User login
Experts Highlight Challenges That Remain for AI Devices in Triaging Skin Cancer
Emerging according to researchers and dermatologists investigating AI.
While some AI-integrated devices designed to triage skin lesions have emerged, including one that received Food and Drug Administration (FDA) clearance earlier in 2024, it may be some time before AI has a meaningful clinical impact in dermatology and, more specifically, the diagnosis of skin cancer, Ivy Lee, MD, a dermatologist in Pasadena, California, and chair of the American Academy of Dermatology’s augmented intelligence committee, told this news organization.
“It hasn’t really translated into clinical practice yet,” Dr. Lee said of AI in dermatology. “There have been significant advances in terms of the technical possibility and feasibility of these tools, but the translation and integration of AI into actual clinical work flows to benefit patients beyond academic research studies has been limited.” More studies and more “easily accessible and digestible information” are needed to evaluate AI tools in dermatologic practice.
“In dermatology, we’re on a cusp with AI,” said Rebecca Hartman, MD, MPH, chief of dermatology at the VA Boston Healthcare System and director of melanoma epidemiology at Brigham and Women’s Hospital, Boston, Massachusetts. “I think it’s going to come and change what we do,” which is especially true for any image-based specialty,” including radiology and pathology, in addition to dermatology.

Dr. Hartman led a study of one of these emerging technologies, the handheld elastic scattering spectroscopy device DermaSensor, which was cleared by the FDA in January for evaluating skin lesions suggestive of skin cancer.
Early AI Devices for Skin Cancer Detection
At the American Society for Laser Medicine and Surgery (ASLMS) meeting in April, a panel explored a number of algorithms with dermatologic applications that use AI to triage skin lesions, including DermaSensor.
Raman spectroscopy, which contains a handheld Raman probe, a diode laser, and a detecting spectrograph. A laser beam — which at 1.56 W/cm2 is below the maximum permissible exposure — focuses on the skin target with a 3.5-mm spot, gathers data on the target, and feeds it back into the unit that houses the algorithm that evaluates the spot analysis. It’s still in the investigative phase. A clinical trial, published almost 5 years ago, demonstrated a sensitivity of 90%-99% and a specificity of 24%-66% for skin cancer.
A dermatoscope called Sklip clips onto a smartphone and performs what company cofounder Alexander Witkowski, MD, PhD, described as an “optical painless virtual biopsy” for at-home use. The device uploads the captured image to an AI platform for analysis. It received FDA breakthrough device designation in 2022. At the ASLMS meeting, Dr. Witkowski said that clinical performance showed the device had a 97% sensitivity and 30% specificity for skin cancer.

DermaSensor, described in the study conducted by Dr. Hartman and others as a noninvasive, point-and-click spectrometer, is a wireless handheld piece that weighs about 10 ounces. The unit captures five recordings to generate a spectral reading, which an algorithm in the software unit analyzes. The study found a sensitivity of 95.5% and specificity of 32.5% for melanoma detection with the device.
The target market for DermaSensor is primary care physicians, and, according to the FDA announcement in January, it is indicated for evaluating skin lesions “suggestive” of melanoma, basal cell carcinoma (BCC), and/or squamous cell carcinoma (SCC) in patients aged 40 and older to “assist healthcare providers in determining whether to refer a patient to a dermatologist.”
So Many Cases, So Few Dermatologists
In dermatology, AI devices have the potential to streamline the crushing burden of diagnosing skin cancer, said Yun Liu, PhD, a senior staff scientist at Google Research, Mountain View, California, who’s worked on developing machine-learning tools in dermatology among other medical fields. “Many people cannot access dermatology expertise when they most need it, ie, without waiting a long time. This causes substantial morbidity for patients,” Dr. Liu said in an interview.

His own research of an AI-based tool to help primary care physicians and nurse practitioners in teledermatology practices diagnose skin conditions documented the shortage of dermatologists to triage lesions, including a finding that only about one quarter of skin conditions are seen by a specialist and that nonspecialists play a pivotal role in the management of skin lesions.
The Centers for Disease Control and Prevention reports that about 6.1 million adults are treated for BCC and SCCs each year. The American Medical Association estimates that 13,200 active dermatologists practice in the United States.
Overcoming Barriers to AI in Dermatology
Before AI makes significant inroads in dermatology, clinicians need to see more verifiable data, said Roxana Daneshjou, MD, PhD, assistant professor of biomedical data science and dermatology at Stanford University, Stanford, California. “One of the challenges is having the availability of models that actually improve clinical care because we have some very early prospective trials on different devices, but we don’t have large-scale randomized clinical trials of AI devices showing definitive behaviors such as improved patient outcomes, that it helps curb skin cancer, or it catches it like dermatologists but helps reduce the biopsy load,” she said. “You need good data.”

Another challenge she noted was overcoming biases built into medicine. “A lot of the image-based models are built on datasets depicting skin disease on White skin, and those models don’t work so well on people with brown and black skin, who have historically had worse outcomes and also have been underrepresented in dermatology,” said Dr. Daneshjou, an associate editor of NEJM AI.
There’s also the challenge of getting verified AI models into the clinic. “Similar to many medical AI endeavors, developing a proof-of-concept or research prototype is far easier and faster than bringing the development to real users,” Dr. Liu said. “In particular, it is important to conduct thorough validation studies on various patient populations and settings and understand how these AI tools can best fit into the workflow or patient journey.”
A study published in 2023 documented progress Google made in deploying AI models in retina specialty clinics in India and Thailand, Dr. Liu noted.
Another challenge is to avoid overdiagnosis with these new technologies, Dr. Hartman said. Her group’s study showed the DermaSensor had a positive predictive value of 16% and a negative predictive value of 98.5%. “I think there’s some question about how this will factor into overdiagnosis. Could this actually bombard dermatologists more if the positive predictive value’s only 16%?”
One key to dermatologists accepting AI tools is having a transparent process for validating them, Dr. Lee said. “Even with FDA clearance, we don’t have the transparency we need as clinicians, researchers, and advocates of machine learning and AI in healthcare.”
But, Dr. Lee noted, the FDA in June took a step toward illuminating its validation process when it adopted guiding principles for transparency for machine learning–enabled devices. “Once we can get more access to this information and have more transparency, that’s where we can think about actually about making the decision to implement or not implement into local healthcare settings,” she said. The process was further enabled by a White House executive order in October 2023 on the safe, secure, and trustworthy development and use of AI.
The experience with telehealth during the COVID-19 pandemic, when patients and providers quickly embraced the technology to stay connected, serves as a potential template for AI, Dr. Lee noted. “As we’d seen with telehealth through the pandemic, you also need the cultural evolution and the development of the infrastructure around it to actually make sure this is a sustainable implementation and a scalable implementation in healthcare.”
Dr. Lee had no relevant relationships to disclose. Dr. Hartman received funding from DermaSensor for a study. Dr. Witkowski is a cofounder of Sklip. Dr. Liu is an employee of Google Research. Dr. Daneshjou reported financial relationships with MD Algorithms, Revea, and L’Oreal.
A version of this article first appeared on Medscape.com.
Emerging according to researchers and dermatologists investigating AI.
While some AI-integrated devices designed to triage skin lesions have emerged, including one that received Food and Drug Administration (FDA) clearance earlier in 2024, it may be some time before AI has a meaningful clinical impact in dermatology and, more specifically, the diagnosis of skin cancer, Ivy Lee, MD, a dermatologist in Pasadena, California, and chair of the American Academy of Dermatology’s augmented intelligence committee, told this news organization.
“It hasn’t really translated into clinical practice yet,” Dr. Lee said of AI in dermatology. “There have been significant advances in terms of the technical possibility and feasibility of these tools, but the translation and integration of AI into actual clinical work flows to benefit patients beyond academic research studies has been limited.” More studies and more “easily accessible and digestible information” are needed to evaluate AI tools in dermatologic practice.
“In dermatology, we’re on a cusp with AI,” said Rebecca Hartman, MD, MPH, chief of dermatology at the VA Boston Healthcare System and director of melanoma epidemiology at Brigham and Women’s Hospital, Boston, Massachusetts. “I think it’s going to come and change what we do,” which is especially true for any image-based specialty,” including radiology and pathology, in addition to dermatology.
Dr. Hartman led a study of one of these emerging technologies, the handheld elastic scattering spectroscopy device DermaSensor, which was cleared by the FDA in January for evaluating skin lesions suggestive of skin cancer.
Early AI Devices for Skin Cancer Detection
At the American Society for Laser Medicine and Surgery (ASLMS) meeting in April, a panel explored a number of algorithms with dermatologic applications that use AI to triage skin lesions, including DermaSensor.
Raman spectroscopy, which contains a handheld Raman probe, a diode laser, and a detecting spectrograph. A laser beam — which at 1.56 W/cm2 is below the maximum permissible exposure — focuses on the skin target with a 3.5-mm spot, gathers data on the target, and feeds it back into the unit that houses the algorithm that evaluates the spot analysis. It’s still in the investigative phase. A clinical trial, published almost 5 years ago, demonstrated a sensitivity of 90%-99% and a specificity of 24%-66% for skin cancer.
A dermatoscope called Sklip clips onto a smartphone and performs what company cofounder Alexander Witkowski, MD, PhD, described as an “optical painless virtual biopsy” for at-home use. The device uploads the captured image to an AI platform for analysis. It received FDA breakthrough device designation in 2022. At the ASLMS meeting, Dr. Witkowski said that clinical performance showed the device had a 97% sensitivity and 30% specificity for skin cancer.
DermaSensor, described in the study conducted by Dr. Hartman and others as a noninvasive, point-and-click spectrometer, is a wireless handheld piece that weighs about 10 ounces. The unit captures five recordings to generate a spectral reading, which an algorithm in the software unit analyzes. The study found a sensitivity of 95.5% and specificity of 32.5% for melanoma detection with the device.
The target market for DermaSensor is primary care physicians, and, according to the FDA announcement in January, it is indicated for evaluating skin lesions “suggestive” of melanoma, basal cell carcinoma (BCC), and/or squamous cell carcinoma (SCC) in patients aged 40 and older to “assist healthcare providers in determining whether to refer a patient to a dermatologist.”
So Many Cases, So Few Dermatologists
In dermatology, AI devices have the potential to streamline the crushing burden of diagnosing skin cancer, said Yun Liu, PhD, a senior staff scientist at Google Research, Mountain View, California, who’s worked on developing machine-learning tools in dermatology among other medical fields. “Many people cannot access dermatology expertise when they most need it, ie, without waiting a long time. This causes substantial morbidity for patients,” Dr. Liu said in an interview.
His own research of an AI-based tool to help primary care physicians and nurse practitioners in teledermatology practices diagnose skin conditions documented the shortage of dermatologists to triage lesions, including a finding that only about one quarter of skin conditions are seen by a specialist and that nonspecialists play a pivotal role in the management of skin lesions.
The Centers for Disease Control and Prevention reports that about 6.1 million adults are treated for BCC and SCCs each year. The American Medical Association estimates that 13,200 active dermatologists practice in the United States.
Overcoming Barriers to AI in Dermatology
Before AI makes significant inroads in dermatology, clinicians need to see more verifiable data, said Roxana Daneshjou, MD, PhD, assistant professor of biomedical data science and dermatology at Stanford University, Stanford, California. “One of the challenges is having the availability of models that actually improve clinical care because we have some very early prospective trials on different devices, but we don’t have large-scale randomized clinical trials of AI devices showing definitive behaviors such as improved patient outcomes, that it helps curb skin cancer, or it catches it like dermatologists but helps reduce the biopsy load,” she said. “You need good data.”
Another challenge she noted was overcoming biases built into medicine. “A lot of the image-based models are built on datasets depicting skin disease on White skin, and those models don’t work so well on people with brown and black skin, who have historically had worse outcomes and also have been underrepresented in dermatology,” said Dr. Daneshjou, an associate editor of NEJM AI.
There’s also the challenge of getting verified AI models into the clinic. “Similar to many medical AI endeavors, developing a proof-of-concept or research prototype is far easier and faster than bringing the development to real users,” Dr. Liu said. “In particular, it is important to conduct thorough validation studies on various patient populations and settings and understand how these AI tools can best fit into the workflow or patient journey.”
A study published in 2023 documented progress Google made in deploying AI models in retina specialty clinics in India and Thailand, Dr. Liu noted.
Another challenge is to avoid overdiagnosis with these new technologies, Dr. Hartman said. Her group’s study showed the DermaSensor had a positive predictive value of 16% and a negative predictive value of 98.5%. “I think there’s some question about how this will factor into overdiagnosis. Could this actually bombard dermatologists more if the positive predictive value’s only 16%?”
One key to dermatologists accepting AI tools is having a transparent process for validating them, Dr. Lee said. “Even with FDA clearance, we don’t have the transparency we need as clinicians, researchers, and advocates of machine learning and AI in healthcare.”
But, Dr. Lee noted, the FDA in June took a step toward illuminating its validation process when it adopted guiding principles for transparency for machine learning–enabled devices. “Once we can get more access to this information and have more transparency, that’s where we can think about actually about making the decision to implement or not implement into local healthcare settings,” she said. The process was further enabled by a White House executive order in October 2023 on the safe, secure, and trustworthy development and use of AI.
The experience with telehealth during the COVID-19 pandemic, when patients and providers quickly embraced the technology to stay connected, serves as a potential template for AI, Dr. Lee noted. “As we’d seen with telehealth through the pandemic, you also need the cultural evolution and the development of the infrastructure around it to actually make sure this is a sustainable implementation and a scalable implementation in healthcare.”
Dr. Lee had no relevant relationships to disclose. Dr. Hartman received funding from DermaSensor for a study. Dr. Witkowski is a cofounder of Sklip. Dr. Liu is an employee of Google Research. Dr. Daneshjou reported financial relationships with MD Algorithms, Revea, and L’Oreal.
A version of this article first appeared on Medscape.com.
Emerging according to researchers and dermatologists investigating AI.
While some AI-integrated devices designed to triage skin lesions have emerged, including one that received Food and Drug Administration (FDA) clearance earlier in 2024, it may be some time before AI has a meaningful clinical impact in dermatology and, more specifically, the diagnosis of skin cancer, Ivy Lee, MD, a dermatologist in Pasadena, California, and chair of the American Academy of Dermatology’s augmented intelligence committee, told this news organization.
“It hasn’t really translated into clinical practice yet,” Dr. Lee said of AI in dermatology. “There have been significant advances in terms of the technical possibility and feasibility of these tools, but the translation and integration of AI into actual clinical work flows to benefit patients beyond academic research studies has been limited.” More studies and more “easily accessible and digestible information” are needed to evaluate AI tools in dermatologic practice.
“In dermatology, we’re on a cusp with AI,” said Rebecca Hartman, MD, MPH, chief of dermatology at the VA Boston Healthcare System and director of melanoma epidemiology at Brigham and Women’s Hospital, Boston, Massachusetts. “I think it’s going to come and change what we do,” which is especially true for any image-based specialty,” including radiology and pathology, in addition to dermatology.
Dr. Hartman led a study of one of these emerging technologies, the handheld elastic scattering spectroscopy device DermaSensor, which was cleared by the FDA in January for evaluating skin lesions suggestive of skin cancer.
Early AI Devices for Skin Cancer Detection
At the American Society for Laser Medicine and Surgery (ASLMS) meeting in April, a panel explored a number of algorithms with dermatologic applications that use AI to triage skin lesions, including DermaSensor.
Raman spectroscopy, which contains a handheld Raman probe, a diode laser, and a detecting spectrograph. A laser beam — which at 1.56 W/cm2 is below the maximum permissible exposure — focuses on the skin target with a 3.5-mm spot, gathers data on the target, and feeds it back into the unit that houses the algorithm that evaluates the spot analysis. It’s still in the investigative phase. A clinical trial, published almost 5 years ago, demonstrated a sensitivity of 90%-99% and a specificity of 24%-66% for skin cancer.
A dermatoscope called Sklip clips onto a smartphone and performs what company cofounder Alexander Witkowski, MD, PhD, described as an “optical painless virtual biopsy” for at-home use. The device uploads the captured image to an AI platform for analysis. It received FDA breakthrough device designation in 2022. At the ASLMS meeting, Dr. Witkowski said that clinical performance showed the device had a 97% sensitivity and 30% specificity for skin cancer.
DermaSensor, described in the study conducted by Dr. Hartman and others as a noninvasive, point-and-click spectrometer, is a wireless handheld piece that weighs about 10 ounces. The unit captures five recordings to generate a spectral reading, which an algorithm in the software unit analyzes. The study found a sensitivity of 95.5% and specificity of 32.5% for melanoma detection with the device.
The target market for DermaSensor is primary care physicians, and, according to the FDA announcement in January, it is indicated for evaluating skin lesions “suggestive” of melanoma, basal cell carcinoma (BCC), and/or squamous cell carcinoma (SCC) in patients aged 40 and older to “assist healthcare providers in determining whether to refer a patient to a dermatologist.”
So Many Cases, So Few Dermatologists
In dermatology, AI devices have the potential to streamline the crushing burden of diagnosing skin cancer, said Yun Liu, PhD, a senior staff scientist at Google Research, Mountain View, California, who’s worked on developing machine-learning tools in dermatology among other medical fields. “Many people cannot access dermatology expertise when they most need it, ie, without waiting a long time. This causes substantial morbidity for patients,” Dr. Liu said in an interview.
His own research of an AI-based tool to help primary care physicians and nurse practitioners in teledermatology practices diagnose skin conditions documented the shortage of dermatologists to triage lesions, including a finding that only about one quarter of skin conditions are seen by a specialist and that nonspecialists play a pivotal role in the management of skin lesions.
The Centers for Disease Control and Prevention reports that about 6.1 million adults are treated for BCC and SCCs each year. The American Medical Association estimates that 13,200 active dermatologists practice in the United States.
Overcoming Barriers to AI in Dermatology
Before AI makes significant inroads in dermatology, clinicians need to see more verifiable data, said Roxana Daneshjou, MD, PhD, assistant professor of biomedical data science and dermatology at Stanford University, Stanford, California. “One of the challenges is having the availability of models that actually improve clinical care because we have some very early prospective trials on different devices, but we don’t have large-scale randomized clinical trials of AI devices showing definitive behaviors such as improved patient outcomes, that it helps curb skin cancer, or it catches it like dermatologists but helps reduce the biopsy load,” she said. “You need good data.”
Another challenge she noted was overcoming biases built into medicine. “A lot of the image-based models are built on datasets depicting skin disease on White skin, and those models don’t work so well on people with brown and black skin, who have historically had worse outcomes and also have been underrepresented in dermatology,” said Dr. Daneshjou, an associate editor of NEJM AI.
There’s also the challenge of getting verified AI models into the clinic. “Similar to many medical AI endeavors, developing a proof-of-concept or research prototype is far easier and faster than bringing the development to real users,” Dr. Liu said. “In particular, it is important to conduct thorough validation studies on various patient populations and settings and understand how these AI tools can best fit into the workflow or patient journey.”
A study published in 2023 documented progress Google made in deploying AI models in retina specialty clinics in India and Thailand, Dr. Liu noted.
Another challenge is to avoid overdiagnosis with these new technologies, Dr. Hartman said. Her group’s study showed the DermaSensor had a positive predictive value of 16% and a negative predictive value of 98.5%. “I think there’s some question about how this will factor into overdiagnosis. Could this actually bombard dermatologists more if the positive predictive value’s only 16%?”
One key to dermatologists accepting AI tools is having a transparent process for validating them, Dr. Lee said. “Even with FDA clearance, we don’t have the transparency we need as clinicians, researchers, and advocates of machine learning and AI in healthcare.”
But, Dr. Lee noted, the FDA in June took a step toward illuminating its validation process when it adopted guiding principles for transparency for machine learning–enabled devices. “Once we can get more access to this information and have more transparency, that’s where we can think about actually about making the decision to implement or not implement into local healthcare settings,” she said. The process was further enabled by a White House executive order in October 2023 on the safe, secure, and trustworthy development and use of AI.
The experience with telehealth during the COVID-19 pandemic, when patients and providers quickly embraced the technology to stay connected, serves as a potential template for AI, Dr. Lee noted. “As we’d seen with telehealth through the pandemic, you also need the cultural evolution and the development of the infrastructure around it to actually make sure this is a sustainable implementation and a scalable implementation in healthcare.”
Dr. Lee had no relevant relationships to disclose. Dr. Hartman received funding from DermaSensor for a study. Dr. Witkowski is a cofounder of Sklip. Dr. Liu is an employee of Google Research. Dr. Daneshjou reported financial relationships with MD Algorithms, Revea, and L’Oreal.
A version of this article first appeared on Medscape.com.
Who’s Behind Cosmetic Procedures at MedSpas?
CARLSBAD, CALIFORNIA — according to Sara Hogan, MD.

“I’m not anti-MedSpa; I’m pro-patient safety,” Dr. Hogan, clinical assistant professor of dermatology at George Washington University, Washington, DC, said at the Controversies & Conversations in Laser & Cosmetic Surgery symposium. “The MedSpa industry is booming; it brought in $17 billion in 2023. There are as many MedSpas in the United States as there are practicing dermatologists, and that number is set to exceed the number of dermatologists.”
According to industry data from the American Med Spa Association, 63% of member MedSpas have non-MD ownership. Among MedSpas owned by physicians, 80% are of a non–core specialty, meaning a specialty other than dermatology, plastic surgery, otorhinolaryngology, or ophthalmology. Of MedSpa medical directors, 69% are from non–core physician specialties. “There’s an increasing amount of data that shows a relatively higher incidence of complications from cosmetic procedures that are delivered at MedSpas,” Dr. Hogan said. “A 2020 study suggested that this is likely due to improper training, improper technique, and/or improper device settings.”
Dr. Hogan also cited adverse effects linked to counterfeit or mishandled botulinum toxin injections that prompted the Centers for Disease Control and Prevention to issue an alert to clinicians in April 2024. Clusters of 22 people in 11 states reported adverse effects after receiving injections with counterfeit botulinum toxin or injections administered by unlicensed or untrained individuals or in non-healthcare settings, such as homes or spas.
To better understand who performs cosmetic procedures, provides medical supervision, and follows safety protocols at MedSpas, Dr. Hogan and colleagues conducted a “truth in advertising” study of 127 MedSpas in the greater Chicago area. They chose this geographic location because an analysis published in 2021 identified Chicago as having the third highest number of aesthetic physicians and the fifth highest number of MedSpas in the United States. The researchers enlisted help from “secret shoppers” who contacted the MedSpas by telephone to ask about the level of training, if patients underwent a review of medical history, the level of on-site physician supervision, and the protocol for complications.
