User login
Use of probiotics in hospitalized adults to prevent Clostridium difficile infection
Clinical Question: Does the use and timing of probiotics in hospitalized adult patients with Clostridium difficile infection (CDI) improve clinical outcomes?
Background: The incidence of CDI in hospitalized patients has increased significantly over the past years, resulting in significant morbidity and mortality. Improved prevention of CDI could have substantial public health benefits.
Study design: Systematic review and metaregression analysis.
Setting: 19 studies meeting inclusion criteria.
Synopsis: Computerized bibliography databases were searched for randomized controlled trials (RCTs) evaluating probiotic effects on CDI in hospitalized adults taking antibiotics.
Comprising 6261 subjects, 19 RCTs were analyzed. The incidence of CDI was lower in the probiotic cohort than in the control group (1.6% vs. 3.9%; P less than 0.001). The pooled relative risk of CDI in probiotic users was 0.42 (95% CI, 0.30-0.57). Metaregression analysis demonstrated that probiotics were significantly more effective if given closer to the first antibiotic dose, with a decrease in efficacy for every day of delay in starting probiotics (P = .04). Probiotics given within 2 days of antibiotic initiation produced a greater reduction of risk for CDI (RR, 0.32; 95% CI, 0.22-0.48) than later administration (RR, 0.70; 95% CI, 0.40-1.23; P = .02). There was no increased risk for adverse events among patients receiving probiotics.
Limitations included high risk of bias because of missing data, attrition, restricted patient population, lack of placebo, and conflict of interest.
Bottom Line: Administration of probiotics soon after the first dose of antibiotic reduces the risk of CDI by more than 50% in hospitalized adults without any increased risk of adverse events.
Reference: Shen NT, Maw A, Tmanova LL et al. Timely use of Probiotics in Hospitalized Adults Prevents Clostridium difficile Infection: A Systematic Review with Meta-Regression Analysis. Gastroenterology. Published on 9 Feb 2017. doi: 10.1053/j.gastro.2017.02.003.
Dr. Martin is clinical professor in the division of hospital medicine, department of medicine, University of California, San Diego.
Clinical Question: Does the use and timing of probiotics in hospitalized adult patients with Clostridium difficile infection (CDI) improve clinical outcomes?
Background: The incidence of CDI in hospitalized patients has increased significantly over the past years, resulting in significant morbidity and mortality. Improved prevention of CDI could have substantial public health benefits.
Study design: Systematic review and metaregression analysis.
Setting: 19 studies meeting inclusion criteria.
Synopsis: Computerized bibliography databases were searched for randomized controlled trials (RCTs) evaluating probiotic effects on CDI in hospitalized adults taking antibiotics.
Comprising 6261 subjects, 19 RCTs were analyzed. The incidence of CDI was lower in the probiotic cohort than in the control group (1.6% vs. 3.9%; P less than 0.001). The pooled relative risk of CDI in probiotic users was 0.42 (95% CI, 0.30-0.57). Metaregression analysis demonstrated that probiotics were significantly more effective if given closer to the first antibiotic dose, with a decrease in efficacy for every day of delay in starting probiotics (P = .04). Probiotics given within 2 days of antibiotic initiation produced a greater reduction of risk for CDI (RR, 0.32; 95% CI, 0.22-0.48) than later administration (RR, 0.70; 95% CI, 0.40-1.23; P = .02). There was no increased risk for adverse events among patients receiving probiotics.
Limitations included high risk of bias because of missing data, attrition, restricted patient population, lack of placebo, and conflict of interest.
Bottom Line: Administration of probiotics soon after the first dose of antibiotic reduces the risk of CDI by more than 50% in hospitalized adults without any increased risk of adverse events.
Reference: Shen NT, Maw A, Tmanova LL et al. Timely use of Probiotics in Hospitalized Adults Prevents Clostridium difficile Infection: A Systematic Review with Meta-Regression Analysis. Gastroenterology. Published on 9 Feb 2017. doi: 10.1053/j.gastro.2017.02.003.
Dr. Martin is clinical professor in the division of hospital medicine, department of medicine, University of California, San Diego.
Clinical Question: Does the use and timing of probiotics in hospitalized adult patients with Clostridium difficile infection (CDI) improve clinical outcomes?
Background: The incidence of CDI in hospitalized patients has increased significantly over the past years, resulting in significant morbidity and mortality. Improved prevention of CDI could have substantial public health benefits.
Study design: Systematic review and metaregression analysis.
Setting: 19 studies meeting inclusion criteria.
Synopsis: Computerized bibliography databases were searched for randomized controlled trials (RCTs) evaluating probiotic effects on CDI in hospitalized adults taking antibiotics.
Comprising 6261 subjects, 19 RCTs were analyzed. The incidence of CDI was lower in the probiotic cohort than in the control group (1.6% vs. 3.9%; P less than 0.001). The pooled relative risk of CDI in probiotic users was 0.42 (95% CI, 0.30-0.57). Metaregression analysis demonstrated that probiotics were significantly more effective if given closer to the first antibiotic dose, with a decrease in efficacy for every day of delay in starting probiotics (P = .04). Probiotics given within 2 days of antibiotic initiation produced a greater reduction of risk for CDI (RR, 0.32; 95% CI, 0.22-0.48) than later administration (RR, 0.70; 95% CI, 0.40-1.23; P = .02). There was no increased risk for adverse events among patients receiving probiotics.
Limitations included high risk of bias because of missing data, attrition, restricted patient population, lack of placebo, and conflict of interest.
Bottom Line: Administration of probiotics soon after the first dose of antibiotic reduces the risk of CDI by more than 50% in hospitalized adults without any increased risk of adverse events.
Reference: Shen NT, Maw A, Tmanova LL et al. Timely use of Probiotics in Hospitalized Adults Prevents Clostridium difficile Infection: A Systematic Review with Meta-Regression Analysis. Gastroenterology. Published on 9 Feb 2017. doi: 10.1053/j.gastro.2017.02.003.
Dr. Martin is clinical professor in the division of hospital medicine, department of medicine, University of California, San Diego.
Sooner may not be better: Study shows no benefit of urgent colonoscopy for lower GI bleeding
Clinical Question: In patients hospitalized for a lower gastrointestinal bleeding (LGIB), does an urgent colonoscopy (less than 24 hours after admission) result in any clinical benefits, compared with waiting for an elective colonoscopy?
Background: LGIB is a common cause of morbidity and mortality, often requiring hospitalization. While colonoscopy is necessary for appropriate work-up and treatment, it remains unclear if time to colonoscopy (urgent vs. elective) confers any clinical benefit in hospitalized patients.
Study Design: Systematic review and meta-analysis.
Setting: Twelve studies meeting inclusion criteria.
Synopsis: Computerized bibliography databases were searched for appropriate studies, and 12 met inclusion criteria, resulting in a total sample size of 10,172 patients in the urgent colonoscopy arm and 14,224 patients in the elective colonoscopy.
Outcome measures included bleeding source identified on colonoscopy, therapeutic endoscopic interventions performed, patients requiring blood transfusions, rebleeding, adverse events, and mortality.
Urgent colonoscopy was associated with increased use of endoscopic therapeutic intervention (relative risk, 1.70; 95% CI, 1.08-2.67). There were no significant differences in bleeding source localization (RR, 1.08; 95% CI, 0.92-1.25), adverse event rates (RR, 1.05; 95% CI, 0.65-1.71), rebleeding rates (RR, 1.14; 95% CI, 0.74-1.78), transfusion requirement (RR, 1.02; 95% CI, 0.73-1.41), or mortality (RR, 1.17; 95% CI, 0.45-3.02) between urgent and elective colonoscopy.
Limitations of the study comprise of inclusion of small number of studies, underpowered statistical analysis, and possible variation in quality assessment of articles evaluated.
Bottom Line: Urgent colonoscopy is safe and usually well tolerated in hospitalized patients with LGIB, but, compared with elective colonoscopy, there is no clear evidence it alters important clinical outcomes.
Reference: Kouanda AM, Somsouk M, Sewell JL, Day LW. Urgent colonoscopy in patients with lower GI bleeding: A systematic review and meta-analysis. Gastrointest Endosc. Published online Feb 4, 2017. doi: 10.1016/j.gie.2017.01.035.
Dr. Martin is clinical professor in the division of hospital medicine, department of medicine, University of California, San Diego.
Clinical Question: In patients hospitalized for a lower gastrointestinal bleeding (LGIB), does an urgent colonoscopy (less than 24 hours after admission) result in any clinical benefits, compared with waiting for an elective colonoscopy?
Background: LGIB is a common cause of morbidity and mortality, often requiring hospitalization. While colonoscopy is necessary for appropriate work-up and treatment, it remains unclear if time to colonoscopy (urgent vs. elective) confers any clinical benefit in hospitalized patients.
Study Design: Systematic review and meta-analysis.
Setting: Twelve studies meeting inclusion criteria.
Synopsis: Computerized bibliography databases were searched for appropriate studies, and 12 met inclusion criteria, resulting in a total sample size of 10,172 patients in the urgent colonoscopy arm and 14,224 patients in the elective colonoscopy.
Outcome measures included bleeding source identified on colonoscopy, therapeutic endoscopic interventions performed, patients requiring blood transfusions, rebleeding, adverse events, and mortality.
Urgent colonoscopy was associated with increased use of endoscopic therapeutic intervention (relative risk, 1.70; 95% CI, 1.08-2.67). There were no significant differences in bleeding source localization (RR, 1.08; 95% CI, 0.92-1.25), adverse event rates (RR, 1.05; 95% CI, 0.65-1.71), rebleeding rates (RR, 1.14; 95% CI, 0.74-1.78), transfusion requirement (RR, 1.02; 95% CI, 0.73-1.41), or mortality (RR, 1.17; 95% CI, 0.45-3.02) between urgent and elective colonoscopy.
Limitations of the study comprise of inclusion of small number of studies, underpowered statistical analysis, and possible variation in quality assessment of articles evaluated.
Bottom Line: Urgent colonoscopy is safe and usually well tolerated in hospitalized patients with LGIB, but, compared with elective colonoscopy, there is no clear evidence it alters important clinical outcomes.
Reference: Kouanda AM, Somsouk M, Sewell JL, Day LW. Urgent colonoscopy in patients with lower GI bleeding: A systematic review and meta-analysis. Gastrointest Endosc. Published online Feb 4, 2017. doi: 10.1016/j.gie.2017.01.035.
Dr. Martin is clinical professor in the division of hospital medicine, department of medicine, University of California, San Diego.
Clinical Question: In patients hospitalized for a lower gastrointestinal bleeding (LGIB), does an urgent colonoscopy (less than 24 hours after admission) result in any clinical benefits, compared with waiting for an elective colonoscopy?
Background: LGIB is a common cause of morbidity and mortality, often requiring hospitalization. While colonoscopy is necessary for appropriate work-up and treatment, it remains unclear if time to colonoscopy (urgent vs. elective) confers any clinical benefit in hospitalized patients.
Study Design: Systematic review and meta-analysis.
Setting: Twelve studies meeting inclusion criteria.
Synopsis: Computerized bibliography databases were searched for appropriate studies, and 12 met inclusion criteria, resulting in a total sample size of 10,172 patients in the urgent colonoscopy arm and 14,224 patients in the elective colonoscopy.
Outcome measures included bleeding source identified on colonoscopy, therapeutic endoscopic interventions performed, patients requiring blood transfusions, rebleeding, adverse events, and mortality.
Urgent colonoscopy was associated with increased use of endoscopic therapeutic intervention (relative risk, 1.70; 95% CI, 1.08-2.67). There were no significant differences in bleeding source localization (RR, 1.08; 95% CI, 0.92-1.25), adverse event rates (RR, 1.05; 95% CI, 0.65-1.71), rebleeding rates (RR, 1.14; 95% CI, 0.74-1.78), transfusion requirement (RR, 1.02; 95% CI, 0.73-1.41), or mortality (RR, 1.17; 95% CI, 0.45-3.02) between urgent and elective colonoscopy.
