User login
Endocrine Society and others to FDA: Restrict BPA
The chemical is used to make plastics in items such as food containers, pitchers, and inner linings of metal products. Small amounts of BPA can leak into food and beverages.
The petition points to a December 2021 report by the European Food Safety Authority titled: “Re-evaluation of the risks to public health related to the presence of bisphenol A (BPA) in foodstuffs,” which summarizes evidence gathered since 2013.
It concludes that “there is a health concern from BPA exposure for all age groups.” Specific concerns include harm to the immune system and male and female reproductive systems.
Average American exposed to 5,000 times the safe level of BPA
The EFSA established a new “tolerable daily intake” of BPA of 0.04 ng/kg of body weight per day. By contrast, in 2014 the FDA estimated that the mean BPA intake for the U.S. population older than 2 years was 200 ng/kg bw/day and that the 90th percentile for BPA intake was 500 ng/kg of body weight per day.
“Using FDA’s own exposure estimates, the average American is exposed to more than 5000 times the safe level of 0.04 ng BPA/kg [body weight per day] set by the EFSA expert panel. Without a doubt, these values constitute a high health risk and support the conclusion that uses of BPA are not safe ... Given the magnitude of the overexposure, we request an expedited review by FDA,” the petition reads.
In addition to the Endocrine Society, which has long warned about the dangers of endocrine-disrupting chemicals, other signatories to the petition include the Environmental Defense Fund, Breast Cancer Prevention Partners, Clean Water Action/Clean Water Fund, Consumer Reports, Environmental Working Group, Healthy Babies Bright Futures, and the former director of the National Institute of Environmental Health Sciences and National Toxicology Program.
In a statement, Endocrine Society BPA expert Heather Patisaul, PhD, of North Carolina University, Raleigh, said the report’s findings “are extremely concerning and prove the point that even very low levels of BPA exposure can be harmful and lead to issues with reproductive health, breast cancer risk, behavior, and metabolism.”
“The FDA needs to acknowledge the science behind endocrine-disrupting chemicals and act accordingly to protect public health,” she urged.
The FDA is expected to decide within the next few days whether to open a docket to accept comments.
A final decision could take 6 months or longer, an Endocrine Society spokesperson told this news organization.
A version of this article first appeared on Medscape.com.
The chemical is used to make plastics in items such as food containers, pitchers, and inner linings of metal products. Small amounts of BPA can leak into food and beverages.
The petition points to a December 2021 report by the European Food Safety Authority titled: “Re-evaluation of the risks to public health related to the presence of bisphenol A (BPA) in foodstuffs,” which summarizes evidence gathered since 2013.
It concludes that “there is a health concern from BPA exposure for all age groups.” Specific concerns include harm to the immune system and male and female reproductive systems.
Average American exposed to 5,000 times the safe level of BPA
The EFSA established a new “tolerable daily intake” of BPA of 0.04 ng/kg of body weight per day. By contrast, in 2014 the FDA estimated that the mean BPA intake for the U.S. population older than 2 years was 200 ng/kg bw/day and that the 90th percentile for BPA intake was 500 ng/kg of body weight per day.
“Using FDA’s own exposure estimates, the average American is exposed to more than 5000 times the safe level of 0.04 ng BPA/kg [body weight per day] set by the EFSA expert panel. Without a doubt, these values constitute a high health risk and support the conclusion that uses of BPA are not safe ... Given the magnitude of the overexposure, we request an expedited review by FDA,” the petition reads.
In addition to the Endocrine Society, which has long warned about the dangers of endocrine-disrupting chemicals, other signatories to the petition include the Environmental Defense Fund, Breast Cancer Prevention Partners, Clean Water Action/Clean Water Fund, Consumer Reports, Environmental Working Group, Healthy Babies Bright Futures, and the former director of the National Institute of Environmental Health Sciences and National Toxicology Program.
In a statement, Endocrine Society BPA expert Heather Patisaul, PhD, of North Carolina University, Raleigh, said the report’s findings “are extremely concerning and prove the point that even very low levels of BPA exposure can be harmful and lead to issues with reproductive health, breast cancer risk, behavior, and metabolism.”
“The FDA needs to acknowledge the science behind endocrine-disrupting chemicals and act accordingly to protect public health,” she urged.
The FDA is expected to decide within the next few days whether to open a docket to accept comments.
A final decision could take 6 months or longer, an Endocrine Society spokesperson told this news organization.
A version of this article first appeared on Medscape.com.
The chemical is used to make plastics in items such as food containers, pitchers, and inner linings of metal products. Small amounts of BPA can leak into food and beverages.
The petition points to a December 2021 report by the European Food Safety Authority titled: “Re-evaluation of the risks to public health related to the presence of bisphenol A (BPA) in foodstuffs,” which summarizes evidence gathered since 2013.
It concludes that “there is a health concern from BPA exposure for all age groups.” Specific concerns include harm to the immune system and male and female reproductive systems.
Average American exposed to 5,000 times the safe level of BPA
The EFSA established a new “tolerable daily intake” of BPA of 0.04 ng/kg of body weight per day. By contrast, in 2014 the FDA estimated that the mean BPA intake for the U.S. population older than 2 years was 200 ng/kg bw/day and that the 90th percentile for BPA intake was 500 ng/kg of body weight per day.
“Using FDA’s own exposure estimates, the average American is exposed to more than 5000 times the safe level of 0.04 ng BPA/kg [body weight per day] set by the EFSA expert panel. Without a doubt, these values constitute a high health risk and support the conclusion that uses of BPA are not safe ... Given the magnitude of the overexposure, we request an expedited review by FDA,” the petition reads.
In addition to the Endocrine Society, which has long warned about the dangers of endocrine-disrupting chemicals, other signatories to the petition include the Environmental Defense Fund, Breast Cancer Prevention Partners, Clean Water Action/Clean Water Fund, Consumer Reports, Environmental Working Group, Healthy Babies Bright Futures, and the former director of the National Institute of Environmental Health Sciences and National Toxicology Program.
In a statement, Endocrine Society BPA expert Heather Patisaul, PhD, of North Carolina University, Raleigh, said the report’s findings “are extremely concerning and prove the point that even very low levels of BPA exposure can be harmful and lead to issues with reproductive health, breast cancer risk, behavior, and metabolism.”
“The FDA needs to acknowledge the science behind endocrine-disrupting chemicals and act accordingly to protect public health,” she urged.
The FDA is expected to decide within the next few days whether to open a docket to accept comments.
A final decision could take 6 months or longer, an Endocrine Society spokesperson told this news organization.
A version of this article first appeared on Medscape.com.
Spanish-speaking navigators show Hispanic patients path to CRC screening
A Spanish-speaking patient navigator dramatically increased the percentage of Hispanics undergoing colorectal screening with colonoscopies in Providence, R.I.
Screening colonoscopies are a well-established approach to reducing colorectal cancer mortality by identifying and removing polyps. However, Hispanics in the United States lag behind the general population in completion rates for screening colonoscopies.
“Starting colorectal cancer colonoscopy screening at age 45 saves lives. But this life-saving procedure is underutilized by certain populations, not only because of limited access to care but because of cultural, language, and educational barriers that exist,” Abdul Saied Calvino, MD, MPH, program director of the Complex General Surgical Oncology Fellowship at Roger Williams Medical Center, Providence, R.I., told this news organization.
Tailored patient navigation is effective but has not been widely adopted. The new study is one of the first to look at the ‘real-life’ impact of these types of programs in the Hispanic population, Dr. Calvino and his colleagues reported in the journal Cancer.
Colorectal cancer is the second leading cause of cancer-related death in the United States overall and the third-most diagnosed cancer site, according to the American Cancer Society. Among Hispanics, colorectal cancer is the second leading cause of cancer mortality and the second-most diagnosed site of malignancy.
Dr. Calvino and his colleagues sought to learn if a culturally tailored patient navigation program could improve rates of screening colonoscopies among Hispanic residents in Providence.
The hospital hired a dedicated Spanish-speaking navigator/coordinator and enrolled 698 men and women into the program.
The navigator sent introductory letters in Spanish to study participants, made phone calls to educate patients about the importance of cancer screening, and called again to ensure that all potential barriers to colonoscopy were overcome, Dr. Calvino said. Colonoscopy completion, cancellations, and no-shows were recorded. Participants were followed for 28 months.
The program proved highly successful, according to the researchers. At the end of the study period, 85% of patients – exceeding the national goal of 80% set by the National Colorectal Cancer Roundtable – had completed testing, with no differences between men and women; the cancellation rate was 9% and only 6% of patients failed to show up for endoscopy.*
Among the group that underwent colonoscopy, 254 (43%) had polyps removed and eight (1.3%) required colectomy, the researchers reported. Five patients (0.8%) were diagnosed with malignancy.
Dr. Calvino attributed the 15% combined rate of no-shows and cancellations to the cost of the procedure (copayment, out-of-pocket expense, and loss of wages) and the inability to follow-up with those patients. He added that 90% of those who completed the procedure said that without the patient navigation program they would not have completed the screening colonoscopies.
Aimee Afable, PhD, MPH, an expert on health disparities and immigrant health at Downstate Health Science University, New York, called the new study small but “important.”
Dr. Afable said strong evidence supports the ability of patient navigation programs to improve the reach and impact of screening programs aimed at the underserved. However, hospitals typically do not adequately fund such initiatives. (Dr. Calvino said the program at Roger Williams started with a grant from the OLDCO Foundation and is now supported by his institution.)
“In 2022, post-COVID, it is common to see health care support staff leaving institutions, hospitals because they’re not being paid well, and they are overburdened,” Dr. Afable told this news organization. “Patient navigation is not, unfortunately, a routine part of health care in the U.S. despite its central role in ensuring continuity of care.”
Funding for the study was provided by a grant from the OLDCO Foundation. Coauthor John C. Hardaway, MD, PhD, reports being a cancer liaison physician for the American College of Surgeons. The other authors have disclosed no relevant financial relationships. Dr. Afable has no disclosures.
A version of this article first appeared on Medscape.com.
*Correction, 2/9/22: An earlier version of this article misidentified the group that set the national screening goal.
This article was updated 2/18/22.
A Spanish-speaking patient navigator dramatically increased the percentage of Hispanics undergoing colorectal screening with colonoscopies in Providence, R.I.
Screening colonoscopies are a well-established approach to reducing colorectal cancer mortality by identifying and removing polyps. However, Hispanics in the United States lag behind the general population in completion rates for screening colonoscopies.
“Starting colorectal cancer colonoscopy screening at age 45 saves lives. But this life-saving procedure is underutilized by certain populations, not only because of limited access to care but because of cultural, language, and educational barriers that exist,” Abdul Saied Calvino, MD, MPH, program director of the Complex General Surgical Oncology Fellowship at Roger Williams Medical Center, Providence, R.I., told this news organization.
Tailored patient navigation is effective but has not been widely adopted. The new study is one of the first to look at the ‘real-life’ impact of these types of programs in the Hispanic population, Dr. Calvino and his colleagues reported in the journal Cancer.
Colorectal cancer is the second leading cause of cancer-related death in the United States overall and the third-most diagnosed cancer site, according to the American Cancer Society. Among Hispanics, colorectal cancer is the second leading cause of cancer mortality and the second-most diagnosed site of malignancy.
Dr. Calvino and his colleagues sought to learn if a culturally tailored patient navigation program could improve rates of screening colonoscopies among Hispanic residents in Providence.
The hospital hired a dedicated Spanish-speaking navigator/coordinator and enrolled 698 men and women into the program.
The navigator sent introductory letters in Spanish to study participants, made phone calls to educate patients about the importance of cancer screening, and called again to ensure that all potential barriers to colonoscopy were overcome, Dr. Calvino said. Colonoscopy completion, cancellations, and no-shows were recorded. Participants were followed for 28 months.
The program proved highly successful, according to the researchers. At the end of the study period, 85% of patients – exceeding the national goal of 80% set by the National Colorectal Cancer Roundtable – had completed testing, with no differences between men and women; the cancellation rate was 9% and only 6% of patients failed to show up for endoscopy.*
Among the group that underwent colonoscopy, 254 (43%) had polyps removed and eight (1.3%) required colectomy, the researchers reported. Five patients (0.8%) were diagnosed with malignancy.
Dr. Calvino attributed the 15% combined rate of no-shows and cancellations to the cost of the procedure (copayment, out-of-pocket expense, and loss of wages) and the inability to follow-up with those patients. He added that 90% of those who completed the procedure said that without the patient navigation program they would not have completed the screening colonoscopies.
Aimee Afable, PhD, MPH, an expert on health disparities and immigrant health at Downstate Health Science University, New York, called the new study small but “important.”
Dr. Afable said strong evidence supports the ability of patient navigation programs to improve the reach and impact of screening programs aimed at the underserved. However, hospitals typically do not adequately fund such initiatives. (Dr. Calvino said the program at Roger Williams started with a grant from the OLDCO Foundation and is now supported by his institution.)
“In 2022, post-COVID, it is common to see health care support staff leaving institutions, hospitals because they’re not being paid well, and they are overburdened,” Dr. Afable told this news organization. “Patient navigation is not, unfortunately, a routine part of health care in the U.S. despite its central role in ensuring continuity of care.”
Funding for the study was provided by a grant from the OLDCO Foundation. Coauthor John C. Hardaway, MD, PhD, reports being a cancer liaison physician for the American College of Surgeons. The other authors have disclosed no relevant financial relationships. Dr. Afable has no disclosures.
A version of this article first appeared on Medscape.com.
*Correction, 2/9/22: An earlier version of this article misidentified the group that set the national screening goal.
This article was updated 2/18/22.
A Spanish-speaking patient navigator dramatically increased the percentage of Hispanics undergoing colorectal screening with colonoscopies in Providence, R.I.
Screening colonoscopies are a well-established approach to reducing colorectal cancer mortality by identifying and removing polyps. However, Hispanics in the United States lag behind the general population in completion rates for screening colonoscopies.
“Starting colorectal cancer colonoscopy screening at age 45 saves lives. But this life-saving procedure is underutilized by certain populations, not only because of limited access to care but because of cultural, language, and educational barriers that exist,” Abdul Saied Calvino, MD, MPH, program director of the Complex General Surgical Oncology Fellowship at Roger Williams Medical Center, Providence, R.I., told this news organization.
Tailored patient navigation is effective but has not been widely adopted. The new study is one of the first to look at the ‘real-life’ impact of these types of programs in the Hispanic population, Dr. Calvino and his colleagues reported in the journal Cancer.
Colorectal cancer is the second leading cause of cancer-related death in the United States overall and the third-most diagnosed cancer site, according to the American Cancer Society. Among Hispanics, colorectal cancer is the second leading cause of cancer mortality and the second-most diagnosed site of malignancy.
Dr. Calvino and his colleagues sought to learn if a culturally tailored patient navigation program could improve rates of screening colonoscopies among Hispanic residents in Providence.
The hospital hired a dedicated Spanish-speaking navigator/coordinator and enrolled 698 men and women into the program.
The navigator sent introductory letters in Spanish to study participants, made phone calls to educate patients about the importance of cancer screening, and called again to ensure that all potential barriers to colonoscopy were overcome, Dr. Calvino said. Colonoscopy completion, cancellations, and no-shows were recorded. Participants were followed for 28 months.
The program proved highly successful, according to the researchers. At the end of the study period, 85% of patients – exceeding the national goal of 80% set by the National Colorectal Cancer Roundtable – had completed testing, with no differences between men and women; the cancellation rate was 9% and only 6% of patients failed to show up for endoscopy.*
Among the group that underwent colonoscopy, 254 (43%) had polyps removed and eight (1.3%) required colectomy, the researchers reported. Five patients (0.8%) were diagnosed with malignancy.
Dr. Calvino attributed the 15% combined rate of no-shows and cancellations to the cost of the procedure (copayment, out-of-pocket expense, and loss of wages) and the inability to follow-up with those patients. He added that 90% of those who completed the procedure said that without the patient navigation program they would not have completed the screening colonoscopies.
Aimee Afable, PhD, MPH, an expert on health disparities and immigrant health at Downstate Health Science University, New York, called the new study small but “important.”
Dr. Afable said strong evidence supports the ability of patient navigation programs to improve the reach and impact of screening programs aimed at the underserved. However, hospitals typically do not adequately fund such initiatives. (Dr. Calvino said the program at Roger Williams started with a grant from the OLDCO Foundation and is now supported by his institution.)
“In 2022, post-COVID, it is common to see health care support staff leaving institutions, hospitals because they’re not being paid well, and they are overburdened,” Dr. Afable told this news organization. “Patient navigation is not, unfortunately, a routine part of health care in the U.S. despite its central role in ensuring continuity of care.”
Funding for the study was provided by a grant from the OLDCO Foundation. Coauthor John C. Hardaway, MD, PhD, reports being a cancer liaison physician for the American College of Surgeons. The other authors have disclosed no relevant financial relationships. Dr. Afable has no disclosures.
A version of this article first appeared on Medscape.com.
*Correction, 2/9/22: An earlier version of this article misidentified the group that set the national screening goal.
This article was updated 2/18/22.
Prophylactic meds may prevent cesarean bleeding
Methylergonovine is often used to control severe bleeding immediately after cesarean deliveries. But a new study suggests that the ergot alkaloid agent could benefit these women if administered before delivery, researchers from the University of Iowa Hospitals, Iowa City, reported in the January edition of the American Journal of Obstetrics and Gynecology. The data were presented Feb. 4 at the 2022 virtual Pregnancy Meeting of the Society of Maternal-Fetal Medicine.
The findings have prompted the institution to begin administering prophylactic methylergonovine in addition to oxytocin at the time of cesarean deliveries, according to the researchers.
“The addition of prophylactic methylergonovine improved uterine tone, decreased the requirement of additional uterotonic agents, decreased the risk of postpartum hemorrhage, and decreased the need for blood transfusions,” lead author Nicole Masse, MD, assistant professor of maternal-fetal medicine at the University of Iowa, said in an interview.
Abnormal uterine tone is the leading cause of postpartum hemorrhage, Dr. Masse said. “Satisfactory uterine tone following delivery is essential. This study found a decreased need for blood transfusions in patients who received prophylactic methylergonovine. Given the risks of blood transfusions, which can include disease transmission and allergic reactions, transfusions should be avoided whenever possible.”
Conducted between June 2019 and February 2021, the single-center, randomized controlled trial of 160 women undergoing an intrapartum cesarean birth is the largest of its kind to date, Dr. Masse said. Women received either intravenous oxytocin at a dose of 300 mU per minute plus 1 mL of intramuscular normal saline (n = 80) or intravenous oxytocin at a dose of 300 mU per minute plus 0.2 mg (1 mL) of intramuscular methylergonovine (n = 80).
Women who received prophylactic methylergonovine required significantly less additional uterotonic agents than those who received oxytocin alone (20% vs. 55%; relative risk, 0.36; 95% confidence interval 0.22-0.59), according to the researchers. Those receiving methylergonovine were more likely to experience improved uterine tone (80% vs. 41.2%; RR, 1.94; 95% CI, 1.46-2.56), a lower incidence of postpartum hemorrhage (35% vs. 58.8%; RR, 0.6; 95% CI, 0.42-0.85), decreased need for a blood transfusion (5% vs. 22.5%; RR, 0.22; 95% CI, 0.08-0.63), and lower mean quantitative blood loss (996 mL vs. 1,315 mL; P = .004), they reported.
