User login
Sharpen your ax
Recently, I had a trauma call at my scenic little hospital in Maine. “Bleeding leg wound, Dr, Crosslin. We’ve got pressure on it. Come soon.” During my jog across the parking lot to the ER, I drifted into my residency mantra and started reciting the ABCs of trauma care:
Airway, Breathing, CT scan.
Airway, Breathing, C-spine collar.
Airway, Breathing, Consult with ortho.
Okay, so it’s been a while. Four years doesn’t seem like a long time, but that little span serves up a lot of change. You settle into a routine in your isolated, bucolic New England coastal town, where most trauma is related to hauling up lobster crates and having Massachusetts drivers scare the moxie out of locals in the crosswalks, and you forget about the hundreds of Level 1 traumas you managed over 5 years in Boston. The drilled-down, rapid sequence of the primary and secondary surveys gets lost, if just for a moment. Your confident swagger is replaced with a measured, humble shuffle into Trauma Bay 1. Do I scan the leg now? Did I feel for pulses in the foot? Wait, where do the major vessels branch again?

After addressing the issue at hand (or in this case, at foot), I kept thinking about the woodsman’s statement. I reflected on how I felt when I entered the trauma bay. Had I been doing enough to keep my own mental tools sharp? Well, actually, no. When did things slip just enough to allow hesitation and a bit of doubt to creep in? Probably sooner than I would care to admit. I certainly don’t think it took all of these 4 years for it to happen.
There has been some discussion of late surrounding the changes to maintenance of certification requirements from the American Board of Surgery. As with anything in surgery, we all need a chance to grumble about how things were better in the good old days. But then we grudgingly have to acknowledge that maybe – just maybe – the new approach makes some sense.
Did anyone really enjoy reporting on a 3-year cycle and taking a high-stakes, nausea-inducing exam every 10 years? I certainly wasn’t looking forward to reporting in this year about my “progress,” especially given how dull I seem to have become in so many subcategories just 4 years after graduation. But reporting every 5 years? That appeals to my inner slacker. Having a more-frequent-but-way-less-stressful examination that can be tailored to my practice? Yes, I’ll give that a shot.
It’s no secret we all are driven to care more about the things we enjoy doing, and educational science has established, quite firmly, the increased likelihood of concrete learning in higher numbers of loosely related fields when the primary subject is of particular interest to the learner. Elementary school teachers implemented that particular tidbit a long time ago. For me, the drive to excel leads me to the oncology, endocrine, and complex hernia reconstruction arenas. I do not pretend to be the world’s authority on trauma surgery, or anorectal surgery, or vascular surgery. I leave that expertise to others I secretly have judged to be far more pathological than myself. But I would be willing to glean more from reviewing those particular subjects if the overall focus is geared toward improving my knowledge and skill in cancer surgery.
In this ultramodern era, when the compendium of medical and surgical knowledge infinitely outpaces our ability to provide “one-stop shopping” services, perhaps it is time we accept the limitations of our interests and our abilities as part of the natural, beneficial evolution of good medical practice. The College’s willingness to work with the ABS to address the hot-button issue of continuing education in an interactive, relevant, timely manner should be a major point of pride. Rather than clinging to the dull ways of the past, I think we all are going to benefit from carrying a collectively sharper ax.
Dr. Crosslin is a general surgeon practicing in Rockport, Maine.
Recently, I had a trauma call at my scenic little hospital in Maine. “Bleeding leg wound, Dr, Crosslin. We’ve got pressure on it. Come soon.” During my jog across the parking lot to the ER, I drifted into my residency mantra and started reciting the ABCs of trauma care:
Airway, Breathing, CT scan.
Airway, Breathing, C-spine collar.
Airway, Breathing, Consult with ortho.
Okay, so it’s been a while. Four years doesn’t seem like a long time, but that little span serves up a lot of change. You settle into a routine in your isolated, bucolic New England coastal town, where most trauma is related to hauling up lobster crates and having Massachusetts drivers scare the moxie out of locals in the crosswalks, and you forget about the hundreds of Level 1 traumas you managed over 5 years in Boston. The drilled-down, rapid sequence of the primary and secondary surveys gets lost, if just for a moment. Your confident swagger is replaced with a measured, humble shuffle into Trauma Bay 1. Do I scan the leg now? Did I feel for pulses in the foot? Wait, where do the major vessels branch again?
After addressing the issue at hand (or in this case, at foot), I kept thinking about the woodsman’s statement. I reflected on how I felt when I entered the trauma bay. Had I been doing enough to keep my own mental tools sharp? Well, actually, no. When did things slip just enough to allow hesitation and a bit of doubt to creep in? Probably sooner than I would care to admit. I certainly don’t think it took all of these 4 years for it to happen.
There has been some discussion of late surrounding the changes to maintenance of certification requirements from the American Board of Surgery. As with anything in surgery, we all need a chance to grumble about how things were better in the good old days. But then we grudgingly have to acknowledge that maybe – just maybe – the new approach makes some sense.
Did anyone really enjoy reporting on a 3-year cycle and taking a high-stakes, nausea-inducing exam every 10 years? I certainly wasn’t looking forward to reporting in this year about my “progress,” especially given how dull I seem to have become in so many subcategories just 4 years after graduation. But reporting every 5 years? That appeals to my inner slacker. Having a more-frequent-but-way-less-stressful examination that can be tailored to my practice? Yes, I’ll give that a shot.
It’s no secret we all are driven to care more about the things we enjoy doing, and educational science has established, quite firmly, the increased likelihood of concrete learning in higher numbers of loosely related fields when the primary subject is of particular interest to the learner. Elementary school teachers implemented that particular tidbit a long time ago. For me, the drive to excel leads me to the oncology, endocrine, and complex hernia reconstruction arenas. I do not pretend to be the world’s authority on trauma surgery, or anorectal surgery, or vascular surgery. I leave that expertise to others I secretly have judged to be far more pathological than myself. But I would be willing to glean more from reviewing those particular subjects if the overall focus is geared toward improving my knowledge and skill in cancer surgery.
In this ultramodern era, when the compendium of medical and surgical knowledge infinitely outpaces our ability to provide “one-stop shopping” services, perhaps it is time we accept the limitations of our interests and our abilities as part of the natural, beneficial evolution of good medical practice. The College’s willingness to work with the ABS to address the hot-button issue of continuing education in an interactive, relevant, timely manner should be a major point of pride. Rather than clinging to the dull ways of the past, I think we all are going to benefit from carrying a collectively sharper ax.
Dr. Crosslin is a general surgeon practicing in Rockport, Maine.
Recently, I had a trauma call at my scenic little hospital in Maine. “Bleeding leg wound, Dr, Crosslin. We’ve got pressure on it. Come soon.” During my jog across the parking lot to the ER, I drifted into my residency mantra and started reciting the ABCs of trauma care:
Airway, Breathing, CT scan.
Airway, Breathing, C-spine collar.
Airway, Breathing, Consult with ortho.
Okay, so it’s been a while. Four years doesn’t seem like a long time, but that little span serves up a lot of change. You settle into a routine in your isolated, bucolic New England coastal town, where most trauma is related to hauling up lobster crates and having Massachusetts drivers scare the moxie out of locals in the crosswalks, and you forget about the hundreds of Level 1 traumas you managed over 5 years in Boston. The drilled-down, rapid sequence of the primary and secondary surveys gets lost, if just for a moment. Your confident swagger is replaced with a measured, humble shuffle into Trauma Bay 1. Do I scan the leg now? Did I feel for pulses in the foot? Wait, where do the major vessels branch again?
After addressing the issue at hand (or in this case, at foot), I kept thinking about the woodsman’s statement. I reflected on how I felt when I entered the trauma bay. Had I been doing enough to keep my own mental tools sharp? Well, actually, no. When did things slip just enough to allow hesitation and a bit of doubt to creep in? Probably sooner than I would care to admit. I certainly don’t think it took all of these 4 years for it to happen.
There has been some discussion of late surrounding the changes to maintenance of certification requirements from the American Board of Surgery. As with anything in surgery, we all need a chance to grumble about how things were better in the good old days. But then we grudgingly have to acknowledge that maybe – just maybe – the new approach makes some sense.
Did anyone really enjoy reporting on a 3-year cycle and taking a high-stakes, nausea-inducing exam every 10 years? I certainly wasn’t looking forward to reporting in this year about my “progress,” especially given how dull I seem to have become in so many subcategories just 4 years after graduation. But reporting every 5 years? That appeals to my inner slacker. Having a more-frequent-but-way-less-stressful examination that can be tailored to my practice? Yes, I’ll give that a shot.
It’s no secret we all are driven to care more about the things we enjoy doing, and educational science has established, quite firmly, the increased likelihood of concrete learning in higher numbers of loosely related fields when the primary subject is of particular interest to the learner. Elementary school teachers implemented that particular tidbit a long time ago. For me, the drive to excel leads me to the oncology, endocrine, and complex hernia reconstruction arenas. I do not pretend to be the world’s authority on trauma surgery, or anorectal surgery, or vascular surgery. I leave that expertise to others I secretly have judged to be far more pathological than myself. But I would be willing to glean more from reviewing those particular subjects if the overall focus is geared toward improving my knowledge and skill in cancer surgery.
In this ultramodern era, when the compendium of medical and surgical knowledge infinitely outpaces our ability to provide “one-stop shopping” services, perhaps it is time we accept the limitations of our interests and our abilities as part of the natural, beneficial evolution of good medical practice. The College’s willingness to work with the ABS to address the hot-button issue of continuing education in an interactive, relevant, timely manner should be a major point of pride. Rather than clinging to the dull ways of the past, I think we all are going to benefit from carrying a collectively sharper ax.
Dr. Crosslin is a general surgeon practicing in Rockport, Maine.
Study pinpoints skin cancer risk factors after hematopoietic cell transplant
CHICAGO – The 10-year incidence rates for both squamous cell carcinoma and basal cell carcinoma arising after hematopoietic cell transplantation are impressively high at 17%-plus for each, but the malignancies occur on two very different timelines, according to Jeffrey F. Scott, MD, a fellow in micrographic surgery and dermatologic oncology at Case Western Reserve University in Cleveland.
Most of the squamous cell carcinomas (SCCs) in a large multicenter retrospective study developed within the first 5 years following hematopoietic cell transplantation (HCT), while the majority of the basal cell carcinomas (BCCs) occurred after that point, Dr. Scott reported at the annual meeting of the American College of Mohs Surgery.
He presented the results of the study, which included 876 HCT recipients followed for a mean of 6.1 years. The study objective was to pin down the risk factors for skin cancer after HCT, especially the patient-specific ones. This has become a pressing issue because the use of HCT is steadily growing, and the 5-year survival rate now exceeds 50%.
The transplant-specific risk factors have previously been fairly well described by others. They include the donor source, type of disease, the conditioning regimen, whether whole body irradiation was used, immunosuppression, graft versus host disease (GVHD), and others.
The patient-centric risk factors, in contrast, have not been well characterized. And it’s critical to thoroughly understand these risk factors in order to develop targeted prevention and surveillance strategies, Dr. Scott said.
“There remains a significant knowledge gap within our field. I would venture that the majority of this audience has treated a patient with skin cancer who has had a transplant,” he said. “Yet when a patient asks us, ‘Doc, what is my risk for skin cancer after my HCT?’ we’re really unable to give them an accurate and complete assessment of that risk. That’s because we’re missing the second major category of risk factors: the patient-specific risk factors.”
The reason for that, he added, is that the major population-based studies and national HCT registries are run by hematologists and oncologists, and they haven’t adequately captured the patient-specific skin cancer risk factors. But these are variables very familiar to dermatologists. They include skin phenotype, history of UV radiation exposure, and history of pre-HCT skin cancer.
Dr. Scott said the multicenter study he presented has two major advantages over prior studies: its large size and thorough followup. Nearly all 876 patients were followed by both an oncologist and a dermatologist at the same institution.
During followup, the HCT recipients collectively developed 63 SCCs, 55 BCCs, and 16 malignant melanomas. The 5- and 10-year incidence rates for SCC were 10.6% and 17.2%. For BCC, the 5- and 10-year rates were 5.7% and 17.6%. All 16 cases of melanoma occurred within 5 years after HCT.
In multivariate Cox proportional hazard analyses, photodamage documented on examination was independently associated with a 3.2-fold increased risk of post-HCT SCC and a 3.5-fold increased risk of BCC.
A pre-transplant history of BCC was associated with a 3.9-fold increased likelihood of developing a BCC afterwards. Similarly, a pre-HCT history of SCC conferred a 4.2-fold increased risk of post-transplant SCC and was also independently associated with a 6.6-fold increased risk of developing melanoma post-HCT.
Fitzpatrick skin types I and II were respectively associated with 9.3- and 7.2-fold increased risks of post-HCT nonmelanoma skin cancer, compared with skin types III-VI.
Acute GVHD wasn’t associated with an increased risk of nonmelanoma skin cancer after HCT. However, in an observation that hasn’t previously been reported by others, chronic GVHD with skin involvement was associated with a 2.7-fold increased likelihood of SCC post-HCT, Dr. Scott noted.
What’s next for Dr. Scott and his coinvestigators? “Our ultimate goal with this project is to develop an interactive risk assessment tool like the National Cancer Institute’s Breast Cancer Risk Assessment Tool that can be online and used by patients and providers to estimate their individualized risk of basal cell carcinoma, squamous cell carcinoma, and melanoma after HCT,” he said.
Dr. Scott reported having no financial conflicts related to the study.
CHICAGO – The 10-year incidence rates for both squamous cell carcinoma and basal cell carcinoma arising after hematopoietic cell transplantation are impressively high at 17%-plus for each, but the malignancies occur on two very different timelines, according to Jeffrey F. Scott, MD, a fellow in micrographic surgery and dermatologic oncology at Case Western Reserve University in Cleveland.
