User login
At-home cervical ripening linked with less time in L&D unit
Women who undergo balloon cervical ripening at home spend less time in the labor and delivery unit and have fewer cesarean deliveries than those who have the induction procedure in a hospital, researchers have found.
The findings, from a meta-analysis of eight previously conducted randomized clinical trials involving 740 women, should spur hospitals to “create and adhere to evidence-based guidelines” for outpatient balloon use, according to the researchers.
“Outpatient balloon cervical ripening is a safe alternative for low-risk patients and has the potential for significant benefits to patients and labor and delivery units,” the authors reported Jan. 6 in Obstetrics and Gynecology.
The rate of labor induction in the United States rose to 29.4% in 2019, the year following publication of the ARRIVE trial of low-risk nulliparous pregnant women, which found that induction at 39 weeks resulted in fewer cesarean deliveries with no difference in neonatal outcomes compared with expectant management, defined as continuing pregnancy until at least 40 weeks 5 days unless induction was medically indicated. Most women require preparation with a balloon-tipped catheter that slowly inflates to stretch and thin out the cervix, a process that can take many hours.
The devices have been shown to be safe, effective, and inexpensive, but the data on outpatient use are limited, according to the researchers. The new study is the “most comprehensive” examination of randomized clinical trials comparing outpatient and inpatient balloon cervical ripening, they say.
The trials included singleton gestations of at least 37 weeks of primarily low-risk patients. Body mass index was slightly lower in the outpatient group, with no differences in maternal age, gestational age at induction, or parity.
Six studies with 571 patients reported on the primary outcome, defined as time from labor unit admission to delivery. The outpatient group had a mean 16.3 hours compared with 23.8 hours for the inpatient group, a difference of 7.24 hours. However, data from three of the studies showed the inpatient group experienced 5.19 hours on average less between balloon expulsion and delivery, potentially due to more frequent adjustments and evaluation for expulsion.
The researchers observed no differences in adverse maternal or neonatal outcomes, and no stillbirths were reported among 378 patients who had the outpatient procedure. Cesarean delivery occurred less often in the outpatient group (21%) versus the inpatient group (27%) (risk ratio, 0.76; 95% confidence interval, 0.59-0.98).
Corresponding author Vincenzo Berghella, MD, director of the Division of Maternal-Fetal Medicine at Jefferson University Hospitals, Philadelphia, called the data “very assuring.” He said, “We knew induction was good in the hospital for many indications. We now know that induction can be started at home and it’s safe.”
Dr. Berghella added that the lower rate of cesarean delivery in the outpatient group likely reflected less use of fetal heart-rate monitoring, which can produce false-positive predictions of fetal compromise.
Still, too few patients have been studied to completely rule out rare adverse events with use of the balloons in the outpatient setting, the researchers acknowledge.
Aaron B. Caughey, MD, PhD, of Oregon Health and Science University, Portland, who was not involved in the study, said current data do not put to rest all safety concerns with the balloons, and it will be vital for health systems to report outcomes as outpatient use of the devices increases.
“Outcomes such as chorioamnionitis and postpartum hemorrhage will be important to have more data on, though there do not appear to be trends from these data,” Dr. Caughey told this news organization. Rarer outcomes, such as cervical injury, placenta abruption, and fetal injury, he added, “will require much larger studies to examine these potential but unlikely risks.”
The authors and Dr. Caughey have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
*Correction, 1/19/22: An earlier version of the headline of this article misstated a study finding. The study found that women who undergo balloon cervical ripening spend less time in the labor and delivery unit than those who have the induction procedure in a hospital.
Women who undergo balloon cervical ripening at home spend less time in the labor and delivery unit and have fewer cesarean deliveries than those who have the induction procedure in a hospital, researchers have found.
The findings, from a meta-analysis of eight previously conducted randomized clinical trials involving 740 women, should spur hospitals to “create and adhere to evidence-based guidelines” for outpatient balloon use, according to the researchers.
“Outpatient balloon cervical ripening is a safe alternative for low-risk patients and has the potential for significant benefits to patients and labor and delivery units,” the authors reported Jan. 6 in Obstetrics and Gynecology.
The rate of labor induction in the United States rose to 29.4% in 2019, the year following publication of the ARRIVE trial of low-risk nulliparous pregnant women, which found that induction at 39 weeks resulted in fewer cesarean deliveries with no difference in neonatal outcomes compared with expectant management, defined as continuing pregnancy until at least 40 weeks 5 days unless induction was medically indicated. Most women require preparation with a balloon-tipped catheter that slowly inflates to stretch and thin out the cervix, a process that can take many hours.
The devices have been shown to be safe, effective, and inexpensive, but the data on outpatient use are limited, according to the researchers. The new study is the “most comprehensive” examination of randomized clinical trials comparing outpatient and inpatient balloon cervical ripening, they say.
The trials included singleton gestations of at least 37 weeks of primarily low-risk patients. Body mass index was slightly lower in the outpatient group, with no differences in maternal age, gestational age at induction, or parity.
Six studies with 571 patients reported on the primary outcome, defined as time from labor unit admission to delivery. The outpatient group had a mean 16.3 hours compared with 23.8 hours for the inpatient group, a difference of 7.24 hours. However, data from three of the studies showed the inpatient group experienced 5.19 hours on average less between balloon expulsion and delivery, potentially due to more frequent adjustments and evaluation for expulsion.
The researchers observed no differences in adverse maternal or neonatal outcomes, and no stillbirths were reported among 378 patients who had the outpatient procedure. Cesarean delivery occurred less often in the outpatient group (21%) versus the inpatient group (27%) (risk ratio, 0.76; 95% confidence interval, 0.59-0.98).
Corresponding author Vincenzo Berghella, MD, director of the Division of Maternal-Fetal Medicine at Jefferson University Hospitals, Philadelphia, called the data “very assuring.” He said, “We knew induction was good in the hospital for many indications. We now know that induction can be started at home and it’s safe.”
Dr. Berghella added that the lower rate of cesarean delivery in the outpatient group likely reflected less use of fetal heart-rate monitoring, which can produce false-positive predictions of fetal compromise.
Still, too few patients have been studied to completely rule out rare adverse events with use of the balloons in the outpatient setting, the researchers acknowledge.
Aaron B. Caughey, MD, PhD, of Oregon Health and Science University, Portland, who was not involved in the study, said current data do not put to rest all safety concerns with the balloons, and it will be vital for health systems to report outcomes as outpatient use of the devices increases.
“Outcomes such as chorioamnionitis and postpartum hemorrhage will be important to have more data on, though there do not appear to be trends from these data,” Dr. Caughey told this news organization. Rarer outcomes, such as cervical injury, placenta abruption, and fetal injury, he added, “will require much larger studies to examine these potential but unlikely risks.”
The authors and Dr. Caughey have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
*Correction, 1/19/22: An earlier version of the headline of this article misstated a study finding. The study found that women who undergo balloon cervical ripening spend less time in the labor and delivery unit than those who have the induction procedure in a hospital.
Women who undergo balloon cervical ripening at home spend less time in the labor and delivery unit and have fewer cesarean deliveries than those who have the induction procedure in a hospital, researchers have found.
The findings, from a meta-analysis of eight previously conducted randomized clinical trials involving 740 women, should spur hospitals to “create and adhere to evidence-based guidelines” for outpatient balloon use, according to the researchers.
“Outpatient balloon cervical ripening is a safe alternative for low-risk patients and has the potential for significant benefits to patients and labor and delivery units,” the authors reported Jan. 6 in Obstetrics and Gynecology.
The rate of labor induction in the United States rose to 29.4% in 2019, the year following publication of the ARRIVE trial of low-risk nulliparous pregnant women, which found that induction at 39 weeks resulted in fewer cesarean deliveries with no difference in neonatal outcomes compared with expectant management, defined as continuing pregnancy until at least 40 weeks 5 days unless induction was medically indicated. Most women require preparation with a balloon-tipped catheter that slowly inflates to stretch and thin out the cervix, a process that can take many hours.
The devices have been shown to be safe, effective, and inexpensive, but the data on outpatient use are limited, according to the researchers. The new study is the “most comprehensive” examination of randomized clinical trials comparing outpatient and inpatient balloon cervical ripening, they say.
The trials included singleton gestations of at least 37 weeks of primarily low-risk patients. Body mass index was slightly lower in the outpatient group, with no differences in maternal age, gestational age at induction, or parity.
Six studies with 571 patients reported on the primary outcome, defined as time from labor unit admission to delivery. The outpatient group had a mean 16.3 hours compared with 23.8 hours for the inpatient group, a difference of 7.24 hours. However, data from three of the studies showed the inpatient group experienced 5.19 hours on average less between balloon expulsion and delivery, potentially due to more frequent adjustments and evaluation for expulsion.
The researchers observed no differences in adverse maternal or neonatal outcomes, and no stillbirths were reported among 378 patients who had the outpatient procedure. Cesarean delivery occurred less often in the outpatient group (21%) versus the inpatient group (27%) (risk ratio, 0.76; 95% confidence interval, 0.59-0.98).
Corresponding author Vincenzo Berghella, MD, director of the Division of Maternal-Fetal Medicine at Jefferson University Hospitals, Philadelphia, called the data “very assuring.” He said, “We knew induction was good in the hospital for many indications. We now know that induction can be started at home and it’s safe.”
Dr. Berghella added that the lower rate of cesarean delivery in the outpatient group likely reflected less use of fetal heart-rate monitoring, which can produce false-positive predictions of fetal compromise.
Still, too few patients have been studied to completely rule out rare adverse events with use of the balloons in the outpatient setting, the researchers acknowledge.
Aaron B. Caughey, MD, PhD, of Oregon Health and Science University, Portland, who was not involved in the study, said current data do not put to rest all safety concerns with the balloons, and it will be vital for health systems to report outcomes as outpatient use of the devices increases.
“Outcomes such as chorioamnionitis and postpartum hemorrhage will be important to have more data on, though there do not appear to be trends from these data,” Dr. Caughey told this news organization. Rarer outcomes, such as cervical injury, placenta abruption, and fetal injury, he added, “will require much larger studies to examine these potential but unlikely risks.”
The authors and Dr. Caughey have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
*Correction, 1/19/22: An earlier version of the headline of this article misstated a study finding. The study found that women who undergo balloon cervical ripening spend less time in the labor and delivery unit than those who have the induction procedure in a hospital.
ACIP releases new dengue vaccine recommendations
The vaccine is only to be used for children aged 9-16 who live in endemic areas and who have evidence with a specific diagnostic test of prior dengue infection.
Dengue is a mosquito-borne virus found throughout the world, primarily in tropical or subtropical climates. Cases had steadily been increasing to 5.2 million in 2019, and the geographic distribution of cases is broadening with climate change and urbanization. About half of the world’s population is now at risk.
The dengue virus has four serotypes. The first infection may be mild or asymptomatic, but the second one can be life-threatening because of a phenomenon called antibody-dependent enhancement.
The lead author of the new recommendations is Gabriela Paz-Bailey, MD, PhD, division of vector-borne diseases, dengue branch, CDC. She told this news organization that, during the second infection, when there are “low levels of antibodies from that first infection, the antibodies help the virus get inside the cells. There the virus is not killed, and that results in increased viral load, and then that can result in more severe disease and the plasma leakage” syndrome, which can lead to shock, severe bleeding, and organ failure. The death rate for severe dengue is up to 13%.
Previous infection with Zika virus, common in the same areas where dengue is endemic, can also increase the risk for symptomatic and severe dengue for subsequent infections.
In the United States, Puerto Rico is the main focus of control efforts because 95% of domestic dengue cases originate there – almost 30,000 cases between 2010 and 2020, with 11,000 cases and 4,000 hospitalizations occurring in children between the ages of 10 and 19.
Because Aedes aegypti, the primary mosquito vector transmitting dengue, is resistant to all commonly used insecticides in Puerto Rico, preventive efforts have shifted from insecticides to vaccination.
Antibody tests prevaccination
The main concern with the Sanofi’s dengue vaccine is that it could act as an asymptomatic primary dengue infection, in effect priming the body for a severe reaction from antibody-dependent enhancement with a subsequent infection. That is why it’s critical that the vaccine only be given to children with evidence of prior disease.
Dr. Paz-Bailey said: “The CDC came up with recommendations of what the performance of the test used for prevaccination screening should be. And it was 98% specificity and 75% sensitivity. ... But no test by itself was found to have a specificity of 98%, and this is why we’re recommending the two-test algorithm,” in which two different assays are run off the same blood sample, drawn at a prevaccination visit.
If the child has evidence of prior dengue, they can proceed with vaccination to protect against recurrent infection. Dengvaxia is given as a series of three shots over 6 months. Vaccine efficacy is 82% – so not everyone is protected, and additionally, that protection declines over time.
There is concern that it will be difficult to achieve compliance with such a complex regimen. Dr. Paz-Bailey said, “But I think that the trust in vaccines that is highly prevalent for [Puerto] Rico and trusting the health care system, and sort of the importance that is assigned to dengue by providers and by parents because of previous outbreaks and previous experiences is going to help us.” She added, “I think that the COVID experience has been very revealing. And what we have learned is that Puerto Rico has a very strong health care system, a very strong network of vaccine providers. ... Coverage for COVID vaccine is higher than in other parts of the U.S.”
One of the interesting things about dengue is that the first infection can range from asymptomatic to life-threatening. The second infection is generally worse because of this antibody-dependent enhancement phenomenon. Eng Eong Ooi, MD, PhD, professor of microbiology and immunology, National University of Singapore, told this news organization, “After you have two infections, you seem to be protected quite well against the remaining two [serotypes]. The vaccine serves as another episode of infection in those who had prior dengue, so then any natural infections after the vaccination in the seropositive become like the outcome of a third or fourth infection.”
Vaccination alone will not solve dengue. Dr. Ooi said, “There’s not one method that would fully control dengue. You need both vaccines as well as control measures, whether it’s Wolbachia or something else. At the same time, I think we need antiviral drugs, because hitting this virus in just one part of its life cycle wouldn’t make a huge, lasting impact.” Dr. Ooi added that as “the spread of the virus and the population immunity drops, you’re actually now more vulnerable to dengue outbreaks when they do get introduced. So, suppressing transmission alone isn’t the answer. You also have to keep herd immunity levels high. So if we can reduce the virus transmission by controlling either mosquito population or transmission and at the same time vaccinate to keep the immunity levels high, then I think we have a chance of controlling dengue.”
Dr. Paz-Bailey concluded: “I do want to emphasize that we are excited about having these tools, because for years and years, we have had really limited options to prevent and control dengue. It’s an important addition to have the vaccine be approved to be used within the U.S., and it’s going to pave the road for future vaccines.”
Dr. Paz-Bailey and Dr. Ooi reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The vaccine is only to be used for children aged 9-16 who live in endemic areas and who have evidence with a specific diagnostic test of prior dengue infection.
Dengue is a mosquito-borne virus found throughout the world, primarily in tropical or subtropical climates. Cases had steadily been increasing to 5.2 million in 2019, and the geographic distribution of cases is broadening with climate change and urbanization. About half of the world’s population is now at risk.
The dengue virus has four serotypes. The first infection may be mild or asymptomatic, but the second one can be life-threatening because of a phenomenon called antibody-dependent enhancement.
The lead author of the new recommendations is Gabriela Paz-Bailey, MD, PhD, division of vector-borne diseases, dengue branch, CDC. She told this news organization that, during the second infection, when there are “low levels of antibodies from that first infection, the antibodies help the virus get inside the cells. There the virus is not killed, and that results in increased viral load, and then that can result in more severe disease and the plasma leakage” syndrome, which can lead to shock, severe bleeding, and organ failure. The death rate for severe dengue is up to 13%.
Previous infection with Zika virus, common in the same areas where dengue is endemic, can also increase the risk for symptomatic and severe dengue for subsequent infections.
In the United States, Puerto Rico is the main focus of control efforts because 95% of domestic dengue cases originate there – almost 30,000 cases between 2010 and 2020, with 11,000 cases and 4,000 hospitalizations occurring in children between the ages of 10 and 19.
Because Aedes aegypti, the primary mosquito vector transmitting dengue, is resistant to all commonly used insecticides in Puerto Rico, preventive efforts have shifted from insecticides to vaccination.
Antibody tests prevaccination
The main concern with the Sanofi’s dengue vaccine is that it could act as an asymptomatic primary dengue infection, in effect priming the body for a severe reaction from antibody-dependent enhancement with a subsequent infection. That is why it’s critical that the vaccine only be given to children with evidence of prior disease.
Dr. Paz-Bailey said: “The CDC came up with recommendations of what the performance of the test used for prevaccination screening should be. And it was 98% specificity and 75% sensitivity. ... But no test by itself was found to have a specificity of 98%, and this is why we’re recommending the two-test algorithm,” in which two different assays are run off the same blood sample, drawn at a prevaccination visit.
If the child has evidence of prior dengue, they can proceed with vaccination to protect against recurrent infection. Dengvaxia is given as a series of three shots over 6 months. Vaccine efficacy is 82% – so not everyone is protected, and additionally, that protection declines over time.
There is concern that it will be difficult to achieve compliance with such a complex regimen. Dr. Paz-Bailey said, “But I think that the trust in vaccines that is highly prevalent for [Puerto] Rico and trusting the health care system, and sort of the importance that is assigned to dengue by providers and by parents because of previous outbreaks and previous experiences is going to help us.” She added, “I think that the COVID experience has been very revealing. And what we have learned is that Puerto Rico has a very strong health care system, a very strong network of vaccine providers. ... Coverage for COVID vaccine is higher than in other parts of the U.S.”
One of the interesting things about dengue is that the first infection can range from asymptomatic to life-threatening. The second infection is generally worse because of this antibody-dependent enhancement phenomenon. Eng Eong Ooi, MD, PhD, professor of microbiology and immunology, National University of Singapore, told this news organization, “After you have two infections, you seem to be protected quite well against the remaining two [serotypes]. The vaccine serves as another episode of infection in those who had prior dengue, so then any natural infections after the vaccination in the seropositive become like the outcome of a third or fourth infection.”
Vaccination alone will not solve dengue. Dr. Ooi said, “There’s not one method that would fully control dengue. You need both vaccines as well as control measures, whether it’s Wolbachia or something else. At the same time, I think we need antiviral drugs, because hitting this virus in just one part of its life cycle wouldn’t make a huge, lasting impact.” Dr. Ooi added that as “the spread of the virus and the population immunity drops, you’re actually now more vulnerable to dengue outbreaks when they do get introduced. So, suppressing transmission alone isn’t the answer. You also have to keep herd immunity levels high. So if we can reduce the virus transmission by controlling either mosquito population or transmission and at the same time vaccinate to keep the immunity levels high, then I think we have a chance of controlling dengue.”
Dr. Paz-Bailey concluded: “I do want to emphasize that we are excited about having these tools, because for years and years, we have had really limited options to prevent and control dengue. It’s an important addition to have the vaccine be approved to be used within the U.S., and it’s going to pave the road for future vaccines.”
Dr. Paz-Bailey and Dr. Ooi reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The vaccine is only to be used for children aged 9-16 who live in endemic areas and who have evidence with a specific diagnostic test of prior dengue infection.
Dengue is a mosquito-borne virus found throughout the world, primarily in tropical or subtropical climates. Cases had steadily been increasing to 5.2 million in 2019, and the geographic distribution of cases is broadening with climate change and urbanization. About half of the world’s population is now at risk.
The dengue virus has four serotypes. The first infection may be mild or asymptomatic, but the second one can be life-threatening because of a phenomenon called antibody-dependent enhancement.
The lead author of the new recommendations is Gabriela Paz-Bailey, MD, PhD, division of vector-borne diseases, dengue branch, CDC. She told this news organization that, during the second infection, when there are “low levels of antibodies from that first infection, the antibodies help the virus get inside the cells. There the virus is not killed, and that results in increased viral load, and then that can result in more severe disease and the plasma leakage” syndrome, which can lead to shock, severe bleeding, and organ failure. The death rate for severe dengue is up to 13%.
Previous infection with Zika virus, common in the same areas where dengue is endemic, can also increase the risk for symptomatic and severe dengue for subsequent infections.
In the United States, Puerto Rico is the main focus of control efforts because 95% of domestic dengue cases originate there – almost 30,000 cases between 2010 and 2020, with 11,000 cases and 4,000 hospitalizations occurring in children between the ages of 10 and 19.
Because Aedes aegypti, the primary mosquito vector transmitting dengue, is resistant to all commonly used insecticides in Puerto Rico, preventive efforts have shifted from insecticides to vaccination.
Antibody tests prevaccination
The main concern with the Sanofi’s dengue vaccine is that it could act as an asymptomatic primary dengue infection, in effect priming the body for a severe reaction from antibody-dependent enhancement with a subsequent infection. That is why it’s critical that the vaccine only be given to children with evidence of prior disease.
Dr. Paz-Bailey said: “The CDC came up with recommendations of what the performance of the test used for prevaccination screening should be. And it was 98% specificity and 75% sensitivity. ... But no test by itself was found to have a specificity of 98%, and this is why we’re recommending the two-test algorithm,” in which two different assays are run off the same blood sample, drawn at a prevaccination visit.
If the child has evidence of prior dengue, they can proceed with vaccination to protect against recurrent infection. Dengvaxia is given as a series of three shots over 6 months. Vaccine efficacy is 82% – so not everyone is protected, and additionally, that protection declines over time.
There is concern that it will be difficult to achieve compliance with such a complex regimen. Dr. Paz-Bailey said, “But I think that the trust in vaccines that is highly prevalent for [Puerto] Rico and trusting the health care system, and sort of the importance that is assigned to dengue by providers and by parents because of previous outbreaks and previous experiences is going to help us.” She added, “I think that the COVID experience has been very revealing. And what we have learned is that Puerto Rico has a very strong health care system, a very strong network of vaccine providers. ... Coverage for COVID vaccine is higher than in other parts of the U.S.”
One of the interesting things about dengue is that the first infection can range from asymptomatic to life-threatening. The second infection is generally worse because of this antibody-dependent enhancement phenomenon. Eng Eong Ooi, MD, PhD, professor of microbiology and immunology, National University of Singapore, told this news organization, “After you have two infections, you seem to be protected quite well against the remaining two [serotypes]. The vaccine serves as another episode of infection in those who had prior dengue, so then any natural infections after the vaccination in the seropositive become like the outcome of a third or fourth infection.”
Vaccination alone will not solve dengue. Dr. Ooi said, “There’s not one method that would fully control dengue. You need both vaccines as well as control measures, whether it’s Wolbachia or something else. At the same time, I think we need antiviral drugs, because hitting this virus in just one part of its life cycle wouldn’t make a huge, lasting impact.” Dr. Ooi added that as “the spread of the virus and the population immunity drops, you’re actually now more vulnerable to dengue outbreaks when they do get introduced. So, suppressing transmission alone isn’t the answer. You also have to keep herd immunity levels high. So if we can reduce the virus transmission by controlling either mosquito population or transmission and at the same time vaccinate to keep the immunity levels high, then I think we have a chance of controlling dengue.”
Dr. Paz-Bailey concluded: “I do want to emphasize that we are excited about having these tools, because for years and years, we have had really limited options to prevent and control dengue. It’s an important addition to have the vaccine be approved to be used within the U.S., and it’s going to pave the road for future vaccines.”
Dr. Paz-Bailey and Dr. Ooi reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM MMWR RECOMMENDATIONS AND REPORTS
Pregnancy diet linked to risk of obesity in child
A new study suggests that a healthy diet initiated by women before conception could lower the risk of obesity in the offspring.
Childhood obesity is a major public health concern in the United Kingdom, with nearly a quarter of children under 5 and more than a third of children starting secondary school being overweight or obese. Furthermore, childhood obesity is likely to persist in adulthood and have long-term health consequences.
Researchers at the University of Southampton (England) analyzed dietary data of 2,963 mother-child dyads identified from the U.K. Southampton Women’s Survey. Using the dietary data, each mother-child dyad was assigned combined diet quality score, based on which they were categorized into 5 groups: poor, poor-medium, medium, medium-better and best. Childhood adiposity was evaluated using dual-energy x-ray absorptiometry (DXA) and body mass index (BMI) z-scores.
