User login
Portal allows hemophilia patients to share data with providers

Novo Nordisk has launched a web-based portal that allows hemophilia patients to share real-time data on their treatment and bleeding events with their healthcare providers.
The portal, HemaGo™ XChange, is an extension of Novo Nordisk’s HemaGo™ mobile application and website, which were launched in 2012.
Data a patient enters into the HemaGo™ diary can be shared through the HemaGo™ XChange with the patient’s hemophilia treatment network.
Patients may also choose to have these data entered into the American Thrombosis and Hemostasis Network’s (ATHN) national database of bleeding disorder treatment information.
“We developed HemaGo™ XChange to help drive progress in hemophilia management by turning static data into usable information for people with hemophilia, their care teams, and even researchers,” said John Spera, vice-president of biopharmaceuticals marketing at Novo Nordisk Inc.
“With timely information about the daily experiences of patients, including bleeds, healthcare providers can adjust their care to better fit patient lives.”
Patients using HemaGo™ can:
- Provide information to their healthcare team, including access to treatment and bleed data, in real time through the HemaGo™ XChange web portal
- Choose to email data directly from the app or website at any time
- Opt-in through their hemophilia treatment center to have their data integrated into ATHN’s national database of bleeding disorder treatment information. ATHN will use and share these data with hemophilia treatment centers to foster its mission of advancing knowledge and transforming care for the bleeding and clotting disorders community.
Providers invited by patients to connect via the HemaGo™ XChange portal can:
- View details about treatments, bleeds, and more for multiple patients
- Track when and how much factor is used; the type of infusion, vial, and dosing amounts; and information about any other medications
- View data on the type, location, duration, frequency, and status of bleeds
- View patient and caregiver life experiences, such as pain and health scores or how a bleeding disorder has affected work, school, or other activities
- Download in-depth reports for all recorded information.
Novo Nordisk does not have access to patient-specific information. The company’s access is restricted to de-identified data in which the individual sources of the data cannot be identified, in accordance with Health Insurance Portability and Accountability Act of 1996 (HIPAA) Privacy and Security Rules.
To download the HemaGo™ app or join the HemaGo™ XChange, visit www.HemaGo.com and www.HGXchange.com. The HemaGo™ app is available for iPhone and Android phones. ![]()
Novo Nordisk has launched a web-based portal that allows hemophilia patients to share real-time data on their treatment and bleeding events with their healthcare providers.
The portal, HemaGo™ XChange, is an extension of Novo Nordisk’s HemaGo™ mobile application and website, which were launched in 2012.
Data a patient enters into the HemaGo™ diary can be shared through the HemaGo™ XChange with the patient’s hemophilia treatment network.
Patients may also choose to have these data entered into the American Thrombosis and Hemostasis Network’s (ATHN) national database of bleeding disorder treatment information.
“We developed HemaGo™ XChange to help drive progress in hemophilia management by turning static data into usable information for people with hemophilia, their care teams, and even researchers,” said John Spera, vice-president of biopharmaceuticals marketing at Novo Nordisk Inc.
“With timely information about the daily experiences of patients, including bleeds, healthcare providers can adjust their care to better fit patient lives.”
Patients using HemaGo™ can:
- Provide information to their healthcare team, including access to treatment and bleed data, in real time through the HemaGo™ XChange web portal
- Choose to email data directly from the app or website at any time
- Opt-in through their hemophilia treatment center to have their data integrated into ATHN’s national database of bleeding disorder treatment information. ATHN will use and share these data with hemophilia treatment centers to foster its mission of advancing knowledge and transforming care for the bleeding and clotting disorders community.
Providers invited by patients to connect via the HemaGo™ XChange portal can:
- View details about treatments, bleeds, and more for multiple patients
- Track when and how much factor is used; the type of infusion, vial, and dosing amounts; and information about any other medications
- View data on the type, location, duration, frequency, and status of bleeds
- View patient and caregiver life experiences, such as pain and health scores or how a bleeding disorder has affected work, school, or other activities
- Download in-depth reports for all recorded information.
Novo Nordisk does not have access to patient-specific information. The company’s access is restricted to de-identified data in which the individual sources of the data cannot be identified, in accordance with Health Insurance Portability and Accountability Act of 1996 (HIPAA) Privacy and Security Rules.
To download the HemaGo™ app or join the HemaGo™ XChange, visit www.HemaGo.com and www.HGXchange.com. The HemaGo™ app is available for iPhone and Android phones. ![]()
Novo Nordisk has launched a web-based portal that allows hemophilia patients to share real-time data on their treatment and bleeding events with their healthcare providers.
The portal, HemaGo™ XChange, is an extension of Novo Nordisk’s HemaGo™ mobile application and website, which were launched in 2012.
Data a patient enters into the HemaGo™ diary can be shared through the HemaGo™ XChange with the patient’s hemophilia treatment network.
Patients may also choose to have these data entered into the American Thrombosis and Hemostasis Network’s (ATHN) national database of bleeding disorder treatment information.
“We developed HemaGo™ XChange to help drive progress in hemophilia management by turning static data into usable information for people with hemophilia, their care teams, and even researchers,” said John Spera, vice-president of biopharmaceuticals marketing at Novo Nordisk Inc.
“With timely information about the daily experiences of patients, including bleeds, healthcare providers can adjust their care to better fit patient lives.”
Patients using HemaGo™ can:
- Provide information to their healthcare team, including access to treatment and bleed data, in real time through the HemaGo™ XChange web portal
- Choose to email data directly from the app or website at any time
- Opt-in through their hemophilia treatment center to have their data integrated into ATHN’s national database of bleeding disorder treatment information. ATHN will use and share these data with hemophilia treatment centers to foster its mission of advancing knowledge and transforming care for the bleeding and clotting disorders community.
Providers invited by patients to connect via the HemaGo™ XChange portal can:
- View details about treatments, bleeds, and more for multiple patients
- Track when and how much factor is used; the type of infusion, vial, and dosing amounts; and information about any other medications
- View data on the type, location, duration, frequency, and status of bleeds
- View patient and caregiver life experiences, such as pain and health scores or how a bleeding disorder has affected work, school, or other activities
- Download in-depth reports for all recorded information.
Novo Nordisk does not have access to patient-specific information. The company’s access is restricted to de-identified data in which the individual sources of the data cannot be identified, in accordance with Health Insurance Portability and Accountability Act of 1996 (HIPAA) Privacy and Security Rules.
To download the HemaGo™ app or join the HemaGo™ XChange, visit www.HemaGo.com and www.HGXchange.com. The HemaGo™ app is available for iPhone and Android phones. ![]()
Dry, thickened skin on hand

The FP asked the patient to show him how he moved about and immediately noticed that the involved area corresponded directly to the part of the hand that pressed upon his cane. He then diagnosed the patient with unilateral hand eczema related to friction.
The FP asked the patient if he would be willing to get a soft glove to wear on his hand while walking. The patient was amenable to this suggestion, but also asked if something could be done for the dry, thickened area that had already built up on his palm.
The FP prescribed ammonium lactate 12% to be applied twice daily, as it is a good moisturizing keratolytic that helps to break down keratin and soften the skin. He also gave the patient a prescription for 0.1% triamcinolone ointment to rub into the affected area at night before going to sleep. The FP recommended not using this during the daytime as it might make the patient’s hand slippery, leading to a fall if he lost his grip on the cane. At a follow-up visit 2 months later, the patient had improved and was very happy with the result.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R. Hand eczema. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:597-602.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP asked the patient to show him how he moved about and immediately noticed that the involved area corresponded directly to the part of the hand that pressed upon his cane. He then diagnosed the patient with unilateral hand eczema related to friction.
The FP asked the patient if he would be willing to get a soft glove to wear on his hand while walking. The patient was amenable to this suggestion, but also asked if something could be done for the dry, thickened area that had already built up on his palm.
The FP prescribed ammonium lactate 12% to be applied twice daily, as it is a good moisturizing keratolytic that helps to break down keratin and soften the skin. He also gave the patient a prescription for 0.1% triamcinolone ointment to rub into the affected area at night before going to sleep. The FP recommended not using this during the daytime as it might make the patient’s hand slippery, leading to a fall if he lost his grip on the cane. At a follow-up visit 2 months later, the patient had improved and was very happy with the result.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R. Hand eczema. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:597-602.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP asked the patient to show him how he moved about and immediately noticed that the involved area corresponded directly to the part of the hand that pressed upon his cane. He then diagnosed the patient with unilateral hand eczema related to friction.
The FP asked the patient if he would be willing to get a soft glove to wear on his hand while walking. The patient was amenable to this suggestion, but also asked if something could be done for the dry, thickened area that had already built up on his palm.
The FP prescribed ammonium lactate 12% to be applied twice daily, as it is a good moisturizing keratolytic that helps to break down keratin and soften the skin. He also gave the patient a prescription for 0.1% triamcinolone ointment to rub into the affected area at night before going to sleep. The FP recommended not using this during the daytime as it might make the patient’s hand slippery, leading to a fall if he lost his grip on the cane. At a follow-up visit 2 months later, the patient had improved and was very happy with the result.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R. Hand eczema. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:597-602.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

When You Can’t Make a Rash Diagnosis
ANSWER
The false statement—and therefore the correct choice—is that MF is almost always fatal (choice “a”). MF can often be controlled, if not completely cured.
DISCUSSION
In its early stages, cutaneous T-cell lymphoma (CTCL) can manifest with an innocuous-appearing rash, notable for its chronicity and resistance to treatment. One example is poikiloderma vasculare atrophicans (PVA), which is identified by nonblanchable atrophic patches with fine surface vascularity that often manifest around the waistline or groin. Left undiagnosed and untreated, PVA can slowly progress to a more advanced stage, as was the case with this patient.
Several cancers can present with rash, including extramammary Paget disease, superficial squamous cell carcinoma (Bowen disease), and various types of metastatic cancer (eg, breast, colon, lung).
The confirmation of CTCL/MF may require serial biopsies over time, as the diagnostic signs can take years to become detectable. These specimens must be accompanied by pertinent clinical information to suggest a differential that includes this lymphoma.