Most of the squamous cell carcinomas (SCCs) in a large multicenter retrospective study developed within the first 5 years following hematopoietic cell transplantation (HCT), while the majority of the basal cell carcinomas (BCCs) occurred after that point, Dr. Scott reported at the annual meeting of the American College of Mohs Surgery.
He presented the results of the study, which included 876 HCT recipients followed for a mean of 6.1 years. The study objective was to pin down the risk factors for skin cancer after HCT, especially the patient-specific ones. This has become a pressing issue because the use of HCT is steadily growing, and the 5-year survival rate now exceeds 50%.
The transplant-specific risk factors have previously been fairly well described by others. They include the donor source, type of disease, the conditioning regimen, whether whole body irradiation was used, immunosuppression, graft versus host disease (GVHD), and others.
The patient-centric risk factors, in contrast, have not been well characterized. And it’s critical to thoroughly understand these risk factors in order to develop targeted prevention and surveillance strategies, Dr. Scott said.
“There remains a significant knowledge gap within our field. I would venture that the majority of this audience has treated a patient with skin cancer who has had a transplant,” he said. “Yet when a patient asks us, ‘Doc, what is my risk for skin cancer after my HCT?’ we’re really unable to give them an accurate and complete assessment of that risk. That’s because we’re missing the second major category of risk factors: the patient-specific risk factors.”
The reason for that, he added, is that the major population-based studies and national HCT registries are run by hematologists and oncologists, and they haven’t adequately captured the patient-specific skin cancer risk factors. But these are variables very familiar to dermatologists. They include skin phenotype, history of UV radiation exposure, and history of pre-HCT skin cancer.
Dr. Scott said the multicenter study he presented has two major advantages over prior studies: its large size and thorough followup. Nearly all 876 patients were followed by both an oncologist and a dermatologist at the same institution.
During followup, the HCT recipients collectively developed 63 SCCs, 55 BCCs, and 16 malignant melanomas. The 5- and 10-year incidence rates for SCC were 10.6% and 17.2%. For BCC, the 5- and 10-year rates were 5.7% and 17.6%. All 16 cases of melanoma occurred within 5 years after HCT.
In multivariate Cox proportional hazard analyses, photodamage documented on examination was independently associated with a 3.2-fold increased risk of post-HCT SCC and a 3.5-fold increased risk of BCC.
A pre-transplant history of BCC was associated with a 3.9-fold increased likelihood of developing a BCC afterwards. Similarly, a pre-HCT history of SCC conferred a 4.2-fold increased risk of post-transplant SCC and was also independently associated with a 6.6-fold increased risk of developing melanoma post-HCT.
Fitzpatrick skin types I and II were respectively associated with 9.3- and 7.2-fold increased risks of post-HCT nonmelanoma skin cancer, compared with skin types III-VI.
Acute GVHD wasn’t associated with an increased risk of nonmelanoma skin cancer after HCT. However, in an observation that hasn’t previously been reported by others, chronic GVHD with skin involvement was associated with a 2.7-fold increased likelihood of SCC post-HCT, Dr. Scott noted.
What’s next for Dr. Scott and his coinvestigators? “Our ultimate goal with this project is to develop an interactive risk assessment tool like the National Cancer Institute’s Breast Cancer Risk Assessment Tool that can be online and used by patients and providers to estimate their individualized risk of basal cell carcinoma, squamous cell carcinoma, and melanoma after HCT,” he said.
Dr. Scott reported having no financial conflicts related to the study.
CHICAGO – The 10-year incidence rates for both squamous cell carcinoma and basal cell carcinoma arising after hematopoietic cell transplantation are impressively high at 17%-plus for each, but the malignancies occur on two very different timelines, according to Jeffrey F. Scott, MD, a fellow in micrographic surgery and dermatologic oncology at Case Western Reserve University in Cleveland.
Most of the squamous cell carcinomas (SCCs) in a large multicenter retrospective study developed within the first 5 years following hematopoietic cell transplantation (HCT), while the majority of the basal cell carcinomas (BCCs) occurred after that point, Dr. Scott reported at the annual meeting of the American College of Mohs Surgery.
He presented the results of the study, which included 876 HCT recipients followed for a mean of 6.1 years. The study objective was to pin down the risk factors for skin cancer after HCT, especially the patient-specific ones. This has become a pressing issue because the use of HCT is steadily growing, and the 5-year survival rate now exceeds 50%.
The transplant-specific risk factors have previously been fairly well described by others. They include the donor source, type of disease, the conditioning regimen, whether whole body irradiation was used, immunosuppression, graft versus host disease (GVHD), and others.
The patient-centric risk factors, in contrast, have not been well characterized. And it’s critical to thoroughly understand these risk factors in order to develop targeted prevention and surveillance strategies, Dr. Scott said.
“There remains a significant knowledge gap within our field. I would venture that the majority of this audience has treated a patient with skin cancer who has had a transplant,” he said. “Yet when a patient asks us, ‘Doc, what is my risk for skin cancer after my HCT?’ we’re really unable to give them an accurate and complete assessment of that risk. That’s because we’re missing the second major category of risk factors: the patient-specific risk factors.”
The reason for that, he added, is that the major population-based studies and national HCT registries are run by hematologists and oncologists, and they haven’t adequately captured the patient-specific skin cancer risk factors. But these are variables very familiar to dermatologists. They include skin phenotype, history of UV radiation exposure, and history of pre-HCT skin cancer.
Dr. Scott said the multicenter study he presented has two major advantages over prior studies: its large size and thorough followup. Nearly all 876 patients were followed by both an oncologist and a dermatologist at the same institution.
During followup, the HCT recipients collectively developed 63 SCCs, 55 BCCs, and 16 malignant melanomas. The 5- and 10-year incidence rates for SCC were 10.6% and 17.2%. For BCC, the 5- and 10-year rates were 5.7% and 17.6%. All 16 cases of melanoma occurred within 5 years after HCT.
In multivariate Cox proportional hazard analyses, photodamage documented on examination was independently associated with a 3.2-fold increased risk of post-HCT SCC and a 3.5-fold increased risk of BCC.
A pre-transplant history of BCC was associated with a 3.9-fold increased likelihood of developing a BCC afterwards. Similarly, a pre-HCT history of SCC conferred a 4.2-fold increased risk of post-transplant SCC and was also independently associated with a 6.6-fold increased risk of developing melanoma post-HCT.
Fitzpatrick skin types I and II were respectively associated with 9.3- and 7.2-fold increased risks of post-HCT nonmelanoma skin cancer, compared with skin types III-VI.
Acute GVHD wasn’t associated with an increased risk of nonmelanoma skin cancer after HCT. However, in an observation that hasn’t previously been reported by others, chronic GVHD with skin involvement was associated with a 2.7-fold increased likelihood of SCC post-HCT, Dr. Scott noted.
What’s next for Dr. Scott and his coinvestigators? “Our ultimate goal with this project is to develop an interactive risk assessment tool like the National Cancer Institute’s Breast Cancer Risk Assessment Tool that can be online and used by patients and providers to estimate their individualized risk of basal cell carcinoma, squamous cell carcinoma, and melanoma after HCT,” he said.
Dr. Scott reported having no financial conflicts related to the study.
REPORTING FROM THE ACMS ANNUAL MEETING
Key clinical point:
Major finding: Photodamage documented on examination more than triples the risk of developing nonmelanoma skin cancer after hematopoietic cell transplantation.
Study details: A multicenter retrospective study of 876 hematopoietic cell recipients followed for a mean of 6.1 years.
Disclosures: The presenter reported having no financial conflicts related to the study, which was conducted without commercial support.
FDA already balances safety, access to investigational drugs
The Food and Drug Administration is generally achieving the balance between ensuring safety and providing access to investigational drugs through compassionate use programs, according to results from a new analysis that found that most of these drugs are available within 6 months of an application to the FDA.
But that balance may be threatened by the recently enacted Right to Try Act, Jeremy Puthumana, of Yale University, New Haven, Conn., and his colleagues reported in an article published on JAMA Network Open. They said the new law encourages sponsors to make investigational drugs available earlier in the clinical development period, potentially jeopardizing safety.
“These findings suggest the FDA and the pharmaceutical industry have established a balance between investigational new drug access and protection of patients from therapies without established safety, which may be compromised by policy makers seeking to speed access to investigational medicines through the Right to Try Act by removing the requirements for FDA oversight and approval of expanded access requests,” the researchers wrote.
The cross-sectional study examined all expanded access programs registered with ClinicalTrials.gov through Aug. 1, 2017. Of 92 expanded access programs for investigational drugs, 69.6% were initiated within 6 months following (43.5%) or preceding (26.1%) submission of a new drug application. Ninety of the 92 drugs ultimately went on to receive FDA approval.
Of the most common uses of the 92 drugs registered in expanded access programs between September 1996 and June 2017, half were used for the treatment of cancer; 16 drugs were used to treat metabolic, endocrine, and genetic diseases; and 14 drugs were used for the treatment of infectious diseases. But there were no significant differences in the timing of program initiation by therapeutic characteristics, the researchers found.
President Donald Trump signed the Right To Try Act of 2017 (S. 204) into law on May 30, 2018, despite opposition from physician and patient groups who expressed concerns that the law will remove FDA safeguards.
The study was funded by a grant from the National Institutes of Health. The researchers reported research support from the Laura and John Arnold Foundation, Johnson and Johnson, Medtronic, the Blue Cross-Blue Shield Association, the FDA, and other federal agencies.
SOURCE: Puthumana J et al. JAMA Network Open. 2018 Jun 15. doi:10.1001/jamanetworkopen.2018.0283.
The Food and Drug Administration is generally achieving the balance between ensuring safety and providing access to investigational drugs through compassionate use programs, according to results from a new analysis that found that most of these drugs are available within 6 months of an application to the FDA.
But that balance may be threatened by the recently enacted Right to Try Act, Jeremy Puthumana, of Yale University, New Haven, Conn., and his colleagues reported in an article published on JAMA Network Open. They said the new law encourages sponsors to make investigational drugs available earlier in the clinical development period, potentially jeopardizing safety.
“These findings suggest the FDA and the pharmaceutical industry have established a balance between investigational new drug access and protection of patients from therapies without established safety, which may be compromised by policy makers seeking to speed access to investigational medicines through the Right to Try Act by removing the requirements for FDA oversight and approval of expanded access requests,” the researchers wrote.
The cross-sectional study examined all expanded access programs registered with ClinicalTrials.gov through Aug. 1, 2017. Of 92 expanded access programs for investigational drugs, 69.6% were initiated within 6 months following (43.5%) or preceding (26.1%) submission of a new drug application. Ninety of the 92 drugs ultimately went on to receive FDA approval.
Of the most common uses of the 92 drugs registered in expanded access programs between September 1996 and June 2017, half were used for the treatment of cancer; 16 drugs were used to treat metabolic, endocrine, and genetic diseases; and 14 drugs were used for the treatment of infectious diseases. But there were no significant differences in the timing of program initiation by therapeutic characteristics, the researchers found.
President Donald Trump signed the Right To Try Act of 2017 (S. 204) into law on May 30, 2018, despite opposition from physician and patient groups who expressed concerns that the law will remove FDA safeguards.
The study was funded by a grant from the National Institutes of Health. The researchers reported research support from the Laura and John Arnold Foundation, Johnson and Johnson, Medtronic, the Blue Cross-Blue Shield Association, the FDA, and other federal agencies.
SOURCE: Puthumana J et al. JAMA Network Open. 2018 Jun 15. doi:10.1001/jamanetworkopen.2018.0283.
The Food and Drug Administration is generally achieving the balance between ensuring safety and providing access to investigational drugs through compassionate use programs, according to results from a new analysis that found that most of these drugs are available within 6 months of an application to the FDA.
But that balance may be threatened by the recently enacted Right to Try Act, Jeremy Puthumana, of Yale University, New Haven, Conn., and his colleagues reported in an article published on JAMA Network Open. They said the new law encourages sponsors to make investigational drugs available earlier in the clinical development period, potentially jeopardizing safety.
“These findings suggest the FDA and the pharmaceutical industry have established a balance between investigational new drug access and protection of patients from therapies without established safety, which may be compromised by policy makers seeking to speed access to investigational medicines through the Right to Try Act by removing the requirements for FDA oversight and approval of expanded access requests,” the researchers wrote.
The cross-sectional study examined all expanded access programs registered with ClinicalTrials.gov through Aug. 1, 2017. Of 92 expanded access programs for investigational drugs, 69.6% were initiated within 6 months following (43.5%) or preceding (26.1%) submission of a new drug application. Ninety of the 92 drugs ultimately went on to receive FDA approval.
Of the most common uses of the 92 drugs registered in expanded access programs between September 1996 and June 2017, half were used for the treatment of cancer; 16 drugs were used to treat metabolic, endocrine, and genetic diseases; and 14 drugs were used for the treatment of infectious diseases. But there were no significant differences in the timing of program initiation by therapeutic characteristics, the researchers found.
President Donald Trump signed the Right To Try Act of 2017 (S. 204) into law on May 30, 2018, despite opposition from physician and patient groups who expressed concerns that the law will remove FDA safeguards.
The study was funded by a grant from the National Institutes of Health. The researchers reported research support from the Laura and John Arnold Foundation, Johnson and Johnson, Medtronic, the Blue Cross-Blue Shield Association, the FDA, and other federal agencies.
SOURCE: Puthumana J et al. JAMA Network Open. 2018 Jun 15. doi:10.1001/jamanetworkopen.2018.0283.
FROM JAMA NETWORK OPEN
Key clinical point: Major finding: Nearly 70% of investigational drugs registered in expanded access programs were made available outside of clinical trials within 6 months of submission of a new drug application.
