User login
New international consensus document on treating OSA
The Spanish Society of Pulmonology and Thoracic Surgery (SEPAR) has issued a new international consensus document (ICD) on obstructive sleep apnea (OSA). The objective is to improve the diagnosis and treatment of one of the most prevalent sleep disorders.
It provides a series of clinical guidelines to help health care professionals make the best decisions for adult patients with OSA. Notably, the authors propose changing the name from sleep apnea syndrome. In recommending the term OSA, they reintroduce the term “obstructive” – to differentiate the disorder from central sleep apnea – and remove the outdated word “syndrome.”
“The definition has also been changed, as it was a bit vague and difficult to understand. And there are significant changes to the treatment and to the diagnostic algorithms – one for primary care and another for sleep units,” Olga Mediano, MD, said in an interview. She is a SEPAR pulmonologist, first author of the ICD, and the coordinator of SEPAR 2022 Year of Intermediate Respiratory Care Units.
Diagnosis in primary care
The ICD indicates that all levels of care must be involved in the management of OSA, a condition in which complete or partial upper airway blockage occurs during sleep, causing the individual to stop breathing for a few seconds. These pauses, which produce hypoxia and sleep fragmentation, increase the risk of workplace and traffic accidents, affect cardiovascular health, and contribute to uncontrolled or resistant hypertension.
The recommendations in the ICD aim at increasing the role of primary care physicians so as to reduce underdiagnosis of OSA in primary care. “The vast majority of patients with OSA haven’t been diagnosed. In fact, those whom we have diagnosed are the patients with the most severe cases – in other words, patients who present with the most symptoms,” said Dr. Mediano. She explained that many patients with OSA don’t consider it a medical condition, so they do not go to the doctor.
“The other big problem is that, before, there was a preconceived notion of the typical OSA patient: A middle-aged obese man who’s fallen asleep in the waiting room. However, there are many other profiles: thin build, women. ... Sleep has a heterogeneous profile, and all profiles need to be known,” said Dr. Mediano. The difficulties in carrying out a sleep study with the various patients are an added problem that the new consensus document also seeks to resolve. “The step we’ve taken is to involve the primary care physician in super-simplified studies to reach more people,” she said. For this, the primary care site must work in coordination with a sleep unit.
“In the super-simplified study, the patient is given a machine to use at home; they hook themselves up to it when they go to sleep. This machine records the number of apnea episodes the patient experiences during the night, as well as the oxygen level. The next day, the patient returns the machine. The data are downloaded to a computer. The software analyzes the breathing pauses that the patient had during the night and automatically gives a series of values that, if very pronounced, as the document indicates, would lead to a diagnosis of OSA. Once diagnosed by a primary care physician, the patient is referred to a sleep unit where treatment can then be assessed,” explained Dr. Mediano.
Different treatments
The new ICD’s approach incorporates therapeutic alternatives as well. Until now, many consensus documents and clinical guidelines have focused on continuous positive airway pressure therapy, in which a machine delivers continuous airflow to help keep the patient’s airway open and unobstructed during sleep. Some guidelines recommend its use, and others do not. “However, in this new document, management of the patient is much more multidisciplinary. What changes, with respect to the treatment, is the philosophy. It’s not one single type of treatment; rather, other therapeutic options are kept in mind,” said Dr. Mediano.
First, treatment of reversible causes of OSA must be offered. The conditions that lead to OSA and that can be reversed are addressed. These include overweight and obesity; heavy drinking; tonsillar hypertrophy, or severe dental or facial alterations, for which surgery can be considered; and gastroesophageal reflux or hypothyroidism, both of which can be treated. “For example, the leading cause of sleep apnea is obesity. If we can get the patient to lose weight, that can end up making the OSA go away. What does the document say? Well, you have to try to implement intensive strategies regarding diet, exercise, etc. And if that’s not enough, you need to consider using drugs or even bariatric surgery,” said Dr. Mediano.
“If there’s no one definitive treatment, we highly recommend that all patients implement hygienic-dietary measures and then assess all the therapeutic options. In some cases, several can be in place at the same time,” she said. Various medical specialists can play a role in the treatment of OSA, said Dr. Mediano. They include otolaryngologists, maxillofacial surgeons, dentists, cardiologists, and neurophysiologists, to mention a few.
A website has been created to explain the ICD. There, visitors will be able to find the most up-to-date version of the ICD as well as related information, news, and materials.
A version of this article appeared on Medscape.com. This article was translated from Univadis Spain.
The Spanish Society of Pulmonology and Thoracic Surgery (SEPAR) has issued a new international consensus document (ICD) on obstructive sleep apnea (OSA). The objective is to improve the diagnosis and treatment of one of the most prevalent sleep disorders.
It provides a series of clinical guidelines to help health care professionals make the best decisions for adult patients with OSA. Notably, the authors propose changing the name from sleep apnea syndrome. In recommending the term OSA, they reintroduce the term “obstructive” – to differentiate the disorder from central sleep apnea – and remove the outdated word “syndrome.”
“The definition has also been changed, as it was a bit vague and difficult to understand. And there are significant changes to the treatment and to the diagnostic algorithms – one for primary care and another for sleep units,” Olga Mediano, MD, said in an interview. She is a SEPAR pulmonologist, first author of the ICD, and the coordinator of SEPAR 2022 Year of Intermediate Respiratory Care Units.
Diagnosis in primary care
The ICD indicates that all levels of care must be involved in the management of OSA, a condition in which complete or partial upper airway blockage occurs during sleep, causing the individual to stop breathing for a few seconds. These pauses, which produce hypoxia and sleep fragmentation, increase the risk of workplace and traffic accidents, affect cardiovascular health, and contribute to uncontrolled or resistant hypertension.
The recommendations in the ICD aim at increasing the role of primary care physicians so as to reduce underdiagnosis of OSA in primary care. “The vast majority of patients with OSA haven’t been diagnosed. In fact, those whom we have diagnosed are the patients with the most severe cases – in other words, patients who present with the most symptoms,” said Dr. Mediano. She explained that many patients with OSA don’t consider it a medical condition, so they do not go to the doctor.
“The other big problem is that, before, there was a preconceived notion of the typical OSA patient: A middle-aged obese man who’s fallen asleep in the waiting room. However, there are many other profiles: thin build, women. ... Sleep has a heterogeneous profile, and all profiles need to be known,” said Dr. Mediano. The difficulties in carrying out a sleep study with the various patients are an added problem that the new consensus document also seeks to resolve. “The step we’ve taken is to involve the primary care physician in super-simplified studies to reach more people,” she said. For this, the primary care site must work in coordination with a sleep unit.
“In the super-simplified study, the patient is given a machine to use at home; they hook themselves up to it when they go to sleep. This machine records the number of apnea episodes the patient experiences during the night, as well as the oxygen level. The next day, the patient returns the machine. The data are downloaded to a computer. The software analyzes the breathing pauses that the patient had during the night and automatically gives a series of values that, if very pronounced, as the document indicates, would lead to a diagnosis of OSA. Once diagnosed by a primary care physician, the patient is referred to a sleep unit where treatment can then be assessed,” explained Dr. Mediano.
Different treatments
The new ICD’s approach incorporates therapeutic alternatives as well. Until now, many consensus documents and clinical guidelines have focused on continuous positive airway pressure therapy, in which a machine delivers continuous airflow to help keep the patient’s airway open and unobstructed during sleep. Some guidelines recommend its use, and others do not. “However, in this new document, management of the patient is much more multidisciplinary. What changes, with respect to the treatment, is the philosophy. It’s not one single type of treatment; rather, other therapeutic options are kept in mind,” said Dr. Mediano.
First, treatment of reversible causes of OSA must be offered. The conditions that lead to OSA and that can be reversed are addressed. These include overweight and obesity; heavy drinking; tonsillar hypertrophy, or severe dental or facial alterations, for which surgery can be considered; and gastroesophageal reflux or hypothyroidism, both of which can be treated. “For example, the leading cause of sleep apnea is obesity. If we can get the patient to lose weight, that can end up making the OSA go away. What does the document say? Well, you have to try to implement intensive strategies regarding diet, exercise, etc. And if that’s not enough, you need to consider using drugs or even bariatric surgery,” said Dr. Mediano.
“If there’s no one definitive treatment, we highly recommend that all patients implement hygienic-dietary measures and then assess all the therapeutic options. In some cases, several can be in place at the same time,” she said. Various medical specialists can play a role in the treatment of OSA, said Dr. Mediano. They include otolaryngologists, maxillofacial surgeons, dentists, cardiologists, and neurophysiologists, to mention a few.
A website has been created to explain the ICD. There, visitors will be able to find the most up-to-date version of the ICD as well as related information, news, and materials.
A version of this article appeared on Medscape.com. This article was translated from Univadis Spain.
The Spanish Society of Pulmonology and Thoracic Surgery (SEPAR) has issued a new international consensus document (ICD) on obstructive sleep apnea (OSA). The objective is to improve the diagnosis and treatment of one of the most prevalent sleep disorders.
It provides a series of clinical guidelines to help health care professionals make the best decisions for adult patients with OSA. Notably, the authors propose changing the name from sleep apnea syndrome. In recommending the term OSA, they reintroduce the term “obstructive” – to differentiate the disorder from central sleep apnea – and remove the outdated word “syndrome.”
“The definition has also been changed, as it was a bit vague and difficult to understand. And there are significant changes to the treatment and to the diagnostic algorithms – one for primary care and another for sleep units,” Olga Mediano, MD, said in an interview. She is a SEPAR pulmonologist, first author of the ICD, and the coordinator of SEPAR 2022 Year of Intermediate Respiratory Care Units.
Diagnosis in primary care
The ICD indicates that all levels of care must be involved in the management of OSA, a condition in which complete or partial upper airway blockage occurs during sleep, causing the individual to stop breathing for a few seconds. These pauses, which produce hypoxia and sleep fragmentation, increase the risk of workplace and traffic accidents, affect cardiovascular health, and contribute to uncontrolled or resistant hypertension.
The recommendations in the ICD aim at increasing the role of primary care physicians so as to reduce underdiagnosis of OSA in primary care. “The vast majority of patients with OSA haven’t been diagnosed. In fact, those whom we have diagnosed are the patients with the most severe cases – in other words, patients who present with the most symptoms,” said Dr. Mediano. She explained that many patients with OSA don’t consider it a medical condition, so they do not go to the doctor.
“The other big problem is that, before, there was a preconceived notion of the typical OSA patient: A middle-aged obese man who’s fallen asleep in the waiting room. However, there are many other profiles: thin build, women. ... Sleep has a heterogeneous profile, and all profiles need to be known,” said Dr. Mediano. The difficulties in carrying out a sleep study with the various patients are an added problem that the new consensus document also seeks to resolve. “The step we’ve taken is to involve the primary care physician in super-simplified studies to reach more people,” she said. For this, the primary care site must work in coordination with a sleep unit.
“In the super-simplified study, the patient is given a machine to use at home; they hook themselves up to it when they go to sleep. This machine records the number of apnea episodes the patient experiences during the night, as well as the oxygen level. The next day, the patient returns the machine. The data are downloaded to a computer. The software analyzes the breathing pauses that the patient had during the night and automatically gives a series of values that, if very pronounced, as the document indicates, would lead to a diagnosis of OSA. Once diagnosed by a primary care physician, the patient is referred to a sleep unit where treatment can then be assessed,” explained Dr. Mediano.
Different treatments
The new ICD’s approach incorporates therapeutic alternatives as well. Until now, many consensus documents and clinical guidelines have focused on continuous positive airway pressure therapy, in which a machine delivers continuous airflow to help keep the patient’s airway open and unobstructed during sleep. Some guidelines recommend its use, and others do not. “However, in this new document, management of the patient is much more multidisciplinary. What changes, with respect to the treatment, is the philosophy. It’s not one single type of treatment; rather, other therapeutic options are kept in mind,” said Dr. Mediano.
First, treatment of reversible causes of OSA must be offered. The conditions that lead to OSA and that can be reversed are addressed. These include overweight and obesity; heavy drinking; tonsillar hypertrophy, or severe dental or facial alterations, for which surgery can be considered; and gastroesophageal reflux or hypothyroidism, both of which can be treated. “For example, the leading cause of sleep apnea is obesity. If we can get the patient to lose weight, that can end up making the OSA go away. What does the document say? Well, you have to try to implement intensive strategies regarding diet, exercise, etc. And if that’s not enough, you need to consider using drugs or even bariatric surgery,” said Dr. Mediano.
“If there’s no one definitive treatment, we highly recommend that all patients implement hygienic-dietary measures and then assess all the therapeutic options. In some cases, several can be in place at the same time,” she said. Various medical specialists can play a role in the treatment of OSA, said Dr. Mediano. They include otolaryngologists, maxillofacial surgeons, dentists, cardiologists, and neurophysiologists, to mention a few.
A website has been created to explain the ICD. There, visitors will be able to find the most up-to-date version of the ICD as well as related information, news, and materials.
A version of this article appeared on Medscape.com. This article was translated from Univadis Spain.
First drug therapy approved for childhood GVHD
Specifically, the indication is for pediatric patients with cGVHD who have already been treated with one or more lines of systemic therapy. The manufacturers have also launched a new oral suspension formulation, in addition to capsules and tablets, which were already available.
Ibrutinib is already approved for use in adults with cGVHD.
The drug is also approved for use in several blood cancers, including chronic lymphocytic leukemia, mantle cell lymphoma, and Waldenström’s macroglobulinemia. All these approvals are for adult patients.
This is the first pediatric indication for the product and is “incredibly meaningful,” said Gauri Sunkersett, DO, associate medical director at AbbVie, which markets the drug together with Jansen. “As a pediatric oncologist, when my patients describe the physical pain they experience from simply hugging their parents, due to their cGVHD, the importance of researching alternative treatment options in this patient population is further validated.”
These children have already been through a lot, having been diagnosed with a leukemia or lymphoma and then undergoing chemotherapy and/or radiotherapy for a stem cell transplant. Just over half (52%-65%) of children who receive allogeneic transplants go on to develop cGVHD, in which the donor bone marrow or stem cells attack the recipient.