The top five cosmetic procedures offered by the 127 surveyed MedSpas were facials (85.0%), hair removal (85.0%), botulinum toxin injections (83.5%), dermal fillers (82.7%), and chemical peels (76.4%). About two thirds of cosmetic procedures were performed by aestheticians (66.9%), followed by registered nurses or licensed practical nurses (52.8%), board-certified physicians (48.8%, mostly plastic and reconstructive surgeons), nurse practitioners (27.6%), and physician assistants (9.4%).
In the realm of supervision, 16.5% of MedSpas surveyed reported that a medical director or supervising physician is always on site. “If not located on site, when asked where the physicians are, the majority of the time they were at the physician’s primary practice, clinic, or hospital,” Dr. Hogan said. “Only 65% of the MedSpas surveyed stated that they informed the patient that the supervising physician is not on site. In addition, a patient’s medical history is reviewed at only 40% of the MedSpas. To give context, in Illinois, a physician can only deliver care after a physician-patient relationship has been established, meaning that a good faith exam has been performed. And if they are to delegate any type of service, they must always be on site to provide assistance.”
Dr. Hogan noted that there are no federal statutes or agencies that regulate or oversee MedSpas. “Regulation and oversight are often delegated to state licensing agencies that are overwhelmed and often stretched thin regarding personnel and budgets,” she said. To raise awareness of this issue, the American Society for Dermatologic Surgery Association (ASDSA) launched the Medical Spa Safety Coalition, which aims to promote model legislation for states known as the Medical Spa Safety Act. Highlights of the bill include clear definitions of medical spa and medical director, as well as the requirement of an on-site medical director who must be a physician trained in all procedures performed at the MedSpa. Coalition members include 16 state dermatology boards as well as the ASDSA, the American Academy of Dermatology Association, the American Society for Laser Medicine & Surgery, and the American Society of Plastic Surgeons.
The ASDSA provided funding to support the published study. Dr. Hogan reported having no financial disclosures.
A version of this article appeared on Medscape.com.
CARLSBAD, CALIFORNIA — according to Sara Hogan, MD.
“I’m not anti-MedSpa; I’m pro-patient safety,” Dr. Hogan, clinical assistant professor of dermatology at George Washington University, Washington, DC, said at the Controversies & Conversations in Laser & Cosmetic Surgery symposium. “The MedSpa industry is booming; it brought in $17 billion in 2023. There are as many MedSpas in the United States as there are practicing dermatologists, and that number is set to exceed the number of dermatologists.”
According to industry data from the American Med Spa Association, 63% of member MedSpas have non-MD ownership. Among MedSpas owned by physicians, 80% are of a non–core specialty, meaning a specialty other than dermatology, plastic surgery, otorhinolaryngology, or ophthalmology. Of MedSpa medical directors, 69% are from non–core physician specialties. “There’s an increasing amount of data that shows a relatively higher incidence of complications from cosmetic procedures that are delivered at MedSpas,” Dr. Hogan said. “A 2020 study suggested that this is likely due to improper training, improper technique, and/or improper device settings.”
Dr. Hogan also cited adverse effects linked to counterfeit or mishandled botulinum toxin injections that prompted the Centers for Disease Control and Prevention to issue an alert to clinicians in April 2024. Clusters of 22 people in 11 states reported adverse effects after receiving injections with counterfeit botulinum toxin or injections administered by unlicensed or untrained individuals or in non-healthcare settings, such as homes or spas.
To better understand who performs cosmetic procedures, provides medical supervision, and follows safety protocols at MedSpas, Dr. Hogan and colleagues conducted a “truth in advertising” study of 127 MedSpas in the greater Chicago area. They chose this geographic location because an analysis published in 2021 identified Chicago as having the third highest number of aesthetic physicians and the fifth highest number of MedSpas in the United States. The researchers enlisted help from “secret shoppers” who contacted the MedSpas by telephone to ask about the level of training, if patients underwent a review of medical history, the level of on-site physician supervision, and the protocol for complications.
The top five cosmetic procedures offered by the 127 surveyed MedSpas were facials (85.0%), hair removal (85.0%), botulinum toxin injections (83.5%), dermal fillers (82.7%), and chemical peels (76.4%). About two thirds of cosmetic procedures were performed by aestheticians (66.9%), followed by registered nurses or licensed practical nurses (52.8%), board-certified physicians (48.8%, mostly plastic and reconstructive surgeons), nurse practitioners (27.6%), and physician assistants (9.4%).
In the realm of supervision, 16.5% of MedSpas surveyed reported that a medical director or supervising physician is always on site. “If not located on site, when asked where the physicians are, the majority of the time they were at the physician’s primary practice, clinic, or hospital,” Dr. Hogan said. “Only 65% of the MedSpas surveyed stated that they informed the patient that the supervising physician is not on site. In addition, a patient’s medical history is reviewed at only 40% of the MedSpas. To give context, in Illinois, a physician can only deliver care after a physician-patient relationship has been established, meaning that a good faith exam has been performed. And if they are to delegate any type of service, they must always be on site to provide assistance.”
Dr. Hogan noted that there are no federal statutes or agencies that regulate or oversee MedSpas. “Regulation and oversight are often delegated to state licensing agencies that are overwhelmed and often stretched thin regarding personnel and budgets,” she said. To raise awareness of this issue, the American Society for Dermatologic Surgery Association (ASDSA) launched the Medical Spa Safety Coalition, which aims to promote model legislation for states known as the Medical Spa Safety Act. Highlights of the bill include clear definitions of medical spa and medical director, as well as the requirement of an on-site medical director who must be a physician trained in all procedures performed at the MedSpa. Coalition members include 16 state dermatology boards as well as the ASDSA, the American Academy of Dermatology Association, the American Society for Laser Medicine & Surgery, and the American Society of Plastic Surgeons.
The ASDSA provided funding to support the published study. Dr. Hogan reported having no financial disclosures.
A version of this article appeared on Medscape.com.
CARLSBAD, CALIFORNIA — according to Sara Hogan, MD.
“I’m not anti-MedSpa; I’m pro-patient safety,” Dr. Hogan, clinical assistant professor of dermatology at George Washington University, Washington, DC, said at the Controversies & Conversations in Laser & Cosmetic Surgery symposium. “The MedSpa industry is booming; it brought in $17 billion in 2023. There are as many MedSpas in the United States as there are practicing dermatologists, and that number is set to exceed the number of dermatologists.”
According to industry data from the American Med Spa Association, 63% of member MedSpas have non-MD ownership. Among MedSpas owned by physicians, 80% are of a non–core specialty, meaning a specialty other than dermatology, plastic surgery, otorhinolaryngology, or ophthalmology. Of MedSpa medical directors, 69% are from non–core physician specialties. “There’s an increasing amount of data that shows a relatively higher incidence of complications from cosmetic procedures that are delivered at MedSpas,” Dr. Hogan said. “A 2020 study suggested that this is likely due to improper training, improper technique, and/or improper device settings.”
Dr. Hogan also cited adverse effects linked to counterfeit or mishandled botulinum toxin injections that prompted the Centers for Disease Control and Prevention to issue an alert to clinicians in April 2024. Clusters of 22 people in 11 states reported adverse effects after receiving injections with counterfeit botulinum toxin or injections administered by unlicensed or untrained individuals or in non-healthcare settings, such as homes or spas.
To better understand who performs cosmetic procedures, provides medical supervision, and follows safety protocols at MedSpas, Dr. Hogan and colleagues conducted a “truth in advertising” study of 127 MedSpas in the greater Chicago area. They chose this geographic location because an analysis published in 2021 identified Chicago as having the third highest number of aesthetic physicians and the fifth highest number of MedSpas in the United States. The researchers enlisted help from “secret shoppers” who contacted the MedSpas by telephone to ask about the level of training, if patients underwent a review of medical history, the level of on-site physician supervision, and the protocol for complications.
The top five cosmetic procedures offered by the 127 surveyed MedSpas were facials (85.0%), hair removal (85.0%), botulinum toxin injections (83.5%), dermal fillers (82.7%), and chemical peels (76.4%). About two thirds of cosmetic procedures were performed by aestheticians (66.9%), followed by registered nurses or licensed practical nurses (52.8%), board-certified physicians (48.8%, mostly plastic and reconstructive surgeons), nurse practitioners (27.6%), and physician assistants (9.4%).
In the realm of supervision, 16.5% of MedSpas surveyed reported that a medical director or supervising physician is always on site. “If not located on site, when asked where the physicians are, the majority of the time they were at the physician’s primary practice, clinic, or hospital,” Dr. Hogan said. “Only 65% of the MedSpas surveyed stated that they informed the patient that the supervising physician is not on site. In addition, a patient’s medical history is reviewed at only 40% of the MedSpas. To give context, in Illinois, a physician can only deliver care after a physician-patient relationship has been established, meaning that a good faith exam has been performed. And if they are to delegate any type of service, they must always be on site to provide assistance.”
Dr. Hogan noted that there are no federal statutes or agencies that regulate or oversee MedSpas. “Regulation and oversight are often delegated to state licensing agencies that are overwhelmed and often stretched thin regarding personnel and budgets,” she said. To raise awareness of this issue, the American Society for Dermatologic Surgery Association (ASDSA) launched the Medical Spa Safety Coalition, which aims to promote model legislation for states known as the Medical Spa Safety Act. Highlights of the bill include clear definitions of medical spa and medical director, as well as the requirement of an on-site medical director who must be a physician trained in all procedures performed at the MedSpa. Coalition members include 16 state dermatology boards as well as the ASDSA, the American Academy of Dermatology Association, the American Society for Laser Medicine & Surgery, and the American Society of Plastic Surgeons.
The ASDSA provided funding to support the published study. Dr. Hogan reported having no financial disclosures.
A version of this article appeared on Medscape.com.
Hip Fractures in Patients With Dementia: To Operate or Not?
In the case of a hip fracture, operating on a patient with dementia can be a difficult decision to make. Indeed, surgery exposes patients with dementia to a higher mortality rate, more delirium and postoperative complications, and a greater loss of mobility than patients of the same age without cognitive impairments. For patients with dementia in institutional settings, survival is better for those who undergo surgery than for those who do not. But what about the prognosis of surgery vs no surgery for patients with dementia who live at home?
To answer this question, researchers in the United States conducted a cohort study using Medicare data. This retrospective study included patients aged 66 years and older with dementia who were living at home and not placed in institutions and who had a hip fracture between January 2017 and June 2018. Patients with incomplete observations, particularly regarding the location and type of residence (home/institution), were excluded from the analysis. Fractures were categorized as (i) fractures of the head and neck, (ii) pertrochanteric, (iii) subtrochanteric, and (iv) multiple/complex. The type and severity (mild, moderate, or severe) of dementia were identified using the diagnostic code list in the International Statistical Classification of Diseases, Tenth Revision.
Examining Mortality
The primary outcome was mortality at 30, 90, and 180 days. Secondary outcomes included hospital delirium; the need for subsequent hospitalization (within 6 months) or home health services (within 10 days); and intensive care interventions such as dialysis, intubation, resuscitation maneuvers, mechanical ventilation, or the insertion of a feeding tube.
Postoperative medical facility admissions were distinguished according to whether there was a plan to return home. To compare the surgery and nonsurgery groups, an inverse propensity score analysis was conducted within subgroups determined by fracture type, comorbidities (using the Elixhauser score), the person or entity responsible for admission (ie, physician, clinic, hospital, etc.), dual eligibility (Medicare and Medicaid), place of residence (ie, urban or rural), race, and sex. Dementia severity was estimated using a frailty index on the basis of evaluation tests that were systematically collected in the Medicare database.
Results Favored Surgery
Among 56,209 patients with dementia who were admitted for a hip fracture (73.0% women; mean age, 86.4 ± 7.0 years), 33,142 (59.0%) underwent surgery and 23,067 (41.0%) did not. Among surgically treated patients, 73.3% had fractures of the head or neck of the femur, and 40.2% had moderate to severe dementia. The nonsurgically treated fractures were 78.5% pertrochanteric. Comorbidities were evenly distributed between the two groups.
At 180 days, mortality was 31.8% in the surgery group compared with 45.7% in the nonsurgery group, resulting in a significant reduction in the unadjusted relative risk (RR) for death in favor of surgery (RR, 0.67; 95% CI, 0.60-0.76; P < .001). Among patients with mild dementia and a fracture of the head or neck of the femur, mortality at 180 days was 26.5% among surgical patients and 34.9% among nonsurgical patients (RR, 0.67; 95% CI, 0.60-0.76; P < .001). After the investigators adjusted for risk according to propensity score, the benefit of surgery remained significant at 30, 90, and 180 days, regardless of dementia severity. There was no significant difference in mortality for other types of hip fractures between the surgery and nonsurgery groups, however.
The adjusted RR for in-hospital delirium was 1.23 (P = .008), which was significant for the surgery group, but only for those with moderate to severe dementia. There were also fewer permanent placements (P < .001) among the surgically treated patients, and fewer patients with mild dementia required nurse care at home. There was no difference in resuscitation maneuvers between surgery and nonsurgery patients, whether the dementia was mild or not. For patients with a fracture of the head or neck of the femur, there was no difference in the likelihood of rehabilitation admission within 180 days, whether they were operated on or not.
Ethical Considerations
This study can inform discussions among healthcare professionals, patients, and patients’ families about which goals to set and which strategy to choose. The main interest of this study lies in its comparison of outcomes between patients with dementia who were operated on and those who were not, rather than comparing patients with and without dementia. Among patients with dementia living at home with a fracture of the head or neck of the femur, those who underwent surgery had a lower risk for death than those who did not, regardless of the severity of dementia.
It is noteworthy that less than two thirds of patients with dementia underwent surgery, which contradicts recommendations for almost routine surgery for patients with dementia. This observation raises questions about respecting patient wishes and advance directives when known, possible detrimental delays in referrals, and legal-medical issues.
Furthermore, the treatment choices of American surgeons are clearly influenced by the type of hip fracture. Fractures of the head and neck of the femur are typically treated with prosthetic arthroplasty, which simplifies postoperative care, compared with osteosynthesis. The latter procedure is more often used for extra-articular hip fractures but entails higher risks. While survival is an apparently more easily achievable goal through surgery, ethical considerations about other treatment objectives such as pain control, functional recovery, and treatment adequacy cannot be overlooked. It is worth noting that the French National Authority for Health issued recommendations in 2018 regarding the care pathway for patients hospitalized for a hip fracture within an orthogeriatric organization.
This story was translated from JIM, which is part of the Medscape Medical News professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
In the case of a hip fracture, operating on a patient with dementia can be a difficult decision to make. Indeed, surgery exposes patients with dementia to a higher mortality rate, more delirium and postoperative complications, and a greater loss of mobility than patients of the same age without cognitive impairments. For patients with dementia in institutional settings, survival is better for those who undergo surgery than for those who do not. But what about the prognosis of surgery vs no surgery for patients with dementia who live at home?
To answer this question, researchers in the United States conducted a cohort study using Medicare data. This retrospective study included patients aged 66 years and older with dementia who were living at home and not placed in institutions and who had a hip fracture between January 2017 and June 2018. Patients with incomplete observations, particularly regarding the location and type of residence (home/institution), were excluded from the analysis. Fractures were categorized as (i) fractures of the head and neck, (ii) pertrochanteric, (iii) subtrochanteric, and (iv) multiple/complex. The type and severity (mild, moderate, or severe) of dementia were identified using the diagnostic code list in the International Statistical Classification of Diseases, Tenth Revision.
Examining Mortality
The primary outcome was mortality at 30, 90, and 180 days. Secondary outcomes included hospital delirium; the need for subsequent hospitalization (within 6 months) or home health services (within 10 days); and intensive care interventions such as dialysis, intubation, resuscitation maneuvers, mechanical ventilation, or the insertion of a feeding tube.
Postoperative medical facility admissions were distinguished according to whether there was a plan to return home. To compare the surgery and nonsurgery groups, an inverse propensity score analysis was conducted within subgroups determined by fracture type, comorbidities (using the Elixhauser score), the person or entity responsible for admission (ie, physician, clinic, hospital, etc.), dual eligibility (Medicare and Medicaid), place of residence (ie, urban or rural), race, and sex. Dementia severity was estimated using a frailty index on the basis of evaluation tests that were systematically collected in the Medicare database.
Results Favored Surgery
Among 56,209 patients with dementia who were admitted for a hip fracture (73.0% women; mean age, 86.4 ± 7.0 years), 33,142 (59.0%) underwent surgery and 23,067 (41.0%) did not. Among surgically treated patients, 73.3% had fractures of the head or neck of the femur, and 40.2% had moderate to severe dementia. The nonsurgically treated fractures were 78.5% pertrochanteric. Comorbidities were evenly distributed between the two groups.
At 180 days, mortality was 31.8% in the surgery group compared with 45.7% in the nonsurgery group, resulting in a significant reduction in the unadjusted relative risk (RR) for death in favor of surgery (RR, 0.67; 95% CI, 0.60-0.76; P < .001). Among patients with mild dementia and a fracture of the head or neck of the femur, mortality at 180 days was 26.5% among surgical patients and 34.9% among nonsurgical patients (RR, 0.67; 95% CI, 0.60-0.76; P < .001). After the investigators adjusted for risk according to propensity score, the benefit of surgery remained significant at 30, 90, and 180 days, regardless of dementia severity. There was no significant difference in mortality for other types of hip fractures between the surgery and nonsurgery groups, however.
The adjusted RR for in-hospital delirium was 1.23 (P = .008), which was significant for the surgery group, but only for those with moderate to severe dementia. There were also fewer permanent placements (P < .001) among the surgically treated patients, and fewer patients with mild dementia required nurse care at home. There was no difference in resuscitation maneuvers between surgery and nonsurgery patients, whether the dementia was mild or not. For patients with a fracture of the head or neck of the femur, there was no difference in the likelihood of rehabilitation admission within 180 days, whether they were operated on or not.
Ethical Considerations
This study can inform discussions among healthcare professionals, patients, and patients’ families about which goals to set and which strategy to choose. The main interest of this study lies in its comparison of outcomes between patients with dementia who were operated on and those who were not, rather than comparing patients with and without dementia. Among patients with dementia living at home with a fracture of the head or neck of the femur, those who underwent surgery had a lower risk for death than those who did not, regardless of the severity of dementia.
It is noteworthy that less than two thirds of patients with dementia underwent surgery, which contradicts recommendations for almost routine surgery for patients with dementia. This observation raises questions about respecting patient wishes and advance directives when known, possible detrimental delays in referrals, and legal-medical issues.
Furthermore, the treatment choices of American surgeons are clearly influenced by the type of hip fracture. Fractures of the head and neck of the femur are typically treated with prosthetic arthroplasty, which simplifies postoperative care, compared with osteosynthesis. The latter procedure is more often used for extra-articular hip fractures but entails higher risks. While survival is an apparently more easily achievable goal through surgery, ethical considerations about other treatment objectives such as pain control, functional recovery, and treatment adequacy cannot be overlooked. It is worth noting that the French National Authority for Health issued recommendations in 2018 regarding the care pathway for patients hospitalized for a hip fracture within an orthogeriatric organization.
This story was translated from JIM, which is part of the Medscape Medical News professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
In the case of a hip fracture, operating on a patient with dementia can be a difficult decision to make. Indeed, surgery exposes patients with dementia to a higher mortality rate, more delirium and postoperative complications, and a greater loss of mobility than patients of the same age without cognitive impairments. For patients with dementia in institutional settings, survival is better for those who undergo surgery than for those who do not. But what about the prognosis of surgery vs no surgery for patients with dementia who live at home?
To answer this question, researchers in the United States conducted a cohort study using Medicare data. This retrospective study included patients aged 66 years and older with dementia who were living at home and not placed in institutions and who had a hip fracture between January 2017 and June 2018. Patients with incomplete observations, particularly regarding the location and type of residence (home/institution), were excluded from the analysis. Fractures were categorized as (i) fractures of the head and neck, (ii) pertrochanteric, (iii) subtrochanteric, and (iv) multiple/complex. The type and severity (mild, moderate, or severe) of dementia were identified using the diagnostic code list in the International Statistical Classification of Diseases, Tenth Revision.
Examining Mortality
The primary outcome was mortality at 30, 90, and 180 days. Secondary outcomes included hospital delirium; the need for subsequent hospitalization (within 6 months) or home health services (within 10 days); and intensive care interventions such as dialysis, intubation, resuscitation maneuvers, mechanical ventilation, or the insertion of a feeding tube.
Postoperative medical facility admissions were distinguished according to whether there was a plan to return home. To compare the surgery and nonsurgery groups, an inverse propensity score analysis was conducted within subgroups determined by fracture type, comorbidities (using the Elixhauser score), the person or entity responsible for admission (ie, physician, clinic, hospital, etc.), dual eligibility (Medicare and Medicaid), place of residence (ie, urban or rural), race, and sex. Dementia severity was estimated using a frailty index on the basis of evaluation tests that were systematically collected in the Medicare database.
Results Favored Surgery
Among 56,209 patients with dementia who were admitted for a hip fracture (73.0% women; mean age, 86.4 ± 7.0 years), 33,142 (59.0%) underwent surgery and 23,067 (41.0%) did not. Among surgically treated patients, 73.3% had fractures of the head or neck of the femur, and 40.2% had moderate to severe dementia. The nonsurgically treated fractures were 78.5% pertrochanteric. Comorbidities were evenly distributed between the two groups.
At 180 days, mortality was 31.8% in the surgery group compared with 45.7% in the nonsurgery group, resulting in a significant reduction in the unadjusted relative risk (RR) for death in favor of surgery (RR, 0.67; 95% CI, 0.60-0.76; P < .001). Among patients with mild dementia and a fracture of the head or neck of the femur, mortality at 180 days was 26.5% among surgical patients and 34.9% among nonsurgical patients (RR, 0.67; 95% CI, 0.60-0.76; P < .001). After the investigators adjusted for risk according to propensity score, the benefit of surgery remained significant at 30, 90, and 180 days, regardless of dementia severity. There was no significant difference in mortality for other types of hip fractures between the surgery and nonsurgery groups, however.
The adjusted RR for in-hospital delirium was 1.23 (P = .008), which was significant for the surgery group, but only for those with moderate to severe dementia. There were also fewer permanent placements (P < .001) among the surgically treated patients, and fewer patients with mild dementia required nurse care at home. There was no difference in resuscitation maneuvers between surgery and nonsurgery patients, whether the dementia was mild or not. For patients with a fracture of the head or neck of the femur, there was no difference in the likelihood of rehabilitation admission within 180 days, whether they were operated on or not.