Limitations of the study comprise of inclusion of small number of studies, underpowered statistical analysis, and possible variation in quality assessment of articles evaluated.
Bottom Line: Urgent colonoscopy is safe and usually well tolerated in hospitalized patients with LGIB, but, compared with elective colonoscopy, there is no clear evidence it alters important clinical outcomes.
Reference: Kouanda AM, Somsouk M, Sewell JL, Day LW. Urgent colonoscopy in patients with lower GI bleeding: A systematic review and meta-analysis. Gastrointest Endosc. Published online Feb 4, 2017. doi: 10.1016/j.gie.2017.01.035.
Dr. Martin is clinical professor in the division of hospital medicine, department of medicine, University of California, San Diego.
CANVAS: Canagliflozin cuts cardiovascular events, doubles risk of amputations
SAN DIEGO –
After an average of 188 weeks of follow-up, the combined rate of cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke was 26.9 events per 1,000 person-years of canagliflozin treatment and 31.5 events per 1,000 person-years of placebo treatment (hazard ratio, 0.86; 95% confidence interval, 0.75-0.97; P less than .001 for noninferiority; P = .02 for superiority) in the Canagliflozin Cardiovascular Assessment Study (CANVAS) and its sister trial, CANVAS-R, investigators reported at the annual scientific sessions of the American Diabetes Association. The report was published simultaneously in the New England Journal of Medicine (N Engl J Med. 2017 Jun 12. doi: 10.1056/NEJMoa1611925).

But unexpectedly, canagliflozin also doubled the risk of amputations, said Dr. Neal, who is with the University of New South Wales and the George Institute for Global Health in Sydney. Treating 1,000 patients for 5 years would lead to 15 excess amputations, including 10 amputations of the toes or forefoot and five amputations at the ankle or above, he said.
The reason for this heightened risk is unknown. Other sodium-glucose co-transporter 2 (SGLT-2) development programs did not comprehensively monitor amputations, so it is unclear whether this is a class effect, Dr. Neal said. For now, the Food and Drug Administration is requiring a boxed warning for canagliflozin, while its European Union product label recommends carefully monitoring patients, emphasizing foot care and hydration, and considering stopping treatment if patients develop lower-extremity ulcers, infection, osteomyelitis, or gangrene.
Canagliflozin might also increase the risk of fractures, Dr. Bruce and his coinvestigators noted. Hazard ratios for overall and low-trauma fractures reached statistical significance in CANVAS, but not in CANVAS-R. As in other trials of SGLT-2 inhibitors, canagliflozin significantly increased the risk of female and male genital mycotic infections (respective HR, 4.27 and 3.76) and was associated with osmotic diuresis (HR, 2.80), and volume depletion (HR, 1.44). However, canagliflozin was not associated with malignancies, hepatic injury, pancreatitis, diabetic ketoacidosis, photosensitivity, hypersensitivity reactions, hypoglycemia, venous thrombotic events, or urinary tract infections.
Canagliflozin (Invokana, Janssen) inhibits SGLT-2, which is responsible for about 90% of renal glucose reabsorption. The FDA approved the medication in 2013 based on interim results from the CANVAS trial, which included 4,330 adults with type 2 diabetes and a history of symptomatic atherosclerotic cardiovascular disease or multiple cardiovascular risk factors. Patients were usually in their 60s, male, and hypertensive. Two-thirds had atherosclerotic cardiovascular disease and about 14% had heart failure. Background medications included metformin, insulin, sulfonylurea, DPP-4 inhibitors, GLP-1 receptor agonists, and cardioprotective agents. Patients were randomly assigned to receive canagliflozin 300 mg or 100 mg or placebo.
Investigators designed the CANVAS-R trial to further evaluate canagliflozin in another 5,813 patients with type 2 diabetes. The SGLT-2 inhibitor met its primary MACE endpoint in the overall pooled analysis and in numerous demographic and clinical subgroups, Dr. Neal said. Canagliflozin also significantly cut the risk of hospitalization for heart failure (HR, 0.67), and met a “hard” composite endpoint of renal death, end-stage renal disease, or a 40% reduction in estimated glomerular filtration rate (HR, 0.60).
Compared with placebo, treatment induced regression of albuminuria and reduced loss of renal function, said coinvestigator Dick de Zeeuw, MD, PhD, of the University of Groningen (the Netherlands). “These data suggest a potential renoprotective effect of canagliflozin treatment in patients with type 2 diabetes at high cardiovascular risk, on top of treatment with angiotensin-converting-enzyme inhibitors and angiotensin receptor blockers,” he said.
However, patients were twice as likely to undergo amputations on canagliflozin, compared with those on placebo (HR, 1.97; 95% CI, 1.41-2.75). Risks were similar for amputation of the toe or forefoot, at the ankle, below the knee, and above the knee, Dr. Neal said. Predictors of amputation also were similar in all arms of the trials, and included peripheral vascular disease, male sex, neuropathy, and hemoglobin A1c above 8%. Amputation was not associated with non-loop diuretic therapy, smoking, hypertension, or age.
Janssen Research and Development makes canagliflozin and sponsored the trials. Dr. Neal and Dr. Zeeuw disclosed consultancy, travel support, or grants from Janssen paid to their institutions, and ties to several other pharmaceutical companies.
SAN DIEGO –
After an average of 188 weeks of follow-up, the combined rate of cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke was 26.9 events per 1,000 person-years of canagliflozin treatment and 31.5 events per 1,000 person-years of placebo treatment (hazard ratio, 0.86; 95% confidence interval, 0.75-0.97; P less than .001 for noninferiority; P = .02 for superiority) in the Canagliflozin Cardiovascular Assessment Study (CANVAS) and its sister trial, CANVAS-R, investigators reported at the annual scientific sessions of the American Diabetes Association. The report was published simultaneously in the New England Journal of Medicine (N Engl J Med. 2017 Jun 12. doi: 10.1056/NEJMoa1611925).
But unexpectedly, canagliflozin also doubled the risk of amputations, said Dr. Neal, who is with the University of New South Wales and the George Institute for Global Health in Sydney. Treating 1,000 patients for 5 years would lead to 15 excess amputations, including 10 amputations of the toes or forefoot and five amputations at the ankle or above, he said.
The reason for this heightened risk is unknown. Other sodium-glucose co-transporter 2 (SGLT-2) development programs did not comprehensively monitor amputations, so it is unclear whether this is a class effect, Dr. Neal said. For now, the Food and Drug Administration is requiring a boxed warning for canagliflozin, while its European Union product label recommends carefully monitoring patients, emphasizing foot care and hydration, and considering stopping treatment if patients develop lower-extremity ulcers, infection, osteomyelitis, or gangrene.
Canagliflozin might also increase the risk of fractures, Dr. Bruce and his coinvestigators noted. Hazard ratios for overall and low-trauma fractures reached statistical significance in CANVAS, but not in CANVAS-R. As in other trials of SGLT-2 inhibitors, canagliflozin significantly increased the risk of female and male genital mycotic infections (respective HR, 4.27 and 3.76) and was associated with osmotic diuresis (HR, 2.80), and volume depletion (HR, 1.44). However, canagliflozin was not associated with malignancies, hepatic injury, pancreatitis, diabetic ketoacidosis, photosensitivity, hypersensitivity reactions, hypoglycemia, venous thrombotic events, or urinary tract infections.
Canagliflozin (Invokana, Janssen) inhibits SGLT-2, which is responsible for about 90% of renal glucose reabsorption. The FDA approved the medication in 2013 based on interim results from the CANVAS trial, which included 4,330 adults with type 2 diabetes and a history of symptomatic atherosclerotic cardiovascular disease or multiple cardiovascular risk factors. Patients were usually in their 60s, male, and hypertensive. Two-thirds had atherosclerotic cardiovascular disease and about 14% had heart failure. Background medications included metformin, insulin, sulfonylurea, DPP-4 inhibitors, GLP-1 receptor agonists, and cardioprotective agents. Patients were randomly assigned to receive canagliflozin 300 mg or 100 mg or placebo.
Investigators designed the CANVAS-R trial to further evaluate canagliflozin in another 5,813 patients with type 2 diabetes. The SGLT-2 inhibitor met its primary MACE endpoint in the overall pooled analysis and in numerous demographic and clinical subgroups, Dr. Neal said. Canagliflozin also significantly cut the risk of hospitalization for heart failure (HR, 0.67), and met a “hard” composite endpoint of renal death, end-stage renal disease, or a 40% reduction in estimated glomerular filtration rate (HR, 0.60).
Compared with placebo, treatment induced regression of albuminuria and reduced loss of renal function, said coinvestigator Dick de Zeeuw, MD, PhD, of the University of Groningen (the Netherlands). “These data suggest a potential renoprotective effect of canagliflozin treatment in patients with type 2 diabetes at high cardiovascular risk, on top of treatment with angiotensin-converting-enzyme inhibitors and angiotensin receptor blockers,” he said.
However, patients were twice as likely to undergo amputations on canagliflozin, compared with those on placebo (HR, 1.97; 95% CI, 1.41-2.75). Risks were similar for amputation of the toe or forefoot, at the ankle, below the knee, and above the knee, Dr. Neal said. Predictors of amputation also were similar in all arms of the trials, and included peripheral vascular disease, male sex, neuropathy, and hemoglobin A1c above 8%. Amputation was not associated with non-loop diuretic therapy, smoking, hypertension, or age.
Janssen Research and Development makes canagliflozin and sponsored the trials. Dr. Neal and Dr. Zeeuw disclosed consultancy, travel support, or grants from Janssen paid to their institutions, and ties to several other pharmaceutical companies.
SAN DIEGO –
After an average of 188 weeks of follow-up, the combined rate of cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke was 26.9 events per 1,000 person-years of canagliflozin treatment and 31.5 events per 1,000 person-years of placebo treatment (hazard ratio, 0.86; 95% confidence interval, 0.75-0.97; P less than .001 for noninferiority; P = .02 for superiority) in the Canagliflozin Cardiovascular Assessment Study (CANVAS) and its sister trial, CANVAS-R, investigators reported at the annual scientific sessions of the American Diabetes Association. The report was published simultaneously in the New England Journal of Medicine (N Engl J Med. 2017 Jun 12. doi: 10.1056/NEJMoa1611925).
But unexpectedly, canagliflozin also doubled the risk of amputations, said Dr. Neal, who is with the University of New South Wales and the George Institute for Global Health in Sydney. Treating 1,000 patients for 5 years would lead to 15 excess amputations, including 10 amputations of the toes or forefoot and five amputations at the ankle or above, he said.
The reason for this heightened risk is unknown. Other sodium-glucose co-transporter 2 (SGLT-2) development programs did not comprehensively monitor amputations, so it is unclear whether this is a class effect, Dr. Neal said. For now, the Food and Drug Administration is requiring a boxed warning for canagliflozin, while its European Union product label recommends carefully monitoring patients, emphasizing foot care and hydration, and considering stopping treatment if patients develop lower-extremity ulcers, infection, osteomyelitis, or gangrene.
Canagliflozin might also increase the risk of fractures, Dr. Bruce and his coinvestigators noted. Hazard ratios for overall and low-trauma fractures reached statistical significance in CANVAS, but not in CANVAS-R. As in other trials of SGLT-2 inhibitors, canagliflozin significantly increased the risk of female and male genital mycotic infections (respective HR, 4.27 and 3.76) and was associated with osmotic diuresis (HR, 2.80), and volume depletion (HR, 1.44). However, canagliflozin was not associated with malignancies, hepatic injury, pancreatitis, diabetic ketoacidosis, photosensitivity, hypersensitivity reactions, hypoglycemia, venous thrombotic events, or urinary tract infections.