“Imagine going through a transplant and then being told you have a moderate to severe chronic disease that can sometimes also be life-threatening,” commented Paul A. Carpenter, MD, attending physician at Seattle Children’s Hospital. “If these children were between 1 and 12 and didn’t respond to steroid treatment, we didn’t have any rigorously studied treatment options – until now.”
The new indication was approved by the U.S. Food and Drug Administration on the basis of results from the iMAGINE trial, for which Dr. Carpenter was a principal investigator.
The phase 1/2 iMAGINE trial was an open-label, multicenter, single-arm trial conducted with 47 patients (mean age, 13 years; range, 1-19 years) with relapsed/refractory cGVHD who had received at least one prior systemic therapy. Ibrutinib was given at a dose of 420 mg orally once daily to patients aged 12 and older and at a dose of 240 mg/m2 orally once daily to patients who were younger than 12 years.
The overall response rate through week 25 was 60% (confidence interval, 95%, 44%-74%). The median duration of response was 5.3 months (95% CI, 2.8-8.8).
The safety profile was consistent with the established profile for ibrutinib. Observed adverse events in pediatric patients were consistent with those observed in adult patients with moderate to severe cGVHD, the companies noted.
The FDA noted that the most common (≥ 20%) adverse reactions, including laboratory abnormalities, were anemia, musculoskeletal pain, pyrexia, diarrhea, pneumonia, abdominal pain, stomatitis, thrombocytopenia, and headache.
Full prescribing information for ibrutinib is available here.
A version of this article first appeared on Medscape.com.
Specifically, the indication is for pediatric patients with cGVHD who have already been treated with one or more lines of systemic therapy. The manufacturers have also launched a new oral suspension formulation, in addition to capsules and tablets, which were already available.
Ibrutinib is already approved for use in adults with cGVHD.
The drug is also approved for use in several blood cancers, including chronic lymphocytic leukemia, mantle cell lymphoma, and Waldenström’s macroglobulinemia. All these approvals are for adult patients.
This is the first pediatric indication for the product and is “incredibly meaningful,” said Gauri Sunkersett, DO, associate medical director at AbbVie, which markets the drug together with Jansen. “As a pediatric oncologist, when my patients describe the physical pain they experience from simply hugging their parents, due to their cGVHD, the importance of researching alternative treatment options in this patient population is further validated.”
These children have already been through a lot, having been diagnosed with a leukemia or lymphoma and then undergoing chemotherapy and/or radiotherapy for a stem cell transplant. Just over half (52%-65%) of children who receive allogeneic transplants go on to develop cGVHD, in which the donor bone marrow or stem cells attack the recipient.
“Imagine going through a transplant and then being told you have a moderate to severe chronic disease that can sometimes also be life-threatening,” commented Paul A. Carpenter, MD, attending physician at Seattle Children’s Hospital. “If these children were between 1 and 12 and didn’t respond to steroid treatment, we didn’t have any rigorously studied treatment options – until now.”
The new indication was approved by the U.S. Food and Drug Administration on the basis of results from the iMAGINE trial, for which Dr. Carpenter was a principal investigator.
The phase 1/2 iMAGINE trial was an open-label, multicenter, single-arm trial conducted with 47 patients (mean age, 13 years; range, 1-19 years) with relapsed/refractory cGVHD who had received at least one prior systemic therapy. Ibrutinib was given at a dose of 420 mg orally once daily to patients aged 12 and older and at a dose of 240 mg/m2 orally once daily to patients who were younger than 12 years.
The overall response rate through week 25 was 60% (confidence interval, 95%, 44%-74%). The median duration of response was 5.3 months (95% CI, 2.8-8.8).
The safety profile was consistent with the established profile for ibrutinib. Observed adverse events in pediatric patients were consistent with those observed in adult patients with moderate to severe cGVHD, the companies noted.
The FDA noted that the most common (≥ 20%) adverse reactions, including laboratory abnormalities, were anemia, musculoskeletal pain, pyrexia, diarrhea, pneumonia, abdominal pain, stomatitis, thrombocytopenia, and headache.
Full prescribing information for ibrutinib is available here.
A version of this article first appeared on Medscape.com.
Specifically, the indication is for pediatric patients with cGVHD who have already been treated with one or more lines of systemic therapy. The manufacturers have also launched a new oral suspension formulation, in addition to capsules and tablets, which were already available.
Ibrutinib is already approved for use in adults with cGVHD.
The drug is also approved for use in several blood cancers, including chronic lymphocytic leukemia, mantle cell lymphoma, and Waldenström’s macroglobulinemia. All these approvals are for adult patients.
This is the first pediatric indication for the product and is “incredibly meaningful,” said Gauri Sunkersett, DO, associate medical director at AbbVie, which markets the drug together with Jansen. “As a pediatric oncologist, when my patients describe the physical pain they experience from simply hugging their parents, due to their cGVHD, the importance of researching alternative treatment options in this patient population is further validated.”
These children have already been through a lot, having been diagnosed with a leukemia or lymphoma and then undergoing chemotherapy and/or radiotherapy for a stem cell transplant. Just over half (52%-65%) of children who receive allogeneic transplants go on to develop cGVHD, in which the donor bone marrow or stem cells attack the recipient.
“Imagine going through a transplant and then being told you have a moderate to severe chronic disease that can sometimes also be life-threatening,” commented Paul A. Carpenter, MD, attending physician at Seattle Children’s Hospital. “If these children were between 1 and 12 and didn’t respond to steroid treatment, we didn’t have any rigorously studied treatment options – until now.”
The new indication was approved by the U.S. Food and Drug Administration on the basis of results from the iMAGINE trial, for which Dr. Carpenter was a principal investigator.
The phase 1/2 iMAGINE trial was an open-label, multicenter, single-arm trial conducted with 47 patients (mean age, 13 years; range, 1-19 years) with relapsed/refractory cGVHD who had received at least one prior systemic therapy. Ibrutinib was given at a dose of 420 mg orally once daily to patients aged 12 and older and at a dose of 240 mg/m2 orally once daily to patients who were younger than 12 years.
The overall response rate through week 25 was 60% (confidence interval, 95%, 44%-74%). The median duration of response was 5.3 months (95% CI, 2.8-8.8).
The safety profile was consistent with the established profile for ibrutinib. Observed adverse events in pediatric patients were consistent with those observed in adult patients with moderate to severe cGVHD, the companies noted.
The FDA noted that the most common (≥ 20%) adverse reactions, including laboratory abnormalities, were anemia, musculoskeletal pain, pyrexia, diarrhea, pneumonia, abdominal pain, stomatitis, thrombocytopenia, and headache.
Full prescribing information for ibrutinib is available here.
A version of this article first appeared on Medscape.com.
Hospitalized COVID-19 patients with GI symptoms have worse outcomes
Patients with COVID-19 who experience gastrointestinal symptoms have overall worse in-hospital complications but less cardiomyopathy and mortality, according to a new study.
About 20% of COVID-19 patients experience gastrointestinal symptoms, such as abdominal pain, diarrhea, nausea, and vomiting, which clinicians should consider when treating their hospitalized patients, wrote researchers led by Nikita Patil, MD, a hospitalist at Nash General Hospital–UNC Nash Healthcare in Rocky Mount, N.C., in Gastro Hep Advances.

“It’s important to know that certain complications are higher in people with GI symptoms,” she said in an interview. “Even without an increased risk of death, there are many problems that affect quality of life and lead to people not being able to do the things they were able to do before.”
Dr. Patil and colleagues analyzed the association of GI symptoms with adverse outcomes in 100,902 patients from the Cerner Real-World Data COVID-19 Database, which included hospital encounters and ED visits for COVID-19 between December 2019 to November 2020; the data were taken from EMRs at centers with which Cerner has a data use agreement. They also looked at factors associated with poor outcomes such as acute respiratory distress syndrome, sepsis, and ventilator requirement or oxygen dependence.
The average age of the patients was 52, and a higher proportion of patients with GI symptoms were 50 and older. Of those with GI symptoms, 54.5% were women. Overall, patients with GI symptoms were more likely to have higher Charlson Comorbidity Index scores and have comorbidities such as acute liver failure, gastroesophageal reflux disease, GI malignancy, and inflammatory bowel disease.
The research team found that COVID-19 patients with GI symptoms were more likely to have acute respiratory distress syndrome (odds ratio, 1.20; 95% confidence interval, 1.11-1.29), sepsis (OR, 1.19; 95% CI, 1.14-1.24), acute kidney injury (OR, 1.30; 95% CI, 1.24-1.36), venous thromboembolism (OR, 1.36; 95% CI, 1.22-1.52), and GI bleeding (OR 1.62; 95% CI, 1.47-1.79), as compared with COVID-19 patients without GI symptoms (P < .0001 for all comparisons). At the same time, those with GI symptoms were less likely to experience cardiomyopathy (OR, 0.87; 95% CI, 0.77-0.99; P = .027), respiratory failure (OR, 0.92; 95% CI, 0.88-0.95; P < .0001), or death (OR, 0.71; 95% CI, 0.67-0.75; P < .0001).
GI bleed was the most common GI complication, found among 2% of all patients, and was more likely in patients with GI symptoms than in those without (3.5% vs. 1.6%). Intestinal ischemia, pancreatitis, acute liver injury, and intestinal pseudo-obstruction weren’t associated with GI symptoms.
Among the 19,915 patients with GI symptoms, older age, higher Charlson Comorbidity Index scores, use of proton pump inhibitors, and use of H2 receptor antagonists were associated with higher mortality, acute respiratory distress syndrome, sepsis, and ventilator or oxygen requirement. Men with GI symptoms also had a higher risk of mortality, acute respiratory distress syndrome, and sepsis.
In particular, proton pump inhibitor use was associated with more than twice the risk of acute respiratory distress syndrome (OR, 2.19; 95% CI, 1.32-1.66; P < .0001). Similarly, H2 receptor antagonist use was associated with higher likelihood of death (OR, 1.78; 95% CI, 1.57-2.02), as well as more than three times the risk of acute respiratory distress syndrome (OR, 3.75; 95% CI, 3.29-4.28), more than twice the risk of sepsis (OR, 2.50; 95% CI, 2.28-2.73), and nearly twice the risk of ventilator or oxygen dependence (OR, 1.97; 95% CI, 1.68-2.30) (P < .0001 for all).
The findings could guide risk stratification, prognosis, and treatment decisions in COVID-19 patients with GI symptoms, as well as inform future research focused on risk mitigation and improvement of COVID-19 outcomes, Dr. Patil said.
“The protocols for COVID-19 treatment have changed over the past 2 years with blood thinners and steroids,” she said. “Although we likely can’t avoid anti-reflux medicines entirely, it’s something we need to be cognizant of and look out for in our hospitalized patients.”
One study limitation was its inclusion of only inpatient or ED encounters and, therefore, omission of those treated at home; this confers bias toward those with more aggressive disease, according to the authors.
The authors reported no grant support or funding sources for this study. One author declared grant support and consultant fees from several companies, including some medical and pharmaceutical companies, which were unrelated to this research. Dr. Patil reported no disclosures.
This article was updated Aug. 26, 2022.
Patients with COVID-19 who experience gastrointestinal symptoms have overall worse in-hospital complications but less cardiomyopathy and mortality, according to a new study.
About 20% of COVID-19 patients experience gastrointestinal symptoms, such as abdominal pain, diarrhea, nausea, and vomiting, which clinicians should consider when treating their hospitalized patients, wrote researchers led by Nikita Patil, MD, a hospitalist at Nash General Hospital–UNC Nash Healthcare in Rocky Mount, N.C., in Gastro Hep Advances.
“It’s important to know that certain complications are higher in people with GI symptoms,” she said in an interview. “Even without an increased risk of death, there are many problems that affect quality of life and lead to people not being able to do the things they were able to do before.”
Dr. Patil and colleagues analyzed the association of GI symptoms with adverse outcomes in 100,902 patients from the Cerner Real-World Data COVID-19 Database, which included hospital encounters and ED visits for COVID-19 between December 2019 to November 2020; the data were taken from EMRs at centers with which Cerner has a data use agreement. They also looked at factors associated with poor outcomes such as acute respiratory distress syndrome, sepsis, and ventilator requirement or oxygen dependence.
The average age of the patients was 52, and a higher proportion of patients with GI symptoms were 50 and older. Of those with GI symptoms, 54.5% were women. Overall, patients with GI symptoms were more likely to have higher Charlson Comorbidity Index scores and have comorbidities such as acute liver failure, gastroesophageal reflux disease, GI malignancy, and inflammatory bowel disease.
The research team found that COVID-19 patients with GI symptoms were more likely to have acute respiratory distress syndrome (odds ratio, 1.20; 95% confidence interval, 1.11-1.29), sepsis (OR, 1.19; 95% CI, 1.14-1.24), acute kidney injury (OR, 1.30; 95% CI, 1.24-1.36), venous thromboembolism (OR, 1.36; 95% CI, 1.22-1.52), and GI bleeding (OR 1.62; 95% CI, 1.47-1.79), as compared with COVID-19 patients without GI symptoms (P < .0001 for all comparisons). At the same time, those with GI symptoms were less likely to experience cardiomyopathy (OR, 0.87; 95% CI, 0.77-0.99; P = .027), respiratory failure (OR, 0.92; 95% CI, 0.88-0.95; P < .0001), or death (OR, 0.71; 95% CI, 0.67-0.75; P < .0001).
GI bleed was the most common GI complication, found among 2% of all patients, and was more likely in patients with GI symptoms than in those without (3.5% vs. 1.6%). Intestinal ischemia, pancreatitis, acute liver injury, and intestinal pseudo-obstruction weren’t associated with GI symptoms.
Among the 19,915 patients with GI symptoms, older age, higher Charlson Comorbidity Index scores, use of proton pump inhibitors, and use of H2 receptor antagonists were associated with higher mortality, acute respiratory distress syndrome, sepsis, and ventilator or oxygen requirement. Men with GI symptoms also had a higher risk of mortality, acute respiratory distress syndrome, and sepsis.