Ethical Considerations
This study can inform discussions among healthcare professionals, patients, and patients’ families about which goals to set and which strategy to choose. The main interest of this study lies in its comparison of outcomes between patients with dementia who were operated on and those who were not, rather than comparing patients with and without dementia. Among patients with dementia living at home with a fracture of the head or neck of the femur, those who underwent surgery had a lower risk for death than those who did not, regardless of the severity of dementia.
It is noteworthy that less than two thirds of patients with dementia underwent surgery, which contradicts recommendations for almost routine surgery for patients with dementia. This observation raises questions about respecting patient wishes and advance directives when known, possible detrimental delays in referrals, and legal-medical issues.
Furthermore, the treatment choices of American surgeons are clearly influenced by the type of hip fracture. Fractures of the head and neck of the femur are typically treated with prosthetic arthroplasty, which simplifies postoperative care, compared with osteosynthesis. The latter procedure is more often used for extra-articular hip fractures but entails higher risks. While survival is an apparently more easily achievable goal through surgery, ethical considerations about other treatment objectives such as pain control, functional recovery, and treatment adequacy cannot be overlooked. It is worth noting that the French National Authority for Health issued recommendations in 2018 regarding the care pathway for patients hospitalized for a hip fracture within an orthogeriatric organization.
This story was translated from JIM, which is part of the Medscape Medical News professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Predicting RSV’s Role in the Upcoming Winter Respiratory Season
For children younger than 5 years old, RSV is the main drive — approximately 2,000,000 outpatient/ED visits and about 75,000 hospitalizations annually. RSV disease ranges from upper respiratory tract infections, eg, in older children and healthy adults, to more severe lower tract disease in young children and the elderly. Premature infants and high-risk groups are particularly prone to severe disease.1 Up to 300 pediatric RSV deaths occur yearly. “Normal” RSV seasons start in mid-November, peak in late December-January, and end after April. Note: More drawn out seasons occur in southern latitudes, eg Texas or Florida. But lately RSV seasons have been anything but normal.
2015-2016 to 2022-2023
RSV data from the Pediatric Health Information System (PHIS), collected at over 49 US children’s hospitals during 2015 to early 2023, show how crazy RSV seasons have been lately.2 The involved months, intensity, and duration of four prepandemic seasons were pretty “normal” (Figure 1). The 2019-2020 season started normally, peaked in January 2020, and was slowing as expected by February. But when SARS-Cov-2 restrictions kicked in during mid-March, RSV detections tanked to almost nothing (ditto other respiratory viruses). A near 14-month RSV hiatus meant that the 2020-2021 RSV season never materialized. However, RSV was not done with us in 2021. It rebounded in May with weekly hospitalizations peaking in late July; this “rebound season” lasted 9 months, not dropping to baseline until February 2022 (Figure 1).
I guess we should have expected a post-pandemic “disturbance in the Force,” as Yoda once said; but I sure didn’t see a prolonged summer/fall/early winter RSV season coming. It was like two “normal” seasons mashed up into one late-but-long season. Not to be outdone, the 2022-2023 RSV season started early (September) and hospitalizations skyrocketed to peak in November at over twice the peak number from any year since 2015, overloading hospitals (influenza and SARS-Cov-2 seasons were co-circulating). The season terminated early though (March 2023).
Okay, so RSV seasonality/intensity were weird post pandemic, but was anything else different? Some 2021-2023 data suggest more RSV disease in older children, rather than the usual younger than 18 month-olds going through their first winter.3 More medically attended RSV in older ages (2-4 years of life) may have been due to the pandemic year without RSV circulation distorting herd immunity, ie older children remained RSV naive. Other data suggest the apparent increase was really just more frequent multiplex viral testing in older children triggered by SARS-CoV-2 co-circulation.4 More data are needed to decide.
CDC 2023-2024 RESP-NET data
The 2023-2024 winter surge (Figure 2), as measured by RESP-NET’s cumulative RSV, influenza and SARS-CoV-2 hospitalization rates for 0- to 5-year-olds,5 shows that all three viruses’ seasonal months were normal-ish: late October 2023 start, late December-early January peak, and mid-May 2024 return to baseline. RSV season was approximately 22% less severe by area-under-the-curve calculations compared with 2022-2023, but still worse than prepandemic years.6 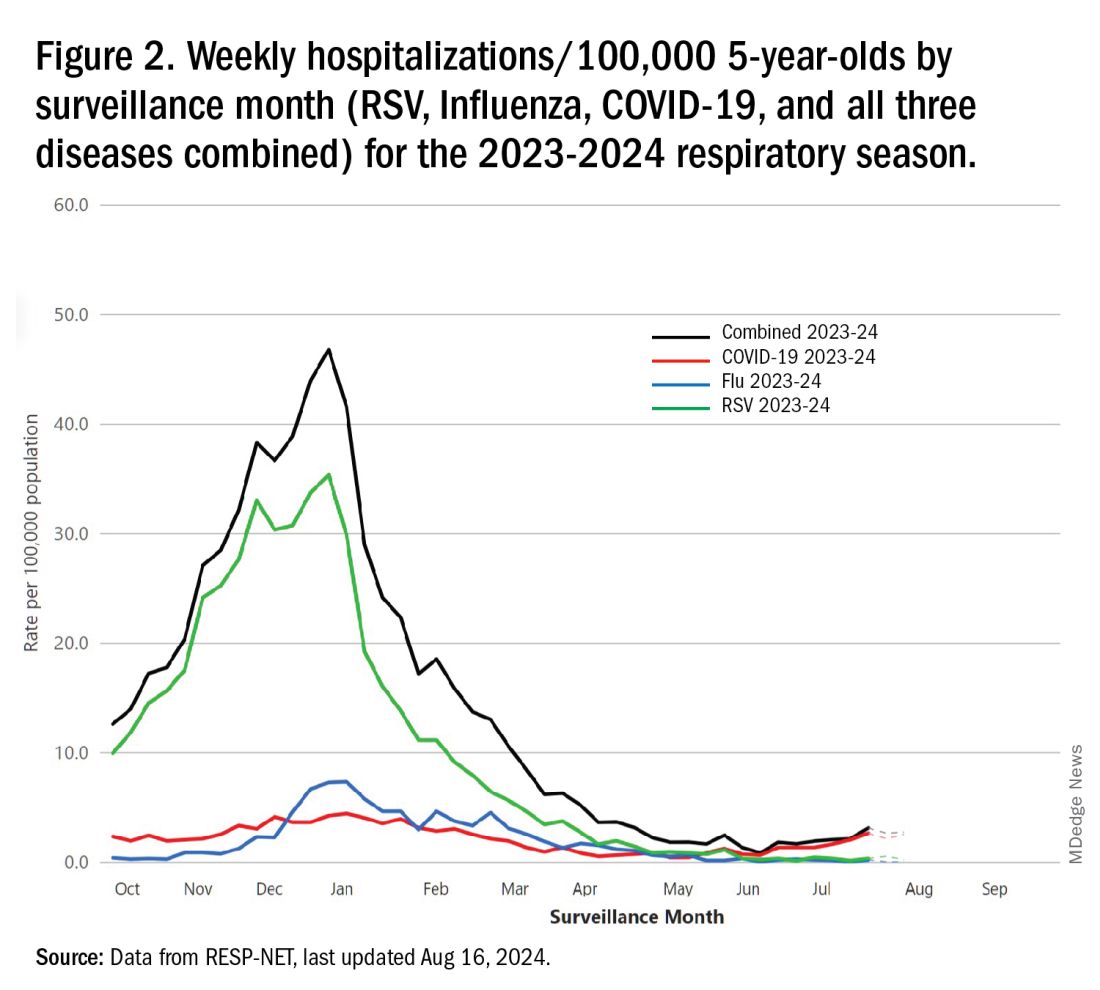
One wonders if the 2022-2023 RSV season might have been worse but for use of the limited supply of nirsevimab.7
Viral Parade
Now we ready ourselves for the 2024-2025 respiratory surge, wondering what nature has in store for us. Will the usual “respiratory virus parade” occur? Will rhinovirus and parainfluenza prevalence bump after a few weeks of schools being in session, adding to the now-usual summer/fall SARS-CoV-2 surge? Note: Twenty-seven states as of Aug. 16 had high SARS-CoV-2 detection in wastewater. Will RSV and influenza start sometime in October/November, peak in January (along with rising SARS-CoV2 activity), followed by a second parainfluenza bump as SARS-CoV-2, influenza, and RSV drop off in April/May? Further, will RSV and influenza seasons be more or less severe than the last 2 years?
Prediction
The overall 2024-2025 respiratory season will be less severe than the past 2 years and hopefully than recent prepandemic years. What is the blueprint for a milder season? First, herd immunity to non-RSV and non-influenza viruses (parainfluenza, rhinovirus, metapneumovirus, adenovirus) in older children should be normalized after 2 years back to usual social activity. So, I expect no mega-seasons from them. The emerging SARS-CoV-2 virus (LB.1) is immunologically close to its recent still-circulating ancestors (KP.2, KP.2.3, KP.3 and KP.3.1.1), so existing SARS-CoV2 herd immunity along with recommended booster vaccine uptake should keep the lid on SARS-CoV2.

Influenza Could Be the Bad News
Which type will dominate? Will a drift/shift occur or vaccine-mismatch reduce vaccine effectiveness? Can we get at least half the population influenza vaccinated, given the vaccine fatigue permeating the US population? The influenza season now underway in the Southern Hemisphere usually helps us predict our season. The Australian May-August 2024 experience (still on an upward trajectory for severity in mid-August) saw no drift/shift or vaccine mismatch. However, this 2024 season has been as severe as 2022 (their worst in a decade). That said, more than 95% has been type A (mostly H1N1 but H3N2 increased in July). So, if our overall 2024-2025 respiratory season is not milder, influenza is the most likely culprit. To reduce chances of influenza being the fly-in-the-ointment, we need to be particularly proactive with seasonal influenza vaccine which is back to the traditional trivalent formulation (one H1N1, one H3N2, and one B type).8 All of this could go out the window if avian influenza becomes more transmissible, but that seems unlikely at present.
Mild RSV Season?
RSV season should be blunted because of the increased use of both the remarkably effective CDC-recommended maternal RSV vaccine9 (one dose during pregnancy weeks 32 through 36, administered September through January) and of nirsevimab (up to 90% reduction in hospitalizations and ED visits).10 (See Figure 3.) 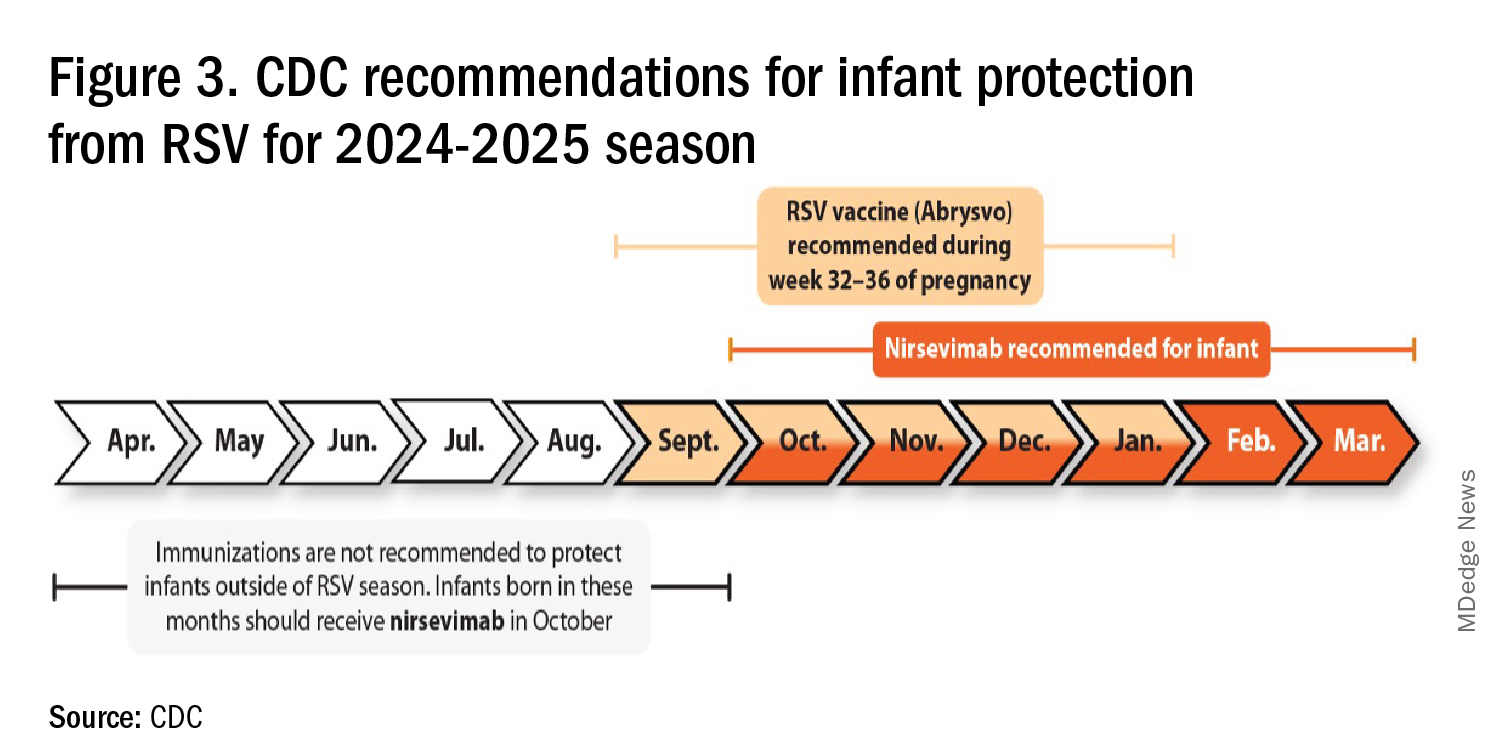
I also expect residual disease to occur mostly in younger than 18 month-olds (the “normal” aged population experiencing their first winter), who received no passive immunity (mother RSV unvaccinated and child did not receive nirsevimab). Some disease will still occur in high-risk infants/children. However, unlike active vaccination strategies, a competent immune system is not required to benefit from passive antibody, whether transplacental or directly administered.
Deep Thought
What if the traditional RSV seasonal hospitalization surge fails to materialize this season? It could happen. If we could get high acceptance/uptake of maternal vaccine and infant nirsevimab, RSV season could resemble the dramatic drop in rotavirus disease the second year after rotavirus vaccine introduction. We could be asking ourselves — “What happened to RSV?”
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics, Kansas City, Missouri. He said he had no relevant financial disclosures. Email him at [email protected].
References
1. CDC. RSV in Infants and Young Children. Respiratory Syncytial Virus Infection (RSV). June 18, 2024. https://www.cdc.gov/rsv/infants-young-children/index.html.
2. Suss RJ and Simões EAF. Respiratory Syncytial Virus Hospital-Based Burden of Disease in Children Younger Than 5 Respiratory Syncytial Virus Hospital-Based Burden of Disease in Children Younger Than 5 Years, 2015-2022. JAMA Netw Open. 2024;7(4):e247125. doi:10.1001/jamanetworkopen.2024.7125.
3. Winthrop ZA et al. Pediatric Respiratory Syncytial Virus Hospitalizations and Respiratory Support After the COVID-19 Pandemic. JAMA Netw Open. 2024;7(6):e2416852. doi:10.1001/jamanetworkopen.2024.16852.
4. Petros BA et al. Increased Pediatric RSV Case Counts Following the Emergence of SARS-CoV-2 Are Attributable to Increased Testing. medRxiv [Preprint]. 2024 Feb 12:2024.02.06.24302387. doi: 10.1101/2024.02.06.24302387.
5. Rates of Laboratory-Confirmed RSV, COVID-19, and Flu Hospitalizations from the RESP-NET Surveillance Systems. Centers for Disease Control and Prevention. https://data.cdc.gov/Public-Health-Surveillance/Rates-of-Laboratory-Confirmed-RSV-COVID-19-and-Flu/kvib-3txy/about_data.
6. CDC. Evaluating the 2023-2024 Respiratory Disease Season Outlook. CFA: Qualitative Assessments. August 14, 2024. https://www.cdc.gov/cfa-qualitative-assessments/php/data-research/2023-2024-season-outlook-retro.html.
7. Health Alert Network (HAN). Limited Availability of Nirsevimab in the United States—Interim CDC Recommendations to Protect Infants from Respiratory Syncytial Virus (RSV) during the 2023–2024 Respiratory Virus Season. October 23, 2023. https://emergency.cdc.gov/han/2023/han00499.asp.
8. CDC. Information for the 2024-2025 Flu Season. Centers for Disease Control and Prevention. March 14, 2024. https://www.cdc.gov/flu/season/faq-flu-season-2024-2025.htm.
9. Kampmann B et al. Bivalent Prefusion F Vaccine in Pregnancy to Prevent RSV Illness in Infants. N Engl J Med. 2023 Apr 20;388(16):1451-1464. doi: 10.1056/NEJMoa2216480.
10. Moline HL. Early Estimate of Nirsevimab Effectiveness for Prevention of Respiratory Syncytial Virus–Associated Hospitalization Among Infants Entering Their First Respiratory Syncytial Virus Season — New Vaccine Surveillance Network, October 2023–February 2024. MMWR Morb Mortal Wkly Rep. 2024;73. doi: 10.15585/mmwr.mm7309a4.
For children younger than 5 years old, RSV is the main drive — approximately 2,000,000 outpatient/ED visits and about 75,000 hospitalizations annually. RSV disease ranges from upper respiratory tract infections, eg, in older children and healthy adults, to more severe lower tract disease in young children and the elderly. Premature infants and high-risk groups are particularly prone to severe disease.1 Up to 300 pediatric RSV deaths occur yearly. “Normal” RSV seasons start in mid-November, peak in late December-January, and end after April. Note: More drawn out seasons occur in southern latitudes, eg Texas or Florida. But lately RSV seasons have been anything but normal.
2015-2016 to 2022-2023
RSV data from the Pediatric Health Information System (PHIS), collected at over 49 US children’s hospitals during 2015 to early 2023, show how crazy RSV seasons have been lately.2 The involved months, intensity, and duration of four prepandemic seasons were pretty “normal” (Figure 1). The 2019-2020 season started normally, peaked in January 2020, and was slowing as expected by February. But when SARS-Cov-2 restrictions kicked in during mid-March, RSV detections tanked to almost nothing (ditto other respiratory viruses). A near 14-month RSV hiatus meant that the 2020-2021 RSV season never materialized. However, RSV was not done with us in 2021. It rebounded in May with weekly hospitalizations peaking in late July; this “rebound season” lasted 9 months, not dropping to baseline until February 2022 (Figure 1).
I guess we should have expected a post-pandemic “disturbance in the Force,” as Yoda once said; but I sure didn’t see a prolonged summer/fall/early winter RSV season coming. It was like two “normal” seasons mashed up into one late-but-long season. Not to be outdone, the 2022-2023 RSV season started early (September) and hospitalizations skyrocketed to peak in November at over twice the peak number from any year since 2015, overloading hospitals (influenza and SARS-Cov-2 seasons were co-circulating). The season terminated early though (March 2023).
Okay, so RSV seasonality/intensity were weird post pandemic, but was anything else different? Some 2021-2023 data suggest more RSV disease in older children, rather than the usual younger than 18 month-olds going through their first winter.3 More medically attended RSV in older ages (2-4 years of life) may have been due to the pandemic year without RSV circulation distorting herd immunity, ie older children remained RSV naive. Other data suggest the apparent increase was really just more frequent multiplex viral testing in older children triggered by SARS-CoV-2 co-circulation.4 More data are needed to decide.
CDC 2023-2024 RESP-NET data
The 2023-2024 winter surge (Figure 2), as measured by RESP-NET’s cumulative RSV, influenza and SARS-CoV-2 hospitalization rates for 0- to 5-year-olds,5 shows that all three viruses’ seasonal months were normal-ish: late October 2023 start, late December-early January peak, and mid-May 2024 return to baseline. RSV season was approximately 22% less severe by area-under-the-curve calculations compared with 2022-2023, but still worse than prepandemic years.6
One wonders if the 2022-2023 RSV season might have been worse but for use of the limited supply of nirsevimab.7
Viral Parade
Now we ready ourselves for the 2024-2025 respiratory surge, wondering what nature has in store for us. Will the usual “respiratory virus parade” occur? Will rhinovirus and parainfluenza prevalence bump after a few weeks of schools being in session, adding to the now-usual summer/fall SARS-CoV-2 surge? Note: Twenty-seven states as of Aug. 16 had high SARS-CoV-2 detection in wastewater. Will RSV and influenza start sometime in October/November, peak in January (along with rising SARS-CoV2 activity), followed by a second parainfluenza bump as SARS-CoV-2, influenza, and RSV drop off in April/May? Further, will RSV and influenza seasons be more or less severe than the last 2 years?
Prediction
The overall 2024-2025 respiratory season will be less severe than the past 2 years and hopefully than recent prepandemic years. What is the blueprint for a milder season? First, herd immunity to non-RSV and non-influenza viruses (parainfluenza, rhinovirus, metapneumovirus, adenovirus) in older children should be normalized after 2 years back to usual social activity. So, I expect no mega-seasons from them. The emerging SARS-CoV-2 virus (LB.1) is immunologically close to its recent still-circulating ancestors (KP.2, KP.2.3, KP.3 and KP.3.1.1), so existing SARS-CoV2 herd immunity along with recommended booster vaccine uptake should keep the lid on SARS-CoV2.
Influenza Could Be the Bad News
Which type will dominate? Will a drift/shift occur or vaccine-mismatch reduce vaccine effectiveness? Can we get at least half the population influenza vaccinated, given the vaccine fatigue permeating the US population? The influenza season now underway in the Southern Hemisphere usually helps us predict our season. The Australian May-August 2024 experience (still on an upward trajectory for severity in mid-August) saw no drift/shift or vaccine mismatch. However, this 2024 season has been as severe as 2022 (their worst in a decade). That said, more than 95% has been type A (mostly H1N1 but H3N2 increased in July). So, if our overall 2024-2025 respiratory season is not milder, influenza is the most likely culprit. To reduce chances of influenza being the fly-in-the-ointment, we need to be particularly proactive with seasonal influenza vaccine which is back to the traditional trivalent formulation (one H1N1, one H3N2, and one B type).8 All of this could go out the window if avian influenza becomes more transmissible, but that seems unlikely at present.
Mild RSV Season?
