User login
Prescribing Patterns Shift After Detailing-Policy Change
In the past decade, medical institutions have begun to check the practice of detailing—pharmaceutical reps promoting medications during sales visits to physicians. This NIH study is one of the first to document the effect of these restrictions. The researchers compared prescribing at 19 academic medical centers (AMCs) that, between 2006 and 2012 instituted policies restricting detailing.
The study compared prescribing by 2,126 physicians at AMCs with that by 24,593 physicians from a pharmacy benefits database. The analysis covered 16.1 million prescriptions in 8 major drug classes: lipid lowering, gastroesophageal reflux disease, diabetes, hypertension, sleep, attention deficit hyperactivity disorder, depression, and antipsychosis.
At the centers with restrictions, physicians prescribed fewer of the promoted drugs and more nonpromoted drugs in the same drug classes. The mean market share of detailed drugs (across all the drug classes) in AMCs before the policy changes was 19.3%. Over the study period, the market share of detailed drugs prescribed by AMC physicians declined by 1.67 percentage point, an 8.7% decrease relative to the prechange level. The comparison group of physicians saw a slight decline over the same period. Although the drop was “modest,” NIH notes, proportionally small changes can represent thousands of prescriptions. The market share of nondetailed drugs increased by a relative 5.6%.
The changes were statistically significant for 6 of the 8 drug classes and for all drugs in the aggregate. The magnitude of changes differed across AMCs, the researchers found. The decline was greatest at centers with the most stringent policies, such as bans on salespeople in patient care areas. In 8 of 11 AMCs with more stringent policies, the changes in prescribing were significant, compared with only 1 of 8 AMCs with more limited measures.
In the past decade, medical institutions have begun to check the practice of detailing—pharmaceutical reps promoting medications during sales visits to physicians. This NIH study is one of the first to document the effect of these restrictions. The researchers compared prescribing at 19 academic medical centers (AMCs) that, between 2006 and 2012 instituted policies restricting detailing.
The study compared prescribing by 2,126 physicians at AMCs with that by 24,593 physicians from a pharmacy benefits database. The analysis covered 16.1 million prescriptions in 8 major drug classes: lipid lowering, gastroesophageal reflux disease, diabetes, hypertension, sleep, attention deficit hyperactivity disorder, depression, and antipsychosis.
At the centers with restrictions, physicians prescribed fewer of the promoted drugs and more nonpromoted drugs in the same drug classes. The mean market share of detailed drugs (across all the drug classes) in AMCs before the policy changes was 19.3%. Over the study period, the market share of detailed drugs prescribed by AMC physicians declined by 1.67 percentage point, an 8.7% decrease relative to the prechange level. The comparison group of physicians saw a slight decline over the same period. Although the drop was “modest,” NIH notes, proportionally small changes can represent thousands of prescriptions. The market share of nondetailed drugs increased by a relative 5.6%.
The changes were statistically significant for 6 of the 8 drug classes and for all drugs in the aggregate. The magnitude of changes differed across AMCs, the researchers found. The decline was greatest at centers with the most stringent policies, such as bans on salespeople in patient care areas. In 8 of 11 AMCs with more stringent policies, the changes in prescribing were significant, compared with only 1 of 8 AMCs with more limited measures.
In the past decade, medical institutions have begun to check the practice of detailing—pharmaceutical reps promoting medications during sales visits to physicians. This NIH study is one of the first to document the effect of these restrictions. The researchers compared prescribing at 19 academic medical centers (AMCs) that, between 2006 and 2012 instituted policies restricting detailing.
The study compared prescribing by 2,126 physicians at AMCs with that by 24,593 physicians from a pharmacy benefits database. The analysis covered 16.1 million prescriptions in 8 major drug classes: lipid lowering, gastroesophageal reflux disease, diabetes, hypertension, sleep, attention deficit hyperactivity disorder, depression, and antipsychosis.
At the centers with restrictions, physicians prescribed fewer of the promoted drugs and more nonpromoted drugs in the same drug classes. The mean market share of detailed drugs (across all the drug classes) in AMCs before the policy changes was 19.3%. Over the study period, the market share of detailed drugs prescribed by AMC physicians declined by 1.67 percentage point, an 8.7% decrease relative to the prechange level. The comparison group of physicians saw a slight decline over the same period. Although the drop was “modest,” NIH notes, proportionally small changes can represent thousands of prescriptions. The market share of nondetailed drugs increased by a relative 5.6%.
The changes were statistically significant for 6 of the 8 drug classes and for all drugs in the aggregate. The magnitude of changes differed across AMCs, the researchers found. The decline was greatest at centers with the most stringent policies, such as bans on salespeople in patient care areas. In 8 of 11 AMCs with more stringent policies, the changes in prescribing were significant, compared with only 1 of 8 AMCs with more limited measures.
Interprofessional Education in Patient Aligned Care Team Primary Care-Mental Health Integration
Over the past 10 years, the VHA has been a national leader in primary care-mental health integration (PC-MHI) within patient aligned care teams (PACTs).1,2 Studies of the PC-MHI collaborative care model consistently have shown increased access to MH services, higher levels of MH treatment engagement, improved MH treatment outcomes, and high patient and provider satisfaction.3-7 Primary care-mental health integration relies heavily on interprofessional team-based practice with providers from diverse educational and clinical backgrounds who work together to deliver integrated mental and behavioral health services within PACTs. This model requires a unique blending of professional cultures and communication and practice styles.
To sustain PC-MHI in PACT, health care professionals (HCPs) must be well trained to work effectively in interprofessional teams. Across health care organizations, training in collaborative interprofessional team-based practice has been identified as an important and challenging task.8-11
Integrating educational experiences among different HCP learners is an approach to developing competency in interprofessional collaboration early in training. The World Health Organization defined interprofessional education (IPE) as occurring “when students from two or more professions learn about, from, and with each other to enable effective collaboration and improve health outcomes.”9 Fundamental to this definition is the belief that interaction among learners from different disciplines during their training develops competency in subsequent effective collaborative practice. Studies of IPE in MH professional training have found that prelicensure IPE contributes to increased knowledge of roles and responsibilities of different disciplines, improved interprofessional communication and attitudes, and increased willingness to work in teams.12-17
Interprofessional education is a valuable training model, but developing interprofessional learning experiences in a system of diverse and often siloed training programs is difficult. More information about design and implementation of IPE training experiences is needed, particularly in outpatient settings in which integration of traditionally separate discipline-specific care is central to the health care mission. The VA PACT PC-MHI is a strong team-based care model that represents a unique opportunity for training across disciplines in interprofessional collaborative care.
To find innovative approaches to meeting the need for IPE in PACT PC-MHI, the authors developed a new IPE program in PC-MHI at the William S. Middleton Memorial Veterans Hospital (WSMMVH) in Madison, Wisconsin. This article reviews the development, implementation, and first-year evaluation of the training program and discusses the challenges and the IPE areas in need of improvement in PACT PC-MHI.
Methods
In 2012, the VHA launched phase 1 of the Mental Health Education Expansion Initiative (MHEEI), a collaboration of the Office of Academic Affiliations (OAA), VHA Mental Health Services (VHA-MHS), and the Office of Mental Health Operations (OMHO).18 The MHEEI was intended to “increase expertise in critical areas of need, expand the recruitment pipeline of well-trained, highly qualified health care providers in behavioral and mental health disciplines, and promote the utilization of interprofessional team-based care.”18 In response, WSMMVH organized a planning committee and submitted a funding request through the section of MHEEI called PACT With Integrated Behavioral Health Providers. The planning committee included training program directors and staff from psychiatry, pharmacy, social work, psychology, and primary care. The authors received funding for trainees in psychiatry (postgraduate year 4 [PGY-4]), pharmacy/MH residency (PGY-2), pharmacy/ambulatory care (PGY-1), and social work (interns).
Curriculum Development
The planning committee met regularly for 6 months to develop the organization, learning objectives, educational strategies, and implementation plan for the IPE program. The program was organized as a 4- to 12-month clinical rotation with the PC-MHI team in PACT, combined with 12 months of protected weekly IPE time (Table 1). 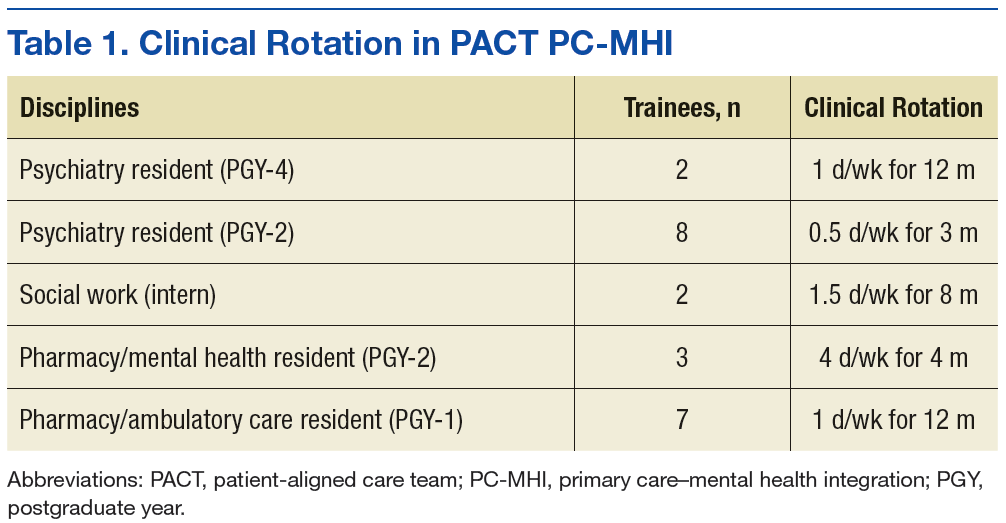
Learning Objectives
To better understand the educational needs and foci for learning objectives, the interprofessional planning committee reviewed guidelines on training in integrated care and collaborative team-based practice.2,9,10,19-21 These guidelines were compared with existing training opportunities for each discipline to identify training gaps and needs.
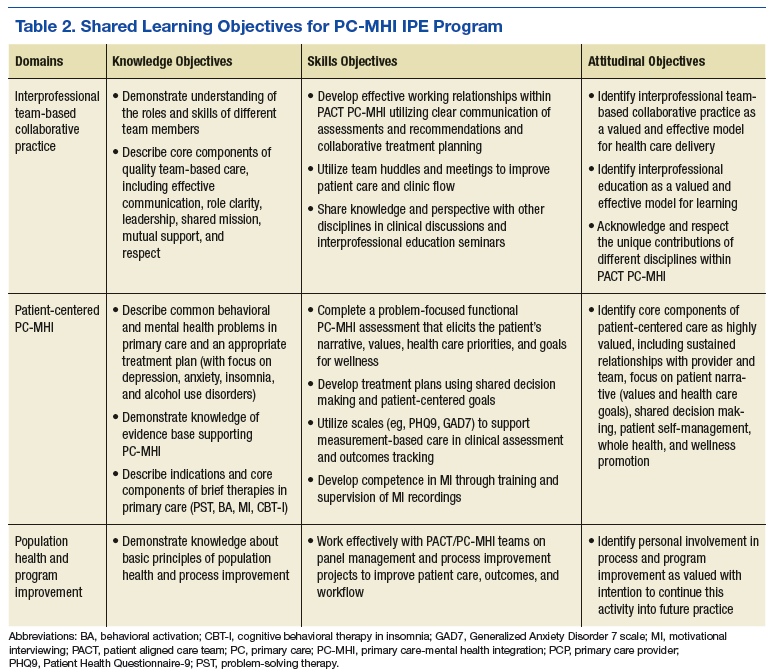
Learning objectives were organized into 3 domains: patient-centered PC-MHI, collaborative team-based practice, and population health and program improvement. Table 2 outlines the shared learning objectives linked to each domain that were common to the psychiatry, pharmacy, and social work disciplines. Although many of the learning objectives were shared among all disciplines, each trainee also had discipline-specific clinical activities and learning objectives. Psychiatry and pharmacy residents focused on primary care psychiatric medication consultation and care management for antidepressant medication starts. Social work interns focused on psychosocial and functional assessment and brief problem-focused psychotherapies. Learning objectives were met through direct veteran care in the primary care clinic as part of the PACT PC-MHI team and through interprofessional learning activities during protected weekly education time.
Implementation
Critical stakeholders in implementing the IPE program involved themselves early and throughout the planning process. Stakeholders included VAMC leadership, primary care and MH service line chiefs and clinic managers, training program directors, and PACT staff. Planning committee members gave presentations on the IPE program at MH service line and PACT meetings in the 2 months before program initiation in order to orient staff to learning objectives, program structure, and impact on PACT PC-MHI operations. Throughout the first year, the planning committee continued to meet every 2 weeks to review progress, solve implementation problems, and revise learning objectives and activities.
Trainee Clinical Activities
A wide range of educational strategies were planned to meet learning objectives across the 3 domains. There was strong emphasis on experiential learning through daily PACT and PC-MHI clinical work, team huddles and meetings, and trainee-led program improvement projects.
Psychiatry and PGY-2 pharmacy/MH residents focused on direct and indirect medication consultation and problem-focused assessments. Their clinical activities included PC-MHI medication evaluation and follow-up visits; chart reviews and e-consults for medication recommendations to PACT providers; reviews of care management data and consultations on veterans enrolled in depression and anxiety care management; “curbside consultations” for providers in PACT huddles and meetings and throughout the clinic day; and “warm handoffs,” same-day initial PC-MHI problem-focused assessments performed on PACT provider request. The residents were part of a pool of staff and trainees who performed these assessments.
PGY-1 pharmacy residents made care management phone calls for antidepressant trials for depression and anxiety. These residents were trained in motivational interviewing (MI). They applied their MI skills during care management calls focused on medication adherence and behavioral interventions for depression (eg, exercise, planning pleasurable activity) and during other clinical rotations, including tobacco cessation and medication management for diabetes and hypertension. Particularly challenging veteran cases from these clinics were cosupervised with medication management and PC-MHIstaff for added consultation on engagement, behavior change, and treatment plan adherence.
Social work interns completed initial PC-MHI psychosocial and functional assessments by phone and directly by same-day warm handoffs from PACT staff. The PC-MHI therapies they provided included problem-solving therapy, behavioral activation, stress management based on cognitive behavioral therapy, and brief alcohol interventions.
Group IPE Activities
All trainees had a weekly protected block of 3 hours during which they came together for group IPE that was designed to elicit active participation; facilitate interprofessional communication; and develop an understanding of and respect for the knowledge, culture, and practice style of the different disciplines.
Trainees participated in a Herrmann Brain Dominance Instrument (HBDI) workshop focused on developing a better understanding of individual differences in thinking and problem solving, with the goal of improving communication and learning within teams.22 In a seminar series on professionalism and boundaries in health care, trainees from each discipline gave a presentation on the traditional structure and content of their discipline’s training and discussed similarities and differences in their disciplines’ professional oaths, codes of ethics, and boundary guidelines.
Motivational interviewing training was conducted early in the year so trainees would be prepared to apply MI skills in their daily PACT PC-MHI clinical work. Motivational inteviewing is a patient-centered approach to engaging patients in health promoting behavior change. It is defined as a “directive, client-centered counseling style for eliciting behavior change by helping clients to explore and resolve ambivalence.”23
Trainees recorded MI sessions with at least 2 live-patient visits and at least 2 simulated-patient interviews (with staff serving as patient actors). The structure of MI training and supervision was deliberately designed to facilitate interprofessional communication and learning. In accord with a group supervision model for MI recorded reviews, the trainees presented their tapes to the entire learning group in the presence of a facilitating supervisor. Trainees had the opportunity to observe different interview styles and exchange feedback within a peer group of interprofessional learners.
Seminars were focused on core PC-MHI clinical content (eg, depression, anxiety, alcohol use disorders) and organized around case-based learning. Trainees divided into small teams in which representatives of each discipline offered their perspective on how to approach planning patient assessment and treatment. During the seminars, the authors engaged trainees as teachers and leaders whenever possible. All trainees presented on a topic in which they had some discipline expertise. For example, social work interns led a seminar on support and social services for victims of domestic violence, and PGY-1 pharmacy/ambulatory care residents led seminars and a panel management project focused on diabetes and depression.
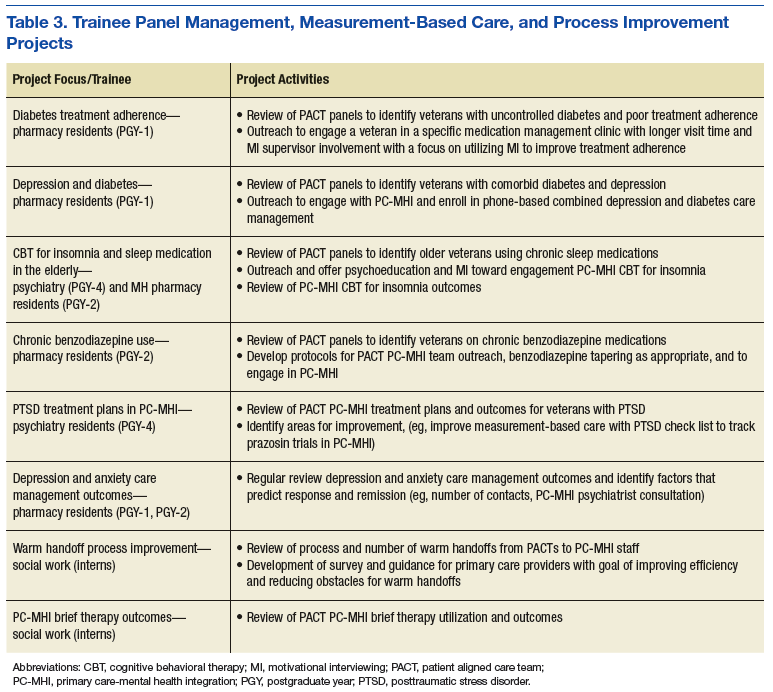
Trainees participated in several PACT PC-MHI projects focused on population- and measurement-based care, panel management, and program improvement (Table 3). Protected IPE time was used to teach trainees about population health principles and different tools for process improvement (eg, Vision-Analysis Team-Aim-Map-Measure-Change-Sustain) and provide a forum in which trainees could share their work with one another.
