User login
Stimulus Offers Cash for Quality
The economic stimulus bill that became law last week includes several items on SHM's healthcare policy wish list.
"It clearly hits some key issues," Eric Siegal, MD, chair of SHM's Public Policy Committee, says in regard to the American Recovery and Reinvestment Act. "This is a step in the right direction."
The $787 billion stimulus package includes:
- $1.1 billion for comparative effectiveness research (CER). Funding for CER is one of SHM's top policy priorities, says Laura Allendorf, SHM's senior advisor for advocacy and government affairs. CER examines the effectiveness of multiple therapies for specific medical conditions, or for a specific set of patients, to determine the best care options. "Funding for this is long overdue and key to healthcare reform," Dr. Siegal says. CER money will be split among the major players in this research, including the National Institutes of Health (NIH) and the Agency for Healthcare Research and Quality (AHRQ).
- A 34% increase in NIH funding. This includes $8.5 billion for research grants and programs that will allow for as many as 15,000 additional grants. "We know that an investment in biomedical research is an investment in the future of healthcare," says David Meltzer, MD, PhD, chair of SHM's Research Committee.
- $19 billion for health information technology. Incentives—and penalties—will target adoption of electronic health records by hospitals and office-based practices. "This will help improve patient safety, as well as care coordination," Allendorf says.
Other healthcare provisions in the package include an additional $86.6 billion in federal Medicaid funds, as well as temporary Medicaid coverage for the recently unemployed.
To keep up with public policy initiatives, check out SHM's advocacy portal.
The economic stimulus bill that became law last week includes several items on SHM's healthcare policy wish list.
"It clearly hits some key issues," Eric Siegal, MD, chair of SHM's Public Policy Committee, says in regard to the American Recovery and Reinvestment Act. "This is a step in the right direction."
The $787 billion stimulus package includes:
- $1.1 billion for comparative effectiveness research (CER). Funding for CER is one of SHM's top policy priorities, says Laura Allendorf, SHM's senior advisor for advocacy and government affairs. CER examines the effectiveness of multiple therapies for specific medical conditions, or for a specific set of patients, to determine the best care options. "Funding for this is long overdue and key to healthcare reform," Dr. Siegal says. CER money will be split among the major players in this research, including the National Institutes of Health (NIH) and the Agency for Healthcare Research and Quality (AHRQ).
- A 34% increase in NIH funding. This includes $8.5 billion for research grants and programs that will allow for as many as 15,000 additional grants. "We know that an investment in biomedical research is an investment in the future of healthcare," says David Meltzer, MD, PhD, chair of SHM's Research Committee.
- $19 billion for health information technology. Incentives—and penalties—will target adoption of electronic health records by hospitals and office-based practices. "This will help improve patient safety, as well as care coordination," Allendorf says.
Other healthcare provisions in the package include an additional $86.6 billion in federal Medicaid funds, as well as temporary Medicaid coverage for the recently unemployed.
To keep up with public policy initiatives, check out SHM's advocacy portal.
The economic stimulus bill that became law last week includes several items on SHM's healthcare policy wish list.
"It clearly hits some key issues," Eric Siegal, MD, chair of SHM's Public Policy Committee, says in regard to the American Recovery and Reinvestment Act. "This is a step in the right direction."
The $787 billion stimulus package includes:
- $1.1 billion for comparative effectiveness research (CER). Funding for CER is one of SHM's top policy priorities, says Laura Allendorf, SHM's senior advisor for advocacy and government affairs. CER examines the effectiveness of multiple therapies for specific medical conditions, or for a specific set of patients, to determine the best care options. "Funding for this is long overdue and key to healthcare reform," Dr. Siegal says. CER money will be split among the major players in this research, including the National Institutes of Health (NIH) and the Agency for Healthcare Research and Quality (AHRQ).
- A 34% increase in NIH funding. This includes $8.5 billion for research grants and programs that will allow for as many as 15,000 additional grants. "We know that an investment in biomedical research is an investment in the future of healthcare," says David Meltzer, MD, PhD, chair of SHM's Research Committee.
- $19 billion for health information technology. Incentives—and penalties—will target adoption of electronic health records by hospitals and office-based practices. "This will help improve patient safety, as well as care coordination," Allendorf says.
Other healthcare provisions in the package include an additional $86.6 billion in federal Medicaid funds, as well as temporary Medicaid coverage for the recently unemployed.
To keep up with public policy initiatives, check out SHM's advocacy portal.
Model's Death Sheds Spotlight on Sepsis Treatment
The recent death of an up-and-coming Brazilian model due to sepsis has again drawn attention to the common disease and how hospitalists should be wary not to miss its diagnosis in hospitalized patients.
Mariana Bridi da Costa, a 20-year-old beauty queen who participated in international competitions, died Jan. 24 from septicemia that began with a urinary tract infection. The original diagnosis did not include the urinary tract infection, leading to severe sepsis. Septicemia kills about 1,400 people a day worldwide, according to the Society of Critical Care Medicine (SCCM). The sepsis mortality rate is on a similar scale to lung, breast, and colon cancer, SCCM data shows.
"When someone comes in with high fever, high heart rate, high respiratory rate, and low blood pressure, you have to begin thinking about how well their organs are working," says Jeffrey Dichter, MD, medical director of cardiovascular intensive care at Regions Hospital in St. Paul, Minn., and former HM program director. "How sick are they? ... Hospitalists should look for the source of infection and evidence of organ failure."
According to the Mayo Clinic, about 750,000 people in the U.S. contract severe sepsis each year, and more than 200,000 people die of it.
Dr. Dichter notes that hospitalists in any setting—from acute-care hospitals to off-site clinics—can run blood tests for kidney and liver functions, as well as electrolyte levels, that serve as quick windows into the presence of sepsis. He also promotes www.survivingsepsis.org, the SCCM's program that aims to reduce sepsis mortality by 25% in five years by defining the disease more clearly and improving its diagnosis.
"Sometimes the symptoms patients come in with seem subtle," Dr. Dichter says. "Sometimes they may come in with evidence of an infection or low blood pressure, but they're awake and alert and talking and seem very normal. … Hospitalists need to be attune."
The recent death of an up-and-coming Brazilian model due to sepsis has again drawn attention to the common disease and how hospitalists should be wary not to miss its diagnosis in hospitalized patients.
Mariana Bridi da Costa, a 20-year-old beauty queen who participated in international competitions, died Jan. 24 from septicemia that began with a urinary tract infection. The original diagnosis did not include the urinary tract infection, leading to severe sepsis. Septicemia kills about 1,400 people a day worldwide, according to the Society of Critical Care Medicine (SCCM). The sepsis mortality rate is on a similar scale to lung, breast, and colon cancer, SCCM data shows.
"When someone comes in with high fever, high heart rate, high respiratory rate, and low blood pressure, you have to begin thinking about how well their organs are working," says Jeffrey Dichter, MD, medical director of cardiovascular intensive care at Regions Hospital in St. Paul, Minn., and former HM program director. "How sick are they? ... Hospitalists should look for the source of infection and evidence of organ failure."
According to the Mayo Clinic, about 750,000 people in the U.S. contract severe sepsis each year, and more than 200,000 people die of it.
Dr. Dichter notes that hospitalists in any setting—from acute-care hospitals to off-site clinics—can run blood tests for kidney and liver functions, as well as electrolyte levels, that serve as quick windows into the presence of sepsis. He also promotes www.survivingsepsis.org, the SCCM's program that aims to reduce sepsis mortality by 25% in five years by defining the disease more clearly and improving its diagnosis.
"Sometimes the symptoms patients come in with seem subtle," Dr. Dichter says. "Sometimes they may come in with evidence of an infection or low blood pressure, but they're awake and alert and talking and seem very normal. … Hospitalists need to be attune."
The recent death of an up-and-coming Brazilian model due to sepsis has again drawn attention to the common disease and how hospitalists should be wary not to miss its diagnosis in hospitalized patients.
Mariana Bridi da Costa, a 20-year-old beauty queen who participated in international competitions, died Jan. 24 from septicemia that began with a urinary tract infection. The original diagnosis did not include the urinary tract infection, leading to severe sepsis. Septicemia kills about 1,400 people a day worldwide, according to the Society of Critical Care Medicine (SCCM). The sepsis mortality rate is on a similar scale to lung, breast, and colon cancer, SCCM data shows.
"When someone comes in with high fever, high heart rate, high respiratory rate, and low blood pressure, you have to begin thinking about how well their organs are working," says Jeffrey Dichter, MD, medical director of cardiovascular intensive care at Regions Hospital in St. Paul, Minn., and former HM program director. "How sick are they? ... Hospitalists should look for the source of infection and evidence of organ failure."
According to the Mayo Clinic, about 750,000 people in the U.S. contract severe sepsis each year, and more than 200,000 people die of it.
Dr. Dichter notes that hospitalists in any setting—from acute-care hospitals to off-site clinics—can run blood tests for kidney and liver functions, as well as electrolyte levels, that serve as quick windows into the presence of sepsis. He also promotes www.survivingsepsis.org, the SCCM's program that aims to reduce sepsis mortality by 25% in five years by defining the disease more clearly and improving its diagnosis.
"Sometimes the symptoms patients come in with seem subtle," Dr. Dichter says. "Sometimes they may come in with evidence of an infection or low blood pressure, but they're awake and alert and talking and seem very normal. … Hospitalists need to be attune."
Research Roundup
Question: Do blood transfusions in hospitalized cancer patients with anemia or thrombocytopenia affect thrombotic event and in-hospital mortality rates?
Background: Erythropoiesis-stimulating agents have recently been shown to increase thrombotic risk and decrease survival in cancer patients. Blood transfusions are a common alternative for anemic patients. However, there are no randomized trials demonstrating improved outcomes in cancer patients receiving transfusions. Furthermore, the safety of transfusions has not been clearly defined.
Study design: Retrospective, cohort study.
Setting: 60 U.S. medical centers.
Synopsis: Using discharge data from the University Health System Consortium, 504,208 hospitalizations of cancer patients revealed that 14% of patients received at least one RBC transfusion and 3% of patients received a platelet transfusion. RBC and platelet transfusions were associated with increased risk of arterial thrombosis (RBCs: OR 1.53; 95% CI 1.46-1.61; platelets: OR 1.55; 1.4-1.71, P<0.001) and venous thrombotic events (RBCs: OR 1.34; 1.29-1.38; platelets: OR 1.2; 1.11-1.29, P<0.001). Additionally, transfusions were associated with increased in-hospital mortality (RBCs: OR 1.34; 1.29-1.38; platelets: OR 2.4; 2.27-2.52, P<0.001). Study results are limited by several factors, including the observational nature and the use of administrative coding data. Information on venous thromboembolism prophylaxis was not available, and the timing of transfusions in relation to the diagnosis of thrombotic events is unknown. Finally, anemia-necessitating transfusions may be a surrogate for "sicker" patients, explaining the increased in-hospital mortality. Blood transfusions in hospitalized patients require further study to determine whether there is a causal relationship between transfusions and increased thrombotic events and mortality.
Bottom line: Blood transfusions in hospitalized cancer patients should be used cautiously, as they are associated with increased thrombotic events and in-hospital mortality.
Citation: Arch Int Med. 2008;168:2377-2381
—Reviewed for the eWire by Kerry Will, MD, Jayne Barr, MD, Kim Tartaglia, MD, Aaron Wenger, MD, Jonathan Wynbrandt, MD, Nathan J. O’Dorisio, MD, The Ohio State University Medical Center, Columbus, OH.
Question: Do blood transfusions in hospitalized cancer patients with anemia or thrombocytopenia affect thrombotic event and in-hospital mortality rates?
Background: Erythropoiesis-stimulating agents have recently been shown to increase thrombotic risk and decrease survival in cancer patients. Blood transfusions are a common alternative for anemic patients. However, there are no randomized trials demonstrating improved outcomes in cancer patients receiving transfusions. Furthermore, the safety of transfusions has not been clearly defined.
Study design: Retrospective, cohort study.
Setting: 60 U.S. medical centers.
Synopsis: Using discharge data from the University Health System Consortium, 504,208 hospitalizations of cancer patients revealed that 14% of patients received at least one RBC transfusion and 3% of patients received a platelet transfusion. RBC and platelet transfusions were associated with increased risk of arterial thrombosis (RBCs: OR 1.53; 95% CI 1.46-1.61; platelets: OR 1.55; 1.4-1.71, P<0.001) and venous thrombotic events (RBCs: OR 1.34; 1.29-1.38; platelets: OR 1.2; 1.11-1.29, P<0.001). Additionally, transfusions were associated with increased in-hospital mortality (RBCs: OR 1.34; 1.29-1.38; platelets: OR 2.4; 2.27-2.52, P<0.001). Study results are limited by several factors, including the observational nature and the use of administrative coding data. Information on venous thromboembolism prophylaxis was not available, and the timing of transfusions in relation to the diagnosis of thrombotic events is unknown. Finally, anemia-necessitating transfusions may be a surrogate for "sicker" patients, explaining the increased in-hospital mortality. Blood transfusions in hospitalized patients require further study to determine whether there is a causal relationship between transfusions and increased thrombotic events and mortality.
Bottom line: Blood transfusions in hospitalized cancer patients should be used cautiously, as they are associated with increased thrombotic events and in-hospital mortality.
Citation: Arch Int Med. 2008;168:2377-2381
—Reviewed for the eWire by Kerry Will, MD, Jayne Barr, MD, Kim Tartaglia, MD, Aaron Wenger, MD, Jonathan Wynbrandt, MD, Nathan J. O’Dorisio, MD, The Ohio State University Medical Center, Columbus, OH.
Question: Do blood transfusions in hospitalized cancer patients with anemia or thrombocytopenia affect thrombotic event and in-hospital mortality rates?
Background: Erythropoiesis-stimulating agents have recently been shown to increase thrombotic risk and decrease survival in cancer patients. Blood transfusions are a common alternative for anemic patients. However, there are no randomized trials demonstrating improved outcomes in cancer patients receiving transfusions. Furthermore, the safety of transfusions has not been clearly defined.
Study design: Retrospective, cohort study.
Setting: 60 U.S. medical centers.
Synopsis: Using discharge data from the University Health System Consortium, 504,208 hospitalizations of cancer patients revealed that 14% of patients received at least one RBC transfusion and 3% of patients received a platelet transfusion. RBC and platelet transfusions were associated with increased risk of arterial thrombosis (RBCs: OR 1.53; 95% CI 1.46-1.61; platelets: OR 1.55; 1.4-1.71, P<0.001) and venous thrombotic events (RBCs: OR 1.34; 1.29-1.38; platelets: OR 1.2; 1.11-1.29, P<0.001). Additionally, transfusions were associated with increased in-hospital mortality (RBCs: OR 1.34; 1.29-1.38; platelets: OR 2.4; 2.27-2.52, P<0.001). Study results are limited by several factors, including the observational nature and the use of administrative coding data. Information on venous thromboembolism prophylaxis was not available, and the timing of transfusions in relation to the diagnosis of thrombotic events is unknown. Finally, anemia-necessitating transfusions may be a surrogate for "sicker" patients, explaining the increased in-hospital mortality. Blood transfusions in hospitalized patients require further study to determine whether there is a causal relationship between transfusions and increased thrombotic events and mortality.
Bottom line: Blood transfusions in hospitalized cancer patients should be used cautiously, as they are associated with increased thrombotic events and in-hospital mortality.
Citation: Arch Int Med. 2008;168:2377-2381
—Reviewed for the eWire by Kerry Will, MD, Jayne Barr, MD, Kim Tartaglia, MD, Aaron Wenger, MD, Jonathan Wynbrandt, MD, Nathan J. O’Dorisio, MD, The Ohio State University Medical Center, Columbus, OH.
Discharge Development
A multidisciplinary pre-discharge intervention—one that hospitalists can advocate for and help lead—resulted in a 30% reduction in hospital utilization within 30 days, according to a single-center study published in the Feb. 3 Annals of Internal Medicine (2009;150(3):178-187).
Researchers, including hospitalist Jeffrey Greenwald, MD, followed 749 adult patients over 30-day periods at Boston Medical Center to test the effects of a nurse discharge advocate program. A nurse arranged follow-up appointments and confirmed medication, while a clinical pharmacist called patients two to four days after discharge to reinforce the discharge plan.
"It isn't realistic that the hospitalists become the primary-care doctors after the discharge," says Dr. Greenwald, director of HM at Boston Medical Center and associate professor of medicine at Boston University School of Medicine. "It's critical that the hospitalists take a lead role in taking responsibility for the pitfalls into which the patients are likely to fall."
Dr. Greenwald thinks hospitalists can push for interventions at their respective centers to reduce rehospitalizations. The research team already is working on a new study to determine which measures could be automated to ensure their completion.
"All we're asking is that, as a team, you put in place the common stopgaps. ... None of this is gene therapy," Dr. Greenwald says. "This is low brain activity. The problem is that it's not low resource intense, and it's not low culture change."
Dr. Greenwald plans to submit information about his study to SHM's Project BOOST (Better Outcomes for Older Adults through Safe Transitions), a mentoring program meant to help hospitalists redesign their discharge process to improve patient outcomes. He says programs like Project BOOST are helping to draw attention to post-discharge protocols at hospitals around the country.
A multidisciplinary pre-discharge intervention—one that hospitalists can advocate for and help lead—resulted in a 30% reduction in hospital utilization within 30 days, according to a single-center study published in the Feb. 3 Annals of Internal Medicine (2009;150(3):178-187).
Researchers, including hospitalist Jeffrey Greenwald, MD, followed 749 adult patients over 30-day periods at Boston Medical Center to test the effects of a nurse discharge advocate program. A nurse arranged follow-up appointments and confirmed medication, while a clinical pharmacist called patients two to four days after discharge to reinforce the discharge plan.
"It isn't realistic that the hospitalists become the primary-care doctors after the discharge," says Dr. Greenwald, director of HM at Boston Medical Center and associate professor of medicine at Boston University School of Medicine. "It's critical that the hospitalists take a lead role in taking responsibility for the pitfalls into which the patients are likely to fall."
Dr. Greenwald thinks hospitalists can push for interventions at their respective centers to reduce rehospitalizations. The research team already is working on a new study to determine which measures could be automated to ensure their completion.
"All we're asking is that, as a team, you put in place the common stopgaps. ... None of this is gene therapy," Dr. Greenwald says. "This is low brain activity. The problem is that it's not low resource intense, and it's not low culture change."
Dr. Greenwald plans to submit information about his study to SHM's Project BOOST (Better Outcomes for Older Adults through Safe Transitions), a mentoring program meant to help hospitalists redesign their discharge process to improve patient outcomes. He says programs like Project BOOST are helping to draw attention to post-discharge protocols at hospitals around the country.
A multidisciplinary pre-discharge intervention—one that hospitalists can advocate for and help lead—resulted in a 30% reduction in hospital utilization within 30 days, according to a single-center study published in the Feb. 3 Annals of Internal Medicine (2009;150(3):178-187).
Researchers, including hospitalist Jeffrey Greenwald, MD, followed 749 adult patients over 30-day periods at Boston Medical Center to test the effects of a nurse discharge advocate program. A nurse arranged follow-up appointments and confirmed medication, while a clinical pharmacist called patients two to four days after discharge to reinforce the discharge plan.
"It isn't realistic that the hospitalists become the primary-care doctors after the discharge," says Dr. Greenwald, director of HM at Boston Medical Center and associate professor of medicine at Boston University School of Medicine. "It's critical that the hospitalists take a lead role in taking responsibility for the pitfalls into which the patients are likely to fall."
Dr. Greenwald thinks hospitalists can push for interventions at their respective centers to reduce rehospitalizations. The research team already is working on a new study to determine which measures could be automated to ensure their completion.
"All we're asking is that, as a team, you put in place the common stopgaps. ... None of this is gene therapy," Dr. Greenwald says. "This is low brain activity. The problem is that it's not low resource intense, and it's not low culture change."
Dr. Greenwald plans to submit information about his study to SHM's Project BOOST (Better Outcomes for Older Adults through Safe Transitions), a mentoring program meant to help hospitalists redesign their discharge process to improve patient outcomes. He says programs like Project BOOST are helping to draw attention to post-discharge protocols at hospitals around the country.
Pin the Pinworm
An 84‐year‐old female patient with hypertension, osteoarthritis, hypothyroidism, and remote breast cancer was admitted with complaints of generalized abdominal pain of 2 months' duration. Pain was described as noncolicky in nature and was associated with diarrhea. She reported 78 daily episodes of watery, non‐foul‐smelling diarrhea. She denied any nausea, vomiting, fever, joint pains, oral ulcers, eye redness, stool incontinence, melena, hematochezia, or weight loss. There was no history of recent travel, antibiotic use, or exposure to sick contacts. She had no risk factors for HIV infection or other sexually transmitted infections. Her social history was significant for dining out on a regular basis and living in an assisted living facility. However, she denied any relationship between her abdominal symptoms and any particular food intake or with bowel movements. She denied any anal pruritis but reported seeing white squiggly things on tissue paper after bowel movements. She denied use of over‐the‐counter laxatives or herbal supplements. None of her prescription medications had diarrhea as a major side effect. Her social history was unremarkable for smoking, alcohol use, or illicit drug use. There were no prior abdominal surgeries. The patient's physical exam showed normal vitals on presentation and was unremarkable except for vague, generalized abdominal tenderness with no involuntary guarding or rebound pain. Her initial laboratory evaluation showed normal complete blood counts with no eosinophilia and normal serum electrolytes and liver and thyroid panel. Acute‐phase reactants, erythrocyte sedimentation rate, and C‐reactive protein were not elevated. Stool evaluation was unremarkable for Clostridium difficile toxin, fat droplets, leukocytes, erythrocytes, ova, parasites, or any bacterial growth on cultures. Computed tomography scans of the abdomen and pelvis were nonrevealing. Her colonoscopic examination 1 year prior was significant only for diverticulosis.1, 2
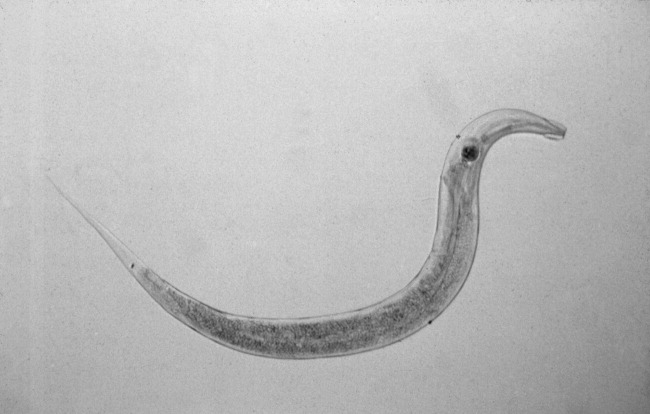
The patient was treated with loperamide as an outpatient with no relief. She was then admitted to the hospital for further diagnostic workup. Hospital workup included a Scotch tape test, which showed adult pinworms. She was treated with a single dose of 400 mg of albendazole with complete resolution of her symptoms within 2 days. No further workup was done. Patient was discharged with advice to contact her primary care doctor for reevaluation if symptoms recurred. However, the patient remained symptom free 1 year after discharge.
DISCUSSION
Enterobius vermicularis is a parasite that infects 2040 million people annually in the United States and about 200 million people worldwide. Equal infection rates are seen in all races, socioeconomic classes, and cultures.1 It is more prevalent among those in crowded living conditions. Humans are the primary natural host for the parasite, although it has been documented in cockroaches and primates. Transmission occurs via the feco‐oral route or via airborne eggs that are dislodged from contaminated clothing or bed linen. Its life cycle begins with parasite eggs hatching in the duodenum, usually within 6 hours of ingestion. They mature into adults in as little as 2 weeks and have a life span of approximately 2 months. Enterobius vermicularis normally inhabits distal small bowel including the terminal ileum, cecum, and vermiform appendix, as well as the proximal ascending colon. After copulation, an adult female will migrate to the perineum, often at night, and lay an average of 10,00015,000 eggs. These eggs mature in about 6 hours and are then transmitted to a new host by the feco‐oral route. The worms live mainly in the intestinal lumen and do not invade tissue. Hence, pinworm infections, unlike many other parasitic infections, are rarely associated with serum eosinophilia or elevated serum IgE levels.
E. vermicularis is generally considered to be an innocuous parasite. Perianal pruritis, especially during the nighttime, is the most common symptom. Patients may develop secondary bacterial infection of the irritated anal skin. Rarely, E. vermicularis infection may result in a life‐threatening illness. A literature review showed pinworm infection to be an infrequent cause of eosinophilic enterocolitis, appendicitis, intestinal obstruction, intestinal perforation, hepatic infection, urinary tract infection, sialoadenitis, salpingitis, enterocolitis, eosinophilic ileocolitis, vulvovaginitis, pelvic inflammatory disease, conditions mimicking inflammatory bowel diseases, perianal abscesses, and perianal granulomas. In a retrospective review of 180 colonoscopies done on patients with rectal bleeding or suspected inflammatory bowel disease, E. vermicularis was identified macroscopically in 31 cases (17.2%). Data collected on 23 of these cases showed that symptoms were present for a mean of 17 months; the symptoms with the highest frequency were abdominal pain (73%), rectal bleeding (62%), chronic diarrhea (50%), and weight loss (42%). None of these patients experienced perianal pruritis or developed inflammatory bowel disease during the follow‐up period of up to 5 years, although 21 patients demonstrated histopathological evidence of nonspecific colitis.6
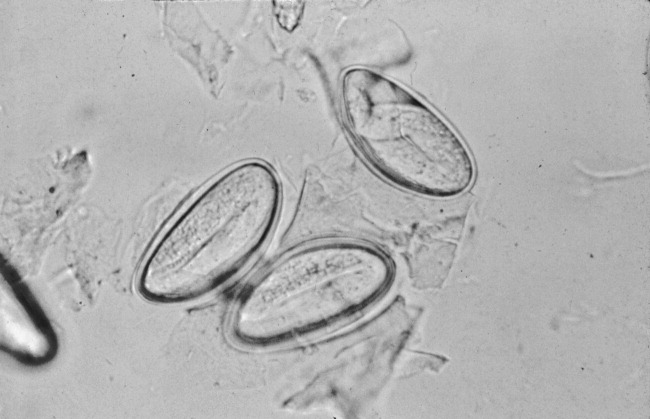
The gold standard for diagnosing E. vermicularis infection is by visualizing the worms directly or by examination of the parasitic eggs under a microscope. The Scotch tape test is a simple, inexpensive, and quick way for confirming the infection. It is performed by doubling clear cellophane Scotch tape onto a wooden stick so that the sticky side points outward and pressing it against the perianal skin. The kidney‐bean‐shaped eggs (50 25 m) will stick to the tape and can then be directly visualized under a microscope. Pinworms are most active during the night, and eggs are deposited around the perianal region and are best recovered before defecation, early in the morning. The sensitivity of this test is 90% if done on 3 consecutive mornings and goes up to 99% when performed on 5 consecutive mornings.2, 3 Female adult worms are pin‐shaped, about 813 mm long, and white in color. They may be seen by direct visualization in the perianal region or more invasively by an anoscopic or colonoscopic examination. However, endoscopic examination may sometimes give false‐negative results as the worms are small, (ie, only a few millimeters in length) and may be missed if the endoscopist is not actively looking for them.
A single oral dose of benzimidazoles (100 mg of mebendazole or 400 mg of albendazole) results in a cure of rate of 95% and 100%, respectively. Despite the high initial cure rates, reinfection remains common; hence, a second dose 12 weeks after the initial treatment is often given to prevent it.4, 5 Pyrantel pamoate and piperazine are alternate treatments. However, they have lower efficacy and are more toxic than benzimidazoles.
Close contacts such as household members are often concurrently infected, and treatment of the remaining household members or of the group institution is also indicated. All bedding and clothes should be laundered. Personal hygiene such as fingernail clipping, frequent hand washing, and bathing should also be encouraged.
