User login
Bilateral cellulitis on legs? Think venous stasis dermatitis
SAN FRANCISCO – If a patient presents with bilateral cellulitis on both legs, think venous stasis dermatitis, which is the number one misdiagnosis of cellulitis and a frequent cause of unnecessary hospitalization for so-called “red leg,” according to Kanade Shinkai, MD, PhD.
“It’s easy to make that mistake, because you have a red, hot leg that’s painful, and the patient is having difficulty walking,” Dr. Shinkai said at the UCSF Annual Advances in Internal Medicine meeting. “Venous stasis dermatitis is one of the things you want to learn to recognize, as hospitalization is typically not needed.”

“That has to do with the venous return back to the heart,” said Dr. Shinkai, a dermatologist at UCSF Medical Center. “If it’s unilateral, it’s almost always on the left side.”
Patients often have features of venous insufficiency that cause stasis, including varicose veins and brawny hyperpigmentation on the medial aspects of the ankles. “They have almost no systemic features: no fever, no white count, no lymphadenopathy,” she said. “These patients need some kind of anti-inflammatory medication because the skin is very inflamed. If you happened to take a biopsy, you would see inflammation as well as lymphatic congestion.”
Dr. Shinkai recommends that patients apply a midpotency topical steroid such as triamcinolone to the affected area, followed by compression, ideally antiembolism stockings (TED hose) – but that can be a hard sell.
“When your legs are that swollen, they’re really painful to wear,” she said. “Patients will say, ‘Don’t you come near me with those TED hose.’ If you’re in that situation, tell them to use an Ace wrap with light compression and each day tighten the Ace wrap a little more until they are able to use TED hose with minimal discomfort.”
The differential diagnosis for venous stasis dermatitis includes cellulitis (which rarely presents bilaterally), deep vein thrombosis, asteatotic dermatitis, erysipelas (more superficial cellulitis that results in elevated, shiny plaques), pyomyositis, necrotizing fasciitis, leukocytoclastic vasculitis, and allergic contact dermatitis.
Dr. Shinkai reported having no relevant financial disclosures.
SAN FRANCISCO – If a patient presents with bilateral cellulitis on both legs, think venous stasis dermatitis, which is the number one misdiagnosis of cellulitis and a frequent cause of unnecessary hospitalization for so-called “red leg,” according to Kanade Shinkai, MD, PhD.
“It’s easy to make that mistake, because you have a red, hot leg that’s painful, and the patient is having difficulty walking,” Dr. Shinkai said at the UCSF Annual Advances in Internal Medicine meeting. “Venous stasis dermatitis is one of the things you want to learn to recognize, as hospitalization is typically not needed.”
“That has to do with the venous return back to the heart,” said Dr. Shinkai, a dermatologist at UCSF Medical Center. “If it’s unilateral, it’s almost always on the left side.”
Patients often have features of venous insufficiency that cause stasis, including varicose veins and brawny hyperpigmentation on the medial aspects of the ankles. “They have almost no systemic features: no fever, no white count, no lymphadenopathy,” she said. “These patients need some kind of anti-inflammatory medication because the skin is very inflamed. If you happened to take a biopsy, you would see inflammation as well as lymphatic congestion.”
Dr. Shinkai recommends that patients apply a midpotency topical steroid such as triamcinolone to the affected area, followed by compression, ideally antiembolism stockings (TED hose) – but that can be a hard sell.
“When your legs are that swollen, they’re really painful to wear,” she said. “Patients will say, ‘Don’t you come near me with those TED hose.’ If you’re in that situation, tell them to use an Ace wrap with light compression and each day tighten the Ace wrap a little more until they are able to use TED hose with minimal discomfort.”
The differential diagnosis for venous stasis dermatitis includes cellulitis (which rarely presents bilaterally), deep vein thrombosis, asteatotic dermatitis, erysipelas (more superficial cellulitis that results in elevated, shiny plaques), pyomyositis, necrotizing fasciitis, leukocytoclastic vasculitis, and allergic contact dermatitis.
Dr. Shinkai reported having no relevant financial disclosures.
SAN FRANCISCO – If a patient presents with bilateral cellulitis on both legs, think venous stasis dermatitis, which is the number one misdiagnosis of cellulitis and a frequent cause of unnecessary hospitalization for so-called “red leg,” according to Kanade Shinkai, MD, PhD.
“It’s easy to make that mistake, because you have a red, hot leg that’s painful, and the patient is having difficulty walking,” Dr. Shinkai said at the UCSF Annual Advances in Internal Medicine meeting. “Venous stasis dermatitis is one of the things you want to learn to recognize, as hospitalization is typically not needed.”
“That has to do with the venous return back to the heart,” said Dr. Shinkai, a dermatologist at UCSF Medical Center. “If it’s unilateral, it’s almost always on the left side.”
Patients often have features of venous insufficiency that cause stasis, including varicose veins and brawny hyperpigmentation on the medial aspects of the ankles. “They have almost no systemic features: no fever, no white count, no lymphadenopathy,” she said. “These patients need some kind of anti-inflammatory medication because the skin is very inflamed. If you happened to take a biopsy, you would see inflammation as well as lymphatic congestion.”
Dr. Shinkai recommends that patients apply a midpotency topical steroid such as triamcinolone to the affected area, followed by compression, ideally antiembolism stockings (TED hose) – but that can be a hard sell.
“When your legs are that swollen, they’re really painful to wear,” she said. “Patients will say, ‘Don’t you come near me with those TED hose.’ If you’re in that situation, tell them to use an Ace wrap with light compression and each day tighten the Ace wrap a little more until they are able to use TED hose with minimal discomfort.”
The differential diagnosis for venous stasis dermatitis includes cellulitis (which rarely presents bilaterally), deep vein thrombosis, asteatotic dermatitis, erysipelas (more superficial cellulitis that results in elevated, shiny plaques), pyomyositis, necrotizing fasciitis, leukocytoclastic vasculitis, and allergic contact dermatitis.
Dr. Shinkai reported having no relevant financial disclosures.
AT THE ANNUAL ADVANCES IN INTERNAL MEDICINE
Endo hubris
I began to write this opinion piece on the red-eye flying back from the outstanding Vascular Annual Meeting, recently held in San Diego. I attended breakfast sessions at 6 a.m., as well as presentations and meetings going on well into the evening. I now have bloodshot eyes, tachycardia, and a heightened perception of things.
It is possible that I am just sleep deprived or maybe it’s a result of inhaling the ubiquitous “medical” marijuana vapors that constantly wafted outside the convention center. Whatever the reason, I have returned in a feverish state of excitement that accompanies a sudden significant insight ... that some of us are under the influence, not of some hallucinogenic, but rather an endovascular- induced euphoria whose spell has made us forget that we are still surgeons.

The exhibition hall had the few customary surgical equipment companies with their surgical loupes, vascular clamps, and needle holders. But it was the expansive displays of every type of endovascular tool, guidewires, catheters, x-ray equipment, endografts, and stents, that attracted the crowds. Not a single vascular ultrasound company showed off their duplex scanners despite the fact that vascular surgeons advanced the use of these instruments and made them as omnipresent as they now are in clinical practice. These companies now find it more profitable to show off their wares at cardiology and radiology meetings.
In the lecture hall, audiences packed in to hear the latest method to treat aortic aneurysms with every variety of endovascular device, but there was not a single presentation on open surgical alternatives. Further, an excellent vascular surgery resident was asked how he would handle a pararenal aneurysm in community practice. He admitted that, unless he could be assisted by an experienced surgeon, he would be uncomfortable performing an open surgical repair. Thus, he would be forced to perform an endovascular treatment even if it would not be the best alternative for the patient. But in the future, will there actually be accomplished surgeons who can assist the newly minted vascular surgeon with open procedures? At a breakfast session dedicated to the aging vascular surgeon, we learned that many will soon be retiring since 46% of the Society are now over the age of 50, and 30% are more than 60 years of age.
Where am I going with this? It is apparent my aphorism that a vascular surgeon can “Operate, Medicate, and Dilate” may no longer hold. Perhaps it should now be “Stent, Ablate, Dilate, and Dilate Again.” Future generations of vascular “surgeons” may be no more than cardiologists who don’t treat the heart, able to perform endovascular revascularizations but unable to perform open operations.
Training paradigms may be affected by middle-aged attending surgeons attempting to prove that they are current by adopting endo-treatments rather than open surgery. Some academic surgeons may see the need to experiment with new endo-techniques to advance their careers. Some may see profit patenting new devices. Some may just be enthralled by what Bruce Brenner refers to as “Endo hubris.” Irrespective, dwindling open procedures will inevitably result in inexperienced open surgeons who will feel comfortable only in an endovascular suite.
Payment inequities that undervalue open procedures and overvalue endovascular ones will promote a preference for endovascular alternatives, many of which are less physically demanding than open surgical procedures and bypasses. Thus, the preference for endovascular procedures will be perpetuated.
Concurrently, our cardiology colleagues will be honing their endovascular skills not only in the coronary arteries but also on the periphery. Soon they will claim superiority. Hospital administrators, already under the spell of Cardiology, will notice the declining profit generated by poorly performed open surgery and resultant prolonged hospitalizations. They will then continue to relegate vascular surgeons to even lesser roles than they now have in so-called Heart and Vascular Centers.
As our open skills deteriorate, patients will be forced to travel to the few centers where some exhausted elderly surgeons will perform the occasional open aortic procedure, distal bypass, or, heaven forbid, some ancient procedure referred to as a carotid endarterectomy.
Of course, some may argue that it is time that endovascular procedures replace “barbaric” or disfiguring open procedures. In fact, this may already be the case for the treatment of thoracic aortic pathology. However, I propose that the time for abandoning surgery has not arrived. There are now sufficient data to show that many endo-procedures are no panacea nor are they without significant limitations. Furthermore, if we abandon open surgery we essentially abandon our raison d’etre. What will then distinguish us from interventional radiologists and cardiologists?
I propose it is time for us to embrace our surgical prowess rather than to treat open procedures like Cinderella’s ugly sisters. I would encourage program directors not to stretch indications for use to justify endovascular treatments but rather adopt standard open procedures. If the volume of indicated open procedures is insufficient, then arrange for the trainee to visit another institution.
We must educate referring physicians and hospital administrators about the benefits of well performed open surgery, and we must make sure that such procedures are, in fact, successfully and expeditiously executed. Non-surgeons also need to be informed about some of the drawbacks of endovascular procedures so that they gain a realistic understanding of the pros and cons.
This does not mean being disparaging, but they should be educated about the occurrence and significance of endoleaks, stent fractures, early recurrence, and other complications. Thus informed, they will better understand the rationale for choosing a vascular surgeon to take care of their patients. They will realize that we remain the only specialists devoted to the understanding and treatment of vascular pathology and consequently able to perform the most appropriate and best treatment for that patient.
I am now fully awake. I am convinced that my evaluation of the events at the meeting were not some sleep-deprived or hallucinogenic aberration. I sincerely believe that it is time for drastic adjustments in our thinking about endovascular and open procedures. If not, vascular surgeons and our specialty may become irrelevant and the repercussions for our survival and that of our patients may be devastating. ■
Russell Samson, MD, a physician in the practice of Sarasota Vascular Specialists, Sarasota, Fl., and a clinical professor of surgery, Florida State University, Tallahassee. He is the medical editor of Vascular Specialist.
I began to write this opinion piece on the red-eye flying back from the outstanding Vascular Annual Meeting, recently held in San Diego. I attended breakfast sessions at 6 a.m., as well as presentations and meetings going on well into the evening. I now have bloodshot eyes, tachycardia, and a heightened perception of things.
It is possible that I am just sleep deprived or maybe it’s a result of inhaling the ubiquitous “medical” marijuana vapors that constantly wafted outside the convention center. Whatever the reason, I have returned in a feverish state of excitement that accompanies a sudden significant insight ... that some of us are under the influence, not of some hallucinogenic, but rather an endovascular- induced euphoria whose spell has made us forget that we are still surgeons.
The exhibition hall had the few customary surgical equipment companies with their surgical loupes, vascular clamps, and needle holders. But it was the expansive displays of every type of endovascular tool, guidewires, catheters, x-ray equipment, endografts, and stents, that attracted the crowds. Not a single vascular ultrasound company showed off their duplex scanners despite the fact that vascular surgeons advanced the use of these instruments and made them as omnipresent as they now are in clinical practice. These companies now find it more profitable to show off their wares at cardiology and radiology meetings.
In the lecture hall, audiences packed in to hear the latest method to treat aortic aneurysms with every variety of endovascular device, but there was not a single presentation on open surgical alternatives. Further, an excellent vascular surgery resident was asked how he would handle a pararenal aneurysm in community practice. He admitted that, unless he could be assisted by an experienced surgeon, he would be uncomfortable performing an open surgical repair. Thus, he would be forced to perform an endovascular treatment even if it would not be the best alternative for the patient. But in the future, will there actually be accomplished surgeons who can assist the newly minted vascular surgeon with open procedures? At a breakfast session dedicated to the aging vascular surgeon, we learned that many will soon be retiring since 46% of the Society are now over the age of 50, and 30% are more than 60 years of age.
Where am I going with this? It is apparent my aphorism that a vascular surgeon can “Operate, Medicate, and Dilate” may no longer hold. Perhaps it should now be “Stent, Ablate, Dilate, and Dilate Again.” Future generations of vascular “surgeons” may be no more than cardiologists who don’t treat the heart, able to perform endovascular revascularizations but unable to perform open operations.
Training paradigms may be affected by middle-aged attending surgeons attempting to prove that they are current by adopting endo-treatments rather than open surgery. Some academic surgeons may see the need to experiment with new endo-techniques to advance their careers. Some may see profit patenting new devices. Some may just be enthralled by what Bruce Brenner refers to as “Endo hubris.” Irrespective, dwindling open procedures will inevitably result in inexperienced open surgeons who will feel comfortable only in an endovascular suite.
Payment inequities that undervalue open procedures and overvalue endovascular ones will promote a preference for endovascular alternatives, many of which are less physically demanding than open surgical procedures and bypasses. Thus, the preference for endovascular procedures will be perpetuated.
Concurrently, our cardiology colleagues will be honing their endovascular skills not only in the coronary arteries but also on the periphery. Soon they will claim superiority. Hospital administrators, already under the spell of Cardiology, will notice the declining profit generated by poorly performed open surgery and resultant prolonged hospitalizations. They will then continue to relegate vascular surgeons to even lesser roles than they now have in so-called Heart and Vascular Centers.
As our open skills deteriorate, patients will be forced to travel to the few centers where some exhausted elderly surgeons will perform the occasional open aortic procedure, distal bypass, or, heaven forbid, some ancient procedure referred to as a carotid endarterectomy.
Of course, some may argue that it is time that endovascular procedures replace “barbaric” or disfiguring open procedures. In fact, this may already be the case for the treatment of thoracic aortic pathology. However, I propose that the time for abandoning surgery has not arrived. There are now sufficient data to show that many endo-procedures are no panacea nor are they without significant limitations. Furthermore, if we abandon open surgery we essentially abandon our raison d’etre. What will then distinguish us from interventional radiologists and cardiologists?
I propose it is time for us to embrace our surgical prowess rather than to treat open procedures like Cinderella’s ugly sisters. I would encourage program directors not to stretch indications for use to justify endovascular treatments but rather adopt standard open procedures. If the volume of indicated open procedures is insufficient, then arrange for the trainee to visit another institution.
We must educate referring physicians and hospital administrators about the benefits of well performed open surgery, and we must make sure that such procedures are, in fact, successfully and expeditiously executed. Non-surgeons also need to be informed about some of the drawbacks of endovascular procedures so that they gain a realistic understanding of the pros and cons.
This does not mean being disparaging, but they should be educated about the occurrence and significance of endoleaks, stent fractures, early recurrence, and other complications. Thus informed, they will better understand the rationale for choosing a vascular surgeon to take care of their patients. They will realize that we remain the only specialists devoted to the understanding and treatment of vascular pathology and consequently able to perform the most appropriate and best treatment for that patient.
I am now fully awake. I am convinced that my evaluation of the events at the meeting were not some sleep-deprived or hallucinogenic aberration. I sincerely believe that it is time for drastic adjustments in our thinking about endovascular and open procedures. If not, vascular surgeons and our specialty may become irrelevant and the repercussions for our survival and that of our patients may be devastating. ■
Russell Samson, MD, a physician in the practice of Sarasota Vascular Specialists, Sarasota, Fl., and a clinical professor of surgery, Florida State University, Tallahassee. He is the medical editor of Vascular Specialist.
I began to write this opinion piece on the red-eye flying back from the outstanding Vascular Annual Meeting, recently held in San Diego. I attended breakfast sessions at 6 a.m., as well as presentations and meetings going on well into the evening. I now have bloodshot eyes, tachycardia, and a heightened perception of things.
It is possible that I am just sleep deprived or maybe it’s a result of inhaling the ubiquitous “medical” marijuana vapors that constantly wafted outside the convention center. Whatever the reason, I have returned in a feverish state of excitement that accompanies a sudden significant insight ... that some of us are under the influence, not of some hallucinogenic, but rather an endovascular- induced euphoria whose spell has made us forget that we are still surgeons.
The exhibition hall had the few customary surgical equipment companies with their surgical loupes, vascular clamps, and needle holders. But it was the expansive displays of every type of endovascular tool, guidewires, catheters, x-ray equipment, endografts, and stents, that attracted the crowds. Not a single vascular ultrasound company showed off their duplex scanners despite the fact that vascular surgeons advanced the use of these instruments and made them as omnipresent as they now are in clinical practice. These companies now find it more profitable to show off their wares at cardiology and radiology meetings.
