User login
Pediatric ED diagnoses vary with the season
The two most common reasons for pediatric emergency department visits exhibit considerable and opposing seasonal variations, according to the Agency for Healthcare Research and Quality.
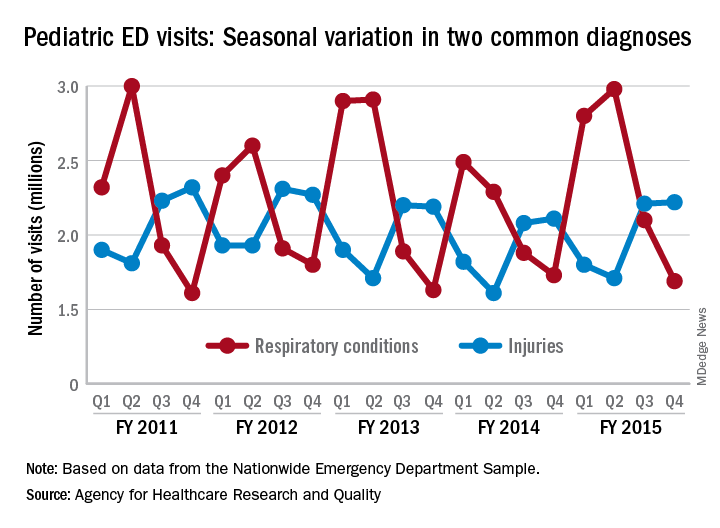
Of the 30 million ED visits by children aged 18 years and younger during fiscal year 2015, about 9.6 million, or just under 24%, were for respiratory disorders, making it the most common diagnosis by body system. The second-most common reason, injuries, was associated with approximately 7.9 million visits in 2015, the AHRQ reported recently in a statistical brief.
Over the 4-year period from 2011 to 2015, pediatric ED visits for respiratory disorders peaked during the months from October to March and dropped during April-September. In 2015, for example, there was a 43% difference between October-December, which was the highest-volume quarter, and July-September, which had the lowest volume of visits, the report showed.
The opposite pattern of seasonality was seen with visits for injury-related visits: The high point each year occurs in April-September, with the low in October-March. In 2015, there was a 30% difference between the lowest-volume quarter of January-March and the highest-volume quarter of July-September, based on the analysis of data from the Nationwide Emergency Department Sample.
The two most common reasons for pediatric emergency department visits exhibit considerable and opposing seasonal variations, according to the Agency for Healthcare Research and Quality.
Of the 30 million ED visits by children aged 18 years and younger during fiscal year 2015, about 9.6 million, or just under 24%, were for respiratory disorders, making it the most common diagnosis by body system. The second-most common reason, injuries, was associated with approximately 7.9 million visits in 2015, the AHRQ reported recently in a statistical brief.
Over the 4-year period from 2011 to 2015, pediatric ED visits for respiratory disorders peaked during the months from October to March and dropped during April-September. In 2015, for example, there was a 43% difference between October-December, which was the highest-volume quarter, and July-September, which had the lowest volume of visits, the report showed.
The opposite pattern of seasonality was seen with visits for injury-related visits: The high point each year occurs in April-September, with the low in October-March. In 2015, there was a 30% difference between the lowest-volume quarter of January-March and the highest-volume quarter of July-September, based on the analysis of data from the Nationwide Emergency Department Sample.
The two most common reasons for pediatric emergency department visits exhibit considerable and opposing seasonal variations, according to the Agency for Healthcare Research and Quality.
Of the 30 million ED visits by children aged 18 years and younger during fiscal year 2015, about 9.6 million, or just under 24%, were for respiratory disorders, making it the most common diagnosis by body system. The second-most common reason, injuries, was associated with approximately 7.9 million visits in 2015, the AHRQ reported recently in a statistical brief.
Over the 4-year period from 2011 to 2015, pediatric ED visits for respiratory disorders peaked during the months from October to March and dropped during April-September. In 2015, for example, there was a 43% difference between October-December, which was the highest-volume quarter, and July-September, which had the lowest volume of visits, the report showed.
The opposite pattern of seasonality was seen with visits for injury-related visits: The high point each year occurs in April-September, with the low in October-March. In 2015, there was a 30% difference between the lowest-volume quarter of January-March and the highest-volume quarter of July-September, based on the analysis of data from the Nationwide Emergency Department Sample.
Social media: ‘The more you do, the easier it gets’
SAN DIEGO – , the first question to ask yourself is why.

“Why are you doing this, and why does it matter?” she asked attendees at the annual Masters of Aesthetics Symposium. “If you know why, then you can answer a lot of questions.”
Dr. Day of the department of dermatology at New York University, said there are at least four quadrants of personal branding. The first is personal (who you are, where you live, family, hobbies, interests, education), and the second is professional (where you work, training, important skills and experience, and what sets you apart). The last two are thought leadership and legacy, “which is not your image,” she said. “It’s what you do for others; it’s the teaching you do from day to day.”
She noted that 74% of people look to social media networks for advice on buying decisions, and 40% of people purchased an item based on seeing it promoted by an influencer via Instagram or Twitter. This extends to aesthetics as well. “We need to become the influencers,” Dr. Day said. However, social media “is not all always about you; it’s the message, so knowing your medium is important. Each medium has its own velocity, its own type of follower, its own best practice to attract the best amount of viewers. Consistency is important. You have to reach your target generation.”
According to Dr. Day, Millennials (those aged 20-35 years) spend an average of 8 hours per day online; 70% use Facebook, 63% use YouTube, and 43% want brands to reach them via e-mail. “They’re a little more concerned about their financial future than other generations,” she said. Meanwhile, 76% of the demographic Generation X (those aged 36-49) access some form of social media. They have an annual buying power of $200 million, and 68% make decisions based on reviews like those on Yelp. “Reviews matter,” she said. “It’s only the people who are unhappy with you who are happy to go out and talk about it. People who are happy with you are going to need more encouragement to write a review.” On average, baby boomers (those aged 50-65 years) spend 27 hours per week online, and nearly 16% spend at least 11 hours on Facebook. Nearly half (48%) rely on credit cards for their purchases, and 13% use LinkedIn.![]()
Achieving success in social media takes patience, perseverance, and authenticity. “The more you do, the easier it gets,” said Dr. Day, who earned a master’s degree in journalism from NYU. “I have a group of people who tend to like my posts consistently, comment consistently, share consistently, and I respond consistently. That’s how you build relationships. When somebody posts, respond.”
Video content is being consumed online more than ever before, but Dr. Day emphasized that such visual content should “have a purpose and be directed to your specific audience – not just making video for the sake of it.” She recommends being selective when choosing your content, and where you post it. “Don’t stretch your brand over multiple [social media] channels if your team can’t support it.” If you thrive in a multichannel environment, BuzzBundle integrates Facebook, Twitter, Google+, LinkedIn, blogs, forums, and Q&A sites for posting with a purpose and a converged strategy across all sites.
“As with any smart strategy, make sure you are tracking your progress,” she said, suggesting AddThis analytics as one way to track how, where, and by whom your content is being shared.
Dr. Day reported having no relevant financial disclosures.
SAN DIEGO – , the first question to ask yourself is why.
“Why are you doing this, and why does it matter?” she asked attendees at the annual Masters of Aesthetics Symposium. “If you know why, then you can answer a lot of questions.”
Dr. Day of the department of dermatology at New York University, said there are at least four quadrants of personal branding. The first is personal (who you are, where you live, family, hobbies, interests, education), and the second is professional (where you work, training, important skills and experience, and what sets you apart). The last two are thought leadership and legacy, “which is not your image,” she said. “It’s what you do for others; it’s the teaching you do from day to day.”
She noted that 74% of people look to social media networks for advice on buying decisions, and 40% of people purchased an item based on seeing it promoted by an influencer via Instagram or Twitter. This extends to aesthetics as well. “We need to become the influencers,” Dr. Day said. However, social media “is not all always about you; it’s the message, so knowing your medium is important. Each medium has its own velocity, its own type of follower, its own best practice to attract the best amount of viewers. Consistency is important. You have to reach your target generation.”
According to Dr. Day, Millennials (those aged 20-35 years) spend an average of 8 hours per day online; 70% use Facebook, 63% use YouTube, and 43% want brands to reach them via e-mail. “They’re a little more concerned about their financial future than other generations,” she said. Meanwhile, 76% of the demographic Generation X (those aged 36-49) access some form of social media. They have an annual buying power of $200 million, and 68% make decisions based on reviews like those on Yelp. “Reviews matter,” she said. “It’s only the people who are unhappy with you who are happy to go out and talk about it. People who are happy with you are going to need more encouragement to write a review.” On average, baby boomers (those aged 50-65 years) spend 27 hours per week online, and nearly 16% spend at least 11 hours on Facebook. Nearly half (48%) rely on credit cards for their purchases, and 13% use LinkedIn.![]()
Achieving success in social media takes patience, perseverance, and authenticity. “The more you do, the easier it gets,” said Dr. Day, who earned a master’s degree in journalism from NYU. “I have a group of people who tend to like my posts consistently, comment consistently, share consistently, and I respond consistently. That’s how you build relationships. When somebody posts, respond.”
Video content is being consumed online more than ever before, but Dr. Day emphasized that such visual content should “have a purpose and be directed to your specific audience – not just making video for the sake of it.” She recommends being selective when choosing your content, and where you post it. “Don’t stretch your brand over multiple [social media] channels if your team can’t support it.” If you thrive in a multichannel environment, BuzzBundle integrates Facebook, Twitter, Google+, LinkedIn, blogs, forums, and Q&A sites for posting with a purpose and a converged strategy across all sites.
“As with any smart strategy, make sure you are tracking your progress,” she said, suggesting AddThis analytics as one way to track how, where, and by whom your content is being shared.
Dr. Day reported having no relevant financial disclosures.
SAN DIEGO – , the first question to ask yourself is why.
“Why are you doing this, and why does it matter?” she asked attendees at the annual Masters of Aesthetics Symposium. “If you know why, then you can answer a lot of questions.”
Dr. Day of the department of dermatology at New York University, said there are at least four quadrants of personal branding. The first is personal (who you are, where you live, family, hobbies, interests, education), and the second is professional (where you work, training, important skills and experience, and what sets you apart). The last two are thought leadership and legacy, “which is not your image,” she said. “It’s what you do for others; it’s the teaching you do from day to day.”
She noted that 74% of people look to social media networks for advice on buying decisions, and 40% of people purchased an item based on seeing it promoted by an influencer via Instagram or Twitter. This extends to aesthetics as well. “We need to become the influencers,” Dr. Day said. However, social media “is not all always about you; it’s the message, so knowing your medium is important. Each medium has its own velocity, its own type of follower, its own best practice to attract the best amount of viewers. Consistency is important. You have to reach your target generation.”
