User login
Selection of strategy for high-risk early RA remission induction hinges on safety
MADRID – Two-year results from the Care in early RA (CareRA) trial demonstrated the sustained effectiveness of a treat-to-target approach in patients with early rheumatoid arthritis at high risk for progression.
The percentage of patients who achieved clinical remission with one of three disease-modifying antirheumatic drug (DMARD) and glucocorticoid-containing regimens ranged from 60% to 65% at 1 year, and the percentage of those patients who were able to maintain their remission at all time points in year 2 ranged from 55% to 70%, none of which were significantly different from each other.

Ms. Stouten added that, according to international guidelines, achieving clinical remission means treating patients early, as soon as possible after the diagnosis of rheumatoid arthritis is made; intensively, with a DMARD, preferably methotrexate if not contraindicated, combined with short-term glucocorticoids; and to target, meaning treatment should be targeted at achieving remission or at least low disease activity in every patient.
The CareRA trial was a prospective, randomized, multicenter trial set up to see which of three methotrexate-based, steroid-containing intensive regimens would be best for inducing remission in patients with high-risk RA. The pragmatic trial was conducted in 13 Belgian rheumatology practices recruiting 400 patients, 300 of whom were designated as high risk for progression based on factors such as their antibody status and presence of joint erosions. CareRA trial investigators defined clinical remission as less than 2.6 on the 28-joint Disease Activity Score using C-reactive protein (DAS28-CRP).
The three regimens all contained a weekly 15-mg dose of methotrexate and prednisone 30 mg or 60 mg that was then tapered weekly after the first 6-7 weeks.
In the COBRA Classic regimen, methotrexate was partnered with sulfasalazine, given as a 2-g daily dose. Prednisone was initially given at a dose of 60 mg and then taped to 5.7 mg starting at week 7.
For the COBRA Slim regimen, just methotrexate and prednisone were used, with the latter started at a dose of 30 mg and then tapered to 5 mg starting at week 6.
Lastly, the COBRA Avant-Garde regimen saw methotrexate combined with leflunomide, 10 mg daily, and the same step-down prednisone regimen as COBRA Slim.
In the first year, treatment in each group was adjusted to achieve a target of low disease activity (DAS28-CRP of 3.2 or lower), with measurements taken every 3 months. The steroid component was stepped down further after 28 weeks and stopped altogether by 34 weeks. The aim was also to reduce the number of DMARDs used, such that everyone was on DMARD monotherapy if possible. In the second year, rheumatologists could treat patients at their own discretion, with adjustments to treatment made according to DAS28-CRP at visits every 3 months.
Ms. Stouten reported that all three of the intensive induction regimens “were very effective in our high-risk population and that they showed persistently high remission rates at year 2.”
The percentage of patients with a DAS28-CRP of less than 2.6 at 2 years was 65.3% for the COBRA Classic regimen, 73.5% for COBRA Slim, and 73.1% for COBRA Avant-Garde.
For inducing remission, however, she suggested that the COBRA Slim regimen might have the edge from a benefit-to-risk perspective.
A total of 60.2% of COBRA Slim patients were in remission at year 1, and 67.8% of them remained in remission throughout year 2. Also, fewer COBRA Slim patients needed biologic therapy, both overall (n = 11) and in the first year (n = 2), when compared with the other two regimens. However, in the COBRA Classic arm, 65.3% were in remission at year 1, and 54.7% of those patients maintained it throughout year 2, whereas in the COBRA Avant-Garde arm the rates were 61.3% at year 1, with 70.2% of those maintaining remission throughout year 2. A total of 18 patients in the COBRA Classic group started biologics, including 10 in the first year, compared with 15 in the COBRA Avant-Garde group, 7 of those in the first year.
“For maintaining remission, there were no statistically significant differences observed in remission rates at year 2 between treatment groups,” Ms. Stouten observed. “However, COBRA Avant-Garde had numerically better CDAI [clinical disease activity index] remission rates at year 2 [48.2% vs. 33.7% for COBRA Slim and 34.7% for COBRA Classic; P = .068].”
The total numbers of patients reporting adverse events related to treatment were lower with the COBRA Slim regimen (n = 164) than with COBRA Classic (n = 209) and COBRA Avant-Garde (n = 208). Fewer COBRA Slim patients also had to stop treatment (5 vs. 9 with COBRA Classic and 12 with COBRA Avant-Garde) or have interrupted treatment (12 vs. 17 and 19, respectively) because of adverse events.
Ms. Stouten had no personal disclosures. The study was supported by a Flemish governmental grant provided by IWT (Innovatie door Wetenschap en Technologie).
[email protected]
On Twitter @rheumnews1
MADRID – Two-year results from the Care in early RA (CareRA) trial demonstrated the sustained effectiveness of a treat-to-target approach in patients with early rheumatoid arthritis at high risk for progression.
The percentage of patients who achieved clinical remission with one of three disease-modifying antirheumatic drug (DMARD) and glucocorticoid-containing regimens ranged from 60% to 65% at 1 year, and the percentage of those patients who were able to maintain their remission at all time points in year 2 ranged from 55% to 70%, none of which were significantly different from each other.
Ms. Stouten added that, according to international guidelines, achieving clinical remission means treating patients early, as soon as possible after the diagnosis of rheumatoid arthritis is made; intensively, with a DMARD, preferably methotrexate if not contraindicated, combined with short-term glucocorticoids; and to target, meaning treatment should be targeted at achieving remission or at least low disease activity in every patient.
The CareRA trial was a prospective, randomized, multicenter trial set up to see which of three methotrexate-based, steroid-containing intensive regimens would be best for inducing remission in patients with high-risk RA. The pragmatic trial was conducted in 13 Belgian rheumatology practices recruiting 400 patients, 300 of whom were designated as high risk for progression based on factors such as their antibody status and presence of joint erosions. CareRA trial investigators defined clinical remission as less than 2.6 on the 28-joint Disease Activity Score using C-reactive protein (DAS28-CRP).
The three regimens all contained a weekly 15-mg dose of methotrexate and prednisone 30 mg or 60 mg that was then tapered weekly after the first 6-7 weeks.
In the COBRA Classic regimen, methotrexate was partnered with sulfasalazine, given as a 2-g daily dose. Prednisone was initially given at a dose of 60 mg and then taped to 5.7 mg starting at week 7.
For the COBRA Slim regimen, just methotrexate and prednisone were used, with the latter started at a dose of 30 mg and then tapered to 5 mg starting at week 6.
Lastly, the COBRA Avant-Garde regimen saw methotrexate combined with leflunomide, 10 mg daily, and the same step-down prednisone regimen as COBRA Slim.
In the first year, treatment in each group was adjusted to achieve a target of low disease activity (DAS28-CRP of 3.2 or lower), with measurements taken every 3 months. The steroid component was stepped down further after 28 weeks and stopped altogether by 34 weeks. The aim was also to reduce the number of DMARDs used, such that everyone was on DMARD monotherapy if possible. In the second year, rheumatologists could treat patients at their own discretion, with adjustments to treatment made according to DAS28-CRP at visits every 3 months.
Ms. Stouten reported that all three of the intensive induction regimens “were very effective in our high-risk population and that they showed persistently high remission rates at year 2.”
The percentage of patients with a DAS28-CRP of less than 2.6 at 2 years was 65.3% for the COBRA Classic regimen, 73.5% for COBRA Slim, and 73.1% for COBRA Avant-Garde.
For inducing remission, however, she suggested that the COBRA Slim regimen might have the edge from a benefit-to-risk perspective.
A total of 60.2% of COBRA Slim patients were in remission at year 1, and 67.8% of them remained in remission throughout year 2. Also, fewer COBRA Slim patients needed biologic therapy, both overall (n = 11) and in the first year (n = 2), when compared with the other two regimens. However, in the COBRA Classic arm, 65.3% were in remission at year 1, and 54.7% of those patients maintained it throughout year 2, whereas in the COBRA Avant-Garde arm the rates were 61.3% at year 1, with 70.2% of those maintaining remission throughout year 2. A total of 18 patients in the COBRA Classic group started biologics, including 10 in the first year, compared with 15 in the COBRA Avant-Garde group, 7 of those in the first year.
“For maintaining remission, there were no statistically significant differences observed in remission rates at year 2 between treatment groups,” Ms. Stouten observed. “However, COBRA Avant-Garde had numerically better CDAI [clinical disease activity index] remission rates at year 2 [48.2% vs. 33.7% for COBRA Slim and 34.7% for COBRA Classic; P = .068].”
The total numbers of patients reporting adverse events related to treatment were lower with the COBRA Slim regimen (n = 164) than with COBRA Classic (n = 209) and COBRA Avant-Garde (n = 208). Fewer COBRA Slim patients also had to stop treatment (5 vs. 9 with COBRA Classic and 12 with COBRA Avant-Garde) or have interrupted treatment (12 vs. 17 and 19, respectively) because of adverse events.
Ms. Stouten had no personal disclosures. The study was supported by a Flemish governmental grant provided by IWT (Innovatie door Wetenschap en Technologie).
[email protected]
On Twitter @rheumnews1
MADRID – Two-year results from the Care in early RA (CareRA) trial demonstrated the sustained effectiveness of a treat-to-target approach in patients with early rheumatoid arthritis at high risk for progression.
The percentage of patients who achieved clinical remission with one of three disease-modifying antirheumatic drug (DMARD) and glucocorticoid-containing regimens ranged from 60% to 65% at 1 year, and the percentage of those patients who were able to maintain their remission at all time points in year 2 ranged from 55% to 70%, none of which were significantly different from each other.
Ms. Stouten added that, according to international guidelines, achieving clinical remission means treating patients early, as soon as possible after the diagnosis of rheumatoid arthritis is made; intensively, with a DMARD, preferably methotrexate if not contraindicated, combined with short-term glucocorticoids; and to target, meaning treatment should be targeted at achieving remission or at least low disease activity in every patient.
The CareRA trial was a prospective, randomized, multicenter trial set up to see which of three methotrexate-based, steroid-containing intensive regimens would be best for inducing remission in patients with high-risk RA. The pragmatic trial was conducted in 13 Belgian rheumatology practices recruiting 400 patients, 300 of whom were designated as high risk for progression based on factors such as their antibody status and presence of joint erosions. CareRA trial investigators defined clinical remission as less than 2.6 on the 28-joint Disease Activity Score using C-reactive protein (DAS28-CRP).
The three regimens all contained a weekly 15-mg dose of methotrexate and prednisone 30 mg or 60 mg that was then tapered weekly after the first 6-7 weeks.
In the COBRA Classic regimen, methotrexate was partnered with sulfasalazine, given as a 2-g daily dose. Prednisone was initially given at a dose of 60 mg and then taped to 5.7 mg starting at week 7.
For the COBRA Slim regimen, just methotrexate and prednisone were used, with the latter started at a dose of 30 mg and then tapered to 5 mg starting at week 6.
Lastly, the COBRA Avant-Garde regimen saw methotrexate combined with leflunomide, 10 mg daily, and the same step-down prednisone regimen as COBRA Slim.
In the first year, treatment in each group was adjusted to achieve a target of low disease activity (DAS28-CRP of 3.2 or lower), with measurements taken every 3 months. The steroid component was stepped down further after 28 weeks and stopped altogether by 34 weeks. The aim was also to reduce the number of DMARDs used, such that everyone was on DMARD monotherapy if possible. In the second year, rheumatologists could treat patients at their own discretion, with adjustments to treatment made according to DAS28-CRP at visits every 3 months.
Ms. Stouten reported that all three of the intensive induction regimens “were very effective in our high-risk population and that they showed persistently high remission rates at year 2.”
The percentage of patients with a DAS28-CRP of less than 2.6 at 2 years was 65.3% for the COBRA Classic regimen, 73.5% for COBRA Slim, and 73.1% for COBRA Avant-Garde.
For inducing remission, however, she suggested that the COBRA Slim regimen might have the edge from a benefit-to-risk perspective.
A total of 60.2% of COBRA Slim patients were in remission at year 1, and 67.8% of them remained in remission throughout year 2. Also, fewer COBRA Slim patients needed biologic therapy, both overall (n = 11) and in the first year (n = 2), when compared with the other two regimens. However, in the COBRA Classic arm, 65.3% were in remission at year 1, and 54.7% of those patients maintained it throughout year 2, whereas in the COBRA Avant-Garde arm the rates were 61.3% at year 1, with 70.2% of those maintaining remission throughout year 2. A total of 18 patients in the COBRA Classic group started biologics, including 10 in the first year, compared with 15 in the COBRA Avant-Garde group, 7 of those in the first year.
“For maintaining remission, there were no statistically significant differences observed in remission rates at year 2 between treatment groups,” Ms. Stouten observed. “However, COBRA Avant-Garde had numerically better CDAI [clinical disease activity index] remission rates at year 2 [48.2% vs. 33.7% for COBRA Slim and 34.7% for COBRA Classic; P = .068].”
The total numbers of patients reporting adverse events related to treatment were lower with the COBRA Slim regimen (n = 164) than with COBRA Classic (n = 209) and COBRA Avant-Garde (n = 208). Fewer COBRA Slim patients also had to stop treatment (5 vs. 9 with COBRA Classic and 12 with COBRA Avant-Garde) or have interrupted treatment (12 vs. 17 and 19, respectively) because of adverse events.
Ms. Stouten had no personal disclosures. The study was supported by a Flemish governmental grant provided by IWT (Innovatie door Wetenschap en Technologie).
[email protected]
On Twitter @rheumnews1
AT THE EULAR 2017 CONGRESS
Key clinical point:
Major finding: The percentage of patients with a DAS28-CRP of less than 2.6 at 2 years was 73.5% for the COBRA Slim regimen, 73.1% for COBRA Avant-Garde, and 65.3% for COBRA Classic.
Data source: The Care in early RA (CareRA) trial, a prospective, randomized, multicenter trial of 379 patients with treatment-naive, early rheumatoid arthritis.