Evaluations
Several tools were used for trainee and program evaluations. Clinical skills were evaluated during daily supervision. Trainees began the year with PC-MHI staff directly observing all their clinical contacts with veterans. Staff evaluated and offered feedback on trainee clinical interviewing and on assessment and treatment planning skills. Once they were assessed to be ready to see veterans on their own, trainees were advanced by staff to “drop-in” direct supervision: Toward the end of a veteran’s visit, a staff preceptor entered the room to review relevant clinical findings, assessment and finalized treatment planning with the trainee and veteran. When appropriate for trainee competence level, clinical contacts were indirectly supervised: Trainees discussed their assessment and treatment plan with a staff supervisor at the end of the day.
Motivational interviewing recordings were reviewed during group supervision. To objectively evaluate MI skills, supervisors who were VA-certified in MI used the Motivational Interviewing Treatment Integrity (MITI) coding tool to review and code both the live- and simulated-patient recordings.24 The MITI coding involves quantitative and qualitative analysis using standardized coding items.
Quantitative items included percentage of open-ended questions (Proficiency: 50%; competency: 70%); percentage of reflections considered complex reflections, or reflective statements adding substantial meaning or emphasis and conveying a deeper or more complex picture of what patients say (Proficiency: 40%; competency: 50%); reflection-to-question ratio (Proficiency: 1:1; competency: 2:1); and percentage of MI-adherent provider statements (Proficiency: 90%; competency: 100%).
Qualitative coding items were a global rating of therapist “empathy,” which evaluated the extent to which the trainee understood or made an effort to grasp the patient’s perspective, and “MI spirit.” This coding intended to capture the overall competence of the trainee in emphasizing collaboration, patient autonomy, and evocation of the patient experience (Proficiency score: 5; competency score: 6).
The PC-MHI teaching staff met midyear and end of year as a team to complete trainee evaluations focused on the 3 areas of learning objectives: patient-centered PC-MHI, collaborative team-based practice, and population health and program improvement. Patient-centered PC-MHI involves direct observation and supervision of trainee clinical contacts with veterans, including assessment and treatment planning, clinical documentation, and review of live- and simulated-patient MI recordings. Collaborative team-based practice involves review of trainee participation in day-to-day teamwork, huddles, team meetings, and IPE activities. Population health and program improvement involves review of trainee work on a panel measurement-based care management or program improvement project. In each learning objectives area, trainees were rated on a 3-point scale: needs improvement (1); satisfactory (2); achieved (3). Core knowledge about PC-MHI evidence base, structure, and clinical topics was assessed with case-based written examination at midyear and end of year.
Surveys and qualitative interviews were used to assess trainee perceptions about the IPE program. A midyear and end-of-year survey assessed trainee satisfaction and perceived efficacy of the IPE training program in meeting core learning objectives. A midyear survey designed by pharmacy residents as part of their program improvement project evaluated attitudes around interprofessional learning and team practice. Trainees met individually with the PC-MHI IPE director at midyear and end of year to gather qualitative feedback on the IPE program.
Outcomes
All trainees advanced to the expected level of supervision for clinical contacts (drop-in or indirect clinical supervision). Over the year, there was significant improvement in trainees’ MI skills as measured by MITI coding of at least 2 live-patient or 2 simulated-patient recordings (Figures 1A and 1B). By end of year, most trainees had reached proficiency or competency in several MITI coded items: percentage of open-ended questions (4/12 proficient, 8/12 competent), percentage of complex reflections (2/12 less than proficient, 3/12 proficient, 7/12 competent), MI adherence (1/12 proficient, 11/12 competent), global empathy rating (2/12 proficient, 10/12 competent), and global MI spirit rating (12/12 competent). Average reflection-to-question ratio for the trainee group increased from 0.63 to 0.96 from midyear to end of year, but only 3 of 12 trainees reached the proficiency level of a 1:1 ratio, and no trainee reached the competency level of a 2:1 ratio. 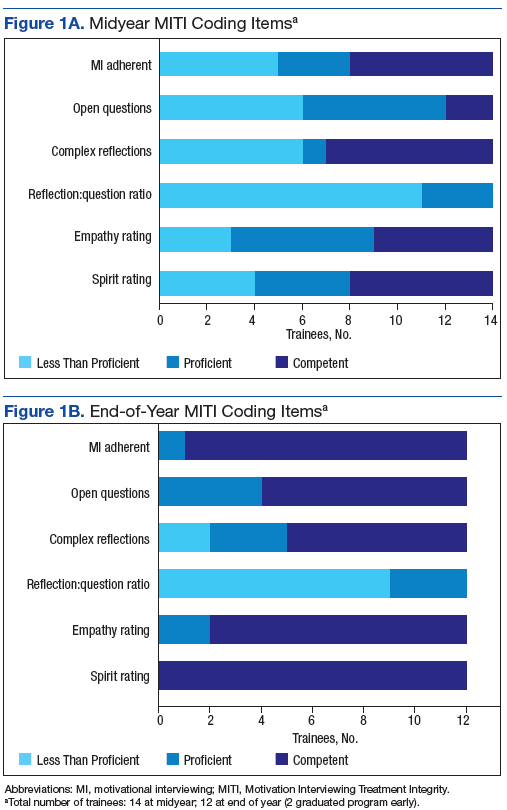
According to the PC-MHI team’s midyear evaluation, most trainees were already making satisfactory progress in the 3 domains of learning objectives for the training program. At end of year, 13 of 14 trainees were assessed as competent in all 3 domains (Figures 2A and B). All trainees passed the midyear and end-of-year written examinations with overall high scores (average score, 82%) demonstrating acquisition of core PC-MHI clinical knowledge. 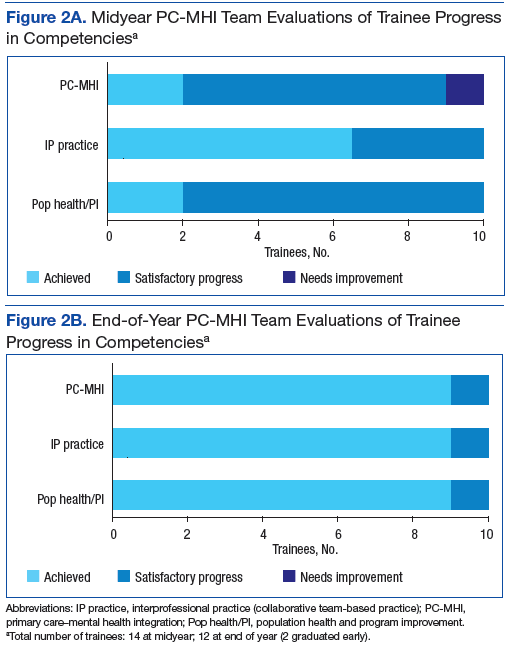
Trainee evaluations of the IPE program were overall highly favorable at both midyear and at end of year. Trainees rated the program effective or extremely effective in developing their skills in patient-centered care, interprofessional communication, and collaborative team-based practice. They also rated the program highly effective in preparing them to use team-based practice skills in other settings. On a midyear survey, trainees moderately to strongly agreed with several positive beliefs and attitudes about team-based care.
In qualitative interviews at program completion, trainees across disciplines rated the MI training with group supervision as one of their most valuable interprofessional learning experiences. Other highly valued training experiences were PACT PC-MHI panel management projects, team-based clinical case reviews, and cross-disciplinary supervision.
Discussion
This article describes the successful development and implementation of a VA-based IPE program in PACT PC-MHI. Interprofessional clinical training and educational experiences were highly valued, and trainees identified positive attitudes and improved skills related to team-based care. These findings support previous findings that IPE is associated with high satisfaction and positive attitudes toward team-based collaborative practice.12-17 Program implementation presented several challenges: nonsynchronous academic calendars and rotation schedules, cross-disciplinary supervision regulations, variations in clinical and supervisory requirements for accreditation standards, the traditional health care hierarchy, and measurement of the impact of IPE experiences.11,25,26
Rotation schedules and academic calendars varied across the psychiatry, pharmacy, and social work home programs. Organizing different trainee rotation schedules was a significant challenge. Collaboration with training directors and support staff was crucial in planning rotations that offered a longitudinal training experience in PACT PC-MHI. Given the participants’ different starting dates, protected IPE time early in the calendar year was focused on developing clinical skills specific to the pharmacy and psychiatry trainees who would be starting in July, and IPE activities that required the presence of all trainee disciplines (eg, MI training, HBDI) were planned for after the September start of the social work interns.
Cross-disciplinary supervision was highly valued by trainees because it offered exposure to the disciplines’ different communication styles and approaches to clinical assessment and decision making. Throughout the year, however, trainees encountered several obstacles to cross-disciplinary supervision, with respect to coding/billing and home program supervisory policies. The authors worked closely with the VA administration and each training program to develop and revise supervising policies and procedures to meet the necessary administrative and program supervisory requirements for accreditation standards.
In some cases, this work resulted in dual supervision by a preceptor of the same discipline (to meet requirements for coding/billing and home program supervision) and clinical supervision by a preceptor of a different discipline (eg, in team meetings or in clinical case reviews during protected IPE time). Preceptors from each discipline met regularly to discuss challenges in cross-disciplinary supervision, review scope-of-practice issues, share information on discipline-specific training, and revise supervisory procedures.
Interprofessional education activities during weekly protected time were designed to improve collaboration and to challenge trainees to examine traditional hierarchical roles and patterns of communication in health care. An emphasis on case-based learning in small groups encouraged trainees to share perspectives on their discipline-specific approach to assessment and treatment planning. Motivational interviewing training, one of the IPE experiences most valued by trainees and staff, created the opportunity for a truly shared learning environment, as trainees largely started at about the same skill level despite having different educational backgrounds. Group supervision of MI recordings offered trainees the opportunity to learn from each other and develop comfort in offering and receiving interprofessional constructive feedback.
Limitations
There were considerable methodologic limitations in the authors’ efforts to evaluate the impact of this training program on trainee attitudes and skills in collaborative team-based practice. Although trainee surveys revealed highly positive attitudes and beliefs about team-based care as well as perceived competence in collaborative practice, these were not validated surveys, and changes could not be accurately measured over time (trainees were not assessed at baseline). Trainees also were involved in other clinical teams within the VA during the year, and it is difficult to assess the specific impact of their PC-MHI IPE experiences. The PC-MHI staff evaluations of trainee competence in collaborative team-based practice were largely observational and potentially vulnerable to biases, as the staff evaluating trainee competence also were part of the IPE program planning process and invested in its success.
To address these limitations in the future, the authors will use better assessment tools at baseline and end of year to more effectively evaluate the impact of the training program on teamwork skills as well changes in attitudes and beliefs about interprofessional learning and teamwork. The Attitudes Toward Interprofessional Health Care Teams Scale and the Perceptions of Effective Interpersonal Teams Scale should be considered as they have published reliability and validity.27,28 The authors could improve the reliability and depth of trainee evaluations with use of a “360-degree evaluation” model for trainee evaluations that includes other PACT members (beyond PC-MHI staff) as well as veterans.
Assessment of MI skills and competency was limited by use of both live- and simulated-patient recordings. Simulation is a valuable learning tool but often does not accurately represent actual clinical situations and challenges. To appropriately assess MI competence, future MI training should emphasize live-patient recordings over simulated-patient visits. Furthermore, whereas trainees reached competency in several MI coding items, none reached competency in the reflection-to-question ratio, and only about half reached competency in percentage of complex reflections. Future MI training will need to focus on further development of reflection skills.
Trainee intentions to remain involved in program improvement and collaborative team-based care in future professional work were core attitudinal learning objectives, but neither was adequately assessed in end-of-year surveys. Ideally, future evaluations will assess subjective trainee intentions and goals around team-based work and objectively measure future professional choices and activities. For example, it would be interesting to determine whether trainees who participated in this program will choose to practice in an interprofessional team-based model or participate in program improvement activities.
Last, the absence of psychology interns was considered a weakness in the learning environment, resulting in a relatively “prescriber-heavy” balance in discipline perspectives for IPE-focused case discussions and other training. Furthermore, the discipline representation in the IPE program did not exemplify the typical PC-MHI team in most VA clinic settings and community practices in which psychology has a strong presence. Adding psychology trainees was an important goal for the IPE program leadership. In 2015, WSMMVH was awarded additional funding for a PACT PC-MHI predoctoral psychology intern through the phase 4 MHEEI. The PC-MHI track psychology intern joined the IPE program in the 2016-2017 training year.
Conclusion
There is broad consensus that interprofessional team-based practice is crucial for providers in the VA and all health care systems. Primary care-mental health integration is an area of VA care in which interprofessional collaboration is uniquely important to implementation and sustainability of the model. Interprofessional education is an effective approach for preparing HCPs for team-based practice, but implementation is challenging. Several factors crucially contributed to the successful implementation of this program: collaboration of the interprofessional planning team with representation from key stakeholders in different departments and training programs; a well-established PACT PC-MHI team with experience in collaborative team-based care; a curriculum structure that emphasized experiential educational strategies designed to promote interprofessional learning and communication; VA leadership support at the national level (MHEEI funding) and local level; and PACT PC-MHI clinical staff committed to teaching and to the IPE mission.
1. Wray LO, Szymanski BR, Kearney LK, McCarthy JF. Implementation of primary care-mental health integration services in the Veterans Health Administration: program activity and associations with engagement in specialty mental health services. J Clin Psychol Med Settings. 2012;19(1):105-116.
2. Kearney LK, Post EP, Pomerantz AS, Zeiss AM. Applying the interprofessional patient aligned care team in the Department of Veterans Affairs: transforming primary care. Am Psychol. 2014;69(4):399-408.
3. Gilbody S, Bower P, Fletcher J, Richards D, Sutton AJ. Collaborative care for depression: a cumulative meta-analysis and review of loner-term outcomes. Arch Intern Med. 2006;166(21):2314-2321.
4. Unützer J, Katon W, Callahan CM, et al; IMPACT (Improving Mood-Promoting Access to Collaborative Treatment) Investigators. Collaborative care management in late-life depression in the primary care setting: a randomized control trial. JAMA. 2002;288(22):2836-2845.
5. Katon W, Unützer J. Consultation psychiatry in the medical home and accountable care organizations: achieving the triple aim. Gen Hosp Psychiatry. 2011;3(4):305-310.
6. Bruce ML, Tenhave TR, Reynolds CF III, et al. Reducing suicidal ideation and depressive symptoms in depressed older primary care patients: a randomized controlled trial. JAMA. 2004;291(9):1081-1091.
7. Alexopoulos GS, Reynolds CF III , Bruce ML, et al; PROSPECT Group. Reducing suicidal ideation and depression in older primary care patients: 24-month outcomes of the PROSPECT study. Am J Psychiatry. 2009;166(8):882-890.
8. Cox M, Cuff P, Brandt B, Reeves S, Zierler B. Measuring the impact of interprofessional education on collaborative practice and patient outcomes. J Interprof Care. 2016;30(1):1-3.
9. World Health Organization, Study Group on Interprofessional Education and Collaborative Practice. Framework for Action on Interprofessional Education and Collaborative Practice. Geneva, Switzerland: World Health Organization; 2010.
10. Interprofessional Education Collaborative Expert Panel. Core Competencies for Interprofessional Collaborative Practice: Report of an Expert Panel. Washington, DC: Interprofessional Education Collaborative; 2011.
11. Blue AV, Mitcham M, Smith T, Raymond J, Greenburg R. Changing the future of health professions: embedding interprofessional education within an academic health center. Acad Med. 2010;85(8):1290-1295.
12. Priest HM, Roberts P, Dent H, Blincoe C, Lawton D, Armstrong C. Interprofessional education and working in mental health: in search of the evidence base. J Nurs Manag. 2008;16(4):474-485.
13. Reeves S. A systematic review of the effects of interprofessional education on staff involved in the care of adults with mental health problems. J Psychiatr Ment Health Nurs. 2001;8(6):533-542.
14. Carpenter J, Barnes D, Dickinson C, Wooff D. Outcomes of interprofessional education for community mental health services in England: the longitudinal evaluation of a postgraduate programme. J Interprof Care. 2006;20(2):145-161.
15. Hammick M, Freeth D, Koppel I, Reeves S, Barr H. A best evidence systematic review of interprofessional education: BEME guide no. 9. Med Teach. 2007;29(8):735-751.
16. Pauzé E, Reeves S. Examining the effects of interprofessional education on mental health providers: findings from an updated systematic review. J Ment Health. 2010;19(3):258-271.
17. Curran V, Heath O, Adey T, et al. An approach to integrating interprofessional education in collaborative mental health care. Acad Psychiatry. 2012;36(2):91-95.
18. Veterans Health Administration. VA Interprofessional Mental Health Education Expansion Initiative, Phase I. Washington, DC; Department of Veterans Affairs; 2012.
19. Dundon M, Dollar K, Schohn M, Lantinga LJ. Primary care–mental health integration: co-located, collaborative care: an operations manual. https://www.mirecc.va.gov/cih-visn2/Documents/Clinical/MH-IPC_CCC_Operations_Manual_Version_2_1.pdf. Published February 2011. Accessed May 19, 2017.
20. McDaniel SH, Grus CL, Cubic BA, et al. Competencies for psychology practice in primary care. Am Psychol. 2014;69(4):409-429.
21. Cowley D, Dunaway K, Forstein M, et al. Teaching psychiatry residents to work at the interface of mental health and primary care. Acad Psychiatry. 2014;38(4):398-404.
22. Herrmann N. The creative brain. J Creat Behav. 1991;25:275-295.
23. Rollnick S, Miller WR. What is motivational interviewing? Behav Cogn Psychother. 1995;23(4):325-334.
24. Pierson HM, Hayes SC, Gifford EV, et al. An examination of the Motivational Interviewing Treatment Integrity code. J Subst Abuse Treat. 2007;32(1):11-17.