According to Dr. Day, Millennials (those aged 20-35 years) spend an average of 8 hours per day online; 70% use Facebook, 63% use YouTube, and 43% want brands to reach them via e-mail. “They’re a little more concerned about their financial future than other generations,” she said. Meanwhile, 76% of the demographic Generation X (those aged 36-49) access some form of social media. They have an annual buying power of $200 million, and 68% make decisions based on reviews like those on Yelp. “Reviews matter,” she said. “It’s only the people who are unhappy with you who are happy to go out and talk about it. People who are happy with you are going to need more encouragement to write a review.” On average, baby boomers (those aged 50-65 years) spend 27 hours per week online, and nearly 16% spend at least 11 hours on Facebook. Nearly half (48%) rely on credit cards for their purchases, and 13% use LinkedIn.![]()
Achieving success in social media takes patience, perseverance, and authenticity. “The more you do, the easier it gets,” said Dr. Day, who earned a master’s degree in journalism from NYU. “I have a group of people who tend to like my posts consistently, comment consistently, share consistently, and I respond consistently. That’s how you build relationships. When somebody posts, respond.”
Video content is being consumed online more than ever before, but Dr. Day emphasized that such visual content should “have a purpose and be directed to your specific audience – not just making video for the sake of it.” She recommends being selective when choosing your content, and where you post it. “Don’t stretch your brand over multiple [social media] channels if your team can’t support it.” If you thrive in a multichannel environment, BuzzBundle integrates Facebook, Twitter, Google+, LinkedIn, blogs, forums, and Q&A sites for posting with a purpose and a converged strategy across all sites.
“As with any smart strategy, make sure you are tracking your progress,” she said, suggesting AddThis analytics as one way to track how, where, and by whom your content is being shared.
Dr. Day reported having no relevant financial disclosures.
AT MOAS 2018
Reflectance confocal microscopy: The future looks bright
CHICAGO – The future looks bright for to rule out malignancy, Ann M. John, MD, asserted at the annual meeting of the American College of Mohs Surgery.

“With the advent of dermoscopy, dermatologists were able to elucidate both benign and malignant patterns to help further guide their decision to biopsy or not. This increased diagnostic accuracy of suspicious lesions by 30%, while reducing the benign to malignant ratio of biopsies performed from 18:1 to 4:1. However, there are still lesions that are equivocal on dermoscopy, as we all know, and for this, there’s reflectance confocal microscopy,” observed Dr. John, of Robert Wood Johnson Medical School, New Brunswick, N.J.
RCM is a device technology that’s been cleared by the Food and Drug Administration since 2008 for the imaging of clinically suspicious lesions. It employs laser scanning to assess the light-scattering properties of cells in the epidermis and dermis, generating images with resolution comparable to histology.
RCM took a back seat initially while American dermatologists were gradually coming to embrace dermoscopy, which their European colleagues had done years earlier. Now, with the availability of handheld RCM for use in the dermatology clinic, expect RCM to assume a growing role in daily practice.
To illustrate the power of RCM as a diagnostic aid, she presented a single-center retrospective study of 1,189 clinically suspicious skin lesions that were equivocal on dermoscopy and then assessed using RCM with 1 year of subsequent patient follow-up. Overall, 155 lesions were deemed positive for cancer or atypia by RCM, while 1,034 were determined to be benign. Of those 155, 46 lesions were considered false positives because of their benign appearance on histologic inspection of the biopsy sample. Only 2 of the 1,034 lesions identified as negative by RCM proved to be false negatives on the basis of clinical changes within 1 year.
The overall sensitivity and specificity of RCM was 98.2% and 99.8%, respectively, with a positive predictive value of 70.3% and a negative predictive value of 99.8%.
The entire RCM procedure takes a skilled technician 15-20 minutes per lesion. As a practical matter, other investigators have estimated that RCM results in a cost savings of about $308,000 per million health plan members per year by reducing the need for biopsies (Dermatol Clin. 2016 Oct;34[4]:367-75).
In addition to evaluating clinically suspicious lesions, other situations in which RCM offers practical value include its use directly before the first cut during Mohs surgery in order to determine the margins of atypia; ex vivo imaging of Mohs margins, which has been shown to be comparable with frozen sections in accuracy but takes only one-third of the time; and imaging of biopsied lesions in order to determine the diagnosis relatively quickly, Dr. John noted.
She reported having no financial conflicts regarding her study.
CHICAGO – The future looks bright for to rule out malignancy, Ann M. John, MD, asserted at the annual meeting of the American College of Mohs Surgery.
“With the advent of dermoscopy, dermatologists were able to elucidate both benign and malignant patterns to help further guide their decision to biopsy or not. This increased diagnostic accuracy of suspicious lesions by 30%, while reducing the benign to malignant ratio of biopsies performed from 18:1 to 4:1. However, there are still lesions that are equivocal on dermoscopy, as we all know, and for this, there’s reflectance confocal microscopy,” observed Dr. John, of Robert Wood Johnson Medical School, New Brunswick, N.J.
RCM is a device technology that’s been cleared by the Food and Drug Administration since 2008 for the imaging of clinically suspicious lesions. It employs laser scanning to assess the light-scattering properties of cells in the epidermis and dermis, generating images with resolution comparable to histology.
RCM took a back seat initially while American dermatologists were gradually coming to embrace dermoscopy, which their European colleagues had done years earlier. Now, with the availability of handheld RCM for use in the dermatology clinic, expect RCM to assume a growing role in daily practice.
To illustrate the power of RCM as a diagnostic aid, she presented a single-center retrospective study of 1,189 clinically suspicious skin lesions that were equivocal on dermoscopy and then assessed using RCM with 1 year of subsequent patient follow-up. Overall, 155 lesions were deemed positive for cancer or atypia by RCM, while 1,034 were determined to be benign. Of those 155, 46 lesions were considered false positives because of their benign appearance on histologic inspection of the biopsy sample. Only 2 of the 1,034 lesions identified as negative by RCM proved to be false negatives on the basis of clinical changes within 1 year.
The overall sensitivity and specificity of RCM was 98.2% and 99.8%, respectively, with a positive predictive value of 70.3% and a negative predictive value of 99.8%.
The entire RCM procedure takes a skilled technician 15-20 minutes per lesion. As a practical matter, other investigators have estimated that RCM results in a cost savings of about $308,000 per million health plan members per year by reducing the need for biopsies (Dermatol Clin. 2016 Oct;34[4]:367-75).
In addition to evaluating clinically suspicious lesions, other situations in which RCM offers practical value include its use directly before the first cut during Mohs surgery in order to determine the margins of atypia; ex vivo imaging of Mohs margins, which has been shown to be comparable with frozen sections in accuracy but takes only one-third of the time; and imaging of biopsied lesions in order to determine the diagnosis relatively quickly, Dr. John noted.
She reported having no financial conflicts regarding her study.
CHICAGO – The future looks bright for to rule out malignancy, Ann M. John, MD, asserted at the annual meeting of the American College of Mohs Surgery.
“With the advent of dermoscopy, dermatologists were able to elucidate both benign and malignant patterns to help further guide their decision to biopsy or not. This increased diagnostic accuracy of suspicious lesions by 30%, while reducing the benign to malignant ratio of biopsies performed from 18:1 to 4:1. However, there are still lesions that are equivocal on dermoscopy, as we all know, and for this, there’s reflectance confocal microscopy,” observed Dr. John, of Robert Wood Johnson Medical School, New Brunswick, N.J.
RCM is a device technology that’s been cleared by the Food and Drug Administration since 2008 for the imaging of clinically suspicious lesions. It employs laser scanning to assess the light-scattering properties of cells in the epidermis and dermis, generating images with resolution comparable to histology.
RCM took a back seat initially while American dermatologists were gradually coming to embrace dermoscopy, which their European colleagues had done years earlier. Now, with the availability of handheld RCM for use in the dermatology clinic, expect RCM to assume a growing role in daily practice.
To illustrate the power of RCM as a diagnostic aid, she presented a single-center retrospective study of 1,189 clinically suspicious skin lesions that were equivocal on dermoscopy and then assessed using RCM with 1 year of subsequent patient follow-up. Overall, 155 lesions were deemed positive for cancer or atypia by RCM, while 1,034 were determined to be benign. Of those 155, 46 lesions were considered false positives because of their benign appearance on histologic inspection of the biopsy sample. Only 2 of the 1,034 lesions identified as negative by RCM proved to be false negatives on the basis of clinical changes within 1 year.
The overall sensitivity and specificity of RCM was 98.2% and 99.8%, respectively, with a positive predictive value of 70.3% and a negative predictive value of 99.8%.
The entire RCM procedure takes a skilled technician 15-20 minutes per lesion. As a practical matter, other investigators have estimated that RCM results in a cost savings of about $308,000 per million health plan members per year by reducing the need for biopsies (Dermatol Clin. 2016 Oct;34[4]:367-75).
In addition to evaluating clinically suspicious lesions, other situations in which RCM offers practical value include its use directly before the first cut during Mohs surgery in order to determine the margins of atypia; ex vivo imaging of Mohs margins, which has been shown to be comparable with frozen sections in accuracy but takes only one-third of the time; and imaging of biopsied lesions in order to determine the diagnosis relatively quickly, Dr. John noted.
She reported having no financial conflicts regarding her study.
REPORTING FROM THE ACMS ANNUAL MEETING
Key clinical point: The future looks bright for reflectance confocal microscopy in dermatology.
Major finding: The sensitivity and specificity of reflectance confocal microscopy for diagnosis of skin cancer in patients with equivocal dermoscopic findings was 98.2% and 99.8%, respectively.
Study details: This retrospective single center study included 1,189 clinically suspicious skin lesions with equivocal dermoscopy findings, which were then evaluated using reflectance confocal microscopy.
Disclosures: The presenter reported having no financial conflicts regarding her study.
Mohs underutilized for melanoma of head and neck
CHICAGO – Contemporary national guidelines undervalue the benefits of Mohs micrographic surgery for patients with melanoma of the head and neck, William C. Fix asserted at the annual meeting of the American College of Mohs Surgery.
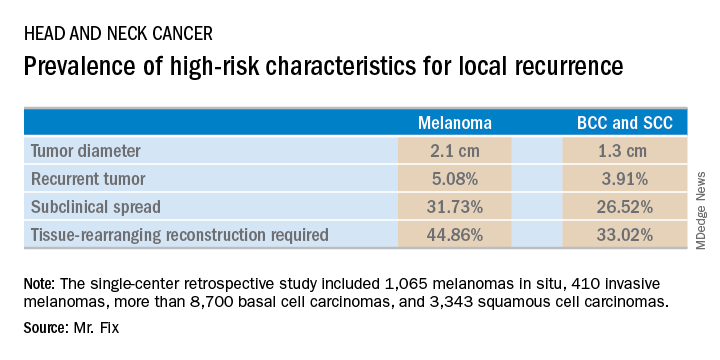
Mr. Fix, a medical student at the University of Pennsylvania, Philadelphia, presented a single-center retrospective study of 13,644 cases of head and neck skin cancer treated with Mohs micrographic surgery (MMS) for margin control. The cohort included 1,065 melanomas in situ, 410 invasive melanomas, more than 8,700 basal cell carcinomas, and 3,343 squamous cell carcinomas.
Mr. Fix and his coinvestigators undertook this observational study because they identified a gap in current guidelines for treatment of skin cancers of the head and neck. For example, the National Comprehensive Cancer Network recommends margin control at the time of primary surgery for BCCs and SCCs deemed at high risk for local recurrence and defines what those high-risk features are. For melanomas, however, the guidelines recommend wide local excision, even though that approach has roughly a 10% recurrence rate, compared with less than 1% for MMS.