Early-stage CTCL can be controlled with topical steroids, but as the condition advances, specialized treatment is needed. The tumor stage observed in
ANSWER
The false statement—and therefore the correct choice—is that MF is almost always fatal (choice “a”). MF can often be controlled, if not completely cured.
DISCUSSION
In its early stages, cutaneous T-cell lymphoma (CTCL) can manifest with an innocuous-appearing rash, notable for its chronicity and resistance to treatment. One example is poikiloderma vasculare atrophicans (PVA), which is identified by nonblanchable atrophic patches with fine surface vascularity that often manifest around the waistline or groin. Left undiagnosed and untreated, PVA can slowly progress to a more advanced stage, as was the case with this patient.
Several cancers can present with rash, including extramammary Paget disease, superficial squamous cell carcinoma (Bowen disease), and various types of metastatic cancer (eg, breast, colon, lung).
The confirmation of CTCL/MF may require serial biopsies over time, as the diagnostic signs can take years to become detectable. These specimens must be accompanied by pertinent clinical information to suggest a differential that includes this lymphoma.
Early-stage CTCL can be controlled with topical steroids, but as the condition advances, specialized treatment is needed. The tumor stage observed in
ANSWER
The false statement—and therefore the correct choice—is that MF is almost always fatal (choice “a”). MF can often be controlled, if not completely cured.
DISCUSSION
In its early stages, cutaneous T-cell lymphoma (CTCL) can manifest with an innocuous-appearing rash, notable for its chronicity and resistance to treatment. One example is poikiloderma vasculare atrophicans (PVA), which is identified by nonblanchable atrophic patches with fine surface vascularity that often manifest around the waistline or groin. Left undiagnosed and untreated, PVA can slowly progress to a more advanced stage, as was the case with this patient.
Several cancers can present with rash, including extramammary Paget disease, superficial squamous cell carcinoma (Bowen disease), and various types of metastatic cancer (eg, breast, colon, lung).
The confirmation of CTCL/MF may require serial biopsies over time, as the diagnostic signs can take years to become detectable. These specimens must be accompanied by pertinent clinical information to suggest a differential that includes this lymphoma.
Early-stage CTCL can be controlled with topical steroids, but as the condition advances, specialized treatment is needed. The tumor stage observed in

For years, this 64-year-old man has complained of itching and a rash around his head and neck. He has consulted several primary care providers—and even a dermatologist. A punch biopsy performed by that provider yielded no clear diagnosis. The patient was advised to return for follow-up but never did so.
Treatment was attempted with a succession of medications; none resulted in any improvement. The list includes antifungal creams (econazole, clotrimazole, and miconazole), an oral antifungal medication (a one-month course of terbinafine 250 mg/d), and a corticosteroid (a one-month course of prednisone 20 mg/d).
In addition to the rash and pruritus, the patient feels “lumps” in the affected areas. He also reports feeling more tired than usual. Prior to the onset of these symptoms, his only complaint was lifelong eczema.
Large infiltrative plaques are seen on both sides of his neck, extending into his ears and onto his scalp. A few exceed 8 cm in diameter, and all have smooth surfaces with no epidermal disturbance. Several discrete, 2- to 4-cm, fixed nodules are also seen and felt on his neck below these plaques.
A 5-mm punch biopsy is performed on one of the plaques on his occipital scalp; the pathology report shows only chronic changes consistent with eczema. The decision is made to perform another biopsy. A deeper, wider, 5-cm wedge from the left preauricular plaque is taken and submitted. The report shows changes consistent with tumor-stage mycosis fungoides (MF).

Both diabetes types increase markedly among youths
The annual incidence of both types 1 and 2 diabetes markedly increased among youths between 2002 and 2012, especially among those in minority racial and ethnic groups, according to a report published online April 13 in the New England Journal of Medicine.
Researchers analyzed trends in diabetes incidence in the observational Search for Diabetes in Youth study, which conducts annual population-based case ascertainment of the disease in people aged 0-20 years. SEARCH is funded by the Centers for Disease Control and Prevention and the National Institute of Diabetes and Digestive and Kidney Diseases.
In this analysis of SEARCH data, there were 11,245 youths with type 1 diabetes in 54,239,600 person-years of surveillance and 2,846 with type 2 diabetes in 28,029,000 person-years of surveillance.
“We estimated that approximately 15,900 cases of type 1 diabetes were diagnosed annually in the U.S. in the 2002-2003 period, and this number increased to 17,900 annually in the 2011-2012 period. Overall, the adjusted annual relative increase in the incidence of type 1 diabetes was 1.8%,” noted Elizabeth J. Mayer-Davis, PhD, of the departments of nutrition and medicine, University of North Carolina, Chapel Hill, and her associates (N Engl J Med. 2017 April 13. doi: 101056/NEJMoa1610187).
Similarly, they estimated that approximately 3,800 cases of type 2 diabetes were diagnosed in the first year of the study, increasing to 5,300 in the final year. The annual relative increase in type 2 diabetes was 4.8%.
The rate of increase varied across the five major ethnic groups studied: non-Hispanic whites, non-Hispanic blacks, Hispanics, Asians or Pacific Islanders, and Native Americans. Type 1 diabetes incidence rose rapidly among Hispanic youths, and type 2 diabetes rose rapidly in all racial and ethnic groups other than whites, with the greatest rate of increase among Native Americans.
These increases suggest “a growing disease burden that will not be shared equally” because of differences among ethnic groups in barriers to care, methods of treatment, and clinical outcomes. “These findings highlight the critical need to identify approaches to reduce disparities among racial and ethnic groups,” Dr. Mayer-Davis and her associates noted.
The National Institute of Diabetes and Digestive and Kidney Diseases and the Centers for Disease Control and Prevention funded the study. Dr. Mayer-Davis reported having no relevant disclosures. One of her associates reported serving as a consultant to Denka-Seiken and MedTest DX.
This study by Mayer-Davis et al. provides the most current data available on the incidence of diabetes in this age group.
The consequence of this increase in diabetes among youths is that the overall disease burden on public health is actually increasing, despite improvements in mortality and CVD rates among older diabetes patients.
According to the 2015 Global Burden of Disease report, the number of years lived with disability has increased by 32.5% and the number of years of life lost has increased by 25.4%.
What do the marked increase in the incidence of diabetes and more people at risk imply about therapy? Data from two large studies over the past several decades support that intensive glycemic control improved outcomes in persons with type 1 or type 2 diabetes mellitus. But what is missing, despite a growing understanding about the pathogenesis of each condition, is knowledge about how best to lower the number of new cases and how best to treat problems once they arise in persons with diabetes.
It is clear that we are far from controlling the negative effects of diabetes on health worldwide. As the prevalence increases, we clearly need new approaches to reduce the burden of this disease on public health.
Julie R. Ingelfinger, M.D., and John A. Jarcho, M.D., are deputy editors of The New England Journal of Medicine. They reported having no relevant disclosures. Dr. Ingelfinger and Dr. Jarcho made these remarks in an editorial accompanying Dr. Mayer-Davis’s report (N Engl J Med. 2017 April 13. doi: 10.1056/NEJMe1616575).
This study by Mayer-Davis et al. provides the most current data available on the incidence of diabetes in this age group.
The consequence of this increase in diabetes among youths is that the overall disease burden on public health is actually increasing, despite improvements in mortality and CVD rates among older diabetes patients.
According to the 2015 Global Burden of Disease report, the number of years lived with disability has increased by 32.5% and the number of years of life lost has increased by 25.4%.
What do the marked increase in the incidence of diabetes and more people at risk imply about therapy? Data from two large studies over the past several decades support that intensive glycemic control improved outcomes in persons with type 1 or type 2 diabetes mellitus. But what is missing, despite a growing understanding about the pathogenesis of each condition, is knowledge about how best to lower the number of new cases and how best to treat problems once they arise in persons with diabetes.
It is clear that we are far from controlling the negative effects of diabetes on health worldwide. As the prevalence increases, we clearly need new approaches to reduce the burden of this disease on public health.
Julie R. Ingelfinger, M.D., and John A. Jarcho, M.D., are deputy editors of The New England Journal of Medicine. They reported having no relevant disclosures. Dr. Ingelfinger and Dr. Jarcho made these remarks in an editorial accompanying Dr. Mayer-Davis’s report (N Engl J Med. 2017 April 13. doi: 10.1056/NEJMe1616575).
This study by Mayer-Davis et al. provides the most current data available on the incidence of diabetes in this age group.
The consequence of this increase in diabetes among youths is that the overall disease burden on public health is actually increasing, despite improvements in mortality and CVD rates among older diabetes patients.
According to the 2015 Global Burden of Disease report, the number of years lived with disability has increased by 32.5% and the number of years of life lost has increased by 25.4%.
What do the marked increase in the incidence of diabetes and more people at risk imply about therapy? Data from two large studies over the past several decades support that intensive glycemic control improved outcomes in persons with type 1 or type 2 diabetes mellitus. But what is missing, despite a growing understanding about the pathogenesis of each condition, is knowledge about how best to lower the number of new cases and how best to treat problems once they arise in persons with diabetes.
It is clear that we are far from controlling the negative effects of diabetes on health worldwide. As the prevalence increases, we clearly need new approaches to reduce the burden of this disease on public health.
Julie R. Ingelfinger, M.D., and John A. Jarcho, M.D., are deputy editors of The New England Journal of Medicine. They reported having no relevant disclosures. Dr. Ingelfinger and Dr. Jarcho made these remarks in an editorial accompanying Dr. Mayer-Davis’s report (N Engl J Med. 2017 April 13. doi: 10.1056/NEJMe1616575).
The annual incidence of both types 1 and 2 diabetes markedly increased among youths between 2002 and 2012, especially among those in minority racial and ethnic groups, according to a report published online April 13 in the New England Journal of Medicine.
Researchers analyzed trends in diabetes incidence in the observational Search for Diabetes in Youth study, which conducts annual population-based case ascertainment of the disease in people aged 0-20 years. SEARCH is funded by the Centers for Disease Control and Prevention and the National Institute of Diabetes and Digestive and Kidney Diseases.
