User login
CDC supports Ebola response in DRC
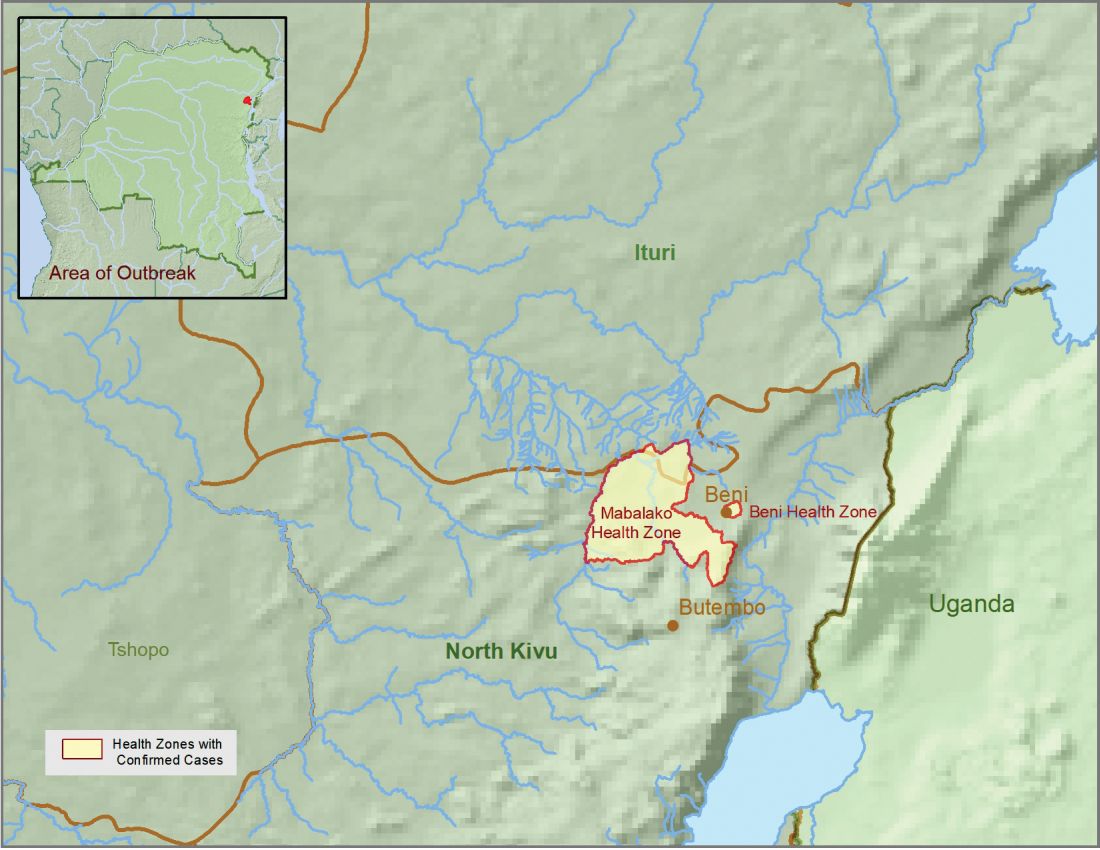
The Centers for Disease Control and Prevention has been working with the Ministry of Health of the Democratic Republic of the Congo (DRC) on a new Ebola outbreak reported on Aug, 1, 2018, in North Kivu province.
![]()
“For the current outbreak, CDC has deployed experienced Ebola experts to DRC and the World Health Organization [WHO] to provide guidance on coordination of outbreak response, laboratory testing, disease contact tracing, infection control, and health communication,” according to a CDC press release.
The CDC’s online response also provides a Traveler’s Health notice of Watch Level 1 for the DRC, which advises standard precautions and avoiding infected individuals, but not an advisory against travel.
The Ebola virus associated with the current outbreak is Zaire ebolavirus, according to genetic testing by scientists in the DRC. This is the same species that caused an outbreak earlier this year in Equateur province in northwestern DRC, although differences between the genes of the viruses suggest the two outbreaks are not linked, according to the CDC media announcement.
As of Aug. 12, 2018, the following statistics were reported by the WHO on the outbreak:
- Confirmed cases: 30
- Probable cases: 27
- Total cases: 57
- Deaths: 41 (14 confirmed, 27 probable)
The outbreak is of particular concern because of the instability of the area, which hampers relief and quarantine efforts. The outbreak is in a part of the country identified by the U.S. State Department as a “restricted travel” zone due to armed conflict and violence targeting civilians, according to the CDC.
The Centers for Disease Control and Prevention has been working with the Ministry of Health of the Democratic Republic of the Congo (DRC) on a new Ebola outbreak reported on Aug, 1, 2018, in North Kivu province.
![]()
“For the current outbreak, CDC has deployed experienced Ebola experts to DRC and the World Health Organization [WHO] to provide guidance on coordination of outbreak response, laboratory testing, disease contact tracing, infection control, and health communication,” according to a CDC press release.
The CDC’s online response also provides a Traveler’s Health notice of Watch Level 1 for the DRC, which advises standard precautions and avoiding infected individuals, but not an advisory against travel.
The Ebola virus associated with the current outbreak is Zaire ebolavirus, according to genetic testing by scientists in the DRC. This is the same species that caused an outbreak earlier this year in Equateur province in northwestern DRC, although differences between the genes of the viruses suggest the two outbreaks are not linked, according to the CDC media announcement.
As of Aug. 12, 2018, the following statistics were reported by the WHO on the outbreak:
- Confirmed cases: 30
- Probable cases: 27
- Total cases: 57
- Deaths: 41 (14 confirmed, 27 probable)
The outbreak is of particular concern because of the instability of the area, which hampers relief and quarantine efforts. The outbreak is in a part of the country identified by the U.S. State Department as a “restricted travel” zone due to armed conflict and violence targeting civilians, according to the CDC.
The Centers for Disease Control and Prevention has been working with the Ministry of Health of the Democratic Republic of the Congo (DRC) on a new Ebola outbreak reported on Aug, 1, 2018, in North Kivu province.
![]()
“For the current outbreak, CDC has deployed experienced Ebola experts to DRC and the World Health Organization [WHO] to provide guidance on coordination of outbreak response, laboratory testing, disease contact tracing, infection control, and health communication,” according to a CDC press release.
The CDC’s online response also provides a Traveler’s Health notice of Watch Level 1 for the DRC, which advises standard precautions and avoiding infected individuals, but not an advisory against travel.
The Ebola virus associated with the current outbreak is Zaire ebolavirus, according to genetic testing by scientists in the DRC. This is the same species that caused an outbreak earlier this year in Equateur province in northwestern DRC, although differences between the genes of the viruses suggest the two outbreaks are not linked, according to the CDC media announcement.
As of Aug. 12, 2018, the following statistics were reported by the WHO on the outbreak:
- Confirmed cases: 30
- Probable cases: 27
- Total cases: 57
- Deaths: 41 (14 confirmed, 27 probable)
The outbreak is of particular concern because of the instability of the area, which hampers relief and quarantine efforts. The outbreak is in a part of the country identified by the U.S. State Department as a “restricted travel” zone due to armed conflict and violence targeting civilians, according to the CDC.
French warn of upsurge in pneumococcal meningitis
MALMO, SWEDEN – A French national study has documented a sharp increase in pneumococcal meningitis since 2015 in children under age 15 years.

The culprit has been identified as serotype 24F, which is not covered by the infant 13-valent conjugate pneumococcal vaccine (PCV13), Naim Ouldali, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
The rapid emergence of serotype 24F has been accompanied by a disturbing change in its penicillin susceptibility. Indeed, penicillin resistance was present in only 18% of serotype 24F isolates in France during 2000-2014, then jumped to 74% during 2015-2016, according to Dr. Ouldali of René Descartes University in Paris.
“PCV13 has strongly reduced the pneumococcal meningitis burden in children, but its benefit now seems to be jeopardized, at least in France. So serum 24F could become a major concern in the coming years because of its characteristics. And now the question is, is this emergence an epidemic phenomenon or not? And if it’s confirmed in future studies and in other countries, probably it should drive the development of next-generation PCV formulations,” he said.
Dr. Ouldali presented a population-based interrupted time-series analysis of a nationwide prospective survey conducted in France during 2001-2016. He noted that the Cochrane Collaboration has deemed this study design second only to the randomized controlled trial in terms of quality of evidence.
The study, which included 227 French pediatric wards and 168 microbiology departments, identified 1,778 children under age 15 years with pneumococcal meningitis. This is believed to be more than 60% of all cases that occurred in the country during the study years.
The purpose of the study was to determine the impact of implementation of routine PCV13 as part of the national vaccine strategy. Rates of PCV13 coverage in French children are very high: in excess of 90% during 2015 to 2016.
Implementation of PCV13 led to a dramatic 38% reduction in the monthly incidence of pneumococcal meningitis, from 0.12 cases per 100,000 children before PCV13 to a low of 0.07 cases per 100,000 in December 2014. But after that the rate rebounded sharply, by 2.3% per month during 2015-2016, to a high of 0.13 cases per 100,000 per month by the end of 2016. Drilling down into the data, Dr. Ouldali and his coinvestigators learned that the resurgence of pneumococcal meningitis was due largely to the emergence of serotype 24F.
“This serotype is of particular concern because of two characteristics: First, it is already known to have a high disease potential – one of the highest, along with serotype 12F – and second, this rapid emergence was accompanied by a change in its penicillin susceptibility,” he noted.
Most of the French rebound in pneumococcal meningitis has occurred in children under 2 years of age. Of note, German investigators also have recently reported a rebound in invasive pneumococcal disease in German children under 16 years of age. Non-PCV13 serotypes accounted for 84% of all invasive pneumococcal disease during 2015-2016, with serotypes 10A and 24F leading the way. As in France, most of the resurgence has involved children less than 2 years old. However, unlike in France, most of the German increase has been in nonmeningitis forms of invasive pneumococcal disease (Vaccine. 2018 Jan 25;36[4]:572-7).
In response to a question from a concerned audience member, Dr. Ouldali said that while the penicillin susceptibility of serotype 24F has taken a sharp turn for the worse, cephalosporin susceptibility has not.
“To date, we have not seen any cephalosporin-resistant strains. To date, there is no need to use vancomycin,” he said.
Dr. Ouldali said the next step he and his colleagues plan to take is to see if there is a clonal expansion or a particular underlying genetic pattern which could explain the explosive emergence of 24F.
The study was funded by a research grant from Pfizer and by the French Pediatric Infectious Diseases Group.
MALMO, SWEDEN – A French national study has documented a sharp increase in pneumococcal meningitis since 2015 in children under age 15 years.
The culprit has been identified as serotype 24F, which is not covered by the infant 13-valent conjugate pneumococcal vaccine (PCV13), Naim Ouldali, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
The rapid emergence of serotype 24F has been accompanied by a disturbing change in its penicillin susceptibility. Indeed, penicillin resistance was present in only 18% of serotype 24F isolates in France during 2000-2014, then jumped to 74% during 2015-2016, according to Dr. Ouldali of René Descartes University in Paris.
“PCV13 has strongly reduced the pneumococcal meningitis burden in children, but its benefit now seems to be jeopardized, at least in France. So serum 24F could become a major concern in the coming years because of its characteristics. And now the question is, is this emergence an epidemic phenomenon or not? And if it’s confirmed in future studies and in other countries, probably it should drive the development of next-generation PCV formulations,” he said.
Dr. Ouldali presented a population-based interrupted time-series analysis of a nationwide prospective survey conducted in France during 2001-2016. He noted that the Cochrane Collaboration has deemed this study design second only to the randomized controlled trial in terms of quality of evidence.
The study, which included 227 French pediatric wards and 168 microbiology departments, identified 1,778 children under age 15 years with pneumococcal meningitis. This is believed to be more than 60% of all cases that occurred in the country during the study years.
The purpose of the study was to determine the impact of implementation of routine PCV13 as part of the national vaccine strategy. Rates of PCV13 coverage in French children are very high: in excess of 90% during 2015 to 2016.
Implementation of PCV13 led to a dramatic 38% reduction in the monthly incidence of pneumococcal meningitis, from 0.12 cases per 100,000 children before PCV13 to a low of 0.07 cases per 100,000 in December 2014. But after that the rate rebounded sharply, by 2.3% per month during 2015-2016, to a high of 0.13 cases per 100,000 per month by the end of 2016. Drilling down into the data, Dr. Ouldali and his coinvestigators learned that the resurgence of pneumococcal meningitis was due largely to the emergence of serotype 24F.
“This serotype is of particular concern because of two characteristics: First, it is already known to have a high disease potential – one of the highest, along with serotype 12F – and second, this rapid emergence was accompanied by a change in its penicillin susceptibility,” he noted.
Most of the French rebound in pneumococcal meningitis has occurred in children under 2 years of age. Of note, German investigators also have recently reported a rebound in invasive pneumococcal disease in German children under 16 years of age. Non-PCV13 serotypes accounted for 84% of all invasive pneumococcal disease during 2015-2016, with serotypes 10A and 24F leading the way. As in France, most of the resurgence has involved children less than 2 years old. However, unlike in France, most of the German increase has been in nonmeningitis forms of invasive pneumococcal disease (Vaccine. 2018 Jan 25;36[4]:572-7).
In response to a question from a concerned audience member, Dr. Ouldali said that while the penicillin susceptibility of serotype 24F has taken a sharp turn for the worse, cephalosporin susceptibility has not.
“To date, we have not seen any cephalosporin-resistant strains. To date, there is no need to use vancomycin,” he said.
Dr. Ouldali said the next step he and his colleagues plan to take is to see if there is a clonal expansion or a particular underlying genetic pattern which could explain the explosive emergence of 24F.
The study was funded by a research grant from Pfizer and by the French Pediatric Infectious Diseases Group.
MALMO, SWEDEN – A French national study has documented a sharp increase in pneumococcal meningitis since 2015 in children under age 15 years.
The culprit has been identified as serotype 24F, which is not covered by the infant 13-valent conjugate pneumococcal vaccine (PCV13), Naim Ouldali, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
The rapid emergence of serotype 24F has been accompanied by a disturbing change in its penicillin susceptibility. Indeed, penicillin resistance was present in only 18% of serotype 24F isolates in France during 2000-2014, then jumped to 74% during 2015-2016, according to Dr. Ouldali of René Descartes University in Paris.
“PCV13 has strongly reduced the pneumococcal meningitis burden in children, but its benefit now seems to be jeopardized, at least in France. So serum 24F could become a major concern in the coming years because of its characteristics. And now the question is, is this emergence an epidemic phenomenon or not? And if it’s confirmed in future studies and in other countries, probably it should drive the development of next-generation PCV formulations,” he said.
Dr. Ouldali presented a population-based interrupted time-series analysis of a nationwide prospective survey conducted in France during 2001-2016. He noted that the Cochrane Collaboration has deemed this study design second only to the randomized controlled trial in terms of quality of evidence.
The study, which included 227 French pediatric wards and 168 microbiology departments, identified 1,778 children under age 15 years with pneumococcal meningitis. This is believed to be more than 60% of all cases that occurred in the country during the study years.
The purpose of the study was to determine the impact of implementation of routine PCV13 as part of the national vaccine strategy. Rates of PCV13 coverage in French children are very high: in excess of 90% during 2015 to 2016.
Implementation of PCV13 led to a dramatic 38% reduction in the monthly incidence of pneumococcal meningitis, from 0.12 cases per 100,000 children before PCV13 to a low of 0.07 cases per 100,000 in December 2014. But after that the rate rebounded sharply, by 2.3% per month during 2015-2016, to a high of 0.13 cases per 100,000 per month by the end of 2016. Drilling down into the data, Dr. Ouldali and his coinvestigators learned that the resurgence of pneumococcal meningitis was due largely to the emergence of serotype 24F.
“This serotype is of particular concern because of two characteristics: First, it is already known to have a high disease potential – one of the highest, along with serotype 12F – and second, this rapid emergence was accompanied by a change in its penicillin susceptibility,” he noted.
Most of the French rebound in pneumococcal meningitis has occurred in children under 2 years of age. Of note, German investigators also have recently reported a rebound in invasive pneumococcal disease in German children under 16 years of age. Non-PCV13 serotypes accounted for 84% of all invasive pneumococcal disease during 2015-2016, with serotypes 10A and 24F leading the way. As in France, most of the resurgence has involved children less than 2 years old. However, unlike in France, most of the German increase has been in nonmeningitis forms of invasive pneumococcal disease (Vaccine. 2018 Jan 25;36[4]:572-7).
In response to a question from a concerned audience member, Dr. Ouldali said that while the penicillin susceptibility of serotype 24F has taken a sharp turn for the worse, cephalosporin susceptibility has not.
“To date, we have not seen any cephalosporin-resistant strains. To date, there is no need to use vancomycin,” he said.
Dr. Ouldali said the next step he and his colleagues plan to take is to see if there is a clonal expansion or a particular underlying genetic pattern which could explain the explosive emergence of 24F.
The study was funded by a research grant from Pfizer and by the French Pediatric Infectious Diseases Group.
REPORTING FROM ESPID 2018
Key clinical point:
Major finding: The incidence of pneumococcal meningitis in French children jumped by 2.3% per month during 2015-2016.
Study details: This population-based interrupted time-series analysis included all 1,778 cases of pneumococcal meningitis in children under age 15 years during 2001-2016 in 227 French pediatric wards.
Disclosures: The study was funded by a grant from Pfizer and by the French Pediatric Infectious Diseases Group.
TBI linked to increased suicide risk
Traumatic brain injury might be associated with an increased risk of suicide, according to results published Aug. 14 in JAMA.
In a retrospective cohort study of 7,418,391 Danish individuals, including 34,529 who died by suicide, patients with medical contact for traumatic brain injury (TBI) had increased suicide risk, compared with the general population (adjusted incidence rate ratio [IRR] = 1.90; 95% confidence interval, 1.83-1.97).
Patients were aged 10 years or older, and follow-up was conducted from Jan. 1, 1980, until date of death, emigration from Denmark, or Dec. 31, 2014, whichever came first. Data were obtained from national registries, including the Danish Civil Registration System, the Database for Integrated Labour Market Research, the National Hospital Register, the Psychiatric Central Research Register, and the Cause of Death Register. Associations between the separate registries were possible because of unique identification numbers assigned to every resident of Denmark, wrote Trine Madsen, PhD, of the Danish Research Institute of Suicide Prevention at the Mental Health Centre Copenhagen, Capital Region of Denmark, and her coauthors.
TBI was recorded in the National Patient Register and was categorized into three types of injury: mild TBI (concussion), skull fracture without documented TBI, and severe TBI (head injury with evidence of structural brain injury). The number of medical contacts for distinct TBI events, accumulated number of days in hospital treatment, age at first TBI, and time since last medical contact for TBI also were assessed.
Data on psychiatric illness and nonfatal self-harm were obtained from the Psychiatric Central Research Register, because of their association with suicide. Data for deaths by suicide were obtained from the Cause of Death Register. Demographic data collected from other registries included sex, age, marital status, cohabitation status, education, and socioeconomic status. IRRs were calculated using adjusted Poisson regression models.
Of 7,418,391 residents of Denmark included in the follow-up period from 1980 to 2014; 567,823 had a TBI diagnosis. Dr. Madsen and her coauthors also found that 423,502 patients (5.7%) were diagnosed with mild TBI, 24,221 (0.3%) with skull fracture, and 120,100 (1.6%) with severe TBI. A total of 34,529 died by suicide.
Of those who died by suicide, 3,536 (10.2%) had a previous TBI diagnosis (2,701 with mild TBI, 174 with skull fracture, and 661 with severe TBI). The absolute rate of suicide in individuals with hospital contact for TBI was 40.6 per 100,000 person-years (95% CI, 39.2-41.9), compared with 19.9 per 100,000 person-years (95% CI, 19.7-20.1) in those with no hospital contact for TBI.
The fully adjusted analysis showed an IRR of 1.90 (95% CI, 1.83-1.97), as well as an increased risk of suicide by TBI severity. The absolute rate for mild TBI was 38.6 per 100,000 person-years (95% CI, 37.1-40.0) with an IRR of 1.81 (95% CI, 1.74-1.88); 42.4 per 100,000 person-years for skull fracture (95% CI, 36.1-48.7) with an IRR of 2.01 (95% CI, 1.73-2.34, P less than .001), and 50.8 per 100,000 person-years for severe TBI (95% CI, 46.9-54.6) with an IRR of 2.38 (95% CI, 2.20-2.58, P less than .001), compared with individuals with no TBI, the authors wrote.
Patients with a first medical contact between 16 and 20 years of age had the highest suicide risk, compared with individuals with no TBI (IRR, 3.01; 95% CI, 2.74-3.30). In addition, individuals who were diagnosed with a psychiatric illness after TBI had a higher risk of suicide than that of those with TBI only (IRR, 4.90; 95% CI, 4.55-5.29; P less than .001), as did those who had engaged in self-harm after TBI (IRR, 7.54; 95% CI, 6.91-8.22; P less than .001). Patients diagnosed with a psychological illness before their TBI had a higher risk of suicide than did those with TBI only (IRR, 2.32; 95% CI, 2.10-2.55; P less than .001), as did those who had engaged self-harm before TBI (IRR, 2.85; 95% CI, 2.53-3.19; P less than .001), the authors noted.
Dr. Madsen and her coauthors cited several limitations. One is that information was not available on which treatment patients with TBIs received. This information “would have been useful to estimate whether different treatment regimens or subsequent follow-up would have reduced the suicide risk,” they wrote.
“Traumatic brain injury is a major public health problem that has many serious consequences, including suicide,” Dr. Madsen and her colleagues wrote. Since falls and traffic accidents account for the largest share of TBIs, helmet use may be a useful protective measure, particularly for injuries related to bicycling and falls that occur at work, the researchers wrote.
“The high prevalence of TBI globally emphasizes the importance for preventing TBI in order to ameliorate its sequelae, such as increased suicide risk,” they concluded.
The study was funded in part by the Mental Health Services Capital Region Denmark and the Lundbeck Foundation. No other disclosures were reported.
SOURCE: Madsen T et al. JAMA. 2018 Aug 14;320(6):580-8.
The results of this study “add to a growing body of evidence pointing to traumatic brain injury (TBI) as an important risk factor for suicide,” Lee Goldstein, MD, PhD, and Ramon Diaz-Arrastia, MD, PhD, wrote in an editorial published with the study (JAMA. 2018 Aug 14;320:[6]:554-6).
The study also stimulates key questions for research, Dr. Goldstein and Dr. Diaz-Arrastia wrote. “How exactly do TBIs increase suicide risk?” they wrote. “What are the substrates and processes that causally link TBI, a highly heterogeneous condition, to a singular catastrophic outcome? The answers are undoubtedly multifactorial and complex.”
Nevertheless, they wrote, the study provides important insights into the “underappreciated relationship” between TBI and suicide, including evidence of a clinical “triad”: TBI history, recent injury, and more numerous post-injury medical contacts for TBI – that may serve as “red flags” for increased suicide risk. “Notably, the results of this study indicate that increased suicide risk is relevant across all TBI severity levels, including the far more common mild injuries. Clinicians, health care professionals, and mental health practitioners must take notice of this important information.”
Dr. Goldstein is affiliated with the department of psychiatry at Boston University and reported no conflicts of interest. Dr. Diaz-Arrastia is affiliated with the department of neurology at the University of Pennsylvania, Philadelphia, and also reported no conflicts of interest.
The results of this study “add to a growing body of evidence pointing to traumatic brain injury (TBI) as an important risk factor for suicide,” Lee Goldstein, MD, PhD, and Ramon Diaz-Arrastia, MD, PhD, wrote in an editorial published with the study (JAMA. 2018 Aug 14;320:[6]:554-6).
The study also stimulates key questions for research, Dr. Goldstein and Dr. Diaz-Arrastia wrote. “How exactly do TBIs increase suicide risk?” they wrote. “What are the substrates and processes that causally link TBI, a highly heterogeneous condition, to a singular catastrophic outcome? The answers are undoubtedly multifactorial and complex.”
Nevertheless, they wrote, the study provides important insights into the “underappreciated relationship” between TBI and suicide, including evidence of a clinical “triad”: TBI history, recent injury, and more numerous post-injury medical contacts for TBI – that may serve as “red flags” for increased suicide risk. “Notably, the results of this study indicate that increased suicide risk is relevant across all TBI severity levels, including the far more common mild injuries. Clinicians, health care professionals, and mental health practitioners must take notice of this important information.”
Dr. Goldstein is affiliated with the department of psychiatry at Boston University and reported no conflicts of interest. Dr. Diaz-Arrastia is affiliated with the department of neurology at the University of Pennsylvania, Philadelphia, and also reported no conflicts of interest.
The results of this study “add to a growing body of evidence pointing to traumatic brain injury (TBI) as an important risk factor for suicide,” Lee Goldstein, MD, PhD, and Ramon Diaz-Arrastia, MD, PhD, wrote in an editorial published with the study (JAMA. 2018 Aug 14;320:[6]:554-6).
The study also stimulates key questions for research, Dr. Goldstein and Dr. Diaz-Arrastia wrote. “How exactly do TBIs increase suicide risk?” they wrote. “What are the substrates and processes that causally link TBI, a highly heterogeneous condition, to a singular catastrophic outcome? The answers are undoubtedly multifactorial and complex.”
Nevertheless, they wrote, the study provides important insights into the “underappreciated relationship” between TBI and suicide, including evidence of a clinical “triad”: TBI history, recent injury, and more numerous post-injury medical contacts for TBI – that may serve as “red flags” for increased suicide risk. “Notably, the results of this study indicate that increased suicide risk is relevant across all TBI severity levels, including the far more common mild injuries. Clinicians, health care professionals, and mental health practitioners must take notice of this important information.”
Dr. Goldstein is affiliated with the department of psychiatry at Boston University and reported no conflicts of interest. Dr. Diaz-Arrastia is affiliated with the department of neurology at the University of Pennsylvania, Philadelphia, and also reported no conflicts of interest.
Traumatic brain injury might be associated with an increased risk of suicide, according to results published Aug. 14 in JAMA.
In a retrospective cohort study of 7,418,391 Danish individuals, including 34,529 who died by suicide, patients with medical contact for traumatic brain injury (TBI) had increased suicide risk, compared with the general population (adjusted incidence rate ratio [IRR] = 1.90; 95% confidence interval, 1.83-1.97).
Patients were aged 10 years or older, and follow-up was conducted from Jan. 1, 1980, until date of death, emigration from Denmark, or Dec. 31, 2014, whichever came first. Data were obtained from national registries, including the Danish Civil Registration System, the Database for Integrated Labour Market Research, the National Hospital Register, the Psychiatric Central Research Register, and the Cause of Death Register. Associations between the separate registries were possible because of unique identification numbers assigned to every resident of Denmark, wrote Trine Madsen, PhD, of the Danish Research Institute of Suicide Prevention at the Mental Health Centre Copenhagen, Capital Region of Denmark, and her coauthors.
TBI was recorded in the National Patient Register and was categorized into three types of injury: mild TBI (concussion), skull fracture without documented TBI, and severe TBI (head injury with evidence of structural brain injury). The number of medical contacts for distinct TBI events, accumulated number of days in hospital treatment, age at first TBI, and time since last medical contact for TBI also were assessed.
Data on psychiatric illness and nonfatal self-harm were obtained from the Psychiatric Central Research Register, because of their association with suicide. Data for deaths by suicide were obtained from the Cause of Death Register. Demographic data collected from other registries included sex, age, marital status, cohabitation status, education, and socioeconomic status. IRRs were calculated using adjusted Poisson regression models.
Of 7,418,391 residents of Denmark included in the follow-up period from 1980 to 2014; 567,823 had a TBI diagnosis. Dr. Madsen and her coauthors also found that 423,502 patients (5.7%) were diagnosed with mild TBI, 24,221 (0.3%) with skull fracture, and 120,100 (1.6%) with severe TBI. A total of 34,529 died by suicide.
Of those who died by suicide, 3,536 (10.2%) had a previous TBI diagnosis (2,701 with mild TBI, 174 with skull fracture, and 661 with severe TBI). The absolute rate of suicide in individuals with hospital contact for TBI was 40.6 per 100,000 person-years (95% CI, 39.2-41.9), compared with 19.9 per 100,000 person-years (95% CI, 19.7-20.1) in those with no hospital contact for TBI.
The fully adjusted analysis showed an IRR of 1.90 (95% CI, 1.83-1.97), as well as an increased risk of suicide by TBI severity. The absolute rate for mild TBI was 38.6 per 100,000 person-years (95% CI, 37.1-40.0) with an IRR of 1.81 (95% CI, 1.74-1.88); 42.4 per 100,000 person-years for skull fracture (95% CI, 36.1-48.7) with an IRR of 2.01 (95% CI, 1.73-2.34, P less than .001), and 50.8 per 100,000 person-years for severe TBI (95% CI, 46.9-54.6) with an IRR of 2.38 (95% CI, 2.20-2.58, P less than .001), compared with individuals with no TBI, the authors wrote.
Patients with a first medical contact between 16 and 20 years of age had the highest suicide risk, compared with individuals with no TBI (IRR, 3.01; 95% CI, 2.74-3.30). In addition, individuals who were diagnosed with a psychiatric illness after TBI had a higher risk of suicide than that of those with TBI only (IRR, 4.90; 95% CI, 4.55-5.29; P less than .001), as did those who had engaged in self-harm after TBI (IRR, 7.54; 95% CI, 6.91-8.22; P less than .001). Patients diagnosed with a psychological illness before their TBI had a higher risk of suicide than did those with TBI only (IRR, 2.32; 95% CI, 2.10-2.55; P less than .001), as did those who had engaged self-harm before TBI (IRR, 2.85; 95% CI, 2.53-3.19; P less than .001), the authors noted.
Dr. Madsen and her coauthors cited several limitations. One is that information was not available on which treatment patients with TBIs received. This information “would have been useful to estimate whether different treatment regimens or subsequent follow-up would have reduced the suicide risk,” they wrote.
“Traumatic brain injury is a major public health problem that has many serious consequences, including suicide,” Dr. Madsen and her colleagues wrote. Since falls and traffic accidents account for the largest share of TBIs, helmet use may be a useful protective measure, particularly for injuries related to bicycling and falls that occur at work, the researchers wrote.
“The high prevalence of TBI globally emphasizes the importance for preventing TBI in order to ameliorate its sequelae, such as increased suicide risk,” they concluded.
The study was funded in part by the Mental Health Services Capital Region Denmark and the Lundbeck Foundation. No other disclosures were reported.
SOURCE: Madsen T et al. JAMA. 2018 Aug 14;320(6):580-8.
Traumatic brain injury might be associated with an increased risk of suicide, according to results published Aug. 14 in JAMA.
In a retrospective cohort study of 7,418,391 Danish individuals, including 34,529 who died by suicide, patients with medical contact for traumatic brain injury (TBI) had increased suicide risk, compared with the general population (adjusted incidence rate ratio [IRR] = 1.90; 95% confidence interval, 1.83-1.97).
Patients were aged 10 years or older, and follow-up was conducted from Jan. 1, 1980, until date of death, emigration from Denmark, or Dec. 31, 2014, whichever came first. Data were obtained from national registries, including the Danish Civil Registration System, the Database for Integrated Labour Market Research, the National Hospital Register, the Psychiatric Central Research Register, and the Cause of Death Register. Associations between the separate registries were possible because of unique identification numbers assigned to every resident of Denmark, wrote Trine Madsen, PhD, of the Danish Research Institute of Suicide Prevention at the Mental Health Centre Copenhagen, Capital Region of Denmark, and her coauthors.
TBI was recorded in the National Patient Register and was categorized into three types of injury: mild TBI (concussion), skull fracture without documented TBI, and severe TBI (head injury with evidence of structural brain injury). The number of medical contacts for distinct TBI events, accumulated number of days in hospital treatment, age at first TBI, and time since last medical contact for TBI also were assessed.
Data on psychiatric illness and nonfatal self-harm were obtained from the Psychiatric Central Research Register, because of their association with suicide. Data for deaths by suicide were obtained from the Cause of Death Register. Demographic data collected from other registries included sex, age, marital status, cohabitation status, education, and socioeconomic status. IRRs were calculated using adjusted Poisson regression models.
Of 7,418,391 residents of Denmark included in the follow-up period from 1980 to 2014; 567,823 had a TBI diagnosis. Dr. Madsen and her coauthors also found that 423,502 patients (5.7%) were diagnosed with mild TBI, 24,221 (0.3%) with skull fracture, and 120,100 (1.6%) with severe TBI. A total of 34,529 died by suicide.
Of those who died by suicide, 3,536 (10.2%) had a previous TBI diagnosis (2,701 with mild TBI, 174 with skull fracture, and 661 with severe TBI). The absolute rate of suicide in individuals with hospital contact for TBI was 40.6 per 100,000 person-years (95% CI, 39.2-41.9), compared with 19.9 per 100,000 person-years (95% CI, 19.7-20.1) in those with no hospital contact for TBI.
The fully adjusted analysis showed an IRR of 1.90 (95% CI, 1.83-1.97), as well as an increased risk of suicide by TBI severity. The absolute rate for mild TBI was 38.6 per 100,000 person-years (95% CI, 37.1-40.0) with an IRR of 1.81 (95% CI, 1.74-1.88); 42.4 per 100,000 person-years for skull fracture (95% CI, 36.1-48.7) with an IRR of 2.01 (95% CI, 1.73-2.34, P less than .001), and 50.8 per 100,000 person-years for severe TBI (95% CI, 46.9-54.6) with an IRR of 2.38 (95% CI, 2.20-2.58, P less than .001), compared with individuals with no TBI, the authors wrote.
Patients with a first medical contact between 16 and 20 years of age had the highest suicide risk, compared with individuals with no TBI (IRR, 3.01; 95% CI, 2.74-3.30). In addition, individuals who were diagnosed with a psychiatric illness after TBI had a higher risk of suicide than that of those with TBI only (IRR, 4.90; 95% CI, 4.55-5.29; P less than .001), as did those who had engaged in self-harm after TBI (IRR, 7.54; 95% CI, 6.91-8.22; P less than .001). Patients diagnosed with a psychological illness before their TBI had a higher risk of suicide than did those with TBI only (IRR, 2.32; 95% CI, 2.10-2.55; P less than .001), as did those who had engaged self-harm before TBI (IRR, 2.85; 95% CI, 2.53-3.19; P less than .001), the authors noted.
Dr. Madsen and her coauthors cited several limitations. One is that information was not available on which treatment patients with TBIs received. This information “would have been useful to estimate whether different treatment regimens or subsequent follow-up would have reduced the suicide risk,” they wrote.
“Traumatic brain injury is a major public health problem that has many serious consequences, including suicide,” Dr. Madsen and her colleagues wrote. Since falls and traffic accidents account for the largest share of TBIs, helmet use may be a useful protective measure, particularly for injuries related to bicycling and falls that occur at work, the researchers wrote.
“The high prevalence of TBI globally emphasizes the importance for preventing TBI in order to ameliorate its sequelae, such as increased suicide risk,” they concluded.
The study was funded in part by the Mental Health Services Capital Region Denmark and the Lundbeck Foundation. No other disclosures were reported.
SOURCE: Madsen T et al. JAMA. 2018 Aug 14;320(6):580-8.
FROM JAMA
Key clinical point: Helmet use might be a useful protective measure against TBI, particularly for injuries related to bicycling and falls that occur at work.
Major finding: Patients with medical contact for TBI had increased suicide risk, compared with the general population (adjusted incidence rate ratio =1.90; 95% confidence interval, 1.83-1.97).
Study details: A retrospective cohort study of 7,418,391 Danish individuals, including 34,529 who died by suicide between 1980 and 2014.
Disclosures: The study was funded in part by the Mental Health Services Capital Region Denmark and the Lundbeck Foundation. No other disclosures were reported.
Source: Madsen T et al. JAMA. 2018 Aug 14;320:(6):580-8.
Long-acting beta2 agonists don’t impact cardiovascular risk factors
Neither heart rate nor blood pressure worsened under long-term use of , according to a post hoc pooled analysis published in Pulmonary Pharmacology & Therapeutics.
The study was conducted by Stefan Andreas, MD, department of cardiology and pneumology, University Medical Centre Göttingen, and Lung Clinic Immenhausen, Germany. The analysis evaluated data from four studies and included a total of 3,104 patients with moderate to very severe COPD, which was defined as Global Initiative for Chronic Obstructive Lung Disease stage 2-4. Patients were randomized to either once-daily olodaterol (5 or 10 mcg), twice-daily formoterol (12 mcg), or placebo. Heart rate and blood pressure were measured before and after dosing at baseline and at four time points during the study: 6 weeks, 12 weeks, 24 weeks, and 48 weeks.
At all time points, the increases seen in the placebo group were greater than seen in the treatment groups; both systolic and diastolic blood pressure showed either slight decreases from or similarities with those seen at baseline, depending on time point. Furthermore, short-term effects were seen around dosing, from before administration to after, although these changes were quantitatively small.
One limitation of the study is that it couldn’t include patients with unstable COPD because of safety reasons; this prevents the findings from being more broadly generalizable.
“These findings, in a large COPD database, speak against the potential negative cardiovascular effects of olodaterol, as well as those of formoterol,” the researchers concluded.
They reported personal fees from various industry entities, such as Novartis, AstraZeneca, and GlaxoSmithKline. Some also reported receiving personal fees from or working for Boehringer Ingelheim, which funded the work.
SOURCE: Andreas S et al. Pulm Pharmacol Ther. 2018 Aug 2. doi: 10.1016/j.pupt.2018.08.002.
Neither heart rate nor blood pressure worsened under long-term use of , according to a post hoc pooled analysis published in Pulmonary Pharmacology & Therapeutics.
The study was conducted by Stefan Andreas, MD, department of cardiology and pneumology, University Medical Centre Göttingen, and Lung Clinic Immenhausen, Germany. The analysis evaluated data from four studies and included a total of 3,104 patients with moderate to very severe COPD, which was defined as Global Initiative for Chronic Obstructive Lung Disease stage 2-4. Patients were randomized to either once-daily olodaterol (5 or 10 mcg), twice-daily formoterol (12 mcg), or placebo. Heart rate and blood pressure were measured before and after dosing at baseline and at four time points during the study: 6 weeks, 12 weeks, 24 weeks, and 48 weeks.
At all time points, the increases seen in the placebo group were greater than seen in the treatment groups; both systolic and diastolic blood pressure showed either slight decreases from or similarities with those seen at baseline, depending on time point. Furthermore, short-term effects were seen around dosing, from before administration to after, although these changes were quantitatively small.
One limitation of the study is that it couldn’t include patients with unstable COPD because of safety reasons; this prevents the findings from being more broadly generalizable.
“These findings, in a large COPD database, speak against the potential negative cardiovascular effects of olodaterol, as well as those of formoterol,” the researchers concluded.
They reported personal fees from various industry entities, such as Novartis, AstraZeneca, and GlaxoSmithKline. Some also reported receiving personal fees from or working for Boehringer Ingelheim, which funded the work.
SOURCE: Andreas S et al. Pulm Pharmacol Ther. 2018 Aug 2. doi: 10.1016/j.pupt.2018.08.002.
Neither heart rate nor blood pressure worsened under long-term use of , according to a post hoc pooled analysis published in Pulmonary Pharmacology & Therapeutics.
The study was conducted by Stefan Andreas, MD, department of cardiology and pneumology, University Medical Centre Göttingen, and Lung Clinic Immenhausen, Germany. The analysis evaluated data from four studies and included a total of 3,104 patients with moderate to very severe COPD, which was defined as Global Initiative for Chronic Obstructive Lung Disease stage 2-4. Patients were randomized to either once-daily olodaterol (5 or 10 mcg), twice-daily formoterol (12 mcg), or placebo. Heart rate and blood pressure were measured before and after dosing at baseline and at four time points during the study: 6 weeks, 12 weeks, 24 weeks, and 48 weeks.
At all time points, the increases seen in the placebo group were greater than seen in the treatment groups; both systolic and diastolic blood pressure showed either slight decreases from or similarities with those seen at baseline, depending on time point. Furthermore, short-term effects were seen around dosing, from before administration to after, although these changes were quantitatively small.
One limitation of the study is that it couldn’t include patients with unstable COPD because of safety reasons; this prevents the findings from being more broadly generalizable.
“These findings, in a large COPD database, speak against the potential negative cardiovascular effects of olodaterol, as well as those of formoterol,” the researchers concluded.
They reported personal fees from various industry entities, such as Novartis, AstraZeneca, and GlaxoSmithKline. Some also reported receiving personal fees from or working for Boehringer Ingelheim, which funded the work.
SOURCE: Andreas S et al. Pulm Pharmacol Ther. 2018 Aug 2. doi: 10.1016/j.pupt.2018.08.002.
FROM PULMONARY PHARMACOLOGY & THERAPEUTICS
Key clinical point: Olodaterol and formoterol had a minimal impact on cardiovascular factors.
Major finding: Patients who were randomized to once-daily olodaterol (5 or 10 mcg), twice-daily formoterol (12 mcg), or placebo showed little change in heart rate and blood pressure at 6, 12, 24, or 48 weeks.
Study details: Post hoc pooled analysis from four studies comprising a total of 3,104 patients with moderate to very severe COPD.
Disclosures: Investigators reported personal fees from various industry entities, such as Novartis, AstraZeneca, and GlaxoSmithKline. Some also reported receiving personal fees from or working for Boehringer Ingelheim.
Source: Andreas S et al. Pulm Pharmacol Ther. 2018 Aug 2. doi: 10.1016/j.pupt.2018.08.002.
Plasma GAG provides prognostic info for RCC
Plasma glycosaminoglycan (GAG) measurements can accurately distinguish metastatic clear-cell renal cell carcinoma (ccRCC) from healthy samples, and can provide accurate diagnostic and prognostic information that may be of value in managing the disease, according to new findings.
A new GAG score had 93.5% sensitivity and 94.7% specificity (discovery set) for differentiating RCC from healthy samples, and the sensitivity estimate was independently validated. The score remained independent and uncorrelated to tumor stage, grade, size, and histology, or confounders such as age or gender, according to investigators. The report is in European Oncology Urology.
The authors note that in both retrospective and prospective studies of metastatic ccRCC cases, the composition and levels of plasma and urine GAGs are significantly different when compared with healthy specimens, and GAG scores have correlated with patient outcomes including progression free and overall survival in some cohorts. But it remains unclear if the alterations in plasma and urine GAGs are limited to just metastatic cases of ccRCC or if they correlate with other histopathologic characteristics in RCC. It is also unclear if the correlation between GAG scores and prognosis is limited to patients who receive systemic therapy or if it is applicable to those who are surgically treated RCC as well.
“These results expand our knowledge on the diagnostic and prognostic potential of plasma GAGs in RCC, which was so far limited to metastatic ccRCC in our previous studies,” wrote Francesco Gatto, MD, of Chalmers University of Technology, Göteborg, Sweden, and his colleagues. “Plasma GAG alterations appear to originate as a response to the tumor and occur early if not concomitantly with tumor formation, and probably independent of its progression.”
To investigate the sensitivity and specificity of plasma GAGs for detection of early-stage RCC as well as its utility in predicting recurrence and death after RCC surgery, Dr. Gatto and his team conducted a retrospective case-control study that included 175 RCC patients who underwent surgery between May 2011 and February 2014 and 19 healthy controls.
Plasma GAGs were measured in both preoperative and postoperative RCC cases and the control group, and a discovery set was analyzed to update the historical GAG score. The sensitivity of the new GAG score that was developed for detecting RCC versus controls was then validated using the remaining samples.
In the first discovery set, which included 67 participants, the new GAG score distinguished RCC from controls with an area under the receiver operating characteristic curve (AUC) of 0.999. In their validation cohort (n = 108), the new GAG score achieved an AUC of 0.991 (95% CI 0.977-1) and at the prespecified cutoff, the validated sensitivity was 93.5%. Specificity could not be validated because the same control group was used in both sets.
Factors including tumor size, grade, and stage, radical nephrectomy, and positive surgical margins were significantly associated with overall survival as were three of five GAG properties in the new scoring system, although the new GAG score did not reach significance by itself (hazard ratio, 1.25; P = 0.08). When looking at whether the new GAG score changed after surgery, the authors found that it was quite variable across patients, and an increased score was observed for 53% of cases and a decrease for 47% after surgery. This change did not appear correlated with outcomes as shown by the recurrence rate within 2 years of surgery.
SOURCE: Gatto F et al. Eur Urol Oncol. 2018 Jun 13. doi: 10.1016/j.euo.2018.04.015.
Plasma glycosaminoglycan (GAG) measurements can accurately distinguish metastatic clear-cell renal cell carcinoma (ccRCC) from healthy samples, and can provide accurate diagnostic and prognostic information that may be of value in managing the disease, according to new findings.
A new GAG score had 93.5% sensitivity and 94.7% specificity (discovery set) for differentiating RCC from healthy samples, and the sensitivity estimate was independently validated. The score remained independent and uncorrelated to tumor stage, grade, size, and histology, or confounders such as age or gender, according to investigators. The report is in European Oncology Urology.
The authors note that in both retrospective and prospective studies of metastatic ccRCC cases, the composition and levels of plasma and urine GAGs are significantly different when compared with healthy specimens, and GAG scores have correlated with patient outcomes including progression free and overall survival in some cohorts. But it remains unclear if the alterations in plasma and urine GAGs are limited to just metastatic cases of ccRCC or if they correlate with other histopathologic characteristics in RCC. It is also unclear if the correlation between GAG scores and prognosis is limited to patients who receive systemic therapy or if it is applicable to those who are surgically treated RCC as well.
“These results expand our knowledge on the diagnostic and prognostic potential of plasma GAGs in RCC, which was so far limited to metastatic ccRCC in our previous studies,” wrote Francesco Gatto, MD, of Chalmers University of Technology, Göteborg, Sweden, and his colleagues. “Plasma GAG alterations appear to originate as a response to the tumor and occur early if not concomitantly with tumor formation, and probably independent of its progression.”
To investigate the sensitivity and specificity of plasma GAGs for detection of early-stage RCC as well as its utility in predicting recurrence and death after RCC surgery, Dr. Gatto and his team conducted a retrospective case-control study that included 175 RCC patients who underwent surgery between May 2011 and February 2014 and 19 healthy controls.
Plasma GAGs were measured in both preoperative and postoperative RCC cases and the control group, and a discovery set was analyzed to update the historical GAG score. The sensitivity of the new GAG score that was developed for detecting RCC versus controls was then validated using the remaining samples.
In the first discovery set, which included 67 participants, the new GAG score distinguished RCC from controls with an area under the receiver operating characteristic curve (AUC) of 0.999. In their validation cohort (n = 108), the new GAG score achieved an AUC of 0.991 (95% CI 0.977-1) and at the prespecified cutoff, the validated sensitivity was 93.5%. Specificity could not be validated because the same control group was used in both sets.
Factors including tumor size, grade, and stage, radical nephrectomy, and positive surgical margins were significantly associated with overall survival as were three of five GAG properties in the new scoring system, although the new GAG score did not reach significance by itself (hazard ratio, 1.25; P = 0.08). When looking at whether the new GAG score changed after surgery, the authors found that it was quite variable across patients, and an increased score was observed for 53% of cases and a decrease for 47% after surgery. This change did not appear correlated with outcomes as shown by the recurrence rate within 2 years of surgery.
SOURCE: Gatto F et al. Eur Urol Oncol. 2018 Jun 13. doi: 10.1016/j.euo.2018.04.015.
Plasma glycosaminoglycan (GAG) measurements can accurately distinguish metastatic clear-cell renal cell carcinoma (ccRCC) from healthy samples, and can provide accurate diagnostic and prognostic information that may be of value in managing the disease, according to new findings.
A new GAG score had 93.5% sensitivity and 94.7% specificity (discovery set) for differentiating RCC from healthy samples, and the sensitivity estimate was independently validated. The score remained independent and uncorrelated to tumor stage, grade, size, and histology, or confounders such as age or gender, according to investigators. The report is in European Oncology Urology.
The authors note that in both retrospective and prospective studies of metastatic ccRCC cases, the composition and levels of plasma and urine GAGs are significantly different when compared with healthy specimens, and GAG scores have correlated with patient outcomes including progression free and overall survival in some cohorts. But it remains unclear if the alterations in plasma and urine GAGs are limited to just metastatic cases of ccRCC or if they correlate with other histopathologic characteristics in RCC. It is also unclear if the correlation between GAG scores and prognosis is limited to patients who receive systemic therapy or if it is applicable to those who are surgically treated RCC as well.
“These results expand our knowledge on the diagnostic and prognostic potential of plasma GAGs in RCC, which was so far limited to metastatic ccRCC in our previous studies,” wrote Francesco Gatto, MD, of Chalmers University of Technology, Göteborg, Sweden, and his colleagues. “Plasma GAG alterations appear to originate as a response to the tumor and occur early if not concomitantly with tumor formation, and probably independent of its progression.”
To investigate the sensitivity and specificity of plasma GAGs for detection of early-stage RCC as well as its utility in predicting recurrence and death after RCC surgery, Dr. Gatto and his team conducted a retrospective case-control study that included 175 RCC patients who underwent surgery between May 2011 and February 2014 and 19 healthy controls.
Plasma GAGs were measured in both preoperative and postoperative RCC cases and the control group, and a discovery set was analyzed to update the historical GAG score. The sensitivity of the new GAG score that was developed for detecting RCC versus controls was then validated using the remaining samples.
In the first discovery set, which included 67 participants, the new GAG score distinguished RCC from controls with an area under the receiver operating characteristic curve (AUC) of 0.999. In their validation cohort (n = 108), the new GAG score achieved an AUC of 0.991 (95% CI 0.977-1) and at the prespecified cutoff, the validated sensitivity was 93.5%. Specificity could not be validated because the same control group was used in both sets.
Factors including tumor size, grade, and stage, radical nephrectomy, and positive surgical margins were significantly associated with overall survival as were three of five GAG properties in the new scoring system, although the new GAG score did not reach significance by itself (hazard ratio, 1.25; P = 0.08). When looking at whether the new GAG score changed after surgery, the authors found that it was quite variable across patients, and an increased score was observed for 53% of cases and a decrease for 47% after surgery. This change did not appear correlated with outcomes as shown by the recurrence rate within 2 years of surgery.
SOURCE: Gatto F et al. Eur Urol Oncol. 2018 Jun 13. doi: 10.1016/j.euo.2018.04.015.
FROM EUROPEAN ONCOLOGY UROLOGY
Key clinical point: GAG measurements can provide accurate diagnostic and prognostic information for surgically treated renal cell carcinoma.
Major finding: A new GAG score had 93.5% sensitivity and 94.7% specificity for differentiating RCC from controls.
Study details: Retrospective case-control study that included 175 RCC patients and 19 controls.
Disclosures: The study was funded by the Knut and Alice Wallenberg Foundation to Chalmers University of Technology and MSK Cancer Center Support Grant P30-CA008748 to the Memorial Sloan Kettering Cancer Center. Dr. Francesco Gatto and Dr. Jens Nielsen were listed as coinventors on patent applications related to the biomarkers described in this study and both are shareholders in Elypta AB, which owned the above-mentioned patent applications. There are no other disclosures.
Source: Gatto F et al. Eur Urol Oncol. 2018 Jun 13. doi: 10.1016/j.euo.2018.04.015.
AGA Clinical Practice Update: Tumor seeding with endoscopic procedures
Certain endoscopic procedures carry the risk of tumor seeding. In prior studies, these rates were 0.005% to 0.009% for patients undergoing percutaneous abdominal biopsy, 1.6% for percutaneous radiofrequency ablation of hepatocellular carcinoma, and 2.7% for needle biopsy of hepatocellular carcinoma. When placing percutaneous endoscopic gastrostomy tubes, the “pull-through” technique is most common but “should be avoided in all patients with oropharyngeal or esophageal cancer,” the clinical practice update states. The authors cite multiple studies linking the pull-through technique to metastasis.
Clinicians also should avoid fine needle aspiration (FNA) of primary hilar cholangiocarcinomas, especially in patients who are surgical or transplant candidates, wrote Ferga C. Gleeson, MB, BCh, and her associates, MD Anderson Cancer Center, Houston. The report is in the September issue of Clinical Gastroenterology and Hepatology (doi: 10.1016/j.cgh.2018.05.014).
For patients with suspected pancreatic cancer, the clinical practice update recommends endoscopic ultrasound (EUS)–guided FNA “in any site within the gland when a confirmatory diagnosis of cancer would alter patient management.” The authors also emphasize promptly closing iatrogenic perforations during endoscopic mucosal resection and endoscopic submucosal dissection and practicing nonexposure techniques during endoscopic resection of subepithelial lesions.
For patients with cholangiocarcinoma, primary tumor FNA is controversial because it can be the sole means of cancer diagnosis but also significantly increases the risk of peritoneal metastasis, especially in the setting of larger tumor size, thicker needles, multiple passes, high-grade tumors, and scanty normal tissue along the needle tract, the experts note. Because FNA “may render a patient with cholangiocarcinoma ineligible for entry into a liver transplantation protocol,” it is “best to avoid” or at least discuss with a transplant hepatologist, they add.
However, EUS is appropriate when evaluating suspicious lymphadenopathy in liver transplantation candidates with cholangiocarcinoma, they note. This is because imaging techniques have inadequate sensitivity and a positive EUS result would preclude unnecessary neoadjuvant chemoradiation and staging laparotomy. If FNA is negative, patients do require staging laparotomy to verify the absence of nodal disease before transplantation, according to the clinical practice update.
Endoscopic mucosal and submucosal resection are valuable treatment options for esophageal, gastric, and colonic dysplasia and early carcinoma, but they also can lead to unintended gastrointestinal perforation. In past studies, rates of iatrogenic perforation were 1% when patients underwent endoscopic mucosal resection and 5% when they underwent submucosal resection. For patients with any stage of gastric cancer, an accidental perforation can seed the peritoneum with cancer cells from the contents of the stomach. Contact with a primary tumor also can cause shedding of tumor cells that can enter the peritoneal cavity through a perforation. Although most of these cases do not have clinically significant outcomes, perforations need to be promptly closed and should be avoided, if at all possible, during endoscopic full-thickness resections, the experts wrote.
They recommend using nonexposure techniques while resecting subepithelial tumors and call for more safety studies of endoscopic submucosal dissection of malignancies and endoscopic full-thickness resection of subepithelial lesions. “These studies should focus on individual reports or case series of peritoneal or mediastinal examination during surgery following failed resection of these lesions,” the authors concluded.
Dr. Gleeson and her associates disclosed no funding sources and reported having no conflicts of interest.
SOURCE: Gleeson FC et al. Clin Gastroenterol Hepatol. 2018 May 17. doi: 10.1016/j.cgh.2018.05.014.
Certain endoscopic procedures carry the risk of tumor seeding. In prior studies, these rates were 0.005% to 0.009% for patients undergoing percutaneous abdominal biopsy, 1.6% for percutaneous radiofrequency ablation of hepatocellular carcinoma, and 2.7% for needle biopsy of hepatocellular carcinoma. When placing percutaneous endoscopic gastrostomy tubes, the “pull-through” technique is most common but “should be avoided in all patients with oropharyngeal or esophageal cancer,” the clinical practice update states. The authors cite multiple studies linking the pull-through technique to metastasis.
Clinicians also should avoid fine needle aspiration (FNA) of primary hilar cholangiocarcinomas, especially in patients who are surgical or transplant candidates, wrote Ferga C. Gleeson, MB, BCh, and her associates, MD Anderson Cancer Center, Houston. The report is in the September issue of Clinical Gastroenterology and Hepatology (doi: 10.1016/j.cgh.2018.05.014).
For patients with suspected pancreatic cancer, the clinical practice update recommends endoscopic ultrasound (EUS)–guided FNA “in any site within the gland when a confirmatory diagnosis of cancer would alter patient management.” The authors also emphasize promptly closing iatrogenic perforations during endoscopic mucosal resection and endoscopic submucosal dissection and practicing nonexposure techniques during endoscopic resection of subepithelial lesions.
For patients with cholangiocarcinoma, primary tumor FNA is controversial because it can be the sole means of cancer diagnosis but also significantly increases the risk of peritoneal metastasis, especially in the setting of larger tumor size, thicker needles, multiple passes, high-grade tumors, and scanty normal tissue along the needle tract, the experts note. Because FNA “may render a patient with cholangiocarcinoma ineligible for entry into a liver transplantation protocol,” it is “best to avoid” or at least discuss with a transplant hepatologist, they add.
However, EUS is appropriate when evaluating suspicious lymphadenopathy in liver transplantation candidates with cholangiocarcinoma, they note. This is because imaging techniques have inadequate sensitivity and a positive EUS result would preclude unnecessary neoadjuvant chemoradiation and staging laparotomy. If FNA is negative, patients do require staging laparotomy to verify the absence of nodal disease before transplantation, according to the clinical practice update.
Endoscopic mucosal and submucosal resection are valuable treatment options for esophageal, gastric, and colonic dysplasia and early carcinoma, but they also can lead to unintended gastrointestinal perforation. In past studies, rates of iatrogenic perforation were 1% when patients underwent endoscopic mucosal resection and 5% when they underwent submucosal resection. For patients with any stage of gastric cancer, an accidental perforation can seed the peritoneum with cancer cells from the contents of the stomach. Contact with a primary tumor also can cause shedding of tumor cells that can enter the peritoneal cavity through a perforation. Although most of these cases do not have clinically significant outcomes, perforations need to be promptly closed and should be avoided, if at all possible, during endoscopic full-thickness resections, the experts wrote.
They recommend using nonexposure techniques while resecting subepithelial tumors and call for more safety studies of endoscopic submucosal dissection of malignancies and endoscopic full-thickness resection of subepithelial lesions. “These studies should focus on individual reports or case series of peritoneal or mediastinal examination during surgery following failed resection of these lesions,” the authors concluded.
Dr. Gleeson and her associates disclosed no funding sources and reported having no conflicts of interest.
SOURCE: Gleeson FC et al. Clin Gastroenterol Hepatol. 2018 May 17. doi: 10.1016/j.cgh.2018.05.014.
Certain endoscopic procedures carry the risk of tumor seeding. In prior studies, these rates were 0.005% to 0.009% for patients undergoing percutaneous abdominal biopsy, 1.6% for percutaneous radiofrequency ablation of hepatocellular carcinoma, and 2.7% for needle biopsy of hepatocellular carcinoma. When placing percutaneous endoscopic gastrostomy tubes, the “pull-through” technique is most common but “should be avoided in all patients with oropharyngeal or esophageal cancer,” the clinical practice update states. The authors cite multiple studies linking the pull-through technique to metastasis.
Clinicians also should avoid fine needle aspiration (FNA) of primary hilar cholangiocarcinomas, especially in patients who are surgical or transplant candidates, wrote Ferga C. Gleeson, MB, BCh, and her associates, MD Anderson Cancer Center, Houston. The report is in the September issue of Clinical Gastroenterology and Hepatology (doi: 10.1016/j.cgh.2018.05.014).
For patients with suspected pancreatic cancer, the clinical practice update recommends endoscopic ultrasound (EUS)–guided FNA “in any site within the gland when a confirmatory diagnosis of cancer would alter patient management.” The authors also emphasize promptly closing iatrogenic perforations during endoscopic mucosal resection and endoscopic submucosal dissection and practicing nonexposure techniques during endoscopic resection of subepithelial lesions.
For patients with cholangiocarcinoma, primary tumor FNA is controversial because it can be the sole means of cancer diagnosis but also significantly increases the risk of peritoneal metastasis, especially in the setting of larger tumor size, thicker needles, multiple passes, high-grade tumors, and scanty normal tissue along the needle tract, the experts note. Because FNA “may render a patient with cholangiocarcinoma ineligible for entry into a liver transplantation protocol,” it is “best to avoid” or at least discuss with a transplant hepatologist, they add.
However, EUS is appropriate when evaluating suspicious lymphadenopathy in liver transplantation candidates with cholangiocarcinoma, they note. This is because imaging techniques have inadequate sensitivity and a positive EUS result would preclude unnecessary neoadjuvant chemoradiation and staging laparotomy. If FNA is negative, patients do require staging laparotomy to verify the absence of nodal disease before transplantation, according to the clinical practice update.
Endoscopic mucosal and submucosal resection are valuable treatment options for esophageal, gastric, and colonic dysplasia and early carcinoma, but they also can lead to unintended gastrointestinal perforation. In past studies, rates of iatrogenic perforation were 1% when patients underwent endoscopic mucosal resection and 5% when they underwent submucosal resection. For patients with any stage of gastric cancer, an accidental perforation can seed the peritoneum with cancer cells from the contents of the stomach. Contact with a primary tumor also can cause shedding of tumor cells that can enter the peritoneal cavity through a perforation. Although most of these cases do not have clinically significant outcomes, perforations need to be promptly closed and should be avoided, if at all possible, during endoscopic full-thickness resections, the experts wrote.
They recommend using nonexposure techniques while resecting subepithelial tumors and call for more safety studies of endoscopic submucosal dissection of malignancies and endoscopic full-thickness resection of subepithelial lesions. “These studies should focus on individual reports or case series of peritoneal or mediastinal examination during surgery following failed resection of these lesions,” the authors concluded.
Dr. Gleeson and her associates disclosed no funding sources and reported having no conflicts of interest.
SOURCE: Gleeson FC et al. Clin Gastroenterol Hepatol. 2018 May 17. doi: 10.1016/j.cgh.2018.05.014.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
CT features associated with (some) ccRCC subtypes
In patients with clear cell renal cell carcinoma (ccRCC), radiogenomic analysis can reveal associations between specific features on CT imaging and messenger RNA-based tumor subtyping, authors of a preliminary analysis contend.
Among 177 patients with ccRCC for whom CT data and molecular subtyping information were available, well-defined vs. poorly-defined tumor margins were significantly associated with messenger RNA (mRNA) subtype m1 tumors, and a combination of margin definition and other qualitative tumor features was significantly associated with m3 subtype, reported Lan Bowen, MD, and Li Xiaojing, MD, from Huizhou (China) Central People’s Hospital.
“We demonstrated m1-subtype is positively associated with well-defined margin while m3-subtype is positively associated with ill-defined margin, renal vein invasion, and collecting-system invasion. These findings should be further investigated and validated in other cohorts,” they wrote. The report was published in Academic Radiology.
Radiogenomic analysis is a method for identifying associations between imaging features and gene expression profiles to provide information that can be used for clinical decision making.
The investigators used the technique to retrospectively explore associations between ccRCC mRNA-based subtyping and CT features.
They identified data on a total of 177 patients with ccRCC from The Cancer Genome Atlas for whom complete CT imaging, including contrast-enhanced images, and mRNA-based subtyping were available.
CT features studied included calcifications, margin definition, renal vein invasion, collecting-system invasion, multicystic tumors, nodular tumor enhancement, and intratumoral vasculature.
In univariate logistic regression analysis, well-defined tumor margins (vs. poorly-defined margins) were significant associated with m1 subtype (odd ratio [OR] 2.104, P = .041).
Similarly, a combination of well-defined tumor margins (OR 2.104, P = .013), no collecting system invasion (OR 0.421, P = .028), and renal vein invasion (OR 2.164, P = .026) were significantly associated with the m3 subtype.
They were no significant associations between CT imaging features and either the m2 or m4 subtypes, the authors found.
The authors did not report study funding sources or potential conflicts of interest.
SOURCE: Bowen L, Xiaojing L. Acad Radiol. doi: 10.1016/j.acra.2018.05.002.
In patients with clear cell renal cell carcinoma (ccRCC), radiogenomic analysis can reveal associations between specific features on CT imaging and messenger RNA-based tumor subtyping, authors of a preliminary analysis contend.
Among 177 patients with ccRCC for whom CT data and molecular subtyping information were available, well-defined vs. poorly-defined tumor margins were significantly associated with messenger RNA (mRNA) subtype m1 tumors, and a combination of margin definition and other qualitative tumor features was significantly associated with m3 subtype, reported Lan Bowen, MD, and Li Xiaojing, MD, from Huizhou (China) Central People’s Hospital.
“We demonstrated m1-subtype is positively associated with well-defined margin while m3-subtype is positively associated with ill-defined margin, renal vein invasion, and collecting-system invasion. These findings should be further investigated and validated in other cohorts,” they wrote. The report was published in Academic Radiology.
Radiogenomic analysis is a method for identifying associations between imaging features and gene expression profiles to provide information that can be used for clinical decision making.
The investigators used the technique to retrospectively explore associations between ccRCC mRNA-based subtyping and CT features.
They identified data on a total of 177 patients with ccRCC from The Cancer Genome Atlas for whom complete CT imaging, including contrast-enhanced images, and mRNA-based subtyping were available.
CT features studied included calcifications, margin definition, renal vein invasion, collecting-system invasion, multicystic tumors, nodular tumor enhancement, and intratumoral vasculature.
In univariate logistic regression analysis, well-defined tumor margins (vs. poorly-defined margins) were significant associated with m1 subtype (odd ratio [OR] 2.104, P = .041).
Similarly, a combination of well-defined tumor margins (OR 2.104, P = .013), no collecting system invasion (OR 0.421, P = .028), and renal vein invasion (OR 2.164, P = .026) were significantly associated with the m3 subtype.
They were no significant associations between CT imaging features and either the m2 or m4 subtypes, the authors found.
The authors did not report study funding sources or potential conflicts of interest.
SOURCE: Bowen L, Xiaojing L. Acad Radiol. doi: 10.1016/j.acra.2018.05.002.
In patients with clear cell renal cell carcinoma (ccRCC), radiogenomic analysis can reveal associations between specific features on CT imaging and messenger RNA-based tumor subtyping, authors of a preliminary analysis contend.
Among 177 patients with ccRCC for whom CT data and molecular subtyping information were available, well-defined vs. poorly-defined tumor margins were significantly associated with messenger RNA (mRNA) subtype m1 tumors, and a combination of margin definition and other qualitative tumor features was significantly associated with m3 subtype, reported Lan Bowen, MD, and Li Xiaojing, MD, from Huizhou (China) Central People’s Hospital.
“We demonstrated m1-subtype is positively associated with well-defined margin while m3-subtype is positively associated with ill-defined margin, renal vein invasion, and collecting-system invasion. These findings should be further investigated and validated in other cohorts,” they wrote. The report was published in Academic Radiology.
Radiogenomic analysis is a method for identifying associations between imaging features and gene expression profiles to provide information that can be used for clinical decision making.
The investigators used the technique to retrospectively explore associations between ccRCC mRNA-based subtyping and CT features.
They identified data on a total of 177 patients with ccRCC from The Cancer Genome Atlas for whom complete CT imaging, including contrast-enhanced images, and mRNA-based subtyping were available.
CT features studied included calcifications, margin definition, renal vein invasion, collecting-system invasion, multicystic tumors, nodular tumor enhancement, and intratumoral vasculature.
In univariate logistic regression analysis, well-defined tumor margins (vs. poorly-defined margins) were significant associated with m1 subtype (odd ratio [OR] 2.104, P = .041).
Similarly, a combination of well-defined tumor margins (OR 2.104, P = .013), no collecting system invasion (OR 0.421, P = .028), and renal vein invasion (OR 2.164, P = .026) were significantly associated with the m3 subtype.
They were no significant associations between CT imaging features and either the m2 or m4 subtypes, the authors found.
The authors did not report study funding sources or potential conflicts of interest.
SOURCE: Bowen L, Xiaojing L. Acad Radiol. doi: 10.1016/j.acra.2018.05.002.
FROM ACADEMIC RADIOLOGY
Key clinical point: Radiogenomic analysis may allow detection of clear cell renal cell carcinoma (ccRCC) subtypes.
Major finding: Well-defined tumor margins on CT were significantly associated with the ccRCC m1 subtype.
Study details: Retrospective analysis of the association between CT features and molecular subtype in 177 patients with ccRCC.
Disclosures: The authors did not report study funding sources or potential conflicts of interest.
Source: Bowen L, Xiaojing L. Acad Radiol. 2018 Jul 29. doi: 10.1016/j.acra.2018.05.002.
Fighting fires
When I grow up, I want to be a fireman. Not long ago, I had occasion to revisit why firefighters are such heroes to young and old. In the process, I learned quite a bit about how fires are managed and realized that a really good surgeon has much in common with a fire Incident Commander.

In late June 2018, a man started a fire in Southern Colorado. That small campfire became the Spring Fire, the third-largest forest fire in Colorado history, which is saying a lot. By the time the fire was mostly contained 2 weeks later, 175 square miles of land had been burned and 1,800 firefighters were involved in the disaster. More than 150 homes were destroyed. Not one person died in or as a result of this fire. Only the most grudging of critics would deny that, while the fire itself was a disaster, the response and outcome constituted a good definition of success.
This story was more than just 30 seconds on the nightly news to me because I was one of the people whose property and 32 years of precious family memories were in danger. I clung to any news of the fire. My own daughter had to evacuate our place there when smoke and flame were visible just a few miles away. I was helpless to do anything but hoped that somehow this conflagration could be stopped.
Within 48 hours, Rocky Mountain Black Team – headed by a man named Shane Greer – arrived in the area. Mr. Greer is the Incident Commander of the Black Team. Over the next 10 days he was the personification of the response to the Spring Fire. He was the main person carrying the overall responsibility for controlling the fire.
The fire is over now, but I reflect frequently on the parallels between surgery and firefighting. I identified with Mr. Greer as probably many did. He didn’t actually stop the fire, but he led the people who did. I was intrigued by this role and I did a little research in fire Incident Commanders. Here’s a list of their numerous roles and responsibilities that I gleaned from an article on the website Firehouse by editor Dennis Rubin from several years ago:
- The Incident Commander (IC) must be a qualified, single, central, and well-supported individual.
- The IC’s main concern is safety of lives and must be conversant in fire-safety procedures.
- The IC must have an understanding of his/her personal limitations. An IC must have firsthand experience at firefighting so that the IC is an individual well informed of the difficulties being experienced on the front line of the fire.
- The priorities of the IC are a) life safety; b) incident stabilization; and c) property conservation.
- The IC develops strategies (what to do) and tactics (how to do it) and follows action plans to achieve these goals.
- The IC develops a management structure that uses span of control (one supervisor per five subordinates) with each unit having a single boss.
- A good IC is a good delegator and calls for help early in the incident including placement of resources in staging areas.
- The IC is responsible for all communication among the team and to the media/public.
- The IC coordinates with outside agencies.
Does this sound familiar to you? Substitute surgeon for IC and you have today’s profile of a good surgeon. When executed well, everyone involved in an incident gets to be a hero and feels a part of something bigger than themselves. The IC (surgeon) gets a lot of credit, but that person also makes sure the whole team gets all the credit and thanks they deserve.
What I see happening in some situations is that we in medicine are putting the wrong ICs in charge or abdicating our positions as IC to others because being an IC is a hard, demanding, full-time job. I also see medicine violating the principles in the first bullet point above – a single, central, and well-supported individual. We get the job of IC and then payers, administrators, and outside agencies drop the support part of the ball. We also have a tendency to violate the “qualified” part of the job description. Someone who has put on the gown and gloves and borne the responsibility of operating should be the quarterback and not someone who has only observed that process.
I can’t thank enough the Black Team and all those who fought the Spring Fire. I hope we all aspire to be ICs in our surgical world. There is a great nobility in such professions as firefighting and surgery, where we jump in to help others who can’t help themselves. The Black Team showed that to me and my community in Colorado. It makes one proud of what we human beings can do when we decide to work together.
True leadership and teamwork do not fragment but instead pull resources together. Patients need that. They need to know that a qualified, single, central, and well-supported person is directing their incident. The existence of such a person fulfilling that role is key to keep the trust that the public places in us. May all our “fires” be led by a good surgeon, er, Incident Commander surgeon.

Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and Co-Editor of ACS Surgery News.
When I grow up, I want to be a fireman. Not long ago, I had occasion to revisit why firefighters are such heroes to young and old. In the process, I learned quite a bit about how fires are managed and realized that a really good surgeon has much in common with a fire Incident Commander.
In late June 2018, a man started a fire in Southern Colorado. That small campfire became the Spring Fire, the third-largest forest fire in Colorado history, which is saying a lot. By the time the fire was mostly contained 2 weeks later, 175 square miles of land had been burned and 1,800 firefighters were involved in the disaster. More than 150 homes were destroyed. Not one person died in or as a result of this fire. Only the most grudging of critics would deny that, while the fire itself was a disaster, the response and outcome constituted a good definition of success.
This story was more than just 30 seconds on the nightly news to me because I was one of the people whose property and 32 years of precious family memories were in danger. I clung to any news of the fire. My own daughter had to evacuate our place there when smoke and flame were visible just a few miles away. I was helpless to do anything but hoped that somehow this conflagration could be stopped.
Within 48 hours, Rocky Mountain Black Team – headed by a man named Shane Greer – arrived in the area. Mr. Greer is the Incident Commander of the Black Team. Over the next 10 days he was the personification of the response to the Spring Fire. He was the main person carrying the overall responsibility for controlling the fire.
The fire is over now, but I reflect frequently on the parallels between surgery and firefighting. I identified with Mr. Greer as probably many did. He didn’t actually stop the fire, but he led the people who did. I was intrigued by this role and I did a little research in fire Incident Commanders. Here’s a list of their numerous roles and responsibilities that I gleaned from an article on the website Firehouse by editor Dennis Rubin from several years ago:
- The Incident Commander (IC) must be a qualified, single, central, and well-supported individual.
- The IC’s main concern is safety of lives and must be conversant in fire-safety procedures.
- The IC must have an understanding of his/her personal limitations. An IC must have firsthand experience at firefighting so that the IC is an individual well informed of the difficulties being experienced on the front line of the fire.
- The priorities of the IC are a) life safety; b) incident stabilization; and c) property conservation.
- The IC develops strategies (what to do) and tactics (how to do it) and follows action plans to achieve these goals.
- The IC develops a management structure that uses span of control (one supervisor per five subordinates) with each unit having a single boss.
- A good IC is a good delegator and calls for help early in the incident including placement of resources in staging areas.
- The IC is responsible for all communication among the team and to the media/public.
- The IC coordinates with outside agencies.
Does this sound familiar to you? Substitute surgeon for IC and you have today’s profile of a good surgeon. When executed well, everyone involved in an incident gets to be a hero and feels a part of something bigger than themselves. The IC (surgeon) gets a lot of credit, but that person also makes sure the whole team gets all the credit and thanks they deserve.
What I see happening in some situations is that we in medicine are putting the wrong ICs in charge or abdicating our positions as IC to others because being an IC is a hard, demanding, full-time job. I also see medicine violating the principles in the first bullet point above – a single, central, and well-supported individual. We get the job of IC and then payers, administrators, and outside agencies drop the support part of the ball. We also have a tendency to violate the “qualified” part of the job description. Someone who has put on the gown and gloves and borne the responsibility of operating should be the quarterback and not someone who has only observed that process.
I can’t thank enough the Black Team and all those who fought the Spring Fire. I hope we all aspire to be ICs in our surgical world. There is a great nobility in such professions as firefighting and surgery, where we jump in to help others who can’t help themselves. The Black Team showed that to me and my community in Colorado. It makes one proud of what we human beings can do when we decide to work together.
True leadership and teamwork do not fragment but instead pull resources together. Patients need that. They need to know that a qualified, single, central, and well-supported person is directing their incident. The existence of such a person fulfilling that role is key to keep the trust that the public places in us. May all our “fires” be led by a good surgeon, er, Incident Commander surgeon.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and Co-Editor of ACS Surgery News.
When I grow up, I want to be a fireman. Not long ago, I had occasion to revisit why firefighters are such heroes to young and old. In the process, I learned quite a bit about how fires are managed and realized that a really good surgeon has much in common with a fire Incident Commander.
In late June 2018, a man started a fire in Southern Colorado. That small campfire became the Spring Fire, the third-largest forest fire in Colorado history, which is saying a lot. By the time the fire was mostly contained 2 weeks later, 175 square miles of land had been burned and 1,800 firefighters were involved in the disaster. More than 150 homes were destroyed. Not one person died in or as a result of this fire. Only the most grudging of critics would deny that, while the fire itself was a disaster, the response and outcome constituted a good definition of success.
This story was more than just 30 seconds on the nightly news to me because I was one of the people whose property and 32 years of precious family memories were in danger. I clung to any news of the fire. My own daughter had to evacuate our place there when smoke and flame were visible just a few miles away. I was helpless to do anything but hoped that somehow this conflagration could be stopped.
Within 48 hours, Rocky Mountain Black Team – headed by a man named Shane Greer – arrived in the area. Mr. Greer is the Incident Commander of the Black Team. Over the next 10 days he was the personification of the response to the Spring Fire. He was the main person carrying the overall responsibility for controlling the fire.
The fire is over now, but I reflect frequently on the parallels between surgery and firefighting. I identified with Mr. Greer as probably many did. He didn’t actually stop the fire, but he led the people who did. I was intrigued by this role and I did a little research in fire Incident Commanders. Here’s a list of their numerous roles and responsibilities that I gleaned from an article on the website Firehouse by editor Dennis Rubin from several years ago:
- The Incident Commander (IC) must be a qualified, single, central, and well-supported individual.
- The IC’s main concern is safety of lives and must be conversant in fire-safety procedures.
- The IC must have an understanding of his/her personal limitations. An IC must have firsthand experience at firefighting so that the IC is an individual well informed of the difficulties being experienced on the front line of the fire.
- The priorities of the IC are a) life safety; b) incident stabilization; and c) property conservation.
- The IC develops strategies (what to do) and tactics (how to do it) and follows action plans to achieve these goals.
- The IC develops a management structure that uses span of control (one supervisor per five subordinates) with each unit having a single boss.
- A good IC is a good delegator and calls for help early in the incident including placement of resources in staging areas.
- The IC is responsible for all communication among the team and to the media/public.
- The IC coordinates with outside agencies.
Does this sound familiar to you? Substitute surgeon for IC and you have today’s profile of a good surgeon. When executed well, everyone involved in an incident gets to be a hero and feels a part of something bigger than themselves. The IC (surgeon) gets a lot of credit, but that person also makes sure the whole team gets all the credit and thanks they deserve.
What I see happening in some situations is that we in medicine are putting the wrong ICs in charge or abdicating our positions as IC to others because being an IC is a hard, demanding, full-time job. I also see medicine violating the principles in the first bullet point above – a single, central, and well-supported individual. We get the job of IC and then payers, administrators, and outside agencies drop the support part of the ball. We also have a tendency to violate the “qualified” part of the job description. Someone who has put on the gown and gloves and borne the responsibility of operating should be the quarterback and not someone who has only observed that process.
I can’t thank enough the Black Team and all those who fought the Spring Fire. I hope we all aspire to be ICs in our surgical world. There is a great nobility in such professions as firefighting and surgery, where we jump in to help others who can’t help themselves. The Black Team showed that to me and my community in Colorado. It makes one proud of what we human beings can do when we decide to work together.
True leadership and teamwork do not fragment but instead pull resources together. Patients need that. They need to know that a qualified, single, central, and well-supported person is directing their incident. The existence of such a person fulfilling that role is key to keep the trust that the public places in us. May all our “fires” be led by a good surgeon, er, Incident Commander surgeon.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and Co-Editor of ACS Surgery News.
ANZ, Japan, and German Exchange Travelers for 2018 Announced
The International Relations Committee of the American College of Surgeons (ACS) sponsors three academic surgeon exchange programs to send a talented young U.S. or Canadian Fellow to the annual surgical meeting of each participating country. Afterwards, the Fellows tour several sites tailored to their specific research interests. In exchange, the College accepts fine young academic surgeon-scholars from the participating societies to attend the annual ACS Clinical Congress. This exchange is with the Royal Australasian College of Surgeons with the ACS Australia-New Zealand Chapter, the Japan Surgical Society with the ACS Japan Chapter, and the German Surgical Society with the ACS Germany Chapter.


The 2018 ANZ Exchange Fellow is Yiu Ming Ho, MB, BS, MS, FRACS, a general and colorectal surgeon University of Sydney, Australia. His recent research has been on examining personalized radiation therapy for low-risk early breast cancer. His U.S. counterpart, Mayur B. Patel, MD, MPH, FACS, is associate professor of surgery, Vanderbilt University Medical Center, TN, specializing in neurotrauma and traumatic brain injury. He attended the Annual Scientific Congress of the Royal Australasian College of Surgeons held in Sydney, Australia, in May.

This October, the College will welcome Japan Exchange Fellow Kenichiro Araki, MD, PhD, assistant professor, division of hepatobiliary and pancreatic surgery, Gunma University Graduate School of Medicine, Maebashi, Japan. Dr. Araki performs research on carcinoma of the liver and pancreas and laparoscopic hepato-pancreato-biliary (HPB) surgery. Brian D. Badgwell, MD, FACS, associate professor, MD Anderson Cancer Center, Houston, TX, attended the Japan Surgical Society meeting in Tokyo in April. Dr. Badgwell specializes in gastrointestinal surgery and acute and palliative surgical oncology. Read about Dr. Bagdwell’s experience in the July Bulletin at bit.ly/2z5UNBA

The ACS Traveling Fellow to Germany, Paul J. Karanicolas, MD, PhD, FACS, FRCSC, associate professor, HPB surgical oncology, Sunnybrook Health Sciences Centre, Toronto, ON, attended the German Surgical Society’s annual meeting in Berlin in April. His German counterpart, Carsten Kamphues, MD, PhD, a senior physician, department for general, visceral and vascular Surgery, Charité-University Medicine, Berlin, will attend the ACS Clinical Congress this year in Boston, MA, and visit several surgical sites under the guidance of his U.S. and German mentors. Dr. Kamphues’s work centers on pancreatic and gastric cancer surgery.
The International Relations Committee of the American College of Surgeons (ACS) sponsors three academic surgeon exchange programs to send a talented young U.S. or Canadian Fellow to the annual surgical meeting of each participating country. Afterwards, the Fellows tour several sites tailored to their specific research interests. In exchange, the College accepts fine young academic surgeon-scholars from the participating societies to attend the annual ACS Clinical Congress. This exchange is with the Royal Australasian College of Surgeons with the ACS Australia-New Zealand Chapter, the Japan Surgical Society with the ACS Japan Chapter, and the German Surgical Society with the ACS Germany Chapter.
The 2018 ANZ Exchange Fellow is Yiu Ming Ho, MB, BS, MS, FRACS, a general and colorectal surgeon University of Sydney, Australia. His recent research has been on examining personalized radiation therapy for low-risk early breast cancer. His U.S. counterpart, Mayur B. Patel, MD, MPH, FACS, is associate professor of surgery, Vanderbilt University Medical Center, TN, specializing in neurotrauma and traumatic brain injury. He attended the Annual Scientific Congress of the Royal Australasian College of Surgeons held in Sydney, Australia, in May.
This October, the College will welcome Japan Exchange Fellow Kenichiro Araki, MD, PhD, assistant professor, division of hepatobiliary and pancreatic surgery, Gunma University Graduate School of Medicine, Maebashi, Japan. Dr. Araki performs research on carcinoma of the liver and pancreas and laparoscopic hepato-pancreato-biliary (HPB) surgery. Brian D. Badgwell, MD, FACS, associate professor, MD Anderson Cancer Center, Houston, TX, attended the Japan Surgical Society meeting in Tokyo in April. Dr. Badgwell specializes in gastrointestinal surgery and acute and palliative surgical oncology. Read about Dr. Bagdwell’s experience in the July Bulletin at bit.ly/2z5UNBA
The ACS Traveling Fellow to Germany, Paul J. Karanicolas, MD, PhD, FACS, FRCSC, associate professor, HPB surgical oncology, Sunnybrook Health Sciences Centre, Toronto, ON, attended the German Surgical Society’s annual meeting in Berlin in April. His German counterpart, Carsten Kamphues, MD, PhD, a senior physician, department for general, visceral and vascular Surgery, Charité-University Medicine, Berlin, will attend the ACS Clinical Congress this year in Boston, MA, and visit several surgical sites under the guidance of his U.S. and German mentors. Dr. Kamphues’s work centers on pancreatic and gastric cancer surgery.
The International Relations Committee of the American College of Surgeons (ACS) sponsors three academic surgeon exchange programs to send a talented young U.S. or Canadian Fellow to the annual surgical meeting of each participating country. Afterwards, the Fellows tour several sites tailored to their specific research interests. In exchange, the College accepts fine young academic surgeon-scholars from the participating societies to attend the annual ACS Clinical Congress. This exchange is with the Royal Australasian College of Surgeons with the ACS Australia-New Zealand Chapter, the Japan Surgical Society with the ACS Japan Chapter, and the German Surgical Society with the ACS Germany Chapter.
The 2018 ANZ Exchange Fellow is Yiu Ming Ho, MB, BS, MS, FRACS, a general and colorectal surgeon University of Sydney, Australia. His recent research has been on examining personalized radiation therapy for low-risk early breast cancer. His U.S. counterpart, Mayur B. Patel, MD, MPH, FACS, is associate professor of surgery, Vanderbilt University Medical Center, TN, specializing in neurotrauma and traumatic brain injury. He attended the Annual Scientific Congress of the Royal Australasian College of Surgeons held in Sydney, Australia, in May.
This October, the College will welcome Japan Exchange Fellow Kenichiro Araki, MD, PhD, assistant professor, division of hepatobiliary and pancreatic surgery, Gunma University Graduate School of Medicine, Maebashi, Japan. Dr. Araki performs research on carcinoma of the liver and pancreas and laparoscopic hepato-pancreato-biliary (HPB) surgery. Brian D. Badgwell, MD, FACS, associate professor, MD Anderson Cancer Center, Houston, TX, attended the Japan Surgical Society meeting in Tokyo in April. Dr. Badgwell specializes in gastrointestinal surgery and acute and palliative surgical oncology. Read about Dr. Bagdwell’s experience in the July Bulletin at bit.ly/2z5UNBA
The ACS Traveling Fellow to Germany, Paul J. Karanicolas, MD, PhD, FACS, FRCSC, associate professor, HPB surgical oncology, Sunnybrook Health Sciences Centre, Toronto, ON, attended the German Surgical Society’s annual meeting in Berlin in April. His German counterpart, Carsten Kamphues, MD, PhD, a senior physician, department for general, visceral and vascular Surgery, Charité-University Medicine, Berlin, will attend the ACS Clinical Congress this year in Boston, MA, and visit several surgical sites under the guidance of his U.S. and German mentors. Dr. Kamphues’s work centers on pancreatic and gastric cancer surgery.
CoC Grants Outstanding Achievement Award to 16 Cancer Care Facilitiesteaser
The Commission on Cancer (CoC) of the American College of Surgeons (ACS) has granted its year-end 2017 Outstanding Achievement Award to a select group of 16 accredited cancer programs throughout the U.S. Award criteria were based on qualitative and quantitative surveys of cancer programs conducted in the second half of 2017.
The purpose of the award is to raise the bar on quality cancer care, with the ultimate goal of increasing awareness about quality care choices among cancer patients and their loved ones. In addition, the award is intended to accomplish the following:
• Recognize those cancer programs that achieve excellence in providing quality care to cancer patients
• Motivate other cancer programs to work toward improving their level of care
• Facilitate a dialogue between award recipients and health care professionals at other cancer facilities for the purpose of sharing best practices
• Encourage honorees to serve as quality-care resources to other cancer programs
The 16 award-winning cancer care programs represent approximately 7 percent of programs surveyed by the CoC July 1–December 31, 2017. “These cancer programs currently represent the best of the best when it comes to cancer care,” said Lawrence N. Shulman, MD, FACP, Chair of the CoC. “Each of these facilities is not just meeting nationally recognized standards for the delivery of quality cancer care, they are exceeding them.”
Visit the ACS website for a list of these award-winning cancer programs at facs.org/quality-programs/cancer/coc/info/outstanding/2017-part-2.
The Commission on Cancer (CoC) of the American College of Surgeons (ACS) has granted its year-end 2017 Outstanding Achievement Award to a select group of 16 accredited cancer programs throughout the U.S. Award criteria were based on qualitative and quantitative surveys of cancer programs conducted in the second half of 2017.
The purpose of the award is to raise the bar on quality cancer care, with the ultimate goal of increasing awareness about quality care choices among cancer patients and their loved ones. In addition, the award is intended to accomplish the following:
• Recognize those cancer programs that achieve excellence in providing quality care to cancer patients
• Motivate other cancer programs to work toward improving their level of care
• Facilitate a dialogue between award recipients and health care professionals at other cancer facilities for the purpose of sharing best practices
• Encourage honorees to serve as quality-care resources to other cancer programs
The 16 award-winning cancer care programs represent approximately 7 percent of programs surveyed by the CoC July 1–December 31, 2017. “These cancer programs currently represent the best of the best when it comes to cancer care,” said Lawrence N. Shulman, MD, FACP, Chair of the CoC. “Each of these facilities is not just meeting nationally recognized standards for the delivery of quality cancer care, they are exceeding them.”
Visit the ACS website for a list of these award-winning cancer programs at facs.org/quality-programs/cancer/coc/info/outstanding/2017-part-2.
The Commission on Cancer (CoC) of the American College of Surgeons (ACS) has granted its year-end 2017 Outstanding Achievement Award to a select group of 16 accredited cancer programs throughout the U.S. Award criteria were based on qualitative and quantitative surveys of cancer programs conducted in the second half of 2017.
The purpose of the award is to raise the bar on quality cancer care, with the ultimate goal of increasing awareness about quality care choices among cancer patients and their loved ones. In addition, the award is intended to accomplish the following:
• Recognize those cancer programs that achieve excellence in providing quality care to cancer patients
• Motivate other cancer programs to work toward improving their level of care
• Facilitate a dialogue between award recipients and health care professionals at other cancer facilities for the purpose of sharing best practices
• Encourage honorees to serve as quality-care resources to other cancer programs
The 16 award-winning cancer care programs represent approximately 7 percent of programs surveyed by the CoC July 1–December 31, 2017. “These cancer programs currently represent the best of the best when it comes to cancer care,” said Lawrence N. Shulman, MD, FACP, Chair of the CoC. “Each of these facilities is not just meeting nationally recognized standards for the delivery of quality cancer care, they are exceeding them.”
Visit the ACS website for a list of these award-winning cancer programs at facs.org/quality-programs/cancer/coc/info/outstanding/2017-part-2.