Moreover, the 2012 appropriate use criteria for MMS put forth by the American Academy of Dermatology in concert with several other medical societies are unclear about invasive melanoma. As a result of this lack of guidance, the use of margin control in primary surgery for melanoma is applied in less than 4% of cases, according to Mr. Fix.
The University of Pennsylvania data he presented showed that melanomas of the head and neck were significantly more likely to be large in size, to be poorly defined, and to have other high-risk features for local recurrence than were the BCCs and SCCs. In a multivariate logistic regression analysis controlling for high-risk characteristics, melanomas were independently associated with a twofold increased likelihood of requiring flap reconstruction compared with BCCs and SCCs of the head and neck.
“We’ve shown that melanomas have high-risk features for local recurrence, possibly to a greater extent than BCCs and SCCs. These features help us triage resource use for BCC and SCC. Could these same features help us make decisions for melanomas?” he asked rhetorically.
Mr. Fix reported having no financial conflicts of interest regarding his study, which was conducted free of commercial support.
CHICAGO – Contemporary national guidelines undervalue the benefits of Mohs micrographic surgery for patients with melanoma of the head and neck, William C. Fix asserted at the annual meeting of the American College of Mohs Surgery.
Mr. Fix, a medical student at the University of Pennsylvania, Philadelphia, presented a single-center retrospective study of 13,644 cases of head and neck skin cancer treated with Mohs micrographic surgery (MMS) for margin control. The cohort included 1,065 melanomas in situ, 410 invasive melanomas, more than 8,700 basal cell carcinomas, and 3,343 squamous cell carcinomas.
Mr. Fix and his coinvestigators undertook this observational study because they identified a gap in current guidelines for treatment of skin cancers of the head and neck. For example, the National Comprehensive Cancer Network recommends margin control at the time of primary surgery for BCCs and SCCs deemed at high risk for local recurrence and defines what those high-risk features are. For melanomas, however, the guidelines recommend wide local excision, even though that approach has roughly a 10% recurrence rate, compared with less than 1% for MMS.
Moreover, the 2012 appropriate use criteria for MMS put forth by the American Academy of Dermatology in concert with several other medical societies are unclear about invasive melanoma. As a result of this lack of guidance, the use of margin control in primary surgery for melanoma is applied in less than 4% of cases, according to Mr. Fix.
The University of Pennsylvania data he presented showed that melanomas of the head and neck were significantly more likely to be large in size, to be poorly defined, and to have other high-risk features for local recurrence than were the BCCs and SCCs. In a multivariate logistic regression analysis controlling for high-risk characteristics, melanomas were independently associated with a twofold increased likelihood of requiring flap reconstruction compared with BCCs and SCCs of the head and neck.
“We’ve shown that melanomas have high-risk features for local recurrence, possibly to a greater extent than BCCs and SCCs. These features help us triage resource use for BCC and SCC. Could these same features help us make decisions for melanomas?” he asked rhetorically.
Mr. Fix reported having no financial conflicts of interest regarding his study, which was conducted free of commercial support.
CHICAGO – Contemporary national guidelines undervalue the benefits of Mohs micrographic surgery for patients with melanoma of the head and neck, William C. Fix asserted at the annual meeting of the American College of Mohs Surgery.
Mr. Fix, a medical student at the University of Pennsylvania, Philadelphia, presented a single-center retrospective study of 13,644 cases of head and neck skin cancer treated with Mohs micrographic surgery (MMS) for margin control. The cohort included 1,065 melanomas in situ, 410 invasive melanomas, more than 8,700 basal cell carcinomas, and 3,343 squamous cell carcinomas.
Mr. Fix and his coinvestigators undertook this observational study because they identified a gap in current guidelines for treatment of skin cancers of the head and neck. For example, the National Comprehensive Cancer Network recommends margin control at the time of primary surgery for BCCs and SCCs deemed at high risk for local recurrence and defines what those high-risk features are. For melanomas, however, the guidelines recommend wide local excision, even though that approach has roughly a 10% recurrence rate, compared with less than 1% for MMS.
Moreover, the 2012 appropriate use criteria for MMS put forth by the American Academy of Dermatology in concert with several other medical societies are unclear about invasive melanoma. As a result of this lack of guidance, the use of margin control in primary surgery for melanoma is applied in less than 4% of cases, according to Mr. Fix.
The University of Pennsylvania data he presented showed that melanomas of the head and neck were significantly more likely to be large in size, to be poorly defined, and to have other high-risk features for local recurrence than were the BCCs and SCCs. In a multivariate logistic regression analysis controlling for high-risk characteristics, melanomas were independently associated with a twofold increased likelihood of requiring flap reconstruction compared with BCCs and SCCs of the head and neck.
“We’ve shown that melanomas have high-risk features for local recurrence, possibly to a greater extent than BCCs and SCCs. These features help us triage resource use for BCC and SCC. Could these same features help us make decisions for melanomas?” he asked rhetorically.
Mr. Fix reported having no financial conflicts of interest regarding his study, which was conducted free of commercial support.
REPORTING FROM THE ACMS ANNUAL MEETING
Key clinical point: Margin control at the time of primary surgery for melanoma of the head and neck makes sense.
Major finding: Patients with a melanoma of the head and neck were twice as likely to require secondary flap reconstruction compared with patients with a basal cell carcinoma or squamous cell carcinoma of the head and neck.
Study details: A retrospective single-center study of 13,644 cases of skin cancer of the head and neck treated with Mohs surgery.
Disclosures: The presenter reported having no financial conflicts regarding the study, which was conducted free of commercial support.
One-quarter of ED sprained ankle diagnoses result in opioid prescription
One-quarter of patients who present at the ED with a , according to the findings of a large study using a national insurance claims database.
M. Kit Delgado, MD, of the Center for Emergency Care Policy and Research at the Perelman School of Medicine, University of Pennsylvania, Philadelphia, and his coauthors analyzed private insurance claims for 30,832 opioid-naive patients who were treated in the emergency department for ankle sprains.
The researchers looked at the initial opioid prescription intensity and duration of subsequent opioid use. The study, published online in Annals of Emergency Medicine, also found a wide variation in prescribing by hospital and geographic region, and an association between higher-potency opioid prescriptions (hydrocodone and oxycodone) and likelihood of extended or prolonged opioid use.
Overall, 25.1% of patients received an opioid prescription, the median tablet quantity was 15 tablets, and median days of opioids supplied was 3 days. Only 5% of patients were prescribed more than 30 tablets, which suggested that the majority of prescriptions written were in agreement with guidelines, the authors wrote.
They noted that nonsteroidal anti-inflammatory drugs are the first-line treatment for ankle sprains, rather than opioids, and are as effective for pain reduction.
Among patients prescribed the equivalent of more than 30 tabs of oxycodone 5 mg, 4.9% of them showed prolonged opioid use – defined as filling four or more subsequent opioid prescriptions in the 30-180 days after the index visit – compared with 1.1% of patients who received fewer than 10 tabs, and 0.5% of those who did not fill an opioid prescription. This represented a nearly fivefold increased probability of transition to prolonged use. For every 26 patients exposed to the higher intensity prescription, 1 would go on to prolonged opioid use.
“We confirmed that the majority of subsequent prescriptions were unlikely to be related to the initial ankle sprain or chronic ankle pain,” the researchers wrote. “This suggests that association between larger prescriptions and increased likelihood of prolonged use could be due to other factors such as patients requesting opioids as default pain control, or the development of dependence or misuse.”
The most commonly prescribed opioid was hydrocodone (64.9%), followed by tramadol (16.2%), oxycodone (14.4%), and codeine (5.5%). The analysis found that patients prescribed higher-potency drugs – namely hydrocodone and oxycodone – were at even greater risk of developing prolonged use.
The researchers noted significant geographic differences in prescribing habits, with 40% of study participants in Arkansas receiving an opioid prescription, compared with 2.8% in North Dakota. Overall, southern states were more likely to overprescribe, and northern states more likely to underprescribe.
Women were at greater risk of transitioning to high-risk prolonged use, as were individuals aged 35-44 years, those with a higher comorbidity burden, or those with a history of drug abuse.
The study was supported by the National Institute on Drug Abuse, the National Institute of Child Health and Human Development, and the Leonard Davis Institute of Health Economics at the University of Pennsylvania. One author declared an honorarium from the United Health Group.
SOURCE: Delgado MK et al. Ann Emerg Med. 2018. Jul 24. doi: 10.1016/j.annemergmed.2018.06.003.
One-quarter of patients who present at the ED with a , according to the findings of a large study using a national insurance claims database.
M. Kit Delgado, MD, of the Center for Emergency Care Policy and Research at the Perelman School of Medicine, University of Pennsylvania, Philadelphia, and his coauthors analyzed private insurance claims for 30,832 opioid-naive patients who were treated in the emergency department for ankle sprains.
The researchers looked at the initial opioid prescription intensity and duration of subsequent opioid use. The study, published online in Annals of Emergency Medicine, also found a wide variation in prescribing by hospital and geographic region, and an association between higher-potency opioid prescriptions (hydrocodone and oxycodone) and likelihood of extended or prolonged opioid use.
Overall, 25.1% of patients received an opioid prescription, the median tablet quantity was 15 tablets, and median days of opioids supplied was 3 days. Only 5% of patients were prescribed more than 30 tablets, which suggested that the majority of prescriptions written were in agreement with guidelines, the authors wrote.
They noted that nonsteroidal anti-inflammatory drugs are the first-line treatment for ankle sprains, rather than opioids, and are as effective for pain reduction.
Among patients prescribed the equivalent of more than 30 tabs of oxycodone 5 mg, 4.9% of them showed prolonged opioid use – defined as filling four or more subsequent opioid prescriptions in the 30-180 days after the index visit – compared with 1.1% of patients who received fewer than 10 tabs, and 0.5% of those who did not fill an opioid prescription. This represented a nearly fivefold increased probability of transition to prolonged use. For every 26 patients exposed to the higher intensity prescription, 1 would go on to prolonged opioid use.
“We confirmed that the majority of subsequent prescriptions were unlikely to be related to the initial ankle sprain or chronic ankle pain,” the researchers wrote. “This suggests that association between larger prescriptions and increased likelihood of prolonged use could be due to other factors such as patients requesting opioids as default pain control, or the development of dependence or misuse.”
The most commonly prescribed opioid was hydrocodone (64.9%), followed by tramadol (16.2%), oxycodone (14.4%), and codeine (5.5%). The analysis found that patients prescribed higher-potency drugs – namely hydrocodone and oxycodone – were at even greater risk of developing prolonged use.
The researchers noted significant geographic differences in prescribing habits, with 40% of study participants in Arkansas receiving an opioid prescription, compared with 2.8% in North Dakota. Overall, southern states were more likely to overprescribe, and northern states more likely to underprescribe.
Women were at greater risk of transitioning to high-risk prolonged use, as were individuals aged 35-44 years, those with a higher comorbidity burden, or those with a history of drug abuse.
The study was supported by the National Institute on Drug Abuse, the National Institute of Child Health and Human Development, and the Leonard Davis Institute of Health Economics at the University of Pennsylvania. One author declared an honorarium from the United Health Group.
SOURCE: Delgado MK et al. Ann Emerg Med. 2018. Jul 24. doi: 10.1016/j.annemergmed.2018.06.003.