25. Shaw D, Blue A. Should psychiatry champion interprofessional education? Acad Psychiatry. 2012;36(3):163-166.
26. Gilbert JH. Interprofessional learning and higher education structural barriers. J Interprof Care. 2005;19(suppl 1):87-106.
27. Heinemann GD, Schmitt MH, Farrell PP, Brallier SA. Development of an Attitudes Toward Health Care Teams Scale. Eval Health Prof. 1999;22(1):123-142.
28. Hepburn K, Tsukuda RA, Fasser C. Team Skills Scale. In: Heinemann GD, Zeiss AM, eds. Team Performance in Healthcare: Assessment and Development. New York, NY: Kluwer Academic/Plenum; 2002:159-163.
Over the past 10 years, the VHA has been a national leader in primary care-mental health integration (PC-MHI) within patient aligned care teams (PACTs).1,2 Studies of the PC-MHI collaborative care model consistently have shown increased access to MH services, higher levels of MH treatment engagement, improved MH treatment outcomes, and high patient and provider satisfaction.3-7 Primary care-mental health integration relies heavily on interprofessional team-based practice with providers from diverse educational and clinical backgrounds who work together to deliver integrated mental and behavioral health services within PACTs. This model requires a unique blending of professional cultures and communication and practice styles.
To sustain PC-MHI in PACT, health care professionals (HCPs) must be well trained to work effectively in interprofessional teams. Across health care organizations, training in collaborative interprofessional team-based practice has been identified as an important and challenging task.8-11
Integrating educational experiences among different HCP learners is an approach to developing competency in interprofessional collaboration early in training. The World Health Organization defined interprofessional education (IPE) as occurring “when students from two or more professions learn about, from, and with each other to enable effective collaboration and improve health outcomes.”9 Fundamental to this definition is the belief that interaction among learners from different disciplines during their training develops competency in subsequent effective collaborative practice. Studies of IPE in MH professional training have found that prelicensure IPE contributes to increased knowledge of roles and responsibilities of different disciplines, improved interprofessional communication and attitudes, and increased willingness to work in teams.12-17
Interprofessional education is a valuable training model, but developing interprofessional learning experiences in a system of diverse and often siloed training programs is difficult. More information about design and implementation of IPE training experiences is needed, particularly in outpatient settings in which integration of traditionally separate discipline-specific care is central to the health care mission. The VA PACT PC-MHI is a strong team-based care model that represents a unique opportunity for training across disciplines in interprofessional collaborative care.
To find innovative approaches to meeting the need for IPE in PACT PC-MHI, the authors developed a new IPE program in PC-MHI at the William S. Middleton Memorial Veterans Hospital (WSMMVH) in Madison, Wisconsin. This article reviews the development, implementation, and first-year evaluation of the training program and discusses the challenges and the IPE areas in need of improvement in PACT PC-MHI.
Methods
In 2012, the VHA launched phase 1 of the Mental Health Education Expansion Initiative (MHEEI), a collaboration of the Office of Academic Affiliations (OAA), VHA Mental Health Services (VHA-MHS), and the Office of Mental Health Operations (OMHO).18 The MHEEI was intended to “increase expertise in critical areas of need, expand the recruitment pipeline of well-trained, highly qualified health care providers in behavioral and mental health disciplines, and promote the utilization of interprofessional team-based care.”18 In response, WSMMVH organized a planning committee and submitted a funding request through the section of MHEEI called PACT With Integrated Behavioral Health Providers. The planning committee included training program directors and staff from psychiatry, pharmacy, social work, psychology, and primary care. The authors received funding for trainees in psychiatry (postgraduate year 4 [PGY-4]), pharmacy/MH residency (PGY-2), pharmacy/ambulatory care (PGY-1), and social work (interns).
Curriculum Development
The planning committee met regularly for 6 months to develop the organization, learning objectives, educational strategies, and implementation plan for the IPE program. The program was organized as a 4- to 12-month clinical rotation with the PC-MHI team in PACT, combined with 12 months of protected weekly IPE time (Table 1).
Learning Objectives
To better understand the educational needs and foci for learning objectives, the interprofessional planning committee reviewed guidelines on training in integrated care and collaborative team-based practice.2,9,10,19-21 These guidelines were compared with existing training opportunities for each discipline to identify training gaps and needs.
Learning objectives were organized into 3 domains: patient-centered PC-MHI, collaborative team-based practice, and population health and program improvement. Table 2 outlines the shared learning objectives linked to each domain that were common to the psychiatry, pharmacy, and social work disciplines. Although many of the learning objectives were shared among all disciplines, each trainee also had discipline-specific clinical activities and learning objectives. Psychiatry and pharmacy residents focused on primary care psychiatric medication consultation and care management for antidepressant medication starts. Social work interns focused on psychosocial and functional assessment and brief problem-focused psychotherapies. Learning objectives were met through direct veteran care in the primary care clinic as part of the PACT PC-MHI team and through interprofessional learning activities during protected weekly education time.
Implementation
Critical stakeholders in implementing the IPE program involved themselves early and throughout the planning process. Stakeholders included VAMC leadership, primary care and MH service line chiefs and clinic managers, training program directors, and PACT staff. Planning committee members gave presentations on the IPE program at MH service line and PACT meetings in the 2 months before program initiation in order to orient staff to learning objectives, program structure, and impact on PACT PC-MHI operations. Throughout the first year, the planning committee continued to meet every 2 weeks to review progress, solve implementation problems, and revise learning objectives and activities.
Trainee Clinical Activities
A wide range of educational strategies were planned to meet learning objectives across the 3 domains. There was strong emphasis on experiential learning through daily PACT and PC-MHI clinical work, team huddles and meetings, and trainee-led program improvement projects.
Psychiatry and PGY-2 pharmacy/MH residents focused on direct and indirect medication consultation and problem-focused assessments. Their clinical activities included PC-MHI medication evaluation and follow-up visits; chart reviews and e-consults for medication recommendations to PACT providers; reviews of care management data and consultations on veterans enrolled in depression and anxiety care management; “curbside consultations” for providers in PACT huddles and meetings and throughout the clinic day; and “warm handoffs,” same-day initial PC-MHI problem-focused assessments performed on PACT provider request. The residents were part of a pool of staff and trainees who performed these assessments.
PGY-1 pharmacy residents made care management phone calls for antidepressant trials for depression and anxiety. These residents were trained in motivational interviewing (MI). They applied their MI skills during care management calls focused on medication adherence and behavioral interventions for depression (eg, exercise, planning pleasurable activity) and during other clinical rotations, including tobacco cessation and medication management for diabetes and hypertension. Particularly challenging veteran cases from these clinics were cosupervised with medication management and PC-MHIstaff for added consultation on engagement, behavior change, and treatment plan adherence.
Social work interns completed initial PC-MHI psychosocial and functional assessments by phone and directly by same-day warm handoffs from PACT staff. The PC-MHI therapies they provided included problem-solving therapy, behavioral activation, stress management based on cognitive behavioral therapy, and brief alcohol interventions.
Group IPE Activities
All trainees had a weekly protected block of 3 hours during which they came together for group IPE that was designed to elicit active participation; facilitate interprofessional communication; and develop an understanding of and respect for the knowledge, culture, and practice style of the different disciplines.
Trainees participated in a Herrmann Brain Dominance Instrument (HBDI) workshop focused on developing a better understanding of individual differences in thinking and problem solving, with the goal of improving communication and learning within teams.22 In a seminar series on professionalism and boundaries in health care, trainees from each discipline gave a presentation on the traditional structure and content of their discipline’s training and discussed similarities and differences in their disciplines’ professional oaths, codes of ethics, and boundary guidelines.
Motivational interviewing training was conducted early in the year so trainees would be prepared to apply MI skills in their daily PACT PC-MHI clinical work. Motivational inteviewing is a patient-centered approach to engaging patients in health promoting behavior change. It is defined as a “directive, client-centered counseling style for eliciting behavior change by helping clients to explore and resolve ambivalence.”23
Trainees recorded MI sessions with at least 2 live-patient visits and at least 2 simulated-patient interviews (with staff serving as patient actors). The structure of MI training and supervision was deliberately designed to facilitate interprofessional communication and learning. In accord with a group supervision model for MI recorded reviews, the trainees presented their tapes to the entire learning group in the presence of a facilitating supervisor. Trainees had the opportunity to observe different interview styles and exchange feedback within a peer group of interprofessional learners.
Seminars were focused on core PC-MHI clinical content (eg, depression, anxiety, alcohol use disorders) and organized around case-based learning. Trainees divided into small teams in which representatives of each discipline offered their perspective on how to approach planning patient assessment and treatment. During the seminars, the authors engaged trainees as teachers and leaders whenever possible. All trainees presented on a topic in which they had some discipline expertise. For example, social work interns led a seminar on support and social services for victims of domestic violence, and PGY-1 pharmacy/ambulatory care residents led seminars and a panel management project focused on diabetes and depression.
Trainees participated in several PACT PC-MHI projects focused on population- and measurement-based care, panel management, and program improvement (Table 3). Protected IPE time was used to teach trainees about population health principles and different tools for process improvement (eg, Vision-Analysis Team-Aim-Map-Measure-Change-Sustain) and provide a forum in which trainees could share their work with one another.
Evaluations
Several tools were used for trainee and program evaluations. Clinical skills were evaluated during daily supervision. Trainees began the year with PC-MHI staff directly observing all their clinical contacts with veterans. Staff evaluated and offered feedback on trainee clinical interviewing and on assessment and treatment planning skills. Once they were assessed to be ready to see veterans on their own, trainees were advanced by staff to “drop-in” direct supervision: Toward the end of a veteran’s visit, a staff preceptor entered the room to review relevant clinical findings, assessment and finalized treatment planning with the trainee and veteran. When appropriate for trainee competence level, clinical contacts were indirectly supervised: Trainees discussed their assessment and treatment plan with a staff supervisor at the end of the day.
Motivational interviewing recordings were reviewed during group supervision. To objectively evaluate MI skills, supervisors who were VA-certified in MI used the Motivational Interviewing Treatment Integrity (MITI) coding tool to review and code both the live- and simulated-patient recordings.24 The MITI coding involves quantitative and qualitative analysis using standardized coding items.
Quantitative items included percentage of open-ended questions (Proficiency: 50%; competency: 70%); percentage of reflections considered complex reflections, or reflective statements adding substantial meaning or emphasis and conveying a deeper or more complex picture of what patients say (Proficiency: 40%; competency: 50%); reflection-to-question ratio (Proficiency: 1:1; competency: 2:1); and percentage of MI-adherent provider statements (Proficiency: 90%; competency: 100%).
Qualitative coding items were a global rating of therapist “empathy,” which evaluated the extent to which the trainee understood or made an effort to grasp the patient’s perspective, and “MI spirit.” This coding intended to capture the overall competence of the trainee in emphasizing collaboration, patient autonomy, and evocation of the patient experience (Proficiency score: 5; competency score: 6).
The PC-MHI teaching staff met midyear and end of year as a team to complete trainee evaluations focused on the 3 areas of learning objectives: patient-centered PC-MHI, collaborative team-based practice, and population health and program improvement. Patient-centered PC-MHI involves direct observation and supervision of trainee clinical contacts with veterans, including assessment and treatment planning, clinical documentation, and review of live- and simulated-patient MI recordings. Collaborative team-based practice involves review of trainee participation in day-to-day teamwork, huddles, team meetings, and IPE activities. Population health and program improvement involves review of trainee work on a panel measurement-based care management or program improvement project. In each learning objectives area, trainees were rated on a 3-point scale: needs improvement (1); satisfactory (2); achieved (3). Core knowledge about PC-MHI evidence base, structure, and clinical topics was assessed with case-based written examination at midyear and end of year.
Surveys and qualitative interviews were used to assess trainee perceptions about the IPE program. A midyear and end-of-year survey assessed trainee satisfaction and perceived efficacy of the IPE training program in meeting core learning objectives. A midyear survey designed by pharmacy residents as part of their program improvement project evaluated attitudes around interprofessional learning and team practice. Trainees met individually with the PC-MHI IPE director at midyear and end of year to gather qualitative feedback on the IPE program.
Outcomes
All trainees advanced to the expected level of supervision for clinical contacts (drop-in or indirect clinical supervision). Over the year, there was significant improvement in trainees’ MI skills as measured by MITI coding of at least 2 live-patient or 2 simulated-patient recordings (Figures 1A and 1B). By end of year, most trainees had reached proficiency or competency in several MITI coded items: percentage of open-ended questions (4/12 proficient, 8/12 competent), percentage of complex reflections (2/12 less than proficient, 3/12 proficient, 7/12 competent), MI adherence (1/12 proficient, 11/12 competent), global empathy rating (2/12 proficient, 10/12 competent), and global MI spirit rating (12/12 competent). Average reflection-to-question ratio for the trainee group increased from 0.63 to 0.96 from midyear to end of year, but only 3 of 12 trainees reached the proficiency level of a 1:1 ratio, and no trainee reached the competency level of a 2:1 ratio.
According to the PC-MHI team’s midyear evaluation, most trainees were already making satisfactory progress in the 3 domains of learning objectives for the training program. At end of year, 13 of 14 trainees were assessed as competent in all 3 domains (Figures 2A and B). All trainees passed the midyear and end-of-year written examinations with overall high scores (average score, 82%) demonstrating acquisition of core PC-MHI clinical knowledge.
Trainee evaluations of the IPE program were overall highly favorable at both midyear and at end of year. Trainees rated the program effective or extremely effective in developing their skills in patient-centered care, interprofessional communication, and collaborative team-based practice. They also rated the program highly effective in preparing them to use team-based practice skills in other settings. On a midyear survey, trainees moderately to strongly agreed with several positive beliefs and attitudes about team-based care.
In qualitative interviews at program completion, trainees across disciplines rated the MI training with group supervision as one of their most valuable interprofessional learning experiences. Other highly valued training experiences were PACT PC-MHI panel management projects, team-based clinical case reviews, and cross-disciplinary supervision.
Discussion
This article describes the successful development and implementation of a VA-based IPE program in PACT PC-MHI. Interprofessional clinical training and educational experiences were highly valued, and trainees identified positive attitudes and improved skills related to team-based care. These findings support previous findings that IPE is associated with high satisfaction and positive attitudes toward team-based collaborative practice.12-17 Program implementation presented several challenges: nonsynchronous academic calendars and rotation schedules, cross-disciplinary supervision regulations, variations in clinical and supervisory requirements for accreditation standards, the traditional health care hierarchy, and measurement of the impact of IPE experiences.11,25,26
Rotation schedules and academic calendars varied across the psychiatry, pharmacy, and social work home programs. Organizing different trainee rotation schedules was a significant challenge. Collaboration with training directors and support staff was crucial in planning rotations that offered a longitudinal training experience in PACT PC-MHI. Given the participants’ different starting dates, protected IPE time early in the calendar year was focused on developing clinical skills specific to the pharmacy and psychiatry trainees who would be starting in July, and IPE activities that required the presence of all trainee disciplines (eg, MI training, HBDI) were planned for after the September start of the social work interns.
Cross-disciplinary supervision was highly valued by trainees because it offered exposure to the disciplines’ different communication styles and approaches to clinical assessment and decision making. Throughout the year, however, trainees encountered several obstacles to cross-disciplinary supervision, with respect to coding/billing and home program supervisory policies. The authors worked closely with the VA administration and each training program to develop and revise supervising policies and procedures to meet the necessary administrative and program supervisory requirements for accreditation standards.
In some cases, this work resulted in dual supervision by a preceptor of the same discipline (to meet requirements for coding/billing and home program supervision) and clinical supervision by a preceptor of a different discipline (eg, in team meetings or in clinical case reviews during protected IPE time). Preceptors from each discipline met regularly to discuss challenges in cross-disciplinary supervision, review scope-of-practice issues, share information on discipline-specific training, and revise supervisory procedures.
Interprofessional education activities during weekly protected time were designed to improve collaboration and to challenge trainees to examine traditional hierarchical roles and patterns of communication in health care. An emphasis on case-based learning in small groups encouraged trainees to share perspectives on their discipline-specific approach to assessment and treatment planning. Motivational interviewing training, one of the IPE experiences most valued by trainees and staff, created the opportunity for a truly shared learning environment, as trainees largely started at about the same skill level despite having different educational backgrounds. Group supervision of MI recordings offered trainees the opportunity to learn from each other and develop comfort in offering and receiving interprofessional constructive feedback.
Limitations
There were considerable methodologic limitations in the authors’ efforts to evaluate the impact of this training program on trainee attitudes and skills in collaborative team-based practice. Although trainee surveys revealed highly positive attitudes and beliefs about team-based care as well as perceived competence in collaborative practice, these were not validated surveys, and changes could not be accurately measured over time (trainees were not assessed at baseline). Trainees also were involved in other clinical teams within the VA during the year, and it is difficult to assess the specific impact of their PC-MHI IPE experiences. The PC-MHI staff evaluations of trainee competence in collaborative team-based practice were largely observational and potentially vulnerable to biases, as the staff evaluating trainee competence also were part of the IPE program planning process and invested in its success.
To address these limitations in the future, the authors will use better assessment tools at baseline and end of year to more effectively evaluate the impact of the training program on teamwork skills as well changes in attitudes and beliefs about interprofessional learning and teamwork. The Attitudes Toward Interprofessional Health Care Teams Scale and the Perceptions of Effective Interpersonal Teams Scale should be considered as they have published reliability and validity.27,28 The authors could improve the reliability and depth of trainee evaluations with use of a “360-degree evaluation” model for trainee evaluations that includes other PACT members (beyond PC-MHI staff) as well as veterans.
Assessment of MI skills and competency was limited by use of both live- and simulated-patient recordings. Simulation is a valuable learning tool but often does not accurately represent actual clinical situations and challenges. To appropriately assess MI competence, future MI training should emphasize live-patient recordings over simulated-patient visits. Furthermore, whereas trainees reached competency in several MI coding items, none reached competency in the reflection-to-question ratio, and only about half reached competency in percentage of complex reflections. Future MI training will need to focus on further development of reflection skills.
