User login
CAR T in DLBCL: Liso-cel has ‘remarkable’ efficacy in cohort
CHICAGO – The CD19–directed chimeric antigen receptor (CAR) T-cell product lisocabtagene maraleucel (liso-cel, JCAR017) produced durable responses in poor-prognosis patients with relapsed/refractory diffuse large B-cell lymphoma (DLBCL), follow-up results of a phase 1 trial show.
Nearly 90% of DLBCL patients who achieved complete response as their best response on liso-cel were alive at 1 year in the study, according to investigator Jeremy S. Abramson, MD, of Massachusetts General Hospital Cancer Center in Boston.
That result is “far superior to what we would have anticipated with conventional therapies in a largely chemorefractory DLBCL population,” Dr. Abramson said at the annual meeting of the American Society of Clinical Oncology.
The new data on liso-cel come on the heels of a second approval of a CAR T-cell therapy for DLBCL, noted Caron Jacobson, MD, of Dana-Farber Cancer Institute, Boston.
Axicabtagene ciloleucel (Yescarta) was approved in October 2017 by the U.S. Food and Drug Administration for relapsed or refractory large B-cell lymphomas, including DLBCL. In May 2018, tisagenlecleucel (Kymriah) received its second FDA approval to treat relapsed or refractory large B-cell lymphomas, including DLBCL.
CAR T-cell therapy “really has transformed outcomes for a group of patients who previously had no other standard of care and who… have a relatively short overall survival,” Dr. Jacobson said.
At the meeting, Dr. Abramson presented findings on DLBCL patients in TRANSCEND NHL 001, a phase 1, multicenter, open-label study of the CD-19 targeted CAR T-cell therapy in relapsed and refractory B-cell non-Hodgkin lymphoma.
About 90% of treated DLBCL patients had one or more poor-risk disease features, such as ECOG performance status 2 and primary refractory disease, which predict poor overall survival, according to Dr. Abramson.
Dr. Abramson’s presentation focused on 102 evaluable DLBCL patients in the dose-finding and dose-expansion cohorts of the TRANSCEND study, including a subset analysis of a core group of 73 patients who met the criteria for pivotal dose cohort of the study (1 x 108 cells given as a single dose).
For the full set of 102 DLBCL patients, the best overall response rate was 75%, including a best complete remission rate of 55%, according to presented data. In the core group of 73 DLBCL patients, best overall response and complete remission rates were 80% and 59%, respectively.
Investigators saw “encouraging” durable response rates at 6 months and beyond in the core DLBCL population, according to Dr. Abramson. Of patients with a complete remission at 3 months, 88% remained in complete remission at the 6-month follow-up, and 93% of those in remission at the 6-month time point were in ongoing response at a median follow-up of 8 months.
Median overall survival had not been reached in either the full or core DLBCL cohorts with a median of 12 months follow-up, he added, noting that 90% of patients who achieved complete remission as their best response remained alive at 1 year.
In terms of adverse effects, liso-cel is showing a low and manageable toxicity profile, with very low rates of severe cytokine release syndrome (CRS) and neurotoxicity at 1% and 13%, respectively, Dr. Abramson reported.
“This anti-CD19 CAR T cell has remarkable efficacy in a group of highly refractory aggressive B-cell non-Hodgkin lymphoma patients,” said Dr. Jacobson, commenting on results of the DLBCL subset.
Based on the data presented, liso-cel is “clearly competitive” with the approved CAR T-cell therapies, though she advised caution in comparing across studies. “I don’t think that there will be a randomized study of all three agents, but I do think that we’ll start to get comparative data from single institution experiences that are using all three products,” she said.
The pivotal DLBCL cohort of TRANSCEND NHL 001 has completed accrual and results will be presented at a future meeting, Dr. Abramson said.
Dr. Abramson reported disclosures related to Celgene, Genentech/Roche, Gilead Sciences, Novartis, Seattle Genetics, and Millennium.
SOURCE: Abramson JS et al. ASCO 2018. Abstract 7505.
CHICAGO – The CD19–directed chimeric antigen receptor (CAR) T-cell product lisocabtagene maraleucel (liso-cel, JCAR017) produced durable responses in poor-prognosis patients with relapsed/refractory diffuse large B-cell lymphoma (DLBCL), follow-up results of a phase 1 trial show.
Nearly 90% of DLBCL patients who achieved complete response as their best response on liso-cel were alive at 1 year in the study, according to investigator Jeremy S. Abramson, MD, of Massachusetts General Hospital Cancer Center in Boston.
That result is “far superior to what we would have anticipated with conventional therapies in a largely chemorefractory DLBCL population,” Dr. Abramson said at the annual meeting of the American Society of Clinical Oncology.
The new data on liso-cel come on the heels of a second approval of a CAR T-cell therapy for DLBCL, noted Caron Jacobson, MD, of Dana-Farber Cancer Institute, Boston.
Axicabtagene ciloleucel (Yescarta) was approved in October 2017 by the U.S. Food and Drug Administration for relapsed or refractory large B-cell lymphomas, including DLBCL. In May 2018, tisagenlecleucel (Kymriah) received its second FDA approval to treat relapsed or refractory large B-cell lymphomas, including DLBCL.
CAR T-cell therapy “really has transformed outcomes for a group of patients who previously had no other standard of care and who… have a relatively short overall survival,” Dr. Jacobson said.
At the meeting, Dr. Abramson presented findings on DLBCL patients in TRANSCEND NHL 001, a phase 1, multicenter, open-label study of the CD-19 targeted CAR T-cell therapy in relapsed and refractory B-cell non-Hodgkin lymphoma.
About 90% of treated DLBCL patients had one or more poor-risk disease features, such as ECOG performance status 2 and primary refractory disease, which predict poor overall survival, according to Dr. Abramson.
Dr. Abramson’s presentation focused on 102 evaluable DLBCL patients in the dose-finding and dose-expansion cohorts of the TRANSCEND study, including a subset analysis of a core group of 73 patients who met the criteria for pivotal dose cohort of the study (1 x 108 cells given as a single dose).
For the full set of 102 DLBCL patients, the best overall response rate was 75%, including a best complete remission rate of 55%, according to presented data. In the core group of 73 DLBCL patients, best overall response and complete remission rates were 80% and 59%, respectively.
Investigators saw “encouraging” durable response rates at 6 months and beyond in the core DLBCL population, according to Dr. Abramson. Of patients with a complete remission at 3 months, 88% remained in complete remission at the 6-month follow-up, and 93% of those in remission at the 6-month time point were in ongoing response at a median follow-up of 8 months.
Median overall survival had not been reached in either the full or core DLBCL cohorts with a median of 12 months follow-up, he added, noting that 90% of patients who achieved complete remission as their best response remained alive at 1 year.
In terms of adverse effects, liso-cel is showing a low and manageable toxicity profile, with very low rates of severe cytokine release syndrome (CRS) and neurotoxicity at 1% and 13%, respectively, Dr. Abramson reported.
“This anti-CD19 CAR T cell has remarkable efficacy in a group of highly refractory aggressive B-cell non-Hodgkin lymphoma patients,” said Dr. Jacobson, commenting on results of the DLBCL subset.
Based on the data presented, liso-cel is “clearly competitive” with the approved CAR T-cell therapies, though she advised caution in comparing across studies. “I don’t think that there will be a randomized study of all three agents, but I do think that we’ll start to get comparative data from single institution experiences that are using all three products,” she said.
The pivotal DLBCL cohort of TRANSCEND NHL 001 has completed accrual and results will be presented at a future meeting, Dr. Abramson said.
Dr. Abramson reported disclosures related to Celgene, Genentech/Roche, Gilead Sciences, Novartis, Seattle Genetics, and Millennium.
SOURCE: Abramson JS et al. ASCO 2018. Abstract 7505.
CHICAGO – The CD19–directed chimeric antigen receptor (CAR) T-cell product lisocabtagene maraleucel (liso-cel, JCAR017) produced durable responses in poor-prognosis patients with relapsed/refractory diffuse large B-cell lymphoma (DLBCL), follow-up results of a phase 1 trial show.
Nearly 90% of DLBCL patients who achieved complete response as their best response on liso-cel were alive at 1 year in the study, according to investigator Jeremy S. Abramson, MD, of Massachusetts General Hospital Cancer Center in Boston.
That result is “far superior to what we would have anticipated with conventional therapies in a largely chemorefractory DLBCL population,” Dr. Abramson said at the annual meeting of the American Society of Clinical Oncology.
The new data on liso-cel come on the heels of a second approval of a CAR T-cell therapy for DLBCL, noted Caron Jacobson, MD, of Dana-Farber Cancer Institute, Boston.
Axicabtagene ciloleucel (Yescarta) was approved in October 2017 by the U.S. Food and Drug Administration for relapsed or refractory large B-cell lymphomas, including DLBCL. In May 2018, tisagenlecleucel (Kymriah) received its second FDA approval to treat relapsed or refractory large B-cell lymphomas, including DLBCL.
CAR T-cell therapy “really has transformed outcomes for a group of patients who previously had no other standard of care and who… have a relatively short overall survival,” Dr. Jacobson said.
At the meeting, Dr. Abramson presented findings on DLBCL patients in TRANSCEND NHL 001, a phase 1, multicenter, open-label study of the CD-19 targeted CAR T-cell therapy in relapsed and refractory B-cell non-Hodgkin lymphoma.
About 90% of treated DLBCL patients had one or more poor-risk disease features, such as ECOG performance status 2 and primary refractory disease, which predict poor overall survival, according to Dr. Abramson.
Dr. Abramson’s presentation focused on 102 evaluable DLBCL patients in the dose-finding and dose-expansion cohorts of the TRANSCEND study, including a subset analysis of a core group of 73 patients who met the criteria for pivotal dose cohort of the study (1 x 108 cells given as a single dose).
For the full set of 102 DLBCL patients, the best overall response rate was 75%, including a best complete remission rate of 55%, according to presented data. In the core group of 73 DLBCL patients, best overall response and complete remission rates were 80% and 59%, respectively.
Investigators saw “encouraging” durable response rates at 6 months and beyond in the core DLBCL population, according to Dr. Abramson. Of patients with a complete remission at 3 months, 88% remained in complete remission at the 6-month follow-up, and 93% of those in remission at the 6-month time point were in ongoing response at a median follow-up of 8 months.
Median overall survival had not been reached in either the full or core DLBCL cohorts with a median of 12 months follow-up, he added, noting that 90% of patients who achieved complete remission as their best response remained alive at 1 year.
In terms of adverse effects, liso-cel is showing a low and manageable toxicity profile, with very low rates of severe cytokine release syndrome (CRS) and neurotoxicity at 1% and 13%, respectively, Dr. Abramson reported.
“This anti-CD19 CAR T cell has remarkable efficacy in a group of highly refractory aggressive B-cell non-Hodgkin lymphoma patients,” said Dr. Jacobson, commenting on results of the DLBCL subset.
Based on the data presented, liso-cel is “clearly competitive” with the approved CAR T-cell therapies, though she advised caution in comparing across studies. “I don’t think that there will be a randomized study of all three agents, but I do think that we’ll start to get comparative data from single institution experiences that are using all three products,” she said.
The pivotal DLBCL cohort of TRANSCEND NHL 001 has completed accrual and results will be presented at a future meeting, Dr. Abramson said.
Dr. Abramson reported disclosures related to Celgene, Genentech/Roche, Gilead Sciences, Novartis, Seattle Genetics, and Millennium.
SOURCE: Abramson JS et al. ASCO 2018. Abstract 7505.
REPORTING FROM ASCO 2018
Key clinical point: (DLBCL).
Major finding: Among DLBCL patients treated with the pivotal dose of liso-cel, 88% who were in complete remission at 3 months remained in complete remission at the 6 month follow-up.