One-quarter of patients who present at the ED with a , according to the findings of a large study using a national insurance claims database.
M. Kit Delgado, MD, of the Center for Emergency Care Policy and Research at the Perelman School of Medicine, University of Pennsylvania, Philadelphia, and his coauthors analyzed private insurance claims for 30,832 opioid-naive patients who were treated in the emergency department for ankle sprains.
The researchers looked at the initial opioid prescription intensity and duration of subsequent opioid use. The study, published online in Annals of Emergency Medicine, also found a wide variation in prescribing by hospital and geographic region, and an association between higher-potency opioid prescriptions (hydrocodone and oxycodone) and likelihood of extended or prolonged opioid use.
Overall, 25.1% of patients received an opioid prescription, the median tablet quantity was 15 tablets, and median days of opioids supplied was 3 days. Only 5% of patients were prescribed more than 30 tablets, which suggested that the majority of prescriptions written were in agreement with guidelines, the authors wrote.
They noted that nonsteroidal anti-inflammatory drugs are the first-line treatment for ankle sprains, rather than opioids, and are as effective for pain reduction.
Among patients prescribed the equivalent of more than 30 tabs of oxycodone 5 mg, 4.9% of them showed prolonged opioid use – defined as filling four or more subsequent opioid prescriptions in the 30-180 days after the index visit – compared with 1.1% of patients who received fewer than 10 tabs, and 0.5% of those who did not fill an opioid prescription. This represented a nearly fivefold increased probability of transition to prolonged use. For every 26 patients exposed to the higher intensity prescription, 1 would go on to prolonged opioid use.
“We confirmed that the majority of subsequent prescriptions were unlikely to be related to the initial ankle sprain or chronic ankle pain,” the researchers wrote. “This suggests that association between larger prescriptions and increased likelihood of prolonged use could be due to other factors such as patients requesting opioids as default pain control, or the development of dependence or misuse.”
The most commonly prescribed opioid was hydrocodone (64.9%), followed by tramadol (16.2%), oxycodone (14.4%), and codeine (5.5%). The analysis found that patients prescribed higher-potency drugs – namely hydrocodone and oxycodone – were at even greater risk of developing prolonged use.
The researchers noted significant geographic differences in prescribing habits, with 40% of study participants in Arkansas receiving an opioid prescription, compared with 2.8% in North Dakota. Overall, southern states were more likely to overprescribe, and northern states more likely to underprescribe.
Women were at greater risk of transitioning to high-risk prolonged use, as were individuals aged 35-44 years, those with a higher comorbidity burden, or those with a history of drug abuse.
The study was supported by the National Institute on Drug Abuse, the National Institute of Child Health and Human Development, and the Leonard Davis Institute of Health Economics at the University of Pennsylvania. One author declared an honorarium from the United Health Group.
SOURCE: Delgado MK et al. Ann Emerg Med. 2018. Jul 24. doi: 10.1016/j.annemergmed.2018.06.003.
FROM ANNALS OF EMERGENCY MEDICINE
Key clinical point: Opioids prescribed for sprained ankles increase the risk of prolonged use.
Major finding: High-intensity opioid prescriptions after a sprained ankle were linked to a fivefold higher risk of prolonged use.
Study details: Analysis of health insurance data from 30,832 patients treated in the emergency department for ankle sprains.
Disclosures: The study was supported by the National Institute on Drug Abuse, the National Institute of Child Health and Human Development, and the Leonard Davis Institute of Health Economics at the University of Pennsylvania. One author declared an honorarium from the United Health Group.
Source: Delgado MK et al. Ann Emerg Med. 2018 Jul 24. doi: 10.1016/j.annemergmed.2018.06.003.
Increased COPD mortality with secondhand smoke exposure in childhood
Prolonged exposure to in adulthood, new research has found.

With data from 70,900 never-smoking men and women, most aged 50 years or over, in the Cancer Prevention Study–II Nutrition Cohort, researchers examined associations between childhood and adult secondhand smoke exposure and the risk of death during adulthood from all causes, heart disease, stroke, and COPD. Participants were followed from enrollment in 1992-1993 to 2016-2017.
In a paper published in the September issue of the American Journal of Preventive Medicine, they reported that individuals who had lived with a smoker throughout childhood (16-18 years) had a 31% higher risk of dying from COPD, compared with individuals not exposed to secondhand smoke during childhood (95% confidence interval 1.05-1.65, P = .06). Any exposure to secondhand smoke in childhood – defined as one or more hours of exposure per week – was associated with a 21% higher risk of COPD mortality.
“It is established that SHS [secondhand smoke] exposure in childhood can result in asthma, chronic wheezing, respiratory infections, and decreased lung function and growth in children,” wrote W. Ryan Diver, a cancer epidemiologist, and his colleagues from the Epidemiology Research Program at the American Cancer Society. “These respiratory illnesses in early life are associated with worse lung function in adolescence and adulthood, as indicated by a lower forced expiratory volume in a 1 second plateau, and ultimately diagnosis of COPD.”
The researchers did not see a significant association between childhood secondhand smoke exposure and the risk of death from ischemic heart disease or stroke in adulthood. But the authors said that there was compelling evidence that secondhand smoke exposure during childhood contributed to increased arterial stiffness, autonomic dysfunction, and other vascular effects, which had led to the hypothesis that such exposure might influence the risk of heart disease and stroke mortality in adulthood. They suggested that this effect might have been more apparent in generations born in the 1950s and 1960s, where both parents were likely to smoke at home, as opposed to just one parent, which would have meant higher levels of exposure to secondhand smoke.
Adult exposure to secondhand smoke showed a significant dose-response relationship with overall mortality. Those exposed for 10 or more hours a week showed a 9% higher risk of death from all causes (95% CI 1.04-1.14, P less than .0001), as well as a significant 27% higher risk of death from ischemic heart disease.
Any exposure to secondhand smoke in adulthood was associated with a 14% higher risk of stroke, with a trend of increasing risk with increasing exposure.
The researchers also saw a significant association between secondhand smoke exposure and COPD mortality, but only in adults who reported being exposed both outside and inside the home.
The authors noted that the most recent Surgeon General’s report found that the evidence on secondhand smoke and increased risk of death from COPD was “suggestive but not sufficient,” and further research was needed.
“The associations observed with both childhood exposure to SHS and adult exposure to SHS add to the mounting data relating SHS to COPD,” they wrote.
One limitation of the study was that it relied on self-report, which in the case of childhood exposure would have required some participants to recall at least 3 decades back. It also did not capture whether it was the mother or father who smoked, which meant the authors could not account for possible effects of smoking during pregnancy.
The investigators noted that “more than 50 years after the publication of the first Surgeon General report on smoking and health, these findings suggest that researchers and scientists still do not fully understand the long-term health consequences of smoking, particularly, the potential delayed effects of childhood SHS exposure in later adulthood.” Despite this, the authors said the findings “provide further support for implementation of smoke-free air laws, smoke-free home policies, and clinical interventions to reduce SHS exposure.”
No conflicts of interest were declared.
SOURCE: Diver WR et al. Am J Prev Med 2018;55[3]:345-52. doi: 10.1016/j.amepre.2018.05.005.
Prolonged exposure to in adulthood, new research has found.
With data from 70,900 never-smoking men and women, most aged 50 years or over, in the Cancer Prevention Study–II Nutrition Cohort, researchers examined associations between childhood and adult secondhand smoke exposure and the risk of death during adulthood from all causes, heart disease, stroke, and COPD. Participants were followed from enrollment in 1992-1993 to 2016-2017.
In a paper published in the September issue of the American Journal of Preventive Medicine, they reported that individuals who had lived with a smoker throughout childhood (16-18 years) had a 31% higher risk of dying from COPD, compared with individuals not exposed to secondhand smoke during childhood (95% confidence interval 1.05-1.65, P = .06). Any exposure to secondhand smoke in childhood – defined as one or more hours of exposure per week – was associated with a 21% higher risk of COPD mortality.
“It is established that SHS [secondhand smoke] exposure in childhood can result in asthma, chronic wheezing, respiratory infections, and decreased lung function and growth in children,” wrote W. Ryan Diver, a cancer epidemiologist, and his colleagues from the Epidemiology Research Program at the American Cancer Society. “These respiratory illnesses in early life are associated with worse lung function in adolescence and adulthood, as indicated by a lower forced expiratory volume in a 1 second plateau, and ultimately diagnosis of COPD.”
The researchers did not see a significant association between childhood secondhand smoke exposure and the risk of death from ischemic heart disease or stroke in adulthood. But the authors said that there was compelling evidence that secondhand smoke exposure during childhood contributed to increased arterial stiffness, autonomic dysfunction, and other vascular effects, which had led to the hypothesis that such exposure might influence the risk of heart disease and stroke mortality in adulthood. They suggested that this effect might have been more apparent in generations born in the 1950s and 1960s, where both parents were likely to smoke at home, as opposed to just one parent, which would have meant higher levels of exposure to secondhand smoke.
Adult exposure to secondhand smoke showed a significant dose-response relationship with overall mortality. Those exposed for 10 or more hours a week showed a 9% higher risk of death from all causes (95% CI 1.04-1.14, P less than .0001), as well as a significant 27% higher risk of death from ischemic heart disease.
Any exposure to secondhand smoke in adulthood was associated with a 14% higher risk of stroke, with a trend of increasing risk with increasing exposure.
The researchers also saw a significant association between secondhand smoke exposure and COPD mortality, but only in adults who reported being exposed both outside and inside the home.
The authors noted that the most recent Surgeon General’s report found that the evidence on secondhand smoke and increased risk of death from COPD was “suggestive but not sufficient,” and further research was needed.
“The associations observed with both childhood exposure to SHS and adult exposure to SHS add to the mounting data relating SHS to COPD,” they wrote.
One limitation of the study was that it relied on self-report, which in the case of childhood exposure would have required some participants to recall at least 3 decades back. It also did not capture whether it was the mother or father who smoked, which meant the authors could not account for possible effects of smoking during pregnancy.
The investigators noted that “more than 50 years after the publication of the first Surgeon General report on smoking and health, these findings suggest that researchers and scientists still do not fully understand the long-term health consequences of smoking, particularly, the potential delayed effects of childhood SHS exposure in later adulthood.” Despite this, the authors said the findings “provide further support for implementation of smoke-free air laws, smoke-free home policies, and clinical interventions to reduce SHS exposure.”
No conflicts of interest were declared.
SOURCE: Diver WR et al. Am J Prev Med 2018;55[3]:345-52. doi: 10.1016/j.amepre.2018.05.005.
Prolonged exposure to in adulthood, new research has found.
With data from 70,900 never-smoking men and women, most aged 50 years or over, in the Cancer Prevention Study–II Nutrition Cohort, researchers examined associations between childhood and adult secondhand smoke exposure and the risk of death during adulthood from all causes, heart disease, stroke, and COPD. Participants were followed from enrollment in 1992-1993 to 2016-2017.
In a paper published in the September issue of the American Journal of Preventive Medicine, they reported that individuals who had lived with a smoker throughout childhood (16-18 years) had a 31% higher risk of dying from COPD, compared with individuals not exposed to secondhand smoke during childhood (95% confidence interval 1.05-1.65, P = .06). Any exposure to secondhand smoke in childhood – defined as one or more hours of exposure per week – was associated with a 21% higher risk of COPD mortality.
