User login
Functional disability prevails despite rheumatoid arthritis treatment
AMSTERDAM – Functional disability remains a significant problem for people with rheumatoid arthritis, with the prevalence remaining at least 15% higher over time than in individuals without the disease.

“We found a higher prevalence of functional disability in patients with RA versus non-RA,” the presenting study investigator Elena Myasoedova, MD, PhD, said at the European Congress of Rheumatology.
Dr. Myasoedova, who is a clinical fellow in rheumatology at the Mayo Clinic in Rochester, Minn., added that the increase in prevalence over time was significantly higher in subjects with RA than in those without RA (P = .003), but that there was no difference in the pace of this increase with adjustment for the duration of RA disease (P = .51).
There was also no difference in functional disability between the two groups of patients by about the 8th or 9th decade.
RA remains one of the most common conditions associated with functional disability, Dr. Myasoedova said, with several risk factors for physical impairment identified, including being female, of older age, smoking, and the use of certain medications (glucocorticoids and antidepressants), as well as sociodemographic factors.
A discrepancy between improved RA disease control and persistent impairment in physical function has been noted in prior studies, but there are few data on how this might change over time. Dr. Myasoedova and her associates investigated this by analyzing data from the Rochester Epidemiology Project, which collects medical data on individuals living in Olmsted County, Minnesota. They identified two populations of adults aged 18 and older: one diagnosed with RA according to 1987 American College of Rheumatology criteria between 1999 and 2013, and one without RA but who were of a similar age and sex and enrolled in the project around the same time.
As part of the project, participants completed an annual questionnaire asking about their health and ability to perform six activities of daily living (ADL). These include the ability to wash, dress, feed, and toilet oneself without assistance, as well as perform normal household chores and walk unaided. Over the course of study, 7,466 questionnaires have been completed by the participants and functional disability was defined as having difficulty with at least one of these six ADLs, Dr. Myasoedova explained.
At baseline, subjects with and without RA were aged a mean of 55 and 56 years, respectively, and 70% in both groups were female. Similar percentages were current (about 15%), former (about 30%), or never smokers (about 55%), and about 40% were obese.
Just under two-thirds (64.4%) of patients in the RA cohort were positive for rheumatoid factor (RF) or anti–cyclic citrullinated peptide (CCP) antibodies. While there was a similar prevalence of functional disability in RA patients who were or were not RF or CCP positive (both 25%, P = .67), there was an increasing prevalence noted in those who were positive versus those who were negative over time (P = .027).
Although the investigators did not conduct an objective assessment for functional disability, these findings highlight the need for vigilant management of patients with RA, Dr. Myasoedova proposed.
“Early and aggressive treatment regimens aimed at tight inflammation control can help prevent the disabling effects of high disease activity and joint damage, thereby lowering functional disability,” she said in an interview ahead of the congress.
Future work, she observed, should look at how the pattern of functional disability changes and the use of transition modeling to understand the bidirectional pattern of potential change and accumulation of functional disability in RA. The investigators also plan to look at risk factors for persistent and worsening functional disability and how treatment – including “treat to target” and biologics – might affect this.
The National Institute of Arthritis and Musculoskeletal and Skin Diseases supported the study. Dr. Myasoedova had no conflicts of interest.
SOURCE: Myasoedova E et al. Ann Rheum Dis. 2018;77(Suppl 2):54. Abstract OP0009.
AMSTERDAM – Functional disability remains a significant problem for people with rheumatoid arthritis, with the prevalence remaining at least 15% higher over time than in individuals without the disease.
“We found a higher prevalence of functional disability in patients with RA versus non-RA,” the presenting study investigator Elena Myasoedova, MD, PhD, said at the European Congress of Rheumatology.
Dr. Myasoedova, who is a clinical fellow in rheumatology at the Mayo Clinic in Rochester, Minn., added that the increase in prevalence over time was significantly higher in subjects with RA than in those without RA (P = .003), but that there was no difference in the pace of this increase with adjustment for the duration of RA disease (P = .51).
There was also no difference in functional disability between the two groups of patients by about the 8th or 9th decade.
RA remains one of the most common conditions associated with functional disability, Dr. Myasoedova said, with several risk factors for physical impairment identified, including being female, of older age, smoking, and the use of certain medications (glucocorticoids and antidepressants), as well as sociodemographic factors.
A discrepancy between improved RA disease control and persistent impairment in physical function has been noted in prior studies, but there are few data on how this might change over time. Dr. Myasoedova and her associates investigated this by analyzing data from the Rochester Epidemiology Project, which collects medical data on individuals living in Olmsted County, Minnesota. They identified two populations of adults aged 18 and older: one diagnosed with RA according to 1987 American College of Rheumatology criteria between 1999 and 2013, and one without RA but who were of a similar age and sex and enrolled in the project around the same time.
As part of the project, participants completed an annual questionnaire asking about their health and ability to perform six activities of daily living (ADL). These include the ability to wash, dress, feed, and toilet oneself without assistance, as well as perform normal household chores and walk unaided. Over the course of study, 7,466 questionnaires have been completed by the participants and functional disability was defined as having difficulty with at least one of these six ADLs, Dr. Myasoedova explained.
At baseline, subjects with and without RA were aged a mean of 55 and 56 years, respectively, and 70% in both groups were female. Similar percentages were current (about 15%), former (about 30%), or never smokers (about 55%), and about 40% were obese.
Just under two-thirds (64.4%) of patients in the RA cohort were positive for rheumatoid factor (RF) or anti–cyclic citrullinated peptide (CCP) antibodies. While there was a similar prevalence of functional disability in RA patients who were or were not RF or CCP positive (both 25%, P = .67), there was an increasing prevalence noted in those who were positive versus those who were negative over time (P = .027).
Although the investigators did not conduct an objective assessment for functional disability, these findings highlight the need for vigilant management of patients with RA, Dr. Myasoedova proposed.
“Early and aggressive treatment regimens aimed at tight inflammation control can help prevent the disabling effects of high disease activity and joint damage, thereby lowering functional disability,” she said in an interview ahead of the congress.
Future work, she observed, should look at how the pattern of functional disability changes and the use of transition modeling to understand the bidirectional pattern of potential change and accumulation of functional disability in RA. The investigators also plan to look at risk factors for persistent and worsening functional disability and how treatment – including “treat to target” and biologics – might affect this.
The National Institute of Arthritis and Musculoskeletal and Skin Diseases supported the study. Dr. Myasoedova had no conflicts of interest.
SOURCE: Myasoedova E et al. Ann Rheum Dis. 2018;77(Suppl 2):54. Abstract OP0009.
AMSTERDAM – Functional disability remains a significant problem for people with rheumatoid arthritis, with the prevalence remaining at least 15% higher over time than in individuals without the disease.
“We found a higher prevalence of functional disability in patients with RA versus non-RA,” the presenting study investigator Elena Myasoedova, MD, PhD, said at the European Congress of Rheumatology.
Dr. Myasoedova, who is a clinical fellow in rheumatology at the Mayo Clinic in Rochester, Minn., added that the increase in prevalence over time was significantly higher in subjects with RA than in those without RA (P = .003), but that there was no difference in the pace of this increase with adjustment for the duration of RA disease (P = .51).
There was also no difference in functional disability between the two groups of patients by about the 8th or 9th decade.
RA remains one of the most common conditions associated with functional disability, Dr. Myasoedova said, with several risk factors for physical impairment identified, including being female, of older age, smoking, and the use of certain medications (glucocorticoids and antidepressants), as well as sociodemographic factors.
A discrepancy between improved RA disease control and persistent impairment in physical function has been noted in prior studies, but there are few data on how this might change over time. Dr. Myasoedova and her associates investigated this by analyzing data from the Rochester Epidemiology Project, which collects medical data on individuals living in Olmsted County, Minnesota. They identified two populations of adults aged 18 and older: one diagnosed with RA according to 1987 American College of Rheumatology criteria between 1999 and 2013, and one without RA but who were of a similar age and sex and enrolled in the project around the same time.
As part of the project, participants completed an annual questionnaire asking about their health and ability to perform six activities of daily living (ADL). These include the ability to wash, dress, feed, and toilet oneself without assistance, as well as perform normal household chores and walk unaided. Over the course of study, 7,466 questionnaires have been completed by the participants and functional disability was defined as having difficulty with at least one of these six ADLs, Dr. Myasoedova explained.
At baseline, subjects with and without RA were aged a mean of 55 and 56 years, respectively, and 70% in both groups were female. Similar percentages were current (about 15%), former (about 30%), or never smokers (about 55%), and about 40% were obese.
Just under two-thirds (64.4%) of patients in the RA cohort were positive for rheumatoid factor (RF) or anti–cyclic citrullinated peptide (CCP) antibodies. While there was a similar prevalence of functional disability in RA patients who were or were not RF or CCP positive (both 25%, P = .67), there was an increasing prevalence noted in those who were positive versus those who were negative over time (P = .027).
Although the investigators did not conduct an objective assessment for functional disability, these findings highlight the need for vigilant management of patients with RA, Dr. Myasoedova proposed.
“Early and aggressive treatment regimens aimed at tight inflammation control can help prevent the disabling effects of high disease activity and joint damage, thereby lowering functional disability,” she said in an interview ahead of the congress.
Future work, she observed, should look at how the pattern of functional disability changes and the use of transition modeling to understand the bidirectional pattern of potential change and accumulation of functional disability in RA. The investigators also plan to look at risk factors for persistent and worsening functional disability and how treatment – including “treat to target” and biologics – might affect this.
The National Institute of Arthritis and Musculoskeletal and Skin Diseases supported the study. Dr. Myasoedova had no conflicts of interest.
SOURCE: Myasoedova E et al. Ann Rheum Dis. 2018;77(Suppl 2):54. Abstract OP0009.
REPORTING FROM THE EULAR 2018 CONGRESS
Key clinical point: Functional disability remains higher over time in patients with rheumatoid arthritis, compared with people without the disease.
Major finding: The prevalence of functional disability was 26% vs. 11% at baseline, a 15% difference that persisted over more than 18 years of follow-up.