In this analysis of SEARCH data, there were 11,245 youths with type 1 diabetes in 54,239,600 person-years of surveillance and 2,846 with type 2 diabetes in 28,029,000 person-years of surveillance.
“We estimated that approximately 15,900 cases of type 1 diabetes were diagnosed annually in the U.S. in the 2002-2003 period, and this number increased to 17,900 annually in the 2011-2012 period. Overall, the adjusted annual relative increase in the incidence of type 1 diabetes was 1.8%,” noted Elizabeth J. Mayer-Davis, PhD, of the departments of nutrition and medicine, University of North Carolina, Chapel Hill, and her associates (N Engl J Med. 2017 April 13. doi: 101056/NEJMoa1610187).
Similarly, they estimated that approximately 3,800 cases of type 2 diabetes were diagnosed in the first year of the study, increasing to 5,300 in the final year. The annual relative increase in type 2 diabetes was 4.8%.
The rate of increase varied across the five major ethnic groups studied: non-Hispanic whites, non-Hispanic blacks, Hispanics, Asians or Pacific Islanders, and Native Americans. Type 1 diabetes incidence rose rapidly among Hispanic youths, and type 2 diabetes rose rapidly in all racial and ethnic groups other than whites, with the greatest rate of increase among Native Americans.
These increases suggest “a growing disease burden that will not be shared equally” because of differences among ethnic groups in barriers to care, methods of treatment, and clinical outcomes. “These findings highlight the critical need to identify approaches to reduce disparities among racial and ethnic groups,” Dr. Mayer-Davis and her associates noted.
The National Institute of Diabetes and Digestive and Kidney Diseases and the Centers for Disease Control and Prevention funded the study. Dr. Mayer-Davis reported having no relevant disclosures. One of her associates reported serving as a consultant to Denka-Seiken and MedTest DX.
The annual incidence of both types 1 and 2 diabetes markedly increased among youths between 2002 and 2012, especially among those in minority racial and ethnic groups, according to a report published online April 13 in the New England Journal of Medicine.
Researchers analyzed trends in diabetes incidence in the observational Search for Diabetes in Youth study, which conducts annual population-based case ascertainment of the disease in people aged 0-20 years. SEARCH is funded by the Centers for Disease Control and Prevention and the National Institute of Diabetes and Digestive and Kidney Diseases.
In this analysis of SEARCH data, there were 11,245 youths with type 1 diabetes in 54,239,600 person-years of surveillance and 2,846 with type 2 diabetes in 28,029,000 person-years of surveillance.
“We estimated that approximately 15,900 cases of type 1 diabetes were diagnosed annually in the U.S. in the 2002-2003 period, and this number increased to 17,900 annually in the 2011-2012 period. Overall, the adjusted annual relative increase in the incidence of type 1 diabetes was 1.8%,” noted Elizabeth J. Mayer-Davis, PhD, of the departments of nutrition and medicine, University of North Carolina, Chapel Hill, and her associates (N Engl J Med. 2017 April 13. doi: 101056/NEJMoa1610187).
Similarly, they estimated that approximately 3,800 cases of type 2 diabetes were diagnosed in the first year of the study, increasing to 5,300 in the final year. The annual relative increase in type 2 diabetes was 4.8%.
The rate of increase varied across the five major ethnic groups studied: non-Hispanic whites, non-Hispanic blacks, Hispanics, Asians or Pacific Islanders, and Native Americans. Type 1 diabetes incidence rose rapidly among Hispanic youths, and type 2 diabetes rose rapidly in all racial and ethnic groups other than whites, with the greatest rate of increase among Native Americans.
These increases suggest “a growing disease burden that will not be shared equally” because of differences among ethnic groups in barriers to care, methods of treatment, and clinical outcomes. “These findings highlight the critical need to identify approaches to reduce disparities among racial and ethnic groups,” Dr. Mayer-Davis and her associates noted.
The National Institute of Diabetes and Digestive and Kidney Diseases and the Centers for Disease Control and Prevention funded the study. Dr. Mayer-Davis reported having no relevant disclosures. One of her associates reported serving as a consultant to Denka-Seiken and MedTest DX.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Both types 1 and 2 diabetes increased markedly among youths between 2002 and 2012, especially among those in minority racial and ethnic groups.
Major finding: The incidence of type 1 diabetes increased an estimated 1.8% per year and that of type 2 diabetes increased 4.8% per year between 2002 and 2012.
Data source: An observational study assessing a nationally representative sample of youths aged 0-20 years in five states, including 11,245 with type 1 and 2,846 with type 2 diabetes.
Disclosures: The National Institute of Diabetes and Digestive and Kidney Diseases and the Centers for Disease Control and Prevention funded the study. Dr. Mayer-Davis reported having no relevant disclosures. One of her associates reported serving as a consultant to Denka-Seiken and MedTest DX.
Coverage denials plague U.S. PCSK9-inhibitor prescriptions
WASHINGTON – During the first year that the lipid-lowering PCSK9 inhibitors were on the U.S. market, 2015-2016, fewer than half the patients prescribed the drug had it covered through their health insurance, based on an analysis of prescriptions written for more than 45,000 patients.
On top of that, about a third of patients with health insurance that eventually agreed to cover the notoriously expensive PCSK (proprotein convertase subtilisin–kexin type) 9 inhibitors failed to actually collect their medication, possibly because of a sizable copay, which meant that, in total, fewer than a third of U.S. patients prescribed these drugs actually began using them, Ann Marie Navar, MD, said at the annual meeting of the American College of Cardiology.
The recent PCSK9-inhibitor experience highlighting the frequent preauthorization roadblocks and denied coverage that providers and patients must navigate is “one of the dirty little secrets of American medicine,” commented Mariell Jessup, MD, a discussant for the study and professor of medicine at the University of Pennsylvania in Philadelphia.
Dr. Navar countered that these problems may be a secret for many Americans “but it’s not a secret for providers. We know the problems patients have getting drugs covered through the prior authorization process.”

Symphony Health’s records included 45,029 U.S. patients who received a first-time PCSK9-inhibitor prescription during the 12 months studied. Just over half were prescriptions exclusively covered by government-funded insurance (with 90% of these covered through Medicaid), 40% exclusively by a commercial insurer, and the balance subject to dual coverage. Nearly half the prescriptions were written by cardiologists, 37% by primary care physicians, and most of the remaining 15% came from endocrinologists.
Among these prescriptions, 79% received an initial rejection. Following appeals, 53% were rejected and 47% covered. Among the more than 21,000 prescriptions approved for coverage, 13,892 (31% of the 45,029) were actually received by patients, Dr. Navar reported.
During the first several months following availability of the PCSK9 inhibitors, the number of new prescriptions steadily rose until a plateau occurred by about April 2016 of about 6,000 new prescriptions written per month. During each of the 12 months examined, the proportion of prescriptions denied coverage remained roughly constant, suggesting that clinicians developed no insights over time into how to better the prospect for ultimate insurance coverage.
In a multivariate analysis certain aspects of the prescribing and coverage process linked with significantly better rates of patients actually receiving the PCSK9 inhibitor. Prescriptions filled at mail-order pharmacies were over fourfold more likely to be received by patients than those filled at retail pharmacies. Prescriptions written by cardiologists were 80% more likely to be received than those written by primary care physicians; those written by endocrinologists were 30% more likely to be filled. Patients who relied exclusively on a government insurance plan had a threefold greater filling rate than those who exclusively had commercial insurance, and patients with both government and commercial insurance had a fourfold greater rate of receiving their prescription, compared with commercial-only patients. Patients who used a manufacturer’s coupon to help reduce the cost of their prescription had a 17-fold higher rate of receiving the drug, compared with patients who did not use a coupon.
A final set of findings underscored the great variability in the approval process that patients encountered. Among the 13,892 prescriptions that were actually dispensed, 45% were dispensed within 1 day of when the prescription was written, but the median time for dispensing wasn’t reached until the tenth day, and for a quarter of the dispenses the lag from writing the prescription to getting it into patients’ hands was greater than 1 month. Rates of coverage denials also varied widely depending on the specific commercial insurers involved and the specific pharmacy benefit manager. Among the top 10 commercial insurers included in the data set, the rate of coverage denial ranged from 33% to 78%.
This variability suggested that many denials were not simply because of clinical factors. Some commercial insurers “introduce vigorous and sometimes burdensome prior authorization procedures,” Dr. Navar said.
[email protected]
On Twitter @mitchelzoler
WASHINGTON – During the first year that the lipid-lowering PCSK9 inhibitors were on the U.S. market, 2015-2016, fewer than half the patients prescribed the drug had it covered through their health insurance, based on an analysis of prescriptions written for more than 45,000 patients.
On top of that, about a third of patients with health insurance that eventually agreed to cover the notoriously expensive PCSK (proprotein convertase subtilisin–kexin type) 9 inhibitors failed to actually collect their medication, possibly because of a sizable copay, which meant that, in total, fewer than a third of U.S. patients prescribed these drugs actually began using them, Ann Marie Navar, MD, said at the annual meeting of the American College of Cardiology.
The recent PCSK9-inhibitor experience highlighting the frequent preauthorization roadblocks and denied coverage that providers and patients must navigate is “one of the dirty little secrets of American medicine,” commented Mariell Jessup, MD, a discussant for the study and professor of medicine at the University of Pennsylvania in Philadelphia.
Dr. Navar countered that these problems may be a secret for many Americans “but it’s not a secret for providers. We know the problems patients have getting drugs covered through the prior authorization process.”
Symphony Health’s records included 45,029 U.S. patients who received a first-time PCSK9-inhibitor prescription during the 12 months studied. Just over half were prescriptions exclusively covered by government-funded insurance (with 90% of these covered through Medicaid), 40% exclusively by a commercial insurer, and the balance subject to dual coverage. Nearly half the prescriptions were written by cardiologists, 37% by primary care physicians, and most of the remaining 15% came from endocrinologists.
Among these prescriptions, 79% received an initial rejection. Following appeals, 53% were rejected and 47% covered. Among the more than 21,000 prescriptions approved for coverage, 13,892 (31% of the 45,029) were actually received by patients, Dr. Navar reported.
