User login
Growth on nose

The FP made the presumptive diagnosis of a nodular basal cell carcinoma.
He explained the importance of performing a biopsy and obtained informed consent. On the same day of the patient’s visit, he injected 1% lidocaine with epinephrine under the lesion with a single stick of a 30 gauge needle. He knew that it was safe to use epinephrine on the nose, and that it would prevent excessive bleeding during the biopsy. Contrary to the myth frequently taught in medical school, the nose is a very vascular area. The physician performed a shave biopsy that removed the top of the lesion flush with the skin around it. (See the Watch & Learn video on “Shave biopsy.”)
The pathology report came back as a nodular basal cell carcinoma. On the following visit, the physician recommended Mohs surgery as a way to preserve the vital anatomy of the nasal ala and achieve the highest cure rate.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Karnes J, Usatine R. Basal cell carcinoma. In: Usatine R, Smith M, Mayeaux EJ, et al. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:989-998.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/.
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com.
The FP made the presumptive diagnosis of a nodular basal cell carcinoma.
He explained the importance of performing a biopsy and obtained informed consent. On the same day of the patient’s visit, he injected 1% lidocaine with epinephrine under the lesion with a single stick of a 30 gauge needle. He knew that it was safe to use epinephrine on the nose, and that it would prevent excessive bleeding during the biopsy. Contrary to the myth frequently taught in medical school, the nose is a very vascular area. The physician performed a shave biopsy that removed the top of the lesion flush with the skin around it. (See the Watch & Learn video on “Shave biopsy.”)
The pathology report came back as a nodular basal cell carcinoma. On the following visit, the physician recommended Mohs surgery as a way to preserve the vital anatomy of the nasal ala and achieve the highest cure rate.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Karnes J, Usatine R. Basal cell carcinoma. In: Usatine R, Smith M, Mayeaux EJ, et al. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:989-998.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/.
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com.
The FP made the presumptive diagnosis of a nodular basal cell carcinoma.
He explained the importance of performing a biopsy and obtained informed consent. On the same day of the patient’s visit, he injected 1% lidocaine with epinephrine under the lesion with a single stick of a 30 gauge needle. He knew that it was safe to use epinephrine on the nose, and that it would prevent excessive bleeding during the biopsy. Contrary to the myth frequently taught in medical school, the nose is a very vascular area. The physician performed a shave biopsy that removed the top of the lesion flush with the skin around it. (See the Watch & Learn video on “Shave biopsy.”)
The pathology report came back as a nodular basal cell carcinoma. On the following visit, the physician recommended Mohs surgery as a way to preserve the vital anatomy of the nasal ala and achieve the highest cure rate.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Karnes J, Usatine R. Basal cell carcinoma. In: Usatine R, Smith M, Mayeaux EJ, et al. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:989-998.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/.
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com.

Ultrasound can’t rule out pulmonary embolism in the ED
SAN DIEGO – In the ICU, ultrasound has been shown to reduce the need for CT to evaluate potential pulmonary embolism. But in the ED, this strategy hasn’t worked out so far, according to Joseph Brown, MD, of the department of emergency medicine at the University of California, San Francisco.

Based on the data so far, the ED patients were less likely than the ICU patients to have another etiology identified on ultrasound that explained their symptoms. Further, ultrasound alone missed small subsegmental pulmonary emboli that were detected on subsequent CT scans in 2 of 11 patients.
The study is continuing, and Dr. Brown explains in this interview how ultrasound might be combined with other risk stratification measures to safely achieve reductions in CT scans.
SAN DIEGO – In the ICU, ultrasound has been shown to reduce the need for CT to evaluate potential pulmonary embolism. But in the ED, this strategy hasn’t worked out so far, according to Joseph Brown, MD, of the department of emergency medicine at the University of California, San Francisco.
Based on the data so far, the ED patients were less likely than the ICU patients to have another etiology identified on ultrasound that explained their symptoms. Further, ultrasound alone missed small subsegmental pulmonary emboli that were detected on subsequent CT scans in 2 of 11 patients.
The study is continuing, and Dr. Brown explains in this interview how ultrasound might be combined with other risk stratification measures to safely achieve reductions in CT scans.
SAN DIEGO – In the ICU, ultrasound has been shown to reduce the need for CT to evaluate potential pulmonary embolism. But in the ED, this strategy hasn’t worked out so far, according to Joseph Brown, MD, of the department of emergency medicine at the University of California, San Francisco.
Based on the data so far, the ED patients were less likely than the ICU patients to have another etiology identified on ultrasound that explained their symptoms. Further, ultrasound alone missed small subsegmental pulmonary emboli that were detected on subsequent CT scans in 2 of 11 patients.
The study is continuing, and Dr. Brown explains in this interview how ultrasound might be combined with other risk stratification measures to safely achieve reductions in CT scans.
REPORTING FROM ACEP18

This is a drill
She had fallen on a garden implement, lacerating her superficial femoral artery. She used her cell phone to call 911. Thanks to an alert EMS crew and the Stop the Bleed training they recently received, a tourniquet was placed without delay. She got to our trauma bay in about 15 minutes after the tourniquet was applied. Although the patient made it abundantly clear that she was in pain, she was stable with moderate tachycardia and a good blood pressure.

Our trauma team leaped into action. The leader took report from the EMS while two nurses and a second surgeon assessed the patient, got her clothes cut off, and applied monitors. A third nurse got a second IV going. Primary survey was done in less than 90 seconds. The patient then underwent a focused exam including a log roll for back injuries.
The leg wound was still oozing a bit, so a second tourniquet was called for and pressure applied until it could be acquired. The patient was given 5 mg of morphine sulfate, which calmed her down a bit. Labs and x-rays were done quickly. The nursing staff suggested a tetanus booster, and the second surgeon who had gotten a basic past medical history suggested vancomycin since the patient said she was allergic to penicillin. Fifteen minutes after she hit the trauma bay, she was on her way to the OR for exploration, debridement, and vascular repair of her injury.
This was all done by four M2 medical students and five N4 nursing students, none of whom had had previous experience with this type of trauma patient
The students were managing this trauma situation in the simulation center of their medical school with four staff watching. This was their second run through for the afternoon. At debriefing, they compared their work on the first trauma of the day (a stab wound to the right chest) to their second attempt. They were satisfied with their efforts and so were we, the faculty who ran the simulation. Comparing their response to those I’ve seen in real life, I’d say these students understood their roles and responsibilities as well as the sort of thrown-together teams I’ve seen at places where trauma is not the main focus. While these young men and women are in the early stage of training and not ready for a real-world trauma emergency, they have gained knowledge about this kind of situation that I didn’t see until I was in residency and beyond. The times they are a-changing.
A couple of days later I was in Rochester, Minn., attending an American College of Surgeons Advanced Education Institute (ACS/AEI) course on simulations. At the end of that course, we participants were challenged by a manikin in extremis. Everyone there was an expert, had an advanced degree, had some experience in simulation, or were surgeons interested in simulation. I found that, even though this was a simulation and the patient was only a pretend human being, my adrenal cortex performed almost as if I were doing a real resuscitation. Previous training I’d had on teamwork, crew resource management, and ACLS all kicked in, and we got it done. But interestingly, we weren’t perfect. We debriefed and found that, even at our level of experience and training, a simple simulation could be very instructive. Seeing/doing is believing.
High-tech skills in high-risk occupations are well served by simulation training. Much of the airline piloting training is done by simulation. It works well for aviation, nuclear reactors, high voltage line work, and medicine. Most of these disciplines have embraced simulation as an essential part of training. Simulation is part of many surgical training programs, but it has other uses.
When was the last time you practiced a trauma resuscitation, an ultrasound fine-needle biopsy, laparoscopic maneuvers, or an unusual technique that you seldom perform, but when needed, must be pulled off very well? Most of us taking this simulation course agreed that time, money, and ego may get in the way of maintaining those skills for those rare instances when they are needed. Surgeons might want to consider simulation to keep some of our rarely used skills from getting rusty.
If you’re going to make a costly error, I would very much like you to do it on a piece of plastic, not on a patient. There are no consequences for messing up a procedure on a manikin and this kind of practice might teach you something critical. Practicing reduces stress and improves the performance of those placed on the spot by real-life events. Do you think Captain “Sully” Sullenberger could have landed that airliner in the Hudson River safely if he hadn’t practiced with countless mind-numbingly complex simulations? Sure, luck plays a part, and innate ability plays a part. But skill, knowledge, and practice are your best bet when all the eyes in the room swivel to you in a moment of crisis.
You may think that simulators have to cost $100,000 and be completely realistic to do the job. That’s not true. A banana, orange, or stick of butter can be fabulous sims for a med student. Felt and cardboard can make a realistic cricothyroidotomy model.
Surgeons all over the country are using simulation training to learn how to be better without getting real blood on their shoes. If you haven’t participated in a training simulation recently, I double-dog dare you to try it and tell me you found it without merit. The ACS Surgical Simulation Summit is being held in March 2019 in Chicago. You might want to check that out.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the University of Kansas School of Medicine, Salina, and Coeditor of ACS Surgery News.
She had fallen on a garden implement, lacerating her superficial femoral artery. She used her cell phone to call 911. Thanks to an alert EMS crew and the Stop the Bleed training they recently received, a tourniquet was placed without delay. She got to our trauma bay in about 15 minutes after the tourniquet was applied. Although the patient made it abundantly clear that she was in pain, she was stable with moderate tachycardia and a good blood pressure.
Our trauma team leaped into action. The leader took report from the EMS while two nurses and a second surgeon assessed the patient, got her clothes cut off, and applied monitors. A third nurse got a second IV going. Primary survey was done in less than 90 seconds. The patient then underwent a focused exam including a log roll for back injuries.
The leg wound was still oozing a bit, so a second tourniquet was called for and pressure applied until it could be acquired. The patient was given 5 mg of morphine sulfate, which calmed her down a bit. Labs and x-rays were done quickly. The nursing staff suggested a tetanus booster, and the second surgeon who had gotten a basic past medical history suggested vancomycin since the patient said she was allergic to penicillin. Fifteen minutes after she hit the trauma bay, she was on her way to the OR for exploration, debridement, and vascular repair of her injury.
This was all done by four M2 medical students and five N4 nursing students, none of whom had had previous experience with this type of trauma patient
The students were managing this trauma situation in the simulation center of their medical school with four staff watching. This was their second run through for the afternoon. At debriefing, they compared their work on the first trauma of the day (a stab wound to the right chest) to their second attempt. They were satisfied with their efforts and so were we, the faculty who ran the simulation. Comparing their response to those I’ve seen in real life, I’d say these students understood their roles and responsibilities as well as the sort of thrown-together teams I’ve seen at places where trauma is not the main focus. While these young men and women are in the early stage of training and not ready for a real-world trauma emergency, they have gained knowledge about this kind of situation that I didn’t see until I was in residency and beyond. The times they are a-changing.
