User login
Fine-needle aspiration alternative allows closer look at pancreatic cystic lesions
Endoscopic ultrasound (EUS)–guided through-the-needle biopsies (TTNBs) of pancreatic cystic lesions are sufficient for accurate molecular analysis, which offers a superior alternative to cyst fluid obtained via fine-needle aspiration, based on a prospective study.
For highest diagnostic clarity, next-generation sequencing (NGS) of TTNBs can be paired with histology, lead author Charlotte Vestrup Rift, MD, PhD, of Copenhagen University Hospital, and colleagues reported.
“The diagnostic algorithm for the management of [pancreatic cystic lesions] includes endoscopic ultrasound examination with aspiration of cyst fluid for cytology,” the investigators wrote in Gastrointestinal Endoscopy. “However, the reported sensitivity of cytology is low [at 54%]. A new microforceps, introduced through a 19-gauge needle, has proven useful for procurement of [TTNBs] that represent both the epithelial and stromal component of the cyst wall. TTNBs have a high sensitivity of 86% for the diagnosis of mucinous cysts.”
Dr. Rift and colleagues evaluated the impact of introducing NGS to the diagnostic process. They noted that concomitant mutations in GNAS and KRAS are diagnostic for intraductal papillary mucinous neoplasms (IPMNs), while other mutations have been linked with progression to cancer.
The study involved 101 patients with pancreatic cystic lesions larger than 15 mm in diameter, mean age of 68 years, among whom 91 had residual TTNBs available after microscopic analysis. These samples underwent a 51-gene NGS panel that included the “most prevalent hot-spot mutations.” Diagnoses were sorted into four categories: neoplastic cyst, mucinous cyst, IPMN, or serous cystic neoplasm.
The primary endpoint was diagnostic yield, both for molecular analysis of TTNBs and for molecular analysis plus histopathology of TTNBs. Sensitivity and specificity of NGS were also determined using histopathology as the gold standard.
Relying on NGS alone, diagnostic yields were 44.5% and 27.7% for detecting a mucinous cyst and determining type of cyst, respectively. These yields rose to 73.3% and 70.3%, respectively, when NGS was used with microscopic evaluation. Continuing with this combined approach, sensitivity and specificity were 83.7% and 81.8%, respectively, for the diagnosis of a mucinous cyst. Sensitivity and specificity were higher still, at 87.2% and 84.6%, respectively, for identifying IPMNs.
The adverse-event rate was 9.9%, with a risk of postprocedure acute pancreatitis of 8.9 % and procedure-associated intracystic bleeding of 3%, according to the authors.
Limitations of the study include the relatively small sample size and the single-center design.
“TTNB-NGS is not sufficient as a stand-alone diagnostic tool as of yet but has a high diagnostic yield when combined with microscopic evaluation and subtyping by immunohistochemistry,” the investigators concluded. “The advantage of EUS-TTNB over EUS–[fine-needle aspiration] is the ability to perform detailed cyst subtyping and the high technical success rate of the procedure. ... However, the procedure comes with a risk of adverse events and thus should be offered to patients where the value of an exact diagnosis outweighs the risks.”
“Molecular subtyping is emerging as a useful clinical test for diagnosing pancreatic cysts,” said Margaret Geraldine Keane, MBBS, MSc, of Johns Hopkins Medicine, Baltimore, although she noted that NGS remains expensive and sporadically available, “which limits its clinical utility and incorporation into diagnostic algorithms for pancreatic cysts. In the future, as the cost of sequencing reduces, and availability improves, this may change.”
For now, Dr. Keane advised physicians to reserve molecular subtyping for cases in which “accurate cyst subtyping will change management ... or when other tests have not provided a clear diagnosis.”
She said the present study is valuable because better diagnostic tests are badly needed for patients with pancreatic cysts, considering the high rate of surgical overtreatment.
“Having more diagnostic tests, such as those described in this publication [to be used on their own or in combination] to decide which patients need surgery, is important,” Dr. Keane said who was not involved in the study.
Better diagnostic tests could also improve outcomes for patients with pancreatic cancer, she said, noting a 5-year survival rate of 10%.
“This outcome is in large part attributable to the late stage at which the majority of patients are diagnosed,” Dr. Keane said. “If patients can be diagnosed earlier, survival dramatically improves. Improvements in diagnostic tests for premalignant pancreatic cystic lesions are therefore vital.”
The study was supported by Rigshospitalets Research Foundation, The Novo Nordisk Foundation, The Danish Cancer Society, and others, although they did not have a role in conducting the study or preparing the manuscript. One investigator disclosed a relationship with MediGlobe. The other investigators reported no conflicts of interest. Dr. Keane disclosed no conflicts of interest.
Endoscopic ultrasound (EUS)–guided through-the-needle biopsies (TTNBs) of pancreatic cystic lesions are sufficient for accurate molecular analysis, which offers a superior alternative to cyst fluid obtained via fine-needle aspiration, based on a prospective study.
For highest diagnostic clarity, next-generation sequencing (NGS) of TTNBs can be paired with histology, lead author Charlotte Vestrup Rift, MD, PhD, of Copenhagen University Hospital, and colleagues reported.
“The diagnostic algorithm for the management of [pancreatic cystic lesions] includes endoscopic ultrasound examination with aspiration of cyst fluid for cytology,” the investigators wrote in Gastrointestinal Endoscopy. “However, the reported sensitivity of cytology is low [at 54%]. A new microforceps, introduced through a 19-gauge needle, has proven useful for procurement of [TTNBs] that represent both the epithelial and stromal component of the cyst wall. TTNBs have a high sensitivity of 86% for the diagnosis of mucinous cysts.”
Dr. Rift and colleagues evaluated the impact of introducing NGS to the diagnostic process. They noted that concomitant mutations in GNAS and KRAS are diagnostic for intraductal papillary mucinous neoplasms (IPMNs), while other mutations have been linked with progression to cancer.
The study involved 101 patients with pancreatic cystic lesions larger than 15 mm in diameter, mean age of 68 years, among whom 91 had residual TTNBs available after microscopic analysis. These samples underwent a 51-gene NGS panel that included the “most prevalent hot-spot mutations.” Diagnoses were sorted into four categories: neoplastic cyst, mucinous cyst, IPMN, or serous cystic neoplasm.
The primary endpoint was diagnostic yield, both for molecular analysis of TTNBs and for molecular analysis plus histopathology of TTNBs. Sensitivity and specificity of NGS were also determined using histopathology as the gold standard.
Relying on NGS alone, diagnostic yields were 44.5% and 27.7% for detecting a mucinous cyst and determining type of cyst, respectively. These yields rose to 73.3% and 70.3%, respectively, when NGS was used with microscopic evaluation. Continuing with this combined approach, sensitivity and specificity were 83.7% and 81.8%, respectively, for the diagnosis of a mucinous cyst. Sensitivity and specificity were higher still, at 87.2% and 84.6%, respectively, for identifying IPMNs.
The adverse-event rate was 9.9%, with a risk of postprocedure acute pancreatitis of 8.9 % and procedure-associated intracystic bleeding of 3%, according to the authors.
Limitations of the study include the relatively small sample size and the single-center design.
“TTNB-NGS is not sufficient as a stand-alone diagnostic tool as of yet but has a high diagnostic yield when combined with microscopic evaluation and subtyping by immunohistochemistry,” the investigators concluded. “The advantage of EUS-TTNB over EUS–[fine-needle aspiration] is the ability to perform detailed cyst subtyping and the high technical success rate of the procedure. ... However, the procedure comes with a risk of adverse events and thus should be offered to patients where the value of an exact diagnosis outweighs the risks.”
“Molecular subtyping is emerging as a useful clinical test for diagnosing pancreatic cysts,” said Margaret Geraldine Keane, MBBS, MSc, of Johns Hopkins Medicine, Baltimore, although she noted that NGS remains expensive and sporadically available, “which limits its clinical utility and incorporation into diagnostic algorithms for pancreatic cysts. In the future, as the cost of sequencing reduces, and availability improves, this may change.”
For now, Dr. Keane advised physicians to reserve molecular subtyping for cases in which “accurate cyst subtyping will change management ... or when other tests have not provided a clear diagnosis.”
She said the present study is valuable because better diagnostic tests are badly needed for patients with pancreatic cysts, considering the high rate of surgical overtreatment.
“Having more diagnostic tests, such as those described in this publication [to be used on their own or in combination] to decide which patients need surgery, is important,” Dr. Keane said who was not involved in the study.
Better diagnostic tests could also improve outcomes for patients with pancreatic cancer, she said, noting a 5-year survival rate of 10%.
“This outcome is in large part attributable to the late stage at which the majority of patients are diagnosed,” Dr. Keane said. “If patients can be diagnosed earlier, survival dramatically improves. Improvements in diagnostic tests for premalignant pancreatic cystic lesions are therefore vital.”
The study was supported by Rigshospitalets Research Foundation, The Novo Nordisk Foundation, The Danish Cancer Society, and others, although they did not have a role in conducting the study or preparing the manuscript. One investigator disclosed a relationship with MediGlobe. The other investigators reported no conflicts of interest. Dr. Keane disclosed no conflicts of interest.
Endoscopic ultrasound (EUS)–guided through-the-needle biopsies (TTNBs) of pancreatic cystic lesions are sufficient for accurate molecular analysis, which offers a superior alternative to cyst fluid obtained via fine-needle aspiration, based on a prospective study.
For highest diagnostic clarity, next-generation sequencing (NGS) of TTNBs can be paired with histology, lead author Charlotte Vestrup Rift, MD, PhD, of Copenhagen University Hospital, and colleagues reported.
“The diagnostic algorithm for the management of [pancreatic cystic lesions] includes endoscopic ultrasound examination with aspiration of cyst fluid for cytology,” the investigators wrote in Gastrointestinal Endoscopy. “However, the reported sensitivity of cytology is low [at 54%]. A new microforceps, introduced through a 19-gauge needle, has proven useful for procurement of [TTNBs] that represent both the epithelial and stromal component of the cyst wall. TTNBs have a high sensitivity of 86% for the diagnosis of mucinous cysts.”
Dr. Rift and colleagues evaluated the impact of introducing NGS to the diagnostic process. They noted that concomitant mutations in GNAS and KRAS are diagnostic for intraductal papillary mucinous neoplasms (IPMNs), while other mutations have been linked with progression to cancer.
The study involved 101 patients with pancreatic cystic lesions larger than 15 mm in diameter, mean age of 68 years, among whom 91 had residual TTNBs available after microscopic analysis. These samples underwent a 51-gene NGS panel that included the “most prevalent hot-spot mutations.” Diagnoses were sorted into four categories: neoplastic cyst, mucinous cyst, IPMN, or serous cystic neoplasm.
The primary endpoint was diagnostic yield, both for molecular analysis of TTNBs and for molecular analysis plus histopathology of TTNBs. Sensitivity and specificity of NGS were also determined using histopathology as the gold standard.
Relying on NGS alone, diagnostic yields were 44.5% and 27.7% for detecting a mucinous cyst and determining type of cyst, respectively. These yields rose to 73.3% and 70.3%, respectively, when NGS was used with microscopic evaluation. Continuing with this combined approach, sensitivity and specificity were 83.7% and 81.8%, respectively, for the diagnosis of a mucinous cyst. Sensitivity and specificity were higher still, at 87.2% and 84.6%, respectively, for identifying IPMNs.
The adverse-event rate was 9.9%, with a risk of postprocedure acute pancreatitis of 8.9 % and procedure-associated intracystic bleeding of 3%, according to the authors.
Limitations of the study include the relatively small sample size and the single-center design.
“TTNB-NGS is not sufficient as a stand-alone diagnostic tool as of yet but has a high diagnostic yield when combined with microscopic evaluation and subtyping by immunohistochemistry,” the investigators concluded. “The advantage of EUS-TTNB over EUS–[fine-needle aspiration] is the ability to perform detailed cyst subtyping and the high technical success rate of the procedure. ... However, the procedure comes with a risk of adverse events and thus should be offered to patients where the value of an exact diagnosis outweighs the risks.”
“Molecular subtyping is emerging as a useful clinical test for diagnosing pancreatic cysts,” said Margaret Geraldine Keane, MBBS, MSc, of Johns Hopkins Medicine, Baltimore, although she noted that NGS remains expensive and sporadically available, “which limits its clinical utility and incorporation into diagnostic algorithms for pancreatic cysts. In the future, as the cost of sequencing reduces, and availability improves, this may change.”
For now, Dr. Keane advised physicians to reserve molecular subtyping for cases in which “accurate cyst subtyping will change management ... or when other tests have not provided a clear diagnosis.”
She said the present study is valuable because better diagnostic tests are badly needed for patients with pancreatic cysts, considering the high rate of surgical overtreatment.
“Having more diagnostic tests, such as those described in this publication [to be used on their own or in combination] to decide which patients need surgery, is important,” Dr. Keane said who was not involved in the study.
Better diagnostic tests could also improve outcomes for patients with pancreatic cancer, she said, noting a 5-year survival rate of 10%.
“This outcome is in large part attributable to the late stage at which the majority of patients are diagnosed,” Dr. Keane said. “If patients can be diagnosed earlier, survival dramatically improves. Improvements in diagnostic tests for premalignant pancreatic cystic lesions are therefore vital.”
The study was supported by Rigshospitalets Research Foundation, The Novo Nordisk Foundation, The Danish Cancer Society, and others, although they did not have a role in conducting the study or preparing the manuscript. One investigator disclosed a relationship with MediGlobe. The other investigators reported no conflicts of interest. Dr. Keane disclosed no conflicts of interest.