Canagliflozin (Invokana, Janssen) inhibits SGLT-2, which is responsible for about 90% of renal glucose reabsorption. The FDA approved the medication in 2013 based on interim results from the CANVAS trial, which included 4,330 adults with type 2 diabetes and a history of symptomatic atherosclerotic cardiovascular disease or multiple cardiovascular risk factors. Patients were usually in their 60s, male, and hypertensive. Two-thirds had atherosclerotic cardiovascular disease and about 14% had heart failure. Background medications included metformin, insulin, sulfonylurea, DPP-4 inhibitors, GLP-1 receptor agonists, and cardioprotective agents. Patients were randomly assigned to receive canagliflozin 300 mg or 100 mg or placebo.
Investigators designed the CANVAS-R trial to further evaluate canagliflozin in another 5,813 patients with type 2 diabetes. The SGLT-2 inhibitor met its primary MACE endpoint in the overall pooled analysis and in numerous demographic and clinical subgroups, Dr. Neal said. Canagliflozin also significantly cut the risk of hospitalization for heart failure (HR, 0.67), and met a “hard” composite endpoint of renal death, end-stage renal disease, or a 40% reduction in estimated glomerular filtration rate (HR, 0.60).
Compared with placebo, treatment induced regression of albuminuria and reduced loss of renal function, said coinvestigator Dick de Zeeuw, MD, PhD, of the University of Groningen (the Netherlands). “These data suggest a potential renoprotective effect of canagliflozin treatment in patients with type 2 diabetes at high cardiovascular risk, on top of treatment with angiotensin-converting-enzyme inhibitors and angiotensin receptor blockers,” he said.
However, patients were twice as likely to undergo amputations on canagliflozin, compared with those on placebo (HR, 1.97; 95% CI, 1.41-2.75). Risks were similar for amputation of the toe or forefoot, at the ankle, below the knee, and above the knee, Dr. Neal said. Predictors of amputation also were similar in all arms of the trials, and included peripheral vascular disease, male sex, neuropathy, and hemoglobin A1c above 8%. Amputation was not associated with non-loop diuretic therapy, smoking, hypertension, or age.
Janssen Research and Development makes canagliflozin and sponsored the trials. Dr. Neal and Dr. Zeeuw disclosed consultancy, travel support, or grants from Janssen paid to their institutions, and ties to several other pharmaceutical companies.
AT THE ADA ANNUAL SCIENTIFIC SESSIONS
Key clinical point: Canagliflozin significantly reduced the risk of cardiovascular and renal events but doubled the risk of amputation, compared with placebo, in patients with type 2 diabetes.
Major finding: The hazard ratio for cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke was 0.86 in favor of canagliflozin (P = .02 for superiority). Patients on treatment were twice as likely to undergo amputations, compared to those on placebo (HR, 1.97).
Data source: Two international, randomized, double-blind trials of more than 10,000 adults with type 2 diabetes at high risk of cardiovascular disease.
Disclosures: Janssen Research and Development makes canagliflozin and sponsored the trials. Dr. Neal and Dr. Zeeuw disclosed consultancy, travel support, or grants from Janssen paid to their institutions and ties to several other pharmaceutical companies.
Recurring Yellowish Papules and Plaques on the Back
The Diagnosis: Nevus Lipomatosus Cutaneous Superficialis
A punch biopsy was obtained from a skin lesion, which showed orthokeratosis, irregular acanthosis, papillomatosis, intense edema in the upper dermis, and mature fat lobules that dissected collagen fibers in the reticular dermis (Figure). Classical-type nevus lipomatosus cutaneous superficialis (NLCS) was diagnosed based on these clinical and histopathological findings. The patient was referred to the plastic surgery clinic for total excision of all lesions.
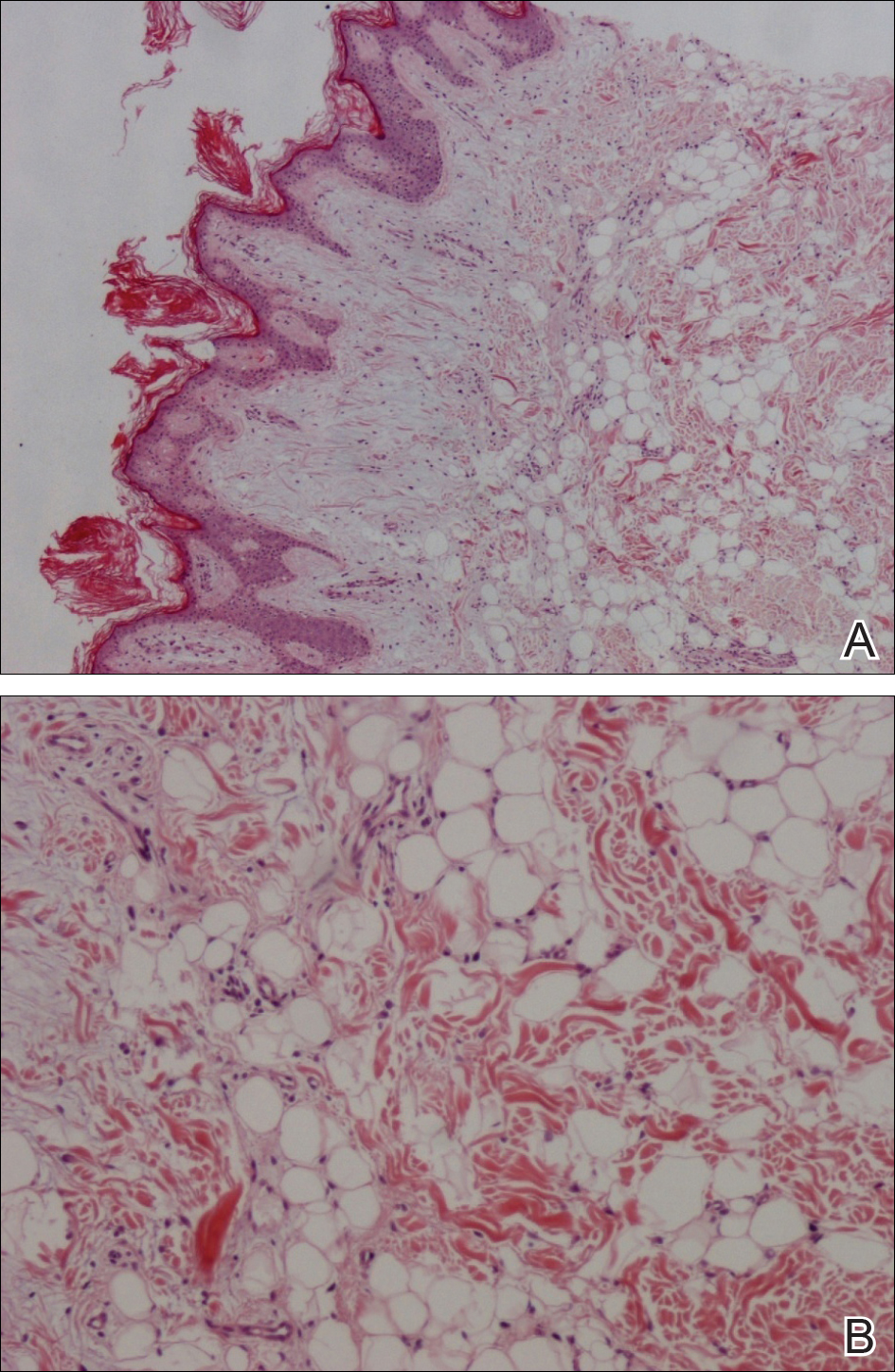
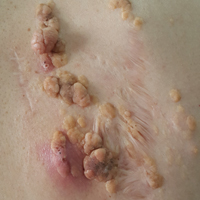
Nevus lipomatosus cutaneous superficialis is a rare hamartoma characterized by ectopic deposition of mature adipose tissue in the dermis.1 It was first described by Hoffmann and Zurhelle2 in 1921. Clinically, NLCS is classified into 2 subtypes: classical (multiple) and solitary. Classical-type NLCS is characterized by multiple pedunculated or sessile, soft, cerebriform, yellowish papules and nodules, especially in the pelvic area. Solitary-type NLCS presents as a sessile papule or nodule with no predilection for localization. Although the classical form of NLCS generally occurs in the first 2 decades of life, the solitary form usually appears in adulthood.3 Nevus lipomatosus cutaneous superficialis has no gender predilection and there is no genetic or congenital defect association.1,4
The pathogenesis of NLCS still is unknown, but some theories have been proposed, such as the development of adipose metaplasia secondary to degeneration of connective tissue, the formation of a true nevus resulting from heterotopic development of adipose tissue, and the development of mature adipocytes from pericytes in dermal vessels.1,5
Histopathology of NLCS shows clusters of ectopic mature adipose tissue in varying rates (10%-50%) between collagen bundles in the dermis. Characteristically, there is no connection between the ectopic mature adipose tissue and the subcutaneous adipose tissue.3 The differential diagnosis of NLCS includes neurofibroma, lymphangioma, sebaceous nevus, fibroepithelial polyps, leiomyoma, and lipomas.1,6
Treatment of NLCS generally involves basic surgical excision; however, patients treated with CO2 laser also have been reported in the literature.5 Because of the growth tendency and the large size of the classical form of NLCS, recurrence may occur, as in our case. In such cases, gradual surgical excision is recommended.5 We present this case to indicate that undesirable surgical results or relapse may occur in untreated patients because of lesion growth and delayed diagnosis.
- Goucha S, Khaled A, Zéglaoui F, et al. Nevus lipomatosus cutaneous superficialis: report of eight cases. Dermatol Ther (Heidelb). 2011;1:25-30.
- Hoffmann E, Zurhelle E. Ubereinen nevus lipomatodes cutaneous superficialis der linkenglutaalgegend. Arch Dermatol Syph. 1921;130:327-333.
- Patil SB, Narchal S, Paricharak M, et al. Nevus lipomatosus cutaneous superficialis: a rare case report. Iran J Med Sci. 2014;39:304-307.
- Bancalari E, Martínez-Sánchez D, Tardío JC. Nevus lipomatosus superficialis with a folliculosebaceous component: report of 2 cases. Patholog Res Int. 2011;2011:105973.
- Kim YJ, Choi JH, Kim H, et al. Recurrence of nevus lipomatosus cutaneous superficialis after CO(2) laser treatment [published online November 14, 2012]. Arch Plast Surg. 2012;39:671-673.
- Wollina U. Photoletter to the editor - nevus lipomatosus superficialis (Hoffmann-Zurhelle). three new cases including one with ulceration and one with ipsilateral gluteal hypertrophy. J Dermatol Case Rep. 2013;7:71-73.
The Diagnosis: Nevus Lipomatosus Cutaneous Superficialis
A punch biopsy was obtained from a skin lesion, which showed orthokeratosis, irregular acanthosis, papillomatosis, intense edema in the upper dermis, and mature fat lobules that dissected collagen fibers in the reticular dermis (Figure). Classical-type nevus lipomatosus cutaneous superficialis (NLCS) was diagnosed based on these clinical and histopathological findings. The patient was referred to the plastic surgery clinic for total excision of all lesions.
Nevus lipomatosus cutaneous superficialis is a rare hamartoma characterized by ectopic deposition of mature adipose tissue in the dermis.1 It was first described by Hoffmann and Zurhelle2 in 1921. Clinically, NLCS is classified into 2 subtypes: classical (multiple) and solitary. Classical-type NLCS is characterized by multiple pedunculated or sessile, soft, cerebriform, yellowish papules and nodules, especially in the pelvic area. Solitary-type NLCS presents as a sessile papule or nodule with no predilection for localization. Although the classical form of NLCS generally occurs in the first 2 decades of life, the solitary form usually appears in adulthood.3 Nevus lipomatosus cutaneous superficialis has no gender predilection and there is no genetic or congenital defect association.1,4
The pathogenesis of NLCS still is unknown, but some theories have been proposed, such as the development of adipose metaplasia secondary to degeneration of connective tissue, the formation of a true nevus resulting from heterotopic development of adipose tissue, and the development of mature adipocytes from pericytes in dermal vessels.1,5
Histopathology of NLCS shows clusters of ectopic mature adipose tissue in varying rates (10%-50%) between collagen bundles in the dermis. Characteristically, there is no connection between the ectopic mature adipose tissue and the subcutaneous adipose tissue.3 The differential diagnosis of NLCS includes neurofibroma, lymphangioma, sebaceous nevus, fibroepithelial polyps, leiomyoma, and lipomas.1,6
Treatment of NLCS generally involves basic surgical excision; however, patients treated with CO2 laser also have been reported in the literature.5 Because of the growth tendency and the large size of the classical form of NLCS, recurrence may occur, as in our case. In such cases, gradual surgical excision is recommended.5 We present this case to indicate that undesirable surgical results or relapse may occur in untreated patients because of lesion growth and delayed diagnosis.