Study details: Retrospective, longitudinal, population-based cohort study of 586 individuals with RA, and 531 without.
Disclosures: The National Institute of Arthritis and Musculoskeletal and Skin Diseases supported the study. Dr. Myasoedova had no conflicts of interest.
Source: Myasoedova E et al. Ann Rheum Dis. 2018;77(Suppl 2):54. Abstract OP0009.
Scaly Annular and Concentric Plaques
The Diagnosis: Annular Psoriasis
Because the patient's history was nonconcordant with the clinical appearance, a 4-mm punch biopsy was performed from a lesion on the left hip. Hematoxylin and eosin-stained sections demonstrated mild irregular acanthosis of the epidermis with discrete mounds of parakeratin (Figure 1A). Higher power revealed numerous neutrophils entrapped within focal scale crusts (Figure 1B). Periodic acid-Schiff stain for fungus demonstrated no hyphal elements or yeast forms in the stratum corneum. These histopathology findings were consistent with the diagnosis of annular psoriasis.
(H&E, original magnification ×4) with neutrophils entrapped in thescale (B)(H&E, original magnification ×20).")
The manifestation of psoriasis may take many forms, ranging from classic plaques to pustular eruptions--either annular or generalized--and erythroderma. Primarily annular plaque-type psoriasis without pustules, however, remains an uncommon finding.1 Psoriatic plaques may become annular or arcuate with central clearing from partial treatment with topical medications, though our patient reported annular plaques prior to any treatment. His presentation was notably different than annular pustular psoriasis in that there were no pustules in the leading edge, and there was no trailing scale, which is typical of annular pustular psoriasis.
Topical triamcinolone prescribed at the initial presentation to the dermatology department helped with pruritus, but due to the large body surface area involved, methotrexate later was initiated. After a 10-mg test dose of methotrexate and titration to 15 mg weekly, dramatic improvement in the rash was noted after 8 weeks. As the rash resolved, only faint hyperpigmented patches remained (Figure 2).

Erythema gyratum repens is a rare paraneoplastic syndrome that presents with annular scaly plaques with concentric circles with a wood grain-like appearance. The borders can advance up to 1 cm daily and show nonspecific findings on histopathology.2 Due to the observation that approximately 80% of cases of erythema gyratum repens were associated with an underlying malignancy, most often of the lung,3 this diagnosis was entertained given our patient's clinical presentation.
Erythema annulare centrifugum (EAC) historically has been divided into 2 forms: superficial and deep.4 Both present with slowly expanding, annular, pink plaques. Superficial EAC demonstrates parakeratosis and trailing scale and has not been proven to be associated with other systemic diseases, while deep EAC has infiltrated borders without scale, and many cases of EAC may represent annular forms of tumid lupus.4 Inflammatory cells may cuff vessels tightly, resulting in so-called coat sleeve infiltrate in superficial EAC. Along with trailing scale, this finding suggests the diagnosis. It has been argued that EAC is not an entity on its own and should prompt evaluation for lupus erythematosus, dermatitis, hypersensitivity to tinea pedis, and Lyme disease in appropriate circumstances.5
Tinea corporis always should be considered when evaluating annular scaly plaques with central clearing. Diagnosis and treatment are straightforward when hyphae are found on microscopy of skin scrapings or seen on periodic acid-Schiff stains of formalin-fixed tissue. Tinea imbricata presents with an interesting morphology and appears more ornate or cerebriform than tinea corporis caused by Trichophyton rubrum. It is caused by infection with Trichophyton circumscriptum and occurs in certain regions in the South Pacific, Southeast Asia, and Central and South America, making the diagnosis within the United States unlikely for a patient who has not traveled to these areas.6
Erythema chronicum migrans is diagnostic of Lyme disease infection with Borrelia burgdorferi, and solitary lesions occur surrounding the site of a tick bite in the majority of patients. Only 20% of patients will develop multiple lesions consistent with erythema chronicum migrans due to multiple tick bites, spirochetemia, or lymphatic spread.7 Up to one-third of patients are unaware that they were bitten by a tick. In endemic areas, this diagnosis must be entertained in any patient presenting with an annular rash, as treatment may prevent notable morbidity.
- Guill C, Hoang M, Carder K. Primary annular plaque-type psoriasis. Pediatr Dermatol. 2005;22:15-18.
- Boyd A, Neldner K, Menter A. Erythema gyratum repens: a paraneoplastic eruption. J Am Acad Dermatol. 1992;26:757-762.
- Kawakami T, Saito R. Erythema gyratum repens unassociated with underlying malignancy. J Dermatol. 1995;22:587-589.
- Weyers W, Diaz-Cascajo C, Weyers I. Erythema annulare centrifugum: results of a clinicopathologic study of 73 patients. Am J Dermatopathol. 2003;25:451-462.
- Ziemer M, Eisendle K, Zelger B. New concepts on erythema annulare centrifugum: a clinical reaction pattern that does notrepresent a specific clinicopathological entity. Br J Dermatol. 2009;160:119-126.
- Bonifaz A, Vázquez-González D. Tinea imbricata in the Americas. Curr Opin Infect Dis. 2011;24:106-111.
- Müllegger R, Glatz M. Skin manifestations of Lyme borreliosis: diagnosis and management. Am J Clin Dermatol. 2008;9:355-368.
The Diagnosis: Annular Psoriasis
Because the patient's history was nonconcordant with the clinical appearance, a 4-mm punch biopsy was performed from a lesion on the left hip. Hematoxylin and eosin-stained sections demonstrated mild irregular acanthosis of the epidermis with discrete mounds of parakeratin (Figure 1A). Higher power revealed numerous neutrophils entrapped within focal scale crusts (Figure 1B). Periodic acid-Schiff stain for fungus demonstrated no hyphal elements or yeast forms in the stratum corneum. These histopathology findings were consistent with the diagnosis of annular psoriasis.
The manifestation of psoriasis may take many forms, ranging from classic plaques to pustular eruptions--either annular or generalized--and erythroderma. Primarily annular plaque-type psoriasis without pustules, however, remains an uncommon finding.1 Psoriatic plaques may become annular or arcuate with central clearing from partial treatment with topical medications, though our patient reported annular plaques prior to any treatment. His presentation was notably different than annular pustular psoriasis in that there were no pustules in the leading edge, and there was no trailing scale, which is typical of annular pustular psoriasis.
Topical triamcinolone prescribed at the initial presentation to the dermatology department helped with pruritus, but due to the large body surface area involved, methotrexate later was initiated. After a 10-mg test dose of methotrexate and titration to 15 mg weekly, dramatic improvement in the rash was noted after 8 weeks. As the rash resolved, only faint hyperpigmented patches remained (Figure 2).
Erythema gyratum repens is a rare paraneoplastic syndrome that presents with annular scaly plaques with concentric circles with a wood grain-like appearance. The borders can advance up to 1 cm daily and show nonspecific findings on histopathology.2 Due to the observation that approximately 80% of cases of erythema gyratum repens were associated with an underlying malignancy, most often of the lung,3 this diagnosis was entertained given our patient's clinical presentation.
Erythema annulare centrifugum (EAC) historically has been divided into 2 forms: superficial and deep.4 Both present with slowly expanding, annular, pink plaques. Superficial EAC demonstrates parakeratosis and trailing scale and has not been proven to be associated with other systemic diseases, while deep EAC has infiltrated borders without scale, and many cases of EAC may represent annular forms of tumid lupus.4 Inflammatory cells may cuff vessels tightly, resulting in so-called coat sleeve infiltrate in superficial EAC. Along with trailing scale, this finding suggests the diagnosis. It has been argued that EAC is not an entity on its own and should prompt evaluation for lupus erythematosus, dermatitis, hypersensitivity to tinea pedis, and Lyme disease in appropriate circumstances.5
Tinea corporis always should be considered when evaluating annular scaly plaques with central clearing. Diagnosis and treatment are straightforward when hyphae are found on microscopy of skin scrapings or seen on periodic acid-Schiff stains of formalin-fixed tissue. Tinea imbricata presents with an interesting morphology and appears more ornate or cerebriform than tinea corporis caused by Trichophyton rubrum. It is caused by infection with Trichophyton circumscriptum and occurs in certain regions in the South Pacific, Southeast Asia, and Central and South America, making the diagnosis within the United States unlikely for a patient who has not traveled to these areas.6
Erythema chronicum migrans is diagnostic of Lyme disease infection with Borrelia burgdorferi, and solitary lesions occur surrounding the site of a tick bite in the majority of patients. Only 20% of patients will develop multiple lesions consistent with erythema chronicum migrans due to multiple tick bites, spirochetemia, or lymphatic spread.7 Up to one-third of patients are unaware that they were bitten by a tick. In endemic areas, this diagnosis must be entertained in any patient presenting with an annular rash, as treatment may prevent notable morbidity.
The Diagnosis: Annular Psoriasis
Because the patient's history was nonconcordant with the clinical appearance, a 4-mm punch biopsy was performed from a lesion on the left hip. Hematoxylin and eosin-stained sections demonstrated mild irregular acanthosis of the epidermis with discrete mounds of parakeratin (Figure 1A). Higher power revealed numerous neutrophils entrapped within focal scale crusts (Figure 1B). Periodic acid-Schiff stain for fungus demonstrated no hyphal elements or yeast forms in the stratum corneum. These histopathology findings were consistent with the diagnosis of annular psoriasis.
The manifestation of psoriasis may take many forms, ranging from classic plaques to pustular eruptions--either annular or generalized--and erythroderma. Primarily annular plaque-type psoriasis without pustules, however, remains an uncommon finding.1 Psoriatic plaques may become annular or arcuate with central clearing from partial treatment with topical medications, though our patient reported annular plaques prior to any treatment. His presentation was notably different than annular pustular psoriasis in that there were no pustules in the leading edge, and there was no trailing scale, which is typical of annular pustular psoriasis.
Topical triamcinolone prescribed at the initial presentation to the dermatology department helped with pruritus, but due to the large body surface area involved, methotrexate later was initiated. After a 10-mg test dose of methotrexate and titration to 15 mg weekly, dramatic improvement in the rash was noted after 8 weeks. As the rash resolved, only faint hyperpigmented patches remained (Figure 2).