FROM GASTROINTESTINAL ENDOSCOPY
Superolateral knee injection with a patellar tilt for osteoarthritis pain


Levels of West Nile virus higher than normal in northern Italy
Climate change has affected the spread of West Nile fever. This observation was confirmed in an Italian Ministry of Health note reporting 94 confirmed cases of infection. Of those cases, 55 were neuroinvasive, 19 were from blood donors, 19 were associated with fever, and in one case, the patient was symptomatic. Seven deaths have occurred since the start of the summer season, particularly in northern Italy.
Entomologists and veterinarians have confirmed the presence of West Nile virus (WNV) in a pool of 100 mosquitoes, 15 birds from targeted species, and 10 wild birds from passive surveillance. Four cases have been reported in horses in which clinical symptoms were attributable to a WNV infection. No cases of infection with Usutu virus (USUV) have been registered in humans. USUV is a virus in the same family as WNV. It was first identified in South Africa in the 1950s and is capable of causing encephalitis. The viral genome has been detected in a pool of 33 mosquitoes and four birds.
Currently, the regions where the circulation of WNV has been confirmed are Emilia-Romagna, Veneto, Piedmont, Lombardy, Sardinia, and Friuli Venezia Giulia. To date, USUV has been detected in Le Marche, Lombardy, Umbria, Emilia Romagna, Friuli Venezia Giulia, Lazio, and Veneto.
Current climate conditions favor the reproduction of the vector (mosquitoes of the Culex genus) and the subsequent viral circulation among wildlife, the natural reservoir of the virus, and mammals (including humans). The 2022 epidemic season is peculiar in comparison with seasons from the past 3 years. Viral circulation has started early, and a greater number of cases have been observed in the avifauna and in the mosquito pool, and there has been an increase in the number of cases in humans.
For these reasons, and considering the significance of the infection for public health, it is necessary to put all useful measures in place to limit the risk of further transmission among humans and animals.
As specified on the Italian National Institute for Health website, West Nile fever is caused by the homonymous virus of the Flaviviridae family, which was isolated for the first time in Uganda in 1937. The virus has spread to almost all continents.
The virus reservoirs are wild birds and mosquitoes (more frequently of the Culex genus). Other means of transmission, although very rare, are organ transplants, blood transfusions, and transmission from mother to fetus. West Nile fever cannot be transmitted from person to person. The virus infects other mammals, especially horses, and in some cases, dogs and rabbits.
Incubation and symptoms
The incubation period from the time of being bitten by an infected mosquito ranges from 2 to 14 days but can be up to 21 days in immunocompromised patients.
Most infected people do not show any symptoms. In around 20% of symptomatic cases, patients present with mild symptoms: fever, headache, nausea, vomiting, enlarged lymph nodes, and skin rashes. These symptoms may only last a few hours, but in rare cases, they may last a few weeks. Symptoms vary significantly, depending on the patient’s age. In children, a mild fever is most common, whereas in young people, symptoms are characterized by a fairly high fever, redness of the eyes, headache, and muscle pains. In the elderly and in debilitated patients, symptoms can be more severe.
The most serious symptoms are seen in fewer than 1% of infected patients (1 in 150 people) and include a high fever, a severe headache, muscle weakness, disorientation, tremors, visual disturbances, listlessness, and seizures, leading to paralysis and coma. Some neurologic effects may be permanent. In the most severe cases (around 1 in 1,000), the virus can cause terminal encephalitis.
Diagnosis
Diagnosis is mostly made through laboratory testing for IgM antibodies on serum and, where indicated, cerebrospinal fluid (CSF). Antibodies can persist beyond the patient’s period of illness (up to 1 year). Therefore, a positive result may indicate a previous infection. Samples collected within 8 days of the onset of symptoms may appear negative; it is therefore advisable to repeat the laboratory test further down the line before excluding the disease. Alternatively, diagnosis may be obtained through polymerase chain reaction or viral culture testing on samples of serum or CSF.
Prevention
A vaccine for West Nile fever does not exist. Prevention consists, above all, of reducing exposure to mosquito bites.
It is advisable that people protect themselves against bites and avoid places where mosquitoes can reproduce easily. The following are recommended:
- Using repellents and wearing of trousers and long-sleeve tops when out in the open, especially at dawn and sunset.
- Using mosquito nets on windows.
- Frequently emptying vases or other containers (for example, buckets) that contain stagnant water.
- Frequently changing the water in animal drinking bowls.
- Keeping child paddling pools in a vertical position when not in use.
- Using authorized repellents and insecticides where the vector may reproduce, such as in stables. For horses, a vaccine is available for veterinary use, which can further reduce the reservoir of viral circulation.
It is important that physicians inform patients in at-risk areas of the presence of this virus, the possible symptoms, and the preventive measures to adopt.
Therapy and treatment
There is no specific therapy for West Nile fever. In most cases, symptoms appear after a few days, but they can last for a few weeks. For the most severe cases, hospital admission is necessary; occasionally, treatment in the intensive care unit is necessary.
This article was translated from Univadis Italy. A version appeared on Medscape.com.
Climate change has affected the spread of West Nile fever. This observation was confirmed in an Italian Ministry of Health note reporting 94 confirmed cases of infection. Of those cases, 55 were neuroinvasive, 19 were from blood donors, 19 were associated with fever, and in one case, the patient was symptomatic. Seven deaths have occurred since the start of the summer season, particularly in northern Italy.
Entomologists and veterinarians have confirmed the presence of West Nile virus (WNV) in a pool of 100 mosquitoes, 15 birds from targeted species, and 10 wild birds from passive surveillance. Four cases have been reported in horses in which clinical symptoms were attributable to a WNV infection. No cases of infection with Usutu virus (USUV) have been registered in humans. USUV is a virus in the same family as WNV. It was first identified in South Africa in the 1950s and is capable of causing encephalitis. The viral genome has been detected in a pool of 33 mosquitoes and four birds.
Currently, the regions where the circulation of WNV has been confirmed are Emilia-Romagna, Veneto, Piedmont, Lombardy, Sardinia, and Friuli Venezia Giulia. To date, USUV has been detected in Le Marche, Lombardy, Umbria, Emilia Romagna, Friuli Venezia Giulia, Lazio, and Veneto.
Current climate conditions favor the reproduction of the vector (mosquitoes of the Culex genus) and the subsequent viral circulation among wildlife, the natural reservoir of the virus, and mammals (including humans). The 2022 epidemic season is peculiar in comparison with seasons from the past 3 years. Viral circulation has started early, and a greater number of cases have been observed in the avifauna and in the mosquito pool, and there has been an increase in the number of cases in humans.
For these reasons, and considering the significance of the infection for public health, it is necessary to put all useful measures in place to limit the risk of further transmission among humans and animals.
As specified on the Italian National Institute for Health website, West Nile fever is caused by the homonymous virus of the Flaviviridae family, which was isolated for the first time in Uganda in 1937. The virus has spread to almost all continents.
The virus reservoirs are wild birds and mosquitoes (more frequently of the Culex genus). Other means of transmission, although very rare, are organ transplants, blood transfusions, and transmission from mother to fetus. West Nile fever cannot be transmitted from person to person. The virus infects other mammals, especially horses, and in some cases, dogs and rabbits.
Incubation and symptoms
The incubation period from the time of being bitten by an infected mosquito ranges from 2 to 14 days but can be up to 21 days in immunocompromised patients.
Most infected people do not show any symptoms. In around 20% of symptomatic cases, patients present with mild symptoms: fever, headache, nausea, vomiting, enlarged lymph nodes, and skin rashes. These symptoms may only last a few hours, but in rare cases, they may last a few weeks. Symptoms vary significantly, depending on the patient’s age. In children, a mild fever is most common, whereas in young people, symptoms are characterized by a fairly high fever, redness of the eyes, headache, and muscle pains. In the elderly and in debilitated patients, symptoms can be more severe.
The most serious symptoms are seen in fewer than 1% of infected patients (1 in 150 people) and include a high fever, a severe headache, muscle weakness, disorientation, tremors, visual disturbances, listlessness, and seizures, leading to paralysis and coma. Some neurologic effects may be permanent. In the most severe cases (around 1 in 1,000), the virus can cause terminal encephalitis.
Diagnosis
Diagnosis is mostly made through laboratory testing for IgM antibodies on serum and, where indicated, cerebrospinal fluid (CSF). Antibodies can persist beyond the patient’s period of illness (up to 1 year). Therefore, a positive result may indicate a previous infection. Samples collected within 8 days of the onset of symptoms may appear negative; it is therefore advisable to repeat the laboratory test further down the line before excluding the disease. Alternatively, diagnosis may be obtained through polymerase chain reaction or viral culture testing on samples of serum or CSF.
Prevention
A vaccine for West Nile fever does not exist. Prevention consists, above all, of reducing exposure to mosquito bites.
It is advisable that people protect themselves against bites and avoid places where mosquitoes can reproduce easily. The following are recommended:
- Using repellents and wearing of trousers and long-sleeve tops when out in the open, especially at dawn and sunset.
- Using mosquito nets on windows.
- Frequently emptying vases or other containers (for example, buckets) that contain stagnant water.
- Frequently changing the water in animal drinking bowls.
- Keeping child paddling pools in a vertical position when not in use.
- Using authorized repellents and insecticides where the vector may reproduce, such as in stables. For horses, a vaccine is available for veterinary use, which can further reduce the reservoir of viral circulation.
It is important that physicians inform patients in at-risk areas of the presence of this virus, the possible symptoms, and the preventive measures to adopt.
Therapy and treatment
There is no specific therapy for West Nile fever. In most cases, symptoms appear after a few days, but they can last for a few weeks. For the most severe cases, hospital admission is necessary; occasionally, treatment in the intensive care unit is necessary.
This article was translated from Univadis Italy. A version appeared on Medscape.com.
Climate change has affected the spread of West Nile fever. This observation was confirmed in an Italian Ministry of Health note reporting 94 confirmed cases of infection. Of those cases, 55 were neuroinvasive, 19 were from blood donors, 19 were associated with fever, and in one case, the patient was symptomatic. Seven deaths have occurred since the start of the summer season, particularly in northern Italy.
Entomologists and veterinarians have confirmed the presence of West Nile virus (WNV) in a pool of 100 mosquitoes, 15 birds from targeted species, and 10 wild birds from passive surveillance. Four cases have been reported in horses in which clinical symptoms were attributable to a WNV infection. No cases of infection with Usutu virus (USUV) have been registered in humans. USUV is a virus in the same family as WNV. It was first identified in South Africa in the 1950s and is capable of causing encephalitis. The viral genome has been detected in a pool of 33 mosquitoes and four birds.
Currently, the regions where the circulation of WNV has been confirmed are Emilia-Romagna, Veneto, Piedmont, Lombardy, Sardinia, and Friuli Venezia Giulia. To date, USUV has been detected in Le Marche, Lombardy, Umbria, Emilia Romagna, Friuli Venezia Giulia, Lazio, and Veneto.
Current climate conditions favor the reproduction of the vector (mosquitoes of the Culex genus) and the subsequent viral circulation among wildlife, the natural reservoir of the virus, and mammals (including humans). The 2022 epidemic season is peculiar in comparison with seasons from the past 3 years. Viral circulation has started early, and a greater number of cases have been observed in the avifauna and in the mosquito pool, and there has been an increase in the number of cases in humans.
For these reasons, and considering the significance of the infection for public health, it is necessary to put all useful measures in place to limit the risk of further transmission among humans and animals.
As specified on the Italian National Institute for Health website, West Nile fever is caused by the homonymous virus of the Flaviviridae family, which was isolated for the first time in Uganda in 1937. The virus has spread to almost all continents.
The virus reservoirs are wild birds and mosquitoes (more frequently of the Culex genus). Other means of transmission, although very rare, are organ transplants, blood transfusions, and transmission from mother to fetus. West Nile fever cannot be transmitted from person to person. The virus infects other mammals, especially horses, and in some cases, dogs and rabbits.
Incubation and symptoms
The incubation period from the time of being bitten by an infected mosquito ranges from 2 to 14 days but can be up to 21 days in immunocompromised patients.
Most infected people do not show any symptoms. In around 20% of symptomatic cases, patients present with mild symptoms: fever, headache, nausea, vomiting, enlarged lymph nodes, and skin rashes. These symptoms may only last a few hours, but in rare cases, they may last a few weeks. Symptoms vary significantly, depending on the patient’s age. In children, a mild fever is most common, whereas in young people, symptoms are characterized by a fairly high fever, redness of the eyes, headache, and muscle pains. In the elderly and in debilitated patients, symptoms can be more severe.
The most serious symptoms are seen in fewer than 1% of infected patients (1 in 150 people) and include a high fever, a severe headache, muscle weakness, disorientation, tremors, visual disturbances, listlessness, and seizures, leading to paralysis and coma. Some neurologic effects may be permanent. In the most severe cases (around 1 in 1,000), the virus can cause terminal encephalitis.
Diagnosis
Diagnosis is mostly made through laboratory testing for IgM antibodies on serum and, where indicated, cerebrospinal fluid (CSF). Antibodies can persist beyond the patient’s period of illness (up to 1 year). Therefore, a positive result may indicate a previous infection. Samples collected within 8 days of the onset of symptoms may appear negative; it is therefore advisable to repeat the laboratory test further down the line before excluding the disease. Alternatively, diagnosis may be obtained through polymerase chain reaction or viral culture testing on samples of serum or CSF.
