User login
Ultraprocessed foods and cancer: Small changes may lower risk
Processed and ultraprocessed food consumption has been shown to increase the risk for various cancers. A new analysis suggests that replacing even a small amount of such foods with an equal amount of minimally processed options may reduce that risk.
Using data from more than 450,000 participants, the dietary substitution analysis found that as well as the risk for several cancer types, including esophageal squamous cell carcinoma by 43% and hepatocellular carcinoma by 23%.
Making this substitution with ultraprocessed foods also appeared to lower cancer risk but often to a lesser degree. For instance, swapping 10% of ultraprocessed foods for minimally processed foods lowered the overall cancer risk by just 1%, the risk of hepatocellular carcinoma by 27%, and the risk of esophageal squamous cell carcinoma by 20%.
Overall, “this study suggests that the replacement of processed and ultraprocessed foods and drinks with an equal amount of minimally processed foods might reduce the risk of various cancer types,” Nathalie Kliemann, PhD, from the World Health Organization’s International Agency for Research on Cancer, Lyon, France, and colleagues concluded.
The findings were published in The Lancet Planetary Health.
Processed and ultraprocessed foods tend to have high-energy density and low nutritional value, and some epidemiological evidence indicates a possible link between consuming ultraprocessed food and cancer outcomes.
Dr. Kliemann and colleagues, for instance, recently published a study showing a link between ultraprocessed food consumption and increased risk for cancer, particularly ovarian cancer, as well as increased risk of dying from cancer. That study of nearly 200,000 middle-aged adults in the UK Biobank database showed that, for each 10 percentage point increase in the consumption of ultraprocessed foods, there was a 2% increase in the overall incidence of cancer and a 19% increase in ovarian cancer incidence.
However, conflicting reports exist, and research exploring associations between processed foods and cancer remains limited.
The researchers wanted to better understand the potential association between the degree of food processing and risk for cancer in a larger cohort of individuals.
The investigators performed a dietary substitution analysis using data from more than 450,000 participants from the European Prospective Investigation into Cancer and Nutrition (EPIC) study and looking at 25 anatomical sites. EPIC study participants, who had no cancer diagnoses prior to enrollment, were identified between March 1991 and July 2001. Of the 450,111 included in the analysis, 47,573 were diagnosed with cancer during a mean follow-up of 14.1 years. Mean age at recruitment was 51 years, and mean BMI was 25.3 kg/m2.
Food items were classified according to their level of processing using the NOVA classification system: minimally or nonprocessed foods (NOVA 1), processed culinary ingredients (NOVA 2), processed foods (NOVA 3), and ultraprocessed foods (NOVA 4). The investigators highlighted comparisons between NOVA 1 and NOVA 3 and between NOVA 1 and NOVA 4.
The analysis revealed that swapping out just 10% of processed foods with minimally processed foods significantly lowered the risk for cancer overall (hazard ratio, 0.96) as well as for esophageal squamous cell carcinoma (HR, 0.57), hepatocellular carcinoma (HR, 0.77), head and neck cancers (HR, 0.80), colon cancer (HR, 0,88), rectal cancer (HR, 0.90), and postmenopausal breast cancer (HR, 0.93)
Swapping 10% of ultraprocessed foods for minimally processed foods lowered the risk of cancer overall only slightly (HR, 0.99) as well as the risk for various cancer types, including hepatocellular carcinoma (HR, 0.73), head and neck cancers (HR, 0.80), esophageal adenocarcinoma (HR, 0.80), and colon cancer (HR, 0.93).
The authors noted several limitations to the analysis, perhaps most notably that intake of ultraprocessed foods contributed to about 32% of total daily energy intake among study participants, but today that percentage could be nearly double across European countries.
“This discrepancy might explain the fewer significant associations observed between ultraprocessed foods and cancer risk than in processed foods and cancer risk,” the authors suggested.
The findings are “broadly in line with current evidence,” but the authors also noted some inconsistencies. For example, the current study showed a positive association between processed food consumption and risk for colorectal cancer and postmenopausal breast cancer, whereas other studies have not.
Overall, though, the authors concluded that increased consumption of minimally processed and fresh foods was associated with reduced overall risk for cancer and risk for specific cancers, and increased consumption of processed and ultraprocessed foods was associated with increased cancer risks.
This study “is the largest study investigating these associations between food processing and cancer risk and therefore has greater power to detect differences in populations, potentially explaining why we found overall more significant results for different cancer sites than other cohorts,” Dr. Kliemann and colleagues wrote.
This study was funded by Cancer Research UK, the French National Cancer Institute, and World Cancer Research Fund International. The authors declared no competing interests.
A version of this article originally appeared on Medscape.com.
Processed and ultraprocessed food consumption has been shown to increase the risk for various cancers. A new analysis suggests that replacing even a small amount of such foods with an equal amount of minimally processed options may reduce that risk.
Using data from more than 450,000 participants, the dietary substitution analysis found that as well as the risk for several cancer types, including esophageal squamous cell carcinoma by 43% and hepatocellular carcinoma by 23%.
Making this substitution with ultraprocessed foods also appeared to lower cancer risk but often to a lesser degree. For instance, swapping 10% of ultraprocessed foods for minimally processed foods lowered the overall cancer risk by just 1%, the risk of hepatocellular carcinoma by 27%, and the risk of esophageal squamous cell carcinoma by 20%.
Overall, “this study suggests that the replacement of processed and ultraprocessed foods and drinks with an equal amount of minimally processed foods might reduce the risk of various cancer types,” Nathalie Kliemann, PhD, from the World Health Organization’s International Agency for Research on Cancer, Lyon, France, and colleagues concluded.
The findings were published in The Lancet Planetary Health.
Processed and ultraprocessed foods tend to have high-energy density and low nutritional value, and some epidemiological evidence indicates a possible link between consuming ultraprocessed food and cancer outcomes.
Dr. Kliemann and colleagues, for instance, recently published a study showing a link between ultraprocessed food consumption and increased risk for cancer, particularly ovarian cancer, as well as increased risk of dying from cancer. That study of nearly 200,000 middle-aged adults in the UK Biobank database showed that, for each 10 percentage point increase in the consumption of ultraprocessed foods, there was a 2% increase in the overall incidence of cancer and a 19% increase in ovarian cancer incidence.
However, conflicting reports exist, and research exploring associations between processed foods and cancer remains limited.
The researchers wanted to better understand the potential association between the degree of food processing and risk for cancer in a larger cohort of individuals.
The investigators performed a dietary substitution analysis using data from more than 450,000 participants from the European Prospective Investigation into Cancer and Nutrition (EPIC) study and looking at 25 anatomical sites. EPIC study participants, who had no cancer diagnoses prior to enrollment, were identified between March 1991 and July 2001. Of the 450,111 included in the analysis, 47,573 were diagnosed with cancer during a mean follow-up of 14.1 years. Mean age at recruitment was 51 years, and mean BMI was 25.3 kg/m2.
Food items were classified according to their level of processing using the NOVA classification system: minimally or nonprocessed foods (NOVA 1), processed culinary ingredients (NOVA 2), processed foods (NOVA 3), and ultraprocessed foods (NOVA 4). The investigators highlighted comparisons between NOVA 1 and NOVA 3 and between NOVA 1 and NOVA 4.
The analysis revealed that swapping out just 10% of processed foods with minimally processed foods significantly lowered the risk for cancer overall (hazard ratio, 0.96) as well as for esophageal squamous cell carcinoma (HR, 0.57), hepatocellular carcinoma (HR, 0.77), head and neck cancers (HR, 0.80), colon cancer (HR, 0,88), rectal cancer (HR, 0.90), and postmenopausal breast cancer (HR, 0.93)
Swapping 10% of ultraprocessed foods for minimally processed foods lowered the risk of cancer overall only slightly (HR, 0.99) as well as the risk for various cancer types, including hepatocellular carcinoma (HR, 0.73), head and neck cancers (HR, 0.80), esophageal adenocarcinoma (HR, 0.80), and colon cancer (HR, 0.93).
The authors noted several limitations to the analysis, perhaps most notably that intake of ultraprocessed foods contributed to about 32% of total daily energy intake among study participants, but today that percentage could be nearly double across European countries.
“This discrepancy might explain the fewer significant associations observed between ultraprocessed foods and cancer risk than in processed foods and cancer risk,” the authors suggested.
The findings are “broadly in line with current evidence,” but the authors also noted some inconsistencies. For example, the current study showed a positive association between processed food consumption and risk for colorectal cancer and postmenopausal breast cancer, whereas other studies have not.
Overall, though, the authors concluded that increased consumption of minimally processed and fresh foods was associated with reduced overall risk for cancer and risk for specific cancers, and increased consumption of processed and ultraprocessed foods was associated with increased cancer risks.
This study “is the largest study investigating these associations between food processing and cancer risk and therefore has greater power to detect differences in populations, potentially explaining why we found overall more significant results for different cancer sites than other cohorts,” Dr. Kliemann and colleagues wrote.
This study was funded by Cancer Research UK, the French National Cancer Institute, and World Cancer Research Fund International. The authors declared no competing interests.
A version of this article originally appeared on Medscape.com.
Processed and ultraprocessed food consumption has been shown to increase the risk for various cancers. A new analysis suggests that replacing even a small amount of such foods with an equal amount of minimally processed options may reduce that risk.
Using data from more than 450,000 participants, the dietary substitution analysis found that as well as the risk for several cancer types, including esophageal squamous cell carcinoma by 43% and hepatocellular carcinoma by 23%.
Making this substitution with ultraprocessed foods also appeared to lower cancer risk but often to a lesser degree. For instance, swapping 10% of ultraprocessed foods for minimally processed foods lowered the overall cancer risk by just 1%, the risk of hepatocellular carcinoma by 27%, and the risk of esophageal squamous cell carcinoma by 20%.
Overall, “this study suggests that the replacement of processed and ultraprocessed foods and drinks with an equal amount of minimally processed foods might reduce the risk of various cancer types,” Nathalie Kliemann, PhD, from the World Health Organization’s International Agency for Research on Cancer, Lyon, France, and colleagues concluded.
The findings were published in The Lancet Planetary Health.
Processed and ultraprocessed foods tend to have high-energy density and low nutritional value, and some epidemiological evidence indicates a possible link between consuming ultraprocessed food and cancer outcomes.
Dr. Kliemann and colleagues, for instance, recently published a study showing a link between ultraprocessed food consumption and increased risk for cancer, particularly ovarian cancer, as well as increased risk of dying from cancer. That study of nearly 200,000 middle-aged adults in the UK Biobank database showed that, for each 10 percentage point increase in the consumption of ultraprocessed foods, there was a 2% increase in the overall incidence of cancer and a 19% increase in ovarian cancer incidence.
However, conflicting reports exist, and research exploring associations between processed foods and cancer remains limited.
The researchers wanted to better understand the potential association between the degree of food processing and risk for cancer in a larger cohort of individuals.
The investigators performed a dietary substitution analysis using data from more than 450,000 participants from the European Prospective Investigation into Cancer and Nutrition (EPIC) study and looking at 25 anatomical sites. EPIC study participants, who had no cancer diagnoses prior to enrollment, were identified between March 1991 and July 2001. Of the 450,111 included in the analysis, 47,573 were diagnosed with cancer during a mean follow-up of 14.1 years. Mean age at recruitment was 51 years, and mean BMI was 25.3 kg/m2.
Food items were classified according to their level of processing using the NOVA classification system: minimally or nonprocessed foods (NOVA 1), processed culinary ingredients (NOVA 2), processed foods (NOVA 3), and ultraprocessed foods (NOVA 4). The investigators highlighted comparisons between NOVA 1 and NOVA 3 and between NOVA 1 and NOVA 4.
The analysis revealed that swapping out just 10% of processed foods with minimally processed foods significantly lowered the risk for cancer overall (hazard ratio, 0.96) as well as for esophageal squamous cell carcinoma (HR, 0.57), hepatocellular carcinoma (HR, 0.77), head and neck cancers (HR, 0.80), colon cancer (HR, 0,88), rectal cancer (HR, 0.90), and postmenopausal breast cancer (HR, 0.93)
Swapping 10% of ultraprocessed foods for minimally processed foods lowered the risk of cancer overall only slightly (HR, 0.99) as well as the risk for various cancer types, including hepatocellular carcinoma (HR, 0.73), head and neck cancers (HR, 0.80), esophageal adenocarcinoma (HR, 0.80), and colon cancer (HR, 0.93).
The authors noted several limitations to the analysis, perhaps most notably that intake of ultraprocessed foods contributed to about 32% of total daily energy intake among study participants, but today that percentage could be nearly double across European countries.
“This discrepancy might explain the fewer significant associations observed between ultraprocessed foods and cancer risk than in processed foods and cancer risk,” the authors suggested.
The findings are “broadly in line with current evidence,” but the authors also noted some inconsistencies. For example, the current study showed a positive association between processed food consumption and risk for colorectal cancer and postmenopausal breast cancer, whereas other studies have not.
Overall, though, the authors concluded that increased consumption of minimally processed and fresh foods was associated with reduced overall risk for cancer and risk for specific cancers, and increased consumption of processed and ultraprocessed foods was associated with increased cancer risks.
This study “is the largest study investigating these associations between food processing and cancer risk and therefore has greater power to detect differences in populations, potentially explaining why we found overall more significant results for different cancer sites than other cohorts,” Dr. Kliemann and colleagues wrote.
This study was funded by Cancer Research UK, the French National Cancer Institute, and World Cancer Research Fund International. The authors declared no competing interests.
A version of this article originally appeared on Medscape.com.
FROM THE LANCET PLANETARY HEALTH
Lack of food for thought: Starve a bacterium, feed an infection
A whole new, tiny level of hangry
Ever been so hungry that everything just got on your nerves? Maybe you feel a little snappy right now? Like you’ll just lash out unless you get something to eat? Been there. And so have bacteria.
New research shows that some bacteria go into a full-on Hulk smash if they’re not getting the nutrients they need by releasing toxins into the body. Sounds like a bacterial temper tantrum.
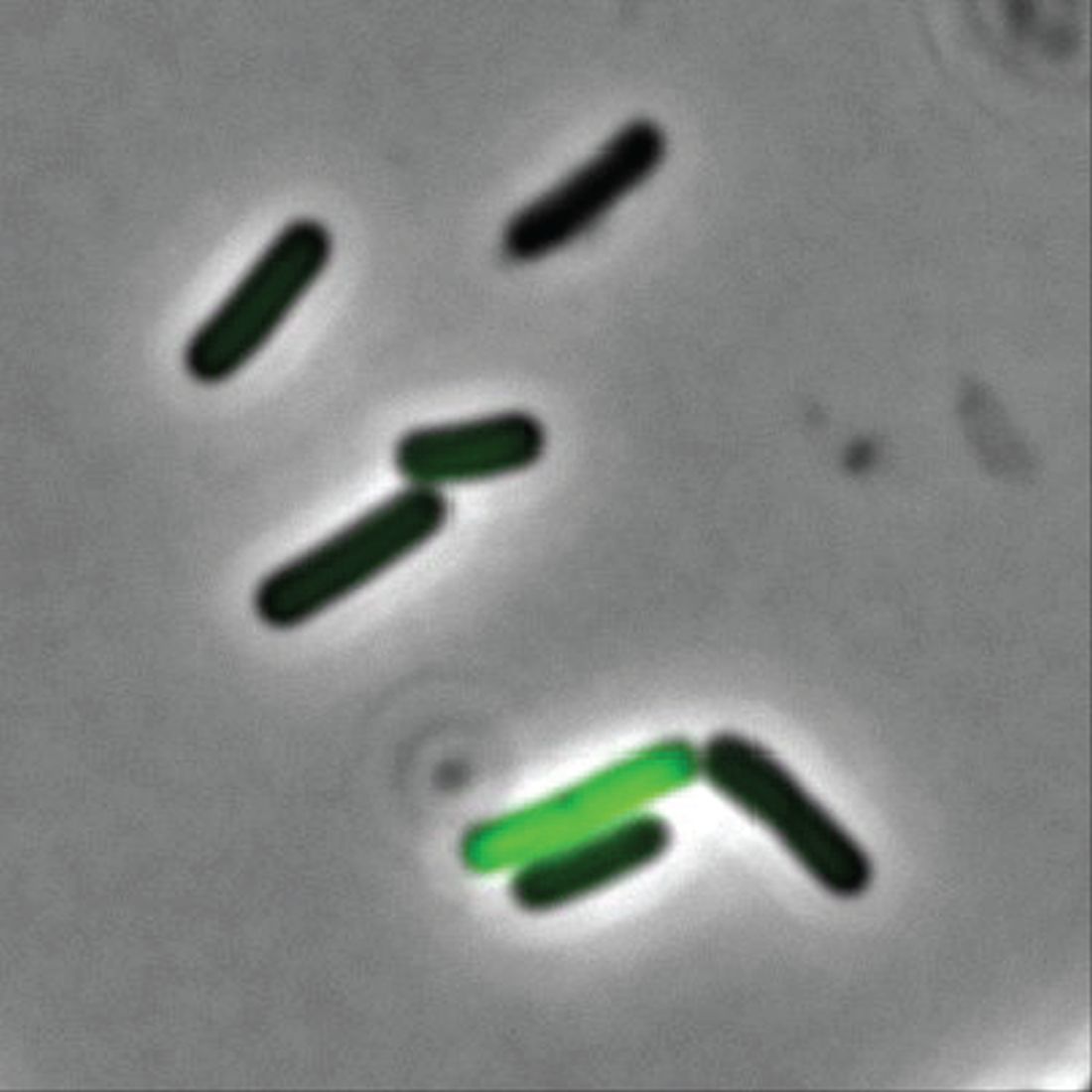
Even though two cells may be genetically identical, they don’t always behave the same in a bacterial community. Some do their job and stay in line, but some evil twins rage out and make people sick by releasing toxins into the environment, Adam Rosenthal, PhD, of the University of North Carolina and his colleagues discovered.
To figure out why some cells were all business as usual while others were not, the investigators looked at Clostridium perfringens, a bacterium found in the intestines of humans and other vertebrates. When the C. perfringens cells were fed a little acetate to munch on, the hangry cells calmed down faster than a kid with a bag of fruit snacks, reducing toxin levels. Some cells even disappeared, falling in line with their model-citizen counterparts.