In the lecture hall, audiences packed in to hear the latest method to treat aortic aneurysms with every variety of endovascular device, but there was not a single presentation on open surgical alternatives. Further, an excellent vascular surgery resident was asked how he would handle a pararenal aneurysm in community practice. He admitted that, unless he could be assisted by an experienced surgeon, he would be uncomfortable performing an open surgical repair. Thus, he would be forced to perform an endovascular treatment even if it would not be the best alternative for the patient. But in the future, will there actually be accomplished surgeons who can assist the newly minted vascular surgeon with open procedures? At a breakfast session dedicated to the aging vascular surgeon, we learned that many will soon be retiring since 46% of the Society are now over the age of 50, and 30% are more than 60 years of age.
Where am I going with this? It is apparent my aphorism that a vascular surgeon can “Operate, Medicate, and Dilate” may no longer hold. Perhaps it should now be “Stent, Ablate, Dilate, and Dilate Again.” Future generations of vascular “surgeons” may be no more than cardiologists who don’t treat the heart, able to perform endovascular revascularizations but unable to perform open operations.
Training paradigms may be affected by middle-aged attending surgeons attempting to prove that they are current by adopting endo-treatments rather than open surgery. Some academic surgeons may see the need to experiment with new endo-techniques to advance their careers. Some may see profit patenting new devices. Some may just be enthralled by what Bruce Brenner refers to as “Endo hubris.” Irrespective, dwindling open procedures will inevitably result in inexperienced open surgeons who will feel comfortable only in an endovascular suite.
Payment inequities that undervalue open procedures and overvalue endovascular ones will promote a preference for endovascular alternatives, many of which are less physically demanding than open surgical procedures and bypasses. Thus, the preference for endovascular procedures will be perpetuated.
Concurrently, our cardiology colleagues will be honing their endovascular skills not only in the coronary arteries but also on the periphery. Soon they will claim superiority. Hospital administrators, already under the spell of Cardiology, will notice the declining profit generated by poorly performed open surgery and resultant prolonged hospitalizations. They will then continue to relegate vascular surgeons to even lesser roles than they now have in so-called Heart and Vascular Centers.
As our open skills deteriorate, patients will be forced to travel to the few centers where some exhausted elderly surgeons will perform the occasional open aortic procedure, distal bypass, or, heaven forbid, some ancient procedure referred to as a carotid endarterectomy.
Of course, some may argue that it is time that endovascular procedures replace “barbaric” or disfiguring open procedures. In fact, this may already be the case for the treatment of thoracic aortic pathology. However, I propose that the time for abandoning surgery has not arrived. There are now sufficient data to show that many endo-procedures are no panacea nor are they without significant limitations. Furthermore, if we abandon open surgery we essentially abandon our raison d’etre. What will then distinguish us from interventional radiologists and cardiologists?
I propose it is time for us to embrace our surgical prowess rather than to treat open procedures like Cinderella’s ugly sisters. I would encourage program directors not to stretch indications for use to justify endovascular treatments but rather adopt standard open procedures. If the volume of indicated open procedures is insufficient, then arrange for the trainee to visit another institution.
We must educate referring physicians and hospital administrators about the benefits of well performed open surgery, and we must make sure that such procedures are, in fact, successfully and expeditiously executed. Non-surgeons also need to be informed about some of the drawbacks of endovascular procedures so that they gain a realistic understanding of the pros and cons.
This does not mean being disparaging, but they should be educated about the occurrence and significance of endoleaks, stent fractures, early recurrence, and other complications. Thus informed, they will better understand the rationale for choosing a vascular surgeon to take care of their patients. They will realize that we remain the only specialists devoted to the understanding and treatment of vascular pathology and consequently able to perform the most appropriate and best treatment for that patient.
I am now fully awake. I am convinced that my evaluation of the events at the meeting were not some sleep-deprived or hallucinogenic aberration. I sincerely believe that it is time for drastic adjustments in our thinking about endovascular and open procedures. If not, vascular surgeons and our specialty may become irrelevant and the repercussions for our survival and that of our patients may be devastating. ■
Russell Samson, MD, a physician in the practice of Sarasota Vascular Specialists, Sarasota, Fl., and a clinical professor of surgery, Florida State University, Tallahassee. He is the medical editor of Vascular Specialist.

Cirrhosis Is Linked to an Increased Risk of Stroke
All forms of cirrhosis are associated with an increased risk of stroke, especially hemorrhagic stroke, according to a large, nationally representative cohort study published online ahead of print June 5 in JAMA Neurology.
Cirrhosis is commonly associated with “extrahepatic hemorrhagic and thrombotic processes, such as gastrointestinal bleeding and venous thromboembolism. [But] the cerebrovascular complications of cirrhosis are comparatively less well understood,” said Neal S. Parikh, MD, Resident Physician Neurologist at New York-Presbyterian Hospital in New York City, and colleagues. Previous studies of the association between cirrhosis and stroke have been small and have yielded conflicting results.

To examine the association between cirrhosis and stroke, Dr. Parikh and colleagues conducted a retrospective study that involved 1,618,059 Medicare beneficiaries hospitalized during a six-year period. In all, 15,586 patients (1%) had cirrhosis at baseline, and 77,268 patients developed stroke during a mean of 4.3 years of follow-up. In addition, the overall incidence of stroke was 2.17% per year among patients with cirrhosis, compared with 1.11% per year among patients without cirrhosis. After the data were adjusted to account for stroke risk factors, relevant comorbidities, and demographic traits, the annual incidence of any type of stroke was significantly higher with cirrhosis than without cirrhosis (hazard ratio [HR], 1.4). The association was stronger for intracranial hemorrhage (HR, 1.9) and subarachnoid hemorrhage (HR, 2.4) than for ischemic stroke (HR, 1.3).
The results of several secondary and sensitivity analyses were consistent with those of the primary analysis, regardless of whether the cirrhosis was alcohol-related or the stroke was fatal. The association was strongest among patients who had decompensated cirrhosis and was not evident at all among patients who had mild liver disease, said Dr. Parikh and colleagues.
Although this study was not designed to explore the reasons for an association between cirrhosis and stroke, the investigators noted several possible explanations. First, “cirrhosis is accompanied by a mixed coagulopathy, with potential implications for hemorrhagic and thrombotic processes.” It has been linked to many bleeding complications, including, most recently, cerebral microhemorrhages detectable on brain MRI. In addition, the underlying causes of cirrhosis, including alcohol abuse, hepatitis infection, and metabolic disease, may also contribute to stroke risk.
Alternatively, clinicians caring for patients with cirrhosis “may limit the aggressiveness of stroke prevention”—for example, by limiting antithrombotic medications or statins—because they are mindful of the patient’s increased risk of bleeding and hepatic toxicity, the authors said.
—Mary Ann Moon
Suggested Reading
Parikh NS, Navi BB, Schneider Y, et al. Association between cirrhosis and stroke in a nationally representative cohort. JAMA Neurol. 2017 Jun 5 [Epub ahead of print].
All forms of cirrhosis are associated with an increased risk of stroke, especially hemorrhagic stroke, according to a large, nationally representative cohort study published online ahead of print June 5 in JAMA Neurology.
Cirrhosis is commonly associated with “extrahepatic hemorrhagic and thrombotic processes, such as gastrointestinal bleeding and venous thromboembolism. [But] the cerebrovascular complications of cirrhosis are comparatively less well understood,” said Neal S. Parikh, MD, Resident Physician Neurologist at New York-Presbyterian Hospital in New York City, and colleagues. Previous studies of the association between cirrhosis and stroke have been small and have yielded conflicting results.
To examine the association between cirrhosis and stroke, Dr. Parikh and colleagues conducted a retrospective study that involved 1,618,059 Medicare beneficiaries hospitalized during a six-year period. In all, 15,586 patients (1%) had cirrhosis at baseline, and 77,268 patients developed stroke during a mean of 4.3 years of follow-up. In addition, the overall incidence of stroke was 2.17% per year among patients with cirrhosis, compared with 1.11% per year among patients without cirrhosis. After the data were adjusted to account for stroke risk factors, relevant comorbidities, and demographic traits, the annual incidence of any type of stroke was significantly higher with cirrhosis than without cirrhosis (hazard ratio [HR], 1.4). The association was stronger for intracranial hemorrhage (HR, 1.9) and subarachnoid hemorrhage (HR, 2.4) than for ischemic stroke (HR, 1.3).
The results of several secondary and sensitivity analyses were consistent with those of the primary analysis, regardless of whether the cirrhosis was alcohol-related or the stroke was fatal. The association was strongest among patients who had decompensated cirrhosis and was not evident at all among patients who had mild liver disease, said Dr. Parikh and colleagues.
Although this study was not designed to explore the reasons for an association between cirrhosis and stroke, the investigators noted several possible explanations. First, “cirrhosis is accompanied by a mixed coagulopathy, with potential implications for hemorrhagic and thrombotic processes.” It has been linked to many bleeding complications, including, most recently, cerebral microhemorrhages detectable on brain MRI. In addition, the underlying causes of cirrhosis, including alcohol abuse, hepatitis infection, and metabolic disease, may also contribute to stroke risk.
Alternatively, clinicians caring for patients with cirrhosis “may limit the aggressiveness of stroke prevention”—for example, by limiting antithrombotic medications or statins—because they are mindful of the patient’s increased risk of bleeding and hepatic toxicity, the authors said.
—Mary Ann Moon
Suggested Reading
Parikh NS, Navi BB, Schneider Y, et al. Association between cirrhosis and stroke in a nationally representative cohort. JAMA Neurol. 2017 Jun 5 [Epub ahead of print].
All forms of cirrhosis are associated with an increased risk of stroke, especially hemorrhagic stroke, according to a large, nationally representative cohort study published online ahead of print June 5 in JAMA Neurology.
Cirrhosis is commonly associated with “extrahepatic hemorrhagic and thrombotic processes, such as gastrointestinal bleeding and venous thromboembolism. [But] the cerebrovascular complications of cirrhosis are comparatively less well understood,” said Neal S. Parikh, MD, Resident Physician Neurologist at New York-Presbyterian Hospital in New York City, and colleagues. Previous studies of the association between cirrhosis and stroke have been small and have yielded conflicting results.
To examine the association between cirrhosis and stroke, Dr. Parikh and colleagues conducted a retrospective study that involved 1,618,059 Medicare beneficiaries hospitalized during a six-year period. In all, 15,586 patients (1%) had cirrhosis at baseline, and 77,268 patients developed stroke during a mean of 4.3 years of follow-up. In addition, the overall incidence of stroke was 2.17% per year among patients with cirrhosis, compared with 1.11% per year among patients without cirrhosis. After the data were adjusted to account for stroke risk factors, relevant comorbidities, and demographic traits, the annual incidence of any type of stroke was significantly higher with cirrhosis than without cirrhosis (hazard ratio [HR], 1.4). The association was stronger for intracranial hemorrhage (HR, 1.9) and subarachnoid hemorrhage (HR, 2.4) than for ischemic stroke (HR, 1.3).
The results of several secondary and sensitivity analyses were consistent with those of the primary analysis, regardless of whether the cirrhosis was alcohol-related or the stroke was fatal. The association was strongest among patients who had decompensated cirrhosis and was not evident at all among patients who had mild liver disease, said Dr. Parikh and colleagues.
Although this study was not designed to explore the reasons for an association between cirrhosis and stroke, the investigators noted several possible explanations. First, “cirrhosis is accompanied by a mixed coagulopathy, with potential implications for hemorrhagic and thrombotic processes.” It has been linked to many bleeding complications, including, most recently, cerebral microhemorrhages detectable on brain MRI. In addition, the underlying causes of cirrhosis, including alcohol abuse, hepatitis infection, and metabolic disease, may also contribute to stroke risk.
Alternatively, clinicians caring for patients with cirrhosis “may limit the aggressiveness of stroke prevention”—for example, by limiting antithrombotic medications or statins—because they are mindful of the patient’s increased risk of bleeding and hepatic toxicity, the authors said.
—Mary Ann Moon
Suggested Reading
Parikh NS, Navi BB, Schneider Y, et al. Association between cirrhosis and stroke in a nationally representative cohort. JAMA Neurol. 2017 Jun 5 [Epub ahead of print].
Dr. Turner concludes term as SBAS president teaser
Patricia L. Turner, MD, FACS, Director, American College of Surgeons (ACS) Division of Member Services, recently concluded her term (2016–2017) as president of the Society of Black Academic Surgeons (SBAS). She is the first woman to have served in that role.
Dr. Turner addressed attendees during the April 27–29 SBAS annual meeting, cohosted with the University of Chicago Medicine and Department of Surgery, IL, which is chaired by Jeffrey B. Matthews, MD, FACS, Dallas B. Phemister Professor of Surgery. In her presidential address, The Enduring Influence of Surgical Societies, she described the first time she attended an SBAS meeting as a medical student and expressed her gratitude for being able to lead the meeting as its 22nd president. “I am also grateful to SBAS for the privilege of serving as its first female president,” she said. (Watch a video from the meeting on the Women of SBAS, including Dr. Turner, at www.sbas.net/media/surgeon-spotlight.aspx?id=13).
In her address, Dr. Turner highlighted historical elements of surgery and the activities of surgical societies. She challenged SBAS to continue to expand diversity in all contexts, including age, specialty, gender, and representative institutional members. She urged the organization to extend its influence by amplifying existing relationships with other organizations, such as the ACS, National Institutes of Health, and the Association of American Medical Colleges, while developing new partnerships with other societies and institutions. She also noted that mentorship and excellence in the surgical sciences continue to be the hallmarks of SBAS.
“SBAS has become a formidable scientific forum for surgeons of all backgrounds interested in quality and excellence,” Dr. Turner said. “[Our membership is] small in number, but the power invested in our members and leaders is substantial; we are influential.”
Anthony Stallion, MD, FACS, chief of pediatric surgery, Carolinas HealthCare System, Charlotte, NC, was installed as Dr. Turner’s successor.
Patricia L. Turner, MD, FACS, Director, American College of Surgeons (ACS) Division of Member Services, recently concluded her term (2016–2017) as president of the Society of Black Academic Surgeons (SBAS). She is the first woman to have served in that role.
Dr. Turner addressed attendees during the April 27–29 SBAS annual meeting, cohosted with the University of Chicago Medicine and Department of Surgery, IL, which is chaired by Jeffrey B. Matthews, MD, FACS, Dallas B. Phemister Professor of Surgery. In her presidential address, The Enduring Influence of Surgical Societies, she described the first time she attended an SBAS meeting as a medical student and expressed her gratitude for being able to lead the meeting as its 22nd president. “I am also grateful to SBAS for the privilege of serving as its first female president,” she said. (Watch a video from the meeting on the Women of SBAS, including Dr. Turner, at www.sbas.net/media/surgeon-spotlight.aspx?id=13).
In her address, Dr. Turner highlighted historical elements of surgery and the activities of surgical societies. She challenged SBAS to continue to expand diversity in all contexts, including age, specialty, gender, and representative institutional members. She urged the organization to extend its influence by amplifying existing relationships with other organizations, such as the ACS, National Institutes of Health, and the Association of American Medical Colleges, while developing new partnerships with other societies and institutions. She also noted that mentorship and excellence in the surgical sciences continue to be the hallmarks of SBAS.
“SBAS has become a formidable scientific forum for surgeons of all backgrounds interested in quality and excellence,” Dr. Turner said. “[Our membership is] small in number, but the power invested in our members and leaders is substantial; we are influential.”
Anthony Stallion, MD, FACS, chief of pediatric surgery, Carolinas HealthCare System, Charlotte, NC, was installed as Dr. Turner’s successor.
Patricia L. Turner, MD, FACS, Director, American College of Surgeons (ACS) Division of Member Services, recently concluded her term (2016–2017) as president of the Society of Black Academic Surgeons (SBAS). She is the first woman to have served in that role.
Dr. Turner addressed attendees during the April 27–29 SBAS annual meeting, cohosted with the University of Chicago Medicine and Department of Surgery, IL, which is chaired by Jeffrey B. Matthews, MD, FACS, Dallas B. Phemister Professor of Surgery. In her presidential address, The Enduring Influence of Surgical Societies, she described the first time she attended an SBAS meeting as a medical student and expressed her gratitude for being able to lead the meeting as its 22nd president. “I am also grateful to SBAS for the privilege of serving as its first female president,” she said. (Watch a video from the meeting on the Women of SBAS, including Dr. Turner, at www.sbas.net/media/surgeon-spotlight.aspx?id=13).
In her address, Dr. Turner highlighted historical elements of surgery and the activities of surgical societies. She challenged SBAS to continue to expand diversity in all contexts, including age, specialty, gender, and representative institutional members. She urged the organization to extend its influence by amplifying existing relationships with other organizations, such as the ACS, National Institutes of Health, and the Association of American Medical Colleges, while developing new partnerships with other societies and institutions. She also noted that mentorship and excellence in the surgical sciences continue to be the hallmarks of SBAS.
“SBAS has become a formidable scientific forum for surgeons of all backgrounds interested in quality and excellence,” Dr. Turner said. “[Our membership is] small in number, but the power invested in our members and leaders is substantial; we are influential.”
Anthony Stallion, MD, FACS, chief of pediatric surgery, Carolinas HealthCare System, Charlotte, NC, was installed as Dr. Turner’s successor.
NSAIDs remain a concern in colorectal ERAS protocols
SEATTLE – Nonselective NSAIDs increase the risk of anastomotic leaks after colorectal surgery, according to a meta-analysis from the University of Sydney, Australia.
After combing results from six randomized, controlled trials and seven retrospective studies involving a total of 23,508 patients, investigators found that postop nonselective NSAIDs (odds ratio, 0.54; 95% CI, 0.43-0.67; P less than .00001), and especially diclofenac (OR, 0.39; 95% CI, 0.28-0.55; P less than .00001), were both associated with an increased risk of leakage.