Prevention
A vaccine for West Nile fever does not exist. Prevention consists, above all, of reducing exposure to mosquito bites.
It is advisable that people protect themselves against bites and avoid places where mosquitoes can reproduce easily. The following are recommended:
- Using repellents and wearing of trousers and long-sleeve tops when out in the open, especially at dawn and sunset.
- Using mosquito nets on windows.
- Frequently emptying vases or other containers (for example, buckets) that contain stagnant water.
- Frequently changing the water in animal drinking bowls.
- Keeping child paddling pools in a vertical position when not in use.
- Using authorized repellents and insecticides where the vector may reproduce, such as in stables. For horses, a vaccine is available for veterinary use, which can further reduce the reservoir of viral circulation.
It is important that physicians inform patients in at-risk areas of the presence of this virus, the possible symptoms, and the preventive measures to adopt.
Therapy and treatment
There is no specific therapy for West Nile fever. In most cases, symptoms appear after a few days, but they can last for a few weeks. For the most severe cases, hospital admission is necessary; occasionally, treatment in the intensive care unit is necessary.
This article was translated from Univadis Italy. A version appeared on Medscape.com.
How docs in firearm-friendly states talk gun safety
Samuel Mathis, MD, tries to cover a lot of ground during a wellness exam for his patients. Nutrition, immunizations, dental hygiene, and staying safe at school are a few of the topics on his list. And the Texas pediatrician asks one more question of children and their parents: “Are there any firearms in the house?”
If the answer is “yes,” Dr. Mathis discusses safety courses and other ideas with the families. “Rather than ask a bunch of questions, often I will say it’s recommended to keep them locked up and don’t forget toddlers can climb heights that you never would have envisioned,” said Dr. Mathis, an assistant professor at the University of Texas Medical Branch, Galveston.
Dr. Mathis said some of his physician colleagues are wary of bringing up the topic of guns in a state that leads the nation with more than 1 million registered firearms. “My discussion is more on firearm responsibility and just making sure they are taking extra steps to keep themselves and everyone around them safe. That works much better in these discussions.”
Gun safety: Public health concern, not politics
The statistics tell why:
- Unintentional shooting deaths by children rose by nearly one third in a 3-month period in 2020, compared with the same period in 2019.
- Of every 10 gun deaths in the United States, 6 are by suicide.
- As of July 28, 372 mass shootings have occured.
- Firearms now represent the leading cause of death among the nation’s youth.
In 2018, the editors of Annals of Internal Medicine urged physicians in the United States to sign a pledge to talk with their patients about guns in the home. To date, at least 3,664 have done so.
In 2019, the American Academy of Family Medicine, with other leading physician and public health organizations, issued a “call to action,” recommending ways to reduce firearm-related injury and death in the United States. Physicians can and should address the issue, it said, by counseling patients about firearm safety.
“This is just another part of healthcare,” said Sarah C. Nosal, MD, a member of the board of directors of the AAFP, who practices at the Urban Horizons Family Health Center, New York.
Dr. Nosal said she asks about firearms during every well-child visit. She also focuses on patients with a history of depression or suicide attempts and those who have experienced domestic violence.
Are physicians counseling patients about gun safety?
A 2018 survey of physicians found that 73% of the 71 who responded agreed to discuss gun safety with at-risk patients. But just 5% said they always talk to those at-risk patients, according to Melanie G. Hagen, MD, professor of internal medicine at the University of Florida, Gainesville, who led the study. While the overwhelming majority agreed that gun safety is a public health issue, only 55% said they felt comfortable initiating conversations about firearms with their patients.
Have things changed since then? “Probably not,” Dr. Hagen said in an interview. She cited some reasons, at least in her state.
One obstacle is that many people, including physicians, believe that Florida’s physician gag law, which prohibited physicians from asking about a patient’s firearm ownership, was still in effect. The law, passed in 2011, was overturned in 2017. In her survey, 76% said they were aware it had been overturned. But that awareness appears not to be universal, she said.
In a 2020 report about physician involvement in promoting gun safety, researchers noted four main challenges: lingering fears about the overturned law and potential liability from violating it, feeling unprepared, worry that patients don’t want to discuss the topic, and lack of time to talk about it during a rushed office visit.
But recent research suggests that patients are often open to talking about gun safety, and another study found that if physicians are given educational materials on firearm safety, more will counsel patients about gun safety.
Are patients and parents receptive?
Parents welcome discussion from health care providers about gun safety, according to a study from the University of Pennsylvania, Philadelphia.
Researchers asked roughly 100 parents to watch a short video about a firearm safety program designed to prevent accidents and suicides from guns. The program, still under study, involves a discussion between a parent and a pediatrician, with information given on secure storage of guns and the offering of a free cable lock.
The parents, about equally divided between gun owners and non–gun owners, said they were open to discussion about firearm safety, especially when the conversation involves their child’s pediatrician. Among the gun owners, only one in three said all their firearms were locked, unloaded, and stored properly. But after getting the safety information, 64% said they would change the way they stored their firearms.
A different program that offered pediatricians educational materials on firearm safety, as well as free firearm locks for distribution, increased the likelihood that the physicians would counsel patients on gun safety, other researchers reported.
Getting the conversation started
Some patients “bristle” when they’re asked about guns, Dr. Hagen said. Focusing on the “why” of the question can soften their response. One of her patients, a man in his 80s, had worked as a prison guard. After he was diagnosed with clinical depression, she asked him if he ever thought about ending his life. He said yes.
“And in Florida, I know a lot of people have guns,” she said. The state ranks second in the nation, with more than a half million registered weapons.
When Dr. Hagen asked him if he had firearms at home, he balked. Why did she need to know? “People do get defensive,” she said. “Luckily, I had a good relationship with this man, and he was willing to listen to me. If it’s someone I have a good relationship with, and I have this initial bristling, if I say: ‘I’m worried about you, I’m worried about your safety,’ that changes the entire conversation.”
She talked through the best plan for this patient, and he agreed to give his weapons to his son to keep.
Likewise, she talks with family members of dementia patients, urging them to be sure the weapons are stored and locked to prevent tragic accidents.
Dr. Nosal said reading the room is key. “Often, we are having the conversation with a parent with a child present,” she said. “Perhaps that is not the conversation the parent or guardian wanted to have with the child present.” In such a situation, she suggests asking the parent if they would talk about it solo.
“It can be a challenge to know the appropriate way to start the conversation,” Dr. Mathis said. The topic is not taught in medical school, although many experts think it should be. Dr. Hagen recently delivered a lecture to medical students about how to broach the topic with patients. She said she hopes it will become a regular event.
“It really comes down to being willing to be open and just ask that first question in a nonjudgmental way,” Dr. Mathis said. It helps, too, he said, for physicians to remember what he always tries to keep in mind: “My job isn’t politics, my job is health.”
Among the points Dr. Hagen makes in her lecture about talking to patients about guns are the following:
- Every day, more than 110 Americans are killed with guns.
- Gun violence accounts for just 1%-2% of those deaths, but mass shootings serve to shine a light on the issue of gun safety.
- 110,000 firearm injuries a year require medical or legal attention. Each year, more than 1,200 children in this country die from gun-related injuries.
- More than 33,000 people, on average, die in the United States each year from gun violence, including more than 21,000 from suicide.
- About 31% of all U.S. households have firearms; 22% of U.S. adults own one or more.
- Guns are 70% less likely to be stored locked and unloaded in homes where suicides or unintentional gun injuries occur.
- Action points: Identify risk, counsel patients at risk, act when someone is in imminent danger (such as unsafe practices or suicide threats).
- Focus on identifying adults who have a risk of inflicting violence on self or others.
- Focus on health and well-being with all; be conversational and educational.
- Clinicians should ask five crucial questions, all with an “L,” if firearms are in the home: Is it Loaded? Locked? Are Little children present? Is the owner feeling Low? Are they Learned [educated] in gun safety?
A version of this article first appeared on Medscape.com.
Samuel Mathis, MD, tries to cover a lot of ground during a wellness exam for his patients. Nutrition, immunizations, dental hygiene, and staying safe at school are a few of the topics on his list. And the Texas pediatrician asks one more question of children and their parents: “Are there any firearms in the house?”
If the answer is “yes,” Dr. Mathis discusses safety courses and other ideas with the families. “Rather than ask a bunch of questions, often I will say it’s recommended to keep them locked up and don’t forget toddlers can climb heights that you never would have envisioned,” said Dr. Mathis, an assistant professor at the University of Texas Medical Branch, Galveston.
Dr. Mathis said some of his physician colleagues are wary of bringing up the topic of guns in a state that leads the nation with more than 1 million registered firearms. “My discussion is more on firearm responsibility and just making sure they are taking extra steps to keep themselves and everyone around them safe. That works much better in these discussions.”
Gun safety: Public health concern, not politics
The statistics tell why:
- Unintentional shooting deaths by children rose by nearly one third in a 3-month period in 2020, compared with the same period in 2019.
- Of every 10 gun deaths in the United States, 6 are by suicide.
- As of July 28, 372 mass shootings have occured.
- Firearms now represent the leading cause of death among the nation’s youth.
In 2018, the editors of Annals of Internal Medicine urged physicians in the United States to sign a pledge to talk with their patients about guns in the home. To date, at least 3,664 have done so.
In 2019, the American Academy of Family Medicine, with other leading physician and public health organizations, issued a “call to action,” recommending ways to reduce firearm-related injury and death in the United States. Physicians can and should address the issue, it said, by counseling patients about firearm safety.
“This is just another part of healthcare,” said Sarah C. Nosal, MD, a member of the board of directors of the AAFP, who practices at the Urban Horizons Family Health Center, New York.
Dr. Nosal said she asks about firearms during every well-child visit. She also focuses on patients with a history of depression or suicide attempts and those who have experienced domestic violence.
Are physicians counseling patients about gun safety?
A 2018 survey of physicians found that 73% of the 71 who responded agreed to discuss gun safety with at-risk patients. But just 5% said they always talk to those at-risk patients, according to Melanie G. Hagen, MD, professor of internal medicine at the University of Florida, Gainesville, who led the study. While the overwhelming majority agreed that gun safety is a public health issue, only 55% said they felt comfortable initiating conversations about firearms with their patients.
Have things changed since then? “Probably not,” Dr. Hagen said in an interview. She cited some reasons, at least in her state.
One obstacle is that many people, including physicians, believe that Florida’s physician gag law, which prohibited physicians from asking about a patient’s firearm ownership, was still in effect. The law, passed in 2011, was overturned in 2017. In her survey, 76% said they were aware it had been overturned. But that awareness appears not to be universal, she said.
In a 2020 report about physician involvement in promoting gun safety, researchers noted four main challenges: lingering fears about the overturned law and potential liability from violating it, feeling unprepared, worry that patients don’t want to discuss the topic, and lack of time to talk about it during a rushed office visit.
But recent research suggests that patients are often open to talking about gun safety, and another study found that if physicians are given educational materials on firearm safety, more will counsel patients about gun safety.
Are patients and parents receptive?
Parents welcome discussion from health care providers about gun safety, according to a study from the University of Pennsylvania, Philadelphia.
Researchers asked roughly 100 parents to watch a short video about a firearm safety program designed to prevent accidents and suicides from guns. The program, still under study, involves a discussion between a parent and a pediatrician, with information given on secure storage of guns and the offering of a free cable lock.
The parents, about equally divided between gun owners and non–gun owners, said they were open to discussion about firearm safety, especially when the conversation involves their child’s pediatrician. Among the gun owners, only one in three said all their firearms were locked, unloaded, and stored properly. But after getting the safety information, 64% said they would change the way they stored their firearms.
A different program that offered pediatricians educational materials on firearm safety, as well as free firearm locks for distribution, increased the likelihood that the physicians would counsel patients on gun safety, other researchers reported.
Getting the conversation started
Some patients “bristle” when they’re asked about guns, Dr. Hagen said. Focusing on the “why” of the question can soften their response. One of her patients, a man in his 80s, had worked as a prison guard. After he was diagnosed with clinical depression, she asked him if he ever thought about ending his life. He said yes.
“And in Florida, I know a lot of people have guns,” she said. The state ranks second in the nation, with more than a half million registered weapons.
When Dr. Hagen asked him if he had firearms at home, he balked. Why did she need to know? “People do get defensive,” she said. “Luckily, I had a good relationship with this man, and he was willing to listen to me. If it’s someone I have a good relationship with, and I have this initial bristling, if I say: ‘I’m worried about you, I’m worried about your safety,’ that changes the entire conversation.”
She talked through the best plan for this patient, and he agreed to give his weapons to his son to keep.
Likewise, she talks with family members of dementia patients, urging them to be sure the weapons are stored and locked to prevent tragic accidents.
Dr. Nosal said reading the room is key. “Often, we are having the conversation with a parent with a child present,” she said. “Perhaps that is not the conversation the parent or guardian wanted to have with the child present.” In such a situation, she suggests asking the parent if they would talk about it solo.
“It can be a challenge to know the appropriate way to start the conversation,” Dr. Mathis said. The topic is not taught in medical school, although many experts think it should be. Dr. Hagen recently delivered a lecture to medical students about how to broach the topic with patients. She said she hopes it will become a regular event.
“It really comes down to being willing to be open and just ask that first question in a nonjudgmental way,” Dr. Mathis said. It helps, too, he said, for physicians to remember what he always tries to keep in mind: “My job isn’t politics, my job is health.”
