User login
For MD-IQ use only
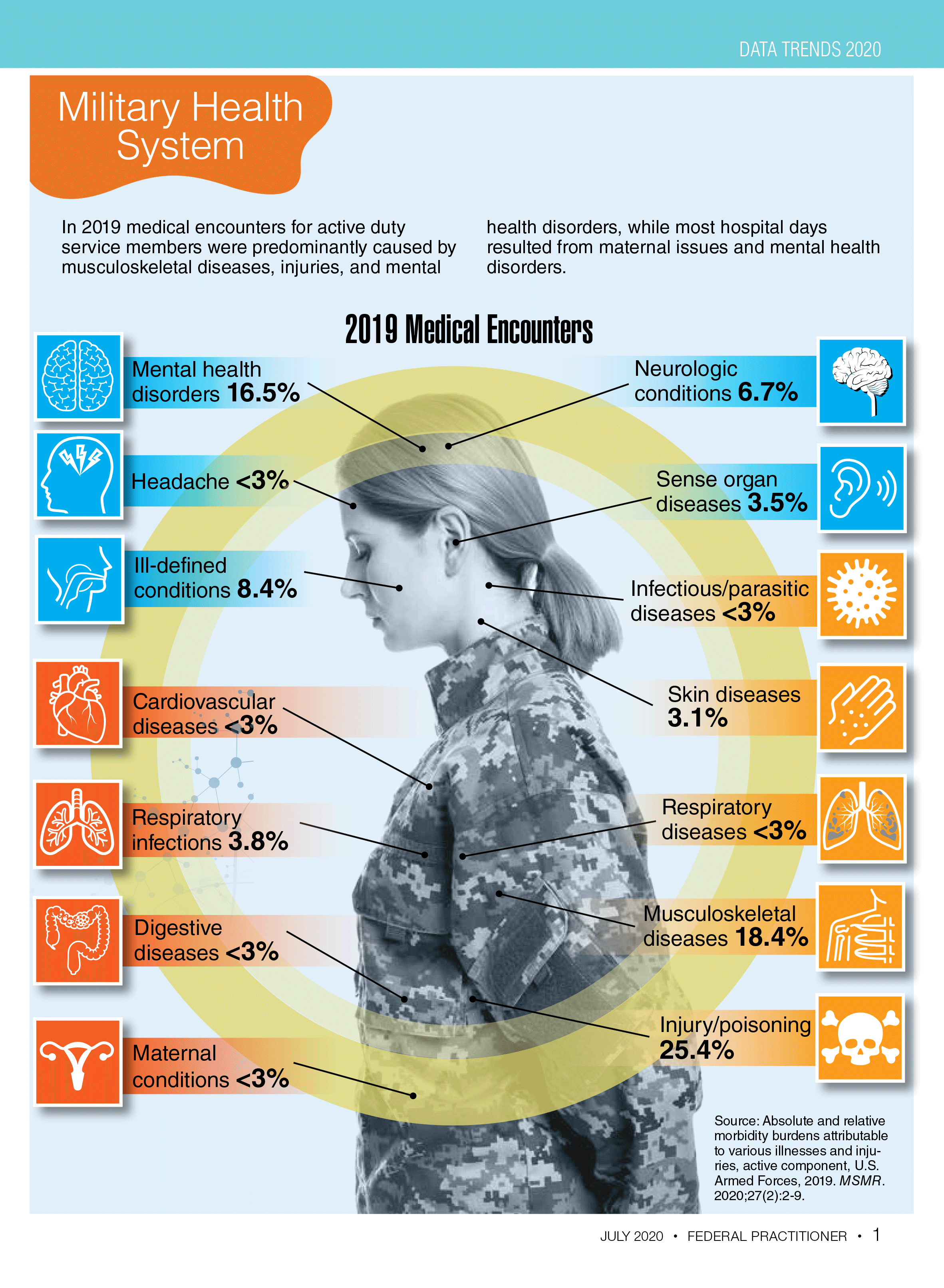
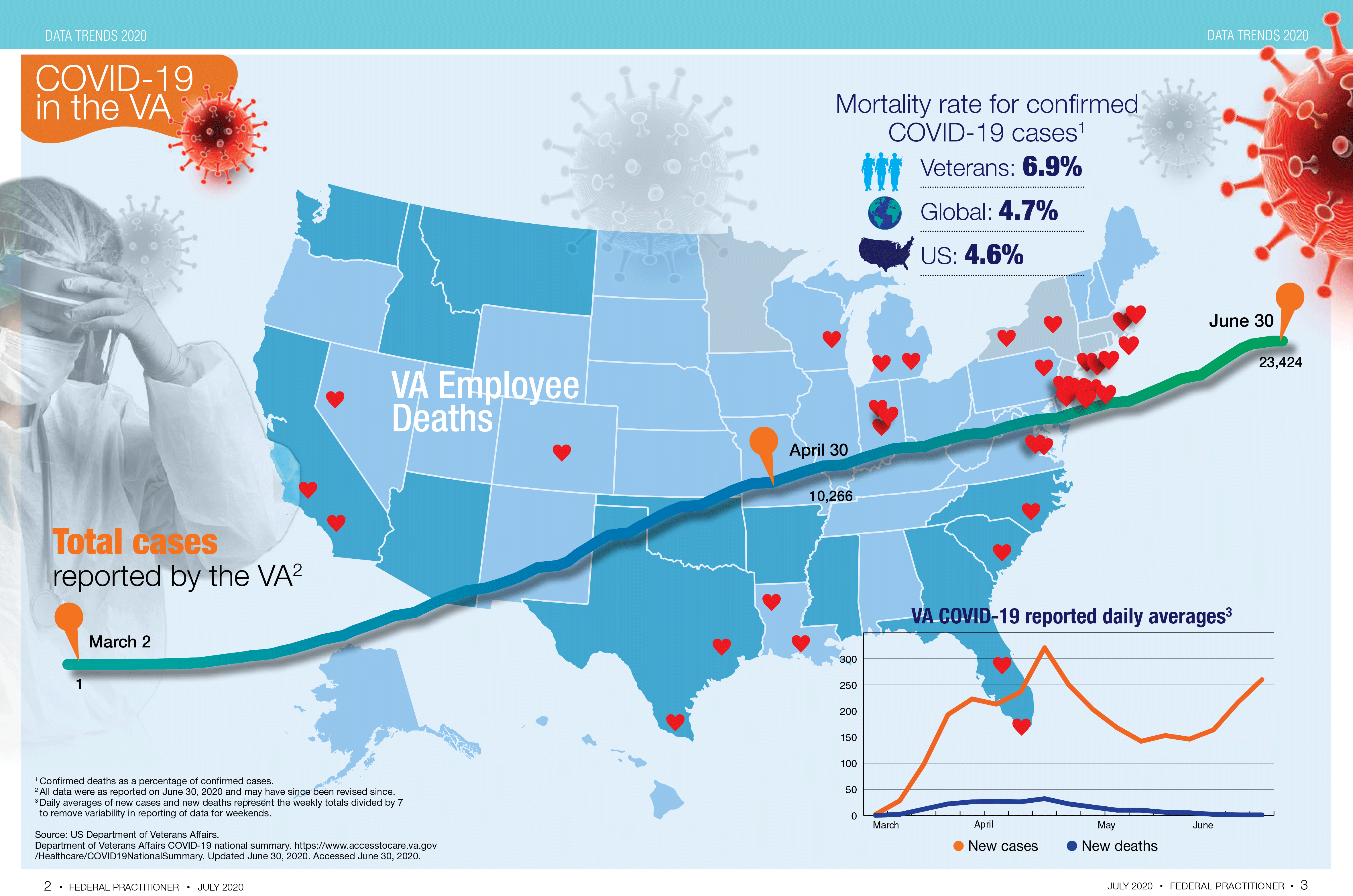
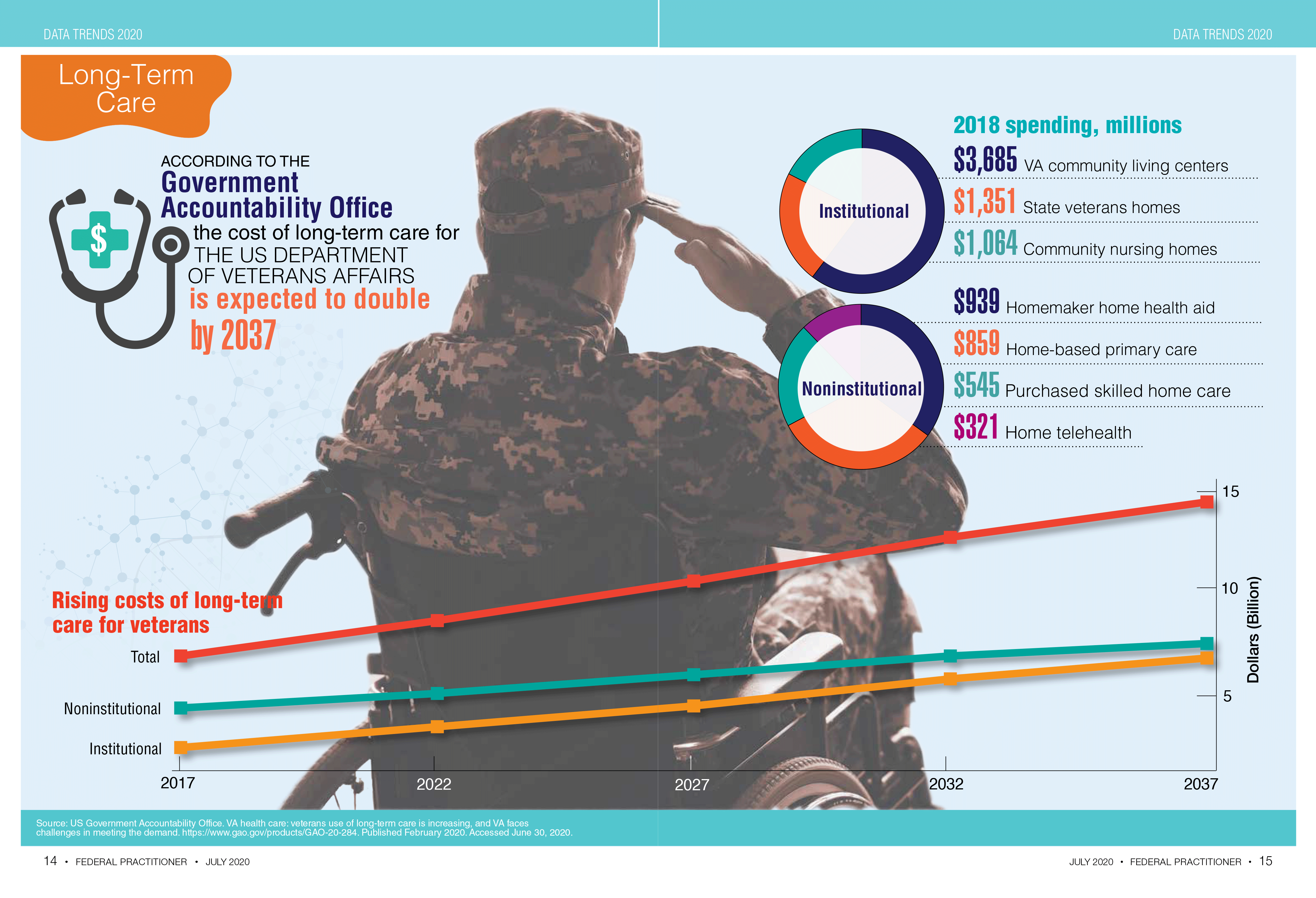
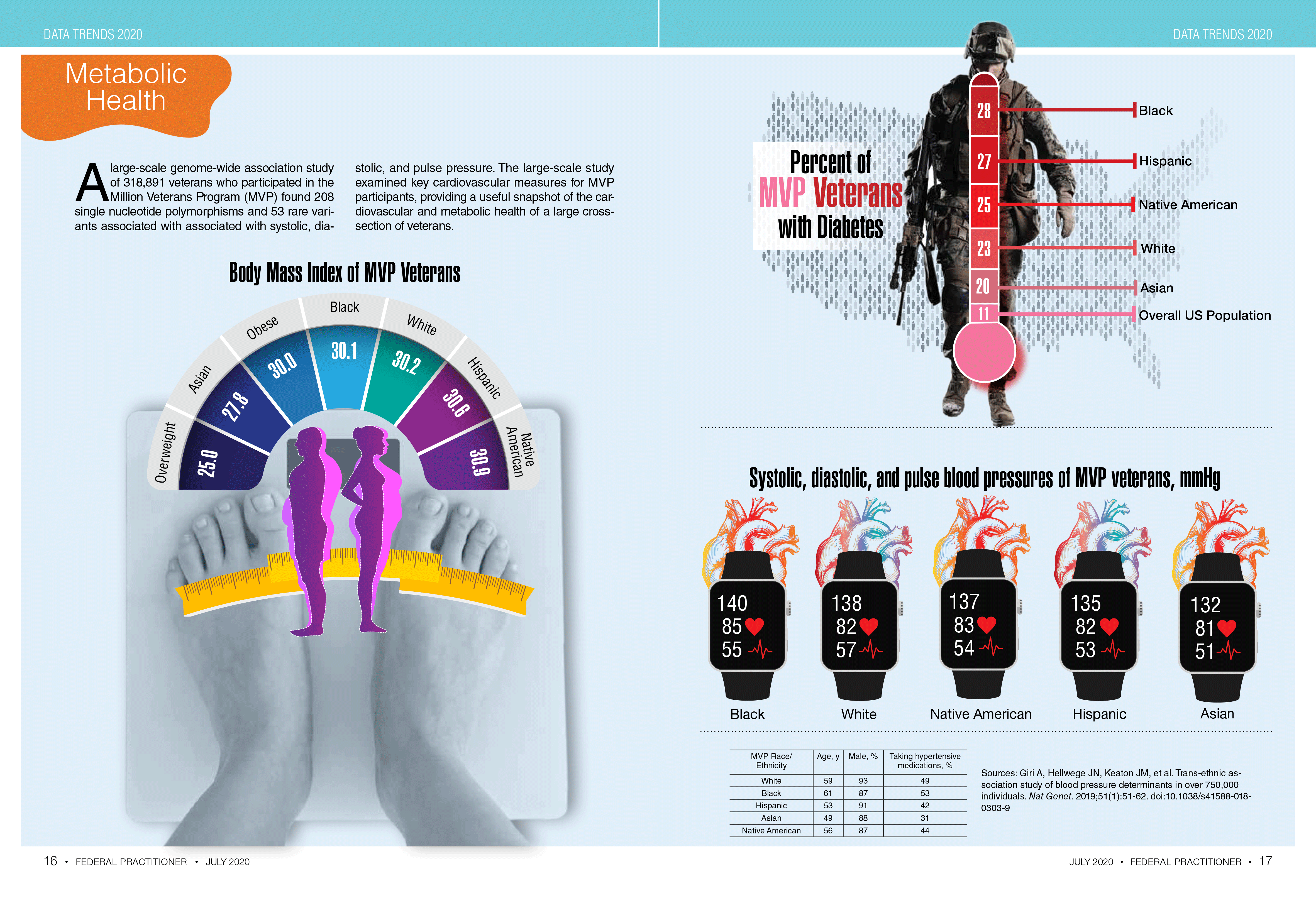
Federal Health Care Data Trends 2020

E.U. gives thumbs up for belantamab in R/R multiple myeloma
The first-in-class drug belantamab mafodotin (Blenrep, GlaxoSmithKline) has been recommended for conditional marketing approval in the European Union (EU) for use in the treatment of relapsed and refractory multiple myeloma in patients who have already tried other therapies.