RSV season should be blunted because of the increased use of both the remarkably effective CDC-recommended maternal RSV vaccine9 (one dose during pregnancy weeks 32 through 36, administered September through January) and of nirsevimab (up to 90% reduction in hospitalizations and ED visits).10 (See Figure 3.)
I also expect residual disease to occur mostly in younger than 18 month-olds (the “normal” aged population experiencing their first winter), who received no passive immunity (mother RSV unvaccinated and child did not receive nirsevimab). Some disease will still occur in high-risk infants/children. However, unlike active vaccination strategies, a competent immune system is not required to benefit from passive antibody, whether transplacental or directly administered.
Deep Thought
What if the traditional RSV seasonal hospitalization surge fails to materialize this season? It could happen. If we could get high acceptance/uptake of maternal vaccine and infant nirsevimab, RSV season could resemble the dramatic drop in rotavirus disease the second year after rotavirus vaccine introduction. We could be asking ourselves — “What happened to RSV?”
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics, Kansas City, Missouri. He said he had no relevant financial disclosures. Email him at [email protected].
References
1. CDC. RSV in Infants and Young Children. Respiratory Syncytial Virus Infection (RSV). June 18, 2024. https://www.cdc.gov/rsv/infants-young-children/index.html.
2. Suss RJ and Simões EAF. Respiratory Syncytial Virus Hospital-Based Burden of Disease in Children Younger Than 5 Respiratory Syncytial Virus Hospital-Based Burden of Disease in Children Younger Than 5 Years, 2015-2022. JAMA Netw Open. 2024;7(4):e247125. doi:10.1001/jamanetworkopen.2024.7125.
3. Winthrop ZA et al. Pediatric Respiratory Syncytial Virus Hospitalizations and Respiratory Support After the COVID-19 Pandemic. JAMA Netw Open. 2024;7(6):e2416852. doi:10.1001/jamanetworkopen.2024.16852.
4. Petros BA et al. Increased Pediatric RSV Case Counts Following the Emergence of SARS-CoV-2 Are Attributable to Increased Testing. medRxiv [Preprint]. 2024 Feb 12:2024.02.06.24302387. doi: 10.1101/2024.02.06.24302387.
5. Rates of Laboratory-Confirmed RSV, COVID-19, and Flu Hospitalizations from the RESP-NET Surveillance Systems. Centers for Disease Control and Prevention. https://data.cdc.gov/Public-Health-Surveillance/Rates-of-Laboratory-Confirmed-RSV-COVID-19-and-Flu/kvib-3txy/about_data.
6. CDC. Evaluating the 2023-2024 Respiratory Disease Season Outlook. CFA: Qualitative Assessments. August 14, 2024. https://www.cdc.gov/cfa-qualitative-assessments/php/data-research/2023-2024-season-outlook-retro.html.
7. Health Alert Network (HAN). Limited Availability of Nirsevimab in the United States—Interim CDC Recommendations to Protect Infants from Respiratory Syncytial Virus (RSV) during the 2023–2024 Respiratory Virus Season. October 23, 2023. https://emergency.cdc.gov/han/2023/han00499.asp.
8. CDC. Information for the 2024-2025 Flu Season. Centers for Disease Control and Prevention. March 14, 2024. https://www.cdc.gov/flu/season/faq-flu-season-2024-2025.htm.
9. Kampmann B et al. Bivalent Prefusion F Vaccine in Pregnancy to Prevent RSV Illness in Infants. N Engl J Med. 2023 Apr 20;388(16):1451-1464. doi: 10.1056/NEJMoa2216480.
10. Moline HL. Early Estimate of Nirsevimab Effectiveness for Prevention of Respiratory Syncytial Virus–Associated Hospitalization Among Infants Entering Their First Respiratory Syncytial Virus Season — New Vaccine Surveillance Network, October 2023–February 2024. MMWR Morb Mortal Wkly Rep. 2024;73. doi: 10.15585/mmwr.mm7309a4.
For children younger than 5 years old, RSV is the main drive — approximately 2,000,000 outpatient/ED visits and about 75,000 hospitalizations annually. RSV disease ranges from upper respiratory tract infections, eg, in older children and healthy adults, to more severe lower tract disease in young children and the elderly. Premature infants and high-risk groups are particularly prone to severe disease.1 Up to 300 pediatric RSV deaths occur yearly. “Normal” RSV seasons start in mid-November, peak in late December-January, and end after April. Note: More drawn out seasons occur in southern latitudes, eg Texas or Florida. But lately RSV seasons have been anything but normal.
2015-2016 to 2022-2023
RSV data from the Pediatric Health Information System (PHIS), collected at over 49 US children’s hospitals during 2015 to early 2023, show how crazy RSV seasons have been lately.2 The involved months, intensity, and duration of four prepandemic seasons were pretty “normal” (Figure 1). The 2019-2020 season started normally, peaked in January 2020, and was slowing as expected by February. But when SARS-Cov-2 restrictions kicked in during mid-March, RSV detections tanked to almost nothing (ditto other respiratory viruses). A near 14-month RSV hiatus meant that the 2020-2021 RSV season never materialized. However, RSV was not done with us in 2021. It rebounded in May with weekly hospitalizations peaking in late July; this “rebound season” lasted 9 months, not dropping to baseline until February 2022 (Figure 1).
I guess we should have expected a post-pandemic “disturbance in the Force,” as Yoda once said; but I sure didn’t see a prolonged summer/fall/early winter RSV season coming. It was like two “normal” seasons mashed up into one late-but-long season. Not to be outdone, the 2022-2023 RSV season started early (September) and hospitalizations skyrocketed to peak in November at over twice the peak number from any year since 2015, overloading hospitals (influenza and SARS-Cov-2 seasons were co-circulating). The season terminated early though (March 2023).
Okay, so RSV seasonality/intensity were weird post pandemic, but was anything else different? Some 2021-2023 data suggest more RSV disease in older children, rather than the usual younger than 18 month-olds going through their first winter.3 More medically attended RSV in older ages (2-4 years of life) may have been due to the pandemic year without RSV circulation distorting herd immunity, ie older children remained RSV naive. Other data suggest the apparent increase was really just more frequent multiplex viral testing in older children triggered by SARS-CoV-2 co-circulation.4 More data are needed to decide.
CDC 2023-2024 RESP-NET data
The 2023-2024 winter surge (Figure 2), as measured by RESP-NET’s cumulative RSV, influenza and SARS-CoV-2 hospitalization rates for 0- to 5-year-olds,5 shows that all three viruses’ seasonal months were normal-ish: late October 2023 start, late December-early January peak, and mid-May 2024 return to baseline. RSV season was approximately 22% less severe by area-under-the-curve calculations compared with 2022-2023, but still worse than prepandemic years.6
One wonders if the 2022-2023 RSV season might have been worse but for use of the limited supply of nirsevimab.7
Viral Parade
Now we ready ourselves for the 2024-2025 respiratory surge, wondering what nature has in store for us. Will the usual “respiratory virus parade” occur? Will rhinovirus and parainfluenza prevalence bump after a few weeks of schools being in session, adding to the now-usual summer/fall SARS-CoV-2 surge? Note: Twenty-seven states as of Aug. 16 had high SARS-CoV-2 detection in wastewater. Will RSV and influenza start sometime in October/November, peak in January (along with rising SARS-CoV2 activity), followed by a second parainfluenza bump as SARS-CoV-2, influenza, and RSV drop off in April/May? Further, will RSV and influenza seasons be more or less severe than the last 2 years?
Prediction
The overall 2024-2025 respiratory season will be less severe than the past 2 years and hopefully than recent prepandemic years. What is the blueprint for a milder season? First, herd immunity to non-RSV and non-influenza viruses (parainfluenza, rhinovirus, metapneumovirus, adenovirus) in older children should be normalized after 2 years back to usual social activity. So, I expect no mega-seasons from them. The emerging SARS-CoV-2 virus (LB.1) is immunologically close to its recent still-circulating ancestors (KP.2, KP.2.3, KP.3 and KP.3.1.1), so existing SARS-CoV2 herd immunity along with recommended booster vaccine uptake should keep the lid on SARS-CoV2.
Influenza Could Be the Bad News
Which type will dominate? Will a drift/shift occur or vaccine-mismatch reduce vaccine effectiveness? Can we get at least half the population influenza vaccinated, given the vaccine fatigue permeating the US population? The influenza season now underway in the Southern Hemisphere usually helps us predict our season. The Australian May-August 2024 experience (still on an upward trajectory for severity in mid-August) saw no drift/shift or vaccine mismatch. However, this 2024 season has been as severe as 2022 (their worst in a decade). That said, more than 95% has been type A (mostly H1N1 but H3N2 increased in July). So, if our overall 2024-2025 respiratory season is not milder, influenza is the most likely culprit. To reduce chances of influenza being the fly-in-the-ointment, we need to be particularly proactive with seasonal influenza vaccine which is back to the traditional trivalent formulation (one H1N1, one H3N2, and one B type).8 All of this could go out the window if avian influenza becomes more transmissible, but that seems unlikely at present.
Mild RSV Season?
RSV season should be blunted because of the increased use of both the remarkably effective CDC-recommended maternal RSV vaccine9 (one dose during pregnancy weeks 32 through 36, administered September through January) and of nirsevimab (up to 90% reduction in hospitalizations and ED visits).10 (See Figure 3.)
I also expect residual disease to occur mostly in younger than 18 month-olds (the “normal” aged population experiencing their first winter), who received no passive immunity (mother RSV unvaccinated and child did not receive nirsevimab). Some disease will still occur in high-risk infants/children. However, unlike active vaccination strategies, a competent immune system is not required to benefit from passive antibody, whether transplacental or directly administered.
Deep Thought
What if the traditional RSV seasonal hospitalization surge fails to materialize this season? It could happen. If we could get high acceptance/uptake of maternal vaccine and infant nirsevimab, RSV season could resemble the dramatic drop in rotavirus disease the second year after rotavirus vaccine introduction. We could be asking ourselves — “What happened to RSV?”
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics, Kansas City, Missouri. He said he had no relevant financial disclosures. Email him at [email protected].
References
1. CDC. RSV in Infants and Young Children. Respiratory Syncytial Virus Infection (RSV). June 18, 2024. https://www.cdc.gov/rsv/infants-young-children/index.html.
2. Suss RJ and Simões EAF. Respiratory Syncytial Virus Hospital-Based Burden of Disease in Children Younger Than 5 Respiratory Syncytial Virus Hospital-Based Burden of Disease in Children Younger Than 5 Years, 2015-2022. JAMA Netw Open. 2024;7(4):e247125. doi:10.1001/jamanetworkopen.2024.7125.
3. Winthrop ZA et al. Pediatric Respiratory Syncytial Virus Hospitalizations and Respiratory Support After the COVID-19 Pandemic. JAMA Netw Open. 2024;7(6):e2416852. doi:10.1001/jamanetworkopen.2024.16852.
4. Petros BA et al. Increased Pediatric RSV Case Counts Following the Emergence of SARS-CoV-2 Are Attributable to Increased Testing. medRxiv [Preprint]. 2024 Feb 12:2024.02.06.24302387. doi: 10.1101/2024.02.06.24302387.
5. Rates of Laboratory-Confirmed RSV, COVID-19, and Flu Hospitalizations from the RESP-NET Surveillance Systems. Centers for Disease Control and Prevention. https://data.cdc.gov/Public-Health-Surveillance/Rates-of-Laboratory-Confirmed-RSV-COVID-19-and-Flu/kvib-3txy/about_data.
6. CDC. Evaluating the 2023-2024 Respiratory Disease Season Outlook. CFA: Qualitative Assessments. August 14, 2024. https://www.cdc.gov/cfa-qualitative-assessments/php/data-research/2023-2024-season-outlook-retro.html.
7. Health Alert Network (HAN). Limited Availability of Nirsevimab in the United States—Interim CDC Recommendations to Protect Infants from Respiratory Syncytial Virus (RSV) during the 2023–2024 Respiratory Virus Season. October 23, 2023. https://emergency.cdc.gov/han/2023/han00499.asp.
8. CDC. Information for the 2024-2025 Flu Season. Centers for Disease Control and Prevention. March 14, 2024. https://www.cdc.gov/flu/season/faq-flu-season-2024-2025.htm.
9. Kampmann B et al. Bivalent Prefusion F Vaccine in Pregnancy to Prevent RSV Illness in Infants. N Engl J Med. 2023 Apr 20;388(16):1451-1464. doi: 10.1056/NEJMoa2216480.
10. Moline HL. Early Estimate of Nirsevimab Effectiveness for Prevention of Respiratory Syncytial Virus–Associated Hospitalization Among Infants Entering Their First Respiratory Syncytial Virus Season — New Vaccine Surveillance Network, October 2023–February 2024. MMWR Morb Mortal Wkly Rep. 2024;73. doi: 10.15585/mmwr.mm7309a4.
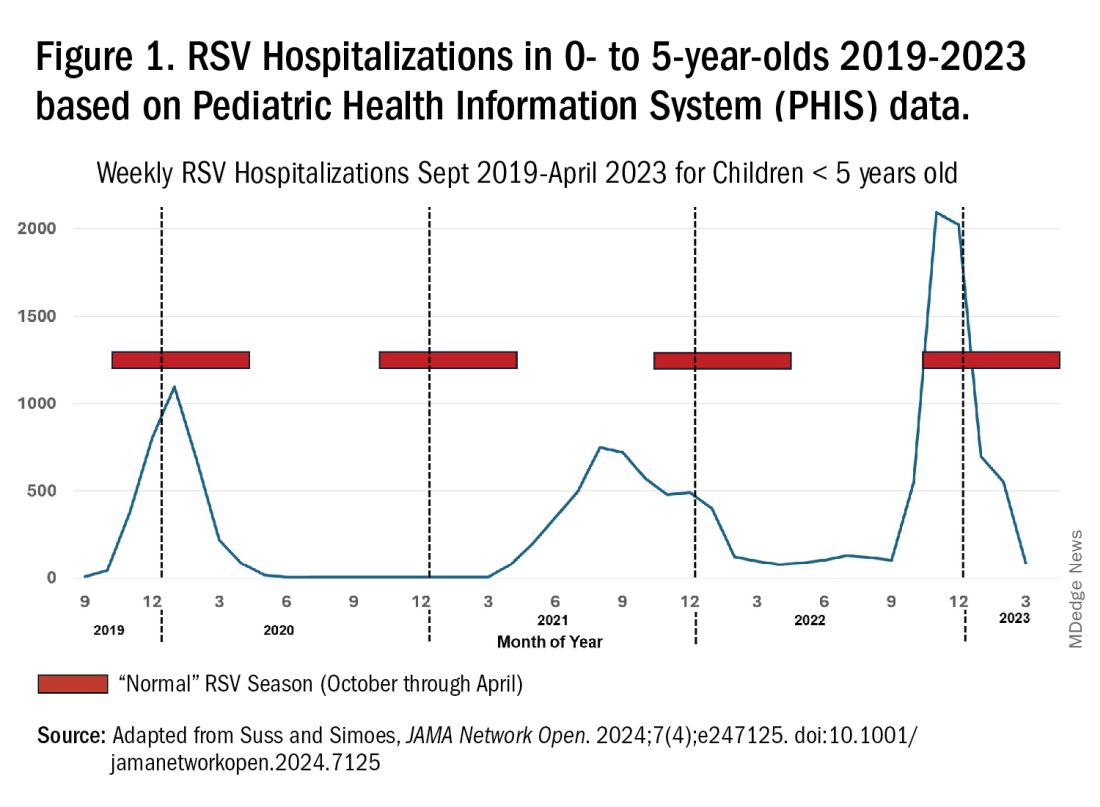
Uterus Transplants in Women With Uterine-Factor Infertility Show High Rate of Live Births
TOPLINE:
Uterus transplants in women with absolute uterine-factor infertility resulted in a 70% success rate of women later giving birth.
METHODOLOGY:
- The study included 20 women with uterine-factor infertility, a condition in which women do not have a uterus or have one that is not functional; each patient had at least one functioning ovary and uterine abnormalities.
- All patients underwent womb transplantation at a large US specialized care center between 2016 and 2019.
- The transplant was performed using grafts from 18 living donors and two deceased donors.
- Patients received anti-rejection medication until the transplanted uterus was removed following one or two live births or graft failure.
- Researchers measured uterus graft survival and subsequent live births.
TAKEAWAY:
- Out of the 20 participants, 14 (70%) had successful uterus transplants and all 14 gave birth to at least one healthy infant.
- Half of the successful pregnancies had complications, which included gestational hypertension (14%), cervical insufficiency (14%), and preterm labor (14%).
- None of the 16 live-born infants had congenital malformations, and no developmental delays were observed as of May 2024.
- Four of the 18 living donors experienced grade 3 complications, including ureteral obstruction and thermal injury to the ureters.
IN PRACTICE:
“Uterus transplant was technically feasible and was associated with a high live birth rate following successful graft survival,” wrote the authors of the study. “Adverse events were common, with medical and surgical risks affecting recipients as well as donors.”
SOURCE:
The study was led by Giuliano Testa, MD, MBA, of Baylor University Medical Center in Dallas, Texas, and was published online in JAMA Network.
LIMITATIONS:
The findings are based on data from a single center. The sample size was small. The high cost of uterus transplants limits generalizability.
DISCLOSURES:
No disclosures were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Uterus transplants in women with absolute uterine-factor infertility resulted in a 70% success rate of women later giving birth.
METHODOLOGY:
- The study included 20 women with uterine-factor infertility, a condition in which women do not have a uterus or have one that is not functional; each patient had at least one functioning ovary and uterine abnormalities.
- All patients underwent womb transplantation at a large US specialized care center between 2016 and 2019.
- The transplant was performed using grafts from 18 living donors and two deceased donors.
- Patients received anti-rejection medication until the transplanted uterus was removed following one or two live births or graft failure.
- Researchers measured uterus graft survival and subsequent live births.
TAKEAWAY:
- Out of the 20 participants, 14 (70%) had successful uterus transplants and all 14 gave birth to at least one healthy infant.
- Half of the successful pregnancies had complications, which included gestational hypertension (14%), cervical insufficiency (14%), and preterm labor (14%).
- None of the 16 live-born infants had congenital malformations, and no developmental delays were observed as of May 2024.
- Four of the 18 living donors experienced grade 3 complications, including ureteral obstruction and thermal injury to the ureters.
IN PRACTICE:
“Uterus transplant was technically feasible and was associated with a high live birth rate following successful graft survival,” wrote the authors of the study. “Adverse events were common, with medical and surgical risks affecting recipients as well as donors.”
SOURCE:
The study was led by Giuliano Testa, MD, MBA, of Baylor University Medical Center in Dallas, Texas, and was published online in JAMA Network.
LIMITATIONS:
The findings are based on data from a single center. The sample size was small. The high cost of uterus transplants limits generalizability.
DISCLOSURES:
No disclosures were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Uterus transplants in women with absolute uterine-factor infertility resulted in a 70% success rate of women later giving birth.
METHODOLOGY:
- The study included 20 women with uterine-factor infertility, a condition in which women do not have a uterus or have one that is not functional; each patient had at least one functioning ovary and uterine abnormalities.
- All patients underwent womb transplantation at a large US specialized care center between 2016 and 2019.
- The transplant was performed using grafts from 18 living donors and two deceased donors.
- Patients received anti-rejection medication until the transplanted uterus was removed following one or two live births or graft failure.
- Researchers measured uterus graft survival and subsequent live births.
TAKEAWAY:
- Out of the 20 participants, 14 (70%) had successful uterus transplants and all 14 gave birth to at least one healthy infant.
- Half of the successful pregnancies had complications, which included gestational hypertension (14%), cervical insufficiency (14%), and preterm labor (14%).
- None of the 16 live-born infants had congenital malformations, and no developmental delays were observed as of May 2024.
- Four of the 18 living donors experienced grade 3 complications, including ureteral obstruction and thermal injury to the ureters.
IN PRACTICE:
“Uterus transplant was technically feasible and was associated with a high live birth rate following successful graft survival,” wrote the authors of the study. “Adverse events were common, with medical and surgical risks affecting recipients as well as donors.”
SOURCE:
The study was led by Giuliano Testa, MD, MBA, of Baylor University Medical Center in Dallas, Texas, and was published online in JAMA Network.
LIMITATIONS:
The findings are based on data from a single center. The sample size was small. The high cost of uterus transplants limits generalizability.
DISCLOSURES:
No disclosures were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
It’s Never Too Late to Convince Patients to Quit Smoking
An estimated 450,000 US deaths are expected this year from conditions attributed to cigarette smoking. Although the percentage of adults who smoke declined from 21% in 2005 to 11% in 2022, the annual death toll has been stable since 2005 and isn’t expected to decline until 2030, owing to an aging population of current and former smokers.
In 2022, based on a national survey, two thirds of the 28.8 million US adult smokers wanted to quit, and more than half tried quitting on their own or with the help of clinicians, but less than 9% succeeded in kicking the habit. The health benefits of quitting, summarized in a patient education handout from the American Cancer Society, include a lower risk for cancer, diabetes, and cardiovascular disease. Furthermore, the handout states, “quitting smoking can add as much as 10 years to your life, compared to if you continued to smoke.”
For my patients older than age 50 who are lifelong smokers, the qualifier “as much as” can be a sticking point. Although most recognize that continuing to smoke exposes them to greater health risks and are willing to undergo lung cancer screening and receive pneumococcal vaccines, a kind of fatalism frequently sets in. I’ve heard more times than I can recall some version of the declaration, “It’s too late for quitting to make much difference for me.” Many smokers think that once they reach middle age, gains in life expectancy will be too small to be worth the intense effort and multiple failed attempts that are typically required to quit permanently. Until recently, there were few data I could call on to persuade them they were wrong.
In February 2024, Dr. Eo Rin Cho and colleagues pooled data from four national cohort studies (United States, United Kingdom, Norway, and Canada) to calculate mortality differences among current, former, and never smokers aged 20-79 years. Compared with never smokers, lifelong smokers died an average of 12-13 years earlier. However, quitting before age 50 nearly eliminated the excess mortality associated with smoking, and in the 50- to 59-year-old age group, cessation eventually reduced excess mortality by 92%-95%. Better yet, more than half of the benefits occurred within the first 3 years after cessation.