So what does this really mean? More research, duh. Now that we know nutrients play a role in toxicity, it may open the door to finding a way to fight against antibiotic resistance in humans and reduce antibiotic use in the food industry.
So think to yourself. Are you bothered for no reason? Getting a little testy with your friends and coworkers? Maybe you just haven’t eaten in a while. You’re literally not alone. Even a single-cell organism can behave based on its hunger levels.
Now go have a snack. Your bacteria are getting restless.
The very hangry iguana?
Imagine yourself on a warm, sunny tropical beach. You are enjoying a piece of cake as you take in the slow beat of the waves lapping against the shore. Life is as good as it could be.
Then you feel a presence nearby. Hostility. Hunger. A set of feral, covetous eyes in the nearby jungle. A reptilian beast stalks you, and its all-encompassing sweet tooth desires your cake.
Wait, hold on, what?
As an unfortunate 3-year-old on vacation in Costa Rica found out, there’s at least one iguana in the world out there with a taste for sugar (better than a taste for blood, we suppose).

While out on the beach, the lizard darted out of nowhere, bit the girl on the back of the hand, and stole her cake. Still not the worst party guest ever. The child was taken to a local clinic, where the wound was cleaned and a 5-day antibiotic treatment (lizards carry salmonella) was provided. Things seemed fine, and the girl returned home without incident.
But of course, that’s not the end of the story. Five months later, the girl’s parents noticed a red bump at the wound site. Over the next 3 months, the surrounding skin grew red and painful. A trip to the hospital in California revealed that she had a ganglion cyst and a discharge of pus. Turns out our cake-obsessed lizard friend did give the little girl a gift: the first known human case of Mycobacterium marinum infection following an iguana bite on record.
M. marinum, which causes a disease similar to tuberculosis, typically infects fish but can infect humans if skin wounds are exposed to contaminated water. It’s also resistant to most antibiotics, which is why the first round didn’t clear up the infection. A second round of more-potent antibiotics seems to be working well.
So, to sum up, this poor child got bitten by a lizard, had her cake stolen, and contracted a rare illness in exchange. For a 3-year-old, that’s gotta be in the top-10 worst days ever. Unless, of course, we’re actually living in the Marvel universe (sorry, multiverse at this point). Then we’re totally going to see the emergence of the new superhero Iguana Girl in 15 years or so. Keep your eyes open.
No allergies? Let them give up cake
Allergy season is already here – starting earlier every year, it seems – and many people are not happy about it. So unhappy, actually, that there’s a list of things they would be willing to give up for a year to get rid of their of allergies, according to a survey conducted by OnePoll on behalf of Flonase.

Nearly 40% of 2,000 respondents with allergies would go a year without eating cake or chocolate or playing video games in exchange for allergy-free status, the survey results show. Almost as many would forgo coffee (38%) or pizza (37%) for a year, while 36% would stay off social media and 31% would take a pay cut or give up their smartphones, the Independent reported.
More than half of the allergic Americans – 54%, to be exact – who were polled this past winter – Feb. 24 to March 1, to be exact – consider allergy symptoms to be the most frustrating part of the spring. Annoying things that were less frustrating to the group included mosquitoes (41%), filing tax returns (38%), and daylight savings time (37%).
The Trump arraignment circus, of course, occurred too late to make the list, as did the big “We’re going back to the office! No wait, we’re closing the office forever!” email extravaganza and emotional roller coaster. That second one, however, did not get nearly as much media coverage.
A whole new, tiny level of hangry
Ever been so hungry that everything just got on your nerves? Maybe you feel a little snappy right now? Like you’ll just lash out unless you get something to eat? Been there. And so have bacteria.
New research shows that some bacteria go into a full-on Hulk smash if they’re not getting the nutrients they need by releasing toxins into the body. Sounds like a bacterial temper tantrum.
Even though two cells may be genetically identical, they don’t always behave the same in a bacterial community. Some do their job and stay in line, but some evil twins rage out and make people sick by releasing toxins into the environment, Adam Rosenthal, PhD, of the University of North Carolina and his colleagues discovered.
To figure out why some cells were all business as usual while others were not, the investigators looked at Clostridium perfringens, a bacterium found in the intestines of humans and other vertebrates. When the C. perfringens cells were fed a little acetate to munch on, the hangry cells calmed down faster than a kid with a bag of fruit snacks, reducing toxin levels. Some cells even disappeared, falling in line with their model-citizen counterparts.
So what does this really mean? More research, duh. Now that we know nutrients play a role in toxicity, it may open the door to finding a way to fight against antibiotic resistance in humans and reduce antibiotic use in the food industry.
So think to yourself. Are you bothered for no reason? Getting a little testy with your friends and coworkers? Maybe you just haven’t eaten in a while. You’re literally not alone. Even a single-cell organism can behave based on its hunger levels.
Now go have a snack. Your bacteria are getting restless.
The very hangry iguana?
Imagine yourself on a warm, sunny tropical beach. You are enjoying a piece of cake as you take in the slow beat of the waves lapping against the shore. Life is as good as it could be.
Then you feel a presence nearby. Hostility. Hunger. A set of feral, covetous eyes in the nearby jungle. A reptilian beast stalks you, and its all-encompassing sweet tooth desires your cake.
Wait, hold on, what?
As an unfortunate 3-year-old on vacation in Costa Rica found out, there’s at least one iguana in the world out there with a taste for sugar (better than a taste for blood, we suppose).
While out on the beach, the lizard darted out of nowhere, bit the girl on the back of the hand, and stole her cake. Still not the worst party guest ever. The child was taken to a local clinic, where the wound was cleaned and a 5-day antibiotic treatment (lizards carry salmonella) was provided. Things seemed fine, and the girl returned home without incident.
But of course, that’s not the end of the story. Five months later, the girl’s parents noticed a red bump at the wound site. Over the next 3 months, the surrounding skin grew red and painful. A trip to the hospital in California revealed that she had a ganglion cyst and a discharge of pus. Turns out our cake-obsessed lizard friend did give the little girl a gift: the first known human case of Mycobacterium marinum infection following an iguana bite on record.
M. marinum, which causes a disease similar to tuberculosis, typically infects fish but can infect humans if skin wounds are exposed to contaminated water. It’s also resistant to most antibiotics, which is why the first round didn’t clear up the infection. A second round of more-potent antibiotics seems to be working well.
So, to sum up, this poor child got bitten by a lizard, had her cake stolen, and contracted a rare illness in exchange. For a 3-year-old, that’s gotta be in the top-10 worst days ever. Unless, of course, we’re actually living in the Marvel universe (sorry, multiverse at this point). Then we’re totally going to see the emergence of the new superhero Iguana Girl in 15 years or so. Keep your eyes open.
No allergies? Let them give up cake
Allergy season is already here – starting earlier every year, it seems – and many people are not happy about it. So unhappy, actually, that there’s a list of things they would be willing to give up for a year to get rid of their of allergies, according to a survey conducted by OnePoll on behalf of Flonase.
Nearly 40% of 2,000 respondents with allergies would go a year without eating cake or chocolate or playing video games in exchange for allergy-free status, the survey results show. Almost as many would forgo coffee (38%) or pizza (37%) for a year, while 36% would stay off social media and 31% would take a pay cut or give up their smartphones, the Independent reported.
More than half of the allergic Americans – 54%, to be exact – who were polled this past winter – Feb. 24 to March 1, to be exact – consider allergy symptoms to be the most frustrating part of the spring. Annoying things that were less frustrating to the group included mosquitoes (41%), filing tax returns (38%), and daylight savings time (37%).
The Trump arraignment circus, of course, occurred too late to make the list, as did the big “We’re going back to the office! No wait, we’re closing the office forever!” email extravaganza and emotional roller coaster. That second one, however, did not get nearly as much media coverage.
A whole new, tiny level of hangry
Ever been so hungry that everything just got on your nerves? Maybe you feel a little snappy right now? Like you’ll just lash out unless you get something to eat? Been there. And so have bacteria.
New research shows that some bacteria go into a full-on Hulk smash if they’re not getting the nutrients they need by releasing toxins into the body. Sounds like a bacterial temper tantrum.
Even though two cells may be genetically identical, they don’t always behave the same in a bacterial community. Some do their job and stay in line, but some evil twins rage out and make people sick by releasing toxins into the environment, Adam Rosenthal, PhD, of the University of North Carolina and his colleagues discovered.
To figure out why some cells were all business as usual while others were not, the investigators looked at Clostridium perfringens, a bacterium found in the intestines of humans and other vertebrates. When the C. perfringens cells were fed a little acetate to munch on, the hangry cells calmed down faster than a kid with a bag of fruit snacks, reducing toxin levels. Some cells even disappeared, falling in line with their model-citizen counterparts.
So what does this really mean? More research, duh. Now that we know nutrients play a role in toxicity, it may open the door to finding a way to fight against antibiotic resistance in humans and reduce antibiotic use in the food industry.
So think to yourself. Are you bothered for no reason? Getting a little testy with your friends and coworkers? Maybe you just haven’t eaten in a while. You’re literally not alone. Even a single-cell organism can behave based on its hunger levels.
Now go have a snack. Your bacteria are getting restless.
The very hangry iguana?
Imagine yourself on a warm, sunny tropical beach. You are enjoying a piece of cake as you take in the slow beat of the waves lapping against the shore. Life is as good as it could be.
Then you feel a presence nearby. Hostility. Hunger. A set of feral, covetous eyes in the nearby jungle. A reptilian beast stalks you, and its all-encompassing sweet tooth desires your cake.
Wait, hold on, what?
As an unfortunate 3-year-old on vacation in Costa Rica found out, there’s at least one iguana in the world out there with a taste for sugar (better than a taste for blood, we suppose).
While out on the beach, the lizard darted out of nowhere, bit the girl on the back of the hand, and stole her cake. Still not the worst party guest ever. The child was taken to a local clinic, where the wound was cleaned and a 5-day antibiotic treatment (lizards carry salmonella) was provided. Things seemed fine, and the girl returned home without incident.
But of course, that’s not the end of the story. Five months later, the girl’s parents noticed a red bump at the wound site. Over the next 3 months, the surrounding skin grew red and painful. A trip to the hospital in California revealed that she had a ganglion cyst and a discharge of pus. Turns out our cake-obsessed lizard friend did give the little girl a gift: the first known human case of Mycobacterium marinum infection following an iguana bite on record.
M. marinum, which causes a disease similar to tuberculosis, typically infects fish but can infect humans if skin wounds are exposed to contaminated water. It’s also resistant to most antibiotics, which is why the first round didn’t clear up the infection. A second round of more-potent antibiotics seems to be working well.
So, to sum up, this poor child got bitten by a lizard, had her cake stolen, and contracted a rare illness in exchange. For a 3-year-old, that’s gotta be in the top-10 worst days ever. Unless, of course, we’re actually living in the Marvel universe (sorry, multiverse at this point). Then we’re totally going to see the emergence of the new superhero Iguana Girl in 15 years or so. Keep your eyes open.
No allergies? Let them give up cake
Allergy season is already here – starting earlier every year, it seems – and many people are not happy about it. So unhappy, actually, that there’s a list of things they would be willing to give up for a year to get rid of their of allergies, according to a survey conducted by OnePoll on behalf of Flonase.
Nearly 40% of 2,000 respondents with allergies would go a year without eating cake or chocolate or playing video games in exchange for allergy-free status, the survey results show. Almost as many would forgo coffee (38%) or pizza (37%) for a year, while 36% would stay off social media and 31% would take a pay cut or give up their smartphones, the Independent reported.
More than half of the allergic Americans – 54%, to be exact – who were polled this past winter – Feb. 24 to March 1, to be exact – consider allergy symptoms to be the most frustrating part of the spring. Annoying things that were less frustrating to the group included mosquitoes (41%), filing tax returns (38%), and daylight savings time (37%).
The Trump arraignment circus, of course, occurred too late to make the list, as did the big “We’re going back to the office! No wait, we’re closing the office forever!” email extravaganza and emotional roller coaster. That second one, however, did not get nearly as much media coverage.
AGA clinical practice update addresses role of endoscopic ultrasound–guided gallbladder drainage in acute cholecystitis
according to a recent clinical practice update by the American Gastroenterological Association.
The update, written by Shayan S. Irani, MD, of Virginia Mason Medical Center, Seattle, and colleagues, also covers techniques and outcomes of EUS-GBD and provides suggestions for training and patient selection.

“In this clinical practice update, we comment on the role of EUS-GBD (compared with ET-GBD [endoscopic treatment via transpapillary gallbladder drainage] and PT [percutaneous transhepatic]-GBD) in the management of acute cholecystitis, and describe its indications, contraindications, procedural considerations, and associated adverse events,” the authors wrote in Clinical Gastroenterology and Hepatology.
Dr. Irani and colleagues noted that EUS-GBD is a valuable alternative to PT-GBD, which can have a significant morbidity, and ET-GBD has been associated with relatively lower technical and clinical success rates in the presence of obstructing pathology of the cystic duct. Advances in lumen-apposing metal stents have further improved outcomes in EUS-GBD, as demonstrated by multiple case series and comparative trials.
According to the update, EUS-GBD is suggested in three scenarios: for draining the gallbladder in patients with acute cholecystitis who are at high risk for surgery, for removing percutaneous cholecystostomy drains in patients who cannot undergo cholecystectomy, and for draining malignant biliary obstruction in patients who have not responded to other treatments. EUS-GBD is contraindicated in patients with significant coagulopathy, large-volume uncontrolled ascites, or gallbladder perforation.
Dr. Irani and colleagues also noted that, between the three main techniques mentioned above, EUS-GBD has the lowest risk of recurrent cholecystitis, whereas ET-GBD and PT-GBD present slightly lower mortality rates.
While the update provides technical guidance on performing EUS-GBD, Dr. Irani and colleagues make clear that EUS-GBD is a highly specialized procedure that requires sufficient training to optimal results.
“Performing the procedure has an associated learning curve and requires advanced EUS training,” they wrote. “Two recent publications have suggested that the minimum number of procedures to gain competency should be approximately 19-25 procedures.”
Addressing unmet needs, Dr. Irani and colleagues suggested that more research is needed to standardize patient selection, procedure technique, and stent follow-up evaluation.
Ongoing studies aim to address whether endoscopic management of cholecystitis and symptomatic gallstones could become a mainstream treatment in the future, they wrote, but “we are still a long way from abandoning standard of care with cholecystectomy.”
This clinical practice update was commissioned by the AGA. Dr. Irani is a consultant for Boston Scientific, ConMed, and GORE; one coauthor received research support from Boston Scientific and Olympus and is a consultant and speaker for Boston Scientific, Cook, Medtronic, Olympus and ConMed. The remaining coauthor disclosed no conflicts.
according to a recent clinical practice update by the American Gastroenterological Association.
The update, written by Shayan S. Irani, MD, of Virginia Mason Medical Center, Seattle, and colleagues, also covers techniques and outcomes of EUS-GBD and provides suggestions for training and patient selection.
“In this clinical practice update, we comment on the role of EUS-GBD (compared with ET-GBD [endoscopic treatment via transpapillary gallbladder drainage] and PT [percutaneous transhepatic]-GBD) in the management of acute cholecystitis, and describe its indications, contraindications, procedural considerations, and associated adverse events,” the authors wrote in Clinical Gastroenterology and Hepatology.
Dr. Irani and colleagues noted that EUS-GBD is a valuable alternative to PT-GBD, which can have a significant morbidity, and ET-GBD has been associated with relatively lower technical and clinical success rates in the presence of obstructing pathology of the cystic duct. Advances in lumen-apposing metal stents have further improved outcomes in EUS-GBD, as demonstrated by multiple case series and comparative trials.
According to the update, EUS-GBD is suggested in three scenarios: for draining the gallbladder in patients with acute cholecystitis who are at high risk for surgery, for removing percutaneous cholecystostomy drains in patients who cannot undergo cholecystectomy, and for draining malignant biliary obstruction in patients who have not responded to other treatments. EUS-GBD is contraindicated in patients with significant coagulopathy, large-volume uncontrolled ascites, or gallbladder perforation.
Dr. Irani and colleagues also noted that, between the three main techniques mentioned above, EUS-GBD has the lowest risk of recurrent cholecystitis, whereas ET-GBD and PT-GBD present slightly lower mortality rates.
While the update provides technical guidance on performing EUS-GBD, Dr. Irani and colleagues make clear that EUS-GBD is a highly specialized procedure that requires sufficient training to optimal results.
“Performing the procedure has an associated learning curve and requires advanced EUS training,” they wrote. “Two recent publications have suggested that the minimum number of procedures to gain competency should be approximately 19-25 procedures.”
Addressing unmet needs, Dr. Irani and colleagues suggested that more research is needed to standardize patient selection, procedure technique, and stent follow-up evaluation.
Ongoing studies aim to address whether endoscopic management of cholecystitis and symptomatic gallstones could become a mainstream treatment in the future, they wrote, but “we are still a long way from abandoning standard of care with cholecystectomy.”
This clinical practice update was commissioned by the AGA. Dr. Irani is a consultant for Boston Scientific, ConMed, and GORE; one coauthor received research support from Boston Scientific and Olympus and is a consultant and speaker for Boston Scientific, Cook, Medtronic, Olympus and ConMed. The remaining coauthor disclosed no conflicts.
according to a recent clinical practice update by the American Gastroenterological Association.
The update, written by Shayan S. Irani, MD, of Virginia Mason Medical Center, Seattle, and colleagues, also covers techniques and outcomes of EUS-GBD and provides suggestions for training and patient selection.
“In this clinical practice update, we comment on the role of EUS-GBD (compared with ET-GBD [endoscopic treatment via transpapillary gallbladder drainage] and PT [percutaneous transhepatic]-GBD) in the management of acute cholecystitis, and describe its indications, contraindications, procedural considerations, and associated adverse events,” the authors wrote in Clinical Gastroenterology and Hepatology.
Dr. Irani and colleagues noted that EUS-GBD is a valuable alternative to PT-GBD, which can have a significant morbidity, and ET-GBD has been associated with relatively lower technical and clinical success rates in the presence of obstructing pathology of the cystic duct. Advances in lumen-apposing metal stents have further improved outcomes in EUS-GBD, as demonstrated by multiple case series and comparative trials.
