User login
Health reform action shifts to Senate, exacerbated by poor AHCA CBO score
With a highly anticipated impact analysis from the nonpartisan Congressional Budget Office, the much maligned American Health Care Act seems relegated to a Capitol Hill recycling bin and repeal/replace focus has moved to the Senate.
Sen. Orrin Hatch (R-Utah), chairman of the Senate Finance Committee, has reached out to physicians’ organizations to learn their priorities.
The organization also called for the reduction of regulatory burdens and increased cost transparency.
Additional recommendations include
• Support for advanceable, refundable tax credits to help individuals purchase private health care coverage, with the current tax credit structure in the ACA maintained.
• Maintenance of the ACA cost-sharing reductions for 2017 and 2018.
• Enhanced tax credits for young adults aged 19-30 years and modest funding of health savings accounts to help counter high deductibles.
The AMA also supports maintenance of the current Medicaid expansion while offering states even more flexibility for innovation.
Similarly, the American Osteopathic Association noted that any policy changes “should be to expand or at least maintain access to comprehensive, affordable coverage and care. With that said, we are also concerned about the growing potential for market instability and the deleterious effect that a collapse would have on patients’ access to insurance coverage and health care services,” according to a May 23 letter from Boyd Buser, DO, president of AOA.
The organization called for continued coverage of preventive care services with no copayment and expressed concern that “the changes being considered for the Medicaid program as part of health reform discussions will significantly impact coverage for these Americans.”
The House-passed American Health Care Act (H.R. 1628) would repeal the ACA’s Medicaid expansion provisions and implement a per-capita funding scheme for state Medicaid programs. “The AOA is concerned that this will leave states with insufficient funds to provide care to the most vulnerable in our society,” Dr. Buser wrote.
AOA recommended a number of consumer protections, including adequate funding of an invisible risk-sharing program that is maintained by an organization outside of the government; efforts to improve health literacy, and other cost-containment recommendations, particularly the maintenance of the cost-sharing reduction payments.
Even if the Senate were able to incorporate these recommendations, its leaders face an uphill battle to get enough support for passage.
“If, on the Republican side, they can come to an agreement on the bill, I think they have a chance of passing it,” Julius Hobson, senior policy analyst at the Washington law firm Polsinelli, said in an interview. “The GOP is not taking up the House-passed AHCA but is proceeding with writing its own reform legislation.
However, he pointed out that there is very little margin for error because the party only holds a two-seat majority and moderates Republican senators have expressed concerns about cuts to Medicaid.
If Senate Republicans do pass a bill that appeals to its more moderate members, that legislation is likely to face stiff opposition in the House.
“Given what we just saw the House go through, I don’t know” if a more moderate bill could pass in that chamber, he said, adding that, if “they don’t do this by the end of the calendar year, you can forget it.”
The potential death blow to the AHCA came in the form of a financial impact “score” from the Congressional Budget Office (CBO).
The government budget watchdog estimated the AHCA would reduce the budget deficit by $119 billion from 2017 to 2026, with the largest savings coming from “reductions in outlays for Medicaid and from the replacement of the Affordable Care Act’s subsidies for nongroup health insurance with new tax credits for nongroup health insurance. Those savings would be partially offset by other changes in coverage provisions – spending for a new Patient and State Stability Fund, designed to reduce premiums, and a reduction in revenues from repealing penalties on employers who do not offer insurance and on people who do not purchase insurance.”
The CBO score also predicted that an additional 23 million patients would be uninsured by 2026 – for a total of 51 million – compared with a total of 28 million uninsured under the ACA.
CBO analysts predicted that nongroup health insurance markets would stabilize before 2020 under the AHCA, but instability could increased if states seek waivers to modify the essential health benefits and community rating requirements.
Although premiums overall would decrease under the AHCA, certain subpopulations could see substantial increases under state waivers.
Additionally, the waivers could also impact the provision of care.
Analysis of the impact of the waiving of essential health benefits is the part doctors should be paying most attention to, Laura Wooster, AOA senior vice president of public policy, said in an interview.
“They would start seeing patients who potentially would have insurance plans that only cover certain benefits,” she said. That would “prevent them from providing certain services or care for their patients under the patients’ coverage. Even a more immediate administrative aspect of it that things would become more complicated if there isn’t a uniform standard, then it is going to be even more complicated for patients to navigate what’s covered, what’s not, and, if the physician takes the insurance, which services are they able to provide.”
She added that, if states waive any or all of the essential health benefits, those benefits would no longer be subject to lifetime and annual caps on spending.
Mr. Hobson suggested that the biggest part of the CBO score that doctors should be worried about is the spike in uninsured that could result from any reform effort.
“The concern for physicians will be that they are more likely to see more patients who don’t have insurance depending on the specialty,” Mr. Hobson said. “Primary care will certainly see a lot of that. Physicians in emergency departments will see more of them because, as you well know, when people don’t have insurance, that’s where they show up when they are at their sickest.”
He added that a “patient can come in, a physician can diagnose the problem, but, if the patient doesn’t have the insurance, he or she may not have the ability to spend the money to do what they need to do, which means they will be back.”
With a highly anticipated impact analysis from the nonpartisan Congressional Budget Office, the much maligned American Health Care Act seems relegated to a Capitol Hill recycling bin and repeal/replace focus has moved to the Senate.
Sen. Orrin Hatch (R-Utah), chairman of the Senate Finance Committee, has reached out to physicians’ organizations to learn their priorities.
The organization also called for the reduction of regulatory burdens and increased cost transparency.
Additional recommendations include
• Support for advanceable, refundable tax credits to help individuals purchase private health care coverage, with the current tax credit structure in the ACA maintained.
• Maintenance of the ACA cost-sharing reductions for 2017 and 2018.
• Enhanced tax credits for young adults aged 19-30 years and modest funding of health savings accounts to help counter high deductibles.
The AMA also supports maintenance of the current Medicaid expansion while offering states even more flexibility for innovation.
Similarly, the American Osteopathic Association noted that any policy changes “should be to expand or at least maintain access to comprehensive, affordable coverage and care. With that said, we are also concerned about the growing potential for market instability and the deleterious effect that a collapse would have on patients’ access to insurance coverage and health care services,” according to a May 23 letter from Boyd Buser, DO, president of AOA.
The organization called for continued coverage of preventive care services with no copayment and expressed concern that “the changes being considered for the Medicaid program as part of health reform discussions will significantly impact coverage for these Americans.”
The House-passed American Health Care Act (H.R. 1628) would repeal the ACA’s Medicaid expansion provisions and implement a per-capita funding scheme for state Medicaid programs. “The AOA is concerned that this will leave states with insufficient funds to provide care to the most vulnerable in our society,” Dr. Buser wrote.
AOA recommended a number of consumer protections, including adequate funding of an invisible risk-sharing program that is maintained by an organization outside of the government; efforts to improve health literacy, and other cost-containment recommendations, particularly the maintenance of the cost-sharing reduction payments.
Even if the Senate were able to incorporate these recommendations, its leaders face an uphill battle to get enough support for passage.
“If, on the Republican side, they can come to an agreement on the bill, I think they have a chance of passing it,” Julius Hobson, senior policy analyst at the Washington law firm Polsinelli, said in an interview. “The GOP is not taking up the House-passed AHCA but is proceeding with writing its own reform legislation.
However, he pointed out that there is very little margin for error because the party only holds a two-seat majority and moderates Republican senators have expressed concerns about cuts to Medicaid.
If Senate Republicans do pass a bill that appeals to its more moderate members, that legislation is likely to face stiff opposition in the House.
“Given what we just saw the House go through, I don’t know” if a more moderate bill could pass in that chamber, he said, adding that, if “they don’t do this by the end of the calendar year, you can forget it.”
The potential death blow to the AHCA came in the form of a financial impact “score” from the Congressional Budget Office (CBO).
The government budget watchdog estimated the AHCA would reduce the budget deficit by $119 billion from 2017 to 2026, with the largest savings coming from “reductions in outlays for Medicaid and from the replacement of the Affordable Care Act’s subsidies for nongroup health insurance with new tax credits for nongroup health insurance. Those savings would be partially offset by other changes in coverage provisions – spending for a new Patient and State Stability Fund, designed to reduce premiums, and a reduction in revenues from repealing penalties on employers who do not offer insurance and on people who do not purchase insurance.”
The CBO score also predicted that an additional 23 million patients would be uninsured by 2026 – for a total of 51 million – compared with a total of 28 million uninsured under the ACA.
CBO analysts predicted that nongroup health insurance markets would stabilize before 2020 under the AHCA, but instability could increased if states seek waivers to modify the essential health benefits and community rating requirements.
Although premiums overall would decrease under the AHCA, certain subpopulations could see substantial increases under state waivers.
Additionally, the waivers could also impact the provision of care.
Analysis of the impact of the waiving of essential health benefits is the part doctors should be paying most attention to, Laura Wooster, AOA senior vice president of public policy, said in an interview.
“They would start seeing patients who potentially would have insurance plans that only cover certain benefits,” she said. That would “prevent them from providing certain services or care for their patients under the patients’ coverage. Even a more immediate administrative aspect of it that things would become more complicated if there isn’t a uniform standard, then it is going to be even more complicated for patients to navigate what’s covered, what’s not, and, if the physician takes the insurance, which services are they able to provide.”
She added that, if states waive any or all of the essential health benefits, those benefits would no longer be subject to lifetime and annual caps on spending.
Mr. Hobson suggested that the biggest part of the CBO score that doctors should be worried about is the spike in uninsured that could result from any reform effort.
“The concern for physicians will be that they are more likely to see more patients who don’t have insurance depending on the specialty,” Mr. Hobson said. “Primary care will certainly see a lot of that. Physicians in emergency departments will see more of them because, as you well know, when people don’t have insurance, that’s where they show up when they are at their sickest.”
He added that a “patient can come in, a physician can diagnose the problem, but, if the patient doesn’t have the insurance, he or she may not have the ability to spend the money to do what they need to do, which means they will be back.”
With a highly anticipated impact analysis from the nonpartisan Congressional Budget Office, the much maligned American Health Care Act seems relegated to a Capitol Hill recycling bin and repeal/replace focus has moved to the Senate.
Sen. Orrin Hatch (R-Utah), chairman of the Senate Finance Committee, has reached out to physicians’ organizations to learn their priorities.
The organization also called for the reduction of regulatory burdens and increased cost transparency.
Additional recommendations include
• Support for advanceable, refundable tax credits to help individuals purchase private health care coverage, with the current tax credit structure in the ACA maintained.
• Maintenance of the ACA cost-sharing reductions for 2017 and 2018.
• Enhanced tax credits for young adults aged 19-30 years and modest funding of health savings accounts to help counter high deductibles.
The AMA also supports maintenance of the current Medicaid expansion while offering states even more flexibility for innovation.
Similarly, the American Osteopathic Association noted that any policy changes “should be to expand or at least maintain access to comprehensive, affordable coverage and care. With that said, we are also concerned about the growing potential for market instability and the deleterious effect that a collapse would have on patients’ access to insurance coverage and health care services,” according to a May 23 letter from Boyd Buser, DO, president of AOA.
The organization called for continued coverage of preventive care services with no copayment and expressed concern that “the changes being considered for the Medicaid program as part of health reform discussions will significantly impact coverage for these Americans.”
The House-passed American Health Care Act (H.R. 1628) would repeal the ACA’s Medicaid expansion provisions and implement a per-capita funding scheme for state Medicaid programs. “The AOA is concerned that this will leave states with insufficient funds to provide care to the most vulnerable in our society,” Dr. Buser wrote.
AOA recommended a number of consumer protections, including adequate funding of an invisible risk-sharing program that is maintained by an organization outside of the government; efforts to improve health literacy, and other cost-containment recommendations, particularly the maintenance of the cost-sharing reduction payments.
Even if the Senate were able to incorporate these recommendations, its leaders face an uphill battle to get enough support for passage.
“If, on the Republican side, they can come to an agreement on the bill, I think they have a chance of passing it,” Julius Hobson, senior policy analyst at the Washington law firm Polsinelli, said in an interview. “The GOP is not taking up the House-passed AHCA but is proceeding with writing its own reform legislation.
However, he pointed out that there is very little margin for error because the party only holds a two-seat majority and moderates Republican senators have expressed concerns about cuts to Medicaid.
If Senate Republicans do pass a bill that appeals to its more moderate members, that legislation is likely to face stiff opposition in the House.
“Given what we just saw the House go through, I don’t know” if a more moderate bill could pass in that chamber, he said, adding that, if “they don’t do this by the end of the calendar year, you can forget it.”
The potential death blow to the AHCA came in the form of a financial impact “score” from the Congressional Budget Office (CBO).
The government budget watchdog estimated the AHCA would reduce the budget deficit by $119 billion from 2017 to 2026, with the largest savings coming from “reductions in outlays for Medicaid and from the replacement of the Affordable Care Act’s subsidies for nongroup health insurance with new tax credits for nongroup health insurance. Those savings would be partially offset by other changes in coverage provisions – spending for a new Patient and State Stability Fund, designed to reduce premiums, and a reduction in revenues from repealing penalties on employers who do not offer insurance and on people who do not purchase insurance.”
The CBO score also predicted that an additional 23 million patients would be uninsured by 2026 – for a total of 51 million – compared with a total of 28 million uninsured under the ACA.
CBO analysts predicted that nongroup health insurance markets would stabilize before 2020 under the AHCA, but instability could increased if states seek waivers to modify the essential health benefits and community rating requirements.
Although premiums overall would decrease under the AHCA, certain subpopulations could see substantial increases under state waivers.
Additionally, the waivers could also impact the provision of care.
Analysis of the impact of the waiving of essential health benefits is the part doctors should be paying most attention to, Laura Wooster, AOA senior vice president of public policy, said in an interview.
“They would start seeing patients who potentially would have insurance plans that only cover certain benefits,” she said. That would “prevent them from providing certain services or care for their patients under the patients’ coverage. Even a more immediate administrative aspect of it that things would become more complicated if there isn’t a uniform standard, then it is going to be even more complicated for patients to navigate what’s covered, what’s not, and, if the physician takes the insurance, which services are they able to provide.”