“As the majority of postpartum hemorrhages are preventable, this study is clinically relevant and can serve to decrease the morbidity associated with postpartum hemorrhage,” Dr. Masse said.
Jennifer Choi, DO, clinical assistant professor of maternal-fetal medicine at Stony Brook University Hospital, New York, said the Iowa team’s results are contrary to prior studies showing no benefit with simultaneous use of oxytocin and ergot alkaloids.
“It would be interesting to see long-term benefits across a diverse population,” she said. “But as methylergonovine is a known contraindication to hypertensive and cardiovascular disorders, including pre-eclampsia, patients would have to be carefully screened.”
Kecia Gaither, MD, MPH, associate professor of clinical obstetrics and gynecology at Weill Cornell Medicine, New York, called the study “a novel idea, but more research and higher numbers are needed for a substantive conclusion.”
Additional studies should look at variables such as the number of prior cesarean deliveries, body mass index, presence of uterine myomas, presence of abnormal placentation (placenta accreta, increta, percreta), and presence of multiple gestation, said Dr. Gaither, who also is director of perinatal services at NYC Health + Hospitals/Lincoln.
“Methergine [methylergonovine] use is contraindicated in women with hypertension/pre-eclampsia spectrum, mitral valve prolapse, history of coronary artery disease, and liver pathology,” she noted.
The researchers reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Methylergonovine is often used to control severe bleeding immediately after cesarean deliveries. But a new study suggests that the ergot alkaloid agent could benefit these women if administered before delivery, researchers from the University of Iowa Hospitals, Iowa City, reported in the January edition of the American Journal of Obstetrics and Gynecology. The data were presented Feb. 4 at the 2022 virtual Pregnancy Meeting of the Society of Maternal-Fetal Medicine.
The findings have prompted the institution to begin administering prophylactic methylergonovine in addition to oxytocin at the time of cesarean deliveries, according to the researchers.
“The addition of prophylactic methylergonovine improved uterine tone, decreased the requirement of additional uterotonic agents, decreased the risk of postpartum hemorrhage, and decreased the need for blood transfusions,” lead author Nicole Masse, MD, assistant professor of maternal-fetal medicine at the University of Iowa, said in an interview.
Abnormal uterine tone is the leading cause of postpartum hemorrhage, Dr. Masse said. “Satisfactory uterine tone following delivery is essential. This study found a decreased need for blood transfusions in patients who received prophylactic methylergonovine. Given the risks of blood transfusions, which can include disease transmission and allergic reactions, transfusions should be avoided whenever possible.”
Conducted between June 2019 and February 2021, the single-center, randomized controlled trial of 160 women undergoing an intrapartum cesarean birth is the largest of its kind to date, Dr. Masse said. Women received either intravenous oxytocin at a dose of 300 mU per minute plus 1 mL of intramuscular normal saline (n = 80) or intravenous oxytocin at a dose of 300 mU per minute plus 0.2 mg (1 mL) of intramuscular methylergonovine (n = 80).
Women who received prophylactic methylergonovine required significantly less additional uterotonic agents than those who received oxytocin alone (20% vs. 55%; relative risk, 0.36; 95% confidence interval 0.22-0.59), according to the researchers. Those receiving methylergonovine were more likely to experience improved uterine tone (80% vs. 41.2%; RR, 1.94; 95% CI, 1.46-2.56), a lower incidence of postpartum hemorrhage (35% vs. 58.8%; RR, 0.6; 95% CI, 0.42-0.85), decreased need for a blood transfusion (5% vs. 22.5%; RR, 0.22; 95% CI, 0.08-0.63), and lower mean quantitative blood loss (996 mL vs. 1,315 mL; P = .004), they reported.
“As the majority of postpartum hemorrhages are preventable, this study is clinically relevant and can serve to decrease the morbidity associated with postpartum hemorrhage,” Dr. Masse said.
Jennifer Choi, DO, clinical assistant professor of maternal-fetal medicine at Stony Brook University Hospital, New York, said the Iowa team’s results are contrary to prior studies showing no benefit with simultaneous use of oxytocin and ergot alkaloids.
“It would be interesting to see long-term benefits across a diverse population,” she said. “But as methylergonovine is a known contraindication to hypertensive and cardiovascular disorders, including pre-eclampsia, patients would have to be carefully screened.”
Kecia Gaither, MD, MPH, associate professor of clinical obstetrics and gynecology at Weill Cornell Medicine, New York, called the study “a novel idea, but more research and higher numbers are needed for a substantive conclusion.”
Additional studies should look at variables such as the number of prior cesarean deliveries, body mass index, presence of uterine myomas, presence of abnormal placentation (placenta accreta, increta, percreta), and presence of multiple gestation, said Dr. Gaither, who also is director of perinatal services at NYC Health + Hospitals/Lincoln.
“Methergine [methylergonovine] use is contraindicated in women with hypertension/pre-eclampsia spectrum, mitral valve prolapse, history of coronary artery disease, and liver pathology,” she noted.
The researchers reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Methylergonovine is often used to control severe bleeding immediately after cesarean deliveries. But a new study suggests that the ergot alkaloid agent could benefit these women if administered before delivery, researchers from the University of Iowa Hospitals, Iowa City, reported in the January edition of the American Journal of Obstetrics and Gynecology. The data were presented Feb. 4 at the 2022 virtual Pregnancy Meeting of the Society of Maternal-Fetal Medicine.
The findings have prompted the institution to begin administering prophylactic methylergonovine in addition to oxytocin at the time of cesarean deliveries, according to the researchers.
“The addition of prophylactic methylergonovine improved uterine tone, decreased the requirement of additional uterotonic agents, decreased the risk of postpartum hemorrhage, and decreased the need for blood transfusions,” lead author Nicole Masse, MD, assistant professor of maternal-fetal medicine at the University of Iowa, said in an interview.
Abnormal uterine tone is the leading cause of postpartum hemorrhage, Dr. Masse said. “Satisfactory uterine tone following delivery is essential. This study found a decreased need for blood transfusions in patients who received prophylactic methylergonovine. Given the risks of blood transfusions, which can include disease transmission and allergic reactions, transfusions should be avoided whenever possible.”
Conducted between June 2019 and February 2021, the single-center, randomized controlled trial of 160 women undergoing an intrapartum cesarean birth is the largest of its kind to date, Dr. Masse said. Women received either intravenous oxytocin at a dose of 300 mU per minute plus 1 mL of intramuscular normal saline (n = 80) or intravenous oxytocin at a dose of 300 mU per minute plus 0.2 mg (1 mL) of intramuscular methylergonovine (n = 80).
Women who received prophylactic methylergonovine required significantly less additional uterotonic agents than those who received oxytocin alone (20% vs. 55%; relative risk, 0.36; 95% confidence interval 0.22-0.59), according to the researchers. Those receiving methylergonovine were more likely to experience improved uterine tone (80% vs. 41.2%; RR, 1.94; 95% CI, 1.46-2.56), a lower incidence of postpartum hemorrhage (35% vs. 58.8%; RR, 0.6; 95% CI, 0.42-0.85), decreased need for a blood transfusion (5% vs. 22.5%; RR, 0.22; 95% CI, 0.08-0.63), and lower mean quantitative blood loss (996 mL vs. 1,315 mL; P = .004), they reported.
“As the majority of postpartum hemorrhages are preventable, this study is clinically relevant and can serve to decrease the morbidity associated with postpartum hemorrhage,” Dr. Masse said.
Jennifer Choi, DO, clinical assistant professor of maternal-fetal medicine at Stony Brook University Hospital, New York, said the Iowa team’s results are contrary to prior studies showing no benefit with simultaneous use of oxytocin and ergot alkaloids.
“It would be interesting to see long-term benefits across a diverse population,” she said. “But as methylergonovine is a known contraindication to hypertensive and cardiovascular disorders, including pre-eclampsia, patients would have to be carefully screened.”
Kecia Gaither, MD, MPH, associate professor of clinical obstetrics and gynecology at Weill Cornell Medicine, New York, called the study “a novel idea, but more research and higher numbers are needed for a substantive conclusion.”
Additional studies should look at variables such as the number of prior cesarean deliveries, body mass index, presence of uterine myomas, presence of abnormal placentation (placenta accreta, increta, percreta), and presence of multiple gestation, said Dr. Gaither, who also is director of perinatal services at NYC Health + Hospitals/Lincoln.
“Methergine [methylergonovine] use is contraindicated in women with hypertension/pre-eclampsia spectrum, mitral valve prolapse, history of coronary artery disease, and liver pathology,” she noted.
The researchers reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Cystic fibrosis in retreat, but still unbeaten
In 1938, the year that cystic fibrosis (CF) was first described clinically, four of five children born with the disease did not live past their first birthdays.
In 2019, the median age at death for patients enrolled in the Cystic Fibrosis Foundation (CFF) registry was 32 years, and the predicted life expectancy for patients with CF who were born from 2015 through 2019 was 46 years.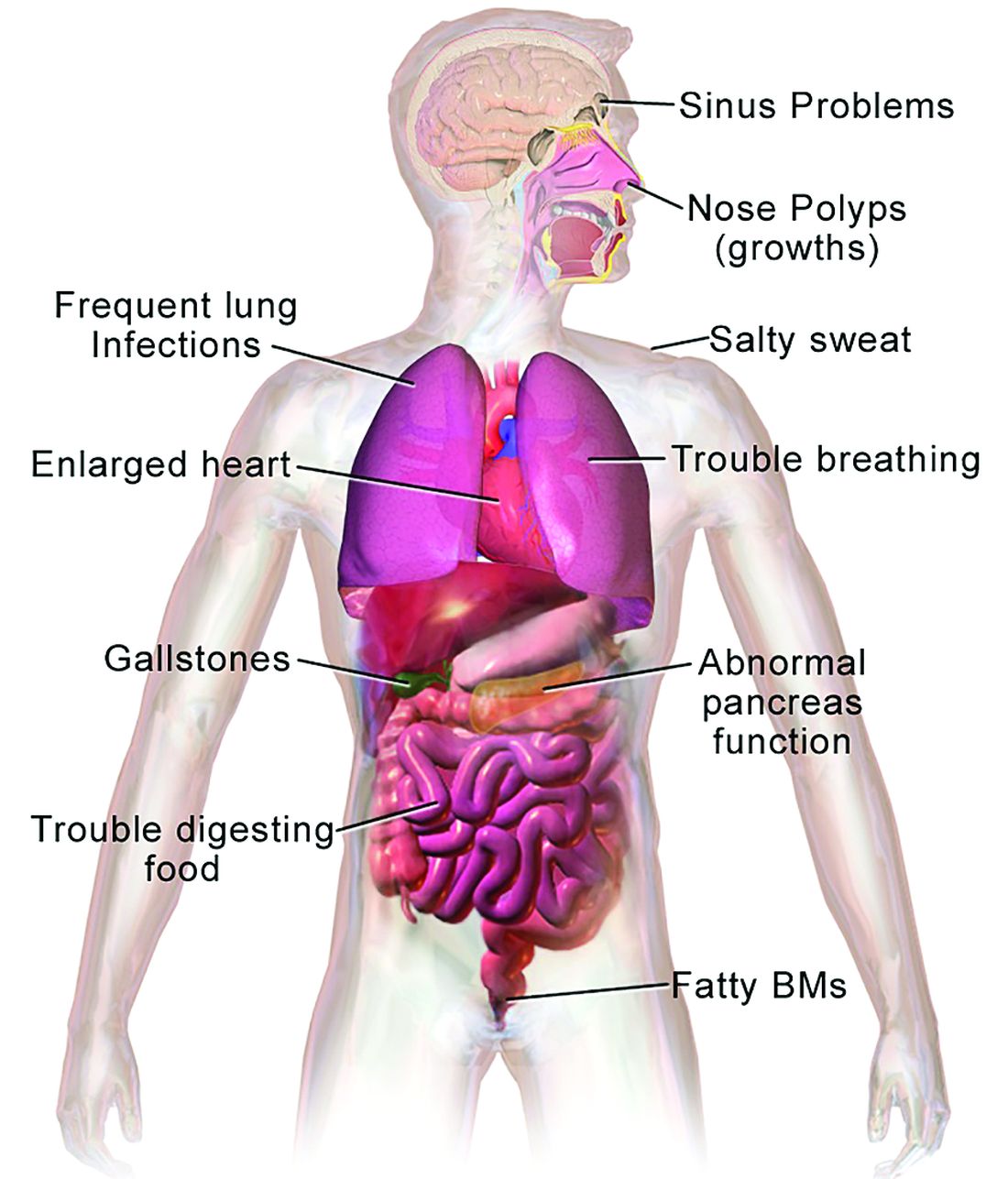
Those numbers reflect the remarkable progress made in the past 4 decades in the care of patients with CF, but also highlight the obstacles ahead, given that the predicted life expectancy for the overall U.S. population in 2019 (pre–COVID-19) was 78.9 years.
Julie Desch, MD, is a CF survivor who has beaten the odds and then some. At age 61, the retired surgical pathologist is a CF patient advocate, speaker, and a board member of the Cystic Fibrosis Research Institute, a not-for-profit organization that funds CF research and offers education, advocacy, and psychosocial support for persons with CF and their families and caregivers.
In an interview, Dr. Desch said that while there has been remarkable progress in her lifetime in the field of CF research and treatment, particularly in the development of drugs that modulate function of the underlying cause of approximately 90% of CF cases, there are still many CF patients who cannot benefit from these therapies.
“There are still 10% of people who don’t make a protein to be modified, so that’s a huge unmet need,” she said.
Genetic disorder
CF is a chronic autosomal recessive disorder with multiorgan and multisystem manifestations. It is caused by mutations in the CFTR gene, which codes for the protein CF transmembrane conductance regulator. CFTR controls transport of chloride ions across cell membranes, specifically the apical membrane of epithelial cells in tissues of the airways, intestinal tract, pancreas, kidneys, sweat glands, and the reproductive system, notably the vas deferens in males.

The F508 deletion (F508del) mutation is the most common, occurring in approximately 70% of persons with CF. It is a class 2-type protein processing mutation, leading to defects in cellular processing, protein stability, and chloride channel gating defects.
The CFTR protein also secretes bicarbonate to regulate the pH of airway surface liquid, and inhibits the epithelial sodium channel, which mediates passive sodium transport across apical membranes of sodium-absorbing epithelial cells in the kidneys, intestine, and airways.
CF typically presents with the buildup in the lungs of abnormally viscous and sticky mucus leading to frequent, severe infections, particularly with Pseudomonas aeruginosa, progressive lung damage and, prior to the development of effective disease management, to premature death. The phenotype often includes malnutrition due to malabsorption, and failure to thrive.
Diagnosis
In all 50 U.S. states and the District of Columbia, newborns are screened for CF with an assay for immunoreactive trypsinogen (IRT) an indirect marker for pancreatic injury that is elevated in serum in most newborns with CF, but also detected in premature infants or those delivered under stressful circumstances. In some states newborns are tested only for IRT, with a diagnosis confirmed with a sweat chloride test and/or a CFTR mutation panel.
Treatment
There is no cure for CF, but the discovery of the gene in 1989 by Canadian and U.S. investigators has led to life-prolonging therapeutic interventions, specifically the development of CFTR modulators.
CFTR modulators include potentiators such as ivacaftor (Kalydeco), and correctors such as lumacaftor and tezacaftor (available in the combination Orkambi), and most recently in the triple combination of elexacaftor, tezacaftor, and ivacaftor (Trikafta; ETI).
Neil Sweezey, MD, FRCPC, a CF expert at The Hospital for Sick Children (SickKids) in Toronto, told this news organization that the ideal therapy for CF, genetic correction of the underlying mutations, is still not feasible, but that CFTR modulators are a close second.
“For 90% of patients, the three-drug combination Trikafta has been shown to be quite safe, quite tolerable, and quite remarkably beneficial,” he said.
In a study reported at CHEST 2021 by investigators from Nationwide Children’s Hospital in Columbus, Ohio, 32 adults who were started on the triple combination had significantly improved in forced expiratory volume in 1 second (FEV1), gain in body mass index, decreased sweat chloride and decreased colonization by Pseudomonas species. In addition, patients had significant improvements in blood inflammatory markers.
Christopher H. Goss, MD, FCCP, professor of pulmonary critical care and sleep medicine and professor of pediatrics at the University of Washington in Seattle, agreed that with the availability of the triple combination, “these are extraordinary times. An astounding fact is that most patients have complete resolution of cough, and the exacerbation rates have just plummeted,” he said in an interview.
Some of the reductions in exacerbations may be attributable to the COVID-19 pandemic, he noted, because patients in isolation have less exposure to circulating respiratory viruses.
“But it has been miraculous, and the clinical effect is certainly still more astounding than the effects of ivacaftor, which was the first truly breakthrough drug. Weight goes up, well-being increases, and the population lung function has shifted up to better grade lung function, in the entire population,” he said.
In addition, the need for lung and heart transplantation has sharply declined.
“I had a patient who had decided to forgo transplantation, despite absolutely horrible lung function, and he’s now bowling and leading a very productive life, when before he had been preparing for end of life,” Dr. Goss said.
Dr. Sweezey emphasized that as with all medications, patients being started on the triple combination require close monitoring for potential adverse events that might require dose modification or, for a small number of patients, withdrawal.
Burden of care
CFTR modulators have reduced but not eliminated the need for some patients to have mucolytic therapy, which may include dornase alfa, a recombinant human deoxyribonuclease (DNase) that reduces the viscosity of lung secretions, hypertonic saline inhaled twice daily (for patients 12 and older), mannitol, and physical manipulations to help patients clear mucus. This can include both manual percussion and the use of devices for high-frequency chest wall oscillation.
The complex nature of CF often requires a combination of other therapies to address comorbidities. These therapies may include infection prophylaxis and treatment with antibiotics and antifungals, nutrition support, and therapy for CF-related complications, including gastrointestinal issues, liver diseases, diabetes, and osteopenia that may be related to poor nutrient absorption, chronic inflammation, or other sequelae of CF.
In addition, patients often require frequent CF care center visits – ideally a minimum of every 3 months – which can result in significant loss of work or school time.
“Outcomes for patients in the long run have been absolutely proven to be best if they’re followed in big, established, multidisciplinary well-organized CF centers,” Dr. Sweezey said. “In the United States and Canada if you’re looked after on a regular basis, which means quarterly, every 3 months – whether you need it or not, you really do need it – and if the patients are seen and assessed and checked every 3 months all of their lives, they have small changes caught early, whether it’s an infection you can slap down with medication or a nutrition problem that may be affecting a child’s growth and development.”
“We’re really kind of at a pivotal moment in CF, where we realize things are changing,” said A. Whitney Brown, MD, senior director for clinical affairs at the Cystic Fibrosis Foundation, and an adult CF and lung transplant physician in the Inova Advanced Lung Disease Program in Falls Church, Va.
“Patient needs and interest have evolved, because of the pandemic and because of the highly effective modulator therapy, but we want to take great effort to study it in a rigorous way, to make sure that as we are agile and adapt the care model, that we can maintain the same quality outcomes that we have traditionally done,” she said in an interview.
The Lancet Respiratory Medicine Commission on the future of CF care states that models of care “need to consider management approaches (including disease monitoring) to maintain health and delay lung transplantation, while minimizing the burden of care for patients and their families.”
