User login
Intra-Articular Steroids May Hasten Cartilage Loss in Knee Osteoarthritis
Study Overview
Objective. To determine the effects of intra-articular triamcinolone acetonide at a dose of 40 mg administered at 3-month intervals on knee pain and progression of knee cartilage loss.
Design. Randomized, double-blind, placebo-controlled trial.
Setting and participants. 140 patients with ultrasonic features of synovitis and symptomatic knee osteoarthritis were selected from the patient pool at Tufts Medical Center in Boston, Massachusetts, between June 2011 and January 2015. Patients selected were age 45 years or older and met American College of Rheumatology osteoarthritis diagnostic criteria. Western Ontario and McMaster Universities (WOMAC) pain scores were between 2 and 8 on weight-bearing questions. Tibiofemoral osteoarthritis on posteroanterior weight bearing semi-flexed radiographs was evident in participants at a Kellegren-Lawrence grade 2 or 3. Eligible patients also had ultra-sonographic evidence of synovitis with an effusion larger than 2 mm in the study knee. Participants were excluded if they had undergone any trauma to the study joint such as osteonecrosis or a poorly controlled systemic illness. If the patient had used antibiotics, hyaluronic acid, glucosamine, chondroitin or had undergone recent intra-articular steroids in 3 months or fewer prior to the enrollment period the patient was excluded from the study. Further, patients were excluded if they were unable to undergo an MRI. Prior to pain assessments, patients were to discontinue any analgesics for 48 hours with the exception of acetaminophen if needed. The mean age of patients in this study was 58 years and the mean body mass index was 30. Half of patients had malalignment of the knee joint.
Intervention. 40 mg of a preparation of 40 mg/mL (total volume 1 mL) was injected into the intervention patients’ affected knees while 1 mL of 0.9% sodium chloride (saline solution) was injected into the control patients’ affected knees. Local anesthetic was not used. If present, synovial fluid was aspirated from the knee prior to injection. Injections were administered every 12 weeks for 2 years. Needle placement by ultrasound was utilized to ensure accurate injections, however, the probe was removed prior to injection. The injecting clinician was not involved in measuring outcomes in the study. Both intervention solutions were in identical syringes and were masked so the patient was blinded to which intervention he or she may have received.
Main outcome measure. Cartilage loss, pain, articular structural damage and physical function were the main outcome measures. Cartilage loss and structural damage were determined by MRI using validated quantitative and semi-quantitative assessments. Pain was measured with WOMAC scores and physical function was assessed using the 20-m walk test and the chair stand test. Patients were assessed during 9 scheduled visits at 3-month intervals when subjective data, blood pressure, and hemoglobin A1c levels were obtained. At 6-month intervals, patients underwent objective measures of function measured by a timed 20-m walk and chair stand testing. Evaluation of quantitative measures of cartilage analysis, semi-quantitative assessment of cartilage damage, bone marrow lesion and effusion volume measurement by MRI were done at time zero, 12 months and 24 months. The 36-Item Short-Form Health Survey was administered at these times as well. Results were computed with intention-to-treat analysis for all outcomes.
Main results. 140 patients were randomized out of 445 patients who were assessed for eligibility. Ten patients in the saline arm and 11 in the glucocorticoid arm were lost to follow-up. Groups were similar in age, BMI, varus or valgus malalignment, ultrasound measures, pain, and function measures. The group injected with triamcinolone had a higher rate of cartilage loss than the group injected with saline (–0.21 mm vs. –0.10 mm, P = 0.01) and had a higher rate of cartilage damage (–133.66 vs –72.41, P = 0.048). Cartilage denudation, bone marrow lesions, trabecular morphology and effusion volumes were not significantly different between groups. WOMAC pain measure differences from baseline in the groups were similar (–1.2 for triamcinolone group vs. –1.9 for the saline group, P = 0.17). There were also no differences between groups for the Visual Analog Scale pain score, stiffness, the 20-m walk test, or the chair stand test. Adverse events were similar between groups. At the end of the study protocol, only 45% of patients were able to correctly identify the group to which they were assigned.
Conclusion. In patients meeting American College of Rheumatology diagnostic criteria for osteoarthritis and evidence of inflammation in the affected joint, 40 mg of triamcinolone administered intra-articularly is no more effective in relieving pain or physical functioning after 2 years of injections every 3 months than normal saline. Injecting 40 mg of triamcinolone may hasten cartilage loss and damage as measured by MRI.
Commentary
In the current study, the rate of cartilage loss in the saline group was on par with prior studies examining the natural history of cartilage loss, suggesting that intra-articular steroid may actually be hastening the loss of cartilage observed in this study. The effect size was deemed moderate by the authors, though clinically significant minimal change has not been determined. Intra-articular cartilage loss is positively correlated with arthroplasty rates [1]. While this study was not designed to investigate the rate of joint replacement after intra-articular corticosteroid measurement, this may be an area for future study. Interestingly, pain and function scores were not significantly different between the 2 groups, despite the changes in cartilage. Of note, prior studies have shown the largest gains in pain relief occur during the first 4 weeks after an injection and pain measurements in this study were performed 3 months after the injections. While helpful for determining the long-term effects of intra-articular glucocorticoid administration, short-term benefits were not measured.
The Osteoarthritis Research Society International guidelines for the nonpharmacologic management of knee osteoarthritis recommend intra-articular steroids for short-term pain management based on meta-analysis of randomized controlled trials [2]. Guidelines set forth by the American College of Rheumatology in 2012 for management of osteoarthritis of the knee also recommend intra-articular steroids [3]. Intra-articular corticosteroid injections were listed as interchangeable, in the absence of comorbid conditions leading to contraindications, with oral acetaminophen, oral and topical NSAIDs, and tramadol.
Hemoglobin A1c and blood pressure were not negatively affected by intra-articular steroids in this study.
Applications for Clinical Practice
While this study overall showed hastening of cartilage loss/damage without long-term pain relief benefit, there are instances where intra-articular steroid injection may still be appropriate. For example, in patients for whom joint replacement therapy has been scheduled and temporary pain relief is needed prior to surgery, intra-articular steroids may provide the pain relief desired without cartilage loss being a clinical concern. Further, if a patient is in need of temporary pain relief to attend an important event and is at a level of marginal functional status due to pain, the benefit may outweigh the risk of hastening cartilage damage/loss to that particular patient. In light of the knowledge gained by this study, any time an intra-articular steroid injection is offered to a patient it should be made clear that the pain relief gained may be temporary and could result in faster deterioration of the cartilage.
Nonpharmacologic therapies for osteoarthritis, including water-based and land-based physical therapy and weight reduction, should be utilized before offering intra-articular corticosteroid injections. These interventions not only have a positive effect on knee osteoarthritis [2] but also promote general health and well-being.
—Christina Downey, MD, Geisinger Medical Center, Danville, PA
1. Eckstein F, Boudreau RM, Wang Z, et al; OAI investigators. Trajectory of cartilage loss within 4 years of knee replacement—a nested case-control study from the osteoarthritis initiative. Osteoarthritis Cartilage 2014;22:1542–9.
2. McAlindon TE, Bannuru RR, Sullivan MC, et al. OARSI Guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis Cartilage 2014; 22:363–88.
3. Hochberg MC, Altman RD, Toupon K, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip and knee. Arthritis Care Res 2012;64:465–74.
Study Overview
Objective. To determine the effects of intra-articular triamcinolone acetonide at a dose of 40 mg administered at 3-month intervals on knee pain and progression of knee cartilage loss.
Design. Randomized, double-blind, placebo-controlled trial.
Setting and participants. 140 patients with ultrasonic features of synovitis and symptomatic knee osteoarthritis were selected from the patient pool at Tufts Medical Center in Boston, Massachusetts, between June 2011 and January 2015. Patients selected were age 45 years or older and met American College of Rheumatology osteoarthritis diagnostic criteria. Western Ontario and McMaster Universities (WOMAC) pain scores were between 2 and 8 on weight-bearing questions. Tibiofemoral osteoarthritis on posteroanterior weight bearing semi-flexed radiographs was evident in participants at a Kellegren-Lawrence grade 2 or 3. Eligible patients also had ultra-sonographic evidence of synovitis with an effusion larger than 2 mm in the study knee. Participants were excluded if they had undergone any trauma to the study joint such as osteonecrosis or a poorly controlled systemic illness. If the patient had used antibiotics, hyaluronic acid, glucosamine, chondroitin or had undergone recent intra-articular steroids in 3 months or fewer prior to the enrollment period the patient was excluded from the study. Further, patients were excluded if they were unable to undergo an MRI. Prior to pain assessments, patients were to discontinue any analgesics for 48 hours with the exception of acetaminophen if needed. The mean age of patients in this study was 58 years and the mean body mass index was 30. Half of patients had malalignment of the knee joint.
Intervention. 40 mg of a preparation of 40 mg/mL (total volume 1 mL) was injected into the intervention patients’ affected knees while 1 mL of 0.9% sodium chloride (saline solution) was injected into the control patients’ affected knees. Local anesthetic was not used. If present, synovial fluid was aspirated from the knee prior to injection. Injections were administered every 12 weeks for 2 years. Needle placement by ultrasound was utilized to ensure accurate injections, however, the probe was removed prior to injection. The injecting clinician was not involved in measuring outcomes in the study. Both intervention solutions were in identical syringes and were masked so the patient was blinded to which intervention he or she may have received.
Main outcome measure. Cartilage loss, pain, articular structural damage and physical function were the main outcome measures. Cartilage loss and structural damage were determined by MRI using validated quantitative and semi-quantitative assessments. Pain was measured with WOMAC scores and physical function was assessed using the 20-m walk test and the chair stand test. Patients were assessed during 9 scheduled visits at 3-month intervals when subjective data, blood pressure, and hemoglobin A1c levels were obtained. At 6-month intervals, patients underwent objective measures of function measured by a timed 20-m walk and chair stand testing. Evaluation of quantitative measures of cartilage analysis, semi-quantitative assessment of cartilage damage, bone marrow lesion and effusion volume measurement by MRI were done at time zero, 12 months and 24 months. The 36-Item Short-Form Health Survey was administered at these times as well. Results were computed with intention-to-treat analysis for all outcomes.
Main results. 140 patients were randomized out of 445 patients who were assessed for eligibility. Ten patients in the saline arm and 11 in the glucocorticoid arm were lost to follow-up. Groups were similar in age, BMI, varus or valgus malalignment, ultrasound measures, pain, and function measures. The group injected with triamcinolone had a higher rate of cartilage loss than the group injected with saline (–0.21 mm vs. –0.10 mm, P = 0.01) and had a higher rate of cartilage damage (–133.66 vs –72.41, P = 0.048). Cartilage denudation, bone marrow lesions, trabecular morphology and effusion volumes were not significantly different between groups. WOMAC pain measure differences from baseline in the groups were similar (–1.2 for triamcinolone group vs. –1.9 for the saline group, P = 0.17). There were also no differences between groups for the Visual Analog Scale pain score, stiffness, the 20-m walk test, or the chair stand test. Adverse events were similar between groups. At the end of the study protocol, only 45% of patients were able to correctly identify the group to which they were assigned.
Conclusion. In patients meeting American College of Rheumatology diagnostic criteria for osteoarthritis and evidence of inflammation in the affected joint, 40 mg of triamcinolone administered intra-articularly is no more effective in relieving pain or physical functioning after 2 years of injections every 3 months than normal saline. Injecting 40 mg of triamcinolone may hasten cartilage loss and damage as measured by MRI.
Commentary
In the current study, the rate of cartilage loss in the saline group was on par with prior studies examining the natural history of cartilage loss, suggesting that intra-articular steroid may actually be hastening the loss of cartilage observed in this study. The effect size was deemed moderate by the authors, though clinically significant minimal change has not been determined. Intra-articular cartilage loss is positively correlated with arthroplasty rates [1]. While this study was not designed to investigate the rate of joint replacement after intra-articular corticosteroid measurement, this may be an area for future study. Interestingly, pain and function scores were not significantly different between the 2 groups, despite the changes in cartilage. Of note, prior studies have shown the largest gains in pain relief occur during the first 4 weeks after an injection and pain measurements in this study were performed 3 months after the injections. While helpful for determining the long-term effects of intra-articular glucocorticoid administration, short-term benefits were not measured.
The Osteoarthritis Research Society International guidelines for the nonpharmacologic management of knee osteoarthritis recommend intra-articular steroids for short-term pain management based on meta-analysis of randomized controlled trials [2]. Guidelines set forth by the American College of Rheumatology in 2012 for management of osteoarthritis of the knee also recommend intra-articular steroids [3]. Intra-articular corticosteroid injections were listed as interchangeable, in the absence of comorbid conditions leading to contraindications, with oral acetaminophen, oral and topical NSAIDs, and tramadol.
Hemoglobin A1c and blood pressure were not negatively affected by intra-articular steroids in this study.
Applications for Clinical Practice
While this study overall showed hastening of cartilage loss/damage without long-term pain relief benefit, there are instances where intra-articular steroid injection may still be appropriate. For example, in patients for whom joint replacement therapy has been scheduled and temporary pain relief is needed prior to surgery, intra-articular steroids may provide the pain relief desired without cartilage loss being a clinical concern. Further, if a patient is in need of temporary pain relief to attend an important event and is at a level of marginal functional status due to pain, the benefit may outweigh the risk of hastening cartilage damage/loss to that particular patient. In light of the knowledge gained by this study, any time an intra-articular steroid injection is offered to a patient it should be made clear that the pain relief gained may be temporary and could result in faster deterioration of the cartilage.
Nonpharmacologic therapies for osteoarthritis, including water-based and land-based physical therapy and weight reduction, should be utilized before offering intra-articular corticosteroid injections. These interventions not only have a positive effect on knee osteoarthritis [2] but also promote general health and well-being.
—Christina Downey, MD, Geisinger Medical Center, Danville, PA
Study Overview
Objective. To determine the effects of intra-articular triamcinolone acetonide at a dose of 40 mg administered at 3-month intervals on knee pain and progression of knee cartilage loss.
Design. Randomized, double-blind, placebo-controlled trial.
Setting and participants. 140 patients with ultrasonic features of synovitis and symptomatic knee osteoarthritis were selected from the patient pool at Tufts Medical Center in Boston, Massachusetts, between June 2011 and January 2015. Patients selected were age 45 years or older and met American College of Rheumatology osteoarthritis diagnostic criteria. Western Ontario and McMaster Universities (WOMAC) pain scores were between 2 and 8 on weight-bearing questions. Tibiofemoral osteoarthritis on posteroanterior weight bearing semi-flexed radiographs was evident in participants at a Kellegren-Lawrence grade 2 or 3. Eligible patients also had ultra-sonographic evidence of synovitis with an effusion larger than 2 mm in the study knee. Participants were excluded if they had undergone any trauma to the study joint such as osteonecrosis or a poorly controlled systemic illness. If the patient had used antibiotics, hyaluronic acid, glucosamine, chondroitin or had undergone recent intra-articular steroids in 3 months or fewer prior to the enrollment period the patient was excluded from the study. Further, patients were excluded if they were unable to undergo an MRI. Prior to pain assessments, patients were to discontinue any analgesics for 48 hours with the exception of acetaminophen if needed. The mean age of patients in this study was 58 years and the mean body mass index was 30. Half of patients had malalignment of the knee joint.
Intervention. 40 mg of a preparation of 40 mg/mL (total volume 1 mL) was injected into the intervention patients’ affected knees while 1 mL of 0.9% sodium chloride (saline solution) was injected into the control patients’ affected knees. Local anesthetic was not used. If present, synovial fluid was aspirated from the knee prior to injection. Injections were administered every 12 weeks for 2 years. Needle placement by ultrasound was utilized to ensure accurate injections, however, the probe was removed prior to injection. The injecting clinician was not involved in measuring outcomes in the study. Both intervention solutions were in identical syringes and were masked so the patient was blinded to which intervention he or she may have received.
Main outcome measure. Cartilage loss, pain, articular structural damage and physical function were the main outcome measures. Cartilage loss and structural damage were determined by MRI using validated quantitative and semi-quantitative assessments. Pain was measured with WOMAC scores and physical function was assessed using the 20-m walk test and the chair stand test. Patients were assessed during 9 scheduled visits at 3-month intervals when subjective data, blood pressure, and hemoglobin A1c levels were obtained. At 6-month intervals, patients underwent objective measures of function measured by a timed 20-m walk and chair stand testing. Evaluation of quantitative measures of cartilage analysis, semi-quantitative assessment of cartilage damage, bone marrow lesion and effusion volume measurement by MRI were done at time zero, 12 months and 24 months. The 36-Item Short-Form Health Survey was administered at these times as well. Results were computed with intention-to-treat analysis for all outcomes.
Main results. 140 patients were randomized out of 445 patients who were assessed for eligibility. Ten patients in the saline arm and 11 in the glucocorticoid arm were lost to follow-up. Groups were similar in age, BMI, varus or valgus malalignment, ultrasound measures, pain, and function measures. The group injected with triamcinolone had a higher rate of cartilage loss than the group injected with saline (–0.21 mm vs. –0.10 mm, P = 0.01) and had a higher rate of cartilage damage (–133.66 vs –72.41, P = 0.048). Cartilage denudation, bone marrow lesions, trabecular morphology and effusion volumes were not significantly different between groups. WOMAC pain measure differences from baseline in the groups were similar (–1.2 for triamcinolone group vs. –1.9 for the saline group, P = 0.17). There were also no differences between groups for the Visual Analog Scale pain score, stiffness, the 20-m walk test, or the chair stand test. Adverse events were similar between groups. At the end of the study protocol, only 45% of patients were able to correctly identify the group to which they were assigned.
Conclusion. In patients meeting American College of Rheumatology diagnostic criteria for osteoarthritis and evidence of inflammation in the affected joint, 40 mg of triamcinolone administered intra-articularly is no more effective in relieving pain or physical functioning after 2 years of injections every 3 months than normal saline. Injecting 40 mg of triamcinolone may hasten cartilage loss and damage as measured by MRI.
Commentary
In the current study, the rate of cartilage loss in the saline group was on par with prior studies examining the natural history of cartilage loss, suggesting that intra-articular steroid may actually be hastening the loss of cartilage observed in this study. The effect size was deemed moderate by the authors, though clinically significant minimal change has not been determined. Intra-articular cartilage loss is positively correlated with arthroplasty rates [1]. While this study was not designed to investigate the rate of joint replacement after intra-articular corticosteroid measurement, this may be an area for future study. Interestingly, pain and function scores were not significantly different between the 2 groups, despite the changes in cartilage. Of note, prior studies have shown the largest gains in pain relief occur during the first 4 weeks after an injection and pain measurements in this study were performed 3 months after the injections. While helpful for determining the long-term effects of intra-articular glucocorticoid administration, short-term benefits were not measured.
The Osteoarthritis Research Society International guidelines for the nonpharmacologic management of knee osteoarthritis recommend intra-articular steroids for short-term pain management based on meta-analysis of randomized controlled trials [2]. Guidelines set forth by the American College of Rheumatology in 2012 for management of osteoarthritis of the knee also recommend intra-articular steroids [3]. Intra-articular corticosteroid injections were listed as interchangeable, in the absence of comorbid conditions leading to contraindications, with oral acetaminophen, oral and topical NSAIDs, and tramadol.
Hemoglobin A1c and blood pressure were not negatively affected by intra-articular steroids in this study.
Applications for Clinical Practice
While this study overall showed hastening of cartilage loss/damage without long-term pain relief benefit, there are instances where intra-articular steroid injection may still be appropriate. For example, in patients for whom joint replacement therapy has been scheduled and temporary pain relief is needed prior to surgery, intra-articular steroids may provide the pain relief desired without cartilage loss being a clinical concern. Further, if a patient is in need of temporary pain relief to attend an important event and is at a level of marginal functional status due to pain, the benefit may outweigh the risk of hastening cartilage damage/loss to that particular patient. In light of the knowledge gained by this study, any time an intra-articular steroid injection is offered to a patient it should be made clear that the pain relief gained may be temporary and could result in faster deterioration of the cartilage.
Nonpharmacologic therapies for osteoarthritis, including water-based and land-based physical therapy and weight reduction, should be utilized before offering intra-articular corticosteroid injections. These interventions not only have a positive effect on knee osteoarthritis [2] but also promote general health and well-being.
—Christina Downey, MD, Geisinger Medical Center, Danville, PA
1. Eckstein F, Boudreau RM, Wang Z, et al; OAI investigators. Trajectory of cartilage loss within 4 years of knee replacement—a nested case-control study from the osteoarthritis initiative. Osteoarthritis Cartilage 2014;22:1542–9.
2. McAlindon TE, Bannuru RR, Sullivan MC, et al. OARSI Guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis Cartilage 2014; 22:363–88.
3. Hochberg MC, Altman RD, Toupon K, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip and knee. Arthritis Care Res 2012;64:465–74.
1. Eckstein F, Boudreau RM, Wang Z, et al; OAI investigators. Trajectory of cartilage loss within 4 years of knee replacement—a nested case-control study from the osteoarthritis initiative. Osteoarthritis Cartilage 2014;22:1542–9.
2. McAlindon TE, Bannuru RR, Sullivan MC, et al. OARSI Guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis Cartilage 2014; 22:363–88.
3. Hochberg MC, Altman RD, Toupon K, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip and knee. Arthritis Care Res 2012;64:465–74.
Nearly half of patients who stop taking opioids for 6 months resume use later
SAN DIEGO – A new study of medical records offers insights into the persistence of opioid use: Most patients who were prescribed opioid painkillers did not go back for a refill right away, but nearly half of patients who stopped taking the drugs for at least 6 months ended up using them again over a 3-year period.
“This key finding indicates that programs that address opioid use need to focus on long-term support and education to ensure that individuals do not become long-term users,” psychiatrist and lead author Shareh Ghani, MD, vice president and medical director of Magellan Health Services, San Francisco, said in an interview.
Researchers also found that opioid use appeared linked to three unexpected conditions – lipid disorders, hypertension, and sleep-wake disorders – and found that more than half of those who had at least two prescriptions for high-dose opioids kept taking the drugs over 18 months after an initial 90-day period.

Dr. Ghani and his colleague, Gowri Shetty, MPH, analyzed medical and pharmacy data from 2009-2012 for 2.5 million people. The participants, aged 20-64 years, came from across the United States and were part of a commercial health plan.
The researchers found that 21% had received one prescription for an opioid. Users considered at risk for persistent use – more than one prescription over 3 years – were more likely than were nonusers to have these characteristics: spondylosis and other back problems (odds ratio, 5.3), substance-related and addictive disorders (OR, 4.6), sleep-wake disorders (OR, 2.2), depressive disorders (OR, 1.7), headaches (OR, 2.1), and anxiety disorders (OR, 1.5.) The P values for all of those characteristics were less than .001.
They also found that patients who received certain kinds of treatment were at higher risk, compared with nonusers: those who were treated for substance abuse treatment (OR, 4.5), in emergency departments (OR, 3.2), with anesthesia (OR, 4.2), for mental health issues (OR, 2.3), and with surgery (OR, 2.0). The P values for all of those characteristics also were less than .001.
“The unexpected findings were the presence of lipid disorders, hypertension, and sleep-wake disorders. These diagnoses were not found in other literature,” Dr. Ghani said in an interview. “These conditions, however, are related to others that are known. For instance, a person with knee joint pain who is overweight – a known risk factor – may also have hypertension and lipid disorders.”
The researchers also discovered that 80% of patients who received an opioid prescription did not get a refill. Of those who had at least two prescriptions and a stable dose over an initial 90 days, 14% went on to have more prescriptions and a boost in dosage over 18 months, while 12% stayed the same and almost 74% took less.
But the situation was different for those with at least two prescriptions and a high dose (more than 120 mg) over an initial 90 days: 56% of them stayed at that level over 18 months.
The researchers also found that 48% of those who had stopped using opioids for at least 6 months went on to use them again. This high rate “suggests that physicians and patients need to be aware of the high risk of dependence and addiction for some individuals,” Dr. Ghani said. “Studying prescription fill behaviors and the persistence of prescription opioid users helps identify individuals at high risk for persistent use and may provide a better understanding of how to target interventions for inappropriate opioid use.”
The study has limitations. It does not indicate whether patients became substance abusers, nor does it provide details about opioids obtained illegally. Still, “we do know from literature and clinical experience that staying on prescription opioids may lead to dependence, escalation of dose, and increased risk of developing addictions that can lead to using street drugs like heroin,” Dr. Ghani said.
Magellan funded the study. Dr. Ghani reported no additional disclosures.
SAN DIEGO – A new study of medical records offers insights into the persistence of opioid use: Most patients who were prescribed opioid painkillers did not go back for a refill right away, but nearly half of patients who stopped taking the drugs for at least 6 months ended up using them again over a 3-year period.
“This key finding indicates that programs that address opioid use need to focus on long-term support and education to ensure that individuals do not become long-term users,” psychiatrist and lead author Shareh Ghani, MD, vice president and medical director of Magellan Health Services, San Francisco, said in an interview.
Researchers also found that opioid use appeared linked to three unexpected conditions – lipid disorders, hypertension, and sleep-wake disorders – and found that more than half of those who had at least two prescriptions for high-dose opioids kept taking the drugs over 18 months after an initial 90-day period.
Dr. Ghani and his colleague, Gowri Shetty, MPH, analyzed medical and pharmacy data from 2009-2012 for 2.5 million people. The participants, aged 20-64 years, came from across the United States and were part of a commercial health plan.
The researchers found that 21% had received one prescription for an opioid. Users considered at risk for persistent use – more than one prescription over 3 years – were more likely than were nonusers to have these characteristics: spondylosis and other back problems (odds ratio, 5.3), substance-related and addictive disorders (OR, 4.6), sleep-wake disorders (OR, 2.2), depressive disorders (OR, 1.7), headaches (OR, 2.1), and anxiety disorders (OR, 1.5.) The P values for all of those characteristics were less than .001.