During the first several months following availability of the PCSK9 inhibitors, the number of new prescriptions steadily rose until a plateau occurred by about April 2016 of about 6,000 new prescriptions written per month. During each of the 12 months examined, the proportion of prescriptions denied coverage remained roughly constant, suggesting that clinicians developed no insights over time into how to better the prospect for ultimate insurance coverage.
In a multivariate analysis certain aspects of the prescribing and coverage process linked with significantly better rates of patients actually receiving the PCSK9 inhibitor. Prescriptions filled at mail-order pharmacies were over fourfold more likely to be received by patients than those filled at retail pharmacies. Prescriptions written by cardiologists were 80% more likely to be received than those written by primary care physicians; those written by endocrinologists were 30% more likely to be filled. Patients who relied exclusively on a government insurance plan had a threefold greater filling rate than those who exclusively had commercial insurance, and patients with both government and commercial insurance had a fourfold greater rate of receiving their prescription, compared with commercial-only patients. Patients who used a manufacturer’s coupon to help reduce the cost of their prescription had a 17-fold higher rate of receiving the drug, compared with patients who did not use a coupon.
A final set of findings underscored the great variability in the approval process that patients encountered. Among the 13,892 prescriptions that were actually dispensed, 45% were dispensed within 1 day of when the prescription was written, but the median time for dispensing wasn’t reached until the tenth day, and for a quarter of the dispenses the lag from writing the prescription to getting it into patients’ hands was greater than 1 month. Rates of coverage denials also varied widely depending on the specific commercial insurers involved and the specific pharmacy benefit manager. Among the top 10 commercial insurers included in the data set, the rate of coverage denial ranged from 33% to 78%.
This variability suggested that many denials were not simply because of clinical factors. Some commercial insurers “introduce vigorous and sometimes burdensome prior authorization procedures,” Dr. Navar said.
[email protected]
On Twitter @mitchelzoler
WASHINGTON – During the first year that the lipid-lowering PCSK9 inhibitors were on the U.S. market, 2015-2016, fewer than half the patients prescribed the drug had it covered through their health insurance, based on an analysis of prescriptions written for more than 45,000 patients.
On top of that, about a third of patients with health insurance that eventually agreed to cover the notoriously expensive PCSK (proprotein convertase subtilisin–kexin type) 9 inhibitors failed to actually collect their medication, possibly because of a sizable copay, which meant that, in total, fewer than a third of U.S. patients prescribed these drugs actually began using them, Ann Marie Navar, MD, said at the annual meeting of the American College of Cardiology.
The recent PCSK9-inhibitor experience highlighting the frequent preauthorization roadblocks and denied coverage that providers and patients must navigate is “one of the dirty little secrets of American medicine,” commented Mariell Jessup, MD, a discussant for the study and professor of medicine at the University of Pennsylvania in Philadelphia.
Dr. Navar countered that these problems may be a secret for many Americans “but it’s not a secret for providers. We know the problems patients have getting drugs covered through the prior authorization process.”
Symphony Health’s records included 45,029 U.S. patients who received a first-time PCSK9-inhibitor prescription during the 12 months studied. Just over half were prescriptions exclusively covered by government-funded insurance (with 90% of these covered through Medicaid), 40% exclusively by a commercial insurer, and the balance subject to dual coverage. Nearly half the prescriptions were written by cardiologists, 37% by primary care physicians, and most of the remaining 15% came from endocrinologists.
Among these prescriptions, 79% received an initial rejection. Following appeals, 53% were rejected and 47% covered. Among the more than 21,000 prescriptions approved for coverage, 13,892 (31% of the 45,029) were actually received by patients, Dr. Navar reported.
During the first several months following availability of the PCSK9 inhibitors, the number of new prescriptions steadily rose until a plateau occurred by about April 2016 of about 6,000 new prescriptions written per month. During each of the 12 months examined, the proportion of prescriptions denied coverage remained roughly constant, suggesting that clinicians developed no insights over time into how to better the prospect for ultimate insurance coverage.
In a multivariate analysis certain aspects of the prescribing and coverage process linked with significantly better rates of patients actually receiving the PCSK9 inhibitor. Prescriptions filled at mail-order pharmacies were over fourfold more likely to be received by patients than those filled at retail pharmacies. Prescriptions written by cardiologists were 80% more likely to be received than those written by primary care physicians; those written by endocrinologists were 30% more likely to be filled. Patients who relied exclusively on a government insurance plan had a threefold greater filling rate than those who exclusively had commercial insurance, and patients with both government and commercial insurance had a fourfold greater rate of receiving their prescription, compared with commercial-only patients. Patients who used a manufacturer’s coupon to help reduce the cost of their prescription had a 17-fold higher rate of receiving the drug, compared with patients who did not use a coupon.
A final set of findings underscored the great variability in the approval process that patients encountered. Among the 13,892 prescriptions that were actually dispensed, 45% were dispensed within 1 day of when the prescription was written, but the median time for dispensing wasn’t reached until the tenth day, and for a quarter of the dispenses the lag from writing the prescription to getting it into patients’ hands was greater than 1 month. Rates of coverage denials also varied widely depending on the specific commercial insurers involved and the specific pharmacy benefit manager. Among the top 10 commercial insurers included in the data set, the rate of coverage denial ranged from 33% to 78%.
This variability suggested that many denials were not simply because of clinical factors. Some commercial insurers “introduce vigorous and sometimes burdensome prior authorization procedures,” Dr. Navar said.
[email protected]
On Twitter @mitchelzoler
AT ACC 17
Key clinical point:
Major finding: Coverage denials occurred for 53% of U.S. patients who received a new prescription for a PCSK9 inhibitor during 2015-2016.
Data source: Review of 45,029 U.S. patients who received a new prescription for a PCSK9 inhibitor in a Symphony Health database.
Disclosures: The study was sponsored by Amgen, the company that markets evolocumab (Repatha). Dr. Navar has received research support from Amgen, Sanofi, and Regeneron and has been a consultant to Sanofi.
APA Presidential Symposium will focus on trials in geriatric psychiatry
Designing clinical trials within a psychiatric practice is a challenging endeavor, regardless of the population. But, setting up trials for older adults can involve unique ethical and economic considerations.
On Saturday, May 20, a panel of four experts will explore these issues in an Invited Presidential Symposium at this year’s annual meeting of the American Psychiatric Association in San Diego. The symposium, which will be held that morning from 8 to 11 a.m., will feature Mary Sano, PhD, of the Mount Sinai School of Medicine, New York; Joan A. Mackell, PhD, of JM Neuroscience, New York; Olga Brawman-Mintzer, MD, of the Medical University of South Carolina, Charleston; and Maria I. Lapid, MD, of the Mayo Clinic, Rochester, Minn. Dr. Sano will chair the symposium, and Dr. Brawman-Mintzer will be the cochair.
The discussion will examine some of the basics of clinical trial design for geriatric psychiatry for several disorders, including dementia and depression, and for numerous conditions, including agitation and behavioral disturbances. It will also explore other key issues, such as the regulatory knowledge needed to conduct clinical trials, the role of the institutional review board in protecting human subjects, and whether the protocol works and will pay the bills.
It will take place on the upper level of the San Diego Convention Center (session ID: 8012). To look up other sessions, check out the APA’s search function.
Designing clinical trials within a psychiatric practice is a challenging endeavor, regardless of the population. But, setting up trials for older adults can involve unique ethical and economic considerations.
On Saturday, May 20, a panel of four experts will explore these issues in an Invited Presidential Symposium at this year’s annual meeting of the American Psychiatric Association in San Diego. The symposium, which will be held that morning from 8 to 11 a.m., will feature Mary Sano, PhD, of the Mount Sinai School of Medicine, New York; Joan A. Mackell, PhD, of JM Neuroscience, New York; Olga Brawman-Mintzer, MD, of the Medical University of South Carolina, Charleston; and Maria I. Lapid, MD, of the Mayo Clinic, Rochester, Minn. Dr. Sano will chair the symposium, and Dr. Brawman-Mintzer will be the cochair.
The discussion will examine some of the basics of clinical trial design for geriatric psychiatry for several disorders, including dementia and depression, and for numerous conditions, including agitation and behavioral disturbances. It will also explore other key issues, such as the regulatory knowledge needed to conduct clinical trials, the role of the institutional review board in protecting human subjects, and whether the protocol works and will pay the bills.
It will take place on the upper level of the San Diego Convention Center (session ID: 8012). To look up other sessions, check out the APA’s search function.
Designing clinical trials within a psychiatric practice is a challenging endeavor, regardless of the population. But, setting up trials for older adults can involve unique ethical and economic considerations.
On Saturday, May 20, a panel of four experts will explore these issues in an Invited Presidential Symposium at this year’s annual meeting of the American Psychiatric Association in San Diego. The symposium, which will be held that morning from 8 to 11 a.m., will feature Mary Sano, PhD, of the Mount Sinai School of Medicine, New York; Joan A. Mackell, PhD, of JM Neuroscience, New York; Olga Brawman-Mintzer, MD, of the Medical University of South Carolina, Charleston; and Maria I. Lapid, MD, of the Mayo Clinic, Rochester, Minn. Dr. Sano will chair the symposium, and Dr. Brawman-Mintzer will be the cochair.
The discussion will examine some of the basics of clinical trial design for geriatric psychiatry for several disorders, including dementia and depression, and for numerous conditions, including agitation and behavioral disturbances. It will also explore other key issues, such as the regulatory knowledge needed to conduct clinical trials, the role of the institutional review board in protecting human subjects, and whether the protocol works and will pay the bills.
It will take place on the upper level of the San Diego Convention Center (session ID: 8012). To look up other sessions, check out the APA’s search function.
In ‘stealth move,’ Mich. refines vaccine waivers, improves rate among kids
Just 3 years ago, Michigan had the fourth-highest rate of unvaccinated kindergartners in the nation. But, when a charter school in northwestern Traverse City reported nearly two dozen cases of whooping cough and several cases of measles that November, state officials were jolted to action.