Although the pinworm's entire life cycle is in the human intestinal tract, gastrointestinal symptoms have seldom been reported. However, this may be because of underreporting. Given the increasing number of patients living in institutionalized environments such as nursing homes and assisted living, it is important to consider the possibility of E. vermicularis infection early on in a diagnostic workup of patients presenting with symptoms of colitis, even when not accompanied by anal pruritis. In a patient presenting with symptoms of inflammatory bowel disease with histopathological evaluation of nonspecific colitis should prompt clinicians to consider E. vermicularis infection.6 On the other hand, in patients who fail to respond to antiparasitic therapy or those who present with weight loss, change in bowel habits, or melena, colonscopic examination is warranted. Considering pinworm infection early during evaluation of nonspecific abdominal complaints may avoid an unnecessary and expensive diagnostic workup.
KEY POINTS
-
Recognize early on that Enterobius vermicularis infection is an important differential diagnosis for patients presenting with symptoms of colitis, thus avoiding unnecessary, expensive, and potentially harmful invasive testing.
-
Recognize that a simple and inexpensive Scotch tape test and/or direct visualization is an easy and effective way of confirming diagnosis and that stool examination may be unhelpful.
-
Recognize that reinfection may be prevented using a second dose of the antiparasitic drug.
- .The pinworm, Enterobius vermicularis.Prim Care.1991;18:13–24.
- ,,,,.Prevalence of intestinal parasites in three socioeconomically‐different regions of Sivas, Turkey.J Health Popul Nutr.2005;23:184–191.
- ,,,.Pinworm infection.Gastrointest Endosc.2001;53:210.
- ,,.Mebendazole (R 17635) in enterobiasis. A clinical trial in mental retardates.Chemotherapy.1975;21:255–260.
- ,,, et al.Field trials on the efficacy of albendazole composite against intestinal nematodiasis.Chung Kuo Chi Sheng Chung Hsueh Yu Chi Sheng Chung Ping Tsa Chih.1998;16:1–5.
- ,,.Enterobius vermicularis and colitis in children.J Pediatr Gastroenterol Nutr.2006;43:610–612.
An 84‐year‐old female patient with hypertension, osteoarthritis, hypothyroidism, and remote breast cancer was admitted with complaints of generalized abdominal pain of 2 months' duration. Pain was described as noncolicky in nature and was associated with diarrhea. She reported 78 daily episodes of watery, non‐foul‐smelling diarrhea. She denied any nausea, vomiting, fever, joint pains, oral ulcers, eye redness, stool incontinence, melena, hematochezia, or weight loss. There was no history of recent travel, antibiotic use, or exposure to sick contacts. She had no risk factors for HIV infection or other sexually transmitted infections. Her social history was significant for dining out on a regular basis and living in an assisted living facility. However, she denied any relationship between her abdominal symptoms and any particular food intake or with bowel movements. She denied any anal pruritis but reported seeing white squiggly things on tissue paper after bowel movements. She denied use of over‐the‐counter laxatives or herbal supplements. None of her prescription medications had diarrhea as a major side effect. Her social history was unremarkable for smoking, alcohol use, or illicit drug use. There were no prior abdominal surgeries. The patient's physical exam showed normal vitals on presentation and was unremarkable except for vague, generalized abdominal tenderness with no involuntary guarding or rebound pain. Her initial laboratory evaluation showed normal complete blood counts with no eosinophilia and normal serum electrolytes and liver and thyroid panel. Acute‐phase reactants, erythrocyte sedimentation rate, and C‐reactive protein were not elevated. Stool evaluation was unremarkable for Clostridium difficile toxin, fat droplets, leukocytes, erythrocytes, ova, parasites, or any bacterial growth on cultures. Computed tomography scans of the abdomen and pelvis were nonrevealing. Her colonoscopic examination 1 year prior was significant only for diverticulosis.1, 2
The patient was treated with loperamide as an outpatient with no relief. She was then admitted to the hospital for further diagnostic workup. Hospital workup included a Scotch tape test, which showed adult pinworms. She was treated with a single dose of 400 mg of albendazole with complete resolution of her symptoms within 2 days. No further workup was done. Patient was discharged with advice to contact her primary care doctor for reevaluation if symptoms recurred. However, the patient remained symptom free 1 year after discharge.
DISCUSSION
Enterobius vermicularis is a parasite that infects 2040 million people annually in the United States and about 200 million people worldwide. Equal infection rates are seen in all races, socioeconomic classes, and cultures.1 It is more prevalent among those in crowded living conditions. Humans are the primary natural host for the parasite, although it has been documented in cockroaches and primates. Transmission occurs via the feco‐oral route or via airborne eggs that are dislodged from contaminated clothing or bed linen. Its life cycle begins with parasite eggs hatching in the duodenum, usually within 6 hours of ingestion. They mature into adults in as little as 2 weeks and have a life span of approximately 2 months. Enterobius vermicularis normally inhabits distal small bowel including the terminal ileum, cecum, and vermiform appendix, as well as the proximal ascending colon. After copulation, an adult female will migrate to the perineum, often at night, and lay an average of 10,00015,000 eggs. These eggs mature in about 6 hours and are then transmitted to a new host by the feco‐oral route. The worms live mainly in the intestinal lumen and do not invade tissue. Hence, pinworm infections, unlike many other parasitic infections, are rarely associated with serum eosinophilia or elevated serum IgE levels.
E. vermicularis is generally considered to be an innocuous parasite. Perianal pruritis, especially during the nighttime, is the most common symptom. Patients may develop secondary bacterial infection of the irritated anal skin. Rarely, E. vermicularis infection may result in a life‐threatening illness. A literature review showed pinworm infection to be an infrequent cause of eosinophilic enterocolitis, appendicitis, intestinal obstruction, intestinal perforation, hepatic infection, urinary tract infection, sialoadenitis, salpingitis, enterocolitis, eosinophilic ileocolitis, vulvovaginitis, pelvic inflammatory disease, conditions mimicking inflammatory bowel diseases, perianal abscesses, and perianal granulomas. In a retrospective review of 180 colonoscopies done on patients with rectal bleeding or suspected inflammatory bowel disease, E. vermicularis was identified macroscopically in 31 cases (17.2%). Data collected on 23 of these cases showed that symptoms were present for a mean of 17 months; the symptoms with the highest frequency were abdominal pain (73%), rectal bleeding (62%), chronic diarrhea (50%), and weight loss (42%). None of these patients experienced perianal pruritis or developed inflammatory bowel disease during the follow‐up period of up to 5 years, although 21 patients demonstrated histopathological evidence of nonspecific colitis.6
The gold standard for diagnosing E. vermicularis infection is by visualizing the worms directly or by examination of the parasitic eggs under a microscope. The Scotch tape test is a simple, inexpensive, and quick way for confirming the infection. It is performed by doubling clear cellophane Scotch tape onto a wooden stick so that the sticky side points outward and pressing it against the perianal skin. The kidney‐bean‐shaped eggs (50 25 m) will stick to the tape and can then be directly visualized under a microscope. Pinworms are most active during the night, and eggs are deposited around the perianal region and are best recovered before defecation, early in the morning. The sensitivity of this test is 90% if done on 3 consecutive mornings and goes up to 99% when performed on 5 consecutive mornings.2, 3 Female adult worms are pin‐shaped, about 813 mm long, and white in color. They may be seen by direct visualization in the perianal region or more invasively by an anoscopic or colonoscopic examination. However, endoscopic examination may sometimes give false‐negative results as the worms are small, (ie, only a few millimeters in length) and may be missed if the endoscopist is not actively looking for them.
A single oral dose of benzimidazoles (100 mg of mebendazole or 400 mg of albendazole) results in a cure of rate of 95% and 100%, respectively. Despite the high initial cure rates, reinfection remains common; hence, a second dose 12 weeks after the initial treatment is often given to prevent it.4, 5 Pyrantel pamoate and piperazine are alternate treatments. However, they have lower efficacy and are more toxic than benzimidazoles.
Close contacts such as household members are often concurrently infected, and treatment of the remaining household members or of the group institution is also indicated. All bedding and clothes should be laundered. Personal hygiene such as fingernail clipping, frequent hand washing, and bathing should also be encouraged.
Although the pinworm's entire life cycle is in the human intestinal tract, gastrointestinal symptoms have seldom been reported. However, this may be because of underreporting. Given the increasing number of patients living in institutionalized environments such as nursing homes and assisted living, it is important to consider the possibility of E. vermicularis infection early on in a diagnostic workup of patients presenting with symptoms of colitis, even when not accompanied by anal pruritis. In a patient presenting with symptoms of inflammatory bowel disease with histopathological evaluation of nonspecific colitis should prompt clinicians to consider E. vermicularis infection.6 On the other hand, in patients who fail to respond to antiparasitic therapy or those who present with weight loss, change in bowel habits, or melena, colonscopic examination is warranted. Considering pinworm infection early during evaluation of nonspecific abdominal complaints may avoid an unnecessary and expensive diagnostic workup.
KEY POINTS
-
Recognize early on that Enterobius vermicularis infection is an important differential diagnosis for patients presenting with symptoms of colitis, thus avoiding unnecessary, expensive, and potentially harmful invasive testing.
-
Recognize that a simple and inexpensive Scotch tape test and/or direct visualization is an easy and effective way of confirming diagnosis and that stool examination may be unhelpful.
-
Recognize that reinfection may be prevented using a second dose of the antiparasitic drug.
An 84‐year‐old female patient with hypertension, osteoarthritis, hypothyroidism, and remote breast cancer was admitted with complaints of generalized abdominal pain of 2 months' duration. Pain was described as noncolicky in nature and was associated with diarrhea. She reported 78 daily episodes of watery, non‐foul‐smelling diarrhea. She denied any nausea, vomiting, fever, joint pains, oral ulcers, eye redness, stool incontinence, melena, hematochezia, or weight loss. There was no history of recent travel, antibiotic use, or exposure to sick contacts. She had no risk factors for HIV infection or other sexually transmitted infections. Her social history was significant for dining out on a regular basis and living in an assisted living facility. However, she denied any relationship between her abdominal symptoms and any particular food intake or with bowel movements. She denied any anal pruritis but reported seeing white squiggly things on tissue paper after bowel movements. She denied use of over‐the‐counter laxatives or herbal supplements. None of her prescription medications had diarrhea as a major side effect. Her social history was unremarkable for smoking, alcohol use, or illicit drug use. There were no prior abdominal surgeries. The patient's physical exam showed normal vitals on presentation and was unremarkable except for vague, generalized abdominal tenderness with no involuntary guarding or rebound pain. Her initial laboratory evaluation showed normal complete blood counts with no eosinophilia and normal serum electrolytes and liver and thyroid panel. Acute‐phase reactants, erythrocyte sedimentation rate, and C‐reactive protein were not elevated. Stool evaluation was unremarkable for Clostridium difficile toxin, fat droplets, leukocytes, erythrocytes, ova, parasites, or any bacterial growth on cultures. Computed tomography scans of the abdomen and pelvis were nonrevealing. Her colonoscopic examination 1 year prior was significant only for diverticulosis.1, 2
The patient was treated with loperamide as an outpatient with no relief. She was then admitted to the hospital for further diagnostic workup. Hospital workup included a Scotch tape test, which showed adult pinworms. She was treated with a single dose of 400 mg of albendazole with complete resolution of her symptoms within 2 days. No further workup was done. Patient was discharged with advice to contact her primary care doctor for reevaluation if symptoms recurred. However, the patient remained symptom free 1 year after discharge.
DISCUSSION
Enterobius vermicularis is a parasite that infects 2040 million people annually in the United States and about 200 million people worldwide. Equal infection rates are seen in all races, socioeconomic classes, and cultures.1 It is more prevalent among those in crowded living conditions. Humans are the primary natural host for the parasite, although it has been documented in cockroaches and primates. Transmission occurs via the feco‐oral route or via airborne eggs that are dislodged from contaminated clothing or bed linen. Its life cycle begins with parasite eggs hatching in the duodenum, usually within 6 hours of ingestion. They mature into adults in as little as 2 weeks and have a life span of approximately 2 months. Enterobius vermicularis normally inhabits distal small bowel including the terminal ileum, cecum, and vermiform appendix, as well as the proximal ascending colon. After copulation, an adult female will migrate to the perineum, often at night, and lay an average of 10,00015,000 eggs. These eggs mature in about 6 hours and are then transmitted to a new host by the feco‐oral route. The worms live mainly in the intestinal lumen and do not invade tissue. Hence, pinworm infections, unlike many other parasitic infections, are rarely associated with serum eosinophilia or elevated serum IgE levels.
E. vermicularis is generally considered to be an innocuous parasite. Perianal pruritis, especially during the nighttime, is the most common symptom. Patients may develop secondary bacterial infection of the irritated anal skin. Rarely, E. vermicularis infection may result in a life‐threatening illness. A literature review showed pinworm infection to be an infrequent cause of eosinophilic enterocolitis, appendicitis, intestinal obstruction, intestinal perforation, hepatic infection, urinary tract infection, sialoadenitis, salpingitis, enterocolitis, eosinophilic ileocolitis, vulvovaginitis, pelvic inflammatory disease, conditions mimicking inflammatory bowel diseases, perianal abscesses, and perianal granulomas. In a retrospective review of 180 colonoscopies done on patients with rectal bleeding or suspected inflammatory bowel disease, E. vermicularis was identified macroscopically in 31 cases (17.2%). Data collected on 23 of these cases showed that symptoms were present for a mean of 17 months; the symptoms with the highest frequency were abdominal pain (73%), rectal bleeding (62%), chronic diarrhea (50%), and weight loss (42%). None of these patients experienced perianal pruritis or developed inflammatory bowel disease during the follow‐up period of up to 5 years, although 21 patients demonstrated histopathological evidence of nonspecific colitis.6
The gold standard for diagnosing E. vermicularis infection is by visualizing the worms directly or by examination of the parasitic eggs under a microscope. The Scotch tape test is a simple, inexpensive, and quick way for confirming the infection. It is performed by doubling clear cellophane Scotch tape onto a wooden stick so that the sticky side points outward and pressing it against the perianal skin. The kidney‐bean‐shaped eggs (50 25 m) will stick to the tape and can then be directly visualized under a microscope. Pinworms are most active during the night, and eggs are deposited around the perianal region and are best recovered before defecation, early in the morning. The sensitivity of this test is 90% if done on 3 consecutive mornings and goes up to 99% when performed on 5 consecutive mornings.2, 3 Female adult worms are pin‐shaped, about 813 mm long, and white in color. They may be seen by direct visualization in the perianal region or more invasively by an anoscopic or colonoscopic examination. However, endoscopic examination may sometimes give false‐negative results as the worms are small, (ie, only a few millimeters in length) and may be missed if the endoscopist is not actively looking for them.
A single oral dose of benzimidazoles (100 mg of mebendazole or 400 mg of albendazole) results in a cure of rate of 95% and 100%, respectively. Despite the high initial cure rates, reinfection remains common; hence, a second dose 12 weeks after the initial treatment is often given to prevent it.4, 5 Pyrantel pamoate and piperazine are alternate treatments. However, they have lower efficacy and are more toxic than benzimidazoles.
Close contacts such as household members are often concurrently infected, and treatment of the remaining household members or of the group institution is also indicated. All bedding and clothes should be laundered. Personal hygiene such as fingernail clipping, frequent hand washing, and bathing should also be encouraged.
Although the pinworm's entire life cycle is in the human intestinal tract, gastrointestinal symptoms have seldom been reported. However, this may be because of underreporting. Given the increasing number of patients living in institutionalized environments such as nursing homes and assisted living, it is important to consider the possibility of E. vermicularis infection early on in a diagnostic workup of patients presenting with symptoms of colitis, even when not accompanied by anal pruritis. In a patient presenting with symptoms of inflammatory bowel disease with histopathological evaluation of nonspecific colitis should prompt clinicians to consider E. vermicularis infection.6 On the other hand, in patients who fail to respond to antiparasitic therapy or those who present with weight loss, change in bowel habits, or melena, colonscopic examination is warranted. Considering pinworm infection early during evaluation of nonspecific abdominal complaints may avoid an unnecessary and expensive diagnostic workup.
KEY POINTS
-
Recognize early on that Enterobius vermicularis infection is an important differential diagnosis for patients presenting with symptoms of colitis, thus avoiding unnecessary, expensive, and potentially harmful invasive testing.
-
Recognize that a simple and inexpensive Scotch tape test and/or direct visualization is an easy and effective way of confirming diagnosis and that stool examination may be unhelpful.
-
Recognize that reinfection may be prevented using a second dose of the antiparasitic drug.
- .The pinworm, Enterobius vermicularis.Prim Care.1991;18:13–24.
- ,,,,.Prevalence of intestinal parasites in three socioeconomically‐different regions of Sivas, Turkey.J Health Popul Nutr.2005;23:184–191.
- ,,,.Pinworm infection.Gastrointest Endosc.2001;53:210.
- ,,.Mebendazole (R 17635) in enterobiasis. A clinical trial in mental retardates.Chemotherapy.1975;21:255–260.
- ,,, et al.Field trials on the efficacy of albendazole composite against intestinal nematodiasis.Chung Kuo Chi Sheng Chung Hsueh Yu Chi Sheng Chung Ping Tsa Chih.1998;16:1–5.
- ,,.Enterobius vermicularis and colitis in children.J Pediatr Gastroenterol Nutr.2006;43:610–612.
- .The pinworm, Enterobius vermicularis.Prim Care.1991;18:13–24.
- ,,,,.Prevalence of intestinal parasites in three socioeconomically‐different regions of Sivas, Turkey.J Health Popul Nutr.2005;23:184–191.
- ,,,.Pinworm infection.Gastrointest Endosc.2001;53:210.
- ,,.Mebendazole (R 17635) in enterobiasis. A clinical trial in mental retardates.Chemotherapy.1975;21:255–260.
- ,,, et al.Field trials on the efficacy of albendazole composite against intestinal nematodiasis.Chung Kuo Chi Sheng Chung Hsueh Yu Chi Sheng Chung Ping Tsa Chih.1998;16:1–5.
- ,,.Enterobius vermicularis and colitis in children.J Pediatr Gastroenterol Nutr.2006;43:610–612.

Polymorphic Ventricular Tachycardia?
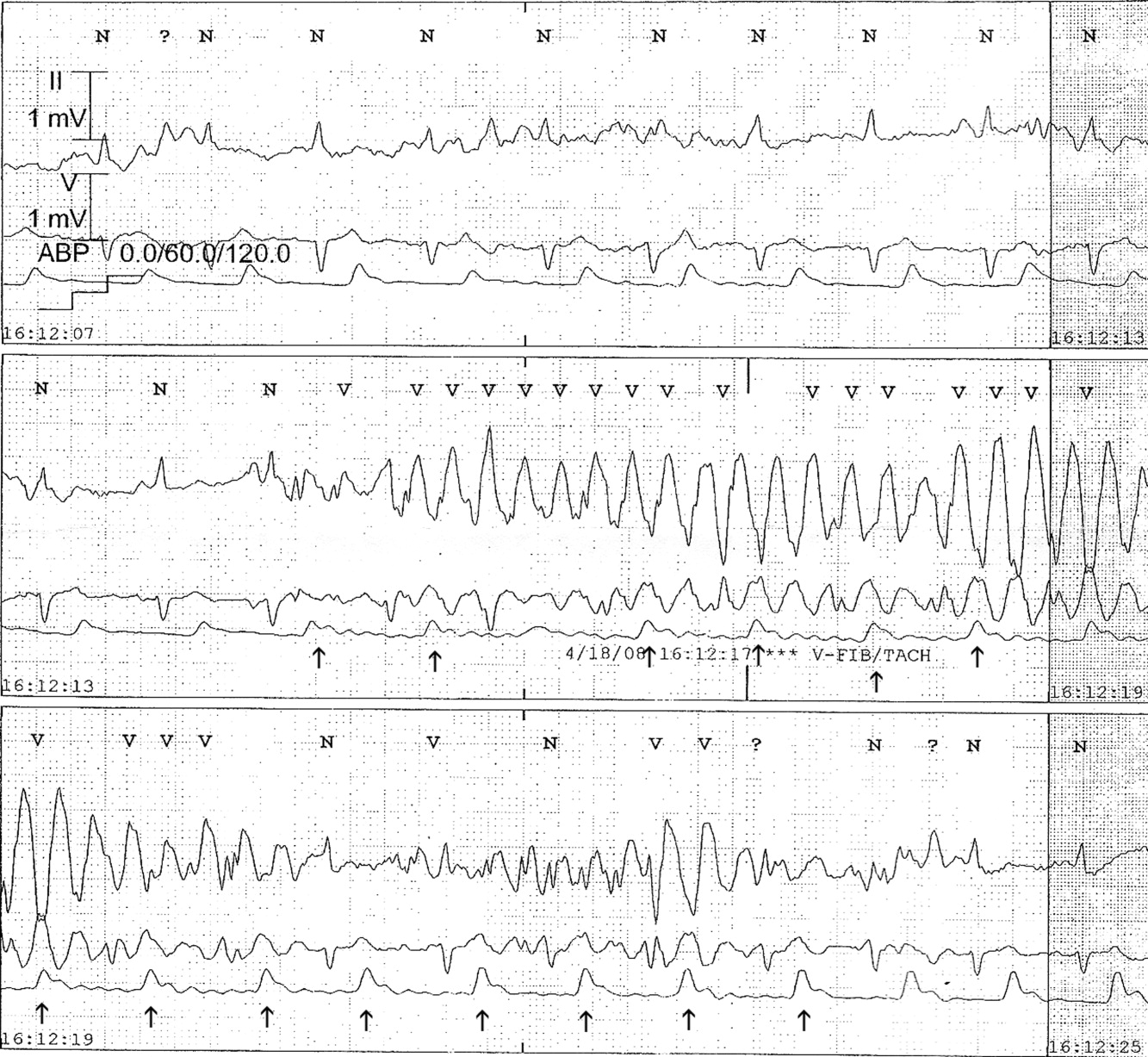
The medical team was called emergently from the telemetry station in response to the tracing shown in Figure 1. The patient was a 65‐year‐old woman with paroxysmal atrial fibrillation and no structural heart disease. The medical team arrived at the bedside to find the patient chatting with her family with a heart rate of 95 and blood pressure of 144/92. The patient had been awake and alert throughout the episode. Initial inspection of the rhythm strip (Figure 1) shows what appears to be nonsustained polymorphic ventricular tachycardia followed by normal QRS complexes. Upon careful inspection of the V1 (lower) tracing, the QRS complexes can be marched backward through the wide complexes to the beginning of the strip, as shown in Figure 2 (arrows), indicating that the wide complexes are artifact.


The presence of artifact is confirmed in Figure 3, in which the arterial blood pressure (ABP) waveform follows the QRS complexes. In polymorphic ventricular tachycardia, the ABP would have fallen and the waveform would have been chaotic. Failure to differentiate between artifact and ventricular tachycardia can lead to inappropriate management.1, 2 The artifact in this case is likely due to electrode motion and emphasizes the importance of using all the available data when evaluating rhythm strips. Critical evaluation of multiple electrocardiographic (ECG) leads is the cornerstone of diagnosis; continuous arterial monitoring, if available, can be useful for confirmation.
- ,,.Approach to the diagnosis and initial management of the stable adult patient with a wide complex tachycardia.Am J Cardiol.2008;101(10):1456–1466.
- ,,,,.Physician interpretation of electrocardiographic artifact that mimics ventricular tachycardia.Am J Med.2001;110(5):335–338.
The medical team was called emergently from the telemetry station in response to the tracing shown in Figure 1. The patient was a 65‐year‐old woman with paroxysmal atrial fibrillation and no structural heart disease. The medical team arrived at the bedside to find the patient chatting with her family with a heart rate of 95 and blood pressure of 144/92. The patient had been awake and alert throughout the episode. Initial inspection of the rhythm strip (Figure 1) shows what appears to be nonsustained polymorphic ventricular tachycardia followed by normal QRS complexes. Upon careful inspection of the V1 (lower) tracing, the QRS complexes can be marched backward through the wide complexes to the beginning of the strip, as shown in Figure 2 (arrows), indicating that the wide complexes are artifact.
The presence of artifact is confirmed in Figure 3, in which the arterial blood pressure (ABP) waveform follows the QRS complexes. In polymorphic ventricular tachycardia, the ABP would have fallen and the waveform would have been chaotic. Failure to differentiate between artifact and ventricular tachycardia can lead to inappropriate management.1, 2 The artifact in this case is likely due to electrode motion and emphasizes the importance of using all the available data when evaluating rhythm strips. Critical evaluation of multiple electrocardiographic (ECG) leads is the cornerstone of diagnosis; continuous arterial monitoring, if available, can be useful for confirmation.
The medical team was called emergently from the telemetry station in response to the tracing shown in Figure 1. The patient was a 65‐year‐old woman with paroxysmal atrial fibrillation and no structural heart disease. The medical team arrived at the bedside to find the patient chatting with her family with a heart rate of 95 and blood pressure of 144/92. The patient had been awake and alert throughout the episode. Initial inspection of the rhythm strip (Figure 1) shows what appears to be nonsustained polymorphic ventricular tachycardia followed by normal QRS complexes. Upon careful inspection of the V1 (lower) tracing, the QRS complexes can be marched backward through the wide complexes to the beginning of the strip, as shown in Figure 2 (arrows), indicating that the wide complexes are artifact.
The presence of artifact is confirmed in Figure 3, in which the arterial blood pressure (ABP) waveform follows the QRS complexes. In polymorphic ventricular tachycardia, the ABP would have fallen and the waveform would have been chaotic. Failure to differentiate between artifact and ventricular tachycardia can lead to inappropriate management.1, 2 The artifact in this case is likely due to electrode motion and emphasizes the importance of using all the available data when evaluating rhythm strips. Critical evaluation of multiple electrocardiographic (ECG) leads is the cornerstone of diagnosis; continuous arterial monitoring, if available, can be useful for confirmation.
- ,,.Approach to the diagnosis and initial management of the stable adult patient with a wide complex tachycardia.Am J Cardiol.2008;101(10):1456–1466.
- ,,,,.Physician interpretation of electrocardiographic artifact that mimics ventricular tachycardia.Am J Med.2001;110(5):335–338.
- ,,.Approach to the diagnosis and initial management of the stable adult patient with a wide complex tachycardia.Am J Cardiol.2008;101(10):1456–1466.
- ,,,,.Physician interpretation of electrocardiographic artifact that mimics ventricular tachycardia.Am J Med.2001;110(5):335–338.

CIPNM in Disseminated Cryptococcal Infection
Critical illness polyneuromyopathy (CIPNM) is frequent among critically‐ill patients.1, 2 CIPNM develops in critically‐ill patients with systemic inflammatory response syndrome, sepsis, or multiple organ failure. We report a case of disseminated cryptococcal infection in a critically‐ill patient who presented with treatment‐refractory cellulitis. His recovery was complicated by difficulty in weaning from mechanical ventilation due to CIPNM.
CASE REPORT
A 49‐year‐old man developed skin swelling and tenderness over his right thigh 1 month prior to admission at a local hospital. He was a pigeon breeder by profession. His medical history was significant for hypertension and poorly controlled diabetes mellitus. His medications included prednisolone (15 mg per day), which he was taking for his chronic arthritis for about 6 months. He was admitted for treatment of cellulitis. Despite antibiotic treatment with ampicillin and sulbactam, his skin lesion became necrotic and gangrenous. Wound healing remained poor even after wound debridement. Patient developed dyspnea 2 weeks after admission and was transferred to the intensive care unit (ICU) of National Taiwan University Hospital for further management.