Trainee intentions to remain involved in program improvement and collaborative team-based care in future professional work were core attitudinal learning objectives, but neither was adequately assessed in end-of-year surveys. Ideally, future evaluations will assess subjective trainee intentions and goals around team-based work and objectively measure future professional choices and activities. For example, it would be interesting to determine whether trainees who participated in this program will choose to practice in an interprofessional team-based model or participate in program improvement activities.
Last, the absence of psychology interns was considered a weakness in the learning environment, resulting in a relatively “prescriber-heavy” balance in discipline perspectives for IPE-focused case discussions and other training. Furthermore, the discipline representation in the IPE program did not exemplify the typical PC-MHI team in most VA clinic settings and community practices in which psychology has a strong presence. Adding psychology trainees was an important goal for the IPE program leadership. In 2015, WSMMVH was awarded additional funding for a PACT PC-MHI predoctoral psychology intern through the phase 4 MHEEI. The PC-MHI track psychology intern joined the IPE program in the 2016-2017 training year.
Conclusion
There is broad consensus that interprofessional team-based practice is crucial for providers in the VA and all health care systems. Primary care-mental health integration is an area of VA care in which interprofessional collaboration is uniquely important to implementation and sustainability of the model. Interprofessional education is an effective approach for preparing HCPs for team-based practice, but implementation is challenging. Several factors crucially contributed to the successful implementation of this program: collaboration of the interprofessional planning team with representation from key stakeholders in different departments and training programs; a well-established PACT PC-MHI team with experience in collaborative team-based care; a curriculum structure that emphasized experiential educational strategies designed to promote interprofessional learning and communication; VA leadership support at the national level (MHEEI funding) and local level; and PACT PC-MHI clinical staff committed to teaching and to the IPE mission.
Over the past 10 years, the VHA has been a national leader in primary care-mental health integration (PC-MHI) within patient aligned care teams (PACTs).1,2 Studies of the PC-MHI collaborative care model consistently have shown increased access to MH services, higher levels of MH treatment engagement, improved MH treatment outcomes, and high patient and provider satisfaction.3-7 Primary care-mental health integration relies heavily on interprofessional team-based practice with providers from diverse educational and clinical backgrounds who work together to deliver integrated mental and behavioral health services within PACTs. This model requires a unique blending of professional cultures and communication and practice styles.
To sustain PC-MHI in PACT, health care professionals (HCPs) must be well trained to work effectively in interprofessional teams. Across health care organizations, training in collaborative interprofessional team-based practice has been identified as an important and challenging task.8-11
Integrating educational experiences among different HCP learners is an approach to developing competency in interprofessional collaboration early in training. The World Health Organization defined interprofessional education (IPE) as occurring “when students from two or more professions learn about, from, and with each other to enable effective collaboration and improve health outcomes.”9 Fundamental to this definition is the belief that interaction among learners from different disciplines during their training develops competency in subsequent effective collaborative practice. Studies of IPE in MH professional training have found that prelicensure IPE contributes to increased knowledge of roles and responsibilities of different disciplines, improved interprofessional communication and attitudes, and increased willingness to work in teams.12-17
Interprofessional education is a valuable training model, but developing interprofessional learning experiences in a system of diverse and often siloed training programs is difficult. More information about design and implementation of IPE training experiences is needed, particularly in outpatient settings in which integration of traditionally separate discipline-specific care is central to the health care mission. The VA PACT PC-MHI is a strong team-based care model that represents a unique opportunity for training across disciplines in interprofessional collaborative care.
To find innovative approaches to meeting the need for IPE in PACT PC-MHI, the authors developed a new IPE program in PC-MHI at the William S. Middleton Memorial Veterans Hospital (WSMMVH) in Madison, Wisconsin. This article reviews the development, implementation, and first-year evaluation of the training program and discusses the challenges and the IPE areas in need of improvement in PACT PC-MHI.
Methods
In 2012, the VHA launched phase 1 of the Mental Health Education Expansion Initiative (MHEEI), a collaboration of the Office of Academic Affiliations (OAA), VHA Mental Health Services (VHA-MHS), and the Office of Mental Health Operations (OMHO).18 The MHEEI was intended to “increase expertise in critical areas of need, expand the recruitment pipeline of well-trained, highly qualified health care providers in behavioral and mental health disciplines, and promote the utilization of interprofessional team-based care.”18 In response, WSMMVH organized a planning committee and submitted a funding request through the section of MHEEI called PACT With Integrated Behavioral Health Providers. The planning committee included training program directors and staff from psychiatry, pharmacy, social work, psychology, and primary care. The authors received funding for trainees in psychiatry (postgraduate year 4 [PGY-4]), pharmacy/MH residency (PGY-2), pharmacy/ambulatory care (PGY-1), and social work (interns).
Curriculum Development
The planning committee met regularly for 6 months to develop the organization, learning objectives, educational strategies, and implementation plan for the IPE program. The program was organized as a 4- to 12-month clinical rotation with the PC-MHI team in PACT, combined with 12 months of protected weekly IPE time (Table 1).
Learning Objectives
To better understand the educational needs and foci for learning objectives, the interprofessional planning committee reviewed guidelines on training in integrated care and collaborative team-based practice.2,9,10,19-21 These guidelines were compared with existing training opportunities for each discipline to identify training gaps and needs.
Learning objectives were organized into 3 domains: patient-centered PC-MHI, collaborative team-based practice, and population health and program improvement. Table 2 outlines the shared learning objectives linked to each domain that were common to the psychiatry, pharmacy, and social work disciplines. Although many of the learning objectives were shared among all disciplines, each trainee also had discipline-specific clinical activities and learning objectives. Psychiatry and pharmacy residents focused on primary care psychiatric medication consultation and care management for antidepressant medication starts. Social work interns focused on psychosocial and functional assessment and brief problem-focused psychotherapies. Learning objectives were met through direct veteran care in the primary care clinic as part of the PACT PC-MHI team and through interprofessional learning activities during protected weekly education time.
Implementation
Critical stakeholders in implementing the IPE program involved themselves early and throughout the planning process. Stakeholders included VAMC leadership, primary care and MH service line chiefs and clinic managers, training program directors, and PACT staff. Planning committee members gave presentations on the IPE program at MH service line and PACT meetings in the 2 months before program initiation in order to orient staff to learning objectives, program structure, and impact on PACT PC-MHI operations. Throughout the first year, the planning committee continued to meet every 2 weeks to review progress, solve implementation problems, and revise learning objectives and activities.
Trainee Clinical Activities
A wide range of educational strategies were planned to meet learning objectives across the 3 domains. There was strong emphasis on experiential learning through daily PACT and PC-MHI clinical work, team huddles and meetings, and trainee-led program improvement projects.
Psychiatry and PGY-2 pharmacy/MH residents focused on direct and indirect medication consultation and problem-focused assessments. Their clinical activities included PC-MHI medication evaluation and follow-up visits; chart reviews and e-consults for medication recommendations to PACT providers; reviews of care management data and consultations on veterans enrolled in depression and anxiety care management; “curbside consultations” for providers in PACT huddles and meetings and throughout the clinic day; and “warm handoffs,” same-day initial PC-MHI problem-focused assessments performed on PACT provider request. The residents were part of a pool of staff and trainees who performed these assessments.
PGY-1 pharmacy residents made care management phone calls for antidepressant trials for depression and anxiety. These residents were trained in motivational interviewing (MI). They applied their MI skills during care management calls focused on medication adherence and behavioral interventions for depression (eg, exercise, planning pleasurable activity) and during other clinical rotations, including tobacco cessation and medication management for diabetes and hypertension. Particularly challenging veteran cases from these clinics were cosupervised with medication management and PC-MHIstaff for added consultation on engagement, behavior change, and treatment plan adherence.
Social work interns completed initial PC-MHI psychosocial and functional assessments by phone and directly by same-day warm handoffs from PACT staff. The PC-MHI therapies they provided included problem-solving therapy, behavioral activation, stress management based on cognitive behavioral therapy, and brief alcohol interventions.
Group IPE Activities
All trainees had a weekly protected block of 3 hours during which they came together for group IPE that was designed to elicit active participation; facilitate interprofessional communication; and develop an understanding of and respect for the knowledge, culture, and practice style of the different disciplines.
Trainees participated in a Herrmann Brain Dominance Instrument (HBDI) workshop focused on developing a better understanding of individual differences in thinking and problem solving, with the goal of improving communication and learning within teams.22 In a seminar series on professionalism and boundaries in health care, trainees from each discipline gave a presentation on the traditional structure and content of their discipline’s training and discussed similarities and differences in their disciplines’ professional oaths, codes of ethics, and boundary guidelines.
Motivational interviewing training was conducted early in the year so trainees would be prepared to apply MI skills in their daily PACT PC-MHI clinical work. Motivational inteviewing is a patient-centered approach to engaging patients in health promoting behavior change. It is defined as a “directive, client-centered counseling style for eliciting behavior change by helping clients to explore and resolve ambivalence.”23
Trainees recorded MI sessions with at least 2 live-patient visits and at least 2 simulated-patient interviews (with staff serving as patient actors). The structure of MI training and supervision was deliberately designed to facilitate interprofessional communication and learning. In accord with a group supervision model for MI recorded reviews, the trainees presented their tapes to the entire learning group in the presence of a facilitating supervisor. Trainees had the opportunity to observe different interview styles and exchange feedback within a peer group of interprofessional learners.
Seminars were focused on core PC-MHI clinical content (eg, depression, anxiety, alcohol use disorders) and organized around case-based learning. Trainees divided into small teams in which representatives of each discipline offered their perspective on how to approach planning patient assessment and treatment. During the seminars, the authors engaged trainees as teachers and leaders whenever possible. All trainees presented on a topic in which they had some discipline expertise. For example, social work interns led a seminar on support and social services for victims of domestic violence, and PGY-1 pharmacy/ambulatory care residents led seminars and a panel management project focused on diabetes and depression.
Trainees participated in several PACT PC-MHI projects focused on population- and measurement-based care, panel management, and program improvement (Table 3). Protected IPE time was used to teach trainees about population health principles and different tools for process improvement (eg, Vision-Analysis Team-Aim-Map-Measure-Change-Sustain) and provide a forum in which trainees could share their work with one another.
Evaluations
Several tools were used for trainee and program evaluations. Clinical skills were evaluated during daily supervision. Trainees began the year with PC-MHI staff directly observing all their clinical contacts with veterans. Staff evaluated and offered feedback on trainee clinical interviewing and on assessment and treatment planning skills. Once they were assessed to be ready to see veterans on their own, trainees were advanced by staff to “drop-in” direct supervision: Toward the end of a veteran’s visit, a staff preceptor entered the room to review relevant clinical findings, assessment and finalized treatment planning with the trainee and veteran. When appropriate for trainee competence level, clinical contacts were indirectly supervised: Trainees discussed their assessment and treatment plan with a staff supervisor at the end of the day.
Motivational interviewing recordings were reviewed during group supervision. To objectively evaluate MI skills, supervisors who were VA-certified in MI used the Motivational Interviewing Treatment Integrity (MITI) coding tool to review and code both the live- and simulated-patient recordings.24 The MITI coding involves quantitative and qualitative analysis using standardized coding items.
Quantitative items included percentage of open-ended questions (Proficiency: 50%; competency: 70%); percentage of reflections considered complex reflections, or reflective statements adding substantial meaning or emphasis and conveying a deeper or more complex picture of what patients say (Proficiency: 40%; competency: 50%); reflection-to-question ratio (Proficiency: 1:1; competency: 2:1); and percentage of MI-adherent provider statements (Proficiency: 90%; competency: 100%).
Qualitative coding items were a global rating of therapist “empathy,” which evaluated the extent to which the trainee understood or made an effort to grasp the patient’s perspective, and “MI spirit.” This coding intended to capture the overall competence of the trainee in emphasizing collaboration, patient autonomy, and evocation of the patient experience (Proficiency score: 5; competency score: 6).
The PC-MHI teaching staff met midyear and end of year as a team to complete trainee evaluations focused on the 3 areas of learning objectives: patient-centered PC-MHI, collaborative team-based practice, and population health and program improvement. Patient-centered PC-MHI involves direct observation and supervision of trainee clinical contacts with veterans, including assessment and treatment planning, clinical documentation, and review of live- and simulated-patient MI recordings. Collaborative team-based practice involves review of trainee participation in day-to-day teamwork, huddles, team meetings, and IPE activities. Population health and program improvement involves review of trainee work on a panel measurement-based care management or program improvement project. In each learning objectives area, trainees were rated on a 3-point scale: needs improvement (1); satisfactory (2); achieved (3). Core knowledge about PC-MHI evidence base, structure, and clinical topics was assessed with case-based written examination at midyear and end of year.
Surveys and qualitative interviews were used to assess trainee perceptions about the IPE program. A midyear and end-of-year survey assessed trainee satisfaction and perceived efficacy of the IPE training program in meeting core learning objectives. A midyear survey designed by pharmacy residents as part of their program improvement project evaluated attitudes around interprofessional learning and team practice. Trainees met individually with the PC-MHI IPE director at midyear and end of year to gather qualitative feedback on the IPE program.
Outcomes
All trainees advanced to the expected level of supervision for clinical contacts (drop-in or indirect clinical supervision). Over the year, there was significant improvement in trainees’ MI skills as measured by MITI coding of at least 2 live-patient or 2 simulated-patient recordings (Figures 1A and 1B). By end of year, most trainees had reached proficiency or competency in several MITI coded items: percentage of open-ended questions (4/12 proficient, 8/12 competent), percentage of complex reflections (2/12 less than proficient, 3/12 proficient, 7/12 competent), MI adherence (1/12 proficient, 11/12 competent), global empathy rating (2/12 proficient, 10/12 competent), and global MI spirit rating (12/12 competent). Average reflection-to-question ratio for the trainee group increased from 0.63 to 0.96 from midyear to end of year, but only 3 of 12 trainees reached the proficiency level of a 1:1 ratio, and no trainee reached the competency level of a 2:1 ratio.
According to the PC-MHI team’s midyear evaluation, most trainees were already making satisfactory progress in the 3 domains of learning objectives for the training program. At end of year, 13 of 14 trainees were assessed as competent in all 3 domains (Figures 2A and B). All trainees passed the midyear and end-of-year written examinations with overall high scores (average score, 82%) demonstrating acquisition of core PC-MHI clinical knowledge.
Trainee evaluations of the IPE program were overall highly favorable at both midyear and at end of year. Trainees rated the program effective or extremely effective in developing their skills in patient-centered care, interprofessional communication, and collaborative team-based practice. They also rated the program highly effective in preparing them to use team-based practice skills in other settings. On a midyear survey, trainees moderately to strongly agreed with several positive beliefs and attitudes about team-based care.
In qualitative interviews at program completion, trainees across disciplines rated the MI training with group supervision as one of their most valuable interprofessional learning experiences. Other highly valued training experiences were PACT PC-MHI panel management projects, team-based clinical case reviews, and cross-disciplinary supervision.
Discussion
This article describes the successful development and implementation of a VA-based IPE program in PACT PC-MHI. Interprofessional clinical training and educational experiences were highly valued, and trainees identified positive attitudes and improved skills related to team-based care. These findings support previous findings that IPE is associated with high satisfaction and positive attitudes toward team-based collaborative practice.12-17 Program implementation presented several challenges: nonsynchronous academic calendars and rotation schedules, cross-disciplinary supervision regulations, variations in clinical and supervisory requirements for accreditation standards, the traditional health care hierarchy, and measurement of the impact of IPE experiences.11,25,26
Rotation schedules and academic calendars varied across the psychiatry, pharmacy, and social work home programs. Organizing different trainee rotation schedules was a significant challenge. Collaboration with training directors and support staff was crucial in planning rotations that offered a longitudinal training experience in PACT PC-MHI. Given the participants’ different starting dates, protected IPE time early in the calendar year was focused on developing clinical skills specific to the pharmacy and psychiatry trainees who would be starting in July, and IPE activities that required the presence of all trainee disciplines (eg, MI training, HBDI) were planned for after the September start of the social work interns.
Cross-disciplinary supervision was highly valued by trainees because it offered exposure to the disciplines’ different communication styles and approaches to clinical assessment and decision making. Throughout the year, however, trainees encountered several obstacles to cross-disciplinary supervision, with respect to coding/billing and home program supervisory policies. The authors worked closely with the VA administration and each training program to develop and revise supervising policies and procedures to meet the necessary administrative and program supervisory requirements for accreditation standards.
In some cases, this work resulted in dual supervision by a preceptor of the same discipline (to meet requirements for coding/billing and home program supervision) and clinical supervision by a preceptor of a different discipline (eg, in team meetings or in clinical case reviews during protected IPE time). Preceptors from each discipline met regularly to discuss challenges in cross-disciplinary supervision, review scope-of-practice issues, share information on discipline-specific training, and revise supervisory procedures.
Interprofessional education activities during weekly protected time were designed to improve collaboration and to challenge trainees to examine traditional hierarchical roles and patterns of communication in health care. An emphasis on case-based learning in small groups encouraged trainees to share perspectives on their discipline-specific approach to assessment and treatment planning. Motivational interviewing training, one of the IPE experiences most valued by trainees and staff, created the opportunity for a truly shared learning environment, as trainees largely started at about the same skill level despite having different educational backgrounds. Group supervision of MI recordings offered trainees the opportunity to learn from each other and develop comfort in offering and receiving interprofessional constructive feedback.
Limitations
There were considerable methodologic limitations in the authors’ efforts to evaluate the impact of this training program on trainee attitudes and skills in collaborative team-based practice. Although trainee surveys revealed highly positive attitudes and beliefs about team-based care as well as perceived competence in collaborative practice, these were not validated surveys, and changes could not be accurately measured over time (trainees were not assessed at baseline). Trainees also were involved in other clinical teams within the VA during the year, and it is difficult to assess the specific impact of their PC-MHI IPE experiences. The PC-MHI staff evaluations of trainee competence in collaborative team-based practice were largely observational and potentially vulnerable to biases, as the staff evaluating trainee competence also were part of the IPE program planning process and invested in its success.