She added that, if states waive any or all of the essential health benefits, those benefits would no longer be subject to lifetime and annual caps on spending.
Mr. Hobson suggested that the biggest part of the CBO score that doctors should be worried about is the spike in uninsured that could result from any reform effort.
“The concern for physicians will be that they are more likely to see more patients who don’t have insurance depending on the specialty,” Mr. Hobson said. “Primary care will certainly see a lot of that. Physicians in emergency departments will see more of them because, as you well know, when people don’t have insurance, that’s where they show up when they are at their sickest.”
He added that a “patient can come in, a physician can diagnose the problem, but, if the patient doesn’t have the insurance, he or she may not have the ability to spend the money to do what they need to do, which means they will be back.”
ATS conference participants shout for science
WASHINGTON – A group of about 60 individuals in lab coats marched through the rain from buses to Upper Senate Park on the evening of May 23, gathering in front of a raised podium in the park shadowed by the Capitol Building.
The demonstrators were trying to bring attention to recent policies that threaten to undermine research funding, tobacco regulation, affordable health care, clean air, and other advocacy priorities of the American Thoracic Society. The ATS had organized this rally – “Lab Coats for Lungs” – in conjunction with its international conference, which took place in Washington May 19-24.
“We rally today because we share growing anxiety that science in general, and our field in particular, is being dismissed in the halls of power,” ATS Vice President Polly Parsons, MD, announced from the podium.
Other speakers condemned the Trump administration’s proposals to scale down on environmental, health, and safety regulations, as well as proposed cuts to federal funding for scientific research, including an 18% reduction to National Institutes of Health funding.
Some speakers, including Gary Ewart, ATS chief of advocacy and government relations, and the event’s organizer, encouraged the crowd to raise their voices.
“Tell me what democracy looks like,” he yelled several times.
“This is what democracy looked like,” his fellow marchers shouted.

“What brought us the ability to transplant a lung and save a patient’s life who is dying of respiratory failure? What will cause the next breakthrough discovery? When our elected officials are looking for answers to challenging questions, what should they use for their guiding light?”
“Science!” bellowed the demonstrators, following each of Dr. Moss’s inquiries.
Some of the marchers wore pink lab coats rather than white, as a demonstration of women’s rights and gender equality in the field of science and medicine.
“The idea to wear pink coats was a result of discussions that mentioned that women’s rights were an integral part of the campaign for science, health, and clean air,” said ATS member Naftali Kaminski, MD. “Access to health care is critical to women, as is clean air. This why we chose to wear pink instead of white coats.”
Other speakers included Sen. Tom Carper (D-DE), Sen. Ed Markey (D-MA), pulmonary fibrosis patient advocate Teresa Barnes, and past ATS President David Gozal, MD.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – A group of about 60 individuals in lab coats marched through the rain from buses to Upper Senate Park on the evening of May 23, gathering in front of a raised podium in the park shadowed by the Capitol Building.
The demonstrators were trying to bring attention to recent policies that threaten to undermine research funding, tobacco regulation, affordable health care, clean air, and other advocacy priorities of the American Thoracic Society. The ATS had organized this rally – “Lab Coats for Lungs” – in conjunction with its international conference, which took place in Washington May 19-24.
“We rally today because we share growing anxiety that science in general, and our field in particular, is being dismissed in the halls of power,” ATS Vice President Polly Parsons, MD, announced from the podium.
Other speakers condemned the Trump administration’s proposals to scale down on environmental, health, and safety regulations, as well as proposed cuts to federal funding for scientific research, including an 18% reduction to National Institutes of Health funding.
Some speakers, including Gary Ewart, ATS chief of advocacy and government relations, and the event’s organizer, encouraged the crowd to raise their voices.
“Tell me what democracy looks like,” he yelled several times.
“This is what democracy looked like,” his fellow marchers shouted.
“What brought us the ability to transplant a lung and save a patient’s life who is dying of respiratory failure? What will cause the next breakthrough discovery? When our elected officials are looking for answers to challenging questions, what should they use for their guiding light?”
“Science!” bellowed the demonstrators, following each of Dr. Moss’s inquiries.
Some of the marchers wore pink lab coats rather than white, as a demonstration of women’s rights and gender equality in the field of science and medicine.
“The idea to wear pink coats was a result of discussions that mentioned that women’s rights were an integral part of the campaign for science, health, and clean air,” said ATS member Naftali Kaminski, MD. “Access to health care is critical to women, as is clean air. This why we chose to wear pink instead of white coats.”
Other speakers included Sen. Tom Carper (D-DE), Sen. Ed Markey (D-MA), pulmonary fibrosis patient advocate Teresa Barnes, and past ATS President David Gozal, MD.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – A group of about 60 individuals in lab coats marched through the rain from buses to Upper Senate Park on the evening of May 23, gathering in front of a raised podium in the park shadowed by the Capitol Building.
The demonstrators were trying to bring attention to recent policies that threaten to undermine research funding, tobacco regulation, affordable health care, clean air, and other advocacy priorities of the American Thoracic Society. The ATS had organized this rally – “Lab Coats for Lungs” – in conjunction with its international conference, which took place in Washington May 19-24.
“We rally today because we share growing anxiety that science in general, and our field in particular, is being dismissed in the halls of power,” ATS Vice President Polly Parsons, MD, announced from the podium.
Other speakers condemned the Trump administration’s proposals to scale down on environmental, health, and safety regulations, as well as proposed cuts to federal funding for scientific research, including an 18% reduction to National Institutes of Health funding.
Some speakers, including Gary Ewart, ATS chief of advocacy and government relations, and the event’s organizer, encouraged the crowd to raise their voices.
“Tell me what democracy looks like,” he yelled several times.
“This is what democracy looked like,” his fellow marchers shouted.
“What brought us the ability to transplant a lung and save a patient’s life who is dying of respiratory failure? What will cause the next breakthrough discovery? When our elected officials are looking for answers to challenging questions, what should they use for their guiding light?”
“Science!” bellowed the demonstrators, following each of Dr. Moss’s inquiries.
Some of the marchers wore pink lab coats rather than white, as a demonstration of women’s rights and gender equality in the field of science and medicine.
“The idea to wear pink coats was a result of discussions that mentioned that women’s rights were an integral part of the campaign for science, health, and clean air,” said ATS member Naftali Kaminski, MD. “Access to health care is critical to women, as is clean air. This why we chose to wear pink instead of white coats.”
Other speakers included Sen. Tom Carper (D-DE), Sen. Ed Markey (D-MA), pulmonary fibrosis patient advocate Teresa Barnes, and past ATS President David Gozal, MD.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT ATS 2017
Does a High-Quality Diet Affect Disability Status in Patients With MS?
NEW ORLEANS—A diet high in fruits, vegetables, legumes, and whole grains and low in sugar and red meat is associated with less disability and fewer depressive symptoms in patients with multiple sclerosis (MS), according to research presented at the 31st Annual Meeting of the Consortium of MS Centers.

“Our findings suggest that people with MS who have a healthier diet have less disability, and that a generally healthy lifestyle is associated with a lower burden of severe depression, pain, fatigue, and cognitive problems. Therefore, modifying diet may offer a way of improving symptoms,” said Ruth Ann Marrie, MD, PhD, Associate Professor of Neurology and Director of the MS Clinic at the University of Manitoba in Winnipeg, Canada.
Many patients with MS ask whether their diet could influence their disease status. To address this question, Dr. Marrie and colleagues assessed the association between overall diet quality and disability and physical and mental functioning in a large cohort of people with MS. They conducted a cross-sectional study of North American Research Committee on MS (NARCOMS) registry participants who had completed a dietary screener questionnaire. The questionnaire, created by the National Health and Nutrition Examination Survey, provides an assessment of diet composition when full information on diet is unavailable. The survey estimates intake of fruits, vegetables and legumes, whole grains, added sugars, and red and processed meats.
The researchers constructed an overall diet-quality score based on responses to the questionnaire and assigned participants to sex-specific quintiles of each of the questionnaire’s five food groups. They then assigned scores for fruits, vegetables, legumes, and whole grains based on the patient’s quintile ranking. The investigators inverted scores for red and processed meats and added sugar. The researchers summed individual food-group scores to obtain an overall diet score, ranging from 4 (poor quality) to 20 (high quality).
Dr. Marrie and colleagues assessed the association between diet quality and disability status (using the Patient-Determined Disease Steps) and mental and physical functioning (ie, depression, fatigue, cognition, mobility, vision, pain, spasticity, tremor, and sensory function) using proportional odds models adjusting for age, gender, income, BMI, smoking status, and disease duration.
In all, 7,418 responders had an average quality-diet score of 11.9. Patients with higher scores tended to be older, leaner, and nonsmokers. People with diet-quality scores in the top quintile had lower levels of disability and lower depression scores. Diet-quality scores were not associated with other physical or mental functioning scores, however.
A lack of details about potentially important dietary factors, such as types of fat, is one limitation of the study, said Dr. Marrie.
“While our study does not prove that diet change will improve symptoms, a high-quality diet that emphasizes intake of fruits, vegetables, and whole grains, and lower intake of red meat, can be encouraged, given the known benefits for general health,” said Dr. Marrie. “Future studies should look at the relationship between diet and disability, as well as symptoms over time, so that we can establish whether changing diet will improve outcomes in MS. These studies should also look at diet in more detail.”
The National MS Society supported this study.
—Erica Tricarico
NEW ORLEANS—A diet high in fruits, vegetables, legumes, and whole grains and low in sugar and red meat is associated with less disability and fewer depressive symptoms in patients with multiple sclerosis (MS), according to research presented at the 31st Annual Meeting of the Consortium of MS Centers.
“Our findings suggest that people with MS who have a healthier diet have less disability, and that a generally healthy lifestyle is associated with a lower burden of severe depression, pain, fatigue, and cognitive problems. Therefore, modifying diet may offer a way of improving symptoms,” said Ruth Ann Marrie, MD, PhD, Associate Professor of Neurology and Director of the MS Clinic at the University of Manitoba in Winnipeg, Canada.
Many patients with MS ask whether their diet could influence their disease status. To address this question, Dr. Marrie and colleagues assessed the association between overall diet quality and disability and physical and mental functioning in a large cohort of people with MS. They conducted a cross-sectional study of North American Research Committee on MS (NARCOMS) registry participants who had completed a dietary screener questionnaire. The questionnaire, created by the National Health and Nutrition Examination Survey, provides an assessment of diet composition when full information on diet is unavailable. The survey estimates intake of fruits, vegetables and legumes, whole grains, added sugars, and red and processed meats.
The researchers constructed an overall diet-quality score based on responses to the questionnaire and assigned participants to sex-specific quintiles of each of the questionnaire’s five food groups. They then assigned scores for fruits, vegetables, legumes, and whole grains based on the patient’s quintile ranking. The investigators inverted scores for red and processed meats and added sugar. The researchers summed individual food-group scores to obtain an overall diet score, ranging from 4 (poor quality) to 20 (high quality).
Dr. Marrie and colleagues assessed the association between diet quality and disability status (using the Patient-Determined Disease Steps) and mental and physical functioning (ie, depression, fatigue, cognition, mobility, vision, pain, spasticity, tremor, and sensory function) using proportional odds models adjusting for age, gender, income, BMI, smoking status, and disease duration.
In all, 7,418 responders had an average quality-diet score of 11.9. Patients with higher scores tended to be older, leaner, and nonsmokers. People with diet-quality scores in the top quintile had lower levels of disability and lower depression scores. Diet-quality scores were not associated with other physical or mental functioning scores, however.
A lack of details about potentially important dietary factors, such as types of fat, is one limitation of the study, said Dr. Marrie.
“While our study does not prove that diet change will improve symptoms, a high-quality diet that emphasizes intake of fruits, vegetables, and whole grains, and lower intake of red meat, can be encouraged, given the known benefits for general health,” said Dr. Marrie. “Future studies should look at the relationship between diet and disability, as well as symptoms over time, so that we can establish whether changing diet will improve outcomes in MS. These studies should also look at diet in more detail.”
The National MS Society supported this study.
—Erica Tricarico
NEW ORLEANS—A diet high in fruits, vegetables, legumes, and whole grains and low in sugar and red meat is associated with less disability and fewer depressive symptoms in patients with multiple sclerosis (MS), according to research presented at the 31st Annual Meeting of the Consortium of MS Centers.
“Our findings suggest that people with MS who have a healthier diet have less disability, and that a generally healthy lifestyle is associated with a lower burden of severe depression, pain, fatigue, and cognitive problems. Therefore, modifying diet may offer a way of improving symptoms,” said Ruth Ann Marrie, MD, PhD, Associate Professor of Neurology and Director of the MS Clinic at the University of Manitoba in Winnipeg, Canada.
Many patients with MS ask whether their diet could influence their disease status. To address this question, Dr. Marrie and colleagues assessed the association between overall diet quality and disability and physical and mental functioning in a large cohort of people with MS. They conducted a cross-sectional study of North American Research Committee on MS (NARCOMS) registry participants who had completed a dietary screener questionnaire. The questionnaire, created by the National Health and Nutrition Examination Survey, provides an assessment of diet composition when full information on diet is unavailable. The survey estimates intake of fruits, vegetables and legumes, whole grains, added sugars, and red and processed meats.
The researchers constructed an overall diet-quality score based on responses to the questionnaire and assigned participants to sex-specific quintiles of each of the questionnaire’s five food groups. They then assigned scores for fruits, vegetables, legumes, and whole grains based on the patient’s quintile ranking. The investigators inverted scores for red and processed meats and added sugar. The researchers summed individual food-group scores to obtain an overall diet score, ranging from 4 (poor quality) to 20 (high quality).
Dr. Marrie and colleagues assessed the association between diet quality and disability status (using the Patient-Determined Disease Steps) and mental and physical functioning (ie, depression, fatigue, cognition, mobility, vision, pain, spasticity, tremor, and sensory function) using proportional odds models adjusting for age, gender, income, BMI, smoking status, and disease duration.