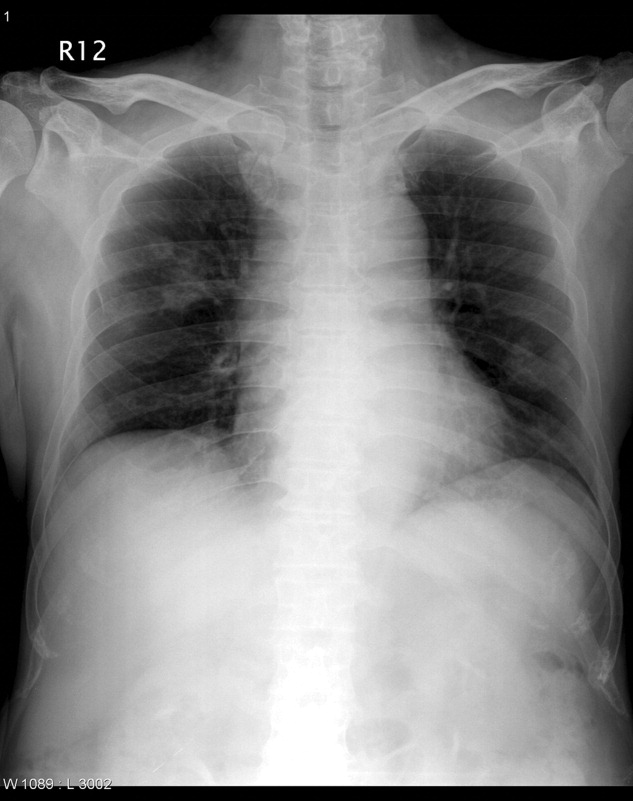
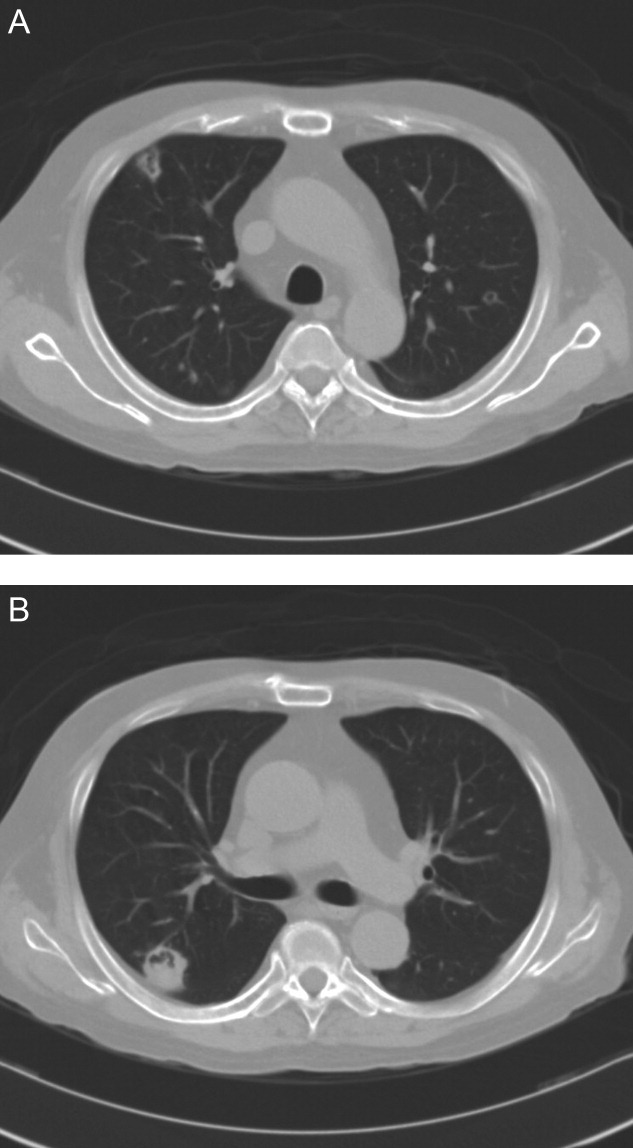
On transfer to ICU, he was drowsy and had an ear temperature of 37.1C, pulse rate of 108 beats/minute, blood pressure of 132/82 mm Hg, and respiratory rate of 20 breaths/minutes. His pupils were isocoric with prompt light reflex. His right thigh wound was 6 cm in length with eschar formation and focal erythema. His total white blood cell count was 14.08 109 cells/L with 72.2% polymorphonuclear leukocytes. His blood glucose level was 326 mg/dL. Other blood work, including hemoglobin, coagulation studies, and renal and liver function tests, were within normal range. Urinalysis was positive for glucose, but there was no hematuria, pyuria, or ketonuria. The chest radiograph (Figure 1) showed small nodules and peripheral infiltrates in both lung fields. Chest computerized tomogram (CT) scans found multiple cavitated lung nodules (Figure 2A,B). Human immunodeficiency virus (HIV) screening test was negative.
Soon after transfer to the ICU, the patient developed respiratory distress and became hemodynamically unstable. He was intubated and resuscitation efforts were started to stabilize him. Yeast‐like organisms were found in the debrided tissue. CT‐guided biopsy of the pulmonary nodules also found yeast‐like organisms. Tissue cultures of skin wound and lung biopsy grew Cryptococcus neoformans. He was diagnosed with disseminated cryptococcal infection and Amphotericin B was started. His hemodynamic status stabilized 2 days after the start of Amphotericin B. Follow‐up chest radiograph 1 week after starting Amphotericin B treatment showed resolution of pulmonary nodules. His right thigh skin lesion also healed gradually.
Unfortunately, he developed severe weakness of all extremities on the fourteenth ICU day, and had difficulty weaning from mechanical ventilation. Neurological examination found diffuse hyporeflexia. The nerve conduction velocity (NCV) study showed decreased amplitude in nerve conduction, with normal velocity. Electromyogram (EMG) found diffuse muscular fibrillation. Based on these findings, CIPNM was diagnosed. Patient underwent tracheostomy on the twenty‐sixth ICU day due to the need for prolonged mechanical ventilation. His antifungal therapy was changed to intravenous fluconazole 600 mg per day. Blood glucose levels were controlled with continuous insulin infusion and insulin dose was titrated to keep the blood glucose below 120 mg/dL. He was finally weaned from mechanical ventilation on the forty‐seventh day of ICU admission, and was transferred to the general ward. With physical therapy, he resumed his daily activities and was discharged from the hospital.
DISCUSSION
Cryptococcus rarely causes disseminated infection in healthy individuals. The vast majority of patients with cryptococcosis are immunocompromised due to conditions such as acquired immunodeficiency syndrome, prolonged treatment with corticosteroids, organ transplantation, malignancy, or diabetes mellitus.3, 4 The patient in this report had 2 of the documented risk factors. In a study of 52 disseminated cryptococcosis patients, the most prevalent underlying condition was HIV infection (46%). Out of these 52 patients, 28 were HIV‐negative, and only 3 of them had no predisposing condition.4 Cutaneous cryptococcus infection could be a manifestation of disseminated cryptococcal infection, or may be a primary disease that would evolve into systemic disease several months later.5, 6 The incidence of primary cutaneous cryptococcosis is much lower than systemic disease with cutaneous manifestation. Cellulitis, which is refractory to treatment with traditional antibacterial agents, should lead to consideration of fungal cellulites, such as cutaneous cryptococcosis or aspergillosis. Once cryptococcal cellulitis is diagnosed, other foci of cryptococcal infection should be sought.
CIPNM includes myopathies, acute neuropathies, neuromuscular transmission defects, or any combination of these disorders.2, 7 CIPNM might arise in ICU patients who have systemic inflammatory response syndrome (SIRS), sepsis, or multiple organ failure. In patients with new onset limb weakness, disuse hyporeflexia, and difficulty in weaning from mechanical ventilation, CIPNM should be among the differential diagnoses. In 1 prospective trial, de Letter et al.8 found CIPNM incidence of 33% in 98 ICU patients. A high APACHE III score, SIRS, and the use of aminoglycoside antibiotics are significant risk factors for the development of CIPNM. In various studies, the incidence of CIPNM ranges from 13% to 76%.2, 710
The definitive diagnosis of CIPNM is established by EMG and NCV studies, which are characterized by (1) reduced amplitudes of compound muscles and sensory action potentials, (2) relatively normal conduction studies, and (3) widespread fibrillations and sharp waves.2 The mean mortality of patients who have developed CIPNM is 35%, with a range from 0% to 73%. About 45% of patients completely recover from CIPNM within 6 weeks to 12 months (with a mean duration of 4.5 months), with good supportive care, provided the underlying condition has been treated.2, 9 There is little evidence to support a specific treatment modality for CIPNM. Mohr et al.1 reported that intravenous immunoglobulin may prevent or ameliorate CIPNM in the ICU, but more prospective and placebo‐controlled studies are needed to confirm their result. In recent studies,11 strict blood glucose control with insulin was found to reduce the risk of CIPNM and duration of mechanical ventilation in both medical and surgical ICU patients.
In conclusion, CIPNM occurs frequently in ICU patients with SIRS, sepsis, or multiple organ failure, leading to prolonged ventilator dependence and increased morbidity and mortality. Risk factor prevention and intensive insulin treatment may reduce the incident of CIPNM and the duration of mechanical ventilation in ICU patients.
- ,,,,.Effects of early treatment with immunoglobulin on critical illness polyneuropathy following multiple organ failure and gram‐negative sepsis.Intensive Care Med.1997;23:1144–1149.
- .Critical illness polyneuropathy and myopathy: clinical features, risk factors and prognosis.Eur J Neurol.2006;13:1203–1212.
- .Cryptococcus neoformans. In:Mandell GL,Bennett JE,Dolin R, eds.Principles and Practice of Infectious Diseases.Philadelphia:Churchill Livingstone;2000:2707–2718.
- ,,, et al.Cryptococcameia: clinical features and prognostic factors.Q J Med.2002;95:511–518.
- ,,.Primary cutaneous cryptococcal cellulitis secondary to insect bite in an immunosuppressed patient after liver transplantation.Clin Exp Dermatol.2005;30:241–243.
- ,.Primary cutaneous cryptococcosis as the presenting manifestation of AIDS.Plast Reconstr Surg.1992;90:1065–1067.
- ,,,,.Effect of critical illness polyneuropathy on the withdrawal from mechanical ventilation and the length of stay in septic patients.Crit Care Med.2005;33:349–354.
- ,,, et al.Critical illness polyneuropathy and myopathy (CIPNM): evidence for local immune activation by cytokine‐expression in the muscle tissue.J Neuroimmunol.2000;106:206–213.
- ,.Critical illness neuromuscular abnormalities.Crit Care Clin.2002;18:553–568.
- ,,,,,.Neuromuscular disorders associated with failure to wean from the ventilator.Intensive Care Med.1995;21:737–743.
- ,,, et al.Impact of intensive insulin therapy on neuromuscular complications and ventilator‐dependency in MICU.Am J Respir Crit Care Med.2007;175:480–489.
Critical illness polyneuromyopathy (CIPNM) is frequent among critically‐ill patients.1, 2 CIPNM develops in critically‐ill patients with systemic inflammatory response syndrome, sepsis, or multiple organ failure. We report a case of disseminated cryptococcal infection in a critically‐ill patient who presented with treatment‐refractory cellulitis. His recovery was complicated by difficulty in weaning from mechanical ventilation due to CIPNM.
CASE REPORT
A 49‐year‐old man developed skin swelling and tenderness over his right thigh 1 month prior to admission at a local hospital. He was a pigeon breeder by profession. His medical history was significant for hypertension and poorly controlled diabetes mellitus. His medications included prednisolone (15 mg per day), which he was taking for his chronic arthritis for about 6 months. He was admitted for treatment of cellulitis. Despite antibiotic treatment with ampicillin and sulbactam, his skin lesion became necrotic and gangrenous. Wound healing remained poor even after wound debridement. Patient developed dyspnea 2 weeks after admission and was transferred to the intensive care unit (ICU) of National Taiwan University Hospital for further management.
On transfer to ICU, he was drowsy and had an ear temperature of 37.1C, pulse rate of 108 beats/minute, blood pressure of 132/82 mm Hg, and respiratory rate of 20 breaths/minutes. His pupils were isocoric with prompt light reflex. His right thigh wound was 6 cm in length with eschar formation and focal erythema. His total white blood cell count was 14.08 109 cells/L with 72.2% polymorphonuclear leukocytes. His blood glucose level was 326 mg/dL. Other blood work, including hemoglobin, coagulation studies, and renal and liver function tests, were within normal range. Urinalysis was positive for glucose, but there was no hematuria, pyuria, or ketonuria. The chest radiograph (Figure 1) showed small nodules and peripheral infiltrates in both lung fields. Chest computerized tomogram (CT) scans found multiple cavitated lung nodules (Figure 2A,B). Human immunodeficiency virus (HIV) screening test was negative.
Soon after transfer to the ICU, the patient developed respiratory distress and became hemodynamically unstable. He was intubated and resuscitation efforts were started to stabilize him. Yeast‐like organisms were found in the debrided tissue. CT‐guided biopsy of the pulmonary nodules also found yeast‐like organisms. Tissue cultures of skin wound and lung biopsy grew Cryptococcus neoformans. He was diagnosed with disseminated cryptococcal infection and Amphotericin B was started. His hemodynamic status stabilized 2 days after the start of Amphotericin B. Follow‐up chest radiograph 1 week after starting Amphotericin B treatment showed resolution of pulmonary nodules. His right thigh skin lesion also healed gradually.
Unfortunately, he developed severe weakness of all extremities on the fourteenth ICU day, and had difficulty weaning from mechanical ventilation. Neurological examination found diffuse hyporeflexia. The nerve conduction velocity (NCV) study showed decreased amplitude in nerve conduction, with normal velocity. Electromyogram (EMG) found diffuse muscular fibrillation. Based on these findings, CIPNM was diagnosed. Patient underwent tracheostomy on the twenty‐sixth ICU day due to the need for prolonged mechanical ventilation. His antifungal therapy was changed to intravenous fluconazole 600 mg per day. Blood glucose levels were controlled with continuous insulin infusion and insulin dose was titrated to keep the blood glucose below 120 mg/dL. He was finally weaned from mechanical ventilation on the forty‐seventh day of ICU admission, and was transferred to the general ward. With physical therapy, he resumed his daily activities and was discharged from the hospital.
DISCUSSION
Cryptococcus rarely causes disseminated infection in healthy individuals. The vast majority of patients with cryptococcosis are immunocompromised due to conditions such as acquired immunodeficiency syndrome, prolonged treatment with corticosteroids, organ transplantation, malignancy, or diabetes mellitus.3, 4 The patient in this report had 2 of the documented risk factors. In a study of 52 disseminated cryptococcosis patients, the most prevalent underlying condition was HIV infection (46%). Out of these 52 patients, 28 were HIV‐negative, and only 3 of them had no predisposing condition.4 Cutaneous cryptococcus infection could be a manifestation of disseminated cryptococcal infection, or may be a primary disease that would evolve into systemic disease several months later.5, 6 The incidence of primary cutaneous cryptococcosis is much lower than systemic disease with cutaneous manifestation. Cellulitis, which is refractory to treatment with traditional antibacterial agents, should lead to consideration of fungal cellulites, such as cutaneous cryptococcosis or aspergillosis. Once cryptococcal cellulitis is diagnosed, other foci of cryptococcal infection should be sought.
CIPNM includes myopathies, acute neuropathies, neuromuscular transmission defects, or any combination of these disorders.2, 7 CIPNM might arise in ICU patients who have systemic inflammatory response syndrome (SIRS), sepsis, or multiple organ failure. In patients with new onset limb weakness, disuse hyporeflexia, and difficulty in weaning from mechanical ventilation, CIPNM should be among the differential diagnoses. In 1 prospective trial, de Letter et al.8 found CIPNM incidence of 33% in 98 ICU patients. A high APACHE III score, SIRS, and the use of aminoglycoside antibiotics are significant risk factors for the development of CIPNM. In various studies, the incidence of CIPNM ranges from 13% to 76%.2, 710
The definitive diagnosis of CIPNM is established by EMG and NCV studies, which are characterized by (1) reduced amplitudes of compound muscles and sensory action potentials, (2) relatively normal conduction studies, and (3) widespread fibrillations and sharp waves.2 The mean mortality of patients who have developed CIPNM is 35%, with a range from 0% to 73%. About 45% of patients completely recover from CIPNM within 6 weeks to 12 months (with a mean duration of 4.5 months), with good supportive care, provided the underlying condition has been treated.2, 9 There is little evidence to support a specific treatment modality for CIPNM. Mohr et al.1 reported that intravenous immunoglobulin may prevent or ameliorate CIPNM in the ICU, but more prospective and placebo‐controlled studies are needed to confirm their result. In recent studies,11 strict blood glucose control with insulin was found to reduce the risk of CIPNM and duration of mechanical ventilation in both medical and surgical ICU patients.
In conclusion, CIPNM occurs frequently in ICU patients with SIRS, sepsis, or multiple organ failure, leading to prolonged ventilator dependence and increased morbidity and mortality. Risk factor prevention and intensive insulin treatment may reduce the incident of CIPNM and the duration of mechanical ventilation in ICU patients.
Critical illness polyneuromyopathy (CIPNM) is frequent among critically‐ill patients.1, 2 CIPNM develops in critically‐ill patients with systemic inflammatory response syndrome, sepsis, or multiple organ failure. We report a case of disseminated cryptococcal infection in a critically‐ill patient who presented with treatment‐refractory cellulitis. His recovery was complicated by difficulty in weaning from mechanical ventilation due to CIPNM.
CASE REPORT
A 49‐year‐old man developed skin swelling and tenderness over his right thigh 1 month prior to admission at a local hospital. He was a pigeon breeder by profession. His medical history was significant for hypertension and poorly controlled diabetes mellitus. His medications included prednisolone (15 mg per day), which he was taking for his chronic arthritis for about 6 months. He was admitted for treatment of cellulitis. Despite antibiotic treatment with ampicillin and sulbactam, his skin lesion became necrotic and gangrenous. Wound healing remained poor even after wound debridement. Patient developed dyspnea 2 weeks after admission and was transferred to the intensive care unit (ICU) of National Taiwan University Hospital for further management.
On transfer to ICU, he was drowsy and had an ear temperature of 37.1C, pulse rate of 108 beats/minute, blood pressure of 132/82 mm Hg, and respiratory rate of 20 breaths/minutes. His pupils were isocoric with prompt light reflex. His right thigh wound was 6 cm in length with eschar formation and focal erythema. His total white blood cell count was 14.08 109 cells/L with 72.2% polymorphonuclear leukocytes. His blood glucose level was 326 mg/dL. Other blood work, including hemoglobin, coagulation studies, and renal and liver function tests, were within normal range. Urinalysis was positive for glucose, but there was no hematuria, pyuria, or ketonuria. The chest radiograph (Figure 1) showed small nodules and peripheral infiltrates in both lung fields. Chest computerized tomogram (CT) scans found multiple cavitated lung nodules (Figure 2A,B). Human immunodeficiency virus (HIV) screening test was negative.
Soon after transfer to the ICU, the patient developed respiratory distress and became hemodynamically unstable. He was intubated and resuscitation efforts were started to stabilize him. Yeast‐like organisms were found in the debrided tissue. CT‐guided biopsy of the pulmonary nodules also found yeast‐like organisms. Tissue cultures of skin wound and lung biopsy grew Cryptococcus neoformans. He was diagnosed with disseminated cryptococcal infection and Amphotericin B was started. His hemodynamic status stabilized 2 days after the start of Amphotericin B. Follow‐up chest radiograph 1 week after starting Amphotericin B treatment showed resolution of pulmonary nodules. His right thigh skin lesion also healed gradually.
Unfortunately, he developed severe weakness of all extremities on the fourteenth ICU day, and had difficulty weaning from mechanical ventilation. Neurological examination found diffuse hyporeflexia. The nerve conduction velocity (NCV) study showed decreased amplitude in nerve conduction, with normal velocity. Electromyogram (EMG) found diffuse muscular fibrillation. Based on these findings, CIPNM was diagnosed. Patient underwent tracheostomy on the twenty‐sixth ICU day due to the need for prolonged mechanical ventilation. His antifungal therapy was changed to intravenous fluconazole 600 mg per day. Blood glucose levels were controlled with continuous insulin infusion and insulin dose was titrated to keep the blood glucose below 120 mg/dL. He was finally weaned from mechanical ventilation on the forty‐seventh day of ICU admission, and was transferred to the general ward. With physical therapy, he resumed his daily activities and was discharged from the hospital.
DISCUSSION
Cryptococcus rarely causes disseminated infection in healthy individuals. The vast majority of patients with cryptococcosis are immunocompromised due to conditions such as acquired immunodeficiency syndrome, prolonged treatment with corticosteroids, organ transplantation, malignancy, or diabetes mellitus.3, 4 The patient in this report had 2 of the documented risk factors. In a study of 52 disseminated cryptococcosis patients, the most prevalent underlying condition was HIV infection (46%). Out of these 52 patients, 28 were HIV‐negative, and only 3 of them had no predisposing condition.4 Cutaneous cryptococcus infection could be a manifestation of disseminated cryptococcal infection, or may be a primary disease that would evolve into systemic disease several months later.5, 6 The incidence of primary cutaneous cryptococcosis is much lower than systemic disease with cutaneous manifestation. Cellulitis, which is refractory to treatment with traditional antibacterial agents, should lead to consideration of fungal cellulites, such as cutaneous cryptococcosis or aspergillosis. Once cryptococcal cellulitis is diagnosed, other foci of cryptococcal infection should be sought.
CIPNM includes myopathies, acute neuropathies, neuromuscular transmission defects, or any combination of these disorders.2, 7 CIPNM might arise in ICU patients who have systemic inflammatory response syndrome (SIRS), sepsis, or multiple organ failure. In patients with new onset limb weakness, disuse hyporeflexia, and difficulty in weaning from mechanical ventilation, CIPNM should be among the differential diagnoses. In 1 prospective trial, de Letter et al.8 found CIPNM incidence of 33% in 98 ICU patients. A high APACHE III score, SIRS, and the use of aminoglycoside antibiotics are significant risk factors for the development of CIPNM. In various studies, the incidence of CIPNM ranges from 13% to 76%.2, 710
The definitive diagnosis of CIPNM is established by EMG and NCV studies, which are characterized by (1) reduced amplitudes of compound muscles and sensory action potentials, (2) relatively normal conduction studies, and (3) widespread fibrillations and sharp waves.2 The mean mortality of patients who have developed CIPNM is 35%, with a range from 0% to 73%. About 45% of patients completely recover from CIPNM within 6 weeks to 12 months (with a mean duration of 4.5 months), with good supportive care, provided the underlying condition has been treated.2, 9 There is little evidence to support a specific treatment modality for CIPNM. Mohr et al.1 reported that intravenous immunoglobulin may prevent or ameliorate CIPNM in the ICU, but more prospective and placebo‐controlled studies are needed to confirm their result. In recent studies,11 strict blood glucose control with insulin was found to reduce the risk of CIPNM and duration of mechanical ventilation in both medical and surgical ICU patients.
In conclusion, CIPNM occurs frequently in ICU patients with SIRS, sepsis, or multiple organ failure, leading to prolonged ventilator dependence and increased morbidity and mortality. Risk factor prevention and intensive insulin treatment may reduce the incident of CIPNM and the duration of mechanical ventilation in ICU patients.
- ,,,,.Effects of early treatment with immunoglobulin on critical illness polyneuropathy following multiple organ failure and gram‐negative sepsis.Intensive Care Med.1997;23:1144–1149.
- .Critical illness polyneuropathy and myopathy: clinical features, risk factors and prognosis.Eur J Neurol.2006;13:1203–1212.
- .Cryptococcus neoformans. In:Mandell GL,Bennett JE,Dolin R, eds.Principles and Practice of Infectious Diseases.Philadelphia:Churchill Livingstone;2000:2707–2718.
- ,,, et al.Cryptococcameia: clinical features and prognostic factors.Q J Med.2002;95:511–518.
- ,,.Primary cutaneous cryptococcal cellulitis secondary to insect bite in an immunosuppressed patient after liver transplantation.Clin Exp Dermatol.2005;30:241–243.
- ,.Primary cutaneous cryptococcosis as the presenting manifestation of AIDS.Plast Reconstr Surg.1992;90:1065–1067.
- ,,,,.Effect of critical illness polyneuropathy on the withdrawal from mechanical ventilation and the length of stay in septic patients.Crit Care Med.2005;33:349–354.
- ,,, et al.Critical illness polyneuropathy and myopathy (CIPNM): evidence for local immune activation by cytokine‐expression in the muscle tissue.J Neuroimmunol.2000;106:206–213.
- ,.Critical illness neuromuscular abnormalities.Crit Care Clin.2002;18:553–568.
- ,,,,,.Neuromuscular disorders associated with failure to wean from the ventilator.Intensive Care Med.1995;21:737–743.
- ,,, et al.Impact of intensive insulin therapy on neuromuscular complications and ventilator‐dependency in MICU.Am J Respir Crit Care Med.2007;175:480–489.
- ,,,,.Effects of early treatment with immunoglobulin on critical illness polyneuropathy following multiple organ failure and gram‐negative sepsis.Intensive Care Med.1997;23:1144–1149.
- .Critical illness polyneuropathy and myopathy: clinical features, risk factors and prognosis.Eur J Neurol.2006;13:1203–1212.
- .Cryptococcus neoformans. In:Mandell GL,Bennett JE,Dolin R, eds.Principles and Practice of Infectious Diseases.Philadelphia:Churchill Livingstone;2000:2707–2718.
- ,,, et al.Cryptococcameia: clinical features and prognostic factors.Q J Med.2002;95:511–518.
- ,,.Primary cutaneous cryptococcal cellulitis secondary to insect bite in an immunosuppressed patient after liver transplantation.Clin Exp Dermatol.2005;30:241–243.
- ,.Primary cutaneous cryptococcosis as the presenting manifestation of AIDS.Plast Reconstr Surg.1992;90:1065–1067.
- ,,,,.Effect of critical illness polyneuropathy on the withdrawal from mechanical ventilation and the length of stay in septic patients.Crit Care Med.2005;33:349–354.
- ,,, et al.Critical illness polyneuropathy and myopathy (CIPNM): evidence for local immune activation by cytokine‐expression in the muscle tissue.J Neuroimmunol.2000;106:206–213.
- ,.Critical illness neuromuscular abnormalities.Crit Care Clin.2002;18:553–568.
- ,,,,,.Neuromuscular disorders associated with failure to wean from the ventilator.Intensive Care Med.1995;21:737–743.
- ,,, et al.Impact of intensive insulin therapy on neuromuscular complications and ventilator‐dependency in MICU.Am J Respir Crit Care Med.2007;175:480–489.

Coding and Documentation
You admitted a patient to the hospital for an upper gastrointestinal bleed. At the time of admission, the patient's mucous membranes were dry, and he was mildly orthostatic and tachycardic. He was given several boluses of normal saline, and he improved. All of this was carefully documented in the medical record. Shortly after discharge, the following cryptic message arrives in your mailbox:
The patient was admitted with gastrointestinal bleeding and noted to have dry mucous membranes, orthostatic hypotension, and tachycardia. He was given intravenous saline. What diagnosis, if any, required treatment with 2 boluses of normal saline?
You remember the patient well but still pull the chart to review the case. It appears obvious that the patient was dry and needed fluid resuscitation. You are confused and do not know how to respond. Your response is just that: Patient was dry and needed fluid resuscitation.
Several days later, you get another message thanking you for your reply but describing what the coder actually needed to be able to code appropriately. Had you answered hypovolemia or dehydration, it would have changed the diagnosis‐related group (DRG) and reimbursement from gastrointestinal hemorrhage ($2700) to gastrointestinal hemorrhage with complications ($4600). Because you did not provide the right answer, the institution was reimbursed for the lesser amount. Now you are left with more questions. Hypovolemia is exactly what the patient had; you basically said so, and it was described throughout the chart, although not in so many words. Why did the coder not just say what was needed? Why can you not just answer again? Why are you being asked to play what appears to be a stupid game when you have sick patients to care for and never enough time? What can you do to prevent this from happening the next time? What other surprises are in store for you?