They also found that patients who received certain kinds of treatment were at higher risk, compared with nonusers: those who were treated for substance abuse treatment (OR, 4.5), in emergency departments (OR, 3.2), with anesthesia (OR, 4.2), for mental health issues (OR, 2.3), and with surgery (OR, 2.0). The P values for all of those characteristics also were less than .001.
“The unexpected findings were the presence of lipid disorders, hypertension, and sleep-wake disorders. These diagnoses were not found in other literature,” Dr. Ghani said in an interview. “These conditions, however, are related to others that are known. For instance, a person with knee joint pain who is overweight – a known risk factor – may also have hypertension and lipid disorders.”
The researchers also discovered that 80% of patients who received an opioid prescription did not get a refill. Of those who had at least two prescriptions and a stable dose over an initial 90 days, 14% went on to have more prescriptions and a boost in dosage over 18 months, while 12% stayed the same and almost 74% took less.
But the situation was different for those with at least two prescriptions and a high dose (more than 120 mg) over an initial 90 days: 56% of them stayed at that level over 18 months.
The researchers also found that 48% of those who had stopped using opioids for at least 6 months went on to use them again. This high rate “suggests that physicians and patients need to be aware of the high risk of dependence and addiction for some individuals,” Dr. Ghani said. “Studying prescription fill behaviors and the persistence of prescription opioid users helps identify individuals at high risk for persistent use and may provide a better understanding of how to target interventions for inappropriate opioid use.”
The study has limitations. It does not indicate whether patients became substance abusers, nor does it provide details about opioids obtained illegally. Still, “we do know from literature and clinical experience that staying on prescription opioids may lead to dependence, escalation of dose, and increased risk of developing addictions that can lead to using street drugs like heroin,” Dr. Ghani said.
Magellan funded the study. Dr. Ghani reported no additional disclosures.
SAN DIEGO – A new study of medical records offers insights into the persistence of opioid use: Most patients who were prescribed opioid painkillers did not go back for a refill right away, but nearly half of patients who stopped taking the drugs for at least 6 months ended up using them again over a 3-year period.
“This key finding indicates that programs that address opioid use need to focus on long-term support and education to ensure that individuals do not become long-term users,” psychiatrist and lead author Shareh Ghani, MD, vice president and medical director of Magellan Health Services, San Francisco, said in an interview.
Researchers also found that opioid use appeared linked to three unexpected conditions – lipid disorders, hypertension, and sleep-wake disorders – and found that more than half of those who had at least two prescriptions for high-dose opioids kept taking the drugs over 18 months after an initial 90-day period.
Dr. Ghani and his colleague, Gowri Shetty, MPH, analyzed medical and pharmacy data from 2009-2012 for 2.5 million people. The participants, aged 20-64 years, came from across the United States and were part of a commercial health plan.
The researchers found that 21% had received one prescription for an opioid. Users considered at risk for persistent use – more than one prescription over 3 years – were more likely than were nonusers to have these characteristics: spondylosis and other back problems (odds ratio, 5.3), substance-related and addictive disorders (OR, 4.6), sleep-wake disorders (OR, 2.2), depressive disorders (OR, 1.7), headaches (OR, 2.1), and anxiety disorders (OR, 1.5.) The P values for all of those characteristics were less than .001.
They also found that patients who received certain kinds of treatment were at higher risk, compared with nonusers: those who were treated for substance abuse treatment (OR, 4.5), in emergency departments (OR, 3.2), with anesthesia (OR, 4.2), for mental health issues (OR, 2.3), and with surgery (OR, 2.0). The P values for all of those characteristics also were less than .001.
“The unexpected findings were the presence of lipid disorders, hypertension, and sleep-wake disorders. These diagnoses were not found in other literature,” Dr. Ghani said in an interview. “These conditions, however, are related to others that are known. For instance, a person with knee joint pain who is overweight – a known risk factor – may also have hypertension and lipid disorders.”
The researchers also discovered that 80% of patients who received an opioid prescription did not get a refill. Of those who had at least two prescriptions and a stable dose over an initial 90 days, 14% went on to have more prescriptions and a boost in dosage over 18 months, while 12% stayed the same and almost 74% took less.
But the situation was different for those with at least two prescriptions and a high dose (more than 120 mg) over an initial 90 days: 56% of them stayed at that level over 18 months.
The researchers also found that 48% of those who had stopped using opioids for at least 6 months went on to use them again. This high rate “suggests that physicians and patients need to be aware of the high risk of dependence and addiction for some individuals,” Dr. Ghani said. “Studying prescription fill behaviors and the persistence of prescription opioid users helps identify individuals at high risk for persistent use and may provide a better understanding of how to target interventions for inappropriate opioid use.”
The study has limitations. It does not indicate whether patients became substance abusers, nor does it provide details about opioids obtained illegally. Still, “we do know from literature and clinical experience that staying on prescription opioids may lead to dependence, escalation of dose, and increased risk of developing addictions that can lead to using street drugs like heroin,” Dr. Ghani said.
Magellan funded the study. Dr. Ghani reported no additional disclosures.
AT APA
Key clinical point:
Major finding: Forty-eight percent of patients who had stopped using opioids for at least 6 months went on to use them again.
Data source: An analysis of medical and pharmacy data from 2009-2012 for 2.5 million people aged 20-64 who were part of a commercial health plan.
Disclosures: Dr. Ghani is vice president and medical director of Magellan Health Services, which funded the study.
Anabolic agents for osteoporosis have limited role so far
SAN FRANCISCO – Parathyroid hormone and parathyroid hormone–related protein analogs show promise for treating osteoporosis, but, for now, they’re reserved for the most severe cases.
Teriparatide, a parathyroid hormone analog, is the first treatment that stimulates bone formation instead of inhibiting bone resorption, but studies to date are too small to evaluate its effect on hip fractures, Jeffrey A. Tice, MD, said at the UCSF Annual Advances in Internal Medicine meeting.

Abaloparatide, a parathyroid hormone-related protein analog approved in April 2017, requires subcutaneous dosing of 80 mcg daily for up to 2 years and has been found to increase bone density in the spine by 11% and in the hip by 4%, compared with placebo, over 18 months. In women with pre-existing vertebral fractures, the agent was found to reduce the incidence of vertebral fractures by 86% and nonvertebral fragility fractures by 43%, but data are not adequate to evaluate its effect on hip fractures. Adverse reactions include hypercalciuria, nausea, hypercalcemia, orthostatic hypotension, tachycardia, and injection site reactions.
Studies to date have shown that combining either teriparatide or abaloparatide with an antiresorptive drug is less effective than either agent alone. However, both agents must be followed by an antiresorptive agent. “These drugs are expensive,” Dr. Tice said. “Right now, they’re reserved for patients with severe osteoporosis.”
The lifetime risk for osteoporotic fractures is 50% in women and 20% in men, and they cause significant morbidity and mortality. Among U.S. hospitalizations for women 55 years and older between 2000 and 2012, Dr. Tice noted, 4.9 million were for osteoporotic fractures, 3 million were for stroke, and 2.9 million were for myocardial infarction.
“Osteoporosis is a very common condition, but it’s under-recognized, in part because it’s a silent disease,” he said. “Only 20%-30% of patients with bone mineral densities less than –2.5 are treated in this country. And, 12 months after hip fracture, only 2% had a dual-energy x-ray absorptiometry [DXA] test, and only 15% were treated with an appropriate drug. We should be asking about fracture history, note vertebral fractures, treat those patients, and we should remember to use chart reminders for DXA.”
Clinical guidelines from the American College of Physicians and other groups recommend alendronate, risedronate, zoledronic acid, or denosumab as first-line therapy for women with osteoporosis. “There are no head to head trials to indicate which agent is best,” Dr. Tice said. “They reduce the fracture risk by 30%-50%, primarily in patients with an existing vertebral fracture or a T score below –2.5.” The use of hormone therapy and raloxifene are generally not recommended.
In a review published in the New England Journal of Medicine, researchers Dennis M. Black, MD, and Clifford J. Rosen, MD, estimated the number of patients needed to treat for 3 years to prevent various fractures (N Engl J Med. 2016 Jan 21;374[3]:254-62). They found that, for nonvertebral fractures, including hip, 35 patients need to be treated for 3 years to prevent one of those fractures, 90 patients for 3 years to prevent one hip fracture, and 14 patients for 3 years to prevent one vertebral fracture.
In the FIT trial, 20% of women taking alendronate lost BMD during the first year (JAMA. 1998 Dec 23-30;280[24]:2077-82). However, those same patients had a 50% fracture reduction, and 92% regained the lost bone mineral density (BMD) by the next measurement. “Using DXA to measure BMD after 1 year of therapy does not accurately predict what will happen over time or reflect fracture reduction,” Dr. Tice said. “Effective treatment for osteoporosis should not be changed because of loss of BMD during the first year of use.”
A rare but potential harm from treatment with bisphosphonates includes osteonecrosis of the jaw, which is believed to affect only 1 in 10,000 patients who are treated for 10 years. Most of these cases (94%) were caused by IV bisphosphonates. Only 4% of cases were being treated for osteoporosis, and 60% were caused by tooth extraction. Because of this, a dental exam is recommended before starting patients on bisphosphonate therapy, but this small risk of osteonecrosis of the jaw “is not a reason to stop bisphosphonate therapy,” Dr. Tice said.
Other concerns include an increased risk for atrial fibrillation that has been observed in randomized, controlled trials of zoledronate and alendronate. “There has been no association in other trials,” Dr. Tice said. “This is likely a chance finding, likely spurious.”
Reports of an increased risk of esophageal cancer from bisphosphonate use have also been suggested, but these come from case series and from two conflicting cohorts of data. “This is most likely not a real finding but is a concern because of clinical reports of esophagitis associated with oral bisphosphonates,” he said.
Another concern from long-term bisphosphonate use is the development of atypical femoral fractures, a subtrochanteric fracture with atypical features. “These are transverse fractures of the femur and are likely a real effect of bisphosphonates,” Dr. Tice said. “They are characterized by transverse fractures, cortical thickening, and the 10-year risk is about 1:200. It’s similar to a stress fracture, and it’s often preceded by pain.”
To bring perspective on the risk of developing an atypical femoral fracture, Dr. Tice offered a comparison. If 1,000 women are treated for 3 years with zoledronic acid, it will prevent 71 vertebral fractures, 11 hip fractures, and 18 other fractures. “So, the best estimate is that you would cause 0.1 atypical femoral fractures,” he said. “That really means that, for every one atypical femoral fracture caused, you’ve prevented 110 hip fractures. So, yes, there’s a risk of harm – but there is so much more benefit.”
Dr. Tice reported having no relevant financial disclosures.
SAN FRANCISCO – Parathyroid hormone and parathyroid hormone–related protein analogs show promise for treating osteoporosis, but, for now, they’re reserved for the most severe cases.
Teriparatide, a parathyroid hormone analog, is the first treatment that stimulates bone formation instead of inhibiting bone resorption, but studies to date are too small to evaluate its effect on hip fractures, Jeffrey A. Tice, MD, said at the UCSF Annual Advances in Internal Medicine meeting.
Abaloparatide, a parathyroid hormone-related protein analog approved in April 2017, requires subcutaneous dosing of 80 mcg daily for up to 2 years and has been found to increase bone density in the spine by 11% and in the hip by 4%, compared with placebo, over 18 months. In women with pre-existing vertebral fractures, the agent was found to reduce the incidence of vertebral fractures by 86% and nonvertebral fragility fractures by 43%, but data are not adequate to evaluate its effect on hip fractures. Adverse reactions include hypercalciuria, nausea, hypercalcemia, orthostatic hypotension, tachycardia, and injection site reactions.
Studies to date have shown that combining either teriparatide or abaloparatide with an antiresorptive drug is less effective than either agent alone. However, both agents must be followed by an antiresorptive agent. “These drugs are expensive,” Dr. Tice said. “Right now, they’re reserved for patients with severe osteoporosis.”
The lifetime risk for osteoporotic fractures is 50% in women and 20% in men, and they cause significant morbidity and mortality. Among U.S. hospitalizations for women 55 years and older between 2000 and 2012, Dr. Tice noted, 4.9 million were for osteoporotic fractures, 3 million were for stroke, and 2.9 million were for myocardial infarction.
“Osteoporosis is a very common condition, but it’s under-recognized, in part because it’s a silent disease,” he said. “Only 20%-30% of patients with bone mineral densities less than –2.5 are treated in this country. And, 12 months after hip fracture, only 2% had a dual-energy x-ray absorptiometry [DXA] test, and only 15% were treated with an appropriate drug. We should be asking about fracture history, note vertebral fractures, treat those patients, and we should remember to use chart reminders for DXA.”
Clinical guidelines from the American College of Physicians and other groups recommend alendronate, risedronate, zoledronic acid, or denosumab as first-line therapy for women with osteoporosis. “There are no head to head trials to indicate which agent is best,” Dr. Tice said. “They reduce the fracture risk by 30%-50%, primarily in patients with an existing vertebral fracture or a T score below –2.5.” The use of hormone therapy and raloxifene are generally not recommended.
In a review published in the New England Journal of Medicine, researchers Dennis M. Black, MD, and Clifford J. Rosen, MD, estimated the number of patients needed to treat for 3 years to prevent various fractures (N Engl J Med. 2016 Jan 21;374[3]:254-62). They found that, for nonvertebral fractures, including hip, 35 patients need to be treated for 3 years to prevent one of those fractures, 90 patients for 3 years to prevent one hip fracture, and 14 patients for 3 years to prevent one vertebral fracture.
In the FIT trial, 20% of women taking alendronate lost BMD during the first year (JAMA. 1998 Dec 23-30;280[24]:2077-82). However, those same patients had a 50% fracture reduction, and 92% regained the lost bone mineral density (BMD) by the next measurement. “Using DXA to measure BMD after 1 year of therapy does not accurately predict what will happen over time or reflect fracture reduction,” Dr. Tice said. “Effective treatment for osteoporosis should not be changed because of loss of BMD during the first year of use.”
A rare but potential harm from treatment with bisphosphonates includes osteonecrosis of the jaw, which is believed to affect only 1 in 10,000 patients who are treated for 10 years. Most of these cases (94%) were caused by IV bisphosphonates. Only 4% of cases were being treated for osteoporosis, and 60% were caused by tooth extraction. Because of this, a dental exam is recommended before starting patients on bisphosphonate therapy, but this small risk of osteonecrosis of the jaw “is not a reason to stop bisphosphonate therapy,” Dr. Tice said.
Other concerns include an increased risk for atrial fibrillation that has been observed in randomized, controlled trials of zoledronate and alendronate. “There has been no association in other trials,” Dr. Tice said. “This is likely a chance finding, likely spurious.”
Reports of an increased risk of esophageal cancer from bisphosphonate use have also been suggested, but these come from case series and from two conflicting cohorts of data. “This is most likely not a real finding but is a concern because of clinical reports of esophagitis associated with oral bisphosphonates,” he said.
Another concern from long-term bisphosphonate use is the development of atypical femoral fractures, a subtrochanteric fracture with atypical features. “These are transverse fractures of the femur and are likely a real effect of bisphosphonates,” Dr. Tice said. “They are characterized by transverse fractures, cortical thickening, and the 10-year risk is about 1:200. It’s similar to a stress fracture, and it’s often preceded by pain.”
To bring perspective on the risk of developing an atypical femoral fracture, Dr. Tice offered a comparison. If 1,000 women are treated for 3 years with zoledronic acid, it will prevent 71 vertebral fractures, 11 hip fractures, and 18 other fractures. “So, the best estimate is that you would cause 0.1 atypical femoral fractures,” he said. “That really means that, for every one atypical femoral fracture caused, you’ve prevented 110 hip fractures. So, yes, there’s a risk of harm – but there is so much more benefit.”
Dr. Tice reported having no relevant financial disclosures.
SAN FRANCISCO – Parathyroid hormone and parathyroid hormone–related protein analogs show promise for treating osteoporosis, but, for now, they’re reserved for the most severe cases.
Teriparatide, a parathyroid hormone analog, is the first treatment that stimulates bone formation instead of inhibiting bone resorption, but studies to date are too small to evaluate its effect on hip fractures, Jeffrey A. Tice, MD, said at the UCSF Annual Advances in Internal Medicine meeting.
Abaloparatide, a parathyroid hormone-related protein analog approved in April 2017, requires subcutaneous dosing of 80 mcg daily for up to 2 years and has been found to increase bone density in the spine by 11% and in the hip by 4%, compared with placebo, over 18 months. In women with pre-existing vertebral fractures, the agent was found to reduce the incidence of vertebral fractures by 86% and nonvertebral fragility fractures by 43%, but data are not adequate to evaluate its effect on hip fractures. Adverse reactions include hypercalciuria, nausea, hypercalcemia, orthostatic hypotension, tachycardia, and injection site reactions.
Studies to date have shown that combining either teriparatide or abaloparatide with an antiresorptive drug is less effective than either agent alone. However, both agents must be followed by an antiresorptive agent. “These drugs are expensive,” Dr. Tice said. “Right now, they’re reserved for patients with severe osteoporosis.”
The lifetime risk for osteoporotic fractures is 50% in women and 20% in men, and they cause significant morbidity and mortality. Among U.S. hospitalizations for women 55 years and older between 2000 and 2012, Dr. Tice noted, 4.9 million were for osteoporotic fractures, 3 million were for stroke, and 2.9 million were for myocardial infarction.
“Osteoporosis is a very common condition, but it’s under-recognized, in part because it’s a silent disease,” he said. “Only 20%-30% of patients with bone mineral densities less than –2.5 are treated in this country. And, 12 months after hip fracture, only 2% had a dual-energy x-ray absorptiometry [DXA] test, and only 15% were treated with an appropriate drug. We should be asking about fracture history, note vertebral fractures, treat those patients, and we should remember to use chart reminders for DXA.”
Clinical guidelines from the American College of Physicians and other groups recommend alendronate, risedronate, zoledronic acid, or denosumab as first-line therapy for women with osteoporosis. “There are no head to head trials to indicate which agent is best,” Dr. Tice said. “They reduce the fracture risk by 30%-50%, primarily in patients with an existing vertebral fracture or a T score below –2.5.” The use of hormone therapy and raloxifene are generally not recommended.
In a review published in the New England Journal of Medicine, researchers Dennis M. Black, MD, and Clifford J. Rosen, MD, estimated the number of patients needed to treat for 3 years to prevent various fractures (N Engl J Med. 2016 Jan 21;374[3]:254-62). They found that, for nonvertebral fractures, including hip, 35 patients need to be treated for 3 years to prevent one of those fractures, 90 patients for 3 years to prevent one hip fracture, and 14 patients for 3 years to prevent one vertebral fracture.
In the FIT trial, 20% of women taking alendronate lost BMD during the first year (JAMA. 1998 Dec 23-30;280[24]:2077-82). However, those same patients had a 50% fracture reduction, and 92% regained the lost bone mineral density (BMD) by the next measurement. “Using DXA to measure BMD after 1 year of therapy does not accurately predict what will happen over time or reflect fracture reduction,” Dr. Tice said. “Effective treatment for osteoporosis should not be changed because of loss of BMD during the first year of use.”
A rare but potential harm from treatment with bisphosphonates includes osteonecrosis of the jaw, which is believed to affect only 1 in 10,000 patients who are treated for 10 years. Most of these cases (94%) were caused by IV bisphosphonates. Only 4% of cases were being treated for osteoporosis, and 60% were caused by tooth extraction. Because of this, a dental exam is recommended before starting patients on bisphosphonate therapy, but this small risk of osteonecrosis of the jaw “is not a reason to stop bisphosphonate therapy,” Dr. Tice said.
Other concerns include an increased risk for atrial fibrillation that has been observed in randomized, controlled trials of zoledronate and alendronate. “There has been no association in other trials,” Dr. Tice said. “This is likely a chance finding, likely spurious.”
Reports of an increased risk of esophageal cancer from bisphosphonate use have also been suggested, but these come from case series and from two conflicting cohorts of data. “This is most likely not a real finding but is a concern because of clinical reports of esophagitis associated with oral bisphosphonates,” he said.
Another concern from long-term bisphosphonate use is the development of atypical femoral fractures, a subtrochanteric fracture with atypical features. “These are transverse fractures of the femur and are likely a real effect of bisphosphonates,” Dr. Tice said. “They are characterized by transverse fractures, cortical thickening, and the 10-year risk is about 1:200. It’s similar to a stress fracture, and it’s often preceded by pain.”
To bring perspective on the risk of developing an atypical femoral fracture, Dr. Tice offered a comparison. If 1,000 women are treated for 3 years with zoledronic acid, it will prevent 71 vertebral fractures, 11 hip fractures, and 18 other fractures. “So, the best estimate is that you would cause 0.1 atypical femoral fractures,” he said. “That really means that, for every one atypical femoral fracture caused, you’ve prevented 110 hip fractures. So, yes, there’s a risk of harm – but there is so much more benefit.”
Dr. Tice reported having no relevant financial disclosures.
EXPERT ANALYSIS FROM THE ANNUAL ADVANCES IN INTERNAL MEDICINE
Antimicrobial Stewardship Programs: Effects on Clinical and Economic Outcomes and Future Directions
From the Ernest Mario School of Pharmacy, Rutgers, The State University of New Jersey, Piscataway, NJ.
Abstract
- Objective: To review the evidence evaluating inpatient antimicrobial stewardship programs (ASPs) with a focus on clinical and economic outcomes.
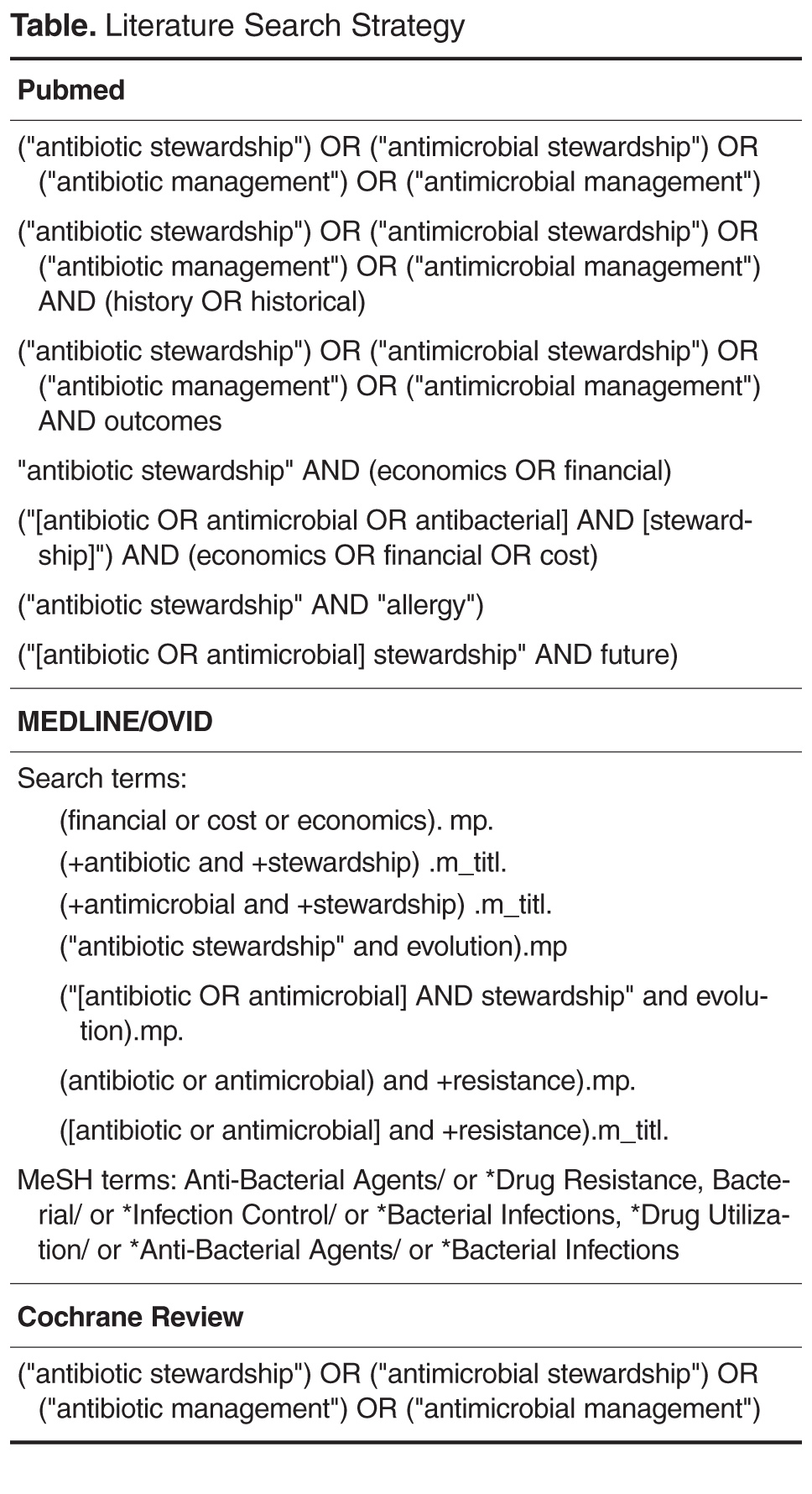
- Methods: Pubmed/MEDLINE and the Cochrane Database of Systematic Reviews were used to identify systematic reviews, meta-analyses, randomized controlled trials, and other relevant literature evaluating the clinical and economic impact of ASP interventions.
- Results: A total of 5 meta-analyses, 3 systematic reviews, and 10 clinical studies (2 randomized controlled, 5 observational, and 3 quasi-experimental studies) were identified for analysis. ASPs were associated with a reduction in antimicrobial consumption and use. However, due to the heterogeneity of outcomes measured among studies, the effectiveness of ASPs varied with the measures used. There are data supporting the cost savings associated with ASPs, but these studies are more sparse. Most of the available evidence supporting ASPs is of low quality, and intervention strategies vary widely among available studies.
