User login
Antibiotics or appendectomy? Both good options
Patients given antibiotics for appendicitis fared no worse in quality of life, at least in the short term, than did patients whose appendix was removed, according to a large, randomized, nonblinded, noninferiority study published online Oct. 5 in The New England Journal of Medicine.
One expert says the body of data, including this trial, indicates that the best appendicitis treatment now comes down to individual patients and choice.
David Flum, MD, director of the Surgical Outcomes Research Center at the University of Washington in Seattle, and colleagues conducted the Comparison of Outcomes of Antibiotic Drugs and Appendectomy (CODA) trial, which compared a 10-day course of antibiotics with appendectomy for patients with appendicitis at 25 US centers.
Although some may interpret the study as praising the potential role of antibiotics, the author of an accompanying editorial warns against rushing to antibiotics, even during a pandemic when hospital resources may be strained.
In the study of 1552 adults (414 with an appendicolith), 776 were randomly assigned to the antibiotics group and 776 to appendectomy (96% of whom underwent a laparoscopic procedure).
After 30 days, antibiotics were found to be noninferior to appendectomy, the standard of treatment for 120 years, as determined on the basis of 30-day scores for the European Quality of Life–5 Dimensions (EQ-5D) questionnaire (mean difference, 0.01 points; 95% CI, −0.001 to 0.03).
EQ-5D at 30 days was chosen as the primary endpoint because it has been validated as an overall measure of health after appendicitis treatment and the 30-day time frame mimics the typical recovery period for appendectomy, Flum and colleagues explain.
Some results favored appendectomy
However, editorialist Danny Jacobs, MD, MPH, president of Oregon Health and Science University in Portland, points out that about a third (29%) of the patients in the antibiotics group had undergone appendectomy by 90 days.
Appendicolith, a well-established potential complication, he acknowledges, was the main driver of the need for surgery (41% with that complication needed appendectomy), but it was not the sole reason.
Complications were more common in the antibiotics group than in the appendectomy group (8.1 vs 3.5 per 100 participants; rate ratio, 2.28; 95% CI, 1.30 – 3.98). The rate of serious adverse events was 4.0 per 100 participants in the antibiotics group and 3.0 per 100 participants in the appendectomy group (rate ratio, 1.29; 95% CI, 0.67 – 2.50). Additionally, the number of emergency department visits was nearly three times higher in the antibiotics group, and more time was spent in the hospital by that group, Jacobs points out.
He notes that the article mentions circumstances such as the COVID-19 pandemic may figure into consideration when weighing antibiotics against appendectomy. But he warns that there also may be a danger of treatment bias in vulnerable populations and that COVID-19 has highlighted disparities in care overall.
“It will be important to ensure that some people, in particular vulnerable populations, are not offered antibiotic therapy preferentially or without adequate education regarding the longer-term implications,” Jacobs writes.
Flum told Medscape Medical News he agrees with Jacobs that the potential for bias is important.
“We should all be worried that new healthcare options won’t be equally applied,” he said.
But he and his coauthors offer an alternative view of the results of the study.
“In the antibiotics group,” they write, “more than 7 in 10 participants avoided surgery, many were treated on an outpatient basis, and participants and caregivers missed less time at work than with appendectomy.”
Flum said, “[T]hat’s going to be attractive to some patients. Not all, but some.”
Douglas Smink, MD, MPH, chief of surgery at Brigham and Women’s Faulkner Hospital in Boston, told Medscape Medical News that he sees this study as an argument for surgery remaining the go-to option for appendicitis, unless there is a safety reason for not performing the surgery.
Patients come in and want their appendix out immediately, he said, and surgery offers a quick option with short length of stay and few complications.
Additionally, he said, if patients are told that, with antibiotics, “there’s a 1 in 3 chance you’re going to need [an appendectomy] in the next 3 months, I think most people would say, ‘Just take it out then,’ ” he said.
Can research decide which is best?
The controversy has been well studied. But with no clear answer in any of the studies about whether appendectomy or use of antibiotics is better, should the current study put the research to rest?
Flum told Medscape Medical News that this study, which is three times the size of the next-largest study, makes clear “there are choices.”
Previous trials in Europe “did not move the needle” on the issue, he said, “in part because they didn’t include the patients who typically get appendectomies.”
He said their team tried to build on those studies and include “typical patients in typical hospitals with typical appendicitis” and found that both surgery and antibiotics are safe and have advantages and disadvantages, depending on the patient.
Smink says one thing that has been definitively answered with this trial is that patients with appendicolith are “more likely to fail with antibiotics.”
Previous trials have excluded patients with appendicolith, and this one did not.
“That’s something we’ve not really known for sure but we’ve assumed,” he said.
But now, Smink says, he thinks the research on the topic has gone about as far as it can go.
He notes that none of the trials has shown antibiotics to be better than appendectomy. “I have a hard time believing we are going to find anything different if we did another study like this. This is a really well-done one,” he said.
“If the best you can do is show noninferiority, which is where we are with these studies on appendicitis, you’re always going to have both options, which is great for patients and doctors,” he said.
The study was funded by the Patient-Centered Outcomes Research Institute. The original article lists the authors’ relevant financial relationships. Jacobs and Smink reported no such relationships.
This article first appeared on Medscape.com.
Patients given antibiotics for appendicitis fared no worse in quality of life, at least in the short term, than did patients whose appendix was removed, according to a large, randomized, nonblinded, noninferiority study published online Oct. 5 in The New England Journal of Medicine.
One expert says the body of data, including this trial, indicates that the best appendicitis treatment now comes down to individual patients and choice.
David Flum, MD, director of the Surgical Outcomes Research Center at the University of Washington in Seattle, and colleagues conducted the Comparison of Outcomes of Antibiotic Drugs and Appendectomy (CODA) trial, which compared a 10-day course of antibiotics with appendectomy for patients with appendicitis at 25 US centers.
Although some may interpret the study as praising the potential role of antibiotics, the author of an accompanying editorial warns against rushing to antibiotics, even during a pandemic when hospital resources may be strained.
In the study of 1552 adults (414 with an appendicolith), 776 were randomly assigned to the antibiotics group and 776 to appendectomy (96% of whom underwent a laparoscopic procedure).
After 30 days, antibiotics were found to be noninferior to appendectomy, the standard of treatment for 120 years, as determined on the basis of 30-day scores for the European Quality of Life–5 Dimensions (EQ-5D) questionnaire (mean difference, 0.01 points; 95% CI, −0.001 to 0.03).
EQ-5D at 30 days was chosen as the primary endpoint because it has been validated as an overall measure of health after appendicitis treatment and the 30-day time frame mimics the typical recovery period for appendectomy, Flum and colleagues explain.
Some results favored appendectomy
However, editorialist Danny Jacobs, MD, MPH, president of Oregon Health and Science University in Portland, points out that about a third (29%) of the patients in the antibiotics group had undergone appendectomy by 90 days.
Appendicolith, a well-established potential complication, he acknowledges, was the main driver of the need for surgery (41% with that complication needed appendectomy), but it was not the sole reason.
Complications were more common in the antibiotics group than in the appendectomy group (8.1 vs 3.5 per 100 participants; rate ratio, 2.28; 95% CI, 1.30 – 3.98). The rate of serious adverse events was 4.0 per 100 participants in the antibiotics group and 3.0 per 100 participants in the appendectomy group (rate ratio, 1.29; 95% CI, 0.67 – 2.50). Additionally, the number of emergency department visits was nearly three times higher in the antibiotics group, and more time was spent in the hospital by that group, Jacobs points out.
He notes that the article mentions circumstances such as the COVID-19 pandemic may figure into consideration when weighing antibiotics against appendectomy. But he warns that there also may be a danger of treatment bias in vulnerable populations and that COVID-19 has highlighted disparities in care overall.
“It will be important to ensure that some people, in particular vulnerable populations, are not offered antibiotic therapy preferentially or without adequate education regarding the longer-term implications,” Jacobs writes.
Flum told Medscape Medical News he agrees with Jacobs that the potential for bias is important.
“We should all be worried that new healthcare options won’t be equally applied,” he said.
But he and his coauthors offer an alternative view of the results of the study.
“In the antibiotics group,” they write, “more than 7 in 10 participants avoided surgery, many were treated on an outpatient basis, and participants and caregivers missed less time at work than with appendectomy.”
Flum said, “[T]hat’s going to be attractive to some patients. Not all, but some.”
Douglas Smink, MD, MPH, chief of surgery at Brigham and Women’s Faulkner Hospital in Boston, told Medscape Medical News that he sees this study as an argument for surgery remaining the go-to option for appendicitis, unless there is a safety reason for not performing the surgery.
Patients come in and want their appendix out immediately, he said, and surgery offers a quick option with short length of stay and few complications.
Additionally, he said, if patients are told that, with antibiotics, “there’s a 1 in 3 chance you’re going to need [an appendectomy] in the next 3 months, I think most people would say, ‘Just take it out then,’ ” he said.
Can research decide which is best?
The controversy has been well studied. But with no clear answer in any of the studies about whether appendectomy or use of antibiotics is better, should the current study put the research to rest?
Flum told Medscape Medical News that this study, which is three times the size of the next-largest study, makes clear “there are choices.”
Previous trials in Europe “did not move the needle” on the issue, he said, “in part because they didn’t include the patients who typically get appendectomies.”
He said their team tried to build on those studies and include “typical patients in typical hospitals with typical appendicitis” and found that both surgery and antibiotics are safe and have advantages and disadvantages, depending on the patient.
Smink says one thing that has been definitively answered with this trial is that patients with appendicolith are “more likely to fail with antibiotics.”
Previous trials have excluded patients with appendicolith, and this one did not.
“That’s something we’ve not really known for sure but we’ve assumed,” he said.
But now, Smink says, he thinks the research on the topic has gone about as far as it can go.
He notes that none of the trials has shown antibiotics to be better than appendectomy. “I have a hard time believing we are going to find anything different if we did another study like this. This is a really well-done one,” he said.
“If the best you can do is show noninferiority, which is where we are with these studies on appendicitis, you’re always going to have both options, which is great for patients and doctors,” he said.
The study was funded by the Patient-Centered Outcomes Research Institute. The original article lists the authors’ relevant financial relationships. Jacobs and Smink reported no such relationships.
This article first appeared on Medscape.com.
Patients given antibiotics for appendicitis fared no worse in quality of life, at least in the short term, than did patients whose appendix was removed, according to a large, randomized, nonblinded, noninferiority study published online Oct. 5 in The New England Journal of Medicine.
One expert says the body of data, including this trial, indicates that the best appendicitis treatment now comes down to individual patients and choice.
David Flum, MD, director of the Surgical Outcomes Research Center at the University of Washington in Seattle, and colleagues conducted the Comparison of Outcomes of Antibiotic Drugs and Appendectomy (CODA) trial, which compared a 10-day course of antibiotics with appendectomy for patients with appendicitis at 25 US centers.
Although some may interpret the study as praising the potential role of antibiotics, the author of an accompanying editorial warns against rushing to antibiotics, even during a pandemic when hospital resources may be strained.
In the study of 1552 adults (414 with an appendicolith), 776 were randomly assigned to the antibiotics group and 776 to appendectomy (96% of whom underwent a laparoscopic procedure).
After 30 days, antibiotics were found to be noninferior to appendectomy, the standard of treatment for 120 years, as determined on the basis of 30-day scores for the European Quality of Life–5 Dimensions (EQ-5D) questionnaire (mean difference, 0.01 points; 95% CI, −0.001 to 0.03).
EQ-5D at 30 days was chosen as the primary endpoint because it has been validated as an overall measure of health after appendicitis treatment and the 30-day time frame mimics the typical recovery period for appendectomy, Flum and colleagues explain.
Some results favored appendectomy
However, editorialist Danny Jacobs, MD, MPH, president of Oregon Health and Science University in Portland, points out that about a third (29%) of the patients in the antibiotics group had undergone appendectomy by 90 days.
Appendicolith, a well-established potential complication, he acknowledges, was the main driver of the need for surgery (41% with that complication needed appendectomy), but it was not the sole reason.
Complications were more common in the antibiotics group than in the appendectomy group (8.1 vs 3.5 per 100 participants; rate ratio, 2.28; 95% CI, 1.30 – 3.98). The rate of serious adverse events was 4.0 per 100 participants in the antibiotics group and 3.0 per 100 participants in the appendectomy group (rate ratio, 1.29; 95% CI, 0.67 – 2.50). Additionally, the number of emergency department visits was nearly three times higher in the antibiotics group, and more time was spent in the hospital by that group, Jacobs points out.
He notes that the article mentions circumstances such as the COVID-19 pandemic may figure into consideration when weighing antibiotics against appendectomy. But he warns that there also may be a danger of treatment bias in vulnerable populations and that COVID-19 has highlighted disparities in care overall.
“It will be important to ensure that some people, in particular vulnerable populations, are not offered antibiotic therapy preferentially or without adequate education regarding the longer-term implications,” Jacobs writes.
Flum told Medscape Medical News he agrees with Jacobs that the potential for bias is important.
“We should all be worried that new healthcare options won’t be equally applied,” he said.
But he and his coauthors offer an alternative view of the results of the study.
“In the antibiotics group,” they write, “more than 7 in 10 participants avoided surgery, many were treated on an outpatient basis, and participants and caregivers missed less time at work than with appendectomy.”
Flum said, “[T]hat’s going to be attractive to some patients. Not all, but some.”
Douglas Smink, MD, MPH, chief of surgery at Brigham and Women’s Faulkner Hospital in Boston, told Medscape Medical News that he sees this study as an argument for surgery remaining the go-to option for appendicitis, unless there is a safety reason for not performing the surgery.
Patients come in and want their appendix out immediately, he said, and surgery offers a quick option with short length of stay and few complications.
Additionally, he said, if patients are told that, with antibiotics, “there’s a 1 in 3 chance you’re going to need [an appendectomy] in the next 3 months, I think most people would say, ‘Just take it out then,’ ” he said.
Can research decide which is best?
The controversy has been well studied. But with no clear answer in any of the studies about whether appendectomy or use of antibiotics is better, should the current study put the research to rest?
Flum told Medscape Medical News that this study, which is three times the size of the next-largest study, makes clear “there are choices.”
Previous trials in Europe “did not move the needle” on the issue, he said, “in part because they didn’t include the patients who typically get appendectomies.”
He said their team tried to build on those studies and include “typical patients in typical hospitals with typical appendicitis” and found that both surgery and antibiotics are safe and have advantages and disadvantages, depending on the patient.
Smink says one thing that has been definitively answered with this trial is that patients with appendicolith are “more likely to fail with antibiotics.”
Previous trials have excluded patients with appendicolith, and this one did not.
“That’s something we’ve not really known for sure but we’ve assumed,” he said.
But now, Smink says, he thinks the research on the topic has gone about as far as it can go.
He notes that none of the trials has shown antibiotics to be better than appendectomy. “I have a hard time believing we are going to find anything different if we did another study like this. This is a really well-done one,” he said.
“If the best you can do is show noninferiority, which is where we are with these studies on appendicitis, you’re always going to have both options, which is great for patients and doctors,” he said.
The study was funded by the Patient-Centered Outcomes Research Institute. The original article lists the authors’ relevant financial relationships. Jacobs and Smink reported no such relationships.
This article first appeared on Medscape.com.
A cure for dementia? Not so fast
“Diabetes drugs may cure dementia.”
How many of you saw that headline (or similar) earlier this year, before the pandemic took over the news?

My patients sure did. And their families. And people who aren’t my patients but found my name in the phone book after reading the headline. Of course, all of them wanted to be put on diabetes drugs to cure or prevent dementia, like the headline said.
The key word in the headline, though, is “may,” which promises nothing. Not only that, but if you actually read the story you quickly learn that the study was done in people who have diabetes, and lowers the risk of dementia.
While there could, possibly, maybe, be something interesting underlying the finding, it could also be as simple as controlling your vascular risk factors, which is good for you.
Of course, the lay public rarely reads past the first few paragraphs. To the nonmedical reader, the cure has been found, and they want it. Where’s the phone?
I’m sure this is good for business in the lay press. People see the headline and don’t bother to read the story but they immediately forward it to friends, family, Facebook and Twitter groups ... That’s a lot of clicks and advertising.
The study might genuinely mean something, but that’s a big “might.” A lot of common drugs have been hyped as being treatments for dementia – statins, ibuprofen, estrogen patches, to name a few – only to quietly die in larger controlled trials. But that part of the research never seems to make the news, only the first small, preliminary, results.
People want us to find answers. Isn’t that what doctors and scientists are supposed to do? I understand that. But by the same token, it’s generally not that easy. And if we try to explain the difficulty, then we’re often accused of being part of “them,” some secretive group trying to hide inexpensive miracle cures from the public to keep Big Pharma in business.
The real truth is that a lot of things initially seem to be good (or bad) and these things change like the seasons. Everyone should be on daily aspirin, oops, maybe not. Saccharine causes bladder cancer, wait, I take that back. And so on.
While diabetes treatments may indeed lower the risk of dementia in patients who have diabetes, people too often extrapolate that to everyone, and wishfully think the headline says “does cure” instead of “may cure.”
I have nothing against research. Everything we have now came from it. But preliminary results are just that – preliminary. Like many other things in this world, they have to be taken with a grain of salt.
Dr. Block has a solo neurology practice in Scottsdale, Arizona. He has no relevant disclosures.
“Diabetes drugs may cure dementia.”
How many of you saw that headline (or similar) earlier this year, before the pandemic took over the news?
My patients sure did. And their families. And people who aren’t my patients but found my name in the phone book after reading the headline. Of course, all of them wanted to be put on diabetes drugs to cure or prevent dementia, like the headline said.
The key word in the headline, though, is “may,” which promises nothing. Not only that, but if you actually read the story you quickly learn that the study was done in people who have diabetes, and lowers the risk of dementia.
While there could, possibly, maybe, be something interesting underlying the finding, it could also be as simple as controlling your vascular risk factors, which is good for you.
Of course, the lay public rarely reads past the first few paragraphs. To the nonmedical reader, the cure has been found, and they want it. Where’s the phone?
I’m sure this is good for business in the lay press. People see the headline and don’t bother to read the story but they immediately forward it to friends, family, Facebook and Twitter groups ... That’s a lot of clicks and advertising.
The study might genuinely mean something, but that’s a big “might.” A lot of common drugs have been hyped as being treatments for dementia – statins, ibuprofen, estrogen patches, to name a few – only to quietly die in larger controlled trials. But that part of the research never seems to make the news, only the first small, preliminary, results.
People want us to find answers. Isn’t that what doctors and scientists are supposed to do? I understand that. But by the same token, it’s generally not that easy. And if we try to explain the difficulty, then we’re often accused of being part of “them,” some secretive group trying to hide inexpensive miracle cures from the public to keep Big Pharma in business.
The real truth is that a lot of things initially seem to be good (or bad) and these things change like the seasons. Everyone should be on daily aspirin, oops, maybe not. Saccharine causes bladder cancer, wait, I take that back. And so on.
While diabetes treatments may indeed lower the risk of dementia in patients who have diabetes, people too often extrapolate that to everyone, and wishfully think the headline says “does cure” instead of “may cure.”
I have nothing against research. Everything we have now came from it. But preliminary results are just that – preliminary. Like many other things in this world, they have to be taken with a grain of salt.
Dr. Block has a solo neurology practice in Scottsdale, Arizona. He has no relevant disclosures.
“Diabetes drugs may cure dementia.”
How many of you saw that headline (or similar) earlier this year, before the pandemic took over the news?
My patients sure did. And their families. And people who aren’t my patients but found my name in the phone book after reading the headline. Of course, all of them wanted to be put on diabetes drugs to cure or prevent dementia, like the headline said.
The key word in the headline, though, is “may,” which promises nothing. Not only that, but if you actually read the story you quickly learn that the study was done in people who have diabetes, and lowers the risk of dementia.
While there could, possibly, maybe, be something interesting underlying the finding, it could also be as simple as controlling your vascular risk factors, which is good for you.
Of course, the lay public rarely reads past the first few paragraphs. To the nonmedical reader, the cure has been found, and they want it. Where’s the phone?
I’m sure this is good for business in the lay press. People see the headline and don’t bother to read the story but they immediately forward it to friends, family, Facebook and Twitter groups ... That’s a lot of clicks and advertising.
The study might genuinely mean something, but that’s a big “might.” A lot of common drugs have been hyped as being treatments for dementia – statins, ibuprofen, estrogen patches, to name a few – only to quietly die in larger controlled trials. But that part of the research never seems to make the news, only the first small, preliminary, results.
People want us to find answers. Isn’t that what doctors and scientists are supposed to do? I understand that. But by the same token, it’s generally not that easy. And if we try to explain the difficulty, then we’re often accused of being part of “them,” some secretive group trying to hide inexpensive miracle cures from the public to keep Big Pharma in business.
The real truth is that a lot of things initially seem to be good (or bad) and these things change like the seasons. Everyone should be on daily aspirin, oops, maybe not. Saccharine causes bladder cancer, wait, I take that back. And so on.
While diabetes treatments may indeed lower the risk of dementia in patients who have diabetes, people too often extrapolate that to everyone, and wishfully think the headline says “does cure” instead of “may cure.”
I have nothing against research. Everything we have now came from it. But preliminary results are just that – preliminary. Like many other things in this world, they have to be taken with a grain of salt.
Dr. Block has a solo neurology practice in Scottsdale, Arizona. He has no relevant disclosures.
Everything I want to tell my adult ADHD patients during the pandemic
An ADHD brain thrives with daily routines, and requires spontaneity and challenge to remain engaged in work, academics, relationships, and even leisure activities. ADHD is a performance issue and not one of intellectual understanding. It is not a problem of knowing what to do, but rather, difficulty doing it.

The COVID-19 pandemic has led to the loss of structure, with many parents working out of their homes alongside their children engaged in virtual learning. There has been a significant loss of impromptu events, since all activities outside of the house require proper planning and safety precautions.
To help normalize the struggles of the adult patient with ADHD during the pandemic, when others’ coping strategies do not work for their ADHD brains.
Adult ADHD is a misnomer – and not just a disorder of inattention and hyperactivity
A better name for this often misconstrued disorder is inconsistent attention and motivation disorder with internal or external hyperactivity/impulsivity.
An ADHD brain vacillates between inattention and hyperfocus. It is not uncommon for individuals with ADHD to lose interest in a new television series when they become hyperfocused on finding the best pandemic-friendly toy for their 5-year-olds, which inevitably turns into a 3-hour Google rabbit-hole search.