According to the update, EUS-GBD is suggested in three scenarios: for draining the gallbladder in patients with acute cholecystitis who are at high risk for surgery, for removing percutaneous cholecystostomy drains in patients who cannot undergo cholecystectomy, and for draining malignant biliary obstruction in patients who have not responded to other treatments. EUS-GBD is contraindicated in patients with significant coagulopathy, large-volume uncontrolled ascites, or gallbladder perforation.
Dr. Irani and colleagues also noted that, between the three main techniques mentioned above, EUS-GBD has the lowest risk of recurrent cholecystitis, whereas ET-GBD and PT-GBD present slightly lower mortality rates.
While the update provides technical guidance on performing EUS-GBD, Dr. Irani and colleagues make clear that EUS-GBD is a highly specialized procedure that requires sufficient training to optimal results.
“Performing the procedure has an associated learning curve and requires advanced EUS training,” they wrote. “Two recent publications have suggested that the minimum number of procedures to gain competency should be approximately 19-25 procedures.”
Addressing unmet needs, Dr. Irani and colleagues suggested that more research is needed to standardize patient selection, procedure technique, and stent follow-up evaluation.
Ongoing studies aim to address whether endoscopic management of cholecystitis and symptomatic gallstones could become a mainstream treatment in the future, they wrote, but “we are still a long way from abandoning standard of care with cholecystectomy.”
This clinical practice update was commissioned by the AGA. Dr. Irani is a consultant for Boston Scientific, ConMed, and GORE; one coauthor received research support from Boston Scientific and Olympus and is a consultant and speaker for Boston Scientific, Cook, Medtronic, Olympus and ConMed. The remaining coauthor disclosed no conflicts.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
SARS-CoV-2 crosses placenta and infects brains of two infants: ‘This is a first’
, according to a study published online today in Pediatrics .
One of the infants died at 13 months and the other remained in hospice care at time of manuscript submission.
Lead author Merline Benny, MD, with the division of neonatology, department of pediatrics at University of Miami, and colleagues briefed reporters today ahead of the release.

“This is a first,” said senior author Shahnaz Duara, MD, medical director of the Neonatal Intensive Care Unit at Holtz Children’s Hospital, Miami, explaining it is the first study to confirm cross-placental SARS-CoV-2 transmission leading to brain injury in a newborn.
Both infants negative for the virus at birth
The two infants were admitted in the early days of the pandemic in the Delta wave to the neonatal ICU at Holtz Children’s Hospital at University of Miami/Jackson Memorial Medical Center.
Both infants tested negative for the virus at birth, but had significantly elevated SARS-CoV-2 antibodies in their blood, indicating that either antibodies crossed the placenta, or the virus crossed and the immune response was the baby’s.
Dr. Benny explained that the researchers have seen, to this point, more than 700 mother/infant pairs in whom the mother tested positive for COVID in Jackson hospital.
Most who tested positive for COVID were asymptomatic and most of the mothers and infants left the hospital without complications.
“However, (these) two babies had a very unusual clinical picture,” Dr. Benny said.
Those infants were born to mothers who became COVID positive in the second trimester and delivered a few weeks later.
Seizures started on day 1 of life
The babies began to seize from the first day of life. They had profound low tone (hypotonia) in their clinical exam, Dr. Benny explained.
“We had absolutely no good explanation for the early seizures and the degree of brain injury we saw,” Dr. Duara said.
Dr. Benny said that as their bodies grew, they had very small head circumference. Unlike some babies born with the Zika virus, these babies were not microcephalic at birth. Brain imaging on the two babies indicated significant brain atrophy, and neurodevelopment exams showed significant delay.
Discussions began with the center’s multidisciplinary team including neurologists, pathologists, neuroradiologists, and obstetricians who cared for both the mothers and the babies.
The experts examined the placentas and found some characteristic COVID changes and presence of the COVID virus. This was accompanied by increased markers for inflammation and a severe reduction in a hormone critical for placental health and brain development.
Examining the infant’s autopsy findings further raised suspicions of maternal transmission, something that had not been documented before.
Coauthor Ali G. Saad, MD, pediatric and perinatal pathology director at Miami, said, “I have seen literally thousands of brains in autopsies over the last 14 years, and this was the most dramatic case of leukoencephalopathy or loss of white matter in a patient with no significant reason. That’s what triggered the investigation.”
Mothers had very different presentations
Coauthor Michael J. Paidas, MD, with the department of obstetrics, gynecology, and reproductive sciences at Miami, pointed out that the circumstances of the two mothers, who were in their 20s, were very different.
One mother delivered at 32 weeks and had a very severe COVID presentation and spent a month in the intensive care unit. The team decided to deliver the child to save the mother, Dr. Paidas said.
In contrast, the other mother had asymptomatic COVID infection in the second trimester and delivered at full term.
He said one of the early suspicions in the babies’ presentations was hypoxic ischemic encephalopathy. “But it wasn’t lack of blood flow to the placenta that caused this,” he said. “As best we can tell, it was the viral infection.”
Instances are rare
The researchers emphasized that these instances are rare and have not been seen before or since the period of this study to their knowledge.
Dr. Duara said, “This is something we want to alert the medical community to more than the general public. We do not want the lay public to be panicked. We’re trying to understand what made these two pregnancies different, so we can direct research towards protecting vulnerable babies.”
Previous data have indicated a relatively benign status in infants who test negative for the COVID virus after birth. Dr. Benny added that COVID vaccination has been found safe in pregnancy and both vaccination and breastfeeding can help passage of antibodies to the infant and help protect the baby. Because these cases happened in the early days of the pandemic, no vaccines were available.
Dr. Paidas received funding from BioIncept to study hypoxic-ischemic encephalopathy with Preimplantation Factor, is a scientific advisory board member, and has stock options. Dr. Paidas and coauthor Dr. Jayakumar are coinventors of SPIKENET, University of Miami, patent pending 2023. The other authors have no conflicts of interest to disclose.
, according to a study published online today in Pediatrics .
One of the infants died at 13 months and the other remained in hospice care at time of manuscript submission.
Lead author Merline Benny, MD, with the division of neonatology, department of pediatrics at University of Miami, and colleagues briefed reporters today ahead of the release.
“This is a first,” said senior author Shahnaz Duara, MD, medical director of the Neonatal Intensive Care Unit at Holtz Children’s Hospital, Miami, explaining it is the first study to confirm cross-placental SARS-CoV-2 transmission leading to brain injury in a newborn.
Both infants negative for the virus at birth
The two infants were admitted in the early days of the pandemic in the Delta wave to the neonatal ICU at Holtz Children’s Hospital at University of Miami/Jackson Memorial Medical Center.
Both infants tested negative for the virus at birth, but had significantly elevated SARS-CoV-2 antibodies in their blood, indicating that either antibodies crossed the placenta, or the virus crossed and the immune response was the baby’s.
Dr. Benny explained that the researchers have seen, to this point, more than 700 mother/infant pairs in whom the mother tested positive for COVID in Jackson hospital.
Most who tested positive for COVID were asymptomatic and most of the mothers and infants left the hospital without complications.
“However, (these) two babies had a very unusual clinical picture,” Dr. Benny said.
Those infants were born to mothers who became COVID positive in the second trimester and delivered a few weeks later.
Seizures started on day 1 of life
The babies began to seize from the first day of life. They had profound low tone (hypotonia) in their clinical exam, Dr. Benny explained.
“We had absolutely no good explanation for the early seizures and the degree of brain injury we saw,” Dr. Duara said.
Dr. Benny said that as their bodies grew, they had very small head circumference. Unlike some babies born with the Zika virus, these babies were not microcephalic at birth. Brain imaging on the two babies indicated significant brain atrophy, and neurodevelopment exams showed significant delay.
Discussions began with the center’s multidisciplinary team including neurologists, pathologists, neuroradiologists, and obstetricians who cared for both the mothers and the babies.
The experts examined the placentas and found some characteristic COVID changes and presence of the COVID virus. This was accompanied by increased markers for inflammation and a severe reduction in a hormone critical for placental health and brain development.
Examining the infant’s autopsy findings further raised suspicions of maternal transmission, something that had not been documented before.
Coauthor Ali G. Saad, MD, pediatric and perinatal pathology director at Miami, said, “I have seen literally thousands of brains in autopsies over the last 14 years, and this was the most dramatic case of leukoencephalopathy or loss of white matter in a patient with no significant reason. That’s what triggered the investigation.”
Mothers had very different presentations
Coauthor Michael J. Paidas, MD, with the department of obstetrics, gynecology, and reproductive sciences at Miami, pointed out that the circumstances of the two mothers, who were in their 20s, were very different.
One mother delivered at 32 weeks and had a very severe COVID presentation and spent a month in the intensive care unit. The team decided to deliver the child to save the mother, Dr. Paidas said.
In contrast, the other mother had asymptomatic COVID infection in the second trimester and delivered at full term.
He said one of the early suspicions in the babies’ presentations was hypoxic ischemic encephalopathy. “But it wasn’t lack of blood flow to the placenta that caused this,” he said. “As best we can tell, it was the viral infection.”
Instances are rare
The researchers emphasized that these instances are rare and have not been seen before or since the period of this study to their knowledge.
Dr. Duara said, “This is something we want to alert the medical community to more than the general public. We do not want the lay public to be panicked. We’re trying to understand what made these two pregnancies different, so we can direct research towards protecting vulnerable babies.”
Previous data have indicated a relatively benign status in infants who test negative for the COVID virus after birth. Dr. Benny added that COVID vaccination has been found safe in pregnancy and both vaccination and breastfeeding can help passage of antibodies to the infant and help protect the baby. Because these cases happened in the early days of the pandemic, no vaccines were available.
Dr. Paidas received funding from BioIncept to study hypoxic-ischemic encephalopathy with Preimplantation Factor, is a scientific advisory board member, and has stock options. Dr. Paidas and coauthor Dr. Jayakumar are coinventors of SPIKENET, University of Miami, patent pending 2023. The other authors have no conflicts of interest to disclose.
, according to a study published online today in Pediatrics .
One of the infants died at 13 months and the other remained in hospice care at time of manuscript submission.
Lead author Merline Benny, MD, with the division of neonatology, department of pediatrics at University of Miami, and colleagues briefed reporters today ahead of the release.
“This is a first,” said senior author Shahnaz Duara, MD, medical director of the Neonatal Intensive Care Unit at Holtz Children’s Hospital, Miami, explaining it is the first study to confirm cross-placental SARS-CoV-2 transmission leading to brain injury in a newborn.
Both infants negative for the virus at birth
The two infants were admitted in the early days of the pandemic in the Delta wave to the neonatal ICU at Holtz Children’s Hospital at University of Miami/Jackson Memorial Medical Center.
Both infants tested negative for the virus at birth, but had significantly elevated SARS-CoV-2 antibodies in their blood, indicating that either antibodies crossed the placenta, or the virus crossed and the immune response was the baby’s.
Dr. Benny explained that the researchers have seen, to this point, more than 700 mother/infant pairs in whom the mother tested positive for COVID in Jackson hospital.
Most who tested positive for COVID were asymptomatic and most of the mothers and infants left the hospital without complications.
“However, (these) two babies had a very unusual clinical picture,” Dr. Benny said.
Those infants were born to mothers who became COVID positive in the second trimester and delivered a few weeks later.
Seizures started on day 1 of life
The babies began to seize from the first day of life. They had profound low tone (hypotonia) in their clinical exam, Dr. Benny explained.
“We had absolutely no good explanation for the early seizures and the degree of brain injury we saw,” Dr. Duara said.
Dr. Benny said that as their bodies grew, they had very small head circumference. Unlike some babies born with the Zika virus, these babies were not microcephalic at birth. Brain imaging on the two babies indicated significant brain atrophy, and neurodevelopment exams showed significant delay.
Discussions began with the center’s multidisciplinary team including neurologists, pathologists, neuroradiologists, and obstetricians who cared for both the mothers and the babies.
The experts examined the placentas and found some characteristic COVID changes and presence of the COVID virus. This was accompanied by increased markers for inflammation and a severe reduction in a hormone critical for placental health and brain development.
Examining the infant’s autopsy findings further raised suspicions of maternal transmission, something that had not been documented before.
Coauthor Ali G. Saad, MD, pediatric and perinatal pathology director at Miami, said, “I have seen literally thousands of brains in autopsies over the last 14 years, and this was the most dramatic case of leukoencephalopathy or loss of white matter in a patient with no significant reason. That’s what triggered the investigation.”
Mothers had very different presentations
Coauthor Michael J. Paidas, MD, with the department of obstetrics, gynecology, and reproductive sciences at Miami, pointed out that the circumstances of the two mothers, who were in their 20s, were very different.
One mother delivered at 32 weeks and had a very severe COVID presentation and spent a month in the intensive care unit. The team decided to deliver the child to save the mother, Dr. Paidas said.
In contrast, the other mother had asymptomatic COVID infection in the second trimester and delivered at full term.
He said one of the early suspicions in the babies’ presentations was hypoxic ischemic encephalopathy. “But it wasn’t lack of blood flow to the placenta that caused this,” he said. “As best we can tell, it was the viral infection.”
Instances are rare
The researchers emphasized that these instances are rare and have not been seen before or since the period of this study to their knowledge.
Dr. Duara said, “This is something we want to alert the medical community to more than the general public. We do not want the lay public to be panicked. We’re trying to understand what made these two pregnancies different, so we can direct research towards protecting vulnerable babies.”
Previous data have indicated a relatively benign status in infants who test negative for the COVID virus after birth. Dr. Benny added that COVID vaccination has been found safe in pregnancy and both vaccination and breastfeeding can help passage of antibodies to the infant and help protect the baby. Because these cases happened in the early days of the pandemic, no vaccines were available.
Dr. Paidas received funding from BioIncept to study hypoxic-ischemic encephalopathy with Preimplantation Factor, is a scientific advisory board member, and has stock options. Dr. Paidas and coauthor Dr. Jayakumar are coinventors of SPIKENET, University of Miami, patent pending 2023. The other authors have no conflicts of interest to disclose.
FROM PEDIATRICS
Infant and maternal weight gain together amplify obesity risk
Rapid weight gain (RWG) in infants and the mother’s prepregnancy overweight have a synergistic effect in increasing the odds that a child will develop overweight or obesity, new research suggests.
Findings were published online in Pediatrics.
Each factor has independently been associated with higher risk of childhood obesity but whether the two factors together exacerbate the risk has not been well studied, according to the authors led by Stephanie Gilley, MD, PhD, department of pediatrics, section of nutrition, University of Colorado at Denver, Aurora.
“Pediatric providers should monitor infants for RWG, especially in the context of maternal obesity, to reduce future risk of obesity,” the authors conclude.
Dr. Gilley’s team studied mother-infant dyads (n = 414) from the Healthy Start Study, an observational prebirth cohort. RWG was defined as a weight-for-age z score increase of at least 0.67 from birth to 3-7 months.
They found that RWG boosted the link between prepregnancy body mass index (ppBMI) and BMI z score, especially in female infants. Females exposed to both maternal obesity with RWG had an average BMI at the 94th percentile (1.50 increase in childhood BMI z score) “nearly at the cutoff for classification of obesity,” compared with those exposed to normal ppBMI with no RWG, who had an average childhood BMI at the 51st percentile.
“Currently, our nutrition recommendations as pediatricians are that all children are fed the same, essentially, after they’re born. We don’t have different growth parameters or different trajectories or targets for children who may have had different in utero exposures,” Dr. Gilley said.
Do some children need more monitoring for RWG?
Though we can’t necessarily draw conclusions from this one study, she says, the findings raise the question of whether children who were exposed in utero to obesity should be monitored for RWG more closely.
Lydia Shook, MD, Mass General Brigham maternal-fetal specialist and codirector of the Diabetes in Pregnancy Program at Massachusetts General Hospital in Boston, said she was struck by the finding in this study that with female infants, but not males, RWG significantly modified the association between ppBMI and early childhood BMI z scores.
“It’s an interesting finding and should be followed up with larger cohorts,” she said, noting that some previous studies have shown males are more vulnerable to maternal obesity and RWG.
“[Often] when we stratify by sex, you really need larger groups to be able to see the differences well,” Dr. Shook said.
She said she also found it interesting that when the researchers adjusted for breastfeeding status or caloric intake in childhood, the findings did not substantially change.
“That’s something that would warrant further investigation in an observational study or controlled trial,” Dr. Shook said.
Preventing rapid weight gain
The authors note that they did not consider possible interventions for preventing RGW in the study, although there are many, Dr. Gilley said.
Dr. Gilley also noted that a limitation of this study is that the population studied was primarily White.
Recent studies have shown the benefits of responsive parenting (RP) interventions, including a large study in 2022 geared toward Black families to teach better infant sleep practices as a way to prevent rapid weight gain.
That study, which tested the SAAF intervention, (Strong African American Families) found that “RP infants were nearly half as likely to experience upward crossing of two major weight-for-age percentile lines (14.1%), compared with control infants (24.2%); P = .09; odds ratio, 0.52; 95% confidence interval, 0.24-1.12.”
Along with sleep interventions, Dr. Gilley said, some researchers are studying the effects on RWG of better paternal engagement, or more involvement with the Women, Infants, and Children program, particularly with lower-income families.
Other studies have looked at breastfeeding vs. formula feeding – “but there have been mixed results there” – and responsive feeding practices, such as teaching families to recognize when a baby is full.
Dr. Gilley said she hopes this work will help broaden the thinking when it comes to infant weight gain.
“We spend a lot of time thinking about babies who are not growing fast enough and very little time thinking about babies who are growing too fast,” she said, “especially in those first 4-6 months of life.”
Dr. Gilley points to a study that illustrates that point. Pesch et al. concluded in a 2021 study based on interviews that pediatricians “are uncertain about the concept, definition, management, and long-term risks of rapid infant weight gain.”
Authors and Dr. Gilley declare no relevant financial relationships.
Rapid weight gain (RWG) in infants and the mother’s prepregnancy overweight have a synergistic effect in increasing the odds that a child will develop overweight or obesity, new research suggests.
Findings were published online in Pediatrics.
Each factor has independently been associated with higher risk of childhood obesity but whether the two factors together exacerbate the risk has not been well studied, according to the authors led by Stephanie Gilley, MD, PhD, department of pediatrics, section of nutrition, University of Colorado at Denver, Aurora.