The product was accepted into the European Medicines Agency (EMA) PRIME program for medicines that have potential to address unmet medical needs, the agency noted.
Belantamab mafodotin was also recently recommended for U.S. approval when a Food and Drug Administration advisory committee voted 12-0 in favor of the drug’s benefits outweighing risks in this patient population.
Specifically, these patients with refractory or relapsed multiple myeloma should have already tried treatment with one of the three major classes of drugs, namely an immunomodulatory agent, a proteasome inhibitor, and a CD-38 monoclonal antibody.
For patients who no longer respond to these drugs, the outlook is bleak, the EMA said. There is an unmet medical need for new treatments that improve survival of these patients beyond the currently observed 3 months or less.
Belantamab mafodotin has a novel mechanism of action: It targets B-cell maturation antigen (BCMA), a protein present on the surface of virtually all multiple myeloma cells, but is absent from normal B-cells, thus “making it an ideal drug target,” the agency remarked.
The product is an antibody–drug conjugate that combines a monoclonal antibody that targets BCMA with the cytotoxic agent maleimidocaproyl monomethylauristatin F (mcMMAF). It homes in on BCMA on myeloma cell surfaces, and once inside the myeloma cell, the cytotoxic agent is released leading to apoptosis, the “programmed” death of the cancerous plasma cells, the agency explained.
Results from open-label study
The recommendation for conditional marketing authorization comes from the EMA Committee for Medicinal Products for Human Use (CHMP) and was based on a phase 2, open-label, randomized, two-arm study, DREAMM-2.
The study investigated the efficacy and safety of two doses of belantamab mafodotin in patients with multiple myeloma who still had active disease after three or more lines of therapy and who no longer responded to treatment with immunomodulatory drugs, proteasome inhibitors, and an anti-CD38 monoclonal antibody.
Six-month results were published in December in The Lancet Oncology. The overall response rate was 31% in the cohort given a 2.5-mg/kg dose of the drug; 30 of 97 patients had outcomes that met the study’s positive threshold.
Another 99 patients in DREAMM-2 received a dose of 3.4 mg/kg, which was judged to have a less favorable safety profile.
The EMA has requested further clinical data, including final results from the phase 2 study, as well as results from a confirmatory phase 3 trial comparing belantamab mafodotin with pomalidomide plus low-dose dexamethasone (a standard treatment option for relapsed and refractory multiple myeloma).
Ocular toxicity
One of the most common side effects of the new drug experienced by participants in clinical trials was keratopathy, which affects the cornea. This ocular toxicity was seen at both drug doses.
The EMA noted that patients taking the drug would need to undergo specific ophthalmic examinations so that any findings can be promptly and adequately managed. As for all medicines, a risk management plan (RMP) will ensure rigorous safety monitoring of the medicine once authorized across the European Union, it added.
At the FDA advisory committee meeting, it was noted that 44% of patients in the group that received the 2.5-mg/kg dose experienced at least one episode of severe keratopathy. In some patients, the ocular side effects caused severe vision loss that interfered with patients’ activities of daily living, such as driving and reading, FDA staff said.
For the United States, the manufacturer proposed a risk evaluation and mitigation strategy (REMS) for the detection and treatment of potential complications of belantamab. This includes recommendations for ophthalmic examinations, including assessment of best corrected visual acuity prior to each treatment cycle and promptly for patients with worsening symptoms.
One of the FDA advisory committee panelists, Gita Thanarajasingam, MD, assistant professor of medicine at the Mayo Clinic, in Rochester, Minn., said belantamab appeared to be well tolerated with the exception of ocular toxicity. Physicians need to acknowledge how severe this risk may be for patients while keeping in mind that belantamab still may be more tolerable for some than current treatments, she said.
“It’s reasonable to leave open the option for decision-making. Patients can express their values and preferences,” Thanarajasingam said. “There’s adequate, albeit not complete, information to guide this risk–benefit discussion in a REMS program.”
Heidi D. Klepin, MD, a professor at Wake Forest University Health Sciences, Winston Salem, N.C., agreed that the informed consent process should allow patients “to choose whether the trade-off is worth it” with belantamab.
This article first appeared on Medscape.com.
The first-in-class drug belantamab mafodotin (Blenrep, GlaxoSmithKline) has been recommended for conditional marketing approval in the European Union (EU) for use in the treatment of relapsed and refractory multiple myeloma in patients who have already tried other therapies.
The product was accepted into the European Medicines Agency (EMA) PRIME program for medicines that have potential to address unmet medical needs, the agency noted.
Belantamab mafodotin was also recently recommended for U.S. approval when a Food and Drug Administration advisory committee voted 12-0 in favor of the drug’s benefits outweighing risks in this patient population.
Specifically, these patients with refractory or relapsed multiple myeloma should have already tried treatment with one of the three major classes of drugs, namely an immunomodulatory agent, a proteasome inhibitor, and a CD-38 monoclonal antibody.
For patients who no longer respond to these drugs, the outlook is bleak, the EMA said. There is an unmet medical need for new treatments that improve survival of these patients beyond the currently observed 3 months or less.
Belantamab mafodotin has a novel mechanism of action: It targets B-cell maturation antigen (BCMA), a protein present on the surface of virtually all multiple myeloma cells, but is absent from normal B-cells, thus “making it an ideal drug target,” the agency remarked.
The product is an antibody–drug conjugate that combines a monoclonal antibody that targets BCMA with the cytotoxic agent maleimidocaproyl monomethylauristatin F (mcMMAF). It homes in on BCMA on myeloma cell surfaces, and once inside the myeloma cell, the cytotoxic agent is released leading to apoptosis, the “programmed” death of the cancerous plasma cells, the agency explained.
Results from open-label study
The recommendation for conditional marketing authorization comes from the EMA Committee for Medicinal Products for Human Use (CHMP) and was based on a phase 2, open-label, randomized, two-arm study, DREAMM-2.
The study investigated the efficacy and safety of two doses of belantamab mafodotin in patients with multiple myeloma who still had active disease after three or more lines of therapy and who no longer responded to treatment with immunomodulatory drugs, proteasome inhibitors, and an anti-CD38 monoclonal antibody.
Six-month results were published in December in The Lancet Oncology. The overall response rate was 31% in the cohort given a 2.5-mg/kg dose of the drug; 30 of 97 patients had outcomes that met the study’s positive threshold.
Another 99 patients in DREAMM-2 received a dose of 3.4 mg/kg, which was judged to have a less favorable safety profile.
The EMA has requested further clinical data, including final results from the phase 2 study, as well as results from a confirmatory phase 3 trial comparing belantamab mafodotin with pomalidomide plus low-dose dexamethasone (a standard treatment option for relapsed and refractory multiple myeloma).
Ocular toxicity
One of the most common side effects of the new drug experienced by participants in clinical trials was keratopathy, which affects the cornea. This ocular toxicity was seen at both drug doses.
The EMA noted that patients taking the drug would need to undergo specific ophthalmic examinations so that any findings can be promptly and adequately managed. As for all medicines, a risk management plan (RMP) will ensure rigorous safety monitoring of the medicine once authorized across the European Union, it added.
At the FDA advisory committee meeting, it was noted that 44% of patients in the group that received the 2.5-mg/kg dose experienced at least one episode of severe keratopathy. In some patients, the ocular side effects caused severe vision loss that interfered with patients’ activities of daily living, such as driving and reading, FDA staff said.
For the United States, the manufacturer proposed a risk evaluation and mitigation strategy (REMS) for the detection and treatment of potential complications of belantamab. This includes recommendations for ophthalmic examinations, including assessment of best corrected visual acuity prior to each treatment cycle and promptly for patients with worsening symptoms.
One of the FDA advisory committee panelists, Gita Thanarajasingam, MD, assistant professor of medicine at the Mayo Clinic, in Rochester, Minn., said belantamab appeared to be well tolerated with the exception of ocular toxicity. Physicians need to acknowledge how severe this risk may be for patients while keeping in mind that belantamab still may be more tolerable for some than current treatments, she said.
“It’s reasonable to leave open the option for decision-making. Patients can express their values and preferences,” Thanarajasingam said. “There’s adequate, albeit not complete, information to guide this risk–benefit discussion in a REMS program.”
Heidi D. Klepin, MD, a professor at Wake Forest University Health Sciences, Winston Salem, N.C., agreed that the informed consent process should allow patients “to choose whether the trade-off is worth it” with belantamab.
This article first appeared on Medscape.com.
The first-in-class drug belantamab mafodotin (Blenrep, GlaxoSmithKline) has been recommended for conditional marketing approval in the European Union (EU) for use in the treatment of relapsed and refractory multiple myeloma in patients who have already tried other therapies.
The product was accepted into the European Medicines Agency (EMA) PRIME program for medicines that have potential to address unmet medical needs, the agency noted.
Belantamab mafodotin was also recently recommended for U.S. approval when a Food and Drug Administration advisory committee voted 12-0 in favor of the drug’s benefits outweighing risks in this patient population.
Specifically, these patients with refractory or relapsed multiple myeloma should have already tried treatment with one of the three major classes of drugs, namely an immunomodulatory agent, a proteasome inhibitor, and a CD-38 monoclonal antibody.
For patients who no longer respond to these drugs, the outlook is bleak, the EMA said. There is an unmet medical need for new treatments that improve survival of these patients beyond the currently observed 3 months or less.
Belantamab mafodotin has a novel mechanism of action: It targets B-cell maturation antigen (BCMA), a protein present on the surface of virtually all multiple myeloma cells, but is absent from normal B-cells, thus “making it an ideal drug target,” the agency remarked.
The product is an antibody–drug conjugate that combines a monoclonal antibody that targets BCMA with the cytotoxic agent maleimidocaproyl monomethylauristatin F (mcMMAF). It homes in on BCMA on myeloma cell surfaces, and once inside the myeloma cell, the cytotoxic agent is released leading to apoptosis, the “programmed” death of the cancerous plasma cells, the agency explained.
Results from open-label study
The recommendation for conditional marketing authorization comes from the EMA Committee for Medicinal Products for Human Use (CHMP) and was based on a phase 2, open-label, randomized, two-arm study, DREAMM-2.
The study investigated the efficacy and safety of two doses of belantamab mafodotin in patients with multiple myeloma who still had active disease after three or more lines of therapy and who no longer responded to treatment with immunomodulatory drugs, proteasome inhibitors, and an anti-CD38 monoclonal antibody.
Six-month results were published in December in The Lancet Oncology. The overall response rate was 31% in the cohort given a 2.5-mg/kg dose of the drug; 30 of 97 patients had outcomes that met the study’s positive threshold.
Another 99 patients in DREAMM-2 received a dose of 3.4 mg/kg, which was judged to have a less favorable safety profile.
The EMA has requested further clinical data, including final results from the phase 2 study, as well as results from a confirmatory phase 3 trial comparing belantamab mafodotin with pomalidomide plus low-dose dexamethasone (a standard treatment option for relapsed and refractory multiple myeloma).
Ocular toxicity
One of the most common side effects of the new drug experienced by participants in clinical trials was keratopathy, which affects the cornea. This ocular toxicity was seen at both drug doses.
The EMA noted that patients taking the drug would need to undergo specific ophthalmic examinations so that any findings can be promptly and adequately managed. As for all medicines, a risk management plan (RMP) will ensure rigorous safety monitoring of the medicine once authorized across the European Union, it added.
At the FDA advisory committee meeting, it was noted that 44% of patients in the group that received the 2.5-mg/kg dose experienced at least one episode of severe keratopathy. In some patients, the ocular side effects caused severe vision loss that interfered with patients’ activities of daily living, such as driving and reading, FDA staff said.
For the United States, the manufacturer proposed a risk evaluation and mitigation strategy (REMS) for the detection and treatment of potential complications of belantamab. This includes recommendations for ophthalmic examinations, including assessment of best corrected visual acuity prior to each treatment cycle and promptly for patients with worsening symptoms.
One of the FDA advisory committee panelists, Gita Thanarajasingam, MD, assistant professor of medicine at the Mayo Clinic, in Rochester, Minn., said belantamab appeared to be well tolerated with the exception of ocular toxicity. Physicians need to acknowledge how severe this risk may be for patients while keeping in mind that belantamab still may be more tolerable for some than current treatments, she said.
“It’s reasonable to leave open the option for decision-making. Patients can express their values and preferences,” Thanarajasingam said. “There’s adequate, albeit not complete, information to guide this risk–benefit discussion in a REMS program.”
Heidi D. Klepin, MD, a professor at Wake Forest University Health Sciences, Winston Salem, N.C., agreed that the informed consent process should allow patients “to choose whether the trade-off is worth it” with belantamab.
This article first appeared on Medscape.com.
New realities
Dear colleagues,
The August issue of The New Gastroenterologist has arrived! The summer of 2020 certainly looks different from years past, as the COVID-19 pandemic rages on and we continue to adjust to the new realities of our personal and professional lives. Our third-year fellows have graduated amidst these unusual circumstances, some facing an uncertain job landscape. Yet their hard work is not lost upon us – as we must step back to recognize their achievements and bid them congratulations on the culmination of several years of training.

The pandemic has been pervasive in medical education with a profound effect on our training programs. Two very resourceful fellows, Indira Bhavsar-Burke and Claire Jansson-Knodell (Indiana University), share their experience with COVID-19 and how they used this time to create an online curriculum for medical students who were pulled from their gastroenterology clinical rotations.
As we remain socially distanced, connecting through virtual platforms and social media seems more important than ever, but digital media can be difficult to navigate as physicians. Austin Chiang (Thomas Jefferson University) offers a candid snapshot of the benefits and pitfalls of social media as a gastroenterologist, with advice on how to optimize one’s professional presence online.