Disclosures: The presenter had no personal disclosures. The study was supported by a Flemish governmental grant provided by IWT (Innovatie door Wetenschap en Technologie).
Children with HIV benefit from double dose of PCV13 vaccine
, while children with kidney or lung disease may need only one dose, reported Sabelle Jallow, PhD, of the University of the Witwatersrand, Johannesburg, South Africa, and associates.
An open-label study was conducted at Chris Hani Baragwanath Academic Hospital (CHBAH) in Soweto, South Africa, to determine the immunogenicity of one and two doses of PCV13 in vaccine-naive children with HIV infection, kidney disease, or lung disease. Of the 112 children in the study, there were 50 HIV-infected children, 8 children with kidney disease, 9 with lung disease, and 45 HIV-uninfected control children with no chronic illness. The average age at enrollment was 62 months, 53% of participants were female, and 96% were of black African descent. At-risk children were given two doses of PCV13, 2 months apart, while control children received only one PCV13 dose (Vaccine. 2017. doi: 10.1016/j.vaccine.2017.06.081).
“In future studies, a larger spectrum of comorbidities should be included to determine the most cost-effective vaccination regimens particularly in low income countries,” the researchers noted.
, while children with kidney or lung disease may need only one dose, reported Sabelle Jallow, PhD, of the University of the Witwatersrand, Johannesburg, South Africa, and associates.
An open-label study was conducted at Chris Hani Baragwanath Academic Hospital (CHBAH) in Soweto, South Africa, to determine the immunogenicity of one and two doses of PCV13 in vaccine-naive children with HIV infection, kidney disease, or lung disease. Of the 112 children in the study, there were 50 HIV-infected children, 8 children with kidney disease, 9 with lung disease, and 45 HIV-uninfected control children with no chronic illness. The average age at enrollment was 62 months, 53% of participants were female, and 96% were of black African descent. At-risk children were given two doses of PCV13, 2 months apart, while control children received only one PCV13 dose (Vaccine. 2017. doi: 10.1016/j.vaccine.2017.06.081).
“In future studies, a larger spectrum of comorbidities should be included to determine the most cost-effective vaccination regimens particularly in low income countries,” the researchers noted.
, while children with kidney or lung disease may need only one dose, reported Sabelle Jallow, PhD, of the University of the Witwatersrand, Johannesburg, South Africa, and associates.
An open-label study was conducted at Chris Hani Baragwanath Academic Hospital (CHBAH) in Soweto, South Africa, to determine the immunogenicity of one and two doses of PCV13 in vaccine-naive children with HIV infection, kidney disease, or lung disease. Of the 112 children in the study, there were 50 HIV-infected children, 8 children with kidney disease, 9 with lung disease, and 45 HIV-uninfected control children with no chronic illness. The average age at enrollment was 62 months, 53% of participants were female, and 96% were of black African descent. At-risk children were given two doses of PCV13, 2 months apart, while control children received only one PCV13 dose (Vaccine. 2017. doi: 10.1016/j.vaccine.2017.06.081).
“In future studies, a larger spectrum of comorbidities should be included to determine the most cost-effective vaccination regimens particularly in low income countries,” the researchers noted.
FROM VACCINE
Watchman device for AF patients ineligible for oral anticoagulation gains support from 1-year registry outcomes
PARIS – Patients with atrial fibrillation at high stroke risk and a contraindication for oral anticoagulation experienced an 83% reduction in their risk of ischemic stroke and transient ischemic attack during their first year after receiving the Watchman left atrial appendage closure device backed by limited-duration dual-antiplatelet therapy, according to a report from the EWOLUTION registry.
Of 605 participants in the European registry who went on dual-antiplatelet treatment (DAPT) in conjunction with receiving the Watchman device, 39% discontinued DAPT within 3 months and 72% were off DAPT by 6 months. Yet the 1-year rate of ischemic stroke or TIA in the EWOLUTION group was just 1.8%, an 83% relative risk reduction compared with the expected 10.5% rate based on the participants’ mean CHA2DS2-VASc score of 4.6 in the absence of oral anticoagulation, Martin W. Bergmann, MD, said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“Obviously this isn’t a randomized trial. This is just reassuring data that we are going in the right direction in terms of efficacy,” said Dr. Bergmann of Cardiologicum Hamburg, a large German group practice.

However, the ESC guidelines were largely based on randomized trials of the Watchman versus oral anticoagulation, including PREVAIL and PROTECT-AF, showing noninferiority. The safety and efficacy of the device in warfarin-ineligible patients was less well studied at the time the guidelines were formulated. And in fact, such patients are excluded from the Food and Drug Administration’s approved indication, which is specifically for patients judged “suitable for warfarin.”
“This gap is now filled by EWOLUTION. This is a registry that’s as good as it gets. We have all the things in place that you need these days to be able to rely on the outcome data,” according to the cardiologist.
EWOLUTION is a prospective, multicenter, all-comers registry. The EWOLUTION population of AF patients on DAPT was high risk: 89% had a CHA2DS2-VASc score of 3 or more, 31% were at least 80 years old, the mean HAS-BLED score was 2.4, and oral anticoagulation was contraindicated in 84% of participants.
Eighty-seven percent of subjects underwent follow-up transesophageal echocardiography. The imaging study showed the Watchman effectively sealed the left atrial appendage in 99.2% of patients as defined by no leak greater than 5 mm. The echo exam also showed the presence of thrombus on the device at follow-up in 4% of patients, although only 1 of the 22 patients with device thrombus experienced a stroke.
“We can conclude two things from this which are in line with earlier studies. First, the rate of thrombus on the device is equal to the rate reported in the randomized controlled trials, which was also 4%, even if the patients were on warfarin for the first 45 days. And second, these thrombi are not related to stroke,” Dr. Bergmann said.
At the 1-year mark, 71% of patients had switched to a single antiplatelet agent, while 17% remained on DAPT, mainly because of comorbid coronary disease for which DAPT is indicated. Seven percent of patients were on no antithrombotic medications. The remaining 5% were transiently on warfarin or a novel oral anticoagulant.
The 1-year cumulative rate of ischemic stroke or TIA was 1.8%, with no instances of systemic embolism. Of note, there were no hemorrhagic strokes. And of the 11 cases of ischemic stroke, none were fatal and only one was disabling.
“This is a sign that comes also from the PREVAIL trial, that if you have a stroke while on left atrial appendage–closure therapy, most of the time it’s not disabling. It’s much less severe on the modified Rankin Scale than if you’re on oral anticoagulation,” said Dr. Bergmann.
The 1.4% rate of ischemic stroke at 1 year in Watchman recipients represents an 81% reduction in risk compared with the expected 7.5% rate in patients with similar CHA2DS2-VASc scores not on oral anticoagulation. This level of stroke risk reduction is similar to that seen in the pivotal ARISTOTLE trial of apixaban (Eliquis) in a high-risk AF population (Lancet. 2012 Nov 17;380[9855]:1749-58).
Major bleeding occurred in 2.5% of patients. The rate of fatal bleeding was 0.5%. To put that in perspective, the 2.5% major bleeding rate was 52% lower than would be expected based upon similar HAS-BLED scores in patients on warfarin. Still, 2.5% is unacceptably high.
“The major serious adverse event is not pericardial effusion or late device embolization, it’s major bleeding occurring during the time the patient is on DAPT, mostly within the first 3 months. So I think we have to do something about this,” he said.
One possibility worthy of formal study is 3 months of periprocedural NOAC monotherapy. “Maybe even low-dose therapy, like 75 mg of dabigatran [Pradaxa] twice daily. We have an antidote that works nicely [idarucizumab, Praxbind] so I think maybe this is the way to go,” Dr. Bergmann observed.
The ongoing EWOLUTION registry is sponsored by Boston Scientific. Dr. Bergmann is a consultant to that company as well as Bayer AG, Daiichi Sankyo, Eli Lilly, and St. Jude Medical.
PARIS – Patients with atrial fibrillation at high stroke risk and a contraindication for oral anticoagulation experienced an 83% reduction in their risk of ischemic stroke and transient ischemic attack during their first year after receiving the Watchman left atrial appendage closure device backed by limited-duration dual-antiplatelet therapy, according to a report from the EWOLUTION registry.
Of 605 participants in the European registry who went on dual-antiplatelet treatment (DAPT) in conjunction with receiving the Watchman device, 39% discontinued DAPT within 3 months and 72% were off DAPT by 6 months. Yet the 1-year rate of ischemic stroke or TIA in the EWOLUTION group was just 1.8%, an 83% relative risk reduction compared with the expected 10.5% rate based on the participants’ mean CHA2DS2-VASc score of 4.6 in the absence of oral anticoagulation, Martin W. Bergmann, MD, said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“Obviously this isn’t a randomized trial. This is just reassuring data that we are going in the right direction in terms of efficacy,” said Dr. Bergmann of Cardiologicum Hamburg, a large German group practice.
However, the ESC guidelines were largely based on randomized trials of the Watchman versus oral anticoagulation, including PREVAIL and PROTECT-AF, showing noninferiority. The safety and efficacy of the device in warfarin-ineligible patients was less well studied at the time the guidelines were formulated. And in fact, such patients are excluded from the Food and Drug Administration’s approved indication, which is specifically for patients judged “suitable for warfarin.”
“This gap is now filled by EWOLUTION. This is a registry that’s as good as it gets. We have all the things in place that you need these days to be able to rely on the outcome data,” according to the cardiologist.
EWOLUTION is a prospective, multicenter, all-comers registry. The EWOLUTION population of AF patients on DAPT was high risk: 89% had a CHA2DS2-VASc score of 3 or more, 31% were at least 80 years old, the mean HAS-BLED score was 2.4, and oral anticoagulation was contraindicated in 84% of participants.
Eighty-seven percent of subjects underwent follow-up transesophageal echocardiography. The imaging study showed the Watchman effectively sealed the left atrial appendage in 99.2% of patients as defined by no leak greater than 5 mm. The echo exam also showed the presence of thrombus on the device at follow-up in 4% of patients, although only 1 of the 22 patients with device thrombus experienced a stroke.
“We can conclude two things from this which are in line with earlier studies. First, the rate of thrombus on the device is equal to the rate reported in the randomized controlled trials, which was also 4%, even if the patients were on warfarin for the first 45 days. And second, these thrombi are not related to stroke,” Dr. Bergmann said.
At the 1-year mark, 71% of patients had switched to a single antiplatelet agent, while 17% remained on DAPT, mainly because of comorbid coronary disease for which DAPT is indicated. Seven percent of patients were on no antithrombotic medications. The remaining 5% were transiently on warfarin or a novel oral anticoagulant.
The 1-year cumulative rate of ischemic stroke or TIA was 1.8%, with no instances of systemic embolism. Of note, there were no hemorrhagic strokes. And of the 11 cases of ischemic stroke, none were fatal and only one was disabling.
“This is a sign that comes also from the PREVAIL trial, that if you have a stroke while on left atrial appendage–closure therapy, most of the time it’s not disabling. It’s much less severe on the modified Rankin Scale than if you’re on oral anticoagulation,” said Dr. Bergmann.
The 1.4% rate of ischemic stroke at 1 year in Watchman recipients represents an 81% reduction in risk compared with the expected 7.5% rate in patients with similar CHA2DS2-VASc scores not on oral anticoagulation. This level of stroke risk reduction is similar to that seen in the pivotal ARISTOTLE trial of apixaban (Eliquis) in a high-risk AF population (Lancet. 2012 Nov 17;380[9855]:1749-58).
Major bleeding occurred in 2.5% of patients. The rate of fatal bleeding was 0.5%. To put that in perspective, the 2.5% major bleeding rate was 52% lower than would be expected based upon similar HAS-BLED scores in patients on warfarin. Still, 2.5% is unacceptably high.
“The major serious adverse event is not pericardial effusion or late device embolization, it’s major bleeding occurring during the time the patient is on DAPT, mostly within the first 3 months. So I think we have to do something about this,” he said.
One possibility worthy of formal study is 3 months of periprocedural NOAC monotherapy. “Maybe even low-dose therapy, like 75 mg of dabigatran [Pradaxa] twice daily. We have an antidote that works nicely [idarucizumab, Praxbind] so I think maybe this is the way to go,” Dr. Bergmann observed.
The ongoing EWOLUTION registry is sponsored by Boston Scientific. Dr. Bergmann is a consultant to that company as well as Bayer AG, Daiichi Sankyo, Eli Lilly, and St. Jude Medical.
PARIS – Patients with atrial fibrillation at high stroke risk and a contraindication for oral anticoagulation experienced an 83% reduction in their risk of ischemic stroke and transient ischemic attack during their first year after receiving the Watchman left atrial appendage closure device backed by limited-duration dual-antiplatelet therapy, according to a report from the EWOLUTION registry.
Of 605 participants in the European registry who went on dual-antiplatelet treatment (DAPT) in conjunction with receiving the Watchman device, 39% discontinued DAPT within 3 months and 72% were off DAPT by 6 months. Yet the 1-year rate of ischemic stroke or TIA in the EWOLUTION group was just 1.8%, an 83% relative risk reduction compared with the expected 10.5% rate based on the participants’ mean CHA2DS2-VASc score of 4.6 in the absence of oral anticoagulation, Martin W. Bergmann, MD, said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“Obviously this isn’t a randomized trial. This is just reassuring data that we are going in the right direction in terms of efficacy,” said Dr. Bergmann of Cardiologicum Hamburg, a large German group practice.
However, the ESC guidelines were largely based on randomized trials of the Watchman versus oral anticoagulation, including PREVAIL and PROTECT-AF, showing noninferiority. The safety and efficacy of the device in warfarin-ineligible patients was less well studied at the time the guidelines were formulated. And in fact, such patients are excluded from the Food and Drug Administration’s approved indication, which is specifically for patients judged “suitable for warfarin.”