“It is established that SHS [secondhand smoke] exposure in childhood can result in asthma, chronic wheezing, respiratory infections, and decreased lung function and growth in children,” wrote W. Ryan Diver, a cancer epidemiologist, and his colleagues from the Epidemiology Research Program at the American Cancer Society. “These respiratory illnesses in early life are associated with worse lung function in adolescence and adulthood, as indicated by a lower forced expiratory volume in a 1 second plateau, and ultimately diagnosis of COPD.”
The researchers did not see a significant association between childhood secondhand smoke exposure and the risk of death from ischemic heart disease or stroke in adulthood. But the authors said that there was compelling evidence that secondhand smoke exposure during childhood contributed to increased arterial stiffness, autonomic dysfunction, and other vascular effects, which had led to the hypothesis that such exposure might influence the risk of heart disease and stroke mortality in adulthood. They suggested that this effect might have been more apparent in generations born in the 1950s and 1960s, where both parents were likely to smoke at home, as opposed to just one parent, which would have meant higher levels of exposure to secondhand smoke.
Adult exposure to secondhand smoke showed a significant dose-response relationship with overall mortality. Those exposed for 10 or more hours a week showed a 9% higher risk of death from all causes (95% CI 1.04-1.14, P less than .0001), as well as a significant 27% higher risk of death from ischemic heart disease.
Any exposure to secondhand smoke in adulthood was associated with a 14% higher risk of stroke, with a trend of increasing risk with increasing exposure.
The researchers also saw a significant association between secondhand smoke exposure and COPD mortality, but only in adults who reported being exposed both outside and inside the home.
The authors noted that the most recent Surgeon General’s report found that the evidence on secondhand smoke and increased risk of death from COPD was “suggestive but not sufficient,” and further research was needed.
“The associations observed with both childhood exposure to SHS and adult exposure to SHS add to the mounting data relating SHS to COPD,” they wrote.
One limitation of the study was that it relied on self-report, which in the case of childhood exposure would have required some participants to recall at least 3 decades back. It also did not capture whether it was the mother or father who smoked, which meant the authors could not account for possible effects of smoking during pregnancy.
The investigators noted that “more than 50 years after the publication of the first Surgeon General report on smoking and health, these findings suggest that researchers and scientists still do not fully understand the long-term health consequences of smoking, particularly, the potential delayed effects of childhood SHS exposure in later adulthood.” Despite this, the authors said the findings “provide further support for implementation of smoke-free air laws, smoke-free home policies, and clinical interventions to reduce SHS exposure.”
No conflicts of interest were declared.
SOURCE: Diver WR et al. Am J Prev Med 2018;55[3]:345-52. doi: 10.1016/j.amepre.2018.05.005.
FROM THE AMERICAN JOURNAL OF PREVENTIVE MEDICINE
Key clinical point: Childhood secondhand smoke exposure is linked to increased COPD mortality in adulthood.
Major finding: Adults who were exposed to secondhand smoke throughout childhood have a 31% higher risk of COPD mortality than do those not exposed.
Study details: Retrospective cohort study of 70,900 never-smoking men and women enrolled in the Cancer Prevention Study–II Nutrition Cohort.
Disclosures: No conflicts of interest were declared.
Source: Diver W et al. Am J Prev Med. 2018;55[3]:345-52. doi: 10.1016/j.amepre.2018.05.005.
Don’t forget about OSHA
With the bewildering array of new bureaucracies that private practices are now forced to contend with, it is easy to forget about the older ones – especially the Occupational Health and Safety Administration (OSHA).

with all the applicable regulations. Even if you hold regular safety meetings (which all too often is not the case), the occasional comprehensive review is always a good idea, and could save you a bundle in fines.
For starters, do you have an official OSHA poster, enumerating employee rights and explaining how to file complaints? Every office must have one posted in plain site, and it is the first thing an OSHA inspector will look for. You can download one from OSHA’s Web site or order it at no charge by calling 800-321-OSHA.
Next, how old is your written exposure control plan for blood-borne pathogens? It should document your use of such protective equipment as gloves, face and eye protection, needle guards, and gowns, and your implementation of universal precautions – and it is supposed to be updated annually, to reflect changes in technology.
You need not adopt every new safety device as it comes on the market, but you should document which ones you are using – and which you pass up – and why. For example, you and your employees may decide not to purchase a new safety needle because you don’t think it will improve safety, or that it will be more trouble than it’s worth; but you should document how you arrived at your decision and why you feel that your current protocol is as good or better.
Review your list of hazardous substances, which all employees have a right to know about. Keep in mind that OSHA’s list includes alcohol, hydrogen peroxide, acetone, and other substances that you might not consider particularly dangerous, but are nevertheless classified as “hazardous.” (My favorite in that category is liquid nitrogen; it’s hard to envision anything less hazardous, since it evaporates instantly if spilled, and cannot injure skin, or anything else, without purposeful, sustained exposure – and is great, incidentally, for extinguishing small fires.) For each substance, your employees must have access to the manufacturer-supplied Material Safety Data Sheet, which outlines the proper procedures for working with a specific material, and for handling and containing it in a spill or other emergency.
Check out your building’s exits. Everyone must be able to evacuate your office quickly in case of fire or other emergencies. At a minimum, you (or the owner of the building) are expected to establish exit routes to accommodate all employees and to post easily visible evacuation diagrams.
Examine all electrical devices and their power sources. All electrically powered equipment – medical, clerical, or anything else in the office – must operate safely. Pay particular attention to the way wall outlets are set up. Make sure each outlet has sufficient power to run the equipment plugged into it and that circuit breakers are present and functioning. And beware the common situation of too many gadgets running off a single circuit.
You must provide all at-risk employees with hepatitis B vaccine at no cost to them. You also must provide and pay for appropriate medical treatment and follow-up after any exposure to a dangerous pathogen.
Other components of the rule include proper containment of regulated medical waste, identification of regulated-waste containers, sharps disposal boxes, and periodic employee training regarding all of these things.
Federal OSHA regulations do not require medical and dental offices to keep an injury and illness log, as other businesses must; but your state may have a requirement that supersedes the federal law. Check with your state, or with your local OSHA office, regarding any such requirements.
It is a mistake to take OSHA regulations lightly; failure to comply with them can result in stiff penalties running into many thousands of dollars.
How can you be certain you are complying with all the rules? The easiest and cheapest way is to call your local OSHA office and request an inspection. Why would you do that? Because OSHA issues no citations during voluntary inspections, as long as you agree to remedy any violations they find.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
With the bewildering array of new bureaucracies that private practices are now forced to contend with, it is easy to forget about the older ones – especially the Occupational Health and Safety Administration (OSHA).
with all the applicable regulations. Even if you hold regular safety meetings (which all too often is not the case), the occasional comprehensive review is always a good idea, and could save you a bundle in fines.
For starters, do you have an official OSHA poster, enumerating employee rights and explaining how to file complaints? Every office must have one posted in plain site, and it is the first thing an OSHA inspector will look for. You can download one from OSHA’s Web site or order it at no charge by calling 800-321-OSHA.
Next, how old is your written exposure control plan for blood-borne pathogens? It should document your use of such protective equipment as gloves, face and eye protection, needle guards, and gowns, and your implementation of universal precautions – and it is supposed to be updated annually, to reflect changes in technology.
You need not adopt every new safety device as it comes on the market, but you should document which ones you are using – and which you pass up – and why. For example, you and your employees may decide not to purchase a new safety needle because you don’t think it will improve safety, or that it will be more trouble than it’s worth; but you should document how you arrived at your decision and why you feel that your current protocol is as good or better.
Review your list of hazardous substances, which all employees have a right to know about. Keep in mind that OSHA’s list includes alcohol, hydrogen peroxide, acetone, and other substances that you might not consider particularly dangerous, but are nevertheless classified as “hazardous.” (My favorite in that category is liquid nitrogen; it’s hard to envision anything less hazardous, since it evaporates instantly if spilled, and cannot injure skin, or anything else, without purposeful, sustained exposure – and is great, incidentally, for extinguishing small fires.) For each substance, your employees must have access to the manufacturer-supplied Material Safety Data Sheet, which outlines the proper procedures for working with a specific material, and for handling and containing it in a spill or other emergency.
Check out your building’s exits. Everyone must be able to evacuate your office quickly in case of fire or other emergencies. At a minimum, you (or the owner of the building) are expected to establish exit routes to accommodate all employees and to post easily visible evacuation diagrams.
Examine all electrical devices and their power sources. All electrically powered equipment – medical, clerical, or anything else in the office – must operate safely. Pay particular attention to the way wall outlets are set up. Make sure each outlet has sufficient power to run the equipment plugged into it and that circuit breakers are present and functioning. And beware the common situation of too many gadgets running off a single circuit.
You must provide all at-risk employees with hepatitis B vaccine at no cost to them. You also must provide and pay for appropriate medical treatment and follow-up after any exposure to a dangerous pathogen.
Other components of the rule include proper containment of regulated medical waste, identification of regulated-waste containers, sharps disposal boxes, and periodic employee training regarding all of these things.
Federal OSHA regulations do not require medical and dental offices to keep an injury and illness log, as other businesses must; but your state may have a requirement that supersedes the federal law. Check with your state, or with your local OSHA office, regarding any such requirements.
It is a mistake to take OSHA regulations lightly; failure to comply with them can result in stiff penalties running into many thousands of dollars.
How can you be certain you are complying with all the rules? The easiest and cheapest way is to call your local OSHA office and request an inspection. Why would you do that? Because OSHA issues no citations during voluntary inspections, as long as you agree to remedy any violations they find.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
With the bewildering array of new bureaucracies that private practices are now forced to contend with, it is easy to forget about the older ones – especially the Occupational Health and Safety Administration (OSHA).
with all the applicable regulations. Even if you hold regular safety meetings (which all too often is not the case), the occasional comprehensive review is always a good idea, and could save you a bundle in fines.
For starters, do you have an official OSHA poster, enumerating employee rights and explaining how to file complaints? Every office must have one posted in plain site, and it is the first thing an OSHA inspector will look for. You can download one from OSHA’s Web site or order it at no charge by calling 800-321-OSHA.
Next, how old is your written exposure control plan for blood-borne pathogens? It should document your use of such protective equipment as gloves, face and eye protection, needle guards, and gowns, and your implementation of universal precautions – and it is supposed to be updated annually, to reflect changes in technology.
You need not adopt every new safety device as it comes on the market, but you should document which ones you are using – and which you pass up – and why. For example, you and your employees may decide not to purchase a new safety needle because you don’t think it will improve safety, or that it will be more trouble than it’s worth; but you should document how you arrived at your decision and why you feel that your current protocol is as good or better.
Review your list of hazardous substances, which all employees have a right to know about. Keep in mind that OSHA’s list includes alcohol, hydrogen peroxide, acetone, and other substances that you might not consider particularly dangerous, but are nevertheless classified as “hazardous.” (My favorite in that category is liquid nitrogen; it’s hard to envision anything less hazardous, since it evaporates instantly if spilled, and cannot injure skin, or anything else, without purposeful, sustained exposure – and is great, incidentally, for extinguishing small fires.) For each substance, your employees must have access to the manufacturer-supplied Material Safety Data Sheet, which outlines the proper procedures for working with a specific material, and for handling and containing it in a spill or other emergency.