This quarter’s “In Focus” feature is an excellent, high-yield review of eosinophilic esophagitis. Ronak Vashi Patel and Ikuo Hirano (Northwestern University) seek to answer frequently asked questions about diagnostic considerations and the approach to management by reviewing therapeutic options – a truly valuable clinical piece to guide any young gastroenterologist.
Our medical ethics series features a poignant piece written by Diana Anderson (University of California, San Francisco) and David Seres (Columbia University) on the role of nutritional support in patients with restrictive eating disorders. The article addresses the complex interplay between certain diagnoses and our emotive response as clinicians – a critical piece of patient care that is seldom discussed. The authors implore us to consider this difficult question: Could our unconscious partiality as physicians be worse than intentional harm?
Adjoa Anyane-Yeboa (Harvard University) discusses how her interest in health equity and health care policy led her to the Commonwealth Fund Fellowship in Minority Health Policy. Her passion for health care delivery reform and the care of vulnerable populations shines through as she describes how this post-GI fellowship pathway has been formative in shaping her career as a dynamic new gastroenterologist.
For those interested in serving as an expert witness, seasoned malpractice attorneys Daniel Mills and Courtney Lindbert (Cunningham, Meyer & Vedrine P.C.) offer a salient list of the “do’s and don’ts” of the medical expert. Finally, this summer’s DHPA Private Practice Perspectives article, written by Michael Weinstein (Capital Digestive Care), offers important considerations for evaluating independent GI practices and how their response to COVID-19 can dictate their preparedness for future crises.
If you have interest in contributing or have ideas for future TNG topics, please contact me ([email protected]), or Ryan Farrell ([email protected]), managing editor of TNG.
Stay well,
Vijaya L. Rao, MD
Editor-in-Chief
Assistant professor of medicine, University of Chicago, section of gastroenterology, hepatology & nutrition
Dear colleagues,
The August issue of The New Gastroenterologist has arrived! The summer of 2020 certainly looks different from years past, as the COVID-19 pandemic rages on and we continue to adjust to the new realities of our personal and professional lives. Our third-year fellows have graduated amidst these unusual circumstances, some facing an uncertain job landscape. Yet their hard work is not lost upon us – as we must step back to recognize their achievements and bid them congratulations on the culmination of several years of training.
The pandemic has been pervasive in medical education with a profound effect on our training programs. Two very resourceful fellows, Indira Bhavsar-Burke and Claire Jansson-Knodell (Indiana University), share their experience with COVID-19 and how they used this time to create an online curriculum for medical students who were pulled from their gastroenterology clinical rotations.
As we remain socially distanced, connecting through virtual platforms and social media seems more important than ever, but digital media can be difficult to navigate as physicians. Austin Chiang (Thomas Jefferson University) offers a candid snapshot of the benefits and pitfalls of social media as a gastroenterologist, with advice on how to optimize one’s professional presence online.
This quarter’s “In Focus” feature is an excellent, high-yield review of eosinophilic esophagitis. Ronak Vashi Patel and Ikuo Hirano (Northwestern University) seek to answer frequently asked questions about diagnostic considerations and the approach to management by reviewing therapeutic options – a truly valuable clinical piece to guide any young gastroenterologist.
Our medical ethics series features a poignant piece written by Diana Anderson (University of California, San Francisco) and David Seres (Columbia University) on the role of nutritional support in patients with restrictive eating disorders. The article addresses the complex interplay between certain diagnoses and our emotive response as clinicians – a critical piece of patient care that is seldom discussed. The authors implore us to consider this difficult question: Could our unconscious partiality as physicians be worse than intentional harm?
Adjoa Anyane-Yeboa (Harvard University) discusses how her interest in health equity and health care policy led her to the Commonwealth Fund Fellowship in Minority Health Policy. Her passion for health care delivery reform and the care of vulnerable populations shines through as she describes how this post-GI fellowship pathway has been formative in shaping her career as a dynamic new gastroenterologist.
For those interested in serving as an expert witness, seasoned malpractice attorneys Daniel Mills and Courtney Lindbert (Cunningham, Meyer & Vedrine P.C.) offer a salient list of the “do’s and don’ts” of the medical expert. Finally, this summer’s DHPA Private Practice Perspectives article, written by Michael Weinstein (Capital Digestive Care), offers important considerations for evaluating independent GI practices and how their response to COVID-19 can dictate their preparedness for future crises.
If you have interest in contributing or have ideas for future TNG topics, please contact me ([email protected]), or Ryan Farrell ([email protected]), managing editor of TNG.
Stay well,
Vijaya L. Rao, MD
Editor-in-Chief
Assistant professor of medicine, University of Chicago, section of gastroenterology, hepatology & nutrition
Dear colleagues,
The August issue of The New Gastroenterologist has arrived! The summer of 2020 certainly looks different from years past, as the COVID-19 pandemic rages on and we continue to adjust to the new realities of our personal and professional lives. Our third-year fellows have graduated amidst these unusual circumstances, some facing an uncertain job landscape. Yet their hard work is not lost upon us – as we must step back to recognize their achievements and bid them congratulations on the culmination of several years of training.
The pandemic has been pervasive in medical education with a profound effect on our training programs. Two very resourceful fellows, Indira Bhavsar-Burke and Claire Jansson-Knodell (Indiana University), share their experience with COVID-19 and how they used this time to create an online curriculum for medical students who were pulled from their gastroenterology clinical rotations.
As we remain socially distanced, connecting through virtual platforms and social media seems more important than ever, but digital media can be difficult to navigate as physicians. Austin Chiang (Thomas Jefferson University) offers a candid snapshot of the benefits and pitfalls of social media as a gastroenterologist, with advice on how to optimize one’s professional presence online.
This quarter’s “In Focus” feature is an excellent, high-yield review of eosinophilic esophagitis. Ronak Vashi Patel and Ikuo Hirano (Northwestern University) seek to answer frequently asked questions about diagnostic considerations and the approach to management by reviewing therapeutic options – a truly valuable clinical piece to guide any young gastroenterologist.
Our medical ethics series features a poignant piece written by Diana Anderson (University of California, San Francisco) and David Seres (Columbia University) on the role of nutritional support in patients with restrictive eating disorders. The article addresses the complex interplay between certain diagnoses and our emotive response as clinicians – a critical piece of patient care that is seldom discussed. The authors implore us to consider this difficult question: Could our unconscious partiality as physicians be worse than intentional harm?
Adjoa Anyane-Yeboa (Harvard University) discusses how her interest in health equity and health care policy led her to the Commonwealth Fund Fellowship in Minority Health Policy. Her passion for health care delivery reform and the care of vulnerable populations shines through as she describes how this post-GI fellowship pathway has been formative in shaping her career as a dynamic new gastroenterologist.
For those interested in serving as an expert witness, seasoned malpractice attorneys Daniel Mills and Courtney Lindbert (Cunningham, Meyer & Vedrine P.C.) offer a salient list of the “do’s and don’ts” of the medical expert. Finally, this summer’s DHPA Private Practice Perspectives article, written by Michael Weinstein (Capital Digestive Care), offers important considerations for evaluating independent GI practices and how their response to COVID-19 can dictate their preparedness for future crises.
If you have interest in contributing or have ideas for future TNG topics, please contact me ([email protected]), or Ryan Farrell ([email protected]), managing editor of TNG.
Stay well,
Vijaya L. Rao, MD
Editor-in-Chief
Assistant professor of medicine, University of Chicago, section of gastroenterology, hepatology & nutrition
US News releases latest top hospitals list, adds COVID heroes
This year’s rankings include special recognition of the “herculean efforts” by the nation’s healthcare professionals in fighting COVID-19, often at great personal risk.
“The US News Hospital Heroes series is a cornerstone of this year’s rankings package, profiling more than 65 health care heroes from across the country, along with commentary from top executives at hospitals who faced the pandemic head on,” a news release from the magazine explains.
“The pandemic has altered, perhaps permanently, how patients get care and from whom they get it. Amid the disruption, we are steadfastly committed to providing the public with authoritative data for comparing hospital quality,” Ben Harder, managing editor and chief of health analysis at US News, said in the release.
“No hospital’s clinical team came through this unprecedented health crisis unscathed. Our Hospital Heroes series is a tribute to recognizing individuals at urban and rural hospitals in communities across the country who have gone above and beyond during this unparalleled time in history,” said Harder.
Mayo Clinic Still Number One
Following Mayo Clinic, Cleveland Clinic in Ohio takes the number two spot this year (up from number four last year) in the magazine’s annual honor roll, which highlights hospitals that deliver “exceptional treatment across multiple areas of care.”
Johns Hopkins Hospital in Baltimore, Maryland, holds the number three spot, while New York-Presbyterian Hospital–Columbia and Cornell in New York City and UCLA Medical Center, Los Angeles, tie for the number four spot.
Massachusetts General Hospital in Boston, which held the number two spot last year, has fallen to number six. Rounding out the top 10, in order, are Cedars-Sinai Medical Center, Los Angeles; UCSF Medical Center, San Francisco; NYU Langone Hospitals, New York City; Northwestern Memorial Hospital, Chicago, Illinois.
2020–2021 Best Hospitals Honor Roll
1. Mayo Clinic, Rochester, Minnesota
2. Cleveland Clinic, Ohio
3. Johns Hopkins Hospital, Baltimore, Maryland
4. (tie) New York–Presbyterian Hospital–Columbia and Cornell, New York City
4. (tie) UCLA Medical Center, Los Angeles
6. Massachusetts General Hospital, Boston
7. Cedars-Sinai Medical Center, San Francisco
8. UCSF Medical Center, San Francisco
9. NYU Langone Hospitals, New York, New York City
10. Northwestern Memorial Hospital, Chicago
11. University of Michigan Hospitals–Michigan Medicine, Ann Arbor
12. Brigham and Women’s Hospital, Boston
13. Stanford Health Care–Stanford Hospital, Palo Alto, California
14. Mount Sinai Hospital, New York City
15. Hospitals of the University of Pennsylvania–Penn Presbyterian, Philadelphia
16. Mayo Clinic–Phoenix
17. Rush University Medical Center, Chicago
18. (tie) Barnes-Jewish Hospital, Saint Louis
18. (tie) Keck Hospital of USC, Los Angeles
20. Houston Methodist Hospital, Texas
In the 2020–2021 Best Hospitals: Specialty Rankings, University of Texas MD Anderson Cancer Center continues to hold the number one spot in cancer, the Hospital for Special Surgery is number one in orthopedics, and the Cleveland Clinic is number one in cardiology and heart surgery.
For this year’s rankings, US News developed a new cardiac rating that measures the quality of hospitals› transcatheter aortic valve replacement, which is rapidly being adopted as a minimally invasive alternative to aortic valve surgery.
Top Five for Cancer
1. University of Texas MD Anderson Cancer Center, Houston
2. Memorial Sloan Kettering Cancer Center, New York City
3. Mayo Clinic, Rochester, Minnesota
4. Johns Hopkins Hospital, Baltimore, Maryland
5. Cleveland Clinic, Ohio
Top Five for Cardiology and Heart Surgery
1. Cleveland Clinic, Ohio
2. Mayo Clinic, Rochester, Minnesota
3. Cedars-Sinai Medical Center, Los Angeles
4. New York–Presbyterian Hospital–Columbia and Cornell, NYC
5. Massachusetts General Hospital, Boston
Top Five for Orthopedics
1. Hospital for Special Surgery, New York City
2. Mayo Clinic, Rochester, Minnesota
3. Cedars-Sinai Medical Center, Los Angeles
4. NYU Langone Orthopedic Hospital, New York City
5. Rush University Medical Center, Chicago
For the 2020–2021 rankings and ratings, US News compared more than 4500 medical centers across the country in 16 specialties and 10 procedures and conditions. Of these, 563 were recognized as Best Regional Hospitals on the basis of their strong performance in multiple areas of care. The top 20 hospitals, which deliver exceptional treatment across many areas of care, were also named to the honor roll.
The magazine notes that data for the 2020–2021 Best Hospitals rankings and ratings come from a period predating the COVID-19 pandemic and were not affected by the pandemic’s impact on hospitals. The methodologies are based largely on objective measures, such as risk-adjusted survival and discharge-to-home rates, volume, and quality of nursing, among other care-related indicators.
The full report on hospital ranking is available online.
This article first appeared on Medscape.com.
This year’s rankings include special recognition of the “herculean efforts” by the nation’s healthcare professionals in fighting COVID-19, often at great personal risk.
“The US News Hospital Heroes series is a cornerstone of this year’s rankings package, profiling more than 65 health care heroes from across the country, along with commentary from top executives at hospitals who faced the pandemic head on,” a news release from the magazine explains.
“The pandemic has altered, perhaps permanently, how patients get care and from whom they get it. Amid the disruption, we are steadfastly committed to providing the public with authoritative data for comparing hospital quality,” Ben Harder, managing editor and chief of health analysis at US News, said in the release.
“No hospital’s clinical team came through this unprecedented health crisis unscathed. Our Hospital Heroes series is a tribute to recognizing individuals at urban and rural hospitals in communities across the country who have gone above and beyond during this unparalleled time in history,” said Harder.
Mayo Clinic Still Number One
Following Mayo Clinic, Cleveland Clinic in Ohio takes the number two spot this year (up from number four last year) in the magazine’s annual honor roll, which highlights hospitals that deliver “exceptional treatment across multiple areas of care.”
Johns Hopkins Hospital in Baltimore, Maryland, holds the number three spot, while New York-Presbyterian Hospital–Columbia and Cornell in New York City and UCLA Medical Center, Los Angeles, tie for the number four spot.
Massachusetts General Hospital in Boston, which held the number two spot last year, has fallen to number six. Rounding out the top 10, in order, are Cedars-Sinai Medical Center, Los Angeles; UCSF Medical Center, San Francisco; NYU Langone Hospitals, New York City; Northwestern Memorial Hospital, Chicago, Illinois.
2020–2021 Best Hospitals Honor Roll
1. Mayo Clinic, Rochester, Minnesota
2. Cleveland Clinic, Ohio
3. Johns Hopkins Hospital, Baltimore, Maryland
4. (tie) New York–Presbyterian Hospital–Columbia and Cornell, New York City
4. (tie) UCLA Medical Center, Los Angeles
6. Massachusetts General Hospital, Boston
7. Cedars-Sinai Medical Center, San Francisco
8. UCSF Medical Center, San Francisco
9. NYU Langone Hospitals, New York, New York City
10. Northwestern Memorial Hospital, Chicago
11. University of Michigan Hospitals–Michigan Medicine, Ann Arbor
12. Brigham and Women’s Hospital, Boston
13. Stanford Health Care–Stanford Hospital, Palo Alto, California
14. Mount Sinai Hospital, New York City
15. Hospitals of the University of Pennsylvania–Penn Presbyterian, Philadelphia
16. Mayo Clinic–Phoenix
17. Rush University Medical Center, Chicago
18. (tie) Barnes-Jewish Hospital, Saint Louis
18. (tie) Keck Hospital of USC, Los Angeles
20. Houston Methodist Hospital, Texas
In the 2020–2021 Best Hospitals: Specialty Rankings, University of Texas MD Anderson Cancer Center continues to hold the number one spot in cancer, the Hospital for Special Surgery is number one in orthopedics, and the Cleveland Clinic is number one in cardiology and heart surgery.