To address these limitations in the future, the authors will use better assessment tools at baseline and end of year to more effectively evaluate the impact of the training program on teamwork skills as well changes in attitudes and beliefs about interprofessional learning and teamwork. The Attitudes Toward Interprofessional Health Care Teams Scale and the Perceptions of Effective Interpersonal Teams Scale should be considered as they have published reliability and validity.27,28 The authors could improve the reliability and depth of trainee evaluations with use of a “360-degree evaluation” model for trainee evaluations that includes other PACT members (beyond PC-MHI staff) as well as veterans.
Assessment of MI skills and competency was limited by use of both live- and simulated-patient recordings. Simulation is a valuable learning tool but often does not accurately represent actual clinical situations and challenges. To appropriately assess MI competence, future MI training should emphasize live-patient recordings over simulated-patient visits. Furthermore, whereas trainees reached competency in several MI coding items, none reached competency in the reflection-to-question ratio, and only about half reached competency in percentage of complex reflections. Future MI training will need to focus on further development of reflection skills.
Trainee intentions to remain involved in program improvement and collaborative team-based care in future professional work were core attitudinal learning objectives, but neither was adequately assessed in end-of-year surveys. Ideally, future evaluations will assess subjective trainee intentions and goals around team-based work and objectively measure future professional choices and activities. For example, it would be interesting to determine whether trainees who participated in this program will choose to practice in an interprofessional team-based model or participate in program improvement activities.
Last, the absence of psychology interns was considered a weakness in the learning environment, resulting in a relatively “prescriber-heavy” balance in discipline perspectives for IPE-focused case discussions and other training. Furthermore, the discipline representation in the IPE program did not exemplify the typical PC-MHI team in most VA clinic settings and community practices in which psychology has a strong presence. Adding psychology trainees was an important goal for the IPE program leadership. In 2015, WSMMVH was awarded additional funding for a PACT PC-MHI predoctoral psychology intern through the phase 4 MHEEI. The PC-MHI track psychology intern joined the IPE program in the 2016-2017 training year.
Conclusion
There is broad consensus that interprofessional team-based practice is crucial for providers in the VA and all health care systems. Primary care-mental health integration is an area of VA care in which interprofessional collaboration is uniquely important to implementation and sustainability of the model. Interprofessional education is an effective approach for preparing HCPs for team-based practice, but implementation is challenging. Several factors crucially contributed to the successful implementation of this program: collaboration of the interprofessional planning team with representation from key stakeholders in different departments and training programs; a well-established PACT PC-MHI team with experience in collaborative team-based care; a curriculum structure that emphasized experiential educational strategies designed to promote interprofessional learning and communication; VA leadership support at the national level (MHEEI funding) and local level; and PACT PC-MHI clinical staff committed to teaching and to the IPE mission.
1. Wray LO, Szymanski BR, Kearney LK, McCarthy JF. Implementation of primary care-mental health integration services in the Veterans Health Administration: program activity and associations with engagement in specialty mental health services. J Clin Psychol Med Settings. 2012;19(1):105-116.
2. Kearney LK, Post EP, Pomerantz AS, Zeiss AM. Applying the interprofessional patient aligned care team in the Department of Veterans Affairs: transforming primary care. Am Psychol. 2014;69(4):399-408.
3. Gilbody S, Bower P, Fletcher J, Richards D, Sutton AJ. Collaborative care for depression: a cumulative meta-analysis and review of loner-term outcomes. Arch Intern Med. 2006;166(21):2314-2321.
4. Unützer J, Katon W, Callahan CM, et al; IMPACT (Improving Mood-Promoting Access to Collaborative Treatment) Investigators. Collaborative care management in late-life depression in the primary care setting: a randomized control trial. JAMA. 2002;288(22):2836-2845.
5. Katon W, Unützer J. Consultation psychiatry in the medical home and accountable care organizations: achieving the triple aim. Gen Hosp Psychiatry. 2011;3(4):305-310.
6. Bruce ML, Tenhave TR, Reynolds CF III, et al. Reducing suicidal ideation and depressive symptoms in depressed older primary care patients: a randomized controlled trial. JAMA. 2004;291(9):1081-1091.
7. Alexopoulos GS, Reynolds CF III , Bruce ML, et al; PROSPECT Group. Reducing suicidal ideation and depression in older primary care patients: 24-month outcomes of the PROSPECT study. Am J Psychiatry. 2009;166(8):882-890.
8. Cox M, Cuff P, Brandt B, Reeves S, Zierler B. Measuring the impact of interprofessional education on collaborative practice and patient outcomes. J Interprof Care. 2016;30(1):1-3.
9. World Health Organization, Study Group on Interprofessional Education and Collaborative Practice. Framework for Action on Interprofessional Education and Collaborative Practice. Geneva, Switzerland: World Health Organization; 2010.
10. Interprofessional Education Collaborative Expert Panel. Core Competencies for Interprofessional Collaborative Practice: Report of an Expert Panel. Washington, DC: Interprofessional Education Collaborative; 2011.
11. Blue AV, Mitcham M, Smith T, Raymond J, Greenburg R. Changing the future of health professions: embedding interprofessional education within an academic health center. Acad Med. 2010;85(8):1290-1295.
12. Priest HM, Roberts P, Dent H, Blincoe C, Lawton D, Armstrong C. Interprofessional education and working in mental health: in search of the evidence base. J Nurs Manag. 2008;16(4):474-485.
13. Reeves S. A systematic review of the effects of interprofessional education on staff involved in the care of adults with mental health problems. J Psychiatr Ment Health Nurs. 2001;8(6):533-542.
14. Carpenter J, Barnes D, Dickinson C, Wooff D. Outcomes of interprofessional education for community mental health services in England: the longitudinal evaluation of a postgraduate programme. J Interprof Care. 2006;20(2):145-161.
15. Hammick M, Freeth D, Koppel I, Reeves S, Barr H. A best evidence systematic review of interprofessional education: BEME guide no. 9. Med Teach. 2007;29(8):735-751.
16. Pauzé E, Reeves S. Examining the effects of interprofessional education on mental health providers: findings from an updated systematic review. J Ment Health. 2010;19(3):258-271.
17. Curran V, Heath O, Adey T, et al. An approach to integrating interprofessional education in collaborative mental health care. Acad Psychiatry. 2012;36(2):91-95.
18. Veterans Health Administration. VA Interprofessional Mental Health Education Expansion Initiative, Phase I. Washington, DC; Department of Veterans Affairs; 2012.
19. Dundon M, Dollar K, Schohn M, Lantinga LJ. Primary care–mental health integration: co-located, collaborative care: an operations manual. https://www.mirecc.va.gov/cih-visn2/Documents/Clinical/MH-IPC_CCC_Operations_Manual_Version_2_1.pdf. Published February 2011. Accessed May 19, 2017.
20. McDaniel SH, Grus CL, Cubic BA, et al. Competencies for psychology practice in primary care. Am Psychol. 2014;69(4):409-429.
21. Cowley D, Dunaway K, Forstein M, et al. Teaching psychiatry residents to work at the interface of mental health and primary care. Acad Psychiatry. 2014;38(4):398-404.
22. Herrmann N. The creative brain. J Creat Behav. 1991;25:275-295.
23. Rollnick S, Miller WR. What is motivational interviewing? Behav Cogn Psychother. 1995;23(4):325-334.
24. Pierson HM, Hayes SC, Gifford EV, et al. An examination of the Motivational Interviewing Treatment Integrity code. J Subst Abuse Treat. 2007;32(1):11-17.
25. Shaw D, Blue A. Should psychiatry champion interprofessional education? Acad Psychiatry. 2012;36(3):163-166.
26. Gilbert JH. Interprofessional learning and higher education structural barriers. J Interprof Care. 2005;19(suppl 1):87-106.
27. Heinemann GD, Schmitt MH, Farrell PP, Brallier SA. Development of an Attitudes Toward Health Care Teams Scale. Eval Health Prof. 1999;22(1):123-142.
28. Hepburn K, Tsukuda RA, Fasser C. Team Skills Scale. In: Heinemann GD, Zeiss AM, eds. Team Performance in Healthcare: Assessment and Development. New York, NY: Kluwer Academic/Plenum; 2002:159-163.
1. Wray LO, Szymanski BR, Kearney LK, McCarthy JF. Implementation of primary care-mental health integration services in the Veterans Health Administration: program activity and associations with engagement in specialty mental health services. J Clin Psychol Med Settings. 2012;19(1):105-116.
2. Kearney LK, Post EP, Pomerantz AS, Zeiss AM. Applying the interprofessional patient aligned care team in the Department of Veterans Affairs: transforming primary care. Am Psychol. 2014;69(4):399-408.
3. Gilbody S, Bower P, Fletcher J, Richards D, Sutton AJ. Collaborative care for depression: a cumulative meta-analysis and review of loner-term outcomes. Arch Intern Med. 2006;166(21):2314-2321.
4. Unützer J, Katon W, Callahan CM, et al; IMPACT (Improving Mood-Promoting Access to Collaborative Treatment) Investigators. Collaborative care management in late-life depression in the primary care setting: a randomized control trial. JAMA. 2002;288(22):2836-2845.
5. Katon W, Unützer J. Consultation psychiatry in the medical home and accountable care organizations: achieving the triple aim. Gen Hosp Psychiatry. 2011;3(4):305-310.
6. Bruce ML, Tenhave TR, Reynolds CF III, et al. Reducing suicidal ideation and depressive symptoms in depressed older primary care patients: a randomized controlled trial. JAMA. 2004;291(9):1081-1091.
7. Alexopoulos GS, Reynolds CF III , Bruce ML, et al; PROSPECT Group. Reducing suicidal ideation and depression in older primary care patients: 24-month outcomes of the PROSPECT study. Am J Psychiatry. 2009;166(8):882-890.
8. Cox M, Cuff P, Brandt B, Reeves S, Zierler B. Measuring the impact of interprofessional education on collaborative practice and patient outcomes. J Interprof Care. 2016;30(1):1-3.
9. World Health Organization, Study Group on Interprofessional Education and Collaborative Practice. Framework for Action on Interprofessional Education and Collaborative Practice. Geneva, Switzerland: World Health Organization; 2010.
10. Interprofessional Education Collaborative Expert Panel. Core Competencies for Interprofessional Collaborative Practice: Report of an Expert Panel. Washington, DC: Interprofessional Education Collaborative; 2011.
11. Blue AV, Mitcham M, Smith T, Raymond J, Greenburg R. Changing the future of health professions: embedding interprofessional education within an academic health center. Acad Med. 2010;85(8):1290-1295.
12. Priest HM, Roberts P, Dent H, Blincoe C, Lawton D, Armstrong C. Interprofessional education and working in mental health: in search of the evidence base. J Nurs Manag. 2008;16(4):474-485.
13. Reeves S. A systematic review of the effects of interprofessional education on staff involved in the care of adults with mental health problems. J Psychiatr Ment Health Nurs. 2001;8(6):533-542.
14. Carpenter J, Barnes D, Dickinson C, Wooff D. Outcomes of interprofessional education for community mental health services in England: the longitudinal evaluation of a postgraduate programme. J Interprof Care. 2006;20(2):145-161.
15. Hammick M, Freeth D, Koppel I, Reeves S, Barr H. A best evidence systematic review of interprofessional education: BEME guide no. 9. Med Teach. 2007;29(8):735-751.
16. Pauzé E, Reeves S. Examining the effects of interprofessional education on mental health providers: findings from an updated systematic review. J Ment Health. 2010;19(3):258-271.
17. Curran V, Heath O, Adey T, et al. An approach to integrating interprofessional education in collaborative mental health care. Acad Psychiatry. 2012;36(2):91-95.
18. Veterans Health Administration. VA Interprofessional Mental Health Education Expansion Initiative, Phase I. Washington, DC; Department of Veterans Affairs; 2012.
19. Dundon M, Dollar K, Schohn M, Lantinga LJ. Primary care–mental health integration: co-located, collaborative care: an operations manual. https://www.mirecc.va.gov/cih-visn2/Documents/Clinical/MH-IPC_CCC_Operations_Manual_Version_2_1.pdf. Published February 2011. Accessed May 19, 2017.
20. McDaniel SH, Grus CL, Cubic BA, et al. Competencies for psychology practice in primary care. Am Psychol. 2014;69(4):409-429.
21. Cowley D, Dunaway K, Forstein M, et al. Teaching psychiatry residents to work at the interface of mental health and primary care. Acad Psychiatry. 2014;38(4):398-404.
22. Herrmann N. The creative brain. J Creat Behav. 1991;25:275-295.
23. Rollnick S, Miller WR. What is motivational interviewing? Behav Cogn Psychother. 1995;23(4):325-334.
24. Pierson HM, Hayes SC, Gifford EV, et al. An examination of the Motivational Interviewing Treatment Integrity code. J Subst Abuse Treat. 2007;32(1):11-17.
25. Shaw D, Blue A. Should psychiatry champion interprofessional education? Acad Psychiatry. 2012;36(3):163-166.
26. Gilbert JH. Interprofessional learning and higher education structural barriers. J Interprof Care. 2005;19(suppl 1):87-106.
27. Heinemann GD, Schmitt MH, Farrell PP, Brallier SA. Development of an Attitudes Toward Health Care Teams Scale. Eval Health Prof. 1999;22(1):123-142.
28. Hepburn K, Tsukuda RA, Fasser C. Team Skills Scale. In: Heinemann GD, Zeiss AM, eds. Team Performance in Healthcare: Assessment and Development. New York, NY: Kluwer Academic/Plenum; 2002:159-163.
Getting a Candle on Her Condition
A 15-year-old girl is brought in by her mother for evaluation of a rash that developed following a “candling” treatment she underwent two weeks ago at a beauty spa.
The treatment, which was performed to eliminate scaling in her external ear canal, involved dripping hot wax from a burning candle into the external auditory meatus. The cooled wax was peeled away, along with the attached scaling. A new, asymptomatic, scaly rash has since appeared in the same area—far worse than the original.
There is no history of recent infection or joint pain, or family history of skin disease.
EXAMINATION
Heavy, uniform, white scaling on a salmon-colored base covers the external auditory meatus, extending 3 or 4 mm into the concha. Similar, milder changes are observed in the left ear.

There are scattered pits in three fingernails, white scaling in the scalp above and behind both ears, and faint pink scaly patches on both knees and elbows.
What is the diagnosis?
DISCUSSION
Psoriasis is extremely common, affecting about 3% of the white population in this country, and is one of a handful of conditions that manifest with the Koebner phenomenon. This means that any trauma (ie, scrapes, burns, scratches, or cuts) can trigger or extend the condition. In this case, the hot wax was likely the culprit.
The patient’s primary care provider, it turns out, was treating the elbow and knee rashes with antifungal creams (to no avail). He hadn’t made the connection between her various skin problems. It was the acute manifestation in the ear that prompted a broader assessment of the patient’s condition—proving the maxim that to find a diagnosis, you have to look for it.
Given its mild nature, this patient’s condition was easily treated with topical steroids and vitamin D-derived cream (calcipotriene). She was advised of the need to avoid exacerbating factors, such as smoking, obesity, excess alcohol intake, and stress.
There is the possibility of the disease worsening despite treatment. The patient also has about a 25% chance of developing psoriatic arthropathy. For these reasons, she will need to be followed by dermatology.
TAKE-HOME LEARNING POINTS
- Psoriasis, though very common, does not always manifest in its typical form.
- Any trauma (ie, burn, scrape, or cut) can trigger preexisting psoriasis, a response called the Koebner phenomenon.
- Several other conditions—including lichen planus, warts, and molluscum—can exhibit this same phenomenon.
- When psoriasis is suspected, potential corroboratory sites of involvement (eg, knees, elbows, nails, and scalp) should be examined. Biopsy is often needed to confirm the diagnosis.
A 15-year-old girl is brought in by her mother for evaluation of a rash that developed following a “candling” treatment she underwent two weeks ago at a beauty spa.
The treatment, which was performed to eliminate scaling in her external ear canal, involved dripping hot wax from a burning candle into the external auditory meatus. The cooled wax was peeled away, along with the attached scaling. A new, asymptomatic, scaly rash has since appeared in the same area—far worse than the original.
There is no history of recent infection or joint pain, or family history of skin disease.
EXAMINATION
Heavy, uniform, white scaling on a salmon-colored base covers the external auditory meatus, extending 3 or 4 mm into the concha. Similar, milder changes are observed in the left ear.
There are scattered pits in three fingernails, white scaling in the scalp above and behind both ears, and faint pink scaly patches on both knees and elbows.
What is the diagnosis?
DISCUSSION
Psoriasis is extremely common, affecting about 3% of the white population in this country, and is one of a handful of conditions that manifest with the Koebner phenomenon. This means that any trauma (ie, scrapes, burns, scratches, or cuts) can trigger or extend the condition. In this case, the hot wax was likely the culprit.
The patient’s primary care provider, it turns out, was treating the elbow and knee rashes with antifungal creams (to no avail). He hadn’t made the connection between her various skin problems. It was the acute manifestation in the ear that prompted a broader assessment of the patient’s condition—proving the maxim that to find a diagnosis, you have to look for it.
Given its mild nature, this patient’s condition was easily treated with topical steroids and vitamin D-derived cream (calcipotriene). She was advised of the need to avoid exacerbating factors, such as smoking, obesity, excess alcohol intake, and stress.
There is the possibility of the disease worsening despite treatment. The patient also has about a 25% chance of developing psoriatic arthropathy. For these reasons, she will need to be followed by dermatology.
TAKE-HOME LEARNING POINTS
- Psoriasis, though very common, does not always manifest in its typical form.
- Any trauma (ie, burn, scrape, or cut) can trigger preexisting psoriasis, a response called the Koebner phenomenon.
- Several other conditions—including lichen planus, warts, and molluscum—can exhibit this same phenomenon.
- When psoriasis is suspected, potential corroboratory sites of involvement (eg, knees, elbows, nails, and scalp) should be examined. Biopsy is often needed to confirm the diagnosis.