In particular, proton pump inhibitor use was associated with more than twice the risk of acute respiratory distress syndrome (OR, 2.19; 95% CI, 1.32-1.66; P < .0001). Similarly, H2 receptor antagonist use was associated with higher likelihood of death (OR, 1.78; 95% CI, 1.57-2.02), as well as more than three times the risk of acute respiratory distress syndrome (OR, 3.75; 95% CI, 3.29-4.28), more than twice the risk of sepsis (OR, 2.50; 95% CI, 2.28-2.73), and nearly twice the risk of ventilator or oxygen dependence (OR, 1.97; 95% CI, 1.68-2.30) (P < .0001 for all).
The findings could guide risk stratification, prognosis, and treatment decisions in COVID-19 patients with GI symptoms, as well as inform future research focused on risk mitigation and improvement of COVID-19 outcomes, Dr. Patil said.
“The protocols for COVID-19 treatment have changed over the past 2 years with blood thinners and steroids,” she said. “Although we likely can’t avoid anti-reflux medicines entirely, it’s something we need to be cognizant of and look out for in our hospitalized patients.”
One study limitation was its inclusion of only inpatient or ED encounters and, therefore, omission of those treated at home; this confers bias toward those with more aggressive disease, according to the authors.
The authors reported no grant support or funding sources for this study. One author declared grant support and consultant fees from several companies, including some medical and pharmaceutical companies, which were unrelated to this research. Dr. Patil reported no disclosures.
This article was updated Aug. 26, 2022.
Patients with COVID-19 who experience gastrointestinal symptoms have overall worse in-hospital complications but less cardiomyopathy and mortality, according to a new study.
About 20% of COVID-19 patients experience gastrointestinal symptoms, such as abdominal pain, diarrhea, nausea, and vomiting, which clinicians should consider when treating their hospitalized patients, wrote researchers led by Nikita Patil, MD, a hospitalist at Nash General Hospital–UNC Nash Healthcare in Rocky Mount, N.C., in Gastro Hep Advances.
“It’s important to know that certain complications are higher in people with GI symptoms,” she said in an interview. “Even without an increased risk of death, there are many problems that affect quality of life and lead to people not being able to do the things they were able to do before.”
Dr. Patil and colleagues analyzed the association of GI symptoms with adverse outcomes in 100,902 patients from the Cerner Real-World Data COVID-19 Database, which included hospital encounters and ED visits for COVID-19 between December 2019 to November 2020; the data were taken from EMRs at centers with which Cerner has a data use agreement. They also looked at factors associated with poor outcomes such as acute respiratory distress syndrome, sepsis, and ventilator requirement or oxygen dependence.
The average age of the patients was 52, and a higher proportion of patients with GI symptoms were 50 and older. Of those with GI symptoms, 54.5% were women. Overall, patients with GI symptoms were more likely to have higher Charlson Comorbidity Index scores and have comorbidities such as acute liver failure, gastroesophageal reflux disease, GI malignancy, and inflammatory bowel disease.
The research team found that COVID-19 patients with GI symptoms were more likely to have acute respiratory distress syndrome (odds ratio, 1.20; 95% confidence interval, 1.11-1.29), sepsis (OR, 1.19; 95% CI, 1.14-1.24), acute kidney injury (OR, 1.30; 95% CI, 1.24-1.36), venous thromboembolism (OR, 1.36; 95% CI, 1.22-1.52), and GI bleeding (OR 1.62; 95% CI, 1.47-1.79), as compared with COVID-19 patients without GI symptoms (P < .0001 for all comparisons). At the same time, those with GI symptoms were less likely to experience cardiomyopathy (OR, 0.87; 95% CI, 0.77-0.99; P = .027), respiratory failure (OR, 0.92; 95% CI, 0.88-0.95; P < .0001), or death (OR, 0.71; 95% CI, 0.67-0.75; P < .0001).
GI bleed was the most common GI complication, found among 2% of all patients, and was more likely in patients with GI symptoms than in those without (3.5% vs. 1.6%). Intestinal ischemia, pancreatitis, acute liver injury, and intestinal pseudo-obstruction weren’t associated with GI symptoms.
Among the 19,915 patients with GI symptoms, older age, higher Charlson Comorbidity Index scores, use of proton pump inhibitors, and use of H2 receptor antagonists were associated with higher mortality, acute respiratory distress syndrome, sepsis, and ventilator or oxygen requirement. Men with GI symptoms also had a higher risk of mortality, acute respiratory distress syndrome, and sepsis.
In particular, proton pump inhibitor use was associated with more than twice the risk of acute respiratory distress syndrome (OR, 2.19; 95% CI, 1.32-1.66; P < .0001). Similarly, H2 receptor antagonist use was associated with higher likelihood of death (OR, 1.78; 95% CI, 1.57-2.02), as well as more than three times the risk of acute respiratory distress syndrome (OR, 3.75; 95% CI, 3.29-4.28), more than twice the risk of sepsis (OR, 2.50; 95% CI, 2.28-2.73), and nearly twice the risk of ventilator or oxygen dependence (OR, 1.97; 95% CI, 1.68-2.30) (P < .0001 for all).
The findings could guide risk stratification, prognosis, and treatment decisions in COVID-19 patients with GI symptoms, as well as inform future research focused on risk mitigation and improvement of COVID-19 outcomes, Dr. Patil said.
“The protocols for COVID-19 treatment have changed over the past 2 years with blood thinners and steroids,” she said. “Although we likely can’t avoid anti-reflux medicines entirely, it’s something we need to be cognizant of and look out for in our hospitalized patients.”
One study limitation was its inclusion of only inpatient or ED encounters and, therefore, omission of those treated at home; this confers bias toward those with more aggressive disease, according to the authors.
The authors reported no grant support or funding sources for this study. One author declared grant support and consultant fees from several companies, including some medical and pharmaceutical companies, which were unrelated to this research. Dr. Patil reported no disclosures.
This article was updated Aug. 26, 2022.
FROM GASTRO HEP ADVANCES
Early menopause linked with increased risk of heart problems
SEOUL, South Korea – Menopause before age 40 is associated with elevated risk of heart failure and atrial fibrillation, according to a study published in European Heart Journal, from the European Society of Cardiology (ESC). The study of more than 1.4 million women revealed that the younger the age at menopause, the higher the risk of heart failure and atrial fibrillation.
“Women with premature menopause should be aware that they may be more likely to develop heart failure or atrial fibrillation than their peers,” said study author Ga Eun Nam, MD, PhD, of Korea University College of Medicine, Seoul. “This may be good motivation to improve lifestyle habits known to be linked with heart disease, such as quitting smoking and exercising.”
Cardiovascular disease typically occurs up to 10 years later in women than men. Premenopausal women are thought to benefit from estrogen’s protective effect on the cardiovascular system. The cessation of menstruation and subsequent decline of estrogen levels may make women more vulnerable to cardiovascular disease.
A national population
Premature menopause affects 1% of women younger than 40 years, the ESC press release stated. Prior studies have found a link between premature (before age 40 years) and early (before age 45 years) menopause and cardiovascular disease overall, but the evidence for heart failure or atrial fibrillation alone is limited. This study examined the associations between premature menopause, age at menopause, and incident heart failure and atrial fibrillation. Data were obtained from the Korean National Health Insurance System (NHIS), which provides health screening at least every 2 years and includes 97% of the population.
The study included 1,401,175 postmenopausal women aged 30 years and older who completed the NHIS health checkup in 2009. Participants were monitored until the end of 2018 for new-onset heart failure and atrial fibrillation. Information was collected on demographics, health behaviors, and reproductive factors, including age at menopause and use of hormone replacement therapy (HRT). Age at menopause was split into four categories: younger than 40 years, 40-44 years, 45-49 years, and 50 years or older. Premature menopause was defined as having the final menstrual period before age 40 years.
Some 28,111 (2%) participants had a history of premature menopause. For these women, the average age at menopause was 36.7 years. The average age at study enrollment for women with and for those without a history of premature menopause was 60 and 61.5 years, respectively. During an average follow-up of 9.1 years, 42,699 (3.0%) developed heart failure, and 44,834 (3.2%) developed atrial fibrillation.
The researchers analyzed the association between history of premature menopause and incident heart failure and atrial fibrillation after adjusting for age, smoking, alcohol use, physical activity, income, body mass index, hypertension, type 2 diabetes, dyslipidemia, chronic kidney disease, coronary heart disease, HRT, and age at menarche. Women who experienced premature menopause had a 33% higher risk for heart failure and 9% higher risk for atrial fibrillation, compared with those who did not.
Reproductive history
The researchers then analyzed the associations between age at menopause and incidence of heart failure and atrial fibrillation after adjusting for the same factors as in the previous analyses. The risk for incident heart failure increased as the age at menopause decreased. Compared with women aged 50 years and older at menopause, those aged 45-49 years, 40-44 years, and younger than 40 years at menopause had 11%, 23%, and 39% greater risk for incident heart failure, respectively. Similarly, the risk for incident atrial fibrillation increased as the age at menopause decreased; the risk was 4%, 10%, and 11% higher for those aged 45-49 years, 40-44 years, and younger than 40 years at menopause, respectively, compared with women aged 50 years and older at menopause.
The authors said that several factors may explain the associations between menopausal age, heart failure, and atrial fibrillation, such as the drop in estrogen levels and changes in body fat distribution.
Dr. Nam concluded, “The misconception that heart disease primarily affects men has meant that sex-specific risk factors have been largely ignored. Evidence is growing that undergoing menopause before the age of 40 years may increase the likelihood of heart disease later in life. Our study indicates that reproductive history should be routinely considered in addition to traditional risk factors such as smoking when evaluating the future likelihood of heart failure and atrial fibrillation.”
A version of this article appeared on Medscape.com. This article was translated from the Medscape French edition.
SEOUL, South Korea – Menopause before age 40 is associated with elevated risk of heart failure and atrial fibrillation, according to a study published in European Heart Journal, from the European Society of Cardiology (ESC). The study of more than 1.4 million women revealed that the younger the age at menopause, the higher the risk of heart failure and atrial fibrillation.
“Women with premature menopause should be aware that they may be more likely to develop heart failure or atrial fibrillation than their peers,” said study author Ga Eun Nam, MD, PhD, of Korea University College of Medicine, Seoul. “This may be good motivation to improve lifestyle habits known to be linked with heart disease, such as quitting smoking and exercising.”
Cardiovascular disease typically occurs up to 10 years later in women than men. Premenopausal women are thought to benefit from estrogen’s protective effect on the cardiovascular system. The cessation of menstruation and subsequent decline of estrogen levels may make women more vulnerable to cardiovascular disease.
A national population
Premature menopause affects 1% of women younger than 40 years, the ESC press release stated. Prior studies have found a link between premature (before age 40 years) and early (before age 45 years) menopause and cardiovascular disease overall, but the evidence for heart failure or atrial fibrillation alone is limited. This study examined the associations between premature menopause, age at menopause, and incident heart failure and atrial fibrillation. Data were obtained from the Korean National Health Insurance System (NHIS), which provides health screening at least every 2 years and includes 97% of the population.
The study included 1,401,175 postmenopausal women aged 30 years and older who completed the NHIS health checkup in 2009. Participants were monitored until the end of 2018 for new-onset heart failure and atrial fibrillation. Information was collected on demographics, health behaviors, and reproductive factors, including age at menopause and use of hormone replacement therapy (HRT). Age at menopause was split into four categories: younger than 40 years, 40-44 years, 45-49 years, and 50 years or older. Premature menopause was defined as having the final menstrual period before age 40 years.
Some 28,111 (2%) participants had a history of premature menopause. For these women, the average age at menopause was 36.7 years. The average age at study enrollment for women with and for those without a history of premature menopause was 60 and 61.5 years, respectively. During an average follow-up of 9.1 years, 42,699 (3.0%) developed heart failure, and 44,834 (3.2%) developed atrial fibrillation.
The researchers analyzed the association between history of premature menopause and incident heart failure and atrial fibrillation after adjusting for age, smoking, alcohol use, physical activity, income, body mass index, hypertension, type 2 diabetes, dyslipidemia, chronic kidney disease, coronary heart disease, HRT, and age at menarche. Women who experienced premature menopause had a 33% higher risk for heart failure and 9% higher risk for atrial fibrillation, compared with those who did not.
Reproductive history
The researchers then analyzed the associations between age at menopause and incidence of heart failure and atrial fibrillation after adjusting for the same factors as in the previous analyses. The risk for incident heart failure increased as the age at menopause decreased. Compared with women aged 50 years and older at menopause, those aged 45-49 years, 40-44 years, and younger than 40 years at menopause had 11%, 23%, and 39% greater risk for incident heart failure, respectively. Similarly, the risk for incident atrial fibrillation increased as the age at menopause decreased; the risk was 4%, 10%, and 11% higher for those aged 45-49 years, 40-44 years, and younger than 40 years at menopause, respectively, compared with women aged 50 years and older at menopause.
The authors said that several factors may explain the associations between menopausal age, heart failure, and atrial fibrillation, such as the drop in estrogen levels and changes in body fat distribution.
Dr. Nam concluded, “The misconception that heart disease primarily affects men has meant that sex-specific risk factors have been largely ignored. Evidence is growing that undergoing menopause before the age of 40 years may increase the likelihood of heart disease later in life. Our study indicates that reproductive history should be routinely considered in addition to traditional risk factors such as smoking when evaluating the future likelihood of heart failure and atrial fibrillation.”
A version of this article appeared on Medscape.com. This article was translated from the Medscape French edition.
SEOUL, South Korea – Menopause before age 40 is associated with elevated risk of heart failure and atrial fibrillation, according to a study published in European Heart Journal, from the European Society of Cardiology (ESC). The study of more than 1.4 million women revealed that the younger the age at menopause, the higher the risk of heart failure and atrial fibrillation.
“Women with premature menopause should be aware that they may be more likely to develop heart failure or atrial fibrillation than their peers,” said study author Ga Eun Nam, MD, PhD, of Korea University College of Medicine, Seoul. “This may be good motivation to improve lifestyle habits known to be linked with heart disease, such as quitting smoking and exercising.”