For this year’s rankings, US News developed a new cardiac rating that measures the quality of hospitals› transcatheter aortic valve replacement, which is rapidly being adopted as a minimally invasive alternative to aortic valve surgery.
Top Five for Cancer
1. University of Texas MD Anderson Cancer Center, Houston
2. Memorial Sloan Kettering Cancer Center, New York City
3. Mayo Clinic, Rochester, Minnesota
4. Johns Hopkins Hospital, Baltimore, Maryland
5. Cleveland Clinic, Ohio
Top Five for Cardiology and Heart Surgery
1. Cleveland Clinic, Ohio
2. Mayo Clinic, Rochester, Minnesota
3. Cedars-Sinai Medical Center, Los Angeles
4. New York–Presbyterian Hospital–Columbia and Cornell, NYC
5. Massachusetts General Hospital, Boston
Top Five for Orthopedics
1. Hospital for Special Surgery, New York City
2. Mayo Clinic, Rochester, Minnesota
3. Cedars-Sinai Medical Center, Los Angeles
4. NYU Langone Orthopedic Hospital, New York City
5. Rush University Medical Center, Chicago
For the 2020–2021 rankings and ratings, US News compared more than 4500 medical centers across the country in 16 specialties and 10 procedures and conditions. Of these, 563 were recognized as Best Regional Hospitals on the basis of their strong performance in multiple areas of care. The top 20 hospitals, which deliver exceptional treatment across many areas of care, were also named to the honor roll.
The magazine notes that data for the 2020–2021 Best Hospitals rankings and ratings come from a period predating the COVID-19 pandemic and were not affected by the pandemic’s impact on hospitals. The methodologies are based largely on objective measures, such as risk-adjusted survival and discharge-to-home rates, volume, and quality of nursing, among other care-related indicators.
The full report on hospital ranking is available online.
This article first appeared on Medscape.com.
This year’s rankings include special recognition of the “herculean efforts” by the nation’s healthcare professionals in fighting COVID-19, often at great personal risk.
“The US News Hospital Heroes series is a cornerstone of this year’s rankings package, profiling more than 65 health care heroes from across the country, along with commentary from top executives at hospitals who faced the pandemic head on,” a news release from the magazine explains.
“The pandemic has altered, perhaps permanently, how patients get care and from whom they get it. Amid the disruption, we are steadfastly committed to providing the public with authoritative data for comparing hospital quality,” Ben Harder, managing editor and chief of health analysis at US News, said in the release.
“No hospital’s clinical team came through this unprecedented health crisis unscathed. Our Hospital Heroes series is a tribute to recognizing individuals at urban and rural hospitals in communities across the country who have gone above and beyond during this unparalleled time in history,” said Harder.
Mayo Clinic Still Number One
Following Mayo Clinic, Cleveland Clinic in Ohio takes the number two spot this year (up from number four last year) in the magazine’s annual honor roll, which highlights hospitals that deliver “exceptional treatment across multiple areas of care.”
Johns Hopkins Hospital in Baltimore, Maryland, holds the number three spot, while New York-Presbyterian Hospital–Columbia and Cornell in New York City and UCLA Medical Center, Los Angeles, tie for the number four spot.
Massachusetts General Hospital in Boston, which held the number two spot last year, has fallen to number six. Rounding out the top 10, in order, are Cedars-Sinai Medical Center, Los Angeles; UCSF Medical Center, San Francisco; NYU Langone Hospitals, New York City; Northwestern Memorial Hospital, Chicago, Illinois.
2020–2021 Best Hospitals Honor Roll
1. Mayo Clinic, Rochester, Minnesota
2. Cleveland Clinic, Ohio
3. Johns Hopkins Hospital, Baltimore, Maryland
4. (tie) New York–Presbyterian Hospital–Columbia and Cornell, New York City
4. (tie) UCLA Medical Center, Los Angeles
6. Massachusetts General Hospital, Boston
7. Cedars-Sinai Medical Center, San Francisco
8. UCSF Medical Center, San Francisco
9. NYU Langone Hospitals, New York, New York City
10. Northwestern Memorial Hospital, Chicago
11. University of Michigan Hospitals–Michigan Medicine, Ann Arbor
12. Brigham and Women’s Hospital, Boston
13. Stanford Health Care–Stanford Hospital, Palo Alto, California
14. Mount Sinai Hospital, New York City
15. Hospitals of the University of Pennsylvania–Penn Presbyterian, Philadelphia
16. Mayo Clinic–Phoenix
17. Rush University Medical Center, Chicago
18. (tie) Barnes-Jewish Hospital, Saint Louis
18. (tie) Keck Hospital of USC, Los Angeles
20. Houston Methodist Hospital, Texas
In the 2020–2021 Best Hospitals: Specialty Rankings, University of Texas MD Anderson Cancer Center continues to hold the number one spot in cancer, the Hospital for Special Surgery is number one in orthopedics, and the Cleveland Clinic is number one in cardiology and heart surgery.
For this year’s rankings, US News developed a new cardiac rating that measures the quality of hospitals› transcatheter aortic valve replacement, which is rapidly being adopted as a minimally invasive alternative to aortic valve surgery.
Top Five for Cancer
1. University of Texas MD Anderson Cancer Center, Houston
2. Memorial Sloan Kettering Cancer Center, New York City
3. Mayo Clinic, Rochester, Minnesota
4. Johns Hopkins Hospital, Baltimore, Maryland
5. Cleveland Clinic, Ohio
Top Five for Cardiology and Heart Surgery
1. Cleveland Clinic, Ohio
2. Mayo Clinic, Rochester, Minnesota
3. Cedars-Sinai Medical Center, Los Angeles
4. New York–Presbyterian Hospital–Columbia and Cornell, NYC
5. Massachusetts General Hospital, Boston
Top Five for Orthopedics
1. Hospital for Special Surgery, New York City
2. Mayo Clinic, Rochester, Minnesota
3. Cedars-Sinai Medical Center, Los Angeles
4. NYU Langone Orthopedic Hospital, New York City
5. Rush University Medical Center, Chicago
For the 2020–2021 rankings and ratings, US News compared more than 4500 medical centers across the country in 16 specialties and 10 procedures and conditions. Of these, 563 were recognized as Best Regional Hospitals on the basis of their strong performance in multiple areas of care. The top 20 hospitals, which deliver exceptional treatment across many areas of care, were also named to the honor roll.
The magazine notes that data for the 2020–2021 Best Hospitals rankings and ratings come from a period predating the COVID-19 pandemic and were not affected by the pandemic’s impact on hospitals. The methodologies are based largely on objective measures, such as risk-adjusted survival and discharge-to-home rates, volume, and quality of nursing, among other care-related indicators.
The full report on hospital ranking is available online.
This article first appeared on Medscape.com.
Updated EULAR/ACR criteria identify more lupus patients
Use of the 2019 EULAR/ACR criteria for systemic lupus erythematosus identified an additional 17% of lupus patients in a cohort of 133 women with undifferentiated connective tissue disease.
Several studies have applied the 2019 EULAR/ACR criteria for systemic lupus erythematosus (SLE) to different patient populations, wrote Massimo Radin, MD, of S. Giovanni Bosco Hospital, Turin, Italy, and colleagues.
“However, it is unknown if the new classifications criteria for SLE might impact on the categorization of patients previously diagnosed with undifferentiated connective tissue disease (UCTD),” they said in a brief report published in Arthritis Care & Research.
In addition, “being classified or not as having SLE may pose clinical and logistic consequences, as patients with a diagnosis of ‘SLE’ might be followed up according to a specific local protocol and have in-label access to certain medications (such as biologics) or may be eligible for the participation in clinical trials,” they wrote.
The investigators applied the 2019 EULAR/ACR criteria to a cohort of 133 women with UCTD but no other diagnosis. The average age of the women was 38 years; the average disease duration was 10 years. Patients who scored 10 points or more on positive clinical and immunological domains at the start of the study were classified as SLE under the 2019 EULAR/ACR criteria.
Overall, 22 patients (17%) met the classification criteria for SLE at the time of their first pregnancy.
Compared with the other patients in the cohort who were not classified as SLE, patients classified as SLE under the 2019 EULAR/ACR criteria had significantly higher frequency of mucocutaneous manifestations (5% vs. 23%), arthritis (17% vs. 59%), isolated urine abnormalities (1% vs. 18%), and highly specific antibodies (15% vs. 50%).
In addition, patients who met the 2019 EULAR/ACR SLE criteria were significantly more likely to meet the ACR 1997 and SLICC criteria after an average follow-up of 9 years compared with the rest of the cohort (18.2% vs. 1.8%). Patients who met the 2019 EULAR/ACR criteria also had significantly shorter disease duration than that of the other patients in the UCTD cohort (8.23 years vs. 10.7 years) and were significantly more likely to develop preeclampsia during pregnancy (18% vs. 0%).
The findings were limited by several factors including the retrospective design of the study and possible lack of generalizability to male patients, the researchers noted.
The results support the need for improved classification criteria for UCTD, as early identification of specific conditions can help guide treatment and reduce the risk of more severe symptoms and complications, the authors said.
“When discriminating between conditions with a marked overlap, such as SLE and UCTD, the proposal of new classification criteria should balance specificity and sensitivity,” the researchers wrote. “When developing new classification criteria, one approach is to select patients and the control groups as representative as possible of the settings (the medical practices) in which these criteria will be used.”
The study received no outside funding. The researchers had no financial conflicts to disclose.
SOURCE: Radin M et al. Art
Use of the 2019 EULAR/ACR criteria for systemic lupus erythematosus identified an additional 17% of lupus patients in a cohort of 133 women with undifferentiated connective tissue disease.
Several studies have applied the 2019 EULAR/ACR criteria for systemic lupus erythematosus (SLE) to different patient populations, wrote Massimo Radin, MD, of S. Giovanni Bosco Hospital, Turin, Italy, and colleagues.
“However, it is unknown if the new classifications criteria for SLE might impact on the categorization of patients previously diagnosed with undifferentiated connective tissue disease (UCTD),” they said in a brief report published in Arthritis Care & Research.
In addition, “being classified or not as having SLE may pose clinical and logistic consequences, as patients with a diagnosis of ‘SLE’ might be followed up according to a specific local protocol and have in-label access to certain medications (such as biologics) or may be eligible for the participation in clinical trials,” they wrote.
The investigators applied the 2019 EULAR/ACR criteria to a cohort of 133 women with UCTD but no other diagnosis. The average age of the women was 38 years; the average disease duration was 10 years. Patients who scored 10 points or more on positive clinical and immunological domains at the start of the study were classified as SLE under the 2019 EULAR/ACR criteria.
Overall, 22 patients (17%) met the classification criteria for SLE at the time of their first pregnancy.
Compared with the other patients in the cohort who were not classified as SLE, patients classified as SLE under the 2019 EULAR/ACR criteria had significantly higher frequency of mucocutaneous manifestations (5% vs. 23%), arthritis (17% vs. 59%), isolated urine abnormalities (1% vs. 18%), and highly specific antibodies (15% vs. 50%).
In addition, patients who met the 2019 EULAR/ACR SLE criteria were significantly more likely to meet the ACR 1997 and SLICC criteria after an average follow-up of 9 years compared with the rest of the cohort (18.2% vs. 1.8%). Patients who met the 2019 EULAR/ACR criteria also had significantly shorter disease duration than that of the other patients in the UCTD cohort (8.23 years vs. 10.7 years) and were significantly more likely to develop preeclampsia during pregnancy (18% vs. 0%).
The findings were limited by several factors including the retrospective design of the study and possible lack of generalizability to male patients, the researchers noted.
The results support the need for improved classification criteria for UCTD, as early identification of specific conditions can help guide treatment and reduce the risk of more severe symptoms and complications, the authors said.
“When discriminating between conditions with a marked overlap, such as SLE and UCTD, the proposal of new classification criteria should balance specificity and sensitivity,” the researchers wrote. “When developing new classification criteria, one approach is to select patients and the control groups as representative as possible of the settings (the medical practices) in which these criteria will be used.”
The study received no outside funding. The researchers had no financial conflicts to disclose.
SOURCE: Radin M et al. Art
Use of the 2019 EULAR/ACR criteria for systemic lupus erythematosus identified an additional 17% of lupus patients in a cohort of 133 women with undifferentiated connective tissue disease.
Several studies have applied the 2019 EULAR/ACR criteria for systemic lupus erythematosus (SLE) to different patient populations, wrote Massimo Radin, MD, of S. Giovanni Bosco Hospital, Turin, Italy, and colleagues.
“However, it is unknown if the new classifications criteria for SLE might impact on the categorization of patients previously diagnosed with undifferentiated connective tissue disease (UCTD),” they said in a brief report published in Arthritis Care & Research.
In addition, “being classified or not as having SLE may pose clinical and logistic consequences, as patients with a diagnosis of ‘SLE’ might be followed up according to a specific local protocol and have in-label access to certain medications (such as biologics) or may be eligible for the participation in clinical trials,” they wrote.
The investigators applied the 2019 EULAR/ACR criteria to a cohort of 133 women with UCTD but no other diagnosis. The average age of the women was 38 years; the average disease duration was 10 years. Patients who scored 10 points or more on positive clinical and immunological domains at the start of the study were classified as SLE under the 2019 EULAR/ACR criteria.
Overall, 22 patients (17%) met the classification criteria for SLE at the time of their first pregnancy.
Compared with the other patients in the cohort who were not classified as SLE, patients classified as SLE under the 2019 EULAR/ACR criteria had significantly higher frequency of mucocutaneous manifestations (5% vs. 23%), arthritis (17% vs. 59%), isolated urine abnormalities (1% vs. 18%), and highly specific antibodies (15% vs. 50%).
In addition, patients who met the 2019 EULAR/ACR SLE criteria were significantly more likely to meet the ACR 1997 and SLICC criteria after an average follow-up of 9 years compared with the rest of the cohort (18.2% vs. 1.8%). Patients who met the 2019 EULAR/ACR criteria also had significantly shorter disease duration than that of the other patients in the UCTD cohort (8.23 years vs. 10.7 years) and were significantly more likely to develop preeclampsia during pregnancy (18% vs. 0%).