A couple of days later I was in Rochester, Minn., attending an American College of Surgeons Advanced Education Institute (ACS/AEI) course on simulations. At the end of that course, we participants were challenged by a manikin in extremis. Everyone there was an expert, had an advanced degree, had some experience in simulation, or were surgeons interested in simulation. I found that, even though this was a simulation and the patient was only a pretend human being, my adrenal cortex performed almost as if I were doing a real resuscitation. Previous training I’d had on teamwork, crew resource management, and ACLS all kicked in, and we got it done. But interestingly, we weren’t perfect. We debriefed and found that, even at our level of experience and training, a simple simulation could be very instructive. Seeing/doing is believing.
High-tech skills in high-risk occupations are well served by simulation training. Much of the airline piloting training is done by simulation. It works well for aviation, nuclear reactors, high voltage line work, and medicine. Most of these disciplines have embraced simulation as an essential part of training. Simulation is part of many surgical training programs, but it has other uses.
When was the last time you practiced a trauma resuscitation, an ultrasound fine-needle biopsy, laparoscopic maneuvers, or an unusual technique that you seldom perform, but when needed, must be pulled off very well? Most of us taking this simulation course agreed that time, money, and ego may get in the way of maintaining those skills for those rare instances when they are needed. Surgeons might want to consider simulation to keep some of our rarely used skills from getting rusty.
If you’re going to make a costly error, I would very much like you to do it on a piece of plastic, not on a patient. There are no consequences for messing up a procedure on a manikin and this kind of practice might teach you something critical. Practicing reduces stress and improves the performance of those placed on the spot by real-life events. Do you think Captain “Sully” Sullenberger could have landed that airliner in the Hudson River safely if he hadn’t practiced with countless mind-numbingly complex simulations? Sure, luck plays a part, and innate ability plays a part. But skill, knowledge, and practice are your best bet when all the eyes in the room swivel to you in a moment of crisis.
You may think that simulators have to cost $100,000 and be completely realistic to do the job. That’s not true. A banana, orange, or stick of butter can be fabulous sims for a med student. Felt and cardboard can make a realistic cricothyroidotomy model.
Surgeons all over the country are using simulation training to learn how to be better without getting real blood on their shoes. If you haven’t participated in a training simulation recently, I double-dog dare you to try it and tell me you found it without merit. The ACS Surgical Simulation Summit is being held in March 2019 in Chicago. You might want to check that out.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the University of Kansas School of Medicine, Salina, and Coeditor of ACS Surgery News.
She had fallen on a garden implement, lacerating her superficial femoral artery. She used her cell phone to call 911. Thanks to an alert EMS crew and the Stop the Bleed training they recently received, a tourniquet was placed without delay. She got to our trauma bay in about 15 minutes after the tourniquet was applied. Although the patient made it abundantly clear that she was in pain, she was stable with moderate tachycardia and a good blood pressure.
Our trauma team leaped into action. The leader took report from the EMS while two nurses and a second surgeon assessed the patient, got her clothes cut off, and applied monitors. A third nurse got a second IV going. Primary survey was done in less than 90 seconds. The patient then underwent a focused exam including a log roll for back injuries.
The leg wound was still oozing a bit, so a second tourniquet was called for and pressure applied until it could be acquired. The patient was given 5 mg of morphine sulfate, which calmed her down a bit. Labs and x-rays were done quickly. The nursing staff suggested a tetanus booster, and the second surgeon who had gotten a basic past medical history suggested vancomycin since the patient said she was allergic to penicillin. Fifteen minutes after she hit the trauma bay, she was on her way to the OR for exploration, debridement, and vascular repair of her injury.
This was all done by four M2 medical students and five N4 nursing students, none of whom had had previous experience with this type of trauma patient
The students were managing this trauma situation in the simulation center of their medical school with four staff watching. This was their second run through for the afternoon. At debriefing, they compared their work on the first trauma of the day (a stab wound to the right chest) to their second attempt. They were satisfied with their efforts and so were we, the faculty who ran the simulation. Comparing their response to those I’ve seen in real life, I’d say these students understood their roles and responsibilities as well as the sort of thrown-together teams I’ve seen at places where trauma is not the main focus. While these young men and women are in the early stage of training and not ready for a real-world trauma emergency, they have gained knowledge about this kind of situation that I didn’t see until I was in residency and beyond. The times they are a-changing.
A couple of days later I was in Rochester, Minn., attending an American College of Surgeons Advanced Education Institute (ACS/AEI) course on simulations. At the end of that course, we participants were challenged by a manikin in extremis. Everyone there was an expert, had an advanced degree, had some experience in simulation, or were surgeons interested in simulation. I found that, even though this was a simulation and the patient was only a pretend human being, my adrenal cortex performed almost as if I were doing a real resuscitation. Previous training I’d had on teamwork, crew resource management, and ACLS all kicked in, and we got it done. But interestingly, we weren’t perfect. We debriefed and found that, even at our level of experience and training, a simple simulation could be very instructive. Seeing/doing is believing.
High-tech skills in high-risk occupations are well served by simulation training. Much of the airline piloting training is done by simulation. It works well for aviation, nuclear reactors, high voltage line work, and medicine. Most of these disciplines have embraced simulation as an essential part of training. Simulation is part of many surgical training programs, but it has other uses.
When was the last time you practiced a trauma resuscitation, an ultrasound fine-needle biopsy, laparoscopic maneuvers, or an unusual technique that you seldom perform, but when needed, must be pulled off very well? Most of us taking this simulation course agreed that time, money, and ego may get in the way of maintaining those skills for those rare instances when they are needed. Surgeons might want to consider simulation to keep some of our rarely used skills from getting rusty.
If you’re going to make a costly error, I would very much like you to do it on a piece of plastic, not on a patient. There are no consequences for messing up a procedure on a manikin and this kind of practice might teach you something critical. Practicing reduces stress and improves the performance of those placed on the spot by real-life events. Do you think Captain “Sully” Sullenberger could have landed that airliner in the Hudson River safely if he hadn’t practiced with countless mind-numbingly complex simulations? Sure, luck plays a part, and innate ability plays a part. But skill, knowledge, and practice are your best bet when all the eyes in the room swivel to you in a moment of crisis.
You may think that simulators have to cost $100,000 and be completely realistic to do the job. That’s not true. A banana, orange, or stick of butter can be fabulous sims for a med student. Felt and cardboard can make a realistic cricothyroidotomy model.
Surgeons all over the country are using simulation training to learn how to be better without getting real blood on their shoes. If you haven’t participated in a training simulation recently, I double-dog dare you to try it and tell me you found it without merit. The ACS Surgical Simulation Summit is being held in March 2019 in Chicago. You might want to check that out.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the University of Kansas School of Medicine, Salina, and Coeditor of ACS Surgery News.
New Updates to Afib Guidelines from CHEST
The American College of Chest Physicians® announced updates to the evidence-based guidelines on antithrombotic therapy for atrial fibrillation. The guideline panel submitted the manuscript, Antithrombotic Therapy for Atrial Fibrillation: CHEST Guideline and Expert Panel Report, for publication in the journal CHEST®.
Key recommendations and shifts from previous guidelines include:
• For patients with atrial fibrillation without valvular heart disease, including those with paroxysmal atrial fibrillation who are at low risk of stroke (eg, CHA2DS2VASc score of 0 in males or 1 in females), we suggest no antithrombotic therapy.
• For patients with a single non-sex CHA2DS2VASc stroke risk factor, we suggest oral anticoagulation rather than no therapy, aspirin or combination therapy with aspirin and clopidogrel.
• For those at high risk of stroke, we recommend oral anticoagulation rather than no therapy, aspirin or combination therapy with aspirin and clopidogrel.
• Where we recommend or suggest in favor of oral anticoagulation, we suggest using a novel oral anticoagulant (NOAC) rather than adjusted-dose vitamin K antagonist therapy. With the latter, it is important to aim for good quality anticoagulation control with a time in therapeutic range (TTR) >70%.
• Attention to modifiable bleeding risk factors should be made at each patient contact, and HAS-BLED score should be used to assess the risk of bleeding where high-risk patients (>=3) can be identified for earlier review and follow-up visits.
The complete guideline article is free to view in the Online First section of the journal CHEST.
The American College of Chest Physicians® announced updates to the evidence-based guidelines on antithrombotic therapy for atrial fibrillation. The guideline panel submitted the manuscript, Antithrombotic Therapy for Atrial Fibrillation: CHEST Guideline and Expert Panel Report, for publication in the journal CHEST®.
Key recommendations and shifts from previous guidelines include:
• For patients with atrial fibrillation without valvular heart disease, including those with paroxysmal atrial fibrillation who are at low risk of stroke (eg, CHA2DS2VASc score of 0 in males or 1 in females), we suggest no antithrombotic therapy.
• For patients with a single non-sex CHA2DS2VASc stroke risk factor, we suggest oral anticoagulation rather than no therapy, aspirin or combination therapy with aspirin and clopidogrel.
• For those at high risk of stroke, we recommend oral anticoagulation rather than no therapy, aspirin or combination therapy with aspirin and clopidogrel.
• Where we recommend or suggest in favor of oral anticoagulation, we suggest using a novel oral anticoagulant (NOAC) rather than adjusted-dose vitamin K antagonist therapy. With the latter, it is important to aim for good quality anticoagulation control with a time in therapeutic range (TTR) >70%.
• Attention to modifiable bleeding risk factors should be made at each patient contact, and HAS-BLED score should be used to assess the risk of bleeding where high-risk patients (>=3) can be identified for earlier review and follow-up visits.
The complete guideline article is free to view in the Online First section of the journal CHEST.
The American College of Chest Physicians® announced updates to the evidence-based guidelines on antithrombotic therapy for atrial fibrillation. The guideline panel submitted the manuscript, Antithrombotic Therapy for Atrial Fibrillation: CHEST Guideline and Expert Panel Report, for publication in the journal CHEST®.
Key recommendations and shifts from previous guidelines include:
• For patients with atrial fibrillation without valvular heart disease, including those with paroxysmal atrial fibrillation who are at low risk of stroke (eg, CHA2DS2VASc score of 0 in males or 1 in females), we suggest no antithrombotic therapy.
• For patients with a single non-sex CHA2DS2VASc stroke risk factor, we suggest oral anticoagulation rather than no therapy, aspirin or combination therapy with aspirin and clopidogrel.
• For those at high risk of stroke, we recommend oral anticoagulation rather than no therapy, aspirin or combination therapy with aspirin and clopidogrel.
• Where we recommend or suggest in favor of oral anticoagulation, we suggest using a novel oral anticoagulant (NOAC) rather than adjusted-dose vitamin K antagonist therapy. With the latter, it is important to aim for good quality anticoagulation control with a time in therapeutic range (TTR) >70%.
• Attention to modifiable bleeding risk factors should be made at each patient contact, and HAS-BLED score should be used to assess the risk of bleeding where high-risk patients (>=3) can be identified for earlier review and follow-up visits.
The complete guideline article is free to view in the Online First section of the journal CHEST.