Study details: A cross-sectional study examining expanded access and compassionate use programs registered through Aug. 1, 2017.
Disclosures: The study was funded by grant from the National Institutes of Health. The researchers reported research support from the Laura and John Arnold Foundation, Johnson and Johnson, Medtronic, the Blue Cross-Blue Shield Association, the FDA and other federal agencies.
Source: Puthumana J et al., JAMA Network Open. 2018 Jun 15. doi:10.1001/jamanetworkopen.2018.0283.
Low vitamin D linked with DVT in lupus patients
AMSTERDAM – Low blood levels of vitamin D were linked with a roughly doubled risk for deep vein thrombosis in a review of nearly 1,400 patients with systemic lupus erythematosus at one U.S. center.
Based on these findings, patients with systemic lupus erythematosus (SLE) should have their blood vitamin D monitored regularly, and if it’s less than 40 ng/mL – the level that was linked with this thrombotic risk – they should receive a vitamin D supplement, Michelle A. Petri, MD, said while presenting a poster at the European Congress of Rheumatology.
She recommended supplementation that provides 50,000 IU of vitamin D weekly, a treatment that appears safe to add to two other routine treatments she recommends for SLE patients – aspirin and hydroxychloroquine.
SLE patients should also have their vitamin D level rechecked on a regular basis, perhaps annually, to confirm that their level remains above 40 ng/mL, said Dr. Petri, professor of medicine and director of the Lupus Center at Johns Hopkins Medicine in Baltimore. She acknowledged that this level is above the target level often applied to the general population, but remains safe.
“It looks like vitamin D may be a useful treatment to add to aspirin and hydroxychloroquine in patients with SLE. It looks very simple and important, but this finding should be repeated and validated by other groups,” commented John D. Isaacs, MD, professor of clinical rheumatology at Newcastle University in Newcastle upon Tyne, England.
Dr. Petri and her associates reviewed records for 1,392 SLE patients enrolled in a Johns Hopkins registry. The patients averaged about 43 years old, 92% were women, and 27% had a history of a thrombotic event, either prior to or after their enrollment. The most common thrombotic event was deep vein thrombosis (DVT), in 14%, and also included stroke in 7%, myocardial infarction in 4%, and a smaller number with other types of arterial or venous thromboses. All these patients also had their blood vitamin D level checked at least once, at the time of enrollment, and 77% had a level below 40 ng/mL.
The first analysis looked at the link between any thrombotic event and vitamin D levels, and included adjustment for age, race, sex, and level of lupus anticoagulant. This showed a statistically significant 2.3-fold increased risk for DVT among patients with a vitamin D level of less than 40 ng/mL, compared with those with a higher level. The researchers did not find a significant association between low vitamin D levels and the rates of total thrombotic events or any arterial thrombotic event.
A second analysis censored out thrombotic events that occurred prior to enrollment and focused on incident thromboses after enrollment into the registry. This analysis showed a statistically significant 75% increased rate of new onset DVT episodes among patients with low vitamin D at entry after adjustment for age, race, and sex. The researchers found no significant associations between low vitamin D and the incidence of any other type of incident thrombosis.
Dr. Petri and Dr. Isaacs reported having no relevant financial disclosures.
SOURCE: Petri MA et al. Ann Rheum Dis. 2018;77(Suppl 2):388, Abstract THU0341.
AMSTERDAM – Low blood levels of vitamin D were linked with a roughly doubled risk for deep vein thrombosis in a review of nearly 1,400 patients with systemic lupus erythematosus at one U.S. center.
Based on these findings, patients with systemic lupus erythematosus (SLE) should have their blood vitamin D monitored regularly, and if it’s less than 40 ng/mL – the level that was linked with this thrombotic risk – they should receive a vitamin D supplement, Michelle A. Petri, MD, said while presenting a poster at the European Congress of Rheumatology.
She recommended supplementation that provides 50,000 IU of vitamin D weekly, a treatment that appears safe to add to two other routine treatments she recommends for SLE patients – aspirin and hydroxychloroquine.
SLE patients should also have their vitamin D level rechecked on a regular basis, perhaps annually, to confirm that their level remains above 40 ng/mL, said Dr. Petri, professor of medicine and director of the Lupus Center at Johns Hopkins Medicine in Baltimore. She acknowledged that this level is above the target level often applied to the general population, but remains safe.
“It looks like vitamin D may be a useful treatment to add to aspirin and hydroxychloroquine in patients with SLE. It looks very simple and important, but this finding should be repeated and validated by other groups,” commented John D. Isaacs, MD, professor of clinical rheumatology at Newcastle University in Newcastle upon Tyne, England.
Dr. Petri and her associates reviewed records for 1,392 SLE patients enrolled in a Johns Hopkins registry. The patients averaged about 43 years old, 92% were women, and 27% had a history of a thrombotic event, either prior to or after their enrollment. The most common thrombotic event was deep vein thrombosis (DVT), in 14%, and also included stroke in 7%, myocardial infarction in 4%, and a smaller number with other types of arterial or venous thromboses. All these patients also had their blood vitamin D level checked at least once, at the time of enrollment, and 77% had a level below 40 ng/mL.
The first analysis looked at the link between any thrombotic event and vitamin D levels, and included adjustment for age, race, sex, and level of lupus anticoagulant. This showed a statistically significant 2.3-fold increased risk for DVT among patients with a vitamin D level of less than 40 ng/mL, compared with those with a higher level. The researchers did not find a significant association between low vitamin D levels and the rates of total thrombotic events or any arterial thrombotic event.
A second analysis censored out thrombotic events that occurred prior to enrollment and focused on incident thromboses after enrollment into the registry. This analysis showed a statistically significant 75% increased rate of new onset DVT episodes among patients with low vitamin D at entry after adjustment for age, race, and sex. The researchers found no significant associations between low vitamin D and the incidence of any other type of incident thrombosis.
Dr. Petri and Dr. Isaacs reported having no relevant financial disclosures.
SOURCE: Petri MA et al. Ann Rheum Dis. 2018;77(Suppl 2):388, Abstract THU0341.
AMSTERDAM – Low blood levels of vitamin D were linked with a roughly doubled risk for deep vein thrombosis in a review of nearly 1,400 patients with systemic lupus erythematosus at one U.S. center.
Based on these findings, patients with systemic lupus erythematosus (SLE) should have their blood vitamin D monitored regularly, and if it’s less than 40 ng/mL – the level that was linked with this thrombotic risk – they should receive a vitamin D supplement, Michelle A. Petri, MD, said while presenting a poster at the European Congress of Rheumatology.
She recommended supplementation that provides 50,000 IU of vitamin D weekly, a treatment that appears safe to add to two other routine treatments she recommends for SLE patients – aspirin and hydroxychloroquine.
SLE patients should also have their vitamin D level rechecked on a regular basis, perhaps annually, to confirm that their level remains above 40 ng/mL, said Dr. Petri, professor of medicine and director of the Lupus Center at Johns Hopkins Medicine in Baltimore. She acknowledged that this level is above the target level often applied to the general population, but remains safe.
“It looks like vitamin D may be a useful treatment to add to aspirin and hydroxychloroquine in patients with SLE. It looks very simple and important, but this finding should be repeated and validated by other groups,” commented John D. Isaacs, MD, professor of clinical rheumatology at Newcastle University in Newcastle upon Tyne, England.
Dr. Petri and her associates reviewed records for 1,392 SLE patients enrolled in a Johns Hopkins registry. The patients averaged about 43 years old, 92% were women, and 27% had a history of a thrombotic event, either prior to or after their enrollment. The most common thrombotic event was deep vein thrombosis (DVT), in 14%, and also included stroke in 7%, myocardial infarction in 4%, and a smaller number with other types of arterial or venous thromboses. All these patients also had their blood vitamin D level checked at least once, at the time of enrollment, and 77% had a level below 40 ng/mL.
The first analysis looked at the link between any thrombotic event and vitamin D levels, and included adjustment for age, race, sex, and level of lupus anticoagulant. This showed a statistically significant 2.3-fold increased risk for DVT among patients with a vitamin D level of less than 40 ng/mL, compared with those with a higher level. The researchers did not find a significant association between low vitamin D levels and the rates of total thrombotic events or any arterial thrombotic event.
A second analysis censored out thrombotic events that occurred prior to enrollment and focused on incident thromboses after enrollment into the registry. This analysis showed a statistically significant 75% increased rate of new onset DVT episodes among patients with low vitamin D at entry after adjustment for age, race, and sex. The researchers found no significant associations between low vitamin D and the incidence of any other type of incident thrombosis.
Dr. Petri and Dr. Isaacs reported having no relevant financial disclosures.
SOURCE: Petri MA et al. Ann Rheum Dis. 2018;77(Suppl 2):388, Abstract THU0341.
REPORTING FROM THE EULAR 2018 CONGRESS
Key clinical point:
Major finding: Lupus patients with a vitamin D level below 40 ng/mL had 2.3-fold more DVT events, compared with those with higher levels.
Study details: A review of 1,392 lupus patients at one U.S. center.
Disclosures: Dr. Petri and Dr. Isaacs reported having no relevant financial disclosures.
Source: Petri MA et al. Ann Rheum Dis. 2018;77(Suppl 2):388. Abstract THU0341.
Anti-CD22 CAR T rescues kids with ALL after CD19 failure
STOCKHOLM, SWEDEN – A novel chimeric antigen receptor T-cell construct directed against CD22 was able to rescue children with relapsed or refractory B-cell acute lymphoblastic leukemia for whom CD19-directed CAR T therapy had failed, investigators from China reported.
Thirty days after CAR T cell infusion, 12 of 15 children (80%) treated with the unnamed CD22 CAR T product had a complete response (CR) and one (6.7%) had a partial response (PR), for an overall response rate (ORR) of 86.7%, said Jing Pan, MD, from the Beijing Boren Hospital in China.
Surprisingly for a therapy of its type, the CD22 CAR T was well tolerated, with only mild cases of the cytokine release syndrome (CRS), and it could be delivered safely in children with relapsed disease after hematopoietic cell transplants (HCT), she reported in a briefing and in an oral abstract session at the annual congress of the European Hematology Association.
“CD22 CAR T immunotherapy brings hope for patients with refractory or relapsed B-ALL who failed on CD19 CAR T immunotherapy, and we think it’s quite safe. No children died and no children had severe side effects during the study, even in post-HCT patients,” Dr. Pan said.
She noted that in a previous clinical trial by her group, some patients experienced relapses and were resistant to retreatment with CD19-directed CAR T therapy due to mutations or loss of the CD19 antigen (Leukemia. 2017 Dec;31[12]:2587-93).
Since CD22 is highly expressed on leukemic cells in children with B-ALL, the investigators decided to evaluate the safety and efficacy of a CD22 CAR T as a rescue strategy. They enrolled 15 patients who either experienced relapse or did not have a response to CD19 CAR T immunotherapy. The CAR T construct they used contains an anti-CD22 single-chain variable fragment derived from a humanized CD22 antibody.
Patient conditioning with fludarabine and cyclophosphamide was performed simultaneously with CAR T transfection and expansion. After about 7 days, the expanded and transformed CAR T cells were infused at a dose of 8.2 x 105/kg in patients who had not undergone HCT, and 0.9 x 105 in patients who had received a transplant.
The patients ranged from 2 to 18 years old (median 8 years), had a median disease course of 21 months (range 5-84 months), and had a median of 42% bone marrow blasts (range 5%-95.5%).
Four of the 15 patients had relapses following allogeneic HCT, and the remaining 11 had relapses following chemotherapy. Two of the patients were found to be minimal residual disease (MRD)-positive by flow cytometry. Two patients had extramedullary disease only at relapse.
Ten of 11 patients who had experienced a hematologic relapse had either a CR or CR with incomplete recovery of counts (CRi), and of these 10 patients, nine were determined on follow-up to be MRD-negative by flow cytometry.
One of the two patients with extramedullary disease had a CR, and the other had a partial response.
Although two patients had no response to CD22 CAR T therapy, expression of the antigen was strong on leukemia cells from these patients, Dr. Pan said.
All patients experienced CRS, but none had greater than grade 2, Dr. Pan said, although she did not provide give specific numbers. Two patients had grade 1 neurotoxicity, two patients had grade 2 hypoxemia, and one patient had grade 2 liver enzyme elevation.
At a median follow-up of 108 days, six patients had been bridged to allogeneic HCT, and eleven of 12 patients who had a CR or CRi at 30 days had no evidence of disease progression. The remaining patient with an initial CR or CRi had a relapse at day 50. The 6-month progression-free survival rate was 91.7%.
Anton Hagenbeek, MD, PhD, from the Academic Medical Center at the University of Amsterdam, the Netherlands, who moderated the briefing but was not involved in the study, commented that given the high leukemia burden of the patients and the apparent efficacy of the therapy, one would expect to see higher grades of CRS, and asked Dr. Pan whether she could account for the CRS findings in her study, compared with those of trials for CD19-directed CAR T therapy.
It may have to do with differences in density of CD22 expression, compared with CD19 expression on leukemia cells, or on differences in the antibody used to target the cells, Dr. Pan said.
SOURCE: Pan J et al. EHA Congress, Abstract S832.
STOCKHOLM, SWEDEN – A novel chimeric antigen receptor T-cell construct directed against CD22 was able to rescue children with relapsed or refractory B-cell acute lymphoblastic leukemia for whom CD19-directed CAR T therapy had failed, investigators from China reported.
Thirty days after CAR T cell infusion, 12 of 15 children (80%) treated with the unnamed CD22 CAR T product had a complete response (CR) and one (6.7%) had a partial response (PR), for an overall response rate (ORR) of 86.7%, said Jing Pan, MD, from the Beijing Boren Hospital in China.
