, showed no active urinary sediments, less than five red blood cells or white blood cells in urine, and proteinuria below 1 g/24 hours.
After analyzing 300-400 microRNAs in these biopsies, the investigators identified 6 that were significantly upregulated in association with treatment outcome in both the first cohort as well as a second validation cohort of 22 responders and 17 nonresponders.
When the researchers looked at the most likely genetic targets of these microRNAs, they identified genes associated with G2/M DNA damage checkpoint regulation, which points to a link with cyclophosphamide efficacy, as well as associations with immunological disease and renal inflammation.
Dr. Hasni said that previous studies of microRNA had looked in the peripheral blood but suggested this may not necessarily reflect what was happening in the kidney.
The next step for researchers is to see if upregulation of these microRNAs is predictive of treatment response.
“If you are giving cyclophosphamide for 2 years, it comes with a high risk of side effects, especially in young women because there is potential for premature ovarian failure,” Dr. Hasni said in an interview. “If we can predict that this patient is not going to respond to cyclophosphamide or will not have a good outcome, we can use alternative therapy, or perhaps use more aggressive or a combination therapy approach rather than keep doing the same thing and 2 years later find out the patient is not going to respond.”
The researchers are also keen to investigate whether these same microRNAs can be isolated from serum or urine, which would reduce the need for kidney biopsy.
“The testing for microRNA is not that hard – it’s the biopsy and extracting the tissue from the biopsy... that’s obviously cumbersome and can only be done in a research setting.”
No conflicts of interest were declared.
MELBOURNE – Researchers have identified six microRNAs that may indicate a better likelihood of response to cyclophosphamide in patients with lupus nephritis, according to a study presented at an international conference on systemic lupus erythematosus.
“MicroRNA has been shown to be important in systemic lupus in several studies, and they’ve identified several microRNA that have been shown to affect the outcome measures in patients,” said Sarfaraz Hasni, MD, director of the Lupus Clinical Research Program at the National Institute of Arthritis and Musculoskeletal and Skin Diseases in Bethesda, Md., who presented a poster on the study at the meeting.
The aim of this study, involving 71 patients with lupus nephritis, was to look for microRNAs associated with treatment response to cyclophosphamide.
The first stage of the study involved isolating microRNAs from kidney biopsies taken from a first cohort of 17 responders and 15 nonresponders.
Responders were patients who, after 2 years of intravenous cyclophosphamide, showed no active urinary sediments, less than five red blood cells or white blood cells in urine, and proteinuria below 1 g/24 hours.
After analyzing 300-400 microRNAs in these biopsies, the investigators identified 6 that were significantly upregulated in association with treatment outcome in both the first cohort as well as a second validation cohort of 22 responders and 17 nonresponders.
When the researchers looked at the most likely genetic targets of these microRNAs, they identified genes associated with G2/M DNA damage checkpoint regulation, which points to a link with cyclophosphamide efficacy, as well as associations with immunological disease and renal inflammation.
Dr. Hasni said that previous studies of microRNA had looked in the peripheral blood but suggested this may not necessarily reflect what was happening in the kidney.
The next step for researchers is to see if upregulation of these microRNAs is predictive of treatment response.
“If you are giving cyclophosphamide for 2 years, it comes with a high risk of side effects, especially in young women because there is potential for premature ovarian failure,” Dr. Hasni said in an interview. “If we can predict that this patient is not going to respond to cyclophosphamide or will not have a good outcome, we can use alternative therapy, or perhaps use more aggressive or a combination therapy approach rather than keep doing the same thing and 2 years later find out the patient is not going to respond.”
The researchers are also keen to investigate whether these same microRNAs can be isolated from serum or urine, which would reduce the need for kidney biopsy.
“The testing for microRNA is not that hard – it’s the biopsy and extracting the tissue from the biopsy... that’s obviously cumbersome and can only be done in a research setting.”
No conflicts of interest were declared.
AT LUPUS 2017
Key clinical point:
Major finding: Researchers have identified six microRNAs from kidney biopsies that are significantly upregulated in patients who respond to cyclophosphamide treatment for lupus nephritis.
Data source: Prospective cohort study in 71 patients with lupus nephritis.
Disclosures: No conflicts of interest were declared.
Metformin linked with better survival in RCC patients with diabetes
Metformin use was associated with better survival for patients with renal cell carcinoma and diabetes in a meta-analysis, investigators report.
Yang Li, MD, and associates at Chongqing (China) Medical University, performed a pooled analysis of data from 254,329 patients with both localized and metastatic renal cell carcinoma, and found the risk of mortality was reduced in patients exposed to metformin (hazard ratio, 0.41; P less than .001).
However, there was significant heterogeneity among the eight eligible studies included in the meta-analysis, Dr. Li and associates reported (Int Urol Nephrol. 2017 Mar 7. doi: 10.1007/s11255-017-1548-4).
In a subgroup analysis, the association held in patients with localized disease, but was not significant in those with metastatic disease.
The current meta-analysis suggests that the use of metformin could improve the survival of kidney cancer patients, particularly those with localized disease; however, further studies are needed, the investigators conclude.
The authors declared that they had no conflicts of interest.
Metformin use was associated with better survival for patients with renal cell carcinoma and diabetes in a meta-analysis, investigators report.
Yang Li, MD, and associates at Chongqing (China) Medical University, performed a pooled analysis of data from 254,329 patients with both localized and metastatic renal cell carcinoma, and found the risk of mortality was reduced in patients exposed to metformin (hazard ratio, 0.41; P less than .001).
However, there was significant heterogeneity among the eight eligible studies included in the meta-analysis, Dr. Li and associates reported (Int Urol Nephrol. 2017 Mar 7. doi: 10.1007/s11255-017-1548-4).
In a subgroup analysis, the association held in patients with localized disease, but was not significant in those with metastatic disease.
The current meta-analysis suggests that the use of metformin could improve the survival of kidney cancer patients, particularly those with localized disease; however, further studies are needed, the investigators conclude.
The authors declared that they had no conflicts of interest.
Metformin use was associated with better survival for patients with renal cell carcinoma and diabetes in a meta-analysis, investigators report.
Yang Li, MD, and associates at Chongqing (China) Medical University, performed a pooled analysis of data from 254,329 patients with both localized and metastatic renal cell carcinoma, and found the risk of mortality was reduced in patients exposed to metformin (hazard ratio, 0.41; P less than .001).
However, there was significant heterogeneity among the eight eligible studies included in the meta-analysis, Dr. Li and associates reported (Int Urol Nephrol. 2017 Mar 7. doi: 10.1007/s11255-017-1548-4).
In a subgroup analysis, the association held in patients with localized disease, but was not significant in those with metastatic disease.
The current meta-analysis suggests that the use of metformin could improve the survival of kidney cancer patients, particularly those with localized disease; however, further studies are needed, the investigators conclude.
The authors declared that they had no conflicts of interest.