‘A great problem to have’
One of the most significant changes in CF care has been the growing population of CF patients like Dr. Desch who are living well into adulthood, with some approaching Medicare eligibility.
With the advent of triple therapy and CFTR modulators being started earlier in life, lung function can be preserved, damage to other organs can be minimized, and life expectancy for patients with CF will continue to improve.
“We’re anticipating that there may be some needs in the aging CF population that are different than what we have historically had,” Dr. Brown said. “Will there be geriatric providers that need to become experts in CF care? That’s a great problem to have,” she said.
Dr. Goss agreed, noting that CF is steadily shifting from a near uniformly fatal disease to a chronic disorder that in many cases can be managed “with a complex regimen of novel drugs, much like HIV.”
He noted that there are multiple drug interactions with the triple combination, “so it’s really important that people don’t start a CF patient on a drug without consulting a pharmacist, because you can totally inactivate ETI, or augment it dramatically, and we’ve seen both happen.”
Cost and access
All experts interviewed for this article agreed that while the care of patients with CF has improved exponentially over the last few decades, there are still troubling inequities in care.
One of the largest impediments is the cost of care, with the triple combination costing more than $300,000 per year.
“Clearly patients aren’t paying that, but insurance companies are, and that’s causing all kinds of trickle-down effects that definitely affect patients. The patients like myself who are able to have insurance that covers it benefit, but there are so many people that don’t,” Dr. Desch said.
Dr. Sweezey noted that prior to the advent of ETI, patients with CF in Canada had better outcomes and longer life expectancy than did similar patients in the United States because of universal access to care and coordinated services under Canada’s health care system, compared with the highly fragmented and inefficient U.S. system. He added that the wider availability of ETI in the United States vs. Canada may begin to narrow that gap, however.
As noted before, there is a substantial proportion of patients – an estimated 10% – who have CFTR mutations that are not correctable by currently available CFTR modulators, and these patients are at significant risk for irreversible airway complications and lung damage.
In addition, although CF occurs most frequently among people of White ancestry, the disease does not respect distinctions of race or ethnicity.
“It’s not just [Whites] – a lot of people from different racial backgrounds, ethnic backgrounds, are not being diagnosed or are not being diagnosed soon enough to have effective care early enough,” Dr. Desch said.
That statement is supported by the Lancet Respiratory Medicine Commission on the future of cystic fibrosis care, whose members noted in 2019 that “epidemiological studies in the past 2 decades have shown that cystic fibrosis occurs and is more frequent than was previously thought in populations of non-European descent, and the disease is now recognized in many regions of the world.”
The commission members noted that the costs of adequate CF care may be beyond the reach of many patients in developing nations.
Still, if the substantial barriers of cost and access can be overcome, the future will continue to look brighter for patients with CF. As Dr. Sweezey put it: “There are studies that are pushing lower age limits for using these modulators, and as the evidence builds for the efficacy and safety at younger ages, I think all of us are hoping that we’ll end up being able to use either the current or future modulators to actually prevent trouble in CF, rather than trying to come along and fix it after it’s been there.”
Dr. Brown disclosed advisory board activity for Vertex that ended prior to her joining the CF Foundation. Dr. Desch, Dr. Goss, and Dr. Sweezey reported no relevant conflicts of interest.
In 1938, the year that cystic fibrosis (CF) was first described clinically, four of five children born with the disease did not live past their first birthdays.
In 2019, the median age at death for patients enrolled in the Cystic Fibrosis Foundation (CFF) registry was 32 years, and the predicted life expectancy for patients with CF who were born from 2015 through 2019 was 46 years.
Those numbers reflect the remarkable progress made in the past 4 decades in the care of patients with CF, but also highlight the obstacles ahead, given that the predicted life expectancy for the overall U.S. population in 2019 (pre–COVID-19) was 78.9 years.
Julie Desch, MD, is a CF survivor who has beaten the odds and then some. At age 61, the retired surgical pathologist is a CF patient advocate, speaker, and a board member of the Cystic Fibrosis Research Institute, a not-for-profit organization that funds CF research and offers education, advocacy, and psychosocial support for persons with CF and their families and caregivers.
In an interview, Dr. Desch said that while there has been remarkable progress in her lifetime in the field of CF research and treatment, particularly in the development of drugs that modulate function of the underlying cause of approximately 90% of CF cases, there are still many CF patients who cannot benefit from these therapies.
“There are still 10% of people who don’t make a protein to be modified, so that’s a huge unmet need,” she said.
Genetic disorder
CF is a chronic autosomal recessive disorder with multiorgan and multisystem manifestations. It is caused by mutations in the CFTR gene, which codes for the protein CF transmembrane conductance regulator. CFTR controls transport of chloride ions across cell membranes, specifically the apical membrane of epithelial cells in tissues of the airways, intestinal tract, pancreas, kidneys, sweat glands, and the reproductive system, notably the vas deferens in males.
The F508 deletion (F508del) mutation is the most common, occurring in approximately 70% of persons with CF. It is a class 2-type protein processing mutation, leading to defects in cellular processing, protein stability, and chloride channel gating defects.
The CFTR protein also secretes bicarbonate to regulate the pH of airway surface liquid, and inhibits the epithelial sodium channel, which mediates passive sodium transport across apical membranes of sodium-absorbing epithelial cells in the kidneys, intestine, and airways.
CF typically presents with the buildup in the lungs of abnormally viscous and sticky mucus leading to frequent, severe infections, particularly with Pseudomonas aeruginosa, progressive lung damage and, prior to the development of effective disease management, to premature death. The phenotype often includes malnutrition due to malabsorption, and failure to thrive.
Diagnosis
In all 50 U.S. states and the District of Columbia, newborns are screened for CF with an assay for immunoreactive trypsinogen (IRT) an indirect marker for pancreatic injury that is elevated in serum in most newborns with CF, but also detected in premature infants or those delivered under stressful circumstances. In some states newborns are tested only for IRT, with a diagnosis confirmed with a sweat chloride test and/or a CFTR mutation panel.
Treatment
There is no cure for CF, but the discovery of the gene in 1989 by Canadian and U.S. investigators has led to life-prolonging therapeutic interventions, specifically the development of CFTR modulators.
CFTR modulators include potentiators such as ivacaftor (Kalydeco), and correctors such as lumacaftor and tezacaftor (available in the combination Orkambi), and most recently in the triple combination of elexacaftor, tezacaftor, and ivacaftor (Trikafta; ETI).
Neil Sweezey, MD, FRCPC, a CF expert at The Hospital for Sick Children (SickKids) in Toronto, told this news organization that the ideal therapy for CF, genetic correction of the underlying mutations, is still not feasible, but that CFTR modulators are a close second.
“For 90% of patients, the three-drug combination Trikafta has been shown to be quite safe, quite tolerable, and quite remarkably beneficial,” he said.
In a study reported at CHEST 2021 by investigators from Nationwide Children’s Hospital in Columbus, Ohio, 32 adults who were started on the triple combination had significantly improved in forced expiratory volume in 1 second (FEV1), gain in body mass index, decreased sweat chloride and decreased colonization by Pseudomonas species. In addition, patients had significant improvements in blood inflammatory markers.
Christopher H. Goss, MD, FCCP, professor of pulmonary critical care and sleep medicine and professor of pediatrics at the University of Washington in Seattle, agreed that with the availability of the triple combination, “these are extraordinary times. An astounding fact is that most patients have complete resolution of cough, and the exacerbation rates have just plummeted,” he said in an interview.
Some of the reductions in exacerbations may be attributable to the COVID-19 pandemic, he noted, because patients in isolation have less exposure to circulating respiratory viruses.
“But it has been miraculous, and the clinical effect is certainly still more astounding than the effects of ivacaftor, which was the first truly breakthrough drug. Weight goes up, well-being increases, and the population lung function has shifted up to better grade lung function, in the entire population,” he said.
In addition, the need for lung and heart transplantation has sharply declined.
“I had a patient who had decided to forgo transplantation, despite absolutely horrible lung function, and he’s now bowling and leading a very productive life, when before he had been preparing for end of life,” Dr. Goss said.
Dr. Sweezey emphasized that as with all medications, patients being started on the triple combination require close monitoring for potential adverse events that might require dose modification or, for a small number of patients, withdrawal.
Burden of care
CFTR modulators have reduced but not eliminated the need for some patients to have mucolytic therapy, which may include dornase alfa, a recombinant human deoxyribonuclease (DNase) that reduces the viscosity of lung secretions, hypertonic saline inhaled twice daily (for patients 12 and older), mannitol, and physical manipulations to help patients clear mucus. This can include both manual percussion and the use of devices for high-frequency chest wall oscillation.
The complex nature of CF often requires a combination of other therapies to address comorbidities. These therapies may include infection prophylaxis and treatment with antibiotics and antifungals, nutrition support, and therapy for CF-related complications, including gastrointestinal issues, liver diseases, diabetes, and osteopenia that may be related to poor nutrient absorption, chronic inflammation, or other sequelae of CF.
In addition, patients often require frequent CF care center visits – ideally a minimum of every 3 months – which can result in significant loss of work or school time.
“Outcomes for patients in the long run have been absolutely proven to be best if they’re followed in big, established, multidisciplinary well-organized CF centers,” Dr. Sweezey said. “In the United States and Canada if you’re looked after on a regular basis, which means quarterly, every 3 months – whether you need it or not, you really do need it – and if the patients are seen and assessed and checked every 3 months all of their lives, they have small changes caught early, whether it’s an infection you can slap down with medication or a nutrition problem that may be affecting a child’s growth and development.”
“We’re really kind of at a pivotal moment in CF, where we realize things are changing,” said A. Whitney Brown, MD, senior director for clinical affairs at the Cystic Fibrosis Foundation, and an adult CF and lung transplant physician in the Inova Advanced Lung Disease Program in Falls Church, Va.
“Patient needs and interest have evolved, because of the pandemic and because of the highly effective modulator therapy, but we want to take great effort to study it in a rigorous way, to make sure that as we are agile and adapt the care model, that we can maintain the same quality outcomes that we have traditionally done,” she said in an interview.
The Lancet Respiratory Medicine Commission on the future of CF care states that models of care “need to consider management approaches (including disease monitoring) to maintain health and delay lung transplantation, while minimizing the burden of care for patients and their families.”
‘A great problem to have’
One of the most significant changes in CF care has been the growing population of CF patients like Dr. Desch who are living well into adulthood, with some approaching Medicare eligibility.
With the advent of triple therapy and CFTR modulators being started earlier in life, lung function can be preserved, damage to other organs can be minimized, and life expectancy for patients with CF will continue to improve.
“We’re anticipating that there may be some needs in the aging CF population that are different than what we have historically had,” Dr. Brown said. “Will there be geriatric providers that need to become experts in CF care? That’s a great problem to have,” she said.
Dr. Goss agreed, noting that CF is steadily shifting from a near uniformly fatal disease to a chronic disorder that in many cases can be managed “with a complex regimen of novel drugs, much like HIV.”
He noted that there are multiple drug interactions with the triple combination, “so it’s really important that people don’t start a CF patient on a drug without consulting a pharmacist, because you can totally inactivate ETI, or augment it dramatically, and we’ve seen both happen.”
Cost and access
All experts interviewed for this article agreed that while the care of patients with CF has improved exponentially over the last few decades, there are still troubling inequities in care.
One of the largest impediments is the cost of care, with the triple combination costing more than $300,000 per year.
“Clearly patients aren’t paying that, but insurance companies are, and that’s causing all kinds of trickle-down effects that definitely affect patients. The patients like myself who are able to have insurance that covers it benefit, but there are so many people that don’t,” Dr. Desch said.
Dr. Sweezey noted that prior to the advent of ETI, patients with CF in Canada had better outcomes and longer life expectancy than did similar patients in the United States because of universal access to care and coordinated services under Canada’s health care system, compared with the highly fragmented and inefficient U.S. system. He added that the wider availability of ETI in the United States vs. Canada may begin to narrow that gap, however.
As noted before, there is a substantial proportion of patients – an estimated 10% – who have CFTR mutations that are not correctable by currently available CFTR modulators, and these patients are at significant risk for irreversible airway complications and lung damage.
In addition, although CF occurs most frequently among people of White ancestry, the disease does not respect distinctions of race or ethnicity.
“It’s not just [Whites] – a lot of people from different racial backgrounds, ethnic backgrounds, are not being diagnosed or are not being diagnosed soon enough to have effective care early enough,” Dr. Desch said.
That statement is supported by the Lancet Respiratory Medicine Commission on the future of cystic fibrosis care, whose members noted in 2019 that “epidemiological studies in the past 2 decades have shown that cystic fibrosis occurs and is more frequent than was previously thought in populations of non-European descent, and the disease is now recognized in many regions of the world.”
The commission members noted that the costs of adequate CF care may be beyond the reach of many patients in developing nations.
Still, if the substantial barriers of cost and access can be overcome, the future will continue to look brighter for patients with CF. As Dr. Sweezey put it: “There are studies that are pushing lower age limits for using these modulators, and as the evidence builds for the efficacy and safety at younger ages, I think all of us are hoping that we’ll end up being able to use either the current or future modulators to actually prevent trouble in CF, rather than trying to come along and fix it after it’s been there.”
Dr. Brown disclosed advisory board activity for Vertex that ended prior to her joining the CF Foundation. Dr. Desch, Dr. Goss, and Dr. Sweezey reported no relevant conflicts of interest.
In 1938, the year that cystic fibrosis (CF) was first described clinically, four of five children born with the disease did not live past their first birthdays.
In 2019, the median age at death for patients enrolled in the Cystic Fibrosis Foundation (CFF) registry was 32 years, and the predicted life expectancy for patients with CF who were born from 2015 through 2019 was 46 years.
Those numbers reflect the remarkable progress made in the past 4 decades in the care of patients with CF, but also highlight the obstacles ahead, given that the predicted life expectancy for the overall U.S. population in 2019 (pre–COVID-19) was 78.9 years.
Julie Desch, MD, is a CF survivor who has beaten the odds and then some. At age 61, the retired surgical pathologist is a CF patient advocate, speaker, and a board member of the Cystic Fibrosis Research Institute, a not-for-profit organization that funds CF research and offers education, advocacy, and psychosocial support for persons with CF and their families and caregivers.
In an interview, Dr. Desch said that while there has been remarkable progress in her lifetime in the field of CF research and treatment, particularly in the development of drugs that modulate function of the underlying cause of approximately 90% of CF cases, there are still many CF patients who cannot benefit from these therapies.
“There are still 10% of people who don’t make a protein to be modified, so that’s a huge unmet need,” she said.
Genetic disorder
CF is a chronic autosomal recessive disorder with multiorgan and multisystem manifestations. It is caused by mutations in the CFTR gene, which codes for the protein CF transmembrane conductance regulator. CFTR controls transport of chloride ions across cell membranes, specifically the apical membrane of epithelial cells in tissues of the airways, intestinal tract, pancreas, kidneys, sweat glands, and the reproductive system, notably the vas deferens in males.
The F508 deletion (F508del) mutation is the most common, occurring in approximately 70% of persons with CF. It is a class 2-type protein processing mutation, leading to defects in cellular processing, protein stability, and chloride channel gating defects.
The CFTR protein also secretes bicarbonate to regulate the pH of airway surface liquid, and inhibits the epithelial sodium channel, which mediates passive sodium transport across apical membranes of sodium-absorbing epithelial cells in the kidneys, intestine, and airways.
CF typically presents with the buildup in the lungs of abnormally viscous and sticky mucus leading to frequent, severe infections, particularly with Pseudomonas aeruginosa, progressive lung damage and, prior to the development of effective disease management, to premature death. The phenotype often includes malnutrition due to malabsorption, and failure to thrive.
Diagnosis
In all 50 U.S. states and the District of Columbia, newborns are screened for CF with an assay for immunoreactive trypsinogen (IRT) an indirect marker for pancreatic injury that is elevated in serum in most newborns with CF, but also detected in premature infants or those delivered under stressful circumstances. In some states newborns are tested only for IRT, with a diagnosis confirmed with a sweat chloride test and/or a CFTR mutation panel.
Treatment
There is no cure for CF, but the discovery of the gene in 1989 by Canadian and U.S. investigators has led to life-prolonging therapeutic interventions, specifically the development of CFTR modulators.
CFTR modulators include potentiators such as ivacaftor (Kalydeco), and correctors such as lumacaftor and tezacaftor (available in the combination Orkambi), and most recently in the triple combination of elexacaftor, tezacaftor, and ivacaftor (Trikafta; ETI).
Neil Sweezey, MD, FRCPC, a CF expert at The Hospital for Sick Children (SickKids) in Toronto, told this news organization that the ideal therapy for CF, genetic correction of the underlying mutations, is still not feasible, but that CFTR modulators are a close second.
“For 90% of patients, the three-drug combination Trikafta has been shown to be quite safe, quite tolerable, and quite remarkably beneficial,” he said.
In a study reported at CHEST 2021 by investigators from Nationwide Children’s Hospital in Columbus, Ohio, 32 adults who were started on the triple combination had significantly improved in forced expiratory volume in 1 second (FEV1), gain in body mass index, decreased sweat chloride and decreased colonization by Pseudomonas species. In addition, patients had significant improvements in blood inflammatory markers.
Christopher H. Goss, MD, FCCP, professor of pulmonary critical care and sleep medicine and professor of pediatrics at the University of Washington in Seattle, agreed that with the availability of the triple combination, “these are extraordinary times. An astounding fact is that most patients have complete resolution of cough, and the exacerbation rates have just plummeted,” he said in an interview.
Some of the reductions in exacerbations may be attributable to the COVID-19 pandemic, he noted, because patients in isolation have less exposure to circulating respiratory viruses.
“But it has been miraculous, and the clinical effect is certainly still more astounding than the effects of ivacaftor, which was the first truly breakthrough drug. Weight goes up, well-being increases, and the population lung function has shifted up to better grade lung function, in the entire population,” he said.
In addition, the need for lung and heart transplantation has sharply declined.
“I had a patient who had decided to forgo transplantation, despite absolutely horrible lung function, and he’s now bowling and leading a very productive life, when before he had been preparing for end of life,” Dr. Goss said.
Dr. Sweezey emphasized that as with all medications, patients being started on the triple combination require close monitoring for potential adverse events that might require dose modification or, for a small number of patients, withdrawal.
Burden of care
CFTR modulators have reduced but not eliminated the need for some patients to have mucolytic therapy, which may include dornase alfa, a recombinant human deoxyribonuclease (DNase) that reduces the viscosity of lung secretions, hypertonic saline inhaled twice daily (for patients 12 and older), mannitol, and physical manipulations to help patients clear mucus. This can include both manual percussion and the use of devices for high-frequency chest wall oscillation.
The complex nature of CF often requires a combination of other therapies to address comorbidities. These therapies may include infection prophylaxis and treatment with antibiotics and antifungals, nutrition support, and therapy for CF-related complications, including gastrointestinal issues, liver diseases, diabetes, and osteopenia that may be related to poor nutrient absorption, chronic inflammation, or other sequelae of CF.
In addition, patients often require frequent CF care center visits – ideally a minimum of every 3 months – which can result in significant loss of work or school time.
