User login
Peer Support for Whistleblowers
Whistleblowers report illegalities, improprieties, or injustices. They step forward wittingly or unwittingly to report perceived wrongdoing. But when a whistleblower takes on powerful and entrenched systems or people, retribution and retaliation often ensue, endangering their career and reputation. These negative consequences can have longterm impacts on the lives of those who believed they were acting in the public interest especially when patient care or public safety was at risk.
The following account is based on personal and professional experiences, conversations with more than a dozen other whistleblowers at the DoD, VA, several other organizations, and a literature review. This documentation of those informal peer conversations, combined with the research, is meant to provide insight into the experiences of a whistleblower and the need for peer support so that employees can remain resilient.
Adverse Whistleblower Experiences
Most employees do not set out to be whistleblowers. The process begins when the whistleblower perceives wrongdoing or harm that is being committed in their workplace. At a health care organization, whistleblowing often is focused on individual or organizational illegal or unethical activities, such as funding or contracting fraud, corruption, theft, discrimination, sexual harassment, public health safety or security violations, persistent medical errors, nepotism, or other violations of workplace rules and regulations. VA employees who experience, witness, or discover wrongdoing may choose to disclose their concerns to a supervisor, senior leader, the Office of the Inspector General (OIG), Human Resources or Equal Employment Opportunity (EEO) Office, Employee Assistance Program (EAP), Office of Special Counsel (OSC), Congress, or to a news organization.
According to the 2013 National Business Ethics Survey, more than 6 million American workers who reported misconduct experienced some form of retaliation.1,2 Retribution can manifest in various overt or covert ways, ranging from outright retaliation and further discrimination to other forms of marginalization. For example, a VA physician alleged that he was detailed to an empty office with no patients after reporting patient wait list mismanagement at his hospital. Other whistleblowers report having misconduct charges levied against them, demotions or loss of position, obstruction from promotion, poor performance evaluations, details to more minor assignments, relocation to more meager office space, or pressure to resign or retire.3
Whistleblowers are rarely rewarded for reporting misconduct within their organization. The Joint Commission describes barriers to reporting sentinel events by medical professionals fearing humiliation, litigation, peer pressure, and oversight investigations if they identify medical errors.4
Once allegations are made, the information often is conveyed to a supervisor or leader. For example, some whistleblowers who have reported a hostile work environment to the DoD EAP have noted that the EAP representative contacted the whistleblower’s manager to mediate the situation. This process can take months or years to resolve. In those instances, the managers are rarely relocated. The whistleblower usually is the one forced to move or take another job, which is not always consistent with their job description, and in turn, may impact their performance rating and opportunities for promotion.
Often, OIG and OSC investigations at the VA and other federal agencies can take as long as 2 years. During that time the whistleblower may remain in a lesser or unwanted position or leave the agency. However, even when OIG substantiates claims of wrongdoing, the agency can make recommendations only to leadership, which may or may not be enacted. Whistleblowers report having to submit Freedom of Information Act requests to learn of the outcome of an OIG investigation when leadership chooses to ignore the recommendation.
Civilian government employees are undervalued by society in general, and the negative stereotypes of lazy, shiftless workers abound, even though many civil servants work to protect the nation’s health, welfare, and safety. Civil servants are familiar with derogatory expressions, such as “bureaucratic bean-counter,” and “good enough for government work.” Even President Trump stated that he would come to Washington, DC, and “drain the swamp.” Yet civil servants can go years without a cost of living increase, a promotion, or a bonus but still be asked to perform additional duties or work long hours to the sacrifice of a work/life balance.
In the Federal Employee Viewpoints Survey and other employee environmental climate scans, high levels of workforce stress often are related to the number of grievances filed, the level of morale, the rates of absenteeism and retention, recruitment shortages, and lost productivity.5 Success in toxic environments usually is based on trying to maintain a “go along to get along” status quo, which means looking the other way when contracts are fraudulently awarded or employee discrimination occurs. If leadership is antagonistic to reform, then identifying wrongdoing may come at significant personal risk.
Retaliatory Practices
Once a whistleblower has stepped forward, retaliatory practices may follow. There are tangible legal, financial, social, emotional, and physical tolls to whistleblowing. “Be in for a penny. Be in for a pound,” an OIG official advised one whistleblower. Once a disclosure is made, the process may become arduous for the whistleblower and require individual resilience to face adversity.
Keeping in mind that OIG, EEO, EAP, and OSC are government agencies that investigate, police, and monitor the system, they do not represent the civil servants who document and identify much of the evidence of wrongdoing on their own. Most civil service employees are not subject matter experts on the U.S. legal code that outlines prohibited personal practices or the Federal Acquisition Regulation.
The Notification and Federal Employee Antidiscrimination and Retaliation (NO FEAR) Act authorized in 2002 (U.S. Code § 2301) is designed to inform and protect those who file grievances or disclosures, but operationalizing those protections can be overwhelming and confusing. If a whistleblower wants advice, he or she must retain legal counsel often at a substantial personal cost. Whistleblowers report spending from $10,000 to more than $100,000 in legal fees for a 1- to 2-year investigation.
These legal fees may force whistleblowers to use family finances or borrow money while hoping for justice along with remuneration in the end. In some cases, the financial impact is compounded when the whistleblower has been demoted, denied a promotion, or fired. For medical professionals, the impact might result in the loss of hospital privileges, professional credentials, or state licensure. The loss of income also can lead to loss of health insurance. The legal and financial burdens impact marriages, spousal job options, retirement, and other family choices (eg, vacations, children’s schools, and caregiving obligations).
During investigations, social status and the reputation of the whistleblower are often impugned. For example, whistleblowers are sometimes depicted as snitches, moles, spies, or tattletales and may be categorized as paranoid, disloyal, or disgruntled by leadership. Rarely are whistleblowers labeled protectors, patriots, or heroes, despite the few high profile cases that come to light, such as Karen Silkwood, Erin Brockovich, or Frank Serpico.
More often, whistleblowers’ reputations, especially in civil sectors, are damaged through acts of discrimination, such as bullying; mobbing (asking other employees to monitor and report on the activities of the whistleblower); ostracizing the employee from the team; devaluing the contributions or the performance of the whistleblower; blackballing from other jobs or opportunities; doublebinding with difficult tasks to complete; gaslighting by calling into question the memory of the whistleblower, the reality of the accusation, or its scope; and marginalization. Accusations of misusing funds, inaccurately recording time and attendance, and disputing their judgement are all tactics used to socially isolate and harass whistleblowers into dropping their case or leaving the organization.3
Furthermore, this level of ostracism has documented impact on the psychological and physical well-being of the employee and negative consequences to the overall functioning of the organization.6 Consequences, such as physical violence and property damage at the time of termination and at other betrayals have occurred.3,7 Other whistleblowers have reported being threatened in person or on social media, harassed, and assaulted, especially in the military.
Whistleblowers, similar to others who are bullied in the workplace often described feelings such as fear, depression, anxiety, loneliness, and humiliation.8 These feelings can lead to whistleblowers needing treatment for substance abuse, depression, anxiety, posttraumatic stress disorder (PTSD) and suicidal ideation.9 Multiple studies on depression and PTSD show a correlation to increased morbidity and mortality.10 However, whistleblowing retaliation is not clearly established as a traumatic stressor in relation to PTSD.11
Insomnia and other sleep disturbances are not uncommon among whistleblowers who also note they have resorted to smoking, overeating, alcohol misuse, or medication to manage their distress. Health consequences also include migraines, muscle tension, gastrointestinal conditions, increased blood pressure, and cardiovascular disease.12
Peer Support Models
Studies of peer-to-peer programs for veterans, law enforcement officers, widows, cancer patients, disaster victims, and others bound by survivorship suggest that peer groups can be an effective means of support, even though the model may vary or be adapted to a specific population. In general, peer support is centered on a common experience, shared credibility, confidentiality, and trust. The approach is meant to provide nonjudgmental support that assists with decision making and resilience and provides comfort and hope. Most peer support or mentorship models require some level of peer counselor screening, competency training on an intervention model, supervision, monitoring, and case management by a more senior or credentialed mental health professional.13
The Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury (DCoE) recognized that health care systems that support civil servants, military members, and veterans can benefit from partnerships with internal (eg, human resources, unions, or dedicated EAP) or external (eg, nonprofit and service organizations) employee peer support programs. The DCoE noted that peer networks facilitate referrals to medical care when threats of suicide or harm to others exists, offer additional case management support, and assist professionals in understanding the patient experience.13
Peer support offered at VA hospitals is conducted by peers who are supervised by mental health clinic staff (usually social workers).14 Law enforcement EAP is another example of peer support within an organization to augment mental health and resilience among officers who have experienced first-responder trauma.
External peer support resources can be accessed through partnerships or referrals. For example, the Tragedy Assistance Program for Survivors (TAPS) relies on survivors of military deaths to support each other through bereavement. Although the DoD offers casualty assistance and mental health care to grieving families, the level of peer support differs from TAPS.15 In another example, Castellano documented the benefits of a reciprocal peer support model implemented across 10 peer-based call center programs that manage high risk-populations.16 Core training was consistent across all programs, and mental health professionals supervised call center peer support providers. This peer/clinician collaboration enhances the overall community mental health efforts.
Temple University documented the patient care benefits for behavioral health services that augmented treatment with evidence-based peer support interventions.17 The researchers found that hospitals that used a peer model improved patient outcomes as demonstrated by fewer hospitalizations, increased life satisfaction and enhanced coping skills, increased medication adherence, and reduced substance abuse or suicidal ideation. Additionally, the peer providers themselves experienced positive health benefits based on their ability to help others, improved their own self-efficacy and gained social and economic growth based on their employment satisfaction.17
Peer Support Interventions
Peer support interventions have been effective with various populations and may be effective for whistleblowers as well. Since whistleblowing tends to involve legal processes that call for privacy and the confidentiality of all parties, whistleblowers experience isolation and alienation. Other whistleblowers can better understand the retaliation, discrimination, and isolation that results. In some instances, whistleblowers discovered years later that other employees had similar experiences. An organized, structured program dedicated to peer support can help employees within a health care system or EAP manage the impacts of identifying wrongdoing.18 Peers may be able to break down this isolation and help establish a new network of support for those involved in whistleblowing cases. Restoring a sense of purpose, meaning, and belonging in the workplace is of significant value for the whistleblower.19 Peers can mentor a whistleblower through the investigative process and help determine next steps. Peers can address building, maintaining, and sustaining resilience to overcome adversity.
Peers who already have experienced their own legal, financial, social, emotional, and physical risks and have developed the necessary resiliency skills to survive make ideal peer counselors.20 These peers have faced similar challenges but have perservered.21
Although peer counselors cannot replace an attorney or mental health provider, they can provide background information on the roles and functions of EEO, EAP, OIG, OSC, and the MSPB and how to navigate those systems. Peers can assist whistleblowers in preparing testimony before congressional hearings or for press interviews. Peer supporters also can encourage whistleblowers to seek care for mental and physical health care and to remain adherent to treatment regimens. They case manage a team effort to enable the whistleblower to overcome the adversity of retaliation.
Creating A New Normal
After the Civil War, the False Claims Act, known as the Lincoln Law, served to protect federal reconstruction activities in the South from individuals who attempted to defraud the federal government.22 Today, most Americans are familiar with WikiLeaks. For generations, whistleblowers have exposed wrongdoing in order to protect or reform governmen programs. Whistleblowers have exposed graft and corruption at the highest levels and in daily operations. They have fought for diversity and inclusion and a workplace free of sexual harassment and assault. They have protected taxpayer dollars from waste, fraud, and abuse.
Despite the personal sacrifices often required, most whistleblowers’ spirits are bolstered by the positive outcomes that their disclosures may produce. However, whistleblowers need compassionate and competent assistance throughout the process. Peers can foster the resilience needed to survive the adversarial nature of the whistleblowing process. Therefore, whistleblowers need to be viewed in a new light that involves advocacy, transparency, and peer support so that positive outcomes in government can be realized for all Americans.
1. Ethics and Compliance Initiative. National Business Ethics Survey (NBES) 2013. http://www.ethics.org/ecihome/research/nbes/nbes-reports/nbes-2013. Published 2013. Accessed June 5, 2017.
2. Schnell G. Whistleblower retaliation on the rise—bad news for whistleblowers and their employers alike. http://constantinecannon.com/whistleblower/whistleblower-retaliation-on-the-rise-bad-news-for-whistleblowers-and-their-employers-alike/#.WNJ1s4WcEYh. Published January 18, 2013. Accessed June 5, 2017.
3. Devine T, Maassarani T. The Corporate Whistleblower’s Survival Guide: A Handbook for Committing the Truth. San Francisco, CA. Berrett-Koehler Publishers; 2011:19-40.
4. The Joint Commission. What Every Hospital Should Know About Sentinel Events. Oakbrook Terrace, IL: Joint Commission on Accreditation of Healthcare Organizations; 2000.
5. Reed GE. Tarnished: Toxic Leadership in the U.S. Military. Lincoln, NE; University of Nebraska Press, Potomac Books; 2015:60.
6. McGraw K. Mental health of women warriors: the power of belonging. In: Ritchie EC, Naclerio AL, eds. Women at War. New York, NY. Oxford University Press; 2015:311-320.
7. Blythe B. Blindsided: A Manager’s Guide to Catastrophic Incidents in the Workplace. New York, NY: Penguin Group; 2002:136-145.
8. Dehue F, Bolman C, Völlink T, Pouwelse M. Coping with bullying at work and health related problems. Int J Stress Manage. 2012;19(3):175-197.
9. Panagioti M, Gooding PA, Dunn G, Tarrier N. Pathways to suicidal behavior in posttraumatic stress disorder. J Trauma Stress. 2011;24(2):137-145.
10. World Health Organization. Meeting report on excess mortality in persons with severe mental disorders. November 18-20, 2015. https://www.fountainhouse.org/sites/default/files/ExcessMortalityMeetingReport.pdf. Accessed June 6, 2017.
11. American Psychiatric Association. Trauma- and Stressor-Related Disorders. In: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA: American Psychiatric Association;2013:265-268, 749-750.
12. Ford DE. Depression, trauma, and cardiovascular health. In: Schnurr PP, Green BL, eds. Trauma and Health: Physical Health Consequences of Exposure to Extreme Stress. Washington, DC: American Psychological Association; 2004:chap 4.
13. Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury. Best practices identified for peer support programs. http://www.dcoe.mil/file/Best_Practices_Identified_for_Peer_Support_Programs_Jan_2011.pdf. Published January 2011. Accessed June 6, 2017.
14. O’Brian-Mazza D, Zimmerman J. The power of peer support: VHA mental health services. https://www.mentalhealth.va.gov/docs/peersupport.pdf. Published September 21, 2012. Accessed June 6, 2017.
15. Bartone PT. Peer support for bereaved survivors: systematic review of evidence and identification of best practices. https://www.taps.org/globalassets/pdf/about-taps/tapspeersupportreport2016.pdf. Published January 2017. Accessed June 6, 2017.
16. Castellano C. Reciprocal peer support (RPS): a decade of not so random acts of kindness. Int J Emerg Ment Health. 2012;14(2):105-110.
17. Salzer M. Consumer-delivered services as a best practice in mental health care delivery and the development of practice guidelines. http://www.cdsdirectory.org/SalzeretalBPPS2002.pdf. Published 2002. Accessed June 14, 2017.
18. Robinson R, Murdoch P. Establishing and Maintaining Peer Support Programs in the Workplace. 3rd ed. Ellicott City, MD: Chevron Publishing Corporation; 2003:1-24.