Key clinical point:
Major finding: In a pooled analysis of data from eight studies, the risk of mortality was reduced in patients exposed to metformin (hazard ratio, 0.41; P less than .001).
Data source: A meta-analysis of eight studies including 254,329 patients with renal cell carcinoma.
Disclosures: The authors declared that they had no conflicts of interest.
Robot-assisted laparoscopic excision of a rectovaginal endometriotic nodule
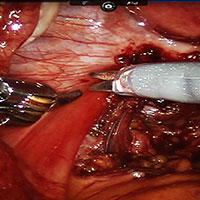
A rectovaginal endometriosis (RVE) is the most severe form of endometriosis. The gold standard for diagnosis is laparoscopy with histologic confirmation. A review of the literature suggests that surgery improves up to 70% of symptoms with generally favorable outcomes.
In this video, we provide a general introduction to endometriosis and a discussion of disease treatment options, ranging from hormonal suppression to radical bowel resections. We also illustrate the steps in robot-assisted laparoscopic excision of an RVE nodule:
- identify the borders of the rectosigmoid
- dissect the pararectal spaces
- release the rectosigmoid from its attachment to the RVE nodule
- identify and isolate the ureter(s)
- determine the margins of the nodule
- ensure complete resection.
Excision of an RVE nodule is a technically challenging surgical procedure. Use of the robot for resection is safe and feasible when performed by a trained and experienced surgeon.
I am pleased to bring you this video, and I hope that it is helpful to your practice.
>> Arnold P. Advincula, MD

Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
A rectovaginal endometriosis (RVE) is the most severe form of endometriosis. The gold standard for diagnosis is laparoscopy with histologic confirmation. A review of the literature suggests that surgery improves up to 70% of symptoms with generally favorable outcomes.
In this video, we provide a general introduction to endometriosis and a discussion of disease treatment options, ranging from hormonal suppression to radical bowel resections. We also illustrate the steps in robot-assisted laparoscopic excision of an RVE nodule:
- identify the borders of the rectosigmoid
- dissect the pararectal spaces
- release the rectosigmoid from its attachment to the RVE nodule
- identify and isolate the ureter(s)
- determine the margins of the nodule
- ensure complete resection.
Excision of an RVE nodule is a technically challenging surgical procedure. Use of the robot for resection is safe and feasible when performed by a trained and experienced surgeon.
I am pleased to bring you this video, and I hope that it is helpful to your practice.
>> Arnold P. Advincula, MD
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
A rectovaginal endometriosis (RVE) is the most severe form of endometriosis. The gold standard for diagnosis is laparoscopy with histologic confirmation. A review of the literature suggests that surgery improves up to 70% of symptoms with generally favorable outcomes.
In this video, we provide a general introduction to endometriosis and a discussion of disease treatment options, ranging from hormonal suppression to radical bowel resections. We also illustrate the steps in robot-assisted laparoscopic excision of an RVE nodule:
- identify the borders of the rectosigmoid
- dissect the pararectal spaces
- release the rectosigmoid from its attachment to the RVE nodule
- identify and isolate the ureter(s)
- determine the margins of the nodule
- ensure complete resection.
Excision of an RVE nodule is a technically challenging surgical procedure. Use of the robot for resection is safe and feasible when performed by a trained and experienced surgeon.
I am pleased to bring you this video, and I hope that it is helpful to your practice.
>> Arnold P. Advincula, MD
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Tapering opioids
The Centers for Disease Control and Prevention guideline for prescribing opioids for chronic pain released in March 2016 suggests that if “patients are found to be receiving high total daily dosages of opioids, clinicians should discuss their safety concerns with the patient [and] consider tapering to a safer dosage...”
All of us who prescribe opioids have had these discussions with patients. They are frequently fraught with hand-wringing and, all-too-often, a “steeling” for battle. We may have a general sense for what these discussions are like from the provider perspective, but what are they like for patients?

Interestingly, patients had an overall low self-perceived risk of opioid overdose. Patients attributed reports of overdose to intent or risky behaviors. Patients rated the importance of treatment of current pain higher than the future potential risk of opioid use and had little faith in nonopioid pain management strategies. Patients reported fear of opioid withdrawal. They also reported the importance of social support and a healthy, trusting relationship with their provider for the facilitation of tapering. None of the patients reported switching providers who had recommended tapering. Patients who had tapered off opioids reported improved quality of life and a level of pain that was largely unchanged.
This work provides critical insight into the fears and reservations of patients facing the prospect of life on lower doses of opioids or life without them altogether. Addressing these fears directly may facilitate the discussions with patients when discussing the tapering of opioids.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article.
The Centers for Disease Control and Prevention guideline for prescribing opioids for chronic pain released in March 2016 suggests that if “patients are found to be receiving high total daily dosages of opioids, clinicians should discuss their safety concerns with the patient [and] consider tapering to a safer dosage...”
All of us who prescribe opioids have had these discussions with patients. They are frequently fraught with hand-wringing and, all-too-often, a “steeling” for battle. We may have a general sense for what these discussions are like from the provider perspective, but what are they like for patients?
Interestingly, patients had an overall low self-perceived risk of opioid overdose. Patients attributed reports of overdose to intent or risky behaviors. Patients rated the importance of treatment of current pain higher than the future potential risk of opioid use and had little faith in nonopioid pain management strategies. Patients reported fear of opioid withdrawal. They also reported the importance of social support and a healthy, trusting relationship with their provider for the facilitation of tapering. None of the patients reported switching providers who had recommended tapering. Patients who had tapered off opioids reported improved quality of life and a level of pain that was largely unchanged.
This work provides critical insight into the fears and reservations of patients facing the prospect of life on lower doses of opioids or life without them altogether. Addressing these fears directly may facilitate the discussions with patients when discussing the tapering of opioids.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article.
The Centers for Disease Control and Prevention guideline for prescribing opioids for chronic pain released in March 2016 suggests that if “patients are found to be receiving high total daily dosages of opioids, clinicians should discuss their safety concerns with the patient [and] consider tapering to a safer dosage...”
All of us who prescribe opioids have had these discussions with patients. They are frequently fraught with hand-wringing and, all-too-often, a “steeling” for battle. We may have a general sense for what these discussions are like from the provider perspective, but what are they like for patients?
Interestingly, patients had an overall low self-perceived risk of opioid overdose. Patients attributed reports of overdose to intent or risky behaviors. Patients rated the importance of treatment of current pain higher than the future potential risk of opioid use and had little faith in nonopioid pain management strategies. Patients reported fear of opioid withdrawal. They also reported the importance of social support and a healthy, trusting relationship with their provider for the facilitation of tapering. None of the patients reported switching providers who had recommended tapering. Patients who had tapered off opioids reported improved quality of life and a level of pain that was largely unchanged.
This work provides critical insight into the fears and reservations of patients facing the prospect of life on lower doses of opioids or life without them altogether. Addressing these fears directly may facilitate the discussions with patients when discussing the tapering of opioids.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article.