- Conclusion: Much of the evidence reviewed supports the assertion that ASPs result in a more judicious use of antimicrobials and lead to better patient care in the inpatient setting. While clinical outcomes vary between programs, there are ubiquitous positive benefits associated with ASPs in terms of antimicrobial consumption, C. difficile infection rates, and resistance, with few adverse effects. To date, economic outcomes have been difficult to uniformly quantify, but there are data supporting the economic benefits of ASPs. As the number of ASPs continues to grow, it is imperative that standardized metrics are considered in order to accurately measure the benefits of these essential programs.
Key words: Antimicrobial stewardship; antimicrobial consumption; resistance.
Antimicrobial resistance is a public health concern that has been escalating over the years and is now identified as a global crisis [1–3]. This is partly due to the widespread use of the same antibiotics that have existed for decades, combined with a lack of sufficient novel antibiotic discovery and development [4]. Bacteria that are resistant to our last-line-of-defense medications have recently emerged, and these resistant organisms may spread to treatment-naive patients [5]. Multidrug-resistant organisms are often found, treated, and likely originate within the hospital practice setting, where antimicrobials can be prescribed by any licensed provider [6]. Upwards of 50% of antibiotics administered are unnecessary and contribute to the problem of increasing resistance [7]. The seriousness of this situation is increasingly apparent; in 2014 the World Health Organization (WHO), President Obama, and Prime Minister Cameron issued statements urging solutions to the resistance crisis [8].
While the urgency of the situation is recognized today, efforts aimed at a more judicious use of antibiotics to curb resistance began as early as the 1960s and led to the first antimicrobial stewardship programs (ASPs) [9–11]. ASPs have since been defined as “coordinated interventions designed to improve and measure the appropriate use of antimicrobial agents by promoting the selection of the optimal antimicrobial drug regimen including dosing, duration of therapy, and route of administration” [1]. The primary objectives of these types of programs are to avoid or reduce adverse events (eg, Clostridium difficile infection) and resistance driven by a shift in minimum inhibitory concentrations (MICs) and to reverse the unnecessary economic burden caused by the inappropriate prescribing of these agents [1].
This article examines the evidence evaluating the reported effectiveness of inpatient ASPs, examining both clinical and economic outcomes. In addition, we touch on ASP history, current status, and future directions in light of current trends. While ASPs are expanding into the outpatient and nursing home settings, we will limit our review here to the inpatient setting.
Historical Background
Modern antibiotics date back to the late 1930s when penicillin and sulfonamides were introduced to the medical market, and resistance to these drug classes was reported just a few years after their introduction. The same bacterial resistance mechanisms that neutralized their efficacy then exist today, and these mechanisms continue to confer resistance among those classes [5].
While “stewardship” was not described as such until the late 1990s [12], institutions have historically been proactive in creating standards around antimicrobial utilization to encourage judicious use of these agents. The earliest form of tracking antibiotic use was in the form of paper charts as “antibiotic logs” [9] and “punch cards” [10] in the 1960s. The idea of a team approach to stewardship dates back to the 1970s, with the example of Hartford Hospital in Hartford, Connecticut, which employed an antimicrobial standards model run by an infectious disease (ID) physician and clinical pharmacists [11]. In 1977, the Infectious Diseases Society of America (IDSA) released a statement that clinical pharmacists may have a substantial impact on patient care, including in ID, contributing to the idea that a team of physicians collaborating with pharmacists presents the best way to combat inappropriate medication use. Pharmacist involvement has since been shown to restrict broad overutilized antimicrobial agents and reduce the rate of C. difficile infection by a significant amount [13].
In 1997 the IDSA and the Society for Healthcare Epidemiology of America (SHEA) published guidelines to assist in the prevention of the growing issue of resistance, mentioning the importance of antimicrobial stewardship [14]. A decade later they released joint guidelines for ASP implementation [15], and the Pediatric Infectious Disease Society (PIDS) joined them in 2012 to publish a joint statement acknowledging and endorsing stewardship [16]. In 2014, the Centers of Disease Control and Prevention (CDC) recommended that every hospital should have an ASP. As of 1 January 2017, the Joint Commission requires an ASP as a standard for accreditation at hospitals, critical access hospitals, and nursing care [17]. Guidelines for implementation of an ASP are currently available through the IDSA and SHEA [1,16].
ASP Interventions
There are 2 main strategies that ASPs have to combat inappropriate antimicrobial use, and each has its own set of systematic interventions. These strategies are referred to as “prospective audit with intervention and feedback” and “prior authorization” [6]. Although most ASPs will incorporate these main strategies, each institution typically creates its own strategies and regulations independently.
Prospective audit with intervention and feedback describes the process of providing recommendations after reviewing utilization and trends of antimicrobial use. This is sometimes referred to as the “back-end” intervention, in which decisions are made after antibiotics have been administered. Interventions that are commonly used under this strategy include discontinuation of antibiotics due to culture data, de-escalation to drugs with narrower spectra, IV to oral conversions, and cessation of surgical prophylaxis [6].
Prior authorization, also referred to as a “front-end” intervention, is the process of approving medications before they are used. Interventions include a restricted formulary for antimicrobials that can be managed through a paging system or a built-in computer restriction program, as well as other guidelines and protocols for dosing and duration of therapy. Restrictions typically focus on broad spectrum antibiotics as well as the more costly drugs on formularies. These solutions reduce the need for manual intervention as technology makes it possible to create automated restriction-based services that prevent inappropriate prescribing [6].
Aside from these main techniques, other strategies are taken to achieve the goal of attaining optimal clinical outcomes while limiting further antimicrobial resistance and adverse effects. Different clinical settings have different needs, and ASPs are customized to each setting’s resources, prescribing habits, and other local specificities [1]. These differences present difficulty with interpreting diverse datasets, but certain themes arise in the literature: commonly assessed clinical outcomes of inpatient ASPs include hospital length of stay (LOS) and readmission, reinfection, mortality, and resistance rates. These outcomes are putatively driven by the more prudent use of antimicrobials, particularly by decreased rates of antimicrobial consumption.
ASP Team Members
While ASPs may differ between institutions, the staff members involved are typically the same, and leadership is always an important aspect of a program. The CDC recommends that ASP leadership consist of a program leader (an ID physician) and a pharmacy leader, who co-lead the team [18]. In addition, the Joint Commission recommends that the multidisciplinary team should include an infection preventionist (ie, infection control and hospital epidemiologist) and practitioner [17]; these specialists have a role in prevention, awareness, and policy [19]. The integration of infection control with stewardship yields the best results [15], as infection control aims to prevent antibiotic use altogether, while stewardship increases the quality of antibiotic regimens that are being prescribed [20].
It is also beneficial to incorporate a microbiologist as an integral part of the team, responsible for performing and interpreting laboratory data (ie, cultures). Nurses should be integrated into ASPs due to the overlap of their routine activities with ASP interventions [21]; other clinicians (regardless of their infectious disease clinical background), quality control, information technology, and environmental services should all collaborate in the hospital-wide systems related to the program where appropriate [18].
Evidence Review
Results
Antimicrobial Usage
The most widely studied aspect of ASPs in the current review was the effect of ASP interventions on antimicrobial consumption and use. Three systematic reviews [22–24] showed improved antibiotic prescribing practices and reduced consumption rates overall, as did several studies inside and outside the intensive care unit (ICU) [25–31].One study found an insignificant declining usage trend [32]. An important underlying facet of this observation is that even as total antibiotic consumption decreases, certain antibiotic and antibiotic class consumption may increase. This is evident in several studies, which showed that as aminoglycoside, carbapenem, and β-lactam-β-lactamase inhibitor use increased, clindamycin (1 case), glycopeptide, fluoroquinolone, and macrolide use decreased [27,28,30]. A potential confounding factor relating to decreased glycopeptide use in Bevilacqua et al [30] was that there was an epidemic of glycopeptide-resistant enterococci during the study period, potentially causing prescribers to naturally avoid it. In any case, since the aim of ASPs is to encourage a more judicious usage of antimicrobials, the observed decreases in consumption of those restricted medications is intuitive. These observations about antimicrobial consumption related to ASPs are relevant because they putatively drive improvements in clinical outcomes, especially those related to reduced adverse events associated with these agents, such as the risk of C. difficile infection with certain drugs (eg, fluoroquinolones, clindamycin, and broad-spectrum antibiotics) and prolonged antibiotic usage [33–35]. There is evidence that these benefits are not limited to antibiotics but extend to antifungal agents and possibly antivirals [22,27,36].
Utilization, Mortality, and Infection Rates
ASPs typically intend to improve patient-focused clinical parameters such as hospital LOS, hospital readmissions, mortality, and incidence of infections acquired secondary to antibiotic usage during a hospital stay, especially C. difficile infection. Most of the reviewed evidence indicates that there has been no significant LOS benefit due to stewardship interventions [24–26,32,37], and one meta-analysis noted that when overall hospital LOS was significantly reduced, ICU-specific LOS was not [22]. Generally, there was also not a significant change in hospital readmission rates [24,26,32]. However, 2 retrospective observational studies found mixed results for both LOS and readmission rates relative to ASP interventions; while both noted a significantly reduced LOS, one study [38] showed an all-cause readmission benefit in a fairly healthy patient population (but no benefit for readmissions due to the specific infections of interest), and the another [29] showed a benefit for readmissions due to infections but an increased rate of readmissions in the intervention group overall. In this latter study, hospitalizations within the previous 3 months were significantly higher at baseline for the intervention group (55% vs. 46%, P = 0.042), suggesting sicker patients and possibly providing an explanation for this unique observation. Even so, a meta-analysis of 5 studies found a significantly elevated risk of readmission associated with ASP interventions (RR 1.26, 95% CI 1.02–1.57; P = 0.03); the authors noted that non–infection-related readmissions accounted for 61% of readmissions, but this was not significantly different between intervention and non-intervention arms [37].
With regard to mortality, most studies found no significant reductions related to stewardship interventions [22,24,26,29,32]. In a prospective randomized controlled trial, all reported deaths (7/160, 4.4%) were in the ASP intervention arm, but these were attributed to the severities of infection or an underlying, chronic disease [25]. One meta-analysis, however, found that there were significant mortality reductions related to stewardship guidelines for empirical antibiotic treatment (OR 0.65, 95% CI 0.54–0.80, P < 0.001; I2 = 65%) and to de-escalation of therapy based on culture results (RR 0.44, 95% CI 0.30–0.66, P < 0.001; I2 = 59%), based on 40 and 25 studies, respectively [39]; but both results exhibited substantial heterogeneity (defined as I2 = 50%–90% [40]) among the relevant studies. Another meta-analysis found that there was no significant change in mortality related to stewardship interventions intending to improve antibiotic appropriateness (RR 0.92, 95% CI 0.69–1.2, P = 0.56; I2 = 72%) or intending to reduce excessive prescribing (RR 0.92, 95% CI 0.81–1.06, P = 0.25; I2 = 0%), but that there was a significant mortality benefit associated with interventions aimed at increasing guideline compliance for pneumonia diagnoses (RR 0.89, 95% CI 0.82–0.97, P = 0.005; I2 = 0%) [37]. In the case of Schuts et al [39], search criteria specifically sought studies that assessed clinical outcomes (eg, mortality), whereas the search of Davey et al [37] focused on studies whose aim was to improve antibiotic prescribing, with a main comparison being between restrictive and persuasive interventions; while the difference may seem subtle, the body of data compiled from these searches may characterize the ASP effect of mortality differently. No significant evidence was found to suggest that reduced antimicrobial consumption increases mortality.
Improving the use of antimicrobial agents should limit collateral damage associated with their use (eg, damage to normal flora and increased resistance), and ideally infections should be better managed. As previously mentioned, one of the concerns with antibiotic usage (particularly fluoroquinolones, macrolides, and broad-spectrum agents) is that collateral damage could lead to increased rates of C. difficile infection. One meta-analysis showed no significant reduction in the rate of C. difficile infection (as well as overall infection rate) relative to ASPs [22]; however, this finding was based on only 3 of the 26 studies analyzed, and only 1 of those 3 studies utilized restrictions for flouroquinolones and cephalosporins. An interrupted time series (ITS) study similarly found no significant reduction in C. difficile infection rate [32]; however, this study was conducted in a hospital with low baseline antibiotic prescribing (it was ranked second-to-last in terms of antibiotic usage among its peer institutions), inherently limiting the risk of C. difficile infection among patients in the pre-ASP setting. In contrast to these findings, a meta-analysis specifically designed to assess the incidence of C. difficile infection relative to stewardship programs found a significantly reduced risk of infection based on 16 studies (RR 0.48, 95% CI 0.38–0.62, P < 0.001; I2 = 76%) [41], and the systematic review conducted by Filice et al [24] found a significant benefit with regard to the C. difficile infection rate in 4 of 6 studies. These results are consistent with those presented as evidence for the impact of stewardship on C. difficile infection by the CDC [42]. Aside from C. difficile infection, one retrospective observational study found that the 14-day reinfection rate (ie, reinfection with the same infection at the same anatomical location) was significantly reduced following stewardship intervention (0% vs. 10%, P = 0.009) [29]. This finding, combined with the C. difficile infection examples, provide evidence for better infection management of ASPs.
While the general trend seems to suggest mixed or no significant benefit for several clinical outcomes, it is important to note that variation in outcomes could be due to differences in the types of ASP interventions and intervention study periods across differing programs. Davey et al [37] found variation in prescribing outcomes based on whether restrictive (ie, restrict prescriber freedom with antimicrobials) or persuasive (ie, suggest changes to prescriber) interventions were used, and on the timeframe in which they were used. At one month into an ASP, restrictive interventions resulted in better prescribing practices relative to persuasive interventions based on 27 studies (effect size 32.0%, 95% CI 2.5%–61.4%), but by 6 months the 2 were not statistically different (effect size 10.1%, 95% CI –47.5% to 66.0%). At 12 and 24 months, persuasive interventions demonstrated greater effects on prescribing outcomes, but these were not significant. These findings provide evidence that different study timeframes can impact ASP practices differently (and these already vary widely in the literature). Considering the variety of ASP interventions employed across the different studies, these factors almost certainly impact the reported antimicrobial consumption rates and outcomes to different degrees as a consequence. A high degree of heterogeneity among an analyzed dataset could itself be the reason for net non-significance within single systematic reviews and meta-analyses.
Resistance
Another goal of ASPs is the prevention of antimicrobial resistance, an area where the evidence generally suggests benefit associated with ASP interventions. Resistance rates to common troublesome organisms, such as methicillin-resistant S. aureus (MRSA), imipenem-resistant P. aeruginosa, and extended-spectrum β-lactamase (ESBL)–producing Klebsiella spp were significantly reduced in a meta-analysis; ESBL-producing E. coli infections were not, however [22]. An ITS study found significantly reduced MRSA resistance, as well as reduced Pseudomonal resistance to imipenem-cilastin and levofloxacin (all P < 0.001), but no significant changes with respect to piperacillin/tazobactam, cefepime, or amikacin resistance [32]. This study also noted increased E. coli resistance to levofloxacin and ceftriaxone (both P < 0.001). No significant changes in resistance were noted for vancomycin-resistant enterococci. It may be a reasonable expectation that decreasing inappropriate antimicrobial use may decrease long-term antimicrobial resistance; but as most studies only span a few years, only the minute changes in resistance are understood [23]. Longer duration studies are needed to better understand resistance outcomes.
Of note is a phenomenon known as the “squeezing the balloon” effect. This can be associated with ASPs, potentially resulting in paradoxically increased resistance [43]. That is, when usage restrictions are placed on certain antibiotics, the use of other non-restricted antibiotics may increase, possibly leading to increased resistance of those non-restricted antibiotics [22] (“constraining one end [of a balloon] causes the other end to bulge … limiting the use of one class of compounds may be counteracted by corresponding changes in prescribing and drug resistance that are even more ominous” [43]). Karanika et al [22] took this phenomonen into consideration, and assessed restricted and non-restricted antimicrobial consumption separately. They found a reduction in consumption for both restricted and non-restricted antibiotics, which included “high potential resistance” antibiotics, specifically carbapenems and glycopeptides. In the study conducted by Cairns et al [28], a similar effect was observed; while the use of other classes of antibiotics decreased (eg, cephalosporins and aminoglycosides), the use of β–lactam–β–lactamase inhibitor combinations actually increased by 48% (change in use: +48.2% [95% CI 21.8%–47.9%]). Hohn et al [26] noted an increased usage rate of carbapenems, even though several other classes of antibiotics had reduced usage. Unfortunately, neither study reported resistance rates, so the impact of these findings is unknown. Finally, Jenkins et al [32] assessed trends in antimicrobial use as changes in rates of consumption. Among the various antibiotics assessed in this study, the rate of flouroquinolone use decreased both before and after the intervention period, although the rate of decreased usage slowed post-ASP (the change in rate post-ASP was +2.2% [95% CI 1.4%–3.1%], P < 0.001). They observed a small (but significant) increase in resistance of E. coli to levofloxacin pre- vs. post-intervention (11.0% vs. 13.9%, P < 0.001); in contrast, a significant decrease in resistance of P. aeruginosa was observed (30.5% vs. 21.4%, P < 0.001). While these examples help illustrate the concept of changes in antibiotic usage patterns associated with an ASP, at best they approximate the “squeezing the balloon” effect since these studies present data for antibiotics that were either restricted or for which restriction was not clearly specified. The “squeezing the balloon” effect is most relevant for the unintended, potentially increased usage of non-restricted drugs secondary to ASP restrictions. Higher resistance rates among certain drug classes observed in the context of this effect would constitute a drawback to an ASP program.
Adverse Effects
Reduced toxicities and adverse effects are expected with reduced usage of antimicrobials. The systematic review conducted by Filice et al [24] examined the incidence of adverse effects related to antibiotic usage, and their findings suggest, at the least, that stewardship programs generally do not cause harm, as only 2 of the studies they examined reported adverse events. Following stewardship interventions, 5.5% of the patients deteriorated; and of those, the large majority (75%) deteriorated due to progression of oncological malignancies. To further illustrate the effect of stewardship interventions on toxicities and side effects of antimicrobials, Schuts et al demonstrated that the risk of nephrotoxicity while on antimicrobial therapy was reduced based on 14 studies of moderate heterogeneity as a result of an ASP (OR 0.46, 95% CI 0.28–0.77, P = 0.003; I2 = 34%) [39,44]. It is intuitive that reduced drug exposure results in reduced adverse effects, as such these results are expected.
Economic Outcomes
Although the focus of ASPs is often to improve clinical outcomes, economic outcomes are an important component of ASPs; these programs bring associated economic value that should be highlighted and further detailed [22,45,46]. Since clinical outcomes are often the main objective of ASPs, most available studies have been clinical effect studies (rather than economic analyses), in which economic assessments are often a secondary consideration, if included.
As a result, cost evaluations are conducted on direct cost reductions whereas indirect cost reductions are often not critically evaluated. ASPs reduce hospital expenditures by limiting hospital-acquired infections and the associated medical costs where they are effective at decreasing consumption of antimicrobials [22,45], and by reducing antibiotic misuse, iatrogenic infections, and the rates of antibiotic-resistant organisms [47]. In one retrospective observational study, annual costs of antibiotics dropped by 33% with re-implementation of an ASP, mirrored by an overall decrease in antibiotic consumption of about 10%, over the course of the intervention study period [30]. Of note is that at 1 year post-ASP re-implementation, antibiotic consumption actually increased (by 5.4%); however, because antibiotic usage had changed to more appropriate and cost-effective therapies, cost expenditures associated with antibiotics were still reduced by 13% for that year relative to pre-ASP re-implementation. Aside from economic evaluations centered on consumption rates, there is the potential to further evaluate economic benefits associated with stewardship when looking at other outcomes, including hospital LOS [22], as well as indirect costs such as morbidity and mortality, societal, and operational costs [46]. Currently, these detailed analyses are lacking. In conjunction with more standardized clinical metrics, these assessments are needed to better delineate the full cost effectiveness of ASPs.
Evidence Summary
The evidence for inpatient ASP effectiveness is promising but mixed. Much of the evidence is low-level, based on observational studies that are retrospective in nature, and systematic reviews and meta-analyses are based on these types of studies. Studies have been conducted over a range of years, and the duration of intervention periods often vary widely between studies; it is difficult to capture and account for all of the infection, prescribing, and drug availability patterns (as well as the intervention differences or new drug approvals) throughout these time periods. To complicate the matter, both the quality of data as well as the quality of the ASPs are highly variable.
As such, the findings across pooled studies for ASPs are hard to amalgamate and draw concrete conclusions from. This difficulty is due to the inherent heterogeneity when comparing smaller individual studies in systematic reviews and meta-analyses. Currently, there are numerous ways to implement an ASP, but there is not a standardized system of specific interventions or metrics. Until we can directly compare similar ASPs and interventions among various institutions, it will be challenging to generalize positive benefits from systematic reviews and meta-analyses. Currently, the CDC is involved in a new initiative in which data from various hospitals are compiled to create a surveillance database [48]. Although this is a step in the right direction for standardized metrics for stewardship, for the current review the lack of standard metrics leads to conflicting results of heterogenic studies, making it difficult to show clear benefits in clinical outcomes.
Despite the vast array of ASPs, their differences, and a range of clinical measures—many with conflicting evidence—there is a noticeable trend toward a more prudent use of antimicrobials. Based on the review of available evidence, inpatient ASPs improve patient care and preserve an important health care resource—antibiotics. As has been presented, this is demonstrated by the alterations in consumption of these agents, has ramifications for secondary outcomes such as reduced instances of C. difficile infections, resistance, and adverse effects, and overall translates into better patient care and reduced costs. But while we can conclude that the direct interventions of stewardship in reducing and restricting antibiotic use have been effective, we cannot clearly state the overall magnitude of benefit, the effectiveness of various ASP structures and components on clinical outcomes (such as LOS, mortality, etc.), and the cost savings due to the heterogeneity of the available evidence.
Future Directions
Moving forward, the future of ASPs encompasses several potential developments. First and foremost, as technological advancements continue to develop, there is a need to integrate and utilize developments in information technology (IT). Baysari et al conducted a review on the value of utilizing IT interventions, focusing mainly on decision support (stand-alone or as a component of other hospital procedures), approval, and surveillance systems [49]. There was benefit associated with these IT interventions in terms of the improvement in the appropriate use of antimicrobials (RR 1.49, 95% CI, 1.07–2.08, P < 0.05; I2 = 93%), but there was no demonstrated benefit in terms of patient mortality or hospital LOS. Aside from this study, broad evidence is still lacking to support the use of IT systems in ASPs because meaningful comparisons amongst the interventions have not been made due to widespread variability in study design and outcome measures. However, it is generally agreed that ASPs must integrate with IT systems as the widespread use of technology within the healthcare field continues to grow. Evidence needs to be provided in the form of higher quality studies centered on similar outcomes to show appropriate approaches for ASPs to leverage IT systems. At a minimum, the integration of IT into ASPs should not hinder clinical outcomes. An important consideration is the variation in practice settings where antibiotic stewardship is to be implemented; eg, a small community hospital will be less equipped to incorporate and support technological tools compared to a large tertiary teaching hospital. Therefore, any antibiotic stewardship IT intervention must be customized to meet local needs, prescriber behaviors, minimize barriers to implementation, and utilize available resources.
Another area of focus for future ASPs is the use of rapid diagnostics. Currently, when patients present with signs and symptoms of an infection, an empiric antimicrobial regimen is started that is then de-escalated as necessary; rapid testing will help to initiate appropriate therapy more quickly and increase antimicrobial effectiveness. Rapid tests range from rapid polymerase chain reaction (PCR)-based screening [50], to Verigene gram-positive blood culture (BC-GP) tests [51], next-generation sequencing methods, and matrix assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) [52]. Rapid diagnostic tools should be viewed as aides to assist ASPs in decreasing antibiotic consumption and improving patient outcomes; these various tools have been shown to improve clinical outcomes when integrated into ASPs, but offer little value addressing the goals of ASPs when used outside of stewardship programs and their sensitive timeframes [53].
In terms of future ASP expansion, stewardship implementation can become more unified and broad in scope. ASPs should expand to include antifungal interventions, an area which is showing progress [36]. ASPs can also be implemented in new areas throughout the hospital (eg, pediatrics and emergency room), as well as areas outside of the hospital setting, including long-term care facilities, dialysis centers, and other institutions [54–56]. A prospective randomized control study was conducted in 30 nursing homes to evaluate the use of a novel resident antimicrobial management plan (RAMP) for improved use of antimicrobials [57]. This study found that the RAMP had no associated adverse effects and suggests that ASP is an important tool in nursing homes. In addition, the general outpatient and pediatric settings show promise for ASPs [56,58,59], but more research is needed to support expansion and to identify how ASP interventions should be applied in these various practice settings. The antimicrobial stewardship interventions that will be utilized will need to be carefully delineated to consider the scale, underlying need, and potential challenges in those settings.
While the future of antibiotic stewardship is unclear, there is certainty that it will continue to develop in both scope and depth to encompass new areas of focus, new settings to improve outcomes, and employ new tools to refine approaches. An important first step for the continued development of ASPs is alignment and standardization, since without alignment it will continue to be difficult to compare outcomes. This issue is currently being addressed by a number of different organizations. With current support from the Joint Commission, the CDC, as well as the President’s Council of Advisors on Science and Technology (PCAST) [8], regulatory requirements for ASPs are well underway, and these drivers will appropriately position ASPs for further advancements. By reducing variability amongst ASPs and delineating implementation of ASPs, there can be a clear identification of both economic and clinical benefits associated with specific interventions.
Corresponding author: Luigi Brunetti, PharmD, MPH, Rutgers, The State University of New Jersey, 160 Frelinghuysen Rd., Piscataway, NJ 08854, [email protected].
Financial disclosures: None.
1. Barlam TF, Cosgrove SE, Abbo AM, et al. Implementing an antimicrobial stewardship program: guidelines by the Infectious Diseases Society of America and the Society of Healthcare Epidemiology of America. Clin Infect Dis 2016;62:e51–77.
2. Hughes D. Selection and evolution of resistance to antimicrobial drugs. IUBMB Life 2014;66:521–9.
3. World Health Organzation. The evolving threat of antimicrobial resistance – options for action. Geneva: WHO Press; 2012.