“Pediatric providers should monitor infants for RWG, especially in the context of maternal obesity, to reduce future risk of obesity,” the authors conclude.
Dr. Gilley’s team studied mother-infant dyads (n = 414) from the Healthy Start Study, an observational prebirth cohort. RWG was defined as a weight-for-age z score increase of at least 0.67 from birth to 3-7 months.
They found that RWG boosted the link between prepregnancy body mass index (ppBMI) and BMI z score, especially in female infants. Females exposed to both maternal obesity with RWG had an average BMI at the 94th percentile (1.50 increase in childhood BMI z score) “nearly at the cutoff for classification of obesity,” compared with those exposed to normal ppBMI with no RWG, who had an average childhood BMI at the 51st percentile.
“Currently, our nutrition recommendations as pediatricians are that all children are fed the same, essentially, after they’re born. We don’t have different growth parameters or different trajectories or targets for children who may have had different in utero exposures,” Dr. Gilley said.
Do some children need more monitoring for RWG?
Though we can’t necessarily draw conclusions from this one study, she says, the findings raise the question of whether children who were exposed in utero to obesity should be monitored for RWG more closely.
Lydia Shook, MD, Mass General Brigham maternal-fetal specialist and codirector of the Diabetes in Pregnancy Program at Massachusetts General Hospital in Boston, said she was struck by the finding in this study that with female infants, but not males, RWG significantly modified the association between ppBMI and early childhood BMI z scores.
“It’s an interesting finding and should be followed up with larger cohorts,” she said, noting that some previous studies have shown males are more vulnerable to maternal obesity and RWG.
“[Often] when we stratify by sex, you really need larger groups to be able to see the differences well,” Dr. Shook said.
She said she also found it interesting that when the researchers adjusted for breastfeeding status or caloric intake in childhood, the findings did not substantially change.
“That’s something that would warrant further investigation in an observational study or controlled trial,” Dr. Shook said.
Preventing rapid weight gain
The authors note that they did not consider possible interventions for preventing RGW in the study, although there are many, Dr. Gilley said.
Dr. Gilley also noted that a limitation of this study is that the population studied was primarily White.
Recent studies have shown the benefits of responsive parenting (RP) interventions, including a large study in 2022 geared toward Black families to teach better infant sleep practices as a way to prevent rapid weight gain.
That study, which tested the SAAF intervention, (Strong African American Families) found that “RP infants were nearly half as likely to experience upward crossing of two major weight-for-age percentile lines (14.1%), compared with control infants (24.2%); P = .09; odds ratio, 0.52; 95% confidence interval, 0.24-1.12.”
Along with sleep interventions, Dr. Gilley said, some researchers are studying the effects on RWG of better paternal engagement, or more involvement with the Women, Infants, and Children program, particularly with lower-income families.
Other studies have looked at breastfeeding vs. formula feeding – “but there have been mixed results there” – and responsive feeding practices, such as teaching families to recognize when a baby is full.
Dr. Gilley said she hopes this work will help broaden the thinking when it comes to infant weight gain.
“We spend a lot of time thinking about babies who are not growing fast enough and very little time thinking about babies who are growing too fast,” she said, “especially in those first 4-6 months of life.”
Dr. Gilley points to a study that illustrates that point. Pesch et al. concluded in a 2021 study based on interviews that pediatricians “are uncertain about the concept, definition, management, and long-term risks of rapid infant weight gain.”
Authors and Dr. Gilley declare no relevant financial relationships.
Rapid weight gain (RWG) in infants and the mother’s prepregnancy overweight have a synergistic effect in increasing the odds that a child will develop overweight or obesity, new research suggests.
Findings were published online in Pediatrics.
Each factor has independently been associated with higher risk of childhood obesity but whether the two factors together exacerbate the risk has not been well studied, according to the authors led by Stephanie Gilley, MD, PhD, department of pediatrics, section of nutrition, University of Colorado at Denver, Aurora.
“Pediatric providers should monitor infants for RWG, especially in the context of maternal obesity, to reduce future risk of obesity,” the authors conclude.
Dr. Gilley’s team studied mother-infant dyads (n = 414) from the Healthy Start Study, an observational prebirth cohort. RWG was defined as a weight-for-age z score increase of at least 0.67 from birth to 3-7 months.
They found that RWG boosted the link between prepregnancy body mass index (ppBMI) and BMI z score, especially in female infants. Females exposed to both maternal obesity with RWG had an average BMI at the 94th percentile (1.50 increase in childhood BMI z score) “nearly at the cutoff for classification of obesity,” compared with those exposed to normal ppBMI with no RWG, who had an average childhood BMI at the 51st percentile.
“Currently, our nutrition recommendations as pediatricians are that all children are fed the same, essentially, after they’re born. We don’t have different growth parameters or different trajectories or targets for children who may have had different in utero exposures,” Dr. Gilley said.
Do some children need more monitoring for RWG?
Though we can’t necessarily draw conclusions from this one study, she says, the findings raise the question of whether children who were exposed in utero to obesity should be monitored for RWG more closely.
Lydia Shook, MD, Mass General Brigham maternal-fetal specialist and codirector of the Diabetes in Pregnancy Program at Massachusetts General Hospital in Boston, said she was struck by the finding in this study that with female infants, but not males, RWG significantly modified the association between ppBMI and early childhood BMI z scores.
“It’s an interesting finding and should be followed up with larger cohorts,” she said, noting that some previous studies have shown males are more vulnerable to maternal obesity and RWG.
“[Often] when we stratify by sex, you really need larger groups to be able to see the differences well,” Dr. Shook said.
She said she also found it interesting that when the researchers adjusted for breastfeeding status or caloric intake in childhood, the findings did not substantially change.
“That’s something that would warrant further investigation in an observational study or controlled trial,” Dr. Shook said.
Preventing rapid weight gain
The authors note that they did not consider possible interventions for preventing RGW in the study, although there are many, Dr. Gilley said.
Dr. Gilley also noted that a limitation of this study is that the population studied was primarily White.
Recent studies have shown the benefits of responsive parenting (RP) interventions, including a large study in 2022 geared toward Black families to teach better infant sleep practices as a way to prevent rapid weight gain.
That study, which tested the SAAF intervention, (Strong African American Families) found that “RP infants were nearly half as likely to experience upward crossing of two major weight-for-age percentile lines (14.1%), compared with control infants (24.2%); P = .09; odds ratio, 0.52; 95% confidence interval, 0.24-1.12.”
Along with sleep interventions, Dr. Gilley said, some researchers are studying the effects on RWG of better paternal engagement, or more involvement with the Women, Infants, and Children program, particularly with lower-income families.
Other studies have looked at breastfeeding vs. formula feeding – “but there have been mixed results there” – and responsive feeding practices, such as teaching families to recognize when a baby is full.
Dr. Gilley said she hopes this work will help broaden the thinking when it comes to infant weight gain.
“We spend a lot of time thinking about babies who are not growing fast enough and very little time thinking about babies who are growing too fast,” she said, “especially in those first 4-6 months of life.”
Dr. Gilley points to a study that illustrates that point. Pesch et al. concluded in a 2021 study based on interviews that pediatricians “are uncertain about the concept, definition, management, and long-term risks of rapid infant weight gain.”
Authors and Dr. Gilley declare no relevant financial relationships.
FROM PEDIATRICS
New update on left atrial appendage closure recommendations
An updated consensus statement on transcatheter left atrial appendage closure (LAAC) has put a newfound focus on patient selection for the procedure, specifically recommending that the procedure is appropriate for patients with nonvalvular atrial fibrillation who have risk for thromboembolism, aren’t well suited for direct oral anticoagulants (DOACs) and have a good chance of living for at least another year.
The statement, published online in the Journal of the Society for Cardiovascular Angiography & Interventions, also makes recommendations for how much experience operators should have, how many procedures they should perform to keep their skills up, and when and how to use imaging and prescribe DOACs, among other suggestions.
The statement represents the first updated guidance for LAAC since 2015. “Since then this field has really expanded and evolved,” writing group chair Jacqueline Saw, MD, said in an interview. “For instance, the indications are more matured and specific, and the procedural technical steps have matured. Imaging has also advanced, there’s more understanding about postprocedural care and there are also new devices that have been approved.”

Dr. Saw, an interventional cardiologist at Vancouver General Hospital and St. Paul’s Hospital, and a professor at the University of British Columbia in Vancouver, called the statement “a piece that puts everything together.”
“This document really summarizes the whole practice for doing transcatheter procedures,” she added, “so it’s all-in-one document in terms of recommendation of who we do the procedure for, how we should do it, how we should image and guide the procedure, and what complications to look out for and how to manage patients post procedure, be it with antithrombotic therapy and/or device surveillance.”
13 recommendations
In all, the statement carries 13 recommendations for LAAC. The Society for Cardiovascular Angiography & Interventions and the Heart Rhythm Society commissioned the writing group. The American College of Cardiology and Society of Cardiovascular Computed Tomography have endorsed the statement. The following are among the recommendations:
- Transcatheter LAAC is appropriate for patients with nonvalvular atrial fibrillation with high thromboembolic risk but for whom long-term oral anticoagulation may be contraindicated and who have at least 1 year’s life expectancy.
- Operators should have performed at least 50 prior left-sided ablations or structural procedures and at least 25 transseptal punctures (TSPs). Interventional-imaging physicians should have experience in guiding 25 or more TSPs before supporting LAAC procedures independently.
- To maintain skills, operators should do 25 or more TSPs and at least 12 LAACs over each 2-year period.
- On-site cardiovascular surgery backup should be available for new programs and for operators early in their learning curve.
- Baseline imaging with transesophageal echocardiography (TEE) or cardiac computed tomography should be performed before LAAC.
- Intraprocedural imaging guidance with TEE or intracardiac echocardiography.
- Follow labeling of each specific LAAC device for technical aspects of the procedure.
- Familiarity with avoiding, recognizing, and managing LAAC complications.
- Predischarge 2-dimensional TEE to rule out pericardial effusion and device embolization.
- Anticoagulation for device-related thrombus.
- Make all efforts to minimize peridevice leaks during implantation because their clinical impact and management isn’t well understood.
- Antithrombotic therapy with warfarin, DOAC, or dual-antiplatelet therapy after LAAC based on the studied regimen and instructions for each specific device, tailored to the bleeding risks for each patient.
- TEE or cardiac computed tomography at 45-90 days after LAAC for device surveillance to assess for peridevice leak and device-related thrombus.
The statement also includes precautionary recommendations. It advises against using routine closure of LAAC-associated iatrogenic atrial septal defects and states that combined procedures with LAAC, such as structural interventions and pulmonary vein isolation, should be avoided because randomized controlled trial data are pending.
“These recommendations are based upon data from updated publications and randomized trial data as well as large registries, including the National Cardiovascular Data Registry, so I think this is a very practical statement that puts all these pieces together for any budding interventionalist doing this procedure and even experienced operations,” Dr. Saw said.
Authors of an accompanying editorial agreed that the “rigorous standards” set out in the statement will help maintain “a high level of procedural safety in the setting of rapid expansion.”
The editorialists, Faisal M. Merchant, MD, of Emory University, Atlanta, and Mohamad Alkhouli, MD, professor of medicine at Mayo Clinic School of Medicine, Rochester, Minn., point out that the incidence of pericardial effusion has decreased from more than 5% in the pivotal Watchman trials to less than 1.5% in the most recent report from the National Cardiovascular Data Registry, which shows that more than 100,000 procedures have been performed in the United States.
But most important as the field moves forward, they stress, is patient selection. The recommendation of limiting patients to those with a life expectancy of 1 year “is a tacit recognition of the fact that the benefits of LAAC take time to accrue, and many older and frail patients are unlikely to derive meaningful benefit.”
Dr. Merchant and Dr. Alkhouli also note that there remains a conundrum in patient selection that remains from the original LAAC trials, which enrolled patients who were eligible for anticoagulation. “Somewhat paradoxically, after its approval, LAAC is mostly prescribed to patients who are not felt to be good anticoagulation candidates.” This leaves physicians “in the precarious position of extrapolating data to patients who were excluded from the original clinical trials.”
Therefore, the consensus statement “is right to put patient selection front and center in its recommendations, but as the field of LAAC comes of age, better evidence to support patient selection will be the real sign of maturity.”
Dr. Saw said she envisions another update over the next 2 years or so as ongoing clinical trials comparing DOAC and LAAC, namely the CHAMPION-AF and OPTION trials, report results.
Dr. Saw and Dr. Merchant, reported no conflicts of interest. Dr. Alkhouli has financial ties to Boston Scientific, Abbott, and Philips.
An updated consensus statement on transcatheter left atrial appendage closure (LAAC) has put a newfound focus on patient selection for the procedure, specifically recommending that the procedure is appropriate for patients with nonvalvular atrial fibrillation who have risk for thromboembolism, aren’t well suited for direct oral anticoagulants (DOACs) and have a good chance of living for at least another year.
The statement, published online in the Journal of the Society for Cardiovascular Angiography & Interventions, also makes recommendations for how much experience operators should have, how many procedures they should perform to keep their skills up, and when and how to use imaging and prescribe DOACs, among other suggestions.
The statement represents the first updated guidance for LAAC since 2015. “Since then this field has really expanded and evolved,” writing group chair Jacqueline Saw, MD, said in an interview. “For instance, the indications are more matured and specific, and the procedural technical steps have matured. Imaging has also advanced, there’s more understanding about postprocedural care and there are also new devices that have been approved.”
Dr. Saw, an interventional cardiologist at Vancouver General Hospital and St. Paul’s Hospital, and a professor at the University of British Columbia in Vancouver, called the statement “a piece that puts everything together.”
“This document really summarizes the whole practice for doing transcatheter procedures,” she added, “so it’s all-in-one document in terms of recommendation of who we do the procedure for, how we should do it, how we should image and guide the procedure, and what complications to look out for and how to manage patients post procedure, be it with antithrombotic therapy and/or device surveillance.”
13 recommendations
In all, the statement carries 13 recommendations for LAAC. The Society for Cardiovascular Angiography & Interventions and the Heart Rhythm Society commissioned the writing group. The American College of Cardiology and Society of Cardiovascular Computed Tomography have endorsed the statement. The following are among the recommendations:
- Transcatheter LAAC is appropriate for patients with nonvalvular atrial fibrillation with high thromboembolic risk but for whom long-term oral anticoagulation may be contraindicated and who have at least 1 year’s life expectancy.
- Operators should have performed at least 50 prior left-sided ablations or structural procedures and at least 25 transseptal punctures (TSPs). Interventional-imaging physicians should have experience in guiding 25 or more TSPs before supporting LAAC procedures independently.
- To maintain skills, operators should do 25 or more TSPs and at least 12 LAACs over each 2-year period.
- On-site cardiovascular surgery backup should be available for new programs and for operators early in their learning curve.
- Baseline imaging with transesophageal echocardiography (TEE) or cardiac computed tomography should be performed before LAAC.
- Intraprocedural imaging guidance with TEE or intracardiac echocardiography.
- Follow labeling of each specific LAAC device for technical aspects of the procedure.
- Familiarity with avoiding, recognizing, and managing LAAC complications.
- Predischarge 2-dimensional TEE to rule out pericardial effusion and device embolization.
- Anticoagulation for device-related thrombus.
- Make all efforts to minimize peridevice leaks during implantation because their clinical impact and management isn’t well understood.
- Antithrombotic therapy with warfarin, DOAC, or dual-antiplatelet therapy after LAAC based on the studied regimen and instructions for each specific device, tailored to the bleeding risks for each patient.
- TEE or cardiac computed tomography at 45-90 days after LAAC for device surveillance to assess for peridevice leak and device-related thrombus.
The statement also includes precautionary recommendations. It advises against using routine closure of LAAC-associated iatrogenic atrial septal defects and states that combined procedures with LAAC, such as structural interventions and pulmonary vein isolation, should be avoided because randomized controlled trial data are pending.
“These recommendations are based upon data from updated publications and randomized trial data as well as large registries, including the National Cardiovascular Data Registry, so I think this is a very practical statement that puts all these pieces together for any budding interventionalist doing this procedure and even experienced operations,” Dr. Saw said.
Authors of an accompanying editorial agreed that the “rigorous standards” set out in the statement will help maintain “a high level of procedural safety in the setting of rapid expansion.”
The editorialists, Faisal M. Merchant, MD, of Emory University, Atlanta, and Mohamad Alkhouli, MD, professor of medicine at Mayo Clinic School of Medicine, Rochester, Minn., point out that the incidence of pericardial effusion has decreased from more than 5% in the pivotal Watchman trials to less than 1.5% in the most recent report from the National Cardiovascular Data Registry, which shows that more than 100,000 procedures have been performed in the United States.
But most important as the field moves forward, they stress, is patient selection. The recommendation of limiting patients to those with a life expectancy of 1 year “is a tacit recognition of the fact that the benefits of LAAC take time to accrue, and many older and frail patients are unlikely to derive meaningful benefit.”
Dr. Merchant and Dr. Alkhouli also note that there remains a conundrum in patient selection that remains from the original LAAC trials, which enrolled patients who were eligible for anticoagulation. “Somewhat paradoxically, after its approval, LAAC is mostly prescribed to patients who are not felt to be good anticoagulation candidates.” This leaves physicians “in the precarious position of extrapolating data to patients who were excluded from the original clinical trials.”
Therefore, the consensus statement “is right to put patient selection front and center in its recommendations, but as the field of LAAC comes of age, better evidence to support patient selection will be the real sign of maturity.”
Dr. Saw said she envisions another update over the next 2 years or so as ongoing clinical trials comparing DOAC and LAAC, namely the CHAMPION-AF and OPTION trials, report results.
Dr. Saw and Dr. Merchant, reported no conflicts of interest. Dr. Alkhouli has financial ties to Boston Scientific, Abbott, and Philips.
An updated consensus statement on transcatheter left atrial appendage closure (LAAC) has put a newfound focus on patient selection for the procedure, specifically recommending that the procedure is appropriate for patients with nonvalvular atrial fibrillation who have risk for thromboembolism, aren’t well suited for direct oral anticoagulants (DOACs) and have a good chance of living for at least another year.
