User login
Predicting stent failure in the treatment of May-Thurner syndrome
BOSTON – The use of an intravascular ultrasound (IVUS)–based scoring system could predict stent failure at 2 years in the treatment of May-Thurner syndrome, according to Steven D. Abramowitz, MD, of the MedStar Washington Hospital Center, Washington, and his colleagues.

Dr. Abramowitz presented their research in the Vascular and Endovascular Society (VESS) sessions held at the Vascular Annual Meeting.
“IVUS has become an important adjuvant diagnostic tool in the treatment of deep venous disease, and as such may provide a useful assessment and predictive tool for treatment success in stenting of May-Thurner syndrome,” said Dr. Abramowitz.
In their study, 118 consecutive patients with May-Thurner syndrome underwent IVUS-guided stent placement from April 2009 through May 2015 at two collaborating institutions. Patients had a mean age of 46 years and included 86 (73%) women. At the time of treatment, 45, 30, 25, and 18 patients had Clinical Etiology Anatomy Pathophysiology disease 3, 4, 5, and 6, respectively.
Dr. Abramowitz described how he and his colleagues derived an IVUS-driven scoring system to assess the following categories of May-Thurner syndrome (nonocclusive or occlusive), disease chronicity (nonthrombotic, acute, or chronic), venous disease length (less than 180 mm or greater than 181 mm), venous inflow compliance (presence or absence of respiratory variation), iliocaval confluence disease involvement (present or absent), iliocaval con-fluence stenting obligation (stented or spared), and presence of perivenous collaterals before and after stenting (none or resolved).
Six of the categories were scored with 0 or 1 and one category was scored with 0, 1, or 2. Scores were tabulated for each patient at the time of initial intervention.
All 118 (100%) patients received anticoagulation and 78 (66%) were on an antiplatelet agent. Thirty-eight (32%) developed moderate in-stent stenosis, required thrombolysis, or underwent additional stenting procedures and were considered treatment failures during the observed period.
Eighty patients (68%) required no additional intervention and were considered treatment successes. The mean IVUS score for all patients was 5.22. The mean IVUS score in the treatment failure cohort was 5.64 compared with a score of 4.67 in the treatment success group, a significant difference. Patients with a score above 4 on this 7-point scale had an increased relative risk (1.6) of stent failure at 2 years.
“An IVUS-driven scoring system score of 4 or greater during initial intervention for May-Thurner syndrome predicts failure at 2 years. Additional treatment modalities should be considered at implantation to prevent failure,” said Dr. Abramowitz.
In an interview, Dr. Abramowitz added: “There is an emerging body of research regarding outcomes of deep venous intervention. However, we are still looking to generate clinically relevant data that will help guide interventionists to achieve durable technical success and long-term positive clinical outcomes for our patients.
“At this time, there is very little data to help correlate what physicians see on venography and IVUS during the treatment of May-Thurner Lesions. This data is hopefully the first step in allowing us to guide intra-operative decision making. IVUS is an excellent tool that has been proven by other studies to aid in the diagnosis and management of venous disease. With this data we also hope that it becomes a drive of patient management as well. Ideally, this data will transition into also guiding anticoagulation management, postoperative surveillance strategies and outcomes stratification for patients,” Dr. Abramowitz concluded.
BOSTON – The use of an intravascular ultrasound (IVUS)–based scoring system could predict stent failure at 2 years in the treatment of May-Thurner syndrome, according to Steven D. Abramowitz, MD, of the MedStar Washington Hospital Center, Washington, and his colleagues.
Dr. Abramowitz presented their research in the Vascular and Endovascular Society (VESS) sessions held at the Vascular Annual Meeting.
“IVUS has become an important adjuvant diagnostic tool in the treatment of deep venous disease, and as such may provide a useful assessment and predictive tool for treatment success in stenting of May-Thurner syndrome,” said Dr. Abramowitz.
In their study, 118 consecutive patients with May-Thurner syndrome underwent IVUS-guided stent placement from April 2009 through May 2015 at two collaborating institutions. Patients had a mean age of 46 years and included 86 (73%) women. At the time of treatment, 45, 30, 25, and 18 patients had Clinical Etiology Anatomy Pathophysiology disease 3, 4, 5, and 6, respectively.
Dr. Abramowitz described how he and his colleagues derived an IVUS-driven scoring system to assess the following categories of May-Thurner syndrome (nonocclusive or occlusive), disease chronicity (nonthrombotic, acute, or chronic), venous disease length (less than 180 mm or greater than 181 mm), venous inflow compliance (presence or absence of respiratory variation), iliocaval confluence disease involvement (present or absent), iliocaval con-fluence stenting obligation (stented or spared), and presence of perivenous collaterals before and after stenting (none or resolved).
Six of the categories were scored with 0 or 1 and one category was scored with 0, 1, or 2. Scores were tabulated for each patient at the time of initial intervention.
All 118 (100%) patients received anticoagulation and 78 (66%) were on an antiplatelet agent. Thirty-eight (32%) developed moderate in-stent stenosis, required thrombolysis, or underwent additional stenting procedures and were considered treatment failures during the observed period.
Eighty patients (68%) required no additional intervention and were considered treatment successes. The mean IVUS score for all patients was 5.22. The mean IVUS score in the treatment failure cohort was 5.64 compared with a score of 4.67 in the treatment success group, a significant difference. Patients with a score above 4 on this 7-point scale had an increased relative risk (1.6) of stent failure at 2 years.
“An IVUS-driven scoring system score of 4 or greater during initial intervention for May-Thurner syndrome predicts failure at 2 years. Additional treatment modalities should be considered at implantation to prevent failure,” said Dr. Abramowitz.
In an interview, Dr. Abramowitz added: “There is an emerging body of research regarding outcomes of deep venous intervention. However, we are still looking to generate clinically relevant data that will help guide interventionists to achieve durable technical success and long-term positive clinical outcomes for our patients.
“At this time, there is very little data to help correlate what physicians see on venography and IVUS during the treatment of May-Thurner Lesions. This data is hopefully the first step in allowing us to guide intra-operative decision making. IVUS is an excellent tool that has been proven by other studies to aid in the diagnosis and management of venous disease. With this data we also hope that it becomes a drive of patient management as well. Ideally, this data will transition into also guiding anticoagulation management, postoperative surveillance strategies and outcomes stratification for patients,” Dr. Abramowitz concluded.
BOSTON – The use of an intravascular ultrasound (IVUS)–based scoring system could predict stent failure at 2 years in the treatment of May-Thurner syndrome, according to Steven D. Abramowitz, MD, of the MedStar Washington Hospital Center, Washington, and his colleagues.
Dr. Abramowitz presented their research in the Vascular and Endovascular Society (VESS) sessions held at the Vascular Annual Meeting.
“IVUS has become an important adjuvant diagnostic tool in the treatment of deep venous disease, and as such may provide a useful assessment and predictive tool for treatment success in stenting of May-Thurner syndrome,” said Dr. Abramowitz.
In their study, 118 consecutive patients with May-Thurner syndrome underwent IVUS-guided stent placement from April 2009 through May 2015 at two collaborating institutions. Patients had a mean age of 46 years and included 86 (73%) women. At the time of treatment, 45, 30, 25, and 18 patients had Clinical Etiology Anatomy Pathophysiology disease 3, 4, 5, and 6, respectively.
Dr. Abramowitz described how he and his colleagues derived an IVUS-driven scoring system to assess the following categories of May-Thurner syndrome (nonocclusive or occlusive), disease chronicity (nonthrombotic, acute, or chronic), venous disease length (less than 180 mm or greater than 181 mm), venous inflow compliance (presence or absence of respiratory variation), iliocaval confluence disease involvement (present or absent), iliocaval con-fluence stenting obligation (stented or spared), and presence of perivenous collaterals before and after stenting (none or resolved).
Six of the categories were scored with 0 or 1 and one category was scored with 0, 1, or 2. Scores were tabulated for each patient at the time of initial intervention.
All 118 (100%) patients received anticoagulation and 78 (66%) were on an antiplatelet agent. Thirty-eight (32%) developed moderate in-stent stenosis, required thrombolysis, or underwent additional stenting procedures and were considered treatment failures during the observed period.
Eighty patients (68%) required no additional intervention and were considered treatment successes. The mean IVUS score for all patients was 5.22. The mean IVUS score in the treatment failure cohort was 5.64 compared with a score of 4.67 in the treatment success group, a significant difference. Patients with a score above 4 on this 7-point scale had an increased relative risk (1.6) of stent failure at 2 years.
“An IVUS-driven scoring system score of 4 or greater during initial intervention for May-Thurner syndrome predicts failure at 2 years. Additional treatment modalities should be considered at implantation to prevent failure,” said Dr. Abramowitz.
In an interview, Dr. Abramowitz added: “There is an emerging body of research regarding outcomes of deep venous intervention. However, we are still looking to generate clinically relevant data that will help guide interventionists to achieve durable technical success and long-term positive clinical outcomes for our patients.
“At this time, there is very little data to help correlate what physicians see on venography and IVUS during the treatment of May-Thurner Lesions. This data is hopefully the first step in allowing us to guide intra-operative decision making. IVUS is an excellent tool that has been proven by other studies to aid in the diagnosis and management of venous disease. With this data we also hope that it becomes a drive of patient management as well. Ideally, this data will transition into also guiding anticoagulation management, postoperative surveillance strategies and outcomes stratification for patients,” Dr. Abramowitz concluded.
FROM THE VASCULAR ANNUAL MEETING
Factor Xa inhibitors versus vitamin K antagonists for preventing embolism in AF patients
Clinical question: Do factor Xa inhibitors reduce the incidence of strokes and systemic embolic events, compared with warfarin, in people with atrial fibrillation?
Background: Factor Xa inhibitors, called DOACs or direct-acting anticoagulants, and vitamin K antagonists (VKAs) are part of treatment guidelines for preventing stroke and systemic embolic events in people with atrial fibrillation (AF). This study assessed the effectiveness and safety of treatment with factor Xa inhibitors versus VKAs for preventing cerebral or systemic embolic events in AF.
Study design: Cochrane Review update.

Setting: Data obtained from trial registers of the Cochrane Central Register of Controlled Trials (August 2017), the Cochrane Heart Group and the Cochrane Stroke Group (September 2016), Embase (1980 to April 2017), and MEDLINE (1950 to April 2017). Authors also screened reference lists and contacted pharmaceutical companies, authors, and sponsors of relevant published trials.
Synopsis: The study included 42,084 participants from 10 trials with a diagnosis of AF who were eligible for long-term anticoagulation with warfarin (target INR 2-3).
The trials directly compared dose-adjusted warfarin with factor Xa inhibitors. Median follow-up ranged from 12 weeks to 1.9 years, and composite primary endpoint was all strokes (both ischemic and hemorrhagic) and non–central nervous systemic embolic events. Factor Xa inhibitor significantly decreased the number of strokes and systemic embolic events, compared with dose-adjusted warfarin (odds ratio, 0.81; 95% confidence interval, 0.72-0.91), reduced the number of major bleeding events (OR, 0.92; 95% CI, 0.63-1.34), and significantly reduced the risk of intracranial hemorrhage (OR, 0.56; 95% CI, 0.45-0.70). They also significantly reduced the number of all-cause deaths (OR, 0.88; 95% CI, 0.81-0.97). One limitation of this study is the heterogeneity and hence lower quality of evidence. This study shows a small net clinical benefit of using factor Xa inhibitors in AF because of a reduction in strokes and systemic embolic events and also a lower risk of bleeding (including intracranial hemorrhages), compared with using warfarin.
Bottom line: Patients with AF have a lower incidence of strokes and systemic embolic events when treated with factor Xa inhibitors, compared with those treated with warfarin.
Citation: Bruins Slot KM et al. Factor Xa inhibitors versus vitamin K antagonists for preventing cerebral or systemic embolism in patients with atrial fibrillation. Cochrane Database Syst Rev. 2018 Mar 6. doi: 10.1002/14651858.CD008980.pub3.
Dr. Veedu is a hospitalist and instructor in the division of hospital medicine at the University of Kentucky, Lexington.
Clinical question: Do factor Xa inhibitors reduce the incidence of strokes and systemic embolic events, compared with warfarin, in people with atrial fibrillation?
Background: Factor Xa inhibitors, called DOACs or direct-acting anticoagulants, and vitamin K antagonists (VKAs) are part of treatment guidelines for preventing stroke and systemic embolic events in people with atrial fibrillation (AF). This study assessed the effectiveness and safety of treatment with factor Xa inhibitors versus VKAs for preventing cerebral or systemic embolic events in AF.
Study design: Cochrane Review update.
Setting: Data obtained from trial registers of the Cochrane Central Register of Controlled Trials (August 2017), the Cochrane Heart Group and the Cochrane Stroke Group (September 2016), Embase (1980 to April 2017), and MEDLINE (1950 to April 2017). Authors also screened reference lists and contacted pharmaceutical companies, authors, and sponsors of relevant published trials.
Synopsis: The study included 42,084 participants from 10 trials with a diagnosis of AF who were eligible for long-term anticoagulation with warfarin (target INR 2-3).
The trials directly compared dose-adjusted warfarin with factor Xa inhibitors. Median follow-up ranged from 12 weeks to 1.9 years, and composite primary endpoint was all strokes (both ischemic and hemorrhagic) and non–central nervous systemic embolic events. Factor Xa inhibitor significantly decreased the number of strokes and systemic embolic events, compared with dose-adjusted warfarin (odds ratio, 0.81; 95% confidence interval, 0.72-0.91), reduced the number of major bleeding events (OR, 0.92; 95% CI, 0.63-1.34), and significantly reduced the risk of intracranial hemorrhage (OR, 0.56; 95% CI, 0.45-0.70). They also significantly reduced the number of all-cause deaths (OR, 0.88; 95% CI, 0.81-0.97). One limitation of this study is the heterogeneity and hence lower quality of evidence. This study shows a small net clinical benefit of using factor Xa inhibitors in AF because of a reduction in strokes and systemic embolic events and also a lower risk of bleeding (including intracranial hemorrhages), compared with using warfarin.
Bottom line: Patients with AF have a lower incidence of strokes and systemic embolic events when treated with factor Xa inhibitors, compared with those treated with warfarin.
Citation: Bruins Slot KM et al. Factor Xa inhibitors versus vitamin K antagonists for preventing cerebral or systemic embolism in patients with atrial fibrillation. Cochrane Database Syst Rev. 2018 Mar 6. doi: 10.1002/14651858.CD008980.pub3.
Dr. Veedu is a hospitalist and instructor in the division of hospital medicine at the University of Kentucky, Lexington.
Clinical question: Do factor Xa inhibitors reduce the incidence of strokes and systemic embolic events, compared with warfarin, in people with atrial fibrillation?
Background: Factor Xa inhibitors, called DOACs or direct-acting anticoagulants, and vitamin K antagonists (VKAs) are part of treatment guidelines for preventing stroke and systemic embolic events in people with atrial fibrillation (AF). This study assessed the effectiveness and safety of treatment with factor Xa inhibitors versus VKAs for preventing cerebral or systemic embolic events in AF.
Study design: Cochrane Review update.
Setting: Data obtained from trial registers of the Cochrane Central Register of Controlled Trials (August 2017), the Cochrane Heart Group and the Cochrane Stroke Group (September 2016), Embase (1980 to April 2017), and MEDLINE (1950 to April 2017). Authors also screened reference lists and contacted pharmaceutical companies, authors, and sponsors of relevant published trials.
Synopsis: The study included 42,084 participants from 10 trials with a diagnosis of AF who were eligible for long-term anticoagulation with warfarin (target INR 2-3).
The trials directly compared dose-adjusted warfarin with factor Xa inhibitors. Median follow-up ranged from 12 weeks to 1.9 years, and composite primary endpoint was all strokes (both ischemic and hemorrhagic) and non–central nervous systemic embolic events. Factor Xa inhibitor significantly decreased the number of strokes and systemic embolic events, compared with dose-adjusted warfarin (odds ratio, 0.81; 95% confidence interval, 0.72-0.91), reduced the number of major bleeding events (OR, 0.92; 95% CI, 0.63-1.34), and significantly reduced the risk of intracranial hemorrhage (OR, 0.56; 95% CI, 0.45-0.70). They also significantly reduced the number of all-cause deaths (OR, 0.88; 95% CI, 0.81-0.97). One limitation of this study is the heterogeneity and hence lower quality of evidence. This study shows a small net clinical benefit of using factor Xa inhibitors in AF because of a reduction in strokes and systemic embolic events and also a lower risk of bleeding (including intracranial hemorrhages), compared with using warfarin.
Bottom line: Patients with AF have a lower incidence of strokes and systemic embolic events when treated with factor Xa inhibitors, compared with those treated with warfarin.
Citation: Bruins Slot KM et al. Factor Xa inhibitors versus vitamin K antagonists for preventing cerebral or systemic embolism in patients with atrial fibrillation. Cochrane Database Syst Rev. 2018 Mar 6. doi: 10.1002/14651858.CD008980.pub3.
Dr. Veedu is a hospitalist and instructor in the division of hospital medicine at the University of Kentucky, Lexington.
No-shows: Trying to predict and reduce the unpredictable
Why do patients no-show?
The reasons are, obviously, widely variable among patients and circumstances. Some are more understandable than others, but all of them add up to an empty chair across the desk and loss of income for that time slot.