“This gap is now filled by EWOLUTION. This is a registry that’s as good as it gets. We have all the things in place that you need these days to be able to rely on the outcome data,” according to the cardiologist.
EWOLUTION is a prospective, multicenter, all-comers registry. The EWOLUTION population of AF patients on DAPT was high risk: 89% had a CHA2DS2-VASc score of 3 or more, 31% were at least 80 years old, the mean HAS-BLED score was 2.4, and oral anticoagulation was contraindicated in 84% of participants.
Eighty-seven percent of subjects underwent follow-up transesophageal echocardiography. The imaging study showed the Watchman effectively sealed the left atrial appendage in 99.2% of patients as defined by no leak greater than 5 mm. The echo exam also showed the presence of thrombus on the device at follow-up in 4% of patients, although only 1 of the 22 patients with device thrombus experienced a stroke.
“We can conclude two things from this which are in line with earlier studies. First, the rate of thrombus on the device is equal to the rate reported in the randomized controlled trials, which was also 4%, even if the patients were on warfarin for the first 45 days. And second, these thrombi are not related to stroke,” Dr. Bergmann said.
At the 1-year mark, 71% of patients had switched to a single antiplatelet agent, while 17% remained on DAPT, mainly because of comorbid coronary disease for which DAPT is indicated. Seven percent of patients were on no antithrombotic medications. The remaining 5% were transiently on warfarin or a novel oral anticoagulant.
The 1-year cumulative rate of ischemic stroke or TIA was 1.8%, with no instances of systemic embolism. Of note, there were no hemorrhagic strokes. And of the 11 cases of ischemic stroke, none were fatal and only one was disabling.
“This is a sign that comes also from the PREVAIL trial, that if you have a stroke while on left atrial appendage–closure therapy, most of the time it’s not disabling. It’s much less severe on the modified Rankin Scale than if you’re on oral anticoagulation,” said Dr. Bergmann.
The 1.4% rate of ischemic stroke at 1 year in Watchman recipients represents an 81% reduction in risk compared with the expected 7.5% rate in patients with similar CHA2DS2-VASc scores not on oral anticoagulation. This level of stroke risk reduction is similar to that seen in the pivotal ARISTOTLE trial of apixaban (Eliquis) in a high-risk AF population (Lancet. 2012 Nov 17;380[9855]:1749-58).
Major bleeding occurred in 2.5% of patients. The rate of fatal bleeding was 0.5%. To put that in perspective, the 2.5% major bleeding rate was 52% lower than would be expected based upon similar HAS-BLED scores in patients on warfarin. Still, 2.5% is unacceptably high.
“The major serious adverse event is not pericardial effusion or late device embolization, it’s major bleeding occurring during the time the patient is on DAPT, mostly within the first 3 months. So I think we have to do something about this,” he said.
One possibility worthy of formal study is 3 months of periprocedural NOAC monotherapy. “Maybe even low-dose therapy, like 75 mg of dabigatran [Pradaxa] twice daily. We have an antidote that works nicely [idarucizumab, Praxbind] so I think maybe this is the way to go,” Dr. Bergmann observed.
The ongoing EWOLUTION registry is sponsored by Boston Scientific. Dr. Bergmann is a consultant to that company as well as Bayer AG, Daiichi Sankyo, Eli Lilly, and St. Jude Medical.
AT EUROPCR
Key clinical point:
Major finding: Patients with AF at high stroke risk and ineligible for oral anticoagulation experienced an 81% reduction in their expected risk of ischemic stroke during their first year of LAA closure with the Watchman device backed by limited-duration dual-antiplatelet therapy
Data source: A prospective, multicenter, single-arm registry that includes 605 patients with AF who underwent left atrial appendage closure with the WATCHMAN device supported by limited-duration dual-antiplatelet therapy.
Disclosures: The ongoing EWOLUTION registry is sponsored by Boston Scientific. The presenter is a consultant to that company and several others.
Statins linked to fewer deaths, slightly higher HbA1c in T2DM
SAN DIEGO – Findings from a study of 12,725 new insulin users with type 2 diabetes mellitus (T2DM) show that those who did not take statins were slightly better able to control their blood sugar, but those who used the cholesterol-lowering drugs lived longer and had fewer cardiac events.
“It is clear that, in this high-risk population, the benefits of statins on cardiovascular outcomes outweigh the small adverse metabolic effects on glycemic control,” study lead author Uche Anyanwagu, MBBS, MSc, a graduate student and research fellow at the University of Nottingham (England), said in an interview about his data presented in a poster at the annual scientific sessions of the American Diabetes Association.

However, “there remain great concerns about statins and their modest adverse effects on glucose and insulin metabolism in increasing the risk of new-onset diabetes or worsening glycemic control, especially in higher doses and with the more potent statins,” Dr. Anyanwagu said. “Very little is known about the relationship between statin use and glycemic control in patients with established T2DM.”
The study authors retrospectively analyzed medical records of 12,725 new insulin users with T2DM from a British primary care database. “The commencement of insulin represents a group of patients with T2DM with longer disease duration and more complex needs, many of whom have other comorbid illnesses,” Dr. Anyanwagu said.
The average age of the subjects was 58.6 years (standard deviation, 13.8), and 50% were female (P less than 0.001 for both). Their average HbA1c level was 8.7 (SD, 1.8; P = .556), and 63% were obese.
The numbers of statin users and nonstatin users were 10,682 and 2,043, respectively. Researchers found that the statin users performed better in measures of all-cause mortality, nonfatal stroke, and a composite outcome measure but not in acute myocardial infarction.
In all-cause mortality, the absolute rate over 5 years was 9.5 deaths per 1,000 person years (95% confidence interval, 8.7-10.5) for statin users and 24.9 (95% CI, 21.5-28.9) for nonusers. After adjustment for age, gender, duration of insulin use, albumin, glomerular filtration rate, lipid profile, and coronary heart disease, the hazard ratio was 1.89 (95% CI, 1.51-2.37) for nonusers, compared with a reference of 1 for users. (P less than .0001).
The absolute rate for a composite outcome – encompassing measures of all-cause mortality, nonfatal acute myocardial infarction, and nonfatal stroke – was 20.7 (95% CI, 19.3-22.1) for statin users and 30.9 (95% CI , 27-35.3) for nonusers (P less than .0001).
As for HbA1c levels, at 12 months, they’d fallen by an average of 0.29% in the statin group and 0.37% in the nonuser group (P = .021). At 36 months, there was a smaller difference (–0.31% vs. –0.35%, respectively), and it wasn’t statistically significant (P = .344).
The study was funded by the University of Nottingham. (England). Dr. Anyanwagu reports no relevant disclosures.
SAN DIEGO – Findings from a study of 12,725 new insulin users with type 2 diabetes mellitus (T2DM) show that those who did not take statins were slightly better able to control their blood sugar, but those who used the cholesterol-lowering drugs lived longer and had fewer cardiac events.
“It is clear that, in this high-risk population, the benefits of statins on cardiovascular outcomes outweigh the small adverse metabolic effects on glycemic control,” study lead author Uche Anyanwagu, MBBS, MSc, a graduate student and research fellow at the University of Nottingham (England), said in an interview about his data presented in a poster at the annual scientific sessions of the American Diabetes Association.
However, “there remain great concerns about statins and their modest adverse effects on glucose and insulin metabolism in increasing the risk of new-onset diabetes or worsening glycemic control, especially in higher doses and with the more potent statins,” Dr. Anyanwagu said. “Very little is known about the relationship between statin use and glycemic control in patients with established T2DM.”
The study authors retrospectively analyzed medical records of 12,725 new insulin users with T2DM from a British primary care database. “The commencement of insulin represents a group of patients with T2DM with longer disease duration and more complex needs, many of whom have other comorbid illnesses,” Dr. Anyanwagu said.
The average age of the subjects was 58.6 years (standard deviation, 13.8), and 50% were female (P less than 0.001 for both). Their average HbA1c level was 8.7 (SD, 1.8; P = .556), and 63% were obese.
The numbers of statin users and nonstatin users were 10,682 and 2,043, respectively. Researchers found that the statin users performed better in measures of all-cause mortality, nonfatal stroke, and a composite outcome measure but not in acute myocardial infarction.
In all-cause mortality, the absolute rate over 5 years was 9.5 deaths per 1,000 person years (95% confidence interval, 8.7-10.5) for statin users and 24.9 (95% CI, 21.5-28.9) for nonusers. After adjustment for age, gender, duration of insulin use, albumin, glomerular filtration rate, lipid profile, and coronary heart disease, the hazard ratio was 1.89 (95% CI, 1.51-2.37) for nonusers, compared with a reference of 1 for users. (P less than .0001).
The absolute rate for a composite outcome – encompassing measures of all-cause mortality, nonfatal acute myocardial infarction, and nonfatal stroke – was 20.7 (95% CI, 19.3-22.1) for statin users and 30.9 (95% CI , 27-35.3) for nonusers (P less than .0001).
As for HbA1c levels, at 12 months, they’d fallen by an average of 0.29% in the statin group and 0.37% in the nonuser group (P = .021). At 36 months, there was a smaller difference (–0.31% vs. –0.35%, respectively), and it wasn’t statistically significant (P = .344).
The study was funded by the University of Nottingham. (England). Dr. Anyanwagu reports no relevant disclosures.
SAN DIEGO – Findings from a study of 12,725 new insulin users with type 2 diabetes mellitus (T2DM) show that those who did not take statins were slightly better able to control their blood sugar, but those who used the cholesterol-lowering drugs lived longer and had fewer cardiac events.
“It is clear that, in this high-risk population, the benefits of statins on cardiovascular outcomes outweigh the small adverse metabolic effects on glycemic control,” study lead author Uche Anyanwagu, MBBS, MSc, a graduate student and research fellow at the University of Nottingham (England), said in an interview about his data presented in a poster at the annual scientific sessions of the American Diabetes Association.
However, “there remain great concerns about statins and their modest adverse effects on glucose and insulin metabolism in increasing the risk of new-onset diabetes or worsening glycemic control, especially in higher doses and with the more potent statins,” Dr. Anyanwagu said. “Very little is known about the relationship between statin use and glycemic control in patients with established T2DM.”
The study authors retrospectively analyzed medical records of 12,725 new insulin users with T2DM from a British primary care database. “The commencement of insulin represents a group of patients with T2DM with longer disease duration and more complex needs, many of whom have other comorbid illnesses,” Dr. Anyanwagu said.
The average age of the subjects was 58.6 years (standard deviation, 13.8), and 50% were female (P less than 0.001 for both). Their average HbA1c level was 8.7 (SD, 1.8; P = .556), and 63% were obese.
The numbers of statin users and nonstatin users were 10,682 and 2,043, respectively. Researchers found that the statin users performed better in measures of all-cause mortality, nonfatal stroke, and a composite outcome measure but not in acute myocardial infarction.
In all-cause mortality, the absolute rate over 5 years was 9.5 deaths per 1,000 person years (95% confidence interval, 8.7-10.5) for statin users and 24.9 (95% CI, 21.5-28.9) for nonusers. After adjustment for age, gender, duration of insulin use, albumin, glomerular filtration rate, lipid profile, and coronary heart disease, the hazard ratio was 1.89 (95% CI, 1.51-2.37) for nonusers, compared with a reference of 1 for users. (P less than .0001).
The absolute rate for a composite outcome – encompassing measures of all-cause mortality, nonfatal acute myocardial infarction, and nonfatal stroke – was 20.7 (95% CI, 19.3-22.1) for statin users and 30.9 (95% CI , 27-35.3) for nonusers (P less than .0001).
As for HbA1c levels, at 12 months, they’d fallen by an average of 0.29% in the statin group and 0.37% in the nonuser group (P = .021). At 36 months, there was a smaller difference (–0.31% vs. –0.35%, respectively), and it wasn’t statistically significant (P = .344).
The study was funded by the University of Nottingham. (England). Dr. Anyanwagu reports no relevant disclosures.
AT THE ADA ANNUAL SCIENTIFIC SESSIONS
Key clinical point: In new insulin users with T2DM, statin use appears to slightly lower the decline in HbA1c, compared with nonuse, but the drug improved all-cause mortality.
Major finding: The adjusted hazard ratio of 5-year all-cause mortality was 1.89 in nonstatin users, vs. a reference of 1 for statin users. At 12 months, HbA1c fell by an average of 0.29% in the statin group and 0.37% in the nonuser group, but the difference wasn’t statistically significant at 36 months.
Data source: A retrospective study of 10,682 stain users and 2,043 nonusers, all of whom were new insulin users, from a British primary care database.
Disclosures: The study was funded by the University of Nottingham (England).
Drug combo improves RV contractility in scleroderma-PAH
A combination of ambrisentan (Letairis) and tadalafil (Cialis) improves regional and global right ventricular contractility in patients with scleroderma-associated pulmonary arterial hypertension, according to an open-label investigation of 23 patients.
The project was a follow-up to a previous report showing that the upfront combination – tadalafil 40 mg and ambrisentan 10 mg oral once daily – improved hemodynamics, right ventricular (RV) structure and function, and functional status in treatment-naive patients after 36 weeks and “may represent a very effective therapy for this patient population” (Am J Respir Crit Care Med. 2015 Nov 1;192(9):1102-10).

At baseline, the subjects had normal left ventricular (LV) size and function, with borderline left atrial enlargement and mild LV diastolic dysfunction. Their right heart chambers were significantly dilated, with RV hypertrophy. Conventional RV function parameters – tricuspid annular systolic plane excursion (TAPSE) and fractional area change (FAC) – were impaired. RV systolic pressure (RVSP) was severely elevated. There was also a marked reduction of global RV longitudinal systolic strain (RVLSS), compared with normal values mainly because of a reduction in midventricular and apical RVLSS, with relative hyperkinesis of basal RVLSS
After 36 weeks of treatment, right heart chamber sizes were significantly reduced. There was also a decrease in RV free wall thickness, which coincided with a significant reduction in RV mass on cardiac MRI. TAPSE, FAC, and global RVLSS improved significantly, and RVSP decreased significantly. LV end-diastolic and end-systolic diameters and volumes increased significantly.
