User login
Ob.gyn. workforce shortage looms
The average age of ob.gyns. is rising across the country, signaling physician shortages that are projected to worsen over the next several decades. The pinch may be felt especially in areas with high birth rates and few younger ob.gyns., according to a report from Doximity.
Doximity’s geographic projections paint a fine-grained picture in agreement with the American College of Obstetricians and Gynecologists’ projections of a national shortfall of up to 8,800 ob.gyns. by 2020, with the deficit of ob.gyns. potentially climbing to 22,000 by 2050.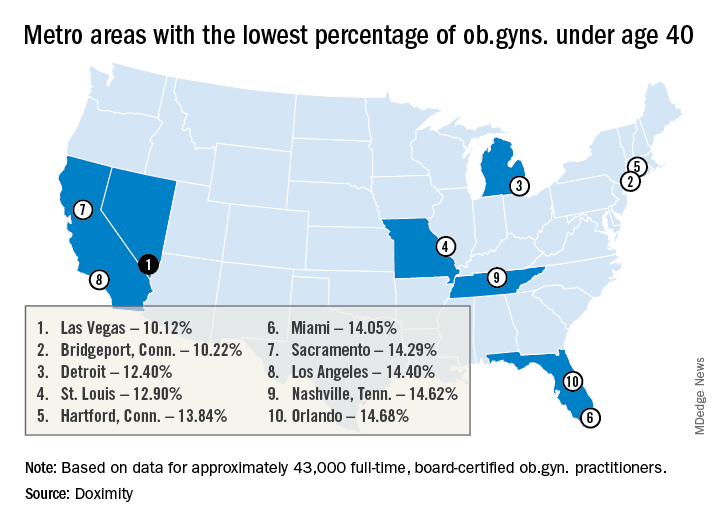
Pittsburgh and Bridgeport, Conn. top the list of metropolitan areas with the oldest average age of practicing ob.gyns., with average ages of 52.32 and 52.12 years, respectively. Las Vegas, Detroit, Miami, Los Angeles, New York, Boston, and Chicago all also made the top 15 cities in this list.
Because ob.gyns. start to leave the work force at age 59 years and retire at a median age of 64 years, this aging physician population could affect access to women’s health services within the decade, said Dr. Whaley. The fact that the burnout rate for ob.gyns. is only topped by emergency room physicians represents another area for concern, said Dr. Whaley of the University of California, Berkeley.
The report drew on data from the Centers for Medicare and Medicaid Services and board certification data. Doximity’s self-reported information from about 43,000 full-time board-certified ob.gyns. was also factored in. The top metropolitan areas were determined by 2010 census data and birth statistics came from federal databases.
With the data sliced another way, Pittsburgh also had the highest percentage of ob.gyns. aged 55 years or older, with 41.92% falling into this age group. Of the 50 metropolitan areas included in the Doximity report, 32 have an ob.gyn. workforce with at least one-third aged 55 years and up.
And there are many metropolitan areas where there’s a paucity of young ob.gyns., signaling future serious shortages, according to Doximity. In 12 of the metropolitan areas studied, less than 15% of the ob.gyn. workforce is aged 40 years or younger. Some of the cities with a potential “double hit” of older ob.gyns. and few younger physicians entering the profession include Las Vegas, Miami, Los Angeles, New York, and Chicago.
The Doximity methodology also took into account the average workload, in terms of the number of live births per physician per year, for ob.gyns. in the various metropolitan areas. There was a large variation in workload calculated this way: St. Louis has 247 live births per ob.gyn per year, while Louisville, Ky., has just 64, according to the report.
Factoring in workload information as well, the report gives a “shortage risk index” listing. Here, Las Vegas, Los Angeles, and Miami top the list. Cities considered at lowest risk for shortages according to this methodology include Baltimore, Denver, Portland, Ore., and Cleveland.
According to a 2017 ACOG workforce report, though women make up nearly half of those entering medical school, over four in five physicians entering ob.gyn. residencies (82.3% in 2016) are women. Further, women made up 58.7% of the ob.gyns. in active practice in 2017, outstripping all other surgical and medical specialties save pediatrics. Within 10 years, two-thirds of all ob.gyns. will be female, according to ACOG.
“While this study cannot determine causation for the variation in workloads, compensation, or shortages across metropolitan areas, we hope it will continue to serve as a baseline for the size of the challenge and prove helpful to health care employers, policymakers, patient advocates, and others interested in further study of this topic,” wrote Dr. Whaley and the report’s coauthors. “This information may also be helpful for ob.gyns. looking to live in areas with an increasing need for their expertise,” they said.
Dr. Whaley has received consulting fees from Castlight Health, Crossover Health, Doximity, Livongo, and Norwest Venture Partners. Doximity funded the production of the report.
The average age of ob.gyns. is rising across the country, signaling physician shortages that are projected to worsen over the next several decades. The pinch may be felt especially in areas with high birth rates and few younger ob.gyns., according to a report from Doximity.
Doximity’s geographic projections paint a fine-grained picture in agreement with the American College of Obstetricians and Gynecologists’ projections of a national shortfall of up to 8,800 ob.gyns. by 2020, with the deficit of ob.gyns. potentially climbing to 22,000 by 2050.
Pittsburgh and Bridgeport, Conn. top the list of metropolitan areas with the oldest average age of practicing ob.gyns., with average ages of 52.32 and 52.12 years, respectively. Las Vegas, Detroit, Miami, Los Angeles, New York, Boston, and Chicago all also made the top 15 cities in this list.
Because ob.gyns. start to leave the work force at age 59 years and retire at a median age of 64 years, this aging physician population could affect access to women’s health services within the decade, said Dr. Whaley. The fact that the burnout rate for ob.gyns. is only topped by emergency room physicians represents another area for concern, said Dr. Whaley of the University of California, Berkeley.
The report drew on data from the Centers for Medicare and Medicaid Services and board certification data. Doximity’s self-reported information from about 43,000 full-time board-certified ob.gyns. was also factored in. The top metropolitan areas were determined by 2010 census data and birth statistics came from federal databases.
With the data sliced another way, Pittsburgh also had the highest percentage of ob.gyns. aged 55 years or older, with 41.92% falling into this age group. Of the 50 metropolitan areas included in the Doximity report, 32 have an ob.gyn. workforce with at least one-third aged 55 years and up.
And there are many metropolitan areas where there’s a paucity of young ob.gyns., signaling future serious shortages, according to Doximity. In 12 of the metropolitan areas studied, less than 15% of the ob.gyn. workforce is aged 40 years or younger. Some of the cities with a potential “double hit” of older ob.gyns. and few younger physicians entering the profession include Las Vegas, Miami, Los Angeles, New York, and Chicago.
The Doximity methodology also took into account the average workload, in terms of the number of live births per physician per year, for ob.gyns. in the various metropolitan areas. There was a large variation in workload calculated this way: St. Louis has 247 live births per ob.gyn per year, while Louisville, Ky., has just 64, according to the report.
Factoring in workload information as well, the report gives a “shortage risk index” listing. Here, Las Vegas, Los Angeles, and Miami top the list. Cities considered at lowest risk for shortages according to this methodology include Baltimore, Denver, Portland, Ore., and Cleveland.
According to a 2017 ACOG workforce report, though women make up nearly half of those entering medical school, over four in five physicians entering ob.gyn. residencies (82.3% in 2016) are women. Further, women made up 58.7% of the ob.gyns. in active practice in 2017, outstripping all other surgical and medical specialties save pediatrics. Within 10 years, two-thirds of all ob.gyns. will be female, according to ACOG.
“While this study cannot determine causation for the variation in workloads, compensation, or shortages across metropolitan areas, we hope it will continue to serve as a baseline for the size of the challenge and prove helpful to health care employers, policymakers, patient advocates, and others interested in further study of this topic,” wrote Dr. Whaley and the report’s coauthors. “This information may also be helpful for ob.gyns. looking to live in areas with an increasing need for their expertise,” they said.
Dr. Whaley has received consulting fees from Castlight Health, Crossover Health, Doximity, Livongo, and Norwest Venture Partners. Doximity funded the production of the report.
The average age of ob.gyns. is rising across the country, signaling physician shortages that are projected to worsen over the next several decades. The pinch may be felt especially in areas with high birth rates and few younger ob.gyns., according to a report from Doximity.
Doximity’s geographic projections paint a fine-grained picture in agreement with the American College of Obstetricians and Gynecologists’ projections of a national shortfall of up to 8,800 ob.gyns. by 2020, with the deficit of ob.gyns. potentially climbing to 22,000 by 2050.
Pittsburgh and Bridgeport, Conn. top the list of metropolitan areas with the oldest average age of practicing ob.gyns., with average ages of 52.32 and 52.12 years, respectively. Las Vegas, Detroit, Miami, Los Angeles, New York, Boston, and Chicago all also made the top 15 cities in this list.
Because ob.gyns. start to leave the work force at age 59 years and retire at a median age of 64 years, this aging physician population could affect access to women’s health services within the decade, said Dr. Whaley. The fact that the burnout rate for ob.gyns. is only topped by emergency room physicians represents another area for concern, said Dr. Whaley of the University of California, Berkeley.
The report drew on data from the Centers for Medicare and Medicaid Services and board certification data. Doximity’s self-reported information from about 43,000 full-time board-certified ob.gyns. was also factored in. The top metropolitan areas were determined by 2010 census data and birth statistics came from federal databases.
With the data sliced another way, Pittsburgh also had the highest percentage of ob.gyns. aged 55 years or older, with 41.92% falling into this age group. Of the 50 metropolitan areas included in the Doximity report, 32 have an ob.gyn. workforce with at least one-third aged 55 years and up.
And there are many metropolitan areas where there’s a paucity of young ob.gyns., signaling future serious shortages, according to Doximity. In 12 of the metropolitan areas studied, less than 15% of the ob.gyn. workforce is aged 40 years or younger. Some of the cities with a potential “double hit” of older ob.gyns. and few younger physicians entering the profession include Las Vegas, Miami, Los Angeles, New York, and Chicago.
The Doximity methodology also took into account the average workload, in terms of the number of live births per physician per year, for ob.gyns. in the various metropolitan areas. There was a large variation in workload calculated this way: St. Louis has 247 live births per ob.gyn per year, while Louisville, Ky., has just 64, according to the report.
Factoring in workload information as well, the report gives a “shortage risk index” listing. Here, Las Vegas, Los Angeles, and Miami top the list. Cities considered at lowest risk for shortages according to this methodology include Baltimore, Denver, Portland, Ore., and Cleveland.
According to a 2017 ACOG workforce report, though women make up nearly half of those entering medical school, over four in five physicians entering ob.gyn. residencies (82.3% in 2016) are women. Further, women made up 58.7% of the ob.gyns. in active practice in 2017, outstripping all other surgical and medical specialties save pediatrics. Within 10 years, two-thirds of all ob.gyns. will be female, according to ACOG.
“While this study cannot determine causation for the variation in workloads, compensation, or shortages across metropolitan areas, we hope it will continue to serve as a baseline for the size of the challenge and prove helpful to health care employers, policymakers, patient advocates, and others interested in further study of this topic,” wrote Dr. Whaley and the report’s coauthors. “This information may also be helpful for ob.gyns. looking to live in areas with an increasing need for their expertise,” they said.
Dr. Whaley has received consulting fees from Castlight Health, Crossover Health, Doximity, Livongo, and Norwest Venture Partners. Doximity funded the production of the report.
Geriatric assessments could fine-tune cancer care for older adults

Fewer than 25% of older cancer patients currently get these assessments, which evaluate a person’s functioning (what he can and cannot do), psychological status, nutrition, cognition, social circumstances, and other, coexisting medical conditions, and which can predict the potential toxicity of chemotherapy.
The new guideline, ASCO’s first in the field of “geriatric oncology,” may have significant potential to change medical practice. “These recommendations will capture the attention of oncologists, I think, and that will be incredibly valuable,” said Corinne Leach, PhD, strategic director of cancer and aging research at the American Cancer Society.
They recognize a shifting demographic reality for cancer specialists, who are treating increasingly older patients as life spans lengthen across the globe. In the United States, 60% of patients newly diagnosed with cancer (an estimated 1.7 million people this year) are aged 65 years or older, as are more than 60% of cancer survivors.
Yet evidence about how best to treat older adults with cancer is weak because older adults are underrepresented in clinical trials. And most oncologists have received little training in how to manage older patients’ unique vulnerabilities.
When researchers asked 305 community oncologists about evaluating older patients, 89% acknowledged “the care of older adults with cancer needs to be improved,” according to a recently published study. Fewer than 25% said they were “very confident” they could identify dementia or accurately assess a patient’s functioning or risk of falling – factors associated with poorer outcomes for cancer treatment.
Still, resistance to change is evident. “We’re all inundated with trying to keep up with new standards of care, and I doubt there will be any broad acceptance of the rigor called for in this guideline,” said Frederick Schnell, MD, medical director of the Community Oncology Alliance.
The burden on physicians shouldn’t be significant, however: The streamlined assessments recommended in the ASCO guideline take only about 20 minutes to complete. Patients fill out surveys during most of that time; about five minutes is required for a nurse or physician assistant to administer several brief tests.
The assessment can identify people at increased risk of experiencing serious side effects from chemotherapy – infections, fatigue, diarrhea, dehydration and other problems that affect more than half of older patients. Physicians can then take steps to address these vulnerabilities, such as prescribing physical therapy for an older patient with muscle weakness or ordering a nutritional consultation for someone who has become malnourished. Also, they can alter chemotherapy regimens to minimize the potential for harm.
Currently, most oncologists decide whether older patients can benefit from chemotherapy by using the “eyeball test,” an assessment that relies primarily on their experience and judgment. “This isn’t enough to understand factors that put older adults at risk; it takes a deeper dive,” said Arti Hurria, MD, director of the Center for Cancer and Aging and professor of medical oncology and therapeutics research at City of Hope, a comprehensive cancer center in Duarte, Calif., and cochair of the panel that produced the new guidelines.
An oncologist walking into a room in a busy clinic might find an older patient already on the exam table, for instance, and miss the fact that he needed assistance getting out of a chair and getting into a gown – important signs of functional impairment that could be aggravated by chemotherapy, Dr. Hurria said. Or, “a very pleasant older patient might smile kindly at you and agree with everything you’re saying, and she might not have understood a thing you said” because of undetected cognitive impairment that could worsen and interfere with treatment, she explained.
William Dale, MD, a geriatrician and Arthur M. Coppola Family Chair in Supportive Care Medicine at City of Hope and another cochair of the guideline panel, tells of an 83-year-old woman whom he saw several years ago, with lung cancer metastasized to her brain. Her family requested a consultation because she’d become withdrawn and forgetful – a sign of accelerating cognitive impairment, they suspected.
Should she have chemotherapy and whole brain radiation, or would that worsen her memory lapses, the patient and family wondered?
One result stood out when Dale ordered a geriatric assessment: This older woman wasn’t cognitively impaired, she was psychologically distressed. “She wasn’t eating, she wasn’t interacting with other people, she appeared not to want treatment, but all this was due to depression,” Dr. Dale recalled. With counseling, the patient decided to undergo chemotherapy and radiation treatment, which he called “remarkably successful.”