The findings, published in the International Journal of Obesity, showed that mother-offspring diet quality trajectories were stable from preconception in mothers to age 8-9 years in the offspring. A poorer diet quality trajectory was linked to higher prepregnancy maternal BMI, lower maternal age at birth, lower educational levels, smoking, and multiparity.
After adjusting for confounders, a 1-category reduction in the dietary trajectory was associated with higher DXA percentage body fat (standard deviation, 0.08; 95% confidence interval, 0.01-0.15) and BMI z-score (SD, 0.08; 95% CI, 0.00-0.16) in the offspring aged 8-9 years.
Lead author Sarah Crozier, PhD, University of Southampton, said: “This research shows the importance of intervening at the earliest possible stage in a child’s life, in pregnancy or even before conception, to enable us to tackle it.” The authors believe that the preconception period serves as a crucial window to introduce favorable changes in the maternal dietary quality.
The research was funded by grants from the Medical Research Council, Project EarlyNutrition, and the European Union’s Seventh Framework and Horizon 2020 programs. The study also received support from National Institute for Health Research Southampton Biomedical Research Centre, the University of Southampton and University Hospital Southampton NHS Foundation Trust. The authors reported no competing interests.
A version of this article first appeared on Medscape UK.
A new study suggests that a healthy diet initiated by women before conception could lower the risk of obesity in the offspring.
Childhood obesity is a major public health concern in the United Kingdom, with nearly a quarter of children under 5 and more than a third of children starting secondary school being overweight or obese. Furthermore, childhood obesity is likely to persist in adulthood and have long-term health consequences.
Researchers at the University of Southampton (England) analyzed dietary data of 2,963 mother-child dyads identified from the U.K. Southampton Women’s Survey. Using the dietary data, each mother-child dyad was assigned combined diet quality score, based on which they were categorized into 5 groups: poor, poor-medium, medium, medium-better and best. Childhood adiposity was evaluated using dual-energy x-ray absorptiometry (DXA) and body mass index (BMI) z-scores.
The findings, published in the International Journal of Obesity, showed that mother-offspring diet quality trajectories were stable from preconception in mothers to age 8-9 years in the offspring. A poorer diet quality trajectory was linked to higher prepregnancy maternal BMI, lower maternal age at birth, lower educational levels, smoking, and multiparity.
After adjusting for confounders, a 1-category reduction in the dietary trajectory was associated with higher DXA percentage body fat (standard deviation, 0.08; 95% confidence interval, 0.01-0.15) and BMI z-score (SD, 0.08; 95% CI, 0.00-0.16) in the offspring aged 8-9 years.
Lead author Sarah Crozier, PhD, University of Southampton, said: “This research shows the importance of intervening at the earliest possible stage in a child’s life, in pregnancy or even before conception, to enable us to tackle it.” The authors believe that the preconception period serves as a crucial window to introduce favorable changes in the maternal dietary quality.
The research was funded by grants from the Medical Research Council, Project EarlyNutrition, and the European Union’s Seventh Framework and Horizon 2020 programs. The study also received support from National Institute for Health Research Southampton Biomedical Research Centre, the University of Southampton and University Hospital Southampton NHS Foundation Trust. The authors reported no competing interests.
A version of this article first appeared on Medscape UK.
A new study suggests that a healthy diet initiated by women before conception could lower the risk of obesity in the offspring.
Childhood obesity is a major public health concern in the United Kingdom, with nearly a quarter of children under 5 and more than a third of children starting secondary school being overweight or obese. Furthermore, childhood obesity is likely to persist in adulthood and have long-term health consequences.
Researchers at the University of Southampton (England) analyzed dietary data of 2,963 mother-child dyads identified from the U.K. Southampton Women’s Survey. Using the dietary data, each mother-child dyad was assigned combined diet quality score, based on which they were categorized into 5 groups: poor, poor-medium, medium, medium-better and best. Childhood adiposity was evaluated using dual-energy x-ray absorptiometry (DXA) and body mass index (BMI) z-scores.
The findings, published in the International Journal of Obesity, showed that mother-offspring diet quality trajectories were stable from preconception in mothers to age 8-9 years in the offspring. A poorer diet quality trajectory was linked to higher prepregnancy maternal BMI, lower maternal age at birth, lower educational levels, smoking, and multiparity.
After adjusting for confounders, a 1-category reduction in the dietary trajectory was associated with higher DXA percentage body fat (standard deviation, 0.08; 95% confidence interval, 0.01-0.15) and BMI z-score (SD, 0.08; 95% CI, 0.00-0.16) in the offspring aged 8-9 years.
Lead author Sarah Crozier, PhD, University of Southampton, said: “This research shows the importance of intervening at the earliest possible stage in a child’s life, in pregnancy or even before conception, to enable us to tackle it.” The authors believe that the preconception period serves as a crucial window to introduce favorable changes in the maternal dietary quality.
The research was funded by grants from the Medical Research Council, Project EarlyNutrition, and the European Union’s Seventh Framework and Horizon 2020 programs. The study also received support from National Institute for Health Research Southampton Biomedical Research Centre, the University of Southampton and University Hospital Southampton NHS Foundation Trust. The authors reported no competing interests.
A version of this article first appeared on Medscape UK.
FROM THE INTERNATIONAL JOURNAL OF OBESITY
Clinician experience, life stressors drive HIV adherence, retention in new patients
A novel twist on the concept of “meeting people where they are” may hold the key to retaining new HIV patients, and even bringing the elusive goal of ending the AIDS epidemic a bit closer. While the concept commonly refers to community outreach and engagement, understanding patient experiences and expectations and personal life stressors in the actual clinic setting may improve overall outcomes, according to new research.
In fact,
“Medical science is not necessarily [at the forefront] of where we want to focus our efforts right now,” Emmanuel Guajardo, MD, lead study author and instructor of infectious diseases at Baylor College of Medicine, Houston, told this news organization.
Rather, “we need to focus on retention in care and adherence to medications. Doubling down on these efforts could really go a long way toward ending the HIV epidemic,” he said.
Study findings were published online Jan. 5, 2022, in AIDS and Behavior.
First time’s a charm
A total of 450 patients attending an HIV clinic in Houston were asked to complete a postvisit survey detailing their experience with the HIV clinician, as well as personal life stressors in the preceding 6 months. Study participants were predominantly non-Hispanic Black (54.2%) or Hispanic (30.7%) and mostly men who have sex with men (MSM), populations that mimic the patients seen at Dr. Guajardo’s clinic. Patients were given the option of survey completion while awaiting discharge, within 2 weeks at the clinic, or (as a last resort) by phone.
Overall scores were based on a composite of validated scales: patient experience scores were defined dichotomously (best experience, most positive experience vs. not the best experience), and life stressor events (death, relationship, economic) were assigned weighted scores based on life change impact (for example, death of a spouse received a score of 100 while moved/changed living location was assigned a score of 25).
“We found that patients who reported better initial experiences with their provider at the first visit were less likely to be lost to follow-up at 6 and 12 months,” explained Dr. Guajardo. “Having fewer life stressors at the first visit [was] also [protective].”
At 6 months, mean overall patient experience scores were 8.60 for those LTFU versus and 8.98 for those not LTFU (P = .011); corresponding mean scores at 12 months were 8.43 and 8.98 respectively (P = .001).
For the dichotomized scoring, patients reporting the best experience with the health care professional were significantly less likely to be LTFU at 6 months (adjusted odd ratio, 0.866; P = .038) and 12 months (aOR, 1.263; P = .029) versus those not reporting the best experience.
Mean life change scores appeared to portend patient drop-off; patients reporting more stressful life events were likelier to be LTFU at 6 months (mean life change score, 129 vs. 100 for those retained in care) and at 12 months (126 vs. 101).
Corresponding multivariate logistic regression models controlling for age, baseline CD4 cell count less than 200, and diagnosis of at least 3 months showed that patients with higher life stressor burdens were significantly more likely to be LTFU at both 6 months (aOR, 1.232, P = .037) and 12 months (aOR, 1.263, P = .029).
Approach matters
“The [study] really hits the nail on the head in terms of identifying a couple of these very salient issues that affect people’s care, especially concerning HIV,” Philip A. Chan, MD, infectious disease specialist and associate professor of medicine at Brown University, Providence, R.I, told this news organization.
“It highlights things that we see on the ground that can interfere with HIV care or [pre-exposure prophylaxis] care, just health care in general, certainly one’s relationship with the physician or provider, and also, you know, real-life stressors,” said Dr. Chan, who was not involved with the study.
Relationship building is especially important for historically underserved populations, a point that’s hardly lost on either Dr. Chan or Dr. Guajardo, who both pointed to higher levels of mistrust among certain patient populations because of their mistreatment by the health care system. The answer? Let the patient lead the initial discussion, allow them to feel comfortable and participate in their care in ways that are most beneficial to them.
“There’s so much miscommunication, misunderstanding, and stigma related to HIV out in the community. So, it’s important to really open the floor for whatever they want to talk about first, before I push any agenda on a new patient.” Dr. Guajardo said. Thereafter, he relies on open-ended questions such as ‘tell me about your sexual partners?’ or ‘what sort of sexual practices do you engage in?’
“At the end of the day, you just need someone dedicated, who can be respectful and listening and caring, and dedicate time to patients to help keep them in care, to listen, and to navigate our incredibly, incredibly complex health care system,” Dr. Chan added.
This study was partly supported by use of the facilities and resources of the Houston Veterans Affairs Center for Innovations in Quality, Effectiveness, and Safety and Harris Health System. Support for the study was also provided by the National Institute of Mental Health and the University of Texas MD Anderson Foundation Chair at Baylor College of Medicine. Dr. Guajardo and Dr. Chan disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A novel twist on the concept of “meeting people where they are” may hold the key to retaining new HIV patients, and even bringing the elusive goal of ending the AIDS epidemic a bit closer. While the concept commonly refers to community outreach and engagement, understanding patient experiences and expectations and personal life stressors in the actual clinic setting may improve overall outcomes, according to new research.
In fact,
“Medical science is not necessarily [at the forefront] of where we want to focus our efforts right now,” Emmanuel Guajardo, MD, lead study author and instructor of infectious diseases at Baylor College of Medicine, Houston, told this news organization.
Rather, “we need to focus on retention in care and adherence to medications. Doubling down on these efforts could really go a long way toward ending the HIV epidemic,” he said.
Study findings were published online Jan. 5, 2022, in AIDS and Behavior.
First time’s a charm
A total of 450 patients attending an HIV clinic in Houston were asked to complete a postvisit survey detailing their experience with the HIV clinician, as well as personal life stressors in the preceding 6 months. Study participants were predominantly non-Hispanic Black (54.2%) or Hispanic (30.7%) and mostly men who have sex with men (MSM), populations that mimic the patients seen at Dr. Guajardo’s clinic. Patients were given the option of survey completion while awaiting discharge, within 2 weeks at the clinic, or (as a last resort) by phone.
Overall scores were based on a composite of validated scales: patient experience scores were defined dichotomously (best experience, most positive experience vs. not the best experience), and life stressor events (death, relationship, economic) were assigned weighted scores based on life change impact (for example, death of a spouse received a score of 100 while moved/changed living location was assigned a score of 25).
“We found that patients who reported better initial experiences with their provider at the first visit were less likely to be lost to follow-up at 6 and 12 months,” explained Dr. Guajardo. “Having fewer life stressors at the first visit [was] also [protective].”
At 6 months, mean overall patient experience scores were 8.60 for those LTFU versus and 8.98 for those not LTFU (P = .011); corresponding mean scores at 12 months were 8.43 and 8.98 respectively (P = .001).
For the dichotomized scoring, patients reporting the best experience with the health care professional were significantly less likely to be LTFU at 6 months (adjusted odd ratio, 0.866; P = .038) and 12 months (aOR, 1.263; P = .029) versus those not reporting the best experience.
Mean life change scores appeared to portend patient drop-off; patients reporting more stressful life events were likelier to be LTFU at 6 months (mean life change score, 129 vs. 100 for those retained in care) and at 12 months (126 vs. 101).
Corresponding multivariate logistic regression models controlling for age, baseline CD4 cell count less than 200, and diagnosis of at least 3 months showed that patients with higher life stressor burdens were significantly more likely to be LTFU at both 6 months (aOR, 1.232, P = .037) and 12 months (aOR, 1.263, P = .029).
Approach matters
“The [study] really hits the nail on the head in terms of identifying a couple of these very salient issues that affect people’s care, especially concerning HIV,” Philip A. Chan, MD, infectious disease specialist and associate professor of medicine at Brown University, Providence, R.I, told this news organization.
“It highlights things that we see on the ground that can interfere with HIV care or [pre-exposure prophylaxis] care, just health care in general, certainly one’s relationship with the physician or provider, and also, you know, real-life stressors,” said Dr. Chan, who was not involved with the study.
Relationship building is especially important for historically underserved populations, a point that’s hardly lost on either Dr. Chan or Dr. Guajardo, who both pointed to higher levels of mistrust among certain patient populations because of their mistreatment by the health care system. The answer? Let the patient lead the initial discussion, allow them to feel comfortable and participate in their care in ways that are most beneficial to them.
“There’s so much miscommunication, misunderstanding, and stigma related to HIV out in the community. So, it’s important to really open the floor for whatever they want to talk about first, before I push any agenda on a new patient.” Dr. Guajardo said. Thereafter, he relies on open-ended questions such as ‘tell me about your sexual partners?’ or ‘what sort of sexual practices do you engage in?’
“At the end of the day, you just need someone dedicated, who can be respectful and listening and caring, and dedicate time to patients to help keep them in care, to listen, and to navigate our incredibly, incredibly complex health care system,” Dr. Chan added.
This study was partly supported by use of the facilities and resources of the Houston Veterans Affairs Center for Innovations in Quality, Effectiveness, and Safety and Harris Health System. Support for the study was also provided by the National Institute of Mental Health and the University of Texas MD Anderson Foundation Chair at Baylor College of Medicine. Dr. Guajardo and Dr. Chan disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A novel twist on the concept of “meeting people where they are” may hold the key to retaining new HIV patients, and even bringing the elusive goal of ending the AIDS epidemic a bit closer. While the concept commonly refers to community outreach and engagement, understanding patient experiences and expectations and personal life stressors in the actual clinic setting may improve overall outcomes, according to new research.
In fact,
“Medical science is not necessarily [at the forefront] of where we want to focus our efforts right now,” Emmanuel Guajardo, MD, lead study author and instructor of infectious diseases at Baylor College of Medicine, Houston, told this news organization.
Rather, “we need to focus on retention in care and adherence to medications. Doubling down on these efforts could really go a long way toward ending the HIV epidemic,” he said.
Study findings were published online Jan. 5, 2022, in AIDS and Behavior.
First time’s a charm
A total of 450 patients attending an HIV clinic in Houston were asked to complete a postvisit survey detailing their experience with the HIV clinician, as well as personal life stressors in the preceding 6 months. Study participants were predominantly non-Hispanic Black (54.2%) or Hispanic (30.7%) and mostly men who have sex with men (MSM), populations that mimic the patients seen at Dr. Guajardo’s clinic. Patients were given the option of survey completion while awaiting discharge, within 2 weeks at the clinic, or (as a last resort) by phone.
Overall scores were based on a composite of validated scales: patient experience scores were defined dichotomously (best experience, most positive experience vs. not the best experience), and life stressor events (death, relationship, economic) were assigned weighted scores based on life change impact (for example, death of a spouse received a score of 100 while moved/changed living location was assigned a score of 25).
“We found that patients who reported better initial experiences with their provider at the first visit were less likely to be lost to follow-up at 6 and 12 months,” explained Dr. Guajardo. “Having fewer life stressors at the first visit [was] also [protective].”
At 6 months, mean overall patient experience scores were 8.60 for those LTFU versus and 8.98 for those not LTFU (P = .011); corresponding mean scores at 12 months were 8.43 and 8.98 respectively (P = .001).
For the dichotomized scoring, patients reporting the best experience with the health care professional were significantly less likely to be LTFU at 6 months (adjusted odd ratio, 0.866; P = .038) and 12 months (aOR, 1.263; P = .029) versus those not reporting the best experience.
Mean life change scores appeared to portend patient drop-off; patients reporting more stressful life events were likelier to be LTFU at 6 months (mean life change score, 129 vs. 100 for those retained in care) and at 12 months (126 vs. 101).
Corresponding multivariate logistic regression models controlling for age, baseline CD4 cell count less than 200, and diagnosis of at least 3 months showed that patients with higher life stressor burdens were significantly more likely to be LTFU at both 6 months (aOR, 1.232, P = .037) and 12 months (aOR, 1.263, P = .029).
Approach matters
“The [study] really hits the nail on the head in terms of identifying a couple of these very salient issues that affect people’s care, especially concerning HIV,” Philip A. Chan, MD, infectious disease specialist and associate professor of medicine at Brown University, Providence, R.I, told this news organization.
“It highlights things that we see on the ground that can interfere with HIV care or [pre-exposure prophylaxis] care, just health care in general, certainly one’s relationship with the physician or provider, and also, you know, real-life stressors,” said Dr. Chan, who was not involved with the study.
Relationship building is especially important for historically underserved populations, a point that’s hardly lost on either Dr. Chan or Dr. Guajardo, who both pointed to higher levels of mistrust among certain patient populations because of their mistreatment by the health care system. The answer? Let the patient lead the initial discussion, allow them to feel comfortable and participate in their care in ways that are most beneficial to them.
“There’s so much miscommunication, misunderstanding, and stigma related to HIV out in the community. So, it’s important to really open the floor for whatever they want to talk about first, before I push any agenda on a new patient.” Dr. Guajardo said. Thereafter, he relies on open-ended questions such as ‘tell me about your sexual partners?’ or ‘what sort of sexual practices do you engage in?’
“At the end of the day, you just need someone dedicated, who can be respectful and listening and caring, and dedicate time to patients to help keep them in care, to listen, and to navigate our incredibly, incredibly complex health care system,” Dr. Chan added.
This study was partly supported by use of the facilities and resources of the Houston Veterans Affairs Center for Innovations in Quality, Effectiveness, and Safety and Harris Health System. Support for the study was also provided by the National Institute of Mental Health and the University of Texas MD Anderson Foundation Chair at Baylor College of Medicine. Dr. Guajardo and Dr. Chan disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AIDS AND BEHAVIOR
Lifestyle changes can lead to remission, but not a cure, in type 2 diabetes
Whenever I get a new patient with type 2 diabetes, who is generally on metformin, one of the very first questions they ask me is, “Can I get off my medication?” Everybody, it seems, who gets diabetes wants to not have diabetes.
So, what does this really mean? What does this mean to me as a clinician? And what does this mean to my patients? The American Diabetes Association recently came out with a consensus statement that defines and interprets the definition of remission in people with type 2 diabetes. Basically, if the hemoglobin A1c is less than 6.5% without diabetes medications for at least 3 months, that’s considered remission.
There are other considerations, such as metabolic surgery, that can lead to remission. But again, such patients should be 3 months post surgery and at least 3 months off diabetes medication. As for a lifestyle intervention, the authors state that remission really happens within about 6 months.

That leads me to wonder: What is remission? Remission really means temporary recovery, so it doesn’t mean a cure. Now, I’m not against curing diabetes. In fact, I’m all for it. But when somebody gets diabetes – and honestly, it doesn’t matter whether it’s type 1 or type 2 – the first thing I think of, and I think the first thing that my patients are taught, is how important it is to have a healthy lifestyle. This healthy lifestyle isn’t just for people with diabetes; it largely means the healthy lifestyle that all of us should follow, one where we eat fewer simple carbs, less processed food, more vegetables, more lean proteins and meats – all of the things that we know we should do. And all of the things that keep us healthy. To some degree, I don’t think you can ever get “remission” from diabetes, because if having diabetes points an individual toward having a healthier lifestyle, I think that’s great.
I think people should exercise more. When it comes to treating diabetes, exercise is key. When you think about obesity, we want to help people who are overweight or obese lose weight as part of their treatment for diabetes. And that doesn’t go away, either.
So, no, people who are diagnosed with diabetes don’t really go into remission if they keep their same old habits and don’t lose weight and don’t exercise. But many people with diabetes can get off medication if they do those things.
However, it’s not true for everybody, and I don’t want people to get unrealistic expectations because I think there are probably about a thousand different subtypes of type 2 diabetes. And I’ve definitely seen people who are lean with type 2 diabetes who don’t respond as well to a lifestyle intervention, or people who are more insulin deficient, who also need medication.
I think it’s really important to frame the expectation that, if remission means going back to the way it was before, when they didn’t have to think about what they ate or whether or not they exercised, that’s not going to happen. I think diabetes should really be a wake-up call that people need to be healthier in terms of their lifestyle habits.
The issue of medication is really an individual one, and I think we need to help patients look for what’s best for the individual, what their targets are, what their goals are. But we also have to think that diabetes isn’t just about glucose.
So remission in terms of the ADA’s definition looks at glucose, but I look at more than glucose. You have to look at lipids and blood pressure. And, as I mentioned earlier, you have to look at whether or not a person has preexisting cardiovascular disease or has the presence of microvascular complications that need to be screened for and treated.
I actually think that, in some ways, the diagnosis of diabetes is helpful simply because it helps put people on a better path to health. I don’t want people to think that remission means that they can go back to unhealthy habits. I really encourage all people to live a healthier lifestyle, and if it leads to improvements in glucose levels and getting off medication, I think that’s wonderful and a worthy goal. But remember, health and meeting one’s targets remain key in the treatment of type 2 diabetes.
Dr. Peters is a professor in the department of clinical medicine at the University of Southern California, Los Angeles. She reported serving on the advisory board or speakers’ bureau of Medscape and several pharmaceutical companies, and has received research support from Dexcom, MannKind, and AstraZeneca. This perspective and an accompanying video first appeared on Medscape.com.
Whenever I get a new patient with type 2 diabetes, who is generally on metformin, one of the very first questions they ask me is, “Can I get off my medication?” Everybody, it seems, who gets diabetes wants to not have diabetes.
So, what does this really mean? What does this mean to me as a clinician? And what does this mean to my patients? The American Diabetes Association recently came out with a consensus statement that defines and interprets the definition of remission in people with type 2 diabetes. Basically, if the hemoglobin A1c is less than 6.5% without diabetes medications for at least 3 months, that’s considered remission.
There are other considerations, such as metabolic surgery, that can lead to remission. But again, such patients should be 3 months post surgery and at least 3 months off diabetes medication. As for a lifestyle intervention, the authors state that remission really happens within about 6 months.
That leads me to wonder: What is remission? Remission really means temporary recovery, so it doesn’t mean a cure. Now, I’m not against curing diabetes. In fact, I’m all for it. But when somebody gets diabetes – and honestly, it doesn’t matter whether it’s type 1 or type 2 – the first thing I think of, and I think the first thing that my patients are taught, is how important it is to have a healthy lifestyle. This healthy lifestyle isn’t just for people with diabetes; it largely means the healthy lifestyle that all of us should follow, one where we eat fewer simple carbs, less processed food, more vegetables, more lean proteins and meats – all of the things that we know we should do. And all of the things that keep us healthy. To some degree, I don’t think you can ever get “remission” from diabetes, because if having diabetes points an individual toward having a healthier lifestyle, I think that’s great.
I think people should exercise more. When it comes to treating diabetes, exercise is key. When you think about obesity, we want to help people who are overweight or obese lose weight as part of their treatment for diabetes. And that doesn’t go away, either.
So, no, people who are diagnosed with diabetes don’t really go into remission if they keep their same old habits and don’t lose weight and don’t exercise. But many people with diabetes can get off medication if they do those things.
However, it’s not true for everybody, and I don’t want people to get unrealistic expectations because I think there are probably about a thousand different subtypes of type 2 diabetes. And I’ve definitely seen people who are lean with type 2 diabetes who don’t respond as well to a lifestyle intervention, or people who are more insulin deficient, who also need medication.
I think it’s really important to frame the expectation that, if remission means going back to the way it was before, when they didn’t have to think about what they ate or whether or not they exercised, that’s not going to happen. I think diabetes should really be a wake-up call that people need to be healthier in terms of their lifestyle habits.
The issue of medication is really an individual one, and I think we need to help patients look for what’s best for the individual, what their targets are, what their goals are. But we also have to think that diabetes isn’t just about glucose.