There was an increased risk with all NSAIDs compared to patients who did not receive them after surgery, but the risk was statistically significant only for nonselective options like diclofenac on subgroup analysis. There was a trend for increased leakage with the nonselective agent ketorolac, as well, but it was not significant (OR, 0.71; 95% CI, 0.35-1.43; P = .34).

“I’m not going to say we need to wait for more studies; there’s something here. We have to be aware there could be a high risk of leakage with nonsteroidals, and we have to be mindful of that with our ERAS [Enhanced Recovery after Surgery] protocols. I don’t think you should be using nonsteroidals unless you are using them in a trial” and collecting data, “because of the uncertainty,” lead investigator and colorectal surgeon Christopher Young, MD, a clinical associate professor of surgery at the University of Sydney, said at the American Society of Colon and Rectal Surgeons annual meeting.
NSAIDS are a routine part of colorectal ERAS protocols in some places to limit opioid use and hasten recovery and hospital discharge, but there’s been concern for some time that they might also increase the risk of anastomotic leakage. The new Australian findings fit in with previous investigations that raised concerns.
A 2016 review, for instance, found that among 856 patients undergoing an elective colon or rectal resection for cancer, the anastomotic leakage rate was significantly higher in the group that received nonsteroidal anti-inflammatory drugs compared to patients who did not (9.2% versus 5.3%). The higher rate was only seen in patients receiving diclofenac. “The use of diclofenac in colorectal surgery can no longer be recommended. Alternatives for postoperative analgesia need to be explored within an enhanced recovery program,” the investigators concluded (J Gastrointest Surg. 2016 Apr;20[4]:776-82. doi: 10.1007/s11605-015-3010-1).
A review of 13,082 bariatric and colorectal surgery patients in Washington State found that NSAIDs beginning within 24 hours after surgery were associated with a 70% increased risk of anastomotic leaks in nonelective colorectal surgery, with a leak rate of 12.3% in the NSAID group and 8.3% in the non-NSAID group (OR, 1.70; 95% CI, 1.11–2.68; P = .01). Although it was unclear which nonsteroidals patients received, intravenous ketorolac or ibuprofen were likely the most common (JAMA Surg. 2015 Mar 1;150[3]: 223–8).
It’s unknown why, exactly, NSAIDs impair healing and anastomotic strength, but it’s thought to be related to effects on prostaglandin synthesis, Dr. Young noted.
Dr. Young had no disclosures.
SEATTLE – Nonselective NSAIDs increase the risk of anastomotic leaks after colorectal surgery, according to a meta-analysis from the University of Sydney, Australia.
After combing results from six randomized, controlled trials and seven retrospective studies involving a total of 23,508 patients, investigators found that postop nonselective NSAIDs (odds ratio, 0.54; 95% CI, 0.43-0.67; P less than .00001), and especially diclofenac (OR, 0.39; 95% CI, 0.28-0.55; P less than .00001), were both associated with an increased risk of leakage.
There was an increased risk with all NSAIDs compared to patients who did not receive them after surgery, but the risk was statistically significant only for nonselective options like diclofenac on subgroup analysis. There was a trend for increased leakage with the nonselective agent ketorolac, as well, but it was not significant (OR, 0.71; 95% CI, 0.35-1.43; P = .34).
“I’m not going to say we need to wait for more studies; there’s something here. We have to be aware there could be a high risk of leakage with nonsteroidals, and we have to be mindful of that with our ERAS [Enhanced Recovery after Surgery] protocols. I don’t think you should be using nonsteroidals unless you are using them in a trial” and collecting data, “because of the uncertainty,” lead investigator and colorectal surgeon Christopher Young, MD, a clinical associate professor of surgery at the University of Sydney, said at the American Society of Colon and Rectal Surgeons annual meeting.
NSAIDS are a routine part of colorectal ERAS protocols in some places to limit opioid use and hasten recovery and hospital discharge, but there’s been concern for some time that they might also increase the risk of anastomotic leakage. The new Australian findings fit in with previous investigations that raised concerns.
A 2016 review, for instance, found that among 856 patients undergoing an elective colon or rectal resection for cancer, the anastomotic leakage rate was significantly higher in the group that received nonsteroidal anti-inflammatory drugs compared to patients who did not (9.2% versus 5.3%). The higher rate was only seen in patients receiving diclofenac. “The use of diclofenac in colorectal surgery can no longer be recommended. Alternatives for postoperative analgesia need to be explored within an enhanced recovery program,” the investigators concluded (J Gastrointest Surg. 2016 Apr;20[4]:776-82. doi: 10.1007/s11605-015-3010-1).
A review of 13,082 bariatric and colorectal surgery patients in Washington State found that NSAIDs beginning within 24 hours after surgery were associated with a 70% increased risk of anastomotic leaks in nonelective colorectal surgery, with a leak rate of 12.3% in the NSAID group and 8.3% in the non-NSAID group (OR, 1.70; 95% CI, 1.11–2.68; P = .01). Although it was unclear which nonsteroidals patients received, intravenous ketorolac or ibuprofen were likely the most common (JAMA Surg. 2015 Mar 1;150[3]: 223–8).
It’s unknown why, exactly, NSAIDs impair healing and anastomotic strength, but it’s thought to be related to effects on prostaglandin synthesis, Dr. Young noted.
Dr. Young had no disclosures.
SEATTLE – Nonselective NSAIDs increase the risk of anastomotic leaks after colorectal surgery, according to a meta-analysis from the University of Sydney, Australia.
After combing results from six randomized, controlled trials and seven retrospective studies involving a total of 23,508 patients, investigators found that postop nonselective NSAIDs (odds ratio, 0.54; 95% CI, 0.43-0.67; P less than .00001), and especially diclofenac (OR, 0.39; 95% CI, 0.28-0.55; P less than .00001), were both associated with an increased risk of leakage.
There was an increased risk with all NSAIDs compared to patients who did not receive them after surgery, but the risk was statistically significant only for nonselective options like diclofenac on subgroup analysis. There was a trend for increased leakage with the nonselective agent ketorolac, as well, but it was not significant (OR, 0.71; 95% CI, 0.35-1.43; P = .34).
“I’m not going to say we need to wait for more studies; there’s something here. We have to be aware there could be a high risk of leakage with nonsteroidals, and we have to be mindful of that with our ERAS [Enhanced Recovery after Surgery] protocols. I don’t think you should be using nonsteroidals unless you are using them in a trial” and collecting data, “because of the uncertainty,” lead investigator and colorectal surgeon Christopher Young, MD, a clinical associate professor of surgery at the University of Sydney, said at the American Society of Colon and Rectal Surgeons annual meeting.
NSAIDS are a routine part of colorectal ERAS protocols in some places to limit opioid use and hasten recovery and hospital discharge, but there’s been concern for some time that they might also increase the risk of anastomotic leakage. The new Australian findings fit in with previous investigations that raised concerns.
A 2016 review, for instance, found that among 856 patients undergoing an elective colon or rectal resection for cancer, the anastomotic leakage rate was significantly higher in the group that received nonsteroidal anti-inflammatory drugs compared to patients who did not (9.2% versus 5.3%). The higher rate was only seen in patients receiving diclofenac. “The use of diclofenac in colorectal surgery can no longer be recommended. Alternatives for postoperative analgesia need to be explored within an enhanced recovery program,” the investigators concluded (J Gastrointest Surg. 2016 Apr;20[4]:776-82. doi: 10.1007/s11605-015-3010-1).
A review of 13,082 bariatric and colorectal surgery patients in Washington State found that NSAIDs beginning within 24 hours after surgery were associated with a 70% increased risk of anastomotic leaks in nonelective colorectal surgery, with a leak rate of 12.3% in the NSAID group and 8.3% in the non-NSAID group (OR, 1.70; 95% CI, 1.11–2.68; P = .01). Although it was unclear which nonsteroidals patients received, intravenous ketorolac or ibuprofen were likely the most common (JAMA Surg. 2015 Mar 1;150[3]: 223–8).
It’s unknown why, exactly, NSAIDs impair healing and anastomotic strength, but it’s thought to be related to effects on prostaglandin synthesis, Dr. Young noted.
Dr. Young had no disclosures.
AT ASCRS 2017
Key clinical point:
Major finding: Postop nonselective NSAIDs (OR, 0.54; 95% CI, 0.43-0.67; P less than .00001), and especially diclofenac (OR, 0.39; 95% CI, 0.28-0.55; P less than .00001), were both associated with an increased risk of leakage.
Data source: Meta-analysis involving 23,508 patients
Disclosures: The presenter had no disclosures.
Study shows that 20% of inpatients given antibiotics develop adverse reactions
Twenty percent of hospitalized adults given antibiotics develop adverse drug events, including GI, nephrotoxic, hematologic, cardiac, and neurotoxic effects, according to a report in JAMA Internal Medicine.
This high frequency of adverse reactions “may not be recognized by clinicians because [these events] have varied manifestations, clinicians may be unaware of the risks associated with specific antibiotic agents, or because they occur after patients are discharged from the hospital,” said Pranita D. Tamma, MD, of the division of pediatric infectious diseases, Johns Hopkins University, Baltimore, and her associates.
They assessed antibiotic-associated adverse drug events in all 1,488 adults admitted to four general medicine services at a single medical center during a 9-month period and given at least 24 hours of any antibiotic therapy. The most common indications for antibiotics were urinary tract infections (12%), skin and soft-tissue infections (8%), and community-acquired pneumonia (7%).
Perhaps as important, the researchers noted, 19% of these adverse drug events were attributed to unnecessary antibiotics – drugs given for conditions for which they were not clinically indicated according to the hospital’s own antibiotic guidelines. These included asymptomatic bacteriuria, aspiration pneumonitis, and heart failure (JAMA Intern. Med. 2017 June 12. doi: 10.1001/jamainternmed.2017.1938).
The most common adverse reactions that developed within 30 days were GI, renal, and hematologic abnormalities. Neurotoxic effects included encephalopathy and seizures; cardiotoxic effects included QTc prolongation. Less frequent adverse events included anaphylaxis, daptomycin-associated myositis, trimethoprim/sulfamethoxazole-associated pancreatitis, linezolid-associated neuropathy, and ciprofloxacin-related tendinitis. The most common adverse reactions that developed within 90 days were C. difficile infections and infections involving multidrug-resistant organisms.
“Our findings underscore the importance of avoiding unnecessary antibiotic prescribing to reduce the harm that can result from antibiotic-associated adverse drug events,” Dr. Tamma and her associates said.
Twenty percent of hospitalized adults given antibiotics develop adverse drug events, including GI, nephrotoxic, hematologic, cardiac, and neurotoxic effects, according to a report in JAMA Internal Medicine.
This high frequency of adverse reactions “may not be recognized by clinicians because [these events] have varied manifestations, clinicians may be unaware of the risks associated with specific antibiotic agents, or because they occur after patients are discharged from the hospital,” said Pranita D. Tamma, MD, of the division of pediatric infectious diseases, Johns Hopkins University, Baltimore, and her associates.
They assessed antibiotic-associated adverse drug events in all 1,488 adults admitted to four general medicine services at a single medical center during a 9-month period and given at least 24 hours of any antibiotic therapy. The most common indications for antibiotics were urinary tract infections (12%), skin and soft-tissue infections (8%), and community-acquired pneumonia (7%).
Perhaps as important, the researchers noted, 19% of these adverse drug events were attributed to unnecessary antibiotics – drugs given for conditions for which they were not clinically indicated according to the hospital’s own antibiotic guidelines. These included asymptomatic bacteriuria, aspiration pneumonitis, and heart failure (JAMA Intern. Med. 2017 June 12. doi: 10.1001/jamainternmed.2017.1938).
The most common adverse reactions that developed within 30 days were GI, renal, and hematologic abnormalities. Neurotoxic effects included encephalopathy and seizures; cardiotoxic effects included QTc prolongation. Less frequent adverse events included anaphylaxis, daptomycin-associated myositis, trimethoprim/sulfamethoxazole-associated pancreatitis, linezolid-associated neuropathy, and ciprofloxacin-related tendinitis. The most common adverse reactions that developed within 90 days were C. difficile infections and infections involving multidrug-resistant organisms.
“Our findings underscore the importance of avoiding unnecessary antibiotic prescribing to reduce the harm that can result from antibiotic-associated adverse drug events,” Dr. Tamma and her associates said.
Twenty percent of hospitalized adults given antibiotics develop adverse drug events, including GI, nephrotoxic, hematologic, cardiac, and neurotoxic effects, according to a report in JAMA Internal Medicine.
This high frequency of adverse reactions “may not be recognized by clinicians because [these events] have varied manifestations, clinicians may be unaware of the risks associated with specific antibiotic agents, or because they occur after patients are discharged from the hospital,” said Pranita D. Tamma, MD, of the division of pediatric infectious diseases, Johns Hopkins University, Baltimore, and her associates.
They assessed antibiotic-associated adverse drug events in all 1,488 adults admitted to four general medicine services at a single medical center during a 9-month period and given at least 24 hours of any antibiotic therapy. The most common indications for antibiotics were urinary tract infections (12%), skin and soft-tissue infections (8%), and community-acquired pneumonia (7%).
Perhaps as important, the researchers noted, 19% of these adverse drug events were attributed to unnecessary antibiotics – drugs given for conditions for which they were not clinically indicated according to the hospital’s own antibiotic guidelines. These included asymptomatic bacteriuria, aspiration pneumonitis, and heart failure (JAMA Intern. Med. 2017 June 12. doi: 10.1001/jamainternmed.2017.1938).
The most common adverse reactions that developed within 30 days were GI, renal, and hematologic abnormalities. Neurotoxic effects included encephalopathy and seizures; cardiotoxic effects included QTc prolongation. Less frequent adverse events included anaphylaxis, daptomycin-associated myositis, trimethoprim/sulfamethoxazole-associated pancreatitis, linezolid-associated neuropathy, and ciprofloxacin-related tendinitis. The most common adverse reactions that developed within 90 days were C. difficile infections and infections involving multidrug-resistant organisms.
“Our findings underscore the importance of avoiding unnecessary antibiotic prescribing to reduce the harm that can result from antibiotic-associated adverse drug events,” Dr. Tamma and her associates said.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Among hospitalized adults given antibiotics, 20% develop adverse reactions, including GI, nephrotoxic, hematologic, cardiac, and neurotoxic effects.
Major finding: Among 1,488 patients, 298 (20%) developed 324 adverse reactions to antibiotics – 73% during hospitalization and 27% after discharge – requiring prolonged hospitalization; a subsequent hospitalization; an ED visit; or additional lab tests, ECGs, or imaging studies.
Data source: A single-center retrospective cohort study involving all 1,488 general medicine inpatients admitted during a 9-month period who received any antibiotic for at least 24 hours.
Disclosures: This study was supported by Pfizer Independent Grants for Learning and Change and the Joint Commission. Dr. Tamma and her associates reported having no relevant financial disclosures.
Meet the two newest SHM board members
SHM’s two newest board members – pediatric hospitalist Kris Rehm, MD, SFHM, and perioperative specialist Rachel Thompson, MD, MPH, SFHM – will bring their expertise to bear on the society’s top panel.
However, neither woman sees her role as shaping the board. In fact, they see themselves as lucky to be joining the team.

“I really want to hear everyone’s voice, and I hope to see how we can all move to better places together,” added Dr. Rehm, associate professor of clinical pediatrics and director of the division of hospital medicine at Vanderbilt University in Nashville.
Both board members were officially seated for three-year terms at HM17 in Las Vegas. They replace former SHM president Robert Harrington, MD, SFHM, and veteran pediatric hospitalist Erin Stucky Fisher, MD, MHM.
Each of the new board members brings a strong perspective to the panel.
For Dr. Thompson, that viewpoint is based in engagement. She is the former chair of SHM’s Pacific Northwest chapter and has spent the past few years leading the perioperative issues for the society’s work group.
“We get to a certain point of our career as hospitalists, and if we’re just plugging in and working, doing our shifts, somewhere in that 8- to 10-year range, we might get a little bored, tired, worn out,” Dr. Thompson said. “I believe, if we have the community and professional home to keep us engaged, that helps us see the value in what we’re doing every day. It helps us continue to grow, so we don’t hit that wall.”
Given Dr. Thompson’s involvement both with her chapter and the society’s chapter support committee, she will likely continue that effort to make sure SHM’s board sees the value of encouraging and partnering with local chapters. She will also work with SHM president Ron Greeno, MD, FCCP, MHM, on policy issues, as her background in public health has aligned her interests on health care reform and other headwinds facing the specialty.
“I went in to do my masters in public health with the idea that I wanted to build the skill set so that I could be more analytical in how I approach our problem solving, our discovery in the hospital setting,” she said. “It really speaks to a part of me that has always been interested in finding ways to prevent illness and moving beyond that reactivity that we have in medicine into a prevention-based [approach].”
Dr. Thompson noted that her background in perioperative medicine helps her work as part of a team because it “entirely relies on collaboration and coordination of care, which is pretty much the basis of what we do in the hospital any day.”
Dr. Rehm, who serves as a pediatric hospitalist at the Monroe Carell Jr. Children’s Hospital at Vanderbilt, said she will also bring a teamwork-focused perspective to the SHM board.
She could be expected to view everything through the lens of inpatient pediatrics, but that’s not her style.
“I think we have so many similarities and so many things that [pediatric and adult hospitalists] can partner to do together,” she said. “We all are involved in, for example, medication reconciliation or discharge-management planning or postacute care follow-up. There’s a lot of synergy, and I think we can learn so much from each other.”
Dr. Rehm, who chairs SHM’s Pediatrics Committee and the 2017 Pediatric Hospital Medicine meeting, pointed out that working well with others is a natural skill set for hospitalists.
“Collaboration is probably my biggest skill set and that of many hospital medicine providers,” she said. “I think I do that in my job here at Vanderbilt in thinking about complicated patients that requirement multiple subspecialists and in bringing together people to figure out the question at hand. That is definitely my leadership style.”