Without much fanfare – or time for opponents to respond – they abandoned the state’s relatively loose rules for getting an exemption and issued a regulation requiring families to consult personally with local public health departments before obtaining an immunization waiver.
The new rule sidestepped potential ideological firefights in the state legislature, which have plagued lawmakers in other states who are trying to crack down on vaccination waivers. The regulation had a dramatic effect. In the first year, the Michigan Department of Health & Human Services reported that the number of statewide waivers issued had plunged 35%. Today, Michigan is in the middle of the pack among vaccination rates.
“The idea was to make the process more burdensome,” said Michigan State University health policy specialist Mark Largent, PhD, who has written extensively about vaccines. “Research has shown that, if you make it more inconvenient to apply for a waiver, fewer people get them.”
Michigan’s experience demonstrates a way for governments to increase immunization rates without having to address religious or philosophical opposition to vaccines.
For many years, opposition to mandatory childhood vaccines has served as a frequent rallying point for those who see immunizations as interference with nature’s intentions, rebel against them as government meddling in family affairs, or raise concerns about their safety.
Vaccine advocates and health professionals regard these views as dangerous, noting that the drugs have dramatically lowered the number of serious childhood illnesses and that studies suggesting they are not safe have been debunked. They also note that vaccines’ proven effectiveness lies in “herd immunity” – the higher the participation rate, the greater the community’s protection against outbreaks of infectious disease.
Many states adopt strategies to curb exemptions “by making applications complicated to fill out or complete,” according to University of Georgia public policy expert W. David Bradford, PhD, who studies immunization. Some states require parents to notarize applications or have them certified by a physician before sending them in, and, “generally speaking, anything that raises the opportunity cost [of exemptions] works to some degree,” Bradford said. “Michigan took it a step further.”
Increasing the number of vaccinated kids in Michigan, which has a Republican governor and Republican majorities in both legislative houses, took a degree of political finesse.
“Health & Human Services wanted to do something, but the legislative option wasn’t there,” Dr. Largent said. Instead, Michigan decided to use a strategy he calls “inconvenience.”
Since 1978, Michigan had required schoolchildren entering kindergarten and middle school to obtain vaccination waiver certificates from county officials. “Some counties allowed you to do it over the phone; in others you mailed in a form and some even let you do it online,” Dr. Largent said. But, in studying vaccine policy across the country, he noted, “One thing is really clear – health departments that require you to go in and get the waiver have much lower rates.”
Michigan offered the perfect vehicle for introducing inconvenience into the process. The Joint Committee on Administrative Rules reviews state agency regulations and, if it takes no action, allows them to go into effect after 15 legislative days. The committee is composed of lawmakers, giving it a legislative imprimatur, but it is not the legislature itself, thus avoiding the political rancor that can accompany debate on controversial issues.
During the 2013-14 school year, the federal Centers for Disease Control and Prevention found that Michigan had the fourth-highest rate of children entering kindergarten who had been exempted from vaccinations. The state Health & Human Services officials proposed a simple requirement: Parents seeking vaccine waivers must be briefed in person by a county health educator before a waiver would be granted. The joint committee approved the rule Dec. 11, 2014. It took effect Jan. 1, 2015.
“We were not aware of the rule until the day it happened,” said Suzanne Waltman, president of Michigan for Vaccine Choice, an antivaccine organization. “We thought it was a stealth move.”
The office of Gov. Rick Snyder did not respond directly to requests for comment on the political hazards of vaccine policy. Retired Republican state Sen. John Pappageorge, cochair of the administrative rules committee in 2014, voted to adopt the rule and described the procedure as a simple one designed to ensure “that implementation is in concurrence with the law.” Republican Rep. Tom McMillin, who was cochair of the committee at the time and voted against the rule, did not respond to requests for an interview.
In a look at one key metric, before 2015, about 22% of Michigan children did not get the fourth round of immunizations for diphtheria, tetanus, and pertussis that is required by the state. That had fallen to 15% 1 year later, slightly better than the national average.
The Traverse City outbreaks were overshadowed in the national media by a more dramatic measles outbreak in Southern California’s Disneyland, which also occurred over the 2014-15 holidays and ultimately led to 150 cases of the disease. But the states’ responses were quite different.
California’s solution was what Dr. Largent calls “eliminationism.” The state Legislature, with Democratic supermajorities, passed a measure doing away with religious and philosophical vaccine exemptions. Passage of the law triggered widespread protests among opponents of vaccines. Besides California, only West Virginia and Mississippi disallow nonmedical waivers.
Dr. Largent said a small number of children need waivers for medical reasons, usually because of allergies or immune deficiencies. Much larger numbers seek waivers for religious or philosophical reasons.
“The idea was to bring the waiver rate down,” Michigan Health & Human Services spokeswoman Angela Minicuci said. “From the perspective of the general population, vaccinations are recommended. This doesn’t take away choice. It simply ensures that people have education.”
But, Dr. Largent said most vaccine opponents are not necessarily swayed by arguments in favor of immunization. Instead, “by heightening the burden, you change some of the incentives” for obtaining waivers. “Moral claims and ideology don’t matter as much when it’s inconvenient.”
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Just 3 years ago, Michigan had the fourth-highest rate of unvaccinated kindergartners in the nation. But, when a charter school in northwestern Traverse City reported nearly two dozen cases of whooping cough and several cases of measles that November, state officials were jolted to action.
Without much fanfare – or time for opponents to respond – they abandoned the state’s relatively loose rules for getting an exemption and issued a regulation requiring families to consult personally with local public health departments before obtaining an immunization waiver.
The new rule sidestepped potential ideological firefights in the state legislature, which have plagued lawmakers in other states who are trying to crack down on vaccination waivers. The regulation had a dramatic effect. In the first year, the Michigan Department of Health & Human Services reported that the number of statewide waivers issued had plunged 35%. Today, Michigan is in the middle of the pack among vaccination rates.
“The idea was to make the process more burdensome,” said Michigan State University health policy specialist Mark Largent, PhD, who has written extensively about vaccines. “Research has shown that, if you make it more inconvenient to apply for a waiver, fewer people get them.”
Michigan’s experience demonstrates a way for governments to increase immunization rates without having to address religious or philosophical opposition to vaccines.
For many years, opposition to mandatory childhood vaccines has served as a frequent rallying point for those who see immunizations as interference with nature’s intentions, rebel against them as government meddling in family affairs, or raise concerns about their safety.
Vaccine advocates and health professionals regard these views as dangerous, noting that the drugs have dramatically lowered the number of serious childhood illnesses and that studies suggesting they are not safe have been debunked. They also note that vaccines’ proven effectiveness lies in “herd immunity” – the higher the participation rate, the greater the community’s protection against outbreaks of infectious disease.
Many states adopt strategies to curb exemptions “by making applications complicated to fill out or complete,” according to University of Georgia public policy expert W. David Bradford, PhD, who studies immunization. Some states require parents to notarize applications or have them certified by a physician before sending them in, and, “generally speaking, anything that raises the opportunity cost [of exemptions] works to some degree,” Bradford said. “Michigan took it a step further.”
Increasing the number of vaccinated kids in Michigan, which has a Republican governor and Republican majorities in both legislative houses, took a degree of political finesse.
“Health & Human Services wanted to do something, but the legislative option wasn’t there,” Dr. Largent said. Instead, Michigan decided to use a strategy he calls “inconvenience.”
Since 1978, Michigan had required schoolchildren entering kindergarten and middle school to obtain vaccination waiver certificates from county officials. “Some counties allowed you to do it over the phone; in others you mailed in a form and some even let you do it online,” Dr. Largent said. But, in studying vaccine policy across the country, he noted, “One thing is really clear – health departments that require you to go in and get the waiver have much lower rates.”
Michigan offered the perfect vehicle for introducing inconvenience into the process. The Joint Committee on Administrative Rules reviews state agency regulations and, if it takes no action, allows them to go into effect after 15 legislative days. The committee is composed of lawmakers, giving it a legislative imprimatur, but it is not the legislature itself, thus avoiding the political rancor that can accompany debate on controversial issues.
During the 2013-14 school year, the federal Centers for Disease Control and Prevention found that Michigan had the fourth-highest rate of children entering kindergarten who had been exempted from vaccinations. The state Health & Human Services officials proposed a simple requirement: Parents seeking vaccine waivers must be briefed in person by a county health educator before a waiver would be granted. The joint committee approved the rule Dec. 11, 2014. It took effect Jan. 1, 2015.
“We were not aware of the rule until the day it happened,” said Suzanne Waltman, president of Michigan for Vaccine Choice, an antivaccine organization. “We thought it was a stealth move.”
The office of Gov. Rick Snyder did not respond directly to requests for comment on the political hazards of vaccine policy. Retired Republican state Sen. John Pappageorge, cochair of the administrative rules committee in 2014, voted to adopt the rule and described the procedure as a simple one designed to ensure “that implementation is in concurrence with the law.” Republican Rep. Tom McMillin, who was cochair of the committee at the time and voted against the rule, did not respond to requests for an interview.
In a look at one key metric, before 2015, about 22% of Michigan children did not get the fourth round of immunizations for diphtheria, tetanus, and pertussis that is required by the state. That had fallen to 15% 1 year later, slightly better than the national average.
The Traverse City outbreaks were overshadowed in the national media by a more dramatic measles outbreak in Southern California’s Disneyland, which also occurred over the 2014-15 holidays and ultimately led to 150 cases of the disease. But the states’ responses were quite different.
California’s solution was what Dr. Largent calls “eliminationism.” The state Legislature, with Democratic supermajorities, passed a measure doing away with religious and philosophical vaccine exemptions. Passage of the law triggered widespread protests among opponents of vaccines. Besides California, only West Virginia and Mississippi disallow nonmedical waivers.
Dr. Largent said a small number of children need waivers for medical reasons, usually because of allergies or immune deficiencies. Much larger numbers seek waivers for religious or philosophical reasons.
“The idea was to bring the waiver rate down,” Michigan Health & Human Services spokeswoman Angela Minicuci said. “From the perspective of the general population, vaccinations are recommended. This doesn’t take away choice. It simply ensures that people have education.”