The statement, published online in the Journal of the Society for Cardiovascular Angiography & Interventions, also makes recommendations for how much experience operators should have, how many procedures they should perform to keep their skills up, and when and how to use imaging and prescribe DOACs, among other suggestions.
The statement represents the first updated guidance for LAAC since 2015. “Since then this field has really expanded and evolved,” writing group chair Jacqueline Saw, MD, said in an interview. “For instance, the indications are more matured and specific, and the procedural technical steps have matured. Imaging has also advanced, there’s more understanding about postprocedural care and there are also new devices that have been approved.”
Dr. Saw, an interventional cardiologist at Vancouver General Hospital and St. Paul’s Hospital, and a professor at the University of British Columbia in Vancouver, called the statement “a piece that puts everything together.”
“This document really summarizes the whole practice for doing transcatheter procedures,” she added, “so it’s all-in-one document in terms of recommendation of who we do the procedure for, how we should do it, how we should image and guide the procedure, and what complications to look out for and how to manage patients post procedure, be it with antithrombotic therapy and/or device surveillance.”
13 recommendations
In all, the statement carries 13 recommendations for LAAC. The Society for Cardiovascular Angiography & Interventions and the Heart Rhythm Society commissioned the writing group. The American College of Cardiology and Society of Cardiovascular Computed Tomography have endorsed the statement. The following are among the recommendations:
- Transcatheter LAAC is appropriate for patients with nonvalvular atrial fibrillation with high thromboembolic risk but for whom long-term oral anticoagulation may be contraindicated and who have at least 1 year’s life expectancy.
- Operators should have performed at least 50 prior left-sided ablations or structural procedures and at least 25 transseptal punctures (TSPs). Interventional-imaging physicians should have experience in guiding 25 or more TSPs before supporting LAAC procedures independently.
- To maintain skills, operators should do 25 or more TSPs and at least 12 LAACs over each 2-year period.
- On-site cardiovascular surgery backup should be available for new programs and for operators early in their learning curve.
- Baseline imaging with transesophageal echocardiography (TEE) or cardiac computed tomography should be performed before LAAC.
- Intraprocedural imaging guidance with TEE or intracardiac echocardiography.
- Follow labeling of each specific LAAC device for technical aspects of the procedure.
- Familiarity with avoiding, recognizing, and managing LAAC complications.
- Predischarge 2-dimensional TEE to rule out pericardial effusion and device embolization.
- Anticoagulation for device-related thrombus.
- Make all efforts to minimize peridevice leaks during implantation because their clinical impact and management isn’t well understood.
- Antithrombotic therapy with warfarin, DOAC, or dual-antiplatelet therapy after LAAC based on the studied regimen and instructions for each specific device, tailored to the bleeding risks for each patient.
- TEE or cardiac computed tomography at 45-90 days after LAAC for device surveillance to assess for peridevice leak and device-related thrombus.
The statement also includes precautionary recommendations. It advises against using routine closure of LAAC-associated iatrogenic atrial septal defects and states that combined procedures with LAAC, such as structural interventions and pulmonary vein isolation, should be avoided because randomized controlled trial data are pending.
“These recommendations are based upon data from updated publications and randomized trial data as well as large registries, including the National Cardiovascular Data Registry, so I think this is a very practical statement that puts all these pieces together for any budding interventionalist doing this procedure and even experienced operations,” Dr. Saw said.
Authors of an accompanying editorial agreed that the “rigorous standards” set out in the statement will help maintain “a high level of procedural safety in the setting of rapid expansion.”
The editorialists, Faisal M. Merchant, MD, of Emory University, Atlanta, and Mohamad Alkhouli, MD, professor of medicine at Mayo Clinic School of Medicine, Rochester, Minn., point out that the incidence of pericardial effusion has decreased from more than 5% in the pivotal Watchman trials to less than 1.5% in the most recent report from the National Cardiovascular Data Registry, which shows that more than 100,000 procedures have been performed in the United States.
But most important as the field moves forward, they stress, is patient selection. The recommendation of limiting patients to those with a life expectancy of 1 year “is a tacit recognition of the fact that the benefits of LAAC take time to accrue, and many older and frail patients are unlikely to derive meaningful benefit.”
Dr. Merchant and Dr. Alkhouli also note that there remains a conundrum in patient selection that remains from the original LAAC trials, which enrolled patients who were eligible for anticoagulation. “Somewhat paradoxically, after its approval, LAAC is mostly prescribed to patients who are not felt to be good anticoagulation candidates.” This leaves physicians “in the precarious position of extrapolating data to patients who were excluded from the original clinical trials.”
Therefore, the consensus statement “is right to put patient selection front and center in its recommendations, but as the field of LAAC comes of age, better evidence to support patient selection will be the real sign of maturity.”
Dr. Saw said she envisions another update over the next 2 years or so as ongoing clinical trials comparing DOAC and LAAC, namely the CHAMPION-AF and OPTION trials, report results.
Dr. Saw and Dr. Merchant, reported no conflicts of interest. Dr. Alkhouli has financial ties to Boston Scientific, Abbott, and Philips.
FROM THE JOURNAL OF THE SOCIETY FOR CARDIOVASCULAR ANGIOGRAPHY & INTERVENTIONS
Practicing ethical medicine ‘is a requirement,’ not a luxury, expert says
NEW ORLEANS – , but results from a national survey of dermatology residency program directors suggest that ethics training is not a priority.
Of the 139 dermatology residency program or associate program directors surveyed in 2022, only 43% responded. Of these, 55% said that their program had no ethics curriculum. Among programs with an ethics curriculum, 75% were implemented in the past 10 years, and the most common settings for teaching ethics were formal didactics (32%) and ad hoc during clinical encounters (28%). Reported barriers to implementing and/or maintaining an ethics curriculum included a lack of time (30%), lack of faculty with expertise (24%), and lack of useful resources (20%).
“Clearly, medical ethics is needed more to be part of our dermatology residency curriculum,” one of the study authors, Jane M. Grant-Kels, MD, professor of dermatology, pathology, and pediatrics, and founding chair of dermatology at the University of Connecticut, Farmington, said during a plenary lecture at the annual meeting of the American Academy of Dermatology. “Why? Because even though we’re physicians, and some of us have big egos, we are just human beings. We have all the faults and frailties of other humans. What we do as doctors often has unintended consequences that impact patients and society at large.”

Dr. Grant-Kels, one of the editors of the textbook “Dermatoethics”, said that, while she does not believe that physicians are intentionally unethical, “we stumble into bad behavior because we fool ourselves. We think that we are ethical. We think our colleagues are ethical, and we don’t view them with a clear, transparent eye. This is referred to as ethical fading or bounded ethicality.”
Similar to religion and good behavior, one can’t really teach someone to be ethical, she continued. “But you can teach people to think about ethics and to recognize an ethical dilemma when they’re in one,” she said. “Most articles that are available [pertain to] whether ethics can be taught or not, but there are very few resources available on how to actually teach ethics.”
That, she added, has been her goal for the last 2 decades: “How do I teach ethics without sounding like I’m more ethical than anybody else, and how do I make it relevant and fun? It’s a difficult challenge.”
Pillars of medical ethics
Dr. Grant-Kels defined ethics as a way of determining how individuals ought to act based on concepts of right and wrong. An ethical dilemma is when an individual faces two competing possibilities: either both justifiable or both unjustifiable, and you have to make a decision. The four pillars of medical ethics, she noted, are beneficence (the notion that the patient’s best interests come first); nonmaleficence (do no intentional harm); autonomy (the patient’s right to refuse or choose a treatment); and justice (fairness in how health care is distributed).
“Medical ethics are the moral principles by which physicians should conduct themselves,” she said. “There is normative ethics, which involves decisions about which moral norms or ethical arguments should we accept and why; and applied ethics, or applications of these norms to specific problems or cases. No ethics is better than bad ethics, and we can see that even in today’s world. The lack of ethics, or poor ethics, or the wrong ethics has terrible consequences.”
Ethics instruction
Dr. Grant-Kels provided a “top 10 list” of tips for incorporating ethics instruction into dermatology residency programs and clinical practices:
- Make room for ethics in your curriculum. “It’s not science, and it needs to be discussed and developed with faculty and residents,” she said.
- Focus on real situations that residents will experience. Discuss what you should do, what you might have done, and why.
- Share stories and be truthful. Include other faculty members, “because you need different perspectives,” she said.
- Go beyond what is right and wrong, and the rationale. “You have to talk about the impact, because decisions you make have unintended consequences for individual patients and for patient care in general,” Dr. Grant-Kels said.
- Practice, practice, practice. Make time for discussions involving ethics, “because it takes a lot of education to be able to identify ethical issues and process them,” she said. “The truth is, we can rationalize almost anything and convince ourselves that we made the right choice. That’s why we need to continue to practice good ethics.”
- Challenge the residents. “Decisions are not always straightforward,” she said. “Pressures push us and we start to justify small decisions and then bigger decisions. This is a very gray zone. What’s ethical for one person may not be ethical to another.”
- Encourage residents and colleagues to ask the right questions and give them confidence to make the right decisions. “We have to work in an environment of ethics,” Dr. Grant-Kels said. “Many of us are role models, and we are not always behaving the way we should be. As role models, we need to be aware of that.”
- Expose residents to a variety of issues. Ethics vary depending on the situation, the people involved, and the information presented.
- Ethics cannot just come up in an ethics class. “We need to foster a culture of ethics,” she said. “If things go wrong and unethical behavior is noted, it needs to be brought to the floor and discussed.”
- Discuss the misguided pursuit of happiness and ethical decision-making. In the opinion of Dr. Grant-Kels, people can behave badly when they’re pursuing something like a career advancement, a new house, or an expensive object like a car or a boat. “They think that if they get that job or get that promotion or if they buy that big house or they buy that sports car, they’re going to be really happy,” she said.
“That’s called impact bias, which causes focalism, where you focus on that one thing, like ‘I’m going to make a lot of money’ or ‘I’m going to buy that big house on the mountain.’ The truth is, buying that car doesn’t make you happy. Buying that big house doesn’t make you happy. We need to combat focalism with professionalism, which means conducting oneself with responsibility, integrity, accountability, and excellence. Practicing ethical medicine is not a luxury; it’s a requirement. We should all try for aspirational ethics.”
Dr. Grant-Kels reported having no relevant financial disclosures.
NEW ORLEANS – , but results from a national survey of dermatology residency program directors suggest that ethics training is not a priority.
Of the 139 dermatology residency program or associate program directors surveyed in 2022, only 43% responded. Of these, 55% said that their program had no ethics curriculum. Among programs with an ethics curriculum, 75% were implemented in the past 10 years, and the most common settings for teaching ethics were formal didactics (32%) and ad hoc during clinical encounters (28%). Reported barriers to implementing and/or maintaining an ethics curriculum included a lack of time (30%), lack of faculty with expertise (24%), and lack of useful resources (20%).
“Clearly, medical ethics is needed more to be part of our dermatology residency curriculum,” one of the study authors, Jane M. Grant-Kels, MD, professor of dermatology, pathology, and pediatrics, and founding chair of dermatology at the University of Connecticut, Farmington, said during a plenary lecture at the annual meeting of the American Academy of Dermatology. “Why? Because even though we’re physicians, and some of us have big egos, we are just human beings. We have all the faults and frailties of other humans. What we do as doctors often has unintended consequences that impact patients and society at large.”
Dr. Grant-Kels, one of the editors of the textbook “Dermatoethics”, said that, while she does not believe that physicians are intentionally unethical, “we stumble into bad behavior because we fool ourselves. We think that we are ethical. We think our colleagues are ethical, and we don’t view them with a clear, transparent eye. This is referred to as ethical fading or bounded ethicality.”
Similar to religion and good behavior, one can’t really teach someone to be ethical, she continued. “But you can teach people to think about ethics and to recognize an ethical dilemma when they’re in one,” she said. “Most articles that are available [pertain to] whether ethics can be taught or not, but there are very few resources available on how to actually teach ethics.”
That, she added, has been her goal for the last 2 decades: “How do I teach ethics without sounding like I’m more ethical than anybody else, and how do I make it relevant and fun? It’s a difficult challenge.”
Pillars of medical ethics
Dr. Grant-Kels defined ethics as a way of determining how individuals ought to act based on concepts of right and wrong. An ethical dilemma is when an individual faces two competing possibilities: either both justifiable or both unjustifiable, and you have to make a decision. The four pillars of medical ethics, she noted, are beneficence (the notion that the patient’s best interests come first); nonmaleficence (do no intentional harm); autonomy (the patient’s right to refuse or choose a treatment); and justice (fairness in how health care is distributed).
“Medical ethics are the moral principles by which physicians should conduct themselves,” she said. “There is normative ethics, which involves decisions about which moral norms or ethical arguments should we accept and why; and applied ethics, or applications of these norms to specific problems or cases. No ethics is better than bad ethics, and we can see that even in today’s world. The lack of ethics, or poor ethics, or the wrong ethics has terrible consequences.”
Ethics instruction
Dr. Grant-Kels provided a “top 10 list” of tips for incorporating ethics instruction into dermatology residency programs and clinical practices:
- Make room for ethics in your curriculum. “It’s not science, and it needs to be discussed and developed with faculty and residents,” she said.
- Focus on real situations that residents will experience. Discuss what you should do, what you might have done, and why.
- Share stories and be truthful. Include other faculty members, “because you need different perspectives,” she said.
- Go beyond what is right and wrong, and the rationale. “You have to talk about the impact, because decisions you make have unintended consequences for individual patients and for patient care in general,” Dr. Grant-Kels said.
- Practice, practice, practice. Make time for discussions involving ethics, “because it takes a lot of education to be able to identify ethical issues and process them,” she said. “The truth is, we can rationalize almost anything and convince ourselves that we made the right choice. That’s why we need to continue to practice good ethics.”
- Challenge the residents. “Decisions are not always straightforward,” she said. “Pressures push us and we start to justify small decisions and then bigger decisions. This is a very gray zone. What’s ethical for one person may not be ethical to another.”
- Encourage residents and colleagues to ask the right questions and give them confidence to make the right decisions. “We have to work in an environment of ethics,” Dr. Grant-Kels said. “Many of us are role models, and we are not always behaving the way we should be. As role models, we need to be aware of that.”
- Expose residents to a variety of issues. Ethics vary depending on the situation, the people involved, and the information presented.
- Ethics cannot just come up in an ethics class. “We need to foster a culture of ethics,” she said. “If things go wrong and unethical behavior is noted, it needs to be brought to the floor and discussed.”
- Discuss the misguided pursuit of happiness and ethical decision-making. In the opinion of Dr. Grant-Kels, people can behave badly when they’re pursuing something like a career advancement, a new house, or an expensive object like a car or a boat. “They think that if they get that job or get that promotion or if they buy that big house or they buy that sports car, they’re going to be really happy,” she said.
“That’s called impact bias, which causes focalism, where you focus on that one thing, like ‘I’m going to make a lot of money’ or ‘I’m going to buy that big house on the mountain.’ The truth is, buying that car doesn’t make you happy. Buying that big house doesn’t make you happy. We need to combat focalism with professionalism, which means conducting oneself with responsibility, integrity, accountability, and excellence. Practicing ethical medicine is not a luxury; it’s a requirement. We should all try for aspirational ethics.”
Dr. Grant-Kels reported having no relevant financial disclosures.
NEW ORLEANS – , but results from a national survey of dermatology residency program directors suggest that ethics training is not a priority.
Of the 139 dermatology residency program or associate program directors surveyed in 2022, only 43% responded. Of these, 55% said that their program had no ethics curriculum. Among programs with an ethics curriculum, 75% were implemented in the past 10 years, and the most common settings for teaching ethics were formal didactics (32%) and ad hoc during clinical encounters (28%). Reported barriers to implementing and/or maintaining an ethics curriculum included a lack of time (30%), lack of faculty with expertise (24%), and lack of useful resources (20%).
“Clearly, medical ethics is needed more to be part of our dermatology residency curriculum,” one of the study authors, Jane M. Grant-Kels, MD, professor of dermatology, pathology, and pediatrics, and founding chair of dermatology at the University of Connecticut, Farmington, said during a plenary lecture at the annual meeting of the American Academy of Dermatology. “Why? Because even though we’re physicians, and some of us have big egos, we are just human beings. We have all the faults and frailties of other humans. What we do as doctors often has unintended consequences that impact patients and society at large.”
Dr. Grant-Kels, one of the editors of the textbook “Dermatoethics”, said that, while she does not believe that physicians are intentionally unethical, “we stumble into bad behavior because we fool ourselves. We think that we are ethical. We think our colleagues are ethical, and we don’t view them with a clear, transparent eye. This is referred to as ethical fading or bounded ethicality.”
Similar to religion and good behavior, one can’t really teach someone to be ethical, she continued. “But you can teach people to think about ethics and to recognize an ethical dilemma when they’re in one,” she said. “Most articles that are available [pertain to] whether ethics can be taught or not, but there are very few resources available on how to actually teach ethics.”
That, she added, has been her goal for the last 2 decades: “How do I teach ethics without sounding like I’m more ethical than anybody else, and how do I make it relevant and fun? It’s a difficult challenge.”
Pillars of medical ethics
Dr. Grant-Kels defined ethics as a way of determining how individuals ought to act based on concepts of right and wrong. An ethical dilemma is when an individual faces two competing possibilities: either both justifiable or both unjustifiable, and you have to make a decision. The four pillars of medical ethics, she noted, are beneficence (the notion that the patient’s best interests come first); nonmaleficence (do no intentional harm); autonomy (the patient’s right to refuse or choose a treatment); and justice (fairness in how health care is distributed).
“Medical ethics are the moral principles by which physicians should conduct themselves,” she said. “There is normative ethics, which involves decisions about which moral norms or ethical arguments should we accept and why; and applied ethics, or applications of these norms to specific problems or cases. No ethics is better than bad ethics, and we can see that even in today’s world. The lack of ethics, or poor ethics, or the wrong ethics has terrible consequences.”
Ethics instruction
Dr. Grant-Kels provided a “top 10 list” of tips for incorporating ethics instruction into dermatology residency programs and clinical practices:
- Make room for ethics in your curriculum. “It’s not science, and it needs to be discussed and developed with faculty and residents,” she said.