4. Gould IM, Bal AM. New antibiotic agents in the pipeline and how they can help overcome microbial resistance. Virulence 2013;4:185–91.
5. Davies J, Davies D. Origins and evolution of antibiotic resistance. Microbiol Mol Biol Rev 2010;74:417–33.
6. Owens RC Jr. Antimicrobial stewardship: concepts and strategies in the 21st century. Diagn Microbiol Infect Dis 2008;61:110–28.
7. Antibiotic resistance threats in the United States, 2013 [Internet]. Centers for Disease Control and Prevention. Available at www.cdc.gov/drugresistance/pdf/ar-threats-2013-508.pdf.
8. Nathan C, Cars O. Antibiotic resistance – problems, progress, prospects. N Engl J Med 2014;371:1761–3.
9. McGoldrick, M. Antimicrobial stewardship. Home Healthc Nurse 2014;32:559–60.
10. Ruedy J. A method of determining patterns of use of antibacterial drugs. Can Med Assoc J 1966;95:807–12.
11. Briceland LL, Nightingdale CH, Quintiliani R, et al. Antibiotic streamlining from combination therapy to monotherapy utilizing an interdisciplinary approach. Arch Inter Med 1988;148:2019–22.
12. McGowan JE Jr, Gerding DN. Does antibiotic restriction prevent resistance? New Horiz 1996;4: 370–6.
13. Cappelletty D, Jacobs D. Evaluating the impact of a pharmacist’s absence from an antimicrobial stewardship team. Am J Health Syst Pharm 2013;70:1065–69.
14. Shales DM, Gerding DN, John JF Jr, et al. Society for Healthcare Epidemiology of America and Infectious Diseases Society of America Joint Committee on the prevention of antimicrobial resistance: guidelines for the prevention of antimicrobial resistance in hospitals. Infect Control Hosp Epidemiol 1997;18:275–91.
15. Dellit TH, Owens RC, McGowan JE, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis 2007;44:159–77.
16. Policy statement on antimicrobial stewardship by the Society for Healthcare Epidemiology of America (SHEA), the Infectious Diseases Society of America (IDSA), and the Pediatric Infectious Diseases Society (PIDS). Infect Ctrl Hosp Epidemiol 2012;33:322–7.
17. The Joint Commission. Approved: New antimicrobial stewardship standard. Joint Commission Perspectives 2016;36:1–8.
18. Pollack LA, Srinivasan A. Core elements of hospital antibiotic stewardship programs from the Centers for Disease Control and Prevention. Clin Infect Dis 2014;59(Suppl 3):S97–100.
19. Moody J. Infection preventionists have a role in accelerating progress toward preventing the emergence and cross-transmission of MDROs. Prevention Strategist 2012 Summer:52–6.
20. Spellberg B, Bartlett JG, Gilbert DN. The future of antibiotics and resistance. N Engl J Med 2013;368:299–302.
21. Olans RN, Olans RD, Demaria A. The critical role of the staff nurse in antimicrobial stewardship--unrecognized, but already there. Clin Infect Dis 2016;62:84–9.
22. Karanika S, Paudel S, Grigoras C, et al. Systematic review and meta-analysis of clinical and economic outcomes from the implementation of hospital-based antimicrobial stewardship programs. Antimicrob Agents Chemother 2016;60:4840–52.
23. Wagner B, Filice GA, Drekonja D, et al. Antimicrobial stewardship programs in inpatient hospital settings: a systematic review. Infect Control Hosp Epidemiol 2014;35:1209–28.
24. Filice G, Drekonja D, Greer N, et al. Antimicrobial stewardship programs in inpatient settings: a systematic review. VA-ESP Project #09-009; 2013.
25. Cairns KA, Doyle JS, Trevillyan JM, et al. The impact of a multidisciplinary antimicrobial stewardship team on the timeliness of antimicrobial therapy in patients with positive blood cultures: a randomized controlled trial. J Antimicrob Chemother 2016;71:3276–83.
26. Hohn A, Heising B, Hertel S, et al. Antibiotic consumption after implementation of a procalcitonin-guided antimicrobial stewardship programme in surgical patients admitted to an intensive care unit: a retrospective before-and-after analysis. Infection 2015;43:405–12.
27. Singh S, Zhang YZ, Chalkley S, et al. A three-point time series study of antibiotic usage on an intensive care unit, following an antibiotic stewardship programme, after an outbreak of multi-resistant Acinetobacter baumannii. Eur J Clin Microbiol Infect Dis 2015;34:1893–900.
28. Cairns KA, Jenney AW, Abbott IJ, et al. Prescribing trends before and after implementation of an antimicrobial stewardship program. Med J Aust 2013;198:262–6.
29. Liew YX, Lee W, Loh JC, et al. Impact of an antimicrobial stewardship programme on patient safety in Singapore General Hospital. Int J Antimicrob Agents 2012;40:55–60.
30. Bevilacqua S, Demoré B, Boschetti E, et al. 15 years of antibiotic stewardship policy in the Nancy Teaching Hospital. Med Mal Infect 2011;41:532–9.
31. Danaher PJ, Milazzo NA, Kerr KJ, et al. The antibiotic support team--a successful educational approach to antibiotic stewardship. Mil Med 2009;174:201–5.
32. Jenkins TC, Knepper BC, Shihadeh K, et al. Long-term outcomes of an antimicrobial stewardship program implemented in a hospital with low baseline antibiotic use. Infect Control Hosp Epidemiol 2015;36:664–72.
33. Brown KA, Khanafer N, Daneman N, Fisman DN. Meta-analysis of antibiotics and the risk of community-associated Clostridium difficile infection. Antimicrob Agents Chemother 2013;57:2326–32.
34. Deshpande A, Pasupuleti V, Thota P, et al. Community-associated Clostridium difficile infection and antibiotics: a meta-analysis. J Antimicrob Chemother 2013;68:1951–61.
35. Slimings C, Riley TV. Antibiotics and hospital-acquired Clostridium difficile infection: update of systematic review and meta-analysis. J Antimicrob Chemother 2014;69:881–91.
36. Antworth A, Collins CD, Kunapuli A, et al. Impact of an antimicrobial stewardship program comprehensive care bundle on management of candidemia. Pharmacotherapy 2013;33:137–43.
37. Davey P, Brown E, Charani E, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev 2013;4:CD003543.
38. Pasquale TR, Trienski TL, Olexia DE, et al. Impact of an antimicrobial stewardship program on patients with acute bacterial skin and skin structure infections. Am J Health Syst Pharm 2014;71:1136–9.
39. Schuts EC, Hulscher ME, Mouton JW, et al. Current evidence on hospital antimicrobial stewardship objectives: a systematic review and meta-analysis. Lancet Infect Dis 2016;16:847–56.
40. Higgins JPT, Green S, editors. Identifying and measuring heterogeneity. Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0. [Internet]. The Cochrane Collaboration, March 2011. Available at http://handbook.cochrane.org/chapter_9/9_5_2_identifying_and_measuring_heterogeneity.htm.
41. Feazel LM, Malhotra A, Perencevich EN, et al. Effect of antibiotic stewardship programmes on Clostridium difficile incidence: a systematic review and meta-analysis. J Antimicrob Chemother 2014;69:1748–54.
42. Impact of antibiotic stewardship programs on Clostridium difficile (C. diff) infections [Internet]. Centers for Disease Control and Prevention. [Updated 2016 May 13; cited 2016 Oct 11]. Available at www.cdc.gov/getsmart/healthcare/evidence/asp-int-cdiff.html.
43. Burke JP. Antibiotic resistance – squeezing the balloon? JAMA 1998;280:1270–1.
44. This nephrotoxicity result is corrected from the originally published result; communicated by Jan M Prins on behalf of the authors for reference [39]. Prins, JM (Department of Internal Medicine, Division of Infectious Diseases, Academic Medical Centre, Amsterdam, Netherlands). Email communication with Joseph Eckart (Pharmacy Practice & Administration, Ernest Mario School of Pharmacy, Rutgers University, Piscataway, NJ). 2016 Oct 9.
45. Coulter S, Merollini K, Roberts JA, et al. The need for cost-effectiveness analyses of antimicrobial stewardship programmes: a structured review. Int J Antimicrob Agents 2015;46:140–9.
46. Dik J, Vemer P, Friedrich A, et al. Financial evaluations of antibiotic stewardship programs—a systematic review. Frontiers Microbiol 2015;6:317.
47. Campbell KA, Stein S, Looze C, Bosco JA. Antibiotic stewardship in orthopaedic surgery: principles and practice. J Am Acad Orthop Surg 2014;22:772–81.
48. Surveillance for antimicrobial use and antimicrobial resistance options, 2015 [Internet]. Centers for Disease Control and Prevention. [Updated 2016 May 3; cited 2016 Nov 22]. Available at www.cdc.gov/nhsn/acute-care-hospital/aur/index.html.
49. Baysari MT, Lehnbom EC, Li L, Hargreaves A, et al. The effectiveness of information technology to improve antimicrobial prescribing in hospitals: a systematic review and meta-analysis. Int J Med Inform. 2016;92:15-34.
50. Bauer KA, West JE, Balada-llasat JM, et al. An antimicrobial stewardship program’s impact with rapid polymerase chain reaction methicillin-resistant Staphylococcus aureus/S. aureus blood culture test in patients with S. aureus bacteremia. Clin Infect Dis 2010;51:1074–80.
51. Sango A, Mccarter YS, Johnson D, et al. Stewardship approach for optimizing antimicrobial therapy through use of a rapid microarray assay on blood cultures positive for Enterococcus species. J Clin Microbiol 2013;51:4008–11.
52. Perez KK, Olsen RJ, Musick WL, et al. Integrating rapid diagnostics and antimicrobial stewardship improves outcomes in patients with antibiotic-resistant Gram-negative bacteremia. J Infect 2014;69:216–25.
53. Bauer KA, Perez KK, Forrest GN, Goff DA. Review of rapid diagnostic tests used by antimicrobial stewardship programs. Clin Infect Dis 2014;59 Suppl 3:S134–145.
54. Dyar OJ, Pagani L, Pulcini C. Strategies and challenges of antimicrobial stewardship in long-term care facilities. Clin Microbiol Infect 2015;21:10–9.
55. D’Agata EM. Antimicrobial use and stewardship programs among dialysis centers. Semin Dial 2013;26:457–64.
56. Smith MJ, Gerber JS, Hersh AL. Inpatient antimicrobial stewardship in pediatrics: a systematic review. J Pediatric Infect Dis Soc 2015;4:e127–135.
57. Fleet E, Gopal Rao G, Patel B, et al. Impact of implementation of a novel antimicrobial stewardship tool on antibiotic use in nursing homes: a prospective cluster randomized control pilot study. J Antimicrob Chemother 2014;69:2265–73.
58. Drekonja DM, Filice GA, Greer N, et al. Antimicrobial stewardship in outpatient settings: a systematic review. Infect Control Hosp Epidemiol 2015;36:142–52.
59. Drekonja D, Filice G, Greer N, et al. Antimicrobial stewardship programs in outpatient settings: a systematic review. VA-ESP Project #09-009; 2014.
60. Zhang YZ, Singh S. Antibiotic stewardship programmes in intensive care units: why, how, and where are they leading us. World J Crit Care Med 2015;4:13–28. (referenced in online Table)
From the Ernest Mario School of Pharmacy, Rutgers, The State University of New Jersey, Piscataway, NJ.
Abstract
- Objective: To review the evidence evaluating inpatient antimicrobial stewardship programs (ASPs) with a focus on clinical and economic outcomes.
- Methods: Pubmed/MEDLINE and the Cochrane Database of Systematic Reviews were used to identify systematic reviews, meta-analyses, randomized controlled trials, and other relevant literature evaluating the clinical and economic impact of ASP interventions.
- Results: A total of 5 meta-analyses, 3 systematic reviews, and 10 clinical studies (2 randomized controlled, 5 observational, and 3 quasi-experimental studies) were identified for analysis. ASPs were associated with a reduction in antimicrobial consumption and use. However, due to the heterogeneity of outcomes measured among studies, the effectiveness of ASPs varied with the measures used. There are data supporting the cost savings associated with ASPs, but these studies are more sparse. Most of the available evidence supporting ASPs is of low quality, and intervention strategies vary widely among available studies.
- Conclusion: Much of the evidence reviewed supports the assertion that ASPs result in a more judicious use of antimicrobials and lead to better patient care in the inpatient setting. While clinical outcomes vary between programs, there are ubiquitous positive benefits associated with ASPs in terms of antimicrobial consumption, C. difficile infection rates, and resistance, with few adverse effects. To date, economic outcomes have been difficult to uniformly quantify, but there are data supporting the economic benefits of ASPs. As the number of ASPs continues to grow, it is imperative that standardized metrics are considered in order to accurately measure the benefits of these essential programs.
Key words: Antimicrobial stewardship; antimicrobial consumption; resistance.
Antimicrobial resistance is a public health concern that has been escalating over the years and is now identified as a global crisis [1–3]. This is partly due to the widespread use of the same antibiotics that have existed for decades, combined with a lack of sufficient novel antibiotic discovery and development [4]. Bacteria that are resistant to our last-line-of-defense medications have recently emerged, and these resistant organisms may spread to treatment-naive patients [5]. Multidrug-resistant organisms are often found, treated, and likely originate within the hospital practice setting, where antimicrobials can be prescribed by any licensed provider [6]. Upwards of 50% of antibiotics administered are unnecessary and contribute to the problem of increasing resistance [7]. The seriousness of this situation is increasingly apparent; in 2014 the World Health Organization (WHO), President Obama, and Prime Minister Cameron issued statements urging solutions to the resistance crisis [8].
While the urgency of the situation is recognized today, efforts aimed at a more judicious use of antibiotics to curb resistance began as early as the 1960s and led to the first antimicrobial stewardship programs (ASPs) [9–11]. ASPs have since been defined as “coordinated interventions designed to improve and measure the appropriate use of antimicrobial agents by promoting the selection of the optimal antimicrobial drug regimen including dosing, duration of therapy, and route of administration” [1]. The primary objectives of these types of programs are to avoid or reduce adverse events (eg, Clostridium difficile infection) and resistance driven by a shift in minimum inhibitory concentrations (MICs) and to reverse the unnecessary economic burden caused by the inappropriate prescribing of these agents [1].
This article examines the evidence evaluating the reported effectiveness of inpatient ASPs, examining both clinical and economic outcomes. In addition, we touch on ASP history, current status, and future directions in light of current trends. While ASPs are expanding into the outpatient and nursing home settings, we will limit our review here to the inpatient setting.
Historical Background
Modern antibiotics date back to the late 1930s when penicillin and sulfonamides were introduced to the medical market, and resistance to these drug classes was reported just a few years after their introduction. The same bacterial resistance mechanisms that neutralized their efficacy then exist today, and these mechanisms continue to confer resistance among those classes [5].
While “stewardship” was not described as such until the late 1990s [12], institutions have historically been proactive in creating standards around antimicrobial utilization to encourage judicious use of these agents. The earliest form of tracking antibiotic use was in the form of paper charts as “antibiotic logs” [9] and “punch cards” [10] in the 1960s. The idea of a team approach to stewardship dates back to the 1970s, with the example of Hartford Hospital in Hartford, Connecticut, which employed an antimicrobial standards model run by an infectious disease (ID) physician and clinical pharmacists [11]. In 1977, the Infectious Diseases Society of America (IDSA) released a statement that clinical pharmacists may have a substantial impact on patient care, including in ID, contributing to the idea that a team of physicians collaborating with pharmacists presents the best way to combat inappropriate medication use. Pharmacist involvement has since been shown to restrict broad overutilized antimicrobial agents and reduce the rate of C. difficile infection by a significant amount [13].
In 1997 the IDSA and the Society for Healthcare Epidemiology of America (SHEA) published guidelines to assist in the prevention of the growing issue of resistance, mentioning the importance of antimicrobial stewardship [14]. A decade later they released joint guidelines for ASP implementation [15], and the Pediatric Infectious Disease Society (PIDS) joined them in 2012 to publish a joint statement acknowledging and endorsing stewardship [16]. In 2014, the Centers of Disease Control and Prevention (CDC) recommended that every hospital should have an ASP. As of 1 January 2017, the Joint Commission requires an ASP as a standard for accreditation at hospitals, critical access hospitals, and nursing care [17]. Guidelines for implementation of an ASP are currently available through the IDSA and SHEA [1,16].
ASP Interventions
There are 2 main strategies that ASPs have to combat inappropriate antimicrobial use, and each has its own set of systematic interventions. These strategies are referred to as “prospective audit with intervention and feedback” and “prior authorization” [6]. Although most ASPs will incorporate these main strategies, each institution typically creates its own strategies and regulations independently.
Prospective audit with intervention and feedback describes the process of providing recommendations after reviewing utilization and trends of antimicrobial use. This is sometimes referred to as the “back-end” intervention, in which decisions are made after antibiotics have been administered. Interventions that are commonly used under this strategy include discontinuation of antibiotics due to culture data, de-escalation to drugs with narrower spectra, IV to oral conversions, and cessation of surgical prophylaxis [6].
Prior authorization, also referred to as a “front-end” intervention, is the process of approving medications before they are used. Interventions include a restricted formulary for antimicrobials that can be managed through a paging system or a built-in computer restriction program, as well as other guidelines and protocols for dosing and duration of therapy. Restrictions typically focus on broad spectrum antibiotics as well as the more costly drugs on formularies. These solutions reduce the need for manual intervention as technology makes it possible to create automated restriction-based services that prevent inappropriate prescribing [6].
Aside from these main techniques, other strategies are taken to achieve the goal of attaining optimal clinical outcomes while limiting further antimicrobial resistance and adverse effects. Different clinical settings have different needs, and ASPs are customized to each setting’s resources, prescribing habits, and other local specificities [1]. These differences present difficulty with interpreting diverse datasets, but certain themes arise in the literature: commonly assessed clinical outcomes of inpatient ASPs include hospital length of stay (LOS) and readmission, reinfection, mortality, and resistance rates. These outcomes are putatively driven by the more prudent use of antimicrobials, particularly by decreased rates of antimicrobial consumption.
ASP Team Members
While ASPs may differ between institutions, the staff members involved are typically the same, and leadership is always an important aspect of a program. The CDC recommends that ASP leadership consist of a program leader (an ID physician) and a pharmacy leader, who co-lead the team [18]. In addition, the Joint Commission recommends that the multidisciplinary team should include an infection preventionist (ie, infection control and hospital epidemiologist) and practitioner [17]; these specialists have a role in prevention, awareness, and policy [19]. The integration of infection control with stewardship yields the best results [15], as infection control aims to prevent antibiotic use altogether, while stewardship increases the quality of antibiotic regimens that are being prescribed [20].
It is also beneficial to incorporate a microbiologist as an integral part of the team, responsible for performing and interpreting laboratory data (ie, cultures). Nurses should be integrated into ASPs due to the overlap of their routine activities with ASP interventions [21]; other clinicians (regardless of their infectious disease clinical background), quality control, information technology, and environmental services should all collaborate in the hospital-wide systems related to the program where appropriate [18].
Evidence Review
Results
Antimicrobial Usage
The most widely studied aspect of ASPs in the current review was the effect of ASP interventions on antimicrobial consumption and use. Three systematic reviews [22–24] showed improved antibiotic prescribing practices and reduced consumption rates overall, as did several studies inside and outside the intensive care unit (ICU) [25–31].One study found an insignificant declining usage trend [32]. An important underlying facet of this observation is that even as total antibiotic consumption decreases, certain antibiotic and antibiotic class consumption may increase. This is evident in several studies, which showed that as aminoglycoside, carbapenem, and β-lactam-β-lactamase inhibitor use increased, clindamycin (1 case), glycopeptide, fluoroquinolone, and macrolide use decreased [27,28,30]. A potential confounding factor relating to decreased glycopeptide use in Bevilacqua et al [30] was that there was an epidemic of glycopeptide-resistant enterococci during the study period, potentially causing prescribers to naturally avoid it. In any case, since the aim of ASPs is to encourage a more judicious usage of antimicrobials, the observed decreases in consumption of those restricted medications is intuitive. These observations about antimicrobial consumption related to ASPs are relevant because they putatively drive improvements in clinical outcomes, especially those related to reduced adverse events associated with these agents, such as the risk of C. difficile infection with certain drugs (eg, fluoroquinolones, clindamycin, and broad-spectrum antibiotics) and prolonged antibiotic usage [33–35]. There is evidence that these benefits are not limited to antibiotics but extend to antifungal agents and possibly antivirals [22,27,36].
Utilization, Mortality, and Infection Rates
ASPs typically intend to improve patient-focused clinical parameters such as hospital LOS, hospital readmissions, mortality, and incidence of infections acquired secondary to antibiotic usage during a hospital stay, especially C. difficile infection. Most of the reviewed evidence indicates that there has been no significant LOS benefit due to stewardship interventions [24–26,32,37], and one meta-analysis noted that when overall hospital LOS was significantly reduced, ICU-specific LOS was not [22]. Generally, there was also not a significant change in hospital readmission rates [24,26,32]. However, 2 retrospective observational studies found mixed results for both LOS and readmission rates relative to ASP interventions; while both noted a significantly reduced LOS, one study [38] showed an all-cause readmission benefit in a fairly healthy patient population (but no benefit for readmissions due to the specific infections of interest), and the another [29] showed a benefit for readmissions due to infections but an increased rate of readmissions in the intervention group overall. In this latter study, hospitalizations within the previous 3 months were significantly higher at baseline for the intervention group (55% vs. 46%, P = 0.042), suggesting sicker patients and possibly providing an explanation for this unique observation. Even so, a meta-analysis of 5 studies found a significantly elevated risk of readmission associated with ASP interventions (RR 1.26, 95% CI 1.02–1.57; P = 0.03); the authors noted that non–infection-related readmissions accounted for 61% of readmissions, but this was not significantly different between intervention and non-intervention arms [37].
With regard to mortality, most studies found no significant reductions related to stewardship interventions [22,24,26,29,32]. In a prospective randomized controlled trial, all reported deaths (7/160, 4.4%) were in the ASP intervention arm, but these were attributed to the severities of infection or an underlying, chronic disease [25]. One meta-analysis, however, found that there were significant mortality reductions related to stewardship guidelines for empirical antibiotic treatment (OR 0.65, 95% CI 0.54–0.80, P < 0.001; I2 = 65%) and to de-escalation of therapy based on culture results (RR 0.44, 95% CI 0.30–0.66, P < 0.001; I2 = 59%), based on 40 and 25 studies, respectively [39]; but both results exhibited substantial heterogeneity (defined as I2 = 50%–90% [40]) among the relevant studies. Another meta-analysis found that there was no significant change in mortality related to stewardship interventions intending to improve antibiotic appropriateness (RR 0.92, 95% CI 0.69–1.2, P = 0.56; I2 = 72%) or intending to reduce excessive prescribing (RR 0.92, 95% CI 0.81–1.06, P = 0.25; I2 = 0%), but that there was a significant mortality benefit associated with interventions aimed at increasing guideline compliance for pneumonia diagnoses (RR 0.89, 95% CI 0.82–0.97, P = 0.005; I2 = 0%) [37]. In the case of Schuts et al [39], search criteria specifically sought studies that assessed clinical outcomes (eg, mortality), whereas the search of Davey et al [37] focused on studies whose aim was to improve antibiotic prescribing, with a main comparison being between restrictive and persuasive interventions; while the difference may seem subtle, the body of data compiled from these searches may characterize the ASP effect of mortality differently. No significant evidence was found to suggest that reduced antimicrobial consumption increases mortality.
Improving the use of antimicrobial agents should limit collateral damage associated with their use (eg, damage to normal flora and increased resistance), and ideally infections should be better managed. As previously mentioned, one of the concerns with antibiotic usage (particularly fluoroquinolones, macrolides, and broad-spectrum agents) is that collateral damage could lead to increased rates of C. difficile infection. One meta-analysis showed no significant reduction in the rate of C. difficile infection (as well as overall infection rate) relative to ASPs [22]; however, this finding was based on only 3 of the 26 studies analyzed, and only 1 of those 3 studies utilized restrictions for flouroquinolones and cephalosporins. An interrupted time series (ITS) study similarly found no significant reduction in C. difficile infection rate [32]; however, this study was conducted in a hospital with low baseline antibiotic prescribing (it was ranked second-to-last in terms of antibiotic usage among its peer institutions), inherently limiting the risk of C. difficile infection among patients in the pre-ASP setting. In contrast to these findings, a meta-analysis specifically designed to assess the incidence of C. difficile infection relative to stewardship programs found a significantly reduced risk of infection based on 16 studies (RR 0.48, 95% CI 0.38–0.62, P < 0.001; I2 = 76%) [41], and the systematic review conducted by Filice et al [24] found a significant benefit with regard to the C. difficile infection rate in 4 of 6 studies. These results are consistent with those presented as evidence for the impact of stewardship on C. difficile infection by the CDC [42]. Aside from C. difficile infection, one retrospective observational study found that the 14-day reinfection rate (ie, reinfection with the same infection at the same anatomical location) was significantly reduced following stewardship intervention (0% vs. 10%, P = 0.009) [29]. This finding, combined with the C. difficile infection examples, provide evidence for better infection management of ASPs.
While the general trend seems to suggest mixed or no significant benefit for several clinical outcomes, it is important to note that variation in outcomes could be due to differences in the types of ASP interventions and intervention study periods across differing programs. Davey et al [37] found variation in prescribing outcomes based on whether restrictive (ie, restrict prescriber freedom with antimicrobials) or persuasive (ie, suggest changes to prescriber) interventions were used, and on the timeframe in which they were used. At one month into an ASP, restrictive interventions resulted in better prescribing practices relative to persuasive interventions based on 27 studies (effect size 32.0%, 95% CI 2.5%–61.4%), but by 6 months the 2 were not statistically different (effect size 10.1%, 95% CI –47.5% to 66.0%). At 12 and 24 months, persuasive interventions demonstrated greater effects on prescribing outcomes, but these were not significant. These findings provide evidence that different study timeframes can impact ASP practices differently (and these already vary widely in the literature). Considering the variety of ASP interventions employed across the different studies, these factors almost certainly impact the reported antimicrobial consumption rates and outcomes to different degrees as a consequence. A high degree of heterogeneity among an analyzed dataset could itself be the reason for net non-significance within single systematic reviews and meta-analyses.
