User login
We're on Instagram!
We're now on Instagram, a social media app designed for sharing photos and videos from a smartphone. Be sure to follow us!
We're now on Instagram, a social media app designed for sharing photos and videos from a smartphone. Be sure to follow us!
We're now on Instagram, a social media app designed for sharing photos and videos from a smartphone. Be sure to follow us!
Is the rise of suicide a medical or societal issue?
It’s hard to ignore the recent report from the Centers for Disease Control and Prevention revealing suicide rates went up by more than 30% in half of states since 1999 (“Suicide rates rising across the U.S.,” CDC Newsroom, June 7, 2018). My professional experience with suicide is limited to one former patient who died several years after aging out of my practice. His death was not a total surprise. The cornerstones of the situation he felt he couldn’t escape were well in place when he was a freshman in high school. I’m sure there was more I could have tried to do at that early stage. Although he was anxious and mildly depressed he never admitted to being suicidal.

Just as in Ms. Roberts’ family, the CDC report has elicited a fresh round of finger pointing and introspection in our country at a time when it is already struggling to find a sense of its own identity. Is it too many guns? Or too few mental health professionals? Or a broken health delivery system?
Dr. Richard A. Friedman, a psychiatrist at Weill Cornell Medical College, writes in the New York Times that “suicide is a medical problem” and that we should declare war on it “as we’ve done with other public health threats like HIV and heart disease” (“Suicide Rates Are Rising. What Should We Do About It?” June 11, 2018). Although it may be contagious with outbreaks and clusters, particularly in the wake of celebrity suicides (“The Science Behind Suicide Contagion,” by Margot Sanger-Katz, The New York Times, Aug 13, 2014), I’m not so sure that suicide is a medical problem. Certainly, it can be spread by a vector, in this case the ubiquitous news media. With more exposure, suicide has become if not the norm, at least in certain subgroups a socially acceptable management option for an unhappy life. But while there are other features of suicide that tempt us to retreat into our comfort zone of the medical model, we need to face the more realistic and unsettling explanation that the increase in the suicide rate is the symptom of a sick society.

We already are making a mistake by interpreting the apparent rise in distractible behavior as a disease that requires medication. Let’s spread a broader net as we search for answers to the alarming suicide death statistics.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
It’s hard to ignore the recent report from the Centers for Disease Control and Prevention revealing suicide rates went up by more than 30% in half of states since 1999 (“Suicide rates rising across the U.S.,” CDC Newsroom, June 7, 2018). My professional experience with suicide is limited to one former patient who died several years after aging out of my practice. His death was not a total surprise. The cornerstones of the situation he felt he couldn’t escape were well in place when he was a freshman in high school. I’m sure there was more I could have tried to do at that early stage. Although he was anxious and mildly depressed he never admitted to being suicidal.
Just as in Ms. Roberts’ family, the CDC report has elicited a fresh round of finger pointing and introspection in our country at a time when it is already struggling to find a sense of its own identity. Is it too many guns? Or too few mental health professionals? Or a broken health delivery system?
Dr. Richard A. Friedman, a psychiatrist at Weill Cornell Medical College, writes in the New York Times that “suicide is a medical problem” and that we should declare war on it “as we’ve done with other public health threats like HIV and heart disease” (“Suicide Rates Are Rising. What Should We Do About It?” June 11, 2018). Although it may be contagious with outbreaks and clusters, particularly in the wake of celebrity suicides (“The Science Behind Suicide Contagion,” by Margot Sanger-Katz, The New York Times, Aug 13, 2014), I’m not so sure that suicide is a medical problem. Certainly, it can be spread by a vector, in this case the ubiquitous news media. With more exposure, suicide has become if not the norm, at least in certain subgroups a socially acceptable management option for an unhappy life. But while there are other features of suicide that tempt us to retreat into our comfort zone of the medical model, we need to face the more realistic and unsettling explanation that the increase in the suicide rate is the symptom of a sick society.
We already are making a mistake by interpreting the apparent rise in distractible behavior as a disease that requires medication. Let’s spread a broader net as we search for answers to the alarming suicide death statistics.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
It’s hard to ignore the recent report from the Centers for Disease Control and Prevention revealing suicide rates went up by more than 30% in half of states since 1999 (“Suicide rates rising across the U.S.,” CDC Newsroom, June 7, 2018). My professional experience with suicide is limited to one former patient who died several years after aging out of my practice. His death was not a total surprise. The cornerstones of the situation he felt he couldn’t escape were well in place when he was a freshman in high school. I’m sure there was more I could have tried to do at that early stage. Although he was anxious and mildly depressed he never admitted to being suicidal.
Just as in Ms. Roberts’ family, the CDC report has elicited a fresh round of finger pointing and introspection in our country at a time when it is already struggling to find a sense of its own identity. Is it too many guns? Or too few mental health professionals? Or a broken health delivery system?
Dr. Richard A. Friedman, a psychiatrist at Weill Cornell Medical College, writes in the New York Times that “suicide is a medical problem” and that we should declare war on it “as we’ve done with other public health threats like HIV and heart disease” (“Suicide Rates Are Rising. What Should We Do About It?” June 11, 2018). Although it may be contagious with outbreaks and clusters, particularly in the wake of celebrity suicides (“The Science Behind Suicide Contagion,” by Margot Sanger-Katz, The New York Times, Aug 13, 2014), I’m not so sure that suicide is a medical problem. Certainly, it can be spread by a vector, in this case the ubiquitous news media. With more exposure, suicide has become if not the norm, at least in certain subgroups a socially acceptable management option for an unhappy life. But while there are other features of suicide that tempt us to retreat into our comfort zone of the medical model, we need to face the more realistic and unsettling explanation that the increase in the suicide rate is the symptom of a sick society.
We already are making a mistake by interpreting the apparent rise in distractible behavior as a disease that requires medication. Let’s spread a broader net as we search for answers to the alarming suicide death statistics.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
Invasive cardiology sets starting salary standard
A 5% increase in average starting salary for the 2017-2018 recruiting year enabled invasive cardiologists to replace orthopedic surgeons as the top physician earners, according to physician recruitment firm Merritt Hawkins.