Surprisingly for a therapy of its type, the CD22 CAR T was well tolerated, with only mild cases of the cytokine release syndrome (CRS), and it could be delivered safely in children with relapsed disease after hematopoietic cell transplants (HCT), she reported in a briefing and in an oral abstract session at the annual congress of the European Hematology Association.
“CD22 CAR T immunotherapy brings hope for patients with refractory or relapsed B-ALL who failed on CD19 CAR T immunotherapy, and we think it’s quite safe. No children died and no children had severe side effects during the study, even in post-HCT patients,” Dr. Pan said.
She noted that in a previous clinical trial by her group, some patients experienced relapses and were resistant to retreatment with CD19-directed CAR T therapy due to mutations or loss of the CD19 antigen (Leukemia. 2017 Dec;31[12]:2587-93).
Since CD22 is highly expressed on leukemic cells in children with B-ALL, the investigators decided to evaluate the safety and efficacy of a CD22 CAR T as a rescue strategy. They enrolled 15 patients who either experienced relapse or did not have a response to CD19 CAR T immunotherapy. The CAR T construct they used contains an anti-CD22 single-chain variable fragment derived from a humanized CD22 antibody.
Patient conditioning with fludarabine and cyclophosphamide was performed simultaneously with CAR T transfection and expansion. After about 7 days, the expanded and transformed CAR T cells were infused at a dose of 8.2 x 105/kg in patients who had not undergone HCT, and 0.9 x 105 in patients who had received a transplant.
The patients ranged from 2 to 18 years old (median 8 years), had a median disease course of 21 months (range 5-84 months), and had a median of 42% bone marrow blasts (range 5%-95.5%).
Four of the 15 patients had relapses following allogeneic HCT, and the remaining 11 had relapses following chemotherapy. Two of the patients were found to be minimal residual disease (MRD)-positive by flow cytometry. Two patients had extramedullary disease only at relapse.
Ten of 11 patients who had experienced a hematologic relapse had either a CR or CR with incomplete recovery of counts (CRi), and of these 10 patients, nine were determined on follow-up to be MRD-negative by flow cytometry.
One of the two patients with extramedullary disease had a CR, and the other had a partial response.
Although two patients had no response to CD22 CAR T therapy, expression of the antigen was strong on leukemia cells from these patients, Dr. Pan said.
All patients experienced CRS, but none had greater than grade 2, Dr. Pan said, although she did not provide give specific numbers. Two patients had grade 1 neurotoxicity, two patients had grade 2 hypoxemia, and one patient had grade 2 liver enzyme elevation.
At a median follow-up of 108 days, six patients had been bridged to allogeneic HCT, and eleven of 12 patients who had a CR or CRi at 30 days had no evidence of disease progression. The remaining patient with an initial CR or CRi had a relapse at day 50. The 6-month progression-free survival rate was 91.7%.
Anton Hagenbeek, MD, PhD, from the Academic Medical Center at the University of Amsterdam, the Netherlands, who moderated the briefing but was not involved in the study, commented that given the high leukemia burden of the patients and the apparent efficacy of the therapy, one would expect to see higher grades of CRS, and asked Dr. Pan whether she could account for the CRS findings in her study, compared with those of trials for CD19-directed CAR T therapy.
It may have to do with differences in density of CD22 expression, compared with CD19 expression on leukemia cells, or on differences in the antibody used to target the cells, Dr. Pan said.
SOURCE: Pan J et al. EHA Congress, Abstract S832.
STOCKHOLM, SWEDEN – A novel chimeric antigen receptor T-cell construct directed against CD22 was able to rescue children with relapsed or refractory B-cell acute lymphoblastic leukemia for whom CD19-directed CAR T therapy had failed, investigators from China reported.
Thirty days after CAR T cell infusion, 12 of 15 children (80%) treated with the unnamed CD22 CAR T product had a complete response (CR) and one (6.7%) had a partial response (PR), for an overall response rate (ORR) of 86.7%, said Jing Pan, MD, from the Beijing Boren Hospital in China.
Surprisingly for a therapy of its type, the CD22 CAR T was well tolerated, with only mild cases of the cytokine release syndrome (CRS), and it could be delivered safely in children with relapsed disease after hematopoietic cell transplants (HCT), she reported in a briefing and in an oral abstract session at the annual congress of the European Hematology Association.
“CD22 CAR T immunotherapy brings hope for patients with refractory or relapsed B-ALL who failed on CD19 CAR T immunotherapy, and we think it’s quite safe. No children died and no children had severe side effects during the study, even in post-HCT patients,” Dr. Pan said.
She noted that in a previous clinical trial by her group, some patients experienced relapses and were resistant to retreatment with CD19-directed CAR T therapy due to mutations or loss of the CD19 antigen (Leukemia. 2017 Dec;31[12]:2587-93).
Since CD22 is highly expressed on leukemic cells in children with B-ALL, the investigators decided to evaluate the safety and efficacy of a CD22 CAR T as a rescue strategy. They enrolled 15 patients who either experienced relapse or did not have a response to CD19 CAR T immunotherapy. The CAR T construct they used contains an anti-CD22 single-chain variable fragment derived from a humanized CD22 antibody.
Patient conditioning with fludarabine and cyclophosphamide was performed simultaneously with CAR T transfection and expansion. After about 7 days, the expanded and transformed CAR T cells were infused at a dose of 8.2 x 105/kg in patients who had not undergone HCT, and 0.9 x 105 in patients who had received a transplant.
The patients ranged from 2 to 18 years old (median 8 years), had a median disease course of 21 months (range 5-84 months), and had a median of 42% bone marrow blasts (range 5%-95.5%).
Four of the 15 patients had relapses following allogeneic HCT, and the remaining 11 had relapses following chemotherapy. Two of the patients were found to be minimal residual disease (MRD)-positive by flow cytometry. Two patients had extramedullary disease only at relapse.
Ten of 11 patients who had experienced a hematologic relapse had either a CR or CR with incomplete recovery of counts (CRi), and of these 10 patients, nine were determined on follow-up to be MRD-negative by flow cytometry.
One of the two patients with extramedullary disease had a CR, and the other had a partial response.
Although two patients had no response to CD22 CAR T therapy, expression of the antigen was strong on leukemia cells from these patients, Dr. Pan said.
All patients experienced CRS, but none had greater than grade 2, Dr. Pan said, although she did not provide give specific numbers. Two patients had grade 1 neurotoxicity, two patients had grade 2 hypoxemia, and one patient had grade 2 liver enzyme elevation.
At a median follow-up of 108 days, six patients had been bridged to allogeneic HCT, and eleven of 12 patients who had a CR or CRi at 30 days had no evidence of disease progression. The remaining patient with an initial CR or CRi had a relapse at day 50. The 6-month progression-free survival rate was 91.7%.
Anton Hagenbeek, MD, PhD, from the Academic Medical Center at the University of Amsterdam, the Netherlands, who moderated the briefing but was not involved in the study, commented that given the high leukemia burden of the patients and the apparent efficacy of the therapy, one would expect to see higher grades of CRS, and asked Dr. Pan whether she could account for the CRS findings in her study, compared with those of trials for CD19-directed CAR T therapy.
It may have to do with differences in density of CD22 expression, compared with CD19 expression on leukemia cells, or on differences in the antibody used to target the cells, Dr. Pan said.
SOURCE: Pan J et al. EHA Congress, Abstract S832.
REPORTING FROM THE EHA CONGRESS
Key clinical point: A CD22-directed chimeric antigen receptor T cell construct may be a highly effective salvage therapy in children with acute lymphoblastic leukemia that has relapsed after, or is resistant to, CD19-direct CAR T therapy.
Major finding: In total, 12 of 15 children (80%) treated with the CD22 CAR T product had a complete response 30 days after infusion.
Study details: Open-label, single-center, single-arm study in 15 children with ALL that is resistant to, or relapsed after, prior CD19 CAR T therapy.
Disclosures: Dr. Pan and colleagues did not disclose a funding source for the study. She reported having no conflicts of interest.
Source: Pan J et al. EHA Congress, Abstract S832.
DLBCL survival improved with novel antibody-drug conjugate
STOCKHOLM, SWEDEN – Adding an experimental antibody-drug conjugate to bendamustine and rituximab more than doubled overall survival over bendamustine/rituximab alone in patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL), investigators reported.
Among 80 transplant-ineligible patients with relapsed or refractory DLBCL in a phase 2 trial, the combination of the antibody-drug conjugate (ADC) polatuzumab vedotin plus bendamustine/rituximab (BR) was associated with a 40% complete response rate, compared with 15% for BR alone.
More importantly, the ADC was associated with 6.7 months median progression-free survival (PFS) versus 2 months for BR, and 11.8 months median overall survival (OS), versus 4.7 months for BR alone, reported Laurie Sehn, MD, from BC Cancer in Vancouver, British Columbia, Canada.
“This randomized phase 2 trial really is, so far, the only head-to-head comparison of a novel targeted agent against a standard therapy in this patient population that’s ineligible for transplant, and it demonstrated that the combination polatuzumab vedotin with BR significantly improved the response rates and progression-free survival, as well as overall survival,” she said at the annual congress of the European Hematology Association.
However, in a separate cohort of patients with follicular lymphoma in the same trial, there was no difference in either PFS or OS during follow-up to date, Dr. Sehn reported.

Polatuzumab vedotin consists of an antibody targeted against CD79b, an antigenic protein expressed on the surface of normal B cells, as well as DLBCL and follicular lymphoma cells.
Dr. Sehn and her colleagues enrolled 80 patients with DLBCL for whom first-line chemoimmunotherapy had failed and who were ineligible for stem cell transplant due to age and/or comorbidities.
A second cohort included 80 patients with follicular lymphoma. In this group, median PFS with polatuzumab vedotin/BR was 17 months versus 17.3 months for BR alone, and median overall survival had not been reached in either arm at the time of the data cutoff.
In the DLBCL cohort, patients were randomized to receive polatuzumab vedotin 1.8 mg/kg plus bendamustine 90mg/m2 for 2 days and rituximab 375mg/m2) or BR alone for six 21-day cycles.
The complete response rate by PET scan – the primary endpoint – was significantly higher with polatuzmab/BR at 40% versus 15% for BR alone (P = .012). Respective overall response rates were 45% versus 18% (P = .008). Also, median PFS with the polatuzmab/BR therapy was 6.7 months versus 2.0 months for BR alone, translating into a hazard ratio of 0.31 (P less than .0001).
Respective median overall survival was 11.8 versus 4.7 months, translating into a hazard ratio for the polatuzmab/BR combination of 0.35 (P = .0008).
The PET complete response rates were higher with polatuzmab/BR regardless of prior lines of therapy or refractory status, Dr. Sehn noted.
“In terms of the safety, I think importantly in the combination there were no unexpected toxicities, so typical to what we would expect with what’s known with this drug alone,” Dr. Sehn said.
Grade 3 or greater toxicities that were higher with the polatuzmab/BR combination included cytopenias, febrile neutropenia, and infections. The single serious adverse event that had a higher incidence in the polatuzumab/BR arm was febrile neutropenia (DLBCL). In total, 12% of patients in the polatuzumab-containing arm and 11% of patients in the BR-only arm died on study. Many of the deaths were due to disease progression.
Anton Hagenbeek, MD, PhD, from the Academic Medical Center at the University of Amsterdam, the Netherlands, who moderated the briefing but was not involved in the study, said that about 20%-30% of patients with relapsed/refractory DLBCL are positive for the CD33 antigen, the target of brentuximab vedotin (Adcetris), and noted that this agent is also being tested in a phase 2 trial.
Martin Hutchings, MD, PhD, from Rigshospitalet in Copenhagen, the Netherlands, who co-moderated the oral abstract session, commented that “it’s not so often that we see significant overall survival differences in a phase 2 study with 80 patients.”
Based on the results of this trial, polatuzumab has been granted breakthrough therapy designation by the U.S. Food and Drug Administration and a PRIME (priority medicine) designation from the European Medicines Agency.
SOURCE: Sehn LH et al. EHA Congress, Abstract S802.
STOCKHOLM, SWEDEN – Adding an experimental antibody-drug conjugate to bendamustine and rituximab more than doubled overall survival over bendamustine/rituximab alone in patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL), investigators reported.
Among 80 transplant-ineligible patients with relapsed or refractory DLBCL in a phase 2 trial, the combination of the antibody-drug conjugate (ADC) polatuzumab vedotin plus bendamustine/rituximab (BR) was associated with a 40% complete response rate, compared with 15% for BR alone.
More importantly, the ADC was associated with 6.7 months median progression-free survival (PFS) versus 2 months for BR, and 11.8 months median overall survival (OS), versus 4.7 months for BR alone, reported Laurie Sehn, MD, from BC Cancer in Vancouver, British Columbia, Canada.
“This randomized phase 2 trial really is, so far, the only head-to-head comparison of a novel targeted agent against a standard therapy in this patient population that’s ineligible for transplant, and it demonstrated that the combination polatuzumab vedotin with BR significantly improved the response rates and progression-free survival, as well as overall survival,” she said at the annual congress of the European Hematology Association.
However, in a separate cohort of patients with follicular lymphoma in the same trial, there was no difference in either PFS or OS during follow-up to date, Dr. Sehn reported.
Polatuzumab vedotin consists of an antibody targeted against CD79b, an antigenic protein expressed on the surface of normal B cells, as well as DLBCL and follicular lymphoma cells.
Dr. Sehn and her colleagues enrolled 80 patients with DLBCL for whom first-line chemoimmunotherapy had failed and who were ineligible for stem cell transplant due to age and/or comorbidities.