A recent study in Neurology: Clinical Practice looked into this question. Interestingly, it found that people with certain chronic diseases, such as medication-overuse headaches, chronic daily headaches, and seizures, were among those with the highest no-show rates.
These are all conditions that require medication fine tuning, but this can be difficult without the patient coming in. There’s only so much that can be done on the phone, and in this business a direct face-to-face conversation is often needed.
On the opposite side, they noted that people with degenerative disorders that have more limited treatments, such as Alzheimer’s and Parkinson’s diseases, had the highest rate of making it to the appointment, though this may be due more to caretakers than the patients themselves.
Financial issues come into play. Younger patients with chronic diseases may have more difficulty taking time off work, or may just simply not have the money for a copay. They could also be too depressed from their situation to come in. Granted, it would be nice if they’d call to let us know they weren’t coming (at my office we don’t ask questions), but many don’t bother.
All of us are affected by this problem. Seeing patients is what drives the economics of every medical practice. An empty exam room is a financial hit, and it denies another patient who needs help a chance to be seen.
Fifteen years ago, my billing company ran some numbers and found that patients on one specific insurance plan had two to three times the rate of no-shows of any of my other contracts. With a number like that, I couldn’t see a reason to stay with them, and I dropped that plan. I felt bad for the reliable patients affected, but the hard truth is that if I can’t keep my practice open, I can’t help anyone. Why this plan had so many no-shows could be from a number of factors, but the end result was the same. Regardless of the reason, it was having a negative impact on my bottom line.

We try all kinds of different ways to remind people of their appointments. My secretary makes reminder calls. Other offices send texts or emails, or have a robocall system. These can only help to a certain degree. At some point, this becomes the “you can lead a horse to water ...” adage.
There’s no real easy answer, either. At my office, we don’t overbook. It seems to be an unwritten rule that every time we gamble that someone won’t come in and then put someone else in the slot, they both show up.
Research like this is interesting, and maybe helpful at making a predictive model about no-shows. But I’m not convinced it will eventually have everyday use in a real-world practice.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Why do patients no-show?
The reasons are, obviously, widely variable among patients and circumstances. Some are more understandable than others, but all of them add up to an empty chair across the desk and loss of income for that time slot.
A recent study in Neurology: Clinical Practice looked into this question. Interestingly, it found that people with certain chronic diseases, such as medication-overuse headaches, chronic daily headaches, and seizures, were among those with the highest no-show rates.
These are all conditions that require medication fine tuning, but this can be difficult without the patient coming in. There’s only so much that can be done on the phone, and in this business a direct face-to-face conversation is often needed.
On the opposite side, they noted that people with degenerative disorders that have more limited treatments, such as Alzheimer’s and Parkinson’s diseases, had the highest rate of making it to the appointment, though this may be due more to caretakers than the patients themselves.
Financial issues come into play. Younger patients with chronic diseases may have more difficulty taking time off work, or may just simply not have the money for a copay. They could also be too depressed from their situation to come in. Granted, it would be nice if they’d call to let us know they weren’t coming (at my office we don’t ask questions), but many don’t bother.
All of us are affected by this problem. Seeing patients is what drives the economics of every medical practice. An empty exam room is a financial hit, and it denies another patient who needs help a chance to be seen.
Fifteen years ago, my billing company ran some numbers and found that patients on one specific insurance plan had two to three times the rate of no-shows of any of my other contracts. With a number like that, I couldn’t see a reason to stay with them, and I dropped that plan. I felt bad for the reliable patients affected, but the hard truth is that if I can’t keep my practice open, I can’t help anyone. Why this plan had so many no-shows could be from a number of factors, but the end result was the same. Regardless of the reason, it was having a negative impact on my bottom line.
We try all kinds of different ways to remind people of their appointments. My secretary makes reminder calls. Other offices send texts or emails, or have a robocall system. These can only help to a certain degree. At some point, this becomes the “you can lead a horse to water ...” adage.
There’s no real easy answer, either. At my office, we don’t overbook. It seems to be an unwritten rule that every time we gamble that someone won’t come in and then put someone else in the slot, they both show up.
Research like this is interesting, and maybe helpful at making a predictive model about no-shows. But I’m not convinced it will eventually have everyday use in a real-world practice.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Why do patients no-show?
The reasons are, obviously, widely variable among patients and circumstances. Some are more understandable than others, but all of them add up to an empty chair across the desk and loss of income for that time slot.
A recent study in Neurology: Clinical Practice looked into this question. Interestingly, it found that people with certain chronic diseases, such as medication-overuse headaches, chronic daily headaches, and seizures, were among those with the highest no-show rates.
These are all conditions that require medication fine tuning, but this can be difficult without the patient coming in. There’s only so much that can be done on the phone, and in this business a direct face-to-face conversation is often needed.
On the opposite side, they noted that people with degenerative disorders that have more limited treatments, such as Alzheimer’s and Parkinson’s diseases, had the highest rate of making it to the appointment, though this may be due more to caretakers than the patients themselves.
Financial issues come into play. Younger patients with chronic diseases may have more difficulty taking time off work, or may just simply not have the money for a copay. They could also be too depressed from their situation to come in. Granted, it would be nice if they’d call to let us know they weren’t coming (at my office we don’t ask questions), but many don’t bother.
All of us are affected by this problem. Seeing patients is what drives the economics of every medical practice. An empty exam room is a financial hit, and it denies another patient who needs help a chance to be seen.
Fifteen years ago, my billing company ran some numbers and found that patients on one specific insurance plan had two to three times the rate of no-shows of any of my other contracts. With a number like that, I couldn’t see a reason to stay with them, and I dropped that plan. I felt bad for the reliable patients affected, but the hard truth is that if I can’t keep my practice open, I can’t help anyone. Why this plan had so many no-shows could be from a number of factors, but the end result was the same. Regardless of the reason, it was having a negative impact on my bottom line.
We try all kinds of different ways to remind people of their appointments. My secretary makes reminder calls. Other offices send texts or emails, or have a robocall system. These can only help to a certain degree. At some point, this becomes the “you can lead a horse to water ...” adage.
There’s no real easy answer, either. At my office, we don’t overbook. It seems to be an unwritten rule that every time we gamble that someone won’t come in and then put someone else in the slot, they both show up.
Research like this is interesting, and maybe helpful at making a predictive model about no-shows. But I’m not convinced it will eventually have everyday use in a real-world practice.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
How to handle anorexia in community hospitals
Food is nonnegotiable
ATLANTA – Everyone has to be on the same page when it comes to anorexia nervosa in a community hospital, according to pediatric hospitalists at Moses H. Cone Memorial Hospital in Greensboro, N.C.

Anorexia cases used to be rare there. When one came in, “everyone was anxious because we just didn’t know quite what to do,” said Suresh Nagappan, MD, a pediatrician and member of the teaching faculty at the hospital. Parents would hear one thing from one provider, something else from the next, and leave angry and confused. “Basically, it was a mess. We needed to standardize it,” he added.
So Dr. Nagappan and his colleagues created guidelines for treating patients with eating disorders about 3 years ago. “It was meeting after meeting for months, but well worth it,” he said at Pediatric Hospital Medicine.
Word of the hospital’s newfound expertise in anorexia has spread since then, and now it’s not unusual for Moses H. Cone to handle a few cases a week.
The pediatric hospitalist team has come to realize that, first and foremost, patients and families need to know why they are there; it’s about medical stabilization, not treating the eating disorder. That comes after discharge. Families need help sometimes to understand that it’s not a quick fix.
To make things clear, there’s strict criteria now for admission, based on American Academy of Pediatrics guidance. The main trigger is being under 75% of ideal body weight, but patients must also have systolic blood pressure below 90 mm Hg and other worrisome signs. “Sometimes, it feels like we’re splitting hairs” on who gets admitted, “but if we don’t have strict criteria on admission, we don’t have an end goal for discharge,” said pediatrician Maggie S. Hall, MD, also on the Moses H. Cone teaching faculty.
As for treatment, “food is medicine, and it’s not negotiable. We make that clear to everyone on day 1. If patients don’t eat their actual meal, they have 20 minutes to drink a supplement. If they can’t do that, they get a nasogastric tube,” Dr. Nagappan said. The tube is pulled after each meal, so that it remains an incentive to eat.
The team start patients with 1,600 calories a day and increase the intake by 200-250 calories a day. The goal is for a patient to gain 100-200 grams per day. Patients pick out what they want to eat with the help of a dietitian. When meals set off overwhelming anxiety, the Moses H. Cone team has learned that benzodiazepines can help.
Ironically, the initiation of regular meals is the most dangerous time for patients. As anorexic bodies switch from catabolic to anabolic metabolism, electrolytes can drop to dangerously low levels, causing arrhythmias, heart failure, and death. In general, “the reason these kids die is cardiac,” Dr. Nagappan said at the meeting, sponsored by the Society of Hospital Medicine, the AAP, and the Academic Pediatric Association.
Refeeding syndrome, as it’s known, is clinically significant in perhaps 6% of patients. The risk goes up if they are below 70% of their ideal body weight; have a prolonged QTc interval; or begin treatment with low phosphorous, magnesium, or potassium.

To counter the threat, electrolytes are measured twice a day at Moses H. Cone during the first week of treatment, and ECGs are taken daily for the first few days. “One thing to be really careful about is when you notice their heart rate beginning to creep up during rest. That can be a sign of developing cardiomyopathy; it’s an indication for us to get echocardiograms,” Dr. Hall said.
The Moses H. Cone team like to include families in meal times – it’s been shown to help – but family members need to be coached beforehand. They can’t be punitive. Mealtime talk has to be positive, and can’t focus on eating. Parents often need help handling their own anger and guilt before trying to eat with their child. Progress has to be monitored, but Dr. Nagappan cautioned that “you have to be really careful about how you get weights”; it should always be in the morning after the first void. Urine needs to be checked to make sure patients aren’t water loading.
Staff should be neutral about weight results, and keep them to themselves. Even something as benign as “good job” can be a problem. “You don’t want these patients focused on their weight. You want them focused on getting better and eating and taking it step by step,” he said.
The presenters had no disclosures to report.
Food is nonnegotiable
Food is nonnegotiable
ATLANTA – Everyone has to be on the same page when it comes to anorexia nervosa in a community hospital, according to pediatric hospitalists at Moses H. Cone Memorial Hospital in Greensboro, N.C.
Anorexia cases used to be rare there. When one came in, “everyone was anxious because we just didn’t know quite what to do,” said Suresh Nagappan, MD, a pediatrician and member of the teaching faculty at the hospital. Parents would hear one thing from one provider, something else from the next, and leave angry and confused. “Basically, it was a mess. We needed to standardize it,” he added.
So Dr. Nagappan and his colleagues created guidelines for treating patients with eating disorders about 3 years ago. “It was meeting after meeting for months, but well worth it,” he said at Pediatric Hospital Medicine.
Word of the hospital’s newfound expertise in anorexia has spread since then, and now it’s not unusual for Moses H. Cone to handle a few cases a week.
The pediatric hospitalist team has come to realize that, first and foremost, patients and families need to know why they are there; it’s about medical stabilization, not treating the eating disorder. That comes after discharge. Families need help sometimes to understand that it’s not a quick fix.
To make things clear, there’s strict criteria now for admission, based on American Academy of Pediatrics guidance. The main trigger is being under 75% of ideal body weight, but patients must also have systolic blood pressure below 90 mm Hg and other worrisome signs. “Sometimes, it feels like we’re splitting hairs” on who gets admitted, “but if we don’t have strict criteria on admission, we don’t have an end goal for discharge,” said pediatrician Maggie S. Hall, MD, also on the Moses H. Cone teaching faculty.
As for treatment, “food is medicine, and it’s not negotiable. We make that clear to everyone on day 1. If patients don’t eat their actual meal, they have 20 minutes to drink a supplement. If they can’t do that, they get a nasogastric tube,” Dr. Nagappan said. The tube is pulled after each meal, so that it remains an incentive to eat.
The team start patients with 1,600 calories a day and increase the intake by 200-250 calories a day. The goal is for a patient to gain 100-200 grams per day. Patients pick out what they want to eat with the help of a dietitian. When meals set off overwhelming anxiety, the Moses H. Cone team has learned that benzodiazepines can help.
Ironically, the initiation of regular meals is the most dangerous time for patients. As anorexic bodies switch from catabolic to anabolic metabolism, electrolytes can drop to dangerously low levels, causing arrhythmias, heart failure, and death. In general, “the reason these kids die is cardiac,” Dr. Nagappan said at the meeting, sponsored by the Society of Hospital Medicine, the AAP, and the Academic Pediatric Association.
Refeeding syndrome, as it’s known, is clinically significant in perhaps 6% of patients. The risk goes up if they are below 70% of their ideal body weight; have a prolonged QTc interval; or begin treatment with low phosphorous, magnesium, or potassium.
To counter the threat, electrolytes are measured twice a day at Moses H. Cone during the first week of treatment, and ECGs are taken daily for the first few days. “One thing to be really careful about is when you notice their heart rate beginning to creep up during rest. That can be a sign of developing cardiomyopathy; it’s an indication for us to get echocardiograms,” Dr. Hall said.
The Moses H. Cone team like to include families in meal times – it’s been shown to help – but family members need to be coached beforehand. They can’t be punitive. Mealtime talk has to be positive, and can’t focus on eating. Parents often need help handling their own anger and guilt before trying to eat with their child. Progress has to be monitored, but Dr. Nagappan cautioned that “you have to be really careful about how you get weights”; it should always be in the morning after the first void. Urine needs to be checked to make sure patients aren’t water loading.
Staff should be neutral about weight results, and keep them to themselves. Even something as benign as “good job” can be a problem. “You don’t want these patients focused on their weight. You want them focused on getting better and eating and taking it step by step,” he said.
The presenters had no disclosures to report.
ATLANTA – Everyone has to be on the same page when it comes to anorexia nervosa in a community hospital, according to pediatric hospitalists at Moses H. Cone Memorial Hospital in Greensboro, N.C.
Anorexia cases used to be rare there. When one came in, “everyone was anxious because we just didn’t know quite what to do,” said Suresh Nagappan, MD, a pediatrician and member of the teaching faculty at the hospital. Parents would hear one thing from one provider, something else from the next, and leave angry and confused. “Basically, it was a mess. We needed to standardize it,” he added.
So Dr. Nagappan and his colleagues created guidelines for treating patients with eating disorders about 3 years ago. “It was meeting after meeting for months, but well worth it,” he said at Pediatric Hospital Medicine.
Word of the hospital’s newfound expertise in anorexia has spread since then, and now it’s not unusual for Moses H. Cone to handle a few cases a week.
The pediatric hospitalist team has come to realize that, first and foremost, patients and families need to know why they are there; it’s about medical stabilization, not treating the eating disorder. That comes after discharge. Families need help sometimes to understand that it’s not a quick fix.
To make things clear, there’s strict criteria now for admission, based on American Academy of Pediatrics guidance. The main trigger is being under 75% of ideal body weight, but patients must also have systolic blood pressure below 90 mm Hg and other worrisome signs. “Sometimes, it feels like we’re splitting hairs” on who gets admitted, “but if we don’t have strict criteria on admission, we don’t have an end goal for discharge,” said pediatrician Maggie S. Hall, MD, also on the Moses H. Cone teaching faculty.
As for treatment, “food is medicine, and it’s not negotiable. We make that clear to everyone on day 1. If patients don’t eat their actual meal, they have 20 minutes to drink a supplement. If they can’t do that, they get a nasogastric tube,” Dr. Nagappan said. The tube is pulled after each meal, so that it remains an incentive to eat.
The team start patients with 1,600 calories a day and increase the intake by 200-250 calories a day. The goal is for a patient to gain 100-200 grams per day. Patients pick out what they want to eat with the help of a dietitian. When meals set off overwhelming anxiety, the Moses H. Cone team has learned that benzodiazepines can help.
Ironically, the initiation of regular meals is the most dangerous time for patients. As anorexic bodies switch from catabolic to anabolic metabolism, electrolytes can drop to dangerously low levels, causing arrhythmias, heart failure, and death. In general, “the reason these kids die is cardiac,” Dr. Nagappan said at the meeting, sponsored by the Society of Hospital Medicine, the AAP, and the Academic Pediatric Association.
Refeeding syndrome, as it’s known, is clinically significant in perhaps 6% of patients. The risk goes up if they are below 70% of their ideal body weight; have a prolonged QTc interval; or begin treatment with low phosphorous, magnesium, or potassium.
To counter the threat, electrolytes are measured twice a day at Moses H. Cone during the first week of treatment, and ECGs are taken daily for the first few days. “One thing to be really careful about is when you notice their heart rate beginning to creep up during rest. That can be a sign of developing cardiomyopathy; it’s an indication for us to get echocardiograms,” Dr. Hall said.
The Moses H. Cone team like to include families in meal times – it’s been shown to help – but family members need to be coached beforehand. They can’t be punitive. Mealtime talk has to be positive, and can’t focus on eating. Parents often need help handling their own anger and guilt before trying to eat with their child. Progress has to be monitored, but Dr. Nagappan cautioned that “you have to be really careful about how you get weights”; it should always be in the morning after the first void. Urine needs to be checked to make sure patients aren’t water loading.
Staff should be neutral about weight results, and keep them to themselves. Even something as benign as “good job” can be a problem. “You don’t want these patients focused on their weight. You want them focused on getting better and eating and taking it step by step,” he said.
The presenters had no disclosures to report.
EXPERT ANALYSIS FROM PHM 2018
Professional psychology
, the ability to figure out how to get people to accept what you’re trying to do for them.