19. Baron SA. Violence in the Workplace: A Prevention and Management Guide for Businesses. Ventura, CA: Pathfinding Publishing; 1995:99-106.
20. Southwick SM, Charney DS. Social support: learning the Tap Code. In: Resilience: The Science of Mastering Life’s Greatest Challenges. Cambridge, United Kingdom: Cambridge University Press; 2012:100-114.
21. Creamer MC, Varker T, Bisson J, et al. Guidelines for peer support in high-risk organizations: an international consensus study using Delphi method. J Trauma Stress. 2012;25(2):134-141.
22. Downs RB. Afterword. In: Sinclair U. The Jungle. New York, NY. Signet Classics; 1906:343-350.
Whistleblowers report illegalities, improprieties, or injustices. They step forward wittingly or unwittingly to report perceived wrongdoing. But when a whistleblower takes on powerful and entrenched systems or people, retribution and retaliation often ensue, endangering their career and reputation. These negative consequences can have longterm impacts on the lives of those who believed they were acting in the public interest especially when patient care or public safety was at risk.
The following account is based on personal and professional experiences, conversations with more than a dozen other whistleblowers at the DoD, VA, several other organizations, and a literature review. This documentation of those informal peer conversations, combined with the research, is meant to provide insight into the experiences of a whistleblower and the need for peer support so that employees can remain resilient.
Adverse Whistleblower Experiences
Most employees do not set out to be whistleblowers. The process begins when the whistleblower perceives wrongdoing or harm that is being committed in their workplace. At a health care organization, whistleblowing often is focused on individual or organizational illegal or unethical activities, such as funding or contracting fraud, corruption, theft, discrimination, sexual harassment, public health safety or security violations, persistent medical errors, nepotism, or other violations of workplace rules and regulations. VA employees who experience, witness, or discover wrongdoing may choose to disclose their concerns to a supervisor, senior leader, the Office of the Inspector General (OIG), Human Resources or Equal Employment Opportunity (EEO) Office, Employee Assistance Program (EAP), Office of Special Counsel (OSC), Congress, or to a news organization.
According to the 2013 National Business Ethics Survey, more than 6 million American workers who reported misconduct experienced some form of retaliation.1,2 Retribution can manifest in various overt or covert ways, ranging from outright retaliation and further discrimination to other forms of marginalization. For example, a VA physician alleged that he was detailed to an empty office with no patients after reporting patient wait list mismanagement at his hospital. Other whistleblowers report having misconduct charges levied against them, demotions or loss of position, obstruction from promotion, poor performance evaluations, details to more minor assignments, relocation to more meager office space, or pressure to resign or retire.3
Whistleblowers are rarely rewarded for reporting misconduct within their organization. The Joint Commission describes barriers to reporting sentinel events by medical professionals fearing humiliation, litigation, peer pressure, and oversight investigations if they identify medical errors.4
Once allegations are made, the information often is conveyed to a supervisor or leader. For example, some whistleblowers who have reported a hostile work environment to the DoD EAP have noted that the EAP representative contacted the whistleblower’s manager to mediate the situation. This process can take months or years to resolve. In those instances, the managers are rarely relocated. The whistleblower usually is the one forced to move or take another job, which is not always consistent with their job description, and in turn, may impact their performance rating and opportunities for promotion.
Often, OIG and OSC investigations at the VA and other federal agencies can take as long as 2 years. During that time the whistleblower may remain in a lesser or unwanted position or leave the agency. However, even when OIG substantiates claims of wrongdoing, the agency can make recommendations only to leadership, which may or may not be enacted. Whistleblowers report having to submit Freedom of Information Act requests to learn of the outcome of an OIG investigation when leadership chooses to ignore the recommendation.
Civilian government employees are undervalued by society in general, and the negative stereotypes of lazy, shiftless workers abound, even though many civil servants work to protect the nation’s health, welfare, and safety. Civil servants are familiar with derogatory expressions, such as “bureaucratic bean-counter,” and “good enough for government work.” Even President Trump stated that he would come to Washington, DC, and “drain the swamp.” Yet civil servants can go years without a cost of living increase, a promotion, or a bonus but still be asked to perform additional duties or work long hours to the sacrifice of a work/life balance.
In the Federal Employee Viewpoints Survey and other employee environmental climate scans, high levels of workforce stress often are related to the number of grievances filed, the level of morale, the rates of absenteeism and retention, recruitment shortages, and lost productivity.5 Success in toxic environments usually is based on trying to maintain a “go along to get along” status quo, which means looking the other way when contracts are fraudulently awarded or employee discrimination occurs. If leadership is antagonistic to reform, then identifying wrongdoing may come at significant personal risk.
Retaliatory Practices
Once a whistleblower has stepped forward, retaliatory practices may follow. There are tangible legal, financial, social, emotional, and physical tolls to whistleblowing. “Be in for a penny. Be in for a pound,” an OIG official advised one whistleblower. Once a disclosure is made, the process may become arduous for the whistleblower and require individual resilience to face adversity.
Keeping in mind that OIG, EEO, EAP, and OSC are government agencies that investigate, police, and monitor the system, they do not represent the civil servants who document and identify much of the evidence of wrongdoing on their own. Most civil service employees are not subject matter experts on the U.S. legal code that outlines prohibited personal practices or the Federal Acquisition Regulation.
The Notification and Federal Employee Antidiscrimination and Retaliation (NO FEAR) Act authorized in 2002 (U.S. Code § 2301) is designed to inform and protect those who file grievances or disclosures, but operationalizing those protections can be overwhelming and confusing. If a whistleblower wants advice, he or she must retain legal counsel often at a substantial personal cost. Whistleblowers report spending from $10,000 to more than $100,000 in legal fees for a 1- to 2-year investigation.
These legal fees may force whistleblowers to use family finances or borrow money while hoping for justice along with remuneration in the end. In some cases, the financial impact is compounded when the whistleblower has been demoted, denied a promotion, or fired. For medical professionals, the impact might result in the loss of hospital privileges, professional credentials, or state licensure. The loss of income also can lead to loss of health insurance. The legal and financial burdens impact marriages, spousal job options, retirement, and other family choices (eg, vacations, children’s schools, and caregiving obligations).
During investigations, social status and the reputation of the whistleblower are often impugned. For example, whistleblowers are sometimes depicted as snitches, moles, spies, or tattletales and may be categorized as paranoid, disloyal, or disgruntled by leadership. Rarely are whistleblowers labeled protectors, patriots, or heroes, despite the few high profile cases that come to light, such as Karen Silkwood, Erin Brockovich, or Frank Serpico.
More often, whistleblowers’ reputations, especially in civil sectors, are damaged through acts of discrimination, such as bullying; mobbing (asking other employees to monitor and report on the activities of the whistleblower); ostracizing the employee from the team; devaluing the contributions or the performance of the whistleblower; blackballing from other jobs or opportunities; doublebinding with difficult tasks to complete; gaslighting by calling into question the memory of the whistleblower, the reality of the accusation, or its scope; and marginalization. Accusations of misusing funds, inaccurately recording time and attendance, and disputing their judgement are all tactics used to socially isolate and harass whistleblowers into dropping their case or leaving the organization.3
Furthermore, this level of ostracism has documented impact on the psychological and physical well-being of the employee and negative consequences to the overall functioning of the organization.6 Consequences, such as physical violence and property damage at the time of termination and at other betrayals have occurred.3,7 Other whistleblowers have reported being threatened in person or on social media, harassed, and assaulted, especially in the military.
Whistleblowers, similar to others who are bullied in the workplace often described feelings such as fear, depression, anxiety, loneliness, and humiliation.8 These feelings can lead to whistleblowers needing treatment for substance abuse, depression, anxiety, posttraumatic stress disorder (PTSD) and suicidal ideation.9 Multiple studies on depression and PTSD show a correlation to increased morbidity and mortality.10 However, whistleblowing retaliation is not clearly established as a traumatic stressor in relation to PTSD.11
Insomnia and other sleep disturbances are not uncommon among whistleblowers who also note they have resorted to smoking, overeating, alcohol misuse, or medication to manage their distress. Health consequences also include migraines, muscle tension, gastrointestinal conditions, increased blood pressure, and cardiovascular disease.12
Peer Support Models
Studies of peer-to-peer programs for veterans, law enforcement officers, widows, cancer patients, disaster victims, and others bound by survivorship suggest that peer groups can be an effective means of support, even though the model may vary or be adapted to a specific population. In general, peer support is centered on a common experience, shared credibility, confidentiality, and trust. The approach is meant to provide nonjudgmental support that assists with decision making and resilience and provides comfort and hope. Most peer support or mentorship models require some level of peer counselor screening, competency training on an intervention model, supervision, monitoring, and case management by a more senior or credentialed mental health professional.13
The Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury (DCoE) recognized that health care systems that support civil servants, military members, and veterans can benefit from partnerships with internal (eg, human resources, unions, or dedicated EAP) or external (eg, nonprofit and service organizations) employee peer support programs. The DCoE noted that peer networks facilitate referrals to medical care when threats of suicide or harm to others exists, offer additional case management support, and assist professionals in understanding the patient experience.13
Peer support offered at VA hospitals is conducted by peers who are supervised by mental health clinic staff (usually social workers).14 Law enforcement EAP is another example of peer support within an organization to augment mental health and resilience among officers who have experienced first-responder trauma.
External peer support resources can be accessed through partnerships or referrals. For example, the Tragedy Assistance Program for Survivors (TAPS) relies on survivors of military deaths to support each other through bereavement. Although the DoD offers casualty assistance and mental health care to grieving families, the level of peer support differs from TAPS.15 In another example, Castellano documented the benefits of a reciprocal peer support model implemented across 10 peer-based call center programs that manage high risk-populations.16 Core training was consistent across all programs, and mental health professionals supervised call center peer support providers. This peer/clinician collaboration enhances the overall community mental health efforts.
Temple University documented the patient care benefits for behavioral health services that augmented treatment with evidence-based peer support interventions.17 The researchers found that hospitals that used a peer model improved patient outcomes as demonstrated by fewer hospitalizations, increased life satisfaction and enhanced coping skills, increased medication adherence, and reduced substance abuse or suicidal ideation. Additionally, the peer providers themselves experienced positive health benefits based on their ability to help others, improved their own self-efficacy and gained social and economic growth based on their employment satisfaction.17
Peer Support Interventions
Peer support interventions have been effective with various populations and may be effective for whistleblowers as well. Since whistleblowing tends to involve legal processes that call for privacy and the confidentiality of all parties, whistleblowers experience isolation and alienation. Other whistleblowers can better understand the retaliation, discrimination, and isolation that results. In some instances, whistleblowers discovered years later that other employees had similar experiences. An organized, structured program dedicated to peer support can help employees within a health care system or EAP manage the impacts of identifying wrongdoing.18 Peers may be able to break down this isolation and help establish a new network of support for those involved in whistleblowing cases. Restoring a sense of purpose, meaning, and belonging in the workplace is of significant value for the whistleblower.19 Peers can mentor a whistleblower through the investigative process and help determine next steps. Peers can address building, maintaining, and sustaining resilience to overcome adversity.
Peers who already have experienced their own legal, financial, social, emotional, and physical risks and have developed the necessary resiliency skills to survive make ideal peer counselors.20 These peers have faced similar challenges but have perservered.21
Although peer counselors cannot replace an attorney or mental health provider, they can provide background information on the roles and functions of EEO, EAP, OIG, OSC, and the MSPB and how to navigate those systems. Peers can assist whistleblowers in preparing testimony before congressional hearings or for press interviews. Peer supporters also can encourage whistleblowers to seek care for mental and physical health care and to remain adherent to treatment regimens. They case manage a team effort to enable the whistleblower to overcome the adversity of retaliation.
Creating A New Normal
After the Civil War, the False Claims Act, known as the Lincoln Law, served to protect federal reconstruction activities in the South from individuals who attempted to defraud the federal government.22 Today, most Americans are familiar with WikiLeaks. For generations, whistleblowers have exposed wrongdoing in order to protect or reform governmen programs. Whistleblowers have exposed graft and corruption at the highest levels and in daily operations. They have fought for diversity and inclusion and a workplace free of sexual harassment and assault. They have protected taxpayer dollars from waste, fraud, and abuse.
Despite the personal sacrifices often required, most whistleblowers’ spirits are bolstered by the positive outcomes that their disclosures may produce. However, whistleblowers need compassionate and competent assistance throughout the process. Peers can foster the resilience needed to survive the adversarial nature of the whistleblowing process. Therefore, whistleblowers need to be viewed in a new light that involves advocacy, transparency, and peer support so that positive outcomes in government can be realized for all Americans.
Whistleblowers report illegalities, improprieties, or injustices. They step forward wittingly or unwittingly to report perceived wrongdoing. But when a whistleblower takes on powerful and entrenched systems or people, retribution and retaliation often ensue, endangering their career and reputation. These negative consequences can have longterm impacts on the lives of those who believed they were acting in the public interest especially when patient care or public safety was at risk.
The following account is based on personal and professional experiences, conversations with more than a dozen other whistleblowers at the DoD, VA, several other organizations, and a literature review. This documentation of those informal peer conversations, combined with the research, is meant to provide insight into the experiences of a whistleblower and the need for peer support so that employees can remain resilient.
Adverse Whistleblower Experiences
Most employees do not set out to be whistleblowers. The process begins when the whistleblower perceives wrongdoing or harm that is being committed in their workplace. At a health care organization, whistleblowing often is focused on individual or organizational illegal or unethical activities, such as funding or contracting fraud, corruption, theft, discrimination, sexual harassment, public health safety or security violations, persistent medical errors, nepotism, or other violations of workplace rules and regulations. VA employees who experience, witness, or discover wrongdoing may choose to disclose their concerns to a supervisor, senior leader, the Office of the Inspector General (OIG), Human Resources or Equal Employment Opportunity (EEO) Office, Employee Assistance Program (EAP), Office of Special Counsel (OSC), Congress, or to a news organization.
According to the 2013 National Business Ethics Survey, more than 6 million American workers who reported misconduct experienced some form of retaliation.1,2 Retribution can manifest in various overt or covert ways, ranging from outright retaliation and further discrimination to other forms of marginalization. For example, a VA physician alleged that he was detailed to an empty office with no patients after reporting patient wait list mismanagement at his hospital. Other whistleblowers report having misconduct charges levied against them, demotions or loss of position, obstruction from promotion, poor performance evaluations, details to more minor assignments, relocation to more meager office space, or pressure to resign or retire.3
Whistleblowers are rarely rewarded for reporting misconduct within their organization. The Joint Commission describes barriers to reporting sentinel events by medical professionals fearing humiliation, litigation, peer pressure, and oversight investigations if they identify medical errors.4
Once allegations are made, the information often is conveyed to a supervisor or leader. For example, some whistleblowers who have reported a hostile work environment to the DoD EAP have noted that the EAP representative contacted the whistleblower’s manager to mediate the situation. This process can take months or years to resolve. In those instances, the managers are rarely relocated. The whistleblower usually is the one forced to move or take another job, which is not always consistent with their job description, and in turn, may impact their performance rating and opportunities for promotion.
Often, OIG and OSC investigations at the VA and other federal agencies can take as long as 2 years. During that time the whistleblower may remain in a lesser or unwanted position or leave the agency. However, even when OIG substantiates claims of wrongdoing, the agency can make recommendations only to leadership, which may or may not be enacted. Whistleblowers report having to submit Freedom of Information Act requests to learn of the outcome of an OIG investigation when leadership chooses to ignore the recommendation.