ECMO for ARDS in the modern era
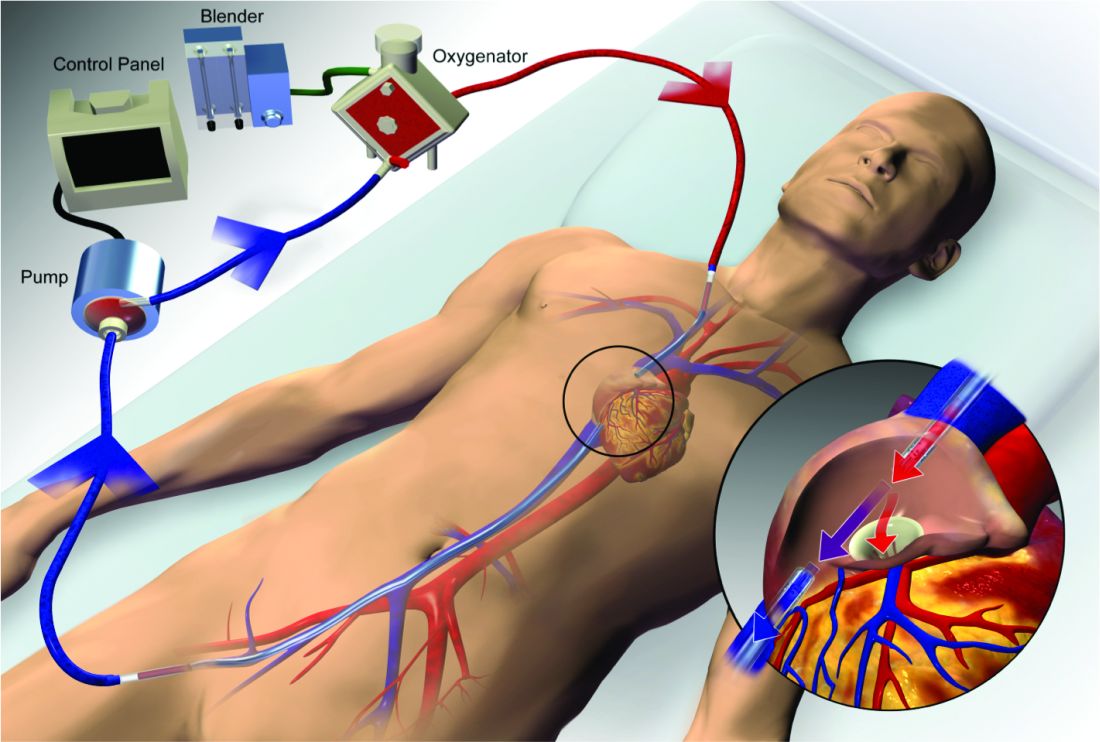
Extracorporeal membrane oxygenation (ECMO) has become increasingly accepted as a rescue therapy for severe respiratory failure from a variety of conditions, though most commonly, the acute respiratory distress syndrome (ARDS) (Thiagarajan R, et al. ASAIO. 2017;63[1]:60). ECMO can provide respiratory or cardiorespiratory support for failing lungs, heart, or both. The most common ECMO configuration used in ARDS is venovenous ECMO, in which blood is withdrawn from a catheter placed in a central vein, pumped through a gas exchange device known as an oxygenator, and returned to the venous system via another catheter. The blood flowing through the oxygenator is separated from a continuous supply of oxygen-rich sweep gas by a semipermeable membrane, across which diffusion-mediated gas exchange occurs, so that the blood exiting it is rich in oxygen and low in carbon dioxide. As venovenous ECMO functions in series with the native circulation, the well-oxygenated blood exiting the ECMO circuit mixes with poorly oxygenated blood flowing through the lungs. Therefore, oxygenation is dependent on native cardiac output to achieve systemic oxygen delivery (Figure 1).
ECMO been used successfully in adults with ARDS since the early 1970s (Hill JD, et al. N Engl J Med. 1972;286[12]:629-34) but, until recently, was limited to small numbers of patients at select global centers and associated with a high-risk profile. In the last decade, however, driven by improvements in ECMO circuit components making the device safer and easier to use, encouraging worldwide experience during the 2009 influenza A (H1N1) pandemic (Davies A, et al. JAMA. 2009;302[17]1888-95), and publication of the Efficacy and Economic Assessment of Conventional Ventilatory Support versus Extracorporeal Membrane Oxygenation for Severe Adult Respiratory Failure (CESAR) trial (Peek GJ, et al. Lancet. 2009;374[9698]:1351-63), ECMO use has markedly increased.
Despite its rapid growth, however, rigorous evidence supporting the use of ECMO has been lacking. The CESAR trial, while impressive in execution, had methodological issues that limited the strength of its conclusions. CESAR was a pragmatic trial that randomized 180 adults with severe respiratory failure from multiple etiologies to conventional management or transfer to an experienced, ECMO-capable center. CESAR met its primary outcome of improved survival without disability in the ECMO-referred group (63% vs 47%, relative risk [RR] 0.69; 95% confidence interval [CI] 0.05 to 0.97, P=.03), but not all patients in that group ultimately received ECMO. In addition, the use of lung protective ventilation was significantly higher in the ECMO-referred group, making it difficult to separate its benefit from that of ECMO. A conservative interpretation is that CESAR showed the clinical benefit of treatment at an ECMO-capable center, experienced in the management of patients with severe respiratory failure.
Not until the release of the Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome (EOLIA) trial earlier this year (Combes A, et al. N Engl J Med. 2018;378[21]:1965-75), did a modern, randomized controlled trial evaluating the use of ECMO itself exist. The EOLIA trial addressed the limitations of CESAR and randomized adult patients with early, severe ARDS to conventional, standard of care management that included a protocolized lung protective strategy in the control group vs immediate initiation of ECMO combined with an ultra-lung protective strategy (targeting end-inspiratory plateau pressure ≤24 cmH2O) in the intervention group. The primary outcome was all-cause mortality at 60 days. Of note, patients enrolled in EOLIA met entry criteria despite greater than 90% of patients receiving neuromuscular blockade and around 60% treated with prone positioning at the time of randomization (importantly, 90% of control group patients ultimately underwent prone positioning).
EOLIA was powered to detect a 20% decrease in mortality in the ECMO group. Based on trial design and the results of the fourth interim analysis, the trial was stopped for futility to reach that endpoint after enrollment of 249 of a maximum 331 patients. Although a 20% mortality reduction was not achieved, 60-day mortality was notably lower in the ECMO-treated group (35% vs 46%, RR 0.76, 95% CI 0.55 to 1.04, P=.09). The key secondary outcome of risk of treatment failure (defined as death in the ECMO group and death or crossover to ECMO in the control group) favored the ECMO group with a RR for mortality of 0.62 (95% CI, 0.47 to 0.82; P<.001), as did other secondary endpoints such as days free of renal and other organ failure.
A major limitation of the trial was that 35 (28%) of control group patients ultimately crossed over to ECMO, which diluted the effect of ECMO observed in the intention-to-treat analysis. Crossover occurred at clinician discretion an average of 6.5 days after randomization and after stringent criteria for crossover was met. These patients were incredibly ill, with a median oxygen saturation of 77%, rapidly worsening inotropic scores, and lactic acidosis; nine individuals had already suffered cardiac arrest, and six had received ECMO as part of extracorporeal cardiopulmonary resuscitation (ECPR), the initiation of venoarterial ECMO during cardiac arrest in attempt to restore spontaneous circulation. Mortality was considerably worse in the crossover group than in conventionally managed cohort overall, and, notably, 33% of patients crossed over to ECMO still survived.
In order to estimate the effect of ECMO on survival times if crossover had not occurred, the authors performed a post-hoc, rank-preserving structural failure time analysis. Though this relies on some assessment regarding the effect of the treatment itself, it showed a hazard ratio for mortality in the ECMO group of 0.51 (95% CI 0.24 to 1.02, P=.055). Although the EOLIA trial was not positive by traditional interpretation, all three major analyses and all secondary endpoints suggest some degree of benefit in patients with severe ARDS managed with ECMO.
Importantly, ECMO was well tolerated (at least when performed at expert centers, as done in this trial). There were significantly more bleeding events and cases of severe thrombocytopenia in the ECMO-treated group, but massive hemorrhage, ischemic and hemorrhagic stroke, arrhythmias, and other complications were similar.
Where do we go from here? Based on the totality of information, it is reasonable to consider ECMO for cases of severe ARDS not responsive to conventional measures, such as a lung protective ventilator strategy, neuromuscular blockade, and prone positioning. Initiation of ECMO may be reasonable prior to implementation of standard of care therapies, in order to permit safe transfer to an experienced center from a center not able to provide them.

Two take-away points: First, it is important to recognize that much of the clinical benefit derived from ECMO may be beyond its ability to normalize gas exchange and be due, at least in part, to the fact that ECMO allows the enhancement of proven lung protective ventilatory strategies. Initiation of ECMO and the “lung rest” it permits reduce the mechanical power applied to the injured alveoli and may attenuate ventilator-induced lung injury, cytokine release, and multiorgan failure that portend poor clinical outcomes in ARDS. Second, ECMO in EOLIA was conducted at expert centers with relatively low rates of complications.
It is too early to know how the critical care community will view ECMO for ARDS in light of EOLIA as well as a growing body of global ECMO experience, or how its wider application may impact the distribution and organization of ECMO centers. Regardless, of paramount importance in using ECMO as a treatment modality is optimizing patient management both prior to and after its initiation.
Dr. Agerstrand is Assistant Professor of Medicine, Director of the Medical ECMO Program, Columbia University College of Physicians and Surgeons, New York-Presbyterian Hospital.
Extracorporeal membrane oxygenation (ECMO) has become increasingly accepted as a rescue therapy for severe respiratory failure from a variety of conditions, though most commonly, the acute respiratory distress syndrome (ARDS) (Thiagarajan R, et al. ASAIO. 2017;63[1]:60). ECMO can provide respiratory or cardiorespiratory support for failing lungs, heart, or both. The most common ECMO configuration used in ARDS is venovenous ECMO, in which blood is withdrawn from a catheter placed in a central vein, pumped through a gas exchange device known as an oxygenator, and returned to the venous system via another catheter. The blood flowing through the oxygenator is separated from a continuous supply of oxygen-rich sweep gas by a semipermeable membrane, across which diffusion-mediated gas exchange occurs, so that the blood exiting it is rich in oxygen and low in carbon dioxide. As venovenous ECMO functions in series with the native circulation, the well-oxygenated blood exiting the ECMO circuit mixes with poorly oxygenated blood flowing through the lungs. Therefore, oxygenation is dependent on native cardiac output to achieve systemic oxygen delivery (Figure 1).
ECMO been used successfully in adults with ARDS since the early 1970s (Hill JD, et al. N Engl J Med. 1972;286[12]:629-34) but, until recently, was limited to small numbers of patients at select global centers and associated with a high-risk profile. In the last decade, however, driven by improvements in ECMO circuit components making the device safer and easier to use, encouraging worldwide experience during the 2009 influenza A (H1N1) pandemic (Davies A, et al. JAMA. 2009;302[17]1888-95), and publication of the Efficacy and Economic Assessment of Conventional Ventilatory Support versus Extracorporeal Membrane Oxygenation for Severe Adult Respiratory Failure (CESAR) trial (Peek GJ, et al. Lancet. 2009;374[9698]:1351-63), ECMO use has markedly increased.