Study details: Follow-up report on a cohort of DLBCL patients from TRANSCEND NHL 001, a phase 1 trial of liso-cel in relapsed and refractory B-cell NHL.
Disclosures: Dr. Abramson reported disclosures related to Celgene, Genentech/Roche, Gilead Sciences, Novartis, Seattle Genetics, and Millennium.
Source: Abramson JS et al. ASCO 2018. Abstract 7505.
Presidential Address: 'Changing Me to We in Vascular Care'
When R. Clement Darling III, MD, took to the podium at the Vascular Annual Meeting to present his presidential address, he highlighted the importance of teamwork and collaboration in training, in maintaining personal well-being, and most importantly, in patient care.

His talk, titled, “Looking Forward Through the Past: Changing Me to We in the Evolution of Team-based Vascular Care,” addressed these issues through a very personal lens. To make his point, Dr. Darling outlined four key take-home concepts that he had found useful “over five decades of working in an operating room as a technologist, a student and a surgeon,” and as chief of the division of vascular surgery at Albany Medical Center Hospital (N.Y.). These formed the basis of his entire address:
1. “None of us is as smart as all of us.” We learn from each other which is the foundation of team-based training.
2. The key to resilience, healing and health, whether for our patients or for ourselves, is caring and supporting each other more.
3. Failure is not an end result. It is the path to success through learning.
4. Remember the past but look to the future. The best predictor of future behavior is the past, but the future we are experiencing now, is like no other!”
Dr. Darling spoke from the heart about the importance of his colleagues and his parents, especially the role of his father as a pioneer in vascular surgery, and of the women in his life as role models.
He stressed how “one of the invaluable things I have learned is the value of failure, evaluating the past to avoid the same mistakes and the benefit of the TEAM in providing support and care.”
“Every day we’re asked to do the impossible and every day we get up, go to work. We do the best we can. We can make the best plans, treat the sickest patients and get a tremendous fulfillment for what we do in what we do. We do the right thing for the patient,” Dr. Darling explained, in summarizing the passion that he feels for vascular surgery.
“We are always willing to do and try the impossible. We’re always willing to be the last person to call when things look bleak. It brings me great glee whenever we get called to the operating room and people look around and go, ‘oh thank God, the vascular surgeon’s here.’ Our colleagues in other specialties are often afraid of blood vessels, afraid of death, afraid of complications. We thrust ourselves every day into situations where nobody else will go,” he added.
“As vascular surgeons we face failure and roadblocks daily yet still persist where others are scared to tread. Many of you have faced far worse barriers of discrimination and unreasonable arbitrary barriers, and I am constantly humbled by your ability to overcome them,” Dr. Darling said. He pointed out that: “This innate ability to focus on the problem is what makes vascular surgeons great. No problem is too complex, no detail is too small. We do the right thing despite the odds against us. We do right by the patient.”
After telling some of his own stories of “failure,” to illustrate its importance as a learning tool, Dr. Darling spoke of one person’s reception of his application to join the SVS: “When I applied for membership to the Society for Vascular Surgery, someone had written a note saying that ‘I should never be considered, nor was I deserving to be a member of the SVS, and never should I be admitted into this austere society.’”
Throughout his address, Dr. Darling re-emphasized the importance of teams and the collaborative nature of patient care. “The SVS has developed strong partnerships with the Society for Vascular Nursing, The American Venous Forum, The Society for Vascular Ultrasound, and is seeking to strengthen relationships with the regional vascular societies, VESS, the Society for Clinical Vascular Surgery, The Society for Vascular Medicine, the American Heart Association, and many others.
“The SVS is developing these relationships with the patient at the center, and with purpose, focusing on ‘shared vision,’ of specific advancements, programs, and initiatives that will advance quality of care. By tapping into this vast array of talent Vascular Surgery will become more agile, intelligent and thoughtful in our care of vascular patients,” Dr. Darling predicted.
But vascular surgeons must become comfortable with moving from the concept of “captain of the ship” to the role of team leadership, he emphasized, if they are to truly succeed in their careers and in providing optimal patient care.
“Currently, each patient coming to your service touches over 100 staff during their experience. This includes your office, vascular lab, angio suite, recovery room, hospital floor, ICU, CT scanner to name a few.” This is part of the need for the evolution from ‘captain’ to ‘leader,’ he added.
“If you have not had any formal training in leadership or team development, I strongly suggest you add this to your learning portfolio,” Dr. Darling counseled. “The SVS is addressing this through its Leadership and Diversity Committee, and you will see an expanding array of learning opportunities in the future.”
With regard to his own tenure as SVS President: “I am proud that during my year as president, the SVS has invested in several new Task Forces to address critical future issues including: Alternative Payment Models for vascular surgery; a national inpatient and outpatient vascular certification program; a focus on our own health, wellness, and potential ways to mitigate potential burnout; and Dr. Makaroun will be taking on the issues of vascular surgery valuation and workforce in the new Task Force on the Future of Vascular Surgery.”
He further discussed the role SVS is playing in helping to define the future of vascular surgery.
“As we work to strengthen our brand and identity, the SVS Executive Board has supported, and thanks, Amy Reed and Will Jordan for their leadership in the APDVS [Association of Program Directors of Vascular Surgery], and for taking the first step toward attaining a separate Vascular Residency Review Committee or RRC.” In addition, he described how “SVS is also working closely, and collaboratively, with the American Board of Surgery, and the Vascular Surgery Board, to complete the work that was begun a decade ago, and achieve an autonomous vascular surgery board that is an equal partner and stakeholder in the ABS.”
Dr. Darling then outlined one of his major concerns and interests: the exit path of senior vascular surgeons, and how this is often a tremendous waste of talent and expertise. “In the last decade of work when senior surgeons are trying to transition to non-clinical work, I think we throw away much of their intellectual skill and experience in dealing with vascular surgery problems,” he said. He urged that “as our senior surgeons leave clinical practice, we need to use their intellectual expertise and experience in a more productive way.”
The Society for Vascular Surgery is establishing pathways for leadership and pathways to train people in administration, he added.
Turning back to the extreme importance of teamwork, Dr. Darling addressed the future.
“We, physicians, nurses, PAs, technologists, staff, and administrators, need to work together, think together, to grow together, not only for our patients, but for our partners and our families. We are all part of the vascular team,” Dr. Darling said.
When R. Clement Darling III, MD, took to the podium at the Vascular Annual Meeting to present his presidential address, he highlighted the importance of teamwork and collaboration in training, in maintaining personal well-being, and most importantly, in patient care.
His talk, titled, “Looking Forward Through the Past: Changing Me to We in the Evolution of Team-based Vascular Care,” addressed these issues through a very personal lens. To make his point, Dr. Darling outlined four key take-home concepts that he had found useful “over five decades of working in an operating room as a technologist, a student and a surgeon,” and as chief of the division of vascular surgery at Albany Medical Center Hospital (N.Y.). These formed the basis of his entire address:
1. “None of us is as smart as all of us.” We learn from each other which is the foundation of team-based training.
2. The key to resilience, healing and health, whether for our patients or for ourselves, is caring and supporting each other more.
3. Failure is not an end result. It is the path to success through learning.
4. Remember the past but look to the future. The best predictor of future behavior is the past, but the future we are experiencing now, is like no other!”
Dr. Darling spoke from the heart about the importance of his colleagues and his parents, especially the role of his father as a pioneer in vascular surgery, and of the women in his life as role models.
He stressed how “one of the invaluable things I have learned is the value of failure, evaluating the past to avoid the same mistakes and the benefit of the TEAM in providing support and care.”
“Every day we’re asked to do the impossible and every day we get up, go to work. We do the best we can. We can make the best plans, treat the sickest patients and get a tremendous fulfillment for what we do in what we do. We do the right thing for the patient,” Dr. Darling explained, in summarizing the passion that he feels for vascular surgery.
“We are always willing to do and try the impossible. We’re always willing to be the last person to call when things look bleak. It brings me great glee whenever we get called to the operating room and people look around and go, ‘oh thank God, the vascular surgeon’s here.’ Our colleagues in other specialties are often afraid of blood vessels, afraid of death, afraid of complications. We thrust ourselves every day into situations where nobody else will go,” he added.
“As vascular surgeons we face failure and roadblocks daily yet still persist where others are scared to tread. Many of you have faced far worse barriers of discrimination and unreasonable arbitrary barriers, and I am constantly humbled by your ability to overcome them,” Dr. Darling said. He pointed out that: “This innate ability to focus on the problem is what makes vascular surgeons great. No problem is too complex, no detail is too small. We do the right thing despite the odds against us. We do right by the patient.”
After telling some of his own stories of “failure,” to illustrate its importance as a learning tool, Dr. Darling spoke of one person’s reception of his application to join the SVS: “When I applied for membership to the Society for Vascular Surgery, someone had written a note saying that ‘I should never be considered, nor was I deserving to be a member of the SVS, and never should I be admitted into this austere society.’”
Throughout his address, Dr. Darling re-emphasized the importance of teams and the collaborative nature of patient care. “The SVS has developed strong partnerships with the Society for Vascular Nursing, The American Venous Forum, The Society for Vascular Ultrasound, and is seeking to strengthen relationships with the regional vascular societies, VESS, the Society for Clinical Vascular Surgery, The Society for Vascular Medicine, the American Heart Association, and many others.
“The SVS is developing these relationships with the patient at the center, and with purpose, focusing on ‘shared vision,’ of specific advancements, programs, and initiatives that will advance quality of care. By tapping into this vast array of talent Vascular Surgery will become more agile, intelligent and thoughtful in our care of vascular patients,” Dr. Darling predicted.
But vascular surgeons must become comfortable with moving from the concept of “captain of the ship” to the role of team leadership, he emphasized, if they are to truly succeed in their careers and in providing optimal patient care.
“Currently, each patient coming to your service touches over 100 staff during their experience. This includes your office, vascular lab, angio suite, recovery room, hospital floor, ICU, CT scanner to name a few.” This is part of the need for the evolution from ‘captain’ to ‘leader,’ he added.
“If you have not had any formal training in leadership or team development, I strongly suggest you add this to your learning portfolio,” Dr. Darling counseled. “The SVS is addressing this through its Leadership and Diversity Committee, and you will see an expanding array of learning opportunities in the future.”
With regard to his own tenure as SVS President: “I am proud that during my year as president, the SVS has invested in several new Task Forces to address critical future issues including: Alternative Payment Models for vascular surgery; a national inpatient and outpatient vascular certification program; a focus on our own health, wellness, and potential ways to mitigate potential burnout; and Dr. Makaroun will be taking on the issues of vascular surgery valuation and workforce in the new Task Force on the Future of Vascular Surgery.”
He further discussed the role SVS is playing in helping to define the future of vascular surgery.
“As we work to strengthen our brand and identity, the SVS Executive Board has supported, and thanks, Amy Reed and Will Jordan for their leadership in the APDVS [Association of Program Directors of Vascular Surgery], and for taking the first step toward attaining a separate Vascular Residency Review Committee or RRC.” In addition, he described how “SVS is also working closely, and collaboratively, with the American Board of Surgery, and the Vascular Surgery Board, to complete the work that was begun a decade ago, and achieve an autonomous vascular surgery board that is an equal partner and stakeholder in the ABS.”
Dr. Darling then outlined one of his major concerns and interests: the exit path of senior vascular surgeons, and how this is often a tremendous waste of talent and expertise. “In the last decade of work when senior surgeons are trying to transition to non-clinical work, I think we throw away much of their intellectual skill and experience in dealing with vascular surgery problems,” he said. He urged that “as our senior surgeons leave clinical practice, we need to use their intellectual expertise and experience in a more productive way.”
The Society for Vascular Surgery is establishing pathways for leadership and pathways to train people in administration, he added.