So remission in terms of the ADA’s definition looks at glucose, but I look at more than glucose. You have to look at lipids and blood pressure. And, as I mentioned earlier, you have to look at whether or not a person has preexisting cardiovascular disease or has the presence of microvascular complications that need to be screened for and treated.
I actually think that, in some ways, the diagnosis of diabetes is helpful simply because it helps put people on a better path to health. I don’t want people to think that remission means that they can go back to unhealthy habits. I really encourage all people to live a healthier lifestyle, and if it leads to improvements in glucose levels and getting off medication, I think that’s wonderful and a worthy goal. But remember, health and meeting one’s targets remain key in the treatment of type 2 diabetes.
Dr. Peters is a professor in the department of clinical medicine at the University of Southern California, Los Angeles. She reported serving on the advisory board or speakers’ bureau of Medscape and several pharmaceutical companies, and has received research support from Dexcom, MannKind, and AstraZeneca. This perspective and an accompanying video first appeared on Medscape.com.
Whenever I get a new patient with type 2 diabetes, who is generally on metformin, one of the very first questions they ask me is, “Can I get off my medication?” Everybody, it seems, who gets diabetes wants to not have diabetes.
So, what does this really mean? What does this mean to me as a clinician? And what does this mean to my patients? The American Diabetes Association recently came out with a consensus statement that defines and interprets the definition of remission in people with type 2 diabetes. Basically, if the hemoglobin A1c is less than 6.5% without diabetes medications for at least 3 months, that’s considered remission.
There are other considerations, such as metabolic surgery, that can lead to remission. But again, such patients should be 3 months post surgery and at least 3 months off diabetes medication. As for a lifestyle intervention, the authors state that remission really happens within about 6 months.
That leads me to wonder: What is remission? Remission really means temporary recovery, so it doesn’t mean a cure. Now, I’m not against curing diabetes. In fact, I’m all for it. But when somebody gets diabetes – and honestly, it doesn’t matter whether it’s type 1 or type 2 – the first thing I think of, and I think the first thing that my patients are taught, is how important it is to have a healthy lifestyle. This healthy lifestyle isn’t just for people with diabetes; it largely means the healthy lifestyle that all of us should follow, one where we eat fewer simple carbs, less processed food, more vegetables, more lean proteins and meats – all of the things that we know we should do. And all of the things that keep us healthy. To some degree, I don’t think you can ever get “remission” from diabetes, because if having diabetes points an individual toward having a healthier lifestyle, I think that’s great.
I think people should exercise more. When it comes to treating diabetes, exercise is key. When you think about obesity, we want to help people who are overweight or obese lose weight as part of their treatment for diabetes. And that doesn’t go away, either.
So, no, people who are diagnosed with diabetes don’t really go into remission if they keep their same old habits and don’t lose weight and don’t exercise. But many people with diabetes can get off medication if they do those things.
However, it’s not true for everybody, and I don’t want people to get unrealistic expectations because I think there are probably about a thousand different subtypes of type 2 diabetes. And I’ve definitely seen people who are lean with type 2 diabetes who don’t respond as well to a lifestyle intervention, or people who are more insulin deficient, who also need medication.
I think it’s really important to frame the expectation that, if remission means going back to the way it was before, when they didn’t have to think about what they ate or whether or not they exercised, that’s not going to happen. I think diabetes should really be a wake-up call that people need to be healthier in terms of their lifestyle habits.
The issue of medication is really an individual one, and I think we need to help patients look for what’s best for the individual, what their targets are, what their goals are. But we also have to think that diabetes isn’t just about glucose.
So remission in terms of the ADA’s definition looks at glucose, but I look at more than glucose. You have to look at lipids and blood pressure. And, as I mentioned earlier, you have to look at whether or not a person has preexisting cardiovascular disease or has the presence of microvascular complications that need to be screened for and treated.
I actually think that, in some ways, the diagnosis of diabetes is helpful simply because it helps put people on a better path to health. I don’t want people to think that remission means that they can go back to unhealthy habits. I really encourage all people to live a healthier lifestyle, and if it leads to improvements in glucose levels and getting off medication, I think that’s wonderful and a worthy goal. But remember, health and meeting one’s targets remain key in the treatment of type 2 diabetes.
Dr. Peters is a professor in the department of clinical medicine at the University of Southern California, Los Angeles. She reported serving on the advisory board or speakers’ bureau of Medscape and several pharmaceutical companies, and has received research support from Dexcom, MannKind, and AstraZeneca. This perspective and an accompanying video first appeared on Medscape.com.
Docs react: Crowd crush survival guide, more dewormer, sizzling earwax
New year, same old TikTok.
You would think after 2021’s often perilous online health trends that the people of the internet would learn a thing or two. Just kidding, who actually thought that? Luckily,
Here’s to another year of “wow,” “ugh,” and “omg” moments. But let’s start with great advice from a doctor using TikTok to help save lives.
The good: Doctor explains how to survive crowd crush
J. Mack Slaughter, MD, (@drjmackslaughter_md) is an emergency physician who’s built his platform by engaging with and educating people on TikTok and Instagram. He recently reacted to the tragedy at the Travis Scott Astroworld music festival in Houston, where 10 people died due to a crowd surge. “This isn’t the first time this has happened, and it won’t be the last,” Dr. Slaughter captioned his post.
He used a video to spread awareness of how to best react to a crowd surge to his audience of over 368,000 followers, laying out four tips that people can use in case this ever happens to them.
Dr. Slaughter’s four tips are to (1) keep your arms up in front of you to give your chest as much room between someone in front of you as possible; (2) stay upright in order to avoid collapsing; (3) go with the flow of the crowd’s movement to conserve energy; (4) stay away from hard surfaces like walls or barriers “that can’t ebb and flow with the crowd.”
“When you get a densely packed area of people, not only can you lose control over your own movements, but you can have your chest compressed to the point where you can’t inhale,” Dr. Slaughter says. Hopefully, this crowd crush phenomenon is something that no one ever has to experience, but it’s better to have the knowledge on how to get through it.
The bad: Papaya seeds and parasites
TikTok user Jacqueline Rae posted about using papaya seeds as a detox method and dewormer in a video that has more than 32.5K likes and over a thousand comments – and she is just one of many TikTok users to promote this. “Papaya seeds on an empty stomach first thing in the morning is an antiparasitic,” Ms. Rae claims.
The papaya seed trend doesn’t come out of thin air, though. There was a study in 2007 where 60 Nigerian children who showed evidence of having intestinal parasites received papaya seeds as a treatment. For 71% of them, the treatment worked to clear their stool of the parasites. However, this is just one study with a pretty small sample size.
Unfortunately, TikTok’s algorithm can cater to hypochondriacs, and after scrolling through dewormer video after dewormer video, where people tout various products and cleanses, patients may really be convinced they have something they don’t.
Terry Simpson, MD, is a California-based physician and weight loss surgeon whose TikTok (@drterrysimpson) bio says: “Know your guts inside and out.” Dr. Simpson made his own video responding to the papaya seed craze, assuaging any anxiety or fears about contracting parasites.
In his video, Dr. Simpson says that most first-world countries like the United States have very few parasites, so patients shouldn’t be worried about them if they haven’t traveled to other countries recently. Additionally, he explains that what many people are seeing expelled after papaya seed cleanses is just fiber, and parasites aren’t visible to the naked eye.
“Papaya seeds are not a cure for parasites,” Dr. Simpson explains. “If you think you have parasites, see a doctor. One pill will get rid of all of the parasites that you can have, but the chances are you don’t have them.”
Symptoms that make people point toward parasites, such as low energy, frequent diarrhea, or other gut issues, can be symptoms of other issues unrelated to parasites, like irritable bowel syndrome or celiac disease. Because of this, it’s important to get a proper diagnosis amid signs of gut trouble.
The ugly: Hydrogen peroxide ear wax cleanse
TikTok user Ayisha Friedman-Negrin (@ayishafrita) got a whopping 2.7 million likes on her video where she puts hydrogen peroxide in her ear (yes, 2.7 million likes). This home remedy, she says, dissolves earwax that is stuck together. She lays her head on one side and waits for the hydrogen peroxide to “sizzle.” It bubbles like a hot spring before yellow-tinged liquid drips out. Yuck.
She isn’t totally wrong – hydrogen peroxide has been used for years to irrigate ears and help soften earwax. But there’s a lot of important information that people replicating this trend on TikTok tend to leave out of their videos. Thankfully, Sina Joorabchi, MD, is here to make sure TikTokers (and the rest of us) aren’t damaging their ears.
Dr. Joorabchi is a board-certified ear, nose, and throat doctor with his own TikTok account (@doctor.sina). He recommends in his video that if hydrogen peroxide is a patient’s go-to ear cleaner, it’s best to stick with one that’s of a 3% hydrogen peroxide concentration, as anything more can damage ears. Additionally, in the original video, Ms. Friedman-Negrin uses too much liquid, and 5 drops a day should work just fine for helping soften earwax.
“Definitely do not attempt [this] if you have an ear infection or history of ear perforation,” Dr. Joorabchi says. “And you don’t want to be using peroxide for an extended period of time. That can cause a lot of ear itching.”
A version of this article first appeared on Medscape.com.
New year, same old TikTok.
You would think after 2021’s often perilous online health trends that the people of the internet would learn a thing or two. Just kidding, who actually thought that? Luckily,
Here’s to another year of “wow,” “ugh,” and “omg” moments. But let’s start with great advice from a doctor using TikTok to help save lives.
The good: Doctor explains how to survive crowd crush
J. Mack Slaughter, MD, (@drjmackslaughter_md) is an emergency physician who’s built his platform by engaging with and educating people on TikTok and Instagram. He recently reacted to the tragedy at the Travis Scott Astroworld music festival in Houston, where 10 people died due to a crowd surge. “This isn’t the first time this has happened, and it won’t be the last,” Dr. Slaughter captioned his post.
He used a video to spread awareness of how to best react to a crowd surge to his audience of over 368,000 followers, laying out four tips that people can use in case this ever happens to them.
Dr. Slaughter’s four tips are to (1) keep your arms up in front of you to give your chest as much room between someone in front of you as possible; (2) stay upright in order to avoid collapsing; (3) go with the flow of the crowd’s movement to conserve energy; (4) stay away from hard surfaces like walls or barriers “that can’t ebb and flow with the crowd.”
“When you get a densely packed area of people, not only can you lose control over your own movements, but you can have your chest compressed to the point where you can’t inhale,” Dr. Slaughter says. Hopefully, this crowd crush phenomenon is something that no one ever has to experience, but it’s better to have the knowledge on how to get through it.
The bad: Papaya seeds and parasites
TikTok user Jacqueline Rae posted about using papaya seeds as a detox method and dewormer in a video that has more than 32.5K likes and over a thousand comments – and she is just one of many TikTok users to promote this. “Papaya seeds on an empty stomach first thing in the morning is an antiparasitic,” Ms. Rae claims.
The papaya seed trend doesn’t come out of thin air, though. There was a study in 2007 where 60 Nigerian children who showed evidence of having intestinal parasites received papaya seeds as a treatment. For 71% of them, the treatment worked to clear their stool of the parasites. However, this is just one study with a pretty small sample size.
Unfortunately, TikTok’s algorithm can cater to hypochondriacs, and after scrolling through dewormer video after dewormer video, where people tout various products and cleanses, patients may really be convinced they have something they don’t.
Terry Simpson, MD, is a California-based physician and weight loss surgeon whose TikTok (@drterrysimpson) bio says: “Know your guts inside and out.” Dr. Simpson made his own video responding to the papaya seed craze, assuaging any anxiety or fears about contracting parasites.
In his video, Dr. Simpson says that most first-world countries like the United States have very few parasites, so patients shouldn’t be worried about them if they haven’t traveled to other countries recently. Additionally, he explains that what many people are seeing expelled after papaya seed cleanses is just fiber, and parasites aren’t visible to the naked eye.
“Papaya seeds are not a cure for parasites,” Dr. Simpson explains. “If you think you have parasites, see a doctor. One pill will get rid of all of the parasites that you can have, but the chances are you don’t have them.”
Symptoms that make people point toward parasites, such as low energy, frequent diarrhea, or other gut issues, can be symptoms of other issues unrelated to parasites, like irritable bowel syndrome or celiac disease. Because of this, it’s important to get a proper diagnosis amid signs of gut trouble.
The ugly: Hydrogen peroxide ear wax cleanse
TikTok user Ayisha Friedman-Negrin (@ayishafrita) got a whopping 2.7 million likes on her video where she puts hydrogen peroxide in her ear (yes, 2.7 million likes). This home remedy, she says, dissolves earwax that is stuck together. She lays her head on one side and waits for the hydrogen peroxide to “sizzle.” It bubbles like a hot spring before yellow-tinged liquid drips out. Yuck.
She isn’t totally wrong – hydrogen peroxide has been used for years to irrigate ears and help soften earwax. But there’s a lot of important information that people replicating this trend on TikTok tend to leave out of their videos. Thankfully, Sina Joorabchi, MD, is here to make sure TikTokers (and the rest of us) aren’t damaging their ears.
Dr. Joorabchi is a board-certified ear, nose, and throat doctor with his own TikTok account (@doctor.sina). He recommends in his video that if hydrogen peroxide is a patient’s go-to ear cleaner, it’s best to stick with one that’s of a 3% hydrogen peroxide concentration, as anything more can damage ears. Additionally, in the original video, Ms. Friedman-Negrin uses too much liquid, and 5 drops a day should work just fine for helping soften earwax.
“Definitely do not attempt [this] if you have an ear infection or history of ear perforation,” Dr. Joorabchi says. “And you don’t want to be using peroxide for an extended period of time. That can cause a lot of ear itching.”
A version of this article first appeared on Medscape.com.
New year, same old TikTok.
You would think after 2021’s often perilous online health trends that the people of the internet would learn a thing or two. Just kidding, who actually thought that? Luckily,
Here’s to another year of “wow,” “ugh,” and “omg” moments. But let’s start with great advice from a doctor using TikTok to help save lives.
The good: Doctor explains how to survive crowd crush
J. Mack Slaughter, MD, (@drjmackslaughter_md) is an emergency physician who’s built his platform by engaging with and educating people on TikTok and Instagram. He recently reacted to the tragedy at the Travis Scott Astroworld music festival in Houston, where 10 people died due to a crowd surge. “This isn’t the first time this has happened, and it won’t be the last,” Dr. Slaughter captioned his post.
He used a video to spread awareness of how to best react to a crowd surge to his audience of over 368,000 followers, laying out four tips that people can use in case this ever happens to them.
Dr. Slaughter’s four tips are to (1) keep your arms up in front of you to give your chest as much room between someone in front of you as possible; (2) stay upright in order to avoid collapsing; (3) go with the flow of the crowd’s movement to conserve energy; (4) stay away from hard surfaces like walls or barriers “that can’t ebb and flow with the crowd.”
“When you get a densely packed area of people, not only can you lose control over your own movements, but you can have your chest compressed to the point where you can’t inhale,” Dr. Slaughter says. Hopefully, this crowd crush phenomenon is something that no one ever has to experience, but it’s better to have the knowledge on how to get through it.
The bad: Papaya seeds and parasites
TikTok user Jacqueline Rae posted about using papaya seeds as a detox method and dewormer in a video that has more than 32.5K likes and over a thousand comments – and she is just one of many TikTok users to promote this. “Papaya seeds on an empty stomach first thing in the morning is an antiparasitic,” Ms. Rae claims.
The papaya seed trend doesn’t come out of thin air, though. There was a study in 2007 where 60 Nigerian children who showed evidence of having intestinal parasites received papaya seeds as a treatment. For 71% of them, the treatment worked to clear their stool of the parasites. However, this is just one study with a pretty small sample size.
Unfortunately, TikTok’s algorithm can cater to hypochondriacs, and after scrolling through dewormer video after dewormer video, where people tout various products and cleanses, patients may really be convinced they have something they don’t.
Terry Simpson, MD, is a California-based physician and weight loss surgeon whose TikTok (@drterrysimpson) bio says: “Know your guts inside and out.” Dr. Simpson made his own video responding to the papaya seed craze, assuaging any anxiety or fears about contracting parasites.
In his video, Dr. Simpson says that most first-world countries like the United States have very few parasites, so patients shouldn’t be worried about them if they haven’t traveled to other countries recently. Additionally, he explains that what many people are seeing expelled after papaya seed cleanses is just fiber, and parasites aren’t visible to the naked eye.
“Papaya seeds are not a cure for parasites,” Dr. Simpson explains. “If you think you have parasites, see a doctor. One pill will get rid of all of the parasites that you can have, but the chances are you don’t have them.”
Symptoms that make people point toward parasites, such as low energy, frequent diarrhea, or other gut issues, can be symptoms of other issues unrelated to parasites, like irritable bowel syndrome or celiac disease. Because of this, it’s important to get a proper diagnosis amid signs of gut trouble.
The ugly: Hydrogen peroxide ear wax cleanse
TikTok user Ayisha Friedman-Negrin (@ayishafrita) got a whopping 2.7 million likes on her video where she puts hydrogen peroxide in her ear (yes, 2.7 million likes). This home remedy, she says, dissolves earwax that is stuck together. She lays her head on one side and waits for the hydrogen peroxide to “sizzle.” It bubbles like a hot spring before yellow-tinged liquid drips out. Yuck.
She isn’t totally wrong – hydrogen peroxide has been used for years to irrigate ears and help soften earwax. But there’s a lot of important information that people replicating this trend on TikTok tend to leave out of their videos. Thankfully, Sina Joorabchi, MD, is here to make sure TikTokers (and the rest of us) aren’t damaging their ears.
Dr. Joorabchi is a board-certified ear, nose, and throat doctor with his own TikTok account (@doctor.sina). He recommends in his video that if hydrogen peroxide is a patient’s go-to ear cleaner, it’s best to stick with one that’s of a 3% hydrogen peroxide concentration, as anything more can damage ears. Additionally, in the original video, Ms. Friedman-Negrin uses too much liquid, and 5 drops a day should work just fine for helping soften earwax.
“Definitely do not attempt [this] if you have an ear infection or history of ear perforation,” Dr. Joorabchi says. “And you don’t want to be using peroxide for an extended period of time. That can cause a lot of ear itching.”
A version of this article first appeared on Medscape.com.
U.S. cancer deaths continue to fall, especially lung cancer
There has been an overall decline of 32% in cancer deaths as of 2019, or approximately 3.5 million cancer deaths averted, the report noted.
“This success is largely because of reductions in smoking that resulted in downstream declines in lung and other smoking-related cancers,” lead author Rebecca L. Siegel of the ACS, and colleagues, noted in the latest edition of the society’s annual report on cancer rates and trends.
The paper was published online Jan. 12 in CA: A Cancer Journal for Clinicians.
In particular, there has been a fall in both the incidence of and mortality from lung cancer, largely due to successful efforts to get people to quit smoking, but also from earlier diagnosis at a stage when the disease is far more amenable to treatment, noted the authors.
For example, the incidence of lung cancer declined by almost 3% per year in men between the years 2009 and 2018 and by 1% a year in women. Currently, the historically large gender gap in lung cancer incidence is disappearing such that in 2018, lung cancer rates were 24% higher in men than they were in women, and rates in women were actually higher in some younger age groups than they were in men.
Moreover, 28% of lung cancers detected in 2018 were found at a localized stage of disease compared with 17% in 2004.
Patients diagnosed with lung cancer are also living longer, with almost one-third of lung cancer patients still alive 3 years after their diagnosis compared with 21% a decade ago.
However, lung cancer is still the biggest contributor to cancer-related mortality overall, at a death toll of 350 per day – more than breast, prostate, and pancreatic cancer combined, the authors wrote.
This is 2.5 times higher than the death rate from colorectal cancer (CRC), the second leading cause of cancer death in the United States, they added.
Nevertheless, the decrease in lung cancer mortality accelerated from 3.1% per year between 2010 and 2014 to 5.4% per year during 2015 to 2019 in men and from 1.8% to 4.3% in women. “Overall, the lung cancer death rate has dropped by 56% from 1990 to 2019 in men and by 32% from 2002 to 2019 in women,” Ms. Siegel and colleagues emphasized.
Overall, the ACS projects there will be over 1.9 million new cancer cases and over 600,000 cancer deaths across the United States in 2022.
Patterns are changing
With prostate cancer now accounting for some 27% of all cancer diagnoses in men, recent trends in the incidence of prostate cancer are somewhat worrisome, the authors wrote. While the incidence for local-stage disease remained stable from 2014 through to 2018, the incidence of advanced-stage disease has increased by 6% a year since 2011. “Consequently, the proportion of distant-stage diagnoses has more than doubled,” the authors noted, “from a low of 3.9% in 2007 to 8.2% in 2018.”
The incidence of breast cancer among women has been slowly increasing by 0.5% per year since about the mid-2000s. This increase is due at least in part to declines in fertility and increases in body weight among women, the authors suggested. Declines in breast cancer mortality have slowed in recent years, dropping from 1% per year from 2013 to 2019 from 2%-3% per year seen during the 1990s and the early 2000s.
As for CRC, incidence patterns are similar by sex but differ by age. For example, incidence rates of CRC declined by about 2% per year between 2014 and 2018 in individuals 50 years and older, but they increased by 1.5% per year in adults under the age of 50. Overall, however, mortality from CRC decreased by about 2% per year between 2010 and 2019, although this trend again masks increasing mortality from CRC among younger adults, where death rates rose by 1.2% per year from 2005 through 2019 in patients under the age of 50.
The third leading cause of death in men and women combined is pancreatic cancer. Here again, mortality rates slowly increased in men between 2000 and 2013 but have remained relatively stable in women.
Between 2010 and 2019, cancers of the tongue, tonsils, and oropharynx caused by human papilloma virus (HPV) increased by about 2% per year in men and by 1% per year in women.
Death from cervical cancer – despite its being one of the most preventable cancers overall – is still the second leading cause of cancer death in women between 20 and 39 years of age. “Most of these women have never been screened so this is low-hanging fruit easily addressed by increasing access to screening and [HPV] vaccination among underserved women,” Ms. Siegel said in a statement.
On the other hand, mortality from liver cancer – having increased rapidly over the past number of decades – appears to have stabilized in more recent years.
Survival at 5 years
For all cancers combined, survival at 5 years between the mid-1970s and 2011 through 2017 increased from 50% to 68% for White patients and by 39% to 63% for Black patients. “For all stages combined, survival is highest for prostate cancer (98%), melanoma of the skin (93%) and female breast cancer (90%),” the authors pointed out.
In contrast, survival at 5 years is lowest, at 11% for pancreatic cancer, 20% for cancers of the liver and esophagus, and 22% for lung cancer.
Indeed, for most of the common cancers, cancer survival has improved since the mid-1970s with the exception or uterine and cervical cancer, the latter because there have been few advancements in treatment.
Even among the more rare blood and lymphoid malignancies, improvements in treatment strategies, including the use of targeted therapies, have resulted in major survival gains from around 20% in the mid-1970s for chronic myeloid leukemia (CML) patients to over 70% for CML patients diagnosed between 2011 and 2017.
Similarly, the discovery and use of immunotherapy has doubled 5-year survival rates to 30% for patients with metastatic melanoma from 15% in 2004. On the other hand, racial disparities in survival odds continue to persist. For every cancer type except for cancer of the pancreas and kidney, survival rates were lower for Black patients than for White patients, the researchers pointed out.
“Black individuals also have lower stage-specific survival for most cancer types,” the report authors noted. Indeed, after adjustment for sex, age, and stage at diagnosis, the risk of death is 33% higher in Black patients than White patients and 51% higher in American Indian/Alaska Natives compared to White patients.
That said, the overall incidence of cancer is still highest among White individuals, in part because of high rates of breast cancer in White women, which may in part reflect overdiagnosis of breast cancer in this patient population, as the authors suggested.
“However, Black women have the highest cancer mortality rates – 12% higher than White women,” they observed. Even more striking, Black women have a 4% lower incidence of breast cancer than White women but a 41% higher mortality risk from it.
As for pediatric and adolescent cancers, incidence rates may be increasing slightly among both age groups, but dramatic reductions in death by 71% among children and by 61% among adolescents from the mid-70s until now continue as a singular success story in the treatment of cancer overall.
All the authors are employed by the ACS.