Check out your building’s exits. Everyone must be able to evacuate your office quickly in case of fire or other emergencies. At a minimum, you (or the owner of the building) are expected to establish exit routes to accommodate all employees and to post easily visible evacuation diagrams.
Examine all electrical devices and their power sources. All electrically powered equipment – medical, clerical, or anything else in the office – must operate safely. Pay particular attention to the way wall outlets are set up. Make sure each outlet has sufficient power to run the equipment plugged into it and that circuit breakers are present and functioning. And beware the common situation of too many gadgets running off a single circuit.
You must provide all at-risk employees with hepatitis B vaccine at no cost to them. You also must provide and pay for appropriate medical treatment and follow-up after any exposure to a dangerous pathogen.
Other components of the rule include proper containment of regulated medical waste, identification of regulated-waste containers, sharps disposal boxes, and periodic employee training regarding all of these things.
Federal OSHA regulations do not require medical and dental offices to keep an injury and illness log, as other businesses must; but your state may have a requirement that supersedes the federal law. Check with your state, or with your local OSHA office, regarding any such requirements.
It is a mistake to take OSHA regulations lightly; failure to comply with them can result in stiff penalties running into many thousands of dollars.
How can you be certain you are complying with all the rules? The easiest and cheapest way is to call your local OSHA office and request an inspection. Why would you do that? Because OSHA issues no citations during voluntary inspections, as long as you agree to remedy any violations they find.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].

Review protocols, follow reprocessing guidelines to cut device-related HAIs
ATLANTA – Ongoing vigilance regarding the role of and transmission of antimicrobial-resistant pathogen is needed, according to Isaac Benowitz, MD, of the Centers for Disease Control and Prevention’s Division of Healthcare Quality Promotion (DHQP).
A review of records from the DHQP, which investigates and responds to infections and related adverse events in health care settings upon invitation, showed that in 2017 environmental pathogens were most often the triggers for these investigations, said Dr. Benowitz, a medical epidemiologist.
He reviewed internal records for consultations with state and local health departments involving medical devices and collected data on health care setting, pathogen, investigation findings including possible exposure or transmission, and public health actions.
Of 285 consultations, 48 involved a specific medical device or general medical device reprocessing, he said, noting that most of those 48 were in an acute care hospital (63%) or clinic (19%).
“The most frequent pathogens noted in these consultations were nontuberculous mycobacteria at 21%, Candida species ... at 10%, and Burkholderia species ... at 8%,” he said, noting that a wide variety of devices were implicated.
In the inpatient setting these devices included ventilators, dialysis machines, breast pumps, central lines, and respiratory therapy equipment. In the outpatient setting they included glucometers and opthalmic equipment.
“In many settings we saw issues with endoscopes, including duodenoscopes, but also bronchoscopes,” he added.
Actions taken as part of the investigations included medical device recalls, improved infection control and reprocessing procedures, and patient notification, education, guidance, testing, and treatment.
In some cases there was disciplinary action or oversight for health care professionals, he added.
Investigations identified medical devices contaminated in manufacturing, incorrect reprocessing of endoscopes or ventilators, and inappropriate medical device use or reuse, he said.
A number of lessons can be learned from these and other investigations, he added.
“First, devices can be reservoirs and transmission vectors for health care–associated infections. Second, health care facilities, health care facility staff, and public health partners should take opportunities to review protocols and the practices within those protocol,” he said. “These are opportunities to strengthen infection control practices even in the absence of documented transmission.”
In fact, in most of the investigations he discussed, transmission was rarely confirmed to be associated with a medical device. This was largely because of a lack of “epidemiological rigor,” but associations between health care–associated infections and medical devices “are still quite meaningful and often actionable,” he said.
Dr. Benowitz stressed the importance of engaging public health partners to discuss findings and actions, explaining that “what may look like a single-facility issue may have a very different perspective when you realize that there’s a similar issue at another facility elsewhere.”
“For all devices, it’s important to ensure adherence to the device reprocessing guidelines, “ he added, noting that these include a combination of facility protocols, manufacturer instructions for use, and guidance from organizations like the Food and Drug Administration and the CDC.
Dr. Benowitz reported having no disclosures.
[email protected]
SOURCE: Benowitz I et al. ICEID 2018, Oral Abstract Presentation E2.
ATLANTA – Ongoing vigilance regarding the role of and transmission of antimicrobial-resistant pathogen is needed, according to Isaac Benowitz, MD, of the Centers for Disease Control and Prevention’s Division of Healthcare Quality Promotion (DHQP).
A review of records from the DHQP, which investigates and responds to infections and related adverse events in health care settings upon invitation, showed that in 2017 environmental pathogens were most often the triggers for these investigations, said Dr. Benowitz, a medical epidemiologist.
He reviewed internal records for consultations with state and local health departments involving medical devices and collected data on health care setting, pathogen, investigation findings including possible exposure or transmission, and public health actions.
Of 285 consultations, 48 involved a specific medical device or general medical device reprocessing, he said, noting that most of those 48 were in an acute care hospital (63%) or clinic (19%).
“The most frequent pathogens noted in these consultations were nontuberculous mycobacteria at 21%, Candida species ... at 10%, and Burkholderia species ... at 8%,” he said, noting that a wide variety of devices were implicated.
In the inpatient setting these devices included ventilators, dialysis machines, breast pumps, central lines, and respiratory therapy equipment. In the outpatient setting they included glucometers and opthalmic equipment.
“In many settings we saw issues with endoscopes, including duodenoscopes, but also bronchoscopes,” he added.
Actions taken as part of the investigations included medical device recalls, improved infection control and reprocessing procedures, and patient notification, education, guidance, testing, and treatment.
In some cases there was disciplinary action or oversight for health care professionals, he added.
Investigations identified medical devices contaminated in manufacturing, incorrect reprocessing of endoscopes or ventilators, and inappropriate medical device use or reuse, he said.
A number of lessons can be learned from these and other investigations, he added.
“First, devices can be reservoirs and transmission vectors for health care–associated infections. Second, health care facilities, health care facility staff, and public health partners should take opportunities to review protocols and the practices within those protocol,” he said. “These are opportunities to strengthen infection control practices even in the absence of documented transmission.”
In fact, in most of the investigations he discussed, transmission was rarely confirmed to be associated with a medical device. This was largely because of a lack of “epidemiological rigor,” but associations between health care–associated infections and medical devices “are still quite meaningful and often actionable,” he said.
Dr. Benowitz stressed the importance of engaging public health partners to discuss findings and actions, explaining that “what may look like a single-facility issue may have a very different perspective when you realize that there’s a similar issue at another facility elsewhere.”
“For all devices, it’s important to ensure adherence to the device reprocessing guidelines, “ he added, noting that these include a combination of facility protocols, manufacturer instructions for use, and guidance from organizations like the Food and Drug Administration and the CDC.
Dr. Benowitz reported having no disclosures.
[email protected]
SOURCE: Benowitz I et al. ICEID 2018, Oral Abstract Presentation E2.
ATLANTA – Ongoing vigilance regarding the role of and transmission of antimicrobial-resistant pathogen is needed, according to Isaac Benowitz, MD, of the Centers for Disease Control and Prevention’s Division of Healthcare Quality Promotion (DHQP).
A review of records from the DHQP, which investigates and responds to infections and related adverse events in health care settings upon invitation, showed that in 2017 environmental pathogens were most often the triggers for these investigations, said Dr. Benowitz, a medical epidemiologist.
He reviewed internal records for consultations with state and local health departments involving medical devices and collected data on health care setting, pathogen, investigation findings including possible exposure or transmission, and public health actions.
Of 285 consultations, 48 involved a specific medical device or general medical device reprocessing, he said, noting that most of those 48 were in an acute care hospital (63%) or clinic (19%).
“The most frequent pathogens noted in these consultations were nontuberculous mycobacteria at 21%, Candida species ... at 10%, and Burkholderia species ... at 8%,” he said, noting that a wide variety of devices were implicated.
In the inpatient setting these devices included ventilators, dialysis machines, breast pumps, central lines, and respiratory therapy equipment. In the outpatient setting they included glucometers and opthalmic equipment.
“In many settings we saw issues with endoscopes, including duodenoscopes, but also bronchoscopes,” he added.
Actions taken as part of the investigations included medical device recalls, improved infection control and reprocessing procedures, and patient notification, education, guidance, testing, and treatment.
In some cases there was disciplinary action or oversight for health care professionals, he added.
Investigations identified medical devices contaminated in manufacturing, incorrect reprocessing of endoscopes or ventilators, and inappropriate medical device use or reuse, he said.
A number of lessons can be learned from these and other investigations, he added.
“First, devices can be reservoirs and transmission vectors for health care–associated infections. Second, health care facilities, health care facility staff, and public health partners should take opportunities to review protocols and the practices within those protocol,” he said. “These are opportunities to strengthen infection control practices even in the absence of documented transmission.”
In fact, in most of the investigations he discussed, transmission was rarely confirmed to be associated with a medical device. This was largely because of a lack of “epidemiological rigor,” but associations between health care–associated infections and medical devices “are still quite meaningful and often actionable,” he said.
Dr. Benowitz stressed the importance of engaging public health partners to discuss findings and actions, explaining that “what may look like a single-facility issue may have a very different perspective when you realize that there’s a similar issue at another facility elsewhere.”
“For all devices, it’s important to ensure adherence to the device reprocessing guidelines, “ he added, noting that these include a combination of facility protocols, manufacturer instructions for use, and guidance from organizations like the Food and Drug Administration and the CDC.
Dr. Benowitz reported having no disclosures.
[email protected]
SOURCE: Benowitz I et al. ICEID 2018, Oral Abstract Presentation E2.
REPORTING FROM ICEID 2018
Key clinical point: Medical devices can be reservoirs and transmission vectors for health care–associated infections.
Major finding: Of 285 consultations, 48 involved medical devices or device reprocessing.
Study details: A review of records from 285 consultations
Disclosures: Dr. Benowitz reported having no disclosures
Source: Benowitz I et al. ICEID 2018, Oral Abstract Presentation E2.
Coronary CT angiography radiation dose fell 78% from 2007-2017
MUNICH – The median radiation dosage received by patients worldwide undergoing coronary CT angiography fell by 78% from 2007 to 2017, according to a prospective study with more than 4,500 patients.

This substantial drop in radiation occurred with a steady rate of nondiagnostic CT scans, less than 2% in both 2007 and 2017.
“Given the high diagnostic accuracy and the low radiation dose, coronary CT angiography should be considered as a first-line diagnostic test,” Jörg Hausleiter, MD, said at the annual congress of the European Society of Cardiology.
The results also showed a huge disparity in the range of radiation doses used worldwide, with a 37-fold intersite variability in the median dose. This finding “underlines the need for further site-specific training and adaptation of contemporary cardiac scan protocols,” said Dr. Hausleiter, professor of medicine at the University of Munich Clinic. He suggested updated imaging guidelines on radiation levels, more educational sessions on how to perform coronary CT angiography, and actions by vendors to adjust their standard imaging protocols.