The changes “may represent transition from maladaptive RV remodeling ... to a more physiological and adaptive RV remodeling;” however, “the effects of treatment should be interpreted with caution, as this was an open-label study without a placebo or a single-drug control group,” said investigators led by Valentina Mercurio, MD, a postdoc fellow at Johns Hopkins University, Baltimore.
“It is conceivable that a heterogeneous RVLSS pattern exists in [scleroderma] patients with longitudinal hyperkinetic basal segment as the predominant vector of contraction early in the disease course. As PAH develops, the ability of the basal segment to compensate decreases, and RV failure ensues, suggesting a ‘two-hit’ hypothesis, in which a preexisting RV contractile dysfunction may predispose to further RV impairment when a second insult (PAH development) occurs,” they said.
Subjects were about 60 years old on average, and most were women. The majority shifted from World Health Organization PAH functional class 3 to 2 during the original trial. Mean 6 minute walk tests increased from 341 m to 401 m.
Gilead and United Therapeutics provided the ambrisentan and tadalafil. Dr. Mercurio reported funding from both companies and Merck. The original study was sponsored by United Therapeutics.

A combination of ambrisentan (Letairis) and tadalafil (Cialis) improves regional and global right ventricular contractility in patients with scleroderma-associated pulmonary arterial hypertension, according to an open-label investigation of 23 patients.
The project was a follow-up to a previous report showing that the upfront combination – tadalafil 40 mg and ambrisentan 10 mg oral once daily – improved hemodynamics, right ventricular (RV) structure and function, and functional status in treatment-naive patients after 36 weeks and “may represent a very effective therapy for this patient population” (Am J Respir Crit Care Med. 2015 Nov 1;192(9):1102-10).
At baseline, the subjects had normal left ventricular (LV) size and function, with borderline left atrial enlargement and mild LV diastolic dysfunction. Their right heart chambers were significantly dilated, with RV hypertrophy. Conventional RV function parameters – tricuspid annular systolic plane excursion (TAPSE) and fractional area change (FAC) – were impaired. RV systolic pressure (RVSP) was severely elevated. There was also a marked reduction of global RV longitudinal systolic strain (RVLSS), compared with normal values mainly because of a reduction in midventricular and apical RVLSS, with relative hyperkinesis of basal RVLSS
After 36 weeks of treatment, right heart chamber sizes were significantly reduced. There was also a decrease in RV free wall thickness, which coincided with a significant reduction in RV mass on cardiac MRI. TAPSE, FAC, and global RVLSS improved significantly, and RVSP decreased significantly. LV end-diastolic and end-systolic diameters and volumes increased significantly.
The changes “may represent transition from maladaptive RV remodeling ... to a more physiological and adaptive RV remodeling;” however, “the effects of treatment should be interpreted with caution, as this was an open-label study without a placebo or a single-drug control group,” said investigators led by Valentina Mercurio, MD, a postdoc fellow at Johns Hopkins University, Baltimore.
“It is conceivable that a heterogeneous RVLSS pattern exists in [scleroderma] patients with longitudinal hyperkinetic basal segment as the predominant vector of contraction early in the disease course. As PAH develops, the ability of the basal segment to compensate decreases, and RV failure ensues, suggesting a ‘two-hit’ hypothesis, in which a preexisting RV contractile dysfunction may predispose to further RV impairment when a second insult (PAH development) occurs,” they said.
Subjects were about 60 years old on average, and most were women. The majority shifted from World Health Organization PAH functional class 3 to 2 during the original trial. Mean 6 minute walk tests increased from 341 m to 401 m.
Gilead and United Therapeutics provided the ambrisentan and tadalafil. Dr. Mercurio reported funding from both companies and Merck. The original study was sponsored by United Therapeutics.
A combination of ambrisentan (Letairis) and tadalafil (Cialis) improves regional and global right ventricular contractility in patients with scleroderma-associated pulmonary arterial hypertension, according to an open-label investigation of 23 patients.
The project was a follow-up to a previous report showing that the upfront combination – tadalafil 40 mg and ambrisentan 10 mg oral once daily – improved hemodynamics, right ventricular (RV) structure and function, and functional status in treatment-naive patients after 36 weeks and “may represent a very effective therapy for this patient population” (Am J Respir Crit Care Med. 2015 Nov 1;192(9):1102-10).
At baseline, the subjects had normal left ventricular (LV) size and function, with borderline left atrial enlargement and mild LV diastolic dysfunction. Their right heart chambers were significantly dilated, with RV hypertrophy. Conventional RV function parameters – tricuspid annular systolic plane excursion (TAPSE) and fractional area change (FAC) – were impaired. RV systolic pressure (RVSP) was severely elevated. There was also a marked reduction of global RV longitudinal systolic strain (RVLSS), compared with normal values mainly because of a reduction in midventricular and apical RVLSS, with relative hyperkinesis of basal RVLSS
After 36 weeks of treatment, right heart chamber sizes were significantly reduced. There was also a decrease in RV free wall thickness, which coincided with a significant reduction in RV mass on cardiac MRI. TAPSE, FAC, and global RVLSS improved significantly, and RVSP decreased significantly. LV end-diastolic and end-systolic diameters and volumes increased significantly.
The changes “may represent transition from maladaptive RV remodeling ... to a more physiological and adaptive RV remodeling;” however, “the effects of treatment should be interpreted with caution, as this was an open-label study without a placebo or a single-drug control group,” said investigators led by Valentina Mercurio, MD, a postdoc fellow at Johns Hopkins University, Baltimore.
“It is conceivable that a heterogeneous RVLSS pattern exists in [scleroderma] patients with longitudinal hyperkinetic basal segment as the predominant vector of contraction early in the disease course. As PAH develops, the ability of the basal segment to compensate decreases, and RV failure ensues, suggesting a ‘two-hit’ hypothesis, in which a preexisting RV contractile dysfunction may predispose to further RV impairment when a second insult (PAH development) occurs,” they said.
Subjects were about 60 years old on average, and most were women. The majority shifted from World Health Organization PAH functional class 3 to 2 during the original trial. Mean 6 minute walk tests increased from 341 m to 401 m.
Gilead and United Therapeutics provided the ambrisentan and tadalafil. Dr. Mercurio reported funding from both companies and Merck. The original study was sponsored by United Therapeutics.
FROM THE AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Key clinical point:
Major finding: After 36 weeks of treatment, TAPSE, FAC, and global RVLSS improved significantly, and RV systolic pressure decreased significantly.
Data source: Cardiac imaging of 23 patients.
Disclosures: Gilead and United Therapeutics provided the ambrisentan and tadalafil. The lead investigator reported funding from both companies and Merck. The original study was sponsored by United Therapeutics.
ANCA-associated vasculitis appears to increase risk of stroke, death
MADRID – Small-vessel vasculitis associated with antineutrophil cytoplasmic autoantibodies (ANCAs) appears to increase the risk of stroke and overall mortality, results of a French retrospective study suggest.
Patients with ANCA-associated vasculitis (AAV) were twice as likely as those without to experience a stroke over 7.5 years, Grégory Pugnet, MD, reported at the European Congress of Rheumatology. Their all-cause mortality was also significantly higher, with 30% of the deaths attributed to cardiovascular causes, said Dr. Pugnet of the Internal Medicine Service at Purpan Hospital in Toulouse, France.
“We think this [shows that it] is very important to monitor [these patients] and to be vigilant in our search for cardiovascular complications and cardiovascular risk factors in this population,” he said.
Dr. Pugnet and his colleagues conducted a retrospective study of 125 patients with AAV who were diagnosed in a teaching hospital between 1981 and 2015. He compared cardiovascular outcomes and mortality between this cohort and two French regional registries: the Midi-Pyrénées County Mortality and Acute Myocardial Infarction Registry and the Dijon Stroke Registry. Outcomes were the date of first acute myocardial infarction, date of first stroke, and date of death; the mean follow-up was about 90 months.
Of the 125 patients with AAV, 99 had granulomatosis with polyangiitis, and 26 had microscopic polyangiitis. Preexisting cardiovascular disease was present in 23. Patients were a mean of 61 years old. Hypertension, peripheral artery disease, and coronary artery disease were all more common among those with cardiovascular disease. These patients were also more likely to smoke.
Over the follow-up period, there were 10 acute myocardial infarctions for an incidence of 8.5 per 1,000 person-years. The MI incidence in the Midi-Pyrénées registry was 2.2 per 1,000 person-years, which was a significant difference in an unadjusted analysis. But after adjusting for age, AAV patients were not significantly more likely to experience a heart attack than were those in the registry.
There were nine strokes during the follow-up period for an incidence of 10.2 per 1,000 person-years. After adjusting for age, this was more than three times higher than the rate of 1.9 per 1,000 person-year in the Dijon Stroke Registry – a significant difference.
A total of 22 AAV patients died during the follow-up period, translating to a mortality of 22.5 per 1,000 person-years. Mortality in the stroke registry was 1.9 per 1,000 person-years. An age-adjusted analysis found that AAV patients were about 1.6 times more likely to die than were those in the Midi-Pyrénées registry.
A multivariate regression analysis identified some factors that were independently associated with the outcomes. Smoking almost quadrupled the risk of having any cardiovascular event (hazard ratio, 3.7), and having had a plasma exchange tripled it (HR, 2.9). Smoking and a history of coronary artery disease were significant risk factors for myocardial infarction (HRs of 8.8 and 10.3, respectively). Dr. Pugnet and his associates didn’t find any significant independent risk factors for stroke. Age was not independently associated with any of the outcomes.
Dr. Pugnet reported receiving travel support from AbbVie and Actelion, fees for serving on an advisory board from Grifols, and lecture fees from AbbVie.
[email protected]
On Twitter @alz_gal
MADRID – Small-vessel vasculitis associated with antineutrophil cytoplasmic autoantibodies (ANCAs) appears to increase the risk of stroke and overall mortality, results of a French retrospective study suggest.
Patients with ANCA-associated vasculitis (AAV) were twice as likely as those without to experience a stroke over 7.5 years, Grégory Pugnet, MD, reported at the European Congress of Rheumatology. Their all-cause mortality was also significantly higher, with 30% of the deaths attributed to cardiovascular causes, said Dr. Pugnet of the Internal Medicine Service at Purpan Hospital in Toulouse, France.
“We think this [shows that it] is very important to monitor [these patients] and to be vigilant in our search for cardiovascular complications and cardiovascular risk factors in this population,” he said.
Dr. Pugnet and his colleagues conducted a retrospective study of 125 patients with AAV who were diagnosed in a teaching hospital between 1981 and 2015. He compared cardiovascular outcomes and mortality between this cohort and two French regional registries: the Midi-Pyrénées County Mortality and Acute Myocardial Infarction Registry and the Dijon Stroke Registry. Outcomes were the date of first acute myocardial infarction, date of first stroke, and date of death; the mean follow-up was about 90 months.
Of the 125 patients with AAV, 99 had granulomatosis with polyangiitis, and 26 had microscopic polyangiitis. Preexisting cardiovascular disease was present in 23. Patients were a mean of 61 years old. Hypertension, peripheral artery disease, and coronary artery disease were all more common among those with cardiovascular disease. These patients were also more likely to smoke.
Over the follow-up period, there were 10 acute myocardial infarctions for an incidence of 8.5 per 1,000 person-years. The MI incidence in the Midi-Pyrénées registry was 2.2 per 1,000 person-years, which was a significant difference in an unadjusted analysis. But after adjusting for age, AAV patients were not significantly more likely to experience a heart attack than were those in the registry.
There were nine strokes during the follow-up period for an incidence of 10.2 per 1,000 person-years. After adjusting for age, this was more than three times higher than the rate of 1.9 per 1,000 person-year in the Dijon Stroke Registry – a significant difference.
A total of 22 AAV patients died during the follow-up period, translating to a mortality of 22.5 per 1,000 person-years. Mortality in the stroke registry was 1.9 per 1,000 person-years. An age-adjusted analysis found that AAV patients were about 1.6 times more likely to die than were those in the Midi-Pyrénées registry.
A multivariate regression analysis identified some factors that were independently associated with the outcomes. Smoking almost quadrupled the risk of having any cardiovascular event (hazard ratio, 3.7), and having had a plasma exchange tripled it (HR, 2.9). Smoking and a history of coronary artery disease were significant risk factors for myocardial infarction (HRs of 8.8 and 10.3, respectively). Dr. Pugnet and his associates didn’t find any significant independent risk factors for stroke. Age was not independently associated with any of the outcomes.
Dr. Pugnet reported receiving travel support from AbbVie and Actelion, fees for serving on an advisory board from Grifols, and lecture fees from AbbVie.
[email protected]
On Twitter @alz_gal
MADRID – Small-vessel vasculitis associated with antineutrophil cytoplasmic autoantibodies (ANCAs) appears to increase the risk of stroke and overall mortality, results of a French retrospective study suggest.
Patients with ANCA-associated vasculitis (AAV) were twice as likely as those without to experience a stroke over 7.5 years, Grégory Pugnet, MD, reported at the European Congress of Rheumatology. Their all-cause mortality was also significantly higher, with 30% of the deaths attributed to cardiovascular causes, said Dr. Pugnet of the Internal Medicine Service at Purpan Hospital in Toulouse, France.
“We think this [shows that it] is very important to monitor [these patients] and to be vigilant in our search for cardiovascular complications and cardiovascular risk factors in this population,” he said.
Dr. Pugnet and his colleagues conducted a retrospective study of 125 patients with AAV who were diagnosed in a teaching hospital between 1981 and 2015. He compared cardiovascular outcomes and mortality between this cohort and two French regional registries: the Midi-Pyrénées County Mortality and Acute Myocardial Infarction Registry and the Dijon Stroke Registry. Outcomes were the date of first acute myocardial infarction, date of first stroke, and date of death; the mean follow-up was about 90 months.