“Outcomes for patients in the long run have been absolutely proven to be best if they’re followed in big, established, multidisciplinary well-organized CF centers,” Dr. Sweezey said. “In the United States and Canada if you’re looked after on a regular basis, which means quarterly, every 3 months – whether you need it or not, you really do need it – and if the patients are seen and assessed and checked every 3 months all of their lives, they have small changes caught early, whether it’s an infection you can slap down with medication or a nutrition problem that may be affecting a child’s growth and development.”
“We’re really kind of at a pivotal moment in CF, where we realize things are changing,” said A. Whitney Brown, MD, senior director for clinical affairs at the Cystic Fibrosis Foundation, and an adult CF and lung transplant physician in the Inova Advanced Lung Disease Program in Falls Church, Va.
“Patient needs and interest have evolved, because of the pandemic and because of the highly effective modulator therapy, but we want to take great effort to study it in a rigorous way, to make sure that as we are agile and adapt the care model, that we can maintain the same quality outcomes that we have traditionally done,” she said in an interview.
The Lancet Respiratory Medicine Commission on the future of CF care states that models of care “need to consider management approaches (including disease monitoring) to maintain health and delay lung transplantation, while minimizing the burden of care for patients and their families.”
‘A great problem to have’
One of the most significant changes in CF care has been the growing population of CF patients like Dr. Desch who are living well into adulthood, with some approaching Medicare eligibility.
With the advent of triple therapy and CFTR modulators being started earlier in life, lung function can be preserved, damage to other organs can be minimized, and life expectancy for patients with CF will continue to improve.
“We’re anticipating that there may be some needs in the aging CF population that are different than what we have historically had,” Dr. Brown said. “Will there be geriatric providers that need to become experts in CF care? That’s a great problem to have,” she said.
Dr. Goss agreed, noting that CF is steadily shifting from a near uniformly fatal disease to a chronic disorder that in many cases can be managed “with a complex regimen of novel drugs, much like HIV.”
He noted that there are multiple drug interactions with the triple combination, “so it’s really important that people don’t start a CF patient on a drug without consulting a pharmacist, because you can totally inactivate ETI, or augment it dramatically, and we’ve seen both happen.”
Cost and access
All experts interviewed for this article agreed that while the care of patients with CF has improved exponentially over the last few decades, there are still troubling inequities in care.
One of the largest impediments is the cost of care, with the triple combination costing more than $300,000 per year.
“Clearly patients aren’t paying that, but insurance companies are, and that’s causing all kinds of trickle-down effects that definitely affect patients. The patients like myself who are able to have insurance that covers it benefit, but there are so many people that don’t,” Dr. Desch said.
Dr. Sweezey noted that prior to the advent of ETI, patients with CF in Canada had better outcomes and longer life expectancy than did similar patients in the United States because of universal access to care and coordinated services under Canada’s health care system, compared with the highly fragmented and inefficient U.S. system. He added that the wider availability of ETI in the United States vs. Canada may begin to narrow that gap, however.
As noted before, there is a substantial proportion of patients – an estimated 10% – who have CFTR mutations that are not correctable by currently available CFTR modulators, and these patients are at significant risk for irreversible airway complications and lung damage.
In addition, although CF occurs most frequently among people of White ancestry, the disease does not respect distinctions of race or ethnicity.
“It’s not just [Whites] – a lot of people from different racial backgrounds, ethnic backgrounds, are not being diagnosed or are not being diagnosed soon enough to have effective care early enough,” Dr. Desch said.
That statement is supported by the Lancet Respiratory Medicine Commission on the future of cystic fibrosis care, whose members noted in 2019 that “epidemiological studies in the past 2 decades have shown that cystic fibrosis occurs and is more frequent than was previously thought in populations of non-European descent, and the disease is now recognized in many regions of the world.”
The commission members noted that the costs of adequate CF care may be beyond the reach of many patients in developing nations.
Still, if the substantial barriers of cost and access can be overcome, the future will continue to look brighter for patients with CF. As Dr. Sweezey put it: “There are studies that are pushing lower age limits for using these modulators, and as the evidence builds for the efficacy and safety at younger ages, I think all of us are hoping that we’ll end up being able to use either the current or future modulators to actually prevent trouble in CF, rather than trying to come along and fix it after it’s been there.”
Dr. Brown disclosed advisory board activity for Vertex that ended prior to her joining the CF Foundation. Dr. Desch, Dr. Goss, and Dr. Sweezey reported no relevant conflicts of interest.
Study questions reliability of maternal drug testing
A new study finding that samples from maternal urine and the meconium of their newborn babies frequently produce different results is raising more questions about drug testing of pregnant women.
The study found concerningly high rates of disagreement (or “discordance”) in biochemical testing between maternal urine in women with a documented history of or active drug use and the meconium in their newborns. In some cases, such discordance might be triggering the inappropriate intervention of childcare protective services, including the separation of infants from their mothers, according to the researchers, who presented their findings Feb. 4 at the meeting sponsored by the Society for Maternal-Fetal Medicine.
“There’s a very big debate right now in the obstetrics and perinatology communities about the utility of biochemical testing and the identification of high-risk women,” lead author Cassandra Heiselman, DO, MPH, clinical assistant professor in the department of obstetrics, gynecology and reproductive medicine at Stony Brook (N.Y.) University, said in an interview. “We know that each biochemical test has limitations, which can include basically the inability to detect all substances, especially synthetic opioids like fentanyl, [and] the possibility for false results.”
Inaccuracies in testing can potentially result in inappropriate separation of mother and baby. “Careful scrutiny of results is needed,” Dr. Heiselman said.
The Stony Brook team conducted a retrospective cohort study that identified women presenting for delivery from January 2017 to March 2021 with indications for drug testing, including a known history of or current substance use disorder/misuse, and late or no prenatal care. A standardized panel was used for testing maternal urine and newborn meconium.
Urine tests of 327 women resulted in 187 (57%) positive and 98 (30%) negative results, along with 42 (13%) samples with incomplete data, the researchers reported. In contrast, drug testing of newborn meconium was positive in 273 (83%) cases, negative in 42 (13%), and was not performed in 12 (4%) – for a rate of concordance of 41%.
Concordance of urine/meconium occurred more frequently in male newborns (65%), compared with females (35%). “It is unclear biologically why there is such a difference based on the sex of the infants’ test and is an area that needs further investigation,” Dr. Heiselman said.
Comparing urine and meconium tests for 11 substances resulted in 195/483 (40%) concordance, the researchers said; 18% were discordant with positive maternal urine, and 41% were discordant with newborn positive meconium.
Oxycodone and fentanyl were significantly discordant with positive maternal urine. Cannabis use was the most common factor associated with a positive test of meconium, according to the researchers.
“Some studies have shown cannabis use in the second trimester can show up in meconium testing even if the mother has stopped that behavior,” Dr. Heiselman said. “Then there is also cross-reactivity with other substances that can lead to higher false positive results, especially in the urine toxicology.”
The reasons for the discordant results are not clear and vary by substance, Dr. Heiselman said.
“Cannabis and methadone were the significant factors leading to discordance with positive newborn meconium, which may reflect prior use earlier in pregnancy without recent use before delivery,” she said in an interview. “Urine and meconium reflect potentially different timing in perinatal exposure and the potential differences in windows of detection for different substances. Therefore, we would expect some discordance in our comparisons, just not the extent that we saw.”
Some test results might also have been false positives. Many commonly used medications, from cough syrups to proton pump inhibitors, have the potential to generate positive results for illicit drugs, Dr. Heiselman said.
“The issue of discordance is a complex one, where there are limitations of the tests being performed, possible cross-reactivity with false positives, and the difference in what test reflects as far as timing of prenatal exposure. Furthermore, a negative test does not rule out sporadic use, nor does a positive result diagnose substance use disorder or its severity,” she said.
Lack of standards
Dr. Heiselman said states and the federal government lack standards to biochemically evaluate women at risk for drug abuse and their newborns.
“My institution uses a risk-based protocol. Basically, we test cases where we have a known history of substance use disorder or active use, a history in the last 3 years of any kind of substance use, initiation of late prenatal care after 20 weeks, or no prenatal care at all,” she said. “And then the pediatricians on the other side will test neonates if the mother has any of that history or if the neonates themselves have unexplained complications or drug withdrawal symptoms.”
High rates of discordance can result in the inappropriate intervention by childcare protective service agencies when the mother may not have a substance use disorder, she noted.
Perinatologist Kecia Gaither, MD, MPH, associate professor of clinical obstetrics and gynecology at Weill Cornell Medicine, New York, called the findings “no surprise,” but added that negative findings in neonates “do not exclude the possibility of substance abuse by the mother. It is important to recognize the limitations inherent with screening tests for illicit substances in neonates from substance-abusing mothers.”
Dr. Heiselman added that understanding what maternal and infant drug tests truly reflect “can help us as clinicians in deciding when we test, whether it’s medically necessary, instead of just thinking biochemical tests are the best screening tool, because we know that we are screening. We must engage these women in empathetic and nonjudgmental discussions, which often will elucidate a substance use disorder history more so than just biochemical testing, negative or positive.”
The researchers disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study finding that samples from maternal urine and the meconium of their newborn babies frequently produce different results is raising more questions about drug testing of pregnant women.
The study found concerningly high rates of disagreement (or “discordance”) in biochemical testing between maternal urine in women with a documented history of or active drug use and the meconium in their newborns. In some cases, such discordance might be triggering the inappropriate intervention of childcare protective services, including the separation of infants from their mothers, according to the researchers, who presented their findings Feb. 4 at the meeting sponsored by the Society for Maternal-Fetal Medicine.
“There’s a very big debate right now in the obstetrics and perinatology communities about the utility of biochemical testing and the identification of high-risk women,” lead author Cassandra Heiselman, DO, MPH, clinical assistant professor in the department of obstetrics, gynecology and reproductive medicine at Stony Brook (N.Y.) University, said in an interview. “We know that each biochemical test has limitations, which can include basically the inability to detect all substances, especially synthetic opioids like fentanyl, [and] the possibility for false results.”
Inaccuracies in testing can potentially result in inappropriate separation of mother and baby. “Careful scrutiny of results is needed,” Dr. Heiselman said.
The Stony Brook team conducted a retrospective cohort study that identified women presenting for delivery from January 2017 to March 2021 with indications for drug testing, including a known history of or current substance use disorder/misuse, and late or no prenatal care. A standardized panel was used for testing maternal urine and newborn meconium.
Urine tests of 327 women resulted in 187 (57%) positive and 98 (30%) negative results, along with 42 (13%) samples with incomplete data, the researchers reported. In contrast, drug testing of newborn meconium was positive in 273 (83%) cases, negative in 42 (13%), and was not performed in 12 (4%) – for a rate of concordance of 41%.
Concordance of urine/meconium occurred more frequently in male newborns (65%), compared with females (35%). “It is unclear biologically why there is such a difference based on the sex of the infants’ test and is an area that needs further investigation,” Dr. Heiselman said.
Comparing urine and meconium tests for 11 substances resulted in 195/483 (40%) concordance, the researchers said; 18% were discordant with positive maternal urine, and 41% were discordant with newborn positive meconium.
Oxycodone and fentanyl were significantly discordant with positive maternal urine. Cannabis use was the most common factor associated with a positive test of meconium, according to the researchers.
“Some studies have shown cannabis use in the second trimester can show up in meconium testing even if the mother has stopped that behavior,” Dr. Heiselman said. “Then there is also cross-reactivity with other substances that can lead to higher false positive results, especially in the urine toxicology.”
The reasons for the discordant results are not clear and vary by substance, Dr. Heiselman said.
“Cannabis and methadone were the significant factors leading to discordance with positive newborn meconium, which may reflect prior use earlier in pregnancy without recent use before delivery,” she said in an interview. “Urine and meconium reflect potentially different timing in perinatal exposure and the potential differences in windows of detection for different substances. Therefore, we would expect some discordance in our comparisons, just not the extent that we saw.”
Some test results might also have been false positives. Many commonly used medications, from cough syrups to proton pump inhibitors, have the potential to generate positive results for illicit drugs, Dr. Heiselman said.
“The issue of discordance is a complex one, where there are limitations of the tests being performed, possible cross-reactivity with false positives, and the difference in what test reflects as far as timing of prenatal exposure. Furthermore, a negative test does not rule out sporadic use, nor does a positive result diagnose substance use disorder or its severity,” she said.
Lack of standards
Dr. Heiselman said states and the federal government lack standards to biochemically evaluate women at risk for drug abuse and their newborns.
“My institution uses a risk-based protocol. Basically, we test cases where we have a known history of substance use disorder or active use, a history in the last 3 years of any kind of substance use, initiation of late prenatal care after 20 weeks, or no prenatal care at all,” she said. “And then the pediatricians on the other side will test neonates if the mother has any of that history or if the neonates themselves have unexplained complications or drug withdrawal symptoms.”
High rates of discordance can result in the inappropriate intervention by childcare protective service agencies when the mother may not have a substance use disorder, she noted.
Perinatologist Kecia Gaither, MD, MPH, associate professor of clinical obstetrics and gynecology at Weill Cornell Medicine, New York, called the findings “no surprise,” but added that negative findings in neonates “do not exclude the possibility of substance abuse by the mother. It is important to recognize the limitations inherent with screening tests for illicit substances in neonates from substance-abusing mothers.”
Dr. Heiselman added that understanding what maternal and infant drug tests truly reflect “can help us as clinicians in deciding when we test, whether it’s medically necessary, instead of just thinking biochemical tests are the best screening tool, because we know that we are screening. We must engage these women in empathetic and nonjudgmental discussions, which often will elucidate a substance use disorder history more so than just biochemical testing, negative or positive.”
The researchers disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study finding that samples from maternal urine and the meconium of their newborn babies frequently produce different results is raising more questions about drug testing of pregnant women.
The study found concerningly high rates of disagreement (or “discordance”) in biochemical testing between maternal urine in women with a documented history of or active drug use and the meconium in their newborns. In some cases, such discordance might be triggering the inappropriate intervention of childcare protective services, including the separation of infants from their mothers, according to the researchers, who presented their findings Feb. 4 at the meeting sponsored by the Society for Maternal-Fetal Medicine.
“There’s a very big debate right now in the obstetrics and perinatology communities about the utility of biochemical testing and the identification of high-risk women,” lead author Cassandra Heiselman, DO, MPH, clinical assistant professor in the department of obstetrics, gynecology and reproductive medicine at Stony Brook (N.Y.) University, said in an interview. “We know that each biochemical test has limitations, which can include basically the inability to detect all substances, especially synthetic opioids like fentanyl, [and] the possibility for false results.”
Inaccuracies in testing can potentially result in inappropriate separation of mother and baby. “Careful scrutiny of results is needed,” Dr. Heiselman said.
The Stony Brook team conducted a retrospective cohort study that identified women presenting for delivery from January 2017 to March 2021 with indications for drug testing, including a known history of or current substance use disorder/misuse, and late or no prenatal care. A standardized panel was used for testing maternal urine and newborn meconium.
Urine tests of 327 women resulted in 187 (57%) positive and 98 (30%) negative results, along with 42 (13%) samples with incomplete data, the researchers reported. In contrast, drug testing of newborn meconium was positive in 273 (83%) cases, negative in 42 (13%), and was not performed in 12 (4%) – for a rate of concordance of 41%.
Concordance of urine/meconium occurred more frequently in male newborns (65%), compared with females (35%). “It is unclear biologically why there is such a difference based on the sex of the infants’ test and is an area that needs further investigation,” Dr. Heiselman said.
Comparing urine and meconium tests for 11 substances resulted in 195/483 (40%) concordance, the researchers said; 18% were discordant with positive maternal urine, and 41% were discordant with newborn positive meconium.
Oxycodone and fentanyl were significantly discordant with positive maternal urine. Cannabis use was the most common factor associated with a positive test of meconium, according to the researchers.
“Some studies have shown cannabis use in the second trimester can show up in meconium testing even if the mother has stopped that behavior,” Dr. Heiselman said. “Then there is also cross-reactivity with other substances that can lead to higher false positive results, especially in the urine toxicology.”
The reasons for the discordant results are not clear and vary by substance, Dr. Heiselman said.
“Cannabis and methadone were the significant factors leading to discordance with positive newborn meconium, which may reflect prior use earlier in pregnancy without recent use before delivery,” she said in an interview. “Urine and meconium reflect potentially different timing in perinatal exposure and the potential differences in windows of detection for different substances. Therefore, we would expect some discordance in our comparisons, just not the extent that we saw.”
Some test results might also have been false positives. Many commonly used medications, from cough syrups to proton pump inhibitors, have the potential to generate positive results for illicit drugs, Dr. Heiselman said.
“The issue of discordance is a complex one, where there are limitations of the tests being performed, possible cross-reactivity with false positives, and the difference in what test reflects as far as timing of prenatal exposure. Furthermore, a negative test does not rule out sporadic use, nor does a positive result diagnose substance use disorder or its severity,” she said.
Lack of standards
Dr. Heiselman said states and the federal government lack standards to biochemically evaluate women at risk for drug abuse and their newborns.
“My institution uses a risk-based protocol. Basically, we test cases where we have a known history of substance use disorder or active use, a history in the last 3 years of any kind of substance use, initiation of late prenatal care after 20 weeks, or no prenatal care at all,” she said. “And then the pediatricians on the other side will test neonates if the mother has any of that history or if the neonates themselves have unexplained complications or drug withdrawal symptoms.”
High rates of discordance can result in the inappropriate intervention by childcare protective service agencies when the mother may not have a substance use disorder, she noted.
Perinatologist Kecia Gaither, MD, MPH, associate professor of clinical obstetrics and gynecology at Weill Cornell Medicine, New York, called the findings “no surprise,” but added that negative findings in neonates “do not exclude the possibility of substance abuse by the mother. It is important to recognize the limitations inherent with screening tests for illicit substances in neonates from substance-abusing mothers.”
Dr. Heiselman added that understanding what maternal and infant drug tests truly reflect “can help us as clinicians in deciding when we test, whether it’s medically necessary, instead of just thinking biochemical tests are the best screening tool, because we know that we are screening. We must engage these women in empathetic and nonjudgmental discussions, which often will elucidate a substance use disorder history more so than just biochemical testing, negative or positive.”
The researchers disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE PREGNANCY MEETING
ctDNA identifies CRC patients who benefit from adjuvant therapy
SAN FRANCISCO — A
The team used a personalized tumor-informed assay (Signatera bespoke multiplex-PCR NGS assay) to measure molecular residual disease (MRD) 4 weeks after surgery.
Among patients who were ctDNA positive at 4 weeks post-op, those who received adjuvant chemotherapy had significantly longer disease-free survival (DFS) at 6 months, compared with patients who didn’t receive it.
The adjuvant chemotherapy was able to clear ctDNA in 68% of that subgroup by 24 weeks, noted study author Masahito Kotaka, MD, PhD, from the gastrointestinal cancer center, Sano Hospital, Hyogo, Japan
“Even with an extended follow-up time, ctDNA positivity at 4 weeks post-op was significantly associated with inferior disease-free survival,” he said.
“Two out of three post-op patients who were positive at 4 weeks recurred, even in stage I or low-risk stage II.”
However, he noted that “patients who were 4 weeks post-op and ctDNA negative did not derive significant benefit from adjuvant chemotherapy in high- risk stage II and III.”
Overall, the study shows that stratifying postsurgical treatment decisions using the assay can identify patients likely to benefit from adjuvant chemotherapy across all stages of the disease, explained Dr. Kotaka.