Just as genetic tests are being used to personalize care for older cancer patients, geriatric assessments can be employed for this purpose – at considerably less expense, said Supriya Gupta Mohile, MD, editor in chief of the Journal of Geriatric Oncology and director of geriatric oncology at the James Wilmot Cancer Institute at the University of Rochester (N.Y.).
She tells of a 78-year-old man with invasive bladder cancer who came in for a consultation. From the medical chart, she learned the patient had hypertension, diabetes, and depression, all reasonably well controlled. From a geriatric assessment, she discovered that he lived alone, had cognitive impairment, relied on his daughter to deliver meals, and was at high risk of falling.
“The patient and his daughter were worried about his safety at home, his cognition getting worse, and fatigue [he was dealing with] and how that might affect his ability to function,” Dr. Mohile said. “His goal was to stay independent, at home, and not be hospitalized or go to rehabilitation.”
The standard of care for this condition was 3-4 months of chemotherapy before surgery, but Dr. Mohile recommended that the older patient skip chemotherapy and have surgery immediately, after reviewing the geriatric assessment with her patient and his family.
Every older patient considering chemotherapy should request an evaluation of this kind, even if your physician doesn’t offer it, said Heidi D. Klepin, MD, associate professor of hematology and oncology at Wake Forest University, Winston-Salem, N.C. “Ask for your doctor to consider your ability to do the things you most care about doing and for care to be individualized to your unique circumstances.”
KHN’s coverage of these topics is supported by John A. Hartford Foundation, Gordon and Betty Moore Foundation, and The SCAN Foundation. Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Fewer than 25% of older cancer patients currently get these assessments, which evaluate a person’s functioning (what he can and cannot do), psychological status, nutrition, cognition, social circumstances, and other, coexisting medical conditions, and which can predict the potential toxicity of chemotherapy.
The new guideline, ASCO’s first in the field of “geriatric oncology,” may have significant potential to change medical practice. “These recommendations will capture the attention of oncologists, I think, and that will be incredibly valuable,” said Corinne Leach, PhD, strategic director of cancer and aging research at the American Cancer Society.
They recognize a shifting demographic reality for cancer specialists, who are treating increasingly older patients as life spans lengthen across the globe. In the United States, 60% of patients newly diagnosed with cancer (an estimated 1.7 million people this year) are aged 65 years or older, as are more than 60% of cancer survivors.
Yet evidence about how best to treat older adults with cancer is weak because older adults are underrepresented in clinical trials. And most oncologists have received little training in how to manage older patients’ unique vulnerabilities.
When researchers asked 305 community oncologists about evaluating older patients, 89% acknowledged “the care of older adults with cancer needs to be improved,” according to a recently published study. Fewer than 25% said they were “very confident” they could identify dementia or accurately assess a patient’s functioning or risk of falling – factors associated with poorer outcomes for cancer treatment.
Still, resistance to change is evident. “We’re all inundated with trying to keep up with new standards of care, and I doubt there will be any broad acceptance of the rigor called for in this guideline,” said Frederick Schnell, MD, medical director of the Community Oncology Alliance.
The burden on physicians shouldn’t be significant, however: The streamlined assessments recommended in the ASCO guideline take only about 20 minutes to complete. Patients fill out surveys during most of that time; about five minutes is required for a nurse or physician assistant to administer several brief tests.
The assessment can identify people at increased risk of experiencing serious side effects from chemotherapy – infections, fatigue, diarrhea, dehydration and other problems that affect more than half of older patients. Physicians can then take steps to address these vulnerabilities, such as prescribing physical therapy for an older patient with muscle weakness or ordering a nutritional consultation for someone who has become malnourished. Also, they can alter chemotherapy regimens to minimize the potential for harm.
Currently, most oncologists decide whether older patients can benefit from chemotherapy by using the “eyeball test,” an assessment that relies primarily on their experience and judgment. “This isn’t enough to understand factors that put older adults at risk; it takes a deeper dive,” said Arti Hurria, MD, director of the Center for Cancer and Aging and professor of medical oncology and therapeutics research at City of Hope, a comprehensive cancer center in Duarte, Calif., and cochair of the panel that produced the new guidelines.
An oncologist walking into a room in a busy clinic might find an older patient already on the exam table, for instance, and miss the fact that he needed assistance getting out of a chair and getting into a gown – important signs of functional impairment that could be aggravated by chemotherapy, Dr. Hurria said. Or, “a very pleasant older patient might smile kindly at you and agree with everything you’re saying, and she might not have understood a thing you said” because of undetected cognitive impairment that could worsen and interfere with treatment, she explained.
William Dale, MD, a geriatrician and Arthur M. Coppola Family Chair in Supportive Care Medicine at City of Hope and another cochair of the guideline panel, tells of an 83-year-old woman whom he saw several years ago, with lung cancer metastasized to her brain. Her family requested a consultation because she’d become withdrawn and forgetful – a sign of accelerating cognitive impairment, they suspected.
Should she have chemotherapy and whole brain radiation, or would that worsen her memory lapses, the patient and family wondered?
One result stood out when Dale ordered a geriatric assessment: This older woman wasn’t cognitively impaired, she was psychologically distressed. “She wasn’t eating, she wasn’t interacting with other people, she appeared not to want treatment, but all this was due to depression,” Dr. Dale recalled. With counseling, the patient decided to undergo chemotherapy and radiation treatment, which he called “remarkably successful.”
Just as genetic tests are being used to personalize care for older cancer patients, geriatric assessments can be employed for this purpose – at considerably less expense, said Supriya Gupta Mohile, MD, editor in chief of the Journal of Geriatric Oncology and director of geriatric oncology at the James Wilmot Cancer Institute at the University of Rochester (N.Y.).
She tells of a 78-year-old man with invasive bladder cancer who came in for a consultation. From the medical chart, she learned the patient had hypertension, diabetes, and depression, all reasonably well controlled. From a geriatric assessment, she discovered that he lived alone, had cognitive impairment, relied on his daughter to deliver meals, and was at high risk of falling.
“The patient and his daughter were worried about his safety at home, his cognition getting worse, and fatigue [he was dealing with] and how that might affect his ability to function,” Dr. Mohile said. “His goal was to stay independent, at home, and not be hospitalized or go to rehabilitation.”
The standard of care for this condition was 3-4 months of chemotherapy before surgery, but Dr. Mohile recommended that the older patient skip chemotherapy and have surgery immediately, after reviewing the geriatric assessment with her patient and his family.
Every older patient considering chemotherapy should request an evaluation of this kind, even if your physician doesn’t offer it, said Heidi D. Klepin, MD, associate professor of hematology and oncology at Wake Forest University, Winston-Salem, N.C. “Ask for your doctor to consider your ability to do the things you most care about doing and for care to be individualized to your unique circumstances.”
KHN’s coverage of these topics is supported by John A. Hartford Foundation, Gordon and Betty Moore Foundation, and The SCAN Foundation. Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Fewer than 25% of older cancer patients currently get these assessments, which evaluate a person’s functioning (what he can and cannot do), psychological status, nutrition, cognition, social circumstances, and other, coexisting medical conditions, and which can predict the potential toxicity of chemotherapy.
The new guideline, ASCO’s first in the field of “geriatric oncology,” may have significant potential to change medical practice. “These recommendations will capture the attention of oncologists, I think, and that will be incredibly valuable,” said Corinne Leach, PhD, strategic director of cancer and aging research at the American Cancer Society.
They recognize a shifting demographic reality for cancer specialists, who are treating increasingly older patients as life spans lengthen across the globe. In the United States, 60% of patients newly diagnosed with cancer (an estimated 1.7 million people this year) are aged 65 years or older, as are more than 60% of cancer survivors.
Yet evidence about how best to treat older adults with cancer is weak because older adults are underrepresented in clinical trials. And most oncologists have received little training in how to manage older patients’ unique vulnerabilities.
When researchers asked 305 community oncologists about evaluating older patients, 89% acknowledged “the care of older adults with cancer needs to be improved,” according to a recently published study. Fewer than 25% said they were “very confident” they could identify dementia or accurately assess a patient’s functioning or risk of falling – factors associated with poorer outcomes for cancer treatment.
Still, resistance to change is evident. “We’re all inundated with trying to keep up with new standards of care, and I doubt there will be any broad acceptance of the rigor called for in this guideline,” said Frederick Schnell, MD, medical director of the Community Oncology Alliance.
The burden on physicians shouldn’t be significant, however: The streamlined assessments recommended in the ASCO guideline take only about 20 minutes to complete. Patients fill out surveys during most of that time; about five minutes is required for a nurse or physician assistant to administer several brief tests.
The assessment can identify people at increased risk of experiencing serious side effects from chemotherapy – infections, fatigue, diarrhea, dehydration and other problems that affect more than half of older patients. Physicians can then take steps to address these vulnerabilities, such as prescribing physical therapy for an older patient with muscle weakness or ordering a nutritional consultation for someone who has become malnourished. Also, they can alter chemotherapy regimens to minimize the potential for harm.
Currently, most oncologists decide whether older patients can benefit from chemotherapy by using the “eyeball test,” an assessment that relies primarily on their experience and judgment. “This isn’t enough to understand factors that put older adults at risk; it takes a deeper dive,” said Arti Hurria, MD, director of the Center for Cancer and Aging and professor of medical oncology and therapeutics research at City of Hope, a comprehensive cancer center in Duarte, Calif., and cochair of the panel that produced the new guidelines.
An oncologist walking into a room in a busy clinic might find an older patient already on the exam table, for instance, and miss the fact that he needed assistance getting out of a chair and getting into a gown – important signs of functional impairment that could be aggravated by chemotherapy, Dr. Hurria said. Or, “a very pleasant older patient might smile kindly at you and agree with everything you’re saying, and she might not have understood a thing you said” because of undetected cognitive impairment that could worsen and interfere with treatment, she explained.
William Dale, MD, a geriatrician and Arthur M. Coppola Family Chair in Supportive Care Medicine at City of Hope and another cochair of the guideline panel, tells of an 83-year-old woman whom he saw several years ago, with lung cancer metastasized to her brain. Her family requested a consultation because she’d become withdrawn and forgetful – a sign of accelerating cognitive impairment, they suspected.
Should she have chemotherapy and whole brain radiation, or would that worsen her memory lapses, the patient and family wondered?
One result stood out when Dale ordered a geriatric assessment: This older woman wasn’t cognitively impaired, she was psychologically distressed. “She wasn’t eating, she wasn’t interacting with other people, she appeared not to want treatment, but all this was due to depression,” Dr. Dale recalled. With counseling, the patient decided to undergo chemotherapy and radiation treatment, which he called “remarkably successful.”
Just as genetic tests are being used to personalize care for older cancer patients, geriatric assessments can be employed for this purpose – at considerably less expense, said Supriya Gupta Mohile, MD, editor in chief of the Journal of Geriatric Oncology and director of geriatric oncology at the James Wilmot Cancer Institute at the University of Rochester (N.Y.).
She tells of a 78-year-old man with invasive bladder cancer who came in for a consultation. From the medical chart, she learned the patient had hypertension, diabetes, and depression, all reasonably well controlled. From a geriatric assessment, she discovered that he lived alone, had cognitive impairment, relied on his daughter to deliver meals, and was at high risk of falling.
“The patient and his daughter were worried about his safety at home, his cognition getting worse, and fatigue [he was dealing with] and how that might affect his ability to function,” Dr. Mohile said. “His goal was to stay independent, at home, and not be hospitalized or go to rehabilitation.”
The standard of care for this condition was 3-4 months of chemotherapy before surgery, but Dr. Mohile recommended that the older patient skip chemotherapy and have surgery immediately, after reviewing the geriatric assessment with her patient and his family.
Every older patient considering chemotherapy should request an evaluation of this kind, even if your physician doesn’t offer it, said Heidi D. Klepin, MD, associate professor of hematology and oncology at Wake Forest University, Winston-Salem, N.C. “Ask for your doctor to consider your ability to do the things you most care about doing and for care to be individualized to your unique circumstances.”
KHN’s coverage of these topics is supported by John A. Hartford Foundation, Gordon and Betty Moore Foundation, and The SCAN Foundation. Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Dupilumab reduces exacerbations, cuts glucocorticoid use in moderate to severe asthma
Among patients with moderate to severe asthma, dupilumab reduced exacerbations by almost 50%, while also allowing glucocorticoid-treated patients to cut their use of that medication by 70%, with no increased risk of exacerbation.
The pair of placebo-controlled studies – Liberty Asthma Quest and Liberty Asthma Venture – also showed treatment-associated stability in forced expiratory volume (FEV1) evidence of lung remodeling among those who took the antibody, Mario Castro, MD, of Washington University, St. Louis, and his colleagues reported in the New England Journal of Medicine.
By week 12, FEV1 it had already increased by 0.32 L, they said.
“An analysis of the postbronchodilator FEV1 slope showed a loss of lung function in patients who received placebo and no loss in those who received dupilumab, findings that suggest a potential effect of dupilumab on airway remodeling,” wrote Dr. Castro and his colleagues. “The slope analysis showed that patients who received placebo lost, on average, approximately 40 mL annually, which is consistent with data from other cohorts of patients with asthma.”
Dupilumab is an anti–interleukin-4 alpha antibody that blocks both IL-4 and IL-13. The Quest trial examined efficacy and safety of two doses (200 mg and 300 mg every 2 weeks), compared with placebo in patients with uncontrolled asthma. Venture examined efficacy and safety of 300 mg or placebo as add-on therapy for patients with severe asthma who were taking glucocorticoids.
Liberty Asthma Quest
This 52-week study randomized 1,902 patients with severe, uncontrolled asthma to placebo or dupilumab 200 mg or 300 mg every other week. The primary endpoints were annual rate of severe asthma exacerbations and the change in FEV1 by week 12. The study also looked at these endpoints in patients whose baseline eosinophil count was greater than 300 per cubic millimeter.
Patients were a mean of 48 years old with a mean baseline FEV1 of about 1.75 L (about 58% of the predicted normal value). They had a mean of two exacerbations per year and an average eosinophil count of about 350 per cubic millimeter.
Both doses outperformed placebo in all endpoints.
Among those taking 200 mg, the annual relapse rate was 0.46 versus 0.87 among those taking placebo – a significant 47.7% risk reduction. Among those taking 300 mg, the exacerbation rate was 0.52 versus 0.97; this translated to a significant 46% risk reduction.
The response rate was even greater among those with an eosinophil count greater than 300 per cubic millimeter: 0.37 for 200 mg and 0.40 for 300 mg versus the placebo rates of 1.08 and 1.24. This translated to risk reductions of 65.8% and 67.4%, respectively.
By week 12, FEV1 had significantly increased by 0.32 L in the 200-mg group and by 0.34 L in the 300-mg group, compared with nonsignificant increases among those taking placebo.
Again, patients with the high eosinophil counts experienced the greatest benefits, with FEV1 increasing by a mean of 0.43 L at 12 weeks in the 200-mg group and by 0.47 L in the 300-mg group, significantly better than either placebo comparator.