Expertise and psychology: Every profession needs both, including our own. Over my years in practice, I’ve met people in many walks of life who develop the same combination. Here are some favorites:
1. Wedding planners
Venues, décor, dresses, floral arrangements, caterers, bands. Wedding planners must know about all of these. And that’s just the start.
Weddings make everyone a bit crazy, or more than a bit. There are parents trying not to let go, children trying to pull away (a Destination Wedding in Patagonia – perfect – none of the family can come!), cultural and taste gaps between the sides (tipplers from Tinseltown and teetotalers from Tupelo), culling the guest list (see Patagonia). Every wedding planner I’ve met could write a book, but won’t. Legal fees would be too high.
Given all this turmoil, some wedding planners might advise elopement and put themselves out of business. No fear of that happening.
2. Event planners
See Wedding Planners, only add: arbitrary and capricious bosses, incompetent implementers, acts of God, acts of man, and everything that goes wrong when there are too many moving parts. One close friend who organizes professional conventions says that every year one attendee posts this complaint on the message board: “Why is there no Diet Mountain Dew?!!!”
3. Dressmakers
Again, see Wedding Planners. Knowing how to design, create, and fit a dress demands a set of skills that earns my admiration and respect. Knowing how to deal with the people who are going to wear the dresses deserves not respect but awe. Even if I knew how to sew, I wouldn’t last a week in this business.
4. Financial planners
Every financial planner I meet describes what they do as “mostly psychology.” Of course, they need to recommend investments that suit the age, life status, and plans of their clients. That’s the easy part.
“When the market is dropping,” says Phil, “people call to scream that they’re losing their shirt. When the market is going up, they call to scream that they’re not making out as well as their friends claim they are.
“Either way, I just hold the phone far enough away from my ear to save my hearing until they’re done venting. Then I try to calm them down and assure them that investing is a long game, and over time they’ll do better staying the course we agreed on than jumping around with every market swing, up or down.”
“Do they listen?”
“Most of them. Eventually.”
4. Speakers’ booking agents
Matching clients with speakers can bring curious challenges. Celebrity speakers in particular may have unique requirements that the agents who book them must figure out and comply with. Or else.
For instance, one young man I met had to book a distinguished jurist. He needed to be picked up in a limo. The limo had to be a Bentley. And the Bentley had to be gray.
Well, excuse me.
5. Waiters
I think the favored term these days is “Servers.” Servers serve strangers. Some strangers are pleasant and courteous. Not all. Waiters mean to please, but to do that they have to put up with a lot. Always with a smile, of course.
Customers ask silly questions. (“What’s good here?”) Some don’t find the menu detailed enough. (“Can I have half of this and some of that, with the sauce on the side?”) They may find the food too hot. Or too cold. Or too spicy. Or too bland. After all that, they may tip a little. Or not.
But the server still has to ask, “Is everything satisfactory?”
6. Psychologists
Never mind.
7. Parking meter readers
Just kidding. Meter readers write parking tickets.

They know perfectly well that everyone knows exactly what they do. And they don’t care.
8. People who field complaints at call centers
Requirement: Patience, savvy, Xanax.
9. Dermatologists
You bet, in spades. I wrote a whole book on the subject. You can read it if you want to. If you disagree, don’t tell me.
I don’t need readers to disagree with me. I already have patients.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at [email protected] .
, the ability to figure out how to get people to accept what you’re trying to do for them.
Expertise and psychology: Every profession needs both, including our own. Over my years in practice, I’ve met people in many walks of life who develop the same combination. Here are some favorites:
1. Wedding planners
Venues, décor, dresses, floral arrangements, caterers, bands. Wedding planners must know about all of these. And that’s just the start.
Weddings make everyone a bit crazy, or more than a bit. There are parents trying not to let go, children trying to pull away (a Destination Wedding in Patagonia – perfect – none of the family can come!), cultural and taste gaps between the sides (tipplers from Tinseltown and teetotalers from Tupelo), culling the guest list (see Patagonia). Every wedding planner I’ve met could write a book, but won’t. Legal fees would be too high.
Given all this turmoil, some wedding planners might advise elopement and put themselves out of business. No fear of that happening.
2. Event planners
See Wedding Planners, only add: arbitrary and capricious bosses, incompetent implementers, acts of God, acts of man, and everything that goes wrong when there are too many moving parts. One close friend who organizes professional conventions says that every year one attendee posts this complaint on the message board: “Why is there no Diet Mountain Dew?!!!”
3. Dressmakers
Again, see Wedding Planners. Knowing how to design, create, and fit a dress demands a set of skills that earns my admiration and respect. Knowing how to deal with the people who are going to wear the dresses deserves not respect but awe. Even if I knew how to sew, I wouldn’t last a week in this business.
4. Financial planners
Every financial planner I meet describes what they do as “mostly psychology.” Of course, they need to recommend investments that suit the age, life status, and plans of their clients. That’s the easy part.
“When the market is dropping,” says Phil, “people call to scream that they’re losing their shirt. When the market is going up, they call to scream that they’re not making out as well as their friends claim they are.
“Either way, I just hold the phone far enough away from my ear to save my hearing until they’re done venting. Then I try to calm them down and assure them that investing is a long game, and over time they’ll do better staying the course we agreed on than jumping around with every market swing, up or down.”
“Do they listen?”
“Most of them. Eventually.”
4. Speakers’ booking agents
Matching clients with speakers can bring curious challenges. Celebrity speakers in particular may have unique requirements that the agents who book them must figure out and comply with. Or else.
For instance, one young man I met had to book a distinguished jurist. He needed to be picked up in a limo. The limo had to be a Bentley. And the Bentley had to be gray.
Well, excuse me.
5. Waiters
I think the favored term these days is “Servers.” Servers serve strangers. Some strangers are pleasant and courteous. Not all. Waiters mean to please, but to do that they have to put up with a lot. Always with a smile, of course.
Customers ask silly questions. (“What’s good here?”) Some don’t find the menu detailed enough. (“Can I have half of this and some of that, with the sauce on the side?”) They may find the food too hot. Or too cold. Or too spicy. Or too bland. After all that, they may tip a little. Or not.
But the server still has to ask, “Is everything satisfactory?”
6. Psychologists
Never mind.
7. Parking meter readers
Just kidding. Meter readers write parking tickets.
They know perfectly well that everyone knows exactly what they do. And they don’t care.
8. People who field complaints at call centers
Requirement: Patience, savvy, Xanax.
9. Dermatologists
You bet, in spades. I wrote a whole book on the subject. You can read it if you want to. If you disagree, don’t tell me.
I don’t need readers to disagree with me. I already have patients.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at [email protected] .
, the ability to figure out how to get people to accept what you’re trying to do for them.
Expertise and psychology: Every profession needs both, including our own. Over my years in practice, I’ve met people in many walks of life who develop the same combination. Here are some favorites:
1. Wedding planners
Venues, décor, dresses, floral arrangements, caterers, bands. Wedding planners must know about all of these. And that’s just the start.
Weddings make everyone a bit crazy, or more than a bit. There are parents trying not to let go, children trying to pull away (a Destination Wedding in Patagonia – perfect – none of the family can come!), cultural and taste gaps between the sides (tipplers from Tinseltown and teetotalers from Tupelo), culling the guest list (see Patagonia). Every wedding planner I’ve met could write a book, but won’t. Legal fees would be too high.
Given all this turmoil, some wedding planners might advise elopement and put themselves out of business. No fear of that happening.
2. Event planners
See Wedding Planners, only add: arbitrary and capricious bosses, incompetent implementers, acts of God, acts of man, and everything that goes wrong when there are too many moving parts. One close friend who organizes professional conventions says that every year one attendee posts this complaint on the message board: “Why is there no Diet Mountain Dew?!!!”
3. Dressmakers
Again, see Wedding Planners. Knowing how to design, create, and fit a dress demands a set of skills that earns my admiration and respect. Knowing how to deal with the people who are going to wear the dresses deserves not respect but awe. Even if I knew how to sew, I wouldn’t last a week in this business.
4. Financial planners
Every financial planner I meet describes what they do as “mostly psychology.” Of course, they need to recommend investments that suit the age, life status, and plans of their clients. That’s the easy part.
“When the market is dropping,” says Phil, “people call to scream that they’re losing their shirt. When the market is going up, they call to scream that they’re not making out as well as their friends claim they are.
“Either way, I just hold the phone far enough away from my ear to save my hearing until they’re done venting. Then I try to calm them down and assure them that investing is a long game, and over time they’ll do better staying the course we agreed on than jumping around with every market swing, up or down.”
“Do they listen?”
“Most of them. Eventually.”
4. Speakers’ booking agents
Matching clients with speakers can bring curious challenges. Celebrity speakers in particular may have unique requirements that the agents who book them must figure out and comply with. Or else.
For instance, one young man I met had to book a distinguished jurist. He needed to be picked up in a limo. The limo had to be a Bentley. And the Bentley had to be gray.
Well, excuse me.
5. Waiters
I think the favored term these days is “Servers.” Servers serve strangers. Some strangers are pleasant and courteous. Not all. Waiters mean to please, but to do that they have to put up with a lot. Always with a smile, of course.
Customers ask silly questions. (“What’s good here?”) Some don’t find the menu detailed enough. (“Can I have half of this and some of that, with the sauce on the side?”) They may find the food too hot. Or too cold. Or too spicy. Or too bland. After all that, they may tip a little. Or not.
But the server still has to ask, “Is everything satisfactory?”
6. Psychologists
Never mind.
7. Parking meter readers
Just kidding. Meter readers write parking tickets.
They know perfectly well that everyone knows exactly what they do. And they don’t care.
8. People who field complaints at call centers
Requirement: Patience, savvy, Xanax.
9. Dermatologists
You bet, in spades. I wrote a whole book on the subject. You can read it if you want to. If you disagree, don’t tell me.
I don’t need readers to disagree with me. I already have patients.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at [email protected] .
Telemedicine: Three fraud and abuse triggers
The practice of telemedicine is rapidly growing as more health professionals discover the value in treating patients via technology. Lisa S. Mazur, a Chicago-based health law attorney specializing in telemedicine, shares guidance on how to avoid running afoul of fraud and abuse regulations when using telehealth.

1. Improper coding. Incorrect billing for telemedicine services is a top trigger for federal fraud and abuse scrutiny. A 2018 Office of Inspector General (OIG) report found that 31% of a sample of 100 telehealth claims did not meet Medicare conditions for payment. Primary reasons for inaccurate billing included ineligible institutional providers; services provided by unacceptable means of communication; claims for noncovered services; and claims for patients who received services at nonrural originating sites. The inspector general estimated that Centers for Medicare & Medicaid Services wasted $3.7 million in improper telehealth payments during the audit period (2014 and 2015) and recommended that CMS conduct more audits going forward to identify telehealth overpayments.
“The error rate is shocking,” Ms. Mazur said in an interview. “The problem is the providers know what they need to do for traditional in-person services, but they don’t fully understand the complexities and nuances that can be implicated by telemedicine. [For instance], they know how to bill for an in-person E/M [evaluation and management] service, but they don’t know to bill for it properly for when it’s done virtually.”
To ensure correct billing, it’s critical for providers and billing staff to review CMS’ resources on requirements for telehealth payments and make sure they’re up to date with any changes.

