User login
HM17 session summary: Rheumatology pearls for the inpatient provider
Presenter
Neal Birnbaum, MD
Session Summary
Dr. Birnbaum began with the differential diagnosis of acute monoarthritis, which is one of the more common reasons for inpatient rheumatology consultation and includes crystalline (e.g., gout), septic, autoimmune (psoriasis), traumatic, and hemorrhagic.
The synovial fluid will give an idea as to whether one is more likely than the other, he said. Normal synovial fluid is transparent, clear, has a low cell count, and is very viscous in nature. Noninflammatory etiologies (osteoarthritis) will have some cells but will largely be similar to normal synovial fluid. Inflammatory causes will have higher cell counts (2-10K WBC) but will have much lower viscosity. Septic joints will look pustular with very high cell counts (sometimes too high to be recorded) and will be positive on fluid culture (unless the patient has already received antimicrobial therapy). Hemorrhagic fluid will look like blood, and the history will give clues as to whether that is the case (recent trauma, history of hemophilia).

Pseudogout (CPPD) is more likely to manifest in different joints (knees more so than wrist more so than shoulders/hips). One should suspect pseudogout in patients with acute arthritis in patients more than 70 years old. Crystals will be positively bifringent and more rectangular or square shaped, compared with gout crystals. Finding chondrocalcinosis on x-ray on a symptomatic patient can make the diagnosis much more likely. However, a patient can have chondrocalcinosis on an x-ray and not have CPPD. A patient can also have no chondrocalcinosis and have CPPD. It is the combination of the x-ray sign and symptoms that creates the high accuracy of the test.
The treatment for both in the acute setting includes colchicine (2 tabs x 1, then 1 more 1 hour later), NSAIDS (although may not be ideal inpatient because of potential toxicities), and corticosteroids (this can be either oral [prednisone 40 mg q24 with rapid taper], intraarticular [triamcinolone 10 mg-40 mg depending on the joint size], or IV [solumedrol or solucortef equivalent to prednisone 40 q24]).
For management of gout chronically, one should strive for a uric acid level of less than 6.0. Contrary to what is commonly believed, one can start urate lowering agents like allopurinol acutely (start with 100 mg for 2 weeks, then titrate up every 2 weeks until one hits the target uric acid level). Clinicians can consider using febuxostat for those patients who have renal insufficiency. While on the urate lowering agent, use low dose colchicine or NSAIDS for the first few months. Unfortunately, there is no long-term chronic strategy to prevent pseudogout flares. If there is an underlying cause for the pseudogout, then try to address it.
Consults for positive antinuclear antibodies (ANA) are common reasons for rheumatology referrals. The patterns of the ANA and the titer are important to the differential diagnosis. Up to 30% of healthy individuals have a positive ANA. ANA can be helpful as a rule out test for systemic lupus erythematosus (SLE), as it has a high sensitivity and a low specificity. However, because SLE is a clinical diagnosis and because of the high ANA positivity in the population, a high ANA alone does not prove a patient has SLE.
Concerning vasculitis, Dr. Birnbaum recommended thinking about it in terms of small versus large vessel disease. For initial evaluation, one should draw a CBC, erythrocyte sedimentation rate/C-reactive protein, urinalysis, chemistry panel, ANA, antineutrophil cytoplasmic antibodies, rheumatoid factor, hepatitis C antibody, and complement levels (C3, C4, CH50). One can also think of drawing cryoglobulins, especially in settings where one is suspicious that hepatitis C may be present. The differential diagnosis for vasculitis includes drug reactions, infections (mostly viral), malignancy, collagen vascular disease, and idiopathic causes (33%-50% of cases). The treatment is to remove offending agents (i.e., drug-induced vasculitis), treat infections (if applicable), and use steroids (the dosing depends on the situation).
Dr. Birnbaum finished with two relatively new illnesses that should be on clinicians’ radars. Chikungunya virus is transmitted by mosquitoes in the same distribution that one may see Zika virus. The symptoms include headaches, fevers, extreme joint pain, and joint swelling (this aspect is different from many other viral illnesses). The illness is usually acute. However, some patients will continue to have symptoms for up to a year. There is no specific treatment other than symptom relief (pain medications, NSAIDs).
Finally, immunoglobulin G4–related disease can affect virtually any organ system, but seems to manifest frequently as pancreatitis in the hospital setting. Think about this in patients with pancreatitis not secondary to the usual alcoholic or gallstone variety. The gold standard for diagnosis is biopsy with histologic findings of IgG4 in plasma cells. Most patients will be noted to have elevated IgG4 levels. The treatment is prednisone 40mg q24 with a taper over 2 months. For those who cannot be weaned or for those with recurrent disease, rituximab (1000mg IV x 1 then approximately 2 weeks later) can be used.
Key takeaways for HM
- Know the differential diagnosis of acute monoarticular arthritis and how the synovial fluid will vary depending on the diagnosis.
- Gout can manifest in other joints besides the first toe. One can use allopurinol even in the acute setting. The goal is to attain a uric acid level of less than 6.0.
- Pseudogout should be considered in patients older than 70 years with acute arthritis. There is no allopurinol equivalent for chronic management.
- Positive ANAs are common, but they do not make the diagnosis of SLE (although a negative ANA generally does rule out SLE).
- SLE is a clinical diagnosis that requires multiple symptoms and findings to make the diagnosis. Please refer to the ACR classification criteria.
- Think of vasculitis in terms of small versus large vessel disease and think of the differential diagnosis as to the etiology (realizing that 33%-50% will end up being idiopathic).
- Chikungunya is mosquito-borne and associated with severe joint pains, headaches, and fevers but can also have joint swelling. While often acute, the symptoms can last for up to a year. Treatment is symptomatic management.
- Think of IgG4-related disease in patients with pancreatitis without the usual causes (alcohol, gallstones). Diagnosis is based on pathology and IgG4 levels. Treatment is with steroids and/or rituximab.
Dr. Kim is a hospitalist who works at Emory University Hospital in Atlanta and is an editorial board member of The Hospitalist.
Presenter
Neal Birnbaum, MD
Session Summary
Dr. Birnbaum began with the differential diagnosis of acute monoarthritis, which is one of the more common reasons for inpatient rheumatology consultation and includes crystalline (e.g., gout), septic, autoimmune (psoriasis), traumatic, and hemorrhagic.
The synovial fluid will give an idea as to whether one is more likely than the other, he said. Normal synovial fluid is transparent, clear, has a low cell count, and is very viscous in nature. Noninflammatory etiologies (osteoarthritis) will have some cells but will largely be similar to normal synovial fluid. Inflammatory causes will have higher cell counts (2-10K WBC) but will have much lower viscosity. Septic joints will look pustular with very high cell counts (sometimes too high to be recorded) and will be positive on fluid culture (unless the patient has already received antimicrobial therapy). Hemorrhagic fluid will look like blood, and the history will give clues as to whether that is the case (recent trauma, history of hemophilia).
Pseudogout (CPPD) is more likely to manifest in different joints (knees more so than wrist more so than shoulders/hips). One should suspect pseudogout in patients with acute arthritis in patients more than 70 years old. Crystals will be positively bifringent and more rectangular or square shaped, compared with gout crystals. Finding chondrocalcinosis on x-ray on a symptomatic patient can make the diagnosis much more likely. However, a patient can have chondrocalcinosis on an x-ray and not have CPPD. A patient can also have no chondrocalcinosis and have CPPD. It is the combination of the x-ray sign and symptoms that creates the high accuracy of the test.
The treatment for both in the acute setting includes colchicine (2 tabs x 1, then 1 more 1 hour later), NSAIDS (although may not be ideal inpatient because of potential toxicities), and corticosteroids (this can be either oral [prednisone 40 mg q24 with rapid taper], intraarticular [triamcinolone 10 mg-40 mg depending on the joint size], or IV [solumedrol or solucortef equivalent to prednisone 40 q24]).
For management of gout chronically, one should strive for a uric acid level of less than 6.0. Contrary to what is commonly believed, one can start urate lowering agents like allopurinol acutely (start with 100 mg for 2 weeks, then titrate up every 2 weeks until one hits the target uric acid level). Clinicians can consider using febuxostat for those patients who have renal insufficiency. While on the urate lowering agent, use low dose colchicine or NSAIDS for the first few months. Unfortunately, there is no long-term chronic strategy to prevent pseudogout flares. If there is an underlying cause for the pseudogout, then try to address it.
Consults for positive antinuclear antibodies (ANA) are common reasons for rheumatology referrals. The patterns of the ANA and the titer are important to the differential diagnosis. Up to 30% of healthy individuals have a positive ANA. ANA can be helpful as a rule out test for systemic lupus erythematosus (SLE), as it has a high sensitivity and a low specificity. However, because SLE is a clinical diagnosis and because of the high ANA positivity in the population, a high ANA alone does not prove a patient has SLE.
Concerning vasculitis, Dr. Birnbaum recommended thinking about it in terms of small versus large vessel disease. For initial evaluation, one should draw a CBC, erythrocyte sedimentation rate/C-reactive protein, urinalysis, chemistry panel, ANA, antineutrophil cytoplasmic antibodies, rheumatoid factor, hepatitis C antibody, and complement levels (C3, C4, CH50). One can also think of drawing cryoglobulins, especially in settings where one is suspicious that hepatitis C may be present. The differential diagnosis for vasculitis includes drug reactions, infections (mostly viral), malignancy, collagen vascular disease, and idiopathic causes (33%-50% of cases). The treatment is to remove offending agents (i.e., drug-induced vasculitis), treat infections (if applicable), and use steroids (the dosing depends on the situation).
Dr. Birnbaum finished with two relatively new illnesses that should be on clinicians’ radars. Chikungunya virus is transmitted by mosquitoes in the same distribution that one may see Zika virus. The symptoms include headaches, fevers, extreme joint pain, and joint swelling (this aspect is different from many other viral illnesses). The illness is usually acute. However, some patients will continue to have symptoms for up to a year. There is no specific treatment other than symptom relief (pain medications, NSAIDs).
Finally, immunoglobulin G4–related disease can affect virtually any organ system, but seems to manifest frequently as pancreatitis in the hospital setting. Think about this in patients with pancreatitis not secondary to the usual alcoholic or gallstone variety. The gold standard for diagnosis is biopsy with histologic findings of IgG4 in plasma cells. Most patients will be noted to have elevated IgG4 levels. The treatment is prednisone 40mg q24 with a taper over 2 months. For those who cannot be weaned or for those with recurrent disease, rituximab (1000mg IV x 1 then approximately 2 weeks later) can be used.
Key takeaways for HM
- Know the differential diagnosis of acute monoarticular arthritis and how the synovial fluid will vary depending on the diagnosis.
- Gout can manifest in other joints besides the first toe. One can use allopurinol even in the acute setting. The goal is to attain a uric acid level of less than 6.0.
- Pseudogout should be considered in patients older than 70 years with acute arthritis. There is no allopurinol equivalent for chronic management.
- Positive ANAs are common, but they do not make the diagnosis of SLE (although a negative ANA generally does rule out SLE).
- SLE is a clinical diagnosis that requires multiple symptoms and findings to make the diagnosis. Please refer to the ACR classification criteria.
- Think of vasculitis in terms of small versus large vessel disease and think of the differential diagnosis as to the etiology (realizing that 33%-50% will end up being idiopathic).
- Chikungunya is mosquito-borne and associated with severe joint pains, headaches, and fevers but can also have joint swelling. While often acute, the symptoms can last for up to a year. Treatment is symptomatic management.
- Think of IgG4-related disease in patients with pancreatitis without the usual causes (alcohol, gallstones). Diagnosis is based on pathology and IgG4 levels. Treatment is with steroids and/or rituximab.
Dr. Kim is a hospitalist who works at Emory University Hospital in Atlanta and is an editorial board member of The Hospitalist.
Presenter
Neal Birnbaum, MD
Session Summary
Dr. Birnbaum began with the differential diagnosis of acute monoarthritis, which is one of the more common reasons for inpatient rheumatology consultation and includes crystalline (e.g., gout), septic, autoimmune (psoriasis), traumatic, and hemorrhagic.
The synovial fluid will give an idea as to whether one is more likely than the other, he said. Normal synovial fluid is transparent, clear, has a low cell count, and is very viscous in nature. Noninflammatory etiologies (osteoarthritis) will have some cells but will largely be similar to normal synovial fluid. Inflammatory causes will have higher cell counts (2-10K WBC) but will have much lower viscosity. Septic joints will look pustular with very high cell counts (sometimes too high to be recorded) and will be positive on fluid culture (unless the patient has already received antimicrobial therapy). Hemorrhagic fluid will look like blood, and the history will give clues as to whether that is the case (recent trauma, history of hemophilia).
Pseudogout (CPPD) is more likely to manifest in different joints (knees more so than wrist more so than shoulders/hips). One should suspect pseudogout in patients with acute arthritis in patients more than 70 years old. Crystals will be positively bifringent and more rectangular or square shaped, compared with gout crystals. Finding chondrocalcinosis on x-ray on a symptomatic patient can make the diagnosis much more likely. However, a patient can have chondrocalcinosis on an x-ray and not have CPPD. A patient can also have no chondrocalcinosis and have CPPD. It is the combination of the x-ray sign and symptoms that creates the high accuracy of the test.
The treatment for both in the acute setting includes colchicine (2 tabs x 1, then 1 more 1 hour later), NSAIDS (although may not be ideal inpatient because of potential toxicities), and corticosteroids (this can be either oral [prednisone 40 mg q24 with rapid taper], intraarticular [triamcinolone 10 mg-40 mg depending on the joint size], or IV [solumedrol or solucortef equivalent to prednisone 40 q24]).
For management of gout chronically, one should strive for a uric acid level of less than 6.0. Contrary to what is commonly believed, one can start urate lowering agents like allopurinol acutely (start with 100 mg for 2 weeks, then titrate up every 2 weeks until one hits the target uric acid level). Clinicians can consider using febuxostat for those patients who have renal insufficiency. While on the urate lowering agent, use low dose colchicine or NSAIDS for the first few months. Unfortunately, there is no long-term chronic strategy to prevent pseudogout flares. If there is an underlying cause for the pseudogout, then try to address it.
Consults for positive antinuclear antibodies (ANA) are common reasons for rheumatology referrals. The patterns of the ANA and the titer are important to the differential diagnosis. Up to 30% of healthy individuals have a positive ANA. ANA can be helpful as a rule out test for systemic lupus erythematosus (SLE), as it has a high sensitivity and a low specificity. However, because SLE is a clinical diagnosis and because of the high ANA positivity in the population, a high ANA alone does not prove a patient has SLE.
Concerning vasculitis, Dr. Birnbaum recommended thinking about it in terms of small versus large vessel disease. For initial evaluation, one should draw a CBC, erythrocyte sedimentation rate/C-reactive protein, urinalysis, chemistry panel, ANA, antineutrophil cytoplasmic antibodies, rheumatoid factor, hepatitis C antibody, and complement levels (C3, C4, CH50). One can also think of drawing cryoglobulins, especially in settings where one is suspicious that hepatitis C may be present. The differential diagnosis for vasculitis includes drug reactions, infections (mostly viral), malignancy, collagen vascular disease, and idiopathic causes (33%-50% of cases). The treatment is to remove offending agents (i.e., drug-induced vasculitis), treat infections (if applicable), and use steroids (the dosing depends on the situation).
Dr. Birnbaum finished with two relatively new illnesses that should be on clinicians’ radars. Chikungunya virus is transmitted by mosquitoes in the same distribution that one may see Zika virus. The symptoms include headaches, fevers, extreme joint pain, and joint swelling (this aspect is different from many other viral illnesses). The illness is usually acute. However, some patients will continue to have symptoms for up to a year. There is no specific treatment other than symptom relief (pain medications, NSAIDs).
Finally, immunoglobulin G4–related disease can affect virtually any organ system, but seems to manifest frequently as pancreatitis in the hospital setting. Think about this in patients with pancreatitis not secondary to the usual alcoholic or gallstone variety. The gold standard for diagnosis is biopsy with histologic findings of IgG4 in plasma cells. Most patients will be noted to have elevated IgG4 levels. The treatment is prednisone 40mg q24 with a taper over 2 months. For those who cannot be weaned or for those with recurrent disease, rituximab (1000mg IV x 1 then approximately 2 weeks later) can be used.
Key takeaways for HM
- Know the differential diagnosis of acute monoarticular arthritis and how the synovial fluid will vary depending on the diagnosis.
- Gout can manifest in other joints besides the first toe. One can use allopurinol even in the acute setting. The goal is to attain a uric acid level of less than 6.0.
- Pseudogout should be considered in patients older than 70 years with acute arthritis. There is no allopurinol equivalent for chronic management.
- Positive ANAs are common, but they do not make the diagnosis of SLE (although a negative ANA generally does rule out SLE).
- SLE is a clinical diagnosis that requires multiple symptoms and findings to make the diagnosis. Please refer to the ACR classification criteria.
- Think of vasculitis in terms of small versus large vessel disease and think of the differential diagnosis as to the etiology (realizing that 33%-50% will end up being idiopathic).
- Chikungunya is mosquito-borne and associated with severe joint pains, headaches, and fevers but can also have joint swelling. While often acute, the symptoms can last for up to a year. Treatment is symptomatic management.
- Think of IgG4-related disease in patients with pancreatitis without the usual causes (alcohol, gallstones). Diagnosis is based on pathology and IgG4 levels. Treatment is with steroids and/or rituximab.
Dr. Kim is a hospitalist who works at Emory University Hospital in Atlanta and is an editorial board member of The Hospitalist.
