User login
How safe is a drug holiday from bisphosphonates for osteoporosis?
Researchers found a small but greater risk of a hip fracture after 2 years of taking a “drug holiday” – stopping therapy – after long-term (≥3-year) use of one bisphosphonate, risedronate, versus another, alendronate.
The risk of a hip fracture after stopping either of these oral bisphosphonate osteoporosis drugs was similar until 2 years, suggesting that patients who take a drug holiday from risedronate should be revaluated before 2 years.
These top-line findings from a propensity-matched cohort study of older patients in Ontario, Canada, were reported at the annual American Society of Bone and Mineral Research (ASBMR) last fall.
The full study, led by Kaleen N. Hayes, PharmD, PhD, Brown University School of Public Health, Providence, R.I., was published online in the Annals of Internal Medicine.
“We emphasize that our results do not indicate that alendronate therapy should be preferred over risedronate therapy,” the researchers stress, as several real-world studies found a similar risk of fractures while patients were receiving either drug.
“The decision to initiate alendronate or risedronate therapy [the two most commonly prescribed bisphosphonates] is driven by the prescriber,” they note, adding that some patients may prefer risedronate because it is available as a monthly dose or a weekly delayed-release formula that does not require fasting.
“We found little difference in the association between risedronate versus alendronate drug holidays and hip fractures until approximately 2 years of not receiving therapy,” Dr. Hayes and colleagues summarize.
Over 3 years, risedronate drug holidays were associated with an 18% relative and 0.6% absolute increased risk for hip fracture compared with alendronate drug holidays.
“To further inform clinical decision-making on drug holidays,” they conclude, “future research should examine when to start and restart osteoporosis therapy on the basis of initial length and type of treatment, patient characteristics, and relative risk for hip fractures versus [atypical femoral fracture].”
Hip fracture risk with risedronate vs. alendronate drug holiday
Long-term bisphosphonate use is associated with a rare risk of osteonecrosis of the jaw or atypical femoral fractures. At the same time, bisphosphonates continue to have a therapeutic effect after therapy is discontinued.
Guidelines recommend that patients at low risk of fracture should therefore have a “drug holiday” after 3 to 5 years of bisphosphonate use and be reassessed 2 to 3 years later, largely based on the Fracture Intervention Trial Long-Term Extension (FLEX) study of alendronate. But risedronate has a shorter half-life, so it may provide shorter residual fracture protection.
Using Ontario administrative data, Dr. Hayes and associates identified more than 60,000 patients who were over aged 65, had received at least 3 years of continuous alendronate or risedronate, and had a subsequent 3-year drug holiday between 2000 and 2020.
They excluded patients who had a fracture or entered a nursing home within 120 days of starting a drug holiday who may have stopped the bisphosphonate due to declining health rather than a drug holiday.
Roughly half (55%) had been taking risedronate and 45% had been taking alendronate.
Using propensity scores, the researchers matched 25,077 patients who had been taking risedronate with an equal number who had been taking alendronate.
Most of the patients were women (82%) and were White.
They started the drug holiday when they were on average 81 years old, after taking the bisphosphonate for 5.9 years on average.
During the 3-year drug holiday, 915 of the 50,154 patients had hip fractures.
This was equivalent to 12.4 hip fractures per 1,000 patients per year during a risedronate holiday and 10.6 hip fractures per 1,000 patients per year during an alendronate holiday (hazard ratio, 1.18).
The risk of hip fracture was not significantly higher at 1 year (HR, 1.03) or at 2 years of a risedronate holiday versus an alendronate holiday (HR, 1.14).
However, the risk of a hip fracture was significantly higher at 2 to 3 years of a risedronate holiday than after an alendronate holiday (HR, 1.34).
There was no significant difference in the risk of any osteoporotic fracture overall (including hip, vertebrae, pelvis, ribs, forearm), however, during a 3-year risedronate versus alendronate drug holiday (HR, 1.07).
The research was supported by the Canadian Institutes of Health Research and Institute for Clinical Evaluative Sciences. Dr. Hayes was supported by a CIHR doctoral research award. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Researchers found a small but greater risk of a hip fracture after 2 years of taking a “drug holiday” – stopping therapy – after long-term (≥3-year) use of one bisphosphonate, risedronate, versus another, alendronate.
The risk of a hip fracture after stopping either of these oral bisphosphonate osteoporosis drugs was similar until 2 years, suggesting that patients who take a drug holiday from risedronate should be revaluated before 2 years.
These top-line findings from a propensity-matched cohort study of older patients in Ontario, Canada, were reported at the annual American Society of Bone and Mineral Research (ASBMR) last fall.
The full study, led by Kaleen N. Hayes, PharmD, PhD, Brown University School of Public Health, Providence, R.I., was published online in the Annals of Internal Medicine.
“We emphasize that our results do not indicate that alendronate therapy should be preferred over risedronate therapy,” the researchers stress, as several real-world studies found a similar risk of fractures while patients were receiving either drug.
“The decision to initiate alendronate or risedronate therapy [the two most commonly prescribed bisphosphonates] is driven by the prescriber,” they note, adding that some patients may prefer risedronate because it is available as a monthly dose or a weekly delayed-release formula that does not require fasting.
“We found little difference in the association between risedronate versus alendronate drug holidays and hip fractures until approximately 2 years of not receiving therapy,” Dr. Hayes and colleagues summarize.
Over 3 years, risedronate drug holidays were associated with an 18% relative and 0.6% absolute increased risk for hip fracture compared with alendronate drug holidays.
“To further inform clinical decision-making on drug holidays,” they conclude, “future research should examine when to start and restart osteoporosis therapy on the basis of initial length and type of treatment, patient characteristics, and relative risk for hip fractures versus [atypical femoral fracture].”
Hip fracture risk with risedronate vs. alendronate drug holiday
Long-term bisphosphonate use is associated with a rare risk of osteonecrosis of the jaw or atypical femoral fractures. At the same time, bisphosphonates continue to have a therapeutic effect after therapy is discontinued.
Guidelines recommend that patients at low risk of fracture should therefore have a “drug holiday” after 3 to 5 years of bisphosphonate use and be reassessed 2 to 3 years later, largely based on the Fracture Intervention Trial Long-Term Extension (FLEX) study of alendronate. But risedronate has a shorter half-life, so it may provide shorter residual fracture protection.
Using Ontario administrative data, Dr. Hayes and associates identified more than 60,000 patients who were over aged 65, had received at least 3 years of continuous alendronate or risedronate, and had a subsequent 3-year drug holiday between 2000 and 2020.
They excluded patients who had a fracture or entered a nursing home within 120 days of starting a drug holiday who may have stopped the bisphosphonate due to declining health rather than a drug holiday.
Roughly half (55%) had been taking risedronate and 45% had been taking alendronate.
Using propensity scores, the researchers matched 25,077 patients who had been taking risedronate with an equal number who had been taking alendronate.
Most of the patients were women (82%) and were White.
They started the drug holiday when they were on average 81 years old, after taking the bisphosphonate for 5.9 years on average.
During the 3-year drug holiday, 915 of the 50,154 patients had hip fractures.
This was equivalent to 12.4 hip fractures per 1,000 patients per year during a risedronate holiday and 10.6 hip fractures per 1,000 patients per year during an alendronate holiday (hazard ratio, 1.18).
The risk of hip fracture was not significantly higher at 1 year (HR, 1.03) or at 2 years of a risedronate holiday versus an alendronate holiday (HR, 1.14).
However, the risk of a hip fracture was significantly higher at 2 to 3 years of a risedronate holiday than after an alendronate holiday (HR, 1.34).
There was no significant difference in the risk of any osteoporotic fracture overall (including hip, vertebrae, pelvis, ribs, forearm), however, during a 3-year risedronate versus alendronate drug holiday (HR, 1.07).
The research was supported by the Canadian Institutes of Health Research and Institute for Clinical Evaluative Sciences. Dr. Hayes was supported by a CIHR doctoral research award. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Researchers found a small but greater risk of a hip fracture after 2 years of taking a “drug holiday” – stopping therapy – after long-term (≥3-year) use of one bisphosphonate, risedronate, versus another, alendronate.
The risk of a hip fracture after stopping either of these oral bisphosphonate osteoporosis drugs was similar until 2 years, suggesting that patients who take a drug holiday from risedronate should be revaluated before 2 years.
These top-line findings from a propensity-matched cohort study of older patients in Ontario, Canada, were reported at the annual American Society of Bone and Mineral Research (ASBMR) last fall.
The full study, led by Kaleen N. Hayes, PharmD, PhD, Brown University School of Public Health, Providence, R.I., was published online in the Annals of Internal Medicine.
“We emphasize that our results do not indicate that alendronate therapy should be preferred over risedronate therapy,” the researchers stress, as several real-world studies found a similar risk of fractures while patients were receiving either drug.
“The decision to initiate alendronate or risedronate therapy [the two most commonly prescribed bisphosphonates] is driven by the prescriber,” they note, adding that some patients may prefer risedronate because it is available as a monthly dose or a weekly delayed-release formula that does not require fasting.
“We found little difference in the association between risedronate versus alendronate drug holidays and hip fractures until approximately 2 years of not receiving therapy,” Dr. Hayes and colleagues summarize.
Over 3 years, risedronate drug holidays were associated with an 18% relative and 0.6% absolute increased risk for hip fracture compared with alendronate drug holidays.
“To further inform clinical decision-making on drug holidays,” they conclude, “future research should examine when to start and restart osteoporosis therapy on the basis of initial length and type of treatment, patient characteristics, and relative risk for hip fractures versus [atypical femoral fracture].”
Hip fracture risk with risedronate vs. alendronate drug holiday
Long-term bisphosphonate use is associated with a rare risk of osteonecrosis of the jaw or atypical femoral fractures. At the same time, bisphosphonates continue to have a therapeutic effect after therapy is discontinued.
Guidelines recommend that patients at low risk of fracture should therefore have a “drug holiday” after 3 to 5 years of bisphosphonate use and be reassessed 2 to 3 years later, largely based on the Fracture Intervention Trial Long-Term Extension (FLEX) study of alendronate. But risedronate has a shorter half-life, so it may provide shorter residual fracture protection.
Using Ontario administrative data, Dr. Hayes and associates identified more than 60,000 patients who were over aged 65, had received at least 3 years of continuous alendronate or risedronate, and had a subsequent 3-year drug holiday between 2000 and 2020.
They excluded patients who had a fracture or entered a nursing home within 120 days of starting a drug holiday who may have stopped the bisphosphonate due to declining health rather than a drug holiday.
Roughly half (55%) had been taking risedronate and 45% had been taking alendronate.
Using propensity scores, the researchers matched 25,077 patients who had been taking risedronate with an equal number who had been taking alendronate.
Most of the patients were women (82%) and were White.
They started the drug holiday when they were on average 81 years old, after taking the bisphosphonate for 5.9 years on average.
During the 3-year drug holiday, 915 of the 50,154 patients had hip fractures.
This was equivalent to 12.4 hip fractures per 1,000 patients per year during a risedronate holiday and 10.6 hip fractures per 1,000 patients per year during an alendronate holiday (hazard ratio, 1.18).
The risk of hip fracture was not significantly higher at 1 year (HR, 1.03) or at 2 years of a risedronate holiday versus an alendronate holiday (HR, 1.14).
However, the risk of a hip fracture was significantly higher at 2 to 3 years of a risedronate holiday than after an alendronate holiday (HR, 1.34).
There was no significant difference in the risk of any osteoporotic fracture overall (including hip, vertebrae, pelvis, ribs, forearm), however, during a 3-year risedronate versus alendronate drug holiday (HR, 1.07).
The research was supported by the Canadian Institutes of Health Research and Institute for Clinical Evaluative Sciences. Dr. Hayes was supported by a CIHR doctoral research award. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Hypertension protocols curb racial bias in therapeutic inertia
Therapeutic inertia regarding intensification of blood pressure treatment has been shown to be more of an issue in Black patients, but this was not the case in the SPRINT trial, which involved a strict standardized approach to blood pressure management, a new analysis shows.