Erythema gyratum repens is a rare paraneoplastic syndrome that presents with annular scaly plaques with concentric circles with a wood grain-like appearance. The borders can advance up to 1 cm daily and show nonspecific findings on histopathology.2 Due to the observation that approximately 80% of cases of erythema gyratum repens were associated with an underlying malignancy, most often of the lung,3 this diagnosis was entertained given our patient's clinical presentation.
Erythema annulare centrifugum (EAC) historically has been divided into 2 forms: superficial and deep.4 Both present with slowly expanding, annular, pink plaques. Superficial EAC demonstrates parakeratosis and trailing scale and has not been proven to be associated with other systemic diseases, while deep EAC has infiltrated borders without scale, and many cases of EAC may represent annular forms of tumid lupus.4 Inflammatory cells may cuff vessels tightly, resulting in so-called coat sleeve infiltrate in superficial EAC. Along with trailing scale, this finding suggests the diagnosis. It has been argued that EAC is not an entity on its own and should prompt evaluation for lupus erythematosus, dermatitis, hypersensitivity to tinea pedis, and Lyme disease in appropriate circumstances.5
Tinea corporis always should be considered when evaluating annular scaly plaques with central clearing. Diagnosis and treatment are straightforward when hyphae are found on microscopy of skin scrapings or seen on periodic acid-Schiff stains of formalin-fixed tissue. Tinea imbricata presents with an interesting morphology and appears more ornate or cerebriform than tinea corporis caused by Trichophyton rubrum. It is caused by infection with Trichophyton circumscriptum and occurs in certain regions in the South Pacific, Southeast Asia, and Central and South America, making the diagnosis within the United States unlikely for a patient who has not traveled to these areas.6
Erythema chronicum migrans is diagnostic of Lyme disease infection with Borrelia burgdorferi, and solitary lesions occur surrounding the site of a tick bite in the majority of patients. Only 20% of patients will develop multiple lesions consistent with erythema chronicum migrans due to multiple tick bites, spirochetemia, or lymphatic spread.7 Up to one-third of patients are unaware that they were bitten by a tick. In endemic areas, this diagnosis must be entertained in any patient presenting with an annular rash, as treatment may prevent notable morbidity.
- Guill C, Hoang M, Carder K. Primary annular plaque-type psoriasis. Pediatr Dermatol. 2005;22:15-18.
- Boyd A, Neldner K, Menter A. Erythema gyratum repens: a paraneoplastic eruption. J Am Acad Dermatol. 1992;26:757-762.
- Kawakami T, Saito R. Erythema gyratum repens unassociated with underlying malignancy. J Dermatol. 1995;22:587-589.
- Weyers W, Diaz-Cascajo C, Weyers I. Erythema annulare centrifugum: results of a clinicopathologic study of 73 patients. Am J Dermatopathol. 2003;25:451-462.
- Ziemer M, Eisendle K, Zelger B. New concepts on erythema annulare centrifugum: a clinical reaction pattern that does notrepresent a specific clinicopathological entity. Br J Dermatol. 2009;160:119-126.
- Bonifaz A, Vázquez-González D. Tinea imbricata in the Americas. Curr Opin Infect Dis. 2011;24:106-111.
- Müllegger R, Glatz M. Skin manifestations of Lyme borreliosis: diagnosis and management. Am J Clin Dermatol. 2008;9:355-368.
- Guill C, Hoang M, Carder K. Primary annular plaque-type psoriasis. Pediatr Dermatol. 2005;22:15-18.
- Boyd A, Neldner K, Menter A. Erythema gyratum repens: a paraneoplastic eruption. J Am Acad Dermatol. 1992;26:757-762.
- Kawakami T, Saito R. Erythema gyratum repens unassociated with underlying malignancy. J Dermatol. 1995;22:587-589.
- Weyers W, Diaz-Cascajo C, Weyers I. Erythema annulare centrifugum: results of a clinicopathologic study of 73 patients. Am J Dermatopathol. 2003;25:451-462.
- Ziemer M, Eisendle K, Zelger B. New concepts on erythema annulare centrifugum: a clinical reaction pattern that does notrepresent a specific clinicopathological entity. Br J Dermatol. 2009;160:119-126.
- Bonifaz A, Vázquez-González D. Tinea imbricata in the Americas. Curr Opin Infect Dis. 2011;24:106-111.
- Müllegger R, Glatz M. Skin manifestations of Lyme borreliosis: diagnosis and management. Am J Clin Dermatol. 2008;9:355-368.

A healthy 23-year-old man presented for evaluation of an enlarging annular pruritic rash of 1.5 years' duration. Treatment with ciclopirox cream 0.77%, calcipotriene cream 0.005%, tacrolimus ointment 0.1%, fluticasone cream 0.05%, and halobetasol cream 0.05% prescribed by an outside physician provided only modest temporary improvement. The patient reported no history of travel outside of western New York, camping, tick bites, or medications. He denied any joint swelling or morning stiffness. Physical examination revealed multiple 4- to 6-cm pink, annular, scaly plaques with central clearing on the abdomen (top) and thighs. A few 1-cm pink scaly patches were present on the back (bottom), and few 2- to 3-mm pink scaly papules were noted on the extensor aspects of the elbows and forearms. A potassium hydroxide examination revealed no hyphal elements or yeast forms.

Is the suicide story fake – or just misleading?
Recently, a lot has been in the news about the increasing rates of suicide in all communities, including among African American youth, and two high-profile celebrities. Now that we have a CEO in the White House who has made the phrase “fake news” part of the national lexicon (and as a former CEO myself), I feel compelled to take a critical, clinical look at the way the suicide story has been reported.
CEOs tend to be unique people, and many of them are fond of hyperbole – as it promotes “followship” in employees and fosters business deals. I interpret fake news as the kind of information, or maybe spin is a better word, promulgated by CEOs.

While following a research letter published recently in JAMA Pediatrics – “Age-Related Racial Disparity in Suicide Rates Among U.S. Youths From 2001 Through 2015” (2018 May 21. doi: 10.001/jamapediatrics.2018.0399) – it occurred to me that this struck me as fake news. But as I thought about it, I realized that the conclusions in the research letter would be better characterized as perhaps misleading news. My basis for reaching those conclusions is rooted in the lessons I learned as a 2-year member of the Institute of Medicine’s Board on Neuroscience and Behavioral Health, Committee on Pathophysiology & Prevention of Adolescent & Adult Suicide. In fact, the report we produced was the first one referenced in the research letter. Unfortunately, however, the research letter’s authors seemed to miss the IOM report’s major take-away messages.
For example, the research letter authors compared the suicide rates among black children and white children in this way: “However, suicide rates increased from 1993 to 1997 and 2008 to 2012 among black children aged 5 to 11 years (from 1.36 to 2.54 per million) and decreased among white children of the same age (from 1.14 to 0.77 per million).” That sentence supports the conclusions of the IOM’s “Reducing Suicide” report, as it confirms that those are very low base rates. However, because the base rates are so low in most populations, it is difficult to determine scientifically whether a significant rise or decrease in rates occurred.
To quote page 377 of IOM report: “The base rate of completed suicide is sufficiently low to preclude all but the largest of studies. When such studies are performed, resultant comparisons are between extremely small and large groups of individuals (suicide completers versus non–suicide completers, or suicide attempters versus non–suicide attempters). Use of suicidal ideation as an outcome can increase incidence and alleviate the problem to some extent; however, it is unclear whether suicidal ideation is a strong predictor of suicide completion. Using both attempts and completions can confound the analysis since attempters may account for some of the suicides completed within the study period. Because the duration of the prevention studies is frequently too brief to collect sufficient data on the low frequency endpoints of suicide or suicide attempt, proximal measures such as changes in knowledge or attitude are used. Yet the predictive value of these variables is unconfirmed.”
Further, according to page 410 of the report: “As the statistical analysis above points out, at a suicide rate of 10 per 100,000 population, approximately 100,000 participants are needed to achieve statistical significance in an experimental context. In studying suicide among low-risk groups, the numbers needed are even greater.”
Let me break this down a bit. , because the numerator is so small and the dominator is so large. Let me put it this way – if the black female suicide rates are 2/100,000, and those rates quadrupled (sounds impressive, doesn’t it?) then there would be 8/100,000 black female suicides; the difference between 2 and 8 per 100,000 is not really a significant difference because the base-rates are so small. But to say the rates quadrupled sounds scary and impressive. “Figures don’t lie, but liars can figure.”
So, the premise of the research letter is whack.
I am not impressed that the rates of black children aged 5-7 increased from 1.36/1,000,000 to 2.54/1,000,000. I am not even sure those two numbers are significantly different, much less have clinical relevance. I have tried to make this point before, but it always gets lost by the hyperbolic press – which continues to yell about suicides in the United States rising by 30% or doubling, even quadrupling. The low base rates make drawing firm conclusions from this data like spitting into the ocean. I understand that one suicide is one suicide too many. But this is not science.
The characterizations about soaring U.S. suicide rates are not exactly fake news. Instead, I would call these interpretations misleading science and news.
Dr. Bell is staff psychiatrist at Jackson Park Hospital’s surgical-medical/psychiatric inpatient unit; clinical professor emeritus, department of psychiatry, University of Illinois at Chicago; former director of the Institute for Juvenile Research (the birthplace of child psychiatry), and former president/CEO of the Community Mental Health Council, all in Chicago. He also serves as chair of psychiatry at Windsor University, St. Kitts.
Recently, a lot has been in the news about the increasing rates of suicide in all communities, including among African American youth, and two high-profile celebrities. Now that we have a CEO in the White House who has made the phrase “fake news” part of the national lexicon (and as a former CEO myself), I feel compelled to take a critical, clinical look at the way the suicide story has been reported.
CEOs tend to be unique people, and many of them are fond of hyperbole – as it promotes “followship” in employees and fosters business deals. I interpret fake news as the kind of information, or maybe spin is a better word, promulgated by CEOs.