These same individuals with ADHD may have low motivation for mundane household chores but become highly motivated when their nonessential Amazon purchases arrive. They may even go as far as pulling an all-nighter to have an electric toy jeep built and ready for the youngster by morning.
Adults with ADHD can also exhibit hyperactive symptoms, such as physical restlessness with fidgeting, and an internal restlessness with anxious and repetitive thoughts that affect their ability to unwind, relax, and even sleep. Impulsivity in adults with ADHD can present as rushing through tasks that one finds uninteresting or unimportant, interrupting others on a Zoom work call, or impulse buying an expensive hot tub instead of a more affordable on their spouse agreed to.
ADHD is a risk factor for contracting COVID-19
Untreated ADHD can increase one’s risk of contracting COVID-19. Israeli researchers published a study in the Journal of Attention Disorders showing that individuals with ADHD are 52% more likely to test positive for COVID-19, compared with those without ADHD, because of risk-taking behaviors, impulsivity, and carelessness. However, individuals whose ADHD symptoms are treated with stimulant medication do not increase their risk of contracting COVID-19, the researchers wrote.
ADHD might be noticed in family members
ADHD is a neurodevelopmental disorder that affects the development of the brain. We know that structural, functional, and chemical differences affect our patients’ ability to regulate attention, motivation, impulses, and emotions. ADHD tends to run in families and is highly genetic. Since spending more time with family members during the pandemic, patients might even recognize ADHD symptoms in siblings, children, and one or both of parents. A child who has ADHD has a 25% chance of having a parent with ADHD.
Strengths and attributes are related to ADHD
Your ability to thrive in new, stressful, and challenging situations is an ADHD attribute that will be beneficial during the pandemic. Creativity, great problem-solving skills, and ability to be flexible will be admired and helpful to our patients with ADHD and others during these uncertain times.
Those with ADHD might be highly sensitive to their environments
As previously mentioned, ADHD is a misnomer and not just a disorder of inattention but also too much attention. Unfortunately, this hyperfocused attention is usually on the wrong things. Those with ADHD might find it difficult to filter and process sensory information correctly and, therefore, can be easily distracted by auditory, visual, tactile, and olfactory stimuli. The change to working at home during the pandemic might make it hard to ignore children’s voices, the uncomfortable new mask bought after losing yet another mask over the weekend, and the smell of cookies emanating from the kitchen. This increased sensitivity may affect one’s emotions.
Heightened emotions are expected during the pandemic and even more so among adults with ADHD. The inability of adults with ADHD to properly filter information can also affect emotional stimuli. These intense emotions, coupled with impulsive behaviors, can cause disagreements with partners, lack of patience with children, and conflict with colleagues. When individuals with ADHD feel attacked or invalidated, they can become emotionally dysregulated and “vomit” their pent up feelings.
ADHD may affect interpersonal relationships
ADHD symptoms of inattention and impulsivity can affect the ability to connect with friends and family. When one is easily distracted by the pandemic’s chaos, it is harder to be mindful and emotionally and physically connected to one’s partner, which also disrupts their sex life and intimacy.
ADHD sensory integration issues can make people sensitive to particular touches, smells, and sensory information. A gentle touch from one’s partner might be annoying during the pandemic, since other senses may already be overstimulated by the loud sounds of children screaming, the visual and auditory distractions of a neighbor mowing the lawn, and the sun beating down because one forgot to get blinds in the home office before the pandemic.
These minor distractions that are usually insignificant to a non-ADHD brain can profoundly affect an ADHD brain since one must use valuable energy to tune out these unwanted disturbances.
Your brain uses a different motivational system than a non-ADHD brain
You have a deficiency in the neurotransmitter dopamine, which affects your motivational system. Your motivational system is based on what you find interesting, challenging, new, exciting, and urgent. Your non-ADHD partner, family members, friends, and colleagues motivate and accomplish their daily tasks differently from you and most likely use a system based on rewards and consequences.
Do not be surprised if you notice that your motivation is diminished during the pandemic because of less novelty and excitement in your life. The coronavirus’s chronic importance level may make everything else in your life not as essential and, therefore, less urgent, which indirectly also lowers your motivation.
Your non-ADHD partner may see that you can focus, prioritize, initiate, and complete tasks when you “choose” to, and confuse your inconsistent behaviors as being within your control. However, this lack of motivation for things that do not pique your interest, challenge you, and are not urgent is not voluntary. It is caused by a lack of neural connections in the area of the brain that controls motivation.
You can still have ADHD even though you were not diagnosed as a child or adolescent
Your symptoms of ADHD may not affect your level of functioning until you go away to college, obtain your first job, marry your partner, start a family, or even until a global pandemic alters every aspect of your daily life.
It is, therefore, never too late to get assessed and treated for ADHD. Stimulants are the first line of treatment for adult ADHD. Nonstimulants may also be prescribed if you do not tolerate the side effects of stimulants or have a history of certain medical conditions. These options include some antidepressants and high blood pressure medicines. Sometimes, just identifying the deficits of those with ADHD and how they may affect their performance at work, school, and interpersonal relationships can help the person living with ADHD. Many other any nonmedication types of effective treatment are available for adults with ADHD, including therapy, executive skills, and mindfulness training.
- ADHD focused cognitive-behavioral therapy can help one change your distorted, negative, and irrational thoughts about themselves, others, and situations and replace them with more realistic and rational thoughts that allow for helpful and adaptive behaviors.
- Executive skills training is a type of ADHD treatment that focuses on developing effective systems, routines, improving time management, organization, planning, productivity, and emotional self-regulation.
- Mindfulness meditation training is an additional treatment for adult ADHD. Mindfulness training teaches skills to focus on the present moment and become aware of one’s thoughts, emotions, and actions without judgment. The goal is to learn to accept your ADHD deficits and all that is out of your control while remaining mindful of your ADHD strengths and focusing on the daily choices within your control.
Silver linings of the pandemic
Numerous underserved and rural geographic areas lack adequate psychiatric care. Many primary care physicians and even some psychiatrists are uncomfortable diagnosing and treating attentional disorders because of a lack of proper training in medical school and fear related to the fact that the first-line treatment for adult ADHD is a controlled substance.
In response to the pandemic, the expansion of telepsychiatry services, state waivers that allow clinicians to practice across state lines, exemptions that enable the prescribing of controlled substances without an in-person medical evaluation, and the acceptance of employees working from home during the COVID-19 pandemic have increased the accessibility of adult ADHD psychiatric assessments and treatment.
It is hoped that when the COVID-19 pandemic is behind us, many of the benefits that have emerged, such as the growth of telepsychiatry, changes in state licensure and prescriber regulations, and reduced work commutes will continue into our postpandemic lives.
Dr. Abraham is a psychiatrist in private practice in Philadelphia. She has no disclosures.
An ADHD brain thrives with daily routines, and requires spontaneity and challenge to remain engaged in work, academics, relationships, and even leisure activities. ADHD is a performance issue and not one of intellectual understanding. It is not a problem of knowing what to do, but rather, difficulty doing it.
The COVID-19 pandemic has led to the loss of structure, with many parents working out of their homes alongside their children engaged in virtual learning. There has been a significant loss of impromptu events, since all activities outside of the house require proper planning and safety precautions.
To help normalize the struggles of the adult patient with ADHD during the pandemic, when others’ coping strategies do not work for their ADHD brains.
Adult ADHD is a misnomer – and not just a disorder of inattention and hyperactivity
A better name for this often misconstrued disorder is inconsistent attention and motivation disorder with internal or external hyperactivity/impulsivity.
An ADHD brain vacillates between inattention and hyperfocus. It is not uncommon for individuals with ADHD to lose interest in a new television series when they become hyperfocused on finding the best pandemic-friendly toy for their 5-year-olds, which inevitably turns into a 3-hour Google rabbit-hole search.
These same individuals with ADHD may have low motivation for mundane household chores but become highly motivated when their nonessential Amazon purchases arrive. They may even go as far as pulling an all-nighter to have an electric toy jeep built and ready for the youngster by morning.
Adults with ADHD can also exhibit hyperactive symptoms, such as physical restlessness with fidgeting, and an internal restlessness with anxious and repetitive thoughts that affect their ability to unwind, relax, and even sleep. Impulsivity in adults with ADHD can present as rushing through tasks that one finds uninteresting or unimportant, interrupting others on a Zoom work call, or impulse buying an expensive hot tub instead of a more affordable on their spouse agreed to.
ADHD is a risk factor for contracting COVID-19
Untreated ADHD can increase one’s risk of contracting COVID-19. Israeli researchers published a study in the Journal of Attention Disorders showing that individuals with ADHD are 52% more likely to test positive for COVID-19, compared with those without ADHD, because of risk-taking behaviors, impulsivity, and carelessness. However, individuals whose ADHD symptoms are treated with stimulant medication do not increase their risk of contracting COVID-19, the researchers wrote.
ADHD might be noticed in family members
ADHD is a neurodevelopmental disorder that affects the development of the brain. We know that structural, functional, and chemical differences affect our patients’ ability to regulate attention, motivation, impulses, and emotions. ADHD tends to run in families and is highly genetic. Since spending more time with family members during the pandemic, patients might even recognize ADHD symptoms in siblings, children, and one or both of parents. A child who has ADHD has a 25% chance of having a parent with ADHD.
Strengths and attributes are related to ADHD
Your ability to thrive in new, stressful, and challenging situations is an ADHD attribute that will be beneficial during the pandemic. Creativity, great problem-solving skills, and ability to be flexible will be admired and helpful to our patients with ADHD and others during these uncertain times.
Those with ADHD might be highly sensitive to their environments
As previously mentioned, ADHD is a misnomer and not just a disorder of inattention but also too much attention. Unfortunately, this hyperfocused attention is usually on the wrong things. Those with ADHD might find it difficult to filter and process sensory information correctly and, therefore, can be easily distracted by auditory, visual, tactile, and olfactory stimuli. The change to working at home during the pandemic might make it hard to ignore children’s voices, the uncomfortable new mask bought after losing yet another mask over the weekend, and the smell of cookies emanating from the kitchen. This increased sensitivity may affect one’s emotions.
Heightened emotions are expected during the pandemic and even more so among adults with ADHD. The inability of adults with ADHD to properly filter information can also affect emotional stimuli. These intense emotions, coupled with impulsive behaviors, can cause disagreements with partners, lack of patience with children, and conflict with colleagues. When individuals with ADHD feel attacked or invalidated, they can become emotionally dysregulated and “vomit” their pent up feelings.
ADHD may affect interpersonal relationships
ADHD symptoms of inattention and impulsivity can affect the ability to connect with friends and family. When one is easily distracted by the pandemic’s chaos, it is harder to be mindful and emotionally and physically connected to one’s partner, which also disrupts their sex life and intimacy.
ADHD sensory integration issues can make people sensitive to particular touches, smells, and sensory information. A gentle touch from one’s partner might be annoying during the pandemic, since other senses may already be overstimulated by the loud sounds of children screaming, the visual and auditory distractions of a neighbor mowing the lawn, and the sun beating down because one forgot to get blinds in the home office before the pandemic.
These minor distractions that are usually insignificant to a non-ADHD brain can profoundly affect an ADHD brain since one must use valuable energy to tune out these unwanted disturbances.
Your brain uses a different motivational system than a non-ADHD brain
You have a deficiency in the neurotransmitter dopamine, which affects your motivational system. Your motivational system is based on what you find interesting, challenging, new, exciting, and urgent. Your non-ADHD partner, family members, friends, and colleagues motivate and accomplish their daily tasks differently from you and most likely use a system based on rewards and consequences.
Do not be surprised if you notice that your motivation is diminished during the pandemic because of less novelty and excitement in your life. The coronavirus’s chronic importance level may make everything else in your life not as essential and, therefore, less urgent, which indirectly also lowers your motivation.
Your non-ADHD partner may see that you can focus, prioritize, initiate, and complete tasks when you “choose” to, and confuse your inconsistent behaviors as being within your control. However, this lack of motivation for things that do not pique your interest, challenge you, and are not urgent is not voluntary. It is caused by a lack of neural connections in the area of the brain that controls motivation.
You can still have ADHD even though you were not diagnosed as a child or adolescent
Your symptoms of ADHD may not affect your level of functioning until you go away to college, obtain your first job, marry your partner, start a family, or even until a global pandemic alters every aspect of your daily life.
It is, therefore, never too late to get assessed and treated for ADHD. Stimulants are the first line of treatment for adult ADHD. Nonstimulants may also be prescribed if you do not tolerate the side effects of stimulants or have a history of certain medical conditions. These options include some antidepressants and high blood pressure medicines. Sometimes, just identifying the deficits of those with ADHD and how they may affect their performance at work, school, and interpersonal relationships can help the person living with ADHD. Many other any nonmedication types of effective treatment are available for adults with ADHD, including therapy, executive skills, and mindfulness training.
- ADHD focused cognitive-behavioral therapy can help one change your distorted, negative, and irrational thoughts about themselves, others, and situations and replace them with more realistic and rational thoughts that allow for helpful and adaptive behaviors.
- Executive skills training is a type of ADHD treatment that focuses on developing effective systems, routines, improving time management, organization, planning, productivity, and emotional self-regulation.
- Mindfulness meditation training is an additional treatment for adult ADHD. Mindfulness training teaches skills to focus on the present moment and become aware of one’s thoughts, emotions, and actions without judgment. The goal is to learn to accept your ADHD deficits and all that is out of your control while remaining mindful of your ADHD strengths and focusing on the daily choices within your control.
Silver linings of the pandemic
Numerous underserved and rural geographic areas lack adequate psychiatric care. Many primary care physicians and even some psychiatrists are uncomfortable diagnosing and treating attentional disorders because of a lack of proper training in medical school and fear related to the fact that the first-line treatment for adult ADHD is a controlled substance.
In response to the pandemic, the expansion of telepsychiatry services, state waivers that allow clinicians to practice across state lines, exemptions that enable the prescribing of controlled substances without an in-person medical evaluation, and the acceptance of employees working from home during the COVID-19 pandemic have increased the accessibility of adult ADHD psychiatric assessments and treatment.
It is hoped that when the COVID-19 pandemic is behind us, many of the benefits that have emerged, such as the growth of telepsychiatry, changes in state licensure and prescriber regulations, and reduced work commutes will continue into our postpandemic lives.
Dr. Abraham is a psychiatrist in private practice in Philadelphia. She has no disclosures.
An ADHD brain thrives with daily routines, and requires spontaneity and challenge to remain engaged in work, academics, relationships, and even leisure activities. ADHD is a performance issue and not one of intellectual understanding. It is not a problem of knowing what to do, but rather, difficulty doing it.
The COVID-19 pandemic has led to the loss of structure, with many parents working out of their homes alongside their children engaged in virtual learning. There has been a significant loss of impromptu events, since all activities outside of the house require proper planning and safety precautions.
To help normalize the struggles of the adult patient with ADHD during the pandemic, when others’ coping strategies do not work for their ADHD brains.
Adult ADHD is a misnomer – and not just a disorder of inattention and hyperactivity
A better name for this often misconstrued disorder is inconsistent attention and motivation disorder with internal or external hyperactivity/impulsivity.
An ADHD brain vacillates between inattention and hyperfocus. It is not uncommon for individuals with ADHD to lose interest in a new television series when they become hyperfocused on finding the best pandemic-friendly toy for their 5-year-olds, which inevitably turns into a 3-hour Google rabbit-hole search.
These same individuals with ADHD may have low motivation for mundane household chores but become highly motivated when their nonessential Amazon purchases arrive. They may even go as far as pulling an all-nighter to have an electric toy jeep built and ready for the youngster by morning.
Adults with ADHD can also exhibit hyperactive symptoms, such as physical restlessness with fidgeting, and an internal restlessness with anxious and repetitive thoughts that affect their ability to unwind, relax, and even sleep. Impulsivity in adults with ADHD can present as rushing through tasks that one finds uninteresting or unimportant, interrupting others on a Zoom work call, or impulse buying an expensive hot tub instead of a more affordable on their spouse agreed to.
ADHD is a risk factor for contracting COVID-19
Untreated ADHD can increase one’s risk of contracting COVID-19. Israeli researchers published a study in the Journal of Attention Disorders showing that individuals with ADHD are 52% more likely to test positive for COVID-19, compared with those without ADHD, because of risk-taking behaviors, impulsivity, and carelessness. However, individuals whose ADHD symptoms are treated with stimulant medication do not increase their risk of contracting COVID-19, the researchers wrote.
ADHD might be noticed in family members
ADHD is a neurodevelopmental disorder that affects the development of the brain. We know that structural, functional, and chemical differences affect our patients’ ability to regulate attention, motivation, impulses, and emotions. ADHD tends to run in families and is highly genetic. Since spending more time with family members during the pandemic, patients might even recognize ADHD symptoms in siblings, children, and one or both of parents. A child who has ADHD has a 25% chance of having a parent with ADHD.
Strengths and attributes are related to ADHD
Your ability to thrive in new, stressful, and challenging situations is an ADHD attribute that will be beneficial during the pandemic. Creativity, great problem-solving skills, and ability to be flexible will be admired and helpful to our patients with ADHD and others during these uncertain times.
Those with ADHD might be highly sensitive to their environments
As previously mentioned, ADHD is a misnomer and not just a disorder of inattention but also too much attention. Unfortunately, this hyperfocused attention is usually on the wrong things. Those with ADHD might find it difficult to filter and process sensory information correctly and, therefore, can be easily distracted by auditory, visual, tactile, and olfactory stimuli. The change to working at home during the pandemic might make it hard to ignore children’s voices, the uncomfortable new mask bought after losing yet another mask over the weekend, and the smell of cookies emanating from the kitchen. This increased sensitivity may affect one’s emotions.
Heightened emotions are expected during the pandemic and even more so among adults with ADHD. The inability of adults with ADHD to properly filter information can also affect emotional stimuli. These intense emotions, coupled with impulsive behaviors, can cause disagreements with partners, lack of patience with children, and conflict with colleagues. When individuals with ADHD feel attacked or invalidated, they can become emotionally dysregulated and “vomit” their pent up feelings.
ADHD may affect interpersonal relationships
ADHD symptoms of inattention and impulsivity can affect the ability to connect with friends and family. When one is easily distracted by the pandemic’s chaos, it is harder to be mindful and emotionally and physically connected to one’s partner, which also disrupts their sex life and intimacy.
ADHD sensory integration issues can make people sensitive to particular touches, smells, and sensory information. A gentle touch from one’s partner might be annoying during the pandemic, since other senses may already be overstimulated by the loud sounds of children screaming, the visual and auditory distractions of a neighbor mowing the lawn, and the sun beating down because one forgot to get blinds in the home office before the pandemic.
These minor distractions that are usually insignificant to a non-ADHD brain can profoundly affect an ADHD brain since one must use valuable energy to tune out these unwanted disturbances.
Your brain uses a different motivational system than a non-ADHD brain
You have a deficiency in the neurotransmitter dopamine, which affects your motivational system. Your motivational system is based on what you find interesting, challenging, new, exciting, and urgent. Your non-ADHD partner, family members, friends, and colleagues motivate and accomplish their daily tasks differently from you and most likely use a system based on rewards and consequences.
Do not be surprised if you notice that your motivation is diminished during the pandemic because of less novelty and excitement in your life. The coronavirus’s chronic importance level may make everything else in your life not as essential and, therefore, less urgent, which indirectly also lowers your motivation.
Your non-ADHD partner may see that you can focus, prioritize, initiate, and complete tasks when you “choose” to, and confuse your inconsistent behaviors as being within your control. However, this lack of motivation for things that do not pique your interest, challenge you, and are not urgent is not voluntary. It is caused by a lack of neural connections in the area of the brain that controls motivation.
You can still have ADHD even though you were not diagnosed as a child or adolescent
Your symptoms of ADHD may not affect your level of functioning until you go away to college, obtain your first job, marry your partner, start a family, or even until a global pandemic alters every aspect of your daily life.
It is, therefore, never too late to get assessed and treated for ADHD. Stimulants are the first line of treatment for adult ADHD. Nonstimulants may also be prescribed if you do not tolerate the side effects of stimulants or have a history of certain medical conditions. These options include some antidepressants and high blood pressure medicines. Sometimes, just identifying the deficits of those with ADHD and how they may affect their performance at work, school, and interpersonal relationships can help the person living with ADHD. Many other any nonmedication types of effective treatment are available for adults with ADHD, including therapy, executive skills, and mindfulness training.
- ADHD focused cognitive-behavioral therapy can help one change your distorted, negative, and irrational thoughts about themselves, others, and situations and replace them with more realistic and rational thoughts that allow for helpful and adaptive behaviors.
- Executive skills training is a type of ADHD treatment that focuses on developing effective systems, routines, improving time management, organization, planning, productivity, and emotional self-regulation.
- Mindfulness meditation training is an additional treatment for adult ADHD. Mindfulness training teaches skills to focus on the present moment and become aware of one’s thoughts, emotions, and actions without judgment. The goal is to learn to accept your ADHD deficits and all that is out of your control while remaining mindful of your ADHD strengths and focusing on the daily choices within your control.
Silver linings of the pandemic
Numerous underserved and rural geographic areas lack adequate psychiatric care. Many primary care physicians and even some psychiatrists are uncomfortable diagnosing and treating attentional disorders because of a lack of proper training in medical school and fear related to the fact that the first-line treatment for adult ADHD is a controlled substance.
In response to the pandemic, the expansion of telepsychiatry services, state waivers that allow clinicians to practice across state lines, exemptions that enable the prescribing of controlled substances without an in-person medical evaluation, and the acceptance of employees working from home during the COVID-19 pandemic have increased the accessibility of adult ADHD psychiatric assessments and treatment.
It is hoped that when the COVID-19 pandemic is behind us, many of the benefits that have emerged, such as the growth of telepsychiatry, changes in state licensure and prescriber regulations, and reduced work commutes will continue into our postpandemic lives.
Dr. Abraham is a psychiatrist in private practice in Philadelphia. She has no disclosures.
FDA posts COVID vaccine guidance amid White House pushback
while medical and trade associations called for a thorough review of any such product before approval.
The FDA took the unusual step of posting background materials much earlier than usual for its planned Oct. 22 advisory committee meeting on potential vaccines for COVID-19. The FDA also on Tuesday afternoon released a new guidance document, expanding on a previous set of recommendations the agency released in June.