Invasive cardiologists who started new jobs in the past year received an average starting salary of $590,000, compared with $563,000 in 2016-2017, while orthopedic surgeons took an 8% cut as their starting salaries dropped from $579,000 to $533,000, Merritt Hawkins reported in its 2018 Review of Physician and Advanced Practitioners Recruiting Incentives.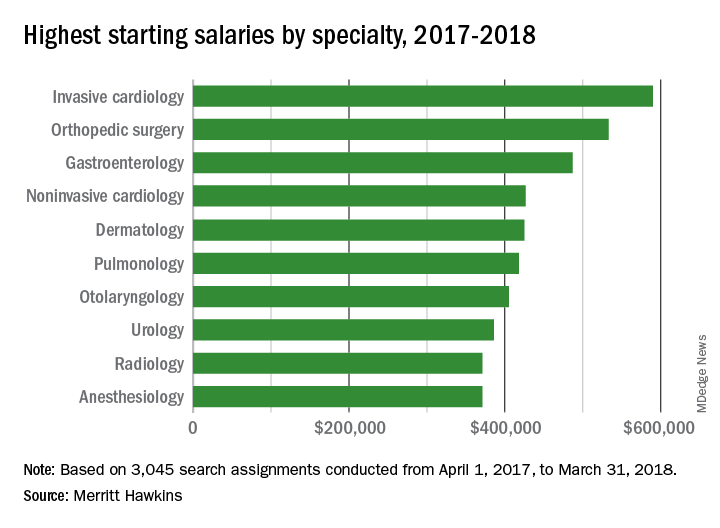
Besides the orthopedic surgeons, specialists who saw considerable drops in pay from 2016 to 2017 included otolaryngologists (–13%), radiologists (–15%), and urologists (–16%), according to the report.
“Demand for specialists is being driven upward by population aging and other factors. Average salaries, however, do not always correspond to increases in demand, at least not initially, as the market needs time to adjust to changing supply and demand dynamics,” Merritt Hawkins noted.
A 5% increase in average starting salary for the 2017-2018 recruiting year enabled invasive cardiologists to replace orthopedic surgeons as the top physician earners, according to physician recruitment firm Merritt Hawkins.
Invasive cardiologists who started new jobs in the past year received an average starting salary of $590,000, compared with $563,000 in 2016-2017, while orthopedic surgeons took an 8% cut as their starting salaries dropped from $579,000 to $533,000, Merritt Hawkins reported in its 2018 Review of Physician and Advanced Practitioners Recruiting Incentives.
Besides the orthopedic surgeons, specialists who saw considerable drops in pay from 2016 to 2017 included otolaryngologists (–13%), radiologists (–15%), and urologists (–16%), according to the report.
“Demand for specialists is being driven upward by population aging and other factors. Average salaries, however, do not always correspond to increases in demand, at least not initially, as the market needs time to adjust to changing supply and demand dynamics,” Merritt Hawkins noted.
A 5% increase in average starting salary for the 2017-2018 recruiting year enabled invasive cardiologists to replace orthopedic surgeons as the top physician earners, according to physician recruitment firm Merritt Hawkins.
Invasive cardiologists who started new jobs in the past year received an average starting salary of $590,000, compared with $563,000 in 2016-2017, while orthopedic surgeons took an 8% cut as their starting salaries dropped from $579,000 to $533,000, Merritt Hawkins reported in its 2018 Review of Physician and Advanced Practitioners Recruiting Incentives.
Besides the orthopedic surgeons, specialists who saw considerable drops in pay from 2016 to 2017 included otolaryngologists (–13%), radiologists (–15%), and urologists (–16%), according to the report.
“Demand for specialists is being driven upward by population aging and other factors. Average salaries, however, do not always correspond to increases in demand, at least not initially, as the market needs time to adjust to changing supply and demand dynamics,” Merritt Hawkins noted.
Size can matter: Laparoscopic hysterectomy for the very large uterus

Visit the Society of Gynecologic Surgeons online: sgsonline.org
Additional videos from SGS are available here, including these recent offerings:
Visit the Society of Gynecologic Surgeons online: sgsonline.org
Additional videos from SGS are available here, including these recent offerings:
Visit the Society of Gynecologic Surgeons online: sgsonline.org
Additional videos from SGS are available here, including these recent offerings:
This video is brought to you by![]()
Register for ACS Comprehensive General Surgery Review Course
The 2018 American College of Surgeons (ACS) Comprehensive General Surgery Review Course, July 26–29 in Chicago, IL, is an intensive three-and-a-half-day review course that will cover essential content areas in general surgery, including alimentary tract, endocrine and soft tissue, oncology, skin and breast, surgical critical care, trauma, and vascular operations, as well as perioperative care.
Course Chair John A. Weigelt, MD, DVM, MMA, FACS, and a distinguished faculty will use didactic and case-based formats to present a comprehensive and practical review. Dr. Weigelt recently retired from the Medical College of Wisconsin, where he was the Milt & Lidy Lunda/Charles Aprahamian Professor of Trauma Surgery, as well as professor and chief, division of trauma and critical care. He is joining the University of South Dakota and the Sanford Health System, Sioux Falls, this summer as professor of surgery. Dr. Weigelt is Medical Director of the ACS Surgical Education and Self-Assessment Program (SESAP®).
The course is a pragmatic review designed to focus on practice issues and will offer several special features, including self-assessment materials, such as pre- and posttests. It may be helpful in preparing for examinations. Self-assessment credit will be available.
The ACS is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide Continuing Medical Education for physicians.
The ACS designates this liv
Register today at bit.ly/2s19VtX, and read more about the course at www.facs.org/gsreviewcourse. Space is limited and registration will be accepted on a first-come, first-served basis. For more information and registration, visit the ACS website or e-mail [email protected] or [email protected].
The 2018 American College of Surgeons (ACS) Comprehensive General Surgery Review Course, July 26–29 in Chicago, IL, is an intensive three-and-a-half-day review course that will cover essential content areas in general surgery, including alimentary tract, endocrine and soft tissue, oncology, skin and breast, surgical critical care, trauma, and vascular operations, as well as perioperative care.
Course Chair John A. Weigelt, MD, DVM, MMA, FACS, and a distinguished faculty will use didactic and case-based formats to present a comprehensive and practical review. Dr. Weigelt recently retired from the Medical College of Wisconsin, where he was the Milt & Lidy Lunda/Charles Aprahamian Professor of Trauma Surgery, as well as professor and chief, division of trauma and critical care. He is joining the University of South Dakota and the Sanford Health System, Sioux Falls, this summer as professor of surgery. Dr. Weigelt is Medical Director of the ACS Surgical Education and Self-Assessment Program (SESAP®).