In all, 7,418 responders had an average quality-diet score of 11.9. Patients with higher scores tended to be older, leaner, and nonsmokers. People with diet-quality scores in the top quintile had lower levels of disability and lower depression scores. Diet-quality scores were not associated with other physical or mental functioning scores, however.
A lack of details about potentially important dietary factors, such as types of fat, is one limitation of the study, said Dr. Marrie.
“While our study does not prove that diet change will improve symptoms, a high-quality diet that emphasizes intake of fruits, vegetables, and whole grains, and lower intake of red meat, can be encouraged, given the known benefits for general health,” said Dr. Marrie. “Future studies should look at the relationship between diet and disability, as well as symptoms over time, so that we can establish whether changing diet will improve outcomes in MS. These studies should also look at diet in more detail.”
The National MS Society supported this study.
—Erica Tricarico

Light Physical Activity May Improve Physical Function in Older Patients With MS
NEW ORLEANS—Older adults with multiple sclerosis (MS) who engaged more in light physical activity demonstrated better physical function independent of sedentary behavior and moderate-to-vigorous activity, according to research presented at the 31st Annual Meeting of the Consortium of MS Centers.

“Such results might underscore light physical activity as a suitable target of future rehabilitative interventions for improving physical function in older adults with MS,” said Katie L.J. Cederberg, a doctoral student at the University of Alabama at Birmingham.
Rate and pattern of participation in physical activity and sedentary behavior might be associated with a reduction of physical function among older adults with MS. Ms. Cederberg conducted a study that examined the associations among levels of light and moderate-to-vigorous physical activity, sedentary behavior, and physical function in older adults with MS.
Ms. Cederberg’s study sample included 40 older adults with MS with a median age of 60. Participants wore an accelerometer during the waking hours of a seven-day period. In addition, Ms. Cederberg used cut-points for MS to process data for time spent in moderate-to-vigorous physical activity, light physical activity, and sedentary behavior. Finally, patients completed the Short Physical Performance Battery (SPPB), the Six-Minute Walk Test, and the Timed 25-Foot Walk.
The median scores for time spent in moderate-to-vigorous physical activity and light physical activity were lower, and sedentary behavior was significantly greater, than those reported for older adults in the general population.
In addition, bivariate correlation analyses suggested that light physical activity and moderate to vigorous physical activity were associated with SPPB, Six-Minute Walk Test, and Timed 25-Foot Walk scores, but the association was stronger for light physical activity. Regression analyses yielded significant associations between light physical activity, but not moderate-to-vigorous physical activity or sedentary behavior, and SPPB, Six-Minute Walk Test, and Timed 25-Foot Walk scores.
NEW ORLEANS—Older adults with multiple sclerosis (MS) who engaged more in light physical activity demonstrated better physical function independent of sedentary behavior and moderate-to-vigorous activity, according to research presented at the 31st Annual Meeting of the Consortium of MS Centers.
“Such results might underscore light physical activity as a suitable target of future rehabilitative interventions for improving physical function in older adults with MS,” said Katie L.J. Cederberg, a doctoral student at the University of Alabama at Birmingham.
Rate and pattern of participation in physical activity and sedentary behavior might be associated with a reduction of physical function among older adults with MS. Ms. Cederberg conducted a study that examined the associations among levels of light and moderate-to-vigorous physical activity, sedentary behavior, and physical function in older adults with MS.
Ms. Cederberg’s study sample included 40 older adults with MS with a median age of 60. Participants wore an accelerometer during the waking hours of a seven-day period. In addition, Ms. Cederberg used cut-points for MS to process data for time spent in moderate-to-vigorous physical activity, light physical activity, and sedentary behavior. Finally, patients completed the Short Physical Performance Battery (SPPB), the Six-Minute Walk Test, and the Timed 25-Foot Walk.
The median scores for time spent in moderate-to-vigorous physical activity and light physical activity were lower, and sedentary behavior was significantly greater, than those reported for older adults in the general population.
In addition, bivariate correlation analyses suggested that light physical activity and moderate to vigorous physical activity were associated with SPPB, Six-Minute Walk Test, and Timed 25-Foot Walk scores, but the association was stronger for light physical activity. Regression analyses yielded significant associations between light physical activity, but not moderate-to-vigorous physical activity or sedentary behavior, and SPPB, Six-Minute Walk Test, and Timed 25-Foot Walk scores.
NEW ORLEANS—Older adults with multiple sclerosis (MS) who engaged more in light physical activity demonstrated better physical function independent of sedentary behavior and moderate-to-vigorous activity, according to research presented at the 31st Annual Meeting of the Consortium of MS Centers.
“Such results might underscore light physical activity as a suitable target of future rehabilitative interventions for improving physical function in older adults with MS,” said Katie L.J. Cederberg, a doctoral student at the University of Alabama at Birmingham.
Rate and pattern of participation in physical activity and sedentary behavior might be associated with a reduction of physical function among older adults with MS. Ms. Cederberg conducted a study that examined the associations among levels of light and moderate-to-vigorous physical activity, sedentary behavior, and physical function in older adults with MS.
Ms. Cederberg’s study sample included 40 older adults with MS with a median age of 60. Participants wore an accelerometer during the waking hours of a seven-day period. In addition, Ms. Cederberg used cut-points for MS to process data for time spent in moderate-to-vigorous physical activity, light physical activity, and sedentary behavior. Finally, patients completed the Short Physical Performance Battery (SPPB), the Six-Minute Walk Test, and the Timed 25-Foot Walk.
The median scores for time spent in moderate-to-vigorous physical activity and light physical activity were lower, and sedentary behavior was significantly greater, than those reported for older adults in the general population.
In addition, bivariate correlation analyses suggested that light physical activity and moderate to vigorous physical activity were associated with SPPB, Six-Minute Walk Test, and Timed 25-Foot Walk scores, but the association was stronger for light physical activity. Regression analyses yielded significant associations between light physical activity, but not moderate-to-vigorous physical activity or sedentary behavior, and SPPB, Six-Minute Walk Test, and Timed 25-Foot Walk scores.
FDA panel backs licensure for epoetin alfa biosimilar
A Food and Drug Administration advisory committee voted overwhelmingly in support of licensure for Epoetin Hospira as a biosimilar product to epoetin alfa (Epogen/Procrit) for all approved Epogen/Procrit indications.
Most committee members who voted “yes” said they were hesitant to do so, however, because of safety concerns, particularly in HIV and oncology patients.
“I voted yes. I came in with concerns about the HIV and oncology patients. However, I do believe ... after hearing the justification, that it meets the [FDA regulatory guideline],” said temporary voting member and patient representative Karen E. Arscott, DO, of the Commonwealth Medical College, Scranton, Penn. “I would like to see extensive follow-up in these two population groups,” she said.
The concerns about HIV and oncology patients are related to the potential for immunogenicity-related events. Some members noted that the study populations were likely too small to detect these rare events.
Scott A. Waldman, MD, of Thomas Jefferson University, Philadelphia, also a temporary member, said he voted “yes” because there was “no substantial difference analytically, biologically, or clinically in what was tested.”
“I think the residual uncertainty of immunogenicity and hypersensitivity and the extrapolation across different patient populations will emerge in postmarketing surveillance. I think that’s when we’ll get the clearest picture of whether there really is any uncertainty in how these drugs perform,” he said.
For one member, however, the concerns were enough for a “no” vote.
“The analytical, clinical, and preclinical data support biosimilarity, and I strongly support approval for indications 1 and 4 based on the clinical data ... but I have residual concerns about lack of data, immunogenicity, basic safety data in patients with HIV and cancer and, for that reason, voted no for the broader indication,” said Thomas S. Uldrick, MD, of the HIV & AIDS Malignancy Branch at the Center for Cancer Research, National Cancer Institute, Bethesda, Md.
Gregory J. Riely, MD, of Memorial Sloan-Kettering Cancer Center in New York expressed similar concerns but said he found the data compelling.
“I understand the concerns around immunogenicity for HIV and cancer patients. I was somewhat reassured by the nonclinical data showing an absence of increased immunogenicity for this biosimilar,” he said.
To support its BLA for Epoetin Hospira, Hospira submitted data from four studies comparing it with the U.S.-licensed Epogen/Procrit and presented an analytical biosimilarity assessment and a nonclinical, clinical pharmacology and clinical biosimilarity assessment. The FDA analysis of the data considered chemistry, manufacturing, and controls, as well as pharmacology/toxicology, immunogenicity, clinical pharmacology, and clinical efficacy and safety.
Sumant Ramachandra, MD, of Pfizer Essential Health noted that the company is not currently seeking an interchangeability designation and that, while this is the first application for a biosimilar product to Amgen’s Epogen/Procrit product, which was approved in 1989, a “highly related epoetin product” from Pfizer (Retacrit) has been available in Europe for 9 years, with more than 363,000 patient years of treatment administered.
The demonstration of biosimilarity in the Epoetin Hospira data presented to the FDA, coupled with well-characterized nature of the reference product, “together support extrapolation across all conditions of use for the reference product,” he said, noting that the data demonstrate that the mechanism of action for both the biosimilar and reference product is the same, and that the immunogenicity profiles are consistent.
The FDA assessment of the data led to a similar conclusion that no clinically significant differences were found between the biosimilar and reference product.
Among other concerns expressed by advisory committee members and/or the public were in regard to the extrapolation of data from patients with chronic kidney disease on hemodialysis to other indications (although this is considered acceptable, according to FDA regulations) and to populations that weren’t studied and about the possibility that Epoetin Hospira would be forced on patients inappropriately, despite the fact that Hospira is not seeking an interchangeability designation. Patients and others speaking on behalf of various patient groups and advocacy organizations called for safeguards against such inappropriate substitution.
Acting committee chair, Brian I. Rini, MD, of the Cleveland Clinic Taussig Cancer Clinic, Ohio, said he voted “yes” because the product met all regulatory requirements but agreed that the “need for vigilance is exceedingly important not only for this drug but for all drugs in this circumstance.”
The FDA, which usually follows the recommendations of its advisory committees, will now consider the BLA for Epoetin Hospira.
In a statement released after the vote, Diem Nguyen, Pfizer Essential Health global president, Americas, said the committee’s recommendation for approval “reinforces the potential value of biosimilars in expanding access to additional high-quality treatment options for the patients in the U.S. who need them.”
The advisory committee members were screened and found to have no relevant conflicts of interest.
A Food and Drug Administration advisory committee voted overwhelmingly in support of licensure for Epoetin Hospira as a biosimilar product to epoetin alfa (Epogen/Procrit) for all approved Epogen/Procrit indications.
Most committee members who voted “yes” said they were hesitant to do so, however, because of safety concerns, particularly in HIV and oncology patients.
“I voted yes. I came in with concerns about the HIV and oncology patients. However, I do believe ... after hearing the justification, that it meets the [FDA regulatory guideline],” said temporary voting member and patient representative Karen E. Arscott, DO, of the Commonwealth Medical College, Scranton, Penn. “I would like to see extensive follow-up in these two population groups,” she said.
The concerns about HIV and oncology patients are related to the potential for immunogenicity-related events. Some members noted that the study populations were likely too small to detect these rare events.
Scott A. Waldman, MD, of Thomas Jefferson University, Philadelphia, also a temporary member, said he voted “yes” because there was “no substantial difference analytically, biologically, or clinically in what was tested.”
“I think the residual uncertainty of immunogenicity and hypersensitivity and the extrapolation across different patient populations will emerge in postmarketing surveillance. I think that’s when we’ll get the clearest picture of whether there really is any uncertainty in how these drugs perform,” he said.
For one member, however, the concerns were enough for a “no” vote.
“The analytical, clinical, and preclinical data support biosimilarity, and I strongly support approval for indications 1 and 4 based on the clinical data ... but I have residual concerns about lack of data, immunogenicity, basic safety data in patients with HIV and cancer and, for that reason, voted no for the broader indication,” said Thomas S. Uldrick, MD, of the HIV & AIDS Malignancy Branch at the Center for Cancer Research, National Cancer Institute, Bethesda, Md.
Gregory J. Riely, MD, of Memorial Sloan-Kettering Cancer Center in New York expressed similar concerns but said he found the data compelling.
“I understand the concerns around immunogenicity for HIV and cancer patients. I was somewhat reassured by the nonclinical data showing an absence of increased immunogenicity for this biosimilar,” he said.
To support its BLA for Epoetin Hospira, Hospira submitted data from four studies comparing it with the U.S.-licensed Epogen/Procrit and presented an analytical biosimilarity assessment and a nonclinical, clinical pharmacology and clinical biosimilarity assessment. The FDA analysis of the data considered chemistry, manufacturing, and controls, as well as pharmacology/toxicology, immunogenicity, clinical pharmacology, and clinical efficacy and safety.
Sumant Ramachandra, MD, of Pfizer Essential Health noted that the company is not currently seeking an interchangeability designation and that, while this is the first application for a biosimilar product to Amgen’s Epogen/Procrit product, which was approved in 1989, a “highly related epoetin product” from Pfizer (Retacrit) has been available in Europe for 9 years, with more than 363,000 patient years of treatment administered.
The demonstration of biosimilarity in the Epoetin Hospira data presented to the FDA, coupled with well-characterized nature of the reference product, “together support extrapolation across all conditions of use for the reference product,” he said, noting that the data demonstrate that the mechanism of action for both the biosimilar and reference product is the same, and that the immunogenicity profiles are consistent.
The FDA assessment of the data led to a similar conclusion that no clinically significant differences were found between the biosimilar and reference product.
Among other concerns expressed by advisory committee members and/or the public were in regard to the extrapolation of data from patients with chronic kidney disease on hemodialysis to other indications (although this is considered acceptable, according to FDA regulations) and to populations that weren’t studied and about the possibility that Epoetin Hospira would be forced on patients inappropriately, despite the fact that Hospira is not seeking an interchangeability designation. Patients and others speaking on behalf of various patient groups and advocacy organizations called for safeguards against such inappropriate substitution.
Acting committee chair, Brian I. Rini, MD, of the Cleveland Clinic Taussig Cancer Clinic, Ohio, said he voted “yes” because the product met all regulatory requirements but agreed that the “need for vigilance is exceedingly important not only for this drug but for all drugs in this circumstance.”