AGA Tech Summit offers packed agenda of innovation and technology
The 2017 AGA Tech Summit, sponsored by the AGA Center for GI Innovation and Technology, promises to provide gastroenterologists and gastrointestinal surgeons with an insider’s perspective on regulators, payors, and companies in the medtech space during its 2017 session from April 12-14 in Boston. “This year’s agenda will highlight personalized diagnostics and the impact of MACRA on gastroenterology,” said Michael L. Kochman, MD, AGAF, of Penn Medicine, Philadelphia, who is executive committee chair of the center. “The intimate nature of the meeting will allow attendees to interact with fellow gastroenterologists and GI surgeons while benefiting from sessions on critical innovation and technology issues in our field.”
Development of the program started at the 2016 conference, building on that session’s highlights, as well as on the needs and interests of its attendees and speakers. “It takes a full 9 months to lock down the topics and find appropriate presenters,” explained Dr. Kochman. “The program is continually assessed and updated to keep up with medtech developments. Handpicked faculty members include prominent leaders in the medical, medtech, and regulatory communities.”

“Two important sessions demonstrate the breadth of the meeting,” stated Dr. Kochman. “This year’s Shark Tank will cover novel developments in GI medtech.” Participating companies and entrepreneurs will have 5 minutes to present their projects to an expert panel of venture capitalists, physicians, and industry executives who make acquisition decisions. “There will also be a cutting-edge session covering liquid biopsy and personalized medicine in gastroenterology,” he added. Other highlights include presentations on “The Macroeconomics of Care Delivery: MACRA and the Change to Come” and practice and device development.
The event includes a wide range of opportunities for networking with faculty and attendees, including during the breaks on both days, a Thursday night reception, and luncheons.
Summit sessions will span critical elements affecting how innovation in the GI space evolves from concept to reality. Other topics covered will include a digestive world outlook, driving innovation adoption, research updates, quality outcomes, raising capital, medtech success in GI and metabolic diseases from 2016, opportunities and challenges in personalized medicine, and improving patient outcomes via quality efforts.
Those who cannot attend the conference can look forward to “Highlights of the 2017 AGA Tech Summit,” which will be published as a supplement to GI & Hepatology News. “There will be writers in Boston attending and capturing highlights of the event sessions,” said Dr. Kochman. “AGA members will have the opportunity to experience the salient points of the presentations through this publication.”
The AGA Tech Summit will foster innovation and technology in the field of digestive health. “The keynote speakers and presenters, along with the audience’s multiple perspectives will be something we can build on to hopefully shape the future of gastroenterology,” concluded Dr. Kochman.
Dr. Kochman disclosed that he serves as a consultant for Boston Scientific Corp. and Dark Canyon Labs.
The 2017 AGA Tech Summit, sponsored by the AGA Center for GI Innovation and Technology, promises to provide gastroenterologists and gastrointestinal surgeons with an insider’s perspective on regulators, payors, and companies in the medtech space during its 2017 session from April 12-14 in Boston. “This year’s agenda will highlight personalized diagnostics and the impact of MACRA on gastroenterology,” said Michael L. Kochman, MD, AGAF, of Penn Medicine, Philadelphia, who is executive committee chair of the center. “The intimate nature of the meeting will allow attendees to interact with fellow gastroenterologists and GI surgeons while benefiting from sessions on critical innovation and technology issues in our field.”
Development of the program started at the 2016 conference, building on that session’s highlights, as well as on the needs and interests of its attendees and speakers. “It takes a full 9 months to lock down the topics and find appropriate presenters,” explained Dr. Kochman. “The program is continually assessed and updated to keep up with medtech developments. Handpicked faculty members include prominent leaders in the medical, medtech, and regulatory communities.”
“Two important sessions demonstrate the breadth of the meeting,” stated Dr. Kochman. “This year’s Shark Tank will cover novel developments in GI medtech.” Participating companies and entrepreneurs will have 5 minutes to present their projects to an expert panel of venture capitalists, physicians, and industry executives who make acquisition decisions. “There will also be a cutting-edge session covering liquid biopsy and personalized medicine in gastroenterology,” he added. Other highlights include presentations on “The Macroeconomics of Care Delivery: MACRA and the Change to Come” and practice and device development.
The event includes a wide range of opportunities for networking with faculty and attendees, including during the breaks on both days, a Thursday night reception, and luncheons.
Summit sessions will span critical elements affecting how innovation in the GI space evolves from concept to reality. Other topics covered will include a digestive world outlook, driving innovation adoption, research updates, quality outcomes, raising capital, medtech success in GI and metabolic diseases from 2016, opportunities and challenges in personalized medicine, and improving patient outcomes via quality efforts.
Those who cannot attend the conference can look forward to “Highlights of the 2017 AGA Tech Summit,” which will be published as a supplement to GI & Hepatology News. “There will be writers in Boston attending and capturing highlights of the event sessions,” said Dr. Kochman. “AGA members will have the opportunity to experience the salient points of the presentations through this publication.”
The AGA Tech Summit will foster innovation and technology in the field of digestive health. “The keynote speakers and presenters, along with the audience’s multiple perspectives will be something we can build on to hopefully shape the future of gastroenterology,” concluded Dr. Kochman.
Dr. Kochman disclosed that he serves as a consultant for Boston Scientific Corp. and Dark Canyon Labs.
The 2017 AGA Tech Summit, sponsored by the AGA Center for GI Innovation and Technology, promises to provide gastroenterologists and gastrointestinal surgeons with an insider’s perspective on regulators, payors, and companies in the medtech space during its 2017 session from April 12-14 in Boston. “This year’s agenda will highlight personalized diagnostics and the impact of MACRA on gastroenterology,” said Michael L. Kochman, MD, AGAF, of Penn Medicine, Philadelphia, who is executive committee chair of the center. “The intimate nature of the meeting will allow attendees to interact with fellow gastroenterologists and GI surgeons while benefiting from sessions on critical innovation and technology issues in our field.”
Development of the program started at the 2016 conference, building on that session’s highlights, as well as on the needs and interests of its attendees and speakers. “It takes a full 9 months to lock down the topics and find appropriate presenters,” explained Dr. Kochman. “The program is continually assessed and updated to keep up with medtech developments. Handpicked faculty members include prominent leaders in the medical, medtech, and regulatory communities.”
“Two important sessions demonstrate the breadth of the meeting,” stated Dr. Kochman. “This year’s Shark Tank will cover novel developments in GI medtech.” Participating companies and entrepreneurs will have 5 minutes to present their projects to an expert panel of venture capitalists, physicians, and industry executives who make acquisition decisions. “There will also be a cutting-edge session covering liquid biopsy and personalized medicine in gastroenterology,” he added. Other highlights include presentations on “The Macroeconomics of Care Delivery: MACRA and the Change to Come” and practice and device development.
The event includes a wide range of opportunities for networking with faculty and attendees, including during the breaks on both days, a Thursday night reception, and luncheons.