The course is a pragmatic review designed to focus on practice issues and will offer several special features, including self-assessment materials, such as pre- and posttests. It may be helpful in preparing for examinations. Self-assessment credit will be available.
The ACS is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide Continuing Medical Education for physicians.
The ACS designates this liv
Register today at bit.ly/2s19VtX, and read more about the course at www.facs.org/gsreviewcourse. Space is limited and registration will be accepted on a first-come, first-served basis. For more information and registration, visit the ACS website or e-mail [email protected] or [email protected].
The 2018 American College of Surgeons (ACS) Comprehensive General Surgery Review Course, July 26–29 in Chicago, IL, is an intensive three-and-a-half-day review course that will cover essential content areas in general surgery, including alimentary tract, endocrine and soft tissue, oncology, skin and breast, surgical critical care, trauma, and vascular operations, as well as perioperative care.
Course Chair John A. Weigelt, MD, DVM, MMA, FACS, and a distinguished faculty will use didactic and case-based formats to present a comprehensive and practical review. Dr. Weigelt recently retired from the Medical College of Wisconsin, where he was the Milt & Lidy Lunda/Charles Aprahamian Professor of Trauma Surgery, as well as professor and chief, division of trauma and critical care. He is joining the University of South Dakota and the Sanford Health System, Sioux Falls, this summer as professor of surgery. Dr. Weigelt is Medical Director of the ACS Surgical Education and Self-Assessment Program (SESAP®).
The course is a pragmatic review designed to focus on practice issues and will offer several special features, including self-assessment materials, such as pre- and posttests. It may be helpful in preparing for examinations. Self-assessment credit will be available.
The ACS is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide Continuing Medical Education for physicians.
The ACS designates this liv
Register today at bit.ly/2s19VtX, and read more about the course at www.facs.org/gsreviewcourse. Space is limited and registration will be accepted on a first-come, first-served basis. For more information and registration, visit the ACS website or e-mail [email protected] or [email protected].
ACS, other organizations concerned with patient safety offer recommendations on OR attire
The American College of Surgeons (ACS), the American Society of Anesthesiologists, the Association of periOperative Registered Nurses, the Association for Professionals in Infection Control and Epidemiology, the Association of Surgical Technologists, the Council on Surgical and Perioperative Safety, and The Joint Commission recently developed consensus recommendations on operating room (OR) attire. The recommendations focus specifically on ear and hair covering.
The group has reached the following conclusions:
Evidence-based recommendations on surgical attire developed for perioperative policies and procedures are best created collaboratively, with a multidisciplinary team representing surgery, anesthesia, nursing, and infection prevention.
The requirement for ear coverage is not supported by sufficient evidence.
At present, available scientific evidence does not demonstrate any association between the type of hat or extent of hair coverage and surgical site infection rates. In fact, a recent report in the
Other issues regarding areas of surgical attire need further evaluation.
For details, read the consensus statement on the ACS website at facs.org/about-acs/consensus-statements/or-attire.
In addition, the ACS recently received notification from The Joint Commission indicating that the accrediting body will incorporate the specifications outlined in the consensus statement into its survey procedures for hospitals and other relevant health care facilities.
The American College of Surgeons (ACS), the American Society of Anesthesiologists, the Association of periOperative Registered Nurses, the Association for Professionals in Infection Control and Epidemiology, the Association of Surgical Technologists, the Council on Surgical and Perioperative Safety, and The Joint Commission recently developed consensus recommendations on operating room (OR) attire. The recommendations focus specifically on ear and hair covering.
The group has reached the following conclusions:
Evidence-based recommendations on surgical attire developed for perioperative policies and procedures are best created collaboratively, with a multidisciplinary team representing surgery, anesthesia, nursing, and infection prevention.
The requirement for ear coverage is not supported by sufficient evidence.
At present, available scientific evidence does not demonstrate any association between the type of hat or extent of hair coverage and surgical site infection rates. In fact, a recent report in the
Other issues regarding areas of surgical attire need further evaluation.
For details, read the consensus statement on the ACS website at facs.org/about-acs/consensus-statements/or-attire.
In addition, the ACS recently received notification from The Joint Commission indicating that the accrediting body will incorporate the specifications outlined in the consensus statement into its survey procedures for hospitals and other relevant health care facilities.
The American College of Surgeons (ACS), the American Society of Anesthesiologists, the Association of periOperative Registered Nurses, the Association for Professionals in Infection Control and Epidemiology, the Association of Surgical Technologists, the Council on Surgical and Perioperative Safety, and The Joint Commission recently developed consensus recommendations on operating room (OR) attire. The recommendations focus specifically on ear and hair covering.
The group has reached the following conclusions:
Evidence-based recommendations on surgical attire developed for perioperative policies and procedures are best created collaboratively, with a multidisciplinary team representing surgery, anesthesia, nursing, and infection prevention.
The requirement for ear coverage is not supported by sufficient evidence.
At present, available scientific evidence does not demonstrate any association between the type of hat or extent of hair coverage and surgical site infection rates. In fact, a recent report in the
Other issues regarding areas of surgical attire need further evaluation.
For details, read the consensus statement on the ACS website at facs.org/about-acs/consensus-statements/or-attire.
In addition, the ACS recently received notification from The Joint Commission indicating that the accrediting body will incorporate the specifications outlined in the consensus statement into its survey procedures for hospitals and other relevant health care facilities.
ACS Clinical Scholars in Residence Program Application Deadline Extended
The American College of Surgeons (ACS) is offering a two-year, onsite fellowship in surgical outcomes research, health services research, and health care policy through the Clinical Scholars in Residence program. The application deadline for positions starting in 2019 has been extended to June 29, 2018.
Applicants must have completed two years of clinical training, be U.S. citizens, and obtained two years of program funding from their home institution or other granting agency. The applicant also must be a member of the ACS and in good standing with the College.
The Clinical Scholar will have the opportunity to work in multiple areas within the ACS Division of Research and Optimal Patient Care at the ACS headquarters in Chicago, IL, to advance the quality improvement initiatives of the ACS and to perform research relevant to ongoing projects within the ACS. Participants also will earn a masters degree after the two years program. The Clinical Scholar will receive strong mentorship in clinical, statistical, and health services research. Previous ACS Clinical Scholars in Residence since 2005 have had excellent, productive experiences that have launched careers in the field.
Important dates for Clinical Scholars in Residence program follow:
Application deadline extended: June 29, 2018
Interview notification: July 13, 2018
Interview Process: July 16–31, 2018
Notification of appointment: August 1, 2018
Starting date: July 1, 2019
For more information, go to facs.org/quality-programs/about/clinical-scholars-program. Contact the ACS Clinical Scholars in Residence Program at [email protected] with additional questions.