The Diagnosis: Nevus Lipomatosus Cutaneous Superficialis
A punch biopsy was obtained from a skin lesion, which showed orthokeratosis, irregular acanthosis, papillomatosis, intense edema in the upper dermis, and mature fat lobules that dissected collagen fibers in the reticular dermis (Figure). Classical-type nevus lipomatosus cutaneous superficialis (NLCS) was diagnosed based on these clinical and histopathological findings. The patient was referred to the plastic surgery clinic for total excision of all lesions.
Nevus lipomatosus cutaneous superficialis is a rare hamartoma characterized by ectopic deposition of mature adipose tissue in the dermis.1 It was first described by Hoffmann and Zurhelle2 in 1921. Clinically, NLCS is classified into 2 subtypes: classical (multiple) and solitary. Classical-type NLCS is characterized by multiple pedunculated or sessile, soft, cerebriform, yellowish papules and nodules, especially in the pelvic area. Solitary-type NLCS presents as a sessile papule or nodule with no predilection for localization. Although the classical form of NLCS generally occurs in the first 2 decades of life, the solitary form usually appears in adulthood.3 Nevus lipomatosus cutaneous superficialis has no gender predilection and there is no genetic or congenital defect association.1,4
The pathogenesis of NLCS still is unknown, but some theories have been proposed, such as the development of adipose metaplasia secondary to degeneration of connective tissue, the formation of a true nevus resulting from heterotopic development of adipose tissue, and the development of mature adipocytes from pericytes in dermal vessels.1,5
Histopathology of NLCS shows clusters of ectopic mature adipose tissue in varying rates (10%-50%) between collagen bundles in the dermis. Characteristically, there is no connection between the ectopic mature adipose tissue and the subcutaneous adipose tissue.3 The differential diagnosis of NLCS includes neurofibroma, lymphangioma, sebaceous nevus, fibroepithelial polyps, leiomyoma, and lipomas.1,6
Treatment of NLCS generally involves basic surgical excision; however, patients treated with CO2 laser also have been reported in the literature.5 Because of the growth tendency and the large size of the classical form of NLCS, recurrence may occur, as in our case. In such cases, gradual surgical excision is recommended.5 We present this case to indicate that undesirable surgical results or relapse may occur in untreated patients because of lesion growth and delayed diagnosis.
- Goucha S, Khaled A, Zéglaoui F, et al. Nevus lipomatosus cutaneous superficialis: report of eight cases. Dermatol Ther (Heidelb). 2011;1:25-30.
- Hoffmann E, Zurhelle E. Ubereinen nevus lipomatodes cutaneous superficialis der linkenglutaalgegend. Arch Dermatol Syph. 1921;130:327-333.
- Patil SB, Narchal S, Paricharak M, et al. Nevus lipomatosus cutaneous superficialis: a rare case report. Iran J Med Sci. 2014;39:304-307.
- Bancalari E, Martínez-Sánchez D, Tardío JC. Nevus lipomatosus superficialis with a folliculosebaceous component: report of 2 cases. Patholog Res Int. 2011;2011:105973.
- Kim YJ, Choi JH, Kim H, et al. Recurrence of nevus lipomatosus cutaneous superficialis after CO(2) laser treatment [published online November 14, 2012]. Arch Plast Surg. 2012;39:671-673.
- Wollina U. Photoletter to the editor - nevus lipomatosus superficialis (Hoffmann-Zurhelle). three new cases including one with ulceration and one with ipsilateral gluteal hypertrophy. J Dermatol Case Rep. 2013;7:71-73.
- Goucha S, Khaled A, Zéglaoui F, et al. Nevus lipomatosus cutaneous superficialis: report of eight cases. Dermatol Ther (Heidelb). 2011;1:25-30.
- Hoffmann E, Zurhelle E. Ubereinen nevus lipomatodes cutaneous superficialis der linkenglutaalgegend. Arch Dermatol Syph. 1921;130:327-333.
- Patil SB, Narchal S, Paricharak M, et al. Nevus lipomatosus cutaneous superficialis: a rare case report. Iran J Med Sci. 2014;39:304-307.
- Bancalari E, Martínez-Sánchez D, Tardío JC. Nevus lipomatosus superficialis with a folliculosebaceous component: report of 2 cases. Patholog Res Int. 2011;2011:105973.
- Kim YJ, Choi JH, Kim H, et al. Recurrence of nevus lipomatosus cutaneous superficialis after CO(2) laser treatment [published online November 14, 2012]. Arch Plast Surg. 2012;39:671-673.
- Wollina U. Photoletter to the editor - nevus lipomatosus superficialis (Hoffmann-Zurhelle). three new cases including one with ulceration and one with ipsilateral gluteal hypertrophy. J Dermatol Case Rep. 2013;7:71-73.

A 36-year-old man presented with a group of partially erythematous, yellowish papules and plaques ranging from 5 to 20 mm in diameter on the right side of the upper back of 20 years' duration. They were surgically excised 8 years prior but recurred and spread. The lesions occasionally were painful and tender with redness and discharge.
Investigational flu vaccine finds way around pyrogenicity problem
aged 5-17 years, Jolanta Airey, MD, of Seqirus in Parkville, Australia, and her associates reported.
In 2010, in Australia and New Zealand, use of a trivalent flu vaccine was associated with unexpected reports of fever and febrile seizures in children aged younger than 9 years. Research into the issue suggested that “degraded RNA fragments delivered by residual lipids activated the release of proinflammatory cytokines, which stimulated the pyrogenic response in children,” the study authors noted. “Increasing the level of sodium taurodeoxycholate (TDOC) to split the B strain in particular resulted in decreased levels of residual lipids and attenuated proinflammatory cytokine signals.”
In a phase III, randomized, observer-blinded study of the two flu vaccines at 32 centers in the United States between September 2015 and June 2016, 1,709 children aged 5-17 years received IIV4, and 569 children the same age received comparator IIV4 (Fluarix Quadrivalent). The two vaccines generated strong immune responses against all the vaccine strains in the children, with the hemagglutination inhibition geometric mean titers similar for all strains and higher for A strains than B strains for both vaccines.
In the 5- to 8-year-old group, fever was reported by 4.5% of those in the IIV4 group and 3.6% of children in the comparator IIV4 group (relative risk, 1.22). In the 9- to 17-year-old group, fever was reported by 2.1% of children in the IIV4 group and 0.8% of those in the comparator IIV4 group (RR, 2.80). Severe fever was reported by 1% or less of any of the groups of children.
Read more in the journal Vaccine (2017 May 9;35[20]:2745-52).
aged 5-17 years, Jolanta Airey, MD, of Seqirus in Parkville, Australia, and her associates reported.
In 2010, in Australia and New Zealand, use of a trivalent flu vaccine was associated with unexpected reports of fever and febrile seizures in children aged younger than 9 years. Research into the issue suggested that “degraded RNA fragments delivered by residual lipids activated the release of proinflammatory cytokines, which stimulated the pyrogenic response in children,” the study authors noted. “Increasing the level of sodium taurodeoxycholate (TDOC) to split the B strain in particular resulted in decreased levels of residual lipids and attenuated proinflammatory cytokine signals.”
In a phase III, randomized, observer-blinded study of the two flu vaccines at 32 centers in the United States between September 2015 and June 2016, 1,709 children aged 5-17 years received IIV4, and 569 children the same age received comparator IIV4 (Fluarix Quadrivalent). The two vaccines generated strong immune responses against all the vaccine strains in the children, with the hemagglutination inhibition geometric mean titers similar for all strains and higher for A strains than B strains for both vaccines.
In the 5- to 8-year-old group, fever was reported by 4.5% of those in the IIV4 group and 3.6% of children in the comparator IIV4 group (relative risk, 1.22). In the 9- to 17-year-old group, fever was reported by 2.1% of children in the IIV4 group and 0.8% of those in the comparator IIV4 group (RR, 2.80). Severe fever was reported by 1% or less of any of the groups of children.
Read more in the journal Vaccine (2017 May 9;35[20]:2745-52).
aged 5-17 years, Jolanta Airey, MD, of Seqirus in Parkville, Australia, and her associates reported.
In 2010, in Australia and New Zealand, use of a trivalent flu vaccine was associated with unexpected reports of fever and febrile seizures in children aged younger than 9 years. Research into the issue suggested that “degraded RNA fragments delivered by residual lipids activated the release of proinflammatory cytokines, which stimulated the pyrogenic response in children,” the study authors noted. “Increasing the level of sodium taurodeoxycholate (TDOC) to split the B strain in particular resulted in decreased levels of residual lipids and attenuated proinflammatory cytokine signals.”
In a phase III, randomized, observer-blinded study of the two flu vaccines at 32 centers in the United States between September 2015 and June 2016, 1,709 children aged 5-17 years received IIV4, and 569 children the same age received comparator IIV4 (Fluarix Quadrivalent). The two vaccines generated strong immune responses against all the vaccine strains in the children, with the hemagglutination inhibition geometric mean titers similar for all strains and higher for A strains than B strains for both vaccines.
In the 5- to 8-year-old group, fever was reported by 4.5% of those in the IIV4 group and 3.6% of children in the comparator IIV4 group (relative risk, 1.22). In the 9- to 17-year-old group, fever was reported by 2.1% of children in the IIV4 group and 0.8% of those in the comparator IIV4 group (RR, 2.80). Severe fever was reported by 1% or less of any of the groups of children.
Read more in the journal Vaccine (2017 May 9;35[20]:2745-52).
FROM VACCINE
Five Steps for Delivering an Effective and Educational Lecture
As lifelong learners, physicians are encouraged and expected to share their knowledge base with budding residents and students. Effective communication is essential to the utmost delivery of clinical knowledge and pearls. Lecture delivery is important for all stages of learning, and adapting efficient techniques early in one's career is critical for the transmission of ideas and teaching points. These tips were created to help formulate guidelines for physician presentations and are open for interpretation. These well-meaning suggestions can be integrated into one's toolbox to foster an enthusiastic educational arena.
Step 1: Know Your Key Message
First and foremost, one should ruminate over the overall message of the lecture. Consider at least 3 main points you want the learner to gain and remember on completion of the lecture. Additionally, it is crucial to think about the audience who will be present for your message and how to deliver your ideas clearly and effectively. Be cognizant of the knowledge base of your listeners and gauge how much initial background information is needed; conversely, if the audience is familiar with the material, excessive introductory material may be unnecessary and cause inattentiveness. Simplicity, both within the inherent message itself and the content and layout, can ameliorate the transmission of data regardless of the audience. A mentor once told me that no slide should contain more than 13 lines of text. Furthermore, if you are counting the number of lines, then you likely need to reduce the text and simplify the slide. Each slide should contain a maximum of 3 or 4 bullet points.1 Convoluted figures should be avoided and key points should be highlighted. Overall, know your take-home message and provide the listener with simplistic text and images to convey the key ideas at their educational level.