INTRODUCTION
Beginning October 1, 2007 the Centers for Medicare and Medicaid Services (CMS) implemented changes in the hospital inpatient prospective payment system that have profound implications for how physicians code and document hospital care. These changes were implemented in an effort to better recognize severity of illness,1 and the information will be used to plan for current and future needs of hospitals, insurers, caregivers, and patients. Severity of illness is a measure of the patient's overall health status reflected by the resources necessary for care and the risk of morbidity and mortality. Factors including the presenting illness, comorbid conditions, functional status, nutritional status, and age contribute to the severity of illness. From a physiologic perspective, factors reflecting loss of homeostatic control such as abnormal vital signs, poor oxygenation, and altered sensorium are determinants of severity of illness. For hospitals, severity of illness is generally reflected by the case mix of concomitant illness. Thus, a patient with community‐acquired pneumonia without other comorbidities requires fewer resources and has a greater chance of a good outcome than the same patient with complications such as acute congestive heart failure. In the context of this article, severity of illness should be considered an indication of the complexity of the patient's presentation. Reporting comorbidities and illness severity will help better define quality of care and medical necessity for that care.
The DRG system provided a set payment for a given hospitalization based on primary and sometimes secondary diagnoses. The new system, using Medicare severity diagnosis‐related groups (MS‐DRGs), accounts for all diagnoses present at the time of admission and all diagnoses made during the hospitalization.
This article discusses the value of appropriate documentation and outlines changes that physicians will need to make to ensure optimal coding. The value of appropriate documentation is described. Specific terminology is illustrated so physicians can document properly and coders can easily extract the necessary information from the medical record to code appropriately. Finally, specific strategies institutions can implement to support physicians and coders are suggested.
A PRIMER ON CODING AND MEDICAL DOCUMENTATION
Prior to October 1, 2007, the DRG for a given hospitalization was calculated from the principle diagnosis and in some cases 1 secondary diagnosis that represented a significant complication or comorbidity. For example, a patient admitted to the hospital with abdominal pain diagnosed as a peptic ulcer would have a DRG to reflect the ulcer. If the patient also had anemia secondary to blood loss from the ulcer, this would serve as a complication, and a DRG with a comorbidity or complication and a higher case weight would be assigned. Additional significant complications would not further alter the DRG.
The new guidelines recognize 3 levels of severity for secondary diagnoses. The DRG from the principal diagnosis can be associated with other diagnoses that recognize no complication or comorbidity, a complication or comorbidity, or a major complication or comorbidity. Thus, a patient admitted with a duodenal ulcer may have a secondary diagnosis such as hypertension, which is not considered significant enough to complicate the DRG, a complication such as ileus, or a major complication such as perforation or heart failure. Depending on the clinical circumstances, a patient admitted with a principal diagnosis of duodenal ulcer could have any of 3 DRGs.
Of all the information contained in the medical record, coders can use only documentation by physicians who are directly caring for the patient during that admission. This includes documentation by resident physicians, physician assistants, or nurse practitioners if the attending documents agreement. Notes of nurses and allied health professionals cannot be used. Consultants' notes can also be used for coding, except when their findings contradict those of the attending physician. In this case, 1 of 2 things can happen. The coder may use the documentation of the attending physician or, if clarification of the appropriate diagnosis or procedure is necessary, query the attending physician. Pathology and radiology reports and laboratory findings cannot be used unless the diagnoses are documented by the attending.
Because coders can use only documentation that follows universal terminology, physicians need to understand coding principles and learn to document using appropriate terminology.2, 3 This includes documentation of diagnoses, conditions, symptoms, or procedures defined by CMS. The large number of vagaries in the coding vernacular used by CMS sometimes makes this lexicon confusing and difficult for physicians. To ensure appropriate documentation, physicians must abandon doctorese, the shorthand vernacular that is commonly used for documentation. Even when a coder is able to correctly infer the diagnosis, he or she cannot use this information because the diagnosis was not specifically documented. It will either be lost or generate a query; both are negative consequences for the hospital and physician because reimbursement might be inappropriately low and the true level of severity of illness might not be appreciated.
Examples of this are myriad (see Appendix B) and include the following:
-
Shorthand notation, such as Na (hyponatremia) and plts, (thrombocytopenia) is not acceptable; the actual diagnosis must be written.
-
Often, there is no documentation of the diagnosis at all, but physicians read between the lines to glean the diagnosis. A note states dysuria followed by +U/A, leaving the assessment blank. The plan says ciprofloxin 500BID X 3d. Most physicians recognize this as shorthand for an uncomplicated urinary tract infection, but the documentation is incomplete because the assessment is omitted, and the coders will not be able to code.
-
A note documents an abnormal laboratory value that is intended to reflect a diagnosis (eg, Na+ = 117, restrict fluids). Coders likely understand that hyponatremia is the diagnosis, but they cannot code it because coding rules state it is only an abnormal laboratory value, not a diagnosis. Hyponatremia must be written in the medical record.
In most circumstances, a few simple guidelines will help:
-
Avoid abbreviations. Full diagnoses should be written in longhand rather than abbreviations or symbols. Use a diagnosis when appropriate, rather than just the symptom, such as hypoxia for dyspnea.
-
Write complete SOAP notes. Always document the diagnosis for which any treatment is rendered or evaluation performed. In other words, always write complete SOAP notes, not SOP notes.
-
Become familiar with rules and concepts of coding and documentation. Some peculiarities of coding rules make little sense to physicians and may appear arbitrary. Certain diagnoses, conditions, or descriptive terms that physicians commonly use cannot be used for coding purposes. These peculiarities will simply need to be learned or handled by queries from coders or real‐time chart review by coding personnel. For example, although exacerbation of chronic obstructive pulmonary disease is recognized in coding rules, exacerbation of congestive heart failure codes to a nonspecific code, and the physician must document it as acute on chronic or acute congestive heart failure. Likewise, the new terminology adopted by the National Kidney Foundation for acute renal failure, acute kidney injury, has no code. Because both of these diagnoses serve as major comorbidities, they have major financial implications for hospitals.
-
Be thorough. All clinically significant conditions noted should be documented and coded. According to CMS rules, a condition, whether major or minor, is clinically significant if it requires any of the following:4
-
Clinical evaluation
-
Therapeutic treatment
-
Diagnostic procedures
-
Extended length of hospital stay
-
Increased nursing care and/or monitoring.
-
Avoid rule‐out diagnoses. It is perfectly acceptable to qualify an uncertain diagnosis. For example, suspected pneumonia can be documented as probable or possible. If you document it as such and empirically treat for pneumonia, the coder may document pneumonia as the diagnosis. Diagnoses that have been ruled out should not be documented. For example, a patient is admitted with neutropenic fever and suspected sepsis. The patient may be given empirical therapy, but if sepsis is ruled out and the treatment is stopped, sepsis is not an appropriate diagnosis.
-
Identify the principal diagnosis. The principal diagnosis is defined as the condition responsible for the patient's admission to the hospital. All other diagnoses are secondary. If a patient enters the hospital because of sepsis of urinary origin but during the hospitalization develops pneumonia that extends the stay, the principal diagnosis from which the DRG is derived remains sepsis of urinary origin. The only exception is the patient with several conditions, any of which would have independently required hospitalization and treatment. In this case, the coders have the option of selecting the principal diagnosis from among the possible principal diagnoses if each is treated with essentially equal effort.
-
Include relevant secondary diagnoses. Another complexity and frustration regarding the coding rules is that they are often highly specific and follow a logic of their own. For coding purposes, upper gastrointestinal bleeding is a diagnosis without comorbidity. However, adding the secondary diagnosis of blood loss anemia increases the case weight by adding a comorbidity, and documenting esophageal hemorrhage adds a major comorbidity, further increasing the case weight. Coders may not, by Medicare rules, prompt or lead physicians to the proper term. If the physician documents upper gastrointestinal bleed, anemia, and esophagitis, the coder cannot ask, Was the esophagitis the cause of the anemia?
Other Considerations
Although coders cannot use documentation from nurses and allied health professionals, their notes often provide clues to issues that the physician may have failed to document. For example, a patient with significant postoperative nausea and vomiting may be treated and followed carefully by the physicians and improve despite no physician documentation. The information contained in the nursing notes can generate a query to the physician to clarify the diagnosis that required treatment for significant nausea and vomiting.
Under the new guidelines, diagnoses present on admission must be distinguished from diagnoses occurring after admission. CMS is very concerned about reducing the incidence of preventable nosocomial events such as decubitus ulcers and catheter‐associated infections. In an attempt to push hospitals to reduce or eliminate the incidence of these adverse events, CMS no longer reimburses certain diagnoses for the added cost of care when these events occur. If a patient leaves the hospital with a catheter‐associated urinary tract infection, CMS assumes that it was hospital‐acquired unless it was clearly documented as present on admission (see Appendix A). It is likely that the list will grow over time; in fact, CMS is considering adding ventilator‐associated pneumonia, Staphylococcus aureus septicemia, and deep venous thrombosis/pulmonary embolism in 2009. Thus, it is important to develop systematic methods to ensure that all diagnoses present on admission are captured and that diagnoses which developed during the hospitalization are acknowledged. A diagnosis present on admission but not recognized until after admission can be documented as present on admission. Another category will also be apparent occasionally in which it cannot be known whether a condition was present on admission or occurred following hospitalization.
PREPARING TO COMPLY WITH MS‐DRG GUIDELINES
Information from Maryland hospitals that have piloted the MS‐DRG methodology indicates that coders will be 25% to 50% less efficient (private communication), largely because of increased communication (queries) between coders and physicians to clarify medical documentation. Queries may be generated whenever the record lacks codable documentation or information is missing, conflicting, ambiguous, or illegible. Most hospitals will need to increase their coding staff and hire or develop educators to teach coders and physicians medical terminology. Many of these educators will need experience in both coding and medicine and will generally require at least an RN degree or the equivalent.5, 6 Hiring experienced coders with a medical background is currently a challenge as many hospitals are responding to the new guidelines, and they are in high demand. Many hospitals will need to upgrade the skills of existing coders or medical personnel to fill these roles. Hospitals that invest in additional coders to train physicians in coding terminology may eventually regain efficiency in the coding process; however, it seems likely that some degree of additional clarification will always be needed.
Hospitals should develop educational programs, including didactic presentations that define the new MS‐DRGs, outline the risks and benefits of the new rules, and provide examples of universal terminology. They should provide handouts, pocket guides, and electronic medical record prompts with coding terminology and frequently asked questions. Specific physician feedback may occur on an individual, departmental, or DRG basis or on the basis of the International Statistical Classification of Diseases and Related Health Problems, 9th edition. Coding specialists need to be available to provide real‐time chart review and answer specific physician inquiries on coding and documentation questions. Physician buy‐in is essential and can be encouraged through careful education, administrative support, and physician champions.
INCENTIVE AND DISINCENTIVES: HOW TO MAXIMIZE COMPLIANCE AMONG PHYSICIANS AND HOSPITALS (AND WHY IT IS SO IMPORTANT)
The new coding rules affect only hospital reimbursement, so physicians get no direct benefit from ensuring that hospitals obtain the maximum appropriate reimbursement. However, physicians indirectly benefit when hospitals have strong profit margins, which allow for improved staffing levels, capital expenditures, additional services, programs, and growth. Any physician who has worked in institutions that operate in the red and in the black fully understands how important hospital revenue is to morale, efficiency, and work satisfaction.
The importance of properly evaluating quality of care cannot be overestimated. CMS, the Joint Commission on the Accreditation of Healthcare Organizations, and other oversight bodies have emphasized this through guidelines, legislation, and financial incentives.7 Pay for performance, value‐based purchasing, and performance indicator data are terms commonly understood by physicians. Hospitals and physicians benefit from improved quality measurements, which are affected by coding and documentation. Without appropriate coding and documentation, institutions that care for the very sickest patients cannot demonstrate their true severity of illness. Increases in morbidity, mortality, and length of stay will not correlate with the documented severity of illness, adversely skewing quality data and affecting hospitals' reputations. Hospitals that do not adequately account for the severity of the patients that they treat and accurately adjust their performance measures for severity will face increasingly difficult challenges to their financial stability and reputation in the future.8 The ability to demonstrate favorable quality report cards2, 3 represents an increasingly important incentive for hospitals.9 Finally, it is important to realize the multitude of functions supported by good documentation in the medical record. The record is also important for quality measurement, protection from liability, evaluation of resource utilization, tumor and other medical data registries, and other uses (see Appendix A).
CONCLUSION
The MS‐DRG system has important implications for physicians and hospitals. The changes will allow CMS to understand more fully the severity of illness of hospitalized patients. It replaces a system that derived a DRG from a single principle diagnosis and in some cases a single comorbidity with one that reflects all conditions. Comorbidities and complications are designated as major, minor, or no complication. Because multiple parties use the medical record for many different functions, better documentation of specificity of severity of illness will affect hospitals in many ways. Importantly, one of these will be reimbursement. Hospitals that historically have had a higher level of severity will now see that reflected in their case mix and may actually see improved reimbursement. Another area that will be affected is quality measurement. If severity of illness is not appropriately documented and accounted for, hospitals could exhibit skewed outcomes of care. For example, if hospitals with sicker (on average) patients document a lower indicator of severity than the true severity of its patients, their mortality experience might appear to be abnormally high in comparison with other hospitals. This can damage reputations and thus affect many things such as patient referrals and utilization of services. This becomes particularly important in a competitive medical market and at a time when patients have increased access to hospital‐specific data on quality of care.
The new guidelines also require medical documentation to capture diagnoses present on admission as opposed to conditions that arise during hospitalization. If not recorded as present on admission, selected conditions will be considered iatrogenic complications and will not receive additional reimbursement. CMS intends this as an incentive for hospitals to improve quality of care by developing safeguards against complications.
It is likely that hospitals will take different approaches to ensuring that medical record documentation skills are taught and adopted by physicians. As different approaches evolve, hopefully best practices will emerge that can be disseminated. These efforts should be taken to ensure appropriate documentation prospectively rather than heavy reliance on a retrospective review and query process, which can be inefficient and expensive, intrusive to physician workflow, and possibly subject to third‐party criticism.
It is vital for hospital senior managers to gain physician input and involvement in both the design and implementation of the programs outlined in this article and to provide them with adequate resources and administrative support throughout the educational process. Ultimately, developing a program that enhances and sustains the medical record documentation skills of its medical staff is critical to the well‐being of any hospital. Accepting the new changes and making the changes necessary to ensure success is certainly an additional burden on physicians; many, if not most, of whom likely feel overworked and overburdened by the many demands on their time. Although they may not derive personal benefit for changing their behaviors, physicians should nevertheless understand the importance of appropriate documentation for the purposes of quality assessment, reimbursement, and resource allocation.
Appendix
APPENDIX A: SELECTED PENNSYLVANIA AND NATIONAL DATABASES USING MEDICAL RECORDS
| Joint Commission on Accreditation of Healthcare Organizations (JCAHO) |
| United Hospital Consortium (UHC) |
| Pennsylvania Health Center Cost Containment Council (PHC4) |
| United Network for Organ Sharing (UNOS) |
| National Cancer Data Base (NCDB) |
| National Database of Nursing Quality Indicators (NDNQI) |
| National Association of Children's Hospitals and Related Institutions (NACHRI) |
| Pennsylvania Trauma Systems Foundation (PTSF) |
| American College of Cardiology (ACC) |
| National Endoscopy Data Base (NEDB) |
| National Surgery Quality Improvement Program (NSQIP) |
| Society of Thoracic Surgery (STS) |
| Uniform Data System for Medical Rehabilitation (UDSMR) |
Appendix
APPENDIX B: NOTES TAKEN DIRECTLY FROM THE MEDICAL RECORD
| What the MDs Document (Doctorese) | What They Mean (Diagnosis/ Universal Terminology) | Coding Result |
|---|---|---|
| plts, Tx 4U plts | Thrombocytopenia | Coders cannot decipher |
| Na+ = 117, fluid restrict | Hyponatremia | Abnormal laboratory test; cannot code |
| O2 sat 80, NC @ 4 l/min | Hypoxia | Coders cannot decipher |
| Alb = 2.4, diet consult, start suppl | Malnutrition | Abnormal laboratory test; cannot code |
| IV NS 250/hr, 2U Tx, GI bleed | Hypovolemia, blood loss anemia | Coders cannot decipher |
| BP, fever, MS, +UA | Sepsis of urinary origin | Urinary tract infection |
Appendix
APPENDIX C: HOSPITAL‐ACQUIRED CONDITIONS OF FOCUS TO THE CENTERS FOR MEDICARE AND MEDICAID SERVICES FOR 2008
| Serious preventable event: object left in surgery |
| Serious preventable event: air embolism |
| Serious preventable event: blood incompatibility |
| Catheter‐associated urinary tract infections |
| Vascular catheterassociated infections |
| Surgical site infection: mediastinitis after coronary artery bypass surgery |
| Hospital‐acquired injuries: fractures, dislocations, intracranial injury, crushing injury, burn, and other unspecified effects of external causes |
Appendix
APPENDIX D: STRATEGIES FOR SUCCESS WITH MEDICARE SEVERITY DIAGNOSIS‐RELATED GROUPS
| Educational initiatives |
| Introductory didactic presentations |
| Online tutorial: coding and documentation |
| Periodic memos with coding tips (Tip of the Month) |
| Web site references on coding tips (comprehensive list) |
| Posters, announcements, and branding |
| Physician support services |
| Web site reference with FAQs |
| Direct contact with coding specialists |
| RN/coding specialist liaison |
| Computerized medical record |
| Staff feedback associated with query process |
| Physician champions |
| Coding department changes |
| Increased staffing |
| RN/coding specialist: real‐time chart reviews |
| Physician coding specialist |
| Standing Coding and Documentation Committee |
Appendix
APPENDIX E: SELECTED CODING TIPS FOR GENERAL MEDICINE
|
| Disease/condition specific tips |
| Gastrointestinal bleed with anemia does not mean that the patient is anemic from the hemorrhage: write blood loss anemia (chronic or acute). |
| Urosepsis codes to urinary tract infection site NOS: write sepsis with urinary origin. |
| CVA or stroke does not mean infarction: write CVA with infarction. |
| Common complications and comorbidities |
| Cardiac: acute myocardial infarction, congestive heart failure, atrial flutter, paroxysmal supraventricular tachycardia, heart block, and second‐degree heart block |
| Gastrointestinal: melena, ascites, hepatitis, and hematemesis |
| Genitourinary: urinary retention, hematuria, urinary tract infection, hydronephrosis, and renal failure |
| Nutritional: dehydration, malnutrition, cachexia, and volume overload |
| Gastrointestinal: peritonitis, perforation, bleeding esophageal varices, ascites, and ileus |
| Genitourinary: acute renal failure, end‐stage renal disease, urinary tract infection, and nephritic syndrome |
| Nutritional: severe malnutrition, body mass index > 40, malnutrition NOS, and cachexia |
| Pulmonary: respiratory failure, aspiration pneumonia, pneumothorax, atelectasis, and hemoptysis |
| General tips |
| A culture must be linked to the site of infection: write pseudomonas pneumonia. |
| Ambulatory dysfunction and deconditioning lack the required specificity to ensure accurate coding; when possible, use abnormal gait, difficulty walking, muscle weakness, and so forth. |
| If the patient appears to be septic, positive blood cultures are not necessary to document sepsis. |
| Discriminate between acute, chronic, and acute on chronic. |
| If the problem is active, do not write history of , which implies that the condition no longer exists: write PMH: chronic (diagnosis). |
| Be specific in documenting congestive heart failure (acute/chronic, systolic/diastolic failure, L/R). |
- Centers for Medicare and Medicaid Services. Medicare Program: Changes to the Hospital Inpatient Prospective Payment Systems and Fiscal Year 2008 Rates. Available at:http://www.cms.hhs.gov/acuteinpatientpps/downloads/cms‐1533‐fc.pdf. Accessed October2008.
- ,,,,.Straight talk: new approaches in healthcare. Rx for reimbursement woes: high‐quality medical documentation and coding. Panel discussion.Mod Healthc.2007;32(29):35–38.
- ,,.Optimizing hospital reimbursement through physician awareness: a step toward better patient care.Orthopedics.1998;21(1):79–83.
- ICD‐9‐CM Official Guidelines for Coding and Reporting (effective October 1, 2007). Available at:http://www.cdc.gov/nchs/datawh/ftpserv/ftpicd9/icdguide07.pdf. Accessed October2008.
- ,.Improving physician documentation through a clinical documentation management program.Nurs Adm.2003;27(4):285–289.
- .A primer for understanding diagnosis‐related groups and inpatient hospital reimbursement with nursing implications.Crit Care Nurs.2005;28(4):360–369.
- US Department of Health and Human Services. Report to Congress: Plan To Implement a Medicare Hospital Value‐Based Purchasing Program. Available at:http://www.cms.hhs.gov/acuteinpatientpps/downloads/hospitalvbpplanrtcfinalsubmitted2007.pdf. Accessed October2008.
- ,,, et al.Results of report cards for patients with congestive heart failure depend on the method used to adjust for severity.Ann Intern Med.2000;133:10–20.
- ,,, et al.Assessment of the Medicare quality improvement organization program.Ann Intern Med.2006;145(5):342–353.
You admitted a patient to the hospital for an upper gastrointestinal bleed. At the time of admission, the patient's mucous membranes were dry, and he was mildly orthostatic and tachycardic. He was given several boluses of normal saline, and he improved. All of this was carefully documented in the medical record. Shortly after discharge, the following cryptic message arrives in your mailbox:
The patient was admitted with gastrointestinal bleeding and noted to have dry mucous membranes, orthostatic hypotension, and tachycardia. He was given intravenous saline. What diagnosis, if any, required treatment with 2 boluses of normal saline?
You remember the patient well but still pull the chart to review the case. It appears obvious that the patient was dry and needed fluid resuscitation. You are confused and do not know how to respond. Your response is just that: Patient was dry and needed fluid resuscitation.
Several days later, you get another message thanking you for your reply but describing what the coder actually needed to be able to code appropriately. Had you answered hypovolemia or dehydration, it would have changed the diagnosis‐related group (DRG) and reimbursement from gastrointestinal hemorrhage ($2700) to gastrointestinal hemorrhage with complications ($4600). Because you did not provide the right answer, the institution was reimbursed for the lesser amount. Now you are left with more questions. Hypovolemia is exactly what the patient had; you basically said so, and it was described throughout the chart, although not in so many words. Why did the coder not just say what was needed? Why can you not just answer again? Why are you being asked to play what appears to be a stupid game when you have sick patients to care for and never enough time? What can you do to prevent this from happening the next time? What other surprises are in store for you?
INTRODUCTION
Beginning October 1, 2007 the Centers for Medicare and Medicaid Services (CMS) implemented changes in the hospital inpatient prospective payment system that have profound implications for how physicians code and document hospital care. These changes were implemented in an effort to better recognize severity of illness,1 and the information will be used to plan for current and future needs of hospitals, insurers, caregivers, and patients. Severity of illness is a measure of the patient's overall health status reflected by the resources necessary for care and the risk of morbidity and mortality. Factors including the presenting illness, comorbid conditions, functional status, nutritional status, and age contribute to the severity of illness. From a physiologic perspective, factors reflecting loss of homeostatic control such as abnormal vital signs, poor oxygenation, and altered sensorium are determinants of severity of illness. For hospitals, severity of illness is generally reflected by the case mix of concomitant illness. Thus, a patient with community‐acquired pneumonia without other comorbidities requires fewer resources and has a greater chance of a good outcome than the same patient with complications such as acute congestive heart failure. In the context of this article, severity of illness should be considered an indication of the complexity of the patient's presentation. Reporting comorbidities and illness severity will help better define quality of care and medical necessity for that care.
The DRG system provided a set payment for a given hospitalization based on primary and sometimes secondary diagnoses. The new system, using Medicare severity diagnosis‐related groups (MS‐DRGs), accounts for all diagnoses present at the time of admission and all diagnoses made during the hospitalization.
This article discusses the value of appropriate documentation and outlines changes that physicians will need to make to ensure optimal coding. The value of appropriate documentation is described. Specific terminology is illustrated so physicians can document properly and coders can easily extract the necessary information from the medical record to code appropriately. Finally, specific strategies institutions can implement to support physicians and coders are suggested.
A PRIMER ON CODING AND MEDICAL DOCUMENTATION
Prior to October 1, 2007, the DRG for a given hospitalization was calculated from the principle diagnosis and in some cases 1 secondary diagnosis that represented a significant complication or comorbidity. For example, a patient admitted to the hospital with abdominal pain diagnosed as a peptic ulcer would have a DRG to reflect the ulcer. If the patient also had anemia secondary to blood loss from the ulcer, this would serve as a complication, and a DRG with a comorbidity or complication and a higher case weight would be assigned. Additional significant complications would not further alter the DRG.
The new guidelines recognize 3 levels of severity for secondary diagnoses. The DRG from the principal diagnosis can be associated with other diagnoses that recognize no complication or comorbidity, a complication or comorbidity, or a major complication or comorbidity. Thus, a patient admitted with a duodenal ulcer may have a secondary diagnosis such as hypertension, which is not considered significant enough to complicate the DRG, a complication such as ileus, or a major complication such as perforation or heart failure. Depending on the clinical circumstances, a patient admitted with a principal diagnosis of duodenal ulcer could have any of 3 DRGs.
Of all the information contained in the medical record, coders can use only documentation by physicians who are directly caring for the patient during that admission. This includes documentation by resident physicians, physician assistants, or nurse practitioners if the attending documents agreement. Notes of nurses and allied health professionals cannot be used. Consultants' notes can also be used for coding, except when their findings contradict those of the attending physician. In this case, 1 of 2 things can happen. The coder may use the documentation of the attending physician or, if clarification of the appropriate diagnosis or procedure is necessary, query the attending physician. Pathology and radiology reports and laboratory findings cannot be used unless the diagnoses are documented by the attending.
Because coders can use only documentation that follows universal terminology, physicians need to understand coding principles and learn to document using appropriate terminology.2, 3 This includes documentation of diagnoses, conditions, symptoms, or procedures defined by CMS. The large number of vagaries in the coding vernacular used by CMS sometimes makes this lexicon confusing and difficult for physicians. To ensure appropriate documentation, physicians must abandon doctorese, the shorthand vernacular that is commonly used for documentation. Even when a coder is able to correctly infer the diagnosis, he or she cannot use this information because the diagnosis was not specifically documented. It will either be lost or generate a query; both are negative consequences for the hospital and physician because reimbursement might be inappropriately low and the true level of severity of illness might not be appreciated.
Examples of this are myriad (see Appendix B) and include the following:
-
Shorthand notation, such as Na (hyponatremia) and plts, (thrombocytopenia) is not acceptable; the actual diagnosis must be written.
-
Often, there is no documentation of the diagnosis at all, but physicians read between the lines to glean the diagnosis. A note states dysuria followed by +U/A, leaving the assessment blank. The plan says ciprofloxin 500BID X 3d. Most physicians recognize this as shorthand for an uncomplicated urinary tract infection, but the documentation is incomplete because the assessment is omitted, and the coders will not be able to code.
-
A note documents an abnormal laboratory value that is intended to reflect a diagnosis (eg, Na+ = 117, restrict fluids). Coders likely understand that hyponatremia is the diagnosis, but they cannot code it because coding rules state it is only an abnormal laboratory value, not a diagnosis. Hyponatremia must be written in the medical record.
In most circumstances, a few simple guidelines will help:
-
Avoid abbreviations. Full diagnoses should be written in longhand rather than abbreviations or symbols. Use a diagnosis when appropriate, rather than just the symptom, such as hypoxia for dyspnea.
-
Write complete SOAP notes. Always document the diagnosis for which any treatment is rendered or evaluation performed. In other words, always write complete SOAP notes, not SOP notes.
-
Become familiar with rules and concepts of coding and documentation. Some peculiarities of coding rules make little sense to physicians and may appear arbitrary. Certain diagnoses, conditions, or descriptive terms that physicians commonly use cannot be used for coding purposes. These peculiarities will simply need to be learned or handled by queries from coders or real‐time chart review by coding personnel. For example, although exacerbation of chronic obstructive pulmonary disease is recognized in coding rules, exacerbation of congestive heart failure codes to a nonspecific code, and the physician must document it as acute on chronic or acute congestive heart failure. Likewise, the new terminology adopted by the National Kidney Foundation for acute renal failure, acute kidney injury, has no code. Because both of these diagnoses serve as major comorbidities, they have major financial implications for hospitals.