While following a research letter published recently in JAMA Pediatrics – “Age-Related Racial Disparity in Suicide Rates Among U.S. Youths From 2001 Through 2015” (2018 May 21. doi: 10.001/jamapediatrics.2018.0399) – it occurred to me that this struck me as fake news. But as I thought about it, I realized that the conclusions in the research letter would be better characterized as perhaps misleading news. My basis for reaching those conclusions is rooted in the lessons I learned as a 2-year member of the Institute of Medicine’s Board on Neuroscience and Behavioral Health, Committee on Pathophysiology & Prevention of Adolescent & Adult Suicide. In fact, the report we produced was the first one referenced in the research letter. Unfortunately, however, the research letter’s authors seemed to miss the IOM report’s major take-away messages.
For example, the research letter authors compared the suicide rates among black children and white children in this way: “However, suicide rates increased from 1993 to 1997 and 2008 to 2012 among black children aged 5 to 11 years (from 1.36 to 2.54 per million) and decreased among white children of the same age (from 1.14 to 0.77 per million).” That sentence supports the conclusions of the IOM’s “Reducing Suicide” report, as it confirms that those are very low base rates. However, because the base rates are so low in most populations, it is difficult to determine scientifically whether a significant rise or decrease in rates occurred.
To quote page 377 of IOM report: “The base rate of completed suicide is sufficiently low to preclude all but the largest of studies. When such studies are performed, resultant comparisons are between extremely small and large groups of individuals (suicide completers versus non–suicide completers, or suicide attempters versus non–suicide attempters). Use of suicidal ideation as an outcome can increase incidence and alleviate the problem to some extent; however, it is unclear whether suicidal ideation is a strong predictor of suicide completion. Using both attempts and completions can confound the analysis since attempters may account for some of the suicides completed within the study period. Because the duration of the prevention studies is frequently too brief to collect sufficient data on the low frequency endpoints of suicide or suicide attempt, proximal measures such as changes in knowledge or attitude are used. Yet the predictive value of these variables is unconfirmed.”
Further, according to page 410 of the report: “As the statistical analysis above points out, at a suicide rate of 10 per 100,000 population, approximately 100,000 participants are needed to achieve statistical significance in an experimental context. In studying suicide among low-risk groups, the numbers needed are even greater.”
Let me break this down a bit. , because the numerator is so small and the dominator is so large. Let me put it this way – if the black female suicide rates are 2/100,000, and those rates quadrupled (sounds impressive, doesn’t it?) then there would be 8/100,000 black female suicides; the difference between 2 and 8 per 100,000 is not really a significant difference because the base-rates are so small. But to say the rates quadrupled sounds scary and impressive. “Figures don’t lie, but liars can figure.”
So, the premise of the research letter is whack.
I am not impressed that the rates of black children aged 5-7 increased from 1.36/1,000,000 to 2.54/1,000,000. I am not even sure those two numbers are significantly different, much less have clinical relevance. I have tried to make this point before, but it always gets lost by the hyperbolic press – which continues to yell about suicides in the United States rising by 30% or doubling, even quadrupling. The low base rates make drawing firm conclusions from this data like spitting into the ocean. I understand that one suicide is one suicide too many. But this is not science.
The characterizations about soaring U.S. suicide rates are not exactly fake news. Instead, I would call these interpretations misleading science and news.
Dr. Bell is staff psychiatrist at Jackson Park Hospital’s surgical-medical/psychiatric inpatient unit; clinical professor emeritus, department of psychiatry, University of Illinois at Chicago; former director of the Institute for Juvenile Research (the birthplace of child psychiatry), and former president/CEO of the Community Mental Health Council, all in Chicago. He also serves as chair of psychiatry at Windsor University, St. Kitts.
Recently, a lot has been in the news about the increasing rates of suicide in all communities, including among African American youth, and two high-profile celebrities. Now that we have a CEO in the White House who has made the phrase “fake news” part of the national lexicon (and as a former CEO myself), I feel compelled to take a critical, clinical look at the way the suicide story has been reported.
CEOs tend to be unique people, and many of them are fond of hyperbole – as it promotes “followship” in employees and fosters business deals. I interpret fake news as the kind of information, or maybe spin is a better word, promulgated by CEOs.
While following a research letter published recently in JAMA Pediatrics – “Age-Related Racial Disparity in Suicide Rates Among U.S. Youths From 2001 Through 2015” (2018 May 21. doi: 10.001/jamapediatrics.2018.0399) – it occurred to me that this struck me as fake news. But as I thought about it, I realized that the conclusions in the research letter would be better characterized as perhaps misleading news. My basis for reaching those conclusions is rooted in the lessons I learned as a 2-year member of the Institute of Medicine’s Board on Neuroscience and Behavioral Health, Committee on Pathophysiology & Prevention of Adolescent & Adult Suicide. In fact, the report we produced was the first one referenced in the research letter. Unfortunately, however, the research letter’s authors seemed to miss the IOM report’s major take-away messages.
For example, the research letter authors compared the suicide rates among black children and white children in this way: “However, suicide rates increased from 1993 to 1997 and 2008 to 2012 among black children aged 5 to 11 years (from 1.36 to 2.54 per million) and decreased among white children of the same age (from 1.14 to 0.77 per million).” That sentence supports the conclusions of the IOM’s “Reducing Suicide” report, as it confirms that those are very low base rates. However, because the base rates are so low in most populations, it is difficult to determine scientifically whether a significant rise or decrease in rates occurred.
To quote page 377 of IOM report: “The base rate of completed suicide is sufficiently low to preclude all but the largest of studies. When such studies are performed, resultant comparisons are between extremely small and large groups of individuals (suicide completers versus non–suicide completers, or suicide attempters versus non–suicide attempters). Use of suicidal ideation as an outcome can increase incidence and alleviate the problem to some extent; however, it is unclear whether suicidal ideation is a strong predictor of suicide completion. Using both attempts and completions can confound the analysis since attempters may account for some of the suicides completed within the study period. Because the duration of the prevention studies is frequently too brief to collect sufficient data on the low frequency endpoints of suicide or suicide attempt, proximal measures such as changes in knowledge or attitude are used. Yet the predictive value of these variables is unconfirmed.”
Further, according to page 410 of the report: “As the statistical analysis above points out, at a suicide rate of 10 per 100,000 population, approximately 100,000 participants are needed to achieve statistical significance in an experimental context. In studying suicide among low-risk groups, the numbers needed are even greater.”
Let me break this down a bit. , because the numerator is so small and the dominator is so large. Let me put it this way – if the black female suicide rates are 2/100,000, and those rates quadrupled (sounds impressive, doesn’t it?) then there would be 8/100,000 black female suicides; the difference between 2 and 8 per 100,000 is not really a significant difference because the base-rates are so small. But to say the rates quadrupled sounds scary and impressive. “Figures don’t lie, but liars can figure.”
So, the premise of the research letter is whack.
I am not impressed that the rates of black children aged 5-7 increased from 1.36/1,000,000 to 2.54/1,000,000. I am not even sure those two numbers are significantly different, much less have clinical relevance. I have tried to make this point before, but it always gets lost by the hyperbolic press – which continues to yell about suicides in the United States rising by 30% or doubling, even quadrupling. The low base rates make drawing firm conclusions from this data like spitting into the ocean. I understand that one suicide is one suicide too many. But this is not science.
The characterizations about soaring U.S. suicide rates are not exactly fake news. Instead, I would call these interpretations misleading science and news.
Dr. Bell is staff psychiatrist at Jackson Park Hospital’s surgical-medical/psychiatric inpatient unit; clinical professor emeritus, department of psychiatry, University of Illinois at Chicago; former director of the Institute for Juvenile Research (the birthplace of child psychiatry), and former president/CEO of the Community Mental Health Council, all in Chicago. He also serves as chair of psychiatry at Windsor University, St. Kitts.
Most Medicaid enrollees exempt from work requirements
Only 6% of the Medicaid population would be unlikely to qualify for an exemption from work requirements for “able-bodied adults” that states are in the process of being implementing, according to a new report from the Kaiser Family Foundation.
Another 15% were in fair or poor health or didn’t work because of illness or disability, 11% didn’t work because they were providing care for family members, and 6% were attending school, Kaiser wrote in an issue brief.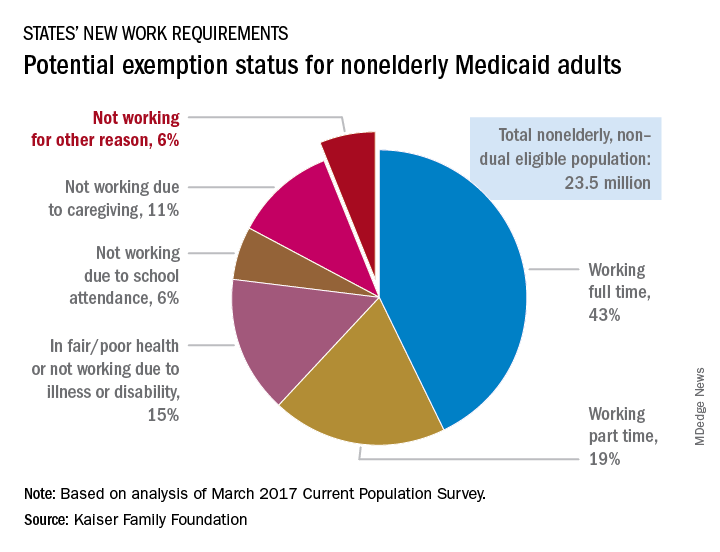
“This target population is much smaller than the groups of enrollees who are already working but would need to comply with new reporting requirements and those who could be exempt and would have to navigate an exemption process,” the Kaiser investigators said.
States will need to set up systems to deal with these issues, but many enrollees face barriers to complying. The waiver program in Arkansas – one of the first four states to receive permission to impose work requirements – “requires beneficiaries to set up an online account and use this account as the sole means of periodic reporting related to work requirements and exemptions,” they noted, but 30% of all nonelderly Medicaid adults say that they have never used a computer, 21% do not use the Internet, and 41% do not use email, based on analysis of 2016 National Health Interview Survey data.