But, Dr. Largent said most vaccine opponents are not necessarily swayed by arguments in favor of immunization. Instead, “by heightening the burden, you change some of the incentives” for obtaining waivers. “Moral claims and ideology don’t matter as much when it’s inconvenient.”
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Just 3 years ago, Michigan had the fourth-highest rate of unvaccinated kindergartners in the nation. But, when a charter school in northwestern Traverse City reported nearly two dozen cases of whooping cough and several cases of measles that November, state officials were jolted to action.
Without much fanfare – or time for opponents to respond – they abandoned the state’s relatively loose rules for getting an exemption and issued a regulation requiring families to consult personally with local public health departments before obtaining an immunization waiver.
The new rule sidestepped potential ideological firefights in the state legislature, which have plagued lawmakers in other states who are trying to crack down on vaccination waivers. The regulation had a dramatic effect. In the first year, the Michigan Department of Health & Human Services reported that the number of statewide waivers issued had plunged 35%. Today, Michigan is in the middle of the pack among vaccination rates.
“The idea was to make the process more burdensome,” said Michigan State University health policy specialist Mark Largent, PhD, who has written extensively about vaccines. “Research has shown that, if you make it more inconvenient to apply for a waiver, fewer people get them.”
Michigan’s experience demonstrates a way for governments to increase immunization rates without having to address religious or philosophical opposition to vaccines.
For many years, opposition to mandatory childhood vaccines has served as a frequent rallying point for those who see immunizations as interference with nature’s intentions, rebel against them as government meddling in family affairs, or raise concerns about their safety.
Vaccine advocates and health professionals regard these views as dangerous, noting that the drugs have dramatically lowered the number of serious childhood illnesses and that studies suggesting they are not safe have been debunked. They also note that vaccines’ proven effectiveness lies in “herd immunity” – the higher the participation rate, the greater the community’s protection against outbreaks of infectious disease.
Many states adopt strategies to curb exemptions “by making applications complicated to fill out or complete,” according to University of Georgia public policy expert W. David Bradford, PhD, who studies immunization. Some states require parents to notarize applications or have them certified by a physician before sending them in, and, “generally speaking, anything that raises the opportunity cost [of exemptions] works to some degree,” Bradford said. “Michigan took it a step further.”
Increasing the number of vaccinated kids in Michigan, which has a Republican governor and Republican majorities in both legislative houses, took a degree of political finesse.
“Health & Human Services wanted to do something, but the legislative option wasn’t there,” Dr. Largent said. Instead, Michigan decided to use a strategy he calls “inconvenience.”
Since 1978, Michigan had required schoolchildren entering kindergarten and middle school to obtain vaccination waiver certificates from county officials. “Some counties allowed you to do it over the phone; in others you mailed in a form and some even let you do it online,” Dr. Largent said. But, in studying vaccine policy across the country, he noted, “One thing is really clear – health departments that require you to go in and get the waiver have much lower rates.”
Michigan offered the perfect vehicle for introducing inconvenience into the process. The Joint Committee on Administrative Rules reviews state agency regulations and, if it takes no action, allows them to go into effect after 15 legislative days. The committee is composed of lawmakers, giving it a legislative imprimatur, but it is not the legislature itself, thus avoiding the political rancor that can accompany debate on controversial issues.
During the 2013-14 school year, the federal Centers for Disease Control and Prevention found that Michigan had the fourth-highest rate of children entering kindergarten who had been exempted from vaccinations. The state Health & Human Services officials proposed a simple requirement: Parents seeking vaccine waivers must be briefed in person by a county health educator before a waiver would be granted. The joint committee approved the rule Dec. 11, 2014. It took effect Jan. 1, 2015.
“We were not aware of the rule until the day it happened,” said Suzanne Waltman, president of Michigan for Vaccine Choice, an antivaccine organization. “We thought it was a stealth move.”
The office of Gov. Rick Snyder did not respond directly to requests for comment on the political hazards of vaccine policy. Retired Republican state Sen. John Pappageorge, cochair of the administrative rules committee in 2014, voted to adopt the rule and described the procedure as a simple one designed to ensure “that implementation is in concurrence with the law.” Republican Rep. Tom McMillin, who was cochair of the committee at the time and voted against the rule, did not respond to requests for an interview.
In a look at one key metric, before 2015, about 22% of Michigan children did not get the fourth round of immunizations for diphtheria, tetanus, and pertussis that is required by the state. That had fallen to 15% 1 year later, slightly better than the national average.
The Traverse City outbreaks were overshadowed in the national media by a more dramatic measles outbreak in Southern California’s Disneyland, which also occurred over the 2014-15 holidays and ultimately led to 150 cases of the disease. But the states’ responses were quite different.
California’s solution was what Dr. Largent calls “eliminationism.” The state Legislature, with Democratic supermajorities, passed a measure doing away with religious and philosophical vaccine exemptions. Passage of the law triggered widespread protests among opponents of vaccines. Besides California, only West Virginia and Mississippi disallow nonmedical waivers.
Dr. Largent said a small number of children need waivers for medical reasons, usually because of allergies or immune deficiencies. Much larger numbers seek waivers for religious or philosophical reasons.
“The idea was to bring the waiver rate down,” Michigan Health & Human Services spokeswoman Angela Minicuci said. “From the perspective of the general population, vaccinations are recommended. This doesn’t take away choice. It simply ensures that people have education.”
But, Dr. Largent said most vaccine opponents are not necessarily swayed by arguments in favor of immunization. Instead, “by heightening the burden, you change some of the incentives” for obtaining waivers. “Moral claims and ideology don’t matter as much when it’s inconvenient.”
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Neurologists weigh in on rising drug prices
Neurologists will tackle the issues surrounding rising prices for neurological drug treatments in a set of presentations during the annual meeting of the American Academy of Neurology in Boston.
During the Contemporary Clinical Issues Plenary Session on April 24, Dennis N. Bourdette, MD, of Oregon Health and Science University, Portland, will give his presentation, “High Drug Prices: The Elephant in the Clinic.”
Dr. Bourdette will also address the problem on April 26 in a session called “Section Topic Controversies,” in which he and Dennis W. Choi, MD, PhD, of the State University of New York at Stony Brook will offer their opinions on how “Neurologists Should Take a Position Regarding the Cost of Neurological Treatments.” Dr. Bourdette is set to illustrate how “Neurologists Should More Vocally Protest Some of the Marked Price Increases Involving Neurological Treatments,” while Dr. Choi will provide rationale for his argument on why “Neurologists Should Influence Policies that Allow Companies to Commit More Resources to R&D for Neurological Diseases While Not Allowing for Rapacious Pricing Practices.” Following the discussion, Dr. Bourdette, Dr. Choi, and session moderators will have a panel discussion on the ways in which AAN members can work most productively for the benefit of their patients.
Sure to be discussed in the series of talks is a recent AAN position paper on prescription drug prices released in March that identified three distinct drug pricing challenges:
- Massive increase in the pricing of previously low-cost generic drugs used to treat common disorders without obvious increases in cost of production or distribution.
- Massive increase in the pricing for high-priced generic and brand name drugs used to treat serious disorders that are not protected by the Orphan Drug Act.
- The high cost of new medications used to treat rare disorders as defined by the Orphan Drug Act.
Neurologists will tackle the issues surrounding rising prices for neurological drug treatments in a set of presentations during the annual meeting of the American Academy of Neurology in Boston.
During the Contemporary Clinical Issues Plenary Session on April 24, Dennis N. Bourdette, MD, of Oregon Health and Science University, Portland, will give his presentation, “High Drug Prices: The Elephant in the Clinic.”
Dr. Bourdette will also address the problem on April 26 in a session called “Section Topic Controversies,” in which he and Dennis W. Choi, MD, PhD, of the State University of New York at Stony Brook will offer their opinions on how “Neurologists Should Take a Position Regarding the Cost of Neurological Treatments.” Dr. Bourdette is set to illustrate how “Neurologists Should More Vocally Protest Some of the Marked Price Increases Involving Neurological Treatments,” while Dr. Choi will provide rationale for his argument on why “Neurologists Should Influence Policies that Allow Companies to Commit More Resources to R&D for Neurological Diseases While Not Allowing for Rapacious Pricing Practices.” Following the discussion, Dr. Bourdette, Dr. Choi, and session moderators will have a panel discussion on the ways in which AAN members can work most productively for the benefit of their patients.
Sure to be discussed in the series of talks is a recent AAN position paper on prescription drug prices released in March that identified three distinct drug pricing challenges:
- Massive increase in the pricing of previously low-cost generic drugs used to treat common disorders without obvious increases in cost of production or distribution.
- Massive increase in the pricing for high-priced generic and brand name drugs used to treat serious disorders that are not protected by the Orphan Drug Act.
- The high cost of new medications used to treat rare disorders as defined by the Orphan Drug Act.
Neurologists will tackle the issues surrounding rising prices for neurological drug treatments in a set of presentations during the annual meeting of the American Academy of Neurology in Boston.
During the Contemporary Clinical Issues Plenary Session on April 24, Dennis N. Bourdette, MD, of Oregon Health and Science University, Portland, will give his presentation, “High Drug Prices: The Elephant in the Clinic.”
Dr. Bourdette will also address the problem on April 26 in a session called “Section Topic Controversies,” in which he and Dennis W. Choi, MD, PhD, of the State University of New York at Stony Brook will offer their opinions on how “Neurologists Should Take a Position Regarding the Cost of Neurological Treatments.” Dr. Bourdette is set to illustrate how “Neurologists Should More Vocally Protest Some of the Marked Price Increases Involving Neurological Treatments,” while Dr. Choi will provide rationale for his argument on why “Neurologists Should Influence Policies that Allow Companies to Commit More Resources to R&D for Neurological Diseases While Not Allowing for Rapacious Pricing Practices.” Following the discussion, Dr. Bourdette, Dr. Choi, and session moderators will have a panel discussion on the ways in which AAN members can work most productively for the benefit of their patients.