2. Kickback skepticism in arrangements. Some telemedicine arrangements can raise kickback concerns if not properly defined. The federal Anti-Kickback Statute prohibits the exchange of anything of value in an effort to induce the referral of business in federal health care programs. For example, if a large hospital system purchases or leases telemedicine equipment at a discounted rate to a rural practice, the hospital could be accused of providing equipment at less than fair market value to secure referrals, Ms. Mazur explained.
Such arrangements should not raise alarm as long as certain conditions are met, according to a 2018 OIG advisory opinion. The opinion stemmed from an inquiry from a nonprofit, federally qualified health center that planned to provide free telemedicine equipment to a county clinic providing HIV testing and treatment. In his opinion, Robert K. DeConti, OIG assistant inspector general for legal affairs, wrote that the arrangement in question was low risk because it included safeguards to prevent inappropriate patient steering, it did not inappropriately increase costs to federal health programs, and it improved access to care.
Essentially, if health professionals can show that their telemedicine arrangement legitimately benefits patient care and improves patient outcomes, they are not likely to draw scrutiny, Ms. Mazur said. Because fraud and abuse laws can be complicated, she recommended having an attorney review telemedicine arrangements before they launch to spot any potential risks. Ensure the purpose of the arrangement can be clearly outlined should questions arise.
3. Free patient technology. The Civil Monetary Penalties Law is another fraud and abuse statute that can come into play in the telemedicine setting. Under this law, health professionals cannot knowingly solicit or receive remuneration for a patient referral nor can they induce patients to visit them via incentives such as free products. In the telemedicine context, the law can be triggered when practices offer patients free remote monitoring devices or apps that help track medical data.
“Hospitals and groups have very legitimate reasons to want to provide their patients with these types of tools for free,” Ms. Mazur said. “But anytime a health professional who is billing Medicare for services provides some to a patient for free, there’s a concern that you’re giving that service or product because you’re trying to induce them to come to you for care.”
The right parameters around free telemedicine tools can make all the difference, she said. For example, it’s important that practices do not market the free or discounted product to patients, according to Ms. Mazur. Also, make clear that the free products do not increase profits for the practice and that the offerings do not raise federal health care billings. Another way to go about it is to include the practice of providing a free telemedicine product or device under the scope of their charity policy by including language outlining when free or discounted products or services can be provided to underinsured patients, Ms. Mazur said.
Another good idea is for practices to integrate telemedicine into their corporate compliance programs. All health care entities are encouraged to have a corporate compliance program that outlines policies, training protocols, and standards of conduct to prevent, identify, and mitigate fraud and abuse.
Practices “need to make sure their existing compliance programs, including policies and procedures, take into account the nuances that are implicated by telemedicine,” Ms. Mazur said.
The practice of telemedicine is rapidly growing as more health professionals discover the value in treating patients via technology. Lisa S. Mazur, a Chicago-based health law attorney specializing in telemedicine, shares guidance on how to avoid running afoul of fraud and abuse regulations when using telehealth.
1. Improper coding. Incorrect billing for telemedicine services is a top trigger for federal fraud and abuse scrutiny. A 2018 Office of Inspector General (OIG) report found that 31% of a sample of 100 telehealth claims did not meet Medicare conditions for payment. Primary reasons for inaccurate billing included ineligible institutional providers; services provided by unacceptable means of communication; claims for noncovered services; and claims for patients who received services at nonrural originating sites. The inspector general estimated that Centers for Medicare & Medicaid Services wasted $3.7 million in improper telehealth payments during the audit period (2014 and 2015) and recommended that CMS conduct more audits going forward to identify telehealth overpayments.
“The error rate is shocking,” Ms. Mazur said in an interview. “The problem is the providers know what they need to do for traditional in-person services, but they don’t fully understand the complexities and nuances that can be implicated by telemedicine. [For instance], they know how to bill for an in-person E/M [evaluation and management] service, but they don’t know to bill for it properly for when it’s done virtually.”
To ensure correct billing, it’s critical for providers and billing staff to review CMS’ resources on requirements for telehealth payments and make sure they’re up to date with any changes.
2. Kickback skepticism in arrangements. Some telemedicine arrangements can raise kickback concerns if not properly defined. The federal Anti-Kickback Statute prohibits the exchange of anything of value in an effort to induce the referral of business in federal health care programs. For example, if a large hospital system purchases or leases telemedicine equipment at a discounted rate to a rural practice, the hospital could be accused of providing equipment at less than fair market value to secure referrals, Ms. Mazur explained.
Such arrangements should not raise alarm as long as certain conditions are met, according to a 2018 OIG advisory opinion. The opinion stemmed from an inquiry from a nonprofit, federally qualified health center that planned to provide free telemedicine equipment to a county clinic providing HIV testing and treatment. In his opinion, Robert K. DeConti, OIG assistant inspector general for legal affairs, wrote that the arrangement in question was low risk because it included safeguards to prevent inappropriate patient steering, it did not inappropriately increase costs to federal health programs, and it improved access to care.
Essentially, if health professionals can show that their telemedicine arrangement legitimately benefits patient care and improves patient outcomes, they are not likely to draw scrutiny, Ms. Mazur said. Because fraud and abuse laws can be complicated, she recommended having an attorney review telemedicine arrangements before they launch to spot any potential risks. Ensure the purpose of the arrangement can be clearly outlined should questions arise.
3. Free patient technology. The Civil Monetary Penalties Law is another fraud and abuse statute that can come into play in the telemedicine setting. Under this law, health professionals cannot knowingly solicit or receive remuneration for a patient referral nor can they induce patients to visit them via incentives such as free products. In the telemedicine context, the law can be triggered when practices offer patients free remote monitoring devices or apps that help track medical data.
“Hospitals and groups have very legitimate reasons to want to provide their patients with these types of tools for free,” Ms. Mazur said. “But anytime a health professional who is billing Medicare for services provides some to a patient for free, there’s a concern that you’re giving that service or product because you’re trying to induce them to come to you for care.”
The right parameters around free telemedicine tools can make all the difference, she said. For example, it’s important that practices do not market the free or discounted product to patients, according to Ms. Mazur. Also, make clear that the free products do not increase profits for the practice and that the offerings do not raise federal health care billings. Another way to go about it is to include the practice of providing a free telemedicine product or device under the scope of their charity policy by including language outlining when free or discounted products or services can be provided to underinsured patients, Ms. Mazur said.
Another good idea is for practices to integrate telemedicine into their corporate compliance programs. All health care entities are encouraged to have a corporate compliance program that outlines policies, training protocols, and standards of conduct to prevent, identify, and mitigate fraud and abuse.
Practices “need to make sure their existing compliance programs, including policies and procedures, take into account the nuances that are implicated by telemedicine,” Ms. Mazur said.
The practice of telemedicine is rapidly growing as more health professionals discover the value in treating patients via technology. Lisa S. Mazur, a Chicago-based health law attorney specializing in telemedicine, shares guidance on how to avoid running afoul of fraud and abuse regulations when using telehealth.
1. Improper coding. Incorrect billing for telemedicine services is a top trigger for federal fraud and abuse scrutiny. A 2018 Office of Inspector General (OIG) report found that 31% of a sample of 100 telehealth claims did not meet Medicare conditions for payment. Primary reasons for inaccurate billing included ineligible institutional providers; services provided by unacceptable means of communication; claims for noncovered services; and claims for patients who received services at nonrural originating sites. The inspector general estimated that Centers for Medicare & Medicaid Services wasted $3.7 million in improper telehealth payments during the audit period (2014 and 2015) and recommended that CMS conduct more audits going forward to identify telehealth overpayments.
“The error rate is shocking,” Ms. Mazur said in an interview. “The problem is the providers know what they need to do for traditional in-person services, but they don’t fully understand the complexities and nuances that can be implicated by telemedicine. [For instance], they know how to bill for an in-person E/M [evaluation and management] service, but they don’t know to bill for it properly for when it’s done virtually.”
To ensure correct billing, it’s critical for providers and billing staff to review CMS’ resources on requirements for telehealth payments and make sure they’re up to date with any changes.
2. Kickback skepticism in arrangements. Some telemedicine arrangements can raise kickback concerns if not properly defined. The federal Anti-Kickback Statute prohibits the exchange of anything of value in an effort to induce the referral of business in federal health care programs. For example, if a large hospital system purchases or leases telemedicine equipment at a discounted rate to a rural practice, the hospital could be accused of providing equipment at less than fair market value to secure referrals, Ms. Mazur explained.
Such arrangements should not raise alarm as long as certain conditions are met, according to a 2018 OIG advisory opinion. The opinion stemmed from an inquiry from a nonprofit, federally qualified health center that planned to provide free telemedicine equipment to a county clinic providing HIV testing and treatment. In his opinion, Robert K. DeConti, OIG assistant inspector general for legal affairs, wrote that the arrangement in question was low risk because it included safeguards to prevent inappropriate patient steering, it did not inappropriately increase costs to federal health programs, and it improved access to care.
Essentially, if health professionals can show that their telemedicine arrangement legitimately benefits patient care and improves patient outcomes, they are not likely to draw scrutiny, Ms. Mazur said. Because fraud and abuse laws can be complicated, she recommended having an attorney review telemedicine arrangements before they launch to spot any potential risks. Ensure the purpose of the arrangement can be clearly outlined should questions arise.
3. Free patient technology. The Civil Monetary Penalties Law is another fraud and abuse statute that can come into play in the telemedicine setting. Under this law, health professionals cannot knowingly solicit or receive remuneration for a patient referral nor can they induce patients to visit them via incentives such as free products. In the telemedicine context, the law can be triggered when practices offer patients free remote monitoring devices or apps that help track medical data.
“Hospitals and groups have very legitimate reasons to want to provide their patients with these types of tools for free,” Ms. Mazur said. “But anytime a health professional who is billing Medicare for services provides some to a patient for free, there’s a concern that you’re giving that service or product because you’re trying to induce them to come to you for care.”
The right parameters around free telemedicine tools can make all the difference, she said. For example, it’s important that practices do not market the free or discounted product to patients, according to Ms. Mazur. Also, make clear that the free products do not increase profits for the practice and that the offerings do not raise federal health care billings. Another way to go about it is to include the practice of providing a free telemedicine product or device under the scope of their charity policy by including language outlining when free or discounted products or services can be provided to underinsured patients, Ms. Mazur said.
Another good idea is for practices to integrate telemedicine into their corporate compliance programs. All health care entities are encouraged to have a corporate compliance program that outlines policies, training protocols, and standards of conduct to prevent, identify, and mitigate fraud and abuse.
Practices “need to make sure their existing compliance programs, including policies and procedures, take into account the nuances that are implicated by telemedicine,” Ms. Mazur said.
Preappointment consults: Evidence builds for boosting access, revenue
About 15 years ago, rheumatologists at the University of Colorado School of Medicine, Aurora, implemented a preappointment consult triage system as a way to identify rheumatology patients who require timely evaluation and treatment.

Over time, the endeavor caused some soul searching. They wondered how effective their consult triage system was in identifying all patients with inflammatory rheumatic diseases and in ensuring they were seen promptly. They also wondered about the revenue implications of routine outpatient care of autoimmune and inflammatory rheumatic disease (AIRD) patients, compared with that of non-AIRD patients.
“Hospital leadership is very interested in making sure that all patients have access to specialty care in a timely manner,” said Sterling G. West, MD, one of the study authors who is also professor of medicine at the university. “However, there are not enough rheumatologists to see all patients with rheumatic complaints, and this deficit is likely to get worse. Although all patients with a rheumatic complaint would likely benefit from a rheumatology consultation, it is clear that timely access to rheumatologic care is most beneficial for patients with inflammatory rheumatic diseases to prevent future morbidity and disability.”
Year-long follow-up finds high sensitivity, more revenue
What started out as a quality improvement project morphed into a robust study that was published online July 12, 2018, in Arthritis Care & Research. Using data recorded in the electronic medical record, Dr. West and his colleagues retrospectively reviewed 961 new outpatient rheumatology consults sent during a 9-month period for final diagnosis and revenue generation for routine outpatient care over 1 year following consult review or initial evaluation. The first step of the consult management involves an intake access coordinator, Ryan Goecker, obtaining information about the patient from the referring clinician. Next, one of three experienced rheumatologists at the university – Duane W. Pearson, MD, Christopher C. Striebich, MD, or Jason R. Kolfenbach, MD – reviews the information about the case. “We do request that labs and x-rays be done ahead of time, depending on what the consult question is, so that we have the data to be able to decide whether a patient likely has an inflammatory process that we need to see or not,” Dr. West explained. “It takes somewhere between 5 and 20 minutes per consult. In total, it takes our rheumatologists about 5 hours a week to do the consults. However, even after subtracting the physician time spent screening consults, the time saved by the consult triage system enabled over 200 more time slots per year to be available to see new AIRD patients than would have been possible without the triage system.”
Following review of the data supplied about the case, patients who may have acute inflammatory monoarticular arthritis or some other rheumatologic emergency are seen within 24-48 hours, while consults with a possible AIRD are approved and seen within 1-4 weeks. Priority is given to those with suspected vasculitis, systemic lupus erythematosus, myositis, and disabling inflammatory arthritis. Patients with probable noninflammatory conditions such as osteoarthritis, fibromyalgia, and mechanical low back pain are not scheduled for an in-person visit. “Instead of simply declining the consult, we try to give some direction, or we say, ‘Why don’t you try this, this, and this, sort of a miniconsult,” Dr. West noted. “One of the potential adverse reactions to doing consult triage would be that the referring provider would be upset if we decline their consult. We acknowledge that. But over time we’ve been able to convince them that this is best for all concerned, so that the inflammatory disease group gets in to see us in an appropriate amount of time.”
Of the 961 consults, 673 were scheduled for an in-person AIRD evaluation and 288 consults were not scheduled. Patients were seen an average of 13 days after consult review. Of the 673 approved consults, 597 (89%) came for evaluation. Of these, 357 were diagnosed as having an AIRD, while 240 were diagnosed as having a non-AIRD. Among the patients not scheduled for a rheumatology visit, 128 had 1-year follow-up data, with 6 patients eventually diagnosed as having an AIRD. This translated into a consult triage sensitivity of 98% and a positive predictive value of 60%. “There’s a fair number of people with noninflammatory disease who do get into see us,” Dr. West said. “That has to do with our desire to not be overly rigid. The sensitivity, specificity, and positive predictive value were not quite as high as some people would like to see, but we really weren’t missing people who really needed to be seen.”
In their conservative cost analysis, revenue data for outpatient care was available for 318 of the 357 AIRD patients and 192 of 240 non-AIRD patients. It demonstrated that care of AIRD patients generates 44 times more revenue, compared with non-AIRD patients ($5,877 vs. $134 per patient, respectively; P less than .001).
“Our consult triage protocol appears to be an effective method to assure that patients with inflammatory rheumatic diseases get expedited access to appropriate rheumatologic care,” Dr. West concluded. “Using conservative measures, caring for patients with inflammatory rheumatic diseases results in significantly more revenue generation.” Generalizability of such a protocol to other practice settings depends on the time rheumatologists are willing to commit to it. “That’s the big thing,” he said. “The question comes up, could a nurse or a nurse practitioner learn the skills over time to be able to do efficient consult triage, to free up the doc from that? Yes. I think that’s absolutely possible.”
Going forward, Dr. Pearson and Dr. Kolfenbach, who are authors on the paper, have launched a pilot project in which the rheumatologist is compensated for doing a record review and e-consult on patients not recommended to be seen in the rheumatology clinic. “For consults who do not have inflammatory disease, we can say [to the referring clinician], ‘If we did see them, this is what we would be doing,’ ” Dr. West said. “Sometimes if there are still questions, we’ll say something like, ‘Once you get the results back, let us know and we can look at it again.’ That way they are getting similar compensation as telemedicine and other forms of consultation.”