Summit sessions will span critical elements affecting how innovation in the GI space evolves from concept to reality. Other topics covered will include a digestive world outlook, driving innovation adoption, research updates, quality outcomes, raising capital, medtech success in GI and metabolic diseases from 2016, opportunities and challenges in personalized medicine, and improving patient outcomes via quality efforts.
Those who cannot attend the conference can look forward to “Highlights of the 2017 AGA Tech Summit,” which will be published as a supplement to GI & Hepatology News. “There will be writers in Boston attending and capturing highlights of the event sessions,” said Dr. Kochman. “AGA members will have the opportunity to experience the salient points of the presentations through this publication.”
The AGA Tech Summit will foster innovation and technology in the field of digestive health. “The keynote speakers and presenters, along with the audience’s multiple perspectives will be something we can build on to hopefully shape the future of gastroenterology,” concluded Dr. Kochman.
Dr. Kochman disclosed that he serves as a consultant for Boston Scientific Corp. and Dark Canyon Labs.

Septic shock patients suffer most from delayed antibiotics
Hospital mortality for sepsis patients was 9% more likely with each hour of delayed administration of antibiotics, and the mortality rates increased with the severity of sepsis, based on data from 35,000 randomly selected sepsis patients.
Early administration of antibiotics in sepsis cases has become accepted as a way to improve outcomes, but the benefits have not been well studied, wrote Vincent X Liu, MD, MS, of Kaiser Permanente Division of Research, Oakland, Calif., and his colleagues.
To quantify the impact of antibiotic timing on mortality rates in different types of sepsis patients, the researchers reviewed data from 35,000 adults treated for sepsis at 21 emergency departments in northern California between 2010 and 2013. The time from registration at the emergency department to administration of the first antibiotics was less than 6 hours (Am J Respir Crit Care Med. 2017 March 27. doi: 10.1164/rccm.201609-1848OC).
The overall mortality rates were 3.9%, 8.8%, and 26.0% for sepsis, severe sepsis, and septic shock, respectively. Absolute mortality increased by 0.3% for sepsis, 0.4% for severe sepsis, and 1.8% for septic shock patients after an hour’s delay in the administration of antibiotics, and the adjusted odds ratio for hospital mortality was 1.09 for each hour between patient registration and antibiotic administration. The median time to the first administration of antibiotics was 2.1 hours, ranging from 1.7 hours for septic shock patients to 2.3 hours for sepsis patients, with ceftriaxone having been the most commonly used antibiotic across all groups.
Approximately 42% of patients received one antibiotic and 43% received two antibiotics. The odds of receiving two or more antibiotics were significantly higher for septic shock patients compared with sepsis patients (72% vs. 52%, respectively).
The findings were limited by several factors, including the inability to adjust for concomitant sepsis treatments and preexisting antibiotic treatments, the researchers said.
The study results do not resolve all questions about the timing of antibiotic administration for sepsis patients, such as whether there is additional benefit to giving the medications at 2 hours rather than 3 hours or 4 hours after ED admission, the researchers noted. However, “our findings support currently held beliefs that administering early antibiotics to infected patients with systemic inflammation is beneficial for reducing mortality,” they said.
The study was supported in part by the Permanente Medical Group and Kaiser Foundation Hospitals, the National Institute of General Medical Sciences, and the Veterans Affairs Health Services Research and Development Service.
In medicine, we strive to increase our understanding of disease states and improve outcomes for patients. This study supports the belief that timing of the admin

In medicine, we strive to increase our understanding of disease states and improve outcomes for patients. This study supports the belief that timing of the admin
In medicine, we strive to increase our understanding of disease states and improve outcomes for patients. This study supports the belief that timing of the admin
Hospital mortality for sepsis patients was 9% more likely with each hour of delayed administration of antibiotics, and the mortality rates increased with the severity of sepsis, based on data from 35,000 randomly selected sepsis patients.
Early administration of antibiotics in sepsis cases has become accepted as a way to improve outcomes, but the benefits have not been well studied, wrote Vincent X Liu, MD, MS, of Kaiser Permanente Division of Research, Oakland, Calif., and his colleagues.
To quantify the impact of antibiotic timing on mortality rates in different types of sepsis patients, the researchers reviewed data from 35,000 adults treated for sepsis at 21 emergency departments in northern California between 2010 and 2013. The time from registration at the emergency department to administration of the first antibiotics was less than 6 hours (Am J Respir Crit Care Med. 2017 March 27. doi: 10.1164/rccm.201609-1848OC).
The overall mortality rates were 3.9%, 8.8%, and 26.0% for sepsis, severe sepsis, and septic shock, respectively. Absolute mortality increased by 0.3% for sepsis, 0.4% for severe sepsis, and 1.8% for septic shock patients after an hour’s delay in the administration of antibiotics, and the adjusted odds ratio for hospital mortality was 1.09 for each hour between patient registration and antibiotic administration. The median time to the first administration of antibiotics was 2.1 hours, ranging from 1.7 hours for septic shock patients to 2.3 hours for sepsis patients, with ceftriaxone having been the most commonly used antibiotic across all groups.
Approximately 42% of patients received one antibiotic and 43% received two antibiotics. The odds of receiving two or more antibiotics were significantly higher for septic shock patients compared with sepsis patients (72% vs. 52%, respectively).
The findings were limited by several factors, including the inability to adjust for concomitant sepsis treatments and preexisting antibiotic treatments, the researchers said.
The study results do not resolve all questions about the timing of antibiotic administration for sepsis patients, such as whether there is additional benefit to giving the medications at 2 hours rather than 3 hours or 4 hours after ED admission, the researchers noted. However, “our findings support currently held beliefs that administering early antibiotics to infected patients with systemic inflammation is beneficial for reducing mortality,” they said.
The study was supported in part by the Permanente Medical Group and Kaiser Foundation Hospitals, the National Institute of General Medical Sciences, and the Veterans Affairs Health Services Research and Development Service.
Hospital mortality for sepsis patients was 9% more likely with each hour of delayed administration of antibiotics, and the mortality rates increased with the severity of sepsis, based on data from 35,000 randomly selected sepsis patients.
Early administration of antibiotics in sepsis cases has become accepted as a way to improve outcomes, but the benefits have not been well studied, wrote Vincent X Liu, MD, MS, of Kaiser Permanente Division of Research, Oakland, Calif., and his colleagues.
To quantify the impact of antibiotic timing on mortality rates in different types of sepsis patients, the researchers reviewed data from 35,000 adults treated for sepsis at 21 emergency departments in northern California between 2010 and 2013. The time from registration at the emergency department to administration of the first antibiotics was less than 6 hours (Am J Respir Crit Care Med. 2017 March 27. doi: 10.1164/rccm.201609-1848OC).