Cardiovascular disease typically occurs up to 10 years later in women than men. Premenopausal women are thought to benefit from estrogen’s protective effect on the cardiovascular system. The cessation of menstruation and subsequent decline of estrogen levels may make women more vulnerable to cardiovascular disease.
A national population
Premature menopause affects 1% of women younger than 40 years, the ESC press release stated. Prior studies have found a link between premature (before age 40 years) and early (before age 45 years) menopause and cardiovascular disease overall, but the evidence for heart failure or atrial fibrillation alone is limited. This study examined the associations between premature menopause, age at menopause, and incident heart failure and atrial fibrillation. Data were obtained from the Korean National Health Insurance System (NHIS), which provides health screening at least every 2 years and includes 97% of the population.
The study included 1,401,175 postmenopausal women aged 30 years and older who completed the NHIS health checkup in 2009. Participants were monitored until the end of 2018 for new-onset heart failure and atrial fibrillation. Information was collected on demographics, health behaviors, and reproductive factors, including age at menopause and use of hormone replacement therapy (HRT). Age at menopause was split into four categories: younger than 40 years, 40-44 years, 45-49 years, and 50 years or older. Premature menopause was defined as having the final menstrual period before age 40 years.
Some 28,111 (2%) participants had a history of premature menopause. For these women, the average age at menopause was 36.7 years. The average age at study enrollment for women with and for those without a history of premature menopause was 60 and 61.5 years, respectively. During an average follow-up of 9.1 years, 42,699 (3.0%) developed heart failure, and 44,834 (3.2%) developed atrial fibrillation.
The researchers analyzed the association between history of premature menopause and incident heart failure and atrial fibrillation after adjusting for age, smoking, alcohol use, physical activity, income, body mass index, hypertension, type 2 diabetes, dyslipidemia, chronic kidney disease, coronary heart disease, HRT, and age at menarche. Women who experienced premature menopause had a 33% higher risk for heart failure and 9% higher risk for atrial fibrillation, compared with those who did not.
Reproductive history
The researchers then analyzed the associations between age at menopause and incidence of heart failure and atrial fibrillation after adjusting for the same factors as in the previous analyses. The risk for incident heart failure increased as the age at menopause decreased. Compared with women aged 50 years and older at menopause, those aged 45-49 years, 40-44 years, and younger than 40 years at menopause had 11%, 23%, and 39% greater risk for incident heart failure, respectively. Similarly, the risk for incident atrial fibrillation increased as the age at menopause decreased; the risk was 4%, 10%, and 11% higher for those aged 45-49 years, 40-44 years, and younger than 40 years at menopause, respectively, compared with women aged 50 years and older at menopause.
The authors said that several factors may explain the associations between menopausal age, heart failure, and atrial fibrillation, such as the drop in estrogen levels and changes in body fat distribution.
Dr. Nam concluded, “The misconception that heart disease primarily affects men has meant that sex-specific risk factors have been largely ignored. Evidence is growing that undergoing menopause before the age of 40 years may increase the likelihood of heart disease later in life. Our study indicates that reproductive history should be routinely considered in addition to traditional risk factors such as smoking when evaluating the future likelihood of heart failure and atrial fibrillation.”
A version of this article appeared on Medscape.com. This article was translated from the Medscape French edition.
Monkeypox in children and women remains rare, CDC data show
Monkeypox cases in the United States continue to be rare in children younger than 15, women, and in individuals older than 60, according to new data released by the Centers for Disease Control and Prevention. Men aged 26-40 make up the highest proportion of cases.
The age distribution of cases is similar to those of sexually transmitted infections, said Monica Gandhi, MD, MPH, associate chief of the division of HIV, infectious diseases, and global medicine at the University of California, San Francisco. It is most common in younger to middle-aged age groups, and less common in children and older individuals. As of Aug. 21, only 17 children younger than 15 have been diagnosed with monkeypox in the United States, and women make up fewer than 1.5% of cases.
“This data should be very reassuring to parents and to children going to back to school,” Dr. Gandhi said in an interview. After 3 months of monitoring the virus, the data suggest that monkeypox is primarily spreading in networks of men who have sex with men (MSM) through sexual activity, “and that isn’t something we worry about with school-spread illness.”
In addition to the reassuring data about children and monkeypox, the CDC released laboratory testing data, a behavioral survey of MSM, patient data on the antiviral medication tecovirimat (TPOXX), and other case demographics and symptoms.
Though the number of positive monkeypox tests have continued to rise, the test-positivity rates have declined over the past month, data show. Since July 16, the positivity rate has dipped from 54% to 23%. This trend is likely because of an increase in testing availability, said Randolph Hubach, PhD, MPH, the director of the Sexual Health Research Lab at Purdue University, West Lafayette, Ind.
“We also saw this with COVID early on with testing: it was really limited to folks who were symptomatic,” he said in an interview . “As testing ramped up in accessibility, you had a lot more negative results, but because testing was more widely available, you were able to capture more positive results.”
The data also show that case numbers continue to grow in the United States, whereas in other countries that identified cases before the United States – Spain, the United Kingdom, and France, for example – cases have been leveling off, noted Dr. Gandhi.
The CDC also shared responses from a survey of gay, bisexual, and other MSM conducted from Aug. 5-15, about how they have changed their sexual behaviors in response to the monkeypox outbreak. Half of respondents reported reduced one-time sexual encounters, 49% reported reducing sex with partners met on dating apps or at sex venues, and 48% reported reducing their number of sex partners. These responses are “heartening to see,” Dr. Gandhi said, and shows that individuals are taking proactive steps to reduce their potential exposure risk to monkeypox.
More detailed demographic data showed that Black, Hispanic, or Latinx individuals make up an increasing proportion of cases in the United States. In May, 71% of people with reported monkeypox infection were White and 29% were Black. For the week of August 8-14, about a third (31%) of monkeypox cases were in White people, 32% were in Hispanic or Latinx people, and 33% were in Black people.
The most common symptoms of monkeypox were rash (98.6%), malaise (72.7%), fever (72.1%), and chills (68.9%). Rectal pain was reported in 43.9% of patients, and 25% had rectal bleeding.
The CDC also released information on 288 patients with monkeypox treated with TPOXX under compassionate use. The median age of patients was 37 and 98.9% were male. About 40% of recipients were White, 35% were Hispanic, and about 16% were Black. This information does not include every patient treated with TPOXX, the agency said, as providers can begin treatment before submitting paperwork. As of Aug. 18, the CDC had received 400 patient intake forms for TPOXX, according to its website.
The agency has yet to release data on vaccination rates, which Dr. Hubach is eager to see. Demographic information on who is receiving vaccinations, and where, can illuminate issues with access as vaccine eligibility continues to expand. “Vaccination is probably going to be the largest tool within our toolbox to try to inhibit disease acquisition and spread,” he said.
A version of this article first appeared on Medscape.com.
Monkeypox cases in the United States continue to be rare in children younger than 15, women, and in individuals older than 60, according to new data released by the Centers for Disease Control and Prevention. Men aged 26-40 make up the highest proportion of cases.
The age distribution of cases is similar to those of sexually transmitted infections, said Monica Gandhi, MD, MPH, associate chief of the division of HIV, infectious diseases, and global medicine at the University of California, San Francisco. It is most common in younger to middle-aged age groups, and less common in children and older individuals. As of Aug. 21, only 17 children younger than 15 have been diagnosed with monkeypox in the United States, and women make up fewer than 1.5% of cases.
“This data should be very reassuring to parents and to children going to back to school,” Dr. Gandhi said in an interview. After 3 months of monitoring the virus, the data suggest that monkeypox is primarily spreading in networks of men who have sex with men (MSM) through sexual activity, “and that isn’t something we worry about with school-spread illness.”
In addition to the reassuring data about children and monkeypox, the CDC released laboratory testing data, a behavioral survey of MSM, patient data on the antiviral medication tecovirimat (TPOXX), and other case demographics and symptoms.
Though the number of positive monkeypox tests have continued to rise, the test-positivity rates have declined over the past month, data show. Since July 16, the positivity rate has dipped from 54% to 23%. This trend is likely because of an increase in testing availability, said Randolph Hubach, PhD, MPH, the director of the Sexual Health Research Lab at Purdue University, West Lafayette, Ind.
“We also saw this with COVID early on with testing: it was really limited to folks who were symptomatic,” he said in an interview . “As testing ramped up in accessibility, you had a lot more negative results, but because testing was more widely available, you were able to capture more positive results.”
The data also show that case numbers continue to grow in the United States, whereas in other countries that identified cases before the United States – Spain, the United Kingdom, and France, for example – cases have been leveling off, noted Dr. Gandhi.
The CDC also shared responses from a survey of gay, bisexual, and other MSM conducted from Aug. 5-15, about how they have changed their sexual behaviors in response to the monkeypox outbreak. Half of respondents reported reduced one-time sexual encounters, 49% reported reducing sex with partners met on dating apps or at sex venues, and 48% reported reducing their number of sex partners. These responses are “heartening to see,” Dr. Gandhi said, and shows that individuals are taking proactive steps to reduce their potential exposure risk to monkeypox.
More detailed demographic data showed that Black, Hispanic, or Latinx individuals make up an increasing proportion of cases in the United States. In May, 71% of people with reported monkeypox infection were White and 29% were Black. For the week of August 8-14, about a third (31%) of monkeypox cases were in White people, 32% were in Hispanic or Latinx people, and 33% were in Black people.
The most common symptoms of monkeypox were rash (98.6%), malaise (72.7%), fever (72.1%), and chills (68.9%). Rectal pain was reported in 43.9% of patients, and 25% had rectal bleeding.
The CDC also released information on 288 patients with monkeypox treated with TPOXX under compassionate use. The median age of patients was 37 and 98.9% were male. About 40% of recipients were White, 35% were Hispanic, and about 16% were Black. This information does not include every patient treated with TPOXX, the agency said, as providers can begin treatment before submitting paperwork. As of Aug. 18, the CDC had received 400 patient intake forms for TPOXX, according to its website.
The agency has yet to release data on vaccination rates, which Dr. Hubach is eager to see. Demographic information on who is receiving vaccinations, and where, can illuminate issues with access as vaccine eligibility continues to expand. “Vaccination is probably going to be the largest tool within our toolbox to try to inhibit disease acquisition and spread,” he said.
A version of this article first appeared on Medscape.com.
Monkeypox cases in the United States continue to be rare in children younger than 15, women, and in individuals older than 60, according to new data released by the Centers for Disease Control and Prevention. Men aged 26-40 make up the highest proportion of cases.
The age distribution of cases is similar to those of sexually transmitted infections, said Monica Gandhi, MD, MPH, associate chief of the division of HIV, infectious diseases, and global medicine at the University of California, San Francisco. It is most common in younger to middle-aged age groups, and less common in children and older individuals. As of Aug. 21, only 17 children younger than 15 have been diagnosed with monkeypox in the United States, and women make up fewer than 1.5% of cases.
“This data should be very reassuring to parents and to children going to back to school,” Dr. Gandhi said in an interview. After 3 months of monitoring the virus, the data suggest that monkeypox is primarily spreading in networks of men who have sex with men (MSM) through sexual activity, “and that isn’t something we worry about with school-spread illness.”
In addition to the reassuring data about children and monkeypox, the CDC released laboratory testing data, a behavioral survey of MSM, patient data on the antiviral medication tecovirimat (TPOXX), and other case demographics and symptoms.
Though the number of positive monkeypox tests have continued to rise, the test-positivity rates have declined over the past month, data show. Since July 16, the positivity rate has dipped from 54% to 23%. This trend is likely because of an increase in testing availability, said Randolph Hubach, PhD, MPH, the director of the Sexual Health Research Lab at Purdue University, West Lafayette, Ind.
“We also saw this with COVID early on with testing: it was really limited to folks who were symptomatic,” he said in an interview . “As testing ramped up in accessibility, you had a lot more negative results, but because testing was more widely available, you were able to capture more positive results.”
The data also show that case numbers continue to grow in the United States, whereas in other countries that identified cases before the United States – Spain, the United Kingdom, and France, for example – cases have been leveling off, noted Dr. Gandhi.
The CDC also shared responses from a survey of gay, bisexual, and other MSM conducted from Aug. 5-15, about how they have changed their sexual behaviors in response to the monkeypox outbreak. Half of respondents reported reduced one-time sexual encounters, 49% reported reducing sex with partners met on dating apps or at sex venues, and 48% reported reducing their number of sex partners. These responses are “heartening to see,” Dr. Gandhi said, and shows that individuals are taking proactive steps to reduce their potential exposure risk to monkeypox.
More detailed demographic data showed that Black, Hispanic, or Latinx individuals make up an increasing proportion of cases in the United States. In May, 71% of people with reported monkeypox infection were White and 29% were Black. For the week of August 8-14, about a third (31%) of monkeypox cases were in White people, 32% were in Hispanic or Latinx people, and 33% were in Black people.
The most common symptoms of monkeypox were rash (98.6%), malaise (72.7%), fever (72.1%), and chills (68.9%). Rectal pain was reported in 43.9% of patients, and 25% had rectal bleeding.
The CDC also released information on 288 patients with monkeypox treated with TPOXX under compassionate use. The median age of patients was 37 and 98.9% were male. About 40% of recipients were White, 35% were Hispanic, and about 16% were Black. This information does not include every patient treated with TPOXX, the agency said, as providers can begin treatment before submitting paperwork. As of Aug. 18, the CDC had received 400 patient intake forms for TPOXX, according to its website.
The agency has yet to release data on vaccination rates, which Dr. Hubach is eager to see. Demographic information on who is receiving vaccinations, and where, can illuminate issues with access as vaccine eligibility continues to expand. “Vaccination is probably going to be the largest tool within our toolbox to try to inhibit disease acquisition and spread,” he said.
A version of this article first appeared on Medscape.com.