A second cohort included 80 patients with follicular lymphoma. In this group, median PFS with polatuzumab vedotin/BR was 17 months versus 17.3 months for BR alone, and median overall survival had not been reached in either arm at the time of the data cutoff.
In the DLBCL cohort, patients were randomized to receive polatuzumab vedotin 1.8 mg/kg plus bendamustine 90mg/m2 for 2 days and rituximab 375mg/m2) or BR alone for six 21-day cycles.
The complete response rate by PET scan – the primary endpoint – was significantly higher with polatuzmab/BR at 40% versus 15% for BR alone (P = .012). Respective overall response rates were 45% versus 18% (P = .008). Also, median PFS with the polatuzmab/BR therapy was 6.7 months versus 2.0 months for BR alone, translating into a hazard ratio of 0.31 (P less than .0001).
Respective median overall survival was 11.8 versus 4.7 months, translating into a hazard ratio for the polatuzmab/BR combination of 0.35 (P = .0008).
The PET complete response rates were higher with polatuzmab/BR regardless of prior lines of therapy or refractory status, Dr. Sehn noted.
“In terms of the safety, I think importantly in the combination there were no unexpected toxicities, so typical to what we would expect with what’s known with this drug alone,” Dr. Sehn said.
Grade 3 or greater toxicities that were higher with the polatuzmab/BR combination included cytopenias, febrile neutropenia, and infections. The single serious adverse event that had a higher incidence in the polatuzumab/BR arm was febrile neutropenia (DLBCL). In total, 12% of patients in the polatuzumab-containing arm and 11% of patients in the BR-only arm died on study. Many of the deaths were due to disease progression.
Anton Hagenbeek, MD, PhD, from the Academic Medical Center at the University of Amsterdam, the Netherlands, who moderated the briefing but was not involved in the study, said that about 20%-30% of patients with relapsed/refractory DLBCL are positive for the CD33 antigen, the target of brentuximab vedotin (Adcetris), and noted that this agent is also being tested in a phase 2 trial.
Martin Hutchings, MD, PhD, from Rigshospitalet in Copenhagen, the Netherlands, who co-moderated the oral abstract session, commented that “it’s not so often that we see significant overall survival differences in a phase 2 study with 80 patients.”
Based on the results of this trial, polatuzumab has been granted breakthrough therapy designation by the U.S. Food and Drug Administration and a PRIME (priority medicine) designation from the European Medicines Agency.
SOURCE: Sehn LH et al. EHA Congress, Abstract S802.
STOCKHOLM, SWEDEN – Adding an experimental antibody-drug conjugate to bendamustine and rituximab more than doubled overall survival over bendamustine/rituximab alone in patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL), investigators reported.
Among 80 transplant-ineligible patients with relapsed or refractory DLBCL in a phase 2 trial, the combination of the antibody-drug conjugate (ADC) polatuzumab vedotin plus bendamustine/rituximab (BR) was associated with a 40% complete response rate, compared with 15% for BR alone.
More importantly, the ADC was associated with 6.7 months median progression-free survival (PFS) versus 2 months for BR, and 11.8 months median overall survival (OS), versus 4.7 months for BR alone, reported Laurie Sehn, MD, from BC Cancer in Vancouver, British Columbia, Canada.
“This randomized phase 2 trial really is, so far, the only head-to-head comparison of a novel targeted agent against a standard therapy in this patient population that’s ineligible for transplant, and it demonstrated that the combination polatuzumab vedotin with BR significantly improved the response rates and progression-free survival, as well as overall survival,” she said at the annual congress of the European Hematology Association.
However, in a separate cohort of patients with follicular lymphoma in the same trial, there was no difference in either PFS or OS during follow-up to date, Dr. Sehn reported.
Polatuzumab vedotin consists of an antibody targeted against CD79b, an antigenic protein expressed on the surface of normal B cells, as well as DLBCL and follicular lymphoma cells.
Dr. Sehn and her colleagues enrolled 80 patients with DLBCL for whom first-line chemoimmunotherapy had failed and who were ineligible for stem cell transplant due to age and/or comorbidities.
A second cohort included 80 patients with follicular lymphoma. In this group, median PFS with polatuzumab vedotin/BR was 17 months versus 17.3 months for BR alone, and median overall survival had not been reached in either arm at the time of the data cutoff.
In the DLBCL cohort, patients were randomized to receive polatuzumab vedotin 1.8 mg/kg plus bendamustine 90mg/m2 for 2 days and rituximab 375mg/m2) or BR alone for six 21-day cycles.
The complete response rate by PET scan – the primary endpoint – was significantly higher with polatuzmab/BR at 40% versus 15% for BR alone (P = .012). Respective overall response rates were 45% versus 18% (P = .008). Also, median PFS with the polatuzmab/BR therapy was 6.7 months versus 2.0 months for BR alone, translating into a hazard ratio of 0.31 (P less than .0001).
Respective median overall survival was 11.8 versus 4.7 months, translating into a hazard ratio for the polatuzmab/BR combination of 0.35 (P = .0008).
The PET complete response rates were higher with polatuzmab/BR regardless of prior lines of therapy or refractory status, Dr. Sehn noted.
“In terms of the safety, I think importantly in the combination there were no unexpected toxicities, so typical to what we would expect with what’s known with this drug alone,” Dr. Sehn said.
Grade 3 or greater toxicities that were higher with the polatuzmab/BR combination included cytopenias, febrile neutropenia, and infections. The single serious adverse event that had a higher incidence in the polatuzumab/BR arm was febrile neutropenia (DLBCL). In total, 12% of patients in the polatuzumab-containing arm and 11% of patients in the BR-only arm died on study. Many of the deaths were due to disease progression.
Anton Hagenbeek, MD, PhD, from the Academic Medical Center at the University of Amsterdam, the Netherlands, who moderated the briefing but was not involved in the study, said that about 20%-30% of patients with relapsed/refractory DLBCL are positive for the CD33 antigen, the target of brentuximab vedotin (Adcetris), and noted that this agent is also being tested in a phase 2 trial.
Martin Hutchings, MD, PhD, from Rigshospitalet in Copenhagen, the Netherlands, who co-moderated the oral abstract session, commented that “it’s not so often that we see significant overall survival differences in a phase 2 study with 80 patients.”
Based on the results of this trial, polatuzumab has been granted breakthrough therapy designation by the U.S. Food and Drug Administration and a PRIME (priority medicine) designation from the European Medicines Agency.
SOURCE: Sehn LH et al. EHA Congress, Abstract S802.
REPORTING FROM THE EHA CONGRESS
Key clinical point:
Major finding: The complete response rate with polatuzumab vedotin plus bendamustine/rituximab (BR) was 40%, compared with 15% for BR alone.
Study details: Randomized controlled phase 2 trial in 80 patients with relapsed/refractory DLBCL.
Disclosures: The study was funded by Hoffman-La Roche. Dr. Sehn reported ties to Roche/Genentech and others.
Source: Sehn LH et al. EHA Congress, Abstract S802.
Vitreous Hemorrhage in the Setting of a Vascular Loop
Vascular loops are rare congenital optic nerve anomalies that originate from the arterial or venous circulation; 90% arise from the arterial circulation.1 Vascular loops are usually asymptomatic unless an arterial or venous occlusion, hyphema, and vitreous or preretinal hemorrhage should arise.1-8 This article describes a patient who presented with a vitreous hemorrhage secondary to a vascular loop.
Case Presentation
A 67-year-old white male presented to the eye clinic at the Providence VA Medical Center in Rhode Island after experiencing floaters and “snowflakes” in the left eye for 2 days. The patient reported having no photopsias, loss of vision, preceding eye/head trauma, or Valsalva maneuver. His medical history was significant for well-controlled type 2 diabetes mellitus (known duration of 5 years), hypertension, hyperlipidemia, coronary artery disease, and anemia. His medications included aspirin 81 mg, furosemide, clonidine, labetalol, valsartan, glipizide, and lantus injections.
The patient’s ocular history was significant for cataracts in both eyes. On examination, best-corrected visual acuity was 20/20 in each eye with intraocular pressures of 15 mm Hg in the right eye and 14 mm Hg in the left eye. Anterior segment examination was notable for 1+ nuclear sclerotic cataracts in both eyes with red blood cells visible in the anterior chamber in the left eye. 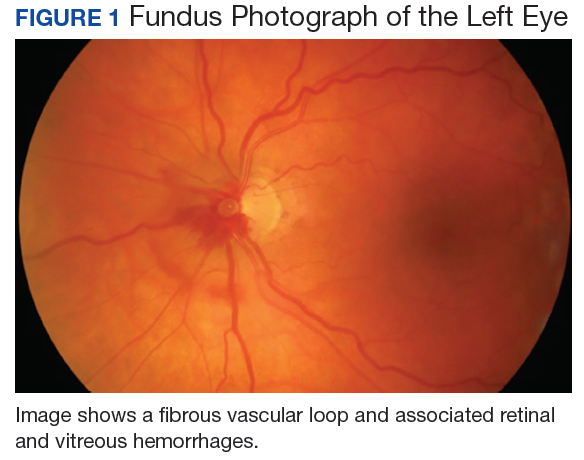
No PVD, retinal break, or detachment was present in the left eye with scleral depression. No background diabetic retinopathy was present in either eye. 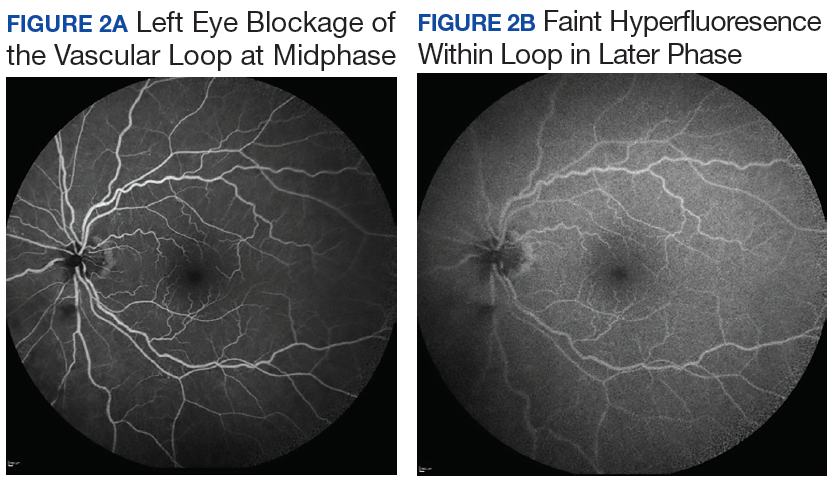
The patient was diagnosed with a vitreous hemorrhage associated with a vascular loop in the left eye. 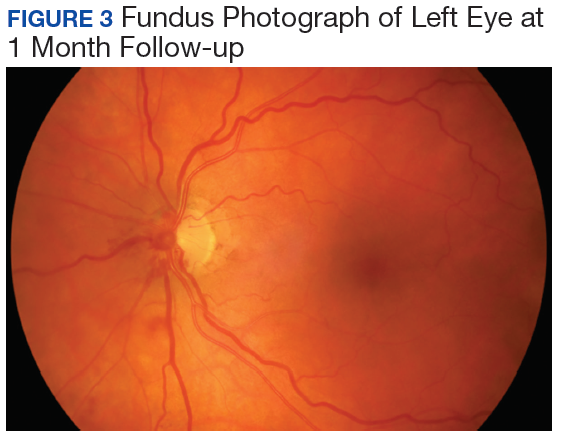
Discussion
Salient features of this case include the prominent vascular loop at the disc extending anteriorly into the vitreous and an absence of features suggestive of one of the more common etiologies of vitreous hemorrhage, such as PVD, retinal tear/detachment, proliferative diabetic retinopathy (PDR), or retinal vein occlusion.
The incidence of venous loops is 1 in 9,000 with no associated systemic conditions.2,3 Typically unilateral, vascular loops arise at the optic disc from the central retinal artery or vein.1-4 An arterial loop is a separate entity from a hyaloid artery.2 The authors were unable to definitively determine whether the loop in this patient was arterial or venous in origin due to blockage from the associated retinal hemorrhage on FA.
Valsalva maneuver, vitreous traction, trauma, and loop torsion in patients with vascular loops can lead to amaurosis fugax, PVD, and hemorrhagic complications, such as hyphema and vitreous and retinal hemorrhages.1,3,6-8 In addition, retinal ischemia and thrombosis from the vascular loops can lead to retinal artery or vein occlusions.1-8 Vitreous and retinal hemorrhages, such as in this patient, are often observed with complete resolution and visual acuity returning to baseline.4,5 For recurrent or nonresolving vitreous hemorrhages, a vitrectomy can be performed.3,6
Conclusion
Patients with vascular loops should be educated to seek eye care if experiencing new onset floaters or visual loss.
1. Codenotti M, Fogliato G, De Benedetto U, Iuliano L, Bandello F. Simultaneous vitreous hemorrhage and branch retinal artery occlusion after prepapillary arterial loop rupture. J Fr Ophtalmol. 2013;36(4):e63-e65.
2. Brown GC, Magargal L, Augsburger JJ, Shields JA. Preretinal arterial loops and retinal arterial occlusion. Am J Ophthalmol. 1979;87(5):646-651.
3. Degenhart W, Brown GC, Augsburger JJ, Magargal L. Prepapillary vascular loops. Ophthalmology. 1981;88(11):1126-1131.
4. Soltau JB, Olk RJ, Gordon JM. Prepapillary arterial loop associated with vitreous hemorrhage and venous retinal macrovessel. Retina. 1996;16(1):74-75.
5. Fujiwara T, Machida S, Herai T, Tazawa Y. Case of subretinal hemorrhage that developed from a prepapillary vascular loop. Jpn J Ophthalmol. 2004;48(2):175-177.