The American College of Surgeons (ACS) is offering a two-year, onsite fellowship in surgical outcomes research, health services research, and health care policy through the Clinical Scholars in Residence program. The application deadline for positions starting in 2019 has been extended to June 29, 2018.
Applicants must have completed two years of clinical training, be U.S. citizens, and obtained two years of program funding from their home institution or other granting agency. The applicant also must be a member of the ACS and in good standing with the College.
The Clinical Scholar will have the opportunity to work in multiple areas within the ACS Division of Research and Optimal Patient Care at the ACS headquarters in Chicago, IL, to advance the quality improvement initiatives of the ACS and to perform research relevant to ongoing projects within the ACS. Participants also will earn a masters degree after the two years program. The Clinical Scholar will receive strong mentorship in clinical, statistical, and health services research. Previous ACS Clinical Scholars in Residence since 2005 have had excellent, productive experiences that have launched careers in the field.
Important dates for Clinical Scholars in Residence program follow:
Application deadline extended: June 29, 2018
Interview notification: July 13, 2018
Interview Process: July 16–31, 2018
Notification of appointment: August 1, 2018
Starting date: July 1, 2019
For more information, go to facs.org/quality-programs/about/clinical-scholars-program. Contact the ACS Clinical Scholars in Residence Program at [email protected] with additional questions.
The American College of Surgeons (ACS) is offering a two-year, onsite fellowship in surgical outcomes research, health services research, and health care policy through the Clinical Scholars in Residence program. The application deadline for positions starting in 2019 has been extended to June 29, 2018.
Applicants must have completed two years of clinical training, be U.S. citizens, and obtained two years of program funding from their home institution or other granting agency. The applicant also must be a member of the ACS and in good standing with the College.
The Clinical Scholar will have the opportunity to work in multiple areas within the ACS Division of Research and Optimal Patient Care at the ACS headquarters in Chicago, IL, to advance the quality improvement initiatives of the ACS and to perform research relevant to ongoing projects within the ACS. Participants also will earn a masters degree after the two years program. The Clinical Scholar will receive strong mentorship in clinical, statistical, and health services research. Previous ACS Clinical Scholars in Residence since 2005 have had excellent, productive experiences that have launched careers in the field.
Important dates for Clinical Scholars in Residence program follow:
Application deadline extended: June 29, 2018
Interview notification: July 13, 2018
Interview Process: July 16–31, 2018
Notification of appointment: August 1, 2018
Starting date: July 1, 2019
For more information, go to facs.org/quality-programs/about/clinical-scholars-program. Contact the ACS Clinical Scholars in Residence Program at [email protected] with additional questions.
Veterans Can Now Access Medical Images and Reports Online
Veterans with a premium account on My HealtheVet no longer need to make an in-person visit to get their medical images and associated study reports—now they can do it online. VA Medical Images and Reports allows users to view, download, and share copies of their radiology studies, including x-rays, mammograms, MRIs, and CTs, from the VA Electronic Health Record.
Radiology studies are available in My HealtheVet 3 calendar days after the study report has been verified. When a request for a specific study is completed, veterans can view a lower resolution thumbnail copy of the images and the radiology report online or download a zip file with the information. For studies with large files, the user can opt to receive an e-mail notification when the download request is complete.
To view diagnostic-quality images, veterans may install a free medical image viewer on their computer. The images and reports can be copied to a CD, DVD, USB flash drive, or any portable drive to share with providers, across VA settings and outside the VA.
Veterans with a premium account on My HealtheVet no longer need to make an in-person visit to get their medical images and associated study reports—now they can do it online. VA Medical Images and Reports allows users to view, download, and share copies of their radiology studies, including x-rays, mammograms, MRIs, and CTs, from the VA Electronic Health Record.
Radiology studies are available in My HealtheVet 3 calendar days after the study report has been verified. When a request for a specific study is completed, veterans can view a lower resolution thumbnail copy of the images and the radiology report online or download a zip file with the information. For studies with large files, the user can opt to receive an e-mail notification when the download request is complete.
To view diagnostic-quality images, veterans may install a free medical image viewer on their computer. The images and reports can be copied to a CD, DVD, USB flash drive, or any portable drive to share with providers, across VA settings and outside the VA.
Veterans with a premium account on My HealtheVet no longer need to make an in-person visit to get their medical images and associated study reports—now they can do it online. VA Medical Images and Reports allows users to view, download, and share copies of their radiology studies, including x-rays, mammograms, MRIs, and CTs, from the VA Electronic Health Record.
Radiology studies are available in My HealtheVet 3 calendar days after the study report has been verified. When a request for a specific study is completed, veterans can view a lower resolution thumbnail copy of the images and the radiology report online or download a zip file with the information. For studies with large files, the user can opt to receive an e-mail notification when the download request is complete.
To view diagnostic-quality images, veterans may install a free medical image viewer on their computer. The images and reports can be copied to a CD, DVD, USB flash drive, or any portable drive to share with providers, across VA settings and outside the VA.
Quizartinib can prolong OS in rel/ref, FLT3-ITD AML

STOCKHOLM—Phase 3 results suggest the FLT3 inhibitor quizartinib can prolong overall survival (OS) in patients with relapsed/refractory, FLT3-ITD acute myeloid leukemia (AML).
In the QuANTUM-R study, patients who received single-agent quizartinib had a significantly longer median OS than patients who received salvage chemotherapy.
There was a trend toward improved event-free survival (EFS) with quizartinib as well.
“QuANTUM-R represents the first study that shows a significant improvement in overall survival for a single agent—a FLT3 inhibitor or any other targeted agent—in this population of FLT3-mutated AML patients with refractory or relapsed disease . . .,” said study investigator Jorge Cortes, MD, of MD Anderson Cancer Center in Houston, Texas.
Dr Cortes presented results from QuANTUM-R at the 23rd Congress of the European Hematology Association (EHA). The research was selected as the best late-breaking abstract (LB2600).
The study was funded by Daiichi Sankyo, Inc., and Dr Cortes is a consultant for the company.
Patients and treatment
QuANTUM-R enrolled adults with FLT3-ITD AML (at least 3% FLT3-ITD allelic ratio) who had refractory disease or had relapsed within 6 months of their first complete remission. They had received at least 1 cycle of an induction regimen containing standard-dose anthracycline or mitoxantrone.