If Dr. Rehm has one goal on the board, it is to become a little bit more like Dr. Thompson and focus on chapter development for pediatric hospitalists.
“I’m really interested in engaging with members to better understand the struggles on the front line so that we can make sure that, as an organization, we’re offering a brand of things that our membership needs,” she said. “So, I’m really looking forward to becoming more involved in the chapter engagement and development. The Nashville chapter is getting re-engaged now and I’m excited to be involved.”
To prepare for her debut board meeting in Las Vegas, Dr. Rehm attended SHM board meetings at the group’s Philadelphia headquarters over the past two years.
“I’ve been lucky enough to attend the fall board meeting in Philadelphia and observe the board in action, and I think that has helped me get to know some of the current board members and to have a little bit of a vision of what the meetings will be like,” she said.
SHM’s two newest board members – pediatric hospitalist Kris Rehm, MD, SFHM, and perioperative specialist Rachel Thompson, MD, MPH, SFHM – will bring their expertise to bear on the society’s top panel.
However, neither woman sees her role as shaping the board. In fact, they see themselves as lucky to be joining the team.
“I really want to hear everyone’s voice, and I hope to see how we can all move to better places together,” added Dr. Rehm, associate professor of clinical pediatrics and director of the division of hospital medicine at Vanderbilt University in Nashville.
Both board members were officially seated for three-year terms at HM17 in Las Vegas. They replace former SHM president Robert Harrington, MD, SFHM, and veteran pediatric hospitalist Erin Stucky Fisher, MD, MHM.
Each of the new board members brings a strong perspective to the panel.
For Dr. Thompson, that viewpoint is based in engagement. She is the former chair of SHM’s Pacific Northwest chapter and has spent the past few years leading the perioperative issues for the society’s work group.
“We get to a certain point of our career as hospitalists, and if we’re just plugging in and working, doing our shifts, somewhere in that 8- to 10-year range, we might get a little bored, tired, worn out,” Dr. Thompson said. “I believe, if we have the community and professional home to keep us engaged, that helps us see the value in what we’re doing every day. It helps us continue to grow, so we don’t hit that wall.”
Given Dr. Thompson’s involvement both with her chapter and the society’s chapter support committee, she will likely continue that effort to make sure SHM’s board sees the value of encouraging and partnering with local chapters. She will also work with SHM president Ron Greeno, MD, FCCP, MHM, on policy issues, as her background in public health has aligned her interests on health care reform and other headwinds facing the specialty.
“I went in to do my masters in public health with the idea that I wanted to build the skill set so that I could be more analytical in how I approach our problem solving, our discovery in the hospital setting,” she said. “It really speaks to a part of me that has always been interested in finding ways to prevent illness and moving beyond that reactivity that we have in medicine into a prevention-based [approach].”
Dr. Thompson noted that her background in perioperative medicine helps her work as part of a team because it “entirely relies on collaboration and coordination of care, which is pretty much the basis of what we do in the hospital any day.”
Dr. Rehm, who serves as a pediatric hospitalist at the Monroe Carell Jr. Children’s Hospital at Vanderbilt, said she will also bring a teamwork-focused perspective to the SHM board.
She could be expected to view everything through the lens of inpatient pediatrics, but that’s not her style.
“I think we have so many similarities and so many things that [pediatric and adult hospitalists] can partner to do together,” she said. “We all are involved in, for example, medication reconciliation or discharge-management planning or postacute care follow-up. There’s a lot of synergy, and I think we can learn so much from each other.”
Dr. Rehm, who chairs SHM’s Pediatrics Committee and the 2017 Pediatric Hospital Medicine meeting, pointed out that working well with others is a natural skill set for hospitalists.
“Collaboration is probably my biggest skill set and that of many hospital medicine providers,” she said. “I think I do that in my job here at Vanderbilt in thinking about complicated patients that requirement multiple subspecialists and in bringing together people to figure out the question at hand. That is definitely my leadership style.”
If Dr. Rehm has one goal on the board, it is to become a little bit more like Dr. Thompson and focus on chapter development for pediatric hospitalists.
“I’m really interested in engaging with members to better understand the struggles on the front line so that we can make sure that, as an organization, we’re offering a brand of things that our membership needs,” she said. “So, I’m really looking forward to becoming more involved in the chapter engagement and development. The Nashville chapter is getting re-engaged now and I’m excited to be involved.”
To prepare for her debut board meeting in Las Vegas, Dr. Rehm attended SHM board meetings at the group’s Philadelphia headquarters over the past two years.
“I’ve been lucky enough to attend the fall board meeting in Philadelphia and observe the board in action, and I think that has helped me get to know some of the current board members and to have a little bit of a vision of what the meetings will be like,” she said.
SHM’s two newest board members – pediatric hospitalist Kris Rehm, MD, SFHM, and perioperative specialist Rachel Thompson, MD, MPH, SFHM – will bring their expertise to bear on the society’s top panel.
However, neither woman sees her role as shaping the board. In fact, they see themselves as lucky to be joining the team.
“I really want to hear everyone’s voice, and I hope to see how we can all move to better places together,” added Dr. Rehm, associate professor of clinical pediatrics and director of the division of hospital medicine at Vanderbilt University in Nashville.
Both board members were officially seated for three-year terms at HM17 in Las Vegas. They replace former SHM president Robert Harrington, MD, SFHM, and veteran pediatric hospitalist Erin Stucky Fisher, MD, MHM.
Each of the new board members brings a strong perspective to the panel.
For Dr. Thompson, that viewpoint is based in engagement. She is the former chair of SHM’s Pacific Northwest chapter and has spent the past few years leading the perioperative issues for the society’s work group.
“We get to a certain point of our career as hospitalists, and if we’re just plugging in and working, doing our shifts, somewhere in that 8- to 10-year range, we might get a little bored, tired, worn out,” Dr. Thompson said. “I believe, if we have the community and professional home to keep us engaged, that helps us see the value in what we’re doing every day. It helps us continue to grow, so we don’t hit that wall.”
Given Dr. Thompson’s involvement both with her chapter and the society’s chapter support committee, she will likely continue that effort to make sure SHM’s board sees the value of encouraging and partnering with local chapters. She will also work with SHM president Ron Greeno, MD, FCCP, MHM, on policy issues, as her background in public health has aligned her interests on health care reform and other headwinds facing the specialty.
“I went in to do my masters in public health with the idea that I wanted to build the skill set so that I could be more analytical in how I approach our problem solving, our discovery in the hospital setting,” she said. “It really speaks to a part of me that has always been interested in finding ways to prevent illness and moving beyond that reactivity that we have in medicine into a prevention-based [approach].”
Dr. Thompson noted that her background in perioperative medicine helps her work as part of a team because it “entirely relies on collaboration and coordination of care, which is pretty much the basis of what we do in the hospital any day.”
Dr. Rehm, who serves as a pediatric hospitalist at the Monroe Carell Jr. Children’s Hospital at Vanderbilt, said she will also bring a teamwork-focused perspective to the SHM board.
She could be expected to view everything through the lens of inpatient pediatrics, but that’s not her style.
“I think we have so many similarities and so many things that [pediatric and adult hospitalists] can partner to do together,” she said. “We all are involved in, for example, medication reconciliation or discharge-management planning or postacute care follow-up. There’s a lot of synergy, and I think we can learn so much from each other.”
Dr. Rehm, who chairs SHM’s Pediatrics Committee and the 2017 Pediatric Hospital Medicine meeting, pointed out that working well with others is a natural skill set for hospitalists.
“Collaboration is probably my biggest skill set and that of many hospital medicine providers,” she said. “I think I do that in my job here at Vanderbilt in thinking about complicated patients that requirement multiple subspecialists and in bringing together people to figure out the question at hand. That is definitely my leadership style.”
If Dr. Rehm has one goal on the board, it is to become a little bit more like Dr. Thompson and focus on chapter development for pediatric hospitalists.
“I’m really interested in engaging with members to better understand the struggles on the front line so that we can make sure that, as an organization, we’re offering a brand of things that our membership needs,” she said. “So, I’m really looking forward to becoming more involved in the chapter engagement and development. The Nashville chapter is getting re-engaged now and I’m excited to be involved.”
To prepare for her debut board meeting in Las Vegas, Dr. Rehm attended SHM board meetings at the group’s Philadelphia headquarters over the past two years.
“I’ve been lucky enough to attend the fall board meeting in Philadelphia and observe the board in action, and I think that has helped me get to know some of the current board members and to have a little bit of a vision of what the meetings will be like,” she said.
What Does the Accountability Act Mean for VA Employees?
On Friday June 23, President Trump signed into law the VA Accountability and Whistleblower Protection Act, which established a revised disciplinary system for VA employees who are accused of poor performance or misconduct and protects those who report them. The bill amends Title 38 of the U.S. Code, adding VA employees to the list of those that the VA Secretary can remove if necessary. The act speeds up the termination and suspension processes for civil servants. The VA also claims that the bill will shorten the process of hiring new administrators. Still unclear is what this bill means for VA health care providers.
VA employees are protected under both Title 5 and Title 38 of the U.S. code. Title 5 governs the employment of all federal civil servants. Title 38 specifically governs the employment of VA employees in certain health care fields. Both titles specify processes for termination, demotion, or suspension and an appeals process.
Critics, including VA Secretary David J. Shulkin, MD, have complained that the previous civil service protections were time consuming and made it difficult to penalize or remove problem employees. Supporters insist that Title 5 and Title 38 protected the rights of good employees and whistleblowers from unfair workplace retaliation.
Under the new law, the VA Secretary can more easily remove, demote, or suspend any employee who warrants a penalty, including executives and supervisors. Although many of the Title 5 and Title 38 protections still cover VA employees, there are several notable changes.
What’s changing for VA employees?
- Time line: The act shortens time between the initial report, employee notification, Secretary’s decision, and appeal request/decision.
- Standard of proof: Previously, the standard of proof for misconduct was “preponderance of evidence.” The new bill lowers this standard to “supported by substantial evidence.” Changing the standard of proof effectively means that the Secretary will need to present less evidence of wrongdoing/negligence for the employee to be removed, demoted, or suspended.
- Appeals: Employees may still appeal removal, demotion, or suspension decisions, but rather than going through the Disciplinary Appeals Board, the Merit Systems Protection Board will hear appeals. Appeals must be filed within 10 days of the Secretary’s final decision. Additionally, administrative judges are instructed to uphold the decision of the Secretary if the evidence meets the “substantial evidence” standard. Administrative judges are prohibited from reducing the penalty.
Analysis
Although these changes are meant to increase the accountability of health care providers in the VA, there are several other legal implications for VA employees. Ultimately, the bill gives the VA Secretary more discretion. Whether this is a good or bad change is open to debate. Even though the bill easily passed in both the House of Representatives and the Senate, some lawmakers remain skeptical because the act increases the power of the Secretary and limits due process for VA employees. Under the new law, VA employees will have less time to prepare their defense and be held to a lower standard of proof, which will make it easier to remove VA employees from their jobs.
The Fifth Amendment of the U.S. Constitution guarantees that all Americans shall not be “deprived of life, liberty, or property, without due process of law.” Furthermore, due process rights increase when the limitations on ones’ rights are greater; this is why the burden of proof falls on the prosecution and why the standard of proof is “beyond a reasonable doubt” in criminal cases, because the rights that are at risk are liberty and, in some cases, life.
Due process is particularly important for civil servants because they are employed by the federal government. The rights to property are at risk of being limited if they are to be removed, demoted, or suspended from their jobs. The VA Accountability and Whistleblower Protection Act limits the due process of VA civil servants. However, it also is important to highlight that under this law, the VA Secretary has the right to remove, demote, or suspend any person who threatens the function and service of the VA or endangers veterans. In other words, while the VA employee’s due process may have decreased, it has increased for those whose lives depend on their service.
On Friday June 23, President Trump signed into law the VA Accountability and Whistleblower Protection Act, which established a revised disciplinary system for VA employees who are accused of poor performance or misconduct and protects those who report them. The bill amends Title 38 of the U.S. Code, adding VA employees to the list of those that the VA Secretary can remove if necessary. The act speeds up the termination and suspension processes for civil servants. The VA also claims that the bill will shorten the process of hiring new administrators. Still unclear is what this bill means for VA health care providers.
VA employees are protected under both Title 5 and Title 38 of the U.S. code. Title 5 governs the employment of all federal civil servants. Title 38 specifically governs the employment of VA employees in certain health care fields. Both titles specify processes for termination, demotion, or suspension and an appeals process.
Critics, including VA Secretary David J. Shulkin, MD, have complained that the previous civil service protections were time consuming and made it difficult to penalize or remove problem employees. Supporters insist that Title 5 and Title 38 protected the rights of good employees and whistleblowers from unfair workplace retaliation.
Under the new law, the VA Secretary can more easily remove, demote, or suspend any employee who warrants a penalty, including executives and supervisors. Although many of the Title 5 and Title 38 protections still cover VA employees, there are several notable changes.
What’s changing for VA employees?
- Time line: The act shortens time between the initial report, employee notification, Secretary’s decision, and appeal request/decision.
- Standard of proof: Previously, the standard of proof for misconduct was “preponderance of evidence.” The new bill lowers this standard to “supported by substantial evidence.” Changing the standard of proof effectively means that the Secretary will need to present less evidence of wrongdoing/negligence for the employee to be removed, demoted, or suspended.
- Appeals: Employees may still appeal removal, demotion, or suspension decisions, but rather than going through the Disciplinary Appeals Board, the Merit Systems Protection Board will hear appeals. Appeals must be filed within 10 days of the Secretary’s final decision. Additionally, administrative judges are instructed to uphold the decision of the Secretary if the evidence meets the “substantial evidence” standard. Administrative judges are prohibited from reducing the penalty.
Analysis
Although these changes are meant to increase the accountability of health care providers in the VA, there are several other legal implications for VA employees. Ultimately, the bill gives the VA Secretary more discretion. Whether this is a good or bad change is open to debate. Even though the bill easily passed in both the House of Representatives and the Senate, some lawmakers remain skeptical because the act increases the power of the Secretary and limits due process for VA employees. Under the new law, VA employees will have less time to prepare their defense and be held to a lower standard of proof, which will make it easier to remove VA employees from their jobs.
The Fifth Amendment of the U.S. Constitution guarantees that all Americans shall not be “deprived of life, liberty, or property, without due process of law.” Furthermore, due process rights increase when the limitations on ones’ rights are greater; this is why the burden of proof falls on the prosecution and why the standard of proof is “beyond a reasonable doubt” in criminal cases, because the rights that are at risk are liberty and, in some cases, life.
Due process is particularly important for civil servants because they are employed by the federal government. The rights to property are at risk of being limited if they are to be removed, demoted, or suspended from their jobs. The VA Accountability and Whistleblower Protection Act limits the due process of VA civil servants. However, it also is important to highlight that under this law, the VA Secretary has the right to remove, demote, or suspend any person who threatens the function and service of the VA or endangers veterans. In other words, while the VA employee’s due process may have decreased, it has increased for those whose lives depend on their service.
On Friday June 23, President Trump signed into law the VA Accountability and Whistleblower Protection Act, which established a revised disciplinary system for VA employees who are accused of poor performance or misconduct and protects those who report them. The bill amends Title 38 of the U.S. Code, adding VA employees to the list of those that the VA Secretary can remove if necessary. The act speeds up the termination and suspension processes for civil servants. The VA also claims that the bill will shorten the process of hiring new administrators. Still unclear is what this bill means for VA health care providers.
VA employees are protected under both Title 5 and Title 38 of the U.S. code. Title 5 governs the employment of all federal civil servants. Title 38 specifically governs the employment of VA employees in certain health care fields. Both titles specify processes for termination, demotion, or suspension and an appeals process.
Critics, including VA Secretary David J. Shulkin, MD, have complained that the previous civil service protections were time consuming and made it difficult to penalize or remove problem employees. Supporters insist that Title 5 and Title 38 protected the rights of good employees and whistleblowers from unfair workplace retaliation.
Under the new law, the VA Secretary can more easily remove, demote, or suspend any employee who warrants a penalty, including executives and supervisors. Although many of the Title 5 and Title 38 protections still cover VA employees, there are several notable changes.
What’s changing for VA employees?
- Time line: The act shortens time between the initial report, employee notification, Secretary’s decision, and appeal request/decision.
- Standard of proof: Previously, the standard of proof for misconduct was “preponderance of evidence.” The new bill lowers this standard to “supported by substantial evidence.” Changing the standard of proof effectively means that the Secretary will need to present less evidence of wrongdoing/negligence for the employee to be removed, demoted, or suspended.
- Appeals: Employees may still appeal removal, demotion, or suspension decisions, but rather than going through the Disciplinary Appeals Board, the Merit Systems Protection Board will hear appeals. Appeals must be filed within 10 days of the Secretary’s final decision. Additionally, administrative judges are instructed to uphold the decision of the Secretary if the evidence meets the “substantial evidence” standard. Administrative judges are prohibited from reducing the penalty.
Analysis
Although these changes are meant to increase the accountability of health care providers in the VA, there are several other legal implications for VA employees. Ultimately, the bill gives the VA Secretary more discretion. Whether this is a good or bad change is open to debate. Even though the bill easily passed in both the House of Representatives and the Senate, some lawmakers remain skeptical because the act increases the power of the Secretary and limits due process for VA employees. Under the new law, VA employees will have less time to prepare their defense and be held to a lower standard of proof, which will make it easier to remove VA employees from their jobs.
The Fifth Amendment of the U.S. Constitution guarantees that all Americans shall not be “deprived of life, liberty, or property, without due process of law.” Furthermore, due process rights increase when the limitations on ones’ rights are greater; this is why the burden of proof falls on the prosecution and why the standard of proof is “beyond a reasonable doubt” in criminal cases, because the rights that are at risk are liberty and, in some cases, life.