Sure to be discussed in the series of talks is a recent AAN position paper on prescription drug prices released in March that identified three distinct drug pricing challenges:
- Massive increase in the pricing of previously low-cost generic drugs used to treat common disorders without obvious increases in cost of production or distribution.
- Massive increase in the pricing for high-priced generic and brand name drugs used to treat serious disorders that are not protected by the Orphan Drug Act.
- The high cost of new medications used to treat rare disorders as defined by the Orphan Drug Act.
Dulera inhaler linked to adrenocorticotropic suppression in small case series
ORLANDO – A combination corticosteroid asthma inhaler has, for the first time, been associated with growth delay and adrenocorticotropic suppression in children.
The single-center case series is small, but the results highlight the need to regularly monitor growth and adrenal function in children using inhaled mometasone furoate/formoterol fumarate (Dulera; Merck), investigators said at the annual meeting of the Endocrine Society.
“We are hoping to raise awareness of this risk in our pediatric endocrinology colleagues, as well as among allergists, pulmonologists, and pediatricians who treat these children,” said Fadi Al Muhaisen, MD. “These kids should be regularly screened for growth delay and adrenal insufficiency and have their growth plotted at every visit as well.”

Dulera was approved in the United States in 2010 as a maintenance therapy for chronic asthma in adults and children aged 12 years and older. Mometasone furoate is a potent corticosteroid, and formoterol fumarate is a long-acting beta2-adrenergic agonist. The prescribing information says that mometasone furoate exerts less effect on the hypothalamic-pituitary-adrenal axis than other inhaled corticosteroids, and that adrenal suppression is unlikely to occur when used at recommended dosages. These range from a low of 100 mcg/5 mcg, two puffs daily to a maximum dose of 800 mcg/20 mcg daily.
The review involved 18 children, all of whom were seen in the endocrinology clinic for growth failure or short stature and were receiving Dulera for management of their asthma. Of these, eight (44%) had a full adrenal evaluation. Six had biochemical evidence of adrenal suppression and two had normal adrenal function. The remaining 10 patients had not undergone an adrenal evaluation. None of them were on any other inhaled corticosteroid. The six children diagnosed with adrenal insufficiency had a mean age of 9.7 years, but ranged in age from 7 to 12 years. They had been using the medication for a mean of 1.3 years, although that varied widely, from just a few months to about 2 years. Only one had been on oral steroids in the preceding 6 months before coming to the endocrinology clinic. Five were using the 200 mcg/5 mcg dose, two puffs daily; one child was taking one puff daily of 100 mcg/5 mcg at the time of diagnosis but had been using the higher dose for the preceding 18 months. Three were using concomitant nasal steroids.
The six children evaluated had been using the medication for a mean of 1.3 years, although that varied widely, from just a few months to about 2 years. Only one had been on oral steroids during the 2 years before coming to the endocrinology clinic. Five were using the 200 mcg/5 mcg dose, two puffs daily; one child was taking one puff daily of 100 mcg/5 mcg at time of diagnosis, but had been using the higher dose for 18 months before that. Three were using concomitant nasal steroids.
All presented with growth failure, with bone age 1-3 years behind chronological age. One child was referred to the clinic after an emergency department visit for headache, nausea, diarrhea, and fatigue – symptoms of adrenal failure. That child had an adrenocroticotropin (ACTH) level of 10 pg/mL. Both his random peak cortisol measures after ACTH stimulation were less than 1 mcg/mL.
ACTH levels in four of the children were less than 5-6 pg/ml, with random and peak stimulated cortisols of around 1 mcg/mL. One patient had an ACTH level of 68 pg/mL, a random cortisol of less than 1 mcg/mL, and a peak stimulated cortisol of 8.7 mcg/mL.
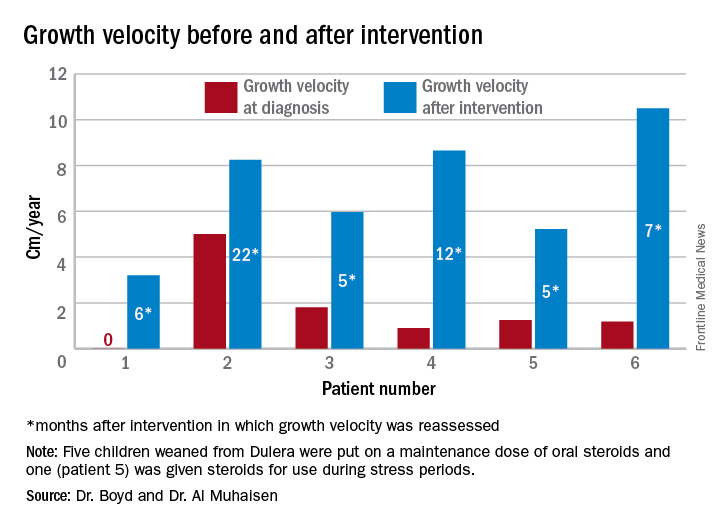
The results were all normal in the four subjects who had repeat adrenal function evaluation after intervention. Adrenal recovery took a mean of 20 months (5-30 months).
Growth accelerated rapidly after intervention, which was either initiation of maintenance oral steroids and discontinuation of Dulera or, in one patient, after Dulera was weaned. At time of adrenal insufficiency diagnosis, four patients had grown 1-2 cm in the prior year; one had not grown at all, and one had grown about 4.5 cm. After discontinuing or weaning the medication, all experienced growth spurts: 3 cm/year in 6 months; 8 cm/year in 22 months; 6 cm/year in 5 months; 8 cm/year in 12 months; 5 cm/year in 5 months; and 10 cm/year in 7 months.
There were no exacerbations in asthma, despite discontinuing the inhaled medication, Dr. Al Muhaisen said. Changing the asthma treatment required some open discussion between the investigators and the treating pulmonologists, he noted.
“We had some back-and-forth discussions, being very frank that we thought the adrenal insufficiency was directly related to this medication and that we needed to wean it and stop it as soon as possible.”
Neither Dr. Al Muhaisen nor Dr. Boyd had any financial disclosures.
ORLANDO – A combination corticosteroid asthma inhaler has, for the first time, been associated with growth delay and adrenocorticotropic suppression in children.
The single-center case series is small, but the results highlight the need to regularly monitor growth and adrenal function in children using inhaled mometasone furoate/formoterol fumarate (Dulera; Merck), investigators said at the annual meeting of the Endocrine Society.
“We are hoping to raise awareness of this risk in our pediatric endocrinology colleagues, as well as among allergists, pulmonologists, and pediatricians who treat these children,” said Fadi Al Muhaisen, MD. “These kids should be regularly screened for growth delay and adrenal insufficiency and have their growth plotted at every visit as well.”
Dulera was approved in the United States in 2010 as a maintenance therapy for chronic asthma in adults and children aged 12 years and older. Mometasone furoate is a potent corticosteroid, and formoterol fumarate is a long-acting beta2-adrenergic agonist. The prescribing information says that mometasone furoate exerts less effect on the hypothalamic-pituitary-adrenal axis than other inhaled corticosteroids, and that adrenal suppression is unlikely to occur when used at recommended dosages. These range from a low of 100 mcg/5 mcg, two puffs daily to a maximum dose of 800 mcg/20 mcg daily.
The review involved 18 children, all of whom were seen in the endocrinology clinic for growth failure or short stature and were receiving Dulera for management of their asthma. Of these, eight (44%) had a full adrenal evaluation. Six had biochemical evidence of adrenal suppression and two had normal adrenal function. The remaining 10 patients had not undergone an adrenal evaluation. None of them were on any other inhaled corticosteroid. The six children diagnosed with adrenal insufficiency had a mean age of 9.7 years, but ranged in age from 7 to 12 years. They had been using the medication for a mean of 1.3 years, although that varied widely, from just a few months to about 2 years. Only one had been on oral steroids in the preceding 6 months before coming to the endocrinology clinic. Five were using the 200 mcg/5 mcg dose, two puffs daily; one child was taking one puff daily of 100 mcg/5 mcg at the time of diagnosis but had been using the higher dose for the preceding 18 months. Three were using concomitant nasal steroids.
The six children evaluated had been using the medication for a mean of 1.3 years, although that varied widely, from just a few months to about 2 years. Only one had been on oral steroids during the 2 years before coming to the endocrinology clinic. Five were using the 200 mcg/5 mcg dose, two puffs daily; one child was taking one puff daily of 100 mcg/5 mcg at time of diagnosis, but had been using the higher dose for 18 months before that. Three were using concomitant nasal steroids.
All presented with growth failure, with bone age 1-3 years behind chronological age. One child was referred to the clinic after an emergency department visit for headache, nausea, diarrhea, and fatigue – symptoms of adrenal failure. That child had an adrenocroticotropin (ACTH) level of 10 pg/mL. Both his random peak cortisol measures after ACTH stimulation were less than 1 mcg/mL.
ACTH levels in four of the children were less than 5-6 pg/ml, with random and peak stimulated cortisols of around 1 mcg/mL. One patient had an ACTH level of 68 pg/mL, a random cortisol of less than 1 mcg/mL, and a peak stimulated cortisol of 8.7 mcg/mL.
The results were all normal in the four subjects who had repeat adrenal function evaluation after intervention. Adrenal recovery took a mean of 20 months (5-30 months).
Growth accelerated rapidly after intervention, which was either initiation of maintenance oral steroids and discontinuation of Dulera or, in one patient, after Dulera was weaned. At time of adrenal insufficiency diagnosis, four patients had grown 1-2 cm in the prior year; one had not grown at all, and one had grown about 4.5 cm. After discontinuing or weaning the medication, all experienced growth spurts: 3 cm/year in 6 months; 8 cm/year in 22 months; 6 cm/year in 5 months; 8 cm/year in 12 months; 5 cm/year in 5 months; and 10 cm/year in 7 months.
There were no exacerbations in asthma, despite discontinuing the inhaled medication, Dr. Al Muhaisen said. Changing the asthma treatment required some open discussion between the investigators and the treating pulmonologists, he noted.
“We had some back-and-forth discussions, being very frank that we thought the adrenal insufficiency was directly related to this medication and that we needed to wean it and stop it as soon as possible.”