The findings were limited by several factors including the retrospective design of the study and possible lack of generalizability to male patients, the researchers noted.
The results support the need for improved classification criteria for UCTD, as early identification of specific conditions can help guide treatment and reduce the risk of more severe symptoms and complications, the authors said.
“When discriminating between conditions with a marked overlap, such as SLE and UCTD, the proposal of new classification criteria should balance specificity and sensitivity,” the researchers wrote. “When developing new classification criteria, one approach is to select patients and the control groups as representative as possible of the settings (the medical practices) in which these criteria will be used.”
The study received no outside funding. The researchers had no financial conflicts to disclose.
SOURCE: Radin M et al. Art
FROM ARTHRITIS CARE & RESEARCH
Hypertension medication adjustment less likely with polypill
A secondary analysis of a major study of polypill therapy for hypertension found that patients who don’t reach blood pressure targets are less likely to have their medications adjusted if they’re on fixed-dose combination therapy.

However, hypertension patients on low-dose, triple-pill combination therapy are more likely to achieve blood pressure control than are those on usual care.
The secondary analysis of Triple Pill vs. Usual Care Management for Patients with Mild-to-Moderate Hypertension (TRIUMPH) was published online in JAMA Cardiology (2020 Jul 22. doi: 10.1001/jamacardio.2020.2739). The trial randomized 700 patients with hypertension in Sri Lanka to triple-pill fixed-dose combination (FDC) therapy or usual care during February 2016–May 2017, with follow-up ending in October 2017.
A greater proportion of FDC patients reached target BP by the end of the study compared with usual care, 70% vs. 55%. However, the study found that therapeutic inertia – the failure to intensify therapy in nonresponsive patients – was more common in the FDC group at 6- and 12-week follow-up: 87% vs. 64% and 90% vs. 65%, respectively; both differences were significant different at P < .001).
The once-daily FDC pill contained telmisartan 20 mg, amlodipine 2.5 mg; and chlorthalidone 12.5 mg.
“Using a triple low-dose combination blood-pressure pill reduced the need to uptitrate BP therapy as more patients are at target, but doctors were less likely to uptitrate with triple-pill therapy when it was needed,” lead author Nelson Wang, MD, a research fellow at the George Institute for Global Health in suburban Sydney, said in an interview.
“Overall, there were fewer treatment inertia episodes in the triple-pill group than in the usual care group, but this was driven by the fact that fewer triple-pill patients needed uptitration when coming to their follow-up visits,” Dr. Wang added.
The analysis found that clinicians who prescribed triple-pill FDC used 23 unique drug treatment regimens per 100 treated patients compared with 54 different regiments with usual care (P < .001). “There was a large simplification in care,” Dr. Wang said of the FDC approach.
Dr. Wang and colleagues called for greater efforts to address therapeutic inertia, particularly with FDC therapies, and suggested potential strategies consisting of patient education, incentives for appropriate treatment adjustments, and feedback mechanisms and reminders for physicians.
“There may also be a need for more dosage options with the FDC triple pill to allow physicians to intensify therapy without fear of overtreatment and adverse drug effects,” they wrote.
In an accompanying editorial (JAMA Cardiol. 2020 Jul 22. doi: 10.1001/jamacardio.2020.2693), Ann Marie Navar, MD, PhD, associate professor of cardiology at Duke Clinical Research Institute, Durham, N.C., noted that initiating treatment with FDC therapy doesn’t preclude a more personalized approach for patients who don’t achieve their BP target. “The real choice now is the choice of initial treatment,” she wrote, adding that future treatment guidelines should consider extending an FDC-first approach to patients with less severe levels of hypertension.

“The study showed there’s room for a both a population-based fixed-drug combination approach and a personalized approach to how we think about hypertension management with fixed-dose therapy,” she said in an interview. “It’s not a one-and-done situation.”
Dr. Wang has no financial relationships to disclose. Study coauthors received funding from the Australian National Health and Medical Research Council and the U.K. National Institute for Health Research. Dr. Navar has no relevant financial relationships to report.
SOURCE: Wang N et al. JAMA Cardiol. 2020. doi: 10.1001/jamacardio.2020.2739.
A secondary analysis of a major study of polypill therapy for hypertension found that patients who don’t reach blood pressure targets are less likely to have their medications adjusted if they’re on fixed-dose combination therapy.
However, hypertension patients on low-dose, triple-pill combination therapy are more likely to achieve blood pressure control than are those on usual care.
The secondary analysis of Triple Pill vs. Usual Care Management for Patients with Mild-to-Moderate Hypertension (TRIUMPH) was published online in JAMA Cardiology (2020 Jul 22. doi: 10.1001/jamacardio.2020.2739). The trial randomized 700 patients with hypertension in Sri Lanka to triple-pill fixed-dose combination (FDC) therapy or usual care during February 2016–May 2017, with follow-up ending in October 2017.
A greater proportion of FDC patients reached target BP by the end of the study compared with usual care, 70% vs. 55%. However, the study found that therapeutic inertia – the failure to intensify therapy in nonresponsive patients – was more common in the FDC group at 6- and 12-week follow-up: 87% vs. 64% and 90% vs. 65%, respectively; both differences were significant different at P < .001).
The once-daily FDC pill contained telmisartan 20 mg, amlodipine 2.5 mg; and chlorthalidone 12.5 mg.
“Using a triple low-dose combination blood-pressure pill reduced the need to uptitrate BP therapy as more patients are at target, but doctors were less likely to uptitrate with triple-pill therapy when it was needed,” lead author Nelson Wang, MD, a research fellow at the George Institute for Global Health in suburban Sydney, said in an interview.
“Overall, there were fewer treatment inertia episodes in the triple-pill group than in the usual care group, but this was driven by the fact that fewer triple-pill patients needed uptitration when coming to their follow-up visits,” Dr. Wang added.
The analysis found that clinicians who prescribed triple-pill FDC used 23 unique drug treatment regimens per 100 treated patients compared with 54 different regiments with usual care (P < .001). “There was a large simplification in care,” Dr. Wang said of the FDC approach.
Dr. Wang and colleagues called for greater efforts to address therapeutic inertia, particularly with FDC therapies, and suggested potential strategies consisting of patient education, incentives for appropriate treatment adjustments, and feedback mechanisms and reminders for physicians.
“There may also be a need for more dosage options with the FDC triple pill to allow physicians to intensify therapy without fear of overtreatment and adverse drug effects,” they wrote.
In an accompanying editorial (JAMA Cardiol. 2020 Jul 22. doi: 10.1001/jamacardio.2020.2693), Ann Marie Navar, MD, PhD, associate professor of cardiology at Duke Clinical Research Institute, Durham, N.C., noted that initiating treatment with FDC therapy doesn’t preclude a more personalized approach for patients who don’t achieve their BP target. “The real choice now is the choice of initial treatment,” she wrote, adding that future treatment guidelines should consider extending an FDC-first approach to patients with less severe levels of hypertension.
“The study showed there’s room for a both a population-based fixed-drug combination approach and a personalized approach to how we think about hypertension management with fixed-dose therapy,” she said in an interview. “It’s not a one-and-done situation.”
Dr. Wang has no financial relationships to disclose. Study coauthors received funding from the Australian National Health and Medical Research Council and the U.K. National Institute for Health Research. Dr. Navar has no relevant financial relationships to report.
SOURCE: Wang N et al. JAMA Cardiol. 2020. doi: 10.1001/jamacardio.2020.2739.
A secondary analysis of a major study of polypill therapy for hypertension found that patients who don’t reach blood pressure targets are less likely to have their medications adjusted if they’re on fixed-dose combination therapy.
However, hypertension patients on low-dose, triple-pill combination therapy are more likely to achieve blood pressure control than are those on usual care.
The secondary analysis of Triple Pill vs. Usual Care Management for Patients with Mild-to-Moderate Hypertension (TRIUMPH) was published online in JAMA Cardiology (2020 Jul 22. doi: 10.1001/jamacardio.2020.2739). The trial randomized 700 patients with hypertension in Sri Lanka to triple-pill fixed-dose combination (FDC) therapy or usual care during February 2016–May 2017, with follow-up ending in October 2017.
A greater proportion of FDC patients reached target BP by the end of the study compared with usual care, 70% vs. 55%. However, the study found that therapeutic inertia – the failure to intensify therapy in nonresponsive patients – was more common in the FDC group at 6- and 12-week follow-up: 87% vs. 64% and 90% vs. 65%, respectively; both differences were significant different at P < .001).
The once-daily FDC pill contained telmisartan 20 mg, amlodipine 2.5 mg; and chlorthalidone 12.5 mg.
“Using a triple low-dose combination blood-pressure pill reduced the need to uptitrate BP therapy as more patients are at target, but doctors were less likely to uptitrate with triple-pill therapy when it was needed,” lead author Nelson Wang, MD, a research fellow at the George Institute for Global Health in suburban Sydney, said in an interview.
“Overall, there were fewer treatment inertia episodes in the triple-pill group than in the usual care group, but this was driven by the fact that fewer triple-pill patients needed uptitration when coming to their follow-up visits,” Dr. Wang added.
The analysis found that clinicians who prescribed triple-pill FDC used 23 unique drug treatment regimens per 100 treated patients compared with 54 different regiments with usual care (P < .001). “There was a large simplification in care,” Dr. Wang said of the FDC approach.
Dr. Wang and colleagues called for greater efforts to address therapeutic inertia, particularly with FDC therapies, and suggested potential strategies consisting of patient education, incentives for appropriate treatment adjustments, and feedback mechanisms and reminders for physicians.
“There may also be a need for more dosage options with the FDC triple pill to allow physicians to intensify therapy without fear of overtreatment and adverse drug effects,” they wrote.
In an accompanying editorial (JAMA Cardiol. 2020 Jul 22. doi: 10.1001/jamacardio.2020.2693), Ann Marie Navar, MD, PhD, associate professor of cardiology at Duke Clinical Research Institute, Durham, N.C., noted that initiating treatment with FDC therapy doesn’t preclude a more personalized approach for patients who don’t achieve their BP target. “The real choice now is the choice of initial treatment,” she wrote, adding that future treatment guidelines should consider extending an FDC-first approach to patients with less severe levels of hypertension.
“The study showed there’s room for a both a population-based fixed-drug combination approach and a personalized approach to how we think about hypertension management with fixed-dose therapy,” she said in an interview. “It’s not a one-and-done situation.”
Dr. Wang has no financial relationships to disclose. Study coauthors received funding from the Australian National Health and Medical Research Council and the U.K. National Institute for Health Research. Dr. Navar has no relevant financial relationships to report.
SOURCE: Wang N et al. JAMA Cardiol. 2020. doi: 10.1001/jamacardio.2020.2739.
FROM JAMA CARDIOLOGY
Hospitalist movers and shakers – July 2020
Rupesh Prasad, MD, SFHM, recently started a new role as medical director of care management for Advocate Aurora Health in Milwaukee. His focus areas include clinical documentation and care transition for inpatients. He was previously the quality and utilization officer for Aurora Sinai Medical Center. Dr. Prasad is a hospitalist with 15 years of experience and has served as the chief of staff at Aurora Sinai Medical Center. He is the cochair for the Advocate Aurora Health Inpatient Physician Informatics Committee, where his focus is on optimization of EHR for the end user.

Dr. Prasad cochairs the Society of Hospital Medicine’s IT Special Interest Group and sits on the Hospital Quality and Patient Safety Committee. He is the president of SHM’s Wisconsin Chapter.
David Rice, MD, recently earned promotion to chief medical officer for Baptist Health, a nonprofit health care system based in Jacksonville, Fla. In addition to his role as CMO, Dr. Rice will maintain the titles of senior vice president and chief quality officer.
Dr. Rice, who has spent the past 5 years as chief quality officer at Baptist Health, will oversee clinical quality, patient safety, and performance improvement. The Baptist Health system includes 200 different points of care.
Dr. Rice takes over for Keith Stein, MD, who had served as Baptist’s CMO since 1999.

Alabama hospitalist Jade Brice-Roshell, MD, has been named one of the “70 African American Leaders in Health Care to Know in 2020” list by Becker’s Hospital Review.
Dr. Brice-Roshell has served as Shelby Baptist Medical Center’s (Alabaster, Ala.) CMO for the past year and has been a Shelby staff member since 2015. It is the second year in a row that she has been honored by Becker’s on this list.
After a nationwide search, executive leaders at Bassett Medical Center in Cooperstown, N.Y., have elected to elevate hospitalist Kai Mebust, MD, FHM, to the role of chief of the department of medicine, succeeding Charles Hyman, MD. Dr. Mebust had been working alongside Dr. Hyman as associate chief since March 2019 while the network was seeking a successor. It turns out they had their man in house all along.

Dr. Mebust has 16 years of experience with Bassett, including 10 years as chief of the hospitalist division and 4 years as medical director of the network’s hospitalist program. In his new position, he will be charged with directing care and providing leadership for the system’s physicians.
Prisma Health Tuomey Hospital (Sumter, S.C.) has raised its level of care for children, newborns, and infants by creating a new pediatric hospitalist program through a strengthened relationship with Children’s Hospital-Midlands in Columbia, S.C.
The rural community has been affiliated with Children’s for a long time, but the new setup places full-time physicians in the Sumter facility that are part of the Children’s team. Residents in and around Sumter will no longer need to travel to Columbia to take advantage of the high-level service.
The pediatric hospitalist team will work closely with local pediatricians and family physicians to ensure that follow-ups and other preventative treatments are handled once a child is discharged from Tuomey Hospital.
Rupesh Prasad, MD, SFHM, recently started a new role as medical director of care management for Advocate Aurora Health in Milwaukee. His focus areas include clinical documentation and care transition for inpatients. He was previously the quality and utilization officer for Aurora Sinai Medical Center. Dr. Prasad is a hospitalist with 15 years of experience and has served as the chief of staff at Aurora Sinai Medical Center. He is the cochair for the Advocate Aurora Health Inpatient Physician Informatics Committee, where his focus is on optimization of EHR for the end user.
Dr. Prasad cochairs the Society of Hospital Medicine’s IT Special Interest Group and sits on the Hospital Quality and Patient Safety Committee. He is the president of SHM’s Wisconsin Chapter.
David Rice, MD, recently earned promotion to chief medical officer for Baptist Health, a nonprofit health care system based in Jacksonville, Fla. In addition to his role as CMO, Dr. Rice will maintain the titles of senior vice president and chief quality officer.
Dr. Rice, who has spent the past 5 years as chief quality officer at Baptist Health, will oversee clinical quality, patient safety, and performance improvement. The Baptist Health system includes 200 different points of care.