Of the 125 patients with AAV, 99 had granulomatosis with polyangiitis, and 26 had microscopic polyangiitis. Preexisting cardiovascular disease was present in 23. Patients were a mean of 61 years old. Hypertension, peripheral artery disease, and coronary artery disease were all more common among those with cardiovascular disease. These patients were also more likely to smoke.
Over the follow-up period, there were 10 acute myocardial infarctions for an incidence of 8.5 per 1,000 person-years. The MI incidence in the Midi-Pyrénées registry was 2.2 per 1,000 person-years, which was a significant difference in an unadjusted analysis. But after adjusting for age, AAV patients were not significantly more likely to experience a heart attack than were those in the registry.
There were nine strokes during the follow-up period for an incidence of 10.2 per 1,000 person-years. After adjusting for age, this was more than three times higher than the rate of 1.9 per 1,000 person-year in the Dijon Stroke Registry – a significant difference.
A total of 22 AAV patients died during the follow-up period, translating to a mortality of 22.5 per 1,000 person-years. Mortality in the stroke registry was 1.9 per 1,000 person-years. An age-adjusted analysis found that AAV patients were about 1.6 times more likely to die than were those in the Midi-Pyrénées registry.
A multivariate regression analysis identified some factors that were independently associated with the outcomes. Smoking almost quadrupled the risk of having any cardiovascular event (hazard ratio, 3.7), and having had a plasma exchange tripled it (HR, 2.9). Smoking and a history of coronary artery disease were significant risk factors for myocardial infarction (HRs of 8.8 and 10.3, respectively). Dr. Pugnet and his associates didn’t find any significant independent risk factors for stroke. Age was not independently associated with any of the outcomes.
Dr. Pugnet reported receiving travel support from AbbVie and Actelion, fees for serving on an advisory board from Grifols, and lecture fees from AbbVie.
[email protected]
On Twitter @alz_gal
AT THE EULAR 2017 CONGRESS
Key clinical point:
Major finding: AAV patients were twice as likely as those without the vasculitis to experience a stroke over 7.5 years.
Data source: A retrospective comparison of 125 AAV patients and patients from two French regional registries: the Midi-Pyrénées County Mortality and Acute Myocardial Infarction Registry and the Dijon Stroke Registry.
Disclosures: Dr. Pugnet reported receiving travel support from AbbVie and Actelion, fees for serving on an advisory board from Grifols, and lecture fees from AbbVie.
Studies examine methotrexate starting dose for RA in monotherapy and combinations
MADRID – A low versus high starting dose of methotrexate given as monotherapy or in combination with glucocorticoids or conventional synthetic disease-modifying antirheumatic drugs to newly diagnosed rheumatoid arthritis patients doesn’t seem to make a difference in short-term disease activity and physical functioning responses, but a higher starting dose of at least 15 mg/week may provide a better chance at achieving a good response at 6 months, according to two separate observational studies presented at the European Congress of Rheumatology.
One of the studies looked at 3- to 6-month disease activity and physical functioning responses to methotrexate used as mono- or combination therapy and the other assessed EULAR clinical responses at 6 months in mostly monotherapy-treated patients.
Low vs. high dose in combination treatments
“Methotrexate is the anchor drug in the treatment of rheumatoid arthritis patients. Current guidelines for methotrexate monotherapy recommend initiating 15 mg/week orally then escalating to 25-30 mg/week or the highest tolerable dose, but no recommendations exist for the drug’s use in combination therapy,” said Sytske Anne Bergstra, first author of a study using the international, observational METEOR database, a cohort with real-world clinical data.

The investigators selected 1,404 RA patients from the METEOR database who had a symptom duration of less than 5 years, had less than 2 months between diagnosis and first visit, and did not change medications (only dose adjustments were allowed). They were divided into three groups: methotrexate monotherapy, methotrexate plus conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), and methotrexate plus glucocorticoids (and possibly csDMARDs). The investigators defined initial starting doses of methotrexate as low (10 mg/week or less) or high (15 mg/week or more) based on the last reported dose of methotrexate at no later than 8 weeks of follow-up.
In each group, females comprised about 80% of patients, and the mean age was 45-48 years. The group that received methotrexate plus csDMARDs had a median symptom duration nearly twice that of the other groups (730 days vs. 365 for monotherapy and 458 for methotrexate plus glucocorticoids). Rheumatoid factor positivity ranged from 77% to 84% and anticitrullinated peptide autoantibody positivity from 72% to 85%.
The use of a high methotrexate starting dose generally trended upward in patients enrolled in the database through 2015, whereas the high point for use of a low dose was 2010 and declined thereafter. Overall, a high starting dose was used in 28% of monotherapy patients, 14% with methotrexate plus csDMARDs, and 46% with methotrexate plus glucocorticoids.
In propensity score–adjusted analyses that helped to control for confounding by indication, there were no differences in the effectiveness of low or high methotrexate starting doses for all three groups after follow-up between 3 and 6 months on Disease Activity Score (DAS), 28-joint DAS, or the Health Assessment Questionnaire (HAQ).
“Our findings seem to contradict the general trend of starting with high methotrexate doses. They indicate that higher doses did not provide better short-term clinical outcome in either monotherapy or combination therapy,” Ms. Bergstra observed.
She continued: “For the moment, we suggest that rheumatologists consider starting with a lower initial methotrexate dose, especially when prescribing in combination with other synthetic DMARDS or glucocorticoids.”
Effect of initial dose on EULAR response
Rebecca Davies of the Centre for Musculoskeletal Research at the University of Manchester (England) presented data from a separate study that examined the effect of giving a low versus a high dose of methotrexate on patients’ rate of response to EULAR criteria at 6 months.
“Methotrexate is the recommended first line treatment for rheumatoid arthritis; however, we have not yet established [a] clear optimal strategy for the starting dose of this therapy,” Ms. Davies said.

The aim of the study was therefore to assess the two most commonly used methotrexate starting doses used in the United Kingdom (7.5 mg/week or less vs. 15 mg/week or more) and how they affected the DAS28 of patients.
A total of 810 patients with rheumatoid arthritis who were starting methotrexate were recruited from the U.K. national, multicenter, longitudinal, observational Rheumatoid Arthritis Medication Study. For inclusion in the study, patients had to have complete DAS28 data at baseline and at 6 months.
The median age of patients was similar among the low- and high-dose groups, at 58 and 61 years, respectively. Most of the participants were female (70% vs. 60%), with a median disease duration of 6 years. Median baseline DAS28 scores were 4.2 in low- and 4.1 in high-dose groups, and baseline HAQ scores were 1.3 and 0.9, respectively.
Ms. Davies noted that 627 (77%) of the patients newly initiated on methotrexate received 15 mg/week, 10 received 20 mg, and 2 received 25 mg. The low dose of 7.5 mg/week was started by 165 patients (20%), 4 started on 5 mg, and 2 started on 2.5 mg. In more than 90% of patients, methotrexate was given orally in both the low- and high-dose groups.
Patients who were initiated on the lower methotrexate dose were more often prescribed concomitant nonbiologic DMARDs (17% vs. 10% of those in the high-dose group). Half of patients in both high- and low-dose groups used oral steroids, and a quarter used intramuscular steroids.
According to the EULAR response criteria, a good response is seen if the final DAS28 drops to 3.2 or below and there is also an improvement of 1.2 or more from baseline values. This was achieved in 23% of patients in the low-dose group and in 33% of patients in the high-dose group. Moderate EULAR clinical responses were seen in 32% and 25%, and nonresponses seen in a respective 45% and 42%.
However, findings on a multinomial logistic regression model “showed that RA patients starting methotrexate on a higher dose have a higher probability of having a good EULAR clinical response, as opposed to nonresponse, at 6 months,” Ms. Davies said.
The unadjusted relative risk ratio in patients starting a high versus low dose was 0.8 for a moderate EULAR response and 1.5 for a good EULAR response. The respective adjusted RRR was 1.0 and 2.7, suggesting that there is no difference between the doses in achieving a moderate response, but the higher dose has the edge at helping patients achieve a good EULAR response by 6 months.
During the discussion following Ms. Davies’ presentation, Roy Fleischmann, MD, of the department of internal medicine at the University of Texas Southwestern Medical Center, Dallas, asked whether a high dose had actually been used at all in the study. Dr. Fleischmann observed that both 7.5 mg/week and 15 mg/week could be considered low doses.
However, one of the chairs of the session, Peter Taylor, PhD , of the University of Oxford (England) noted that the bioavailability of methotrexate does not change much when the dose is above 15 mg via the oral route.
Kimme Hyrich, MD, of the University of Manchester (England) and senior author on the study, pointed out that the point of the analysis was to compare the starting doses of methotrexate among patients, and there might have been patients who received higher doses (25 mg or more) during the 6-month follow-up period. It is expected that future work will look at the change in the dose response over the 6-month time period, she said.
Ms. Bergstra and Ms. Davies reported that they had no relevant financial disclosures. Several coauthors for the METEOR database study disclosed financial relationships with numerous companies that market drugs for RA.
MADRID – A low versus high starting dose of methotrexate given as monotherapy or in combination with glucocorticoids or conventional synthetic disease-modifying antirheumatic drugs to newly diagnosed rheumatoid arthritis patients doesn’t seem to make a difference in short-term disease activity and physical functioning responses, but a higher starting dose of at least 15 mg/week may provide a better chance at achieving a good response at 6 months, according to two separate observational studies presented at the European Congress of Rheumatology.
One of the studies looked at 3- to 6-month disease activity and physical functioning responses to methotrexate used as mono- or combination therapy and the other assessed EULAR clinical responses at 6 months in mostly monotherapy-treated patients.
Low vs. high dose in combination treatments
“Methotrexate is the anchor drug in the treatment of rheumatoid arthritis patients. Current guidelines for methotrexate monotherapy recommend initiating 15 mg/week orally then escalating to 25-30 mg/week or the highest tolerable dose, but no recommendations exist for the drug’s use in combination therapy,” said Sytske Anne Bergstra, first author of a study using the international, observational METEOR database, a cohort with real-world clinical data.
The investigators selected 1,404 RA patients from the METEOR database who had a symptom duration of less than 5 years, had less than 2 months between diagnosis and first visit, and did not change medications (only dose adjustments were allowed). They were divided into three groups: methotrexate monotherapy, methotrexate plus conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), and methotrexate plus glucocorticoids (and possibly csDMARDs). The investigators defined initial starting doses of methotrexate as low (10 mg/week or less) or high (15 mg/week or more) based on the last reported dose of methotrexate at no later than 8 weeks of follow-up.
In each group, females comprised about 80% of patients, and the mean age was 45-48 years. The group that received methotrexate plus csDMARDs had a median symptom duration nearly twice that of the other groups (730 days vs. 365 for monotherapy and 458 for methotrexate plus glucocorticoids). Rheumatoid factor positivity ranged from 77% to 84% and anticitrullinated peptide autoantibody positivity from 72% to 85%.
The use of a high methotrexate starting dose generally trended upward in patients enrolled in the database through 2015, whereas the high point for use of a low dose was 2010 and declined thereafter. Overall, a high starting dose was used in 28% of monotherapy patients, 14% with methotrexate plus csDMARDs, and 46% with methotrexate plus glucocorticoids.
In propensity score–adjusted analyses that helped to control for confounding by indication, there were no differences in the effectiveness of low or high methotrexate starting doses for all three groups after follow-up between 3 and 6 months on Disease Activity Score (DAS), 28-joint DAS, or the Health Assessment Questionnaire (HAQ).
“Our findings seem to contradict the general trend of starting with high methotrexate doses. They indicate that higher doses did not provide better short-term clinical outcome in either monotherapy or combination therapy,” Ms. Bergstra observed.
She continued: “For the moment, we suggest that rheumatologists consider starting with a lower initial methotrexate dose, especially when prescribing in combination with other synthetic DMARDS or glucocorticoids.”
Effect of initial dose on EULAR response
Rebecca Davies of the Centre for Musculoskeletal Research at the University of Manchester (England) presented data from a separate study that examined the effect of giving a low versus a high dose of methotrexate on patients’ rate of response to EULAR criteria at 6 months.
“Methotrexate is the recommended first line treatment for rheumatoid arthritis; however, we have not yet established [a] clear optimal strategy for the starting dose of this therapy,” Ms. Davies said.
The aim of the study was therefore to assess the two most commonly used methotrexate starting doses used in the United Kingdom (7.5 mg/week or less vs. 15 mg/week or more) and how they affected the DAS28 of patients.
A total of 810 patients with rheumatoid arthritis who were starting methotrexate were recruited from the U.K. national, multicenter, longitudinal, observational Rheumatoid Arthritis Medication Study. For inclusion in the study, patients had to have complete DAS28 data at baseline and at 6 months.
The median age of patients was similar among the low- and high-dose groups, at 58 and 61 years, respectively. Most of the participants were female (70% vs. 60%), with a median disease duration of 6 years. Median baseline DAS28 scores were 4.2 in low- and 4.1 in high-dose groups, and baseline HAQ scores were 1.3 and 0.9, respectively.
Ms. Davies noted that 627 (77%) of the patients newly initiated on methotrexate received 15 mg/week, 10 received 20 mg, and 2 received 25 mg. The low dose of 7.5 mg/week was started by 165 patients (20%), 4 started on 5 mg, and 2 started on 2.5 mg. In more than 90% of patients, methotrexate was given orally in both the low- and high-dose groups.
Patients who were initiated on the lower methotrexate dose were more often prescribed concomitant nonbiologic DMARDs (17% vs. 10% of those in the high-dose group). Half of patients in both high- and low-dose groups used oral steroids, and a quarter used intramuscular steroids.
According to the EULAR response criteria, a good response is seen if the final DAS28 drops to 3.2 or below and there is also an improvement of 1.2 or more from baseline values. This was achieved in 23% of patients in the low-dose group and in 33% of patients in the high-dose group. Moderate EULAR clinical responses were seen in 32% and 25%, and nonresponses seen in a respective 45% and 42%.