-
Be thorough. All clinically significant conditions noted should be documented and coded. According to CMS rules, a condition, whether major or minor, is clinically significant if it requires any of the following:4
-
Clinical evaluation
-
Therapeutic treatment
-
Diagnostic procedures
-
Extended length of hospital stay
-
Increased nursing care and/or monitoring.
-
Avoid rule‐out diagnoses. It is perfectly acceptable to qualify an uncertain diagnosis. For example, suspected pneumonia can be documented as probable or possible. If you document it as such and empirically treat for pneumonia, the coder may document pneumonia as the diagnosis. Diagnoses that have been ruled out should not be documented. For example, a patient is admitted with neutropenic fever and suspected sepsis. The patient may be given empirical therapy, but if sepsis is ruled out and the treatment is stopped, sepsis is not an appropriate diagnosis.
-
Identify the principal diagnosis. The principal diagnosis is defined as the condition responsible for the patient's admission to the hospital. All other diagnoses are secondary. If a patient enters the hospital because of sepsis of urinary origin but during the hospitalization develops pneumonia that extends the stay, the principal diagnosis from which the DRG is derived remains sepsis of urinary origin. The only exception is the patient with several conditions, any of which would have independently required hospitalization and treatment. In this case, the coders have the option of selecting the principal diagnosis from among the possible principal diagnoses if each is treated with essentially equal effort.
-
Include relevant secondary diagnoses. Another complexity and frustration regarding the coding rules is that they are often highly specific and follow a logic of their own. For coding purposes, upper gastrointestinal bleeding is a diagnosis without comorbidity. However, adding the secondary diagnosis of blood loss anemia increases the case weight by adding a comorbidity, and documenting esophageal hemorrhage adds a major comorbidity, further increasing the case weight. Coders may not, by Medicare rules, prompt or lead physicians to the proper term. If the physician documents upper gastrointestinal bleed, anemia, and esophagitis, the coder cannot ask, Was the esophagitis the cause of the anemia?
Other Considerations
Although coders cannot use documentation from nurses and allied health professionals, their notes often provide clues to issues that the physician may have failed to document. For example, a patient with significant postoperative nausea and vomiting may be treated and followed carefully by the physicians and improve despite no physician documentation. The information contained in the nursing notes can generate a query to the physician to clarify the diagnosis that required treatment for significant nausea and vomiting.
Under the new guidelines, diagnoses present on admission must be distinguished from diagnoses occurring after admission. CMS is very concerned about reducing the incidence of preventable nosocomial events such as decubitus ulcers and catheter‐associated infections. In an attempt to push hospitals to reduce or eliminate the incidence of these adverse events, CMS no longer reimburses certain diagnoses for the added cost of care when these events occur. If a patient leaves the hospital with a catheter‐associated urinary tract infection, CMS assumes that it was hospital‐acquired unless it was clearly documented as present on admission (see Appendix A). It is likely that the list will grow over time; in fact, CMS is considering adding ventilator‐associated pneumonia, Staphylococcus aureus septicemia, and deep venous thrombosis/pulmonary embolism in 2009. Thus, it is important to develop systematic methods to ensure that all diagnoses present on admission are captured and that diagnoses which developed during the hospitalization are acknowledged. A diagnosis present on admission but not recognized until after admission can be documented as present on admission. Another category will also be apparent occasionally in which it cannot be known whether a condition was present on admission or occurred following hospitalization.
PREPARING TO COMPLY WITH MS‐DRG GUIDELINES
Information from Maryland hospitals that have piloted the MS‐DRG methodology indicates that coders will be 25% to 50% less efficient (private communication), largely because of increased communication (queries) between coders and physicians to clarify medical documentation. Queries may be generated whenever the record lacks codable documentation or information is missing, conflicting, ambiguous, or illegible. Most hospitals will need to increase their coding staff and hire or develop educators to teach coders and physicians medical terminology. Many of these educators will need experience in both coding and medicine and will generally require at least an RN degree or the equivalent.5, 6 Hiring experienced coders with a medical background is currently a challenge as many hospitals are responding to the new guidelines, and they are in high demand. Many hospitals will need to upgrade the skills of existing coders or medical personnel to fill these roles. Hospitals that invest in additional coders to train physicians in coding terminology may eventually regain efficiency in the coding process; however, it seems likely that some degree of additional clarification will always be needed.
Hospitals should develop educational programs, including didactic presentations that define the new MS‐DRGs, outline the risks and benefits of the new rules, and provide examples of universal terminology. They should provide handouts, pocket guides, and electronic medical record prompts with coding terminology and frequently asked questions. Specific physician feedback may occur on an individual, departmental, or DRG basis or on the basis of the International Statistical Classification of Diseases and Related Health Problems, 9th edition. Coding specialists need to be available to provide real‐time chart review and answer specific physician inquiries on coding and documentation questions. Physician buy‐in is essential and can be encouraged through careful education, administrative support, and physician champions.
INCENTIVE AND DISINCENTIVES: HOW TO MAXIMIZE COMPLIANCE AMONG PHYSICIANS AND HOSPITALS (AND WHY IT IS SO IMPORTANT)
The new coding rules affect only hospital reimbursement, so physicians get no direct benefit from ensuring that hospitals obtain the maximum appropriate reimbursement. However, physicians indirectly benefit when hospitals have strong profit margins, which allow for improved staffing levels, capital expenditures, additional services, programs, and growth. Any physician who has worked in institutions that operate in the red and in the black fully understands how important hospital revenue is to morale, efficiency, and work satisfaction.
The importance of properly evaluating quality of care cannot be overestimated. CMS, the Joint Commission on the Accreditation of Healthcare Organizations, and other oversight bodies have emphasized this through guidelines, legislation, and financial incentives.7 Pay for performance, value‐based purchasing, and performance indicator data are terms commonly understood by physicians. Hospitals and physicians benefit from improved quality measurements, which are affected by coding and documentation. Without appropriate coding and documentation, institutions that care for the very sickest patients cannot demonstrate their true severity of illness. Increases in morbidity, mortality, and length of stay will not correlate with the documented severity of illness, adversely skewing quality data and affecting hospitals' reputations. Hospitals that do not adequately account for the severity of the patients that they treat and accurately adjust their performance measures for severity will face increasingly difficult challenges to their financial stability and reputation in the future.8 The ability to demonstrate favorable quality report cards2, 3 represents an increasingly important incentive for hospitals.9 Finally, it is important to realize the multitude of functions supported by good documentation in the medical record. The record is also important for quality measurement, protection from liability, evaluation of resource utilization, tumor and other medical data registries, and other uses (see Appendix A).
CONCLUSION
The MS‐DRG system has important implications for physicians and hospitals. The changes will allow CMS to understand more fully the severity of illness of hospitalized patients. It replaces a system that derived a DRG from a single principle diagnosis and in some cases a single comorbidity with one that reflects all conditions. Comorbidities and complications are designated as major, minor, or no complication. Because multiple parties use the medical record for many different functions, better documentation of specificity of severity of illness will affect hospitals in many ways. Importantly, one of these will be reimbursement. Hospitals that historically have had a higher level of severity will now see that reflected in their case mix and may actually see improved reimbursement. Another area that will be affected is quality measurement. If severity of illness is not appropriately documented and accounted for, hospitals could exhibit skewed outcomes of care. For example, if hospitals with sicker (on average) patients document a lower indicator of severity than the true severity of its patients, their mortality experience might appear to be abnormally high in comparison with other hospitals. This can damage reputations and thus affect many things such as patient referrals and utilization of services. This becomes particularly important in a competitive medical market and at a time when patients have increased access to hospital‐specific data on quality of care.
The new guidelines also require medical documentation to capture diagnoses present on admission as opposed to conditions that arise during hospitalization. If not recorded as present on admission, selected conditions will be considered iatrogenic complications and will not receive additional reimbursement. CMS intends this as an incentive for hospitals to improve quality of care by developing safeguards against complications.
It is likely that hospitals will take different approaches to ensuring that medical record documentation skills are taught and adopted by physicians. As different approaches evolve, hopefully best practices will emerge that can be disseminated. These efforts should be taken to ensure appropriate documentation prospectively rather than heavy reliance on a retrospective review and query process, which can be inefficient and expensive, intrusive to physician workflow, and possibly subject to third‐party criticism.
It is vital for hospital senior managers to gain physician input and involvement in both the design and implementation of the programs outlined in this article and to provide them with adequate resources and administrative support throughout the educational process. Ultimately, developing a program that enhances and sustains the medical record documentation skills of its medical staff is critical to the well‐being of any hospital. Accepting the new changes and making the changes necessary to ensure success is certainly an additional burden on physicians; many, if not most, of whom likely feel overworked and overburdened by the many demands on their time. Although they may not derive personal benefit for changing their behaviors, physicians should nevertheless understand the importance of appropriate documentation for the purposes of quality assessment, reimbursement, and resource allocation.
Appendix
APPENDIX A: SELECTED PENNSYLVANIA AND NATIONAL DATABASES USING MEDICAL RECORDS
| Joint Commission on Accreditation of Healthcare Organizations (JCAHO) |
| United Hospital Consortium (UHC) |
| Pennsylvania Health Center Cost Containment Council (PHC4) |
| United Network for Organ Sharing (UNOS) |
| National Cancer Data Base (NCDB) |
| National Database of Nursing Quality Indicators (NDNQI) |
| National Association of Children's Hospitals and Related Institutions (NACHRI) |
| Pennsylvania Trauma Systems Foundation (PTSF) |
| American College of Cardiology (ACC) |
| National Endoscopy Data Base (NEDB) |
| National Surgery Quality Improvement Program (NSQIP) |
| Society of Thoracic Surgery (STS) |
| Uniform Data System for Medical Rehabilitation (UDSMR) |
Appendix
APPENDIX B: NOTES TAKEN DIRECTLY FROM THE MEDICAL RECORD
| What the MDs Document (Doctorese) | What They Mean (Diagnosis/ Universal Terminology) | Coding Result |
|---|---|---|
| plts, Tx 4U plts | Thrombocytopenia | Coders cannot decipher |
| Na+ = 117, fluid restrict | Hyponatremia | Abnormal laboratory test; cannot code |
| O2 sat 80, NC @ 4 l/min | Hypoxia | Coders cannot decipher |
| Alb = 2.4, diet consult, start suppl | Malnutrition | Abnormal laboratory test; cannot code |
| IV NS 250/hr, 2U Tx, GI bleed | Hypovolemia, blood loss anemia | Coders cannot decipher |
| BP, fever, MS, +UA | Sepsis of urinary origin | Urinary tract infection |
Appendix
APPENDIX C: HOSPITAL‐ACQUIRED CONDITIONS OF FOCUS TO THE CENTERS FOR MEDICARE AND MEDICAID SERVICES FOR 2008
| Serious preventable event: object left in surgery |
| Serious preventable event: air embolism |
| Serious preventable event: blood incompatibility |
| Catheter‐associated urinary tract infections |
| Vascular catheterassociated infections |
| Surgical site infection: mediastinitis after coronary artery bypass surgery |
| Hospital‐acquired injuries: fractures, dislocations, intracranial injury, crushing injury, burn, and other unspecified effects of external causes |
Appendix
APPENDIX D: STRATEGIES FOR SUCCESS WITH MEDICARE SEVERITY DIAGNOSIS‐RELATED GROUPS
| Educational initiatives |
| Introductory didactic presentations |
| Online tutorial: coding and documentation |
| Periodic memos with coding tips (Tip of the Month) |
| Web site references on coding tips (comprehensive list) |
| Posters, announcements, and branding |
| Physician support services |
| Web site reference with FAQs |
| Direct contact with coding specialists |
| RN/coding specialist liaison |
| Computerized medical record |
| Staff feedback associated with query process |
| Physician champions |
| Coding department changes |
| Increased staffing |
| RN/coding specialist: real‐time chart reviews |
| Physician coding specialist |
| Standing Coding and Documentation Committee |
Appendix
APPENDIX E: SELECTED CODING TIPS FOR GENERAL MEDICINE
|
| Disease/condition specific tips |
| Gastrointestinal bleed with anemia does not mean that the patient is anemic from the hemorrhage: write blood loss anemia (chronic or acute). |
| Urosepsis codes to urinary tract infection site NOS: write sepsis with urinary origin. |
| CVA or stroke does not mean infarction: write CVA with infarction. |
| Common complications and comorbidities |
| Cardiac: acute myocardial infarction, congestive heart failure, atrial flutter, paroxysmal supraventricular tachycardia, heart block, and second‐degree heart block |
| Gastrointestinal: melena, ascites, hepatitis, and hematemesis |
| Genitourinary: urinary retention, hematuria, urinary tract infection, hydronephrosis, and renal failure |
| Nutritional: dehydration, malnutrition, cachexia, and volume overload |
| Gastrointestinal: peritonitis, perforation, bleeding esophageal varices, ascites, and ileus |
| Genitourinary: acute renal failure, end‐stage renal disease, urinary tract infection, and nephritic syndrome |
| Nutritional: severe malnutrition, body mass index > 40, malnutrition NOS, and cachexia |
| Pulmonary: respiratory failure, aspiration pneumonia, pneumothorax, atelectasis, and hemoptysis |
| General tips |
| A culture must be linked to the site of infection: write pseudomonas pneumonia. |
| Ambulatory dysfunction and deconditioning lack the required specificity to ensure accurate coding; when possible, use abnormal gait, difficulty walking, muscle weakness, and so forth. |
| If the patient appears to be septic, positive blood cultures are not necessary to document sepsis. |
| Discriminate between acute, chronic, and acute on chronic. |
| If the problem is active, do not write history of , which implies that the condition no longer exists: write PMH: chronic (diagnosis). |
| Be specific in documenting congestive heart failure (acute/chronic, systolic/diastolic failure, L/R). |
You admitted a patient to the hospital for an upper gastrointestinal bleed. At the time of admission, the patient's mucous membranes were dry, and he was mildly orthostatic and tachycardic. He was given several boluses of normal saline, and he improved. All of this was carefully documented in the medical record. Shortly after discharge, the following cryptic message arrives in your mailbox:
The patient was admitted with gastrointestinal bleeding and noted to have dry mucous membranes, orthostatic hypotension, and tachycardia. He was given intravenous saline. What diagnosis, if any, required treatment with 2 boluses of normal saline?
You remember the patient well but still pull the chart to review the case. It appears obvious that the patient was dry and needed fluid resuscitation. You are confused and do not know how to respond. Your response is just that: Patient was dry and needed fluid resuscitation.
Several days later, you get another message thanking you for your reply but describing what the coder actually needed to be able to code appropriately. Had you answered hypovolemia or dehydration, it would have changed the diagnosis‐related group (DRG) and reimbursement from gastrointestinal hemorrhage ($2700) to gastrointestinal hemorrhage with complications ($4600). Because you did not provide the right answer, the institution was reimbursed for the lesser amount. Now you are left with more questions. Hypovolemia is exactly what the patient had; you basically said so, and it was described throughout the chart, although not in so many words. Why did the coder not just say what was needed? Why can you not just answer again? Why are you being asked to play what appears to be a stupid game when you have sick patients to care for and never enough time? What can you do to prevent this from happening the next time? What other surprises are in store for you?
INTRODUCTION
Beginning October 1, 2007 the Centers for Medicare and Medicaid Services (CMS) implemented changes in the hospital inpatient prospective payment system that have profound implications for how physicians code and document hospital care. These changes were implemented in an effort to better recognize severity of illness,1 and the information will be used to plan for current and future needs of hospitals, insurers, caregivers, and patients. Severity of illness is a measure of the patient's overall health status reflected by the resources necessary for care and the risk of morbidity and mortality. Factors including the presenting illness, comorbid conditions, functional status, nutritional status, and age contribute to the severity of illness. From a physiologic perspective, factors reflecting loss of homeostatic control such as abnormal vital signs, poor oxygenation, and altered sensorium are determinants of severity of illness. For hospitals, severity of illness is generally reflected by the case mix of concomitant illness. Thus, a patient with community‐acquired pneumonia without other comorbidities requires fewer resources and has a greater chance of a good outcome than the same patient with complications such as acute congestive heart failure. In the context of this article, severity of illness should be considered an indication of the complexity of the patient's presentation. Reporting comorbidities and illness severity will help better define quality of care and medical necessity for that care.
The DRG system provided a set payment for a given hospitalization based on primary and sometimes secondary diagnoses. The new system, using Medicare severity diagnosis‐related groups (MS‐DRGs), accounts for all diagnoses present at the time of admission and all diagnoses made during the hospitalization.
This article discusses the value of appropriate documentation and outlines changes that physicians will need to make to ensure optimal coding. The value of appropriate documentation is described. Specific terminology is illustrated so physicians can document properly and coders can easily extract the necessary information from the medical record to code appropriately. Finally, specific strategies institutions can implement to support physicians and coders are suggested.
A PRIMER ON CODING AND MEDICAL DOCUMENTATION
Prior to October 1, 2007, the DRG for a given hospitalization was calculated from the principle diagnosis and in some cases 1 secondary diagnosis that represented a significant complication or comorbidity. For example, a patient admitted to the hospital with abdominal pain diagnosed as a peptic ulcer would have a DRG to reflect the ulcer. If the patient also had anemia secondary to blood loss from the ulcer, this would serve as a complication, and a DRG with a comorbidity or complication and a higher case weight would be assigned. Additional significant complications would not further alter the DRG.
The new guidelines recognize 3 levels of severity for secondary diagnoses. The DRG from the principal diagnosis can be associated with other diagnoses that recognize no complication or comorbidity, a complication or comorbidity, or a major complication or comorbidity. Thus, a patient admitted with a duodenal ulcer may have a secondary diagnosis such as hypertension, which is not considered significant enough to complicate the DRG, a complication such as ileus, or a major complication such as perforation or heart failure. Depending on the clinical circumstances, a patient admitted with a principal diagnosis of duodenal ulcer could have any of 3 DRGs.
Of all the information contained in the medical record, coders can use only documentation by physicians who are directly caring for the patient during that admission. This includes documentation by resident physicians, physician assistants, or nurse practitioners if the attending documents agreement. Notes of nurses and allied health professionals cannot be used. Consultants' notes can also be used for coding, except when their findings contradict those of the attending physician. In this case, 1 of 2 things can happen. The coder may use the documentation of the attending physician or, if clarification of the appropriate diagnosis or procedure is necessary, query the attending physician. Pathology and radiology reports and laboratory findings cannot be used unless the diagnoses are documented by the attending.
Because coders can use only documentation that follows universal terminology, physicians need to understand coding principles and learn to document using appropriate terminology.2, 3 This includes documentation of diagnoses, conditions, symptoms, or procedures defined by CMS. The large number of vagaries in the coding vernacular used by CMS sometimes makes this lexicon confusing and difficult for physicians. To ensure appropriate documentation, physicians must abandon doctorese, the shorthand vernacular that is commonly used for documentation. Even when a coder is able to correctly infer the diagnosis, he or she cannot use this information because the diagnosis was not specifically documented. It will either be lost or generate a query; both are negative consequences for the hospital and physician because reimbursement might be inappropriately low and the true level of severity of illness might not be appreciated.
Examples of this are myriad (see Appendix B) and include the following:
-
Shorthand notation, such as Na (hyponatremia) and plts, (thrombocytopenia) is not acceptable; the actual diagnosis must be written.
-
Often, there is no documentation of the diagnosis at all, but physicians read between the lines to glean the diagnosis. A note states dysuria followed by +U/A, leaving the assessment blank. The plan says ciprofloxin 500BID X 3d. Most physicians recognize this as shorthand for an uncomplicated urinary tract infection, but the documentation is incomplete because the assessment is omitted, and the coders will not be able to code.
-
A note documents an abnormal laboratory value that is intended to reflect a diagnosis (eg, Na+ = 117, restrict fluids). Coders likely understand that hyponatremia is the diagnosis, but they cannot code it because coding rules state it is only an abnormal laboratory value, not a diagnosis. Hyponatremia must be written in the medical record.
In most circumstances, a few simple guidelines will help:
-
Avoid abbreviations. Full diagnoses should be written in longhand rather than abbreviations or symbols. Use a diagnosis when appropriate, rather than just the symptom, such as hypoxia for dyspnea.
-
Write complete SOAP notes. Always document the diagnosis for which any treatment is rendered or evaluation performed. In other words, always write complete SOAP notes, not SOP notes.
-
Become familiar with rules and concepts of coding and documentation. Some peculiarities of coding rules make little sense to physicians and may appear arbitrary. Certain diagnoses, conditions, or descriptive terms that physicians commonly use cannot be used for coding purposes. These peculiarities will simply need to be learned or handled by queries from coders or real‐time chart review by coding personnel. For example, although exacerbation of chronic obstructive pulmonary disease is recognized in coding rules, exacerbation of congestive heart failure codes to a nonspecific code, and the physician must document it as acute on chronic or acute congestive heart failure. Likewise, the new terminology adopted by the National Kidney Foundation for acute renal failure, acute kidney injury, has no code. Because both of these diagnoses serve as major comorbidities, they have major financial implications for hospitals.
-
Be thorough. All clinically significant conditions noted should be documented and coded. According to CMS rules, a condition, whether major or minor, is clinically significant if it requires any of the following:4
-
Clinical evaluation
-
Therapeutic treatment
-
Diagnostic procedures
-
Extended length of hospital stay
-
Increased nursing care and/or monitoring.
-
Avoid rule‐out diagnoses. It is perfectly acceptable to qualify an uncertain diagnosis. For example, suspected pneumonia can be documented as probable or possible. If you document it as such and empirically treat for pneumonia, the coder may document pneumonia as the diagnosis. Diagnoses that have been ruled out should not be documented. For example, a patient is admitted with neutropenic fever and suspected sepsis. The patient may be given empirical therapy, but if sepsis is ruled out and the treatment is stopped, sepsis is not an appropriate diagnosis.
-
Identify the principal diagnosis. The principal diagnosis is defined as the condition responsible for the patient's admission to the hospital. All other diagnoses are secondary. If a patient enters the hospital because of sepsis of urinary origin but during the hospitalization develops pneumonia that extends the stay, the principal diagnosis from which the DRG is derived remains sepsis of urinary origin. The only exception is the patient with several conditions, any of which would have independently required hospitalization and treatment. In this case, the coders have the option of selecting the principal diagnosis from among the possible principal diagnoses if each is treated with essentially equal effort.
-
Include relevant secondary diagnoses. Another complexity and frustration regarding the coding rules is that they are often highly specific and follow a logic of their own. For coding purposes, upper gastrointestinal bleeding is a diagnosis without comorbidity. However, adding the secondary diagnosis of blood loss anemia increases the case weight by adding a comorbidity, and documenting esophageal hemorrhage adds a major comorbidity, further increasing the case weight. Coders may not, by Medicare rules, prompt or lead physicians to the proper term. If the physician documents upper gastrointestinal bleed, anemia, and esophagitis, the coder cannot ask, Was the esophagitis the cause of the anemia?
Other Considerations
Although coders cannot use documentation from nurses and allied health professionals, their notes often provide clues to issues that the physician may have failed to document. For example, a patient with significant postoperative nausea and vomiting may be treated and followed carefully by the physicians and improve despite no physician documentation. The information contained in the nursing notes can generate a query to the physician to clarify the diagnosis that required treatment for significant nausea and vomiting.
Under the new guidelines, diagnoses present on admission must be distinguished from diagnoses occurring after admission. CMS is very concerned about reducing the incidence of preventable nosocomial events such as decubitus ulcers and catheter‐associated infections. In an attempt to push hospitals to reduce or eliminate the incidence of these adverse events, CMS no longer reimburses certain diagnoses for the added cost of care when these events occur. If a patient leaves the hospital with a catheter‐associated urinary tract infection, CMS assumes that it was hospital‐acquired unless it was clearly documented as present on admission (see Appendix A). It is likely that the list will grow over time; in fact, CMS is considering adding ventilator‐associated pneumonia, Staphylococcus aureus septicemia, and deep venous thrombosis/pulmonary embolism in 2009. Thus, it is important to develop systematic methods to ensure that all diagnoses present on admission are captured and that diagnoses which developed during the hospitalization are acknowledged. A diagnosis present on admission but not recognized until after admission can be documented as present on admission. Another category will also be apparent occasionally in which it cannot be known whether a condition was present on admission or occurred following hospitalization.
PREPARING TO COMPLY WITH MS‐DRG GUIDELINES
Information from Maryland hospitals that have piloted the MS‐DRG methodology indicates that coders will be 25% to 50% less efficient (private communication), largely because of increased communication (queries) between coders and physicians to clarify medical documentation. Queries may be generated whenever the record lacks codable documentation or information is missing, conflicting, ambiguous, or illegible. Most hospitals will need to increase their coding staff and hire or develop educators to teach coders and physicians medical terminology. Many of these educators will need experience in both coding and medicine and will generally require at least an RN degree or the equivalent.5, 6 Hiring experienced coders with a medical background is currently a challenge as many hospitals are responding to the new guidelines, and they are in high demand. Many hospitals will need to upgrade the skills of existing coders or medical personnel to fill these roles. Hospitals that invest in additional coders to train physicians in coding terminology may eventually regain efficiency in the coding process; however, it seems likely that some degree of additional clarification will always be needed.
Hospitals should develop educational programs, including didactic presentations that define the new MS‐DRGs, outline the risks and benefits of the new rules, and provide examples of universal terminology. They should provide handouts, pocket guides, and electronic medical record prompts with coding terminology and frequently asked questions. Specific physician feedback may occur on an individual, departmental, or DRG basis or on the basis of the International Statistical Classification of Diseases and Related Health Problems, 9th edition. Coding specialists need to be available to provide real‐time chart review and answer specific physician inquiries on coding and documentation questions. Physician buy‐in is essential and can be encouraged through careful education, administrative support, and physician champions.
INCENTIVE AND DISINCENTIVES: HOW TO MAXIMIZE COMPLIANCE AMONG PHYSICIANS AND HOSPITALS (AND WHY IT IS SO IMPORTANT)
The new coding rules affect only hospital reimbursement, so physicians get no direct benefit from ensuring that hospitals obtain the maximum appropriate reimbursement. However, physicians indirectly benefit when hospitals have strong profit margins, which allow for improved staffing levels, capital expenditures, additional services, programs, and growth. Any physician who has worked in institutions that operate in the red and in the black fully understands how important hospital revenue is to morale, efficiency, and work satisfaction.
The importance of properly evaluating quality of care cannot be overestimated. CMS, the Joint Commission on the Accreditation of Healthcare Organizations, and other oversight bodies have emphasized this through guidelines, legislation, and financial incentives.7 Pay for performance, value‐based purchasing, and performance indicator data are terms commonly understood by physicians. Hospitals and physicians benefit from improved quality measurements, which are affected by coding and documentation. Without appropriate coding and documentation, institutions that care for the very sickest patients cannot demonstrate their true severity of illness. Increases in morbidity, mortality, and length of stay will not correlate with the documented severity of illness, adversely skewing quality data and affecting hospitals' reputations. Hospitals that do not adequately account for the severity of the patients that they treat and accurately adjust their performance measures for severity will face increasingly difficult challenges to their financial stability and reputation in the future.8 The ability to demonstrate favorable quality report cards2, 3 represents an increasingly important incentive for hospitals.9 Finally, it is important to realize the multitude of functions supported by good documentation in the medical record. The record is also important for quality measurement, protection from liability, evaluation of resource utilization, tumor and other medical data registries, and other uses (see Appendix A).