VIDEO: NCI estimation of MBC numbers a start, but more is needed
CHICAGO – After Shirley A. Mertz, JD, was diagnosed with metastatic breast cancer, she was surprised to learn the government wasn’t counting people like her in data gathered on the disease. Only a minority of women with the disease – those diagnosed de novo – are included in Surveillance, Epidemiology and End Results (SEER) data, she said in a video interview at the annual meeting of the American Society of Clinical Oncology.
A recently published report by a National Cancer Institute mathematician and her associates estimates that about 155,000 women are living with metastatic breast cancer and that three-quarters of those women were initially diagnosed with lower-stage disease that progressed to stage IV. Ms. Mertz, president of the Metastatic Breast Cancer Network, says the estimate is a good start, but it’s important to go further and include those diagnosed with a metastatic recurrence in SEER data to get an accurate view.
“If we are not counted, then it appears we don’t matter, and how can we know if we are doing better if we don’t know how many of us are out there,” she said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @NikolaidesLaura
CHICAGO – After Shirley A. Mertz, JD, was diagnosed with metastatic breast cancer, she was surprised to learn the government wasn’t counting people like her in data gathered on the disease. Only a minority of women with the disease – those diagnosed de novo – are included in Surveillance, Epidemiology and End Results (SEER) data, she said in a video interview at the annual meeting of the American Society of Clinical Oncology.
A recently published report by a National Cancer Institute mathematician and her associates estimates that about 155,000 women are living with metastatic breast cancer and that three-quarters of those women were initially diagnosed with lower-stage disease that progressed to stage IV. Ms. Mertz, president of the Metastatic Breast Cancer Network, says the estimate is a good start, but it’s important to go further and include those diagnosed with a metastatic recurrence in SEER data to get an accurate view.
“If we are not counted, then it appears we don’t matter, and how can we know if we are doing better if we don’t know how many of us are out there,” she said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @NikolaidesLaura
CHICAGO – After Shirley A. Mertz, JD, was diagnosed with metastatic breast cancer, she was surprised to learn the government wasn’t counting people like her in data gathered on the disease. Only a minority of women with the disease – those diagnosed de novo – are included in Surveillance, Epidemiology and End Results (SEER) data, she said in a video interview at the annual meeting of the American Society of Clinical Oncology.
A recently published report by a National Cancer Institute mathematician and her associates estimates that about 155,000 women are living with metastatic breast cancer and that three-quarters of those women were initially diagnosed with lower-stage disease that progressed to stage IV. Ms. Mertz, president of the Metastatic Breast Cancer Network, says the estimate is a good start, but it’s important to go further and include those diagnosed with a metastatic recurrence in SEER data to get an accurate view.
“If we are not counted, then it appears we don’t matter, and how can we know if we are doing better if we don’t know how many of us are out there,” she said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @NikolaidesLaura
AT ASCO 2017

Most veterans with schizophrenia or bipolar I report suicide attempts
SAN DIEGO – A new study reports that about half of assessed U.S. veterans with schizophrenia or bipolar I disorder have tried to kill themselves. Nearly 70% of those with schizophrenia had documented suicidal behavior or ideation, as did more than 82% of those with bipolar I disorder.
“The VA struggles to predict suicidal ideation and behavior,” said study lead author Philip D. Harvey, PhD, of the Carter VA Medical Center in Miami, in an interview. “These data suggest that having one of these diagnoses is a major risk factor. Regular assessment makes considerable sense.”
Dr. Harvey released the study findings in a poster at the annual meeting of the American Psychiatric Association.
For the study, Dr. Harvey and his colleagues examined findings from a VA research project into the genetics behind functional disability in schizophrenia and bipolar illness.
“We know that suicide risk is higher in veterans than in the general population. We also know that the current focus is on returning veterans who were deployed in combat operations,” said Dr. Harvey, who also is affiliated with the University of Miami. “We wanted to evaluate the risk for suicidal ideation and behavior in the segment of the veteran population who have recently or ever been exposed to military trauma.”
The project assessed VA patients with schizophrenia (N = 3,941) or bipolar I disorder (N = 5,414) through in-person evaluations regarding issues like cognitive and functional status, and history of posttraumatic stress disorder. All of the subjects were outpatients at 26 VA medical centers.
Combined, the mean age of the study participants was 53.6 years, plus or minus 11 years, and 86.2% were male. Whites made up 57.4% of the sample, followed by blacks (37.0%) and other (5.6%). A total of 27% had no comorbid psychiatric conditions.
The study authors found documented suicidal ideation or suicidal behavior in 69.9% of veterans with schizophrenia and 82.3% of those with bipolar disorder; the percentages who reported making actual suicide attempts was 46.1% schizophrenia and 54.5% bipolar disorder.
The risk of suicidal ideation was lower in schizophrenia vs. bipolar disorder (odds ratio, 0.82; 95% confidence interval, 0.71-0.95), as was suicidal behavior (OR, 0.81; 95% CI, 0.71-0.93).
Dr. Harvey said this is not surprising. “The combination of a history of euphoric mood and significant depression [characteristic of bipolar disorder] is very challenging.”
Other factors lowered risk: College education vs. high school or less (OR, 0.82; 95% CI, 0.67-1.00 for ideation; OR, 0.70; 95% CI, 0.58-0.84 for behavior). In addition, lower risk was found among black vs. white patients (OR, 0.72; 95% CI, 0.63-0.84 for ideation; OR, 0.82; 95% CI, 0.72-0.93, for behavior).
These factors boosted risk: multiple psychiatric comorbidities vs. none (OR, 2.61; 95% CI, 2.22-3.07 for ideation; OR, 3.82; 95% CI, 3.30-4.41, for behavior), and those with a history of being ever vs. never married (OR, 1.18; 95% CI, 1.02-1.37 for ideation; OR, 1.36; 95% CI, 1.19-1.55, for behavior). Most of those who had been married later were divorced.
“These findings underscore the need for continuous monitoring for suicidality in veteran populations, regardless of age or psychiatric diagnosis, and especially with multiple psychiatric comorbidities,” the authors wrote.
The study was funded by the Department of Veterans Affairs Cooperative Study Program. Dr. Harvey reported no relevant disclosures.
SAN DIEGO – A new study reports that about half of assessed U.S. veterans with schizophrenia or bipolar I disorder have tried to kill themselves. Nearly 70% of those with schizophrenia had documented suicidal behavior or ideation, as did more than 82% of those with bipolar I disorder.
“The VA struggles to predict suicidal ideation and behavior,” said study lead author Philip D. Harvey, PhD, of the Carter VA Medical Center in Miami, in an interview. “These data suggest that having one of these diagnoses is a major risk factor. Regular assessment makes considerable sense.”
Dr. Harvey released the study findings in a poster at the annual meeting of the American Psychiatric Association.
For the study, Dr. Harvey and his colleagues examined findings from a VA research project into the genetics behind functional disability in schizophrenia and bipolar illness.
“We know that suicide risk is higher in veterans than in the general population. We also know that the current focus is on returning veterans who were deployed in combat operations,” said Dr. Harvey, who also is affiliated with the University of Miami. “We wanted to evaluate the risk for suicidal ideation and behavior in the segment of the veteran population who have recently or ever been exposed to military trauma.”
The project assessed VA patients with schizophrenia (N = 3,941) or bipolar I disorder (N = 5,414) through in-person evaluations regarding issues like cognitive and functional status, and history of posttraumatic stress disorder. All of the subjects were outpatients at 26 VA medical centers.
Combined, the mean age of the study participants was 53.6 years, plus or minus 11 years, and 86.2% were male. Whites made up 57.4% of the sample, followed by blacks (37.0%) and other (5.6%). A total of 27% had no comorbid psychiatric conditions.
The study authors found documented suicidal ideation or suicidal behavior in 69.9% of veterans with schizophrenia and 82.3% of those with bipolar disorder; the percentages who reported making actual suicide attempts was 46.1% schizophrenia and 54.5% bipolar disorder.
The risk of suicidal ideation was lower in schizophrenia vs. bipolar disorder (odds ratio, 0.82; 95% confidence interval, 0.71-0.95), as was suicidal behavior (OR, 0.81; 95% CI, 0.71-0.93).
Dr. Harvey said this is not surprising. “The combination of a history of euphoric mood and significant depression [characteristic of bipolar disorder] is very challenging.”
Other factors lowered risk: College education vs. high school or less (OR, 0.82; 95% CI, 0.67-1.00 for ideation; OR, 0.70; 95% CI, 0.58-0.84 for behavior). In addition, lower risk was found among black vs. white patients (OR, 0.72; 95% CI, 0.63-0.84 for ideation; OR, 0.82; 95% CI, 0.72-0.93, for behavior).
These factors boosted risk: multiple psychiatric comorbidities vs. none (OR, 2.61; 95% CI, 2.22-3.07 for ideation; OR, 3.82; 95% CI, 3.30-4.41, for behavior), and those with a history of being ever vs. never married (OR, 1.18; 95% CI, 1.02-1.37 for ideation; OR, 1.36; 95% CI, 1.19-1.55, for behavior). Most of those who had been married later were divorced.
“These findings underscore the need for continuous monitoring for suicidality in veteran populations, regardless of age or psychiatric diagnosis, and especially with multiple psychiatric comorbidities,” the authors wrote.
The study was funded by the Department of Veterans Affairs Cooperative Study Program. Dr. Harvey reported no relevant disclosures.
SAN DIEGO – A new study reports that about half of assessed U.S. veterans with schizophrenia or bipolar I disorder have tried to kill themselves. Nearly 70% of those with schizophrenia had documented suicidal behavior or ideation, as did more than 82% of those with bipolar I disorder.
“The VA struggles to predict suicidal ideation and behavior,” said study lead author Philip D. Harvey, PhD, of the Carter VA Medical Center in Miami, in an interview. “These data suggest that having one of these diagnoses is a major risk factor. Regular assessment makes considerable sense.”
Dr. Harvey released the study findings in a poster at the annual meeting of the American Psychiatric Association.
For the study, Dr. Harvey and his colleagues examined findings from a VA research project into the genetics behind functional disability in schizophrenia and bipolar illness.
“We know that suicide risk is higher in veterans than in the general population. We also know that the current focus is on returning veterans who were deployed in combat operations,” said Dr. Harvey, who also is affiliated with the University of Miami. “We wanted to evaluate the risk for suicidal ideation and behavior in the segment of the veteran population who have recently or ever been exposed to military trauma.”
The project assessed VA patients with schizophrenia (N = 3,941) or bipolar I disorder (N = 5,414) through in-person evaluations regarding issues like cognitive and functional status, and history of posttraumatic stress disorder. All of the subjects were outpatients at 26 VA medical centers.
Combined, the mean age of the study participants was 53.6 years, plus or minus 11 years, and 86.2% were male. Whites made up 57.4% of the sample, followed by blacks (37.0%) and other (5.6%). A total of 27% had no comorbid psychiatric conditions.
The study authors found documented suicidal ideation or suicidal behavior in 69.9% of veterans with schizophrenia and 82.3% of those with bipolar disorder; the percentages who reported making actual suicide attempts was 46.1% schizophrenia and 54.5% bipolar disorder.
The risk of suicidal ideation was lower in schizophrenia vs. bipolar disorder (odds ratio, 0.82; 95% confidence interval, 0.71-0.95), as was suicidal behavior (OR, 0.81; 95% CI, 0.71-0.93).
Dr. Harvey said this is not surprising. “The combination of a history of euphoric mood and significant depression [characteristic of bipolar disorder] is very challenging.”
Other factors lowered risk: College education vs. high school or less (OR, 0.82; 95% CI, 0.67-1.00 for ideation; OR, 0.70; 95% CI, 0.58-0.84 for behavior). In addition, lower risk was found among black vs. white patients (OR, 0.72; 95% CI, 0.63-0.84 for ideation; OR, 0.82; 95% CI, 0.72-0.93, for behavior).
These factors boosted risk: multiple psychiatric comorbidities vs. none (OR, 2.61; 95% CI, 2.22-3.07 for ideation; OR, 3.82; 95% CI, 3.30-4.41, for behavior), and those with a history of being ever vs. never married (OR, 1.18; 95% CI, 1.02-1.37 for ideation; OR, 1.36; 95% CI, 1.19-1.55, for behavior). Most of those who had been married later were divorced.
“These findings underscore the need for continuous monitoring for suicidality in veteran populations, regardless of age or psychiatric diagnosis, and especially with multiple psychiatric comorbidities,” the authors wrote.
The study was funded by the Department of Veterans Affairs Cooperative Study Program. Dr. Harvey reported no relevant disclosures.
AT APA
Key clinical point: Roughly half of U.S. veterans with schizophrenia or bipolar I disorder have tried to kill themselves, and most of these veterans have histories of suicidal ideation or behavior.
Major finding: Suicide attempts are reported in 46.1% of patients with schizophrenia and 54.5% of those with bipolar I disorder. Documented suicidal ideation or behavior is reported in 69.9% of veterans with schizophrenia and 82.3% of those with bipolar disorder.
Data source: A genomic study with in-person assessments of VA patients with schizophrenia (N = 3,941) or bipolar disorder (N = 5,414). The mean age was 53.6 years, plus or minus 11 years; 86.2% were male, and 57.4% were white.
Disclosures: The study was funded by the Department of Veterans Affairs Cooperative Study Program.
‘Admirable’ overall survival attainable in AML with enasidenib

CHICAGO—The experimental mutant IDH2 (mIDH2) inhibitor enasidenib has produced “admirable” overall survival in patients with mIDH2 relapsed or refractory acute myeloid leukemia (AML), according to Eytan M. Stein, MD, an investigator on the phase 1 dose escalation and expansion study.
Patients who achieved a complete remission (CR) had a median overall survival (OS) of 19.7 months and non-CR responders, 13.8 months.
“I really want to make the point,” Dr Stein said, “this is a group of patients that are highly refractory, either refractory to induction chemotherapy, refractory to standard of care approaches for patients who are unable to get induction chemotherapy, so refractory to hypomethylating agents or low-dose cytarabine.”
Mutations in IDH2 occur in approximately 12% of AML patients.
Dr Stein explained that the mutant protein converts alpha ketoglutarate to beta hydroxyglutarate (2-HG). And increased levels of intracellular 2-HG lead to methylation changes in the cell that cause a block in myeloid differentiation.
Enasidenib, also known as AG-221, is a selective, oral, potent inhibitor of the mIDH2 enzyyme.
Dr Stein, of Memorial Sloan Kettering Cancer Center in New York, New York, presented the results during the ASCO 2017 Annual Meeting (abstract 7004).
The clinical and translational papers were published simultaneously in Blood.
Study design
The phase 1/2 study had a large dose-escalation component, with 113 patients enrolled. Patients had to have an advanced hematologic malignancy with an IDH2 mutation.
Patients received cumulative daily doses of 50 mg – 650 mg of enasidenib in continuous 28-day cycles.
Four expansion arms were added, with 126 patients.
Two expansion arms were in relapsed/refractory AML patients: one in patients 60 years or older or any age if they had relapsed after bone marrow transplant (BMT), and the other in patients younger than 60 excluding those relapsed after BMT.
The other 2 expansion arms were in untreated AML patients and in patients with any hematologic malignancy ineligible for the other arms.
Dr Stein presented results for the relapsed/refractory AML patients in the dose escalation and expansion phases of the study.
The key endpoints were safety, tolerability, maximum tolerated dose (MTD), and dose-limiting toxicities; response rates as assessed by the local investigator according to IWG criteria; and assessment of clinical activity.
Dr Stein noted the phase 2 study is now completely accrued (n=91) and the recommended enasidenib dose is 100 mg/day in relapsed/refractory AML.
The MTD was not reached at doses up to 650 mg/day.
Baseline characteristics
Median age of all 239 phase 1 patients was 70 years (range, 19-100), 57% were male, and almost all patients had intermediate- or poor-risk disease.
The investigators were also interested in the co-occurring mutations in patients on screening and whether there were differences between patients with mIDH2 at R172 and R140.
Seventy-five percent of the patients (n=179) had R140 and 24% had R172 (n=57).
There was a statistically significant difference in the number of co-occurring mutations in the R140 and R172 patients, with the R140 patients having a higher co-mutation burden compared with the R172 patients, (P=0.020).
The most frequent mutations co-occurring in R140 patients were SRSF2, followed by, in descending order of frequency, DNMT3A, RUNX1, ASXL1, and 24 others.
SFSR2 does not occur in R172 patients. DNMT3A was the most frequently co-occurring mutation in R172, followed by ASXL1, BCOR, NRAS, RUNX1, KMT2A, KRAS, and STAG2.
Safety
The most common treatment-emergent adverse events (TEAE) that occurred in 20% or more of all patients of any grade included nausea (46%), hyperbilirubinemia (45%), diarrhea and fatigue (40% each), decreased appetite (38%), vomiting (32%), dyspnea (31%), cough (29%), pyrexia and febrile neutropenia (28% each), thrombocytopenia, anemia, constipation, hypokalemia, and peripheral edema (27% each), pneumonia (21%), and hyperuricemia (20%).
The only 2 grade 3/4 TEAEs that rose above the level of 5% were hyperbilirubinemia (12%) and thrombocytopenia (6%).
“The hyperbilirubinemia, as I’ve mentioned in a number of meetings before this,” Dr Stein clarified, “is one that occurs because the enzyme is an off-target effect of inhibiting the UGT1A1 enzyme, which conjugates bilirubin.”