In the new guidance document, FDA officials outline what will be required for even a limited clearance, known as an emergency use authorization (EUA), for a COVID-19 vaccine.
“Data from phase 3 studies should include a median follow-up duration of at least 2 months after completion of the full vaccination regimen to help provide adequate information to assess a vaccine’s benefit-risk profile,” the FDA said in the document.
FDA staff have emphasized the higher bar that drugmakers and regulators face in considering approval of a COVID-19 vaccine.
“Vaccines are complex biological products, and an EUA for a COVID-19 vaccine may allow for rapid and widespread deployment for administration of the vaccine to millions of individuals, including healthy people,” the agency staff said in the briefing documents.
The FDA’s briefing document for the Oct. 22 meeting appears to be markedly at odds with the claim Trump made in a video Monday night, in which he told the American public that “vaccines are coming momentarily.”
Trump, who is in a tightly contested presidential race against Democratic candidate Joe Biden, has repeatedly made claims of the potential arrival of COVID vaccines that are at odds with timelines offered with guarded optimism by experts in infectious diseases.
But based on these new guidelines from the FDA, it appears that the White House may now endorse the FDA’s stance, according to a Wall Street Journal report based on “people familiar with the matter.”
The publication reports that the White House, which has yet to officially comment, “endorsed the U.S. Food and Drug Administration’s plans for assessing whether a Covid-19 vaccine should be given widely, casting aside objections to requirements that would likely mean a shot won’t be cleared until after Election Day, people familiar with the matter said.”
Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, on Monday night said during a virtual appearance at the twenty-first annual New Yorker Festival that there could be evidence as early as November or December about whether one of the vaccines now in testing will work out. He declared himself to have “cautious optimism” about potential rollout of vaccines as early as late 2020 or early 2021.
Peter Lurie, MD, MPH, who earlier served as the FDA’s associate commissioner for public health strategy and analysis, described the agency’s release of the briefing document as being a positive development.
News organizations, including the New York Times, have reported that the White House had sought to block the FDA from releasing further instructions for companies developing COVID-19 vaccines. The Associated Press on Tuesday said that a senior Trump administration official confirmed that the White House had blocked earlier FDA plans to formally publish the safety guidelines based on the 2-month data requirement, arguing that there was “no clinical or medical reason” for it.
“It is an encouraging sign that, despite opposition from the White House, the Food and Drug Administration has effectively published guidelines for emergency release of a vaccine for COVID-19 by disclosing the advice it has been providing to individual sponsors,” said Dr. Lurie, who is now executive director and president of the Center for Science in the Public Interest.
In a news release, he said the White House had sought to keep the FDA guidance under wraps “so it could maintain the public fiction that a safe and effective vaccine could be available before Election Day or even so that it could force emergency authorization of a vaccine with more limited follow-up.”
“Even the pharmaceutical industry has been clamoring for the release of these guidelines. We all want a safe and effective vaccine to end the pandemic, and we want it sooner rather than later,” Dr. Lurie said. “But we can’t afford for the Trump administration to bungle vaccine review the way they’ve bungled nearly every other aspect of its pandemic response.”
Tuesday also saw a flood of statements in support of FDA officials, including tweets from the chief executive of Pfizer, which is among the leaders in the race to develop a COVID-19 vaccine. Pfizer’s Albert Bourla, DVM, PhD, said that the FDA’s “public servants are known for their high integrity and scientific expertise and we have full faith in their ability to set appropriate standards for the approval of a COVID vaccine or treatment.”
The American Medical Association on Tuesday announced a public webinar on Wednesday where its president, Susan R. Bailey, MD, will discuss the COVID-19 vaccine review process with Peter Marks, MD, PhD, director of the Center for Biologics Evaluation and Research at the FDA. The AMA described this webinar as part of work “to restore trust in science and science-based decision-making among policymakers and the public.”
“To ensure media and the physician community are continuously informed about the federal review process for COVID-19 vaccine candidates, the AMA will host a webinar series to gain fact-based insights from the nation’s highest-ranking subject matter experts working to protect the health of the public,” the organization said in announcing the webinar.
In a statement, leaders of the Association of American Medical Colleges said that the FDA’s Vaccines and Related Biological Products Advisory Committee should evaluate any COVID-19 candidate vaccines prior to the FDA issuing an EUA.
“Full approval of a new vaccine or biologic requires demonstration of safety and effectiveness through a process that includes evaluation by the VRBPAC. Their recommendations are considered by FDA staff who ultimately have the authority to approve the new product,” said AAMC chief scientific officer Ross McKinney Jr, MD, and AAMC CEO David J. Skorton, MD, in the statement.
Thomas M. File Jr., MD, president of the Infectious Diseases Society of America, said in a statement that his association again asked the White House to “follow medical and scientific expertise in efforts to combat COVID-19.”
“It is imperative that a vaccine be approved on the basis of FDA’s quality standards and that its safety and efficacy are established before it is authorized,” Dr. File said. “A vaccine that has been approved with speed, rather than safety and efficacy, at the forefront will compound the challenges posed by this pandemic. FDA guidelines for approval that set standards the American people can trust are essential to the success of a vaccine.”
Stephen J. Ubl, chief executive of the Pharmaceutical Research and Manufacturers of America, said in a statement that his association “supports any efforts by FDA to provide clarifying guidance and we have engaged with the agency to support bringing greater transparency to the review process for COVID-19 vaccines.”
“To help address this public health crisis, our companies have also taken unprecedented steps to share vaccine clinical trial protocols and data in real time,” Mr. Ubl said. “We welcome the agency’s efforts to instill confidence in the rigorous safety of these potential vaccines.”
On Oct. 1, Michelle McMurry-Heath, MD, PhD, president and chief executive of the Biotechnology Innovation Organization, released publicly her letter urging Department of Health & Human Services Secretary Alex Azar to “publicly release all new guidance” related to a COVID-19 vaccine. Such a move would bolster public confidence in the vaccine, she said.
“We cannot allow a lack of transparency to undermine confidence in the vaccine development process. The public must have full faith in the scientific process and the rigor of FDA’s regulatory oversight if we are to end the pandemic,” she wrote in the Oct. 1 letter to Azar. “Releasing any additional guidance on granting emergency use authorization for a vaccine will go a long way in accomplishing this critical goal.”
{kind=link}
This article first appeared on Medscape.com.
while medical and trade associations called for a thorough review of any such product before approval.
The FDA took the unusual step of posting background materials much earlier than usual for its planned Oct. 22 advisory committee meeting on potential vaccines for COVID-19. The FDA also on Tuesday afternoon released a new guidance document, expanding on a previous set of recommendations the agency released in June.
In the new guidance document, FDA officials outline what will be required for even a limited clearance, known as an emergency use authorization (EUA), for a COVID-19 vaccine.
“Data from phase 3 studies should include a median follow-up duration of at least 2 months after completion of the full vaccination regimen to help provide adequate information to assess a vaccine’s benefit-risk profile,” the FDA said in the document.
FDA staff have emphasized the higher bar that drugmakers and regulators face in considering approval of a COVID-19 vaccine.
“Vaccines are complex biological products, and an EUA for a COVID-19 vaccine may allow for rapid and widespread deployment for administration of the vaccine to millions of individuals, including healthy people,” the agency staff said in the briefing documents.
The FDA’s briefing document for the Oct. 22 meeting appears to be markedly at odds with the claim Trump made in a video Monday night, in which he told the American public that “vaccines are coming momentarily.”
Trump, who is in a tightly contested presidential race against Democratic candidate Joe Biden, has repeatedly made claims of the potential arrival of COVID vaccines that are at odds with timelines offered with guarded optimism by experts in infectious diseases.
But based on these new guidelines from the FDA, it appears that the White House may now endorse the FDA’s stance, according to a Wall Street Journal report based on “people familiar with the matter.”
The publication reports that the White House, which has yet to officially comment, “endorsed the U.S. Food and Drug Administration’s plans for assessing whether a Covid-19 vaccine should be given widely, casting aside objections to requirements that would likely mean a shot won’t be cleared until after Election Day, people familiar with the matter said.”
Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, on Monday night said during a virtual appearance at the twenty-first annual New Yorker Festival that there could be evidence as early as November or December about whether one of the vaccines now in testing will work out. He declared himself to have “cautious optimism” about potential rollout of vaccines as early as late 2020 or early 2021.
Peter Lurie, MD, MPH, who earlier served as the FDA’s associate commissioner for public health strategy and analysis, described the agency’s release of the briefing document as being a positive development.
News organizations, including the New York Times, have reported that the White House had sought to block the FDA from releasing further instructions for companies developing COVID-19 vaccines. The Associated Press on Tuesday said that a senior Trump administration official confirmed that the White House had blocked earlier FDA plans to formally publish the safety guidelines based on the 2-month data requirement, arguing that there was “no clinical or medical reason” for it.
“It is an encouraging sign that, despite opposition from the White House, the Food and Drug Administration has effectively published guidelines for emergency release of a vaccine for COVID-19 by disclosing the advice it has been providing to individual sponsors,” said Dr. Lurie, who is now executive director and president of the Center for Science in the Public Interest.
In a news release, he said the White House had sought to keep the FDA guidance under wraps “so it could maintain the public fiction that a safe and effective vaccine could be available before Election Day or even so that it could force emergency authorization of a vaccine with more limited follow-up.”
“Even the pharmaceutical industry has been clamoring for the release of these guidelines. We all want a safe and effective vaccine to end the pandemic, and we want it sooner rather than later,” Dr. Lurie said. “But we can’t afford for the Trump administration to bungle vaccine review the way they’ve bungled nearly every other aspect of its pandemic response.”
Tuesday also saw a flood of statements in support of FDA officials, including tweets from the chief executive of Pfizer, which is among the leaders in the race to develop a COVID-19 vaccine. Pfizer’s Albert Bourla, DVM, PhD, said that the FDA’s “public servants are known for their high integrity and scientific expertise and we have full faith in their ability to set appropriate standards for the approval of a COVID vaccine or treatment.”
The American Medical Association on Tuesday announced a public webinar on Wednesday where its president, Susan R. Bailey, MD, will discuss the COVID-19 vaccine review process with Peter Marks, MD, PhD, director of the Center for Biologics Evaluation and Research at the FDA. The AMA described this webinar as part of work “to restore trust in science and science-based decision-making among policymakers and the public.”
“To ensure media and the physician community are continuously informed about the federal review process for COVID-19 vaccine candidates, the AMA will host a webinar series to gain fact-based insights from the nation’s highest-ranking subject matter experts working to protect the health of the public,” the organization said in announcing the webinar.
In a statement, leaders of the Association of American Medical Colleges said that the FDA’s Vaccines and Related Biological Products Advisory Committee should evaluate any COVID-19 candidate vaccines prior to the FDA issuing an EUA.
“Full approval of a new vaccine or biologic requires demonstration of safety and effectiveness through a process that includes evaluation by the VRBPAC. Their recommendations are considered by FDA staff who ultimately have the authority to approve the new product,” said AAMC chief scientific officer Ross McKinney Jr, MD, and AAMC CEO David J. Skorton, MD, in the statement.
Thomas M. File Jr., MD, president of the Infectious Diseases Society of America, said in a statement that his association again asked the White House to “follow medical and scientific expertise in efforts to combat COVID-19.”
“It is imperative that a vaccine be approved on the basis of FDA’s quality standards and that its safety and efficacy are established before it is authorized,” Dr. File said. “A vaccine that has been approved with speed, rather than safety and efficacy, at the forefront will compound the challenges posed by this pandemic. FDA guidelines for approval that set standards the American people can trust are essential to the success of a vaccine.”
Stephen J. Ubl, chief executive of the Pharmaceutical Research and Manufacturers of America, said in a statement that his association “supports any efforts by FDA to provide clarifying guidance and we have engaged with the agency to support bringing greater transparency to the review process for COVID-19 vaccines.”
“To help address this public health crisis, our companies have also taken unprecedented steps to share vaccine clinical trial protocols and data in real time,” Mr. Ubl said. “We welcome the agency’s efforts to instill confidence in the rigorous safety of these potential vaccines.”
On Oct. 1, Michelle McMurry-Heath, MD, PhD, president and chief executive of the Biotechnology Innovation Organization, released publicly her letter urging Department of Health & Human Services Secretary Alex Azar to “publicly release all new guidance” related to a COVID-19 vaccine. Such a move would bolster public confidence in the vaccine, she said.
“We cannot allow a lack of transparency to undermine confidence in the vaccine development process. The public must have full faith in the scientific process and the rigor of FDA’s regulatory oversight if we are to end the pandemic,” she wrote in the Oct. 1 letter to Azar. “Releasing any additional guidance on granting emergency use authorization for a vaccine will go a long way in accomplishing this critical goal.”
This article first appeared on Medscape.com.
while medical and trade associations called for a thorough review of any such product before approval.
The FDA took the unusual step of posting background materials much earlier than usual for its planned Oct. 22 advisory committee meeting on potential vaccines for COVID-19. The FDA also on Tuesday afternoon released a new guidance document, expanding on a previous set of recommendations the agency released in June.
In the new guidance document, FDA officials outline what will be required for even a limited clearance, known as an emergency use authorization (EUA), for a COVID-19 vaccine.
“Data from phase 3 studies should include a median follow-up duration of at least 2 months after completion of the full vaccination regimen to help provide adequate information to assess a vaccine’s benefit-risk profile,” the FDA said in the document.
FDA staff have emphasized the higher bar that drugmakers and regulators face in considering approval of a COVID-19 vaccine.
“Vaccines are complex biological products, and an EUA for a COVID-19 vaccine may allow for rapid and widespread deployment for administration of the vaccine to millions of individuals, including healthy people,” the agency staff said in the briefing documents.
The FDA’s briefing document for the Oct. 22 meeting appears to be markedly at odds with the claim Trump made in a video Monday night, in which he told the American public that “vaccines are coming momentarily.”
Trump, who is in a tightly contested presidential race against Democratic candidate Joe Biden, has repeatedly made claims of the potential arrival of COVID vaccines that are at odds with timelines offered with guarded optimism by experts in infectious diseases.
But based on these new guidelines from the FDA, it appears that the White House may now endorse the FDA’s stance, according to a Wall Street Journal report based on “people familiar with the matter.”
The publication reports that the White House, which has yet to officially comment, “endorsed the U.S. Food and Drug Administration’s plans for assessing whether a Covid-19 vaccine should be given widely, casting aside objections to requirements that would likely mean a shot won’t be cleared until after Election Day, people familiar with the matter said.”
Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, on Monday night said during a virtual appearance at the twenty-first annual New Yorker Festival that there could be evidence as early as November or December about whether one of the vaccines now in testing will work out. He declared himself to have “cautious optimism” about potential rollout of vaccines as early as late 2020 or early 2021.
Peter Lurie, MD, MPH, who earlier served as the FDA’s associate commissioner for public health strategy and analysis, described the agency’s release of the briefing document as being a positive development.
News organizations, including the New York Times, have reported that the White House had sought to block the FDA from releasing further instructions for companies developing COVID-19 vaccines. The Associated Press on Tuesday said that a senior Trump administration official confirmed that the White House had blocked earlier FDA plans to formally publish the safety guidelines based on the 2-month data requirement, arguing that there was “no clinical or medical reason” for it.
“It is an encouraging sign that, despite opposition from the White House, the Food and Drug Administration has effectively published guidelines for emergency release of a vaccine for COVID-19 by disclosing the advice it has been providing to individual sponsors,” said Dr. Lurie, who is now executive director and president of the Center for Science in the Public Interest.
In a news release, he said the White House had sought to keep the FDA guidance under wraps “so it could maintain the public fiction that a safe and effective vaccine could be available before Election Day or even so that it could force emergency authorization of a vaccine with more limited follow-up.”
“Even the pharmaceutical industry has been clamoring for the release of these guidelines. We all want a safe and effective vaccine to end the pandemic, and we want it sooner rather than later,” Dr. Lurie said. “But we can’t afford for the Trump administration to bungle vaccine review the way they’ve bungled nearly every other aspect of its pandemic response.”
Tuesday also saw a flood of statements in support of FDA officials, including tweets from the chief executive of Pfizer, which is among the leaders in the race to develop a COVID-19 vaccine. Pfizer’s Albert Bourla, DVM, PhD, said that the FDA’s “public servants are known for their high integrity and scientific expertise and we have full faith in their ability to set appropriate standards for the approval of a COVID vaccine or treatment.”
The American Medical Association on Tuesday announced a public webinar on Wednesday where its president, Susan R. Bailey, MD, will discuss the COVID-19 vaccine review process with Peter Marks, MD, PhD, director of the Center for Biologics Evaluation and Research at the FDA. The AMA described this webinar as part of work “to restore trust in science and science-based decision-making among policymakers and the public.”
“To ensure media and the physician community are continuously informed about the federal review process for COVID-19 vaccine candidates, the AMA will host a webinar series to gain fact-based insights from the nation’s highest-ranking subject matter experts working to protect the health of the public,” the organization said in announcing the webinar.
In a statement, leaders of the Association of American Medical Colleges said that the FDA’s Vaccines and Related Biological Products Advisory Committee should evaluate any COVID-19 candidate vaccines prior to the FDA issuing an EUA.
“Full approval of a new vaccine or biologic requires demonstration of safety and effectiveness through a process that includes evaluation by the VRBPAC. Their recommendations are considered by FDA staff who ultimately have the authority to approve the new product,” said AAMC chief scientific officer Ross McKinney Jr, MD, and AAMC CEO David J. Skorton, MD, in the statement.
Thomas M. File Jr., MD, president of the Infectious Diseases Society of America, said in a statement that his association again asked the White House to “follow medical and scientific expertise in efforts to combat COVID-19.”
“It is imperative that a vaccine be approved on the basis of FDA’s quality standards and that its safety and efficacy are established before it is authorized,” Dr. File said. “A vaccine that has been approved with speed, rather than safety and efficacy, at the forefront will compound the challenges posed by this pandemic. FDA guidelines for approval that set standards the American people can trust are essential to the success of a vaccine.”
Stephen J. Ubl, chief executive of the Pharmaceutical Research and Manufacturers of America, said in a statement that his association “supports any efforts by FDA to provide clarifying guidance and we have engaged with the agency to support bringing greater transparency to the review process for COVID-19 vaccines.”
“To help address this public health crisis, our companies have also taken unprecedented steps to share vaccine clinical trial protocols and data in real time,” Mr. Ubl said. “We welcome the agency’s efforts to instill confidence in the rigorous safety of these potential vaccines.”
On Oct. 1, Michelle McMurry-Heath, MD, PhD, president and chief executive of the Biotechnology Innovation Organization, released publicly her letter urging Department of Health & Human Services Secretary Alex Azar to “publicly release all new guidance” related to a COVID-19 vaccine. Such a move would bolster public confidence in the vaccine, she said.
“We cannot allow a lack of transparency to undermine confidence in the vaccine development process. The public must have full faith in the scientific process and the rigor of FDA’s regulatory oversight if we are to end the pandemic,” she wrote in the Oct. 1 letter to Azar. “Releasing any additional guidance on granting emergency use authorization for a vaccine will go a long way in accomplishing this critical goal.”
This article first appeared on Medscape.com.
Long-Term Oxygen Therapy and Risk of Fire-Related Events
Chronic obstructive pulmonary disease (COPD) has been the third leading cause of death in the US since 2008.1 Current management of COPD includes smoking cessation, adequate nutrition, medication therapy, pulmonary rehabilitation, and vaccines.2 Outside of pharmacologic management, oxygen therapy has become a staple treatment of chronic hypoxemic respiratory failure due to COPD. Landmark trials, including the Nocturnal Oxygen Therapy Trial (NOTT) and Medical Research Council (MRC) study, demonstrated improved survival in patients with COPD and hypoxemia, particularly if these patients received oxygen for 18 hours per day.3,4 NOTT prospectively evaluated 203 patients at 6 centers who were randomly allocated to either continuous oxygen therapy or 12-hour nocturnal oxygen therapy. The overall mortality in the nocturnal oxygen therapy group was 1.94 times that in the continuous oxygen therapy group (P = .01).3 The MRC study included 87 patients who were randomized to oxygen therapy or no oxygen; risk of death was 12% per year in the treated group vs 29% per year in the control group (P = .04).4 The effectiveness of long-term oxygen therapy (LTOT) in active smokers continues to be a source of debate; although 50% of patients in the NOTT trial were smokers, there was no subgroup analysis of whether smoking status had an impact on survival in those on continuous oxygen therapy.
Although many therapies are available for the treatment of COPD, the most effective treatment to prevent the progression of COPD is smoking cessation. Resources like smoking cessation programs, nicotine patches, and medications, such as bupropion and varenicline, are available to aid smoking cessation.5 However, many patients are unable to quit tobacco use despite their best efforts using available resources, and they continue to smoke even with progressive COPD. Long-time smokers also are likely to continue smoking while on LTOT, which increases their risk for fire-related injury.6-8
Traditional indications are being scrutinized after the LTOT trial found no benefit with respect to time to death or first hospitalization among patients with stable COPD and resting or exercise-induced moderate desaturation.9
Although oxygen accelerates combustion and is a potential fire hazard, LTOT has been prescribed even to active smokers as the 2 landmark trials did not exclude patients who were active smokers from receiving oxygen therapy.3,4 Therefore, LTOT has traditionally been prescribed to veterans who are actively smoking, despite the fire hazard. Attempts at mitigating hazards related to oxygen therapy in active smokers include counseling extensively about safety measures (which includes avoiding open flames such as candles, large fires, or sparks when on LTOT and providing Home Safety Agreements—a written contract between prescriber and patient wherein the patient agrees to abide by the terms of the US Department of Veterans Affairs (VA) to mitigate hazards related to LTOT in order to receive LTOT (eAppendix
Methods
With this practice in mind, we conducted an institutional review board approved retrospective chart review of all veterans with diagnosis of COPD within the Central Texas Veterans Health Care System (CTVHCS) who were prescribed new LTOT between October 1, 2010 and September 30, 2015. Given the retrospective nature of the chart review, patient consent was not obtained. Inclusion criteria were veterans aged > 18 years who had a confirmed diagnosis of COPD by spirometry and who met criteria for either continuous or ambulation- only oxygen therapy.