A version of this article first appeared on Medscape.com.
There has been an overall decline of 32% in cancer deaths as of 2019, or approximately 3.5 million cancer deaths averted, the report noted.
“This success is largely because of reductions in smoking that resulted in downstream declines in lung and other smoking-related cancers,” lead author Rebecca L. Siegel of the ACS, and colleagues, noted in the latest edition of the society’s annual report on cancer rates and trends.
The paper was published online Jan. 12 in CA: A Cancer Journal for Clinicians.
In particular, there has been a fall in both the incidence of and mortality from lung cancer, largely due to successful efforts to get people to quit smoking, but also from earlier diagnosis at a stage when the disease is far more amenable to treatment, noted the authors.
For example, the incidence of lung cancer declined by almost 3% per year in men between the years 2009 and 2018 and by 1% a year in women. Currently, the historically large gender gap in lung cancer incidence is disappearing such that in 2018, lung cancer rates were 24% higher in men than they were in women, and rates in women were actually higher in some younger age groups than they were in men.
Moreover, 28% of lung cancers detected in 2018 were found at a localized stage of disease compared with 17% in 2004.
Patients diagnosed with lung cancer are also living longer, with almost one-third of lung cancer patients still alive 3 years after their diagnosis compared with 21% a decade ago.
However, lung cancer is still the biggest contributor to cancer-related mortality overall, at a death toll of 350 per day – more than breast, prostate, and pancreatic cancer combined, the authors wrote.
This is 2.5 times higher than the death rate from colorectal cancer (CRC), the second leading cause of cancer death in the United States, they added.
Nevertheless, the decrease in lung cancer mortality accelerated from 3.1% per year between 2010 and 2014 to 5.4% per year during 2015 to 2019 in men and from 1.8% to 4.3% in women. “Overall, the lung cancer death rate has dropped by 56% from 1990 to 2019 in men and by 32% from 2002 to 2019 in women,” Ms. Siegel and colleagues emphasized.
Overall, the ACS projects there will be over 1.9 million new cancer cases and over 600,000 cancer deaths across the United States in 2022.
Patterns are changing
With prostate cancer now accounting for some 27% of all cancer diagnoses in men, recent trends in the incidence of prostate cancer are somewhat worrisome, the authors wrote. While the incidence for local-stage disease remained stable from 2014 through to 2018, the incidence of advanced-stage disease has increased by 6% a year since 2011. “Consequently, the proportion of distant-stage diagnoses has more than doubled,” the authors noted, “from a low of 3.9% in 2007 to 8.2% in 2018.”
The incidence of breast cancer among women has been slowly increasing by 0.5% per year since about the mid-2000s. This increase is due at least in part to declines in fertility and increases in body weight among women, the authors suggested. Declines in breast cancer mortality have slowed in recent years, dropping from 1% per year from 2013 to 2019 from 2%-3% per year seen during the 1990s and the early 2000s.
As for CRC, incidence patterns are similar by sex but differ by age. For example, incidence rates of CRC declined by about 2% per year between 2014 and 2018 in individuals 50 years and older, but they increased by 1.5% per year in adults under the age of 50. Overall, however, mortality from CRC decreased by about 2% per year between 2010 and 2019, although this trend again masks increasing mortality from CRC among younger adults, where death rates rose by 1.2% per year from 2005 through 2019 in patients under the age of 50.
The third leading cause of death in men and women combined is pancreatic cancer. Here again, mortality rates slowly increased in men between 2000 and 2013 but have remained relatively stable in women.
Between 2010 and 2019, cancers of the tongue, tonsils, and oropharynx caused by human papilloma virus (HPV) increased by about 2% per year in men and by 1% per year in women.
Death from cervical cancer – despite its being one of the most preventable cancers overall – is still the second leading cause of cancer death in women between 20 and 39 years of age. “Most of these women have never been screened so this is low-hanging fruit easily addressed by increasing access to screening and [HPV] vaccination among underserved women,” Ms. Siegel said in a statement.
On the other hand, mortality from liver cancer – having increased rapidly over the past number of decades – appears to have stabilized in more recent years.
Survival at 5 years
For all cancers combined, survival at 5 years between the mid-1970s and 2011 through 2017 increased from 50% to 68% for White patients and by 39% to 63% for Black patients. “For all stages combined, survival is highest for prostate cancer (98%), melanoma of the skin (93%) and female breast cancer (90%),” the authors pointed out.
In contrast, survival at 5 years is lowest, at 11% for pancreatic cancer, 20% for cancers of the liver and esophagus, and 22% for lung cancer.
Indeed, for most of the common cancers, cancer survival has improved since the mid-1970s with the exception or uterine and cervical cancer, the latter because there have been few advancements in treatment.
Even among the more rare blood and lymphoid malignancies, improvements in treatment strategies, including the use of targeted therapies, have resulted in major survival gains from around 20% in the mid-1970s for chronic myeloid leukemia (CML) patients to over 70% for CML patients diagnosed between 2011 and 2017.
Similarly, the discovery and use of immunotherapy has doubled 5-year survival rates to 30% for patients with metastatic melanoma from 15% in 2004. On the other hand, racial disparities in survival odds continue to persist. For every cancer type except for cancer of the pancreas and kidney, survival rates were lower for Black patients than for White patients, the researchers pointed out.
“Black individuals also have lower stage-specific survival for most cancer types,” the report authors noted. Indeed, after adjustment for sex, age, and stage at diagnosis, the risk of death is 33% higher in Black patients than White patients and 51% higher in American Indian/Alaska Natives compared to White patients.
That said, the overall incidence of cancer is still highest among White individuals, in part because of high rates of breast cancer in White women, which may in part reflect overdiagnosis of breast cancer in this patient population, as the authors suggested.
“However, Black women have the highest cancer mortality rates – 12% higher than White women,” they observed. Even more striking, Black women have a 4% lower incidence of breast cancer than White women but a 41% higher mortality risk from it.
As for pediatric and adolescent cancers, incidence rates may be increasing slightly among both age groups, but dramatic reductions in death by 71% among children and by 61% among adolescents from the mid-70s until now continue as a singular success story in the treatment of cancer overall.
All the authors are employed by the ACS.
A version of this article first appeared on Medscape.com.
There has been an overall decline of 32% in cancer deaths as of 2019, or approximately 3.5 million cancer deaths averted, the report noted.
“This success is largely because of reductions in smoking that resulted in downstream declines in lung and other smoking-related cancers,” lead author Rebecca L. Siegel of the ACS, and colleagues, noted in the latest edition of the society’s annual report on cancer rates and trends.
The paper was published online Jan. 12 in CA: A Cancer Journal for Clinicians.
In particular, there has been a fall in both the incidence of and mortality from lung cancer, largely due to successful efforts to get people to quit smoking, but also from earlier diagnosis at a stage when the disease is far more amenable to treatment, noted the authors.
For example, the incidence of lung cancer declined by almost 3% per year in men between the years 2009 and 2018 and by 1% a year in women. Currently, the historically large gender gap in lung cancer incidence is disappearing such that in 2018, lung cancer rates were 24% higher in men than they were in women, and rates in women were actually higher in some younger age groups than they were in men.
Moreover, 28% of lung cancers detected in 2018 were found at a localized stage of disease compared with 17% in 2004.
Patients diagnosed with lung cancer are also living longer, with almost one-third of lung cancer patients still alive 3 years after their diagnosis compared with 21% a decade ago.
However, lung cancer is still the biggest contributor to cancer-related mortality overall, at a death toll of 350 per day – more than breast, prostate, and pancreatic cancer combined, the authors wrote.
This is 2.5 times higher than the death rate from colorectal cancer (CRC), the second leading cause of cancer death in the United States, they added.
Nevertheless, the decrease in lung cancer mortality accelerated from 3.1% per year between 2010 and 2014 to 5.4% per year during 2015 to 2019 in men and from 1.8% to 4.3% in women. “Overall, the lung cancer death rate has dropped by 56% from 1990 to 2019 in men and by 32% from 2002 to 2019 in women,” Ms. Siegel and colleagues emphasized.
Overall, the ACS projects there will be over 1.9 million new cancer cases and over 600,000 cancer deaths across the United States in 2022.
Patterns are changing
With prostate cancer now accounting for some 27% of all cancer diagnoses in men, recent trends in the incidence of prostate cancer are somewhat worrisome, the authors wrote. While the incidence for local-stage disease remained stable from 2014 through to 2018, the incidence of advanced-stage disease has increased by 6% a year since 2011. “Consequently, the proportion of distant-stage diagnoses has more than doubled,” the authors noted, “from a low of 3.9% in 2007 to 8.2% in 2018.”
The incidence of breast cancer among women has been slowly increasing by 0.5% per year since about the mid-2000s. This increase is due at least in part to declines in fertility and increases in body weight among women, the authors suggested. Declines in breast cancer mortality have slowed in recent years, dropping from 1% per year from 2013 to 2019 from 2%-3% per year seen during the 1990s and the early 2000s.
As for CRC, incidence patterns are similar by sex but differ by age. For example, incidence rates of CRC declined by about 2% per year between 2014 and 2018 in individuals 50 years and older, but they increased by 1.5% per year in adults under the age of 50. Overall, however, mortality from CRC decreased by about 2% per year between 2010 and 2019, although this trend again masks increasing mortality from CRC among younger adults, where death rates rose by 1.2% per year from 2005 through 2019 in patients under the age of 50.
The third leading cause of death in men and women combined is pancreatic cancer. Here again, mortality rates slowly increased in men between 2000 and 2013 but have remained relatively stable in women.
Between 2010 and 2019, cancers of the tongue, tonsils, and oropharynx caused by human papilloma virus (HPV) increased by about 2% per year in men and by 1% per year in women.
Death from cervical cancer – despite its being one of the most preventable cancers overall – is still the second leading cause of cancer death in women between 20 and 39 years of age. “Most of these women have never been screened so this is low-hanging fruit easily addressed by increasing access to screening and [HPV] vaccination among underserved women,” Ms. Siegel said in a statement.
On the other hand, mortality from liver cancer – having increased rapidly over the past number of decades – appears to have stabilized in more recent years.
Survival at 5 years
For all cancers combined, survival at 5 years between the mid-1970s and 2011 through 2017 increased from 50% to 68% for White patients and by 39% to 63% for Black patients. “For all stages combined, survival is highest for prostate cancer (98%), melanoma of the skin (93%) and female breast cancer (90%),” the authors pointed out.
In contrast, survival at 5 years is lowest, at 11% for pancreatic cancer, 20% for cancers of the liver and esophagus, and 22% for lung cancer.
Indeed, for most of the common cancers, cancer survival has improved since the mid-1970s with the exception or uterine and cervical cancer, the latter because there have been few advancements in treatment.
Even among the more rare blood and lymphoid malignancies, improvements in treatment strategies, including the use of targeted therapies, have resulted in major survival gains from around 20% in the mid-1970s for chronic myeloid leukemia (CML) patients to over 70% for CML patients diagnosed between 2011 and 2017.
Similarly, the discovery and use of immunotherapy has doubled 5-year survival rates to 30% for patients with metastatic melanoma from 15% in 2004. On the other hand, racial disparities in survival odds continue to persist. For every cancer type except for cancer of the pancreas and kidney, survival rates were lower for Black patients than for White patients, the researchers pointed out.
“Black individuals also have lower stage-specific survival for most cancer types,” the report authors noted. Indeed, after adjustment for sex, age, and stage at diagnosis, the risk of death is 33% higher in Black patients than White patients and 51% higher in American Indian/Alaska Natives compared to White patients.
That said, the overall incidence of cancer is still highest among White individuals, in part because of high rates of breast cancer in White women, which may in part reflect overdiagnosis of breast cancer in this patient population, as the authors suggested.
“However, Black women have the highest cancer mortality rates – 12% higher than White women,” they observed. Even more striking, Black women have a 4% lower incidence of breast cancer than White women but a 41% higher mortality risk from it.
As for pediatric and adolescent cancers, incidence rates may be increasing slightly among both age groups, but dramatic reductions in death by 71% among children and by 61% among adolescents from the mid-70s until now continue as a singular success story in the treatment of cancer overall.
All the authors are employed by the ACS.
A version of this article first appeared on Medscape.com.
FROM CA: A CANCER JOURNAL FOR CLINICIANS
Swallowable intragastric balloon shows significant weight loss
results from a meta-analysis show.
“We believe this analysis to be the most comprehensive review [of the Allurion balloon],” reported first author Daryl Ramai, MD, of the division of gastroenterology and hepatology, University of Utah, Salt Lake City, and colleagues in the research, published in the November/December 2021 issue of the Journal of Clinical Gastroenterology.
“Our study showed that the Allurion balloon reduces waist circumference and triglyceride levels and [is] associated with less adverse events when compared with other intragastric balloons,” the authors concluded.
Unlike other balloons, the Allurion gastric balloon is compressed into a small capsule that is connected to a thin catheter and, once swallowed, it is then inflated with 550 mL of liquid through the catheter to create a feeling of fullness and help control hunger.
The procedure can be performed on an outpatient basis in approximately 20 minutes, potentially avoiding the burden and extra costs of surgery or endoscopic placement and removal. After approximately 4 months, the balloon is designed to empty through a valve that spontaneously opens, and the balloon is then passed in the stool.
Though currently used around the world, the balloon does not yet have approval from the Food and Drug Administration.
Meta-analysis shows 12.2% average weight loss across studies
To assess the balloon’s performance, the authors identified 7 out of 273 published studies that met the analysis criteria. The studies included 2,152 patients, ranging in age from 18 to 65 years, with a mean baseline body mass index of 32.1-38.6 kg/m2.
All of the studies were prospective, with reported outcomes at 3-4 months, when the Allurion balloon typically deflates. Three of the studies were multicenter, while four were single center.
In terms of improvements in BMI, the results showed the pooled mean difference from baseline through to the end of the studies was 0.88 (P = .001), and the weighted average percentage of total body weight loss during treatment across the studies was 12.2%.
The mean excess body weight loss across the Allurion studies was 49.1%.
The analysis was not designed to directly compare outcomes with other balloons, but the authors note, for instance, that the ReShape Duo intragastric balloon (an FDA-approved dual-balloon system) has been reported in a previous study to be associated with a percentage of total body weight loss of 7.6% at 6 months, compared with 3.6% observed among those with lifestyle modifications.
However, a separate meta-analysis showed the pooled percentage of total body weight loss with the FDA-approved Orbera balloon to be about the same as the current Allurion analysis, at 12.3% at 3 months after implantation (followed by 13.2% at 6 months and 11.3% at 12 months). The analysis further showed excess body weight loss with the Orbera balloon at 12 months to be 25.4%.
In other outcomes, the current meta-analysis also showed significant improvements with the Allurion balloon in waist circumference of 0.89 (P = .001) and in triglyceride levels of 0.66 (P = .004) versus baseline.
Previous research involving the FDA-approved Obalon intragastric balloon, which is inflated with gas rather than liquid, showed a significant reduction in waist circumference from 109 cm (±12.3) to 99 cm (±10.5) (P < .05), and another study showed that 37.5% of patients receiving the Orbera balloon had normalized triglyceride levels after 4 months, without concomitant medical therapy.
Adverse events appear lower vs. other balloons
Potential risks associated with the Allurion balloon include the potential for early deflation; however, the pooled rate of early balloon deflation observed in the meta-analysis was relatively low at 1.8%.
Other adverse events reported with the Allurion balloon were abdominal pain (37.5%), vomiting (29.6%), diarrhea (15.4%), and small bowel obstruction (0.5%).
The corresponding rates of abdominal pain with the ReShape Duo and Orbera balloons have been reported at 54.5% and 57.5%, respectively, with the effects possibly caused by overinflation, the authors noted.
And rates of vomiting with the ReShape Duo and Orbera balloons have been reported as much higher, at 86.7% and 86.8%, respectively.
Of note, there were no deaths or cases of acute pancreatitis reported in the meta-analysis studies of Allurion.
As reported by this news organization, such concerns have been raised in previous FDA alerts regarding the Orbera and ReShape Duo liquid-filled intragastric balloons.
In the most recent update, issued in April 2020, the FDA described receiving reports of 18 deaths that had occurred worldwide since the approvals of the Orbera and ReShape balloons, including eight in the United States.
Dr. Ramai noted that the concern about the issues is warranted.
“These concerns are valid,” he told this news organization. “Theoretically, since the Allurion balloon is placed for a shorter time span, it is conceivable that there may be less adverse events. However, comparative trials are needed to confirm this.”
Although the balloons show efficacy in patients struggling with weight loss, metabolic syndrome, and fatty liver disease, “the type and duration of intragastric balloons should be tailored to the patient,” Dr. Ramai said.
“Clinicians should thoroughly discuss with their patients the benefits and risks of using an intragastric balloon,” he added. “Furthermore, placement of intragastric balloons should only be attempted by clinicians with expertise in bariatric endoscopy.”
The study received no financial support. Dr. Ramai reported no relevant financial relationships.
A version of this article first appeared on Medscape.com,
results from a meta-analysis show.
“We believe this analysis to be the most comprehensive review [of the Allurion balloon],” reported first author Daryl Ramai, MD, of the division of gastroenterology and hepatology, University of Utah, Salt Lake City, and colleagues in the research, published in the November/December 2021 issue of the Journal of Clinical Gastroenterology.
“Our study showed that the Allurion balloon reduces waist circumference and triglyceride levels and [is] associated with less adverse events when compared with other intragastric balloons,” the authors concluded.
Unlike other balloons, the Allurion gastric balloon is compressed into a small capsule that is connected to a thin catheter and, once swallowed, it is then inflated with 550 mL of liquid through the catheter to create a feeling of fullness and help control hunger.
The procedure can be performed on an outpatient basis in approximately 20 minutes, potentially avoiding the burden and extra costs of surgery or endoscopic placement and removal. After approximately 4 months, the balloon is designed to empty through a valve that spontaneously opens, and the balloon is then passed in the stool.
Though currently used around the world, the balloon does not yet have approval from the Food and Drug Administration.
Meta-analysis shows 12.2% average weight loss across studies
To assess the balloon’s performance, the authors identified 7 out of 273 published studies that met the analysis criteria. The studies included 2,152 patients, ranging in age from 18 to 65 years, with a mean baseline body mass index of 32.1-38.6 kg/m2.
All of the studies were prospective, with reported outcomes at 3-4 months, when the Allurion balloon typically deflates. Three of the studies were multicenter, while four were single center.
In terms of improvements in BMI, the results showed the pooled mean difference from baseline through to the end of the studies was 0.88 (P = .001), and the weighted average percentage of total body weight loss during treatment across the studies was 12.2%.
The mean excess body weight loss across the Allurion studies was 49.1%.
The analysis was not designed to directly compare outcomes with other balloons, but the authors note, for instance, that the ReShape Duo intragastric balloon (an FDA-approved dual-balloon system) has been reported in a previous study to be associated with a percentage of total body weight loss of 7.6% at 6 months, compared with 3.6% observed among those with lifestyle modifications.
However, a separate meta-analysis showed the pooled percentage of total body weight loss with the FDA-approved Orbera balloon to be about the same as the current Allurion analysis, at 12.3% at 3 months after implantation (followed by 13.2% at 6 months and 11.3% at 12 months). The analysis further showed excess body weight loss with the Orbera balloon at 12 months to be 25.4%.
In other outcomes, the current meta-analysis also showed significant improvements with the Allurion balloon in waist circumference of 0.89 (P = .001) and in triglyceride levels of 0.66 (P = .004) versus baseline.
Previous research involving the FDA-approved Obalon intragastric balloon, which is inflated with gas rather than liquid, showed a significant reduction in waist circumference from 109 cm (±12.3) to 99 cm (±10.5) (P < .05), and another study showed that 37.5% of patients receiving the Orbera balloon had normalized triglyceride levels after 4 months, without concomitant medical therapy.
Adverse events appear lower vs. other balloons
Potential risks associated with the Allurion balloon include the potential for early deflation; however, the pooled rate of early balloon deflation observed in the meta-analysis was relatively low at 1.8%.
Other adverse events reported with the Allurion balloon were abdominal pain (37.5%), vomiting (29.6%), diarrhea (15.4%), and small bowel obstruction (0.5%).
The corresponding rates of abdominal pain with the ReShape Duo and Orbera balloons have been reported at 54.5% and 57.5%, respectively, with the effects possibly caused by overinflation, the authors noted.
And rates of vomiting with the ReShape Duo and Orbera balloons have been reported as much higher, at 86.7% and 86.8%, respectively.
Of note, there were no deaths or cases of acute pancreatitis reported in the meta-analysis studies of Allurion.
As reported by this news organization, such concerns have been raised in previous FDA alerts regarding the Orbera and ReShape Duo liquid-filled intragastric balloons.
In the most recent update, issued in April 2020, the FDA described receiving reports of 18 deaths that had occurred worldwide since the approvals of the Orbera and ReShape balloons, including eight in the United States.
Dr. Ramai noted that the concern about the issues is warranted.
“These concerns are valid,” he told this news organization. “Theoretically, since the Allurion balloon is placed for a shorter time span, it is conceivable that there may be less adverse events. However, comparative trials are needed to confirm this.”
Although the balloons show efficacy in patients struggling with weight loss, metabolic syndrome, and fatty liver disease, “the type and duration of intragastric balloons should be tailored to the patient,” Dr. Ramai said.
“Clinicians should thoroughly discuss with their patients the benefits and risks of using an intragastric balloon,” he added. “Furthermore, placement of intragastric balloons should only be attempted by clinicians with expertise in bariatric endoscopy.”
The study received no financial support. Dr. Ramai reported no relevant financial relationships.
A version of this article first appeared on Medscape.com,
results from a meta-analysis show.
“We believe this analysis to be the most comprehensive review [of the Allurion balloon],” reported first author Daryl Ramai, MD, of the division of gastroenterology and hepatology, University of Utah, Salt Lake City, and colleagues in the research, published in the November/December 2021 issue of the Journal of Clinical Gastroenterology.
“Our study showed that the Allurion balloon reduces waist circumference and triglyceride levels and [is] associated with less adverse events when compared with other intragastric balloons,” the authors concluded.
Unlike other balloons, the Allurion gastric balloon is compressed into a small capsule that is connected to a thin catheter and, once swallowed, it is then inflated with 550 mL of liquid through the catheter to create a feeling of fullness and help control hunger.
The procedure can be performed on an outpatient basis in approximately 20 minutes, potentially avoiding the burden and extra costs of surgery or endoscopic placement and removal. After approximately 4 months, the balloon is designed to empty through a valve that spontaneously opens, and the balloon is then passed in the stool.
Though currently used around the world, the balloon does not yet have approval from the Food and Drug Administration.
Meta-analysis shows 12.2% average weight loss across studies
To assess the balloon’s performance, the authors identified 7 out of 273 published studies that met the analysis criteria. The studies included 2,152 patients, ranging in age from 18 to 65 years, with a mean baseline body mass index of 32.1-38.6 kg/m2.
All of the studies were prospective, with reported outcomes at 3-4 months, when the Allurion balloon typically deflates. Three of the studies were multicenter, while four were single center.
In terms of improvements in BMI, the results showed the pooled mean difference from baseline through to the end of the studies was 0.88 (P = .001), and the weighted average percentage of total body weight loss during treatment across the studies was 12.2%.
The mean excess body weight loss across the Allurion studies was 49.1%.
The analysis was not designed to directly compare outcomes with other balloons, but the authors note, for instance, that the ReShape Duo intragastric balloon (an FDA-approved dual-balloon system) has been reported in a previous study to be associated with a percentage of total body weight loss of 7.6% at 6 months, compared with 3.6% observed among those with lifestyle modifications.
However, a separate meta-analysis showed the pooled percentage of total body weight loss with the FDA-approved Orbera balloon to be about the same as the current Allurion analysis, at 12.3% at 3 months after implantation (followed by 13.2% at 6 months and 11.3% at 12 months). The analysis further showed excess body weight loss with the Orbera balloon at 12 months to be 25.4%.
In other outcomes, the current meta-analysis also showed significant improvements with the Allurion balloon in waist circumference of 0.89 (P = .001) and in triglyceride levels of 0.66 (P = .004) versus baseline.