Despite its rapid growth, however, rigorous evidence supporting the use of ECMO has been lacking. The CESAR trial, while impressive in execution, had methodological issues that limited the strength of its conclusions. CESAR was a pragmatic trial that randomized 180 adults with severe respiratory failure from multiple etiologies to conventional management or transfer to an experienced, ECMO-capable center. CESAR met its primary outcome of improved survival without disability in the ECMO-referred group (63% vs 47%, relative risk [RR] 0.69; 95% confidence interval [CI] 0.05 to 0.97, P=.03), but not all patients in that group ultimately received ECMO. In addition, the use of lung protective ventilation was significantly higher in the ECMO-referred group, making it difficult to separate its benefit from that of ECMO. A conservative interpretation is that CESAR showed the clinical benefit of treatment at an ECMO-capable center, experienced in the management of patients with severe respiratory failure.
Not until the release of the Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome (EOLIA) trial earlier this year (Combes A, et al. N Engl J Med. 2018;378[21]:1965-75), did a modern, randomized controlled trial evaluating the use of ECMO itself exist. The EOLIA trial addressed the limitations of CESAR and randomized adult patients with early, severe ARDS to conventional, standard of care management that included a protocolized lung protective strategy in the control group vs immediate initiation of ECMO combined with an ultra-lung protective strategy (targeting end-inspiratory plateau pressure ≤24 cmH2O) in the intervention group. The primary outcome was all-cause mortality at 60 days. Of note, patients enrolled in EOLIA met entry criteria despite greater than 90% of patients receiving neuromuscular blockade and around 60% treated with prone positioning at the time of randomization (importantly, 90% of control group patients ultimately underwent prone positioning).
EOLIA was powered to detect a 20% decrease in mortality in the ECMO group. Based on trial design and the results of the fourth interim analysis, the trial was stopped for futility to reach that endpoint after enrollment of 249 of a maximum 331 patients. Although a 20% mortality reduction was not achieved, 60-day mortality was notably lower in the ECMO-treated group (35% vs 46%, RR 0.76, 95% CI 0.55 to 1.04, P=.09). The key secondary outcome of risk of treatment failure (defined as death in the ECMO group and death or crossover to ECMO in the control group) favored the ECMO group with a RR for mortality of 0.62 (95% CI, 0.47 to 0.82; P<.001), as did other secondary endpoints such as days free of renal and other organ failure.
A major limitation of the trial was that 35 (28%) of control group patients ultimately crossed over to ECMO, which diluted the effect of ECMO observed in the intention-to-treat analysis. Crossover occurred at clinician discretion an average of 6.5 days after randomization and after stringent criteria for crossover was met. These patients were incredibly ill, with a median oxygen saturation of 77%, rapidly worsening inotropic scores, and lactic acidosis; nine individuals had already suffered cardiac arrest, and six had received ECMO as part of extracorporeal cardiopulmonary resuscitation (ECPR), the initiation of venoarterial ECMO during cardiac arrest in attempt to restore spontaneous circulation. Mortality was considerably worse in the crossover group than in conventionally managed cohort overall, and, notably, 33% of patients crossed over to ECMO still survived.
In order to estimate the effect of ECMO on survival times if crossover had not occurred, the authors performed a post-hoc, rank-preserving structural failure time analysis. Though this relies on some assessment regarding the effect of the treatment itself, it showed a hazard ratio for mortality in the ECMO group of 0.51 (95% CI 0.24 to 1.02, P=.055). Although the EOLIA trial was not positive by traditional interpretation, all three major analyses and all secondary endpoints suggest some degree of benefit in patients with severe ARDS managed with ECMO.
Importantly, ECMO was well tolerated (at least when performed at expert centers, as done in this trial). There were significantly more bleeding events and cases of severe thrombocytopenia in the ECMO-treated group, but massive hemorrhage, ischemic and hemorrhagic stroke, arrhythmias, and other complications were similar.
Where do we go from here? Based on the totality of information, it is reasonable to consider ECMO for cases of severe ARDS not responsive to conventional measures, such as a lung protective ventilator strategy, neuromuscular blockade, and prone positioning. Initiation of ECMO may be reasonable prior to implementation of standard of care therapies, in order to permit safe transfer to an experienced center from a center not able to provide them.
Two take-away points: First, it is important to recognize that much of the clinical benefit derived from ECMO may be beyond its ability to normalize gas exchange and be due, at least in part, to the fact that ECMO allows the enhancement of proven lung protective ventilatory strategies. Initiation of ECMO and the “lung rest” it permits reduce the mechanical power applied to the injured alveoli and may attenuate ventilator-induced lung injury, cytokine release, and multiorgan failure that portend poor clinical outcomes in ARDS. Second, ECMO in EOLIA was conducted at expert centers with relatively low rates of complications.
It is too early to know how the critical care community will view ECMO for ARDS in light of EOLIA as well as a growing body of global ECMO experience, or how its wider application may impact the distribution and organization of ECMO centers. Regardless, of paramount importance in using ECMO as a treatment modality is optimizing patient management both prior to and after its initiation.
Dr. Agerstrand is Assistant Professor of Medicine, Director of the Medical ECMO Program, Columbia University College of Physicians and Surgeons, New York-Presbyterian Hospital.
Extracorporeal membrane oxygenation (ECMO) has become increasingly accepted as a rescue therapy for severe respiratory failure from a variety of conditions, though most commonly, the acute respiratory distress syndrome (ARDS) (Thiagarajan R, et al. ASAIO. 2017;63[1]:60). ECMO can provide respiratory or cardiorespiratory support for failing lungs, heart, or both. The most common ECMO configuration used in ARDS is venovenous ECMO, in which blood is withdrawn from a catheter placed in a central vein, pumped through a gas exchange device known as an oxygenator, and returned to the venous system via another catheter. The blood flowing through the oxygenator is separated from a continuous supply of oxygen-rich sweep gas by a semipermeable membrane, across which diffusion-mediated gas exchange occurs, so that the blood exiting it is rich in oxygen and low in carbon dioxide. As venovenous ECMO functions in series with the native circulation, the well-oxygenated blood exiting the ECMO circuit mixes with poorly oxygenated blood flowing through the lungs. Therefore, oxygenation is dependent on native cardiac output to achieve systemic oxygen delivery (Figure 1).
ECMO been used successfully in adults with ARDS since the early 1970s (Hill JD, et al. N Engl J Med. 1972;286[12]:629-34) but, until recently, was limited to small numbers of patients at select global centers and associated with a high-risk profile. In the last decade, however, driven by improvements in ECMO circuit components making the device safer and easier to use, encouraging worldwide experience during the 2009 influenza A (H1N1) pandemic (Davies A, et al. JAMA. 2009;302[17]1888-95), and publication of the Efficacy and Economic Assessment of Conventional Ventilatory Support versus Extracorporeal Membrane Oxygenation for Severe Adult Respiratory Failure (CESAR) trial (Peek GJ, et al. Lancet. 2009;374[9698]:1351-63), ECMO use has markedly increased.
Despite its rapid growth, however, rigorous evidence supporting the use of ECMO has been lacking. The CESAR trial, while impressive in execution, had methodological issues that limited the strength of its conclusions. CESAR was a pragmatic trial that randomized 180 adults with severe respiratory failure from multiple etiologies to conventional management or transfer to an experienced, ECMO-capable center. CESAR met its primary outcome of improved survival without disability in the ECMO-referred group (63% vs 47%, relative risk [RR] 0.69; 95% confidence interval [CI] 0.05 to 0.97, P=.03), but not all patients in that group ultimately received ECMO. In addition, the use of lung protective ventilation was significantly higher in the ECMO-referred group, making it difficult to separate its benefit from that of ECMO. A conservative interpretation is that CESAR showed the clinical benefit of treatment at an ECMO-capable center, experienced in the management of patients with severe respiratory failure.
Not until the release of the Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome (EOLIA) trial earlier this year (Combes A, et al. N Engl J Med. 2018;378[21]:1965-75), did a modern, randomized controlled trial evaluating the use of ECMO itself exist. The EOLIA trial addressed the limitations of CESAR and randomized adult patients with early, severe ARDS to conventional, standard of care management that included a protocolized lung protective strategy in the control group vs immediate initiation of ECMO combined with an ultra-lung protective strategy (targeting end-inspiratory plateau pressure ≤24 cmH2O) in the intervention group. The primary outcome was all-cause mortality at 60 days. Of note, patients enrolled in EOLIA met entry criteria despite greater than 90% of patients receiving neuromuscular blockade and around 60% treated with prone positioning at the time of randomization (importantly, 90% of control group patients ultimately underwent prone positioning).
EOLIA was powered to detect a 20% decrease in mortality in the ECMO group. Based on trial design and the results of the fourth interim analysis, the trial was stopped for futility to reach that endpoint after enrollment of 249 of a maximum 331 patients. Although a 20% mortality reduction was not achieved, 60-day mortality was notably lower in the ECMO-treated group (35% vs 46%, RR 0.76, 95% CI 0.55 to 1.04, P=.09). The key secondary outcome of risk of treatment failure (defined as death in the ECMO group and death or crossover to ECMO in the control group) favored the ECMO group with a RR for mortality of 0.62 (95% CI, 0.47 to 0.82; P<.001), as did other secondary endpoints such as days free of renal and other organ failure.
A major limitation of the trial was that 35 (28%) of control group patients ultimately crossed over to ECMO, which diluted the effect of ECMO observed in the intention-to-treat analysis. Crossover occurred at clinician discretion an average of 6.5 days after randomization and after stringent criteria for crossover was met. These patients were incredibly ill, with a median oxygen saturation of 77%, rapidly worsening inotropic scores, and lactic acidosis; nine individuals had already suffered cardiac arrest, and six had received ECMO as part of extracorporeal cardiopulmonary resuscitation (ECPR), the initiation of venoarterial ECMO during cardiac arrest in attempt to restore spontaneous circulation. Mortality was considerably worse in the crossover group than in conventionally managed cohort overall, and, notably, 33% of patients crossed over to ECMO still survived.
In order to estimate the effect of ECMO on survival times if crossover had not occurred, the authors performed a post-hoc, rank-preserving structural failure time analysis. Though this relies on some assessment regarding the effect of the treatment itself, it showed a hazard ratio for mortality in the ECMO group of 0.51 (95% CI 0.24 to 1.02, P=.055). Although the EOLIA trial was not positive by traditional interpretation, all three major analyses and all secondary endpoints suggest some degree of benefit in patients with severe ARDS managed with ECMO.
Importantly, ECMO was well tolerated (at least when performed at expert centers, as done in this trial). There were significantly more bleeding events and cases of severe thrombocytopenia in the ECMO-treated group, but massive hemorrhage, ischemic and hemorrhagic stroke, arrhythmias, and other complications were similar.
Where do we go from here? Based on the totality of information, it is reasonable to consider ECMO for cases of severe ARDS not responsive to conventional measures, such as a lung protective ventilator strategy, neuromuscular blockade, and prone positioning. Initiation of ECMO may be reasonable prior to implementation of standard of care therapies, in order to permit safe transfer to an experienced center from a center not able to provide them.