A 15-year-old girl is brought in by her mother for evaluation of a rash that developed following a “candling” treatment she underwent two weeks ago at a beauty spa.
The treatment, which was performed to eliminate scaling in her external ear canal, involved dripping hot wax from a burning candle into the external auditory meatus. The cooled wax was peeled away, along with the attached scaling. A new, asymptomatic, scaly rash has since appeared in the same area—far worse than the original.
There is no history of recent infection or joint pain, or family history of skin disease.
EXAMINATION
Heavy, uniform, white scaling on a salmon-colored base covers the external auditory meatus, extending 3 or 4 mm into the concha. Similar, milder changes are observed in the left ear.
There are scattered pits in three fingernails, white scaling in the scalp above and behind both ears, and faint pink scaly patches on both knees and elbows.
What is the diagnosis?
DISCUSSION
Psoriasis is extremely common, affecting about 3% of the white population in this country, and is one of a handful of conditions that manifest with the Koebner phenomenon. This means that any trauma (ie, scrapes, burns, scratches, or cuts) can trigger or extend the condition. In this case, the hot wax was likely the culprit.
The patient’s primary care provider, it turns out, was treating the elbow and knee rashes with antifungal creams (to no avail). He hadn’t made the connection between her various skin problems. It was the acute manifestation in the ear that prompted a broader assessment of the patient’s condition—proving the maxim that to find a diagnosis, you have to look for it.
Given its mild nature, this patient’s condition was easily treated with topical steroids and vitamin D-derived cream (calcipotriene). She was advised of the need to avoid exacerbating factors, such as smoking, obesity, excess alcohol intake, and stress.
There is the possibility of the disease worsening despite treatment. The patient also has about a 25% chance of developing psoriatic arthropathy. For these reasons, she will need to be followed by dermatology.
TAKE-HOME LEARNING POINTS
- Psoriasis, though very common, does not always manifest in its typical form.
- Any trauma (ie, burn, scrape, or cut) can trigger preexisting psoriasis, a response called the Koebner phenomenon.
- Several other conditions—including lichen planus, warts, and molluscum—can exhibit this same phenomenon.
- When psoriasis is suspected, potential corroboratory sites of involvement (eg, knees, elbows, nails, and scalp) should be examined. Biopsy is often needed to confirm the diagnosis.
Ferrous sulfate bests iron complex in treating IDA in infants, young kids

A trial comparing ferrous sulfate with iron polysaccharide complex to treat infants and young children with nutritional iron-deficiency anemia (IDA) has shown ferrous sulfate to be more effective at raising hemoglobin levels in this population, according to researchers.
Dozens of oral iron supplements exist for IDA treatment, ferrous sulfate being the most commonly used. Iron polysaccharide complex, however, may be better tolerated.
Investigators undertook the BESTIRON study (NCT01904864) to determine whether the iron complex was more efficacious than ferrous sulfate in increasing hemoglobin concentrations in infants and young children aged 9 to 48 months.
Up to 3% of children aged 1 to 2 years in the United States have IDA, as do millions worldwide. IDA is associated with impaired neurodevelopment in the young.
Inadequate dietary iron intake in this group is the most common cause of IDA. It most often results from excessive cow milk consumption and/or prolonged breastfeeding without appropriate iron supplementation.
For this study, investigators randomized 80 infants and young children with nutritional IDA to receive 3 mg/kg of ferrous sulfate (n=40) or iron complex (n=40) drops once daily for 12 weeks.
Patients had to have hemoglobin concentrations of 10 g/dL or less, mean corpuscular volumes of 70 fL or less, reticulocyte hemoglobin equivalents of 25 pg or less, and either serum ferritin level of 15 ng/mL or less or total iron-binding capacity of 425 μg/dL or greater.
And they could have no clinical or laboratory evidence of other causes of anemia.
All 80 patients were included in the primary analysis evaluating change in hemoglobin concentration during the 12 weeks after starting oral iron therapy.
Patient characteristics
Patient characteristics were similar between the groups. The mean age was 23 months and 55% were male.
Most patients (61%) were Hispanic white, 9% were non-Hispanic white, and 11% were black.
Ten patients in the ferrous sulfate group and 8 in the iron complex group had received a packed red blood cell transfusion prior to study enrollment.
Results
Fifty-nine patients completed all study visits, 28 in the ferrous sulfate group and 31 in the iron complex group.
Patients’ mean hemoglobin level in the ferrous sulfate group increased from 7.9 g/dL to 11.9 g/dL over the 12 weeks. In the iron complex group, the patients’ hemoglobin level increased from 7.7 g/dL to 11.1 g/dL.
Using a linear mixed model, the primary outcome demonstrated a significant difference in the change in hemoglobin concentration of 1.0 g/dL (95% CI, 0.4-1.6; P < .001) between the groups, favoring ferrous sulfate.
IDA completely resolved in 8 of 28 (29%) patients in the ferrous sulfate group and 2 of 31 (6%) in the iron complex group (P=0.04).
However, successful administration of the supplement—meaning he child did not spit out the medication—was higher in the iron complex group (94%) than the iron sulfate group (82%), P=0.009.
The median serum ferritin level increased from 3.0 ng/mL to 15.6 ng/mL in the ferrous sulfate arm, which was significantly better than in the iron complex arm, which increased from 2.0 ng/mL to 7.5 ng/mL, P<0.001.
And the mean total iron binding capacity significantly increased in the ferrous sulfate group compared with the iron oxide group (P<0.001).
Safety
The investigators reported that patients treated with iron complex had significantly more diahrrea, while patients treated with ferrous sulfate had more vomiting, although the latter was not statistically significant.
A gastrointestinal adverse effect profile created at the end of the study showed no significant differences between the groups.
The investigators noted a few limitations of the study.
First, it was conducted in a single tertiary-care children’s hospital, the Children’s Medical Center in Dallas, Texas.
Second, a disproportionate number of patients were from lower income and minority families and frequently had severe anemia, with approximately 23% requiring blood transfusion prior to study start.
And third, the trial had a high lost-to-follow-up rate of 25% at the final visit.
So the results may not be generalizable to the general pediatric population.
Nevertheless, the investigators concluded, “Once daily, low-dose ferrous sulfate should be considered for children with nutritional iron-deficiency anemia.”
The team reported their findings in JAMA.
The study was an investigator-initiated trial with sponsorship from Gensavis Pharmaceuticals LLC, the manufacturer of the iron polysaccharide complex used in the trial. The company provided funding for both trial drugs.
The study received additional grant support from the National Center for Advancing Translational Sciences and the National Heart, Lung, and Blood Institute. ![]()
A trial comparing ferrous sulfate with iron polysaccharide complex to treat infants and young children with nutritional iron-deficiency anemia (IDA) has shown ferrous sulfate to be more effective at raising hemoglobin levels in this population, according to researchers.
Dozens of oral iron supplements exist for IDA treatment, ferrous sulfate being the most commonly used. Iron polysaccharide complex, however, may be better tolerated.
Investigators undertook the BESTIRON study (NCT01904864) to determine whether the iron complex was more efficacious than ferrous sulfate in increasing hemoglobin concentrations in infants and young children aged 9 to 48 months.
Up to 3% of children aged 1 to 2 years in the United States have IDA, as do millions worldwide. IDA is associated with impaired neurodevelopment in the young.
Inadequate dietary iron intake in this group is the most common cause of IDA. It most often results from excessive cow milk consumption and/or prolonged breastfeeding without appropriate iron supplementation.
For this study, investigators randomized 80 infants and young children with nutritional IDA to receive 3 mg/kg of ferrous sulfate (n=40) or iron complex (n=40) drops once daily for 12 weeks.
Patients had to have hemoglobin concentrations of 10 g/dL or less, mean corpuscular volumes of 70 fL or less, reticulocyte hemoglobin equivalents of 25 pg or less, and either serum ferritin level of 15 ng/mL or less or total iron-binding capacity of 425 μg/dL or greater.
And they could have no clinical or laboratory evidence of other causes of anemia.
All 80 patients were included in the primary analysis evaluating change in hemoglobin concentration during the 12 weeks after starting oral iron therapy.
Patient characteristics
Patient characteristics were similar between the groups. The mean age was 23 months and 55% were male.
Most patients (61%) were Hispanic white, 9% were non-Hispanic white, and 11% were black.
Ten patients in the ferrous sulfate group and 8 in the iron complex group had received a packed red blood cell transfusion prior to study enrollment.
Results
Fifty-nine patients completed all study visits, 28 in the ferrous sulfate group and 31 in the iron complex group.
Patients’ mean hemoglobin level in the ferrous sulfate group increased from 7.9 g/dL to 11.9 g/dL over the 12 weeks. In the iron complex group, the patients’ hemoglobin level increased from 7.7 g/dL to 11.1 g/dL.
Using a linear mixed model, the primary outcome demonstrated a significant difference in the change in hemoglobin concentration of 1.0 g/dL (95% CI, 0.4-1.6; P < .001) between the groups, favoring ferrous sulfate.
IDA completely resolved in 8 of 28 (29%) patients in the ferrous sulfate group and 2 of 31 (6%) in the iron complex group (P=0.04).
However, successful administration of the supplement—meaning he child did not spit out the medication—was higher in the iron complex group (94%) than the iron sulfate group (82%), P=0.009.
The median serum ferritin level increased from 3.0 ng/mL to 15.6 ng/mL in the ferrous sulfate arm, which was significantly better than in the iron complex arm, which increased from 2.0 ng/mL to 7.5 ng/mL, P<0.001.
And the mean total iron binding capacity significantly increased in the ferrous sulfate group compared with the iron oxide group (P<0.001).
Safety
The investigators reported that patients treated with iron complex had significantly more diahrrea, while patients treated with ferrous sulfate had more vomiting, although the latter was not statistically significant.
A gastrointestinal adverse effect profile created at the end of the study showed no significant differences between the groups.
The investigators noted a few limitations of the study.
First, it was conducted in a single tertiary-care children’s hospital, the Children’s Medical Center in Dallas, Texas.
Second, a disproportionate number of patients were from lower income and minority families and frequently had severe anemia, with approximately 23% requiring blood transfusion prior to study start.
And third, the trial had a high lost-to-follow-up rate of 25% at the final visit.
So the results may not be generalizable to the general pediatric population.
Nevertheless, the investigators concluded, “Once daily, low-dose ferrous sulfate should be considered for children with nutritional iron-deficiency anemia.”
The team reported their findings in JAMA.
The study was an investigator-initiated trial with sponsorship from Gensavis Pharmaceuticals LLC, the manufacturer of the iron polysaccharide complex used in the trial. The company provided funding for both trial drugs.
The study received additional grant support from the National Center for Advancing Translational Sciences and the National Heart, Lung, and Blood Institute. ![]()
A trial comparing ferrous sulfate with iron polysaccharide complex to treat infants and young children with nutritional iron-deficiency anemia (IDA) has shown ferrous sulfate to be more effective at raising hemoglobin levels in this population, according to researchers.
Dozens of oral iron supplements exist for IDA treatment, ferrous sulfate being the most commonly used. Iron polysaccharide complex, however, may be better tolerated.
Investigators undertook the BESTIRON study (NCT01904864) to determine whether the iron complex was more efficacious than ferrous sulfate in increasing hemoglobin concentrations in infants and young children aged 9 to 48 months.
Up to 3% of children aged 1 to 2 years in the United States have IDA, as do millions worldwide. IDA is associated with impaired neurodevelopment in the young.
Inadequate dietary iron intake in this group is the most common cause of IDA. It most often results from excessive cow milk consumption and/or prolonged breastfeeding without appropriate iron supplementation.
For this study, investigators randomized 80 infants and young children with nutritional IDA to receive 3 mg/kg of ferrous sulfate (n=40) or iron complex (n=40) drops once daily for 12 weeks.
Patients had to have hemoglobin concentrations of 10 g/dL or less, mean corpuscular volumes of 70 fL or less, reticulocyte hemoglobin equivalents of 25 pg or less, and either serum ferritin level of 15 ng/mL or less or total iron-binding capacity of 425 μg/dL or greater.
And they could have no clinical or laboratory evidence of other causes of anemia.
All 80 patients were included in the primary analysis evaluating change in hemoglobin concentration during the 12 weeks after starting oral iron therapy.
Patient characteristics
Patient characteristics were similar between the groups. The mean age was 23 months and 55% were male.
Most patients (61%) were Hispanic white, 9% were non-Hispanic white, and 11% were black.
Ten patients in the ferrous sulfate group and 8 in the iron complex group had received a packed red blood cell transfusion prior to study enrollment.
Results
Fifty-nine patients completed all study visits, 28 in the ferrous sulfate group and 31 in the iron complex group.
Patients’ mean hemoglobin level in the ferrous sulfate group increased from 7.9 g/dL to 11.9 g/dL over the 12 weeks. In the iron complex group, the patients’ hemoglobin level increased from 7.7 g/dL to 11.1 g/dL.
Using a linear mixed model, the primary outcome demonstrated a significant difference in the change in hemoglobin concentration of 1.0 g/dL (95% CI, 0.4-1.6; P < .001) between the groups, favoring ferrous sulfate.
IDA completely resolved in 8 of 28 (29%) patients in the ferrous sulfate group and 2 of 31 (6%) in the iron complex group (P=0.04).
However, successful administration of the supplement—meaning he child did not spit out the medication—was higher in the iron complex group (94%) than the iron sulfate group (82%), P=0.009.
The median serum ferritin level increased from 3.0 ng/mL to 15.6 ng/mL in the ferrous sulfate arm, which was significantly better than in the iron complex arm, which increased from 2.0 ng/mL to 7.5 ng/mL, P<0.001.
And the mean total iron binding capacity significantly increased in the ferrous sulfate group compared with the iron oxide group (P<0.001).
Safety
The investigators reported that patients treated with iron complex had significantly more diahrrea, while patients treated with ferrous sulfate had more vomiting, although the latter was not statistically significant.
A gastrointestinal adverse effect profile created at the end of the study showed no significant differences between the groups.
The investigators noted a few limitations of the study.
First, it was conducted in a single tertiary-care children’s hospital, the Children’s Medical Center in Dallas, Texas.
Second, a disproportionate number of patients were from lower income and minority families and frequently had severe anemia, with approximately 23% requiring blood transfusion prior to study start.
And third, the trial had a high lost-to-follow-up rate of 25% at the final visit.
So the results may not be generalizable to the general pediatric population.
Nevertheless, the investigators concluded, “Once daily, low-dose ferrous sulfate should be considered for children with nutritional iron-deficiency anemia.”
The team reported their findings in JAMA.
The study was an investigator-initiated trial with sponsorship from Gensavis Pharmaceuticals LLC, the manufacturer of the iron polysaccharide complex used in the trial. The company provided funding for both trial drugs.
The study received additional grant support from the National Center for Advancing Translational Sciences and the National Heart, Lung, and Blood Institute. ![]()
Itchy nodules on legs

The FP did a 4-mm punch biopsy to confirm that this was a case of prurigo nodularis and prescribed clobetasol cream to be applied twice daily to the pruritic nodules. The FP recommended that the patient apply the cream instead of scratching the area. The FP also said that if the patient couldn’t avoid touching the area, it would be better to lightly rub the area over his clothing instead.
The biopsy results subsequently confirmed a diagnosis of prurigo nodularis. At the patient’s 2-week follow-up, he indicated that his symptoms were 50% better since using the clobetasol. The FP explained to the patient the nature of prurigo nodularis, including the patient’s itch-scratch cycle and how stress was making it worse. The patient acknowledged that his symptoms had become worse when he began having financial trouble. The FP asked the patient if he wanted to see a counselor, but the patient declined, saying that he just needed to get more work.
At a one-month follow-up, 90% of the nodules were resolved, although there were still some stubborn areas that continued to itch. The patient could not control scratching these areas at times. The FP offered intralesional injections with triamcinolone and/or cryotherapy. The patient consented to liquid nitrogen therapy and the remaining nodules were frozen for approximately 10 seconds each using a liquid nitrogen spray.
Four weeks later, the patient had 4 remaining nodules. The FP injected the nodules with 10 mg/mL triamcinolone and refilled the clobetasol cream. At the next appointment, 2 nodules remained. The patient indicated that he would continue using the cream until the nodules went away. In many cases, prurigo nodularis does not respond especially well to treatment, so this patient was fortunate that standard treatments provided a good outcome.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Johnson A. Self-inflicted dermatosis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013: 856-862.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP did a 4-mm punch biopsy to confirm that this was a case of prurigo nodularis and prescribed clobetasol cream to be applied twice daily to the pruritic nodules. The FP recommended that the patient apply the cream instead of scratching the area. The FP also said that if the patient couldn’t avoid touching the area, it would be better to lightly rub the area over his clothing instead.
The biopsy results subsequently confirmed a diagnosis of prurigo nodularis. At the patient’s 2-week follow-up, he indicated that his symptoms were 50% better since using the clobetasol. The FP explained to the patient the nature of prurigo nodularis, including the patient’s itch-scratch cycle and how stress was making it worse. The patient acknowledged that his symptoms had become worse when he began having financial trouble. The FP asked the patient if he wanted to see a counselor, but the patient declined, saying that he just needed to get more work.
At a one-month follow-up, 90% of the nodules were resolved, although there were still some stubborn areas that continued to itch. The patient could not control scratching these areas at times. The FP offered intralesional injections with triamcinolone and/or cryotherapy. The patient consented to liquid nitrogen therapy and the remaining nodules were frozen for approximately 10 seconds each using a liquid nitrogen spray.
Four weeks later, the patient had 4 remaining nodules. The FP injected the nodules with 10 mg/mL triamcinolone and refilled the clobetasol cream. At the next appointment, 2 nodules remained. The patient indicated that he would continue using the cream until the nodules went away. In many cases, prurigo nodularis does not respond especially well to treatment, so this patient was fortunate that standard treatments provided a good outcome.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Johnson A. Self-inflicted dermatosis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013: 856-862.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP did a 4-mm punch biopsy to confirm that this was a case of prurigo nodularis and prescribed clobetasol cream to be applied twice daily to the pruritic nodules. The FP recommended that the patient apply the cream instead of scratching the area. The FP also said that if the patient couldn’t avoid touching the area, it would be better to lightly rub the area over his clothing instead.