“Overall, we found that therapeutic inertia was similar in different races in the SPRINT trial. We did not see disparities that have been reported in previous observational studies,” lead author, Alexander Zheutlin, MD, University of Utah School of Medicine, Salt Lake City, told this news organization.
“These results show that a well-resourced approach in which a standardized approach to blood pressure measurement and treatment intensification is followed can overcome the racial disparity that is seen in therapeutic inertia and the treatment of blood pressure,” he added.
The study was published online in JAMA Network Open on Jan. 10.
The authors explain that hypertension remains a leading modifiable cause of racial disparities in cardiovascular disease. Despite similar treatment rates and increased availability of safe, effective, and affordable antihypertensive medications, blood pressure control rates among Black and Hispanic adults remain significantly lower than among White adults in the United States, and one of the factors contributing to this is thought to be therapeutic inertia – the phenomenon of clinicians not initiating or up-titrating clinically indicated therapy in the setting of unmet treatment goals.
The current analysis of the SPRINT trial was conducted to investigate whether racial and ethnic differences in therapeutic inertia in hypertension were present when blood pressure care was standardized and protocolized.
The landmark SPRINT trial compared intensive (<120 mm Hg) with standard (<140 mm Hg) systolic blood pressure treatment goals in adults 50 years and older at high risk for cardiovascular disease. The present analysis was restricted to participant visits with measured blood pressure above the target goal and included 4,141 patients in the standard group and 4,415 patients in the intensive group.
Results showed that the overall prevalence of therapeutic inertia – defined as no antihypertensive medication intensification at each study visit where the blood pressure was above target goal – was either similar or lower for Black and Hispanic participants than for White participants. This pattern was observed whether participants were randomized to the standard or intensive treatment group.
“These findings support the idea that a standardized approach to blood pressure management, as implemented in SPRINT, may help ensure equitable care is provided to all patients and could reduce the contribution of therapeutic inertia to disparities in uncontrolled blood pressure,” the authors say.
They point out that therapeutic inertia has been identified as a key clinician-level barrier to blood pressure control and is estimated to be present in more than 80% of clinic visits in community practice, whereas in the current analysis of the SPRINT trial, therapeutic inertia was present in 50% to 60% of participant visits with uncontrolled blood pressure.
“In SPRINT, blood pressure had to be measured at defined intervals with a specific method, and there were clear instructions on intensifying treatment if blood pressure was above a certain goal,” Dr. Zheutlin noted. “Our results show that within such strict confines, therapeutic inertia does not seem to be different between different racial groups. This suggests that we could make better gains in blood pressure control and more equitable treatment if we adopted a standardized approach to hypertension management.”
He added: “Many guidelines have been published on when to start treatment and the targets for blood pressure, but there is a lot of variation in how we turn these guidelines into protocols. We need to bring in more consistent protocols on blood pressure measurement and intensification and ensure they are followed. In practice, if the BP is 5 or 10 mm Hg above target, a clinician may defer a decision to intensify treatment and intensification never gets done. But if there was a strict protocol to follow, there would be less chance of this happening.”
Therapeutic inertia still high
In an accompanying commentary, Matthew Rivara, MD, Nisha Bansal, MD, and Bessie Young, MD, University of Washington, Seattle, say the current SPRINT analysis has broad implications for reducing racial and ethnic disparities in achievement of evidence-based treatment targets in the general population.
“In hypertension management, standardized protocols for medication adjustments may limit clinician practice heterogeneity to ultimately reduce differences in blood pressure control among racial and ethnic minority populations,” they write. But they add that such protocols must be implemented thoughtfully to incorporate individualized clinical assessment and clinician-patient shared decision-making.
Dr. Rivara et al. point out that the rates of therapeutic inertia in SPRINT, while lower than community-based estimates, were still very high. They suggest reasons for this could include clinician concerns about medication efficacy, adverse effects, and patient mistrust of medical professionals. Outside the clinical trial environment, additional considerations may include prescription drug and laboratory test costs, pharmacy access, and competing demands during busy clinic visits.
To address these challenges, they say that clinicians need education on current clinical practice guidelines, managing complications of intensified antihypertensive therapies, and shared decisionmaking, including culturally sensitive collaborative care. Similarly, care systems must support patients on how to address concerns about treatments.
Finally, further research is needed to better define the specific factors associated with therapeutic inertia to allow tailored interventions to overcome this inertia.
“In designing and performing such research, it is vital that investigators engage with racial and ethnic minority groups to better explore the intersection of race, ethnicity, therapeutic decision-making, trust, and shared decisionmaking,” they add.
The SPRINT trial was funded with federal funds from the National Institutes of Health. Dr. Zheutlin reported receiving grants from the NIH during the conduct of the study.
A version of this article first appeared on Medscape.com.
Therapeutic inertia regarding intensification of blood pressure treatment has been shown to be more of an issue in Black patients, but this was not the case in the SPRINT trial, which involved a strict standardized approach to blood pressure management, a new analysis shows.
“Overall, we found that therapeutic inertia was similar in different races in the SPRINT trial. We did not see disparities that have been reported in previous observational studies,” lead author, Alexander Zheutlin, MD, University of Utah School of Medicine, Salt Lake City, told this news organization.
“These results show that a well-resourced approach in which a standardized approach to blood pressure measurement and treatment intensification is followed can overcome the racial disparity that is seen in therapeutic inertia and the treatment of blood pressure,” he added.
The study was published online in JAMA Network Open on Jan. 10.
The authors explain that hypertension remains a leading modifiable cause of racial disparities in cardiovascular disease. Despite similar treatment rates and increased availability of safe, effective, and affordable antihypertensive medications, blood pressure control rates among Black and Hispanic adults remain significantly lower than among White adults in the United States, and one of the factors contributing to this is thought to be therapeutic inertia – the phenomenon of clinicians not initiating or up-titrating clinically indicated therapy in the setting of unmet treatment goals.
The current analysis of the SPRINT trial was conducted to investigate whether racial and ethnic differences in therapeutic inertia in hypertension were present when blood pressure care was standardized and protocolized.
The landmark SPRINT trial compared intensive (<120 mm Hg) with standard (<140 mm Hg) systolic blood pressure treatment goals in adults 50 years and older at high risk for cardiovascular disease. The present analysis was restricted to participant visits with measured blood pressure above the target goal and included 4,141 patients in the standard group and 4,415 patients in the intensive group.
Results showed that the overall prevalence of therapeutic inertia – defined as no antihypertensive medication intensification at each study visit where the blood pressure was above target goal – was either similar or lower for Black and Hispanic participants than for White participants. This pattern was observed whether participants were randomized to the standard or intensive treatment group.
“These findings support the idea that a standardized approach to blood pressure management, as implemented in SPRINT, may help ensure equitable care is provided to all patients and could reduce the contribution of therapeutic inertia to disparities in uncontrolled blood pressure,” the authors say.
They point out that therapeutic inertia has been identified as a key clinician-level barrier to blood pressure control and is estimated to be present in more than 80% of clinic visits in community practice, whereas in the current analysis of the SPRINT trial, therapeutic inertia was present in 50% to 60% of participant visits with uncontrolled blood pressure.
“In SPRINT, blood pressure had to be measured at defined intervals with a specific method, and there were clear instructions on intensifying treatment if blood pressure was above a certain goal,” Dr. Zheutlin noted. “Our results show that within such strict confines, therapeutic inertia does not seem to be different between different racial groups. This suggests that we could make better gains in blood pressure control and more equitable treatment if we adopted a standardized approach to hypertension management.”
He added: “Many guidelines have been published on when to start treatment and the targets for blood pressure, but there is a lot of variation in how we turn these guidelines into protocols. We need to bring in more consistent protocols on blood pressure measurement and intensification and ensure they are followed. In practice, if the BP is 5 or 10 mm Hg above target, a clinician may defer a decision to intensify treatment and intensification never gets done. But if there was a strict protocol to follow, there would be less chance of this happening.”
Therapeutic inertia still high
In an accompanying commentary, Matthew Rivara, MD, Nisha Bansal, MD, and Bessie Young, MD, University of Washington, Seattle, say the current SPRINT analysis has broad implications for reducing racial and ethnic disparities in achievement of evidence-based treatment targets in the general population.
“In hypertension management, standardized protocols for medication adjustments may limit clinician practice heterogeneity to ultimately reduce differences in blood pressure control among racial and ethnic minority populations,” they write. But they add that such protocols must be implemented thoughtfully to incorporate individualized clinical assessment and clinician-patient shared decision-making.
Dr. Rivara et al. point out that the rates of therapeutic inertia in SPRINT, while lower than community-based estimates, were still very high. They suggest reasons for this could include clinician concerns about medication efficacy, adverse effects, and patient mistrust of medical professionals. Outside the clinical trial environment, additional considerations may include prescription drug and laboratory test costs, pharmacy access, and competing demands during busy clinic visits.
To address these challenges, they say that clinicians need education on current clinical practice guidelines, managing complications of intensified antihypertensive therapies, and shared decisionmaking, including culturally sensitive collaborative care. Similarly, care systems must support patients on how to address concerns about treatments.
Finally, further research is needed to better define the specific factors associated with therapeutic inertia to allow tailored interventions to overcome this inertia.
“In designing and performing such research, it is vital that investigators engage with racial and ethnic minority groups to better explore the intersection of race, ethnicity, therapeutic decision-making, trust, and shared decisionmaking,” they add.
The SPRINT trial was funded with federal funds from the National Institutes of Health. Dr. Zheutlin reported receiving grants from the NIH during the conduct of the study.
A version of this article first appeared on Medscape.com.
Therapeutic inertia regarding intensification of blood pressure treatment has been shown to be more of an issue in Black patients, but this was not the case in the SPRINT trial, which involved a strict standardized approach to blood pressure management, a new analysis shows.
“Overall, we found that therapeutic inertia was similar in different races in the SPRINT trial. We did not see disparities that have been reported in previous observational studies,” lead author, Alexander Zheutlin, MD, University of Utah School of Medicine, Salt Lake City, told this news organization.
“These results show that a well-resourced approach in which a standardized approach to blood pressure measurement and treatment intensification is followed can overcome the racial disparity that is seen in therapeutic inertia and the treatment of blood pressure,” he added.
The study was published online in JAMA Network Open on Jan. 10.
The authors explain that hypertension remains a leading modifiable cause of racial disparities in cardiovascular disease. Despite similar treatment rates and increased availability of safe, effective, and affordable antihypertensive medications, blood pressure control rates among Black and Hispanic adults remain significantly lower than among White adults in the United States, and one of the factors contributing to this is thought to be therapeutic inertia – the phenomenon of clinicians not initiating or up-titrating clinically indicated therapy in the setting of unmet treatment goals.
The current analysis of the SPRINT trial was conducted to investigate whether racial and ethnic differences in therapeutic inertia in hypertension were present when blood pressure care was standardized and protocolized.
The landmark SPRINT trial compared intensive (<120 mm Hg) with standard (<140 mm Hg) systolic blood pressure treatment goals in adults 50 years and older at high risk for cardiovascular disease. The present analysis was restricted to participant visits with measured blood pressure above the target goal and included 4,141 patients in the standard group and 4,415 patients in the intensive group.
Results showed that the overall prevalence of therapeutic inertia – defined as no antihypertensive medication intensification at each study visit where the blood pressure was above target goal – was either similar or lower for Black and Hispanic participants than for White participants. This pattern was observed whether participants were randomized to the standard or intensive treatment group.
“These findings support the idea that a standardized approach to blood pressure management, as implemented in SPRINT, may help ensure equitable care is provided to all patients and could reduce the contribution of therapeutic inertia to disparities in uncontrolled blood pressure,” the authors say.
They point out that therapeutic inertia has been identified as a key clinician-level barrier to blood pressure control and is estimated to be present in more than 80% of clinic visits in community practice, whereas in the current analysis of the SPRINT trial, therapeutic inertia was present in 50% to 60% of participant visits with uncontrolled blood pressure.