However, findings on a multinomial logistic regression model “showed that RA patients starting methotrexate on a higher dose have a higher probability of having a good EULAR clinical response, as opposed to nonresponse, at 6 months,” Ms. Davies said.
The unadjusted relative risk ratio in patients starting a high versus low dose was 0.8 for a moderate EULAR response and 1.5 for a good EULAR response. The respective adjusted RRR was 1.0 and 2.7, suggesting that there is no difference between the doses in achieving a moderate response, but the higher dose has the edge at helping patients achieve a good EULAR response by 6 months.
During the discussion following Ms. Davies’ presentation, Roy Fleischmann, MD, of the department of internal medicine at the University of Texas Southwestern Medical Center, Dallas, asked whether a high dose had actually been used at all in the study. Dr. Fleischmann observed that both 7.5 mg/week and 15 mg/week could be considered low doses.
However, one of the chairs of the session, Peter Taylor, PhD , of the University of Oxford (England) noted that the bioavailability of methotrexate does not change much when the dose is above 15 mg via the oral route.
Kimme Hyrich, MD, of the University of Manchester (England) and senior author on the study, pointed out that the point of the analysis was to compare the starting doses of methotrexate among patients, and there might have been patients who received higher doses (25 mg or more) during the 6-month follow-up period. It is expected that future work will look at the change in the dose response over the 6-month time period, she said.
Ms. Bergstra and Ms. Davies reported that they had no relevant financial disclosures. Several coauthors for the METEOR database study disclosed financial relationships with numerous companies that market drugs for RA.
MADRID – A low versus high starting dose of methotrexate given as monotherapy or in combination with glucocorticoids or conventional synthetic disease-modifying antirheumatic drugs to newly diagnosed rheumatoid arthritis patients doesn’t seem to make a difference in short-term disease activity and physical functioning responses, but a higher starting dose of at least 15 mg/week may provide a better chance at achieving a good response at 6 months, according to two separate observational studies presented at the European Congress of Rheumatology.
One of the studies looked at 3- to 6-month disease activity and physical functioning responses to methotrexate used as mono- or combination therapy and the other assessed EULAR clinical responses at 6 months in mostly monotherapy-treated patients.
Low vs. high dose in combination treatments
“Methotrexate is the anchor drug in the treatment of rheumatoid arthritis patients. Current guidelines for methotrexate monotherapy recommend initiating 15 mg/week orally then escalating to 25-30 mg/week or the highest tolerable dose, but no recommendations exist for the drug’s use in combination therapy,” said Sytske Anne Bergstra, first author of a study using the international, observational METEOR database, a cohort with real-world clinical data.
The investigators selected 1,404 RA patients from the METEOR database who had a symptom duration of less than 5 years, had less than 2 months between diagnosis and first visit, and did not change medications (only dose adjustments were allowed). They were divided into three groups: methotrexate monotherapy, methotrexate plus conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), and methotrexate plus glucocorticoids (and possibly csDMARDs). The investigators defined initial starting doses of methotrexate as low (10 mg/week or less) or high (15 mg/week or more) based on the last reported dose of methotrexate at no later than 8 weeks of follow-up.
In each group, females comprised about 80% of patients, and the mean age was 45-48 years. The group that received methotrexate plus csDMARDs had a median symptom duration nearly twice that of the other groups (730 days vs. 365 for monotherapy and 458 for methotrexate plus glucocorticoids). Rheumatoid factor positivity ranged from 77% to 84% and anticitrullinated peptide autoantibody positivity from 72% to 85%.
The use of a high methotrexate starting dose generally trended upward in patients enrolled in the database through 2015, whereas the high point for use of a low dose was 2010 and declined thereafter. Overall, a high starting dose was used in 28% of monotherapy patients, 14% with methotrexate plus csDMARDs, and 46% with methotrexate plus glucocorticoids.
In propensity score–adjusted analyses that helped to control for confounding by indication, there were no differences in the effectiveness of low or high methotrexate starting doses for all three groups after follow-up between 3 and 6 months on Disease Activity Score (DAS), 28-joint DAS, or the Health Assessment Questionnaire (HAQ).
“Our findings seem to contradict the general trend of starting with high methotrexate doses. They indicate that higher doses did not provide better short-term clinical outcome in either monotherapy or combination therapy,” Ms. Bergstra observed.
She continued: “For the moment, we suggest that rheumatologists consider starting with a lower initial methotrexate dose, especially when prescribing in combination with other synthetic DMARDS or glucocorticoids.”
Effect of initial dose on EULAR response
Rebecca Davies of the Centre for Musculoskeletal Research at the University of Manchester (England) presented data from a separate study that examined the effect of giving a low versus a high dose of methotrexate on patients’ rate of response to EULAR criteria at 6 months.
“Methotrexate is the recommended first line treatment for rheumatoid arthritis; however, we have not yet established [a] clear optimal strategy for the starting dose of this therapy,” Ms. Davies said.
The aim of the study was therefore to assess the two most commonly used methotrexate starting doses used in the United Kingdom (7.5 mg/week or less vs. 15 mg/week or more) and how they affected the DAS28 of patients.
A total of 810 patients with rheumatoid arthritis who were starting methotrexate were recruited from the U.K. national, multicenter, longitudinal, observational Rheumatoid Arthritis Medication Study. For inclusion in the study, patients had to have complete DAS28 data at baseline and at 6 months.
The median age of patients was similar among the low- and high-dose groups, at 58 and 61 years, respectively. Most of the participants were female (70% vs. 60%), with a median disease duration of 6 years. Median baseline DAS28 scores were 4.2 in low- and 4.1 in high-dose groups, and baseline HAQ scores were 1.3 and 0.9, respectively.
Ms. Davies noted that 627 (77%) of the patients newly initiated on methotrexate received 15 mg/week, 10 received 20 mg, and 2 received 25 mg. The low dose of 7.5 mg/week was started by 165 patients (20%), 4 started on 5 mg, and 2 started on 2.5 mg. In more than 90% of patients, methotrexate was given orally in both the low- and high-dose groups.
Patients who were initiated on the lower methotrexate dose were more often prescribed concomitant nonbiologic DMARDs (17% vs. 10% of those in the high-dose group). Half of patients in both high- and low-dose groups used oral steroids, and a quarter used intramuscular steroids.
According to the EULAR response criteria, a good response is seen if the final DAS28 drops to 3.2 or below and there is also an improvement of 1.2 or more from baseline values. This was achieved in 23% of patients in the low-dose group and in 33% of patients in the high-dose group. Moderate EULAR clinical responses were seen in 32% and 25%, and nonresponses seen in a respective 45% and 42%.
However, findings on a multinomial logistic regression model “showed that RA patients starting methotrexate on a higher dose have a higher probability of having a good EULAR clinical response, as opposed to nonresponse, at 6 months,” Ms. Davies said.
The unadjusted relative risk ratio in patients starting a high versus low dose was 0.8 for a moderate EULAR response and 1.5 for a good EULAR response. The respective adjusted RRR was 1.0 and 2.7, suggesting that there is no difference between the doses in achieving a moderate response, but the higher dose has the edge at helping patients achieve a good EULAR response by 6 months.
During the discussion following Ms. Davies’ presentation, Roy Fleischmann, MD, of the department of internal medicine at the University of Texas Southwestern Medical Center, Dallas, asked whether a high dose had actually been used at all in the study. Dr. Fleischmann observed that both 7.5 mg/week and 15 mg/week could be considered low doses.
However, one of the chairs of the session, Peter Taylor, PhD , of the University of Oxford (England) noted that the bioavailability of methotrexate does not change much when the dose is above 15 mg via the oral route.
Kimme Hyrich, MD, of the University of Manchester (England) and senior author on the study, pointed out that the point of the analysis was to compare the starting doses of methotrexate among patients, and there might have been patients who received higher doses (25 mg or more) during the 6-month follow-up period. It is expected that future work will look at the change in the dose response over the 6-month time period, she said.
Ms. Bergstra and Ms. Davies reported that they had no relevant financial disclosures. Several coauthors for the METEOR database study disclosed financial relationships with numerous companies that market drugs for RA.
AT THE EULAR 2017 CONGRESS
Key clinical point: For newly diagnosed RA, consider using a lower methotrexate starting dose with combination therapy and a higher dose of 15 mg/week or more in monotherapy.
Major finding: In one study, 23% and 33% of patients taking low-dose or high-dose methotrexate, respectively, achieved a good EULAR clinical response.
Data source: Two studies (METEOR and RAMS) evaluating the comparative effects of initiating low versus high doses of methotrexate for newly diagnosed rheumatoid arthritis.
Disclosures: The presenters reported they had no relevant financial disclosures. Several coauthors for the METEOR database study disclosed financial relationships with numerous companies that market drugs for RA.
Pediatric Dermatology Consult - July 2017
BY JUSLEEN AHLUWALIA, MD, AND LAWRENCE F. EICHENFIELD, MD
Consider immunologic blistering diseases in the differential diagnosis of unusual vesicles and bullae in infants and children.
The patient was diagnosed with infantile bullous pemphigoid. Treatment was initiated with clobetasol 0.05% ointment twice daily to the affected areas. Despite treatment with topical corticosteroids, the patient continued to manifest bullae and urticariforme plaques on his legs and trunk. He was then started on oral prednisolone 1 mg/kg per day with gastrointestinal ulcer prophylaxis. He improved within 3 weeks of treatment.

Overall, childhood BP carries a good prognosis and responds well to topical or oral steroids.1 Most patients achieve remission within a few weeks to months of treatments; however, disease course can vary with several relapses over a few years. The longest duration of disease that has been reported is 3 years.1 Second-line treatments – such as dapsone, sulfapyridine, mycophenolate mofetil, administered alone or concurrently with steroids – may be considered for those who fail to respond to conventional treatment.1,5 Intravenous immunoglobulin has reported to be efficacious and well-tolerated in a few cases of treatment-resistant childhood BP.1,5
Differentiation of infantile bullous pemphigoid from other common and uncommon vesiculobullous diseases is necessary. Bullous impetigo (A), caused by Streptococcus pyogenes or Staphylococcus aureus can present with vesicles and bullae due to staphylococcal exfoliative toxins (exfoliatin A-D) which cause separation at the superficial epidermal level. Hand, foot, and mouth disease (HFMD) (B) is an acute Coxsackie viral infection, classically involving the oral mucosa, palms, and soles, although broad variations in presentations include “eczema coxsackium,” Gianotti-Crosti–type lesions, and petechiae.6 Linear IgA dermatosis (C) is an immunobullous condition occurring most frequently in perioral and perineal regions. The disease is characterized by a linear deposition of IgA along the dermal-epidermal junction. Dermatitis herpetiformis (E) is an autoimmune, papulovesicular eruption most commonly involving extensor surfaces of extremities and is characterized by granular deposition of IgA in the papillary dermis.
This patient’s systemic steroids were successfully tapered over several months without disease recurrence. It is unknown why this immunobullous disease is usually self-limited in children, unlike BP in adults, which has significant morbidity or mortality. While uncommon, it is important to consider immunologic blistering diseases in the differential diagnosis of unusual vesicles and bullae in infants and children.
Dr. Ahluwalia is with the division of pediatric and adolescent dermatology, Rady Children’s Hospital, San Diego, and the departments of dermatology and pediatrics at the University of California, San Diego. Dr. Eichenfield is chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego and professor of dermatology and pediatrics at the University of California, San Diego. Neither of the physicians has relevant financial disclosures. Email them at [email protected].
References
1. Pediatr Dermatol. 2016 Mar-Apr;33(2):e77-81.
2. Orphanet J Rare Dis. 2014 Dec 10;9:185.
3. J Am Acad Dermatol. 2008 Jan;58(1):41-8.
4. Arch Dermatol. 1991 Mar;127(3):378-86.
BY JUSLEEN AHLUWALIA, MD, AND LAWRENCE F. EICHENFIELD, MD
Consider immunologic blistering diseases in the differential diagnosis of unusual vesicles and bullae in infants and children.
The patient was diagnosed with infantile bullous pemphigoid. Treatment was initiated with clobetasol 0.05% ointment twice daily to the affected areas. Despite treatment with topical corticosteroids, the patient continued to manifest bullae and urticariforme plaques on his legs and trunk. He was then started on oral prednisolone 1 mg/kg per day with gastrointestinal ulcer prophylaxis. He improved within 3 weeks of treatment.
Overall, childhood BP carries a good prognosis and responds well to topical or oral steroids.1 Most patients achieve remission within a few weeks to months of treatments; however, disease course can vary with several relapses over a few years. The longest duration of disease that has been reported is 3 years.1 Second-line treatments – such as dapsone, sulfapyridine, mycophenolate mofetil, administered alone or concurrently with steroids – may be considered for those who fail to respond to conventional treatment.1,5 Intravenous immunoglobulin has reported to be efficacious and well-tolerated in a few cases of treatment-resistant childhood BP.1,5
Differentiation of infantile bullous pemphigoid from other common and uncommon vesiculobullous diseases is necessary. Bullous impetigo (A), caused by Streptococcus pyogenes or Staphylococcus aureus can present with vesicles and bullae due to staphylococcal exfoliative toxins (exfoliatin A-D) which cause separation at the superficial epidermal level. Hand, foot, and mouth disease (HFMD) (B) is an acute Coxsackie viral infection, classically involving the oral mucosa, palms, and soles, although broad variations in presentations include “eczema coxsackium,” Gianotti-Crosti–type lesions, and petechiae.6 Linear IgA dermatosis (C) is an immunobullous condition occurring most frequently in perioral and perineal regions. The disease is characterized by a linear deposition of IgA along the dermal-epidermal junction. Dermatitis herpetiformis (E) is an autoimmune, papulovesicular eruption most commonly involving extensor surfaces of extremities and is characterized by granular deposition of IgA in the papillary dermis.