“So a patient who goes on this study who has a defect in bilirubin conjugation because they have Gilbert’s disease, they will have a higher level of bilirubin compared to a patient who doesn’t have Gilbert’s disease. This does not appear to have any clinical sequelae. You’ll also notice AST, ALT, alkaline phosphatase or any liver failure is not on this [TEAE] list.”
Response
The overall response rate for the patients who received enasidenib 100 mg/day was 38.5% (42/109) and for all doses 40.3% (71/176).
The true CR rate was 20.2% (100 mg/day) and 19.3% for all doses.
An additional 20% achieved a CR with incomplete hematologic recovery, CR with incomplete platelet recovery, partial response (PR), and morphologic leukemia-free state with either 100 mg enasidenib daily or all doses.
“Time to first response is not immediate,” Dr Stein pointed out. “It takes a median of 1.9 months to get there, and the time to complete remission takes even longer, a median of 3.7 months in the 100-mg experience, 3.8 months in all doses, to get to that best response.”
“I think the clinical importance of this is,” he added, “for a patient that one might have who is on this drug, it is important to keep them on the drug for a prolonged period of time so that they have the opportunity to have that response.”
Hematologic parameters also improved gradually.
Increases in platelet count, absolute neutrophil count, and hemoglobin level did not rise exponentially upon administration of study drug, but rather they slowly rose, “again getting to this point, that the drug takes time to work,” Dr Stein emphasized.
Patients in CR had very high transfusion independence rates, “which is what I would expect,” Dr Stein said. “If you are in complete remission, you should be transfusion independent.”
“What’s a little bit more interesting, though,” Dr Stein added, “is those patients who are non-CR responders. [I]n those patients who have responded but have less than a complete remission, 50% of them are independent of red cell transfusions and 50% of them are independent of platelet transfusions.”
Survival
The CR data and transfusion independence data translated into a median OS in these relapsed and refractory AML patients of 9.3 months.
And about 10% - 15% of the patients had prolonged survival up to 2 years and longer on the single agent.
Analysis of OS by best response revealed that for patients with a CR, “they really have an admirable overall survival of 19.7 months, almost 20 months,” Dr Stein said.
Patients who had a non-CR response had a median OS of 13.8 months, and non-responders had a median OS of 7.0 months.
And there was a qualitative improvement in response over time: the number of patients with CRs and PRs increased, while the number with stable disease decreased.
“Again, I think getting at the point it takes time for these responses to occur,” Dr Stein iterated.
Over the course of therapy, some responders had a differentiation of myeloblasts, so that by cycle 3, the marrow looked largely normal.
The investigators did not observe any morphological evidence of cytotoxicity or cellular aplasia.
But they did observe myeloid differentiation using FISH.
Trisomy 8 that was evident at the time of screening in responders’ myeloblasts, persisted in the promyelocytes and mature granulocyte population, and was no longer evident in the lymphoid compartment.
Baseline 2-HG levels and mIDH2 variant allele frequency were similar for responding and non-responding patients.
The investigators believe that differentiation of myeloblsts, not cytotoxicity, may drive the clinical efficacy of enasidenib.
A phase 3 trial of enasidenib monotherapy versus conventional care regimens is underway in older patients with late-stage AML, and phase 1/2 studies of enasidenib combinations are ongoing in newly diagnosed AML patients.
Enasidenib, which also has efficacy in myelodysplastic syndromes, has been granted priority review for relapsed/refractory AML by the US Food and Drug Administration. ![]()
CHICAGO—The experimental mutant IDH2 (mIDH2) inhibitor enasidenib has produced “admirable” overall survival in patients with mIDH2 relapsed or refractory acute myeloid leukemia (AML), according to Eytan M. Stein, MD, an investigator on the phase 1 dose escalation and expansion study.
Patients who achieved a complete remission (CR) had a median overall survival (OS) of 19.7 months and non-CR responders, 13.8 months.
“I really want to make the point,” Dr Stein said, “this is a group of patients that are highly refractory, either refractory to induction chemotherapy, refractory to standard of care approaches for patients who are unable to get induction chemotherapy, so refractory to hypomethylating agents or low-dose cytarabine.”
Mutations in IDH2 occur in approximately 12% of AML patients.
Dr Stein explained that the mutant protein converts alpha ketoglutarate to beta hydroxyglutarate (2-HG). And increased levels of intracellular 2-HG lead to methylation changes in the cell that cause a block in myeloid differentiation.
Enasidenib, also known as AG-221, is a selective, oral, potent inhibitor of the mIDH2 enzyyme.
Dr Stein, of Memorial Sloan Kettering Cancer Center in New York, New York, presented the results during the ASCO 2017 Annual Meeting (abstract 7004).
The clinical and translational papers were published simultaneously in Blood.
Study design
The phase 1/2 study had a large dose-escalation component, with 113 patients enrolled. Patients had to have an advanced hematologic malignancy with an IDH2 mutation.
Patients received cumulative daily doses of 50 mg – 650 mg of enasidenib in continuous 28-day cycles.
Four expansion arms were added, with 126 patients.
Two expansion arms were in relapsed/refractory AML patients: one in patients 60 years or older or any age if they had relapsed after bone marrow transplant (BMT), and the other in patients younger than 60 excluding those relapsed after BMT.
The other 2 expansion arms were in untreated AML patients and in patients with any hematologic malignancy ineligible for the other arms.
Dr Stein presented results for the relapsed/refractory AML patients in the dose escalation and expansion phases of the study.
The key endpoints were safety, tolerability, maximum tolerated dose (MTD), and dose-limiting toxicities; response rates as assessed by the local investigator according to IWG criteria; and assessment of clinical activity.
Dr Stein noted the phase 2 study is now completely accrued (n=91) and the recommended enasidenib dose is 100 mg/day in relapsed/refractory AML.
The MTD was not reached at doses up to 650 mg/day.
Baseline characteristics
Median age of all 239 phase 1 patients was 70 years (range, 19-100), 57% were male, and almost all patients had intermediate- or poor-risk disease.
The investigators were also interested in the co-occurring mutations in patients on screening and whether there were differences between patients with mIDH2 at R172 and R140.
Seventy-five percent of the patients (n=179) had R140 and 24% had R172 (n=57).
There was a statistically significant difference in the number of co-occurring mutations in the R140 and R172 patients, with the R140 patients having a higher co-mutation burden compared with the R172 patients, (P=0.020).
The most frequent mutations co-occurring in R140 patients were SRSF2, followed by, in descending order of frequency, DNMT3A, RUNX1, ASXL1, and 24 others.
SFSR2 does not occur in R172 patients. DNMT3A was the most frequently co-occurring mutation in R172, followed by ASXL1, BCOR, NRAS, RUNX1, KMT2A, KRAS, and STAG2.
Safety
The most common treatment-emergent adverse events (TEAE) that occurred in 20% or more of all patients of any grade included nausea (46%), hyperbilirubinemia (45%), diarrhea and fatigue (40% each), decreased appetite (38%), vomiting (32%), dyspnea (31%), cough (29%), pyrexia and febrile neutropenia (28% each), thrombocytopenia, anemia, constipation, hypokalemia, and peripheral edema (27% each), pneumonia (21%), and hyperuricemia (20%).
The only 2 grade 3/4 TEAEs that rose above the level of 5% were hyperbilirubinemia (12%) and thrombocytopenia (6%).
“The hyperbilirubinemia, as I’ve mentioned in a number of meetings before this,” Dr Stein clarified, “is one that occurs because the enzyme is an off-target effect of inhibiting the UGT1A1 enzyme, which conjugates bilirubin.”
“So a patient who goes on this study who has a defect in bilirubin conjugation because they have Gilbert’s disease, they will have a higher level of bilirubin compared to a patient who doesn’t have Gilbert’s disease. This does not appear to have any clinical sequelae. You’ll also notice AST, ALT, alkaline phosphatase or any liver failure is not on this [TEAE] list.”
Response
The overall response rate for the patients who received enasidenib 100 mg/day was 38.5% (42/109) and for all doses 40.3% (71/176).
The true CR rate was 20.2% (100 mg/day) and 19.3% for all doses.
An additional 20% achieved a CR with incomplete hematologic recovery, CR with incomplete platelet recovery, partial response (PR), and morphologic leukemia-free state with either 100 mg enasidenib daily or all doses.
“Time to first response is not immediate,” Dr Stein pointed out. “It takes a median of 1.9 months to get there, and the time to complete remission takes even longer, a median of 3.7 months in the 100-mg experience, 3.8 months in all doses, to get to that best response.”
“I think the clinical importance of this is,” he added, “for a patient that one might have who is on this drug, it is important to keep them on the drug for a prolonged period of time so that they have the opportunity to have that response.”
Hematologic parameters also improved gradually.
Increases in platelet count, absolute neutrophil count, and hemoglobin level did not rise exponentially upon administration of study drug, but rather they slowly rose, “again getting to this point, that the drug takes time to work,” Dr Stein emphasized.
Patients in CR had very high transfusion independence rates, “which is what I would expect,” Dr Stein said. “If you are in complete remission, you should be transfusion independent.”
“What’s a little bit more interesting, though,” Dr Stein added, “is those patients who are non-CR responders. [I]n those patients who have responded but have less than a complete remission, 50% of them are independent of red cell transfusions and 50% of them are independent of platelet transfusions.”
Survival
The CR data and transfusion independence data translated into a median OS in these relapsed and refractory AML patients of 9.3 months.
And about 10% - 15% of the patients had prolonged survival up to 2 years and longer on the single agent.
Analysis of OS by best response revealed that for patients with a CR, “they really have an admirable overall survival of 19.7 months, almost 20 months,” Dr Stein said.
Patients who had a non-CR response had a median OS of 13.8 months, and non-responders had a median OS of 7.0 months.
And there was a qualitative improvement in response over time: the number of patients with CRs and PRs increased, while the number with stable disease decreased.
“Again, I think getting at the point it takes time for these responses to occur,” Dr Stein iterated.
Over the course of therapy, some responders had a differentiation of myeloblasts, so that by cycle 3, the marrow looked largely normal.
The investigators did not observe any morphological evidence of cytotoxicity or cellular aplasia.
But they did observe myeloid differentiation using FISH.
Trisomy 8 that was evident at the time of screening in responders’ myeloblasts, persisted in the promyelocytes and mature granulocyte population, and was no longer evident in the lymphoid compartment.
Baseline 2-HG levels and mIDH2 variant allele frequency were similar for responding and non-responding patients.
The investigators believe that differentiation of myeloblsts, not cytotoxicity, may drive the clinical efficacy of enasidenib.
A phase 3 trial of enasidenib monotherapy versus conventional care regimens is underway in older patients with late-stage AML, and phase 1/2 studies of enasidenib combinations are ongoing in newly diagnosed AML patients.
Enasidenib, which also has efficacy in myelodysplastic syndromes, has been granted priority review for relapsed/refractory AML by the US Food and Drug Administration. ![]()
CHICAGO—The experimental mutant IDH2 (mIDH2) inhibitor enasidenib has produced “admirable” overall survival in patients with mIDH2 relapsed or refractory acute myeloid leukemia (AML), according to Eytan M. Stein, MD, an investigator on the phase 1 dose escalation and expansion study.
Patients who achieved a complete remission (CR) had a median overall survival (OS) of 19.7 months and non-CR responders, 13.8 months.
“I really want to make the point,” Dr Stein said, “this is a group of patients that are highly refractory, either refractory to induction chemotherapy, refractory to standard of care approaches for patients who are unable to get induction chemotherapy, so refractory to hypomethylating agents or low-dose cytarabine.”
Mutations in IDH2 occur in approximately 12% of AML patients.
Dr Stein explained that the mutant protein converts alpha ketoglutarate to beta hydroxyglutarate (2-HG). And increased levels of intracellular 2-HG lead to methylation changes in the cell that cause a block in myeloid differentiation.
Enasidenib, also known as AG-221, is a selective, oral, potent inhibitor of the mIDH2 enzyyme.
Dr Stein, of Memorial Sloan Kettering Cancer Center in New York, New York, presented the results during the ASCO 2017 Annual Meeting (abstract 7004).
The clinical and translational papers were published simultaneously in Blood.
Study design
The phase 1/2 study had a large dose-escalation component, with 113 patients enrolled. Patients had to have an advanced hematologic malignancy with an IDH2 mutation.
Patients received cumulative daily doses of 50 mg – 650 mg of enasidenib in continuous 28-day cycles.
Four expansion arms were added, with 126 patients.
Two expansion arms were in relapsed/refractory AML patients: one in patients 60 years or older or any age if they had relapsed after bone marrow transplant (BMT), and the other in patients younger than 60 excluding those relapsed after BMT.
The other 2 expansion arms were in untreated AML patients and in patients with any hematologic malignancy ineligible for the other arms.
Dr Stein presented results for the relapsed/refractory AML patients in the dose escalation and expansion phases of the study.
The key endpoints were safety, tolerability, maximum tolerated dose (MTD), and dose-limiting toxicities; response rates as assessed by the local investigator according to IWG criteria; and assessment of clinical activity.
Dr Stein noted the phase 2 study is now completely accrued (n=91) and the recommended enasidenib dose is 100 mg/day in relapsed/refractory AML.
The MTD was not reached at doses up to 650 mg/day.
Baseline characteristics
Median age of all 239 phase 1 patients was 70 years (range, 19-100), 57% were male, and almost all patients had intermediate- or poor-risk disease.
The investigators were also interested in the co-occurring mutations in patients on screening and whether there were differences between patients with mIDH2 at R172 and R140.
Seventy-five percent of the patients (n=179) had R140 and 24% had R172 (n=57).
There was a statistically significant difference in the number of co-occurring mutations in the R140 and R172 patients, with the R140 patients having a higher co-mutation burden compared with the R172 patients, (P=0.020).
The most frequent mutations co-occurring in R140 patients were SRSF2, followed by, in descending order of frequency, DNMT3A, RUNX1, ASXL1, and 24 others.
SFSR2 does not occur in R172 patients. DNMT3A was the most frequently co-occurring mutation in R172, followed by ASXL1, BCOR, NRAS, RUNX1, KMT2A, KRAS, and STAG2.
Safety
The most common treatment-emergent adverse events (TEAE) that occurred in 20% or more of all patients of any grade included nausea (46%), hyperbilirubinemia (45%), diarrhea and fatigue (40% each), decreased appetite (38%), vomiting (32%), dyspnea (31%), cough (29%), pyrexia and febrile neutropenia (28% each), thrombocytopenia, anemia, constipation, hypokalemia, and peripheral edema (27% each), pneumonia (21%), and hyperuricemia (20%).
The only 2 grade 3/4 TEAEs that rose above the level of 5% were hyperbilirubinemia (12%) and thrombocytopenia (6%).
“The hyperbilirubinemia, as I’ve mentioned in a number of meetings before this,” Dr Stein clarified, “is one that occurs because the enzyme is an off-target effect of inhibiting the UGT1A1 enzyme, which conjugates bilirubin.”
“So a patient who goes on this study who has a defect in bilirubin conjugation because they have Gilbert’s disease, they will have a higher level of bilirubin compared to a patient who doesn’t have Gilbert’s disease. This does not appear to have any clinical sequelae. You’ll also notice AST, ALT, alkaline phosphatase or any liver failure is not on this [TEAE] list.”
Response
The overall response rate for the patients who received enasidenib 100 mg/day was 38.5% (42/109) and for all doses 40.3% (71/176).
The true CR rate was 20.2% (100 mg/day) and 19.3% for all doses.
An additional 20% achieved a CR with incomplete hematologic recovery, CR with incomplete platelet recovery, partial response (PR), and morphologic leukemia-free state with either 100 mg enasidenib daily or all doses.
“Time to first response is not immediate,” Dr Stein pointed out. “It takes a median of 1.9 months to get there, and the time to complete remission takes even longer, a median of 3.7 months in the 100-mg experience, 3.8 months in all doses, to get to that best response.”
“I think the clinical importance of this is,” he added, “for a patient that one might have who is on this drug, it is important to keep them on the drug for a prolonged period of time so that they have the opportunity to have that response.”
Hematologic parameters also improved gradually.
Increases in platelet count, absolute neutrophil count, and hemoglobin level did not rise exponentially upon administration of study drug, but rather they slowly rose, “again getting to this point, that the drug takes time to work,” Dr Stein emphasized.
Patients in CR had very high transfusion independence rates, “which is what I would expect,” Dr Stein said. “If you are in complete remission, you should be transfusion independent.”
“What’s a little bit more interesting, though,” Dr Stein added, “is those patients who are non-CR responders. [I]n those patients who have responded but have less than a complete remission, 50% of them are independent of red cell transfusions and 50% of them are independent of platelet transfusions.”
Survival
The CR data and transfusion independence data translated into a median OS in these relapsed and refractory AML patients of 9.3 months.
And about 10% - 15% of the patients had prolonged survival up to 2 years and longer on the single agent.
Analysis of OS by best response revealed that for patients with a CR, “they really have an admirable overall survival of 19.7 months, almost 20 months,” Dr Stein said.
Patients who had a non-CR response had a median OS of 13.8 months, and non-responders had a median OS of 7.0 months.
And there was a qualitative improvement in response over time: the number of patients with CRs and PRs increased, while the number with stable disease decreased.
“Again, I think getting at the point it takes time for these responses to occur,” Dr Stein iterated.
Over the course of therapy, some responders had a differentiation of myeloblasts, so that by cycle 3, the marrow looked largely normal.
The investigators did not observe any morphological evidence of cytotoxicity or cellular aplasia.
But they did observe myeloid differentiation using FISH.
Trisomy 8 that was evident at the time of screening in responders’ myeloblasts, persisted in the promyelocytes and mature granulocyte population, and was no longer evident in the lymphoid compartment.