Dr. Rice takes over for Keith Stein, MD, who had served as Baptist’s CMO since 1999.
Alabama hospitalist Jade Brice-Roshell, MD, has been named one of the “70 African American Leaders in Health Care to Know in 2020” list by Becker’s Hospital Review.
Dr. Brice-Roshell has served as Shelby Baptist Medical Center’s (Alabaster, Ala.) CMO for the past year and has been a Shelby staff member since 2015. It is the second year in a row that she has been honored by Becker’s on this list.
After a nationwide search, executive leaders at Bassett Medical Center in Cooperstown, N.Y., have elected to elevate hospitalist Kai Mebust, MD, FHM, to the role of chief of the department of medicine, succeeding Charles Hyman, MD. Dr. Mebust had been working alongside Dr. Hyman as associate chief since March 2019 while the network was seeking a successor. It turns out they had their man in house all along.
Dr. Mebust has 16 years of experience with Bassett, including 10 years as chief of the hospitalist division and 4 years as medical director of the network’s hospitalist program. In his new position, he will be charged with directing care and providing leadership for the system’s physicians.
Prisma Health Tuomey Hospital (Sumter, S.C.) has raised its level of care for children, newborns, and infants by creating a new pediatric hospitalist program through a strengthened relationship with Children’s Hospital-Midlands in Columbia, S.C.
The rural community has been affiliated with Children’s for a long time, but the new setup places full-time physicians in the Sumter facility that are part of the Children’s team. Residents in and around Sumter will no longer need to travel to Columbia to take advantage of the high-level service.
The pediatric hospitalist team will work closely with local pediatricians and family physicians to ensure that follow-ups and other preventative treatments are handled once a child is discharged from Tuomey Hospital.
Rupesh Prasad, MD, SFHM, recently started a new role as medical director of care management for Advocate Aurora Health in Milwaukee. His focus areas include clinical documentation and care transition for inpatients. He was previously the quality and utilization officer for Aurora Sinai Medical Center. Dr. Prasad is a hospitalist with 15 years of experience and has served as the chief of staff at Aurora Sinai Medical Center. He is the cochair for the Advocate Aurora Health Inpatient Physician Informatics Committee, where his focus is on optimization of EHR for the end user.
Dr. Prasad cochairs the Society of Hospital Medicine’s IT Special Interest Group and sits on the Hospital Quality and Patient Safety Committee. He is the president of SHM’s Wisconsin Chapter.
David Rice, MD, recently earned promotion to chief medical officer for Baptist Health, a nonprofit health care system based in Jacksonville, Fla. In addition to his role as CMO, Dr. Rice will maintain the titles of senior vice president and chief quality officer.
Dr. Rice, who has spent the past 5 years as chief quality officer at Baptist Health, will oversee clinical quality, patient safety, and performance improvement. The Baptist Health system includes 200 different points of care.
Dr. Rice takes over for Keith Stein, MD, who had served as Baptist’s CMO since 1999.
Alabama hospitalist Jade Brice-Roshell, MD, has been named one of the “70 African American Leaders in Health Care to Know in 2020” list by Becker’s Hospital Review.
Dr. Brice-Roshell has served as Shelby Baptist Medical Center’s (Alabaster, Ala.) CMO for the past year and has been a Shelby staff member since 2015. It is the second year in a row that she has been honored by Becker’s on this list.
After a nationwide search, executive leaders at Bassett Medical Center in Cooperstown, N.Y., have elected to elevate hospitalist Kai Mebust, MD, FHM, to the role of chief of the department of medicine, succeeding Charles Hyman, MD. Dr. Mebust had been working alongside Dr. Hyman as associate chief since March 2019 while the network was seeking a successor. It turns out they had their man in house all along.
Dr. Mebust has 16 years of experience with Bassett, including 10 years as chief of the hospitalist division and 4 years as medical director of the network’s hospitalist program. In his new position, he will be charged with directing care and providing leadership for the system’s physicians.
Prisma Health Tuomey Hospital (Sumter, S.C.) has raised its level of care for children, newborns, and infants by creating a new pediatric hospitalist program through a strengthened relationship with Children’s Hospital-Midlands in Columbia, S.C.
The rural community has been affiliated with Children’s for a long time, but the new setup places full-time physicians in the Sumter facility that are part of the Children’s team. Residents in and around Sumter will no longer need to travel to Columbia to take advantage of the high-level service.
The pediatric hospitalist team will work closely with local pediatricians and family physicians to ensure that follow-ups and other preventative treatments are handled once a child is discharged from Tuomey Hospital.
Americans getting more sunburns
, for reasons that are unclear, Nicole L. Bolick, MD, reported at the virtual annual meeting of the American Academy of Dermatology.

On the plus side, utilization of indoor tanning plunged in the United States during the same period, a statistic worth celebrating as a public health and legislative success, noted Dr. Bolick, who was at the Harvard T.H. Chan School of Public Health, Boston, when she conducted her study and is now at East Carolina University, Greenville, N.C.
More good news: Her analysis of data from 67,471 nationally representative participants in the Centers for Disease Control and Prevention’s National Health Information Survey for the years 2005, 2010, and 2015 also demonstrated that the public’s adoption of several key skin cancer prevention behaviors is on the rise, although she added that rates clearly remain suboptimal.
For example, the proportion of Americans who practice sun avoidance climbed from 31.7% in 2005 to 35.5% in 2010, and 36.8% in 2015 in a multivariate logistic regression analysis adjusted for demographics, alcohol use, location, smoking status, education level, health insurance, and family and personal history of skin cancer.
Similarly, the use of sunscreen always or most of the time when outdoors for more than 1 hour on a warm, sunny day rose from an adjusted 31.5% in 2005 to 33.1% in 2010 and to 34.3% in 2015.
Also, sun protective clothing – long pants, hats, and/or long-sleeved shirts – was utilized always or most of the time by 35.9% of respondents in 2005, 38.4% in 2010, and 37.2% in 2015.
In 2005, 19% of Americans reported having a lifetime history of a physician-performed full body skin examination. The prevalence of this secondary skin cancer prevention measure rose to 22.4% in 2010 and remained the same in 2015.
In the 2005 national survey, 14.1% of respondents reported engaging in indoor tanning within the past year. This figure dropped to 6.2% in 2010 and fell further to 4.1% in 2015.
A history of two or more sunburns within the past year was reported by 18.2% of subjects in 2005, by 21.1% in 2010, and by 19.9% in 2015. It’s unclear whether this unwelcome phenomenon is due to inadequate use of sun protection or increased awareness of the link between sun exposure and skin cancer, with a resultant increase in reporting of sunburns. The influence of climate change is another possible explanation worthy of further study, according to Dr. Bolick.
She reported having no financial conflicts regarding her study, conducted free of commercial support.
, for reasons that are unclear, Nicole L. Bolick, MD, reported at the virtual annual meeting of the American Academy of Dermatology.
On the plus side, utilization of indoor tanning plunged in the United States during the same period, a statistic worth celebrating as a public health and legislative success, noted Dr. Bolick, who was at the Harvard T.H. Chan School of Public Health, Boston, when she conducted her study and is now at East Carolina University, Greenville, N.C.
More good news: Her analysis of data from 67,471 nationally representative participants in the Centers for Disease Control and Prevention’s National Health Information Survey for the years 2005, 2010, and 2015 also demonstrated that the public’s adoption of several key skin cancer prevention behaviors is on the rise, although she added that rates clearly remain suboptimal.
For example, the proportion of Americans who practice sun avoidance climbed from 31.7% in 2005 to 35.5% in 2010, and 36.8% in 2015 in a multivariate logistic regression analysis adjusted for demographics, alcohol use, location, smoking status, education level, health insurance, and family and personal history of skin cancer.
Similarly, the use of sunscreen always or most of the time when outdoors for more than 1 hour on a warm, sunny day rose from an adjusted 31.5% in 2005 to 33.1% in 2010 and to 34.3% in 2015.
Also, sun protective clothing – long pants, hats, and/or long-sleeved shirts – was utilized always or most of the time by 35.9% of respondents in 2005, 38.4% in 2010, and 37.2% in 2015.
In 2005, 19% of Americans reported having a lifetime history of a physician-performed full body skin examination. The prevalence of this secondary skin cancer prevention measure rose to 22.4% in 2010 and remained the same in 2015.
In the 2005 national survey, 14.1% of respondents reported engaging in indoor tanning within the past year. This figure dropped to 6.2% in 2010 and fell further to 4.1% in 2015.
A history of two or more sunburns within the past year was reported by 18.2% of subjects in 2005, by 21.1% in 2010, and by 19.9% in 2015. It’s unclear whether this unwelcome phenomenon is due to inadequate use of sun protection or increased awareness of the link between sun exposure and skin cancer, with a resultant increase in reporting of sunburns. The influence of climate change is another possible explanation worthy of further study, according to Dr. Bolick.
She reported having no financial conflicts regarding her study, conducted free of commercial support.
, for reasons that are unclear, Nicole L. Bolick, MD, reported at the virtual annual meeting of the American Academy of Dermatology.
On the plus side, utilization of indoor tanning plunged in the United States during the same period, a statistic worth celebrating as a public health and legislative success, noted Dr. Bolick, who was at the Harvard T.H. Chan School of Public Health, Boston, when she conducted her study and is now at East Carolina University, Greenville, N.C.
More good news: Her analysis of data from 67,471 nationally representative participants in the Centers for Disease Control and Prevention’s National Health Information Survey for the years 2005, 2010, and 2015 also demonstrated that the public’s adoption of several key skin cancer prevention behaviors is on the rise, although she added that rates clearly remain suboptimal.
For example, the proportion of Americans who practice sun avoidance climbed from 31.7% in 2005 to 35.5% in 2010, and 36.8% in 2015 in a multivariate logistic regression analysis adjusted for demographics, alcohol use, location, smoking status, education level, health insurance, and family and personal history of skin cancer.
Similarly, the use of sunscreen always or most of the time when outdoors for more than 1 hour on a warm, sunny day rose from an adjusted 31.5% in 2005 to 33.1% in 2010 and to 34.3% in 2015.
Also, sun protective clothing – long pants, hats, and/or long-sleeved shirts – was utilized always or most of the time by 35.9% of respondents in 2005, 38.4% in 2010, and 37.2% in 2015.
In 2005, 19% of Americans reported having a lifetime history of a physician-performed full body skin examination. The prevalence of this secondary skin cancer prevention measure rose to 22.4% in 2010 and remained the same in 2015.
In the 2005 national survey, 14.1% of respondents reported engaging in indoor tanning within the past year. This figure dropped to 6.2% in 2010 and fell further to 4.1% in 2015.
A history of two or more sunburns within the past year was reported by 18.2% of subjects in 2005, by 21.1% in 2010, and by 19.9% in 2015. It’s unclear whether this unwelcome phenomenon is due to inadequate use of sun protection or increased awareness of the link between sun exposure and skin cancer, with a resultant increase in reporting of sunburns. The influence of climate change is another possible explanation worthy of further study, according to Dr. Bolick.
She reported having no financial conflicts regarding her study, conducted free of commercial support.
FROM AAD 20

Men occupy most leadership roles in medicine
Since the early 2000s, approximately half of medical students in the United States – and in many years, more than half – have been women, but according to an update provided at the virtual Pediatric Hospital Medicine.
In pediatrics, a specialty in which approximately 70% of physicians are now women, there has been progress, but still less than 30% of pediatric department chairs are female, said Vincent Chiang, MD, chief medical officer of Boston Children’s Hospital, during a presentation at the virtual meeting sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
Citing published data and a survey he personally conducted of the top children’s hospitals identified by the U.S. News and World Report, Dr. Chiang said a minority of division chiefs, chief medical officers, chief financial officers, and other leaders are female. At his institution, only 2 of 16 division chiefs are female.
“No matter how you slice it, women are underrepresented in leadership positions,” he noted.
The problem is certainly not confined to medicine. Dr. Chiang cited data showing that women and men have reached “near parity” in workforce participation in the United States even though the 20% earnings gap has changed little over time.
According to 2020 data from the World Economic Forum, the United States ranked 51 for the gender gap calculated on the basis of economic, political, educational, and health attainment. Even if this places the United States in the top third of the rankings, it is far behind Iceland and the Scandinavian countries that lead the list.
Efforts to reduce structural biases are part of the fix, but Dr. Chiang cautioned that fundamental changes might never occur if the plan is to wait for an approach based on meritocracy. He said that existing structural biases are “slanted away from women,” who are not necessarily granted the opportunities that are readily available to men.
“A meritocracy only works if the initial playing field was level. Otherwise, it just perpetuates the inequalities,” he said.
The problem is not a shortage of women with the skills to lead. In a study by Zenger/Folkman, a consulting company that works on leadership skill development, women performed better than men in 16 of 18 leadership categories, according to Dr. Chiang.
“There is certainly no shortage of capable women,” he noted.
Of the many issues, Dr. Chiang highlighted two. The first is the challenge of placing women on leadership pathways. This is likely to require proactive strategies, such as fast-track advancement programs that guide female candidates toward leadership roles.
The second is more nuanced. According to Dr. Chiang, women who want to assume a leadership role should think more actively about how and who is making decisions at their institution so they can position themselves appropriately. This is nuanced because “there is a certain amount of gamesmanship,” he said. The rise to leadership “has never been a pure meritocracy.”
Importantly, many of the key decisions in any institution involve money, according to Dr. Chiang. As a result, he advised those seeking leadership roles to join audit committees or otherwise take on responsibility for profit-and-loss management. Even in a nonprofit institution, “you need to make the numbers work,” he said, citing the common catchphrase: “No margin, no mission.”
However, Dr. Chiang acknowledged the many obstacles that prevent women from working their way into positions of leadership. For example, networking is important, but women are not necessarily attracted or invited to some of the social engagements, such as golf outings, where strong relationships are created.
In a survey of 100,000 people working at Fortune 500 companies, “82% of women say they feel excluded at work and much of that comes from that informal networking,” Dr. Chiang said. “Whereas 92% of men think they are not excluding women in their daily work.”
There is no single solution, but Dr. Chiang believes that concrete structural changes are needed. Female doctors remain grossly underrepresented in leadership roles even as they now represent more than half of the workforce for many specialties. Based on the need for proactive approaches outlined by Dr. Chiang, it appears unlikely that gender inequality will ever resolve itself.
Lisa S. Rotenstein, MD, who has written on fixing the gender imbalance in health care, including for the Harvard Business Review, said she agreed during an interview that structural changes are critical.