The FDA, which usually follows the recommendations of its advisory committees, will now consider the BLA for Epoetin Hospira.
In a statement released after the vote, Diem Nguyen, Pfizer Essential Health global president, Americas, said the committee’s recommendation for approval “reinforces the potential value of biosimilars in expanding access to additional high-quality treatment options for the patients in the U.S. who need them.”
The advisory committee members were screened and found to have no relevant conflicts of interest.
A Food and Drug Administration advisory committee voted overwhelmingly in support of licensure for Epoetin Hospira as a biosimilar product to epoetin alfa (Epogen/Procrit) for all approved Epogen/Procrit indications.
Most committee members who voted “yes” said they were hesitant to do so, however, because of safety concerns, particularly in HIV and oncology patients.
“I voted yes. I came in with concerns about the HIV and oncology patients. However, I do believe ... after hearing the justification, that it meets the [FDA regulatory guideline],” said temporary voting member and patient representative Karen E. Arscott, DO, of the Commonwealth Medical College, Scranton, Penn. “I would like to see extensive follow-up in these two population groups,” she said.
The concerns about HIV and oncology patients are related to the potential for immunogenicity-related events. Some members noted that the study populations were likely too small to detect these rare events.
Scott A. Waldman, MD, of Thomas Jefferson University, Philadelphia, also a temporary member, said he voted “yes” because there was “no substantial difference analytically, biologically, or clinically in what was tested.”
“I think the residual uncertainty of immunogenicity and hypersensitivity and the extrapolation across different patient populations will emerge in postmarketing surveillance. I think that’s when we’ll get the clearest picture of whether there really is any uncertainty in how these drugs perform,” he said.
For one member, however, the concerns were enough for a “no” vote.
“The analytical, clinical, and preclinical data support biosimilarity, and I strongly support approval for indications 1 and 4 based on the clinical data ... but I have residual concerns about lack of data, immunogenicity, basic safety data in patients with HIV and cancer and, for that reason, voted no for the broader indication,” said Thomas S. Uldrick, MD, of the HIV & AIDS Malignancy Branch at the Center for Cancer Research, National Cancer Institute, Bethesda, Md.
Gregory J. Riely, MD, of Memorial Sloan-Kettering Cancer Center in New York expressed similar concerns but said he found the data compelling.
“I understand the concerns around immunogenicity for HIV and cancer patients. I was somewhat reassured by the nonclinical data showing an absence of increased immunogenicity for this biosimilar,” he said.
To support its BLA for Epoetin Hospira, Hospira submitted data from four studies comparing it with the U.S.-licensed Epogen/Procrit and presented an analytical biosimilarity assessment and a nonclinical, clinical pharmacology and clinical biosimilarity assessment. The FDA analysis of the data considered chemistry, manufacturing, and controls, as well as pharmacology/toxicology, immunogenicity, clinical pharmacology, and clinical efficacy and safety.
Sumant Ramachandra, MD, of Pfizer Essential Health noted that the company is not currently seeking an interchangeability designation and that, while this is the first application for a biosimilar product to Amgen’s Epogen/Procrit product, which was approved in 1989, a “highly related epoetin product” from Pfizer (Retacrit) has been available in Europe for 9 years, with more than 363,000 patient years of treatment administered.
The demonstration of biosimilarity in the Epoetin Hospira data presented to the FDA, coupled with well-characterized nature of the reference product, “together support extrapolation across all conditions of use for the reference product,” he said, noting that the data demonstrate that the mechanism of action for both the biosimilar and reference product is the same, and that the immunogenicity profiles are consistent.
The FDA assessment of the data led to a similar conclusion that no clinically significant differences were found between the biosimilar and reference product.
Among other concerns expressed by advisory committee members and/or the public were in regard to the extrapolation of data from patients with chronic kidney disease on hemodialysis to other indications (although this is considered acceptable, according to FDA regulations) and to populations that weren’t studied and about the possibility that Epoetin Hospira would be forced on patients inappropriately, despite the fact that Hospira is not seeking an interchangeability designation. Patients and others speaking on behalf of various patient groups and advocacy organizations called for safeguards against such inappropriate substitution.
Acting committee chair, Brian I. Rini, MD, of the Cleveland Clinic Taussig Cancer Clinic, Ohio, said he voted “yes” because the product met all regulatory requirements but agreed that the “need for vigilance is exceedingly important not only for this drug but for all drugs in this circumstance.”
The FDA, which usually follows the recommendations of its advisory committees, will now consider the BLA for Epoetin Hospira.
In a statement released after the vote, Diem Nguyen, Pfizer Essential Health global president, Americas, said the committee’s recommendation for approval “reinforces the potential value of biosimilars in expanding access to additional high-quality treatment options for the patients in the U.S. who need them.”
The advisory committee members were screened and found to have no relevant conflicts of interest.
Key clinical point:
Major finding: The data demonstrate that the mechanism of action for both the biosimilar and reference product is the same, and that the immunogenicity profiles are consistent.
Data source: An FDA advisory committee review of epoetin alfa biosimilar Epoetin Hospira.
Disclosures: The advisory committee members were screened and found to have no relevant conflicts of interest.
Guideline May Enhance Conversations About SUDEP
A new guideline codeveloped by the American Academy of Neurology and the American Epilepsy Society is intended to aid clinicians as they counsel patients about SUDEP. The practice guideline, published in the April 25 issue of Neurology, provides information about SUDEP incidence in different epilepsy populations, data about risk factors, and recommendations for patient care.

“Our guideline brings clarity to the [SUDEP] discussion, giving health care providers practical information they can use to help people with epilepsy reduce their risk,” said Cynthia Harden, MD, Director of Epilepsy Services for the Mount Sinai Health System in New York City.
A panel of experts searched the MEDLINE and Embase databases from the earliest available article to November 2010. An identical search was performed in April 2015 for articles published since November 2010. The keywords for both searches were “SUDEP” and other traditional medical subheadings for epilepsy (eg, “epilepsy/abnormalities,” “epilepsy/drug effects,” or “epilepsy/therapy”).
After reviewing more than 1,000 abstracts, the panel selected 70 relevant articles. The team then conducted a systematic review and developed conclusions using the modified Grading Recommendations Assessment, Development, and Evaluation process. All recommendations were made by consensus.
Incidence rates were based on 12 Class I studies. The systematic review found that SUDEP affects one in 4,500 children with epilepsy per year. Based on these findings, the experts recommend that clinicians inform parents or guardians about this low risk of SUDEP in children (Level B). In addition, the panel recommends that clinicians inform adult patients about the small risk of SUDEP, which typically affects one in 1,000 adults with epilepsy annually (Level B).
The panel also found that generalized tonic-clonic seizures, which involve convulsions and loss of consciousness, are a major risk factor for SUDEP. In addition, they noted that patients who have three or more of these seizures per year have a 15-fold increased risk of SUDEP. To reduce this risk, clinicians are advised to manage epilepsy therapies actively in these patients to reduce seizures (Level B).
The guideline also recommends nocturnal supervision or other nocturnal precautions for patients who experience frequent generalized tonic-clonic seizures and nocturnal seizures (Level C). Furthermore, the presence of an additional person age 10 or older in the bedroom is associated with a decreased SUDEP risk. If individualized epilepsy and psychosocial circumstances permit, such a person should be present, said the panel. Providing nighttime observation might be overly burdensome or intrusive for some patients, the authors added.
Finally, clinicians are advised to inform patients that seizure freedom, especially freedom from generalized tonic-clonic seizures, is strongly associated with a decreased risk of SUDEP (Level B). The panel also analyzed other SUDEP risk factors (eg, lamotrigine use in women, heart rate variability, and male gender), but too little evidence was available to support recommendations.
“Research to identify preventable risk factors should be supported and encouraged so that future clinical trials will be conducted to reduce SUDEP occurrence,” said Dr. Harden.
—Erica Tricarico
Suggested Reading
Harden C, Tomson T, Gloss D, et al. Practice guideline summary: Sudden unexpected death in epilepsy incidence rates and risk factors: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology. 2017;88(17):1674-1680.
A new guideline codeveloped by the American Academy of Neurology and the American Epilepsy Society is intended to aid clinicians as they counsel patients about SUDEP. The practice guideline, published in the April 25 issue of Neurology, provides information about SUDEP incidence in different epilepsy populations, data about risk factors, and recommendations for patient care.
“Our guideline brings clarity to the [SUDEP] discussion, giving health care providers practical information they can use to help people with epilepsy reduce their risk,” said Cynthia Harden, MD, Director of Epilepsy Services for the Mount Sinai Health System in New York City.
A panel of experts searched the MEDLINE and Embase databases from the earliest available article to November 2010. An identical search was performed in April 2015 for articles published since November 2010. The keywords for both searches were “SUDEP” and other traditional medical subheadings for epilepsy (eg, “epilepsy/abnormalities,” “epilepsy/drug effects,” or “epilepsy/therapy”).
After reviewing more than 1,000 abstracts, the panel selected 70 relevant articles. The team then conducted a systematic review and developed conclusions using the modified Grading Recommendations Assessment, Development, and Evaluation process. All recommendations were made by consensus.
Incidence rates were based on 12 Class I studies. The systematic review found that SUDEP affects one in 4,500 children with epilepsy per year. Based on these findings, the experts recommend that clinicians inform parents or guardians about this low risk of SUDEP in children (Level B). In addition, the panel recommends that clinicians inform adult patients about the small risk of SUDEP, which typically affects one in 1,000 adults with epilepsy annually (Level B).
The panel also found that generalized tonic-clonic seizures, which involve convulsions and loss of consciousness, are a major risk factor for SUDEP. In addition, they noted that patients who have three or more of these seizures per year have a 15-fold increased risk of SUDEP. To reduce this risk, clinicians are advised to manage epilepsy therapies actively in these patients to reduce seizures (Level B).
The guideline also recommends nocturnal supervision or other nocturnal precautions for patients who experience frequent generalized tonic-clonic seizures and nocturnal seizures (Level C). Furthermore, the presence of an additional person age 10 or older in the bedroom is associated with a decreased SUDEP risk. If individualized epilepsy and psychosocial circumstances permit, such a person should be present, said the panel. Providing nighttime observation might be overly burdensome or intrusive for some patients, the authors added.
Finally, clinicians are advised to inform patients that seizure freedom, especially freedom from generalized tonic-clonic seizures, is strongly associated with a decreased risk of SUDEP (Level B). The panel also analyzed other SUDEP risk factors (eg, lamotrigine use in women, heart rate variability, and male gender), but too little evidence was available to support recommendations.
“Research to identify preventable risk factors should be supported and encouraged so that future clinical trials will be conducted to reduce SUDEP occurrence,” said Dr. Harden.
—Erica Tricarico
Suggested Reading
Harden C, Tomson T, Gloss D, et al. Practice guideline summary: Sudden unexpected death in epilepsy incidence rates and risk factors: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology. 2017;88(17):1674-1680.
A new guideline codeveloped by the American Academy of Neurology and the American Epilepsy Society is intended to aid clinicians as they counsel patients about SUDEP. The practice guideline, published in the April 25 issue of Neurology, provides information about SUDEP incidence in different epilepsy populations, data about risk factors, and recommendations for patient care.
“Our guideline brings clarity to the [SUDEP] discussion, giving health care providers practical information they can use to help people with epilepsy reduce their risk,” said Cynthia Harden, MD, Director of Epilepsy Services for the Mount Sinai Health System in New York City.
A panel of experts searched the MEDLINE and Embase databases from the earliest available article to November 2010. An identical search was performed in April 2015 for articles published since November 2010. The keywords for both searches were “SUDEP” and other traditional medical subheadings for epilepsy (eg, “epilepsy/abnormalities,” “epilepsy/drug effects,” or “epilepsy/therapy”).
After reviewing more than 1,000 abstracts, the panel selected 70 relevant articles. The team then conducted a systematic review and developed conclusions using the modified Grading Recommendations Assessment, Development, and Evaluation process. All recommendations were made by consensus.
Incidence rates were based on 12 Class I studies. The systematic review found that SUDEP affects one in 4,500 children with epilepsy per year. Based on these findings, the experts recommend that clinicians inform parents or guardians about this low risk of SUDEP in children (Level B). In addition, the panel recommends that clinicians inform adult patients about the small risk of SUDEP, which typically affects one in 1,000 adults with epilepsy annually (Level B).
The panel also found that generalized tonic-clonic seizures, which involve convulsions and loss of consciousness, are a major risk factor for SUDEP. In addition, they noted that patients who have three or more of these seizures per year have a 15-fold increased risk of SUDEP. To reduce this risk, clinicians are advised to manage epilepsy therapies actively in these patients to reduce seizures (Level B).
The guideline also recommends nocturnal supervision or other nocturnal precautions for patients who experience frequent generalized tonic-clonic seizures and nocturnal seizures (Level C). Furthermore, the presence of an additional person age 10 or older in the bedroom is associated with a decreased SUDEP risk. If individualized epilepsy and psychosocial circumstances permit, such a person should be present, said the panel. Providing nighttime observation might be overly burdensome or intrusive for some patients, the authors added.
Finally, clinicians are advised to inform patients that seizure freedom, especially freedom from generalized tonic-clonic seizures, is strongly associated with a decreased risk of SUDEP (Level B). The panel also analyzed other SUDEP risk factors (eg, lamotrigine use in women, heart rate variability, and male gender), but too little evidence was available to support recommendations.
“Research to identify preventable risk factors should be supported and encouraged so that future clinical trials will be conducted to reduce SUDEP occurrence,” said Dr. Harden.
—Erica Tricarico
Suggested Reading
Harden C, Tomson T, Gloss D, et al. Practice guideline summary: Sudden unexpected death in epilepsy incidence rates and risk factors: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology. 2017;88(17):1674-1680.
Number Needed to Treat Analyses Comparing Alemtuzumab With Ocrelizumab
NEW ORLEANS—Two-year analyses show that fewer patients required treatment with alemtuzumab than ocrelizumab to prevent one relapse, to prevent relapse in one patient, and to prevent six-month confirmed disability worsening in one patient versus subcutaneous interferon beta-1a, according to a report presented at the 31st Annual Meeting of the Consortium of Multiple Sclerosis Centers.