At first glance, these estimates may seem too good to be true. A few months later, though, a different research group, using data from a large cancer prevention study and 2018 US population census and mortality rates, largely confirmed their findings. Dr. Thuy Le and colleagues found that quitting at age 35, 45, 55, 65, or 75 years resulted in average life gains of 8, 5.6, 3.5, 1.7, and 0.7 years, respectively, relative to continuing to smoke. Because no patient is average, the analysis also presented some helpful probabilities. For example, a smoker who quits at age 65 has about a 1 in 4 chance of gaining at least 1 full year of life and a 1 in 6 chance of gaining at least 4 years. In other words, from a life expectancy perspective alone, it’s almost never too late to quit smoking.
Dr. Lin is a family physician and Associate Director, Family Medicine Residency Program, Lancaster General Hospital, Lancaster, Pennsylvania. He blogs at Common Sense Family Doctor. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
An estimated 450,000 US deaths are expected this year from conditions attributed to cigarette smoking. Although the percentage of adults who smoke declined from 21% in 2005 to 11% in 2022, the annual death toll has been stable since 2005 and isn’t expected to decline until 2030, owing to an aging population of current and former smokers.
In 2022, based on a national survey, two thirds of the 28.8 million US adult smokers wanted to quit, and more than half tried quitting on their own or with the help of clinicians, but less than 9% succeeded in kicking the habit. The health benefits of quitting, summarized in a patient education handout from the American Cancer Society, include a lower risk for cancer, diabetes, and cardiovascular disease. Furthermore, the handout states, “quitting smoking can add as much as 10 years to your life, compared to if you continued to smoke.”
For my patients older than age 50 who are lifelong smokers, the qualifier “as much as” can be a sticking point. Although most recognize that continuing to smoke exposes them to greater health risks and are willing to undergo lung cancer screening and receive pneumococcal vaccines, a kind of fatalism frequently sets in. I’ve heard more times than I can recall some version of the declaration, “It’s too late for quitting to make much difference for me.” Many smokers think that once they reach middle age, gains in life expectancy will be too small to be worth the intense effort and multiple failed attempts that are typically required to quit permanently. Until recently, there were few data I could call on to persuade them they were wrong.
In February 2024, Dr. Eo Rin Cho and colleagues pooled data from four national cohort studies (United States, United Kingdom, Norway, and Canada) to calculate mortality differences among current, former, and never smokers aged 20-79 years. Compared with never smokers, lifelong smokers died an average of 12-13 years earlier. However, quitting before age 50 nearly eliminated the excess mortality associated with smoking, and in the 50- to 59-year-old age group, cessation eventually reduced excess mortality by 92%-95%. Better yet, more than half of the benefits occurred within the first 3 years after cessation.
At first glance, these estimates may seem too good to be true. A few months later, though, a different research group, using data from a large cancer prevention study and 2018 US population census and mortality rates, largely confirmed their findings. Dr. Thuy Le and colleagues found that quitting at age 35, 45, 55, 65, or 75 years resulted in average life gains of 8, 5.6, 3.5, 1.7, and 0.7 years, respectively, relative to continuing to smoke. Because no patient is average, the analysis also presented some helpful probabilities. For example, a smoker who quits at age 65 has about a 1 in 4 chance of gaining at least 1 full year of life and a 1 in 6 chance of gaining at least 4 years. In other words, from a life expectancy perspective alone, it’s almost never too late to quit smoking.
Dr. Lin is a family physician and Associate Director, Family Medicine Residency Program, Lancaster General Hospital, Lancaster, Pennsylvania. He blogs at Common Sense Family Doctor. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
An estimated 450,000 US deaths are expected this year from conditions attributed to cigarette smoking. Although the percentage of adults who smoke declined from 21% in 2005 to 11% in 2022, the annual death toll has been stable since 2005 and isn’t expected to decline until 2030, owing to an aging population of current and former smokers.
In 2022, based on a national survey, two thirds of the 28.8 million US adult smokers wanted to quit, and more than half tried quitting on their own or with the help of clinicians, but less than 9% succeeded in kicking the habit. The health benefits of quitting, summarized in a patient education handout from the American Cancer Society, include a lower risk for cancer, diabetes, and cardiovascular disease. Furthermore, the handout states, “quitting smoking can add as much as 10 years to your life, compared to if you continued to smoke.”
For my patients older than age 50 who are lifelong smokers, the qualifier “as much as” can be a sticking point. Although most recognize that continuing to smoke exposes them to greater health risks and are willing to undergo lung cancer screening and receive pneumococcal vaccines, a kind of fatalism frequently sets in. I’ve heard more times than I can recall some version of the declaration, “It’s too late for quitting to make much difference for me.” Many smokers think that once they reach middle age, gains in life expectancy will be too small to be worth the intense effort and multiple failed attempts that are typically required to quit permanently. Until recently, there were few data I could call on to persuade them they were wrong.
In February 2024, Dr. Eo Rin Cho and colleagues pooled data from four national cohort studies (United States, United Kingdom, Norway, and Canada) to calculate mortality differences among current, former, and never smokers aged 20-79 years. Compared with never smokers, lifelong smokers died an average of 12-13 years earlier. However, quitting before age 50 nearly eliminated the excess mortality associated with smoking, and in the 50- to 59-year-old age group, cessation eventually reduced excess mortality by 92%-95%. Better yet, more than half of the benefits occurred within the first 3 years after cessation.
At first glance, these estimates may seem too good to be true. A few months later, though, a different research group, using data from a large cancer prevention study and 2018 US population census and mortality rates, largely confirmed their findings. Dr. Thuy Le and colleagues found that quitting at age 35, 45, 55, 65, or 75 years resulted in average life gains of 8, 5.6, 3.5, 1.7, and 0.7 years, respectively, relative to continuing to smoke. Because no patient is average, the analysis also presented some helpful probabilities. For example, a smoker who quits at age 65 has about a 1 in 4 chance of gaining at least 1 full year of life and a 1 in 6 chance of gaining at least 4 years. In other words, from a life expectancy perspective alone, it’s almost never too late to quit smoking.
Dr. Lin is a family physician and Associate Director, Family Medicine Residency Program, Lancaster General Hospital, Lancaster, Pennsylvania. He blogs at Common Sense Family Doctor. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Primary Care: Re Carpe Your Diem
William Fox, MD, a self-described “dinosaur,” works in an independent internal medicine practice with two other physicians in Charlottesville, Virginia. He is rarely able to accept new patients, and when he does see one, they often have to wait months for the appointment. He accepts the burden of many pent-up needs, along with the huge administrative chore of coordinating their care with subspecialists.
“I will probably have to make multiple visits in a quick succession in order to make sure that I stabilize all the various issues,” Dr. Fox said. Doing so for a complicated new patient is nearly impossible because of time pressures, especially as it has become increasingly difficult for his patients to access subspecialists.
Dr. Fox traced the roots of the problem to a shortage of primary care physicians.
“Primary care is a vital part of healthcare and infrastructure in the United States, and it is being eroded unfortunately, as fewer and fewer medical students and residents choose to go into the primary care field,” Fox said. “And the reason it’s being eroded partly is because it is undervalued” and under-reimbursed, he added.
A study published 2 years ago in the Journal of General Internal Medicine proved what every primary care clinician already knows: The 24-hour day simply isn’t long enough.
Assuming an average panel of 2500 patients, the authors estimated the average time needed to provide currently recommended preventive care services and vaccines, chronic disease care, and management of acute illnesses. The answer: 26.7 hours a day.
However, using a team-based approach in which the necessary care was divided between physicians, advanced practice providers, and medical assistants, the physician component could be whittled down to 9 hours.
As chair of the Board of Regents of the American College of Physicians (ACP), Dr. Fox champions the ACP’s endorsement of physician-led team-based care, which improves patient outcomes and increases well-being among health professionals. But practices like his rarely have the necessary resources to support advanced practice clinicians or social workers. “Team-based care can be achieved in larger healthcare systems that have the resources to do it,” said Dr. Fox. “We need to find a way for smaller independent practices to also participate in team-based care.”
The solution? Major reform in the current fee-for-service payment structure, which incentivizes patient volume over patient outcomes. Dr. Fox co-authored a 2022 position statement from ACP outlining strategies such as prospective payment models that could achieve high-quality care and address social inequities. “We need to evolve our payment system from a fee-for-service system into a blended system where you have some population-based payments along with fee-for-service, or a fully capitated system,” he said.
Advantages of Team-Based Care
When a patient wrote on a satisfaction survey “the doctor spent more time examining the computer than examining me,” Kevin Hopkins, MD, decided he needed to change some things. Now the vice chief of Cleveland Clinic’s Primary Care Institute in Cleveland, in 2010, he developed a rudimentary team-based care model consisting of himself and two medical assistants at Cleveland Clinic.
The assistants did much of the patient intake, served as scribes while Dr. Hopkins saw his patients, and completed most of the required documentation. “I was able to see 30% more patients in a day and still take great care of them,” Dr. Hopkins said.
The concept of team-based care has evolved since then, often including some combination of advanced practice providers such as physician assistants (PAs) or nurse practitioners (NPs), nurses or medical assistants, and social workers or case managers working under the leadership of a physician. According to Dr. Hopkins, the basic strategy should be that “the physician does what only the physician is uniquely trained and qualified to do.” All other tasks, such as data entry, handling refill requests and messages from the patient portal, scheduling, or patient education, can — and should — be done by someone else.
Dr. Hopkins also serves as a senior physician advisor to the American Medical Association (AMA) and an instructor for workshops like “Saving Time: Practice Innovation Boot Camp.” His advice for clinicians who would like to streamline their workflow is to start with small steps.
“You’re not going to be able to hire all the people that you’d like to have,” he said. “I encourage physicians to look around at the people that they have and what they are currently doing as a part of their roles and responsibilities.”
The AMA Team-Based Care and Workflow website provides brief continuing medical education activities on topics such as implementing lab testing prior to office visits or advanced protocols for rooming and discharge; adopting any of these strategies can help save steps during office visits.
Dr. Hopkins said the AMA is committed to reducing the regulatory burden on clinicians. Clinical compliance officers may misinterpret regulatory requirements, putting into place overly conservative internal policies and procedures. The AMA’s “Reducing Regulatory Burden Playbook” offers advice on practices that could be stopped, such as two-factor authentication for approving or signing orders unless they are for controlled substances, or started, such as writing prescriptions for chronic daily medications for the maximum allowed length. Reducing a few clicks with each log-on to the electronic health record or reducing the number of tasks physicians must complete to log on can dramatically reduce hours spent on the computer.
Telehealth Changes Everything
But it might be even more efficient to keep patients out of the office.
Initially piloted in Palo Alto, California, from 2018 to 2022, the Tera Practice adopted team-based care strategies in a practice that conducts most of its work virtually. Sutter Health has since expanded the concept to three “Connected Care Clinics” in the San Francisco area, which provide 80% of their care via secure messaging, telephone, or video visit. Staff work primarily from home, and patients do not need to take off work or spend time driving to in-person visits to access care.
Matthew Sakumoto, MD, is a virtualist primary care physician at Sutter Health’s San Francisco clinic and an adjunct assistant clinical professor at the University of California, San Francisco. He leads a three-person team, which typically has included either an NP or a PA, along with a licensed vocational nurse or medical assistant.
“I go into clinic once a week, but a lot of the visits are video visits, so I don’t feel the pressure to address everything all in one visit,” Dr. Sakumoto said. “It is really freeing for both me and the patient.”
For more complex patients, for example, he prioritizes one problem at a visit because his team will follow up virtually for administrative issues like refills or specialty referrals. He can easily find time to schedule a patient for a follow-up virtual visit in the next week or 2 weeks to address additional needs. And on days he and his staff work from home, patients who message with an urgent concern can often be seen by video that same day.
Dr. Sakumoto and his team have a traditional huddle in the office the morning of their clinic day to plan for the scheduled visits, but most of their days are less structured. On non-clinic days, their morning Zoom huddle has a much different focus.
“We’re saying, ‘Okay, who are our high-risk patients? Who haven’t we seen in a while?’ ” Dr. Sakumoto said. They group patients into tiers based on factors such as age, number of complex medical needs, and frequency of emergency visits or hospitalizations. They also check in with higher-risk patients who haven’t contacted the office or been seen recently.
Dr. Sakumoto noticed in medical school doctors take excellent care of the patients who show up to the clinic. “We don’t do quite as well for those that don’t show up,” he said. The hybrid-virtual model gives him time to think in a more population-based way about engaging his entire panel of patients. The majority have capitated or value-based insurance plans, providing a dedicated monthly revenue stream that funds his virtual practice.
More clinicians may be able to hire staff and adopt some of these innovative approaches if Congress approves proposed changes to Medicare and Medicaid increasing the use of value-based payment systems. Although these changes may not provide all the funding needed to reinvigorate the field of primary care medicine, Dr. Fox said, “at least some people in positions of power and responsibility are beginning to think more seriously about these issues.”
Dr. Sakumoto reported personal fees from the following companies within the past 24 months: Clearstep Health, Carbon Health, Matter Health, CareAlign, PlushCare, Teladoc, and Nabla Health. Dr. Fox and Dr. Hopkins reported no financial conflicts of interest.
A former pediatrician and disease detective, Ann Thomas, MD, MPH, is a freelance science writer living in Portland, Oregon.
A version of this article first appeared on Medscape.com.
William Fox, MD, a self-described “dinosaur,” works in an independent internal medicine practice with two other physicians in Charlottesville, Virginia. He is rarely able to accept new patients, and when he does see one, they often have to wait months for the appointment. He accepts the burden of many pent-up needs, along with the huge administrative chore of coordinating their care with subspecialists.
“I will probably have to make multiple visits in a quick succession in order to make sure that I stabilize all the various issues,” Dr. Fox said. Doing so for a complicated new patient is nearly impossible because of time pressures, especially as it has become increasingly difficult for his patients to access subspecialists.
Dr. Fox traced the roots of the problem to a shortage of primary care physicians.
“Primary care is a vital part of healthcare and infrastructure in the United States, and it is being eroded unfortunately, as fewer and fewer medical students and residents choose to go into the primary care field,” Fox said. “And the reason it’s being eroded partly is because it is undervalued” and under-reimbursed, he added.
A study published 2 years ago in the Journal of General Internal Medicine proved what every primary care clinician already knows: The 24-hour day simply isn’t long enough.
Assuming an average panel of 2500 patients, the authors estimated the average time needed to provide currently recommended preventive care services and vaccines, chronic disease care, and management of acute illnesses. The answer: 26.7 hours a day.
However, using a team-based approach in which the necessary care was divided between physicians, advanced practice providers, and medical assistants, the physician component could be whittled down to 9 hours.
As chair of the Board of Regents of the American College of Physicians (ACP), Dr. Fox champions the ACP’s endorsement of physician-led team-based care, which improves patient outcomes and increases well-being among health professionals. But practices like his rarely have the necessary resources to support advanced practice clinicians or social workers. “Team-based care can be achieved in larger healthcare systems that have the resources to do it,” said Dr. Fox. “We need to find a way for smaller independent practices to also participate in team-based care.”
The solution? Major reform in the current fee-for-service payment structure, which incentivizes patient volume over patient outcomes. Dr. Fox co-authored a 2022 position statement from ACP outlining strategies such as prospective payment models that could achieve high-quality care and address social inequities. “We need to evolve our payment system from a fee-for-service system into a blended system where you have some population-based payments along with fee-for-service, or a fully capitated system,” he said.
Advantages of Team-Based Care
When a patient wrote on a satisfaction survey “the doctor spent more time examining the computer than examining me,” Kevin Hopkins, MD, decided he needed to change some things. Now the vice chief of Cleveland Clinic’s Primary Care Institute in Cleveland, in 2010, he developed a rudimentary team-based care model consisting of himself and two medical assistants at Cleveland Clinic.
The assistants did much of the patient intake, served as scribes while Dr. Hopkins saw his patients, and completed most of the required documentation. “I was able to see 30% more patients in a day and still take great care of them,” Dr. Hopkins said.
The concept of team-based care has evolved since then, often including some combination of advanced practice providers such as physician assistants (PAs) or nurse practitioners (NPs), nurses or medical assistants, and social workers or case managers working under the leadership of a physician. According to Dr. Hopkins, the basic strategy should be that “the physician does what only the physician is uniquely trained and qualified to do.” All other tasks, such as data entry, handling refill requests and messages from the patient portal, scheduling, or patient education, can — and should — be done by someone else.
Dr. Hopkins also serves as a senior physician advisor to the American Medical Association (AMA) and an instructor for workshops like “Saving Time: Practice Innovation Boot Camp.” His advice for clinicians who would like to streamline their workflow is to start with small steps.
“You’re not going to be able to hire all the people that you’d like to have,” he said. “I encourage physicians to look around at the people that they have and what they are currently doing as a part of their roles and responsibilities.”
The AMA Team-Based Care and Workflow website provides brief continuing medical education activities on topics such as implementing lab testing prior to office visits or advanced protocols for rooming and discharge; adopting any of these strategies can help save steps during office visits.
Dr. Hopkins said the AMA is committed to reducing the regulatory burden on clinicians. Clinical compliance officers may misinterpret regulatory requirements, putting into place overly conservative internal policies and procedures. The AMA’s “Reducing Regulatory Burden Playbook” offers advice on practices that could be stopped, such as two-factor authentication for approving or signing orders unless they are for controlled substances, or started, such as writing prescriptions for chronic daily medications for the maximum allowed length. Reducing a few clicks with each log-on to the electronic health record or reducing the number of tasks physicians must complete to log on can dramatically reduce hours spent on the computer.
Telehealth Changes Everything
But it might be even more efficient to keep patients out of the office.
Initially piloted in Palo Alto, California, from 2018 to 2022, the Tera Practice adopted team-based care strategies in a practice that conducts most of its work virtually. Sutter Health has since expanded the concept to three “Connected Care Clinics” in the San Francisco area, which provide 80% of their care via secure messaging, telephone, or video visit. Staff work primarily from home, and patients do not need to take off work or spend time driving to in-person visits to access care.
Matthew Sakumoto, MD, is a virtualist primary care physician at Sutter Health’s San Francisco clinic and an adjunct assistant clinical professor at the University of California, San Francisco. He leads a three-person team, which typically has included either an NP or a PA, along with a licensed vocational nurse or medical assistant.
“I go into clinic once a week, but a lot of the visits are video visits, so I don’t feel the pressure to address everything all in one visit,” Dr. Sakumoto said. “It is really freeing for both me and the patient.”
For more complex patients, for example, he prioritizes one problem at a visit because his team will follow up virtually for administrative issues like refills or specialty referrals. He can easily find time to schedule a patient for a follow-up virtual visit in the next week or 2 weeks to address additional needs. And on days he and his staff work from home, patients who message with an urgent concern can often be seen by video that same day.
Dr. Sakumoto and his team have a traditional huddle in the office the morning of their clinic day to plan for the scheduled visits, but most of their days are less structured. On non-clinic days, their morning Zoom huddle has a much different focus.
“We’re saying, ‘Okay, who are our high-risk patients? Who haven’t we seen in a while?’ ” Dr. Sakumoto said. They group patients into tiers based on factors such as age, number of complex medical needs, and frequency of emergency visits or hospitalizations. They also check in with higher-risk patients who haven’t contacted the office or been seen recently.
Dr. Sakumoto noticed in medical school doctors take excellent care of the patients who show up to the clinic. “We don’t do quite as well for those that don’t show up,” he said. The hybrid-virtual model gives him time to think in a more population-based way about engaging his entire panel of patients. The majority have capitated or value-based insurance plans, providing a dedicated monthly revenue stream that funds his virtual practice.
More clinicians may be able to hire staff and adopt some of these innovative approaches if Congress approves proposed changes to Medicare and Medicaid increasing the use of value-based payment systems. Although these changes may not provide all the funding needed to reinvigorate the field of primary care medicine, Dr. Fox said, “at least some people in positions of power and responsibility are beginning to think more seriously about these issues.”
Dr. Sakumoto reported personal fees from the following companies within the past 24 months: Clearstep Health, Carbon Health, Matter Health, CareAlign, PlushCare, Teladoc, and Nabla Health. Dr. Fox and Dr. Hopkins reported no financial conflicts of interest.
A former pediatrician and disease detective, Ann Thomas, MD, MPH, is a freelance science writer living in Portland, Oregon.
A version of this article first appeared on Medscape.com.
William Fox, MD, a self-described “dinosaur,” works in an independent internal medicine practice with two other physicians in Charlottesville, Virginia. He is rarely able to accept new patients, and when he does see one, they often have to wait months for the appointment. He accepts the burden of many pent-up needs, along with the huge administrative chore of coordinating their care with subspecialists.
“I will probably have to make multiple visits in a quick succession in order to make sure that I stabilize all the various issues,” Dr. Fox said. Doing so for a complicated new patient is nearly impossible because of time pressures, especially as it has become increasingly difficult for his patients to access subspecialists.
Dr. Fox traced the roots of the problem to a shortage of primary care physicians.
“Primary care is a vital part of healthcare and infrastructure in the United States, and it is being eroded unfortunately, as fewer and fewer medical students and residents choose to go into the primary care field,” Fox said. “And the reason it’s being eroded partly is because it is undervalued” and under-reimbursed, he added.
A study published 2 years ago in the Journal of General Internal Medicine proved what every primary care clinician already knows: The 24-hour day simply isn’t long enough.
Assuming an average panel of 2500 patients, the authors estimated the average time needed to provide currently recommended preventive care services and vaccines, chronic disease care, and management of acute illnesses. The answer: 26.7 hours a day.
However, using a team-based approach in which the necessary care was divided between physicians, advanced practice providers, and medical assistants, the physician component could be whittled down to 9 hours.
As chair of the Board of Regents of the American College of Physicians (ACP), Dr. Fox champions the ACP’s endorsement of physician-led team-based care, which improves patient outcomes and increases well-being among health professionals. But practices like his rarely have the necessary resources to support advanced practice clinicians or social workers. “Team-based care can be achieved in larger healthcare systems that have the resources to do it,” said Dr. Fox. “We need to find a way for smaller independent practices to also participate in team-based care.”
The solution? Major reform in the current fee-for-service payment structure, which incentivizes patient volume over patient outcomes. Dr. Fox co-authored a 2022 position statement from ACP outlining strategies such as prospective payment models that could achieve high-quality care and address social inequities. “We need to evolve our payment system from a fee-for-service system into a blended system where you have some population-based payments along with fee-for-service, or a fully capitated system,” he said.
Advantages of Team-Based Care
When a patient wrote on a satisfaction survey “the doctor spent more time examining the computer than examining me,” Kevin Hopkins, MD, decided he needed to change some things. Now the vice chief of Cleveland Clinic’s Primary Care Institute in Cleveland, in 2010, he developed a rudimentary team-based care model consisting of himself and two medical assistants at Cleveland Clinic.