Commentary: Gastric Cancer Surgery Trials, September 2022
Surgical resection plays a critical role in the management of early-stage gastric cancer. Depending on the tumor stage and location, there are different surgical approaches. Complications associated with surgical resection can significantly affect quality of life and ability to receive subsequent treatment. With recent advances in minimally invasive approaches, laparoscopic resections are emerging as an attractive option for patients undergoing oncologic surgeries.
The KLASS-02 trial was a multicenter, randomized, controlled, noninferiority clinical trial, which enrolled 1050 patients with locally advanced gastric cancer. Of the enrolled patients, 974 patients underwent R0 resection either by laparoscopic (n = 492) or open (n = 482) distal gastrectomy. In the previous readout of this study with 3 years of follow-up, laparoscopic distal gastrectomy had noninferior oncologic outcomes compared with open surgery for locally advanced gastric cancer. Son and colleagues are now reporting 5-year follow-up results. Overall survival (OS; 88.9% vs 88.7%; P = .30) and relapse-free survival (79.5% vs 81.1%; P = .658) rates were similar in both surgical groups. The pattern of recurrences was similar between the two groups as well, with peroneal (42.1% of patients) and hematogenous (20.8%) being the most frequent ones. However, patients who underwent laparoscopic vs open distal gastrectomy had a significantly lower late complication rate (6.5% vs 11.0%; P = .01). This study demonstrates that laparoscopic distal gastrectomy is an appropriate alternative to open distal gastrectomy and should be offered to patients who are treated in centers with experience in performing these types of operations.
Peritoneal metastasis is a common site for the spread of gastric cancer. As such, the role of hyperthermic intraperitoneal chemotherapy (HIPEC) in the management of this disease has been explored in a number of studies. The effectiveness of prophylactic HIPEC during resection of early-stage gastric cancer remains unknown.
Shen and colleagues conducted a propensity score-matching analysis looking at the efficacy and safety of HIPEC in this setting. The study evaluated outcomes of 395 patients with locally advanced gastric cancer who underwent resection with (n = 146) or without HIPEC (n = 248). In the HIPEC group, OS compared favorably to the surgery-only group (69.9% vs 40.8%, P = .049) and 2-year relapse-free survival was higher with HIPEC (60.7% vs 31.6%, P = .049).
Previously, the CYTO-CHIP propensity score analysis study performed in France demonstrated that HIPEC in addition to cytoreductive surgery resulted in improved OS in patients with advanced gastric cancer and peritoneal metastasis compared to cytoreduction surgery alone.1 However, with both of these reports, interpretation of the results carries inherent limitations that are associated with retrospective study design. Prior prospective studies, on the other hand, had mixed results. An ongoing phase 3 prospective study of D2 resection and HIPEC in locally advanced gastric carcinoma (GASTRICHIP) will hopefully provide a definitive answer regarding the benefit of HIPEC in early-stage gastric cancer management (NCT01882933). Ultimately, going forward, the role of HIPEC in early-stage disease will need to be examined in a prospective study with carefully selected patients, using the latest biomarkers and systemic therapies.
Mismatch repair protein deficient (dMMR) or microsatellite unstable gastric cancer (MSI-H) have distinct biologic behaviors and treatment responses. They are much more responsive to immune checkpoint inhibitors in the metastatic setting. In early-stage disease, exploratory analysis of patients with MSI-H tumors previously enrolled in the perioperative MAGIC trial, revealed that patients with MSI-H tumors had a better prognosis when treated with surgery alone, and they potentially experienced detrimental effects from chemotherapy.2
The GERCOR NEONIPIGA single-arm phase 2 study enrolled 32 patients with resectable dMMR/MSI-H gastric and gastroesophageal junction tumors.3 Patients were treated with 240-mg neoadjuvant nivolumab once every 2 weeks six times and 1-mg/kg ipilimumab once every 6 weeks twice, followed by surgery and 480-mg adjuvant nivolumab once every 4 weeks nine times. Twenty-nine patients underwent resection. All resections were with negative margins (R0). Pathologic complete response was seen in 17 (58.6%) of patients. As of the February 2022 data cutoff, with a median duration of follow-up of 14.9 months, 30 out of 31 patients with early-stage disease remained alive and without recurrence or progression (one evaluable patient had metastatic disease).
These results certainly support further investigation of immunotherapy use in this patient population. However, in the absence of prospective randomized data, the combination of fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) remains the standard of care in those who can tolerate it. For patients with MSI-H tumors who are not candidates for combination chemotherapy or whose tumors are progressing on chemotherapy, neoadjuvant immunotherapy is certainly a good option to consider.
Additional References
1. Bonnot P-E et al. Cytoreductive surgery with or without hyperthermic intraperitoneal chemotherapy for gastric cancer with peritoneal metastases (CYTO-CHIP study): A propensity score analysis. J Clin Oncol. 2019;37:2028-2040. Doi: 10.1200/JCO.18.01688
2. Smyth EC et al. Mismatch repair deficiency, microsatellite instability, and survival: An exploratory analysis of the Medical Research Council Adjuvant Gastric Infusional Chemotherapy (MAGIC) trial. JAMA Oncol. 2017;3:1197-1203. Doi: 10.1001/jamaoncol.2016.6762
3. André T et al. Neoadjuvant nivolumab plus ipilimumab and adjuvant nivolumab in localized deficient mismatch repair/microsatellite instability-high gastric or esophagogastric junction adenocarcinoma: The GERCOR NEONIPIGA phase II study. J Clin Oncol. 2022 (Aug 15. Doi: 10.1200/JCO.22.00686
Surgical resection plays a critical role in the management of early-stage gastric cancer. Depending on the tumor stage and location, there are different surgical approaches. Complications associated with surgical resection can significantly affect quality of life and ability to receive subsequent treatment. With recent advances in minimally invasive approaches, laparoscopic resections are emerging as an attractive option for patients undergoing oncologic surgeries.
The KLASS-02 trial was a multicenter, randomized, controlled, noninferiority clinical trial, which enrolled 1050 patients with locally advanced gastric cancer. Of the enrolled patients, 974 patients underwent R0 resection either by laparoscopic (n = 492) or open (n = 482) distal gastrectomy. In the previous readout of this study with 3 years of follow-up, laparoscopic distal gastrectomy had noninferior oncologic outcomes compared with open surgery for locally advanced gastric cancer. Son and colleagues are now reporting 5-year follow-up results. Overall survival (OS; 88.9% vs 88.7%; P = .30) and relapse-free survival (79.5% vs 81.1%; P = .658) rates were similar in both surgical groups. The pattern of recurrences was similar between the two groups as well, with peroneal (42.1% of patients) and hematogenous (20.8%) being the most frequent ones. However, patients who underwent laparoscopic vs open distal gastrectomy had a significantly lower late complication rate (6.5% vs 11.0%; P = .01). This study demonstrates that laparoscopic distal gastrectomy is an appropriate alternative to open distal gastrectomy and should be offered to patients who are treated in centers with experience in performing these types of operations.
Peritoneal metastasis is a common site for the spread of gastric cancer. As such, the role of hyperthermic intraperitoneal chemotherapy (HIPEC) in the management of this disease has been explored in a number of studies. The effectiveness of prophylactic HIPEC during resection of early-stage gastric cancer remains unknown.
Shen and colleagues conducted a propensity score-matching analysis looking at the efficacy and safety of HIPEC in this setting. The study evaluated outcomes of 395 patients with locally advanced gastric cancer who underwent resection with (n = 146) or without HIPEC (n = 248). In the HIPEC group, OS compared favorably to the surgery-only group (69.9% vs 40.8%, P = .049) and 2-year relapse-free survival was higher with HIPEC (60.7% vs 31.6%, P = .049).
Previously, the CYTO-CHIP propensity score analysis study performed in France demonstrated that HIPEC in addition to cytoreductive surgery resulted in improved OS in patients with advanced gastric cancer and peritoneal metastasis compared to cytoreduction surgery alone.1 However, with both of these reports, interpretation of the results carries inherent limitations that are associated with retrospective study design. Prior prospective studies, on the other hand, had mixed results. An ongoing phase 3 prospective study of D2 resection and HIPEC in locally advanced gastric carcinoma (GASTRICHIP) will hopefully provide a definitive answer regarding the benefit of HIPEC in early-stage gastric cancer management (NCT01882933). Ultimately, going forward, the role of HIPEC in early-stage disease will need to be examined in a prospective study with carefully selected patients, using the latest biomarkers and systemic therapies.
Mismatch repair protein deficient (dMMR) or microsatellite unstable gastric cancer (MSI-H) have distinct biologic behaviors and treatment responses. They are much more responsive to immune checkpoint inhibitors in the metastatic setting. In early-stage disease, exploratory analysis of patients with MSI-H tumors previously enrolled in the perioperative MAGIC trial, revealed that patients with MSI-H tumors had a better prognosis when treated with surgery alone, and they potentially experienced detrimental effects from chemotherapy.2
The GERCOR NEONIPIGA single-arm phase 2 study enrolled 32 patients with resectable dMMR/MSI-H gastric and gastroesophageal junction tumors.3 Patients were treated with 240-mg neoadjuvant nivolumab once every 2 weeks six times and 1-mg/kg ipilimumab once every 6 weeks twice, followed by surgery and 480-mg adjuvant nivolumab once every 4 weeks nine times. Twenty-nine patients underwent resection. All resections were with negative margins (R0). Pathologic complete response was seen in 17 (58.6%) of patients. As of the February 2022 data cutoff, with a median duration of follow-up of 14.9 months, 30 out of 31 patients with early-stage disease remained alive and without recurrence or progression (one evaluable patient had metastatic disease).
These results certainly support further investigation of immunotherapy use in this patient population. However, in the absence of prospective randomized data, the combination of fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) remains the standard of care in those who can tolerate it. For patients with MSI-H tumors who are not candidates for combination chemotherapy or whose tumors are progressing on chemotherapy, neoadjuvant immunotherapy is certainly a good option to consider.
Additional References
1. Bonnot P-E et al. Cytoreductive surgery with or without hyperthermic intraperitoneal chemotherapy for gastric cancer with peritoneal metastases (CYTO-CHIP study): A propensity score analysis. J Clin Oncol. 2019;37:2028-2040. Doi: 10.1200/JCO.18.01688
2. Smyth EC et al. Mismatch repair deficiency, microsatellite instability, and survival: An exploratory analysis of the Medical Research Council Adjuvant Gastric Infusional Chemotherapy (MAGIC) trial. JAMA Oncol. 2017;3:1197-1203. Doi: 10.1001/jamaoncol.2016.6762
3. André T et al. Neoadjuvant nivolumab plus ipilimumab and adjuvant nivolumab in localized deficient mismatch repair/microsatellite instability-high gastric or esophagogastric junction adenocarcinoma: The GERCOR NEONIPIGA phase II study. J Clin Oncol. 2022 (Aug 15. Doi: 10.1200/JCO.22.00686
Surgical resection plays a critical role in the management of early-stage gastric cancer. Depending on the tumor stage and location, there are different surgical approaches. Complications associated with surgical resection can significantly affect quality of life and ability to receive subsequent treatment. With recent advances in minimally invasive approaches, laparoscopic resections are emerging as an attractive option for patients undergoing oncologic surgeries.
The KLASS-02 trial was a multicenter, randomized, controlled, noninferiority clinical trial, which enrolled 1050 patients with locally advanced gastric cancer. Of the enrolled patients, 974 patients underwent R0 resection either by laparoscopic (n = 492) or open (n = 482) distal gastrectomy. In the previous readout of this study with 3 years of follow-up, laparoscopic distal gastrectomy had noninferior oncologic outcomes compared with open surgery for locally advanced gastric cancer. Son and colleagues are now reporting 5-year follow-up results. Overall survival (OS; 88.9% vs 88.7%; P = .30) and relapse-free survival (79.5% vs 81.1%; P = .658) rates were similar in both surgical groups. The pattern of recurrences was similar between the two groups as well, with peroneal (42.1% of patients) and hematogenous (20.8%) being the most frequent ones. However, patients who underwent laparoscopic vs open distal gastrectomy had a significantly lower late complication rate (6.5% vs 11.0%; P = .01). This study demonstrates that laparoscopic distal gastrectomy is an appropriate alternative to open distal gastrectomy and should be offered to patients who are treated in centers with experience in performing these types of operations.
Peritoneal metastasis is a common site for the spread of gastric cancer. As such, the role of hyperthermic intraperitoneal chemotherapy (HIPEC) in the management of this disease has been explored in a number of studies. The effectiveness of prophylactic HIPEC during resection of early-stage gastric cancer remains unknown.
Shen and colleagues conducted a propensity score-matching analysis looking at the efficacy and safety of HIPEC in this setting. The study evaluated outcomes of 395 patients with locally advanced gastric cancer who underwent resection with (n = 146) or without HIPEC (n = 248). In the HIPEC group, OS compared favorably to the surgery-only group (69.9% vs 40.8%, P = .049) and 2-year relapse-free survival was higher with HIPEC (60.7% vs 31.6%, P = .049).
Previously, the CYTO-CHIP propensity score analysis study performed in France demonstrated that HIPEC in addition to cytoreductive surgery resulted in improved OS in patients with advanced gastric cancer and peritoneal metastasis compared to cytoreduction surgery alone.1 However, with both of these reports, interpretation of the results carries inherent limitations that are associated with retrospective study design. Prior prospective studies, on the other hand, had mixed results. An ongoing phase 3 prospective study of D2 resection and HIPEC in locally advanced gastric carcinoma (GASTRICHIP) will hopefully provide a definitive answer regarding the benefit of HIPEC in early-stage gastric cancer management (NCT01882933). Ultimately, going forward, the role of HIPEC in early-stage disease will need to be examined in a prospective study with carefully selected patients, using the latest biomarkers and systemic therapies.