Patients were randomized to receive once-daily treatment with quizartinib (n=245) or a salvage chemotherapy regimen (n=122)—low-dose cytarabine (LoDAC, n=29); combination mitoxantrone, etoposide, and cytarabine (MEC, n=40); or combination fludarabine, cytarabine, and idarubicin (FLAG-IDA, n=53).
Responders could proceed to hematopoietic stem cell transplant (HSCT), and those in the quizartinib arm could resume quizartinib after HSCT.
Baseline characteristics were similar between the treatment arms. The median age was 55 (range, 19-81) for patients receiving quizartinib and 58 (range, 18-78) for those receiving chemotherapy.
Thirty-three percent of the quizartinib arm had refractory disease, and 67% had relapsed disease. Thirty-four percent of the chemotherapy arm had refractory disease, and 66% had relapsed disease.
The percentage of patients with a prior allogeneic HSCT was 25% in the quizartinib arm and 23% in the chemotherapy arm. Most patients in both arms had intermediate-risk cytogenetics—78% of the quizartinib arm and 66% of the chemotherapy arm.
In all, 241 patients received quizartinib, and 94 received salvage chemotherapy—LoDAC (n=22), MEC (n=25), and FLAG-IDA (n=47). Of the 28 patients in the chemotherapy group who were not treated, most withdrew consent.
The median treatment duration was 4 cycles (range, 1-3) in the quizartinib arm and 1 cycle (range, 1-2) for patients who received LoDAC, MEC, and FLAG-IDA.
The most common reason for discontinuation of chemotherapy was lack of response/progression (n=49), followed by death (n=6). Twenty-four patients completed salvage chemotherapy.
In the quizarinib arm, the most common reasons for treatment discontinuation were HSCT (n=79), relapse (n=60), or lack of response/progression (n=47).
Thirty-two percent of quizartinib-treated patients and 12% of the chemotherapy group went on to HSCT.
Results
The median follow-up was 23.5 months. The efficacy results include all randomized patients, and the safety results include only those who received their assigned treatment.
The study’s primary endpoint was OS. The median OS was 6.2 months in the quizartinib arm and 4.7 months in the chemotherapy arm (hazard ratio=0.76, P=0.0177). The 1-year OS rate was 27% and 20%, respectively.
The median EFS was 6.0 weeks in the quizartinib arm and 3.7 weeks in the chemotherapy arm (hazard ratio=0.90, P=0.1071). Dr Cortes noted that patients who did not receive treatment were censored on day 1, and partial responses were counted as failures in the EFS analysis.
The overall response rate was 69% in the quizartinib arm and 30% in the chemotherapy arm.
The composite complete response (CR) rate was 48% in the quizartinib arm and 27% in the chemotherapy arm. This includes the CR rate (4% and 1%, respectively), the rate of CR with incomplete platelet recovery (4% and 0%, respectively), and the rate of CR with incomplete hematologic recovery (40% and 26%, respectively). The rate of partial response was 21% and 3%, respectively.
Dr Cortes said rates of treatment-emergent adverse events (TEAEs) were similar between the treatment arms.
Grade 3 or higher hematologic TEAEs occurring in at least 5% of patients (in the quizartinib and chemotherapy groups, respectively) included thrombocytopenia (35% and 34%), anemia (30% and 29%), neutropenia (32% and 25%), febrile neutropenia (31% and 21%), and leukopenia (17% and 16%).
Grade 3 or higher nonhematologic TEAEs occurring in at least 5% of patients (in the quizartinib and chemotherapy groups, respectively) included fatigue (8% and 1%), hypokalemia (12% and 9%), sepsis/septic shock (16% and 18%), dyspnea (5% for both), hypophosphatemia (5% for both), and pneumonia (12% and 9%).
Three percent of patients in the quizartinib arm had grade 3 QTcF prolongation, but there were no grade 4 cases. Two patients discontinued quizartinib due to QTcF prolongation.
“The safety of this drug has remained constant across over 1600 patients that have been treated with quizartinib across a variety of studies,” Dr Cortes said.
He added that QuANTUM-R results open up the possibility that quizartinib could be used in other settings. Researchers are already testing standard chemotherapy with and without quizartinib in a phase 3 trial of patients with newly diagnosed, FLT-ITD AML (QuANTUM-First).
STOCKHOLM—Phase 3 results suggest the FLT3 inhibitor quizartinib can prolong overall survival (OS) in patients with relapsed/refractory, FLT3-ITD acute myeloid leukemia (AML).
In the QuANTUM-R study, patients who received single-agent quizartinib had a significantly longer median OS than patients who received salvage chemotherapy.
There was a trend toward improved event-free survival (EFS) with quizartinib as well.
“QuANTUM-R represents the first study that shows a significant improvement in overall survival for a single agent—a FLT3 inhibitor or any other targeted agent—in this population of FLT3-mutated AML patients with refractory or relapsed disease . . .,” said study investigator Jorge Cortes, MD, of MD Anderson Cancer Center in Houston, Texas.
Dr Cortes presented results from QuANTUM-R at the 23rd Congress of the European Hematology Association (EHA). The research was selected as the best late-breaking abstract (LB2600).
The study was funded by Daiichi Sankyo, Inc., and Dr Cortes is a consultant for the company.
Patients and treatment
QuANTUM-R enrolled adults with FLT3-ITD AML (at least 3% FLT3-ITD allelic ratio) who had refractory disease or had relapsed within 6 months of their first complete remission. They had received at least 1 cycle of an induction regimen containing standard-dose anthracycline or mitoxantrone.
Patients were randomized to receive once-daily treatment with quizartinib (n=245) or a salvage chemotherapy regimen (n=122)—low-dose cytarabine (LoDAC, n=29); combination mitoxantrone, etoposide, and cytarabine (MEC, n=40); or combination fludarabine, cytarabine, and idarubicin (FLAG-IDA, n=53).
Responders could proceed to hematopoietic stem cell transplant (HSCT), and those in the quizartinib arm could resume quizartinib after HSCT.
Baseline characteristics were similar between the treatment arms. The median age was 55 (range, 19-81) for patients receiving quizartinib and 58 (range, 18-78) for those receiving chemotherapy.
Thirty-three percent of the quizartinib arm had refractory disease, and 67% had relapsed disease. Thirty-four percent of the chemotherapy arm had refractory disease, and 66% had relapsed disease.