CONCLUSION
The MS‐DRG system has important implications for physicians and hospitals. The changes will allow CMS to understand more fully the severity of illness of hospitalized patients. It replaces a system that derived a DRG from a single principle diagnosis and in some cases a single comorbidity with one that reflects all conditions. Comorbidities and complications are designated as major, minor, or no complication. Because multiple parties use the medical record for many different functions, better documentation of specificity of severity of illness will affect hospitals in many ways. Importantly, one of these will be reimbursement. Hospitals that historically have had a higher level of severity will now see that reflected in their case mix and may actually see improved reimbursement. Another area that will be affected is quality measurement. If severity of illness is not appropriately documented and accounted for, hospitals could exhibit skewed outcomes of care. For example, if hospitals with sicker (on average) patients document a lower indicator of severity than the true severity of its patients, their mortality experience might appear to be abnormally high in comparison with other hospitals. This can damage reputations and thus affect many things such as patient referrals and utilization of services. This becomes particularly important in a competitive medical market and at a time when patients have increased access to hospital‐specific data on quality of care.
The new guidelines also require medical documentation to capture diagnoses present on admission as opposed to conditions that arise during hospitalization. If not recorded as present on admission, selected conditions will be considered iatrogenic complications and will not receive additional reimbursement. CMS intends this as an incentive for hospitals to improve quality of care by developing safeguards against complications.
It is likely that hospitals will take different approaches to ensuring that medical record documentation skills are taught and adopted by physicians. As different approaches evolve, hopefully best practices will emerge that can be disseminated. These efforts should be taken to ensure appropriate documentation prospectively rather than heavy reliance on a retrospective review and query process, which can be inefficient and expensive, intrusive to physician workflow, and possibly subject to third‐party criticism.
It is vital for hospital senior managers to gain physician input and involvement in both the design and implementation of the programs outlined in this article and to provide them with adequate resources and administrative support throughout the educational process. Ultimately, developing a program that enhances and sustains the medical record documentation skills of its medical staff is critical to the well‐being of any hospital. Accepting the new changes and making the changes necessary to ensure success is certainly an additional burden on physicians; many, if not most, of whom likely feel overworked and overburdened by the many demands on their time. Although they may not derive personal benefit for changing their behaviors, physicians should nevertheless understand the importance of appropriate documentation for the purposes of quality assessment, reimbursement, and resource allocation.
Appendix
APPENDIX A: SELECTED PENNSYLVANIA AND NATIONAL DATABASES USING MEDICAL RECORDS
| Joint Commission on Accreditation of Healthcare Organizations (JCAHO) |
| United Hospital Consortium (UHC) |
| Pennsylvania Health Center Cost Containment Council (PHC4) |
| United Network for Organ Sharing (UNOS) |
| National Cancer Data Base (NCDB) |
| National Database of Nursing Quality Indicators (NDNQI) |
| National Association of Children's Hospitals and Related Institutions (NACHRI) |
| Pennsylvania Trauma Systems Foundation (PTSF) |
| American College of Cardiology (ACC) |
| National Endoscopy Data Base (NEDB) |
| National Surgery Quality Improvement Program (NSQIP) |
| Society of Thoracic Surgery (STS) |
| Uniform Data System for Medical Rehabilitation (UDSMR) |
Appendix
APPENDIX B: NOTES TAKEN DIRECTLY FROM THE MEDICAL RECORD
| What the MDs Document (Doctorese) | What They Mean (Diagnosis/ Universal Terminology) | Coding Result |
|---|---|---|
| plts, Tx 4U plts | Thrombocytopenia | Coders cannot decipher |
| Na+ = 117, fluid restrict | Hyponatremia | Abnormal laboratory test; cannot code |
| O2 sat 80, NC @ 4 l/min | Hypoxia | Coders cannot decipher |
| Alb = 2.4, diet consult, start suppl | Malnutrition | Abnormal laboratory test; cannot code |
| IV NS 250/hr, 2U Tx, GI bleed | Hypovolemia, blood loss anemia | Coders cannot decipher |
| BP, fever, MS, +UA | Sepsis of urinary origin | Urinary tract infection |
Appendix
APPENDIX C: HOSPITAL‐ACQUIRED CONDITIONS OF FOCUS TO THE CENTERS FOR MEDICARE AND MEDICAID SERVICES FOR 2008
| Serious preventable event: object left in surgery |
| Serious preventable event: air embolism |
| Serious preventable event: blood incompatibility |
| Catheter‐associated urinary tract infections |
| Vascular catheterassociated infections |
| Surgical site infection: mediastinitis after coronary artery bypass surgery |
| Hospital‐acquired injuries: fractures, dislocations, intracranial injury, crushing injury, burn, and other unspecified effects of external causes |
Appendix
APPENDIX D: STRATEGIES FOR SUCCESS WITH MEDICARE SEVERITY DIAGNOSIS‐RELATED GROUPS
| Educational initiatives |
| Introductory didactic presentations |
| Online tutorial: coding and documentation |
| Periodic memos with coding tips (Tip of the Month) |
| Web site references on coding tips (comprehensive list) |
| Posters, announcements, and branding |
| Physician support services |
| Web site reference with FAQs |
| Direct contact with coding specialists |
| RN/coding specialist liaison |
| Computerized medical record |
| Staff feedback associated with query process |
| Physician champions |
| Coding department changes |
| Increased staffing |
| RN/coding specialist: real‐time chart reviews |
| Physician coding specialist |
| Standing Coding and Documentation Committee |
Appendix
APPENDIX E: SELECTED CODING TIPS FOR GENERAL MEDICINE
|
| Disease/condition specific tips |
| Gastrointestinal bleed with anemia does not mean that the patient is anemic from the hemorrhage: write blood loss anemia (chronic or acute). |
| Urosepsis codes to urinary tract infection site NOS: write sepsis with urinary origin. |
| CVA or stroke does not mean infarction: write CVA with infarction. |
| Common complications and comorbidities |
| Cardiac: acute myocardial infarction, congestive heart failure, atrial flutter, paroxysmal supraventricular tachycardia, heart block, and second‐degree heart block |
| Gastrointestinal: melena, ascites, hepatitis, and hematemesis |
| Genitourinary: urinary retention, hematuria, urinary tract infection, hydronephrosis, and renal failure |
| Nutritional: dehydration, malnutrition, cachexia, and volume overload |
| Gastrointestinal: peritonitis, perforation, bleeding esophageal varices, ascites, and ileus |
| Genitourinary: acute renal failure, end‐stage renal disease, urinary tract infection, and nephritic syndrome |
| Nutritional: severe malnutrition, body mass index > 40, malnutrition NOS, and cachexia |
| Pulmonary: respiratory failure, aspiration pneumonia, pneumothorax, atelectasis, and hemoptysis |
| General tips |
| A culture must be linked to the site of infection: write pseudomonas pneumonia. |
| Ambulatory dysfunction and deconditioning lack the required specificity to ensure accurate coding; when possible, use abnormal gait, difficulty walking, muscle weakness, and so forth. |
| If the patient appears to be septic, positive blood cultures are not necessary to document sepsis. |
| Discriminate between acute, chronic, and acute on chronic. |
| If the problem is active, do not write history of , which implies that the condition no longer exists: write PMH: chronic (diagnosis). |
| Be specific in documenting congestive heart failure (acute/chronic, systolic/diastolic failure, L/R). |
- Centers for Medicare and Medicaid Services. Medicare Program: Changes to the Hospital Inpatient Prospective Payment Systems and Fiscal Year 2008 Rates. Available at:http://www.cms.hhs.gov/acuteinpatientpps/downloads/cms‐1533‐fc.pdf. Accessed October2008.
- ,,,,.Straight talk: new approaches in healthcare. Rx for reimbursement woes: high‐quality medical documentation and coding. Panel discussion.Mod Healthc.2007;32(29):35–38.
- ,,.Optimizing hospital reimbursement through physician awareness: a step toward better patient care.Orthopedics.1998;21(1):79–83.
- ICD‐9‐CM Official Guidelines for Coding and Reporting (effective October 1, 2007). Available at:http://www.cdc.gov/nchs/datawh/ftpserv/ftpicd9/icdguide07.pdf. Accessed October2008.
- ,.Improving physician documentation through a clinical documentation management program.Nurs Adm.2003;27(4):285–289.
- .A primer for understanding diagnosis‐related groups and inpatient hospital reimbursement with nursing implications.Crit Care Nurs.2005;28(4):360–369.
- US Department of Health and Human Services. Report to Congress: Plan To Implement a Medicare Hospital Value‐Based Purchasing Program. Available at:http://www.cms.hhs.gov/acuteinpatientpps/downloads/hospitalvbpplanrtcfinalsubmitted2007.pdf. Accessed October2008.
- ,,, et al.Results of report cards for patients with congestive heart failure depend on the method used to adjust for severity.Ann Intern Med.2000;133:10–20.
- ,,, et al.Assessment of the Medicare quality improvement organization program.Ann Intern Med.2006;145(5):342–353.
- Centers for Medicare and Medicaid Services. Medicare Program: Changes to the Hospital Inpatient Prospective Payment Systems and Fiscal Year 2008 Rates. Available at:http://www.cms.hhs.gov/acuteinpatientpps/downloads/cms‐1533‐fc.pdf. Accessed October2008.
- ,,,,.Straight talk: new approaches in healthcare. Rx for reimbursement woes: high‐quality medical documentation and coding. Panel discussion.Mod Healthc.2007;32(29):35–38.
- ,,.Optimizing hospital reimbursement through physician awareness: a step toward better patient care.Orthopedics.1998;21(1):79–83.
- ICD‐9‐CM Official Guidelines for Coding and Reporting (effective October 1, 2007). Available at:http://www.cdc.gov/nchs/datawh/ftpserv/ftpicd9/icdguide07.pdf. Accessed October2008.
- ,.Improving physician documentation through a clinical documentation management program.Nurs Adm.2003;27(4):285–289.
- .A primer for understanding diagnosis‐related groups and inpatient hospital reimbursement with nursing implications.Crit Care Nurs.2005;28(4):360–369.
- US Department of Health and Human Services. Report to Congress: Plan To Implement a Medicare Hospital Value‐Based Purchasing Program. Available at:http://www.cms.hhs.gov/acuteinpatientpps/downloads/hospitalvbpplanrtcfinalsubmitted2007.pdf. Accessed October2008.
- ,,, et al.Results of report cards for patients with congestive heart failure depend on the method used to adjust for severity.Ann Intern Med.2000;133:10–20.
- ,,, et al.Assessment of the Medicare quality improvement organization program.Ann Intern Med.2006;145(5):342–353.
Newer Antifungal Agents
Therapy of serious fungal infections, for decades largely limited to the deoxycholate (regular) preparation of amphotericin B (D‐AmB), expanded significantly with the introduction of fluconazole, followed by lipid‐based formulations of amphotericin B (L‐AmB) and itraconazole. More recently the antifungal armamentarium has broadened further with the approval of voriconazole and posaconazole, as well as the echinocandins caspofungin, micafungin, and anidulafungin. Clinicians, including hospitalists, primary care, emergency medicine, and critical care physicians, may find it challenging to remain abreast of indications for these novel agents, and we review these below, with a focus on adult patients. Manuscripts used in the review were identified by a search of English‐language articles in the PubMed MEDLINE database from 1994 to the present, using the keywords triazoles, echinocandins, voriconazole, posaconazole, caspofungin, micafungin, anidulafungin, candidemia, candidiasis, aspergillosis, invasive Aspergillus, zygomycosis, febrile neutropenia, endemic mycosis, histoplasmosis, and coccidioidomycosis. In addition, reference lists for the majority of the identified manuscripts were hand‐searched for additional pertinent citations.
Table 1 summarizes the newer systemic antifungal therapies and Table 2 summarizes the significant drug‐drug interactions with the newer antifungals.
| Antifungals | Trade Name | FDA‐Approved Indications | Usual Adult Dosing | Adverse Effects |
|---|---|---|---|---|
| ||||
| Azoles | ||||
| Voriconazole | Vfend | Invasive aspergillosis. | Intravenous: 6 mg/kg IV every 12 hours, then 4 mg/kg IV every 12 hours. | Transient visual disturbances (up to 30% in trials), rash, increases in hepatic enzymes, severe hepatotoxicity, and hallucinations. |
| Candidemia in nonneutropenic patients and the following Candida infections: disseminated infections in skin and infections in abdomen, kidney, bladder wall, and wounds. | Oral: 200 mg PO every 12 hours if 40 kg, 100 mg PO every 12 hours if 40 kg. | Accumulation of sulfobutyl ester ‐cyclodextrin, a solubilizing excipient, may occur in patients with creatinine clearance 50 mL/minute receiving the intravenous formulation. | ||
| Esophageal candidiasis. | ||||
| Fungal infections due to Scedosporium apiospermum (asexual form of Pseudallescheria boydii) and Fusarium spp. including Fusarium solani, in patients intolerant of, or refractory to, other therapy. | ||||
| Posaconazole | Noxafil | Prophylaxis of invasive Aspergillus and Candida infections in patients, 13 years of age and older, who are at high risk of developing these infections due to being severely immunocompromised, such as HSCT recipients with graft‐versus‐host disease or those with hematologic malignancies with prolonged neutropenia from chemotherapy. | Prophylaxis of invasive fungal infections: 200 mg (5 mL) PO TID. | Fever, headache, dry mouth, dizziness, fatigue, nausea, vomiting, diarrhea, rash, QT interval prolongation, and elevation of hepatic enzymes. |
| Oropharyngeal candidiasis, including oropharyngeal candidiasis refractory to itraconazole and/or fluconazole. | Oropharyngeal candidiasis: loading dose of 100 mg (2.5 mL) PO BID on day 1, then 100 mg (2.5 mL) PO once daily. | |||
| Oropharyngeal candidiasis refractory to itraconazole and/or fluconazole: 400 mg (10 mL) PO BID. | ||||
| To enhance oral absorption, administer with a full meal or liquid nutritional supplement. | ||||
| Echinocandins | ||||
| Caspofungin | Cancidas | Empirical therapy for presumed fungal infections in febrile, neutropenic patients. | All indications: 70 mg IV loading dose 1, followed by 50 mg IV daily. | Phlebitis, elevation of hepatic enzymes, headache, fever, nausea, vomiting, leukopenia, and histamine mediated symptoms including rash, pruritus, facial swelling, and vasodilatation. |
| Candidemia and the following Candida infections: intraabdominal abscesses, peritonitis, and pleural space infections. | No loading dose required for esophageal candidiasis. | |||
| Esophageal candidiasis. | ||||
| Invasive aspergillosis in patients who are refractory to or intolerant of other therapies (ie, amphotericin B, lipid formulations of amphotericin B, and/or itraconazole). | ||||
| Micafungin | Mycamine | Candidemia, acute disseminated candidiasis, Candida peritonitis and abscesses. | Candidemia, acute disseminated candidiasis, Candida peritonitis and abscesses: 100 mg IV daily. | Similar to caspofungin. |
| Esophageal candidiasis. | Esophageal candidiasis: 150 mg IV daily. | |||
| Prophylaxis of Candida infections in patients undergoing HSCT. | Prophylaxis of Candida infections in HSCT recipients: 50 mg IV daily. | |||
| Anidulafungin | Eraxis | Candidemia and other forms of Candida infections (intraabdominal abscess, peritonitis). | Candidemia/other Candida infections: 200 mg IV loading dose 1, followed by 100 mg IV daily. | Similar to caspofungin. |
| Esophageal candidiasis. | Esophageal candidiasis: 100 mg IV loading dose 1, followed by 50 mg IV Q daily thereafter. | |||
| Antifungal | Effect | Interacting Drugs |
|---|---|---|
| ||
| Voriconazole | Decreased azole serum concentration | Rifampin, rifabutin, carbamazepine, long‐acting barbiturates, efavirenz, high‐dose ritonavir (400 mg twice daily), phenytoin |
| Increased azole serum concentration | Oral contraceptives containing ethinyl estradiol and norethindrone, HIV protease inhibitors other than ritonavir, and nonnucleoside reverse transcriptase inhibitors other than efavirenz | |
| Increased serum concentration of coadministered drug | Sirolimus, rifabutin, efavirenz, terfenadine, astemizole, cisapride, pimozide, quinine, cyclosporine, methadone, tacrolimus, oral contraceptives containing ethinyl estradiol and norethindrone, HIV protease inhibitors other than ritonavir, nonnucleoside reverse transcriptase inhibitors other than efavirenz, benzodiazepines, HMG‐CoA reductase inhibitors, dihydropyridine calcium channel blockers, vinca alkaloids, omeprazole, phenytoin, warfarin, sulfonylurea oral hypoglycemics, and ergot alkaloids | |
| Posaconazole | Decreased azole serum concentration | Cimetidine, rifabutin, phenytoin |
| Increased serum concentration of coadministered drug | Cyclosporine, tacrolimus, rifabutin, midazolam, pheytoin, terfenidine, astemizole, pimozide, cisapride, quinidine, ergot alkaloids, vinca alkaloids, sirolimus, HMG Co‐A reductase inhibitors, and calcium channel blockers | |
| Caspofungin | Decreased serum concentration of caspofungin | Efavirenz, nevirapine, phenytoin, dexamethasone, and carbamazepine |
| Increased serum concentration of caspofungin | Cyclosporine | |
| Decreased serum concentration of coadministered drug | Tacrolimus | |
| Micafungin | Increased serum concentration of coadministered drug | Sirolimus, nifedipine, and itraconazole |
| Anidulafungin | No clinically relevant drug‐drug interactions | |
INVASIVE CANDIDIASIS
Candida has become a leading cause of nosocomial bloodstream infections, and is associated with an attributable mortality of 15% to 25%.1 Candidemia results in an estimated 10‐day increase in hospital length of stay, as well as an average $40,000 (US) increase in costs.2 Invasive candidiasis may be defined as catheter‐related candidemia, other hematogenously disseminated disease, or visceral involvement.3 Risk factors are present in most patients with invasive candidiasis, and include broad‐spectrum antibiotics; parenteral nutrition; central catheters; hospitalization in the intensive care unit setting; renal failure; burns; gastrointestinal and cardiac surgery; and colonization with Candida, particularly at multiple sites.1, 2
Historically, treatment of invasive candidiasis consisted of D‐AmB, with fluconazole largely but not completely replacing amphotericin after prospective trials demonstrated comparable efficacy with markedly improved tolerability. Fluconazole has poor or uncertain activity against C. krusei and C. glabrata, however, leading to reluctance on the part of many clinicians to use it for non‐C. albicans infection (or empirically in the unstable patient). Others have raised concerns regarding the use of fluconazole even for C. albicans in the setting of an unstable or neutropenic patient, given its fungistatic rather than fungicidal activity, although this is a theoretical rather than proven shortcoming.1 Current Infectious Diseases Society of America (IDSA) guidelines for the treatment of candidemia recommend the use of caspofungin, fluconazole, D‐AmB, or the combination of D‐AmB and fluconazole.4 The IDSA recommendations are under revision, however, and we summarize newer evidence below.
Mora‐Duarte et al.,5 in a 2002 trial, randomized patients with invasive candidiasis to caspofungin or D‐AmB, and found a favorable response in 73% and 62%, respectively, which fell just short of statistical significance. Caspofungin was better tolerated than D‐AmB, and the authors concluded that caspofungin was at least as effective as D‐AmB, with fewer adverse effects.5 A 2007 study randomized invasive candidiasis patients to micafungin or L‐AmB, and reported similar efficacy in both arms, with less drug‐related adverse events in the echinocandin‐treated group.6 Reboli et al.7 conducted a noninferiority trial comparing anidulafungin to fluconazole, and found a significantly superior outcome in the anidulafungin arm. Perhaps surprisingly, the outcome difference between the 2 groups was greater for C. albicans than for any other species.7 Although the large majority of patients in the preceding trials had candidemia, one study demonstrated a favorable response to caspofungin in 81% of patients with invasive candidal infections other than candidemia.8
Fewer data exist regarding the use of newer azoles for the treatment of invasive candidiasis. Ostrosky‐Zeichner et al.3 utilized voriconazole as salvage therapy in 52 patients with invasive candidiasis either refractory to or intolerant of other antifungals (almost all of whom had failed therapy with D‐AmB and/or other azoles), and found a 56% favorable response rate in this challenging population. More recently, Kullberg et al.9 studied voriconazole versus D‐AmB followed by fluconazole in candidemic patients, with a similar outcome but somewhat better tolerability in the voriconazole arm. We are unaware of comparative studies involving posaconazole for invasive candidiasis.
In summary, although fluconazole is the drug of choice for most invasive candidal infections, the initial use of an echinocandin should be considered when infection with a non‐C. albicans species is likely, particularly if the patient is unstable. Provided the organism later proves likely to be sensitive, switching to fluconazole is reasonable, particularly given the absence of an oral echinocandin formulation. The 3 currently available echinocandins appear to be interchangeable for the treatment of serious Candida infections.
NEUTROPENIC FEVER
Neutropenia is the most critical factor leading to infection in patients with cancer. Empiric treatment with broad‐spectrum antimicrobials should be initiated at the first sign of infection, since delay can lead to increased mortality.10 There are numerous causes for fever in the neutropenic host, although bacterial infection is most common. Fungal infections can cause unexplained fever and should be considered in neutropenic patients who remain febrile despite broad‐spectrum antibiotics.
Fungal infections in the neutropenic host can have severe consequences. Given their high morbidity and mortality and a lack of effective diagnostic techniques for early detection, empiric antifungal therapy is mandatory in the appropriate setting. Antifungal therapy should be considered in patients who remain febrile and neutropenic for 5 days despite broad‐spectrum antibiotics. The most common fungal pathogens include Candida and Aspergillus spp.11 Other considerations include the emergence of non‐albicans Candida infections and other opportunistic pathogens such as Zygomycetes (Mucor and related pathogens), Fusarium spp, and Scedosporium spp.
Empiric antifungal coverage in the neutropenic host has evolved over the past 2 decades, with the first trials demonstrating the utility of empiric antifungal treatment in the neutropenic host published in the 1980s. These trials demonstrated that addition of D‐AmB to broad spectrum antibiotics decreased development of fungal infections, and led to better outcomes.12, 13 While these studies established D‐AmB as standard empiric antifungal therapy in neutropenic fever, nephrotoxicity and infusion‐related reactions limited its subsequent use as less toxic alternatives were developed. The lipid formulations of amphotericin B, in particular liposomal AmB and amphotericin B lipid complex, have been shown to be as effective as D‐AmB for empiric treatment of febrile neutropenia, with less toxicities but significantly higher expense.14, 15 The older generation azoles itraconazole and fluconazole have also been studied. Itraconazole has been proven to be as effective as D‐AmB in febrile neutropenia with less toxicity; however, the oral capsule has erratic absorption and should be used cautiously.16
Newer agents studied for use in febrile neutropenia include caspofungin and voriconazole. Caspofungin is active against azole‐resistant Candida spp and Aspergillus spp with a favorable toxicity profile, making it an attractive candidate for use in febrile neutropenia. Caspofungin was compared to L‐AmB as empiric antifungal therapy in a randomized double‐blind trial of 1,095 patients with febrile neutropenia.17 The overall success rate was essentially identical for both agents, demonstrating noninferiority of caspofungin therapy. Among patients with baseline fungal infections, significantly more patients receiving caspofungin than L‐AmB had successful outcomes (52% versus 26%, P = 0.04). Overall, caspofungin was better tolerated and associated with fewer complications than L‐AmB.17 The other available echinocandins, micafungin and anidulafungin, have not yet been studied for febrile neutropenia in randomized, controlled fashion.
Voriconazole is a second‐generation azole with activity against fluconazole‐resistant Candida strains; however, the minimum inhibitory concentrations (MICs) are proportionally higher, suggesting a possible cross‐resistance mechanism among highly azole‐resistant strains.18 Voriconazole is active against most Aspergillus spp, Fusarium spp, and Scedosporium apiospermum.19 Voriconazole was compared to L‐AmB in an open‐label, randomized trial of 837 patients with febrile neutropenia.20 Patients were stratified according to risk of fungal infection and previous antifungal prophylaxis. Toxic side effects were similar in both groups. Less breakthrough fungal infections were seen in the voriconazole group; however, there were more discontinuations due to lack of efficacy in patients receiving voriconazole compared to L‐AmB. The overall success rate was 26% with voriconazole and 31% with L‐AmB (95% confidence interval [CI] for absolute difference in success rates: 10.6% to 1.6%), with the low figures reflective not only of infection severity, but also gravity of underlying disease, persistent fever presumably not of fungal origin, and adverse drug effects. Because the predetermined definition of noninferiority for the confidence interval difference between the groups was not met, the U.S. Food and Drug Administration (FDA) voted against approval of voriconazole for febrile neutropenia.
Overall, the role of newer antifungals in the treatment of febrile neutropenia is evolving. Based on current evidence, we prefer caspofungin as the treatment of choice for patients with febrile neutropenia because of its low toxicity profile and good clinical spectrum against most likely pathogens. D‐AmB has long been the gold standard; however, due to toxicity concerns, lipid‐based formulations have largely replaced it, with a notable increase in cost. Voriconazole cannot be recommended at this time based on failure to meet the noninferiority endpoint when compared to L‐AmB. However, for cases in which there is a high suspicion of invasive aspergillosis infection, voriconazole should be considered.
INVASIVE ASPERGILLOSIS
Invasive aspergillosis infection has become an increasing threat in immunocompromised patients, including those treated for cancer, undergoing organ transplantation, or with advanced human immunodeficiency virus (HIV) infection. In particular, patients being treated for hematologic malignancies and those undergoing hematopoietic stem cell transplant (HSCT) are at highest risk, due to prolonged, severe neutropenia. Infection with invasive aspergillosis also occurs when steroids are used for treatment of graft‐versus‐host disease in the HSCT population.
Aspergillus species are saprobic molds found ubiquitously in nature. Most diseases are caused by Aspergillus fumigatus, followed by A. flavus, A. niger, and A. terreus. Infection with Aspergillus can cause a wide spectrum of illnesses, ranging from allergic reactions to fulminant, lethal infections. The lungs are the most common site of primary invasive disease and are associated with high mortality, especially in severely immunocompromised patients.21 Infection is rapidly progressive and can be refractory to treatment, due to the organism's ability to grow quickly and invade blood vessels. Susceptible patients are unable to control infection and thus at high risk for dissemination and death. Prompt administration of an effective antifungal agent is necessary upon suspicion of invasive disease.
The choice of antifungals for invasive Aspergillus infection has grown significantly over the past decade. Current FDA‐approved agents with activity and indications for Aspergillus infection include D‐AmB and its lipid formulations, itraconazole, voriconazole, posaconazole, and caspofungin. D‐AmB and voriconazole are the only agents licensed in the US for the primary treatment of invasive aspergillosis, with D‐AmB the sole therapeutic option until recently. The lipid formulations of amphotericin B, itraconazole, and caspofungin are approved for salvage therapy. Posaconazole is licensed for prophylaxis of invasive aspergillosis in patients who are severely immunocompromised, including those with HSCT and graft‐versus‐host disease as well as those with hematologic malignancies and prolonged neutropenia. Besides caspofungin, the other available echinocandins, micafungin and anidulafungin, are active against Aspergillus species, but not yet FDA‐approved for this indication.
Voriconazole has replaced D‐AmB as the primary treatment of invasive pulmonary aspergillosis.21 Voriconazole was compared to D‐AmB in a randomized, multicenter, open‐label trial of 277 immunocompromised patients with definite or probable disease. The underlying condition in most patients was acute leukemia or allogeneic HSCT, and the majority of patients had invasive pulmonary disease. A successful outcome at week 12 was seen in 53% in the voriconazole group and 32% in the D‐AmB group, with survival rates of 71% and 58%, respectively; both differences were statistically significant. There were more adverse events in the D‐AmB group. Overall, the authors concluded that initial therapy with voriconazole led to better responses, improved survival and fewer side effects than D‐AmB.22
Caspofungin and micafungin have been studied for use as salvage therapy in invasive Aspergillus infection. Caspofungin was studied in 83 patients with invasive aspergillosis refractory to or intolerant of D‐AmB, lipid formulations of amphotericin B, or triazoles, most of whom had hematologic malignancy and allogeneic HSCT. The majority of patients had invasive pulmonary aspergillosis, and a favorable response was seen in 45% of this extremely high‐risk population.23 Micafungin was evaluated in a phase II study as primary or salvage therapy for invasive aspergillosis in adults and children. Of the patients receiving micafungin alone, those receiving the drug as primary therapy had a 50% (n = 6/12) response rate, compared to 41% (9/22) in the salvage therapy group.24 Optimal dosing of micafungin for the treatment of Aspergillus has not yet been established.