Criteria for exclusion included patients with hypoxemia not solely attributable to COPD or due to diseases other than COPD. We reviewed encounters in these patients’ charts, including follow-up in the clinic of the providers prescribing oxygen, to assess for fire-related incidents, defined as events wherein fire was visualized by the patient or by individuals living with the patient and with report provided to medical equipment company providing oxygen; the patient did not have to seek medical care to qualify for fire-related incident. Of the 158 patients who met the criteria for inclusion in the study, 152 were male.
Statistics
Bayesian logistic regression was used to model the outcome variable fire-related incident with the predictors smoking status, age, race, depression, PTSD, and type of oxygen used. Mental health disorders have significant effect on substance use disorders, such as alcohol use. Depression and PTSD were more common mental health diagnoses found in our patient population. Additionally, due to the small sample size, these psychiatric diagnoses were chosen to evaluate the impact of mental health disorders on firerelated events.
Although the sample size of events was small, weakly informative normal priors (0, 2.5) were used to shrink parameter estimates toward 0 and minimize overfitting. Weakly informative normal priors have also been suggested to deal with the problem of quasi-complete separation, where in our case, both smoking and no-PTSD perfectly predicted the 9 fire-related incidents.10 All input variables were centered and scaled as recommended. 9 The model fit well as assessed by posterior predictive checks, and Rhat was 1.00 for all parameters, indicating that all chains converged. Analysis was completed in R version 3.5.1 using the ‘brms’ package for Bayesian modeling.11
Results
The mean age for the 158 included patients was 71.3 years in nonsmokers and 65.9 years in smokers. Fifty-three of the included patients were active smokers when LTOT was initiated. Nine veterans had fire-related incidents during the study period. All 9 patients were actively smoking (about 17%) at the time of the fire incidents. There were no deaths, and 5 patients required hospitalization due to facial burns resulting from the fire-related incidents. Our study focused on 5 baseline characteristics in our population (Table 1). After gathering data, our group inferred that these characteristics had a potential relationship to fire-related incidents compared with other variables that were studied. Future studies could look at other patient characteristics that may be linked to fire-related incidents in patients on LTOT. For example, not having PTSD also perfectly predicts fire-related incidents in our data (ie, none of the participants who had fire-related incidents had PTSD). Although this finding was not within the 95% confidence interval (CI) in the model, it does show that care must be taken when interpreting effects from small samples (Table 2). The modelestimated odds of a fire-related incident occurring in a smoker were 31.6 (5.1-372.7) times more likely than were the odds of a firerelated incident occurring in a nonsmoker, holding all other predictors at their reference level; 95% CI for the odds ratios for all other predictors in the model included a value of 1.
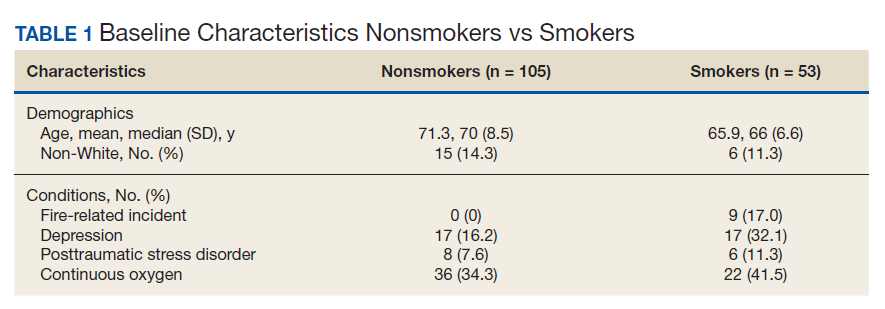

Discussion
This study showed evidence of increased odds of fire-related events in actively smoking patients receiving LTOT compared with patients who do not actively smoke while attempting to adjust for potential confounders. Of the 9 patients who had fire events, 5 required hospitalization for burns.
A similar retrospective cohort study by Sharma and colleagues in 2015 demonstrated an increased risk of burn-related injury when on LTOT but reiterated that the benefit of oxygen outweighs the risk of burn-related injury in patients requiring oxygen therapy.12 Interestingly, Sharma and colleagues were unable to identify smoking status for the patients studied but further identified factors associated with burn injury to include male sex, low socioeconomic status, oxygen therapy use, and ≥ 3 comorbidities. The study’s conclusion recommended continued education by health care professionals (HCPs) to their patients on LTOT regarding potential for burn injury. In the same vein, the VA National Center for Ethics in Health Care noted that “clinicians should familiarize themselves with the risks and benefits of LTOT; should inform their patients of the risks and benefits without exaggerating the risk associated with smoking; avoid undue coercion inherent in the clinician’s ability to withdraw LTOT; reduce the risk to the greatest degree possible; and consider termination of LTOT in very extreme cases and in consultation with a multidisciplinary committee.”13
This statement is in contrast to the guidelines and policies of other countries, such as Sweden, where smoking is a direct contraindication for prescription of oxygen therapy, or in Australia and New Zealand, where the Thoracic Society of Australia and New Zealand oxygen therapy guidelines recommend against prescription of LTOT, citing “increased fire risk and the probability that the poorer prognosis conferred by smoking will offset treatment benefit.”6,14
The prevalence of oxygen therapy introduces the potential for fire-related incidents with subsequent injury requiring medical care. There are few studies regarding home oxygen fire in the US due to the lack of a uniform reporting system. One study by Wendling and Pelletier analyzed deaths in Maine, Massachusetts, New Hampshire, and Oklahoma between 2000 and 2007 and found 38 deaths directly attributable to home oxygen fires as a result of smoking.15 Further, the Consumer Product Safety Commission’s National Electronic Injury Surveillance System between 2003 and 2006 attributed 1,190 thermal burns related to home oxygen fires; the majority of which were ignited by tobacco smoking.15 The Swedish National Register of Respiratory Failure (Swedevox) published prospective population-based, consecutive cohort study that collected data over 17 years and evaluated the risk of fire-related incident in those on LTOT. Of the 12,497 patients sampled, 17 had a burn injury and 2 patients died. The low incidence of burn injury on LTOT was attributed to the strict guidelines instituted in Sweden for doctors to avoid prescribing LTOT to actively smoking patients.6 A follow-up study by Tanash and colleagues compared the risk of burn injury in each country, respectively. The results found an increased number of burn injuries in those on oxygen therapy in Denmark, a country with fewer restrictions on smoking compared with those of Sweden.7 Similarly, our results showed that the rate of fire and burn injuries was exclusively among veterans who were active smokers. All patients who were prescribed oxygen therapy at CTVHCS received counseling and signed Home Safety Agreements. Despite following the recommendations set forth by the VA on counseling, extensive harm reduction techniques, and close follow-up, we found there was still a high incidence of fires in veterans with COPD on LTOT who continue to smoke.
The findings from our study concur with those previously published regarding the risk of home oxygen fire and concomitant smoking, supporting the idea for more regulated and concrete guidelines for prescribing LTOT to those requiring it.8
Limitations
The major limitation was the small sample size of our study. Another limitation was that our study population is predominantly male as is common in veteran cohorts. In fiscal year 2016, the veteran population of Texas was 1,434,361 males and 168,967 females.16 According to Franklin and colleagues, HCPs noticed an increase use of long-term oxygen among women compared with that of men.17
Conclusions
Our study showed an increased odds of firerelated incidents of patients while on LTOT, strengthening the argument that even with extensive education, those who smoke and are on LTOT continue to put themselves at risk of a fire-related incident. This finding stresses the importance of continuing patient education on the importance of smoking cessation prior to administration of LTOT or avoiding fire hazards while on LTOT. Further research into LTOT and fire hazards could help in implementing a more structured approval process for patients who want to obtain LTOT. We propose further studies evaluating risk factors for the incidence of fire events among patients prescribed LTOT. A growing and aging population with a need for LTOT necessitates examination of oxygen safe prescribing.
1. Ni H, Xu J. COPD-related mortality by sex and race among adults aged 25 and over: United States 2000-2014. https:// www.cdc.gov/nchs/data/databriefs/db256.pdf. Published September 2016. Accessed September 10, 2020.
2. Itoh M, Tsuji T, Nemoto K, Nakamura H, Aoshiba K. Undernutrition in patients with COPD and its treatment. Nutrients. 2013;5(4):1316-1335. doi:10.3390/nu5041316
3. Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease: a clinical trial. Nocturnal Oxygen Therapy Trial Group. Ann Intern Med. 1980;93(3):391. doi:10.7326/0003-4819-93-3-391
4. Long term domiciliary oxygen therapy in chronic hypoxic cor pulmonale complicating chronic bronchitis and emphysema. Report of the Medical Research Council Working Party. Lancet. 1981;1(8222):681-686. doi:10.1016/S0140-6736(81)91970-X
5. Anthonisen NR, Skeans MA, Wise RA, Manfreda J, Kanner RE, Connett JE. The effects of a smoking cessation intervention on 14.5-year mortality. Ann Intern Med. 2005;142(4):233-239. doi:10.7326/0003-4819-142-4 -200502150-00005
6. Tanash HA, Huss F, Ekström M. The risk of burn injury during long-term oxygen therapy: a 17-year longitudinal national study in Sweden. Int J Chron Obstruct Pulmon Dis. 2015;10:2479-2484. doi:10.2147/COPD.S91508
7. Tanash HA, Ringbaek T, Huss F, Ekström M. Burn injury during long-term oxygen therapy in Denmark and Sweden: the potential role of smoking. Int J Chronic Obstruct Pulmon Dis. 2017;12:193-197. doi:10.2147/COPD.S119949
8. Kassis SA, Savetamal A, Assi R, et al. Characteristics of patients with injury secondary to smoking on home oxygen therapy transferred intubated to a burn center. J Am Coll Surg. 2014;218(6):1182-1186. doi:10.1016/j.jamcollsurg.2013.12.055
9. Long-Term Oxygen Treatment Trial Research Group, Albert RK, Au DH, et al. A Randomized Trial of Long-Term Oxygen for COPD with Moderate Desaturation. N Engl J Med. 2016;375(17):1617-1627. doi:10.1056/NEJMoa1604344
10. Ghosh J, Li Y, Mitra R. On the use of Cauchy prior distributions for Bayesian logistic regression. Bayesian Anal. 2018;13(2):359-383. doi:10.1214/17-ba1051
11. Bürkner P-C. brms: An R package for Bayesian multilevel models using Stan. J Stat Software. 2017;80(1). doi:10.18637/jss.v080.i01
12. Sharma G, Meena R, Goodwin JS, Zhang W, Kuo Y-F, Duarte AG. Burn injury associated with home oxygen use in patients with chronic obstructive pulmonary disease. Mayo Clin Proc. 2015;90(4):492-499. doi:10.1016/j.mayocp.2014.12.024
13. US Department of Veterans Affairs, National Ethics Committee. Ethical considerations that arise when a home care patient on long term oxygen therapy continues to smoke. http://vaww.ethics.va.gov/docs/necrpts/NEC_Report_20100301_Smoking_while_on_LTOT.pdf. Published March 2010. [Nonpublic, source not verified.]
14. McDonald C F, Whyte K, Jenkins S, Serginson J. Frith P. Clinical practice guideline on adult domiciliary oxygen therapy: executive summary from the Thoracic Society of Australia and New Zealand. Respirology. 2016;21(1):76-78. doi:10.1111/resp.12678
15. Centers for Disease Control and Prevention (CDC). Fatal fires associated with smoking during long-term oxygen therapy--Maine, Massachusetts, New Hampshire, and Oklahoma, 2000-2007. MMWR Morb Mortal Wkly Rep. 2008;57(31):852-854.
16. US Department of Veteran Affairs. National Center for Veterans Analysis and Statistics. Population tables: the state, age/gender, 2016. https://www.va.gov/vetdata/Veteran_ Population.asp. Updated August 5, 2020. Accessed September 11, 2020.
17. Franklin KA, Gustafson T, Ranstam J, Ström K. Survival and future need of long-term oxygen therapy for chronic obstructive pulmonary disease--gender differences. Respir Med. 2007;101(7):1506-1511. doi:10.1016/j.rmed.2007.01.009
Chronic obstructive pulmonary disease (COPD) has been the third leading cause of death in the US since 2008.1 Current management of COPD includes smoking cessation, adequate nutrition, medication therapy, pulmonary rehabilitation, and vaccines.2 Outside of pharmacologic management, oxygen therapy has become a staple treatment of chronic hypoxemic respiratory failure due to COPD. Landmark trials, including the Nocturnal Oxygen Therapy Trial (NOTT) and Medical Research Council (MRC) study, demonstrated improved survival in patients with COPD and hypoxemia, particularly if these patients received oxygen for 18 hours per day.3,4 NOTT prospectively evaluated 203 patients at 6 centers who were randomly allocated to either continuous oxygen therapy or 12-hour nocturnal oxygen therapy. The overall mortality in the nocturnal oxygen therapy group was 1.94 times that in the continuous oxygen therapy group (P = .01).3 The MRC study included 87 patients who were randomized to oxygen therapy or no oxygen; risk of death was 12% per year in the treated group vs 29% per year in the control group (P = .04).4 The effectiveness of long-term oxygen therapy (LTOT) in active smokers continues to be a source of debate; although 50% of patients in the NOTT trial were smokers, there was no subgroup analysis of whether smoking status had an impact on survival in those on continuous oxygen therapy.
Although many therapies are available for the treatment of COPD, the most effective treatment to prevent the progression of COPD is smoking cessation. Resources like smoking cessation programs, nicotine patches, and medications, such as bupropion and varenicline, are available to aid smoking cessation.5 However, many patients are unable to quit tobacco use despite their best efforts using available resources, and they continue to smoke even with progressive COPD. Long-time smokers also are likely to continue smoking while on LTOT, which increases their risk for fire-related injury.6-8
Traditional indications are being scrutinized after the LTOT trial found no benefit with respect to time to death or first hospitalization among patients with stable COPD and resting or exercise-induced moderate desaturation.9
Although oxygen accelerates combustion and is a potential fire hazard, LTOT has been prescribed even to active smokers as the 2 landmark trials did not exclude patients who were active smokers from receiving oxygen therapy.3,4 Therefore, LTOT has traditionally been prescribed to veterans who are actively smoking, despite the fire hazard. Attempts at mitigating hazards related to oxygen therapy in active smokers include counseling extensively about safety measures (which includes avoiding open flames such as candles, large fires, or sparks when on LTOT and providing Home Safety Agreements—a written contract between prescriber and patient wherein the patient agrees to abide by the terms of the US Department of Veterans Affairs (VA) to mitigate hazards related to LTOT in order to receive LTOT (eAppendix
Methods
With this practice in mind, we conducted an institutional review board approved retrospective chart review of all veterans with diagnosis of COPD within the Central Texas Veterans Health Care System (CTVHCS) who were prescribed new LTOT between October 1, 2010 and September 30, 2015. Given the retrospective nature of the chart review, patient consent was not obtained. Inclusion criteria were veterans aged > 18 years who had a confirmed diagnosis of COPD by spirometry and who met criteria for either continuous or ambulation- only oxygen therapy.
Criteria for exclusion included patients with hypoxemia not solely attributable to COPD or due to diseases other than COPD. We reviewed encounters in these patients’ charts, including follow-up in the clinic of the providers prescribing oxygen, to assess for fire-related incidents, defined as events wherein fire was visualized by the patient or by individuals living with the patient and with report provided to medical equipment company providing oxygen; the patient did not have to seek medical care to qualify for fire-related incident. Of the 158 patients who met the criteria for inclusion in the study, 152 were male.
Statistics
Bayesian logistic regression was used to model the outcome variable fire-related incident with the predictors smoking status, age, race, depression, PTSD, and type of oxygen used. Mental health disorders have significant effect on substance use disorders, such as alcohol use. Depression and PTSD were more common mental health diagnoses found in our patient population. Additionally, due to the small sample size, these psychiatric diagnoses were chosen to evaluate the impact of mental health disorders on firerelated events.
Although the sample size of events was small, weakly informative normal priors (0, 2.5) were used to shrink parameter estimates toward 0 and minimize overfitting. Weakly informative normal priors have also been suggested to deal with the problem of quasi-complete separation, where in our case, both smoking and no-PTSD perfectly predicted the 9 fire-related incidents.10 All input variables were centered and scaled as recommended. 9 The model fit well as assessed by posterior predictive checks, and Rhat was 1.00 for all parameters, indicating that all chains converged. Analysis was completed in R version 3.5.1 using the ‘brms’ package for Bayesian modeling.11
Results
The mean age for the 158 included patients was 71.3 years in nonsmokers and 65.9 years in smokers. Fifty-three of the included patients were active smokers when LTOT was initiated. Nine veterans had fire-related incidents during the study period. All 9 patients were actively smoking (about 17%) at the time of the fire incidents. There were no deaths, and 5 patients required hospitalization due to facial burns resulting from the fire-related incidents. Our study focused on 5 baseline characteristics in our population (Table 1). After gathering data, our group inferred that these characteristics had a potential relationship to fire-related incidents compared with other variables that were studied. Future studies could look at other patient characteristics that may be linked to fire-related incidents in patients on LTOT. For example, not having PTSD also perfectly predicts fire-related incidents in our data (ie, none of the participants who had fire-related incidents had PTSD). Although this finding was not within the 95% confidence interval (CI) in the model, it does show that care must be taken when interpreting effects from small samples (Table 2). The modelestimated odds of a fire-related incident occurring in a smoker were 31.6 (5.1-372.7) times more likely than were the odds of a firerelated incident occurring in a nonsmoker, holding all other predictors at their reference level; 95% CI for the odds ratios for all other predictors in the model included a value of 1.
Discussion
This study showed evidence of increased odds of fire-related events in actively smoking patients receiving LTOT compared with patients who do not actively smoke while attempting to adjust for potential confounders. Of the 9 patients who had fire events, 5 required hospitalization for burns.
A similar retrospective cohort study by Sharma and colleagues in 2015 demonstrated an increased risk of burn-related injury when on LTOT but reiterated that the benefit of oxygen outweighs the risk of burn-related injury in patients requiring oxygen therapy.12 Interestingly, Sharma and colleagues were unable to identify smoking status for the patients studied but further identified factors associated with burn injury to include male sex, low socioeconomic status, oxygen therapy use, and ≥ 3 comorbidities. The study’s conclusion recommended continued education by health care professionals (HCPs) to their patients on LTOT regarding potential for burn injury. In the same vein, the VA National Center for Ethics in Health Care noted that “clinicians should familiarize themselves with the risks and benefits of LTOT; should inform their patients of the risks and benefits without exaggerating the risk associated with smoking; avoid undue coercion inherent in the clinician’s ability to withdraw LTOT; reduce the risk to the greatest degree possible; and consider termination of LTOT in very extreme cases and in consultation with a multidisciplinary committee.”13
This statement is in contrast to the guidelines and policies of other countries, such as Sweden, where smoking is a direct contraindication for prescription of oxygen therapy, or in Australia and New Zealand, where the Thoracic Society of Australia and New Zealand oxygen therapy guidelines recommend against prescription of LTOT, citing “increased fire risk and the probability that the poorer prognosis conferred by smoking will offset treatment benefit.”6,14
The prevalence of oxygen therapy introduces the potential for fire-related incidents with subsequent injury requiring medical care. There are few studies regarding home oxygen fire in the US due to the lack of a uniform reporting system. One study by Wendling and Pelletier analyzed deaths in Maine, Massachusetts, New Hampshire, and Oklahoma between 2000 and 2007 and found 38 deaths directly attributable to home oxygen fires as a result of smoking.15 Further, the Consumer Product Safety Commission’s National Electronic Injury Surveillance System between 2003 and 2006 attributed 1,190 thermal burns related to home oxygen fires; the majority of which were ignited by tobacco smoking.15 The Swedish National Register of Respiratory Failure (Swedevox) published prospective population-based, consecutive cohort study that collected data over 17 years and evaluated the risk of fire-related incident in those on LTOT. Of the 12,497 patients sampled, 17 had a burn injury and 2 patients died. The low incidence of burn injury on LTOT was attributed to the strict guidelines instituted in Sweden for doctors to avoid prescribing LTOT to actively smoking patients.6 A follow-up study by Tanash and colleagues compared the risk of burn injury in each country, respectively. The results found an increased number of burn injuries in those on oxygen therapy in Denmark, a country with fewer restrictions on smoking compared with those of Sweden.7 Similarly, our results showed that the rate of fire and burn injuries was exclusively among veterans who were active smokers. All patients who were prescribed oxygen therapy at CTVHCS received counseling and signed Home Safety Agreements. Despite following the recommendations set forth by the VA on counseling, extensive harm reduction techniques, and close follow-up, we found there was still a high incidence of fires in veterans with COPD on LTOT who continue to smoke.
The findings from our study concur with those previously published regarding the risk of home oxygen fire and concomitant smoking, supporting the idea for more regulated and concrete guidelines for prescribing LTOT to those requiring it.8
Limitations
The major limitation was the small sample size of our study. Another limitation was that our study population is predominantly male as is common in veteran cohorts. In fiscal year 2016, the veteran population of Texas was 1,434,361 males and 168,967 females.16 According to Franklin and colleagues, HCPs noticed an increase use of long-term oxygen among women compared with that of men.17
Conclusions
Our study showed an increased odds of firerelated incidents of patients while on LTOT, strengthening the argument that even with extensive education, those who smoke and are on LTOT continue to put themselves at risk of a fire-related incident. This finding stresses the importance of continuing patient education on the importance of smoking cessation prior to administration of LTOT or avoiding fire hazards while on LTOT. Further research into LTOT and fire hazards could help in implementing a more structured approval process for patients who want to obtain LTOT. We propose further studies evaluating risk factors for the incidence of fire events among patients prescribed LTOT. A growing and aging population with a need for LTOT necessitates examination of oxygen safe prescribing.
Chronic obstructive pulmonary disease (COPD) has been the third leading cause of death in the US since 2008.1 Current management of COPD includes smoking cessation, adequate nutrition, medication therapy, pulmonary rehabilitation, and vaccines.2 Outside of pharmacologic management, oxygen therapy has become a staple treatment of chronic hypoxemic respiratory failure due to COPD. Landmark trials, including the Nocturnal Oxygen Therapy Trial (NOTT) and Medical Research Council (MRC) study, demonstrated improved survival in patients with COPD and hypoxemia, particularly if these patients received oxygen for 18 hours per day.3,4 NOTT prospectively evaluated 203 patients at 6 centers who were randomly allocated to either continuous oxygen therapy or 12-hour nocturnal oxygen therapy. The overall mortality in the nocturnal oxygen therapy group was 1.94 times that in the continuous oxygen therapy group (P = .01).3 The MRC study included 87 patients who were randomized to oxygen therapy or no oxygen; risk of death was 12% per year in the treated group vs 29% per year in the control group (P = .04).4 The effectiveness of long-term oxygen therapy (LTOT) in active smokers continues to be a source of debate; although 50% of patients in the NOTT trial were smokers, there was no subgroup analysis of whether smoking status had an impact on survival in those on continuous oxygen therapy.