Dr. Kotaka presented the new results at the Gastrointestinal Cancers Symposium.
“ctDNA dynamics from 4-week post-op positivity to 12 weeks afterwards could become new surrogate endpoints beyond disease-free survival,” he suggested.
However, the discussant for this abstract, Rona Yaeger, MD, from Memorial Sloan Kettering Cancer Center in New York, cautioned that this is not yet ready for clinical use.
“There was a clear prognostic effect,” she said. “This was a very large sample size and validates some of the earlier studies showing that ctDNA is a very important prognostic marker.” This study “gives us a tighter confidence interval due to the large size.”
However, there are limitations, one being that it was not a randomized study so it is unknown who received adjuvant therapy, she pointed out. “Since it is not randomized, the groups are not equal.”
Summarizing, she said that ctDNA is a strong prognostic marker that identifies MRD. “But it is expensive and currently doesn’t guide our adjuvant decisions,” she said. “It is not ready yet for standard evaluation of early-stage colorectal cancer patients, and we don’t know yet if additional therapy after adjuvant therapy in ctDNA-positive patients will change outcomes.”
Study details
The new results come from the GALAXY study, which is part of a large platform in Japan, called CIRCULATE, that is evaluating the clinical utility of ctDNA in patients with resectable colorectal cancer. Aside from GALAXY, which is a prospective observational trial, CIRCULATE also includes two phase 3 randomized trials: VEGA and ALTAIR.
For their study, Dr. Kotaka and colleagues monitored ctDNA status in patients with clinical stage l to IV colorectal cancer who underwent complete surgical resection and then evaluated the association of ctDNA dynamics with a short-term clinical outcome and adjuvant therapy efficacy.
A total of 1,040 patients were included in the current analysis. They were stratified into subgroups that were either ctDNA positive (n = 183) or ctDNA negative (n = 531) 4 weeks post surgery. The cohort included 116 patients with stage I disease, 478 with stage II, 503 with stage III, and 268 patients with oligomet resectable stage IV (of whom 16% received neoadjuvant chemotherapy).
Blood samples were collected before surgery and at 4, 12, 24, 36, 48, 72, and 96 weeks following resection.
The team looked at 6-month disease-free survival rates. Among patients with high-risk stage II disease and with a positive ctDNA assay at 4 weeks post-op, those who received adjuvant chemotherapy had a 6-month DFS rate of 100% vs. 53.8% who did not receive adjuvant chemotherapy.
For stage III disease, those rates were 89.2% vs. 32.0%, and for stage IV disease, they were 72.7% vs. 28.3%.
At a median follow-up of 11.4 months, the 6- and 12-month DFS was 96.5% and 92.7% for all patients who were ctDNA negative at 4 weeks post-op. Outcomes for patients who were ctDNA positive were significantly poorer, at 62.8% and 47.5% (hazard ratio, 10.9; P <.001; sensitivity for recurrence, 63.6%).
Of the 188 patients who were MRD positive at 4 weeks post-op with available MRD status at 12 weeks, 95 received adjuvant therapy. The ctDNA clearance rate at 12 weeks was significantly higher in the adjuvant therapy group vs. no adjuvant therapy; 57% vs. 8% in stage I-IV (P < .001), and 58% vs. 11% (4/37) in stage II–III (P < .001).
Additionally, the ctDNA clearance rate at 24 weeks was also significantly higher in adjuvant vs. no adjuvant therapy arms; 26% vs. 0% in patients with stage I-IV disease (P = .003), and 33% vs. 0% in patients with stage II-III disease (P = .03).
Cumulative clearance of ctDNA at 6 months post-op was significantly higher in the adjuvant vs. no adjuvant therapy arms (67% vs. 7% by 24 weeks; cumulative HR, 17.1; P < .001). For patients MRD positive at 4 weeks, the 6-month DFS was also significantly higher in adjuvant vs. no adjuvant therapy arms; 84% vs 34% (HR, 0.15; P < .001), which was observed across all stages.
Upon multivariate analysis, the highest risk of recurrence for patients with stage II-III cancer correlated with ctDNA-positive vs. ctDNA-negative status (HR, 15.3; P <. 001), mutant vs. wild-type RAS (HR, 1.8; P = .04), or mutant vs. wild-type BRAF (HR, 5.2; P < .001).
The group is continuing with its research into a ctDNA-guided adjuvant strategy. More data will be available soon from the ongoing randomized VEGA and ALTAIR studies and will be presented at future conference, Dr. Kotaka commented.
CIRCULATE‐Japan receives financial supports from the Japan Agency for Medical Research and Development and from Taiho Pharmaceutical, through Alpha‐A. Dr. Kotaka reported relationships with Chugai, Lilly Japan, Taiho, Takeda, and Yakult Honsha. Dr. Yaeger reported relationships with Array BioPharma, Boehringer Ingelheim, Mirati Therapeutics, Natera, and Pfizer.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO — A
The team used a personalized tumor-informed assay (Signatera bespoke multiplex-PCR NGS assay) to measure molecular residual disease (MRD) 4 weeks after surgery.
Among patients who were ctDNA positive at 4 weeks post-op, those who received adjuvant chemotherapy had significantly longer disease-free survival (DFS) at 6 months, compared with patients who didn’t receive it.
The adjuvant chemotherapy was able to clear ctDNA in 68% of that subgroup by 24 weeks, noted study author Masahito Kotaka, MD, PhD, from the gastrointestinal cancer center, Sano Hospital, Hyogo, Japan
“Even with an extended follow-up time, ctDNA positivity at 4 weeks post-op was significantly associated with inferior disease-free survival,” he said.
“Two out of three post-op patients who were positive at 4 weeks recurred, even in stage I or low-risk stage II.”
However, he noted that “patients who were 4 weeks post-op and ctDNA negative did not derive significant benefit from adjuvant chemotherapy in high- risk stage II and III.”
Overall, the study shows that stratifying postsurgical treatment decisions using the assay can identify patients likely to benefit from adjuvant chemotherapy across all stages of the disease, explained Dr. Kotaka.
Dr. Kotaka presented the new results at the Gastrointestinal Cancers Symposium.
“ctDNA dynamics from 4-week post-op positivity to 12 weeks afterwards could become new surrogate endpoints beyond disease-free survival,” he suggested.
However, the discussant for this abstract, Rona Yaeger, MD, from Memorial Sloan Kettering Cancer Center in New York, cautioned that this is not yet ready for clinical use.
“There was a clear prognostic effect,” she said. “This was a very large sample size and validates some of the earlier studies showing that ctDNA is a very important prognostic marker.” This study “gives us a tighter confidence interval due to the large size.”
However, there are limitations, one being that it was not a randomized study so it is unknown who received adjuvant therapy, she pointed out. “Since it is not randomized, the groups are not equal.”
Summarizing, she said that ctDNA is a strong prognostic marker that identifies MRD. “But it is expensive and currently doesn’t guide our adjuvant decisions,” she said. “It is not ready yet for standard evaluation of early-stage colorectal cancer patients, and we don’t know yet if additional therapy after adjuvant therapy in ctDNA-positive patients will change outcomes.”
Study details
The new results come from the GALAXY study, which is part of a large platform in Japan, called CIRCULATE, that is evaluating the clinical utility of ctDNA in patients with resectable colorectal cancer. Aside from GALAXY, which is a prospective observational trial, CIRCULATE also includes two phase 3 randomized trials: VEGA and ALTAIR.
For their study, Dr. Kotaka and colleagues monitored ctDNA status in patients with clinical stage l to IV colorectal cancer who underwent complete surgical resection and then evaluated the association of ctDNA dynamics with a short-term clinical outcome and adjuvant therapy efficacy.
A total of 1,040 patients were included in the current analysis. They were stratified into subgroups that were either ctDNA positive (n = 183) or ctDNA negative (n = 531) 4 weeks post surgery. The cohort included 116 patients with stage I disease, 478 with stage II, 503 with stage III, and 268 patients with oligomet resectable stage IV (of whom 16% received neoadjuvant chemotherapy).
Blood samples were collected before surgery and at 4, 12, 24, 36, 48, 72, and 96 weeks following resection.
The team looked at 6-month disease-free survival rates. Among patients with high-risk stage II disease and with a positive ctDNA assay at 4 weeks post-op, those who received adjuvant chemotherapy had a 6-month DFS rate of 100% vs. 53.8% who did not receive adjuvant chemotherapy.
For stage III disease, those rates were 89.2% vs. 32.0%, and for stage IV disease, they were 72.7% vs. 28.3%.
At a median follow-up of 11.4 months, the 6- and 12-month DFS was 96.5% and 92.7% for all patients who were ctDNA negative at 4 weeks post-op. Outcomes for patients who were ctDNA positive were significantly poorer, at 62.8% and 47.5% (hazard ratio, 10.9; P <.001; sensitivity for recurrence, 63.6%).
Of the 188 patients who were MRD positive at 4 weeks post-op with available MRD status at 12 weeks, 95 received adjuvant therapy. The ctDNA clearance rate at 12 weeks was significantly higher in the adjuvant therapy group vs. no adjuvant therapy; 57% vs. 8% in stage I-IV (P < .001), and 58% vs. 11% (4/37) in stage II–III (P < .001).
Additionally, the ctDNA clearance rate at 24 weeks was also significantly higher in adjuvant vs. no adjuvant therapy arms; 26% vs. 0% in patients with stage I-IV disease (P = .003), and 33% vs. 0% in patients with stage II-III disease (P = .03).
Cumulative clearance of ctDNA at 6 months post-op was significantly higher in the adjuvant vs. no adjuvant therapy arms (67% vs. 7% by 24 weeks; cumulative HR, 17.1; P < .001). For patients MRD positive at 4 weeks, the 6-month DFS was also significantly higher in adjuvant vs. no adjuvant therapy arms; 84% vs 34% (HR, 0.15; P < .001), which was observed across all stages.
Upon multivariate analysis, the highest risk of recurrence for patients with stage II-III cancer correlated with ctDNA-positive vs. ctDNA-negative status (HR, 15.3; P <. 001), mutant vs. wild-type RAS (HR, 1.8; P = .04), or mutant vs. wild-type BRAF (HR, 5.2; P < .001).
The group is continuing with its research into a ctDNA-guided adjuvant strategy. More data will be available soon from the ongoing randomized VEGA and ALTAIR studies and will be presented at future conference, Dr. Kotaka commented.
CIRCULATE‐Japan receives financial supports from the Japan Agency for Medical Research and Development and from Taiho Pharmaceutical, through Alpha‐A. Dr. Kotaka reported relationships with Chugai, Lilly Japan, Taiho, Takeda, and Yakult Honsha. Dr. Yaeger reported relationships with Array BioPharma, Boehringer Ingelheim, Mirati Therapeutics, Natera, and Pfizer.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO — A
The team used a personalized tumor-informed assay (Signatera bespoke multiplex-PCR NGS assay) to measure molecular residual disease (MRD) 4 weeks after surgery.
Among patients who were ctDNA positive at 4 weeks post-op, those who received adjuvant chemotherapy had significantly longer disease-free survival (DFS) at 6 months, compared with patients who didn’t receive it.
The adjuvant chemotherapy was able to clear ctDNA in 68% of that subgroup by 24 weeks, noted study author Masahito Kotaka, MD, PhD, from the gastrointestinal cancer center, Sano Hospital, Hyogo, Japan
“Even with an extended follow-up time, ctDNA positivity at 4 weeks post-op was significantly associated with inferior disease-free survival,” he said.
“Two out of three post-op patients who were positive at 4 weeks recurred, even in stage I or low-risk stage II.”
However, he noted that “patients who were 4 weeks post-op and ctDNA negative did not derive significant benefit from adjuvant chemotherapy in high- risk stage II and III.”
Overall, the study shows that stratifying postsurgical treatment decisions using the assay can identify patients likely to benefit from adjuvant chemotherapy across all stages of the disease, explained Dr. Kotaka.
Dr. Kotaka presented the new results at the Gastrointestinal Cancers Symposium.
“ctDNA dynamics from 4-week post-op positivity to 12 weeks afterwards could become new surrogate endpoints beyond disease-free survival,” he suggested.
However, the discussant for this abstract, Rona Yaeger, MD, from Memorial Sloan Kettering Cancer Center in New York, cautioned that this is not yet ready for clinical use.
“There was a clear prognostic effect,” she said. “This was a very large sample size and validates some of the earlier studies showing that ctDNA is a very important prognostic marker.” This study “gives us a tighter confidence interval due to the large size.”
However, there are limitations, one being that it was not a randomized study so it is unknown who received adjuvant therapy, she pointed out. “Since it is not randomized, the groups are not equal.”
Summarizing, she said that ctDNA is a strong prognostic marker that identifies MRD. “But it is expensive and currently doesn’t guide our adjuvant decisions,” she said. “It is not ready yet for standard evaluation of early-stage colorectal cancer patients, and we don’t know yet if additional therapy after adjuvant therapy in ctDNA-positive patients will change outcomes.”
Study details
The new results come from the GALAXY study, which is part of a large platform in Japan, called CIRCULATE, that is evaluating the clinical utility of ctDNA in patients with resectable colorectal cancer. Aside from GALAXY, which is a prospective observational trial, CIRCULATE also includes two phase 3 randomized trials: VEGA and ALTAIR.
For their study, Dr. Kotaka and colleagues monitored ctDNA status in patients with clinical stage l to IV colorectal cancer who underwent complete surgical resection and then evaluated the association of ctDNA dynamics with a short-term clinical outcome and adjuvant therapy efficacy.
A total of 1,040 patients were included in the current analysis. They were stratified into subgroups that were either ctDNA positive (n = 183) or ctDNA negative (n = 531) 4 weeks post surgery. The cohort included 116 patients with stage I disease, 478 with stage II, 503 with stage III, and 268 patients with oligomet resectable stage IV (of whom 16% received neoadjuvant chemotherapy).
Blood samples were collected before surgery and at 4, 12, 24, 36, 48, 72, and 96 weeks following resection.
The team looked at 6-month disease-free survival rates. Among patients with high-risk stage II disease and with a positive ctDNA assay at 4 weeks post-op, those who received adjuvant chemotherapy had a 6-month DFS rate of 100% vs. 53.8% who did not receive adjuvant chemotherapy.
For stage III disease, those rates were 89.2% vs. 32.0%, and for stage IV disease, they were 72.7% vs. 28.3%.
At a median follow-up of 11.4 months, the 6- and 12-month DFS was 96.5% and 92.7% for all patients who were ctDNA negative at 4 weeks post-op. Outcomes for patients who were ctDNA positive were significantly poorer, at 62.8% and 47.5% (hazard ratio, 10.9; P <.001; sensitivity for recurrence, 63.6%).
Of the 188 patients who were MRD positive at 4 weeks post-op with available MRD status at 12 weeks, 95 received adjuvant therapy. The ctDNA clearance rate at 12 weeks was significantly higher in the adjuvant therapy group vs. no adjuvant therapy; 57% vs. 8% in stage I-IV (P < .001), and 58% vs. 11% (4/37) in stage II–III (P < .001).
Additionally, the ctDNA clearance rate at 24 weeks was also significantly higher in adjuvant vs. no adjuvant therapy arms; 26% vs. 0% in patients with stage I-IV disease (P = .003), and 33% vs. 0% in patients with stage II-III disease (P = .03).
Cumulative clearance of ctDNA at 6 months post-op was significantly higher in the adjuvant vs. no adjuvant therapy arms (67% vs. 7% by 24 weeks; cumulative HR, 17.1; P < .001). For patients MRD positive at 4 weeks, the 6-month DFS was also significantly higher in adjuvant vs. no adjuvant therapy arms; 84% vs 34% (HR, 0.15; P < .001), which was observed across all stages.
Upon multivariate analysis, the highest risk of recurrence for patients with stage II-III cancer correlated with ctDNA-positive vs. ctDNA-negative status (HR, 15.3; P <. 001), mutant vs. wild-type RAS (HR, 1.8; P = .04), or mutant vs. wild-type BRAF (HR, 5.2; P < .001).
The group is continuing with its research into a ctDNA-guided adjuvant strategy. More data will be available soon from the ongoing randomized VEGA and ALTAIR studies and will be presented at future conference, Dr. Kotaka commented.
CIRCULATE‐Japan receives financial supports from the Japan Agency for Medical Research and Development and from Taiho Pharmaceutical, through Alpha‐A. Dr. Kotaka reported relationships with Chugai, Lilly Japan, Taiho, Takeda, and Yakult Honsha. Dr. Yaeger reported relationships with Array BioPharma, Boehringer Ingelheim, Mirati Therapeutics, Natera, and Pfizer.
A version of this article first appeared on Medscape.com.
FROM GI CANCERS SYMPOSIUM 2022
Dual immunotherapy promising new option for liver cancer
The novel regimen, dubbed STRIDE (Single T Regular Interval D), comprised a single priming dose of the investigational agent tremelimumab followed by regular doses of durvalumab (Imfinzi).
Patients on this regimen experienced a 22% lower risk of death than patients treated with sorafenib (Nexavar), which at the time the trial began was the only approved frontline standard of care for patients with advanced HCC.
At 3 years, almost 31% of patients treated with combination therapy were still alive, versus 24.7% for durvalumab alone and 20.2% for sorafenib.
This novel regimen “may represent new treatment options for patients with untreated hepatocellular carcinoma,” said lead author Ghassan Abou-Alfa, MD, MBA, an attending physician at Memorial Sloan Kettering Comprehensive Cancer Center, New York. “Pending FDA approval, this novel dual immunotherapy regimen could be readily available to all patients and would not require additional safety assessments prior to treatment.”
He presented the new results here at the Gastrointestinal Cancers Symposium (GICS) 2022.
Discussing the abstract, Anthony B. El-Khoueiry, MD, from the University of Southern California, Norris Comprehensive Cancer Center, Los Angeles, agreed that the STRIDE regimen, with the combination of one priming dose of tremelimumab and regular interval durvalumab, is a new first-line treatment option for advanced HCC patients.
“But there are some limitations to the study and topics that will require further additional investigation,” he added.
Liver cancer increasing
Liver cancer is one of the few cancers for which deaths rates are increasing. In the United States. The overall rate of death due to liver cancer has doubled since 1980, Dr. Abou-Alfa told the audience. The most recent 5-year survival rates are 32.6% for localized disease, 10.8% with regional disease, and 2.4% with distant disease.
Until recently, first-line treatment for untreated HCC was limited to the multikinase inhibitors sorafenib and lenvatinib (Lenvima), which have been associated with median overall survival of approximately 1 year but also with toxicities that impact the quality of life, he commented.
“More recently, the anti-PD-L1 agent atezolizumab plus bevacizumab showed significant survival benefit versus sorafenib and have become a standard of care following approval in 2020,” Dr. Abou-Alfa said.
Tremelimumab is an experimental immunotherapy that targets the CTLA-4 receptor, and in 2020 it received orphan drug status for the treatment of HCC from the U.S. Food and Drug Administration. The authors hypothesized that tremelimumab would boost the response to durvalumab, a PDL-1 inhibitor, as this had been observed in the phase 2 Study 22 trial, which had tested the STRIDE regimen.
Now in the phase 3 HIMALAYA trial, the STRIDE regimen was compared to durvalumab used alone and to sorafenib used alone.