Previous research involving the FDA-approved Obalon intragastric balloon, which is inflated with gas rather than liquid, showed a significant reduction in waist circumference from 109 cm (±12.3) to 99 cm (±10.5) (P < .05), and another study showed that 37.5% of patients receiving the Orbera balloon had normalized triglyceride levels after 4 months, without concomitant medical therapy.
Adverse events appear lower vs. other balloons
Potential risks associated with the Allurion balloon include the potential for early deflation; however, the pooled rate of early balloon deflation observed in the meta-analysis was relatively low at 1.8%.
Other adverse events reported with the Allurion balloon were abdominal pain (37.5%), vomiting (29.6%), diarrhea (15.4%), and small bowel obstruction (0.5%).
The corresponding rates of abdominal pain with the ReShape Duo and Orbera balloons have been reported at 54.5% and 57.5%, respectively, with the effects possibly caused by overinflation, the authors noted.
And rates of vomiting with the ReShape Duo and Orbera balloons have been reported as much higher, at 86.7% and 86.8%, respectively.
Of note, there were no deaths or cases of acute pancreatitis reported in the meta-analysis studies of Allurion.
As reported by this news organization, such concerns have been raised in previous FDA alerts regarding the Orbera and ReShape Duo liquid-filled intragastric balloons.
In the most recent update, issued in April 2020, the FDA described receiving reports of 18 deaths that had occurred worldwide since the approvals of the Orbera and ReShape balloons, including eight in the United States.
Dr. Ramai noted that the concern about the issues is warranted.
“These concerns are valid,” he told this news organization. “Theoretically, since the Allurion balloon is placed for a shorter time span, it is conceivable that there may be less adverse events. However, comparative trials are needed to confirm this.”
Although the balloons show efficacy in patients struggling with weight loss, metabolic syndrome, and fatty liver disease, “the type and duration of intragastric balloons should be tailored to the patient,” Dr. Ramai said.
“Clinicians should thoroughly discuss with their patients the benefits and risks of using an intragastric balloon,” he added. “Furthermore, placement of intragastric balloons should only be attempted by clinicians with expertise in bariatric endoscopy.”
The study received no financial support. Dr. Ramai reported no relevant financial relationships.
A version of this article first appeared on Medscape.com,
FROM THE JOURNAL OF CLINICAL GASTROENTEROLOGY
UTIs in pregnancy: Managing urethritis, asymptomatic bacteriuria, cystitis, and pyelonephritis
CASE Pregnant woman with dysuria and suprapubic pain
A 25-year-old primigravid woman at 18 weeks of gestation requests evaluation because of the acute onset of frequent urination, dysuria, urination hesitancy, and suprapubic pain on the morning following intercourse. She has not experienced similar symptoms in the past. On physical examination, her temperature is 38 °C, pulse is 96 beats per minute, respirations are 18 per minute, and blood pressure is 100/76 mm Hg. She has no urethral discharge but is tender to palpation in the suprapubic area.
- What is the most likely diagnosis?
- What tests would be of greatest value in confirming the diagnosis?
- What is the most appropriate treatment for this patient?
Meet our perpetrator
Urinary tract infections (UTIs) are among the most common infections that occur during pregnancy. They may take one of 4 forms: acute urethritis, asymptomatic bacteriuria, acute cystitis, and acute pyelonephritis.1 The first 3 conditions usually are straightforward to diagnose and treat, and they usually do not cause major problems for the mother or fetus. The latter, however, can cause serious complications that pose risk to the mother and fetus.
This article will review the microbiology, clinical manifestations, diagnosis, and treatment of these 4 disorders in pregnancy. Particular emphasis will be placed on measures to avoid adverse effects on the mother and fetus from antimicrobial agents.
Acute urethritis
Acute urethritis can be caused by low concentrations of coliform organisms in the lower urinary tract, but it usually is secondary to infection by Neisseria gonorrhea or Chlamydia trachomatis. In most prenatal populations, the prevalence of one or the other of these 2 infections is approximately 5%.1
The most common clinical manifestations of acute urethritis are a purulent urethral discharge, increased frequency of urination, dysuria, and urination hesitancy. The diagnosis most easily is confirmed by obtaining a specimen of urethral discharge or urine and evaluating the sample by a nucleic acid amplification test for both gonorrhea and chlamydia.
Antibiotic therapy is preferred. The current recommended treatment for gonococcal urethritis is a single intramuscular injection of ceftriaxone 500 mg. If the patient prefers oral therapy, she can receive cefixime 800 mg in a single dose. For patients with an allergy to beta-lactam antibiotics, the alternative regimen is gentamicin 240 mg in a single intramuscular injection, combined with oral azithromycin in a single 2,000-mg dose. For treatment of chlamydia in pregnancy, the recommended therapy is azithromycin 1,000 mg in a single oral dose.2 A test of cure should be performed within 4 weeks of treatment.
Asymptomatic bacteriuria
Asymptomatic bacteriuria (ASB) is the most common UTI in women. Approximately 5% to 8% of all sexually active women have ASB. The condition is not unique to pregnancy; it is associated primarily with the assumption of coital activity. In point of fact, the ASB typically precedes pregnancy by several years.1
The principal pathogens responsible for ASB are shown in the FIGURE. Over 80% of first-time infections are secondary to Escherichia coli. As more recurrent episodes occur, the other Gram-negative bacilli (ie, Klebsiella pneumoniae, Proteus species) become more prevalent. The 3 major Gram-positive cocci that cause UTIs are enterococci, Staphylococcus saprophyticus, and group B streptococci.1,3,4
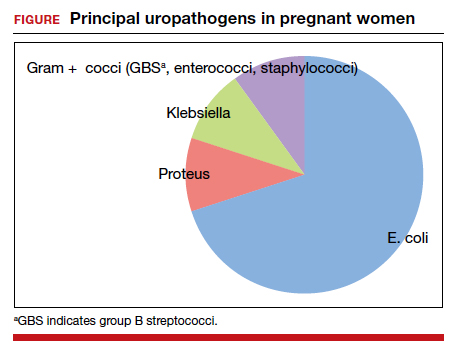
In nonpregnant women, ASB usually remains completely asymptomatic, and ascending infections only rarely occur. In pregnancy, however, urinary stasis is present due to the effects of progesterone on ureteral peristalsis and because of pressure on the ureters (particularly the right) by the expanding gravid uterus. As a result, ascending infection may occur in approximately 20% of patients if the lower tract infection is not identified and treated adequately.1
Clean-catch specimens and treatment
The standard criterion for the diagnosis of ASB is a urine culture that shows greater than 100,000 colonies/mL of a recognized uropathogen.1 The urine usually is obtained as a midstream, clean-catch specimen, and the test should be performed at the time of the first prenatal appointment. Once identified, ASB should be treated promptly with one of the antibiotics listed in the TABLE. Nitrofurantoin monohydrate macrocrystals (nitrofurantoin) and trimethoprim-sulfamethoxazole should be avoided in the first trimester unless no other drug is active against the identified microorganism.
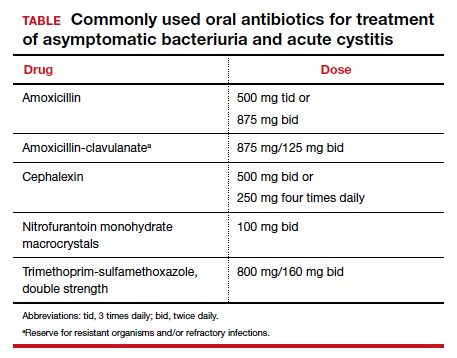
Both have been linked to teratogenic fetal effects.5-8 The defects associated with the former drug include eye abnormalities, heart defects, and facial clefts. The abnormalities associated with the latter include neural tube defects, heart defects, choanal atresia, and diaphragmatic hernia. In the first trimester, amoxicillin and cephalexin are reasonable choices for treatment. As a general rule, a 3-day course of antibiotics will be effective for eradicating the initial episode of ASB. For recurrent infections, a 7- to 10-day course is indicated.1,3,4
Acute cystitis
The microbiology of acute cystitis essentially is identical to that of asymptomatic bacteriuria. The usual clinical manifestations include increased frequency of urination, dysuria, and urination hesitancy in association with suprapubic discomfort and a lowgrade fever.
The diagnosis can be quickly confirmed by testing the urine pH and assessing for leukocyte esterase and nitrites. If both the leukocyte esterase and nitrite test are positive, the probability of a positive urine culture is high; however, the nitrite test can be falsely negative if the urine has been incubating in the bladder for only a short period of time or if a Gram-positive organism is responsible for the infection. The urine pH is particularly helpful if it is elevated in the range of 8. This finding strongly is associated with a Proteus infection.1,9-11
Continue to: In-out catheterization is ideal...
In-out catheterization is ideal
I recommend that the urine sample be obtained by an in-out catheterization in symptomatic patients. This technique eliminates any concern about contamination of the specimen by vaginal organisms and provides a “pure” sample for culture. When urine is obtained by this method, the criterion for a positive culture result is greater than 100 colonies/mL.3 If the urine is obtained by the midstream clean-catch method, the cutoff for a positive culture remains greater than 100,000 colonies/mL.1,3
Unless the clinician is working in a low resource environment, the culture should always be obtained even though the patient will be empirically treated prior to the culture result being available. The culture can be helpful in guiding changes in antibiotic therapy if the initial response to treatment is poor.
In the first trimester, empiric treatment should be with amoxicillin or cephalexin. Beyond the first trimester, nitrofurantoin should be the drug of choice. This antibiotic is inexpensive and well-tolerated. It has limited effect on the bowel or vaginal flora and is unlikely to cause a secondary yeast infection or diarrhea. If a Proteus infection is suspected, however, trimethoprim-sulfamethoxazole double strength (800 mg/ 160 mg) should be used because this organism is not susceptible to nitrofurantoin. The duration of therapy should be a minimum of 3 days with the first infection and 7 to 10 days with recurrent infections.1,3,4
Acute pyelonephritis
Pyelonephritis may develop de novo or may result from inadequate treatment of lower urinary tract infection. The right kidney is affected in approximately 75% of cases because the right ureter is more subject to compression by the gravid uterus. The principal pathogen is E coli, although Klebsiella pneumoniae and Proteus species also are of importance. Other aerobic Gram-negative bacilli, such as Pseudomonas and Serratia species, are much less common unless the patient is immunosuppressed or has an indwelling catheter.1
The characteristic clinical manifestations of acute pyelonephritis are high fever (>39 °C), shaking chills, nausea and vomiting, and flank pain and tenderness. Increased frequency of urination and dysuria also may be present. In addition, pyelonephritis may be accompanied by preterm labor, sepsis, and acute respiratory distress syndrome (ARDS). The diagnosis is established by clinical findings, urinalysis, and urine culture. The urine specimen should be obtained by an in-out catheterization, analyzed initially by dipstick for nitrites and leukocyte esterase, and submitted for culture and sensitivity. Blood cultures should be obtained, and chest radiography should be performed if ARDS is suspected.
Empiric treatment should be started as soon as these initial diagnostic tests are completed. Many women in the first 20 weeks of pregnancy will not be seriously ill and may be treated as outpatients. I recommend an initial dose of intramuscular ceftriaxone 2 g followed by oral amoxicillin-clavulanate (875 mg twice daily) for a total of 10 days. If the patient is allergic to beta-lactam antibiotics, oral trimethoprim-sulfamethoxazole double strength (800 mg/160 mg) twice daily would be an excellent alternative.1,12
Treating seriously ill patients
Patients who are more seriously ill, particularly in the second half of pregnancy when preterm labor is more likely, should be hospitalized for supportive care (intravenous [IV] fluids, antipyretics, anti-emetics) and treatment with parenteral antibiotics.1,12 At our medical center, IV ceftriaxone (2 g every 24 hours), is the agent of choice. It has a convenient dosing schedule and covers almost all of the potential uropathogens. If an unusually drug-resistant organism is suspected, gentamicin or aztreonam can be combined with ceftriaxone to ensure complete coverage (see dosage recommendations below).
If the patient is allergic to beta-lactam antibiotics, alternative IV agents include:
- trimethoprim-sulfamethoxazole (8–10 mg/kg/d in 2 divided doses)
- gentamicin (5 mg/kg of ideal body weight every 24 hours)
- aztreonam (2 g every 8 hours)
Parenteral antibiotics should be administered until the patient has been afebrile and asymptomatic for 24 hours. At this point, oral antibiotics, based on sensitivity testing, can be started, and the patient can be discharged to complete a 10-day course of therapy.
Continue to: Treatment failure...
Treatment failure
Obstetric patients with pyelonephritis usually respond promptly to antibiotics. More than 75% will be afebrile within 48 hours, and more than 90% will be afebrile within 72 hours. When patients fail to respond promptly, 2 major causes should be considered. The first is antibiotic resistance, and this problem can be corrected on the basis of the sensitivity studies. The second is ureteral obstruction, secondary either to the effect of the gravid uterus or a urinary stone. If obstruction is suspected, renal ultrasonography should be performed. Depending upon the cause of the obstruction, a procedure such as a percutaneous nephrostomy or cystoscopic removal of the stone may be necessary.
Recurrence is possible. Following an initial episode of pyelonephritis, approximately 20% of patients will experience a recurrent lower or upper tract infection.1 Because of this recurrence rate, I recommend that these patients receive suppressive doses of antibiotics for the remainder of pregnancy. An ideal agent for suppression is nitrofurantoin (100 mg at bedtime). An alternative agent is trimethoprim-sulfamethoxazole double strength (800 mg/160 mg) once daily. Amoxicillin and cephalexin are less desirable for prophylaxis because of their adverse effects on vaginal and bowel flora and their propensity for precipitating yeast infection and/or diarrhea.
CASE Resolved
The most likely diagnosis in this patient is acute cystitis. An in-out catheterization should be performed to obtain an uncontaminated urine specimen. A portion of the specimen should be forwarded to the laboratory for urine culture and sensitivity. Another portion should be used for assessment by dipstick. If the nitrite and leukocyte tests are positive, the diagnosis of acute cystitis is confirmed. Since this infection is the patient’s first episode, a reasonable antibiotic regimen would be oral nitrofurantoin (100 mg twice daily) for 3 days. The course should be extended to 7 days if symptoms persist at the end of 3 days. ●
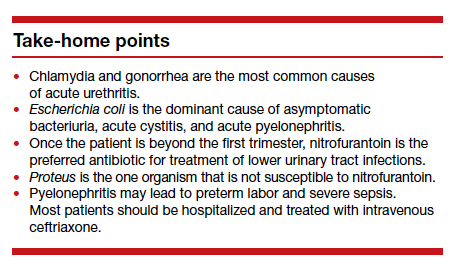
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TR, et al, eds. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862- 919.
- St Cyr S, Barbee L, Workowski KA, et al. Update to CDC’s Treatment Guidelines for Gonococcal Infection, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1911-1916.
- Hooton TM. Uncomplicated urinary tract infection. N Engl J Med. 2012;366:1028-1037.
- Finn SD. Acute uncomplicated urinary tract infection in women. N Engl J Med. 2003;349:259-266.
- Crider KS, Cleves MA, Reefhuis J, et al. Antibacterial medication use during pregnancy and risk of birth defects. Arch Pediatr Adolesc Med. 2009;163:978-985.
- Ailes EC, Gilboa SM, Gill SK, et al. Association between antibiotic use among pregnant women with urinary tract infections in the first trimester and birth defects, National Birth Defects Prevention Study 1997 to 2011. Birth Defects Res A Clin Mol Teratol. 2016;106:940-949.
- ACOG Committee Opinion No. 717 summary: sulfonamides, nitrofurantoin, and risk of birth defects. Obstet Gynecol. 2017;130:666-667.
- Duff P. Which antibiotics should be used with caution in pregnant women with UTI? OBG Manag. 2018;30:14-17.
- Hooton TM, Roberts PL, Cox ME, et al. Voided midstream urine culture and acute cystitis in premenopausal women. N Engl J Med. 2013;369:1883-1891.
- Mignini L, Carroli G, Abalos E, et al. Accuracy of diagnostic tests to detect asymptomatic bacteriuria during pregnancy. Obstet Gynecol. 2009;113:346-352.
- Schneeberger C, van den Heuvel ER, Erwich JJHM, et al. Contamination rates of three urine-sampling methods to assess bacteriuria in pregnant women. Obstet Gynecol. 2013;121:299-305.
- Duff P. Antibiotic selection in obstetrics: making cost-effective choices. Clin Obstet Gynecol. 2002;45:59-72.

Dr. Duff is Professor of MaternalFetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine.
The author reports no financial relationships relevant to this article.
Dr. Duff is Professor of MaternalFetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine.
The author reports no financial relationships relevant to this article.
Dr. Duff is Professor of MaternalFetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine.
The author reports no financial relationships relevant to this article.
CASE Pregnant woman with dysuria and suprapubic pain
A 25-year-old primigravid woman at 18 weeks of gestation requests evaluation because of the acute onset of frequent urination, dysuria, urination hesitancy, and suprapubic pain on the morning following intercourse. She has not experienced similar symptoms in the past. On physical examination, her temperature is 38 °C, pulse is 96 beats per minute, respirations are 18 per minute, and blood pressure is 100/76 mm Hg. She has no urethral discharge but is tender to palpation in the suprapubic area.
- What is the most likely diagnosis?
- What tests would be of greatest value in confirming the diagnosis?
- What is the most appropriate treatment for this patient?
Meet our perpetrator
Urinary tract infections (UTIs) are among the most common infections that occur during pregnancy. They may take one of 4 forms: acute urethritis, asymptomatic bacteriuria, acute cystitis, and acute pyelonephritis.1 The first 3 conditions usually are straightforward to diagnose and treat, and they usually do not cause major problems for the mother or fetus. The latter, however, can cause serious complications that pose risk to the mother and fetus.
This article will review the microbiology, clinical manifestations, diagnosis, and treatment of these 4 disorders in pregnancy. Particular emphasis will be placed on measures to avoid adverse effects on the mother and fetus from antimicrobial agents.
Acute urethritis
Acute urethritis can be caused by low concentrations of coliform organisms in the lower urinary tract, but it usually is secondary to infection by Neisseria gonorrhea or Chlamydia trachomatis. In most prenatal populations, the prevalence of one or the other of these 2 infections is approximately 5%.1
The most common clinical manifestations of acute urethritis are a purulent urethral discharge, increased frequency of urination, dysuria, and urination hesitancy. The diagnosis most easily is confirmed by obtaining a specimen of urethral discharge or urine and evaluating the sample by a nucleic acid amplification test for both gonorrhea and chlamydia.
Antibiotic therapy is preferred. The current recommended treatment for gonococcal urethritis is a single intramuscular injection of ceftriaxone 500 mg. If the patient prefers oral therapy, she can receive cefixime 800 mg in a single dose. For patients with an allergy to beta-lactam antibiotics, the alternative regimen is gentamicin 240 mg in a single intramuscular injection, combined with oral azithromycin in a single 2,000-mg dose. For treatment of chlamydia in pregnancy, the recommended therapy is azithromycin 1,000 mg in a single oral dose.2 A test of cure should be performed within 4 weeks of treatment.
Asymptomatic bacteriuria
Asymptomatic bacteriuria (ASB) is the most common UTI in women. Approximately 5% to 8% of all sexually active women have ASB. The condition is not unique to pregnancy; it is associated primarily with the assumption of coital activity. In point of fact, the ASB typically precedes pregnancy by several years.1
The principal pathogens responsible for ASB are shown in the FIGURE. Over 80% of first-time infections are secondary to Escherichia coli. As more recurrent episodes occur, the other Gram-negative bacilli (ie, Klebsiella pneumoniae, Proteus species) become more prevalent. The 3 major Gram-positive cocci that cause UTIs are enterococci, Staphylococcus saprophyticus, and group B streptococci.1,3,4
In nonpregnant women, ASB usually remains completely asymptomatic, and ascending infections only rarely occur. In pregnancy, however, urinary stasis is present due to the effects of progesterone on ureteral peristalsis and because of pressure on the ureters (particularly the right) by the expanding gravid uterus. As a result, ascending infection may occur in approximately 20% of patients if the lower tract infection is not identified and treated adequately.1
Clean-catch specimens and treatment
The standard criterion for the diagnosis of ASB is a urine culture that shows greater than 100,000 colonies/mL of a recognized uropathogen.1 The urine usually is obtained as a midstream, clean-catch specimen, and the test should be performed at the time of the first prenatal appointment. Once identified, ASB should be treated promptly with one of the antibiotics listed in the TABLE. Nitrofurantoin monohydrate macrocrystals (nitrofurantoin) and trimethoprim-sulfamethoxazole should be avoided in the first trimester unless no other drug is active against the identified microorganism.
Both have been linked to teratogenic fetal effects.5-8 The defects associated with the former drug include eye abnormalities, heart defects, and facial clefts. The abnormalities associated with the latter include neural tube defects, heart defects, choanal atresia, and diaphragmatic hernia. In the first trimester, amoxicillin and cephalexin are reasonable choices for treatment. As a general rule, a 3-day course of antibiotics will be effective for eradicating the initial episode of ASB. For recurrent infections, a 7- to 10-day course is indicated.1,3,4
Acute cystitis
The microbiology of acute cystitis essentially is identical to that of asymptomatic bacteriuria. The usual clinical manifestations include increased frequency of urination, dysuria, and urination hesitancy in association with suprapubic discomfort and a lowgrade fever.
The diagnosis can be quickly confirmed by testing the urine pH and assessing for leukocyte esterase and nitrites. If both the leukocyte esterase and nitrite test are positive, the probability of a positive urine culture is high; however, the nitrite test can be falsely negative if the urine has been incubating in the bladder for only a short period of time or if a Gram-positive organism is responsible for the infection. The urine pH is particularly helpful if it is elevated in the range of 8. This finding strongly is associated with a Proteus infection.1,9-11
Continue to: In-out catheterization is ideal...
In-out catheterization is ideal
I recommend that the urine sample be obtained by an in-out catheterization in symptomatic patients. This technique eliminates any concern about contamination of the specimen by vaginal organisms and provides a “pure” sample for culture. When urine is obtained by this method, the criterion for a positive culture result is greater than 100 colonies/mL.3 If the urine is obtained by the midstream clean-catch method, the cutoff for a positive culture remains greater than 100,000 colonies/mL.1,3
Unless the clinician is working in a low resource environment, the culture should always be obtained even though the patient will be empirically treated prior to the culture result being available. The culture can be helpful in guiding changes in antibiotic therapy if the initial response to treatment is poor.
In the first trimester, empiric treatment should be with amoxicillin or cephalexin. Beyond the first trimester, nitrofurantoin should be the drug of choice. This antibiotic is inexpensive and well-tolerated. It has limited effect on the bowel or vaginal flora and is unlikely to cause a secondary yeast infection or diarrhea. If a Proteus infection is suspected, however, trimethoprim-sulfamethoxazole double strength (800 mg/ 160 mg) should be used because this organism is not susceptible to nitrofurantoin. The duration of therapy should be a minimum of 3 days with the first infection and 7 to 10 days with recurrent infections.1,3,4
Acute pyelonephritis
Pyelonephritis may develop de novo or may result from inadequate treatment of lower urinary tract infection. The right kidney is affected in approximately 75% of cases because the right ureter is more subject to compression by the gravid uterus. The principal pathogen is E coli, although Klebsiella pneumoniae and Proteus species also are of importance. Other aerobic Gram-negative bacilli, such as Pseudomonas and Serratia species, are much less common unless the patient is immunosuppressed or has an indwelling catheter.1
The characteristic clinical manifestations of acute pyelonephritis are high fever (>39 °C), shaking chills, nausea and vomiting, and flank pain and tenderness. Increased frequency of urination and dysuria also may be present. In addition, pyelonephritis may be accompanied by preterm labor, sepsis, and acute respiratory distress syndrome (ARDS). The diagnosis is established by clinical findings, urinalysis, and urine culture. The urine specimen should be obtained by an in-out catheterization, analyzed initially by dipstick for nitrites and leukocyte esterase, and submitted for culture and sensitivity. Blood cultures should be obtained, and chest radiography should be performed if ARDS is suspected.