Although many therapies are available for the treatment of COPD, the most effective treatment to prevent the progression of COPD is smoking cessation. Resources like smoking cessation programs, nicotine patches, and medications, such as bupropion and varenicline, are available to aid smoking cessation.5 However, many patients are unable to quit tobacco use despite their best efforts using available resources, and they continue to smoke even with progressive COPD. Long-time smokers also are likely to continue smoking while on LTOT, which increases their risk for fire-related injury.6-8
Traditional indications are being scrutinized after the LTOT trial found no benefit with respect to time to death or first hospitalization among patients with stable COPD and resting or exercise-induced moderate desaturation.9
Although oxygen accelerates combustion and is a potential fire hazard, LTOT has been prescribed even to active smokers as the 2 landmark trials did not exclude patients who were active smokers from receiving oxygen therapy.3,4 Therefore, LTOT has traditionally been prescribed to veterans who are actively smoking, despite the fire hazard. Attempts at mitigating hazards related to oxygen therapy in active smokers include counseling extensively about safety measures (which includes avoiding open flames such as candles, large fires, or sparks when on LTOT and providing Home Safety Agreements—a written contract between prescriber and patient wherein the patient agrees to abide by the terms of the US Department of Veterans Affairs (VA) to mitigate hazards related to LTOT in order to receive LTOT (eAppendix
Methods
With this practice in mind, we conducted an institutional review board approved retrospective chart review of all veterans with diagnosis of COPD within the Central Texas Veterans Health Care System (CTVHCS) who were prescribed new LTOT between October 1, 2010 and September 30, 2015. Given the retrospective nature of the chart review, patient consent was not obtained. Inclusion criteria were veterans aged > 18 years who had a confirmed diagnosis of COPD by spirometry and who met criteria for either continuous or ambulation- only oxygen therapy.
Criteria for exclusion included patients with hypoxemia not solely attributable to COPD or due to diseases other than COPD. We reviewed encounters in these patients’ charts, including follow-up in the clinic of the providers prescribing oxygen, to assess for fire-related incidents, defined as events wherein fire was visualized by the patient or by individuals living with the patient and with report provided to medical equipment company providing oxygen; the patient did not have to seek medical care to qualify for fire-related incident. Of the 158 patients who met the criteria for inclusion in the study, 152 were male.
Statistics
Bayesian logistic regression was used to model the outcome variable fire-related incident with the predictors smoking status, age, race, depression, PTSD, and type of oxygen used. Mental health disorders have significant effect on substance use disorders, such as alcohol use. Depression and PTSD were more common mental health diagnoses found in our patient population. Additionally, due to the small sample size, these psychiatric diagnoses were chosen to evaluate the impact of mental health disorders on firerelated events.
Although the sample size of events was small, weakly informative normal priors (0, 2.5) were used to shrink parameter estimates toward 0 and minimize overfitting. Weakly informative normal priors have also been suggested to deal with the problem of quasi-complete separation, where in our case, both smoking and no-PTSD perfectly predicted the 9 fire-related incidents.10 All input variables were centered and scaled as recommended. 9 The model fit well as assessed by posterior predictive checks, and Rhat was 1.00 for all parameters, indicating that all chains converged. Analysis was completed in R version 3.5.1 using the ‘brms’ package for Bayesian modeling.11
Results
The mean age for the 158 included patients was 71.3 years in nonsmokers and 65.9 years in smokers. Fifty-three of the included patients were active smokers when LTOT was initiated. Nine veterans had fire-related incidents during the study period. All 9 patients were actively smoking (about 17%) at the time of the fire incidents. There were no deaths, and 5 patients required hospitalization due to facial burns resulting from the fire-related incidents. Our study focused on 5 baseline characteristics in our population (Table 1). After gathering data, our group inferred that these characteristics had a potential relationship to fire-related incidents compared with other variables that were studied. Future studies could look at other patient characteristics that may be linked to fire-related incidents in patients on LTOT. For example, not having PTSD also perfectly predicts fire-related incidents in our data (ie, none of the participants who had fire-related incidents had PTSD). Although this finding was not within the 95% confidence interval (CI) in the model, it does show that care must be taken when interpreting effects from small samples (Table 2). The modelestimated odds of a fire-related incident occurring in a smoker were 31.6 (5.1-372.7) times more likely than were the odds of a firerelated incident occurring in a nonsmoker, holding all other predictors at their reference level; 95% CI for the odds ratios for all other predictors in the model included a value of 1.
Discussion
This study showed evidence of increased odds of fire-related events in actively smoking patients receiving LTOT compared with patients who do not actively smoke while attempting to adjust for potential confounders. Of the 9 patients who had fire events, 5 required hospitalization for burns.
A similar retrospective cohort study by Sharma and colleagues in 2015 demonstrated an increased risk of burn-related injury when on LTOT but reiterated that the benefit of oxygen outweighs the risk of burn-related injury in patients requiring oxygen therapy.12 Interestingly, Sharma and colleagues were unable to identify smoking status for the patients studied but further identified factors associated with burn injury to include male sex, low socioeconomic status, oxygen therapy use, and ≥ 3 comorbidities. The study’s conclusion recommended continued education by health care professionals (HCPs) to their patients on LTOT regarding potential for burn injury. In the same vein, the VA National Center for Ethics in Health Care noted that “clinicians should familiarize themselves with the risks and benefits of LTOT; should inform their patients of the risks and benefits without exaggerating the risk associated with smoking; avoid undue coercion inherent in the clinician’s ability to withdraw LTOT; reduce the risk to the greatest degree possible; and consider termination of LTOT in very extreme cases and in consultation with a multidisciplinary committee.”13
This statement is in contrast to the guidelines and policies of other countries, such as Sweden, where smoking is a direct contraindication for prescription of oxygen therapy, or in Australia and New Zealand, where the Thoracic Society of Australia and New Zealand oxygen therapy guidelines recommend against prescription of LTOT, citing “increased fire risk and the probability that the poorer prognosis conferred by smoking will offset treatment benefit.”6,14
The prevalence of oxygen therapy introduces the potential for fire-related incidents with subsequent injury requiring medical care. There are few studies regarding home oxygen fire in the US due to the lack of a uniform reporting system. One study by Wendling and Pelletier analyzed deaths in Maine, Massachusetts, New Hampshire, and Oklahoma between 2000 and 2007 and found 38 deaths directly attributable to home oxygen fires as a result of smoking.15 Further, the Consumer Product Safety Commission’s National Electronic Injury Surveillance System between 2003 and 2006 attributed 1,190 thermal burns related to home oxygen fires; the majority of which were ignited by tobacco smoking.15 The Swedish National Register of Respiratory Failure (Swedevox) published prospective population-based, consecutive cohort study that collected data over 17 years and evaluated the risk of fire-related incident in those on LTOT. Of the 12,497 patients sampled, 17 had a burn injury and 2 patients died. The low incidence of burn injury on LTOT was attributed to the strict guidelines instituted in Sweden for doctors to avoid prescribing LTOT to actively smoking patients.6 A follow-up study by Tanash and colleagues compared the risk of burn injury in each country, respectively. The results found an increased number of burn injuries in those on oxygen therapy in Denmark, a country with fewer restrictions on smoking compared with those of Sweden.7 Similarly, our results showed that the rate of fire and burn injuries was exclusively among veterans who were active smokers. All patients who were prescribed oxygen therapy at CTVHCS received counseling and signed Home Safety Agreements. Despite following the recommendations set forth by the VA on counseling, extensive harm reduction techniques, and close follow-up, we found there was still a high incidence of fires in veterans with COPD on LTOT who continue to smoke.
The findings from our study concur with those previously published regarding the risk of home oxygen fire and concomitant smoking, supporting the idea for more regulated and concrete guidelines for prescribing LTOT to those requiring it.8
Limitations
The major limitation was the small sample size of our study. Another limitation was that our study population is predominantly male as is common in veteran cohorts. In fiscal year 2016, the veteran population of Texas was 1,434,361 males and 168,967 females.16 According to Franklin and colleagues, HCPs noticed an increase use of long-term oxygen among women compared with that of men.17
Conclusions
Our study showed an increased odds of firerelated incidents of patients while on LTOT, strengthening the argument that even with extensive education, those who smoke and are on LTOT continue to put themselves at risk of a fire-related incident. This finding stresses the importance of continuing patient education on the importance of smoking cessation prior to administration of LTOT or avoiding fire hazards while on LTOT. Further research into LTOT and fire hazards could help in implementing a more structured approval process for patients who want to obtain LTOT. We propose further studies evaluating risk factors for the incidence of fire events among patients prescribed LTOT. A growing and aging population with a need for LTOT necessitates examination of oxygen safe prescribing.
1. Ni H, Xu J. COPD-related mortality by sex and race among adults aged 25 and over: United States 2000-2014. https:// www.cdc.gov/nchs/data/databriefs/db256.pdf. Published September 2016. Accessed September 10, 2020.
2. Itoh M, Tsuji T, Nemoto K, Nakamura H, Aoshiba K. Undernutrition in patients with COPD and its treatment. Nutrients. 2013;5(4):1316-1335. doi:10.3390/nu5041316
3. Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease: a clinical trial. Nocturnal Oxygen Therapy Trial Group. Ann Intern Med. 1980;93(3):391. doi:10.7326/0003-4819-93-3-391
4. Long term domiciliary oxygen therapy in chronic hypoxic cor pulmonale complicating chronic bronchitis and emphysema. Report of the Medical Research Council Working Party. Lancet. 1981;1(8222):681-686. doi:10.1016/S0140-6736(81)91970-X
5. Anthonisen NR, Skeans MA, Wise RA, Manfreda J, Kanner RE, Connett JE. The effects of a smoking cessation intervention on 14.5-year mortality. Ann Intern Med. 2005;142(4):233-239. doi:10.7326/0003-4819-142-4 -200502150-00005
6. Tanash HA, Huss F, Ekström M. The risk of burn injury during long-term oxygen therapy: a 17-year longitudinal national study in Sweden. Int J Chron Obstruct Pulmon Dis. 2015;10:2479-2484. doi:10.2147/COPD.S91508
7. Tanash HA, Ringbaek T, Huss F, Ekström M. Burn injury during long-term oxygen therapy in Denmark and Sweden: the potential role of smoking. Int J Chronic Obstruct Pulmon Dis. 2017;12:193-197. doi:10.2147/COPD.S119949
8. Kassis SA, Savetamal A, Assi R, et al. Characteristics of patients with injury secondary to smoking on home oxygen therapy transferred intubated to a burn center. J Am Coll Surg. 2014;218(6):1182-1186. doi:10.1016/j.jamcollsurg.2013.12.055
9. Long-Term Oxygen Treatment Trial Research Group, Albert RK, Au DH, et al. A Randomized Trial of Long-Term Oxygen for COPD with Moderate Desaturation. N Engl J Med. 2016;375(17):1617-1627. doi:10.1056/NEJMoa1604344
10. Ghosh J, Li Y, Mitra R. On the use of Cauchy prior distributions for Bayesian logistic regression. Bayesian Anal. 2018;13(2):359-383. doi:10.1214/17-ba1051
11. Bürkner P-C. brms: An R package for Bayesian multilevel models using Stan. J Stat Software. 2017;80(1). doi:10.18637/jss.v080.i01
12. Sharma G, Meena R, Goodwin JS, Zhang W, Kuo Y-F, Duarte AG. Burn injury associated with home oxygen use in patients with chronic obstructive pulmonary disease. Mayo Clin Proc. 2015;90(4):492-499. doi:10.1016/j.mayocp.2014.12.024
13. US Department of Veterans Affairs, National Ethics Committee. Ethical considerations that arise when a home care patient on long term oxygen therapy continues to smoke. http://vaww.ethics.va.gov/docs/necrpts/NEC_Report_20100301_Smoking_while_on_LTOT.pdf. Published March 2010. [Nonpublic, source not verified.]
14. McDonald C F, Whyte K, Jenkins S, Serginson J. Frith P. Clinical practice guideline on adult domiciliary oxygen therapy: executive summary from the Thoracic Society of Australia and New Zealand. Respirology. 2016;21(1):76-78. doi:10.1111/resp.12678
15. Centers for Disease Control and Prevention (CDC). Fatal fires associated with smoking during long-term oxygen therapy--Maine, Massachusetts, New Hampshire, and Oklahoma, 2000-2007. MMWR Morb Mortal Wkly Rep. 2008;57(31):852-854.
16. US Department of Veteran Affairs. National Center for Veterans Analysis and Statistics. Population tables: the state, age/gender, 2016. https://www.va.gov/vetdata/Veteran_ Population.asp. Updated August 5, 2020. Accessed September 11, 2020.
17. Franklin KA, Gustafson T, Ranstam J, Ström K. Survival and future need of long-term oxygen therapy for chronic obstructive pulmonary disease--gender differences. Respir Med. 2007;101(7):1506-1511. doi:10.1016/j.rmed.2007.01.009
1. Ni H, Xu J. COPD-related mortality by sex and race among adults aged 25 and over: United States 2000-2014. https:// www.cdc.gov/nchs/data/databriefs/db256.pdf. Published September 2016. Accessed September 10, 2020.
2. Itoh M, Tsuji T, Nemoto K, Nakamura H, Aoshiba K. Undernutrition in patients with COPD and its treatment. Nutrients. 2013;5(4):1316-1335. doi:10.3390/nu5041316
3. Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease: a clinical trial. Nocturnal Oxygen Therapy Trial Group. Ann Intern Med. 1980;93(3):391. doi:10.7326/0003-4819-93-3-391
4. Long term domiciliary oxygen therapy in chronic hypoxic cor pulmonale complicating chronic bronchitis and emphysema. Report of the Medical Research Council Working Party. Lancet. 1981;1(8222):681-686. doi:10.1016/S0140-6736(81)91970-X
5. Anthonisen NR, Skeans MA, Wise RA, Manfreda J, Kanner RE, Connett JE. The effects of a smoking cessation intervention on 14.5-year mortality. Ann Intern Med. 2005;142(4):233-239. doi:10.7326/0003-4819-142-4 -200502150-00005
6. Tanash HA, Huss F, Ekström M. The risk of burn injury during long-term oxygen therapy: a 17-year longitudinal national study in Sweden. Int J Chron Obstruct Pulmon Dis. 2015;10:2479-2484. doi:10.2147/COPD.S91508
7. Tanash HA, Ringbaek T, Huss F, Ekström M. Burn injury during long-term oxygen therapy in Denmark and Sweden: the potential role of smoking. Int J Chronic Obstruct Pulmon Dis. 2017;12:193-197. doi:10.2147/COPD.S119949
8. Kassis SA, Savetamal A, Assi R, et al. Characteristics of patients with injury secondary to smoking on home oxygen therapy transferred intubated to a burn center. J Am Coll Surg. 2014;218(6):1182-1186. doi:10.1016/j.jamcollsurg.2013.12.055
9. Long-Term Oxygen Treatment Trial Research Group, Albert RK, Au DH, et al. A Randomized Trial of Long-Term Oxygen for COPD with Moderate Desaturation. N Engl J Med. 2016;375(17):1617-1627. doi:10.1056/NEJMoa1604344
10. Ghosh J, Li Y, Mitra R. On the use of Cauchy prior distributions for Bayesian logistic regression. Bayesian Anal. 2018;13(2):359-383. doi:10.1214/17-ba1051
11. Bürkner P-C. brms: An R package for Bayesian multilevel models using Stan. J Stat Software. 2017;80(1). doi:10.18637/jss.v080.i01
12. Sharma G, Meena R, Goodwin JS, Zhang W, Kuo Y-F, Duarte AG. Burn injury associated with home oxygen use in patients with chronic obstructive pulmonary disease. Mayo Clin Proc. 2015;90(4):492-499. doi:10.1016/j.mayocp.2014.12.024
13. US Department of Veterans Affairs, National Ethics Committee. Ethical considerations that arise when a home care patient on long term oxygen therapy continues to smoke. http://vaww.ethics.va.gov/docs/necrpts/NEC_Report_20100301_Smoking_while_on_LTOT.pdf. Published March 2010. [Nonpublic, source not verified.]
14. McDonald C F, Whyte K, Jenkins S, Serginson J. Frith P. Clinical practice guideline on adult domiciliary oxygen therapy: executive summary from the Thoracic Society of Australia and New Zealand. Respirology. 2016;21(1):76-78. doi:10.1111/resp.12678
15. Centers for Disease Control and Prevention (CDC). Fatal fires associated with smoking during long-term oxygen therapy--Maine, Massachusetts, New Hampshire, and Oklahoma, 2000-2007. MMWR Morb Mortal Wkly Rep. 2008;57(31):852-854.
16. US Department of Veteran Affairs. National Center for Veterans Analysis and Statistics. Population tables: the state, age/gender, 2016. https://www.va.gov/vetdata/Veteran_ Population.asp. Updated August 5, 2020. Accessed September 11, 2020.
17. Franklin KA, Gustafson T, Ranstam J, Ström K. Survival and future need of long-term oxygen therapy for chronic obstructive pulmonary disease--gender differences. Respir Med. 2007;101(7):1506-1511. doi:10.1016/j.rmed.2007.01.009
Restarting breast cancer screening after disruption not so simple
according to a modeling study reported at the 12th European Breast Cancer Conference.
Fallout of the pandemic has included reductions in cancer screening and diagnosis, said study investigator Lindy M. Kregting, a PhD student in the department of public health at Erasmus Medical Center, University Medical Center Rotterdam (the Netherlands).
In the Netherlands, new breast cancer diagnoses fell dramatically from historical levels starting in February. The number in April was less than half of that expected.
Ms. Kregting and colleagues used modeling to assess the impact of four strategies for restarting breast cancer screening in the Netherlands. The strategies differed regarding the population affected, the duration of the effects, and changes in stopping age. The usual situation, without any disruption, served as the comparator.
Results showed wide variation across strategies with respect to the increase in screening capacity needed during the latter half of this year – from 0% to 100% – and the excess breast cancer mortality occurring during 2020-2030 – from as many as 181 excess breast cancer deaths to as few as 14.
“The effects of the disruption are dependent on the chosen restart strategy,” Ms. Kregting summarized. “It would be preferred to immediately catch up because this minimizes the impact, but it also requires a very high capacity, so it may not always be possible. A proper alternative would be to increase the stopping age, so no screens are omitted, because this requires a rather normal capacity, and it will result in only small effects on incidence and mortality.”
As screening programs restart in some countries, there are still a lot of unknowns that could affect outcomes, including how many women will attend given that some may stay away out of fear, Ms. Kregting cautioned.
“We plan to do further model calculations when we know exactly what has happened. ... For now, we just assumed some reasonable disruption periods, and we assumed that capacity would be back to the original, before COVID-19, but I think we can say this is probably not the case,” she added.
Study details
Ms. Kregting and colleagues used Dutch breast cancer screening program parameters (biennial digital mammography for women aged 50-75 years) and a microsimulation screening analysis model to simulate four strategies for restarting breast cancer screening after a 6-month disruption:
- “Everyone delay,” a strategy in which all screening continues in the order planned with no change in the stopping age of 75 years (so that one in four women ultimately miss a screening during their lifetime)
- “First rounds no delay,” in which there is a delay in screening except for women having their first screening
- “Continue after stopping age,” in which there is a delay in screening but temporary increasing of the stopping age (to 76.5 years) to ensure all women get their final screen
- “Catch-up after stop,” in which capacity is increased to ensure full catch-up, with all delayed screens caught up in a 6-month period (the second half of 2020).
Results showed that 5,872 women would be screened in the latter half of 2020 if screening proceeded as usual without disruption. The necessary capacity was essentially the same with all of the restarting strategies, except for the catch-up-after-stop strategy, which would require a doubling of that number.
The temporal pattern of breast cancer incidence varied according to restart strategy early on, but incidence essentially returned to that expected with undisrupted screening by 2025 for all four strategies, with some small fluctuations thereafter.
The impact on breast cancer mortality differed considerably long term. It increased slightly and transiently above the expected level with the catch-up-after-stop strategy, but there were sizable, long-lasting increases with the other strategies, with excess deaths still seen in 2060 for the everyone-delay strategy.
In absolute terms, the excess number of breast cancer deaths during 2020-2030, compared with undisrupted screening, was 181 with the everyone-delay strategy, 155 with the first-rounds-no-delay strategy, 145 with the continue-after-stopping-age strategy, and just 14 with the catch-up-after-stop strategy. Ms. Kregting declined to provide numbers for other countries, given that the model is based on the Dutch population and screening program.
Results in context
“The unprecedented burden of COVID-19 on health systems worldwide has important implications for cancer care,” said invited discussant Alessandra Gennari, MD, PhD, of the University of Eastern Piedmont and Maggiore della Carità Hospital, both in Novara, Italy.
“There is a delay in diagnosis due to the fact that screening programs and diagnostic programs have been decreased or suspended in many Western countries where this is standard of care. Patients also are more reluctant to present to health care services, delaying their diagnosis,” Dr. Gennari said.
Findings of this new study add to those of similar studies undertaken in Italy (published in In Vivo) and the United Kingdom (published in The Lancet Oncology) showing the likely marked toll of the pandemic on cancer diagnosis and mortality, Dr. Gennari noted. Taken together, the findings underscore the urgent need for policy interventions to mitigate this impact.
“These interventions should focus on increasing routine diagnostic capacity, through which up to 40% of patients with cancer are diagnosed,” Dr. Gennari recommended. “Public health messaging is needed that accurately conveys the risk of severe illness from COVID-19 versus the risks of not seeking health care advice if patients are symptomatic. Finally, there is a need for provision of evidence-based data on which clinicians can adequately base their decision on how to manage the risks of cancer patients and the risks and benefits of procedures during the pandemic.”
The current study did not have any specific funding, and Ms. Kregting disclosed no conflicts of interest. Dr. Gennari disclosed relationships with Roche, Eisai, Lilly, AstraZeneca, Daiichi Sankyo, Merck, Novartis, and Pfizer.