Civilian government employees are undervalued by society in general, and the negative stereotypes of lazy, shiftless workers abound, even though many civil servants work to protect the nation’s health, welfare, and safety. Civil servants are familiar with derogatory expressions, such as “bureaucratic bean-counter,” and “good enough for government work.” Even President Trump stated that he would come to Washington, DC, and “drain the swamp.” Yet civil servants can go years without a cost of living increase, a promotion, or a bonus but still be asked to perform additional duties or work long hours to the sacrifice of a work/life balance.
In the Federal Employee Viewpoints Survey and other employee environmental climate scans, high levels of workforce stress often are related to the number of grievances filed, the level of morale, the rates of absenteeism and retention, recruitment shortages, and lost productivity.5 Success in toxic environments usually is based on trying to maintain a “go along to get along” status quo, which means looking the other way when contracts are fraudulently awarded or employee discrimination occurs. If leadership is antagonistic to reform, then identifying wrongdoing may come at significant personal risk.
Retaliatory Practices
Once a whistleblower has stepped forward, retaliatory practices may follow. There are tangible legal, financial, social, emotional, and physical tolls to whistleblowing. “Be in for a penny. Be in for a pound,” an OIG official advised one whistleblower. Once a disclosure is made, the process may become arduous for the whistleblower and require individual resilience to face adversity.
Keeping in mind that OIG, EEO, EAP, and OSC are government agencies that investigate, police, and monitor the system, they do not represent the civil servants who document and identify much of the evidence of wrongdoing on their own. Most civil service employees are not subject matter experts on the U.S. legal code that outlines prohibited personal practices or the Federal Acquisition Regulation.
The Notification and Federal Employee Antidiscrimination and Retaliation (NO FEAR) Act authorized in 2002 (U.S. Code § 2301) is designed to inform and protect those who file grievances or disclosures, but operationalizing those protections can be overwhelming and confusing. If a whistleblower wants advice, he or she must retain legal counsel often at a substantial personal cost. Whistleblowers report spending from $10,000 to more than $100,000 in legal fees for a 1- to 2-year investigation.
These legal fees may force whistleblowers to use family finances or borrow money while hoping for justice along with remuneration in the end. In some cases, the financial impact is compounded when the whistleblower has been demoted, denied a promotion, or fired. For medical professionals, the impact might result in the loss of hospital privileges, professional credentials, or state licensure. The loss of income also can lead to loss of health insurance. The legal and financial burdens impact marriages, spousal job options, retirement, and other family choices (eg, vacations, children’s schools, and caregiving obligations).
During investigations, social status and the reputation of the whistleblower are often impugned. For example, whistleblowers are sometimes depicted as snitches, moles, spies, or tattletales and may be categorized as paranoid, disloyal, or disgruntled by leadership. Rarely are whistleblowers labeled protectors, patriots, or heroes, despite the few high profile cases that come to light, such as Karen Silkwood, Erin Brockovich, or Frank Serpico.
More often, whistleblowers’ reputations, especially in civil sectors, are damaged through acts of discrimination, such as bullying; mobbing (asking other employees to monitor and report on the activities of the whistleblower); ostracizing the employee from the team; devaluing the contributions or the performance of the whistleblower; blackballing from other jobs or opportunities; doublebinding with difficult tasks to complete; gaslighting by calling into question the memory of the whistleblower, the reality of the accusation, or its scope; and marginalization. Accusations of misusing funds, inaccurately recording time and attendance, and disputing their judgement are all tactics used to socially isolate and harass whistleblowers into dropping their case or leaving the organization.3
Furthermore, this level of ostracism has documented impact on the psychological and physical well-being of the employee and negative consequences to the overall functioning of the organization.6 Consequences, such as physical violence and property damage at the time of termination and at other betrayals have occurred.3,7 Other whistleblowers have reported being threatened in person or on social media, harassed, and assaulted, especially in the military.
Whistleblowers, similar to others who are bullied in the workplace often described feelings such as fear, depression, anxiety, loneliness, and humiliation.8 These feelings can lead to whistleblowers needing treatment for substance abuse, depression, anxiety, posttraumatic stress disorder (PTSD) and suicidal ideation.9 Multiple studies on depression and PTSD show a correlation to increased morbidity and mortality.10 However, whistleblowing retaliation is not clearly established as a traumatic stressor in relation to PTSD.11
Insomnia and other sleep disturbances are not uncommon among whistleblowers who also note they have resorted to smoking, overeating, alcohol misuse, or medication to manage their distress. Health consequences also include migraines, muscle tension, gastrointestinal conditions, increased blood pressure, and cardiovascular disease.12
Peer Support Models
Studies of peer-to-peer programs for veterans, law enforcement officers, widows, cancer patients, disaster victims, and others bound by survivorship suggest that peer groups can be an effective means of support, even though the model may vary or be adapted to a specific population. In general, peer support is centered on a common experience, shared credibility, confidentiality, and trust. The approach is meant to provide nonjudgmental support that assists with decision making and resilience and provides comfort and hope. Most peer support or mentorship models require some level of peer counselor screening, competency training on an intervention model, supervision, monitoring, and case management by a more senior or credentialed mental health professional.13
The Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury (DCoE) recognized that health care systems that support civil servants, military members, and veterans can benefit from partnerships with internal (eg, human resources, unions, or dedicated EAP) or external (eg, nonprofit and service organizations) employee peer support programs. The DCoE noted that peer networks facilitate referrals to medical care when threats of suicide or harm to others exists, offer additional case management support, and assist professionals in understanding the patient experience.13
Peer support offered at VA hospitals is conducted by peers who are supervised by mental health clinic staff (usually social workers).14 Law enforcement EAP is another example of peer support within an organization to augment mental health and resilience among officers who have experienced first-responder trauma.
External peer support resources can be accessed through partnerships or referrals. For example, the Tragedy Assistance Program for Survivors (TAPS) relies on survivors of military deaths to support each other through bereavement. Although the DoD offers casualty assistance and mental health care to grieving families, the level of peer support differs from TAPS.15 In another example, Castellano documented the benefits of a reciprocal peer support model implemented across 10 peer-based call center programs that manage high risk-populations.16 Core training was consistent across all programs, and mental health professionals supervised call center peer support providers. This peer/clinician collaboration enhances the overall community mental health efforts.
Temple University documented the patient care benefits for behavioral health services that augmented treatment with evidence-based peer support interventions.17 The researchers found that hospitals that used a peer model improved patient outcomes as demonstrated by fewer hospitalizations, increased life satisfaction and enhanced coping skills, increased medication adherence, and reduced substance abuse or suicidal ideation. Additionally, the peer providers themselves experienced positive health benefits based on their ability to help others, improved their own self-efficacy and gained social and economic growth based on their employment satisfaction.17
Peer Support Interventions
Peer support interventions have been effective with various populations and may be effective for whistleblowers as well. Since whistleblowing tends to involve legal processes that call for privacy and the confidentiality of all parties, whistleblowers experience isolation and alienation. Other whistleblowers can better understand the retaliation, discrimination, and isolation that results. In some instances, whistleblowers discovered years later that other employees had similar experiences. An organized, structured program dedicated to peer support can help employees within a health care system or EAP manage the impacts of identifying wrongdoing.18 Peers may be able to break down this isolation and help establish a new network of support for those involved in whistleblowing cases. Restoring a sense of purpose, meaning, and belonging in the workplace is of significant value for the whistleblower.19 Peers can mentor a whistleblower through the investigative process and help determine next steps. Peers can address building, maintaining, and sustaining resilience to overcome adversity.
Peers who already have experienced their own legal, financial, social, emotional, and physical risks and have developed the necessary resiliency skills to survive make ideal peer counselors.20 These peers have faced similar challenges but have perservered.21
Although peer counselors cannot replace an attorney or mental health provider, they can provide background information on the roles and functions of EEO, EAP, OIG, OSC, and the MSPB and how to navigate those systems. Peers can assist whistleblowers in preparing testimony before congressional hearings or for press interviews. Peer supporters also can encourage whistleblowers to seek care for mental and physical health care and to remain adherent to treatment regimens. They case manage a team effort to enable the whistleblower to overcome the adversity of retaliation.
Creating A New Normal
After the Civil War, the False Claims Act, known as the Lincoln Law, served to protect federal reconstruction activities in the South from individuals who attempted to defraud the federal government.22 Today, most Americans are familiar with WikiLeaks. For generations, whistleblowers have exposed wrongdoing in order to protect or reform governmen programs. Whistleblowers have exposed graft and corruption at the highest levels and in daily operations. They have fought for diversity and inclusion and a workplace free of sexual harassment and assault. They have protected taxpayer dollars from waste, fraud, and abuse.
Despite the personal sacrifices often required, most whistleblowers’ spirits are bolstered by the positive outcomes that their disclosures may produce. However, whistleblowers need compassionate and competent assistance throughout the process. Peers can foster the resilience needed to survive the adversarial nature of the whistleblowing process. Therefore, whistleblowers need to be viewed in a new light that involves advocacy, transparency, and peer support so that positive outcomes in government can be realized for all Americans.
1. Ethics and Compliance Initiative. National Business Ethics Survey (NBES) 2013. http://www.ethics.org/ecihome/research/nbes/nbes-reports/nbes-2013. Published 2013. Accessed June 5, 2017.
2. Schnell G. Whistleblower retaliation on the rise—bad news for whistleblowers and their employers alike. http://constantinecannon.com/whistleblower/whistleblower-retaliation-on-the-rise-bad-news-for-whistleblowers-and-their-employers-alike/#.WNJ1s4WcEYh. Published January 18, 2013. Accessed June 5, 2017.
3. Devine T, Maassarani T. The Corporate Whistleblower’s Survival Guide: A Handbook for Committing the Truth. San Francisco, CA. Berrett-Koehler Publishers; 2011:19-40.
4. The Joint Commission. What Every Hospital Should Know About Sentinel Events. Oakbrook Terrace, IL: Joint Commission on Accreditation of Healthcare Organizations; 2000.
5. Reed GE. Tarnished: Toxic Leadership in the U.S. Military. Lincoln, NE; University of Nebraska Press, Potomac Books; 2015:60.
6. McGraw K. Mental health of women warriors: the power of belonging. In: Ritchie EC, Naclerio AL, eds. Women at War. New York, NY. Oxford University Press; 2015:311-320.
7. Blythe B. Blindsided: A Manager’s Guide to Catastrophic Incidents in the Workplace. New York, NY: Penguin Group; 2002:136-145.
8. Dehue F, Bolman C, Völlink T, Pouwelse M. Coping with bullying at work and health related problems. Int J Stress Manage. 2012;19(3):175-197.
9. Panagioti M, Gooding PA, Dunn G, Tarrier N. Pathways to suicidal behavior in posttraumatic stress disorder. J Trauma Stress. 2011;24(2):137-145.
10. World Health Organization. Meeting report on excess mortality in persons with severe mental disorders. November 18-20, 2015. https://www.fountainhouse.org/sites/default/files/ExcessMortalityMeetingReport.pdf. Accessed June 6, 2017.
11. American Psychiatric Association. Trauma- and Stressor-Related Disorders. In: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA: American Psychiatric Association;2013:265-268, 749-750.
12. Ford DE. Depression, trauma, and cardiovascular health. In: Schnurr PP, Green BL, eds. Trauma and Health: Physical Health Consequences of Exposure to Extreme Stress. Washington, DC: American Psychological Association; 2004:chap 4.
13. Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury. Best practices identified for peer support programs. http://www.dcoe.mil/file/Best_Practices_Identified_for_Peer_Support_Programs_Jan_2011.pdf. Published January 2011. Accessed June 6, 2017.
14. O’Brian-Mazza D, Zimmerman J. The power of peer support: VHA mental health services. https://www.mentalhealth.va.gov/docs/peersupport.pdf. Published September 21, 2012. Accessed June 6, 2017.
15. Bartone PT. Peer support for bereaved survivors: systematic review of evidence and identification of best practices. https://www.taps.org/globalassets/pdf/about-taps/tapspeersupportreport2016.pdf. Published January 2017. Accessed June 6, 2017.
16. Castellano C. Reciprocal peer support (RPS): a decade of not so random acts of kindness. Int J Emerg Ment Health. 2012;14(2):105-110.
17. Salzer M. Consumer-delivered services as a best practice in mental health care delivery and the development of practice guidelines. http://www.cdsdirectory.org/SalzeretalBPPS2002.pdf. Published 2002. Accessed June 14, 2017.
18. Robinson R, Murdoch P. Establishing and Maintaining Peer Support Programs in the Workplace. 3rd ed. Ellicott City, MD: Chevron Publishing Corporation; 2003:1-24.
19. Baron SA. Violence in the Workplace: A Prevention and Management Guide for Businesses. Ventura, CA: Pathfinding Publishing; 1995:99-106.
20. Southwick SM, Charney DS. Social support: learning the Tap Code. In: Resilience: The Science of Mastering Life’s Greatest Challenges. Cambridge, United Kingdom: Cambridge University Press; 2012:100-114.
21. Creamer MC, Varker T, Bisson J, et al. Guidelines for peer support in high-risk organizations: an international consensus study using Delphi method. J Trauma Stress. 2012;25(2):134-141.
22. Downs RB. Afterword. In: Sinclair U. The Jungle. New York, NY. Signet Classics; 1906:343-350.
1. Ethics and Compliance Initiative. National Business Ethics Survey (NBES) 2013. http://www.ethics.org/ecihome/research/nbes/nbes-reports/nbes-2013. Published 2013. Accessed June 5, 2017.
2. Schnell G. Whistleblower retaliation on the rise—bad news for whistleblowers and their employers alike. http://constantinecannon.com/whistleblower/whistleblower-retaliation-on-the-rise-bad-news-for-whistleblowers-and-their-employers-alike/#.WNJ1s4WcEYh. Published January 18, 2013. Accessed June 5, 2017.
3. Devine T, Maassarani T. The Corporate Whistleblower’s Survival Guide: A Handbook for Committing the Truth. San Francisco, CA. Berrett-Koehler Publishers; 2011:19-40.
4. The Joint Commission. What Every Hospital Should Know About Sentinel Events. Oakbrook Terrace, IL: Joint Commission on Accreditation of Healthcare Organizations; 2000.
5. Reed GE. Tarnished: Toxic Leadership in the U.S. Military. Lincoln, NE; University of Nebraska Press, Potomac Books; 2015:60.
6. McGraw K. Mental health of women warriors: the power of belonging. In: Ritchie EC, Naclerio AL, eds. Women at War. New York, NY. Oxford University Press; 2015:311-320.
7. Blythe B. Blindsided: A Manager’s Guide to Catastrophic Incidents in the Workplace. New York, NY: Penguin Group; 2002:136-145.
8. Dehue F, Bolman C, Völlink T, Pouwelse M. Coping with bullying at work and health related problems. Int J Stress Manage. 2012;19(3):175-197.
9. Panagioti M, Gooding PA, Dunn G, Tarrier N. Pathways to suicidal behavior in posttraumatic stress disorder. J Trauma Stress. 2011;24(2):137-145.
10. World Health Organization. Meeting report on excess mortality in persons with severe mental disorders. November 18-20, 2015. https://www.fountainhouse.org/sites/default/files/ExcessMortalityMeetingReport.pdf. Accessed June 6, 2017.
11. American Psychiatric Association. Trauma- and Stressor-Related Disorders. In: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA: American Psychiatric Association;2013:265-268, 749-750.