Turning back to the extreme importance of teamwork, Dr. Darling addressed the future.
“We, physicians, nurses, PAs, technologists, staff, and administrators, need to work together, think together, to grow together, not only for our patients, but for our partners and our families. We are all part of the vascular team,” Dr. Darling said.
When R. Clement Darling III, MD, took to the podium at the Vascular Annual Meeting to present his presidential address, he highlighted the importance of teamwork and collaboration in training, in maintaining personal well-being, and most importantly, in patient care.
His talk, titled, “Looking Forward Through the Past: Changing Me to We in the Evolution of Team-based Vascular Care,” addressed these issues through a very personal lens. To make his point, Dr. Darling outlined four key take-home concepts that he had found useful “over five decades of working in an operating room as a technologist, a student and a surgeon,” and as chief of the division of vascular surgery at Albany Medical Center Hospital (N.Y.). These formed the basis of his entire address:
1. “None of us is as smart as all of us.” We learn from each other which is the foundation of team-based training.
2. The key to resilience, healing and health, whether for our patients or for ourselves, is caring and supporting each other more.
3. Failure is not an end result. It is the path to success through learning.
4. Remember the past but look to the future. The best predictor of future behavior is the past, but the future we are experiencing now, is like no other!”
Dr. Darling spoke from the heart about the importance of his colleagues and his parents, especially the role of his father as a pioneer in vascular surgery, and of the women in his life as role models.
He stressed how “one of the invaluable things I have learned is the value of failure, evaluating the past to avoid the same mistakes and the benefit of the TEAM in providing support and care.”
“Every day we’re asked to do the impossible and every day we get up, go to work. We do the best we can. We can make the best plans, treat the sickest patients and get a tremendous fulfillment for what we do in what we do. We do the right thing for the patient,” Dr. Darling explained, in summarizing the passion that he feels for vascular surgery.
“We are always willing to do and try the impossible. We’re always willing to be the last person to call when things look bleak. It brings me great glee whenever we get called to the operating room and people look around and go, ‘oh thank God, the vascular surgeon’s here.’ Our colleagues in other specialties are often afraid of blood vessels, afraid of death, afraid of complications. We thrust ourselves every day into situations where nobody else will go,” he added.
“As vascular surgeons we face failure and roadblocks daily yet still persist where others are scared to tread. Many of you have faced far worse barriers of discrimination and unreasonable arbitrary barriers, and I am constantly humbled by your ability to overcome them,” Dr. Darling said. He pointed out that: “This innate ability to focus on the problem is what makes vascular surgeons great. No problem is too complex, no detail is too small. We do the right thing despite the odds against us. We do right by the patient.”
After telling some of his own stories of “failure,” to illustrate its importance as a learning tool, Dr. Darling spoke of one person’s reception of his application to join the SVS: “When I applied for membership to the Society for Vascular Surgery, someone had written a note saying that ‘I should never be considered, nor was I deserving to be a member of the SVS, and never should I be admitted into this austere society.’”
Throughout his address, Dr. Darling re-emphasized the importance of teams and the collaborative nature of patient care. “The SVS has developed strong partnerships with the Society for Vascular Nursing, The American Venous Forum, The Society for Vascular Ultrasound, and is seeking to strengthen relationships with the regional vascular societies, VESS, the Society for Clinical Vascular Surgery, The Society for Vascular Medicine, the American Heart Association, and many others.
“The SVS is developing these relationships with the patient at the center, and with purpose, focusing on ‘shared vision,’ of specific advancements, programs, and initiatives that will advance quality of care. By tapping into this vast array of talent Vascular Surgery will become more agile, intelligent and thoughtful in our care of vascular patients,” Dr. Darling predicted.
But vascular surgeons must become comfortable with moving from the concept of “captain of the ship” to the role of team leadership, he emphasized, if they are to truly succeed in their careers and in providing optimal patient care.
“Currently, each patient coming to your service touches over 100 staff during their experience. This includes your office, vascular lab, angio suite, recovery room, hospital floor, ICU, CT scanner to name a few.” This is part of the need for the evolution from ‘captain’ to ‘leader,’ he added.
“If you have not had any formal training in leadership or team development, I strongly suggest you add this to your learning portfolio,” Dr. Darling counseled. “The SVS is addressing this through its Leadership and Diversity Committee, and you will see an expanding array of learning opportunities in the future.”
With regard to his own tenure as SVS President: “I am proud that during my year as president, the SVS has invested in several new Task Forces to address critical future issues including: Alternative Payment Models for vascular surgery; a national inpatient and outpatient vascular certification program; a focus on our own health, wellness, and potential ways to mitigate potential burnout; and Dr. Makaroun will be taking on the issues of vascular surgery valuation and workforce in the new Task Force on the Future of Vascular Surgery.”
He further discussed the role SVS is playing in helping to define the future of vascular surgery.
“As we work to strengthen our brand and identity, the SVS Executive Board has supported, and thanks, Amy Reed and Will Jordan for their leadership in the APDVS [Association of Program Directors of Vascular Surgery], and for taking the first step toward attaining a separate Vascular Residency Review Committee or RRC.” In addition, he described how “SVS is also working closely, and collaboratively, with the American Board of Surgery, and the Vascular Surgery Board, to complete the work that was begun a decade ago, and achieve an autonomous vascular surgery board that is an equal partner and stakeholder in the ABS.”
Dr. Darling then outlined one of his major concerns and interests: the exit path of senior vascular surgeons, and how this is often a tremendous waste of talent and expertise. “In the last decade of work when senior surgeons are trying to transition to non-clinical work, I think we throw away much of their intellectual skill and experience in dealing with vascular surgery problems,” he said. He urged that “as our senior surgeons leave clinical practice, we need to use their intellectual expertise and experience in a more productive way.”
The Society for Vascular Surgery is establishing pathways for leadership and pathways to train people in administration, he added.
Turning back to the extreme importance of teamwork, Dr. Darling addressed the future.
“We, physicians, nurses, PAs, technologists, staff, and administrators, need to work together, think together, to grow together, not only for our patients, but for our partners and our families. We are all part of the vascular team,” Dr. Darling said.
Cutavirus shows no association with primary cutaneous lymphoma
The parvovirus known as cutavirus appears unlikely to play a pathogenic role in primary cutaneous B- and T-cell lymphoma, based on data from 189 biopsies.
Although researchers have long suspected viruses of a role in primary cutaneous lymphomas, “all of the so-far-suspected viruses including retroviruses, herpesviruses, and polyomaviruses have failed to reveal a consistent association with both cutaneous B-cell lymphoma [CBCL] and cutaneous T-cell lymphoma [CTCL],” wrote Alexander Kreuter, MD, of the department of dermatology, venereology, and allergology at Helios St. Elisabeth Hospital Oberhausen, Germany, and his colleagues.
In a research letter published in JAMA Dermatology, the researchers analyzed 189 paraffin-embedded biopsy specimens from 130 adults with CBCL or CTCL.
Overall, cutavirus DNA was identified in 6 (3.2%) of the 189 lymphoma biopsies and in 6 (4.6%) of 130 patients. Cutavirus was identified only in male patients with mycosis fungoides, and no cutavirus was identified in patients or biopsies without mycosis fungoides, the researchers noted. Viral DNA loads in the cutavirus-positive biopsies ranged from 1.3 to 85.0 cutavirus DNA copies per beta globin gene copy.
The findings were limited by several factors, such as the lack of biopsy samples for some lymphoma subtypes and the availability of a single specimen from most patients, the researchers noted. However, the analysis of a large number of samples suggested that cutavirus is not associated with the development of most primary cutaneous lymphomas, they said.
The study was funded by the German National Reference Center for Papilloma- and Polyomaviruses. The researchers had no financial conflicts to disclose.
SOURCE: Kreuter A et al. JAMA Dermatol. 2018 Jun 27. doi:10.1001/jamadermatol.2018.1628.
The parvovirus known as cutavirus appears unlikely to play a pathogenic role in primary cutaneous B- and T-cell lymphoma, based on data from 189 biopsies.
Although researchers have long suspected viruses of a role in primary cutaneous lymphomas, “all of the so-far-suspected viruses including retroviruses, herpesviruses, and polyomaviruses have failed to reveal a consistent association with both cutaneous B-cell lymphoma [CBCL] and cutaneous T-cell lymphoma [CTCL],” wrote Alexander Kreuter, MD, of the department of dermatology, venereology, and allergology at Helios St. Elisabeth Hospital Oberhausen, Germany, and his colleagues.
In a research letter published in JAMA Dermatology, the researchers analyzed 189 paraffin-embedded biopsy specimens from 130 adults with CBCL or CTCL.
Overall, cutavirus DNA was identified in 6 (3.2%) of the 189 lymphoma biopsies and in 6 (4.6%) of 130 patients. Cutavirus was identified only in male patients with mycosis fungoides, and no cutavirus was identified in patients or biopsies without mycosis fungoides, the researchers noted. Viral DNA loads in the cutavirus-positive biopsies ranged from 1.3 to 85.0 cutavirus DNA copies per beta globin gene copy.
The findings were limited by several factors, such as the lack of biopsy samples for some lymphoma subtypes and the availability of a single specimen from most patients, the researchers noted. However, the analysis of a large number of samples suggested that cutavirus is not associated with the development of most primary cutaneous lymphomas, they said.
The study was funded by the German National Reference Center for Papilloma- and Polyomaviruses. The researchers had no financial conflicts to disclose.
SOURCE: Kreuter A et al. JAMA Dermatol. 2018 Jun 27. doi:10.1001/jamadermatol.2018.1628.
The parvovirus known as cutavirus appears unlikely to play a pathogenic role in primary cutaneous B- and T-cell lymphoma, based on data from 189 biopsies.
Although researchers have long suspected viruses of a role in primary cutaneous lymphomas, “all of the so-far-suspected viruses including retroviruses, herpesviruses, and polyomaviruses have failed to reveal a consistent association with both cutaneous B-cell lymphoma [CBCL] and cutaneous T-cell lymphoma [CTCL],” wrote Alexander Kreuter, MD, of the department of dermatology, venereology, and allergology at Helios St. Elisabeth Hospital Oberhausen, Germany, and his colleagues.
In a research letter published in JAMA Dermatology, the researchers analyzed 189 paraffin-embedded biopsy specimens from 130 adults with CBCL or CTCL.
Overall, cutavirus DNA was identified in 6 (3.2%) of the 189 lymphoma biopsies and in 6 (4.6%) of 130 patients. Cutavirus was identified only in male patients with mycosis fungoides, and no cutavirus was identified in patients or biopsies without mycosis fungoides, the researchers noted. Viral DNA loads in the cutavirus-positive biopsies ranged from 1.3 to 85.0 cutavirus DNA copies per beta globin gene copy.
The findings were limited by several factors, such as the lack of biopsy samples for some lymphoma subtypes and the availability of a single specimen from most patients, the researchers noted. However, the analysis of a large number of samples suggested that cutavirus is not associated with the development of most primary cutaneous lymphomas, they said.
The study was funded by the German National Reference Center for Papilloma- and Polyomaviruses. The researchers had no financial conflicts to disclose.
SOURCE: Kreuter A et al. JAMA Dermatol. 2018 Jun 27. doi:10.1001/jamadermatol.2018.1628.
FROM JAMA DERMATOLOGY
Key clinical point: Cutavirus may not have a primary role in cutaneous lymphomas.
Major finding: Cutavirus was identified in 6 (3.2%) of 189 lymphoma biopsies.
Study details: The data come from 130 patients with cutaneous B-cell lymphoma or cutaneous T-cell lymphoma and a total of 189 biopsy specimens.
Disclosures: The study was funded by the German National Reference Center for Papilloma- and Polyomaviruses. The researchers had no financial conflicts to disclose.