The percentage of patients with a prior allogeneic HSCT was 25% in the quizartinib arm and 23% in the chemotherapy arm. Most patients in both arms had intermediate-risk cytogenetics—78% of the quizartinib arm and 66% of the chemotherapy arm.
In all, 241 patients received quizartinib, and 94 received salvage chemotherapy—LoDAC (n=22), MEC (n=25), and FLAG-IDA (n=47). Of the 28 patients in the chemotherapy group who were not treated, most withdrew consent.
The median treatment duration was 4 cycles (range, 1-3) in the quizartinib arm and 1 cycle (range, 1-2) for patients who received LoDAC, MEC, and FLAG-IDA.
The most common reason for discontinuation of chemotherapy was lack of response/progression (n=49), followed by death (n=6). Twenty-four patients completed salvage chemotherapy.
In the quizarinib arm, the most common reasons for treatment discontinuation were HSCT (n=79), relapse (n=60), or lack of response/progression (n=47).
Thirty-two percent of quizartinib-treated patients and 12% of the chemotherapy group went on to HSCT.
Results
The median follow-up was 23.5 months. The efficacy results include all randomized patients, and the safety results include only those who received their assigned treatment.
The study’s primary endpoint was OS. The median OS was 6.2 months in the quizartinib arm and 4.7 months in the chemotherapy arm (hazard ratio=0.76, P=0.0177). The 1-year OS rate was 27% and 20%, respectively.
The median EFS was 6.0 weeks in the quizartinib arm and 3.7 weeks in the chemotherapy arm (hazard ratio=0.90, P=0.1071). Dr Cortes noted that patients who did not receive treatment were censored on day 1, and partial responses were counted as failures in the EFS analysis.
The overall response rate was 69% in the quizartinib arm and 30% in the chemotherapy arm.
The composite complete response (CR) rate was 48% in the quizartinib arm and 27% in the chemotherapy arm. This includes the CR rate (4% and 1%, respectively), the rate of CR with incomplete platelet recovery (4% and 0%, respectively), and the rate of CR with incomplete hematologic recovery (40% and 26%, respectively). The rate of partial response was 21% and 3%, respectively.
Dr Cortes said rates of treatment-emergent adverse events (TEAEs) were similar between the treatment arms.
Grade 3 or higher hematologic TEAEs occurring in at least 5% of patients (in the quizartinib and chemotherapy groups, respectively) included thrombocytopenia (35% and 34%), anemia (30% and 29%), neutropenia (32% and 25%), febrile neutropenia (31% and 21%), and leukopenia (17% and 16%).
Grade 3 or higher nonhematologic TEAEs occurring in at least 5% of patients (in the quizartinib and chemotherapy groups, respectively) included fatigue (8% and 1%), hypokalemia (12% and 9%), sepsis/septic shock (16% and 18%), dyspnea (5% for both), hypophosphatemia (5% for both), and pneumonia (12% and 9%).
Three percent of patients in the quizartinib arm had grade 3 QTcF prolongation, but there were no grade 4 cases. Two patients discontinued quizartinib due to QTcF prolongation.
“The safety of this drug has remained constant across over 1600 patients that have been treated with quizartinib across a variety of studies,” Dr Cortes said.
He added that QuANTUM-R results open up the possibility that quizartinib could be used in other settings. Researchers are already testing standard chemotherapy with and without quizartinib in a phase 3 trial of patients with newly diagnosed, FLT-ITD AML (QuANTUM-First).
STOCKHOLM—Phase 3 results suggest the FLT3 inhibitor quizartinib can prolong overall survival (OS) in patients with relapsed/refractory, FLT3-ITD acute myeloid leukemia (AML).
In the QuANTUM-R study, patients who received single-agent quizartinib had a significantly longer median OS than patients who received salvage chemotherapy.
There was a trend toward improved event-free survival (EFS) with quizartinib as well.
“QuANTUM-R represents the first study that shows a significant improvement in overall survival for a single agent—a FLT3 inhibitor or any other targeted agent—in this population of FLT3-mutated AML patients with refractory or relapsed disease . . .,” said study investigator Jorge Cortes, MD, of MD Anderson Cancer Center in Houston, Texas.
Dr Cortes presented results from QuANTUM-R at the 23rd Congress of the European Hematology Association (EHA). The research was selected as the best late-breaking abstract (LB2600).
The study was funded by Daiichi Sankyo, Inc., and Dr Cortes is a consultant for the company.
Patients and treatment
QuANTUM-R enrolled adults with FLT3-ITD AML (at least 3% FLT3-ITD allelic ratio) who had refractory disease or had relapsed within 6 months of their first complete remission. They had received at least 1 cycle of an induction regimen containing standard-dose anthracycline or mitoxantrone.
Patients were randomized to receive once-daily treatment with quizartinib (n=245) or a salvage chemotherapy regimen (n=122)—low-dose cytarabine (LoDAC, n=29); combination mitoxantrone, etoposide, and cytarabine (MEC, n=40); or combination fludarabine, cytarabine, and idarubicin (FLAG-IDA, n=53).
Responders could proceed to hematopoietic stem cell transplant (HSCT), and those in the quizartinib arm could resume quizartinib after HSCT.
Baseline characteristics were similar between the treatment arms. The median age was 55 (range, 19-81) for patients receiving quizartinib and 58 (range, 18-78) for those receiving chemotherapy.
Thirty-three percent of the quizartinib arm had refractory disease, and 67% had relapsed disease. Thirty-four percent of the chemotherapy arm had refractory disease, and 66% had relapsed disease.
The percentage of patients with a prior allogeneic HSCT was 25% in the quizartinib arm and 23% in the chemotherapy arm. Most patients in both arms had intermediate-risk cytogenetics—78% of the quizartinib arm and 66% of the chemotherapy arm.
In all, 241 patients received quizartinib, and 94 received salvage chemotherapy—LoDAC (n=22), MEC (n=25), and FLAG-IDA (n=47). Of the 28 patients in the chemotherapy group who were not treated, most withdrew consent.
The median treatment duration was 4 cycles (range, 1-3) in the quizartinib arm and 1 cycle (range, 1-2) for patients who received LoDAC, MEC, and FLAG-IDA.
The most common reason for discontinuation of chemotherapy was lack of response/progression (n=49), followed by death (n=6). Twenty-four patients completed salvage chemotherapy.
In the quizarinib arm, the most common reasons for treatment discontinuation were HSCT (n=79), relapse (n=60), or lack of response/progression (n=47).