The benefit was already noticeable by the 2-week evaluation, the investigators noted.
Dupilumab appeared safe; injection-site reactions were the most common adverse event, occurring in 15% of the low-dose group and 18% of the high-dose group. However, 52 patients taking the drug experienced eosinophilia, compared with four of those taking placebo (4.1% vs. 0.6%).
Four of those taking the study drug experienced clinical symptoms associated with eosinophilia, including worsening eosinophilia and chronic eosinophilic pneumonia.
Liberty Asthma Venture
In this study, the effect of dupilumab on glucocorticoid use among 210 patients with severe asthma was examined. Patients were randomized to add-on dupilumab 300 mg every 2 weeks for 24 weeks. Glucocorticoids were tapered downward from weeks 4 to 20. The primary endpoints were percent reduction in glucocorticoid dose at week 24, and the percentage of patients who experienced a reduction of at least 50% in glucocorticoid dose.
These patients were a mean of 51 years old, with a mean of two severe asthma exacerbations in the past year. Their mean daily oral glucocorticoid dose at randomization was about 11 mg per day. Their mean prebronchodilator FEV1 was about 1.6 liters – about 52% of predicted value.
Oral glucocorticoid use decreased by a mean of 70.1% in the active group, compared with 41.9% in the placebo group, a statistically significant difference, Klaus F. Rabe, MD, of Christian Albrechts University, Kiel, Germany, and his coauthors wrote in the New England Journal of Medicine. The median change was even better: A 100% reduction in the active group and 50% reduction in the placebo group.
By week 24, 80% of those taking dupilumab had decreased their glucocorticoid intake by at least 50%, compared with 50% of the placebo group reaching this goal. The glucocorticoid dose was less than 5 mg/day in 69% of the dupilumab group, compared with 33% of the placebo group.
Like Quest, Venture showed a treatment advantage among patients with high baseline eosinophil count. “The magnitude of the effect was largest in patients with a higher eosinophil count at baseline,” the investigators wrote. “… The odds ratios [a 50% glucocorticoid reduction] for dupilumab versus placebo were 6.59 among patients with 300 or more cells per cubic millimeter at baseline and 2.91 among those with less than 300 cells per cubic millimeter at baseline.”
In a fully adjusted model at week 24, 48% of the patients in the dupilumab group were able to stop oral glucocorticoids entirely, compared with 25% of the placebo group.
Dupilumab was also associated with a significant 59% reduction in severe annual asthma exacerbations. FEV1 among the active group was 0.22 L better than that in the placebo group at week 24.
Again, patients with a higher baseline blood eosinophil count experienced greater treatment benefit; among these, the rate of severe asthma exacerbations was 71% lower than the rate in the placebo group, and FEV1 was 0.32 L higher.
The most frequent adverse events were viral infections (9% of the patients in the dupilumab group vs. 18% of those in the placebo group), bronchitis (7% vs. 6%), sinusitis (7% vs. 4%), influenza (3% vs. 6%), and eosinophilia (14% vs. 1%). Injection-site reactions occurred in 9% of those taking dupilumab and 4% of those taking placebo.
Antidrug antibodies developed in five patients in each group, without clinical effect.
Both trials were funded by Sanofi and Regeneron. Dr. Castro has received grant support from Sanofi. Dr. Rabe has received consulting and lecture fees from AstraZeneca, Boehringer Ingelheim, Novartis, Sanofi, and Teva Pharmaceutical Industries.
SOURCES: Castro M et al. N Engl J Med. 2018;378:2486-96; KF Rabe et al. N Engl J Med. 2018;378:2475-85.
Among patients with moderate to severe asthma, dupilumab reduced exacerbations by almost 50%, while also allowing glucocorticoid-treated patients to cut their use of that medication by 70%, with no increased risk of exacerbation.
The pair of placebo-controlled studies – Liberty Asthma Quest and Liberty Asthma Venture – also showed treatment-associated stability in forced expiratory volume (FEV1) evidence of lung remodeling among those who took the antibody, Mario Castro, MD, of Washington University, St. Louis, and his colleagues reported in the New England Journal of Medicine.
By week 12, FEV1 it had already increased by 0.32 L, they said.
“An analysis of the postbronchodilator FEV1 slope showed a loss of lung function in patients who received placebo and no loss in those who received dupilumab, findings that suggest a potential effect of dupilumab on airway remodeling,” wrote Dr. Castro and his colleagues. “The slope analysis showed that patients who received placebo lost, on average, approximately 40 mL annually, which is consistent with data from other cohorts of patients with asthma.”
Dupilumab is an anti–interleukin-4 alpha antibody that blocks both IL-4 and IL-13. The Quest trial examined efficacy and safety of two doses (200 mg and 300 mg every 2 weeks), compared with placebo in patients with uncontrolled asthma. Venture examined efficacy and safety of 300 mg or placebo as add-on therapy for patients with severe asthma who were taking glucocorticoids.
Liberty Asthma Quest
This 52-week study randomized 1,902 patients with severe, uncontrolled asthma to placebo or dupilumab 200 mg or 300 mg every other week. The primary endpoints were annual rate of severe asthma exacerbations and the change in FEV1 by week 12. The study also looked at these endpoints in patients whose baseline eosinophil count was greater than 300 per cubic millimeter.
Patients were a mean of 48 years old with a mean baseline FEV1 of about 1.75 L (about 58% of the predicted normal value). They had a mean of two exacerbations per year and an average eosinophil count of about 350 per cubic millimeter.
Both doses outperformed placebo in all endpoints.
Among those taking 200 mg, the annual relapse rate was 0.46 versus 0.87 among those taking placebo – a significant 47.7% risk reduction. Among those taking 300 mg, the exacerbation rate was 0.52 versus 0.97; this translated to a significant 46% risk reduction.
The response rate was even greater among those with an eosinophil count greater than 300 per cubic millimeter: 0.37 for 200 mg and 0.40 for 300 mg versus the placebo rates of 1.08 and 1.24. This translated to risk reductions of 65.8% and 67.4%, respectively.
By week 12, FEV1 had significantly increased by 0.32 L in the 200-mg group and by 0.34 L in the 300-mg group, compared with nonsignificant increases among those taking placebo.
Again, patients with the high eosinophil counts experienced the greatest benefits, with FEV1 increasing by a mean of 0.43 L at 12 weeks in the 200-mg group and by 0.47 L in the 300-mg group, significantly better than either placebo comparator.
The benefit was already noticeable by the 2-week evaluation, the investigators noted.
Dupilumab appeared safe; injection-site reactions were the most common adverse event, occurring in 15% of the low-dose group and 18% of the high-dose group. However, 52 patients taking the drug experienced eosinophilia, compared with four of those taking placebo (4.1% vs. 0.6%).
Four of those taking the study drug experienced clinical symptoms associated with eosinophilia, including worsening eosinophilia and chronic eosinophilic pneumonia.
Liberty Asthma Venture
In this study, the effect of dupilumab on glucocorticoid use among 210 patients with severe asthma was examined. Patients were randomized to add-on dupilumab 300 mg every 2 weeks for 24 weeks. Glucocorticoids were tapered downward from weeks 4 to 20. The primary endpoints were percent reduction in glucocorticoid dose at week 24, and the percentage of patients who experienced a reduction of at least 50% in glucocorticoid dose.
These patients were a mean of 51 years old, with a mean of two severe asthma exacerbations in the past year. Their mean daily oral glucocorticoid dose at randomization was about 11 mg per day. Their mean prebronchodilator FEV1 was about 1.6 liters – about 52% of predicted value.
Oral glucocorticoid use decreased by a mean of 70.1% in the active group, compared with 41.9% in the placebo group, a statistically significant difference, Klaus F. Rabe, MD, of Christian Albrechts University, Kiel, Germany, and his coauthors wrote in the New England Journal of Medicine. The median change was even better: A 100% reduction in the active group and 50% reduction in the placebo group.
By week 24, 80% of those taking dupilumab had decreased their glucocorticoid intake by at least 50%, compared with 50% of the placebo group reaching this goal. The glucocorticoid dose was less than 5 mg/day in 69% of the dupilumab group, compared with 33% of the placebo group.
Like Quest, Venture showed a treatment advantage among patients with high baseline eosinophil count. “The magnitude of the effect was largest in patients with a higher eosinophil count at baseline,” the investigators wrote. “… The odds ratios [a 50% glucocorticoid reduction] for dupilumab versus placebo were 6.59 among patients with 300 or more cells per cubic millimeter at baseline and 2.91 among those with less than 300 cells per cubic millimeter at baseline.”
In a fully adjusted model at week 24, 48% of the patients in the dupilumab group were able to stop oral glucocorticoids entirely, compared with 25% of the placebo group.
Dupilumab was also associated with a significant 59% reduction in severe annual asthma exacerbations. FEV1 among the active group was 0.22 L better than that in the placebo group at week 24.
Again, patients with a higher baseline blood eosinophil count experienced greater treatment benefit; among these, the rate of severe asthma exacerbations was 71% lower than the rate in the placebo group, and FEV1 was 0.32 L higher.
The most frequent adverse events were viral infections (9% of the patients in the dupilumab group vs. 18% of those in the placebo group), bronchitis (7% vs. 6%), sinusitis (7% vs. 4%), influenza (3% vs. 6%), and eosinophilia (14% vs. 1%). Injection-site reactions occurred in 9% of those taking dupilumab and 4% of those taking placebo.
Antidrug antibodies developed in five patients in each group, without clinical effect.
Both trials were funded by Sanofi and Regeneron. Dr. Castro has received grant support from Sanofi. Dr. Rabe has received consulting and lecture fees from AstraZeneca, Boehringer Ingelheim, Novartis, Sanofi, and Teva Pharmaceutical Industries.
SOURCES: Castro M et al. N Engl J Med. 2018;378:2486-96; KF Rabe et al. N Engl J Med. 2018;378:2475-85.
Among patients with moderate to severe asthma, dupilumab reduced exacerbations by almost 50%, while also allowing glucocorticoid-treated patients to cut their use of that medication by 70%, with no increased risk of exacerbation.
The pair of placebo-controlled studies – Liberty Asthma Quest and Liberty Asthma Venture – also showed treatment-associated stability in forced expiratory volume (FEV1) evidence of lung remodeling among those who took the antibody, Mario Castro, MD, of Washington University, St. Louis, and his colleagues reported in the New England Journal of Medicine.
By week 12, FEV1 it had already increased by 0.32 L, they said.
“An analysis of the postbronchodilator FEV1 slope showed a loss of lung function in patients who received placebo and no loss in those who received dupilumab, findings that suggest a potential effect of dupilumab on airway remodeling,” wrote Dr. Castro and his colleagues. “The slope analysis showed that patients who received placebo lost, on average, approximately 40 mL annually, which is consistent with data from other cohorts of patients with asthma.”
Dupilumab is an anti–interleukin-4 alpha antibody that blocks both IL-4 and IL-13. The Quest trial examined efficacy and safety of two doses (200 mg and 300 mg every 2 weeks), compared with placebo in patients with uncontrolled asthma. Venture examined efficacy and safety of 300 mg or placebo as add-on therapy for patients with severe asthma who were taking glucocorticoids.
Liberty Asthma Quest
This 52-week study randomized 1,902 patients with severe, uncontrolled asthma to placebo or dupilumab 200 mg or 300 mg every other week. The primary endpoints were annual rate of severe asthma exacerbations and the change in FEV1 by week 12. The study also looked at these endpoints in patients whose baseline eosinophil count was greater than 300 per cubic millimeter.
Patients were a mean of 48 years old with a mean baseline FEV1 of about 1.75 L (about 58% of the predicted normal value). They had a mean of two exacerbations per year and an average eosinophil count of about 350 per cubic millimeter.
Both doses outperformed placebo in all endpoints.
Among those taking 200 mg, the annual relapse rate was 0.46 versus 0.87 among those taking placebo – a significant 47.7% risk reduction. Among those taking 300 mg, the exacerbation rate was 0.52 versus 0.97; this translated to a significant 46% risk reduction.
The response rate was even greater among those with an eosinophil count greater than 300 per cubic millimeter: 0.37 for 200 mg and 0.40 for 300 mg versus the placebo rates of 1.08 and 1.24. This translated to risk reductions of 65.8% and 67.4%, respectively.
By week 12, FEV1 had significantly increased by 0.32 L in the 200-mg group and by 0.34 L in the 300-mg group, compared with nonsignificant increases among those taking placebo.
Again, patients with the high eosinophil counts experienced the greatest benefits, with FEV1 increasing by a mean of 0.43 L at 12 weeks in the 200-mg group and by 0.47 L in the 300-mg group, significantly better than either placebo comparator.
The benefit was already noticeable by the 2-week evaluation, the investigators noted.
Dupilumab appeared safe; injection-site reactions were the most common adverse event, occurring in 15% of the low-dose group and 18% of the high-dose group. However, 52 patients taking the drug experienced eosinophilia, compared with four of those taking placebo (4.1% vs. 0.6%).
Four of those taking the study drug experienced clinical symptoms associated with eosinophilia, including worsening eosinophilia and chronic eosinophilic pneumonia.
Liberty Asthma Venture
In this study, the effect of dupilumab on glucocorticoid use among 210 patients with severe asthma was examined. Patients were randomized to add-on dupilumab 300 mg every 2 weeks for 24 weeks. Glucocorticoids were tapered downward from weeks 4 to 20. The primary endpoints were percent reduction in glucocorticoid dose at week 24, and the percentage of patients who experienced a reduction of at least 50% in glucocorticoid dose.
These patients were a mean of 51 years old, with a mean of two severe asthma exacerbations in the past year. Their mean daily oral glucocorticoid dose at randomization was about 11 mg per day. Their mean prebronchodilator FEV1 was about 1.6 liters – about 52% of predicted value.
Oral glucocorticoid use decreased by a mean of 70.1% in the active group, compared with 41.9% in the placebo group, a statistically significant difference, Klaus F. Rabe, MD, of Christian Albrechts University, Kiel, Germany, and his coauthors wrote in the New England Journal of Medicine. The median change was even better: A 100% reduction in the active group and 50% reduction in the placebo group.
By week 24, 80% of those taking dupilumab had decreased their glucocorticoid intake by at least 50%, compared with 50% of the placebo group reaching this goal. The glucocorticoid dose was less than 5 mg/day in 69% of the dupilumab group, compared with 33% of the placebo group.
Like Quest, Venture showed a treatment advantage among patients with high baseline eosinophil count. “The magnitude of the effect was largest in patients with a higher eosinophil count at baseline,” the investigators wrote. “… The odds ratios [a 50% glucocorticoid reduction] for dupilumab versus placebo were 6.59 among patients with 300 or more cells per cubic millimeter at baseline and 2.91 among those with less than 300 cells per cubic millimeter at baseline.”
In a fully adjusted model at week 24, 48% of the patients in the dupilumab group were able to stop oral glucocorticoids entirely, compared with 25% of the placebo group.
Dupilumab was also associated with a significant 59% reduction in severe annual asthma exacerbations. FEV1 among the active group was 0.22 L better than that in the placebo group at week 24.