Among the points Dr. Hagen makes in her lecture about talking to patients about guns are the following:
- Every day, more than 110 Americans are killed with guns.
- Gun violence accounts for just 1%-2% of those deaths, but mass shootings serve to shine a light on the issue of gun safety.
- 110,000 firearm injuries a year require medical or legal attention. Each year, more than 1,200 children in this country die from gun-related injuries.
- More than 33,000 people, on average, die in the United States each year from gun violence, including more than 21,000 from suicide.
- About 31% of all U.S. households have firearms; 22% of U.S. adults own one or more.
- Guns are 70% less likely to be stored locked and unloaded in homes where suicides or unintentional gun injuries occur.
- Action points: Identify risk, counsel patients at risk, act when someone is in imminent danger (such as unsafe practices or suicide threats).
- Focus on identifying adults who have a risk of inflicting violence on self or others.
- Focus on health and well-being with all; be conversational and educational.
- Clinicians should ask five crucial questions, all with an “L,” if firearms are in the home: Is it Loaded? Locked? Are Little children present? Is the owner feeling Low? Are they Learned [educated] in gun safety?
A version of this article first appeared on Medscape.com.
Samuel Mathis, MD, tries to cover a lot of ground during a wellness exam for his patients. Nutrition, immunizations, dental hygiene, and staying safe at school are a few of the topics on his list. And the Texas pediatrician asks one more question of children and their parents: “Are there any firearms in the house?”
If the answer is “yes,” Dr. Mathis discusses safety courses and other ideas with the families. “Rather than ask a bunch of questions, often I will say it’s recommended to keep them locked up and don’t forget toddlers can climb heights that you never would have envisioned,” said Dr. Mathis, an assistant professor at the University of Texas Medical Branch, Galveston.
Dr. Mathis said some of his physician colleagues are wary of bringing up the topic of guns in a state that leads the nation with more than 1 million registered firearms. “My discussion is more on firearm responsibility and just making sure they are taking extra steps to keep themselves and everyone around them safe. That works much better in these discussions.”
Gun safety: Public health concern, not politics
The statistics tell why:
- Unintentional shooting deaths by children rose by nearly one third in a 3-month period in 2020, compared with the same period in 2019.
- Of every 10 gun deaths in the United States, 6 are by suicide.
- As of July 28, 372 mass shootings have occured.
- Firearms now represent the leading cause of death among the nation’s youth.
In 2018, the editors of Annals of Internal Medicine urged physicians in the United States to sign a pledge to talk with their patients about guns in the home. To date, at least 3,664 have done so.
In 2019, the American Academy of Family Medicine, with other leading physician and public health organizations, issued a “call to action,” recommending ways to reduce firearm-related injury and death in the United States. Physicians can and should address the issue, it said, by counseling patients about firearm safety.
“This is just another part of healthcare,” said Sarah C. Nosal, MD, a member of the board of directors of the AAFP, who practices at the Urban Horizons Family Health Center, New York.
Dr. Nosal said she asks about firearms during every well-child visit. She also focuses on patients with a history of depression or suicide attempts and those who have experienced domestic violence.
Are physicians counseling patients about gun safety?
A 2018 survey of physicians found that 73% of the 71 who responded agreed to discuss gun safety with at-risk patients. But just 5% said they always talk to those at-risk patients, according to Melanie G. Hagen, MD, professor of internal medicine at the University of Florida, Gainesville, who led the study. While the overwhelming majority agreed that gun safety is a public health issue, only 55% said they felt comfortable initiating conversations about firearms with their patients.
Have things changed since then? “Probably not,” Dr. Hagen said in an interview. She cited some reasons, at least in her state.
One obstacle is that many people, including physicians, believe that Florida’s physician gag law, which prohibited physicians from asking about a patient’s firearm ownership, was still in effect. The law, passed in 2011, was overturned in 2017. In her survey, 76% said they were aware it had been overturned. But that awareness appears not to be universal, she said.
In a 2020 report about physician involvement in promoting gun safety, researchers noted four main challenges: lingering fears about the overturned law and potential liability from violating it, feeling unprepared, worry that patients don’t want to discuss the topic, and lack of time to talk about it during a rushed office visit.
But recent research suggests that patients are often open to talking about gun safety, and another study found that if physicians are given educational materials on firearm safety, more will counsel patients about gun safety.
Are patients and parents receptive?
Parents welcome discussion from health care providers about gun safety, according to a study from the University of Pennsylvania, Philadelphia.
Researchers asked roughly 100 parents to watch a short video about a firearm safety program designed to prevent accidents and suicides from guns. The program, still under study, involves a discussion between a parent and a pediatrician, with information given on secure storage of guns and the offering of a free cable lock.
The parents, about equally divided between gun owners and non–gun owners, said they were open to discussion about firearm safety, especially when the conversation involves their child’s pediatrician. Among the gun owners, only one in three said all their firearms were locked, unloaded, and stored properly. But after getting the safety information, 64% said they would change the way they stored their firearms.
A different program that offered pediatricians educational materials on firearm safety, as well as free firearm locks for distribution, increased the likelihood that the physicians would counsel patients on gun safety, other researchers reported.
Getting the conversation started
Some patients “bristle” when they’re asked about guns, Dr. Hagen said. Focusing on the “why” of the question can soften their response. One of her patients, a man in his 80s, had worked as a prison guard. After he was diagnosed with clinical depression, she asked him if he ever thought about ending his life. He said yes.
“And in Florida, I know a lot of people have guns,” she said. The state ranks second in the nation, with more than a half million registered weapons.
When Dr. Hagen asked him if he had firearms at home, he balked. Why did she need to know? “People do get defensive,” she said. “Luckily, I had a good relationship with this man, and he was willing to listen to me. If it’s someone I have a good relationship with, and I have this initial bristling, if I say: ‘I’m worried about you, I’m worried about your safety,’ that changes the entire conversation.”
She talked through the best plan for this patient, and he agreed to give his weapons to his son to keep.
Likewise, she talks with family members of dementia patients, urging them to be sure the weapons are stored and locked to prevent tragic accidents.
Dr. Nosal said reading the room is key. “Often, we are having the conversation with a parent with a child present,” she said. “Perhaps that is not the conversation the parent or guardian wanted to have with the child present.” In such a situation, she suggests asking the parent if they would talk about it solo.
“It can be a challenge to know the appropriate way to start the conversation,” Dr. Mathis said. The topic is not taught in medical school, although many experts think it should be. Dr. Hagen recently delivered a lecture to medical students about how to broach the topic with patients. She said she hopes it will become a regular event.
“It really comes down to being willing to be open and just ask that first question in a nonjudgmental way,” Dr. Mathis said. It helps, too, he said, for physicians to remember what he always tries to keep in mind: “My job isn’t politics, my job is health.”
Among the points Dr. Hagen makes in her lecture about talking to patients about guns are the following:
- Every day, more than 110 Americans are killed with guns.
- Gun violence accounts for just 1%-2% of those deaths, but mass shootings serve to shine a light on the issue of gun safety.
- 110,000 firearm injuries a year require medical or legal attention. Each year, more than 1,200 children in this country die from gun-related injuries.
- More than 33,000 people, on average, die in the United States each year from gun violence, including more than 21,000 from suicide.
- About 31% of all U.S. households have firearms; 22% of U.S. adults own one or more.
- Guns are 70% less likely to be stored locked and unloaded in homes where suicides or unintentional gun injuries occur.
- Action points: Identify risk, counsel patients at risk, act when someone is in imminent danger (such as unsafe practices or suicide threats).
- Focus on identifying adults who have a risk of inflicting violence on self or others.
- Focus on health and well-being with all; be conversational and educational.
- Clinicians should ask five crucial questions, all with an “L,” if firearms are in the home: Is it Loaded? Locked? Are Little children present? Is the owner feeling Low? Are they Learned [educated] in gun safety?
A version of this article first appeared on Medscape.com.
Autoimmune disease patients’ waxing, waning response to COVID vaccination studied in-depth
A new study in The Lancet Rheumatology examines the strength and duration of SARS-CoV-2 vaccine–induced immunoglobulin-G antibody responses over time for patients with a variety of autoimmune diseases, compared with healthy controls.
The presence of humoral antibodies to SARS-CoV-2 has been shown to correlate with protection against COVID infection. But for patients with immune-mediated inflammatory diseases (IMIDs), host response to COVID infection or to vaccination is affected by the immune dysfunction imposed by the IMID and by the use of immune-modulating drugs to treat it.
This new study finds a weaker – as shown previously – and less sustained immune response to SARS-CoV-2 vaccines in patients with a variety of IMIDs, including rheumatoid arthritis, spondyloarthritis, psoriasis, inflammatory bowel diseases, and other systemic autoimmune diseases such as lupus. It also points toward the possibility of adjusting treatment and vaccination schedules and strategies for these patients based on their antibody levels, among other factors, to preserve best protection against severe COVID.
“It is important to assess immune response in these patients to see if they still have protection against severe COVID infection,” said lead author David Simon, MD, senior clinical scientist in clinical immunology and rheumatology at University Hospital Erlangen (Germany). “We know that antibody response is an immune correlate. Therefore, it is important to see how large and durable the immune response is to the coronavirus vaccine in these IMID patients, and whether specific drugs or therapies have negative effects on their immune response.”
What was studied?
For this large prospective cohort study, researchers registered 5076 coronavirus-vaccinated individuals. They analyzed serum samples obtained between December 15, 2020, and December 1, 2021, from 2,535 patients diagnosed with IMIDs and participating in a prospective coronavirus study program at the Deutsches Zentrum Immuntherapie in Erlangen. The IMID patients had a mean age of 55.0 years, and 58.9% were women.
A healthy control group of 1,198 individuals without IMID who had a mean age of 40.7 years, including 53.8% men, was also recruited for the analysis. All approved coronavirus vaccines were included, following standard vaccination schedules. Antibody response was measured over time by an enzyme-linked immunosorbent assay from 8 weeks after first vaccination to week 40.
Among the findings, the healthy controls had higher postvaccine antibody levels than did those with IMIDs. But the majority of vaccinated patients with IMID were able to build up a humoral immune response to SARS-CoV-2. Patients who were taking B-cell inhibitors like rituximab (Rituxan, Genentech; and biosimilars) and T-cell inhibitors like abatacept (Orencia, Bristol Myers Squibb) for IMIDs had significantly poorer antibody response.
Greater age and the use of combination therapies for IMIDs, compared with monotherapy, further reduced immune response to the vaccine. In terms of vaccination modality, messenger RNA–based vaccines induced higher antibody levels than did vector-based vaccines. The researchers noted that patients with IMID who were given a third vaccine dose could actually catch up well with the antibody responses observed in healthy controls.
“We looked at whether different IMIDs had a different humoral response, and we also assessed if there are effects from different therapeutic strategies,” Dr. Simon explained. “It doesn’t matter so much what kind of IMID patients have; much more important is the specific drug treatment and its impact on their antibody response.” Some participants were advised to briefly stop taking some immunosuppressive treatments before or after vaccination.
One of Dr. Simon’s coauthors, statistician and rheumatologist Koray Tascilar, MD, added, “This research is important because we looked not only at who responded less, which has been previously established, but who are at greater risk of losing their immune response, and how quickly.”
Need to take care
“Most treatments we as rheumatologists give to our patients don’t affect their SARS-CoV-2 humoral response,” Dr. Simon said. “However, there are specific drugs that are associated with lower antibody response. With respect to those drugs, we have to be more careful.”
It is important to be able to tell patients which drugs are safe and won’t have a negative impact on their immune response to vaccinations, Dr. Tascilar said. “But it would be too strong to say we’re ready to choose therapies based on their potential impact on protection against COVID. Yes, there is a risk from catching COVID, but we need to balance that risk with the risk of not giving patients the medications that are necessary to treat their rheumatologic condition.”
These diseases are serious, sometimes life-threatening. “We might think of strategies for how to mitigate the risk of underprotection from COVID that is brought about by these treatments,” he said. For example, offering boosters sooner or more frequently, or prophylactically treating with monoclonal antibodies.
“This study, along other recent studies, has found that antibody levels in patients with immune-mediated diseases wane more rapidly than in healthy controls, and this is especially true of those on medications that interfere with the B and T cells and anticytokine therapies,” Rebecca Haberman, MD, assistant professor, division of rheumatology, New York University Langone Health, noted in an email to this news organization.
“While there is no known antibody level that specifically correlates with clinical protection, and each patient needs to be thought of individually, these findings support the use of supplemental booster dosing in patients with immune-mediated inflammatory diseases,” Dr. Haberman said, adding that her own research in this area has shown similar results.
“As a rheumatologist, I would be more likely to encourage my patients – especially those on immunomodulatory medications – to get boosted.”
Dr. Tascilar said his study does not directly answer the question of whether an earlier booster shot would be an effective strategy for patients with IMID. “In our department, we have an early boosting strategy, based on level of immune response.” But the decision of revaccination or not, and when, is based on a number of factors, not only on the level of antibodies. “It’s just part of the instruments we are using.”
The study was supported by the Deutsche Forschungsgemeinschaft. Dr. Simon and Dr. Tascilar declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study in The Lancet Rheumatology examines the strength and duration of SARS-CoV-2 vaccine–induced immunoglobulin-G antibody responses over time for patients with a variety of autoimmune diseases, compared with healthy controls.
The presence of humoral antibodies to SARS-CoV-2 has been shown to correlate with protection against COVID infection. But for patients with immune-mediated inflammatory diseases (IMIDs), host response to COVID infection or to vaccination is affected by the immune dysfunction imposed by the IMID and by the use of immune-modulating drugs to treat it.