12. Ford DE. Depression, trauma, and cardiovascular health. In: Schnurr PP, Green BL, eds. Trauma and Health: Physical Health Consequences of Exposure to Extreme Stress. Washington, DC: American Psychological Association; 2004:chap 4.
13. Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury. Best practices identified for peer support programs. http://www.dcoe.mil/file/Best_Practices_Identified_for_Peer_Support_Programs_Jan_2011.pdf. Published January 2011. Accessed June 6, 2017.
14. O’Brian-Mazza D, Zimmerman J. The power of peer support: VHA mental health services. https://www.mentalhealth.va.gov/docs/peersupport.pdf. Published September 21, 2012. Accessed June 6, 2017.
15. Bartone PT. Peer support for bereaved survivors: systematic review of evidence and identification of best practices. https://www.taps.org/globalassets/pdf/about-taps/tapspeersupportreport2016.pdf. Published January 2017. Accessed June 6, 2017.
16. Castellano C. Reciprocal peer support (RPS): a decade of not so random acts of kindness. Int J Emerg Ment Health. 2012;14(2):105-110.
17. Salzer M. Consumer-delivered services as a best practice in mental health care delivery and the development of practice guidelines. http://www.cdsdirectory.org/SalzeretalBPPS2002.pdf. Published 2002. Accessed June 14, 2017.
18. Robinson R, Murdoch P. Establishing and Maintaining Peer Support Programs in the Workplace. 3rd ed. Ellicott City, MD: Chevron Publishing Corporation; 2003:1-24.
19. Baron SA. Violence in the Workplace: A Prevention and Management Guide for Businesses. Ventura, CA: Pathfinding Publishing; 1995:99-106.
20. Southwick SM, Charney DS. Social support: learning the Tap Code. In: Resilience: The Science of Mastering Life’s Greatest Challenges. Cambridge, United Kingdom: Cambridge University Press; 2012:100-114.
21. Creamer MC, Varker T, Bisson J, et al. Guidelines for peer support in high-risk organizations: an international consensus study using Delphi method. J Trauma Stress. 2012;25(2):134-141.
22. Downs RB. Afterword. In: Sinclair U. The Jungle. New York, NY. Signet Classics; 1906:343-350.
Genetic Information May Hold Key to Multiple-Substance Addiction
The Million Veteran Program (MVP) is now the largest genomic database in the world, with more than 550,000 veterans enrolled. Researchers have been mining the data for a variety of studies, including studies to examine the genetic risk factors for chronic use of alcohol, tobacco, and opioids.
Most people who smoke or use drugs also drink alcohol, and changes in one behavior are likely to be associated with changes in the others, according to researchers from the VA Connecticut Healthcare System and the Corporal Michael J. Crescenz VAMC. That likelihood suggests a shared genetic risk for multiple-substance use, but to date, studies on the subject have been limited by the small size of the available samples, the researchers say. The MVP is providing a unique opportunity to analyze massive amounts of longitudinal data to discover potential genetic links.
The answers also may provide opportunities for treatment and prevention. For example, it may be possible to reduce the use of multiple harmful substances simultaneously with more than 1 medication.
The first target in this “ambitious effort,” the researchers say, is heavy drinking. They’re using data from the Veterans Aging Cohort Study and from the AUDIT-C, a self-report questionnaire given annually to veterans, which quantifies recent drinking. The researchers plan to validate their initial findings, already published, and then combine that information with the genotype information from the MVP to identify novel genetic predictors of heavy drinking.
The researchers have begun to use a similar approach to study chronic opioid use and smoking. Ultimately, they plan to integrate all the findings to yield genetic profiles for multisubstance use.
The Million Veteran Program (MVP) is now the largest genomic database in the world, with more than 550,000 veterans enrolled. Researchers have been mining the data for a variety of studies, including studies to examine the genetic risk factors for chronic use of alcohol, tobacco, and opioids.
Most people who smoke or use drugs also drink alcohol, and changes in one behavior are likely to be associated with changes in the others, according to researchers from the VA Connecticut Healthcare System and the Corporal Michael J. Crescenz VAMC. That likelihood suggests a shared genetic risk for multiple-substance use, but to date, studies on the subject have been limited by the small size of the available samples, the researchers say. The MVP is providing a unique opportunity to analyze massive amounts of longitudinal data to discover potential genetic links.
The answers also may provide opportunities for treatment and prevention. For example, it may be possible to reduce the use of multiple harmful substances simultaneously with more than 1 medication.
The first target in this “ambitious effort,” the researchers say, is heavy drinking. They’re using data from the Veterans Aging Cohort Study and from the AUDIT-C, a self-report questionnaire given annually to veterans, which quantifies recent drinking. The researchers plan to validate their initial findings, already published, and then combine that information with the genotype information from the MVP to identify novel genetic predictors of heavy drinking.
The researchers have begun to use a similar approach to study chronic opioid use and smoking. Ultimately, they plan to integrate all the findings to yield genetic profiles for multisubstance use.
The Million Veteran Program (MVP) is now the largest genomic database in the world, with more than 550,000 veterans enrolled. Researchers have been mining the data for a variety of studies, including studies to examine the genetic risk factors for chronic use of alcohol, tobacco, and opioids.
Most people who smoke or use drugs also drink alcohol, and changes in one behavior are likely to be associated with changes in the others, according to researchers from the VA Connecticut Healthcare System and the Corporal Michael J. Crescenz VAMC. That likelihood suggests a shared genetic risk for multiple-substance use, but to date, studies on the subject have been limited by the small size of the available samples, the researchers say. The MVP is providing a unique opportunity to analyze massive amounts of longitudinal data to discover potential genetic links.
The answers also may provide opportunities for treatment and prevention. For example, it may be possible to reduce the use of multiple harmful substances simultaneously with more than 1 medication.
The first target in this “ambitious effort,” the researchers say, is heavy drinking. They’re using data from the Veterans Aging Cohort Study and from the AUDIT-C, a self-report questionnaire given annually to veterans, which quantifies recent drinking. The researchers plan to validate their initial findings, already published, and then combine that information with the genotype information from the MVP to identify novel genetic predictors of heavy drinking.
The researchers have begun to use a similar approach to study chronic opioid use and smoking. Ultimately, they plan to integrate all the findings to yield genetic profiles for multisubstance use.
Pregnant Patient Develops a Rare Case of Multiple Sclerosis
Pregnancy is generally found to offer a respite from multiple sclerosis (MS). Pregnant women rarely develop MS or to have relapses. But in a unique and challenging case, a woman in her 14th week of her second pregnancy developed signs and symptoms of tumefactive multiple sclerosis (TMS), a rare subtype of MS. The TMS was only one of several unexpected clinical puzzles, according to the clinicians reporting on the case.
The patient, who had been healthy, was admitted with acute onset of paresthesias and word-finding difficulty. She had just had a long drive from Florida, and the the clinicians first assumed that she was fatigued from the trip and from the pregnancy. A magnetic resonance imaging (MRI) scan of the brain, however, suggested an ischemic event.
While hospitalized, the patient’s condition rapidly worsened. More scan and test findings proved consistent with TMS. A repeat MRI scan showed interval progression with a growing tumefactive demyelinating lesion (TDL) with diffuse surrounding edema and new periventricular signal changes. Although rare, TDLs often represent fulminant forms of MS, the clinicians note. Because the lesions mimic strokes, tumors, and abscesses, diagnosis is difficult. Moreover, the gadolinium (which was avoided because it can cause birth defects) might have helped them visualize lesions sooner.
The patient was started on high-dose IV methylprednisolone and plasma exchange, but the response was mild. The poor response to both treatment modalities is infrequent in TMS, the clinicians say—yet another unforeseen obstacle.
In addition to counseling the patient about the usual protective effects of pregnancy, her clinicians counseled her “extensively” about natalizumab and the possible beneficial effects of disease-modifying therapies. But the patient made the difficult decision to terminate the pregnancy, in part because she felt it was better to focus on her existing child rather than on caring for 2 young children while having a chronic progressive disease with uncertain recovery.
Another surprise was in store. Within 12 hours after an uncomplicated dilatation and curettage, the patient was able to move her right arm. That “drastic improvement” was followed by moderate improvement in her right leg. Her “paradoxical” improvement after the termination might indicate a “different from expected” hormonal influence in the pathogenesis of TMS, the clinicians say, but more likely represents a delayed corroborating effect of steroids and plasma exchange.
In the following weeks, the patient’s recovery was “satisfying” with gradual improvement and partial return of expressive language. Eighteen months later, the patient was clinically stable on natalizumab.
Source:
Pakneshan S, Bernitsas E. BMJ Case Rep. 2017. pii: bcr-2017-219534.
doi: 10.1136/bcr-2017-219534.
Pregnancy is generally found to offer a respite from multiple sclerosis (MS). Pregnant women rarely develop MS or to have relapses. But in a unique and challenging case, a woman in her 14th week of her second pregnancy developed signs and symptoms of tumefactive multiple sclerosis (TMS), a rare subtype of MS. The TMS was only one of several unexpected clinical puzzles, according to the clinicians reporting on the case.
The patient, who had been healthy, was admitted with acute onset of paresthesias and word-finding difficulty. She had just had a long drive from Florida, and the the clinicians first assumed that she was fatigued from the trip and from the pregnancy. A magnetic resonance imaging (MRI) scan of the brain, however, suggested an ischemic event.
While hospitalized, the patient’s condition rapidly worsened. More scan and test findings proved consistent with TMS. A repeat MRI scan showed interval progression with a growing tumefactive demyelinating lesion (TDL) with diffuse surrounding edema and new periventricular signal changes. Although rare, TDLs often represent fulminant forms of MS, the clinicians note. Because the lesions mimic strokes, tumors, and abscesses, diagnosis is difficult. Moreover, the gadolinium (which was avoided because it can cause birth defects) might have helped them visualize lesions sooner.
The patient was started on high-dose IV methylprednisolone and plasma exchange, but the response was mild. The poor response to both treatment modalities is infrequent in TMS, the clinicians say—yet another unforeseen obstacle.
In addition to counseling the patient about the usual protective effects of pregnancy, her clinicians counseled her “extensively” about natalizumab and the possible beneficial effects of disease-modifying therapies. But the patient made the difficult decision to terminate the pregnancy, in part because she felt it was better to focus on her existing child rather than on caring for 2 young children while having a chronic progressive disease with uncertain recovery.
Another surprise was in store. Within 12 hours after an uncomplicated dilatation and curettage, the patient was able to move her right arm. That “drastic improvement” was followed by moderate improvement in her right leg. Her “paradoxical” improvement after the termination might indicate a “different from expected” hormonal influence in the pathogenesis of TMS, the clinicians say, but more likely represents a delayed corroborating effect of steroids and plasma exchange.
In the following weeks, the patient’s recovery was “satisfying” with gradual improvement and partial return of expressive language. Eighteen months later, the patient was clinically stable on natalizumab.
Source:
Pakneshan S, Bernitsas E. BMJ Case Rep. 2017. pii: bcr-2017-219534.
doi: 10.1136/bcr-2017-219534.
Pregnancy is generally found to offer a respite from multiple sclerosis (MS). Pregnant women rarely develop MS or to have relapses. But in a unique and challenging case, a woman in her 14th week of her second pregnancy developed signs and symptoms of tumefactive multiple sclerosis (TMS), a rare subtype of MS. The TMS was only one of several unexpected clinical puzzles, according to the clinicians reporting on the case.
The patient, who had been healthy, was admitted with acute onset of paresthesias and word-finding difficulty. She had just had a long drive from Florida, and the the clinicians first assumed that she was fatigued from the trip and from the pregnancy. A magnetic resonance imaging (MRI) scan of the brain, however, suggested an ischemic event.
While hospitalized, the patient’s condition rapidly worsened. More scan and test findings proved consistent with TMS. A repeat MRI scan showed interval progression with a growing tumefactive demyelinating lesion (TDL) with diffuse surrounding edema and new periventricular signal changes. Although rare, TDLs often represent fulminant forms of MS, the clinicians note. Because the lesions mimic strokes, tumors, and abscesses, diagnosis is difficult. Moreover, the gadolinium (which was avoided because it can cause birth defects) might have helped them visualize lesions sooner.
The patient was started on high-dose IV methylprednisolone and plasma exchange, but the response was mild. The poor response to both treatment modalities is infrequent in TMS, the clinicians say—yet another unforeseen obstacle.
In addition to counseling the patient about the usual protective effects of pregnancy, her clinicians counseled her “extensively” about natalizumab and the possible beneficial effects of disease-modifying therapies. But the patient made the difficult decision to terminate the pregnancy, in part because she felt it was better to focus on her existing child rather than on caring for 2 young children while having a chronic progressive disease with uncertain recovery.
Another surprise was in store. Within 12 hours after an uncomplicated dilatation and curettage, the patient was able to move her right arm. That “drastic improvement” was followed by moderate improvement in her right leg. Her “paradoxical” improvement after the termination might indicate a “different from expected” hormonal influence in the pathogenesis of TMS, the clinicians say, but more likely represents a delayed corroborating effect of steroids and plasma exchange.
In the following weeks, the patient’s recovery was “satisfying” with gradual improvement and partial return of expressive language. Eighteen months later, the patient was clinically stable on natalizumab.
Source:
Pakneshan S, Bernitsas E. BMJ Case Rep. 2017. pii: bcr-2017-219534.
doi: 10.1136/bcr-2017-219534.
Brentuximab meets phase 3 primary endpoint in frontline advanced HL

Brentuximab vedotin (Adcetris®) in combination with a 3-drug chemotherapy regimen has met its primary endpoint of statistically significant improvement in modified progression-free survival (mPFS) compared with standard therapy in frontline treatment of advanced stage Hodgkin lymphoma (HL).
The ECHELON-1 trial tested brentuximab vedotin plus Adriamycin, vinblastine, and dacarbazine (AVD) against Adriamycin, bleomycin, vinblastine, and dacarbazine (ABVD) in 1334 patients with previously untreated advanced HL.
Patients treated with brentuximab showed an 82% lower risk of disease progression compared with 77% in the ABVD arm.
Brentuximab vedotin is currently not approved as a frontline therapy for HL.
“Notably, this is the first clinical trial in frontline advanced Hodgkin lymphoma to show superior efficacy of a regimen that eliminates bleomycin,” said Clay Siegall, PhD, president and CEO of Seattle Genetics.
Dirk Huebner, MD, executive medical director of oncology at Takeda Pharmaceutical Company, said the results of the trial “have the potential to change the treatment approach of frontline advanced Hodgkin lymphoma.”
Seattle Genetics and Takeda are jointly developing brentuximab vedotin. Seattle Genetics has US and Canadian commercialization rights and Takeda has rights to commercialize it in the rest of the world.
Brentuximab vedotin is an antibody-drug conjugate (ADC) made up of an anti-CD30 monoclonal antibody attached by a linker to monomethyl auristatin E (MMAE). The linker system is stable in the bloodstream but releases MMAE when internalized into CD30-expressing tumor cells.
ECHELON-1
ECHELON-1 (NCT01712490) is a randomized, 2-arm, multicenter phase 3 trial comparing brentuximab vedotin plus AVD to ABVD as frontline therapy in treatment-naïve advanced HL.
The trial enrolled 1334 patients with histologically confirmed advanced HL.
The primary endpoint is mPFS by independent review facility.
The investigators, regulatory bodies, and trial sponsors defined mPFS as the time to progression, death, or receipt of additional anticancer therapy for patients who were not in complete response (CR) after completion of frontline therapy.