Again, patients with a higher baseline blood eosinophil count experienced greater treatment benefit; among these, the rate of severe asthma exacerbations was 71% lower than the rate in the placebo group, and FEV1 was 0.32 L higher.
The most frequent adverse events were viral infections (9% of the patients in the dupilumab group vs. 18% of those in the placebo group), bronchitis (7% vs. 6%), sinusitis (7% vs. 4%), influenza (3% vs. 6%), and eosinophilia (14% vs. 1%). Injection-site reactions occurred in 9% of those taking dupilumab and 4% of those taking placebo.
Antidrug antibodies developed in five patients in each group, without clinical effect.
Both trials were funded by Sanofi and Regeneron. Dr. Castro has received grant support from Sanofi. Dr. Rabe has received consulting and lecture fees from AstraZeneca, Boehringer Ingelheim, Novartis, Sanofi, and Teva Pharmaceutical Industries.
SOURCES: Castro M et al. N Engl J Med. 2018;378:2486-96; KF Rabe et al. N Engl J Med. 2018;378:2475-85.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Dupilumab allowed asthma patients to decrease glucocorticoids with no risk of asthma exacerbation.
Major finding: Dupilumab reduced exacerbations by almost 50%, while also allowing glucocorticoid-treated patients to cut their use of that medication by 70%.
Study details: Liberty Asthma Quest comprised 1,902 patients and Liberty Asthma Venture comprised 210. Both were randomized, placebo-controlled trials.
Disclosures: Both trials were funded by Sanofi and Regeneron. Dr. Castro has received grant support from Sanofi. Dr. Rabe has received consulting and lecture fees from AstraZeneca, Boehringer Ingelheim, Novartis, Sanofi, and Teva Pharmaceutical Industries.
Sources: Castro M et al. N Engl J Med. 2018;378:2486-96; Rabe KF et al. N Engl J Med. 2018;378:2475-85.
Intravascular Involvement of Cutaneous Squamous Cell Carcinoma
Cutaneous squamous cell carcinoma (cSCC) is the second most common form of skin cancer after basal cell carcinoma.1 With an estimated 700,000 cases reported annually in the United States, the incidence of cSCC continues to increase.2 Most patients with cSCC have an excellent prognosis after surgical clearance, with Mohs micrographic surgery (MMS) being the most successful treatment, followed by excision and electrodesiccation and curettage. A subset of patients with cSCC carry an increased risk of local recurrence, lymph node metastasis, and disease-specific death. A meta-analysis of 36 studies found that statistically significant risk factors for recurrence of cSCC included thickness greater than 2 mm (risk ratio [RR], 9.64; 95% CI, 1.30-1.52), invasion beyond the subcutaneous fat (RR, 7.61; 95% CI, 4.17-13.88), perineural invasion (RR, 4.30; 95% CI, 2.80-6.60), diameter greater than 20 mm (RR, 3.22; 95% CI, 1.91-5.45), location on temple (RR, 3.20; 95% CI, 1.12-9.15), and poor differentiation (RR, 2.66; 95% CI, 1.72-4.14).3 Additional risk factors for cSCC metastasis included location on the temple, ear, or lip, as well as a history of immunosuppression. Factors for disease-specific death were diameter greater than 20 mm, poor differentiation, location on the ear or lip, invasion beyond the subcutaneous fat, and perineural invasion.3 Perineural and/or lymphovascular invasion is considered high risk, but despite being linked to negative outcomes, there are no treatment guidelines based on lymphovascular (intravascular) invasion.4 We present a case of intravascular involvement found during MMS and treated with adjuvant radiotherapy after surgery. We share this case with the goal of discussing management in such cases and highlighting the need for improved definitive guidelines for high-risk cSCCs.
Case Report
A 72-year-old man presented with a rapidly growing lesion on the left side of the forehead of 1 year’s duration. His medical history was remarkable for B-cell lymphoma, which was currently in remission following chemotherapy 10 years prior. The lesion started as a small, red, dry patch that the patient initially thought was eczema. The site progressively enlarged to a red tumor measuring 2.4×2.0 cm (Figure 1), and the patient presented to the dermatology department for further evaluation. There was no clinical evidence of lymphadenopathy. A skin biopsy confirmed a moderately differentiated cSCC with a positive deep margin (Figure 2). Due to the tumor’s location, histology, size, and poorly defined borders, the patient was referred for treatment with MMS. The lesion was removed in a total of 2 stages and 4 sections. In addition to a proliferation of spindled tumor cells seen during surgery, which was consistent with cSCC, an intravascular component was noted despite clear margins after the surgery (Figure 3). The aggressive histology of intravascular involvement was subsequently confirmed by the academic dermatopathologist at our institution. With the evidence of an intravascular component of this patient’s cSCC, there was concern about further metastatic disease. After discussing the more aggressive histology type and size of the cSCC with the patient, he underwent subsequent computed tomography of the head, neck, and chest. Fortunately, this imaging did not show evidence of metastatic disease; thus, final staging of the cSCC was cT2N0M0. After interdisciplinary discussion and consultation with radiation oncology, the site of the cSCC was treated with adjuvant radiotherapy. The patient received a total of 6600 cGy delivered in 33 fractions of 200 cGy, each using an en face technique and 6 eV over a total treatment course of 48 days.

 noted in surgical debulk for Mohs micrographic surgery (A)(H&E, original magnification ×4)...")
. Of note, stage II revealed no residual tumor.")
One year after undergoing MMS and adjuvant radiotherapy, the patient remains free of cSCC recurrence or metastases and still undergoes regular interdisciplinary monitoring. Without clear guidelines on the treatment of patients with intravascular involvement of cSCC, we relied on prior experience with similar cases.
Comment
This case highlights the challenge in managing patients with high-risk cSCC, as the current guidelines provided by the American Joint Committee on Cancer (AJCC) and the National Comprehensive Cancer Network (NCCN) vary on the inclusion of intravascular involvement of cSCC as high risk and treatment is at the discretion of the provider in such circumstances.5-7 Both the AJCC and the NCCN have defined high-risk factors and staging for cSCC. The AJCC 8th edition (AJCC-8) revised guidelines include several high-risk factors of cSCC, including tumor diameter of 4 cm or larger leading to upstaging of a tumor from T2 to T3, invasion into or beyond the level of the subcutaneous tissue, depth of invasion greater than 6 mm, and large-caliber perineural invasion, and removed poorly differentiated histology from the AJCC-8 guidelines compared to the AJCC-7 guidelines. According to the AJCC-8 guidelines, location on the ear or lip, desmoplastic or spindle cell features, lymphovascular invasion, and immunosuppression do not affect tumor staging. The AJCC’s criteria for its TNM staging system strictly focus on features of the primary tumor and do not include clinical risk factors such as recurrence or immunosuppression. In contrast, the NCCN does include lymphovascular invasion as a high-risk factor of cSCC.
Intravascular invasion plays a considerable role in patient survival in certain cancers (eg, breast, gastric, prostate). In cutaneous malignancies, such as melanoma and SCC, metastasis more commonly occurs via lymphatic spread. When present, vascular invasion typically coexists with lymphatic involvement. The presence of microscopic lymphovascular invasion in cSCCs has not been definitively proven to increase the risk of metastases.8 However, multivariate analysis has shown that lymphovascular invasion independently predicts nodal metastasis and disease-specific death.9 As such, there are no guidelines on sentinel lymph node biopsy or adjuvant therapy in the setting of lymphovascular involvement of cSCCs. A survey-based study of 117 Mohs surgeons found a lack of consistency in their approaches to evaluation and management of high-risk SCCs. Most respondents noted perineural invasion and in-transit metastasis as the main findings that would lead to radiologic nodal staging, sentinel lymph node biopsy, or adjuvant radiotherapy, but they highlighted the lack of evidence-based treatment guidelines.4 High-risk cSCC can be treated via MMS or conventional surgery with safe excision margins. Adjuvant radiotherapy can reduce tumor recurrence and improve survival and therefore should be considered in cases of advanced or high-risk cSCCs, such as in our case.
The lack of consensus over the definition of high-risk cSCCs, a lack of high-quality therapeutic studies, and the absence of a prognostic model that integrates multiple risk factors all have made the prediction of outcomes and the formation of definitive management of cSCCs challenging. Multidisciplinary teams and vigilant monitoring are crucial in the successful management of high-risk cSCC, but further studies and reports are needed to develop definitive treatment algorithms.
- Karia PS, Han J, Schmults CD. Cutaneous squamous cell carcinoma: estimated incidence of disease, nodal metastasis, and deaths from disease in the United States, 2012. J Am Acad Dermatol. 2013;68:957-966.
- Rogers HW, Weinstock MA, Harris AR, et al. Incidence estimate of nonmelanoma skin cancer in the United States, 2006. Arch Dermatol. 2010;146:283-287.
- Thompson AK, Kelley BF, Prokop LJ, et al. Risk factors for cutaneous squamous cell carcinoma recurrence, metastasis, and disease-specific death: a systematic review and meta-analysis. JAMA Dermatol. 2016;152:419-428.
- Jambusaria-Pahlajani A, Hess SD, Katz KA, et al. Uncertainty in the perioperative management of high-risk cutaneous squamous cell carcinoma among Mohs surgeons. Arch Dermatol. 2010;146:1225-1231.
- Motaparthi K, Kapil JP, Velazquez EF. Cutaneous squamous cell carcinoma: review of the eighth edition of the American Joint Committee on Cancer Staging Guidelines, prognostic factors, and histopathologic variants. Adv Anat Pathol. 2017;24:171-194.
- Amin MD, Edge SB, Greene FL, et al, eds. AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer; 2017.
- National Comprehensive Cancer Network. Squamous Cell Skin Cancer (Version 2.2018). https://www.nccn.org/professionals/physician_gls/pdf/squamous.pdf. Accessed June 27, 2018.
- Lonie S, Niumsawatt V, Castley A. A prognostic dilemma of basal cell carcinoma with intravascular invasion. Plast Reconstr Surg Glob Open. 2016;4:e1046.
- Carter JB, Johnson MM, Chua TL, et al. Outcomes of primary cutaneous squamous cell carcinoma with perineural invasion: an 11-year cohort study. JAMA Dermatol. 2013;149:35-41.
Cutaneous squamous cell carcinoma (cSCC) is the second most common form of skin cancer after basal cell carcinoma.1 With an estimated 700,000 cases reported annually in the United States, the incidence of cSCC continues to increase.2 Most patients with cSCC have an excellent prognosis after surgical clearance, with Mohs micrographic surgery (MMS) being the most successful treatment, followed by excision and electrodesiccation and curettage. A subset of patients with cSCC carry an increased risk of local recurrence, lymph node metastasis, and disease-specific death. A meta-analysis of 36 studies found that statistically significant risk factors for recurrence of cSCC included thickness greater than 2 mm (risk ratio [RR], 9.64; 95% CI, 1.30-1.52), invasion beyond the subcutaneous fat (RR, 7.61; 95% CI, 4.17-13.88), perineural invasion (RR, 4.30; 95% CI, 2.80-6.60), diameter greater than 20 mm (RR, 3.22; 95% CI, 1.91-5.45), location on temple (RR, 3.20; 95% CI, 1.12-9.15), and poor differentiation (RR, 2.66; 95% CI, 1.72-4.14).3 Additional risk factors for cSCC metastasis included location on the temple, ear, or lip, as well as a history of immunosuppression. Factors for disease-specific death were diameter greater than 20 mm, poor differentiation, location on the ear or lip, invasion beyond the subcutaneous fat, and perineural invasion.3 Perineural and/or lymphovascular invasion is considered high risk, but despite being linked to negative outcomes, there are no treatment guidelines based on lymphovascular (intravascular) invasion.4 We present a case of intravascular involvement found during MMS and treated with adjuvant radiotherapy after surgery. We share this case with the goal of discussing management in such cases and highlighting the need for improved definitive guidelines for high-risk cSCCs.
Case Report
A 72-year-old man presented with a rapidly growing lesion on the left side of the forehead of 1 year’s duration. His medical history was remarkable for B-cell lymphoma, which was currently in remission following chemotherapy 10 years prior. The lesion started as a small, red, dry patch that the patient initially thought was eczema. The site progressively enlarged to a red tumor measuring 2.4×2.0 cm (Figure 1), and the patient presented to the dermatology department for further evaluation. There was no clinical evidence of lymphadenopathy. A skin biopsy confirmed a moderately differentiated cSCC with a positive deep margin (Figure 2). Due to the tumor’s location, histology, size, and poorly defined borders, the patient was referred for treatment with MMS. The lesion was removed in a total of 2 stages and 4 sections. In addition to a proliferation of spindled tumor cells seen during surgery, which was consistent with cSCC, an intravascular component was noted despite clear margins after the surgery (Figure 3). The aggressive histology of intravascular involvement was subsequently confirmed by the academic dermatopathologist at our institution. With the evidence of an intravascular component of this patient’s cSCC, there was concern about further metastatic disease. After discussing the more aggressive histology type and size of the cSCC with the patient, he underwent subsequent computed tomography of the head, neck, and chest. Fortunately, this imaging did not show evidence of metastatic disease; thus, final staging of the cSCC was cT2N0M0. After interdisciplinary discussion and consultation with radiation oncology, the site of the cSCC was treated with adjuvant radiotherapy. The patient received a total of 6600 cGy delivered in 33 fractions of 200 cGy, each using an en face technique and 6 eV over a total treatment course of 48 days.
One year after undergoing MMS and adjuvant radiotherapy, the patient remains free of cSCC recurrence or metastases and still undergoes regular interdisciplinary monitoring. Without clear guidelines on the treatment of patients with intravascular involvement of cSCC, we relied on prior experience with similar cases.
Comment
This case highlights the challenge in managing patients with high-risk cSCC, as the current guidelines provided by the American Joint Committee on Cancer (AJCC) and the National Comprehensive Cancer Network (NCCN) vary on the inclusion of intravascular involvement of cSCC as high risk and treatment is at the discretion of the provider in such circumstances.5-7 Both the AJCC and the NCCN have defined high-risk factors and staging for cSCC. The AJCC 8th edition (AJCC-8) revised guidelines include several high-risk factors of cSCC, including tumor diameter of 4 cm or larger leading to upstaging of a tumor from T2 to T3, invasion into or beyond the level of the subcutaneous tissue, depth of invasion greater than 6 mm, and large-caliber perineural invasion, and removed poorly differentiated histology from the AJCC-8 guidelines compared to the AJCC-7 guidelines. According to the AJCC-8 guidelines, location on the ear or lip, desmoplastic or spindle cell features, lymphovascular invasion, and immunosuppression do not affect tumor staging. The AJCC’s criteria for its TNM staging system strictly focus on features of the primary tumor and do not include clinical risk factors such as recurrence or immunosuppression. In contrast, the NCCN does include lymphovascular invasion as a high-risk factor of cSCC.