The assistants did much of the patient intake, served as scribes while Dr. Hopkins saw his patients, and completed most of the required documentation. “I was able to see 30% more patients in a day and still take great care of them,” Dr. Hopkins said.
The concept of team-based care has evolved since then, often including some combination of advanced practice providers such as physician assistants (PAs) or nurse practitioners (NPs), nurses or medical assistants, and social workers or case managers working under the leadership of a physician. According to Dr. Hopkins, the basic strategy should be that “the physician does what only the physician is uniquely trained and qualified to do.” All other tasks, such as data entry, handling refill requests and messages from the patient portal, scheduling, or patient education, can — and should — be done by someone else.
Dr. Hopkins also serves as a senior physician advisor to the American Medical Association (AMA) and an instructor for workshops like “Saving Time: Practice Innovation Boot Camp.” His advice for clinicians who would like to streamline their workflow is to start with small steps.
“You’re not going to be able to hire all the people that you’d like to have,” he said. “I encourage physicians to look around at the people that they have and what they are currently doing as a part of their roles and responsibilities.”
The AMA Team-Based Care and Workflow website provides brief continuing medical education activities on topics such as implementing lab testing prior to office visits or advanced protocols for rooming and discharge; adopting any of these strategies can help save steps during office visits.
Dr. Hopkins said the AMA is committed to reducing the regulatory burden on clinicians. Clinical compliance officers may misinterpret regulatory requirements, putting into place overly conservative internal policies and procedures. The AMA’s “Reducing Regulatory Burden Playbook” offers advice on practices that could be stopped, such as two-factor authentication for approving or signing orders unless they are for controlled substances, or started, such as writing prescriptions for chronic daily medications for the maximum allowed length. Reducing a few clicks with each log-on to the electronic health record or reducing the number of tasks physicians must complete to log on can dramatically reduce hours spent on the computer.
Telehealth Changes Everything
But it might be even more efficient to keep patients out of the office.
Initially piloted in Palo Alto, California, from 2018 to 2022, the Tera Practice adopted team-based care strategies in a practice that conducts most of its work virtually. Sutter Health has since expanded the concept to three “Connected Care Clinics” in the San Francisco area, which provide 80% of their care via secure messaging, telephone, or video visit. Staff work primarily from home, and patients do not need to take off work or spend time driving to in-person visits to access care.
Matthew Sakumoto, MD, is a virtualist primary care physician at Sutter Health’s San Francisco clinic and an adjunct assistant clinical professor at the University of California, San Francisco. He leads a three-person team, which typically has included either an NP or a PA, along with a licensed vocational nurse or medical assistant.
“I go into clinic once a week, but a lot of the visits are video visits, so I don’t feel the pressure to address everything all in one visit,” Dr. Sakumoto said. “It is really freeing for both me and the patient.”
For more complex patients, for example, he prioritizes one problem at a visit because his team will follow up virtually for administrative issues like refills or specialty referrals. He can easily find time to schedule a patient for a follow-up virtual visit in the next week or 2 weeks to address additional needs. And on days he and his staff work from home, patients who message with an urgent concern can often be seen by video that same day.
Dr. Sakumoto and his team have a traditional huddle in the office the morning of their clinic day to plan for the scheduled visits, but most of their days are less structured. On non-clinic days, their morning Zoom huddle has a much different focus.
“We’re saying, ‘Okay, who are our high-risk patients? Who haven’t we seen in a while?’ ” Dr. Sakumoto said. They group patients into tiers based on factors such as age, number of complex medical needs, and frequency of emergency visits or hospitalizations. They also check in with higher-risk patients who haven’t contacted the office or been seen recently.
Dr. Sakumoto noticed in medical school doctors take excellent care of the patients who show up to the clinic. “We don’t do quite as well for those that don’t show up,” he said. The hybrid-virtual model gives him time to think in a more population-based way about engaging his entire panel of patients. The majority have capitated or value-based insurance plans, providing a dedicated monthly revenue stream that funds his virtual practice.
More clinicians may be able to hire staff and adopt some of these innovative approaches if Congress approves proposed changes to Medicare and Medicaid increasing the use of value-based payment systems. Although these changes may not provide all the funding needed to reinvigorate the field of primary care medicine, Dr. Fox said, “at least some people in positions of power and responsibility are beginning to think more seriously about these issues.”
Dr. Sakumoto reported personal fees from the following companies within the past 24 months: Clearstep Health, Carbon Health, Matter Health, CareAlign, PlushCare, Teladoc, and Nabla Health. Dr. Fox and Dr. Hopkins reported no financial conflicts of interest.
A former pediatrician and disease detective, Ann Thomas, MD, MPH, is a freelance science writer living in Portland, Oregon.
A version of this article first appeared on Medscape.com.
Rural Women Face Greater Challenges in Perimenopause
Women in the perimenopausal period who live in rural areas have a higher prevalence of symptoms typical of this period and a poorer health-related quality of life than women living in urban areas, according to a cross-sectional study that was conducted in Spain.
Cristina Llaneza Suárez, a specialist in family and community medicine and the lead author of the study, told this news organization that women living in rural areas face greater difficulties with access to healthcare services, employment, and transportation and a heavier burden of caregiving. She mentioned that these barriers “can represent an added challenge during the perimenopausal stage, when significant life changes generally occur for all women.” The challenges may lead to “poorer health-related quality of life during perimenopause, compared with women living in urban areas.”
The research group led by Dr. Llaneza aimed to test the hypothesis that sociodemographic characteristics influence symptoms and quality of life in women in perimenopause. They enrolled 270 women aged 45-55 years from eight autonomous communities in Spain who had variability in their menstrual cycles (lasting more than 7 days or amenorrhea greater than 60 days but less than a year).
This cross-sectional study was conducted from December 2019 to April 2023, using the short version of the Cervantes scale to assess health-related quality of life and the Beck Depression Inventory to evaluate associated depressive symptoms.
Among the main findings of the study was that sociocultural factors can influence the perception of perimenopausal symptoms. Living in rural areas has a negative effect on health-related quality of life scales, and this finding is consistent with those of previous studies conducted on women in India, Turkey, Poland, and Peru.
In addition, the selected sample of women experiencing changes in their menstrual cycles and residing in rural areas showed a high prevalence of hot flashes (70% overall and 80% in rural areas) and a poorer quality of life in women with obesity.
“It is striking that, although there is a worse perception of quality of life during perimenopause in women living in rural areas, the proportion of women experiencing some degree of depressive symptoms, according to the Beck inventory, was similar to that of women residing in urban areas,” said Dr. Llaneza. She noted that “no worse scores were observed in sexuality or in the couple relationship.”
Rural Physicians’ Role
Women in the perimenopausal period face significant challenges resulting from inadequate access to healthcare services and limited awareness about menopause. In many countries, this topic is still taboo, both in the family environment and in workplaces and health centers.
Dr. Llaneza mentioned that when she began her training as a primary care physician in a rural population, she witnessed firsthand some of the barriers that women in this age group face, such as limited access to healthcare due to a lack of public transportation. She added that, coupled with this challenge, “there are no regular public transport services that allow independent access for patients, and many [women] lack a driver’s license, making them dependent on others to receive healthcare.” Another important point that she identified was the lack of health education in rural populations, which leads to a minimization of perimenopausal symptoms and causes delays in prevention and early detection.
According to the World Health Organization, healthcare professionals often lack the necessary training to recognize and treat the symptoms of perimenopause and postmenopause. This situation, coupled with the limited attention given to the sexual well-being of menopausal women, contributes to gynecological problems and risks for sexually transmitted infections in this population. The absence of specific health policies and funding for menopause exacerbates the situation, particularly in regions where other health needs compete for limited resources.
Dr. Llaneza noted that primary care physicians in rural areas are responsible for leading primary prevention actions through community interventions that contribute to improving health. Community physicians in rural areas have a lower patient load than urban physicians do. Therefore, “this allows for a more thorough management and closer monitoring of these conditions, which highlights the importance of prevention of perimenopausal symptoms and community education,” she said.
An important goal in improving the quality of life of women in the perimenopausal period is reducing symptoms. Hormone replacement therapy is the cornerstone of treatment, along with nonhormonal therapies such as the use of isoflavones. However, the aforementioned barriers lead to a delay in initiating effective treatment.
Dr. Llaneza added that the main limitation that she encountered during her clinical practice in rural areas regarding the initiation of hormonal therapy was “the reluctance of certain professionals to start it, as they consider that these drugs should be prescribed by menopause specialists because of potential side effects and the increased risk for developing breast cancer.”
Call for Training
Dr. Llaneza and her research team emphasized the need for further research on new drugs for controlling vasomotor symptoms, expressing their interest in conducting additional studies. “We would like to conduct a study on the use of these therapies in perimenopausal and postmenopausal women residing in rural areas.
“We believe that our data may be of interest to healthcare authorities seeking to combat population exodus in rural areas,” they wrote. In addition, they recommended additional training for rural primary care physicians on perimenopause and menopause topics regarding prevention, management, and access, as well as further awareness about preventing depressive symptoms in this population.
Dr. Llaneza declared that she has no relevant financial relationships.
This story was translated from the Medscape Spanish edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Women in the perimenopausal period who live in rural areas have a higher prevalence of symptoms typical of this period and a poorer health-related quality of life than women living in urban areas, according to a cross-sectional study that was conducted in Spain.
Cristina Llaneza Suárez, a specialist in family and community medicine and the lead author of the study, told this news organization that women living in rural areas face greater difficulties with access to healthcare services, employment, and transportation and a heavier burden of caregiving. She mentioned that these barriers “can represent an added challenge during the perimenopausal stage, when significant life changes generally occur for all women.” The challenges may lead to “poorer health-related quality of life during perimenopause, compared with women living in urban areas.”
The research group led by Dr. Llaneza aimed to test the hypothesis that sociodemographic characteristics influence symptoms and quality of life in women in perimenopause. They enrolled 270 women aged 45-55 years from eight autonomous communities in Spain who had variability in their menstrual cycles (lasting more than 7 days or amenorrhea greater than 60 days but less than a year).
This cross-sectional study was conducted from December 2019 to April 2023, using the short version of the Cervantes scale to assess health-related quality of life and the Beck Depression Inventory to evaluate associated depressive symptoms.
Among the main findings of the study was that sociocultural factors can influence the perception of perimenopausal symptoms. Living in rural areas has a negative effect on health-related quality of life scales, and this finding is consistent with those of previous studies conducted on women in India, Turkey, Poland, and Peru.
In addition, the selected sample of women experiencing changes in their menstrual cycles and residing in rural areas showed a high prevalence of hot flashes (70% overall and 80% in rural areas) and a poorer quality of life in women with obesity.
“It is striking that, although there is a worse perception of quality of life during perimenopause in women living in rural areas, the proportion of women experiencing some degree of depressive symptoms, according to the Beck inventory, was similar to that of women residing in urban areas,” said Dr. Llaneza. She noted that “no worse scores were observed in sexuality or in the couple relationship.”
Rural Physicians’ Role
Women in the perimenopausal period face significant challenges resulting from inadequate access to healthcare services and limited awareness about menopause. In many countries, this topic is still taboo, both in the family environment and in workplaces and health centers.
Dr. Llaneza mentioned that when she began her training as a primary care physician in a rural population, she witnessed firsthand some of the barriers that women in this age group face, such as limited access to healthcare due to a lack of public transportation. She added that, coupled with this challenge, “there are no regular public transport services that allow independent access for patients, and many [women] lack a driver’s license, making them dependent on others to receive healthcare.” Another important point that she identified was the lack of health education in rural populations, which leads to a minimization of perimenopausal symptoms and causes delays in prevention and early detection.
According to the World Health Organization, healthcare professionals often lack the necessary training to recognize and treat the symptoms of perimenopause and postmenopause. This situation, coupled with the limited attention given to the sexual well-being of menopausal women, contributes to gynecological problems and risks for sexually transmitted infections in this population. The absence of specific health policies and funding for menopause exacerbates the situation, particularly in regions where other health needs compete for limited resources.
Dr. Llaneza noted that primary care physicians in rural areas are responsible for leading primary prevention actions through community interventions that contribute to improving health. Community physicians in rural areas have a lower patient load than urban physicians do. Therefore, “this allows for a more thorough management and closer monitoring of these conditions, which highlights the importance of prevention of perimenopausal symptoms and community education,” she said.
An important goal in improving the quality of life of women in the perimenopausal period is reducing symptoms. Hormone replacement therapy is the cornerstone of treatment, along with nonhormonal therapies such as the use of isoflavones. However, the aforementioned barriers lead to a delay in initiating effective treatment.
Dr. Llaneza added that the main limitation that she encountered during her clinical practice in rural areas regarding the initiation of hormonal therapy was “the reluctance of certain professionals to start it, as they consider that these drugs should be prescribed by menopause specialists because of potential side effects and the increased risk for developing breast cancer.”
Call for Training
Dr. Llaneza and her research team emphasized the need for further research on new drugs for controlling vasomotor symptoms, expressing their interest in conducting additional studies. “We would like to conduct a study on the use of these therapies in perimenopausal and postmenopausal women residing in rural areas.
“We believe that our data may be of interest to healthcare authorities seeking to combat population exodus in rural areas,” they wrote. In addition, they recommended additional training for rural primary care physicians on perimenopause and menopause topics regarding prevention, management, and access, as well as further awareness about preventing depressive symptoms in this population.
Dr. Llaneza declared that she has no relevant financial relationships.
This story was translated from the Medscape Spanish edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Women in the perimenopausal period who live in rural areas have a higher prevalence of symptoms typical of this period and a poorer health-related quality of life than women living in urban areas, according to a cross-sectional study that was conducted in Spain.
Cristina Llaneza Suárez, a specialist in family and community medicine and the lead author of the study, told this news organization that women living in rural areas face greater difficulties with access to healthcare services, employment, and transportation and a heavier burden of caregiving. She mentioned that these barriers “can represent an added challenge during the perimenopausal stage, when significant life changes generally occur for all women.” The challenges may lead to “poorer health-related quality of life during perimenopause, compared with women living in urban areas.”
The research group led by Dr. Llaneza aimed to test the hypothesis that sociodemographic characteristics influence symptoms and quality of life in women in perimenopause. They enrolled 270 women aged 45-55 years from eight autonomous communities in Spain who had variability in their menstrual cycles (lasting more than 7 days or amenorrhea greater than 60 days but less than a year).
This cross-sectional study was conducted from December 2019 to April 2023, using the short version of the Cervantes scale to assess health-related quality of life and the Beck Depression Inventory to evaluate associated depressive symptoms.
Among the main findings of the study was that sociocultural factors can influence the perception of perimenopausal symptoms. Living in rural areas has a negative effect on health-related quality of life scales, and this finding is consistent with those of previous studies conducted on women in India, Turkey, Poland, and Peru.
In addition, the selected sample of women experiencing changes in their menstrual cycles and residing in rural areas showed a high prevalence of hot flashes (70% overall and 80% in rural areas) and a poorer quality of life in women with obesity.
“It is striking that, although there is a worse perception of quality of life during perimenopause in women living in rural areas, the proportion of women experiencing some degree of depressive symptoms, according to the Beck inventory, was similar to that of women residing in urban areas,” said Dr. Llaneza. She noted that “no worse scores were observed in sexuality or in the couple relationship.”
Rural Physicians’ Role
Women in the perimenopausal period face significant challenges resulting from inadequate access to healthcare services and limited awareness about menopause. In many countries, this topic is still taboo, both in the family environment and in workplaces and health centers.
Dr. Llaneza mentioned that when she began her training as a primary care physician in a rural population, she witnessed firsthand some of the barriers that women in this age group face, such as limited access to healthcare due to a lack of public transportation. She added that, coupled with this challenge, “there are no regular public transport services that allow independent access for patients, and many [women] lack a driver’s license, making them dependent on others to receive healthcare.” Another important point that she identified was the lack of health education in rural populations, which leads to a minimization of perimenopausal symptoms and causes delays in prevention and early detection.
According to the World Health Organization, healthcare professionals often lack the necessary training to recognize and treat the symptoms of perimenopause and postmenopause. This situation, coupled with the limited attention given to the sexual well-being of menopausal women, contributes to gynecological problems and risks for sexually transmitted infections in this population. The absence of specific health policies and funding for menopause exacerbates the situation, particularly in regions where other health needs compete for limited resources.
Dr. Llaneza noted that primary care physicians in rural areas are responsible for leading primary prevention actions through community interventions that contribute to improving health. Community physicians in rural areas have a lower patient load than urban physicians do. Therefore, “this allows for a more thorough management and closer monitoring of these conditions, which highlights the importance of prevention of perimenopausal symptoms and community education,” she said.
An important goal in improving the quality of life of women in the perimenopausal period is reducing symptoms. Hormone replacement therapy is the cornerstone of treatment, along with nonhormonal therapies such as the use of isoflavones. However, the aforementioned barriers lead to a delay in initiating effective treatment.
Dr. Llaneza added that the main limitation that she encountered during her clinical practice in rural areas regarding the initiation of hormonal therapy was “the reluctance of certain professionals to start it, as they consider that these drugs should be prescribed by menopause specialists because of potential side effects and the increased risk for developing breast cancer.”
Call for Training
Dr. Llaneza and her research team emphasized the need for further research on new drugs for controlling vasomotor symptoms, expressing their interest in conducting additional studies. “We would like to conduct a study on the use of these therapies in perimenopausal and postmenopausal women residing in rural areas.
“We believe that our data may be of interest to healthcare authorities seeking to combat population exodus in rural areas,” they wrote. In addition, they recommended additional training for rural primary care physicians on perimenopause and menopause topics regarding prevention, management, and access, as well as further awareness about preventing depressive symptoms in this population.
Dr. Llaneza declared that she has no relevant financial relationships.
This story was translated from the Medscape Spanish edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Misdiagnosis of Crusted Scabies: Skin Excoriations Resembling Brown Sugar Are Characteristic
To the Editor:
Crusted scabies (formerly known as Norwegian scabies) is a rare and highly contagious variant of scabies, in which the skin is infested with thousands to millions of Sarcoptes scabiei var hominis mites. We present a case of skin changes that were misdiagnosed as atopic dermatitis, seborrhea, xerosis, and drug eruption on initial presentation, which prompted treatment with a corticosteroid that inadvertently caused progression to crusted scabies.
A 79-year-old woman who uses a wheelchair presented to the clinic with skin changes that consisted of diffuse, severely pruritic, erythematous plaques on the head, neck, trunk, face, and extremities of 2 years’ duration. She had a medical history of hyperlipidemia, hypertension, and hyperglycemia, as well as a stroke that required hospitalization 2 years prior to the onset of the skin changes. She had no history of allergies.
Prior clinical diagnoses by primary care and dermatology included xerosis, atopic dermatitis, seborrhea, and drug eruption. She was treated with a mid-potency topical corticosteroid (triamcinolone acetonide cream 0.1%) twice daily and prednisone 40 mg once daily for 2- to 4-week courses over an 8-month period without reduction in symptoms.
Physical examination at the current presentation revealed golden, crusted, fine, powdery but slightly sticky flakes that spread diffusely across the entire body and came off in crumbles with a simple touch. These widespread crusts were easily visible on clothing. There was underlying diffuse erythema beneath the flaking skin on the trunk and proximal extremities. The scale and shedding skin laid in piles on the patient’s lap and resembled brown sugar (Figure 1). The patient also reported decreased hand function and dexterity due to the yellowbrown, thick, crusty plaques that had developed on both the palmar and dorsal sides of the hands (Figure 2). Erythematous plaques on the scalp, forehead, and inner ears resembled seborrhea (Figure 3). Pruritus severity was rated by the patient as 10 of 10, and she scratched her skin the entire time she was in the clinic. The patient was emotional and stated that she had not been able to sleep due to the discomfort. We suspected scabies, and the patient was reassured to learn that it could be confirmed with a simple skin scrape test.

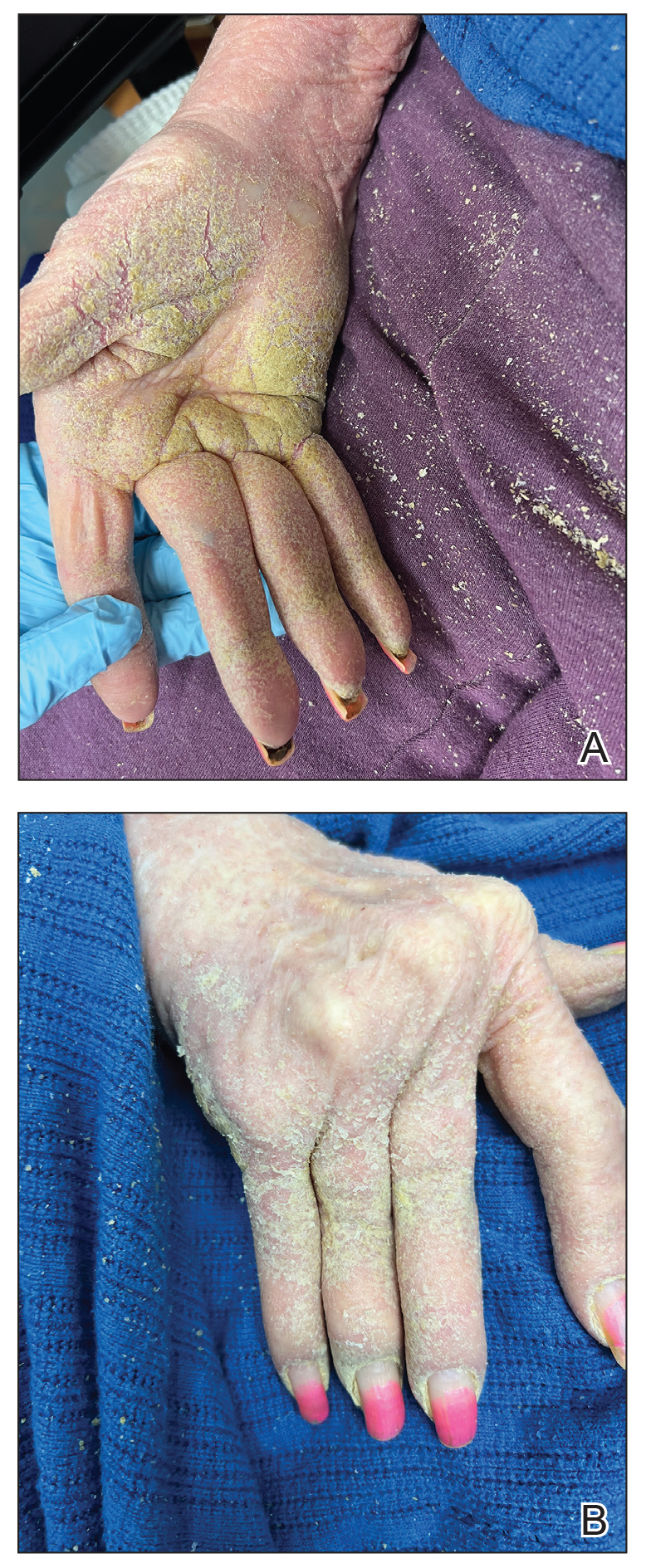

The crusted lesions on the patient's hands were scraped with a #15-blade scalpel, and a routine potassium hydroxide mount was performed. The skin scrapings were placed on a slide with a drop of 10% potassium hydroxide and observed under low-power (×10) and high-power (×40) microscopy, which revealed thousands of mites and eggs (along with previously hatched eggs) (Figure 4) and quickly confirmed a diagnosis of crusted scabies.an extremely contagious form of scabies seen in older patients with compromised immune systems, malnutrition, or disabilities. The patient was prescribed oral ivermectin (3 mg dosed at 200 μg/kg of body weight) and topical permethrin 5%, neither of which she took, as she died of a COVID-19 infection complication 3 days after this diagnostic clinic visit.