In the absence of head-to-head trials, researchers can use the number needed to treat to indirectly assess the comparative efficacy of disease-modifying therapies. Aaron L. Boster, MD, and colleagues analyzed the number needed to treat to prevent clinical disease events in studies of alemtuzumab and ocrelizumab in relapsing-remitting multiple sclerosis (MS). Dr. Boster is a clinical neuroimmunologist at the OhioHealth MS Clinic in Columbus.
Number needed to treat values were derived from post hoc analyses of two-year data from studies of alemtuzumab (12 mg) and ocrelizumab (600 mg). Alemtuzumab data were of pooled treatment-naive patients from the CAMMS223 and CARE-MS I studies (n = 786), and separately, patients with inadequate response to prior therapy from CARE-MS II (n = 628). Ocrelizumab data were derived from the OPERA I and II studies (n = 821 and n = 835, respectively). Alemtuzumab was administered as two annual courses; ocrelizumab was administered at baseline and weeks 24, 48, and 72. Number needed to treat was based on inverse of absolute risk differences versus subcutaneous interferon beta-1a 44 μg three times per week (common comparator) for annualized relapse rate and proportion of patients experiencing relapse, and the Altman method for six-month confirmed disability worsening. Lower number needed to treat values reflect greater efficacy.
Baseline mean Expanded Disability Status Scale (EDSS) scores were 2.0 for CAMMS223 and CARE-MS I, 2.7 for CARE-MS II, 2.9 for OPERA I, and 2.8 for OPERA II. Mean MS duration was 1.9 years in CAMMS223 and CARE-MS I, 4.5 years in CARE-MS II, and 6.7 years in OPERA I and II. Mean number of relapses in the previous two years was 2.5 for CAMMS223 and CARE-MS I, 2.8 for CARE-MS II, and 1.8 in OPERA I and II.
Alemtuzumab and ocrelizumab significantly reduced annualized relapse rates and confirmed disability worsening versus subcutaneous interferon beta-1a. Number needed to treat values to prevent one relapse versus subcutaneous interferon beta-1a were lower with alemtuzumab (CAMMS223/CARE-MS I: five; CARE-MS II: four) than with ocrelizumab (OPERA I/II: eight in each study), as were number needed to treat values to prevent one patient from experiencing relapse (CAMMS223/CARE-MS I and CARE-MS II: six in each study; OPERA I and II: eight in each study), and to prevent one patient from experiencing six-month confirmed disability worsening (CAMMS223/CARE-MS I: 15; CARE-MS II: 13; OPERA I: 23; OPERA II: 21).
Although the populations in the available datasets differ, these findings suggest a benefit of alemtuzumab over ocrelizumab.
This study was supported by Sanofi Genzyme.
NEW ORLEANS—Two-year analyses show that fewer patients required treatment with alemtuzumab than ocrelizumab to prevent one relapse, to prevent relapse in one patient, and to prevent six-month confirmed disability worsening in one patient versus subcutaneous interferon beta-1a, according to a report presented at the 31st Annual Meeting of the Consortium of Multiple Sclerosis Centers.
In the absence of head-to-head trials, researchers can use the number needed to treat to indirectly assess the comparative efficacy of disease-modifying therapies. Aaron L. Boster, MD, and colleagues analyzed the number needed to treat to prevent clinical disease events in studies of alemtuzumab and ocrelizumab in relapsing-remitting multiple sclerosis (MS). Dr. Boster is a clinical neuroimmunologist at the OhioHealth MS Clinic in Columbus.
Number needed to treat values were derived from post hoc analyses of two-year data from studies of alemtuzumab (12 mg) and ocrelizumab (600 mg). Alemtuzumab data were of pooled treatment-naive patients from the CAMMS223 and CARE-MS I studies (n = 786), and separately, patients with inadequate response to prior therapy from CARE-MS II (n = 628). Ocrelizumab data were derived from the OPERA I and II studies (n = 821 and n = 835, respectively). Alemtuzumab was administered as two annual courses; ocrelizumab was administered at baseline and weeks 24, 48, and 72. Number needed to treat was based on inverse of absolute risk differences versus subcutaneous interferon beta-1a 44 μg three times per week (common comparator) for annualized relapse rate and proportion of patients experiencing relapse, and the Altman method for six-month confirmed disability worsening. Lower number needed to treat values reflect greater efficacy.
Baseline mean Expanded Disability Status Scale (EDSS) scores were 2.0 for CAMMS223 and CARE-MS I, 2.7 for CARE-MS II, 2.9 for OPERA I, and 2.8 for OPERA II. Mean MS duration was 1.9 years in CAMMS223 and CARE-MS I, 4.5 years in CARE-MS II, and 6.7 years in OPERA I and II. Mean number of relapses in the previous two years was 2.5 for CAMMS223 and CARE-MS I, 2.8 for CARE-MS II, and 1.8 in OPERA I and II.
Alemtuzumab and ocrelizumab significantly reduced annualized relapse rates and confirmed disability worsening versus subcutaneous interferon beta-1a. Number needed to treat values to prevent one relapse versus subcutaneous interferon beta-1a were lower with alemtuzumab (CAMMS223/CARE-MS I: five; CARE-MS II: four) than with ocrelizumab (OPERA I/II: eight in each study), as were number needed to treat values to prevent one patient from experiencing relapse (CAMMS223/CARE-MS I and CARE-MS II: six in each study; OPERA I and II: eight in each study), and to prevent one patient from experiencing six-month confirmed disability worsening (CAMMS223/CARE-MS I: 15; CARE-MS II: 13; OPERA I: 23; OPERA II: 21).
Although the populations in the available datasets differ, these findings suggest a benefit of alemtuzumab over ocrelizumab.
This study was supported by Sanofi Genzyme.
NEW ORLEANS—Two-year analyses show that fewer patients required treatment with alemtuzumab than ocrelizumab to prevent one relapse, to prevent relapse in one patient, and to prevent six-month confirmed disability worsening in one patient versus subcutaneous interferon beta-1a, according to a report presented at the 31st Annual Meeting of the Consortium of Multiple Sclerosis Centers.
In the absence of head-to-head trials, researchers can use the number needed to treat to indirectly assess the comparative efficacy of disease-modifying therapies. Aaron L. Boster, MD, and colleagues analyzed the number needed to treat to prevent clinical disease events in studies of alemtuzumab and ocrelizumab in relapsing-remitting multiple sclerosis (MS). Dr. Boster is a clinical neuroimmunologist at the OhioHealth MS Clinic in Columbus.
Number needed to treat values were derived from post hoc analyses of two-year data from studies of alemtuzumab (12 mg) and ocrelizumab (600 mg). Alemtuzumab data were of pooled treatment-naive patients from the CAMMS223 and CARE-MS I studies (n = 786), and separately, patients with inadequate response to prior therapy from CARE-MS II (n = 628). Ocrelizumab data were derived from the OPERA I and II studies (n = 821 and n = 835, respectively). Alemtuzumab was administered as two annual courses; ocrelizumab was administered at baseline and weeks 24, 48, and 72. Number needed to treat was based on inverse of absolute risk differences versus subcutaneous interferon beta-1a 44 μg three times per week (common comparator) for annualized relapse rate and proportion of patients experiencing relapse, and the Altman method for six-month confirmed disability worsening. Lower number needed to treat values reflect greater efficacy.
Baseline mean Expanded Disability Status Scale (EDSS) scores were 2.0 for CAMMS223 and CARE-MS I, 2.7 for CARE-MS II, 2.9 for OPERA I, and 2.8 for OPERA II. Mean MS duration was 1.9 years in CAMMS223 and CARE-MS I, 4.5 years in CARE-MS II, and 6.7 years in OPERA I and II. Mean number of relapses in the previous two years was 2.5 for CAMMS223 and CARE-MS I, 2.8 for CARE-MS II, and 1.8 in OPERA I and II.
Alemtuzumab and ocrelizumab significantly reduced annualized relapse rates and confirmed disability worsening versus subcutaneous interferon beta-1a. Number needed to treat values to prevent one relapse versus subcutaneous interferon beta-1a were lower with alemtuzumab (CAMMS223/CARE-MS I: five; CARE-MS II: four) than with ocrelizumab (OPERA I/II: eight in each study), as were number needed to treat values to prevent one patient from experiencing relapse (CAMMS223/CARE-MS I and CARE-MS II: six in each study; OPERA I and II: eight in each study), and to prevent one patient from experiencing six-month confirmed disability worsening (CAMMS223/CARE-MS I: 15; CARE-MS II: 13; OPERA I: 23; OPERA II: 21).
Although the populations in the available datasets differ, these findings suggest a benefit of alemtuzumab over ocrelizumab.
This study was supported by Sanofi Genzyme.
HM17 session summary: The hospitalist’s role in the opioid epidemic
Presenters
Shoshana J. Herzig, MD, MPH, and Hillary J. Mosher, MFA, MD, FHM
Summary
The growth in opiate prescribing and associated increases in adverse events has created unique challenges for hospitalists, including how best to assess pain and opiate use disorders and how to safely prescribe opiates during hospitalization and at discharge.
These challenges are compounded by patient and system factors and a paucity of evidence-based guidelines to help guide safe administration of opiates in hospitalized patients. This can mean frustration for hospitalists and harm for patients.

Key takeaways for HM
- When assessing patients’ pain, it is crucial to differentiate between acute and chronic pain (or both) and whether it is nociceptive or neuropathic. Misclassification of pain contributes to inappropriate exposure and escalation of opiate therapy during hospitalization.
- Always consider nonopioid analgesics such as NSAIDs first and pair them with opiates. Studies in a variety of conditions have demonstrated that these are equally, if not more, effective, even for severe pain, such as with renal colic. Reserve opiates for moderate to severe pain.
- Always assess whether the benefits of initiating or continuing opioid therapy outweigh the risks for individual patients. There is no validated tool to predict risk for adverse events and/or opioid abuse disorder but a careful review of patient history can identify established risk factors (such as a history of mental illness or substance abuse disorders, renal impairment, or other comorbidities). In addition, nearly all states now have Prescription Drug Monitoring Programs, and hospitalists should consult these routinely when prescribing opiates.
- Always clearly discuss expectations and risks of opioid therapy, including the potential for development of opioid use disorders with hospitalized patients prior to initiation. Emphasize pain reduction rather than elimination and focus on functional goals such as improved mobility. Also, set expectations for stepping down treatment up front.
- Use the lowest effective dose of immediate-release opioids (preferably oral route) for shortest duration possible. Long acting opiates are associated with increased risk of adverse events, and their initiation should generally be avoided in hospitalized patients with noncancer pain.
- Minimize risk by avoiding concurrent administration of other medications with sedative properties, especially benzodiazepines, which have been found to significantly increase the risk of adverse events, including overdose.
- Recognize that chronic opioid use often begins with treatment of acute pain during hospitalization. Adopt best practice for discharge, including prescribing shorter courses whenever possible, discussing initiation, and changes or modifications in opiate therapy with patients’ primary care provider, and ensure timely postdischarge follow-up. Also consider coprescription of naloxone at discharge for higher risk patients.
Dr. Stella is a hospitalist in Denver and an editorial board member of The Hospitalist.
Presenters
Shoshana J. Herzig, MD, MPH, and Hillary J. Mosher, MFA, MD, FHM
Summary
The growth in opiate prescribing and associated increases in adverse events has created unique challenges for hospitalists, including how best to assess pain and opiate use disorders and how to safely prescribe opiates during hospitalization and at discharge.
These challenges are compounded by patient and system factors and a paucity of evidence-based guidelines to help guide safe administration of opiates in hospitalized patients. This can mean frustration for hospitalists and harm for patients.
Key takeaways for HM
- When assessing patients’ pain, it is crucial to differentiate between acute and chronic pain (or both) and whether it is nociceptive or neuropathic. Misclassification of pain contributes to inappropriate exposure and escalation of opiate therapy during hospitalization.
- Always consider nonopioid analgesics such as NSAIDs first and pair them with opiates. Studies in a variety of conditions have demonstrated that these are equally, if not more, effective, even for severe pain, such as with renal colic. Reserve opiates for moderate to severe pain.
- Always assess whether the benefits of initiating or continuing opioid therapy outweigh the risks for individual patients. There is no validated tool to predict risk for adverse events and/or opioid abuse disorder but a careful review of patient history can identify established risk factors (such as a history of mental illness or substance abuse disorders, renal impairment, or other comorbidities). In addition, nearly all states now have Prescription Drug Monitoring Programs, and hospitalists should consult these routinely when prescribing opiates.
- Always clearly discuss expectations and risks of opioid therapy, including the potential for development of opioid use disorders with hospitalized patients prior to initiation. Emphasize pain reduction rather than elimination and focus on functional goals such as improved mobility. Also, set expectations for stepping down treatment up front.
- Use the lowest effective dose of immediate-release opioids (preferably oral route) for shortest duration possible. Long acting opiates are associated with increased risk of adverse events, and their initiation should generally be avoided in hospitalized patients with noncancer pain.
- Minimize risk by avoiding concurrent administration of other medications with sedative properties, especially benzodiazepines, which have been found to significantly increase the risk of adverse events, including overdose.
- Recognize that chronic opioid use often begins with treatment of acute pain during hospitalization. Adopt best practice for discharge, including prescribing shorter courses whenever possible, discussing initiation, and changes or modifications in opiate therapy with patients’ primary care provider, and ensure timely postdischarge follow-up. Also consider coprescription of naloxone at discharge for higher risk patients.
Dr. Stella is a hospitalist in Denver and an editorial board member of The Hospitalist.
Presenters
Shoshana J. Herzig, MD, MPH, and Hillary J. Mosher, MFA, MD, FHM
Summary
The growth in opiate prescribing and associated increases in adverse events has created unique challenges for hospitalists, including how best to assess pain and opiate use disorders and how to safely prescribe opiates during hospitalization and at discharge.
These challenges are compounded by patient and system factors and a paucity of evidence-based guidelines to help guide safe administration of opiates in hospitalized patients. This can mean frustration for hospitalists and harm for patients.