Intravascular invasion plays a considerable role in patient survival in certain cancers (eg, breast, gastric, prostate). In cutaneous malignancies, such as melanoma and SCC, metastasis more commonly occurs via lymphatic spread. When present, vascular invasion typically coexists with lymphatic involvement. The presence of microscopic lymphovascular invasion in cSCCs has not been definitively proven to increase the risk of metastases.8 However, multivariate analysis has shown that lymphovascular invasion independently predicts nodal metastasis and disease-specific death.9 As such, there are no guidelines on sentinel lymph node biopsy or adjuvant therapy in the setting of lymphovascular involvement of cSCCs. A survey-based study of 117 Mohs surgeons found a lack of consistency in their approaches to evaluation and management of high-risk SCCs. Most respondents noted perineural invasion and in-transit metastasis as the main findings that would lead to radiologic nodal staging, sentinel lymph node biopsy, or adjuvant radiotherapy, but they highlighted the lack of evidence-based treatment guidelines.4 High-risk cSCC can be treated via MMS or conventional surgery with safe excision margins. Adjuvant radiotherapy can reduce tumor recurrence and improve survival and therefore should be considered in cases of advanced or high-risk cSCCs, such as in our case.
The lack of consensus over the definition of high-risk cSCCs, a lack of high-quality therapeutic studies, and the absence of a prognostic model that integrates multiple risk factors all have made the prediction of outcomes and the formation of definitive management of cSCCs challenging. Multidisciplinary teams and vigilant monitoring are crucial in the successful management of high-risk cSCC, but further studies and reports are needed to develop definitive treatment algorithms.
Cutaneous squamous cell carcinoma (cSCC) is the second most common form of skin cancer after basal cell carcinoma.1 With an estimated 700,000 cases reported annually in the United States, the incidence of cSCC continues to increase.2 Most patients with cSCC have an excellent prognosis after surgical clearance, with Mohs micrographic surgery (MMS) being the most successful treatment, followed by excision and electrodesiccation and curettage. A subset of patients with cSCC carry an increased risk of local recurrence, lymph node metastasis, and disease-specific death. A meta-analysis of 36 studies found that statistically significant risk factors for recurrence of cSCC included thickness greater than 2 mm (risk ratio [RR], 9.64; 95% CI, 1.30-1.52), invasion beyond the subcutaneous fat (RR, 7.61; 95% CI, 4.17-13.88), perineural invasion (RR, 4.30; 95% CI, 2.80-6.60), diameter greater than 20 mm (RR, 3.22; 95% CI, 1.91-5.45), location on temple (RR, 3.20; 95% CI, 1.12-9.15), and poor differentiation (RR, 2.66; 95% CI, 1.72-4.14).3 Additional risk factors for cSCC metastasis included location on the temple, ear, or lip, as well as a history of immunosuppression. Factors for disease-specific death were diameter greater than 20 mm, poor differentiation, location on the ear or lip, invasion beyond the subcutaneous fat, and perineural invasion.3 Perineural and/or lymphovascular invasion is considered high risk, but despite being linked to negative outcomes, there are no treatment guidelines based on lymphovascular (intravascular) invasion.4 We present a case of intravascular involvement found during MMS and treated with adjuvant radiotherapy after surgery. We share this case with the goal of discussing management in such cases and highlighting the need for improved definitive guidelines for high-risk cSCCs.
Case Report
A 72-year-old man presented with a rapidly growing lesion on the left side of the forehead of 1 year’s duration. His medical history was remarkable for B-cell lymphoma, which was currently in remission following chemotherapy 10 years prior. The lesion started as a small, red, dry patch that the patient initially thought was eczema. The site progressively enlarged to a red tumor measuring 2.4×2.0 cm (Figure 1), and the patient presented to the dermatology department for further evaluation. There was no clinical evidence of lymphadenopathy. A skin biopsy confirmed a moderately differentiated cSCC with a positive deep margin (Figure 2). Due to the tumor’s location, histology, size, and poorly defined borders, the patient was referred for treatment with MMS. The lesion was removed in a total of 2 stages and 4 sections. In addition to a proliferation of spindled tumor cells seen during surgery, which was consistent with cSCC, an intravascular component was noted despite clear margins after the surgery (Figure 3). The aggressive histology of intravascular involvement was subsequently confirmed by the academic dermatopathologist at our institution. With the evidence of an intravascular component of this patient’s cSCC, there was concern about further metastatic disease. After discussing the more aggressive histology type and size of the cSCC with the patient, he underwent subsequent computed tomography of the head, neck, and chest. Fortunately, this imaging did not show evidence of metastatic disease; thus, final staging of the cSCC was cT2N0M0. After interdisciplinary discussion and consultation with radiation oncology, the site of the cSCC was treated with adjuvant radiotherapy. The patient received a total of 6600 cGy delivered in 33 fractions of 200 cGy, each using an en face technique and 6 eV over a total treatment course of 48 days.
One year after undergoing MMS and adjuvant radiotherapy, the patient remains free of cSCC recurrence or metastases and still undergoes regular interdisciplinary monitoring. Without clear guidelines on the treatment of patients with intravascular involvement of cSCC, we relied on prior experience with similar cases.
Comment
This case highlights the challenge in managing patients with high-risk cSCC, as the current guidelines provided by the American Joint Committee on Cancer (AJCC) and the National Comprehensive Cancer Network (NCCN) vary on the inclusion of intravascular involvement of cSCC as high risk and treatment is at the discretion of the provider in such circumstances.5-7 Both the AJCC and the NCCN have defined high-risk factors and staging for cSCC. The AJCC 8th edition (AJCC-8) revised guidelines include several high-risk factors of cSCC, including tumor diameter of 4 cm or larger leading to upstaging of a tumor from T2 to T3, invasion into or beyond the level of the subcutaneous tissue, depth of invasion greater than 6 mm, and large-caliber perineural invasion, and removed poorly differentiated histology from the AJCC-8 guidelines compared to the AJCC-7 guidelines. According to the AJCC-8 guidelines, location on the ear or lip, desmoplastic or spindle cell features, lymphovascular invasion, and immunosuppression do not affect tumor staging. The AJCC’s criteria for its TNM staging system strictly focus on features of the primary tumor and do not include clinical risk factors such as recurrence or immunosuppression. In contrast, the NCCN does include lymphovascular invasion as a high-risk factor of cSCC.
Intravascular invasion plays a considerable role in patient survival in certain cancers (eg, breast, gastric, prostate). In cutaneous malignancies, such as melanoma and SCC, metastasis more commonly occurs via lymphatic spread. When present, vascular invasion typically coexists with lymphatic involvement. The presence of microscopic lymphovascular invasion in cSCCs has not been definitively proven to increase the risk of metastases.8 However, multivariate analysis has shown that lymphovascular invasion independently predicts nodal metastasis and disease-specific death.9 As such, there are no guidelines on sentinel lymph node biopsy or adjuvant therapy in the setting of lymphovascular involvement of cSCCs. A survey-based study of 117 Mohs surgeons found a lack of consistency in their approaches to evaluation and management of high-risk SCCs. Most respondents noted perineural invasion and in-transit metastasis as the main findings that would lead to radiologic nodal staging, sentinel lymph node biopsy, or adjuvant radiotherapy, but they highlighted the lack of evidence-based treatment guidelines.4 High-risk cSCC can be treated via MMS or conventional surgery with safe excision margins. Adjuvant radiotherapy can reduce tumor recurrence and improve survival and therefore should be considered in cases of advanced or high-risk cSCCs, such as in our case.
The lack of consensus over the definition of high-risk cSCCs, a lack of high-quality therapeutic studies, and the absence of a prognostic model that integrates multiple risk factors all have made the prediction of outcomes and the formation of definitive management of cSCCs challenging. Multidisciplinary teams and vigilant monitoring are crucial in the successful management of high-risk cSCC, but further studies and reports are needed to develop definitive treatment algorithms.
- Karia PS, Han J, Schmults CD. Cutaneous squamous cell carcinoma: estimated incidence of disease, nodal metastasis, and deaths from disease in the United States, 2012. J Am Acad Dermatol. 2013;68:957-966.
- Rogers HW, Weinstock MA, Harris AR, et al. Incidence estimate of nonmelanoma skin cancer in the United States, 2006. Arch Dermatol. 2010;146:283-287.
- Thompson AK, Kelley BF, Prokop LJ, et al. Risk factors for cutaneous squamous cell carcinoma recurrence, metastasis, and disease-specific death: a systematic review and meta-analysis. JAMA Dermatol. 2016;152:419-428.
- Jambusaria-Pahlajani A, Hess SD, Katz KA, et al. Uncertainty in the perioperative management of high-risk cutaneous squamous cell carcinoma among Mohs surgeons. Arch Dermatol. 2010;146:1225-1231.
- Motaparthi K, Kapil JP, Velazquez EF. Cutaneous squamous cell carcinoma: review of the eighth edition of the American Joint Committee on Cancer Staging Guidelines, prognostic factors, and histopathologic variants. Adv Anat Pathol. 2017;24:171-194.
- Amin MD, Edge SB, Greene FL, et al, eds. AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer; 2017.
- National Comprehensive Cancer Network. Squamous Cell Skin Cancer (Version 2.2018). https://www.nccn.org/professionals/physician_gls/pdf/squamous.pdf. Accessed June 27, 2018.
- Lonie S, Niumsawatt V, Castley A. A prognostic dilemma of basal cell carcinoma with intravascular invasion. Plast Reconstr Surg Glob Open. 2016;4:e1046.
- Carter JB, Johnson MM, Chua TL, et al. Outcomes of primary cutaneous squamous cell carcinoma with perineural invasion: an 11-year cohort study. JAMA Dermatol. 2013;149:35-41.
- Karia PS, Han J, Schmults CD. Cutaneous squamous cell carcinoma: estimated incidence of disease, nodal metastasis, and deaths from disease in the United States, 2012. J Am Acad Dermatol. 2013;68:957-966.
- Rogers HW, Weinstock MA, Harris AR, et al. Incidence estimate of nonmelanoma skin cancer in the United States, 2006. Arch Dermatol. 2010;146:283-287.
- Thompson AK, Kelley BF, Prokop LJ, et al. Risk factors for cutaneous squamous cell carcinoma recurrence, metastasis, and disease-specific death: a systematic review and meta-analysis. JAMA Dermatol. 2016;152:419-428.
- Jambusaria-Pahlajani A, Hess SD, Katz KA, et al. Uncertainty in the perioperative management of high-risk cutaneous squamous cell carcinoma among Mohs surgeons. Arch Dermatol. 2010;146:1225-1231.
- Motaparthi K, Kapil JP, Velazquez EF. Cutaneous squamous cell carcinoma: review of the eighth edition of the American Joint Committee on Cancer Staging Guidelines, prognostic factors, and histopathologic variants. Adv Anat Pathol. 2017;24:171-194.
- Amin MD, Edge SB, Greene FL, et al, eds. AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer; 2017.
- National Comprehensive Cancer Network. Squamous Cell Skin Cancer (Version 2.2018). https://www.nccn.org/professionals/physician_gls/pdf/squamous.pdf. Accessed June 27, 2018.
- Lonie S, Niumsawatt V, Castley A. A prognostic dilemma of basal cell carcinoma with intravascular invasion. Plast Reconstr Surg Glob Open. 2016;4:e1046.
- Carter JB, Johnson MM, Chua TL, et al. Outcomes of primary cutaneous squamous cell carcinoma with perineural invasion: an 11-year cohort study. JAMA Dermatol. 2013;149:35-41.
Resident Pearl
- Intravascular (also referred to as lymphovascular when involving vessels and/or lymphatics) invasion of cutaneous squamous cell carcinoma can be considered a high-risk factor that may warrant adjuvant therapy.

New Survey on Burnout Coming to Members
Society for Vascular Surgery members are receiving an important email from the Mayo Clinic containing a survey from the SVS Wellness Task Force.

It is the second survey the task force has distributed, all aimed at ascertaining burnout and wellness statistics from SVS members.
“We need evidence,” said Malachi Sheahan, MD, who co-chairs the group with Dawn Coleman, MD. “We can’t make change without evidence.”
He issued a “Societal Call to Action” to SVS members at the end of a Friday session addressing burnout issues, “Promoting Physician Well-Being: Achieving Quadruple Aim.”
Dr. Sheahan disclosed statistics from the first task force survey, completed by 860 members. Collectively, members worked an average 73.5 hours a week, with five hours completing electronic medical records and 5.5 hours of administrative/scholarly activities added to 63 hours in the office.
“Eighty-nine percent feel burned out on occasion, everyone thinks they’re working too hard and when there are conflicts between work and personal life, they’re resolved in favor of the personal side only 8 percent of the time,” he said of the just-released data. He believes EMR will be the No. 1 conflict of vascular surgeons, with surgeons reporting they spend one hour charting for every one hour of patient time. “It’s just not working out,” he said.
Twenty percent said they had been sued for malpractice within the past two years, 37 percent reported being depressed within the month prior to completing the survey and the 8 percent who reported suicide ideation within the past year is double the national rate, Dr. Sheahan said. The second survey, launched Monday, focuses more on physical debility and should take fewer than 10 minutes to complete, he said. “Look for the survey, and please take it.”
He added that there are initiatives going forward that aim to change the environment and change the culture, including the SVS task force and the American Board of Surgery’s new lifelong learning initiative. “This is a call to action,” he said. “The main thing I want to say is that this is changeable. I don’t want you to think or say that we can’t do it. “We can. We just need evidence.”
Society for Vascular Surgery members are receiving an important email from the Mayo Clinic containing a survey from the SVS Wellness Task Force.
It is the second survey the task force has distributed, all aimed at ascertaining burnout and wellness statistics from SVS members.
“We need evidence,” said Malachi Sheahan, MD, who co-chairs the group with Dawn Coleman, MD. “We can’t make change without evidence.”
He issued a “Societal Call to Action” to SVS members at the end of a Friday session addressing burnout issues, “Promoting Physician Well-Being: Achieving Quadruple Aim.”
Dr. Sheahan disclosed statistics from the first task force survey, completed by 860 members. Collectively, members worked an average 73.5 hours a week, with five hours completing electronic medical records and 5.5 hours of administrative/scholarly activities added to 63 hours in the office.
“Eighty-nine percent feel burned out on occasion, everyone thinks they’re working too hard and when there are conflicts between work and personal life, they’re resolved in favor of the personal side only 8 percent of the time,” he said of the just-released data. He believes EMR will be the No. 1 conflict of vascular surgeons, with surgeons reporting they spend one hour charting for every one hour of patient time. “It’s just not working out,” he said.
Twenty percent said they had been sued for malpractice within the past two years, 37 percent reported being depressed within the month prior to completing the survey and the 8 percent who reported suicide ideation within the past year is double the national rate, Dr. Sheahan said. The second survey, launched Monday, focuses more on physical debility and should take fewer than 10 minutes to complete, he said. “Look for the survey, and please take it.”
He added that there are initiatives going forward that aim to change the environment and change the culture, including the SVS task force and the American Board of Surgery’s new lifelong learning initiative. “This is a call to action,” he said. “The main thing I want to say is that this is changeable. I don’t want you to think or say that we can’t do it. “We can. We just need evidence.”
Society for Vascular Surgery members are receiving an important email from the Mayo Clinic containing a survey from the SVS Wellness Task Force.