Two take-away points: First, it is important to recognize that much of the clinical benefit derived from ECMO may be beyond its ability to normalize gas exchange and be due, at least in part, to the fact that ECMO allows the enhancement of proven lung protective ventilatory strategies. Initiation of ECMO and the “lung rest” it permits reduce the mechanical power applied to the injured alveoli and may attenuate ventilator-induced lung injury, cytokine release, and multiorgan failure that portend poor clinical outcomes in ARDS. Second, ECMO in EOLIA was conducted at expert centers with relatively low rates of complications.
It is too early to know how the critical care community will view ECMO for ARDS in light of EOLIA as well as a growing body of global ECMO experience, or how its wider application may impact the distribution and organization of ECMO centers. Regardless, of paramount importance in using ECMO as a treatment modality is optimizing patient management both prior to and after its initiation.
Dr. Agerstrand is Assistant Professor of Medicine, Director of the Medical ECMO Program, Columbia University College of Physicians and Surgeons, New York-Presbyterian Hospital.
National Board of Echocardiography offering board exam
Due to significant interest in the pulmonary/critical care community, the National Board of Echocardiography (NBE) has opened registration for a board examination as a requirement for national level certification in advanced critical care echocardiography (ACCE). The examination has been developed by the National Board of Medical Examiners; CHEST and the other professional societies are well represented on the writing committee. The first examination is scheduled to be given on January 15, 2019.
The board of the NBE will be the final arbiter for other requirements for certification. We anticipate that these will be available in 2019.
A few essential questions about the certification:
1. Who will be eligible for certification in ACCE?
The policy of the NBE is that any licensed physician may take the examination. Passing the examination confers testamur status, which is only one of several requirements for certification. The board of the NBE will make the final decision as to how to define the clinical background of the candidate that will be required for certification.
2. What will be the requirements for demonstration of competence at image acquisition for ACCE?
Competence at ACCE requires that the intensivist be expert at image acquisition of a comprehensive image set. The board of the NBE will make the final decision as to what constitutes a full ACCE image set, how many studies must be performed by the candidate, and how the studies will be documented. Regarding the latter question, it is likely that there will be a need for identification of qualified mentors to guide the candidate through the process of demonstrating competence in image acquisition.
3. What resources exist to learn more about the examination?
For some suggestions regarding mastery of the cognitive base, Dr. Yonatan Greenstein has set up an independent website that has recommendations about study material and an example of the full ACCE image set (advancedcriticalcareecho.org). The NBE website has a list of subjects that will be covered in the examination. In addition to passing the examination, there will be other elements required for ACCE certification. The NBE has not yet made final decision on the additional requirements. As soon as they are available, they will be posted on the NBE website (echoboards.org).
There is keen interest amongst fellows and junior attendings in the NBE certification who are already competent in whole body ultrasonography. They see ACCE as a natural and necessary extension of their scope of practice, as a means of better helping their critically ill patients, and as a means of acquiring a unique skill that defines them as having a special skill compared with other intensivists. A smaller group of senior attending intensivists are primarily motivated by a well-defined practice-related need of skill at ACCE and/or a strong perception that knowledge of ACCE may directly improve their ability to care for the critically ill patient. Interest in certification extends across the various specialties that provide critical care services. The NBE has indicated that there has been a strong showing of registrations for the examination thus far.
We recommend that candidates for certification consider that passing the examination should be the priority. Collection of the image set may occur in parallel, as the two will complement each other. Preparation for the examination requires intensive study of the cognitive base of ACCE and mastery of image interpretation.
To aid in preparation for the ACCE examination, CHEST is offering a comprehensive review course, Advanced Critical Care Echocardiography Board Review Exam Course, being held at the CHEST Innovation, Simulation, and Training Center, December 7-8, 2018, in Glenview, Illinois.
Due to significant interest in the pulmonary/critical care community, the National Board of Echocardiography (NBE) has opened registration for a board examination as a requirement for national level certification in advanced critical care echocardiography (ACCE). The examination has been developed by the National Board of Medical Examiners; CHEST and the other professional societies are well represented on the writing committee. The first examination is scheduled to be given on January 15, 2019.
The board of the NBE will be the final arbiter for other requirements for certification. We anticipate that these will be available in 2019.
A few essential questions about the certification:
1. Who will be eligible for certification in ACCE?
The policy of the NBE is that any licensed physician may take the examination. Passing the examination confers testamur status, which is only one of several requirements for certification. The board of the NBE will make the final decision as to how to define the clinical background of the candidate that will be required for certification.
2. What will be the requirements for demonstration of competence at image acquisition for ACCE?
Competence at ACCE requires that the intensivist be expert at image acquisition of a comprehensive image set. The board of the NBE will make the final decision as to what constitutes a full ACCE image set, how many studies must be performed by the candidate, and how the studies will be documented. Regarding the latter question, it is likely that there will be a need for identification of qualified mentors to guide the candidate through the process of demonstrating competence in image acquisition.
3. What resources exist to learn more about the examination?
For some suggestions regarding mastery of the cognitive base, Dr. Yonatan Greenstein has set up an independent website that has recommendations about study material and an example of the full ACCE image set (advancedcriticalcareecho.org). The NBE website has a list of subjects that will be covered in the examination. In addition to passing the examination, there will be other elements required for ACCE certification. The NBE has not yet made final decision on the additional requirements. As soon as they are available, they will be posted on the NBE website (echoboards.org).
There is keen interest amongst fellows and junior attendings in the NBE certification who are already competent in whole body ultrasonography. They see ACCE as a natural and necessary extension of their scope of practice, as a means of better helping their critically ill patients, and as a means of acquiring a unique skill that defines them as having a special skill compared with other intensivists. A smaller group of senior attending intensivists are primarily motivated by a well-defined practice-related need of skill at ACCE and/or a strong perception that knowledge of ACCE may directly improve their ability to care for the critically ill patient. Interest in certification extends across the various specialties that provide critical care services. The NBE has indicated that there has been a strong showing of registrations for the examination thus far.
We recommend that candidates for certification consider that passing the examination should be the priority. Collection of the image set may occur in parallel, as the two will complement each other. Preparation for the examination requires intensive study of the cognitive base of ACCE and mastery of image interpretation.
To aid in preparation for the ACCE examination, CHEST is offering a comprehensive review course, Advanced Critical Care Echocardiography Board Review Exam Course, being held at the CHEST Innovation, Simulation, and Training Center, December 7-8, 2018, in Glenview, Illinois.
Due to significant interest in the pulmonary/critical care community, the National Board of Echocardiography (NBE) has opened registration for a board examination as a requirement for national level certification in advanced critical care echocardiography (ACCE). The examination has been developed by the National Board of Medical Examiners; CHEST and the other professional societies are well represented on the writing committee. The first examination is scheduled to be given on January 15, 2019.
The board of the NBE will be the final arbiter for other requirements for certification. We anticipate that these will be available in 2019.
A few essential questions about the certification:
1. Who will be eligible for certification in ACCE?
The policy of the NBE is that any licensed physician may take the examination. Passing the examination confers testamur status, which is only one of several requirements for certification. The board of the NBE will make the final decision as to how to define the clinical background of the candidate that will be required for certification.
2. What will be the requirements for demonstration of competence at image acquisition for ACCE?
Competence at ACCE requires that the intensivist be expert at image acquisition of a comprehensive image set. The board of the NBE will make the final decision as to what constitutes a full ACCE image set, how many studies must be performed by the candidate, and how the studies will be documented. Regarding the latter question, it is likely that there will be a need for identification of qualified mentors to guide the candidate through the process of demonstrating competence in image acquisition.
3. What resources exist to learn more about the examination?
For some suggestions regarding mastery of the cognitive base, Dr. Yonatan Greenstein has set up an independent website that has recommendations about study material and an example of the full ACCE image set (advancedcriticalcareecho.org). The NBE website has a list of subjects that will be covered in the examination. In addition to passing the examination, there will be other elements required for ACCE certification. The NBE has not yet made final decision on the additional requirements. As soon as they are available, they will be posted on the NBE website (echoboards.org).
There is keen interest amongst fellows and junior attendings in the NBE certification who are already competent in whole body ultrasonography. They see ACCE as a natural and necessary extension of their scope of practice, as a means of better helping their critically ill patients, and as a means of acquiring a unique skill that defines them as having a special skill compared with other intensivists. A smaller group of senior attending intensivists are primarily motivated by a well-defined practice-related need of skill at ACCE and/or a strong perception that knowledge of ACCE may directly improve their ability to care for the critically ill patient. Interest in certification extends across the various specialties that provide critical care services. The NBE has indicated that there has been a strong showing of registrations for the examination thus far.
We recommend that candidates for certification consider that passing the examination should be the priority. Collection of the image set may occur in parallel, as the two will complement each other. Preparation for the examination requires intensive study of the cognitive base of ACCE and mastery of image interpretation.
To aid in preparation for the ACCE examination, CHEST is offering a comprehensive review course, Advanced Critical Care Echocardiography Board Review Exam Course, being held at the CHEST Innovation, Simulation, and Training Center, December 7-8, 2018, in Glenview, Illinois.
Interventional Chest/Diagnostic Procedures
Interventional Chest/Diagnostic Procedures
Endobronchial valve therapy receives FDA approval for bronchoscopic LVR
Lung volume reduction surgery (LVRS) is an established approach to improve exercise capacity and lung function in patients with heterogeneous emphysema and may confer survival benefit in patients with apical-predominant disease (Fishman, et al. N Engl J Med. 2003;348[21]:2059). Despite this, LVRS case numbers remain low due to patient and procedural morbidity. Bronchoscopic alternatives for LVRS have advanced considerably over the last decade with endobronchial valve (EBV) therapy emerging as a viable option for select subsets of patients with heterogeneous emphysema. Endobronchial valves are removable devices placed in segmental/subsegmental airways, which allow efflux of air during exhalation but close during inspiration, resulting in distal atelectasis in the absence of collateral ventilation.
The LIBERATE study, a multicenter randomized controlled trial demonstrated improvement in FEV1 ≥15% in 48% of patients after EBV placement compared with 17% of patients receiving standard medical therapy has resulted in FDA approval (Criner G, et al. Am J Respir Crit Care Med. 2018 May 22. doi: 10.1164/rccm.201803-0590OC. [Epub ahead of print]). Patients with EBV had improved subjective dyspnea scores, residual volume, and 6-minute walk distance; however, the pneumothorax rate was 27%.
All study patients with EBV underwent bronchoscopic evaluation for collateral ventilation using a proprietary digital system, which measures expiratory airflow in target airways to establish the presence of collateral ventilation. Previous data have demonstrated improved transplant-free survival when implanted EBVs result in atelectasis of the target lobe, which requires intact interlobar fissures (Garner, et al. Am J Respir Crit Care Med. 2016;194[4]:519). Ongoing clinical trials are attempting to clarify the role of EBV therapy in different phenotypes of COPD, including patients with homogenous emphysema. Long-term follow-up data will be important in determining the broader implementation of bronchoscopic lung volume reduction moving forward.