Due process is particularly important for civil servants because they are employed by the federal government. The rights to property are at risk of being limited if they are to be removed, demoted, or suspended from their jobs. The VA Accountability and Whistleblower Protection Act limits the due process of VA civil servants. However, it also is important to highlight that under this law, the VA Secretary has the right to remove, demote, or suspend any person who threatens the function and service of the VA or endangers veterans. In other words, while the VA employee’s due process may have decreased, it has increased for those whose lives depend on their service.
Quality of Chronic Obstructive Pulmonary Disease-Related Health Care in Rural and Urban Veterans Affairs Clinics
Chronic obstructive pulmonary disease (COPD) affects between 11 and 24 million people in the U.S. and is the third leading cause of death in this country.1,2 Airflow obstruction on spirometry in addition to respiratory symptoms is required to establish a diagnosis of COPD.3,4 As many as 40% of patients with a clinical diagnosis of COPD have not had spirometry or have spirometry results inconsistent with the diagnosis of COPD.5,6 In addition to recommended spirometry, many patients with COPD do not receive other evidence-based therapies.7,8
About 50% of patients in the Minneapolis VA Health Care System (MVAHCS) receive care in its rural community-based outreach clinics (CBOCs). Data regarding the quality of general medical care between rural and urban populations are sparse; however, studies suggest that the quality of care delivered in rural clinics may be lower than the care provided in an urban setting.9-12 Care for patients with COPD in an urban setting is suboptimal with only 58% of patients receiving guideline-based care, and there are no comparative data for penetrance in the rural setting.8 Most published studies on patients with COPD treated in rural vs urban locations are outcomes studies that queried statewide or national registry data evaluating the frequency of emergency department (ED) visits or hospital admissions for COPD exacerbations, all-cause mortality, or COPD exacerbation-related mortality.13-18 There are no studies examining potential differences in the quality of health care received by patients with COPD in rural vs urban locations or whether these potential differences are associated with changes in health care utilization.
The authors sought to determine whether patients with the diagnosis of COPD treated in the MVAHCS and its 13 CBOCs receive similar quality of disease-related health care in rural vs urban primary care clinic locations. The authors hypothesized that patients who receive their primary care in rural clinics would be less likely to have had spirometry or to receive respiratory immunizations and short- or long-acting inhalers and that discrepancies would be associated with increased health care utilization in rural areas as measured by prescriptions for systemic corticosteroids, antibiotics, ED visits, or hospital admissions for COPD exacerbations.
Methods
The MVAHCS has 14 primary care locations; these locations were designated as rural or urban based on the Rural-Urban Commuting Area codes.19,20 There were 4 urban locations and 10 rural clinics; all rural clinics were farther than 40 miles from the main Minneapolis VAMC.
Patient Selection
The authors performed a retrospective chart review after receiving an institutional review board waiver for this quality assessment study. All patients who had a prior ICD-9 encounter diagnosis of COPD (codes: 491.0, 491.1, 491.2, 491.20, 491.21, 491.22, 491.8, 491.9, 492.0, 492.8, 494, 494.0, 494.1, 496) and who were seen in primary care during March 2015 were identified. Each subject’s first visit during that month was used as the start of the retrospective 1-year look-back period. All eligible subjects were sorted based on their rural or urban location and a randomly assigned number. Patients were then selected according to ascending numbers from each rural and urban clinic in proportion to the clinic’s representation among all eligible patients.
Outcomes
The primary outcomes—possible discrepancies in quality of health care for patients with COPD in rural vs urban primary care clinics—were assessed by (1) prior spirometry; (2) any prior pneumonia vaccination; (3) an influenza vaccination within the past year; (4) prescriptions within the past year for a short-acting beta agonist (SABA) metered-dose inhaler; and (5) prescriptions for a long-acting inhalers, including long-acting beta agonists (LABAs), long-acting muscarinic antagonists (LAMAs), or inhaled corticosteroids (ICSs).
Secondary outcomes included (1) an active prescription for home oxygen within the past calendar year; (2) health care utilization assessed via prescriptions for intermittent courses of oral corticosteroids; (3) prescriptions for respiratory antibiotics (macrolides, tetracyclines, fluoroquinolones) within the past year for COPD exacerbations; (4) ED visits; (5) hospital admissions (and need for mechanical ventilation) for COPD exacerbations within the past year; and (6) whether patients were seen by either VA or Non-VA pulmonology providers.
Data Collection
Patients’ demographic data and comorbidities were collected via chart review. A 1-year prescription medication list was obtained by an electronic database search of the MVAHCS electronic medical record (EMR). Additional antibiotics and corticosteroid prescriptions for COPD exacerbations paid for by the VA but filled at a local pharmacy were manually searched from a separate database to supplement the electronic prescription list. Comparison of the electronic prescription list and pharmacy records in 25% of patients found 100% concordance in the prescription lists. The investigator manually reviewed and extracted the following data from the EMR, scanned-in records, and a Midwest VA COPD registry database: most recent spirometry results; immunization status for influenza in the past year; prior pneumonia vaccination; home oxygen prescription; whether the patient received respiratory antibiotic or intermittent oral corticosteroid treatment for COPD exacerbations; whether the patient had a ED visit or hospital admission for COPD exacerbation with or without need for mechanical ventilation; and whether the patient had been seen by a pulmonology provider. The investigator reviewed all primary care provider notes in the past year for documentation of non-VA ED visits or hospitalizations that were not present in the EMR, Midwest VA COPD registry database, or scanned patient records.
Data Analysis
Results are described as mean ± standard deviation, median (interquartile range) or proportion, expressed as a percentage as appropriate for the level of measurement and distribution. The proportions meeting the COPD quality of health care outcomes in the urban and rural groups were compared using a chi-square test of proportions, and 95% confidence intervals (CI) on the differences were estimated. Samples of 400 patients each from the rural and urban groups were estimated to provide a 95% 2-sided CI on the differences of about ± 0.05 (5%), assuming the proportion meeting the quality of care outcomes in the urban group would be at least 0.8 (80%).
Results
The authors identified 1,538 patients with a previous encounter diagnosis of COPD who were seen in a primary care clinic in the MVAHCS in March of 2015. The authors reviewed the medical records of 801 randomly selected patients: 400 rural clinic patients and 401 urban clinic patients. Demographic characteristics and major comorbidities of rural and urban patients were similar except more rural patients were white, and fewer had a record of obstructive sleep apnea, alcoholism, or addictive disorders (Table 1). Prescriptions for common chronic medical conditions were similar for rural and urban groups, including medications for depression (31% vs 33%) or diabetes mellitus (25% vs 28%). In patients who had spirometry, the severity of COPD, as assessed by mean forced expiratory volume (FEV1), was similar between rural and urban patients (2.06 L vs 2.10 L). 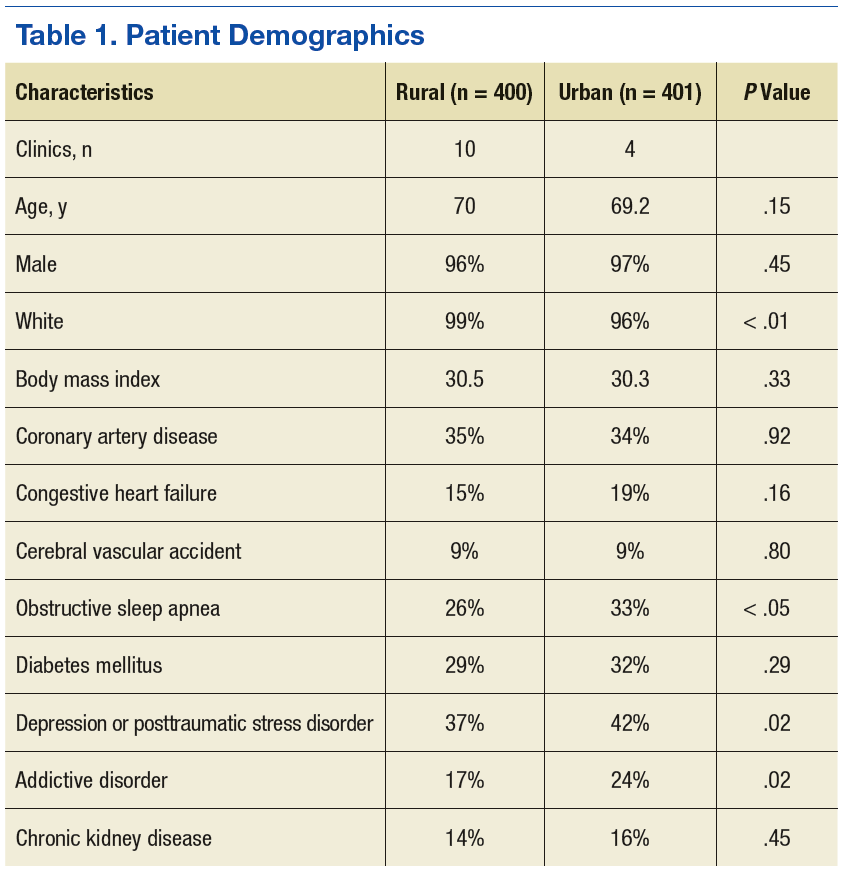
Quality of COPD Care
Spirometry was documented in fewer rural clinic patients than in urban clinic patients (51% vs 82%; difference 31%, 95% CI: 25% to 37%) (Table 2).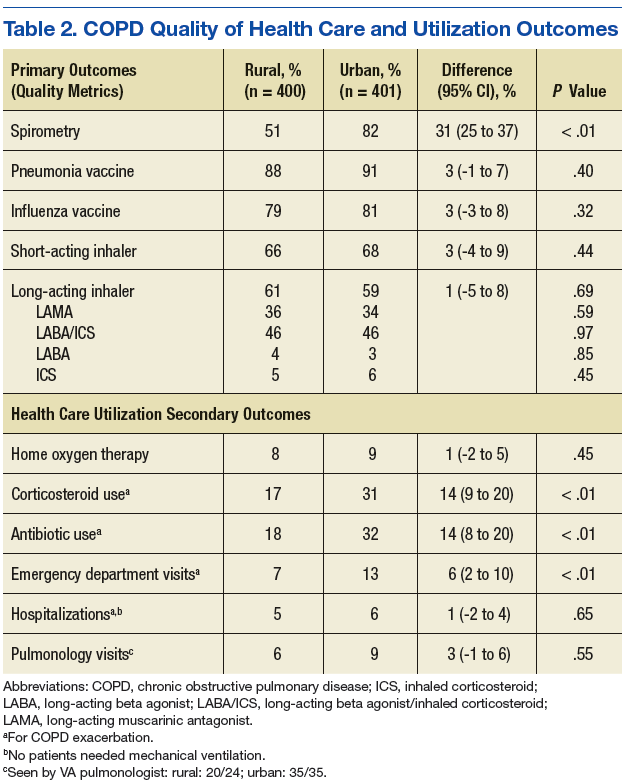
COPD Outcomes
Home oxygen prescription rates were similar for rural and urban clinic patients (8% vs 9%; difference 1%, 95% CI: -2% to 5%). Rural patients received fewer prescriptions for intermittent oral corticosteroids (17% vs 31%; difference 14%, 95% CI: 9% to 20%) and antibiotics for COPD exacerbations (18% vs 32%; difference 14%, 95% CI: 8% to 20%). Rural patients had fewer ED visits for COPD exacerbations (7% vs 13%; difference 6%, 95% CI: 2% to 10%), and similar admission rates for COPD exacerbations (5% vs 6%; difference 1%, 95% CI: -2% to 4%). Of the few patients hospitalized for COPD exacerbations, none required mechanical ventilation. There was no significant difference in the number of rural vs urban patients seen by a pulmonologist in the calendar year of the study (6% vs 9%; difference 3%, 95% CI:-1% to 6%), with the majority seen by VA providers: 20/24 rural patients and 35/35 urban patients.
Discussion
Fewer rural patients had prior spirometry; otherwise, the COPD-related quality metrics were similar between rural and urban patient groups in the MVAHCS, including immunizations for pneumonia and influenza, and prescribing rates for short- and long-acting inhaler therapy. Despite the similarity in these COPD quality measures, rural clinic patients seemed to have less health care utilization related to COPD exacerbations.
Spirometry with airflow obstruction in the presence of respiratory symptoms is required for accurate diagnosis of COPD.3,4 Spirometry has been available at the MVAHCS hospital-based clinic for years. Efforts to address this disparity led to implementation of on-site spirometry at all rural and urban clinics about 2 years prior to the patient enrollment visit date for the study. Fewer rural patients had spirometry, which is possibly from prior disparity in resources; yet rates of spirometry in all patients with a clinical diagnosis of COPD in the MVAHCS are higher (rural 51%, urban 82%) than previously reported. A nationwide study of 94,000 veterans with recent clinical diagnosis of COPD found only 37% had spirometry within 2.5 years of diagnosis,21 and another non-VA study (n = 553) showed only 31% of patients discharged from a hospital with a diagnosis of COPD exacerbation had spirometry performed within a 8-year period prior to hospitalization.22
Annual influenza vaccines are recommended for everyone aged > 6 months, and the pneumonia vaccine is recommended for all patients with COPD in order to reduce the risk of COPD exacerbations and pneumonias.23,24 The rates of vaccination at MVAHCS rural and urban clinics for both influenza (79% vs 81%) and pneumococcus (88% vs 91%) are higher than previously published studies of patients with COPD for influenza vaccination (30%-51%) and pneumonia vaccination (21%-51%) and did not differ between rural and urban clinics.7,25-28 The observed high vaccination rates may be due to EMR prompts and requirements to document vaccination status and offer recommended vaccinations.
Long-acting inhalers have been shown to reduce rates of COPD exacerbations and improve patients’ quality of life.29 The authors found no disparity in the prescription rate of short- or long-acting inhalers between rural and urban patients, and no difference in the severity of COPD, as indicated by FEV1, that might influence prescription rates.
The authors attempted to evaluate health care resource utilization as an indicator of health care quality and outcomes. Based on previous reports, the authors expected to find lower quality of care and increased utilization in rural patients. Previous studies have shown rural patients can be more symptomatic with a higher body mass index, airflow obstruction, dyspnea, and exercise capacity index (BODE index) than are patients in urban settings.16,30 Statewide and national registry data have shown rural patients have higher rates of primary care visits, ER visits, and hospitalizations for COPD exacerbations.
Rural patients also have been shown to have higher mortality rates and were more likely to be in a long-term care center and less likely to have home care or palliative care than were their urban counterparts.13-18,31 If the severity of illness is similar in rural and urban areas, higher health care utilization related to COPD would suggest that patients in rural settings may be receiving inferior quality of health care. The authors could not find any previous reports of the quality of COPD care delivered in rural vs urban settings.
In this study the only difference in quality of care was the lower proportion of rural patients with a record of spirometry that is needed to confirm the diagnosis. The observed differences in the quality of care measures wouldn’t be expected to lead to large differences in the outcome measures. Contrary to the literature and the observed similarity in quality of care, rural patients had better COPD outcomes perhaps due to unmeasured differences in risk or failure to capture medical visits outside of the VA system. The severity of COPD based on FEV1 and concurrent diagnoses, such as heart failure, did not suggest that rural patients in this comparison had a higher burden of illness or risk of poor COPD outcomes.
More than 70,000 patients spanning a large geographic region receive primary care at MVAHCS, which provides comparable care to all COPD patients, regardless of location, by using the same EMR system, providing evidence-based order sets for disease management, proactively offering on-site and remote COPD case managers for high-risk patients, and more recently, implementing on-site spirometry testing in all clinics. This approach as opposed to the traditional outreach clinic model may in part explain the similarity in quality of care in urban and rural clinics that was not reported in previous studies.
Limitations
This study was performed retrospectively, increasing the potential of missing data, especially from outside the VA health care system. Patients were not randomly assigned to rural or urban clinics, so differences in patient characteristics could exist. Alcohol and addictive disorders were more common in urban patients, which might affect adherence to prescribed medications. In addition, lower rate of obstructive sleep apnea was found in the rural population, which has been linked to increased airway inflammation and COPD exacerbations resulting in hospitalization.32,33 Mortality was not assessed as all patients were alive and seen in clinic at time of enrollment.
The authors were not able to record a patients’ residence in a long-term care facility or institutionalization, use of home care, or palliative care services due to limitations in the EMR system. Whether patients received comanaged primary care or underwent pulmonary rehabilitation could not be obtained from the EMR. Most patients never had lung volumes or diffusion capacity and thus were not included. The authors could not report whether inhaler therapy was appropriate compared with the Global Initiative for Chronic Obstructive Lund Disease(GOLD)severity score because most of the spirometry was done at a discordant time to when inhaler therapy was assessed, and new GOLD guidelines include patient symptoms that were not reliably recorded in the EMR. Last, the authors had hoped to include smoking status and cessation practices as part of the quality measures, but due to significant variability in patients’ documented smoking status in the same period, the data were deemed unreliable.
Conclusion
No disparities were found between rural and urban clinics in the quality of health care for patients with COPD in the MVAHCS except that fewer rural patients had prior spirometry; a difference that is likely due to the fact that only recently has spirometry been implemented in the MVAHCS rural clinics. Overall the quality of COPD care was high and above the previously reported rates. Further larger studies of rural and urban quality of health care for patients with COPD are needed in other VA and non-VA systems to determine whether disparities exist and whether they are associated with clinical outcomes, including ED visits, hospitalizations, and mortality.
1. Blackwell DL, Lucas JW, Clarke TC. Summary health statistics for U.S. adults: national health interview survey, 2012. Vital Health Stat 10. 2014(260):1-161.