“In SPRINT, blood pressure had to be measured at defined intervals with a specific method, and there were clear instructions on intensifying treatment if blood pressure was above a certain goal,” Dr. Zheutlin noted. “Our results show that within such strict confines, therapeutic inertia does not seem to be different between different racial groups. This suggests that we could make better gains in blood pressure control and more equitable treatment if we adopted a standardized approach to hypertension management.”
He added: “Many guidelines have been published on when to start treatment and the targets for blood pressure, but there is a lot of variation in how we turn these guidelines into protocols. We need to bring in more consistent protocols on blood pressure measurement and intensification and ensure they are followed. In practice, if the BP is 5 or 10 mm Hg above target, a clinician may defer a decision to intensify treatment and intensification never gets done. But if there was a strict protocol to follow, there would be less chance of this happening.”
Therapeutic inertia still high
In an accompanying commentary, Matthew Rivara, MD, Nisha Bansal, MD, and Bessie Young, MD, University of Washington, Seattle, say the current SPRINT analysis has broad implications for reducing racial and ethnic disparities in achievement of evidence-based treatment targets in the general population.
“In hypertension management, standardized protocols for medication adjustments may limit clinician practice heterogeneity to ultimately reduce differences in blood pressure control among racial and ethnic minority populations,” they write. But they add that such protocols must be implemented thoughtfully to incorporate individualized clinical assessment and clinician-patient shared decision-making.
Dr. Rivara et al. point out that the rates of therapeutic inertia in SPRINT, while lower than community-based estimates, were still very high. They suggest reasons for this could include clinician concerns about medication efficacy, adverse effects, and patient mistrust of medical professionals. Outside the clinical trial environment, additional considerations may include prescription drug and laboratory test costs, pharmacy access, and competing demands during busy clinic visits.
To address these challenges, they say that clinicians need education on current clinical practice guidelines, managing complications of intensified antihypertensive therapies, and shared decisionmaking, including culturally sensitive collaborative care. Similarly, care systems must support patients on how to address concerns about treatments.
Finally, further research is needed to better define the specific factors associated with therapeutic inertia to allow tailored interventions to overcome this inertia.
“In designing and performing such research, it is vital that investigators engage with racial and ethnic minority groups to better explore the intersection of race, ethnicity, therapeutic decision-making, trust, and shared decisionmaking,” they add.
The SPRINT trial was funded with federal funds from the National Institutes of Health. Dr. Zheutlin reported receiving grants from the NIH during the conduct of the study.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Cervical cancer screening rates on the decline in the U.S.
The number of women screened for cervical cancer in the United States declined between 2005 and 2019 with lack of knowledge about the need for screening being cited as the most common reason for not receiving up-to-date screening. These are the results of a population-based, cross-sectional study conducted by the U.S. Preventive Services Task Force and were published online in JAMA Network Open.
“The fact that this reason increased over time across most sociodemographic groups suggests a need for interventions targeting screening awareness for all women,” lead author Ryan Suk, PhD, MS, from the University of Texas Health Science Center, Houston, and colleagues wrote.
Between 2005 and 2019, the researchers evaluated data from 20,557 women (weighted, 113.1 million women) included in the U.S. National Health Interview Survey. The cohort included women aged 21-65 years without previous hysterectomy and included data on sociodemographic factors such as race, ethnicity, sexual orientation, health insurance type, and rurality of residence.
Dr. Suk and colleagues found that the proportion of women without current screening increased from 2005 to 2019 (from 14.4% to 23.0%; P < .001) and that a higher proportion of those women were in the 21- to 29-year age group (weighted, 29.1%), compared with women in the 30- to 65-year age group (weighted, 21.1%; P < .001). Regardless of age, not knowing that screening was indicated was the most common reason cited for not having up-to-date screening.
Sociodemographic factors influence on rates and reasons for overdue screening
Based on weighted population estimates, 6.1% of women included were Asian, 17.2% were Hispanic, 13.1% were non-Hispanic Black, 61% were non-Hispanic White, and 2.7% were other races and/or ethnicities.
Dr. Suk and colleagues found that Asian women had the highest rates of overdue screening, compared with non-Hispanic White women, who had the lowest rates (weighted, 31.4% vs. 20.1%, respectively). The authors also found that reasons for overdue screening varied by sociodemographic factors. For example, while both Asian and Hispanic women cited lack of knowledge as a barrier to routine screening, Asian women were more likely to also report lack of recommendation from a health care professional as a barrier while Hispanic women were more likely to also report lack of access as a barrier to timely screening.
Over the 14-year study period, higher rates of overdue screening were also noted among those identifying as LGBTQ+ versus heterosexual (32.0% vs. 22.2%; P < .001), those with no insurance versus private insurance (41.7% vs. 18.1%; P < .001), and those living in rural versus urban areas (26.2% vs. 22.6%; P = .04).
For the study, guideline-concordant, up-to-date screening in 2005 was defined as screening every 3 years for women aged 21-65 years based on USPSTF guidelines and clinical recommendations. For 2019, up-to-date screening was defined as screening every 3 years with a Papanicolaou (Pap smear) test alone for women aged 21-29 years and screening every 3 years with a Pap smear alone or every 5 years with high-risk human papillomavirus testing or cotesting for women aged 30-65 years.
Dr. Suk and colleagues suggested that guideline updates over the study period could have led to uncertainty regarding appropriate timing and recommended screening intervals, which in turn, may have played a role in decreased cancer screening recommendations.
“Studies have suggested that changing guidelines may produce an increase in both overscreening and underscreening but those already at higher risk of cervical cancer may be most susceptible to underscreening,” wrote the authors.
In an interview, Ruchi Garg, MD, from Mid Atlantic Gynecologic Oncology and Pelvic Surgery Associates, Fairfax, Va., commented: “I think it has been hard to keep up with the guidelines changing so frequently. Furthermore it’s not clearly delineated (or at least there seems to be confusion or extrapolation) that the guidelines are just for Pap smear and that it doesn’t translate into a well woman checkup/pelvic exam; [however], if physicians continue to tell the patients to come in every year, then there won’t be so much underscreening since the physicians/providers will be able to keep track of when the Pap smears need to get done.”
Similar to the study authors, Dr. Garg also suggested that community lectures and public health announcements, particularly when guidelines are updated, will be helpful in enhancing patient education and reducing the rate of this preventable cancer.
The study authors and commentator disclosed no relevant financial relationships.
The number of women screened for cervical cancer in the United States declined between 2005 and 2019 with lack of knowledge about the need for screening being cited as the most common reason for not receiving up-to-date screening. These are the results of a population-based, cross-sectional study conducted by the U.S. Preventive Services Task Force and were published online in JAMA Network Open.
“The fact that this reason increased over time across most sociodemographic groups suggests a need for interventions targeting screening awareness for all women,” lead author Ryan Suk, PhD, MS, from the University of Texas Health Science Center, Houston, and colleagues wrote.
Between 2005 and 2019, the researchers evaluated data from 20,557 women (weighted, 113.1 million women) included in the U.S. National Health Interview Survey. The cohort included women aged 21-65 years without previous hysterectomy and included data on sociodemographic factors such as race, ethnicity, sexual orientation, health insurance type, and rurality of residence.
Dr. Suk and colleagues found that the proportion of women without current screening increased from 2005 to 2019 (from 14.4% to 23.0%; P < .001) and that a higher proportion of those women were in the 21- to 29-year age group (weighted, 29.1%), compared with women in the 30- to 65-year age group (weighted, 21.1%; P < .001). Regardless of age, not knowing that screening was indicated was the most common reason cited for not having up-to-date screening.
Sociodemographic factors influence on rates and reasons for overdue screening
Based on weighted population estimates, 6.1% of women included were Asian, 17.2% were Hispanic, 13.1% were non-Hispanic Black, 61% were non-Hispanic White, and 2.7% were other races and/or ethnicities.
Dr. Suk and colleagues found that Asian women had the highest rates of overdue screening, compared with non-Hispanic White women, who had the lowest rates (weighted, 31.4% vs. 20.1%, respectively). The authors also found that reasons for overdue screening varied by sociodemographic factors. For example, while both Asian and Hispanic women cited lack of knowledge as a barrier to routine screening, Asian women were more likely to also report lack of recommendation from a health care professional as a barrier while Hispanic women were more likely to also report lack of access as a barrier to timely screening.
Over the 14-year study period, higher rates of overdue screening were also noted among those identifying as LGBTQ+ versus heterosexual (32.0% vs. 22.2%; P < .001), those with no insurance versus private insurance (41.7% vs. 18.1%; P < .001), and those living in rural versus urban areas (26.2% vs. 22.6%; P = .04).
For the study, guideline-concordant, up-to-date screening in 2005 was defined as screening every 3 years for women aged 21-65 years based on USPSTF guidelines and clinical recommendations. For 2019, up-to-date screening was defined as screening every 3 years with a Papanicolaou (Pap smear) test alone for women aged 21-29 years and screening every 3 years with a Pap smear alone or every 5 years with high-risk human papillomavirus testing or cotesting for women aged 30-65 years.
Dr. Suk and colleagues suggested that guideline updates over the study period could have led to uncertainty regarding appropriate timing and recommended screening intervals, which in turn, may have played a role in decreased cancer screening recommendations.
“Studies have suggested that changing guidelines may produce an increase in both overscreening and underscreening but those already at higher risk of cervical cancer may be most susceptible to underscreening,” wrote the authors.
In an interview, Ruchi Garg, MD, from Mid Atlantic Gynecologic Oncology and Pelvic Surgery Associates, Fairfax, Va., commented: “I think it has been hard to keep up with the guidelines changing so frequently. Furthermore it’s not clearly delineated (or at least there seems to be confusion or extrapolation) that the guidelines are just for Pap smear and that it doesn’t translate into a well woman checkup/pelvic exam; [however], if physicians continue to tell the patients to come in every year, then there won’t be so much underscreening since the physicians/providers will be able to keep track of when the Pap smears need to get done.”
Similar to the study authors, Dr. Garg also suggested that community lectures and public health announcements, particularly when guidelines are updated, will be helpful in enhancing patient education and reducing the rate of this preventable cancer.
The study authors and commentator disclosed no relevant financial relationships.
The number of women screened for cervical cancer in the United States declined between 2005 and 2019 with lack of knowledge about the need for screening being cited as the most common reason for not receiving up-to-date screening. These are the results of a population-based, cross-sectional study conducted by the U.S. Preventive Services Task Force and were published online in JAMA Network Open.
“The fact that this reason increased over time across most sociodemographic groups suggests a need for interventions targeting screening awareness for all women,” lead author Ryan Suk, PhD, MS, from the University of Texas Health Science Center, Houston, and colleagues wrote.
Between 2005 and 2019, the researchers evaluated data from 20,557 women (weighted, 113.1 million women) included in the U.S. National Health Interview Survey. The cohort included women aged 21-65 years without previous hysterectomy and included data on sociodemographic factors such as race, ethnicity, sexual orientation, health insurance type, and rurality of residence.
Dr. Suk and colleagues found that the proportion of women without current screening increased from 2005 to 2019 (from 14.4% to 23.0%; P < .001) and that a higher proportion of those women were in the 21- to 29-year age group (weighted, 29.1%), compared with women in the 30- to 65-year age group (weighted, 21.1%; P < .001). Regardless of age, not knowing that screening was indicated was the most common reason cited for not having up-to-date screening.
Sociodemographic factors influence on rates and reasons for overdue screening
Based on weighted population estimates, 6.1% of women included were Asian, 17.2% were Hispanic, 13.1% were non-Hispanic Black, 61% were non-Hispanic White, and 2.7% were other races and/or ethnicities.
Dr. Suk and colleagues found that Asian women had the highest rates of overdue screening, compared with non-Hispanic White women, who had the lowest rates (weighted, 31.4% vs. 20.1%, respectively). The authors also found that reasons for overdue screening varied by sociodemographic factors. For example, while both Asian and Hispanic women cited lack of knowledge as a barrier to routine screening, Asian women were more likely to also report lack of recommendation from a health care professional as a barrier while Hispanic women were more likely to also report lack of access as a barrier to timely screening.