Source: Kreuter A et al. JAMA Dermatol. 2018 Jun 27. doi:10.1001/jamadermatol.2018.1628.
Methotrexate proves largely ineffective for maintaining peripheral SpA remission
AMSTERDAM – Starting patients with newly diagnosed, peripheral spondyloarthritis (SpA) on treatment with a tumor necrosis factor (TNF) inhibitor within 12 weeks of symptom onset produced an “amazing,” long-term, complete remission that resembled cure in more than half of the 40 treated patients, a finding that now needs replication in a larger, multicenter study, Philippe Carron, MD, said at the European Congress of Rheumatology.
Ongoing research on patients in the original study cohort also showed that methotrexate is largely ineffective to help wean patients in remission on a tumor necrosis factor inhibitor off the biologic drug, said Dr. Carron, a rheumatologist at the University of Ghent (Belgium). In his group’s most recent experience with 22 patients in remission on a regimen of golimumab and methotrexate, 5 remained in remission (23%) when golimumab treatment stopped, whereas the other 17 patients had to restart golimumab (Simponi) while continuing on methotrexate after relapsing on methotrexate monotherapy, Dr. Carron reported.

Methotrexate has “overall weak efficacy for maintaining biological-free remission” in patients with peripheral SpA, he concluded.
But Dr. Carron remained very positive about the main finding of the CRESPA (Clinical Remission in Patients with Early Peripheral Spondyloarthritis) study, which has now shown a durable complete remission – free from arthritis, enthesitis, and dactylitis – in 21 of 40 (53%) patients who began golimumab treatment within 12 weeks of their symptom onset and then remained in remission when the golimumab was eventually stopped. These patients have now remained in complete remission for 2.4-5.8 years of follow-up, Dr. Carron said. He attributed this very durable remission while off any treatment to the rapid start of TNF-inhibitor therapy within weeks of their symptom onset.
“This is fantastic; these patients are cured. Early treatment is the most important reason why the result is so good,” but it also poses the biggest challenge for using this approach in routine practice, Dr. Carron said in an interview. “It took us 3 years to find the 60 patients” enrolled in CRESPA. “Most of the time, patients go elsewhere for treatment, and it’s several months until they see us. In many countries there are not enough rheumatologists, and patients wait 3, 4 months before we see them.” Another important feature of the intervention was that golimumab treatment continued until patients presented as completely symptom free on two consecutive clinic visits spaced about 12 weeks apart.
Dr. Carron and his associates published their initial findings from CRESPA in 2017 (Ann Rheum Dis. 2017 Aug;76[8]:1389-95), and they also have reported updates on the main results at meetings. At the 2018 EULAR Congress, Dr. Carron reported the outcomes of 31 patients in the study who entered a 2-year period of extended golimumab treatment either because they never reached complete remission or because they relapsed after stopping golimumab and so restarted the drug. Of these patients, 25 completed the full 2 years of the CRESPA extension phase on golimumab. Of those patients, 22 were in complete remission and agreed to continue; they began a tapering phase that started with receiving concurrent treatment with 15 mg/week of oral methotrexate then, after 12 weeks on methotrexate, discontinued their golimumab but continued on the methotrexate regimen.
After an average follow-up of 80 weeks in this postextension phase, 5 patients (23%) remained in remission on methotrexate monotherapy, while the other 17 patients (77%) had to restart golimumab. Of these 17 patients, 15 because of a relapse, and 2 restarted because they had to discontinue methotrexate after developing adverse effects. The median time to restarting golimumab among these 17 patients was 228 days, Dr. Carron said. In all 17 patients, remission returned within 12 weeks of restarting golimumab treatment.
SOURCE: Carron P et al. EULAR 2018 Congress, Abstract OP0335.
AMSTERDAM – Starting patients with newly diagnosed, peripheral spondyloarthritis (SpA) on treatment with a tumor necrosis factor (TNF) inhibitor within 12 weeks of symptom onset produced an “amazing,” long-term, complete remission that resembled cure in more than half of the 40 treated patients, a finding that now needs replication in a larger, multicenter study, Philippe Carron, MD, said at the European Congress of Rheumatology.
Ongoing research on patients in the original study cohort also showed that methotrexate is largely ineffective to help wean patients in remission on a tumor necrosis factor inhibitor off the biologic drug, said Dr. Carron, a rheumatologist at the University of Ghent (Belgium). In his group’s most recent experience with 22 patients in remission on a regimen of golimumab and methotrexate, 5 remained in remission (23%) when golimumab treatment stopped, whereas the other 17 patients had to restart golimumab (Simponi) while continuing on methotrexate after relapsing on methotrexate monotherapy, Dr. Carron reported.
Methotrexate has “overall weak efficacy for maintaining biological-free remission” in patients with peripheral SpA, he concluded.
But Dr. Carron remained very positive about the main finding of the CRESPA (Clinical Remission in Patients with Early Peripheral Spondyloarthritis) study, which has now shown a durable complete remission – free from arthritis, enthesitis, and dactylitis – in 21 of 40 (53%) patients who began golimumab treatment within 12 weeks of their symptom onset and then remained in remission when the golimumab was eventually stopped. These patients have now remained in complete remission for 2.4-5.8 years of follow-up, Dr. Carron said. He attributed this very durable remission while off any treatment to the rapid start of TNF-inhibitor therapy within weeks of their symptom onset.
“This is fantastic; these patients are cured. Early treatment is the most important reason why the result is so good,” but it also poses the biggest challenge for using this approach in routine practice, Dr. Carron said in an interview. “It took us 3 years to find the 60 patients” enrolled in CRESPA. “Most of the time, patients go elsewhere for treatment, and it’s several months until they see us. In many countries there are not enough rheumatologists, and patients wait 3, 4 months before we see them.” Another important feature of the intervention was that golimumab treatment continued until patients presented as completely symptom free on two consecutive clinic visits spaced about 12 weeks apart.
Dr. Carron and his associates published their initial findings from CRESPA in 2017 (Ann Rheum Dis. 2017 Aug;76[8]:1389-95), and they also have reported updates on the main results at meetings. At the 2018 EULAR Congress, Dr. Carron reported the outcomes of 31 patients in the study who entered a 2-year period of extended golimumab treatment either because they never reached complete remission or because they relapsed after stopping golimumab and so restarted the drug. Of these patients, 25 completed the full 2 years of the CRESPA extension phase on golimumab. Of those patients, 22 were in complete remission and agreed to continue; they began a tapering phase that started with receiving concurrent treatment with 15 mg/week of oral methotrexate then, after 12 weeks on methotrexate, discontinued their golimumab but continued on the methotrexate regimen.
After an average follow-up of 80 weeks in this postextension phase, 5 patients (23%) remained in remission on methotrexate monotherapy, while the other 17 patients (77%) had to restart golimumab. Of these 17 patients, 15 because of a relapse, and 2 restarted because they had to discontinue methotrexate after developing adverse effects. The median time to restarting golimumab among these 17 patients was 228 days, Dr. Carron said. In all 17 patients, remission returned within 12 weeks of restarting golimumab treatment.
SOURCE: Carron P et al. EULAR 2018 Congress, Abstract OP0335.
AMSTERDAM – Starting patients with newly diagnosed, peripheral spondyloarthritis (SpA) on treatment with a tumor necrosis factor (TNF) inhibitor within 12 weeks of symptom onset produced an “amazing,” long-term, complete remission that resembled cure in more than half of the 40 treated patients, a finding that now needs replication in a larger, multicenter study, Philippe Carron, MD, said at the European Congress of Rheumatology.
Ongoing research on patients in the original study cohort also showed that methotrexate is largely ineffective to help wean patients in remission on a tumor necrosis factor inhibitor off the biologic drug, said Dr. Carron, a rheumatologist at the University of Ghent (Belgium). In his group’s most recent experience with 22 patients in remission on a regimen of golimumab and methotrexate, 5 remained in remission (23%) when golimumab treatment stopped, whereas the other 17 patients had to restart golimumab (Simponi) while continuing on methotrexate after relapsing on methotrexate monotherapy, Dr. Carron reported.
Methotrexate has “overall weak efficacy for maintaining biological-free remission” in patients with peripheral SpA, he concluded.
But Dr. Carron remained very positive about the main finding of the CRESPA (Clinical Remission in Patients with Early Peripheral Spondyloarthritis) study, which has now shown a durable complete remission – free from arthritis, enthesitis, and dactylitis – in 21 of 40 (53%) patients who began golimumab treatment within 12 weeks of their symptom onset and then remained in remission when the golimumab was eventually stopped. These patients have now remained in complete remission for 2.4-5.8 years of follow-up, Dr. Carron said. He attributed this very durable remission while off any treatment to the rapid start of TNF-inhibitor therapy within weeks of their symptom onset.
“This is fantastic; these patients are cured. Early treatment is the most important reason why the result is so good,” but it also poses the biggest challenge for using this approach in routine practice, Dr. Carron said in an interview. “It took us 3 years to find the 60 patients” enrolled in CRESPA. “Most of the time, patients go elsewhere for treatment, and it’s several months until they see us. In many countries there are not enough rheumatologists, and patients wait 3, 4 months before we see them.” Another important feature of the intervention was that golimumab treatment continued until patients presented as completely symptom free on two consecutive clinic visits spaced about 12 weeks apart.
Dr. Carron and his associates published their initial findings from CRESPA in 2017 (Ann Rheum Dis. 2017 Aug;76[8]:1389-95), and they also have reported updates on the main results at meetings. At the 2018 EULAR Congress, Dr. Carron reported the outcomes of 31 patients in the study who entered a 2-year period of extended golimumab treatment either because they never reached complete remission or because they relapsed after stopping golimumab and so restarted the drug. Of these patients, 25 completed the full 2 years of the CRESPA extension phase on golimumab. Of those patients, 22 were in complete remission and agreed to continue; they began a tapering phase that started with receiving concurrent treatment with 15 mg/week of oral methotrexate then, after 12 weeks on methotrexate, discontinued their golimumab but continued on the methotrexate regimen.
After an average follow-up of 80 weeks in this postextension phase, 5 patients (23%) remained in remission on methotrexate monotherapy, while the other 17 patients (77%) had to restart golimumab. Of these 17 patients, 15 because of a relapse, and 2 restarted because they had to discontinue methotrexate after developing adverse effects. The median time to restarting golimumab among these 17 patients was 228 days, Dr. Carron said. In all 17 patients, remission returned within 12 weeks of restarting golimumab treatment.
SOURCE: Carron P et al. EULAR 2018 Congress, Abstract OP0335.
REPORTING FROM THE EULAR 2018 CONGRESS
Key clinical point:
Major finding: Among 22 patients who stopped golimumab and continued methotrexate, 17 (77%) relapsed and had to restart golimumab.
Study details: CRESPA, a single-center, controlled study of 60 patients with recently diagnosed peripheral spondyloarthritis.
Disclosures: CRESPA received partial funding from Janssen, the company that markets golimumab (Simponi). Dr. Carron had no additional disclosures.
Source: Carron P et al. EULAR 2018 Congress, Abstract OP0335.77.
Midlife fitness tied to lower later-life CVD mortality, depression risk
Higher cardiorespiratory fitness at midlife appears linked to a lower risk of depression in later life. In addition, higher midlife fitness is associated with a lower risk of cardiovascular mortality when depression preceded CVD death, according to a retrospective study published in JAMA Psychiatry.
“These findings ... should encourage physicians to consider fitness and physical activity in promoting healthy aging,” wrote Benjamin L. Willis, MD, MPH, of the Cooper Institute in Dallas, and his associates.
The study included 17,989 participants from the Cooper Center Longitudinal Study and linked data from those participants with a depression diagnosis based on Medicare claims and cardiovascular disease (CVD) mortality rates based on the National Death Index.