Only 6% of the Medicaid population would be unlikely to qualify for an exemption from work requirements for “able-bodied adults” that states are in the process of being implementing, according to a new report from the Kaiser Family Foundation.
Another 15% were in fair or poor health or didn’t work because of illness or disability, 11% didn’t work because they were providing care for family members, and 6% were attending school, Kaiser wrote in an issue brief.
“This target population is much smaller than the groups of enrollees who are already working but would need to comply with new reporting requirements and those who could be exempt and would have to navigate an exemption process,” the Kaiser investigators said.
States will need to set up systems to deal with these issues, but many enrollees face barriers to complying. The waiver program in Arkansas – one of the first four states to receive permission to impose work requirements – “requires beneficiaries to set up an online account and use this account as the sole means of periodic reporting related to work requirements and exemptions,” they noted, but 30% of all nonelderly Medicaid adults say that they have never used a computer, 21% do not use the Internet, and 41% do not use email, based on analysis of 2016 National Health Interview Survey data.
Only 6% of the Medicaid population would be unlikely to qualify for an exemption from work requirements for “able-bodied adults” that states are in the process of being implementing, according to a new report from the Kaiser Family Foundation.
Another 15% were in fair or poor health or didn’t work because of illness or disability, 11% didn’t work because they were providing care for family members, and 6% were attending school, Kaiser wrote in an issue brief.
“This target population is much smaller than the groups of enrollees who are already working but would need to comply with new reporting requirements and those who could be exempt and would have to navigate an exemption process,” the Kaiser investigators said.
States will need to set up systems to deal with these issues, but many enrollees face barriers to complying. The waiver program in Arkansas – one of the first four states to receive permission to impose work requirements – “requires beneficiaries to set up an online account and use this account as the sole means of periodic reporting related to work requirements and exemptions,” they noted, but 30% of all nonelderly Medicaid adults say that they have never used a computer, 21% do not use the Internet, and 41% do not use email, based on analysis of 2016 National Health Interview Survey data.
Malignancy risk of tocilizumab and TNF inhibitors found similar
AMSTERDAM – , according to an analysis of three large databases presented at the European Congress of Rheumatology.
“When we combined the databases, the incidence of any malignancy excluding nonmelanoma skin cancer was 13.09 per 1,000 patient years in the tocilizumab group and 13.46 in the TNF-inhibitor group,” reported Seoyoung C. Kim, MD, ScD, of the division of pharmacoepidemiology & pharmacoeconomics at Brigham and Women’s Hospital, Boston.

The study was conducted with data from 10,393 adult RA patients treated with tocilizumab and 26,357 patients treated with TNFi in the Medicare, QuintilesIMS PharMetrics Plus, and Truven Health MarketScan databases. All patients were new starts on tocilizumab or the TNFi on which they were evaluated, but all were required to have been exposed to at least one different biologic prior to starting the treatment. A diagnosis of RA at least 365 days prior to inclusion in this analysis was required to rule out prevalent cancers, which was an exclusion criterion.
More than 60 covariates were employed in the analysis to minimize the risk of confounders. These included demographics, RA characteristics, comorbidities, and other medications.
There also was no difference in the rates of the 12 most common cancer types when those exposed to tocilizumab were compared with those exposed to TNFi in a secondary analysis of these data, according to Dr. Kim. When expressed as hazard ratios, there were some numerical differences in relative risk among these cancers on both as-treated and intention-to-treat analyses, but confidence intervals were large, and none approached significance.
RA itself has been associated with an increased risk of some malignancies, such as lung cancer, but the relationship between the proinflammatory state of RA, its treatments, and the risk of cancer has been unclear, according to Dr. Kim. She said, “There is some concern relative to use of TNFi or other biologics in regard to developing malignancy, but studies have been inconsistent.”

Dr. Kim conceded that a lack of data on patients’ disease duration or activity is one limitation of this analysis. Another is that residual confounding can never be ruled out from a retrospective analysis. However, she said that, because the two biologics were compared for the same indication in patients exposed to at least one previous biologic, the confounding may be less than it would be if tocilizumab was compared with a conventional synthetic disease modifying antirheumatic drug (csDMARD), such as methotrexate. Again, there also was a requirement for exposure to at least one prior biologic, and this also is reassuring for the final conclusion.
“In other words, even among RA patients who were exposed to more than one biologic, the risk of cancer was similar between tocilizumab and TNF-inhibitor initiators,” Dr. Kim reported.
Roche provided funding for the study. Dr. Kim reports financial relationships with Bristol-Myers Squibb, Pfizer, and Roche.
AMSTERDAM – , according to an analysis of three large databases presented at the European Congress of Rheumatology.
“When we combined the databases, the incidence of any malignancy excluding nonmelanoma skin cancer was 13.09 per 1,000 patient years in the tocilizumab group and 13.46 in the TNF-inhibitor group,” reported Seoyoung C. Kim, MD, ScD, of the division of pharmacoepidemiology & pharmacoeconomics at Brigham and Women’s Hospital, Boston.
The study was conducted with data from 10,393 adult RA patients treated with tocilizumab and 26,357 patients treated with TNFi in the Medicare, QuintilesIMS PharMetrics Plus, and Truven Health MarketScan databases. All patients were new starts on tocilizumab or the TNFi on which they were evaluated, but all were required to have been exposed to at least one different biologic prior to starting the treatment. A diagnosis of RA at least 365 days prior to inclusion in this analysis was required to rule out prevalent cancers, which was an exclusion criterion.
More than 60 covariates were employed in the analysis to minimize the risk of confounders. These included demographics, RA characteristics, comorbidities, and other medications.
There also was no difference in the rates of the 12 most common cancer types when those exposed to tocilizumab were compared with those exposed to TNFi in a secondary analysis of these data, according to Dr. Kim. When expressed as hazard ratios, there were some numerical differences in relative risk among these cancers on both as-treated and intention-to-treat analyses, but confidence intervals were large, and none approached significance.
RA itself has been associated with an increased risk of some malignancies, such as lung cancer, but the relationship between the proinflammatory state of RA, its treatments, and the risk of cancer has been unclear, according to Dr. Kim. She said, “There is some concern relative to use of TNFi or other biologics in regard to developing malignancy, but studies have been inconsistent.”
Dr. Kim conceded that a lack of data on patients’ disease duration or activity is one limitation of this analysis. Another is that residual confounding can never be ruled out from a retrospective analysis. However, she said that, because the two biologics were compared for the same indication in patients exposed to at least one previous biologic, the confounding may be less than it would be if tocilizumab was compared with a conventional synthetic disease modifying antirheumatic drug (csDMARD), such as methotrexate. Again, there also was a requirement for exposure to at least one prior biologic, and this also is reassuring for the final conclusion.
“In other words, even among RA patients who were exposed to more than one biologic, the risk of cancer was similar between tocilizumab and TNF-inhibitor initiators,” Dr. Kim reported.
Roche provided funding for the study. Dr. Kim reports financial relationships with Bristol-Myers Squibb, Pfizer, and Roche.
AMSTERDAM – , according to an analysis of three large databases presented at the European Congress of Rheumatology.
“When we combined the databases, the incidence of any malignancy excluding nonmelanoma skin cancer was 13.09 per 1,000 patient years in the tocilizumab group and 13.46 in the TNF-inhibitor group,” reported Seoyoung C. Kim, MD, ScD, of the division of pharmacoepidemiology & pharmacoeconomics at Brigham and Women’s Hospital, Boston.
The study was conducted with data from 10,393 adult RA patients treated with tocilizumab and 26,357 patients treated with TNFi in the Medicare, QuintilesIMS PharMetrics Plus, and Truven Health MarketScan databases. All patients were new starts on tocilizumab or the TNFi on which they were evaluated, but all were required to have been exposed to at least one different biologic prior to starting the treatment. A diagnosis of RA at least 365 days prior to inclusion in this analysis was required to rule out prevalent cancers, which was an exclusion criterion.
More than 60 covariates were employed in the analysis to minimize the risk of confounders. These included demographics, RA characteristics, comorbidities, and other medications.
There also was no difference in the rates of the 12 most common cancer types when those exposed to tocilizumab were compared with those exposed to TNFi in a secondary analysis of these data, according to Dr. Kim. When expressed as hazard ratios, there were some numerical differences in relative risk among these cancers on both as-treated and intention-to-treat analyses, but confidence intervals were large, and none approached significance.
RA itself has been associated with an increased risk of some malignancies, such as lung cancer, but the relationship between the proinflammatory state of RA, its treatments, and the risk of cancer has been unclear, according to Dr. Kim. She said, “There is some concern relative to use of TNFi or other biologics in regard to developing malignancy, but studies have been inconsistent.”
Dr. Kim conceded that a lack of data on patients’ disease duration or activity is one limitation of this analysis. Another is that residual confounding can never be ruled out from a retrospective analysis. However, she said that, because the two biologics were compared for the same indication in patients exposed to at least one previous biologic, the confounding may be less than it would be if tocilizumab was compared with a conventional synthetic disease modifying antirheumatic drug (csDMARD), such as methotrexate. Again, there also was a requirement for exposure to at least one prior biologic, and this also is reassuring for the final conclusion.
“In other words, even among RA patients who were exposed to more than one biologic, the risk of cancer was similar between tocilizumab and TNF-inhibitor initiators,” Dr. Kim reported.
Roche provided funding for the study. Dr. Kim reports financial relationships with Bristol-Myers Squibb, Pfizer, and Roche.
REPORTING FROM THE EULAR 2018 CONGRESS
Key clinical point: Tocilizumab was not associated with a higher cancer risk in rheumatoid arthritis than TNFi treatment in a cohort study.
Major finding: Relative to TNFI, the hazard ratio for malignancy was 0.98 (95% CI, 0.80-1.19) for tocilizumab relative to TNFi.
Study details: Cohort study with propensity matching with data from 10,393 adult RA patients treated with tocilizumab and 26,357 patients treated with TNFi.
Disclosures: Roche provided funding for the study. Dr. Kim reports financial relationships with Bristol-Myers Squibb, Pfizer, and Roche.
FDA approves pembrolizumab for relapsed/refractory PMBCL
The immune checkpoint inhibitor in adult and pediatric patients.