Posaconazole, the newest triazole antifungal, has been shown to be effective for the prevention of invasive aspergillosis in immunocompromised patients25, 26 and has also been studied for the treatment of invasive disease. In an open‐label trial, patients with invasive aspergillosis refractory or intolerant to conventional therapy were administered posaconazole, with historical controls as a comparator group.27 The majority of patients had underlying hematologic malignancies with approximately half undergoing HSCT, and most patients had pulmonary infection. The overall success rate was 42% for posaconazole and 26% for the control group. Posaconazole appeared to confer a survival benefit over control at 30 days and end of therapy (P = 0.0003).
Based on current data, we recommend voriconazole for primary treatment of invasive pulmonary aspergillosis. Alternatives include L‐AmB, caspofungin, micafungin, or posaconazole; of these agents, only L‐AmB has been studied as primary (as opposed to salvage) therapy for invasive aspergillosis in a reasonably‐powered trial.28 We agree with current IDSA guidelines, which suggest L‐AmB as a possible alternative to voriconazole for primary therapy of invasive aspergillosis in some patients, particularly where drug‐drug interactions make the use of voriconazole problematic.21
MUCOCUTANEOUS CANDIDIASIS
Oropharyngeal candidiasis, or thrush, is a common infection in infants; those receiving antibiotics, chemotherapy or inhaled corticosteroids; and those with underlying immunodeficiency states. Esophageal candidiasis is most common in patients infected with HIV. Oral candidiasis usually does not cause symptoms, while esophageal disease is associated with odynophagia and dysphagia.
Candida albicans is the most common cause of mucocutaneous candidiasis. Treatment of thrush usually entails topical antifungal agents such as clotrimazole troches or nystatin, or oral azoles such as fluconazole or itraconazole. Topical therapy is ineffective for esophageal candidiasis, and oral or intravenous azoles are required as first‐line therapy with fluconazole being preferred. The treatment of oral and esophageal candidiasis is often complicated by recurrence, especially in immunodeficient patients, and resistance to standard treatments occurs frequently. Identification of Candida to the species level should be performed in the setting of refractory mucocutaneous disease, as this may play a role in the choice of therapy. The 2004 IDSA Guidelines, currently under revision, contain recommendations for treatment of refractory mucocutaneous candidiasis.4 The guidelines recommend a trial of oral itraconazole for fluconazole‐refractory thrush. Intravenous caspofungin and D‐AmB are usually effective alternatives. For treatment of fluconazole‐refractory esophageal disease, the guidelines recommend itraconazole solution, voriconazole, or caspofungin, with D‐AmB recommended as second line therapy, though it is now seldom used in this setting due to significant adverse affects. Experience using newer antifungals is increasing, and these data are summarized below.
Voriconazole has been shown at least as effective as fluconazole in the treatment of esophageal candidiasis in immunocompromised patients.29 A study involving 256 patients revealed success rates of 98% for voriconazole and 95% for fluconazole. C. albicans was the most common pathogen isolated. Perfect et al.30 demonstrated the utility of voriconazole for refractory esophageal candidiasis in 38 patients. A successful outcome was seen in 61% of patients treated with intravenous followed by oral voriconazole. The most common pathogen was C. albicans, although the series included several cases of infection with C. krusei.
Caspofungin was compared to D‐AmB for the treatment of esophageal candidiasis in a multicenter, double‐blind, randomized trial of 128 patients.31 Caspofungin appeared to be at least as effective as D‐AmB, with a significantly higher incidence of drug‐related adverse effects seen in the D‐AmB arm. Caspofungin was also compared to fluconazole in a double‐blind, randomized trial of 177 patients with Candida esophagitis. Favorable responses were seen in 81% and 85% of caspofungin and fluconazole treated patients, respectively. A trend toward higher relapse rate 4 weeks after stopping therapy was seen with caspofungin compared to fluconazole, as was a trend toward superior eradication rates for C. glabrata in the caspofungin arm compared to the fluconazole arm, although neither reached statistical significance.32
Micafungin was used for the treatment of esophageal candidiasis in a dose‐ranging trial of 245 HIV‐infected patients.33 Endoscopic combined cure rate for the 100 mg and 150 mg doses of micafungin (84%) was comparable to that of intravenous fluconazole 200 mg/day (87%). In the posttreatment period, 9 patients in the micafungin arm had a worsening of severity score or received nonprophylactic antifungal therapy. No patients in the fluconazole group experienced a relapse.
Anidulafungin has been compared with fluconazole for the treatment of Candida esophagitis in a randomized, double‐blind trial of 601 patients, with an initial endoscopic success rate approaching 100% in both groups.34 The 2‐week follow‐up examination revealed that 64% and 90% of patients treated with anidulafungin and fluconazole, respectively, sustained endoscopic success (P 0.001).
Posaconazole was compared with fluconazole for treatment of thrush in 350 patients with HIV/acquired immunodeficiency syndrome (AIDS) in a randomized, blinded study.35 Both posaconazole and fluconazole were administered at a dose of 200 mg on day 1, followed by 100 mg/day. Clinical success occurred in 92% of patients receiving posaconazole and 93% receiving fluconazole. Mycological success was equivalent on day 14 in both arms; however, by day 42, significantly more posaconazole recipients continued to demonstrate mycological success. Posaconazole was recently evaluated for the treatment of azole‐refractory thrush and esophageal candidiasis in patients with advanced HIV infection, demonstrating a success rate of 75% in this population failing fluconazole or itraconazole therapy.36
Multiple new agents are available for the treatment of mucocutaneous candidiasis. Aside from topical antifungals for the initial treatment of thrush, fluconazole remains first line systemic therapy for both oral and esophageal candidiasis due to safety, tolerability, and cost. For fluconazole‐refractory disease, newer choices include voriconazole, the echinocandins, and posaconazole. Voriconazole and posaconazole are attractive options given their oral availability. The relapse rates seen in trials with the echinocandins are concerning; however, these are useful options when azole resistance is suspected.
ZYGOMYCOSIS
Zygomycosis (often referred to less correctly as mucormycosis) is a devastating opportunistic fungal infection that appears to be increasing in frequency. Historically, zygomycosis has commonly occurred in poorly controlled diabetic patients, particularly in the setting of diabetic ketoacidosis, and classically results in rhinocerebral disease with a relatively poor outcome. In recent years, a striking increase has been seen in patients with more profound immunosuppression, particularly those with hematologic malignancies or undergoing HSCT. Sinopulmonary rather than rhinocerebral disease is the most common manifestation in this population.3739 Other well‐described risk factors include iron chelation therapy with deferoxamine, intravenous drug use, solid organ transplantation, metabolic acidosis, trauma, and burns. Disease is also occasionally seen in the seemingly immunocompetent, with 176 of 929 (19%) patients in a comprehensive review lacking an obvious risk factor.37, 40
Invasive mold infections caused by the Zygomycetes are associated with a poor outcome, with Roden et al.37 reporting mortality in excess of 50% in their series. Mortality in patients with hematological malignancies has been reported to be particularly high.37, 38 The cornerstones of successful therapy include early detection of infection, correction or improvement of immunosuppression when possible, prompt surgical debridement of infected tissue, and appropriate antifungal therapy.40 D‐AmB has constituted standard zygomycosis therapy for decades, although it has recently been largely replaced by L‐AmB. Overall survival rates have been reported to be 61% and 69% with the use of D‐AmB and lipid preparations, respectively.37
Given the relatively poor outcomes and substantial infusion‐related toxicity and nephrotoxicity associated with even liposomal preparations of AmB, considerable interest exists in the identification of alternative therapeutic agents. Unfortunately, echinocandins and most triazoles appear to have modest to no activity against Zygomycetes, with a recent case‐control study indicating that widespread use of voriconazole in high‐risk populations may be helping to drive the emergence of breakthrough zygomycosis.39 Posaconazole appears to be an exception, however; with in vitro and murine studies suggesting it compares favorably to D‐AmB in this setting.4143 Numerous case reports describe favorable outcomes with the use of posaconazole as salvage therapy for zygomycosis, and 2 recent retrospective studies support its role in this setting.44, 45 Currently, use of posaconazole for the treatment of zygomycosis is limited by the absence of an intravenous preparation, although this is reportedly under development.46 At present, the role of posaconazole in this setting appears limited to step‐down therapy in those patients who have responded appropriately to L‐AmB, and for salvage therapy. Although an intravenous preparation of posaconazole appears attractive as a first‐line agent for zygomycosis, currently studied patients (ie, those unresponsive to or intolerant of D‐AmB) may not be fully representative of a broader population, and clinical trials will be necessary before more definitive conclusions may be drawn.47
ENDEMIC MYCOSES
Coccidioidomycosis
Coccidioidomycosis results from environmental exposure to either Coccidioides immitis or C. posadii. At least 50% of infections are asymptomatic, with the majority of the remaining individuals exhibiting acute, self‐limited pulmonary symptoms. A small percentage of patients develop chronic illness, either pulmonary or disseminated disease, including involvement of skin, bone/joint, and central nervous system (CNS).48, 49 Current therapy consists of either fluconazole or itraconazole for CNS disease and non‐life‐threatening disease elsewhere, with D‐AmB reserved for pregnancy and more fulminant illness.49 Unfortunately, response failures and relapses are seen commonly with all of these agents, with a resultant need for alternative antifungals.
The echinocandins have no clear role in the treatment of coccidioidomycosis.49 More interest surrounds the use of the newer azoles, with multiple studies demonstrating excellent in vitro activity of both voriconazole and posaconazole against Coccidioides species.5052 Several recently reported open‐label studies have reported good results with the use of posaconazole for chronic coccidioidomycosis, 2 of which enrolled patients intolerant of or refractory to usual agents.5355 Based on these data, posaconazole appears to be highly active against Coccidioides, and should perhaps be the drug of choice in the majority of patients who fail to respond to or tolerate older triazoles.
Histoplasmosis
Histoplasmosis is particularly endemic in the Ohio and Mississippi valleys, although it occurs less commonly in many other areas as well. Inhaled Histoplasma capsulatum conidia result in subclinical infection in the majority of exposed individuals, with self‐limited pneumonia the rule in most others. A minority of patients will experience chronic pulmonary disease or dissemination.56 Not all disease requires treatment, with most pulmonary disease resolving spontaneously; but definite indications for treatment include moderate or severe pneumonia, chronic cavitary lung disease, CNS involvement, and progressive disseminated disease.56 Standard therapy consists of itraconazole or lipid formulations of amphotericin B, based on severity. Multiple studies have demonstrated excellent in vitro activity of voriconazole and particularly posaconazole against H. capsulatum.52, 5759 Recently, in 2 small series of patients, patients failing either to improve with or tolerate conventional agents demonstrated favorable outcomes when they were treated with voriconazole or posaconazole.60, 61 Both drugs appear to be appropriate second‐line agents, with posaconazole arguably preferable based on current evidence.
CONCLUSIONS
The spectrum of available antifungal agents has expanded considerably in recent years, and the advent of additional drugs is expected shortly. Well‐tolerated and effective drugs are now available for most fungal infections, although the precise role for newer agents in some of these diseases has yet to be defined. Future clinical trials should help resolve these uncertainties.
- ,,.Current treatment strategies for disseminated candidiasis.Clin Infect Dis.2006;42:244–251.
- .Echinocandins for candidemia in adults without neutropenia.N Engl J Med.2006;355:1154–1159.
- ,,,.Voriconazole salvage treatment of invasive candidiasis.Eur J Clin Microbiol Infect Dis.2003;22:651–655.
- ,,, et al.Guidelines for treatment of candidiasis.Clin Infect Dis.2004;38:161–189.
- ,,, et al.Comparison of caspofugin and amphotericin B for invasive candidiasis.N Engl J Med.2002;347:2020–2029.
- ,,, et al.Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomized double‐blind trial.Lancet.2007;369:1519–1527.
- ,,, et al.Anidulafungin versus fluconazole for invasive candidiasis.N Engl J Med.2007;356:2472–2482.
- ,,, et al.Caspofungin for the treatment of less common forms of invasive candidiasis.J Antimicrob Chemother.2007;60:363–369.
- ,,, et al.Voriconazole versus a regimen of amphotericin B followed by fluconazole for candidaemia in non‐neutropenic patients: a randomized non‐inferiority trial.Lancet.2005;366:1435–1442.
- ,.Fever of unknown origin in febrile leucopenia.Infect Dis Clin North Am.2007;21:1055–1090.
- ,,, et al.2002 Guidelines for the use of antimicrobial agents in neutropenic patients with cancer.Clin Infect Dis.2002;34:730–751.
- ,,, et al.Empiric antibiotic and antifungal therapy for cancer patients with prolonged fever and granulocytopenia.Am J Med.1982;72:101–111.
- EORTC International Antimicrobial Therapy Cooperative Group.Empiric antifungal therapy in febrile granulocytopenic patients.Am J Med.1989;86:668–672.
- ,,, et al.Liposomal amphotericin B for empirical therapy in patients with persistent fever and neutropenia.N Engl J Med.1999;340:7644–7671.
- ,,, et al.A randomized comparison of liposomal versus conventional amphotericin B for the treatment of pyrexia of unknown origin in neutropenic patients.Br J Haematol.1997;98:711–718.
- ,,, et al.Pharmacokinetics and safety of a 7 day administration of intravenous itraconazole followed by a 14‐day administration of itraconazole oral solution in patients with hematologic malignancy.Antimicrob Agents Chemother.2001;45:981–985.
- ,,, et al.Caspofungin versus liposomal amphotericin B for empirical antifungal therapy in patients with persistent fever and neutropenia.N Engl J Med.2004;351:1392–1402.
- ,,, et al.In vitro activities of voriconazole and four other antifungal agents against 394 clinical isolates of Candida spp.Antimicrob Agents Chemother.1998;42:161–163.
- ,,, et al.Antifungal activity of a new triazole, voriconazole (UK‐109,496) compared with three other antifungal agents tested against clinical isolates of filamentous fungi.Med Mycol.1998;36:433–436.
- ,,, et al.Voriconazole compared with liposomal amphotericin B for empirical antifungal therapy in patients with neutropenia and persistent fever.N Engl J Med.2002;346:225–234.
- ,,, et al.Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America.Clin Infect Dis.2008;46:327–360.
- ,,, et al.Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis.N Engl J Med.2002;347:408–415.
- ,,, et al.Efficacy and safety of caspofungin for treatment of invasive aspergillosis in patients refractory to or intolerant of conventional antifungal therapy.Clin Infect Dis.2004;39:1563–1571.
- ,,, et al.Micafungin (FK463), alone or in combination with other systemic antifungal agents, for the treatment of acute invasive aspergillosis.J Infect2006;53:337–349.
- ,,, et al.Posaconazole vs. fluconazole or itraconazole prophylaxis in patients with neutropenia.N Engl J Med.2007;356:348–359.
- ,,, et al.Posaconazole or fluconazole for prophylaxis in severe graft versus host disease.N Engl J Med.2007;356:335–347.
- ,,, et al.Treatment of invasive aspergillosis with posaconazole in patients who are refractory to or intolerant of conventional therapy: an externally controlled trial.Clin Infect Dis.2007;44:2–12.
- ,,, et al.Liposomal amphotericin B as initial therapy for invasive mold infection: a randomized trial comparing a high‐loading dose regimen with standard dosing (AmBiLoad trial).Clin Infect Dis.2007;44:1289–1297.
- ,,, et al.A randomized, double‐blind, double‐dummy, multicenter trial of voriconazole and fluconazole in the treatment of esophageal candidiasis in immunocompromised patients.Clin Infect Dis.2001;33:1447–1454.
- ,,, et al.Voriconazole treatment for less‐common, emerging, or refractory fungal infections.Clin Infect Dis.2003;36:1122–1131.
- ,,, et al.A randomized double‐blind study of caspofungin versus amphotericin for the treatment of candidal esophagitis.Clin Infect Dis.2001;33:1529–1535.
- ,,, et al.A randomized double‐blind study of caspofungin versus fluconazole for the treatment of esophageal candidiasis.Am J Med.2002;113:294–299.
- ,,, et al.A randomized, double‐blind, parallel‐group, dose‐response study of micafungin compared with fluconazole for the treatment of esophageal candidiasis in HIV‐positive patients.Clin Infect Dis.2004;39:842–849.
- ,,, et al.A randomized, double‐blind trial of anidulafungin versus fluconazole for the treatment of esophageal candidiasis.Clin Infect Dis.2004;39:770–775.
- ,,, et al.A multicenter randomized trial evaluating posaconazole versus fluconazole for the treatment of oropharyngeal candidiasis in subjects with HIV/AIDS.Clin Infect Dis.2006;42:1179–1186.
- ,,, et al.Posaconazole for the treatment of azole‐refractory oropharyngeal and esophageal candidiasis in subjects with HIV infection.Clin Infect Dis.2007;44:607–614.
- ,,, et al.Epidemiology and outcome of zygomycosis: a review of 929 reported cases.Clin Infect Dis.2005;41:634–653.
- ,,,.Zygomycosis in the 1990s in a tertiary‐care cancer center.Clin Infect Dis.2000;30:851–856.
- ,,, et al.Zygomycosis in a tertiary‐care center in the era of Aspergillus‐active antifungal therapy: a case‐control observational study of 27 recent cases.J Infect Dis.2005;191:1350–1360.
- ,.Invasive zygomycosis: update on pathogenesis, clinical manifestations, and management.Infect Dis Clin North Am.2006;20:581–607.
- ,,,,.In vitro activities of posaconazole itraconazole, voriconazole, amphotericin B, and fluconazole against 37 clinical isolates of zygomycetes.Antimicrob Agents Chemother.2002;46:1581–1582.
- ,,,,.In vivo activity of posaconazole against mucor spp. in an immunosuppressed‐mouse model.Antimicrob Agents Chemother.2002;46:2310–2312.
- ,,,,.In vitro susceptibilities of 217 clinical isolates of zygomycetes to conventional and new antifungal agents.Antimicrob Agents Chemother.2007;51:2587–2590.
- ,,, et al.Posaconazole as salvage therapy for zygomycosis.Antimicrob Agents Chemother.2006;50:126–133.
- ,,,,.Posaconazole is effective as salvage therapy in zygomycosis: a retrospective summary of 91 cases.Clin Infect Dis.2006;42:e61–e65.
- ,.Changing epidemiology of rare mould infections.Drugs.2007;67:1803–1812.
- .Posaconazole.Drugs.2005;65:1568–1569.
- ,,, et al.Coccidioidomycosis.Clin Infect Dis.2005;41:1217–1223.
- ,,.Epidemiologic, clinical, and diagnostic aspects of coccidioidomycosis.J Clin Microbiol.2007;4:26–30.
- ,,,.Therapeutic efficacy of caspofungin alone and in combination with amphotericin B deoxycholate for coccidioidomycosis in a mouse model.J Antimicrob Chemother.2007;60:1341–1346.
- ,.Antifungal susceptibility profiles of Coccidioides immitis and Coccidioides posadasii from endemic and non‐endemic areas.Mycopathologia.2007;163:31–19.
- ,,,,,.In vitro activities of voriconazole, itraconazole, and amphotericin B against Blastomyces dermatitidis, Coccidioides immitis, and Histoplasma capsulatum.Antimicrob Agents Chemother.2000;44:1734–1736.
- ,,,,.Refractory coccidioidomycosis treated with posaconazole.Clin Infect Dis.2005;40:1770–1776.
- ,,, et al.Safety, tolerance, and efficacy of posaconazole therapy in patients with nonmeningeal disseminated or chronic pulmonary coccidioidomycosis.Clin Infect Dis.2007;45:562–568.
- ,,, et al.Posaconazole therapy for chronic refractory coccidioidomycosis.Chest.2007;132:952–958.
- ,,, et al.Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America.Clin Infect Dis.2007;45:807–825.
- ,,,,.In vitro activities of new and established triazoles against opportunistic filamentous and dimorphic fungi.Med Mycol.2005;43:281–284.
- ,,, et al.Comparison of a new triazole antifungal agent, Schering 56592, with itraconazole and amphotericin B for treatment of histoplasmosis in immunocompetent mice.Antimicrob Agents Chemother.1999;439:322–328.
- ,,, et al.Activity of newer triazoles against Histoplasma capsulatum from patients with AIDS who failed fluconazole.J Antimicrob Chemother.2006;57:1235–1239.
- ,,,,,.Histoplasmosis in solid organ transplant recipients at a large midwestern university transplant center.Transpl Infect Dis.2005;7:109–115.
- ,,, et al.Salvage treatment of histoplasmosis with posaconazole.J Infect.2007;54:319–327.
Therapy of serious fungal infections, for decades largely limited to the deoxycholate (regular) preparation of amphotericin B (D‐AmB), expanded significantly with the introduction of fluconazole, followed by lipid‐based formulations of amphotericin B (L‐AmB) and itraconazole. More recently the antifungal armamentarium has broadened further with the approval of voriconazole and posaconazole, as well as the echinocandins caspofungin, micafungin, and anidulafungin. Clinicians, including hospitalists, primary care, emergency medicine, and critical care physicians, may find it challenging to remain abreast of indications for these novel agents, and we review these below, with a focus on adult patients. Manuscripts used in the review were identified by a search of English‐language articles in the PubMed MEDLINE database from 1994 to the present, using the keywords triazoles, echinocandins, voriconazole, posaconazole, caspofungin, micafungin, anidulafungin, candidemia, candidiasis, aspergillosis, invasive Aspergillus, zygomycosis, febrile neutropenia, endemic mycosis, histoplasmosis, and coccidioidomycosis. In addition, reference lists for the majority of the identified manuscripts were hand‐searched for additional pertinent citations.
Table 1 summarizes the newer systemic antifungal therapies and Table 2 summarizes the significant drug‐drug interactions with the newer antifungals.
| Antifungals | Trade Name | FDA‐Approved Indications | Usual Adult Dosing | Adverse Effects |
|---|---|---|---|---|
| ||||
| Azoles | ||||
| Voriconazole | Vfend | Invasive aspergillosis. | Intravenous: 6 mg/kg IV every 12 hours, then 4 mg/kg IV every 12 hours. | Transient visual disturbances (up to 30% in trials), rash, increases in hepatic enzymes, severe hepatotoxicity, and hallucinations. |
| Candidemia in nonneutropenic patients and the following Candida infections: disseminated infections in skin and infections in abdomen, kidney, bladder wall, and wounds. | Oral: 200 mg PO every 12 hours if 40 kg, 100 mg PO every 12 hours if 40 kg. | Accumulation of sulfobutyl ester ‐cyclodextrin, a solubilizing excipient, may occur in patients with creatinine clearance 50 mL/minute receiving the intravenous formulation. | ||
| Esophageal candidiasis. | ||||
| Fungal infections due to Scedosporium apiospermum (asexual form of Pseudallescheria boydii) and Fusarium spp. including Fusarium solani, in patients intolerant of, or refractory to, other therapy. | ||||
| Posaconazole | Noxafil | Prophylaxis of invasive Aspergillus and Candida infections in patients, 13 years of age and older, who are at high risk of developing these infections due to being severely immunocompromised, such as HSCT recipients with graft‐versus‐host disease or those with hematologic malignancies with prolonged neutropenia from chemotherapy. | Prophylaxis of invasive fungal infections: 200 mg (5 mL) PO TID. | Fever, headache, dry mouth, dizziness, fatigue, nausea, vomiting, diarrhea, rash, QT interval prolongation, and elevation of hepatic enzymes. |
| Oropharyngeal candidiasis, including oropharyngeal candidiasis refractory to itraconazole and/or fluconazole. | Oropharyngeal candidiasis: loading dose of 100 mg (2.5 mL) PO BID on day 1, then 100 mg (2.5 mL) PO once daily. | |||
| Oropharyngeal candidiasis refractory to itraconazole and/or fluconazole: 400 mg (10 mL) PO BID. | ||||
| To enhance oral absorption, administer with a full meal or liquid nutritional supplement. | ||||
| Echinocandins | ||||
| Caspofungin | Cancidas | Empirical therapy for presumed fungal infections in febrile, neutropenic patients. | All indications: 70 mg IV loading dose 1, followed by 50 mg IV daily. | Phlebitis, elevation of hepatic enzymes, headache, fever, nausea, vomiting, leukopenia, and histamine mediated symptoms including rash, pruritus, facial swelling, and vasodilatation. |
| Candidemia and the following Candida infections: intraabdominal abscesses, peritonitis, and pleural space infections. | No loading dose required for esophageal candidiasis. | |||
| Esophageal candidiasis. | ||||
| Invasive aspergillosis in patients who are refractory to or intolerant of other therapies (ie, amphotericin B, lipid formulations of amphotericin B, and/or itraconazole). | ||||
| Micafungin | Mycamine | Candidemia, acute disseminated candidiasis, Candida peritonitis and abscesses. | Candidemia, acute disseminated candidiasis, Candida peritonitis and abscesses: 100 mg IV daily. | Similar to caspofungin. |
| Esophageal candidiasis. | Esophageal candidiasis: 150 mg IV daily. | |||
| Prophylaxis of Candida infections in patients undergoing HSCT. | Prophylaxis of Candida infections in HSCT recipients: 50 mg IV daily. | |||
| Anidulafungin | Eraxis | Candidemia and other forms of Candida infections (intraabdominal abscess, peritonitis). | Candidemia/other Candida infections: 200 mg IV loading dose 1, followed by 100 mg IV daily. | Similar to caspofungin. |
| Esophageal candidiasis. | Esophageal candidiasis: 100 mg IV loading dose 1, followed by 50 mg IV Q daily thereafter. | |||
| Antifungal | Effect | Interacting Drugs |
|---|---|---|
| ||
| Voriconazole | Decreased azole serum concentration | Rifampin, rifabutin, carbamazepine, long‐acting barbiturates, efavirenz, high‐dose ritonavir (400 mg twice daily), phenytoin |
| Increased azole serum concentration | Oral contraceptives containing ethinyl estradiol and norethindrone, HIV protease inhibitors other than ritonavir, and nonnucleoside reverse transcriptase inhibitors other than efavirenz | |
| Increased serum concentration of coadministered drug | Sirolimus, rifabutin, efavirenz, terfenadine, astemizole, cisapride, pimozide, quinine, cyclosporine, methadone, tacrolimus, oral contraceptives containing ethinyl estradiol and norethindrone, HIV protease inhibitors other than ritonavir, nonnucleoside reverse transcriptase inhibitors other than efavirenz, benzodiazepines, HMG‐CoA reductase inhibitors, dihydropyridine calcium channel blockers, vinca alkaloids, omeprazole, phenytoin, warfarin, sulfonylurea oral hypoglycemics, and ergot alkaloids | |
| Posaconazole | Decreased azole serum concentration | Cimetidine, rifabutin, phenytoin |
| Increased serum concentration of coadministered drug | Cyclosporine, tacrolimus, rifabutin, midazolam, pheytoin, terfenidine, astemizole, pimozide, cisapride, quinidine, ergot alkaloids, vinca alkaloids, sirolimus, HMG Co‐A reductase inhibitors, and calcium channel blockers | |
| Caspofungin | Decreased serum concentration of caspofungin | Efavirenz, nevirapine, phenytoin, dexamethasone, and carbamazepine |
| Increased serum concentration of caspofungin | Cyclosporine | |
| Decreased serum concentration of coadministered drug | Tacrolimus | |
| Micafungin | Increased serum concentration of coadministered drug | Sirolimus, nifedipine, and itraconazole |
| Anidulafungin | No clinically relevant drug‐drug interactions | |
INVASIVE CANDIDIASIS
Candida has become a leading cause of nosocomial bloodstream infections, and is associated with an attributable mortality of 15% to 25%.1 Candidemia results in an estimated 10‐day increase in hospital length of stay, as well as an average $40,000 (US) increase in costs.2 Invasive candidiasis may be defined as catheter‐related candidemia, other hematogenously disseminated disease, or visceral involvement.3 Risk factors are present in most patients with invasive candidiasis, and include broad‐spectrum antibiotics; parenteral nutrition; central catheters; hospitalization in the intensive care unit setting; renal failure; burns; gastrointestinal and cardiac surgery; and colonization with Candida, particularly at multiple sites.1, 2
Historically, treatment of invasive candidiasis consisted of D‐AmB, with fluconazole largely but not completely replacing amphotericin after prospective trials demonstrated comparable efficacy with markedly improved tolerability. Fluconazole has poor or uncertain activity against C. krusei and C. glabrata, however, leading to reluctance on the part of many clinicians to use it for non‐C. albicans infection (or empirically in the unstable patient). Others have raised concerns regarding the use of fluconazole even for C. albicans in the setting of an unstable or neutropenic patient, given its fungistatic rather than fungicidal activity, although this is a theoretical rather than proven shortcoming.1 Current Infectious Diseases Society of America (IDSA) guidelines for the treatment of candidemia recommend the use of caspofungin, fluconazole, D‐AmB, or the combination of D‐AmB and fluconazole.4 The IDSA recommendations are under revision, however, and we summarize newer evidence below.