The participants were mostly men (80.2%), and their mean age at midlife assessment was 50 years. The participants’ treadmill time at midlife was used to categorize them into age- and sex-specific quintiles, with quintile 1 representing low fitness, quintiles 2 and 3 representing moderate fitness, and quintiles 4 and 5 representing high fitness.
After 117,218 person-years of follow-up, the investigators observed 2,701 depression diagnoses, 610 deaths tied to cardiovascular disease without prior depression, and 231 deaths associated with CVD after depression.
In addition, Dr. Willis and his associates found that (hazard ratio, 0.84; 95% confidence interval, 0.74-0.95), compared with participants with a low level of fitness. Participants with a high level of fitness also had a 61% lower risk of death from CVD without depression (HR, 0.39; 95% CI, 0.31-0.48), compared with those who had low fitness levels. Participants with a high fitness level who received a depression diagnosis had a 56% lower risk of death from CVD (HR, 0.44; 95% CI, 0.31-0.64), compared with those who had a low level of fitness.
The researchers pointed out that cardiovascular disease mortality is higher following depression but that cardiorespiratory fitness at midlife is a modifiable risk factor for both depression and CVD mortality.
Dr. Willis and his associates cited several limitations. Among them was the unavailability of information about participants’ use of medication that could influence either the presence or absence of a depression diagnosis.
Nevertheless, they said, the results provide lessons for clinicians and patients.
“This study shows that being fit at midlife is associated with a lower risk of later-life depression and subsequent CVD mortality, even in the presence of depression,” they wrote. “These findings suggest the importance of fitness in primary prevention of heart disease and associated CVD mortality in older aging adults.”
The investigators reported no conflicts of interest.
SOURCE: Willis BL et al. JAMA Psychiatry. 2018 Jun 27. doi: 10.1001/jamapsychiatry.2018.1467.
Higher cardiorespiratory fitness at midlife appears linked to a lower risk of depression in later life. In addition, higher midlife fitness is associated with a lower risk of cardiovascular mortality when depression preceded CVD death, according to a retrospective study published in JAMA Psychiatry.
“These findings ... should encourage physicians to consider fitness and physical activity in promoting healthy aging,” wrote Benjamin L. Willis, MD, MPH, of the Cooper Institute in Dallas, and his associates.
The study included 17,989 participants from the Cooper Center Longitudinal Study and linked data from those participants with a depression diagnosis based on Medicare claims and cardiovascular disease (CVD) mortality rates based on the National Death Index.
The participants were mostly men (80.2%), and their mean age at midlife assessment was 50 years. The participants’ treadmill time at midlife was used to categorize them into age- and sex-specific quintiles, with quintile 1 representing low fitness, quintiles 2 and 3 representing moderate fitness, and quintiles 4 and 5 representing high fitness.
After 117,218 person-years of follow-up, the investigators observed 2,701 depression diagnoses, 610 deaths tied to cardiovascular disease without prior depression, and 231 deaths associated with CVD after depression.
In addition, Dr. Willis and his associates found that (hazard ratio, 0.84; 95% confidence interval, 0.74-0.95), compared with participants with a low level of fitness. Participants with a high level of fitness also had a 61% lower risk of death from CVD without depression (HR, 0.39; 95% CI, 0.31-0.48), compared with those who had low fitness levels. Participants with a high fitness level who received a depression diagnosis had a 56% lower risk of death from CVD (HR, 0.44; 95% CI, 0.31-0.64), compared with those who had a low level of fitness.
The researchers pointed out that cardiovascular disease mortality is higher following depression but that cardiorespiratory fitness at midlife is a modifiable risk factor for both depression and CVD mortality.
Dr. Willis and his associates cited several limitations. Among them was the unavailability of information about participants’ use of medication that could influence either the presence or absence of a depression diagnosis.
Nevertheless, they said, the results provide lessons for clinicians and patients.
“This study shows that being fit at midlife is associated with a lower risk of later-life depression and subsequent CVD mortality, even in the presence of depression,” they wrote. “These findings suggest the importance of fitness in primary prevention of heart disease and associated CVD mortality in older aging adults.”
The investigators reported no conflicts of interest.
SOURCE: Willis BL et al. JAMA Psychiatry. 2018 Jun 27. doi: 10.1001/jamapsychiatry.2018.1467.
Higher cardiorespiratory fitness at midlife appears linked to a lower risk of depression in later life. In addition, higher midlife fitness is associated with a lower risk of cardiovascular mortality when depression preceded CVD death, according to a retrospective study published in JAMA Psychiatry.
“These findings ... should encourage physicians to consider fitness and physical activity in promoting healthy aging,” wrote Benjamin L. Willis, MD, MPH, of the Cooper Institute in Dallas, and his associates.
The study included 17,989 participants from the Cooper Center Longitudinal Study and linked data from those participants with a depression diagnosis based on Medicare claims and cardiovascular disease (CVD) mortality rates based on the National Death Index.
The participants were mostly men (80.2%), and their mean age at midlife assessment was 50 years. The participants’ treadmill time at midlife was used to categorize them into age- and sex-specific quintiles, with quintile 1 representing low fitness, quintiles 2 and 3 representing moderate fitness, and quintiles 4 and 5 representing high fitness.
After 117,218 person-years of follow-up, the investigators observed 2,701 depression diagnoses, 610 deaths tied to cardiovascular disease without prior depression, and 231 deaths associated with CVD after depression.
In addition, Dr. Willis and his associates found that (hazard ratio, 0.84; 95% confidence interval, 0.74-0.95), compared with participants with a low level of fitness. Participants with a high level of fitness also had a 61% lower risk of death from CVD without depression (HR, 0.39; 95% CI, 0.31-0.48), compared with those who had low fitness levels. Participants with a high fitness level who received a depression diagnosis had a 56% lower risk of death from CVD (HR, 0.44; 95% CI, 0.31-0.64), compared with those who had a low level of fitness.
The researchers pointed out that cardiovascular disease mortality is higher following depression but that cardiorespiratory fitness at midlife is a modifiable risk factor for both depression and CVD mortality.
Dr. Willis and his associates cited several limitations. Among them was the unavailability of information about participants’ use of medication that could influence either the presence or absence of a depression diagnosis.
Nevertheless, they said, the results provide lessons for clinicians and patients.
“This study shows that being fit at midlife is associated with a lower risk of later-life depression and subsequent CVD mortality, even in the presence of depression,” they wrote. “These findings suggest the importance of fitness in primary prevention of heart disease and associated CVD mortality in older aging adults.”
The investigators reported no conflicts of interest.
SOURCE: Willis BL et al. JAMA Psychiatry. 2018 Jun 27. doi: 10.1001/jamapsychiatry.2018.1467.
REPORTING FROM JAMA PSYCHIATRY
IMAGINE-RA: No need for MRI with treat-to-target strategy
AMSTERDAM – Results of the

“Despite patients achieving a target of clinical remission, we still see erosive progression in about 20%-30%,” study investigator Signe Møller-Bisgaard, MD, PhD, said at the European Congress of Rheumatology. That’s regardless of the definition of remission that you use, she added.
Dr. Møller-Bisgaard, a resident in rheumatology and postdoctoral researcher who works at Rigshospitalet and Frederiksberg Hospital in Copenhagen, observed that both synovial inflammation and bone marrow edema seen on MRI had been shown to predict progression in patients with rheumatoid arthritis.
What was not known, however, was whether there was any value in specifically targeting MRI remission in patients who had already achieved clinical remission. This is what the IMAGINE-RA study set out to address. It was a 2-year trial of 200 patients with rheumatoid arthritis in clinical remission who were recruited and randomized to either an MRI or conventional treat-to-target strategy. The study involved nine rheumatology and eight radiological departments, Dr. Møller-Bisgaard said.
The protocol for the study (Trials. 2015;16:178) defined clinical remission as a DAS28-CRP of 3.2 or lower and no swollen joints. Patients had to have erosions on x-ray, be anti–cyclic citrullinated peptide positive, and be treated only with conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) at the time of entry.
During the study patients were assessed every 4 months via the DAS28 or DAS28 plus MRI of the dominant hand and wrist, with radiographs of the hands and feet performed annually in both groups and MRI also performed yearly in the conventional treat-to-target group.
“Treatment was intensified in both arms if the DAS28-CRP was above 3.2, and there was at least one clinical swollen joint,” Dr. Møller-Bisgaard explained. Treatment was also intensified in the MRI group if bone marrow edema was observed. Treatment intensification involved maximal doses of csDMARDs alone or in combinations, and then addition of biologic treatments, such as a tumor necrosis factor inhibitor.
“Targeting absence of MRI bone marrow edema in addition to a conventional treat-to-target strategy in RA patients in clinical remission had no effect on the probability of achieving DAS28-CRP remission or halting radiographic progression,” she said.
However, there were some positive effects on several predefined secondary endpoints. For instance, more patients in the MRI group than in the conventional treat-to-target group achieved American College of Rheumatology/EULAR remission (49% vs. 32%; P = .017). There was a significant improvement in the number of swollen joints and a patient and physician global assessment. “There was also more improvement in HAQ [Health Assessment Questionnaire], with a difference between the groups of .14 [P less than .001], Dr. Møller-Bisgaard reported.
The IMAGINE-RA study is funded by grants from the Danish Rheumatism Association and the Research Fund of Region Zealand. Funding is also provided by AbbVie via a nonrestricted grant, and adalimumab is provided free of charge. Dr. Møller-Bisgaard and coauthors had no personal conflicts of interest to declare.
SOURCE: Møller-Bisgaard S et al. EULAR 2018 Congress. Abstract OP0018.
AMSTERDAM – Results of the
“Despite patients achieving a target of clinical remission, we still see erosive progression in about 20%-30%,” study investigator Signe Møller-Bisgaard, MD, PhD, said at the European Congress of Rheumatology. That’s regardless of the definition of remission that you use, she added.
Dr. Møller-Bisgaard, a resident in rheumatology and postdoctoral researcher who works at Rigshospitalet and Frederiksberg Hospital in Copenhagen, observed that both synovial inflammation and bone marrow edema seen on MRI had been shown to predict progression in patients with rheumatoid arthritis.
What was not known, however, was whether there was any value in specifically targeting MRI remission in patients who had already achieved clinical remission. This is what the IMAGINE-RA study set out to address. It was a 2-year trial of 200 patients with rheumatoid arthritis in clinical remission who were recruited and randomized to either an MRI or conventional treat-to-target strategy. The study involved nine rheumatology and eight radiological departments, Dr. Møller-Bisgaard said.
The protocol for the study (Trials. 2015;16:178) defined clinical remission as a DAS28-CRP of 3.2 or lower and no swollen joints. Patients had to have erosions on x-ray, be anti–cyclic citrullinated peptide positive, and be treated only with conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) at the time of entry.
During the study patients were assessed every 4 months via the DAS28 or DAS28 plus MRI of the dominant hand and wrist, with radiographs of the hands and feet performed annually in both groups and MRI also performed yearly in the conventional treat-to-target group.
“Treatment was intensified in both arms if the DAS28-CRP was above 3.2, and there was at least one clinical swollen joint,” Dr. Møller-Bisgaard explained. Treatment was also intensified in the MRI group if bone marrow edema was observed. Treatment intensification involved maximal doses of csDMARDs alone or in combinations, and then addition of biologic treatments, such as a tumor necrosis factor inhibitor.
“Targeting absence of MRI bone marrow edema in addition to a conventional treat-to-target strategy in RA patients in clinical remission had no effect on the probability of achieving DAS28-CRP remission or halting radiographic progression,” she said.
However, there were some positive effects on several predefined secondary endpoints. For instance, more patients in the MRI group than in the conventional treat-to-target group achieved American College of Rheumatology/EULAR remission (49% vs. 32%; P = .017). There was a significant improvement in the number of swollen joints and a patient and physician global assessment. “There was also more improvement in HAQ [Health Assessment Questionnaire], with a difference between the groups of .14 [P less than .001], Dr. Møller-Bisgaard reported.