SOURCE: Kregting L et al. EBCC-12 Virtual Conference, Abstract 24.
according to a modeling study reported at the 12th European Breast Cancer Conference.
Fallout of the pandemic has included reductions in cancer screening and diagnosis, said study investigator Lindy M. Kregting, a PhD student in the department of public health at Erasmus Medical Center, University Medical Center Rotterdam (the Netherlands).
In the Netherlands, new breast cancer diagnoses fell dramatically from historical levels starting in February. The number in April was less than half of that expected.
Ms. Kregting and colleagues used modeling to assess the impact of four strategies for restarting breast cancer screening in the Netherlands. The strategies differed regarding the population affected, the duration of the effects, and changes in stopping age. The usual situation, without any disruption, served as the comparator.
Results showed wide variation across strategies with respect to the increase in screening capacity needed during the latter half of this year – from 0% to 100% – and the excess breast cancer mortality occurring during 2020-2030 – from as many as 181 excess breast cancer deaths to as few as 14.
“The effects of the disruption are dependent on the chosen restart strategy,” Ms. Kregting summarized. “It would be preferred to immediately catch up because this minimizes the impact, but it also requires a very high capacity, so it may not always be possible. A proper alternative would be to increase the stopping age, so no screens are omitted, because this requires a rather normal capacity, and it will result in only small effects on incidence and mortality.”
As screening programs restart in some countries, there are still a lot of unknowns that could affect outcomes, including how many women will attend given that some may stay away out of fear, Ms. Kregting cautioned.
“We plan to do further model calculations when we know exactly what has happened. ... For now, we just assumed some reasonable disruption periods, and we assumed that capacity would be back to the original, before COVID-19, but I think we can say this is probably not the case,” she added.
Study details
Ms. Kregting and colleagues used Dutch breast cancer screening program parameters (biennial digital mammography for women aged 50-75 years) and a microsimulation screening analysis model to simulate four strategies for restarting breast cancer screening after a 6-month disruption:
- “Everyone delay,” a strategy in which all screening continues in the order planned with no change in the stopping age of 75 years (so that one in four women ultimately miss a screening during their lifetime)
- “First rounds no delay,” in which there is a delay in screening except for women having their first screening
- “Continue after stopping age,” in which there is a delay in screening but temporary increasing of the stopping age (to 76.5 years) to ensure all women get their final screen
- “Catch-up after stop,” in which capacity is increased to ensure full catch-up, with all delayed screens caught up in a 6-month period (the second half of 2020).
Results showed that 5,872 women would be screened in the latter half of 2020 if screening proceeded as usual without disruption. The necessary capacity was essentially the same with all of the restarting strategies, except for the catch-up-after-stop strategy, which would require a doubling of that number.
The temporal pattern of breast cancer incidence varied according to restart strategy early on, but incidence essentially returned to that expected with undisrupted screening by 2025 for all four strategies, with some small fluctuations thereafter.
The impact on breast cancer mortality differed considerably long term. It increased slightly and transiently above the expected level with the catch-up-after-stop strategy, but there were sizable, long-lasting increases with the other strategies, with excess deaths still seen in 2060 for the everyone-delay strategy.
In absolute terms, the excess number of breast cancer deaths during 2020-2030, compared with undisrupted screening, was 181 with the everyone-delay strategy, 155 with the first-rounds-no-delay strategy, 145 with the continue-after-stopping-age strategy, and just 14 with the catch-up-after-stop strategy. Ms. Kregting declined to provide numbers for other countries, given that the model is based on the Dutch population and screening program.
Results in context
“The unprecedented burden of COVID-19 on health systems worldwide has important implications for cancer care,” said invited discussant Alessandra Gennari, MD, PhD, of the University of Eastern Piedmont and Maggiore della Carità Hospital, both in Novara, Italy.
“There is a delay in diagnosis due to the fact that screening programs and diagnostic programs have been decreased or suspended in many Western countries where this is standard of care. Patients also are more reluctant to present to health care services, delaying their diagnosis,” Dr. Gennari said.
Findings of this new study add to those of similar studies undertaken in Italy (published in In Vivo) and the United Kingdom (published in The Lancet Oncology) showing the likely marked toll of the pandemic on cancer diagnosis and mortality, Dr. Gennari noted. Taken together, the findings underscore the urgent need for policy interventions to mitigate this impact.
“These interventions should focus on increasing routine diagnostic capacity, through which up to 40% of patients with cancer are diagnosed,” Dr. Gennari recommended. “Public health messaging is needed that accurately conveys the risk of severe illness from COVID-19 versus the risks of not seeking health care advice if patients are symptomatic. Finally, there is a need for provision of evidence-based data on which clinicians can adequately base their decision on how to manage the risks of cancer patients and the risks and benefits of procedures during the pandemic.”
The current study did not have any specific funding, and Ms. Kregting disclosed no conflicts of interest. Dr. Gennari disclosed relationships with Roche, Eisai, Lilly, AstraZeneca, Daiichi Sankyo, Merck, Novartis, and Pfizer.
SOURCE: Kregting L et al. EBCC-12 Virtual Conference, Abstract 24.
according to a modeling study reported at the 12th European Breast Cancer Conference.
Fallout of the pandemic has included reductions in cancer screening and diagnosis, said study investigator Lindy M. Kregting, a PhD student in the department of public health at Erasmus Medical Center, University Medical Center Rotterdam (the Netherlands).
In the Netherlands, new breast cancer diagnoses fell dramatically from historical levels starting in February. The number in April was less than half of that expected.
Ms. Kregting and colleagues used modeling to assess the impact of four strategies for restarting breast cancer screening in the Netherlands. The strategies differed regarding the population affected, the duration of the effects, and changes in stopping age. The usual situation, without any disruption, served as the comparator.
Results showed wide variation across strategies with respect to the increase in screening capacity needed during the latter half of this year – from 0% to 100% – and the excess breast cancer mortality occurring during 2020-2030 – from as many as 181 excess breast cancer deaths to as few as 14.
“The effects of the disruption are dependent on the chosen restart strategy,” Ms. Kregting summarized. “It would be preferred to immediately catch up because this minimizes the impact, but it also requires a very high capacity, so it may not always be possible. A proper alternative would be to increase the stopping age, so no screens are omitted, because this requires a rather normal capacity, and it will result in only small effects on incidence and mortality.”
As screening programs restart in some countries, there are still a lot of unknowns that could affect outcomes, including how many women will attend given that some may stay away out of fear, Ms. Kregting cautioned.
“We plan to do further model calculations when we know exactly what has happened. ... For now, we just assumed some reasonable disruption periods, and we assumed that capacity would be back to the original, before COVID-19, but I think we can say this is probably not the case,” she added.
Study details
Ms. Kregting and colleagues used Dutch breast cancer screening program parameters (biennial digital mammography for women aged 50-75 years) and a microsimulation screening analysis model to simulate four strategies for restarting breast cancer screening after a 6-month disruption:
- “Everyone delay,” a strategy in which all screening continues in the order planned with no change in the stopping age of 75 years (so that one in four women ultimately miss a screening during their lifetime)
- “First rounds no delay,” in which there is a delay in screening except for women having their first screening
- “Continue after stopping age,” in which there is a delay in screening but temporary increasing of the stopping age (to 76.5 years) to ensure all women get their final screen
- “Catch-up after stop,” in which capacity is increased to ensure full catch-up, with all delayed screens caught up in a 6-month period (the second half of 2020).
Results showed that 5,872 women would be screened in the latter half of 2020 if screening proceeded as usual without disruption. The necessary capacity was essentially the same with all of the restarting strategies, except for the catch-up-after-stop strategy, which would require a doubling of that number.
The temporal pattern of breast cancer incidence varied according to restart strategy early on, but incidence essentially returned to that expected with undisrupted screening by 2025 for all four strategies, with some small fluctuations thereafter.
The impact on breast cancer mortality differed considerably long term. It increased slightly and transiently above the expected level with the catch-up-after-stop strategy, but there were sizable, long-lasting increases with the other strategies, with excess deaths still seen in 2060 for the everyone-delay strategy.
In absolute terms, the excess number of breast cancer deaths during 2020-2030, compared with undisrupted screening, was 181 with the everyone-delay strategy, 155 with the first-rounds-no-delay strategy, 145 with the continue-after-stopping-age strategy, and just 14 with the catch-up-after-stop strategy. Ms. Kregting declined to provide numbers for other countries, given that the model is based on the Dutch population and screening program.
Results in context
“The unprecedented burden of COVID-19 on health systems worldwide has important implications for cancer care,” said invited discussant Alessandra Gennari, MD, PhD, of the University of Eastern Piedmont and Maggiore della Carità Hospital, both in Novara, Italy.
“There is a delay in diagnosis due to the fact that screening programs and diagnostic programs have been decreased or suspended in many Western countries where this is standard of care. Patients also are more reluctant to present to health care services, delaying their diagnosis,” Dr. Gennari said.
Findings of this new study add to those of similar studies undertaken in Italy (published in In Vivo) and the United Kingdom (published in The Lancet Oncology) showing the likely marked toll of the pandemic on cancer diagnosis and mortality, Dr. Gennari noted. Taken together, the findings underscore the urgent need for policy interventions to mitigate this impact.
“These interventions should focus on increasing routine diagnostic capacity, through which up to 40% of patients with cancer are diagnosed,” Dr. Gennari recommended. “Public health messaging is needed that accurately conveys the risk of severe illness from COVID-19 versus the risks of not seeking health care advice if patients are symptomatic. Finally, there is a need for provision of evidence-based data on which clinicians can adequately base their decision on how to manage the risks of cancer patients and the risks and benefits of procedures during the pandemic.”
The current study did not have any specific funding, and Ms. Kregting disclosed no conflicts of interest. Dr. Gennari disclosed relationships with Roche, Eisai, Lilly, AstraZeneca, Daiichi Sankyo, Merck, Novartis, and Pfizer.
SOURCE: Kregting L et al. EBCC-12 Virtual Conference, Abstract 24.
FROM EBCC-12 VIRTUAL CONFERENCE
Chronic, preventive care fell as telemedicine soared during COVID-19
As the COVID-19 pandemic drove down the number of primary care visits and altered the method – moving many to telehealth appointments instead of in-person visits – the content of those appointments also changed, researchers reported in JAMA Network Open.
For the study, G. Caleb Alexander, MD, from the Center for Drug Safety and Effectiveness, Johns Hopkins University, Baltimore, and colleagues analyzed data from the IQVIA National Disease and Therapeutic Index, a nationally representative audit of outpatient care in the United States, from the first quarter of 2018 through the second quarter of 2020.
Most primary care visits in 2018 and 2019 were office based, the authors noted. In the second quarter (Q2, April-May) of 2020, as the COVID-19 pandemic spread across the country, the total number of primary care encounters decreased by 21.4%, and the number of office visits dropped by 50.2%, compared with the average of visits during Q2 in 2018 and 2019.
At the same time, telemedicine visits increased from just 1.1% of total visits in Q2 of 2018 and 2019 to 4.1% of visits in the first quarter (January through March) of 2020 and to 35.3% of visits in Q2 of 2020.
The authors also found that the use of telemedicine in the first half of 2020 varied by geographical region and was not associated with the regional COVID-19 burden. In the Pacific region (Washington, Oregon, and California), 26.8% of encounters were virtual. By contrast, the proportion of telemedicine encounters accounted for only 15.1% of visits in the East North Central states (Wisconsin, Michigan, Illinois, Indiana, and Ohio).
Adults between the ages of 19 and 55 years were more likely to attend telemedicine visits than were those younger or older. Additionally, adults who were commercially insured were more likely to adopt telemedicine versus those with public or no insurance. The study did not find substantial differences in telemedicine use by payer type, nor evidence of a racial disparity between Black and White people in their use of telemedicine.
Drop-off in preventive and chronic care
During the second quarter of this year, the authors reported, the number of visits that included blood pressure assessments dropped by 50.1% and the number of visits in which cholesterol levels were assessed fell by 36.9%, compared with the Q2 of 2018 and 2019.
Visits in which providers prescribed new antihypertensive or cholesterol-lowering medications decreased by 26% in Q2 of 2020 versus the same periods in the previous 2 years. The number of visits in which such prescriptions were renewed dropped by 8.9%.
New treatments also decreased significantly in Q2 of 2020 for patients with chronic conditions, including hypertension, diabetes, high cholesterol, asthma, depression, and insomnia.
When the authors compared the content of telemedicine versus in-person visits in Q2 of 2020, they found a substantial difference. Blood pressure was assessed in 69.7% of office visits, compared with 9.6% of telemedicine. Similarly, cholesterol levels were evaluated in 21.6% of office visits versus 13.5% of telemedicine encounters. New medications were ordered in similar proportions of office-based and telemedicine visits.
The authors concluded that “the COVID-19 pandemic has been associated with changes in the structure of primary care delivery, with the content of telemedicine visits differing from that of office-based encounters.”
While limited in scope, the authors noted, their study is one of the first to evaluate the changes in the content of primary care visits during the pandemic. They attributed the decline in evaluations of cardiovascular risk factors such as blood pressure and cholesterol to “fewer total visits and less frequent assessments during telemedicine encounters.”
While pointing to the inherent limitations of telemedicine, the study did not mention the availability of digital home blood pressure cuffs or home cholesterol test kits. Both kinds of devices are available at consumer-friendly price points and can help people track their indicators, but they’re not considered a substitute for sphygmomanometers used in offices or conventional lab tests. It’s not known how many consumers with cardiovascular risk factors have this kind of home monitoring equipment or how many doctors look at this kind of data.
Dr. Alexander reported serving as a paid adviser to IQVIA; that he is a cofounding principal and equity holder in Monument Analytics, a health care consultancy whose clients include the life sciences industry as well as plaintiffs in opioid litigation; and that he is a member of OptumRx’s National P&T Committee. One coauthor reported serving as an unpaid adviser to IQVIA and receiving personal fees from the states of California, Washington, and Alaska outside the submitted work. No other disclosures were reported.
A version of this article originally appeared on Medscape.com.
As the COVID-19 pandemic drove down the number of primary care visits and altered the method – moving many to telehealth appointments instead of in-person visits – the content of those appointments also changed, researchers reported in JAMA Network Open.
For the study, G. Caleb Alexander, MD, from the Center for Drug Safety and Effectiveness, Johns Hopkins University, Baltimore, and colleagues analyzed data from the IQVIA National Disease and Therapeutic Index, a nationally representative audit of outpatient care in the United States, from the first quarter of 2018 through the second quarter of 2020.
Most primary care visits in 2018 and 2019 were office based, the authors noted. In the second quarter (Q2, April-May) of 2020, as the COVID-19 pandemic spread across the country, the total number of primary care encounters decreased by 21.4%, and the number of office visits dropped by 50.2%, compared with the average of visits during Q2 in 2018 and 2019.
At the same time, telemedicine visits increased from just 1.1% of total visits in Q2 of 2018 and 2019 to 4.1% of visits in the first quarter (January through March) of 2020 and to 35.3% of visits in Q2 of 2020.
The authors also found that the use of telemedicine in the first half of 2020 varied by geographical region and was not associated with the regional COVID-19 burden. In the Pacific region (Washington, Oregon, and California), 26.8% of encounters were virtual. By contrast, the proportion of telemedicine encounters accounted for only 15.1% of visits in the East North Central states (Wisconsin, Michigan, Illinois, Indiana, and Ohio).
Adults between the ages of 19 and 55 years were more likely to attend telemedicine visits than were those younger or older. Additionally, adults who were commercially insured were more likely to adopt telemedicine versus those with public or no insurance. The study did not find substantial differences in telemedicine use by payer type, nor evidence of a racial disparity between Black and White people in their use of telemedicine.
Drop-off in preventive and chronic care
During the second quarter of this year, the authors reported, the number of visits that included blood pressure assessments dropped by 50.1% and the number of visits in which cholesterol levels were assessed fell by 36.9%, compared with the Q2 of 2018 and 2019.
Visits in which providers prescribed new antihypertensive or cholesterol-lowering medications decreased by 26% in Q2 of 2020 versus the same periods in the previous 2 years. The number of visits in which such prescriptions were renewed dropped by 8.9%.
New treatments also decreased significantly in Q2 of 2020 for patients with chronic conditions, including hypertension, diabetes, high cholesterol, asthma, depression, and insomnia.
When the authors compared the content of telemedicine versus in-person visits in Q2 of 2020, they found a substantial difference. Blood pressure was assessed in 69.7% of office visits, compared with 9.6% of telemedicine. Similarly, cholesterol levels were evaluated in 21.6% of office visits versus 13.5% of telemedicine encounters. New medications were ordered in similar proportions of office-based and telemedicine visits.
The authors concluded that “the COVID-19 pandemic has been associated with changes in the structure of primary care delivery, with the content of telemedicine visits differing from that of office-based encounters.”
While limited in scope, the authors noted, their study is one of the first to evaluate the changes in the content of primary care visits during the pandemic. They attributed the decline in evaluations of cardiovascular risk factors such as blood pressure and cholesterol to “fewer total visits and less frequent assessments during telemedicine encounters.”
While pointing to the inherent limitations of telemedicine, the study did not mention the availability of digital home blood pressure cuffs or home cholesterol test kits. Both kinds of devices are available at consumer-friendly price points and can help people track their indicators, but they’re not considered a substitute for sphygmomanometers used in offices or conventional lab tests. It’s not known how many consumers with cardiovascular risk factors have this kind of home monitoring equipment or how many doctors look at this kind of data.
Dr. Alexander reported serving as a paid adviser to IQVIA; that he is a cofounding principal and equity holder in Monument Analytics, a health care consultancy whose clients include the life sciences industry as well as plaintiffs in opioid litigation; and that he is a member of OptumRx’s National P&T Committee. One coauthor reported serving as an unpaid adviser to IQVIA and receiving personal fees from the states of California, Washington, and Alaska outside the submitted work. No other disclosures were reported.
A version of this article originally appeared on Medscape.com.
As the COVID-19 pandemic drove down the number of primary care visits and altered the method – moving many to telehealth appointments instead of in-person visits – the content of those appointments also changed, researchers reported in JAMA Network Open.
For the study, G. Caleb Alexander, MD, from the Center for Drug Safety and Effectiveness, Johns Hopkins University, Baltimore, and colleagues analyzed data from the IQVIA National Disease and Therapeutic Index, a nationally representative audit of outpatient care in the United States, from the first quarter of 2018 through the second quarter of 2020.
Most primary care visits in 2018 and 2019 were office based, the authors noted. In the second quarter (Q2, April-May) of 2020, as the COVID-19 pandemic spread across the country, the total number of primary care encounters decreased by 21.4%, and the number of office visits dropped by 50.2%, compared with the average of visits during Q2 in 2018 and 2019.
At the same time, telemedicine visits increased from just 1.1% of total visits in Q2 of 2018 and 2019 to 4.1% of visits in the first quarter (January through March) of 2020 and to 35.3% of visits in Q2 of 2020.
The authors also found that the use of telemedicine in the first half of 2020 varied by geographical region and was not associated with the regional COVID-19 burden. In the Pacific region (Washington, Oregon, and California), 26.8% of encounters were virtual. By contrast, the proportion of telemedicine encounters accounted for only 15.1% of visits in the East North Central states (Wisconsin, Michigan, Illinois, Indiana, and Ohio).
Adults between the ages of 19 and 55 years were more likely to attend telemedicine visits than were those younger or older. Additionally, adults who were commercially insured were more likely to adopt telemedicine versus those with public or no insurance. The study did not find substantial differences in telemedicine use by payer type, nor evidence of a racial disparity between Black and White people in their use of telemedicine.
Drop-off in preventive and chronic care
During the second quarter of this year, the authors reported, the number of visits that included blood pressure assessments dropped by 50.1% and the number of visits in which cholesterol levels were assessed fell by 36.9%, compared with the Q2 of 2018 and 2019.
Visits in which providers prescribed new antihypertensive or cholesterol-lowering medications decreased by 26% in Q2 of 2020 versus the same periods in the previous 2 years. The number of visits in which such prescriptions were renewed dropped by 8.9%.
New treatments also decreased significantly in Q2 of 2020 for patients with chronic conditions, including hypertension, diabetes, high cholesterol, asthma, depression, and insomnia.
When the authors compared the content of telemedicine versus in-person visits in Q2 of 2020, they found a substantial difference. Blood pressure was assessed in 69.7% of office visits, compared with 9.6% of telemedicine. Similarly, cholesterol levels were evaluated in 21.6% of office visits versus 13.5% of telemedicine encounters. New medications were ordered in similar proportions of office-based and telemedicine visits.
The authors concluded that “the COVID-19 pandemic has been associated with changes in the structure of primary care delivery, with the content of telemedicine visits differing from that of office-based encounters.”
While limited in scope, the authors noted, their study is one of the first to evaluate the changes in the content of primary care visits during the pandemic. They attributed the decline in evaluations of cardiovascular risk factors such as blood pressure and cholesterol to “fewer total visits and less frequent assessments during telemedicine encounters.”
While pointing to the inherent limitations of telemedicine, the study did not mention the availability of digital home blood pressure cuffs or home cholesterol test kits. Both kinds of devices are available at consumer-friendly price points and can help people track their indicators, but they’re not considered a substitute for sphygmomanometers used in offices or conventional lab tests. It’s not known how many consumers with cardiovascular risk factors have this kind of home monitoring equipment or how many doctors look at this kind of data.
Dr. Alexander reported serving as a paid adviser to IQVIA; that he is a cofounding principal and equity holder in Monument Analytics, a health care consultancy whose clients include the life sciences industry as well as plaintiffs in opioid litigation; and that he is a member of OptumRx’s National P&T Committee. One coauthor reported serving as an unpaid adviser to IQVIA and receiving personal fees from the states of California, Washington, and Alaska outside the submitted work. No other disclosures were reported.
A version of this article originally appeared on Medscape.com.
Meta-analysis: Acalabrutinib showed better PFS and OS than other frontline CLL therapies
Acalabrutinib, given alone or in combination with obinutuzumab, showed favorable progression-free survival (PFS) and overall survival (OS), compared with other frontline therapies for chronic lymphocytic leukemia (CLL) in fludarabine-ineligible patients, according to the results of a meta-analysis comparing clinical trial results.