6. Strassman IB, Desai UR. Prepapillary vascular loop and a recurrent vitreous hemorrhage. Retina. 1997;17(2):166-167.
7. Singh R, Fujinami K, Moore AT. Branch retinal artery occlusion secondary to prepapillary arterial loop. Retin Cases Brief Rep. 2014;8(2):124-126.
8. Takahashi K. Hemodynamics of prepapillary vascular loop in hemi-central retinal vein occlusion [in Japanese]. Nippon Ganka Gakkai Zasshi. 1999;103(5):404-408.
Vascular loops are rare congenital optic nerve anomalies that originate from the arterial or venous circulation; 90% arise from the arterial circulation.1 Vascular loops are usually asymptomatic unless an arterial or venous occlusion, hyphema, and vitreous or preretinal hemorrhage should arise.1-8 This article describes a patient who presented with a vitreous hemorrhage secondary to a vascular loop.
Case Presentation
A 67-year-old white male presented to the eye clinic at the Providence VA Medical Center in Rhode Island after experiencing floaters and “snowflakes” in the left eye for 2 days. The patient reported having no photopsias, loss of vision, preceding eye/head trauma, or Valsalva maneuver. His medical history was significant for well-controlled type 2 diabetes mellitus (known duration of 5 years), hypertension, hyperlipidemia, coronary artery disease, and anemia. His medications included aspirin 81 mg, furosemide, clonidine, labetalol, valsartan, glipizide, and lantus injections.
The patient’s ocular history was significant for cataracts in both eyes. On examination, best-corrected visual acuity was 20/20 in each eye with intraocular pressures of 15 mm Hg in the right eye and 14 mm Hg in the left eye. Anterior segment examination was notable for 1+ nuclear sclerotic cataracts in both eyes with red blood cells visible in the anterior chamber in the left eye.
No PVD, retinal break, or detachment was present in the left eye with scleral depression. No background diabetic retinopathy was present in either eye.
The patient was diagnosed with a vitreous hemorrhage associated with a vascular loop in the left eye.
Discussion
Salient features of this case include the prominent vascular loop at the disc extending anteriorly into the vitreous and an absence of features suggestive of one of the more common etiologies of vitreous hemorrhage, such as PVD, retinal tear/detachment, proliferative diabetic retinopathy (PDR), or retinal vein occlusion.
The incidence of venous loops is 1 in 9,000 with no associated systemic conditions.2,3 Typically unilateral, vascular loops arise at the optic disc from the central retinal artery or vein.1-4 An arterial loop is a separate entity from a hyaloid artery.2 The authors were unable to definitively determine whether the loop in this patient was arterial or venous in origin due to blockage from the associated retinal hemorrhage on FA.
Valsalva maneuver, vitreous traction, trauma, and loop torsion in patients with vascular loops can lead to amaurosis fugax, PVD, and hemorrhagic complications, such as hyphema and vitreous and retinal hemorrhages.1,3,6-8 In addition, retinal ischemia and thrombosis from the vascular loops can lead to retinal artery or vein occlusions.1-8 Vitreous and retinal hemorrhages, such as in this patient, are often observed with complete resolution and visual acuity returning to baseline.4,5 For recurrent or nonresolving vitreous hemorrhages, a vitrectomy can be performed.3,6
Conclusion
Patients with vascular loops should be educated to seek eye care if experiencing new onset floaters or visual loss.
Vascular loops are rare congenital optic nerve anomalies that originate from the arterial or venous circulation; 90% arise from the arterial circulation.1 Vascular loops are usually asymptomatic unless an arterial or venous occlusion, hyphema, and vitreous or preretinal hemorrhage should arise.1-8 This article describes a patient who presented with a vitreous hemorrhage secondary to a vascular loop.
Case Presentation
A 67-year-old white male presented to the eye clinic at the Providence VA Medical Center in Rhode Island after experiencing floaters and “snowflakes” in the left eye for 2 days. The patient reported having no photopsias, loss of vision, preceding eye/head trauma, or Valsalva maneuver. His medical history was significant for well-controlled type 2 diabetes mellitus (known duration of 5 years), hypertension, hyperlipidemia, coronary artery disease, and anemia. His medications included aspirin 81 mg, furosemide, clonidine, labetalol, valsartan, glipizide, and lantus injections.
The patient’s ocular history was significant for cataracts in both eyes. On examination, best-corrected visual acuity was 20/20 in each eye with intraocular pressures of 15 mm Hg in the right eye and 14 mm Hg in the left eye. Anterior segment examination was notable for 1+ nuclear sclerotic cataracts in both eyes with red blood cells visible in the anterior chamber in the left eye.
No PVD, retinal break, or detachment was present in the left eye with scleral depression. No background diabetic retinopathy was present in either eye.
The patient was diagnosed with a vitreous hemorrhage associated with a vascular loop in the left eye.
Discussion
Salient features of this case include the prominent vascular loop at the disc extending anteriorly into the vitreous and an absence of features suggestive of one of the more common etiologies of vitreous hemorrhage, such as PVD, retinal tear/detachment, proliferative diabetic retinopathy (PDR), or retinal vein occlusion.
The incidence of venous loops is 1 in 9,000 with no associated systemic conditions.2,3 Typically unilateral, vascular loops arise at the optic disc from the central retinal artery or vein.1-4 An arterial loop is a separate entity from a hyaloid artery.2 The authors were unable to definitively determine whether the loop in this patient was arterial or venous in origin due to blockage from the associated retinal hemorrhage on FA.
Valsalva maneuver, vitreous traction, trauma, and loop torsion in patients with vascular loops can lead to amaurosis fugax, PVD, and hemorrhagic complications, such as hyphema and vitreous and retinal hemorrhages.1,3,6-8 In addition, retinal ischemia and thrombosis from the vascular loops can lead to retinal artery or vein occlusions.1-8 Vitreous and retinal hemorrhages, such as in this patient, are often observed with complete resolution and visual acuity returning to baseline.4,5 For recurrent or nonresolving vitreous hemorrhages, a vitrectomy can be performed.3,6
Conclusion
Patients with vascular loops should be educated to seek eye care if experiencing new onset floaters or visual loss.
1. Codenotti M, Fogliato G, De Benedetto U, Iuliano L, Bandello F. Simultaneous vitreous hemorrhage and branch retinal artery occlusion after prepapillary arterial loop rupture. J Fr Ophtalmol. 2013;36(4):e63-e65.
2. Brown GC, Magargal L, Augsburger JJ, Shields JA. Preretinal arterial loops and retinal arterial occlusion. Am J Ophthalmol. 1979;87(5):646-651.
3. Degenhart W, Brown GC, Augsburger JJ, Magargal L. Prepapillary vascular loops. Ophthalmology. 1981;88(11):1126-1131.
4. Soltau JB, Olk RJ, Gordon JM. Prepapillary arterial loop associated with vitreous hemorrhage and venous retinal macrovessel. Retina. 1996;16(1):74-75.
5. Fujiwara T, Machida S, Herai T, Tazawa Y. Case of subretinal hemorrhage that developed from a prepapillary vascular loop. Jpn J Ophthalmol. 2004;48(2):175-177.
6. Strassman IB, Desai UR. Prepapillary vascular loop and a recurrent vitreous hemorrhage. Retina. 1997;17(2):166-167.
7. Singh R, Fujinami K, Moore AT. Branch retinal artery occlusion secondary to prepapillary arterial loop. Retin Cases Brief Rep. 2014;8(2):124-126.
8. Takahashi K. Hemodynamics of prepapillary vascular loop in hemi-central retinal vein occlusion [in Japanese]. Nippon Ganka Gakkai Zasshi. 1999;103(5):404-408.
1. Codenotti M, Fogliato G, De Benedetto U, Iuliano L, Bandello F. Simultaneous vitreous hemorrhage and branch retinal artery occlusion after prepapillary arterial loop rupture. J Fr Ophtalmol. 2013;36(4):e63-e65.
2. Brown GC, Magargal L, Augsburger JJ, Shields JA. Preretinal arterial loops and retinal arterial occlusion. Am J Ophthalmol. 1979;87(5):646-651.
3. Degenhart W, Brown GC, Augsburger JJ, Magargal L. Prepapillary vascular loops. Ophthalmology. 1981;88(11):1126-1131.
4. Soltau JB, Olk RJ, Gordon JM. Prepapillary arterial loop associated with vitreous hemorrhage and venous retinal macrovessel. Retina. 1996;16(1):74-75.
5. Fujiwara T, Machida S, Herai T, Tazawa Y. Case of subretinal hemorrhage that developed from a prepapillary vascular loop. Jpn J Ophthalmol. 2004;48(2):175-177.
6. Strassman IB, Desai UR. Prepapillary vascular loop and a recurrent vitreous hemorrhage. Retina. 1997;17(2):166-167.
7. Singh R, Fujinami K, Moore AT. Branch retinal artery occlusion secondary to prepapillary arterial loop. Retin Cases Brief Rep. 2014;8(2):124-126.
8. Takahashi K. Hemodynamics of prepapillary vascular loop in hemi-central retinal vein occlusion [in Japanese]. Nippon Ganka Gakkai Zasshi. 1999;103(5):404-408.
Efficacy of KTE-C19 CAR T cells not compromised by prior blinatumomab
CHICAGO—Prior exposure to blinatumomab does not appear to affect the successful manufacture of KTE-C19 or its efficacy in patients with relapsed/refractory acute lymphoblastic leukemia (ALL), an investigator reported at the 2018 ASCO Annual Meeting.
The clinical benefit of KTE-C19, an anti-CD19 chimeric antigen receptor (CAR) T-cell therapy, was preserved regardless of whether patients were exposed to blinatumomab, said Bijal D. Shah, MD, of Moffitt Cancer Center in Tampa, Florida.
High rates of complete response and undetectable minimal residual disease (MRD) were independent of exposure to blinatumomab, a CD19/CD3 bispecific T-cell engager.
“We feel the results of these data support KTE-C19 as an effective option for adults with refractory leukemia, regardless of prior exposure to CD19-directed therapy,” Dr Shah reported at the meeting (abstract 7006*).
The current standard of care for adults with relapsed/refractory ALL includes blinatumomab, raising the question of whether prior exposure to this CD19-directed treatment could influence the manufacture or efficacy of KTE-C19.
Sara Cooley, MD, of Masonic Medical Center, University of Minnesota in Minneapolis, said results of this analysis suggest prior blinatumomab should not be a contraindication or concern in the context of KTE-C19.
“This remains to be shown with other CAR T-cell therapies,” she said in a presentation at ASCO on cellular therapy in leukemia.
The analysis by Dr Shah and co-investigators was based on ZUMA-3 (NCT02614066), a phase 1 study including adults with relapsed/refractory ALL who received KTE-C19 at doses of 0.5, 1, or 2 x 106 cells/kg.
They excluded patients in the highest dose cohort, who were required to be blinatumomab naïve, per protocol. That left 23 patients who received 0.5 or 1 x 106 cells/kg, of whom 11 had prior blinatumomab exposure and 12 did not.
Best overall response appeared to be independent of prior blinatumomab treatment, with a CR rate of 72% overall, and 63% and 80% for blinatumomab-exposed and blinatumomab-naïve patients, respectively.
The rate of undetectable MRD was likewise high at 88% in the prior blinatumomab group and 100% in the no-blinatumomab group.
Product characteristics did not vary according to blinatumomab exposure, though there was a trend toward a more differentiated phenotype in those patients who had received prior CD19-directed treatment, he said.
There were no significant differences between groups in the rate of grade 3 or greater cytokine release syndrome. Neurologic events were higher in the blinatumomab-naïve patients, though a higher percentage of those patients received the 1 x 106 cells/kg dose, Dr Shah reported.
Investigators also looked at CAR T levels by treatment.
“We cannot appreciate any significant differences between the blinatumomab-naïve and the blinatumomab-exposed groups,” Dr Shah told ASCO attendees.
The ZUMA-3 trial was sponsored by Kite, a Gilead Company.
*Data in the abstract differ from the presentation.
CHICAGO—Prior exposure to blinatumomab does not appear to affect the successful manufacture of KTE-C19 or its efficacy in patients with relapsed/refractory acute lymphoblastic leukemia (ALL), an investigator reported at the 2018 ASCO Annual Meeting.
The clinical benefit of KTE-C19, an anti-CD19 chimeric antigen receptor (CAR) T-cell therapy, was preserved regardless of whether patients were exposed to blinatumomab, said Bijal D. Shah, MD, of Moffitt Cancer Center in Tampa, Florida.
High rates of complete response and undetectable minimal residual disease (MRD) were independent of exposure to blinatumomab, a CD19/CD3 bispecific T-cell engager.
“We feel the results of these data support KTE-C19 as an effective option for adults with refractory leukemia, regardless of prior exposure to CD19-directed therapy,” Dr Shah reported at the meeting (abstract 7006*).
The current standard of care for adults with relapsed/refractory ALL includes blinatumomab, raising the question of whether prior exposure to this CD19-directed treatment could influence the manufacture or efficacy of KTE-C19.
Sara Cooley, MD, of Masonic Medical Center, University of Minnesota in Minneapolis, said results of this analysis suggest prior blinatumomab should not be a contraindication or concern in the context of KTE-C19.
“This remains to be shown with other CAR T-cell therapies,” she said in a presentation at ASCO on cellular therapy in leukemia.
The analysis by Dr Shah and co-investigators was based on ZUMA-3 (NCT02614066), a phase 1 study including adults with relapsed/refractory ALL who received KTE-C19 at doses of 0.5, 1, or 2 x 106 cells/kg.
They excluded patients in the highest dose cohort, who were required to be blinatumomab naïve, per protocol. That left 23 patients who received 0.5 or 1 x 106 cells/kg, of whom 11 had prior blinatumomab exposure and 12 did not.