- Focus on real situations that residents will experience. Discuss what you should do, what you might have done, and why.
- Share stories and be truthful. Include other faculty members, “because you need different perspectives,” she said.
- Go beyond what is right and wrong, and the rationale. “You have to talk about the impact, because decisions you make have unintended consequences for individual patients and for patient care in general,” Dr. Grant-Kels said.
- Practice, practice, practice. Make time for discussions involving ethics, “because it takes a lot of education to be able to identify ethical issues and process them,” she said. “The truth is, we can rationalize almost anything and convince ourselves that we made the right choice. That’s why we need to continue to practice good ethics.”
- Challenge the residents. “Decisions are not always straightforward,” she said. “Pressures push us and we start to justify small decisions and then bigger decisions. This is a very gray zone. What’s ethical for one person may not be ethical to another.”
- Encourage residents and colleagues to ask the right questions and give them confidence to make the right decisions. “We have to work in an environment of ethics,” Dr. Grant-Kels said. “Many of us are role models, and we are not always behaving the way we should be. As role models, we need to be aware of that.”
- Expose residents to a variety of issues. Ethics vary depending on the situation, the people involved, and the information presented.
- Ethics cannot just come up in an ethics class. “We need to foster a culture of ethics,” she said. “If things go wrong and unethical behavior is noted, it needs to be brought to the floor and discussed.”
- Discuss the misguided pursuit of happiness and ethical decision-making. In the opinion of Dr. Grant-Kels, people can behave badly when they’re pursuing something like a career advancement, a new house, or an expensive object like a car or a boat. “They think that if they get that job or get that promotion or if they buy that big house or they buy that sports car, they’re going to be really happy,” she said.
“That’s called impact bias, which causes focalism, where you focus on that one thing, like ‘I’m going to make a lot of money’ or ‘I’m going to buy that big house on the mountain.’ The truth is, buying that car doesn’t make you happy. Buying that big house doesn’t make you happy. We need to combat focalism with professionalism, which means conducting oneself with responsibility, integrity, accountability, and excellence. Practicing ethical medicine is not a luxury; it’s a requirement. We should all try for aspirational ethics.”
Dr. Grant-Kels reported having no relevant financial disclosures.
AT AAD 2023
Kidney disease skews Alzheimer’s biomarker testing
New research provides more evidence that
In a cross-sectional study of adults with and those without cognitive impairment, chronic kidney disease was associated with increased plasma concentrations of phosphorylated tau (p-tau) 217 and 181.
However, there were no associations between chronic kidney disease and the ratio of p-tau217 to unphosphorylated tau 217 (pT217/T217), and the associations with p-tau181 to unphosphorylated tau 181 (pT181/T181) were attenuated in patients with cognitive impairment.
“These novel findings suggest that plasma measures of the phosphorylated to unphosphorylated tau ratios are more accurate than p-tau forms alone as they correlate less with individual difference in glomerular filtration rate or impaired kidney function,” reported an investigative team led by Oskar Hansson, MD, PhD, with Lund University in Sweden.
“Thus, to mitigate the effects of non-Alzheimer’s–related comorbidities like chronic kidney disease on the performance of plasma Alzheimer’s disease biomarkers, certain tau ratios, and specifically pT217/T217, should be considered for implementation in clinical practice and drug trials,” they added.
The study was published online in JAMA Neurology to coincide with a presentation at the International Conference on Alzheimer’s and Parkinson’s Diseases in Gothenburg, Sweden.
Skewed tau levels
Plasma biomarkers of amyloid-beta (Abeta) and tau pathologies, and in particular variants in p-tau217 and p-tau181, have shown promise for use in Alzheimer’s disease diagnosis and prognosis. However, previous reports have suggested that chronic kidney disease might influence plasma p-tau217 and p-tau181 concentrations, potentially decreasing their usefulness in the diagnostic workup of dementia.
Researchers investigated associations of chronic kidney disease with plasma ratios of p-tau217 and p-tau181 to the corresponding unphosphorylated peptides in Alzheimer’s disease.
The data came from 473 older adults, with and without cognitive impairment, from the Swedish BioFinder-2 study who had plasma tau assessments and chronic kidney disease status established within 6 months of plasma collection.
The researchers found that lower estimated glomerular filtration rate levels (indicative of kidney dysfunction) were associated with higher plasma concentrations of phosphorylated and unphosphorylated tau peptides measured simultaneously using the tau immunoprecipitation mass spectrometry assay.
However, the correlations with estimated glomerular filtration rate were nonsignificant for the pT217/T217 ratio in individuals with cognitive impairment and were significantly attenuated for pT217/T217 in cognitively unimpaired individuals and for pT181/T181 in both cognitively unimpaired and impaired individuals.
“Importantly, we demonstrate that there were no significant associations between chronic kidney disease and the pT217/T217 ratio and changes in plasma pT181/T181 associated with chronic kidney disease were small or nonsignificant,” the researchers noted.
“Our results indicate that by using p-tau/tau ratios we may be able to reduce the variability in plasma p-tau levels driven by impaired kidney function and consequently such ratios are more robust measures of brain p-tau pathology in individuals with both early- and later-stage Alzheimer’s disease,” they added.
The researchers believe this is likely true for the ratios of other related proteins – a view that is supported by findings of attenuated associations of chronic kidney disease with Abeta42/40, compared with Abeta42 and Abeta40 in the current study and in previous studies.
Important clinical implications
Reached for comment, Rebecca Edelmayer, PhD, Alzheimer’s Association senior director of scientific engagement, noted that research continues to indicate that blood biomarkers have “promise for improving, and possibly even redefining, the clinical workup for Alzheimer’s disease.
“Many of the Alzheimer’s blood tests in development today have focused on core blood biomarkers associated with amyloid accumulation and tau tangle formation in the brain,” Dr. Edelmayer said.
“Before these tests can be used more broadly in the clinic, we need to understand all of the variables that may impact the results of various blood biomarkers, including differences that may be driven by race, ethnicity, sex, and underlying health conditions, such as chronic kidney disease.
“This study corroborates other research suggesting that some Alzheimer’s-associated markers can be affected by chronic kidney disease, but by using ratios of amyloid or tau markers, we may be able to minimize these differences in results caused by underlying disease,” Dr. Edelmayer said.
Howard Fillit, MD, cofounder and chief science officer at the Alzheimer’s Drug Discovery Foundation, said, “Using these ratios makes a lot of sense because the ratios wouldn’t change with kidney function. I think this is an important advance in clinical utilization of these tests.”
Dr. Fillit noted that older people often have declining kidney function, which can be easily measured by glomerular filtration rate. Changes in blood levels of these markers with declining kidney function are “not unexpected, but [it’s] important that it’s been demonstrated.
“As we go forward, maybe the future utilization of these tests will be not only recording the ratios but also reporting the ratios in the context of somebody’s glomerular filtration rate. You could imagine a scenario where when the test is done, it’s automatically done alongside of glomerular filtration rate,” Dr. Fillit said in an interview.
The study was supported by Coins for Alzheimer’s Research Trust, the Tracy Family Stable Isotope Labeling Quantitation Center, and the National Institute of Neurological Disorders and Stroke. Dr. Hansson has received support to his institution from ADx, AVID Radiopharmaceuticals, Biogen, Eli Lilly, Eisai, Fujirebio, GE Healthcare, Pfizer, and Roche; consultancy/speaker fees from Amylyx, Alzpath, Biogen, Cerveau, Fujirebio, Genentech, Novartis, Roche, and Siemens; and personal fees from Eli Lilly, Eisai, Bioarctic, and Biogen outside the submitted work. Dr. Edelmayer and Dr. Fillit have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
New research provides more evidence that
In a cross-sectional study of adults with and those without cognitive impairment, chronic kidney disease was associated with increased plasma concentrations of phosphorylated tau (p-tau) 217 and 181.
However, there were no associations between chronic kidney disease and the ratio of p-tau217 to unphosphorylated tau 217 (pT217/T217), and the associations with p-tau181 to unphosphorylated tau 181 (pT181/T181) were attenuated in patients with cognitive impairment.
“These novel findings suggest that plasma measures of the phosphorylated to unphosphorylated tau ratios are more accurate than p-tau forms alone as they correlate less with individual difference in glomerular filtration rate or impaired kidney function,” reported an investigative team led by Oskar Hansson, MD, PhD, with Lund University in Sweden.
“Thus, to mitigate the effects of non-Alzheimer’s–related comorbidities like chronic kidney disease on the performance of plasma Alzheimer’s disease biomarkers, certain tau ratios, and specifically pT217/T217, should be considered for implementation in clinical practice and drug trials,” they added.
The study was published online in JAMA Neurology to coincide with a presentation at the International Conference on Alzheimer’s and Parkinson’s Diseases in Gothenburg, Sweden.
Skewed tau levels
Plasma biomarkers of amyloid-beta (Abeta) and tau pathologies, and in particular variants in p-tau217 and p-tau181, have shown promise for use in Alzheimer’s disease diagnosis and prognosis. However, previous reports have suggested that chronic kidney disease might influence plasma p-tau217 and p-tau181 concentrations, potentially decreasing their usefulness in the diagnostic workup of dementia.
Researchers investigated associations of chronic kidney disease with plasma ratios of p-tau217 and p-tau181 to the corresponding unphosphorylated peptides in Alzheimer’s disease.
The data came from 473 older adults, with and without cognitive impairment, from the Swedish BioFinder-2 study who had plasma tau assessments and chronic kidney disease status established within 6 months of plasma collection.
The researchers found that lower estimated glomerular filtration rate levels (indicative of kidney dysfunction) were associated with higher plasma concentrations of phosphorylated and unphosphorylated tau peptides measured simultaneously using the tau immunoprecipitation mass spectrometry assay.
However, the correlations with estimated glomerular filtration rate were nonsignificant for the pT217/T217 ratio in individuals with cognitive impairment and were significantly attenuated for pT217/T217 in cognitively unimpaired individuals and for pT181/T181 in both cognitively unimpaired and impaired individuals.
“Importantly, we demonstrate that there were no significant associations between chronic kidney disease and the pT217/T217 ratio and changes in plasma pT181/T181 associated with chronic kidney disease were small or nonsignificant,” the researchers noted.
“Our results indicate that by using p-tau/tau ratios we may be able to reduce the variability in plasma p-tau levels driven by impaired kidney function and consequently such ratios are more robust measures of brain p-tau pathology in individuals with both early- and later-stage Alzheimer’s disease,” they added.
The researchers believe this is likely true for the ratios of other related proteins – a view that is supported by findings of attenuated associations of chronic kidney disease with Abeta42/40, compared with Abeta42 and Abeta40 in the current study and in previous studies.
Important clinical implications
Reached for comment, Rebecca Edelmayer, PhD, Alzheimer’s Association senior director of scientific engagement, noted that research continues to indicate that blood biomarkers have “promise for improving, and possibly even redefining, the clinical workup for Alzheimer’s disease.
“Many of the Alzheimer’s blood tests in development today have focused on core blood biomarkers associated with amyloid accumulation and tau tangle formation in the brain,” Dr. Edelmayer said.
“Before these tests can be used more broadly in the clinic, we need to understand all of the variables that may impact the results of various blood biomarkers, including differences that may be driven by race, ethnicity, sex, and underlying health conditions, such as chronic kidney disease.
“This study corroborates other research suggesting that some Alzheimer’s-associated markers can be affected by chronic kidney disease, but by using ratios of amyloid or tau markers, we may be able to minimize these differences in results caused by underlying disease,” Dr. Edelmayer said.
Howard Fillit, MD, cofounder and chief science officer at the Alzheimer’s Drug Discovery Foundation, said, “Using these ratios makes a lot of sense because the ratios wouldn’t change with kidney function. I think this is an important advance in clinical utilization of these tests.”
Dr. Fillit noted that older people often have declining kidney function, which can be easily measured by glomerular filtration rate. Changes in blood levels of these markers with declining kidney function are “not unexpected, but [it’s] important that it’s been demonstrated.
“As we go forward, maybe the future utilization of these tests will be not only recording the ratios but also reporting the ratios in the context of somebody’s glomerular filtration rate. You could imagine a scenario where when the test is done, it’s automatically done alongside of glomerular filtration rate,” Dr. Fillit said in an interview.
The study was supported by Coins for Alzheimer’s Research Trust, the Tracy Family Stable Isotope Labeling Quantitation Center, and the National Institute of Neurological Disorders and Stroke. Dr. Hansson has received support to his institution from ADx, AVID Radiopharmaceuticals, Biogen, Eli Lilly, Eisai, Fujirebio, GE Healthcare, Pfizer, and Roche; consultancy/speaker fees from Amylyx, Alzpath, Biogen, Cerveau, Fujirebio, Genentech, Novartis, Roche, and Siemens; and personal fees from Eli Lilly, Eisai, Bioarctic, and Biogen outside the submitted work. Dr. Edelmayer and Dr. Fillit have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
New research provides more evidence that
In a cross-sectional study of adults with and those without cognitive impairment, chronic kidney disease was associated with increased plasma concentrations of phosphorylated tau (p-tau) 217 and 181.
However, there were no associations between chronic kidney disease and the ratio of p-tau217 to unphosphorylated tau 217 (pT217/T217), and the associations with p-tau181 to unphosphorylated tau 181 (pT181/T181) were attenuated in patients with cognitive impairment.
“These novel findings suggest that plasma measures of the phosphorylated to unphosphorylated tau ratios are more accurate than p-tau forms alone as they correlate less with individual difference in glomerular filtration rate or impaired kidney function,” reported an investigative team led by Oskar Hansson, MD, PhD, with Lund University in Sweden.
“Thus, to mitigate the effects of non-Alzheimer’s–related comorbidities like chronic kidney disease on the performance of plasma Alzheimer’s disease biomarkers, certain tau ratios, and specifically pT217/T217, should be considered for implementation in clinical practice and drug trials,” they added.
The study was published online in JAMA Neurology to coincide with a presentation at the International Conference on Alzheimer’s and Parkinson’s Diseases in Gothenburg, Sweden.
Skewed tau levels
Plasma biomarkers of amyloid-beta (Abeta) and tau pathologies, and in particular variants in p-tau217 and p-tau181, have shown promise for use in Alzheimer’s disease diagnosis and prognosis. However, previous reports have suggested that chronic kidney disease might influence plasma p-tau217 and p-tau181 concentrations, potentially decreasing their usefulness in the diagnostic workup of dementia.
Researchers investigated associations of chronic kidney disease with plasma ratios of p-tau217 and p-tau181 to the corresponding unphosphorylated peptides in Alzheimer’s disease.
The data came from 473 older adults, with and without cognitive impairment, from the Swedish BioFinder-2 study who had plasma tau assessments and chronic kidney disease status established within 6 months of plasma collection.
The researchers found that lower estimated glomerular filtration rate levels (indicative of kidney dysfunction) were associated with higher plasma concentrations of phosphorylated and unphosphorylated tau peptides measured simultaneously using the tau immunoprecipitation mass spectrometry assay.
However, the correlations with estimated glomerular filtration rate were nonsignificant for the pT217/T217 ratio in individuals with cognitive impairment and were significantly attenuated for pT217/T217 in cognitively unimpaired individuals and for pT181/T181 in both cognitively unimpaired and impaired individuals.
“Importantly, we demonstrate that there were no significant associations between chronic kidney disease and the pT217/T217 ratio and changes in plasma pT181/T181 associated with chronic kidney disease were small or nonsignificant,” the researchers noted.
“Our results indicate that by using p-tau/tau ratios we may be able to reduce the variability in plasma p-tau levels driven by impaired kidney function and consequently such ratios are more robust measures of brain p-tau pathology in individuals with both early- and later-stage Alzheimer’s disease,” they added.
The researchers believe this is likely true for the ratios of other related proteins – a view that is supported by findings of attenuated associations of chronic kidney disease with Abeta42/40, compared with Abeta42 and Abeta40 in the current study and in previous studies.
Important clinical implications
Reached for comment, Rebecca Edelmayer, PhD, Alzheimer’s Association senior director of scientific engagement, noted that research continues to indicate that blood biomarkers have “promise for improving, and possibly even redefining, the clinical workup for Alzheimer’s disease.
“Many of the Alzheimer’s blood tests in development today have focused on core blood biomarkers associated with amyloid accumulation and tau tangle formation in the brain,” Dr. Edelmayer said.
“Before these tests can be used more broadly in the clinic, we need to understand all of the variables that may impact the results of various blood biomarkers, including differences that may be driven by race, ethnicity, sex, and underlying health conditions, such as chronic kidney disease.
“This study corroborates other research suggesting that some Alzheimer’s-associated markers can be affected by chronic kidney disease, but by using ratios of amyloid or tau markers, we may be able to minimize these differences in results caused by underlying disease,” Dr. Edelmayer said.
Howard Fillit, MD, cofounder and chief science officer at the Alzheimer’s Drug Discovery Foundation, said, “Using these ratios makes a lot of sense because the ratios wouldn’t change with kidney function. I think this is an important advance in clinical utilization of these tests.”
Dr. Fillit noted that older people often have declining kidney function, which can be easily measured by glomerular filtration rate. Changes in blood levels of these markers with declining kidney function are “not unexpected, but [it’s] important that it’s been demonstrated.
“As we go forward, maybe the future utilization of these tests will be not only recording the ratios but also reporting the ratios in the context of somebody’s glomerular filtration rate. You could imagine a scenario where when the test is done, it’s automatically done alongside of glomerular filtration rate,” Dr. Fillit said in an interview.
The study was supported by Coins for Alzheimer’s Research Trust, the Tracy Family Stable Isotope Labeling Quantitation Center, and the National Institute of Neurological Disorders and Stroke. Dr. Hansson has received support to his institution from ADx, AVID Radiopharmaceuticals, Biogen, Eli Lilly, Eisai, Fujirebio, GE Healthcare, Pfizer, and Roche; consultancy/speaker fees from Amylyx, Alzpath, Biogen, Cerveau, Fujirebio, Genentech, Novartis, Roche, and Siemens; and personal fees from Eli Lilly, Eisai, Bioarctic, and Biogen outside the submitted work. Dr. Edelmayer and Dr. Fillit have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AD/PD 2023
No added benefit of time-restricted eating in NAFLD
, according to the results of a randomized controlled trial conducted in China.