Key takeaways for HM
- When assessing patients’ pain, it is crucial to differentiate between acute and chronic pain (or both) and whether it is nociceptive or neuropathic. Misclassification of pain contributes to inappropriate exposure and escalation of opiate therapy during hospitalization.
- Always consider nonopioid analgesics such as NSAIDs first and pair them with opiates. Studies in a variety of conditions have demonstrated that these are equally, if not more, effective, even for severe pain, such as with renal colic. Reserve opiates for moderate to severe pain.
- Always assess whether the benefits of initiating or continuing opioid therapy outweigh the risks for individual patients. There is no validated tool to predict risk for adverse events and/or opioid abuse disorder but a careful review of patient history can identify established risk factors (such as a history of mental illness or substance abuse disorders, renal impairment, or other comorbidities). In addition, nearly all states now have Prescription Drug Monitoring Programs, and hospitalists should consult these routinely when prescribing opiates.
- Always clearly discuss expectations and risks of opioid therapy, including the potential for development of opioid use disorders with hospitalized patients prior to initiation. Emphasize pain reduction rather than elimination and focus on functional goals such as improved mobility. Also, set expectations for stepping down treatment up front.
- Use the lowest effective dose of immediate-release opioids (preferably oral route) for shortest duration possible. Long acting opiates are associated with increased risk of adverse events, and their initiation should generally be avoided in hospitalized patients with noncancer pain.
- Minimize risk by avoiding concurrent administration of other medications with sedative properties, especially benzodiazepines, which have been found to significantly increase the risk of adverse events, including overdose.
- Recognize that chronic opioid use often begins with treatment of acute pain during hospitalization. Adopt best practice for discharge, including prescribing shorter courses whenever possible, discussing initiation, and changes or modifications in opiate therapy with patients’ primary care provider, and ensure timely postdischarge follow-up. Also consider coprescription of naloxone at discharge for higher risk patients.
Dr. Stella is a hospitalist in Denver and an editorial board member of The Hospitalist.
FRAX Prediction With and Without Bone Mineral Density Testing
In the U.S. about 2 million men have osteoporosis.1 About 1 in 5 men will experience an osteoporotic-related fracture in his lifetime.2 In addition, men with hip fracture have a higher mortality rate compared with that of women with hip fracture.3 The National Osteoporosis Foundation guidelines and the Endocrine Society guidelines recommend that all men aged ≥ 70 years have bone mineral density (BMD) testing. Depending on risk factors, osteoporosis screening may be appropriate for men aged ≥ 50 years. A BMD with a T-score of -2.5 or lower is classified as osteoporosis.2
In addition to osteoporosis, osteopenia also negatively impacts men. Osteopenia is defined as a BMD with a T-score of -1 to -2.5.2 According to the National Health and Nutrition Examination Survey (NHANES), about 30% of men aged ≥ 50 years have osteopenia.4 FRAX is a fracture risk assessment tool that is used to predict the 10-year risk of fracture in untreated patients with osteopenia. The FRAX tool has been validated with the use of BMD testing only at the femoral neck; it has not been validated in other parts of the body. Treatment is indicated if the 10-year fracture risk is > 20% for major osteoporotic fractures and > 3% for hip fractures, based on the FRAX calculation.2
The following risk factors are used in the FRAX calculation: age; sex; weight (kilograms); height (centimeters); previous fracture (yes or no); parental history of hip fracture (yes or no); current smoker (yes or no); oral glucocorticoid exposure currently or for > 3 months in the past (yes or no); rheumatoid arthritis (yes or no); secondary osteoporosis or a disorder strongly associated with osteoporosis, including type 1 diabetes mellitus, osteogenesis imperfecta in adults, untreated long-standing hyperthyroidism, hypogonadism, premature menopause, chronic malnutrition, malabsorption, or chronic liver disease (yes or no); 3 or more units of alcohol daily (yes or no); and BMD.5
A dual-energy X-ray absorptiometry (DXA) examination is needed to determine BMD. However, a DXA examination is not always feasible for patients who have limited access, transportation challenges, require the use of assistive devices, and may be unaware of the importance of BMD testing.
The FRAX calculation can be obtained with or without BMD. Gadam and colleagues compared FRAX calculations with and without BMD to predict the 10-year risk of fracture.6 Their study found that 84% of patients had an identical fracture risk prediction whether or not BMD was included. The only risk factor evaluated that was significantly different between those with different treatment predictions and those with identical treatment predictions was age. However, the majority of patients included were female (96%).
No studies existed that compared fracture prediction risk with and without BMD in a male-only population. The purpose of this study was to determine whether FRAX without BMD was as effective as FRAX with BMD to predict the risk of osteoporotic fractures and provide an identical treatment recommendation in male veteran patients at the Lexington VAMC in Kentucky.
Methods
A retrospective chart review was conducted at the Lexington VAMC. Approval was obtained from the Lexington VAMC Institutional Review Board and Research and Development Committee. Patients were identified using the computerized patient record system (CPRS). Included patients were male, ≥ 50 years, had a documented DXA in CPRS from January 2006 to September 2015, and had a previous fracture determined by ICD-9 codes. Patients were excluded if they were diagnosed with osteoporosis or were ever treated for osteoporosis before a DXA scan.
Data collection included patient’s age, gender, race, glucocorticoid use for at least 3 months within 1 year prior to DXA, body weight within 3 months prior to DXA, height within 1 year prior to DXA, family history of fracture, previous fall or fracture, diagnosis of rheumatoid arthritis, smoking status at the time of DXA, alcohol intake of at least 3 drinks per day at the time of DXA, and vitamin D level within 1 year prior to DXA. In order to find a clinically significant difference (P < .05) with a power of 80%, a sample size of 64 patients was needed.
Each patient’s FRAX predictions were calculated with and without BMD. Patients were then separated into 2 groups: those who had an identical treatment recommendation when calculating FRAX with and without BMD, and those who had a different treatment recommendation when calculating FRAX with and without BMD. Binary variables for each group were compared using the Fisher exact test, and numeric variables were compared using a simple Student’s t test.
Results
After screening 1,510 patients, only 119 patients met the criteria and were included in the study (Figure). All patients included were male. Mean age was 71.2 years and 113 (95.0%) were white (Table 1).
Of the 119 patients included in the study, 98 patients (82.4%) had the same treatment recommendation when the FRAX score was calculated with and without BMD. The remaining 21 patients (17.6%) had different treatment recommendations when FRAX scores were calculated with BMD compared with FRAX scores calculated without BMD. Treatment was recommended based on risk prediction for 43 of the 98 patients who had identical treatment recommendations. Of the 21 patients who had different treatment recommendations, treatment was recommended based on risk prediction for 14 patients when FRAX scores were calculated with BMD. Treatment was recommended for the other 7 patients when FRAX scores were calculated without BMD.
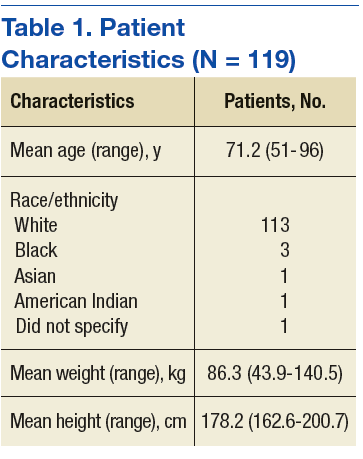
Of the numeric variables evaluated, mean age, femoral neck BMD, and T-score were all significantly different between the 2 groups (Table 2). Patients with an identical treatment recommendation were a mean age of 67.9 years (SD: 10.2 y), and patients with different treatment recommendations were a mean age of 62.2 years (SD: 8.9 y) (P = .011). Patients with an identical treatment recommendation had a mean BMD of 0.9 (SD: 0.2), and patients with different treatment recommendations had a mean BMD of 0.8 (SD: 0.1) (P = .021). Patients with an identical treatment recommendation had a mean T-score of -1.7 (SD: 1.2), and patients with different treatment recommendations had a mean T-score of -2.3 (SD: 1.1) (P = .031). Mean weight, height, and vitamin D level were not statistically significantly different between the 2 groups.
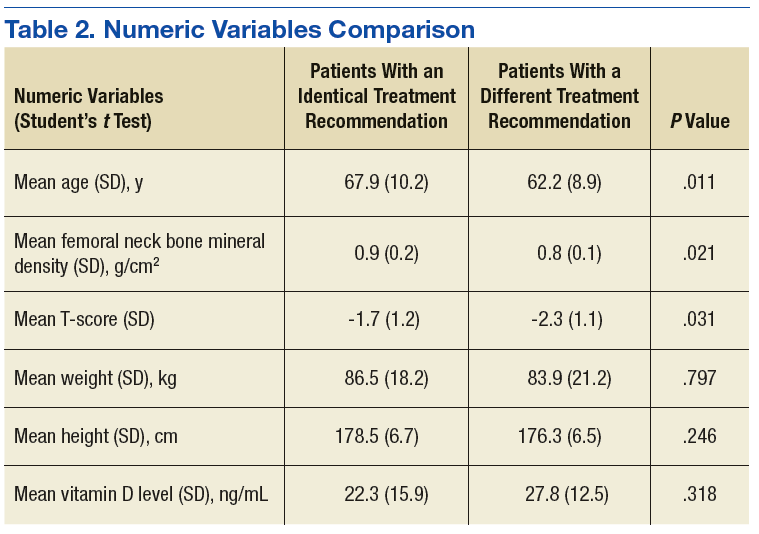
Of the binary variables evaluated, only glucocorticoid use was significantly different between the 2 groups. Of the patients with an identical treatment recommendation, 4 (4.1%) received a glucocorticoid. 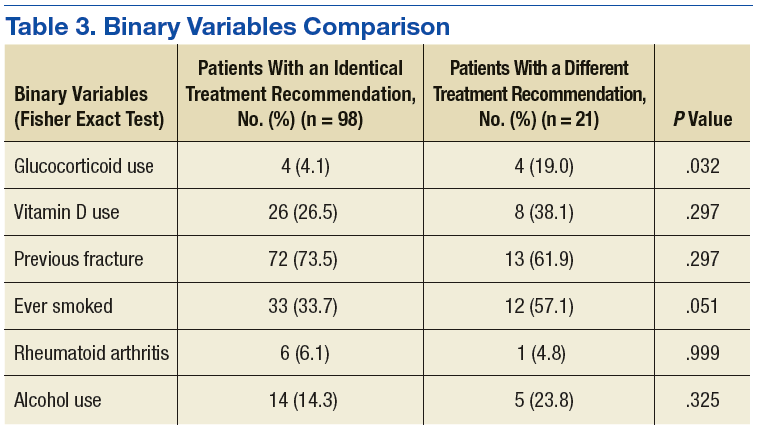
Discussion
The purpose of this retrospective study was to determine whether using FRAX without BMD was as effective as using FRAX with BMD in predicting the risk of osteoporotic fractures and in providing identical treatment recommendations in male veteran patients. The results of this study revealed that FRAX calculations without BMD provided identical treatment recommendations as FRAX calculations with BMD for 82.4% of male veteran patients. These findings were similar to the findings of another study by Gadam and colleagues, in which 84% of patients had identical treatment recommendations when calculating FRAX scores with and without BMD.6 In contrast, a prospective cohort study by Ettinger and colleagues found that the addition of BMD to the FRAX calculation enhanced the performance of the FRAX tool by correctly identifying more patients who experienced a fracture within the following 10 years.8
Several of the risk factors evaluated in the present study were indicative of an identical treatment recommendation. Age was one of the risk factors that differed significantly between the 2 groups. The mean age of patients with an identical treatment recommendation was 67.9 years, and the mean age of patients with different treatment recommendations was 62.2 years (P = .011). These findings opposed the findings in the Gadam and colleagues’ study.6 The results of that study revealed that younger age rather than older age was more indicative of an identical treatment recommendation. The study by Gadam and colleagues included both male and female patients; however, the majority of patients included in the Gadam study were female (96%).6 Because the present study included only male patients, a comparison of the results was difficult because of the different patient populations.
A higher T-score (P = .031) and a higher BMD (P = .021) were the other 2 risk factors associated with an identical treatment recommendation with and without BMD. The Gadam and colleagues study did not find these to be significant risk factors for identifying an identical treatment recommendation.6
The FRAX calculation without BMD identified all the patients meeting treatment criteria based on the FRAX calculation with BMD except for 14 of the 119 patients (11.8%). Therefore, > 88% of patients who met treatment criteria based on FRAX calculated with BMD also met treatment criteria based on FRAX without BMD.
The FRAX calculation has several advantages, including risk stratification in men and identifying those with other conditions that may predispose them to a fracture.7 Therefore, before obtaining a DXA scan, it would be reasonable to calculate a FRAX score without BMD to identify patients who are at high risk for fracture but who may not receive treatment because they are not considered to need a DXA scan or a DXA scan is not feasible.
Limitations
Currently, FRAX is validated only using femoral neck BMD. This study was a retrospective chart review only; no information was obtained from communicating with the patient, including the patient’s past medical history and family history. Also, this study had a small sample size: Of the 1,510 patients screened, only 119 met inclusion criteria. None of the 119 patients evaluated had a family history of fracture documented in their CPRS. Therefore, several of the patient’s 10-year fracture risk scores may be underestimated if one or both of their parents experienced a fracture. Last, the majority of patients included in this study were white, so the results of this study cannot necessarily be generalized to other races.
Conclusion
The majority of male patients had an identical treatment recommendation when a FRAX score was calculated with and without BMD. Older age, higher BMD, and higher T-score were all indicative of an identical treatment recommendation. Larger studies are necessary in order to validate the FRAX tool without the use of femoral neck BMD. However, the FRAX tool alone can be beneficial to identify male patients who should have a DXA scan performed to obtain a BMD. If a male patient’s FRAX score suggests risk for osteoporotic fracture, then a DXA scan should be completed to obtain a BMD if feasible.