The biopsy results subsequently confirmed a diagnosis of prurigo nodularis. At the patient’s 2-week follow-up, he indicated that his symptoms were 50% better since using the clobetasol. The FP explained to the patient the nature of prurigo nodularis, including the patient’s itch-scratch cycle and how stress was making it worse. The patient acknowledged that his symptoms had become worse when he began having financial trouble. The FP asked the patient if he wanted to see a counselor, but the patient declined, saying that he just needed to get more work.
At a one-month follow-up, 90% of the nodules were resolved, although there were still some stubborn areas that continued to itch. The patient could not control scratching these areas at times. The FP offered intralesional injections with triamcinolone and/or cryotherapy. The patient consented to liquid nitrogen therapy and the remaining nodules were frozen for approximately 10 seconds each using a liquid nitrogen spray.
Four weeks later, the patient had 4 remaining nodules. The FP injected the nodules with 10 mg/mL triamcinolone and refilled the clobetasol cream. At the next appointment, 2 nodules remained. The patient indicated that he would continue using the cream until the nodules went away. In many cases, prurigo nodularis does not respond especially well to treatment, so this patient was fortunate that standard treatments provided a good outcome.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Johnson A. Self-inflicted dermatosis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013: 856-862.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

ACS Committee on Diversity Issues seeks two new members
The American College of Surgeons (ACS) Committee on Diversity Issues (CODI) is seeking candidates to fill two vacancies on the committee beginning in October 2017.
The mission of the Committee on Diversity Issues is to study the educational and professional needs of underrepresented surgeons and surgical trainees and the impact that its work may have on the elimination of health care disparities among diverse population groups.
Surgeons interested in developing initiatives to expand diversity within the ACS membership and leadership and to developing resources and programming for surgeons related to diversity and cultural competency should apply. Nominations are open to all, and the committee encourages representation by individuals of diverse cultural, racial, and ethnic backgrounds.
Nominees must meet the following criteria:
- Be an active Fellow of the ACS
- Be able to serve an initial three-year term: 2017–2020
- Attend one in-person meeting at the annual ACS Clinical Congress
- Participate in quarterly conference calls
- Contribute to committee initiatives
To apply, go to www.surveymonkey.com/r/CmteDiversityApp to access the application and submit by June 30.
Applicants will need to do the following:
- Upload a summary of your curriculum vitae (five pages or less)
- Upload a letter of interest highlighting your skills and expertise, along with contributions you would like to make to the committee
Eligible candidates will be selected and notified by the committee in July and will be invited to attend the October 23 meeting of the Committee on Diversity Issues as guests. This meeting is held in conjunction with the 2017 Clinical Congress in San Diego. Travel reimbursement will not be provided.
Direct questions to [email protected].
The American College of Surgeons (ACS) Committee on Diversity Issues (CODI) is seeking candidates to fill two vacancies on the committee beginning in October 2017.
The mission of the Committee on Diversity Issues is to study the educational and professional needs of underrepresented surgeons and surgical trainees and the impact that its work may have on the elimination of health care disparities among diverse population groups.
Surgeons interested in developing initiatives to expand diversity within the ACS membership and leadership and to developing resources and programming for surgeons related to diversity and cultural competency should apply. Nominations are open to all, and the committee encourages representation by individuals of diverse cultural, racial, and ethnic backgrounds.
Nominees must meet the following criteria:
- Be an active Fellow of the ACS
- Be able to serve an initial three-year term: 2017–2020
- Attend one in-person meeting at the annual ACS Clinical Congress
- Participate in quarterly conference calls
- Contribute to committee initiatives
To apply, go to www.surveymonkey.com/r/CmteDiversityApp to access the application and submit by June 30.
Applicants will need to do the following:
- Upload a summary of your curriculum vitae (five pages or less)
- Upload a letter of interest highlighting your skills and expertise, along with contributions you would like to make to the committee
Eligible candidates will be selected and notified by the committee in July and will be invited to attend the October 23 meeting of the Committee on Diversity Issues as guests. This meeting is held in conjunction with the 2017 Clinical Congress in San Diego. Travel reimbursement will not be provided.
Direct questions to [email protected].
The American College of Surgeons (ACS) Committee on Diversity Issues (CODI) is seeking candidates to fill two vacancies on the committee beginning in October 2017.
The mission of the Committee on Diversity Issues is to study the educational and professional needs of underrepresented surgeons and surgical trainees and the impact that its work may have on the elimination of health care disparities among diverse population groups.
Surgeons interested in developing initiatives to expand diversity within the ACS membership and leadership and to developing resources and programming for surgeons related to diversity and cultural competency should apply. Nominations are open to all, and the committee encourages representation by individuals of diverse cultural, racial, and ethnic backgrounds.
Nominees must meet the following criteria:
- Be an active Fellow of the ACS
- Be able to serve an initial three-year term: 2017–2020
- Attend one in-person meeting at the annual ACS Clinical Congress
- Participate in quarterly conference calls
- Contribute to committee initiatives
To apply, go to www.surveymonkey.com/r/CmteDiversityApp to access the application and submit by June 30.
Applicants will need to do the following:
- Upload a summary of your curriculum vitae (five pages or less)
- Upload a letter of interest highlighting your skills and expertise, along with contributions you would like to make to the committee
Eligible candidates will be selected and notified by the committee in July and will be invited to attend the October 23 meeting of the Committee on Diversity Issues as guests. This meeting is held in conjunction with the 2017 Clinical Congress in San Diego. Travel reimbursement will not be provided.
Direct questions to [email protected].
Acute cholecystitis: Not always routine
The more we think we know, the less we actually may know. As new techniques develop and their use is closely examined and reported, details about the patient’s disease and the surgeon’s skill and judgment turn out to matter more and more in the decision-making process. So it is with acute cholecystitis.
I have recently been puzzled and intrigued by changing trends in the management of acute cholecystitis that are apparent in the medical literature, discussions in the ACS Communities, and practice in my local community.
When I was a resident, the debate about early cholecystectomy vs antibiotics with interval operation 6 weeks later was just being settled in the literature in favor of early cholecystectomy. The weight of evidence in the surgical literature found that delay made the eventual operation more difficult and costly.

In the following 2 decades, early cholecystectomy became the indicated treatment for acute cholecystitis. In that era, of course, these operations were open, as that was our only option and one which we all learned to perform with confidence during residency. Tube cholecystostomy was a rarity reserved only for the most severely ill and feeble, and done by surgeons, since interventional radiologists had not yet appeared on the scene.
In the rare instance of acute cholecystitis so severe, and anatomic landmarks so obscured, that the gallbladder could not be safely dissected away from the common bile duct, a remnant of the gallbladder might be left behind, the mucosa cauterized, and the right upper quadrant drained.
Fast forward 40 years, and we find a distinctly different landscape. As the Boomer generation reaches geriatric age in expanding numbers, surgeons encounter an increasingly older patient population, often with numerous comorbidities and high surgical risk. Our increased critical care capability to rescue patients from sepsis and organ failure also introduces new challenges in decision-making about whether immediate cholecystectomy or a temporizing option is better for the elderly septic ICU patient before us.
At the same time, our overwhelmingly most common elective biliary procedure has become a laparoscopic cholecystectomy (LC), with which our younger surgeons have become comfortable and facile. Multiple randomized studies also confirm the superiority of early LC for acute cholecystitis, although LC is associated with a higher rate of conversion to open cholecystectomy in acute cholecystitis than in the elective setting. Since it is acknowledged that the mortality and morbidity of an open cholecystectomy is greater than that of its laparoscopic counterpart, especially in the setting of severe inflammation, and the younger surgeons are less confident in performing open cholecystectomy, it is not surprising that they embrace a strategy that allows them to avoid surgical management of acute cholecystitis in the high-risk patient with severe disease.
The ready availability of interventional radiologists in the past 30 years also offers a less invasive option than surgery – the percutaneous tube cholecystostomy (PC). It is no wonder that PC has increasingly become the “go-to” early option when the patient is old and sick or the surgeon lacks confidence in his/her open surgical skills in a potentially hostile, inflamed right upper quadrant. If the increasing number of articles on PC appearing in the literature is any indication, its use has proliferated in the recent past. As yet, no randomized clinical trials or other high-quality evidence have emerged to support its increased use, but a consensus panel of experts has issued the Tokyo Guidelines, recommending PC as primary therapy for stage III acute cholecystitis, the form of disease associated with organ failure, but not citing evidence to support this recommendation (J Hepatobiliary Pancreat Surg. 2007;14[1]:91-7). Although the rate of PC use in Medicare patients with stage III acute cholecystitis has more than doubled in the past 20 years, Tokyo Guidelines have clearly not been uniformly adopted in the U.S., since PC use in patients with stage III acute cholecystitis is only 10% (J Am Coll Surg. 2017;224[4]: 502-14).
Whether the increase in PC use is appropriate or not remains undetermined. Other uncertainties about PC need clarification. When patients have a PC placed for acute cholecystitis, do they always need their gallbladders removed later? The rate of recurrent acute cholecystitis after PC is variable in the literature, although it appears to be more likely in patients with acute calculous than acalculous cholecystitis. The likelihood that the patient will later undergo a cholecystectomy varies from a low of 3% to a high of 57% in various studies.(Surgery. 2014;155[4]:615-22; J Am Coll Surg. 2012; 214[2]:196-201).
The exact rate may not even accurately be known, since some patients may be lost to follow-up or get subsequent care in another facility. The decision to perform cholecystectomy after PC involves assessment of patient risk for surgery and, ultimately, surgeon judgment. Other questions also remain unanswered: What is the role of surgeon experience in the decision to defer surgical therapy for acute cholecystitis? Is the surgeon even the one who is in charge of the decision in all cases, or is that decision being made by an internist, intensivist, or hospitalist, who may judge the patient’s risk differently than a surgeon would? Are we witnessing an evolution in management of severe cholecystitis in the high-risk, septic and elderly patient towards antibiotics and PC unless the patient fails that treatment? This strategy appears to be gaining in popularity, since several studies have shown that the minority of patients who have PC end up having their gallbladders removed. If symptoms recur and nonoperative treatment has clearly failed, should the decision be made to refer to a highly experienced surgeon (by virtue of laparoscopic skills or reputation as a hepatic-pancreatic biliary specialist)? Recent studies show that 46%-86% of elective interval cholecystectomies after successful PC can be performed laparoscopically with low complication rates, although those studies came from institutions with notable laparoscopic expertise (J Am Coll Surg. 2012;214[2]:196-201; J Gastrointest Surg. 2017; 21[5]:761-69).
One of my most revered senior surgical mentors recently opined that the safest strategy for the high-risk patient with severe acute cholecystitis was indeed PC and antibiotics followed by watchful waiting, and reserving cholecystectomy only for those who fail nonoperative therapy. I initially bristled at that concept as being antithetic to the surgical bias in favor of cholecystectomy as the answer to all gallbladder evils. But after reflecting further on the changing landscape of our therapeutic options and our changing surgical training, I’m thinking that his strategy may be reasonable.
After all, it’s about choosing the safest path for the patient. All cholecystectomies are not routine.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
The more we think we know, the less we actually may know. As new techniques develop and their use is closely examined and reported, details about the patient’s disease and the surgeon’s skill and judgment turn out to matter more and more in the decision-making process. So it is with acute cholecystitis.
I have recently been puzzled and intrigued by changing trends in the management of acute cholecystitis that are apparent in the medical literature, discussions in the ACS Communities, and practice in my local community.
When I was a resident, the debate about early cholecystectomy vs antibiotics with interval operation 6 weeks later was just being settled in the literature in favor of early cholecystectomy. The weight of evidence in the surgical literature found that delay made the eventual operation more difficult and costly.
In the following 2 decades, early cholecystectomy became the indicated treatment for acute cholecystitis. In that era, of course, these operations were open, as that was our only option and one which we all learned to perform with confidence during residency. Tube cholecystostomy was a rarity reserved only for the most severely ill and feeble, and done by surgeons, since interventional radiologists had not yet appeared on the scene.
In the rare instance of acute cholecystitis so severe, and anatomic landmarks so obscured, that the gallbladder could not be safely dissected away from the common bile duct, a remnant of the gallbladder might be left behind, the mucosa cauterized, and the right upper quadrant drained.
Fast forward 40 years, and we find a distinctly different landscape. As the Boomer generation reaches geriatric age in expanding numbers, surgeons encounter an increasingly older patient population, often with numerous comorbidities and high surgical risk. Our increased critical care capability to rescue patients from sepsis and organ failure also introduces new challenges in decision-making about whether immediate cholecystectomy or a temporizing option is better for the elderly septic ICU patient before us.
At the same time, our overwhelmingly most common elective biliary procedure has become a laparoscopic cholecystectomy (LC), with which our younger surgeons have become comfortable and facile. Multiple randomized studies also confirm the superiority of early LC for acute cholecystitis, although LC is associated with a higher rate of conversion to open cholecystectomy in acute cholecystitis than in the elective setting. Since it is acknowledged that the mortality and morbidity of an open cholecystectomy is greater than that of its laparoscopic counterpart, especially in the setting of severe inflammation, and the younger surgeons are less confident in performing open cholecystectomy, it is not surprising that they embrace a strategy that allows them to avoid surgical management of acute cholecystitis in the high-risk patient with severe disease.
The ready availability of interventional radiologists in the past 30 years also offers a less invasive option than surgery – the percutaneous tube cholecystostomy (PC). It is no wonder that PC has increasingly become the “go-to” early option when the patient is old and sick or the surgeon lacks confidence in his/her open surgical skills in a potentially hostile, inflamed right upper quadrant. If the increasing number of articles on PC appearing in the literature is any indication, its use has proliferated in the recent past. As yet, no randomized clinical trials or other high-quality evidence have emerged to support its increased use, but a consensus panel of experts has issued the Tokyo Guidelines, recommending PC as primary therapy for stage III acute cholecystitis, the form of disease associated with organ failure, but not citing evidence to support this recommendation (J Hepatobiliary Pancreat Surg. 2007;14[1]:91-7). Although the rate of PC use in Medicare patients with stage III acute cholecystitis has more than doubled in the past 20 years, Tokyo Guidelines have clearly not been uniformly adopted in the U.S., since PC use in patients with stage III acute cholecystitis is only 10% (J Am Coll Surg. 2017;224[4]: 502-14).
Whether the increase in PC use is appropriate or not remains undetermined. Other uncertainties about PC need clarification. When patients have a PC placed for acute cholecystitis, do they always need their gallbladders removed later? The rate of recurrent acute cholecystitis after PC is variable in the literature, although it appears to be more likely in patients with acute calculous than acalculous cholecystitis. The likelihood that the patient will later undergo a cholecystectomy varies from a low of 3% to a high of 57% in various studies.(Surgery. 2014;155[4]:615-22; J Am Coll Surg. 2012; 214[2]:196-201).
The exact rate may not even accurately be known, since some patients may be lost to follow-up or get subsequent care in another facility. The decision to perform cholecystectomy after PC involves assessment of patient risk for surgery and, ultimately, surgeon judgment. Other questions also remain unanswered: What is the role of surgeon experience in the decision to defer surgical therapy for acute cholecystitis? Is the surgeon even the one who is in charge of the decision in all cases, or is that decision being made by an internist, intensivist, or hospitalist, who may judge the patient’s risk differently than a surgeon would? Are we witnessing an evolution in management of severe cholecystitis in the high-risk, septic and elderly patient towards antibiotics and PC unless the patient fails that treatment? This strategy appears to be gaining in popularity, since several studies have shown that the minority of patients who have PC end up having their gallbladders removed. If symptoms recur and nonoperative treatment has clearly failed, should the decision be made to refer to a highly experienced surgeon (by virtue of laparoscopic skills or reputation as a hepatic-pancreatic biliary specialist)? Recent studies show that 46%-86% of elective interval cholecystectomies after successful PC can be performed laparoscopically with low complication rates, although those studies came from institutions with notable laparoscopic expertise (J Am Coll Surg. 2012;214[2]:196-201; J Gastrointest Surg. 2017; 21[5]:761-69).
One of my most revered senior surgical mentors recently opined that the safest strategy for the high-risk patient with severe acute cholecystitis was indeed PC and antibiotics followed by watchful waiting, and reserving cholecystectomy only for those who fail nonoperative therapy. I initially bristled at that concept as being antithetic to the surgical bias in favor of cholecystectomy as the answer to all gallbladder evils. But after reflecting further on the changing landscape of our therapeutic options and our changing surgical training, I’m thinking that his strategy may be reasonable.
After all, it’s about choosing the safest path for the patient. All cholecystectomies are not routine.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
The more we think we know, the less we actually may know. As new techniques develop and their use is closely examined and reported, details about the patient’s disease and the surgeon’s skill and judgment turn out to matter more and more in the decision-making process. So it is with acute cholecystitis.
I have recently been puzzled and intrigued by changing trends in the management of acute cholecystitis that are apparent in the medical literature, discussions in the ACS Communities, and practice in my local community.
When I was a resident, the debate about early cholecystectomy vs antibiotics with interval operation 6 weeks later was just being settled in the literature in favor of early cholecystectomy. The weight of evidence in the surgical literature found that delay made the eventual operation more difficult and costly.
In the following 2 decades, early cholecystectomy became the indicated treatment for acute cholecystitis. In that era, of course, these operations were open, as that was our only option and one which we all learned to perform with confidence during residency. Tube cholecystostomy was a rarity reserved only for the most severely ill and feeble, and done by surgeons, since interventional radiologists had not yet appeared on the scene.
In the rare instance of acute cholecystitis so severe, and anatomic landmarks so obscured, that the gallbladder could not be safely dissected away from the common bile duct, a remnant of the gallbladder might be left behind, the mucosa cauterized, and the right upper quadrant drained.