Over the 14-year study period, higher rates of overdue screening were also noted among those identifying as LGBTQ+ versus heterosexual (32.0% vs. 22.2%; P < .001), those with no insurance versus private insurance (41.7% vs. 18.1%; P < .001), and those living in rural versus urban areas (26.2% vs. 22.6%; P = .04).
For the study, guideline-concordant, up-to-date screening in 2005 was defined as screening every 3 years for women aged 21-65 years based on USPSTF guidelines and clinical recommendations. For 2019, up-to-date screening was defined as screening every 3 years with a Papanicolaou (Pap smear) test alone for women aged 21-29 years and screening every 3 years with a Pap smear alone or every 5 years with high-risk human papillomavirus testing or cotesting for women aged 30-65 years.
Dr. Suk and colleagues suggested that guideline updates over the study period could have led to uncertainty regarding appropriate timing and recommended screening intervals, which in turn, may have played a role in decreased cancer screening recommendations.
“Studies have suggested that changing guidelines may produce an increase in both overscreening and underscreening but those already at higher risk of cervical cancer may be most susceptible to underscreening,” wrote the authors.
In an interview, Ruchi Garg, MD, from Mid Atlantic Gynecologic Oncology and Pelvic Surgery Associates, Fairfax, Va., commented: “I think it has been hard to keep up with the guidelines changing so frequently. Furthermore it’s not clearly delineated (or at least there seems to be confusion or extrapolation) that the guidelines are just for Pap smear and that it doesn’t translate into a well woman checkup/pelvic exam; [however], if physicians continue to tell the patients to come in every year, then there won’t be so much underscreening since the physicians/providers will be able to keep track of when the Pap smears need to get done.”
Similar to the study authors, Dr. Garg also suggested that community lectures and public health announcements, particularly when guidelines are updated, will be helpful in enhancing patient education and reducing the rate of this preventable cancer.
The study authors and commentator disclosed no relevant financial relationships.
FROM JAMA NETWORK OPEN
Severe pain in the frontotemporal area
Migraine is a neurologic disease characterized by episodes of throbbing, often unilateral, headache. These attacks are associated with visual or other sensory symptoms (classic aura) related to the central nervous system, nausea, and vomiting, and are often set off or exacerbated by physical activity. The age-adjusted prevalence is estimated at 15.9% across all adults, but migraine is much more common in women, with a prevalence of 21% in women and 10.7% in men.
On the basis of the patient's history, clinical suspicion for chronic migraine should be high. Hemiplegic migraine usually presents with temporary unilateral hemiparesis, sometimes with speech disturbance. Attacks of chronic paroxysmal hemicrania are also unilateral but are characterized by their highly intense but short duration. Clinical suspicion for a space-occupying lesion should be raised in cases where patients with a history of headache present with new symptoms or abnormal signs.
The diagnosis of chronic migraine is a clinical one. The American Headache Society defines chronic migraine as at least five attacks of migraine-like or tension type–like headache that must fulfill specific criteria. If the migraine occurs with aura, it must occur 8 days or more per month for more than 3 months and be relieved by a triptan or ergot derivative. If the migraine occurs without aura, the same criteria apply, but it is important that the aforementioned signs and symptoms cannot be accounted for by another diagnosis.
For moderate or severe attacks, migraine-specific agents are recommended: triptans, dihydroergotamine (DHE), small-molecule CGRP receptor antagonists (gepants), and selective serotonin (5-HT1F) receptor agonists (ditans). However, it is accepted that migraine treatment must be individualized, and that a trial-and-error period should be expected. Recent data suggest that about 30% of migraine patients who are prescribed a triptan have an insufficient response to this approach. Some research has shown that such patients have a better response after being switched to a second drug in the triptan class, while other studies have shown no difference. The patient in the current case might also be a candidate for preventive treatment, which should generally be considered when, in spite of acute treatment, migraine interferes with the patient's day-to-day routine or when attacks become frequent. The four CGRP monoclonal antibodies approved in the United States are eptinezumab, erenumab, fremanezumab, and galcanezumab.
Angeliki Vgontzas, MD, Instructor, Department of Neurology, Harvard Medical School; Associate Neurologist, Department of Neurology, Brigham and Women's Hospital/Brigham and Women's Faulkner Hospital, Boston, Massachusetts.
Angeliki Vgontzas, MD, has disclosed no relevant financial relationships.
Migraine is a neurologic disease characterized by episodes of throbbing, often unilateral, headache. These attacks are associated with visual or other sensory symptoms (classic aura) related to the central nervous system, nausea, and vomiting, and are often set off or exacerbated by physical activity. The age-adjusted prevalence is estimated at 15.9% across all adults, but migraine is much more common in women, with a prevalence of 21% in women and 10.7% in men.
On the basis of the patient's history, clinical suspicion for chronic migraine should be high. Hemiplegic migraine usually presents with temporary unilateral hemiparesis, sometimes with speech disturbance. Attacks of chronic paroxysmal hemicrania are also unilateral but are characterized by their highly intense but short duration. Clinical suspicion for a space-occupying lesion should be raised in cases where patients with a history of headache present with new symptoms or abnormal signs.
The diagnosis of chronic migraine is a clinical one. The American Headache Society defines chronic migraine as at least five attacks of migraine-like or tension type–like headache that must fulfill specific criteria. If the migraine occurs with aura, it must occur 8 days or more per month for more than 3 months and be relieved by a triptan or ergot derivative. If the migraine occurs without aura, the same criteria apply, but it is important that the aforementioned signs and symptoms cannot be accounted for by another diagnosis.
For moderate or severe attacks, migraine-specific agents are recommended: triptans, dihydroergotamine (DHE), small-molecule CGRP receptor antagonists (gepants), and selective serotonin (5-HT1F) receptor agonists (ditans). However, it is accepted that migraine treatment must be individualized, and that a trial-and-error period should be expected. Recent data suggest that about 30% of migraine patients who are prescribed a triptan have an insufficient response to this approach. Some research has shown that such patients have a better response after being switched to a second drug in the triptan class, while other studies have shown no difference. The patient in the current case might also be a candidate for preventive treatment, which should generally be considered when, in spite of acute treatment, migraine interferes with the patient's day-to-day routine or when attacks become frequent. The four CGRP monoclonal antibodies approved in the United States are eptinezumab, erenumab, fremanezumab, and galcanezumab.
Angeliki Vgontzas, MD, Instructor, Department of Neurology, Harvard Medical School; Associate Neurologist, Department of Neurology, Brigham and Women's Hospital/Brigham and Women's Faulkner Hospital, Boston, Massachusetts.
Angeliki Vgontzas, MD, has disclosed no relevant financial relationships.
Migraine is a neurologic disease characterized by episodes of throbbing, often unilateral, headache. These attacks are associated with visual or other sensory symptoms (classic aura) related to the central nervous system, nausea, and vomiting, and are often set off or exacerbated by physical activity. The age-adjusted prevalence is estimated at 15.9% across all adults, but migraine is much more common in women, with a prevalence of 21% in women and 10.7% in men.
On the basis of the patient's history, clinical suspicion for chronic migraine should be high. Hemiplegic migraine usually presents with temporary unilateral hemiparesis, sometimes with speech disturbance. Attacks of chronic paroxysmal hemicrania are also unilateral but are characterized by their highly intense but short duration. Clinical suspicion for a space-occupying lesion should be raised in cases where patients with a history of headache present with new symptoms or abnormal signs.
The diagnosis of chronic migraine is a clinical one. The American Headache Society defines chronic migraine as at least five attacks of migraine-like or tension type–like headache that must fulfill specific criteria. If the migraine occurs with aura, it must occur 8 days or more per month for more than 3 months and be relieved by a triptan or ergot derivative. If the migraine occurs without aura, the same criteria apply, but it is important that the aforementioned signs and symptoms cannot be accounted for by another diagnosis.
For moderate or severe attacks, migraine-specific agents are recommended: triptans, dihydroergotamine (DHE), small-molecule CGRP receptor antagonists (gepants), and selective serotonin (5-HT1F) receptor agonists (ditans). However, it is accepted that migraine treatment must be individualized, and that a trial-and-error period should be expected. Recent data suggest that about 30% of migraine patients who are prescribed a triptan have an insufficient response to this approach. Some research has shown that such patients have a better response after being switched to a second drug in the triptan class, while other studies have shown no difference. The patient in the current case might also be a candidate for preventive treatment, which should generally be considered when, in spite of acute treatment, migraine interferes with the patient's day-to-day routine or when attacks become frequent. The four CGRP monoclonal antibodies approved in the United States are eptinezumab, erenumab, fremanezumab, and galcanezumab.
Angeliki Vgontzas, MD, Instructor, Department of Neurology, Harvard Medical School; Associate Neurologist, Department of Neurology, Brigham and Women's Hospital/Brigham and Women's Faulkner Hospital, Boston, Massachusetts.
Angeliki Vgontzas, MD, has disclosed no relevant financial relationships.
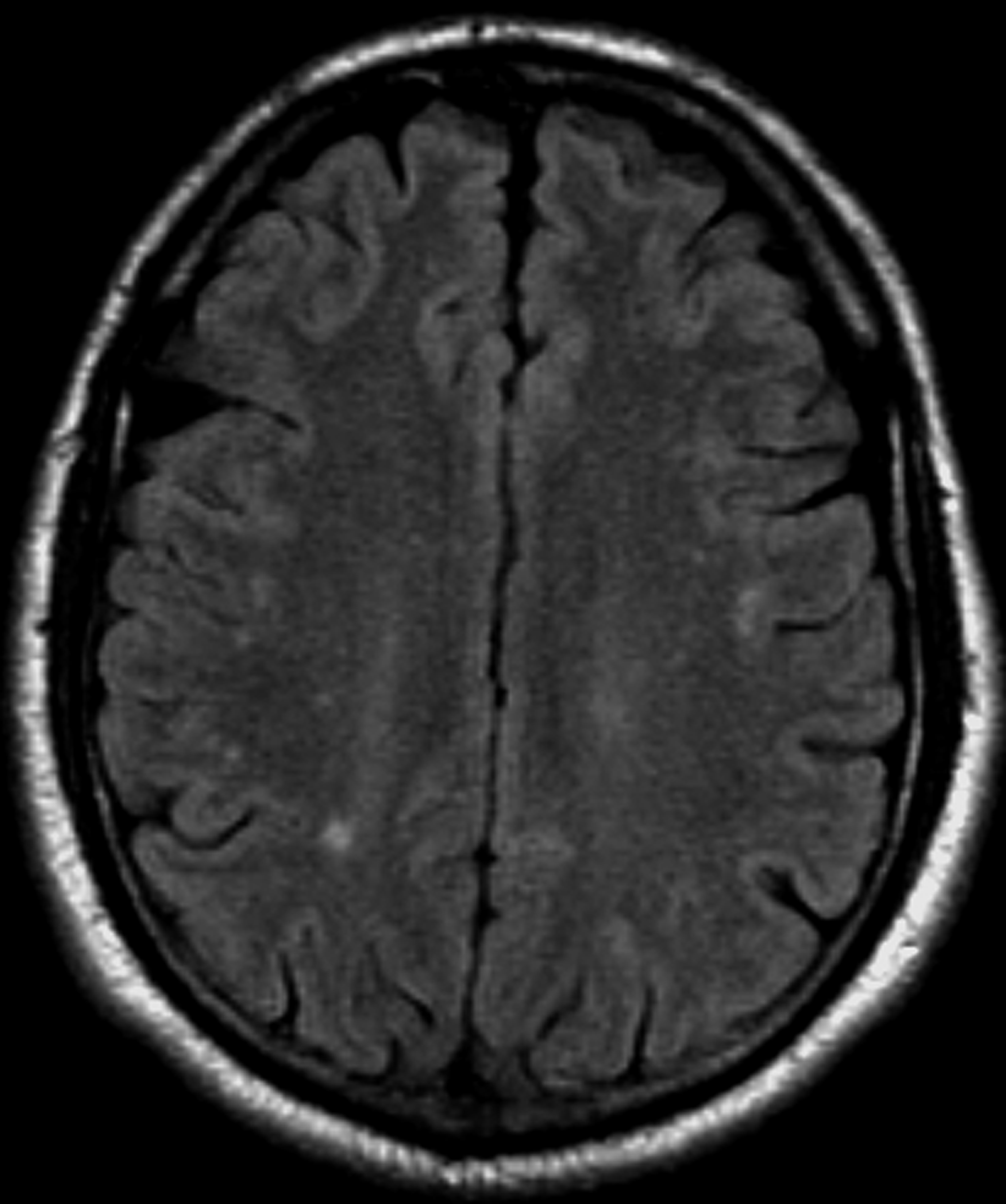
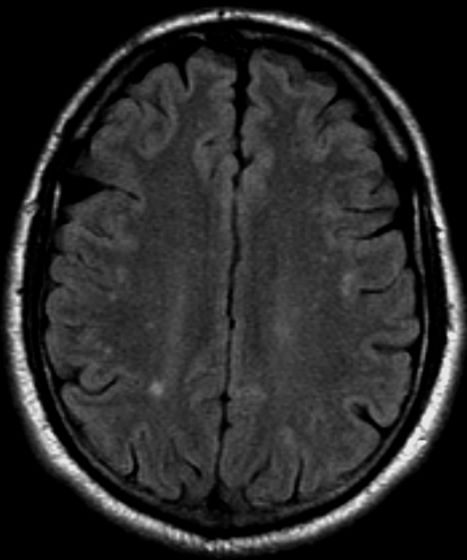
A 36-year-old man presents with severe pain in the frontotemporal area. He reports a history of severe headaches, sometimes with nausea. In the past year, these symptoms have begun to "knock him out" for nearly 2 weeks out of a month. The patient historically has been able to curtail his symptoms with a triptan. Physical examination is remarkable for Adie tonic pupil. A 1.5 T MRI of the brain is performed. Axial FLAIR sequence reveals scattered white matter lesions consistent with foci of demyelination.