Resistance
Another goal of ASPs is the prevention of antimicrobial resistance, an area where the evidence generally suggests benefit associated with ASP interventions. Resistance rates to common troublesome organisms, such as methicillin-resistant S. aureus (MRSA), imipenem-resistant P. aeruginosa, and extended-spectrum β-lactamase (ESBL)–producing Klebsiella spp were significantly reduced in a meta-analysis; ESBL-producing E. coli infections were not, however [22]. An ITS study found significantly reduced MRSA resistance, as well as reduced Pseudomonal resistance to imipenem-cilastin and levofloxacin (all P < 0.001), but no significant changes with respect to piperacillin/tazobactam, cefepime, or amikacin resistance [32]. This study also noted increased E. coli resistance to levofloxacin and ceftriaxone (both P < 0.001). No significant changes in resistance were noted for vancomycin-resistant enterococci. It may be a reasonable expectation that decreasing inappropriate antimicrobial use may decrease long-term antimicrobial resistance; but as most studies only span a few years, only the minute changes in resistance are understood [23]. Longer duration studies are needed to better understand resistance outcomes.
Of note is a phenomenon known as the “squeezing the balloon” effect. This can be associated with ASPs, potentially resulting in paradoxically increased resistance [43]. That is, when usage restrictions are placed on certain antibiotics, the use of other non-restricted antibiotics may increase, possibly leading to increased resistance of those non-restricted antibiotics [22] (“constraining one end [of a balloon] causes the other end to bulge … limiting the use of one class of compounds may be counteracted by corresponding changes in prescribing and drug resistance that are even more ominous” [43]). Karanika et al [22] took this phenomonen into consideration, and assessed restricted and non-restricted antimicrobial consumption separately. They found a reduction in consumption for both restricted and non-restricted antibiotics, which included “high potential resistance” antibiotics, specifically carbapenems and glycopeptides. In the study conducted by Cairns et al [28], a similar effect was observed; while the use of other classes of antibiotics decreased (eg, cephalosporins and aminoglycosides), the use of β–lactam–β–lactamase inhibitor combinations actually increased by 48% (change in use: +48.2% [95% CI 21.8%–47.9%]). Hohn et al [26] noted an increased usage rate of carbapenems, even though several other classes of antibiotics had reduced usage. Unfortunately, neither study reported resistance rates, so the impact of these findings is unknown. Finally, Jenkins et al [32] assessed trends in antimicrobial use as changes in rates of consumption. Among the various antibiotics assessed in this study, the rate of flouroquinolone use decreased both before and after the intervention period, although the rate of decreased usage slowed post-ASP (the change in rate post-ASP was +2.2% [95% CI 1.4%–3.1%], P < 0.001). They observed a small (but significant) increase in resistance of E. coli to levofloxacin pre- vs. post-intervention (11.0% vs. 13.9%, P < 0.001); in contrast, a significant decrease in resistance of P. aeruginosa was observed (30.5% vs. 21.4%, P < 0.001). While these examples help illustrate the concept of changes in antibiotic usage patterns associated with an ASP, at best they approximate the “squeezing the balloon” effect since these studies present data for antibiotics that were either restricted or for which restriction was not clearly specified. The “squeezing the balloon” effect is most relevant for the unintended, potentially increased usage of non-restricted drugs secondary to ASP restrictions. Higher resistance rates among certain drug classes observed in the context of this effect would constitute a drawback to an ASP program.
Adverse Effects
Reduced toxicities and adverse effects are expected with reduced usage of antimicrobials. The systematic review conducted by Filice et al [24] examined the incidence of adverse effects related to antibiotic usage, and their findings suggest, at the least, that stewardship programs generally do not cause harm, as only 2 of the studies they examined reported adverse events. Following stewardship interventions, 5.5% of the patients deteriorated; and of those, the large majority (75%) deteriorated due to progression of oncological malignancies. To further illustrate the effect of stewardship interventions on toxicities and side effects of antimicrobials, Schuts et al demonstrated that the risk of nephrotoxicity while on antimicrobial therapy was reduced based on 14 studies of moderate heterogeneity as a result of an ASP (OR 0.46, 95% CI 0.28–0.77, P = 0.003; I2 = 34%) [39,44]. It is intuitive that reduced drug exposure results in reduced adverse effects, as such these results are expected.
Economic Outcomes
Although the focus of ASPs is often to improve clinical outcomes, economic outcomes are an important component of ASPs; these programs bring associated economic value that should be highlighted and further detailed [22,45,46]. Since clinical outcomes are often the main objective of ASPs, most available studies have been clinical effect studies (rather than economic analyses), in which economic assessments are often a secondary consideration, if included.
As a result, cost evaluations are conducted on direct cost reductions whereas indirect cost reductions are often not critically evaluated. ASPs reduce hospital expenditures by limiting hospital-acquired infections and the associated medical costs where they are effective at decreasing consumption of antimicrobials [22,45], and by reducing antibiotic misuse, iatrogenic infections, and the rates of antibiotic-resistant organisms [47]. In one retrospective observational study, annual costs of antibiotics dropped by 33% with re-implementation of an ASP, mirrored by an overall decrease in antibiotic consumption of about 10%, over the course of the intervention study period [30]. Of note is that at 1 year post-ASP re-implementation, antibiotic consumption actually increased (by 5.4%); however, because antibiotic usage had changed to more appropriate and cost-effective therapies, cost expenditures associated with antibiotics were still reduced by 13% for that year relative to pre-ASP re-implementation. Aside from economic evaluations centered on consumption rates, there is the potential to further evaluate economic benefits associated with stewardship when looking at other outcomes, including hospital LOS [22], as well as indirect costs such as morbidity and mortality, societal, and operational costs [46]. Currently, these detailed analyses are lacking. In conjunction with more standardized clinical metrics, these assessments are needed to better delineate the full cost effectiveness of ASPs.
Evidence Summary
The evidence for inpatient ASP effectiveness is promising but mixed. Much of the evidence is low-level, based on observational studies that are retrospective in nature, and systematic reviews and meta-analyses are based on these types of studies. Studies have been conducted over a range of years, and the duration of intervention periods often vary widely between studies; it is difficult to capture and account for all of the infection, prescribing, and drug availability patterns (as well as the intervention differences or new drug approvals) throughout these time periods. To complicate the matter, both the quality of data as well as the quality of the ASPs are highly variable.
As such, the findings across pooled studies for ASPs are hard to amalgamate and draw concrete conclusions from. This difficulty is due to the inherent heterogeneity when comparing smaller individual studies in systematic reviews and meta-analyses. Currently, there are numerous ways to implement an ASP, but there is not a standardized system of specific interventions or metrics. Until we can directly compare similar ASPs and interventions among various institutions, it will be challenging to generalize positive benefits from systematic reviews and meta-analyses. Currently, the CDC is involved in a new initiative in which data from various hospitals are compiled to create a surveillance database [48]. Although this is a step in the right direction for standardized metrics for stewardship, for the current review the lack of standard metrics leads to conflicting results of heterogenic studies, making it difficult to show clear benefits in clinical outcomes.
Despite the vast array of ASPs, their differences, and a range of clinical measures—many with conflicting evidence—there is a noticeable trend toward a more prudent use of antimicrobials. Based on the review of available evidence, inpatient ASPs improve patient care and preserve an important health care resource—antibiotics. As has been presented, this is demonstrated by the alterations in consumption of these agents, has ramifications for secondary outcomes such as reduced instances of C. difficile infections, resistance, and adverse effects, and overall translates into better patient care and reduced costs. But while we can conclude that the direct interventions of stewardship in reducing and restricting antibiotic use have been effective, we cannot clearly state the overall magnitude of benefit, the effectiveness of various ASP structures and components on clinical outcomes (such as LOS, mortality, etc.), and the cost savings due to the heterogeneity of the available evidence.
Future Directions
Moving forward, the future of ASPs encompasses several potential developments. First and foremost, as technological advancements continue to develop, there is a need to integrate and utilize developments in information technology (IT). Baysari et al conducted a review on the value of utilizing IT interventions, focusing mainly on decision support (stand-alone or as a component of other hospital procedures), approval, and surveillance systems [49]. There was benefit associated with these IT interventions in terms of the improvement in the appropriate use of antimicrobials (RR 1.49, 95% CI, 1.07–2.08, P < 0.05; I2 = 93%), but there was no demonstrated benefit in terms of patient mortality or hospital LOS. Aside from this study, broad evidence is still lacking to support the use of IT systems in ASPs because meaningful comparisons amongst the interventions have not been made due to widespread variability in study design and outcome measures. However, it is generally agreed that ASPs must integrate with IT systems as the widespread use of technology within the healthcare field continues to grow. Evidence needs to be provided in the form of higher quality studies centered on similar outcomes to show appropriate approaches for ASPs to leverage IT systems. At a minimum, the integration of IT into ASPs should not hinder clinical outcomes. An important consideration is the variation in practice settings where antibiotic stewardship is to be implemented; eg, a small community hospital will be less equipped to incorporate and support technological tools compared to a large tertiary teaching hospital. Therefore, any antibiotic stewardship IT intervention must be customized to meet local needs, prescriber behaviors, minimize barriers to implementation, and utilize available resources.
Another area of focus for future ASPs is the use of rapid diagnostics. Currently, when patients present with signs and symptoms of an infection, an empiric antimicrobial regimen is started that is then de-escalated as necessary; rapid testing will help to initiate appropriate therapy more quickly and increase antimicrobial effectiveness. Rapid tests range from rapid polymerase chain reaction (PCR)-based screening [50], to Verigene gram-positive blood culture (BC-GP) tests [51], next-generation sequencing methods, and matrix assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) [52]. Rapid diagnostic tools should be viewed as aides to assist ASPs in decreasing antibiotic consumption and improving patient outcomes; these various tools have been shown to improve clinical outcomes when integrated into ASPs, but offer little value addressing the goals of ASPs when used outside of stewardship programs and their sensitive timeframes [53].
In terms of future ASP expansion, stewardship implementation can become more unified and broad in scope. ASPs should expand to include antifungal interventions, an area which is showing progress [36]. ASPs can also be implemented in new areas throughout the hospital (eg, pediatrics and emergency room), as well as areas outside of the hospital setting, including long-term care facilities, dialysis centers, and other institutions [54–56]. A prospective randomized control study was conducted in 30 nursing homes to evaluate the use of a novel resident antimicrobial management plan (RAMP) for improved use of antimicrobials [57]. This study found that the RAMP had no associated adverse effects and suggests that ASP is an important tool in nursing homes. In addition, the general outpatient and pediatric settings show promise for ASPs [56,58,59], but more research is needed to support expansion and to identify how ASP interventions should be applied in these various practice settings. The antimicrobial stewardship interventions that will be utilized will need to be carefully delineated to consider the scale, underlying need, and potential challenges in those settings.
While the future of antibiotic stewardship is unclear, there is certainty that it will continue to develop in both scope and depth to encompass new areas of focus, new settings to improve outcomes, and employ new tools to refine approaches. An important first step for the continued development of ASPs is alignment and standardization, since without alignment it will continue to be difficult to compare outcomes. This issue is currently being addressed by a number of different organizations. With current support from the Joint Commission, the CDC, as well as the President’s Council of Advisors on Science and Technology (PCAST) [8], regulatory requirements for ASPs are well underway, and these drivers will appropriately position ASPs for further advancements. By reducing variability amongst ASPs and delineating implementation of ASPs, there can be a clear identification of both economic and clinical benefits associated with specific interventions.
Corresponding author: Luigi Brunetti, PharmD, MPH, Rutgers, The State University of New Jersey, 160 Frelinghuysen Rd., Piscataway, NJ 08854, [email protected].
Financial disclosures: None.
From the Ernest Mario School of Pharmacy, Rutgers, The State University of New Jersey, Piscataway, NJ.
Abstract
- Objective: To review the evidence evaluating inpatient antimicrobial stewardship programs (ASPs) with a focus on clinical and economic outcomes.
- Methods: Pubmed/MEDLINE and the Cochrane Database of Systematic Reviews were used to identify systematic reviews, meta-analyses, randomized controlled trials, and other relevant literature evaluating the clinical and economic impact of ASP interventions.
- Results: A total of 5 meta-analyses, 3 systematic reviews, and 10 clinical studies (2 randomized controlled, 5 observational, and 3 quasi-experimental studies) were identified for analysis. ASPs were associated with a reduction in antimicrobial consumption and use. However, due to the heterogeneity of outcomes measured among studies, the effectiveness of ASPs varied with the measures used. There are data supporting the cost savings associated with ASPs, but these studies are more sparse. Most of the available evidence supporting ASPs is of low quality, and intervention strategies vary widely among available studies.
- Conclusion: Much of the evidence reviewed supports the assertion that ASPs result in a more judicious use of antimicrobials and lead to better patient care in the inpatient setting. While clinical outcomes vary between programs, there are ubiquitous positive benefits associated with ASPs in terms of antimicrobial consumption, C. difficile infection rates, and resistance, with few adverse effects. To date, economic outcomes have been difficult to uniformly quantify, but there are data supporting the economic benefits of ASPs. As the number of ASPs continues to grow, it is imperative that standardized metrics are considered in order to accurately measure the benefits of these essential programs.
Key words: Antimicrobial stewardship; antimicrobial consumption; resistance.
Antimicrobial resistance is a public health concern that has been escalating over the years and is now identified as a global crisis [1–3]. This is partly due to the widespread use of the same antibiotics that have existed for decades, combined with a lack of sufficient novel antibiotic discovery and development [4]. Bacteria that are resistant to our last-line-of-defense medications have recently emerged, and these resistant organisms may spread to treatment-naive patients [5]. Multidrug-resistant organisms are often found, treated, and likely originate within the hospital practice setting, where antimicrobials can be prescribed by any licensed provider [6]. Upwards of 50% of antibiotics administered are unnecessary and contribute to the problem of increasing resistance [7]. The seriousness of this situation is increasingly apparent; in 2014 the World Health Organization (WHO), President Obama, and Prime Minister Cameron issued statements urging solutions to the resistance crisis [8].
While the urgency of the situation is recognized today, efforts aimed at a more judicious use of antibiotics to curb resistance began as early as the 1960s and led to the first antimicrobial stewardship programs (ASPs) [9–11]. ASPs have since been defined as “coordinated interventions designed to improve and measure the appropriate use of antimicrobial agents by promoting the selection of the optimal antimicrobial drug regimen including dosing, duration of therapy, and route of administration” [1]. The primary objectives of these types of programs are to avoid or reduce adverse events (eg, Clostridium difficile infection) and resistance driven by a shift in minimum inhibitory concentrations (MICs) and to reverse the unnecessary economic burden caused by the inappropriate prescribing of these agents [1].
This article examines the evidence evaluating the reported effectiveness of inpatient ASPs, examining both clinical and economic outcomes. In addition, we touch on ASP history, current status, and future directions in light of current trends. While ASPs are expanding into the outpatient and nursing home settings, we will limit our review here to the inpatient setting.
Historical Background
Modern antibiotics date back to the late 1930s when penicillin and sulfonamides were introduced to the medical market, and resistance to these drug classes was reported just a few years after their introduction. The same bacterial resistance mechanisms that neutralized their efficacy then exist today, and these mechanisms continue to confer resistance among those classes [5].
While “stewardship” was not described as such until the late 1990s [12], institutions have historically been proactive in creating standards around antimicrobial utilization to encourage judicious use of these agents. The earliest form of tracking antibiotic use was in the form of paper charts as “antibiotic logs” [9] and “punch cards” [10] in the 1960s. The idea of a team approach to stewardship dates back to the 1970s, with the example of Hartford Hospital in Hartford, Connecticut, which employed an antimicrobial standards model run by an infectious disease (ID) physician and clinical pharmacists [11]. In 1977, the Infectious Diseases Society of America (IDSA) released a statement that clinical pharmacists may have a substantial impact on patient care, including in ID, contributing to the idea that a team of physicians collaborating with pharmacists presents the best way to combat inappropriate medication use. Pharmacist involvement has since been shown to restrict broad overutilized antimicrobial agents and reduce the rate of C. difficile infection by a significant amount [13].
In 1997 the IDSA and the Society for Healthcare Epidemiology of America (SHEA) published guidelines to assist in the prevention of the growing issue of resistance, mentioning the importance of antimicrobial stewardship [14]. A decade later they released joint guidelines for ASP implementation [15], and the Pediatric Infectious Disease Society (PIDS) joined them in 2012 to publish a joint statement acknowledging and endorsing stewardship [16]. In 2014, the Centers of Disease Control and Prevention (CDC) recommended that every hospital should have an ASP. As of 1 January 2017, the Joint Commission requires an ASP as a standard for accreditation at hospitals, critical access hospitals, and nursing care [17]. Guidelines for implementation of an ASP are currently available through the IDSA and SHEA [1,16].
ASP Interventions
There are 2 main strategies that ASPs have to combat inappropriate antimicrobial use, and each has its own set of systematic interventions. These strategies are referred to as “prospective audit with intervention and feedback” and “prior authorization” [6]. Although most ASPs will incorporate these main strategies, each institution typically creates its own strategies and regulations independently.
Prospective audit with intervention and feedback describes the process of providing recommendations after reviewing utilization and trends of antimicrobial use. This is sometimes referred to as the “back-end” intervention, in which decisions are made after antibiotics have been administered. Interventions that are commonly used under this strategy include discontinuation of antibiotics due to culture data, de-escalation to drugs with narrower spectra, IV to oral conversions, and cessation of surgical prophylaxis [6].
Prior authorization, also referred to as a “front-end” intervention, is the process of approving medications before they are used. Interventions include a restricted formulary for antimicrobials that can be managed through a paging system or a built-in computer restriction program, as well as other guidelines and protocols for dosing and duration of therapy. Restrictions typically focus on broad spectrum antibiotics as well as the more costly drugs on formularies. These solutions reduce the need for manual intervention as technology makes it possible to create automated restriction-based services that prevent inappropriate prescribing [6].
Aside from these main techniques, other strategies are taken to achieve the goal of attaining optimal clinical outcomes while limiting further antimicrobial resistance and adverse effects. Different clinical settings have different needs, and ASPs are customized to each setting’s resources, prescribing habits, and other local specificities [1]. These differences present difficulty with interpreting diverse datasets, but certain themes arise in the literature: commonly assessed clinical outcomes of inpatient ASPs include hospital length of stay (LOS) and readmission, reinfection, mortality, and resistance rates. These outcomes are putatively driven by the more prudent use of antimicrobials, particularly by decreased rates of antimicrobial consumption.
ASP Team Members
While ASPs may differ between institutions, the staff members involved are typically the same, and leadership is always an important aspect of a program. The CDC recommends that ASP leadership consist of a program leader (an ID physician) and a pharmacy leader, who co-lead the team [18]. In addition, the Joint Commission recommends that the multidisciplinary team should include an infection preventionist (ie, infection control and hospital epidemiologist) and practitioner [17]; these specialists have a role in prevention, awareness, and policy [19]. The integration of infection control with stewardship yields the best results [15], as infection control aims to prevent antibiotic use altogether, while stewardship increases the quality of antibiotic regimens that are being prescribed [20].
It is also beneficial to incorporate a microbiologist as an integral part of the team, responsible for performing and interpreting laboratory data (ie, cultures). Nurses should be integrated into ASPs due to the overlap of their routine activities with ASP interventions [21]; other clinicians (regardless of their infectious disease clinical background), quality control, information technology, and environmental services should all collaborate in the hospital-wide systems related to the program where appropriate [18].
Evidence Review
Results
Antimicrobial Usage
The most widely studied aspect of ASPs in the current review was the effect of ASP interventions on antimicrobial consumption and use. Three systematic reviews [22–24] showed improved antibiotic prescribing practices and reduced consumption rates overall, as did several studies inside and outside the intensive care unit (ICU) [25–31].One study found an insignificant declining usage trend [32]. An important underlying facet of this observation is that even as total antibiotic consumption decreases, certain antibiotic and antibiotic class consumption may increase. This is evident in several studies, which showed that as aminoglycoside, carbapenem, and β-lactam-β-lactamase inhibitor use increased, clindamycin (1 case), glycopeptide, fluoroquinolone, and macrolide use decreased [27,28,30]. A potential confounding factor relating to decreased glycopeptide use in Bevilacqua et al [30] was that there was an epidemic of glycopeptide-resistant enterococci during the study period, potentially causing prescribers to naturally avoid it. In any case, since the aim of ASPs is to encourage a more judicious usage of antimicrobials, the observed decreases in consumption of those restricted medications is intuitive. These observations about antimicrobial consumption related to ASPs are relevant because they putatively drive improvements in clinical outcomes, especially those related to reduced adverse events associated with these agents, such as the risk of C. difficile infection with certain drugs (eg, fluoroquinolones, clindamycin, and broad-spectrum antibiotics) and prolonged antibiotic usage [33–35]. There is evidence that these benefits are not limited to antibiotics but extend to antifungal agents and possibly antivirals [22,27,36].
Utilization, Mortality, and Infection Rates
ASPs typically intend to improve patient-focused clinical parameters such as hospital LOS, hospital readmissions, mortality, and incidence of infections acquired secondary to antibiotic usage during a hospital stay, especially C. difficile infection. Most of the reviewed evidence indicates that there has been no significant LOS benefit due to stewardship interventions [24–26,32,37], and one meta-analysis noted that when overall hospital LOS was significantly reduced, ICU-specific LOS was not [22]. Generally, there was also not a significant change in hospital readmission rates [24,26,32]. However, 2 retrospective observational studies found mixed results for both LOS and readmission rates relative to ASP interventions; while both noted a significantly reduced LOS, one study [38] showed an all-cause readmission benefit in a fairly healthy patient population (but no benefit for readmissions due to the specific infections of interest), and the another [29] showed a benefit for readmissions due to infections but an increased rate of readmissions in the intervention group overall. In this latter study, hospitalizations within the previous 3 months were significantly higher at baseline for the intervention group (55% vs. 46%, P = 0.042), suggesting sicker patients and possibly providing an explanation for this unique observation. Even so, a meta-analysis of 5 studies found a significantly elevated risk of readmission associated with ASP interventions (RR 1.26, 95% CI 1.02–1.57; P = 0.03); the authors noted that non–infection-related readmissions accounted for 61% of readmissions, but this was not significantly different between intervention and non-intervention arms [37].
With regard to mortality, most studies found no significant reductions related to stewardship interventions [22,24,26,29,32]. In a prospective randomized controlled trial, all reported deaths (7/160, 4.4%) were in the ASP intervention arm, but these were attributed to the severities of infection or an underlying, chronic disease [25]. One meta-analysis, however, found that there were significant mortality reductions related to stewardship guidelines for empirical antibiotic treatment (OR 0.65, 95% CI 0.54–0.80, P < 0.001; I2 = 65%) and to de-escalation of therapy based on culture results (RR 0.44, 95% CI 0.30–0.66, P < 0.001; I2 = 59%), based on 40 and 25 studies, respectively [39]; but both results exhibited substantial heterogeneity (defined as I2 = 50%–90% [40]) among the relevant studies. Another meta-analysis found that there was no significant change in mortality related to stewardship interventions intending to improve antibiotic appropriateness (RR 0.92, 95% CI 0.69–1.2, P = 0.56; I2 = 72%) or intending to reduce excessive prescribing (RR 0.92, 95% CI 0.81–1.06, P = 0.25; I2 = 0%), but that there was a significant mortality benefit associated with interventions aimed at increasing guideline compliance for pneumonia diagnoses (RR 0.89, 95% CI 0.82–0.97, P = 0.005; I2 = 0%) [37]. In the case of Schuts et al [39], search criteria specifically sought studies that assessed clinical outcomes (eg, mortality), whereas the search of Davey et al [37] focused on studies whose aim was to improve antibiotic prescribing, with a main comparison being between restrictive and persuasive interventions; while the difference may seem subtle, the body of data compiled from these searches may characterize the ASP effect of mortality differently. No significant evidence was found to suggest that reduced antimicrobial consumption increases mortality.
Improving the use of antimicrobial agents should limit collateral damage associated with their use (eg, damage to normal flora and increased resistance), and ideally infections should be better managed. As previously mentioned, one of the concerns with antibiotic usage (particularly fluoroquinolones, macrolides, and broad-spectrum agents) is that collateral damage could lead to increased rates of C. difficile infection. One meta-analysis showed no significant reduction in the rate of C. difficile infection (as well as overall infection rate) relative to ASPs [22]; however, this finding was based on only 3 of the 26 studies analyzed, and only 1 of those 3 studies utilized restrictions for flouroquinolones and cephalosporins. An interrupted time series (ITS) study similarly found no significant reduction in C. difficile infection rate [32]; however, this study was conducted in a hospital with low baseline antibiotic prescribing (it was ranked second-to-last in terms of antibiotic usage among its peer institutions), inherently limiting the risk of C. difficile infection among patients in the pre-ASP setting. In contrast to these findings, a meta-analysis specifically designed to assess the incidence of C. difficile infection relative to stewardship programs found a significantly reduced risk of infection based on 16 studies (RR 0.48, 95% CI 0.38–0.62, P < 0.001; I2 = 76%) [41], and the systematic review conducted by Filice et al [24] found a significant benefit with regard to the C. difficile infection rate in 4 of 6 studies. These results are consistent with those presented as evidence for the impact of stewardship on C. difficile infection by the CDC [42]. Aside from C. difficile infection, one retrospective observational study found that the 14-day reinfection rate (ie, reinfection with the same infection at the same anatomical location) was significantly reduced following stewardship intervention (0% vs. 10%, P = 0.009) [29]. This finding, combined with the C. difficile infection examples, provide evidence for better infection management of ASPs.