This patient’s systemic steroids were successfully tapered over several months without disease recurrence. It is unknown why this immunobullous disease is usually self-limited in children, unlike BP in adults, which has significant morbidity or mortality. While uncommon, it is important to consider immunologic blistering diseases in the differential diagnosis of unusual vesicles and bullae in infants and children.
Dr. Ahluwalia is with the division of pediatric and adolescent dermatology, Rady Children’s Hospital, San Diego, and the departments of dermatology and pediatrics at the University of California, San Diego. Dr. Eichenfield is chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego and professor of dermatology and pediatrics at the University of California, San Diego. Neither of the physicians has relevant financial disclosures. Email them at [email protected].
References
1. Pediatr Dermatol. 2016 Mar-Apr;33(2):e77-81.
2. Orphanet J Rare Dis. 2014 Dec 10;9:185.
3. J Am Acad Dermatol. 2008 Jan;58(1):41-8.
4. Arch Dermatol. 1991 Mar;127(3):378-86.
BY JUSLEEN AHLUWALIA, MD, AND LAWRENCE F. EICHENFIELD, MD
Consider immunologic blistering diseases in the differential diagnosis of unusual vesicles and bullae in infants and children.
The patient was diagnosed with infantile bullous pemphigoid. Treatment was initiated with clobetasol 0.05% ointment twice daily to the affected areas. Despite treatment with topical corticosteroids, the patient continued to manifest bullae and urticariforme plaques on his legs and trunk. He was then started on oral prednisolone 1 mg/kg per day with gastrointestinal ulcer prophylaxis. He improved within 3 weeks of treatment.
Overall, childhood BP carries a good prognosis and responds well to topical or oral steroids.1 Most patients achieve remission within a few weeks to months of treatments; however, disease course can vary with several relapses over a few years. The longest duration of disease that has been reported is 3 years.1 Second-line treatments – such as dapsone, sulfapyridine, mycophenolate mofetil, administered alone or concurrently with steroids – may be considered for those who fail to respond to conventional treatment.1,5 Intravenous immunoglobulin has reported to be efficacious and well-tolerated in a few cases of treatment-resistant childhood BP.1,5
Differentiation of infantile bullous pemphigoid from other common and uncommon vesiculobullous diseases is necessary. Bullous impetigo (A), caused by Streptococcus pyogenes or Staphylococcus aureus can present with vesicles and bullae due to staphylococcal exfoliative toxins (exfoliatin A-D) which cause separation at the superficial epidermal level. Hand, foot, and mouth disease (HFMD) (B) is an acute Coxsackie viral infection, classically involving the oral mucosa, palms, and soles, although broad variations in presentations include “eczema coxsackium,” Gianotti-Crosti–type lesions, and petechiae.6 Linear IgA dermatosis (C) is an immunobullous condition occurring most frequently in perioral and perineal regions. The disease is characterized by a linear deposition of IgA along the dermal-epidermal junction. Dermatitis herpetiformis (E) is an autoimmune, papulovesicular eruption most commonly involving extensor surfaces of extremities and is characterized by granular deposition of IgA in the papillary dermis.
This patient’s systemic steroids were successfully tapered over several months without disease recurrence. It is unknown why this immunobullous disease is usually self-limited in children, unlike BP in adults, which has significant morbidity or mortality. While uncommon, it is important to consider immunologic blistering diseases in the differential diagnosis of unusual vesicles and bullae in infants and children.
Dr. Ahluwalia is with the division of pediatric and adolescent dermatology, Rady Children’s Hospital, San Diego, and the departments of dermatology and pediatrics at the University of California, San Diego. Dr. Eichenfield is chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego and professor of dermatology and pediatrics at the University of California, San Diego. Neither of the physicians has relevant financial disclosures. Email them at [email protected].
References
1. Pediatr Dermatol. 2016 Mar-Apr;33(2):e77-81.
2. Orphanet J Rare Dis. 2014 Dec 10;9:185.
3. J Am Acad Dermatol. 2008 Jan;58(1):41-8.
4. Arch Dermatol. 1991 Mar;127(3):378-86.

A 3-month-old otherwise healthy boy was referred for a 2-week history of a nonpruritic, urticariforme eruption that progressed to blisters on the trunk, hands, and feet. The patient had a 4-day history of a nonproductive cough preceding the rash. He was otherwise active with normal feeding and bowel habits. His family history was negative for dermatologic or autoimmune disease.
On examination, the patient is a well-developed, active male with widespread erythematous infiltrated papules and arcuate plaques, tense vesiculobullous lesions, and multiple erosions on the trunk and extremities. Mucous membranes and perineum were spared.
Bacterial culture of a lesion was negative. Consult from dermatology was obtained and a biopsy performed.
Histologic examination showed a subepidermal unilocular blister with serous fluid containing predominately eosinophils and lymphocytes. Direct immunofluorescence revealed linear immunoglobulin G and C3 deposition along the basement membrane.
Hospitalists’ scope of services continues to evolve
Over the course of serial iterations of the State of Hospital Medicine (SOHM) Report, SHM has presented survey data that describe the evolving role hospitalists play in patient care. The 2016 SOHM Report shows the continuation of prior trends in hospital medicine groups’ (HMGs) scope of admittance and comanagement services. Some downturns are notable among previously increased specialty services.
The SOHM Report characterizes HMGs by their general scope of admitted patients – as admitters of purely traditional internal medicine or pediatrics hospitalized patients; full-range, nearly universal admitters who admit most patients within their age designation except OB and emergency surgery patients; or traditional admitters with some exceptions (for example, limited classically surgical patients).

As adult and adult-ped HMGs make up almost 97% of survey respondents, the predominance of the “some exceptions” category seems to represent a serious trend in much of Hospital Medicine practice. This could mean that HMGs have worked out more specific arrangements as to which patients they will admit or that the definitions are more in flux. It comes at a time when concerns figure prominently in national discussions over the stretching of hospitalists by their expanding scope of care and the need for ever more coordinated care between hospitalists and specialists.
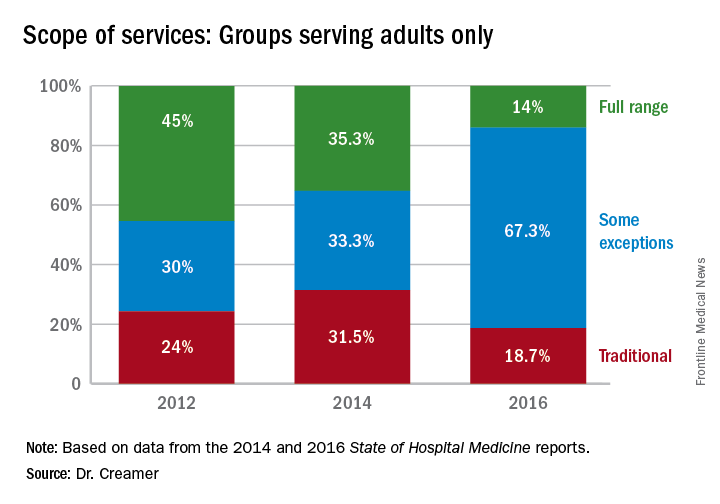
Again, with these opportunities, concerns have arisen about scope-creep and its potential deleterious effects on patient care. Hospitalists have been noted to be prodded into providing critical, geriatric, and palliative care, without specialty training in these areas.1 Interestingly, however, specialty work reported by HMGs has largely shown a downturn since 2014, when most specialty services had appeared to be on the rise.
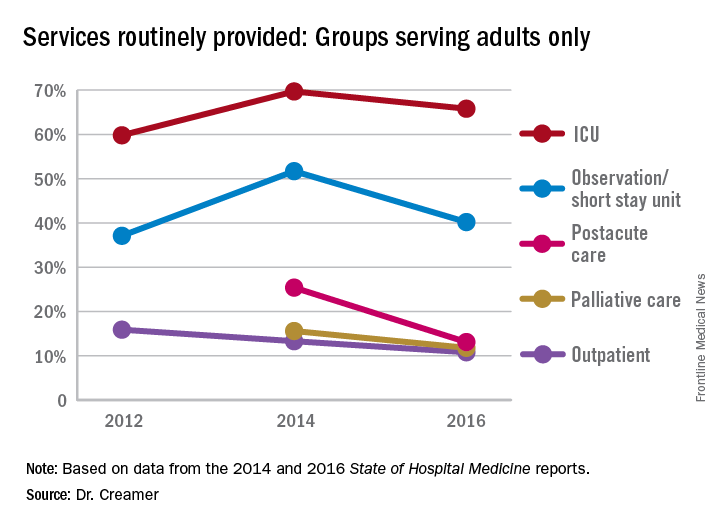
Whether this means that there is relief from scope-creep or that it is “just a blip” will remain to be seen in future data. If HMGs are able to capture the opportunity to improve outcomes through greater involvement in postacute care, this particular area may be one to watch, despite its apparent downturn since the 2014 report.
Thus, it is as imperative as ever that HMGs participate in the State of Hospital Medicine survey.
Dr. Creamer is a member of SHM’s Practice Analysis Committee. He is a hospitalist and informaticist with the MetroHealth System in Cleveland.
References
1. Wellikson, L. Hospitalists Stretched as their Responsibilities Broaden. The Hospitalist. 2016 Nov;2016(11).
Over the course of serial iterations of the State of Hospital Medicine (SOHM) Report, SHM has presented survey data that describe the evolving role hospitalists play in patient care. The 2016 SOHM Report shows the continuation of prior trends in hospital medicine groups’ (HMGs) scope of admittance and comanagement services. Some downturns are notable among previously increased specialty services.
The SOHM Report characterizes HMGs by their general scope of admitted patients – as admitters of purely traditional internal medicine or pediatrics hospitalized patients; full-range, nearly universal admitters who admit most patients within their age designation except OB and emergency surgery patients; or traditional admitters with some exceptions (for example, limited classically surgical patients).
As adult and adult-ped HMGs make up almost 97% of survey respondents, the predominance of the “some exceptions” category seems to represent a serious trend in much of Hospital Medicine practice. This could mean that HMGs have worked out more specific arrangements as to which patients they will admit or that the definitions are more in flux. It comes at a time when concerns figure prominently in national discussions over the stretching of hospitalists by their expanding scope of care and the need for ever more coordinated care between hospitalists and specialists.
Again, with these opportunities, concerns have arisen about scope-creep and its potential deleterious effects on patient care. Hospitalists have been noted to be prodded into providing critical, geriatric, and palliative care, without specialty training in these areas.1 Interestingly, however, specialty work reported by HMGs has largely shown a downturn since 2014, when most specialty services had appeared to be on the rise.
Whether this means that there is relief from scope-creep or that it is “just a blip” will remain to be seen in future data. If HMGs are able to capture the opportunity to improve outcomes through greater involvement in postacute care, this particular area may be one to watch, despite its apparent downturn since the 2014 report.
Thus, it is as imperative as ever that HMGs participate in the State of Hospital Medicine survey.
Dr. Creamer is a member of SHM’s Practice Analysis Committee. He is a hospitalist and informaticist with the MetroHealth System in Cleveland.
References
1. Wellikson, L. Hospitalists Stretched as their Responsibilities Broaden. The Hospitalist. 2016 Nov;2016(11).
Over the course of serial iterations of the State of Hospital Medicine (SOHM) Report, SHM has presented survey data that describe the evolving role hospitalists play in patient care. The 2016 SOHM Report shows the continuation of prior trends in hospital medicine groups’ (HMGs) scope of admittance and comanagement services. Some downturns are notable among previously increased specialty services.
The SOHM Report characterizes HMGs by their general scope of admitted patients – as admitters of purely traditional internal medicine or pediatrics hospitalized patients; full-range, nearly universal admitters who admit most patients within their age designation except OB and emergency surgery patients; or traditional admitters with some exceptions (for example, limited classically surgical patients).
As adult and adult-ped HMGs make up almost 97% of survey respondents, the predominance of the “some exceptions” category seems to represent a serious trend in much of Hospital Medicine practice. This could mean that HMGs have worked out more specific arrangements as to which patients they will admit or that the definitions are more in flux. It comes at a time when concerns figure prominently in national discussions over the stretching of hospitalists by their expanding scope of care and the need for ever more coordinated care between hospitalists and specialists.
Again, with these opportunities, concerns have arisen about scope-creep and its potential deleterious effects on patient care. Hospitalists have been noted to be prodded into providing critical, geriatric, and palliative care, without specialty training in these areas.1 Interestingly, however, specialty work reported by HMGs has largely shown a downturn since 2014, when most specialty services had appeared to be on the rise.
Whether this means that there is relief from scope-creep or that it is “just a blip” will remain to be seen in future data. If HMGs are able to capture the opportunity to improve outcomes through greater involvement in postacute care, this particular area may be one to watch, despite its apparent downturn since the 2014 report.
Thus, it is as imperative as ever that HMGs participate in the State of Hospital Medicine survey.
Dr. Creamer is a member of SHM’s Practice Analysis Committee. He is a hospitalist and informaticist with the MetroHealth System in Cleveland.
References
1. Wellikson, L. Hospitalists Stretched as their Responsibilities Broaden. The Hospitalist. 2016 Nov;2016(11).
Physician liability in opioid deaths
Question: Regarding opioid deaths, which of the following is incorrect?
A. The term refers to accidental or intentional deaths caused mostly by heroin.
B. They are reaching epidemic proportions.
C. May form the basis for a wrongful death lawsuit.
D. May lead to loss of medical license.
E. The physician may face prosecution for homicide.
Answer: A. Opioids are a class of drugs that include the illegal drug heroin, as well as prescription drugs such as fentanyl, oxycodone, hydrocodone, codeine, and morphine. To be sure, opioid deaths occur in addicts from the deliberate or accidental use of heroin; but other opioids, especially painkillers, are also widely implicated. In addition, deaths have resulted from the careless, negligent, reckless, or wanton conduct of doctors who prescribe them without the proper indications or in inappropriate amounts, and then fail to provide careful follow-up.