“In order to address current disparities, leaders should be thinking about how to remove both the formal and informal obstacles that prevent women and minorities from getting into the rooms where these decisions are being made,” said Dr. Rotenstein, who is an instructor in medicine at Brigham and Women’s Hospital, Harvard Medical School in Boston.
“This will need to involve sponsorship that gets women invited to the right committees or in positions with responsibility for profit-and-loss management,” she added.
Dr. Rotenstein spoke about improving “access to the pipeline” that leads to leadership roles. The ways in which women are excluded from opportunities is often subtle and difficult to penetrate without fundamental changes, she explained.
“Institutions need to understand the processes that lead to leadership roles and make the changes that allow women and minorities to participate,” she said. It is not enough to recognize the problem, according to Dr. Rotenstein.
Like Dr. Chiang, she noted that changes are needed in the methods that move underrepresented groups into leadership roles.
Dr. Chiang reported no potential conflicts of interest relevant to this study.
Since the early 2000s, approximately half of medical students in the United States – and in many years, more than half – have been women, but according to an update provided at the virtual Pediatric Hospital Medicine.
In pediatrics, a specialty in which approximately 70% of physicians are now women, there has been progress, but still less than 30% of pediatric department chairs are female, said Vincent Chiang, MD, chief medical officer of Boston Children’s Hospital, during a presentation at the virtual meeting sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
Citing published data and a survey he personally conducted of the top children’s hospitals identified by the U.S. News and World Report, Dr. Chiang said a minority of division chiefs, chief medical officers, chief financial officers, and other leaders are female. At his institution, only 2 of 16 division chiefs are female.
“No matter how you slice it, women are underrepresented in leadership positions,” he noted.
The problem is certainly not confined to medicine. Dr. Chiang cited data showing that women and men have reached “near parity” in workforce participation in the United States even though the 20% earnings gap has changed little over time.
According to 2020 data from the World Economic Forum, the United States ranked 51 for the gender gap calculated on the basis of economic, political, educational, and health attainment. Even if this places the United States in the top third of the rankings, it is far behind Iceland and the Scandinavian countries that lead the list.
Efforts to reduce structural biases are part of the fix, but Dr. Chiang cautioned that fundamental changes might never occur if the plan is to wait for an approach based on meritocracy. He said that existing structural biases are “slanted away from women,” who are not necessarily granted the opportunities that are readily available to men.
“A meritocracy only works if the initial playing field was level. Otherwise, it just perpetuates the inequalities,” he said.
The problem is not a shortage of women with the skills to lead. In a study by Zenger/Folkman, a consulting company that works on leadership skill development, women performed better than men in 16 of 18 leadership categories, according to Dr. Chiang.
“There is certainly no shortage of capable women,” he noted.
Of the many issues, Dr. Chiang highlighted two. The first is the challenge of placing women on leadership pathways. This is likely to require proactive strategies, such as fast-track advancement programs that guide female candidates toward leadership roles.
The second is more nuanced. According to Dr. Chiang, women who want to assume a leadership role should think more actively about how and who is making decisions at their institution so they can position themselves appropriately. This is nuanced because “there is a certain amount of gamesmanship,” he said. The rise to leadership “has never been a pure meritocracy.”
Importantly, many of the key decisions in any institution involve money, according to Dr. Chiang. As a result, he advised those seeking leadership roles to join audit committees or otherwise take on responsibility for profit-and-loss management. Even in a nonprofit institution, “you need to make the numbers work,” he said, citing the common catchphrase: “No margin, no mission.”
However, Dr. Chiang acknowledged the many obstacles that prevent women from working their way into positions of leadership. For example, networking is important, but women are not necessarily attracted or invited to some of the social engagements, such as golf outings, where strong relationships are created.
In a survey of 100,000 people working at Fortune 500 companies, “82% of women say they feel excluded at work and much of that comes from that informal networking,” Dr. Chiang said. “Whereas 92% of men think they are not excluding women in their daily work.”
There is no single solution, but Dr. Chiang believes that concrete structural changes are needed. Female doctors remain grossly underrepresented in leadership roles even as they now represent more than half of the workforce for many specialties. Based on the need for proactive approaches outlined by Dr. Chiang, it appears unlikely that gender inequality will ever resolve itself.
Lisa S. Rotenstein, MD, who has written on fixing the gender imbalance in health care, including for the Harvard Business Review, said she agreed during an interview that structural changes are critical.
“In order to address current disparities, leaders should be thinking about how to remove both the formal and informal obstacles that prevent women and minorities from getting into the rooms where these decisions are being made,” said Dr. Rotenstein, who is an instructor in medicine at Brigham and Women’s Hospital, Harvard Medical School in Boston.
“This will need to involve sponsorship that gets women invited to the right committees or in positions with responsibility for profit-and-loss management,” she added.
Dr. Rotenstein spoke about improving “access to the pipeline” that leads to leadership roles. The ways in which women are excluded from opportunities is often subtle and difficult to penetrate without fundamental changes, she explained.
“Institutions need to understand the processes that lead to leadership roles and make the changes that allow women and minorities to participate,” she said. It is not enough to recognize the problem, according to Dr. Rotenstein.
Like Dr. Chiang, she noted that changes are needed in the methods that move underrepresented groups into leadership roles.
Dr. Chiang reported no potential conflicts of interest relevant to this study.
Since the early 2000s, approximately half of medical students in the United States – and in many years, more than half – have been women, but according to an update provided at the virtual Pediatric Hospital Medicine.
In pediatrics, a specialty in which approximately 70% of physicians are now women, there has been progress, but still less than 30% of pediatric department chairs are female, said Vincent Chiang, MD, chief medical officer of Boston Children’s Hospital, during a presentation at the virtual meeting sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
Citing published data and a survey he personally conducted of the top children’s hospitals identified by the U.S. News and World Report, Dr. Chiang said a minority of division chiefs, chief medical officers, chief financial officers, and other leaders are female. At his institution, only 2 of 16 division chiefs are female.
“No matter how you slice it, women are underrepresented in leadership positions,” he noted.
The problem is certainly not confined to medicine. Dr. Chiang cited data showing that women and men have reached “near parity” in workforce participation in the United States even though the 20% earnings gap has changed little over time.
According to 2020 data from the World Economic Forum, the United States ranked 51 for the gender gap calculated on the basis of economic, political, educational, and health attainment. Even if this places the United States in the top third of the rankings, it is far behind Iceland and the Scandinavian countries that lead the list.
Efforts to reduce structural biases are part of the fix, but Dr. Chiang cautioned that fundamental changes might never occur if the plan is to wait for an approach based on meritocracy. He said that existing structural biases are “slanted away from women,” who are not necessarily granted the opportunities that are readily available to men.
“A meritocracy only works if the initial playing field was level. Otherwise, it just perpetuates the inequalities,” he said.
The problem is not a shortage of women with the skills to lead. In a study by Zenger/Folkman, a consulting company that works on leadership skill development, women performed better than men in 16 of 18 leadership categories, according to Dr. Chiang.
“There is certainly no shortage of capable women,” he noted.
Of the many issues, Dr. Chiang highlighted two. The first is the challenge of placing women on leadership pathways. This is likely to require proactive strategies, such as fast-track advancement programs that guide female candidates toward leadership roles.
The second is more nuanced. According to Dr. Chiang, women who want to assume a leadership role should think more actively about how and who is making decisions at their institution so they can position themselves appropriately. This is nuanced because “there is a certain amount of gamesmanship,” he said. The rise to leadership “has never been a pure meritocracy.”
Importantly, many of the key decisions in any institution involve money, according to Dr. Chiang. As a result, he advised those seeking leadership roles to join audit committees or otherwise take on responsibility for profit-and-loss management. Even in a nonprofit institution, “you need to make the numbers work,” he said, citing the common catchphrase: “No margin, no mission.”
However, Dr. Chiang acknowledged the many obstacles that prevent women from working their way into positions of leadership. For example, networking is important, but women are not necessarily attracted or invited to some of the social engagements, such as golf outings, where strong relationships are created.
In a survey of 100,000 people working at Fortune 500 companies, “82% of women say they feel excluded at work and much of that comes from that informal networking,” Dr. Chiang said. “Whereas 92% of men think they are not excluding women in their daily work.”
There is no single solution, but Dr. Chiang believes that concrete structural changes are needed. Female doctors remain grossly underrepresented in leadership roles even as they now represent more than half of the workforce for many specialties. Based on the need for proactive approaches outlined by Dr. Chiang, it appears unlikely that gender inequality will ever resolve itself.
Lisa S. Rotenstein, MD, who has written on fixing the gender imbalance in health care, including for the Harvard Business Review, said she agreed during an interview that structural changes are critical.
“In order to address current disparities, leaders should be thinking about how to remove both the formal and informal obstacles that prevent women and minorities from getting into the rooms where these decisions are being made,” said Dr. Rotenstein, who is an instructor in medicine at Brigham and Women’s Hospital, Harvard Medical School in Boston.
“This will need to involve sponsorship that gets women invited to the right committees or in positions with responsibility for profit-and-loss management,” she added.
Dr. Rotenstein spoke about improving “access to the pipeline” that leads to leadership roles. The ways in which women are excluded from opportunities is often subtle and difficult to penetrate without fundamental changes, she explained.
“Institutions need to understand the processes that lead to leadership roles and make the changes that allow women and minorities to participate,” she said. It is not enough to recognize the problem, according to Dr. Rotenstein.
Like Dr. Chiang, she noted that changes are needed in the methods that move underrepresented groups into leadership roles.
Dr. Chiang reported no potential conflicts of interest relevant to this study.
FROM PHM20
Erythematous Plaque on the Scalp With Alopecia
The Diagnosis: Tufted Hair Folliculitis
Dermoscopic examination revealed multiple hair tufts of 5 to 20 normal hairs emerging from single dilated follicular openings (Figure 1). The density of hair follicles was reduced with adherent yellow-white scales that encircled the dilated follicular orifices. Histopathology revealed hyperkeratosis and parakeratosis in the stratum corneum. Infiltration of lymphocytes, neutrophils, plasma cells, and eosinophils around the upper portions of the follicles also was found. Multiple hairs emerging from a single dilated follicular ostia with prominent fibrosis of the dermis were seen (Figure 2). Based on the clinical and histopathological findings, the patient was diagnosed with tufted hair folliculitis (THF). She was treated with minocycline 100 mg once daily and an intralesional betamethasone injection 5 mg once daily. After 2 weeks of treatment, the lesion improved and decreased in size to 1×1 cm in diameter; however, the hair tufts and scarring alopecia remained.

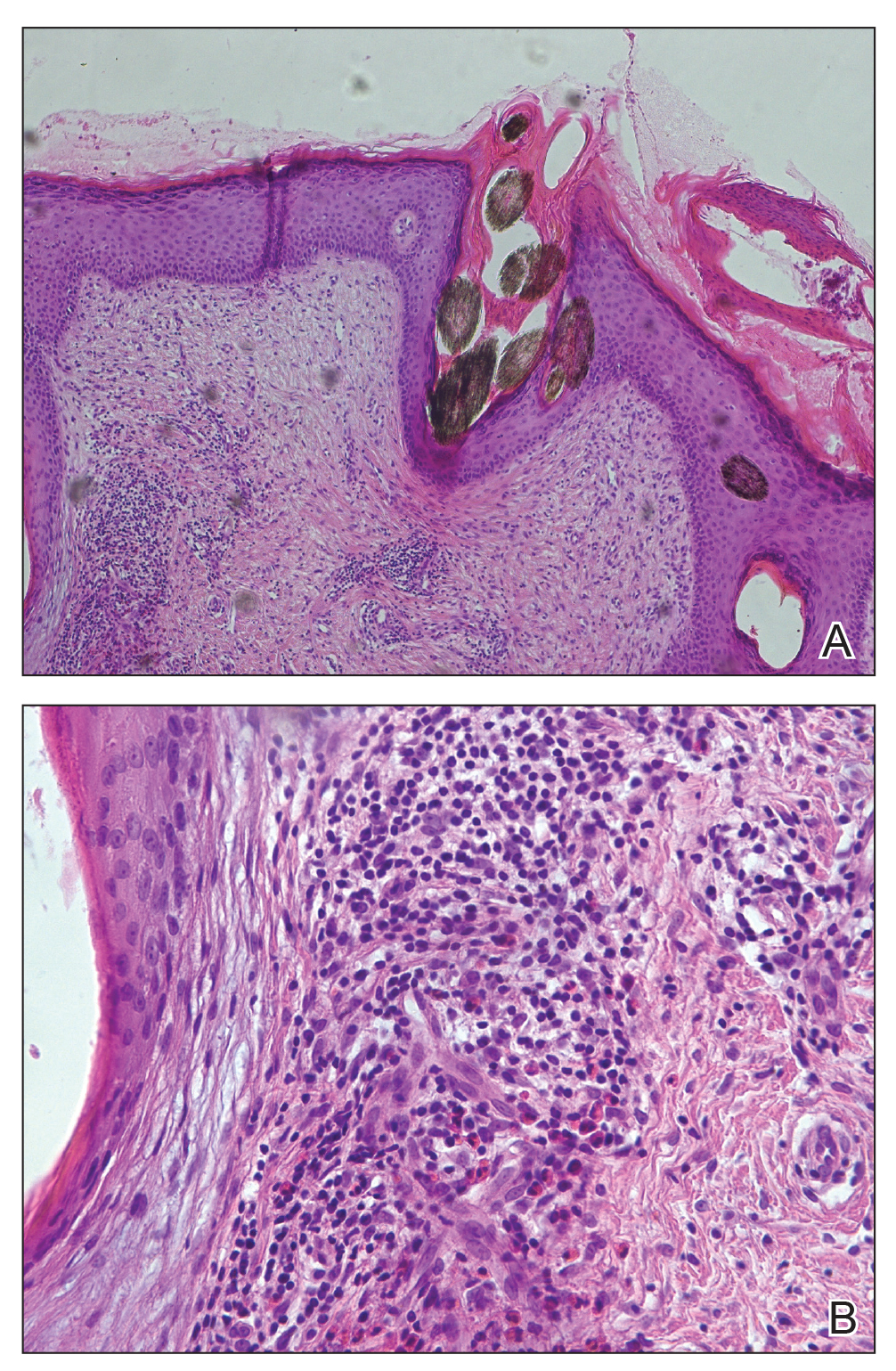
Tufted hair folliculitis is a rare inflammatory condition of the scalp characterized by a peculiar tufting of hair that was first described by Smith and Sanderson1 in 1978. Most patients present with a patch or plaque on the parietal or occipital region of the scalp. The condition may lead to the destruction of follicular units, resulting in permanent scarring alopecia.2 Histopathology in our patient revealed perifollicular inflammation, and several follicles could be seen converging toward a common follicular duct with a widely dilated opening, consistent with the diagnosis of THF.