The trial randomized 1,171 patients to receive either the STRIDE regimen (a single dose of 75 mg tremelimumab plus 1,500 mg durvalumab every 4 weeks) or durvalumab alone (1,500 mg every 4 weeks) or sorafenib alone (400 mg twice daily).
Initially, there was also a lower-dose tremelimumab-containing arm, but recruitment into this arm was halted after a planned analysis of Study 22 failed to show a meaningful efficacy difference between that arm and durvalumab alone.
At data cutoff, the study’s primary objective was met. Overall survival was significantly improved for STRIDE versus sorafenib (hazard ratio; P = .0035). Median overall survival was 16.4 months for the STRIDE group versus 13.8 months for sorafenib and 16.6 months for durvalumab alone.
Median progression-free survival was 3.8 months, 3.7 months, and 41.1 months, respectively.
The overall response rate for the STRIDE arm was 20.1% compared to 17% for durvalumab, and 5.1% for sorafenib, and the median duration of response was 22.3 months, 16.8 months, and 18.4 months, respectively.
Treatment-related grade 3 or 4 adverse events occurred in 25.8% of patients on the combination, compared with 12.9% for durvalumab and 36.9% for sorafenib.
Grade 5 events occurred in 2.3% of the STRIDE group, compared with 0% among those receiving durvalumab alone and 0.8% in the sorafenib group. Treatment discontinuation due to events occurred in 8.2%, 4.1%, and 11.0% of patients, respectively.
New option for first-line treatment
In his discussion of the abstract, Dr. El-Khoueiry raised a few issues with the HIMALAYA trial that he felt needed further investigation.
Due to the study design, no conclusions can be drawn regarding the STRIDE regimen versus durvalumab as a single agent – the study was not powered for that, he said.
Also, the trial excluded patients with main portal vein thrombosis (PVT), he noted, and he felt that the subgroup analysis of hepatitis C patients requires further study.
“Another point is that, compared with other studies, bleeding events were less common in the HIMALAYA trial, but it did exclude patients with main PVT who are at highest risk of bleeding,” he pointed out.
STRIDE has a different toxicity profile from that seen with VEGF-containing combinations (for example, containing bevacizumab) and has a lower bleeding risk and a manageable rate of immune-mediated adverse events that require steroids. “But looking at non-VEGF regimens, is there an advantage to this, since most subsequent therapies target VEGF?” he questioned.
Another question is if there is a role for single agent PD-1/PD-L1 in first-line HCC. “This trial found that durvalumab was noninferior to sorafenib. This could be a first-line treatment option for select patients – maybe those who are poor candidates for combination therapy or have contraindications to VEGF,” said Dr. El-Khoueiry.
Nevertheless, STRIDE represents an emerging treatment option for this population, especially for patients who have contraindications for bevacizumab and a high bleeding risk, he concluded.
“So for HCC, it is amazing that we now have multiple first-line treatment options available,” he said. “The choice of therapy should be guided by toxicity profile and patient specific contraindications.”
For the future, he emphasized that biomarker development is critical to enhance a personalized approach driven by tumor and host biology.
“Sorafenib is no longer an appropriate control arm for first-line trials,” he said. “Timing of transition from liver-directed therapy to systemic therapy is critical given multiple available options.”
HCC in the setting of compromised liver function continues to be an unmet need. “And finally, in the second line and beyond, therapy after first-line immunotherapy combinations is largely empiric,” he said. “Research is needed to establish the efficacy of available and future therapeutic options post immunotherapy and the optimal sequence.”
This study received funding from AstraZeneca, maker of durvalumab. Dr. Abou-Alfa and Dr. El-Khoueiry reported relationships with numerous pharmaceutical companies.
A version of this article first appeared on Medscape.com.
The novel regimen, dubbed STRIDE (Single T Regular Interval D), comprised a single priming dose of the investigational agent tremelimumab followed by regular doses of durvalumab (Imfinzi).
Patients on this regimen experienced a 22% lower risk of death than patients treated with sorafenib (Nexavar), which at the time the trial began was the only approved frontline standard of care for patients with advanced HCC.
At 3 years, almost 31% of patients treated with combination therapy were still alive, versus 24.7% for durvalumab alone and 20.2% for sorafenib.
This novel regimen “may represent new treatment options for patients with untreated hepatocellular carcinoma,” said lead author Ghassan Abou-Alfa, MD, MBA, an attending physician at Memorial Sloan Kettering Comprehensive Cancer Center, New York. “Pending FDA approval, this novel dual immunotherapy regimen could be readily available to all patients and would not require additional safety assessments prior to treatment.”
He presented the new results here at the Gastrointestinal Cancers Symposium (GICS) 2022.
Discussing the abstract, Anthony B. El-Khoueiry, MD, from the University of Southern California, Norris Comprehensive Cancer Center, Los Angeles, agreed that the STRIDE regimen, with the combination of one priming dose of tremelimumab and regular interval durvalumab, is a new first-line treatment option for advanced HCC patients.
“But there are some limitations to the study and topics that will require further additional investigation,” he added.
Liver cancer increasing
Liver cancer is one of the few cancers for which deaths rates are increasing. In the United States. The overall rate of death due to liver cancer has doubled since 1980, Dr. Abou-Alfa told the audience. The most recent 5-year survival rates are 32.6% for localized disease, 10.8% with regional disease, and 2.4% with distant disease.
Until recently, first-line treatment for untreated HCC was limited to the multikinase inhibitors sorafenib and lenvatinib (Lenvima), which have been associated with median overall survival of approximately 1 year but also with toxicities that impact the quality of life, he commented.
“More recently, the anti-PD-L1 agent atezolizumab plus bevacizumab showed significant survival benefit versus sorafenib and have become a standard of care following approval in 2020,” Dr. Abou-Alfa said.
Tremelimumab is an experimental immunotherapy that targets the CTLA-4 receptor, and in 2020 it received orphan drug status for the treatment of HCC from the U.S. Food and Drug Administration. The authors hypothesized that tremelimumab would boost the response to durvalumab, a PDL-1 inhibitor, as this had been observed in the phase 2 Study 22 trial, which had tested the STRIDE regimen.
Now in the phase 3 HIMALAYA trial, the STRIDE regimen was compared to durvalumab used alone and to sorafenib used alone.
The trial randomized 1,171 patients to receive either the STRIDE regimen (a single dose of 75 mg tremelimumab plus 1,500 mg durvalumab every 4 weeks) or durvalumab alone (1,500 mg every 4 weeks) or sorafenib alone (400 mg twice daily).
Initially, there was also a lower-dose tremelimumab-containing arm, but recruitment into this arm was halted after a planned analysis of Study 22 failed to show a meaningful efficacy difference between that arm and durvalumab alone.
At data cutoff, the study’s primary objective was met. Overall survival was significantly improved for STRIDE versus sorafenib (hazard ratio; P = .0035). Median overall survival was 16.4 months for the STRIDE group versus 13.8 months for sorafenib and 16.6 months for durvalumab alone.
Median progression-free survival was 3.8 months, 3.7 months, and 41.1 months, respectively.
The overall response rate for the STRIDE arm was 20.1% compared to 17% for durvalumab, and 5.1% for sorafenib, and the median duration of response was 22.3 months, 16.8 months, and 18.4 months, respectively.
Treatment-related grade 3 or 4 adverse events occurred in 25.8% of patients on the combination, compared with 12.9% for durvalumab and 36.9% for sorafenib.
Grade 5 events occurred in 2.3% of the STRIDE group, compared with 0% among those receiving durvalumab alone and 0.8% in the sorafenib group. Treatment discontinuation due to events occurred in 8.2%, 4.1%, and 11.0% of patients, respectively.
New option for first-line treatment
In his discussion of the abstract, Dr. El-Khoueiry raised a few issues with the HIMALAYA trial that he felt needed further investigation.
Due to the study design, no conclusions can be drawn regarding the STRIDE regimen versus durvalumab as a single agent – the study was not powered for that, he said.
Also, the trial excluded patients with main portal vein thrombosis (PVT), he noted, and he felt that the subgroup analysis of hepatitis C patients requires further study.
“Another point is that, compared with other studies, bleeding events were less common in the HIMALAYA trial, but it did exclude patients with main PVT who are at highest risk of bleeding,” he pointed out.
STRIDE has a different toxicity profile from that seen with VEGF-containing combinations (for example, containing bevacizumab) and has a lower bleeding risk and a manageable rate of immune-mediated adverse events that require steroids. “But looking at non-VEGF regimens, is there an advantage to this, since most subsequent therapies target VEGF?” he questioned.
Another question is if there is a role for single agent PD-1/PD-L1 in first-line HCC. “This trial found that durvalumab was noninferior to sorafenib. This could be a first-line treatment option for select patients – maybe those who are poor candidates for combination therapy or have contraindications to VEGF,” said Dr. El-Khoueiry.
Nevertheless, STRIDE represents an emerging treatment option for this population, especially for patients who have contraindications for bevacizumab and a high bleeding risk, he concluded.
“So for HCC, it is amazing that we now have multiple first-line treatment options available,” he said. “The choice of therapy should be guided by toxicity profile and patient specific contraindications.”
For the future, he emphasized that biomarker development is critical to enhance a personalized approach driven by tumor and host biology.
“Sorafenib is no longer an appropriate control arm for first-line trials,” he said. “Timing of transition from liver-directed therapy to systemic therapy is critical given multiple available options.”
HCC in the setting of compromised liver function continues to be an unmet need. “And finally, in the second line and beyond, therapy after first-line immunotherapy combinations is largely empiric,” he said. “Research is needed to establish the efficacy of available and future therapeutic options post immunotherapy and the optimal sequence.”
This study received funding from AstraZeneca, maker of durvalumab. Dr. Abou-Alfa and Dr. El-Khoueiry reported relationships with numerous pharmaceutical companies.
A version of this article first appeared on Medscape.com.
The novel regimen, dubbed STRIDE (Single T Regular Interval D), comprised a single priming dose of the investigational agent tremelimumab followed by regular doses of durvalumab (Imfinzi).
Patients on this regimen experienced a 22% lower risk of death than patients treated with sorafenib (Nexavar), which at the time the trial began was the only approved frontline standard of care for patients with advanced HCC.
At 3 years, almost 31% of patients treated with combination therapy were still alive, versus 24.7% for durvalumab alone and 20.2% for sorafenib.
This novel regimen “may represent new treatment options for patients with untreated hepatocellular carcinoma,” said lead author Ghassan Abou-Alfa, MD, MBA, an attending physician at Memorial Sloan Kettering Comprehensive Cancer Center, New York. “Pending FDA approval, this novel dual immunotherapy regimen could be readily available to all patients and would not require additional safety assessments prior to treatment.”
He presented the new results here at the Gastrointestinal Cancers Symposium (GICS) 2022.
Discussing the abstract, Anthony B. El-Khoueiry, MD, from the University of Southern California, Norris Comprehensive Cancer Center, Los Angeles, agreed that the STRIDE regimen, with the combination of one priming dose of tremelimumab and regular interval durvalumab, is a new first-line treatment option for advanced HCC patients.
“But there are some limitations to the study and topics that will require further additional investigation,” he added.
Liver cancer increasing
Liver cancer is one of the few cancers for which deaths rates are increasing. In the United States. The overall rate of death due to liver cancer has doubled since 1980, Dr. Abou-Alfa told the audience. The most recent 5-year survival rates are 32.6% for localized disease, 10.8% with regional disease, and 2.4% with distant disease.
Until recently, first-line treatment for untreated HCC was limited to the multikinase inhibitors sorafenib and lenvatinib (Lenvima), which have been associated with median overall survival of approximately 1 year but also with toxicities that impact the quality of life, he commented.
“More recently, the anti-PD-L1 agent atezolizumab plus bevacizumab showed significant survival benefit versus sorafenib and have become a standard of care following approval in 2020,” Dr. Abou-Alfa said.
Tremelimumab is an experimental immunotherapy that targets the CTLA-4 receptor, and in 2020 it received orphan drug status for the treatment of HCC from the U.S. Food and Drug Administration. The authors hypothesized that tremelimumab would boost the response to durvalumab, a PDL-1 inhibitor, as this had been observed in the phase 2 Study 22 trial, which had tested the STRIDE regimen.
Now in the phase 3 HIMALAYA trial, the STRIDE regimen was compared to durvalumab used alone and to sorafenib used alone.
The trial randomized 1,171 patients to receive either the STRIDE regimen (a single dose of 75 mg tremelimumab plus 1,500 mg durvalumab every 4 weeks) or durvalumab alone (1,500 mg every 4 weeks) or sorafenib alone (400 mg twice daily).
Initially, there was also a lower-dose tremelimumab-containing arm, but recruitment into this arm was halted after a planned analysis of Study 22 failed to show a meaningful efficacy difference between that arm and durvalumab alone.
At data cutoff, the study’s primary objective was met. Overall survival was significantly improved for STRIDE versus sorafenib (hazard ratio; P = .0035). Median overall survival was 16.4 months for the STRIDE group versus 13.8 months for sorafenib and 16.6 months for durvalumab alone.
Median progression-free survival was 3.8 months, 3.7 months, and 41.1 months, respectively.
The overall response rate for the STRIDE arm was 20.1% compared to 17% for durvalumab, and 5.1% for sorafenib, and the median duration of response was 22.3 months, 16.8 months, and 18.4 months, respectively.
Treatment-related grade 3 or 4 adverse events occurred in 25.8% of patients on the combination, compared with 12.9% for durvalumab and 36.9% for sorafenib.
Grade 5 events occurred in 2.3% of the STRIDE group, compared with 0% among those receiving durvalumab alone and 0.8% in the sorafenib group. Treatment discontinuation due to events occurred in 8.2%, 4.1%, and 11.0% of patients, respectively.
New option for first-line treatment
In his discussion of the abstract, Dr. El-Khoueiry raised a few issues with the HIMALAYA trial that he felt needed further investigation.
Due to the study design, no conclusions can be drawn regarding the STRIDE regimen versus durvalumab as a single agent – the study was not powered for that, he said.
Also, the trial excluded patients with main portal vein thrombosis (PVT), he noted, and he felt that the subgroup analysis of hepatitis C patients requires further study.
“Another point is that, compared with other studies, bleeding events were less common in the HIMALAYA trial, but it did exclude patients with main PVT who are at highest risk of bleeding,” he pointed out.
STRIDE has a different toxicity profile from that seen with VEGF-containing combinations (for example, containing bevacizumab) and has a lower bleeding risk and a manageable rate of immune-mediated adverse events that require steroids. “But looking at non-VEGF regimens, is there an advantage to this, since most subsequent therapies target VEGF?” he questioned.
Another question is if there is a role for single agent PD-1/PD-L1 in first-line HCC. “This trial found that durvalumab was noninferior to sorafenib. This could be a first-line treatment option for select patients – maybe those who are poor candidates for combination therapy or have contraindications to VEGF,” said Dr. El-Khoueiry.
Nevertheless, STRIDE represents an emerging treatment option for this population, especially for patients who have contraindications for bevacizumab and a high bleeding risk, he concluded.
“So for HCC, it is amazing that we now have multiple first-line treatment options available,” he said. “The choice of therapy should be guided by toxicity profile and patient specific contraindications.”
For the future, he emphasized that biomarker development is critical to enhance a personalized approach driven by tumor and host biology.
“Sorafenib is no longer an appropriate control arm for first-line trials,” he said. “Timing of transition from liver-directed therapy to systemic therapy is critical given multiple available options.”
HCC in the setting of compromised liver function continues to be an unmet need. “And finally, in the second line and beyond, therapy after first-line immunotherapy combinations is largely empiric,” he said. “Research is needed to establish the efficacy of available and future therapeutic options post immunotherapy and the optimal sequence.”
This study received funding from AstraZeneca, maker of durvalumab. Dr. Abou-Alfa and Dr. El-Khoueiry reported relationships with numerous pharmaceutical companies.
A version of this article first appeared on Medscape.com.
FROM GI CANCERS SYMPOSIUM 2022
Primer message boosts colorectal cancer screening rates
Researchers have found a simple, low-cost way to get more adults to complete a fecal immunochemical test (FIT) to screen for colorectal cancer (CRC).
In a randomized controlled trial, patients who received an electronic “primer” message through their patient portal before the test kit arrived in their mailbox were more apt to complete and return the test than peers who didn’t get the electronic message.
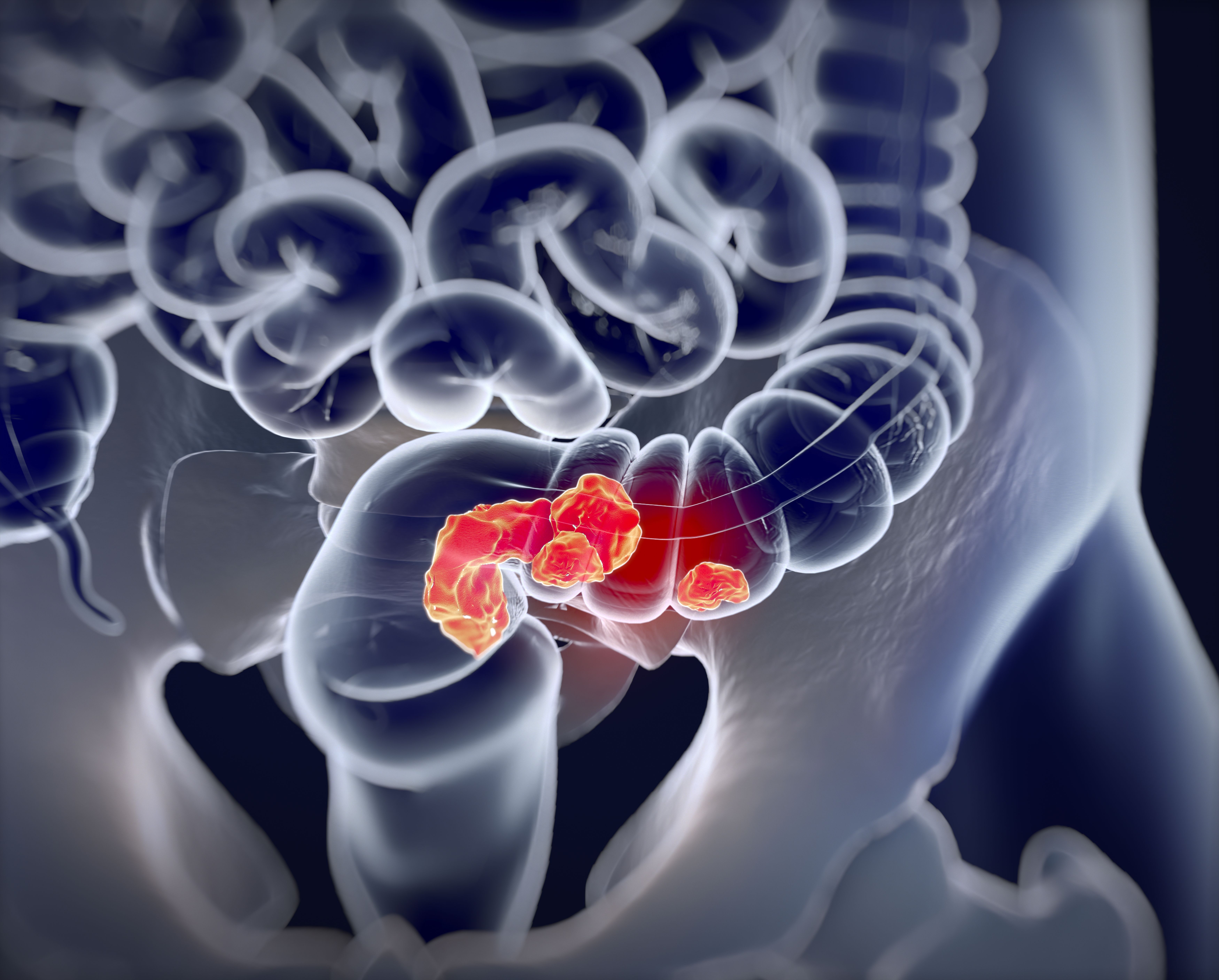
“We were thrilled by the magnitude of the impact,” Gregory Goshgarian, MSc, MPH, and Daniel Croymans, MD, with the department of medicine, David Geffen School of Medicine, University of California, Los Angeles, said in a joint email to this news organization.