Physicians may face both civil and criminal liabilities in such a situation. One remedy sought in wrongful death is a civil action, i.e., a malpractice lawsuit against the negligent doctor. The plaintiff is asserting that by violating community professional standards, the physician’s substandard conduct breached his duty of due care and was a proximate cause of the patient’s death. The evidentiary proof that is required to sustain such an allegation is “more probable than not” or “preponderance of evidence,” and expert medical testimony is typically necessary to establish the requisite standard of care and causation. Where there is gross negligence, i.e., egregious conduct that was reckless, the jury may award punitive damages.
Not infrequently, the wayward doctor faces triple liability: a civil lawsuit, state medical board action, and criminal prosecution for homicide. Given the publicity over soaring opioid death rates, one can expect aggressive prosecution of dealers and doctors alike.

This was not the first such case in Oklahoma. In 2014, a 71-year-old pain management doctor pleaded guilty to eight counts of second-degree murder in connection with several drug overdose deaths and will serve 8 years in prison. The doctor had reportedly prescribed more controlled drugs than any other physician in the state of Oklahoma. These drugs included hydrocodone, oxycodone, alprazolam, diazepam (Valium), and carisoprodol (Soma) – as many as 600 pills at a time. He allegedly accepted only cash payment for the office visits, and a review of his patient files revealed inadequate assessment of patient complaints or physical findings to justify the prescriptions.
Other states have been equally aggressive in prosecuting doctors over opioid deaths from reckless prescribing habits.
For the first time, New York in 2014 convicted a doctor of manslaughter in the overdose deaths of patients from oxycodone and alprazolam (Xanax). Some of the patients were prescribed as many as 500-800 pills over a 5- to 6-week period. The defendant, an anesthesiologist and pain management specialist, allegedly saw upward of 90 patients a day in his Queens weekend storefront clinic, charging them on a per-prescription basis. In his defense, he claimed that he was simply trying to help suffering people who misused medications and who misled him (“tough patients and good liars”).
Likewise, a Los Angeles–area doctor was recently convicted of second-degree murder for prescribing painkillers that killed three patients, and he was sentenced to 30 years to life in prison.
According to the Centers for Disease Control and Prevention, both drug overdose and opioid-involved deaths continue to increase in the United States.2 The majority of drug overdose deaths (more than 6 out of 10) involve an opioid, and the number has quadrupled since 1999.2 It has been estimated that more than 18,000 overdose deaths in 2014 involved prescription painkillers, while an additional 10,000 fatalities were attributed to heroin and 5,000 to fentanyl and other synthetic opioids. Overdose deaths exceed motor vehicle accidents as the leading cause of injury-related deaths. About 90 Americans die every day from an opioid overdose, and opioids have been forecast to kill 500,000 Americans over the next decade.
The CDC acknowledges that prescription opioids are a driving factor, noting that since 1999, the amount sold in the United States has nearly quadrupled, yet there has not been an overall change in the amount of pain that Americans report.
States such as Missouri, faced with the skyrocketing cost of treating the opioid epidemic, have sued the drug manufacturers, blaming them for their “campaign of fraud and deception.” At the same time, doctors have been deemed the “biggest culprit” for the opioid addiction epidemic, and one author has pointedly asserted that “by refusing to accept their inability to separate pain relief from addiction, physicians have long suffered the sin of hubris – and their patients have paid the price.”3
The U.S. Surgeon General recently took the historic step of writing to all American doctors asking for their help. And the American Medical Association has developed an educational module explaining the epidemic and how opioid misuse is linked to heroin addiction. The module also outlines risk-reducing steps when using opioids for pain relief.4
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. Some of the materials here have appeared in previous columns by the author. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at [email protected].
References
1. Available at www.foxnews.om/health/2017/06/26/oklahoma-doctor-charged-in-opioid-deaths-5-patients.html. Accessed June 28, 2017.
2. Available at www.cdc.gov/drugoverdose/epidemic/index.html. Accessed June 28, 2017.
3. Available at www.thedailybeast.com/the-doctors-who-started-the-opioid-epidemic. Accessed June 27, 2017.
4. https://www.end-opioid-epidemic.org. Accessed July 5, 2017.
Question: Regarding opioid deaths, which of the following is incorrect?
A. The term refers to accidental or intentional deaths caused mostly by heroin.
B. They are reaching epidemic proportions.
C. May form the basis for a wrongful death lawsuit.
D. May lead to loss of medical license.
E. The physician may face prosecution for homicide.
Answer: A. Opioids are a class of drugs that include the illegal drug heroin, as well as prescription drugs such as fentanyl, oxycodone, hydrocodone, codeine, and morphine. To be sure, opioid deaths occur in addicts from the deliberate or accidental use of heroin; but other opioids, especially painkillers, are also widely implicated. In addition, deaths have resulted from the careless, negligent, reckless, or wanton conduct of doctors who prescribe them without the proper indications or in inappropriate amounts, and then fail to provide careful follow-up.
Physicians may face both civil and criminal liabilities in such a situation. One remedy sought in wrongful death is a civil action, i.e., a malpractice lawsuit against the negligent doctor. The plaintiff is asserting that by violating community professional standards, the physician’s substandard conduct breached his duty of due care and was a proximate cause of the patient’s death. The evidentiary proof that is required to sustain such an allegation is “more probable than not” or “preponderance of evidence,” and expert medical testimony is typically necessary to establish the requisite standard of care and causation. Where there is gross negligence, i.e., egregious conduct that was reckless, the jury may award punitive damages.
Not infrequently, the wayward doctor faces triple liability: a civil lawsuit, state medical board action, and criminal prosecution for homicide. Given the publicity over soaring opioid death rates, one can expect aggressive prosecution of dealers and doctors alike.
This was not the first such case in Oklahoma. In 2014, a 71-year-old pain management doctor pleaded guilty to eight counts of second-degree murder in connection with several drug overdose deaths and will serve 8 years in prison. The doctor had reportedly prescribed more controlled drugs than any other physician in the state of Oklahoma. These drugs included hydrocodone, oxycodone, alprazolam, diazepam (Valium), and carisoprodol (Soma) – as many as 600 pills at a time. He allegedly accepted only cash payment for the office visits, and a review of his patient files revealed inadequate assessment of patient complaints or physical findings to justify the prescriptions.
Other states have been equally aggressive in prosecuting doctors over opioid deaths from reckless prescribing habits.
For the first time, New York in 2014 convicted a doctor of manslaughter in the overdose deaths of patients from oxycodone and alprazolam (Xanax). Some of the patients were prescribed as many as 500-800 pills over a 5- to 6-week period. The defendant, an anesthesiologist and pain management specialist, allegedly saw upward of 90 patients a day in his Queens weekend storefront clinic, charging them on a per-prescription basis. In his defense, he claimed that he was simply trying to help suffering people who misused medications and who misled him (“tough patients and good liars”).
Likewise, a Los Angeles–area doctor was recently convicted of second-degree murder for prescribing painkillers that killed three patients, and he was sentenced to 30 years to life in prison.
According to the Centers for Disease Control and Prevention, both drug overdose and opioid-involved deaths continue to increase in the United States.2 The majority of drug overdose deaths (more than 6 out of 10) involve an opioid, and the number has quadrupled since 1999.2 It has been estimated that more than 18,000 overdose deaths in 2014 involved prescription painkillers, while an additional 10,000 fatalities were attributed to heroin and 5,000 to fentanyl and other synthetic opioids. Overdose deaths exceed motor vehicle accidents as the leading cause of injury-related deaths. About 90 Americans die every day from an opioid overdose, and opioids have been forecast to kill 500,000 Americans over the next decade.
The CDC acknowledges that prescription opioids are a driving factor, noting that since 1999, the amount sold in the United States has nearly quadrupled, yet there has not been an overall change in the amount of pain that Americans report.
States such as Missouri, faced with the skyrocketing cost of treating the opioid epidemic, have sued the drug manufacturers, blaming them for their “campaign of fraud and deception.” At the same time, doctors have been deemed the “biggest culprit” for the opioid addiction epidemic, and one author has pointedly asserted that “by refusing to accept their inability to separate pain relief from addiction, physicians have long suffered the sin of hubris – and their patients have paid the price.”3
The U.S. Surgeon General recently took the historic step of writing to all American doctors asking for their help. And the American Medical Association has developed an educational module explaining the epidemic and how opioid misuse is linked to heroin addiction. The module also outlines risk-reducing steps when using opioids for pain relief.4
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. Some of the materials here have appeared in previous columns by the author. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at [email protected].
References
1. Available at www.foxnews.om/health/2017/06/26/oklahoma-doctor-charged-in-opioid-deaths-5-patients.html. Accessed June 28, 2017.
2. Available at www.cdc.gov/drugoverdose/epidemic/index.html. Accessed June 28, 2017.
3. Available at www.thedailybeast.com/the-doctors-who-started-the-opioid-epidemic. Accessed June 27, 2017.
4. https://www.end-opioid-epidemic.org. Accessed July 5, 2017.
Question: Regarding opioid deaths, which of the following is incorrect?
A. The term refers to accidental or intentional deaths caused mostly by heroin.
B. They are reaching epidemic proportions.
C. May form the basis for a wrongful death lawsuit.
D. May lead to loss of medical license.
E. The physician may face prosecution for homicide.
Answer: A. Opioids are a class of drugs that include the illegal drug heroin, as well as prescription drugs such as fentanyl, oxycodone, hydrocodone, codeine, and morphine. To be sure, opioid deaths occur in addicts from the deliberate or accidental use of heroin; but other opioids, especially painkillers, are also widely implicated. In addition, deaths have resulted from the careless, negligent, reckless, or wanton conduct of doctors who prescribe them without the proper indications or in inappropriate amounts, and then fail to provide careful follow-up.
Physicians may face both civil and criminal liabilities in such a situation. One remedy sought in wrongful death is a civil action, i.e., a malpractice lawsuit against the negligent doctor. The plaintiff is asserting that by violating community professional standards, the physician’s substandard conduct breached his duty of due care and was a proximate cause of the patient’s death. The evidentiary proof that is required to sustain such an allegation is “more probable than not” or “preponderance of evidence,” and expert medical testimony is typically necessary to establish the requisite standard of care and causation. Where there is gross negligence, i.e., egregious conduct that was reckless, the jury may award punitive damages.
Not infrequently, the wayward doctor faces triple liability: a civil lawsuit, state medical board action, and criminal prosecution for homicide. Given the publicity over soaring opioid death rates, one can expect aggressive prosecution of dealers and doctors alike.
This was not the first such case in Oklahoma. In 2014, a 71-year-old pain management doctor pleaded guilty to eight counts of second-degree murder in connection with several drug overdose deaths and will serve 8 years in prison. The doctor had reportedly prescribed more controlled drugs than any other physician in the state of Oklahoma. These drugs included hydrocodone, oxycodone, alprazolam, diazepam (Valium), and carisoprodol (Soma) – as many as 600 pills at a time. He allegedly accepted only cash payment for the office visits, and a review of his patient files revealed inadequate assessment of patient complaints or physical findings to justify the prescriptions.
Other states have been equally aggressive in prosecuting doctors over opioid deaths from reckless prescribing habits.
For the first time, New York in 2014 convicted a doctor of manslaughter in the overdose deaths of patients from oxycodone and alprazolam (Xanax). Some of the patients were prescribed as many as 500-800 pills over a 5- to 6-week period. The defendant, an anesthesiologist and pain management specialist, allegedly saw upward of 90 patients a day in his Queens weekend storefront clinic, charging them on a per-prescription basis. In his defense, he claimed that he was simply trying to help suffering people who misused medications and who misled him (“tough patients and good liars”).
Likewise, a Los Angeles–area doctor was recently convicted of second-degree murder for prescribing painkillers that killed three patients, and he was sentenced to 30 years to life in prison.
According to the Centers for Disease Control and Prevention, both drug overdose and opioid-involved deaths continue to increase in the United States.2 The majority of drug overdose deaths (more than 6 out of 10) involve an opioid, and the number has quadrupled since 1999.2 It has been estimated that more than 18,000 overdose deaths in 2014 involved prescription painkillers, while an additional 10,000 fatalities were attributed to heroin and 5,000 to fentanyl and other synthetic opioids. Overdose deaths exceed motor vehicle accidents as the leading cause of injury-related deaths. About 90 Americans die every day from an opioid overdose, and opioids have been forecast to kill 500,000 Americans over the next decade.
The CDC acknowledges that prescription opioids are a driving factor, noting that since 1999, the amount sold in the United States has nearly quadrupled, yet there has not been an overall change in the amount of pain that Americans report.
States such as Missouri, faced with the skyrocketing cost of treating the opioid epidemic, have sued the drug manufacturers, blaming them for their “campaign of fraud and deception.” At the same time, doctors have been deemed the “biggest culprit” for the opioid addiction epidemic, and one author has pointedly asserted that “by refusing to accept their inability to separate pain relief from addiction, physicians have long suffered the sin of hubris – and their patients have paid the price.”3
The U.S. Surgeon General recently took the historic step of writing to all American doctors asking for their help. And the American Medical Association has developed an educational module explaining the epidemic and how opioid misuse is linked to heroin addiction. The module also outlines risk-reducing steps when using opioids for pain relief.4
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. Some of the materials here have appeared in previous columns by the author. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at [email protected].
References
1. Available at www.foxnews.om/health/2017/06/26/oklahoma-doctor-charged-in-opioid-deaths-5-patients.html. Accessed June 28, 2017.
2. Available at www.cdc.gov/drugoverdose/epidemic/index.html. Accessed June 28, 2017.
3. Available at www.thedailybeast.com/the-doctors-who-started-the-opioid-epidemic. Accessed June 27, 2017.
4. https://www.end-opioid-epidemic.org. Accessed July 5, 2017.