Empiric treatment should be started as soon as these initial diagnostic tests are completed. Many women in the first 20 weeks of pregnancy will not be seriously ill and may be treated as outpatients. I recommend an initial dose of intramuscular ceftriaxone 2 g followed by oral amoxicillin-clavulanate (875 mg twice daily) for a total of 10 days. If the patient is allergic to beta-lactam antibiotics, oral trimethoprim-sulfamethoxazole double strength (800 mg/160 mg) twice daily would be an excellent alternative.1,12
Treating seriously ill patients
Patients who are more seriously ill, particularly in the second half of pregnancy when preterm labor is more likely, should be hospitalized for supportive care (intravenous [IV] fluids, antipyretics, anti-emetics) and treatment with parenteral antibiotics.1,12 At our medical center, IV ceftriaxone (2 g every 24 hours), is the agent of choice. It has a convenient dosing schedule and covers almost all of the potential uropathogens. If an unusually drug-resistant organism is suspected, gentamicin or aztreonam can be combined with ceftriaxone to ensure complete coverage (see dosage recommendations below).
If the patient is allergic to beta-lactam antibiotics, alternative IV agents include:
- trimethoprim-sulfamethoxazole (8–10 mg/kg/d in 2 divided doses)
- gentamicin (5 mg/kg of ideal body weight every 24 hours)
- aztreonam (2 g every 8 hours)
Parenteral antibiotics should be administered until the patient has been afebrile and asymptomatic for 24 hours. At this point, oral antibiotics, based on sensitivity testing, can be started, and the patient can be discharged to complete a 10-day course of therapy.
Continue to: Treatment failure...
Treatment failure
Obstetric patients with pyelonephritis usually respond promptly to antibiotics. More than 75% will be afebrile within 48 hours, and more than 90% will be afebrile within 72 hours. When patients fail to respond promptly, 2 major causes should be considered. The first is antibiotic resistance, and this problem can be corrected on the basis of the sensitivity studies. The second is ureteral obstruction, secondary either to the effect of the gravid uterus or a urinary stone. If obstruction is suspected, renal ultrasonography should be performed. Depending upon the cause of the obstruction, a procedure such as a percutaneous nephrostomy or cystoscopic removal of the stone may be necessary.
Recurrence is possible. Following an initial episode of pyelonephritis, approximately 20% of patients will experience a recurrent lower or upper tract infection.1 Because of this recurrence rate, I recommend that these patients receive suppressive doses of antibiotics for the remainder of pregnancy. An ideal agent for suppression is nitrofurantoin (100 mg at bedtime). An alternative agent is trimethoprim-sulfamethoxazole double strength (800 mg/160 mg) once daily. Amoxicillin and cephalexin are less desirable for prophylaxis because of their adverse effects on vaginal and bowel flora and their propensity for precipitating yeast infection and/or diarrhea.
CASE Resolved
The most likely diagnosis in this patient is acute cystitis. An in-out catheterization should be performed to obtain an uncontaminated urine specimen. A portion of the specimen should be forwarded to the laboratory for urine culture and sensitivity. Another portion should be used for assessment by dipstick. If the nitrite and leukocyte tests are positive, the diagnosis of acute cystitis is confirmed. Since this infection is the patient’s first episode, a reasonable antibiotic regimen would be oral nitrofurantoin (100 mg twice daily) for 3 days. The course should be extended to 7 days if symptoms persist at the end of 3 days. ●
CASE Pregnant woman with dysuria and suprapubic pain
A 25-year-old primigravid woman at 18 weeks of gestation requests evaluation because of the acute onset of frequent urination, dysuria, urination hesitancy, and suprapubic pain on the morning following intercourse. She has not experienced similar symptoms in the past. On physical examination, her temperature is 38 °C, pulse is 96 beats per minute, respirations are 18 per minute, and blood pressure is 100/76 mm Hg. She has no urethral discharge but is tender to palpation in the suprapubic area.
- What is the most likely diagnosis?
- What tests would be of greatest value in confirming the diagnosis?
- What is the most appropriate treatment for this patient?
Meet our perpetrator
Urinary tract infections (UTIs) are among the most common infections that occur during pregnancy. They may take one of 4 forms: acute urethritis, asymptomatic bacteriuria, acute cystitis, and acute pyelonephritis.1 The first 3 conditions usually are straightforward to diagnose and treat, and they usually do not cause major problems for the mother or fetus. The latter, however, can cause serious complications that pose risk to the mother and fetus.
This article will review the microbiology, clinical manifestations, diagnosis, and treatment of these 4 disorders in pregnancy. Particular emphasis will be placed on measures to avoid adverse effects on the mother and fetus from antimicrobial agents.
Acute urethritis
Acute urethritis can be caused by low concentrations of coliform organisms in the lower urinary tract, but it usually is secondary to infection by Neisseria gonorrhea or Chlamydia trachomatis. In most prenatal populations, the prevalence of one or the other of these 2 infections is approximately 5%.1
The most common clinical manifestations of acute urethritis are a purulent urethral discharge, increased frequency of urination, dysuria, and urination hesitancy. The diagnosis most easily is confirmed by obtaining a specimen of urethral discharge or urine and evaluating the sample by a nucleic acid amplification test for both gonorrhea and chlamydia.
Antibiotic therapy is preferred. The current recommended treatment for gonococcal urethritis is a single intramuscular injection of ceftriaxone 500 mg. If the patient prefers oral therapy, she can receive cefixime 800 mg in a single dose. For patients with an allergy to beta-lactam antibiotics, the alternative regimen is gentamicin 240 mg in a single intramuscular injection, combined with oral azithromycin in a single 2,000-mg dose. For treatment of chlamydia in pregnancy, the recommended therapy is azithromycin 1,000 mg in a single oral dose.2 A test of cure should be performed within 4 weeks of treatment.
Asymptomatic bacteriuria
Asymptomatic bacteriuria (ASB) is the most common UTI in women. Approximately 5% to 8% of all sexually active women have ASB. The condition is not unique to pregnancy; it is associated primarily with the assumption of coital activity. In point of fact, the ASB typically precedes pregnancy by several years.1
The principal pathogens responsible for ASB are shown in the FIGURE. Over 80% of first-time infections are secondary to Escherichia coli. As more recurrent episodes occur, the other Gram-negative bacilli (ie, Klebsiella pneumoniae, Proteus species) become more prevalent. The 3 major Gram-positive cocci that cause UTIs are enterococci, Staphylococcus saprophyticus, and group B streptococci.1,3,4
In nonpregnant women, ASB usually remains completely asymptomatic, and ascending infections only rarely occur. In pregnancy, however, urinary stasis is present due to the effects of progesterone on ureteral peristalsis and because of pressure on the ureters (particularly the right) by the expanding gravid uterus. As a result, ascending infection may occur in approximately 20% of patients if the lower tract infection is not identified and treated adequately.1
Clean-catch specimens and treatment
The standard criterion for the diagnosis of ASB is a urine culture that shows greater than 100,000 colonies/mL of a recognized uropathogen.1 The urine usually is obtained as a midstream, clean-catch specimen, and the test should be performed at the time of the first prenatal appointment. Once identified, ASB should be treated promptly with one of the antibiotics listed in the TABLE. Nitrofurantoin monohydrate macrocrystals (nitrofurantoin) and trimethoprim-sulfamethoxazole should be avoided in the first trimester unless no other drug is active against the identified microorganism.
Both have been linked to teratogenic fetal effects.5-8 The defects associated with the former drug include eye abnormalities, heart defects, and facial clefts. The abnormalities associated with the latter include neural tube defects, heart defects, choanal atresia, and diaphragmatic hernia. In the first trimester, amoxicillin and cephalexin are reasonable choices for treatment. As a general rule, a 3-day course of antibiotics will be effective for eradicating the initial episode of ASB. For recurrent infections, a 7- to 10-day course is indicated.1,3,4
Acute cystitis
The microbiology of acute cystitis essentially is identical to that of asymptomatic bacteriuria. The usual clinical manifestations include increased frequency of urination, dysuria, and urination hesitancy in association with suprapubic discomfort and a lowgrade fever.
The diagnosis can be quickly confirmed by testing the urine pH and assessing for leukocyte esterase and nitrites. If both the leukocyte esterase and nitrite test are positive, the probability of a positive urine culture is high; however, the nitrite test can be falsely negative if the urine has been incubating in the bladder for only a short period of time or if a Gram-positive organism is responsible for the infection. The urine pH is particularly helpful if it is elevated in the range of 8. This finding strongly is associated with a Proteus infection.1,9-11
Continue to: In-out catheterization is ideal...
In-out catheterization is ideal
I recommend that the urine sample be obtained by an in-out catheterization in symptomatic patients. This technique eliminates any concern about contamination of the specimen by vaginal organisms and provides a “pure” sample for culture. When urine is obtained by this method, the criterion for a positive culture result is greater than 100 colonies/mL.3 If the urine is obtained by the midstream clean-catch method, the cutoff for a positive culture remains greater than 100,000 colonies/mL.1,3
Unless the clinician is working in a low resource environment, the culture should always be obtained even though the patient will be empirically treated prior to the culture result being available. The culture can be helpful in guiding changes in antibiotic therapy if the initial response to treatment is poor.
In the first trimester, empiric treatment should be with amoxicillin or cephalexin. Beyond the first trimester, nitrofurantoin should be the drug of choice. This antibiotic is inexpensive and well-tolerated. It has limited effect on the bowel or vaginal flora and is unlikely to cause a secondary yeast infection or diarrhea. If a Proteus infection is suspected, however, trimethoprim-sulfamethoxazole double strength (800 mg/ 160 mg) should be used because this organism is not susceptible to nitrofurantoin. The duration of therapy should be a minimum of 3 days with the first infection and 7 to 10 days with recurrent infections.1,3,4
Acute pyelonephritis
Pyelonephritis may develop de novo or may result from inadequate treatment of lower urinary tract infection. The right kidney is affected in approximately 75% of cases because the right ureter is more subject to compression by the gravid uterus. The principal pathogen is E coli, although Klebsiella pneumoniae and Proteus species also are of importance. Other aerobic Gram-negative bacilli, such as Pseudomonas and Serratia species, are much less common unless the patient is immunosuppressed or has an indwelling catheter.1
The characteristic clinical manifestations of acute pyelonephritis are high fever (>39 °C), shaking chills, nausea and vomiting, and flank pain and tenderness. Increased frequency of urination and dysuria also may be present. In addition, pyelonephritis may be accompanied by preterm labor, sepsis, and acute respiratory distress syndrome (ARDS). The diagnosis is established by clinical findings, urinalysis, and urine culture. The urine specimen should be obtained by an in-out catheterization, analyzed initially by dipstick for nitrites and leukocyte esterase, and submitted for culture and sensitivity. Blood cultures should be obtained, and chest radiography should be performed if ARDS is suspected.
Empiric treatment should be started as soon as these initial diagnostic tests are completed. Many women in the first 20 weeks of pregnancy will not be seriously ill and may be treated as outpatients. I recommend an initial dose of intramuscular ceftriaxone 2 g followed by oral amoxicillin-clavulanate (875 mg twice daily) for a total of 10 days. If the patient is allergic to beta-lactam antibiotics, oral trimethoprim-sulfamethoxazole double strength (800 mg/160 mg) twice daily would be an excellent alternative.1,12
Treating seriously ill patients
Patients who are more seriously ill, particularly in the second half of pregnancy when preterm labor is more likely, should be hospitalized for supportive care (intravenous [IV] fluids, antipyretics, anti-emetics) and treatment with parenteral antibiotics.1,12 At our medical center, IV ceftriaxone (2 g every 24 hours), is the agent of choice. It has a convenient dosing schedule and covers almost all of the potential uropathogens. If an unusually drug-resistant organism is suspected, gentamicin or aztreonam can be combined with ceftriaxone to ensure complete coverage (see dosage recommendations below).
If the patient is allergic to beta-lactam antibiotics, alternative IV agents include:
- trimethoprim-sulfamethoxazole (8–10 mg/kg/d in 2 divided doses)
- gentamicin (5 mg/kg of ideal body weight every 24 hours)
- aztreonam (2 g every 8 hours)
Parenteral antibiotics should be administered until the patient has been afebrile and asymptomatic for 24 hours. At this point, oral antibiotics, based on sensitivity testing, can be started, and the patient can be discharged to complete a 10-day course of therapy.
Continue to: Treatment failure...
Treatment failure
Obstetric patients with pyelonephritis usually respond promptly to antibiotics. More than 75% will be afebrile within 48 hours, and more than 90% will be afebrile within 72 hours. When patients fail to respond promptly, 2 major causes should be considered. The first is antibiotic resistance, and this problem can be corrected on the basis of the sensitivity studies. The second is ureteral obstruction, secondary either to the effect of the gravid uterus or a urinary stone. If obstruction is suspected, renal ultrasonography should be performed. Depending upon the cause of the obstruction, a procedure such as a percutaneous nephrostomy or cystoscopic removal of the stone may be necessary.
Recurrence is possible. Following an initial episode of pyelonephritis, approximately 20% of patients will experience a recurrent lower or upper tract infection.1 Because of this recurrence rate, I recommend that these patients receive suppressive doses of antibiotics for the remainder of pregnancy. An ideal agent for suppression is nitrofurantoin (100 mg at bedtime). An alternative agent is trimethoprim-sulfamethoxazole double strength (800 mg/160 mg) once daily. Amoxicillin and cephalexin are less desirable for prophylaxis because of their adverse effects on vaginal and bowel flora and their propensity for precipitating yeast infection and/or diarrhea.
CASE Resolved
The most likely diagnosis in this patient is acute cystitis. An in-out catheterization should be performed to obtain an uncontaminated urine specimen. A portion of the specimen should be forwarded to the laboratory for urine culture and sensitivity. Another portion should be used for assessment by dipstick. If the nitrite and leukocyte tests are positive, the diagnosis of acute cystitis is confirmed. Since this infection is the patient’s first episode, a reasonable antibiotic regimen would be oral nitrofurantoin (100 mg twice daily) for 3 days. The course should be extended to 7 days if symptoms persist at the end of 3 days. ●
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TR, et al, eds. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862- 919.
- St Cyr S, Barbee L, Workowski KA, et al. Update to CDC’s Treatment Guidelines for Gonococcal Infection, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1911-1916.
- Hooton TM. Uncomplicated urinary tract infection. N Engl J Med. 2012;366:1028-1037.
- Finn SD. Acute uncomplicated urinary tract infection in women. N Engl J Med. 2003;349:259-266.
- Crider KS, Cleves MA, Reefhuis J, et al. Antibacterial medication use during pregnancy and risk of birth defects. Arch Pediatr Adolesc Med. 2009;163:978-985.
- Ailes EC, Gilboa SM, Gill SK, et al. Association between antibiotic use among pregnant women with urinary tract infections in the first trimester and birth defects, National Birth Defects Prevention Study 1997 to 2011. Birth Defects Res A Clin Mol Teratol. 2016;106:940-949.
- ACOG Committee Opinion No. 717 summary: sulfonamides, nitrofurantoin, and risk of birth defects. Obstet Gynecol. 2017;130:666-667.
- Duff P. Which antibiotics should be used with caution in pregnant women with UTI? OBG Manag. 2018;30:14-17.
- Hooton TM, Roberts PL, Cox ME, et al. Voided midstream urine culture and acute cystitis in premenopausal women. N Engl J Med. 2013;369:1883-1891.
- Mignini L, Carroli G, Abalos E, et al. Accuracy of diagnostic tests to detect asymptomatic bacteriuria during pregnancy. Obstet Gynecol. 2009;113:346-352.
- Schneeberger C, van den Heuvel ER, Erwich JJHM, et al. Contamination rates of three urine-sampling methods to assess bacteriuria in pregnant women. Obstet Gynecol. 2013;121:299-305.
- Duff P. Antibiotic selection in obstetrics: making cost-effective choices. Clin Obstet Gynecol. 2002;45:59-72.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TR, et al, eds. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862- 919.
- St Cyr S, Barbee L, Workowski KA, et al. Update to CDC’s Treatment Guidelines for Gonococcal Infection, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1911-1916.
- Hooton TM. Uncomplicated urinary tract infection. N Engl J Med. 2012;366:1028-1037.
- Finn SD. Acute uncomplicated urinary tract infection in women. N Engl J Med. 2003;349:259-266.
- Crider KS, Cleves MA, Reefhuis J, et al. Antibacterial medication use during pregnancy and risk of birth defects. Arch Pediatr Adolesc Med. 2009;163:978-985.
- Ailes EC, Gilboa SM, Gill SK, et al. Association between antibiotic use among pregnant women with urinary tract infections in the first trimester and birth defects, National Birth Defects Prevention Study 1997 to 2011. Birth Defects Res A Clin Mol Teratol. 2016;106:940-949.
- ACOG Committee Opinion No. 717 summary: sulfonamides, nitrofurantoin, and risk of birth defects. Obstet Gynecol. 2017;130:666-667.
- Duff P. Which antibiotics should be used with caution in pregnant women with UTI? OBG Manag. 2018;30:14-17.
- Hooton TM, Roberts PL, Cox ME, et al. Voided midstream urine culture and acute cystitis in premenopausal women. N Engl J Med. 2013;369:1883-1891.
- Mignini L, Carroli G, Abalos E, et al. Accuracy of diagnostic tests to detect asymptomatic bacteriuria during pregnancy. Obstet Gynecol. 2009;113:346-352.
- Schneeberger C, van den Heuvel ER, Erwich JJHM, et al. Contamination rates of three urine-sampling methods to assess bacteriuria in pregnant women. Obstet Gynecol. 2013;121:299-305.
- Duff P. Antibiotic selection in obstetrics: making cost-effective choices. Clin Obstet Gynecol. 2002;45:59-72.
The Supreme Court and reproductive rights

There is now great interest in the Supreme Court’s handling of cases that involve a woman’s ability to have an abortion. Recent decisions, and those planned in the next few months will be the source of intense scrutiny. But the Court’s involvement in reproductive rights did not begin with abortion. In fact, the Supreme Court has a long history of controversial decisions dealing with reproductive rights.
Involuntary sterilization
A notable, even infamous, case was Buck v Bell (1927)—later discredited—in which the Court reviewed a state law that provided for the involuntary sterilization of the “feeble minded.”1 The 8-1 decision was that the state could choose to have such a law to protect the so-called genetic health of the state. The law was based on a theory of eugenics. The opinion by the highly respected Justice Oliver Wendell Holmes included the unfortunate conclusion, “Three generations of imbeciles are enough.”2 As mentioned, the law has since been thoroughly discredited. In 1942, the Court did come to a different result, holding in Skinner v Oklahoma that it was unconstitutional for a state to involuntarily sterilize “habitual criminals.”3
Contraception
Forty years after Buck, in Griswold v Connecticut, the Court reviewed a state law that prohibited the distribution of any drug or device used for contraception (even for married couples).4 In a 7-2 decision, the Supreme Court struck down the state law as violating a marital right of privacy. Beyond its specific holding, Griswold was important in several ways. First, a physician was raising the rights of patients (not specifically his own rights). This is notable because, ordinarily in court, litigants may argue their own rights, not the rights of others. This has been important in later reproductive rights cases because often it has been physicians raising and arguing the rights of patients.
A second interesting part of Griswold was the source of this constitutional right of privacy. The Constitution contains no express privacy provision. In Griswold, the Court found that the 1st, 3rd, 4th, and 9th Amendments create the right to privacy in marital relations. Writing for the majority, Justice Douglas found that “emanations” from these amendments have “penumbras” that create a right of marital privacy.
Although Griswold was based on marital privacy, a few years later, in 1972, the Court essentially converted that right to one of reproductive privacy (“the decision whether to bear or beget a child.”) In Eisenstadt v Baird, the Court held that it was a violation of equal protection (the 14th Amendment) for a state to allow contraception to the married but deny it to an unmarried person.5
Continue to: Abortion...
Abortion
In 1971, the Court had heard arguments in 2 cases that raised issues regarding whether state laws prohibiting abortion were constitutional. The first oral argument in Roe v Wade is widely considered one of the worst oral arguments in modern history, and for several reasons the Court set the case for rehearing the following Term (October 1972). In January 1973, the Court decided Roe v Wade.6 The 7-2 decision was written by Justice Blackmun, who had at one point been the attorney for the Mayo Clinic and might be considered one of the first “health lawyers.” The Court held that the Constitution (perhaps in the 14th or 9th Amendment) includes a right of privacy that includes the right of a woman to choose to have, or not to have, an abortion. In implementing the right, the Court held that a state may impose only modest medical safeguards for the mother (eg, requiring that abortions be performed by a licensed physician). In the second trimester, to the point of viability, a state could impose only limitations on abortion that were reasonably directed to ensure the health of the mother. After a fetus was viable (could live outside the mother’s body), the state was free to regulate or prohibit abortions and protect the fetus. At the time, viability was approximately the beginning of the third trimester.6
The clear majority of the Court in Roe (7-2) may have suggested that there was not strong opposition to the decision. That, of course, was not the case. Legal and political conflict surrounding the case has been, and remains, intense. Since 1973, the Court has been called upon to decide many abortion cases, and each case seems to beget more controversy and still more cases.
Some of the legal objections to Roe and other abortion decisions are that the constitutional basis for the decision remains unclear—a specific right of privacy is not contained in the text of the Constitution. Several locations of a possible right of privacy have been mentioned by various justices, but “substantive due process” became the common constitutional basis for the right. Critics note that “substantive” due process (as opposed to procedural due process) is not mentioned in the Constitution, and it is short on clear guiding principles. Beyond those jurisprudential issues, of course, there were strong religious and philosophical objections to abortion. What followed Roe has been a long series of efforts to limit or discourage access to abortion, and the Supreme Court has had to decide a great many abortion cases (and a few contraception cases) over the last 50 years. Most years (except from 2008‒2013) the Court has heard, on average, at least one abortion case.
By way of examples, here are some of the issues related to abortion that the Court has decided:
- Payment and facilities. States and the federal government are not required to pay for abortions for women who cannot afford them or to provide facilities for abortion.7-10
- Informed consent. Some states’ special informed consent requirements for abortion were upheld, but complex consents that required the father’s participation were not.
- Ability to advertise. Prohibitions on advertisement of abortion services were struck down.
- Location. Requirements for hospital-only abortions (or similar regulations) were struck down.
- Anti-abortion protests. Several cases addressed guidelines involving demonstrations near abortion clinics.
Of particular importance was the case of Planned Parenthood of Southeastern Pennsylvania v Casey—“Casey.”11 In 1992 that case reaffirmed the “essential” holding of Roe v Wade. A plurality in that case de-emphasized the trimester framework and applied an “undue burden” test on limitations on abortion. In the more recent cases argued before the Court, Casey is frequently referred to as specifically reaffirming, and therefore solidifying, Roe.
Consent for minors
There have been several cases since 1973 that involved contraceptives or abortions and “minors” (generally, adolescents aged <18 years, although there are some state-defined exceptions). These cases typically involve 2 issues: the right of minors to consent to treatment and the obligation of the physician to provide information to parents about treatment to their minor daughter. In 1977 the Court struck down a New York law that prohibited the distribution of contraceptives to minors.12 However, abortion issues involving minors have been more complicated. While the Court has struck down “2-parent” consent statutes,13 it has generally upheld 1-parent consent statutes, but only if those statutes contain a “judicial bypass” provision and an emergency medical provision.11,14,15 (This bypass allows a minor to “bypass” parental consent to abortion in some circumstances, and instead seek judicial authorization for an abortion.) Generally, the Court has upheld parental notification for abortions, with exceptions where it would be harmful to the minor who is seeking the abortion.16-19
Continue to: Who can perform an abortion...
Who can perform an abortion
Over the years there have also been several cases raising questions about the professionals who can perform abortions, their hospital privileges, and what facilities can perform abortions. Two of those cases in recent years have, for example, seen the Court strike down state statutes that required the physicians who perform abortions to have admitting privileges at least in 1 nearby hospital.20,21 The basis for these decisions is that the admitting qualification is an “undue burden” because it serves almost no health purpose, while significantly limiting the number of professionals who can perform abortions.
Cases this Term
The current Term of the Court (officially the “October 2021 Term”) may be one of the most significant for reproductive rights in recent history. The Court accepted 6 abortion-related cases to hear. It dismissed 3 of those cases, which had become “moot” because the Biden administration changed the rules that had been legally challenged.22-24 It has heard arguments in the 3 (technically 4) remaining cases, in which decisions will be announced over the next several months.