The overall mortality rates were 3.9%, 8.8%, and 26.0% for sepsis, severe sepsis, and septic shock, respectively. Absolute mortality increased by 0.3% for sepsis, 0.4% for severe sepsis, and 1.8% for septic shock patients after an hour’s delay in the administration of antibiotics, and the adjusted odds ratio for hospital mortality was 1.09 for each hour between patient registration and antibiotic administration. The median time to the first administration of antibiotics was 2.1 hours, ranging from 1.7 hours for septic shock patients to 2.3 hours for sepsis patients, with ceftriaxone having been the most commonly used antibiotic across all groups.
Approximately 42% of patients received one antibiotic and 43% received two antibiotics. The odds of receiving two or more antibiotics were significantly higher for septic shock patients compared with sepsis patients (72% vs. 52%, respectively).
The findings were limited by several factors, including the inability to adjust for concomitant sepsis treatments and preexisting antibiotic treatments, the researchers said.
The study results do not resolve all questions about the timing of antibiotic administration for sepsis patients, such as whether there is additional benefit to giving the medications at 2 hours rather than 3 hours or 4 hours after ED admission, the researchers noted. However, “our findings support currently held beliefs that administering early antibiotics to infected patients with systemic inflammation is beneficial for reducing mortality,” they said.
The study was supported in part by the Permanente Medical Group and Kaiser Foundation Hospitals, the National Institute of General Medical Sciences, and the Veterans Affairs Health Services Research and Development Service.
FROM THE AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Key clinical point: Each hour of delay in antibiotic administration increased the odds of hospital mortality in sepsis patients.
Major finding: An hour delay in antibiotic administration increased the absolute mortality by 0.3% for cases of sepsis, 0.4% for severe sepsis, and 1.8% for septic shock.
Data source: A retrospective study of 35,000 adult patients treated with a sepsis quality improvement program at 21 emergency departments in California.
Disclosures: The study was supported in part by the Permanente Medical Group and Kaiser Foundation Hospitals, the National Institute of General Medical Sciences, and the Veterans Affairs Health Services Research and Development Service.
Get on board with APMs or risk having your practice commoditized
Gastroenterologists need to get on board with assuming risk through the adoption of advanced alternative payment methods under Medicare’s new Quality Payment Program or risk losing money through the commoditization of their services.
That’s the message Lawrence Kosinski, MD, of the Illinois Gastroenterology Group, has for his fellow gastroenterologists.
“To me, MIPS [Merit-based Incentive Payment System] is just an extension of what we were doing with PQRS and meaningful use, value-based modifiers,” Dr. Kosinski, who serves as practice councillor on the AGA Governing Board, said in an interview in advance of his presentation at the 2017 AGA Tech Summit sponsored by the AGA Center for GI Innovation and Technology.

If gastroenterologists choose to stay on that path rather than accept the two-sided risk of following the APM track of the Quality Payment Program, “you are going to have commoditized services and you are going to just make less money and work for somebody else. But if you want to be in control of your own future, we have to strive to work in [the APM] direction.”
To get there, the culture of gastroenterology will need to shift.
“Our culture right now is one where we get paid for making widgets,” he said. “And the more widgets we make, the more money we make. The more colonoscopies we do, the more money we make. The more we can charge for those colonoscopies and get collected, the better things are for us.”
The future could allow gastroenterologists to charge for more and different services, he added.
“A lot of people are working to replace colonoscopies with much less expensive alternative,” Dr. Kosinski said. “So where does a gastroenterologist have a competitive advantage? It’s in the knowledge of these complex diseases that are running up the cost of health care. Over 80% of the cost of health care is for the management of chronic disease. We happen to have a very expensive set of chronic diseases that we take care of in GI, very complicated illnesses. We need to leverage that. We need to leverage the management of those patients, but we need to be able to show how our work decreases the overall cost of care so that we can get a piece of that risk premium.”
He warned: “If we don’t do that, we’re just going to be commoditized proceduralists.”
And the upside will be better reimbursements for doctors and lower overall costs for health systems.
“We may be able to increase our own reimbursement as long as we are critical in lowering the overall cost of care for the entire population,” he said.
To that end, “well-managed GI practices should be able to develop a competitive advantage in a value space to be able to supply the needed services,” he said, adding that “we’re going to have to provide value by improving quality through a focus on patient outcomes. We have to assure a new level of patient relationships and ultimately focus on lowering the cost of care for a population of patients.”
Gastroenterologists need to get on board with assuming risk through the adoption of advanced alternative payment methods under Medicare’s new Quality Payment Program or risk losing money through the commoditization of their services.
That’s the message Lawrence Kosinski, MD, of the Illinois Gastroenterology Group, has for his fellow gastroenterologists.
“To me, MIPS [Merit-based Incentive Payment System] is just an extension of what we were doing with PQRS and meaningful use, value-based modifiers,” Dr. Kosinski, who serves as practice councillor on the AGA Governing Board, said in an interview in advance of his presentation at the 2017 AGA Tech Summit sponsored by the AGA Center for GI Innovation and Technology.
If gastroenterologists choose to stay on that path rather than accept the two-sided risk of following the APM track of the Quality Payment Program, “you are going to have commoditized services and you are going to just make less money and work for somebody else. But if you want to be in control of your own future, we have to strive to work in [the APM] direction.”
To get there, the culture of gastroenterology will need to shift.
“Our culture right now is one where we get paid for making widgets,” he said. “And the more widgets we make, the more money we make. The more colonoscopies we do, the more money we make. The more we can charge for those colonoscopies and get collected, the better things are for us.”
The future could allow gastroenterologists to charge for more and different services, he added.
“A lot of people are working to replace colonoscopies with much less expensive alternative,” Dr. Kosinski said. “So where does a gastroenterologist have a competitive advantage? It’s in the knowledge of these complex diseases that are running up the cost of health care. Over 80% of the cost of health care is for the management of chronic disease. We happen to have a very expensive set of chronic diseases that we take care of in GI, very complicated illnesses. We need to leverage that. We need to leverage the management of those patients, but we need to be able to show how our work decreases the overall cost of care so that we can get a piece of that risk premium.”
He warned: “If we don’t do that, we’re just going to be commoditized proceduralists.”
And the upside will be better reimbursements for doctors and lower overall costs for health systems.
“We may be able to increase our own reimbursement as long as we are critical in lowering the overall cost of care for the entire population,” he said.
To that end, “well-managed GI practices should be able to develop a competitive advantage in a value space to be able to supply the needed services,” he said, adding that “we’re going to have to provide value by improving quality through a focus on patient outcomes. We have to assure a new level of patient relationships and ultimately focus on lowering the cost of care for a population of patients.”
Gastroenterologists need to get on board with assuming risk through the adoption of advanced alternative payment methods under Medicare’s new Quality Payment Program or risk losing money through the commoditization of their services.
That’s the message Lawrence Kosinski, MD, of the Illinois Gastroenterology Group, has for his fellow gastroenterologists.
“To me, MIPS [Merit-based Incentive Payment System] is just an extension of what we were doing with PQRS and meaningful use, value-based modifiers,” Dr. Kosinski, who serves as practice councillor on the AGA Governing Board, said in an interview in advance of his presentation at the 2017 AGA Tech Summit sponsored by the AGA Center for GI Innovation and Technology.