Mismatch repair protein deficient (dMMR) or microsatellite unstable gastric cancer (MSI-H) have distinct biologic behaviors and treatment responses. They are much more responsive to immune checkpoint inhibitors in the metastatic setting. In early-stage disease, exploratory analysis of patients with MSI-H tumors previously enrolled in the perioperative MAGIC trial, revealed that patients with MSI-H tumors had a better prognosis when treated with surgery alone, and they potentially experienced detrimental effects from chemotherapy.2
The GERCOR NEONIPIGA single-arm phase 2 study enrolled 32 patients with resectable dMMR/MSI-H gastric and gastroesophageal junction tumors.3 Patients were treated with 240-mg neoadjuvant nivolumab once every 2 weeks six times and 1-mg/kg ipilimumab once every 6 weeks twice, followed by surgery and 480-mg adjuvant nivolumab once every 4 weeks nine times. Twenty-nine patients underwent resection. All resections were with negative margins (R0). Pathologic complete response was seen in 17 (58.6%) of patients. As of the February 2022 data cutoff, with a median duration of follow-up of 14.9 months, 30 out of 31 patients with early-stage disease remained alive and without recurrence or progression (one evaluable patient had metastatic disease).
These results certainly support further investigation of immunotherapy use in this patient population. However, in the absence of prospective randomized data, the combination of fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) remains the standard of care in those who can tolerate it. For patients with MSI-H tumors who are not candidates for combination chemotherapy or whose tumors are progressing on chemotherapy, neoadjuvant immunotherapy is certainly a good option to consider.
Additional References
1. Bonnot P-E et al. Cytoreductive surgery with or without hyperthermic intraperitoneal chemotherapy for gastric cancer with peritoneal metastases (CYTO-CHIP study): A propensity score analysis. J Clin Oncol. 2019;37:2028-2040. Doi: 10.1200/JCO.18.01688
2. Smyth EC et al. Mismatch repair deficiency, microsatellite instability, and survival: An exploratory analysis of the Medical Research Council Adjuvant Gastric Infusional Chemotherapy (MAGIC) trial. JAMA Oncol. 2017;3:1197-1203. Doi: 10.1001/jamaoncol.2016.6762
3. André T et al. Neoadjuvant nivolumab plus ipilimumab and adjuvant nivolumab in localized deficient mismatch repair/microsatellite instability-high gastric or esophagogastric junction adenocarcinoma: The GERCOR NEONIPIGA phase II study. J Clin Oncol. 2022 (Aug 15. Doi: 10.1200/JCO.22.00686
Commentary: Diet and Colorectal Cancer, September 2022

This month's journal articles in the field of colorectal cancer research lack the cachet of some of the high-profile dispatches we discussed in previous editions of Clinical Edge. Nonetheless, there are several interesting reports this month.
The first is a clinical trial report that came out of China investigating the possible synergistic effect of high-dose vitamin C with chemotherapy in the first-line treatment of metastatic colorectal cancer (mCRC). The study was based on preclinical data that showed a synergistic increase in cancer cell death with chemotherapy plus high-dose vitamin C in in vitro models. Wang and colleagues randomly assigned 442 treatment-naive patients with mCRC to receive folinic acid, fluorouracil, and oxaliplatin (FOLFOX) and bevacizumab with or without 1.5 g/kg vitamin C intravenously on days 1-3 of each chemotherapy cycle.
The study's primary endpoint was progression-free survival (PFS), and patients were stratified on the basis of tumor sidedness and use of bevacizumab. PFS for the intention-to-treat group was unaffected by use of vitamin C (hazard ratio [HR] 0.86; 95% CI 0.70-1.05; P = .1). However, patients whose tumors harbored RAS mutations had a PFS that was significantly improved in the vitamin C arm (9.2 vs 7.8 months; HR 0.67; 95% CI 0.50-0.91; P = .01). Additionally, treatment-related adverse events were no more common in the treatment arm than in the control arm. Although I seldom draw clinical conclusions from subgroup analyses, I find it comforting to know that high-dose vitamin C is at least safe and potentially helpful for some patients. Many of my patients through the years have asked me about the utility of high-dose vitamin C. At least I can now inform them that the treatment is unlikely to cause physical harm or substantially decrease the efficacy of chemotherapy.
The second article I will discuss focuses on dietary fat intake and its potential effects on mortality and cancer progression in patients with mCRC. Using a food-frequency questionnaire, the authors of the study assessed the diets of 1194 patients who had been part of a previous cooperative group study for patients with treatment-naive mCRC (Van Blarigan et al). Over a median follow-up of 6.1 years, patients with the highest median intake of vegetable fats (23.5% kcal/d; interquartile range [IQR] 21.6%-25.7% kcal/d) vs the lowest intake (11.6% kcal/d; IQR 10.1%-12.7% kcal/d) showed a lower risk for all-cause mortality (adjusted HR 0.79; 95% CI 0.63-1.00) and cancer progression or death (adjusted HR 0.71; 95% CI 0.57-0.88). Although this study's results were not unexpected given data that have been published in the past, it builds on previous work as it shows the specific benefits of vegetable fats vis-à-vis animal fats, which are detrimental to survival. Oncologists continue to benefit from these studies because they allow us to give more specific dietary recommendations for high fat-containing vegan foods, such as avocados, olives, and nuts.
This month's journal articles in the field of colorectal cancer research lack the cachet of some of the high-profile dispatches we discussed in previous editions of Clinical Edge. Nonetheless, there are several interesting reports this month.
The first is a clinical trial report that came out of China investigating the possible synergistic effect of high-dose vitamin C with chemotherapy in the first-line treatment of metastatic colorectal cancer (mCRC). The study was based on preclinical data that showed a synergistic increase in cancer cell death with chemotherapy plus high-dose vitamin C in in vitro models. Wang and colleagues randomly assigned 442 treatment-naive patients with mCRC to receive folinic acid, fluorouracil, and oxaliplatin (FOLFOX) and bevacizumab with or without 1.5 g/kg vitamin C intravenously on days 1-3 of each chemotherapy cycle.
The study's primary endpoint was progression-free survival (PFS), and patients were stratified on the basis of tumor sidedness and use of bevacizumab. PFS for the intention-to-treat group was unaffected by use of vitamin C (hazard ratio [HR] 0.86; 95% CI 0.70-1.05; P = .1). However, patients whose tumors harbored RAS mutations had a PFS that was significantly improved in the vitamin C arm (9.2 vs 7.8 months; HR 0.67; 95% CI 0.50-0.91; P = .01). Additionally, treatment-related adverse events were no more common in the treatment arm than in the control arm. Although I seldom draw clinical conclusions from subgroup analyses, I find it comforting to know that high-dose vitamin C is at least safe and potentially helpful for some patients. Many of my patients through the years have asked me about the utility of high-dose vitamin C. At least I can now inform them that the treatment is unlikely to cause physical harm or substantially decrease the efficacy of chemotherapy.
The second article I will discuss focuses on dietary fat intake and its potential effects on mortality and cancer progression in patients with mCRC. Using a food-frequency questionnaire, the authors of the study assessed the diets of 1194 patients who had been part of a previous cooperative group study for patients with treatment-naive mCRC (Van Blarigan et al). Over a median follow-up of 6.1 years, patients with the highest median intake of vegetable fats (23.5% kcal/d; interquartile range [IQR] 21.6%-25.7% kcal/d) vs the lowest intake (11.6% kcal/d; IQR 10.1%-12.7% kcal/d) showed a lower risk for all-cause mortality (adjusted HR 0.79; 95% CI 0.63-1.00) and cancer progression or death (adjusted HR 0.71; 95% CI 0.57-0.88). Although this study's results were not unexpected given data that have been published in the past, it builds on previous work as it shows the specific benefits of vegetable fats vis-à-vis animal fats, which are detrimental to survival. Oncologists continue to benefit from these studies because they allow us to give more specific dietary recommendations for high fat-containing vegan foods, such as avocados, olives, and nuts.
This month's journal articles in the field of colorectal cancer research lack the cachet of some of the high-profile dispatches we discussed in previous editions of Clinical Edge. Nonetheless, there are several interesting reports this month.
The first is a clinical trial report that came out of China investigating the possible synergistic effect of high-dose vitamin C with chemotherapy in the first-line treatment of metastatic colorectal cancer (mCRC). The study was based on preclinical data that showed a synergistic increase in cancer cell death with chemotherapy plus high-dose vitamin C in in vitro models. Wang and colleagues randomly assigned 442 treatment-naive patients with mCRC to receive folinic acid, fluorouracil, and oxaliplatin (FOLFOX) and bevacizumab with or without 1.5 g/kg vitamin C intravenously on days 1-3 of each chemotherapy cycle.
The study's primary endpoint was progression-free survival (PFS), and patients were stratified on the basis of tumor sidedness and use of bevacizumab. PFS for the intention-to-treat group was unaffected by use of vitamin C (hazard ratio [HR] 0.86; 95% CI 0.70-1.05; P = .1). However, patients whose tumors harbored RAS mutations had a PFS that was significantly improved in the vitamin C arm (9.2 vs 7.8 months; HR 0.67; 95% CI 0.50-0.91; P = .01). Additionally, treatment-related adverse events were no more common in the treatment arm than in the control arm. Although I seldom draw clinical conclusions from subgroup analyses, I find it comforting to know that high-dose vitamin C is at least safe and potentially helpful for some patients. Many of my patients through the years have asked me about the utility of high-dose vitamin C. At least I can now inform them that the treatment is unlikely to cause physical harm or substantially decrease the efficacy of chemotherapy.
The second article I will discuss focuses on dietary fat intake and its potential effects on mortality and cancer progression in patients with mCRC. Using a food-frequency questionnaire, the authors of the study assessed the diets of 1194 patients who had been part of a previous cooperative group study for patients with treatment-naive mCRC (Van Blarigan et al). Over a median follow-up of 6.1 years, patients with the highest median intake of vegetable fats (23.5% kcal/d; interquartile range [IQR] 21.6%-25.7% kcal/d) vs the lowest intake (11.6% kcal/d; IQR 10.1%-12.7% kcal/d) showed a lower risk for all-cause mortality (adjusted HR 0.79; 95% CI 0.63-1.00) and cancer progression or death (adjusted HR 0.71; 95% CI 0.57-0.88). Although this study's results were not unexpected given data that have been published in the past, it builds on previous work as it shows the specific benefits of vegetable fats vis-à-vis animal fats, which are detrimental to survival. Oncologists continue to benefit from these studies because they allow us to give more specific dietary recommendations for high fat-containing vegan foods, such as avocados, olives, and nuts.
COMMENT & CONTROVERSY
How common is IUD perforation, expulsion, and malposition?
ROBERT L. BARBIERI, MD (APRIL 2022)
The seriousness of IUD embedment
I appreciated Dr. Barbieri’s comprehensive review of clinical problems regarding the intrauterine device (IUD). It is interesting that, in spite of your mention of IUD embedment in the myometrium, other publications regarding this phenomenon are seemingly absent (except for ours).1 Whether or not there is associated pain (and sometimes there is not), in our experience its removal can result in IUD fracture. As you stated, it is true that 3D transvaginal sonography perfectly enables this visualization, yet it is surprising that others have not experienced what we have. Nonetheless, it is encouraging to see that IUD embedment is seriously mentioned.
- Fernandez CM, Levine EM, Cabiya M, et al. Intrauterine device embedment resulting in its fracture: a case series. Arch Obstet Gynecol. 2021;2:1-4.
Elliot Levine, MD
Chicago, Illinois
Dr. Barbieri responds
I thank Dr. Levine for highlighting the important issue of IUD fracture and providing a reference to a case series of IUD fractures. Although such fracture is not common, when it does occur it may require a hysteroscopic procedure to remove all pieces of the IUD. In the cited case series, fracture was more commonly observed with the copper IUD than with the LNG-IUD. With regard to IUD malposition, 4 publications reviewed in my recent editorial describe the problem of an IUD arm embedded in the myometrium.1-4
References
- Benacerraf BR, Shipp TD, Bromley B. Three-dimensional ultrasound detection of abnormally located intrauterine contraceptive devices which are a source of pelvic pain and abnormal bleeding. Ultrasound Obstet Gynecol. 2009;34:110-115.
- Braaten KP, Benson CB, Maurer R, et al. Malpositioned intrauterine contraceptive devices: risk factors, outcomes and future pregnancies. Obstet Gynecol. 2011;118:1014-1020.
- Gerkowicz SA, Fiorentino DG, Kovacs AP, et al. Uterine structural abnormality and intrauterine device malposition: analysis of ultrasonographic and demographic variables of 517 patients. Am J Obstet Gynecol. 2019;220:183.e1-e8.
- Connolly CT, Fox NS. Incidence and risk factors for a malpositioned intrauterine device detected on three-dimensional ultrasound within eight weeks of placement. J Ultrasound Med. September 27, 2021.
Will NAAT replace microscopy for the identification of organisms causing vaginitis?
ROBERT L. BARBIERI, MD (MARCH 2022)
Follow-up questions on NAAT testing
The sensitivity of NAAT testing, as outlined in Dr. Barbieri’s editorial, is undoubtedly better than the clinical methods most clinicians are using. I appreciate the frustration we providers often experience in drawing conclusions for patients based on the Amsel criteria for bacterial vaginitis (BV). I am surprised by the low sensitivity of microscopy for yeast vaginitis. My follow-up questions are:
- Have the NAATs referenced been validated in clinical trials and proven to improve patient outcomes?
- Will the proposal to begin empiric therapy for both yeast vaginitis and BV in combination while waiting for NAAT results lead to an increase of resistant strains?
- What is the cost of NAAT for vaginitis, and is this cost effective in routine practice?
- Can NAATs be utilized to detect resistant strains of yeast or Gardnerella sp?
Alan Paul Gehrich, MD (COL, MC ret.)