The Food and Drug Administration based the accelerated approval on results from 53 patients with relapsed or refractory primary mediastinal large B-cell lymphoma in the KEYNOTE-170 trial. In the phase 2 trial, patients received 200 mg of pembrolizumab intravenously for 3 weeks until unacceptable toxicity or documented disease progression occurred. This continued for up to 24 months in patients who did not display progression. The overall response rate to pembrolizumab was 45% (95% CI, 32-60), which included both complete (11%) and partial (34%) responses. The median duration of response was not met within the follow-up period (median, 9.7 months) and the median time to first objective response was 2.8 months.
The recommended dose for pembrolizumab in adults is 200 mg every 3 weeks. It is recommended that pediatric patients receive 2 mg/kg every 3 weeks, with a maximum dose of 200 mg.
The most common adverse reactions to pembrolizumab were musculoskeletal pain, upper respiratory tract infection, pyrexia, fatigue, cough, dyspnea, diarrhea, nausea, arrhythmia, and headache. In total, a quarter of patients with adverse reactions required systemic treatment with a corticosteroid and 26% of patients had serious adverse reactions.
Pembrolizumab was approved via the FDA’s accelerated approval process, which allows for earlier approval of drugs that treat serious medical conditions and fulfill an unmet medical need. The drug was approved based on tumor response rate and durability of response, the FDA noted.
The immune checkpoint inhibitor in adult and pediatric patients.
The Food and Drug Administration based the accelerated approval on results from 53 patients with relapsed or refractory primary mediastinal large B-cell lymphoma in the KEYNOTE-170 trial. In the phase 2 trial, patients received 200 mg of pembrolizumab intravenously for 3 weeks until unacceptable toxicity or documented disease progression occurred. This continued for up to 24 months in patients who did not display progression. The overall response rate to pembrolizumab was 45% (95% CI, 32-60), which included both complete (11%) and partial (34%) responses. The median duration of response was not met within the follow-up period (median, 9.7 months) and the median time to first objective response was 2.8 months.
The recommended dose for pembrolizumab in adults is 200 mg every 3 weeks. It is recommended that pediatric patients receive 2 mg/kg every 3 weeks, with a maximum dose of 200 mg.
The most common adverse reactions to pembrolizumab were musculoskeletal pain, upper respiratory tract infection, pyrexia, fatigue, cough, dyspnea, diarrhea, nausea, arrhythmia, and headache. In total, a quarter of patients with adverse reactions required systemic treatment with a corticosteroid and 26% of patients had serious adverse reactions.
Pembrolizumab was approved via the FDA’s accelerated approval process, which allows for earlier approval of drugs that treat serious medical conditions and fulfill an unmet medical need. The drug was approved based on tumor response rate and durability of response, the FDA noted.
The immune checkpoint inhibitor in adult and pediatric patients.
The Food and Drug Administration based the accelerated approval on results from 53 patients with relapsed or refractory primary mediastinal large B-cell lymphoma in the KEYNOTE-170 trial. In the phase 2 trial, patients received 200 mg of pembrolizumab intravenously for 3 weeks until unacceptable toxicity or documented disease progression occurred. This continued for up to 24 months in patients who did not display progression. The overall response rate to pembrolizumab was 45% (95% CI, 32-60), which included both complete (11%) and partial (34%) responses. The median duration of response was not met within the follow-up period (median, 9.7 months) and the median time to first objective response was 2.8 months.
The recommended dose for pembrolizumab in adults is 200 mg every 3 weeks. It is recommended that pediatric patients receive 2 mg/kg every 3 weeks, with a maximum dose of 200 mg.
The most common adverse reactions to pembrolizumab were musculoskeletal pain, upper respiratory tract infection, pyrexia, fatigue, cough, dyspnea, diarrhea, nausea, arrhythmia, and headache. In total, a quarter of patients with adverse reactions required systemic treatment with a corticosteroid and 26% of patients had serious adverse reactions.
Pembrolizumab was approved via the FDA’s accelerated approval process, which allows for earlier approval of drugs that treat serious medical conditions and fulfill an unmet medical need. The drug was approved based on tumor response rate and durability of response, the FDA noted.
Family medicine remains first in recruiting demand
according to physician recruitment firm Merritt Hawkins.
The company conducted 497 searches for family physicians from April 1, 2017, to March 31, 2018, marking the third straight year of decline for the specialty but still more than double the 243 searches conducted for psychiatrists, the medical specialty that was second more frequently requested for recruitment, Merritt Hawkins wrote in its 2018 Survey of Physician and Advanced Practitioners Recruiting Incentives.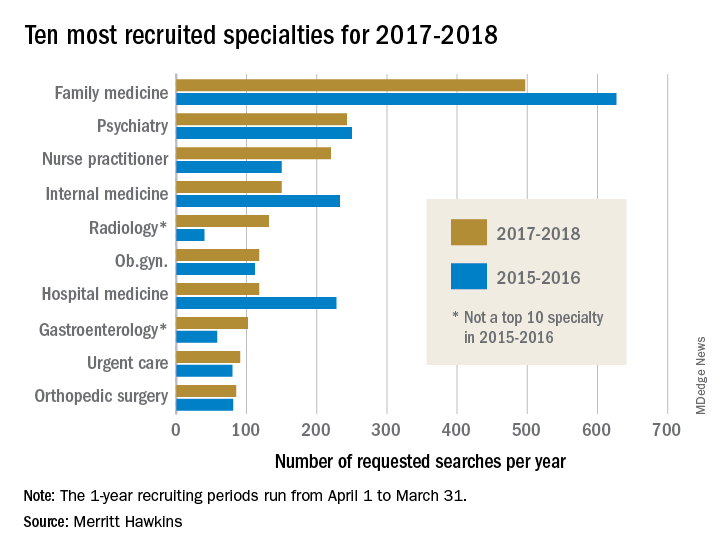
Gastroenterology, with an eighth-place finish in 2017-2018, also showed strong growth by increasing 55% from the year before and rising 137% over the past 3 years. The rise of gastroenterology and radiology over the past 2 years came at the expense of pediatrics, which went from 10th in 2015-2016 to 13th this year, and neurology, which dropped from 7th to 15th, Merritt Hawkins wrote in the report, which was based on a total of 3,045 search assignments conducted in 2017-2018.
“While demand for primary care physicians remains robust, hospitals, medical groups, and other health care facilities are shifting their recruiting efforts to medical specialists,” the company wrote, noting that recruiting assignments for medical specialists have risen from 67% of all searches 3 years ago to 74% in the past year.
“It’s a matter of demographic destiny,” Travis Singleton, senior vice president of Merritt Hawkins, said in a written statement accompanying the report. “Americans are getting older, and it is medical specialists who will be taking care of our aging and ailing bodies and brains. We still need more primary care doctors, but a growing emphasis is being placed on recruiting specialists.”
according to physician recruitment firm Merritt Hawkins.
The company conducted 497 searches for family physicians from April 1, 2017, to March 31, 2018, marking the third straight year of decline for the specialty but still more than double the 243 searches conducted for psychiatrists, the medical specialty that was second more frequently requested for recruitment, Merritt Hawkins wrote in its 2018 Survey of Physician and Advanced Practitioners Recruiting Incentives.
Gastroenterology, with an eighth-place finish in 2017-2018, also showed strong growth by increasing 55% from the year before and rising 137% over the past 3 years. The rise of gastroenterology and radiology over the past 2 years came at the expense of pediatrics, which went from 10th in 2015-2016 to 13th this year, and neurology, which dropped from 7th to 15th, Merritt Hawkins wrote in the report, which was based on a total of 3,045 search assignments conducted in 2017-2018.
“While demand for primary care physicians remains robust, hospitals, medical groups, and other health care facilities are shifting their recruiting efforts to medical specialists,” the company wrote, noting that recruiting assignments for medical specialists have risen from 67% of all searches 3 years ago to 74% in the past year.
“It’s a matter of demographic destiny,” Travis Singleton, senior vice president of Merritt Hawkins, said in a written statement accompanying the report. “Americans are getting older, and it is medical specialists who will be taking care of our aging and ailing bodies and brains. We still need more primary care doctors, but a growing emphasis is being placed on recruiting specialists.”
according to physician recruitment firm Merritt Hawkins.
The company conducted 497 searches for family physicians from April 1, 2017, to March 31, 2018, marking the third straight year of decline for the specialty but still more than double the 243 searches conducted for psychiatrists, the medical specialty that was second more frequently requested for recruitment, Merritt Hawkins wrote in its 2018 Survey of Physician and Advanced Practitioners Recruiting Incentives.
Gastroenterology, with an eighth-place finish in 2017-2018, also showed strong growth by increasing 55% from the year before and rising 137% over the past 3 years. The rise of gastroenterology and radiology over the past 2 years came at the expense of pediatrics, which went from 10th in 2015-2016 to 13th this year, and neurology, which dropped from 7th to 15th, Merritt Hawkins wrote in the report, which was based on a total of 3,045 search assignments conducted in 2017-2018.
“While demand for primary care physicians remains robust, hospitals, medical groups, and other health care facilities are shifting their recruiting efforts to medical specialists,” the company wrote, noting that recruiting assignments for medical specialists have risen from 67% of all searches 3 years ago to 74% in the past year.
“It’s a matter of demographic destiny,” Travis Singleton, senior vice president of Merritt Hawkins, said in a written statement accompanying the report. “Americans are getting older, and it is medical specialists who will be taking care of our aging and ailing bodies and brains. We still need more primary care doctors, but a growing emphasis is being placed on recruiting specialists.”
Benefits of nicotine preloading undercut by reduced varenicline usage
Nicotine preloading with patches 4 weeks before making a quit attempt was not significantly associated with according to Paul Aveyard, PhD, and his associates at Nuffield Department of Primary Care Health Sciences, University of Oxford (England).
The primary study outcome, biochemically validated abstinence at 6 months, was achieved by 17.5% of the 899 people who preloaded with a 21-mg/24-hr nicotine patch for 4 weeks and by 14.4% of the 893 in the control group. After 1 year, 14.0% of people in the preloading group maintained long-term abstinence, compared with 11.3% in the control group. In addition, 35.5% of the preloading group and 32.3% of the control group achieved abstinence 4 weeks from baseline.