The IMAGINE-RA study is funded by grants from the Danish Rheumatism Association and the Research Fund of Region Zealand. Funding is also provided by AbbVie via a nonrestricted grant, and adalimumab is provided free of charge. Dr. Møller-Bisgaard and coauthors had no personal conflicts of interest to declare.
SOURCE: Møller-Bisgaard S et al. EULAR 2018 Congress. Abstract OP0018.
AMSTERDAM – Results of the
“Despite patients achieving a target of clinical remission, we still see erosive progression in about 20%-30%,” study investigator Signe Møller-Bisgaard, MD, PhD, said at the European Congress of Rheumatology. That’s regardless of the definition of remission that you use, she added.
Dr. Møller-Bisgaard, a resident in rheumatology and postdoctoral researcher who works at Rigshospitalet and Frederiksberg Hospital in Copenhagen, observed that both synovial inflammation and bone marrow edema seen on MRI had been shown to predict progression in patients with rheumatoid arthritis.
What was not known, however, was whether there was any value in specifically targeting MRI remission in patients who had already achieved clinical remission. This is what the IMAGINE-RA study set out to address. It was a 2-year trial of 200 patients with rheumatoid arthritis in clinical remission who were recruited and randomized to either an MRI or conventional treat-to-target strategy. The study involved nine rheumatology and eight radiological departments, Dr. Møller-Bisgaard said.
The protocol for the study (Trials. 2015;16:178) defined clinical remission as a DAS28-CRP of 3.2 or lower and no swollen joints. Patients had to have erosions on x-ray, be anti–cyclic citrullinated peptide positive, and be treated only with conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) at the time of entry.
During the study patients were assessed every 4 months via the DAS28 or DAS28 plus MRI of the dominant hand and wrist, with radiographs of the hands and feet performed annually in both groups and MRI also performed yearly in the conventional treat-to-target group.
“Treatment was intensified in both arms if the DAS28-CRP was above 3.2, and there was at least one clinical swollen joint,” Dr. Møller-Bisgaard explained. Treatment was also intensified in the MRI group if bone marrow edema was observed. Treatment intensification involved maximal doses of csDMARDs alone or in combinations, and then addition of biologic treatments, such as a tumor necrosis factor inhibitor.
“Targeting absence of MRI bone marrow edema in addition to a conventional treat-to-target strategy in RA patients in clinical remission had no effect on the probability of achieving DAS28-CRP remission or halting radiographic progression,” she said.
However, there were some positive effects on several predefined secondary endpoints. For instance, more patients in the MRI group than in the conventional treat-to-target group achieved American College of Rheumatology/EULAR remission (49% vs. 32%; P = .017). There was a significant improvement in the number of swollen joints and a patient and physician global assessment. “There was also more improvement in HAQ [Health Assessment Questionnaire], with a difference between the groups of .14 [P less than .001], Dr. Møller-Bisgaard reported.
The IMAGINE-RA study is funded by grants from the Danish Rheumatism Association and the Research Fund of Region Zealand. Funding is also provided by AbbVie via a nonrestricted grant, and adalimumab is provided free of charge. Dr. Møller-Bisgaard and coauthors had no personal conflicts of interest to declare.
SOURCE: Møller-Bisgaard S et al. EULAR 2018 Congress. Abstract OP0018.
REPORTING FROM THE EULAR 2018 CONGRESS
Key clinical point: When a treat-to-target approach is used there is no added benefit of using magnetic resonance imaging.
Major finding: At 2 years, a similar percentage of patients achieved a DAS28-CRP of less than 2.6 and had no radiographic progression with an MRI-guided and conventional treat-to-target strategy.
Study details: The IMAGINE-RA study, a 2-year, prospective, randomized, multicenter trial of 200 patients with rheumatoid arthritis in clinical remission treated at 10 Danish hospitals.
Disclosures: The IMAGINE-RA study is funded by grants from the Danish Rheumatism Association and the Research Fund of Region Zealand. Funding is also provided by AbbVie via a nonrestricted grant and adalimumab is provided free of charge. Dr. Møller-Bisgaard and her coauthors had no personal conflicts of interest to declare.
Source: Møller-Bisgaard S et al. EULAR 2018 Congress. Abstract OP0018.
Many veterans with comorbid pain and OUD not receiving MAT
SAN DIEGO – Less than 30% of veterans on medication-assisted treatment for opioids had a diagnosis of opioid use disorder, and only 7% of veterans with an opioid use disorder initiated medication-assisted treatment.
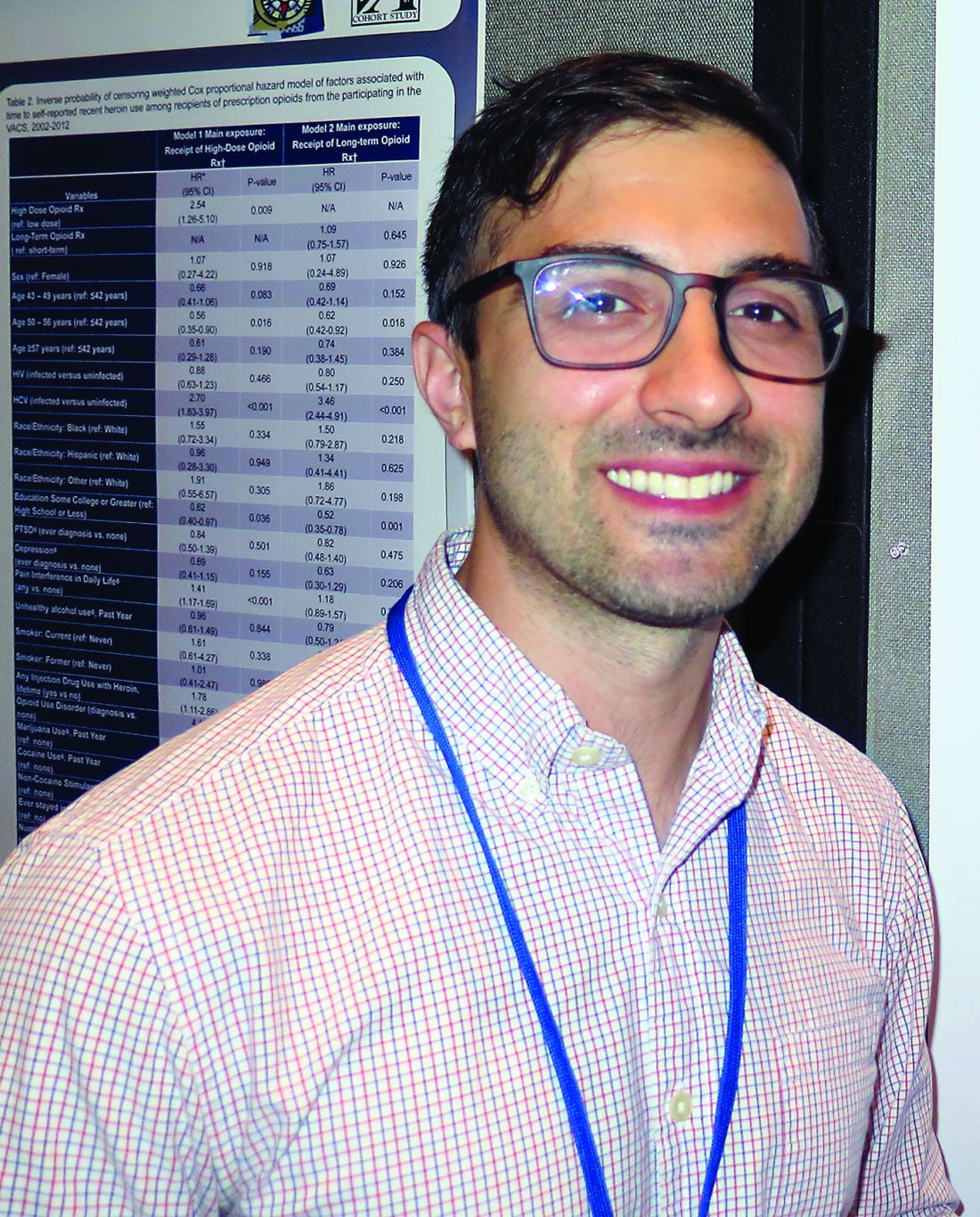
Those are key findings from a large study that set out to assess factors associated with initiating medication-assisted treatment (MAT) among veterans seeking pain care and to characterize the cohort of veterans seeking specialty pain care who initiated MAT.
“ but it was really low,” lead study author Lisham Ashrafioun, PhD, said in an interview at the annual meeting of the College on Problems of Drug Dependence. “These findings are preliminary, but I think we need to understand a lot more about how to treat people with opioid use disorders who are receiving pain care as well.”
Dr. Ashrafioun, a research investigator at the Veteran Affairs Center of Excellence for Suicide Prevention at the Canandaigua VA Medical Center, N.Y., and his associates drew from national VA electronic medical record data to identify 219,443 veterans who initiated specialty pain services during fiscal year 2012-2014. They used procedure and billing codes to identify veterans who started using MAT for opioids within the year following initiation of pain services, and extracted data on demographics, psychiatric and medical diagnoses, and pain intensity scores.
Of the 219,443 veterans, only 2,406 had received MAT in the year following the index visit (1.1%). In addition, only 26.4% of those on MAT had an opioid use disorder and just 6.6% of those with an opioid use disorder initiated MAT.
In adjusted analyses, opioid use disorders (adjusted odds ratio, 5.71) and opioid prescriptions (aOR, 2.33) were significantly associated with greater odds of receiving MAT. Moreover, having a diagnosis of depression was associated with a greater odds of receiving MAT (aOR, 1.26), while having a diagnosis of PTSD was associated with a greater odds of not receiving it (aOR, 0.90). The researchers also found that having a diagnosis of alcohol use disorder was associated with a greater odds of not receiving MAT (aOR, 0.85), while having a diagnosis of drug use disorder was associated with a greater odds of receiving it (aOR, 1.32).
Dr. Ashrafioun, who also holds a faculty position in the department of psychiatry at the University of Rochester (N.Y.), acknowledged certain limitations of the study. For example, the sample was restricted to only those receiving specialty pain care, provider and facility variation was not accounted for, and study participants might have initiated MAT outside of the VA.
He reported having no financial disclosures.
[email protected]
SAN DIEGO – Less than 30% of veterans on medication-assisted treatment for opioids had a diagnosis of opioid use disorder, and only 7% of veterans with an opioid use disorder initiated medication-assisted treatment.
Those are key findings from a large study that set out to assess factors associated with initiating medication-assisted treatment (MAT) among veterans seeking pain care and to characterize the cohort of veterans seeking specialty pain care who initiated MAT.
“ but it was really low,” lead study author Lisham Ashrafioun, PhD, said in an interview at the annual meeting of the College on Problems of Drug Dependence. “These findings are preliminary, but I think we need to understand a lot more about how to treat people with opioid use disorders who are receiving pain care as well.”
Dr. Ashrafioun, a research investigator at the Veteran Affairs Center of Excellence for Suicide Prevention at the Canandaigua VA Medical Center, N.Y., and his associates drew from national VA electronic medical record data to identify 219,443 veterans who initiated specialty pain services during fiscal year 2012-2014. They used procedure and billing codes to identify veterans who started using MAT for opioids within the year following initiation of pain services, and extracted data on demographics, psychiatric and medical diagnoses, and pain intensity scores.
Of the 219,443 veterans, only 2,406 had received MAT in the year following the index visit (1.1%). In addition, only 26.4% of those on MAT had an opioid use disorder and just 6.6% of those with an opioid use disorder initiated MAT.