This new study finds a weaker – as shown previously – and less sustained immune response to SARS-CoV-2 vaccines in patients with a variety of IMIDs, including rheumatoid arthritis, spondyloarthritis, psoriasis, inflammatory bowel diseases, and other systemic autoimmune diseases such as lupus. It also points toward the possibility of adjusting treatment and vaccination schedules and strategies for these patients based on their antibody levels, among other factors, to preserve best protection against severe COVID.
“It is important to assess immune response in these patients to see if they still have protection against severe COVID infection,” said lead author David Simon, MD, senior clinical scientist in clinical immunology and rheumatology at University Hospital Erlangen (Germany). “We know that antibody response is an immune correlate. Therefore, it is important to see how large and durable the immune response is to the coronavirus vaccine in these IMID patients, and whether specific drugs or therapies have negative effects on their immune response.”
What was studied?
For this large prospective cohort study, researchers registered 5076 coronavirus-vaccinated individuals. They analyzed serum samples obtained between December 15, 2020, and December 1, 2021, from 2,535 patients diagnosed with IMIDs and participating in a prospective coronavirus study program at the Deutsches Zentrum Immuntherapie in Erlangen. The IMID patients had a mean age of 55.0 years, and 58.9% were women.
A healthy control group of 1,198 individuals without IMID who had a mean age of 40.7 years, including 53.8% men, was also recruited for the analysis. All approved coronavirus vaccines were included, following standard vaccination schedules. Antibody response was measured over time by an enzyme-linked immunosorbent assay from 8 weeks after first vaccination to week 40.
Among the findings, the healthy controls had higher postvaccine antibody levels than did those with IMIDs. But the majority of vaccinated patients with IMID were able to build up a humoral immune response to SARS-CoV-2. Patients who were taking B-cell inhibitors like rituximab (Rituxan, Genentech; and biosimilars) and T-cell inhibitors like abatacept (Orencia, Bristol Myers Squibb) for IMIDs had significantly poorer antibody response.
Greater age and the use of combination therapies for IMIDs, compared with monotherapy, further reduced immune response to the vaccine. In terms of vaccination modality, messenger RNA–based vaccines induced higher antibody levels than did vector-based vaccines. The researchers noted that patients with IMID who were given a third vaccine dose could actually catch up well with the antibody responses observed in healthy controls.
“We looked at whether different IMIDs had a different humoral response, and we also assessed if there are effects from different therapeutic strategies,” Dr. Simon explained. “It doesn’t matter so much what kind of IMID patients have; much more important is the specific drug treatment and its impact on their antibody response.” Some participants were advised to briefly stop taking some immunosuppressive treatments before or after vaccination.
One of Dr. Simon’s coauthors, statistician and rheumatologist Koray Tascilar, MD, added, “This research is important because we looked not only at who responded less, which has been previously established, but who are at greater risk of losing their immune response, and how quickly.”
Need to take care
“Most treatments we as rheumatologists give to our patients don’t affect their SARS-CoV-2 humoral response,” Dr. Simon said. “However, there are specific drugs that are associated with lower antibody response. With respect to those drugs, we have to be more careful.”
It is important to be able to tell patients which drugs are safe and won’t have a negative impact on their immune response to vaccinations, Dr. Tascilar said. “But it would be too strong to say we’re ready to choose therapies based on their potential impact on protection against COVID. Yes, there is a risk from catching COVID, but we need to balance that risk with the risk of not giving patients the medications that are necessary to treat their rheumatologic condition.”
These diseases are serious, sometimes life-threatening. “We might think of strategies for how to mitigate the risk of underprotection from COVID that is brought about by these treatments,” he said. For example, offering boosters sooner or more frequently, or prophylactically treating with monoclonal antibodies.
“This study, along other recent studies, has found that antibody levels in patients with immune-mediated diseases wane more rapidly than in healthy controls, and this is especially true of those on medications that interfere with the B and T cells and anticytokine therapies,” Rebecca Haberman, MD, assistant professor, division of rheumatology, New York University Langone Health, noted in an email to this news organization.
“While there is no known antibody level that specifically correlates with clinical protection, and each patient needs to be thought of individually, these findings support the use of supplemental booster dosing in patients with immune-mediated inflammatory diseases,” Dr. Haberman said, adding that her own research in this area has shown similar results.
“As a rheumatologist, I would be more likely to encourage my patients – especially those on immunomodulatory medications – to get boosted.”
Dr. Tascilar said his study does not directly answer the question of whether an earlier booster shot would be an effective strategy for patients with IMID. “In our department, we have an early boosting strategy, based on level of immune response.” But the decision of revaccination or not, and when, is based on a number of factors, not only on the level of antibodies. “It’s just part of the instruments we are using.”
The study was supported by the Deutsche Forschungsgemeinschaft. Dr. Simon and Dr. Tascilar declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study in The Lancet Rheumatology examines the strength and duration of SARS-CoV-2 vaccine–induced immunoglobulin-G antibody responses over time for patients with a variety of autoimmune diseases, compared with healthy controls.
The presence of humoral antibodies to SARS-CoV-2 has been shown to correlate with protection against COVID infection. But for patients with immune-mediated inflammatory diseases (IMIDs), host response to COVID infection or to vaccination is affected by the immune dysfunction imposed by the IMID and by the use of immune-modulating drugs to treat it.
This new study finds a weaker – as shown previously – and less sustained immune response to SARS-CoV-2 vaccines in patients with a variety of IMIDs, including rheumatoid arthritis, spondyloarthritis, psoriasis, inflammatory bowel diseases, and other systemic autoimmune diseases such as lupus. It also points toward the possibility of adjusting treatment and vaccination schedules and strategies for these patients based on their antibody levels, among other factors, to preserve best protection against severe COVID.
“It is important to assess immune response in these patients to see if they still have protection against severe COVID infection,” said lead author David Simon, MD, senior clinical scientist in clinical immunology and rheumatology at University Hospital Erlangen (Germany). “We know that antibody response is an immune correlate. Therefore, it is important to see how large and durable the immune response is to the coronavirus vaccine in these IMID patients, and whether specific drugs or therapies have negative effects on their immune response.”
What was studied?
For this large prospective cohort study, researchers registered 5076 coronavirus-vaccinated individuals. They analyzed serum samples obtained between December 15, 2020, and December 1, 2021, from 2,535 patients diagnosed with IMIDs and participating in a prospective coronavirus study program at the Deutsches Zentrum Immuntherapie in Erlangen. The IMID patients had a mean age of 55.0 years, and 58.9% were women.
A healthy control group of 1,198 individuals without IMID who had a mean age of 40.7 years, including 53.8% men, was also recruited for the analysis. All approved coronavirus vaccines were included, following standard vaccination schedules. Antibody response was measured over time by an enzyme-linked immunosorbent assay from 8 weeks after first vaccination to week 40.
Among the findings, the healthy controls had higher postvaccine antibody levels than did those with IMIDs. But the majority of vaccinated patients with IMID were able to build up a humoral immune response to SARS-CoV-2. Patients who were taking B-cell inhibitors like rituximab (Rituxan, Genentech; and biosimilars) and T-cell inhibitors like abatacept (Orencia, Bristol Myers Squibb) for IMIDs had significantly poorer antibody response.
Greater age and the use of combination therapies for IMIDs, compared with monotherapy, further reduced immune response to the vaccine. In terms of vaccination modality, messenger RNA–based vaccines induced higher antibody levels than did vector-based vaccines. The researchers noted that patients with IMID who were given a third vaccine dose could actually catch up well with the antibody responses observed in healthy controls.
“We looked at whether different IMIDs had a different humoral response, and we also assessed if there are effects from different therapeutic strategies,” Dr. Simon explained. “It doesn’t matter so much what kind of IMID patients have; much more important is the specific drug treatment and its impact on their antibody response.” Some participants were advised to briefly stop taking some immunosuppressive treatments before or after vaccination.
One of Dr. Simon’s coauthors, statistician and rheumatologist Koray Tascilar, MD, added, “This research is important because we looked not only at who responded less, which has been previously established, but who are at greater risk of losing their immune response, and how quickly.”
Need to take care
“Most treatments we as rheumatologists give to our patients don’t affect their SARS-CoV-2 humoral response,” Dr. Simon said. “However, there are specific drugs that are associated with lower antibody response. With respect to those drugs, we have to be more careful.”
It is important to be able to tell patients which drugs are safe and won’t have a negative impact on their immune response to vaccinations, Dr. Tascilar said. “But it would be too strong to say we’re ready to choose therapies based on their potential impact on protection against COVID. Yes, there is a risk from catching COVID, but we need to balance that risk with the risk of not giving patients the medications that are necessary to treat their rheumatologic condition.”
These diseases are serious, sometimes life-threatening. “We might think of strategies for how to mitigate the risk of underprotection from COVID that is brought about by these treatments,” he said. For example, offering boosters sooner or more frequently, or prophylactically treating with monoclonal antibodies.
“This study, along other recent studies, has found that antibody levels in patients with immune-mediated diseases wane more rapidly than in healthy controls, and this is especially true of those on medications that interfere with the B and T cells and anticytokine therapies,” Rebecca Haberman, MD, assistant professor, division of rheumatology, New York University Langone Health, noted in an email to this news organization.
“While there is no known antibody level that specifically correlates with clinical protection, and each patient needs to be thought of individually, these findings support the use of supplemental booster dosing in patients with immune-mediated inflammatory diseases,” Dr. Haberman said, adding that her own research in this area has shown similar results.
“As a rheumatologist, I would be more likely to encourage my patients – especially those on immunomodulatory medications – to get boosted.”
Dr. Tascilar said his study does not directly answer the question of whether an earlier booster shot would be an effective strategy for patients with IMID. “In our department, we have an early boosting strategy, based on level of immune response.” But the decision of revaccination or not, and when, is based on a number of factors, not only on the level of antibodies. “It’s just part of the instruments we are using.”
The study was supported by the Deutsche Forschungsgemeinschaft. Dr. Simon and Dr. Tascilar declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE LANCET RHEUMATOLOGY

Infographic: Is physician behavior on social media really so bad?
The medical profession is held to a high standard of personal conduct, so physicians keep a sharp eye out for how fellow doctors behave. That goes for social media as well as in-person conduct.
(and it’s not as egregious as you might think). If you’re interested in delving deeper into the data, check out the Medscape Physicians Behaving Badly Report 2022.
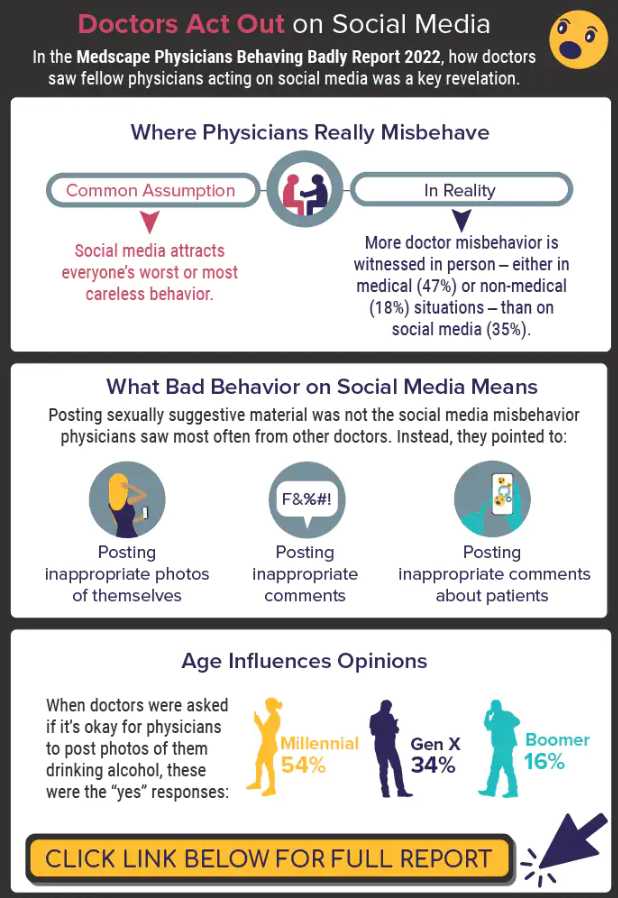
A version of this article first appeared on Medscape.com.
The medical profession is held to a high standard of personal conduct, so physicians keep a sharp eye out for how fellow doctors behave. That goes for social media as well as in-person conduct.
(and it’s not as egregious as you might think). If you’re interested in delving deeper into the data, check out the Medscape Physicians Behaving Badly Report 2022.
A version of this article first appeared on Medscape.com.
The medical profession is held to a high standard of personal conduct, so physicians keep a sharp eye out for how fellow doctors behave. That goes for social media as well as in-person conduct.
(and it’s not as egregious as you might think). If you’re interested in delving deeper into the data, check out the Medscape Physicians Behaving Badly Report 2022.
A version of this article first appeared on Medscape.com.
Home program improves some functional capacity in COPD
A home-based strength training program does not improve dyspnea in patients with chronic obstructive lung disease (COPD), but it does improve some functional capacity and helps patients feel better, a 12-month long HOMEX exercise program shows.
Anja Frei, PhD, University of Zurich, Switzerland, and colleagues reported.
“Our study showed that the HOMEX strength training program had no effect on dyspnea after 12 months in persons with COPD who completed PR, [but] the program improved functional exercise capacity ... and many participants reported having perceived positive effects that they attributed to the training,” investigators add.