Baseline 2-HG levels and mIDH2 variant allele frequency were similar for responding and non-responding patients.
The investigators believe that differentiation of myeloblsts, not cytotoxicity, may drive the clinical efficacy of enasidenib.
A phase 3 trial of enasidenib monotherapy versus conventional care regimens is underway in older patients with late-stage AML, and phase 1/2 studies of enasidenib combinations are ongoing in newly diagnosed AML patients.
Enasidenib, which also has efficacy in myelodysplastic syndromes, has been granted priority review for relapsed/refractory AML by the US Food and Drug Administration. ![]()
Depression not responsible for teen weight gain, but SSRIs may be
Adolescents with major depressive disorder (MDD) were more likely to lose weight, but treatment with some SSRIs was associated with weight gain, based on data from a longitudinal study of 264 participants published online June 16 in Pediatrics.
MDD was associated with decrease in body mass index (BMI), fat mass index (FMI), and lean BMI (LBMI) z scores after controlling for factors including age, sex, physical activity, dietary intake, and length of study participation. However, dosage and duration of treatment with SSRIs were associated with increases in BMI, FMI, and LBMI z scores (Pediatrics. 2017. doi: 10.1542/peds.2016-3943).
The participants were part of a 2-year prospective study on the skeletal impact of SSRI use in older adolescents, and the average length of study participation was 1.5 years. After a baseline visit, they had follow-up visits, at which they completed the Inventory of Depressive Symptomatology (IDS), the Beck Depression Inventory (BDI-II), the Beck Anxiety Inventory (BAI), and the modified version of the Physical Activity Questionnaire for Adolescents, every four months. In addition, height, weight, and grip strength were measured. Body composition was measured using the BMI z score, FMI z score, LBMI z score, and visceral fat (Vfat) score.
Depression and anxiety, based on IDS and BAI scores, were inversely associated with changes in BMI z scores, and longer SSRI use was associated with increased BMI z scores. These changes remained significant when IDS scores and cumulative SSRI doses were included in the analysis.
In addition, use and duration of SSRIs each were significantly associated with increased FMI and LBMI scores after adjusting for standard confounding variables. SSRI use was associated with increased visceral fat mass, but the change was not significant.
When the researchers examined differences among individual drugs, they found that citalopram and escitalopram, but not sertraline, were associated with significant increases in both adiposity and lean mass. Fluoxetine showed a smaller, but still significant, effect.
SSRI use also impacted height over the study period (P less than .05), and fluoxetine had the greatest effect. Depression (IDS score) had no significant impact on height.
No significant differences appeared in the impact of SSRI use according to gender for LBMI, height z scores, or VFat. However, males had a significantly greater increase in BMI and FMI z scores, compared with females, over a longer period of SSRI use, a finding that deserves additional study, Dr. Calarge and associates noted.
The results were limited by several factors including the relatively small sample size, the use of self-reports, and the challenges of accurately documenting medication use, the researchers said.
Fat and lean mass were measured separately in this study, and, “to our surprise, SSRI use was positively associated with both outcome variables in a similar manner,” Dr. Calarge and associates noted. “When we specifically focused on VFat, the association with SSRI use remained positive, albeit weaker. This suggests that, over extended periods of use, SSRIs will cause an overall increase in BMI, comprising an increase in both fat and lean mass. Importantly, this is also associated with an increase in VFat, which is particularly detrimental to health,” and may contribute to the higher incidence of cardiovascular disease in MDD patients, they added. Future research should explore mechanisms of action and interventions to address treatment effects.
The researchers had no relevant financial disclosures. The study was funded by the National Institutes of Health, the National Institute of Mental Health, and the National Center for Research Resources.
Adolescents with major depressive disorder (MDD) were more likely to lose weight, but treatment with some SSRIs was associated with weight gain, based on data from a longitudinal study of 264 participants published online June 16 in Pediatrics.
MDD was associated with decrease in body mass index (BMI), fat mass index (FMI), and lean BMI (LBMI) z scores after controlling for factors including age, sex, physical activity, dietary intake, and length of study participation. However, dosage and duration of treatment with SSRIs were associated with increases in BMI, FMI, and LBMI z scores (Pediatrics. 2017. doi: 10.1542/peds.2016-3943).
The participants were part of a 2-year prospective study on the skeletal impact of SSRI use in older adolescents, and the average length of study participation was 1.5 years. After a baseline visit, they had follow-up visits, at which they completed the Inventory of Depressive Symptomatology (IDS), the Beck Depression Inventory (BDI-II), the Beck Anxiety Inventory (BAI), and the modified version of the Physical Activity Questionnaire for Adolescents, every four months. In addition, height, weight, and grip strength were measured. Body composition was measured using the BMI z score, FMI z score, LBMI z score, and visceral fat (Vfat) score.
Depression and anxiety, based on IDS and BAI scores, were inversely associated with changes in BMI z scores, and longer SSRI use was associated with increased BMI z scores. These changes remained significant when IDS scores and cumulative SSRI doses were included in the analysis.
In addition, use and duration of SSRIs each were significantly associated with increased FMI and LBMI scores after adjusting for standard confounding variables. SSRI use was associated with increased visceral fat mass, but the change was not significant.
When the researchers examined differences among individual drugs, they found that citalopram and escitalopram, but not sertraline, were associated with significant increases in both adiposity and lean mass. Fluoxetine showed a smaller, but still significant, effect.
SSRI use also impacted height over the study period (P less than .05), and fluoxetine had the greatest effect. Depression (IDS score) had no significant impact on height.
No significant differences appeared in the impact of SSRI use according to gender for LBMI, height z scores, or VFat. However, males had a significantly greater increase in BMI and FMI z scores, compared with females, over a longer period of SSRI use, a finding that deserves additional study, Dr. Calarge and associates noted.
The results were limited by several factors including the relatively small sample size, the use of self-reports, and the challenges of accurately documenting medication use, the researchers said.
Fat and lean mass were measured separately in this study, and, “to our surprise, SSRI use was positively associated with both outcome variables in a similar manner,” Dr. Calarge and associates noted. “When we specifically focused on VFat, the association with SSRI use remained positive, albeit weaker. This suggests that, over extended periods of use, SSRIs will cause an overall increase in BMI, comprising an increase in both fat and lean mass. Importantly, this is also associated with an increase in VFat, which is particularly detrimental to health,” and may contribute to the higher incidence of cardiovascular disease in MDD patients, they added. Future research should explore mechanisms of action and interventions to address treatment effects.
The researchers had no relevant financial disclosures. The study was funded by the National Institutes of Health, the National Institute of Mental Health, and the National Center for Research Resources.
Adolescents with major depressive disorder (MDD) were more likely to lose weight, but treatment with some SSRIs was associated with weight gain, based on data from a longitudinal study of 264 participants published online June 16 in Pediatrics.
MDD was associated with decrease in body mass index (BMI), fat mass index (FMI), and lean BMI (LBMI) z scores after controlling for factors including age, sex, physical activity, dietary intake, and length of study participation. However, dosage and duration of treatment with SSRIs were associated with increases in BMI, FMI, and LBMI z scores (Pediatrics. 2017. doi: 10.1542/peds.2016-3943).
The participants were part of a 2-year prospective study on the skeletal impact of SSRI use in older adolescents, and the average length of study participation was 1.5 years. After a baseline visit, they had follow-up visits, at which they completed the Inventory of Depressive Symptomatology (IDS), the Beck Depression Inventory (BDI-II), the Beck Anxiety Inventory (BAI), and the modified version of the Physical Activity Questionnaire for Adolescents, every four months. In addition, height, weight, and grip strength were measured. Body composition was measured using the BMI z score, FMI z score, LBMI z score, and visceral fat (Vfat) score.
Depression and anxiety, based on IDS and BAI scores, were inversely associated with changes in BMI z scores, and longer SSRI use was associated with increased BMI z scores. These changes remained significant when IDS scores and cumulative SSRI doses were included in the analysis.
In addition, use and duration of SSRIs each were significantly associated with increased FMI and LBMI scores after adjusting for standard confounding variables. SSRI use was associated with increased visceral fat mass, but the change was not significant.
When the researchers examined differences among individual drugs, they found that citalopram and escitalopram, but not sertraline, were associated with significant increases in both adiposity and lean mass. Fluoxetine showed a smaller, but still significant, effect.
SSRI use also impacted height over the study period (P less than .05), and fluoxetine had the greatest effect. Depression (IDS score) had no significant impact on height.
No significant differences appeared in the impact of SSRI use according to gender for LBMI, height z scores, or VFat. However, males had a significantly greater increase in BMI and FMI z scores, compared with females, over a longer period of SSRI use, a finding that deserves additional study, Dr. Calarge and associates noted.
The results were limited by several factors including the relatively small sample size, the use of self-reports, and the challenges of accurately documenting medication use, the researchers said.
Fat and lean mass were measured separately in this study, and, “to our surprise, SSRI use was positively associated with both outcome variables in a similar manner,” Dr. Calarge and associates noted. “When we specifically focused on VFat, the association with SSRI use remained positive, albeit weaker. This suggests that, over extended periods of use, SSRIs will cause an overall increase in BMI, comprising an increase in both fat and lean mass. Importantly, this is also associated with an increase in VFat, which is particularly detrimental to health,” and may contribute to the higher incidence of cardiovascular disease in MDD patients, they added. Future research should explore mechanisms of action and interventions to address treatment effects.
The researchers had no relevant financial disclosures. The study was funded by the National Institutes of Health, the National Institute of Mental Health, and the National Center for Research Resources.
FROM PEDIATRICS
Key clinical point: Major depressive disorder failed to promote changes in BMI in older adolescents.
Major finding: (P less than .003).
Data source: The data came from a longitudinal study of 264 adolescents aged 15-20 years.
Disclosures: The researchers had no relevant financial disclosures. The study was funded by the National Institutes of Health, the National Institute of Mental Health, and the National Center for Research Resources.
Fifty-year retrospective by Dr. William G. Wilkoff
When the first issue of Pediatric News was published 50 years ago, I was starting the second half of my first year in medical school. Over the ensuing 50 years, I have lived through and witnessed some dramatic changes in pediatrics. Here are just a few of the transitions that I’ve observed and Pediatric News has covered:
The birth of interventional neonatology
When I was an intern at Duke University Medical Center in Durham, N.C., a paper appeared in the New England Journal of Medicine describing the use of a simple continuous positive pressure apparatus for the treatment of respiratory distress syndrome entitled, “Treatment of idiopathic respiratory-distress syndrome with continuous positive airway pressure,” (1971 Jun 17;284[24]:1333-40). After seeing the paper, George Brumley, MD, the head of nursery, immediately had the hospital engineers build us our own setup, and we became part of what could arguably be called the revolution that turned neonatology into an interventional specialty.

From meningitis to mental health
Although it came gradually, one of the most significant changes over the last 50 years has been the shift in the mix of pathology presenting to the general pediatrician. In the 1970s and 1980s, the threat of invasive bacterial disease, usually from Haemophilus influenzae, was always hanging over us. It was not unusual for a single community pediatrician to see four or five cases of meningitis in a year. The introduction of effective vaccines and more potent antibiotics lessened the threat of serious bacterial infection, and in its place came a flood of mental health complaints, including anxiety (25% prevalence among 13- to 18-year-olds, depression (13% prevalence among 12- to 17-year-olds) and attention-deficit/hyperactivity disorder (ADHD) (9% prevalence among 13- to 18-year-olds). The result is the impression that, at times, being a general pediatrician today feels like being a more than part-time psychiatrist/psychologist.
Mental retardation and autism
In the 1970s and 1980s, the diagnosis of autism was usually reserved for children with serious communication difficulties. Many physicians and the lay public expected that a child who was diagnosed with autism would have no speech at all. The prevalence of the condition in the last quarter of the century was felt to be about 1 in 2,000.
The more common diagnosis during that period was mental retardation. However, as the result of insensitive stereotyping, “mental retardation” has become an offensive term and has vanished from the pediatric lexicon.
Autism, however, has flourished, and a recent estimate cited by the CDC pegs its prevalence at 1 in 68. Based on my observations, I expect that much, if not most, of this increase is the result of expanded diagnostic criteria and relabeling.
Chicken scratches to mouse clicks
In keeping with a long tradition in medicine, my office notes when I began in practice were unreadable by anyone except a very few my long-term coworkers. My scribbles were brief and often included sketches of wounds and body parts. Their primary purpose was to remind me what had transpired at that office visit and to record the biometrics. Unfortunately, as the cloud of malpractice crept over the landscape, with it came the nonsensical mantra, “if it wasn’t documented, it didn’t happen.”
With the introduction of computers, medical records became inflated and often inaccurate, documents to be used primarily for data collection and risk management. The physician now is tasked with being the data entry clerk who must keep her eyes on the computer screen at the expense of a meaningful interaction with the patient. Sadly, the physician-unfriendliness of electronic medical records has driven many older and experienced pediatricians into premature retirement, robbing general pediatrics of their accumulated wisdom.
A part-time job
In 1975, there were 22,730 practicing pediatricians, of whom 23% were women. In 2011, there were 80,992 pediatricians, of whom 56.6% were women. The percentage of women practicing pediatrics continues to climb, with the most recent figure being 58%. From the patient perspective, this shift in gender dominance has been well received.
At the same time, there has been a trend toward more pediatricians of both genders pursuing part-time employment. The model of the physician being the owner/operator of a medical practice that was flourishing when I began in practice has been replaced by one in which the physician is an employee of a much larger entity, which is pressured from all sides to cut costs. To make matters worse, the Medical Home model that currently is in vogue is proving to be a more expensive vehicle for delivering health care. The patient now is asked to view his physician as the director of a team and may see him or her only infrequently, at the expense of the therapeutic benefits of familiarity.
When I was in medical school, the tuition was around $2,500/year, and I graduated with a debt of about $3,000 – with an interest rate so low that I was in no rush to pay it off. Now a student entering medical school can expect to pay around $60,000/year – an amount that has far outstripped inflation.
These realities combine to create a potentially unsustainable economic climate for pediatricians. I have had a wonderful 50 years being a pediatrician. But I can’t promise the same level of enjoyment to the next generation of pediatricians, unless someone can figure how to cut the expense of medical school and/or make part-time employment fit into a health care delivery system that must contain costs to survive.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.” Email him at [email protected].
When the first issue of Pediatric News was published 50 years ago, I was starting the second half of my first year in medical school. Over the ensuing 50 years, I have lived through and witnessed some dramatic changes in pediatrics. Here are just a few of the transitions that I’ve observed and Pediatric News has covered:
The birth of interventional neonatology
When I was an intern at Duke University Medical Center in Durham, N.C., a paper appeared in the New England Journal of Medicine describing the use of a simple continuous positive pressure apparatus for the treatment of respiratory distress syndrome entitled, “Treatment of idiopathic respiratory-distress syndrome with continuous positive airway pressure,” (1971 Jun 17;284[24]:1333-40). After seeing the paper, George Brumley, MD, the head of nursery, immediately had the hospital engineers build us our own setup, and we became part of what could arguably be called the revolution that turned neonatology into an interventional specialty.
From meningitis to mental health
Although it came gradually, one of the most significant changes over the last 50 years has been the shift in the mix of pathology presenting to the general pediatrician. In the 1970s and 1980s, the threat of invasive bacterial disease, usually from Haemophilus influenzae, was always hanging over us. It was not unusual for a single community pediatrician to see four or five cases of meningitis in a year. The introduction of effective vaccines and more potent antibiotics lessened the threat of serious bacterial infection, and in its place came a flood of mental health complaints, including anxiety (25% prevalence among 13- to 18-year-olds, depression (13% prevalence among 12- to 17-year-olds) and attention-deficit/hyperactivity disorder (ADHD) (9% prevalence among 13- to 18-year-olds). The result is the impression that, at times, being a general pediatrician today feels like being a more than part-time psychiatrist/psychologist.
Mental retardation and autism
In the 1970s and 1980s, the diagnosis of autism was usually reserved for children with serious communication difficulties. Many physicians and the lay public expected that a child who was diagnosed with autism would have no speech at all. The prevalence of the condition in the last quarter of the century was felt to be about 1 in 2,000.
The more common diagnosis during that period was mental retardation. However, as the result of insensitive stereotyping, “mental retardation” has become an offensive term and has vanished from the pediatric lexicon.
Autism, however, has flourished, and a recent estimate cited by the CDC pegs its prevalence at 1 in 68. Based on my observations, I expect that much, if not most, of this increase is the result of expanded diagnostic criteria and relabeling.
Chicken scratches to mouse clicks
In keeping with a long tradition in medicine, my office notes when I began in practice were unreadable by anyone except a very few my long-term coworkers. My scribbles were brief and often included sketches of wounds and body parts. Their primary purpose was to remind me what had transpired at that office visit and to record the biometrics. Unfortunately, as the cloud of malpractice crept over the landscape, with it came the nonsensical mantra, “if it wasn’t documented, it didn’t happen.”
With the introduction of computers, medical records became inflated and often inaccurate, documents to be used primarily for data collection and risk management. The physician now is tasked with being the data entry clerk who must keep her eyes on the computer screen at the expense of a meaningful interaction with the patient. Sadly, the physician-unfriendliness of electronic medical records has driven many older and experienced pediatricians into premature retirement, robbing general pediatrics of their accumulated wisdom.
A part-time job
In 1975, there were 22,730 practicing pediatricians, of whom 23% were women. In 2011, there were 80,992 pediatricians, of whom 56.6% were women. The percentage of women practicing pediatrics continues to climb, with the most recent figure being 58%. From the patient perspective, this shift in gender dominance has been well received.