At UCLA Health, “including a primer patient portal message is now standard practice for our FIT mailer program,” they added.
Their study was published online Feb. 4 in JAMA Network Open.
Heads-up message boosts compliance
CRC screening rates in the United States remain well below the national benchmark of 80%, and COVID-19 hasn’t helped. As a result, multiple medical and professional societies have emphasized the use of a mailed FIT outreach program.
As part of the outreach program, researchers at UCLA Health developed an electronic primer message within the electronic patient portal to alert patients due for CRC screening that they would be receiving a FIT kit in the mail.
They tested the impact of the primer messages in a randomized controlled trial involving 2,339 adults (mean age, 59 years, 57.5% women). Out of these, 1,157 received the standard mailed FIT kit (control group) and 1,182 received the standard mailed FIT kit plus a primer message sent through their personal patient portal.
Adding the primer message significantly increased the FIT completion rate at 6 months by 5.5%, with rates of 37.6% in the intervention group versus 32.1% in the control group.
After adjusting for patient demographics, the primer (versus no primer) led to significantly increased odds of completing CRC screening (adjusted odds ratio: 1.29; 95% confidence interval, 1.08-1.53; P = .004).
The primer message also shortened the time to FIT screening by 3 days (35 days with the primer vs. 38 days without).
Dr. Goshgarian and Dr. Croymans believe the priming messages worked well in their patient population because at the beginning of the intervention they identified a potential lack of awareness of the incoming FIT kit mailer as a barrier to uptake.
“We believe patients were receiving the kits with minimal advanced warning and discarding it as a mistake or hesitant to complete it because they did not understand the value to them,” they told this news organization.
“Therefore, a priming message helped to bridge that gap and allowed patients to be aware of the incoming FIT kits, know why it was important to do the FIT kit, and ultimately led to increasing our FIT kit return rates and thus CRC screening,” they said.
The researchers caution that their findings may be more relevant to patient populations who are more engaged in their health or who are more technologically savvy. In the UCLA Health system, roughly 84% of patients have an activated patient portal.
‘Good enhancement’ for health care systems
Reached for comment, Aasma Shaukat, MD, MPH, professor of medicine, NYU Langone Health, and first author of the American College of Gastroenterology (ACG) 2021 CRC screening guidelines, said the results are “interesting but not entirely surprising.”
“There’s literature supporting that a letter or notification prior to the FIT being mailed improves its uptake. Here, the authors applied it to their health care system in a quality improvement study and demonstrated it works,” Dr. Shaukat said.
“This is a good enhancement for health care systems where most of their patients are using or accessing their health chart portal,” added Dr. Shaukat.
“Caveats are that the generalizability is not known. It requires EHR [electronic health record] support tools and patients with access to a computer and enrolled and able to access their electronic chart, likely those with high literacy and English speaking.”
Funding for the study was provided by the UCLA Health Department of Medicine. Dr. Goshgarian, Dr. Croymans, and Dr. Shaukat have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Researchers have found a simple, low-cost way to get more adults to complete a fecal immunochemical test (FIT) to screen for colorectal cancer (CRC).
In a randomized controlled trial, patients who received an electronic “primer” message through their patient portal before the test kit arrived in their mailbox were more apt to complete and return the test than peers who didn’t get the electronic message.
“We were thrilled by the magnitude of the impact,” Gregory Goshgarian, MSc, MPH, and Daniel Croymans, MD, with the department of medicine, David Geffen School of Medicine, University of California, Los Angeles, said in a joint email to this news organization.
At UCLA Health, “including a primer patient portal message is now standard practice for our FIT mailer program,” they added.
Their study was published online Feb. 4 in JAMA Network Open.
Heads-up message boosts compliance
CRC screening rates in the United States remain well below the national benchmark of 80%, and COVID-19 hasn’t helped. As a result, multiple medical and professional societies have emphasized the use of a mailed FIT outreach program.
As part of the outreach program, researchers at UCLA Health developed an electronic primer message within the electronic patient portal to alert patients due for CRC screening that they would be receiving a FIT kit in the mail.
They tested the impact of the primer messages in a randomized controlled trial involving 2,339 adults (mean age, 59 years, 57.5% women). Out of these, 1,157 received the standard mailed FIT kit (control group) and 1,182 received the standard mailed FIT kit plus a primer message sent through their personal patient portal.
Adding the primer message significantly increased the FIT completion rate at 6 months by 5.5%, with rates of 37.6% in the intervention group versus 32.1% in the control group.
After adjusting for patient demographics, the primer (versus no primer) led to significantly increased odds of completing CRC screening (adjusted odds ratio: 1.29; 95% confidence interval, 1.08-1.53; P = .004).
The primer message also shortened the time to FIT screening by 3 days (35 days with the primer vs. 38 days without).
Dr. Goshgarian and Dr. Croymans believe the priming messages worked well in their patient population because at the beginning of the intervention they identified a potential lack of awareness of the incoming FIT kit mailer as a barrier to uptake.
“We believe patients were receiving the kits with minimal advanced warning and discarding it as a mistake or hesitant to complete it because they did not understand the value to them,” they told this news organization.
“Therefore, a priming message helped to bridge that gap and allowed patients to be aware of the incoming FIT kits, know why it was important to do the FIT kit, and ultimately led to increasing our FIT kit return rates and thus CRC screening,” they said.
The researchers caution that their findings may be more relevant to patient populations who are more engaged in their health or who are more technologically savvy. In the UCLA Health system, roughly 84% of patients have an activated patient portal.
‘Good enhancement’ for health care systems
Reached for comment, Aasma Shaukat, MD, MPH, professor of medicine, NYU Langone Health, and first author of the American College of Gastroenterology (ACG) 2021 CRC screening guidelines, said the results are “interesting but not entirely surprising.”
“There’s literature supporting that a letter or notification prior to the FIT being mailed improves its uptake. Here, the authors applied it to their health care system in a quality improvement study and demonstrated it works,” Dr. Shaukat said.
“This is a good enhancement for health care systems where most of their patients are using or accessing their health chart portal,” added Dr. Shaukat.
“Caveats are that the generalizability is not known. It requires EHR [electronic health record] support tools and patients with access to a computer and enrolled and able to access their electronic chart, likely those with high literacy and English speaking.”
Funding for the study was provided by the UCLA Health Department of Medicine. Dr. Goshgarian, Dr. Croymans, and Dr. Shaukat have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Researchers have found a simple, low-cost way to get more adults to complete a fecal immunochemical test (FIT) to screen for colorectal cancer (CRC).
In a randomized controlled trial, patients who received an electronic “primer” message through their patient portal before the test kit arrived in their mailbox were more apt to complete and return the test than peers who didn’t get the electronic message.
“We were thrilled by the magnitude of the impact,” Gregory Goshgarian, MSc, MPH, and Daniel Croymans, MD, with the department of medicine, David Geffen School of Medicine, University of California, Los Angeles, said in a joint email to this news organization.
At UCLA Health, “including a primer patient portal message is now standard practice for our FIT mailer program,” they added.
Their study was published online Feb. 4 in JAMA Network Open.
Heads-up message boosts compliance
CRC screening rates in the United States remain well below the national benchmark of 80%, and COVID-19 hasn’t helped. As a result, multiple medical and professional societies have emphasized the use of a mailed FIT outreach program.
As part of the outreach program, researchers at UCLA Health developed an electronic primer message within the electronic patient portal to alert patients due for CRC screening that they would be receiving a FIT kit in the mail.
They tested the impact of the primer messages in a randomized controlled trial involving 2,339 adults (mean age, 59 years, 57.5% women). Out of these, 1,157 received the standard mailed FIT kit (control group) and 1,182 received the standard mailed FIT kit plus a primer message sent through their personal patient portal.
Adding the primer message significantly increased the FIT completion rate at 6 months by 5.5%, with rates of 37.6% in the intervention group versus 32.1% in the control group.
After adjusting for patient demographics, the primer (versus no primer) led to significantly increased odds of completing CRC screening (adjusted odds ratio: 1.29; 95% confidence interval, 1.08-1.53; P = .004).
The primer message also shortened the time to FIT screening by 3 days (35 days with the primer vs. 38 days without).
Dr. Goshgarian and Dr. Croymans believe the priming messages worked well in their patient population because at the beginning of the intervention they identified a potential lack of awareness of the incoming FIT kit mailer as a barrier to uptake.
“We believe patients were receiving the kits with minimal advanced warning and discarding it as a mistake or hesitant to complete it because they did not understand the value to them,” they told this news organization.
“Therefore, a priming message helped to bridge that gap and allowed patients to be aware of the incoming FIT kits, know why it was important to do the FIT kit, and ultimately led to increasing our FIT kit return rates and thus CRC screening,” they said.
The researchers caution that their findings may be more relevant to patient populations who are more engaged in their health or who are more technologically savvy. In the UCLA Health system, roughly 84% of patients have an activated patient portal.
‘Good enhancement’ for health care systems
Reached for comment, Aasma Shaukat, MD, MPH, professor of medicine, NYU Langone Health, and first author of the American College of Gastroenterology (ACG) 2021 CRC screening guidelines, said the results are “interesting but not entirely surprising.”
“There’s literature supporting that a letter or notification prior to the FIT being mailed improves its uptake. Here, the authors applied it to their health care system in a quality improvement study and demonstrated it works,” Dr. Shaukat said.
“This is a good enhancement for health care systems where most of their patients are using or accessing their health chart portal,” added Dr. Shaukat.
“Caveats are that the generalizability is not known. It requires EHR [electronic health record] support tools and patients with access to a computer and enrolled and able to access their electronic chart, likely those with high literacy and English speaking.”
Funding for the study was provided by the UCLA Health Department of Medicine. Dr. Goshgarian, Dr. Croymans, and Dr. Shaukat have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
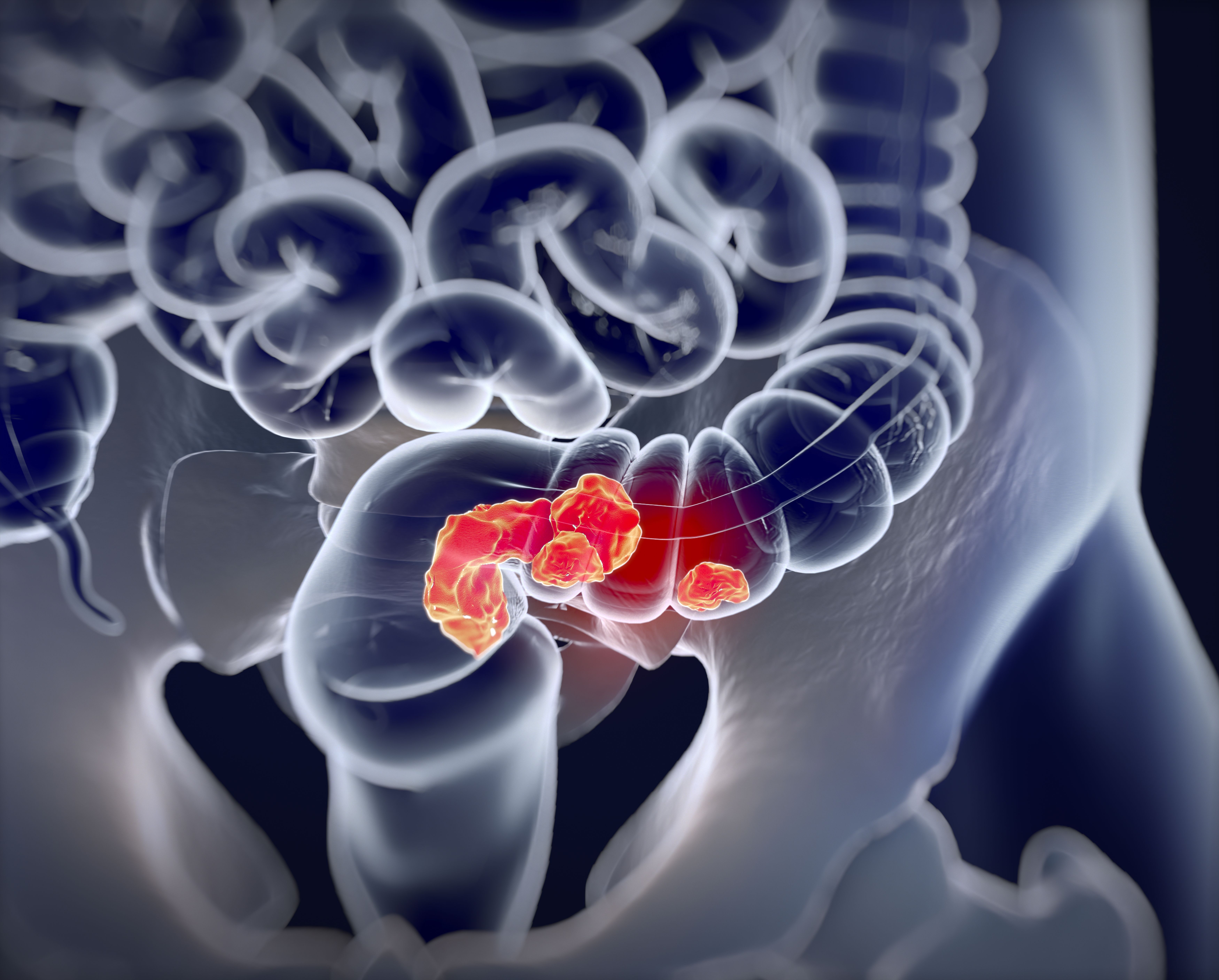
Adding TACE to lenvatinib improves survival in liver cancer
The combination of TACE and lenvatinib “represents a potential new first-line treatment option for patients with advanced HCC,” said study author Ming Kuang, MD, PhD, professor in hepatobiliary surgery and interventional ultrasound and director of the cancer center in the First Affiliated Hospital, Sun Yat-sen University, Guangzhou, China.
The combination of the two approaches was “safe and effective for patients with advanced hepatocellular carcinoma and demonstrated remarkable improvements in overall survival, progression-free survival, and overall response rate, as well as acceptable toxicity,” he said.
Patients receiving combination therapy achieved a median overall survival of 17.8 months, compared with 11.5 months in the lenvatinib arm (hazard ratio, 0.45; P < .001). Similarly, median progression-free survival also favored lenvatinib plus TACE: 10.6 months vs. 6.4 months (HR, 0.43; P < .001).
The study results were presented at the Gastrointestinal Cancers Symposium.
Discussing the abstract, Anthony B. El-Khoueiry, MD, from the University of Southern California, Norris Comprehensive Cancer Center, Los Angeles, said the results are “intriguing,” and he commended the researchers on carrying out this study.
“It reinforces the feasibility of combined liver directed and systemic therapy,” he said.
“However, it does not change the standard of care in the U.S.,” he cautioned.
“Systemic therapy backbone is not the standard of care, and the design of this study was not optimal to answer the question of whether the addition of liver-directed therapy in advanced HCC improves outcomes,” he added.
Dr. EL-Khoueiry pointed out that these new results from the LAUNCH trial contrast with two studies that looked at liver-directed plus a systemic therapy. Both of those previous studies used sorafenib, one utilizing Y-90 and the other conventional TACE.
Both of those studies were negative, he said. “But there were differences between these studies and LAUNCH.”
Aside from the fact that they used sorafenib and not lenvatinib, another difference was that the patient population of LAUNCH was younger than in the other two studies. In addition, most patients in the LAUCH trial had hepatitis B, and they received a higher number of TACE treatments than in the previous studies. “One can argue that maybe treatment selection was more optimal,” Dr. El-Khoueiry commented.
He also noted that “the control arm of lenvatinib underperformed, as sorafenib median overall survival in previous trials ranges from 13 to 15 months. We would have expected lenvatinib to perform at least as well or better.” (The median overall survival was 11.5 months).
Improved outcomes with combination therapy
The LAUNCH study involved 338 treatment-naive patients with advanced HCC from 12 hospitals in China who were randomly assigned to receive either lenvatinib plus TACE (n = 170) or lenvatinib alone (n = 168).
TACE was administered on day 1 following treatment with lenvatinib, which was administered at 8 mg or 12 mg once daily, depending on the patient’s weight.
The majority of patients were 60 years of age or younger, with a median age of 54-56 years. The majority of patients were male (81.8% in the combination group vs. 78.6% in the lenvatinib-alone group), and the majority had hepatitis B (87.1% vs. 85.7%).
At a median follow-up of 18.4 months for the lenvatinib-TACE group and 17.0 months for the lenvatinib group, the results showed a significantly improved overall survival of 17.8 months with the combination vs. 11.5 months for monotherapy (HR, 0.45; P < .001). Median progression-free survival (PFS) was also significantly longer, at 10.6 months vs. 6.4 months, respectively (HR, 0.43; P < .001).
The overall response rate was 54.1% vs. 25.0% (P < .001), and one complete response was observed in each study arm. The complete response rate was 2.9% vs. 0.6%; partial response rate, 51.2% vs. 24.4%; stable disease rate, 40.0% vs. 48.2%; and rate of disease progression, 5.9% vs. 26.8% for the lenvatinib-TACE group and lenvatinib monotherapy groups. The disease control rate was 94.1% vs. 73.2%.
Grade 3-4 adverse events that occurred more frequently in the lenvatinib-TACE group than in the lenvatinib group included increased liver enzymes, with increased ALT in 17.6% vs. 1.2%; increased AST in 22.9% vs. 1.8%; and hyperbilirubinemia in 9.4% vs. 3.0%.
“Subgroup analysis shows that the combination group had better overall survival and progression-free survival in most of the analyzed subgroups,” said Dr. Kuang. “Multivariate analysis also found that portal vein tumor thrombus and treatment allocation were independent risk factors of overall survival, and that age, portal vein tumor thrombus, and treatment allocation were independent risk factors of progression-free survival.”
Study limitations
In his discussion of the abstract, Dr. El-Khoueiry noted that the LAUNCH trial had several limitations, one being the heterogeneity of the patient population and potential imbalance. “There is limited information regarding extrahepatic disease burden and distribution,” he explained. “Another limitation is that the younger population – with the majority having hepatitis B – limits the broad applicability of the result and has a potential impact on the low rate of treatment discontinuation.”
This study received no industry funding. Dr. Kuang has disclosed no relevant financial relationships. Dr. El-Khoueiry reported relationships with ABL bio, Agenus, Astex, AstraZeneca/MedImmune, Bayer, Bristol-Myers Squibb, CytomX Therapeutics, Eisai, EMD Serono, Exelixis, Fulgent Genetics, Gilead Sciences, Merck, Pieris Pharmaceuticals, QED Therapeutics, and Roche/Genentech.