The first of these cases (involving the Texas Heartbeat Act) raises very important, but vexing, procedural issues about a Texas abortion law. The second (Whole Woman’s Health v Jackson) is a direct challenge to Roe v Wade. The third case (Cameron v EMW Women’s Surgical Center) involves the narrow question of whether a state attorney general can intervene in a case to uphold a state abortion law when another state official refuses to defend the law.25 It is worthwhile taking a look at the first 2 of these cases.
Texas Heartbeat Act
In the first case (technically, it is 2 cases, as we will see), the Texas legislature adopted a law that prohibits abortions after there is a discernable heartbeat (around 6 weeks of pregnancy). The law precludes state officials from enforcing the law. Instead, it allows almost any private citizen to seek monetary damages ($10,000 plus fees) from anyone who performs an abortion or “aids and abets” an abortion. (This is in some ways similar to “private attorney general” actions found in the False Claims Act, and in some civil rights and labor laws.) This statute is clearly inconsistent with Roe in that it prohibits abortions before the end of the second trimester. If it were a usual law—a Texas law being enforced by state officials—federal courts would issue injunctions to state officials against enforcing the law. The difficulty with the Texas law (and its very purpose) is that there are procedural limitations in federal law that make it very difficult to find a path for federal courts to review the Texas statute quickly. For example, would federal courts enjoin every private citizen of the state? There is a longstanding Constitutional doctrine that precludes federal courts from enjoining state courts.26 Therefore, it is difficult to challenge the law before someone performing or aiding an abortion has been ordered to pay the private citizen who is enforcing it. In the interim, which could be months or even years, health care providers face uncertainty about continuing to provide abortion services. Some providers would stop providing abortion services, reducing the availability of those services.
Two cases challenge this Texas procedure. In the first, Whole Woman’s Health v Jackson, 27 abortion providers seek to find some way through the procedural thicket to allow an immediate challenge to the statute. It is important because this technique of exclusive private enforcement could be used in any number of ways by the state to chill important constitutional rights (beyond abortion—to speech, to bear arms). In the second case involving the Texas law, U.S. v Texas, the federal government seeks to intervene in the case, which is another unusual procedure.28 The Court found these questions so important and difficult that it allowed 3 hours of argument (and 4 sets of lawyers). It seems likely that the Court will find a mechanism for allowing some early federal court review of individual enforcement of state laws, while minimizing harm to the state-national federalism that is at the heart of the Constitution.
For the recent procedural decisions in the Texas cases, see the “Current Court Decisions” box below.
On December 10, 2021, the Court handed down two decisions in reproductive freedom (abortion) cases, both involving the Texas abortion law (which prohibits most abortions after a fetal heartbeat can be detected and allows only private individuals to enforce the law). The more significant of the two cases, Whole Woman’s Health v Jackson,1 was the request of abortion providers (and others) to allow them to challenge the constitutionality of the Texas law by suing various state officials or a private individual, before the enforcement of the new Texas law.
The decision of the Court was somewhat complex because of the split among justices. Overall:
- The Court held 8-1 that before the law is enforced, providers have the ability to sue executives of medical licensing boards. This was based on the possibility that there could be licensure discipline for professionals who violate the new abortion law. Only Justice Thomas dissented from this part of the decision, which was written by Justice Gorsuch.
- The Court unanimously held that state-court judges could not be sued to stop enforcement of the law, and dismissed them from the suit.
- In a 5-4 split the Court held that state court clerks (and the state attorney general) could not be brought into federal court as a way of challenging the law. This was based on the 11th Amendment, sovereign immunity, and an important precedent from 1908.2 Chief Justice Roberts wrote from the justices who were essentially in dissent (Justices Bryer, Kagan, and Sotomayor). Justice Sotomayor also wrote a dissent (joined by Justices Breyer and Kagan) urging that there should be some way for providers to test the constitutionality of the law before enforcement. Allowing an action against state court clerks would be a good way to do that. She also expressly noted the problem of the Texas law approach being used by other states to attack any number of constitutional rights.
- The Court unanimously dismissed (for lack of standing) the one private citizen who had been sued. He had signed a sworn statement that he did not intend to seek the damages against abortion providers under the Texas law.
- The Court declined again to stay the Texas law while it is being challenged. That is, it left standing the 5th Circuit order allowing the law to go into effect.
- In a second, related case, the Court dismissed, without deciding, the Biden administration’s request to become a party in the Texas abortion case.3
References
- Whole Woman’s Health v Jackson, No. 21–463 (Dec. 10, 2021). https://www.supremecourt.gov /opinions/21pdf/21-463_new_8o6b.pdf.
- Ex parte Young, 209 U.S. 123 (1908).
- U.S. v Texas, 21-588 (Dec. 10, 2021). https://www.supremecourt.gov/opinions/21pdf/21-588 _c07d.pdf
Continue to: Re-evaluating the viability standard...
Re-evaluating the viability standard
The substantive abortion issue in Dobbs v Jackson Women’s Health Organization is the constitutionality of the Mississippi Gestational Age Act, which allows abortions after 15 weeks of pregnancy only for medical emergencies or severe fetal abnormality.29 This case is likely the most watched and controversial case of the Term. Many medical organizations have filed amicus curiae briefs, including the American College of Obstetricians and Gynecologists joined by the American Medical Association,30 the International Federation of Gynecology and Obstetrics,31 and the American Association of Pro-Life Obstetricians and Gynecologists.32 The reason for all this attention is that the Court has accepted to resolve “whether all pre-viability prohibitions on elective abortions are unconstitutional.” Thus, it represents a direct challenge to the trimester/viability structure of Roe.
It appears that there are 3 justices ready to outright overrule Roe, 3 that would uphold it as is, and 3 who are not in favor of Roe, but feel bound by precedent or are not in favor of a traumatic move. For that reason, there may be a narrow decision in this case. For example, the Court might find a procedural way to avoid directly deciding the abortion issue in this case, or it might uphold the right to abortion but change the viability standard. It is also true that predicting what the Court will do in controversial cases is a fool’s errand.
The complexity of reproductive rights and the ObGyn practice
These cases and policies affect the day-to-day practice of obstetrics. It is the most legally complex area of medical practice for several reasons. The law varies considerably from state to state. The clinician who practices both in California and across the border in Arizona will face substantially different laws, especially regarding the treatment of adolescents. And the reproductive rights laws in many states are a complicated mix of state statutes and state court decisions, with an overlay of federal statutes and court decisions, and a series of both state and federal regulations. This article demonstrates an additional complexity for practitioners—the continuous change in the law surrounding reproductive rights—and practice involving adolescent patients is especially difficult.
There are some good state-by-state reviews of laws related to abortion and contraception. We find the Guttmacher Institute particularly helpful. (See “State-by-state reviews of laws related to abortion and contraception”.) Although these are good resources, they are not the basis for legal practice with the current law in a state. The complexity and ever-changing nature of reproductive rights is one of the reasons we believe that it is important that anyone in active ObGyn practice maintain an ongoing professional relationship with a lawyer with expertise in this area of practice. This relationship should establish and update policies and procedures consistent with local law, consent and other forms, reporting of possible child abuse, and the like. An annual legal checkup may be as important for physicians as a physical checkup is for their patients.
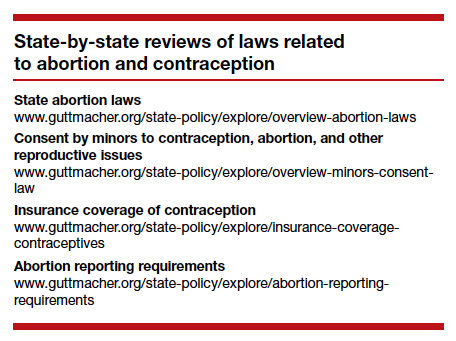
Future outcomes
At the end of the Term, we will review the outcome of the cases noted above—and the possibility of follow-on cases. Whatever the Court does this Term, it will not be the end of the legal and political struggles over abortion and other reproductive issues. These questions deeply divide our society, and the cases and controversies reflect that continuing division. ●
- Buck v Bell, 274 U.S. 200 (1927).
- Id. at 207.
- Skinner v State of Oklahoma, ex rel. Williamson, 316 U.S. 535 (1942).
- Griswold v Connecticut, 381 U.S. 479 (1965)
- Eisenstadt v Baird, 405 U.S. 438 (1972).
- Roe v Wade, 410 U.S. 113 (1973).
- Harris v McRae, 448 U.S. 297 (1980).
- Williams v Zbaraz, 448 U.S 358 (1980).
- Webster v Reproductive Health Services, 492 U.S. 490 (1989).
- Rust v Sullivan, 500 U.S. 173 (1991).
- Planned Parenthood of Southeastern Pennsylvania v Casey, 505 U.S. 833 (1992).
- Carey v Population Services, 431 U.S. 678 (1977).
- Bellotti v Baird, 443 U.S. 622 (1979).
- Planned Parenthood of Kansas City v Ashcroft, 462 U.S. 476 (1983).
- Planned Parenthood of Northern New England v Ayotte, 546 U.S. 320 (2006).
- H.L. v Matheson, 450 U.S. 398 (1981).
- Hodgson v Minnesota, 497 U.S. 417 (1990).
- Ohio v Akron Center for Reproductive Health, 497 U.S. 502 (1990).
- Lambert v Wicklund, 520 U.S. 292 (1997).
- June Medical Services v Russo, 591 U.S. ___ (2020), https:// www.supremecourt.gov/opinions/19pdf/18-1323_c07d.pdf.
- Whole Woman’s Health v Hellerstedt, 579 U.S. 582 (2016).
- AMA v Becerra, dismissed May 17, 2021, https://www .scotusblog.com/case-files/cases/american-medical -association-v-cochran.
- Becerra v Baltimore, dismissed May 17, 2021, https://www .scotusblog.com/case-files/cases/cochran-v-mayor-and-city-council-of-baltimore.
- Oregon v Becerra, dismissed May 17, 2021, https://www .scotusblog.com/case-files/cases/oregon-v-cochran.
- Cameron v EMW Women’s Surgical Center, 20-601. https:// www.scotusblog.com/case-files/cases/cameron-v-emw -womens-surgical-center-p-s-c.
- Ex parte Young, 209 U.S. 123 (1908).
- Whole Woman’s Health v Jackson, 21-463. https://www .scotusblog.com/case-files/cases/whole-womans-health-v -jackson.
- U.S. v Texas, 21-588. https://www.scotusblog.com/case-files /cases/united-states-v-texas-3.
- Dobbs v Jackson Women’s Health Organization, 19-1392. https://www.scotusblog.com/case-files/cases/dobbs-v -jackson-womens-health-organization.
- Brief of Amici Curiae American College of Obstetricians and Gynecologists et al., Dobbs v Jackson Women’s Health Organization (Sep. 2021). https://www.acog.org/ -/media/project/acog/acogorg/files/advocacy/amicus -briefs/2021/20210920-dobbs-v-jwho-amicus-brief.pdf?la=e n&hash=717DFDD07A03B93A04490E66835BB8C5.
- Brief Amicus Curiae of International Federation of Gynecology and Obstetrics, Dobbs v Jackson Women’s Health Organization (Sep. 20, 2021). https://www.supremecourt. gov/DocketPDF/19/19-1392/193019/20210920155508744 _41426%20pdf%20Chen.pdf.
- Brief Amicus Curiae of American Association of Pro-Life Obstetricians and Gynecologists. Dobbs v Jackson Women’s Health Organization (Sep. 2021). https://www.supremecourt .gov/DocketPDF/19/19-1392/185350/20210729163532595 _No.%2019-1392%20-%20American%20Association %20of%20Pro-Life%20Obstetricians%20and%20 Gynecologists%20-%20Amicus%20Brief%20in%20Support %20of%20Petitioner%20-%207-29-21.pdf.

Mr. Smith is Professor Emeritus, Dean Emeritus, California Western School of Law, San Diego, California.
Dr. Sanfilippo is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh; Director, Reproductive Endocrinology and Infertility, Magee-Womens Hospital, Pittsburgh, Pennsylvania. He serves on the OBG Management Board of Editors.
The authors report no financial relationships relevant to this article.
Mr. Smith is Professor Emeritus, Dean Emeritus, California Western School of Law, San Diego, California.
Dr. Sanfilippo is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh; Director, Reproductive Endocrinology and Infertility, Magee-Womens Hospital, Pittsburgh, Pennsylvania. He serves on the OBG Management Board of Editors.
The authors report no financial relationships relevant to this article.
Mr. Smith is Professor Emeritus, Dean Emeritus, California Western School of Law, San Diego, California.
Dr. Sanfilippo is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh; Director, Reproductive Endocrinology and Infertility, Magee-Womens Hospital, Pittsburgh, Pennsylvania. He serves on the OBG Management Board of Editors.
The authors report no financial relationships relevant to this article.
There is now great interest in the Supreme Court’s handling of cases that involve a woman’s ability to have an abortion. Recent decisions, and those planned in the next few months will be the source of intense scrutiny. But the Court’s involvement in reproductive rights did not begin with abortion. In fact, the Supreme Court has a long history of controversial decisions dealing with reproductive rights.
Involuntary sterilization
A notable, even infamous, case was Buck v Bell (1927)—later discredited—in which the Court reviewed a state law that provided for the involuntary sterilization of the “feeble minded.”1 The 8-1 decision was that the state could choose to have such a law to protect the so-called genetic health of the state. The law was based on a theory of eugenics. The opinion by the highly respected Justice Oliver Wendell Holmes included the unfortunate conclusion, “Three generations of imbeciles are enough.”2 As mentioned, the law has since been thoroughly discredited. In 1942, the Court did come to a different result, holding in Skinner v Oklahoma that it was unconstitutional for a state to involuntarily sterilize “habitual criminals.”3
Contraception
Forty years after Buck, in Griswold v Connecticut, the Court reviewed a state law that prohibited the distribution of any drug or device used for contraception (even for married couples).4 In a 7-2 decision, the Supreme Court struck down the state law as violating a marital right of privacy. Beyond its specific holding, Griswold was important in several ways. First, a physician was raising the rights of patients (not specifically his own rights). This is notable because, ordinarily in court, litigants may argue their own rights, not the rights of others. This has been important in later reproductive rights cases because often it has been physicians raising and arguing the rights of patients.
A second interesting part of Griswold was the source of this constitutional right of privacy. The Constitution contains no express privacy provision. In Griswold, the Court found that the 1st, 3rd, 4th, and 9th Amendments create the right to privacy in marital relations. Writing for the majority, Justice Douglas found that “emanations” from these amendments have “penumbras” that create a right of marital privacy.
Although Griswold was based on marital privacy, a few years later, in 1972, the Court essentially converted that right to one of reproductive privacy (“the decision whether to bear or beget a child.”) In Eisenstadt v Baird, the Court held that it was a violation of equal protection (the 14th Amendment) for a state to allow contraception to the married but deny it to an unmarried person.5
Continue to: Abortion...
Abortion
In 1971, the Court had heard arguments in 2 cases that raised issues regarding whether state laws prohibiting abortion were constitutional. The first oral argument in Roe v Wade is widely considered one of the worst oral arguments in modern history, and for several reasons the Court set the case for rehearing the following Term (October 1972). In January 1973, the Court decided Roe v Wade.6 The 7-2 decision was written by Justice Blackmun, who had at one point been the attorney for the Mayo Clinic and might be considered one of the first “health lawyers.” The Court held that the Constitution (perhaps in the 14th or 9th Amendment) includes a right of privacy that includes the right of a woman to choose to have, or not to have, an abortion. In implementing the right, the Court held that a state may impose only modest medical safeguards for the mother (eg, requiring that abortions be performed by a licensed physician). In the second trimester, to the point of viability, a state could impose only limitations on abortion that were reasonably directed to ensure the health of the mother. After a fetus was viable (could live outside the mother’s body), the state was free to regulate or prohibit abortions and protect the fetus. At the time, viability was approximately the beginning of the third trimester.6
The clear majority of the Court in Roe (7-2) may have suggested that there was not strong opposition to the decision. That, of course, was not the case. Legal and political conflict surrounding the case has been, and remains, intense. Since 1973, the Court has been called upon to decide many abortion cases, and each case seems to beget more controversy and still more cases.
Some of the legal objections to Roe and other abortion decisions are that the constitutional basis for the decision remains unclear—a specific right of privacy is not contained in the text of the Constitution. Several locations of a possible right of privacy have been mentioned by various justices, but “substantive due process” became the common constitutional basis for the right. Critics note that “substantive” due process (as opposed to procedural due process) is not mentioned in the Constitution, and it is short on clear guiding principles. Beyond those jurisprudential issues, of course, there were strong religious and philosophical objections to abortion. What followed Roe has been a long series of efforts to limit or discourage access to abortion, and the Supreme Court has had to decide a great many abortion cases (and a few contraception cases) over the last 50 years. Most years (except from 2008‒2013) the Court has heard, on average, at least one abortion case.
By way of examples, here are some of the issues related to abortion that the Court has decided:
- Payment and facilities. States and the federal government are not required to pay for abortions for women who cannot afford them or to provide facilities for abortion.7-10
- Informed consent. Some states’ special informed consent requirements for abortion were upheld, but complex consents that required the father’s participation were not.
- Ability to advertise. Prohibitions on advertisement of abortion services were struck down.
- Location. Requirements for hospital-only abortions (or similar regulations) were struck down.
- Anti-abortion protests. Several cases addressed guidelines involving demonstrations near abortion clinics.
Of particular importance was the case of Planned Parenthood of Southeastern Pennsylvania v Casey—“Casey.”11 In 1992 that case reaffirmed the “essential” holding of Roe v Wade. A plurality in that case de-emphasized the trimester framework and applied an “undue burden” test on limitations on abortion. In the more recent cases argued before the Court, Casey is frequently referred to as specifically reaffirming, and therefore solidifying, Roe.
Consent for minors
There have been several cases since 1973 that involved contraceptives or abortions and “minors” (generally, adolescents aged <18 years, although there are some state-defined exceptions). These cases typically involve 2 issues: the right of minors to consent to treatment and the obligation of the physician to provide information to parents about treatment to their minor daughter. In 1977 the Court struck down a New York law that prohibited the distribution of contraceptives to minors.12 However, abortion issues involving minors have been more complicated. While the Court has struck down “2-parent” consent statutes,13 it has generally upheld 1-parent consent statutes, but only if those statutes contain a “judicial bypass” provision and an emergency medical provision.11,14,15 (This bypass allows a minor to “bypass” parental consent to abortion in some circumstances, and instead seek judicial authorization for an abortion.) Generally, the Court has upheld parental notification for abortions, with exceptions where it would be harmful to the minor who is seeking the abortion.16-19
Continue to: Who can perform an abortion...
Who can perform an abortion
Over the years there have also been several cases raising questions about the professionals who can perform abortions, their hospital privileges, and what facilities can perform abortions. Two of those cases in recent years have, for example, seen the Court strike down state statutes that required the physicians who perform abortions to have admitting privileges at least in 1 nearby hospital.20,21 The basis for these decisions is that the admitting qualification is an “undue burden” because it serves almost no health purpose, while significantly limiting the number of professionals who can perform abortions.
Cases this Term
The current Term of the Court (officially the “October 2021 Term”) may be one of the most significant for reproductive rights in recent history. The Court accepted 6 abortion-related cases to hear. It dismissed 3 of those cases, which had become “moot” because the Biden administration changed the rules that had been legally challenged.22-24 It has heard arguments in the 3 (technically 4) remaining cases, in which decisions will be announced over the next several months.
The first of these cases (involving the Texas Heartbeat Act) raises very important, but vexing, procedural issues about a Texas abortion law. The second (Whole Woman’s Health v Jackson) is a direct challenge to Roe v Wade. The third case (Cameron v EMW Women’s Surgical Center) involves the narrow question of whether a state attorney general can intervene in a case to uphold a state abortion law when another state official refuses to defend the law.25 It is worthwhile taking a look at the first 2 of these cases.
Texas Heartbeat Act
In the first case (technically, it is 2 cases, as we will see), the Texas legislature adopted a law that prohibits abortions after there is a discernable heartbeat (around 6 weeks of pregnancy). The law precludes state officials from enforcing the law. Instead, it allows almost any private citizen to seek monetary damages ($10,000 plus fees) from anyone who performs an abortion or “aids and abets” an abortion. (This is in some ways similar to “private attorney general” actions found in the False Claims Act, and in some civil rights and labor laws.) This statute is clearly inconsistent with Roe in that it prohibits abortions before the end of the second trimester. If it were a usual law—a Texas law being enforced by state officials—federal courts would issue injunctions to state officials against enforcing the law. The difficulty with the Texas law (and its very purpose) is that there are procedural limitations in federal law that make it very difficult to find a path for federal courts to review the Texas statute quickly. For example, would federal courts enjoin every private citizen of the state? There is a longstanding Constitutional doctrine that precludes federal courts from enjoining state courts.26 Therefore, it is difficult to challenge the law before someone performing or aiding an abortion has been ordered to pay the private citizen who is enforcing it. In the interim, which could be months or even years, health care providers face uncertainty about continuing to provide abortion services. Some providers would stop providing abortion services, reducing the availability of those services.
Two cases challenge this Texas procedure. In the first, Whole Woman’s Health v Jackson, 27 abortion providers seek to find some way through the procedural thicket to allow an immediate challenge to the statute. It is important because this technique of exclusive private enforcement could be used in any number of ways by the state to chill important constitutional rights (beyond abortion—to speech, to bear arms). In the second case involving the Texas law, U.S. v Texas, the federal government seeks to intervene in the case, which is another unusual procedure.28 The Court found these questions so important and difficult that it allowed 3 hours of argument (and 4 sets of lawyers). It seems likely that the Court will find a mechanism for allowing some early federal court review of individual enforcement of state laws, while minimizing harm to the state-national federalism that is at the heart of the Constitution.
For the recent procedural decisions in the Texas cases, see the “Current Court Decisions” box below.
On December 10, 2021, the Court handed down two decisions in reproductive freedom (abortion) cases, both involving the Texas abortion law (which prohibits most abortions after a fetal heartbeat can be detected and allows only private individuals to enforce the law). The more significant of the two cases, Whole Woman’s Health v Jackson,1 was the request of abortion providers (and others) to allow them to challenge the constitutionality of the Texas law by suing various state officials or a private individual, before the enforcement of the new Texas law.
The decision of the Court was somewhat complex because of the split among justices. Overall:
- The Court held 8-1 that before the law is enforced, providers have the ability to sue executives of medical licensing boards. This was based on the possibility that there could be licensure discipline for professionals who violate the new abortion law. Only Justice Thomas dissented from this part of the decision, which was written by Justice Gorsuch.
- The Court unanimously held that state-court judges could not be sued to stop enforcement of the law, and dismissed them from the suit.
- In a 5-4 split the Court held that state court clerks (and the state attorney general) could not be brought into federal court as a way of challenging the law. This was based on the 11th Amendment, sovereign immunity, and an important precedent from 1908.2 Chief Justice Roberts wrote from the justices who were essentially in dissent (Justices Bryer, Kagan, and Sotomayor). Justice Sotomayor also wrote a dissent (joined by Justices Breyer and Kagan) urging that there should be some way for providers to test the constitutionality of the law before enforcement. Allowing an action against state court clerks would be a good way to do that. She also expressly noted the problem of the Texas law approach being used by other states to attack any number of constitutional rights.
- The Court unanimously dismissed (for lack of standing) the one private citizen who had been sued. He had signed a sworn statement that he did not intend to seek the damages against abortion providers under the Texas law.
- The Court declined again to stay the Texas law while it is being challenged. That is, it left standing the 5th Circuit order allowing the law to go into effect.
- In a second, related case, the Court dismissed, without deciding, the Biden administration’s request to become a party in the Texas abortion case.3
References
- Whole Woman’s Health v Jackson, No. 21–463 (Dec. 10, 2021). https://www.supremecourt.gov /opinions/21pdf/21-463_new_8o6b.pdf.
- Ex parte Young, 209 U.S. 123 (1908).
- U.S. v Texas, 21-588 (Dec. 10, 2021). https://www.supremecourt.gov/opinions/21pdf/21-588 _c07d.pdf
Continue to: Re-evaluating the viability standard...