Step 2: Prepare
Preparation is of utmost importance. Reading over the slides several times prior to the presentation is vital. You are the assumed expert on the topic and meticulously knowing the subject matter helps with the confidence of your delivery. Ease of subject matter also helps you, as the presenter, to rely less on verbatim reading of the slides and allows you to interact more with your audience. It is important to be familiar with the order of your presentation as well as the phrases and figures provided.2 Flipping back and forth through slides can be distracting to the audience and can make the order of your presentation seem incongruous, presenting as a hastily constructed lecture. If you are prepared, you can engage your audience and provide additional information that is not on the slides to maintain interest. Remember that reading the slides can reduce your voice to a monotone, subtracting enthusiasm and energy from the delivery of your talk.2 Rehearsal helps give you the freedom to confidently and proudly present your subject material.
Step 3: Be Animated
You are the main attraction and the performer of this lecture. Radiate the confidence you gained from being prepared with the ability to engage in eye contact and gestures as needed to convey your point. Regularly shift your focus around the room to attempt to involve as many people as possible in your talk.2 Your main focus should be your audience and not your slides; the slides should simply help guide your talk.3 During your presentation, you also can ask rhetorical questions that you can then answer to keep the group engaged (eg, "So, what does this tell us?" or "What would you do next?"). These questions demonstrate to your audience that you are interested in their attention and can help reciprocate the enthusiasm. Use language that involves your audience as a group participant. For example, when looking at visual aids, introduce them by saying "If we look at this table, we can see that . . ." or "This figure shows us that . . ."2,3 Additionally, be cognizant of the volume and pace of your voice. During key points, you may want to slightly raise your voice and slow your pace for emphasis. Anxiety can make all presenters speed through their material; however, try to be mindful of the rhythm of your speech. With preparation you should be able to accurately gauge the length of your presentation but also adapt to the necessary time constraints if too much time is spent on one point early on. Most would believe that all good lectures end at least a few minutes early to allow for questions and comprehension of the material as well as to provide your audience with time to move on to their next engagement or clinical duty.
Step 4: Encourage Active Participation
Active audience participation is shown by a multitude of studies to provide the highest level of comprehension.4,5 In a crossover study conducted by Bleske et al,4 30 students were divided into 2 groups and were taught 6 therapeutic topics, with 3 topics provided by conventional lecture and 3 topics taught by team-based learning. At the end of the educational series, the students were surveyed to evaluate their confidence and attitudes. Students demonstrated not only higher examination scores with team-based learning but higher confidence in their ability to transmit the information garnered through therapeutic recommendations.4 Although small, this study highlights the intuitive notion that active learning with subject material, either by sharing ideas with colleagues or having small brainstorming discussions throughout lectures, helps consolidate the information for long-term memory and comprehension.
Additionally, teaching in a medical environment can present unique challenges, as participants may feel anxiety over having right or wrong answers due to fear of inadequacy among their scholarly peers. Neher et al6 proposed a 5-step "microskills" model for teaching young physicians, and although it is intended for a clinical setting, it also can be applied to engaging and answering questions from a medical audience in general. Their model focuses on the teacher, or in our case the lecturer, asking a question and then applying the following model: (1) get a commitment, (2) probe for supporting evidence, (3) teach general rules, (4) reinforce what was done right, and (5) correct mistakes.6 After asking your question, the student commits to an answer and must then provide supporting details for their choice, thus feeling more responsible for their collaborative role in problem-solving. Based on their answer, you can then teach your general rule, provide positive feedback on what the student said accurately, and ultimately correct any erroneous information. This prototype of learning is best utilized in the clinical setting but also can enhance participant engagement in lectures while maintaining an inviting educational environment.
Step 5: Summarize
Lastly, conclude your presentation with at least 3 memorable points. What was the point of the presentation? What message do you want your audience to take with them and apply to clinical care? Reiterating the key points through repetition is crucial for long-term memory. Leave the audience with additional thoughts for exploration and subsequent discussion. How can your work or topic be further translated into additional projects for investigation? If the lecture material contains abundant clinical information beyond 3 points, a handout can be helpful to avoid having learners struggling to keep up with notes. This piece of take-home material can serve as a tool for subsequent study and to stimulate enhanced memory of the subject material provided. A strong concluding message can consolidate and remind learners of the scope of the topic and highlight the vital information that should be retained.
Final Thoughts
In summary, the clinical lecturer provides a unique teaching experience, and all physicians should feel proficient in formulating and delivering an educational lecture. These simple tips that call for the teacher to know and prepare his/her key message to deliver an animated and engaged presentation and then to summarize key findings are suggestions for the utmost transmission of data and ideas for all learners.
Acknowledgment
A special thank you to Joan E. St. Onge, MD (Miami, Florida), for her help providing resources for this topic.
- Yeager M. 4 Steps to Giving Effective Presentations. U.S. News & World Report. http://money.usnews.com/money/blogs/outside-voices-careers/2015/04/02/4-steps-to-giving-effective-presentations. Published April 2, 2015. Accessed May 30, 2017.
- Delivering an effective presentation. University of Leicester website. http://www2.le.ac.uk/offices/ld/resources/presentations/delivering-presentation. Accessed May 30, 2017.
- James G. Fix your presentations: 21 quick tips. Inc. http://www.inc.com/geoffrey-james/how-to-fix-your-presentations-21-tips.html. Published February 29, 2012. Accessed May 30, 2017.
- Bleske BE, Remington TL, Wells TD, et al. A randomized crossover comparison of team-based learning and lecture format on learning outcomes. Am J Pharm Educ. 2016;80:120.
- Tsang A, Harris DM. Faculty and second-year medical student perceptions of active learning in an integrated curriculum. Adv Physiol Educ. 2016;40:446-453.
- Neher JO, Gordon KC, Meyer B, et al. A five-step "microskills" model of clinical teaching. J Am Board Fam Pract. 1992;5:419-424.
As lifelong learners, physicians are encouraged and expected to share their knowledge base with budding residents and students. Effective communication is essential to the utmost delivery of clinical knowledge and pearls. Lecture delivery is important for all stages of learning, and adapting efficient techniques early in one's career is critical for the transmission of ideas and teaching points. These tips were created to help formulate guidelines for physician presentations and are open for interpretation. These well-meaning suggestions can be integrated into one's toolbox to foster an enthusiastic educational arena.
Step 1: Know Your Key Message
First and foremost, one should ruminate over the overall message of the lecture. Consider at least 3 main points you want the learner to gain and remember on completion of the lecture. Additionally, it is crucial to think about the audience who will be present for your message and how to deliver your ideas clearly and effectively. Be cognizant of the knowledge base of your listeners and gauge how much initial background information is needed; conversely, if the audience is familiar with the material, excessive introductory material may be unnecessary and cause inattentiveness. Simplicity, both within the inherent message itself and the content and layout, can ameliorate the transmission of data regardless of the audience. A mentor once told me that no slide should contain more than 13 lines of text. Furthermore, if you are counting the number of lines, then you likely need to reduce the text and simplify the slide. Each slide should contain a maximum of 3 or 4 bullet points.1 Convoluted figures should be avoided and key points should be highlighted. Overall, know your take-home message and provide the listener with simplistic text and images to convey the key ideas at their educational level.
Step 2: Prepare
Preparation is of utmost importance. Reading over the slides several times prior to the presentation is vital. You are the assumed expert on the topic and meticulously knowing the subject matter helps with the confidence of your delivery. Ease of subject matter also helps you, as the presenter, to rely less on verbatim reading of the slides and allows you to interact more with your audience. It is important to be familiar with the order of your presentation as well as the phrases and figures provided.2 Flipping back and forth through slides can be distracting to the audience and can make the order of your presentation seem incongruous, presenting as a hastily constructed lecture. If you are prepared, you can engage your audience and provide additional information that is not on the slides to maintain interest. Remember that reading the slides can reduce your voice to a monotone, subtracting enthusiasm and energy from the delivery of your talk.2 Rehearsal helps give you the freedom to confidently and proudly present your subject material.
Step 3: Be Animated
You are the main attraction and the performer of this lecture. Radiate the confidence you gained from being prepared with the ability to engage in eye contact and gestures as needed to convey your point. Regularly shift your focus around the room to attempt to involve as many people as possible in your talk.2 Your main focus should be your audience and not your slides; the slides should simply help guide your talk.3 During your presentation, you also can ask rhetorical questions that you can then answer to keep the group engaged (eg, "So, what does this tell us?" or "What would you do next?"). These questions demonstrate to your audience that you are interested in their attention and can help reciprocate the enthusiasm. Use language that involves your audience as a group participant. For example, when looking at visual aids, introduce them by saying "If we look at this table, we can see that . . ." or "This figure shows us that . . ."2,3 Additionally, be cognizant of the volume and pace of your voice. During key points, you may want to slightly raise your voice and slow your pace for emphasis. Anxiety can make all presenters speed through their material; however, try to be mindful of the rhythm of your speech. With preparation you should be able to accurately gauge the length of your presentation but also adapt to the necessary time constraints if too much time is spent on one point early on. Most would believe that all good lectures end at least a few minutes early to allow for questions and comprehension of the material as well as to provide your audience with time to move on to their next engagement or clinical duty.
Step 4: Encourage Active Participation
Active audience participation is shown by a multitude of studies to provide the highest level of comprehension.4,5 In a crossover study conducted by Bleske et al,4 30 students were divided into 2 groups and were taught 6 therapeutic topics, with 3 topics provided by conventional lecture and 3 topics taught by team-based learning. At the end of the educational series, the students were surveyed to evaluate their confidence and attitudes. Students demonstrated not only higher examination scores with team-based learning but higher confidence in their ability to transmit the information garnered through therapeutic recommendations.4 Although small, this study highlights the intuitive notion that active learning with subject material, either by sharing ideas with colleagues or having small brainstorming discussions throughout lectures, helps consolidate the information for long-term memory and comprehension.
Additionally, teaching in a medical environment can present unique challenges, as participants may feel anxiety over having right or wrong answers due to fear of inadequacy among their scholarly peers. Neher et al6 proposed a 5-step "microskills" model for teaching young physicians, and although it is intended for a clinical setting, it also can be applied to engaging and answering questions from a medical audience in general. Their model focuses on the teacher, or in our case the lecturer, asking a question and then applying the following model: (1) get a commitment, (2) probe for supporting evidence, (3) teach general rules, (4) reinforce what was done right, and (5) correct mistakes.6 After asking your question, the student commits to an answer and must then provide supporting details for their choice, thus feeling more responsible for their collaborative role in problem-solving. Based on their answer, you can then teach your general rule, provide positive feedback on what the student said accurately, and ultimately correct any erroneous information. This prototype of learning is best utilized in the clinical setting but also can enhance participant engagement in lectures while maintaining an inviting educational environment.
Step 5: Summarize
Lastly, conclude your presentation with at least 3 memorable points. What was the point of the presentation? What message do you want your audience to take with them and apply to clinical care? Reiterating the key points through repetition is crucial for long-term memory. Leave the audience with additional thoughts for exploration and subsequent discussion. How can your work or topic be further translated into additional projects for investigation? If the lecture material contains abundant clinical information beyond 3 points, a handout can be helpful to avoid having learners struggling to keep up with notes. This piece of take-home material can serve as a tool for subsequent study and to stimulate enhanced memory of the subject material provided. A strong concluding message can consolidate and remind learners of the scope of the topic and highlight the vital information that should be retained.
Final Thoughts
In summary, the clinical lecturer provides a unique teaching experience, and all physicians should feel proficient in formulating and delivering an educational lecture. These simple tips that call for the teacher to know and prepare his/her key message to deliver an animated and engaged presentation and then to summarize key findings are suggestions for the utmost transmission of data and ideas for all learners.
Acknowledgment
A special thank you to Joan E. St. Onge, MD (Miami, Florida), for her help providing resources for this topic.
As lifelong learners, physicians are encouraged and expected to share their knowledge base with budding residents and students. Effective communication is essential to the utmost delivery of clinical knowledge and pearls. Lecture delivery is important for all stages of learning, and adapting efficient techniques early in one's career is critical for the transmission of ideas and teaching points. These tips were created to help formulate guidelines for physician presentations and are open for interpretation. These well-meaning suggestions can be integrated into one's toolbox to foster an enthusiastic educational arena.