Bethesda, Maryland
Dr. Barbieri responds
I thank Dr. Gehrich for raising the important issue of what is the optimal endpoint to assess the clinical utility of NAAT testing for vaginitis. Most studies of the use of NAAT to diagnose the cause of vaginitis focus on comparing NAAT results to standard clinical practice (microscopy and pH), and to a “gold standard.” In most studies the gold standards are Nugent scoring with Amsel criteria to resolve intermediate Nugent scores for bacterial vaginosis, culture for Candida, and culture for Trichomonas vaginalis. It is clear from multiple studies that NAAT provides superior sensitivity and specificity compared with standard clinical practice.1-3 As noted in the editorial, in a study of 466 patients with symptoms of vaginitis, standard office approaches to the diagnosis of vaginitis resulted in the failure to identify the correct infection in a large number of cases.4 For the diagnosis of BV, clinicians missed 42% of the cases identified by NAAT. For the diagnosis of Candida, clinicians missed 46% of the cases identified by NAAT. For the diagnosis of T vaginalis, clinicians missed 72% of the cases identified by NAAT. This resulted in clinicians not appropriately treating many infections detected by NAAT.
NAAT does provide information about the presence of Candida glabrata and Candida krusei, organisms which may be resistant to fluconazole. I agree with Dr. Gehrich that the optimal use of NAAT testing in practice is poorly studied with regard to treatment between sample collection and NAAT results. Cost of testing is a complex issue. Standard microscopy is relatively inexpensive, but performs poorly in clinical practice, resulting in misdiagnosis. NAAT testing is expensive but correctly identifies causes of vaginitis.
References
- Schwebke JR, Gaydos CA, Hyirjesy P, et al. Diagnostic performance of a molecular test versus clinician assessment of vaginitis. J Clin Microbiol. 2018;56:e00252-18.
- Broache M, Cammarata CL, Stonebraker E, et al. Performance of vaginal panel assay compared with clinical diagnosis of vaginitis. Obstet Gynecol. 2021;138:853-859.
- Schwebke JR, Taylor SN, Ackerman N, et al. Clinical validation of the Aptima bacterial vaginosis and Aptima Candida/Trichomonas vaginalis assays: results from a prospective multi-center study. J Clin Microbiol. 2020;58:e01643-19. 4
- Gaydos CA, Beqaj S, Schwebke JR, et al. Clinical validation of a test for the diagnosis of vaginitis. Obstet Gynecol. 2017;130:181-189.
How common is IUD perforation, expulsion, and malposition?
ROBERT L. BARBIERI, MD (APRIL 2022)
The seriousness of IUD embedment
I appreciated Dr. Barbieri’s comprehensive review of clinical problems regarding the intrauterine device (IUD). It is interesting that, in spite of your mention of IUD embedment in the myometrium, other publications regarding this phenomenon are seemingly absent (except for ours).1 Whether or not there is associated pain (and sometimes there is not), in our experience its removal can result in IUD fracture. As you stated, it is true that 3D transvaginal sonography perfectly enables this visualization, yet it is surprising that others have not experienced what we have. Nonetheless, it is encouraging to see that IUD embedment is seriously mentioned.
- Fernandez CM, Levine EM, Cabiya M, et al. Intrauterine device embedment resulting in its fracture: a case series. Arch Obstet Gynecol. 2021;2:1-4.
Elliot Levine, MD
Chicago, Illinois
Dr. Barbieri responds
I thank Dr. Levine for highlighting the important issue of IUD fracture and providing a reference to a case series of IUD fractures. Although such fracture is not common, when it does occur it may require a hysteroscopic procedure to remove all pieces of the IUD. In the cited case series, fracture was more commonly observed with the copper IUD than with the LNG-IUD. With regard to IUD malposition, 4 publications reviewed in my recent editorial describe the problem of an IUD arm embedded in the myometrium.1-4
References
- Benacerraf BR, Shipp TD, Bromley B. Three-dimensional ultrasound detection of abnormally located intrauterine contraceptive devices which are a source of pelvic pain and abnormal bleeding. Ultrasound Obstet Gynecol. 2009;34:110-115.
- Braaten KP, Benson CB, Maurer R, et al. Malpositioned intrauterine contraceptive devices: risk factors, outcomes and future pregnancies. Obstet Gynecol. 2011;118:1014-1020.
- Gerkowicz SA, Fiorentino DG, Kovacs AP, et al. Uterine structural abnormality and intrauterine device malposition: analysis of ultrasonographic and demographic variables of 517 patients. Am J Obstet Gynecol. 2019;220:183.e1-e8.
- Connolly CT, Fox NS. Incidence and risk factors for a malpositioned intrauterine device detected on three-dimensional ultrasound within eight weeks of placement. J Ultrasound Med. September 27, 2021.
Will NAAT replace microscopy for the identification of organisms causing vaginitis?
ROBERT L. BARBIERI, MD (MARCH 2022)
Follow-up questions on NAAT testing
The sensitivity of NAAT testing, as outlined in Dr. Barbieri’s editorial, is undoubtedly better than the clinical methods most clinicians are using. I appreciate the frustration we providers often experience in drawing conclusions for patients based on the Amsel criteria for bacterial vaginitis (BV). I am surprised by the low sensitivity of microscopy for yeast vaginitis. My follow-up questions are:
- Have the NAATs referenced been validated in clinical trials and proven to improve patient outcomes?
- Will the proposal to begin empiric therapy for both yeast vaginitis and BV in combination while waiting for NAAT results lead to an increase of resistant strains?
- What is the cost of NAAT for vaginitis, and is this cost effective in routine practice?
- Can NAATs be utilized to detect resistant strains of yeast or Gardnerella sp?
Alan Paul Gehrich, MD (COL, MC ret.)
Bethesda, Maryland
Dr. Barbieri responds
I thank Dr. Gehrich for raising the important issue of what is the optimal endpoint to assess the clinical utility of NAAT testing for vaginitis. Most studies of the use of NAAT to diagnose the cause of vaginitis focus on comparing NAAT results to standard clinical practice (microscopy and pH), and to a “gold standard.” In most studies the gold standards are Nugent scoring with Amsel criteria to resolve intermediate Nugent scores for bacterial vaginosis, culture for Candida, and culture for Trichomonas vaginalis. It is clear from multiple studies that NAAT provides superior sensitivity and specificity compared with standard clinical practice.1-3 As noted in the editorial, in a study of 466 patients with symptoms of vaginitis, standard office approaches to the diagnosis of vaginitis resulted in the failure to identify the correct infection in a large number of cases.4 For the diagnosis of BV, clinicians missed 42% of the cases identified by NAAT. For the diagnosis of Candida, clinicians missed 46% of the cases identified by NAAT. For the diagnosis of T vaginalis, clinicians missed 72% of the cases identified by NAAT. This resulted in clinicians not appropriately treating many infections detected by NAAT.
NAAT does provide information about the presence of Candida glabrata and Candida krusei, organisms which may be resistant to fluconazole. I agree with Dr. Gehrich that the optimal use of NAAT testing in practice is poorly studied with regard to treatment between sample collection and NAAT results. Cost of testing is a complex issue. Standard microscopy is relatively inexpensive, but performs poorly in clinical practice, resulting in misdiagnosis. NAAT testing is expensive but correctly identifies causes of vaginitis.
References
- Schwebke JR, Gaydos CA, Hyirjesy P, et al. Diagnostic performance of a molecular test versus clinician assessment of vaginitis. J Clin Microbiol. 2018;56:e00252-18.
- Broache M, Cammarata CL, Stonebraker E, et al. Performance of vaginal panel assay compared with clinical diagnosis of vaginitis. Obstet Gynecol. 2021;138:853-859.
- Schwebke JR, Taylor SN, Ackerman N, et al. Clinical validation of the Aptima bacterial vaginosis and Aptima Candida/Trichomonas vaginalis assays: results from a prospective multi-center study. J Clin Microbiol. 2020;58:e01643-19. 4
- Gaydos CA, Beqaj S, Schwebke JR, et al. Clinical validation of a test for the diagnosis of vaginitis. Obstet Gynecol. 2017;130:181-189.
How common is IUD perforation, expulsion, and malposition?
ROBERT L. BARBIERI, MD (APRIL 2022)
The seriousness of IUD embedment
I appreciated Dr. Barbieri’s comprehensive review of clinical problems regarding the intrauterine device (IUD). It is interesting that, in spite of your mention of IUD embedment in the myometrium, other publications regarding this phenomenon are seemingly absent (except for ours).1 Whether or not there is associated pain (and sometimes there is not), in our experience its removal can result in IUD fracture. As you stated, it is true that 3D transvaginal sonography perfectly enables this visualization, yet it is surprising that others have not experienced what we have. Nonetheless, it is encouraging to see that IUD embedment is seriously mentioned.
- Fernandez CM, Levine EM, Cabiya M, et al. Intrauterine device embedment resulting in its fracture: a case series. Arch Obstet Gynecol. 2021;2:1-4.
Elliot Levine, MD
Chicago, Illinois
Dr. Barbieri responds
I thank Dr. Levine for highlighting the important issue of IUD fracture and providing a reference to a case series of IUD fractures. Although such fracture is not common, when it does occur it may require a hysteroscopic procedure to remove all pieces of the IUD. In the cited case series, fracture was more commonly observed with the copper IUD than with the LNG-IUD. With regard to IUD malposition, 4 publications reviewed in my recent editorial describe the problem of an IUD arm embedded in the myometrium.1-4
References
- Benacerraf BR, Shipp TD, Bromley B. Three-dimensional ultrasound detection of abnormally located intrauterine contraceptive devices which are a source of pelvic pain and abnormal bleeding. Ultrasound Obstet Gynecol. 2009;34:110-115.
- Braaten KP, Benson CB, Maurer R, et al. Malpositioned intrauterine contraceptive devices: risk factors, outcomes and future pregnancies. Obstet Gynecol. 2011;118:1014-1020.
- Gerkowicz SA, Fiorentino DG, Kovacs AP, et al. Uterine structural abnormality and intrauterine device malposition: analysis of ultrasonographic and demographic variables of 517 patients. Am J Obstet Gynecol. 2019;220:183.e1-e8.
- Connolly CT, Fox NS. Incidence and risk factors for a malpositioned intrauterine device detected on three-dimensional ultrasound within eight weeks of placement. J Ultrasound Med. September 27, 2021.
Will NAAT replace microscopy for the identification of organisms causing vaginitis?
ROBERT L. BARBIERI, MD (MARCH 2022)
Follow-up questions on NAAT testing
The sensitivity of NAAT testing, as outlined in Dr. Barbieri’s editorial, is undoubtedly better than the clinical methods most clinicians are using. I appreciate the frustration we providers often experience in drawing conclusions for patients based on the Amsel criteria for bacterial vaginitis (BV). I am surprised by the low sensitivity of microscopy for yeast vaginitis. My follow-up questions are:
- Have the NAATs referenced been validated in clinical trials and proven to improve patient outcomes?
- Will the proposal to begin empiric therapy for both yeast vaginitis and BV in combination while waiting for NAAT results lead to an increase of resistant strains?
- What is the cost of NAAT for vaginitis, and is this cost effective in routine practice?
- Can NAATs be utilized to detect resistant strains of yeast or Gardnerella sp?
Alan Paul Gehrich, MD (COL, MC ret.)
Bethesda, Maryland
Dr. Barbieri responds
I thank Dr. Gehrich for raising the important issue of what is the optimal endpoint to assess the clinical utility of NAAT testing for vaginitis. Most studies of the use of NAAT to diagnose the cause of vaginitis focus on comparing NAAT results to standard clinical practice (microscopy and pH), and to a “gold standard.” In most studies the gold standards are Nugent scoring with Amsel criteria to resolve intermediate Nugent scores for bacterial vaginosis, culture for Candida, and culture for Trichomonas vaginalis. It is clear from multiple studies that NAAT provides superior sensitivity and specificity compared with standard clinical practice.1-3 As noted in the editorial, in a study of 466 patients with symptoms of vaginitis, standard office approaches to the diagnosis of vaginitis resulted in the failure to identify the correct infection in a large number of cases.4 For the diagnosis of BV, clinicians missed 42% of the cases identified by NAAT. For the diagnosis of Candida, clinicians missed 46% of the cases identified by NAAT. For the diagnosis of T vaginalis, clinicians missed 72% of the cases identified by NAAT. This resulted in clinicians not appropriately treating many infections detected by NAAT.
NAAT does provide information about the presence of Candida glabrata and Candida krusei, organisms which may be resistant to fluconazole. I agree with Dr. Gehrich that the optimal use of NAAT testing in practice is poorly studied with regard to treatment between sample collection and NAAT results. Cost of testing is a complex issue. Standard microscopy is relatively inexpensive, but performs poorly in clinical practice, resulting in misdiagnosis. NAAT testing is expensive but correctly identifies causes of vaginitis.
References
- Schwebke JR, Gaydos CA, Hyirjesy P, et al. Diagnostic performance of a molecular test versus clinician assessment of vaginitis. J Clin Microbiol. 2018;56:e00252-18.
- Broache M, Cammarata CL, Stonebraker E, et al. Performance of vaginal panel assay compared with clinical diagnosis of vaginitis. Obstet Gynecol. 2021;138:853-859.
- Schwebke JR, Taylor SN, Ackerman N, et al. Clinical validation of the Aptima bacterial vaginosis and Aptima Candida/Trichomonas vaginalis assays: results from a prospective multi-center study. J Clin Microbiol. 2020;58:e01643-19. 4
- Gaydos CA, Beqaj S, Schwebke JR, et al. Clinical validation of a test for the diagnosis of vaginitis. Obstet Gynecol. 2017;130:181-189.
At what age do ObGyns recommend their patients begin cervical cancer screening?
In their peer-to-peer interview, “Cervical cancer: A path to eradication,” (OBG Manag. May 2022;34:30-34.) David G. Mutch, MD, and Warner Huh, MD, discussed the varying guidelines for cervical cancer screening. Dr. Huh pointed out that the 2020 guidelines for the American Cancer Society recommend cervical cancer screening to begin at age 25 years, although the current guidelines for the American College of Obstetricians and Gynecologists continue to recommend age 21. He noted that “the rate of cervical cancer is extremely low under age 25, and other countries like the United Kingdom already” screen beginning at age 25. OBG Management followed up with a poll for readers to ask: “Guidelines vary on what age to begin screening for cervical cancer. What age do you typically recommend for patients?”