2. Xu J, Murphy SL, Kochanek KD, Bastian BA. Deaths: final data for 2013. Natl Vital Stat Rep. 2016;64(2):1-119.
3. Celli BR, MacNee W, Force AET. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932-946.
4. Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS; GOLD Scientific Committee. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001;163(5):1256-1276.
5. Ghattas C, Dai A, Gemmel DJ, Awad MH. Over diagnosis of chronic obstructive pulmonary disease in an underserved patient population. Int J Chron Obstruct Pulmon Dis. 2013;8:545-549.
6. Zwar NA, Marks GB, Hermiz O, et al. Predictors of accuracy of diagnosis of chronic obstructive pulmonary disease in general practice. Med J Aust. 2011;195(4):168-171.
7. Lopez-Campos JL, Abad Arranz M, Calero-Acuña C, et al. Guideline adherence in outpatient clinics for chronic obstructive pulmonary disease: results from a clinical audit. PLoS One. 2016;11(3):e0151896.
8. McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348(26):2635-2645.
9. Spoont M, Greer N, Su J, Fitzgerald P, Rutks I, Wilt TJ. Rural vs. Urban Ambulatory Health Care: A Systematic Review. Washington, DC: U.S. Department of Veteran Affairs; 2011.
10. Weeks WB, Wallace AE, Wang S, Lee A, Kazis LE. Rural-urban disparities in health-related quality of life within disease categories of Veterans. J Rural Health. 2006;22(3):204-211.
11. Wallace AE, Weeks WB, Wang S, Lee AF, Kazis LE. Rural and urban disparities in health-related quality of life among veterans with psychiatric disorders. Psychiatr Serv. 2006;57(6):851-856.
12. Meit M, Knudson A, Gilbert T, et al; Rural Health Reform Policy Research Center. The 2014 update of the rural-urban chartbook. https://ruralhealth.und .edu/projects/health-reform-policy-research-center/pdf/2014-rural-urban-chartbook-update.pdf. Published October 2014. Accessed April 18, 2017.
13. Jackson BE, Suzuki S, Coultas D, et al. Safety-net facilities and hospitalization rates of chronic obstructive pulmonary disease: a cross-sectional analysis of the 2007 Texas Health Care Information Council inpatient data. Int J Chron Obstruct Pulmon Dis. 2011;6:563-571.
14. Jackson BE, Suzuki S, Lo K, et al. Geographic disparity in COPD hospitalization rates among the Texas population. Respir Med. 2011;105(5):734-739.15. Skinner HG, Blanchard J, Elixhauser A. Trends in emergency department visits, 2006-2011: statistical brief #179. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb179-Emergency-Department-Trends.pdf. Published September 2014. Accessed May 9, 2017.
16. Jackson BE, Coultas DB, Suzuki S, Singh KP, Bae S. Rural-urban disparities in quality of life among patients with COPD. J Rural Health. 2013;29(suppl 1):62S-69S.
17. Singh GK, Siahpush M. Widening rural-urban disparities in life expectancy, U.S., 1969-2009. Am J Prev Med. 2014;46(2):e19-e29.
18. Abrams TE, Vaughan-Sarrazin M, Fan VS, Kaboli PJ. Geographic isolation and the risk for chronic obstructive pulmonary disease-related mortality: a cohort study. Ann Intern Med. 2011;155(2):80-86.
19. Hart LG, Larson EH, Lishner DM. Rural definitions for health policy and research. Am J Public Health. 2005;95(7):1149-1155.
20. U.S. Department of Agriculture, Economic Research Service. Rural-urban commuting area codes. https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes.aspx#U20K1F50H0A. Updated October 12, 2016. Accessed May 9, 2017.
21. Joo MJ, Lee TA, Weiss KB. Geographic variation of spirometry use in newly diagnosed COPD. Chest. 2008;134(1):38-45.
22. Damarla M, Celli BR, Mullerova HX, Pinto-Plata VM. Discrepancy in the use of confirmatory tests in patients hospitalized with the diagnosis of chronic obstructive pulmonary disease or congestive heart failure. Respir Care. 2006;51(10):1120-1124.
23. Grohskopf LA, Sokolow LZ, Olsen SJ, Bresee JS, Broder KR, Karron RA. Prevention and control of influenza with vaccines: recommendations of the advisory committee on immunization practices, United States, 2015-16 influenza season. MMWR Morb Mortal Wkly Rep. 2015;64(30):818-825.
24. Kim DK, Bridges CB, Harriman KH; Advisory Committee on Immunization Practices. Advisory committee on immunization practices recommended immunization schedule for adults aged 19 years or older: United States, 2016. Ann Intern Med. 2016;164(3):184-194.
25. Cimen P, Unlu M, Kirakli C, et al. Should patients with COPD be vaccinated? Respir Care. 2015;60(2):239-243.
26. Mowls DS, Cheruvu VK, Zullo MD. Influenza vaccination in adults with chronic obstructive pulmonary disease: the impact of a diagnostic breathing test on vaccination rates PLoS One. 2013;8(6):e67600.
27. Shoup JA, Madrid C, Koehler C, et al. Effectiveness and cost of influenza vaccine reminders for adults with asthma or chronic obstructive pulmonary disease. Am J Manag Care. 2015;21(7):e405-e413.
28. Arinez-Fernandez MC, Carrasco-Garrido P, Garcia-Carballo M, Hernandez-Barrera V, de Miguel AG, Jimenez-Garcia R. Determinants of pneumococcal vaccination among patients with chronic obstructive pulmonary disease in Spain. Hum Vaccin. 2006;2(3):99-104.29. Qaseem A, Wilt TJ, Weinberger SE, et al. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155(3):179-191.
30. Celli BR, Cote CG, Marin JM, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(10):1005-1012.
31. Goodridge D, Lawson J, Rennie D, Marciniuk D. Rural/urban differences in health care utilization and place of death for persons with respiratory illness in the last year of life. Rural Remote Health. 2010;10(2):1349.
32. Wang Y, Hu K, Liu K, et al. Obstructive sleep apnea exacerbates airway inflammation in patients with chronic obstructive pulmonary disease. Sleep Med. 2015;16(9):1123-1130.
33. Marin JM, Soriano JB, Carrizo SJ, Boldova A, Celli BR. Outcomes in patients with chronic obstructive pulmonary disease and obstructive sleep apnea: the overlap syndrome. Am J Respir Crit Care Med. 2010;182(3):325-331
Chronic obstructive pulmonary disease (COPD) affects between 11 and 24 million people in the U.S. and is the third leading cause of death in this country.1,2 Airflow obstruction on spirometry in addition to respiratory symptoms is required to establish a diagnosis of COPD.3,4 As many as 40% of patients with a clinical diagnosis of COPD have not had spirometry or have spirometry results inconsistent with the diagnosis of COPD.5,6 In addition to recommended spirometry, many patients with COPD do not receive other evidence-based therapies.7,8
About 50% of patients in the Minneapolis VA Health Care System (MVAHCS) receive care in its rural community-based outreach clinics (CBOCs). Data regarding the quality of general medical care between rural and urban populations are sparse; however, studies suggest that the quality of care delivered in rural clinics may be lower than the care provided in an urban setting.9-12 Care for patients with COPD in an urban setting is suboptimal with only 58% of patients receiving guideline-based care, and there are no comparative data for penetrance in the rural setting.8 Most published studies on patients with COPD treated in rural vs urban locations are outcomes studies that queried statewide or national registry data evaluating the frequency of emergency department (ED) visits or hospital admissions for COPD exacerbations, all-cause mortality, or COPD exacerbation-related mortality.13-18 There are no studies examining potential differences in the quality of health care received by patients with COPD in rural vs urban locations or whether these potential differences are associated with changes in health care utilization.
The authors sought to determine whether patients with the diagnosis of COPD treated in the MVAHCS and its 13 CBOCs receive similar quality of disease-related health care in rural vs urban primary care clinic locations. The authors hypothesized that patients who receive their primary care in rural clinics would be less likely to have had spirometry or to receive respiratory immunizations and short- or long-acting inhalers and that discrepancies would be associated with increased health care utilization in rural areas as measured by prescriptions for systemic corticosteroids, antibiotics, ED visits, or hospital admissions for COPD exacerbations.
Methods
The MVAHCS has 14 primary care locations; these locations were designated as rural or urban based on the Rural-Urban Commuting Area codes.19,20 There were 4 urban locations and 10 rural clinics; all rural clinics were farther than 40 miles from the main Minneapolis VAMC.
Patient Selection
The authors performed a retrospective chart review after receiving an institutional review board waiver for this quality assessment study. All patients who had a prior ICD-9 encounter diagnosis of COPD (codes: 491.0, 491.1, 491.2, 491.20, 491.21, 491.22, 491.8, 491.9, 492.0, 492.8, 494, 494.0, 494.1, 496) and who were seen in primary care during March 2015 were identified. Each subject’s first visit during that month was used as the start of the retrospective 1-year look-back period. All eligible subjects were sorted based on their rural or urban location and a randomly assigned number. Patients were then selected according to ascending numbers from each rural and urban clinic in proportion to the clinic’s representation among all eligible patients.
Outcomes
The primary outcomes—possible discrepancies in quality of health care for patients with COPD in rural vs urban primary care clinics—were assessed by (1) prior spirometry; (2) any prior pneumonia vaccination; (3) an influenza vaccination within the past year; (4) prescriptions within the past year for a short-acting beta agonist (SABA) metered-dose inhaler; and (5) prescriptions for a long-acting inhalers, including long-acting beta agonists (LABAs), long-acting muscarinic antagonists (LAMAs), or inhaled corticosteroids (ICSs).
Secondary outcomes included (1) an active prescription for home oxygen within the past calendar year; (2) health care utilization assessed via prescriptions for intermittent courses of oral corticosteroids; (3) prescriptions for respiratory antibiotics (macrolides, tetracyclines, fluoroquinolones) within the past year for COPD exacerbations; (4) ED visits; (5) hospital admissions (and need for mechanical ventilation) for COPD exacerbations within the past year; and (6) whether patients were seen by either VA or Non-VA pulmonology providers.
Data Collection
Patients’ demographic data and comorbidities were collected via chart review. A 1-year prescription medication list was obtained by an electronic database search of the MVAHCS electronic medical record (EMR). Additional antibiotics and corticosteroid prescriptions for COPD exacerbations paid for by the VA but filled at a local pharmacy were manually searched from a separate database to supplement the electronic prescription list. Comparison of the electronic prescription list and pharmacy records in 25% of patients found 100% concordance in the prescription lists. The investigator manually reviewed and extracted the following data from the EMR, scanned-in records, and a Midwest VA COPD registry database: most recent spirometry results; immunization status for influenza in the past year; prior pneumonia vaccination; home oxygen prescription; whether the patient received respiratory antibiotic or intermittent oral corticosteroid treatment for COPD exacerbations; whether the patient had a ED visit or hospital admission for COPD exacerbation with or without need for mechanical ventilation; and whether the patient had been seen by a pulmonology provider. The investigator reviewed all primary care provider notes in the past year for documentation of non-VA ED visits or hospitalizations that were not present in the EMR, Midwest VA COPD registry database, or scanned patient records.
Data Analysis
Results are described as mean ± standard deviation, median (interquartile range) or proportion, expressed as a percentage as appropriate for the level of measurement and distribution. The proportions meeting the COPD quality of health care outcomes in the urban and rural groups were compared using a chi-square test of proportions, and 95% confidence intervals (CI) on the differences were estimated. Samples of 400 patients each from the rural and urban groups were estimated to provide a 95% 2-sided CI on the differences of about ± 0.05 (5%), assuming the proportion meeting the quality of care outcomes in the urban group would be at least 0.8 (80%).
Results
The authors identified 1,538 patients with a previous encounter diagnosis of COPD who were seen in a primary care clinic in the MVAHCS in March of 2015. The authors reviewed the medical records of 801 randomly selected patients: 400 rural clinic patients and 401 urban clinic patients. Demographic characteristics and major comorbidities of rural and urban patients were similar except more rural patients were white, and fewer had a record of obstructive sleep apnea, alcoholism, or addictive disorders (Table 1). Prescriptions for common chronic medical conditions were similar for rural and urban groups, including medications for depression (31% vs 33%) or diabetes mellitus (25% vs 28%). In patients who had spirometry, the severity of COPD, as assessed by mean forced expiratory volume (FEV1), was similar between rural and urban patients (2.06 L vs 2.10 L).
Quality of COPD Care
Spirometry was documented in fewer rural clinic patients than in urban clinic patients (51% vs 82%; difference 31%, 95% CI: 25% to 37%) (Table 2).
COPD Outcomes
Home oxygen prescription rates were similar for rural and urban clinic patients (8% vs 9%; difference 1%, 95% CI: -2% to 5%). Rural patients received fewer prescriptions for intermittent oral corticosteroids (17% vs 31%; difference 14%, 95% CI: 9% to 20%) and antibiotics for COPD exacerbations (18% vs 32%; difference 14%, 95% CI: 8% to 20%). Rural patients had fewer ED visits for COPD exacerbations (7% vs 13%; difference 6%, 95% CI: 2% to 10%), and similar admission rates for COPD exacerbations (5% vs 6%; difference 1%, 95% CI: -2% to 4%). Of the few patients hospitalized for COPD exacerbations, none required mechanical ventilation. There was no significant difference in the number of rural vs urban patients seen by a pulmonologist in the calendar year of the study (6% vs 9%; difference 3%, 95% CI:-1% to 6%), with the majority seen by VA providers: 20/24 rural patients and 35/35 urban patients.
Discussion
Fewer rural patients had prior spirometry; otherwise, the COPD-related quality metrics were similar between rural and urban patient groups in the MVAHCS, including immunizations for pneumonia and influenza, and prescribing rates for short- and long-acting inhaler therapy. Despite the similarity in these COPD quality measures, rural clinic patients seemed to have less health care utilization related to COPD exacerbations.
Spirometry with airflow obstruction in the presence of respiratory symptoms is required for accurate diagnosis of COPD.3,4 Spirometry has been available at the MVAHCS hospital-based clinic for years. Efforts to address this disparity led to implementation of on-site spirometry at all rural and urban clinics about 2 years prior to the patient enrollment visit date for the study. Fewer rural patients had spirometry, which is possibly from prior disparity in resources; yet rates of spirometry in all patients with a clinical diagnosis of COPD in the MVAHCS are higher (rural 51%, urban 82%) than previously reported. A nationwide study of 94,000 veterans with recent clinical diagnosis of COPD found only 37% had spirometry within 2.5 years of diagnosis,21 and another non-VA study (n = 553) showed only 31% of patients discharged from a hospital with a diagnosis of COPD exacerbation had spirometry performed within a 8-year period prior to hospitalization.22
Annual influenza vaccines are recommended for everyone aged > 6 months, and the pneumonia vaccine is recommended for all patients with COPD in order to reduce the risk of COPD exacerbations and pneumonias.23,24 The rates of vaccination at MVAHCS rural and urban clinics for both influenza (79% vs 81%) and pneumococcus (88% vs 91%) are higher than previously published studies of patients with COPD for influenza vaccination (30%-51%) and pneumonia vaccination (21%-51%) and did not differ between rural and urban clinics.7,25-28 The observed high vaccination rates may be due to EMR prompts and requirements to document vaccination status and offer recommended vaccinations.
Long-acting inhalers have been shown to reduce rates of COPD exacerbations and improve patients’ quality of life.29 The authors found no disparity in the prescription rate of short- or long-acting inhalers between rural and urban patients, and no difference in the severity of COPD, as indicated by FEV1, that might influence prescription rates.
The authors attempted to evaluate health care resource utilization as an indicator of health care quality and outcomes. Based on previous reports, the authors expected to find lower quality of care and increased utilization in rural patients. Previous studies have shown rural patients can be more symptomatic with a higher body mass index, airflow obstruction, dyspnea, and exercise capacity index (BODE index) than are patients in urban settings.16,30 Statewide and national registry data have shown rural patients have higher rates of primary care visits, ER visits, and hospitalizations for COPD exacerbations.
Rural patients also have been shown to have higher mortality rates and were more likely to be in a long-term care center and less likely to have home care or palliative care than were their urban counterparts.13-18,31 If the severity of illness is similar in rural and urban areas, higher health care utilization related to COPD would suggest that patients in rural settings may be receiving inferior quality of health care. The authors could not find any previous reports of the quality of COPD care delivered in rural vs urban settings.
In this study the only difference in quality of care was the lower proportion of rural patients with a record of spirometry that is needed to confirm the diagnosis. The observed differences in the quality of care measures wouldn’t be expected to lead to large differences in the outcome measures. Contrary to the literature and the observed similarity in quality of care, rural patients had better COPD outcomes perhaps due to unmeasured differences in risk or failure to capture medical visits outside of the VA system. The severity of COPD based on FEV1 and concurrent diagnoses, such as heart failure, did not suggest that rural patients in this comparison had a higher burden of illness or risk of poor COPD outcomes.
More than 70,000 patients spanning a large geographic region receive primary care at MVAHCS, which provides comparable care to all COPD patients, regardless of location, by using the same EMR system, providing evidence-based order sets for disease management, proactively offering on-site and remote COPD case managers for high-risk patients, and more recently, implementing on-site spirometry testing in all clinics. This approach as opposed to the traditional outreach clinic model may in part explain the similarity in quality of care in urban and rural clinics that was not reported in previous studies.
Limitations
This study was performed retrospectively, increasing the potential of missing data, especially from outside the VA health care system. Patients were not randomly assigned to rural or urban clinics, so differences in patient characteristics could exist. Alcohol and addictive disorders were more common in urban patients, which might affect adherence to prescribed medications. In addition, lower rate of obstructive sleep apnea was found in the rural population, which has been linked to increased airway inflammation and COPD exacerbations resulting in hospitalization.32,33 Mortality was not assessed as all patients were alive and seen in clinic at time of enrollment.