The Prospective Multicenter Registry on Radiation Dose Estimates of Cardiac CT Angiography in Daily Practice in 2017 (PROTECTION-VI) study included 4,502 patients from a total of 61 sites in 32 countries. At each participating site, investigators enrolled consecutive adults during a randomly selected month in 2017, with a median of 51 patients enrolled at each site undergoing diagnostic coronary CT angiography. Comparison data for 2007 came from a similar study run by Dr. Hausleiter and his associates at that time, with 1,965 patients undergoing coronary CT angiography (JAMA. 2009 Feb 4;301[5]:500-7). In 2007, the median dose-length product of radiation for each scan was 885 mGy x cm, which corresponds to a radiation dose of about 12.4 mSv. In 2017, the median dose-length product was 195 mGy x cm, corresponding to a dose of about 2.7 mSv. By both measures the median dose dropped by roughly 78%.
A multivariate analysis identified three changes in the way clinicians obtained most of the CT scans during the two studied time periods that seemed to explain the drop in radiation dose. First, more scan protocols in 2017 used low tube potential; second, more protocols in 2017 used prospectively ECG-triggered axial high-pitch scans; and third, 2017 had increased use of iterative image reconstruction, Dr. Hausleiter said. Patient variables that had modest but significant links with increased radiation doses were higher body weight, higher heart rate, and no sinus rhythm.
Concurrently with Dr. Hausleiter’s talk at the congress, the results appeared in an article online (Euro Heart J. 2018 Aug 25. doi: 10.1093/eurheartj/ehy546).
The results from the PROTECTION VI study show that the radiation doses used today for coronary CT angiography are very low. But the study is limited by looking only at the median doses used at 61 sites worldwide. I hope that the dose level seen in the study is what is now used at community hospitals across the United States, but for the time being we can’t be sure.

With today’s CT technology, as long as the dose-length product a patient receives is less than 200 mGy x cm, the facility is doing a good job of minimizing radiation exposure. As CT technology continues to improve, we can expect the median dose to fall even more in the future.
Todd C. Villines, MD , a cardiologist at Georgetown University in Washington and immediate past president of the Society of Cardiovascular CT, made these comments in an interview. He had no relevant disclosures.
The results from the PROTECTION VI study show that the radiation doses used today for coronary CT angiography are very low. But the study is limited by looking only at the median doses used at 61 sites worldwide. I hope that the dose level seen in the study is what is now used at community hospitals across the United States, but for the time being we can’t be sure.
With today’s CT technology, as long as the dose-length product a patient receives is less than 200 mGy x cm, the facility is doing a good job of minimizing radiation exposure. As CT technology continues to improve, we can expect the median dose to fall even more in the future.
Todd C. Villines, MD , a cardiologist at Georgetown University in Washington and immediate past president of the Society of Cardiovascular CT, made these comments in an interview. He had no relevant disclosures.
The results from the PROTECTION VI study show that the radiation doses used today for coronary CT angiography are very low. But the study is limited by looking only at the median doses used at 61 sites worldwide. I hope that the dose level seen in the study is what is now used at community hospitals across the United States, but for the time being we can’t be sure.
With today’s CT technology, as long as the dose-length product a patient receives is less than 200 mGy x cm, the facility is doing a good job of minimizing radiation exposure. As CT technology continues to improve, we can expect the median dose to fall even more in the future.
Todd C. Villines, MD , a cardiologist at Georgetown University in Washington and immediate past president of the Society of Cardiovascular CT, made these comments in an interview. He had no relevant disclosures.
MUNICH – The median radiation dosage received by patients worldwide undergoing coronary CT angiography fell by 78% from 2007 to 2017, according to a prospective study with more than 4,500 patients.
This substantial drop in radiation occurred with a steady rate of nondiagnostic CT scans, less than 2% in both 2007 and 2017.
“Given the high diagnostic accuracy and the low radiation dose, coronary CT angiography should be considered as a first-line diagnostic test,” Jörg Hausleiter, MD, said at the annual congress of the European Society of Cardiology.
The results also showed a huge disparity in the range of radiation doses used worldwide, with a 37-fold intersite variability in the median dose. This finding “underlines the need for further site-specific training and adaptation of contemporary cardiac scan protocols,” said Dr. Hausleiter, professor of medicine at the University of Munich Clinic. He suggested updated imaging guidelines on radiation levels, more educational sessions on how to perform coronary CT angiography, and actions by vendors to adjust their standard imaging protocols.
The Prospective Multicenter Registry on Radiation Dose Estimates of Cardiac CT Angiography in Daily Practice in 2017 (PROTECTION-VI) study included 4,502 patients from a total of 61 sites in 32 countries. At each participating site, investigators enrolled consecutive adults during a randomly selected month in 2017, with a median of 51 patients enrolled at each site undergoing diagnostic coronary CT angiography. Comparison data for 2007 came from a similar study run by Dr. Hausleiter and his associates at that time, with 1,965 patients undergoing coronary CT angiography (JAMA. 2009 Feb 4;301[5]:500-7). In 2007, the median dose-length product of radiation for each scan was 885 mGy x cm, which corresponds to a radiation dose of about 12.4 mSv. In 2017, the median dose-length product was 195 mGy x cm, corresponding to a dose of about 2.7 mSv. By both measures the median dose dropped by roughly 78%.
A multivariate analysis identified three changes in the way clinicians obtained most of the CT scans during the two studied time periods that seemed to explain the drop in radiation dose. First, more scan protocols in 2017 used low tube potential; second, more protocols in 2017 used prospectively ECG-triggered axial high-pitch scans; and third, 2017 had increased use of iterative image reconstruction, Dr. Hausleiter said. Patient variables that had modest but significant links with increased radiation doses were higher body weight, higher heart rate, and no sinus rhythm.
Concurrently with Dr. Hausleiter’s talk at the congress, the results appeared in an article online (Euro Heart J. 2018 Aug 25. doi: 10.1093/eurheartj/ehy546).
MUNICH – The median radiation dosage received by patients worldwide undergoing coronary CT angiography fell by 78% from 2007 to 2017, according to a prospective study with more than 4,500 patients.
This substantial drop in radiation occurred with a steady rate of nondiagnostic CT scans, less than 2% in both 2007 and 2017.
“Given the high diagnostic accuracy and the low radiation dose, coronary CT angiography should be considered as a first-line diagnostic test,” Jörg Hausleiter, MD, said at the annual congress of the European Society of Cardiology.
The results also showed a huge disparity in the range of radiation doses used worldwide, with a 37-fold intersite variability in the median dose. This finding “underlines the need for further site-specific training and adaptation of contemporary cardiac scan protocols,” said Dr. Hausleiter, professor of medicine at the University of Munich Clinic. He suggested updated imaging guidelines on radiation levels, more educational sessions on how to perform coronary CT angiography, and actions by vendors to adjust their standard imaging protocols.
The Prospective Multicenter Registry on Radiation Dose Estimates of Cardiac CT Angiography in Daily Practice in 2017 (PROTECTION-VI) study included 4,502 patients from a total of 61 sites in 32 countries. At each participating site, investigators enrolled consecutive adults during a randomly selected month in 2017, with a median of 51 patients enrolled at each site undergoing diagnostic coronary CT angiography. Comparison data for 2007 came from a similar study run by Dr. Hausleiter and his associates at that time, with 1,965 patients undergoing coronary CT angiography (JAMA. 2009 Feb 4;301[5]:500-7). In 2007, the median dose-length product of radiation for each scan was 885 mGy x cm, which corresponds to a radiation dose of about 12.4 mSv. In 2017, the median dose-length product was 195 mGy x cm, corresponding to a dose of about 2.7 mSv. By both measures the median dose dropped by roughly 78%.
A multivariate analysis identified three changes in the way clinicians obtained most of the CT scans during the two studied time periods that seemed to explain the drop in radiation dose. First, more scan protocols in 2017 used low tube potential; second, more protocols in 2017 used prospectively ECG-triggered axial high-pitch scans; and third, 2017 had increased use of iterative image reconstruction, Dr. Hausleiter said. Patient variables that had modest but significant links with increased radiation doses were higher body weight, higher heart rate, and no sinus rhythm.
Concurrently with Dr. Hausleiter’s talk at the congress, the results appeared in an article online (Euro Heart J. 2018 Aug 25. doi: 10.1093/eurheartj/ehy546).
REPORTING FROM THE ESC CONGRESS 2018
Key clinical point: The median radiation dose during coronary CT angiography fell from 2007 to 2017.
Major finding: The median dose-length product was 195 mGY x cm in 2017 and 885 mGy x cm in 2007.
Study details: PROTECTION VI, a prospective study run at 61 sites in 32 countries.
Disclosures: PROTECTION VI received no commercial funding. Dr. Hausleiter has received research funding from Abbott Vascular.
Piperacillin-tazobactam fails to outperform meropenem in bloodstream infections
A new study finds that piperacillin-tazobactam doesn’t improve mortality compared to meropenem in patients with ceftriaxone-resistant blood poisoning caused by E. coli or K. pneumoniae. The findings were so striking that the study was ended early.

Courtesy: JAMA
“These findings do not support use of piperacillin-tazobactam in this setting,” wrote the authors. The report was published Sept. 11 in JAMA (2018;320[10]:984-94.)
According to the Centers for Disease Control and Prevention, an estimated 1,700 deaths in the United States in 2011 were caused by gram-negative bacteria that produce extended-spectrum beta-lactamase enzymes.
While carbapenems such as meropenem (Merrem) are “regarded as the treatment of choice for serious infections,” the MERINO trial (NCT02176122) authors wrote, their rising use could lead to drug resistance.
One alternate option is to embrace beta-lactam/beta-lactamase inhibitors such as piperacillin-tazobactam (Zosyn), the researchers noted, but research has produced conflicting results.
Piperacillin-tazobactam is an injected penicillin antibiotic used to treat conditions such as severe pneumonia, complicated urinary tract infections and complicated skin and soft tissue infections.
For the new study, researchers led by Patrick N. A. Harris, MBBS, of the University of Queensland, randomly assigned 188 patients to intravenous piperacillin-tazobactam (4.5 g every 6 hours) and 191 patients to meropenem (1 g every 8 hours) for 4-14 days, depending on clinician’s preference. (12 other patients did not continue with the study after initial randomization due to factors such as errors).
All patients were adults and had at least one blood test showing they were positive for E. coli or K. pneumoniae. They all had to be nonsusceptible to ceftriaxone (Rocephin) but susceptible to piperacillin-tazobactam.
The study was ceased prior to enrollment because of the risk of harm. Interim findings suggested the study was unlikely to show higher effectiveness for piperacillin-tazobactam
The primary analysis included 379 patients (mean age 67 years, 48% were women), and the primary outcome analysis included 378 patients.
A total of 23 (12.3%) of 187 patients in the piperacillin-tazobactam group died by 30 days compared to 7 (3.7%) of 191 in the meropenem group (risk difference: 8.6%, P = .90 for noninferiority).
By day 4, 68% of the piperacillin-tazobactam group and 75% of the meropenem group achieved clinical and microbiological resolution.
Serious adverse effects other than death were rare, occurring in around 3% of the piperacillin-tazobactam group and nearly 2% of the meropenem group.
The researchers note various limitations, including the unblinded nature of the study and the fact that it’s not known if extended or continuous infusions of piperacillin-tazobactam would boost the drug’s effectiveness. They also note that delays resulted in some patients initially receiving treatment with one of the study’s two drugs before being randomized to the other.