If gastroenterologists choose to stay on that path rather than accept the two-sided risk of following the APM track of the Quality Payment Program, “you are going to have commoditized services and you are going to just make less money and work for somebody else. But if you want to be in control of your own future, we have to strive to work in [the APM] direction.”
To get there, the culture of gastroenterology will need to shift.
“Our culture right now is one where we get paid for making widgets,” he said. “And the more widgets we make, the more money we make. The more colonoscopies we do, the more money we make. The more we can charge for those colonoscopies and get collected, the better things are for us.”
The future could allow gastroenterologists to charge for more and different services, he added.
“A lot of people are working to replace colonoscopies with much less expensive alternative,” Dr. Kosinski said. “So where does a gastroenterologist have a competitive advantage? It’s in the knowledge of these complex diseases that are running up the cost of health care. Over 80% of the cost of health care is for the management of chronic disease. We happen to have a very expensive set of chronic diseases that we take care of in GI, very complicated illnesses. We need to leverage that. We need to leverage the management of those patients, but we need to be able to show how our work decreases the overall cost of care so that we can get a piece of that risk premium.”
He warned: “If we don’t do that, we’re just going to be commoditized proceduralists.”
And the upside will be better reimbursements for doctors and lower overall costs for health systems.
“We may be able to increase our own reimbursement as long as we are critical in lowering the overall cost of care for the entire population,” he said.
To that end, “well-managed GI practices should be able to develop a competitive advantage in a value space to be able to supply the needed services,” he said, adding that “we’re going to have to provide value by improving quality through a focus on patient outcomes. We have to assure a new level of patient relationships and ultimately focus on lowering the cost of care for a population of patients.”
Hard water versus your skin
Observational studies suggest that hard water is associated with the development of atopic dermatitis (AD). Studies of children in the United Kingdom, Spain, and Japan show the prevalence of AD is significantly higher in the highest water hardness categories than that in the lowest. Calcium cations in water can interfere with normal epidermal calcium gradients that are necessary for corneocyte development and proper stratum corneum barrier formation.
Water hardness, determined by the amount of dissolved calcium and magnesium in the water, varies by geography and mineral content of the water supply. The hardest water supply in the United States is mostly localized to the Upper Plains and Rocky Mountain areas. General guidelines for classification of waters are: 0-60 mg/L calcium carbonate (soft); 61-120 mg/L (moderately hard); 121-180 mg/L (hard); and more than 180 mg/L (very hard). In regions where there is hard water, the surfactants in soap, such as sodium dodecyl sulfate, react with the calcium and magnesium ions in hard water, resulting in precipitation of the surfactant – leaving a film of residue on the skin, shower tiles, pipes, glassware, etc.

Atopic dermatitis, xerosis, and pruritus are some of the common skin reactions to hard water. Other less-well-defined effects on the skin include clogged pores and acne from surfactant residue left on the skin and altered sebum production. In addition, more surfactants or cleansers are needed to clean the skin and hair in areas with hard water because the abundant cations require a much heavier lather to dissolve.
Calcium and magnesium cations left on the skin can also form free radicals. Free radicals over time can result in collagen and elastin breakdown and in the increased prevalence of fine lines and wrinkles.

Hard water and geography should be considered a possible factor when assessing patients with recalcitrant eczema, pruritus, or xerosis that cannot otherwise be reversed. Water softening treatments are a simple solution in areas where the mineral content of water is elevated or the water plays a role in clinical skin disease.
Dr. Lily Talakoub and Dr. Naissan O. Wesley and are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
References
United States Geological Survey Water Quality Information: Water Hardness and Alkalinity.
J Am Acad Dermatol. 1987 Jun;16(6):1263-4.
Contact Dermatitis. 1996 Dec;35(6):337-43.
Lancet. 1998 Aug 15;352(9127):527-31.
Contact Dermatitis. 1999;41(6):311-4.
Environ Res. 2004 Jan;94(1):33-7.
Observational studies suggest that hard water is associated with the development of atopic dermatitis (AD). Studies of children in the United Kingdom, Spain, and Japan show the prevalence of AD is significantly higher in the highest water hardness categories than that in the lowest. Calcium cations in water can interfere with normal epidermal calcium gradients that are necessary for corneocyte development and proper stratum corneum barrier formation.
Water hardness, determined by the amount of dissolved calcium and magnesium in the water, varies by geography and mineral content of the water supply. The hardest water supply in the United States is mostly localized to the Upper Plains and Rocky Mountain areas. General guidelines for classification of waters are: 0-60 mg/L calcium carbonate (soft); 61-120 mg/L (moderately hard); 121-180 mg/L (hard); and more than 180 mg/L (very hard). In regions where there is hard water, the surfactants in soap, such as sodium dodecyl sulfate, react with the calcium and magnesium ions in hard water, resulting in precipitation of the surfactant – leaving a film of residue on the skin, shower tiles, pipes, glassware, etc.
Atopic dermatitis, xerosis, and pruritus are some of the common skin reactions to hard water. Other less-well-defined effects on the skin include clogged pores and acne from surfactant residue left on the skin and altered sebum production. In addition, more surfactants or cleansers are needed to clean the skin and hair in areas with hard water because the abundant cations require a much heavier lather to dissolve.
Calcium and magnesium cations left on the skin can also form free radicals. Free radicals over time can result in collagen and elastin breakdown and in the increased prevalence of fine lines and wrinkles.
Hard water and geography should be considered a possible factor when assessing patients with recalcitrant eczema, pruritus, or xerosis that cannot otherwise be reversed. Water softening treatments are a simple solution in areas where the mineral content of water is elevated or the water plays a role in clinical skin disease.
Dr. Lily Talakoub and Dr. Naissan O. Wesley and are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
References
United States Geological Survey Water Quality Information: Water Hardness and Alkalinity.
J Am Acad Dermatol. 1987 Jun;16(6):1263-4.
Contact Dermatitis. 1996 Dec;35(6):337-43.
Lancet. 1998 Aug 15;352(9127):527-31.
Contact Dermatitis. 1999;41(6):311-4.
Environ Res. 2004 Jan;94(1):33-7.
Observational studies suggest that hard water is associated with the development of atopic dermatitis (AD). Studies of children in the United Kingdom, Spain, and Japan show the prevalence of AD is significantly higher in the highest water hardness categories than that in the lowest. Calcium cations in water can interfere with normal epidermal calcium gradients that are necessary for corneocyte development and proper stratum corneum barrier formation.
Water hardness, determined by the amount of dissolved calcium and magnesium in the water, varies by geography and mineral content of the water supply. The hardest water supply in the United States is mostly localized to the Upper Plains and Rocky Mountain areas. General guidelines for classification of waters are: 0-60 mg/L calcium carbonate (soft); 61-120 mg/L (moderately hard); 121-180 mg/L (hard); and more than 180 mg/L (very hard). In regions where there is hard water, the surfactants in soap, such as sodium dodecyl sulfate, react with the calcium and magnesium ions in hard water, resulting in precipitation of the surfactant – leaving a film of residue on the skin, shower tiles, pipes, glassware, etc.