They chose mPFS instead of PFS because they say it provides a clearer picture of the efficacy of primary anticancer therapy by eliminating the confounding effects of additional anticancer therapy.
Secondary endpoints include overall survival (OS), CR, and safety.
The results demonstrated that combination treatment with brentuximab resulted in a statistically significant improvement in mPFS versus the control arm (hazard ratio=0.770; P=0.035).
Interim analysis of OS, the key secondary endpoint, also trended in favor of the brentuximab plus AVD arm.
The safety profile of the brentuximab combination was consistent with that of the single-agent components of the regimen.
Patients in the brentuximab arm experienced an increased incidence of febrile neutropenia and peripheral neuropathy compared to the ABVD arm.
Febrile neutropenia was reduced with the use of prophylactic growth factors.
Peripheral neuropathy was managed through dose modifications.
Patients treated with ABVD had an increased rate and severity of pulmonary toxicity.
The companies plan to submit an abstract for presentation at the American Society of Hematology annual meeting in December.
Brentuximab is currently approved by the US Food and Drug Administration (FDA) for the treatment of patients with classical HL who have received a prior stem cell transplant or 2 prior chemotherapy treatments.
Brentuximab is also approved to treat patient with anaplastic large cell lymphoma who have failed one prior treatment.
For more on brentuximab vedotin, see the full prescribing informtion. ![]()
Brentuximab vedotin (Adcetris®) in combination with a 3-drug chemotherapy regimen has met its primary endpoint of statistically significant improvement in modified progression-free survival (mPFS) compared with standard therapy in frontline treatment of advanced stage Hodgkin lymphoma (HL).
The ECHELON-1 trial tested brentuximab vedotin plus Adriamycin, vinblastine, and dacarbazine (AVD) against Adriamycin, bleomycin, vinblastine, and dacarbazine (ABVD) in 1334 patients with previously untreated advanced HL.
Patients treated with brentuximab showed an 82% lower risk of disease progression compared with 77% in the ABVD arm.
Brentuximab vedotin is currently not approved as a frontline therapy for HL.
“Notably, this is the first clinical trial in frontline advanced Hodgkin lymphoma to show superior efficacy of a regimen that eliminates bleomycin,” said Clay Siegall, PhD, president and CEO of Seattle Genetics.
Dirk Huebner, MD, executive medical director of oncology at Takeda Pharmaceutical Company, said the results of the trial “have the potential to change the treatment approach of frontline advanced Hodgkin lymphoma.”
Seattle Genetics and Takeda are jointly developing brentuximab vedotin. Seattle Genetics has US and Canadian commercialization rights and Takeda has rights to commercialize it in the rest of the world.
Brentuximab vedotin is an antibody-drug conjugate (ADC) made up of an anti-CD30 monoclonal antibody attached by a linker to monomethyl auristatin E (MMAE). The linker system is stable in the bloodstream but releases MMAE when internalized into CD30-expressing tumor cells.
ECHELON-1
ECHELON-1 (NCT01712490) is a randomized, 2-arm, multicenter phase 3 trial comparing brentuximab vedotin plus AVD to ABVD as frontline therapy in treatment-naïve advanced HL.
The trial enrolled 1334 patients with histologically confirmed advanced HL.
The primary endpoint is mPFS by independent review facility.
The investigators, regulatory bodies, and trial sponsors defined mPFS as the time to progression, death, or receipt of additional anticancer therapy for patients who were not in complete response (CR) after completion of frontline therapy.
They chose mPFS instead of PFS because they say it provides a clearer picture of the efficacy of primary anticancer therapy by eliminating the confounding effects of additional anticancer therapy.
Secondary endpoints include overall survival (OS), CR, and safety.
The results demonstrated that combination treatment with brentuximab resulted in a statistically significant improvement in mPFS versus the control arm (hazard ratio=0.770; P=0.035).
Interim analysis of OS, the key secondary endpoint, also trended in favor of the brentuximab plus AVD arm.
The safety profile of the brentuximab combination was consistent with that of the single-agent components of the regimen.
Patients in the brentuximab arm experienced an increased incidence of febrile neutropenia and peripheral neuropathy compared to the ABVD arm.
Febrile neutropenia was reduced with the use of prophylactic growth factors.
Peripheral neuropathy was managed through dose modifications.
Patients treated with ABVD had an increased rate and severity of pulmonary toxicity.
The companies plan to submit an abstract for presentation at the American Society of Hematology annual meeting in December.
Brentuximab is currently approved by the US Food and Drug Administration (FDA) for the treatment of patients with classical HL who have received a prior stem cell transplant or 2 prior chemotherapy treatments.
Brentuximab is also approved to treat patient with anaplastic large cell lymphoma who have failed one prior treatment.
For more on brentuximab vedotin, see the full prescribing informtion. ![]()
Brentuximab vedotin (Adcetris®) in combination with a 3-drug chemotherapy regimen has met its primary endpoint of statistically significant improvement in modified progression-free survival (mPFS) compared with standard therapy in frontline treatment of advanced stage Hodgkin lymphoma (HL).
The ECHELON-1 trial tested brentuximab vedotin plus Adriamycin, vinblastine, and dacarbazine (AVD) against Adriamycin, bleomycin, vinblastine, and dacarbazine (ABVD) in 1334 patients with previously untreated advanced HL.
Patients treated with brentuximab showed an 82% lower risk of disease progression compared with 77% in the ABVD arm.
Brentuximab vedotin is currently not approved as a frontline therapy for HL.
“Notably, this is the first clinical trial in frontline advanced Hodgkin lymphoma to show superior efficacy of a regimen that eliminates bleomycin,” said Clay Siegall, PhD, president and CEO of Seattle Genetics.
Dirk Huebner, MD, executive medical director of oncology at Takeda Pharmaceutical Company, said the results of the trial “have the potential to change the treatment approach of frontline advanced Hodgkin lymphoma.”
Seattle Genetics and Takeda are jointly developing brentuximab vedotin. Seattle Genetics has US and Canadian commercialization rights and Takeda has rights to commercialize it in the rest of the world.
Brentuximab vedotin is an antibody-drug conjugate (ADC) made up of an anti-CD30 monoclonal antibody attached by a linker to monomethyl auristatin E (MMAE). The linker system is stable in the bloodstream but releases MMAE when internalized into CD30-expressing tumor cells.
ECHELON-1
ECHELON-1 (NCT01712490) is a randomized, 2-arm, multicenter phase 3 trial comparing brentuximab vedotin plus AVD to ABVD as frontline therapy in treatment-naïve advanced HL.
The trial enrolled 1334 patients with histologically confirmed advanced HL.
The primary endpoint is mPFS by independent review facility.
The investigators, regulatory bodies, and trial sponsors defined mPFS as the time to progression, death, or receipt of additional anticancer therapy for patients who were not in complete response (CR) after completion of frontline therapy.
They chose mPFS instead of PFS because they say it provides a clearer picture of the efficacy of primary anticancer therapy by eliminating the confounding effects of additional anticancer therapy.
Secondary endpoints include overall survival (OS), CR, and safety.
The results demonstrated that combination treatment with brentuximab resulted in a statistically significant improvement in mPFS versus the control arm (hazard ratio=0.770; P=0.035).
Interim analysis of OS, the key secondary endpoint, also trended in favor of the brentuximab plus AVD arm.
The safety profile of the brentuximab combination was consistent with that of the single-agent components of the regimen.
Patients in the brentuximab arm experienced an increased incidence of febrile neutropenia and peripheral neuropathy compared to the ABVD arm.
Febrile neutropenia was reduced with the use of prophylactic growth factors.
Peripheral neuropathy was managed through dose modifications.
Patients treated with ABVD had an increased rate and severity of pulmonary toxicity.
The companies plan to submit an abstract for presentation at the American Society of Hematology annual meeting in December.
Brentuximab is currently approved by the US Food and Drug Administration (FDA) for the treatment of patients with classical HL who have received a prior stem cell transplant or 2 prior chemotherapy treatments.
Brentuximab is also approved to treat patient with anaplastic large cell lymphoma who have failed one prior treatment.
For more on brentuximab vedotin, see the full prescribing informtion. ![]()
Boston Children’s Hospital tops annual ranking
Boston Children’s Hospital is the country’s top hospital for children, according to U.S. New & World Report.
This marks the 3rd consecutive year and the fifth time in 6 years that Boston Children’s Hospital either has earned the honor on its own or been tied for the top spot. This year’s second-place finisher, Children’s Hospital of Philadelphia, was first in 2013-2014 and tied for first in 2014-2015 and 2012-2013.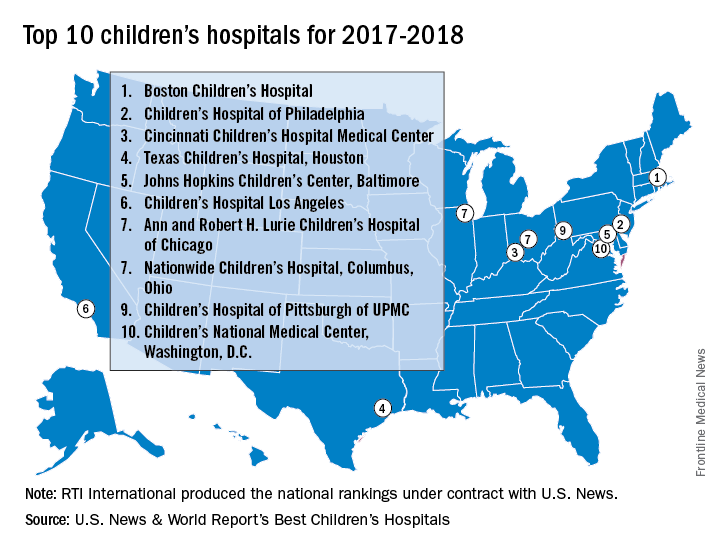
Of the 187 facilities that qualified for inclusion this year, 113 submitted sufficient data to be considered in at least one of the 10 specialties that make up the rating: cancer, cardiology and heart surgery, diabetes and endocrinology, gastroenterology and gastrointestinal surgery, neonatology, nephrology, neurology and neurosurgery, orthopedics, pulmonology, and urology. In addition, a survey of individuals conducted to establish the hospitals’ reputations – generally worth about 15% of a hospital’s score in each specialty – was completed by 3,269 physicians.
Boston Children’s Hospital was ranked first in five of the ten specialties, Children’s Hospital of Philadelphia finished first in diabetes/endocrinology and pulmonology, Texas Children’s Hospital was first in cardiology/heart surgery, Children’s National Medical Center was first in neonatology, and St. Jude Children’s Research Hospital in Memphis topped the cancer ranking, U.S. News & World Report said.
The research organization, RTI International, conducted the physician survey and produced the methodology and national rankings under contract with U.S. News & World Report.
Boston Children’s Hospital is the country’s top hospital for children, according to U.S. New & World Report.
This marks the 3rd consecutive year and the fifth time in 6 years that Boston Children’s Hospital either has earned the honor on its own or been tied for the top spot. This year’s second-place finisher, Children’s Hospital of Philadelphia, was first in 2013-2014 and tied for first in 2014-2015 and 2012-2013.
Of the 187 facilities that qualified for inclusion this year, 113 submitted sufficient data to be considered in at least one of the 10 specialties that make up the rating: cancer, cardiology and heart surgery, diabetes and endocrinology, gastroenterology and gastrointestinal surgery, neonatology, nephrology, neurology and neurosurgery, orthopedics, pulmonology, and urology. In addition, a survey of individuals conducted to establish the hospitals’ reputations – generally worth about 15% of a hospital’s score in each specialty – was completed by 3,269 physicians.
Boston Children’s Hospital was ranked first in five of the ten specialties, Children’s Hospital of Philadelphia finished first in diabetes/endocrinology and pulmonology, Texas Children’s Hospital was first in cardiology/heart surgery, Children’s National Medical Center was first in neonatology, and St. Jude Children’s Research Hospital in Memphis topped the cancer ranking, U.S. News & World Report said.
The research organization, RTI International, conducted the physician survey and produced the methodology and national rankings under contract with U.S. News & World Report.
Boston Children’s Hospital is the country’s top hospital for children, according to U.S. New & World Report.
This marks the 3rd consecutive year and the fifth time in 6 years that Boston Children’s Hospital either has earned the honor on its own or been tied for the top spot. This year’s second-place finisher, Children’s Hospital of Philadelphia, was first in 2013-2014 and tied for first in 2014-2015 and 2012-2013.
Of the 187 facilities that qualified for inclusion this year, 113 submitted sufficient data to be considered in at least one of the 10 specialties that make up the rating: cancer, cardiology and heart surgery, diabetes and endocrinology, gastroenterology and gastrointestinal surgery, neonatology, nephrology, neurology and neurosurgery, orthopedics, pulmonology, and urology. In addition, a survey of individuals conducted to establish the hospitals’ reputations – generally worth about 15% of a hospital’s score in each specialty – was completed by 3,269 physicians.
Boston Children’s Hospital was ranked first in five of the ten specialties, Children’s Hospital of Philadelphia finished first in diabetes/endocrinology and pulmonology, Texas Children’s Hospital was first in cardiology/heart surgery, Children’s National Medical Center was first in neonatology, and St. Jude Children’s Research Hospital in Memphis topped the cancer ranking, U.S. News & World Report said.
The research organization, RTI International, conducted the physician survey and produced the methodology and national rankings under contract with U.S. News & World Report.
Clearer instructions linked to fewer medication dosing errors
In nine pediatric dosing trials, more than 80% of parents made more than one medication dosing error, according to a study by H. Shonna Yin, MD, and associates. Misunderstandings about how to accurately choose the right dosing tools as well as confusion related to units of measure contribute to most errors. Matching dosing tools more closely with prescribed dose volumes, as well as using pictograms, can greatly reduce the number of pediatric medication errors, the researchers noted.
The study shows that 83.5% of parents made at least one dosing error (overdosing was present in 12.1% of errors), and 29.3% of parents made at least one large error in administering their children’s medicine. Parents who received text-only instructions or milliliter/teaspoon labels made more large errors. The biggest influence on errors resulted from providing tools more closely matched to the recommended dose measurements.
The researchers conducted a randomized controlled experiment in three pediatric clinics. Each site’s institutional review board approved the study. An average of 491 parents of children older than 8 years were randomly assigned to one of four groups, and given labels and dosing tools that varied in label instruction format and units. Each parent measured nine doses of liquid medicine in a random order, using three different tools.
Parents in group 1 received text and pictogram dosing instructions with milliliter-only labels and tools. They had decreased odds of making a dosing error compared with parents who received milliliter/teaspoon labels and tools without pictographic instructions in groups 2 and 4, and had lower odds of making large dosing errors compared with group 3, whose participants received text-only instructions (Pediatrics. 2017 June 27. doi: 10.1542/peds.2016-3237).
“Our findings support the use of a specific algorithm to help health care providers and pharmacists determine which dosing tool is most optimal to provide to parents,” said Dr. Yin. “We found that pictograms were associated with statistically significant reductions in large overdosing errors, with a trend for reduction in any error.”
No financial disclosures or conflicts of interest were reported.
In nine pediatric dosing trials, more than 80% of parents made more than one medication dosing error, according to a study by H. Shonna Yin, MD, and associates. Misunderstandings about how to accurately choose the right dosing tools as well as confusion related to units of measure contribute to most errors. Matching dosing tools more closely with prescribed dose volumes, as well as using pictograms, can greatly reduce the number of pediatric medication errors, the researchers noted.