Neither Dr. Al Muhaisen nor Dr. Boyd had any financial disclosures.
ORLANDO – A combination corticosteroid asthma inhaler has, for the first time, been associated with growth delay and adrenocorticotropic suppression in children.
The single-center case series is small, but the results highlight the need to regularly monitor growth and adrenal function in children using inhaled mometasone furoate/formoterol fumarate (Dulera; Merck), investigators said at the annual meeting of the Endocrine Society.
“We are hoping to raise awareness of this risk in our pediatric endocrinology colleagues, as well as among allergists, pulmonologists, and pediatricians who treat these children,” said Fadi Al Muhaisen, MD. “These kids should be regularly screened for growth delay and adrenal insufficiency and have their growth plotted at every visit as well.”
Dulera was approved in the United States in 2010 as a maintenance therapy for chronic asthma in adults and children aged 12 years and older. Mometasone furoate is a potent corticosteroid, and formoterol fumarate is a long-acting beta2-adrenergic agonist. The prescribing information says that mometasone furoate exerts less effect on the hypothalamic-pituitary-adrenal axis than other inhaled corticosteroids, and that adrenal suppression is unlikely to occur when used at recommended dosages. These range from a low of 100 mcg/5 mcg, two puffs daily to a maximum dose of 800 mcg/20 mcg daily.
The review involved 18 children, all of whom were seen in the endocrinology clinic for growth failure or short stature and were receiving Dulera for management of their asthma. Of these, eight (44%) had a full adrenal evaluation. Six had biochemical evidence of adrenal suppression and two had normal adrenal function. The remaining 10 patients had not undergone an adrenal evaluation. None of them were on any other inhaled corticosteroid. The six children diagnosed with adrenal insufficiency had a mean age of 9.7 years, but ranged in age from 7 to 12 years. They had been using the medication for a mean of 1.3 years, although that varied widely, from just a few months to about 2 years. Only one had been on oral steroids in the preceding 6 months before coming to the endocrinology clinic. Five were using the 200 mcg/5 mcg dose, two puffs daily; one child was taking one puff daily of 100 mcg/5 mcg at the time of diagnosis but had been using the higher dose for the preceding 18 months. Three were using concomitant nasal steroids.
The six children evaluated had been using the medication for a mean of 1.3 years, although that varied widely, from just a few months to about 2 years. Only one had been on oral steroids during the 2 years before coming to the endocrinology clinic. Five were using the 200 mcg/5 mcg dose, two puffs daily; one child was taking one puff daily of 100 mcg/5 mcg at time of diagnosis, but had been using the higher dose for 18 months before that. Three were using concomitant nasal steroids.
All presented with growth failure, with bone age 1-3 years behind chronological age. One child was referred to the clinic after an emergency department visit for headache, nausea, diarrhea, and fatigue – symptoms of adrenal failure. That child had an adrenocroticotropin (ACTH) level of 10 pg/mL. Both his random peak cortisol measures after ACTH stimulation were less than 1 mcg/mL.
ACTH levels in four of the children were less than 5-6 pg/ml, with random and peak stimulated cortisols of around 1 mcg/mL. One patient had an ACTH level of 68 pg/mL, a random cortisol of less than 1 mcg/mL, and a peak stimulated cortisol of 8.7 mcg/mL.
The results were all normal in the four subjects who had repeat adrenal function evaluation after intervention. Adrenal recovery took a mean of 20 months (5-30 months).
Growth accelerated rapidly after intervention, which was either initiation of maintenance oral steroids and discontinuation of Dulera or, in one patient, after Dulera was weaned. At time of adrenal insufficiency diagnosis, four patients had grown 1-2 cm in the prior year; one had not grown at all, and one had grown about 4.5 cm. After discontinuing or weaning the medication, all experienced growth spurts: 3 cm/year in 6 months; 8 cm/year in 22 months; 6 cm/year in 5 months; 8 cm/year in 12 months; 5 cm/year in 5 months; and 10 cm/year in 7 months.
There were no exacerbations in asthma, despite discontinuing the inhaled medication, Dr. Al Muhaisen said. Changing the asthma treatment required some open discussion between the investigators and the treating pulmonologists, he noted.
“We had some back-and-forth discussions, being very frank that we thought the adrenal insufficiency was directly related to this medication and that we needed to wean it and stop it as soon as possible.”
Neither Dr. Al Muhaisen nor Dr. Boyd had any financial disclosures.
AT ENDO 2017
Key clinical point:
Major finding: Of eight children who had an adrenal workup at an endocrinology clinic, six had adrenal suppression.
Data source: The case series comprised 18 children taking Dulera who presented with growth failure.
Disclosures: Neither Dr. Al Muhaisen nor Dr. Boyd had any financial disclosures.
FDA approves Ingrezza for tardive dyskinesia in adults
The Food and Drug Administration has approved valbenazine capsules for the treatment of tardive dyskinesia in adults.
The approval, announced April 11, came after a 6-week, placebo-controlled trial of 234 participants that compared valbenazine to placebo. At the end of the trial, those who took valbenazine experienced improvement in the severity of involuntary movements, compared with those who received placebo. As a vesicular monoamine transporter type 2 inhibitor, valbenazine works by regulating the amount of dopamine that is released into nerve cells by blocking a protein in the brain. The drug, the first to receive approval for tardive dyskinesia in adults, will be marketed as Ingrezza by Neurocrine Biosciences. Valbenazine is reportedly being studied as a treatment for Tourette syndrome in children and adolescents.![]()
In a statement, Mitchell Mathis, MD, director of the FDA’s division of psychiatry products in the Center for Drug Evaluation and Research, praised the approval as “an important advance for patients suffering with tardive dyskinesia.”
Characterized by uncontrolled movement of the face and body, tardive dyskinesia is a side effect in up to 8% of patients taking typical and atypical antipsychotics. The movement disorder also can cause other debilitating problems, including difficulty with chewing, speaking, and swallowing. Some data show that in about 87% of cases, the condition is irreversible even 3 years after the inciting agent has been discontinued (Parkinsonism Relat Disord. 2016. 32;124-6).
“Tardive dyskinesia can be disabling and can further stigmatize patients with mental illness,” Dr. Mathis said in the statement.
The side effects of valbenazine include sleepiness and QT prolongation. The agency said the patients taking the drug should not drive, operate heavy machinery, or engage in other potentially dangerous activities. Likewise, the drug should be avoided in patients with congenital long QT syndrome or in those with abnormal heartbeats associated with a prolonged QT interval, the agency said.
[email protected]
On Twitter @ginalhenderson
The Food and Drug Administration has approved valbenazine capsules for the treatment of tardive dyskinesia in adults.
The approval, announced April 11, came after a 6-week, placebo-controlled trial of 234 participants that compared valbenazine to placebo. At the end of the trial, those who took valbenazine experienced improvement in the severity of involuntary movements, compared with those who received placebo. As a vesicular monoamine transporter type 2 inhibitor, valbenazine works by regulating the amount of dopamine that is released into nerve cells by blocking a protein in the brain. The drug, the first to receive approval for tardive dyskinesia in adults, will be marketed as Ingrezza by Neurocrine Biosciences. Valbenazine is reportedly being studied as a treatment for Tourette syndrome in children and adolescents.![]()
In a statement, Mitchell Mathis, MD, director of the FDA’s division of psychiatry products in the Center for Drug Evaluation and Research, praised the approval as “an important advance for patients suffering with tardive dyskinesia.”
Characterized by uncontrolled movement of the face and body, tardive dyskinesia is a side effect in up to 8% of patients taking typical and atypical antipsychotics. The movement disorder also can cause other debilitating problems, including difficulty with chewing, speaking, and swallowing. Some data show that in about 87% of cases, the condition is irreversible even 3 years after the inciting agent has been discontinued (Parkinsonism Relat Disord. 2016. 32;124-6).
“Tardive dyskinesia can be disabling and can further stigmatize patients with mental illness,” Dr. Mathis said in the statement.
The side effects of valbenazine include sleepiness and QT prolongation. The agency said the patients taking the drug should not drive, operate heavy machinery, or engage in other potentially dangerous activities. Likewise, the drug should be avoided in patients with congenital long QT syndrome or in those with abnormal heartbeats associated with a prolonged QT interval, the agency said.
[email protected]
On Twitter @ginalhenderson
The Food and Drug Administration has approved valbenazine capsules for the treatment of tardive dyskinesia in adults.
The approval, announced April 11, came after a 6-week, placebo-controlled trial of 234 participants that compared valbenazine to placebo. At the end of the trial, those who took valbenazine experienced improvement in the severity of involuntary movements, compared with those who received placebo. As a vesicular monoamine transporter type 2 inhibitor, valbenazine works by regulating the amount of dopamine that is released into nerve cells by blocking a protein in the brain. The drug, the first to receive approval for tardive dyskinesia in adults, will be marketed as Ingrezza by Neurocrine Biosciences. Valbenazine is reportedly being studied as a treatment for Tourette syndrome in children and adolescents.![]()
In a statement, Mitchell Mathis, MD, director of the FDA’s division of psychiatry products in the Center for Drug Evaluation and Research, praised the approval as “an important advance for patients suffering with tardive dyskinesia.”
Characterized by uncontrolled movement of the face and body, tardive dyskinesia is a side effect in up to 8% of patients taking typical and atypical antipsychotics. The movement disorder also can cause other debilitating problems, including difficulty with chewing, speaking, and swallowing. Some data show that in about 87% of cases, the condition is irreversible even 3 years after the inciting agent has been discontinued (Parkinsonism Relat Disord. 2016. 32;124-6).
“Tardive dyskinesia can be disabling and can further stigmatize patients with mental illness,” Dr. Mathis said in the statement.
The side effects of valbenazine include sleepiness and QT prolongation. The agency said the patients taking the drug should not drive, operate heavy machinery, or engage in other potentially dangerous activities. Likewise, the drug should be avoided in patients with congenital long QT syndrome or in those with abnormal heartbeats associated with a prolonged QT interval, the agency said.
[email protected]
On Twitter @ginalhenderson