The study was published online in the journal CHEST.
Intervention or controls
A total of 123 patients (mean age, 67 years) with COPD were randomly assigned to the intervention group or to the control group. The mean forced expiratory volume in 1 second (FEV1) was 39.3% of predicted. Three-quarters of participants had severe or very severe COPD.
A total of 104 patients completed the 12-month study. “The primary outcome was change in dyspnea (Chronic Respiratory Questionnaire, CRQ) from baseline to 12 months,” investigators note. Secondary outcomes included change in exercise capacity as assessed by the 1-minute-sit-to-stand test (1-min-STST); the 6-minute walk test (6MWT); health-related quality of life, exacerbations, and symptoms.
The HOMEX program was a structured, home-based strength training program developed for patients with COPD that could be done following the pulmonary rehabilitation program, with the intention of maintaining the training benefits gained during pulmonary rehabilitation.
“We deliberately focused on the strength component of exercise training due to the fact that skeletal muscle dysfunction is prevalent in COPD and [is] associated with lower daily physical activity and poor prognosis,” the authors explain. Patients had completed pulmonary rehabilitation no longer than 1 month prior to starting the training program. The program required a chair and a set of resistance bands and consisted of trunk, upper limb, and lower limb exercises done at different intensity levels.
Participants were instructed to do the exercises 6 days per week for about 20 minutes per day over the 12-month study interval. The dyspnea score dropped from 4.65 to 4.42 from baseline to 12 months in the intervention group, compared with a drop from 4.61 to 4.06 in the control group, the investigators reported. “There was no evidence for a difference between the two groups in change in the 6MWT distance after 12 months ... but moderate evidence for a between-group difference in the change of repetitions in the 1-min-STST favoring the IG (intervention group),” they also noted, at an adjusted mean difference of 2.6 (95% confidence interval, 0.22-5.03, P = .033).
In all other outcomes, no differences were observed between the two groups. Importantly, 70% of participants carried on with the HOMEX training program until study endpoint and at least 79% of them persevered for at least 10 months. Based on results from a satisfaction survey, 81% of participants randomly assigned to the intervention group indicated that they “liked” or “very much liked” participating in the program, and 79% of them reported that they experienced positive effects that they felt were attributed to the training.
“The program was safe and the majority of the multimorbid and severely ill study participants adhered to the training during the study year,” the authors write. And while the program had no effect on functional exercise capacity as measured by the 6MWT, it did improve the strength and intramuscular coordination of the lower leg muscles because the program had repetitive sit-to-stand exercises as a component of the training. “Adherence to this long-term training program was surprisingly high,” the authors say. “It was well accepted by COPD patients and may facilitate continued training at home.”
One limitation of the study was that some participants did not travel to the rehabilitation clinic for a follow-up assessment.
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A home-based strength training program does not improve dyspnea in patients with chronic obstructive lung disease (COPD), but it does improve some functional capacity and helps patients feel better, a 12-month long HOMEX exercise program shows.
Anja Frei, PhD, University of Zurich, Switzerland, and colleagues reported.
“Our study showed that the HOMEX strength training program had no effect on dyspnea after 12 months in persons with COPD who completed PR, [but] the program improved functional exercise capacity ... and many participants reported having perceived positive effects that they attributed to the training,” investigators add.
The study was published online in the journal CHEST.
Intervention or controls
A total of 123 patients (mean age, 67 years) with COPD were randomly assigned to the intervention group or to the control group. The mean forced expiratory volume in 1 second (FEV1) was 39.3% of predicted. Three-quarters of participants had severe or very severe COPD.
A total of 104 patients completed the 12-month study. “The primary outcome was change in dyspnea (Chronic Respiratory Questionnaire, CRQ) from baseline to 12 months,” investigators note. Secondary outcomes included change in exercise capacity as assessed by the 1-minute-sit-to-stand test (1-min-STST); the 6-minute walk test (6MWT); health-related quality of life, exacerbations, and symptoms.
The HOMEX program was a structured, home-based strength training program developed for patients with COPD that could be done following the pulmonary rehabilitation program, with the intention of maintaining the training benefits gained during pulmonary rehabilitation.
“We deliberately focused on the strength component of exercise training due to the fact that skeletal muscle dysfunction is prevalent in COPD and [is] associated with lower daily physical activity and poor prognosis,” the authors explain. Patients had completed pulmonary rehabilitation no longer than 1 month prior to starting the training program. The program required a chair and a set of resistance bands and consisted of trunk, upper limb, and lower limb exercises done at different intensity levels.
Participants were instructed to do the exercises 6 days per week for about 20 minutes per day over the 12-month study interval. The dyspnea score dropped from 4.65 to 4.42 from baseline to 12 months in the intervention group, compared with a drop from 4.61 to 4.06 in the control group, the investigators reported. “There was no evidence for a difference between the two groups in change in the 6MWT distance after 12 months ... but moderate evidence for a between-group difference in the change of repetitions in the 1-min-STST favoring the IG (intervention group),” they also noted, at an adjusted mean difference of 2.6 (95% confidence interval, 0.22-5.03, P = .033).
In all other outcomes, no differences were observed between the two groups. Importantly, 70% of participants carried on with the HOMEX training program until study endpoint and at least 79% of them persevered for at least 10 months. Based on results from a satisfaction survey, 81% of participants randomly assigned to the intervention group indicated that they “liked” or “very much liked” participating in the program, and 79% of them reported that they experienced positive effects that they felt were attributed to the training.
“The program was safe and the majority of the multimorbid and severely ill study participants adhered to the training during the study year,” the authors write. And while the program had no effect on functional exercise capacity as measured by the 6MWT, it did improve the strength and intramuscular coordination of the lower leg muscles because the program had repetitive sit-to-stand exercises as a component of the training. “Adherence to this long-term training program was surprisingly high,” the authors say. “It was well accepted by COPD patients and may facilitate continued training at home.”
One limitation of the study was that some participants did not travel to the rehabilitation clinic for a follow-up assessment.
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A home-based strength training program does not improve dyspnea in patients with chronic obstructive lung disease (COPD), but it does improve some functional capacity and helps patients feel better, a 12-month long HOMEX exercise program shows.
Anja Frei, PhD, University of Zurich, Switzerland, and colleagues reported.
“Our study showed that the HOMEX strength training program had no effect on dyspnea after 12 months in persons with COPD who completed PR, [but] the program improved functional exercise capacity ... and many participants reported having perceived positive effects that they attributed to the training,” investigators add.
The study was published online in the journal CHEST.
Intervention or controls
A total of 123 patients (mean age, 67 years) with COPD were randomly assigned to the intervention group or to the control group. The mean forced expiratory volume in 1 second (FEV1) was 39.3% of predicted. Three-quarters of participants had severe or very severe COPD.
A total of 104 patients completed the 12-month study. “The primary outcome was change in dyspnea (Chronic Respiratory Questionnaire, CRQ) from baseline to 12 months,” investigators note. Secondary outcomes included change in exercise capacity as assessed by the 1-minute-sit-to-stand test (1-min-STST); the 6-minute walk test (6MWT); health-related quality of life, exacerbations, and symptoms.
The HOMEX program was a structured, home-based strength training program developed for patients with COPD that could be done following the pulmonary rehabilitation program, with the intention of maintaining the training benefits gained during pulmonary rehabilitation.
“We deliberately focused on the strength component of exercise training due to the fact that skeletal muscle dysfunction is prevalent in COPD and [is] associated with lower daily physical activity and poor prognosis,” the authors explain. Patients had completed pulmonary rehabilitation no longer than 1 month prior to starting the training program. The program required a chair and a set of resistance bands and consisted of trunk, upper limb, and lower limb exercises done at different intensity levels.
Participants were instructed to do the exercises 6 days per week for about 20 minutes per day over the 12-month study interval. The dyspnea score dropped from 4.65 to 4.42 from baseline to 12 months in the intervention group, compared with a drop from 4.61 to 4.06 in the control group, the investigators reported. “There was no evidence for a difference between the two groups in change in the 6MWT distance after 12 months ... but moderate evidence for a between-group difference in the change of repetitions in the 1-min-STST favoring the IG (intervention group),” they also noted, at an adjusted mean difference of 2.6 (95% confidence interval, 0.22-5.03, P = .033).
In all other outcomes, no differences were observed between the two groups. Importantly, 70% of participants carried on with the HOMEX training program until study endpoint and at least 79% of them persevered for at least 10 months. Based on results from a satisfaction survey, 81% of participants randomly assigned to the intervention group indicated that they “liked” or “very much liked” participating in the program, and 79% of them reported that they experienced positive effects that they felt were attributed to the training.
“The program was safe and the majority of the multimorbid and severely ill study participants adhered to the training during the study year,” the authors write. And while the program had no effect on functional exercise capacity as measured by the 6MWT, it did improve the strength and intramuscular coordination of the lower leg muscles because the program had repetitive sit-to-stand exercises as a component of the training. “Adherence to this long-term training program was surprisingly high,” the authors say. “It was well accepted by COPD patients and may facilitate continued training at home.”
One limitation of the study was that some participants did not travel to the rehabilitation clinic for a follow-up assessment.
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
‘Molecular map’ of CLL yields fresh genetic insights
Released in a report in Nature Genetics, the map has doubled the number of genetic traits linked the disease from around 100 to 202, lead author Binyamin A. Knisbacher, PhD, a postdoctoral fellow at the Broad Institute of MIT and Harvard Medical Schoo, Boston, said in an interview.
“It also delineated the molecular landscape of the two immunoglobulin gene (IGHV) subtypes, refined CLL subtyping, and built richer genetic prognostic models,” he said.
According to Dr. Knisbacher, CLL “has been at the forefront of genomic discovery,” and research has shown that there’s a wide variety of somatic mutations that drive CLL initiation across the patient population. However, as many as 10% of cases don’t appear to be driven by any known genetic variation, he said, and there’s a need to identify more subtypes and “build richer prognostic models of patient survival” based on genetics and multiomics such as genomics, transcriptomics, and epigenomics.
For the new study, researchers analyzed RNA and DNA from 1,095 patients with CLL and 54 patients with monoclonal B cell lymphocytosis and built what they say is the largest CLL dataset in existence. It’s twice the size of previous datasets, Dr. Knisbacher said.
“We found that RNA expression data was extremely informative for characterizing CLL,” Dr. Knisbacher said. “The RNA expression subtypes refined the ‘classic’ two IGHV subtypes. It is well documented that patients with U-CLL (IGHV-unmutated CLL) have substantially worse clinical outcome in comparison to M-CLL patients (IGHV-mutated CLLs). We found that M-CLLs that have RNA expression profiles similar to U-CLLs have worse survival than M-CLLs with a typical expression profile. Failure-free survival was 50% shorter – 5.3 versus 10.7 years median failure-free survival.”
In addition, he said, “U-CLLs with expression similar to M-CLLs had better survival than U-CLLs with an RNA expression profile typical to U-CLLs.”
The researchers have made their molecular map publicly available at https://cllmap.org/. Researchers can use it “to discover more about each subtype of CLL, and these future studies can help to improve clinical prognosis for the benefit of the patient,” Dr. Knisbacher said.
The study authors added that “this molecular foundation may allow for better prediction of response to therapy or provide the basis for rational combination of novel agents.”
Lee Greenberger, PhD, chief science officer of the Leukemia & Lymphoma Society, said in an interview that the study “provides foundational data further subtyping CLL patients and outcomes. It identifies new targets for therapy or diagnostic predictions in the future. This type of foundational work has proven invaluable in the development of new medicines for cancer in general.”
While there are many medications that have improved therapeutic outcomes in CLL, he added, “cures – or life-long disease control –remain elusive for many patients. Therefore, new molecular insights are needed that could personalize therapies or even lead to entirely new therapies.”
In addition, he said, although prevention of CLL still remains elusive, “it is conceivable that some of the mutations found in this paper occur early in the CLL trajectory, perhaps even before the disease is presented clinically.”
The study was funded by the National Institutes of Health and the Broad/IBM Cancer Resistance Research Project. Dr. Knisbacher and several other authors disclose that they are inventors on a patent related to CLL. Several authors report various relationships with industry. Dr. Greenberger has no disclosures.
Released in a report in Nature Genetics, the map has doubled the number of genetic traits linked the disease from around 100 to 202, lead author Binyamin A. Knisbacher, PhD, a postdoctoral fellow at the Broad Institute of MIT and Harvard Medical Schoo, Boston, said in an interview.
“It also delineated the molecular landscape of the two immunoglobulin gene (IGHV) subtypes, refined CLL subtyping, and built richer genetic prognostic models,” he said.
According to Dr. Knisbacher, CLL “has been at the forefront of genomic discovery,” and research has shown that there’s a wide variety of somatic mutations that drive CLL initiation across the patient population. However, as many as 10% of cases don’t appear to be driven by any known genetic variation, he said, and there’s a need to identify more subtypes and “build richer prognostic models of patient survival” based on genetics and multiomics such as genomics, transcriptomics, and epigenomics.
For the new study, researchers analyzed RNA and DNA from 1,095 patients with CLL and 54 patients with monoclonal B cell lymphocytosis and built what they say is the largest CLL dataset in existence. It’s twice the size of previous datasets, Dr. Knisbacher said.