Step 1: Know Your Key Message
First and foremost, one should ruminate over the overall message of the lecture. Consider at least 3 main points you want the learner to gain and remember on completion of the lecture. Additionally, it is crucial to think about the audience who will be present for your message and how to deliver your ideas clearly and effectively. Be cognizant of the knowledge base of your listeners and gauge how much initial background information is needed; conversely, if the audience is familiar with the material, excessive introductory material may be unnecessary and cause inattentiveness. Simplicity, both within the inherent message itself and the content and layout, can ameliorate the transmission of data regardless of the audience. A mentor once told me that no slide should contain more than 13 lines of text. Furthermore, if you are counting the number of lines, then you likely need to reduce the text and simplify the slide. Each slide should contain a maximum of 3 or 4 bullet points.1 Convoluted figures should be avoided and key points should be highlighted. Overall, know your take-home message and provide the listener with simplistic text and images to convey the key ideas at their educational level.
Step 2: Prepare
Preparation is of utmost importance. Reading over the slides several times prior to the presentation is vital. You are the assumed expert on the topic and meticulously knowing the subject matter helps with the confidence of your delivery. Ease of subject matter also helps you, as the presenter, to rely less on verbatim reading of the slides and allows you to interact more with your audience. It is important to be familiar with the order of your presentation as well as the phrases and figures provided.2 Flipping back and forth through slides can be distracting to the audience and can make the order of your presentation seem incongruous, presenting as a hastily constructed lecture. If you are prepared, you can engage your audience and provide additional information that is not on the slides to maintain interest. Remember that reading the slides can reduce your voice to a monotone, subtracting enthusiasm and energy from the delivery of your talk.2 Rehearsal helps give you the freedom to confidently and proudly present your subject material.
Step 3: Be Animated
You are the main attraction and the performer of this lecture. Radiate the confidence you gained from being prepared with the ability to engage in eye contact and gestures as needed to convey your point. Regularly shift your focus around the room to attempt to involve as many people as possible in your talk.2 Your main focus should be your audience and not your slides; the slides should simply help guide your talk.3 During your presentation, you also can ask rhetorical questions that you can then answer to keep the group engaged (eg, "So, what does this tell us?" or "What would you do next?"). These questions demonstrate to your audience that you are interested in their attention and can help reciprocate the enthusiasm. Use language that involves your audience as a group participant. For example, when looking at visual aids, introduce them by saying "If we look at this table, we can see that . . ." or "This figure shows us that . . ."2,3 Additionally, be cognizant of the volume and pace of your voice. During key points, you may want to slightly raise your voice and slow your pace for emphasis. Anxiety can make all presenters speed through their material; however, try to be mindful of the rhythm of your speech. With preparation you should be able to accurately gauge the length of your presentation but also adapt to the necessary time constraints if too much time is spent on one point early on. Most would believe that all good lectures end at least a few minutes early to allow for questions and comprehension of the material as well as to provide your audience with time to move on to their next engagement or clinical duty.
Step 4: Encourage Active Participation
Active audience participation is shown by a multitude of studies to provide the highest level of comprehension.4,5 In a crossover study conducted by Bleske et al,4 30 students were divided into 2 groups and were taught 6 therapeutic topics, with 3 topics provided by conventional lecture and 3 topics taught by team-based learning. At the end of the educational series, the students were surveyed to evaluate their confidence and attitudes. Students demonstrated not only higher examination scores with team-based learning but higher confidence in their ability to transmit the information garnered through therapeutic recommendations.4 Although small, this study highlights the intuitive notion that active learning with subject material, either by sharing ideas with colleagues or having small brainstorming discussions throughout lectures, helps consolidate the information for long-term memory and comprehension.
Additionally, teaching in a medical environment can present unique challenges, as participants may feel anxiety over having right or wrong answers due to fear of inadequacy among their scholarly peers. Neher et al6 proposed a 5-step "microskills" model for teaching young physicians, and although it is intended for a clinical setting, it also can be applied to engaging and answering questions from a medical audience in general. Their model focuses on the teacher, or in our case the lecturer, asking a question and then applying the following model: (1) get a commitment, (2) probe for supporting evidence, (3) teach general rules, (4) reinforce what was done right, and (5) correct mistakes.6 After asking your question, the student commits to an answer and must then provide supporting details for their choice, thus feeling more responsible for their collaborative role in problem-solving. Based on their answer, you can then teach your general rule, provide positive feedback on what the student said accurately, and ultimately correct any erroneous information. This prototype of learning is best utilized in the clinical setting but also can enhance participant engagement in lectures while maintaining an inviting educational environment.
Step 5: Summarize
Lastly, conclude your presentation with at least 3 memorable points. What was the point of the presentation? What message do you want your audience to take with them and apply to clinical care? Reiterating the key points through repetition is crucial for long-term memory. Leave the audience with additional thoughts for exploration and subsequent discussion. How can your work or topic be further translated into additional projects for investigation? If the lecture material contains abundant clinical information beyond 3 points, a handout can be helpful to avoid having learners struggling to keep up with notes. This piece of take-home material can serve as a tool for subsequent study and to stimulate enhanced memory of the subject material provided. A strong concluding message can consolidate and remind learners of the scope of the topic and highlight the vital information that should be retained.
Final Thoughts
In summary, the clinical lecturer provides a unique teaching experience, and all physicians should feel proficient in formulating and delivering an educational lecture. These simple tips that call for the teacher to know and prepare his/her key message to deliver an animated and engaged presentation and then to summarize key findings are suggestions for the utmost transmission of data and ideas for all learners.
Acknowledgment
A special thank you to Joan E. St. Onge, MD (Miami, Florida), for her help providing resources for this topic.
- Yeager M. 4 Steps to Giving Effective Presentations. U.S. News & World Report. http://money.usnews.com/money/blogs/outside-voices-careers/2015/04/02/4-steps-to-giving-effective-presentations. Published April 2, 2015. Accessed May 30, 2017.
- Delivering an effective presentation. University of Leicester website. http://www2.le.ac.uk/offices/ld/resources/presentations/delivering-presentation. Accessed May 30, 2017.
- James G. Fix your presentations: 21 quick tips. Inc. http://www.inc.com/geoffrey-james/how-to-fix-your-presentations-21-tips.html. Published February 29, 2012. Accessed May 30, 2017.
- Bleske BE, Remington TL, Wells TD, et al. A randomized crossover comparison of team-based learning and lecture format on learning outcomes. Am J Pharm Educ. 2016;80:120.
- Tsang A, Harris DM. Faculty and second-year medical student perceptions of active learning in an integrated curriculum. Adv Physiol Educ. 2016;40:446-453.
- Neher JO, Gordon KC, Meyer B, et al. A five-step "microskills" model of clinical teaching. J Am Board Fam Pract. 1992;5:419-424.
- Yeager M. 4 Steps to Giving Effective Presentations. U.S. News & World Report. http://money.usnews.com/money/blogs/outside-voices-careers/2015/04/02/4-steps-to-giving-effective-presentations. Published April 2, 2015. Accessed May 30, 2017.
- Delivering an effective presentation. University of Leicester website. http://www2.le.ac.uk/offices/ld/resources/presentations/delivering-presentation. Accessed May 30, 2017.
- James G. Fix your presentations: 21 quick tips. Inc. http://www.inc.com/geoffrey-james/how-to-fix-your-presentations-21-tips.html. Published February 29, 2012. Accessed May 30, 2017.
- Bleske BE, Remington TL, Wells TD, et al. A randomized crossover comparison of team-based learning and lecture format on learning outcomes. Am J Pharm Educ. 2016;80:120.
- Tsang A, Harris DM. Faculty and second-year medical student perceptions of active learning in an integrated curriculum. Adv Physiol Educ. 2016;40:446-453.
- Neher JO, Gordon KC, Meyer B, et al. A five-step "microskills" model of clinical teaching. J Am Board Fam Pract. 1992;5:419-424.

Mandar Jog, MD
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

DEVOTE: Degludec and glargine had similar risk with less severe hypoglycemia
SAN DIEGO – For patients with type 2 diabetes at high risk of cardiovascular disease, the ultra–long-acting, once-daily basal insulin degludec produced a similar risk of major adverse cardiovascular events as glargine with a significantly lower risk of severe hypoglycemia, new data show.
Nonfatal myocardial infarction, nonfatal stroke, or cardiovascular death occurred in 325 (8.5%) patients on degludec and 356 (9.3%) patients on glargine (hazard ratio, 0.91; 95% confidence interval, 0.78 to 1.06; P = .21) in DEVOTE (the Trial Comparing Cardiovascular Safety of Insulin Degludec versus Insulin Glargine in Patients with Type 2 Diabetes at High Risk of Cardiovascular Events). Rates of severe hypoglycemia were 4.9% and 6.6%, respectively (P less than .001), investigators reported at the annual scientific sessions of the American Diabetes Association and simultaneously in the New England Journal of Medicine (2017 Jun 12. doi: 10.1056/NEJMoa1615692).

Insulin degludec injection (Tresiba®, Novo Nordisk) is a basal insulin analog, the long, soluble hexamer chains of which are metabolized only at the ends, yielding at least a 42-hour duration of action, Todd Hobbs, MD, chief medical officer of Novo Nordisk, Princeton, N.J., explained in an interview. In contrast, glargine has about a 12-hour half-life. Previous trials of degludec did not adjudicate cardiovascular endpoints, which the U.S. Food and Drug Administration only recently began requiring for insulins, Dr. Hobbs said. In response to an FDA request, the phase III, international, randomized, double-blind DEVOTE trial compared the cardiovascular safety of daily basal insulin degludec (100 U per mL) with that of glargine U100 in more than 7,600 adults with type 2 diabetes.

Fully 98% of patients completed the 2-year trial. The overall risk of major adverse cardiac events resembled that of each individual component, including cardiovascular death (HR, 0.96; 95% CI, 0.76-1.21; P = .71), nonfatal myocardial infarction (HR, 0.85; 95% CI, 0.68-1.06; P = .15), and nonfatal stroke (HR, 0.90; 95% CI, 0.65-1.23; P =. 50). Degludec remained noninferior to glargine when researchers added unstable angina to the primary endpoint and accounted for patient location, treatment duration, length of follow-up, and age, sex, body mass index, and renal function.
Both insulins produced similar HbA1c levels of about 7.5%, but degludec cut fasting plasma glucose by about 5 mg per mL more, compared with glargine (P less than .001), the investigators reported. Furthermore, the odds ratio for severe hypoglycemia significantly favored degludec (HR, 0.73; 95% CI, 0.60-0.89; P less than .001). In other words, 40 patients would need to receive degludec rather than glargine to prevent one event of severe hypoglycemia. Previous studies have shown similar results, Dr. Buse said. In a pooled analysis of all five trials of type 2 diabetes in the degludec clinical development program, degludec was associated with a significantly lower risk of hypoglycemia, particularly nocturnal episodes, than was glargine (Diabetes Obes Metab. 2013;15:175-84).
Findings were similar in the double-blind SWITCH 2 trial (Diabetologia. 2016;59[Suppl 1]:1-581).
DEVOTE identified no safety issues for degludec, compared with glargine. Each arm had similar rates of serious or severe adverse events, leading to treatment discontinuation, and neoplasms. Nonetheless, DEVOTE had several limitations, said Elizabeth R. Seaquist, MD, of the University of Minnesota, Minneapolis, who was not involved in the study. “Investigators could modify the titration protocol based on clinical judgment, and it isn’t clear whether this modification was applied equally in both arms,” she said at ADA. “Another weakness is that there were no data collected about moderate symptomatic hypoglycemia, the most common type of hypoglycemia that patients experience.” DEVOTE also did not examine how often blood glucose dropped below 54 mg per dL, the point at which patients often do not know they are hypoglycemic. Investigators also should examine whether degludec cuts health care costs or improves sleep or quality of life, whether its glycemic benefits extends to patients who are insulin-naive or have severe kidney disease, and how it compares with glargine U300, she added.