Clinical Edge Journal Scan Commentary: HCC January 2022

For many years, sorafenib was the only FDA-approved systemic treatment for patients with uHCC. Initial case reports of remarkable responses of tumors to immunotherapy, and results of the Phase I/II CheckMate-040 clinical trial, led to the September 2017 FDA approval of nivolumab for the treatment of patients with uHCC after progression on sorafenib. Thereafter, several randomized clinical trials comparing sorafenib to immunotherapy and immunotherapy combinations were initiated, including the comparison of nivolumab to sorafenib. In June 2019 it was announced that this trial did not reach its prespecified endpoint, and the FDA approval for the uHCC indication was voluntarily withdrawn. In December 2021, Yau et al published the final results of the CheckMate-459 randomized trial that included 743 adult patients with advanced HCC randomly assigned to receive either nivolumab (n=371) or sorafenib (n=372) in the first line setting. The primary endpoint was overall survival (OS) assessed in the intention-to-treat population. The median OS was 16.4 months (95% CI 13.9–18.4) with nivolumab and 14.7 months (11.9–17.2) with sorafenib (hazard ratio 0.85 [95% CI 0.72–1.02]; P = 0.075; minimum follow-up 22.8 months). Serious treatment-related adverse events were reported in 43 (12%) patients receiving nivolumab and 39 (11%) patients receiving sorafenib. The authors concluded that though first-line nivolumab treatment did not significantly improve OS compared with sorafenib, single-agent nivolumab might be considered a treatment option for patients in whom tyrosine kinase inhibitors or antiangiogenic drugs are not safe.
Cheng et al reported an update on the outcomes of the IMbrave150 study, 12 months after the primary analysis. This study established atezolizumab and bevacizumab as the current standard of care for the initial systemic treatment of patients with uHCC. The median OS was 19.2 months (95% CI 17.0-23.7) with atezolizumab/bevacizumab and 13.4 months (95% CI 11.4-16.9) with sorafenib (hazard ratio [HR], 0.66; 95% CI 0.52-0.85; descriptive P < 0.001). The overall response rate (ORR) was 30% with atezolizumab/bevacizumab, while treatment-related grade 3/4 adverse events occurred in 143 (43%) of 329 receiving atezolizumab/bevacizumab and 72 (46%) of 156 receiving sorafenib. Treatment-related grade 5 events occurred in 6 (2%) and 1 (<1%) patients. Therefore, atezolizumab/bevacizumab remains the first-line standard of care for patients with uHCC.
Finally, Jácome et al undertook a combined analysis of 3 randomized controlled trials (KEYNOTE-240, CheckMate-459, and IMbrave150), with 1,657 patients with uHCC and who were treated with either immunotherapy (n=985) or sorafenib (in the first-line setting) or placebo (in the sorafenib-refractory setting) (n=672). The conclusion of the meta-analysis was that checkpoint inhibitors were associated with superior OS (HR, 0.75; P = .006), progression-free survival (HR, 0.74; P = .03), and ORR (odds ratio [OR], 2.82; P < .001) and lower odds of grade 3 or 4 treatment-related adverse events (OR, 0.44; P = .04) than the comparators, confirming that immunotherapy remains an integral part of the treatment of patients with uHCC.
For many years, sorafenib was the only FDA-approved systemic treatment for patients with uHCC. Initial case reports of remarkable responses of tumors to immunotherapy, and results of the Phase I/II CheckMate-040 clinical trial, led to the September 2017 FDA approval of nivolumab for the treatment of patients with uHCC after progression on sorafenib. Thereafter, several randomized clinical trials comparing sorafenib to immunotherapy and immunotherapy combinations were initiated, including the comparison of nivolumab to sorafenib. In June 2019 it was announced that this trial did not reach its prespecified endpoint, and the FDA approval for the uHCC indication was voluntarily withdrawn. In December 2021, Yau et al published the final results of the CheckMate-459 randomized trial that included 743 adult patients with advanced HCC randomly assigned to receive either nivolumab (n=371) or sorafenib (n=372) in the first line setting. The primary endpoint was overall survival (OS) assessed in the intention-to-treat population. The median OS was 16.4 months (95% CI 13.9–18.4) with nivolumab and 14.7 months (11.9–17.2) with sorafenib (hazard ratio 0.85 [95% CI 0.72–1.02]; P = 0.075; minimum follow-up 22.8 months). Serious treatment-related adverse events were reported in 43 (12%) patients receiving nivolumab and 39 (11%) patients receiving sorafenib. The authors concluded that though first-line nivolumab treatment did not significantly improve OS compared with sorafenib, single-agent nivolumab might be considered a treatment option for patients in whom tyrosine kinase inhibitors or antiangiogenic drugs are not safe.
Cheng et al reported an update on the outcomes of the IMbrave150 study, 12 months after the primary analysis. This study established atezolizumab and bevacizumab as the current standard of care for the initial systemic treatment of patients with uHCC. The median OS was 19.2 months (95% CI 17.0-23.7) with atezolizumab/bevacizumab and 13.4 months (95% CI 11.4-16.9) with sorafenib (hazard ratio [HR], 0.66; 95% CI 0.52-0.85; descriptive P < 0.001). The overall response rate (ORR) was 30% with atezolizumab/bevacizumab, while treatment-related grade 3/4 adverse events occurred in 143 (43%) of 329 receiving atezolizumab/bevacizumab and 72 (46%) of 156 receiving sorafenib. Treatment-related grade 5 events occurred in 6 (2%) and 1 (<1%) patients. Therefore, atezolizumab/bevacizumab remains the first-line standard of care for patients with uHCC.
Finally, Jácome et al undertook a combined analysis of 3 randomized controlled trials (KEYNOTE-240, CheckMate-459, and IMbrave150), with 1,657 patients with uHCC and who were treated with either immunotherapy (n=985) or sorafenib (in the first-line setting) or placebo (in the sorafenib-refractory setting) (n=672). The conclusion of the meta-analysis was that checkpoint inhibitors were associated with superior OS (HR, 0.75; P = .006), progression-free survival (HR, 0.74; P = .03), and ORR (odds ratio [OR], 2.82; P < .001) and lower odds of grade 3 or 4 treatment-related adverse events (OR, 0.44; P = .04) than the comparators, confirming that immunotherapy remains an integral part of the treatment of patients with uHCC.
For many years, sorafenib was the only FDA-approved systemic treatment for patients with uHCC. Initial case reports of remarkable responses of tumors to immunotherapy, and results of the Phase I/II CheckMate-040 clinical trial, led to the September 2017 FDA approval of nivolumab for the treatment of patients with uHCC after progression on sorafenib. Thereafter, several randomized clinical trials comparing sorafenib to immunotherapy and immunotherapy combinations were initiated, including the comparison of nivolumab to sorafenib. In June 2019 it was announced that this trial did not reach its prespecified endpoint, and the FDA approval for the uHCC indication was voluntarily withdrawn. In December 2021, Yau et al published the final results of the CheckMate-459 randomized trial that included 743 adult patients with advanced HCC randomly assigned to receive either nivolumab (n=371) or sorafenib (n=372) in the first line setting. The primary endpoint was overall survival (OS) assessed in the intention-to-treat population. The median OS was 16.4 months (95% CI 13.9–18.4) with nivolumab and 14.7 months (11.9–17.2) with sorafenib (hazard ratio 0.85 [95% CI 0.72–1.02]; P = 0.075; minimum follow-up 22.8 months). Serious treatment-related adverse events were reported in 43 (12%) patients receiving nivolumab and 39 (11%) patients receiving sorafenib. The authors concluded that though first-line nivolumab treatment did not significantly improve OS compared with sorafenib, single-agent nivolumab might be considered a treatment option for patients in whom tyrosine kinase inhibitors or antiangiogenic drugs are not safe.
Cheng et al reported an update on the outcomes of the IMbrave150 study, 12 months after the primary analysis. This study established atezolizumab and bevacizumab as the current standard of care for the initial systemic treatment of patients with uHCC. The median OS was 19.2 months (95% CI 17.0-23.7) with atezolizumab/bevacizumab and 13.4 months (95% CI 11.4-16.9) with sorafenib (hazard ratio [HR], 0.66; 95% CI 0.52-0.85; descriptive P < 0.001). The overall response rate (ORR) was 30% with atezolizumab/bevacizumab, while treatment-related grade 3/4 adverse events occurred in 143 (43%) of 329 receiving atezolizumab/bevacizumab and 72 (46%) of 156 receiving sorafenib. Treatment-related grade 5 events occurred in 6 (2%) and 1 (<1%) patients. Therefore, atezolizumab/bevacizumab remains the first-line standard of care for patients with uHCC.
Finally, Jácome et al undertook a combined analysis of 3 randomized controlled trials (KEYNOTE-240, CheckMate-459, and IMbrave150), with 1,657 patients with uHCC and who were treated with either immunotherapy (n=985) or sorafenib (in the first-line setting) or placebo (in the sorafenib-refractory setting) (n=672). The conclusion of the meta-analysis was that checkpoint inhibitors were associated with superior OS (HR, 0.75; P = .006), progression-free survival (HR, 0.74; P = .03), and ORR (odds ratio [OR], 2.82; P < .001) and lower odds of grade 3 or 4 treatment-related adverse events (OR, 0.44; P = .04) than the comparators, confirming that immunotherapy remains an integral part of the treatment of patients with uHCC.
AI holds its own against pathologists for prostate cancer diagnosis
AI has shown promise in the diagnosis and grading of prostate cancer. However studies so far have been siloed, “with limited proof for generalization across diverse multinational cohorts, representing one of the central barriers to implementation of AI algorithms in clinical practice,” the investigators wrote in Nature Medicine.
Wouter Bulten, from the Radboud Institute for Health Sciences, Radboud University Medical Center, Nijmegen, the Netherlands, and coauthors reported the outcomes of the international PANDA histopathology competition, in which 1,290 deep learning algorithm developers were challenged to come up with reproducible algorithms that could match the findings of human experts. Deep learning is a form of machine learning in which artificial neural networks “learn” from large datasets and apply that learning in a similar way to the human brain. At least one AI product for detecting prostate cancer – the Paige Prostate system – has already been approved for clinical use in the United States. The Food and Drug Administration authorized marketing it in September 2021, as an adjunct to – but not replacement for – pathologist review.