While the general trend seems to suggest mixed or no significant benefit for several clinical outcomes, it is important to note that variation in outcomes could be due to differences in the types of ASP interventions and intervention study periods across differing programs. Davey et al [37] found variation in prescribing outcomes based on whether restrictive (ie, restrict prescriber freedom with antimicrobials) or persuasive (ie, suggest changes to prescriber) interventions were used, and on the timeframe in which they were used. At one month into an ASP, restrictive interventions resulted in better prescribing practices relative to persuasive interventions based on 27 studies (effect size 32.0%, 95% CI 2.5%–61.4%), but by 6 months the 2 were not statistically different (effect size 10.1%, 95% CI –47.5% to 66.0%). At 12 and 24 months, persuasive interventions demonstrated greater effects on prescribing outcomes, but these were not significant. These findings provide evidence that different study timeframes can impact ASP practices differently (and these already vary widely in the literature). Considering the variety of ASP interventions employed across the different studies, these factors almost certainly impact the reported antimicrobial consumption rates and outcomes to different degrees as a consequence. A high degree of heterogeneity among an analyzed dataset could itself be the reason for net non-significance within single systematic reviews and meta-analyses.
Resistance
Another goal of ASPs is the prevention of antimicrobial resistance, an area where the evidence generally suggests benefit associated with ASP interventions. Resistance rates to common troublesome organisms, such as methicillin-resistant S. aureus (MRSA), imipenem-resistant P. aeruginosa, and extended-spectrum β-lactamase (ESBL)–producing Klebsiella spp were significantly reduced in a meta-analysis; ESBL-producing E. coli infections were not, however [22]. An ITS study found significantly reduced MRSA resistance, as well as reduced Pseudomonal resistance to imipenem-cilastin and levofloxacin (all P < 0.001), but no significant changes with respect to piperacillin/tazobactam, cefepime, or amikacin resistance [32]. This study also noted increased E. coli resistance to levofloxacin and ceftriaxone (both P < 0.001). No significant changes in resistance were noted for vancomycin-resistant enterococci. It may be a reasonable expectation that decreasing inappropriate antimicrobial use may decrease long-term antimicrobial resistance; but as most studies only span a few years, only the minute changes in resistance are understood [23]. Longer duration studies are needed to better understand resistance outcomes.
Of note is a phenomenon known as the “squeezing the balloon” effect. This can be associated with ASPs, potentially resulting in paradoxically increased resistance [43]. That is, when usage restrictions are placed on certain antibiotics, the use of other non-restricted antibiotics may increase, possibly leading to increased resistance of those non-restricted antibiotics [22] (“constraining one end [of a balloon] causes the other end to bulge … limiting the use of one class of compounds may be counteracted by corresponding changes in prescribing and drug resistance that are even more ominous” [43]). Karanika et al [22] took this phenomonen into consideration, and assessed restricted and non-restricted antimicrobial consumption separately. They found a reduction in consumption for both restricted and non-restricted antibiotics, which included “high potential resistance” antibiotics, specifically carbapenems and glycopeptides. In the study conducted by Cairns et al [28], a similar effect was observed; while the use of other classes of antibiotics decreased (eg, cephalosporins and aminoglycosides), the use of β–lactam–β–lactamase inhibitor combinations actually increased by 48% (change in use: +48.2% [95% CI 21.8%–47.9%]). Hohn et al [26] noted an increased usage rate of carbapenems, even though several other classes of antibiotics had reduced usage. Unfortunately, neither study reported resistance rates, so the impact of these findings is unknown. Finally, Jenkins et al [32] assessed trends in antimicrobial use as changes in rates of consumption. Among the various antibiotics assessed in this study, the rate of flouroquinolone use decreased both before and after the intervention period, although the rate of decreased usage slowed post-ASP (the change in rate post-ASP was +2.2% [95% CI 1.4%–3.1%], P < 0.001). They observed a small (but significant) increase in resistance of E. coli to levofloxacin pre- vs. post-intervention (11.0% vs. 13.9%, P < 0.001); in contrast, a significant decrease in resistance of P. aeruginosa was observed (30.5% vs. 21.4%, P < 0.001). While these examples help illustrate the concept of changes in antibiotic usage patterns associated with an ASP, at best they approximate the “squeezing the balloon” effect since these studies present data for antibiotics that were either restricted or for which restriction was not clearly specified. The “squeezing the balloon” effect is most relevant for the unintended, potentially increased usage of non-restricted drugs secondary to ASP restrictions. Higher resistance rates among certain drug classes observed in the context of this effect would constitute a drawback to an ASP program.
Adverse Effects
Reduced toxicities and adverse effects are expected with reduced usage of antimicrobials. The systematic review conducted by Filice et al [24] examined the incidence of adverse effects related to antibiotic usage, and their findings suggest, at the least, that stewardship programs generally do not cause harm, as only 2 of the studies they examined reported adverse events. Following stewardship interventions, 5.5% of the patients deteriorated; and of those, the large majority (75%) deteriorated due to progression of oncological malignancies. To further illustrate the effect of stewardship interventions on toxicities and side effects of antimicrobials, Schuts et al demonstrated that the risk of nephrotoxicity while on antimicrobial therapy was reduced based on 14 studies of moderate heterogeneity as a result of an ASP (OR 0.46, 95% CI 0.28–0.77, P = 0.003; I2 = 34%) [39,44]. It is intuitive that reduced drug exposure results in reduced adverse effects, as such these results are expected.
Economic Outcomes
Although the focus of ASPs is often to improve clinical outcomes, economic outcomes are an important component of ASPs; these programs bring associated economic value that should be highlighted and further detailed [22,45,46]. Since clinical outcomes are often the main objective of ASPs, most available studies have been clinical effect studies (rather than economic analyses), in which economic assessments are often a secondary consideration, if included.
As a result, cost evaluations are conducted on direct cost reductions whereas indirect cost reductions are often not critically evaluated. ASPs reduce hospital expenditures by limiting hospital-acquired infections and the associated medical costs where they are effective at decreasing consumption of antimicrobials [22,45], and by reducing antibiotic misuse, iatrogenic infections, and the rates of antibiotic-resistant organisms [47]. In one retrospective observational study, annual costs of antibiotics dropped by 33% with re-implementation of an ASP, mirrored by an overall decrease in antibiotic consumption of about 10%, over the course of the intervention study period [30]. Of note is that at 1 year post-ASP re-implementation, antibiotic consumption actually increased (by 5.4%); however, because antibiotic usage had changed to more appropriate and cost-effective therapies, cost expenditures associated with antibiotics were still reduced by 13% for that year relative to pre-ASP re-implementation. Aside from economic evaluations centered on consumption rates, there is the potential to further evaluate economic benefits associated with stewardship when looking at other outcomes, including hospital LOS [22], as well as indirect costs such as morbidity and mortality, societal, and operational costs [46]. Currently, these detailed analyses are lacking. In conjunction with more standardized clinical metrics, these assessments are needed to better delineate the full cost effectiveness of ASPs.
Evidence Summary
The evidence for inpatient ASP effectiveness is promising but mixed. Much of the evidence is low-level, based on observational studies that are retrospective in nature, and systematic reviews and meta-analyses are based on these types of studies. Studies have been conducted over a range of years, and the duration of intervention periods often vary widely between studies; it is difficult to capture and account for all of the infection, prescribing, and drug availability patterns (as well as the intervention differences or new drug approvals) throughout these time periods. To complicate the matter, both the quality of data as well as the quality of the ASPs are highly variable.
As such, the findings across pooled studies for ASPs are hard to amalgamate and draw concrete conclusions from. This difficulty is due to the inherent heterogeneity when comparing smaller individual studies in systematic reviews and meta-analyses. Currently, there are numerous ways to implement an ASP, but there is not a standardized system of specific interventions or metrics. Until we can directly compare similar ASPs and interventions among various institutions, it will be challenging to generalize positive benefits from systematic reviews and meta-analyses. Currently, the CDC is involved in a new initiative in which data from various hospitals are compiled to create a surveillance database [48]. Although this is a step in the right direction for standardized metrics for stewardship, for the current review the lack of standard metrics leads to conflicting results of heterogenic studies, making it difficult to show clear benefits in clinical outcomes.
Despite the vast array of ASPs, their differences, and a range of clinical measures—many with conflicting evidence—there is a noticeable trend toward a more prudent use of antimicrobials. Based on the review of available evidence, inpatient ASPs improve patient care and preserve an important health care resource—antibiotics. As has been presented, this is demonstrated by the alterations in consumption of these agents, has ramifications for secondary outcomes such as reduced instances of C. difficile infections, resistance, and adverse effects, and overall translates into better patient care and reduced costs. But while we can conclude that the direct interventions of stewardship in reducing and restricting antibiotic use have been effective, we cannot clearly state the overall magnitude of benefit, the effectiveness of various ASP structures and components on clinical outcomes (such as LOS, mortality, etc.), and the cost savings due to the heterogeneity of the available evidence.
Future Directions
Moving forward, the future of ASPs encompasses several potential developments. First and foremost, as technological advancements continue to develop, there is a need to integrate and utilize developments in information technology (IT). Baysari et al conducted a review on the value of utilizing IT interventions, focusing mainly on decision support (stand-alone or as a component of other hospital procedures), approval, and surveillance systems [49]. There was benefit associated with these IT interventions in terms of the improvement in the appropriate use of antimicrobials (RR 1.49, 95% CI, 1.07–2.08, P < 0.05; I2 = 93%), but there was no demonstrated benefit in terms of patient mortality or hospital LOS. Aside from this study, broad evidence is still lacking to support the use of IT systems in ASPs because meaningful comparisons amongst the interventions have not been made due to widespread variability in study design and outcome measures. However, it is generally agreed that ASPs must integrate with IT systems as the widespread use of technology within the healthcare field continues to grow. Evidence needs to be provided in the form of higher quality studies centered on similar outcomes to show appropriate approaches for ASPs to leverage IT systems. At a minimum, the integration of IT into ASPs should not hinder clinical outcomes. An important consideration is the variation in practice settings where antibiotic stewardship is to be implemented; eg, a small community hospital will be less equipped to incorporate and support technological tools compared to a large tertiary teaching hospital. Therefore, any antibiotic stewardship IT intervention must be customized to meet local needs, prescriber behaviors, minimize barriers to implementation, and utilize available resources.
Another area of focus for future ASPs is the use of rapid diagnostics. Currently, when patients present with signs and symptoms of an infection, an empiric antimicrobial regimen is started that is then de-escalated as necessary; rapid testing will help to initiate appropriate therapy more quickly and increase antimicrobial effectiveness. Rapid tests range from rapid polymerase chain reaction (PCR)-based screening [50], to Verigene gram-positive blood culture (BC-GP) tests [51], next-generation sequencing methods, and matrix assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) [52]. Rapid diagnostic tools should be viewed as aides to assist ASPs in decreasing antibiotic consumption and improving patient outcomes; these various tools have been shown to improve clinical outcomes when integrated into ASPs, but offer little value addressing the goals of ASPs when used outside of stewardship programs and their sensitive timeframes [53].
In terms of future ASP expansion, stewardship implementation can become more unified and broad in scope. ASPs should expand to include antifungal interventions, an area which is showing progress [36]. ASPs can also be implemented in new areas throughout the hospital (eg, pediatrics and emergency room), as well as areas outside of the hospital setting, including long-term care facilities, dialysis centers, and other institutions [54–56]. A prospective randomized control study was conducted in 30 nursing homes to evaluate the use of a novel resident antimicrobial management plan (RAMP) for improved use of antimicrobials [57]. This study found that the RAMP had no associated adverse effects and suggests that ASP is an important tool in nursing homes. In addition, the general outpatient and pediatric settings show promise for ASPs [56,58,59], but more research is needed to support expansion and to identify how ASP interventions should be applied in these various practice settings. The antimicrobial stewardship interventions that will be utilized will need to be carefully delineated to consider the scale, underlying need, and potential challenges in those settings.
While the future of antibiotic stewardship is unclear, there is certainty that it will continue to develop in both scope and depth to encompass new areas of focus, new settings to improve outcomes, and employ new tools to refine approaches. An important first step for the continued development of ASPs is alignment and standardization, since without alignment it will continue to be difficult to compare outcomes. This issue is currently being addressed by a number of different organizations. With current support from the Joint Commission, the CDC, as well as the President’s Council of Advisors on Science and Technology (PCAST) [8], regulatory requirements for ASPs are well underway, and these drivers will appropriately position ASPs for further advancements. By reducing variability amongst ASPs and delineating implementation of ASPs, there can be a clear identification of both economic and clinical benefits associated with specific interventions.
Corresponding author: Luigi Brunetti, PharmD, MPH, Rutgers, The State University of New Jersey, 160 Frelinghuysen Rd., Piscataway, NJ 08854, [email protected].
Financial disclosures: None.
1. Barlam TF, Cosgrove SE, Abbo AM, et al. Implementing an antimicrobial stewardship program: guidelines by the Infectious Diseases Society of America and the Society of Healthcare Epidemiology of America. Clin Infect Dis 2016;62:e51–77.
2. Hughes D. Selection and evolution of resistance to antimicrobial drugs. IUBMB Life 2014;66:521–9.
3. World Health Organzation. The evolving threat of antimicrobial resistance – options for action. Geneva: WHO Press; 2012.
4. Gould IM, Bal AM. New antibiotic agents in the pipeline and how they can help overcome microbial resistance. Virulence 2013;4:185–91.
5. Davies J, Davies D. Origins and evolution of antibiotic resistance. Microbiol Mol Biol Rev 2010;74:417–33.
6. Owens RC Jr. Antimicrobial stewardship: concepts and strategies in the 21st century. Diagn Microbiol Infect Dis 2008;61:110–28.
7. Antibiotic resistance threats in the United States, 2013 [Internet]. Centers for Disease Control and Prevention. Available at www.cdc.gov/drugresistance/pdf/ar-threats-2013-508.pdf.
8. Nathan C, Cars O. Antibiotic resistance – problems, progress, prospects. N Engl J Med 2014;371:1761–3.
9. McGoldrick, M. Antimicrobial stewardship. Home Healthc Nurse 2014;32:559–60.
10. Ruedy J. A method of determining patterns of use of antibacterial drugs. Can Med Assoc J 1966;95:807–12.
11. Briceland LL, Nightingdale CH, Quintiliani R, et al. Antibiotic streamlining from combination therapy to monotherapy utilizing an interdisciplinary approach. Arch Inter Med 1988;148:2019–22.
12. McGowan JE Jr, Gerding DN. Does antibiotic restriction prevent resistance? New Horiz 1996;4: 370–6.
13. Cappelletty D, Jacobs D. Evaluating the impact of a pharmacist’s absence from an antimicrobial stewardship team. Am J Health Syst Pharm 2013;70:1065–69.
14. Shales DM, Gerding DN, John JF Jr, et al. Society for Healthcare Epidemiology of America and Infectious Diseases Society of America Joint Committee on the prevention of antimicrobial resistance: guidelines for the prevention of antimicrobial resistance in hospitals. Infect Control Hosp Epidemiol 1997;18:275–91.
15. Dellit TH, Owens RC, McGowan JE, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis 2007;44:159–77.
16. Policy statement on antimicrobial stewardship by the Society for Healthcare Epidemiology of America (SHEA), the Infectious Diseases Society of America (IDSA), and the Pediatric Infectious Diseases Society (PIDS). Infect Ctrl Hosp Epidemiol 2012;33:322–7.
17. The Joint Commission. Approved: New antimicrobial stewardship standard. Joint Commission Perspectives 2016;36:1–8.
18. Pollack LA, Srinivasan A. Core elements of hospital antibiotic stewardship programs from the Centers for Disease Control and Prevention. Clin Infect Dis 2014;59(Suppl 3):S97–100.
19. Moody J. Infection preventionists have a role in accelerating progress toward preventing the emergence and cross-transmission of MDROs. Prevention Strategist 2012 Summer:52–6.
20. Spellberg B, Bartlett JG, Gilbert DN. The future of antibiotics and resistance. N Engl J Med 2013;368:299–302.
21. Olans RN, Olans RD, Demaria A. The critical role of the staff nurse in antimicrobial stewardship--unrecognized, but already there. Clin Infect Dis 2016;62:84–9.
22. Karanika S, Paudel S, Grigoras C, et al. Systematic review and meta-analysis of clinical and economic outcomes from the implementation of hospital-based antimicrobial stewardship programs. Antimicrob Agents Chemother 2016;60:4840–52.
23. Wagner B, Filice GA, Drekonja D, et al. Antimicrobial stewardship programs in inpatient hospital settings: a systematic review. Infect Control Hosp Epidemiol 2014;35:1209–28.
24. Filice G, Drekonja D, Greer N, et al. Antimicrobial stewardship programs in inpatient settings: a systematic review. VA-ESP Project #09-009; 2013.
25. Cairns KA, Doyle JS, Trevillyan JM, et al. The impact of a multidisciplinary antimicrobial stewardship team on the timeliness of antimicrobial therapy in patients with positive blood cultures: a randomized controlled trial. J Antimicrob Chemother 2016;71:3276–83.
26. Hohn A, Heising B, Hertel S, et al. Antibiotic consumption after implementation of a procalcitonin-guided antimicrobial stewardship programme in surgical patients admitted to an intensive care unit: a retrospective before-and-after analysis. Infection 2015;43:405–12.
27. Singh S, Zhang YZ, Chalkley S, et al. A three-point time series study of antibiotic usage on an intensive care unit, following an antibiotic stewardship programme, after an outbreak of multi-resistant Acinetobacter baumannii. Eur J Clin Microbiol Infect Dis 2015;34:1893–900.
28. Cairns KA, Jenney AW, Abbott IJ, et al. Prescribing trends before and after implementation of an antimicrobial stewardship program. Med J Aust 2013;198:262–6.
29. Liew YX, Lee W, Loh JC, et al. Impact of an antimicrobial stewardship programme on patient safety in Singapore General Hospital. Int J Antimicrob Agents 2012;40:55–60.
30. Bevilacqua S, Demoré B, Boschetti E, et al. 15 years of antibiotic stewardship policy in the Nancy Teaching Hospital. Med Mal Infect 2011;41:532–9.
31. Danaher PJ, Milazzo NA, Kerr KJ, et al. The antibiotic support team--a successful educational approach to antibiotic stewardship. Mil Med 2009;174:201–5.
32. Jenkins TC, Knepper BC, Shihadeh K, et al. Long-term outcomes of an antimicrobial stewardship program implemented in a hospital with low baseline antibiotic use. Infect Control Hosp Epidemiol 2015;36:664–72.
33. Brown KA, Khanafer N, Daneman N, Fisman DN. Meta-analysis of antibiotics and the risk of community-associated Clostridium difficile infection. Antimicrob Agents Chemother 2013;57:2326–32.
34. Deshpande A, Pasupuleti V, Thota P, et al. Community-associated Clostridium difficile infection and antibiotics: a meta-analysis. J Antimicrob Chemother 2013;68:1951–61.
35. Slimings C, Riley TV. Antibiotics and hospital-acquired Clostridium difficile infection: update of systematic review and meta-analysis. J Antimicrob Chemother 2014;69:881–91.
36. Antworth A, Collins CD, Kunapuli A, et al. Impact of an antimicrobial stewardship program comprehensive care bundle on management of candidemia. Pharmacotherapy 2013;33:137–43.
37. Davey P, Brown E, Charani E, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev 2013;4:CD003543.
38. Pasquale TR, Trienski TL, Olexia DE, et al. Impact of an antimicrobial stewardship program on patients with acute bacterial skin and skin structure infections. Am J Health Syst Pharm 2014;71:1136–9.
39. Schuts EC, Hulscher ME, Mouton JW, et al. Current evidence on hospital antimicrobial stewardship objectives: a systematic review and meta-analysis. Lancet Infect Dis 2016;16:847–56.
40. Higgins JPT, Green S, editors. Identifying and measuring heterogeneity. Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0. [Internet]. The Cochrane Collaboration, March 2011. Available at http://handbook.cochrane.org/chapter_9/9_5_2_identifying_and_measuring_heterogeneity.htm.
41. Feazel LM, Malhotra A, Perencevich EN, et al. Effect of antibiotic stewardship programmes on Clostridium difficile incidence: a systematic review and meta-analysis. J Antimicrob Chemother 2014;69:1748–54.
42. Impact of antibiotic stewardship programs on Clostridium difficile (C. diff) infections [Internet]. Centers for Disease Control and Prevention. [Updated 2016 May 13; cited 2016 Oct 11]. Available at www.cdc.gov/getsmart/healthcare/evidence/asp-int-cdiff.html.
43. Burke JP. Antibiotic resistance – squeezing the balloon? JAMA 1998;280:1270–1.
44. This nephrotoxicity result is corrected from the originally published result; communicated by Jan M Prins on behalf of the authors for reference [39]. Prins, JM (Department of Internal Medicine, Division of Infectious Diseases, Academic Medical Centre, Amsterdam, Netherlands). Email communication with Joseph Eckart (Pharmacy Practice & Administration, Ernest Mario School of Pharmacy, Rutgers University, Piscataway, NJ). 2016 Oct 9.
45. Coulter S, Merollini K, Roberts JA, et al. The need for cost-effectiveness analyses of antimicrobial stewardship programmes: a structured review. Int J Antimicrob Agents 2015;46:140–9.
46. Dik J, Vemer P, Friedrich A, et al. Financial evaluations of antibiotic stewardship programs—a systematic review. Frontiers Microbiol 2015;6:317.
47. Campbell KA, Stein S, Looze C, Bosco JA. Antibiotic stewardship in orthopaedic surgery: principles and practice. J Am Acad Orthop Surg 2014;22:772–81.
48. Surveillance for antimicrobial use and antimicrobial resistance options, 2015 [Internet]. Centers for Disease Control and Prevention. [Updated 2016 May 3; cited 2016 Nov 22]. Available at www.cdc.gov/nhsn/acute-care-hospital/aur/index.html.
49. Baysari MT, Lehnbom EC, Li L, Hargreaves A, et al. The effectiveness of information technology to improve antimicrobial prescribing in hospitals: a systematic review and meta-analysis. Int J Med Inform. 2016;92:15-34.
50. Bauer KA, West JE, Balada-llasat JM, et al. An antimicrobial stewardship program’s impact with rapid polymerase chain reaction methicillin-resistant Staphylococcus aureus/S. aureus blood culture test in patients with S. aureus bacteremia. Clin Infect Dis 2010;51:1074–80.
51. Sango A, Mccarter YS, Johnson D, et al. Stewardship approach for optimizing antimicrobial therapy through use of a rapid microarray assay on blood cultures positive for Enterococcus species. J Clin Microbiol 2013;51:4008–11.
52. Perez KK, Olsen RJ, Musick WL, et al. Integrating rapid diagnostics and antimicrobial stewardship improves outcomes in patients with antibiotic-resistant Gram-negative bacteremia. J Infect 2014;69:216–25.
53. Bauer KA, Perez KK, Forrest GN, Goff DA. Review of rapid diagnostic tests used by antimicrobial stewardship programs. Clin Infect Dis 2014;59 Suppl 3:S134–145.
54. Dyar OJ, Pagani L, Pulcini C. Strategies and challenges of antimicrobial stewardship in long-term care facilities. Clin Microbiol Infect 2015;21:10–9.
55. D’Agata EM. Antimicrobial use and stewardship programs among dialysis centers. Semin Dial 2013;26:457–64.
56. Smith MJ, Gerber JS, Hersh AL. Inpatient antimicrobial stewardship in pediatrics: a systematic review. J Pediatric Infect Dis Soc 2015;4:e127–135.
57. Fleet E, Gopal Rao G, Patel B, et al. Impact of implementation of a novel antimicrobial stewardship tool on antibiotic use in nursing homes: a prospective cluster randomized control pilot study. J Antimicrob Chemother 2014;69:2265–73.
58. Drekonja DM, Filice GA, Greer N, et al. Antimicrobial stewardship in outpatient settings: a systematic review. Infect Control Hosp Epidemiol 2015;36:142–52.
59. Drekonja D, Filice G, Greer N, et al. Antimicrobial stewardship programs in outpatient settings: a systematic review. VA-ESP Project #09-009; 2014.
60. Zhang YZ, Singh S. Antibiotic stewardship programmes in intensive care units: why, how, and where are they leading us. World J Crit Care Med 2015;4:13–28. (referenced in online Table)
1. Barlam TF, Cosgrove SE, Abbo AM, et al. Implementing an antimicrobial stewardship program: guidelines by the Infectious Diseases Society of America and the Society of Healthcare Epidemiology of America. Clin Infect Dis 2016;62:e51–77.
2. Hughes D. Selection and evolution of resistance to antimicrobial drugs. IUBMB Life 2014;66:521–9.
3. World Health Organzation. The evolving threat of antimicrobial resistance – options for action. Geneva: WHO Press; 2012.
4. Gould IM, Bal AM. New antibiotic agents in the pipeline and how they can help overcome microbial resistance. Virulence 2013;4:185–91.
5. Davies J, Davies D. Origins and evolution of antibiotic resistance. Microbiol Mol Biol Rev 2010;74:417–33.
6. Owens RC Jr. Antimicrobial stewardship: concepts and strategies in the 21st century. Diagn Microbiol Infect Dis 2008;61:110–28.
7. Antibiotic resistance threats in the United States, 2013 [Internet]. Centers for Disease Control and Prevention. Available at www.cdc.gov/drugresistance/pdf/ar-threats-2013-508.pdf.
8. Nathan C, Cars O. Antibiotic resistance – problems, progress, prospects. N Engl J Med 2014;371:1761–3.
9. McGoldrick, M. Antimicrobial stewardship. Home Healthc Nurse 2014;32:559–60.
10. Ruedy J. A method of determining patterns of use of antibacterial drugs. Can Med Assoc J 1966;95:807–12.
11. Briceland LL, Nightingdale CH, Quintiliani R, et al. Antibiotic streamlining from combination therapy to monotherapy utilizing an interdisciplinary approach. Arch Inter Med 1988;148:2019–22.