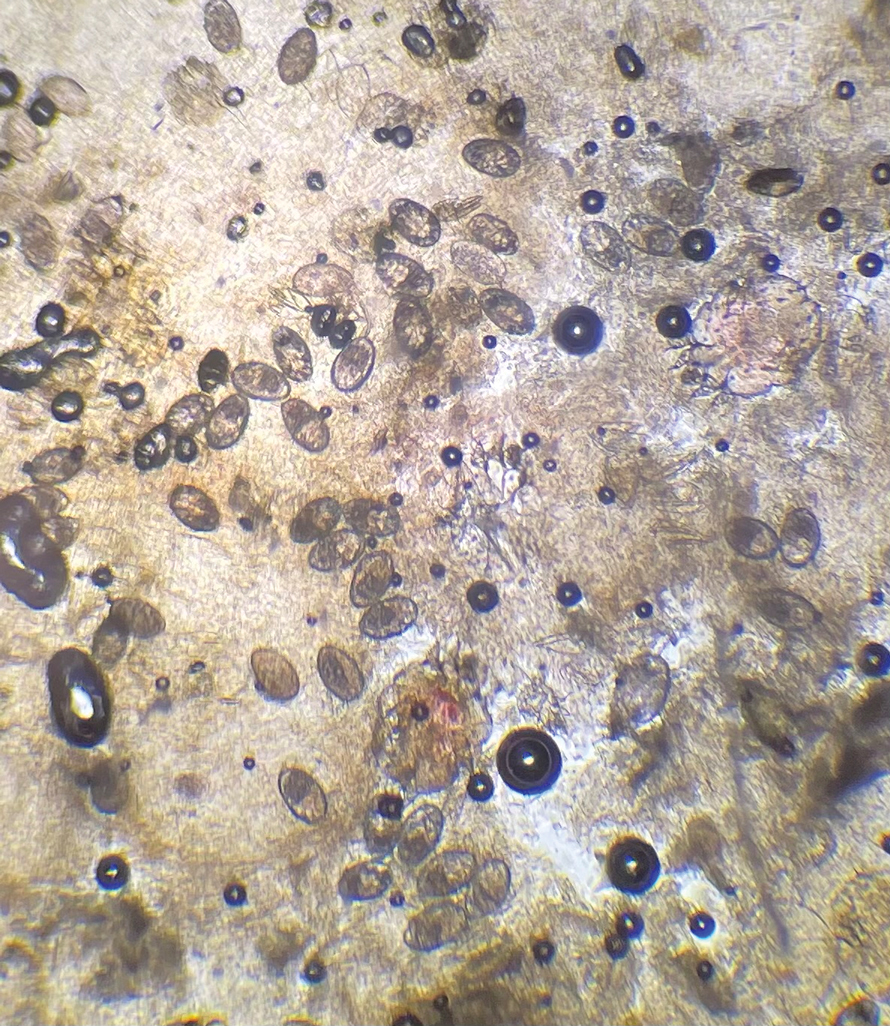
Classic and crusted scabies are both caused by infestation of the Sarcoptes scabiei var hominis mite. Classic scabies is a result of an infestation of a small number of mites (commonly 5–15 mites), while crusted scabies is due to hyperinfestation by as many as millions of mites, the latter often requiring more aggressive treatment. The mites are first transmitted to humans by either skin-toskin contact or fomites on bedding and clothing. The scabies mite undergoes 4 life cycle stages: egg, larvae, nymph, and adult. Once female mites are transmitted, they burrow under the skin and lay 2 to 3 eggs per day. The eggs hatch within 3 to 4 days, after which the larvae migrate to the skin surface. The larval stage lasts for 3 to 4 days, during which the larvae burrow into the stratum corneum to create molting pouches, until they molt into slightly larger nymphs. Nymphs can be found in hair follicles or molting pouches until they further molt within 3 to 4 days into adults, which are round, saclike mites. The adult male and female mites then mate, leaving the female fertile for the rest of her 1- to 2-month lifespan. Impregnated female mites traverse the skin surface in search of a burrow site, using the pulvilli on the anterior aspect of 2 legs to hold onto the skin. Once burrowed, the female mite continues to lay eggs for the rest of her life, with approximately 10% of her eggs resulting in adult mites. Male mites feed in shallow pits of the skin until they find a female burrow site for mating.1 This continuous life cycle of the scabies mite gives rise to highly transmissible, pruritic skin excoriations, as demonstrated in our patient.
The skin has a relatively late inflammatory and adaptive immune response to scabies, typically occurring 4 to 6 weeks after the initial infestation.2 This delayed inflammatory response and onset of symptoms may be due to the scabies mite’s ability to alter aspects of the host’s immune response, which differs in classic vs crusted scabies. In classic scabies, there is a predominance of CD4+ T cells in the dermis and minimal CD8+ T cells. The opposite is true in crusted scabies— there is an overwhelming infiltration of CD8+ T cells and minimal CD4+ T cells.3 The CD8+ T-cell predominance in crusted scabies is hypothesized to be the cause of keratinocyte apoptosis, resulting in epidermal hyperproliferation. Keratinocyte apoptosis also secretes cytokines, which may lead to the immunologic targeting of healthy skin cells. The damage of healthy dermal cells contributes to the inability of the skin’s immune system to mount an effective response, allowing the parasite to grow uncontrollably in patients with crusted scabies.4
This ineffective immune response is further exacerbated by corticosteroids, which are commonly prescribed for pruritus experienced by patients with scabies infestations. The mechanism of action of corticosteroids is the production of anti-inflammatory, antimitotic, and immunosuppressive effects.5 Because the integumentary immune system is imbalanced during crusted scabies infestation, the immunosuppressive mechanism of oral and topical corticosteroids further reduces the cellular immune response to scabies. The flourishing of the scabies mites along with keratinocyte apoptosis4 results in the development of hyperkeratotic skin crusting, most frequently on the palms, soles, arms, and legs. Risk factors for crusted scabies include immunosuppression, hospitalization, crowded living conditions, and poor hygiene, though no known risk factors were documented in up to 42% (33/78) of patients with crusted scabies in one study.6
Patients with crusted scabies typically present with generalized, poorly defined, erythematous, fissured plaques covered by scaling and crusts. Plaques on bony prominences such as finger articulations and elbows may have a thick verrucous aspect.1 Skin flaking that resembles brown sugar—a mixture of white sugar and molasses—is a clue to the diagnosis of crusted scabies. Brown sugar has a slightly sandy and sticky texture that ranges in color from very light brown to very dark brown. When present, flakes always appears slightly lighter than the patient’s skin tone. Although skin burrows are pathognomonic and clinically recognizable features of scabies, these burrows can be disguised by lesions, such as the hyperkeratotic plaques seen in our patient. The lesions may or may not be associated with pruritus, which may occur only at night, and bacterial superinfection has been reported in severe cases of crusted scabies,7 as scratching can cause sores, which may lead to infection. In severe cases, the constant scratching could lead to sepsis if the infection enters the bloodstream.8 Another symptom of scabies is a rash that causes small bumps that tend to form in a line, resembling small bites, hives, or pimples, and scaly plaques can lead to misdiagnosis as atopic dermatitis.
Treatment often is delayed due to misdiagnosis, as seen in our patient. Common misdiagnoses include atopic dermatitis, pityriasis rosea, systemic lupus erythematosus, bullous pemphigoid, lichen planus, pediculosis corporis, seborrheic scalp dermatitis, and adverse drug reactions.9 Patients with extensive infestations of crusted scabies should be treated with a 4-week course of permethrin cream 5% daily for 1 week, then twice per week until resolved, and oral ivermectin 200 μg/kg dosed 1 week apart for up to 4 weeks, if needed.1 Topical permethrin works by producing a selective neurotoxic effect on invertebrates such as scabies mites, which disrupts the function of voltage-gated sodium channels, thereby paralyzing the adult mites to halt the spread of infestation. However, treatment with topical medications can be difficult due to the thick crusts that have formed, which make it more challenging for the skin to properly absorb the treatment. Additionally, surgical debridement as an adjunct procedure has been done to improve the effectiveness of topical medications by removing all the mites in skin.10 On the other hand, the mechanism in which ivermectin treats scabies infestations is poorly understood. Current research suggests that ivermectin works by causing persistent opening of pH-gated chloride channels in scabies mites.11 There is emerging concern for drug resistance to these scabicides,12 revealing a need for further research of treatment options.
Patients with crusted scabies can have an extremely large number of mites (up to 2 million), making them more infectious than patients with classic scabies.13 As a result, it is imperative to reduce environmental transmission and risk for reinfection with mites during treatment. Because crusted scabies is transmitted by prolonged skinto- skin contact or by contact with personal items of an infected person (eg, bedding, clothing), treatment guidelines require all clothing, bedding, and towels of a patient with scabies to be machine-washed and dried with hot water and hot dryer cycles. If an item cannot be washed, it should be stored in a sealed plastic bag for 1 week, as scabies mites cannot survive more than 2 to 3 days away from their host of human skin.13 Treatment of close contacts of patients with scabies is recommended, as well as for those in endemic areas or closed communities, such as nursing homes or jails.
- Salavastru CM, Chosidow O, Boffa MJ, et al. European guideline for the management of scabies. J Eur Acad Dermatol Venereol. 2017;31:1248-1253. doi:10.1111/jdv.14351
- Morgan MS, Arlian LG, Markey MP. Sarcoptes scabiei mites modulate gene expression in human skin equivalents. PLoS One. 2013;8:e71143. doi:10.1371/journal.pone.0071143
- Walton SF, Beroukas D, Roberts-Thomson P, et al. New insights into disease pathogenesis in crusted (Norwegian) scabies: the skin immune response in crusted scabies. Br J Dermatol. 2008;158:1247-1255. doi:10.1111/j.1365-2133.2008.08541.x
- Bhat SA, Mounsey KE, Liu X, et al. Host immune responses to the itch mite, Sarcoptes scabiei, in humans. Parasit Vectors. 2017;10:385. doi:10.1186/s13071-017-2320-4
- Binic´ I, Jankovic´ A, Jovanovic´ D, et al. Crusted (Norwegian) scabies following systemic and topical corticosteroid therapy. J Korean Med Sci. 2009;25:188-191. doi:10.3346/jkms.2010.25.1.188
- Roberts LJ, Huffam SE, Walton SF, et al. Crusted scabies: clinical and immunological findings in seventy-eight patients and a review of the literature. J Infect. 2005;50:375-381. doi:10.1016/j.jinf.2004.08.033
- Yari N, Malone CH, Rivas A. Misdiagnosed crusted scabies in an AIDS patient leads to hyperinfestation. Cutis. 2017;99:202-204.
- American Academy of Dermatology Association. Scabies: signs and symptoms. Accessed July 12, 2024. https://www.aad.org/public/diseases/a-z/scabies-symptoms
- Siegfried EC, Hebert AA. Diagnosis of atopic dermatitis: mimics, overlaps, and complications. J Clin Med. 2015;4:884-917. doi:10.3390/jcm4050884
- Maghrabi MM, Lum S, Joba AT, et al. Norwegian crusted scabies: an unusual case presentation. J Foot Ankle Surg. 2014;53:62-66. doi:10.1053/j.jfas.2013.09.002
- Currie BJ, McCarthy JS. Permethrin and ivermectin for scabies. N Engl J Med. 2010;362:717-725. doi:10.1056/NEJMct0910329
- Andriantsoanirina V, Izri A, Botterel F, et al. Molecular survey of knockdown resistance to pyrethroids in human scabies mites. Clin Microbiol Infect. 2014;20:O139-O141. doi:10.1111/1469-0691.12334
- Centers for Disease Control and Prevention. Preventing scabies. Published December 18, 2023. Accessed August 9, 2024. https://www.cdc.gov/scabies/prevention/index.html
To the Editor:
Crusted scabies (formerly known as Norwegian scabies) is a rare and highly contagious variant of scabies, in which the skin is infested with thousands to millions of Sarcoptes scabiei var hominis mites. We present a case of skin changes that were misdiagnosed as atopic dermatitis, seborrhea, xerosis, and drug eruption on initial presentation, which prompted treatment with a corticosteroid that inadvertently caused progression to crusted scabies.
A 79-year-old woman who uses a wheelchair presented to the clinic with skin changes that consisted of diffuse, severely pruritic, erythematous plaques on the head, neck, trunk, face, and extremities of 2 years’ duration. She had a medical history of hyperlipidemia, hypertension, and hyperglycemia, as well as a stroke that required hospitalization 2 years prior to the onset of the skin changes. She had no history of allergies.
Prior clinical diagnoses by primary care and dermatology included xerosis, atopic dermatitis, seborrhea, and drug eruption. She was treated with a mid-potency topical corticosteroid (triamcinolone acetonide cream 0.1%) twice daily and prednisone 40 mg once daily for 2- to 4-week courses over an 8-month period without reduction in symptoms.
Physical examination at the current presentation revealed golden, crusted, fine, powdery but slightly sticky flakes that spread diffusely across the entire body and came off in crumbles with a simple touch. These widespread crusts were easily visible on clothing. There was underlying diffuse erythema beneath the flaking skin on the trunk and proximal extremities. The scale and shedding skin laid in piles on the patient’s lap and resembled brown sugar (Figure 1). The patient also reported decreased hand function and dexterity due to the yellowbrown, thick, crusty plaques that had developed on both the palmar and dorsal sides of the hands (Figure 2). Erythematous plaques on the scalp, forehead, and inner ears resembled seborrhea (Figure 3). Pruritus severity was rated by the patient as 10 of 10, and she scratched her skin the entire time she was in the clinic. The patient was emotional and stated that she had not been able to sleep due to the discomfort. We suspected scabies, and the patient was reassured to learn that it could be confirmed with a simple skin scrape test.
The crusted lesions on the patient's hands were scraped with a #15-blade scalpel, and a routine potassium hydroxide mount was performed. The skin scrapings were placed on a slide with a drop of 10% potassium hydroxide and observed under low-power (×10) and high-power (×40) microscopy, which revealed thousands of mites and eggs (along with previously hatched eggs) (Figure 4) and quickly confirmed a diagnosis of crusted scabies.an extremely contagious form of scabies seen in older patients with compromised immune systems, malnutrition, or disabilities. The patient was prescribed oral ivermectin (3 mg dosed at 200 μg/kg of body weight) and topical permethrin 5%, neither of which she took, as she died of a COVID-19 infection complication 3 days after this diagnostic clinic visit.
Classic and crusted scabies are both caused by infestation of the Sarcoptes scabiei var hominis mite. Classic scabies is a result of an infestation of a small number of mites (commonly 5–15 mites), while crusted scabies is due to hyperinfestation by as many as millions of mites, the latter often requiring more aggressive treatment. The mites are first transmitted to humans by either skin-toskin contact or fomites on bedding and clothing. The scabies mite undergoes 4 life cycle stages: egg, larvae, nymph, and adult. Once female mites are transmitted, they burrow under the skin and lay 2 to 3 eggs per day. The eggs hatch within 3 to 4 days, after which the larvae migrate to the skin surface. The larval stage lasts for 3 to 4 days, during which the larvae burrow into the stratum corneum to create molting pouches, until they molt into slightly larger nymphs. Nymphs can be found in hair follicles or molting pouches until they further molt within 3 to 4 days into adults, which are round, saclike mites. The adult male and female mites then mate, leaving the female fertile for the rest of her 1- to 2-month lifespan. Impregnated female mites traverse the skin surface in search of a burrow site, using the pulvilli on the anterior aspect of 2 legs to hold onto the skin. Once burrowed, the female mite continues to lay eggs for the rest of her life, with approximately 10% of her eggs resulting in adult mites. Male mites feed in shallow pits of the skin until they find a female burrow site for mating.1 This continuous life cycle of the scabies mite gives rise to highly transmissible, pruritic skin excoriations, as demonstrated in our patient.
The skin has a relatively late inflammatory and adaptive immune response to scabies, typically occurring 4 to 6 weeks after the initial infestation.2 This delayed inflammatory response and onset of symptoms may be due to the scabies mite’s ability to alter aspects of the host’s immune response, which differs in classic vs crusted scabies. In classic scabies, there is a predominance of CD4+ T cells in the dermis and minimal CD8+ T cells. The opposite is true in crusted scabies— there is an overwhelming infiltration of CD8+ T cells and minimal CD4+ T cells.3 The CD8+ T-cell predominance in crusted scabies is hypothesized to be the cause of keratinocyte apoptosis, resulting in epidermal hyperproliferation. Keratinocyte apoptosis also secretes cytokines, which may lead to the immunologic targeting of healthy skin cells. The damage of healthy dermal cells contributes to the inability of the skin’s immune system to mount an effective response, allowing the parasite to grow uncontrollably in patients with crusted scabies.4
This ineffective immune response is further exacerbated by corticosteroids, which are commonly prescribed for pruritus experienced by patients with scabies infestations. The mechanism of action of corticosteroids is the production of anti-inflammatory, antimitotic, and immunosuppressive effects.5 Because the integumentary immune system is imbalanced during crusted scabies infestation, the immunosuppressive mechanism of oral and topical corticosteroids further reduces the cellular immune response to scabies. The flourishing of the scabies mites along with keratinocyte apoptosis4 results in the development of hyperkeratotic skin crusting, most frequently on the palms, soles, arms, and legs. Risk factors for crusted scabies include immunosuppression, hospitalization, crowded living conditions, and poor hygiene, though no known risk factors were documented in up to 42% (33/78) of patients with crusted scabies in one study.6
Patients with crusted scabies typically present with generalized, poorly defined, erythematous, fissured plaques covered by scaling and crusts. Plaques on bony prominences such as finger articulations and elbows may have a thick verrucous aspect.1 Skin flaking that resembles brown sugar—a mixture of white sugar and molasses—is a clue to the diagnosis of crusted scabies. Brown sugar has a slightly sandy and sticky texture that ranges in color from very light brown to very dark brown. When present, flakes always appears slightly lighter than the patient’s skin tone. Although skin burrows are pathognomonic and clinically recognizable features of scabies, these burrows can be disguised by lesions, such as the hyperkeratotic plaques seen in our patient. The lesions may or may not be associated with pruritus, which may occur only at night, and bacterial superinfection has been reported in severe cases of crusted scabies,7 as scratching can cause sores, which may lead to infection. In severe cases, the constant scratching could lead to sepsis if the infection enters the bloodstream.8 Another symptom of scabies is a rash that causes small bumps that tend to form in a line, resembling small bites, hives, or pimples, and scaly plaques can lead to misdiagnosis as atopic dermatitis.
Treatment often is delayed due to misdiagnosis, as seen in our patient. Common misdiagnoses include atopic dermatitis, pityriasis rosea, systemic lupus erythematosus, bullous pemphigoid, lichen planus, pediculosis corporis, seborrheic scalp dermatitis, and adverse drug reactions.9 Patients with extensive infestations of crusted scabies should be treated with a 4-week course of permethrin cream 5% daily for 1 week, then twice per week until resolved, and oral ivermectin 200 μg/kg dosed 1 week apart for up to 4 weeks, if needed.1 Topical permethrin works by producing a selective neurotoxic effect on invertebrates such as scabies mites, which disrupts the function of voltage-gated sodium channels, thereby paralyzing the adult mites to halt the spread of infestation. However, treatment with topical medications can be difficult due to the thick crusts that have formed, which make it more challenging for the skin to properly absorb the treatment. Additionally, surgical debridement as an adjunct procedure has been done to improve the effectiveness of topical medications by removing all the mites in skin.10 On the other hand, the mechanism in which ivermectin treats scabies infestations is poorly understood. Current research suggests that ivermectin works by causing persistent opening of pH-gated chloride channels in scabies mites.11 There is emerging concern for drug resistance to these scabicides,12 revealing a need for further research of treatment options.
Patients with crusted scabies can have an extremely large number of mites (up to 2 million), making them more infectious than patients with classic scabies.13 As a result, it is imperative to reduce environmental transmission and risk for reinfection with mites during treatment. Because crusted scabies is transmitted by prolonged skinto- skin contact or by contact with personal items of an infected person (eg, bedding, clothing), treatment guidelines require all clothing, bedding, and towels of a patient with scabies to be machine-washed and dried with hot water and hot dryer cycles. If an item cannot be washed, it should be stored in a sealed plastic bag for 1 week, as scabies mites cannot survive more than 2 to 3 days away from their host of human skin.13 Treatment of close contacts of patients with scabies is recommended, as well as for those in endemic areas or closed communities, such as nursing homes or jails.
To the Editor:
Crusted scabies (formerly known as Norwegian scabies) is a rare and highly contagious variant of scabies, in which the skin is infested with thousands to millions of Sarcoptes scabiei var hominis mites. We present a case of skin changes that were misdiagnosed as atopic dermatitis, seborrhea, xerosis, and drug eruption on initial presentation, which prompted treatment with a corticosteroid that inadvertently caused progression to crusted scabies.
A 79-year-old woman who uses a wheelchair presented to the clinic with skin changes that consisted of diffuse, severely pruritic, erythematous plaques on the head, neck, trunk, face, and extremities of 2 years’ duration. She had a medical history of hyperlipidemia, hypertension, and hyperglycemia, as well as a stroke that required hospitalization 2 years prior to the onset of the skin changes. She had no history of allergies.
Prior clinical diagnoses by primary care and dermatology included xerosis, atopic dermatitis, seborrhea, and drug eruption. She was treated with a mid-potency topical corticosteroid (triamcinolone acetonide cream 0.1%) twice daily and prednisone 40 mg once daily for 2- to 4-week courses over an 8-month period without reduction in symptoms.