Re-evaluating the viability standard
The substantive abortion issue in Dobbs v Jackson Women’s Health Organization is the constitutionality of the Mississippi Gestational Age Act, which allows abortions after 15 weeks of pregnancy only for medical emergencies or severe fetal abnormality.29 This case is likely the most watched and controversial case of the Term. Many medical organizations have filed amicus curiae briefs, including the American College of Obstetricians and Gynecologists joined by the American Medical Association,30 the International Federation of Gynecology and Obstetrics,31 and the American Association of Pro-Life Obstetricians and Gynecologists.32 The reason for all this attention is that the Court has accepted to resolve “whether all pre-viability prohibitions on elective abortions are unconstitutional.” Thus, it represents a direct challenge to the trimester/viability structure of Roe.
It appears that there are 3 justices ready to outright overrule Roe, 3 that would uphold it as is, and 3 who are not in favor of Roe, but feel bound by precedent or are not in favor of a traumatic move. For that reason, there may be a narrow decision in this case. For example, the Court might find a procedural way to avoid directly deciding the abortion issue in this case, or it might uphold the right to abortion but change the viability standard. It is also true that predicting what the Court will do in controversial cases is a fool’s errand.
The complexity of reproductive rights and the ObGyn practice
These cases and policies affect the day-to-day practice of obstetrics. It is the most legally complex area of medical practice for several reasons. The law varies considerably from state to state. The clinician who practices both in California and across the border in Arizona will face substantially different laws, especially regarding the treatment of adolescents. And the reproductive rights laws in many states are a complicated mix of state statutes and state court decisions, with an overlay of federal statutes and court decisions, and a series of both state and federal regulations. This article demonstrates an additional complexity for practitioners—the continuous change in the law surrounding reproductive rights—and practice involving adolescent patients is especially difficult.
There are some good state-by-state reviews of laws related to abortion and contraception. We find the Guttmacher Institute particularly helpful. (See “State-by-state reviews of laws related to abortion and contraception”.) Although these are good resources, they are not the basis for legal practice with the current law in a state. The complexity and ever-changing nature of reproductive rights is one of the reasons we believe that it is important that anyone in active ObGyn practice maintain an ongoing professional relationship with a lawyer with expertise in this area of practice. This relationship should establish and update policies and procedures consistent with local law, consent and other forms, reporting of possible child abuse, and the like. An annual legal checkup may be as important for physicians as a physical checkup is for their patients.
Future outcomes
At the end of the Term, we will review the outcome of the cases noted above—and the possibility of follow-on cases. Whatever the Court does this Term, it will not be the end of the legal and political struggles over abortion and other reproductive issues. These questions deeply divide our society, and the cases and controversies reflect that continuing division. ●
There is now great interest in the Supreme Court’s handling of cases that involve a woman’s ability to have an abortion. Recent decisions, and those planned in the next few months will be the source of intense scrutiny. But the Court’s involvement in reproductive rights did not begin with abortion. In fact, the Supreme Court has a long history of controversial decisions dealing with reproductive rights.
Involuntary sterilization
A notable, even infamous, case was Buck v Bell (1927)—later discredited—in which the Court reviewed a state law that provided for the involuntary sterilization of the “feeble minded.”1 The 8-1 decision was that the state could choose to have such a law to protect the so-called genetic health of the state. The law was based on a theory of eugenics. The opinion by the highly respected Justice Oliver Wendell Holmes included the unfortunate conclusion, “Three generations of imbeciles are enough.”2 As mentioned, the law has since been thoroughly discredited. In 1942, the Court did come to a different result, holding in Skinner v Oklahoma that it was unconstitutional for a state to involuntarily sterilize “habitual criminals.”3
Contraception
Forty years after Buck, in Griswold v Connecticut, the Court reviewed a state law that prohibited the distribution of any drug or device used for contraception (even for married couples).4 In a 7-2 decision, the Supreme Court struck down the state law as violating a marital right of privacy. Beyond its specific holding, Griswold was important in several ways. First, a physician was raising the rights of patients (not specifically his own rights). This is notable because, ordinarily in court, litigants may argue their own rights, not the rights of others. This has been important in later reproductive rights cases because often it has been physicians raising and arguing the rights of patients.
A second interesting part of Griswold was the source of this constitutional right of privacy. The Constitution contains no express privacy provision. In Griswold, the Court found that the 1st, 3rd, 4th, and 9th Amendments create the right to privacy in marital relations. Writing for the majority, Justice Douglas found that “emanations” from these amendments have “penumbras” that create a right of marital privacy.
Although Griswold was based on marital privacy, a few years later, in 1972, the Court essentially converted that right to one of reproductive privacy (“the decision whether to bear or beget a child.”) In Eisenstadt v Baird, the Court held that it was a violation of equal protection (the 14th Amendment) for a state to allow contraception to the married but deny it to an unmarried person.5
Continue to: Abortion...
Abortion
In 1971, the Court had heard arguments in 2 cases that raised issues regarding whether state laws prohibiting abortion were constitutional. The first oral argument in Roe v Wade is widely considered one of the worst oral arguments in modern history, and for several reasons the Court set the case for rehearing the following Term (October 1972). In January 1973, the Court decided Roe v Wade.6 The 7-2 decision was written by Justice Blackmun, who had at one point been the attorney for the Mayo Clinic and might be considered one of the first “health lawyers.” The Court held that the Constitution (perhaps in the 14th or 9th Amendment) includes a right of privacy that includes the right of a woman to choose to have, or not to have, an abortion. In implementing the right, the Court held that a state may impose only modest medical safeguards for the mother (eg, requiring that abortions be performed by a licensed physician). In the second trimester, to the point of viability, a state could impose only limitations on abortion that were reasonably directed to ensure the health of the mother. After a fetus was viable (could live outside the mother’s body), the state was free to regulate or prohibit abortions and protect the fetus. At the time, viability was approximately the beginning of the third trimester.6
The clear majority of the Court in Roe (7-2) may have suggested that there was not strong opposition to the decision. That, of course, was not the case. Legal and political conflict surrounding the case has been, and remains, intense. Since 1973, the Court has been called upon to decide many abortion cases, and each case seems to beget more controversy and still more cases.
Some of the legal objections to Roe and other abortion decisions are that the constitutional basis for the decision remains unclear—a specific right of privacy is not contained in the text of the Constitution. Several locations of a possible right of privacy have been mentioned by various justices, but “substantive due process” became the common constitutional basis for the right. Critics note that “substantive” due process (as opposed to procedural due process) is not mentioned in the Constitution, and it is short on clear guiding principles. Beyond those jurisprudential issues, of course, there were strong religious and philosophical objections to abortion. What followed Roe has been a long series of efforts to limit or discourage access to abortion, and the Supreme Court has had to decide a great many abortion cases (and a few contraception cases) over the last 50 years. Most years (except from 2008‒2013) the Court has heard, on average, at least one abortion case.
By way of examples, here are some of the issues related to abortion that the Court has decided:
- Payment and facilities. States and the federal government are not required to pay for abortions for women who cannot afford them or to provide facilities for abortion.7-10
- Informed consent. Some states’ special informed consent requirements for abortion were upheld, but complex consents that required the father’s participation were not.
- Ability to advertise. Prohibitions on advertisement of abortion services were struck down.
- Location. Requirements for hospital-only abortions (or similar regulations) were struck down.
- Anti-abortion protests. Several cases addressed guidelines involving demonstrations near abortion clinics.
Of particular importance was the case of Planned Parenthood of Southeastern Pennsylvania v Casey—“Casey.”11 In 1992 that case reaffirmed the “essential” holding of Roe v Wade. A plurality in that case de-emphasized the trimester framework and applied an “undue burden” test on limitations on abortion. In the more recent cases argued before the Court, Casey is frequently referred to as specifically reaffirming, and therefore solidifying, Roe.
Consent for minors
There have been several cases since 1973 that involved contraceptives or abortions and “minors” (generally, adolescents aged <18 years, although there are some state-defined exceptions). These cases typically involve 2 issues: the right of minors to consent to treatment and the obligation of the physician to provide information to parents about treatment to their minor daughter. In 1977 the Court struck down a New York law that prohibited the distribution of contraceptives to minors.12 However, abortion issues involving minors have been more complicated. While the Court has struck down “2-parent” consent statutes,13 it has generally upheld 1-parent consent statutes, but only if those statutes contain a “judicial bypass” provision and an emergency medical provision.11,14,15 (This bypass allows a minor to “bypass” parental consent to abortion in some circumstances, and instead seek judicial authorization for an abortion.) Generally, the Court has upheld parental notification for abortions, with exceptions where it would be harmful to the minor who is seeking the abortion.16-19
Continue to: Who can perform an abortion...
Who can perform an abortion
Over the years there have also been several cases raising questions about the professionals who can perform abortions, their hospital privileges, and what facilities can perform abortions. Two of those cases in recent years have, for example, seen the Court strike down state statutes that required the physicians who perform abortions to have admitting privileges at least in 1 nearby hospital.20,21 The basis for these decisions is that the admitting qualification is an “undue burden” because it serves almost no health purpose, while significantly limiting the number of professionals who can perform abortions.
Cases this Term
The current Term of the Court (officially the “October 2021 Term”) may be one of the most significant for reproductive rights in recent history. The Court accepted 6 abortion-related cases to hear. It dismissed 3 of those cases, which had become “moot” because the Biden administration changed the rules that had been legally challenged.22-24 It has heard arguments in the 3 (technically 4) remaining cases, in which decisions will be announced over the next several months.
The first of these cases (involving the Texas Heartbeat Act) raises very important, but vexing, procedural issues about a Texas abortion law. The second (Whole Woman’s Health v Jackson) is a direct challenge to Roe v Wade. The third case (Cameron v EMW Women’s Surgical Center) involves the narrow question of whether a state attorney general can intervene in a case to uphold a state abortion law when another state official refuses to defend the law.25 It is worthwhile taking a look at the first 2 of these cases.
Texas Heartbeat Act
In the first case (technically, it is 2 cases, as we will see), the Texas legislature adopted a law that prohibits abortions after there is a discernable heartbeat (around 6 weeks of pregnancy). The law precludes state officials from enforcing the law. Instead, it allows almost any private citizen to seek monetary damages ($10,000 plus fees) from anyone who performs an abortion or “aids and abets” an abortion. (This is in some ways similar to “private attorney general” actions found in the False Claims Act, and in some civil rights and labor laws.) This statute is clearly inconsistent with Roe in that it prohibits abortions before the end of the second trimester. If it were a usual law—a Texas law being enforced by state officials—federal courts would issue injunctions to state officials against enforcing the law. The difficulty with the Texas law (and its very purpose) is that there are procedural limitations in federal law that make it very difficult to find a path for federal courts to review the Texas statute quickly. For example, would federal courts enjoin every private citizen of the state? There is a longstanding Constitutional doctrine that precludes federal courts from enjoining state courts.26 Therefore, it is difficult to challenge the law before someone performing or aiding an abortion has been ordered to pay the private citizen who is enforcing it. In the interim, which could be months or even years, health care providers face uncertainty about continuing to provide abortion services. Some providers would stop providing abortion services, reducing the availability of those services.
Two cases challenge this Texas procedure. In the first, Whole Woman’s Health v Jackson, 27 abortion providers seek to find some way through the procedural thicket to allow an immediate challenge to the statute. It is important because this technique of exclusive private enforcement could be used in any number of ways by the state to chill important constitutional rights (beyond abortion—to speech, to bear arms). In the second case involving the Texas law, U.S. v Texas, the federal government seeks to intervene in the case, which is another unusual procedure.28 The Court found these questions so important and difficult that it allowed 3 hours of argument (and 4 sets of lawyers). It seems likely that the Court will find a mechanism for allowing some early federal court review of individual enforcement of state laws, while minimizing harm to the state-national federalism that is at the heart of the Constitution.
For the recent procedural decisions in the Texas cases, see the “Current Court Decisions” box below.
On December 10, 2021, the Court handed down two decisions in reproductive freedom (abortion) cases, both involving the Texas abortion law (which prohibits most abortions after a fetal heartbeat can be detected and allows only private individuals to enforce the law). The more significant of the two cases, Whole Woman’s Health v Jackson,1 was the request of abortion providers (and others) to allow them to challenge the constitutionality of the Texas law by suing various state officials or a private individual, before the enforcement of the new Texas law.
The decision of the Court was somewhat complex because of the split among justices. Overall:
- The Court held 8-1 that before the law is enforced, providers have the ability to sue executives of medical licensing boards. This was based on the possibility that there could be licensure discipline for professionals who violate the new abortion law. Only Justice Thomas dissented from this part of the decision, which was written by Justice Gorsuch.
- The Court unanimously held that state-court judges could not be sued to stop enforcement of the law, and dismissed them from the suit.
- In a 5-4 split the Court held that state court clerks (and the state attorney general) could not be brought into federal court as a way of challenging the law. This was based on the 11th Amendment, sovereign immunity, and an important precedent from 1908.2 Chief Justice Roberts wrote from the justices who were essentially in dissent (Justices Bryer, Kagan, and Sotomayor). Justice Sotomayor also wrote a dissent (joined by Justices Breyer and Kagan) urging that there should be some way for providers to test the constitutionality of the law before enforcement. Allowing an action against state court clerks would be a good way to do that. She also expressly noted the problem of the Texas law approach being used by other states to attack any number of constitutional rights.
- The Court unanimously dismissed (for lack of standing) the one private citizen who had been sued. He had signed a sworn statement that he did not intend to seek the damages against abortion providers under the Texas law.
- The Court declined again to stay the Texas law while it is being challenged. That is, it left standing the 5th Circuit order allowing the law to go into effect.
- In a second, related case, the Court dismissed, without deciding, the Biden administration’s request to become a party in the Texas abortion case.3
References
- Whole Woman’s Health v Jackson, No. 21–463 (Dec. 10, 2021). https://www.supremecourt.gov /opinions/21pdf/21-463_new_8o6b.pdf.
- Ex parte Young, 209 U.S. 123 (1908).
- U.S. v Texas, 21-588 (Dec. 10, 2021). https://www.supremecourt.gov/opinions/21pdf/21-588 _c07d.pdf
Continue to: Re-evaluating the viability standard...
Re-evaluating the viability standard
The substantive abortion issue in Dobbs v Jackson Women’s Health Organization is the constitutionality of the Mississippi Gestational Age Act, which allows abortions after 15 weeks of pregnancy only for medical emergencies or severe fetal abnormality.29 This case is likely the most watched and controversial case of the Term. Many medical organizations have filed amicus curiae briefs, including the American College of Obstetricians and Gynecologists joined by the American Medical Association,30 the International Federation of Gynecology and Obstetrics,31 and the American Association of Pro-Life Obstetricians and Gynecologists.32 The reason for all this attention is that the Court has accepted to resolve “whether all pre-viability prohibitions on elective abortions are unconstitutional.” Thus, it represents a direct challenge to the trimester/viability structure of Roe.
It appears that there are 3 justices ready to outright overrule Roe, 3 that would uphold it as is, and 3 who are not in favor of Roe, but feel bound by precedent or are not in favor of a traumatic move. For that reason, there may be a narrow decision in this case. For example, the Court might find a procedural way to avoid directly deciding the abortion issue in this case, or it might uphold the right to abortion but change the viability standard. It is also true that predicting what the Court will do in controversial cases is a fool’s errand.
The complexity of reproductive rights and the ObGyn practice
These cases and policies affect the day-to-day practice of obstetrics. It is the most legally complex area of medical practice for several reasons. The law varies considerably from state to state. The clinician who practices both in California and across the border in Arizona will face substantially different laws, especially regarding the treatment of adolescents. And the reproductive rights laws in many states are a complicated mix of state statutes and state court decisions, with an overlay of federal statutes and court decisions, and a series of both state and federal regulations. This article demonstrates an additional complexity for practitioners—the continuous change in the law surrounding reproductive rights—and practice involving adolescent patients is especially difficult.
There are some good state-by-state reviews of laws related to abortion and contraception. We find the Guttmacher Institute particularly helpful. (See “State-by-state reviews of laws related to abortion and contraception”.) Although these are good resources, they are not the basis for legal practice with the current law in a state. The complexity and ever-changing nature of reproductive rights is one of the reasons we believe that it is important that anyone in active ObGyn practice maintain an ongoing professional relationship with a lawyer with expertise in this area of practice. This relationship should establish and update policies and procedures consistent with local law, consent and other forms, reporting of possible child abuse, and the like. An annual legal checkup may be as important for physicians as a physical checkup is for their patients.
Future outcomes
At the end of the Term, we will review the outcome of the cases noted above—and the possibility of follow-on cases. Whatever the Court does this Term, it will not be the end of the legal and political struggles over abortion and other reproductive issues. These questions deeply divide our society, and the cases and controversies reflect that continuing division. ●
- Buck v Bell, 274 U.S. 200 (1927).
- Id. at 207.
- Skinner v State of Oklahoma, ex rel. Williamson, 316 U.S. 535 (1942).
- Griswold v Connecticut, 381 U.S. 479 (1965)
- Eisenstadt v Baird, 405 U.S. 438 (1972).
- Roe v Wade, 410 U.S. 113 (1973).
- Harris v McRae, 448 U.S. 297 (1980).
- Williams v Zbaraz, 448 U.S 358 (1980).
- Webster v Reproductive Health Services, 492 U.S. 490 (1989).
- Rust v Sullivan, 500 U.S. 173 (1991).
- Planned Parenthood of Southeastern Pennsylvania v Casey, 505 U.S. 833 (1992).
- Carey v Population Services, 431 U.S. 678 (1977).
- Bellotti v Baird, 443 U.S. 622 (1979).
- Planned Parenthood of Kansas City v Ashcroft, 462 U.S. 476 (1983).
- Planned Parenthood of Northern New England v Ayotte, 546 U.S. 320 (2006).
- H.L. v Matheson, 450 U.S. 398 (1981).
- Hodgson v Minnesota, 497 U.S. 417 (1990).
- Ohio v Akron Center for Reproductive Health, 497 U.S. 502 (1990).
- Lambert v Wicklund, 520 U.S. 292 (1997).
- June Medical Services v Russo, 591 U.S. ___ (2020), https:// www.supremecourt.gov/opinions/19pdf/18-1323_c07d.pdf.
- Whole Woman’s Health v Hellerstedt, 579 U.S. 582 (2016).
- AMA v Becerra, dismissed May 17, 2021, https://www .scotusblog.com/case-files/cases/american-medical -association-v-cochran.
- Becerra v Baltimore, dismissed May 17, 2021, https://www .scotusblog.com/case-files/cases/cochran-v-mayor-and-city-council-of-baltimore.
- Oregon v Becerra, dismissed May 17, 2021, https://www .scotusblog.com/case-files/cases/oregon-v-cochran.
- Cameron v EMW Women’s Surgical Center, 20-601. https:// www.scotusblog.com/case-files/cases/cameron-v-emw -womens-surgical-center-p-s-c.
- Ex parte Young, 209 U.S. 123 (1908).
- Whole Woman’s Health v Jackson, 21-463. https://www .scotusblog.com/case-files/cases/whole-womans-health-v -jackson.
- U.S. v Texas, 21-588. https://www.scotusblog.com/case-files /cases/united-states-v-texas-3.
- Dobbs v Jackson Women’s Health Organization, 19-1392. https://www.scotusblog.com/case-files/cases/dobbs-v -jackson-womens-health-organization.
- Brief of Amici Curiae American College of Obstetricians and Gynecologists et al., Dobbs v Jackson Women’s Health Organization (Sep. 2021). https://www.acog.org/ -/media/project/acog/acogorg/files/advocacy/amicus -briefs/2021/20210920-dobbs-v-jwho-amicus-brief.pdf?la=e n&hash=717DFDD07A03B93A04490E66835BB8C5.
- Brief Amicus Curiae of International Federation of Gynecology and Obstetrics, Dobbs v Jackson Women’s Health Organization (Sep. 20, 2021). https://www.supremecourt. gov/DocketPDF/19/19-1392/193019/20210920155508744 _41426%20pdf%20Chen.pdf.
- Brief Amicus Curiae of American Association of Pro-Life Obstetricians and Gynecologists. Dobbs v Jackson Women’s Health Organization (Sep. 2021). https://www.supremecourt .gov/DocketPDF/19/19-1392/185350/20210729163532595 _No.%2019-1392%20-%20American%20Association %20of%20Pro-Life%20Obstetricians%20and%20 Gynecologists%20-%20Amicus%20Brief%20in%20Support %20of%20Petitioner%20-%207-29-21.pdf.
- Buck v Bell, 274 U.S. 200 (1927).
- Id. at 207.
- Skinner v State of Oklahoma, ex rel. Williamson, 316 U.S. 535 (1942).
- Griswold v Connecticut, 381 U.S. 479 (1965)
- Eisenstadt v Baird, 405 U.S. 438 (1972).
- Roe v Wade, 410 U.S. 113 (1973).
- Harris v McRae, 448 U.S. 297 (1980).
- Williams v Zbaraz, 448 U.S 358 (1980).
- Webster v Reproductive Health Services, 492 U.S. 490 (1989).
- Rust v Sullivan, 500 U.S. 173 (1991).
- Planned Parenthood of Southeastern Pennsylvania v Casey, 505 U.S. 833 (1992).
- Carey v Population Services, 431 U.S. 678 (1977).
- Bellotti v Baird, 443 U.S. 622 (1979).
- Planned Parenthood of Kansas City v Ashcroft, 462 U.S. 476 (1983).
- Planned Parenthood of Northern New England v Ayotte, 546 U.S. 320 (2006).
- H.L. v Matheson, 450 U.S. 398 (1981).
- Hodgson v Minnesota, 497 U.S. 417 (1990).
- Ohio v Akron Center for Reproductive Health, 497 U.S. 502 (1990).
- Lambert v Wicklund, 520 U.S. 292 (1997).
- June Medical Services v Russo, 591 U.S. ___ (2020), https:// www.supremecourt.gov/opinions/19pdf/18-1323_c07d.pdf.
- Whole Woman’s Health v Hellerstedt, 579 U.S. 582 (2016).
- AMA v Becerra, dismissed May 17, 2021, https://www .scotusblog.com/case-files/cases/american-medical -association-v-cochran.
- Becerra v Baltimore, dismissed May 17, 2021, https://www .scotusblog.com/case-files/cases/cochran-v-mayor-and-city-council-of-baltimore.
- Oregon v Becerra, dismissed May 17, 2021, https://www .scotusblog.com/case-files/cases/oregon-v-cochran.
- Cameron v EMW Women’s Surgical Center, 20-601. https:// www.scotusblog.com/case-files/cases/cameron-v-emw -womens-surgical-center-p-s-c.
- Ex parte Young, 209 U.S. 123 (1908).
- Whole Woman’s Health v Jackson, 21-463. https://www .scotusblog.com/case-files/cases/whole-womans-health-v -jackson.
- U.S. v Texas, 21-588. https://www.scotusblog.com/case-files /cases/united-states-v-texas-3.
- Dobbs v Jackson Women’s Health Organization, 19-1392. https://www.scotusblog.com/case-files/cases/dobbs-v -jackson-womens-health-organization.
- Brief of Amici Curiae American College of Obstetricians and Gynecologists et al., Dobbs v Jackson Women’s Health Organization (Sep. 2021). https://www.acog.org/ -/media/project/acog/acogorg/files/advocacy/amicus -briefs/2021/20210920-dobbs-v-jwho-amicus-brief.pdf?la=e n&hash=717DFDD07A03B93A04490E66835BB8C5.
- Brief Amicus Curiae of International Federation of Gynecology and Obstetrics, Dobbs v Jackson Women’s Health Organization (Sep. 20, 2021). https://www.supremecourt. gov/DocketPDF/19/19-1392/193019/20210920155508744 _41426%20pdf%20Chen.pdf.
- Brief Amicus Curiae of American Association of Pro-Life Obstetricians and Gynecologists. Dobbs v Jackson Women’s Health Organization (Sep. 2021). https://www.supremecourt .gov/DocketPDF/19/19-1392/185350/20210729163532595 _No.%2019-1392%20-%20American%20Association %20of%20Pro-Life%20Obstetricians%20and%20 Gynecologists%20-%20Amicus%20Brief%20in%20Support %20of%20Petitioner%20-%207-29-21.pdf.