The developers of the new algorithms participating in the competition were given a set of 10,616 digitized prostate biopsies to learn from, then were tested against a panel of either one to six – depending on the country – experienced uropathologists on a set of 393 digitized slides. A selection of 15 teams were then invited to take part in a validation phase with an additional 1,616 slides.
Within the first 10 days of the competition, one algorithm already achieved greater than 0.90 agreement with the uropathologists; by day 33, the median performance of all the teams in the competition was greater than 0.85 agreement with the human experts.
Algorithms correctly detected tumors in 99.7% of cases
The algorithms selected for validation showed even higher levels of agreement – 0.931 on average (95% confidence interval, 0.918-0.944). These algorithms correctly detected tumors in 99.7% of cases (95% CI, 98.1%-99.7%), and correctly identified 92.9% of negative results (95% CI, 91.9%-96.7%).
When it came to classifying the prostate cancers based on Gleason grade, the algorithms showed significantly more agreement with uropathologists than did an international panel of 13 or 20 general pathologists.
“This higher sensitivity shows promise for reducing pathologist workload by automated identification and exclusion of most benign biopsies from review,” the authors wrote.
The study found that the AI algorithms missed 1%-1.9% of cancers, but the general pathologists missed 1.8%-7.3%. The algorithms demonstrated a sensitivity of 96.4%-98.2% and specificity of 75%-100% for tumors, whereas the pathologists showed a sensitivity of 91.9-96.5% and specificity of 92.3%-95%.
Benign cases were misclassified
The main error that the algorithms made was misclassifying benign cases as ISUP GG 1 cancer. The authors commented that this was likely caused by a shift in the distribution of cases between the training data given to the algorithms and the data set they were validated on.
They also noted that, in one validation set, the algorithms overgraded a “substantial proportion” of ISUP GG 3 cases as GG 4, whereas general pathologists tended to undergrade cases, particularly in the higher-grade cancers.
“These differences suggest that general pathologists supported by AI could reach higher agreements with uropathologists, potentially alleviating some of the rater variability associated with Gleason grading,” they wrote.
The authors also pointed out that the algorithms were validated on individual biopsies from each patient, whereas in the clinical context, a pathologist would likely have multiple biopsies from a single patient.
“Future studies can focus on patient-level evaluation of tissue samples, taking multiple cores and sections into account for the final diagnosis,” they wrote.
The study was supported by the Dutch Cancer Society, Netherlands Organization for Scientific Research, Google, Verily Life Sciences, Swedish Research Council, Swedish Cancer Society, Swedish eScience Research Center, EIT Health, Karolinska Institutet, Åke Wiberg Foundation, Prostatacancerförbundet, Academy of Finland, Cancer Foundation Finland, and ERAPerMed. The authors declared a range of grants and funding outside the study, including from Philips Digital Pathology Solutions. Several authors declared patents related to prostate cancer diagnoses, and 10 were employees of Google.
AI has shown promise in the diagnosis and grading of prostate cancer. However studies so far have been siloed, “with limited proof for generalization across diverse multinational cohorts, representing one of the central barriers to implementation of AI algorithms in clinical practice,” the investigators wrote in Nature Medicine.
Wouter Bulten, from the Radboud Institute for Health Sciences, Radboud University Medical Center, Nijmegen, the Netherlands, and coauthors reported the outcomes of the international PANDA histopathology competition, in which 1,290 deep learning algorithm developers were challenged to come up with reproducible algorithms that could match the findings of human experts. Deep learning is a form of machine learning in which artificial neural networks “learn” from large datasets and apply that learning in a similar way to the human brain. At least one AI product for detecting prostate cancer – the Paige Prostate system – has already been approved for clinical use in the United States. The Food and Drug Administration authorized marketing it in September 2021, as an adjunct to – but not replacement for – pathologist review.
The developers of the new algorithms participating in the competition were given a set of 10,616 digitized prostate biopsies to learn from, then were tested against a panel of either one to six – depending on the country – experienced uropathologists on a set of 393 digitized slides. A selection of 15 teams were then invited to take part in a validation phase with an additional 1,616 slides.
Within the first 10 days of the competition, one algorithm already achieved greater than 0.90 agreement with the uropathologists; by day 33, the median performance of all the teams in the competition was greater than 0.85 agreement with the human experts.
Algorithms correctly detected tumors in 99.7% of cases
The algorithms selected for validation showed even higher levels of agreement – 0.931 on average (95% confidence interval, 0.918-0.944). These algorithms correctly detected tumors in 99.7% of cases (95% CI, 98.1%-99.7%), and correctly identified 92.9% of negative results (95% CI, 91.9%-96.7%).
When it came to classifying the prostate cancers based on Gleason grade, the algorithms showed significantly more agreement with uropathologists than did an international panel of 13 or 20 general pathologists.
“This higher sensitivity shows promise for reducing pathologist workload by automated identification and exclusion of most benign biopsies from review,” the authors wrote.
The study found that the AI algorithms missed 1%-1.9% of cancers, but the general pathologists missed 1.8%-7.3%. The algorithms demonstrated a sensitivity of 96.4%-98.2% and specificity of 75%-100% for tumors, whereas the pathologists showed a sensitivity of 91.9-96.5% and specificity of 92.3%-95%.
Benign cases were misclassified
The main error that the algorithms made was misclassifying benign cases as ISUP GG 1 cancer. The authors commented that this was likely caused by a shift in the distribution of cases between the training data given to the algorithms and the data set they were validated on.
They also noted that, in one validation set, the algorithms overgraded a “substantial proportion” of ISUP GG 3 cases as GG 4, whereas general pathologists tended to undergrade cases, particularly in the higher-grade cancers.
“These differences suggest that general pathologists supported by AI could reach higher agreements with uropathologists, potentially alleviating some of the rater variability associated with Gleason grading,” they wrote.
The authors also pointed out that the algorithms were validated on individual biopsies from each patient, whereas in the clinical context, a pathologist would likely have multiple biopsies from a single patient.
“Future studies can focus on patient-level evaluation of tissue samples, taking multiple cores and sections into account for the final diagnosis,” they wrote.
The study was supported by the Dutch Cancer Society, Netherlands Organization for Scientific Research, Google, Verily Life Sciences, Swedish Research Council, Swedish Cancer Society, Swedish eScience Research Center, EIT Health, Karolinska Institutet, Åke Wiberg Foundation, Prostatacancerförbundet, Academy of Finland, Cancer Foundation Finland, and ERAPerMed. The authors declared a range of grants and funding outside the study, including from Philips Digital Pathology Solutions. Several authors declared patents related to prostate cancer diagnoses, and 10 were employees of Google.
AI has shown promise in the diagnosis and grading of prostate cancer. However studies so far have been siloed, “with limited proof for generalization across diverse multinational cohorts, representing one of the central barriers to implementation of AI algorithms in clinical practice,” the investigators wrote in Nature Medicine.
Wouter Bulten, from the Radboud Institute for Health Sciences, Radboud University Medical Center, Nijmegen, the Netherlands, and coauthors reported the outcomes of the international PANDA histopathology competition, in which 1,290 deep learning algorithm developers were challenged to come up with reproducible algorithms that could match the findings of human experts. Deep learning is a form of machine learning in which artificial neural networks “learn” from large datasets and apply that learning in a similar way to the human brain. At least one AI product for detecting prostate cancer – the Paige Prostate system – has already been approved for clinical use in the United States. The Food and Drug Administration authorized marketing it in September 2021, as an adjunct to – but not replacement for – pathologist review.
The developers of the new algorithms participating in the competition were given a set of 10,616 digitized prostate biopsies to learn from, then were tested against a panel of either one to six – depending on the country – experienced uropathologists on a set of 393 digitized slides. A selection of 15 teams were then invited to take part in a validation phase with an additional 1,616 slides.
Within the first 10 days of the competition, one algorithm already achieved greater than 0.90 agreement with the uropathologists; by day 33, the median performance of all the teams in the competition was greater than 0.85 agreement with the human experts.
Algorithms correctly detected tumors in 99.7% of cases
The algorithms selected for validation showed even higher levels of agreement – 0.931 on average (95% confidence interval, 0.918-0.944). These algorithms correctly detected tumors in 99.7% of cases (95% CI, 98.1%-99.7%), and correctly identified 92.9% of negative results (95% CI, 91.9%-96.7%).
When it came to classifying the prostate cancers based on Gleason grade, the algorithms showed significantly more agreement with uropathologists than did an international panel of 13 or 20 general pathologists.
“This higher sensitivity shows promise for reducing pathologist workload by automated identification and exclusion of most benign biopsies from review,” the authors wrote.
The study found that the AI algorithms missed 1%-1.9% of cancers, but the general pathologists missed 1.8%-7.3%. The algorithms demonstrated a sensitivity of 96.4%-98.2% and specificity of 75%-100% for tumors, whereas the pathologists showed a sensitivity of 91.9-96.5% and specificity of 92.3%-95%.
Benign cases were misclassified
The main error that the algorithms made was misclassifying benign cases as ISUP GG 1 cancer. The authors commented that this was likely caused by a shift in the distribution of cases between the training data given to the algorithms and the data set they were validated on.
They also noted that, in one validation set, the algorithms overgraded a “substantial proportion” of ISUP GG 3 cases as GG 4, whereas general pathologists tended to undergrade cases, particularly in the higher-grade cancers.
“These differences suggest that general pathologists supported by AI could reach higher agreements with uropathologists, potentially alleviating some of the rater variability associated with Gleason grading,” they wrote.
The authors also pointed out that the algorithms were validated on individual biopsies from each patient, whereas in the clinical context, a pathologist would likely have multiple biopsies from a single patient.
“Future studies can focus on patient-level evaluation of tissue samples, taking multiple cores and sections into account for the final diagnosis,” they wrote.
The study was supported by the Dutch Cancer Society, Netherlands Organization for Scientific Research, Google, Verily Life Sciences, Swedish Research Council, Swedish Cancer Society, Swedish eScience Research Center, EIT Health, Karolinska Institutet, Åke Wiberg Foundation, Prostatacancerförbundet, Academy of Finland, Cancer Foundation Finland, and ERAPerMed. The authors declared a range of grants and funding outside the study, including from Philips Digital Pathology Solutions. Several authors declared patents related to prostate cancer diagnoses, and 10 were employees of Google.
FROM FAMILY PRACTICE
SARS-Co-V2 Deserves Our Respect, Can We Provide It Before the Next Variant Arrives?

Health care’s modern-day version of the Greek chorus is growing louder and more persistent. My colleagues and I have long been among them.
In news conferences, journal articles, and podcasts, this chorus is pleading with the public to pay attention to its message: SARs-CoV-2 is not done with us. Omicron can kill; it can infect the vaccinated.
We have found, like everyone else, that Omicron runs on its rules; with Delta, two vaccine shots were able to lower the positivity rate. With Omicron, two shots have not been enough.
The WHO used the word “surprise” in its November announcement that Omicron was a variant of “concern.”
So did Trevor Bedford, a computational biologist and infectious disease scientist at the Fred Hutchinson Cancer Center in Seattle, who said that Omicron “took me and everyone by surprise.”1 Speaking on KevinMD’s podcast, he told his host that with the degree of immunity in the global population, he was expecting subsequent evolving strains to have minor, subtle genetic mutations, akin to how flu varies from year to year. What was a surprise was the giant leap in evolution that occurred with Omicron, which contains 36 mutations in the spike protein and approximately 50 mutations in total. Because of these mutations, the original two-shot mRNA COVID vaccines becomes only 40% effective against symptomatic disease after several months (thankfully a booster shot increases this to ~80%).2 But the decreased vaccine protection without a booster, along with relaxation of mitigation measures, brought us to where we are now.