Researchers conducted a systematic literature review for applicable CLL studies that examined frontline treatments in order to compare the results with data on acalabrutinib (monotherapy and in combination with obinutuzumab) from patients in the ELEVATE-TN study (NCT02475681), according to a report published in Clinical Therapeutics.
Matthew S. Davids, MD, MMSc, of the Dana-Farber Cancer Institute in Boston, and colleagues performed a network meta-analysis (NMA) comparing acalabrutinib versus other standard frontline therapies for CLL in patients for whom fludarabine-based treatment is not appropriate.
“In the absence of head-to-head trial data, NMAs allow for simultaneous comparisons of a number of interventions with multiple comparators, by synthesizing direct and indirect evidence,” the authors stated.
Eight randomized controlled trials (RCTs) met the criteria for comparison.
The researchers constructed two evidence networks: Network A comprised solely RCTs that met the inclusion criteria, and Network B comprised seven RCTs and a published cross-trial comparison of ibrutinib from RESONATE-2 and chlorambucil plus obinutuzumab from iLLUMINATE. PFS and OS results were reported by using hazard ratios and 95% credible intervals.
Overall benefit
Both networks showed a significant improvement in PFS for acalabrutinib plus obinutuzumab over all comparators, according to the researchers. Both networks also showed a significant improvement in PFS for acalabrutinib monotherapy versus most comparators, with a significant difference to ibrutinib monotherapy found in Network A but not Network B.
Conversely, a significant difference in PFS was observed for acalabrutinib monotherapy versus venetoclax plus obinutuzumab in Network B but not Network A.
Overall survival hazard ratios ranged from 0.18 to 0.65 in favor of acalabrutinib-based treatment, but not all were significant. Acalabrutinib plus obinutuzumab ranked highest in terms of PFS and OS improvement, followed by acalabrutinib monotherapy.
“Although our NMAs provide useful insights into the relative efficacy of acalabrutinib, compared with other frontline treatments of CLL, the results cannot be considered confirmatory, and head-to-head randomized trials are needed, especially to compare the efficacy of acalabrutinib versus other targeted agents,” the researchers concluded.
AstraZeneca sponsored the study. The authors reported funding from AstraZeneca and numerous other pharmaceutical companies.
SOURCE: Davids MS et al. Clin Ther. 2020 Oct 5. doi: 10.1016/j.clinthera.2020.08.017.
Acalabrutinib, given alone or in combination with obinutuzumab, showed favorable progression-free survival (PFS) and overall survival (OS), compared with other frontline therapies for chronic lymphocytic leukemia (CLL) in fludarabine-ineligible patients, according to the results of a meta-analysis comparing clinical trial results.
Researchers conducted a systematic literature review for applicable CLL studies that examined frontline treatments in order to compare the results with data on acalabrutinib (monotherapy and in combination with obinutuzumab) from patients in the ELEVATE-TN study (NCT02475681), according to a report published in Clinical Therapeutics.
Matthew S. Davids, MD, MMSc, of the Dana-Farber Cancer Institute in Boston, and colleagues performed a network meta-analysis (NMA) comparing acalabrutinib versus other standard frontline therapies for CLL in patients for whom fludarabine-based treatment is not appropriate.
“In the absence of head-to-head trial data, NMAs allow for simultaneous comparisons of a number of interventions with multiple comparators, by synthesizing direct and indirect evidence,” the authors stated.
Eight randomized controlled trials (RCTs) met the criteria for comparison.
The researchers constructed two evidence networks: Network A comprised solely RCTs that met the inclusion criteria, and Network B comprised seven RCTs and a published cross-trial comparison of ibrutinib from RESONATE-2 and chlorambucil plus obinutuzumab from iLLUMINATE. PFS and OS results were reported by using hazard ratios and 95% credible intervals.
Overall benefit
Both networks showed a significant improvement in PFS for acalabrutinib plus obinutuzumab over all comparators, according to the researchers. Both networks also showed a significant improvement in PFS for acalabrutinib monotherapy versus most comparators, with a significant difference to ibrutinib monotherapy found in Network A but not Network B.
Conversely, a significant difference in PFS was observed for acalabrutinib monotherapy versus venetoclax plus obinutuzumab in Network B but not Network A.
Overall survival hazard ratios ranged from 0.18 to 0.65 in favor of acalabrutinib-based treatment, but not all were significant. Acalabrutinib plus obinutuzumab ranked highest in terms of PFS and OS improvement, followed by acalabrutinib monotherapy.
“Although our NMAs provide useful insights into the relative efficacy of acalabrutinib, compared with other frontline treatments of CLL, the results cannot be considered confirmatory, and head-to-head randomized trials are needed, especially to compare the efficacy of acalabrutinib versus other targeted agents,” the researchers concluded.
AstraZeneca sponsored the study. The authors reported funding from AstraZeneca and numerous other pharmaceutical companies.
SOURCE: Davids MS et al. Clin Ther. 2020 Oct 5. doi: 10.1016/j.clinthera.2020.08.017.
Acalabrutinib, given alone or in combination with obinutuzumab, showed favorable progression-free survival (PFS) and overall survival (OS), compared with other frontline therapies for chronic lymphocytic leukemia (CLL) in fludarabine-ineligible patients, according to the results of a meta-analysis comparing clinical trial results.
Researchers conducted a systematic literature review for applicable CLL studies that examined frontline treatments in order to compare the results with data on acalabrutinib (monotherapy and in combination with obinutuzumab) from patients in the ELEVATE-TN study (NCT02475681), according to a report published in Clinical Therapeutics.
Matthew S. Davids, MD, MMSc, of the Dana-Farber Cancer Institute in Boston, and colleagues performed a network meta-analysis (NMA) comparing acalabrutinib versus other standard frontline therapies for CLL in patients for whom fludarabine-based treatment is not appropriate.
“In the absence of head-to-head trial data, NMAs allow for simultaneous comparisons of a number of interventions with multiple comparators, by synthesizing direct and indirect evidence,” the authors stated.
Eight randomized controlled trials (RCTs) met the criteria for comparison.
The researchers constructed two evidence networks: Network A comprised solely RCTs that met the inclusion criteria, and Network B comprised seven RCTs and a published cross-trial comparison of ibrutinib from RESONATE-2 and chlorambucil plus obinutuzumab from iLLUMINATE. PFS and OS results were reported by using hazard ratios and 95% credible intervals.
Overall benefit
Both networks showed a significant improvement in PFS for acalabrutinib plus obinutuzumab over all comparators, according to the researchers. Both networks also showed a significant improvement in PFS for acalabrutinib monotherapy versus most comparators, with a significant difference to ibrutinib monotherapy found in Network A but not Network B.
Conversely, a significant difference in PFS was observed for acalabrutinib monotherapy versus venetoclax plus obinutuzumab in Network B but not Network A.
Overall survival hazard ratios ranged from 0.18 to 0.65 in favor of acalabrutinib-based treatment, but not all were significant. Acalabrutinib plus obinutuzumab ranked highest in terms of PFS and OS improvement, followed by acalabrutinib monotherapy.
“Although our NMAs provide useful insights into the relative efficacy of acalabrutinib, compared with other frontline treatments of CLL, the results cannot be considered confirmatory, and head-to-head randomized trials are needed, especially to compare the efficacy of acalabrutinib versus other targeted agents,” the researchers concluded.
AstraZeneca sponsored the study. The authors reported funding from AstraZeneca and numerous other pharmaceutical companies.
SOURCE: Davids MS et al. Clin Ther. 2020 Oct 5. doi: 10.1016/j.clinthera.2020.08.017.
FROM CLINICAL THERAPEUTICS
Atezolizumab strikes out in ovarian cancer
“Despite notable success with the incorporation of bevacizumab and atezolizumab in the treatment of other solid tumors ... the first such study in ovarian cancer did not meet its first primary endpoint” of extending PFS in the intention-to-treat population or in patients positive for programmed death-ligand 1 (PD-L1), said investigator Kathleen Moore, MD, of the University of Oklahoma in Oklahoma City.
Dr. Moore presented this study, IMagyn050/GOG 3015/ENGOT-OV39, at the European Society for Medical Oncology Virtual Congress 2020.
Explaining the negative results
The rationale for this study was good, said discussant Isabelle Ray-Coquard, MD, PhD, of the University Claude Bernard Lyon I in Villeurbanne, France, who was an investigator on the study but not an author on the meeting report.
Unfortunately, the study’s results were ultimately negative. A prior phase 3 trial of an immune checkpoint inhibitor in ovarian cancer also had negative results. In the JAVELIN OVARIAN 100 trial, adding avelumab to chemotherapy did not improve PFS, and the trial was stopped early for futility.
Dr. Ray-Coquard posed the question of whether checkpoint inhibitors are “dead” for epithelial ovarian cancer but said the answer isn’t clear.
There might be something unique about the tumor microenvironment that shields ovarian cancer from the immune system, or perhaps the PD-L1 pathway is the wrong target for immunotherapy.
It might also be that the first-line setting is the wrong place for checkpoint inhibitors, and they might work better in the second line, Dr. Ray-Coquard said.
Another possibility is that the delayed effect of immunotherapy means that overall survival – which isn’t yet mature for IMagyn050 – might be a better primary outcome than PFS.
Patient and treatment details
IMagyn050 enrolled 1,301 patients with newly diagnosed, stage III/IV epithelial ovarian, primary peritoneal, or fallopian tube cancer.
Patients were randomized to atezolizumab (n = 651) or placebo (n = 650) in combination with bevacizumab, paclitaxel, and carboplatin every 3 weeks for six cycles. For cycles 7-22, patients received bevacizumab with placebo or atezolizumab.
Most patients had ovarian cancer (73% in the placebo arm and 75% in the atezolizumab arm), followed by fallopian tube cancer (17% and 15%, respectively) and primary peritoneal cancer (10% and 9%, respectively).
In both arms, 31% of patients had stage IV disease, and 60% were PD-L1 positive (at least 1% of tumor cells staining positive).
Treatment was given in the neoadjuvant setting for 25% of patients in both arms and after primary cytoreductive surgery for the remaining patients.
Efficacy and safety
In the intention-to-treat population, the median PFS was 19.5 months with atezolizumab and 18.4 months in the placebo arm. In PD-L1–positive patients, the median PFS was 20.8 months and 18.5 months, respectively.
The differences in PFS were not statistically significant or clinically meaningful, Dr. Ray-Coquard said.
She noted that results were not stratified by BRCA status, which has been linked to PFS in ovarian cancer, and a potential imbalance between the groups might have contributed to the negative results.
Overall survival data won’t be mature until 2023, but, in the first interim analysis, “there was no apparent difference in the curves,” Dr. Moore said.
In the intention-to-treat population, the median overall survival was not reached in either treatment arm. In the PD-L1–positive population, the median overall survival was 31.2 months in the placebo arm and was not reached in the atezolizumab arm.
Adverse events were consistent with the known safety profiles of atezolizumab and the other drugs, Dr. Moore said. There were more serious events and more events leading to discontinuation with atezolizumab.
Adverse events more common with atezolizumab included febrile neutropenia, pyrexia, thyroid abnormalities, and rash, including severe cutaneous reactions. Colitis, pancreatitis, and infusion-related reactions were relatively infrequent but more common with atezolizumab, Dr. Moore said.
What the future holds
Dr. Ray-Coquard said there are signals in IMagyn050 that warrant follow-up, including a trend toward improved PFS among women who had high-grade nonserous clear cell histology. In this group, the median PFS was 12.3 months in the placebo arm and 13.6 months in the atezolizumab arm (hazard ratio, 0.64).
Additionally, there was a significant PFS improvement in women with at least 5% of their tumor cells staining positive for PD-L1. The median PFS was 20.2 months in the placebo arm but was not reached in the atezolizumab arm (HR, 0.64; P = .0278).
Dr. Ray-Coquard said we need to know who these PD-L1–high patients are in terms of BRCA status, histology, and residual disease.
She went on to say that companies haven’t given up on checkpoint inhibitors for ovarian cancer. Phase 3 trials are testing the atezolizumab/bevacizumab/chemotherapy combination for late relapsed disease, atezolizumab with niraparib and chemotherapy for recurrent ovarian cancer, and nivolumab with rucaparib following response to chemotherapy.
The IMagyn050 study was funded by F. Hoffmann-La Roche, the company developing atezolizumab. Dr. Moore and Dr. Ray-Coquard disclosed relationships with Roche and many other companies.
SOURCE: Moore K et al. ESMO 2020, Abstract LBA31.
“Despite notable success with the incorporation of bevacizumab and atezolizumab in the treatment of other solid tumors ... the first such study in ovarian cancer did not meet its first primary endpoint” of extending PFS in the intention-to-treat population or in patients positive for programmed death-ligand 1 (PD-L1), said investigator Kathleen Moore, MD, of the University of Oklahoma in Oklahoma City.
Dr. Moore presented this study, IMagyn050/GOG 3015/ENGOT-OV39, at the European Society for Medical Oncology Virtual Congress 2020.
Explaining the negative results
The rationale for this study was good, said discussant Isabelle Ray-Coquard, MD, PhD, of the University Claude Bernard Lyon I in Villeurbanne, France, who was an investigator on the study but not an author on the meeting report.
Unfortunately, the study’s results were ultimately negative. A prior phase 3 trial of an immune checkpoint inhibitor in ovarian cancer also had negative results. In the JAVELIN OVARIAN 100 trial, adding avelumab to chemotherapy did not improve PFS, and the trial was stopped early for futility.
Dr. Ray-Coquard posed the question of whether checkpoint inhibitors are “dead” for epithelial ovarian cancer but said the answer isn’t clear.
There might be something unique about the tumor microenvironment that shields ovarian cancer from the immune system, or perhaps the PD-L1 pathway is the wrong target for immunotherapy.
It might also be that the first-line setting is the wrong place for checkpoint inhibitors, and they might work better in the second line, Dr. Ray-Coquard said.
Another possibility is that the delayed effect of immunotherapy means that overall survival – which isn’t yet mature for IMagyn050 – might be a better primary outcome than PFS.
Patient and treatment details
IMagyn050 enrolled 1,301 patients with newly diagnosed, stage III/IV epithelial ovarian, primary peritoneal, or fallopian tube cancer.
Patients were randomized to atezolizumab (n = 651) or placebo (n = 650) in combination with bevacizumab, paclitaxel, and carboplatin every 3 weeks for six cycles. For cycles 7-22, patients received bevacizumab with placebo or atezolizumab.
Most patients had ovarian cancer (73% in the placebo arm and 75% in the atezolizumab arm), followed by fallopian tube cancer (17% and 15%, respectively) and primary peritoneal cancer (10% and 9%, respectively).
In both arms, 31% of patients had stage IV disease, and 60% were PD-L1 positive (at least 1% of tumor cells staining positive).
Treatment was given in the neoadjuvant setting for 25% of patients in both arms and after primary cytoreductive surgery for the remaining patients.
Efficacy and safety
In the intention-to-treat population, the median PFS was 19.5 months with atezolizumab and 18.4 months in the placebo arm. In PD-L1–positive patients, the median PFS was 20.8 months and 18.5 months, respectively.
The differences in PFS were not statistically significant or clinically meaningful, Dr. Ray-Coquard said.
She noted that results were not stratified by BRCA status, which has been linked to PFS in ovarian cancer, and a potential imbalance between the groups might have contributed to the negative results.
Overall survival data won’t be mature until 2023, but, in the first interim analysis, “there was no apparent difference in the curves,” Dr. Moore said.
In the intention-to-treat population, the median overall survival was not reached in either treatment arm. In the PD-L1–positive population, the median overall survival was 31.2 months in the placebo arm and was not reached in the atezolizumab arm.
Adverse events were consistent with the known safety profiles of atezolizumab and the other drugs, Dr. Moore said. There were more serious events and more events leading to discontinuation with atezolizumab.
Adverse events more common with atezolizumab included febrile neutropenia, pyrexia, thyroid abnormalities, and rash, including severe cutaneous reactions. Colitis, pancreatitis, and infusion-related reactions were relatively infrequent but more common with atezolizumab, Dr. Moore said.
What the future holds
Dr. Ray-Coquard said there are signals in IMagyn050 that warrant follow-up, including a trend toward improved PFS among women who had high-grade nonserous clear cell histology. In this group, the median PFS was 12.3 months in the placebo arm and 13.6 months in the atezolizumab arm (hazard ratio, 0.64).
Additionally, there was a significant PFS improvement in women with at least 5% of their tumor cells staining positive for PD-L1. The median PFS was 20.2 months in the placebo arm but was not reached in the atezolizumab arm (HR, 0.64; P = .0278).
Dr. Ray-Coquard said we need to know who these PD-L1–high patients are in terms of BRCA status, histology, and residual disease.
She went on to say that companies haven’t given up on checkpoint inhibitors for ovarian cancer. Phase 3 trials are testing the atezolizumab/bevacizumab/chemotherapy combination for late relapsed disease, atezolizumab with niraparib and chemotherapy for recurrent ovarian cancer, and nivolumab with rucaparib following response to chemotherapy.
The IMagyn050 study was funded by F. Hoffmann-La Roche, the company developing atezolizumab. Dr. Moore and Dr. Ray-Coquard disclosed relationships with Roche and many other companies.
SOURCE: Moore K et al. ESMO 2020, Abstract LBA31.
“Despite notable success with the incorporation of bevacizumab and atezolizumab in the treatment of other solid tumors ... the first such study in ovarian cancer did not meet its first primary endpoint” of extending PFS in the intention-to-treat population or in patients positive for programmed death-ligand 1 (PD-L1), said investigator Kathleen Moore, MD, of the University of Oklahoma in Oklahoma City.
Dr. Moore presented this study, IMagyn050/GOG 3015/ENGOT-OV39, at the European Society for Medical Oncology Virtual Congress 2020.
Explaining the negative results
The rationale for this study was good, said discussant Isabelle Ray-Coquard, MD, PhD, of the University Claude Bernard Lyon I in Villeurbanne, France, who was an investigator on the study but not an author on the meeting report.
Unfortunately, the study’s results were ultimately negative. A prior phase 3 trial of an immune checkpoint inhibitor in ovarian cancer also had negative results. In the JAVELIN OVARIAN 100 trial, adding avelumab to chemotherapy did not improve PFS, and the trial was stopped early for futility.
Dr. Ray-Coquard posed the question of whether checkpoint inhibitors are “dead” for epithelial ovarian cancer but said the answer isn’t clear.
There might be something unique about the tumor microenvironment that shields ovarian cancer from the immune system, or perhaps the PD-L1 pathway is the wrong target for immunotherapy.
It might also be that the first-line setting is the wrong place for checkpoint inhibitors, and they might work better in the second line, Dr. Ray-Coquard said.
Another possibility is that the delayed effect of immunotherapy means that overall survival – which isn’t yet mature for IMagyn050 – might be a better primary outcome than PFS.
Patient and treatment details
IMagyn050 enrolled 1,301 patients with newly diagnosed, stage III/IV epithelial ovarian, primary peritoneal, or fallopian tube cancer.
Patients were randomized to atezolizumab (n = 651) or placebo (n = 650) in combination with bevacizumab, paclitaxel, and carboplatin every 3 weeks for six cycles. For cycles 7-22, patients received bevacizumab with placebo or atezolizumab.
Most patients had ovarian cancer (73% in the placebo arm and 75% in the atezolizumab arm), followed by fallopian tube cancer (17% and 15%, respectively) and primary peritoneal cancer (10% and 9%, respectively).
In both arms, 31% of patients had stage IV disease, and 60% were PD-L1 positive (at least 1% of tumor cells staining positive).
Treatment was given in the neoadjuvant setting for 25% of patients in both arms and after primary cytoreductive surgery for the remaining patients.
Efficacy and safety
In the intention-to-treat population, the median PFS was 19.5 months with atezolizumab and 18.4 months in the placebo arm. In PD-L1–positive patients, the median PFS was 20.8 months and 18.5 months, respectively.
The differences in PFS were not statistically significant or clinically meaningful, Dr. Ray-Coquard said.
She noted that results were not stratified by BRCA status, which has been linked to PFS in ovarian cancer, and a potential imbalance between the groups might have contributed to the negative results.
Overall survival data won’t be mature until 2023, but, in the first interim analysis, “there was no apparent difference in the curves,” Dr. Moore said.
In the intention-to-treat population, the median overall survival was not reached in either treatment arm. In the PD-L1–positive population, the median overall survival was 31.2 months in the placebo arm and was not reached in the atezolizumab arm.
Adverse events were consistent with the known safety profiles of atezolizumab and the other drugs, Dr. Moore said. There were more serious events and more events leading to discontinuation with atezolizumab.
Adverse events more common with atezolizumab included febrile neutropenia, pyrexia, thyroid abnormalities, and rash, including severe cutaneous reactions. Colitis, pancreatitis, and infusion-related reactions were relatively infrequent but more common with atezolizumab, Dr. Moore said.
What the future holds
Dr. Ray-Coquard said there are signals in IMagyn050 that warrant follow-up, including a trend toward improved PFS among women who had high-grade nonserous clear cell histology. In this group, the median PFS was 12.3 months in the placebo arm and 13.6 months in the atezolizumab arm (hazard ratio, 0.64).
Additionally, there was a significant PFS improvement in women with at least 5% of their tumor cells staining positive for PD-L1. The median PFS was 20.2 months in the placebo arm but was not reached in the atezolizumab arm (HR, 0.64; P = .0278).
Dr. Ray-Coquard said we need to know who these PD-L1–high patients are in terms of BRCA status, histology, and residual disease.
She went on to say that companies haven’t given up on checkpoint inhibitors for ovarian cancer. Phase 3 trials are testing the atezolizumab/bevacizumab/chemotherapy combination for late relapsed disease, atezolizumab with niraparib and chemotherapy for recurrent ovarian cancer, and nivolumab with rucaparib following response to chemotherapy.
The IMagyn050 study was funded by F. Hoffmann-La Roche, the company developing atezolizumab. Dr. Moore and Dr. Ray-Coquard disclosed relationships with Roche and many other companies.
SOURCE: Moore K et al. ESMO 2020, Abstract LBA31.
FROM ESMO 2020
Deep brain stimulation ‘promising’ in severe schizophrenia
Deep brain stimulation (DBS) may be an effective option for patients with treatment-resistant schizophrenia (TRS), new research suggests. However, until further studies are conducted, the treatment should only be considered for the most severe cases.

The first clinical trial to assess DBS in this challenging patient population included eight patients initially randomly assigned to receive electrode placement in one of two locations in the brain. Once a clinical response was achieved and participants were stabilized, they were randomly assigned to a second crossover phase.