A total of 187 readers cast their vote:
82.4% (154 readers) said age 21
8.0% (15 readers) said age 25
9.6% (18 readers) said other age
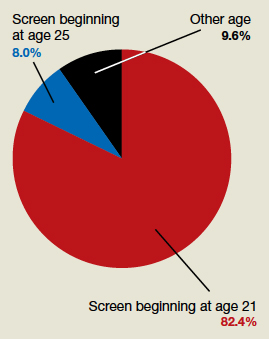
In their peer-to-peer interview, “Cervical cancer: A path to eradication,” (OBG Manag. May 2022;34:30-34.) David G. Mutch, MD, and Warner Huh, MD, discussed the varying guidelines for cervical cancer screening. Dr. Huh pointed out that the 2020 guidelines for the American Cancer Society recommend cervical cancer screening to begin at age 25 years, although the current guidelines for the American College of Obstetricians and Gynecologists continue to recommend age 21. He noted that “the rate of cervical cancer is extremely low under age 25, and other countries like the United Kingdom already” screen beginning at age 25. OBG Management followed up with a poll for readers to ask: “Guidelines vary on what age to begin screening for cervical cancer. What age do you typically recommend for patients?”
A total of 187 readers cast their vote:
82.4% (154 readers) said age 21
8.0% (15 readers) said age 25
9.6% (18 readers) said other age
In their peer-to-peer interview, “Cervical cancer: A path to eradication,” (OBG Manag. May 2022;34:30-34.) David G. Mutch, MD, and Warner Huh, MD, discussed the varying guidelines for cervical cancer screening. Dr. Huh pointed out that the 2020 guidelines for the American Cancer Society recommend cervical cancer screening to begin at age 25 years, although the current guidelines for the American College of Obstetricians and Gynecologists continue to recommend age 21. He noted that “the rate of cervical cancer is extremely low under age 25, and other countries like the United Kingdom already” screen beginning at age 25. OBG Management followed up with a poll for readers to ask: “Guidelines vary on what age to begin screening for cervical cancer. What age do you typically recommend for patients?”
A total of 187 readers cast their vote:
82.4% (154 readers) said age 21
8.0% (15 readers) said age 25
9.6% (18 readers) said other age
Well-child visits rise, but disparities remain
Adherence to well-child visits in the United States increased overall over a 10-year period, but a gap of up to 20% persisted between the highest and lowest adherence groups, reflecting disparities by race and ethnicity, poverty level, geography, and insurance status.
Well-child visits are recommended to provide children with preventive health and development services, ensure immunizations, and allow parents to discuss health concerns, wrote Salam Abdus, PhD, and Thomas M. Selden, PhD, of the Agency for Healthcare Research and Quality, Rockville, Md.
“We know from prior studies that as of 2008, well-child visits were trending upward, but often fell short of recommendations among key socioeconomic groups,” they wrote.
To examine recent trends in well-child visits, the researchers conducted a cross-sectional study of data from the Medical Expenditure Panel Survey (MEPS) on children aged 0 to 18 years. The findings were published in JAMA Pediatrics.
The study population included 19,018 children in 2006 and 2007 and 17,533 children in 2016 and 2017.
Adherence was defined as the ratio of reported well-child visits divided by the recommended number of visits in a calendar year.
Overall, the mean adherence increased from 47.9% in 2006-2007 to 62.3% in 2016-2017.
However, significant gaps persisted across race and ethnicity. Notably, adherence in the Hispanic population increased by nearly 22% between the study dates, compared to a 15.3% increase among White non-Hispanic children. However, Hispanic children still trailed White children overall in 2016-2017 (58% vs. 67.8%).
The smallest increase in adherence occurred among Black non-Hispanic children (5.6%) which further widened the gap between Black and White non-Hispanic children in 2016-2017 (52.5% vs. 67.8%).
Adherence rates increased similarly for children with public and private insurance (15.5% and 13.9%, respectively), but the adherence rates for uninsured children remained stable. Adherence in 2016-2017 for children with private, public, and no insurance were 66.3%, 58.7%, and 31.1%.
Also, despite overall increases in adherence across regions, a gap of more than 20% separated the region with the highest adherence (Northeast) from the lowest (West) in both the 2006-2007 and 2016-2017 periods (69.3% vs. 38.4%, and 79.3% vs. 55.2%, respectively).
The findings show an increase in well-child visits that spanned a time period of increased recommendations, economic changes, and the impact of the Affordable Care Act, but unaddressed disparities remain, the researchers noted.
Reducing disparities and improving adherence, “will require the combined efforts of researchers, policymakers, and clinicians to improve our understanding of adherence, to implement policies improving access to care, and to increase health care professional engagement with disadvantaged communities,” they concluded.
Overall increases are encouraging, but barriers need attention
“Demographic data are critical to determine which groups of children need the most support for recommended well child care,” Susan Boulter, MD, of the Geisel School of Medicine at Dartmouth, Hanover, N.H., said in an interview. In the current study, “it was encouraging to see how either public or private insurance significantly increased the percentage of children receiving well child care,” she said.
The level of increased adherence to AAP-recommended guidelines for well-child visits was surprising, said Dr. Boulter. The overall increase is likely attributable in part to the increased coverage for well-child visits in the wake of the Affordable Care Act, as the study authors mention, she said.
“The gains experienced by Hispanic families were especially encouraging,” she added.
However, ongoing barriers to well-child care include “lack of adequate provider numbers and mix, transportation difficulties for patients, and lack of child care and time away from work for parents so they can complete the recommended well child visit schedule,” Dr. Boulter noted. “Provider schedules and locations of care should be improved so families would have easier access. Also, social media should have more positive well-child messages to counteract the negative messaging.”
More research is needed to examine the impact of COVID-19 on well-child visits, Dr. Boulter emphasized. “Most likely, the percentages in all groups will have changed since COVID-19 has impacted office practices,” she said. “Anxiety about COVID-19 transmissibility in the pediatric office decreased routine office visits, and skepticism about vaccines, including vaccine refusal, has significantly changed the percentage of children who have received the AAP recommended vaccines,” she explained. Ideally, the study authors will review the MEPS data again to examine changes since the COVID-19 pandemic began, she told this news organization.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Boulter had no financial conflicts to disclose and serves on the editorial advisory board of Pediatric News.
Adherence to well-child visits in the United States increased overall over a 10-year period, but a gap of up to 20% persisted between the highest and lowest adherence groups, reflecting disparities by race and ethnicity, poverty level, geography, and insurance status.
Well-child visits are recommended to provide children with preventive health and development services, ensure immunizations, and allow parents to discuss health concerns, wrote Salam Abdus, PhD, and Thomas M. Selden, PhD, of the Agency for Healthcare Research and Quality, Rockville, Md.
“We know from prior studies that as of 2008, well-child visits were trending upward, but often fell short of recommendations among key socioeconomic groups,” they wrote.
To examine recent trends in well-child visits, the researchers conducted a cross-sectional study of data from the Medical Expenditure Panel Survey (MEPS) on children aged 0 to 18 years. The findings were published in JAMA Pediatrics.
The study population included 19,018 children in 2006 and 2007 and 17,533 children in 2016 and 2017.
Adherence was defined as the ratio of reported well-child visits divided by the recommended number of visits in a calendar year.
Overall, the mean adherence increased from 47.9% in 2006-2007 to 62.3% in 2016-2017.
However, significant gaps persisted across race and ethnicity. Notably, adherence in the Hispanic population increased by nearly 22% between the study dates, compared to a 15.3% increase among White non-Hispanic children. However, Hispanic children still trailed White children overall in 2016-2017 (58% vs. 67.8%).
The smallest increase in adherence occurred among Black non-Hispanic children (5.6%) which further widened the gap between Black and White non-Hispanic children in 2016-2017 (52.5% vs. 67.8%).
Adherence rates increased similarly for children with public and private insurance (15.5% and 13.9%, respectively), but the adherence rates for uninsured children remained stable. Adherence in 2016-2017 for children with private, public, and no insurance were 66.3%, 58.7%, and 31.1%.
Also, despite overall increases in adherence across regions, a gap of more than 20% separated the region with the highest adherence (Northeast) from the lowest (West) in both the 2006-2007 and 2016-2017 periods (69.3% vs. 38.4%, and 79.3% vs. 55.2%, respectively).
The findings show an increase in well-child visits that spanned a time period of increased recommendations, economic changes, and the impact of the Affordable Care Act, but unaddressed disparities remain, the researchers noted.
Reducing disparities and improving adherence, “will require the combined efforts of researchers, policymakers, and clinicians to improve our understanding of adherence, to implement policies improving access to care, and to increase health care professional engagement with disadvantaged communities,” they concluded.
Overall increases are encouraging, but barriers need attention
“Demographic data are critical to determine which groups of children need the most support for recommended well child care,” Susan Boulter, MD, of the Geisel School of Medicine at Dartmouth, Hanover, N.H., said in an interview. In the current study, “it was encouraging to see how either public or private insurance significantly increased the percentage of children receiving well child care,” she said.
The level of increased adherence to AAP-recommended guidelines for well-child visits was surprising, said Dr. Boulter. The overall increase is likely attributable in part to the increased coverage for well-child visits in the wake of the Affordable Care Act, as the study authors mention, she said.
“The gains experienced by Hispanic families were especially encouraging,” she added.
However, ongoing barriers to well-child care include “lack of adequate provider numbers and mix, transportation difficulties for patients, and lack of child care and time away from work for parents so they can complete the recommended well child visit schedule,” Dr. Boulter noted. “Provider schedules and locations of care should be improved so families would have easier access. Also, social media should have more positive well-child messages to counteract the negative messaging.”
More research is needed to examine the impact of COVID-19 on well-child visits, Dr. Boulter emphasized. “Most likely, the percentages in all groups will have changed since COVID-19 has impacted office practices,” she said. “Anxiety about COVID-19 transmissibility in the pediatric office decreased routine office visits, and skepticism about vaccines, including vaccine refusal, has significantly changed the percentage of children who have received the AAP recommended vaccines,” she explained. Ideally, the study authors will review the MEPS data again to examine changes since the COVID-19 pandemic began, she told this news organization.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Boulter had no financial conflicts to disclose and serves on the editorial advisory board of Pediatric News.
Adherence to well-child visits in the United States increased overall over a 10-year period, but a gap of up to 20% persisted between the highest and lowest adherence groups, reflecting disparities by race and ethnicity, poverty level, geography, and insurance status.
Well-child visits are recommended to provide children with preventive health and development services, ensure immunizations, and allow parents to discuss health concerns, wrote Salam Abdus, PhD, and Thomas M. Selden, PhD, of the Agency for Healthcare Research and Quality, Rockville, Md.
“We know from prior studies that as of 2008, well-child visits were trending upward, but often fell short of recommendations among key socioeconomic groups,” they wrote.
To examine recent trends in well-child visits, the researchers conducted a cross-sectional study of data from the Medical Expenditure Panel Survey (MEPS) on children aged 0 to 18 years. The findings were published in JAMA Pediatrics.
The study population included 19,018 children in 2006 and 2007 and 17,533 children in 2016 and 2017.
Adherence was defined as the ratio of reported well-child visits divided by the recommended number of visits in a calendar year.
Overall, the mean adherence increased from 47.9% in 2006-2007 to 62.3% in 2016-2017.
However, significant gaps persisted across race and ethnicity. Notably, adherence in the Hispanic population increased by nearly 22% between the study dates, compared to a 15.3% increase among White non-Hispanic children. However, Hispanic children still trailed White children overall in 2016-2017 (58% vs. 67.8%).
The smallest increase in adherence occurred among Black non-Hispanic children (5.6%) which further widened the gap between Black and White non-Hispanic children in 2016-2017 (52.5% vs. 67.8%).
Adherence rates increased similarly for children with public and private insurance (15.5% and 13.9%, respectively), but the adherence rates for uninsured children remained stable. Adherence in 2016-2017 for children with private, public, and no insurance were 66.3%, 58.7%, and 31.1%.
Also, despite overall increases in adherence across regions, a gap of more than 20% separated the region with the highest adherence (Northeast) from the lowest (West) in both the 2006-2007 and 2016-2017 periods (69.3% vs. 38.4%, and 79.3% vs. 55.2%, respectively).
The findings show an increase in well-child visits that spanned a time period of increased recommendations, economic changes, and the impact of the Affordable Care Act, but unaddressed disparities remain, the researchers noted.
Reducing disparities and improving adherence, “will require the combined efforts of researchers, policymakers, and clinicians to improve our understanding of adherence, to implement policies improving access to care, and to increase health care professional engagement with disadvantaged communities,” they concluded.
Overall increases are encouraging, but barriers need attention
“Demographic data are critical to determine which groups of children need the most support for recommended well child care,” Susan Boulter, MD, of the Geisel School of Medicine at Dartmouth, Hanover, N.H., said in an interview. In the current study, “it was encouraging to see how either public or private insurance significantly increased the percentage of children receiving well child care,” she said.
The level of increased adherence to AAP-recommended guidelines for well-child visits was surprising, said Dr. Boulter. The overall increase is likely attributable in part to the increased coverage for well-child visits in the wake of the Affordable Care Act, as the study authors mention, she said.
“The gains experienced by Hispanic families were especially encouraging,” she added.
However, ongoing barriers to well-child care include “lack of adequate provider numbers and mix, transportation difficulties for patients, and lack of child care and time away from work for parents so they can complete the recommended well child visit schedule,” Dr. Boulter noted. “Provider schedules and locations of care should be improved so families would have easier access. Also, social media should have more positive well-child messages to counteract the negative messaging.”
More research is needed to examine the impact of COVID-19 on well-child visits, Dr. Boulter emphasized. “Most likely, the percentages in all groups will have changed since COVID-19 has impacted office practices,” she said. “Anxiety about COVID-19 transmissibility in the pediatric office decreased routine office visits, and skepticism about vaccines, including vaccine refusal, has significantly changed the percentage of children who have received the AAP recommended vaccines,” she explained. Ideally, the study authors will review the MEPS data again to examine changes since the COVID-19 pandemic began, she told this news organization.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Boulter had no financial conflicts to disclose and serves on the editorial advisory board of Pediatric News.
FROM JAMA PEDIATRICS