It is the second survey the task force has distributed, all aimed at ascertaining burnout and wellness statistics from SVS members.
“We need evidence,” said Malachi Sheahan, MD, who co-chairs the group with Dawn Coleman, MD. “We can’t make change without evidence.”
He issued a “Societal Call to Action” to SVS members at the end of a Friday session addressing burnout issues, “Promoting Physician Well-Being: Achieving Quadruple Aim.”
Dr. Sheahan disclosed statistics from the first task force survey, completed by 860 members. Collectively, members worked an average 73.5 hours a week, with five hours completing electronic medical records and 5.5 hours of administrative/scholarly activities added to 63 hours in the office.
“Eighty-nine percent feel burned out on occasion, everyone thinks they’re working too hard and when there are conflicts between work and personal life, they’re resolved in favor of the personal side only 8 percent of the time,” he said of the just-released data. He believes EMR will be the No. 1 conflict of vascular surgeons, with surgeons reporting they spend one hour charting for every one hour of patient time. “It’s just not working out,” he said.
Twenty percent said they had been sued for malpractice within the past two years, 37 percent reported being depressed within the month prior to completing the survey and the 8 percent who reported suicide ideation within the past year is double the national rate, Dr. Sheahan said. The second survey, launched Monday, focuses more on physical debility and should take fewer than 10 minutes to complete, he said. “Look for the survey, and please take it.”
He added that there are initiatives going forward that aim to change the environment and change the culture, including the SVS task force and the American Board of Surgery’s new lifelong learning initiative. “This is a call to action,” he said. “The main thing I want to say is that this is changeable. I don’t want you to think or say that we can’t do it. “We can. We just need evidence.”
Welcoming a New President, Presenting Awards
The Vascular Annual Meeting conducts important Society business at the SVS Annual Business Meeting. During Saturday’s meeting and luncheon, President R. Clement Darling III, MD, will hand over the leadership reins to President-Elect Michel S. Makaroun, MD.

The meeting is from 12 to 1:30 p.m. Saturday in Ballroom C of the Hynes Convention Center. Besides welcoming a new president, the meeting also will include acting on the 2018-2019 slate of officers.

Members also recieved updates from officers and select committees and recognized outstanding achievements and awards from the Journal of Vascular Surgery, SVS Foundation and SVS. Award winners included the first recipients of the new SVS Foundation Community Awareness and Prevention Project Practice Grant.
The following people received awards during the luncheon:
SVS Presidential Citation Award
Drs. Kellie R. Brown, for her work as Chair of the Postgraduate Education Committee; O. William Brown, Chair of the Conflict of Interest Committee; Daniel G. Clair, Chair of the Education Council; Michael C. Dalsing, Chair of the Government Relations Committee; Alan Dardik, Chair of the Research Council; Dennis R. Gable, Chair of the Public and Professional Outreach Committee; Richard J. Fowl, Chair of the Ethics and Professional Conduct Committee; Brad L. Johnson, Chair of the Quality and Performance Measures Committee; Larry Kraiss, Chair of the SVS Patient Safety Organization; Walter J. McCarthy, Chair of the History Committee; Frank B. Pomposelli, Chair of the Clinical Practice Council; Jeffrey Raines; Amy Reed, Chair of the Fellows Committee; Edith Tzeng, Chair of the Research and Education Committee; Robert Zwolak, Chair of the VA Vascular Surgeons Committee; and Roger Gregory and James S.T. Yao, for their dedicated service in capturing the history of SVS.
SVS Awards
Women’s Leadership Training Grants
Drs. Dawn Coleman, Bao-Ngoc Nguyen and Margaret Tracci
SVS Vascular Surgery Trainee Advocacy Travel Scholarship
Dr. Anahita Dua
SVS Foundation Awards
SVS Foundation and American College of Surgeons Mentored Clinical Scientist Research Career Development Award (K08)
Dr. Bao-Ngoc Nguyen
SVS Foundation E.J. Wylie Traveling Fellowship
Dr. Omid Jazaeri
SVS Foundation Clinical Research Seed Grant
Drs. Samantha D. Minc and Bjoern D. Suckow, MD, MS
SVS Foundation Resident Research Award
Dr. Kaspar M. Trocha
SVS Foundation Research Career Development Travel Award
Drs. James Brooks, Kristina Giles, and Samir Shah, MD
Vascular Cures/ SVS Foundation Wylie Scholar Award
John Byrne, MB BCh, MD (by research), FRCSI
SVS Foundation Community Awareness and Prevention Project Practice Grant
Drs. Manish Mehta, MD, MPH; Elizabeth L. Detschelt, MD; and Marcus E. Semel, MD, MPH
Vascular Research Initiatives Conference Trainee Travel Scholarship
Drs. Frank M. Davis, Catherine Go, Omar Saffaf, and Karim M. Salem
SVS Foundation Student Research Fellowship Award
Arash Fereydooni* (Yale School of Medicine), Helen Genis* (University of Toronto), Nikolai Thomas Harroun (Washington University, St.Louis), Alice Jo* (Case Western Reserve University School of Medicine), Revanth Kosaraju* (Beth Israel Deaconess Medical Center), Alexa Mordhorst* (Vancouver General Hospital/University of British Columbia), Lindsey Anne Olivere (Duke University School of Medicine), Suzannah Patterson (Brigham and Women’s Hospital/Harvard Medical School), Joel L. Ramirez* (University of California, San Francisco), Sudie Ann Robinson* (SUNY Upstate Medical University), Muzammil Hussain Syed (St. Michael’s Hospital/McMaster University), Jeffrey W. Zhao* (Northwestern Feinberg School of Medicine)
(*Awarded a Society for Vascular Surgery General Surgery Resident/Medical Student VAM Travel Scholarship)
The Vascular Annual Meeting conducts important Society business at the SVS Annual Business Meeting. During Saturday’s meeting and luncheon, President R. Clement Darling III, MD, will hand over the leadership reins to President-Elect Michel S. Makaroun, MD.
The meeting is from 12 to 1:30 p.m. Saturday in Ballroom C of the Hynes Convention Center. Besides welcoming a new president, the meeting also will include acting on the 2018-2019 slate of officers.
Members also recieved updates from officers and select committees and recognized outstanding achievements and awards from the Journal of Vascular Surgery, SVS Foundation and SVS. Award winners included the first recipients of the new SVS Foundation Community Awareness and Prevention Project Practice Grant.
The following people received awards during the luncheon:
SVS Presidential Citation Award
Drs. Kellie R. Brown, for her work as Chair of the Postgraduate Education Committee; O. William Brown, Chair of the Conflict of Interest Committee; Daniel G. Clair, Chair of the Education Council; Michael C. Dalsing, Chair of the Government Relations Committee; Alan Dardik, Chair of the Research Council; Dennis R. Gable, Chair of the Public and Professional Outreach Committee; Richard J. Fowl, Chair of the Ethics and Professional Conduct Committee; Brad L. Johnson, Chair of the Quality and Performance Measures Committee; Larry Kraiss, Chair of the SVS Patient Safety Organization; Walter J. McCarthy, Chair of the History Committee; Frank B. Pomposelli, Chair of the Clinical Practice Council; Jeffrey Raines; Amy Reed, Chair of the Fellows Committee; Edith Tzeng, Chair of the Research and Education Committee; Robert Zwolak, Chair of the VA Vascular Surgeons Committee; and Roger Gregory and James S.T. Yao, for their dedicated service in capturing the history of SVS.
SVS Awards
Women’s Leadership Training Grants
Drs. Dawn Coleman, Bao-Ngoc Nguyen and Margaret Tracci
SVS Vascular Surgery Trainee Advocacy Travel Scholarship
Dr. Anahita Dua
SVS Foundation Awards
SVS Foundation and American College of Surgeons Mentored Clinical Scientist Research Career Development Award (K08)
Dr. Bao-Ngoc Nguyen
SVS Foundation E.J. Wylie Traveling Fellowship
Dr. Omid Jazaeri
SVS Foundation Clinical Research Seed Grant
Drs. Samantha D. Minc and Bjoern D. Suckow, MD, MS
SVS Foundation Resident Research Award
Dr. Kaspar M. Trocha
SVS Foundation Research Career Development Travel Award
Drs. James Brooks, Kristina Giles, and Samir Shah, MD
Vascular Cures/ SVS Foundation Wylie Scholar Award
John Byrne, MB BCh, MD (by research), FRCSI
SVS Foundation Community Awareness and Prevention Project Practice Grant
Drs. Manish Mehta, MD, MPH; Elizabeth L. Detschelt, MD; and Marcus E. Semel, MD, MPH
Vascular Research Initiatives Conference Trainee Travel Scholarship
Drs. Frank M. Davis, Catherine Go, Omar Saffaf, and Karim M. Salem
SVS Foundation Student Research Fellowship Award
Arash Fereydooni* (Yale School of Medicine), Helen Genis* (University of Toronto), Nikolai Thomas Harroun (Washington University, St.Louis), Alice Jo* (Case Western Reserve University School of Medicine), Revanth Kosaraju* (Beth Israel Deaconess Medical Center), Alexa Mordhorst* (Vancouver General Hospital/University of British Columbia), Lindsey Anne Olivere (Duke University School of Medicine), Suzannah Patterson (Brigham and Women’s Hospital/Harvard Medical School), Joel L. Ramirez* (University of California, San Francisco), Sudie Ann Robinson* (SUNY Upstate Medical University), Muzammil Hussain Syed (St. Michael’s Hospital/McMaster University), Jeffrey W. Zhao* (Northwestern Feinberg School of Medicine)
(*Awarded a Society for Vascular Surgery General Surgery Resident/Medical Student VAM Travel Scholarship)
The Vascular Annual Meeting conducts important Society business at the SVS Annual Business Meeting. During Saturday’s meeting and luncheon, President R. Clement Darling III, MD, will hand over the leadership reins to President-Elect Michel S. Makaroun, MD.
The meeting is from 12 to 1:30 p.m. Saturday in Ballroom C of the Hynes Convention Center. Besides welcoming a new president, the meeting also will include acting on the 2018-2019 slate of officers.
Members also recieved updates from officers and select committees and recognized outstanding achievements and awards from the Journal of Vascular Surgery, SVS Foundation and SVS. Award winners included the first recipients of the new SVS Foundation Community Awareness and Prevention Project Practice Grant.
The following people received awards during the luncheon:
SVS Presidential Citation Award
Drs. Kellie R. Brown, for her work as Chair of the Postgraduate Education Committee; O. William Brown, Chair of the Conflict of Interest Committee; Daniel G. Clair, Chair of the Education Council; Michael C. Dalsing, Chair of the Government Relations Committee; Alan Dardik, Chair of the Research Council; Dennis R. Gable, Chair of the Public and Professional Outreach Committee; Richard J. Fowl, Chair of the Ethics and Professional Conduct Committee; Brad L. Johnson, Chair of the Quality and Performance Measures Committee; Larry Kraiss, Chair of the SVS Patient Safety Organization; Walter J. McCarthy, Chair of the History Committee; Frank B. Pomposelli, Chair of the Clinical Practice Council; Jeffrey Raines; Amy Reed, Chair of the Fellows Committee; Edith Tzeng, Chair of the Research and Education Committee; Robert Zwolak, Chair of the VA Vascular Surgeons Committee; and Roger Gregory and James S.T. Yao, for their dedicated service in capturing the history of SVS.
SVS Awards
Women’s Leadership Training Grants
Drs. Dawn Coleman, Bao-Ngoc Nguyen and Margaret Tracci
SVS Vascular Surgery Trainee Advocacy Travel Scholarship
Dr. Anahita Dua
SVS Foundation Awards
SVS Foundation and American College of Surgeons Mentored Clinical Scientist Research Career Development Award (K08)
Dr. Bao-Ngoc Nguyen
SVS Foundation E.J. Wylie Traveling Fellowship
Dr. Omid Jazaeri
SVS Foundation Clinical Research Seed Grant
Drs. Samantha D. Minc and Bjoern D. Suckow, MD, MS
SVS Foundation Resident Research Award
Dr. Kaspar M. Trocha
SVS Foundation Research Career Development Travel Award
Drs. James Brooks, Kristina Giles, and Samir Shah, MD
Vascular Cures/ SVS Foundation Wylie Scholar Award
John Byrne, MB BCh, MD (by research), FRCSI
SVS Foundation Community Awareness and Prevention Project Practice Grant
Drs. Manish Mehta, MD, MPH; Elizabeth L. Detschelt, MD; and Marcus E. Semel, MD, MPH
Vascular Research Initiatives Conference Trainee Travel Scholarship
Drs. Frank M. Davis, Catherine Go, Omar Saffaf, and Karim M. Salem
SVS Foundation Student Research Fellowship Award
Arash Fereydooni* (Yale School of Medicine), Helen Genis* (University of Toronto), Nikolai Thomas Harroun (Washington University, St.Louis), Alice Jo* (Case Western Reserve University School of Medicine), Revanth Kosaraju* (Beth Israel Deaconess Medical Center), Alexa Mordhorst* (Vancouver General Hospital/University of British Columbia), Lindsey Anne Olivere (Duke University School of Medicine), Suzannah Patterson (Brigham and Women’s Hospital/Harvard Medical School), Joel L. Ramirez* (University of California, San Francisco), Sudie Ann Robinson* (SUNY Upstate Medical University), Muzammil Hussain Syed (St. Michael’s Hospital/McMaster University), Jeffrey W. Zhao* (Northwestern Feinberg School of Medicine)
(*Awarded a Society for Vascular Surgery General Surgery Resident/Medical Student VAM Travel Scholarship)
A Six-Year Review of the First U.S. Vascular Simulation Course
Duty hour restrictions, changing training paradigms, and diminishing open surgical case volumes have caused dramatic shifts in the vascular trainee experience, according to Malachi Sheahan, MD, and his colleagues from Louisiana State University, New Orleans.

Dr. Sheahan and his colleagues examined the benefits of simulation courses as an augment to vascular training. They performed a 6-year review of the first simulation course established for vascular trainees in the United States.
The 3-day vascular simulation course studied was conducted at a dedicated learning center from 2012 to 2017. Attendees rated their confidence pre- and postcourse on a 6-point Likert scale ranging from 1 (none) to 6 (expert) across 8 different technical and cognitive categories. Participants were also asked to rate the value of each activity, according to Dr. Sheahan.
Assessments of each trainee were completed by the course director and sent to their program director. After 6 months, program directors and participants were surveyed on the lasting usefulness of the course. Full data were available for 98 vascular trainees: 59 categorized as Junior (PGY1-2); and 39 as Senior (PGY 3).
“Our study demonstrates that a brief, intensive simulation course can have a valuable and lasting impact on vascular resident education,” said Dr. Sheahan.
Overall, the participants rated all teaching activities as useful (4) or better, with anatomic exposures (5.8) and one-on-one suturing (5.5) rated most valuable. Both groups showed significant improvement in confidence in all measures, with Juniors improving significantly more than did Seniors in anastomoses, abdominal aortic aneurysm measurements, and tibial exposures.
Six-month follow-up with program directors found that 100% reported at least one lasting skill improvement and 85% stated that they modified their trainees curriculum based on the course assessment.