In Chicago, we knew the Omicron variant would move quickly, considering how it moved through South Africa and the United Kingdom. What we didn’t anticipate was that in one week’s time, our hospital would need to add another 100 dedicated COVID ICU beds. Nor did we anticipate the extent that Omicron would affect staffing levels in the same amount of time.
At our hospital, we have eliminated elective surgeries that require a hospital stay, which includes surgeries for cancer. One of my colleagues, Ryan Merkow, MD, a surgical oncologist, remarked recently he had to cancel half of his scheduled surgeries because of a lack of hospital space.3
Dispelling Myths
What is concerning about this current wave is how many unvaccinated are hospitalized. Because Omicron is so infectious and because of lower vaccination rates in younger adults and children, we have a younger group of adults and children admitted with COVID, who had been uninfected by previous surges.
A major myth that makes health care workers so frustrated is the tale that Omicron is milder. Unvaccinated people infected with this variant are seriously ill and are dying. Despite its “mild” label, once a patient is hospitalized, Omicron can be just as severe as its predecessors.4 For many, getting vaccinated is the difference between staying at home with some symptoms and being in the ICU.
As of January 10, according to the CDC, although 88% of people over the age of 65 are vaccinated, only 37.5% have gotten boosters which are key to restoring protection against Omicron. And among children, only 54% between 12- and 17-years-old are fully vaccinated, and a mere 17% of children aged 5 to 11 have gotten both of their shots.
Remember the conversations regarding natural immunity? Omicron has muffled that conversation. Those who have been infected with SARS-Co-V2 before can still get infected and very ill with Omicron. So now is the time to get vaccinated.
Transmissibility
We knew SARS-CoV-2 could spread 1 of 2 ways: large virus-carrying droplets that enter through the nose, mouth, and eyes, as well as miniscule airborne droplets of virus that float in the air and travel further than 6 feet. However, prior to Omicron, transmission of these smaller droplets via the air was not as frequent. But with Omicron, while it still travels by larger respiratory droplets, it appears to have more airborne spread.
In late December, The Lancet Regional Health published results of research conducted one month earlier at a designated quarantine hotel in Hong Kong.5 The index case was housed in the room across a hallway from the second case, who developed their case 8 days into quarantine. Testing showed the Omicron variant in both cases. Environmental testing of the walls and ceiling suggested airborne spread of the virus in places unreachable by large respiratory droplets.
Now with Omicron, people need to wear high-filtering masks that fit tight against the face, such as a N95, KN-95, or KF-94 if possible. And when removing the mask to eat and drink, one should be in well-ventilated areas, away from others.
People should avoid getting Omicron, regardless of vaccination status. This variant is so infectious that, compared to the Delta variant, people are twice as likely to infect others that live with them. And infecting others leads to a chain of transmission that can close schools, take over hospital beds, and disable or kill the most vulnerable in our communities.
Public and private behavior, and public policy
In July, months before that WHO announced Omicron’s existence, Rella and colleagues reported in Scientific Reports on the outcome of a new model designed to show how a vaccine-resistant strain could rapidly transmit through a highly vaccinated population if transmission mitigation interventions are dropped too soon.6
The authors wrote that the success of a vaccine-resistant strain making inroads into a population depends on the obvious – it finds populations with a low rate of vaccination. What is not so obvious, the authors wrote, is that a vaccine-resistant virus does its worst when transmission is not well controlled in a highly vaccinated population. What can prevent a surge like this are social behaviors and public policy that decrease the chain of transmission of SARS-CoV-2, such as vaccination, masking, and testing.
It is people’s behavior, and ineffective public policy, that are so frustrating to us. The WHO’s secretary general warned against relying solely on vaccines in December. “Vaccines alone will not get any country out of this crisis.”
Omicron takes a new mindset. What we were doing before is not protecting now. Unchecked spread is overwhelming our health care systems and putting the vulnerable in our population at risk. The ramification of this unchecked spread reaches everywhere – into the economy, our educational system, and our nation’s mental health.
When the pandemic started, the policies to control its spread rested on local government and public agencies; we all would have been better served had there been a unified, national response to an infectious threat that does not obey municipal or state boundaries.
The universal sentiment among health care workers is frustration with local and state governments that are either dictating policy that can harm the public we are trying to protect.
As of September, at least 23 state legislatures have passed laws changing a governor’s executive power reach. Many have taken it away. Others are fighting in the courts over mask mandates.
As for when the pandemic will subside, that appears to be up to the public and public policy makers. They will determine how long this will last and how many will die or be disabled before its end.
References
- KevinMD.com. Trevor Bedford on Omicron and what about Covid keeps him up at night. Dec. 17 podcast. https://www.kevinmd.com/blog/post-author/the-podcast-by-kevinmd/page/2
- Andrews N, Stowe J, Kirsebom F, et al. Effectiveness of COVID-19 vaccines against the Omicron (B.1.1.529) variant of concern. MedRxiv. Preprint. doi: https://doi.org/10.1101/2021.12.14.21267615
- Weise E and Shamus KJ. (January 13, 2022). As COVID-19 surges, there are no hospital beds for others in need of care. USA Today. As COVID-19 surges, there are no hospital beds for others in need of care (yahoo.com)
- Wolter N, Jassat W, Walaza S, et al. Early assessment of the clinical severity of the SARS-CoV-2 Omicron variant in South Africa. MedRxiv. Preprint. doi: https://doi.org/10.1101/2021.12.21.21268116
- Shuk-Ching Wong, Albert Ka-Wing Au, Hong Chen et al. Transmission of Omicron (B.1.1.529) - SARS-CoV-2 Variant of Concern in a designated quarantine hotel for travelers: a challenge of elimination strategy of COVID-19. The Lancet Regional Health - Western Pacific. Available online 23 December 2021
- Rella SA, Kulikova YA, Dermitzakis ET, et al. Rates of SARS-CoV-2 transmission and vaccination impact the fate of vaccine-resistant strains. Sci Rep 11, 15729 (2021).
- WHO press conference on coronavirus disease (COVID-19) - 14 December 2021.
- Telebriefing on Covid-19 Update. https://www.cdc.gov/media/releases/2022/t0107-Covid-update.html
- Shuk-Ching Wong, Albert Ka-Wing Au, Hong Chen et al. Transmission of Omicron (B.1.1.529) - SARS-CoV-2 Variant of Concern in a designated quarantine hotel for travelers: a challenge of elimination strategy of COVID-1 The Lancet Regional Health - Western Pacific. Available online 23 December 2021
- CDC. Interim Guidance for Managing Healthcare Personnel with SARS-CoV-2 Infection or Exposure to SARS-CoV-2. Dec. 23, 2021.
- Mariah Timms. Tennessee appeals federal court order temporarily blocking new state law on school masks. Nashville Tennessean. Jan. 3, 2022.
- Statewide Number of Covid-19 Hospitalized Pediatric Patients. Jan. 4, 2022.
- National Conference of State Legislatures. Legislative Oversight of Emergency Executive Powers. Jan. 4, 2022.
https://news.yahoo.com/Covid-surges-others-care-theres-105949790.html
Elizabeth Weise and Kristen Jordan Shamus. As COVID-19 surges, there are no hospital beds for others in need of care. USA Today. Jan. 13, 2022.
Health care’s modern-day version of the Greek chorus is growing louder and more persistent. My colleagues and I have long been among them.
In news conferences, journal articles, and podcasts, this chorus is pleading with the public to pay attention to its message: SARs-CoV-2 is not done with us. Omicron can kill; it can infect the vaccinated.
We have found, like everyone else, that Omicron runs on its rules; with Delta, two vaccine shots were able to lower the positivity rate. With Omicron, two shots have not been enough.
The WHO used the word “surprise” in its November announcement that Omicron was a variant of “concern.”
So did Trevor Bedford, a computational biologist and infectious disease scientist at the Fred Hutchinson Cancer Center in Seattle, who said that Omicron “took me and everyone by surprise.”1 Speaking on KevinMD’s podcast, he told his host that with the degree of immunity in the global population, he was expecting subsequent evolving strains to have minor, subtle genetic mutations, akin to how flu varies from year to year. What was a surprise was the giant leap in evolution that occurred with Omicron, which contains 36 mutations in the spike protein and approximately 50 mutations in total. Because of these mutations, the original two-shot mRNA COVID vaccines becomes only 40% effective against symptomatic disease after several months (thankfully a booster shot increases this to ~80%).2 But the decreased vaccine protection without a booster, along with relaxation of mitigation measures, brought us to where we are now.
In Chicago, we knew the Omicron variant would move quickly, considering how it moved through South Africa and the United Kingdom. What we didn’t anticipate was that in one week’s time, our hospital would need to add another 100 dedicated COVID ICU beds. Nor did we anticipate the extent that Omicron would affect staffing levels in the same amount of time.
At our hospital, we have eliminated elective surgeries that require a hospital stay, which includes surgeries for cancer. One of my colleagues, Ryan Merkow, MD, a surgical oncologist, remarked recently he had to cancel half of his scheduled surgeries because of a lack of hospital space.3
Dispelling Myths
What is concerning about this current wave is how many unvaccinated are hospitalized. Because Omicron is so infectious and because of lower vaccination rates in younger adults and children, we have a younger group of adults and children admitted with COVID, who had been uninfected by previous surges.
A major myth that makes health care workers so frustrated is the tale that Omicron is milder. Unvaccinated people infected with this variant are seriously ill and are dying. Despite its “mild” label, once a patient is hospitalized, Omicron can be just as severe as its predecessors.4 For many, getting vaccinated is the difference between staying at home with some symptoms and being in the ICU.
As of January 10, according to the CDC, although 88% of people over the age of 65 are vaccinated, only 37.5% have gotten boosters which are key to restoring protection against Omicron. And among children, only 54% between 12- and 17-years-old are fully vaccinated, and a mere 17% of children aged 5 to 11 have gotten both of their shots.
Remember the conversations regarding natural immunity? Omicron has muffled that conversation. Those who have been infected with SARS-Co-V2 before can still get infected and very ill with Omicron. So now is the time to get vaccinated.
Transmissibility
We knew SARS-CoV-2 could spread 1 of 2 ways: large virus-carrying droplets that enter through the nose, mouth, and eyes, as well as miniscule airborne droplets of virus that float in the air and travel further than 6 feet. However, prior to Omicron, transmission of these smaller droplets via the air was not as frequent. But with Omicron, while it still travels by larger respiratory droplets, it appears to have more airborne spread.
In late December, The Lancet Regional Health published results of research conducted one month earlier at a designated quarantine hotel in Hong Kong.5 The index case was housed in the room across a hallway from the second case, who developed their case 8 days into quarantine. Testing showed the Omicron variant in both cases. Environmental testing of the walls and ceiling suggested airborne spread of the virus in places unreachable by large respiratory droplets.
Now with Omicron, people need to wear high-filtering masks that fit tight against the face, such as a N95, KN-95, or KF-94 if possible. And when removing the mask to eat and drink, one should be in well-ventilated areas, away from others.
People should avoid getting Omicron, regardless of vaccination status. This variant is so infectious that, compared to the Delta variant, people are twice as likely to infect others that live with them. And infecting others leads to a chain of transmission that can close schools, take over hospital beds, and disable or kill the most vulnerable in our communities.
Public and private behavior, and public policy
In July, months before that WHO announced Omicron’s existence, Rella and colleagues reported in Scientific Reports on the outcome of a new model designed to show how a vaccine-resistant strain could rapidly transmit through a highly vaccinated population if transmission mitigation interventions are dropped too soon.6
The authors wrote that the success of a vaccine-resistant strain making inroads into a population depends on the obvious – it finds populations with a low rate of vaccination. What is not so obvious, the authors wrote, is that a vaccine-resistant virus does its worst when transmission is not well controlled in a highly vaccinated population. What can prevent a surge like this are social behaviors and public policy that decrease the chain of transmission of SARS-CoV-2, such as vaccination, masking, and testing.
It is people’s behavior, and ineffective public policy, that are so frustrating to us. The WHO’s secretary general warned against relying solely on vaccines in December. “Vaccines alone will not get any country out of this crisis.”