At the same time, there has been a trend toward more pediatricians of both genders pursuing part-time employment. The model of the physician being the owner/operator of a medical practice that was flourishing when I began in practice has been replaced by one in which the physician is an employee of a much larger entity, which is pressured from all sides to cut costs. To make matters worse, the Medical Home model that currently is in vogue is proving to be a more expensive vehicle for delivering health care. The patient now is asked to view his physician as the director of a team and may see him or her only infrequently, at the expense of the therapeutic benefits of familiarity.
When I was in medical school, the tuition was around $2,500/year, and I graduated with a debt of about $3,000 – with an interest rate so low that I was in no rush to pay it off. Now a student entering medical school can expect to pay around $60,000/year – an amount that has far outstripped inflation.
These realities combine to create a potentially unsustainable economic climate for pediatricians. I have had a wonderful 50 years being a pediatrician. But I can’t promise the same level of enjoyment to the next generation of pediatricians, unless someone can figure how to cut the expense of medical school and/or make part-time employment fit into a health care delivery system that must contain costs to survive.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.” Email him at [email protected].
When the first issue of Pediatric News was published 50 years ago, I was starting the second half of my first year in medical school. Over the ensuing 50 years, I have lived through and witnessed some dramatic changes in pediatrics. Here are just a few of the transitions that I’ve observed and Pediatric News has covered:
The birth of interventional neonatology
When I was an intern at Duke University Medical Center in Durham, N.C., a paper appeared in the New England Journal of Medicine describing the use of a simple continuous positive pressure apparatus for the treatment of respiratory distress syndrome entitled, “Treatment of idiopathic respiratory-distress syndrome with continuous positive airway pressure,” (1971 Jun 17;284[24]:1333-40). After seeing the paper, George Brumley, MD, the head of nursery, immediately had the hospital engineers build us our own setup, and we became part of what could arguably be called the revolution that turned neonatology into an interventional specialty.
From meningitis to mental health
Although it came gradually, one of the most significant changes over the last 50 years has been the shift in the mix of pathology presenting to the general pediatrician. In the 1970s and 1980s, the threat of invasive bacterial disease, usually from Haemophilus influenzae, was always hanging over us. It was not unusual for a single community pediatrician to see four or five cases of meningitis in a year. The introduction of effective vaccines and more potent antibiotics lessened the threat of serious bacterial infection, and in its place came a flood of mental health complaints, including anxiety (25% prevalence among 13- to 18-year-olds, depression (13% prevalence among 12- to 17-year-olds) and attention-deficit/hyperactivity disorder (ADHD) (9% prevalence among 13- to 18-year-olds). The result is the impression that, at times, being a general pediatrician today feels like being a more than part-time psychiatrist/psychologist.
Mental retardation and autism
In the 1970s and 1980s, the diagnosis of autism was usually reserved for children with serious communication difficulties. Many physicians and the lay public expected that a child who was diagnosed with autism would have no speech at all. The prevalence of the condition in the last quarter of the century was felt to be about 1 in 2,000.
The more common diagnosis during that period was mental retardation. However, as the result of insensitive stereotyping, “mental retardation” has become an offensive term and has vanished from the pediatric lexicon.
Autism, however, has flourished, and a recent estimate cited by the CDC pegs its prevalence at 1 in 68. Based on my observations, I expect that much, if not most, of this increase is the result of expanded diagnostic criteria and relabeling.
Chicken scratches to mouse clicks
In keeping with a long tradition in medicine, my office notes when I began in practice were unreadable by anyone except a very few my long-term coworkers. My scribbles were brief and often included sketches of wounds and body parts. Their primary purpose was to remind me what had transpired at that office visit and to record the biometrics. Unfortunately, as the cloud of malpractice crept over the landscape, with it came the nonsensical mantra, “if it wasn’t documented, it didn’t happen.”
With the introduction of computers, medical records became inflated and often inaccurate, documents to be used primarily for data collection and risk management. The physician now is tasked with being the data entry clerk who must keep her eyes on the computer screen at the expense of a meaningful interaction with the patient. Sadly, the physician-unfriendliness of electronic medical records has driven many older and experienced pediatricians into premature retirement, robbing general pediatrics of their accumulated wisdom.
A part-time job
In 1975, there were 22,730 practicing pediatricians, of whom 23% were women. In 2011, there were 80,992 pediatricians, of whom 56.6% were women. The percentage of women practicing pediatrics continues to climb, with the most recent figure being 58%. From the patient perspective, this shift in gender dominance has been well received.
At the same time, there has been a trend toward more pediatricians of both genders pursuing part-time employment. The model of the physician being the owner/operator of a medical practice that was flourishing when I began in practice has been replaced by one in which the physician is an employee of a much larger entity, which is pressured from all sides to cut costs. To make matters worse, the Medical Home model that currently is in vogue is proving to be a more expensive vehicle for delivering health care. The patient now is asked to view his physician as the director of a team and may see him or her only infrequently, at the expense of the therapeutic benefits of familiarity.
When I was in medical school, the tuition was around $2,500/year, and I graduated with a debt of about $3,000 – with an interest rate so low that I was in no rush to pay it off. Now a student entering medical school can expect to pay around $60,000/year – an amount that has far outstripped inflation.
These realities combine to create a potentially unsustainable economic climate for pediatricians. I have had a wonderful 50 years being a pediatrician. But I can’t promise the same level of enjoyment to the next generation of pediatricians, unless someone can figure how to cut the expense of medical school and/or make part-time employment fit into a health care delivery system that must contain costs to survive.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.” Email him at [email protected].
Tweaking CBT to boost outcomes in GAD
SAN FRANCISCO – The search is on for ways to refine cognitive-behavioral therapy for generalized anxiety disorder in order to improve upon current relatively modest success rates.
Cognitive-behavioral therapy (CBT) is less effective for generalized anxiety disorder (GAD) than for the other anxiety disorders. Only about one-half of patients are improved post-treatment, and less than one-third reach recovery, noted Richard E. Zinbarg, PhD, at the annual conference of the Anxiety and Depression Association of America.

At a session on advances in treatment of GAD, investigators presented randomized clinical trials assessing a variety of specific strategies aimed at enhancing the effectiveness of CBT in evidence-based fashion. The trials included a study of the impact of having patients keep a worry outcome journal, an exploration of the potential deleterious effects of a phenomenon known as relaxation-induced anxiety, and a study of the effectiveness of emotion regulation therapy, a relatively recent form of psychotherapy that’s part of the so-called “third wave” of CBT.
Worry outcome journal
Lucas LaFreniere observed that while CBT has been broadly shown to be effective for GAD, the various forms of CBT are packages of components that often include psychoeducation, stimulus control, behavioral experiments, exposure, cognitive reframing, relaxation training, and other elements in various combinations and sequences. Almost none of these specific components has been evaluated formally to learn whether they are pulling their weight therapeutically and making a positive contribution to outcomes.
Mr. LaFreniere, a doctoral student in clinical psychology at Pennsylvania State University in Hershey, presented a randomized trial of one such component, worry outcome monitoring, which currently is incorporated in some but not all CBT programs for GAD. Mr. LaFreniere and his coinvestigators developed a version of worry outcome monitoring they dubbed the worry outcome journal, or WOJ, which he characterized as “a brief ecological momentary intervention for worry.”

The WOJ works like this: At four random times per day, WOJ users receive a phone message to drop what they’re doing and record on a chart what they’re currently worrying about. They briefly note the date and time, the content of their worry, the distress it’s causing on a 1-7 scale, how much time they’re spending thinking about it, and their prediction as to the likelihood that this negative event actually will come to pass, which by the nature of their illness generally is unrealistically sky high early on in treatment. Later, they return to record whether the worrisome outcome occurred. The WOJ data are often reviewed in session.
The hypothesis was that the WOJ would reduce worry by aiding GAD patients in attending to their worries more thoroughly and objectively, recognizing in the moment the high cost of their worrying in terms of distress and cognitive interference, forming more realistic predictions about the future, and changing their conviction that excessive worrying is a worthwhile use of their time.
“One thing that particularly motivates me as a treatment researcher is the idea that those with GAD could be making themselves chronically miserable in an effort to protect themselves from future catastrophes that likely are not even going to happen. That’s a lot of human suffering that isn’t necessary. What we can do to help with that, we should do,” Mr. LaFreniere said.
On the other hand, this was a matter that cried out for a controlled trial because of the possibility that attempts to reduce worry might have unintended harmful consequences.
“Those with GAD have positive beliefs about worry. They believe it’s useful: it motivates, buffers emotional shifts, facilitates problem solving, and marks you as caring and conscientious – good personality traits,” he explained.
His study included 51 GAD patients randomized to 10 days using the WOJ or to a thought log control condition in which prompted by their cell phone four times daily, they recorded whatever everyday thought was on their mind at the moment. An example drawn from personal experience, Mr. LaFreniere said, might be “I love enchiladas!”
Outcome measures evaluated at baseline, again at 10 days upon conclusion of the intervention, and finally at 30 days of follow-up were the Penn State Worry Questionnaire, the GAD Questionnaire for DSM-IV, and the Meta-Cognitions Questionnaire subscales for positive beliefs about worry, uncontrollability of one’s thoughts, and negative beliefs about worry.
“The big reveal was that 91% of their worries did not come true,” he reported.
The primary outcome was reduction in worries as measured by the Penn State Questionnaire. The WOJ group showed a significant reduction, compared with controls, immediately post-treatment – which remained significant, albeit attenuated to a moderate effect size, at 30 days.
At day 10, 18 of 29 WOJ users no longer met diagnostic criteria for GAD, compared with 6 of 22 controls. By day 30, however, there was no significant between-group difference on this secondary endpoint.
The WOJ group showed a significantly greater reduction than controls on the secondary endpoint of uncontrollability of beliefs at both days 10 and 30.
“The WOJ may be a viable ecological momentary intervention for reducing worry in GAD. Therapist-free use of WOJ led to decreased worrying after only 10 days. It’s quite possible that longer practice may yield even stronger results. After all, for a normal CBT protocol, we’re looking at 8-20 weeks of treatment,” Mr. LaFreniere observed.
“I’d like to underscore that there was no harm done: The WOJ didn’t increase detrimental beliefs about worry,” he added. “We had a worry ourselves as researchers – disconfirmed by the trial – that patients may take the non-occurrence of their worries as some kind of proof that worry prevented those bad things from happening.”
Mr. LaFreniere is interested in studying the WOJ for worry reduction in non-GAD populations.
“Worry can be very high in other anxiety disorders, major depressive disorder, bipolar disorders, and in insomnia. The WOJ is highly cost-effective and easy to disseminate. It could very easily be made into a smartphone app,” he said.
Relaxation-induced anxiety
Relaxation training often is incorporated in treatment packages for GAD. Yet, it’s possible that one reason CBT is only modestly effective for GAD is because of relaxation-induced anxiety (RIA), an understudied phenomenon defined as a paradoxical increase in the physiological, behavioral, and cognitive aspects of anxiety when a person tries to relax.
“It has been theorized that individuals who are especially concerned with maintaining control over physical and psychological processes find relaxation vulnerable, unpleasant, and activating. Thus, discomfort with perceived lack of control during relaxed moments – an inability to let go – may result in unsought increase in anxiety during therapeutic attempts at relaxation,” according to Michelle G. Newman, PhD, professor of psychology at Penn State.

She presented a secondary analysis of a published randomized clinical trial she coauthored (J Consult Clin Psychol. 2002 Apr;70[2]:288-98) in which 41 participants with GAD were assigned to CBT with relaxation therapy using standard progressive muscle relaxation techniques or to self-control desensitization. Relaxation therapy and relaxation-induced anxiety ratings were recorded at each session. Outcomes were assessed post-treatment and at 6, 12, and 24 months of follow-up using the Penn State Worry Questionnaire, the State-Trait Anxiety Inventory, the Hamilton Anxiety Rating Scale, and the Clinician Severity Rating for GAD symptoms. In addition, immediately after each in-session relaxation practice, patients were asked to rate on a 9-point scale how much they noticed an increase in anxiety during the relaxation session.
All subjects improved significantly, but those with a lower peak RIA – defined as the highest level of RIA experienced in any of the 14 treatment sessions – had significantly fewer GAD symptoms at the end of therapy as well as at 2-year follow-up. Peak RIA was unrelated to baseline GAD symptom severity or change over time in anxiety symptoms. However, patients whose peak RIA occurred during the last several treatment sessions showed less improvement in GAD symptoms at the conclusion of treatment than those whose peak came earlier.
The clinical implications of these findings are that therapists who use progressive muscle relaxation in the treatment of GAD should assess RIA at the conclusion of every session, and if a patient reports moderate or higher RIA, the duration of the relaxation training portion of therapy should not be shortened until after several consecutive sessions of lower RIA have been reported, according to Dr. Newman.
Emotion regulation therapy
Megan E. Renna brought attendees up to speed on emotion regulation therapy (ERT), a third wave variant of CBT that incorporates principles from more traditional CBT, such as skills training and exposure, supplemented by teaching emotion regulation skills. Those skills include the development of present moment awareness and cultivation of compassion. Both are grounded in research on motivational and regulatory learning mechanisms related to threat vs. safety and reward versus loss.
As detailed in a recent review article for which she was first author (Front Psychol. 2017 Feb 6;8:98), ERT is a manualized, mechanism-targeted treatment for what she termed “distress disorders”; namely, GAD and major depressive disorder, which are highly comorbid, share key underlying temperamental features, and for whom adequate therapeutic success is all too often elusive. ERT appears to be particularly useful during the emerging adulthood years and across a broad range of ethnic and racial patients, according to Ms. Renna, a PhD student in clinical psychology at Hunter College in New York.
The efficacy of the original 20-session, individual therapy version of ERT was established in a study of 20 GAD patients, half of whom also had major depression (Depress Anxiety. 2015 Aug;32[8]:614-23). But Ms. Renna said ERT’s developers – Douglas S. Mennin, PhD, of Hunter College, and David M. Fresco, PhD, of Kent State (Ohio) University, are interested in determining the minimum effective therapeutic dose of ERT. They have conducted an open randomized trial of a 16-session version of ERT in which the results proved similar to those seen with 20 sessions. Now they’re carrying out a study of 8 vs. 16 sessions. The study is ongoing, but at first look, the results with 8 sessions of ERT appear similar to 16, Ms. Renna said.
None of the speakers reported having any financial conflicts of interest.
SAN FRANCISCO – The search is on for ways to refine cognitive-behavioral therapy for generalized anxiety disorder in order to improve upon current relatively modest success rates.
Cognitive-behavioral therapy (CBT) is less effective for generalized anxiety disorder (GAD) than for the other anxiety disorders. Only about one-half of patients are improved post-treatment, and less than one-third reach recovery, noted Richard E. Zinbarg, PhD, at the annual conference of the Anxiety and Depression Association of America.
At a session on advances in treatment of GAD, investigators presented randomized clinical trials assessing a variety of specific strategies aimed at enhancing the effectiveness of CBT in evidence-based fashion. The trials included a study of the impact of having patients keep a worry outcome journal, an exploration of the potential deleterious effects of a phenomenon known as relaxation-induced anxiety, and a study of the effectiveness of emotion regulation therapy, a relatively recent form of psychotherapy that’s part of the so-called “third wave” of CBT.
Worry outcome journal
Lucas LaFreniere observed that while CBT has been broadly shown to be effective for GAD, the various forms of CBT are packages of components that often include psychoeducation, stimulus control, behavioral experiments, exposure, cognitive reframing, relaxation training, and other elements in various combinations and sequences. Almost none of these specific components has been evaluated formally to learn whether they are pulling their weight therapeutically and making a positive contribution to outcomes.
Mr. LaFreniere, a doctoral student in clinical psychology at Pennsylvania State University in Hershey, presented a randomized trial of one such component, worry outcome monitoring, which currently is incorporated in some but not all CBT programs for GAD. Mr. LaFreniere and his coinvestigators developed a version of worry outcome monitoring they dubbed the worry outcome journal, or WOJ, which he characterized as “a brief ecological momentary intervention for worry.”
The WOJ works like this: At four random times per day, WOJ users receive a phone message to drop what they’re doing and record on a chart what they’re currently worrying about. They briefly note the date and time, the content of their worry, the distress it’s causing on a 1-7 scale, how much time they’re spending thinking about it, and their prediction as to the likelihood that this negative event actually will come to pass, which by the nature of their illness generally is unrealistically sky high early on in treatment. Later, they return to record whether the worrisome outcome occurred. The WOJ data are often reviewed in session.
The hypothesis was that the WOJ would reduce worry by aiding GAD patients in attending to their worries more thoroughly and objectively, recognizing in the moment the high cost of their worrying in terms of distress and cognitive interference, forming more realistic predictions about the future, and changing their conviction that excessive worrying is a worthwhile use of their time.
“One thing that particularly motivates me as a treatment researcher is the idea that those with GAD could be making themselves chronically miserable in an effort to protect themselves from future catastrophes that likely are not even going to happen. That’s a lot of human suffering that isn’t necessary. What we can do to help with that, we should do,” Mr. LaFreniere said.
On the other hand, this was a matter that cried out for a controlled trial because of the possibility that attempts to reduce worry might have unintended harmful consequences.
“Those with GAD have positive beliefs about worry. They believe it’s useful: it motivates, buffers emotional shifts, facilitates problem solving, and marks you as caring and conscientious – good personality traits,” he explained.