Best overall response appeared to be independent of prior blinatumomab treatment, with a CR rate of 72% overall, and 63% and 80% for blinatumomab-exposed and blinatumomab-naïve patients, respectively.
The rate of undetectable MRD was likewise high at 88% in the prior blinatumomab group and 100% in the no-blinatumomab group.
Product characteristics did not vary according to blinatumomab exposure, though there was a trend toward a more differentiated phenotype in those patients who had received prior CD19-directed treatment, he said.
There were no significant differences between groups in the rate of grade 3 or greater cytokine release syndrome. Neurologic events were higher in the blinatumomab-naïve patients, though a higher percentage of those patients received the 1 x 106 cells/kg dose, Dr Shah reported.
Investigators also looked at CAR T levels by treatment.
“We cannot appreciate any significant differences between the blinatumomab-naïve and the blinatumomab-exposed groups,” Dr Shah told ASCO attendees.
The ZUMA-3 trial was sponsored by Kite, a Gilead Company.
*Data in the abstract differ from the presentation.
CHICAGO—Prior exposure to blinatumomab does not appear to affect the successful manufacture of KTE-C19 or its efficacy in patients with relapsed/refractory acute lymphoblastic leukemia (ALL), an investigator reported at the 2018 ASCO Annual Meeting.
The clinical benefit of KTE-C19, an anti-CD19 chimeric antigen receptor (CAR) T-cell therapy, was preserved regardless of whether patients were exposed to blinatumomab, said Bijal D. Shah, MD, of Moffitt Cancer Center in Tampa, Florida.
High rates of complete response and undetectable minimal residual disease (MRD) were independent of exposure to blinatumomab, a CD19/CD3 bispecific T-cell engager.
“We feel the results of these data support KTE-C19 as an effective option for adults with refractory leukemia, regardless of prior exposure to CD19-directed therapy,” Dr Shah reported at the meeting (abstract 7006*).
The current standard of care for adults with relapsed/refractory ALL includes blinatumomab, raising the question of whether prior exposure to this CD19-directed treatment could influence the manufacture or efficacy of KTE-C19.
Sara Cooley, MD, of Masonic Medical Center, University of Minnesota in Minneapolis, said results of this analysis suggest prior blinatumomab should not be a contraindication or concern in the context of KTE-C19.
“This remains to be shown with other CAR T-cell therapies,” she said in a presentation at ASCO on cellular therapy in leukemia.
The analysis by Dr Shah and co-investigators was based on ZUMA-3 (NCT02614066), a phase 1 study including adults with relapsed/refractory ALL who received KTE-C19 at doses of 0.5, 1, or 2 x 106 cells/kg.
They excluded patients in the highest dose cohort, who were required to be blinatumomab naïve, per protocol. That left 23 patients who received 0.5 or 1 x 106 cells/kg, of whom 11 had prior blinatumomab exposure and 12 did not.
Best overall response appeared to be independent of prior blinatumomab treatment, with a CR rate of 72% overall, and 63% and 80% for blinatumomab-exposed and blinatumomab-naïve patients, respectively.
The rate of undetectable MRD was likewise high at 88% in the prior blinatumomab group and 100% in the no-blinatumomab group.
Product characteristics did not vary according to blinatumomab exposure, though there was a trend toward a more differentiated phenotype in those patients who had received prior CD19-directed treatment, he said.
There were no significant differences between groups in the rate of grade 3 or greater cytokine release syndrome. Neurologic events were higher in the blinatumomab-naïve patients, though a higher percentage of those patients received the 1 x 106 cells/kg dose, Dr Shah reported.
Investigators also looked at CAR T levels by treatment.
“We cannot appreciate any significant differences between the blinatumomab-naïve and the blinatumomab-exposed groups,” Dr Shah told ASCO attendees.
The ZUMA-3 trial was sponsored by Kite, a Gilead Company.
*Data in the abstract differ from the presentation.
Antipsychotics linked to increased body fat, insulin resistance in children
Twelve weeks of treatment with three different antipsychotics commonly used in children and adolescents with disruptive behavioral disorders was associated with rapid-onset adverse changes in adiposity and insulin sensitivity, results of a randomized clinical trial show.
The adverse effect on adiposity was greatest for children aged 6-18 years who received olanzapine, but was also seen in study participants randomized to receive risperidone or aripiprazole, according to results of the study published in JAMA Psychiatry.
These findings inform the risk-benefit analysis for off-label pediatric use of antipsychotics for disruptive behavior disorders, Ginger E. Nicol, MD, of Washington University, St. Louis, and colleagues wrote.
“The potential psychiatric benefits of antipsychotic use in this population, evident in this trial and others, should be carefully weighed against the potential for childhood onset of abdominal obesity and insulin resistance that – compared with adult onset – further increases long-term risk for [type 2 diabetes], cardiovascular disease, and related conditions,” the researchers wrote.
This randomized, prospective clinical trial included 144 antipsychotic-naive children and adolescents aged 6-18 years who had been diagnosed with one or more psychiatric disorders and clinically significant aggression. They were randomly and evenly assigned to 12 weeks of treatment with oral olanzapine, risperidone, or aripiprazole.
Those who received olanzapine had a 4.12% increase in percentage total body fat from baseline to week 12, as measured by dual-energy x-ray absorptiometry (DXA). That increase was significantly greater than the total body fat increases of 1.18% for risperidone and 1.66% for aripiprazole seen over that same time period (P less than .001 for time-by-treatment interaction), the researchers reported.
Insulin sensitivity decreased over time in the pooled study sample, with significant changes reported in insulin-stimulated glucose rate of disappearance, glucose rate of appearance, and glycerol rate of appearance. The changes did not differ significantly across the three treatment groups.
The lack of a placebo group in this study makes it unclear how much of the body fat and insulin sensitivity changes were attributable to antipsychotic medication. Psychiatric symptoms did improve significantly with treatment, the researchers noted.
Dr. Nicol reported research funding from the National Institute of Mental Health, Otsuka America Pharmaceutical, Alkermes PLC, The Sidney R. Baer Jr. Foundation, and the Center for Brain Research in Mood Disorders at Washington University in St Louis. Co-authors reported financial ties to Reviva Pharmaceuticals, Sunovion Pharmaceuticals, Indivior, Amgen, and other companies.
SOURCE: Nicol GE et al. JAMA Psychiatry. 2018 Jun 13. doi: 10.1001/jamapsychiatry.2018.1088.
The findings of this study by Nicol and colleagues corroborate previous reports that used conventional anthropometry to document the metabolic adverse effects of second-generation antipsychotic medications in children and adolescents, according to authors of an accompanying editorial.
The current study used “gold standard” methods of measurement to demonstrate that 12 weeks of treatment with low-dose olanzapine, risperidone, or aripiprazole led to rapid-onset changes in adiposity and insulin sensitivity, with larger increases in those who received olanzapine.
“As such, the study even more emphatically underlines the risks to which these vulnerable populations are exposed,” Marc De Hert, MD, PhD, and Johan Detraux wrote.
It is now is clear that the potential psychiatric benefits of off-label antipsychotics need to be weighed against the potential for childhood-onset obesity and insulin resistance, they added. However, longer-term studies that use hard end points, such as new-onset diabetes or cardiovascular disease are needed.
Marc De Hert, MD, PhD, and Johan Detraux, are with Katholieke Universiteit Leuven, Kortenberg, Belgium. These comments are from an accompanying editorial (JAMA Psychiatry. 2018 Jun 13. doi: 10.1001/jamapsychiatry.2018.1080 ). Dr. De Hert reported no disclosures. Mr. Detraux reported partial support by the Janssen Academy for work on the the Belgian Discussion Board on Antipsychotic Treatment.
The findings of this study by Nicol and colleagues corroborate previous reports that used conventional anthropometry to document the metabolic adverse effects of second-generation antipsychotic medications in children and adolescents, according to authors of an accompanying editorial.
The current study used “gold standard” methods of measurement to demonstrate that 12 weeks of treatment with low-dose olanzapine, risperidone, or aripiprazole led to rapid-onset changes in adiposity and insulin sensitivity, with larger increases in those who received olanzapine.
“As such, the study even more emphatically underlines the risks to which these vulnerable populations are exposed,” Marc De Hert, MD, PhD, and Johan Detraux wrote.
It is now is clear that the potential psychiatric benefits of off-label antipsychotics need to be weighed against the potential for childhood-onset obesity and insulin resistance, they added. However, longer-term studies that use hard end points, such as new-onset diabetes or cardiovascular disease are needed.
Marc De Hert, MD, PhD, and Johan Detraux, are with Katholieke Universiteit Leuven, Kortenberg, Belgium. These comments are from an accompanying editorial (JAMA Psychiatry. 2018 Jun 13. doi: 10.1001/jamapsychiatry.2018.1080 ). Dr. De Hert reported no disclosures. Mr. Detraux reported partial support by the Janssen Academy for work on the the Belgian Discussion Board on Antipsychotic Treatment.
The findings of this study by Nicol and colleagues corroborate previous reports that used conventional anthropometry to document the metabolic adverse effects of second-generation antipsychotic medications in children and adolescents, according to authors of an accompanying editorial.
The current study used “gold standard” methods of measurement to demonstrate that 12 weeks of treatment with low-dose olanzapine, risperidone, or aripiprazole led to rapid-onset changes in adiposity and insulin sensitivity, with larger increases in those who received olanzapine.
“As such, the study even more emphatically underlines the risks to which these vulnerable populations are exposed,” Marc De Hert, MD, PhD, and Johan Detraux wrote.
It is now is clear that the potential psychiatric benefits of off-label antipsychotics need to be weighed against the potential for childhood-onset obesity and insulin resistance, they added. However, longer-term studies that use hard end points, such as new-onset diabetes or cardiovascular disease are needed.
Marc De Hert, MD, PhD, and Johan Detraux, are with Katholieke Universiteit Leuven, Kortenberg, Belgium. These comments are from an accompanying editorial (JAMA Psychiatry. 2018 Jun 13. doi: 10.1001/jamapsychiatry.2018.1080 ). Dr. De Hert reported no disclosures. Mr. Detraux reported partial support by the Janssen Academy for work on the the Belgian Discussion Board on Antipsychotic Treatment.
Twelve weeks of treatment with three different antipsychotics commonly used in children and adolescents with disruptive behavioral disorders was associated with rapid-onset adverse changes in adiposity and insulin sensitivity, results of a randomized clinical trial show.
The adverse effect on adiposity was greatest for children aged 6-18 years who received olanzapine, but was also seen in study participants randomized to receive risperidone or aripiprazole, according to results of the study published in JAMA Psychiatry.
These findings inform the risk-benefit analysis for off-label pediatric use of antipsychotics for disruptive behavior disorders, Ginger E. Nicol, MD, of Washington University, St. Louis, and colleagues wrote.
“The potential psychiatric benefits of antipsychotic use in this population, evident in this trial and others, should be carefully weighed against the potential for childhood onset of abdominal obesity and insulin resistance that – compared with adult onset – further increases long-term risk for [type 2 diabetes], cardiovascular disease, and related conditions,” the researchers wrote.
This randomized, prospective clinical trial included 144 antipsychotic-naive children and adolescents aged 6-18 years who had been diagnosed with one or more psychiatric disorders and clinically significant aggression. They were randomly and evenly assigned to 12 weeks of treatment with oral olanzapine, risperidone, or aripiprazole.
Those who received olanzapine had a 4.12% increase in percentage total body fat from baseline to week 12, as measured by dual-energy x-ray absorptiometry (DXA). That increase was significantly greater than the total body fat increases of 1.18% for risperidone and 1.66% for aripiprazole seen over that same time period (P less than .001 for time-by-treatment interaction), the researchers reported.
Insulin sensitivity decreased over time in the pooled study sample, with significant changes reported in insulin-stimulated glucose rate of disappearance, glucose rate of appearance, and glycerol rate of appearance. The changes did not differ significantly across the three treatment groups.
The lack of a placebo group in this study makes it unclear how much of the body fat and insulin sensitivity changes were attributable to antipsychotic medication. Psychiatric symptoms did improve significantly with treatment, the researchers noted.
Dr. Nicol reported research funding from the National Institute of Mental Health, Otsuka America Pharmaceutical, Alkermes PLC, The Sidney R. Baer Jr. Foundation, and the Center for Brain Research in Mood Disorders at Washington University in St Louis. Co-authors reported financial ties to Reviva Pharmaceuticals, Sunovion Pharmaceuticals, Indivior, Amgen, and other companies.
SOURCE: Nicol GE et al. JAMA Psychiatry. 2018 Jun 13. doi: 10.1001/jamapsychiatry.2018.1088.
Twelve weeks of treatment with three different antipsychotics commonly used in children and adolescents with disruptive behavioral disorders was associated with rapid-onset adverse changes in adiposity and insulin sensitivity, results of a randomized clinical trial show.
The adverse effect on adiposity was greatest for children aged 6-18 years who received olanzapine, but was also seen in study participants randomized to receive risperidone or aripiprazole, according to results of the study published in JAMA Psychiatry.
These findings inform the risk-benefit analysis for off-label pediatric use of antipsychotics for disruptive behavior disorders, Ginger E. Nicol, MD, of Washington University, St. Louis, and colleagues wrote.
“The potential psychiatric benefits of antipsychotic use in this population, evident in this trial and others, should be carefully weighed against the potential for childhood onset of abdominal obesity and insulin resistance that – compared with adult onset – further increases long-term risk for [type 2 diabetes], cardiovascular disease, and related conditions,” the researchers wrote.
This randomized, prospective clinical trial included 144 antipsychotic-naive children and adolescents aged 6-18 years who had been diagnosed with one or more psychiatric disorders and clinically significant aggression. They were randomly and evenly assigned to 12 weeks of treatment with oral olanzapine, risperidone, or aripiprazole.