A version of this article first appeared on Medscape.com.
The combination of TACE and lenvatinib “represents a potential new first-line treatment option for patients with advanced HCC,” said study author Ming Kuang, MD, PhD, professor in hepatobiliary surgery and interventional ultrasound and director of the cancer center in the First Affiliated Hospital, Sun Yat-sen University, Guangzhou, China.
The combination of the two approaches was “safe and effective for patients with advanced hepatocellular carcinoma and demonstrated remarkable improvements in overall survival, progression-free survival, and overall response rate, as well as acceptable toxicity,” he said.
Patients receiving combination therapy achieved a median overall survival of 17.8 months, compared with 11.5 months in the lenvatinib arm (hazard ratio, 0.45; P < .001). Similarly, median progression-free survival also favored lenvatinib plus TACE: 10.6 months vs. 6.4 months (HR, 0.43; P < .001).
The study results were presented at the Gastrointestinal Cancers Symposium.
Discussing the abstract, Anthony B. El-Khoueiry, MD, from the University of Southern California, Norris Comprehensive Cancer Center, Los Angeles, said the results are “intriguing,” and he commended the researchers on carrying out this study.
“It reinforces the feasibility of combined liver directed and systemic therapy,” he said.
“However, it does not change the standard of care in the U.S.,” he cautioned.
“Systemic therapy backbone is not the standard of care, and the design of this study was not optimal to answer the question of whether the addition of liver-directed therapy in advanced HCC improves outcomes,” he added.
Dr. EL-Khoueiry pointed out that these new results from the LAUNCH trial contrast with two studies that looked at liver-directed plus a systemic therapy. Both of those previous studies used sorafenib, one utilizing Y-90 and the other conventional TACE.
Both of those studies were negative, he said. “But there were differences between these studies and LAUNCH.”
Aside from the fact that they used sorafenib and not lenvatinib, another difference was that the patient population of LAUNCH was younger than in the other two studies. In addition, most patients in the LAUCH trial had hepatitis B, and they received a higher number of TACE treatments than in the previous studies. “One can argue that maybe treatment selection was more optimal,” Dr. El-Khoueiry commented.
He also noted that “the control arm of lenvatinib underperformed, as sorafenib median overall survival in previous trials ranges from 13 to 15 months. We would have expected lenvatinib to perform at least as well or better.” (The median overall survival was 11.5 months).
Improved outcomes with combination therapy
The LAUNCH study involved 338 treatment-naive patients with advanced HCC from 12 hospitals in China who were randomly assigned to receive either lenvatinib plus TACE (n = 170) or lenvatinib alone (n = 168).
TACE was administered on day 1 following treatment with lenvatinib, which was administered at 8 mg or 12 mg once daily, depending on the patient’s weight.
The majority of patients were 60 years of age or younger, with a median age of 54-56 years. The majority of patients were male (81.8% in the combination group vs. 78.6% in the lenvatinib-alone group), and the majority had hepatitis B (87.1% vs. 85.7%).
At a median follow-up of 18.4 months for the lenvatinib-TACE group and 17.0 months for the lenvatinib group, the results showed a significantly improved overall survival of 17.8 months with the combination vs. 11.5 months for monotherapy (HR, 0.45; P < .001). Median progression-free survival (PFS) was also significantly longer, at 10.6 months vs. 6.4 months, respectively (HR, 0.43; P < .001).
The overall response rate was 54.1% vs. 25.0% (P < .001), and one complete response was observed in each study arm. The complete response rate was 2.9% vs. 0.6%; partial response rate, 51.2% vs. 24.4%; stable disease rate, 40.0% vs. 48.2%; and rate of disease progression, 5.9% vs. 26.8% for the lenvatinib-TACE group and lenvatinib monotherapy groups. The disease control rate was 94.1% vs. 73.2%.
Grade 3-4 adverse events that occurred more frequently in the lenvatinib-TACE group than in the lenvatinib group included increased liver enzymes, with increased ALT in 17.6% vs. 1.2%; increased AST in 22.9% vs. 1.8%; and hyperbilirubinemia in 9.4% vs. 3.0%.
“Subgroup analysis shows that the combination group had better overall survival and progression-free survival in most of the analyzed subgroups,” said Dr. Kuang. “Multivariate analysis also found that portal vein tumor thrombus and treatment allocation were independent risk factors of overall survival, and that age, portal vein tumor thrombus, and treatment allocation were independent risk factors of progression-free survival.”
Study limitations
In his discussion of the abstract, Dr. El-Khoueiry noted that the LAUNCH trial had several limitations, one being the heterogeneity of the patient population and potential imbalance. “There is limited information regarding extrahepatic disease burden and distribution,” he explained. “Another limitation is that the younger population – with the majority having hepatitis B – limits the broad applicability of the result and has a potential impact on the low rate of treatment discontinuation.”
This study received no industry funding. Dr. Kuang has disclosed no relevant financial relationships. Dr. El-Khoueiry reported relationships with ABL bio, Agenus, Astex, AstraZeneca/MedImmune, Bayer, Bristol-Myers Squibb, CytomX Therapeutics, Eisai, EMD Serono, Exelixis, Fulgent Genetics, Gilead Sciences, Merck, Pieris Pharmaceuticals, QED Therapeutics, and Roche/Genentech.
A version of this article first appeared on Medscape.com.
The combination of TACE and lenvatinib “represents a potential new first-line treatment option for patients with advanced HCC,” said study author Ming Kuang, MD, PhD, professor in hepatobiliary surgery and interventional ultrasound and director of the cancer center in the First Affiliated Hospital, Sun Yat-sen University, Guangzhou, China.
The combination of the two approaches was “safe and effective for patients with advanced hepatocellular carcinoma and demonstrated remarkable improvements in overall survival, progression-free survival, and overall response rate, as well as acceptable toxicity,” he said.
Patients receiving combination therapy achieved a median overall survival of 17.8 months, compared with 11.5 months in the lenvatinib arm (hazard ratio, 0.45; P < .001). Similarly, median progression-free survival also favored lenvatinib plus TACE: 10.6 months vs. 6.4 months (HR, 0.43; P < .001).
The study results were presented at the Gastrointestinal Cancers Symposium.
Discussing the abstract, Anthony B. El-Khoueiry, MD, from the University of Southern California, Norris Comprehensive Cancer Center, Los Angeles, said the results are “intriguing,” and he commended the researchers on carrying out this study.
“It reinforces the feasibility of combined liver directed and systemic therapy,” he said.
“However, it does not change the standard of care in the U.S.,” he cautioned.
“Systemic therapy backbone is not the standard of care, and the design of this study was not optimal to answer the question of whether the addition of liver-directed therapy in advanced HCC improves outcomes,” he added.
Dr. EL-Khoueiry pointed out that these new results from the LAUNCH trial contrast with two studies that looked at liver-directed plus a systemic therapy. Both of those previous studies used sorafenib, one utilizing Y-90 and the other conventional TACE.
Both of those studies were negative, he said. “But there were differences between these studies and LAUNCH.”
Aside from the fact that they used sorafenib and not lenvatinib, another difference was that the patient population of LAUNCH was younger than in the other two studies. In addition, most patients in the LAUCH trial had hepatitis B, and they received a higher number of TACE treatments than in the previous studies. “One can argue that maybe treatment selection was more optimal,” Dr. El-Khoueiry commented.
He also noted that “the control arm of lenvatinib underperformed, as sorafenib median overall survival in previous trials ranges from 13 to 15 months. We would have expected lenvatinib to perform at least as well or better.” (The median overall survival was 11.5 months).
Improved outcomes with combination therapy
The LAUNCH study involved 338 treatment-naive patients with advanced HCC from 12 hospitals in China who were randomly assigned to receive either lenvatinib plus TACE (n = 170) or lenvatinib alone (n = 168).
TACE was administered on day 1 following treatment with lenvatinib, which was administered at 8 mg or 12 mg once daily, depending on the patient’s weight.
The majority of patients were 60 years of age or younger, with a median age of 54-56 years. The majority of patients were male (81.8% in the combination group vs. 78.6% in the lenvatinib-alone group), and the majority had hepatitis B (87.1% vs. 85.7%).
At a median follow-up of 18.4 months for the lenvatinib-TACE group and 17.0 months for the lenvatinib group, the results showed a significantly improved overall survival of 17.8 months with the combination vs. 11.5 months for monotherapy (HR, 0.45; P < .001). Median progression-free survival (PFS) was also significantly longer, at 10.6 months vs. 6.4 months, respectively (HR, 0.43; P < .001).
The overall response rate was 54.1% vs. 25.0% (P < .001), and one complete response was observed in each study arm. The complete response rate was 2.9% vs. 0.6%; partial response rate, 51.2% vs. 24.4%; stable disease rate, 40.0% vs. 48.2%; and rate of disease progression, 5.9% vs. 26.8% for the lenvatinib-TACE group and lenvatinib monotherapy groups. The disease control rate was 94.1% vs. 73.2%.
Grade 3-4 adverse events that occurred more frequently in the lenvatinib-TACE group than in the lenvatinib group included increased liver enzymes, with increased ALT in 17.6% vs. 1.2%; increased AST in 22.9% vs. 1.8%; and hyperbilirubinemia in 9.4% vs. 3.0%.
“Subgroup analysis shows that the combination group had better overall survival and progression-free survival in most of the analyzed subgroups,” said Dr. Kuang. “Multivariate analysis also found that portal vein tumor thrombus and treatment allocation were independent risk factors of overall survival, and that age, portal vein tumor thrombus, and treatment allocation were independent risk factors of progression-free survival.”
Study limitations
In his discussion of the abstract, Dr. El-Khoueiry noted that the LAUNCH trial had several limitations, one being the heterogeneity of the patient population and potential imbalance. “There is limited information regarding extrahepatic disease burden and distribution,” he explained. “Another limitation is that the younger population – with the majority having hepatitis B – limits the broad applicability of the result and has a potential impact on the low rate of treatment discontinuation.”
This study received no industry funding. Dr. Kuang has disclosed no relevant financial relationships. Dr. El-Khoueiry reported relationships with ABL bio, Agenus, Astex, AstraZeneca/MedImmune, Bayer, Bristol-Myers Squibb, CytomX Therapeutics, Eisai, EMD Serono, Exelixis, Fulgent Genetics, Gilead Sciences, Merck, Pieris Pharmaceuticals, QED Therapeutics, and Roche/Genentech.
A version of this article first appeared on Medscape.com.
FROM GI CANCERS SYMPOSIUM 2022
USDA announces stricter standards for school nutrition
The U.S. Department of Agriculture has announced new changes to school nutrition standards for the next 2 school years, which will reinstate health goals that were rolled back during the Trump administration.
The Biden administration is also tightening rules for fat and salt content in foods after restrictions were eased during the pandemic, according to the Washington Post.
“Nutritious school meals give America’s children the foundation for successful, healthy lives,” Tom Vilsack, the U.S. agriculture secretary, said in a statement on Feb. 4.
“We applaud schools’ heroic efforts throughout the challenges of this pandemic to continue serving kids the most nutritious meals possible,” he said. “The standards we’re putting in place of the next 2 school years will help schools transition to a future that builds on the tremendous strides they’ve made improving school meal nutrition over the past decade.”
For the 2022-2023 school year, schools and childcare providers will be required to offer low-fat or nonfat unflavored milks and limit the fat in sweet flavored milks. In addition, at least 80% of the grains served during school breakfasts and lunches each week must be considered rich in whole grains.
For the 2023-2024 school year, the weekly sodium limit for school lunches will be decreased by 10%.
The changes mark a shift from the Trump administration, which eased policies on whole grains, nonfat milk, and sodium, the newspaper reported. Then the pandemic forced additional changes as school districts scrambled to package meals for students. The USDA granted extra flexibility and eased some guidelines to ensure that children could be fed while schools were closed or focused on remote learning.
Now the USDA is updating the nutrition standards to “give schools clear expectations for gradual transition from current pandemic operations to more nutritious meals,” Stacy Dean, the USDA’s deputy undersecretary for food, nutrition, and consumer services, told reporters.
The Biden administration’s changes represent a shift back to Obama-era nutrition standards from 2012, according to the Post. But some nutrition advocates have said the new changes don’t address enough issues, such as added sugars. Fruit and vegetable requirements, for instance, will remain the same as the 2012 standards.
That said, some advocates have said the transition could be tough as schools move out of pandemic-era protocols. The School Nutrition Association, which represents school food service manufacturers and professionals, has urged Congress to provide additional support and waiver extensions for the next school year.
“School nutrition professionals are frantic just trying to get enough food on the tray for our students amid relentless supply chain disruptions and labor shortages,” Beth Wallace, the association’s president, told the Washington Post.
The shift will likely require a balancing act and slow transition. The USDA has been consulting with stakeholders for months to determine how to move toward stricter school nutrition standards while also acknowledging the pandemic, supply chain disruptions, and labor shortages.
“This approach is really going to help move forward the nutrition of the meals and allows the schools to continue to function effectively,” Geri Henchy, director of nutrition policy at the Food Research and Action Center, told the Post.
“Schools can’t make big changes at this point because of the supply chain and staffing,” she said. “They have a lot of waivers at this point that are helping them, and this balances the needs of all the different sectors.”
The USDA plans to issue a proposed rule in fall 2022 to update nutrition standards for the future, the department said in its announcement, which would be finalized for the 2024-2025 school year.
A version of this article first appeared on WebMD.com.
The U.S. Department of Agriculture has announced new changes to school nutrition standards for the next 2 school years, which will reinstate health goals that were rolled back during the Trump administration.
The Biden administration is also tightening rules for fat and salt content in foods after restrictions were eased during the pandemic, according to the Washington Post.
“Nutritious school meals give America’s children the foundation for successful, healthy lives,” Tom Vilsack, the U.S. agriculture secretary, said in a statement on Feb. 4.
“We applaud schools’ heroic efforts throughout the challenges of this pandemic to continue serving kids the most nutritious meals possible,” he said. “The standards we’re putting in place of the next 2 school years will help schools transition to a future that builds on the tremendous strides they’ve made improving school meal nutrition over the past decade.”
For the 2022-2023 school year, schools and childcare providers will be required to offer low-fat or nonfat unflavored milks and limit the fat in sweet flavored milks. In addition, at least 80% of the grains served during school breakfasts and lunches each week must be considered rich in whole grains.
For the 2023-2024 school year, the weekly sodium limit for school lunches will be decreased by 10%.
The changes mark a shift from the Trump administration, which eased policies on whole grains, nonfat milk, and sodium, the newspaper reported. Then the pandemic forced additional changes as school districts scrambled to package meals for students. The USDA granted extra flexibility and eased some guidelines to ensure that children could be fed while schools were closed or focused on remote learning.
Now the USDA is updating the nutrition standards to “give schools clear expectations for gradual transition from current pandemic operations to more nutritious meals,” Stacy Dean, the USDA’s deputy undersecretary for food, nutrition, and consumer services, told reporters.
The Biden administration’s changes represent a shift back to Obama-era nutrition standards from 2012, according to the Post. But some nutrition advocates have said the new changes don’t address enough issues, such as added sugars. Fruit and vegetable requirements, for instance, will remain the same as the 2012 standards.
That said, some advocates have said the transition could be tough as schools move out of pandemic-era protocols. The School Nutrition Association, which represents school food service manufacturers and professionals, has urged Congress to provide additional support and waiver extensions for the next school year.
“School nutrition professionals are frantic just trying to get enough food on the tray for our students amid relentless supply chain disruptions and labor shortages,” Beth Wallace, the association’s president, told the Washington Post.
The shift will likely require a balancing act and slow transition. The USDA has been consulting with stakeholders for months to determine how to move toward stricter school nutrition standards while also acknowledging the pandemic, supply chain disruptions, and labor shortages.
“This approach is really going to help move forward the nutrition of the meals and allows the schools to continue to function effectively,” Geri Henchy, director of nutrition policy at the Food Research and Action Center, told the Post.
“Schools can’t make big changes at this point because of the supply chain and staffing,” she said. “They have a lot of waivers at this point that are helping them, and this balances the needs of all the different sectors.”
The USDA plans to issue a proposed rule in fall 2022 to update nutrition standards for the future, the department said in its announcement, which would be finalized for the 2024-2025 school year.
A version of this article first appeared on WebMD.com.
The U.S. Department of Agriculture has announced new changes to school nutrition standards for the next 2 school years, which will reinstate health goals that were rolled back during the Trump administration.
The Biden administration is also tightening rules for fat and salt content in foods after restrictions were eased during the pandemic, according to the Washington Post.
“Nutritious school meals give America’s children the foundation for successful, healthy lives,” Tom Vilsack, the U.S. agriculture secretary, said in a statement on Feb. 4.
“We applaud schools’ heroic efforts throughout the challenges of this pandemic to continue serving kids the most nutritious meals possible,” he said. “The standards we’re putting in place of the next 2 school years will help schools transition to a future that builds on the tremendous strides they’ve made improving school meal nutrition over the past decade.”
For the 2022-2023 school year, schools and childcare providers will be required to offer low-fat or nonfat unflavored milks and limit the fat in sweet flavored milks. In addition, at least 80% of the grains served during school breakfasts and lunches each week must be considered rich in whole grains.
For the 2023-2024 school year, the weekly sodium limit for school lunches will be decreased by 10%.
The changes mark a shift from the Trump administration, which eased policies on whole grains, nonfat milk, and sodium, the newspaper reported. Then the pandemic forced additional changes as school districts scrambled to package meals for students. The USDA granted extra flexibility and eased some guidelines to ensure that children could be fed while schools were closed or focused on remote learning.
Now the USDA is updating the nutrition standards to “give schools clear expectations for gradual transition from current pandemic operations to more nutritious meals,” Stacy Dean, the USDA’s deputy undersecretary for food, nutrition, and consumer services, told reporters.
The Biden administration’s changes represent a shift back to Obama-era nutrition standards from 2012, according to the Post. But some nutrition advocates have said the new changes don’t address enough issues, such as added sugars. Fruit and vegetable requirements, for instance, will remain the same as the 2012 standards.
That said, some advocates have said the transition could be tough as schools move out of pandemic-era protocols. The School Nutrition Association, which represents school food service manufacturers and professionals, has urged Congress to provide additional support and waiver extensions for the next school year.
“School nutrition professionals are frantic just trying to get enough food on the tray for our students amid relentless supply chain disruptions and labor shortages,” Beth Wallace, the association’s president, told the Washington Post.
The shift will likely require a balancing act and slow transition. The USDA has been consulting with stakeholders for months to determine how to move toward stricter school nutrition standards while also acknowledging the pandemic, supply chain disruptions, and labor shortages.
“This approach is really going to help move forward the nutrition of the meals and allows the schools to continue to function effectively,” Geri Henchy, director of nutrition policy at the Food Research and Action Center, told the Post.
“Schools can’t make big changes at this point because of the supply chain and staffing,” she said. “They have a lot of waivers at this point that are helping them, and this balances the needs of all the different sectors.”
The USDA plans to issue a proposed rule in fall 2022 to update nutrition standards for the future, the department said in its announcement, which would be finalized for the 2024-2025 school year.
A version of this article first appeared on WebMD.com.