His study included 51 GAD patients randomized to 10 days using the WOJ or to a thought log control condition in which prompted by their cell phone four times daily, they recorded whatever everyday thought was on their mind at the moment. An example drawn from personal experience, Mr. LaFreniere said, might be “I love enchiladas!”
Outcome measures evaluated at baseline, again at 10 days upon conclusion of the intervention, and finally at 30 days of follow-up were the Penn State Worry Questionnaire, the GAD Questionnaire for DSM-IV, and the Meta-Cognitions Questionnaire subscales for positive beliefs about worry, uncontrollability of one’s thoughts, and negative beliefs about worry.
“The big reveal was that 91% of their worries did not come true,” he reported.
The primary outcome was reduction in worries as measured by the Penn State Questionnaire. The WOJ group showed a significant reduction, compared with controls, immediately post-treatment – which remained significant, albeit attenuated to a moderate effect size, at 30 days.
At day 10, 18 of 29 WOJ users no longer met diagnostic criteria for GAD, compared with 6 of 22 controls. By day 30, however, there was no significant between-group difference on this secondary endpoint.
The WOJ group showed a significantly greater reduction than controls on the secondary endpoint of uncontrollability of beliefs at both days 10 and 30.
“The WOJ may be a viable ecological momentary intervention for reducing worry in GAD. Therapist-free use of WOJ led to decreased worrying after only 10 days. It’s quite possible that longer practice may yield even stronger results. After all, for a normal CBT protocol, we’re looking at 8-20 weeks of treatment,” Mr. LaFreniere observed.
“I’d like to underscore that there was no harm done: The WOJ didn’t increase detrimental beliefs about worry,” he added. “We had a worry ourselves as researchers – disconfirmed by the trial – that patients may take the non-occurrence of their worries as some kind of proof that worry prevented those bad things from happening.”
Mr. LaFreniere is interested in studying the WOJ for worry reduction in non-GAD populations.
“Worry can be very high in other anxiety disorders, major depressive disorder, bipolar disorders, and in insomnia. The WOJ is highly cost-effective and easy to disseminate. It could very easily be made into a smartphone app,” he said.
Relaxation-induced anxiety
Relaxation training often is incorporated in treatment packages for GAD. Yet, it’s possible that one reason CBT is only modestly effective for GAD is because of relaxation-induced anxiety (RIA), an understudied phenomenon defined as a paradoxical increase in the physiological, behavioral, and cognitive aspects of anxiety when a person tries to relax.
“It has been theorized that individuals who are especially concerned with maintaining control over physical and psychological processes find relaxation vulnerable, unpleasant, and activating. Thus, discomfort with perceived lack of control during relaxed moments – an inability to let go – may result in unsought increase in anxiety during therapeutic attempts at relaxation,” according to Michelle G. Newman, PhD, professor of psychology at Penn State.
She presented a secondary analysis of a published randomized clinical trial she coauthored (J Consult Clin Psychol. 2002 Apr;70[2]:288-98) in which 41 participants with GAD were assigned to CBT with relaxation therapy using standard progressive muscle relaxation techniques or to self-control desensitization. Relaxation therapy and relaxation-induced anxiety ratings were recorded at each session. Outcomes were assessed post-treatment and at 6, 12, and 24 months of follow-up using the Penn State Worry Questionnaire, the State-Trait Anxiety Inventory, the Hamilton Anxiety Rating Scale, and the Clinician Severity Rating for GAD symptoms. In addition, immediately after each in-session relaxation practice, patients were asked to rate on a 9-point scale how much they noticed an increase in anxiety during the relaxation session.
All subjects improved significantly, but those with a lower peak RIA – defined as the highest level of RIA experienced in any of the 14 treatment sessions – had significantly fewer GAD symptoms at the end of therapy as well as at 2-year follow-up. Peak RIA was unrelated to baseline GAD symptom severity or change over time in anxiety symptoms. However, patients whose peak RIA occurred during the last several treatment sessions showed less improvement in GAD symptoms at the conclusion of treatment than those whose peak came earlier.
The clinical implications of these findings are that therapists who use progressive muscle relaxation in the treatment of GAD should assess RIA at the conclusion of every session, and if a patient reports moderate or higher RIA, the duration of the relaxation training portion of therapy should not be shortened until after several consecutive sessions of lower RIA have been reported, according to Dr. Newman.
Emotion regulation therapy
Megan E. Renna brought attendees up to speed on emotion regulation therapy (ERT), a third wave variant of CBT that incorporates principles from more traditional CBT, such as skills training and exposure, supplemented by teaching emotion regulation skills. Those skills include the development of present moment awareness and cultivation of compassion. Both are grounded in research on motivational and regulatory learning mechanisms related to threat vs. safety and reward versus loss.
As detailed in a recent review article for which she was first author (Front Psychol. 2017 Feb 6;8:98), ERT is a manualized, mechanism-targeted treatment for what she termed “distress disorders”; namely, GAD and major depressive disorder, which are highly comorbid, share key underlying temperamental features, and for whom adequate therapeutic success is all too often elusive. ERT appears to be particularly useful during the emerging adulthood years and across a broad range of ethnic and racial patients, according to Ms. Renna, a PhD student in clinical psychology at Hunter College in New York.
The efficacy of the original 20-session, individual therapy version of ERT was established in a study of 20 GAD patients, half of whom also had major depression (Depress Anxiety. 2015 Aug;32[8]:614-23). But Ms. Renna said ERT’s developers – Douglas S. Mennin, PhD, of Hunter College, and David M. Fresco, PhD, of Kent State (Ohio) University, are interested in determining the minimum effective therapeutic dose of ERT. They have conducted an open randomized trial of a 16-session version of ERT in which the results proved similar to those seen with 20 sessions. Now they’re carrying out a study of 8 vs. 16 sessions. The study is ongoing, but at first look, the results with 8 sessions of ERT appear similar to 16, Ms. Renna said.
None of the speakers reported having any financial conflicts of interest.
SAN FRANCISCO – The search is on for ways to refine cognitive-behavioral therapy for generalized anxiety disorder in order to improve upon current relatively modest success rates.
Cognitive-behavioral therapy (CBT) is less effective for generalized anxiety disorder (GAD) than for the other anxiety disorders. Only about one-half of patients are improved post-treatment, and less than one-third reach recovery, noted Richard E. Zinbarg, PhD, at the annual conference of the Anxiety and Depression Association of America.
At a session on advances in treatment of GAD, investigators presented randomized clinical trials assessing a variety of specific strategies aimed at enhancing the effectiveness of CBT in evidence-based fashion. The trials included a study of the impact of having patients keep a worry outcome journal, an exploration of the potential deleterious effects of a phenomenon known as relaxation-induced anxiety, and a study of the effectiveness of emotion regulation therapy, a relatively recent form of psychotherapy that’s part of the so-called “third wave” of CBT.
Worry outcome journal
Lucas LaFreniere observed that while CBT has been broadly shown to be effective for GAD, the various forms of CBT are packages of components that often include psychoeducation, stimulus control, behavioral experiments, exposure, cognitive reframing, relaxation training, and other elements in various combinations and sequences. Almost none of these specific components has been evaluated formally to learn whether they are pulling their weight therapeutically and making a positive contribution to outcomes.
Mr. LaFreniere, a doctoral student in clinical psychology at Pennsylvania State University in Hershey, presented a randomized trial of one such component, worry outcome monitoring, which currently is incorporated in some but not all CBT programs for GAD. Mr. LaFreniere and his coinvestigators developed a version of worry outcome monitoring they dubbed the worry outcome journal, or WOJ, which he characterized as “a brief ecological momentary intervention for worry.”
The WOJ works like this: At four random times per day, WOJ users receive a phone message to drop what they’re doing and record on a chart what they’re currently worrying about. They briefly note the date and time, the content of their worry, the distress it’s causing on a 1-7 scale, how much time they’re spending thinking about it, and their prediction as to the likelihood that this negative event actually will come to pass, which by the nature of their illness generally is unrealistically sky high early on in treatment. Later, they return to record whether the worrisome outcome occurred. The WOJ data are often reviewed in session.
The hypothesis was that the WOJ would reduce worry by aiding GAD patients in attending to their worries more thoroughly and objectively, recognizing in the moment the high cost of their worrying in terms of distress and cognitive interference, forming more realistic predictions about the future, and changing their conviction that excessive worrying is a worthwhile use of their time.
“One thing that particularly motivates me as a treatment researcher is the idea that those with GAD could be making themselves chronically miserable in an effort to protect themselves from future catastrophes that likely are not even going to happen. That’s a lot of human suffering that isn’t necessary. What we can do to help with that, we should do,” Mr. LaFreniere said.
On the other hand, this was a matter that cried out for a controlled trial because of the possibility that attempts to reduce worry might have unintended harmful consequences.
“Those with GAD have positive beliefs about worry. They believe it’s useful: it motivates, buffers emotional shifts, facilitates problem solving, and marks you as caring and conscientious – good personality traits,” he explained.
His study included 51 GAD patients randomized to 10 days using the WOJ or to a thought log control condition in which prompted by their cell phone four times daily, they recorded whatever everyday thought was on their mind at the moment. An example drawn from personal experience, Mr. LaFreniere said, might be “I love enchiladas!”
Outcome measures evaluated at baseline, again at 10 days upon conclusion of the intervention, and finally at 30 days of follow-up were the Penn State Worry Questionnaire, the GAD Questionnaire for DSM-IV, and the Meta-Cognitions Questionnaire subscales for positive beliefs about worry, uncontrollability of one’s thoughts, and negative beliefs about worry.
“The big reveal was that 91% of their worries did not come true,” he reported.
The primary outcome was reduction in worries as measured by the Penn State Questionnaire. The WOJ group showed a significant reduction, compared with controls, immediately post-treatment – which remained significant, albeit attenuated to a moderate effect size, at 30 days.
At day 10, 18 of 29 WOJ users no longer met diagnostic criteria for GAD, compared with 6 of 22 controls. By day 30, however, there was no significant between-group difference on this secondary endpoint.
The WOJ group showed a significantly greater reduction than controls on the secondary endpoint of uncontrollability of beliefs at both days 10 and 30.
“The WOJ may be a viable ecological momentary intervention for reducing worry in GAD. Therapist-free use of WOJ led to decreased worrying after only 10 days. It’s quite possible that longer practice may yield even stronger results. After all, for a normal CBT protocol, we’re looking at 8-20 weeks of treatment,” Mr. LaFreniere observed.
“I’d like to underscore that there was no harm done: The WOJ didn’t increase detrimental beliefs about worry,” he added. “We had a worry ourselves as researchers – disconfirmed by the trial – that patients may take the non-occurrence of their worries as some kind of proof that worry prevented those bad things from happening.”
Mr. LaFreniere is interested in studying the WOJ for worry reduction in non-GAD populations.
“Worry can be very high in other anxiety disorders, major depressive disorder, bipolar disorders, and in insomnia. The WOJ is highly cost-effective and easy to disseminate. It could very easily be made into a smartphone app,” he said.
Relaxation-induced anxiety
Relaxation training often is incorporated in treatment packages for GAD. Yet, it’s possible that one reason CBT is only modestly effective for GAD is because of relaxation-induced anxiety (RIA), an understudied phenomenon defined as a paradoxical increase in the physiological, behavioral, and cognitive aspects of anxiety when a person tries to relax.
“It has been theorized that individuals who are especially concerned with maintaining control over physical and psychological processes find relaxation vulnerable, unpleasant, and activating. Thus, discomfort with perceived lack of control during relaxed moments – an inability to let go – may result in unsought increase in anxiety during therapeutic attempts at relaxation,” according to Michelle G. Newman, PhD, professor of psychology at Penn State.
She presented a secondary analysis of a published randomized clinical trial she coauthored (J Consult Clin Psychol. 2002 Apr;70[2]:288-98) in which 41 participants with GAD were assigned to CBT with relaxation therapy using standard progressive muscle relaxation techniques or to self-control desensitization. Relaxation therapy and relaxation-induced anxiety ratings were recorded at each session. Outcomes were assessed post-treatment and at 6, 12, and 24 months of follow-up using the Penn State Worry Questionnaire, the State-Trait Anxiety Inventory, the Hamilton Anxiety Rating Scale, and the Clinician Severity Rating for GAD symptoms. In addition, immediately after each in-session relaxation practice, patients were asked to rate on a 9-point scale how much they noticed an increase in anxiety during the relaxation session.
All subjects improved significantly, but those with a lower peak RIA – defined as the highest level of RIA experienced in any of the 14 treatment sessions – had significantly fewer GAD symptoms at the end of therapy as well as at 2-year follow-up. Peak RIA was unrelated to baseline GAD symptom severity or change over time in anxiety symptoms. However, patients whose peak RIA occurred during the last several treatment sessions showed less improvement in GAD symptoms at the conclusion of treatment than those whose peak came earlier.
The clinical implications of these findings are that therapists who use progressive muscle relaxation in the treatment of GAD should assess RIA at the conclusion of every session, and if a patient reports moderate or higher RIA, the duration of the relaxation training portion of therapy should not be shortened until after several consecutive sessions of lower RIA have been reported, according to Dr. Newman.
Emotion regulation therapy
Megan E. Renna brought attendees up to speed on emotion regulation therapy (ERT), a third wave variant of CBT that incorporates principles from more traditional CBT, such as skills training and exposure, supplemented by teaching emotion regulation skills. Those skills include the development of present moment awareness and cultivation of compassion. Both are grounded in research on motivational and regulatory learning mechanisms related to threat vs. safety and reward versus loss.
As detailed in a recent review article for which she was first author (Front Psychol. 2017 Feb 6;8:98), ERT is a manualized, mechanism-targeted treatment for what she termed “distress disorders”; namely, GAD and major depressive disorder, which are highly comorbid, share key underlying temperamental features, and for whom adequate therapeutic success is all too often elusive. ERT appears to be particularly useful during the emerging adulthood years and across a broad range of ethnic and racial patients, according to Ms. Renna, a PhD student in clinical psychology at Hunter College in New York.
The efficacy of the original 20-session, individual therapy version of ERT was established in a study of 20 GAD patients, half of whom also had major depression (Depress Anxiety. 2015 Aug;32[8]:614-23). But Ms. Renna said ERT’s developers – Douglas S. Mennin, PhD, of Hunter College, and David M. Fresco, PhD, of Kent State (Ohio) University, are interested in determining the minimum effective therapeutic dose of ERT. They have conducted an open randomized trial of a 16-session version of ERT in which the results proved similar to those seen with 20 sessions. Now they’re carrying out a study of 8 vs. 16 sessions. The study is ongoing, but at first look, the results with 8 sessions of ERT appear similar to 16, Ms. Renna said.
None of the speakers reported having any financial conflicts of interest.
EXPERT ANALYSIS FROM THE ANXIETY AND DEPRESSION CONFERENCE 2017
Docs to Senate: Abandon your secret efforts on ACA repeal/replace
Six major organizations representing physicians have written to Senate leaders asking them to step back and take a different tack on health reform.
Senators have been meeting behind closed doors to craft health reform legislation as an alternative to the House-passed American Health Care Act (AHCA). To date, no draft legislation has surfaced publicly and no hearings have been held to discuss health reform provisions under consideration.
The letter was signed by the American Academy of Family Physicians, the American Academy of Pediatrics, the American College of Physicians, the American Congress of Obstetricians and Gynecologists, the American Osteopathic Association, and the American Psychiatric Association.
The groups raised their specific objections to two provisions of the AHCA that senators are said to be considering: caps on Medicaid funding and repeal of the Affordable Care Act’s essential benefits package.
Throughout the current health reform efforts “our organizations continually offered constructive ideas on achieving agreement on legislation consistent with our shared principles,” according to the letter. “Regrettably, both the House and Senate seem to be heading to a vote on legislation that would violate those principles by rolling back coverage and patient protections for tens of millions of patients.”
[email protected]
On Twitter @denisefulton
Six major organizations representing physicians have written to Senate leaders asking them to step back and take a different tack on health reform.
Senators have been meeting behind closed doors to craft health reform legislation as an alternative to the House-passed American Health Care Act (AHCA). To date, no draft legislation has surfaced publicly and no hearings have been held to discuss health reform provisions under consideration.
The letter was signed by the American Academy of Family Physicians, the American Academy of Pediatrics, the American College of Physicians, the American Congress of Obstetricians and Gynecologists, the American Osteopathic Association, and the American Psychiatric Association.
The groups raised their specific objections to two provisions of the AHCA that senators are said to be considering: caps on Medicaid funding and repeal of the Affordable Care Act’s essential benefits package.
Throughout the current health reform efforts “our organizations continually offered constructive ideas on achieving agreement on legislation consistent with our shared principles,” according to the letter. “Regrettably, both the House and Senate seem to be heading to a vote on legislation that would violate those principles by rolling back coverage and patient protections for tens of millions of patients.”
[email protected]
On Twitter @denisefulton
Six major organizations representing physicians have written to Senate leaders asking them to step back and take a different tack on health reform.
Senators have been meeting behind closed doors to craft health reform legislation as an alternative to the House-passed American Health Care Act (AHCA). To date, no draft legislation has surfaced publicly and no hearings have been held to discuss health reform provisions under consideration.
The letter was signed by the American Academy of Family Physicians, the American Academy of Pediatrics, the American College of Physicians, the American Congress of Obstetricians and Gynecologists, the American Osteopathic Association, and the American Psychiatric Association.
The groups raised their specific objections to two provisions of the AHCA that senators are said to be considering: caps on Medicaid funding and repeal of the Affordable Care Act’s essential benefits package.