At the Zuckerberg San Francisco General Hospital (ZSFG), use of a novel electronic consultation and referral system that was implemented in 2007 by University of California, San Francisco, providers continues to thrive for rheumatology and other specialty services. With this electronic system, previously called e-referral, all provider communication is captured in real time and recorded within the electronic health record. In a 2015 article from Arthritis Care & Research, researchers led by Jinoos Yazdany, MD, MPH, reviewed 2,105 e-referrals made between 2008 and 2012 (Arthritis Care Res. 2015;67[8]:1158-63). The main outcome of interest was use of preconsultation exchange, defined as back-and-forth communication between referring and specialty care providers, facilitating triage of referrals, requests for more information, or resolution of questions without a visit. The researchers found that about 25% of e-consults were resolved without a clinic visit, and that the proportion of e-consults undergoing preconsultation exchange increased over time, from 55% in 2008 to 74% in 2011.
“We’ve had situations in which somebody within our hospital system has requested a rheumatology referral but did not realize the urgency of the patients’ clinical signs and symptoms,” Dr. Yazdany, a rheumatologist and health services researcher at UCSF, said in an interview. “E-referrals are often responded to within that day. When we see an e-consult for a young woman with a rash and protein in her urine, a rheumatologist will recognize that is very concerning for a serious diagnosis like lupus of the kidney or systemic vasculitis. In that situation, we would pick up the phone and sometimes even call the patient and have them come to the emergency room for an urgent evaluation. Over the years, there have been many situations in which we’ve been able to intervene much earlier than we otherwise would have. In some cases that early intervention was lifesaving, or at least organ-preserving for the patient.”
Two studies from the early 2000s examined the use of preappointment management in rheumatology (see Arthritis Care Res. 2001;45:295-300 and Arthritis Rheum. 2004;51:253-7), but this is among the first to incorporate use of an electronic medical record to provide real-time exchange between the specialist and the referring provider. Clinicians at UCSF are reimbursed for reviewing e-consults in one of two ways. Those at ZSFG have protected and compensated time for the task, “so it’s basically part of their job to spend a half day a week on e-consults,” Dr. Yazdany said. “The department of public health and our health care system fold that into operational costs. That’s absolutely critical for success. To be done well and thoughtfully, managing consults and referrals takes time. It takes a lot of expertise.” Meanwhile, clinicians at UCSF’s main university hospital receive a small payment for each e-consult they review. “If it’s a complex consult it’s a higher reimbursement,” she said. “If it’s a simple one, it’s slightly less reimbursement, so it’s a fee-for-service model. It’s something that the health system funds, because it creates efficiencies and access for patients.”
Gaining popularity across specialties
Delphine S. Tuot, MD, a nephrologist who directs the ZSFG e-consult system, said that the notion of preconsult triage is gaining popularity in all medical specialties. For example, the Blue Shield of California Foundation is funding implementation of e-consult systems across many of California’s safety net health care delivery systems. “We have many health care plans that are interested in this process as well, because it improves access to specialty care, particularly in rural areas or in areas where the specialist workforce is limited,” said Dr. Tuot, who is codirector of the UCSF Center for Innovation in Access and Quality at ZSFG. Such efforts are also being promoted by the Public Hospital Redesign and Incentives in Medi-Cal Program (PRIME), which is part of California’s Medicaid waiver. PRIME “is encouraging health systems to look at innovative ways to deliver specialty care,” Dr. Tuot said. “E-consults and other non–face-to-face ways to deliver specialty care, including telemedicine encounters, count toward that metric for the Medicaid waiver.”

At the national level, the Association of American Medical Colleges has collaborated with more than 20 academic medical centers in 14 states, including Dartmouth-Hitchcock and Yale University, to implement tools built into the electronic medical record system through a program known as Project CORE (Coordinating Optimal Referral Experiences). According to Scott Shipman, MD, MPH, director of clinical innovations for the AAMC, nearly all of the current CORE sites have either gone live with the model in rheumatology or are planning to do so. “Better communication and coordination between primary care providers and specialists is important for all specialties, but because of the complexity of evaluation and management of problems in rheumatology, there is a tremendous opportunity for the CORE model to help get providers on the same page,” Dr. Shipman said in an interview. “We do this through simple decision support that we build into the referral order in the EMR, available at the point of care. Additionally, given the workforce challenges facing rheumatology in most regions of the country and consequent access barriers, offloading some of the demand via e-consults holds great promise.” Current focus areas for Project CORE, he said, include continued support of current CORE sites in their implementation and scaling efforts to maximize impact, advocacy to promote payer engagement in support of e-consult reimbursements, and working to extend the model to additional academic medical centers.

Dr. Tuot emphasized that performing e-consults “takes time and effort on behalf of specialists, so if you’re by yourself in solo practice it probably does not make sense to implement,” she said. “You need to spend your time seeing patients as much as possible. For primary care providers who are asking for curbside consults, it’s probably best to have things in writing from the specialist, such as in an e-consult, to make sure there’s no misunderstanding.”
As demand for rheumatology services increases, clinicians “have to figure out a way to see patients in most urgent need of our services,” Dr. Yazdany said. “That requires that we use technology like the e-consult system to prioritize the patients that we’re seeing. As we look at the rheumatology workforce shortage, especially in some geographic regions, it’s going to be absolutely critical. There are some diseases that no other specialists have experience caring for. In those situations, those patients need to get in to see rheumatologists in a timely fashion.”
Paper-based preconsult triage system
At Essentia Health, an integrated health care system with facilities in Minnesota, Wisconsin, and North Dakota, Meghan Scheibe, MD, a rheumatologist, is currently working with a rheumatologist colleague and a registered nurse to implement a paper-based preconsult triage system, “because our wait times have unfortunately skyrocketed,” she said. “We receive a lot of outside referrals from other health care groups and large health care systems that don’t have access to rheumatology.” Currently, the triage system is comprised of a referral note which includes the reason for consultation. Dr. Scheibe and her colleague rank the referral as expedited, intermediate concern, or low priority based on information provided by the referring clinician. “We mark those for our nurse to help schedule, and we let the referring provider know what the wait time is,” Dr. Scheibe said. “Then they have an opportunity to communicate back to us or say, ‘Yes, that’s fine,’ or, ‘I’m really worried about this patient. Could you get her in sooner?’ ”