Atopic dermatitis, xerosis, and pruritus are some of the common skin reactions to hard water. Other less-well-defined effects on the skin include clogged pores and acne from surfactant residue left on the skin and altered sebum production. In addition, more surfactants or cleansers are needed to clean the skin and hair in areas with hard water because the abundant cations require a much heavier lather to dissolve.
Calcium and magnesium cations left on the skin can also form free radicals. Free radicals over time can result in collagen and elastin breakdown and in the increased prevalence of fine lines and wrinkles.
Hard water and geography should be considered a possible factor when assessing patients with recalcitrant eczema, pruritus, or xerosis that cannot otherwise be reversed. Water softening treatments are a simple solution in areas where the mineral content of water is elevated or the water plays a role in clinical skin disease.
Dr. Lily Talakoub and Dr. Naissan O. Wesley and are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
References
United States Geological Survey Water Quality Information: Water Hardness and Alkalinity.
J Am Acad Dermatol. 1987 Jun;16(6):1263-4.
Contact Dermatitis. 1996 Dec;35(6):337-43.
Lancet. 1998 Aug 15;352(9127):527-31.
Contact Dermatitis. 1999;41(6):311-4.
Environ Res. 2004 Jan;94(1):33-7.
Real-time data, transparency needed to improve safety
With an increasing number of emerging technological advances in both medical devices and procedures, two factors will help improve safety and outcomes for patients: better real-time data and information transparency.
And the key to getting that data will be broader use of registries, according to Dana Telem, MD, director of the Comprehensive Hernia Program at the University of Michigan, Ann Arbor.
Dr. Telem will discuss the importance of real-time information and registries during her April 13 presentation at the 2017 AGA Tech Summit, sponsored by the AGA Center for GI Innovation and Technology.
Speaking in advance of the meeting, Dr. Telem noted that understanding value and finding potential safety issues are among the reasons for using data registries.
“I think that’s really why we need to focus on getting real-time data and that’s why I think registry efforts are so important,” she said. “What registries are really great at [is] identifying those isolated events.”
In addition, they help with another key concept she will highlight during her talk: transparency, something that is especially important as new techniques and devices are introduced.
“We understand that there are going to be early adopters, and you need to have the pioneers in order to take those next steps,” she said.
But to get the most out of those new technologies, data need to be recorded not only for short-term outcomes but over the long term as well “so that we can really assess the value of the techniques or the devices that we are putting out into the community.”
And by providing transparency on what is known, as well as unknown, it also helps patients in making their own decisions on whether to proceed with something new.
She believes that, especially when it comes to newer technologies, patients will be willing to be a part of that data collection if doctors are transparent.
“Many people are willing as long as you are honest with them,” Dr. Telem said. “I think particularly that when newer devices and techniques come out, particularly endoscopic procedures that can save them an operation, they are more willing than not, oftentimes, to do it, which is also where it gets a little bit dangerous if you are not transparent.”
But even being transparent can be a challenge.
“I think a lot of the issue that we have in health care is what type of information we are providing and how are we providing it, and is the receiver of information actually understanding what we are saying?” she pondered.
“I don’t think we know the answers to that, but I think part of the solution at least is to be as open about what we know as well as what we don’t know at the same time and let the patient make a decision based on their value system,” she continued. “A lot of times with these newer technologies or techniques, you really have to sit down with the patient and ask them about their long-term goals, what are acceptable and unacceptable outcomes.”
Recognizing the importance of data registries, in 2014 AGA launched a new initiative working as a neutral, objective broker to establish clinical research studies. Through this program, AGA collects important data to assess the value of new technologies and procedures on patient care. Ultimately, the data AGA collects will support the approval, coverage, and adoption of new technologies that demonstrate promise and merit. To learn more about AGA’s registry initiative or get involved, please contact Sonya Serra, AGA’s senior director of registry development and integrity, at [email protected].
With an increasing number of emerging technological advances in both medical devices and procedures, two factors will help improve safety and outcomes for patients: better real-time data and information transparency.
And the key to getting that data will be broader use of registries, according to Dana Telem, MD, director of the Comprehensive Hernia Program at the University of Michigan, Ann Arbor.
Dr. Telem will discuss the importance of real-time information and registries during her April 13 presentation at the 2017 AGA Tech Summit, sponsored by the AGA Center for GI Innovation and Technology.
Speaking in advance of the meeting, Dr. Telem noted that understanding value and finding potential safety issues are among the reasons for using data registries.
“I think that’s really why we need to focus on getting real-time data and that’s why I think registry efforts are so important,” she said. “What registries are really great at [is] identifying those isolated events.”
In addition, they help with another key concept she will highlight during her talk: transparency, something that is especially important as new techniques and devices are introduced.
“We understand that there are going to be early adopters, and you need to have the pioneers in order to take those next steps,” she said.
But to get the most out of those new technologies, data need to be recorded not only for short-term outcomes but over the long term as well “so that we can really assess the value of the techniques or the devices that we are putting out into the community.”
And by providing transparency on what is known, as well as unknown, it also helps patients in making their own decisions on whether to proceed with something new.
She believes that, especially when it comes to newer technologies, patients will be willing to be a part of that data collection if doctors are transparent.
“Many people are willing as long as you are honest with them,” Dr. Telem said. “I think particularly that when newer devices and techniques come out, particularly endoscopic procedures that can save them an operation, they are more willing than not, oftentimes, to do it, which is also where it gets a little bit dangerous if you are not transparent.”
But even being transparent can be a challenge.
“I think a lot of the issue that we have in health care is what type of information we are providing and how are we providing it, and is the receiver of information actually understanding what we are saying?” she pondered.
“I don’t think we know the answers to that, but I think part of the solution at least is to be as open about what we know as well as what we don’t know at the same time and let the patient make a decision based on their value system,” she continued. “A lot of times with these newer technologies or techniques, you really have to sit down with the patient and ask them about their long-term goals, what are acceptable and unacceptable outcomes.”
Recognizing the importance of data registries, in 2014 AGA launched a new initiative working as a neutral, objective broker to establish clinical research studies. Through this program, AGA collects important data to assess the value of new technologies and procedures on patient care. Ultimately, the data AGA collects will support the approval, coverage, and adoption of new technologies that demonstrate promise and merit. To learn more about AGA’s registry initiative or get involved, please contact Sonya Serra, AGA’s senior director of registry development and integrity, at [email protected].
With an increasing number of emerging technological advances in both medical devices and procedures, two factors will help improve safety and outcomes for patients: better real-time data and information transparency.
And the key to getting that data will be broader use of registries, according to Dana Telem, MD, director of the Comprehensive Hernia Program at the University of Michigan, Ann Arbor.
Dr. Telem will discuss the importance of real-time information and registries during her April 13 presentation at the 2017 AGA Tech Summit, sponsored by the AGA Center for GI Innovation and Technology.