12. McGowan JE Jr, Gerding DN. Does antibiotic restriction prevent resistance? New Horiz 1996;4: 370–6.
13. Cappelletty D, Jacobs D. Evaluating the impact of a pharmacist’s absence from an antimicrobial stewardship team. Am J Health Syst Pharm 2013;70:1065–69.
14. Shales DM, Gerding DN, John JF Jr, et al. Society for Healthcare Epidemiology of America and Infectious Diseases Society of America Joint Committee on the prevention of antimicrobial resistance: guidelines for the prevention of antimicrobial resistance in hospitals. Infect Control Hosp Epidemiol 1997;18:275–91.
15. Dellit TH, Owens RC, McGowan JE, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis 2007;44:159–77.
16. Policy statement on antimicrobial stewardship by the Society for Healthcare Epidemiology of America (SHEA), the Infectious Diseases Society of America (IDSA), and the Pediatric Infectious Diseases Society (PIDS). Infect Ctrl Hosp Epidemiol 2012;33:322–7.
17. The Joint Commission. Approved: New antimicrobial stewardship standard. Joint Commission Perspectives 2016;36:1–8.
18. Pollack LA, Srinivasan A. Core elements of hospital antibiotic stewardship programs from the Centers for Disease Control and Prevention. Clin Infect Dis 2014;59(Suppl 3):S97–100.
19. Moody J. Infection preventionists have a role in accelerating progress toward preventing the emergence and cross-transmission of MDROs. Prevention Strategist 2012 Summer:52–6.
20. Spellberg B, Bartlett JG, Gilbert DN. The future of antibiotics and resistance. N Engl J Med 2013;368:299–302.
21. Olans RN, Olans RD, Demaria A. The critical role of the staff nurse in antimicrobial stewardship--unrecognized, but already there. Clin Infect Dis 2016;62:84–9.
22. Karanika S, Paudel S, Grigoras C, et al. Systematic review and meta-analysis of clinical and economic outcomes from the implementation of hospital-based antimicrobial stewardship programs. Antimicrob Agents Chemother 2016;60:4840–52.
23. Wagner B, Filice GA, Drekonja D, et al. Antimicrobial stewardship programs in inpatient hospital settings: a systematic review. Infect Control Hosp Epidemiol 2014;35:1209–28.
24. Filice G, Drekonja D, Greer N, et al. Antimicrobial stewardship programs in inpatient settings: a systematic review. VA-ESP Project #09-009; 2013.
25. Cairns KA, Doyle JS, Trevillyan JM, et al. The impact of a multidisciplinary antimicrobial stewardship team on the timeliness of antimicrobial therapy in patients with positive blood cultures: a randomized controlled trial. J Antimicrob Chemother 2016;71:3276–83.
26. Hohn A, Heising B, Hertel S, et al. Antibiotic consumption after implementation of a procalcitonin-guided antimicrobial stewardship programme in surgical patients admitted to an intensive care unit: a retrospective before-and-after analysis. Infection 2015;43:405–12.
27. Singh S, Zhang YZ, Chalkley S, et al. A three-point time series study of antibiotic usage on an intensive care unit, following an antibiotic stewardship programme, after an outbreak of multi-resistant Acinetobacter baumannii. Eur J Clin Microbiol Infect Dis 2015;34:1893–900.
28. Cairns KA, Jenney AW, Abbott IJ, et al. Prescribing trends before and after implementation of an antimicrobial stewardship program. Med J Aust 2013;198:262–6.
29. Liew YX, Lee W, Loh JC, et al. Impact of an antimicrobial stewardship programme on patient safety in Singapore General Hospital. Int J Antimicrob Agents 2012;40:55–60.
30. Bevilacqua S, Demoré B, Boschetti E, et al. 15 years of antibiotic stewardship policy in the Nancy Teaching Hospital. Med Mal Infect 2011;41:532–9.
31. Danaher PJ, Milazzo NA, Kerr KJ, et al. The antibiotic support team--a successful educational approach to antibiotic stewardship. Mil Med 2009;174:201–5.
32. Jenkins TC, Knepper BC, Shihadeh K, et al. Long-term outcomes of an antimicrobial stewardship program implemented in a hospital with low baseline antibiotic use. Infect Control Hosp Epidemiol 2015;36:664–72.
33. Brown KA, Khanafer N, Daneman N, Fisman DN. Meta-analysis of antibiotics and the risk of community-associated Clostridium difficile infection. Antimicrob Agents Chemother 2013;57:2326–32.
34. Deshpande A, Pasupuleti V, Thota P, et al. Community-associated Clostridium difficile infection and antibiotics: a meta-analysis. J Antimicrob Chemother 2013;68:1951–61.
35. Slimings C, Riley TV. Antibiotics and hospital-acquired Clostridium difficile infection: update of systematic review and meta-analysis. J Antimicrob Chemother 2014;69:881–91.
36. Antworth A, Collins CD, Kunapuli A, et al. Impact of an antimicrobial stewardship program comprehensive care bundle on management of candidemia. Pharmacotherapy 2013;33:137–43.
37. Davey P, Brown E, Charani E, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev 2013;4:CD003543.
38. Pasquale TR, Trienski TL, Olexia DE, et al. Impact of an antimicrobial stewardship program on patients with acute bacterial skin and skin structure infections. Am J Health Syst Pharm 2014;71:1136–9.
39. Schuts EC, Hulscher ME, Mouton JW, et al. Current evidence on hospital antimicrobial stewardship objectives: a systematic review and meta-analysis. Lancet Infect Dis 2016;16:847–56.
40. Higgins JPT, Green S, editors. Identifying and measuring heterogeneity. Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0. [Internet]. The Cochrane Collaboration, March 2011. Available at http://handbook.cochrane.org/chapter_9/9_5_2_identifying_and_measuring_heterogeneity.htm.
41. Feazel LM, Malhotra A, Perencevich EN, et al. Effect of antibiotic stewardship programmes on Clostridium difficile incidence: a systematic review and meta-analysis. J Antimicrob Chemother 2014;69:1748–54.
42. Impact of antibiotic stewardship programs on Clostridium difficile (C. diff) infections [Internet]. Centers for Disease Control and Prevention. [Updated 2016 May 13; cited 2016 Oct 11]. Available at www.cdc.gov/getsmart/healthcare/evidence/asp-int-cdiff.html.
43. Burke JP. Antibiotic resistance – squeezing the balloon? JAMA 1998;280:1270–1.
44. This nephrotoxicity result is corrected from the originally published result; communicated by Jan M Prins on behalf of the authors for reference [39]. Prins, JM (Department of Internal Medicine, Division of Infectious Diseases, Academic Medical Centre, Amsterdam, Netherlands). Email communication with Joseph Eckart (Pharmacy Practice & Administration, Ernest Mario School of Pharmacy, Rutgers University, Piscataway, NJ). 2016 Oct 9.
45. Coulter S, Merollini K, Roberts JA, et al. The need for cost-effectiveness analyses of antimicrobial stewardship programmes: a structured review. Int J Antimicrob Agents 2015;46:140–9.
46. Dik J, Vemer P, Friedrich A, et al. Financial evaluations of antibiotic stewardship programs—a systematic review. Frontiers Microbiol 2015;6:317.
47. Campbell KA, Stein S, Looze C, Bosco JA. Antibiotic stewardship in orthopaedic surgery: principles and practice. J Am Acad Orthop Surg 2014;22:772–81.
48. Surveillance for antimicrobial use and antimicrobial resistance options, 2015 [Internet]. Centers for Disease Control and Prevention. [Updated 2016 May 3; cited 2016 Nov 22]. Available at www.cdc.gov/nhsn/acute-care-hospital/aur/index.html.
49. Baysari MT, Lehnbom EC, Li L, Hargreaves A, et al. The effectiveness of information technology to improve antimicrobial prescribing in hospitals: a systematic review and meta-analysis. Int J Med Inform. 2016;92:15-34.
50. Bauer KA, West JE, Balada-llasat JM, et al. An antimicrobial stewardship program’s impact with rapid polymerase chain reaction methicillin-resistant Staphylococcus aureus/S. aureus blood culture test in patients with S. aureus bacteremia. Clin Infect Dis 2010;51:1074–80.
51. Sango A, Mccarter YS, Johnson D, et al. Stewardship approach for optimizing antimicrobial therapy through use of a rapid microarray assay on blood cultures positive for Enterococcus species. J Clin Microbiol 2013;51:4008–11.
52. Perez KK, Olsen RJ, Musick WL, et al. Integrating rapid diagnostics and antimicrobial stewardship improves outcomes in patients with antibiotic-resistant Gram-negative bacteremia. J Infect 2014;69:216–25.
53. Bauer KA, Perez KK, Forrest GN, Goff DA. Review of rapid diagnostic tests used by antimicrobial stewardship programs. Clin Infect Dis 2014;59 Suppl 3:S134–145.
54. Dyar OJ, Pagani L, Pulcini C. Strategies and challenges of antimicrobial stewardship in long-term care facilities. Clin Microbiol Infect 2015;21:10–9.
55. D’Agata EM. Antimicrobial use and stewardship programs among dialysis centers. Semin Dial 2013;26:457–64.
56. Smith MJ, Gerber JS, Hersh AL. Inpatient antimicrobial stewardship in pediatrics: a systematic review. J Pediatric Infect Dis Soc 2015;4:e127–135.
57. Fleet E, Gopal Rao G, Patel B, et al. Impact of implementation of a novel antimicrobial stewardship tool on antibiotic use in nursing homes: a prospective cluster randomized control pilot study. J Antimicrob Chemother 2014;69:2265–73.
58. Drekonja DM, Filice GA, Greer N, et al. Antimicrobial stewardship in outpatient settings: a systematic review. Infect Control Hosp Epidemiol 2015;36:142–52.
59. Drekonja D, Filice G, Greer N, et al. Antimicrobial stewardship programs in outpatient settings: a systematic review. VA-ESP Project #09-009; 2014.
60. Zhang YZ, Singh S. Antibiotic stewardship programmes in intensive care units: why, how, and where are they leading us. World J Crit Care Med 2015;4:13–28. (referenced in online Table)
HM17 session summary: Hospitalists as leaders in patient flow and hospital throughput
Presenters
Gaby Berger, MD; Aaron Hamilton, MD, FHM; Christopher Kim, MD, SFHM; Eduardo Margo, MD; Vikas Parekh, MD, FACP, SFHM; Anneliese Schleyer, MD, SFHM; Emily Wang, MD
Session Summary
This HM17 workshop brought together academic and community hospitalists to share effective strategies for improving hospital patient flow.

This was followed by a break-out session, in which hospitalists were encouraged to further explore these and other strategies for improving patient flow.
Key takeaways for HM
- Expedited discharge: Identify patients who can be safely discharged before noon. Consider creating standard work to ensure that key steps in discharge planning process, such as completion of medication reconciliation and discharge instructions and communication with patient and families and the interdisciplinary team, occur the day prior to discharge.
- Length of stay reduction strategies: Partner with utilization management to identify and develop a strategy to actively manage patients with long length of stay. Several institutions have set up committees to review such cases and address barriers, escalating requests for resources to executive leadership as needed.
- Facilitate transfers: Develop a standard process that is streamlined and patient-centered and includes established criteria for deciding whether interhospital transfers are appropriate.
- Short Stay Units: Some hospitals have had success with hospitalist-run short stay units as a strategy to decrease length of stay in observation patients. This strategy is most ideal for patients with a predictable length of stay. If you are thinking of starting an observation unit at your hospital, consider establishing criteria and protocols to expedite care.
- Hospitalist Quarterback: Given their broad perspective and clinical knowledge, hospitalists are uniquely positioned to help manage hospital, and even system-wide, capacity in real time. Some hospitals have successfully employed this strategy in some form to improve throughput. However, hospitalists need tools to help them electronically track incoming patients, integration with utilization management resources, and support from executive leadership to be successful.
Dr. Stella is a hospitalist in Denver and an editorial board member of The Hospitalist.
Presenters
Gaby Berger, MD; Aaron Hamilton, MD, FHM; Christopher Kim, MD, SFHM; Eduardo Margo, MD; Vikas Parekh, MD, FACP, SFHM; Anneliese Schleyer, MD, SFHM; Emily Wang, MD
Session Summary
This HM17 workshop brought together academic and community hospitalists to share effective strategies for improving hospital patient flow.
This was followed by a break-out session, in which hospitalists were encouraged to further explore these and other strategies for improving patient flow.
Key takeaways for HM
- Expedited discharge: Identify patients who can be safely discharged before noon. Consider creating standard work to ensure that key steps in discharge planning process, such as completion of medication reconciliation and discharge instructions and communication with patient and families and the interdisciplinary team, occur the day prior to discharge.
- Length of stay reduction strategies: Partner with utilization management to identify and develop a strategy to actively manage patients with long length of stay. Several institutions have set up committees to review such cases and address barriers, escalating requests for resources to executive leadership as needed.
- Facilitate transfers: Develop a standard process that is streamlined and patient-centered and includes established criteria for deciding whether interhospital transfers are appropriate.
- Short Stay Units: Some hospitals have had success with hospitalist-run short stay units as a strategy to decrease length of stay in observation patients. This strategy is most ideal for patients with a predictable length of stay. If you are thinking of starting an observation unit at your hospital, consider establishing criteria and protocols to expedite care.
- Hospitalist Quarterback: Given their broad perspective and clinical knowledge, hospitalists are uniquely positioned to help manage hospital, and even system-wide, capacity in real time. Some hospitals have successfully employed this strategy in some form to improve throughput. However, hospitalists need tools to help them electronically track incoming patients, integration with utilization management resources, and support from executive leadership to be successful.
Dr. Stella is a hospitalist in Denver and an editorial board member of The Hospitalist.
Presenters
Gaby Berger, MD; Aaron Hamilton, MD, FHM; Christopher Kim, MD, SFHM; Eduardo Margo, MD; Vikas Parekh, MD, FACP, SFHM; Anneliese Schleyer, MD, SFHM; Emily Wang, MD
Session Summary
This HM17 workshop brought together academic and community hospitalists to share effective strategies for improving hospital patient flow.
This was followed by a break-out session, in which hospitalists were encouraged to further explore these and other strategies for improving patient flow.
Key takeaways for HM
- Expedited discharge: Identify patients who can be safely discharged before noon. Consider creating standard work to ensure that key steps in discharge planning process, such as completion of medication reconciliation and discharge instructions and communication with patient and families and the interdisciplinary team, occur the day prior to discharge.
- Length of stay reduction strategies: Partner with utilization management to identify and develop a strategy to actively manage patients with long length of stay. Several institutions have set up committees to review such cases and address barriers, escalating requests for resources to executive leadership as needed.
- Facilitate transfers: Develop a standard process that is streamlined and patient-centered and includes established criteria for deciding whether interhospital transfers are appropriate.
- Short Stay Units: Some hospitals have had success with hospitalist-run short stay units as a strategy to decrease length of stay in observation patients. This strategy is most ideal for patients with a predictable length of stay. If you are thinking of starting an observation unit at your hospital, consider establishing criteria and protocols to expedite care.
- Hospitalist Quarterback: Given their broad perspective and clinical knowledge, hospitalists are uniquely positioned to help manage hospital, and even system-wide, capacity in real time. Some hospitals have successfully employed this strategy in some form to improve throughput. However, hospitalists need tools to help them electronically track incoming patients, integration with utilization management resources, and support from executive leadership to be successful.
Dr. Stella is a hospitalist in Denver and an editorial board member of The Hospitalist.
Tramadol extended-release treated opioid withdrawal symptoms better than clonidine
For patients with opioid use disorders, a 7-day taper with up to 600 mg of extended-release tramadol per day suppressed withdrawal symptoms as well as buprenorphine and significantly better than clonidine, in a randomized, double-blind, double-dummy placebo-controlled trial of 103 patients.
Tramadol ER also produced less severe withdrawal symptoms after taper than did buprenorphine, reported Kelly E. Dunn, PhD, of Johns Hopkins University in Baltimore, and her associates. The study was published online July 12 in JAMA Psychiatry.
“Tramadol ER is a schedule V medication that can be administered once a day and has lower abuse liability than other opioid agonists,” the researchers wrote. “These data suggest that tramadol ER is a promising and valuable medication for the management of opioid withdrawal in patients undergoing treatment for opioid use disorder.”
Successful opioid detoxification hinges on managing withdrawal symptoms, often with clonidine, which is an unscheduled adrenergic agonist, or buprenorphine HCl, which is a partial mu and opioid receptor like–1 receptor agonist and kappa antagonist. Clonidine has low abuse potential, but must be given several times daily, can cause sedation and hypotension, and is less effective than buprenorphine, which is a schedule III drug that requires a specialized waiver to prescribe. In contrast, tramadol ER has lower abuse potential (schedule V), a low affinity for mu, kappa, and delta opioid receptors, and an elimination half-life compatible with once-daily dosing, the investigators reported (JAMA Psychiatry. 2017 Jul 12. doi: 10.1001/jamapsychiatry.2017.1838).
Their study included three phases. First, participants were stabilized with subcutaneous morphine injections four times daily for 7-10 days. Next, they started a 7-day taper with buprenorphine (31 individuals), clonidine (36 individuals), or tramadol ER (36 individuals). Then they crossed over to a 7-day double-blind placebo period. The researchers measured withdrawal symptoms on the 11-item Clinical Opiate Withdrawal Scale (COWS) and the 16-item, 5-point Subjective Opiate Withdrawal Scale (SOWS).
For all three medications, average COWS and SOWS scores rose at the start of taper and subsequently dropped. For example, buprenorphine patients averaged higher SOWS scores after taper (7.2) than did clonidine (3.2) or tramadol ER patients (2.8), but the differences were not statistically significant. Post hoc analyses of SOWS scores linked clonidine with significantly worse withdrawal symptoms than tramadol ER (P = .02) or buprenorphine (P less than .001) during taper.
Patients also reported significant lessening of withdrawal symptoms after tapering off clonidine (P less than .001) and tramadol ER (P = .03), but not buprenorphine. Average pupil diameters increased only after stopping buprenorphine but rose slightly while tapering off the other medications. Patients also used significantly more concomitant medication after stopping buprenorphine. “Together, these findings suggest that buprenorphine participants experienced continued withdrawal following the removal of buprenorphine,” the researchers wrote. “Although a delayed onset of withdrawal has been previously reported following buprenorphine withdrawal, it is notable that this pattern was not observed in the other groups.”
In all, 85% of study participants were male, 42% were white, and the average age was 29 years. Retention rates were 66% for clonidine, 72% for tramadol ER, and 90% for buprenorphine. About half of patients reported adverse effects, and those rates were similar among the groups. Most of the adverse effects were related to opioid withdrawal, and no severe adverse events were reported.
The study “shows that tramadol extended-release suppressed withdrawal more than clonidine and comparably to buprenorphine during a double-blind taper, and did not produce a delayed onset of opioid withdrawal after the taper,” the researchers wrote. However, the findings “are tempered by the high rates of relapse generally associated with supervised withdrawal relative to maintenance treatments, and epidemiologic evidence that tramadol is abusable.” Tramadol ER was previously unscheduled but now is a schedule V medication, which “adds complexity in its use for opioid withdrawal suppression,” they noted. They recommended more studies in patients with worse withdrawal symptoms, outpatient settings, and extended care to prevent overdose.
The National Institute on Drug Abuse funded the work. Reckitt Benckiser Pharmaceuticals provided buprenorphine and placebo tablets and reviewed the report for scientific accuracy. Dr. Dunn and one coinvestigator had no disclosures. The senior author, Eric C. Strain, MD, and another coinvestigator disclosed ties to Indivior Pharmaceuticals, Egalet, and several other pharmaceutical companies.
For patients with opioid use disorders, a 7-day taper with up to 600 mg of extended-release tramadol per day suppressed withdrawal symptoms as well as buprenorphine and significantly better than clonidine, in a randomized, double-blind, double-dummy placebo-controlled trial of 103 patients.
Tramadol ER also produced less severe withdrawal symptoms after taper than did buprenorphine, reported Kelly E. Dunn, PhD, of Johns Hopkins University in Baltimore, and her associates. The study was published online July 12 in JAMA Psychiatry.
“Tramadol ER is a schedule V medication that can be administered once a day and has lower abuse liability than other opioid agonists,” the researchers wrote. “These data suggest that tramadol ER is a promising and valuable medication for the management of opioid withdrawal in patients undergoing treatment for opioid use disorder.”
Successful opioid detoxification hinges on managing withdrawal symptoms, often with clonidine, which is an unscheduled adrenergic agonist, or buprenorphine HCl, which is a partial mu and opioid receptor like–1 receptor agonist and kappa antagonist. Clonidine has low abuse potential, but must be given several times daily, can cause sedation and hypotension, and is less effective than buprenorphine, which is a schedule III drug that requires a specialized waiver to prescribe. In contrast, tramadol ER has lower abuse potential (schedule V), a low affinity for mu, kappa, and delta opioid receptors, and an elimination half-life compatible with once-daily dosing, the investigators reported (JAMA Psychiatry. 2017 Jul 12. doi: 10.1001/jamapsychiatry.2017.1838).
Their study included three phases. First, participants were stabilized with subcutaneous morphine injections four times daily for 7-10 days. Next, they started a 7-day taper with buprenorphine (31 individuals), clonidine (36 individuals), or tramadol ER (36 individuals). Then they crossed over to a 7-day double-blind placebo period. The researchers measured withdrawal symptoms on the 11-item Clinical Opiate Withdrawal Scale (COWS) and the 16-item, 5-point Subjective Opiate Withdrawal Scale (SOWS).
For all three medications, average COWS and SOWS scores rose at the start of taper and subsequently dropped. For example, buprenorphine patients averaged higher SOWS scores after taper (7.2) than did clonidine (3.2) or tramadol ER patients (2.8), but the differences were not statistically significant. Post hoc analyses of SOWS scores linked clonidine with significantly worse withdrawal symptoms than tramadol ER (P = .02) or buprenorphine (P less than .001) during taper.
Patients also reported significant lessening of withdrawal symptoms after tapering off clonidine (P less than .001) and tramadol ER (P = .03), but not buprenorphine. Average pupil diameters increased only after stopping buprenorphine but rose slightly while tapering off the other medications. Patients also used significantly more concomitant medication after stopping buprenorphine. “Together, these findings suggest that buprenorphine participants experienced continued withdrawal following the removal of buprenorphine,” the researchers wrote. “Although a delayed onset of withdrawal has been previously reported following buprenorphine withdrawal, it is notable that this pattern was not observed in the other groups.”
In all, 85% of study participants were male, 42% were white, and the average age was 29 years. Retention rates were 66% for clonidine, 72% for tramadol ER, and 90% for buprenorphine. About half of patients reported adverse effects, and those rates were similar among the groups. Most of the adverse effects were related to opioid withdrawal, and no severe adverse events were reported.
The study “shows that tramadol extended-release suppressed withdrawal more than clonidine and comparably to buprenorphine during a double-blind taper, and did not produce a delayed onset of opioid withdrawal after the taper,” the researchers wrote. However, the findings “are tempered by the high rates of relapse generally associated with supervised withdrawal relative to maintenance treatments, and epidemiologic evidence that tramadol is abusable.” Tramadol ER was previously unscheduled but now is a schedule V medication, which “adds complexity in its use for opioid withdrawal suppression,” they noted. They recommended more studies in patients with worse withdrawal symptoms, outpatient settings, and extended care to prevent overdose.
The National Institute on Drug Abuse funded the work. Reckitt Benckiser Pharmaceuticals provided buprenorphine and placebo tablets and reviewed the report for scientific accuracy. Dr. Dunn and one coinvestigator had no disclosures. The senior author, Eric C. Strain, MD, and another coinvestigator disclosed ties to Indivior Pharmaceuticals, Egalet, and several other pharmaceutical companies.
For patients with opioid use disorders, a 7-day taper with up to 600 mg of extended-release tramadol per day suppressed withdrawal symptoms as well as buprenorphine and significantly better than clonidine, in a randomized, double-blind, double-dummy placebo-controlled trial of 103 patients.
Tramadol ER also produced less severe withdrawal symptoms after taper than did buprenorphine, reported Kelly E. Dunn, PhD, of Johns Hopkins University in Baltimore, and her associates. The study was published online July 12 in JAMA Psychiatry.
“Tramadol ER is a schedule V medication that can be administered once a day and has lower abuse liability than other opioid agonists,” the researchers wrote. “These data suggest that tramadol ER is a promising and valuable medication for the management of opioid withdrawal in patients undergoing treatment for opioid use disorder.”
Successful opioid detoxification hinges on managing withdrawal symptoms, often with clonidine, which is an unscheduled adrenergic agonist, or buprenorphine HCl, which is a partial mu and opioid receptor like–1 receptor agonist and kappa antagonist. Clonidine has low abuse potential, but must be given several times daily, can cause sedation and hypotension, and is less effective than buprenorphine, which is a schedule III drug that requires a specialized waiver to prescribe. In contrast, tramadol ER has lower abuse potential (schedule V), a low affinity for mu, kappa, and delta opioid receptors, and an elimination half-life compatible with once-daily dosing, the investigators reported (JAMA Psychiatry. 2017 Jul 12. doi: 10.1001/jamapsychiatry.2017.1838).
Their study included three phases. First, participants were stabilized with subcutaneous morphine injections four times daily for 7-10 days. Next, they started a 7-day taper with buprenorphine (31 individuals), clonidine (36 individuals), or tramadol ER (36 individuals). Then they crossed over to a 7-day double-blind placebo period. The researchers measured withdrawal symptoms on the 11-item Clinical Opiate Withdrawal Scale (COWS) and the 16-item, 5-point Subjective Opiate Withdrawal Scale (SOWS).