With the same calorie restrictions, an 8-hour time-restricted eating (TRE) pattern was no more effective in lowering intrahepatic triglyceride content or achieving resolution of NAFLD than daily calorie restriction (DCR) without time constraints (habitual meal timing).
TRE also did not provide additional benefits over DCR for reducing body fat or metabolic risk factors.
Calorie intake restriction seems to explain most of the beneficial effects of TRE and supports the importance of calorie restriction in a TRE regimen in adults with obesity and NAFLD, say the investigators, led by Xueyun Wei, MD, with Southern Medical University, Guangzhou (China).
The study “supports some other recent data that kind of disproves that intermittent fasting actually works that well and that it basically comes down to calorie restriction,” said Lisa Ganjhu, DO, who wasn’t involved in the research.
“It doesn’t matter when you are calorie restricting; it’s just that you are restricting calories to a certain amount. We know that works,” Dr. Ganjhu, a clinical associate professor in the division of gastroenterology and hepatology at NYU Grossman School of Medicine, told this news organization.
Results of the TREATY-FLD study were published online in JAMA Network Open.
Calorie reduction is key
NAFLD has become a major worldwide public health challenge, affecting roughly 20%-30% of adults in the general population and more than 70% of adults with obesity and diabetes.
Weight loss through lifestyle modifications has been shown to improve liver fat and metabolic disorders. TRE, a type of intermittent fasting, has garnered attention as a potential alternative to DCR for weight loss. “However, most of the reported benefits of TRE are either ‘untested or under tested’ and can’t isolate the effects of TRE itself,” Dr. Wei and colleagues note.
In the TREATY-FLD study, 88 adults (mean age, 32 years; 56% male) with obesity and NAFLD and similar baseline characteristics were randomly allocated to a TRE or DCR group.
All participants were instructed to maintain a diet of 1,500-1,800 kcal per day for men and 1,200-1,500 kcal per day for women for 12 months. The diets consisted of 40%-55% carbohydrate, 15%-20% protein, and 20%-30% fat. Participants were also given one protein shake per day for the first 6 months and received dietary counseling throughout the study.
Participants in the TRE group were told to eat only between 8 AM and 4 PM each day. Only noncaloric beverages were permitted outside of the daily eating window. Participants in the DCR group had no restrictions on when they could eat.
Investigators found no significant between-group differences in change in MRI-measured IHTG content from baseline to 6 or 12 months (the primary outcome).
At 6 months, IHTG content was reduced by 8.3% in the TRE group and by 8.1% in the DRC group. At 12 months, IHTG content was reduced by 6.9% and 7.9%, respectively. The net change in IHTG content was not significantly different between the groups at 6 months (percentage point difference: −0.2; P = .86) or 12 months (percentage point difference: 1; P = .45)
Liver stiffness was reduced by 2.1 kPa in the TRE group and 1.7 kPa in the DCR group at 12 months, with no significant difference between the groups (P = .33). A percentage of participants in the TRE and DCR groups had resolution of NAFLD (defined as IHTG content less than 5%) at 12 months (33% vs. 49%; P = .31).
During the 12-month intervention, body weight was significantly reduced by 8.4 kg in the TRE group and 7.8 kg in the DCR group, with no significant between-group differences (P = .69).
In addition, waist circumference, body fat percentage, fat mass, lean mass, total abdominal fat, subcutaneous fat, visceral fat, and visceral to subcutaneous fat ratio were all significantly and comparably reduced in the two groups.
Both groups also saw significant and comparable improvement over 12 months in metabolic risk factors, including systolic and diastolic blood pressure, pulse rate, and total cholesterol, triglyceride, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol levels.
However, TRE might be more effective in improving insulin sensitivity than DCR. Both diets significantly reduced fasting plasma glucose level, hemoglobin A1c, and homeostasis model assessment of insulin resistance (HOMA-IR) at 6 months. TRE significantly reduced HOMA-IR, compared with DCR at 12 months.
Both diets significantly reduced levels of liver enzymes, including serum alanine aminotransferase, aspartate aminotransferase, and gamma-glutamyl transferase, with no significant between-group differences.
Eat less, exercise more
Although the study found no additional benefit from TRE, it’s still good advice to skip snacking in the evening, Dr. Ganjhu said in an interview. “No one snacks on anything healthy at night. I mean, who’s chewing on celery?” she added.
Eating late at night can trigger reflux, so “not eating anything for several hours before bed or better yet going for a walk after dinner to kickstart your metabolism is good advice,” Dr. Ganjhu said.
For obesity and fatty liver disease, it really comes down to diet and exercise, she noted.
“For all the money that is going into pharmaceuticals, the long and the short of it is you just have to eat less and work out more and manage all the other factors like diabetes, high blood pressure, and metabolic syndrome. But getting people to follow that is tough,” Dr. Ganjhu said.
The study was supported by grants from the National Key Research and Development Project, Joint Funds of the National Natural Science Foundation of China, and Key-Area Clinical Research Program of Southern Medical University. Dr. Wei and Dr. Ganjhu report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
, according to the results of a randomized controlled trial conducted in China.
With the same calorie restrictions, an 8-hour time-restricted eating (TRE) pattern was no more effective in lowering intrahepatic triglyceride content or achieving resolution of NAFLD than daily calorie restriction (DCR) without time constraints (habitual meal timing).
TRE also did not provide additional benefits over DCR for reducing body fat or metabolic risk factors.
Calorie intake restriction seems to explain most of the beneficial effects of TRE and supports the importance of calorie restriction in a TRE regimen in adults with obesity and NAFLD, say the investigators, led by Xueyun Wei, MD, with Southern Medical University, Guangzhou (China).
The study “supports some other recent data that kind of disproves that intermittent fasting actually works that well and that it basically comes down to calorie restriction,” said Lisa Ganjhu, DO, who wasn’t involved in the research.
“It doesn’t matter when you are calorie restricting; it’s just that you are restricting calories to a certain amount. We know that works,” Dr. Ganjhu, a clinical associate professor in the division of gastroenterology and hepatology at NYU Grossman School of Medicine, told this news organization.
Results of the TREATY-FLD study were published online in JAMA Network Open.
Calorie reduction is key
NAFLD has become a major worldwide public health challenge, affecting roughly 20%-30% of adults in the general population and more than 70% of adults with obesity and diabetes.
Weight loss through lifestyle modifications has been shown to improve liver fat and metabolic disorders. TRE, a type of intermittent fasting, has garnered attention as a potential alternative to DCR for weight loss. “However, most of the reported benefits of TRE are either ‘untested or under tested’ and can’t isolate the effects of TRE itself,” Dr. Wei and colleagues note.
In the TREATY-FLD study, 88 adults (mean age, 32 years; 56% male) with obesity and NAFLD and similar baseline characteristics were randomly allocated to a TRE or DCR group.
All participants were instructed to maintain a diet of 1,500-1,800 kcal per day for men and 1,200-1,500 kcal per day for women for 12 months. The diets consisted of 40%-55% carbohydrate, 15%-20% protein, and 20%-30% fat. Participants were also given one protein shake per day for the first 6 months and received dietary counseling throughout the study.
Participants in the TRE group were told to eat only between 8 AM and 4 PM each day. Only noncaloric beverages were permitted outside of the daily eating window. Participants in the DCR group had no restrictions on when they could eat.
Investigators found no significant between-group differences in change in MRI-measured IHTG content from baseline to 6 or 12 months (the primary outcome).
At 6 months, IHTG content was reduced by 8.3% in the TRE group and by 8.1% in the DRC group. At 12 months, IHTG content was reduced by 6.9% and 7.9%, respectively. The net change in IHTG content was not significantly different between the groups at 6 months (percentage point difference: −0.2; P = .86) or 12 months (percentage point difference: 1; P = .45)
Liver stiffness was reduced by 2.1 kPa in the TRE group and 1.7 kPa in the DCR group at 12 months, with no significant difference between the groups (P = .33). A percentage of participants in the TRE and DCR groups had resolution of NAFLD (defined as IHTG content less than 5%) at 12 months (33% vs. 49%; P = .31).
During the 12-month intervention, body weight was significantly reduced by 8.4 kg in the TRE group and 7.8 kg in the DCR group, with no significant between-group differences (P = .69).
In addition, waist circumference, body fat percentage, fat mass, lean mass, total abdominal fat, subcutaneous fat, visceral fat, and visceral to subcutaneous fat ratio were all significantly and comparably reduced in the two groups.
Both groups also saw significant and comparable improvement over 12 months in metabolic risk factors, including systolic and diastolic blood pressure, pulse rate, and total cholesterol, triglyceride, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol levels.
However, TRE might be more effective in improving insulin sensitivity than DCR. Both diets significantly reduced fasting plasma glucose level, hemoglobin A1c, and homeostasis model assessment of insulin resistance (HOMA-IR) at 6 months. TRE significantly reduced HOMA-IR, compared with DCR at 12 months.
Both diets significantly reduced levels of liver enzymes, including serum alanine aminotransferase, aspartate aminotransferase, and gamma-glutamyl transferase, with no significant between-group differences.
Eat less, exercise more
Although the study found no additional benefit from TRE, it’s still good advice to skip snacking in the evening, Dr. Ganjhu said in an interview. “No one snacks on anything healthy at night. I mean, who’s chewing on celery?” she added.
Eating late at night can trigger reflux, so “not eating anything for several hours before bed or better yet going for a walk after dinner to kickstart your metabolism is good advice,” Dr. Ganjhu said.
For obesity and fatty liver disease, it really comes down to diet and exercise, she noted.
“For all the money that is going into pharmaceuticals, the long and the short of it is you just have to eat less and work out more and manage all the other factors like diabetes, high blood pressure, and metabolic syndrome. But getting people to follow that is tough,” Dr. Ganjhu said.
The study was supported by grants from the National Key Research and Development Project, Joint Funds of the National Natural Science Foundation of China, and Key-Area Clinical Research Program of Southern Medical University. Dr. Wei and Dr. Ganjhu report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
, according to the results of a randomized controlled trial conducted in China.
With the same calorie restrictions, an 8-hour time-restricted eating (TRE) pattern was no more effective in lowering intrahepatic triglyceride content or achieving resolution of NAFLD than daily calorie restriction (DCR) without time constraints (habitual meal timing).
TRE also did not provide additional benefits over DCR for reducing body fat or metabolic risk factors.
Calorie intake restriction seems to explain most of the beneficial effects of TRE and supports the importance of calorie restriction in a TRE regimen in adults with obesity and NAFLD, say the investigators, led by Xueyun Wei, MD, with Southern Medical University, Guangzhou (China).
The study “supports some other recent data that kind of disproves that intermittent fasting actually works that well and that it basically comes down to calorie restriction,” said Lisa Ganjhu, DO, who wasn’t involved in the research.
“It doesn’t matter when you are calorie restricting; it’s just that you are restricting calories to a certain amount. We know that works,” Dr. Ganjhu, a clinical associate professor in the division of gastroenterology and hepatology at NYU Grossman School of Medicine, told this news organization.
Results of the TREATY-FLD study were published online in JAMA Network Open.
Calorie reduction is key
NAFLD has become a major worldwide public health challenge, affecting roughly 20%-30% of adults in the general population and more than 70% of adults with obesity and diabetes.
Weight loss through lifestyle modifications has been shown to improve liver fat and metabolic disorders. TRE, a type of intermittent fasting, has garnered attention as a potential alternative to DCR for weight loss. “However, most of the reported benefits of TRE are either ‘untested or under tested’ and can’t isolate the effects of TRE itself,” Dr. Wei and colleagues note.
In the TREATY-FLD study, 88 adults (mean age, 32 years; 56% male) with obesity and NAFLD and similar baseline characteristics were randomly allocated to a TRE or DCR group.
All participants were instructed to maintain a diet of 1,500-1,800 kcal per day for men and 1,200-1,500 kcal per day for women for 12 months. The diets consisted of 40%-55% carbohydrate, 15%-20% protein, and 20%-30% fat. Participants were also given one protein shake per day for the first 6 months and received dietary counseling throughout the study.
Participants in the TRE group were told to eat only between 8 AM and 4 PM each day. Only noncaloric beverages were permitted outside of the daily eating window. Participants in the DCR group had no restrictions on when they could eat.
Investigators found no significant between-group differences in change in MRI-measured IHTG content from baseline to 6 or 12 months (the primary outcome).
At 6 months, IHTG content was reduced by 8.3% in the TRE group and by 8.1% in the DRC group. At 12 months, IHTG content was reduced by 6.9% and 7.9%, respectively. The net change in IHTG content was not significantly different between the groups at 6 months (percentage point difference: −0.2; P = .86) or 12 months (percentage point difference: 1; P = .45)
Liver stiffness was reduced by 2.1 kPa in the TRE group and 1.7 kPa in the DCR group at 12 months, with no significant difference between the groups (P = .33). A percentage of participants in the TRE and DCR groups had resolution of NAFLD (defined as IHTG content less than 5%) at 12 months (33% vs. 49%; P = .31).
During the 12-month intervention, body weight was significantly reduced by 8.4 kg in the TRE group and 7.8 kg in the DCR group, with no significant between-group differences (P = .69).
In addition, waist circumference, body fat percentage, fat mass, lean mass, total abdominal fat, subcutaneous fat, visceral fat, and visceral to subcutaneous fat ratio were all significantly and comparably reduced in the two groups.
Both groups also saw significant and comparable improvement over 12 months in metabolic risk factors, including systolic and diastolic blood pressure, pulse rate, and total cholesterol, triglyceride, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol levels.
However, TRE might be more effective in improving insulin sensitivity than DCR. Both diets significantly reduced fasting plasma glucose level, hemoglobin A1c, and homeostasis model assessment of insulin resistance (HOMA-IR) at 6 months. TRE significantly reduced HOMA-IR, compared with DCR at 12 months.
Both diets significantly reduced levels of liver enzymes, including serum alanine aminotransferase, aspartate aminotransferase, and gamma-glutamyl transferase, with no significant between-group differences.
Eat less, exercise more
Although the study found no additional benefit from TRE, it’s still good advice to skip snacking in the evening, Dr. Ganjhu said in an interview. “No one snacks on anything healthy at night. I mean, who’s chewing on celery?” she added.
Eating late at night can trigger reflux, so “not eating anything for several hours before bed or better yet going for a walk after dinner to kickstart your metabolism is good advice,” Dr. Ganjhu said.
For obesity and fatty liver disease, it really comes down to diet and exercise, she noted.
“For all the money that is going into pharmaceuticals, the long and the short of it is you just have to eat less and work out more and manage all the other factors like diabetes, high blood pressure, and metabolic syndrome. But getting people to follow that is tough,” Dr. Ganjhu said.
The study was supported by grants from the National Key Research and Development Project, Joint Funds of the National Natural Science Foundation of China, and Key-Area Clinical Research Program of Southern Medical University. Dr. Wei and Dr. Ganjhu report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Vedolizumab appears effective for inducing remission in chronic pouchitis
after undergoing ileal pouch-anal anastomosis (IPAA) for ulcerative colitis, according to a phase 4 trial.
The incidence of modified Pouchitis Disease Activity Index (mPDAI)–defined remission after 14 weeks was 31% for vedolizumab, compared with 10% for placebo.
“Vedolizumab works in both ulcerative colitis and Crohn’s disease, so it appeared rational to test its efficacy in chronic, antibiotic-resistant pouchitis,” lead author Simon Travis, DPhil, professor of clinical gastroenterology at the University of Oxford’s Kennedy Institute of Rheumatology and Translational Gastroenterology Unit in the United Kingdom, said in an interview.
“Vedolizumab works for antibiotic-resistant pouchitis,” he said. “It is the first advanced therapy licensed for chronic pouchitis in Europe and can be a game changer for patients who develop pouchitis after experiencing ulcerative colitis severe enough to need colectomy who might have thought that surgery would be the ultimate solution.”
The study was published online in The New England Journal of Medicine.
Treating chronic pouchitis
About half of patients with ulcerative colitis who undergo restorative proctocolectomy with IPAA will develop pouchitis within 5 years, the authors write. Among those, about one-fifth will have chronic pouchitis, with symptoms that last longer than 4 weeks. Symptoms include increased stool frequency, abdominal pain, fecal urgency, and impaired quality of life.
Typically, antibiotics are recommended as first-line treatment for acute pouchitis, but antibiotic resistance is common. Previous studies have suggested that tumor necrosis factor antagonists and the monoclonal antibodies vedolizumab and ustekinumab may be effective in pouchitis that is refractory to antibiotics.
The U.S. Food and Drug Administration has approved vedolizumab as a treatment for moderate to severe ulcerative colitis and Crohn’s disease. In early 2022, the European Commission approved vedolizumab for adult patients with moderate to severe active chronic pouchitis who had undergone proctocolectomy with IPAA and had an inadequate response to antibiotic therapy. The approval was based on results from the EARNEST trial.
As part of the EARNEST trial, Dr. Travis and colleagues at 31 sites in North America and Europe conducted a phase 4, double-blind, randomized trial to evaluate vedolizumab for chronic pouchitis after IPAA for ulcerative colitis.
Between October 2016 and March 2020, researchers identified 102 adult patients who met the study criteria. They were eligible if they had undergone proctocolectomy at least 1 year before screening and had active chronic pouchitis, which was defined by an mPDAI score of 5 or more and a minimum subscore of 2 on the endoscopic domain.
After a 28-day screening period, patients were randomly assigned in a 1:1 ratio to receive 300 mg of intravenous vedolizumab or placebo on day 1 and at weeks 2, 6, 14, 22, and 30. All patients also received 500 mg of oral ciprofloxacin twice daily from weeks 1 to 4. Additional courses of antibiotics were allowed, as needed, for pouchitis flares that occurred after week 14.
The primary endpoint was mPDAI-defined remission, or an mPDAI score of 4 or less and a reduction of 2 or more points on the 12-point scale at week 14.
Other endpoints included mPDAI-defined remission at week 34, mPDAI-defined response (a reduction of 2 or more points) at weeks 14 and 34, and PDAI-defined remission (a PDAI score of 6 or less and a reduction of 3 or more points on the 18-point scale) at weeks 14 and 34. The mPDAI is based on clinical symptoms and endoscopic findings, whereas the PDAI is based on clinical symptoms, endoscopic findings, and histologic findings.