The study shows that 83.5% of parents made at least one dosing error (overdosing was present in 12.1% of errors), and 29.3% of parents made at least one large error in administering their children’s medicine. Parents who received text-only instructions or milliliter/teaspoon labels made more large errors. The biggest influence on errors resulted from providing tools more closely matched to the recommended dose measurements.
The researchers conducted a randomized controlled experiment in three pediatric clinics. Each site’s institutional review board approved the study. An average of 491 parents of children older than 8 years were randomly assigned to one of four groups, and given labels and dosing tools that varied in label instruction format and units. Each parent measured nine doses of liquid medicine in a random order, using three different tools.
Parents in group 1 received text and pictogram dosing instructions with milliliter-only labels and tools. They had decreased odds of making a dosing error compared with parents who received milliliter/teaspoon labels and tools without pictographic instructions in groups 2 and 4, and had lower odds of making large dosing errors compared with group 3, whose participants received text-only instructions (Pediatrics. 2017 June 27. doi: 10.1542/peds.2016-3237).
“Our findings support the use of a specific algorithm to help health care providers and pharmacists determine which dosing tool is most optimal to provide to parents,” said Dr. Yin. “We found that pictograms were associated with statistically significant reductions in large overdosing errors, with a trend for reduction in any error.”
No financial disclosures or conflicts of interest were reported.
In nine pediatric dosing trials, more than 80% of parents made more than one medication dosing error, according to a study by H. Shonna Yin, MD, and associates. Misunderstandings about how to accurately choose the right dosing tools as well as confusion related to units of measure contribute to most errors. Matching dosing tools more closely with prescribed dose volumes, as well as using pictograms, can greatly reduce the number of pediatric medication errors, the researchers noted.
The study shows that 83.5% of parents made at least one dosing error (overdosing was present in 12.1% of errors), and 29.3% of parents made at least one large error in administering their children’s medicine. Parents who received text-only instructions or milliliter/teaspoon labels made more large errors. The biggest influence on errors resulted from providing tools more closely matched to the recommended dose measurements.
The researchers conducted a randomized controlled experiment in three pediatric clinics. Each site’s institutional review board approved the study. An average of 491 parents of children older than 8 years were randomly assigned to one of four groups, and given labels and dosing tools that varied in label instruction format and units. Each parent measured nine doses of liquid medicine in a random order, using three different tools.
Parents in group 1 received text and pictogram dosing instructions with milliliter-only labels and tools. They had decreased odds of making a dosing error compared with parents who received milliliter/teaspoon labels and tools without pictographic instructions in groups 2 and 4, and had lower odds of making large dosing errors compared with group 3, whose participants received text-only instructions (Pediatrics. 2017 June 27. doi: 10.1542/peds.2016-3237).
“Our findings support the use of a specific algorithm to help health care providers and pharmacists determine which dosing tool is most optimal to provide to parents,” said Dr. Yin. “We found that pictograms were associated with statistically significant reductions in large overdosing errors, with a trend for reduction in any error.”
No financial disclosures or conflicts of interest were reported.
FROM PEDIATRICS
Key clinical point:
Major finding: In nine dosing trials, 83.5% of parents made more than one medication dosing error, mainly overdosing.
Data source: A randomized controlled study. Recruitment took place in pediatric outpatient clinics in New York, California, and Georgia. Each site’s institutional review board approved the study.
Disclosures: The National Institutes of Health/National Institute of Child Health and Human Development funded the study. The authors declared no conflict of interest.
CRPM may be promising predictive biomarker for knee osteoarthritis
LAS VEGAS – , Anne-Christine Bay-Jensen, PhD, said at the World Congress on Osteoarthritis.

That way, investigators maximize the likelihood of obtaining a positive outcome undiluted by giving the therapy to the wrong patients.
CRPM shows preliminary evidence of passing muster on both counts, according to Dr. Bay-Jensen, head of rheumatology at Nordic Bioscience in Herløv, Denmark.
The Danish researcher introduced herself to the Las Vegas audience by announcing, “My purpose in life is to develop biomarkers for identifying phenotypes in osteoarthritis.”
Indeed, she has been a pioneer in investigating the clinical utility of CRPM, a degradation fragment of C-reactive protein that is produced in the joint and thus reflects joint-specific tissue inflammation. Unlike C-reactive protein, which is an acute phase reactant, CRPM reflects chronic inflammation, she explained at the meeting sponsored by the Osteoarthritis Research Society International.
Her early work with CRPM explored its use as a biomarker in rheumatoid arthritis (RA) patients. She demonstrated, for example, in a secondary analysis of the phase III, double-blind, placebo-controlled LITHE trial that an 11% reduction in CRPM at week 4 of treatment with tocilizumab (Actemra) plus methotrexate was associated with a fourfold increased likelihood of a clinical response at week 16. That finding indicates that utilizing CRPM as an early predictor of tocilizumab efficacy promotes a more targeted, cost-effective, and personalized use of the biologic agent.
At OARSI 2017, Dr. Bay-Jensen presented evidence that even though the mean serum CRPM is significantly higher in patients with RA than in those with knee osteoarthritis (KOA), one-third or more of KOA patients have levels of joint tissue inflammation comparable to that seen in RA. That patient subset with a highly inflammatory KOA phenotype would be the logical focus of future clinical trials of agents having potent anti-inflammatory effects, rather than potential therapies with bone- or cartilage-modifying effects.
The data came from a biomarker study of 113 patients with early RA, as well as from two Nordic Bioscience–sponsored phase III randomized, multicenter, placebo-controlled clinical trials of oral salmon calcitonin in a total of 2,306 patients with knee osteoarthritis, both of which proved negative (Osteoarthritis Cartilage. 2015 Apr;23[4]:532-43). The mean baseline CRPM in the early RA patients was 17.1 ng/mL, compared with 8.5 ng/mL in the KOA patients. However, 31% of KOA patients in one phase III oral calcitonin trial and 41% in the other had a baseline serum CRPM greater than 9 ng/mL, a level that overlapped with 75% of the RA patients.
A related substudy of the oral calcitonin trials examined CRPM as a predictive biomarker. It included 153 knees without OA at baseline, 50 of which developed radiographic evidence of KOA, as evidenced by a Kellgren-Lawrence grade of 2 or 3 during 2 years of prospective follow-up. A serum CRPM of 9 ng/mL or more at baseline was associated with a 4.6-fold increased likelihood of incident KOA during follow-up.
Nordic Bioscience, Dr. Bay-Jensen’s employer, markets numerous proprietary biomarker assays, including one for CRPM.
LAS VEGAS – , Anne-Christine Bay-Jensen, PhD, said at the World Congress on Osteoarthritis.
That way, investigators maximize the likelihood of obtaining a positive outcome undiluted by giving the therapy to the wrong patients.
CRPM shows preliminary evidence of passing muster on both counts, according to Dr. Bay-Jensen, head of rheumatology at Nordic Bioscience in Herløv, Denmark.
The Danish researcher introduced herself to the Las Vegas audience by announcing, “My purpose in life is to develop biomarkers for identifying phenotypes in osteoarthritis.”
Indeed, she has been a pioneer in investigating the clinical utility of CRPM, a degradation fragment of C-reactive protein that is produced in the joint and thus reflects joint-specific tissue inflammation. Unlike C-reactive protein, which is an acute phase reactant, CRPM reflects chronic inflammation, she explained at the meeting sponsored by the Osteoarthritis Research Society International.
Her early work with CRPM explored its use as a biomarker in rheumatoid arthritis (RA) patients. She demonstrated, for example, in a secondary analysis of the phase III, double-blind, placebo-controlled LITHE trial that an 11% reduction in CRPM at week 4 of treatment with tocilizumab (Actemra) plus methotrexate was associated with a fourfold increased likelihood of a clinical response at week 16. That finding indicates that utilizing CRPM as an early predictor of tocilizumab efficacy promotes a more targeted, cost-effective, and personalized use of the biologic agent.
At OARSI 2017, Dr. Bay-Jensen presented evidence that even though the mean serum CRPM is significantly higher in patients with RA than in those with knee osteoarthritis (KOA), one-third or more of KOA patients have levels of joint tissue inflammation comparable to that seen in RA. That patient subset with a highly inflammatory KOA phenotype would be the logical focus of future clinical trials of agents having potent anti-inflammatory effects, rather than potential therapies with bone- or cartilage-modifying effects.
The data came from a biomarker study of 113 patients with early RA, as well as from two Nordic Bioscience–sponsored phase III randomized, multicenter, placebo-controlled clinical trials of oral salmon calcitonin in a total of 2,306 patients with knee osteoarthritis, both of which proved negative (Osteoarthritis Cartilage. 2015 Apr;23[4]:532-43). The mean baseline CRPM in the early RA patients was 17.1 ng/mL, compared with 8.5 ng/mL in the KOA patients. However, 31% of KOA patients in one phase III oral calcitonin trial and 41% in the other had a baseline serum CRPM greater than 9 ng/mL, a level that overlapped with 75% of the RA patients.
A related substudy of the oral calcitonin trials examined CRPM as a predictive biomarker. It included 153 knees without OA at baseline, 50 of which developed radiographic evidence of KOA, as evidenced by a Kellgren-Lawrence grade of 2 or 3 during 2 years of prospective follow-up. A serum CRPM of 9 ng/mL or more at baseline was associated with a 4.6-fold increased likelihood of incident KOA during follow-up.
Nordic Bioscience, Dr. Bay-Jensen’s employer, markets numerous proprietary biomarker assays, including one for CRPM.
LAS VEGAS – , Anne-Christine Bay-Jensen, PhD, said at the World Congress on Osteoarthritis.
That way, investigators maximize the likelihood of obtaining a positive outcome undiluted by giving the therapy to the wrong patients.
CRPM shows preliminary evidence of passing muster on both counts, according to Dr. Bay-Jensen, head of rheumatology at Nordic Bioscience in Herløv, Denmark.
The Danish researcher introduced herself to the Las Vegas audience by announcing, “My purpose in life is to develop biomarkers for identifying phenotypes in osteoarthritis.”
Indeed, she has been a pioneer in investigating the clinical utility of CRPM, a degradation fragment of C-reactive protein that is produced in the joint and thus reflects joint-specific tissue inflammation. Unlike C-reactive protein, which is an acute phase reactant, CRPM reflects chronic inflammation, she explained at the meeting sponsored by the Osteoarthritis Research Society International.
Her early work with CRPM explored its use as a biomarker in rheumatoid arthritis (RA) patients. She demonstrated, for example, in a secondary analysis of the phase III, double-blind, placebo-controlled LITHE trial that an 11% reduction in CRPM at week 4 of treatment with tocilizumab (Actemra) plus methotrexate was associated with a fourfold increased likelihood of a clinical response at week 16. That finding indicates that utilizing CRPM as an early predictor of tocilizumab efficacy promotes a more targeted, cost-effective, and personalized use of the biologic agent.
At OARSI 2017, Dr. Bay-Jensen presented evidence that even though the mean serum CRPM is significantly higher in patients with RA than in those with knee osteoarthritis (KOA), one-third or more of KOA patients have levels of joint tissue inflammation comparable to that seen in RA. That patient subset with a highly inflammatory KOA phenotype would be the logical focus of future clinical trials of agents having potent anti-inflammatory effects, rather than potential therapies with bone- or cartilage-modifying effects.
The data came from a biomarker study of 113 patients with early RA, as well as from two Nordic Bioscience–sponsored phase III randomized, multicenter, placebo-controlled clinical trials of oral salmon calcitonin in a total of 2,306 patients with knee osteoarthritis, both of which proved negative (Osteoarthritis Cartilage. 2015 Apr;23[4]:532-43). The mean baseline CRPM in the early RA patients was 17.1 ng/mL, compared with 8.5 ng/mL in the KOA patients. However, 31% of KOA patients in one phase III oral calcitonin trial and 41% in the other had a baseline serum CRPM greater than 9 ng/mL, a level that overlapped with 75% of the RA patients.
A related substudy of the oral calcitonin trials examined CRPM as a predictive biomarker. It included 153 knees without OA at baseline, 50 of which developed radiographic evidence of KOA, as evidenced by a Kellgren-Lawrence grade of 2 or 3 during 2 years of prospective follow-up. A serum CRPM of 9 ng/mL or more at baseline was associated with a 4.6-fold increased likelihood of incident KOA during follow-up.
Nordic Bioscience, Dr. Bay-Jensen’s employer, markets numerous proprietary biomarker assays, including one for CRPM.
EXPERT ANALYSIS FROM OARSI 2017
Very-low-volume vascular surgery practice linked to worse outcomes
The very-low-volume practice of surgeons performing no more than one open abdominal aortic aneurysm repair (OAR) or carotid endarterectomy (CEA) per year has persisted in New York State and was associated with worse postoperative outcomes and longer lengths of stay in a cohort study of statewide hospital data.
The study examined inpatient data on elective OARs and CEAs performed from 2000 to 2014 in every hospital in the state.
While the numbers and proportions of very-low-volume surgeons decreased (44.6%-23% for OAR and 35.2%-18.1% for CEA) and the number of procedures performed by these surgeons also decreased (QAR, 346-47; CEA, 395-90), the data are “concerning” and elucidate the “persistence” of very-low-volume practice in open vascular surgery, said Jialin Mao, MD, of Cornell University, New York, and associates (JAMA Surg. doi: 10:1001/jamasurg.2017.1100).
Very-low-volume surgeons were significantly less likely to be vascular surgeons, compared with higher-volume surgeons for both OAR (23.9% vs. 63.9%) and CEA (14.6% vs. 51.7%), they reported.
Compared with patients treated by higher-volume surgeons, those whose OAR was performed by very-low-volume surgeons had a twofold higher risk of postoperative death (6.7% vs. 3.5%) after adjusting for patient risk factors, surgeon specialty, and facility characteristics. Patients of very-low-volume surgeons also had significantly higher odds of sepsis or shock (odds ratio, 1.45), prolonged length of stay (OR, 1.37) and 30-day readmission (OR, 1.19), although the latter was not significant.
Similarly, patients whose CEA was performed by very-low-volume surgeons had a significant 1.8-fold higher odds of experiencing postoperative acute myocardial infarction (1.5% vs. 0.5%) and stroke (3.5% vs. 2.1%). They also were significantly more likely to have 30-day readmission (OR, 1.30).
With both procedures, patients treated by very-low-volume surgeons tended to be younger and healthier (less likely to have two or more comorbidities). They also were more likely to be nonwhite or insured by Medicaid.
“It is reasonable to speculate,” the researchers wrote, “that those treated by very-low-volume surgeons were more likely to be socioeconomically disadvantaged.”
Notably, 30% of the very-low-volume practice occurred in New York City, “where accessibility to high-volume practitioners should generally be higher,” they said.
The findings “indicate the need to eliminate this type of practice, to restrict the practice of these very-low-volume surgeons or to force referrals to higher-volume and specialized surgeons, and to improve disparity in access to high-quality care for all patients,” they said.
The study was funded in part by the U.S. Food and Drug Administration. The researchers reported having no relevant conflicts of interest.
The delineation of a threshold number of cases of OAR and CEA below which surgeons should not be credentialed remains unclear, despite much discussion of the volume-outcome relationship in vascular surgery.
In the current endovascular era, OAR in particular has become increasingly less frequent, with a dramatic effect on trainee experiences. It is often proposed that these cases be limited to high-volume surgeons. Some are concerned, however, that this action will leave rural surgeons unprepared to deal with ruptured abdominal aortic aneurysm and will force patients to travel long distances.