It’s early in the process, but so far, implementation of the preconsult triage protocol “is allowing us to focus on the consultations on which we can be most impactful and not overwhelm the rheumatology workforce that we have,” she said.
Research reported in the UCSF study was supported by the American College of Rheumatology’s Ephraim P. Engleman Endowed Resident Research Preceptorship and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. None of the sources interviewed for this story reported having relevant financial disclosures.
About 15 years ago, rheumatologists at the University of Colorado School of Medicine, Aurora, implemented a preappointment consult triage system as a way to identify rheumatology patients who require timely evaluation and treatment.
Over time, the endeavor caused some soul searching. They wondered how effective their consult triage system was in identifying all patients with inflammatory rheumatic diseases and in ensuring they were seen promptly. They also wondered about the revenue implications of routine outpatient care of autoimmune and inflammatory rheumatic disease (AIRD) patients, compared with that of non-AIRD patients.
“Hospital leadership is very interested in making sure that all patients have access to specialty care in a timely manner,” said Sterling G. West, MD, one of the study authors who is also professor of medicine at the university. “However, there are not enough rheumatologists to see all patients with rheumatic complaints, and this deficit is likely to get worse. Although all patients with a rheumatic complaint would likely benefit from a rheumatology consultation, it is clear that timely access to rheumatologic care is most beneficial for patients with inflammatory rheumatic diseases to prevent future morbidity and disability.”
Year-long follow-up finds high sensitivity, more revenue
What started out as a quality improvement project morphed into a robust study that was published online July 12, 2018, in Arthritis Care & Research. Using data recorded in the electronic medical record, Dr. West and his colleagues retrospectively reviewed 961 new outpatient rheumatology consults sent during a 9-month period for final diagnosis and revenue generation for routine outpatient care over 1 year following consult review or initial evaluation. The first step of the consult management involves an intake access coordinator, Ryan Goecker, obtaining information about the patient from the referring clinician. Next, one of three experienced rheumatologists at the university – Duane W. Pearson, MD, Christopher C. Striebich, MD, or Jason R. Kolfenbach, MD – reviews the information about the case. “We do request that labs and x-rays be done ahead of time, depending on what the consult question is, so that we have the data to be able to decide whether a patient likely has an inflammatory process that we need to see or not,” Dr. West explained. “It takes somewhere between 5 and 20 minutes per consult. In total, it takes our rheumatologists about 5 hours a week to do the consults. However, even after subtracting the physician time spent screening consults, the time saved by the consult triage system enabled over 200 more time slots per year to be available to see new AIRD patients than would have been possible without the triage system.”
Following review of the data supplied about the case, patients who may have acute inflammatory monoarticular arthritis or some other rheumatologic emergency are seen within 24-48 hours, while consults with a possible AIRD are approved and seen within 1-4 weeks. Priority is given to those with suspected vasculitis, systemic lupus erythematosus, myositis, and disabling inflammatory arthritis. Patients with probable noninflammatory conditions such as osteoarthritis, fibromyalgia, and mechanical low back pain are not scheduled for an in-person visit. “Instead of simply declining the consult, we try to give some direction, or we say, ‘Why don’t you try this, this, and this, sort of a miniconsult,” Dr. West noted. “One of the potential adverse reactions to doing consult triage would be that the referring provider would be upset if we decline their consult. We acknowledge that. But over time we’ve been able to convince them that this is best for all concerned, so that the inflammatory disease group gets in to see us in an appropriate amount of time.”
Of the 961 consults, 673 were scheduled for an in-person AIRD evaluation and 288 consults were not scheduled. Patients were seen an average of 13 days after consult review. Of the 673 approved consults, 597 (89%) came for evaluation. Of these, 357 were diagnosed as having an AIRD, while 240 were diagnosed as having a non-AIRD. Among the patients not scheduled for a rheumatology visit, 128 had 1-year follow-up data, with 6 patients eventually diagnosed as having an AIRD. This translated into a consult triage sensitivity of 98% and a positive predictive value of 60%. “There’s a fair number of people with noninflammatory disease who do get into see us,” Dr. West said. “That has to do with our desire to not be overly rigid. The sensitivity, specificity, and positive predictive value were not quite as high as some people would like to see, but we really weren’t missing people who really needed to be seen.”
In their conservative cost analysis, revenue data for outpatient care was available for 318 of the 357 AIRD patients and 192 of 240 non-AIRD patients. It demonstrated that care of AIRD patients generates 44 times more revenue, compared with non-AIRD patients ($5,877 vs. $134 per patient, respectively; P less than .001).
“Our consult triage protocol appears to be an effective method to assure that patients with inflammatory rheumatic diseases get expedited access to appropriate rheumatologic care,” Dr. West concluded. “Using conservative measures, caring for patients with inflammatory rheumatic diseases results in significantly more revenue generation.” Generalizability of such a protocol to other practice settings depends on the time rheumatologists are willing to commit to it. “That’s the big thing,” he said. “The question comes up, could a nurse or a nurse practitioner learn the skills over time to be able to do efficient consult triage, to free up the doc from that? Yes. I think that’s absolutely possible.”
Going forward, Dr. Pearson and Dr. Kolfenbach, who are authors on the paper, have launched a pilot project in which the rheumatologist is compensated for doing a record review and e-consult on patients not recommended to be seen in the rheumatology clinic. “For consults who do not have inflammatory disease, we can say [to the referring clinician], ‘If we did see them, this is what we would be doing,’ ” Dr. West said. “Sometimes if there are still questions, we’ll say something like, ‘Once you get the results back, let us know and we can look at it again.’ That way they are getting similar compensation as telemedicine and other forms of consultation.”
At the Zuckerberg San Francisco General Hospital (ZSFG), use of a novel electronic consultation and referral system that was implemented in 2007 by University of California, San Francisco, providers continues to thrive for rheumatology and other specialty services. With this electronic system, previously called e-referral, all provider communication is captured in real time and recorded within the electronic health record. In a 2015 article from Arthritis Care & Research, researchers led by Jinoos Yazdany, MD, MPH, reviewed 2,105 e-referrals made between 2008 and 2012 (Arthritis Care Res. 2015;67[8]:1158-63). The main outcome of interest was use of preconsultation exchange, defined as back-and-forth communication between referring and specialty care providers, facilitating triage of referrals, requests for more information, or resolution of questions without a visit. The researchers found that about 25% of e-consults were resolved without a clinic visit, and that the proportion of e-consults undergoing preconsultation exchange increased over time, from 55% in 2008 to 74% in 2011.
“We’ve had situations in which somebody within our hospital system has requested a rheumatology referral but did not realize the urgency of the patients’ clinical signs and symptoms,” Dr. Yazdany, a rheumatologist and health services researcher at UCSF, said in an interview. “E-referrals are often responded to within that day. When we see an e-consult for a young woman with a rash and protein in her urine, a rheumatologist will recognize that is very concerning for a serious diagnosis like lupus of the kidney or systemic vasculitis. In that situation, we would pick up the phone and sometimes even call the patient and have them come to the emergency room for an urgent evaluation. Over the years, there have been many situations in which we’ve been able to intervene much earlier than we otherwise would have. In some cases that early intervention was lifesaving, or at least organ-preserving for the patient.”
Two studies from the early 2000s examined the use of preappointment management in rheumatology (see Arthritis Care Res. 2001;45:295-300 and Arthritis Rheum. 2004;51:253-7), but this is among the first to incorporate use of an electronic medical record to provide real-time exchange between the specialist and the referring provider. Clinicians at UCSF are reimbursed for reviewing e-consults in one of two ways. Those at ZSFG have protected and compensated time for the task, “so it’s basically part of their job to spend a half day a week on e-consults,” Dr. Yazdany said. “The department of public health and our health care system fold that into operational costs. That’s absolutely critical for success. To be done well and thoughtfully, managing consults and referrals takes time. It takes a lot of expertise.” Meanwhile, clinicians at UCSF’s main university hospital receive a small payment for each e-consult they review. “If it’s a complex consult it’s a higher reimbursement,” she said. “If it’s a simple one, it’s slightly less reimbursement, so it’s a fee-for-service model. It’s something that the health system funds, because it creates efficiencies and access for patients.”
Gaining popularity across specialties
Delphine S. Tuot, MD, a nephrologist who directs the ZSFG e-consult system, said that the notion of preconsult triage is gaining popularity in all medical specialties. For example, the Blue Shield of California Foundation is funding implementation of e-consult systems across many of California’s safety net health care delivery systems. “We have many health care plans that are interested in this process as well, because it improves access to specialty care, particularly in rural areas or in areas where the specialist workforce is limited,” said Dr. Tuot, who is codirector of the UCSF Center for Innovation in Access and Quality at ZSFG. Such efforts are also being promoted by the Public Hospital Redesign and Incentives in Medi-Cal Program (PRIME), which is part of California’s Medicaid waiver. PRIME “is encouraging health systems to look at innovative ways to deliver specialty care,” Dr. Tuot said. “E-consults and other non–face-to-face ways to deliver specialty care, including telemedicine encounters, count toward that metric for the Medicaid waiver.”
At the national level, the Association of American Medical Colleges has collaborated with more than 20 academic medical centers in 14 states, including Dartmouth-Hitchcock and Yale University, to implement tools built into the electronic medical record system through a program known as Project CORE (Coordinating Optimal Referral Experiences). According to Scott Shipman, MD, MPH, director of clinical innovations for the AAMC, nearly all of the current CORE sites have either gone live with the model in rheumatology or are planning to do so. “Better communication and coordination between primary care providers and specialists is important for all specialties, but because of the complexity of evaluation and management of problems in rheumatology, there is a tremendous opportunity for the CORE model to help get providers on the same page,” Dr. Shipman said in an interview. “We do this through simple decision support that we build into the referral order in the EMR, available at the point of care. Additionally, given the workforce challenges facing rheumatology in most regions of the country and consequent access barriers, offloading some of the demand via e-consults holds great promise.” Current focus areas for Project CORE, he said, include continued support of current CORE sites in their implementation and scaling efforts to maximize impact, advocacy to promote payer engagement in support of e-consult reimbursements, and working to extend the model to additional academic medical centers.
Dr. Tuot emphasized that performing e-consults “takes time and effort on behalf of specialists, so if you’re by yourself in solo practice it probably does not make sense to implement,” she said. “You need to spend your time seeing patients as much as possible. For primary care providers who are asking for curbside consults, it’s probably best to have things in writing from the specialist, such as in an e-consult, to make sure there’s no misunderstanding.”
As demand for rheumatology services increases, clinicians “have to figure out a way to see patients in most urgent need of our services,” Dr. Yazdany said. “That requires that we use technology like the e-consult system to prioritize the patients that we’re seeing. As we look at the rheumatology workforce shortage, especially in some geographic regions, it’s going to be absolutely critical. There are some diseases that no other specialists have experience caring for. In those situations, those patients need to get in to see rheumatologists in a timely fashion.”
Paper-based preconsult triage system
At Essentia Health, an integrated health care system with facilities in Minnesota, Wisconsin, and North Dakota, Meghan Scheibe, MD, a rheumatologist, is currently working with a rheumatologist colleague and a registered nurse to implement a paper-based preconsult triage system, “because our wait times have unfortunately skyrocketed,” she said. “We receive a lot of outside referrals from other health care groups and large health care systems that don’t have access to rheumatology.” Currently, the triage system is comprised of a referral note which includes the reason for consultation. Dr. Scheibe and her colleague rank the referral as expedited, intermediate concern, or low priority based on information provided by the referring clinician. “We mark those for our nurse to help schedule, and we let the referring provider know what the wait time is,” Dr. Scheibe said. “Then they have an opportunity to communicate back to us or say, ‘Yes, that’s fine,’ or, ‘I’m really worried about this patient. Could you get her in sooner?’ ”
It’s early in the process, but so far, implementation of the preconsult triage protocol “is allowing us to focus on the consultations on which we can be most impactful and not overwhelm the rheumatology workforce that we have,” she said.
Research reported in the UCSF study was supported by the American College of Rheumatology’s Ephraim P. Engleman Endowed Resident Research Preceptorship and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. None of the sources interviewed for this story reported having relevant financial disclosures.
About 15 years ago, rheumatologists at the University of Colorado School of Medicine, Aurora, implemented a preappointment consult triage system as a way to identify rheumatology patients who require timely evaluation and treatment.
Over time, the endeavor caused some soul searching. They wondered how effective their consult triage system was in identifying all patients with inflammatory rheumatic diseases and in ensuring they were seen promptly. They also wondered about the revenue implications of routine outpatient care of autoimmune and inflammatory rheumatic disease (AIRD) patients, compared with that of non-AIRD patients.
“Hospital leadership is very interested in making sure that all patients have access to specialty care in a timely manner,” said Sterling G. West, MD, one of the study authors who is also professor of medicine at the university. “However, there are not enough rheumatologists to see all patients with rheumatic complaints, and this deficit is likely to get worse. Although all patients with a rheumatic complaint would likely benefit from a rheumatology consultation, it is clear that timely access to rheumatologic care is most beneficial for patients with inflammatory rheumatic diseases to prevent future morbidity and disability.”
Year-long follow-up finds high sensitivity, more revenue
What started out as a quality improvement project morphed into a robust study that was published online July 12, 2018, in Arthritis Care & Research. Using data recorded in the electronic medical record, Dr. West and his colleagues retrospectively reviewed 961 new outpatient rheumatology consults sent during a 9-month period for final diagnosis and revenue generation for routine outpatient care over 1 year following consult review or initial evaluation. The first step of the consult management involves an intake access coordinator, Ryan Goecker, obtaining information about the patient from the referring clinician. Next, one of three experienced rheumatologists at the university – Duane W. Pearson, MD, Christopher C. Striebich, MD, or Jason R. Kolfenbach, MD – reviews the information about the case. “We do request that labs and x-rays be done ahead of time, depending on what the consult question is, so that we have the data to be able to decide whether a patient likely has an inflammatory process that we need to see or not,” Dr. West explained. “It takes somewhere between 5 and 20 minutes per consult. In total, it takes our rheumatologists about 5 hours a week to do the consults. However, even after subtracting the physician time spent screening consults, the time saved by the consult triage system enabled over 200 more time slots per year to be available to see new AIRD patients than would have been possible without the triage system.”
Following review of the data supplied about the case, patients who may have acute inflammatory monoarticular arthritis or some other rheumatologic emergency are seen within 24-48 hours, while consults with a possible AIRD are approved and seen within 1-4 weeks. Priority is given to those with suspected vasculitis, systemic lupus erythematosus, myositis, and disabling inflammatory arthritis. Patients with probable noninflammatory conditions such as osteoarthritis, fibromyalgia, and mechanical low back pain are not scheduled for an in-person visit. “Instead of simply declining the consult, we try to give some direction, or we say, ‘Why don’t you try this, this, and this, sort of a miniconsult,” Dr. West noted. “One of the potential adverse reactions to doing consult triage would be that the referring provider would be upset if we decline their consult. We acknowledge that. But over time we’ve been able to convince them that this is best for all concerned, so that the inflammatory disease group gets in to see us in an appropriate amount of time.”
Of the 961 consults, 673 were scheduled for an in-person AIRD evaluation and 288 consults were not scheduled. Patients were seen an average of 13 days after consult review. Of the 673 approved consults, 597 (89%) came for evaluation. Of these, 357 were diagnosed as having an AIRD, while 240 were diagnosed as having a non-AIRD. Among the patients not scheduled for a rheumatology visit, 128 had 1-year follow-up data, with 6 patients eventually diagnosed as having an AIRD. This translated into a consult triage sensitivity of 98% and a positive predictive value of 60%. “There’s a fair number of people with noninflammatory disease who do get into see us,” Dr. West said. “That has to do with our desire to not be overly rigid. The sensitivity, specificity, and positive predictive value were not quite as high as some people would like to see, but we really weren’t missing people who really needed to be seen.”
In their conservative cost analysis, revenue data for outpatient care was available for 318 of the 357 AIRD patients and 192 of 240 non-AIRD patients. It demonstrated that care of AIRD patients generates 44 times more revenue, compared with non-AIRD patients ($5,877 vs. $134 per patient, respectively; P less than .001).
“Our consult triage protocol appears to be an effective method to assure that patients with inflammatory rheumatic diseases get expedited access to appropriate rheumatologic care,” Dr. West concluded. “Using conservative measures, caring for patients with inflammatory rheumatic diseases results in significantly more revenue generation.” Generalizability of such a protocol to other practice settings depends on the time rheumatologists are willing to commit to it. “That’s the big thing,” he said. “The question comes up, could a nurse or a nurse practitioner learn the skills over time to be able to do efficient consult triage, to free up the doc from that? Yes. I think that’s absolutely possible.”
Going forward, Dr. Pearson and Dr. Kolfenbach, who are authors on the paper, have launched a pilot project in which the rheumatologist is compensated for doing a record review and e-consult on patients not recommended to be seen in the rheumatology clinic. “For consults who do not have inflammatory disease, we can say [to the referring clinician], ‘If we did see them, this is what we would be doing,’ ” Dr. West said. “Sometimes if there are still questions, we’ll say something like, ‘Once you get the results back, let us know and we can look at it again.’ That way they are getting similar compensation as telemedicine and other forms of consultation.”
At the Zuckerberg San Francisco General Hospital (ZSFG), use of a novel electronic consultation and referral system that was implemented in 2007 by University of California, San Francisco, providers continues to thrive for rheumatology and other specialty services. With this electronic system, previously called e-referral, all provider communication is captured in real time and recorded within the electronic health record. In a 2015 article from Arthritis Care & Research, researchers led by Jinoos Yazdany, MD, MPH, reviewed 2,105 e-referrals made between 2008 and 2012 (Arthritis Care Res. 2015;67[8]:1158-63). The main outcome of interest was use of preconsultation exchange, defined as back-and-forth communication between referring and specialty care providers, facilitating triage of referrals, requests for more information, or resolution of questions without a visit. The researchers found that about 25% of e-consults were resolved without a clinic visit, and that the proportion of e-consults undergoing preconsultation exchange increased over time, from 55% in 2008 to 74% in 2011.
“We’ve had situations in which somebody within our hospital system has requested a rheumatology referral but did not realize the urgency of the patients’ clinical signs and symptoms,” Dr. Yazdany, a rheumatologist and health services researcher at UCSF, said in an interview. “E-referrals are often responded to within that day. When we see an e-consult for a young woman with a rash and protein in her urine, a rheumatologist will recognize that is very concerning for a serious diagnosis like lupus of the kidney or systemic vasculitis. In that situation, we would pick up the phone and sometimes even call the patient and have them come to the emergency room for an urgent evaluation. Over the years, there have been many situations in which we’ve been able to intervene much earlier than we otherwise would have. In some cases that early intervention was lifesaving, or at least organ-preserving for the patient.”
Two studies from the early 2000s examined the use of preappointment management in rheumatology (see Arthritis Care Res. 2001;45:295-300 and Arthritis Rheum. 2004;51:253-7), but this is among the first to incorporate use of an electronic medical record to provide real-time exchange between the specialist and the referring provider. Clinicians at UCSF are reimbursed for reviewing e-consults in one of two ways. Those at ZSFG have protected and compensated time for the task, “so it’s basically part of their job to spend a half day a week on e-consults,” Dr. Yazdany said. “The department of public health and our health care system fold that into operational costs. That’s absolutely critical for success. To be done well and thoughtfully, managing consults and referrals takes time. It takes a lot of expertise.” Meanwhile, clinicians at UCSF’s main university hospital receive a small payment for each e-consult they review. “If it’s a complex consult it’s a higher reimbursement,” she said. “If it’s a simple one, it’s slightly less reimbursement, so it’s a fee-for-service model. It’s something that the health system funds, because it creates efficiencies and access for patients.”
Gaining popularity across specialties
Delphine S. Tuot, MD, a nephrologist who directs the ZSFG e-consult system, said that the notion of preconsult triage is gaining popularity in all medical specialties. For example, the Blue Shield of California Foundation is funding implementation of e-consult systems across many of California’s safety net health care delivery systems. “We have many health care plans that are interested in this process as well, because it improves access to specialty care, particularly in rural areas or in areas where the specialist workforce is limited,” said Dr. Tuot, who is codirector of the UCSF Center for Innovation in Access and Quality at ZSFG. Such efforts are also being promoted by the Public Hospital Redesign and Incentives in Medi-Cal Program (PRIME), which is part of California’s Medicaid waiver. PRIME “is encouraging health systems to look at innovative ways to deliver specialty care,” Dr. Tuot said. “E-consults and other non–face-to-face ways to deliver specialty care, including telemedicine encounters, count toward that metric for the Medicaid waiver.”
At the national level, the Association of American Medical Colleges has collaborated with more than 20 academic medical centers in 14 states, including Dartmouth-Hitchcock and Yale University, to implement tools built into the electronic medical record system through a program known as Project CORE (Coordinating Optimal Referral Experiences). According to Scott Shipman, MD, MPH, director of clinical innovations for the AAMC, nearly all of the current CORE sites have either gone live with the model in rheumatology or are planning to do so. “Better communication and coordination between primary care providers and specialists is important for all specialties, but because of the complexity of evaluation and management of problems in rheumatology, there is a tremendous opportunity for the CORE model to help get providers on the same page,” Dr. Shipman said in an interview. “We do this through simple decision support that we build into the referral order in the EMR, available at the point of care. Additionally, given the workforce challenges facing rheumatology in most regions of the country and consequent access barriers, offloading some of the demand via e-consults holds great promise.” Current focus areas for Project CORE, he said, include continued support of current CORE sites in their implementation and scaling efforts to maximize impact, advocacy to promote payer engagement in support of e-consult reimbursements, and working to extend the model to additional academic medical centers.
Dr. Tuot emphasized that performing e-consults “takes time and effort on behalf of specialists, so if you’re by yourself in solo practice it probably does not make sense to implement,” she said. “You need to spend your time seeing patients as much as possible. For primary care providers who are asking for curbside consults, it’s probably best to have things in writing from the specialist, such as in an e-consult, to make sure there’s no misunderstanding.”
As demand for rheumatology services increases, clinicians “have to figure out a way to see patients in most urgent need of our services,” Dr. Yazdany said. “That requires that we use technology like the e-consult system to prioritize the patients that we’re seeing. As we look at the rheumatology workforce shortage, especially in some geographic regions, it’s going to be absolutely critical. There are some diseases that no other specialists have experience caring for. In those situations, those patients need to get in to see rheumatologists in a timely fashion.”
Paper-based preconsult triage system
At Essentia Health, an integrated health care system with facilities in Minnesota, Wisconsin, and North Dakota, Meghan Scheibe, MD, a rheumatologist, is currently working with a rheumatologist colleague and a registered nurse to implement a paper-based preconsult triage system, “because our wait times have unfortunately skyrocketed,” she said. “We receive a lot of outside referrals from other health care groups and large health care systems that don’t have access to rheumatology.” Currently, the triage system is comprised of a referral note which includes the reason for consultation. Dr. Scheibe and her colleague rank the referral as expedited, intermediate concern, or low priority based on information provided by the referring clinician. “We mark those for our nurse to help schedule, and we let the referring provider know what the wait time is,” Dr. Scheibe said. “Then they have an opportunity to communicate back to us or say, ‘Yes, that’s fine,’ or, ‘I’m really worried about this patient. Could you get her in sooner?’ ”
It’s early in the process, but so far, implementation of the preconsult triage protocol “is allowing us to focus on the consultations on which we can be most impactful and not overwhelm the rheumatology workforce that we have,” she said.
Research reported in the UCSF study was supported by the American College of Rheumatology’s Ephraim P. Engleman Endowed Resident Research Preceptorship and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. None of the sources interviewed for this story reported having relevant financial disclosures.
Flexible Bronchoscopic Removal of 3 Foreign Objects
Consider flexible bronchoscopy as an option to retrieve aspirated foreign bodies in the airway.
Airway foreign-body aspiration may cause no symptoms, although it can produce acute and life-threatening central airway obstruction.1 In the US, at least 2,700 people, including more than 300 children, die of foreign-body aspiration each year.2 Most foreign-body aspirations occur in children and elderly patients.3 In adults, dementia, drug intoxication, strokes, seizures, and neurologic disorders may predispose patients to aspiration.3 Some of the consequences of an aspirated object are complete or partial airway obstruction, respiratory distress and failure, pneumothorax, and hemorrhage.2 In addition, inadvertent aspiration of foreign objects in asymptomatic patients may not be evident for months, resulting in late complications as postobstructive pneumonia, bronchiectasis, or lung abscess.2
We present a case of a patient with documented schizophrenia with nonadherence to his antipsychotic medications who aspirated different objects. Flexible bronchoscopy was performed since rigid bronchoscopy is not available at our institution. Several bronchoscopy tools were required to successfully remove the objects and avoid further invasive interventions, such as cardiothoracic surgery.
Case Presentation
A 55-year-old man with schizophrenia on antipsychotics developed cough, shortness of breath, and dysphagia of 1-month of evolution. Because his symptoms worsened, his mother brought him to the emergency department. Peripheral oxygen saturation was 97% at room air. Lung auscultation was remarkable for bilateral scattered rhonchi and wheezes.
Laboratory results showed leukocytosis with neutrophilia and hypotonic hypovolemic hyponatremia. 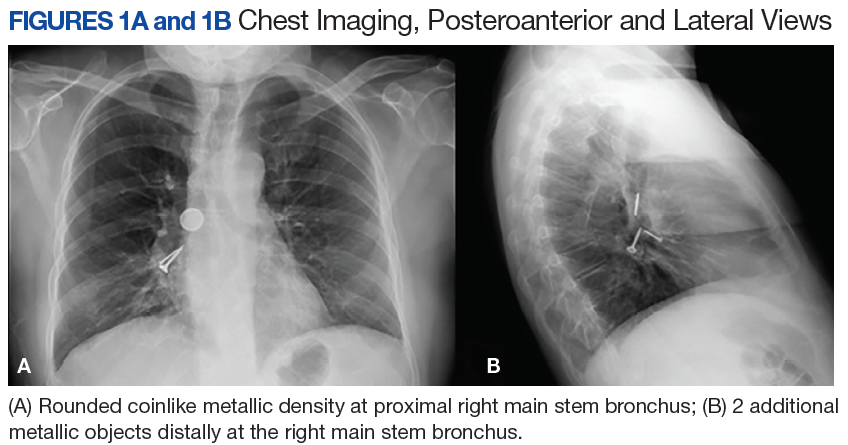
The patient stated that he did not remember swallowing any objects, although his mother confirmed that he was not adherent with his antipsychotic medications, which could have predisposed him to aspiration secondary to possible psychotic episodes. 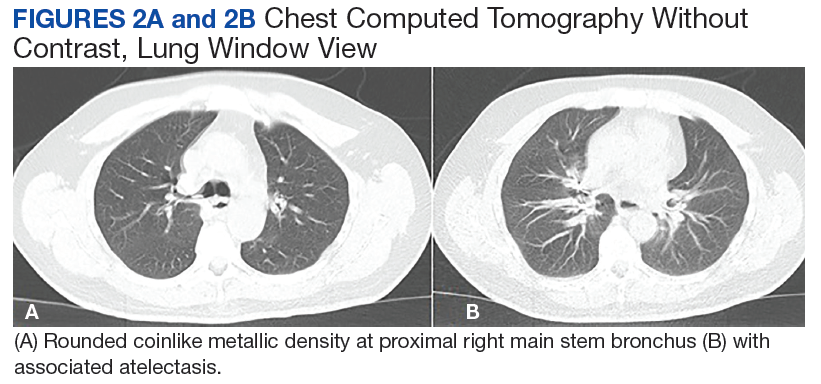
Piperacillin/tazobactam 4.5 g every 8 hours was started to cover anaerobic bacterial organisms causing abscess, and IV fluids were given for hypovolemia. Flexible bronchoscopy (rigid bronchoscopy is superior although not available at our institution) was planned to be performed in the operating room (OR) because we predicted a difficult and prolonged retrieval in view of multiple and different-sized objects.
A bronchoscopy was performed, showing a disk-shaped metallic foreign body at the right main stem bronchus. After multiple attempts using the tripod retrieval tool, a coin was removed (Figures 3A and 3B). 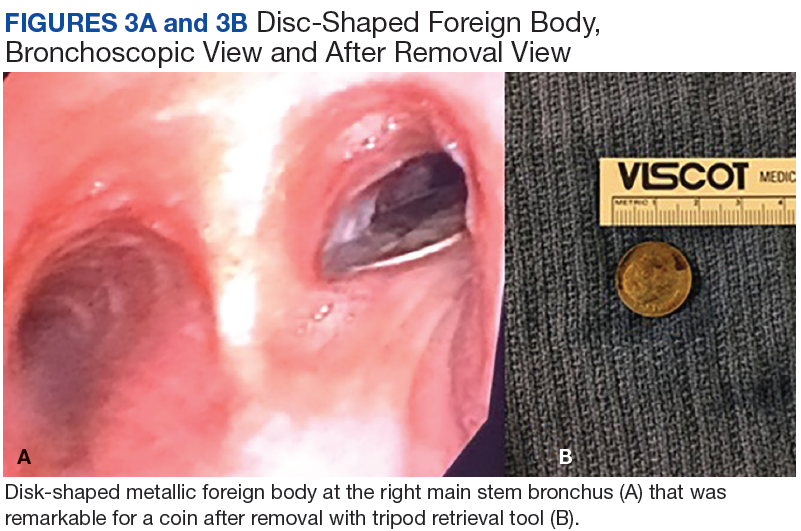