“We found that RNA expression data was extremely informative for characterizing CLL,” Dr. Knisbacher said. “The RNA expression subtypes refined the ‘classic’ two IGHV subtypes. It is well documented that patients with U-CLL (IGHV-unmutated CLL) have substantially worse clinical outcome in comparison to M-CLL patients (IGHV-mutated CLLs). We found that M-CLLs that have RNA expression profiles similar to U-CLLs have worse survival than M-CLLs with a typical expression profile. Failure-free survival was 50% shorter – 5.3 versus 10.7 years median failure-free survival.”
In addition, he said, “U-CLLs with expression similar to M-CLLs had better survival than U-CLLs with an RNA expression profile typical to U-CLLs.”
The researchers have made their molecular map publicly available at https://cllmap.org/. Researchers can use it “to discover more about each subtype of CLL, and these future studies can help to improve clinical prognosis for the benefit of the patient,” Dr. Knisbacher said.
The study authors added that “this molecular foundation may allow for better prediction of response to therapy or provide the basis for rational combination of novel agents.”
Lee Greenberger, PhD, chief science officer of the Leukemia & Lymphoma Society, said in an interview that the study “provides foundational data further subtyping CLL patients and outcomes. It identifies new targets for therapy or diagnostic predictions in the future. This type of foundational work has proven invaluable in the development of new medicines for cancer in general.”
While there are many medications that have improved therapeutic outcomes in CLL, he added, “cures – or life-long disease control –remain elusive for many patients. Therefore, new molecular insights are needed that could personalize therapies or even lead to entirely new therapies.”
In addition, he said, although prevention of CLL still remains elusive, “it is conceivable that some of the mutations found in this paper occur early in the CLL trajectory, perhaps even before the disease is presented clinically.”
The study was funded by the National Institutes of Health and the Broad/IBM Cancer Resistance Research Project. Dr. Knisbacher and several other authors disclose that they are inventors on a patent related to CLL. Several authors report various relationships with industry. Dr. Greenberger has no disclosures.
Released in a report in Nature Genetics, the map has doubled the number of genetic traits linked the disease from around 100 to 202, lead author Binyamin A. Knisbacher, PhD, a postdoctoral fellow at the Broad Institute of MIT and Harvard Medical Schoo, Boston, said in an interview.
“It also delineated the molecular landscape of the two immunoglobulin gene (IGHV) subtypes, refined CLL subtyping, and built richer genetic prognostic models,” he said.
According to Dr. Knisbacher, CLL “has been at the forefront of genomic discovery,” and research has shown that there’s a wide variety of somatic mutations that drive CLL initiation across the patient population. However, as many as 10% of cases don’t appear to be driven by any known genetic variation, he said, and there’s a need to identify more subtypes and “build richer prognostic models of patient survival” based on genetics and multiomics such as genomics, transcriptomics, and epigenomics.
For the new study, researchers analyzed RNA and DNA from 1,095 patients with CLL and 54 patients with monoclonal B cell lymphocytosis and built what they say is the largest CLL dataset in existence. It’s twice the size of previous datasets, Dr. Knisbacher said.
“We found that RNA expression data was extremely informative for characterizing CLL,” Dr. Knisbacher said. “The RNA expression subtypes refined the ‘classic’ two IGHV subtypes. It is well documented that patients with U-CLL (IGHV-unmutated CLL) have substantially worse clinical outcome in comparison to M-CLL patients (IGHV-mutated CLLs). We found that M-CLLs that have RNA expression profiles similar to U-CLLs have worse survival than M-CLLs with a typical expression profile. Failure-free survival was 50% shorter – 5.3 versus 10.7 years median failure-free survival.”
In addition, he said, “U-CLLs with expression similar to M-CLLs had better survival than U-CLLs with an RNA expression profile typical to U-CLLs.”
The researchers have made their molecular map publicly available at https://cllmap.org/. Researchers can use it “to discover more about each subtype of CLL, and these future studies can help to improve clinical prognosis for the benefit of the patient,” Dr. Knisbacher said.
The study authors added that “this molecular foundation may allow for better prediction of response to therapy or provide the basis for rational combination of novel agents.”
Lee Greenberger, PhD, chief science officer of the Leukemia & Lymphoma Society, said in an interview that the study “provides foundational data further subtyping CLL patients and outcomes. It identifies new targets for therapy or diagnostic predictions in the future. This type of foundational work has proven invaluable in the development of new medicines for cancer in general.”
While there are many medications that have improved therapeutic outcomes in CLL, he added, “cures – or life-long disease control –remain elusive for many patients. Therefore, new molecular insights are needed that could personalize therapies or even lead to entirely new therapies.”
In addition, he said, although prevention of CLL still remains elusive, “it is conceivable that some of the mutations found in this paper occur early in the CLL trajectory, perhaps even before the disease is presented clinically.”
The study was funded by the National Institutes of Health and the Broad/IBM Cancer Resistance Research Project. Dr. Knisbacher and several other authors disclose that they are inventors on a patent related to CLL. Several authors report various relationships with industry. Dr. Greenberger has no disclosures.
FROM NATURE GENETICS
Paxlovid reduces risk of COVID death by 79% in older adults
The antiviral drug Paxlovid appears to reduce the risk of dying from COVID-19 by 79% and decrease hospitalizations by 73% in at-risk patients who are ages 65 and older, according to a new study published in The New England Journal of Medicine.
The pill, which is a combination of the drugs nirmatrelvir and ritonavir, received FDA emergency use authorization in December 2021 to treat mild to moderate disease in ages 12 and older who face high risks for having severe COVID-19, hospitalization, and death.
“The results of the study show unequivocally that treatment with Paxlovid significantly reduces the risk of hospitalization and death from COVID-19,” Doron Netzer, MD, the senior study author and a researcher with Clalit Health Services, Tel Aviv, told The Jerusalem Post.
“We are the country’s leader in the provision of giving Paxlovid to relevant patients,” he said. “It was given to patients all over the country, with medical teams monitoring the patients who took the pills.”
, the news outlet reported. The research team analyzed information from Clalit’s electronic medical records. The health care organization covers about 52% of the Israeli population and almost two-thirds of older adults. More than 30,000 COVID-19 patients in Israel have been treated with the drug so far.
Dr. Netzer and colleagues looked at hospitalization and death data for at-risk COVID-19 patients ages 40 and older between Jan. 9 and March 31, when the original Omicron variant was the dominant strain in Israel. During that time, more than 1.1 million Clalit patients were infected with COVID-19, 109,000 patients were considered at-risk, and 3,900 patients received the drug.
The average age of the patients was 60, and 39% of the patients were 65 and older. Overall, 78% of the patients had previous COVID-19 immunity due to vaccination, prior infection, or both.
Among ages 65 and older, the rate of COVID-19 hospitalization was 14.7 cases per 100,000 person-days among treated patients, compared with 58.9 cases per 100,000 person-days among untreated patients. This represented a 73% lower chance of being hospitalized.
Among ages 40-64, the rate of hospitalization due to COVID-19 was 15.2 cases per 100,000 person-days among treated patients, compared with 15.8 cases per 100,000 person-days among untreated patients. The risk of hospitalization wasn’t significantly lower for this age group.
Among ages 65 and older, there were two deaths from COVID-19 in 2,484 treated patients, compared with 158 in the 40,337 untreated patients. This represented a 79% lower chance of dying from COVID-19.
Among ages 40-64, there was one death from COVID-19 in 1,418 treated patients, compared with 16 in the 65,015 untreated patients. The risk of death wasn’t significantly lower for this age group.
For both age groups, a lack of previous COVID-19 immunity and a previous hospitalization were most strongly linked to high rates of hospitalization during the Omicron wave.
The researchers noted that they didn’t break down the data on ages 40-64 who had cancer and other severe conditions that weaken the immune system. These patients may be more likely to benefit from Paxlovid, they said, though future studies will need to analyze the data.
The study didn’t receive any financial or in-kind support, the authors said.
A version of this article first appeared on WebMD.com.
The antiviral drug Paxlovid appears to reduce the risk of dying from COVID-19 by 79% and decrease hospitalizations by 73% in at-risk patients who are ages 65 and older, according to a new study published in The New England Journal of Medicine.
The pill, which is a combination of the drugs nirmatrelvir and ritonavir, received FDA emergency use authorization in December 2021 to treat mild to moderate disease in ages 12 and older who face high risks for having severe COVID-19, hospitalization, and death.
“The results of the study show unequivocally that treatment with Paxlovid significantly reduces the risk of hospitalization and death from COVID-19,” Doron Netzer, MD, the senior study author and a researcher with Clalit Health Services, Tel Aviv, told The Jerusalem Post.
“We are the country’s leader in the provision of giving Paxlovid to relevant patients,” he said. “It was given to patients all over the country, with medical teams monitoring the patients who took the pills.”
, the news outlet reported. The research team analyzed information from Clalit’s electronic medical records. The health care organization covers about 52% of the Israeli population and almost two-thirds of older adults. More than 30,000 COVID-19 patients in Israel have been treated with the drug so far.
Dr. Netzer and colleagues looked at hospitalization and death data for at-risk COVID-19 patients ages 40 and older between Jan. 9 and March 31, when the original Omicron variant was the dominant strain in Israel. During that time, more than 1.1 million Clalit patients were infected with COVID-19, 109,000 patients were considered at-risk, and 3,900 patients received the drug.
The average age of the patients was 60, and 39% of the patients were 65 and older. Overall, 78% of the patients had previous COVID-19 immunity due to vaccination, prior infection, or both.
Among ages 65 and older, the rate of COVID-19 hospitalization was 14.7 cases per 100,000 person-days among treated patients, compared with 58.9 cases per 100,000 person-days among untreated patients. This represented a 73% lower chance of being hospitalized.
Among ages 40-64, the rate of hospitalization due to COVID-19 was 15.2 cases per 100,000 person-days among treated patients, compared with 15.8 cases per 100,000 person-days among untreated patients. The risk of hospitalization wasn’t significantly lower for this age group.
Among ages 65 and older, there were two deaths from COVID-19 in 2,484 treated patients, compared with 158 in the 40,337 untreated patients. This represented a 79% lower chance of dying from COVID-19.
Among ages 40-64, there was one death from COVID-19 in 1,418 treated patients, compared with 16 in the 65,015 untreated patients. The risk of death wasn’t significantly lower for this age group.
For both age groups, a lack of previous COVID-19 immunity and a previous hospitalization were most strongly linked to high rates of hospitalization during the Omicron wave.
The researchers noted that they didn’t break down the data on ages 40-64 who had cancer and other severe conditions that weaken the immune system. These patients may be more likely to benefit from Paxlovid, they said, though future studies will need to analyze the data.
The study didn’t receive any financial or in-kind support, the authors said.
A version of this article first appeared on WebMD.com.
The antiviral drug Paxlovid appears to reduce the risk of dying from COVID-19 by 79% and decrease hospitalizations by 73% in at-risk patients who are ages 65 and older, according to a new study published in The New England Journal of Medicine.
The pill, which is a combination of the drugs nirmatrelvir and ritonavir, received FDA emergency use authorization in December 2021 to treat mild to moderate disease in ages 12 and older who face high risks for having severe COVID-19, hospitalization, and death.
“The results of the study show unequivocally that treatment with Paxlovid significantly reduces the risk of hospitalization and death from COVID-19,” Doron Netzer, MD, the senior study author and a researcher with Clalit Health Services, Tel Aviv, told The Jerusalem Post.
“We are the country’s leader in the provision of giving Paxlovid to relevant patients,” he said. “It was given to patients all over the country, with medical teams monitoring the patients who took the pills.”
, the news outlet reported. The research team analyzed information from Clalit’s electronic medical records. The health care organization covers about 52% of the Israeli population and almost two-thirds of older adults. More than 30,000 COVID-19 patients in Israel have been treated with the drug so far.
Dr. Netzer and colleagues looked at hospitalization and death data for at-risk COVID-19 patients ages 40 and older between Jan. 9 and March 31, when the original Omicron variant was the dominant strain in Israel. During that time, more than 1.1 million Clalit patients were infected with COVID-19, 109,000 patients were considered at-risk, and 3,900 patients received the drug.
The average age of the patients was 60, and 39% of the patients were 65 and older. Overall, 78% of the patients had previous COVID-19 immunity due to vaccination, prior infection, or both.
Among ages 65 and older, the rate of COVID-19 hospitalization was 14.7 cases per 100,000 person-days among treated patients, compared with 58.9 cases per 100,000 person-days among untreated patients. This represented a 73% lower chance of being hospitalized.
Among ages 40-64, the rate of hospitalization due to COVID-19 was 15.2 cases per 100,000 person-days among treated patients, compared with 15.8 cases per 100,000 person-days among untreated patients. The risk of hospitalization wasn’t significantly lower for this age group.
Among ages 65 and older, there were two deaths from COVID-19 in 2,484 treated patients, compared with 158 in the 40,337 untreated patients. This represented a 79% lower chance of dying from COVID-19.
Among ages 40-64, there was one death from COVID-19 in 1,418 treated patients, compared with 16 in the 65,015 untreated patients. The risk of death wasn’t significantly lower for this age group.
For both age groups, a lack of previous COVID-19 immunity and a previous hospitalization were most strongly linked to high rates of hospitalization during the Omicron wave.
The researchers noted that they didn’t break down the data on ages 40-64 who had cancer and other severe conditions that weaken the immune system. These patients may be more likely to benefit from Paxlovid, they said, though future studies will need to analyze the data.
The study didn’t receive any financial or in-kind support, the authors said.