Throughout the current health reform efforts “our organizations continually offered constructive ideas on achieving agreement on legislation consistent with our shared principles,” according to the letter. “Regrettably, both the House and Senate seem to be heading to a vote on legislation that would violate those principles by rolling back coverage and patient protections for tens of millions of patients.”
[email protected]
On Twitter @denisefulton
Vaccine delivery costs challenge physicians
, reported Mandy A. Allison, MD, of the University of Colorado at Denver, Aurora, and her associates.
Using the American Academy of Pediatrics’ recommended level of payment for first vaccine administration at that time – $25 – more than three-quarters of the practices surveyed said that all payer types paid less than the cost of vaccine administration, the researchers noted.
Those reporting that payment for vaccine administration was $11 or more was 74% for FFS, 74% for PPOs, 57% for MCOs/HMOs, 37% for CHIP, and 34% for Medicaid, the investigators reported.
In terms of how profit margins for vaccine delivery had changed in the last 3 years, an increase was reported by 25% of pediatric practices (Ped) and 15% of family physician practices (FP), no change was reported by 38% of Ped and 49% of FP, and a decrease by 37% of Ped and 36% of FP practices.
Of those practices that used strategies to reduce vaccine purchase cost or increase payment, 81% Ped and 36% FP used online purchasing discounts, 78% Ped and 49% FP used prompt pay discounts, 65% Ped and 49% FP used bulk order discounts, 69% Ped and 42% FP used group purchasing, and 69% Ped and 33% FP used promotional pricing.
Fewer than half of the practices said that they negotiated with private insurers regarding payment for vaccines (44% Ped, 33% FP) and administration fees (44% Ped, 35% FP).
When asked if they had stopped purchasing one or more pediatric vaccines for financial reasons, the answer was “yes” for 12% of Ped and 23% of FP, “no, but have seriously considered” for 24% of Ped and 26% of FP, and “no” for 64% of Ped and 51% of FP, reported Dr. Allison and her colleagues.
Read more in Academic Pediatrics (2017. doi: 10.1016/j.acap.2017.06.001).
, reported Mandy A. Allison, MD, of the University of Colorado at Denver, Aurora, and her associates.
Using the American Academy of Pediatrics’ recommended level of payment for first vaccine administration at that time – $25 – more than three-quarters of the practices surveyed said that all payer types paid less than the cost of vaccine administration, the researchers noted.
Those reporting that payment for vaccine administration was $11 or more was 74% for FFS, 74% for PPOs, 57% for MCOs/HMOs, 37% for CHIP, and 34% for Medicaid, the investigators reported.
In terms of how profit margins for vaccine delivery had changed in the last 3 years, an increase was reported by 25% of pediatric practices (Ped) and 15% of family physician practices (FP), no change was reported by 38% of Ped and 49% of FP, and a decrease by 37% of Ped and 36% of FP practices.
Of those practices that used strategies to reduce vaccine purchase cost or increase payment, 81% Ped and 36% FP used online purchasing discounts, 78% Ped and 49% FP used prompt pay discounts, 65% Ped and 49% FP used bulk order discounts, 69% Ped and 42% FP used group purchasing, and 69% Ped and 33% FP used promotional pricing.
Fewer than half of the practices said that they negotiated with private insurers regarding payment for vaccines (44% Ped, 33% FP) and administration fees (44% Ped, 35% FP).
When asked if they had stopped purchasing one or more pediatric vaccines for financial reasons, the answer was “yes” for 12% of Ped and 23% of FP, “no, but have seriously considered” for 24% of Ped and 26% of FP, and “no” for 64% of Ped and 51% of FP, reported Dr. Allison and her colleagues.
Read more in Academic Pediatrics (2017. doi: 10.1016/j.acap.2017.06.001).
, reported Mandy A. Allison, MD, of the University of Colorado at Denver, Aurora, and her associates.
Using the American Academy of Pediatrics’ recommended level of payment for first vaccine administration at that time – $25 – more than three-quarters of the practices surveyed said that all payer types paid less than the cost of vaccine administration, the researchers noted.
Those reporting that payment for vaccine administration was $11 or more was 74% for FFS, 74% for PPOs, 57% for MCOs/HMOs, 37% for CHIP, and 34% for Medicaid, the investigators reported.
In terms of how profit margins for vaccine delivery had changed in the last 3 years, an increase was reported by 25% of pediatric practices (Ped) and 15% of family physician practices (FP), no change was reported by 38% of Ped and 49% of FP, and a decrease by 37% of Ped and 36% of FP practices.
Of those practices that used strategies to reduce vaccine purchase cost or increase payment, 81% Ped and 36% FP used online purchasing discounts, 78% Ped and 49% FP used prompt pay discounts, 65% Ped and 49% FP used bulk order discounts, 69% Ped and 42% FP used group purchasing, and 69% Ped and 33% FP used promotional pricing.
Fewer than half of the practices said that they negotiated with private insurers regarding payment for vaccines (44% Ped, 33% FP) and administration fees (44% Ped, 35% FP).
When asked if they had stopped purchasing one or more pediatric vaccines for financial reasons, the answer was “yes” for 12% of Ped and 23% of FP, “no, but have seriously considered” for 24% of Ped and 26% of FP, and “no” for 64% of Ped and 51% of FP, reported Dr. Allison and her colleagues.
Read more in Academic Pediatrics (2017. doi: 10.1016/j.acap.2017.06.001).
FROM ACADEMIC PEDIATRICS
Painful Necrotic Ulcer on the Vulva
The Diagnosis: Mucormycosis
Skin biopsy and histology revealed broad, wide-angle, branched, nonseptate hyphae suggestive of mucormycosis infection (Figure 1). Computed tomography of the abdomen and pelvis revealed marked stranding in the vulvar region and urothelial thickening and enhancement suggestive of infection (Figure 2). Computed tomography of the chest demonstrated multiple irregular nodules in the bilateral upper lobes consistent with disseminated mucormycosis (Figure 3). The patient was started on intravenous amphotericin B and posaconazole. Surgery was not pursued given the poor prognosis of her refractory acute lymphoblastic leukemia, pancytopenia, and disseminated fungal infection. The patient was discharged home with hospice care.
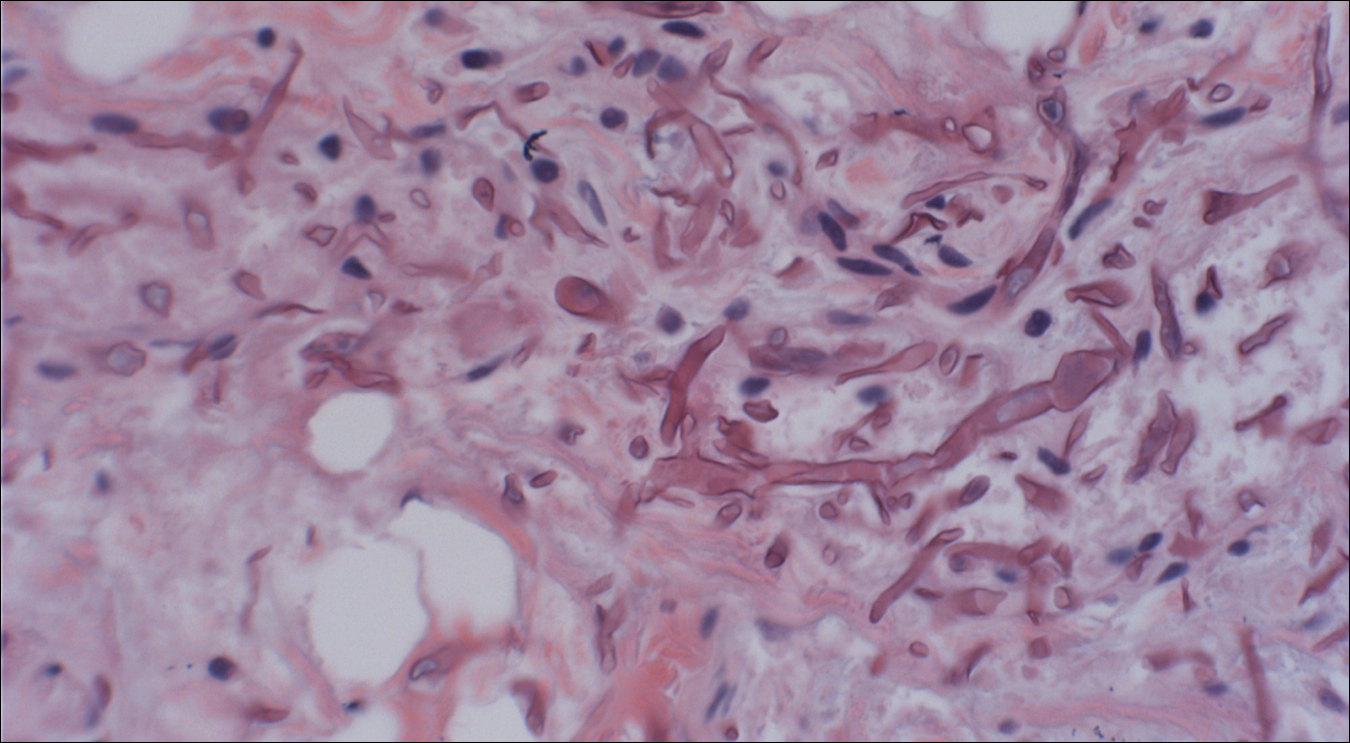
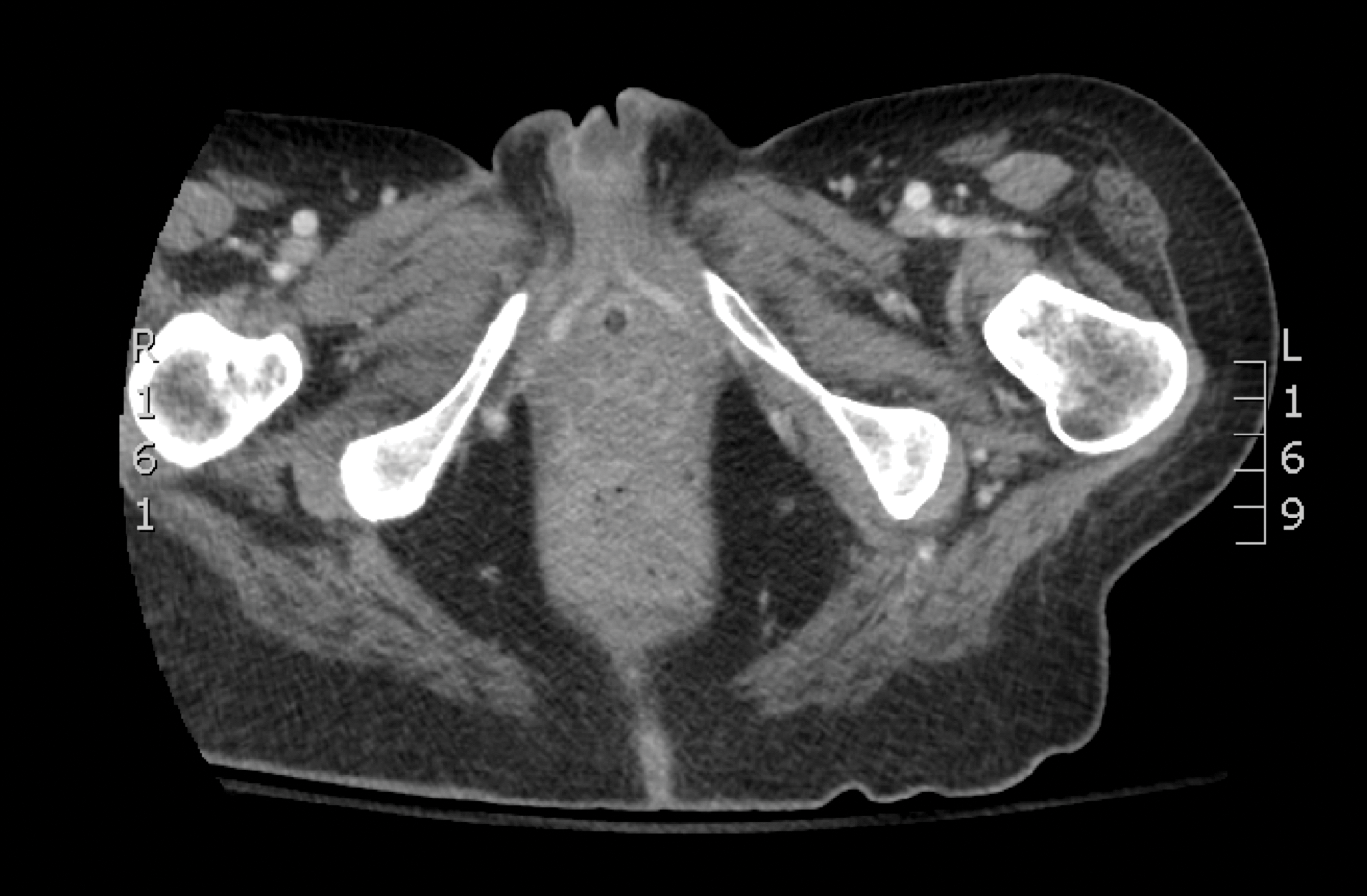
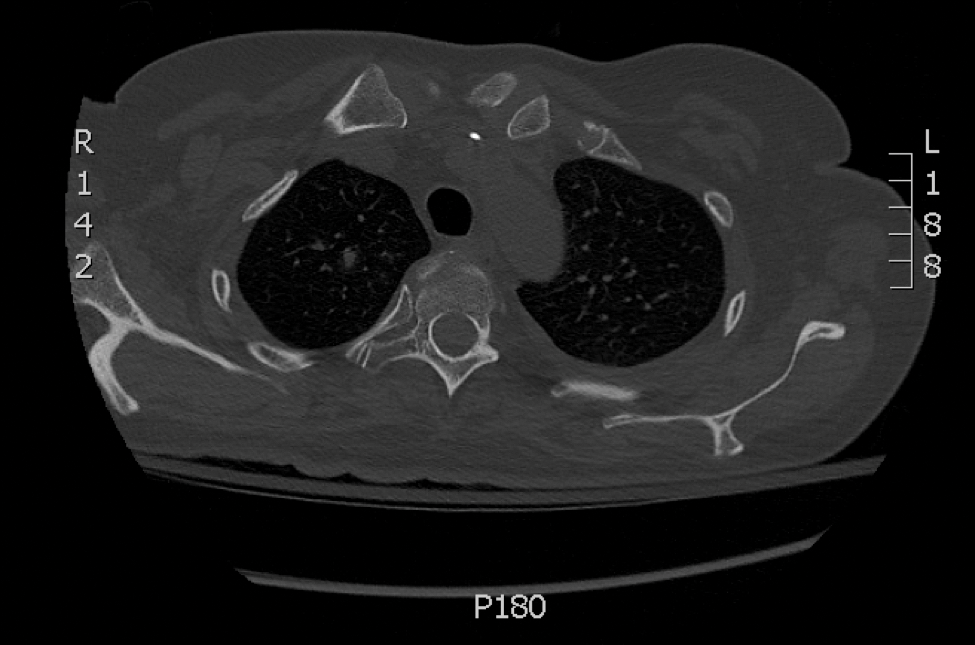
Mucormycosis is an infection caused by fungi that belong to the order Mucorales. The most common genera responsible for human disease are Rhizopus, Mucor, and Rhizomucor, which are organisms ubiquitous in nature and found in soil.1 Mucorales hyphae are widely branched and primarily nonseptate, which distinguishes them from hyphae of ascomycetous molds such as Aspergillus, which are narrowly branched and septate.
Mucormycosis primarily affects immunocompromised individuals. The overall incidence of mucormycosis is difficult to estimate, and the risk for infection varies based on the patient population. For example, the incidence of mucormycosis in hematologic malignancy ranges from 1% to 8% and from 0.4% to 16.0% in solid organ transplant recipients.2 One large series of 929 cases noted that the most common risk factors were associated with impaired immune function including diabetes mellitus and diabetic ketoacidosis (36% of cases), hematologic malignancy (17%), and solid organ (7%) or bone marrow transplantation (5%). Other risk factors include neutropenia, steroid therapy, and other immunocompromising conditions.3 Healthy individuals have a strong natural immunity to mucormycosis and rarely are affected by the disease.2
The host response to Mucorales is primarily driven by phagocyte-mediated killing via oxidative metabolites and cationic peptides called defensins.1 Thus, severely neutropenic patients are at high risk for developing mucormycosis.1 In contrast, it appears as though AIDS patients are not at increased risk for mucormycosis, supporting the theory that T lymphocytes are not involved in the host response.1 The conditions of diabetic ketoacidosis leave patients susceptible to mucormycosis for several reasons. First, hyperglycemia and low pH induce phagocyte dysfunction and thus inhibit the host response to Mucorales.4 Second, these organisms have an active ketone reductase system that may allow them to grow more readily in high glucose, acidic conditions.1 Third, diabetic ketoacidosis conditions increase serum free iron, and Mucorales utilizes host iron for cell growth and development.1 Individuals such as hemodialysis patients receiving the iron chelator deferoxamine also are at risk for mucormycosis, as Rhizopus can bind to this molecule and transport the bound iron intracellularly for growth utilization.1
Mucormycosis infection is characterized by infarction and rapid necrosis of host tissues resulting from vascular infiltration by fungal hyphae. The most common site of infection is rhino-orbital-cerebral (39%), followed by lungs (24%) and skin (19%).3 Dissemination occurs in 23% of cases.3 Inoculation most commonly occurs via inhalation of airborne fungal spores by an immunocompromised host with resultant fungal proliferation in the paranasal sinuses, bronchioles, or alveoli. Gastrointestinal tract infection is presumed to occur via ingestion of spores.5
Cutaneous infection, as in our patient, occurs via the inoculation of spores into the dermis through breaks in the skin such as from intravenous lines, urinary catheters, injection sites, surgical sites, and traumatic wounds. Cutaneous infections typically present as a single erythematous, painful, indurated papule that rapidly progresses to a necrotic ulcer with overlying black eschar. In some cases, the progression may be more indolent over the course of several weeks.2 There are few reported cases of primary vulvar mucormycosis, as in our patient.6,7 The previously reported cases involved severely immunocompromised patients who developed large necrotic lesions over the vulva that demonstrated widely branching, nonseptate hyphae on histologic examination. Each patient required extensive surgical debridement with systemic antifungal treatment.6,7
A timely diagnosis of mucormycosis often hinges on a high index of suspicion on behalf of the clinician. A fungal etiology always should be considered for an infection in an immunocompromised patient. Furthermore, nonresponse to antibiotic treatment should be an important diagnostic clue that the infection could be fungal in origin. The definitive diagnosis of mucormycosis is confirmed by tissue biopsy and the presence of broad, widely branching, nonseptate hyphae seen on histopathologic examination.