Insulin degludec received FDA approval in September 2015, based on interim results of DEVOTE. Novo Nordisk makes insulin degludec and sponsored the trial. Dr. Buse disclosed consulting fees from Novo Nordisk and ties to many other pharmaceutical companies. Dr. Seaquist disclosed ties to Novo Nordisk, Eli Lilly, Locemia, and Lucera. Dr. Hobbs is chief medical officer for Novo Nordisk.
SAN DIEGO – For patients with type 2 diabetes at high risk of cardiovascular disease, the ultra–long-acting, once-daily basal insulin degludec produced a similar risk of major adverse cardiovascular events as glargine with a significantly lower risk of severe hypoglycemia, new data show.
Nonfatal myocardial infarction, nonfatal stroke, or cardiovascular death occurred in 325 (8.5%) patients on degludec and 356 (9.3%) patients on glargine (hazard ratio, 0.91; 95% confidence interval, 0.78 to 1.06; P = .21) in DEVOTE (the Trial Comparing Cardiovascular Safety of Insulin Degludec versus Insulin Glargine in Patients with Type 2 Diabetes at High Risk of Cardiovascular Events). Rates of severe hypoglycemia were 4.9% and 6.6%, respectively (P less than .001), investigators reported at the annual scientific sessions of the American Diabetes Association and simultaneously in the New England Journal of Medicine (2017 Jun 12. doi: 10.1056/NEJMoa1615692).
Insulin degludec injection (Tresiba®, Novo Nordisk) is a basal insulin analog, the long, soluble hexamer chains of which are metabolized only at the ends, yielding at least a 42-hour duration of action, Todd Hobbs, MD, chief medical officer of Novo Nordisk, Princeton, N.J., explained in an interview. In contrast, glargine has about a 12-hour half-life. Previous trials of degludec did not adjudicate cardiovascular endpoints, which the U.S. Food and Drug Administration only recently began requiring for insulins, Dr. Hobbs said. In response to an FDA request, the phase III, international, randomized, double-blind DEVOTE trial compared the cardiovascular safety of daily basal insulin degludec (100 U per mL) with that of glargine U100 in more than 7,600 adults with type 2 diabetes.
Fully 98% of patients completed the 2-year trial. The overall risk of major adverse cardiac events resembled that of each individual component, including cardiovascular death (HR, 0.96; 95% CI, 0.76-1.21; P = .71), nonfatal myocardial infarction (HR, 0.85; 95% CI, 0.68-1.06; P = .15), and nonfatal stroke (HR, 0.90; 95% CI, 0.65-1.23; P =. 50). Degludec remained noninferior to glargine when researchers added unstable angina to the primary endpoint and accounted for patient location, treatment duration, length of follow-up, and age, sex, body mass index, and renal function.
Both insulins produced similar HbA1c levels of about 7.5%, but degludec cut fasting plasma glucose by about 5 mg per mL more, compared with glargine (P less than .001), the investigators reported. Furthermore, the odds ratio for severe hypoglycemia significantly favored degludec (HR, 0.73; 95% CI, 0.60-0.89; P less than .001). In other words, 40 patients would need to receive degludec rather than glargine to prevent one event of severe hypoglycemia. Previous studies have shown similar results, Dr. Buse said. In a pooled analysis of all five trials of type 2 diabetes in the degludec clinical development program, degludec was associated with a significantly lower risk of hypoglycemia, particularly nocturnal episodes, than was glargine (Diabetes Obes Metab. 2013;15:175-84).
Findings were similar in the double-blind SWITCH 2 trial (Diabetologia. 2016;59[Suppl 1]:1-581).
DEVOTE identified no safety issues for degludec, compared with glargine. Each arm had similar rates of serious or severe adverse events, leading to treatment discontinuation, and neoplasms. Nonetheless, DEVOTE had several limitations, said Elizabeth R. Seaquist, MD, of the University of Minnesota, Minneapolis, who was not involved in the study. “Investigators could modify the titration protocol based on clinical judgment, and it isn’t clear whether this modification was applied equally in both arms,” she said at ADA. “Another weakness is that there were no data collected about moderate symptomatic hypoglycemia, the most common type of hypoglycemia that patients experience.” DEVOTE also did not examine how often blood glucose dropped below 54 mg per dL, the point at which patients often do not know they are hypoglycemic. Investigators also should examine whether degludec cuts health care costs or improves sleep or quality of life, whether its glycemic benefits extends to patients who are insulin-naive or have severe kidney disease, and how it compares with glargine U300, she added.
Insulin degludec received FDA approval in September 2015, based on interim results of DEVOTE. Novo Nordisk makes insulin degludec and sponsored the trial. Dr. Buse disclosed consulting fees from Novo Nordisk and ties to many other pharmaceutical companies. Dr. Seaquist disclosed ties to Novo Nordisk, Eli Lilly, Locemia, and Lucera. Dr. Hobbs is chief medical officer for Novo Nordisk.
SAN DIEGO – For patients with type 2 diabetes at high risk of cardiovascular disease, the ultra–long-acting, once-daily basal insulin degludec produced a similar risk of major adverse cardiovascular events as glargine with a significantly lower risk of severe hypoglycemia, new data show.
Nonfatal myocardial infarction, nonfatal stroke, or cardiovascular death occurred in 325 (8.5%) patients on degludec and 356 (9.3%) patients on glargine (hazard ratio, 0.91; 95% confidence interval, 0.78 to 1.06; P = .21) in DEVOTE (the Trial Comparing Cardiovascular Safety of Insulin Degludec versus Insulin Glargine in Patients with Type 2 Diabetes at High Risk of Cardiovascular Events). Rates of severe hypoglycemia were 4.9% and 6.6%, respectively (P less than .001), investigators reported at the annual scientific sessions of the American Diabetes Association and simultaneously in the New England Journal of Medicine (2017 Jun 12. doi: 10.1056/NEJMoa1615692).
Insulin degludec injection (Tresiba®, Novo Nordisk) is a basal insulin analog, the long, soluble hexamer chains of which are metabolized only at the ends, yielding at least a 42-hour duration of action, Todd Hobbs, MD, chief medical officer of Novo Nordisk, Princeton, N.J., explained in an interview. In contrast, glargine has about a 12-hour half-life. Previous trials of degludec did not adjudicate cardiovascular endpoints, which the U.S. Food and Drug Administration only recently began requiring for insulins, Dr. Hobbs said. In response to an FDA request, the phase III, international, randomized, double-blind DEVOTE trial compared the cardiovascular safety of daily basal insulin degludec (100 U per mL) with that of glargine U100 in more than 7,600 adults with type 2 diabetes.
Fully 98% of patients completed the 2-year trial. The overall risk of major adverse cardiac events resembled that of each individual component, including cardiovascular death (HR, 0.96; 95% CI, 0.76-1.21; P = .71), nonfatal myocardial infarction (HR, 0.85; 95% CI, 0.68-1.06; P = .15), and nonfatal stroke (HR, 0.90; 95% CI, 0.65-1.23; P =. 50). Degludec remained noninferior to glargine when researchers added unstable angina to the primary endpoint and accounted for patient location, treatment duration, length of follow-up, and age, sex, body mass index, and renal function.
Both insulins produced similar HbA1c levels of about 7.5%, but degludec cut fasting plasma glucose by about 5 mg per mL more, compared with glargine (P less than .001), the investigators reported. Furthermore, the odds ratio for severe hypoglycemia significantly favored degludec (HR, 0.73; 95% CI, 0.60-0.89; P less than .001). In other words, 40 patients would need to receive degludec rather than glargine to prevent one event of severe hypoglycemia. Previous studies have shown similar results, Dr. Buse said. In a pooled analysis of all five trials of type 2 diabetes in the degludec clinical development program, degludec was associated with a significantly lower risk of hypoglycemia, particularly nocturnal episodes, than was glargine (Diabetes Obes Metab. 2013;15:175-84).
Findings were similar in the double-blind SWITCH 2 trial (Diabetologia. 2016;59[Suppl 1]:1-581).
DEVOTE identified no safety issues for degludec, compared with glargine. Each arm had similar rates of serious or severe adverse events, leading to treatment discontinuation, and neoplasms. Nonetheless, DEVOTE had several limitations, said Elizabeth R. Seaquist, MD, of the University of Minnesota, Minneapolis, who was not involved in the study. “Investigators could modify the titration protocol based on clinical judgment, and it isn’t clear whether this modification was applied equally in both arms,” she said at ADA. “Another weakness is that there were no data collected about moderate symptomatic hypoglycemia, the most common type of hypoglycemia that patients experience.” DEVOTE also did not examine how often blood glucose dropped below 54 mg per dL, the point at which patients often do not know they are hypoglycemic. Investigators also should examine whether degludec cuts health care costs or improves sleep or quality of life, whether its glycemic benefits extends to patients who are insulin-naive or have severe kidney disease, and how it compares with glargine U300, she added.
Insulin degludec received FDA approval in September 2015, based on interim results of DEVOTE. Novo Nordisk makes insulin degludec and sponsored the trial. Dr. Buse disclosed consulting fees from Novo Nordisk and ties to many other pharmaceutical companies. Dr. Seaquist disclosed ties to Novo Nordisk, Eli Lilly, Locemia, and Lucera. Dr. Hobbs is chief medical officer for Novo Nordisk.
AT THE ADA ANNUAL SCIENTIFIC SESSIONS
Key clinical point: The ultra–long-acting basal insulin degludec was noninferior to glargine in terms of cardiovascular risk and was superior in terms of severe hypoglycemia.
Major finding: Nonfatal myocardial infarction, nonfatal stroke, or cardiovascular death occurred in 325 (8.5%) patients on degludec and 356 (9.3%) patients on glargine (HR, 0.91; 95% CI, 0.78-1.06; P = .21). Rates of severe hypoglycemia were 4.9% and 6.6%, respectively (P less than .001).
Data source: A randomized, double-blind, multicenter trial of 7,637 adults with type 2 diabetes at high risk of cardiovascular disease.
Disclosures: Novo Nordisk makes insulin degludec and sponsored the trial. Dr. Buse disclosed consulting fees from Novo Nordisk and ties to many other pharmaceutical companies. Dr. Seaquist disclosed ties to Novo Nordisk, Eli Lilly, Locemia, and Lucera. Dr. Hobbs is chief medical officer for Novo Nordisk.
Angiotensin II may improve vasopressors’ efficacy
WASHINGTON – Adding angiotensin II to available vasopressor therapies correlated with significantly improved arterial pressure in patients with catecholamine-resistant vasodilatory shock and less adverse effects, according to a study presented at the recent international conference of the American Thoracic Society.
In a double blind, controlled, phase III study, 70% of 163 patients given angiotensin II reached arterial pressure of at least 75 mm HG or improved by at least 10 mm Hg three hours later, compared with 23.4% of the 158 patients given a placebo (P less than .001).
Those in the angiotensin II group also saw a mean pressure increase of 12.5 mm Hg in the first 3 hours after initiating treatment, compared with 2.9 mm Hg in the placebo group (P less than .001), according to Ashish Khanna, MD, FCCP, of the Cleveland Clinic, and his fellow researchers (N Engl J Med. 2017 May 21. doi: 10.1056/NEJMoa1704154).
Current vasopressor therapies for vasodilatory patients are associated with dangerous side effects and a 30-day mortality rate of more than 50%, which is a major concern for patients who do not have many options to begin with, the researchers noted.
“Treatment options for patients with catecholamine-resistant vasodilatory shock are limited, and the treatments that are available are often associated with side effects,” said Dr. Khanna and his colleagues.
The researchers added the naturally occurring peptide hormone angiotensin II to vasodilatory patients’ treatment regimen in order to “more closely [mimic] natural physiologic responses to shock, which include increased secretion of catecholamines, vasopressin, and RAAS hormones.”