The unadjusted odds ratio for the effect of preloading at 6 months was 1.25 (95% confidence interval, 0.97-1.62; P = .08) and not statistically significant. However, when reduced varenicline usage in the preloading group was taken into account, the effect of preloading did reach statistical significance (OR, 1.34; 95% CI, 1.03-1.73; P = .03). Similar results were found at 1 year and at 4 weeks, where the preloading effect did not reach significance until adjusted for varenicline usage.
“Nicotine preloading with a 21-mg/24-hr nicotine patch for 4 weeks seems to be efficacious, safe, and well tolerated, but probably deters the use of varenicline, the most effective smoking cessation drug. If it were possible to overcome this unintended consequence, preloading could lead to a worthwhile increase in long-term smoking abstinence,” the investigators concluded.
SOURCE: Aveyard P et al. BMJ. 2018 Jun 13. doi: 10.1136/bmj.k2164.
Nicotine preloading with patches 4 weeks before making a quit attempt was not significantly associated with according to Paul Aveyard, PhD, and his associates at Nuffield Department of Primary Care Health Sciences, University of Oxford (England).
The primary study outcome, biochemically validated abstinence at 6 months, was achieved by 17.5% of the 899 people who preloaded with a 21-mg/24-hr nicotine patch for 4 weeks and by 14.4% of the 893 in the control group. After 1 year, 14.0% of people in the preloading group maintained long-term abstinence, compared with 11.3% in the control group. In addition, 35.5% of the preloading group and 32.3% of the control group achieved abstinence 4 weeks from baseline.
The unadjusted odds ratio for the effect of preloading at 6 months was 1.25 (95% confidence interval, 0.97-1.62; P = .08) and not statistically significant. However, when reduced varenicline usage in the preloading group was taken into account, the effect of preloading did reach statistical significance (OR, 1.34; 95% CI, 1.03-1.73; P = .03). Similar results were found at 1 year and at 4 weeks, where the preloading effect did not reach significance until adjusted for varenicline usage.
“Nicotine preloading with a 21-mg/24-hr nicotine patch for 4 weeks seems to be efficacious, safe, and well tolerated, but probably deters the use of varenicline, the most effective smoking cessation drug. If it were possible to overcome this unintended consequence, preloading could lead to a worthwhile increase in long-term smoking abstinence,” the investigators concluded.
SOURCE: Aveyard P et al. BMJ. 2018 Jun 13. doi: 10.1136/bmj.k2164.
Nicotine preloading with patches 4 weeks before making a quit attempt was not significantly associated with according to Paul Aveyard, PhD, and his associates at Nuffield Department of Primary Care Health Sciences, University of Oxford (England).
The primary study outcome, biochemically validated abstinence at 6 months, was achieved by 17.5% of the 899 people who preloaded with a 21-mg/24-hr nicotine patch for 4 weeks and by 14.4% of the 893 in the control group. After 1 year, 14.0% of people in the preloading group maintained long-term abstinence, compared with 11.3% in the control group. In addition, 35.5% of the preloading group and 32.3% of the control group achieved abstinence 4 weeks from baseline.
The unadjusted odds ratio for the effect of preloading at 6 months was 1.25 (95% confidence interval, 0.97-1.62; P = .08) and not statistically significant. However, when reduced varenicline usage in the preloading group was taken into account, the effect of preloading did reach statistical significance (OR, 1.34; 95% CI, 1.03-1.73; P = .03). Similar results were found at 1 year and at 4 weeks, where the preloading effect did not reach significance until adjusted for varenicline usage.
“Nicotine preloading with a 21-mg/24-hr nicotine patch for 4 weeks seems to be efficacious, safe, and well tolerated, but probably deters the use of varenicline, the most effective smoking cessation drug. If it were possible to overcome this unintended consequence, preloading could lead to a worthwhile increase in long-term smoking abstinence,” the investigators concluded.
SOURCE: Aveyard P et al. BMJ. 2018 Jun 13. doi: 10.1136/bmj.k2164.
FROM THE BMJ
Bisphosphonate ‘holidays’ exceeding 2 years linked to increased fractures
AMSTERDAM – Older women on bisphosphonate treatment for at least 3 years who then stopped taking the drug showed a 40% increased risk for hip fracture after they were off the bisphosphonate for more than 2 years, compared with women who never stopped using the drug, according to an analysis of more than 150,000 women in a Medicare database.
The implication of this observational-data finding is that drug holidays from a bisphosphonate regimen “may not be appropriate for all patients,” Kenneth G. Saag, MD, said at the European Congress of Rheumatology.
The finding seems to dispute a recent recommendation from the American College of Physicians (Ann Intern Med. 2017 June 6;166[11]:818-39) that drug treatment to prevent bone fractures in osteoporotic women should stop after 5 years, noted Dr. Saag, a rheumatologist and professor of medicine at the University of Alabama, Birmingham. The median duration of bisphosphonate treatment in the studied cohort before the drug use stopped was 5.5 years.
“Drug holidays [from a bisphosphonate] have become increasingly common” because of concerns about potential adverse effects from prolonged, continuous bisphosphonate treatment, especially the risk for osteonecrosis of the jaw and atypical femoral fractures, he said. These bisphosphonate stoppages are sometimes permanent and sometimes temporary, Dr. Saag noted. Ideally, assessment of the risks and benefits from a bisphosphonate drug holiday should occur in a randomized study, but in current U.S. practice such a trial would be “impossible because there is not equipoise around the decision of whether or not to stop,” he said.

To try to gain insight into the impact of halting bisphosphonate treatment with observational data, Dr. Saag and his associates used records collected by Medicare on 153,236 women who started a new course of bisphosphonate treatment and remained on it for at least 3 years during 2006 to 2014. When selecting these women, the researchers also focused on those with at least 80% adherence to their bisphosphonate regimen, based on prescription coverage data. The analysis censored women who also received other treatments that can affect bone density, such as estrogen or denosumab (Prolia, Xgeva). The average age of the women was 79 years; two-thirds were aged 75 years or older. The median duration of follow-up information after bisphosphonate stoppage was 2.1 years. Forty percent of the women stopped their bisphosphonate treatment for at least 6 months, and 13% of the women who stopped treatment subsequently restarted a bisphosphonate drug. The most commonly used bisphosphonate was alendronate (Fosamax, Binosto), used by 72%, followed by zoledronic acid (Reclast, Zometa), used by 16%.
The analysis divided women who stopped their bisphosphonate treatment into subgroups based on the duration of stoppage, and showed that the rate of hip fracture was 40% higher among women who stopped treatment for more than 2 years but not more than 3 years, compared with the women who never interrupted their bisphosphonate treatment, a statistically significant difference, Dr. Saag said. In contrast, among women who halted bisphosphonate treatment for more than 1 year but not more than 2 years, the hip fracture risk was 20% higher than that of nonstoppers, also a statistically significant difference. These and all the other analyses the researchers ran adjusted for the possible impact from baseline differences in several demographic and clinical variables.
Dr. Saag cautioned that while the relatively increased risk for hip fracture from a prolonged halt to bisphosphonate treatment was 40%, the absolute increase in risk was “relatively modest,” representing an increased fracture rate of 0.5-1 additional fractures during every 100 patient years of follow-up.
For the endpoint of major osteoporotic fracture at any location, the risk was 10% higher among women who stopped treatment for more than 2 years but not for longer than 3 years, compared with nonstoppers.
The researchers also focused on two key subgroups. Among women who only took alendronate, a drug holiday of more than 2 years was linked with a statistically significant 20% rise in hip fractures, compared with women who never stopped the drug. And among the 4% of studied women who had a history of a bone fracture because of bone fragility, stoppage of their bisphosphonate treatment for more than 2 years doubled their hip fracture rate, compared with similar women who did not stop their treatment.
The study received no commercial funding. Dr. Saag has been a consultant to and has received research funding from Amgen, Lilly, and Radius.
SOURCE: Curtis J et al. EULAR 2018 Congress, abstract OP0017.
AMSTERDAM – Older women on bisphosphonate treatment for at least 3 years who then stopped taking the drug showed a 40% increased risk for hip fracture after they were off the bisphosphonate for more than 2 years, compared with women who never stopped using the drug, according to an analysis of more than 150,000 women in a Medicare database.
The implication of this observational-data finding is that drug holidays from a bisphosphonate regimen “may not be appropriate for all patients,” Kenneth G. Saag, MD, said at the European Congress of Rheumatology.
The finding seems to dispute a recent recommendation from the American College of Physicians (Ann Intern Med. 2017 June 6;166[11]:818-39) that drug treatment to prevent bone fractures in osteoporotic women should stop after 5 years, noted Dr. Saag, a rheumatologist and professor of medicine at the University of Alabama, Birmingham. The median duration of bisphosphonate treatment in the studied cohort before the drug use stopped was 5.5 years.
“Drug holidays [from a bisphosphonate] have become increasingly common” because of concerns about potential adverse effects from prolonged, continuous bisphosphonate treatment, especially the risk for osteonecrosis of the jaw and atypical femoral fractures, he said. These bisphosphonate stoppages are sometimes permanent and sometimes temporary, Dr. Saag noted. Ideally, assessment of the risks and benefits from a bisphosphonate drug holiday should occur in a randomized study, but in current U.S. practice such a trial would be “impossible because there is not equipoise around the decision of whether or not to stop,” he said.
To try to gain insight into the impact of halting bisphosphonate treatment with observational data, Dr. Saag and his associates used records collected by Medicare on 153,236 women who started a new course of bisphosphonate treatment and remained on it for at least 3 years during 2006 to 2014. When selecting these women, the researchers also focused on those with at least 80% adherence to their bisphosphonate regimen, based on prescription coverage data. The analysis censored women who also received other treatments that can affect bone density, such as estrogen or denosumab (Prolia, Xgeva). The average age of the women was 79 years; two-thirds were aged 75 years or older. The median duration of follow-up information after bisphosphonate stoppage was 2.1 years. Forty percent of the women stopped their bisphosphonate treatment for at least 6 months, and 13% of the women who stopped treatment subsequently restarted a bisphosphonate drug. The most commonly used bisphosphonate was alendronate (Fosamax, Binosto), used by 72%, followed by zoledronic acid (Reclast, Zometa), used by 16%.