For all three medications, average COWS and SOWS scores rose at the start of taper and subsequently dropped. For example, buprenorphine patients averaged higher SOWS scores after taper (7.2) than did clonidine (3.2) or tramadol ER patients (2.8), but the differences were not statistically significant. Post hoc analyses of SOWS scores linked clonidine with significantly worse withdrawal symptoms than tramadol ER (P = .02) or buprenorphine (P less than .001) during taper.
Patients also reported significant lessening of withdrawal symptoms after tapering off clonidine (P less than .001) and tramadol ER (P = .03), but not buprenorphine. Average pupil diameters increased only after stopping buprenorphine but rose slightly while tapering off the other medications. Patients also used significantly more concomitant medication after stopping buprenorphine. “Together, these findings suggest that buprenorphine participants experienced continued withdrawal following the removal of buprenorphine,” the researchers wrote. “Although a delayed onset of withdrawal has been previously reported following buprenorphine withdrawal, it is notable that this pattern was not observed in the other groups.”
In all, 85% of study participants were male, 42% were white, and the average age was 29 years. Retention rates were 66% for clonidine, 72% for tramadol ER, and 90% for buprenorphine. About half of patients reported adverse effects, and those rates were similar among the groups. Most of the adverse effects were related to opioid withdrawal, and no severe adverse events were reported.
The study “shows that tramadol extended-release suppressed withdrawal more than clonidine and comparably to buprenorphine during a double-blind taper, and did not produce a delayed onset of opioid withdrawal after the taper,” the researchers wrote. However, the findings “are tempered by the high rates of relapse generally associated with supervised withdrawal relative to maintenance treatments, and epidemiologic evidence that tramadol is abusable.” Tramadol ER was previously unscheduled but now is a schedule V medication, which “adds complexity in its use for opioid withdrawal suppression,” they noted. They recommended more studies in patients with worse withdrawal symptoms, outpatient settings, and extended care to prevent overdose.
The National Institute on Drug Abuse funded the work. Reckitt Benckiser Pharmaceuticals provided buprenorphine and placebo tablets and reviewed the report for scientific accuracy. Dr. Dunn and one coinvestigator had no disclosures. The senior author, Eric C. Strain, MD, and another coinvestigator disclosed ties to Indivior Pharmaceuticals, Egalet, and several other pharmaceutical companies.
FROM JAMA PSYCHIATRY
Key clinical point:
Major finding: Withdrawal symptoms were significantly worse during taper with clonidine than with tramadol ER (P = .02) or buprenorphine (P less than .001), in post hoc analyses of the 5-point Subjective Opiate Withdrawal Scale. Retention rates also were lowest with clonidine (66%).
Data source: A randomized, double-blind, double-dummy placebo-controlled study of 103 patients with opioid use disorder.
Disclosures: The National Institute on Drug Abuse funded the study. Reckitt Benckiser Pharmaceuticals provided the buprenorphine and placebo tablets and reviewed the report for scientific accuracy. Dr. Dunn and one coinvestigator had no disclosures. The senior author, Eric C. Strain, MD, and another coinvestigator disclosed ties to Indivior Pharmaceuticals, Egalet Corporation, and several other pharmaceutical companies.
Prenatal methadone maintenance linked to poorer child neurodevelopment
SAN FRANCISCO – Infants born to mothers receiving methadone maintenance treatment show poorer-than-average neurodevelopment outcomes, a retrospective study found.
Delays or difficulties in motor abilities appeared first in these children, followed by evidence of cognitive problems in their second year of life, reported Cristina Borradori Tolsa, MD, of University Hospital, Geneva.
“Higher methadone doses during pregnancy can have a detrimental effect on neonatal characteristics and children’s psychomotor development,” Dr. Borradori Tolsa said at the Pediatric Academic Societies meeting. She noted the need for long-term follow-up of children prenatally exposed to methadone maintenance therapy to evaluate their cognitive abilities and school readiness at preschool ages.
Only 38% of the women had exclusively used methadone, while the other 62% had used a variety of substances, including cocaine, alcohol, benzodiazepine, marijuana, and antidepressants. The women had a low average socioeconomic status based on their level of education and the occupations of the children’s fathers.
The researchers drew children’s development data from their scores on the Bayley Scales of Infant Development, Second Edition (BSID-II), at 6 months and 18-24 months. The BSID-II has an average score of 100 and includes a mental development index for language and cognitive development, and a psychomotor development index to assess fine and gross motor skills.
At age 6 months, 75% of the 40 children assessed showed some level of motor skills delay, and 33% had a moderate to severe delay in psychomotor skills. A quarter had no delay at all (a score of at least 85). The average psychomotor score at 6 months was 76, and the average cognitive score was 88. Most of the children (60%) did, however, show mental development within the normal range at 6 months.
By the age of 18-24 months, half of the 36 children assessed showed no motor delays, and half showed no cognitive delays. One in five (20%) showed a moderate to severe psychomotor delay, and 14% showed a moderate to severe mental development delay. Mild delays in mental development occurred in 36% of the toddlers assessed, and 30% showed mild delays in psychomotor skills.
A dose-response effect was seen with mothers’ higher doses of methadone at birth and their children’s psychomotor scores at 6 months. No similar association existed for mental development, and the psychomotor association disappeared by 18-24 months. At this older age, however, 68% of children born to mothers taking a high dose of methadone showed cognitive delays, compared with 29% of children born to mothers on a low dose.
Although no differences were seen in newborns’ average gestational age (an average of 37.8 weeks overall) or birth weight between the high-dose and low-dose methadone groups, infants born to mothers with high doses were more likely to be small for gestational age (P = .01) and to need longer treatment duration for neonatal abstinence syndrome (NAS) (P = .03). Overall, 44% of the newborns were small for gestational age, 28% were born microcephalic, and all but three required pharmacologic treatment for NAS. NAS treatment lasted an average 54 days for the cohort, and the average hospital stay for the babies was 76 days.
The researchers did not report having any external funding or relevant financial disclosures.
SAN FRANCISCO – Infants born to mothers receiving methadone maintenance treatment show poorer-than-average neurodevelopment outcomes, a retrospective study found.
Delays or difficulties in motor abilities appeared first in these children, followed by evidence of cognitive problems in their second year of life, reported Cristina Borradori Tolsa, MD, of University Hospital, Geneva.
“Higher methadone doses during pregnancy can have a detrimental effect on neonatal characteristics and children’s psychomotor development,” Dr. Borradori Tolsa said at the Pediatric Academic Societies meeting. She noted the need for long-term follow-up of children prenatally exposed to methadone maintenance therapy to evaluate their cognitive abilities and school readiness at preschool ages.
Only 38% of the women had exclusively used methadone, while the other 62% had used a variety of substances, including cocaine, alcohol, benzodiazepine, marijuana, and antidepressants. The women had a low average socioeconomic status based on their level of education and the occupations of the children’s fathers.
The researchers drew children’s development data from their scores on the Bayley Scales of Infant Development, Second Edition (BSID-II), at 6 months and 18-24 months. The BSID-II has an average score of 100 and includes a mental development index for language and cognitive development, and a psychomotor development index to assess fine and gross motor skills.
At age 6 months, 75% of the 40 children assessed showed some level of motor skills delay, and 33% had a moderate to severe delay in psychomotor skills. A quarter had no delay at all (a score of at least 85). The average psychomotor score at 6 months was 76, and the average cognitive score was 88. Most of the children (60%) did, however, show mental development within the normal range at 6 months.
By the age of 18-24 months, half of the 36 children assessed showed no motor delays, and half showed no cognitive delays. One in five (20%) showed a moderate to severe psychomotor delay, and 14% showed a moderate to severe mental development delay. Mild delays in mental development occurred in 36% of the toddlers assessed, and 30% showed mild delays in psychomotor skills.
A dose-response effect was seen with mothers’ higher doses of methadone at birth and their children’s psychomotor scores at 6 months. No similar association existed for mental development, and the psychomotor association disappeared by 18-24 months. At this older age, however, 68% of children born to mothers taking a high dose of methadone showed cognitive delays, compared with 29% of children born to mothers on a low dose.
Although no differences were seen in newborns’ average gestational age (an average of 37.8 weeks overall) or birth weight between the high-dose and low-dose methadone groups, infants born to mothers with high doses were more likely to be small for gestational age (P = .01) and to need longer treatment duration for neonatal abstinence syndrome (NAS) (P = .03). Overall, 44% of the newborns were small for gestational age, 28% were born microcephalic, and all but three required pharmacologic treatment for NAS. NAS treatment lasted an average 54 days for the cohort, and the average hospital stay for the babies was 76 days.
The researchers did not report having any external funding or relevant financial disclosures.
SAN FRANCISCO – Infants born to mothers receiving methadone maintenance treatment show poorer-than-average neurodevelopment outcomes, a retrospective study found.
Delays or difficulties in motor abilities appeared first in these children, followed by evidence of cognitive problems in their second year of life, reported Cristina Borradori Tolsa, MD, of University Hospital, Geneva.
“Higher methadone doses during pregnancy can have a detrimental effect on neonatal characteristics and children’s psychomotor development,” Dr. Borradori Tolsa said at the Pediatric Academic Societies meeting. She noted the need for long-term follow-up of children prenatally exposed to methadone maintenance therapy to evaluate their cognitive abilities and school readiness at preschool ages.
Only 38% of the women had exclusively used methadone, while the other 62% had used a variety of substances, including cocaine, alcohol, benzodiazepine, marijuana, and antidepressants. The women had a low average socioeconomic status based on their level of education and the occupations of the children’s fathers.
The researchers drew children’s development data from their scores on the Bayley Scales of Infant Development, Second Edition (BSID-II), at 6 months and 18-24 months. The BSID-II has an average score of 100 and includes a mental development index for language and cognitive development, and a psychomotor development index to assess fine and gross motor skills.
At age 6 months, 75% of the 40 children assessed showed some level of motor skills delay, and 33% had a moderate to severe delay in psychomotor skills. A quarter had no delay at all (a score of at least 85). The average psychomotor score at 6 months was 76, and the average cognitive score was 88. Most of the children (60%) did, however, show mental development within the normal range at 6 months.
By the age of 18-24 months, half of the 36 children assessed showed no motor delays, and half showed no cognitive delays. One in five (20%) showed a moderate to severe psychomotor delay, and 14% showed a moderate to severe mental development delay. Mild delays in mental development occurred in 36% of the toddlers assessed, and 30% showed mild delays in psychomotor skills.
A dose-response effect was seen with mothers’ higher doses of methadone at birth and their children’s psychomotor scores at 6 months. No similar association existed for mental development, and the psychomotor association disappeared by 18-24 months. At this older age, however, 68% of children born to mothers taking a high dose of methadone showed cognitive delays, compared with 29% of children born to mothers on a low dose.
Although no differences were seen in newborns’ average gestational age (an average of 37.8 weeks overall) or birth weight between the high-dose and low-dose methadone groups, infants born to mothers with high doses were more likely to be small for gestational age (P = .01) and to need longer treatment duration for neonatal abstinence syndrome (NAS) (P = .03). Overall, 44% of the newborns were small for gestational age, 28% were born microcephalic, and all but three required pharmacologic treatment for NAS. NAS treatment lasted an average 54 days for the cohort, and the average hospital stay for the babies was 76 days.
The researchers did not report having any external funding or relevant financial disclosures.
AT PAS 17
Key clinical point:
Major finding: Three-fourths of methadone-exposed infants showed psychomotor delays at 6 months, and 50% showed cognitive delays and/or psychomotor delays at 18-24 months.
Data source: A retrospective analysis of neurodevelopment scores of children born to 61 mothers in Geneva who received methadone maintenance therapy during pregnancy.
Disclosures: The researchers did not report having any external funding or relevant financial disclosures.
Federal exchanges attract fewer insurers for 2018
The number of health plans submitting applications to offer coverage on the federal insurance exchanges in 2018 was down 38% from last year, officials at the Centers for Medicare & Medicaid announced July 10. At this year’s initial filing deadline for fiscal year 2018, 141 qualified health plans had submitted applications to offer coverage in the 39 states that use healthcare.gov, the federally facilitated exchange platform, compared with 227 last year and 281 the year before, CMS officials said in a statement.
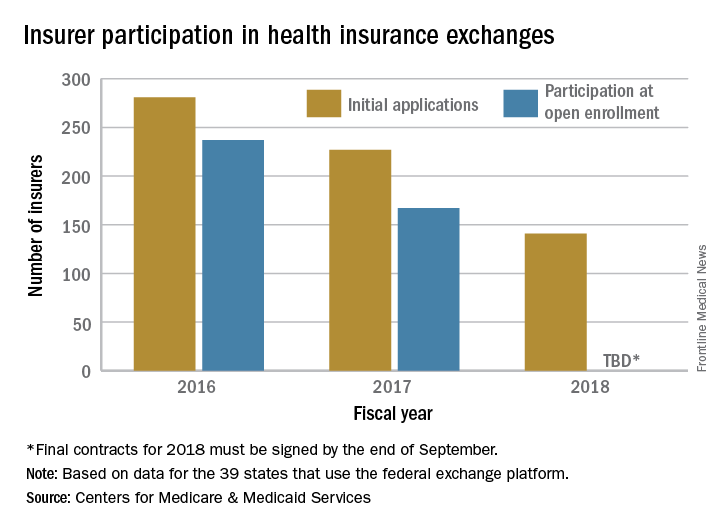
“This is further proof that the Affordable Care Act is failing,” CMS Administrator Seema Verma said in the statement. “Insurers continue to flee the Exchanges, causing Americans to lose their choice for health insurance or lose their coverage all together. These numbers are clear; the status quo is not working. The American people deserve health care choices and access to quality, affordable health care coverage.”
The number of health plans submitting applications to offer coverage on the federal insurance exchanges in 2018 was down 38% from last year, officials at the Centers for Medicare & Medicaid announced July 10. At this year’s initial filing deadline for fiscal year 2018, 141 qualified health plans had submitted applications to offer coverage in the 39 states that use healthcare.gov, the federally facilitated exchange platform, compared with 227 last year and 281 the year before, CMS officials said in a statement.
“This is further proof that the Affordable Care Act is failing,” CMS Administrator Seema Verma said in the statement. “Insurers continue to flee the Exchanges, causing Americans to lose their choice for health insurance or lose their coverage all together. These numbers are clear; the status quo is not working. The American people deserve health care choices and access to quality, affordable health care coverage.”
The number of health plans submitting applications to offer coverage on the federal insurance exchanges in 2018 was down 38% from last year, officials at the Centers for Medicare & Medicaid announced July 10. At this year’s initial filing deadline for fiscal year 2018, 141 qualified health plans had submitted applications to offer coverage in the 39 states that use healthcare.gov, the federally facilitated exchange platform, compared with 227 last year and 281 the year before, CMS officials said in a statement.
“This is further proof that the Affordable Care Act is failing,” CMS Administrator Seema Verma said in the statement. “Insurers continue to flee the Exchanges, causing Americans to lose their choice for health insurance or lose their coverage all together. These numbers are clear; the status quo is not working. The American people deserve health care choices and access to quality, affordable health care coverage.”
Involuntary commitment sought in 5% of anorexia admissions
SAN DIEGO – Court orders were sought to force 5% of patients admitted for anorexia nervosa disorders to remain involuntarily under hospital care, according to findings from a 4-year study of patients treated at a Colorado clinic.
Nearly all of the patients declined to fight those efforts. However, the orders were withdrawn in about one-quarter of cases because treatment was deemed to be futile.
The study findings point to the importance of seeking civil commitment early in the course of illness in patients with anorexia nervosa when it can do the most good, study author Patricia Westmoreland, MD, attending psychiatrist at the Eating Recovery Center in Denver, said in an interview.

Dr. Westmoreland presented the findings at the annual meeting of the American Psychiatric Association, where she contended that anorexia nervosa has the highest mortality of any psychiatric disorder. “If patients are not treated earlier in the course of their illness and when they’re at a younger age,” she said, “they develop severe and enduring eating disorders.”
Anorexia nervosa is estimated to have a prevalence rate of 0.3% in young women. Research suggests that 20% of people with the disease kill themselves (Int J Eat Disord. 2003 Dec;34[4]:383-96), (Arch Gen Psychiatry. 2011;68[7]:724-31).
For the new study, Dr. Westmoreland and her colleagues tracked 2,106 admissions of patients who were treated for two conditions – anorexia nervosa restricting subtype and anorexia nervosa binge purge subtype – at the Eating Recovery Center from April 2012 to March 2016. The ages and genders of the subjects were not available.
Officials sought involuntary care in 109, or 5.2%, of the admissions, including 11 patients who were recommitted at least once.
Of the 109 admissions:
• 85% waived the right to a hearing (94% of those who fought commitment ultimately were committed involuntarily).
• 31% successfully completed treatment.
• 24% had their commitments – also known as certifications – terminated because treatment appeared to be futile.
“These are patients for whom certification is only helpful to a point, beyond which it becomes harmful, i.e., patients harming themselves to leave a locked facility, patients pulling out NG tubes so many times they cause injury, patients who purge continuously despite being tube fed,” Dr. Westmoreland said in an interview. “In other cases, the team evaluated the patient and determined he or she is, in general, being harmed more than helped by trying to attain goal weight. This is where harm reduction may prove useful. And failing that, palliative or hospice care for a patient who has had many treatments over the years and has never recovered for any meaningful period of time.”
Dr. Westmoreland defined harm reduction in this context as “having patient being managed at an agreed-upon weight that is lower than an ideal body weight, but nonetheless a weight at which they can function and have some quality of life, even if that quality of life is not optimal.”
This also means that the patient must regularly check with an outpatient treatment team – dietitian, psychiatrist, and therapist – and be monitored for signs of unacceptable levels of weight loss or abnormal lab results, she said. These problems, she added, will trigger hospitalization.
Dr. Westmoreland reported no relevant disclosures.
SAN DIEGO – Court orders were sought to force 5% of patients admitted for anorexia nervosa disorders to remain involuntarily under hospital care, according to findings from a 4-year study of patients treated at a Colorado clinic.
Nearly all of the patients declined to fight those efforts. However, the orders were withdrawn in about one-quarter of cases because treatment was deemed to be futile.
The study findings point to the importance of seeking civil commitment early in the course of illness in patients with anorexia nervosa when it can do the most good, study author Patricia Westmoreland, MD, attending psychiatrist at the Eating Recovery Center in Denver, said in an interview.
Dr. Westmoreland presented the findings at the annual meeting of the American Psychiatric Association, where she contended that anorexia nervosa has the highest mortality of any psychiatric disorder. “If patients are not treated earlier in the course of their illness and when they’re at a younger age,” she said, “they develop severe and enduring eating disorders.”
Anorexia nervosa is estimated to have a prevalence rate of 0.3% in young women. Research suggests that 20% of people with the disease kill themselves (Int J Eat Disord. 2003 Dec;34[4]:383-96), (Arch Gen Psychiatry. 2011;68[7]:724-31).
For the new study, Dr. Westmoreland and her colleagues tracked 2,106 admissions of patients who were treated for two conditions – anorexia nervosa restricting subtype and anorexia nervosa binge purge subtype – at the Eating Recovery Center from April 2012 to March 2016. The ages and genders of the subjects were not available.
Officials sought involuntary care in 109, or 5.2%, of the admissions, including 11 patients who were recommitted at least once.
Of the 109 admissions:
• 85% waived the right to a hearing (94% of those who fought commitment ultimately were committed involuntarily).
• 31% successfully completed treatment.
• 24% had their commitments – also known as certifications – terminated because treatment appeared to be futile.
“These are patients for whom certification is only helpful to a point, beyond which it becomes harmful, i.e., patients harming themselves to leave a locked facility, patients pulling out NG tubes so many times they cause injury, patients who purge continuously despite being tube fed,” Dr. Westmoreland said in an interview. “In other cases, the team evaluated the patient and determined he or she is, in general, being harmed more than helped by trying to attain goal weight. This is where harm reduction may prove useful. And failing that, palliative or hospice care for a patient who has had many treatments over the years and has never recovered for any meaningful period of time.”
Dr. Westmoreland defined harm reduction in this context as “having patient being managed at an agreed-upon weight that is lower than an ideal body weight, but nonetheless a weight at which they can function and have some quality of life, even if that quality of life is not optimal.”
This also means that the patient must regularly check with an outpatient treatment team – dietitian, psychiatrist, and therapist – and be monitored for signs of unacceptable levels of weight loss or abnormal lab results, she said. These problems, she added, will trigger hospitalization.
Dr. Westmoreland reported no relevant disclosures.
SAN DIEGO – Court orders were sought to force 5% of patients admitted for anorexia nervosa disorders to remain involuntarily under hospital care, according to findings from a 4-year study of patients treated at a Colorado clinic.
Nearly all of the patients declined to fight those efforts. However, the orders were withdrawn in about one-quarter of cases because treatment was deemed to be futile.
The study findings point to the importance of seeking civil commitment early in the course of illness in patients with anorexia nervosa when it can do the most good, study author Patricia Westmoreland, MD, attending psychiatrist at the Eating Recovery Center in Denver, said in an interview.
Dr. Westmoreland presented the findings at the annual meeting of the American Psychiatric Association, where she contended that anorexia nervosa has the highest mortality of any psychiatric disorder. “If patients are not treated earlier in the course of their illness and when they’re at a younger age,” she said, “they develop severe and enduring eating disorders.”
Anorexia nervosa is estimated to have a prevalence rate of 0.3% in young women. Research suggests that 20% of people with the disease kill themselves (Int J Eat Disord. 2003 Dec;34[4]:383-96), (Arch Gen Psychiatry. 2011;68[7]:724-31).
For the new study, Dr. Westmoreland and her colleagues tracked 2,106 admissions of patients who were treated for two conditions – anorexia nervosa restricting subtype and anorexia nervosa binge purge subtype – at the Eating Recovery Center from April 2012 to March 2016. The ages and genders of the subjects were not available.
Officials sought involuntary care in 109, or 5.2%, of the admissions, including 11 patients who were recommitted at least once.
Of the 109 admissions:
• 85% waived the right to a hearing (94% of those who fought commitment ultimately were committed involuntarily).
• 31% successfully completed treatment.
• 24% had their commitments – also known as certifications – terminated because treatment appeared to be futile.
“These are patients for whom certification is only helpful to a point, beyond which it becomes harmful, i.e., patients harming themselves to leave a locked facility, patients pulling out NG tubes so many times they cause injury, patients who purge continuously despite being tube fed,” Dr. Westmoreland said in an interview. “In other cases, the team evaluated the patient and determined he or she is, in general, being harmed more than helped by trying to attain goal weight. This is where harm reduction may prove useful. And failing that, palliative or hospice care for a patient who has had many treatments over the years and has never recovered for any meaningful period of time.”
Dr. Westmoreland defined harm reduction in this context as “having patient being managed at an agreed-upon weight that is lower than an ideal body weight, but nonetheless a weight at which they can function and have some quality of life, even if that quality of life is not optimal.”
This also means that the patient must regularly check with an outpatient treatment team – dietitian, psychiatrist, and therapist – and be monitored for signs of unacceptable levels of weight loss or abnormal lab results, she said. These problems, she added, will trigger hospitalization.
Dr. Westmoreland reported no relevant disclosures.
AT APA
Stopping Prediabetes Before It Becomes Diabetes
In the Navajo area, 1 in 5 Native Americans has diabetes, and about 75,000 have prediabetes. That is the impetus for IHS’s new campaign, launched at the Northern Navajo Medical Center, to raise awareness and knowledge of prediabetes—and to let people know it can be reversed.
The “Do I Have Prediabetes?” campaign by the Shiprock Health Promotion Program is intended to help people assess their risk and reverse prediabetes before their blood sugar level is high enough to be type 2 diabetes. The program builds on the groundwork of a 2016 CDC national prediabetes awareness campaign. Materials include posters, an infographic that depicts the risk factors, roadside billboards, and a video for waiting rooms.
The IHS has already made progress against at least 1 diabetes-related issue: kidney failure. Through the Special Diabetes Program for Indians, innovative evidence-based interventions helped reduce kidney failure from diabetes among Native American adults by 54% between 1996 and 2013. Kidney failure from diabetes in Native Americans was the highest of any ethnic group but now has dropped the fastest. The Shiprock program will continue through early 2018.
In the Navajo area, 1 in 5 Native Americans has diabetes, and about 75,000 have prediabetes. That is the impetus for IHS’s new campaign, launched at the Northern Navajo Medical Center, to raise awareness and knowledge of prediabetes—and to let people know it can be reversed.
The “Do I Have Prediabetes?” campaign by the Shiprock Health Promotion Program is intended to help people assess their risk and reverse prediabetes before their blood sugar level is high enough to be type 2 diabetes. The program builds on the groundwork of a 2016 CDC national prediabetes awareness campaign. Materials include posters, an infographic that depicts the risk factors, roadside billboards, and a video for waiting rooms.
The IHS has already made progress against at least 1 diabetes-related issue: kidney failure. Through the Special Diabetes Program for Indians, innovative evidence-based interventions helped reduce kidney failure from diabetes among Native American adults by 54% between 1996 and 2013. Kidney failure from diabetes in Native Americans was the highest of any ethnic group but now has dropped the fastest. The Shiprock program will continue through early 2018.
In the Navajo area, 1 in 5 Native Americans has diabetes, and about 75,000 have prediabetes. That is the impetus for IHS’s new campaign, launched at the Northern Navajo Medical Center, to raise awareness and knowledge of prediabetes—and to let people know it can be reversed.
The “Do I Have Prediabetes?” campaign by the Shiprock Health Promotion Program is intended to help people assess their risk and reverse prediabetes before their blood sugar level is high enough to be type 2 diabetes. The program builds on the groundwork of a 2016 CDC national prediabetes awareness campaign. Materials include posters, an infographic that depicts the risk factors, roadside billboards, and a video for waiting rooms.
The IHS has already made progress against at least 1 diabetes-related issue: kidney failure. Through the Special Diabetes Program for Indians, innovative evidence-based interventions helped reduce kidney failure from diabetes among Native American adults by 54% between 1996 and 2013. Kidney failure from diabetes in Native Americans was the highest of any ethnic group but now has dropped the fastest. The Shiprock program will continue through early 2018.