The authors were not able to record a patients’ residence in a long-term care facility or institutionalization, use of home care, or palliative care services due to limitations in the EMR system. Whether patients received comanaged primary care or underwent pulmonary rehabilitation could not be obtained from the EMR. Most patients never had lung volumes or diffusion capacity and thus were not included. The authors could not report whether inhaler therapy was appropriate compared with the Global Initiative for Chronic Obstructive Lund Disease(GOLD)severity score because most of the spirometry was done at a discordant time to when inhaler therapy was assessed, and new GOLD guidelines include patient symptoms that were not reliably recorded in the EMR. Last, the authors had hoped to include smoking status and cessation practices as part of the quality measures, but due to significant variability in patients’ documented smoking status in the same period, the data were deemed unreliable.
Conclusion
No disparities were found between rural and urban clinics in the quality of health care for patients with COPD in the MVAHCS except that fewer rural patients had prior spirometry; a difference that is likely due to the fact that only recently has spirometry been implemented in the MVAHCS rural clinics. Overall the quality of COPD care was high and above the previously reported rates. Further larger studies of rural and urban quality of health care for patients with COPD are needed in other VA and non-VA systems to determine whether disparities exist and whether they are associated with clinical outcomes, including ED visits, hospitalizations, and mortality.
Chronic obstructive pulmonary disease (COPD) affects between 11 and 24 million people in the U.S. and is the third leading cause of death in this country.1,2 Airflow obstruction on spirometry in addition to respiratory symptoms is required to establish a diagnosis of COPD.3,4 As many as 40% of patients with a clinical diagnosis of COPD have not had spirometry or have spirometry results inconsistent with the diagnosis of COPD.5,6 In addition to recommended spirometry, many patients with COPD do not receive other evidence-based therapies.7,8
About 50% of patients in the Minneapolis VA Health Care System (MVAHCS) receive care in its rural community-based outreach clinics (CBOCs). Data regarding the quality of general medical care between rural and urban populations are sparse; however, studies suggest that the quality of care delivered in rural clinics may be lower than the care provided in an urban setting.9-12 Care for patients with COPD in an urban setting is suboptimal with only 58% of patients receiving guideline-based care, and there are no comparative data for penetrance in the rural setting.8 Most published studies on patients with COPD treated in rural vs urban locations are outcomes studies that queried statewide or national registry data evaluating the frequency of emergency department (ED) visits or hospital admissions for COPD exacerbations, all-cause mortality, or COPD exacerbation-related mortality.13-18 There are no studies examining potential differences in the quality of health care received by patients with COPD in rural vs urban locations or whether these potential differences are associated with changes in health care utilization.
The authors sought to determine whether patients with the diagnosis of COPD treated in the MVAHCS and its 13 CBOCs receive similar quality of disease-related health care in rural vs urban primary care clinic locations. The authors hypothesized that patients who receive their primary care in rural clinics would be less likely to have had spirometry or to receive respiratory immunizations and short- or long-acting inhalers and that discrepancies would be associated with increased health care utilization in rural areas as measured by prescriptions for systemic corticosteroids, antibiotics, ED visits, or hospital admissions for COPD exacerbations.
Methods
The MVAHCS has 14 primary care locations; these locations were designated as rural or urban based on the Rural-Urban Commuting Area codes.19,20 There were 4 urban locations and 10 rural clinics; all rural clinics were farther than 40 miles from the main Minneapolis VAMC.
Patient Selection
The authors performed a retrospective chart review after receiving an institutional review board waiver for this quality assessment study. All patients who had a prior ICD-9 encounter diagnosis of COPD (codes: 491.0, 491.1, 491.2, 491.20, 491.21, 491.22, 491.8, 491.9, 492.0, 492.8, 494, 494.0, 494.1, 496) and who were seen in primary care during March 2015 were identified. Each subject’s first visit during that month was used as the start of the retrospective 1-year look-back period. All eligible subjects were sorted based on their rural or urban location and a randomly assigned number. Patients were then selected according to ascending numbers from each rural and urban clinic in proportion to the clinic’s representation among all eligible patients.
Outcomes
The primary outcomes—possible discrepancies in quality of health care for patients with COPD in rural vs urban primary care clinics—were assessed by (1) prior spirometry; (2) any prior pneumonia vaccination; (3) an influenza vaccination within the past year; (4) prescriptions within the past year for a short-acting beta agonist (SABA) metered-dose inhaler; and (5) prescriptions for a long-acting inhalers, including long-acting beta agonists (LABAs), long-acting muscarinic antagonists (LAMAs), or inhaled corticosteroids (ICSs).
Secondary outcomes included (1) an active prescription for home oxygen within the past calendar year; (2) health care utilization assessed via prescriptions for intermittent courses of oral corticosteroids; (3) prescriptions for respiratory antibiotics (macrolides, tetracyclines, fluoroquinolones) within the past year for COPD exacerbations; (4) ED visits; (5) hospital admissions (and need for mechanical ventilation) for COPD exacerbations within the past year; and (6) whether patients were seen by either VA or Non-VA pulmonology providers.
Data Collection
Patients’ demographic data and comorbidities were collected via chart review. A 1-year prescription medication list was obtained by an electronic database search of the MVAHCS electronic medical record (EMR). Additional antibiotics and corticosteroid prescriptions for COPD exacerbations paid for by the VA but filled at a local pharmacy were manually searched from a separate database to supplement the electronic prescription list. Comparison of the electronic prescription list and pharmacy records in 25% of patients found 100% concordance in the prescription lists. The investigator manually reviewed and extracted the following data from the EMR, scanned-in records, and a Midwest VA COPD registry database: most recent spirometry results; immunization status for influenza in the past year; prior pneumonia vaccination; home oxygen prescription; whether the patient received respiratory antibiotic or intermittent oral corticosteroid treatment for COPD exacerbations; whether the patient had a ED visit or hospital admission for COPD exacerbation with or without need for mechanical ventilation; and whether the patient had been seen by a pulmonology provider. The investigator reviewed all primary care provider notes in the past year for documentation of non-VA ED visits or hospitalizations that were not present in the EMR, Midwest VA COPD registry database, or scanned patient records.
Data Analysis
Results are described as mean ± standard deviation, median (interquartile range) or proportion, expressed as a percentage as appropriate for the level of measurement and distribution. The proportions meeting the COPD quality of health care outcomes in the urban and rural groups were compared using a chi-square test of proportions, and 95% confidence intervals (CI) on the differences were estimated. Samples of 400 patients each from the rural and urban groups were estimated to provide a 95% 2-sided CI on the differences of about ± 0.05 (5%), assuming the proportion meeting the quality of care outcomes in the urban group would be at least 0.8 (80%).
Results
The authors identified 1,538 patients with a previous encounter diagnosis of COPD who were seen in a primary care clinic in the MVAHCS in March of 2015. The authors reviewed the medical records of 801 randomly selected patients: 400 rural clinic patients and 401 urban clinic patients. Demographic characteristics and major comorbidities of rural and urban patients were similar except more rural patients were white, and fewer had a record of obstructive sleep apnea, alcoholism, or addictive disorders (Table 1). Prescriptions for common chronic medical conditions were similar for rural and urban groups, including medications for depression (31% vs 33%) or diabetes mellitus (25% vs 28%). In patients who had spirometry, the severity of COPD, as assessed by mean forced expiratory volume (FEV1), was similar between rural and urban patients (2.06 L vs 2.10 L).
Quality of COPD Care
Spirometry was documented in fewer rural clinic patients than in urban clinic patients (51% vs 82%; difference 31%, 95% CI: 25% to 37%) (Table 2).
COPD Outcomes
Home oxygen prescription rates were similar for rural and urban clinic patients (8% vs 9%; difference 1%, 95% CI: -2% to 5%). Rural patients received fewer prescriptions for intermittent oral corticosteroids (17% vs 31%; difference 14%, 95% CI: 9% to 20%) and antibiotics for COPD exacerbations (18% vs 32%; difference 14%, 95% CI: 8% to 20%). Rural patients had fewer ED visits for COPD exacerbations (7% vs 13%; difference 6%, 95% CI: 2% to 10%), and similar admission rates for COPD exacerbations (5% vs 6%; difference 1%, 95% CI: -2% to 4%). Of the few patients hospitalized for COPD exacerbations, none required mechanical ventilation. There was no significant difference in the number of rural vs urban patients seen by a pulmonologist in the calendar year of the study (6% vs 9%; difference 3%, 95% CI:-1% to 6%), with the majority seen by VA providers: 20/24 rural patients and 35/35 urban patients.
Discussion
Fewer rural patients had prior spirometry; otherwise, the COPD-related quality metrics were similar between rural and urban patient groups in the MVAHCS, including immunizations for pneumonia and influenza, and prescribing rates for short- and long-acting inhaler therapy. Despite the similarity in these COPD quality measures, rural clinic patients seemed to have less health care utilization related to COPD exacerbations.
Spirometry with airflow obstruction in the presence of respiratory symptoms is required for accurate diagnosis of COPD.3,4 Spirometry has been available at the MVAHCS hospital-based clinic for years. Efforts to address this disparity led to implementation of on-site spirometry at all rural and urban clinics about 2 years prior to the patient enrollment visit date for the study. Fewer rural patients had spirometry, which is possibly from prior disparity in resources; yet rates of spirometry in all patients with a clinical diagnosis of COPD in the MVAHCS are higher (rural 51%, urban 82%) than previously reported. A nationwide study of 94,000 veterans with recent clinical diagnosis of COPD found only 37% had spirometry within 2.5 years of diagnosis,21 and another non-VA study (n = 553) showed only 31% of patients discharged from a hospital with a diagnosis of COPD exacerbation had spirometry performed within a 8-year period prior to hospitalization.22
Annual influenza vaccines are recommended for everyone aged > 6 months, and the pneumonia vaccine is recommended for all patients with COPD in order to reduce the risk of COPD exacerbations and pneumonias.23,24 The rates of vaccination at MVAHCS rural and urban clinics for both influenza (79% vs 81%) and pneumococcus (88% vs 91%) are higher than previously published studies of patients with COPD for influenza vaccination (30%-51%) and pneumonia vaccination (21%-51%) and did not differ between rural and urban clinics.7,25-28 The observed high vaccination rates may be due to EMR prompts and requirements to document vaccination status and offer recommended vaccinations.
Long-acting inhalers have been shown to reduce rates of COPD exacerbations and improve patients’ quality of life.29 The authors found no disparity in the prescription rate of short- or long-acting inhalers between rural and urban patients, and no difference in the severity of COPD, as indicated by FEV1, that might influence prescription rates.
The authors attempted to evaluate health care resource utilization as an indicator of health care quality and outcomes. Based on previous reports, the authors expected to find lower quality of care and increased utilization in rural patients. Previous studies have shown rural patients can be more symptomatic with a higher body mass index, airflow obstruction, dyspnea, and exercise capacity index (BODE index) than are patients in urban settings.16,30 Statewide and national registry data have shown rural patients have higher rates of primary care visits, ER visits, and hospitalizations for COPD exacerbations.
Rural patients also have been shown to have higher mortality rates and were more likely to be in a long-term care center and less likely to have home care or palliative care than were their urban counterparts.13-18,31 If the severity of illness is similar in rural and urban areas, higher health care utilization related to COPD would suggest that patients in rural settings may be receiving inferior quality of health care. The authors could not find any previous reports of the quality of COPD care delivered in rural vs urban settings.
In this study the only difference in quality of care was the lower proportion of rural patients with a record of spirometry that is needed to confirm the diagnosis. The observed differences in the quality of care measures wouldn’t be expected to lead to large differences in the outcome measures. Contrary to the literature and the observed similarity in quality of care, rural patients had better COPD outcomes perhaps due to unmeasured differences in risk or failure to capture medical visits outside of the VA system. The severity of COPD based on FEV1 and concurrent diagnoses, such as heart failure, did not suggest that rural patients in this comparison had a higher burden of illness or risk of poor COPD outcomes.
More than 70,000 patients spanning a large geographic region receive primary care at MVAHCS, which provides comparable care to all COPD patients, regardless of location, by using the same EMR system, providing evidence-based order sets for disease management, proactively offering on-site and remote COPD case managers for high-risk patients, and more recently, implementing on-site spirometry testing in all clinics. This approach as opposed to the traditional outreach clinic model may in part explain the similarity in quality of care in urban and rural clinics that was not reported in previous studies.
Limitations
This study was performed retrospectively, increasing the potential of missing data, especially from outside the VA health care system. Patients were not randomly assigned to rural or urban clinics, so differences in patient characteristics could exist. Alcohol and addictive disorders were more common in urban patients, which might affect adherence to prescribed medications. In addition, lower rate of obstructive sleep apnea was found in the rural population, which has been linked to increased airway inflammation and COPD exacerbations resulting in hospitalization.32,33 Mortality was not assessed as all patients were alive and seen in clinic at time of enrollment.
The authors were not able to record a patients’ residence in a long-term care facility or institutionalization, use of home care, or palliative care services due to limitations in the EMR system. Whether patients received comanaged primary care or underwent pulmonary rehabilitation could not be obtained from the EMR. Most patients never had lung volumes or diffusion capacity and thus were not included. The authors could not report whether inhaler therapy was appropriate compared with the Global Initiative for Chronic Obstructive Lund Disease(GOLD)severity score because most of the spirometry was done at a discordant time to when inhaler therapy was assessed, and new GOLD guidelines include patient symptoms that were not reliably recorded in the EMR. Last, the authors had hoped to include smoking status and cessation practices as part of the quality measures, but due to significant variability in patients’ documented smoking status in the same period, the data were deemed unreliable.
Conclusion
No disparities were found between rural and urban clinics in the quality of health care for patients with COPD in the MVAHCS except that fewer rural patients had prior spirometry; a difference that is likely due to the fact that only recently has spirometry been implemented in the MVAHCS rural clinics. Overall the quality of COPD care was high and above the previously reported rates. Further larger studies of rural and urban quality of health care for patients with COPD are needed in other VA and non-VA systems to determine whether disparities exist and whether they are associated with clinical outcomes, including ED visits, hospitalizations, and mortality.
1. Blackwell DL, Lucas JW, Clarke TC. Summary health statistics for U.S. adults: national health interview survey, 2012. Vital Health Stat 10. 2014(260):1-161.
2. Xu J, Murphy SL, Kochanek KD, Bastian BA. Deaths: final data for 2013. Natl Vital Stat Rep. 2016;64(2):1-119.
3. Celli BR, MacNee W, Force AET. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932-946.
4. Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS; GOLD Scientific Committee. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001;163(5):1256-1276.
5. Ghattas C, Dai A, Gemmel DJ, Awad MH. Over diagnosis of chronic obstructive pulmonary disease in an underserved patient population. Int J Chron Obstruct Pulmon Dis. 2013;8:545-549.
6. Zwar NA, Marks GB, Hermiz O, et al. Predictors of accuracy of diagnosis of chronic obstructive pulmonary disease in general practice. Med J Aust. 2011;195(4):168-171.
7. Lopez-Campos JL, Abad Arranz M, Calero-Acuña C, et al. Guideline adherence in outpatient clinics for chronic obstructive pulmonary disease: results from a clinical audit. PLoS One. 2016;11(3):e0151896.
8. McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348(26):2635-2645.
9. Spoont M, Greer N, Su J, Fitzgerald P, Rutks I, Wilt TJ. Rural vs. Urban Ambulatory Health Care: A Systematic Review. Washington, DC: U.S. Department of Veteran Affairs; 2011.
10. Weeks WB, Wallace AE, Wang S, Lee A, Kazis LE. Rural-urban disparities in health-related quality of life within disease categories of Veterans. J Rural Health. 2006;22(3):204-211.
11. Wallace AE, Weeks WB, Wang S, Lee AF, Kazis LE. Rural and urban disparities in health-related quality of life among veterans with psychiatric disorders. Psychiatr Serv. 2006;57(6):851-856.
12. Meit M, Knudson A, Gilbert T, et al; Rural Health Reform Policy Research Center. The 2014 update of the rural-urban chartbook. https://ruralhealth.und .edu/projects/health-reform-policy-research-center/pdf/2014-rural-urban-chartbook-update.pdf. Published October 2014. Accessed April 18, 2017.
13. Jackson BE, Suzuki S, Coultas D, et al. Safety-net facilities and hospitalization rates of chronic obstructive pulmonary disease: a cross-sectional analysis of the 2007 Texas Health Care Information Council inpatient data. Int J Chron Obstruct Pulmon Dis. 2011;6:563-571.
14. Jackson BE, Suzuki S, Lo K, et al. Geographic disparity in COPD hospitalization rates among the Texas population. Respir Med. 2011;105(5):734-739.15. Skinner HG, Blanchard J, Elixhauser A. Trends in emergency department visits, 2006-2011: statistical brief #179. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb179-Emergency-Department-Trends.pdf. Published September 2014. Accessed May 9, 2017.
16. Jackson BE, Coultas DB, Suzuki S, Singh KP, Bae S. Rural-urban disparities in quality of life among patients with COPD. J Rural Health. 2013;29(suppl 1):62S-69S.
17. Singh GK, Siahpush M. Widening rural-urban disparities in life expectancy, U.S., 1969-2009. Am J Prev Med. 2014;46(2):e19-e29.
18. Abrams TE, Vaughan-Sarrazin M, Fan VS, Kaboli PJ. Geographic isolation and the risk for chronic obstructive pulmonary disease-related mortality: a cohort study. Ann Intern Med. 2011;155(2):80-86.
19. Hart LG, Larson EH, Lishner DM. Rural definitions for health policy and research. Am J Public Health. 2005;95(7):1149-1155.
20. U.S. Department of Agriculture, Economic Research Service. Rural-urban commuting area codes. https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes.aspx#U20K1F50H0A. Updated October 12, 2016. Accessed May 9, 2017.