The pathogenic mechanisms of THF are unclear. Primary hair tufting, local trauma, tinea capitis, nevoid malformation, and Staphylococcus aureus infection have been proposed as causative pathomechanisms.3 Typically there is no history of underlying disease or trauma on the scalp; however, secondary changes may have occurred following unrecognized trauma or repeated stimuli. Staphylococcal infections may play a notable role in inducing THF. Ekmekci and Koslu4 reported that a local inflammatory process led to the destruction of adjacent follicles, which subsequently amalgamated to form a common follicular duct due to local fibrosis and scarring. However, Powell et al5 found no evidence of local immune suppression or immune failure that could explain the abnormal host response to a certain presumptive superantigen. In our patient, the inflammatory injury was mild, and no purulent exudation was found from the dilated follicular openings. Because the patient had applied an antibiotic ointment prior to presentation, bacterial cultures from biopsy specimens were not appropriate.
The differential diagnosis of THF includes folliculitis decalvans, folliculitis keloidalis nuchae, dissecting cellulitis of the scalp, and follicular lichen planus.6 In our patient, folliculitis keloidalis nuchae and dissecting cellulitis of the scalp were excluded because no keloid or purulent inflammation was found. The diagnosis of follicular lichen planus was not taken into consideration because characteristic pathology such as liquefaction degeneration of basal cells was not observed. Folliculitis decalvans was considered to be a possible cause of the alopecia in our patient. It also was suggested that hair tufting could be a secondary phenomenon, occurring in several inflammatory disorders of the scalp. Powell et al5 concluded that THF should be considered as a distinctive clinicohistologic variant of folliculitis decalvans characterized by multiple hair tufts with patches of scarring alopecia. This hypothesis corresponded with our patient's clinical manifestation and histopathology.
Conventional treatment of THF includes topical antiseptics and oral antibiotics (eg, flucloxacillin, erythromycin, tetracycline, doxycycline), but reduction in hair bundling rarely has been observed after antibiotic treatment. Although good prognosis has been reported after surgical excision of the involved areas, it can only be performed in small lesions.6 Pranteda et al7 reported that combination therapy with oral rifampin and oral clindamycin can prevent relapse long-term. Combination therapy for 10 weeks also was effective in 10 of 18 patients with THF.5 Rifampin is an effective therapeutic modality to control the progression of THF as well as prevent relapse; however, long-term use should be avoided to prevent hepatic or renal side effects.7 Our patient was successfully treated with intralesional betamethasone and oral minocycline to reduce the inflammation and prevent the expansion of scarring alopecia.
Acknowledgment
The authors thank Xue Chen, MD (Beijing, China), for writing support.
- Smith NP, Sanderson KV. Tufted folliculitis of the scalp. J R Soc Med. 1978;71:606-608.
- Broshtilova V, Bardarov E, Kazandjieva J, et al. Tufted hair folliculitis: a case report and literature review. Acta Dermatovenerol Alp Pannonica Adriat. 2011;20:27-29.
- Gungor S, Yuksel T, Topal I. Tufted hair folliculitis associated with Melkersson-Rosenthal syndrome and hidradenitis suppurativa. Indian J Dermatol Venereol Leprol. 2014;80:484-487.
- Ekmekci TR, Koslu A. Tufted hair folliculitis causing skullcap-pattern cicatricial alopecia. J Eur Acad Dermatol Venereol. 2006;20:227-229.
- Powell JJ, Dawber RP, Gatter K. Folliculitis decalvans including tufted folliculitis: clinical, histological and therapeutic findings. Br J Dermatol. 1999;140:328-333.
- Baroni A, Romano F. Tufted hair folliculitis in a patient affected by pachydermoperiostosis: case report and videodermoscopic features. Skinmed. 2011;9:186-188.
- Pranteda G, Grimaldi M, Palese E, et al. Tufted hair folliculitis: complete enduring response after treatment with rifampicin. J Dermatolog Treat. 2004;15:396-398.
The Diagnosis: Tufted Hair Folliculitis
Dermoscopic examination revealed multiple hair tufts of 5 to 20 normal hairs emerging from single dilated follicular openings (Figure 1). The density of hair follicles was reduced with adherent yellow-white scales that encircled the dilated follicular orifices. Histopathology revealed hyperkeratosis and parakeratosis in the stratum corneum. Infiltration of lymphocytes, neutrophils, plasma cells, and eosinophils around the upper portions of the follicles also was found. Multiple hairs emerging from a single dilated follicular ostia with prominent fibrosis of the dermis were seen (Figure 2). Based on the clinical and histopathological findings, the patient was diagnosed with tufted hair folliculitis (THF). She was treated with minocycline 100 mg once daily and an intralesional betamethasone injection 5 mg once daily. After 2 weeks of treatment, the lesion improved and decreased in size to 1×1 cm in diameter; however, the hair tufts and scarring alopecia remained.
Tufted hair folliculitis is a rare inflammatory condition of the scalp characterized by a peculiar tufting of hair that was first described by Smith and Sanderson1 in 1978. Most patients present with a patch or plaque on the parietal or occipital region of the scalp. The condition may lead to the destruction of follicular units, resulting in permanent scarring alopecia.2 Histopathology in our patient revealed perifollicular inflammation, and several follicles could be seen converging toward a common follicular duct with a widely dilated opening, consistent with the diagnosis of THF.
The pathogenic mechanisms of THF are unclear. Primary hair tufting, local trauma, tinea capitis, nevoid malformation, and Staphylococcus aureus infection have been proposed as causative pathomechanisms.3 Typically there is no history of underlying disease or trauma on the scalp; however, secondary changes may have occurred following unrecognized trauma or repeated stimuli. Staphylococcal infections may play a notable role in inducing THF. Ekmekci and Koslu4 reported that a local inflammatory process led to the destruction of adjacent follicles, which subsequently amalgamated to form a common follicular duct due to local fibrosis and scarring. However, Powell et al5 found no evidence of local immune suppression or immune failure that could explain the abnormal host response to a certain presumptive superantigen. In our patient, the inflammatory injury was mild, and no purulent exudation was found from the dilated follicular openings. Because the patient had applied an antibiotic ointment prior to presentation, bacterial cultures from biopsy specimens were not appropriate.
The differential diagnosis of THF includes folliculitis decalvans, folliculitis keloidalis nuchae, dissecting cellulitis of the scalp, and follicular lichen planus.6 In our patient, folliculitis keloidalis nuchae and dissecting cellulitis of the scalp were excluded because no keloid or purulent inflammation was found. The diagnosis of follicular lichen planus was not taken into consideration because characteristic pathology such as liquefaction degeneration of basal cells was not observed. Folliculitis decalvans was considered to be a possible cause of the alopecia in our patient. It also was suggested that hair tufting could be a secondary phenomenon, occurring in several inflammatory disorders of the scalp. Powell et al5 concluded that THF should be considered as a distinctive clinicohistologic variant of folliculitis decalvans characterized by multiple hair tufts with patches of scarring alopecia. This hypothesis corresponded with our patient's clinical manifestation and histopathology.
Conventional treatment of THF includes topical antiseptics and oral antibiotics (eg, flucloxacillin, erythromycin, tetracycline, doxycycline), but reduction in hair bundling rarely has been observed after antibiotic treatment. Although good prognosis has been reported after surgical excision of the involved areas, it can only be performed in small lesions.6 Pranteda et al7 reported that combination therapy with oral rifampin and oral clindamycin can prevent relapse long-term. Combination therapy for 10 weeks also was effective in 10 of 18 patients with THF.5 Rifampin is an effective therapeutic modality to control the progression of THF as well as prevent relapse; however, long-term use should be avoided to prevent hepatic or renal side effects.7 Our patient was successfully treated with intralesional betamethasone and oral minocycline to reduce the inflammation and prevent the expansion of scarring alopecia.
Acknowledgment
The authors thank Xue Chen, MD (Beijing, China), for writing support.
The Diagnosis: Tufted Hair Folliculitis
Dermoscopic examination revealed multiple hair tufts of 5 to 20 normal hairs emerging from single dilated follicular openings (Figure 1). The density of hair follicles was reduced with adherent yellow-white scales that encircled the dilated follicular orifices. Histopathology revealed hyperkeratosis and parakeratosis in the stratum corneum. Infiltration of lymphocytes, neutrophils, plasma cells, and eosinophils around the upper portions of the follicles also was found. Multiple hairs emerging from a single dilated follicular ostia with prominent fibrosis of the dermis were seen (Figure 2). Based on the clinical and histopathological findings, the patient was diagnosed with tufted hair folliculitis (THF). She was treated with minocycline 100 mg once daily and an intralesional betamethasone injection 5 mg once daily. After 2 weeks of treatment, the lesion improved and decreased in size to 1×1 cm in diameter; however, the hair tufts and scarring alopecia remained.
Tufted hair folliculitis is a rare inflammatory condition of the scalp characterized by a peculiar tufting of hair that was first described by Smith and Sanderson1 in 1978. Most patients present with a patch or plaque on the parietal or occipital region of the scalp. The condition may lead to the destruction of follicular units, resulting in permanent scarring alopecia.2 Histopathology in our patient revealed perifollicular inflammation, and several follicles could be seen converging toward a common follicular duct with a widely dilated opening, consistent with the diagnosis of THF.
The pathogenic mechanisms of THF are unclear. Primary hair tufting, local trauma, tinea capitis, nevoid malformation, and Staphylococcus aureus infection have been proposed as causative pathomechanisms.3 Typically there is no history of underlying disease or trauma on the scalp; however, secondary changes may have occurred following unrecognized trauma or repeated stimuli. Staphylococcal infections may play a notable role in inducing THF. Ekmekci and Koslu4 reported that a local inflammatory process led to the destruction of adjacent follicles, which subsequently amalgamated to form a common follicular duct due to local fibrosis and scarring. However, Powell et al5 found no evidence of local immune suppression or immune failure that could explain the abnormal host response to a certain presumptive superantigen. In our patient, the inflammatory injury was mild, and no purulent exudation was found from the dilated follicular openings. Because the patient had applied an antibiotic ointment prior to presentation, bacterial cultures from biopsy specimens were not appropriate.
The differential diagnosis of THF includes folliculitis decalvans, folliculitis keloidalis nuchae, dissecting cellulitis of the scalp, and follicular lichen planus.6 In our patient, folliculitis keloidalis nuchae and dissecting cellulitis of the scalp were excluded because no keloid or purulent inflammation was found. The diagnosis of follicular lichen planus was not taken into consideration because characteristic pathology such as liquefaction degeneration of basal cells was not observed. Folliculitis decalvans was considered to be a possible cause of the alopecia in our patient. It also was suggested that hair tufting could be a secondary phenomenon, occurring in several inflammatory disorders of the scalp. Powell et al5 concluded that THF should be considered as a distinctive clinicohistologic variant of folliculitis decalvans characterized by multiple hair tufts with patches of scarring alopecia. This hypothesis corresponded with our patient's clinical manifestation and histopathology.
Conventional treatment of THF includes topical antiseptics and oral antibiotics (eg, flucloxacillin, erythromycin, tetracycline, doxycycline), but reduction in hair bundling rarely has been observed after antibiotic treatment. Although good prognosis has been reported after surgical excision of the involved areas, it can only be performed in small lesions.6 Pranteda et al7 reported that combination therapy with oral rifampin and oral clindamycin can prevent relapse long-term. Combination therapy for 10 weeks also was effective in 10 of 18 patients with THF.5 Rifampin is an effective therapeutic modality to control the progression of THF as well as prevent relapse; however, long-term use should be avoided to prevent hepatic or renal side effects.7 Our patient was successfully treated with intralesional betamethasone and oral minocycline to reduce the inflammation and prevent the expansion of scarring alopecia.
Acknowledgment
The authors thank Xue Chen, MD (Beijing, China), for writing support.
- Smith NP, Sanderson KV. Tufted folliculitis of the scalp. J R Soc Med. 1978;71:606-608.
- Broshtilova V, Bardarov E, Kazandjieva J, et al. Tufted hair folliculitis: a case report and literature review. Acta Dermatovenerol Alp Pannonica Adriat. 2011;20:27-29.
- Gungor S, Yuksel T, Topal I. Tufted hair folliculitis associated with Melkersson-Rosenthal syndrome and hidradenitis suppurativa. Indian J Dermatol Venereol Leprol. 2014;80:484-487.
- Ekmekci TR, Koslu A. Tufted hair folliculitis causing skullcap-pattern cicatricial alopecia. J Eur Acad Dermatol Venereol. 2006;20:227-229.
- Powell JJ, Dawber RP, Gatter K. Folliculitis decalvans including tufted folliculitis: clinical, histological and therapeutic findings. Br J Dermatol. 1999;140:328-333.
- Baroni A, Romano F. Tufted hair folliculitis in a patient affected by pachydermoperiostosis: case report and videodermoscopic features. Skinmed. 2011;9:186-188.
- Pranteda G, Grimaldi M, Palese E, et al. Tufted hair folliculitis: complete enduring response after treatment with rifampicin. J Dermatolog Treat. 2004;15:396-398.
- Smith NP, Sanderson KV. Tufted folliculitis of the scalp. J R Soc Med. 1978;71:606-608.
- Broshtilova V, Bardarov E, Kazandjieva J, et al. Tufted hair folliculitis: a case report and literature review. Acta Dermatovenerol Alp Pannonica Adriat. 2011;20:27-29.
- Gungor S, Yuksel T, Topal I. Tufted hair folliculitis associated with Melkersson-Rosenthal syndrome and hidradenitis suppurativa. Indian J Dermatol Venereol Leprol. 2014;80:484-487.
- Ekmekci TR, Koslu A. Tufted hair folliculitis causing skullcap-pattern cicatricial alopecia. J Eur Acad Dermatol Venereol. 2006;20:227-229.
- Powell JJ, Dawber RP, Gatter K. Folliculitis decalvans including tufted folliculitis: clinical, histological and therapeutic findings. Br J Dermatol. 1999;140:328-333.
- Baroni A, Romano F. Tufted hair folliculitis in a patient affected by pachydermoperiostosis: case report and videodermoscopic features. Skinmed. 2011;9:186-188.
- Pranteda G, Grimaldi M, Palese E, et al. Tufted hair folliculitis: complete enduring response after treatment with rifampicin. J Dermatolog Treat. 2004;15:396-398.

A 37-year-old woman presented with a 2×6-cm, firm, erythematous plaque on the parietal region of the scalp of 1 year’s duration. No history of injury to the scalp was noted. The patient noticed hair loss in the affected area in the month prior to presentation. She was afebrile and otherwise asymptomatic. She denied a family history of similar scalp disorders.