Vivek Murthy, MD
Jason A. Akulian, MD, FCCP
Steering Committee Members
Pediatric Chest Medicine
CFTR modulators
Cystic fibrosis (CF) is a progressive genetic disorder resulting in multiorgan disease with progressive respiratory decline. CF is caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene. This codes for the CFTR anion channel and contributes to the movement of salt in and out of the cell. CFTR dysfunction leads to thickened secretions in the lungs and other organs, such as the gut and pancreas. This leads to more lung infections and other organ dysfunction that ultimately leads to premature death.

Established CF treatments include pulmonary and nutritional interventions. CFTR modulators are recent novel therapies that improve the function of CFTR and target the basic defect. Two types of modulator drugs (potentiators and correctors) have been developed with effectiveness depending upon the kind of CF mutation the person has.
CFTR potentiators, such as Kalydeco® (ivacaftor monotherapy), increase the likelihood that the CFTR channel will transport ions through the cell membrane, ie, they increase the channel’s “open probability.” Kalydeco has been approved for patients 12 months or older with mutations that result in partial CFTR protein function in the cell membrane. CFTR correctors, such as lumacaftor and tezacaftor, increase the amount of normal or mutated CFTR protein that gets transported, increasing the amount of CFTR protein on the cell surface. Combination drugs such as Orkambi® (lumacaftor/ivacaftor) for patients 2 years and older, and Symdeko™ (tezacaftor/ivacaftor) for patients 12 years and older, are considered in patients homozygous for the F508del mutation.
Sumit Bhargava, MBBS, FCCP
Steering Committee Member
Pulmonary Physiology, Function, and Rehabilitation
Wildfires, particulate matter, and lung function
In the last 3 decades, human-caused climate change contributed to wildfires in an additional 4.2 million hectares of land across the western US alone. Human impact on climate is responsible for nearly doubling the expected wildfire area (Abatzoglou, et al. PNAS. 2016;113:11770). Year 2017 saw the most destructive wildfires in California recorded to date, and over $2 billion dollars was spent by the US Forest Service, the most-expensive on record. Besides the devastating effects on the forestry and nearby communities, wildfires also generate a large amount of particulate matter (PM). In western US, wildfires contributed to 71.3% of total PM2.5 on days exceeding regulatory PM2.5 standards during 2004-2009 (Liu et al. Clim Change. 2016;138:655). Acute PM exposure is associated with respiratory health effects, such as exacerbation of asthma and COPD, increased ED visits and hospitalization for pneumonia, and increased mortality. Chronic PM2.5 exposure may also affect lung function. Cross-shift and cross-season FEV1 declined by 0.150 L and 0.104 L, respectively in forest firefighters (Betchley, et al. Am. J Ind Med. 1997;31:503). The Children’s Health Study conducted in California found that subjects who were exposed to the highest level of exposure to PM2.5 were five times more likely to have an FEV1 less than 80% of expected FEV1 when they reached 18 years of age than subjects exposed to the lowest level of PM2.5 (Gauderman et al. N Engl J Med. 2004;351:1057). Clinicians should educate patients and the public how to protect our environment and, when wildfires occur, how to protect themselves from exposure to PM.
Thomas W. DeCato, MD
Fellow-in-Training Committee Member
Yuh-Chin T. Huang, MD, FCCP
Steering Committee Member
Pulmonary Vascular Disease
Small increases in pulmonary pressures—big impact
Pulmonary hypertension (PH) is a progressive, life-limiting pulmonary vascular disease that is diagnosed hemodynamically by right-sided heart catheterization (RHC) and defined by a mean pulmonary artery pressure (mPAP) >25 mm Hg (Hoeper MM, et al. JACC. 2013;62(25 Suppl):D42).

The impact of PH on survival both in its “pure” form, pulmonary arterial hypertension, and in the setting of underlying cardiopulmonary disease, is well established. However, the clinical relevance of mildly elevated mPAP, defined as mPAP between 18 and 24 mm Hg, has been unclear until recently. Two large cohort studies have suggested that mild increases in mPAP are clinically relevant. A large retrospective analysis of hemodynamic data from 21,727 US veterans found mildly increased mPAP (19-24 mm Hg) was associated with increased hospitalization and decreased survival (Maron, et al. Circulation. 2016;133:1240).

While this population was skewed toward elderly men, a study from Vanderbilt University that included equal numbers of men and women showed similar results. Patients with mPAP 19-24 mm Hg experienced incrementally increased mortality (HR:1.31, P=.001). Importantly, in the subset of patients who underwent a repeat RHC in follow-up, 61% developed progressive increases of pulmonary pressures (>25 mm Hg) on follow-up RHC suggesting that the disease process may progress in a substantial proportion of patients (Assad, et al. JAMA Cardiol. 2017;2[1]):1361). Combined with prior data from smaller cohorts, these studies highlight the impact of mildly increased pulmonary pressures on outcomes. Given the dearth of available data regarding interventions for these patients, there is an urgent need to study to role of specific therapy for mildly elevated pulmonary pressures.
Vijay Balasubramanian, MD, FCCP
Steering Committee Member
Jean Elwing, MD, FCCP
Steering Committee Vice-Chair
Thoracic Oncology
Multiple tumor nodules in lung cancer diagnosis
Low dose CT (LDCT) scan screening for lung cancer is a recommended preventative modality for adults with a significant smoking history (Mayer et al. Ann Int Med. 2014;160(5):330). The screening approach aims to identify adults at significant risk for lung cancer. The goal is to discover lung cancers at low stage with benign mediastinal nodes for optimal treatment and potential for cure. In a minority, but significant number of cases, the LDCT demonstrates multiple lung nodules or masses confounding the attempt to adequately stage the tumor. Two tumors representing a primary cancer and separate malignant spread, namely, intra-pulmonary metastases, in the same lobe, different ipsilateral lobe, or contralateral lobe would be staged, respectively, as T3, T4, or M1a (Detterbeck et al. Chest. 2013;143(5):e191S). Clearly, if the two tumors are separate unique primary cancers, independent of one another, then at best they would be considered as multiple T1 tumors. The treatment modalities of and clinical survival outcomes for these multiple conditions would be markedly different.
The identification of additional tumors may be synchronous (at the same time of the primary discovery) or metachronous (at a later time than the primary discovery). The approach is basically the same. Two tumors with different histologic types, or having separate in-situ squamous cell carcinoma patterns, or disparate immunohistochemical or molecular expressions, or different genomic profiles or driver mutations may be considered as separate distinct primary malignancies (Detterbeck et al. J Thorac Oncol. 2016;11:639; Nicholson et al. J Thorac Oncol. 2017;13:205). Separate foci of ground-glass opacities with small solid central component indicative of minimally invasive adenocarcinoma may be designated as the highest T-stage. These cited and more challenging cases should be presented to a lung cancer tumor board with multiple specialties represented for analysis and judgment. The approach to diagnostic decision-making and clinical management should involve the expertise of all specialties in the lung cancer patient care team.
Arnold M. Schwartz, MD, PhD, FCCP
Steering Committee Member
Interventional Chest/Diagnostic Procedures
Endobronchial valve therapy receives FDA approval for bronchoscopic LVR
Lung volume reduction surgery (LVRS) is an established approach to improve exercise capacity and lung function in patients with heterogeneous emphysema and may confer survival benefit in patients with apical-predominant disease (Fishman, et al. N Engl J Med. 2003;348[21]:2059). Despite this, LVRS case numbers remain low due to patient and procedural morbidity. Bronchoscopic alternatives for LVRS have advanced considerably over the last decade with endobronchial valve (EBV) therapy emerging as a viable option for select subsets of patients with heterogeneous emphysema. Endobronchial valves are removable devices placed in segmental/subsegmental airways, which allow efflux of air during exhalation but close during inspiration, resulting in distal atelectasis in the absence of collateral ventilation.
The LIBERATE study, a multicenter randomized controlled trial demonstrated improvement in FEV1 ≥15% in 48% of patients after EBV placement compared with 17% of patients receiving standard medical therapy has resulted in FDA approval (Criner G, et al. Am J Respir Crit Care Med. 2018 May 22. doi: 10.1164/rccm.201803-0590OC. [Epub ahead of print]). Patients with EBV had improved subjective dyspnea scores, residual volume, and 6-minute walk distance; however, the pneumothorax rate was 27%.
All study patients with EBV underwent bronchoscopic evaluation for collateral ventilation using a proprietary digital system, which measures expiratory airflow in target airways to establish the presence of collateral ventilation. Previous data have demonstrated improved transplant-free survival when implanted EBVs result in atelectasis of the target lobe, which requires intact interlobar fissures (Garner, et al. Am J Respir Crit Care Med. 2016;194[4]:519). Ongoing clinical trials are attempting to clarify the role of EBV therapy in different phenotypes of COPD, including patients with homogenous emphysema. Long-term follow-up data will be important in determining the broader implementation of bronchoscopic lung volume reduction moving forward.
Vivek Murthy, MD
Jason A. Akulian, MD, FCCP
Steering Committee Members
Pediatric Chest Medicine
CFTR modulators
Cystic fibrosis (CF) is a progressive genetic disorder resulting in multiorgan disease with progressive respiratory decline. CF is caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene. This codes for the CFTR anion channel and contributes to the movement of salt in and out of the cell. CFTR dysfunction leads to thickened secretions in the lungs and other organs, such as the gut and pancreas. This leads to more lung infections and other organ dysfunction that ultimately leads to premature death.
Established CF treatments include pulmonary and nutritional interventions. CFTR modulators are recent novel therapies that improve the function of CFTR and target the basic defect. Two types of modulator drugs (potentiators and correctors) have been developed with effectiveness depending upon the kind of CF mutation the person has.
CFTR potentiators, such as Kalydeco® (ivacaftor monotherapy), increase the likelihood that the CFTR channel will transport ions through the cell membrane, ie, they increase the channel’s “open probability.” Kalydeco has been approved for patients 12 months or older with mutations that result in partial CFTR protein function in the cell membrane. CFTR correctors, such as lumacaftor and tezacaftor, increase the amount of normal or mutated CFTR protein that gets transported, increasing the amount of CFTR protein on the cell surface. Combination drugs such as Orkambi® (lumacaftor/ivacaftor) for patients 2 years and older, and Symdeko™ (tezacaftor/ivacaftor) for patients 12 years and older, are considered in patients homozygous for the F508del mutation.
Sumit Bhargava, MBBS, FCCP
Steering Committee Member
Pulmonary Physiology, Function, and Rehabilitation
Wildfires, particulate matter, and lung function
In the last 3 decades, human-caused climate change contributed to wildfires in an additional 4.2 million hectares of land across the western US alone. Human impact on climate is responsible for nearly doubling the expected wildfire area (Abatzoglou, et al. PNAS. 2016;113:11770). Year 2017 saw the most destructive wildfires in California recorded to date, and over $2 billion dollars was spent by the US Forest Service, the most-expensive on record. Besides the devastating effects on the forestry and nearby communities, wildfires also generate a large amount of particulate matter (PM). In western US, wildfires contributed to 71.3% of total PM2.5 on days exceeding regulatory PM2.5 standards during 2004-2009 (Liu et al. Clim Change. 2016;138:655). Acute PM exposure is associated with respiratory health effects, such as exacerbation of asthma and COPD, increased ED visits and hospitalization for pneumonia, and increased mortality. Chronic PM2.5 exposure may also affect lung function. Cross-shift and cross-season FEV1 declined by 0.150 L and 0.104 L, respectively in forest firefighters (Betchley, et al. Am. J Ind Med. 1997;31:503). The Children’s Health Study conducted in California found that subjects who were exposed to the highest level of exposure to PM2.5 were five times more likely to have an FEV1 less than 80% of expected FEV1 when they reached 18 years of age than subjects exposed to the lowest level of PM2.5 (Gauderman et al. N Engl J Med. 2004;351:1057). Clinicians should educate patients and the public how to protect our environment and, when wildfires occur, how to protect themselves from exposure to PM.