Preliminary findings from the first phase of the DBS-SCHIZO pilot study, which were reported in 2017, showed promising efficacy.
The newly released final results revealed an association between DBS and significant improvements in Positive and Negative Symptoms Scale (PANSS) scores, as well as reductions in doses of antipsychotic medication. Moreover, the effect reversed when the electrode was switched off.
“DBS may be a potential option for severe treatment-resistant schizophrenia patients,” lead investigator Iluminada Corripio, MD, PhD, department of psychiatry, Hospital de la Santa Creu i Sant Pau, Barcelona, said during her presentation at the virtual congress of the European College of Neuropsychopharmacology. The new data were updated results of a study published in EBioMedicine earlier this year.
Dr. Corripio underlined that it is important to balance the risks and benefits of the intervention. DBS is “not useful for all phenotypes,” and benefits have been seen in patients with hallucinations but not in those with a disorganized phenotype, she added.
High economic burden
Managing TRS is challenging and is associated with a high clinical and economic burden, Corripio noted. Relapse rates can reach 80%, increasing resource use by between 200% and 900%.
There is a strong rationale for studying the use of DBS in schizophrenia, because schizophrenia shares a neurologic basis with other neurologic and psychiatric disorders centered around the cortical-striatal-thalamic-cortical circuit, said Dr. Corripio.
The study included eight patients with a DSM-IV-TR diagnosis of schizophrenia whose conditions were resistant to at least two different atypical antipsychotics and who had not responded to clozapine monotherapy, combination therapy, or electroconvulsive therapy.
All were randomly assigned in a 1:1 ratio to DBS electrode implantation in one of two locations. Investigators chose the nucleus accumbens (NAcc), because recent studies have shown that DBS can increase dopamine levels there, and the subgenual anterior cingulate cortex (ACC). Deactivation failure in the ACC region has been observed in patients with schizophrenia and other mental illnesses.
Stimulation began 48-72 hours postoperatively with unilateral left stimulation at 2.5 volts. It was increased in 0.5 volt increments to a maximum of 7.5 volts. Patients who did not respond were switched to bilateral stimulation.
Follow-up was conducted every 2 weeks for up to 20 months. The study’s primary outcome was a symptomatic response, defined as an improvement of at least 25% on the PANSS.
Once that was achieved, patients could enter a second randomization phase in which they were assigned, in a 24-week, double-blind crossover design, to on- or off-treatment DBS arms such that patients received stimulation for 12 weeks before the device was turned off for 12 weeks, or vice versa.
Those who experienced relapse while off treatment were crossed over to the on-treatment arm; those who experienced relapsed while on treatment were withdrawn from the study. The patients’ average age was 42.5 years, and 50% were women. All were taking clozapine in combination with another antipsychotic.
Adverse events
Five patients experienced adverse events during the first phase, four of which were associated with rechargeable battery replacement. One experienced akathisia, another experienced behavioral changes, and a third experienced electrical disturbances.
A fourth patient experienced postsurgical hemorrhage of the right internal capsule on day 4, followed by encephalitis at week 8. He had a clinical improvement but experienced relapsed during follow-up.
The fifth patient accidentally switched off the device and withdrew from the study.
During the first randomization phase, DBS was associated with significant improvements on total, positive, and negative PANSS scores in comparison with the postoperative baseline measure in the seven remaining patients (P < .001).
When the team compared the baseline measure with the last observation, the improvement in PANSS scores remained significant for total scores (P = .007) and positive scores (P = .002), but not for negative scores (P = .18).
Three patients entered the second crossover phase of the study. Two began in the off-treatment arm and experienced relapsed within 1 and 2 weeks, respectively. Total PANSS scores increased from 79 to 98 for the first patient and from 47 to 93 for the second patient.
Neuroimaging showed that, among patients who responded to DBS, brain metabolism increased in some brain areas and decreased in others. Dr. Corripio said this suggests a “rebalancing” of neural circuits.
As of July 2020, one of three patients with an electrode placed in the NAcc had experienced remission of positive symptoms and now has predominant negative symptoms. Another experienced significant improvements in negative symptoms. Two patients currently require psychosocial rehabilitation.
Patients for whom an electrode was placed in the ACC required higher voltages and more time to achieve an effect in comparison with those for whom an electrode was placed in the NAcc. Two patients required bilateral stimulation.
However, for all three patients who remained in the study, their clozapine dose was reduced.
Dr. Corripio reported that the team has observed negative thoughts and obsessive symptoms in patients with electrodes in the ACC, and all have needed either psychosocial rehabilitation or cognitive-behavioral therapy.
The investigators are now planning another DBS study involving patients with TRS, although this one will include a clinical recovery program focusing on family interventions and cognitive-behavioral therapy.
“Last-resort” treatment
In the postpresentation debate, Damiaan Denys, PhD, professor and chair of the department of psychiatry at the Academic Medical Canter, University of Amsterdam, said that DBS remains a treatment of “last resort” in TRS.
This is because it is both costly and invasive, and although the associated risk of bleeding and infection is low, he noted that the consequences are significant.
Dr. Denys added that patients need to have the potential for improvement; electrodes can be easily implanted, and the approach may tempt clinicians who sometimes “struggle with a huge amount of treatment-refractory cases.”
He also pointed to results achieved in studies of obsessive-compulsive disorder and depression, in which around 50% of patients responded to DBS.
“I think that’s the reason why we should be reluctant and not treat anyone at any stage, but first look for the more severe cases,” Dr. Denys said.
Unmet need
Judith M. Gault, PhD, associate research professor of neurosurgery at the University of Colorado at Denver, Aurora, also took part in the debate.
She said in an interview that patients with TRS have a lot of unmet needs and that DBS is worth trying in this patient population, with the goal being to “conduct a really good clinical trial” similar to the current study.
Antipsychotic drugs work well in responsive patients, but “in some cases the person is treatment refractory ... and in other cases the patient relapses,” Dr. Gault said.
She believes that DBS has the “potential to be more potent than antipsychotics in modulating the circuit of interest” and so fulfills the unmet needs of these patients while alleviating their symptoms.
Dr. Gault added that some patients experience “breakthrough symptoms” even while they are medication adherent. “That is a call for an intervention that is more potent” and suggests another potential role for DBS.
Overall, there are “a lot of really compelling reasons to pursue” DBS. However, there are also questions about how motivated patients with TRS are to participate in a clinical trial, Dr. Gault noted.
Patients with schizophrenia “tend not to be very motivated, especially if they have negative symptoms.” However, “if you were able to consider more of the population and not just the most severely affected, eventually you would find more people who are interested,” she said.
Still, it will take a better understanding of the efficacy and safety of the intervention for more people to be interested in trying it, said Dr. Gault.
“I think it’s hard early on, when you don’t actually know what the outcomes would be, if it’s even effective at all. But as you get more and more data in the population and at the different targets, people would be more open to it,” she said.
Another issue in generating interest among patients with schizophrenia is that many have not considered DBS as an option.
“It takes a while to think about it,” she noted. “You don’t want to rush into something that you just heard about, and so part of it is just education.”
The study was funded by Instituto Carlos III. Dr. Corripio reported having received research grants and conducting consultancy for Otsuka, Ferrer, Janssen, and Lilly. No other relevant financial relationships were reported.
A version of this article originally appeared on Medscape.com.
Deep brain stimulation (DBS) may be an effective option for patients with treatment-resistant schizophrenia (TRS), new research suggests. However, until further studies are conducted, the treatment should only be considered for the most severe cases.
The first clinical trial to assess DBS in this challenging patient population included eight patients initially randomly assigned to receive electrode placement in one of two locations in the brain. Once a clinical response was achieved and participants were stabilized, they were randomly assigned to a second crossover phase.
Preliminary findings from the first phase of the DBS-SCHIZO pilot study, which were reported in 2017, showed promising efficacy.
The newly released final results revealed an association between DBS and significant improvements in Positive and Negative Symptoms Scale (PANSS) scores, as well as reductions in doses of antipsychotic medication. Moreover, the effect reversed when the electrode was switched off.
“DBS may be a potential option for severe treatment-resistant schizophrenia patients,” lead investigator Iluminada Corripio, MD, PhD, department of psychiatry, Hospital de la Santa Creu i Sant Pau, Barcelona, said during her presentation at the virtual congress of the European College of Neuropsychopharmacology. The new data were updated results of a study published in EBioMedicine earlier this year.
Dr. Corripio underlined that it is important to balance the risks and benefits of the intervention. DBS is “not useful for all phenotypes,” and benefits have been seen in patients with hallucinations but not in those with a disorganized phenotype, she added.
High economic burden
Managing TRS is challenging and is associated with a high clinical and economic burden, Corripio noted. Relapse rates can reach 80%, increasing resource use by between 200% and 900%.
There is a strong rationale for studying the use of DBS in schizophrenia, because schizophrenia shares a neurologic basis with other neurologic and psychiatric disorders centered around the cortical-striatal-thalamic-cortical circuit, said Dr. Corripio.
The study included eight patients with a DSM-IV-TR diagnosis of schizophrenia whose conditions were resistant to at least two different atypical antipsychotics and who had not responded to clozapine monotherapy, combination therapy, or electroconvulsive therapy.
All were randomly assigned in a 1:1 ratio to DBS electrode implantation in one of two locations. Investigators chose the nucleus accumbens (NAcc), because recent studies have shown that DBS can increase dopamine levels there, and the subgenual anterior cingulate cortex (ACC). Deactivation failure in the ACC region has been observed in patients with schizophrenia and other mental illnesses.
Stimulation began 48-72 hours postoperatively with unilateral left stimulation at 2.5 volts. It was increased in 0.5 volt increments to a maximum of 7.5 volts. Patients who did not respond were switched to bilateral stimulation.
Follow-up was conducted every 2 weeks for up to 20 months. The study’s primary outcome was a symptomatic response, defined as an improvement of at least 25% on the PANSS.
Once that was achieved, patients could enter a second randomization phase in which they were assigned, in a 24-week, double-blind crossover design, to on- or off-treatment DBS arms such that patients received stimulation for 12 weeks before the device was turned off for 12 weeks, or vice versa.
Those who experienced relapse while off treatment were crossed over to the on-treatment arm; those who experienced relapsed while on treatment were withdrawn from the study. The patients’ average age was 42.5 years, and 50% were women. All were taking clozapine in combination with another antipsychotic.
Adverse events
Five patients experienced adverse events during the first phase, four of which were associated with rechargeable battery replacement. One experienced akathisia, another experienced behavioral changes, and a third experienced electrical disturbances.
A fourth patient experienced postsurgical hemorrhage of the right internal capsule on day 4, followed by encephalitis at week 8. He had a clinical improvement but experienced relapsed during follow-up.
The fifth patient accidentally switched off the device and withdrew from the study.
During the first randomization phase, DBS was associated with significant improvements on total, positive, and negative PANSS scores in comparison with the postoperative baseline measure in the seven remaining patients (P < .001).
When the team compared the baseline measure with the last observation, the improvement in PANSS scores remained significant for total scores (P = .007) and positive scores (P = .002), but not for negative scores (P = .18).
Three patients entered the second crossover phase of the study. Two began in the off-treatment arm and experienced relapsed within 1 and 2 weeks, respectively. Total PANSS scores increased from 79 to 98 for the first patient and from 47 to 93 for the second patient.
Neuroimaging showed that, among patients who responded to DBS, brain metabolism increased in some brain areas and decreased in others. Dr. Corripio said this suggests a “rebalancing” of neural circuits.
As of July 2020, one of three patients with an electrode placed in the NAcc had experienced remission of positive symptoms and now has predominant negative symptoms. Another experienced significant improvements in negative symptoms. Two patients currently require psychosocial rehabilitation.
Patients for whom an electrode was placed in the ACC required higher voltages and more time to achieve an effect in comparison with those for whom an electrode was placed in the NAcc. Two patients required bilateral stimulation.
However, for all three patients who remained in the study, their clozapine dose was reduced.
Dr. Corripio reported that the team has observed negative thoughts and obsessive symptoms in patients with electrodes in the ACC, and all have needed either psychosocial rehabilitation or cognitive-behavioral therapy.
The investigators are now planning another DBS study involving patients with TRS, although this one will include a clinical recovery program focusing on family interventions and cognitive-behavioral therapy.
“Last-resort” treatment
In the postpresentation debate, Damiaan Denys, PhD, professor and chair of the department of psychiatry at the Academic Medical Canter, University of Amsterdam, said that DBS remains a treatment of “last resort” in TRS.
This is because it is both costly and invasive, and although the associated risk of bleeding and infection is low, he noted that the consequences are significant.
Dr. Denys added that patients need to have the potential for improvement; electrodes can be easily implanted, and the approach may tempt clinicians who sometimes “struggle with a huge amount of treatment-refractory cases.”
He also pointed to results achieved in studies of obsessive-compulsive disorder and depression, in which around 50% of patients responded to DBS.
“I think that’s the reason why we should be reluctant and not treat anyone at any stage, but first look for the more severe cases,” Dr. Denys said.
Unmet need
Judith M. Gault, PhD, associate research professor of neurosurgery at the University of Colorado at Denver, Aurora, also took part in the debate.
She said in an interview that patients with TRS have a lot of unmet needs and that DBS is worth trying in this patient population, with the goal being to “conduct a really good clinical trial” similar to the current study.
Antipsychotic drugs work well in responsive patients, but “in some cases the person is treatment refractory ... and in other cases the patient relapses,” Dr. Gault said.
She believes that DBS has the “potential to be more potent than antipsychotics in modulating the circuit of interest” and so fulfills the unmet needs of these patients while alleviating their symptoms.
Dr. Gault added that some patients experience “breakthrough symptoms” even while they are medication adherent. “That is a call for an intervention that is more potent” and suggests another potential role for DBS.
Overall, there are “a lot of really compelling reasons to pursue” DBS. However, there are also questions about how motivated patients with TRS are to participate in a clinical trial, Dr. Gault noted.
Patients with schizophrenia “tend not to be very motivated, especially if they have negative symptoms.” However, “if you were able to consider more of the population and not just the most severely affected, eventually you would find more people who are interested,” she said.
Still, it will take a better understanding of the efficacy and safety of the intervention for more people to be interested in trying it, said Dr. Gault.
“I think it’s hard early on, when you don’t actually know what the outcomes would be, if it’s even effective at all. But as you get more and more data in the population and at the different targets, people would be more open to it,” she said.
Another issue in generating interest among patients with schizophrenia is that many have not considered DBS as an option.
“It takes a while to think about it,” she noted. “You don’t want to rush into something that you just heard about, and so part of it is just education.”
The study was funded by Instituto Carlos III. Dr. Corripio reported having received research grants and conducting consultancy for Otsuka, Ferrer, Janssen, and Lilly. No other relevant financial relationships were reported.
A version of this article originally appeared on Medscape.com.
Deep brain stimulation (DBS) may be an effective option for patients with treatment-resistant schizophrenia (TRS), new research suggests. However, until further studies are conducted, the treatment should only be considered for the most severe cases.
The first clinical trial to assess DBS in this challenging patient population included eight patients initially randomly assigned to receive electrode placement in one of two locations in the brain. Once a clinical response was achieved and participants were stabilized, they were randomly assigned to a second crossover phase.
Preliminary findings from the first phase of the DBS-SCHIZO pilot study, which were reported in 2017, showed promising efficacy.
The newly released final results revealed an association between DBS and significant improvements in Positive and Negative Symptoms Scale (PANSS) scores, as well as reductions in doses of antipsychotic medication. Moreover, the effect reversed when the electrode was switched off.
“DBS may be a potential option for severe treatment-resistant schizophrenia patients,” lead investigator Iluminada Corripio, MD, PhD, department of psychiatry, Hospital de la Santa Creu i Sant Pau, Barcelona, said during her presentation at the virtual congress of the European College of Neuropsychopharmacology. The new data were updated results of a study published in EBioMedicine earlier this year.
Dr. Corripio underlined that it is important to balance the risks and benefits of the intervention. DBS is “not useful for all phenotypes,” and benefits have been seen in patients with hallucinations but not in those with a disorganized phenotype, she added.
High economic burden
Managing TRS is challenging and is associated with a high clinical and economic burden, Corripio noted. Relapse rates can reach 80%, increasing resource use by between 200% and 900%.
There is a strong rationale for studying the use of DBS in schizophrenia, because schizophrenia shares a neurologic basis with other neurologic and psychiatric disorders centered around the cortical-striatal-thalamic-cortical circuit, said Dr. Corripio.
The study included eight patients with a DSM-IV-TR diagnosis of schizophrenia whose conditions were resistant to at least two different atypical antipsychotics and who had not responded to clozapine monotherapy, combination therapy, or electroconvulsive therapy.
All were randomly assigned in a 1:1 ratio to DBS electrode implantation in one of two locations. Investigators chose the nucleus accumbens (NAcc), because recent studies have shown that DBS can increase dopamine levels there, and the subgenual anterior cingulate cortex (ACC). Deactivation failure in the ACC region has been observed in patients with schizophrenia and other mental illnesses.
Stimulation began 48-72 hours postoperatively with unilateral left stimulation at 2.5 volts. It was increased in 0.5 volt increments to a maximum of 7.5 volts. Patients who did not respond were switched to bilateral stimulation.
Follow-up was conducted every 2 weeks for up to 20 months. The study’s primary outcome was a symptomatic response, defined as an improvement of at least 25% on the PANSS.
Once that was achieved, patients could enter a second randomization phase in which they were assigned, in a 24-week, double-blind crossover design, to on- or off-treatment DBS arms such that patients received stimulation for 12 weeks before the device was turned off for 12 weeks, or vice versa.
Those who experienced relapse while off treatment were crossed over to the on-treatment arm; those who experienced relapsed while on treatment were withdrawn from the study. The patients’ average age was 42.5 years, and 50% were women. All were taking clozapine in combination with another antipsychotic.
Adverse events
Five patients experienced adverse events during the first phase, four of which were associated with rechargeable battery replacement. One experienced akathisia, another experienced behavioral changes, and a third experienced electrical disturbances.
A fourth patient experienced postsurgical hemorrhage of the right internal capsule on day 4, followed by encephalitis at week 8. He had a clinical improvement but experienced relapsed during follow-up.
The fifth patient accidentally switched off the device and withdrew from the study.
During the first randomization phase, DBS was associated with significant improvements on total, positive, and negative PANSS scores in comparison with the postoperative baseline measure in the seven remaining patients (P < .001).
When the team compared the baseline measure with the last observation, the improvement in PANSS scores remained significant for total scores (P = .007) and positive scores (P = .002), but not for negative scores (P = .18).
Three patients entered the second crossover phase of the study. Two began in the off-treatment arm and experienced relapsed within 1 and 2 weeks, respectively. Total PANSS scores increased from 79 to 98 for the first patient and from 47 to 93 for the second patient.
Neuroimaging showed that, among patients who responded to DBS, brain metabolism increased in some brain areas and decreased in others. Dr. Corripio said this suggests a “rebalancing” of neural circuits.
As of July 2020, one of three patients with an electrode placed in the NAcc had experienced remission of positive symptoms and now has predominant negative symptoms. Another experienced significant improvements in negative symptoms. Two patients currently require psychosocial rehabilitation.
Patients for whom an electrode was placed in the ACC required higher voltages and more time to achieve an effect in comparison with those for whom an electrode was placed in the NAcc. Two patients required bilateral stimulation.
However, for all three patients who remained in the study, their clozapine dose was reduced.
Dr. Corripio reported that the team has observed negative thoughts and obsessive symptoms in patients with electrodes in the ACC, and all have needed either psychosocial rehabilitation or cognitive-behavioral therapy.
The investigators are now planning another DBS study involving patients with TRS, although this one will include a clinical recovery program focusing on family interventions and cognitive-behavioral therapy.
“Last-resort” treatment
In the postpresentation debate, Damiaan Denys, PhD, professor and chair of the department of psychiatry at the Academic Medical Canter, University of Amsterdam, said that DBS remains a treatment of “last resort” in TRS.
This is because it is both costly and invasive, and although the associated risk of bleeding and infection is low, he noted that the consequences are significant.
Dr. Denys added that patients need to have the potential for improvement; electrodes can be easily implanted, and the approach may tempt clinicians who sometimes “struggle with a huge amount of treatment-refractory cases.”
He also pointed to results achieved in studies of obsessive-compulsive disorder and depression, in which around 50% of patients responded to DBS.
“I think that’s the reason why we should be reluctant and not treat anyone at any stage, but first look for the more severe cases,” Dr. Denys said.
Unmet need
Judith M. Gault, PhD, associate research professor of neurosurgery at the University of Colorado at Denver, Aurora, also took part in the debate.
She said in an interview that patients with TRS have a lot of unmet needs and that DBS is worth trying in this patient population, with the goal being to “conduct a really good clinical trial” similar to the current study.
Antipsychotic drugs work well in responsive patients, but “in some cases the person is treatment refractory ... and in other cases the patient relapses,” Dr. Gault said.
She believes that DBS has the “potential to be more potent than antipsychotics in modulating the circuit of interest” and so fulfills the unmet needs of these patients while alleviating their symptoms.
Dr. Gault added that some patients experience “breakthrough symptoms” even while they are medication adherent. “That is a call for an intervention that is more potent” and suggests another potential role for DBS.
Overall, there are “a lot of really compelling reasons to pursue” DBS. However, there are also questions about how motivated patients with TRS are to participate in a clinical trial, Dr. Gault noted.
Patients with schizophrenia “tend not to be very motivated, especially if they have negative symptoms.” However, “if you were able to consider more of the population and not just the most severely affected, eventually you would find more people who are interested,” she said.
Still, it will take a better understanding of the efficacy and safety of the intervention for more people to be interested in trying it, said Dr. Gault.
“I think it’s hard early on, when you don’t actually know what the outcomes would be, if it’s even effective at all. But as you get more and more data in the population and at the different targets, people would be more open to it,” she said.
Another issue in generating interest among patients with schizophrenia is that many have not considered DBS as an option.
“It takes a while to think about it,” she noted. “You don’t want to rush into something that you just heard about, and so part of it is just education.”
The study was funded by Instituto Carlos III. Dr. Corripio reported having received research grants and conducting consultancy for Otsuka, Ferrer, Janssen, and Lilly. No other relevant financial relationships were reported.
A version of this article originally appeared on Medscape.com.