Omicron takes a new mindset. What we were doing before is not protecting now. Unchecked spread is overwhelming our health care systems and putting the vulnerable in our population at risk. The ramification of this unchecked spread reaches everywhere – into the economy, our educational system, and our nation’s mental health.
When the pandemic started, the policies to control its spread rested on local government and public agencies; we all would have been better served had there been a unified, national response to an infectious threat that does not obey municipal or state boundaries.
The universal sentiment among health care workers is frustration with local and state governments that are either dictating policy that can harm the public we are trying to protect.
As of September, at least 23 state legislatures have passed laws changing a governor’s executive power reach. Many have taken it away. Others are fighting in the courts over mask mandates.
As for when the pandemic will subside, that appears to be up to the public and public policy makers. They will determine how long this will last and how many will die or be disabled before its end.
Health care’s modern-day version of the Greek chorus is growing louder and more persistent. My colleagues and I have long been among them.
In news conferences, journal articles, and podcasts, this chorus is pleading with the public to pay attention to its message: SARs-CoV-2 is not done with us. Omicron can kill; it can infect the vaccinated.
We have found, like everyone else, that Omicron runs on its rules; with Delta, two vaccine shots were able to lower the positivity rate. With Omicron, two shots have not been enough.
The WHO used the word “surprise” in its November announcement that Omicron was a variant of “concern.”
So did Trevor Bedford, a computational biologist and infectious disease scientist at the Fred Hutchinson Cancer Center in Seattle, who said that Omicron “took me and everyone by surprise.”1 Speaking on KevinMD’s podcast, he told his host that with the degree of immunity in the global population, he was expecting subsequent evolving strains to have minor, subtle genetic mutations, akin to how flu varies from year to year. What was a surprise was the giant leap in evolution that occurred with Omicron, which contains 36 mutations in the spike protein and approximately 50 mutations in total. Because of these mutations, the original two-shot mRNA COVID vaccines becomes only 40% effective against symptomatic disease after several months (thankfully a booster shot increases this to ~80%).2 But the decreased vaccine protection without a booster, along with relaxation of mitigation measures, brought us to where we are now.
In Chicago, we knew the Omicron variant would move quickly, considering how it moved through South Africa and the United Kingdom. What we didn’t anticipate was that in one week’s time, our hospital would need to add another 100 dedicated COVID ICU beds. Nor did we anticipate the extent that Omicron would affect staffing levels in the same amount of time.
At our hospital, we have eliminated elective surgeries that require a hospital stay, which includes surgeries for cancer. One of my colleagues, Ryan Merkow, MD, a surgical oncologist, remarked recently he had to cancel half of his scheduled surgeries because of a lack of hospital space.3
Dispelling Myths
What is concerning about this current wave is how many unvaccinated are hospitalized. Because Omicron is so infectious and because of lower vaccination rates in younger adults and children, we have a younger group of adults and children admitted with COVID, who had been uninfected by previous surges.
A major myth that makes health care workers so frustrated is the tale that Omicron is milder. Unvaccinated people infected with this variant are seriously ill and are dying. Despite its “mild” label, once a patient is hospitalized, Omicron can be just as severe as its predecessors.4 For many, getting vaccinated is the difference between staying at home with some symptoms and being in the ICU.
As of January 10, according to the CDC, although 88% of people over the age of 65 are vaccinated, only 37.5% have gotten boosters which are key to restoring protection against Omicron. And among children, only 54% between 12- and 17-years-old are fully vaccinated, and a mere 17% of children aged 5 to 11 have gotten both of their shots.
Remember the conversations regarding natural immunity? Omicron has muffled that conversation. Those who have been infected with SARS-Co-V2 before can still get infected and very ill with Omicron. So now is the time to get vaccinated.
Transmissibility
We knew SARS-CoV-2 could spread 1 of 2 ways: large virus-carrying droplets that enter through the nose, mouth, and eyes, as well as miniscule airborne droplets of virus that float in the air and travel further than 6 feet. However, prior to Omicron, transmission of these smaller droplets via the air was not as frequent. But with Omicron, while it still travels by larger respiratory droplets, it appears to have more airborne spread.
In late December, The Lancet Regional Health published results of research conducted one month earlier at a designated quarantine hotel in Hong Kong.5 The index case was housed in the room across a hallway from the second case, who developed their case 8 days into quarantine. Testing showed the Omicron variant in both cases. Environmental testing of the walls and ceiling suggested airborne spread of the virus in places unreachable by large respiratory droplets.
Now with Omicron, people need to wear high-filtering masks that fit tight against the face, such as a N95, KN-95, or KF-94 if possible. And when removing the mask to eat and drink, one should be in well-ventilated areas, away from others.
People should avoid getting Omicron, regardless of vaccination status. This variant is so infectious that, compared to the Delta variant, people are twice as likely to infect others that live with them. And infecting others leads to a chain of transmission that can close schools, take over hospital beds, and disable or kill the most vulnerable in our communities.
Public and private behavior, and public policy
In July, months before that WHO announced Omicron’s existence, Rella and colleagues reported in Scientific Reports on the outcome of a new model designed to show how a vaccine-resistant strain could rapidly transmit through a highly vaccinated population if transmission mitigation interventions are dropped too soon.6
The authors wrote that the success of a vaccine-resistant strain making inroads into a population depends on the obvious – it finds populations with a low rate of vaccination. What is not so obvious, the authors wrote, is that a vaccine-resistant virus does its worst when transmission is not well controlled in a highly vaccinated population. What can prevent a surge like this are social behaviors and public policy that decrease the chain of transmission of SARS-CoV-2, such as vaccination, masking, and testing.
It is people’s behavior, and ineffective public policy, that are so frustrating to us. The WHO’s secretary general warned against relying solely on vaccines in December. “Vaccines alone will not get any country out of this crisis.”
Omicron takes a new mindset. What we were doing before is not protecting now. Unchecked spread is overwhelming our health care systems and putting the vulnerable in our population at risk. The ramification of this unchecked spread reaches everywhere – into the economy, our educational system, and our nation’s mental health.
When the pandemic started, the policies to control its spread rested on local government and public agencies; we all would have been better served had there been a unified, national response to an infectious threat that does not obey municipal or state boundaries.
The universal sentiment among health care workers is frustration with local and state governments that are either dictating policy that can harm the public we are trying to protect.
As of September, at least 23 state legislatures have passed laws changing a governor’s executive power reach. Many have taken it away. Others are fighting in the courts over mask mandates.
As for when the pandemic will subside, that appears to be up to the public and public policy makers. They will determine how long this will last and how many will die or be disabled before its end.
References
- KevinMD.com. Trevor Bedford on Omicron and what about Covid keeps him up at night. Dec. 17 podcast. https://www.kevinmd.com/blog/post-author/the-podcast-by-kevinmd/page/2
- Andrews N, Stowe J, Kirsebom F, et al. Effectiveness of COVID-19 vaccines against the Omicron (B.1.1.529) variant of concern. MedRxiv. Preprint. doi: https://doi.org/10.1101/2021.12.14.21267615
- Weise E and Shamus KJ. (January 13, 2022). As COVID-19 surges, there are no hospital beds for others in need of care. USA Today. As COVID-19 surges, there are no hospital beds for others in need of care (yahoo.com)
- Wolter N, Jassat W, Walaza S, et al. Early assessment of the clinical severity of the SARS-CoV-2 Omicron variant in South Africa. MedRxiv. Preprint. doi: https://doi.org/10.1101/2021.12.21.21268116
- Shuk-Ching Wong, Albert Ka-Wing Au, Hong Chen et al. Transmission of Omicron (B.1.1.529) - SARS-CoV-2 Variant of Concern in a designated quarantine hotel for travelers: a challenge of elimination strategy of COVID-19. The Lancet Regional Health - Western Pacific. Available online 23 December 2021
- Rella SA, Kulikova YA, Dermitzakis ET, et al. Rates of SARS-CoV-2 transmission and vaccination impact the fate of vaccine-resistant strains. Sci Rep 11, 15729 (2021).
- WHO press conference on coronavirus disease (COVID-19) - 14 December 2021.
- Telebriefing on Covid-19 Update. https://www.cdc.gov/media/releases/2022/t0107-Covid-update.html
- Shuk-Ching Wong, Albert Ka-Wing Au, Hong Chen et al. Transmission of Omicron (B.1.1.529) - SARS-CoV-2 Variant of Concern in a designated quarantine hotel for travelers: a challenge of elimination strategy of COVID-1 The Lancet Regional Health - Western Pacific. Available online 23 December 2021
- CDC. Interim Guidance for Managing Healthcare Personnel with SARS-CoV-2 Infection or Exposure to SARS-CoV-2. Dec. 23, 2021.
- Mariah Timms. Tennessee appeals federal court order temporarily blocking new state law on school masks. Nashville Tennessean. Jan. 3, 2022.
- Statewide Number of Covid-19 Hospitalized Pediatric Patients. Jan. 4, 2022.
- National Conference of State Legislatures. Legislative Oversight of Emergency Executive Powers. Jan. 4, 2022.
https://news.yahoo.com/Covid-surges-others-care-theres-105949790.html
Elizabeth Weise and Kristen Jordan Shamus. As COVID-19 surges, there are no hospital beds for others in need of care. USA Today. Jan. 13, 2022.
References
- KevinMD.com. Trevor Bedford on Omicron and what about Covid keeps him up at night. Dec. 17 podcast. https://www.kevinmd.com/blog/post-author/the-podcast-by-kevinmd/page/2
- Andrews N, Stowe J, Kirsebom F, et al. Effectiveness of COVID-19 vaccines against the Omicron (B.1.1.529) variant of concern. MedRxiv. Preprint. doi: https://doi.org/10.1101/2021.12.14.21267615
- Weise E and Shamus KJ. (January 13, 2022). As COVID-19 surges, there are no hospital beds for others in need of care. USA Today. As COVID-19 surges, there are no hospital beds for others in need of care (yahoo.com)
- Wolter N, Jassat W, Walaza S, et al. Early assessment of the clinical severity of the SARS-CoV-2 Omicron variant in South Africa. MedRxiv. Preprint. doi: https://doi.org/10.1101/2021.12.21.21268116
- Shuk-Ching Wong, Albert Ka-Wing Au, Hong Chen et al. Transmission of Omicron (B.1.1.529) - SARS-CoV-2 Variant of Concern in a designated quarantine hotel for travelers: a challenge of elimination strategy of COVID-19. The Lancet Regional Health - Western Pacific. Available online 23 December 2021
- Rella SA, Kulikova YA, Dermitzakis ET, et al. Rates of SARS-CoV-2 transmission and vaccination impact the fate of vaccine-resistant strains. Sci Rep 11, 15729 (2021).
- WHO press conference on coronavirus disease (COVID-19) - 14 December 2021.
- Telebriefing on Covid-19 Update. https://www.cdc.gov/media/releases/2022/t0107-Covid-update.html
- Shuk-Ching Wong, Albert Ka-Wing Au, Hong Chen et al. Transmission of Omicron (B.1.1.529) - SARS-CoV-2 Variant of Concern in a designated quarantine hotel for travelers: a challenge of elimination strategy of COVID-1 The Lancet Regional Health - Western Pacific. Available online 23 December 2021
- CDC. Interim Guidance for Managing Healthcare Personnel with SARS-CoV-2 Infection or Exposure to SARS-CoV-2. Dec. 23, 2021.
- Mariah Timms. Tennessee appeals federal court order temporarily blocking new state law on school masks. Nashville Tennessean. Jan. 3, 2022.
- Statewide Number of Covid-19 Hospitalized Pediatric Patients. Jan. 4, 2022.
- National Conference of State Legislatures. Legislative Oversight of Emergency Executive Powers. Jan. 4, 2022.
https://news.yahoo.com/Covid-surges-others-care-theres-105949790.html
Elizabeth Weise and Kristen Jordan Shamus. As COVID-19 surges, there are no hospital beds for others in need of care. USA Today. Jan. 13, 2022.