Thirty-two percent of quizartinib-treated patients and 12% of the chemotherapy group went on to HSCT.
Results
The median follow-up was 23.5 months. The efficacy results include all randomized patients, and the safety results include only those who received their assigned treatment.
The study’s primary endpoint was OS. The median OS was 6.2 months in the quizartinib arm and 4.7 months in the chemotherapy arm (hazard ratio=0.76, P=0.0177). The 1-year OS rate was 27% and 20%, respectively.
The median EFS was 6.0 weeks in the quizartinib arm and 3.7 weeks in the chemotherapy arm (hazard ratio=0.90, P=0.1071). Dr Cortes noted that patients who did not receive treatment were censored on day 1, and partial responses were counted as failures in the EFS analysis.
The overall response rate was 69% in the quizartinib arm and 30% in the chemotherapy arm.
The composite complete response (CR) rate was 48% in the quizartinib arm and 27% in the chemotherapy arm. This includes the CR rate (4% and 1%, respectively), the rate of CR with incomplete platelet recovery (4% and 0%, respectively), and the rate of CR with incomplete hematologic recovery (40% and 26%, respectively). The rate of partial response was 21% and 3%, respectively.
Dr Cortes said rates of treatment-emergent adverse events (TEAEs) were similar between the treatment arms.
Grade 3 or higher hematologic TEAEs occurring in at least 5% of patients (in the quizartinib and chemotherapy groups, respectively) included thrombocytopenia (35% and 34%), anemia (30% and 29%), neutropenia (32% and 25%), febrile neutropenia (31% and 21%), and leukopenia (17% and 16%).
Grade 3 or higher nonhematologic TEAEs occurring in at least 5% of patients (in the quizartinib and chemotherapy groups, respectively) included fatigue (8% and 1%), hypokalemia (12% and 9%), sepsis/septic shock (16% and 18%), dyspnea (5% for both), hypophosphatemia (5% for both), and pneumonia (12% and 9%).
Three percent of patients in the quizartinib arm had grade 3 QTcF prolongation, but there were no grade 4 cases. Two patients discontinued quizartinib due to QTcF prolongation.
“The safety of this drug has remained constant across over 1600 patients that have been treated with quizartinib across a variety of studies,” Dr Cortes said.
He added that QuANTUM-R results open up the possibility that quizartinib could be used in other settings. Researchers are already testing standard chemotherapy with and without quizartinib in a phase 3 trial of patients with newly diagnosed, FLT-ITD AML (QuANTUM-First).
Peripheral blood MRD correlates with treatment benefit in CLL
CHICAGO—Minimal residual disease (MRD) kinetics confirms the high, durable MRD-negativity with venetoclax plus rituximab in relapsed/refractory chronic lymphocytic leukemia (CLL), according to a further examination of the phase 3 MURANO study.
Undetectable MRD-negativity is associated with extended progression-free survival (PFS) and overall survival in patients receiving chemoimmunotherapy for CLL.
“Attainment of MRD-negativity in relapsed/refractory CLL is also a desired trial endpoint due to the subjectivity of complete response definition regarding pathologic lymph node size,” said Peter Hillmen, MD, of St James’s University Hospital, Leeds, United Kingdom, at the 2018 ASCO Annual Meeting.
Dr Hillmen reported new data on MRD response in cytogenetic and molecular risk groups, MRD sustainability and kinetics, and MRD conversion in the MURANO trial (abstract 7508).
MURANO trial (NCT02005471)
In the trial, venetoclax-rituximab showed superior PFS and peripheral blood and bone marrow MRD-negativity as compared to bendamustine plus rituximab (BR) in relapsed/refractory CLL patients.
Patients were randomized to venetoclax-rituximab for 6 months, followed by single-agent venetoclax for up to 1.5 years, or BR for 6 months. Peripheral blood samples were serially collected and bone marrow was collected at the end of combination treatment or at best response.
MRD findings
The new results show higher concordance in MRD-negativity between bone marrow and peripheral blood in venetoclax-rituximab (45 of 50 patients, 90%) vs BR (3 of 10 patients, 30%) in paired samples.
Focusing on peripheral blood MRD, Dr Hillmen said the best MRD-negativity rates were higher with venetoclax-rituximab (84%) than BR (23%). These results were independent of high-risk factors—such as del 17p, IGVH unmutated, and mutated TP53—only for venetoclax-rituximab treated patients.
“The superior peripheral blood MRD response with venetoclax-rituximab was consistent across subgroups at the end of completion of treatment,” Dr Hillmen said. “Most patients who achieved peripheral blood MRD-negativity on venetoclax-rituximab remained MRD-negative and were progression-free.”
Among 121 of 194 (62%) patients on venetoclax-rituximab who achieved MRD-negativity at the end of combination therapy, 100 (83%) patients maintained MRD-negativity and were progression-free at a median follow-up of 13.8 months. Two patients developed progressive disease and 2 patients died (unrelated to CLL).
Two patients developed Richter’s disease (with one MRD-positive directly before therapy) and 15 (12%) patients converted to confirmed MRD-positive at a median MRD-positive follow-up of 5.6 months.
“High peripheral blood MRD-negativity at the end of combination treatment and concordance with bone marrow MRD with venetoclax-rituximab,” Dr Hillmen said, “confirms the value of peripheral blood MRD for evaluation of treatment benefit in relapsed/refractory CLL patients. The high rate of peripheral blood MRD-negativity at end of combination treatment with venetoclax-rituximab was attained regardless of risk features.”
Some conversion to MRD-positivity occurred only in a small proportion of patients. Most cases were of intermediate level and remained progression-free, he said.
“MRD kinetics indicate that peripheral blood MRD-negativity with venetoclax-rituximab occurs early and is maintained over time with current follow-up,” Dr Hillmen added. The MRD data now provide a framework for designing response adaptive therapy.
The US Food and Drug Administration recently approved venetoclax-rituximab for CLL or small lymphocytic lymphoma for patients with or without del 17p.
Venetoclax is being developed by Genentech and Abbvie.
CHICAGO—Minimal residual disease (MRD) kinetics confirms the high, durable MRD-negativity with venetoclax plus rituximab in relapsed/refractory chronic lymphocytic leukemia (CLL), according to a further examination of the phase 3 MURANO study.
Undetectable MRD-negativity is associated with extended progression-free survival (PFS) and overall survival in patients receiving chemoimmunotherapy for CLL.