Sarah E. Deery, MD, and Marc L. Schermerhorn, MD, are in the division of vascular and endovascular surgery at Beth Israel Deaconess Medical Center in Boston. These remarks are adapted from an editorial accompanying the study. They reported having no disclosures.
The delineation of a threshold number of cases of OAR and CEA below which surgeons should not be credentialed remains unclear, despite much discussion of the volume-outcome relationship in vascular surgery.
In the current endovascular era, OAR in particular has become increasingly less frequent, with a dramatic effect on trainee experiences. It is often proposed that these cases be limited to high-volume surgeons. Some are concerned, however, that this action will leave rural surgeons unprepared to deal with ruptured abdominal aortic aneurysm and will force patients to travel long distances.
Sarah E. Deery, MD, and Marc L. Schermerhorn, MD, are in the division of vascular and endovascular surgery at Beth Israel Deaconess Medical Center in Boston. These remarks are adapted from an editorial accompanying the study. They reported having no disclosures.
The delineation of a threshold number of cases of OAR and CEA below which surgeons should not be credentialed remains unclear, despite much discussion of the volume-outcome relationship in vascular surgery.
In the current endovascular era, OAR in particular has become increasingly less frequent, with a dramatic effect on trainee experiences. It is often proposed that these cases be limited to high-volume surgeons. Some are concerned, however, that this action will leave rural surgeons unprepared to deal with ruptured abdominal aortic aneurysm and will force patients to travel long distances.
Sarah E. Deery, MD, and Marc L. Schermerhorn, MD, are in the division of vascular and endovascular surgery at Beth Israel Deaconess Medical Center in Boston. These remarks are adapted from an editorial accompanying the study. They reported having no disclosures.
The very-low-volume practice of surgeons performing no more than one open abdominal aortic aneurysm repair (OAR) or carotid endarterectomy (CEA) per year has persisted in New York State and was associated with worse postoperative outcomes and longer lengths of stay in a cohort study of statewide hospital data.
The study examined inpatient data on elective OARs and CEAs performed from 2000 to 2014 in every hospital in the state.
While the numbers and proportions of very-low-volume surgeons decreased (44.6%-23% for OAR and 35.2%-18.1% for CEA) and the number of procedures performed by these surgeons also decreased (QAR, 346-47; CEA, 395-90), the data are “concerning” and elucidate the “persistence” of very-low-volume practice in open vascular surgery, said Jialin Mao, MD, of Cornell University, New York, and associates (JAMA Surg. doi: 10:1001/jamasurg.2017.1100).
Very-low-volume surgeons were significantly less likely to be vascular surgeons, compared with higher-volume surgeons for both OAR (23.9% vs. 63.9%) and CEA (14.6% vs. 51.7%), they reported.
Compared with patients treated by higher-volume surgeons, those whose OAR was performed by very-low-volume surgeons had a twofold higher risk of postoperative death (6.7% vs. 3.5%) after adjusting for patient risk factors, surgeon specialty, and facility characteristics. Patients of very-low-volume surgeons also had significantly higher odds of sepsis or shock (odds ratio, 1.45), prolonged length of stay (OR, 1.37) and 30-day readmission (OR, 1.19), although the latter was not significant.
Similarly, patients whose CEA was performed by very-low-volume surgeons had a significant 1.8-fold higher odds of experiencing postoperative acute myocardial infarction (1.5% vs. 0.5%) and stroke (3.5% vs. 2.1%). They also were significantly more likely to have 30-day readmission (OR, 1.30).
With both procedures, patients treated by very-low-volume surgeons tended to be younger and healthier (less likely to have two or more comorbidities). They also were more likely to be nonwhite or insured by Medicaid.
“It is reasonable to speculate,” the researchers wrote, “that those treated by very-low-volume surgeons were more likely to be socioeconomically disadvantaged.”
Notably, 30% of the very-low-volume practice occurred in New York City, “where accessibility to high-volume practitioners should generally be higher,” they said.
The findings “indicate the need to eliminate this type of practice, to restrict the practice of these very-low-volume surgeons or to force referrals to higher-volume and specialized surgeons, and to improve disparity in access to high-quality care for all patients,” they said.
The study was funded in part by the U.S. Food and Drug Administration. The researchers reported having no relevant conflicts of interest.
The very-low-volume practice of surgeons performing no more than one open abdominal aortic aneurysm repair (OAR) or carotid endarterectomy (CEA) per year has persisted in New York State and was associated with worse postoperative outcomes and longer lengths of stay in a cohort study of statewide hospital data.
The study examined inpatient data on elective OARs and CEAs performed from 2000 to 2014 in every hospital in the state.
While the numbers and proportions of very-low-volume surgeons decreased (44.6%-23% for OAR and 35.2%-18.1% for CEA) and the number of procedures performed by these surgeons also decreased (QAR, 346-47; CEA, 395-90), the data are “concerning” and elucidate the “persistence” of very-low-volume practice in open vascular surgery, said Jialin Mao, MD, of Cornell University, New York, and associates (JAMA Surg. doi: 10:1001/jamasurg.2017.1100).
Very-low-volume surgeons were significantly less likely to be vascular surgeons, compared with higher-volume surgeons for both OAR (23.9% vs. 63.9%) and CEA (14.6% vs. 51.7%), they reported.
Compared with patients treated by higher-volume surgeons, those whose OAR was performed by very-low-volume surgeons had a twofold higher risk of postoperative death (6.7% vs. 3.5%) after adjusting for patient risk factors, surgeon specialty, and facility characteristics. Patients of very-low-volume surgeons also had significantly higher odds of sepsis or shock (odds ratio, 1.45), prolonged length of stay (OR, 1.37) and 30-day readmission (OR, 1.19), although the latter was not significant.
Similarly, patients whose CEA was performed by very-low-volume surgeons had a significant 1.8-fold higher odds of experiencing postoperative acute myocardial infarction (1.5% vs. 0.5%) and stroke (3.5% vs. 2.1%). They also were significantly more likely to have 30-day readmission (OR, 1.30).
With both procedures, patients treated by very-low-volume surgeons tended to be younger and healthier (less likely to have two or more comorbidities). They also were more likely to be nonwhite or insured by Medicaid.
“It is reasonable to speculate,” the researchers wrote, “that those treated by very-low-volume surgeons were more likely to be socioeconomically disadvantaged.”
Notably, 30% of the very-low-volume practice occurred in New York City, “where accessibility to high-volume practitioners should generally be higher,” they said.
The findings “indicate the need to eliminate this type of practice, to restrict the practice of these very-low-volume surgeons or to force referrals to higher-volume and specialized surgeons, and to improve disparity in access to high-quality care for all patients,” they said.
The study was funded in part by the U.S. Food and Drug Administration. The researchers reported having no relevant conflicts of interest.
FROM JAMA SURGERY
Key clinical point: The very-low-volume practice of open abdominal aortic aneurysm repair and carotid endarterectomy (one or fewer annual procedures) is associated with worse postoperative outcomes and greater length of stay.
Major finding: Patients whose procedure was performed by very-low-volume surgeons had a twofold higher risk of postoperative death after OAR or 1.8-fold higher odds of experiencing postoperative acute myocardial infarction or stroke after CEA.
Data source: The study was funded in part by the U.S. Food and Drug Administration.
Disclosures: The researchers reported having no relevant conflicts of interest.
MV disease in children requires modified strategies
NEW YORK – Repairing mitral valves in pediatric patients must overcome two issues: the wide variability in their anatomy and their growth. Using strategies and techniques common in adult mitral surgery can accomplish good mitral valve function in children, but some techniques in children differ, like using combined resorbable material with autologous tissue or transferring native chords instead of placing artificial chords to a malfunctioning leaflet.
Pedro del Nido, MD, of Boston Children’s Hospital, said the spectrum of mitral valve pathology in children goes from congenital mitral stenosis with a thick annulus with leaflet immobility to leaflet hypermobility that involves anterior leaflet prolapse and can involve a cleft that causes regurgitation. Dr. del Nido explained his surgical approaches for mitral valve disease in children at the 2017 Mitral Conclave, sponsored by the American Association of Thoracic Surgery.

Accessing the mitral valve in children requires a different approach than in adults, Dr. del Nido said. “Going through the left atrium is generally difficult, so we often enter through a trans-septal incision,” he said. “The main reason for that is because the tricuspid valve is often associated with the mitral valve problem and this gives us the most direct exposure.”
Once the surgeon gains exposure, the surgical analysis for a diseased adult or child valve is almost identical, with the exception that adult disease is acquired whereas childhood disease tends to be congenital, Dr. del Nido said. “In the congenital patient, we often find fibroelastic tissue that the child is born with,” he said. “We see this in neonates and young infants. It thickens over time; it doesn’t often calcify, but it does often restrict the leaflets and it tends to fuse the chords, so in essence you have direct attachments of the leaflets to the papillaries.”
He explained that this pathology requires an approach similar to that for rheumatic mitral disease in adults. “Start splitting the commissures and start resecting the tissue off the chords creating fenestrations in order to improve the inflow.” Dr. del Nido added, “If you don’t do this, the child will always have a gradient, and if you think about an adult having problems and symptoms with a gradient, think about a 10-year-old running around trying to do athletics; it’s impossible.”
Dysfunctional chords also require a somewhat different approach in children than they require in adults. “We find elongation of the chords and the anterior support structure is abnormal; the secondary chords are totally intact,” Dr. del Nido said. When confronting a torn-edge chord, resection is often an option in adults, but is uncommon in children. “We don’t usually have very much leaflet tissue,” he said. Artificial chords do not accommodate growth.
“We tend to use native tissue,” said Dr. del Nido. “You can transfer the strut chord; you can transfer the secondary chord in order to achieve support for the edge of that prolapsed leaflet.”
Leaflet problems are probably the biggest single source of recurrence in children, Dr. del Nido said. A cleft on the anterior leaflet can be particularly vexing. For example, cleft edges attached to the septum can prevent the valve leaflet from coaptation with the posterior leaflet. “If you don’t recognize that on 3-D echocardiography, you’re going to have a problem; that leaflet will never create the coaptation surface that you want,” he said.
The solution may lie underneath the leaflet. Said Dr. del Nido, “We tend to want to close a cleft, and, yes, that will get you relief of regurgitation in the central portion, but if you end up with immobility of that leaflet, then look underneath. Most often there are very abnormal attachments to the edges of that cleft to the septum. You have to get rid of that; if you don’t resect all that, you’ll never have a leaflet that truly floats up to coapt against the posterior leaflet.”
Annular dilation in children can also challenge a cardiothoracic surgeon’s skill.
In rare cases, a suture commissuroplasty may correct the problem. Sometimes Dr. del Nido will use the DeVega suture annuloplasty – “even though it is very much user dependent; it’s very easy in pediatrics to create stenosis with the DeVega.” As an alternative, synthetic ring annuloplasties can confine valve growth and are rarely used.
Dr. del Nido’s preference is to use a hybrid approach of tissue and resorbable material. “The advantage of the resorbable material is that it will go away, but that’s also the problem with the resorbable material,” he said. “Once it does go away, there’s nothing there to support the annulus, so a combination of tissue and resorbable suture is probably the best answer.”
In posterior leaflet deficiency, a patch of pericardium posteriorly can augment the dysfunctional leaflet. You can also use pericardium as an annuloplasty ring. “You can use it circumferentially,” Dr. del Nido said. “It’s a soft ring; you can certainly use this material which is autologous; it does provide strength to the fibrous annulus; it does support that valve; and you do see growth.” He added that bovine pericardium is not ideal for this use.
Dr. del Nido reported no relevant financial relationships.
NEW YORK – Repairing mitral valves in pediatric patients must overcome two issues: the wide variability in their anatomy and their growth. Using strategies and techniques common in adult mitral surgery can accomplish good mitral valve function in children, but some techniques in children differ, like using combined resorbable material with autologous tissue or transferring native chords instead of placing artificial chords to a malfunctioning leaflet.
Pedro del Nido, MD, of Boston Children’s Hospital, said the spectrum of mitral valve pathology in children goes from congenital mitral stenosis with a thick annulus with leaflet immobility to leaflet hypermobility that involves anterior leaflet prolapse and can involve a cleft that causes regurgitation. Dr. del Nido explained his surgical approaches for mitral valve disease in children at the 2017 Mitral Conclave, sponsored by the American Association of Thoracic Surgery.
Accessing the mitral valve in children requires a different approach than in adults, Dr. del Nido said. “Going through the left atrium is generally difficult, so we often enter through a trans-septal incision,” he said. “The main reason for that is because the tricuspid valve is often associated with the mitral valve problem and this gives us the most direct exposure.”
Once the surgeon gains exposure, the surgical analysis for a diseased adult or child valve is almost identical, with the exception that adult disease is acquired whereas childhood disease tends to be congenital, Dr. del Nido said. “In the congenital patient, we often find fibroelastic tissue that the child is born with,” he said. “We see this in neonates and young infants. It thickens over time; it doesn’t often calcify, but it does often restrict the leaflets and it tends to fuse the chords, so in essence you have direct attachments of the leaflets to the papillaries.”
He explained that this pathology requires an approach similar to that for rheumatic mitral disease in adults. “Start splitting the commissures and start resecting the tissue off the chords creating fenestrations in order to improve the inflow.” Dr. del Nido added, “If you don’t do this, the child will always have a gradient, and if you think about an adult having problems and symptoms with a gradient, think about a 10-year-old running around trying to do athletics; it’s impossible.”
Dysfunctional chords also require a somewhat different approach in children than they require in adults. “We find elongation of the chords and the anterior support structure is abnormal; the secondary chords are totally intact,” Dr. del Nido said. When confronting a torn-edge chord, resection is often an option in adults, but is uncommon in children. “We don’t usually have very much leaflet tissue,” he said. Artificial chords do not accommodate growth.
“We tend to use native tissue,” said Dr. del Nido. “You can transfer the strut chord; you can transfer the secondary chord in order to achieve support for the edge of that prolapsed leaflet.”
Leaflet problems are probably the biggest single source of recurrence in children, Dr. del Nido said. A cleft on the anterior leaflet can be particularly vexing. For example, cleft edges attached to the septum can prevent the valve leaflet from coaptation with the posterior leaflet. “If you don’t recognize that on 3-D echocardiography, you’re going to have a problem; that leaflet will never create the coaptation surface that you want,” he said.
The solution may lie underneath the leaflet. Said Dr. del Nido, “We tend to want to close a cleft, and, yes, that will get you relief of regurgitation in the central portion, but if you end up with immobility of that leaflet, then look underneath. Most often there are very abnormal attachments to the edges of that cleft to the septum. You have to get rid of that; if you don’t resect all that, you’ll never have a leaflet that truly floats up to coapt against the posterior leaflet.”
Annular dilation in children can also challenge a cardiothoracic surgeon’s skill.
In rare cases, a suture commissuroplasty may correct the problem. Sometimes Dr. del Nido will use the DeVega suture annuloplasty – “even though it is very much user dependent; it’s very easy in pediatrics to create stenosis with the DeVega.” As an alternative, synthetic ring annuloplasties can confine valve growth and are rarely used.
Dr. del Nido’s preference is to use a hybrid approach of tissue and resorbable material. “The advantage of the resorbable material is that it will go away, but that’s also the problem with the resorbable material,” he said. “Once it does go away, there’s nothing there to support the annulus, so a combination of tissue and resorbable suture is probably the best answer.”