A version of this article first appeared on WebMD.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Vaccine hope now for leading cause of U.S. infant hospitalizations: RSV
Respiratory syncytial virus (RSV) is the leading cause of U.S. infant hospitalizations overall and across population subgroups, new data published in the Journal of Infectious Diseases confirm.
Acute bronchiolitis caused by RSV accounted for 9.6% (95% confidence interval, 9.4%-9.9%) and 9.3% (95% CI, 9.0%-9.6%) of total infant hospitalizations from January 2009 to September 2015 and October 2015 to December 2019, respectively.
Journal issue includes 14 RSV studies
The latest issue of the journal includes a special section with results from 14 studies related to the widespread, easy-to-catch virus, highlighting the urgency of finding a solution for all infants.
In one study, authors led by Mina Suh, MPH, with EpidStrategies, a division of ToxStrategies in Rockville, Md., reported that, in children under the age of 5 years in the United States, RSV caused 58,000 annual hospitalizations and from 100 to 500 annual deaths from 2009 to 2019 (the latest year data were available).
Globally, in 2015, among infants younger than 6 months, an estimated 1.4 million hospital admissions and 27,300 in-hospital deaths were attributed to RSV lower respiratory tract infection (LRTI).
The researchers used the largest publicly available, all-payer database in the United States – the National (Nationwide) Inpatient Sample – to describe the leading causes of infant hospitalizations.
The authors noted that, because clinicians don’t routinely perform lab tests for RSV, the true health care burden is likely higher and its public health impact greater than these numbers show.
Immunization candidates advance
There are no preventative options currently available to substantially cut RSV infections in all infants, though immunization candidates are advancing, showing safety and efficacy in clinical trials.
Palivizumab is currently the only available option in the United States to prevent RSV and is recommended only for a small group of infants with particular forms of heart or lung disease and those born prematurely at 29 weeks’ gestational age. Further, palivizumab has to be given monthly throughout the RSV season.
Another of the studies in the journal supplement concluded that a universal immunization strategy with one of the candidates, nirsevimab (Sanofi, AstraZeneca), an investigational long-acting monoclonal antibody, could substantially reduce the health burden and economic burden for U.S. infants in their first RSV season.
The researchers, led by Alexia Kieffer, MSc, MPH, with Sanofi, used static decision-analytic modeling for the estimates. Modeled RSV-related outcomes included primary care and ED visits, hospitalizations, including ICU admission and mechanical ventilations, and RSV-related deaths.
“The results of this model suggested that the use of nirsevimab in all infants could reduce health events by 55% and the overall costs to the payer by 49%,” the authors of the study wrote.
According to the study, universal immunization of all infants with nirsevimab is expected to reduce 290,174 RSV-related medically attended LRTI (MALRTI), 24,986 hospitalizations, and cut $612 million in costs to the health care system.
The authors wrote: “While this reduction would be driven by term infants, who account for most of the RSV-MALRTI burden; all infants, including palivizumab-eligible and preterm infants who suffer from significantly higher rates of disease, would benefit from this immunization strategy.”
Excitement for another option
Jörn-Hendrik Weitkamp, MD, professor of pediatrics and director for patient-oriented research at Monroe Carell Jr. Children’s Hospital at Vanderbilt University, Nashville, Tenn., said in an interview there is much excitement in the field for nirsevimab as it has significant advantages over palivizumab.
RSV “is a huge burden to the children, the families, the hospitals, and the medical system,” he said.
Ideally there would be a vaccine to offer the best protection, he noted.
“People have spent their lives, their careers trying to develop a vaccine for RSV,” he said, but that has been elusive for more than 60 years. Therefore, passive immunization is the best of the current options, he says, and nirsevimab “seems to be very effective.”
What’s not clear, Dr. Weitkamp said, is how much nirsevimab will cost as it is not yet approved by the Food and Drug Administration. However, it has the great advantage of being given only once before the season starts instead of monthly (as required for palivizumab) through the season, “which is painful, inconvenient, and traumatizing. We limit that one to the children at highest risk.”
Rolling out an infant nirsevimab program would likely vary by geographic region, Ms. Kieffer and colleagues said, to help ensure infants are protected during the peak of their region’s RSV season.
The journal’s RSV supplement was supported by Sanofi and AstraZeneca. The studies by Ms. Suh and colleagues and Ms. Kieffer and colleagues were supported by AstraZeneca and Sanofi. Ms. Suh and several coauthors are employees of EpidStrategies. One coauthor is an employee of Sanofi and may hold shares and/or stock options in the company. Ms. Kieffer and several coauthors are employees of Sanofi and may hold shares and/or stock options in the company. Dr. Weitkamp reported no relevant financial relationships.
Respiratory syncytial virus (RSV) is the leading cause of U.S. infant hospitalizations overall and across population subgroups, new data published in the Journal of Infectious Diseases confirm.
Acute bronchiolitis caused by RSV accounted for 9.6% (95% confidence interval, 9.4%-9.9%) and 9.3% (95% CI, 9.0%-9.6%) of total infant hospitalizations from January 2009 to September 2015 and October 2015 to December 2019, respectively.
Journal issue includes 14 RSV studies
The latest issue of the journal includes a special section with results from 14 studies related to the widespread, easy-to-catch virus, highlighting the urgency of finding a solution for all infants.
In one study, authors led by Mina Suh, MPH, with EpidStrategies, a division of ToxStrategies in Rockville, Md., reported that, in children under the age of 5 years in the United States, RSV caused 58,000 annual hospitalizations and from 100 to 500 annual deaths from 2009 to 2019 (the latest year data were available).
Globally, in 2015, among infants younger than 6 months, an estimated 1.4 million hospital admissions and 27,300 in-hospital deaths were attributed to RSV lower respiratory tract infection (LRTI).
The researchers used the largest publicly available, all-payer database in the United States – the National (Nationwide) Inpatient Sample – to describe the leading causes of infant hospitalizations.
The authors noted that, because clinicians don’t routinely perform lab tests for RSV, the true health care burden is likely higher and its public health impact greater than these numbers show.
Immunization candidates advance
There are no preventative options currently available to substantially cut RSV infections in all infants, though immunization candidates are advancing, showing safety and efficacy in clinical trials.
Palivizumab is currently the only available option in the United States to prevent RSV and is recommended only for a small group of infants with particular forms of heart or lung disease and those born prematurely at 29 weeks’ gestational age. Further, palivizumab has to be given monthly throughout the RSV season.
Another of the studies in the journal supplement concluded that a universal immunization strategy with one of the candidates, nirsevimab (Sanofi, AstraZeneca), an investigational long-acting monoclonal antibody, could substantially reduce the health burden and economic burden for U.S. infants in their first RSV season.
The researchers, led by Alexia Kieffer, MSc, MPH, with Sanofi, used static decision-analytic modeling for the estimates. Modeled RSV-related outcomes included primary care and ED visits, hospitalizations, including ICU admission and mechanical ventilations, and RSV-related deaths.
“The results of this model suggested that the use of nirsevimab in all infants could reduce health events by 55% and the overall costs to the payer by 49%,” the authors of the study wrote.
According to the study, universal immunization of all infants with nirsevimab is expected to reduce 290,174 RSV-related medically attended LRTI (MALRTI), 24,986 hospitalizations, and cut $612 million in costs to the health care system.
The authors wrote: “While this reduction would be driven by term infants, who account for most of the RSV-MALRTI burden; all infants, including palivizumab-eligible and preterm infants who suffer from significantly higher rates of disease, would benefit from this immunization strategy.”
Excitement for another option
Jörn-Hendrik Weitkamp, MD, professor of pediatrics and director for patient-oriented research at Monroe Carell Jr. Children’s Hospital at Vanderbilt University, Nashville, Tenn., said in an interview there is much excitement in the field for nirsevimab as it has significant advantages over palivizumab.
RSV “is a huge burden to the children, the families, the hospitals, and the medical system,” he said.
Ideally there would be a vaccine to offer the best protection, he noted.
“People have spent their lives, their careers trying to develop a vaccine for RSV,” he said, but that has been elusive for more than 60 years. Therefore, passive immunization is the best of the current options, he says, and nirsevimab “seems to be very effective.”
What’s not clear, Dr. Weitkamp said, is how much nirsevimab will cost as it is not yet approved by the Food and Drug Administration. However, it has the great advantage of being given only once before the season starts instead of monthly (as required for palivizumab) through the season, “which is painful, inconvenient, and traumatizing. We limit that one to the children at highest risk.”
Rolling out an infant nirsevimab program would likely vary by geographic region, Ms. Kieffer and colleagues said, to help ensure infants are protected during the peak of their region’s RSV season.
The journal’s RSV supplement was supported by Sanofi and AstraZeneca. The studies by Ms. Suh and colleagues and Ms. Kieffer and colleagues were supported by AstraZeneca and Sanofi. Ms. Suh and several coauthors are employees of EpidStrategies. One coauthor is an employee of Sanofi and may hold shares and/or stock options in the company. Ms. Kieffer and several coauthors are employees of Sanofi and may hold shares and/or stock options in the company. Dr. Weitkamp reported no relevant financial relationships.
Respiratory syncytial virus (RSV) is the leading cause of U.S. infant hospitalizations overall and across population subgroups, new data published in the Journal of Infectious Diseases confirm.
Acute bronchiolitis caused by RSV accounted for 9.6% (95% confidence interval, 9.4%-9.9%) and 9.3% (95% CI, 9.0%-9.6%) of total infant hospitalizations from January 2009 to September 2015 and October 2015 to December 2019, respectively.
Journal issue includes 14 RSV studies
The latest issue of the journal includes a special section with results from 14 studies related to the widespread, easy-to-catch virus, highlighting the urgency of finding a solution for all infants.
In one study, authors led by Mina Suh, MPH, with EpidStrategies, a division of ToxStrategies in Rockville, Md., reported that, in children under the age of 5 years in the United States, RSV caused 58,000 annual hospitalizations and from 100 to 500 annual deaths from 2009 to 2019 (the latest year data were available).
Globally, in 2015, among infants younger than 6 months, an estimated 1.4 million hospital admissions and 27,300 in-hospital deaths were attributed to RSV lower respiratory tract infection (LRTI).
The researchers used the largest publicly available, all-payer database in the United States – the National (Nationwide) Inpatient Sample – to describe the leading causes of infant hospitalizations.
The authors noted that, because clinicians don’t routinely perform lab tests for RSV, the true health care burden is likely higher and its public health impact greater than these numbers show.
Immunization candidates advance
There are no preventative options currently available to substantially cut RSV infections in all infants, though immunization candidates are advancing, showing safety and efficacy in clinical trials.
Palivizumab is currently the only available option in the United States to prevent RSV and is recommended only for a small group of infants with particular forms of heart or lung disease and those born prematurely at 29 weeks’ gestational age. Further, palivizumab has to be given monthly throughout the RSV season.
Another of the studies in the journal supplement concluded that a universal immunization strategy with one of the candidates, nirsevimab (Sanofi, AstraZeneca), an investigational long-acting monoclonal antibody, could substantially reduce the health burden and economic burden for U.S. infants in their first RSV season.
The researchers, led by Alexia Kieffer, MSc, MPH, with Sanofi, used static decision-analytic modeling for the estimates. Modeled RSV-related outcomes included primary care and ED visits, hospitalizations, including ICU admission and mechanical ventilations, and RSV-related deaths.
“The results of this model suggested that the use of nirsevimab in all infants could reduce health events by 55% and the overall costs to the payer by 49%,” the authors of the study wrote.
According to the study, universal immunization of all infants with nirsevimab is expected to reduce 290,174 RSV-related medically attended LRTI (MALRTI), 24,986 hospitalizations, and cut $612 million in costs to the health care system.
The authors wrote: “While this reduction would be driven by term infants, who account for most of the RSV-MALRTI burden; all infants, including palivizumab-eligible and preterm infants who suffer from significantly higher rates of disease, would benefit from this immunization strategy.”
Excitement for another option
Jörn-Hendrik Weitkamp, MD, professor of pediatrics and director for patient-oriented research at Monroe Carell Jr. Children’s Hospital at Vanderbilt University, Nashville, Tenn., said in an interview there is much excitement in the field for nirsevimab as it has significant advantages over palivizumab.
RSV “is a huge burden to the children, the families, the hospitals, and the medical system,” he said.
Ideally there would be a vaccine to offer the best protection, he noted.
“People have spent their lives, their careers trying to develop a vaccine for RSV,” he said, but that has been elusive for more than 60 years. Therefore, passive immunization is the best of the current options, he says, and nirsevimab “seems to be very effective.”
What’s not clear, Dr. Weitkamp said, is how much nirsevimab will cost as it is not yet approved by the Food and Drug Administration. However, it has the great advantage of being given only once before the season starts instead of monthly (as required for palivizumab) through the season, “which is painful, inconvenient, and traumatizing. We limit that one to the children at highest risk.”
Rolling out an infant nirsevimab program would likely vary by geographic region, Ms. Kieffer and colleagues said, to help ensure infants are protected during the peak of their region’s RSV season.
The journal’s RSV supplement was supported by Sanofi and AstraZeneca. The studies by Ms. Suh and colleagues and Ms. Kieffer and colleagues were supported by AstraZeneca and Sanofi. Ms. Suh and several coauthors are employees of EpidStrategies. One coauthor is an employee of Sanofi and may hold shares and/or stock options in the company. Ms. Kieffer and several coauthors are employees of Sanofi and may hold shares and/or stock options in the company. Dr. Weitkamp reported no relevant financial relationships.
FROM THE JOURNAL OF INFECTIOUS DISEASES