Overall, 36 patients (71%) in the vedolizumab group and 32 patients (63%) in the placebo group completed treatment and received all infusions through week 30. Eight patients in each group discontinued vedolizumab or placebo owing to a lack of efficacy. Demographic and clinical characteristics were similar in the two groups – about 84% of the patients were White, and the majority were men.
At the 14-week mark, 16 of 51 patients (31%) in the vedolizumab group and 5 of 51 patients (10%) in the placebo group achieved mPDAI-defined remission (a 21–percentage point difference; 95% CI, 5-38; P = .01). At week 34, 35% of the vedolizumab group and 18% of the placebo group reached remission. A post hoc analysis found that a high percentage of patients in the vedolizumab group reached remission regardless of whether concomitant antibiotics were used before week 14 or 34.
“Concomitant antibiotic use after week 4 was reported in a higher percentage of patients in the vedolizumab group than in the placebo group, a finding that was unexpected,” the authors write. “However, the use of additional antibiotics was not considered to be a treatment failure because antibiotics are the current standard of care for chronic pouchitis.”
Additional findings
Vedolizumab showed major differences in the other endpoints as well. The percentage of patients with PDAI-defined remission was 35% in the vedolizumab group versus 10% in the placebo group at week 14, and 37% versus 18% at week 34.
The percentage of patients with mPDAI-defined response at week 14 was 63% among the vedolizumab group and 33% among the placebo group. By week 34, the between-group difference was 51% versus 29%.
Vedolizumab also showed greater changes in total PDAI scores, including endoscopic and histologic subscores, as well as remission and response defined by the Inflammatory Bowel Disease Questionnaire (IBDQ). However, there were no significant differences in changes from baseline for the IBDQ or the Cleveland Global Quality of Life (CGQL) score.
The vedolizumab group had a higher percentage of patients with sustained mPDAI-defined remission (difference, 22 percentage points; 95% CI, 6-37) and sustained PDAI-defined remission (difference, 23 percentage points; 95% CI, 8-39).
Adverse events were reported in 47 patients (92%) in the vedolizumab group and 44 patients (86%) in the placebo group. Pouchitis was reported as an adverse event in 24 patients (47%) in the vedolizumab group and 20 patients (39%) in the placebo group. More patients in the vedolizumab group also reported upper respiratory tract infections and headaches.
Serious adverse events occurred in three patients (6%) in the vedolizumab group and four patients (8%) in the placebo group. One adverse event led to discontinuation of vedolizumab, and no serious adverse events were related to vedolizumab or led to discontinuation of vedolizumab.
‘Landmark study’
“This is a landmark study that shows us that a biologic that we have used for Crohn’s disease and ulcerative colitis may also be used to treat chronic pouchitis. This is a large unmet need for our patients and an important advancement for the field,” Miguel Regueiro, MD, chair of the Digestive Disease and Surgery Institute at the Cleveland Clinic, told this news organization.
The Cleveland Clinic has one of the highest referral rates in the country for IPAA, noted Dr. Regueiro, who wasn’t involved with this study. Colleagues are currently conducting studies to determine who may develop pouchitis and understand why certain patients develop pouchitis after the procedure, he said.
One question the EARNEST trial leaves unanswered is whether vedolizumab will be required as a sustained medicine to control pouchitis or could be stopped at some point, he said. “My sense is that, as is the case with any IBD, chronic treatment will be required,” he added.
The higher rate of ciprofloxacin use among patients who received vedolizumab is interesting, Dr. Regueiro said.
“[The researchers] note that ciprofloxacin was used for symptoms and do not know if there was active inflammation. It’s possible that bacterial overgrowth caused symptoms and the antibiotic treated that, and in a study this small, it is difficult to say anything more,” he said.
The study was sponsored by Takeda, the manufacturer of vedolizumab. Several authors reported speaking fees and consultant roles for numerous pharmaceutical companies, including Takeda. Three of the authors are employees of Takeda. Dr. Regueiro reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
after undergoing ileal pouch-anal anastomosis (IPAA) for ulcerative colitis, according to a phase 4 trial.
The incidence of modified Pouchitis Disease Activity Index (mPDAI)–defined remission after 14 weeks was 31% for vedolizumab, compared with 10% for placebo.
“Vedolizumab works in both ulcerative colitis and Crohn’s disease, so it appeared rational to test its efficacy in chronic, antibiotic-resistant pouchitis,” lead author Simon Travis, DPhil, professor of clinical gastroenterology at the University of Oxford’s Kennedy Institute of Rheumatology and Translational Gastroenterology Unit in the United Kingdom, said in an interview.
“Vedolizumab works for antibiotic-resistant pouchitis,” he said. “It is the first advanced therapy licensed for chronic pouchitis in Europe and can be a game changer for patients who develop pouchitis after experiencing ulcerative colitis severe enough to need colectomy who might have thought that surgery would be the ultimate solution.”
The study was published online in The New England Journal of Medicine.
Treating chronic pouchitis
About half of patients with ulcerative colitis who undergo restorative proctocolectomy with IPAA will develop pouchitis within 5 years, the authors write. Among those, about one-fifth will have chronic pouchitis, with symptoms that last longer than 4 weeks. Symptoms include increased stool frequency, abdominal pain, fecal urgency, and impaired quality of life.
Typically, antibiotics are recommended as first-line treatment for acute pouchitis, but antibiotic resistance is common. Previous studies have suggested that tumor necrosis factor antagonists and the monoclonal antibodies vedolizumab and ustekinumab may be effective in pouchitis that is refractory to antibiotics.
The U.S. Food and Drug Administration has approved vedolizumab as a treatment for moderate to severe ulcerative colitis and Crohn’s disease. In early 2022, the European Commission approved vedolizumab for adult patients with moderate to severe active chronic pouchitis who had undergone proctocolectomy with IPAA and had an inadequate response to antibiotic therapy. The approval was based on results from the EARNEST trial.
As part of the EARNEST trial, Dr. Travis and colleagues at 31 sites in North America and Europe conducted a phase 4, double-blind, randomized trial to evaluate vedolizumab for chronic pouchitis after IPAA for ulcerative colitis.
Between October 2016 and March 2020, researchers identified 102 adult patients who met the study criteria. They were eligible if they had undergone proctocolectomy at least 1 year before screening and had active chronic pouchitis, which was defined by an mPDAI score of 5 or more and a minimum subscore of 2 on the endoscopic domain.
After a 28-day screening period, patients were randomly assigned in a 1:1 ratio to receive 300 mg of intravenous vedolizumab or placebo on day 1 and at weeks 2, 6, 14, 22, and 30. All patients also received 500 mg of oral ciprofloxacin twice daily from weeks 1 to 4. Additional courses of antibiotics were allowed, as needed, for pouchitis flares that occurred after week 14.
The primary endpoint was mPDAI-defined remission, or an mPDAI score of 4 or less and a reduction of 2 or more points on the 12-point scale at week 14.
Other endpoints included mPDAI-defined remission at week 34, mPDAI-defined response (a reduction of 2 or more points) at weeks 14 and 34, and PDAI-defined remission (a PDAI score of 6 or less and a reduction of 3 or more points on the 18-point scale) at weeks 14 and 34. The mPDAI is based on clinical symptoms and endoscopic findings, whereas the PDAI is based on clinical symptoms, endoscopic findings, and histologic findings.
Overall, 36 patients (71%) in the vedolizumab group and 32 patients (63%) in the placebo group completed treatment and received all infusions through week 30. Eight patients in each group discontinued vedolizumab or placebo owing to a lack of efficacy. Demographic and clinical characteristics were similar in the two groups – about 84% of the patients were White, and the majority were men.
At the 14-week mark, 16 of 51 patients (31%) in the vedolizumab group and 5 of 51 patients (10%) in the placebo group achieved mPDAI-defined remission (a 21–percentage point difference; 95% CI, 5-38; P = .01). At week 34, 35% of the vedolizumab group and 18% of the placebo group reached remission. A post hoc analysis found that a high percentage of patients in the vedolizumab group reached remission regardless of whether concomitant antibiotics were used before week 14 or 34.
“Concomitant antibiotic use after week 4 was reported in a higher percentage of patients in the vedolizumab group than in the placebo group, a finding that was unexpected,” the authors write. “However, the use of additional antibiotics was not considered to be a treatment failure because antibiotics are the current standard of care for chronic pouchitis.”
Additional findings
Vedolizumab showed major differences in the other endpoints as well. The percentage of patients with PDAI-defined remission was 35% in the vedolizumab group versus 10% in the placebo group at week 14, and 37% versus 18% at week 34.
The percentage of patients with mPDAI-defined response at week 14 was 63% among the vedolizumab group and 33% among the placebo group. By week 34, the between-group difference was 51% versus 29%.
Vedolizumab also showed greater changes in total PDAI scores, including endoscopic and histologic subscores, as well as remission and response defined by the Inflammatory Bowel Disease Questionnaire (IBDQ). However, there were no significant differences in changes from baseline for the IBDQ or the Cleveland Global Quality of Life (CGQL) score.
The vedolizumab group had a higher percentage of patients with sustained mPDAI-defined remission (difference, 22 percentage points; 95% CI, 6-37) and sustained PDAI-defined remission (difference, 23 percentage points; 95% CI, 8-39).
Adverse events were reported in 47 patients (92%) in the vedolizumab group and 44 patients (86%) in the placebo group. Pouchitis was reported as an adverse event in 24 patients (47%) in the vedolizumab group and 20 patients (39%) in the placebo group. More patients in the vedolizumab group also reported upper respiratory tract infections and headaches.
Serious adverse events occurred in three patients (6%) in the vedolizumab group and four patients (8%) in the placebo group. One adverse event led to discontinuation of vedolizumab, and no serious adverse events were related to vedolizumab or led to discontinuation of vedolizumab.
‘Landmark study’
“This is a landmark study that shows us that a biologic that we have used for Crohn’s disease and ulcerative colitis may also be used to treat chronic pouchitis. This is a large unmet need for our patients and an important advancement for the field,” Miguel Regueiro, MD, chair of the Digestive Disease and Surgery Institute at the Cleveland Clinic, told this news organization.
The Cleveland Clinic has one of the highest referral rates in the country for IPAA, noted Dr. Regueiro, who wasn’t involved with this study. Colleagues are currently conducting studies to determine who may develop pouchitis and understand why certain patients develop pouchitis after the procedure, he said.
One question the EARNEST trial leaves unanswered is whether vedolizumab will be required as a sustained medicine to control pouchitis or could be stopped at some point, he said. “My sense is that, as is the case with any IBD, chronic treatment will be required,” he added.
The higher rate of ciprofloxacin use among patients who received vedolizumab is interesting, Dr. Regueiro said.
“[The researchers] note that ciprofloxacin was used for symptoms and do not know if there was active inflammation. It’s possible that bacterial overgrowth caused symptoms and the antibiotic treated that, and in a study this small, it is difficult to say anything more,” he said.
The study was sponsored by Takeda, the manufacturer of vedolizumab. Several authors reported speaking fees and consultant roles for numerous pharmaceutical companies, including Takeda. Three of the authors are employees of Takeda. Dr. Regueiro reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
after undergoing ileal pouch-anal anastomosis (IPAA) for ulcerative colitis, according to a phase 4 trial.
The incidence of modified Pouchitis Disease Activity Index (mPDAI)–defined remission after 14 weeks was 31% for vedolizumab, compared with 10% for placebo.
“Vedolizumab works in both ulcerative colitis and Crohn’s disease, so it appeared rational to test its efficacy in chronic, antibiotic-resistant pouchitis,” lead author Simon Travis, DPhil, professor of clinical gastroenterology at the University of Oxford’s Kennedy Institute of Rheumatology and Translational Gastroenterology Unit in the United Kingdom, said in an interview.
“Vedolizumab works for antibiotic-resistant pouchitis,” he said. “It is the first advanced therapy licensed for chronic pouchitis in Europe and can be a game changer for patients who develop pouchitis after experiencing ulcerative colitis severe enough to need colectomy who might have thought that surgery would be the ultimate solution.”
The study was published online in The New England Journal of Medicine.
Treating chronic pouchitis
About half of patients with ulcerative colitis who undergo restorative proctocolectomy with IPAA will develop pouchitis within 5 years, the authors write. Among those, about one-fifth will have chronic pouchitis, with symptoms that last longer than 4 weeks. Symptoms include increased stool frequency, abdominal pain, fecal urgency, and impaired quality of life.
Typically, antibiotics are recommended as first-line treatment for acute pouchitis, but antibiotic resistance is common. Previous studies have suggested that tumor necrosis factor antagonists and the monoclonal antibodies vedolizumab and ustekinumab may be effective in pouchitis that is refractory to antibiotics.
The U.S. Food and Drug Administration has approved vedolizumab as a treatment for moderate to severe ulcerative colitis and Crohn’s disease. In early 2022, the European Commission approved vedolizumab for adult patients with moderate to severe active chronic pouchitis who had undergone proctocolectomy with IPAA and had an inadequate response to antibiotic therapy. The approval was based on results from the EARNEST trial.
As part of the EARNEST trial, Dr. Travis and colleagues at 31 sites in North America and Europe conducted a phase 4, double-blind, randomized trial to evaluate vedolizumab for chronic pouchitis after IPAA for ulcerative colitis.
Between October 2016 and March 2020, researchers identified 102 adult patients who met the study criteria. They were eligible if they had undergone proctocolectomy at least 1 year before screening and had active chronic pouchitis, which was defined by an mPDAI score of 5 or more and a minimum subscore of 2 on the endoscopic domain.
After a 28-day screening period, patients were randomly assigned in a 1:1 ratio to receive 300 mg of intravenous vedolizumab or placebo on day 1 and at weeks 2, 6, 14, 22, and 30. All patients also received 500 mg of oral ciprofloxacin twice daily from weeks 1 to 4. Additional courses of antibiotics were allowed, as needed, for pouchitis flares that occurred after week 14.
The primary endpoint was mPDAI-defined remission, or an mPDAI score of 4 or less and a reduction of 2 or more points on the 12-point scale at week 14.
Other endpoints included mPDAI-defined remission at week 34, mPDAI-defined response (a reduction of 2 or more points) at weeks 14 and 34, and PDAI-defined remission (a PDAI score of 6 or less and a reduction of 3 or more points on the 18-point scale) at weeks 14 and 34. The mPDAI is based on clinical symptoms and endoscopic findings, whereas the PDAI is based on clinical symptoms, endoscopic findings, and histologic findings.
Overall, 36 patients (71%) in the vedolizumab group and 32 patients (63%) in the placebo group completed treatment and received all infusions through week 30. Eight patients in each group discontinued vedolizumab or placebo owing to a lack of efficacy. Demographic and clinical characteristics were similar in the two groups – about 84% of the patients were White, and the majority were men.
At the 14-week mark, 16 of 51 patients (31%) in the vedolizumab group and 5 of 51 patients (10%) in the placebo group achieved mPDAI-defined remission (a 21–percentage point difference; 95% CI, 5-38; P = .01). At week 34, 35% of the vedolizumab group and 18% of the placebo group reached remission. A post hoc analysis found that a high percentage of patients in the vedolizumab group reached remission regardless of whether concomitant antibiotics were used before week 14 or 34.
“Concomitant antibiotic use after week 4 was reported in a higher percentage of patients in the vedolizumab group than in the placebo group, a finding that was unexpected,” the authors write. “However, the use of additional antibiotics was not considered to be a treatment failure because antibiotics are the current standard of care for chronic pouchitis.”
Additional findings
Vedolizumab showed major differences in the other endpoints as well. The percentage of patients with PDAI-defined remission was 35% in the vedolizumab group versus 10% in the placebo group at week 14, and 37% versus 18% at week 34.
The percentage of patients with mPDAI-defined response at week 14 was 63% among the vedolizumab group and 33% among the placebo group. By week 34, the between-group difference was 51% versus 29%.
Vedolizumab also showed greater changes in total PDAI scores, including endoscopic and histologic subscores, as well as remission and response defined by the Inflammatory Bowel Disease Questionnaire (IBDQ). However, there were no significant differences in changes from baseline for the IBDQ or the Cleveland Global Quality of Life (CGQL) score.
The vedolizumab group had a higher percentage of patients with sustained mPDAI-defined remission (difference, 22 percentage points; 95% CI, 6-37) and sustained PDAI-defined remission (difference, 23 percentage points; 95% CI, 8-39).
Adverse events were reported in 47 patients (92%) in the vedolizumab group and 44 patients (86%) in the placebo group. Pouchitis was reported as an adverse event in 24 patients (47%) in the vedolizumab group and 20 patients (39%) in the placebo group. More patients in the vedolizumab group also reported upper respiratory tract infections and headaches.
Serious adverse events occurred in three patients (6%) in the vedolizumab group and four patients (8%) in the placebo group. One adverse event led to discontinuation of vedolizumab, and no serious adverse events were related to vedolizumab or led to discontinuation of vedolizumab.
‘Landmark study’
“This is a landmark study that shows us that a biologic that we have used for Crohn’s disease and ulcerative colitis may also be used to treat chronic pouchitis. This is a large unmet need for our patients and an important advancement for the field,” Miguel Regueiro, MD, chair of the Digestive Disease and Surgery Institute at the Cleveland Clinic, told this news organization.
The Cleveland Clinic has one of the highest referral rates in the country for IPAA, noted Dr. Regueiro, who wasn’t involved with this study. Colleagues are currently conducting studies to determine who may develop pouchitis and understand why certain patients develop pouchitis after the procedure, he said.
One question the EARNEST trial leaves unanswered is whether vedolizumab will be required as a sustained medicine to control pouchitis or could be stopped at some point, he said. “My sense is that, as is the case with any IBD, chronic treatment will be required,” he added.
The higher rate of ciprofloxacin use among patients who received vedolizumab is interesting, Dr. Regueiro said.
“[The researchers] note that ciprofloxacin was used for symptoms and do not know if there was active inflammation. It’s possible that bacterial overgrowth caused symptoms and the antibiotic treated that, and in a study this small, it is difficult to say anything more,” he said.
The study was sponsored by Takeda, the manufacturer of vedolizumab. Several authors reported speaking fees and consultant roles for numerous pharmaceutical companies, including Takeda. Three of the authors are employees of Takeda. Dr. Regueiro reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE