User login
Itraconazole for BCC: Does it work?
CHICAGO – Justin J. Leitenberger, MD, declared at the annual meeting of the American College of Mohs Surgery.

The oral antifungal inhibits the hedgehog signaling pathway, a key driver of BCC. And while itraconazole is not as potent an inhibitor of hedgehog pathway expression as, say vismodegib (Erivedge), the antifungal acts at a separate site on the pathway, making it an attractive candidate for combination therapy, explained Dr. Leitenberger of Oregon Health & Science University, Portland.
Dermatologists at Stanford University have led the way in exploring oral itraconazole as a treatment for BCC. Among a series of 29 patients with one or more large but nonadvanced BCCs, 19 were treated using oral itraconazole at 200 mg b.i.d. for 1 month or 100 mg b.i.d. for an average of 2.3 months. Hedgehog pathway expression was reduced by 65% in the itraconazole-treated patients, as compared with the 90% reduction which is achieved with vismodegib.
Of more direct clinical relevance, however, itraconazole also reduced tumor area by 24%. Four of eight patients with 57 tumors achieved a partial response, and the other four had stable disease (J Clin Oncol. 2014 Mar 10;32[8]:745-51).
The Stanford group has also shown that combination therapy with oral itraconazole and intravenous arsenic trioxide reduces hedgehog pathway expression by 75%, up by an absolute 10% from itraconazole alone. The two agents inhibit the pathway at different sites.
Five patients with metastatic BCC who relapsed after treatment with vismodegib received intravenous arsenic trioxide for the first 5 days of every month, followed by oral itraconazole at 200 mg b.i.d. on days 6-28. Three patients completed three such cycles, while two discontinued early because of progressive disease or adverse events including a grade 3 infection and grade 2 transaminitis. All three patients who completed three treatment cycles achieved stable disease. The Stanford investigators speculated that concurrent continuous dosing might be required to obtain tumor shrinkage (JAMA Dermatol. 2016 Apr;152[4]:452-6).
Lots more work remains to be done in order to optimize combination therapy utilizing oral itraconazole for advanced BCC. Different dosing regimens and combinations of hedgehog pathway inhibitors need to be studied. Another important question is how effective itraconazole-based combinations will be in vismodegib-naive as compared with vismodegib-resistant patients, Dr. Leitenberger observed.
He reported having no financial conflicts regarding his presentation.
CHICAGO – Justin J. Leitenberger, MD, declared at the annual meeting of the American College of Mohs Surgery.
The oral antifungal inhibits the hedgehog signaling pathway, a key driver of BCC. And while itraconazole is not as potent an inhibitor of hedgehog pathway expression as, say vismodegib (Erivedge), the antifungal acts at a separate site on the pathway, making it an attractive candidate for combination therapy, explained Dr. Leitenberger of Oregon Health & Science University, Portland.
Dermatologists at Stanford University have led the way in exploring oral itraconazole as a treatment for BCC. Among a series of 29 patients with one or more large but nonadvanced BCCs, 19 were treated using oral itraconazole at 200 mg b.i.d. for 1 month or 100 mg b.i.d. for an average of 2.3 months. Hedgehog pathway expression was reduced by 65% in the itraconazole-treated patients, as compared with the 90% reduction which is achieved with vismodegib.
Of more direct clinical relevance, however, itraconazole also reduced tumor area by 24%. Four of eight patients with 57 tumors achieved a partial response, and the other four had stable disease (J Clin Oncol. 2014 Mar 10;32[8]:745-51).
The Stanford group has also shown that combination therapy with oral itraconazole and intravenous arsenic trioxide reduces hedgehog pathway expression by 75%, up by an absolute 10% from itraconazole alone. The two agents inhibit the pathway at different sites.
Five patients with metastatic BCC who relapsed after treatment with vismodegib received intravenous arsenic trioxide for the first 5 days of every month, followed by oral itraconazole at 200 mg b.i.d. on days 6-28. Three patients completed three such cycles, while two discontinued early because of progressive disease or adverse events including a grade 3 infection and grade 2 transaminitis. All three patients who completed three treatment cycles achieved stable disease. The Stanford investigators speculated that concurrent continuous dosing might be required to obtain tumor shrinkage (JAMA Dermatol. 2016 Apr;152[4]:452-6).
Lots more work remains to be done in order to optimize combination therapy utilizing oral itraconazole for advanced BCC. Different dosing regimens and combinations of hedgehog pathway inhibitors need to be studied. Another important question is how effective itraconazole-based combinations will be in vismodegib-naive as compared with vismodegib-resistant patients, Dr. Leitenberger observed.
He reported having no financial conflicts regarding his presentation.
CHICAGO – Justin J. Leitenberger, MD, declared at the annual meeting of the American College of Mohs Surgery.
The oral antifungal inhibits the hedgehog signaling pathway, a key driver of BCC. And while itraconazole is not as potent an inhibitor of hedgehog pathway expression as, say vismodegib (Erivedge), the antifungal acts at a separate site on the pathway, making it an attractive candidate for combination therapy, explained Dr. Leitenberger of Oregon Health & Science University, Portland.
Dermatologists at Stanford University have led the way in exploring oral itraconazole as a treatment for BCC. Among a series of 29 patients with one or more large but nonadvanced BCCs, 19 were treated using oral itraconazole at 200 mg b.i.d. for 1 month or 100 mg b.i.d. for an average of 2.3 months. Hedgehog pathway expression was reduced by 65% in the itraconazole-treated patients, as compared with the 90% reduction which is achieved with vismodegib.
Of more direct clinical relevance, however, itraconazole also reduced tumor area by 24%. Four of eight patients with 57 tumors achieved a partial response, and the other four had stable disease (J Clin Oncol. 2014 Mar 10;32[8]:745-51).
The Stanford group has also shown that combination therapy with oral itraconazole and intravenous arsenic trioxide reduces hedgehog pathway expression by 75%, up by an absolute 10% from itraconazole alone. The two agents inhibit the pathway at different sites.
Five patients with metastatic BCC who relapsed after treatment with vismodegib received intravenous arsenic trioxide for the first 5 days of every month, followed by oral itraconazole at 200 mg b.i.d. on days 6-28. Three patients completed three such cycles, while two discontinued early because of progressive disease or adverse events including a grade 3 infection and grade 2 transaminitis. All three patients who completed three treatment cycles achieved stable disease. The Stanford investigators speculated that concurrent continuous dosing might be required to obtain tumor shrinkage (JAMA Dermatol. 2016 Apr;152[4]:452-6).
Lots more work remains to be done in order to optimize combination therapy utilizing oral itraconazole for advanced BCC. Different dosing regimens and combinations of hedgehog pathway inhibitors need to be studied. Another important question is how effective itraconazole-based combinations will be in vismodegib-naive as compared with vismodegib-resistant patients, Dr. Leitenberger observed.
He reported having no financial conflicts regarding his presentation.
EXPERT ANALYSIS FROM THE ACMS ANNUAL MEETING
Speaking the unspeakable: Talking to children about parental mental illness
You probably think you know how to talk with a child about death. But somehow talking about a parent’s mental illness may seem more difficult. Even medical professionals, as most people, can find themselves feeling more judgmental or uneasy talking about mental illness than about physical problems. But with a prevalence of about one in four people having mental disorders, we need to be prepared for this discussion.

Sometimes family members, or even parents themselves, have asked me to tell a child about a parent’s mental illness or substance use. They know the child is confused and scared but don’t know what to say about this still-hushed issue. Other times, children’s behaviors show that they are struggling – by their aggression, depression, decline in school performance, anger, anxiety, or running away – and I find out only by asking that they are experiencing life with a mentally ill parent.
Both are times to get more information about the nature of the parent’s symptoms, what is being done about it; what the child has seen, heard, or experienced; the child’s safety; and what intrinsic or cultural attitudes the family has about the problem. It is best if the affected parents themselves are able to talk realistically about the illness with the child. Sometimes we, as pediatric professionals, can help get the conversation started or may need to step in.
Teens can understand the nature of mental illness as a brain disorder, but often have acquired misinformation from peers, the other parent who is hurt and angry, or the Internet that needs to be respectfully corrected. They may be less willing to have such a discussion than would younger children, as they may have experienced verbal or physical aggression from the parent, embarrassment in front of peers, or teasing by classmates. They may have developed coping strategies of writing off the parent, defiance, aggressive responses, or denial.
It is important to find a relaxed moment and begin by saying, “May I ask what you have noticed about your parent’s behavior?” and “What did you make of it?” If they do not answer, you could add, “You know, like acting different or strange.” It is very valuable to be able to name it, if you know the diagnosis, to make the illness more objective. Teens are typically egocentric and wonder if they are prone to develop a similar condition, as well as anxious about who will be there for them if the parent does not get better; both are good questions to address.
Both adolescents and school-aged children are very attuned to when things in life are “unfair,” and having an ill parent certainly qualifies. It is important for whoever has this discussion to empathize, and to acknowledge that it is unfair and that feeling angry, sad, or confused is natural – without giving them permission for misbehavior. It may be easier for some children to have a journal in which to write questions to have an adult answer later. Any child can be given hope by knowing that the parent is getting help (or that you will work on this), especially if the parents themselves say they are trying to get better. The children need to know that although mental illness tends to get better and worse at unexpected times, mental health can be improved. It is essential that children of school age and older have a clear plan for what to do if the parent loses control or is in danger. This might include getting out of the house and calling the parent’s partner, a trusted neighbor, or 911.
While teens may feel guilty about their anger or things they might have said or done in reaction to the ill parent, school-aged and preschool children are more likely to feel guilty that they somehow contributed to the parent’s condition through misbehavior or some imagined influence. Eliciting these thoughts may simply require asking, “What thoughts have you had about why this happened?” or having another family member prompting them by saying, “I have been wondering if there is something I should have done. Have you wondered about that, too?”
What is harder to explain is the impression children may get that their depressed or psychotic or drug-abusing parents no longer love them; and the parents may have said hurtful things to them. School-aged children can be told and can understand an illness of “the feelings and thinking parts of the brain” as being similar to other physical illnesses, such as the flu, that “make people act tired or grouchy or say things they do not mean.” Children of all ages need to be reassured that, inside, their parents still love them, and “it is the illness talking” if they act or speak otherwise. In the case of substance abuse disorders, which might seem more of a choice by the parent than would other mental illnesses, it can be helpful to point out that “drugs and alcohol can be stronger than people and can take over their brains.” The National Alliance on Mental Illness (www.nami.org) offers support programs that may be helpful for older children.

Sometimes families may resist telling a child about parental mental illness because of personal beliefs, cultural stigma, or privacy concerns. I try to emphasize that by being honest in giving children an understanding of their parents’ mental illness, one is helping them trust the adults in their lives. They need the truth and also to practice formulating things to say to counter those who have incorrect ideas, or who insult or make fun of them. They need the truth about mental illness to make sense of their experiences so they can feel lovable and hopeful about their own futures and can recognize illness symptoms in themselves. Giving them words, ensuring their safety and support, and strengthening their coping can help buffer the impact of this common adverse childhood experience to help prevent long-term negative effects.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at [email protected].
You probably think you know how to talk with a child about death. But somehow talking about a parent’s mental illness may seem more difficult. Even medical professionals, as most people, can find themselves feeling more judgmental or uneasy talking about mental illness than about physical problems. But with a prevalence of about one in four people having mental disorders, we need to be prepared for this discussion.
Sometimes family members, or even parents themselves, have asked me to tell a child about a parent’s mental illness or substance use. They know the child is confused and scared but don’t know what to say about this still-hushed issue. Other times, children’s behaviors show that they are struggling – by their aggression, depression, decline in school performance, anger, anxiety, or running away – and I find out only by asking that they are experiencing life with a mentally ill parent.
Both are times to get more information about the nature of the parent’s symptoms, what is being done about it; what the child has seen, heard, or experienced; the child’s safety; and what intrinsic or cultural attitudes the family has about the problem. It is best if the affected parents themselves are able to talk realistically about the illness with the child. Sometimes we, as pediatric professionals, can help get the conversation started or may need to step in.
Teens can understand the nature of mental illness as a brain disorder, but often have acquired misinformation from peers, the other parent who is hurt and angry, or the Internet that needs to be respectfully corrected. They may be less willing to have such a discussion than would younger children, as they may have experienced verbal or physical aggression from the parent, embarrassment in front of peers, or teasing by classmates. They may have developed coping strategies of writing off the parent, defiance, aggressive responses, or denial.
It is important to find a relaxed moment and begin by saying, “May I ask what you have noticed about your parent’s behavior?” and “What did you make of it?” If they do not answer, you could add, “You know, like acting different or strange.” It is very valuable to be able to name it, if you know the diagnosis, to make the illness more objective. Teens are typically egocentric and wonder if they are prone to develop a similar condition, as well as anxious about who will be there for them if the parent does not get better; both are good questions to address.
Both adolescents and school-aged children are very attuned to when things in life are “unfair,” and having an ill parent certainly qualifies. It is important for whoever has this discussion to empathize, and to acknowledge that it is unfair and that feeling angry, sad, or confused is natural – without giving them permission for misbehavior. It may be easier for some children to have a journal in which to write questions to have an adult answer later. Any child can be given hope by knowing that the parent is getting help (or that you will work on this), especially if the parents themselves say they are trying to get better. The children need to know that although mental illness tends to get better and worse at unexpected times, mental health can be improved. It is essential that children of school age and older have a clear plan for what to do if the parent loses control or is in danger. This might include getting out of the house and calling the parent’s partner, a trusted neighbor, or 911.
While teens may feel guilty about their anger or things they might have said or done in reaction to the ill parent, school-aged and preschool children are more likely to feel guilty that they somehow contributed to the parent’s condition through misbehavior or some imagined influence. Eliciting these thoughts may simply require asking, “What thoughts have you had about why this happened?” or having another family member prompting them by saying, “I have been wondering if there is something I should have done. Have you wondered about that, too?”
What is harder to explain is the impression children may get that their depressed or psychotic or drug-abusing parents no longer love them; and the parents may have said hurtful things to them. School-aged children can be told and can understand an illness of “the feelings and thinking parts of the brain” as being similar to other physical illnesses, such as the flu, that “make people act tired or grouchy or say things they do not mean.” Children of all ages need to be reassured that, inside, their parents still love them, and “it is the illness talking” if they act or speak otherwise. In the case of substance abuse disorders, which might seem more of a choice by the parent than would other mental illnesses, it can be helpful to point out that “drugs and alcohol can be stronger than people and can take over their brains.” The National Alliance on Mental Illness (www.nami.org) offers support programs that may be helpful for older children.
Sometimes families may resist telling a child about parental mental illness because of personal beliefs, cultural stigma, or privacy concerns. I try to emphasize that by being honest in giving children an understanding of their parents’ mental illness, one is helping them trust the adults in their lives. They need the truth and also to practice formulating things to say to counter those who have incorrect ideas, or who insult or make fun of them. They need the truth about mental illness to make sense of their experiences so they can feel lovable and hopeful about their own futures and can recognize illness symptoms in themselves. Giving them words, ensuring their safety and support, and strengthening their coping can help buffer the impact of this common adverse childhood experience to help prevent long-term negative effects.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at [email protected].
You probably think you know how to talk with a child about death. But somehow talking about a parent’s mental illness may seem more difficult. Even medical professionals, as most people, can find themselves feeling more judgmental or uneasy talking about mental illness than about physical problems. But with a prevalence of about one in four people having mental disorders, we need to be prepared for this discussion.
Sometimes family members, or even parents themselves, have asked me to tell a child about a parent’s mental illness or substance use. They know the child is confused and scared but don’t know what to say about this still-hushed issue. Other times, children’s behaviors show that they are struggling – by their aggression, depression, decline in school performance, anger, anxiety, or running away – and I find out only by asking that they are experiencing life with a mentally ill parent.
Both are times to get more information about the nature of the parent’s symptoms, what is being done about it; what the child has seen, heard, or experienced; the child’s safety; and what intrinsic or cultural attitudes the family has about the problem. It is best if the affected parents themselves are able to talk realistically about the illness with the child. Sometimes we, as pediatric professionals, can help get the conversation started or may need to step in.
Teens can understand the nature of mental illness as a brain disorder, but often have acquired misinformation from peers, the other parent who is hurt and angry, or the Internet that needs to be respectfully corrected. They may be less willing to have such a discussion than would younger children, as they may have experienced verbal or physical aggression from the parent, embarrassment in front of peers, or teasing by classmates. They may have developed coping strategies of writing off the parent, defiance, aggressive responses, or denial.
It is important to find a relaxed moment and begin by saying, “May I ask what you have noticed about your parent’s behavior?” and “What did you make of it?” If they do not answer, you could add, “You know, like acting different or strange.” It is very valuable to be able to name it, if you know the diagnosis, to make the illness more objective. Teens are typically egocentric and wonder if they are prone to develop a similar condition, as well as anxious about who will be there for them if the parent does not get better; both are good questions to address.
Both adolescents and school-aged children are very attuned to when things in life are “unfair,” and having an ill parent certainly qualifies. It is important for whoever has this discussion to empathize, and to acknowledge that it is unfair and that feeling angry, sad, or confused is natural – without giving them permission for misbehavior. It may be easier for some children to have a journal in which to write questions to have an adult answer later. Any child can be given hope by knowing that the parent is getting help (or that you will work on this), especially if the parents themselves say they are trying to get better. The children need to know that although mental illness tends to get better and worse at unexpected times, mental health can be improved. It is essential that children of school age and older have a clear plan for what to do if the parent loses control or is in danger. This might include getting out of the house and calling the parent’s partner, a trusted neighbor, or 911.
While teens may feel guilty about their anger or things they might have said or done in reaction to the ill parent, school-aged and preschool children are more likely to feel guilty that they somehow contributed to the parent’s condition through misbehavior or some imagined influence. Eliciting these thoughts may simply require asking, “What thoughts have you had about why this happened?” or having another family member prompting them by saying, “I have been wondering if there is something I should have done. Have you wondered about that, too?”
What is harder to explain is the impression children may get that their depressed or psychotic or drug-abusing parents no longer love them; and the parents may have said hurtful things to them. School-aged children can be told and can understand an illness of “the feelings and thinking parts of the brain” as being similar to other physical illnesses, such as the flu, that “make people act tired or grouchy or say things they do not mean.” Children of all ages need to be reassured that, inside, their parents still love them, and “it is the illness talking” if they act or speak otherwise. In the case of substance abuse disorders, which might seem more of a choice by the parent than would other mental illnesses, it can be helpful to point out that “drugs and alcohol can be stronger than people and can take over their brains.” The National Alliance on Mental Illness (www.nami.org) offers support programs that may be helpful for older children.
Sometimes families may resist telling a child about parental mental illness because of personal beliefs, cultural stigma, or privacy concerns. I try to emphasize that by being honest in giving children an understanding of their parents’ mental illness, one is helping them trust the adults in their lives. They need the truth and also to practice formulating things to say to counter those who have incorrect ideas, or who insult or make fun of them. They need the truth about mental illness to make sense of their experiences so they can feel lovable and hopeful about their own futures and can recognize illness symptoms in themselves. Giving them words, ensuring their safety and support, and strengthening their coping can help buffer the impact of this common adverse childhood experience to help prevent long-term negative effects.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at [email protected].
Declining lung function linked to heart failure, stroke
Rapid declines in spirometric measures of lung function were associated with higher risks of cardiovascular disease, according to a recent analysis of a large, prospective cohort study.
Rapid declines in forced expiratory volume in 1 second (FEV1) were associated with increased incidence of heart failure, stroke, and death in the analysis of the ARIC (Atherosclerosis Risk in Communities) study.
The risk of incident heart failure among FEV1 rapid decliners was particularly high, with a fourfold increase within 12 months. That suggests clinicians should carefully consider incipient heart failure in patients with rapid changes in FEV1, investigators reported in the Journal of the American College of Cardiology.
Rapid declines in forced vital capacity (FVC) were also associated with higher incidences of heart failure and death in the analysis by Odilson M. Silvestre, MD, of the division of cardiovascular medicine at Brigham and Women’s Hospital, Boston, and colleagues.
The analysis included a total of 10,351 ARIC participants with a mean follow-up of 17 years. All had undergone spirometry at the first study visit between 1987 and 1989, and on the second visit between 1990 and 1992.
One-quarter of participants were classified as FEV1 rapid decliners, defined by an FEV1 decrease of at least 1.9% per year. Likewise, one-quarter of participants were classified as FVC rapid decliners, based on an FVC decrease of at least 2.1%.
Rapid decline in FEV1 was associated with a higher risk of incident heart failure (hazard ratio, 1.17; 95% confidence interval, 1.04-1.33; P = .010), and was most prognostic in the first year of follow-up (HR, 4.22; 95% CI, 1.34-13.26; P = .01), investigators said.
Rapid decline in FVC was likewise associated with a greater heart failure risk (HR, 1.27; 95% CI, 1.12-1.44; P less than .001).
Increased heart failure risk persisted after excluding patients with incident coronary heart disease in both the FEV1 and FVC rapid decliners, the investigators said.
A rapid decline in FEV1 was also associated with a higher stroke risk (HR, 1.25; 95% CI, 1.04-1.50; P = .015).
FEV1 rapid decliners had a higher overall rate of incident cardiovascular disease than those without rapid decline, even after adjustment for baseline variables such as age, sex, race, body mass index, and heart rate (HR, 1.15; 95% CI, 1.04-1.26; P = .004), and FVC rapid decliners likewise had a 19% greater risk of the composite endpoint (HR, 1.19; 95% CI, 1.08-1.32; P less than .001).
The National Heart, Lung, and Blood Institute, the American Heart Association, and other sources supported the study. Dr. Silvestre reported having no relevant conflicts.
SOURCE: Silvestre OM et al. J Am Coll Cardiol. 2018 Sep 4;72(10):1109-22.
Cardiologists and pulmonologists should closely collaborate to better identify the relationship between lung function decline and early cardiovascular disease detection, said the authors of an editorial accompanying the study.
Improved collaboration would help manage these conditions, stopping early disease progression and preventing overt cardiovascular disease, wrote Daniel A. Duprez, MD, PhD, and David R. Jacobs Jr., PhD.
“The resulting symptomatic and prognostic benefits outweigh those attainable by treating either condition alone,” noted Dr. Duprez and Dr. Jacobs.
The study by Dr. Silvestre and coauthors showed that rapid declines in forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) among participants in the ARIC (Atherosclerosis Risk in Communities) study were associated with a higher incidence of composite cardiovascular disease, heart failure, and total death.
The association between FEV1 and new heart failure was substantially impacted by 22 heart failure events occurring in the first year, with a hazard ratio of 4.22 for predicting those cases, the editorial authors noted.
“We suggest that this association with early cases could be the result of reversed causality, reflecting heart failure undiagnosed at the second spirometry test,” they explained (J Am Coll Cardiol. 2018 Sep 4;72[10]:1123-5).
Dr. Duprez is with the cardiovascular division of the University of Minnesota, Minneapolis, and Dr. Jacobs is with the division of epidemiology and community health at the University of Minnesota, Minneapolis. Dr. Duprez and Dr. Jacobs reported they had no relevant disclosures.
Cardiologists and pulmonologists should closely collaborate to better identify the relationship between lung function decline and early cardiovascular disease detection, said the authors of an editorial accompanying the study.
Improved collaboration would help manage these conditions, stopping early disease progression and preventing overt cardiovascular disease, wrote Daniel A. Duprez, MD, PhD, and David R. Jacobs Jr., PhD.
“The resulting symptomatic and prognostic benefits outweigh those attainable by treating either condition alone,” noted Dr. Duprez and Dr. Jacobs.
The study by Dr. Silvestre and coauthors showed that rapid declines in forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) among participants in the ARIC (Atherosclerosis Risk in Communities) study were associated with a higher incidence of composite cardiovascular disease, heart failure, and total death.
The association between FEV1 and new heart failure was substantially impacted by 22 heart failure events occurring in the first year, with a hazard ratio of 4.22 for predicting those cases, the editorial authors noted.
“We suggest that this association with early cases could be the result of reversed causality, reflecting heart failure undiagnosed at the second spirometry test,” they explained (J Am Coll Cardiol. 2018 Sep 4;72[10]:1123-5).
Dr. Duprez is with the cardiovascular division of the University of Minnesota, Minneapolis, and Dr. Jacobs is with the division of epidemiology and community health at the University of Minnesota, Minneapolis. Dr. Duprez and Dr. Jacobs reported they had no relevant disclosures.
Cardiologists and pulmonologists should closely collaborate to better identify the relationship between lung function decline and early cardiovascular disease detection, said the authors of an editorial accompanying the study.
Improved collaboration would help manage these conditions, stopping early disease progression and preventing overt cardiovascular disease, wrote Daniel A. Duprez, MD, PhD, and David R. Jacobs Jr., PhD.
“The resulting symptomatic and prognostic benefits outweigh those attainable by treating either condition alone,” noted Dr. Duprez and Dr. Jacobs.
The study by Dr. Silvestre and coauthors showed that rapid declines in forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) among participants in the ARIC (Atherosclerosis Risk in Communities) study were associated with a higher incidence of composite cardiovascular disease, heart failure, and total death.
The association between FEV1 and new heart failure was substantially impacted by 22 heart failure events occurring in the first year, with a hazard ratio of 4.22 for predicting those cases, the editorial authors noted.
“We suggest that this association with early cases could be the result of reversed causality, reflecting heart failure undiagnosed at the second spirometry test,” they explained (J Am Coll Cardiol. 2018 Sep 4;72[10]:1123-5).
Dr. Duprez is with the cardiovascular division of the University of Minnesota, Minneapolis, and Dr. Jacobs is with the division of epidemiology and community health at the University of Minnesota, Minneapolis. Dr. Duprez and Dr. Jacobs reported they had no relevant disclosures.
Rapid declines in spirometric measures of lung function were associated with higher risks of cardiovascular disease, according to a recent analysis of a large, prospective cohort study.
Rapid declines in forced expiratory volume in 1 second (FEV1) were associated with increased incidence of heart failure, stroke, and death in the analysis of the ARIC (Atherosclerosis Risk in Communities) study.
The risk of incident heart failure among FEV1 rapid decliners was particularly high, with a fourfold increase within 12 months. That suggests clinicians should carefully consider incipient heart failure in patients with rapid changes in FEV1, investigators reported in the Journal of the American College of Cardiology.
Rapid declines in forced vital capacity (FVC) were also associated with higher incidences of heart failure and death in the analysis by Odilson M. Silvestre, MD, of the division of cardiovascular medicine at Brigham and Women’s Hospital, Boston, and colleagues.
The analysis included a total of 10,351 ARIC participants with a mean follow-up of 17 years. All had undergone spirometry at the first study visit between 1987 and 1989, and on the second visit between 1990 and 1992.
One-quarter of participants were classified as FEV1 rapid decliners, defined by an FEV1 decrease of at least 1.9% per year. Likewise, one-quarter of participants were classified as FVC rapid decliners, based on an FVC decrease of at least 2.1%.
Rapid decline in FEV1 was associated with a higher risk of incident heart failure (hazard ratio, 1.17; 95% confidence interval, 1.04-1.33; P = .010), and was most prognostic in the first year of follow-up (HR, 4.22; 95% CI, 1.34-13.26; P = .01), investigators said.
Rapid decline in FVC was likewise associated with a greater heart failure risk (HR, 1.27; 95% CI, 1.12-1.44; P less than .001).
Increased heart failure risk persisted after excluding patients with incident coronary heart disease in both the FEV1 and FVC rapid decliners, the investigators said.
A rapid decline in FEV1 was also associated with a higher stroke risk (HR, 1.25; 95% CI, 1.04-1.50; P = .015).
FEV1 rapid decliners had a higher overall rate of incident cardiovascular disease than those without rapid decline, even after adjustment for baseline variables such as age, sex, race, body mass index, and heart rate (HR, 1.15; 95% CI, 1.04-1.26; P = .004), and FVC rapid decliners likewise had a 19% greater risk of the composite endpoint (HR, 1.19; 95% CI, 1.08-1.32; P less than .001).
The National Heart, Lung, and Blood Institute, the American Heart Association, and other sources supported the study. Dr. Silvestre reported having no relevant conflicts.
SOURCE: Silvestre OM et al. J Am Coll Cardiol. 2018 Sep 4;72(10):1109-22.
Rapid declines in spirometric measures of lung function were associated with higher risks of cardiovascular disease, according to a recent analysis of a large, prospective cohort study.
Rapid declines in forced expiratory volume in 1 second (FEV1) were associated with increased incidence of heart failure, stroke, and death in the analysis of the ARIC (Atherosclerosis Risk in Communities) study.
The risk of incident heart failure among FEV1 rapid decliners was particularly high, with a fourfold increase within 12 months. That suggests clinicians should carefully consider incipient heart failure in patients with rapid changes in FEV1, investigators reported in the Journal of the American College of Cardiology.
Rapid declines in forced vital capacity (FVC) were also associated with higher incidences of heart failure and death in the analysis by Odilson M. Silvestre, MD, of the division of cardiovascular medicine at Brigham and Women’s Hospital, Boston, and colleagues.
The analysis included a total of 10,351 ARIC participants with a mean follow-up of 17 years. All had undergone spirometry at the first study visit between 1987 and 1989, and on the second visit between 1990 and 1992.
One-quarter of participants were classified as FEV1 rapid decliners, defined by an FEV1 decrease of at least 1.9% per year. Likewise, one-quarter of participants were classified as FVC rapid decliners, based on an FVC decrease of at least 2.1%.
Rapid decline in FEV1 was associated with a higher risk of incident heart failure (hazard ratio, 1.17; 95% confidence interval, 1.04-1.33; P = .010), and was most prognostic in the first year of follow-up (HR, 4.22; 95% CI, 1.34-13.26; P = .01), investigators said.
Rapid decline in FVC was likewise associated with a greater heart failure risk (HR, 1.27; 95% CI, 1.12-1.44; P less than .001).
Increased heart failure risk persisted after excluding patients with incident coronary heart disease in both the FEV1 and FVC rapid decliners, the investigators said.
A rapid decline in FEV1 was also associated with a higher stroke risk (HR, 1.25; 95% CI, 1.04-1.50; P = .015).
FEV1 rapid decliners had a higher overall rate of incident cardiovascular disease than those without rapid decline, even after adjustment for baseline variables such as age, sex, race, body mass index, and heart rate (HR, 1.15; 95% CI, 1.04-1.26; P = .004), and FVC rapid decliners likewise had a 19% greater risk of the composite endpoint (HR, 1.19; 95% CI, 1.08-1.32; P less than .001).
The National Heart, Lung, and Blood Institute, the American Heart Association, and other sources supported the study. Dr. Silvestre reported having no relevant conflicts.
SOURCE: Silvestre OM et al. J Am Coll Cardiol. 2018 Sep 4;72(10):1109-22.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Key clinical point: Rapid declines in spirometric measures of lung function were associated with higher risks of heart failure, among other adverse cardiovascular outcomes.
Major finding: Rapid decline in forced expiratory volume in 1 second was associated with higher risk of incident heart failure (HR, 1.17; 95% CI, 1.04-1.33; P = .010), and was most prognostic in the first year of follow-up (HR, 4.22; 95% CI, 1.34-13.26; P = .01).
Study details: An analysis including a total of 10,351 participants in a large, prospective cohort study with a mean follow-up of 17 years.
Disclosures: The National Heart, Lung, and Blood Institute, the American Heart Association, and other sources supported the study. Dr. Silvestre reported having no relevant conflicts.
Source: Silvestre OM et al. J Am Coll Cardiol. 2018 Sep 4;72(10):1109-22.
Children and teens are at risk for drug-drug interactions

“During 2013-2014, one-fifth of children and adolescents used at least one prescription medication and [about] 1 in 10 concurrently used two [or more] prescription medications,” Dima M. Qato, PharmD, MPH, PhD, of the University of Illinois at Chicago, and her colleagues wrote in Pediatrics. “Among children and adolescents concurrently using two [or more] prescription medications, 1 in 12 was at risk for a major DDI.”
The researchers used data from the six most recent cycles of the National Health and Nutrition Examination Survey conducted by the National Center for Health Statistics, beginning with the 2003-2004 cycle through the 2013-2014 cycle, yielding a sample of 23,152 participants aged 0-19 years across the 10-year period. The survey differentiated between prescriptions for acute use (used for 30 days or less) or for chronic use. Concurrent use was defined as using two or more prescription drugs within the 30 days prior to taking the survey. The Micromedex was used to determine the possibility of having a DDI.
The investigators noted a “notable” decrease in the use of acute drug treatments from 11% at the beginning to 7% at the end of the 10-year cycle (P less than .01). This was “driven largely by a decrease in the use of antibiotics.”
They identified the most commonly used prescription drugs, including respiratory agents, especially bronchodilators (the most common type was albuterol); psychotherapeutic agents, especially CNS stimulants (most commonly methylphenidate); and antidepressants (most commonly fluoxetine).
“Among concurrent users of prescription medications, combinations that involved respiratory agents, such as bronchodilators and leukotriene modifiers, and psychotropic medications, including antidepressants, atypical antipsychotics, and CNS stimulants, were the most prevalent,” Dr. Qato and her colleagues wrote. Of the 301 concurrent users in the 2013-2014 survey cycle, 156 unique drugs were used.
Of the children and adolescents who were concurrently using prescription medications, 8% were at risk for major DDIs, the researchers noted. “Nearly half of interacting regimens used involved psychotropic agents, primarily antidepressants, the most common adverse interaction effect being QT prolongation.” About 68% of these regimens included use of at least one acute medication.
They also found that “prescription medications associated with an increased risk of suicidality are commonly used in children and adolescents and are often used together. For example, more than half of adolescent girls taking antidepressants concurrently use at least two additional psychotropic medications or hormonal contraceptives. Although there is some evidence that the combined use of these drugs may increase the onset and severity of suicidal thoughts and behavior, we found no cases of DDIs associated with suicidality.”
Dr. Qato and her colleagues noted some limitations to their study, including using the potential for DDI rather than actual adverse events, survey data being limited to prescription medications and not over-the-counter treatments, and the possible misclassification of chronic medications as acute medications depending on when treatments were initiated.
That being said, the investigators concluded that treatment “and prevention efforts to reduce the burden of adverse drug events in younger populations should be used to consider the role of interacting drug combinations, especially among these individuals.”
Funding for the study was provided by the Robert Woods Johnson Foundation. No relevant financial disclosures were reported.
SOURCE: Qato DM et al. Pediatrics. 2018 Aug 27. doi: 10.1542/peds.2018-1042.
Technology could play a key role in preventing adverse events from drug-drug interactions (DDI) in pediatric patients.
There are apps that can be embedded within EHRs, but there are risks of alert fatigue, which could cause DDI warnings to be ignored altogether, as well as not enough alerts, especially if EHRs are not communicating between doctors, leading to missed DDI avoidance opportunities. The solution is to select alerts that strike the balance between the two.
Stephen Downs, MD , of the University of Indiana, Indianapolis, chairs the advisory board for the American Academy of Pediatrics Child Health Informatics Center. These comments are summarized from a commentary accompanying the article by Qato et al (Pediatrics. 2018 Aug 27. doi: 10.1542/ peds.2018-2023 ).
Technology could play a key role in preventing adverse events from drug-drug interactions (DDI) in pediatric patients.
There are apps that can be embedded within EHRs, but there are risks of alert fatigue, which could cause DDI warnings to be ignored altogether, as well as not enough alerts, especially if EHRs are not communicating between doctors, leading to missed DDI avoidance opportunities. The solution is to select alerts that strike the balance between the two.
Stephen Downs, MD , of the University of Indiana, Indianapolis, chairs the advisory board for the American Academy of Pediatrics Child Health Informatics Center. These comments are summarized from a commentary accompanying the article by Qato et al (Pediatrics. 2018 Aug 27. doi: 10.1542/ peds.2018-2023 ).
Technology could play a key role in preventing adverse events from drug-drug interactions (DDI) in pediatric patients.
There are apps that can be embedded within EHRs, but there are risks of alert fatigue, which could cause DDI warnings to be ignored altogether, as well as not enough alerts, especially if EHRs are not communicating between doctors, leading to missed DDI avoidance opportunities. The solution is to select alerts that strike the balance between the two.
Stephen Downs, MD , of the University of Indiana, Indianapolis, chairs the advisory board for the American Academy of Pediatrics Child Health Informatics Center. These comments are summarized from a commentary accompanying the article by Qato et al (Pediatrics. 2018 Aug 27. doi: 10.1542/ peds.2018-2023 ).
“During 2013-2014, one-fifth of children and adolescents used at least one prescription medication and [about] 1 in 10 concurrently used two [or more] prescription medications,” Dima M. Qato, PharmD, MPH, PhD, of the University of Illinois at Chicago, and her colleagues wrote in Pediatrics. “Among children and adolescents concurrently using two [or more] prescription medications, 1 in 12 was at risk for a major DDI.”
The researchers used data from the six most recent cycles of the National Health and Nutrition Examination Survey conducted by the National Center for Health Statistics, beginning with the 2003-2004 cycle through the 2013-2014 cycle, yielding a sample of 23,152 participants aged 0-19 years across the 10-year period. The survey differentiated between prescriptions for acute use (used for 30 days or less) or for chronic use. Concurrent use was defined as using two or more prescription drugs within the 30 days prior to taking the survey. The Micromedex was used to determine the possibility of having a DDI.
The investigators noted a “notable” decrease in the use of acute drug treatments from 11% at the beginning to 7% at the end of the 10-year cycle (P less than .01). This was “driven largely by a decrease in the use of antibiotics.”
They identified the most commonly used prescription drugs, including respiratory agents, especially bronchodilators (the most common type was albuterol); psychotherapeutic agents, especially CNS stimulants (most commonly methylphenidate); and antidepressants (most commonly fluoxetine).
“Among concurrent users of prescription medications, combinations that involved respiratory agents, such as bronchodilators and leukotriene modifiers, and psychotropic medications, including antidepressants, atypical antipsychotics, and CNS stimulants, were the most prevalent,” Dr. Qato and her colleagues wrote. Of the 301 concurrent users in the 2013-2014 survey cycle, 156 unique drugs were used.
Of the children and adolescents who were concurrently using prescription medications, 8% were at risk for major DDIs, the researchers noted. “Nearly half of interacting regimens used involved psychotropic agents, primarily antidepressants, the most common adverse interaction effect being QT prolongation.” About 68% of these regimens included use of at least one acute medication.
They also found that “prescription medications associated with an increased risk of suicidality are commonly used in children and adolescents and are often used together. For example, more than half of adolescent girls taking antidepressants concurrently use at least two additional psychotropic medications or hormonal contraceptives. Although there is some evidence that the combined use of these drugs may increase the onset and severity of suicidal thoughts and behavior, we found no cases of DDIs associated with suicidality.”
Dr. Qato and her colleagues noted some limitations to their study, including using the potential for DDI rather than actual adverse events, survey data being limited to prescription medications and not over-the-counter treatments, and the possible misclassification of chronic medications as acute medications depending on when treatments were initiated.
That being said, the investigators concluded that treatment “and prevention efforts to reduce the burden of adverse drug events in younger populations should be used to consider the role of interacting drug combinations, especially among these individuals.”
Funding for the study was provided by the Robert Woods Johnson Foundation. No relevant financial disclosures were reported.
SOURCE: Qato DM et al. Pediatrics. 2018 Aug 27. doi: 10.1542/peds.2018-1042.
“During 2013-2014, one-fifth of children and adolescents used at least one prescription medication and [about] 1 in 10 concurrently used two [or more] prescription medications,” Dima M. Qato, PharmD, MPH, PhD, of the University of Illinois at Chicago, and her colleagues wrote in Pediatrics. “Among children and adolescents concurrently using two [or more] prescription medications, 1 in 12 was at risk for a major DDI.”
The researchers used data from the six most recent cycles of the National Health and Nutrition Examination Survey conducted by the National Center for Health Statistics, beginning with the 2003-2004 cycle through the 2013-2014 cycle, yielding a sample of 23,152 participants aged 0-19 years across the 10-year period. The survey differentiated between prescriptions for acute use (used for 30 days or less) or for chronic use. Concurrent use was defined as using two or more prescription drugs within the 30 days prior to taking the survey. The Micromedex was used to determine the possibility of having a DDI.
The investigators noted a “notable” decrease in the use of acute drug treatments from 11% at the beginning to 7% at the end of the 10-year cycle (P less than .01). This was “driven largely by a decrease in the use of antibiotics.”
They identified the most commonly used prescription drugs, including respiratory agents, especially bronchodilators (the most common type was albuterol); psychotherapeutic agents, especially CNS stimulants (most commonly methylphenidate); and antidepressants (most commonly fluoxetine).
“Among concurrent users of prescription medications, combinations that involved respiratory agents, such as bronchodilators and leukotriene modifiers, and psychotropic medications, including antidepressants, atypical antipsychotics, and CNS stimulants, were the most prevalent,” Dr. Qato and her colleagues wrote. Of the 301 concurrent users in the 2013-2014 survey cycle, 156 unique drugs were used.
Of the children and adolescents who were concurrently using prescription medications, 8% were at risk for major DDIs, the researchers noted. “Nearly half of interacting regimens used involved psychotropic agents, primarily antidepressants, the most common adverse interaction effect being QT prolongation.” About 68% of these regimens included use of at least one acute medication.
They also found that “prescription medications associated with an increased risk of suicidality are commonly used in children and adolescents and are often used together. For example, more than half of adolescent girls taking antidepressants concurrently use at least two additional psychotropic medications or hormonal contraceptives. Although there is some evidence that the combined use of these drugs may increase the onset and severity of suicidal thoughts and behavior, we found no cases of DDIs associated with suicidality.”
Dr. Qato and her colleagues noted some limitations to their study, including using the potential for DDI rather than actual adverse events, survey data being limited to prescription medications and not over-the-counter treatments, and the possible misclassification of chronic medications as acute medications depending on when treatments were initiated.
That being said, the investigators concluded that treatment “and prevention efforts to reduce the burden of adverse drug events in younger populations should be used to consider the role of interacting drug combinations, especially among these individuals.”
Funding for the study was provided by the Robert Woods Johnson Foundation. No relevant financial disclosures were reported.
SOURCE: Qato DM et al. Pediatrics. 2018 Aug 27. doi: 10.1542/peds.2018-1042.
FROM PEDIATRICS
Key clinical point: Children are at risk for drug-drug interactions from concurrent use of two or more medications.
Major finding: Of adolescents using two or more drugs, 1 in 12 are at risk for a major drug-drug interaction.
Study details: Researchers used data from the six most recent cycles of the National Health and Nutrition Examination Survey conducted by the National Center for Health Statistics, yielding a sample of 23,152 participants aged 0-19 years across the 10-year period.
Disclosures: Funding for the study was provided by the Robert Woods Johnson Foundation. No relevant financial disclosures were reported.
Source: Qato DM et al. Pediatrics. 2018 Aug 27. doi: 10.1542/peds.2018-1042.
Frailty and risk of postoperative complications
Background: FTR is a quality measure defined as death after a serious, potentially preventable complication. Frailty incorporates different domains including physical performance, gait, mobility, nutritional status, mental health, and cognition. Although there are some studies linking frailty and FTR and postoperative morbidity, the degree and association with low-risk procedures is unclear.

Study design: Retrospective cohort study.
Setting: More than 600 hospitals participating in the American College of Surgeons’ National Surgical Quality Improvement Program database during 2005-2012.
Synopsis: The cohort included 984,550 adult patients who underwent inpatient procedure for general, vascular, thoracic, cardiac, and orthopedic operations. The Risk Analysis Index (RAI) score was used to calculate frailty. The rate of major complications increased as the RAI score was higher for both low-risk and high-risk surgery. For RAI scores less than 10, the rate was 7.4%; for RAI scores 11-20, the rate was 19.8%; for RAI scores 21-30, the rate was 41.1%; and for RAI scores above 40, the rate was 53.6%. Stratifying by the number of complications, significant increases in FTR were observed across the RAI categories for both low-risk and high-risk procedures.
Frailty assessment should be considered a part of the routine perioperative evaluation and should stimulate preoperative interventions aimed at reducing risk for postoperative complications.
Bottom line: This large retrospective study found an association between increasing frailty and both the number of complications and FTR for both low-risk and high-risk surgical procedures.
Citation: Shah R et al. Association of frailty with failure to rescue after low-risk and high-risk inpatient surgery. JAMA Surg. 2018 Mar 21;153(5):e180214.
Dr. Canepa is a hospitalist in the division of hospital medicine at the University of Kentucky, Lexington.
Background: FTR is a quality measure defined as death after a serious, potentially preventable complication. Frailty incorporates different domains including physical performance, gait, mobility, nutritional status, mental health, and cognition. Although there are some studies linking frailty and FTR and postoperative morbidity, the degree and association with low-risk procedures is unclear.
Study design: Retrospective cohort study.
Setting: More than 600 hospitals participating in the American College of Surgeons’ National Surgical Quality Improvement Program database during 2005-2012.
Synopsis: The cohort included 984,550 adult patients who underwent inpatient procedure for general, vascular, thoracic, cardiac, and orthopedic operations. The Risk Analysis Index (RAI) score was used to calculate frailty. The rate of major complications increased as the RAI score was higher for both low-risk and high-risk surgery. For RAI scores less than 10, the rate was 7.4%; for RAI scores 11-20, the rate was 19.8%; for RAI scores 21-30, the rate was 41.1%; and for RAI scores above 40, the rate was 53.6%. Stratifying by the number of complications, significant increases in FTR were observed across the RAI categories for both low-risk and high-risk procedures.
Frailty assessment should be considered a part of the routine perioperative evaluation and should stimulate preoperative interventions aimed at reducing risk for postoperative complications.
Bottom line: This large retrospective study found an association between increasing frailty and both the number of complications and FTR for both low-risk and high-risk surgical procedures.
Citation: Shah R et al. Association of frailty with failure to rescue after low-risk and high-risk inpatient surgery. JAMA Surg. 2018 Mar 21;153(5):e180214.
Dr. Canepa is a hospitalist in the division of hospital medicine at the University of Kentucky, Lexington.
Background: FTR is a quality measure defined as death after a serious, potentially preventable complication. Frailty incorporates different domains including physical performance, gait, mobility, nutritional status, mental health, and cognition. Although there are some studies linking frailty and FTR and postoperative morbidity, the degree and association with low-risk procedures is unclear.
Study design: Retrospective cohort study.
Setting: More than 600 hospitals participating in the American College of Surgeons’ National Surgical Quality Improvement Program database during 2005-2012.
Synopsis: The cohort included 984,550 adult patients who underwent inpatient procedure for general, vascular, thoracic, cardiac, and orthopedic operations. The Risk Analysis Index (RAI) score was used to calculate frailty. The rate of major complications increased as the RAI score was higher for both low-risk and high-risk surgery. For RAI scores less than 10, the rate was 7.4%; for RAI scores 11-20, the rate was 19.8%; for RAI scores 21-30, the rate was 41.1%; and for RAI scores above 40, the rate was 53.6%. Stratifying by the number of complications, significant increases in FTR were observed across the RAI categories for both low-risk and high-risk procedures.
Frailty assessment should be considered a part of the routine perioperative evaluation and should stimulate preoperative interventions aimed at reducing risk for postoperative complications.
Bottom line: This large retrospective study found an association between increasing frailty and both the number of complications and FTR for both low-risk and high-risk surgical procedures.
Citation: Shah R et al. Association of frailty with failure to rescue after low-risk and high-risk inpatient surgery. JAMA Surg. 2018 Mar 21;153(5):e180214.
Dr. Canepa is a hospitalist in the division of hospital medicine at the University of Kentucky, Lexington.
USPSTF releases its first perinatal depression draft recommendations

It has given this draft recommendation a B grade, which means that there is moderate certainty of at least moderate net benefit. This is the first time the USPSTF has reviewed this topic.
It’s estimated that one in seven women are affected by perinatal depression, which can have negative effects on both the mothers affected and their children. In its review of evidence, the USPSTF found convincing evidence that counseling, particularly cognitive-behavioral and interpersonal therapies, can prevent perinatal depression.
The draft recommendation affects women who are pregnant or 1 year post partum; specifically, these women will not have a current diagnosis of depression but are at increased risk for it nonetheless. At this time, there is no accurate screening tool available to determine whether women have perinatal depression or are at increased risk. However, certain risk factors have been associated with it, including current stressful life events, personal or family history of depression, history of physical or sexual abuse, pregestational or gestational diabetes, complications during pregnancy such as hyperemesis or premature contractions, adolescent pregnancy, lack of social or financial support, and low socioeconomic status.
The USPSTF reviewed 50 trials considered to be of good or fair quality, with a mean participant age of 29 years; 26 included pregnant women, 22 included women post partum, and 2 included both. Counseling interventions were the most widely studied and “reduced the likelihood of the onset of perinatal depression by 39%” for a pooled risk ratio of 0.61 (95% confidence interval, 0.47-0.78), compared with control conditions. Two kinds of therapies stood out as especially effective: cognitive-behavioral and interpersonal. Cognitive-behavioral therapy focuses on negative thoughts, moods, behaviors, and attitudes and seeks to increase positive events and activities. Interpersonal therapy focuses on how interpersonal interactions and patterns can contribute to the development and maintenance of psychological issues and distress.
The comment period for these draft recommendations will continue through Sept. 24 at www.uspreventiveservicestaskforce.org/tfcomment.htm.
This article was updated 8/28/18.
It has given this draft recommendation a B grade, which means that there is moderate certainty of at least moderate net benefit. This is the first time the USPSTF has reviewed this topic.
It’s estimated that one in seven women are affected by perinatal depression, which can have negative effects on both the mothers affected and their children. In its review of evidence, the USPSTF found convincing evidence that counseling, particularly cognitive-behavioral and interpersonal therapies, can prevent perinatal depression.
The draft recommendation affects women who are pregnant or 1 year post partum; specifically, these women will not have a current diagnosis of depression but are at increased risk for it nonetheless. At this time, there is no accurate screening tool available to determine whether women have perinatal depression or are at increased risk. However, certain risk factors have been associated with it, including current stressful life events, personal or family history of depression, history of physical or sexual abuse, pregestational or gestational diabetes, complications during pregnancy such as hyperemesis or premature contractions, adolescent pregnancy, lack of social or financial support, and low socioeconomic status.
The USPSTF reviewed 50 trials considered to be of good or fair quality, with a mean participant age of 29 years; 26 included pregnant women, 22 included women post partum, and 2 included both. Counseling interventions were the most widely studied and “reduced the likelihood of the onset of perinatal depression by 39%” for a pooled risk ratio of 0.61 (95% confidence interval, 0.47-0.78), compared with control conditions. Two kinds of therapies stood out as especially effective: cognitive-behavioral and interpersonal. Cognitive-behavioral therapy focuses on negative thoughts, moods, behaviors, and attitudes and seeks to increase positive events and activities. Interpersonal therapy focuses on how interpersonal interactions and patterns can contribute to the development and maintenance of psychological issues and distress.
The comment period for these draft recommendations will continue through Sept. 24 at www.uspreventiveservicestaskforce.org/tfcomment.htm.
This article was updated 8/28/18.
It has given this draft recommendation a B grade, which means that there is moderate certainty of at least moderate net benefit. This is the first time the USPSTF has reviewed this topic.
It’s estimated that one in seven women are affected by perinatal depression, which can have negative effects on both the mothers affected and their children. In its review of evidence, the USPSTF found convincing evidence that counseling, particularly cognitive-behavioral and interpersonal therapies, can prevent perinatal depression.
The draft recommendation affects women who are pregnant or 1 year post partum; specifically, these women will not have a current diagnosis of depression but are at increased risk for it nonetheless. At this time, there is no accurate screening tool available to determine whether women have perinatal depression or are at increased risk. However, certain risk factors have been associated with it, including current stressful life events, personal or family history of depression, history of physical or sexual abuse, pregestational or gestational diabetes, complications during pregnancy such as hyperemesis or premature contractions, adolescent pregnancy, lack of social or financial support, and low socioeconomic status.
The USPSTF reviewed 50 trials considered to be of good or fair quality, with a mean participant age of 29 years; 26 included pregnant women, 22 included women post partum, and 2 included both. Counseling interventions were the most widely studied and “reduced the likelihood of the onset of perinatal depression by 39%” for a pooled risk ratio of 0.61 (95% confidence interval, 0.47-0.78), compared with control conditions. Two kinds of therapies stood out as especially effective: cognitive-behavioral and interpersonal. Cognitive-behavioral therapy focuses on negative thoughts, moods, behaviors, and attitudes and seeks to increase positive events and activities. Interpersonal therapy focuses on how interpersonal interactions and patterns can contribute to the development and maintenance of psychological issues and distress.
The comment period for these draft recommendations will continue through Sept. 24 at www.uspreventiveservicestaskforce.org/tfcomment.htm.
This article was updated 8/28/18.
Not on My Watch!
The itchy patch of skin on this 60-year-old man’s forearm, beneath his watch, has troubled him intermittently for a year. It is unresponsive to topical medications, including tolnaftate cream and 1% hydrocortisone cream; the latter seemed to improve the condition initially, but with time, the patch grew larger and itchier.
The patient’s primary care provider believed the rash might be precancerous and prescribed 5-fluorouracil cream, which showed no benefit. The patient was then referred to a dermatologist, who performed a KOH examination. No fungal elements were found.
At that point, the patient decided to simply ignore the problem. That resolve ended when the itchiness increased—leading to his presentation today. He is in decent health but has had a kidney transplant and is taking the standard immunosuppressant (anti-rejection) medications.
EXAMINATION
A faintly pink, scaly rash is located on the patient’s forearm. It is unimpressive in appearance but very bothersome to the patient.

Despite the patient’s history, fungal origin remains a possibility, as does psoriasis. A punch biopsy is performed.
What is the diagnosis?
DISCUSSION
The biopsy results showed numerous fungal elements crowded around deeper aspects of hair follicles and a granulomatous reaction in the surrounding skin.
Normally, dermatophytes (the organisms that cause superficial fungal infections) are incapable of invading deeper tissues, making KOH exam a simple diagnostic method. But with immune suppression, the infection is able to invade deeper structures, making it more difficult to diagnose and treat. In this patient’s case, the use of steroid creams under occlusion (ie, the watch) had suppressed the body’s immune response to the infection.
The terminology used to describe this phenomenon varies according to the severity of infection. Tinea incognito might be used to describe this patient’s case, in which the steroid rendered the condition almost impossible to diagnose visually. With continued use of stronger topical steroids, the degree of inflammation might have been worse, involving deeper, larger nodules instead of faint pink scaling. In such cases, the term Majocchi fungal granuloma is used.
This patient moved his watch to the other arm temporarily and was successfully treated with twice-daily application of topical econazole cream and a two-week course of oral terbinafine (250 mg/d).
TAKE-HOME LEARNING POINTS
- Immunosuppression can make fungal infections more difficult to diagnose and treat.
- Dermatophytes don’t normally invade deeper structures and can usually be detected with a KOH exam of surface skin cells.
- If the patient is immunocompromised, a fungal diagnosis is best confirmed with a punch biopsy, and treatment achieved with a combination of oral and topical antifungal products.
- Mild cases of this kind are termed tinea incognito, while more severe cases are called Majocchi fungal granuloma.
The itchy patch of skin on this 60-year-old man’s forearm, beneath his watch, has troubled him intermittently for a year. It is unresponsive to topical medications, including tolnaftate cream and 1% hydrocortisone cream; the latter seemed to improve the condition initially, but with time, the patch grew larger and itchier.
The patient’s primary care provider believed the rash might be precancerous and prescribed 5-fluorouracil cream, which showed no benefit. The patient was then referred to a dermatologist, who performed a KOH examination. No fungal elements were found.
At that point, the patient decided to simply ignore the problem. That resolve ended when the itchiness increased—leading to his presentation today. He is in decent health but has had a kidney transplant and is taking the standard immunosuppressant (anti-rejection) medications.
EXAMINATION
A faintly pink, scaly rash is located on the patient’s forearm. It is unimpressive in appearance but very bothersome to the patient.
Despite the patient’s history, fungal origin remains a possibility, as does psoriasis. A punch biopsy is performed.
What is the diagnosis?
DISCUSSION
The biopsy results showed numerous fungal elements crowded around deeper aspects of hair follicles and a granulomatous reaction in the surrounding skin.
Normally, dermatophytes (the organisms that cause superficial fungal infections) are incapable of invading deeper tissues, making KOH exam a simple diagnostic method. But with immune suppression, the infection is able to invade deeper structures, making it more difficult to diagnose and treat. In this patient’s case, the use of steroid creams under occlusion (ie, the watch) had suppressed the body’s immune response to the infection.
The terminology used to describe this phenomenon varies according to the severity of infection. Tinea incognito might be used to describe this patient’s case, in which the steroid rendered the condition almost impossible to diagnose visually. With continued use of stronger topical steroids, the degree of inflammation might have been worse, involving deeper, larger nodules instead of faint pink scaling. In such cases, the term Majocchi fungal granuloma is used.
This patient moved his watch to the other arm temporarily and was successfully treated with twice-daily application of topical econazole cream and a two-week course of oral terbinafine (250 mg/d).
TAKE-HOME LEARNING POINTS
- Immunosuppression can make fungal infections more difficult to diagnose and treat.
- Dermatophytes don’t normally invade deeper structures and can usually be detected with a KOH exam of surface skin cells.
- If the patient is immunocompromised, a fungal diagnosis is best confirmed with a punch biopsy, and treatment achieved with a combination of oral and topical antifungal products.
- Mild cases of this kind are termed tinea incognito, while more severe cases are called Majocchi fungal granuloma.
The itchy patch of skin on this 60-year-old man’s forearm, beneath his watch, has troubled him intermittently for a year. It is unresponsive to topical medications, including tolnaftate cream and 1% hydrocortisone cream; the latter seemed to improve the condition initially, but with time, the patch grew larger and itchier.
The patient’s primary care provider believed the rash might be precancerous and prescribed 5-fluorouracil cream, which showed no benefit. The patient was then referred to a dermatologist, who performed a KOH examination. No fungal elements were found.
At that point, the patient decided to simply ignore the problem. That resolve ended when the itchiness increased—leading to his presentation today. He is in decent health but has had a kidney transplant and is taking the standard immunosuppressant (anti-rejection) medications.
EXAMINATION
A faintly pink, scaly rash is located on the patient’s forearm. It is unimpressive in appearance but very bothersome to the patient.
Despite the patient’s history, fungal origin remains a possibility, as does psoriasis. A punch biopsy is performed.
What is the diagnosis?
DISCUSSION
The biopsy results showed numerous fungal elements crowded around deeper aspects of hair follicles and a granulomatous reaction in the surrounding skin.
Normally, dermatophytes (the organisms that cause superficial fungal infections) are incapable of invading deeper tissues, making KOH exam a simple diagnostic method. But with immune suppression, the infection is able to invade deeper structures, making it more difficult to diagnose and treat. In this patient’s case, the use of steroid creams under occlusion (ie, the watch) had suppressed the body’s immune response to the infection.
The terminology used to describe this phenomenon varies according to the severity of infection. Tinea incognito might be used to describe this patient’s case, in which the steroid rendered the condition almost impossible to diagnose visually. With continued use of stronger topical steroids, the degree of inflammation might have been worse, involving deeper, larger nodules instead of faint pink scaling. In such cases, the term Majocchi fungal granuloma is used.
This patient moved his watch to the other arm temporarily and was successfully treated with twice-daily application of topical econazole cream and a two-week course of oral terbinafine (250 mg/d).
TAKE-HOME LEARNING POINTS
- Immunosuppression can make fungal infections more difficult to diagnose and treat.
- Dermatophytes don’t normally invade deeper structures and can usually be detected with a KOH exam of surface skin cells.
- If the patient is immunocompromised, a fungal diagnosis is best confirmed with a punch biopsy, and treatment achieved with a combination of oral and topical antifungal products.
- Mild cases of this kind are termed tinea incognito, while more severe cases are called Majocchi fungal granuloma.
European Commission approves first CAR T-cell therapies
The , two chimeric antigen receptor (CAR) T-cell therapies.
Tisagenlecleucel is now approved for use in pediatric and young adult patients up to 25 years of age with B-cell acute lymphoblastic leukemia (ALL) that is refractory, in relapse post transplant, or in second or later relapse.
Tisagenlecleucel is also approved to treat adults with relapsed or refractory diffuse large B-cell lymphoma (DLBCL) who have received two or more lines of systemic therapy.
Axicabtagene ciloleucel is approved for adults with relapsed/refractory DLBCL and primary mediastinal large B-cell lymphoma (PMBCL) after two or more lines of systemic therapy. The treatment is marketed by Kite, a Gilead company.
The axicabtagene ciloleucel approval is based on results from the single arm, ZUMA-1 trial. During the study of 101 patients who received a single infusion, 72% responded to therapy and 51% achieved a complete response. At 1 year, median overall survival had not been reached.
Novartis expects to launch tisagenlecleucel initially for pediatric ALL. The company said timing for tisagenlecleucel availability in each country will depend on multiple factors, including the onboarding of qualified treatment centers for the appropriate indications, as well as the completion of national reimbursement procedures.
The EC’s approval of tisagenlecleucel is based on results from the phase 2 JULIET and ELIANA trials.
Updated results from JULIET were presented at the annual congress of the European Hematology Association in June 2018. The trial enrolled 165 adults with relapsed/refractory DLBCL, and 111 of them received a single infusion of tisagenlecleucel. Most of the patients who discontinued before dosing did so because of disease progression or clinical deterioration.
The median time from infusion to data cutoff was 13.9 months.
The overall response rate was 52%, and the complete response (CR) rate was 40%. At the time of data cutoff, none of the responders had gone on to receive a stem cell transplant.
Updated results from ELIANA were published in New England Journal of Medicine (2018;378:439-48).
The trial included 75 children and young adults with relapsed/refractory ALL. The overall remission rate was 81% (61/75), with 60% of patients (n = 45) achieving a complete remission (CR) and 21% (n = 16) achieving a CR with incomplete hematologic recovery (CRi).
All patients whose best response was CR/CRi were negative for minimal residual disease. The median duration of response was not met.
The , two chimeric antigen receptor (CAR) T-cell therapies.
Tisagenlecleucel is now approved for use in pediatric and young adult patients up to 25 years of age with B-cell acute lymphoblastic leukemia (ALL) that is refractory, in relapse post transplant, or in second or later relapse.
Tisagenlecleucel is also approved to treat adults with relapsed or refractory diffuse large B-cell lymphoma (DLBCL) who have received two or more lines of systemic therapy.
Axicabtagene ciloleucel is approved for adults with relapsed/refractory DLBCL and primary mediastinal large B-cell lymphoma (PMBCL) after two or more lines of systemic therapy. The treatment is marketed by Kite, a Gilead company.
The axicabtagene ciloleucel approval is based on results from the single arm, ZUMA-1 trial. During the study of 101 patients who received a single infusion, 72% responded to therapy and 51% achieved a complete response. At 1 year, median overall survival had not been reached.
Novartis expects to launch tisagenlecleucel initially for pediatric ALL. The company said timing for tisagenlecleucel availability in each country will depend on multiple factors, including the onboarding of qualified treatment centers for the appropriate indications, as well as the completion of national reimbursement procedures.
The EC’s approval of tisagenlecleucel is based on results from the phase 2 JULIET and ELIANA trials.
Updated results from JULIET were presented at the annual congress of the European Hematology Association in June 2018. The trial enrolled 165 adults with relapsed/refractory DLBCL, and 111 of them received a single infusion of tisagenlecleucel. Most of the patients who discontinued before dosing did so because of disease progression or clinical deterioration.
The median time from infusion to data cutoff was 13.9 months.
The overall response rate was 52%, and the complete response (CR) rate was 40%. At the time of data cutoff, none of the responders had gone on to receive a stem cell transplant.
Updated results from ELIANA were published in New England Journal of Medicine (2018;378:439-48).
The trial included 75 children and young adults with relapsed/refractory ALL. The overall remission rate was 81% (61/75), with 60% of patients (n = 45) achieving a complete remission (CR) and 21% (n = 16) achieving a CR with incomplete hematologic recovery (CRi).
All patients whose best response was CR/CRi were negative for minimal residual disease. The median duration of response was not met.
The , two chimeric antigen receptor (CAR) T-cell therapies.
Tisagenlecleucel is now approved for use in pediatric and young adult patients up to 25 years of age with B-cell acute lymphoblastic leukemia (ALL) that is refractory, in relapse post transplant, or in second or later relapse.
Tisagenlecleucel is also approved to treat adults with relapsed or refractory diffuse large B-cell lymphoma (DLBCL) who have received two or more lines of systemic therapy.
Axicabtagene ciloleucel is approved for adults with relapsed/refractory DLBCL and primary mediastinal large B-cell lymphoma (PMBCL) after two or more lines of systemic therapy. The treatment is marketed by Kite, a Gilead company.
The axicabtagene ciloleucel approval is based on results from the single arm, ZUMA-1 trial. During the study of 101 patients who received a single infusion, 72% responded to therapy and 51% achieved a complete response. At 1 year, median overall survival had not been reached.
Novartis expects to launch tisagenlecleucel initially for pediatric ALL. The company said timing for tisagenlecleucel availability in each country will depend on multiple factors, including the onboarding of qualified treatment centers for the appropriate indications, as well as the completion of national reimbursement procedures.
The EC’s approval of tisagenlecleucel is based on results from the phase 2 JULIET and ELIANA trials.
Updated results from JULIET were presented at the annual congress of the European Hematology Association in June 2018. The trial enrolled 165 adults with relapsed/refractory DLBCL, and 111 of them received a single infusion of tisagenlecleucel. Most of the patients who discontinued before dosing did so because of disease progression or clinical deterioration.
The median time from infusion to data cutoff was 13.9 months.
The overall response rate was 52%, and the complete response (CR) rate was 40%. At the time of data cutoff, none of the responders had gone on to receive a stem cell transplant.
Updated results from ELIANA were published in New England Journal of Medicine (2018;378:439-48).
The trial included 75 children and young adults with relapsed/refractory ALL. The overall remission rate was 81% (61/75), with 60% of patients (n = 45) achieving a complete remission (CR) and 21% (n = 16) achieving a CR with incomplete hematologic recovery (CRi).
All patients whose best response was CR/CRi were negative for minimal residual disease. The median duration of response was not met.
Agminated Heterogeneous Papules on the Neck
The Diagnosis: Eruptive Blue Nevus
All biopsies demonstrated similar histologic features, including an intradermal proliferation of heavily pigmented, spindle-shaped dendritic melanocytes (Figure). The dermal pigment was most pronounced in the grossly darker papules, and there was not a substantial amount of background pigmentation at the stratum basale. Cytologic atypia, foci of necrosis, and mitotic activity were absent from all sections. There was no definitive junctional component identified, no multinucleated giant cells, and there was no overlying epidermal aberration. With some background pigmentation seen histologically, nevus spilus was considered, but because this acute eruption occurred in a young adult without appreciable gross background hyperpigmentation, the clinical context led to a diagnosis of eruptive blue nevus. After communicating the findings to the patient, he declined further treatment.
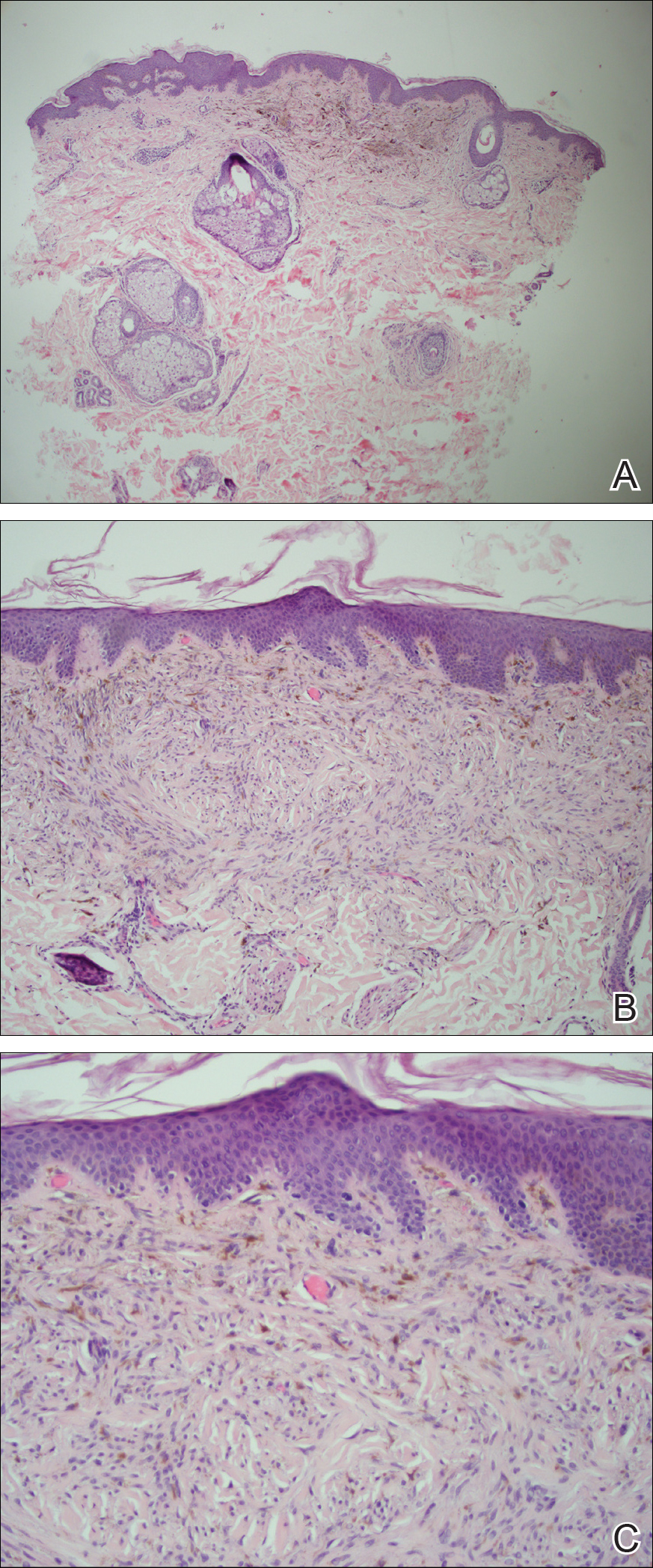
Eruptive blue nevus is an exceptionally rare subtype of blue nevus with few cases reported since the 1940s.1-9 Generally, each case report found a triggering event that could possibly have precipitated the acute proliferation and evolution of nevi. Triggering events can include bullous processes such as erythema multiforme2 and Stevens-Johnson syndrome,3 severe sunburn,4 trauma,5 immunosuppression,6 and a variety of endocrinopathies. No such history could be identified in our patient, except the biopsy.
Common blue nevi are benign, usually congenital, well-circumscribed, solitary, blue-gray macules or papules. Half of blue nevi cases are found on the dorsal aspects of the hands and feet but can present anywhere (eg, face, scalp, wrists, sacrum, buttocks). The blue-gray color appreciated clinically is attributed to the Tyndall effect, which occurs when long-wavelength light--red, orange, and yellow--is absorbed by the melanin deep in the dermis, while short-wavelength visible light--blue, violet, and indigo--is reflected with backscattering. On polarized dermoscopy, a homogeneous blue-gray hue is appreciated, but lighter segments may be present when collagen deposition is robust. Histopathologic findings confirm spindle-shaped dendritic melanocytes in the dermis without epidermal involvement. It generally is accepted that the etiology of these benign nevi is a failed migration of neural crest cells to the epidermis.10,11 Although the common blue nevus may be simple to diagnose, several subtypes have been described in the literature, including combined blue nevus, desmoplastic blue nevus, hypomelanotic/amelanotic blue nevus, and epithelioid blue nevus of Carney complex, and excluding a malignant process is of monumental importance.7,12
Biopsy is recommended for common blue nevi in the evaluation of newly acquired lesions, expansion of previously stable nevi, or for nevi larger than 10 mm in diameter. The nature of eruptive blue nevi warrants a biopsy to exclude melanoma or another malignant process. While the Becker nevus may manifest in adolescent males, it is clinically distinct from an eruptive blue nevus due to the size, relative homogeneity, and presence of hair within the lesion. Cutaneous amyloidosis may appear clinically similar to an eruptive blue nevus, but globular or amorphous material was not present in the papillary dermis of biopsied lesions in our patient. Since there was no cellular atypia or mitotic activity, melanoma and other malignancies were ruled out. Lastly, NAME syndrome by definition must include atrial myxomas, myxoid neurofibromas, and ephelides in addition to the nevi; however, our patient had only nevi and few ephelides. Once the diagnosis is established and benign nature confirmed, treatment is not necessarily required. If the patient elects to remove the lesion for aesthetic reasons, an excision into the subcutaneous fat is required to ensure complete removal of deep dermal melanocytes. Prior excisions of eruptive blue nevi have had no recurrence after more than 10 months.8,9
- Krause M, Bonnekoh B, Weisshaar E, et al. Coincidence of multiple, disseminated, tardive-eruptive blue nevi with cutis marmorata teleangiectatica congenita. Dermatology. 2000;200:134-138.
- Soltani K, Bernstein J, Lorincz A. Eruptive nevocytic nevi after erythema multiforme. J Am Acad Dermatol. 1979;1:503-505.
- Shoji T, Cockerell C, Koff A, et al. Eruptive melanocytic nevi after Stevens-Johnson syndrome. J Am Acad Dermatol. 1997;37:337-339.
- Hendricks W. Eruptive blue nevi. J Am Acad Dermatol. 1981;4:50-53.
- Kesty K, Zargari O. Eruptive blue nevi. Indian J Dermatol Venereol Leprol. 2015;81:198-201.
- Chen T, Kurwa H, Trotter M, et al. Agminated blue nevi in a patient with dermatomyositis. J Am Acad Dermatol. 2013;68:52-53.
- Walsh M. Correspondence: eruptive disseminated blue naevi of the scalp. Br J Dermatol. 1999;141:581-582.
- Nardini P, De Giorgi V, Massi D, et al. Eruptive disseminated blue naevi of the scalp. Br J Dermatol. 1999;140:178-180.
- de Giorgi V, Massi D, Brunasso G, et al. Eruptive multiple blue nevi of the penis: a clinical dermoscopic pathologic case study. J Cutan Pathol. 2004;31:185-188.
- Zimmermann AH, Becker SA. Precursors of epidermal melanocytes in the negro fetus. In: Gordon M, ed. Pigment Cell Biology. New York, NY: Academic Press Inc; 1959:159-170.
- Leopold JG, Richards DB. The interrelationship of blue and common naevi. J Pathol Bacteriol. 1968;95:37-46.
- Zembowicz A, Phadke P. Blue nevi and variants: an update. Arch Pathol Lab Med. 2011;135:327-336.
The Diagnosis: Eruptive Blue Nevus
All biopsies demonstrated similar histologic features, including an intradermal proliferation of heavily pigmented, spindle-shaped dendritic melanocytes (Figure). The dermal pigment was most pronounced in the grossly darker papules, and there was not a substantial amount of background pigmentation at the stratum basale. Cytologic atypia, foci of necrosis, and mitotic activity were absent from all sections. There was no definitive junctional component identified, no multinucleated giant cells, and there was no overlying epidermal aberration. With some background pigmentation seen histologically, nevus spilus was considered, but because this acute eruption occurred in a young adult without appreciable gross background hyperpigmentation, the clinical context led to a diagnosis of eruptive blue nevus. After communicating the findings to the patient, he declined further treatment.
Eruptive blue nevus is an exceptionally rare subtype of blue nevus with few cases reported since the 1940s.1-9 Generally, each case report found a triggering event that could possibly have precipitated the acute proliferation and evolution of nevi. Triggering events can include bullous processes such as erythema multiforme2 and Stevens-Johnson syndrome,3 severe sunburn,4 trauma,5 immunosuppression,6 and a variety of endocrinopathies. No such history could be identified in our patient, except the biopsy.
Common blue nevi are benign, usually congenital, well-circumscribed, solitary, blue-gray macules or papules. Half of blue nevi cases are found on the dorsal aspects of the hands and feet but can present anywhere (eg, face, scalp, wrists, sacrum, buttocks). The blue-gray color appreciated clinically is attributed to the Tyndall effect, which occurs when long-wavelength light--red, orange, and yellow--is absorbed by the melanin deep in the dermis, while short-wavelength visible light--blue, violet, and indigo--is reflected with backscattering. On polarized dermoscopy, a homogeneous blue-gray hue is appreciated, but lighter segments may be present when collagen deposition is robust. Histopathologic findings confirm spindle-shaped dendritic melanocytes in the dermis without epidermal involvement. It generally is accepted that the etiology of these benign nevi is a failed migration of neural crest cells to the epidermis.10,11 Although the common blue nevus may be simple to diagnose, several subtypes have been described in the literature, including combined blue nevus, desmoplastic blue nevus, hypomelanotic/amelanotic blue nevus, and epithelioid blue nevus of Carney complex, and excluding a malignant process is of monumental importance.7,12
Biopsy is recommended for common blue nevi in the evaluation of newly acquired lesions, expansion of previously stable nevi, or for nevi larger than 10 mm in diameter. The nature of eruptive blue nevi warrants a biopsy to exclude melanoma or another malignant process. While the Becker nevus may manifest in adolescent males, it is clinically distinct from an eruptive blue nevus due to the size, relative homogeneity, and presence of hair within the lesion. Cutaneous amyloidosis may appear clinically similar to an eruptive blue nevus, but globular or amorphous material was not present in the papillary dermis of biopsied lesions in our patient. Since there was no cellular atypia or mitotic activity, melanoma and other malignancies were ruled out. Lastly, NAME syndrome by definition must include atrial myxomas, myxoid neurofibromas, and ephelides in addition to the nevi; however, our patient had only nevi and few ephelides. Once the diagnosis is established and benign nature confirmed, treatment is not necessarily required. If the patient elects to remove the lesion for aesthetic reasons, an excision into the subcutaneous fat is required to ensure complete removal of deep dermal melanocytes. Prior excisions of eruptive blue nevi have had no recurrence after more than 10 months.8,9
The Diagnosis: Eruptive Blue Nevus
All biopsies demonstrated similar histologic features, including an intradermal proliferation of heavily pigmented, spindle-shaped dendritic melanocytes (Figure). The dermal pigment was most pronounced in the grossly darker papules, and there was not a substantial amount of background pigmentation at the stratum basale. Cytologic atypia, foci of necrosis, and mitotic activity were absent from all sections. There was no definitive junctional component identified, no multinucleated giant cells, and there was no overlying epidermal aberration. With some background pigmentation seen histologically, nevus spilus was considered, but because this acute eruption occurred in a young adult without appreciable gross background hyperpigmentation, the clinical context led to a diagnosis of eruptive blue nevus. After communicating the findings to the patient, he declined further treatment.
Eruptive blue nevus is an exceptionally rare subtype of blue nevus with few cases reported since the 1940s.1-9 Generally, each case report found a triggering event that could possibly have precipitated the acute proliferation and evolution of nevi. Triggering events can include bullous processes such as erythema multiforme2 and Stevens-Johnson syndrome,3 severe sunburn,4 trauma,5 immunosuppression,6 and a variety of endocrinopathies. No such history could be identified in our patient, except the biopsy.
Common blue nevi are benign, usually congenital, well-circumscribed, solitary, blue-gray macules or papules. Half of blue nevi cases are found on the dorsal aspects of the hands and feet but can present anywhere (eg, face, scalp, wrists, sacrum, buttocks). The blue-gray color appreciated clinically is attributed to the Tyndall effect, which occurs when long-wavelength light--red, orange, and yellow--is absorbed by the melanin deep in the dermis, while short-wavelength visible light--blue, violet, and indigo--is reflected with backscattering. On polarized dermoscopy, a homogeneous blue-gray hue is appreciated, but lighter segments may be present when collagen deposition is robust. Histopathologic findings confirm spindle-shaped dendritic melanocytes in the dermis without epidermal involvement. It generally is accepted that the etiology of these benign nevi is a failed migration of neural crest cells to the epidermis.10,11 Although the common blue nevus may be simple to diagnose, several subtypes have been described in the literature, including combined blue nevus, desmoplastic blue nevus, hypomelanotic/amelanotic blue nevus, and epithelioid blue nevus of Carney complex, and excluding a malignant process is of monumental importance.7,12
Biopsy is recommended for common blue nevi in the evaluation of newly acquired lesions, expansion of previously stable nevi, or for nevi larger than 10 mm in diameter. The nature of eruptive blue nevi warrants a biopsy to exclude melanoma or another malignant process. While the Becker nevus may manifest in adolescent males, it is clinically distinct from an eruptive blue nevus due to the size, relative homogeneity, and presence of hair within the lesion. Cutaneous amyloidosis may appear clinically similar to an eruptive blue nevus, but globular or amorphous material was not present in the papillary dermis of biopsied lesions in our patient. Since there was no cellular atypia or mitotic activity, melanoma and other malignancies were ruled out. Lastly, NAME syndrome by definition must include atrial myxomas, myxoid neurofibromas, and ephelides in addition to the nevi; however, our patient had only nevi and few ephelides. Once the diagnosis is established and benign nature confirmed, treatment is not necessarily required. If the patient elects to remove the lesion for aesthetic reasons, an excision into the subcutaneous fat is required to ensure complete removal of deep dermal melanocytes. Prior excisions of eruptive blue nevi have had no recurrence after more than 10 months.8,9
- Krause M, Bonnekoh B, Weisshaar E, et al. Coincidence of multiple, disseminated, tardive-eruptive blue nevi with cutis marmorata teleangiectatica congenita. Dermatology. 2000;200:134-138.
- Soltani K, Bernstein J, Lorincz A. Eruptive nevocytic nevi after erythema multiforme. J Am Acad Dermatol. 1979;1:503-505.
- Shoji T, Cockerell C, Koff A, et al. Eruptive melanocytic nevi after Stevens-Johnson syndrome. J Am Acad Dermatol. 1997;37:337-339.
- Hendricks W. Eruptive blue nevi. J Am Acad Dermatol. 1981;4:50-53.
- Kesty K, Zargari O. Eruptive blue nevi. Indian J Dermatol Venereol Leprol. 2015;81:198-201.
- Chen T, Kurwa H, Trotter M, et al. Agminated blue nevi in a patient with dermatomyositis. J Am Acad Dermatol. 2013;68:52-53.
- Walsh M. Correspondence: eruptive disseminated blue naevi of the scalp. Br J Dermatol. 1999;141:581-582.
- Nardini P, De Giorgi V, Massi D, et al. Eruptive disseminated blue naevi of the scalp. Br J Dermatol. 1999;140:178-180.
- de Giorgi V, Massi D, Brunasso G, et al. Eruptive multiple blue nevi of the penis: a clinical dermoscopic pathologic case study. J Cutan Pathol. 2004;31:185-188.
- Zimmermann AH, Becker SA. Precursors of epidermal melanocytes in the negro fetus. In: Gordon M, ed. Pigment Cell Biology. New York, NY: Academic Press Inc; 1959:159-170.
- Leopold JG, Richards DB. The interrelationship of blue and common naevi. J Pathol Bacteriol. 1968;95:37-46.
- Zembowicz A, Phadke P. Blue nevi and variants: an update. Arch Pathol Lab Med. 2011;135:327-336.
- Krause M, Bonnekoh B, Weisshaar E, et al. Coincidence of multiple, disseminated, tardive-eruptive blue nevi with cutis marmorata teleangiectatica congenita. Dermatology. 2000;200:134-138.
- Soltani K, Bernstein J, Lorincz A. Eruptive nevocytic nevi after erythema multiforme. J Am Acad Dermatol. 1979;1:503-505.
- Shoji T, Cockerell C, Koff A, et al. Eruptive melanocytic nevi after Stevens-Johnson syndrome. J Am Acad Dermatol. 1997;37:337-339.
- Hendricks W. Eruptive blue nevi. J Am Acad Dermatol. 1981;4:50-53.
- Kesty K, Zargari O. Eruptive blue nevi. Indian J Dermatol Venereol Leprol. 2015;81:198-201.
- Chen T, Kurwa H, Trotter M, et al. Agminated blue nevi in a patient with dermatomyositis. J Am Acad Dermatol. 2013;68:52-53.
- Walsh M. Correspondence: eruptive disseminated blue naevi of the scalp. Br J Dermatol. 1999;141:581-582.
- Nardini P, De Giorgi V, Massi D, et al. Eruptive disseminated blue naevi of the scalp. Br J Dermatol. 1999;140:178-180.
- de Giorgi V, Massi D, Brunasso G, et al. Eruptive multiple blue nevi of the penis: a clinical dermoscopic pathologic case study. J Cutan Pathol. 2004;31:185-188.
- Zimmermann AH, Becker SA. Precursors of epidermal melanocytes in the negro fetus. In: Gordon M, ed. Pigment Cell Biology. New York, NY: Academic Press Inc; 1959:159-170.
- Leopold JG, Richards DB. The interrelationship of blue and common naevi. J Pathol Bacteriol. 1968;95:37-46.
- Zembowicz A, Phadke P. Blue nevi and variants: an update. Arch Pathol Lab Med. 2011;135:327-336.
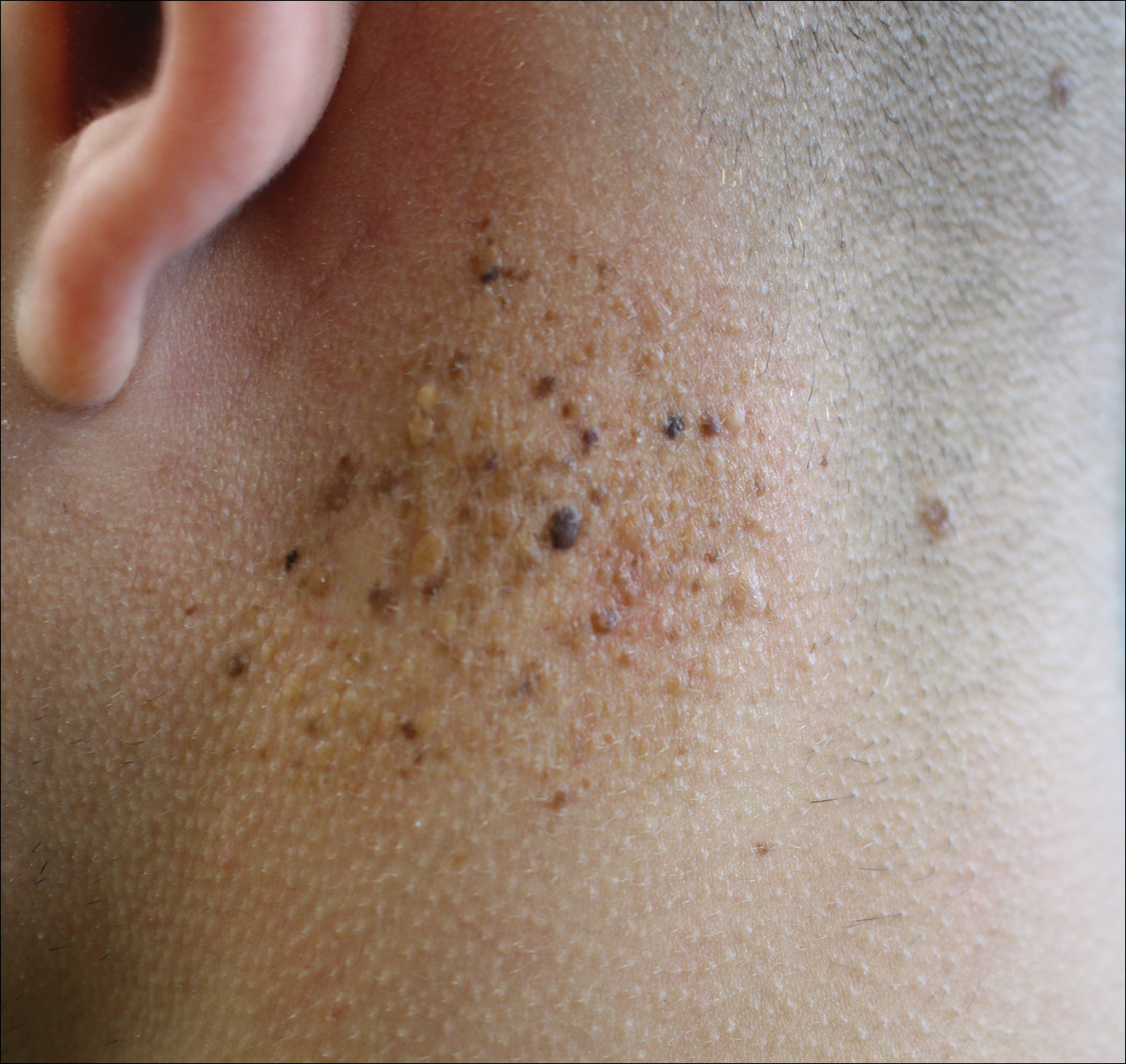
A 19-year-old man presented to the dermatology clinic for evaluation of several new dark papules on the neck of 1 year's duration. He denied any personal or family history of skin cancer, cardiac abnormalities, or endocrine dysfunction. He also denied any recent changes in health or use of medication. A biopsy was performed at the site 2 years prior for a single blue nevus, but the patient denied history of other trauma or cutaneous eruptions localized to the area. Physical examination revealed numerous dark brown, blue, white, and flesh-colored papules and macules agminated into a well-circumscribed plaque on the left posterolateral neck without background hyperpigmentation. The total area of the plaque was roughly 3×4 cm. There was no associated edema or erythema. Cardiac murmur, thyromegaly, exophthalmos, neurologic deficits, regional lymphadenopathy, and similar skin findings on other areas of the body were not appreciated. Three scouting punch biopsies were taken of the various morphologies present.

New MI definition aims to better distinguish infarction from injury
MUNICH – The worldwide cardiology community’s newly revised universal definition of an MI refines the way that cardiologists distinguish between myocardial infarction and myocardial injury, said Joseph S. Alpert, MD, one of the two chairs of the definition-writing panel.
“We had three previous definitions, but there is still a lot of confusion [about distinguishing] between injury and infarction. We definitely hope that this fourth definition will further help people distinguish the two and help people determine whether or not a patient has an MI,” said Dr. Alpert following a session at the annual congress of the European Society of Cardiology that introduced some of the key elements of the new revision.
Days before the ESC congress, a task force formed by the European Society of Cardiology, the American College of Cardiology, the American Heart Association, and the World Heart Federation released the Fourth Universal Definition of Myocardial Infarction (2018) (J Am Coll Cardiol. 2018 Aug 24. doi: 10.1016/j.jacc.2018.08.1038), which follows the series of three prior MI definitions that these groups have issued since the first iteration came out in 2007 (J Am Coll Cardiol. 2007;50[22]:2173-95).
The new revision includes 5 “new concepts,” 14 updated concepts, and 6 new sections since the third universal definition from 2012. The change that topped Dr. Alpert’s list of key messages was the need to determine whether a rise in cardiac troponin, a key biomarker of cardiac damage, resulted from infarction or injury.
These two alternative diagnoses mean “a very different outlook for patients. Treatment is different, and their prognosis is different. It’s important to make the distinction,” said Dr. Alpert, professor of medicine at the University of Arizona in Tucson.
The new changes to making an MI diagnosis will likely help drive a couple of important changes in the way U.S. patients with suspected myocardial injury or infarction get assessed, he said in an interview. The first change will be wide uptake of high sensitivity cardiac troponin (hscTn) assays over the next 5 years or so, as the ability to measure this key diagnostic biomarker progresses from its initial Food and Drug Administration approval for the U.S. market in 2017 to “close to 100% of U.S. hospitals using it,” he predicted. A big issue that is currently slowing even quicker adoption of hscTn is that many hospitals, including the one where Dr. Alpert practices, still have laboratory contracts in place that tether them to older troponin-testing technologies and make it economically unfeasible to change until their contracts expire. The contract in place where Dr. Alpert practices runs out in 2019, and soon after that happens he expects to gain the ability to order a hscTn test.
The new, fourth definition says that hscTn is “recommended for routine clinical use,” but routine U.S. use “won’t be immediate because many hospitals will put in hscTn only when their old contract runs out,” he said.
Another practice-changing impact from the fourth definition may be expanded U.S. availability and use of MR imaging, which the fourth definition identified as the most informative and versatile of the several imaging options used to confirm or rule out an MI.
Cardiac MR “provides both functional and tissue characterization. It’s the technique with the most potential,” able to noninvasively identify “both the nature and extent of myocardial damage,” explained Chiara Bucciarelli-Ducci, MD, a cardiologist and imaging specialist at the Bristol (England) Heart Institute. A single cardiac MR scan “gives many answers,” said Dr. Bucciarelli-Ducci, who also served on the fourth definition task force and spoke at the session about the document’s revised imaging recommendations.

“In the setting of acute MI, cardiac MR can also be used to assess the presence and extent of myocardium at risk (myocardial edema), myocardial salvage, microvascular obstruction, intramyocardial hemorrhage, and infarct size, all markers of myocardial injury that have prognostic value,” according to the fourth definition. “In patients with possible acute MI but unobstructed coronary arteries, cardiac MR can help to diagnose alternative conditions such as myocarditis, Takotsubo syndrome, embolic infarction, or MI with spontaneous recanalization.”
“What’s turning out is that, a large number of patients with chest pain have an infection and not an MI, and cardiac MR can distinguish inflammation and myocarditis from infarction. We’re now doing a lot more MRs,” Dr. Alpert said. Although MR capability is not as widely available today as other imaging methods, like echocardiography and CT, over the next 5 years that will likely change, he said. But Dr. Alpert cautioned that not every patient with a suspected MI needs MR assessment. It’s best focused for selected patients with an uncertain diagnosis based on the core indicators of disease: history, ECG, changes in hscTn levels over time, and a chest x-ray. “MR is for when there are questions,” he said. When patients present with classic MI signs and symptoms the diagnosis can depend just on the basics, perhaps supplemented with a more widely available imaging method like echocardiography to look for wall motion abnormalities, he said. “If echo shows good left ventricular function you probably don’t need MR.” he said.
CT coronary angiography (CTCA) is another useful diagnostic tool, and right now is more widely available than MR. CTCA “may be used to diagnose coronary artery disease in patients with an acute coronary syndrome event in the emergency department or chest pain unit, particularly in low- to intermediate-risk patients with normal hscTn at presentation,” said the fourth definition. But Dr. Alpert cited the radiation dose from CT as a limiting factor. “We have patients who get repeat CT scans, and we know that increases their cancer risk. There is no such thing as a totally safe dose of radiation.” Lack of radiation exposure is another feature that makes MR imaging attractive.
Dr. Alpert had no disclosures. Dr. Bucciarelli-Ducci has had a financial relationship with Circle Cardiovascular Imaging.
MUNICH – The worldwide cardiology community’s newly revised universal definition of an MI refines the way that cardiologists distinguish between myocardial infarction and myocardial injury, said Joseph S. Alpert, MD, one of the two chairs of the definition-writing panel.
“We had three previous definitions, but there is still a lot of confusion [about distinguishing] between injury and infarction. We definitely hope that this fourth definition will further help people distinguish the two and help people determine whether or not a patient has an MI,” said Dr. Alpert following a session at the annual congress of the European Society of Cardiology that introduced some of the key elements of the new revision.
Days before the ESC congress, a task force formed by the European Society of Cardiology, the American College of Cardiology, the American Heart Association, and the World Heart Federation released the Fourth Universal Definition of Myocardial Infarction (2018) (J Am Coll Cardiol. 2018 Aug 24. doi: 10.1016/j.jacc.2018.08.1038), which follows the series of three prior MI definitions that these groups have issued since the first iteration came out in 2007 (J Am Coll Cardiol. 2007;50[22]:2173-95).
The new revision includes 5 “new concepts,” 14 updated concepts, and 6 new sections since the third universal definition from 2012. The change that topped Dr. Alpert’s list of key messages was the need to determine whether a rise in cardiac troponin, a key biomarker of cardiac damage, resulted from infarction or injury.
These two alternative diagnoses mean “a very different outlook for patients. Treatment is different, and their prognosis is different. It’s important to make the distinction,” said Dr. Alpert, professor of medicine at the University of Arizona in Tucson.
The new changes to making an MI diagnosis will likely help drive a couple of important changes in the way U.S. patients with suspected myocardial injury or infarction get assessed, he said in an interview. The first change will be wide uptake of high sensitivity cardiac troponin (hscTn) assays over the next 5 years or so, as the ability to measure this key diagnostic biomarker progresses from its initial Food and Drug Administration approval for the U.S. market in 2017 to “close to 100% of U.S. hospitals using it,” he predicted. A big issue that is currently slowing even quicker adoption of hscTn is that many hospitals, including the one where Dr. Alpert practices, still have laboratory contracts in place that tether them to older troponin-testing technologies and make it economically unfeasible to change until their contracts expire. The contract in place where Dr. Alpert practices runs out in 2019, and soon after that happens he expects to gain the ability to order a hscTn test.
The new, fourth definition says that hscTn is “recommended for routine clinical use,” but routine U.S. use “won’t be immediate because many hospitals will put in hscTn only when their old contract runs out,” he said.
Another practice-changing impact from the fourth definition may be expanded U.S. availability and use of MR imaging, which the fourth definition identified as the most informative and versatile of the several imaging options used to confirm or rule out an MI.
Cardiac MR “provides both functional and tissue characterization. It’s the technique with the most potential,” able to noninvasively identify “both the nature and extent of myocardial damage,” explained Chiara Bucciarelli-Ducci, MD, a cardiologist and imaging specialist at the Bristol (England) Heart Institute. A single cardiac MR scan “gives many answers,” said Dr. Bucciarelli-Ducci, who also served on the fourth definition task force and spoke at the session about the document’s revised imaging recommendations.
“In the setting of acute MI, cardiac MR can also be used to assess the presence and extent of myocardium at risk (myocardial edema), myocardial salvage, microvascular obstruction, intramyocardial hemorrhage, and infarct size, all markers of myocardial injury that have prognostic value,” according to the fourth definition. “In patients with possible acute MI but unobstructed coronary arteries, cardiac MR can help to diagnose alternative conditions such as myocarditis, Takotsubo syndrome, embolic infarction, or MI with spontaneous recanalization.”
“What’s turning out is that, a large number of patients with chest pain have an infection and not an MI, and cardiac MR can distinguish inflammation and myocarditis from infarction. We’re now doing a lot more MRs,” Dr. Alpert said. Although MR capability is not as widely available today as other imaging methods, like echocardiography and CT, over the next 5 years that will likely change, he said. But Dr. Alpert cautioned that not every patient with a suspected MI needs MR assessment. It’s best focused for selected patients with an uncertain diagnosis based on the core indicators of disease: history, ECG, changes in hscTn levels over time, and a chest x-ray. “MR is for when there are questions,” he said. When patients present with classic MI signs and symptoms the diagnosis can depend just on the basics, perhaps supplemented with a more widely available imaging method like echocardiography to look for wall motion abnormalities, he said. “If echo shows good left ventricular function you probably don’t need MR.” he said.
CT coronary angiography (CTCA) is another useful diagnostic tool, and right now is more widely available than MR. CTCA “may be used to diagnose coronary artery disease in patients with an acute coronary syndrome event in the emergency department or chest pain unit, particularly in low- to intermediate-risk patients with normal hscTn at presentation,” said the fourth definition. But Dr. Alpert cited the radiation dose from CT as a limiting factor. “We have patients who get repeat CT scans, and we know that increases their cancer risk. There is no such thing as a totally safe dose of radiation.” Lack of radiation exposure is another feature that makes MR imaging attractive.
Dr. Alpert had no disclosures. Dr. Bucciarelli-Ducci has had a financial relationship with Circle Cardiovascular Imaging.
MUNICH – The worldwide cardiology community’s newly revised universal definition of an MI refines the way that cardiologists distinguish between myocardial infarction and myocardial injury, said Joseph S. Alpert, MD, one of the two chairs of the definition-writing panel.
“We had three previous definitions, but there is still a lot of confusion [about distinguishing] between injury and infarction. We definitely hope that this fourth definition will further help people distinguish the two and help people determine whether or not a patient has an MI,” said Dr. Alpert following a session at the annual congress of the European Society of Cardiology that introduced some of the key elements of the new revision.
Days before the ESC congress, a task force formed by the European Society of Cardiology, the American College of Cardiology, the American Heart Association, and the World Heart Federation released the Fourth Universal Definition of Myocardial Infarction (2018) (J Am Coll Cardiol. 2018 Aug 24. doi: 10.1016/j.jacc.2018.08.1038), which follows the series of three prior MI definitions that these groups have issued since the first iteration came out in 2007 (J Am Coll Cardiol. 2007;50[22]:2173-95).
The new revision includes 5 “new concepts,” 14 updated concepts, and 6 new sections since the third universal definition from 2012. The change that topped Dr. Alpert’s list of key messages was the need to determine whether a rise in cardiac troponin, a key biomarker of cardiac damage, resulted from infarction or injury.
These two alternative diagnoses mean “a very different outlook for patients. Treatment is different, and their prognosis is different. It’s important to make the distinction,” said Dr. Alpert, professor of medicine at the University of Arizona in Tucson.
The new changes to making an MI diagnosis will likely help drive a couple of important changes in the way U.S. patients with suspected myocardial injury or infarction get assessed, he said in an interview. The first change will be wide uptake of high sensitivity cardiac troponin (hscTn) assays over the next 5 years or so, as the ability to measure this key diagnostic biomarker progresses from its initial Food and Drug Administration approval for the U.S. market in 2017 to “close to 100% of U.S. hospitals using it,” he predicted. A big issue that is currently slowing even quicker adoption of hscTn is that many hospitals, including the one where Dr. Alpert practices, still have laboratory contracts in place that tether them to older troponin-testing technologies and make it economically unfeasible to change until their contracts expire. The contract in place where Dr. Alpert practices runs out in 2019, and soon after that happens he expects to gain the ability to order a hscTn test.
The new, fourth definition says that hscTn is “recommended for routine clinical use,” but routine U.S. use “won’t be immediate because many hospitals will put in hscTn only when their old contract runs out,” he said.
Another practice-changing impact from the fourth definition may be expanded U.S. availability and use of MR imaging, which the fourth definition identified as the most informative and versatile of the several imaging options used to confirm or rule out an MI.
Cardiac MR “provides both functional and tissue characterization. It’s the technique with the most potential,” able to noninvasively identify “both the nature and extent of myocardial damage,” explained Chiara Bucciarelli-Ducci, MD, a cardiologist and imaging specialist at the Bristol (England) Heart Institute. A single cardiac MR scan “gives many answers,” said Dr. Bucciarelli-Ducci, who also served on the fourth definition task force and spoke at the session about the document’s revised imaging recommendations.
“In the setting of acute MI, cardiac MR can also be used to assess the presence and extent of myocardium at risk (myocardial edema), myocardial salvage, microvascular obstruction, intramyocardial hemorrhage, and infarct size, all markers of myocardial injury that have prognostic value,” according to the fourth definition. “In patients with possible acute MI but unobstructed coronary arteries, cardiac MR can help to diagnose alternative conditions such as myocarditis, Takotsubo syndrome, embolic infarction, or MI with spontaneous recanalization.”
“What’s turning out is that, a large number of patients with chest pain have an infection and not an MI, and cardiac MR can distinguish inflammation and myocarditis from infarction. We’re now doing a lot more MRs,” Dr. Alpert said. Although MR capability is not as widely available today as other imaging methods, like echocardiography and CT, over the next 5 years that will likely change, he said. But Dr. Alpert cautioned that not every patient with a suspected MI needs MR assessment. It’s best focused for selected patients with an uncertain diagnosis based on the core indicators of disease: history, ECG, changes in hscTn levels over time, and a chest x-ray. “MR is for when there are questions,” he said. When patients present with classic MI signs and symptoms the diagnosis can depend just on the basics, perhaps supplemented with a more widely available imaging method like echocardiography to look for wall motion abnormalities, he said. “If echo shows good left ventricular function you probably don’t need MR.” he said.
CT coronary angiography (CTCA) is another useful diagnostic tool, and right now is more widely available than MR. CTCA “may be used to diagnose coronary artery disease in patients with an acute coronary syndrome event in the emergency department or chest pain unit, particularly in low- to intermediate-risk patients with normal hscTn at presentation,” said the fourth definition. But Dr. Alpert cited the radiation dose from CT as a limiting factor. “We have patients who get repeat CT scans, and we know that increases their cancer risk. There is no such thing as a totally safe dose of radiation.” Lack of radiation exposure is another feature that makes MR imaging attractive.
Dr. Alpert had no disclosures. Dr. Bucciarelli-Ducci has had a financial relationship with Circle Cardiovascular Imaging.
REPORTING FROM THE ESC CONGRESS 2018