Speaking in advance of the meeting, Dr. Telem noted that understanding value and finding potential safety issues are among the reasons for using data registries.
“I think that’s really why we need to focus on getting real-time data and that’s why I think registry efforts are so important,” she said. “What registries are really great at [is] identifying those isolated events.”
In addition, they help with another key concept she will highlight during her talk: transparency, something that is especially important as new techniques and devices are introduced.
“We understand that there are going to be early adopters, and you need to have the pioneers in order to take those next steps,” she said.
But to get the most out of those new technologies, data need to be recorded not only for short-term outcomes but over the long term as well “so that we can really assess the value of the techniques or the devices that we are putting out into the community.”
And by providing transparency on what is known, as well as unknown, it also helps patients in making their own decisions on whether to proceed with something new.
She believes that, especially when it comes to newer technologies, patients will be willing to be a part of that data collection if doctors are transparent.
“Many people are willing as long as you are honest with them,” Dr. Telem said. “I think particularly that when newer devices and techniques come out, particularly endoscopic procedures that can save them an operation, they are more willing than not, oftentimes, to do it, which is also where it gets a little bit dangerous if you are not transparent.”
But even being transparent can be a challenge.
“I think a lot of the issue that we have in health care is what type of information we are providing and how are we providing it, and is the receiver of information actually understanding what we are saying?” she pondered.
“I don’t think we know the answers to that, but I think part of the solution at least is to be as open about what we know as well as what we don’t know at the same time and let the patient make a decision based on their value system,” she continued. “A lot of times with these newer technologies or techniques, you really have to sit down with the patient and ask them about their long-term goals, what are acceptable and unacceptable outcomes.”
Recognizing the importance of data registries, in 2014 AGA launched a new initiative working as a neutral, objective broker to establish clinical research studies. Through this program, AGA collects important data to assess the value of new technologies and procedures on patient care. Ultimately, the data AGA collects will support the approval, coverage, and adoption of new technologies that demonstrate promise and merit. To learn more about AGA’s registry initiative or get involved, please contact Sonya Serra, AGA’s senior director of registry development and integrity, at [email protected].
Physicians favor ACOG mammography recommendations
Primary care physicians tend to follow breast cancer screening recommendations from the American Congress of Obstetricians and Gynecologists, according to findings from a recent survey.
The American Congress of Obstetricians and Gynecologists (ACOG), the American Cancer Society (ACS), and the U.S. Preventive Services Task Force (USPSTF) offer conflicting guidelines on the optimal time to initiate and discontinue screening mammography, as well as the optimal screening interval. ACOG recommends annual screening for women aged 40 and older, while the ACS advises annual screening at age 45, and the USPSTF calls for biennial mammograms starting at age 50, though all three organizations stress individualized management.
There were 871 respondents, including family medicine/general practice physicians (44.2%), internists (29.7%), and gynecologists (26.1%). The average age of the respondents was 53 years, and more than half of them had been in practice for more than 20 years. A slight majority (55%) were men, and most (71%) were white.
A total of 26.0% of the respondents said they trusted ACOG screening guidelines the most, 23.8% said they trusted ACS guidelines, and 22.9% said they trusted USPSTF guidelines the most.
In total, 81% of physicians recommended screening to women aged 40-44 years, 88% recommended screening to women aged 45-49 years, and 67% recommended screening for women 75 years or older. Among physicians who recommended screening, most recommended annual exams.
These findings show that physicians differ sharply in their adherence to practice guidelines. The results also “provide an important benchmark as guidelines continue evolving, and underscore the need to delineate barriers and facilitators to implementing guidelines in clinical practice,” the researchers wrote.
Primary care physicians tend to follow breast cancer screening recommendations from the American Congress of Obstetricians and Gynecologists, according to findings from a recent survey.
The American Congress of Obstetricians and Gynecologists (ACOG), the American Cancer Society (ACS), and the U.S. Preventive Services Task Force (USPSTF) offer conflicting guidelines on the optimal time to initiate and discontinue screening mammography, as well as the optimal screening interval. ACOG recommends annual screening for women aged 40 and older, while the ACS advises annual screening at age 45, and the USPSTF calls for biennial mammograms starting at age 50, though all three organizations stress individualized management.
There were 871 respondents, including family medicine/general practice physicians (44.2%), internists (29.7%), and gynecologists (26.1%). The average age of the respondents was 53 years, and more than half of them had been in practice for more than 20 years. A slight majority (55%) were men, and most (71%) were white.
A total of 26.0% of the respondents said they trusted ACOG screening guidelines the most, 23.8% said they trusted ACS guidelines, and 22.9% said they trusted USPSTF guidelines the most.
In total, 81% of physicians recommended screening to women aged 40-44 years, 88% recommended screening to women aged 45-49 years, and 67% recommended screening for women 75 years or older. Among physicians who recommended screening, most recommended annual exams.
These findings show that physicians differ sharply in their adherence to practice guidelines. The results also “provide an important benchmark as guidelines continue evolving, and underscore the need to delineate barriers and facilitators to implementing guidelines in clinical practice,” the researchers wrote.
Primary care physicians tend to follow breast cancer screening recommendations from the American Congress of Obstetricians and Gynecologists, according to findings from a recent survey.
The American Congress of Obstetricians and Gynecologists (ACOG), the American Cancer Society (ACS), and the U.S. Preventive Services Task Force (USPSTF) offer conflicting guidelines on the optimal time to initiate and discontinue screening mammography, as well as the optimal screening interval. ACOG recommends annual screening for women aged 40 and older, while the ACS advises annual screening at age 45, and the USPSTF calls for biennial mammograms starting at age 50, though all three organizations stress individualized management.
There were 871 respondents, including family medicine/general practice physicians (44.2%), internists (29.7%), and gynecologists (26.1%). The average age of the respondents was 53 years, and more than half of them had been in practice for more than 20 years. A slight majority (55%) were men, and most (71%) were white.
A total of 26.0% of the respondents said they trusted ACOG screening guidelines the most, 23.8% said they trusted ACS guidelines, and 22.9% said they trusted USPSTF guidelines the most.
In total, 81% of physicians recommended screening to women aged 40-44 years, 88% recommended screening to women aged 45-49 years, and 67% recommended screening for women 75 years or older. Among physicians who recommended screening, most recommended annual exams.
These findings show that physicians differ sharply in their adherence to practice guidelines. The results also “provide an important benchmark as guidelines continue evolving, and underscore the need to delineate barriers and facilitators to implementing guidelines in clinical practice,” the researchers wrote.
FROM JAMA INTERNAL MEDICINE
Key clinical point:
Major finding: Across physicians groups, 81% of respondents recommended screening women aged 40-44 years.
Data source: An analysis of survey responses regarding breast cancer care from a nationally representative sample of 871 family/general medicine physicians, internists, and gynecologists.
Disclosures: The researchers reported having no conflicts of interest.