The patient was reintubated without any complications. A postprocedure chest radiograph showed the absence of foreign bodies and no pneumothorax. The patient completed IV antibiotic with piperacillin/tazobactam and supportive therapy with clinical improvement and successful extubation within 2 days. Cardiothoracic surgery was not required. Psychiatry service recommended to continue the same antipsychotic medications, administered only by his mother to assure adherence and to avoid similar future events. The patient was discharged home without any immediate complications despite having had a coin, nail, and screw aspiration (Figure 6).
Discussion
More than 50% of foreign bodies lodge at the right main stem bronchus due to the trachea’s anatomical position.2,4 In adults, foreign-body aspiration may present with nonspecific symptoms, such as cough and dyspnea.4 Other symptoms might include wheezes, chest discomfort, and sputum production. A chest radiograph is helpful as part of the initial diagnostic workup. A chest CT scan without contrast should be performed to confirm the diagnosis and to plan possible foreign-body retrieval.
Bronchoscopy is the gold standard for diagnosis and management of foreign-body aspiration.1 Rigid bronchoscopy is superior to flexible bronchoscopy in removal of large airway foreign bodies.1 The rigid bronchoscopy provides the ability to function as an endotracheal tube, thus allowing control of the airway and a conduit through which foreign bodies can be removed.1 Nonetheless, sometimes retrieval of foreign bodies deeper into the subsegmental bronchi cannot be achieved.1 Moreover, the required equipment or knowledgeable staff is not always available.1 Therefore, flexible bronchoscopy is an option to retrieve airway foreign bodies especially those located distal in the airway and for those medical centers without rigid bronchoscopy as is the case in our institution.
In our case, flexible bronchoscopy was performed in the OR because we predicted a difficult and prolonged retrieval in view of multiple and different-sized objects. Anesthesia Service assistance was requested anticipating need for patient sedation and intubation. We used the tripod and snare retrieval tools to remove 3 foreign objects located at the right main stem bronchus. Even though multiple attempts were made and endotracheal intubation was required, a successful retrieval with flexible bronchoscopy was performed. Moreover, cardiothoracic surgery was not required avoiding more invasive interventions with subsequent morbidity and mortality.
Conclusion
Flexible bronchoscopy is an important tool within the arsenal of the Pulmonology Service. The management of the underlying etiology also should be performed. In our case, the Psychiatry Service recommended that the patient’s medications should be administered by his mother to avoid similar events in the future. Flexible bronchoscopy can be a valuable option for foreign objects removal, especially those distally located in the lung segments as well as in those medical centers where rigid bronchoscopy is not available.
1. Mehta D, Mehta C, Bansal S, Singla S, Tangri N. Flexible bronchoscopic removal of a three piece foreign body from a child’s bronchus. Australas Med J. 2012;5(4):227-230.
2. Mercado JA, Rodríguez W. Occult aspiration of a chicken wishbone as a cause of hemoptysis. P R Health Sci J. 1999;18(1):71-73.
3. Robles-Arias CM, Campos-Santiago Z, Vega MT, Rosa-Cruz F, Rodríguez-Cintrón W. Aspiration of a dental tool during a crown placement procedure. Fed Pract. 2014;31(6):12-14.
4. Blanco-Ramos M, Botana-Rial M, García-Fontán E, Fernández-Villar A, Gallas-Torreira M. Update in the extraction of airway foreign bodies in adults. J Thorac Dis. 2016;8(11):3452-3456.
Consider flexible bronchoscopy as an option to retrieve aspirated foreign bodies in the airway.
Consider flexible bronchoscopy as an option to retrieve aspirated foreign bodies in the airway.
Airway foreign-body aspiration may cause no symptoms, although it can produce acute and life-threatening central airway obstruction.1 In the US, at least 2,700 people, including more than 300 children, die of foreign-body aspiration each year.2 Most foreign-body aspirations occur in children and elderly patients.3 In adults, dementia, drug intoxication, strokes, seizures, and neurologic disorders may predispose patients to aspiration.3 Some of the consequences of an aspirated object are complete or partial airway obstruction, respiratory distress and failure, pneumothorax, and hemorrhage.2 In addition, inadvertent aspiration of foreign objects in asymptomatic patients may not be evident for months, resulting in late complications as postobstructive pneumonia, bronchiectasis, or lung abscess.2
We present a case of a patient with documented schizophrenia with nonadherence to his antipsychotic medications who aspirated different objects. Flexible bronchoscopy was performed since rigid bronchoscopy is not available at our institution. Several bronchoscopy tools were required to successfully remove the objects and avoid further invasive interventions, such as cardiothoracic surgery.
Case Presentation
A 55-year-old man with schizophrenia on antipsychotics developed cough, shortness of breath, and dysphagia of 1-month of evolution. Because his symptoms worsened, his mother brought him to the emergency department. Peripheral oxygen saturation was 97% at room air. Lung auscultation was remarkable for bilateral scattered rhonchi and wheezes.
Laboratory results showed leukocytosis with neutrophilia and hypotonic hypovolemic hyponatremia.
The patient stated that he did not remember swallowing any objects, although his mother confirmed that he was not adherent with his antipsychotic medications, which could have predisposed him to aspiration secondary to possible psychotic episodes.
Piperacillin/tazobactam 4.5 g every 8 hours was started to cover anaerobic bacterial organisms causing abscess, and IV fluids were given for hypovolemia. Flexible bronchoscopy (rigid bronchoscopy is superior although not available at our institution) was planned to be performed in the operating room (OR) because we predicted a difficult and prolonged retrieval in view of multiple and different-sized objects.
A bronchoscopy was performed, showing a disk-shaped metallic foreign body at the right main stem bronchus. After multiple attempts using the tripod retrieval tool, a coin was removed (Figures 3A and 3B).
The patient was reintubated without any complications. A postprocedure chest radiograph showed the absence of foreign bodies and no pneumothorax. The patient completed IV antibiotic with piperacillin/tazobactam and supportive therapy with clinical improvement and successful extubation within 2 days. Cardiothoracic surgery was not required. Psychiatry service recommended to continue the same antipsychotic medications, administered only by his mother to assure adherence and to avoid similar future events. The patient was discharged home without any immediate complications despite having had a coin, nail, and screw aspiration (Figure 6).
Discussion
More than 50% of foreign bodies lodge at the right main stem bronchus due to the trachea’s anatomical position.2,4 In adults, foreign-body aspiration may present with nonspecific symptoms, such as cough and dyspnea.4 Other symptoms might include wheezes, chest discomfort, and sputum production. A chest radiograph is helpful as part of the initial diagnostic workup. A chest CT scan without contrast should be performed to confirm the diagnosis and to plan possible foreign-body retrieval.
Bronchoscopy is the gold standard for diagnosis and management of foreign-body aspiration.1 Rigid bronchoscopy is superior to flexible bronchoscopy in removal of large airway foreign bodies.1 The rigid bronchoscopy provides the ability to function as an endotracheal tube, thus allowing control of the airway and a conduit through which foreign bodies can be removed.1 Nonetheless, sometimes retrieval of foreign bodies deeper into the subsegmental bronchi cannot be achieved.1 Moreover, the required equipment or knowledgeable staff is not always available.1 Therefore, flexible bronchoscopy is an option to retrieve airway foreign bodies especially those located distal in the airway and for those medical centers without rigid bronchoscopy as is the case in our institution.
In our case, flexible bronchoscopy was performed in the OR because we predicted a difficult and prolonged retrieval in view of multiple and different-sized objects. Anesthesia Service assistance was requested anticipating need for patient sedation and intubation. We used the tripod and snare retrieval tools to remove 3 foreign objects located at the right main stem bronchus. Even though multiple attempts were made and endotracheal intubation was required, a successful retrieval with flexible bronchoscopy was performed. Moreover, cardiothoracic surgery was not required avoiding more invasive interventions with subsequent morbidity and mortality.
Conclusion
Flexible bronchoscopy is an important tool within the arsenal of the Pulmonology Service. The management of the underlying etiology also should be performed. In our case, the Psychiatry Service recommended that the patient’s medications should be administered by his mother to avoid similar events in the future. Flexible bronchoscopy can be a valuable option for foreign objects removal, especially those distally located in the lung segments as well as in those medical centers where rigid bronchoscopy is not available.
Airway foreign-body aspiration may cause no symptoms, although it can produce acute and life-threatening central airway obstruction.1 In the US, at least 2,700 people, including more than 300 children, die of foreign-body aspiration each year.2 Most foreign-body aspirations occur in children and elderly patients.3 In adults, dementia, drug intoxication, strokes, seizures, and neurologic disorders may predispose patients to aspiration.3 Some of the consequences of an aspirated object are complete or partial airway obstruction, respiratory distress and failure, pneumothorax, and hemorrhage.2 In addition, inadvertent aspiration of foreign objects in asymptomatic patients may not be evident for months, resulting in late complications as postobstructive pneumonia, bronchiectasis, or lung abscess.2
We present a case of a patient with documented schizophrenia with nonadherence to his antipsychotic medications who aspirated different objects. Flexible bronchoscopy was performed since rigid bronchoscopy is not available at our institution. Several bronchoscopy tools were required to successfully remove the objects and avoid further invasive interventions, such as cardiothoracic surgery.
Case Presentation
A 55-year-old man with schizophrenia on antipsychotics developed cough, shortness of breath, and dysphagia of 1-month of evolution. Because his symptoms worsened, his mother brought him to the emergency department. Peripheral oxygen saturation was 97% at room air. Lung auscultation was remarkable for bilateral scattered rhonchi and wheezes.
Laboratory results showed leukocytosis with neutrophilia and hypotonic hypovolemic hyponatremia.
The patient stated that he did not remember swallowing any objects, although his mother confirmed that he was not adherent with his antipsychotic medications, which could have predisposed him to aspiration secondary to possible psychotic episodes.
Piperacillin/tazobactam 4.5 g every 8 hours was started to cover anaerobic bacterial organisms causing abscess, and IV fluids were given for hypovolemia. Flexible bronchoscopy (rigid bronchoscopy is superior although not available at our institution) was planned to be performed in the operating room (OR) because we predicted a difficult and prolonged retrieval in view of multiple and different-sized objects.
A bronchoscopy was performed, showing a disk-shaped metallic foreign body at the right main stem bronchus. After multiple attempts using the tripod retrieval tool, a coin was removed (Figures 3A and 3B).
The patient was reintubated without any complications. A postprocedure chest radiograph showed the absence of foreign bodies and no pneumothorax. The patient completed IV antibiotic with piperacillin/tazobactam and supportive therapy with clinical improvement and successful extubation within 2 days. Cardiothoracic surgery was not required. Psychiatry service recommended to continue the same antipsychotic medications, administered only by his mother to assure adherence and to avoid similar future events. The patient was discharged home without any immediate complications despite having had a coin, nail, and screw aspiration (Figure 6).
Discussion
More than 50% of foreign bodies lodge at the right main stem bronchus due to the trachea’s anatomical position.2,4 In adults, foreign-body aspiration may present with nonspecific symptoms, such as cough and dyspnea.4 Other symptoms might include wheezes, chest discomfort, and sputum production. A chest radiograph is helpful as part of the initial diagnostic workup. A chest CT scan without contrast should be performed to confirm the diagnosis and to plan possible foreign-body retrieval.
Bronchoscopy is the gold standard for diagnosis and management of foreign-body aspiration.1 Rigid bronchoscopy is superior to flexible bronchoscopy in removal of large airway foreign bodies.1 The rigid bronchoscopy provides the ability to function as an endotracheal tube, thus allowing control of the airway and a conduit through which foreign bodies can be removed.1 Nonetheless, sometimes retrieval of foreign bodies deeper into the subsegmental bronchi cannot be achieved.1 Moreover, the required equipment or knowledgeable staff is not always available.1 Therefore, flexible bronchoscopy is an option to retrieve airway foreign bodies especially those located distal in the airway and for those medical centers without rigid bronchoscopy as is the case in our institution.
In our case, flexible bronchoscopy was performed in the OR because we predicted a difficult and prolonged retrieval in view of multiple and different-sized objects. Anesthesia Service assistance was requested anticipating need for patient sedation and intubation. We used the tripod and snare retrieval tools to remove 3 foreign objects located at the right main stem bronchus. Even though multiple attempts were made and endotracheal intubation was required, a successful retrieval with flexible bronchoscopy was performed. Moreover, cardiothoracic surgery was not required avoiding more invasive interventions with subsequent morbidity and mortality.
Conclusion
Flexible bronchoscopy is an important tool within the arsenal of the Pulmonology Service. The management of the underlying etiology also should be performed. In our case, the Psychiatry Service recommended that the patient’s medications should be administered by his mother to avoid similar events in the future. Flexible bronchoscopy can be a valuable option for foreign objects removal, especially those distally located in the lung segments as well as in those medical centers where rigid bronchoscopy is not available.
1. Mehta D, Mehta C, Bansal S, Singla S, Tangri N. Flexible bronchoscopic removal of a three piece foreign body from a child’s bronchus. Australas Med J. 2012;5(4):227-230.
2. Mercado JA, Rodríguez W. Occult aspiration of a chicken wishbone as a cause of hemoptysis. P R Health Sci J. 1999;18(1):71-73.
3. Robles-Arias CM, Campos-Santiago Z, Vega MT, Rosa-Cruz F, Rodríguez-Cintrón W. Aspiration of a dental tool during a crown placement procedure. Fed Pract. 2014;31(6):12-14.
4. Blanco-Ramos M, Botana-Rial M, García-Fontán E, Fernández-Villar A, Gallas-Torreira M. Update in the extraction of airway foreign bodies in adults. J Thorac Dis. 2016;8(11):3452-3456.
1. Mehta D, Mehta C, Bansal S, Singla S, Tangri N. Flexible bronchoscopic removal of a three piece foreign body from a child’s bronchus. Australas Med J. 2012;5(4):227-230.
2. Mercado JA, Rodríguez W. Occult aspiration of a chicken wishbone as a cause of hemoptysis. P R Health Sci J. 1999;18(1):71-73.
3. Robles-Arias CM, Campos-Santiago Z, Vega MT, Rosa-Cruz F, Rodríguez-Cintrón W. Aspiration of a dental tool during a crown placement procedure. Fed Pract. 2014;31(6):12-14.
4. Blanco-Ramos M, Botana-Rial M, García-Fontán E, Fernández-Villar A, Gallas-Torreira M. Update in the extraction of airway foreign bodies in adults. J Thorac Dis. 2016;8(11):3452-3456.
What’s The Impact of Occult HBV in Chronic HCV?
The reported prevalence of occult hepatitis B infection (OBI) varies widely: from < 1% to as high as 89.5% in HIV patients. Among patients with chronic hepatitis, the prevalence—again—ranges widely, from 0% to 52% but is highest in patients with chronic hepatitis C (CHC).
The clinical impact of OBI on patients with CHC has been extensively investigated, say researchers from the Institute of Liver and Biliary Sciences in New Delhi, India, but the available data are conflicting. In fact, when they conducted their study to assess the prevalence of OBI and evaluate its impact on clinical outcomes and response to antiviral therapy in CHC, the findings were “largely inconclusive.”
The study included 80 patients, of whom 32 (40%) had seropositive OBI. Hepatitis C virus genotype information was available for 59 patients, revealing that genotype 3 was most common.
However, analysis of clinical, biochemical, histopathologic and treatment response based on seropositivity and semiquantitative estimate of anti-HBc did not yield statistically significant results. Plasma samples of 14 were reactive for anti-HBc, 12 for anti-HBs, and 6 for both antibodies. Hepatitis B virus DNA (34 IU/mL) was detected in the plasma sample of only 1 patient by quantitative polymerase chain reaction. Therefore, the researchers say, the prevalence of OBI was 1.25%.
Anti-HBc total antibody levels did not influence clinical outcomes and response to directly acting antiviral therapy. Nor did genotype make a significant difference: 90.7% of genotype 3 patients and 92.8% of genotype 1 patients attained sustained virologic response.
More prospective studies should be conducted, the researchers urge, to further explore “this seemingly enigmatic issue.”
Source:
Bhatia M, Gupta E, Choudhary MC, Jindal A, Sarin SK. J Lab Physicians. 2018;10(3):304-308.
doi: 10.4103/JLP.JLP_12_18.
The reported prevalence of occult hepatitis B infection (OBI) varies widely: from < 1% to as high as 89.5% in HIV patients. Among patients with chronic hepatitis, the prevalence—again—ranges widely, from 0% to 52% but is highest in patients with chronic hepatitis C (CHC).
The clinical impact of OBI on patients with CHC has been extensively investigated, say researchers from the Institute of Liver and Biliary Sciences in New Delhi, India, but the available data are conflicting. In fact, when they conducted their study to assess the prevalence of OBI and evaluate its impact on clinical outcomes and response to antiviral therapy in CHC, the findings were “largely inconclusive.”
The study included 80 patients, of whom 32 (40%) had seropositive OBI. Hepatitis C virus genotype information was available for 59 patients, revealing that genotype 3 was most common.
However, analysis of clinical, biochemical, histopathologic and treatment response based on seropositivity and semiquantitative estimate of anti-HBc did not yield statistically significant results. Plasma samples of 14 were reactive for anti-HBc, 12 for anti-HBs, and 6 for both antibodies. Hepatitis B virus DNA (34 IU/mL) was detected in the plasma sample of only 1 patient by quantitative polymerase chain reaction. Therefore, the researchers say, the prevalence of OBI was 1.25%.
Anti-HBc total antibody levels did not influence clinical outcomes and response to directly acting antiviral therapy. Nor did genotype make a significant difference: 90.7% of genotype 3 patients and 92.8% of genotype 1 patients attained sustained virologic response.
More prospective studies should be conducted, the researchers urge, to further explore “this seemingly enigmatic issue.”
Source:
Bhatia M, Gupta E, Choudhary MC, Jindal A, Sarin SK. J Lab Physicians. 2018;10(3):304-308.
doi: 10.4103/JLP.JLP_12_18.
The reported prevalence of occult hepatitis B infection (OBI) varies widely: from < 1% to as high as 89.5% in HIV patients. Among patients with chronic hepatitis, the prevalence—again—ranges widely, from 0% to 52% but is highest in patients with chronic hepatitis C (CHC).
The clinical impact of OBI on patients with CHC has been extensively investigated, say researchers from the Institute of Liver and Biliary Sciences in New Delhi, India, but the available data are conflicting. In fact, when they conducted their study to assess the prevalence of OBI and evaluate its impact on clinical outcomes and response to antiviral therapy in CHC, the findings were “largely inconclusive.”
The study included 80 patients, of whom 32 (40%) had seropositive OBI. Hepatitis C virus genotype information was available for 59 patients, revealing that genotype 3 was most common.
However, analysis of clinical, biochemical, histopathologic and treatment response based on seropositivity and semiquantitative estimate of anti-HBc did not yield statistically significant results. Plasma samples of 14 were reactive for anti-HBc, 12 for anti-HBs, and 6 for both antibodies. Hepatitis B virus DNA (34 IU/mL) was detected in the plasma sample of only 1 patient by quantitative polymerase chain reaction. Therefore, the researchers say, the prevalence of OBI was 1.25%.
Anti-HBc total antibody levels did not influence clinical outcomes and response to directly acting antiviral therapy. Nor did genotype make a significant difference: 90.7% of genotype 3 patients and 92.8% of genotype 1 patients attained sustained virologic response.
More prospective studies should be conducted, the researchers urge, to further explore “this seemingly enigmatic issue.”
Source:
Bhatia M, Gupta E, Choudhary MC, Jindal A, Sarin SK. J Lab Physicians. 2018;10(3):304-308.
doi: 10.4103/JLP.JLP_12_18.
Team identifies potential immunotherapy target for AML