“Attainment of MRD-negativity in relapsed/refractory CLL is also a desired trial endpoint due to the subjectivity of complete response definition regarding pathologic lymph node size,” said Peter Hillmen, MD, of St James’s University Hospital, Leeds, United Kingdom, at the 2018 ASCO Annual Meeting.
Dr Hillmen reported new data on MRD response in cytogenetic and molecular risk groups, MRD sustainability and kinetics, and MRD conversion in the MURANO trial (abstract 7508).
MURANO trial (NCT02005471)
In the trial, venetoclax-rituximab showed superior PFS and peripheral blood and bone marrow MRD-negativity as compared to bendamustine plus rituximab (BR) in relapsed/refractory CLL patients.
Patients were randomized to venetoclax-rituximab for 6 months, followed by single-agent venetoclax for up to 1.5 years, or BR for 6 months. Peripheral blood samples were serially collected and bone marrow was collected at the end of combination treatment or at best response.
MRD findings
The new results show higher concordance in MRD-negativity between bone marrow and peripheral blood in venetoclax-rituximab (45 of 50 patients, 90%) vs BR (3 of 10 patients, 30%) in paired samples.
Focusing on peripheral blood MRD, Dr Hillmen said the best MRD-negativity rates were higher with venetoclax-rituximab (84%) than BR (23%). These results were independent of high-risk factors—such as del 17p, IGVH unmutated, and mutated TP53—only for venetoclax-rituximab treated patients.
“The superior peripheral blood MRD response with venetoclax-rituximab was consistent across subgroups at the end of completion of treatment,” Dr Hillmen said. “Most patients who achieved peripheral blood MRD-negativity on venetoclax-rituximab remained MRD-negative and were progression-free.”
Among 121 of 194 (62%) patients on venetoclax-rituximab who achieved MRD-negativity at the end of combination therapy, 100 (83%) patients maintained MRD-negativity and were progression-free at a median follow-up of 13.8 months. Two patients developed progressive disease and 2 patients died (unrelated to CLL).
Two patients developed Richter’s disease (with one MRD-positive directly before therapy) and 15 (12%) patients converted to confirmed MRD-positive at a median MRD-positive follow-up of 5.6 months.
“High peripheral blood MRD-negativity at the end of combination treatment and concordance with bone marrow MRD with venetoclax-rituximab,” Dr Hillmen said, “confirms the value of peripheral blood MRD for evaluation of treatment benefit in relapsed/refractory CLL patients. The high rate of peripheral blood MRD-negativity at end of combination treatment with venetoclax-rituximab was attained regardless of risk features.”
Some conversion to MRD-positivity occurred only in a small proportion of patients. Most cases were of intermediate level and remained progression-free, he said.
“MRD kinetics indicate that peripheral blood MRD-negativity with venetoclax-rituximab occurs early and is maintained over time with current follow-up,” Dr Hillmen added. The MRD data now provide a framework for designing response adaptive therapy.
The US Food and Drug Administration recently approved venetoclax-rituximab for CLL or small lymphocytic lymphoma for patients with or without del 17p.
Venetoclax is being developed by Genentech and Abbvie.
CHICAGO—Minimal residual disease (MRD) kinetics confirms the high, durable MRD-negativity with venetoclax plus rituximab in relapsed/refractory chronic lymphocytic leukemia (CLL), according to a further examination of the phase 3 MURANO study.
Undetectable MRD-negativity is associated with extended progression-free survival (PFS) and overall survival in patients receiving chemoimmunotherapy for CLL.
“Attainment of MRD-negativity in relapsed/refractory CLL is also a desired trial endpoint due to the subjectivity of complete response definition regarding pathologic lymph node size,” said Peter Hillmen, MD, of St James’s University Hospital, Leeds, United Kingdom, at the 2018 ASCO Annual Meeting.
Dr Hillmen reported new data on MRD response in cytogenetic and molecular risk groups, MRD sustainability and kinetics, and MRD conversion in the MURANO trial (abstract 7508).
MURANO trial (NCT02005471)
In the trial, venetoclax-rituximab showed superior PFS and peripheral blood and bone marrow MRD-negativity as compared to bendamustine plus rituximab (BR) in relapsed/refractory CLL patients.
Patients were randomized to venetoclax-rituximab for 6 months, followed by single-agent venetoclax for up to 1.5 years, or BR for 6 months. Peripheral blood samples were serially collected and bone marrow was collected at the end of combination treatment or at best response.
MRD findings
The new results show higher concordance in MRD-negativity between bone marrow and peripheral blood in venetoclax-rituximab (45 of 50 patients, 90%) vs BR (3 of 10 patients, 30%) in paired samples.
Focusing on peripheral blood MRD, Dr Hillmen said the best MRD-negativity rates were higher with venetoclax-rituximab (84%) than BR (23%). These results were independent of high-risk factors—such as del 17p, IGVH unmutated, and mutated TP53—only for venetoclax-rituximab treated patients.
“The superior peripheral blood MRD response with venetoclax-rituximab was consistent across subgroups at the end of completion of treatment,” Dr Hillmen said. “Most patients who achieved peripheral blood MRD-negativity on venetoclax-rituximab remained MRD-negative and were progression-free.”
Among 121 of 194 (62%) patients on venetoclax-rituximab who achieved MRD-negativity at the end of combination therapy, 100 (83%) patients maintained MRD-negativity and were progression-free at a median follow-up of 13.8 months. Two patients developed progressive disease and 2 patients died (unrelated to CLL).
Two patients developed Richter’s disease (with one MRD-positive directly before therapy) and 15 (12%) patients converted to confirmed MRD-positive at a median MRD-positive follow-up of 5.6 months.
“High peripheral blood MRD-negativity at the end of combination treatment and concordance with bone marrow MRD with venetoclax-rituximab,” Dr Hillmen said, “confirms the value of peripheral blood MRD for evaluation of treatment benefit in relapsed/refractory CLL patients. The high rate of peripheral blood MRD-negativity at end of combination treatment with venetoclax-rituximab was attained regardless of risk features.”
Some conversion to MRD-positivity occurred only in a small proportion of patients. Most cases were of intermediate level and remained progression-free, he said.
“MRD kinetics indicate that peripheral blood MRD-negativity with venetoclax-rituximab occurs early and is maintained over time with current follow-up,” Dr Hillmen added. The MRD data now provide a framework for designing response adaptive therapy.
The US Food and Drug Administration recently approved venetoclax-rituximab for CLL or small lymphocytic lymphoma for patients with or without del 17p.
Venetoclax is being developed by Genentech and Abbvie.