Fast forward 40 years, and we find a distinctly different landscape. As the Boomer generation reaches geriatric age in expanding numbers, surgeons encounter an increasingly older patient population, often with numerous comorbidities and high surgical risk. Our increased critical care capability to rescue patients from sepsis and organ failure also introduces new challenges in decision-making about whether immediate cholecystectomy or a temporizing option is better for the elderly septic ICU patient before us.
At the same time, our overwhelmingly most common elective biliary procedure has become a laparoscopic cholecystectomy (LC), with which our younger surgeons have become comfortable and facile. Multiple randomized studies also confirm the superiority of early LC for acute cholecystitis, although LC is associated with a higher rate of conversion to open cholecystectomy in acute cholecystitis than in the elective setting. Since it is acknowledged that the mortality and morbidity of an open cholecystectomy is greater than that of its laparoscopic counterpart, especially in the setting of severe inflammation, and the younger surgeons are less confident in performing open cholecystectomy, it is not surprising that they embrace a strategy that allows them to avoid surgical management of acute cholecystitis in the high-risk patient with severe disease.
The ready availability of interventional radiologists in the past 30 years also offers a less invasive option than surgery – the percutaneous tube cholecystostomy (PC). It is no wonder that PC has increasingly become the “go-to” early option when the patient is old and sick or the surgeon lacks confidence in his/her open surgical skills in a potentially hostile, inflamed right upper quadrant. If the increasing number of articles on PC appearing in the literature is any indication, its use has proliferated in the recent past. As yet, no randomized clinical trials or other high-quality evidence have emerged to support its increased use, but a consensus panel of experts has issued the Tokyo Guidelines, recommending PC as primary therapy for stage III acute cholecystitis, the form of disease associated with organ failure, but not citing evidence to support this recommendation (J Hepatobiliary Pancreat Surg. 2007;14[1]:91-7). Although the rate of PC use in Medicare patients with stage III acute cholecystitis has more than doubled in the past 20 years, Tokyo Guidelines have clearly not been uniformly adopted in the U.S., since PC use in patients with stage III acute cholecystitis is only 10% (J Am Coll Surg. 2017;224[4]: 502-14).
Whether the increase in PC use is appropriate or not remains undetermined. Other uncertainties about PC need clarification. When patients have a PC placed for acute cholecystitis, do they always need their gallbladders removed later? The rate of recurrent acute cholecystitis after PC is variable in the literature, although it appears to be more likely in patients with acute calculous than acalculous cholecystitis. The likelihood that the patient will later undergo a cholecystectomy varies from a low of 3% to a high of 57% in various studies.(Surgery. 2014;155[4]:615-22; J Am Coll Surg. 2012; 214[2]:196-201).
The exact rate may not even accurately be known, since some patients may be lost to follow-up or get subsequent care in another facility. The decision to perform cholecystectomy after PC involves assessment of patient risk for surgery and, ultimately, surgeon judgment. Other questions also remain unanswered: What is the role of surgeon experience in the decision to defer surgical therapy for acute cholecystitis? Is the surgeon even the one who is in charge of the decision in all cases, or is that decision being made by an internist, intensivist, or hospitalist, who may judge the patient’s risk differently than a surgeon would? Are we witnessing an evolution in management of severe cholecystitis in the high-risk, septic and elderly patient towards antibiotics and PC unless the patient fails that treatment? This strategy appears to be gaining in popularity, since several studies have shown that the minority of patients who have PC end up having their gallbladders removed. If symptoms recur and nonoperative treatment has clearly failed, should the decision be made to refer to a highly experienced surgeon (by virtue of laparoscopic skills or reputation as a hepatic-pancreatic biliary specialist)? Recent studies show that 46%-86% of elective interval cholecystectomies after successful PC can be performed laparoscopically with low complication rates, although those studies came from institutions with notable laparoscopic expertise (J Am Coll Surg. 2012;214[2]:196-201; J Gastrointest Surg. 2017; 21[5]:761-69).
One of my most revered senior surgical mentors recently opined that the safest strategy for the high-risk patient with severe acute cholecystitis was indeed PC and antibiotics followed by watchful waiting, and reserving cholecystectomy only for those who fail nonoperative therapy. I initially bristled at that concept as being antithetic to the surgical bias in favor of cholecystectomy as the answer to all gallbladder evils. But after reflecting further on the changing landscape of our therapeutic options and our changing surgical training, I’m thinking that his strategy may be reasonable.
After all, it’s about choosing the safest path for the patient. All cholecystectomies are not routine.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
An Act of Service, an Act of Love
Since its foundation in 1913 as the premier surgical professional organization in the United States, and one of the most influential in the world, the American College of Surgeons has shaped the policies and molded the education of numerous generations of surgeons. All young surgeons should aspire to be invested as Fellows some day as the highest honor in their career.
Service is an important factor in the decision to become a surgeon. As a Fellow of the ACS, the young surgeon will find many opportunities for service. Active participation as a Fellow is an act of service and can be an act of love for our patients, our colleagues, and our profession. And, with it, comes loyalty, a spirit of dedication, and a sense of unity. In addition, by joining the College we contribute to influencing our society in a positive way to protect our patients and our profession.
Becoming an active participant in the College means serving on committees, attending the Clinical Congress as frequently as feasible, and encouraging colleagues to aspire to become a Fellow.
In the end, being a part of our College and contributing to its growth and legacy is an act of service and, for many, an act of love.
Dr. Oviedo is with Capital Regional Surgical Associates, Tallahassee, Fla., and is Assistant Professor of Surgery, Florida State University College of Medicine. He serves as the ACS Young Fellow Association Liaison.
Since its foundation in 1913 as the premier surgical professional organization in the United States, and one of the most influential in the world, the American College of Surgeons has shaped the policies and molded the education of numerous generations of surgeons. All young surgeons should aspire to be invested as Fellows some day as the highest honor in their career.
Service is an important factor in the decision to become a surgeon. As a Fellow of the ACS, the young surgeon will find many opportunities for service. Active participation as a Fellow is an act of service and can be an act of love for our patients, our colleagues, and our profession. And, with it, comes loyalty, a spirit of dedication, and a sense of unity. In addition, by joining the College we contribute to influencing our society in a positive way to protect our patients and our profession.
Becoming an active participant in the College means serving on committees, attending the Clinical Congress as frequently as feasible, and encouraging colleagues to aspire to become a Fellow.
In the end, being a part of our College and contributing to its growth and legacy is an act of service and, for many, an act of love.
Dr. Oviedo is with Capital Regional Surgical Associates, Tallahassee, Fla., and is Assistant Professor of Surgery, Florida State University College of Medicine. He serves as the ACS Young Fellow Association Liaison.
Since its foundation in 1913 as the premier surgical professional organization in the United States, and one of the most influential in the world, the American College of Surgeons has shaped the policies and molded the education of numerous generations of surgeons. All young surgeons should aspire to be invested as Fellows some day as the highest honor in their career.
Service is an important factor in the decision to become a surgeon. As a Fellow of the ACS, the young surgeon will find many opportunities for service. Active participation as a Fellow is an act of service and can be an act of love for our patients, our colleagues, and our profession. And, with it, comes loyalty, a spirit of dedication, and a sense of unity. In addition, by joining the College we contribute to influencing our society in a positive way to protect our patients and our profession.
Becoming an active participant in the College means serving on committees, attending the Clinical Congress as frequently as feasible, and encouraging colleagues to aspire to become a Fellow.
In the end, being a part of our College and contributing to its growth and legacy is an act of service and, for many, an act of love.
Dr. Oviedo is with Capital Regional Surgical Associates, Tallahassee, Fla., and is Assistant Professor of Surgery, Florida State University College of Medicine. He serves as the ACS Young Fellow Association Liaison.
New ACS Resources in Surgical Education Online Now
The American College of Surgeons (ACS) Division of Education’s new Resources in Surgical Education (RISE) recently debuted on the ACS website. RISE is headed by Ajit K. Sachdeva, MD, FACS, FRCSC, Director, ACS Division of Education. The RISE web page is available at www.facs.org/education/division-of-education/publications/rise/current.

The inaugural article, “Create a Surgical Faculty Compensation Plan that Supports the Educational Mission,” by David A. Rogers, MD, MHPE, FACS, FAAP, is now available at www.facs.org/education/division-of-education/publications/rise/current. Future articles will be posted every six to eight weeks.
For additional information, contact Krashina Hudson at [email protected] or at 312-202-5335.
The American College of Surgeons (ACS) Division of Education’s new Resources in Surgical Education (RISE) recently debuted on the ACS website. RISE is headed by Ajit K. Sachdeva, MD, FACS, FRCSC, Director, ACS Division of Education. The RISE web page is available at www.facs.org/education/division-of-education/publications/rise/current.
The inaugural article, “Create a Surgical Faculty Compensation Plan that Supports the Educational Mission,” by David A. Rogers, MD, MHPE, FACS, FAAP, is now available at www.facs.org/education/division-of-education/publications/rise/current. Future articles will be posted every six to eight weeks.
For additional information, contact Krashina Hudson at [email protected] or at 312-202-5335.
The American College of Surgeons (ACS) Division of Education’s new Resources in Surgical Education (RISE) recently debuted on the ACS website. RISE is headed by Ajit K. Sachdeva, MD, FACS, FRCSC, Director, ACS Division of Education. The RISE web page is available at www.facs.org/education/division-of-education/publications/rise/current.
The inaugural article, “Create a Surgical Faculty Compensation Plan that Supports the Educational Mission,” by David A. Rogers, MD, MHPE, FACS, FAAP, is now available at www.facs.org/education/division-of-education/publications/rise/current. Future articles will be posted every six to eight weeks.
For additional information, contact Krashina Hudson at [email protected] or at 312-202-5335.
Surgeons learn about leading, influencing policy at 2017 ACS Leadership & Advocacy Summit
The 2017 American College of Surgeons (ACS) Leadership & Advocacy Summit, May 6–9 in Washington, DC, was a well-attended conference that brought together surgeons from across the U.S. to enhance their leadership skills and to learn about how they can advocate for the advancement of issues important to the field of surgery.
Leadership Summit
More than 450 surgeons and residents participated in the ACS Leadership Summit held May 6–7. The Leadership portion of the Leadership & Advocacy Summit included a series of presentations that provided practical, take-home tips on how to be a better leader. Presentations covered such diverse leadership topics as how to handle difficult conversations, manage difficult people, and lead from behind; how it’s not all about you, and leading by example; volunteering in your own backyard; avoiding burnout and promoting resilience; preparing for leadership positions in medicine; and successfully addressing critical situations in the operating room. PowerPoint presentations shown at the 2017 Leadership Summit are available at facs.org/advocacy/participate/summit/2017-presentations.
In addition, ACS chapter leaders shared success stories. Representatives of the Connecticut Chapter focused on resident engagement, representatives of the North Texas Chapter and South Texas Chapter explained the positive results that can be realized by holding joint chapter meetings, and members of the Georgia Society of the ACS discussed their Stop the Bleed® effort. Participants then convened in state breakout sessions during the lunch hour to identify new strategies and initiatives for implementation at the chapter level. ACS Executive Director David B. Hoyt, MD, FACS, provided an update on ACS activities.
Advocacy Summit
More than 300 surgeons and residents participated in the ACS Advocacy Summit, May 7−9. Participants in the Advocacy Summit portion of the ACS Leadership & Advocacy Summit came to Washington primarily to meet with lawmakers and congressional staff to educate them about key ACS legislative priorities that affect surgical patients, including ensuring an adequate surgical workforce in underserved areas; advancing childhood cancer research and surveillance and providing resources for pediatric cancer survivors; allocating funding for the Children’s Health Insurance Program, which provides health care coverage to uninsured children from low-income families; improving liability protections for trauma care providers; and providing greater flexibility for providers during implementation of the Merit-based Incentive Payment System (MIPS). The issue briefs presented during the Advocacy Summit are available on the ACS Professional Association website at web4.facs.org/eBusiness/login.aspx?ReturnURL=~/SAML/SSOService.aspx?r=1.
In addition, health care reform was discussed during a few panel sessions. Just days before the Advocacy Summit, the House of Representatives had passed the American Health Care Act by a vote of 217-213. Summit attendees were educated about the College’s concerns with the legislation and were advised that the Senate bill likely would be dramatically different. The College continues to work to ensure that ACS health care reform principles—patient safety and quality, patient access to surgical care, reduction of health care costs and medical liability reform—are included in a revised Senate bill. The full ACS 2017 statement on health care reform was published in the May issue of the Bulletin and is available at bulletin.facs.org/2017/05/american-college-of-surgeons-2017-statement-on-health-care-reform/.
The 2017 American College of Surgeons (ACS) Leadership & Advocacy Summit, May 6–9 in Washington, DC, was a well-attended conference that brought together surgeons from across the U.S. to enhance their leadership skills and to learn about how they can advocate for the advancement of issues important to the field of surgery.
Leadership Summit
More than 450 surgeons and residents participated in the ACS Leadership Summit held May 6–7. The Leadership portion of the Leadership & Advocacy Summit included a series of presentations that provided practical, take-home tips on how to be a better leader. Presentations covered such diverse leadership topics as how to handle difficult conversations, manage difficult people, and lead from behind; how it’s not all about you, and leading by example; volunteering in your own backyard; avoiding burnout and promoting resilience; preparing for leadership positions in medicine; and successfully addressing critical situations in the operating room. PowerPoint presentations shown at the 2017 Leadership Summit are available at facs.org/advocacy/participate/summit/2017-presentations.
In addition, ACS chapter leaders shared success stories. Representatives of the Connecticut Chapter focused on resident engagement, representatives of the North Texas Chapter and South Texas Chapter explained the positive results that can be realized by holding joint chapter meetings, and members of the Georgia Society of the ACS discussed their Stop the Bleed® effort. Participants then convened in state breakout sessions during the lunch hour to identify new strategies and initiatives for implementation at the chapter level. ACS Executive Director David B. Hoyt, MD, FACS, provided an update on ACS activities.
Advocacy Summit
More than 300 surgeons and residents participated in the ACS Advocacy Summit, May 7−9. Participants in the Advocacy Summit portion of the ACS Leadership & Advocacy Summit came to Washington primarily to meet with lawmakers and congressional staff to educate them about key ACS legislative priorities that affect surgical patients, including ensuring an adequate surgical workforce in underserved areas; advancing childhood cancer research and surveillance and providing resources for pediatric cancer survivors; allocating funding for the Children’s Health Insurance Program, which provides health care coverage to uninsured children from low-income families; improving liability protections for trauma care providers; and providing greater flexibility for providers during implementation of the Merit-based Incentive Payment System (MIPS). The issue briefs presented during the Advocacy Summit are available on the ACS Professional Association website at web4.facs.org/eBusiness/login.aspx?ReturnURL=~/SAML/SSOService.aspx?r=1.
In addition, health care reform was discussed during a few panel sessions. Just days before the Advocacy Summit, the House of Representatives had passed the American Health Care Act by a vote of 217-213. Summit attendees were educated about the College’s concerns with the legislation and were advised that the Senate bill likely would be dramatically different. The College continues to work to ensure that ACS health care reform principles—patient safety and quality, patient access to surgical care, reduction of health care costs and medical liability reform—are included in a revised Senate bill. The full ACS 2017 statement on health care reform was published in the May issue of the Bulletin and is available at bulletin.facs.org/2017/05/american-college-of-surgeons-2017-statement-on-health-care-reform/.
The 2017 American College of Surgeons (ACS) Leadership & Advocacy Summit, May 6–9 in Washington, DC, was a well-attended conference that brought together surgeons from across the U.S. to enhance their leadership skills and to learn about how they can advocate for the advancement of issues important to the field of surgery.
Leadership Summit
More than 450 surgeons and residents participated in the ACS Leadership Summit held May 6–7. The Leadership portion of the Leadership & Advocacy Summit included a series of presentations that provided practical, take-home tips on how to be a better leader. Presentations covered such diverse leadership topics as how to handle difficult conversations, manage difficult people, and lead from behind; how it’s not all about you, and leading by example; volunteering in your own backyard; avoiding burnout and promoting resilience; preparing for leadership positions in medicine; and successfully addressing critical situations in the operating room. PowerPoint presentations shown at the 2017 Leadership Summit are available at facs.org/advocacy/participate/summit/2017-presentations.
In addition, ACS chapter leaders shared success stories. Representatives of the Connecticut Chapter focused on resident engagement, representatives of the North Texas Chapter and South Texas Chapter explained the positive results that can be realized by holding joint chapter meetings, and members of the Georgia Society of the ACS discussed their Stop the Bleed® effort. Participants then convened in state breakout sessions during the lunch hour to identify new strategies and initiatives for implementation at the chapter level. ACS Executive Director David B. Hoyt, MD, FACS, provided an update on ACS activities.
Advocacy Summit
More than 300 surgeons and residents participated in the ACS Advocacy Summit, May 7−9. Participants in the Advocacy Summit portion of the ACS Leadership & Advocacy Summit came to Washington primarily to meet with lawmakers and congressional staff to educate them about key ACS legislative priorities that affect surgical patients, including ensuring an adequate surgical workforce in underserved areas; advancing childhood cancer research and surveillance and providing resources for pediatric cancer survivors; allocating funding for the Children’s Health Insurance Program, which provides health care coverage to uninsured children from low-income families; improving liability protections for trauma care providers; and providing greater flexibility for providers during implementation of the Merit-based Incentive Payment System (MIPS). The issue briefs presented during the Advocacy Summit are available on the ACS Professional Association website at web4.facs.org/eBusiness/login.aspx?ReturnURL=~/SAML/SSOService.aspx?r=1.
In addition, health care reform was discussed during a few panel sessions. Just days before the Advocacy Summit, the House of Representatives had passed the American Health Care Act by a vote of 217-213. Summit attendees were educated about the College’s concerns with the legislation and were advised that the Senate bill likely would be dramatically different. The College continues to work to ensure that ACS health care reform principles—patient safety and quality, patient access to surgical care, reduction of health care costs and medical liability reform—are included in a revised Senate bill. The full ACS 2017 statement on health care reform was published in the May issue of the Bulletin and is available at bulletin.facs.org/2017/05/american-college-of-surgeons-2017-statement-on-health-care-reform/.