Thomas W. DeCato, MD
Fellow-in-Training Committee Member
Yuh-Chin T. Huang, MD, FCCP
Steering Committee Member
Pulmonary Vascular Disease
Small increases in pulmonary pressures—big impact
Pulmonary hypertension (PH) is a progressive, life-limiting pulmonary vascular disease that is diagnosed hemodynamically by right-sided heart catheterization (RHC) and defined by a mean pulmonary artery pressure (mPAP) >25 mm Hg (Hoeper MM, et al. JACC. 2013;62(25 Suppl):D42).
The impact of PH on survival both in its “pure” form, pulmonary arterial hypertension, and in the setting of underlying cardiopulmonary disease, is well established. However, the clinical relevance of mildly elevated mPAP, defined as mPAP between 18 and 24 mm Hg, has been unclear until recently. Two large cohort studies have suggested that mild increases in mPAP are clinically relevant. A large retrospective analysis of hemodynamic data from 21,727 US veterans found mildly increased mPAP (19-24 mm Hg) was associated with increased hospitalization and decreased survival (Maron, et al. Circulation. 2016;133:1240).
While this population was skewed toward elderly men, a study from Vanderbilt University that included equal numbers of men and women showed similar results. Patients with mPAP 19-24 mm Hg experienced incrementally increased mortality (HR:1.31, P=.001). Importantly, in the subset of patients who underwent a repeat RHC in follow-up, 61% developed progressive increases of pulmonary pressures (>25 mm Hg) on follow-up RHC suggesting that the disease process may progress in a substantial proportion of patients (Assad, et al. JAMA Cardiol. 2017;2[1]):1361). Combined with prior data from smaller cohorts, these studies highlight the impact of mildly increased pulmonary pressures on outcomes. Given the dearth of available data regarding interventions for these patients, there is an urgent need to study to role of specific therapy for mildly elevated pulmonary pressures.
Vijay Balasubramanian, MD, FCCP
Steering Committee Member
Jean Elwing, MD, FCCP
Steering Committee Vice-Chair
Thoracic Oncology
Multiple tumor nodules in lung cancer diagnosis
Low dose CT (LDCT) scan screening for lung cancer is a recommended preventative modality for adults with a significant smoking history (Mayer et al. Ann Int Med. 2014;160(5):330). The screening approach aims to identify adults at significant risk for lung cancer. The goal is to discover lung cancers at low stage with benign mediastinal nodes for optimal treatment and potential for cure. In a minority, but significant number of cases, the LDCT demonstrates multiple lung nodules or masses confounding the attempt to adequately stage the tumor. Two tumors representing a primary cancer and separate malignant spread, namely, intra-pulmonary metastases, in the same lobe, different ipsilateral lobe, or contralateral lobe would be staged, respectively, as T3, T4, or M1a (Detterbeck et al. Chest. 2013;143(5):e191S). Clearly, if the two tumors are separate unique primary cancers, independent of one another, then at best they would be considered as multiple T1 tumors. The treatment modalities of and clinical survival outcomes for these multiple conditions would be markedly different.
The identification of additional tumors may be synchronous (at the same time of the primary discovery) or metachronous (at a later time than the primary discovery). The approach is basically the same. Two tumors with different histologic types, or having separate in-situ squamous cell carcinoma patterns, or disparate immunohistochemical or molecular expressions, or different genomic profiles or driver mutations may be considered as separate distinct primary malignancies (Detterbeck et al. J Thorac Oncol. 2016;11:639; Nicholson et al. J Thorac Oncol. 2017;13:205). Separate foci of ground-glass opacities with small solid central component indicative of minimally invasive adenocarcinoma may be designated as the highest T-stage. These cited and more challenging cases should be presented to a lung cancer tumor board with multiple specialties represented for analysis and judgment. The approach to diagnostic decision-making and clinical management should involve the expertise of all specialties in the lung cancer patient care team.
Arnold M. Schwartz, MD, PhD, FCCP
Steering Committee Member
Interventional Chest/Diagnostic Procedures
Endobronchial valve therapy receives FDA approval for bronchoscopic LVR
Lung volume reduction surgery (LVRS) is an established approach to improve exercise capacity and lung function in patients with heterogeneous emphysema and may confer survival benefit in patients with apical-predominant disease (Fishman, et al. N Engl J Med. 2003;348[21]:2059). Despite this, LVRS case numbers remain low due to patient and procedural morbidity. Bronchoscopic alternatives for LVRS have advanced considerably over the last decade with endobronchial valve (EBV) therapy emerging as a viable option for select subsets of patients with heterogeneous emphysema. Endobronchial valves are removable devices placed in segmental/subsegmental airways, which allow efflux of air during exhalation but close during inspiration, resulting in distal atelectasis in the absence of collateral ventilation.
The LIBERATE study, a multicenter randomized controlled trial demonstrated improvement in FEV1 ≥15% in 48% of patients after EBV placement compared with 17% of patients receiving standard medical therapy has resulted in FDA approval (Criner G, et al. Am J Respir Crit Care Med. 2018 May 22. doi: 10.1164/rccm.201803-0590OC. [Epub ahead of print]). Patients with EBV had improved subjective dyspnea scores, residual volume, and 6-minute walk distance; however, the pneumothorax rate was 27%.
All study patients with EBV underwent bronchoscopic evaluation for collateral ventilation using a proprietary digital system, which measures expiratory airflow in target airways to establish the presence of collateral ventilation. Previous data have demonstrated improved transplant-free survival when implanted EBVs result in atelectasis of the target lobe, which requires intact interlobar fissures (Garner, et al. Am J Respir Crit Care Med. 2016;194[4]:519). Ongoing clinical trials are attempting to clarify the role of EBV therapy in different phenotypes of COPD, including patients with homogenous emphysema. Long-term follow-up data will be important in determining the broader implementation of bronchoscopic lung volume reduction moving forward.
Vivek Murthy, MD
Jason A. Akulian, MD, FCCP
Steering Committee Members
Pediatric Chest Medicine
CFTR modulators
Cystic fibrosis (CF) is a progressive genetic disorder resulting in multiorgan disease with progressive respiratory decline. CF is caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene. This codes for the CFTR anion channel and contributes to the movement of salt in and out of the cell. CFTR dysfunction leads to thickened secretions in the lungs and other organs, such as the gut and pancreas. This leads to more lung infections and other organ dysfunction that ultimately leads to premature death.
Established CF treatments include pulmonary and nutritional interventions. CFTR modulators are recent novel therapies that improve the function of CFTR and target the basic defect. Two types of modulator drugs (potentiators and correctors) have been developed with effectiveness depending upon the kind of CF mutation the person has.
CFTR potentiators, such as Kalydeco® (ivacaftor monotherapy), increase the likelihood that the CFTR channel will transport ions through the cell membrane, ie, they increase the channel’s “open probability.” Kalydeco has been approved for patients 12 months or older with mutations that result in partial CFTR protein function in the cell membrane. CFTR correctors, such as lumacaftor and tezacaftor, increase the amount of normal or mutated CFTR protein that gets transported, increasing the amount of CFTR protein on the cell surface. Combination drugs such as Orkambi® (lumacaftor/ivacaftor) for patients 2 years and older, and Symdeko™ (tezacaftor/ivacaftor) for patients 12 years and older, are considered in patients homozygous for the F508del mutation.
Sumit Bhargava, MBBS, FCCP
Steering Committee Member
Pulmonary Physiology, Function, and Rehabilitation
Wildfires, particulate matter, and lung function
In the last 3 decades, human-caused climate change contributed to wildfires in an additional 4.2 million hectares of land across the western US alone. Human impact on climate is responsible for nearly doubling the expected wildfire area (Abatzoglou, et al. PNAS. 2016;113:11770). Year 2017 saw the most destructive wildfires in California recorded to date, and over $2 billion dollars was spent by the US Forest Service, the most-expensive on record. Besides the devastating effects on the forestry and nearby communities, wildfires also generate a large amount of particulate matter (PM). In western US, wildfires contributed to 71.3% of total PM2.5 on days exceeding regulatory PM2.5 standards during 2004-2009 (Liu et al. Clim Change. 2016;138:655). Acute PM exposure is associated with respiratory health effects, such as exacerbation of asthma and COPD, increased ED visits and hospitalization for pneumonia, and increased mortality. Chronic PM2.5 exposure may also affect lung function. Cross-shift and cross-season FEV1 declined by 0.150 L and 0.104 L, respectively in forest firefighters (Betchley, et al. Am. J Ind Med. 1997;31:503). The Children’s Health Study conducted in California found that subjects who were exposed to the highest level of exposure to PM2.5 were five times more likely to have an FEV1 less than 80% of expected FEV1 when they reached 18 years of age than subjects exposed to the lowest level of PM2.5 (Gauderman et al. N Engl J Med. 2004;351:1057). Clinicians should educate patients and the public how to protect our environment and, when wildfires occur, how to protect themselves from exposure to PM.
Thomas W. DeCato, MD
Fellow-in-Training Committee Member
Yuh-Chin T. Huang, MD, FCCP
Steering Committee Member
Pulmonary Vascular Disease
Small increases in pulmonary pressures—big impact
Pulmonary hypertension (PH) is a progressive, life-limiting pulmonary vascular disease that is diagnosed hemodynamically by right-sided heart catheterization (RHC) and defined by a mean pulmonary artery pressure (mPAP) >25 mm Hg (Hoeper MM, et al. JACC. 2013;62(25 Suppl):D42).
The impact of PH on survival both in its “pure” form, pulmonary arterial hypertension, and in the setting of underlying cardiopulmonary disease, is well established. However, the clinical relevance of mildly elevated mPAP, defined as mPAP between 18 and 24 mm Hg, has been unclear until recently. Two large cohort studies have suggested that mild increases in mPAP are clinically relevant. A large retrospective analysis of hemodynamic data from 21,727 US veterans found mildly increased mPAP (19-24 mm Hg) was associated with increased hospitalization and decreased survival (Maron, et al. Circulation. 2016;133:1240).
While this population was skewed toward elderly men, a study from Vanderbilt University that included equal numbers of men and women showed similar results. Patients with mPAP 19-24 mm Hg experienced incrementally increased mortality (HR:1.31, P=.001). Importantly, in the subset of patients who underwent a repeat RHC in follow-up, 61% developed progressive increases of pulmonary pressures (>25 mm Hg) on follow-up RHC suggesting that the disease process may progress in a substantial proportion of patients (Assad, et al. JAMA Cardiol. 2017;2[1]):1361). Combined with prior data from smaller cohorts, these studies highlight the impact of mildly increased pulmonary pressures on outcomes. Given the dearth of available data regarding interventions for these patients, there is an urgent need to study to role of specific therapy for mildly elevated pulmonary pressures.