The study authors caution that it’s not clear if newer beta-lactam/beta-lactamase inhibitors agents such as ceftolozane-tazobactam or ceftazidime-avibactam may be effective in this population.
The study was funded by the University of Queensland, Australian Society for Antimicrobials, International Society for Chemotherapy, and National University Hospital Singapore. Various organizations funded the researchers and the study’s whole-genome sequencing. The study authors report various disclosures, including funding from drugmakers such as Pfizer, maker of Zosyn (through its subsidiary Wyeth) and Merrem.
SOURCE: Harris PNA et al. JAMA 2018 Sep 11;320[10]:984-94. doi: 10.1001/jama.2018.12163.
There may be no greater present-day antibiotic resistance threat than the prospect of nonsusceptibility developing among patients with blood poisoning who receive carbapenems for infections caused by E. coli or K. pneumonia. New antibiotics are being developed and researchers are taking a second look at existing drugs.
The new study aims to shed light on the effectiveness of piperacillin-tazobactam in this population compared to carbapenems. Surprisingly, the researchers failed to show a mortality benefit for the drug vs. meropenem. What now? Future research could shed light on newer beta-lactam/beta-lactamase inhibitors, and studies may also offer insight into alternatives such as short-term antibiotic therapy. The upcoming availability of electronic decision support tools may be helpful, and it remains important to prevent infections in the first place.
This commentary was taken from an editorial by Mary K. Hayden, MD, and Sarah Y. Won, MD, MPH, of Rush University Medical Center (JAMA 2018 Sep 11;320[10]:979-81). Dr. Hayden reports research funding from Colorox and serving as an investigator on research products that received product support from Sage Corporation, Molnlycke, Clorox, OpGen and Medline.
There may be no greater present-day antibiotic resistance threat than the prospect of nonsusceptibility developing among patients with blood poisoning who receive carbapenems for infections caused by E. coli or K. pneumonia. New antibiotics are being developed and researchers are taking a second look at existing drugs.
The new study aims to shed light on the effectiveness of piperacillin-tazobactam in this population compared to carbapenems. Surprisingly, the researchers failed to show a mortality benefit for the drug vs. meropenem. What now? Future research could shed light on newer beta-lactam/beta-lactamase inhibitors, and studies may also offer insight into alternatives such as short-term antibiotic therapy. The upcoming availability of electronic decision support tools may be helpful, and it remains important to prevent infections in the first place.
This commentary was taken from an editorial by Mary K. Hayden, MD, and Sarah Y. Won, MD, MPH, of Rush University Medical Center (JAMA 2018 Sep 11;320[10]:979-81). Dr. Hayden reports research funding from Colorox and serving as an investigator on research products that received product support from Sage Corporation, Molnlycke, Clorox, OpGen and Medline.
There may be no greater present-day antibiotic resistance threat than the prospect of nonsusceptibility developing among patients with blood poisoning who receive carbapenems for infections caused by E. coli or K. pneumonia. New antibiotics are being developed and researchers are taking a second look at existing drugs.
The new study aims to shed light on the effectiveness of piperacillin-tazobactam in this population compared to carbapenems. Surprisingly, the researchers failed to show a mortality benefit for the drug vs. meropenem. What now? Future research could shed light on newer beta-lactam/beta-lactamase inhibitors, and studies may also offer insight into alternatives such as short-term antibiotic therapy. The upcoming availability of electronic decision support tools may be helpful, and it remains important to prevent infections in the first place.
This commentary was taken from an editorial by Mary K. Hayden, MD, and Sarah Y. Won, MD, MPH, of Rush University Medical Center (JAMA 2018 Sep 11;320[10]:979-81). Dr. Hayden reports research funding from Colorox and serving as an investigator on research products that received product support from Sage Corporation, Molnlycke, Clorox, OpGen and Medline.
A new study finds that piperacillin-tazobactam doesn’t improve mortality compared to meropenem in patients with ceftriaxone-resistant blood poisoning caused by E. coli or K. pneumoniae. The findings were so striking that the study was ended early.
Courtesy: JAMA
“These findings do not support use of piperacillin-tazobactam in this setting,” wrote the authors. The report was published Sept. 11 in JAMA (2018;320[10]:984-94.)
According to the Centers for Disease Control and Prevention, an estimated 1,700 deaths in the United States in 2011 were caused by gram-negative bacteria that produce extended-spectrum beta-lactamase enzymes.
While carbapenems such as meropenem (Merrem) are “regarded as the treatment of choice for serious infections,” the MERINO trial (NCT02176122) authors wrote, their rising use could lead to drug resistance.
One alternate option is to embrace beta-lactam/beta-lactamase inhibitors such as piperacillin-tazobactam (Zosyn), the researchers noted, but research has produced conflicting results.
Piperacillin-tazobactam is an injected penicillin antibiotic used to treat conditions such as severe pneumonia, complicated urinary tract infections and complicated skin and soft tissue infections.
For the new study, researchers led by Patrick N. A. Harris, MBBS, of the University of Queensland, randomly assigned 188 patients to intravenous piperacillin-tazobactam (4.5 g every 6 hours) and 191 patients to meropenem (1 g every 8 hours) for 4-14 days, depending on clinician’s preference. (12 other patients did not continue with the study after initial randomization due to factors such as errors).
All patients were adults and had at least one blood test showing they were positive for E. coli or K. pneumoniae. They all had to be nonsusceptible to ceftriaxone (Rocephin) but susceptible to piperacillin-tazobactam.
The study was ceased prior to enrollment because of the risk of harm. Interim findings suggested the study was unlikely to show higher effectiveness for piperacillin-tazobactam
The primary analysis included 379 patients (mean age 67 years, 48% were women), and the primary outcome analysis included 378 patients.
A total of 23 (12.3%) of 187 patients in the piperacillin-tazobactam group died by 30 days compared to 7 (3.7%) of 191 in the meropenem group (risk difference: 8.6%, P = .90 for noninferiority).
By day 4, 68% of the piperacillin-tazobactam group and 75% of the meropenem group achieved clinical and microbiological resolution.
Serious adverse effects other than death were rare, occurring in around 3% of the piperacillin-tazobactam group and nearly 2% of the meropenem group.
The researchers note various limitations, including the unblinded nature of the study and the fact that it’s not known if extended or continuous infusions of piperacillin-tazobactam would boost the drug’s effectiveness. They also note that delays resulted in some patients initially receiving treatment with one of the study’s two drugs before being randomized to the other.
The study authors caution that it’s not clear if newer beta-lactam/beta-lactamase inhibitors agents such as ceftolozane-tazobactam or ceftazidime-avibactam may be effective in this population.
The study was funded by the University of Queensland, Australian Society for Antimicrobials, International Society for Chemotherapy, and National University Hospital Singapore. Various organizations funded the researchers and the study’s whole-genome sequencing. The study authors report various disclosures, including funding from drugmakers such as Pfizer, maker of Zosyn (through its subsidiary Wyeth) and Merrem.
SOURCE: Harris PNA et al. JAMA 2018 Sep 11;320[10]:984-94. doi: 10.1001/jama.2018.12163.
A new study finds that piperacillin-tazobactam doesn’t improve mortality compared to meropenem in patients with ceftriaxone-resistant blood poisoning caused by E. coli or K. pneumoniae. The findings were so striking that the study was ended early.
Courtesy: JAMA
“These findings do not support use of piperacillin-tazobactam in this setting,” wrote the authors. The report was published Sept. 11 in JAMA (2018;320[10]:984-94.)
According to the Centers for Disease Control and Prevention, an estimated 1,700 deaths in the United States in 2011 were caused by gram-negative bacteria that produce extended-spectrum beta-lactamase enzymes.
While carbapenems such as meropenem (Merrem) are “regarded as the treatment of choice for serious infections,” the MERINO trial (NCT02176122) authors wrote, their rising use could lead to drug resistance.
One alternate option is to embrace beta-lactam/beta-lactamase inhibitors such as piperacillin-tazobactam (Zosyn), the researchers noted, but research has produced conflicting results.
Piperacillin-tazobactam is an injected penicillin antibiotic used to treat conditions such as severe pneumonia, complicated urinary tract infections and complicated skin and soft tissue infections.
For the new study, researchers led by Patrick N. A. Harris, MBBS, of the University of Queensland, randomly assigned 188 patients to intravenous piperacillin-tazobactam (4.5 g every 6 hours) and 191 patients to meropenem (1 g every 8 hours) for 4-14 days, depending on clinician’s preference. (12 other patients did not continue with the study after initial randomization due to factors such as errors).
All patients were adults and had at least one blood test showing they were positive for E. coli or K. pneumoniae. They all had to be nonsusceptible to ceftriaxone (Rocephin) but susceptible to piperacillin-tazobactam.
The study was ceased prior to enrollment because of the risk of harm. Interim findings suggested the study was unlikely to show higher effectiveness for piperacillin-tazobactam
The primary analysis included 379 patients (mean age 67 years, 48% were women), and the primary outcome analysis included 378 patients.
A total of 23 (12.3%) of 187 patients in the piperacillin-tazobactam group died by 30 days compared to 7 (3.7%) of 191 in the meropenem group (risk difference: 8.6%, P = .90 for noninferiority).
By day 4, 68% of the piperacillin-tazobactam group and 75% of the meropenem group achieved clinical and microbiological resolution.
Serious adverse effects other than death were rare, occurring in around 3% of the piperacillin-tazobactam group and nearly 2% of the meropenem group.
The researchers note various limitations, including the unblinded nature of the study and the fact that it’s not known if extended or continuous infusions of piperacillin-tazobactam would boost the drug’s effectiveness. They also note that delays resulted in some patients initially receiving treatment with one of the study’s two drugs before being randomized to the other.
The study authors caution that it’s not clear if newer beta-lactam/beta-lactamase inhibitors agents such as ceftolozane-tazobactam or ceftazidime-avibactam may be effective in this population.
The study was funded by the University of Queensland, Australian Society for Antimicrobials, International Society for Chemotherapy, and National University Hospital Singapore. Various organizations funded the researchers and the study’s whole-genome sequencing. The study authors report various disclosures, including funding from drugmakers such as Pfizer, maker of Zosyn (through its subsidiary Wyeth) and Merrem.
SOURCE: Harris PNA et al. JAMA 2018 Sep 11;320[10]:984-94. doi: 10.1001/jama.2018.12163.
FROM JAMA
Key clinical point: Piperacillin-tazobactam isn’t a superior alternative to meropenem in patients with ceftriaxone-resistant blood poisoning caused by E. coli or K. pneumoniae.
Major finding: By 30 days, 12% of patients in the piperacillin-tazobactam group died compared to 4% of the meropenem group.
Study details: Unblinded, randomized, noninferiority trial of 379 patients with bloodstream infection caused by ceftriaxone-nonsusceptible E. coli or K. pneumoniae who received piperacillin-tazobactam (n=188) or meropenem (n = 191).
Disclosures: The study was funded by the University of Queensland, Australian Society for Antimicrobials, International Society for Chemotherapy, and National University Hospital Singapore. Various organizations funded the researchers and the study’s whole-genome sequencing. The study authors report various disclosures.
Source: Harris PNA et al. JAMA 2018 Sep 11. doi: 10.1001/jama.2018.12163.