Physical examination at the current presentation revealed golden, crusted, fine, powdery but slightly sticky flakes that spread diffusely across the entire body and came off in crumbles with a simple touch. These widespread crusts were easily visible on clothing. There was underlying diffuse erythema beneath the flaking skin on the trunk and proximal extremities. The scale and shedding skin laid in piles on the patient’s lap and resembled brown sugar (Figure 1). The patient also reported decreased hand function and dexterity due to the yellowbrown, thick, crusty plaques that had developed on both the palmar and dorsal sides of the hands (Figure 2). Erythematous plaques on the scalp, forehead, and inner ears resembled seborrhea (Figure 3). Pruritus severity was rated by the patient as 10 of 10, and she scratched her skin the entire time she was in the clinic. The patient was emotional and stated that she had not been able to sleep due to the discomfort. We suspected scabies, and the patient was reassured to learn that it could be confirmed with a simple skin scrape test.
The crusted lesions on the patient's hands were scraped with a #15-blade scalpel, and a routine potassium hydroxide mount was performed. The skin scrapings were placed on a slide with a drop of 10% potassium hydroxide and observed under low-power (×10) and high-power (×40) microscopy, which revealed thousands of mites and eggs (along with previously hatched eggs) (Figure 4) and quickly confirmed a diagnosis of crusted scabies.an extremely contagious form of scabies seen in older patients with compromised immune systems, malnutrition, or disabilities. The patient was prescribed oral ivermectin (3 mg dosed at 200 μg/kg of body weight) and topical permethrin 5%, neither of which she took, as she died of a COVID-19 infection complication 3 days after this diagnostic clinic visit.
Classic and crusted scabies are both caused by infestation of the Sarcoptes scabiei var hominis mite. Classic scabies is a result of an infestation of a small number of mites (commonly 5–15 mites), while crusted scabies is due to hyperinfestation by as many as millions of mites, the latter often requiring more aggressive treatment. The mites are first transmitted to humans by either skin-toskin contact or fomites on bedding and clothing. The scabies mite undergoes 4 life cycle stages: egg, larvae, nymph, and adult. Once female mites are transmitted, they burrow under the skin and lay 2 to 3 eggs per day. The eggs hatch within 3 to 4 days, after which the larvae migrate to the skin surface. The larval stage lasts for 3 to 4 days, during which the larvae burrow into the stratum corneum to create molting pouches, until they molt into slightly larger nymphs. Nymphs can be found in hair follicles or molting pouches until they further molt within 3 to 4 days into adults, which are round, saclike mites. The adult male and female mites then mate, leaving the female fertile for the rest of her 1- to 2-month lifespan. Impregnated female mites traverse the skin surface in search of a burrow site, using the pulvilli on the anterior aspect of 2 legs to hold onto the skin. Once burrowed, the female mite continues to lay eggs for the rest of her life, with approximately 10% of her eggs resulting in adult mites. Male mites feed in shallow pits of the skin until they find a female burrow site for mating.1 This continuous life cycle of the scabies mite gives rise to highly transmissible, pruritic skin excoriations, as demonstrated in our patient.
The skin has a relatively late inflammatory and adaptive immune response to scabies, typically occurring 4 to 6 weeks after the initial infestation.2 This delayed inflammatory response and onset of symptoms may be due to the scabies mite’s ability to alter aspects of the host’s immune response, which differs in classic vs crusted scabies. In classic scabies, there is a predominance of CD4+ T cells in the dermis and minimal CD8+ T cells. The opposite is true in crusted scabies— there is an overwhelming infiltration of CD8+ T cells and minimal CD4+ T cells.3 The CD8+ T-cell predominance in crusted scabies is hypothesized to be the cause of keratinocyte apoptosis, resulting in epidermal hyperproliferation. Keratinocyte apoptosis also secretes cytokines, which may lead to the immunologic targeting of healthy skin cells. The damage of healthy dermal cells contributes to the inability of the skin’s immune system to mount an effective response, allowing the parasite to grow uncontrollably in patients with crusted scabies.4
This ineffective immune response is further exacerbated by corticosteroids, which are commonly prescribed for pruritus experienced by patients with scabies infestations. The mechanism of action of corticosteroids is the production of anti-inflammatory, antimitotic, and immunosuppressive effects.5 Because the integumentary immune system is imbalanced during crusted scabies infestation, the immunosuppressive mechanism of oral and topical corticosteroids further reduces the cellular immune response to scabies. The flourishing of the scabies mites along with keratinocyte apoptosis4 results in the development of hyperkeratotic skin crusting, most frequently on the palms, soles, arms, and legs. Risk factors for crusted scabies include immunosuppression, hospitalization, crowded living conditions, and poor hygiene, though no known risk factors were documented in up to 42% (33/78) of patients with crusted scabies in one study.6
Patients with crusted scabies typically present with generalized, poorly defined, erythematous, fissured plaques covered by scaling and crusts. Plaques on bony prominences such as finger articulations and elbows may have a thick verrucous aspect.1 Skin flaking that resembles brown sugar—a mixture of white sugar and molasses—is a clue to the diagnosis of crusted scabies. Brown sugar has a slightly sandy and sticky texture that ranges in color from very light brown to very dark brown. When present, flakes always appears slightly lighter than the patient’s skin tone. Although skin burrows are pathognomonic and clinically recognizable features of scabies, these burrows can be disguised by lesions, such as the hyperkeratotic plaques seen in our patient. The lesions may or may not be associated with pruritus, which may occur only at night, and bacterial superinfection has been reported in severe cases of crusted scabies,7 as scratching can cause sores, which may lead to infection. In severe cases, the constant scratching could lead to sepsis if the infection enters the bloodstream.8 Another symptom of scabies is a rash that causes small bumps that tend to form in a line, resembling small bites, hives, or pimples, and scaly plaques can lead to misdiagnosis as atopic dermatitis.
Treatment often is delayed due to misdiagnosis, as seen in our patient. Common misdiagnoses include atopic dermatitis, pityriasis rosea, systemic lupus erythematosus, bullous pemphigoid, lichen planus, pediculosis corporis, seborrheic scalp dermatitis, and adverse drug reactions.9 Patients with extensive infestations of crusted scabies should be treated with a 4-week course of permethrin cream 5% daily for 1 week, then twice per week until resolved, and oral ivermectin 200 μg/kg dosed 1 week apart for up to 4 weeks, if needed.1 Topical permethrin works by producing a selective neurotoxic effect on invertebrates such as scabies mites, which disrupts the function of voltage-gated sodium channels, thereby paralyzing the adult mites to halt the spread of infestation. However, treatment with topical medications can be difficult due to the thick crusts that have formed, which make it more challenging for the skin to properly absorb the treatment. Additionally, surgical debridement as an adjunct procedure has been done to improve the effectiveness of topical medications by removing all the mites in skin.10 On the other hand, the mechanism in which ivermectin treats scabies infestations is poorly understood. Current research suggests that ivermectin works by causing persistent opening of pH-gated chloride channels in scabies mites.11 There is emerging concern for drug resistance to these scabicides,12 revealing a need for further research of treatment options.
Patients with crusted scabies can have an extremely large number of mites (up to 2 million), making them more infectious than patients with classic scabies.13 As a result, it is imperative to reduce environmental transmission and risk for reinfection with mites during treatment. Because crusted scabies is transmitted by prolonged skinto- skin contact or by contact with personal items of an infected person (eg, bedding, clothing), treatment guidelines require all clothing, bedding, and towels of a patient with scabies to be machine-washed and dried with hot water and hot dryer cycles. If an item cannot be washed, it should be stored in a sealed plastic bag for 1 week, as scabies mites cannot survive more than 2 to 3 days away from their host of human skin.13 Treatment of close contacts of patients with scabies is recommended, as well as for those in endemic areas or closed communities, such as nursing homes or jails.
- Salavastru CM, Chosidow O, Boffa MJ, et al. European guideline for the management of scabies. J Eur Acad Dermatol Venereol. 2017;31:1248-1253. doi:10.1111/jdv.14351
- Morgan MS, Arlian LG, Markey MP. Sarcoptes scabiei mites modulate gene expression in human skin equivalents. PLoS One. 2013;8:e71143. doi:10.1371/journal.pone.0071143
- Walton SF, Beroukas D, Roberts-Thomson P, et al. New insights into disease pathogenesis in crusted (Norwegian) scabies: the skin immune response in crusted scabies. Br J Dermatol. 2008;158:1247-1255. doi:10.1111/j.1365-2133.2008.08541.x
- Bhat SA, Mounsey KE, Liu X, et al. Host immune responses to the itch mite, Sarcoptes scabiei, in humans. Parasit Vectors. 2017;10:385. doi:10.1186/s13071-017-2320-4
- Binic´ I, Jankovic´ A, Jovanovic´ D, et al. Crusted (Norwegian) scabies following systemic and topical corticosteroid therapy. J Korean Med Sci. 2009;25:188-191. doi:10.3346/jkms.2010.25.1.188
- Roberts LJ, Huffam SE, Walton SF, et al. Crusted scabies: clinical and immunological findings in seventy-eight patients and a review of the literature. J Infect. 2005;50:375-381. doi:10.1016/j.jinf.2004.08.033
- Yari N, Malone CH, Rivas A. Misdiagnosed crusted scabies in an AIDS patient leads to hyperinfestation. Cutis. 2017;99:202-204.
- American Academy of Dermatology Association. Scabies: signs and symptoms. Accessed July 12, 2024. https://www.aad.org/public/diseases/a-z/scabies-symptoms
- Siegfried EC, Hebert AA. Diagnosis of atopic dermatitis: mimics, overlaps, and complications. J Clin Med. 2015;4:884-917. doi:10.3390/jcm4050884
- Maghrabi MM, Lum S, Joba AT, et al. Norwegian crusted scabies: an unusual case presentation. J Foot Ankle Surg. 2014;53:62-66. doi:10.1053/j.jfas.2013.09.002
- Currie BJ, McCarthy JS. Permethrin and ivermectin for scabies. N Engl J Med. 2010;362:717-725. doi:10.1056/NEJMct0910329
- Andriantsoanirina V, Izri A, Botterel F, et al. Molecular survey of knockdown resistance to pyrethroids in human scabies mites. Clin Microbiol Infect. 2014;20:O139-O141. doi:10.1111/1469-0691.12334
- Centers for Disease Control and Prevention. Preventing scabies. Published December 18, 2023. Accessed August 9, 2024. https://www.cdc.gov/scabies/prevention/index.html
- Salavastru CM, Chosidow O, Boffa MJ, et al. European guideline for the management of scabies. J Eur Acad Dermatol Venereol. 2017;31:1248-1253. doi:10.1111/jdv.14351
- Morgan MS, Arlian LG, Markey MP. Sarcoptes scabiei mites modulate gene expression in human skin equivalents. PLoS One. 2013;8:e71143. doi:10.1371/journal.pone.0071143
- Walton SF, Beroukas D, Roberts-Thomson P, et al. New insights into disease pathogenesis in crusted (Norwegian) scabies: the skin immune response in crusted scabies. Br J Dermatol. 2008;158:1247-1255. doi:10.1111/j.1365-2133.2008.08541.x
- Bhat SA, Mounsey KE, Liu X, et al. Host immune responses to the itch mite, Sarcoptes scabiei, in humans. Parasit Vectors. 2017;10:385. doi:10.1186/s13071-017-2320-4
- Binic´ I, Jankovic´ A, Jovanovic´ D, et al. Crusted (Norwegian) scabies following systemic and topical corticosteroid therapy. J Korean Med Sci. 2009;25:188-191. doi:10.3346/jkms.2010.25.1.188
- Roberts LJ, Huffam SE, Walton SF, et al. Crusted scabies: clinical and immunological findings in seventy-eight patients and a review of the literature. J Infect. 2005;50:375-381. doi:10.1016/j.jinf.2004.08.033
- Yari N, Malone CH, Rivas A. Misdiagnosed crusted scabies in an AIDS patient leads to hyperinfestation. Cutis. 2017;99:202-204.
- American Academy of Dermatology Association. Scabies: signs and symptoms. Accessed July 12, 2024. https://www.aad.org/public/diseases/a-z/scabies-symptoms
- Siegfried EC, Hebert AA. Diagnosis of atopic dermatitis: mimics, overlaps, and complications. J Clin Med. 2015;4:884-917. doi:10.3390/jcm4050884
- Maghrabi MM, Lum S, Joba AT, et al. Norwegian crusted scabies: an unusual case presentation. J Foot Ankle Surg. 2014;53:62-66. doi:10.1053/j.jfas.2013.09.002
- Currie BJ, McCarthy JS. Permethrin and ivermectin for scabies. N Engl J Med. 2010;362:717-725. doi:10.1056/NEJMct0910329
- Andriantsoanirina V, Izri A, Botterel F, et al. Molecular survey of knockdown resistance to pyrethroids in human scabies mites. Clin Microbiol Infect. 2014;20:O139-O141. doi:10.1111/1469-0691.12334
- Centers for Disease Control and Prevention. Preventing scabies. Published December 18, 2023. Accessed August 9, 2024. https://www.cdc.gov/scabies/prevention/index.html
PRACTICE POINTS
- Crusted scabies often is misdiagnosed because it mimics common dermatologic conditions, such as atopic dermatitis, psoriasis, drug eruption, and seborrhea. A unique feature of crusted scabies is fine or coarse scaling that resembles brown sugar.
- Immunosuppressants, such as topical corticosteroids, worsen the skin’s immune response to classic scabies infestations, which leads to parasitic overgrowth and the development of crusted scabies.
- Treatment of crusted scabies requires topical and oral scabicide; in addition, all clothing, bedding, and towels should be machine-washed and dried with hot water and hot dryer cycles to prevent environmental transmission and reinfection.

Recurrent Pancreatitis Triples Risk for Chronic Disease
TOPLINE:
The overall progression to chronic pancreatitis among adults was three times higher following recurrent episodes of acute pancreatitis than occurring after just the first acute pancreatitis episode.
METHODOLOGY:
- The progression of acute pancreatitis is time-dependent, with the recurrence and progression rates to recurrent acute pancreatitis and chronic pancreatitis varying based on the follow-up duration and may be affected by the cause and severity of the first acute episode.
- To better understand the progression of acute pancreatitis to recurrent acute pancreatitis and chronic pancreatitis, researchers conducted a systematic review and meta-analysis of 119 studies, all of which were used for qualitative and quantitative synthesis and 29 of which also were used for calculating incidence rates.
- The primary outcomes were the incidence rates of recurrent acute and chronic pancreatitis following the initial episode of acute pancreatitis and the incidence rate of chronic pancreatitis after recurrent episodes of acute pancreatitis.
- The secondary outcomes were the cumulative incidences and proportions of recurrent acute and chronic pancreatitis following the initial acute pancreatitis episode and the proportion of chronic pancreatitis occurring after recurrent acute pancreatitis episodes.
TAKEAWAY:
- The incidence rate of recurrent acute pancreatitis after the first acute episode was 5.26 per 100 person-years in adults and 4.64 per 100 person-years in children, a difference that did not reach statistical significance.
- The progression rate to chronic pancreatitis in adults was threefold higher after recurrent acute pancreatitis episodes than after the first acute pancreatitis episode (4.31 vs 1.38 per 100 person-years).
- Hypertriglyceridemia-induced acute pancreatitis had the highest recurrence rates, followed by alcohol-induced, idiopathic, and biliary pancreatitis.
- The overall progression rate into chronic pancreatitis was 8% after the first acute pancreatitis episode and 24% after recurrent episodes of acute pancreatitis. Progression to chronic pancreatitis among adults was highest among those with alcohol-induced disease, followed by idiopathic and biliary pancreatitis.
- A moderately severe first episode of acute pancreatitis was associated with the highest recurrence rate, followed by mild and severe first episodes.
IN PRACTICE:
The authors emphasized the need to develop new interventions to address the factors associated with acute pancreatitis and its progression and to better utilize existing approaches, such as brief and repeated psychological interventions and alcohol and smoking cessation programs. Deeper investigation into the underlying causes of the disease’s etiology is warranted to reduce recurrence and progression rates, they noted.
SOURCE:
The study, led by Endre-Botond Gagyi, MD, of the Center for Translational Medicine, Semmelweis University, Budapest, Hungary, was published online in Therapeutic Advances in Gastroenterology.
LIMITATIONS:
Most of the studies included in the analysis were retrospective, and there was high heterogeneity between them. The researchers could only analyze the presence of recurrent acute pancreatitis but could not explore the number of episodes or their impact on progression due to the lack of reported data.
DISCLOSURES:
The study was funded by the New National Excellence Program of the Ministry for Innovation and Technology from the National Research, Development and Innovation Fund. The authors declared no conflict of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
The overall progression to chronic pancreatitis among adults was three times higher following recurrent episodes of acute pancreatitis than occurring after just the first acute pancreatitis episode.
METHODOLOGY:
- The progression of acute pancreatitis is time-dependent, with the recurrence and progression rates to recurrent acute pancreatitis and chronic pancreatitis varying based on the follow-up duration and may be affected by the cause and severity of the first acute episode.
- To better understand the progression of acute pancreatitis to recurrent acute pancreatitis and chronic pancreatitis, researchers conducted a systematic review and meta-analysis of 119 studies, all of which were used for qualitative and quantitative synthesis and 29 of which also were used for calculating incidence rates.
- The primary outcomes were the incidence rates of recurrent acute and chronic pancreatitis following the initial episode of acute pancreatitis and the incidence rate of chronic pancreatitis after recurrent episodes of acute pancreatitis.
- The secondary outcomes were the cumulative incidences and proportions of recurrent acute and chronic pancreatitis following the initial acute pancreatitis episode and the proportion of chronic pancreatitis occurring after recurrent acute pancreatitis episodes.
TAKEAWAY:
- The incidence rate of recurrent acute pancreatitis after the first acute episode was 5.26 per 100 person-years in adults and 4.64 per 100 person-years in children, a difference that did not reach statistical significance.
- The progression rate to chronic pancreatitis in adults was threefold higher after recurrent acute pancreatitis episodes than after the first acute pancreatitis episode (4.31 vs 1.38 per 100 person-years).
- Hypertriglyceridemia-induced acute pancreatitis had the highest recurrence rates, followed by alcohol-induced, idiopathic, and biliary pancreatitis.
- The overall progression rate into chronic pancreatitis was 8% after the first acute pancreatitis episode and 24% after recurrent episodes of acute pancreatitis. Progression to chronic pancreatitis among adults was highest among those with alcohol-induced disease, followed by idiopathic and biliary pancreatitis.
- A moderately severe first episode of acute pancreatitis was associated with the highest recurrence rate, followed by mild and severe first episodes.
IN PRACTICE:
The authors emphasized the need to develop new interventions to address the factors associated with acute pancreatitis and its progression and to better utilize existing approaches, such as brief and repeated psychological interventions and alcohol and smoking cessation programs. Deeper investigation into the underlying causes of the disease’s etiology is warranted to reduce recurrence and progression rates, they noted.
SOURCE:
The study, led by Endre-Botond Gagyi, MD, of the Center for Translational Medicine, Semmelweis University, Budapest, Hungary, was published online in Therapeutic Advances in Gastroenterology.
LIMITATIONS:
Most of the studies included in the analysis were retrospective, and there was high heterogeneity between them. The researchers could only analyze the presence of recurrent acute pancreatitis but could not explore the number of episodes or their impact on progression due to the lack of reported data.
DISCLOSURES:
The study was funded by the New National Excellence Program of the Ministry for Innovation and Technology from the National Research, Development and Innovation Fund. The authors declared no conflict of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
The overall progression to chronic pancreatitis among adults was three times higher following recurrent episodes of acute pancreatitis than occurring after just the first acute pancreatitis episode.
METHODOLOGY:
- The progression of acute pancreatitis is time-dependent, with the recurrence and progression rates to recurrent acute pancreatitis and chronic pancreatitis varying based on the follow-up duration and may be affected by the cause and severity of the first acute episode.
- To better understand the progression of acute pancreatitis to recurrent acute pancreatitis and chronic pancreatitis, researchers conducted a systematic review and meta-analysis of 119 studies, all of which were used for qualitative and quantitative synthesis and 29 of which also were used for calculating incidence rates.
- The primary outcomes were the incidence rates of recurrent acute and chronic pancreatitis following the initial episode of acute pancreatitis and the incidence rate of chronic pancreatitis after recurrent episodes of acute pancreatitis.
- The secondary outcomes were the cumulative incidences and proportions of recurrent acute and chronic pancreatitis following the initial acute pancreatitis episode and the proportion of chronic pancreatitis occurring after recurrent acute pancreatitis episodes.
TAKEAWAY:
- The incidence rate of recurrent acute pancreatitis after the first acute episode was 5.26 per 100 person-years in adults and 4.64 per 100 person-years in children, a difference that did not reach statistical significance.
- The progression rate to chronic pancreatitis in adults was threefold higher after recurrent acute pancreatitis episodes than after the first acute pancreatitis episode (4.31 vs 1.38 per 100 person-years).
- Hypertriglyceridemia-induced acute pancreatitis had the highest recurrence rates, followed by alcohol-induced, idiopathic, and biliary pancreatitis.
- The overall progression rate into chronic pancreatitis was 8% after the first acute pancreatitis episode and 24% after recurrent episodes of acute pancreatitis. Progression to chronic pancreatitis among adults was highest among those with alcohol-induced disease, followed by idiopathic and biliary pancreatitis.
- A moderately severe first episode of acute pancreatitis was associated with the highest recurrence rate, followed by mild and severe first episodes.
IN PRACTICE:
The authors emphasized the need to develop new interventions to address the factors associated with acute pancreatitis and its progression and to better utilize existing approaches, such as brief and repeated psychological interventions and alcohol and smoking cessation programs. Deeper investigation into the underlying causes of the disease’s etiology is warranted to reduce recurrence and progression rates, they noted.
SOURCE:
The study, led by Endre-Botond Gagyi, MD, of the Center for Translational Medicine, Semmelweis University, Budapest, Hungary, was published online in Therapeutic Advances in Gastroenterology.
LIMITATIONS:
Most of the studies included in the analysis were retrospective, and there was high heterogeneity between them. The researchers could only analyze the presence of recurrent acute pancreatitis but could not explore the number of episodes or their impact on progression due to the lack of reported data.
DISCLOSURES:
The study was funded by the New National Excellence Program of the Ministry for Innovation and Technology from the National Research, Development and Innovation Fund. The authors declared no conflict of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.