In posterior leaflet deficiency, a patch of pericardium posteriorly can augment the dysfunctional leaflet. You can also use pericardium as an annuloplasty ring. “You can use it circumferentially,” Dr. del Nido said. “It’s a soft ring; you can certainly use this material which is autologous; it does provide strength to the fibrous annulus; it does support that valve; and you do see growth.” He added that bovine pericardium is not ideal for this use.
Dr. del Nido reported no relevant financial relationships.
NEW YORK – Repairing mitral valves in pediatric patients must overcome two issues: the wide variability in their anatomy and their growth. Using strategies and techniques common in adult mitral surgery can accomplish good mitral valve function in children, but some techniques in children differ, like using combined resorbable material with autologous tissue or transferring native chords instead of placing artificial chords to a malfunctioning leaflet.
Pedro del Nido, MD, of Boston Children’s Hospital, said the spectrum of mitral valve pathology in children goes from congenital mitral stenosis with a thick annulus with leaflet immobility to leaflet hypermobility that involves anterior leaflet prolapse and can involve a cleft that causes regurgitation. Dr. del Nido explained his surgical approaches for mitral valve disease in children at the 2017 Mitral Conclave, sponsored by the American Association of Thoracic Surgery.
Accessing the mitral valve in children requires a different approach than in adults, Dr. del Nido said. “Going through the left atrium is generally difficult, so we often enter through a trans-septal incision,” he said. “The main reason for that is because the tricuspid valve is often associated with the mitral valve problem and this gives us the most direct exposure.”
Once the surgeon gains exposure, the surgical analysis for a diseased adult or child valve is almost identical, with the exception that adult disease is acquired whereas childhood disease tends to be congenital, Dr. del Nido said. “In the congenital patient, we often find fibroelastic tissue that the child is born with,” he said. “We see this in neonates and young infants. It thickens over time; it doesn’t often calcify, but it does often restrict the leaflets and it tends to fuse the chords, so in essence you have direct attachments of the leaflets to the papillaries.”
He explained that this pathology requires an approach similar to that for rheumatic mitral disease in adults. “Start splitting the commissures and start resecting the tissue off the chords creating fenestrations in order to improve the inflow.” Dr. del Nido added, “If you don’t do this, the child will always have a gradient, and if you think about an adult having problems and symptoms with a gradient, think about a 10-year-old running around trying to do athletics; it’s impossible.”
Dysfunctional chords also require a somewhat different approach in children than they require in adults. “We find elongation of the chords and the anterior support structure is abnormal; the secondary chords are totally intact,” Dr. del Nido said. When confronting a torn-edge chord, resection is often an option in adults, but is uncommon in children. “We don’t usually have very much leaflet tissue,” he said. Artificial chords do not accommodate growth.
“We tend to use native tissue,” said Dr. del Nido. “You can transfer the strut chord; you can transfer the secondary chord in order to achieve support for the edge of that prolapsed leaflet.”
Leaflet problems are probably the biggest single source of recurrence in children, Dr. del Nido said. A cleft on the anterior leaflet can be particularly vexing. For example, cleft edges attached to the septum can prevent the valve leaflet from coaptation with the posterior leaflet. “If you don’t recognize that on 3-D echocardiography, you’re going to have a problem; that leaflet will never create the coaptation surface that you want,” he said.
The solution may lie underneath the leaflet. Said Dr. del Nido, “We tend to want to close a cleft, and, yes, that will get you relief of regurgitation in the central portion, but if you end up with immobility of that leaflet, then look underneath. Most often there are very abnormal attachments to the edges of that cleft to the septum. You have to get rid of that; if you don’t resect all that, you’ll never have a leaflet that truly floats up to coapt against the posterior leaflet.”
Annular dilation in children can also challenge a cardiothoracic surgeon’s skill.
In rare cases, a suture commissuroplasty may correct the problem. Sometimes Dr. del Nido will use the DeVega suture annuloplasty – “even though it is very much user dependent; it’s very easy in pediatrics to create stenosis with the DeVega.” As an alternative, synthetic ring annuloplasties can confine valve growth and are rarely used.
Dr. del Nido’s preference is to use a hybrid approach of tissue and resorbable material. “The advantage of the resorbable material is that it will go away, but that’s also the problem with the resorbable material,” he said. “Once it does go away, there’s nothing there to support the annulus, so a combination of tissue and resorbable suture is probably the best answer.”
In posterior leaflet deficiency, a patch of pericardium posteriorly can augment the dysfunctional leaflet. You can also use pericardium as an annuloplasty ring. “You can use it circumferentially,” Dr. del Nido said. “It’s a soft ring; you can certainly use this material which is autologous; it does provide strength to the fibrous annulus; it does support that valve; and you do see growth.” He added that bovine pericardium is not ideal for this use.
Dr. del Nido reported no relevant financial relationships.
AT THE 2017 MITRAL VALVE CONCLAVE
Key clinical point: Operating on mitral valves in pediatric patients must overcome the wide variability in anatomy among young patients and accommodate growth.
Major finding: Strategies that involve a combination of resorbable material with autologous tissue can accomplish repair in most of these patients.
Data source: Review based on Dr. del Nido’s experience.
Disclosures: Dr. del Nido reported having no relevant financial disclosures.
ALTTO follow-up: Dual HER2 blockade may benefit HER2+/HR- tumors
CHICAGO – HER2-positive/HR-negative breast tumors may have a different biology than HER2+/HR+ tumors and may derive more benefit from dual HER2 blockade, according to 5-year results from the phase III ALTTO trial comparing 1 year of adjuvant anti-HER2 therapy with lapatinib and trastuzumab alone, sequentially, or in combination in patients with HER2-positive early breast cancer.
The hazard ratios for this preplanned updated analysis at a median of 6.9 years of follow-up (when all patients had reached 5 years of follow-up) are similar to those from the primary analysis reported at the 2014 ASCO annual meeting and published in the Journal of Clinical Oncology in 2015 (J Clin Oncol. 2015;34:1034-42) at a median clinical follow-up of 4.5 years, Alvaro Moreno-Aspitia, MD, reported at the annual meeting of the American Society of Clinical Oncology.
In the current analysis, the rate of disease-free survival was 85% with combined lapatinib and trastuzumab (L+T), 84% for sequential trastuzumab and lapatinib (T–L), and 82% with T (hazard ratio for disease-free survival was 0.86 for L+T vs. T and 0.93 for T–L vs. T alone,) said Dr. Moreno-Aspitia of Mayo Clinic, Jacksonville, Fla.
“So, at this time, as noted in the primary analysis, there’s no benefit on the primary endpoint in regard to dual HER2 blockade as provided in this clinical trial,” he said.
There also were no significant differences seen in disease-free survival based on chemotherapy timing, he said.
Notably, disease-free survival was similar across treatment groups among patients with HER2+/HR+ tumors (85% for L+T, 85% to T–L, and 83% for T; HRs, 0.91 and 0.90 vs. T, respectively), but, among those with HER2+/HR– tumors, the 6-year disease-free survival difference for L+T (84%) vs. T (80%) was slightly greater (HR, 0.80).
“This is a hypothesis generating observation that also holds that possibly these patients with hormone receptor–negative tumors may derive benefit from dual HER2 blockade,” Dr. Moreno-Aspitia said, noting that this has also been observed in several other trials.
The 6-year overall survival in ALTTO was 93%, 92%, and 91% for L+T, T–L, and T, respectively (HRs for overall survival, 0.86 for L+T vs. T and 0.88 for T–L).
“At this time, there is absolutely no [overall survival] benefit on dual HER2 blockade over single agent trastuzumab. However, it is very rewarding to see that over 90% of the patients who participated in this trial are alive at this longer-term follow-up,” he said.
As for cardiac events, the numbers remained low as in the primary ALTTO analysis, and no new safety signals had emerged.
ALTTO study subjects were 8,381 patients randomized from 946 sites in 44 countries between June 2007 and July 2011. Those in the L+T group received both agents together for 52 weeks; those in the sequential treatment group received T for 12 weeks followed by a 6-week wash-out period, followed by lapatinib for 34 weeks; and those in the trastuzumab arm (the control arm) and the lapatinib arm each received treatment for 52 weeks. In 2011 the lapatinib arm was closed because of futility, and results for that arm are not included in this analysis.
Long-term follow up of participants continues, a large number of correlative studies are ongoing, and final results will be reported when all patients have been followed for at least 10 years, Dr. Moreno-Aspitia said.
The ALTTO trial was sponsored by GlaxoSmithKline and Novartis. Dr. Moreno-Aspitia reported having no disclosures.
CHICAGO – HER2-positive/HR-negative breast tumors may have a different biology than HER2+/HR+ tumors and may derive more benefit from dual HER2 blockade, according to 5-year results from the phase III ALTTO trial comparing 1 year of adjuvant anti-HER2 therapy with lapatinib and trastuzumab alone, sequentially, or in combination in patients with HER2-positive early breast cancer.
The hazard ratios for this preplanned updated analysis at a median of 6.9 years of follow-up (when all patients had reached 5 years of follow-up) are similar to those from the primary analysis reported at the 2014 ASCO annual meeting and published in the Journal of Clinical Oncology in 2015 (J Clin Oncol. 2015;34:1034-42) at a median clinical follow-up of 4.5 years, Alvaro Moreno-Aspitia, MD, reported at the annual meeting of the American Society of Clinical Oncology.
In the current analysis, the rate of disease-free survival was 85% with combined lapatinib and trastuzumab (L+T), 84% for sequential trastuzumab and lapatinib (T–L), and 82% with T (hazard ratio for disease-free survival was 0.86 for L+T vs. T and 0.93 for T–L vs. T alone,) said Dr. Moreno-Aspitia of Mayo Clinic, Jacksonville, Fla.
“So, at this time, as noted in the primary analysis, there’s no benefit on the primary endpoint in regard to dual HER2 blockade as provided in this clinical trial,” he said.
There also were no significant differences seen in disease-free survival based on chemotherapy timing, he said.
Notably, disease-free survival was similar across treatment groups among patients with HER2+/HR+ tumors (85% for L+T, 85% to T–L, and 83% for T; HRs, 0.91 and 0.90 vs. T, respectively), but, among those with HER2+/HR– tumors, the 6-year disease-free survival difference for L+T (84%) vs. T (80%) was slightly greater (HR, 0.80).
“This is a hypothesis generating observation that also holds that possibly these patients with hormone receptor–negative tumors may derive benefit from dual HER2 blockade,” Dr. Moreno-Aspitia said, noting that this has also been observed in several other trials.
The 6-year overall survival in ALTTO was 93%, 92%, and 91% for L+T, T–L, and T, respectively (HRs for overall survival, 0.86 for L+T vs. T and 0.88 for T–L).
“At this time, there is absolutely no [overall survival] benefit on dual HER2 blockade over single agent trastuzumab. However, it is very rewarding to see that over 90% of the patients who participated in this trial are alive at this longer-term follow-up,” he said.
As for cardiac events, the numbers remained low as in the primary ALTTO analysis, and no new safety signals had emerged.
ALTTO study subjects were 8,381 patients randomized from 946 sites in 44 countries between June 2007 and July 2011. Those in the L+T group received both agents together for 52 weeks; those in the sequential treatment group received T for 12 weeks followed by a 6-week wash-out period, followed by lapatinib for 34 weeks; and those in the trastuzumab arm (the control arm) and the lapatinib arm each received treatment for 52 weeks. In 2011 the lapatinib arm was closed because of futility, and results for that arm are not included in this analysis.
Long-term follow up of participants continues, a large number of correlative studies are ongoing, and final results will be reported when all patients have been followed for at least 10 years, Dr. Moreno-Aspitia said.
The ALTTO trial was sponsored by GlaxoSmithKline and Novartis. Dr. Moreno-Aspitia reported having no disclosures.
CHICAGO – HER2-positive/HR-negative breast tumors may have a different biology than HER2+/HR+ tumors and may derive more benefit from dual HER2 blockade, according to 5-year results from the phase III ALTTO trial comparing 1 year of adjuvant anti-HER2 therapy with lapatinib and trastuzumab alone, sequentially, or in combination in patients with HER2-positive early breast cancer.
The hazard ratios for this preplanned updated analysis at a median of 6.9 years of follow-up (when all patients had reached 5 years of follow-up) are similar to those from the primary analysis reported at the 2014 ASCO annual meeting and published in the Journal of Clinical Oncology in 2015 (J Clin Oncol. 2015;34:1034-42) at a median clinical follow-up of 4.5 years, Alvaro Moreno-Aspitia, MD, reported at the annual meeting of the American Society of Clinical Oncology.
In the current analysis, the rate of disease-free survival was 85% with combined lapatinib and trastuzumab (L+T), 84% for sequential trastuzumab and lapatinib (T–L), and 82% with T (hazard ratio for disease-free survival was 0.86 for L+T vs. T and 0.93 for T–L vs. T alone,) said Dr. Moreno-Aspitia of Mayo Clinic, Jacksonville, Fla.
“So, at this time, as noted in the primary analysis, there’s no benefit on the primary endpoint in regard to dual HER2 blockade as provided in this clinical trial,” he said.
There also were no significant differences seen in disease-free survival based on chemotherapy timing, he said.
Notably, disease-free survival was similar across treatment groups among patients with HER2+/HR+ tumors (85% for L+T, 85% to T–L, and 83% for T; HRs, 0.91 and 0.90 vs. T, respectively), but, among those with HER2+/HR– tumors, the 6-year disease-free survival difference for L+T (84%) vs. T (80%) was slightly greater (HR, 0.80).
“This is a hypothesis generating observation that also holds that possibly these patients with hormone receptor–negative tumors may derive benefit from dual HER2 blockade,” Dr. Moreno-Aspitia said, noting that this has also been observed in several other trials.
The 6-year overall survival in ALTTO was 93%, 92%, and 91% for L+T, T–L, and T, respectively (HRs for overall survival, 0.86 for L+T vs. T and 0.88 for T–L).
“At this time, there is absolutely no [overall survival] benefit on dual HER2 blockade over single agent trastuzumab. However, it is very rewarding to see that over 90% of the patients who participated in this trial are alive at this longer-term follow-up,” he said.
As for cardiac events, the numbers remained low as in the primary ALTTO analysis, and no new safety signals had emerged.
ALTTO study subjects were 8,381 patients randomized from 946 sites in 44 countries between June 2007 and July 2011. Those in the L+T group received both agents together for 52 weeks; those in the sequential treatment group received T for 12 weeks followed by a 6-week wash-out period, followed by lapatinib for 34 weeks; and those in the trastuzumab arm (the control arm) and the lapatinib arm each received treatment for 52 weeks. In 2011 the lapatinib arm was closed because of futility, and results for that arm are not included in this analysis.
Long-term follow up of participants continues, a large number of correlative studies are ongoing, and final results will be reported when all patients have been followed for at least 10 years, Dr. Moreno-Aspitia said.
The ALTTO trial was sponsored by GlaxoSmithKline and Novartis. Dr. Moreno-Aspitia reported having no disclosures.
AT ASCO 2017
Key clinical point:
Major finding: DFS differed slightly between lapatinib plus trastuzumab and trastuzumab alone (84% vs. 80%; HR, 0.80) among those with HER2+/HR-negative tumors but not among those with HER2+/HR+ tumors.
Data source: The phase III ALTTO trial of 8,381 patients.
Disclosures: The ALTTO trial was sponsored by GlaxoSmithKline and Novartis. Dr. Moreno-Aspitia reported having no disclosures.