21. Joo MJ, Lee TA, Weiss KB. Geographic variation of spirometry use in newly diagnosed COPD. Chest. 2008;134(1):38-45.
22. Damarla M, Celli BR, Mullerova HX, Pinto-Plata VM. Discrepancy in the use of confirmatory tests in patients hospitalized with the diagnosis of chronic obstructive pulmonary disease or congestive heart failure. Respir Care. 2006;51(10):1120-1124.
23. Grohskopf LA, Sokolow LZ, Olsen SJ, Bresee JS, Broder KR, Karron RA. Prevention and control of influenza with vaccines: recommendations of the advisory committee on immunization practices, United States, 2015-16 influenza season. MMWR Morb Mortal Wkly Rep. 2015;64(30):818-825.
24. Kim DK, Bridges CB, Harriman KH; Advisory Committee on Immunization Practices. Advisory committee on immunization practices recommended immunization schedule for adults aged 19 years or older: United States, 2016. Ann Intern Med. 2016;164(3):184-194.
25. Cimen P, Unlu M, Kirakli C, et al. Should patients with COPD be vaccinated? Respir Care. 2015;60(2):239-243.
26. Mowls DS, Cheruvu VK, Zullo MD. Influenza vaccination in adults with chronic obstructive pulmonary disease: the impact of a diagnostic breathing test on vaccination rates PLoS One. 2013;8(6):e67600.
27. Shoup JA, Madrid C, Koehler C, et al. Effectiveness and cost of influenza vaccine reminders for adults with asthma or chronic obstructive pulmonary disease. Am J Manag Care. 2015;21(7):e405-e413.
28. Arinez-Fernandez MC, Carrasco-Garrido P, Garcia-Carballo M, Hernandez-Barrera V, de Miguel AG, Jimenez-Garcia R. Determinants of pneumococcal vaccination among patients with chronic obstructive pulmonary disease in Spain. Hum Vaccin. 2006;2(3):99-104.29. Qaseem A, Wilt TJ, Weinberger SE, et al. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155(3):179-191.
30. Celli BR, Cote CG, Marin JM, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(10):1005-1012.
31. Goodridge D, Lawson J, Rennie D, Marciniuk D. Rural/urban differences in health care utilization and place of death for persons with respiratory illness in the last year of life. Rural Remote Health. 2010;10(2):1349.
32. Wang Y, Hu K, Liu K, et al. Obstructive sleep apnea exacerbates airway inflammation in patients with chronic obstructive pulmonary disease. Sleep Med. 2015;16(9):1123-1130.
33. Marin JM, Soriano JB, Carrizo SJ, Boldova A, Celli BR. Outcomes in patients with chronic obstructive pulmonary disease and obstructive sleep apnea: the overlap syndrome. Am J Respir Crit Care Med. 2010;182(3):325-331
1. Blackwell DL, Lucas JW, Clarke TC. Summary health statistics for U.S. adults: national health interview survey, 2012. Vital Health Stat 10. 2014(260):1-161.
2. Xu J, Murphy SL, Kochanek KD, Bastian BA. Deaths: final data for 2013. Natl Vital Stat Rep. 2016;64(2):1-119.
3. Celli BR, MacNee W, Force AET. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932-946.
4. Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS; GOLD Scientific Committee. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001;163(5):1256-1276.
5. Ghattas C, Dai A, Gemmel DJ, Awad MH. Over diagnosis of chronic obstructive pulmonary disease in an underserved patient population. Int J Chron Obstruct Pulmon Dis. 2013;8:545-549.
6. Zwar NA, Marks GB, Hermiz O, et al. Predictors of accuracy of diagnosis of chronic obstructive pulmonary disease in general practice. Med J Aust. 2011;195(4):168-171.
7. Lopez-Campos JL, Abad Arranz M, Calero-Acuña C, et al. Guideline adherence in outpatient clinics for chronic obstructive pulmonary disease: results from a clinical audit. PLoS One. 2016;11(3):e0151896.
8. McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348(26):2635-2645.
9. Spoont M, Greer N, Su J, Fitzgerald P, Rutks I, Wilt TJ. Rural vs. Urban Ambulatory Health Care: A Systematic Review. Washington, DC: U.S. Department of Veteran Affairs; 2011.
10. Weeks WB, Wallace AE, Wang S, Lee A, Kazis LE. Rural-urban disparities in health-related quality of life within disease categories of Veterans. J Rural Health. 2006;22(3):204-211.
11. Wallace AE, Weeks WB, Wang S, Lee AF, Kazis LE. Rural and urban disparities in health-related quality of life among veterans with psychiatric disorders. Psychiatr Serv. 2006;57(6):851-856.
12. Meit M, Knudson A, Gilbert T, et al; Rural Health Reform Policy Research Center. The 2014 update of the rural-urban chartbook. https://ruralhealth.und .edu/projects/health-reform-policy-research-center/pdf/2014-rural-urban-chartbook-update.pdf. Published October 2014. Accessed April 18, 2017.
13. Jackson BE, Suzuki S, Coultas D, et al. Safety-net facilities and hospitalization rates of chronic obstructive pulmonary disease: a cross-sectional analysis of the 2007 Texas Health Care Information Council inpatient data. Int J Chron Obstruct Pulmon Dis. 2011;6:563-571.
14. Jackson BE, Suzuki S, Lo K, et al. Geographic disparity in COPD hospitalization rates among the Texas population. Respir Med. 2011;105(5):734-739.15. Skinner HG, Blanchard J, Elixhauser A. Trends in emergency department visits, 2006-2011: statistical brief #179. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb179-Emergency-Department-Trends.pdf. Published September 2014. Accessed May 9, 2017.
16. Jackson BE, Coultas DB, Suzuki S, Singh KP, Bae S. Rural-urban disparities in quality of life among patients with COPD. J Rural Health. 2013;29(suppl 1):62S-69S.
17. Singh GK, Siahpush M. Widening rural-urban disparities in life expectancy, U.S., 1969-2009. Am J Prev Med. 2014;46(2):e19-e29.
18. Abrams TE, Vaughan-Sarrazin M, Fan VS, Kaboli PJ. Geographic isolation and the risk for chronic obstructive pulmonary disease-related mortality: a cohort study. Ann Intern Med. 2011;155(2):80-86.
19. Hart LG, Larson EH, Lishner DM. Rural definitions for health policy and research. Am J Public Health. 2005;95(7):1149-1155.
20. U.S. Department of Agriculture, Economic Research Service. Rural-urban commuting area codes. https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes.aspx#U20K1F50H0A. Updated October 12, 2016. Accessed May 9, 2017.
21. Joo MJ, Lee TA, Weiss KB. Geographic variation of spirometry use in newly diagnosed COPD. Chest. 2008;134(1):38-45.
22. Damarla M, Celli BR, Mullerova HX, Pinto-Plata VM. Discrepancy in the use of confirmatory tests in patients hospitalized with the diagnosis of chronic obstructive pulmonary disease or congestive heart failure. Respir Care. 2006;51(10):1120-1124.
23. Grohskopf LA, Sokolow LZ, Olsen SJ, Bresee JS, Broder KR, Karron RA. Prevention and control of influenza with vaccines: recommendations of the advisory committee on immunization practices, United States, 2015-16 influenza season. MMWR Morb Mortal Wkly Rep. 2015;64(30):818-825.
24. Kim DK, Bridges CB, Harriman KH; Advisory Committee on Immunization Practices. Advisory committee on immunization practices recommended immunization schedule for adults aged 19 years or older: United States, 2016. Ann Intern Med. 2016;164(3):184-194.
25. Cimen P, Unlu M, Kirakli C, et al. Should patients with COPD be vaccinated? Respir Care. 2015;60(2):239-243.
26. Mowls DS, Cheruvu VK, Zullo MD. Influenza vaccination in adults with chronic obstructive pulmonary disease: the impact of a diagnostic breathing test on vaccination rates PLoS One. 2013;8(6):e67600.
27. Shoup JA, Madrid C, Koehler C, et al. Effectiveness and cost of influenza vaccine reminders for adults with asthma or chronic obstructive pulmonary disease. Am J Manag Care. 2015;21(7):e405-e413.
28. Arinez-Fernandez MC, Carrasco-Garrido P, Garcia-Carballo M, Hernandez-Barrera V, de Miguel AG, Jimenez-Garcia R. Determinants of pneumococcal vaccination among patients with chronic obstructive pulmonary disease in Spain. Hum Vaccin. 2006;2(3):99-104.29. Qaseem A, Wilt TJ, Weinberger SE, et al. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155(3):179-191.
30. Celli BR, Cote CG, Marin JM, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(10):1005-1012.
31. Goodridge D, Lawson J, Rennie D, Marciniuk D. Rural/urban differences in health care utilization and place of death for persons with respiratory illness in the last year of life. Rural Remote Health. 2010;10(2):1349.
32. Wang Y, Hu K, Liu K, et al. Obstructive sleep apnea exacerbates airway inflammation in patients with chronic obstructive pulmonary disease. Sleep Med. 2015;16(9):1123-1130.
33. Marin JM, Soriano JB, Carrizo SJ, Boldova A, Celli BR. Outcomes in patients with chronic obstructive pulmonary disease and obstructive sleep apnea: the overlap syndrome. Am J Respir Crit Care Med. 2010;182(3):325-331
Betrixaban receives FDA approval for VTE prophylaxis in adults

The oral, once-daily factor Xa inhibitor betrixaban (Bevyxxa®) was granted approval by the US Food and Drug Administration (FDA) under priority review.
Betrixaban is the first and only anticoagulant for hospital and extended duration prophylaxis of venous thromboembolism (VTE) in adult patients hospitalized for an acute medical illness at risk for thromboembolic complications due to restricted mobility and other risk factors for VTE, according to Portola Pharmaceuticals, Inc, the drug’s developer.
Betrixaban had also received fast track designation from the FDA.
Betrixaban is Portola’s first commercial product.
The FDA approved betrixaban based on data from the phase 3 APEX trial, a randomized, double-blind multinational clinical trial comparing extended duration betrixaban to short duration of enoxaparin.
The trial enrolled 7513 patients at more than 450 clinical sites worldwide. The patients were acutely ill with medical conditions, hospitalized, and had risk factors for VTE.
Patients who received betrixaban had an initial dose of 160 mg orally on day 1, 80 mg once daily for 35 to 42 days, and a placebo injection once daily for 6 to 14 days.
Patients who received enoxaparin had a 40 mg injection subcutaneously once daily for 6 to 14 days and a placebo pill orally once daily for 35 to 42 days.
Efficacy data was analyzed in 7441 patients and assessed by a composite outcome score comprising either the occurrence of asymptomatic proximal deep vein thrombosis (DVT) or symptomatic DVT, non-fatal pulmonary embolism (PE), or VTE-related death.
Investigators observed fewer events in patients receiving betrixaban (4.4%) compared with those taking enoxaparin (6%) (relative risk 0.75, 95% CI: 0.61, 0.91) with no significant increase in major bleeding (0.67% vs 0.57%, respectively).
The most common adverse reactions with betrixaban occurring in 5% or more of patients were related to bleeding.
Overall, 54% of patients receiving betrixaban experienced at least one adverse reaction compared with 52% taking enoxaparin.
The frequency of patients reporting serious adverse reactions was similar between betrixaban (18%) and enoxaparin (17%).
The most frequent reason for treatment discontinuation was bleeding, with an incidence rate for all bleeding episodes of 2.4% and 1.2% for betrixaban and enoxaparin, respectively.
The incidence rate for major bleeding episodes was 0.67% and 0.57% for betrixaban and enoxaparin, respectively.
Portola expects to launch betrixaban between August and November 2017.
The European Medicines Agency’s Committee for Human Medicinal Products (CHMP) is reviewing betrixaban for marketing authorization under its standard review period.
Portola is also advancing clinical development of andexanet alfa (AndexXa®) and cerdulatinib.
Andexanet alfa is a recombinant protein designed to reverse the anticoagulant effect in patients treated with an oral or injectable factor Xa inhibitor.
Cerdulatinib is a Syk/JAK inhibitor to treat hematologic cancers.
See the full prescribing information for more details on betrixaban. ![]()
The oral, once-daily factor Xa inhibitor betrixaban (Bevyxxa®) was granted approval by the US Food and Drug Administration (FDA) under priority review.
Betrixaban is the first and only anticoagulant for hospital and extended duration prophylaxis of venous thromboembolism (VTE) in adult patients hospitalized for an acute medical illness at risk for thromboembolic complications due to restricted mobility and other risk factors for VTE, according to Portola Pharmaceuticals, Inc, the drug’s developer.
Betrixaban had also received fast track designation from the FDA.
Betrixaban is Portola’s first commercial product.
The FDA approved betrixaban based on data from the phase 3 APEX trial, a randomized, double-blind multinational clinical trial comparing extended duration betrixaban to short duration of enoxaparin.
The trial enrolled 7513 patients at more than 450 clinical sites worldwide. The patients were acutely ill with medical conditions, hospitalized, and had risk factors for VTE.
Patients who received betrixaban had an initial dose of 160 mg orally on day 1, 80 mg once daily for 35 to 42 days, and a placebo injection once daily for 6 to 14 days.
Patients who received enoxaparin had a 40 mg injection subcutaneously once daily for 6 to 14 days and a placebo pill orally once daily for 35 to 42 days.
Efficacy data was analyzed in 7441 patients and assessed by a composite outcome score comprising either the occurrence of asymptomatic proximal deep vein thrombosis (DVT) or symptomatic DVT, non-fatal pulmonary embolism (PE), or VTE-related death.
Investigators observed fewer events in patients receiving betrixaban (4.4%) compared with those taking enoxaparin (6%) (relative risk 0.75, 95% CI: 0.61, 0.91) with no significant increase in major bleeding (0.67% vs 0.57%, respectively).
The most common adverse reactions with betrixaban occurring in 5% or more of patients were related to bleeding.
Overall, 54% of patients receiving betrixaban experienced at least one adverse reaction compared with 52% taking enoxaparin.
The frequency of patients reporting serious adverse reactions was similar between betrixaban (18%) and enoxaparin (17%).
The most frequent reason for treatment discontinuation was bleeding, with an incidence rate for all bleeding episodes of 2.4% and 1.2% for betrixaban and enoxaparin, respectively.
The incidence rate for major bleeding episodes was 0.67% and 0.57% for betrixaban and enoxaparin, respectively.
Portola expects to launch betrixaban between August and November 2017.
The European Medicines Agency’s Committee for Human Medicinal Products (CHMP) is reviewing betrixaban for marketing authorization under its standard review period.
Portola is also advancing clinical development of andexanet alfa (AndexXa®) and cerdulatinib.
Andexanet alfa is a recombinant protein designed to reverse the anticoagulant effect in patients treated with an oral or injectable factor Xa inhibitor.
Cerdulatinib is a Syk/JAK inhibitor to treat hematologic cancers.
See the full prescribing information for more details on betrixaban. ![]()
The oral, once-daily factor Xa inhibitor betrixaban (Bevyxxa®) was granted approval by the US Food and Drug Administration (FDA) under priority review.
Betrixaban is the first and only anticoagulant for hospital and extended duration prophylaxis of venous thromboembolism (VTE) in adult patients hospitalized for an acute medical illness at risk for thromboembolic complications due to restricted mobility and other risk factors for VTE, according to Portola Pharmaceuticals, Inc, the drug’s developer.
Betrixaban had also received fast track designation from the FDA.
Betrixaban is Portola’s first commercial product.
The FDA approved betrixaban based on data from the phase 3 APEX trial, a randomized, double-blind multinational clinical trial comparing extended duration betrixaban to short duration of enoxaparin.
The trial enrolled 7513 patients at more than 450 clinical sites worldwide. The patients were acutely ill with medical conditions, hospitalized, and had risk factors for VTE.
Patients who received betrixaban had an initial dose of 160 mg orally on day 1, 80 mg once daily for 35 to 42 days, and a placebo injection once daily for 6 to 14 days.
Patients who received enoxaparin had a 40 mg injection subcutaneously once daily for 6 to 14 days and a placebo pill orally once daily for 35 to 42 days.
Efficacy data was analyzed in 7441 patients and assessed by a composite outcome score comprising either the occurrence of asymptomatic proximal deep vein thrombosis (DVT) or symptomatic DVT, non-fatal pulmonary embolism (PE), or VTE-related death.
Investigators observed fewer events in patients receiving betrixaban (4.4%) compared with those taking enoxaparin (6%) (relative risk 0.75, 95% CI: 0.61, 0.91) with no significant increase in major bleeding (0.67% vs 0.57%, respectively).
The most common adverse reactions with betrixaban occurring in 5% or more of patients were related to bleeding.
Overall, 54% of patients receiving betrixaban experienced at least one adverse reaction compared with 52% taking enoxaparin.
The frequency of patients reporting serious adverse reactions was similar between betrixaban (18%) and enoxaparin (17%).
The most frequent reason for treatment discontinuation was bleeding, with an incidence rate for all bleeding episodes of 2.4% and 1.2% for betrixaban and enoxaparin, respectively.
The incidence rate for major bleeding episodes was 0.67% and 0.57% for betrixaban and enoxaparin, respectively.
Portola expects to launch betrixaban between August and November 2017.
The European Medicines Agency’s Committee for Human Medicinal Products (CHMP) is reviewing betrixaban for marketing authorization under its standard review period.
Portola is also advancing clinical development of andexanet alfa (AndexXa®) and cerdulatinib.
Andexanet alfa is a recombinant protein designed to reverse the anticoagulant effect in patients treated with an oral or injectable factor Xa inhibitor.
Cerdulatinib is a Syk/JAK inhibitor to treat hematologic cancers.
See the full prescribing information for more details on betrixaban. ![]()