Vijay Balasubramanian, MD, FCCP
Steering Committee Member
Jean Elwing, MD, FCCP
Steering Committee Vice-Chair
Thoracic Oncology
Multiple tumor nodules in lung cancer diagnosis
Low dose CT (LDCT) scan screening for lung cancer is a recommended preventative modality for adults with a significant smoking history (Mayer et al. Ann Int Med. 2014;160(5):330). The screening approach aims to identify adults at significant risk for lung cancer. The goal is to discover lung cancers at low stage with benign mediastinal nodes for optimal treatment and potential for cure. In a minority, but significant number of cases, the LDCT demonstrates multiple lung nodules or masses confounding the attempt to adequately stage the tumor. Two tumors representing a primary cancer and separate malignant spread, namely, intra-pulmonary metastases, in the same lobe, different ipsilateral lobe, or contralateral lobe would be staged, respectively, as T3, T4, or M1a (Detterbeck et al. Chest. 2013;143(5):e191S). Clearly, if the two tumors are separate unique primary cancers, independent of one another, then at best they would be considered as multiple T1 tumors. The treatment modalities of and clinical survival outcomes for these multiple conditions would be markedly different.
The identification of additional tumors may be synchronous (at the same time of the primary discovery) or metachronous (at a later time than the primary discovery). The approach is basically the same. Two tumors with different histologic types, or having separate in-situ squamous cell carcinoma patterns, or disparate immunohistochemical or molecular expressions, or different genomic profiles or driver mutations may be considered as separate distinct primary malignancies (Detterbeck et al. J Thorac Oncol. 2016;11:639; Nicholson et al. J Thorac Oncol. 2017;13:205). Separate foci of ground-glass opacities with small solid central component indicative of minimally invasive adenocarcinoma may be designated as the highest T-stage. These cited and more challenging cases should be presented to a lung cancer tumor board with multiple specialties represented for analysis and judgment. The approach to diagnostic decision-making and clinical management should involve the expertise of all specialties in the lung cancer patient care team.
Arnold M. Schwartz, MD, PhD, FCCP
Steering Committee Member
This month in the journal CHEST®
Editor’s picks
Original Research
Pilot Feasibility Study in Establishing the Role of Ultrasound-Guided Pleural Biopsies in Pleural Infection (The AUDIO Study). By Dr. I. Psallidas, et al.
Commentary
Sleep Apnea Morbidity: A Consequence of Microbial-Immune Cross-Talk? By Dr. N. Farre, et al.
Evidence-Based Medicine
Treatment of Interstitial Lung Disease-Associated Cough: CHEST guideline and expert panel report. By Dr. S. S. Birring, et al.
Editor’s picks
Original Research
Pilot Feasibility Study in Establishing the Role of Ultrasound-Guided Pleural Biopsies in Pleural Infection (The AUDIO Study). By Dr. I. Psallidas, et al.
Commentary
Sleep Apnea Morbidity: A Consequence of Microbial-Immune Cross-Talk? By Dr. N. Farre, et al.
Evidence-Based Medicine
Treatment of Interstitial Lung Disease-Associated Cough: CHEST guideline and expert panel report. By Dr. S. S. Birring, et al.
Editor’s picks
Original Research
Pilot Feasibility Study in Establishing the Role of Ultrasound-Guided Pleural Biopsies in Pleural Infection (The AUDIO Study). By Dr. I. Psallidas, et al.
Commentary
Sleep Apnea Morbidity: A Consequence of Microbial-Immune Cross-Talk? By Dr. N. Farre, et al.
Evidence-Based Medicine
Treatment of Interstitial Lung Disease-Associated Cough: CHEST guideline and expert panel report. By Dr. S. S. Birring, et al.
Perioperative diabetes and HbA1c in mortality
Clinical question: Do preoperative hemoglobin A1c (HbA1c) and perioperative glucose predict outcomes in patients undergoing noncardiac and cardiac surgeries?
Background: Hyperglycemia in the perioperative period has been associated with infection, delayed wound healing, and postoperative mortality. Studies have investigated the effects of HbA1c or hyperglycemia on postoperative outcomes, but none have been performed to assess the effect of one while controlling for the other.
Study design: Retrospective analysis.
Setting: Single-center, Duke University Health System.

Synopsis: Using a database of electronic health records at Duke University Health System, Durham, N.C., investigators reviewed 13,077 surgeries (6,684 noncardiac and 6,393 cardiac) to determine the association of preoperative HbA1c with perioperative glucose and 30-day mortality. For noncardiac surgery, increased average perioperative glucose was associated with increased mortality (P = .04). In cardiac surgery both low and high average glucose was associated with increased mortality (P = .001). By contrast, HbA1c was not a significant predictor of postoperative mortality in cardiac surgery (P = .08), and in noncardiac surgery, HbA1C was negatively associated with 30-day mortality (P = .01). Overall, perioperative glucose was predictive of 30-day mortality, but HbA1c was not associated with 30-day mortality after researchers controlled for glucose.
Because the study is retrospective, no causal relationship can be established. Hospitalists involved in perioperative care should aim for optimization of glucose control regardless of preoperative HbA1c.
Bottom line: Perioperative glucose is related to surgical outcomes, but HbA1c is a less useful indicator of 30-day postoperative mortality.
Citation: Van den Boom W et al. Effect of A1C and glucose on postoperative mortality in noncardiac and cardiac surgeries. Diabetes Care. 2018 Feb;41:782-8.
Clinical question: Do preoperative hemoglobin A1c (HbA1c) and perioperative glucose predict outcomes in patients undergoing noncardiac and cardiac surgeries?
Background: Hyperglycemia in the perioperative period has been associated with infection, delayed wound healing, and postoperative mortality. Studies have investigated the effects of HbA1c or hyperglycemia on postoperative outcomes, but none have been performed to assess the effect of one while controlling for the other.
Study design: Retrospective analysis.
Setting: Single-center, Duke University Health System.
Synopsis: Using a database of electronic health records at Duke University Health System, Durham, N.C., investigators reviewed 13,077 surgeries (6,684 noncardiac and 6,393 cardiac) to determine the association of preoperative HbA1c with perioperative glucose and 30-day mortality. For noncardiac surgery, increased average perioperative glucose was associated with increased mortality (P = .04). In cardiac surgery both low and high average glucose was associated with increased mortality (P = .001). By contrast, HbA1c was not a significant predictor of postoperative mortality in cardiac surgery (P = .08), and in noncardiac surgery, HbA1C was negatively associated with 30-day mortality (P = .01). Overall, perioperative glucose was predictive of 30-day mortality, but HbA1c was not associated with 30-day mortality after researchers controlled for glucose.
Because the study is retrospective, no causal relationship can be established. Hospitalists involved in perioperative care should aim for optimization of glucose control regardless of preoperative HbA1c.
Bottom line: Perioperative glucose is related to surgical outcomes, but HbA1c is a less useful indicator of 30-day postoperative mortality.
Citation: Van den Boom W et al. Effect of A1C and glucose on postoperative mortality in noncardiac and cardiac surgeries. Diabetes Care. 2018 Feb;41:782-8.
Clinical question: Do preoperative hemoglobin A1c (HbA1c) and perioperative glucose predict outcomes in patients undergoing noncardiac and cardiac surgeries?
Background: Hyperglycemia in the perioperative period has been associated with infection, delayed wound healing, and postoperative mortality. Studies have investigated the effects of HbA1c or hyperglycemia on postoperative outcomes, but none have been performed to assess the effect of one while controlling for the other.
Study design: Retrospective analysis.
Setting: Single-center, Duke University Health System.
Synopsis: Using a database of electronic health records at Duke University Health System, Durham, N.C., investigators reviewed 13,077 surgeries (6,684 noncardiac and 6,393 cardiac) to determine the association of preoperative HbA1c with perioperative glucose and 30-day mortality. For noncardiac surgery, increased average perioperative glucose was associated with increased mortality (P = .04). In cardiac surgery both low and high average glucose was associated with increased mortality (P = .001). By contrast, HbA1c was not a significant predictor of postoperative mortality in cardiac surgery (P = .08), and in noncardiac surgery, HbA1C was negatively associated with 30-day mortality (P = .01). Overall, perioperative glucose was predictive of 30-day mortality, but HbA1c was not associated with 30-day mortality after researchers controlled for glucose.
Because the study is retrospective, no causal relationship can be established. Hospitalists involved in perioperative care should aim for optimization of glucose control regardless of preoperative HbA1c.
Bottom line: Perioperative glucose is related to surgical outcomes, but HbA1c is a less useful indicator of 30-day postoperative mortality.
Citation: Van den Boom W et al. Effect of A1C and glucose on postoperative mortality in noncardiac and cardiac surgeries. Diabetes Care. 2018 Feb;41:782-8.
Syncope alone after age 60 does not require admission
SAN DIEGO – Unless the cause of syncope has been identified after a thorough workup in the emergency department, there is no advantage to admitting patients aged 60 years and older who complain of syncope, an ED-based study has found.
Almost 2,500 patients aged 60 or older with unexplained syncope after a thorough workup had similar 30-day outcomes whether they were admitted to the hospital or sent home from the ED, based on the results of a retrospective study presented at the annual meeting of the American College of Emergency Physicians.
Dr. Marc A. Probst of the Icahn School of Medicine at Mount Sinai, New York, who presented the data, reported that many centers admit older patients with syncope, although the benefit of this practice has not been well established.
In a video interview, Dr. Probst points out how the findings may be useful in guiding clinical decisions or counseling patients when admission is being considered.
SAN DIEGO – Unless the cause of syncope has been identified after a thorough workup in the emergency department, there is no advantage to admitting patients aged 60 years and older who complain of syncope, an ED-based study has found.
Almost 2,500 patients aged 60 or older with unexplained syncope after a thorough workup had similar 30-day outcomes whether they were admitted to the hospital or sent home from the ED, based on the results of a retrospective study presented at the annual meeting of the American College of Emergency Physicians.
Dr. Marc A. Probst of the Icahn School of Medicine at Mount Sinai, New York, who presented the data, reported that many centers admit older patients with syncope, although the benefit of this practice has not been well established.
In a video interview, Dr. Probst points out how the findings may be useful in guiding clinical decisions or counseling patients when admission is being considered.
SAN DIEGO – Unless the cause of syncope has been identified after a thorough workup in the emergency department, there is no advantage to admitting patients aged 60 years and older who complain of syncope, an ED-based study has found.
Almost 2,500 patients aged 60 or older with unexplained syncope after a thorough workup had similar 30-day outcomes whether they were admitted to the hospital or sent home from the ED, based on the results of a retrospective study presented at the annual meeting of the American College of Emergency Physicians.
Dr. Marc A. Probst of the Icahn School of Medicine at Mount Sinai, New York, who presented the data, reported that many centers admit older patients with syncope, although the benefit of this practice has not been well established.
In a video interview, Dr. Probst points out how the findings may be useful in guiding clinical decisions or counseling patients when admission is being considered.
REPORTING FROM ACEP18