Treatment involves aggressive surgical debridement of all necrotic tissues and elimination of predisposing factors for infection such as hyperglycemia, metabolic acidosis, deferoxamine administration, and immunosuppressive medications. Early initiation of antifungal therapy with the lipid formulation of amphotericin B is recommended. Oral posaconazole or isavuconazole typically are used as step-down therapy after a favorable clinical response with initial amphotericin B treatment. Deferasirox, in contrast to deferoxamine, is an iron chelator that may reduce the pathogenicity of Mucorales and may help as an adjunctive therapy.8 In addition, hyperbaric oxygen therapy may have limited benefit in some cases.9 In spite of these treatments, the overall mortality of mucormycosis is 50% or higher and approaches nearly 100% in cases of disseminated disease, such as in our patient.1,3
- Ibrahim AS, Spellberg B, Walsh TJ, et al. Pathogenesis of mucormycosis. Clin Infect Dis. 2012;54(suppl 1):S16-S22.
- Petrikkos G, Skiada A, Lortholary O, et al. Epidemiology and clinical manifestations of mucormycosis. Clin Infect Dis. 2012;54(suppl 1):S23-S34.
- Roden MM, Zaoutis TE, Buchanan WL, et al. Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clin Infect Dis. 2005;41:634-653.
- Chinn RY, Diamond RD. Generation of chemotactic factors by Rhizopus oryzae in the presence and absence of serum: relationship to hyphal damage mediated by human neutrophils and effects of hyperglycemia and ketoacidosis. Infect Immun. 1982;38:1123-1129.
- Cheng VC, Chan JF, Ngan AH, et al. Outbreak of intestinal infection due to Rhizopus microsporus [published online July 29, 2009]. J Clin Microbiol. 2009;47:2834-2843.
- Colon M, Romaguera J, Mendez K, et al. Mucormycosis of the vulva in an immunocompromised pediatric patient. Bol Asoc Med P R. 2013;105:65-67.
- Nomura J, Ruskin J, Sahebi F, et al. Mucormycosis of the vulva following bone marrow transplantation. Bone Marrow Transplant. 1997;19:859-860.
- Spellberg B, Andes D, Perez M, et al. Safety and outcomes of open-label deferasirox iron chelation therapy for mucormycosis. Antimicrob Agents Chemother. 2009;53:3122-3125.
- Ferguson BJ, Mitchell TG, Moon R, et al. Adjunctive hyperbaric oxygen for treatment of rhinocerebral mucormycosis. Rev Infect Dis. 1988;10:551-559.
The Diagnosis: Mucormycosis
Skin biopsy and histology revealed broad, wide-angle, branched, nonseptate hyphae suggestive of mucormycosis infection (Figure 1). Computed tomography of the abdomen and pelvis revealed marked stranding in the vulvar region and urothelial thickening and enhancement suggestive of infection (Figure 2). Computed tomography of the chest demonstrated multiple irregular nodules in the bilateral upper lobes consistent with disseminated mucormycosis (Figure 3). The patient was started on intravenous amphotericin B and posaconazole. Surgery was not pursued given the poor prognosis of her refractory acute lymphoblastic leukemia, pancytopenia, and disseminated fungal infection. The patient was discharged home with hospice care.
Mucormycosis is an infection caused by fungi that belong to the order Mucorales. The most common genera responsible for human disease are Rhizopus, Mucor, and Rhizomucor, which are organisms ubiquitous in nature and found in soil.1 Mucorales hyphae are widely branched and primarily nonseptate, which distinguishes them from hyphae of ascomycetous molds such as Aspergillus, which are narrowly branched and septate.
Mucormycosis primarily affects immunocompromised individuals. The overall incidence of mucormycosis is difficult to estimate, and the risk for infection varies based on the patient population. For example, the incidence of mucormycosis in hematologic malignancy ranges from 1% to 8% and from 0.4% to 16.0% in solid organ transplant recipients.2 One large series of 929 cases noted that the most common risk factors were associated with impaired immune function including diabetes mellitus and diabetic ketoacidosis (36% of cases), hematologic malignancy (17%), and solid organ (7%) or bone marrow transplantation (5%). Other risk factors include neutropenia, steroid therapy, and other immunocompromising conditions.3 Healthy individuals have a strong natural immunity to mucormycosis and rarely are affected by the disease.2
The host response to Mucorales is primarily driven by phagocyte-mediated killing via oxidative metabolites and cationic peptides called defensins.1 Thus, severely neutropenic patients are at high risk for developing mucormycosis.1 In contrast, it appears as though AIDS patients are not at increased risk for mucormycosis, supporting the theory that T lymphocytes are not involved in the host response.1 The conditions of diabetic ketoacidosis leave patients susceptible to mucormycosis for several reasons. First, hyperglycemia and low pH induce phagocyte dysfunction and thus inhibit the host response to Mucorales.4 Second, these organisms have an active ketone reductase system that may allow them to grow more readily in high glucose, acidic conditions.1 Third, diabetic ketoacidosis conditions increase serum free iron, and Mucorales utilizes host iron for cell growth and development.1 Individuals such as hemodialysis patients receiving the iron chelator deferoxamine also are at risk for mucormycosis, as Rhizopus can bind to this molecule and transport the bound iron intracellularly for growth utilization.1
Mucormycosis infection is characterized by infarction and rapid necrosis of host tissues resulting from vascular infiltration by fungal hyphae. The most common site of infection is rhino-orbital-cerebral (39%), followed by lungs (24%) and skin (19%).3 Dissemination occurs in 23% of cases.3 Inoculation most commonly occurs via inhalation of airborne fungal spores by an immunocompromised host with resultant fungal proliferation in the paranasal sinuses, bronchioles, or alveoli. Gastrointestinal tract infection is presumed to occur via ingestion of spores.5
Cutaneous infection, as in our patient, occurs via the inoculation of spores into the dermis through breaks in the skin such as from intravenous lines, urinary catheters, injection sites, surgical sites, and traumatic wounds. Cutaneous infections typically present as a single erythematous, painful, indurated papule that rapidly progresses to a necrotic ulcer with overlying black eschar. In some cases, the progression may be more indolent over the course of several weeks.2 There are few reported cases of primary vulvar mucormycosis, as in our patient.6,7 The previously reported cases involved severely immunocompromised patients who developed large necrotic lesions over the vulva that demonstrated widely branching, nonseptate hyphae on histologic examination. Each patient required extensive surgical debridement with systemic antifungal treatment.6,7
A timely diagnosis of mucormycosis often hinges on a high index of suspicion on behalf of the clinician. A fungal etiology always should be considered for an infection in an immunocompromised patient. Furthermore, nonresponse to antibiotic treatment should be an important diagnostic clue that the infection could be fungal in origin. The definitive diagnosis of mucormycosis is confirmed by tissue biopsy and the presence of broad, widely branching, nonseptate hyphae seen on histopathologic examination.
Treatment involves aggressive surgical debridement of all necrotic tissues and elimination of predisposing factors for infection such as hyperglycemia, metabolic acidosis, deferoxamine administration, and immunosuppressive medications. Early initiation of antifungal therapy with the lipid formulation of amphotericin B is recommended. Oral posaconazole or isavuconazole typically are used as step-down therapy after a favorable clinical response with initial amphotericin B treatment. Deferasirox, in contrast to deferoxamine, is an iron chelator that may reduce the pathogenicity of Mucorales and may help as an adjunctive therapy.8 In addition, hyperbaric oxygen therapy may have limited benefit in some cases.9 In spite of these treatments, the overall mortality of mucormycosis is 50% or higher and approaches nearly 100% in cases of disseminated disease, such as in our patient.1,3
The Diagnosis: Mucormycosis
Skin biopsy and histology revealed broad, wide-angle, branched, nonseptate hyphae suggestive of mucormycosis infection (Figure 1). Computed tomography of the abdomen and pelvis revealed marked stranding in the vulvar region and urothelial thickening and enhancement suggestive of infection (Figure 2). Computed tomography of the chest demonstrated multiple irregular nodules in the bilateral upper lobes consistent with disseminated mucormycosis (Figure 3). The patient was started on intravenous amphotericin B and posaconazole. Surgery was not pursued given the poor prognosis of her refractory acute lymphoblastic leukemia, pancytopenia, and disseminated fungal infection. The patient was discharged home with hospice care.
Mucormycosis is an infection caused by fungi that belong to the order Mucorales. The most common genera responsible for human disease are Rhizopus, Mucor, and Rhizomucor, which are organisms ubiquitous in nature and found in soil.1 Mucorales hyphae are widely branched and primarily nonseptate, which distinguishes them from hyphae of ascomycetous molds such as Aspergillus, which are narrowly branched and septate.
Mucormycosis primarily affects immunocompromised individuals. The overall incidence of mucormycosis is difficult to estimate, and the risk for infection varies based on the patient population. For example, the incidence of mucormycosis in hematologic malignancy ranges from 1% to 8% and from 0.4% to 16.0% in solid organ transplant recipients.2 One large series of 929 cases noted that the most common risk factors were associated with impaired immune function including diabetes mellitus and diabetic ketoacidosis (36% of cases), hematologic malignancy (17%), and solid organ (7%) or bone marrow transplantation (5%). Other risk factors include neutropenia, steroid therapy, and other immunocompromising conditions.3 Healthy individuals have a strong natural immunity to mucormycosis and rarely are affected by the disease.2
The host response to Mucorales is primarily driven by phagocyte-mediated killing via oxidative metabolites and cationic peptides called defensins.1 Thus, severely neutropenic patients are at high risk for developing mucormycosis.1 In contrast, it appears as though AIDS patients are not at increased risk for mucormycosis, supporting the theory that T lymphocytes are not involved in the host response.1 The conditions of diabetic ketoacidosis leave patients susceptible to mucormycosis for several reasons. First, hyperglycemia and low pH induce phagocyte dysfunction and thus inhibit the host response to Mucorales.4 Second, these organisms have an active ketone reductase system that may allow them to grow more readily in high glucose, acidic conditions.1 Third, diabetic ketoacidosis conditions increase serum free iron, and Mucorales utilizes host iron for cell growth and development.1 Individuals such as hemodialysis patients receiving the iron chelator deferoxamine also are at risk for mucormycosis, as Rhizopus can bind to this molecule and transport the bound iron intracellularly for growth utilization.1
Mucormycosis infection is characterized by infarction and rapid necrosis of host tissues resulting from vascular infiltration by fungal hyphae. The most common site of infection is rhino-orbital-cerebral (39%), followed by lungs (24%) and skin (19%).3 Dissemination occurs in 23% of cases.3 Inoculation most commonly occurs via inhalation of airborne fungal spores by an immunocompromised host with resultant fungal proliferation in the paranasal sinuses, bronchioles, or alveoli. Gastrointestinal tract infection is presumed to occur via ingestion of spores.5
Cutaneous infection, as in our patient, occurs via the inoculation of spores into the dermis through breaks in the skin such as from intravenous lines, urinary catheters, injection sites, surgical sites, and traumatic wounds. Cutaneous infections typically present as a single erythematous, painful, indurated papule that rapidly progresses to a necrotic ulcer with overlying black eschar. In some cases, the progression may be more indolent over the course of several weeks.2 There are few reported cases of primary vulvar mucormycosis, as in our patient.6,7 The previously reported cases involved severely immunocompromised patients who developed large necrotic lesions over the vulva that demonstrated widely branching, nonseptate hyphae on histologic examination. Each patient required extensive surgical debridement with systemic antifungal treatment.6,7
A timely diagnosis of mucormycosis often hinges on a high index of suspicion on behalf of the clinician. A fungal etiology always should be considered for an infection in an immunocompromised patient. Furthermore, nonresponse to antibiotic treatment should be an important diagnostic clue that the infection could be fungal in origin. The definitive diagnosis of mucormycosis is confirmed by tissue biopsy and the presence of broad, widely branching, nonseptate hyphae seen on histopathologic examination.
Treatment involves aggressive surgical debridement of all necrotic tissues and elimination of predisposing factors for infection such as hyperglycemia, metabolic acidosis, deferoxamine administration, and immunosuppressive medications. Early initiation of antifungal therapy with the lipid formulation of amphotericin B is recommended. Oral posaconazole or isavuconazole typically are used as step-down therapy after a favorable clinical response with initial amphotericin B treatment. Deferasirox, in contrast to deferoxamine, is an iron chelator that may reduce the pathogenicity of Mucorales and may help as an adjunctive therapy.8 In addition, hyperbaric oxygen therapy may have limited benefit in some cases.9 In spite of these treatments, the overall mortality of mucormycosis is 50% or higher and approaches nearly 100% in cases of disseminated disease, such as in our patient.1,3
- Ibrahim AS, Spellberg B, Walsh TJ, et al. Pathogenesis of mucormycosis. Clin Infect Dis. 2012;54(suppl 1):S16-S22.
- Petrikkos G, Skiada A, Lortholary O, et al. Epidemiology and clinical manifestations of mucormycosis. Clin Infect Dis. 2012;54(suppl 1):S23-S34.
- Roden MM, Zaoutis TE, Buchanan WL, et al. Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clin Infect Dis. 2005;41:634-653.
- Chinn RY, Diamond RD. Generation of chemotactic factors by Rhizopus oryzae in the presence and absence of serum: relationship to hyphal damage mediated by human neutrophils and effects of hyperglycemia and ketoacidosis. Infect Immun. 1982;38:1123-1129.
- Cheng VC, Chan JF, Ngan AH, et al. Outbreak of intestinal infection due to Rhizopus microsporus [published online July 29, 2009]. J Clin Microbiol. 2009;47:2834-2843.
- Colon M, Romaguera J, Mendez K, et al. Mucormycosis of the vulva in an immunocompromised pediatric patient. Bol Asoc Med P R. 2013;105:65-67.
- Nomura J, Ruskin J, Sahebi F, et al. Mucormycosis of the vulva following bone marrow transplantation. Bone Marrow Transplant. 1997;19:859-860.
- Spellberg B, Andes D, Perez M, et al. Safety and outcomes of open-label deferasirox iron chelation therapy for mucormycosis. Antimicrob Agents Chemother. 2009;53:3122-3125.
- Ferguson BJ, Mitchell TG, Moon R, et al. Adjunctive hyperbaric oxygen for treatment of rhinocerebral mucormycosis. Rev Infect Dis. 1988;10:551-559.
- Ibrahim AS, Spellberg B, Walsh TJ, et al. Pathogenesis of mucormycosis. Clin Infect Dis. 2012;54(suppl 1):S16-S22.
- Petrikkos G, Skiada A, Lortholary O, et al. Epidemiology and clinical manifestations of mucormycosis. Clin Infect Dis. 2012;54(suppl 1):S23-S34.
- Roden MM, Zaoutis TE, Buchanan WL, et al. Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clin Infect Dis. 2005;41:634-653.
- Chinn RY, Diamond RD. Generation of chemotactic factors by Rhizopus oryzae in the presence and absence of serum: relationship to hyphal damage mediated by human neutrophils and effects of hyperglycemia and ketoacidosis. Infect Immun. 1982;38:1123-1129.
- Cheng VC, Chan JF, Ngan AH, et al. Outbreak of intestinal infection due to Rhizopus microsporus [published online July 29, 2009]. J Clin Microbiol. 2009;47:2834-2843.
- Colon M, Romaguera J, Mendez K, et al. Mucormycosis of the vulva in an immunocompromised pediatric patient. Bol Asoc Med P R. 2013;105:65-67.
- Nomura J, Ruskin J, Sahebi F, et al. Mucormycosis of the vulva following bone marrow transplantation. Bone Marrow Transplant. 1997;19:859-860.
- Spellberg B, Andes D, Perez M, et al. Safety and outcomes of open-label deferasirox iron chelation therapy for mucormycosis. Antimicrob Agents Chemother. 2009;53:3122-3125.
- Ferguson BJ, Mitchell TG, Moon R, et al. Adjunctive hyperbaric oxygen for treatment of rhinocerebral mucormycosis. Rev Infect Dis. 1988;10:551-559.

A 48-year-old woman with relapsed T-cell acute lymphoblastic leukemia was admitted to the oncology service for salvage chemotherapy and allogeneic stem cell transplant. Her admission was complicated by extended-spectrum β-lactamase-producing Escherichia coli sepsis and persistent pancytopenia, which required transfer to the intensive care unit. After 2 weeks and while still in the intensive care unit, she developed a painful necrotic vulvar ulcer over the right labia and clitoris that progressed and formed an overlying black eschar.