In adjusted analyses, opioid use disorders (adjusted odds ratio, 5.71) and opioid prescriptions (aOR, 2.33) were significantly associated with greater odds of receiving MAT. Moreover, having a diagnosis of depression was associated with a greater odds of receiving MAT (aOR, 1.26), while having a diagnosis of PTSD was associated with a greater odds of not receiving it (aOR, 0.90). The researchers also found that having a diagnosis of alcohol use disorder was associated with a greater odds of not receiving MAT (aOR, 0.85), while having a diagnosis of drug use disorder was associated with a greater odds of receiving it (aOR, 1.32).
Dr. Ashrafioun, who also holds a faculty position in the department of psychiatry at the University of Rochester (N.Y.), acknowledged certain limitations of the study. For example, the sample was restricted to only those receiving specialty pain care, provider and facility variation was not accounted for, and study participants might have initiated MAT outside of the VA.
He reported having no financial disclosures.
[email protected]
SAN DIEGO – Less than 30% of veterans on medication-assisted treatment for opioids had a diagnosis of opioid use disorder, and only 7% of veterans with an opioid use disorder initiated medication-assisted treatment.
Those are key findings from a large study that set out to assess factors associated with initiating medication-assisted treatment (MAT) among veterans seeking pain care and to characterize the cohort of veterans seeking specialty pain care who initiated MAT.
“ but it was really low,” lead study author Lisham Ashrafioun, PhD, said in an interview at the annual meeting of the College on Problems of Drug Dependence. “These findings are preliminary, but I think we need to understand a lot more about how to treat people with opioid use disorders who are receiving pain care as well.”
Dr. Ashrafioun, a research investigator at the Veteran Affairs Center of Excellence for Suicide Prevention at the Canandaigua VA Medical Center, N.Y., and his associates drew from national VA electronic medical record data to identify 219,443 veterans who initiated specialty pain services during fiscal year 2012-2014. They used procedure and billing codes to identify veterans who started using MAT for opioids within the year following initiation of pain services, and extracted data on demographics, psychiatric and medical diagnoses, and pain intensity scores.
Of the 219,443 veterans, only 2,406 had received MAT in the year following the index visit (1.1%). In addition, only 26.4% of those on MAT had an opioid use disorder and just 6.6% of those with an opioid use disorder initiated MAT.
In adjusted analyses, opioid use disorders (adjusted odds ratio, 5.71) and opioid prescriptions (aOR, 2.33) were significantly associated with greater odds of receiving MAT. Moreover, having a diagnosis of depression was associated with a greater odds of receiving MAT (aOR, 1.26), while having a diagnosis of PTSD was associated with a greater odds of not receiving it (aOR, 0.90). The researchers also found that having a diagnosis of alcohol use disorder was associated with a greater odds of not receiving MAT (aOR, 0.85), while having a diagnosis of drug use disorder was associated with a greater odds of receiving it (aOR, 1.32).
Dr. Ashrafioun, who also holds a faculty position in the department of psychiatry at the University of Rochester (N.Y.), acknowledged certain limitations of the study. For example, the sample was restricted to only those receiving specialty pain care, provider and facility variation was not accounted for, and study participants might have initiated MAT outside of the VA.
He reported having no financial disclosures.
[email protected]
REPORTING FROM CPDD 2018
Key clinical point: Several clinical features differentiate veterans seeking specialty pain care who receive medication-assisted treatment (MAT) from those who do not.
Major finding: Only 26.5% of veterans on MAT had an opioid use disorder.
Study details: An analysis of 219,443 veterans who initiated specialty pain services during fiscal year 2012-2014.
Disclosures: Dr. Ashrafioun reported having no financial disclosures.
Cocaine use declining among young adults
SAN DIEGO – Use of cocaine by young adults in the United States has declined significantly since the early 2000s, but it remains relatively common. In fact, results from an analysis of national data suggest that about 5% of 18- to 22-year-olds have used cocaine in the past 12 months.
“We don’t typically think of cocaine use amongst young people, but it is of a nontrivial prevalence,” lead study author Kristin E. Schneider said in an interview at the annual meeting of the College on Problems of Drug Dependence. “If someone has risky alcohol use they might also have risky substance use. We need to be screening for those things as well, while most interventions these days focus on problem drinking.”
Ms. Schneider, a graduate student in the department of mental health at Johns Hopkins University, Baltimore, and her associates drew from the 2002-2014 waves of the National Survey on Drug Use and Health to describe trends in cocaine use among young adults by race/ethnicity, sex, and college enrollment. They assessed for lifetime use, any past 12-month cocaine use, past 30-day use, and any past 12-month use disorder. They also tested for linear and quadratic trends over time.

When the researchers averaged across all years, they found that 12.1% of young adults had ever used cocaine, 5.9% had used it in the past 12 months, 1.8% had used in the past 30 days, and 1% had a use disorder in the past 12 months. They also observed significant linear declines in cocaine use across the entire study period. For example, between 2002 and 2014, the prevalence of lifetime cocaine use declined from 13.7% to 8.6%, past 12-month use declined from 6.3% to 4.1%, and past 30-day use declined from 1.8% to 1.4%.
Nonstudents had higher lifetime rates of cocaine use, compared with students (14.8% vs. 7.8%, respectively), but differences between the two groups were small for other indicators. “Perhaps being an emerging environment with other [young] adults who are also making risky health behavior decisions compensates for this baseline difference of risk between people who go to college and those who do not,” Ms. Schneider said. At the same time, the lowest rates of past 12-month cocaine use was observed in black males (1.6%), Asian females (0.8%), and black females (0.8%).
The National Institute on Drug Abuse supported the study. Ms. Schneider reported having no financial disclosures.
SAN DIEGO – Use of cocaine by young adults in the United States has declined significantly since the early 2000s, but it remains relatively common. In fact, results from an analysis of national data suggest that about 5% of 18- to 22-year-olds have used cocaine in the past 12 months.
“We don’t typically think of cocaine use amongst young people, but it is of a nontrivial prevalence,” lead study author Kristin E. Schneider said in an interview at the annual meeting of the College on Problems of Drug Dependence. “If someone has risky alcohol use they might also have risky substance use. We need to be screening for those things as well, while most interventions these days focus on problem drinking.”
Ms. Schneider, a graduate student in the department of mental health at Johns Hopkins University, Baltimore, and her associates drew from the 2002-2014 waves of the National Survey on Drug Use and Health to describe trends in cocaine use among young adults by race/ethnicity, sex, and college enrollment. They assessed for lifetime use, any past 12-month cocaine use, past 30-day use, and any past 12-month use disorder. They also tested for linear and quadratic trends over time.
When the researchers averaged across all years, they found that 12.1% of young adults had ever used cocaine, 5.9% had used it in the past 12 months, 1.8% had used in the past 30 days, and 1% had a use disorder in the past 12 months. They also observed significant linear declines in cocaine use across the entire study period. For example, between 2002 and 2014, the prevalence of lifetime cocaine use declined from 13.7% to 8.6%, past 12-month use declined from 6.3% to 4.1%, and past 30-day use declined from 1.8% to 1.4%.
Nonstudents had higher lifetime rates of cocaine use, compared with students (14.8% vs. 7.8%, respectively), but differences between the two groups were small for other indicators. “Perhaps being an emerging environment with other [young] adults who are also making risky health behavior decisions compensates for this baseline difference of risk between people who go to college and those who do not,” Ms. Schneider said. At the same time, the lowest rates of past 12-month cocaine use was observed in black males (1.6%), Asian females (0.8%), and black females (0.8%).
The National Institute on Drug Abuse supported the study. Ms. Schneider reported having no financial disclosures.
SAN DIEGO – Use of cocaine by young adults in the United States has declined significantly since the early 2000s, but it remains relatively common. In fact, results from an analysis of national data suggest that about 5% of 18- to 22-year-olds have used cocaine in the past 12 months.
“We don’t typically think of cocaine use amongst young people, but it is of a nontrivial prevalence,” lead study author Kristin E. Schneider said in an interview at the annual meeting of the College on Problems of Drug Dependence. “If someone has risky alcohol use they might also have risky substance use. We need to be screening for those things as well, while most interventions these days focus on problem drinking.”
Ms. Schneider, a graduate student in the department of mental health at Johns Hopkins University, Baltimore, and her associates drew from the 2002-2014 waves of the National Survey on Drug Use and Health to describe trends in cocaine use among young adults by race/ethnicity, sex, and college enrollment. They assessed for lifetime use, any past 12-month cocaine use, past 30-day use, and any past 12-month use disorder. They also tested for linear and quadratic trends over time.
When the researchers averaged across all years, they found that 12.1% of young adults had ever used cocaine, 5.9% had used it in the past 12 months, 1.8% had used in the past 30 days, and 1% had a use disorder in the past 12 months. They also observed significant linear declines in cocaine use across the entire study period. For example, between 2002 and 2014, the prevalence of lifetime cocaine use declined from 13.7% to 8.6%, past 12-month use declined from 6.3% to 4.1%, and past 30-day use declined from 1.8% to 1.4%.
Nonstudents had higher lifetime rates of cocaine use, compared with students (14.8% vs. 7.8%, respectively), but differences between the two groups were small for other indicators. “Perhaps being an emerging environment with other [young] adults who are also making risky health behavior decisions compensates for this baseline difference of risk between people who go to college and those who do not,” Ms. Schneider said. At the same time, the lowest rates of past 12-month cocaine use was observed in black males (1.6%), Asian females (0.8%), and black females (0.8%).
The National Institute on Drug Abuse supported the study. Ms. Schneider reported having no financial disclosures.
AT CPDD 2018
Key clinical point: Cocaine use has declined among young adults in the United States.
Major finding: Between 2002 and 2014, the prevalence of lifetime cocaine use declined from 13.7% to 8.6%.
Study details: An analysis drawn from the 2002-2014 waves of the National Survey on Drug Use and Health.
Disclosures: The National Institute on Drug Abuse supported the study. Ms. Schneider reported having no financial disclosures.
Heart failure confers poor prognosis in rheumatoid arthritis
AMSTERDAM – The combination of heart failure and rheumatoid arthritis carries a poor prognosis, according to data from the German biologics register.
Of 393 patients enrolled in RABBIT (Rheumatoide Arthritis: Beobachtung der Biologika-Therapie) who had heart failure in addition to their rheumatoid arthritis, 131 (33%) needed hospital treatment or died over a 10-year period. The mean time to hospitalization or death was 2.5-3.0 years.