The analysis divided women who stopped their bisphosphonate treatment into subgroups based on the duration of stoppage, and showed that the rate of hip fracture was 40% higher among women who stopped treatment for more than 2 years but not more than 3 years, compared with the women who never interrupted their bisphosphonate treatment, a statistically significant difference, Dr. Saag said. In contrast, among women who halted bisphosphonate treatment for more than 1 year but not more than 2 years, the hip fracture risk was 20% higher than that of nonstoppers, also a statistically significant difference. These and all the other analyses the researchers ran adjusted for the possible impact from baseline differences in several demographic and clinical variables.
Dr. Saag cautioned that while the relatively increased risk for hip fracture from a prolonged halt to bisphosphonate treatment was 40%, the absolute increase in risk was “relatively modest,” representing an increased fracture rate of 0.5-1 additional fractures during every 100 patient years of follow-up.
For the endpoint of major osteoporotic fracture at any location, the risk was 10% higher among women who stopped treatment for more than 2 years but not for longer than 3 years, compared with nonstoppers.
The researchers also focused on two key subgroups. Among women who only took alendronate, a drug holiday of more than 2 years was linked with a statistically significant 20% rise in hip fractures, compared with women who never stopped the drug. And among the 4% of studied women who had a history of a bone fracture because of bone fragility, stoppage of their bisphosphonate treatment for more than 2 years doubled their hip fracture rate, compared with similar women who did not stop their treatment.
The study received no commercial funding. Dr. Saag has been a consultant to and has received research funding from Amgen, Lilly, and Radius.
SOURCE: Curtis J et al. EULAR 2018 Congress, abstract OP0017.
AMSTERDAM – Older women on bisphosphonate treatment for at least 3 years who then stopped taking the drug showed a 40% increased risk for hip fracture after they were off the bisphosphonate for more than 2 years, compared with women who never stopped using the drug, according to an analysis of more than 150,000 women in a Medicare database.
The implication of this observational-data finding is that drug holidays from a bisphosphonate regimen “may not be appropriate for all patients,” Kenneth G. Saag, MD, said at the European Congress of Rheumatology.
The finding seems to dispute a recent recommendation from the American College of Physicians (Ann Intern Med. 2017 June 6;166[11]:818-39) that drug treatment to prevent bone fractures in osteoporotic women should stop after 5 years, noted Dr. Saag, a rheumatologist and professor of medicine at the University of Alabama, Birmingham. The median duration of bisphosphonate treatment in the studied cohort before the drug use stopped was 5.5 years.
“Drug holidays [from a bisphosphonate] have become increasingly common” because of concerns about potential adverse effects from prolonged, continuous bisphosphonate treatment, especially the risk for osteonecrosis of the jaw and atypical femoral fractures, he said. These bisphosphonate stoppages are sometimes permanent and sometimes temporary, Dr. Saag noted. Ideally, assessment of the risks and benefits from a bisphosphonate drug holiday should occur in a randomized study, but in current U.S. practice such a trial would be “impossible because there is not equipoise around the decision of whether or not to stop,” he said.
To try to gain insight into the impact of halting bisphosphonate treatment with observational data, Dr. Saag and his associates used records collected by Medicare on 153,236 women who started a new course of bisphosphonate treatment and remained on it for at least 3 years during 2006 to 2014. When selecting these women, the researchers also focused on those with at least 80% adherence to their bisphosphonate regimen, based on prescription coverage data. The analysis censored women who also received other treatments that can affect bone density, such as estrogen or denosumab (Prolia, Xgeva). The average age of the women was 79 years; two-thirds were aged 75 years or older. The median duration of follow-up information after bisphosphonate stoppage was 2.1 years. Forty percent of the women stopped their bisphosphonate treatment for at least 6 months, and 13% of the women who stopped treatment subsequently restarted a bisphosphonate drug. The most commonly used bisphosphonate was alendronate (Fosamax, Binosto), used by 72%, followed by zoledronic acid (Reclast, Zometa), used by 16%.
The analysis divided women who stopped their bisphosphonate treatment into subgroups based on the duration of stoppage, and showed that the rate of hip fracture was 40% higher among women who stopped treatment for more than 2 years but not more than 3 years, compared with the women who never interrupted their bisphosphonate treatment, a statistically significant difference, Dr. Saag said. In contrast, among women who halted bisphosphonate treatment for more than 1 year but not more than 2 years, the hip fracture risk was 20% higher than that of nonstoppers, also a statistically significant difference. These and all the other analyses the researchers ran adjusted for the possible impact from baseline differences in several demographic and clinical variables.
Dr. Saag cautioned that while the relatively increased risk for hip fracture from a prolonged halt to bisphosphonate treatment was 40%, the absolute increase in risk was “relatively modest,” representing an increased fracture rate of 0.5-1 additional fractures during every 100 patient years of follow-up.
For the endpoint of major osteoporotic fracture at any location, the risk was 10% higher among women who stopped treatment for more than 2 years but not for longer than 3 years, compared with nonstoppers.
The researchers also focused on two key subgroups. Among women who only took alendronate, a drug holiday of more than 2 years was linked with a statistically significant 20% rise in hip fractures, compared with women who never stopped the drug. And among the 4% of studied women who had a history of a bone fracture because of bone fragility, stoppage of their bisphosphonate treatment for more than 2 years doubled their hip fracture rate, compared with similar women who did not stop their treatment.
The study received no commercial funding. Dr. Saag has been a consultant to and has received research funding from Amgen, Lilly, and Radius.
SOURCE: Curtis J et al. EULAR 2018 Congress, abstract OP0017.
REPORTING FROM THE EULAR 2018 CONGRESS
Key clinical point: Stopping a bisphosphonate for more than 2 years boosts hip fracture risk.
Major finding: Women stopping bisphosphonate use for more than 2 years had a 40% higher rate of hip fractures compared with women who didn’t stop the drug.
Study details: Review of data collected by Medicare for 153,236 women treated with a bisphosphonate drug.
Disclosures: The study received no commercial funding. Dr. Saag has been a consultant to and has received research funding from Amgen, Lilly, and Radius.
Source: Curtis J et al. EULAR 2018 Congress, abstract OP0017.
FDA approves bevacizumab for advanced ovarian cancer
The Food and Drug Administration has approved bevacizumab (Avastin) for treating stage III or IV ovarian, fallopian tube, or primary peritoneal cancer following initial surgical resection, first in combination with chemotherapy (carboplatin and paclitaxel), then as monotherapy.
The approval was based on an improvement in progression-free survival (PFS) in the phase 3, three-arm GOG-0218 trial, evaluating the addition of bevacizumab to carboplatin and paclitaxel for patients with stage III or IV epithelial ovarian, fallopian tube, or primary peritoneal cancer following initial surgical resection, the FDA said in a press statement.
The most serious adverse events of bevacizumab included gastrointestinal perforation, wounds that don’t heal, and serious bleeding. Other possible adverse events included kidney problems, fistula, severe high blood pressure, severe stroke or heart problems, and problems of the nervous system and vision. Less serious events included headache, nosebleeds, rectal bleeding, and dry skin.
The recommended bevacizumab dose for stage III or IV epithelial ovarian, fallopian tube, or primary peritoneal cancer following initial surgical resection is 15 mg/kg every 3 weeks with carboplatin and paclitaxel for up to 6 cycles, followed by 15 mg/kg every 3 weeks as a single agent, for a total of up to 22 cycles, the FDA said.
The Food and Drug Administration has approved bevacizumab (Avastin) for treating stage III or IV ovarian, fallopian tube, or primary peritoneal cancer following initial surgical resection, first in combination with chemotherapy (carboplatin and paclitaxel), then as monotherapy.
The approval was based on an improvement in progression-free survival (PFS) in the phase 3, three-arm GOG-0218 trial, evaluating the addition of bevacizumab to carboplatin and paclitaxel for patients with stage III or IV epithelial ovarian, fallopian tube, or primary peritoneal cancer following initial surgical resection, the FDA said in a press statement.
The most serious adverse events of bevacizumab included gastrointestinal perforation, wounds that don’t heal, and serious bleeding. Other possible adverse events included kidney problems, fistula, severe high blood pressure, severe stroke or heart problems, and problems of the nervous system and vision. Less serious events included headache, nosebleeds, rectal bleeding, and dry skin.
The recommended bevacizumab dose for stage III or IV epithelial ovarian, fallopian tube, or primary peritoneal cancer following initial surgical resection is 15 mg/kg every 3 weeks with carboplatin and paclitaxel for up to 6 cycles, followed by 15 mg/kg every 3 weeks as a single agent, for a total of up to 22 cycles, the FDA said.
The Food and Drug Administration has approved bevacizumab (Avastin) for treating stage III or IV ovarian, fallopian tube, or primary peritoneal cancer following initial surgical resection, first in combination with chemotherapy (carboplatin and paclitaxel), then as monotherapy.
The approval was based on an improvement in progression-free survival (PFS) in the phase 3, three-arm GOG-0218 trial, evaluating the addition of bevacizumab to carboplatin and paclitaxel for patients with stage III or IV epithelial ovarian, fallopian tube, or primary peritoneal cancer following initial surgical resection, the FDA said in a press statement.
The most serious adverse events of bevacizumab included gastrointestinal perforation, wounds that don’t heal, and serious bleeding. Other possible adverse events included kidney problems, fistula, severe high blood pressure, severe stroke or heart problems, and problems of the nervous system and vision. Less serious events included headache, nosebleeds, rectal bleeding, and dry skin.
The recommended bevacizumab dose for stage III or IV epithelial ovarian, fallopian tube, or primary peritoneal cancer following initial surgical resection is 15 mg/kg every 3 weeks with carboplatin and paclitaxel for up to 6 cycles, followed by 15 mg/kg every 3 weeks as a single agent, for a total of up to 22 cycles, the FDA said.