New research could aid the development of immunotherapies tailored to patients with acute myeloid leukemia (AML) who are undergoing stem cell transplant (SCT).
Researchers found they could use genetic sequencing and computer software to identify minor histocompatibility antigens (mHAs) known to occur in AML.
The team used this method to predict novel graft-versus-leukemia (GVL) mHAs and demonstrated that one of these mHAs could be a “potentially useful” therapeutic target.
Ben Vincent, MD, of the University of North Carolina Lineberger Comprehensive Cancer Center in Chapel Hill, and his colleagues reported these findings in Blood Advances.
In their retrospective study, the researchers tested whether their software could predict antigenic targets in 101 SCT donor-recipient pairs.
The researchers found they could correctly identify 14 of 18 mHAs known to occur in AML, but they were also able to predict 102 new GVL mHAs.
The researchers then confirmed one of these GVL mHAs, called UNC-GRK4-V, as a potential target for immunotherapy. The team observed immune responses to UNC-GRK4-V in four of nine AML patients who had undergone SCT.
Looking ahead, the researchers want to optimize their software to predict the most common AML-associated mHAs present in the U.S. population and confirm these predicted antigens as valid immunotherapy targets.
The team believes they could potentially use their predictions to engineer donor immune cells to specifically target the cancer cell antigens while preventing graft-versus-host disease.
“We’ve developed a software package that predicts leukemia-specific immune targets in any leukemia patient undergoing a stem cell transplant based on DNA and RNA sequencing and demonstrated that these data can lead to actual targets expressed on leukemia cells,” Dr. Vincent said.
“The next step of our work is to use that information for patient-specific therapies to try to improve cure rates without making graft-versus-host disease worse.”
The current research was supported by a National Cancer Institute grant, an ASCO Young Investigator Award, the North Carolina University Cancer Research Fund, and the Scott Neil Schwirck Fellowship.
New research could aid the development of immunotherapies tailored to patients with acute myeloid leukemia (AML) who are undergoing stem cell transplant (SCT).
Researchers found they could use genetic sequencing and computer software to identify minor histocompatibility antigens (mHAs) known to occur in AML.
The team used this method to predict novel graft-versus-leukemia (GVL) mHAs and demonstrated that one of these mHAs could be a “potentially useful” therapeutic target.
Ben Vincent, MD, of the University of North Carolina Lineberger Comprehensive Cancer Center in Chapel Hill, and his colleagues reported these findings in Blood Advances.
In their retrospective study, the researchers tested whether their software could predict antigenic targets in 101 SCT donor-recipient pairs.
The researchers found they could correctly identify 14 of 18 mHAs known to occur in AML, but they were also able to predict 102 new GVL mHAs.
The researchers then confirmed one of these GVL mHAs, called UNC-GRK4-V, as a potential target for immunotherapy. The team observed immune responses to UNC-GRK4-V in four of nine AML patients who had undergone SCT.
Looking ahead, the researchers want to optimize their software to predict the most common AML-associated mHAs present in the U.S. population and confirm these predicted antigens as valid immunotherapy targets.
The team believes they could potentially use their predictions to engineer donor immune cells to specifically target the cancer cell antigens while preventing graft-versus-host disease.
“We’ve developed a software package that predicts leukemia-specific immune targets in any leukemia patient undergoing a stem cell transplant based on DNA and RNA sequencing and demonstrated that these data can lead to actual targets expressed on leukemia cells,” Dr. Vincent said.
“The next step of our work is to use that information for patient-specific therapies to try to improve cure rates without making graft-versus-host disease worse.”
The current research was supported by a National Cancer Institute grant, an ASCO Young Investigator Award, the North Carolina University Cancer Research Fund, and the Scott Neil Schwirck Fellowship.
New research could aid the development of immunotherapies tailored to patients with acute myeloid leukemia (AML) who are undergoing stem cell transplant (SCT).
Researchers found they could use genetic sequencing and computer software to identify minor histocompatibility antigens (mHAs) known to occur in AML.
The team used this method to predict novel graft-versus-leukemia (GVL) mHAs and demonstrated that one of these mHAs could be a “potentially useful” therapeutic target.
Ben Vincent, MD, of the University of North Carolina Lineberger Comprehensive Cancer Center in Chapel Hill, and his colleagues reported these findings in Blood Advances.
In their retrospective study, the researchers tested whether their software could predict antigenic targets in 101 SCT donor-recipient pairs.
The researchers found they could correctly identify 14 of 18 mHAs known to occur in AML, but they were also able to predict 102 new GVL mHAs.
The researchers then confirmed one of these GVL mHAs, called UNC-GRK4-V, as a potential target for immunotherapy. The team observed immune responses to UNC-GRK4-V in four of nine AML patients who had undergone SCT.
Looking ahead, the researchers want to optimize their software to predict the most common AML-associated mHAs present in the U.S. population and confirm these predicted antigens as valid immunotherapy targets.
The team believes they could potentially use their predictions to engineer donor immune cells to specifically target the cancer cell antigens while preventing graft-versus-host disease.
“We’ve developed a software package that predicts leukemia-specific immune targets in any leukemia patient undergoing a stem cell transplant based on DNA and RNA sequencing and demonstrated that these data can lead to actual targets expressed on leukemia cells,” Dr. Vincent said.
“The next step of our work is to use that information for patient-specific therapies to try to improve cure rates without making graft-versus-host disease worse.”
The current research was supported by a National Cancer Institute grant, an ASCO Young Investigator Award, the North Carolina University Cancer Research Fund, and the Scott Neil Schwirck Fellowship.