Those who received olanzapine had a 4.12% increase in percentage total body fat from baseline to week 12, as measured by dual-energy x-ray absorptiometry (DXA). That increase was significantly greater than the total body fat increases of 1.18% for risperidone and 1.66% for aripiprazole seen over that same time period (P less than .001 for time-by-treatment interaction), the researchers reported.
Insulin sensitivity decreased over time in the pooled study sample, with significant changes reported in insulin-stimulated glucose rate of disappearance, glucose rate of appearance, and glycerol rate of appearance. The changes did not differ significantly across the three treatment groups.
The lack of a placebo group in this study makes it unclear how much of the body fat and insulin sensitivity changes were attributable to antipsychotic medication. Psychiatric symptoms did improve significantly with treatment, the researchers noted.
Dr. Nicol reported research funding from the National Institute of Mental Health, Otsuka America Pharmaceutical, Alkermes PLC, The Sidney R. Baer Jr. Foundation, and the Center for Brain Research in Mood Disorders at Washington University in St Louis. Co-authors reported financial ties to Reviva Pharmaceuticals, Sunovion Pharmaceuticals, Indivior, Amgen, and other companies.
SOURCE: Nicol GE et al. JAMA Psychiatry. 2018 Jun 13. doi: 10.1001/jamapsychiatry.2018.1088.
FROM JAMA PSYCHIATRY
Key clinical point:
Major finding: Olanzapine-treated youths had the highest percentage total body fat increase (4.12%), but substantial increases were also noted for risperidone (1.18%) and aripiprazole (1.66%).
Study details: A randomized clinical trial including 144 antipsychotic-naive youths aged 6-18 years with one or more psychiatric disorders and clinically significant aggression.
Disclosures: Study authors reported disclosures related to Otsuka America Pharmaceutical, Alkermes PLC, Reviva Pharmaceuticals, Sunovion Pharmaceuticals, Indivior, Amgen, and other companies.
Source: Nicol GE et al. JAMA Psychiatry. 2018 Jun 13. doi:10.1001/jamapsychiatry.2018.1088.
DEA ruling may have stoked illicit opioid sales
Illicit online sales of opioids increased significantly following a 2014 regulatory decision that restricted the legal supply of opioids in the United States, results of a recent analysis show.
Opioid sales in the so-called cryptomarkets also shifted toward more potent drugs, including fentanyl, after the U.S. Drug Enforcement Administration rescheduled hydrocodone combination products, making them harder to access, authors of the analysis reported.
Those results suggest “the possibility of a causal relation” between the schedule change and sales trends on cryptomarket sites, according to James Martin, PhD, of Swinburne University, Melbourne, Australia, and co-authors.
“Our analysis cannot rule out other possible causal explanatory factors, but our results are consistent with the possibility that the schedule change might have directly contributed to the changes we observed in the supply of illicit opioids,” Dr. Martin and colleagues wrote in the BMJ.
Cryptomarkets outside the United States had no such uptick in opioid traffic over time, reinforcing the possibility that the 2014 DEA decision caused an increase in the illicit opioid supply. The analysis included 31 online illicit markets operating between October 2013 and July 2016.
Investigators collected data using web crawling software that downloaded HTML pages on the cryptomarket sites and extracted relevant information such as listing titles and drug types for later analysis. Generally, each market was fully crawled every 2 weeks. After data was scraped and extracted, they conducted an interrupted time series analysis of drug sales for each day of the data collection period.
Opioids represented 13.7% of all drug sales through U.S. cryptomarkets in July 2016, they found, compared with a modeled estimate of 6.7% of sales that would have occurred in the absence of the new schedule introduction.
“This represents an approximate doubling of the percentage of the total drug sales through cryptomarkets within the United States,” the authors wrote.
Fentanyl was the least purchased product at the beginning of the analysis, but by July 2016 it was the second most frequently purchased. No other drug category had any meaningful changes in the proportion of sales over time.
There was no way for researchers to confirm that U.S.-based cryptomarket sites were selling to customers in the United States or elsewhere. However, they said, cryptomarket buyers often use sites in the same country to avoid shipment losses and increased delivery time.
Part of the study were funded by the Social Sciences and Humanities Research Council of Canada, Macquarie University internal grants, and the Ministry of Justice and Security of the Netherlands. Study authors had no current financial relationships relevant to the study.
SOURCE: Martin J, et al. BMJ. 2018 Jun 13. doi: 10.1136/bmj.k2270.
The overdose crisis in the United States will likely worsen if “supply-side” measures, such as the tighter prescribing regulations evaluated in this study, are not coupled with interventions to reduce harm and decrease demand, according to Scott E. Hadland, MD, and Leo Beletsky.
On a more basic level, the analysis by James Martin and colleagues raises questions about the use of drug scheduling to regulate public health, the authors concluded in an accompanying editorial.
“The U.S. scheduling scheme inexplicably holds such disparate substances as cannabis, heroin, and psilocybin to be equally dangerous,” they wrote. “It is high time to rethink how, why, and when this regulatory framework is deployed to curb drug-related harms.”
The shift from schedule III to schedule II creates barriers to medication access that disproportionately affect individuals in rural areas and those with limited mobility, since refills for schedule II drugs can only be obtained through an in-person visit to a provider and pharmacist, the authors wrote.
Scott E Hadland, MD, is with Grayken Center for Addiction/Department of Pediatrics, Boston Medical Center, and Leo Beletsky is with the School of Law and Bouvé College of Health Sciences, Northeastern University, Boston. Mr. Beletsky reported sitting on the advisory board of a data analytics company that has an interest in the U.S. opioid crisis. These comments are from their accompanying editorial (BMJ. 2018 Jun 13. doi: 10.1136/bmj.k2480 ). Mr. Beletsky reported sitting on the advisory board of a data analytics company that has an interest in the U.S. opioid crisis.
The overdose crisis in the United States will likely worsen if “supply-side” measures, such as the tighter prescribing regulations evaluated in this study, are not coupled with interventions to reduce harm and decrease demand, according to Scott E. Hadland, MD, and Leo Beletsky.
On a more basic level, the analysis by James Martin and colleagues raises questions about the use of drug scheduling to regulate public health, the authors concluded in an accompanying editorial.
“The U.S. scheduling scheme inexplicably holds such disparate substances as cannabis, heroin, and psilocybin to be equally dangerous,” they wrote. “It is high time to rethink how, why, and when this regulatory framework is deployed to curb drug-related harms.”
The shift from schedule III to schedule II creates barriers to medication access that disproportionately affect individuals in rural areas and those with limited mobility, since refills for schedule II drugs can only be obtained through an in-person visit to a provider and pharmacist, the authors wrote.
Scott E Hadland, MD, is with Grayken Center for Addiction/Department of Pediatrics, Boston Medical Center, and Leo Beletsky is with the School of Law and Bouvé College of Health Sciences, Northeastern University, Boston. Mr. Beletsky reported sitting on the advisory board of a data analytics company that has an interest in the U.S. opioid crisis. These comments are from their accompanying editorial (BMJ. 2018 Jun 13. doi: 10.1136/bmj.k2480 ). Mr. Beletsky reported sitting on the advisory board of a data analytics company that has an interest in the U.S. opioid crisis.
The overdose crisis in the United States will likely worsen if “supply-side” measures, such as the tighter prescribing regulations evaluated in this study, are not coupled with interventions to reduce harm and decrease demand, according to Scott E. Hadland, MD, and Leo Beletsky.
On a more basic level, the analysis by James Martin and colleagues raises questions about the use of drug scheduling to regulate public health, the authors concluded in an accompanying editorial.
“The U.S. scheduling scheme inexplicably holds such disparate substances as cannabis, heroin, and psilocybin to be equally dangerous,” they wrote. “It is high time to rethink how, why, and when this regulatory framework is deployed to curb drug-related harms.”
The shift from schedule III to schedule II creates barriers to medication access that disproportionately affect individuals in rural areas and those with limited mobility, since refills for schedule II drugs can only be obtained through an in-person visit to a provider and pharmacist, the authors wrote.
Scott E Hadland, MD, is with Grayken Center for Addiction/Department of Pediatrics, Boston Medical Center, and Leo Beletsky is with the School of Law and Bouvé College of Health Sciences, Northeastern University, Boston. Mr. Beletsky reported sitting on the advisory board of a data analytics company that has an interest in the U.S. opioid crisis. These comments are from their accompanying editorial (BMJ. 2018 Jun 13. doi: 10.1136/bmj.k2480 ). Mr. Beletsky reported sitting on the advisory board of a data analytics company that has an interest in the U.S. opioid crisis.
Illicit online sales of opioids increased significantly following a 2014 regulatory decision that restricted the legal supply of opioids in the United States, results of a recent analysis show.
Opioid sales in the so-called cryptomarkets also shifted toward more potent drugs, including fentanyl, after the U.S. Drug Enforcement Administration rescheduled hydrocodone combination products, making them harder to access, authors of the analysis reported.
Those results suggest “the possibility of a causal relation” between the schedule change and sales trends on cryptomarket sites, according to James Martin, PhD, of Swinburne University, Melbourne, Australia, and co-authors.
“Our analysis cannot rule out other possible causal explanatory factors, but our results are consistent with the possibility that the schedule change might have directly contributed to the changes we observed in the supply of illicit opioids,” Dr. Martin and colleagues wrote in the BMJ.
Cryptomarkets outside the United States had no such uptick in opioid traffic over time, reinforcing the possibility that the 2014 DEA decision caused an increase in the illicit opioid supply. The analysis included 31 online illicit markets operating between October 2013 and July 2016.
Investigators collected data using web crawling software that downloaded HTML pages on the cryptomarket sites and extracted relevant information such as listing titles and drug types for later analysis. Generally, each market was fully crawled every 2 weeks. After data was scraped and extracted, they conducted an interrupted time series analysis of drug sales for each day of the data collection period.
Opioids represented 13.7% of all drug sales through U.S. cryptomarkets in July 2016, they found, compared with a modeled estimate of 6.7% of sales that would have occurred in the absence of the new schedule introduction.
“This represents an approximate doubling of the percentage of the total drug sales through cryptomarkets within the United States,” the authors wrote.
Fentanyl was the least purchased product at the beginning of the analysis, but by July 2016 it was the second most frequently purchased. No other drug category had any meaningful changes in the proportion of sales over time.
There was no way for researchers to confirm that U.S.-based cryptomarket sites were selling to customers in the United States or elsewhere. However, they said, cryptomarket buyers often use sites in the same country to avoid shipment losses and increased delivery time.
Part of the study were funded by the Social Sciences and Humanities Research Council of Canada, Macquarie University internal grants, and the Ministry of Justice and Security of the Netherlands. Study authors had no current financial relationships relevant to the study.
SOURCE: Martin J, et al. BMJ. 2018 Jun 13. doi: 10.1136/bmj.k2270.
Illicit online sales of opioids increased significantly following a 2014 regulatory decision that restricted the legal supply of opioids in the United States, results of a recent analysis show.
Opioid sales in the so-called cryptomarkets also shifted toward more potent drugs, including fentanyl, after the U.S. Drug Enforcement Administration rescheduled hydrocodone combination products, making them harder to access, authors of the analysis reported.
Those results suggest “the possibility of a causal relation” between the schedule change and sales trends on cryptomarket sites, according to James Martin, PhD, of Swinburne University, Melbourne, Australia, and co-authors.
“Our analysis cannot rule out other possible causal explanatory factors, but our results are consistent with the possibility that the schedule change might have directly contributed to the changes we observed in the supply of illicit opioids,” Dr. Martin and colleagues wrote in the BMJ.
Cryptomarkets outside the United States had no such uptick in opioid traffic over time, reinforcing the possibility that the 2014 DEA decision caused an increase in the illicit opioid supply. The analysis included 31 online illicit markets operating between October 2013 and July 2016.
Investigators collected data using web crawling software that downloaded HTML pages on the cryptomarket sites and extracted relevant information such as listing titles and drug types for later analysis. Generally, each market was fully crawled every 2 weeks. After data was scraped and extracted, they conducted an interrupted time series analysis of drug sales for each day of the data collection period.
Opioids represented 13.7% of all drug sales through U.S. cryptomarkets in July 2016, they found, compared with a modeled estimate of 6.7% of sales that would have occurred in the absence of the new schedule introduction.
“This represents an approximate doubling of the percentage of the total drug sales through cryptomarkets within the United States,” the authors wrote.
Fentanyl was the least purchased product at the beginning of the analysis, but by July 2016 it was the second most frequently purchased. No other drug category had any meaningful changes in the proportion of sales over time.
There was no way for researchers to confirm that U.S.-based cryptomarket sites were selling to customers in the United States or elsewhere. However, they said, cryptomarket buyers often use sites in the same country to avoid shipment losses and increased delivery time.
Part of the study were funded by the Social Sciences and Humanities Research Council of Canada, Macquarie University internal grants, and the Ministry of Justice and Security of the Netherlands. Study authors had no current financial relationships relevant to the study.
SOURCE: Martin J, et al. BMJ. 2018 Jun 13. doi: 10.1136/bmj.k2270.
FROM BMJ
Key clinical point: Major finding: Opioids represented 13.7% of all drug sales through U.S. cryptomarkets in July 2016, compared with a modeled estimate of 6.7%.
Study details: An analysis of 31 online cryptomarkets operating between October 2013 and July 2016.
Disclosures: Part of the study were funded by the Social Sciences and Humanities Research Council of Canada, Macquarie University internal grants, and the Ministry of Justice and Security of the Netherlands. Study authors reported having no current financial relationships relevant to the study.
Source: Martin J, et al. BMJ. 2018 Jun 13. doi: 10.1136/bmj.k2270.