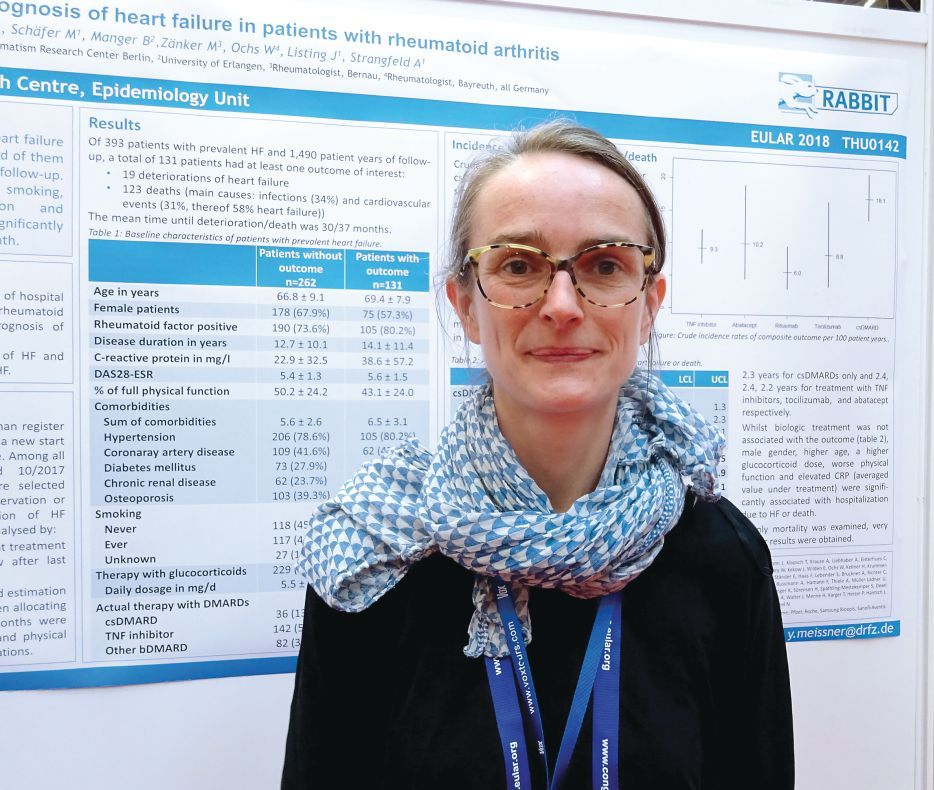
“We include patients at the start of their DMARD [disease modifying antirheumatic drug] treatment and follow them up for at least 5 years,” said Dr. Meissner, explaining how the German biologics register works. “For this analysis, we selected all the patients with prevalent heart failure and followed them up until either the database was closed, they dropped out, or had an event.” In this case, an event was defined as a composite of deterioration in heart failure that required hospitalization or death from any cause.
Dr. Meissner, of the German Rheumatism Research Center in Berlin, noted that 19 (14.5%) patients experienced a deterioration in their heart failure and 123 deaths were recorded during the study period that started in May 2001 and ended in October 2017. Around one-third of deaths were attributable to infections (34%), and one-third were attributable to cardiovascular causes (31%). Of the CV deaths, more than half (58%) were attributed to patients’ heart failure.
“What impressed us the most is the number of comorbidities at baseline,” Dr. Meissner said. Not including heart failure or rheumatoid arthritis, patients who experienced an event had an average of 6.5 comorbidities versus 5.6 for those who did not have an event. These additional comorbidities included hypertension, coronary artery disease, diabetes mellitus, chronic renal disease, and osteoporosis.
Crude incidence rates (IRs) for heart failure deterioration or death were calculated according to the rheumatoid arthritis treatment being used and found to be highest in those treated with conventional DMARDs, at 18.1/100 patient-years. IRs with biologic treatments were lower, at 10.2/100 patient-years for abatacept, 9.3 for TNF inhibitors, 8.8 for tocilizumab, and 6.0 for rituximab. What this suggests it that better control of inflammation results in a lower risk for hospitalization and death, Dr. Meissner and her associates reported in their poster presentation.
“If patients are not effectively treated for rheumatoid arthritis, there might be other consequences like the deterioration of heart failure or death,” Dr. Meissner said.
She noted that investigators also looked at identifying risk factors for hospitalization or death and found that there was a greater adjusted relative risk if patients were male (RR = 2.4), older (RR = 1.3 per 5-year increase in age), or if they smoked (RR = 1.7). Using higher doses of glucocorticoids also was a risk factor, with a RR of 1.4 for every 5 mg/day increase in dose.
Better physical function was associated with a lower risk of an event (RR = 0.9) and, along with smoking and adjustment of the steroid dose, is a risk factor that could potentially be influenced, Dr. Meissner proposed.
No data on how the heart failure was being managed are available for this cohort and more research is needed.
“There is still not enough known about this topic, and we need the research to determine how to best manage these patients,” Dr. Meissner said. “The time to an event was only 3 years from the time of inclusion in the register, so we need better management of those patients with heart failure as a comorbidity.”
RABBIT is supported by a joint, unconditional grant from AbbVie, Bristol-Myers Squibb, Celltrion, Hexal AG, Lilly, MSD Sharp & Dohme, Pfizer, Roche, Samsung Bioepis, Sanofi-Aventis, and UCB. Dr. Meissner disclosed being on a speakers bureau for Pfizer.
SOURCE: Meissner Y et al. EULAR 2018 Congress. Abstract THU0142 .
AMSTERDAM – The combination of heart failure and rheumatoid arthritis carries a poor prognosis, according to data from the German biologics register.
Of 393 patients enrolled in RABBIT (Rheumatoide Arthritis: Beobachtung der Biologika-Therapie) who had heart failure in addition to their rheumatoid arthritis, 131 (33%) needed hospital treatment or died over a 10-year period. The mean time to hospitalization or death was 2.5-3.0 years.
“We include patients at the start of their DMARD [disease modifying antirheumatic drug] treatment and follow them up for at least 5 years,” said Dr. Meissner, explaining how the German biologics register works. “For this analysis, we selected all the patients with prevalent heart failure and followed them up until either the database was closed, they dropped out, or had an event.” In this case, an event was defined as a composite of deterioration in heart failure that required hospitalization or death from any cause.
Dr. Meissner, of the German Rheumatism Research Center in Berlin, noted that 19 (14.5%) patients experienced a deterioration in their heart failure and 123 deaths were recorded during the study period that started in May 2001 and ended in October 2017. Around one-third of deaths were attributable to infections (34%), and one-third were attributable to cardiovascular causes (31%). Of the CV deaths, more than half (58%) were attributed to patients’ heart failure.
“What impressed us the most is the number of comorbidities at baseline,” Dr. Meissner said. Not including heart failure or rheumatoid arthritis, patients who experienced an event had an average of 6.5 comorbidities versus 5.6 for those who did not have an event. These additional comorbidities included hypertension, coronary artery disease, diabetes mellitus, chronic renal disease, and osteoporosis.
Crude incidence rates (IRs) for heart failure deterioration or death were calculated according to the rheumatoid arthritis treatment being used and found to be highest in those treated with conventional DMARDs, at 18.1/100 patient-years. IRs with biologic treatments were lower, at 10.2/100 patient-years for abatacept, 9.3 for TNF inhibitors, 8.8 for tocilizumab, and 6.0 for rituximab. What this suggests it that better control of inflammation results in a lower risk for hospitalization and death, Dr. Meissner and her associates reported in their poster presentation.
“If patients are not effectively treated for rheumatoid arthritis, there might be other consequences like the deterioration of heart failure or death,” Dr. Meissner said.
She noted that investigators also looked at identifying risk factors for hospitalization or death and found that there was a greater adjusted relative risk if patients were male (RR = 2.4), older (RR = 1.3 per 5-year increase in age), or if they smoked (RR = 1.7). Using higher doses of glucocorticoids also was a risk factor, with a RR of 1.4 for every 5 mg/day increase in dose.
Better physical function was associated with a lower risk of an event (RR = 0.9) and, along with smoking and adjustment of the steroid dose, is a risk factor that could potentially be influenced, Dr. Meissner proposed.
No data on how the heart failure was being managed are available for this cohort and more research is needed.
“There is still not enough known about this topic, and we need the research to determine how to best manage these patients,” Dr. Meissner said. “The time to an event was only 3 years from the time of inclusion in the register, so we need better management of those patients with heart failure as a comorbidity.”
RABBIT is supported by a joint, unconditional grant from AbbVie, Bristol-Myers Squibb, Celltrion, Hexal AG, Lilly, MSD Sharp & Dohme, Pfizer, Roche, Samsung Bioepis, Sanofi-Aventis, and UCB. Dr. Meissner disclosed being on a speakers bureau for Pfizer.
SOURCE: Meissner Y et al. EULAR 2018 Congress. Abstract THU0142 .
AMSTERDAM – The combination of heart failure and rheumatoid arthritis carries a poor prognosis, according to data from the German biologics register.
Of 393 patients enrolled in RABBIT (Rheumatoide Arthritis: Beobachtung der Biologika-Therapie) who had heart failure in addition to their rheumatoid arthritis, 131 (33%) needed hospital treatment or died over a 10-year period. The mean time to hospitalization or death was 2.5-3.0 years.
“We include patients at the start of their DMARD [disease modifying antirheumatic drug] treatment and follow them up for at least 5 years,” said Dr. Meissner, explaining how the German biologics register works. “For this analysis, we selected all the patients with prevalent heart failure and followed them up until either the database was closed, they dropped out, or had an event.” In this case, an event was defined as a composite of deterioration in heart failure that required hospitalization or death from any cause.
Dr. Meissner, of the German Rheumatism Research Center in Berlin, noted that 19 (14.5%) patients experienced a deterioration in their heart failure and 123 deaths were recorded during the study period that started in May 2001 and ended in October 2017. Around one-third of deaths were attributable to infections (34%), and one-third were attributable to cardiovascular causes (31%). Of the CV deaths, more than half (58%) were attributed to patients’ heart failure.
“What impressed us the most is the number of comorbidities at baseline,” Dr. Meissner said. Not including heart failure or rheumatoid arthritis, patients who experienced an event had an average of 6.5 comorbidities versus 5.6 for those who did not have an event. These additional comorbidities included hypertension, coronary artery disease, diabetes mellitus, chronic renal disease, and osteoporosis.
Crude incidence rates (IRs) for heart failure deterioration or death were calculated according to the rheumatoid arthritis treatment being used and found to be highest in those treated with conventional DMARDs, at 18.1/100 patient-years. IRs with biologic treatments were lower, at 10.2/100 patient-years for abatacept, 9.3 for TNF inhibitors, 8.8 for tocilizumab, and 6.0 for rituximab. What this suggests it that better control of inflammation results in a lower risk for hospitalization and death, Dr. Meissner and her associates reported in their poster presentation.
“If patients are not effectively treated for rheumatoid arthritis, there might be other consequences like the deterioration of heart failure or death,” Dr. Meissner said.
She noted that investigators also looked at identifying risk factors for hospitalization or death and found that there was a greater adjusted relative risk if patients were male (RR = 2.4), older (RR = 1.3 per 5-year increase in age), or if they smoked (RR = 1.7). Using higher doses of glucocorticoids also was a risk factor, with a RR of 1.4 for every 5 mg/day increase in dose.
Better physical function was associated with a lower risk of an event (RR = 0.9) and, along with smoking and adjustment of the steroid dose, is a risk factor that could potentially be influenced, Dr. Meissner proposed.
No data on how the heart failure was being managed are available for this cohort and more research is needed.
“There is still not enough known about this topic, and we need the research to determine how to best manage these patients,” Dr. Meissner said. “The time to an event was only 3 years from the time of inclusion in the register, so we need better management of those patients with heart failure as a comorbidity.”
RABBIT is supported by a joint, unconditional grant from AbbVie, Bristol-Myers Squibb, Celltrion, Hexal AG, Lilly, MSD Sharp & Dohme, Pfizer, Roche, Samsung Bioepis, Sanofi-Aventis, and UCB. Dr. Meissner disclosed being on a speakers bureau for Pfizer.
SOURCE: Meissner Y et al. EULAR 2018 Congress. Abstract THU0142 .
REPORTING FROM THE EULAR 2018 CONGRESS
Key clinical point: Comorbid heart failure and rheumatoid arthritis carry an unfavorable prognosis, but risk factors have been identified.
Major finding: One-third of patients were hospitalized or died, with a mean time to deterioration or death of 2.5-3 years.
Study details: 393 patients with both heart failure and rheumatoid arthritis enrolled in the German biologics register RABBIT.
Disclosures: RABBIT is supported by a joint, unconditional grant from AbbVie, Bristol-Myers Squibb, Celltrion, Hexal AG, Lilly, MSD Sharp & Dohme, Pfizer, Roche, Samsung Bioepis, Sanofi-Aventis, and UCB. Dr. Meissner disclosed being part of a speakers bureau for Pfizer.
Source: Meissner Y et al. EULAR 2018 Congress, Abstract THU0142.