Additionally, when obtaining a BMD is not feasible to predict fracture risk, the FRAX tool alone may be useful a majority of the time to accurately determine treatment recommendations in male patients aged > 65 years. The results of this study lead the authors to believe that FRAX without BMD in male patients aged > 65 years will appropriately identify more patients for treatment. ˜
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the Lexington VA Medical Center.
1. Sweet MG, Sweet JM, Jeremiah MP, Galazka SS. Diagnosis and treatment of osteoporosis. Am Fam Physician. 2009;79(3):193-200.
2. Cosman F, de Beur SJ, LeBoff MS, et al. Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int. 2014;25(10):2359-2381.
3. Khan AA, Hodsman AB, Papaioannou A, Kendler D, Brown JP, Olszynski WP. Management of osteoporosis in men: an update and case example. CMAJ. 2007;176(3):345-348.
4. Looker AC, Melton LJ III, Harris TB, Borrud LG, Shepherd JA. Prevalence and trends in low femur bone density among older US adults: NHANES 2005-2006 compared with NHANES III. J Bone Miner Res. 2010;25(1):64-71.
5. Kanas JA; World Health Organization Scientific Group. Assessment of osteoporosis at the primary health care level. https://www.shef.ac.uk/FRAX/pdfs/WHO_Technical_Report.pdf. Published 2007. Accessed March 29, 2017.
6. Gadam RK, Schlauch K, Izuora KE. FRAX prediction without BMD for assessment of osteoporotic fracture risk. Endocr Pract. 2013;19(5):780-784.
7. Siris E, Delmas PD. Assessment of 10-year absolute fracture risk: a new paradigm with worldwide application. Osteoporosis Int. 2008;19(4):383-384.
8. Ettinger B, Liu H, Blackwell T, et al. Validation of FRC, a fracture risk assessment tool, in a cohort of older men: the osteoporotic fractures in men (MrOS) study. J Clin Densitom. 2012;15(3):334-342.
In the U.S. about 2 million men have osteoporosis.1 About 1 in 5 men will experience an osteoporotic-related fracture in his lifetime.2 In addition, men with hip fracture have a higher mortality rate compared with that of women with hip fracture.3 The National Osteoporosis Foundation guidelines and the Endocrine Society guidelines recommend that all men aged ≥ 70 years have bone mineral density (BMD) testing. Depending on risk factors, osteoporosis screening may be appropriate for men aged ≥ 50 years. A BMD with a T-score of -2.5 or lower is classified as osteoporosis.2
In addition to osteoporosis, osteopenia also negatively impacts men. Osteopenia is defined as a BMD with a T-score of -1 to -2.5.2 According to the National Health and Nutrition Examination Survey (NHANES), about 30% of men aged ≥ 50 years have osteopenia.4 FRAX is a fracture risk assessment tool that is used to predict the 10-year risk of fracture in untreated patients with osteopenia. The FRAX tool has been validated with the use of BMD testing only at the femoral neck; it has not been validated in other parts of the body. Treatment is indicated if the 10-year fracture risk is > 20% for major osteoporotic fractures and > 3% for hip fractures, based on the FRAX calculation.2
The following risk factors are used in the FRAX calculation: age; sex; weight (kilograms); height (centimeters); previous fracture (yes or no); parental history of hip fracture (yes or no); current smoker (yes or no); oral glucocorticoid exposure currently or for > 3 months in the past (yes or no); rheumatoid arthritis (yes or no); secondary osteoporosis or a disorder strongly associated with osteoporosis, including type 1 diabetes mellitus, osteogenesis imperfecta in adults, untreated long-standing hyperthyroidism, hypogonadism, premature menopause, chronic malnutrition, malabsorption, or chronic liver disease (yes or no); 3 or more units of alcohol daily (yes or no); and BMD.5
A dual-energy X-ray absorptiometry (DXA) examination is needed to determine BMD. However, a DXA examination is not always feasible for patients who have limited access, transportation challenges, require the use of assistive devices, and may be unaware of the importance of BMD testing.
The FRAX calculation can be obtained with or without BMD. Gadam and colleagues compared FRAX calculations with and without BMD to predict the 10-year risk of fracture.6 Their study found that 84% of patients had an identical fracture risk prediction whether or not BMD was included. The only risk factor evaluated that was significantly different between those with different treatment predictions and those with identical treatment predictions was age. However, the majority of patients included were female (96%).
No studies existed that compared fracture prediction risk with and without BMD in a male-only population. The purpose of this study was to determine whether FRAX without BMD was as effective as FRAX with BMD to predict the risk of osteoporotic fractures and provide an identical treatment recommendation in male veteran patients at the Lexington VAMC in Kentucky.
Methods
A retrospective chart review was conducted at the Lexington VAMC. Approval was obtained from the Lexington VAMC Institutional Review Board and Research and Development Committee. Patients were identified using the computerized patient record system (CPRS). Included patients were male, ≥ 50 years, had a documented DXA in CPRS from January 2006 to September 2015, and had a previous fracture determined by ICD-9 codes. Patients were excluded if they were diagnosed with osteoporosis or were ever treated for osteoporosis before a DXA scan.
Data collection included patient’s age, gender, race, glucocorticoid use for at least 3 months within 1 year prior to DXA, body weight within 3 months prior to DXA, height within 1 year prior to DXA, family history of fracture, previous fall or fracture, diagnosis of rheumatoid arthritis, smoking status at the time of DXA, alcohol intake of at least 3 drinks per day at the time of DXA, and vitamin D level within 1 year prior to DXA. In order to find a clinically significant difference (P < .05) with a power of 80%, a sample size of 64 patients was needed.
Each patient’s FRAX predictions were calculated with and without BMD. Patients were then separated into 2 groups: those who had an identical treatment recommendation when calculating FRAX with and without BMD, and those who had a different treatment recommendation when calculating FRAX with and without BMD. Binary variables for each group were compared using the Fisher exact test, and numeric variables were compared using a simple Student’s t test.
Results
After screening 1,510 patients, only 119 patients met the criteria and were included in the study (Figure). All patients included were male. Mean age was 71.2 years and 113 (95.0%) were white (Table 1).
Of the 119 patients included in the study, 98 patients (82.4%) had the same treatment recommendation when the FRAX score was calculated with and without BMD. The remaining 21 patients (17.6%) had different treatment recommendations when FRAX scores were calculated with BMD compared with FRAX scores calculated without BMD. Treatment was recommended based on risk prediction for 43 of the 98 patients who had identical treatment recommendations. Of the 21 patients who had different treatment recommendations, treatment was recommended based on risk prediction for 14 patients when FRAX scores were calculated with BMD. Treatment was recommended for the other 7 patients when FRAX scores were calculated without BMD.
Of the numeric variables evaluated, mean age, femoral neck BMD, and T-score were all significantly different between the 2 groups (Table 2). Patients with an identical treatment recommendation were a mean age of 67.9 years (SD: 10.2 y), and patients with different treatment recommendations were a mean age of 62.2 years (SD: 8.9 y) (P = .011). Patients with an identical treatment recommendation had a mean BMD of 0.9 (SD: 0.2), and patients with different treatment recommendations had a mean BMD of 0.8 (SD: 0.1) (P = .021). Patients with an identical treatment recommendation had a mean T-score of -1.7 (SD: 1.2), and patients with different treatment recommendations had a mean T-score of -2.3 (SD: 1.1) (P = .031). Mean weight, height, and vitamin D level were not statistically significantly different between the 2 groups.
Of the binary variables evaluated, only glucocorticoid use was significantly different between the 2 groups. Of the patients with an identical treatment recommendation, 4 (4.1%) received a glucocorticoid.
Discussion
The purpose of this retrospective study was to determine whether using FRAX without BMD was as effective as using FRAX with BMD in predicting the risk of osteoporotic fractures and in providing identical treatment recommendations in male veteran patients. The results of this study revealed that FRAX calculations without BMD provided identical treatment recommendations as FRAX calculations with BMD for 82.4% of male veteran patients. These findings were similar to the findings of another study by Gadam and colleagues, in which 84% of patients had identical treatment recommendations when calculating FRAX scores with and without BMD.6 In contrast, a prospective cohort study by Ettinger and colleagues found that the addition of BMD to the FRAX calculation enhanced the performance of the FRAX tool by correctly identifying more patients who experienced a fracture within the following 10 years.8
Several of the risk factors evaluated in the present study were indicative of an identical treatment recommendation. Age was one of the risk factors that differed significantly between the 2 groups. The mean age of patients with an identical treatment recommendation was 67.9 years, and the mean age of patients with different treatment recommendations was 62.2 years (P = .011). These findings opposed the findings in the Gadam and colleagues’ study.6 The results of that study revealed that younger age rather than older age was more indicative of an identical treatment recommendation. The study by Gadam and colleagues included both male and female patients; however, the majority of patients included in the Gadam study were female (96%).6 Because the present study included only male patients, a comparison of the results was difficult because of the different patient populations.
A higher T-score (P = .031) and a higher BMD (P = .021) were the other 2 risk factors associated with an identical treatment recommendation with and without BMD. The Gadam and colleagues study did not find these to be significant risk factors for identifying an identical treatment recommendation.6
The FRAX calculation without BMD identified all the patients meeting treatment criteria based on the FRAX calculation with BMD except for 14 of the 119 patients (11.8%). Therefore, > 88% of patients who met treatment criteria based on FRAX calculated with BMD also met treatment criteria based on FRAX without BMD.
The FRAX calculation has several advantages, including risk stratification in men and identifying those with other conditions that may predispose them to a fracture.7 Therefore, before obtaining a DXA scan, it would be reasonable to calculate a FRAX score without BMD to identify patients who are at high risk for fracture but who may not receive treatment because they are not considered to need a DXA scan or a DXA scan is not feasible.
Limitations
Currently, FRAX is validated only using femoral neck BMD. This study was a retrospective chart review only; no information was obtained from communicating with the patient, including the patient’s past medical history and family history. Also, this study had a small sample size: Of the 1,510 patients screened, only 119 met inclusion criteria. None of the 119 patients evaluated had a family history of fracture documented in their CPRS. Therefore, several of the patient’s 10-year fracture risk scores may be underestimated if one or both of their parents experienced a fracture. Last, the majority of patients included in this study were white, so the results of this study cannot necessarily be generalized to other races.
Conclusion
The majority of male patients had an identical treatment recommendation when a FRAX score was calculated with and without BMD. Older age, higher BMD, and higher T-score were all indicative of an identical treatment recommendation. Larger studies are necessary in order to validate the FRAX tool without the use of femoral neck BMD. However, the FRAX tool alone can be beneficial to identify male patients who should have a DXA scan performed to obtain a BMD. If a male patient’s FRAX score suggests risk for osteoporotic fracture, then a DXA scan should be completed to obtain a BMD if feasible.
Additionally, when obtaining a BMD is not feasible to predict fracture risk, the FRAX tool alone may be useful a majority of the time to accurately determine treatment recommendations in male patients aged > 65 years. The results of this study lead the authors to believe that FRAX without BMD in male patients aged > 65 years will appropriately identify more patients for treatment. ˜
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the Lexington VA Medical Center.
In the U.S. about 2 million men have osteoporosis.1 About 1 in 5 men will experience an osteoporotic-related fracture in his lifetime.2 In addition, men with hip fracture have a higher mortality rate compared with that of women with hip fracture.3 The National Osteoporosis Foundation guidelines and the Endocrine Society guidelines recommend that all men aged ≥ 70 years have bone mineral density (BMD) testing. Depending on risk factors, osteoporosis screening may be appropriate for men aged ≥ 50 years. A BMD with a T-score of -2.5 or lower is classified as osteoporosis.2
In addition to osteoporosis, osteopenia also negatively impacts men. Osteopenia is defined as a BMD with a T-score of -1 to -2.5.2 According to the National Health and Nutrition Examination Survey (NHANES), about 30% of men aged ≥ 50 years have osteopenia.4 FRAX is a fracture risk assessment tool that is used to predict the 10-year risk of fracture in untreated patients with osteopenia. The FRAX tool has been validated with the use of BMD testing only at the femoral neck; it has not been validated in other parts of the body. Treatment is indicated if the 10-year fracture risk is > 20% for major osteoporotic fractures and > 3% for hip fractures, based on the FRAX calculation.2
The following risk factors are used in the FRAX calculation: age; sex; weight (kilograms); height (centimeters); previous fracture (yes or no); parental history of hip fracture (yes or no); current smoker (yes or no); oral glucocorticoid exposure currently or for > 3 months in the past (yes or no); rheumatoid arthritis (yes or no); secondary osteoporosis or a disorder strongly associated with osteoporosis, including type 1 diabetes mellitus, osteogenesis imperfecta in adults, untreated long-standing hyperthyroidism, hypogonadism, premature menopause, chronic malnutrition, malabsorption, or chronic liver disease (yes or no); 3 or more units of alcohol daily (yes or no); and BMD.5
A dual-energy X-ray absorptiometry (DXA) examination is needed to determine BMD. However, a DXA examination is not always feasible for patients who have limited access, transportation challenges, require the use of assistive devices, and may be unaware of the importance of BMD testing.
The FRAX calculation can be obtained with or without BMD. Gadam and colleagues compared FRAX calculations with and without BMD to predict the 10-year risk of fracture.6 Their study found that 84% of patients had an identical fracture risk prediction whether or not BMD was included. The only risk factor evaluated that was significantly different between those with different treatment predictions and those with identical treatment predictions was age. However, the majority of patients included were female (96%).
No studies existed that compared fracture prediction risk with and without BMD in a male-only population. The purpose of this study was to determine whether FRAX without BMD was as effective as FRAX with BMD to predict the risk of osteoporotic fractures and provide an identical treatment recommendation in male veteran patients at the Lexington VAMC in Kentucky.
Methods
A retrospective chart review was conducted at the Lexington VAMC. Approval was obtained from the Lexington VAMC Institutional Review Board and Research and Development Committee. Patients were identified using the computerized patient record system (CPRS). Included patients were male, ≥ 50 years, had a documented DXA in CPRS from January 2006 to September 2015, and had a previous fracture determined by ICD-9 codes. Patients were excluded if they were diagnosed with osteoporosis or were ever treated for osteoporosis before a DXA scan.