Duty hour restrictions, changing training paradigms, and diminishing open surgical case volumes have caused dramatic shifts in the vascular trainee experience, according to Malachi Sheahan, MD, and his colleagues from Louisiana State University, New Orleans.
Dr. Sheahan and his colleagues examined the benefits of simulation courses as an augment to vascular training. They performed a 6-year review of the first simulation course established for vascular trainees in the United States.
The 3-day vascular simulation course studied was conducted at a dedicated learning center from 2012 to 2017. Attendees rated their confidence pre- and postcourse on a 6-point Likert scale ranging from 1 (none) to 6 (expert) across 8 different technical and cognitive categories. Participants were also asked to rate the value of each activity, according to Dr. Sheahan.
Assessments of each trainee were completed by the course director and sent to their program director. After 6 months, program directors and participants were surveyed on the lasting usefulness of the course. Full data were available for 98 vascular trainees: 59 categorized as Junior (PGY1-2); and 39 as Senior (PGY 3).
“Our study demonstrates that a brief, intensive simulation course can have a valuable and lasting impact on vascular resident education,” said Dr. Sheahan.
Overall, the participants rated all teaching activities as useful (4) or better, with anatomic exposures (5.8) and one-on-one suturing (5.5) rated most valuable. Both groups showed significant improvement in confidence in all measures, with Juniors improving significantly more than did Seniors in anastomoses, abdominal aortic aneurysm measurements, and tibial exposures.
Six-month follow-up with program directors found that 100% reported at least one lasting skill improvement and 85% stated that they modified their trainees curriculum based on the course assessment.
Duty hour restrictions, changing training paradigms, and diminishing open surgical case volumes have caused dramatic shifts in the vascular trainee experience, according to Malachi Sheahan, MD, and his colleagues from Louisiana State University, New Orleans.
Dr. Sheahan and his colleagues examined the benefits of simulation courses as an augment to vascular training. They performed a 6-year review of the first simulation course established for vascular trainees in the United States.
The 3-day vascular simulation course studied was conducted at a dedicated learning center from 2012 to 2017. Attendees rated their confidence pre- and postcourse on a 6-point Likert scale ranging from 1 (none) to 6 (expert) across 8 different technical and cognitive categories. Participants were also asked to rate the value of each activity, according to Dr. Sheahan.
Assessments of each trainee were completed by the course director and sent to their program director. After 6 months, program directors and participants were surveyed on the lasting usefulness of the course. Full data were available for 98 vascular trainees: 59 categorized as Junior (PGY1-2); and 39 as Senior (PGY 3).
“Our study demonstrates that a brief, intensive simulation course can have a valuable and lasting impact on vascular resident education,” said Dr. Sheahan.
Overall, the participants rated all teaching activities as useful (4) or better, with anatomic exposures (5.8) and one-on-one suturing (5.5) rated most valuable. Both groups showed significant improvement in confidence in all measures, with Juniors improving significantly more than did Seniors in anastomoses, abdominal aortic aneurysm measurements, and tibial exposures.
Six-month follow-up with program directors found that 100% reported at least one lasting skill improvement and 85% stated that they modified their trainees curriculum based on the course assessment.
Crawford Critical Issues Forum Covers the National Shortage of Vascular Surgeons
This year’s E. Stanley Crawford Critical Issues Forum addressed the current status of the vascular surgery workforce, its existing geographic distribution, the potential for a worsening shortage, and proposed solutions to ensure future vascular care delivery.

As is tradition, the forum was organized and moderated by the SVS president-elect, this year Michel S. Makaroun, MD, co-director of the UPMC Heart and Vascular Institute in Pittsburgh. The session began with an overview from Dr. Makaroun on the critical nature of the growing problem.
He described how the current shortage of vascular surgeons is projected to worsen for two main reasons: First, newly trained vascular surgeons are not entering the workforce in adequate numbers to meet the increased demand presented by the nation’s aging population, even with the improvements projected from the new 0-5 training program; second, there is a large percentage of vascular surgeons currently practicing who are expected to retire in the next decade, with estimates reaching 35%-45%. He detailed the results of the 2017 survey of vascular surgeons that showed this and other concerning factors.
“We do not take vacations,” he said. “We have significant overwork.” In addition, “half of the surgeons who said they would retire, said they would retire before the age of 65.” In fact, nearly 50% of those surveyed have firm retirement plans, and nearly 20% were planning on retiring within the next five years.

“To summarize, we have a pipeline, which at maximum would within the next five years introduce 608 new vascular resident and fellow graduates into the workforce, and at the same time we’ll be losing the same number of practicing vascular surgeons. So, at best, we will stay even,” said Dr. Makaroun.
“The Current Landscape of the Vascular Surgery Recruitment Market” was addressed by Jeremy Robinson of Merritt Hawkins. He pointed out the market evidence for a large scarcity of vascular surgeons, with a huge number of positions going unfilled, more than half of new trainees receiving more than 100 offers, and bidding wars going on among employers, including offering expansive salaries and benefits to vascular surgeons as part of recruitment efforts.
In his talk, “Where Did the Vascular Surgeons Go? Seven Years of Futile Recruitment Attempts,” Gerald Goldstein, MD, of the Western Maryland Health System, addressed the problem of attracting new vascular surgeons. His talk was key in pointing out the problems of large health care facilities in poor and rural areas. “We’re not a Band-Aid station. ... we’re a big hospital, we serve a large geographic area and a large cohort of patients,” he said. Still they have failed to recruit a single vascular surgeon. He pointed out how places such as his could not compete for vascular surgeons against more desirable urban centers with more amenities and sufficient backup surgeons to provide lower workloads and improved quality of life, which includes time off, not being on call, and collaboration and teamwork. He was not optimistic about solutions and was fighting the final solution: hospital contraction of services.
“Workforce Targets: How Can We Know Whether We Have Enough Vascular Surgeons?” was discussed by Mark Friedberg, MD, of the RAND Corporation. Dr. Friedberg pointed out that it was important to define what was meant by a shortage of vascular surgeons, asking whether a surgeon/population metric was the most valuable or should it include other components, such as geographic considerations, quality of care issues, patient waiting times, and more. In addition, he asked, for any metric chosen, how was the decision made in choosing the optimal level? What is the best ratio of vascular surgeons to population, and how do you decide it?
Finally, Anton Sidawy, MD, of the George Washington University Hospital, Washington, looked at possible solutions to the problem in his talk, “Pathways to Alleviate Shortages and Maldistributions of Vascular Surgeons.” Dr. Sidawy stressed the need for a multifaceted approach, including government at the federal, state, and local levels, as well as medical schools and training programs. He particularly stressed the need for improving the distribution of vascular surgeons to underserved rural areas, such as described by Dr. Goldstein. However, this would require thinking outside the box, perhaps involving redistribution of training to more underserved areas of the country and also recruitment of more individuals from those areas. This is more likely to produce vascular surgeons willing to remain or return to such areas to practice, as has been well documented.
Another possibility is to provide incentives for older vascular surgeons to delay retirement, perhaps with lowered workload, freedom from being on-call, and other benefits.
But perhaps his most radical suggestion is the idea of rethinking the role of vascular surgeons entirely, to include the ability to perform more general surgery operations, allowing them more flexibility to take on roles in smaller communities and organizations that could not afford a narrowly defined specialist.
The forum concluded with a panel discussion in which the panelists addressed questions from the audience.
This year’s E. Stanley Crawford Critical Issues Forum addressed the current status of the vascular surgery workforce, its existing geographic distribution, the potential for a worsening shortage, and proposed solutions to ensure future vascular care delivery.
As is tradition, the forum was organized and moderated by the SVS president-elect, this year Michel S. Makaroun, MD, co-director of the UPMC Heart and Vascular Institute in Pittsburgh. The session began with an overview from Dr. Makaroun on the critical nature of the growing problem.
He described how the current shortage of vascular surgeons is projected to worsen for two main reasons: First, newly trained vascular surgeons are not entering the workforce in adequate numbers to meet the increased demand presented by the nation’s aging population, even with the improvements projected from the new 0-5 training program; second, there is a large percentage of vascular surgeons currently practicing who are expected to retire in the next decade, with estimates reaching 35%-45%. He detailed the results of the 2017 survey of vascular surgeons that showed this and other concerning factors.
“We do not take vacations,” he said. “We have significant overwork.” In addition, “half of the surgeons who said they would retire, said they would retire before the age of 65.” In fact, nearly 50% of those surveyed have firm retirement plans, and nearly 20% were planning on retiring within the next five years.
“To summarize, we have a pipeline, which at maximum would within the next five years introduce 608 new vascular resident and fellow graduates into the workforce, and at the same time we’ll be losing the same number of practicing vascular surgeons. So, at best, we will stay even,” said Dr. Makaroun.
“The Current Landscape of the Vascular Surgery Recruitment Market” was addressed by Jeremy Robinson of Merritt Hawkins. He pointed out the market evidence for a large scarcity of vascular surgeons, with a huge number of positions going unfilled, more than half of new trainees receiving more than 100 offers, and bidding wars going on among employers, including offering expansive salaries and benefits to vascular surgeons as part of recruitment efforts.
In his talk, “Where Did the Vascular Surgeons Go? Seven Years of Futile Recruitment Attempts,” Gerald Goldstein, MD, of the Western Maryland Health System, addressed the problem of attracting new vascular surgeons. His talk was key in pointing out the problems of large health care facilities in poor and rural areas. “We’re not a Band-Aid station. ... we’re a big hospital, we serve a large geographic area and a large cohort of patients,” he said. Still they have failed to recruit a single vascular surgeon. He pointed out how places such as his could not compete for vascular surgeons against more desirable urban centers with more amenities and sufficient backup surgeons to provide lower workloads and improved quality of life, which includes time off, not being on call, and collaboration and teamwork. He was not optimistic about solutions and was fighting the final solution: hospital contraction of services.
“Workforce Targets: How Can We Know Whether We Have Enough Vascular Surgeons?” was discussed by Mark Friedberg, MD, of the RAND Corporation. Dr. Friedberg pointed out that it was important to define what was meant by a shortage of vascular surgeons, asking whether a surgeon/population metric was the most valuable or should it include other components, such as geographic considerations, quality of care issues, patient waiting times, and more. In addition, he asked, for any metric chosen, how was the decision made in choosing the optimal level? What is the best ratio of vascular surgeons to population, and how do you decide it?
Finally, Anton Sidawy, MD, of the George Washington University Hospital, Washington, looked at possible solutions to the problem in his talk, “Pathways to Alleviate Shortages and Maldistributions of Vascular Surgeons.” Dr. Sidawy stressed the need for a multifaceted approach, including government at the federal, state, and local levels, as well as medical schools and training programs. He particularly stressed the need for improving the distribution of vascular surgeons to underserved rural areas, such as described by Dr. Goldstein. However, this would require thinking outside the box, perhaps involving redistribution of training to more underserved areas of the country and also recruitment of more individuals from those areas. This is more likely to produce vascular surgeons willing to remain or return to such areas to practice, as has been well documented.
Another possibility is to provide incentives for older vascular surgeons to delay retirement, perhaps with lowered workload, freedom from being on-call, and other benefits.
But perhaps his most radical suggestion is the idea of rethinking the role of vascular surgeons entirely, to include the ability to perform more general surgery operations, allowing them more flexibility to take on roles in smaller communities and organizations that could not afford a narrowly defined specialist.
The forum concluded with a panel discussion in which the panelists addressed questions from the audience.
This year’s E. Stanley Crawford Critical Issues Forum addressed the current status of the vascular surgery workforce, its existing geographic distribution, the potential for a worsening shortage, and proposed solutions to ensure future vascular care delivery.
As is tradition, the forum was organized and moderated by the SVS president-elect, this year Michel S. Makaroun, MD, co-director of the UPMC Heart and Vascular Institute in Pittsburgh. The session began with an overview from Dr. Makaroun on the critical nature of the growing problem.
He described how the current shortage of vascular surgeons is projected to worsen for two main reasons: First, newly trained vascular surgeons are not entering the workforce in adequate numbers to meet the increased demand presented by the nation’s aging population, even with the improvements projected from the new 0-5 training program; second, there is a large percentage of vascular surgeons currently practicing who are expected to retire in the next decade, with estimates reaching 35%-45%. He detailed the results of the 2017 survey of vascular surgeons that showed this and other concerning factors.
“We do not take vacations,” he said. “We have significant overwork.” In addition, “half of the surgeons who said they would retire, said they would retire before the age of 65.” In fact, nearly 50% of those surveyed have firm retirement plans, and nearly 20% were planning on retiring within the next five years.
“To summarize, we have a pipeline, which at maximum would within the next five years introduce 608 new vascular resident and fellow graduates into the workforce, and at the same time we’ll be losing the same number of practicing vascular surgeons. So, at best, we will stay even,” said Dr. Makaroun.
“The Current Landscape of the Vascular Surgery Recruitment Market” was addressed by Jeremy Robinson of Merritt Hawkins. He pointed out the market evidence for a large scarcity of vascular surgeons, with a huge number of positions going unfilled, more than half of new trainees receiving more than 100 offers, and bidding wars going on among employers, including offering expansive salaries and benefits to vascular surgeons as part of recruitment efforts.
In his talk, “Where Did the Vascular Surgeons Go? Seven Years of Futile Recruitment Attempts,” Gerald Goldstein, MD, of the Western Maryland Health System, addressed the problem of attracting new vascular surgeons. His talk was key in pointing out the problems of large health care facilities in poor and rural areas. “We’re not a Band-Aid station. ... we’re a big hospital, we serve a large geographic area and a large cohort of patients,” he said. Still they have failed to recruit a single vascular surgeon. He pointed out how places such as his could not compete for vascular surgeons against more desirable urban centers with more amenities and sufficient backup surgeons to provide lower workloads and improved quality of life, which includes time off, not being on call, and collaboration and teamwork. He was not optimistic about solutions and was fighting the final solution: hospital contraction of services.
“Workforce Targets: How Can We Know Whether We Have Enough Vascular Surgeons?” was discussed by Mark Friedberg, MD, of the RAND Corporation. Dr. Friedberg pointed out that it was important to define what was meant by a shortage of vascular surgeons, asking whether a surgeon/population metric was the most valuable or should it include other components, such as geographic considerations, quality of care issues, patient waiting times, and more. In addition, he asked, for any metric chosen, how was the decision made in choosing the optimal level? What is the best ratio of vascular surgeons to population, and how do you decide it?
Finally, Anton Sidawy, MD, of the George Washington University Hospital, Washington, looked at possible solutions to the problem in his talk, “Pathways to Alleviate Shortages and Maldistributions of Vascular Surgeons.” Dr. Sidawy stressed the need for a multifaceted approach, including government at the federal, state, and local levels, as well as medical schools and training programs. He particularly stressed the need for improving the distribution of vascular surgeons to underserved rural areas, such as described by Dr. Goldstein. However, this would require thinking outside the box, perhaps involving redistribution of training to more underserved areas of the country and also recruitment of more individuals from those areas. This is more likely to produce vascular surgeons willing to remain or return to such areas to practice, as has been well documented.