To test the efficacy of angiotensin II, researchers gathered patients with a median age of 64 years and a mean arterial pressure of 66.3 mm Hg.
Sepsis was the predominant cause of shock for 80.7% of the study’s participants.
Patients were injected with either 20 ng/kg of body weight per minute of angiotensin II or an equivalent dose of a placebo until mean arterial pressure reached 75 mm Hg. After 3 hours and 15 minutes of treatment, the dosages were adjusted to keep pressure between 65 and 75 mm Hg for the next 48 hours.
Among patients in the angiotensin II group, 67% of patients were able to decrease angiotensin II and vasopressor doses within 30 minutes of injection, according to researchers.
When researchers measured improvement using the cardiovascular Sequential Organ Failure Assessment, patients in the angiotensin II group saw an average decrease of 1.75 points, compared with 1.28 points in patients in the placebo group (P = .01) 48 hours after treatment.
The Sequential Organ Failure Assessment is scaled from 0-4, with higher scores indicating more severe organ failure.
When measuring for adverse affects, serious effects occurred in 60.7% of the angiotensin II patients, compared with in 67.1% of those in the placebo group.
At the 28-day mark, 75 angiotensin II patients (46.0%) died, compared with 85 patients (53.8%) of the placebo group.
This study was limited by the small sample size, “so the possibility of clinically important side effects attributable to angiotensin II therapy cannot be exuded,” the researches warned.
Also, the follow-up timeline of 28 days, may not have given researchers enough time to uncover the full extent of positive and negative long-term effects associated with angiotensin II.
This study was supported by La Jolla Pharmaceutical, from which multiple researchers reported receiving financial support in the form of personal fees and grants. Two of the researchers reported having patents related to administering angiotensin II and additional patents pending.
[email protected]
On Twitter @eaztweets
WASHINGTON – Adding angiotensin II to available vasopressor therapies correlated with significantly improved arterial pressure in patients with catecholamine-resistant vasodilatory shock and less adverse effects, according to a study presented at the recent international conference of the American Thoracic Society.
In a double blind, controlled, phase III study, 70% of 163 patients given angiotensin II reached arterial pressure of at least 75 mm HG or improved by at least 10 mm Hg three hours later, compared with 23.4% of the 158 patients given a placebo (P less than .001).
Those in the angiotensin II group also saw a mean pressure increase of 12.5 mm Hg in the first 3 hours after initiating treatment, compared with 2.9 mm Hg in the placebo group (P less than .001), according to Ashish Khanna, MD, FCCP, of the Cleveland Clinic, and his fellow researchers (N Engl J Med. 2017 May 21. doi: 10.1056/NEJMoa1704154).
Current vasopressor therapies for vasodilatory patients are associated with dangerous side effects and a 30-day mortality rate of more than 50%, which is a major concern for patients who do not have many options to begin with, the researchers noted.
“Treatment options for patients with catecholamine-resistant vasodilatory shock are limited, and the treatments that are available are often associated with side effects,” said Dr. Khanna and his colleagues.
The researchers added the naturally occurring peptide hormone angiotensin II to vasodilatory patients’ treatment regimen in order to “more closely [mimic] natural physiologic responses to shock, which include increased secretion of catecholamines, vasopressin, and RAAS hormones.”
To test the efficacy of angiotensin II, researchers gathered patients with a median age of 64 years and a mean arterial pressure of 66.3 mm Hg.
Sepsis was the predominant cause of shock for 80.7% of the study’s participants.
Patients were injected with either 20 ng/kg of body weight per minute of angiotensin II or an equivalent dose of a placebo until mean arterial pressure reached 75 mm Hg. After 3 hours and 15 minutes of treatment, the dosages were adjusted to keep pressure between 65 and 75 mm Hg for the next 48 hours.
Among patients in the angiotensin II group, 67% of patients were able to decrease angiotensin II and vasopressor doses within 30 minutes of injection, according to researchers.
When researchers measured improvement using the cardiovascular Sequential Organ Failure Assessment, patients in the angiotensin II group saw an average decrease of 1.75 points, compared with 1.28 points in patients in the placebo group (P = .01) 48 hours after treatment.
The Sequential Organ Failure Assessment is scaled from 0-4, with higher scores indicating more severe organ failure.
When measuring for adverse affects, serious effects occurred in 60.7% of the angiotensin II patients, compared with in 67.1% of those in the placebo group.
At the 28-day mark, 75 angiotensin II patients (46.0%) died, compared with 85 patients (53.8%) of the placebo group.
This study was limited by the small sample size, “so the possibility of clinically important side effects attributable to angiotensin II therapy cannot be exuded,” the researches warned.
Also, the follow-up timeline of 28 days, may not have given researchers enough time to uncover the full extent of positive and negative long-term effects associated with angiotensin II.
This study was supported by La Jolla Pharmaceutical, from which multiple researchers reported receiving financial support in the form of personal fees and grants. Two of the researchers reported having patents related to administering angiotensin II and additional patents pending.
[email protected]
On Twitter @eaztweets
WASHINGTON – Adding angiotensin II to available vasopressor therapies correlated with significantly improved arterial pressure in patients with catecholamine-resistant vasodilatory shock and less adverse effects, according to a study presented at the recent international conference of the American Thoracic Society.
In a double blind, controlled, phase III study, 70% of 163 patients given angiotensin II reached arterial pressure of at least 75 mm HG or improved by at least 10 mm Hg three hours later, compared with 23.4% of the 158 patients given a placebo (P less than .001).
Those in the angiotensin II group also saw a mean pressure increase of 12.5 mm Hg in the first 3 hours after initiating treatment, compared with 2.9 mm Hg in the placebo group (P less than .001), according to Ashish Khanna, MD, FCCP, of the Cleveland Clinic, and his fellow researchers (N Engl J Med. 2017 May 21. doi: 10.1056/NEJMoa1704154).
Current vasopressor therapies for vasodilatory patients are associated with dangerous side effects and a 30-day mortality rate of more than 50%, which is a major concern for patients who do not have many options to begin with, the researchers noted.
“Treatment options for patients with catecholamine-resistant vasodilatory shock are limited, and the treatments that are available are often associated with side effects,” said Dr. Khanna and his colleagues.
The researchers added the naturally occurring peptide hormone angiotensin II to vasodilatory patients’ treatment regimen in order to “more closely [mimic] natural physiologic responses to shock, which include increased secretion of catecholamines, vasopressin, and RAAS hormones.”
To test the efficacy of angiotensin II, researchers gathered patients with a median age of 64 years and a mean arterial pressure of 66.3 mm Hg.
Sepsis was the predominant cause of shock for 80.7% of the study’s participants.
Patients were injected with either 20 ng/kg of body weight per minute of angiotensin II or an equivalent dose of a placebo until mean arterial pressure reached 75 mm Hg. After 3 hours and 15 minutes of treatment, the dosages were adjusted to keep pressure between 65 and 75 mm Hg for the next 48 hours.
Among patients in the angiotensin II group, 67% of patients were able to decrease angiotensin II and vasopressor doses within 30 minutes of injection, according to researchers.
When researchers measured improvement using the cardiovascular Sequential Organ Failure Assessment, patients in the angiotensin II group saw an average decrease of 1.75 points, compared with 1.28 points in patients in the placebo group (P = .01) 48 hours after treatment.
The Sequential Organ Failure Assessment is scaled from 0-4, with higher scores indicating more severe organ failure.
When measuring for adverse affects, serious effects occurred in 60.7% of the angiotensin II patients, compared with in 67.1% of those in the placebo group.
At the 28-day mark, 75 angiotensin II patients (46.0%) died, compared with 85 patients (53.8%) of the placebo group.
This study was limited by the small sample size, “so the possibility of clinically important side effects attributable to angiotensin II therapy cannot be exuded,” the researches warned.
Also, the follow-up timeline of 28 days, may not have given researchers enough time to uncover the full extent of positive and negative long-term effects associated with angiotensin II.
This study was supported by La Jolla Pharmaceutical, from which multiple researchers reported receiving financial support in the form of personal fees and grants. Two of the researchers reported having patents related to administering angiotensin II and additional patents pending.
[email protected]
On Twitter @eaztweets
At ATS 2017
Key clinical point:
Major finding: In the first 3 hours, patients taking angiotensin II improved arterial pressure by an average of 12.5 mm Hg, compared with 2.9 mm Hg in patients taking the placebo (P less than .001)
Data source: Double blind, randomized, control trial of 321 patients with catecholamine-resistant vasodilatory shock collected from 75 intensive care units globally during May 2015-January 2017.
Disclosures: Multiple investigators reported receiving support from La Jolla Pharmaceutical and similar companies in the form of grants and/or personal fees. Two of the researchers reported having patents related to administering angiotensin II and additional patents pending.
VA and DoE to Use Supercomputing for Transformative Science
The VA and the Department of Energy (DoE) have formed a new partnership focused on secure analysis of “big data.” The VA-DoE Big Data Science Initiative will use digital health and genomic data from the Million Veteran Program (MVP), the VA’s electronic health records system, DoD, Centers for Medicare and Medicaid Services, and the CDC’s National Death Index.
The partnership is based in DoE’s National Laboratory system, one of the world’s top resources for supercomputing, where machines are capable of millions of billions of calculations per second. The partnership will allow thousands of researchers access to this unprecedented data resource over time in a secure environment, said VA Secretary David J. Shulkin, MD.
An initial suite of specific studies is already being planned, the VA says. One group of researchers will build algorithms to generate “highly tailored” risk scores for suicide, which could help VA clinicians and researchers predict which patients are at highest risk and evaluate prevention strategies.
Other projects include one to find new ways to distinguish lethal from nonlethal prostate cancer and another to determine which risk factors best predict certain forms of cardiovascular disease.
“The transformative science that will be developed through this partnership,” Shulkin says, “will improve health care for veterans and all Americans.”
The VA and the Department of Energy (DoE) have formed a new partnership focused on secure analysis of “big data.” The VA-DoE Big Data Science Initiative will use digital health and genomic data from the Million Veteran Program (MVP), the VA’s electronic health records system, DoD, Centers for Medicare and Medicaid Services, and the CDC’s National Death Index.
The partnership is based in DoE’s National Laboratory system, one of the world’s top resources for supercomputing, where machines are capable of millions of billions of calculations per second. The partnership will allow thousands of researchers access to this unprecedented data resource over time in a secure environment, said VA Secretary David J. Shulkin, MD.
An initial suite of specific studies is already being planned, the VA says. One group of researchers will build algorithms to generate “highly tailored” risk scores for suicide, which could help VA clinicians and researchers predict which patients are at highest risk and evaluate prevention strategies.
Other projects include one to find new ways to distinguish lethal from nonlethal prostate cancer and another to determine which risk factors best predict certain forms of cardiovascular disease.
“The transformative science that will be developed through this partnership,” Shulkin says, “will improve health care for veterans and all Americans.”
The VA and the Department of Energy (DoE) have formed a new partnership focused on secure analysis of “big data.” The VA-DoE Big Data Science Initiative will use digital health and genomic data from the Million Veteran Program (MVP), the VA’s electronic health records system, DoD, Centers for Medicare and Medicaid Services, and the CDC’s National Death Index.
The partnership is based in DoE’s National Laboratory system, one of the world’s top resources for supercomputing, where machines are capable of millions of billions of calculations per second. The partnership will allow thousands of researchers access to this unprecedented data resource over time in a secure environment, said VA Secretary David J. Shulkin, MD.
An initial suite of specific studies is already being planned, the VA says. One group of researchers will build algorithms to generate “highly tailored” risk scores for suicide, which could help VA clinicians and researchers predict which patients are at highest risk and evaluate prevention strategies.
Other projects include one to find new ways to distinguish lethal from nonlethal prostate cancer and another to determine which risk factors best predict certain forms of cardiovascular disease.
“The transformative science that will be developed through this partnership,” Shulkin says, “will improve health care for veterans and all Americans.”