Data collection included patient’s age, gender, race, glucocorticoid use for at least 3 months within 1 year prior to DXA, body weight within 3 months prior to DXA, height within 1 year prior to DXA, family history of fracture, previous fall or fracture, diagnosis of rheumatoid arthritis, smoking status at the time of DXA, alcohol intake of at least 3 drinks per day at the time of DXA, and vitamin D level within 1 year prior to DXA. In order to find a clinically significant difference (P < .05) with a power of 80%, a sample size of 64 patients was needed.
Each patient’s FRAX predictions were calculated with and without BMD. Patients were then separated into 2 groups: those who had an identical treatment recommendation when calculating FRAX with and without BMD, and those who had a different treatment recommendation when calculating FRAX with and without BMD. Binary variables for each group were compared using the Fisher exact test, and numeric variables were compared using a simple Student’s t test.
Results
After screening 1,510 patients, only 119 patients met the criteria and were included in the study (Figure). All patients included were male. Mean age was 71.2 years and 113 (95.0%) were white (Table 1).
Of the 119 patients included in the study, 98 patients (82.4%) had the same treatment recommendation when the FRAX score was calculated with and without BMD. The remaining 21 patients (17.6%) had different treatment recommendations when FRAX scores were calculated with BMD compared with FRAX scores calculated without BMD. Treatment was recommended based on risk prediction for 43 of the 98 patients who had identical treatment recommendations. Of the 21 patients who had different treatment recommendations, treatment was recommended based on risk prediction for 14 patients when FRAX scores were calculated with BMD. Treatment was recommended for the other 7 patients when FRAX scores were calculated without BMD.
Of the numeric variables evaluated, mean age, femoral neck BMD, and T-score were all significantly different between the 2 groups (Table 2). Patients with an identical treatment recommendation were a mean age of 67.9 years (SD: 10.2 y), and patients with different treatment recommendations were a mean age of 62.2 years (SD: 8.9 y) (P = .011). Patients with an identical treatment recommendation had a mean BMD of 0.9 (SD: 0.2), and patients with different treatment recommendations had a mean BMD of 0.8 (SD: 0.1) (P = .021). Patients with an identical treatment recommendation had a mean T-score of -1.7 (SD: 1.2), and patients with different treatment recommendations had a mean T-score of -2.3 (SD: 1.1) (P = .031). Mean weight, height, and vitamin D level were not statistically significantly different between the 2 groups.
Of the binary variables evaluated, only glucocorticoid use was significantly different between the 2 groups. Of the patients with an identical treatment recommendation, 4 (4.1%) received a glucocorticoid.
Discussion
The purpose of this retrospective study was to determine whether using FRAX without BMD was as effective as using FRAX with BMD in predicting the risk of osteoporotic fractures and in providing identical treatment recommendations in male veteran patients. The results of this study revealed that FRAX calculations without BMD provided identical treatment recommendations as FRAX calculations with BMD for 82.4% of male veteran patients. These findings were similar to the findings of another study by Gadam and colleagues, in which 84% of patients had identical treatment recommendations when calculating FRAX scores with and without BMD.6 In contrast, a prospective cohort study by Ettinger and colleagues found that the addition of BMD to the FRAX calculation enhanced the performance of the FRAX tool by correctly identifying more patients who experienced a fracture within the following 10 years.8
Several of the risk factors evaluated in the present study were indicative of an identical treatment recommendation. Age was one of the risk factors that differed significantly between the 2 groups. The mean age of patients with an identical treatment recommendation was 67.9 years, and the mean age of patients with different treatment recommendations was 62.2 years (P = .011). These findings opposed the findings in the Gadam and colleagues’ study.6 The results of that study revealed that younger age rather than older age was more indicative of an identical treatment recommendation. The study by Gadam and colleagues included both male and female patients; however, the majority of patients included in the Gadam study were female (96%).6 Because the present study included only male patients, a comparison of the results was difficult because of the different patient populations.
A higher T-score (P = .031) and a higher BMD (P = .021) were the other 2 risk factors associated with an identical treatment recommendation with and without BMD. The Gadam and colleagues study did not find these to be significant risk factors for identifying an identical treatment recommendation.6
The FRAX calculation without BMD identified all the patients meeting treatment criteria based on the FRAX calculation with BMD except for 14 of the 119 patients (11.8%). Therefore, > 88% of patients who met treatment criteria based on FRAX calculated with BMD also met treatment criteria based on FRAX without BMD.
The FRAX calculation has several advantages, including risk stratification in men and identifying those with other conditions that may predispose them to a fracture.7 Therefore, before obtaining a DXA scan, it would be reasonable to calculate a FRAX score without BMD to identify patients who are at high risk for fracture but who may not receive treatment because they are not considered to need a DXA scan or a DXA scan is not feasible.
Limitations
Currently, FRAX is validated only using femoral neck BMD. This study was a retrospective chart review only; no information was obtained from communicating with the patient, including the patient’s past medical history and family history. Also, this study had a small sample size: Of the 1,510 patients screened, only 119 met inclusion criteria. None of the 119 patients evaluated had a family history of fracture documented in their CPRS. Therefore, several of the patient’s 10-year fracture risk scores may be underestimated if one or both of their parents experienced a fracture. Last, the majority of patients included in this study were white, so the results of this study cannot necessarily be generalized to other races.
Conclusion
The majority of male patients had an identical treatment recommendation when a FRAX score was calculated with and without BMD. Older age, higher BMD, and higher T-score were all indicative of an identical treatment recommendation. Larger studies are necessary in order to validate the FRAX tool without the use of femoral neck BMD. However, the FRAX tool alone can be beneficial to identify male patients who should have a DXA scan performed to obtain a BMD. If a male patient’s FRAX score suggests risk for osteoporotic fracture, then a DXA scan should be completed to obtain a BMD if feasible.
Additionally, when obtaining a BMD is not feasible to predict fracture risk, the FRAX tool alone may be useful a majority of the time to accurately determine treatment recommendations in male patients aged > 65 years. The results of this study lead the authors to believe that FRAX without BMD in male patients aged > 65 years will appropriately identify more patients for treatment. ˜
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the Lexington VA Medical Center.
1. Sweet MG, Sweet JM, Jeremiah MP, Galazka SS. Diagnosis and treatment of osteoporosis. Am Fam Physician. 2009;79(3):193-200.
2. Cosman F, de Beur SJ, LeBoff MS, et al. Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int. 2014;25(10):2359-2381.
3. Khan AA, Hodsman AB, Papaioannou A, Kendler D, Brown JP, Olszynski WP. Management of osteoporosis in men: an update and case example. CMAJ. 2007;176(3):345-348.
4. Looker AC, Melton LJ III, Harris TB, Borrud LG, Shepherd JA. Prevalence and trends in low femur bone density among older US adults: NHANES 2005-2006 compared with NHANES III. J Bone Miner Res. 2010;25(1):64-71.
5. Kanas JA; World Health Organization Scientific Group. Assessment of osteoporosis at the primary health care level. https://www.shef.ac.uk/FRAX/pdfs/WHO_Technical_Report.pdf. Published 2007. Accessed March 29, 2017.
6. Gadam RK, Schlauch K, Izuora KE. FRAX prediction without BMD for assessment of osteoporotic fracture risk. Endocr Pract. 2013;19(5):780-784.
7. Siris E, Delmas PD. Assessment of 10-year absolute fracture risk: a new paradigm with worldwide application. Osteoporosis Int. 2008;19(4):383-384.
8. Ettinger B, Liu H, Blackwell T, et al. Validation of FRC, a fracture risk assessment tool, in a cohort of older men: the osteoporotic fractures in men (MrOS) study. J Clin Densitom. 2012;15(3):334-342.
1. Sweet MG, Sweet JM, Jeremiah MP, Galazka SS. Diagnosis and treatment of osteoporosis. Am Fam Physician. 2009;79(3):193-200.
2. Cosman F, de Beur SJ, LeBoff MS, et al. Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int. 2014;25(10):2359-2381.
3. Khan AA, Hodsman AB, Papaioannou A, Kendler D, Brown JP, Olszynski WP. Management of osteoporosis in men: an update and case example. CMAJ. 2007;176(3):345-348.
4. Looker AC, Melton LJ III, Harris TB, Borrud LG, Shepherd JA. Prevalence and trends in low femur bone density among older US adults: NHANES 2005-2006 compared with NHANES III. J Bone Miner Res. 2010;25(1):64-71.
5. Kanas JA; World Health Organization Scientific Group. Assessment of osteoporosis at the primary health care level. https://www.shef.ac.uk/FRAX/pdfs/WHO_Technical_Report.pdf. Published 2007. Accessed March 29, 2017.
6. Gadam RK, Schlauch K, Izuora KE. FRAX prediction without BMD for assessment of osteoporotic fracture risk. Endocr Pract. 2013;19(5):780-784.
7. Siris E, Delmas PD. Assessment of 10-year absolute fracture risk: a new paradigm with worldwide application. Osteoporosis Int. 2008;19(4):383-384.
8. Ettinger B, Liu H, Blackwell T, et al. Validation of FRC, a fracture risk assessment tool, in a cohort of older men: the osteoporotic fractures in men (MrOS) study. J Clin Densitom. 2012;15(3):334-342.
Finding could lead to ‘Holy Grail’ of antithrombotic therapy

The protein CIB1 may be a superior target for antithrombotic therapy, according to researchers.
The team found that CIB1 plays a role in thrombus development but not in initial clot formation.
“The Holy Grail of our field is to reduce unwanted thrombus formation without completely blocking other important platelet functions,” said study author Ulhas Naik, PhD, of Thomas Jefferson University in Philadelphia, Pennsylvania.
He and his colleagues believe targeting CIB1 may do just that.
In earlier work, the researchers showed that CIB1 was involved in thrombus formation. They found mice that lacked the CIB1 gene were less likely to form a thrombus.
That work also indicated that mice lacking the CIB1 were still able to form a platelet plug, suggesting this gene was involved only in the process of thrombus formation.
To investigate this possibility further and to demonstrate that the process was relevant to human physiology, Dr Naik and his colleagues conducted the current study.
The team described this work in PLOS ONE.
The researchers studied human platelets and probed the molecules that interacted with CIB1 at different time points after platelet activation.
The team found that CIB1 does not begin to bind and interact with platelet molecular machinery until after filopodia formation, which allows platelets to cross-link to one another and begin to form a plug.
The study also elucidated a number of molecules that CIB1 interacts with during outside-in signaling and thrombus formation.
“This work demonstrates that CIB1 could be a good antithrombotic drug target,” Dr Naik said. “If we block CIB1, it hampers thrombus formation without interfering with platelet plug formation. If developed further, blocking CIB1 could reduce the risk of heart attack and stroke without increasing the risk for excessive bleeding that is the trade-off of current medication.”
The next step for Dr Naik and his colleagues is screening for small-molecule compounds that would inhibit CIB1 and could be developed into new therapies. ![]()
The protein CIB1 may be a superior target for antithrombotic therapy, according to researchers.
The team found that CIB1 plays a role in thrombus development but not in initial clot formation.
“The Holy Grail of our field is to reduce unwanted thrombus formation without completely blocking other important platelet functions,” said study author Ulhas Naik, PhD, of Thomas Jefferson University in Philadelphia, Pennsylvania.
He and his colleagues believe targeting CIB1 may do just that.
In earlier work, the researchers showed that CIB1 was involved in thrombus formation. They found mice that lacked the CIB1 gene were less likely to form a thrombus.
That work also indicated that mice lacking the CIB1 were still able to form a platelet plug, suggesting this gene was involved only in the process of thrombus formation.
To investigate this possibility further and to demonstrate that the process was relevant to human physiology, Dr Naik and his colleagues conducted the current study.
The team described this work in PLOS ONE.
The researchers studied human platelets and probed the molecules that interacted with CIB1 at different time points after platelet activation.
The team found that CIB1 does not begin to bind and interact with platelet molecular machinery until after filopodia formation, which allows platelets to cross-link to one another and begin to form a plug.
The study also elucidated a number of molecules that CIB1 interacts with during outside-in signaling and thrombus formation.
“This work demonstrates that CIB1 could be a good antithrombotic drug target,” Dr Naik said. “If we block CIB1, it hampers thrombus formation without interfering with platelet plug formation. If developed further, blocking CIB1 could reduce the risk of heart attack and stroke without increasing the risk for excessive bleeding that is the trade-off of current medication.”
The next step for Dr Naik and his colleagues is screening for small-molecule compounds that would inhibit CIB1 and could be developed into new therapies. ![]()
The protein CIB1 may be a superior target for antithrombotic therapy, according to researchers.
The team found that CIB1 plays a role in thrombus development but not in initial clot formation.
“The Holy Grail of our field is to reduce unwanted thrombus formation without completely blocking other important platelet functions,” said study author Ulhas Naik, PhD, of Thomas Jefferson University in Philadelphia, Pennsylvania.
He and his colleagues believe targeting CIB1 may do just that.
In earlier work, the researchers showed that CIB1 was involved in thrombus formation. They found mice that lacked the CIB1 gene were less likely to form a thrombus.
That work also indicated that mice lacking the CIB1 were still able to form a platelet plug, suggesting this gene was involved only in the process of thrombus formation.
To investigate this possibility further and to demonstrate that the process was relevant to human physiology, Dr Naik and his colleagues conducted the current study.
The team described this work in PLOS ONE.
The researchers studied human platelets and probed the molecules that interacted with CIB1 at different time points after platelet activation.
The team found that CIB1 does not begin to bind and interact with platelet molecular machinery until after filopodia formation, which allows platelets to cross-link to one another and begin to form a plug.
The study also elucidated a number of molecules that CIB1 interacts with during outside-in signaling and thrombus formation.
“This work demonstrates that CIB1 could be a good antithrombotic drug target,” Dr Naik said. “If we block CIB1, it hampers thrombus formation without interfering with platelet plug formation. If developed further, blocking CIB1 could reduce the risk of heart attack and stroke without increasing the risk for excessive bleeding that is the trade-off of current medication.”
The next step for Dr Naik and his colleagues is screening for small-molecule compounds that would inhibit CIB1 and could be developed into new therapies. ![]()