Another possibility is to provide incentives for older vascular surgeons to delay retirement, perhaps with lowered workload, freedom from being on-call, and other benefits.
But perhaps his most radical suggestion is the idea of rethinking the role of vascular surgeons entirely, to include the ability to perform more general surgery operations, allowing them more flexibility to take on roles in smaller communities and organizations that could not afford a narrowly defined specialist.
The forum concluded with a panel discussion in which the panelists addressed questions from the audience.
Cost led to missed care for 4.5% of Americans in 2017
The percentage of Americans who went without medical care due to cost rose to 4.5% in 2017, reversing a 6-year trend, the National Center for Health Statistics reported.
The rate was 4.4% in 2016, which represented a slowdown in what had been steady decline over the previous 5 years, according to data from the National Health Interview Survey. Declining rates corresponded with the implementation of early provisions of the Affordable Care Act in 2010.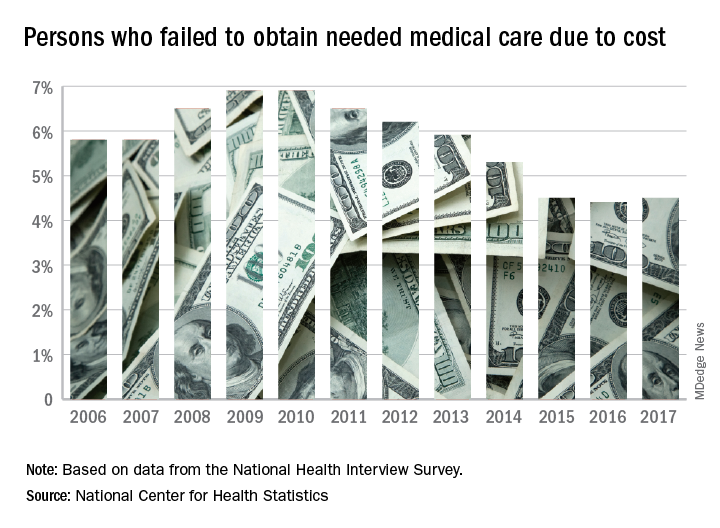
The 2017 rate varied considerably by age group. Not surprisingly, more working-age people – those aged 18-64 years – reported that they did not seek medical care at some point in the previous 12 months due to cost (6.1%). The rate was 1.2% for those under 18 years and 2.7% for the Medicare eligible – those aged 65 years and older.
For 2016, the rates were 6.2% for those aged 18-64 years, 1.2% for the under-18 group, and 2.1% for the 65+ group, the data show.
Among females of all ages in 2017, 4.8% failed to get needed care at some point in the previous year, compared with 4.1% of men. Those numbers were unchanged from 2016 but down from 4.9% for females in 2015 and up from 4.0% for males that year, the NCHS said.
In 2017, the rate also varied by race/ethnicity – 4.1% for whites, 5.3% for Hispanics, 6.1% for blacks – and by location – 4.1% for large metropolitan areas, 4.9% for small metro areas, and 5.5% for rural locales, according to the early release of survey data.
The percentage of Americans who went without medical care due to cost rose to 4.5% in 2017, reversing a 6-year trend, the National Center for Health Statistics reported.
The rate was 4.4% in 2016, which represented a slowdown in what had been steady decline over the previous 5 years, according to data from the National Health Interview Survey. Declining rates corresponded with the implementation of early provisions of the Affordable Care Act in 2010.
The 2017 rate varied considerably by age group. Not surprisingly, more working-age people – those aged 18-64 years – reported that they did not seek medical care at some point in the previous 12 months due to cost (6.1%). The rate was 1.2% for those under 18 years and 2.7% for the Medicare eligible – those aged 65 years and older.
For 2016, the rates were 6.2% for those aged 18-64 years, 1.2% for the under-18 group, and 2.1% for the 65+ group, the data show.
Among females of all ages in 2017, 4.8% failed to get needed care at some point in the previous year, compared with 4.1% of men. Those numbers were unchanged from 2016 but down from 4.9% for females in 2015 and up from 4.0% for males that year, the NCHS said.
In 2017, the rate also varied by race/ethnicity – 4.1% for whites, 5.3% for Hispanics, 6.1% for blacks – and by location – 4.1% for large metropolitan areas, 4.9% for small metro areas, and 5.5% for rural locales, according to the early release of survey data.
The percentage of Americans who went without medical care due to cost rose to 4.5% in 2017, reversing a 6-year trend, the National Center for Health Statistics reported.
The rate was 4.4% in 2016, which represented a slowdown in what had been steady decline over the previous 5 years, according to data from the National Health Interview Survey. Declining rates corresponded with the implementation of early provisions of the Affordable Care Act in 2010.
The 2017 rate varied considerably by age group. Not surprisingly, more working-age people – those aged 18-64 years – reported that they did not seek medical care at some point in the previous 12 months due to cost (6.1%). The rate was 1.2% for those under 18 years and 2.7% for the Medicare eligible – those aged 65 years and older.
For 2016, the rates were 6.2% for those aged 18-64 years, 1.2% for the under-18 group, and 2.1% for the 65+ group, the data show.
Among females of all ages in 2017, 4.8% failed to get needed care at some point in the previous year, compared with 4.1% of men. Those numbers were unchanged from 2016 but down from 4.9% for females in 2015 and up from 4.0% for males that year, the NCHS said.
In 2017, the rate also varied by race/ethnicity – 4.1% for whites, 5.3% for Hispanics, 6.1% for blacks – and by location – 4.1% for large metropolitan areas, 4.9% for small metro areas, and 5.5% for rural locales, according to the early release of survey data.
Glucocorticosteroid use raises sarcopenia risk in RA
AMSTERDAM – Patients with RA have a higher risk of developing sarcopenia if they are treated with glucocorticosteroids, study findings suggested.
“The strength of our study is that it is a prospective, longitudinal study and this study is the first, to our knowledge, to look at risk factors for sarcopenia limited to RA patients,” Yutaro Yamada, MD, said in an interview at the European Congress of Rheumatology.
Dr. Yamada, of the department of orthopedic surgery at Osaka City University, Japan, said that there is a twofold rationale for looking at risk factors for sarcopenia in RA patients. First, RA causes chronic inflammation and this in turn is thought to lead to a metabolic state that then results in muscle loss. Furthermore, joint dysfunction and subsequent disuse likely contribute to weakening muscles. Second, glucocorticosteroids, which are commonly used to treat patients with RA, have themselves been associated with a low muscle area in prior research.
In 2016, the CHIKARA study was initiated “to clarify the correlation between RA disease activity and sarcopenia,” Dr. Yamada and his associates reported in a poster presentation. They recruited 100 patients, of whom 78% were women, and recorded body weight, muscle mass, fat mass, and predicted bone mass using a body composition analyzer at entry and 1 year later. Laboratory data and disease activity parameters were also assessed, along with radiologic findings and ability to perform activities of daily living. Patients’ treatment was also recorded.
At baseline, the mean age of study participants was 68 years with a mean disease duration of 5.5 years. The majority (86%) had been treated with methotrexate, with 26% also using glucocorticosteroids, and 30% using biologic agents.
Just over one-quarter (28%) were diagnosed with sarcopenia over the course of 1 year. Sarcopenia was defined by criteria agreed by the Asia Working Group on Sarcopenia (Am Med Dir Assoc. 2014;15[2]:95-101) that set thresholds for low muscle mass, low muscle strength, and low physical performance.
Comparing the 9 patients who did develop sarcopenia with the 86 who did not, the researchers found that sarcopenia patients tended to be younger (66.7 vs. 80.2 years), although the difference was not statistically significant. Interestingly, however, more than half (55.6%) of patients who developed sarcopenia were using glucocorticosteroids, compared with 22% of those who were not (P = .029). Of note, the average glucocorticosteroid dose was just 2 mg/day. Patients who developed sarcopenia were also observed to have a lower fat mass (11.7 vs. 15.8, P = .058).
A multiple logistic regression analysis found that using a glucocorticosteroid dose of 2 mg/day or more and lower body fat mass (odds ratio, 0.78; 95% CI 0.61-0.98; P = 0.037) were significant variables for the onset of sarcopenia.
Dr. Yamada noted that 2 mg/day is “a relatively low dose” and so avoiding glucocorticosteroid therapy in those at risk of sarcopenia, particularly those with a low fat mass, may be something to consider.
The study did not receive commercial funding, and Dr. Yamada had no conflicts of interest to disclose.
SOURCE: Yamada Y et al. Ann Rheum Dis. 2018;77(Suppl 2):308-9. Abstract THU0181.
AMSTERDAM – Patients with RA have a higher risk of developing sarcopenia if they are treated with glucocorticosteroids, study findings suggested.
“The strength of our study is that it is a prospective, longitudinal study and this study is the first, to our knowledge, to look at risk factors for sarcopenia limited to RA patients,” Yutaro Yamada, MD, said in an interview at the European Congress of Rheumatology.
Dr. Yamada, of the department of orthopedic surgery at Osaka City University, Japan, said that there is a twofold rationale for looking at risk factors for sarcopenia in RA patients. First, RA causes chronic inflammation and this in turn is thought to lead to a metabolic state that then results in muscle loss. Furthermore, joint dysfunction and subsequent disuse likely contribute to weakening muscles. Second, glucocorticosteroids, which are commonly used to treat patients with RA, have themselves been associated with a low muscle area in prior research.
In 2016, the CHIKARA study was initiated “to clarify the correlation between RA disease activity and sarcopenia,” Dr. Yamada and his associates reported in a poster presentation. They recruited 100 patients, of whom 78% were women, and recorded body weight, muscle mass, fat mass, and predicted bone mass using a body composition analyzer at entry and 1 year later. Laboratory data and disease activity parameters were also assessed, along with radiologic findings and ability to perform activities of daily living. Patients’ treatment was also recorded.
At baseline, the mean age of study participants was 68 years with a mean disease duration of 5.5 years. The majority (86%) had been treated with methotrexate, with 26% also using glucocorticosteroids, and 30% using biologic agents.
Just over one-quarter (28%) were diagnosed with sarcopenia over the course of 1 year. Sarcopenia was defined by criteria agreed by the Asia Working Group on Sarcopenia (Am Med Dir Assoc. 2014;15[2]:95-101) that set thresholds for low muscle mass, low muscle strength, and low physical performance.
Comparing the 9 patients who did develop sarcopenia with the 86 who did not, the researchers found that sarcopenia patients tended to be younger (66.7 vs. 80.2 years), although the difference was not statistically significant. Interestingly, however, more than half (55.6%) of patients who developed sarcopenia were using glucocorticosteroids, compared with 22% of those who were not (P = .029). Of note, the average glucocorticosteroid dose was just 2 mg/day. Patients who developed sarcopenia were also observed to have a lower fat mass (11.7 vs. 15.8, P = .058).
A multiple logistic regression analysis found that using a glucocorticosteroid dose of 2 mg/day or more and lower body fat mass (odds ratio, 0.78; 95% CI 0.61-0.98; P = 0.037) were significant variables for the onset of sarcopenia.
Dr. Yamada noted that 2 mg/day is “a relatively low dose” and so avoiding glucocorticosteroid therapy in those at risk of sarcopenia, particularly those with a low fat mass, may be something to consider.
The study did not receive commercial funding, and Dr. Yamada had no conflicts of interest to disclose.
SOURCE: Yamada Y et al. Ann Rheum Dis. 2018;77(Suppl 2):308-9. Abstract THU0181.
AMSTERDAM – Patients with RA have a higher risk of developing sarcopenia if they are treated with glucocorticosteroids, study findings suggested.
“The strength of our study is that it is a prospective, longitudinal study and this study is the first, to our knowledge, to look at risk factors for sarcopenia limited to RA patients,” Yutaro Yamada, MD, said in an interview at the European Congress of Rheumatology.
Dr. Yamada, of the department of orthopedic surgery at Osaka City University, Japan, said that there is a twofold rationale for looking at risk factors for sarcopenia in RA patients. First, RA causes chronic inflammation and this in turn is thought to lead to a metabolic state that then results in muscle loss. Furthermore, joint dysfunction and subsequent disuse likely contribute to weakening muscles. Second, glucocorticosteroids, which are commonly used to treat patients with RA, have themselves been associated with a low muscle area in prior research.
In 2016, the CHIKARA study was initiated “to clarify the correlation between RA disease activity and sarcopenia,” Dr. Yamada and his associates reported in a poster presentation. They recruited 100 patients, of whom 78% were women, and recorded body weight, muscle mass, fat mass, and predicted bone mass using a body composition analyzer at entry and 1 year later. Laboratory data and disease activity parameters were also assessed, along with radiologic findings and ability to perform activities of daily living. Patients’ treatment was also recorded.
At baseline, the mean age of study participants was 68 years with a mean disease duration of 5.5 years. The majority (86%) had been treated with methotrexate, with 26% also using glucocorticosteroids, and 30% using biologic agents.
Just over one-quarter (28%) were diagnosed with sarcopenia over the course of 1 year. Sarcopenia was defined by criteria agreed by the Asia Working Group on Sarcopenia (Am Med Dir Assoc. 2014;15[2]:95-101) that set thresholds for low muscle mass, low muscle strength, and low physical performance.
Comparing the 9 patients who did develop sarcopenia with the 86 who did not, the researchers found that sarcopenia patients tended to be younger (66.7 vs. 80.2 years), although the difference was not statistically significant. Interestingly, however, more than half (55.6%) of patients who developed sarcopenia were using glucocorticosteroids, compared with 22% of those who were not (P = .029). Of note, the average glucocorticosteroid dose was just 2 mg/day. Patients who developed sarcopenia were also observed to have a lower fat mass (11.7 vs. 15.8, P = .058).
A multiple logistic regression analysis found that using a glucocorticosteroid dose of 2 mg/day or more and lower body fat mass (odds ratio, 0.78; 95% CI 0.61-0.98; P = 0.037) were significant variables for the onset of sarcopenia.
Dr. Yamada noted that 2 mg/day is “a relatively low dose” and so avoiding glucocorticosteroid therapy in those at risk of sarcopenia, particularly those with a low fat mass, may be something to consider.
The study did not receive commercial funding, and Dr. Yamada had no conflicts of interest to disclose.
SOURCE: Yamada Y et al. Ann Rheum Dis. 2018;77(Suppl 2):308-9. Abstract THU0181.
REPORTING FROM THE EULAR 2018 CONGRESS
Key clinical point: Patients with RA and a lean body mass have a heightened risk of developing sarcopenia if they are treated with glucocorticosteroids.
Major finding: Using glucocorticosteroids at doses of 2 mg/day or more significantly increased the odds of developing sarcopenia (odds ratio, 8.0; 95% confidence interval, 1.17-54.8; P = .034).
Study details: The CHIKARA study – a prospective, observational study involving 100 patients with RA.
Disclosures: The study did not receive commercial funding, and Dr. Yamada had no conflicts of interest to disclose.
Source: Yamada Y et al. Ann Rheum Dis. 2018;77(Suppl 2):308-9. Abstract THU0181.