Mora‐Duarte et al.,5 in a 2002 trial, randomized patients with invasive candidiasis to caspofungin or D‐AmB, and found a favorable response in 73% and 62%, respectively, which fell just short of statistical significance. Caspofungin was better tolerated than D‐AmB, and the authors concluded that caspofungin was at least as effective as D‐AmB, with fewer adverse effects.5 A 2007 study randomized invasive candidiasis patients to micafungin or L‐AmB, and reported similar efficacy in both arms, with less drug‐related adverse events in the echinocandin‐treated group.6 Reboli et al.7 conducted a noninferiority trial comparing anidulafungin to fluconazole, and found a significantly superior outcome in the anidulafungin arm. Perhaps surprisingly, the outcome difference between the 2 groups was greater for C. albicans than for any other species.7 Although the large majority of patients in the preceding trials had candidemia, one study demonstrated a favorable response to caspofungin in 81% of patients with invasive candidal infections other than candidemia.8
Fewer data exist regarding the use of newer azoles for the treatment of invasive candidiasis. Ostrosky‐Zeichner et al.3 utilized voriconazole as salvage therapy in 52 patients with invasive candidiasis either refractory to or intolerant of other antifungals (almost all of whom had failed therapy with D‐AmB and/or other azoles), and found a 56% favorable response rate in this challenging population. More recently, Kullberg et al.9 studied voriconazole versus D‐AmB followed by fluconazole in candidemic patients, with a similar outcome but somewhat better tolerability in the voriconazole arm. We are unaware of comparative studies involving posaconazole for invasive candidiasis.
In summary, although fluconazole is the drug of choice for most invasive candidal infections, the initial use of an echinocandin should be considered when infection with a non‐C. albicans species is likely, particularly if the patient is unstable. Provided the organism later proves likely to be sensitive, switching to fluconazole is reasonable, particularly given the absence of an oral echinocandin formulation. The 3 currently available echinocandins appear to be interchangeable for the treatment of serious Candida infections.
NEUTROPENIC FEVER
Neutropenia is the most critical factor leading to infection in patients with cancer. Empiric treatment with broad‐spectrum antimicrobials should be initiated at the first sign of infection, since delay can lead to increased mortality.10 There are numerous causes for fever in the neutropenic host, although bacterial infection is most common. Fungal infections can cause unexplained fever and should be considered in neutropenic patients who remain febrile despite broad‐spectrum antibiotics.
Fungal infections in the neutropenic host can have severe consequences. Given their high morbidity and mortality and a lack of effective diagnostic techniques for early detection, empiric antifungal therapy is mandatory in the appropriate setting. Antifungal therapy should be considered in patients who remain febrile and neutropenic for 5 days despite broad‐spectrum antibiotics. The most common fungal pathogens include Candida and Aspergillus spp.11 Other considerations include the emergence of non‐albicans Candida infections and other opportunistic pathogens such as Zygomycetes (Mucor and related pathogens), Fusarium spp, and Scedosporium spp.
Empiric antifungal coverage in the neutropenic host has evolved over the past 2 decades, with the first trials demonstrating the utility of empiric antifungal treatment in the neutropenic host published in the 1980s. These trials demonstrated that addition of D‐AmB to broad spectrum antibiotics decreased development of fungal infections, and led to better outcomes.12, 13 While these studies established D‐AmB as standard empiric antifungal therapy in neutropenic fever, nephrotoxicity and infusion‐related reactions limited its subsequent use as less toxic alternatives were developed. The lipid formulations of amphotericin B, in particular liposomal AmB and amphotericin B lipid complex, have been shown to be as effective as D‐AmB for empiric treatment of febrile neutropenia, with less toxicities but significantly higher expense.14, 15 The older generation azoles itraconazole and fluconazole have also been studied. Itraconazole has been proven to be as effective as D‐AmB in febrile neutropenia with less toxicity; however, the oral capsule has erratic absorption and should be used cautiously.16
Newer agents studied for use in febrile neutropenia include caspofungin and voriconazole. Caspofungin is active against azole‐resistant Candida spp and Aspergillus spp with a favorable toxicity profile, making it an attractive candidate for use in febrile neutropenia. Caspofungin was compared to L‐AmB as empiric antifungal therapy in a randomized double‐blind trial of 1,095 patients with febrile neutropenia.17 The overall success rate was essentially identical for both agents, demonstrating noninferiority of caspofungin therapy. Among patients with baseline fungal infections, significantly more patients receiving caspofungin than L‐AmB had successful outcomes (52% versus 26%, P = 0.04). Overall, caspofungin was better tolerated and associated with fewer complications than L‐AmB.17 The other available echinocandins, micafungin and anidulafungin, have not yet been studied for febrile neutropenia in randomized, controlled fashion.
Voriconazole is a second‐generation azole with activity against fluconazole‐resistant Candida strains; however, the minimum inhibitory concentrations (MICs) are proportionally higher, suggesting a possible cross‐resistance mechanism among highly azole‐resistant strains.18 Voriconazole is active against most Aspergillus spp, Fusarium spp, and Scedosporium apiospermum.19 Voriconazole was compared to L‐AmB in an open‐label, randomized trial of 837 patients with febrile neutropenia.20 Patients were stratified according to risk of fungal infection and previous antifungal prophylaxis. Toxic side effects were similar in both groups. Less breakthrough fungal infections were seen in the voriconazole group; however, there were more discontinuations due to lack of efficacy in patients receiving voriconazole compared to L‐AmB. The overall success rate was 26% with voriconazole and 31% with L‐AmB (95% confidence interval [CI] for absolute difference in success rates: 10.6% to 1.6%), with the low figures reflective not only of infection severity, but also gravity of underlying disease, persistent fever presumably not of fungal origin, and adverse drug effects. Because the predetermined definition of noninferiority for the confidence interval difference between the groups was not met, the U.S. Food and Drug Administration (FDA) voted against approval of voriconazole for febrile neutropenia.
Overall, the role of newer antifungals in the treatment of febrile neutropenia is evolving. Based on current evidence, we prefer caspofungin as the treatment of choice for patients with febrile neutropenia because of its low toxicity profile and good clinical spectrum against most likely pathogens. D‐AmB has long been the gold standard; however, due to toxicity concerns, lipid‐based formulations have largely replaced it, with a notable increase in cost. Voriconazole cannot be recommended at this time based on failure to meet the noninferiority endpoint when compared to L‐AmB. However, for cases in which there is a high suspicion of invasive aspergillosis infection, voriconazole should be considered.
INVASIVE ASPERGILLOSIS
Invasive aspergillosis infection has become an increasing threat in immunocompromised patients, including those treated for cancer, undergoing organ transplantation, or with advanced human immunodeficiency virus (HIV) infection. In particular, patients being treated for hematologic malignancies and those undergoing hematopoietic stem cell transplant (HSCT) are at highest risk, due to prolonged, severe neutropenia. Infection with invasive aspergillosis also occurs when steroids are used for treatment of graft‐versus‐host disease in the HSCT population.
Aspergillus species are saprobic molds found ubiquitously in nature. Most diseases are caused by Aspergillus fumigatus, followed by A. flavus, A. niger, and A. terreus. Infection with Aspergillus can cause a wide spectrum of illnesses, ranging from allergic reactions to fulminant, lethal infections. The lungs are the most common site of primary invasive disease and are associated with high mortality, especially in severely immunocompromised patients.21 Infection is rapidly progressive and can be refractory to treatment, due to the organism's ability to grow quickly and invade blood vessels. Susceptible patients are unable to control infection and thus at high risk for dissemination and death. Prompt administration of an effective antifungal agent is necessary upon suspicion of invasive disease.
The choice of antifungals for invasive Aspergillus infection has grown significantly over the past decade. Current FDA‐approved agents with activity and indications for Aspergillus infection include D‐AmB and its lipid formulations, itraconazole, voriconazole, posaconazole, and caspofungin. D‐AmB and voriconazole are the only agents licensed in the US for the primary treatment of invasive aspergillosis, with D‐AmB the sole therapeutic option until recently. The lipid formulations of amphotericin B, itraconazole, and caspofungin are approved for salvage therapy. Posaconazole is licensed for prophylaxis of invasive aspergillosis in patients who are severely immunocompromised, including those with HSCT and graft‐versus‐host disease as well as those with hematologic malignancies and prolonged neutropenia. Besides caspofungin, the other available echinocandins, micafungin and anidulafungin, are active against Aspergillus species, but not yet FDA‐approved for this indication.
Voriconazole has replaced D‐AmB as the primary treatment of invasive pulmonary aspergillosis.21 Voriconazole was compared to D‐AmB in a randomized, multicenter, open‐label trial of 277 immunocompromised patients with definite or probable disease. The underlying condition in most patients was acute leukemia or allogeneic HSCT, and the majority of patients had invasive pulmonary disease. A successful outcome at week 12 was seen in 53% in the voriconazole group and 32% in the D‐AmB group, with survival rates of 71% and 58%, respectively; both differences were statistically significant. There were more adverse events in the D‐AmB group. Overall, the authors concluded that initial therapy with voriconazole led to better responses, improved survival and fewer side effects than D‐AmB.22
Caspofungin and micafungin have been studied for use as salvage therapy in invasive Aspergillus infection. Caspofungin was studied in 83 patients with invasive aspergillosis refractory to or intolerant of D‐AmB, lipid formulations of amphotericin B, or triazoles, most of whom had hematologic malignancy and allogeneic HSCT. The majority of patients had invasive pulmonary aspergillosis, and a favorable response was seen in 45% of this extremely high‐risk population.23 Micafungin was evaluated in a phase II study as primary or salvage therapy for invasive aspergillosis in adults and children. Of the patients receiving micafungin alone, those receiving the drug as primary therapy had a 50% (n = 6/12) response rate, compared to 41% (9/22) in the salvage therapy group.24 Optimal dosing of micafungin for the treatment of Aspergillus has not yet been established.
Posaconazole, the newest triazole antifungal, has been shown to be effective for the prevention of invasive aspergillosis in immunocompromised patients25, 26 and has also been studied for the treatment of invasive disease. In an open‐label trial, patients with invasive aspergillosis refractory or intolerant to conventional therapy were administered posaconazole, with historical controls as a comparator group.27 The majority of patients had underlying hematologic malignancies with approximately half undergoing HSCT, and most patients had pulmonary infection. The overall success rate was 42% for posaconazole and 26% for the control group. Posaconazole appeared to confer a survival benefit over control at 30 days and end of therapy (P = 0.0003).
Based on current data, we recommend voriconazole for primary treatment of invasive pulmonary aspergillosis. Alternatives include L‐AmB, caspofungin, micafungin, or posaconazole; of these agents, only L‐AmB has been studied as primary (as opposed to salvage) therapy for invasive aspergillosis in a reasonably‐powered trial.28 We agree with current IDSA guidelines, which suggest L‐AmB as a possible alternative to voriconazole for primary therapy of invasive aspergillosis in some patients, particularly where drug‐drug interactions make the use of voriconazole problematic.21
MUCOCUTANEOUS CANDIDIASIS
Oropharyngeal candidiasis, or thrush, is a common infection in infants; those receiving antibiotics, chemotherapy or inhaled corticosteroids; and those with underlying immunodeficiency states. Esophageal candidiasis is most common in patients infected with HIV. Oral candidiasis usually does not cause symptoms, while esophageal disease is associated with odynophagia and dysphagia.
Candida albicans is the most common cause of mucocutaneous candidiasis. Treatment of thrush usually entails topical antifungal agents such as clotrimazole troches or nystatin, or oral azoles such as fluconazole or itraconazole. Topical therapy is ineffective for esophageal candidiasis, and oral or intravenous azoles are required as first‐line therapy with fluconazole being preferred. The treatment of oral and esophageal candidiasis is often complicated by recurrence, especially in immunodeficient patients, and resistance to standard treatments occurs frequently. Identification of Candida to the species level should be performed in the setting of refractory mucocutaneous disease, as this may play a role in the choice of therapy. The 2004 IDSA Guidelines, currently under revision, contain recommendations for treatment of refractory mucocutaneous candidiasis.4 The guidelines recommend a trial of oral itraconazole for fluconazole‐refractory thrush. Intravenous caspofungin and D‐AmB are usually effective alternatives. For treatment of fluconazole‐refractory esophageal disease, the guidelines recommend itraconazole solution, voriconazole, or caspofungin, with D‐AmB recommended as second line therapy, though it is now seldom used in this setting due to significant adverse affects. Experience using newer antifungals is increasing, and these data are summarized below.
Voriconazole has been shown at least as effective as fluconazole in the treatment of esophageal candidiasis in immunocompromised patients.29 A study involving 256 patients revealed success rates of 98% for voriconazole and 95% for fluconazole. C. albicans was the most common pathogen isolated. Perfect et al.30 demonstrated the utility of voriconazole for refractory esophageal candidiasis in 38 patients. A successful outcome was seen in 61% of patients treated with intravenous followed by oral voriconazole. The most common pathogen was C. albicans, although the series included several cases of infection with C. krusei.
Caspofungin was compared to D‐AmB for the treatment of esophageal candidiasis in a multicenter, double‐blind, randomized trial of 128 patients.31 Caspofungin appeared to be at least as effective as D‐AmB, with a significantly higher incidence of drug‐related adverse effects seen in the D‐AmB arm. Caspofungin was also compared to fluconazole in a double‐blind, randomized trial of 177 patients with Candida esophagitis. Favorable responses were seen in 81% and 85% of caspofungin and fluconazole treated patients, respectively. A trend toward higher relapse rate 4 weeks after stopping therapy was seen with caspofungin compared to fluconazole, as was a trend toward superior eradication rates for C. glabrata in the caspofungin arm compared to the fluconazole arm, although neither reached statistical significance.32
Micafungin was used for the treatment of esophageal candidiasis in a dose‐ranging trial of 245 HIV‐infected patients.33 Endoscopic combined cure rate for the 100 mg and 150 mg doses of micafungin (84%) was comparable to that of intravenous fluconazole 200 mg/day (87%). In the posttreatment period, 9 patients in the micafungin arm had a worsening of severity score or received nonprophylactic antifungal therapy. No patients in the fluconazole group experienced a relapse.
Anidulafungin has been compared with fluconazole for the treatment of Candida esophagitis in a randomized, double‐blind trial of 601 patients, with an initial endoscopic success rate approaching 100% in both groups.34 The 2‐week follow‐up examination revealed that 64% and 90% of patients treated with anidulafungin and fluconazole, respectively, sustained endoscopic success (P 0.001).
Posaconazole was compared with fluconazole for treatment of thrush in 350 patients with HIV/acquired immunodeficiency syndrome (AIDS) in a randomized, blinded study.35 Both posaconazole and fluconazole were administered at a dose of 200 mg on day 1, followed by 100 mg/day. Clinical success occurred in 92% of patients receiving posaconazole and 93% receiving fluconazole. Mycological success was equivalent on day 14 in both arms; however, by day 42, significantly more posaconazole recipients continued to demonstrate mycological success. Posaconazole was recently evaluated for the treatment of azole‐refractory thrush and esophageal candidiasis in patients with advanced HIV infection, demonstrating a success rate of 75% in this population failing fluconazole or itraconazole therapy.36
Multiple new agents are available for the treatment of mucocutaneous candidiasis. Aside from topical antifungals for the initial treatment of thrush, fluconazole remains first line systemic therapy for both oral and esophageal candidiasis due to safety, tolerability, and cost. For fluconazole‐refractory disease, newer choices include voriconazole, the echinocandins, and posaconazole. Voriconazole and posaconazole are attractive options given their oral availability. The relapse rates seen in trials with the echinocandins are concerning; however, these are useful options when azole resistance is suspected.
ZYGOMYCOSIS
Zygomycosis (often referred to less correctly as mucormycosis) is a devastating opportunistic fungal infection that appears to be increasing in frequency. Historically, zygomycosis has commonly occurred in poorly controlled diabetic patients, particularly in the setting of diabetic ketoacidosis, and classically results in rhinocerebral disease with a relatively poor outcome. In recent years, a striking increase has been seen in patients with more profound immunosuppression, particularly those with hematologic malignancies or undergoing HSCT. Sinopulmonary rather than rhinocerebral disease is the most common manifestation in this population.3739 Other well‐described risk factors include iron chelation therapy with deferoxamine, intravenous drug use, solid organ transplantation, metabolic acidosis, trauma, and burns. Disease is also occasionally seen in the seemingly immunocompetent, with 176 of 929 (19%) patients in a comprehensive review lacking an obvious risk factor.37, 40
Invasive mold infections caused by the Zygomycetes are associated with a poor outcome, with Roden et al.37 reporting mortality in excess of 50% in their series. Mortality in patients with hematological malignancies has been reported to be particularly high.37, 38 The cornerstones of successful therapy include early detection of infection, correction or improvement of immunosuppression when possible, prompt surgical debridement of infected tissue, and appropriate antifungal therapy.40 D‐AmB has constituted standard zygomycosis therapy for decades, although it has recently been largely replaced by L‐AmB. Overall survival rates have been reported to be 61% and 69% with the use of D‐AmB and lipid preparations, respectively.37
Given the relatively poor outcomes and substantial infusion‐related toxicity and nephrotoxicity associated with even liposomal preparations of AmB, considerable interest exists in the identification of alternative therapeutic agents. Unfortunately, echinocandins and most triazoles appear to have modest to no activity against Zygomycetes, with a recent case‐control study indicating that widespread use of voriconazole in high‐risk populations may be helping to drive the emergence of breakthrough zygomycosis.39 Posaconazole appears to be an exception, however; with in vitro and murine studies suggesting it compares favorably to D‐AmB in this setting.4143 Numerous case reports describe favorable outcomes with the use of posaconazole as salvage therapy for zygomycosis, and 2 recent retrospective studies support its role in this setting.44, 45 Currently, use of posaconazole for the treatment of zygomycosis is limited by the absence of an intravenous preparation, although this is reportedly under development.46 At present, the role of posaconazole in this setting appears limited to step‐down therapy in those patients who have responded appropriately to L‐AmB, and for salvage therapy. Although an intravenous preparation of posaconazole appears attractive as a first‐line agent for zygomycosis, currently studied patients (ie, those unresponsive to or intolerant of D‐AmB) may not be fully representative of a broader population, and clinical trials will be necessary before more definitive conclusions may be drawn.47
ENDEMIC MYCOSES
Coccidioidomycosis
Coccidioidomycosis results from environmental exposure to either Coccidioides immitis or C. posadii. At least 50% of infections are asymptomatic, with the majority of the remaining individuals exhibiting acute, self‐limited pulmonary symptoms. A small percentage of patients develop chronic illness, either pulmonary or disseminated disease, including involvement of skin, bone/joint, and central nervous system (CNS).48, 49 Current therapy consists of either fluconazole or itraconazole for CNS disease and non‐life‐threatening disease elsewhere, with D‐AmB reserved for pregnancy and more fulminant illness.49 Unfortunately, response failures and relapses are seen commonly with all of these agents, with a resultant need for alternative antifungals.
The echinocandins have no clear role in the treatment of coccidioidomycosis.49 More interest surrounds the use of the newer azoles, with multiple studies demonstrating excellent in vitro activity of both voriconazole and posaconazole against Coccidioides species.5052 Several recently reported open‐label studies have reported good results with the use of posaconazole for chronic coccidioidomycosis, 2 of which enrolled patients intolerant of or refractory to usual agents.5355 Based on these data, posaconazole appears to be highly active against Coccidioides, and should perhaps be the drug of choice in the majority of patients who fail to respond to or tolerate older triazoles.
Histoplasmosis
Histoplasmosis is particularly endemic in the Ohio and Mississippi valleys, although it occurs less commonly in many other areas as well. Inhaled Histoplasma capsulatum conidia result in subclinical infection in the majority of exposed individuals, with self‐limited pneumonia the rule in most others. A minority of patients will experience chronic pulmonary disease or dissemination.56 Not all disease requires treatment, with most pulmonary disease resolving spontaneously; but definite indications for treatment include moderate or severe pneumonia, chronic cavitary lung disease, CNS involvement, and progressive disseminated disease.56 Standard therapy consists of itraconazole or lipid formulations of amphotericin B, based on severity. Multiple studies have demonstrated excellent in vitro activity of voriconazole and particularly posaconazole against H. capsulatum.52, 5759 Recently, in 2 small series of patients, patients failing either to improve with or tolerate conventional agents demonstrated favorable outcomes when they were treated with voriconazole or posaconazole.60, 61 Both drugs appear to be appropriate second‐line agents, with posaconazole arguably preferable based on current evidence.
CONCLUSIONS
The spectrum of available antifungal agents has expanded considerably in recent years, and the advent of additional drugs is expected shortly. Well‐tolerated and effective drugs are now available for most fungal infections, although the precise role for newer agents in some of these diseases has yet to be defined. Future clinical trials should help resolve these uncertainties.
Therapy of serious fungal infections, for decades largely limited to the deoxycholate (regular) preparation of amphotericin B (D‐AmB), expanded significantly with the introduction of fluconazole, followed by lipid‐based formulations of amphotericin B (L‐AmB) and itraconazole. More recently the antifungal armamentarium has broadened further with the approval of voriconazole and posaconazole, as well as the echinocandins caspofungin, micafungin, and anidulafungin. Clinicians, including hospitalists, primary care, emergency medicine, and critical care physicians, may find it challenging to remain abreast of indications for these novel agents, and we review these below, with a focus on adult patients. Manuscripts used in the review were identified by a search of English‐language articles in the PubMed MEDLINE database from 1994 to the present, using the keywords triazoles, echinocandins, voriconazole, posaconazole, caspofungin, micafungin, anidulafungin, candidemia, candidiasis, aspergillosis, invasive Aspergillus, zygomycosis, febrile neutropenia, endemic mycosis, histoplasmosis, and coccidioidomycosis. In addition, reference lists for the majority of the identified manuscripts were hand‐searched for additional pertinent citations.
Table 1 summarizes the newer systemic antifungal therapies and Table 2 summarizes the significant drug‐drug interactions with the newer antifungals.
| Antifungals | Trade Name | FDA‐Approved Indications | Usual Adult Dosing | Adverse Effects |
|---|---|---|---|---|
| ||||
| Azoles | ||||
| Voriconazole | Vfend | Invasive aspergillosis. | Intravenous: 6 mg/kg IV every 12 hours, then 4 mg/kg IV every 12 hours. | Transient visual disturbances (up to 30% in trials), rash, increases in hepatic enzymes, severe hepatotoxicity, and hallucinations. |
| Candidemia in nonneutropenic patients and the following Candida infections: disseminated infections in skin and infections in abdomen, kidney, bladder wall, and wounds. | Oral: 200 mg PO every 12 hours if 40 kg, 100 mg PO every 12 hours if 40 kg. | Accumulation of sulfobutyl ester ‐cyclodextrin, a solubilizing excipient, may occur in patients with creatinine clearance 50 mL/minute receiving the intravenous formulation. | ||
| Esophageal candidiasis. | ||||
| Fungal infections due to Scedosporium apiospermum (asexual form of Pseudallescheria boydii) and Fusarium spp. including Fusarium solani, in patients intolerant of, or refractory to, other therapy. | ||||
| Posaconazole | Noxafil | Prophylaxis of invasive Aspergillus and Candida infections in patients, 13 years of age and older, who are at high risk of developing these infections due to being severely immunocompromised, such as HSCT recipients with graft‐versus‐host disease or those with hematologic malignancies with prolonged neutropenia from chemotherapy. | Prophylaxis of invasive fungal infections: 200 mg (5 mL) PO TID. | Fever, headache, dry mouth, dizziness, fatigue, nausea, vomiting, diarrhea, rash, QT interval prolongation, and elevation of hepatic enzymes. |
| Oropharyngeal candidiasis, including oropharyngeal candidiasis refractory to itraconazole and/or fluconazole. | Oropharyngeal candidiasis: loading dose of 100 mg (2.5 mL) PO BID on day 1, then 100 mg (2.5 mL) PO once daily. | |||
| Oropharyngeal candidiasis refractory to itraconazole and/or fluconazole: 400 mg (10 mL) PO BID. | ||||
| To enhance oral absorption, administer with a full meal or liquid nutritional supplement. | ||||
| Echinocandins | ||||
| Caspofungin | Cancidas | Empirical therapy for presumed fungal infections in febrile, neutropenic patients. | All indications: 70 mg IV loading dose 1, followed by 50 mg IV daily. | Phlebitis, elevation of hepatic enzymes, headache, fever, nausea, vomiting, leukopenia, and histamine mediated symptoms including rash, pruritus, facial swelling, and vasodilatation. |
| Candidemia and the following Candida infections: intraabdominal abscesses, peritonitis, and pleural space infections. | No loading dose required for esophageal candidiasis. | |||
| Esophageal candidiasis. | ||||
| Invasive aspergillosis in patients who are refractory to or intolerant of other therapies (ie, amphotericin B, lipid formulations of amphotericin B, and/or itraconazole). | ||||
| Micafungin | Mycamine | Candidemia, acute disseminated candidiasis, Candida peritonitis and abscesses. | Candidemia, acute disseminated candidiasis, Candida peritonitis and abscesses: 100 mg IV daily. | Similar to caspofungin. |
| Esophageal candidiasis. | Esophageal candidiasis: 150 mg IV daily. | |||
| Prophylaxis of Candida infections in patients undergoing HSCT. | Prophylaxis of Candida infections in HSCT recipients: 50 mg IV daily. | |||
| Anidulafungin | Eraxis | Candidemia and other forms of Candida infections (intraabdominal abscess, peritonitis). | Candidemia/other Candida infections: 200 mg IV loading dose 1, followed by 100 mg IV daily. | Similar to caspofungin. |
| Esophageal candidiasis. | Esophageal candidiasis: 100 mg IV loading dose 1, followed by 50 mg IV Q daily thereafter. | |||
| Antifungal | Effect | Interacting Drugs |
|---|---|---|
| ||
| Voriconazole | Decreased azole serum concentration | Rifampin, rifabutin, carbamazepine, long‐acting barbiturates, efavirenz, high‐dose ritonavir (400 mg twice daily), phenytoin |
| Increased azole serum concentration | Oral contraceptives containing ethinyl estradiol and norethindrone, HIV protease inhibitors other than ritonavir, and nonnucleoside reverse transcriptase inhibitors other than efavirenz | |
| Increased serum concentration of coadministered drug | Sirolimus, rifabutin, efavirenz, terfenadine, astemizole, cisapride, pimozide, quinine, cyclosporine, methadone, tacrolimus, oral contraceptives containing ethinyl estradiol and norethindrone, HIV protease inhibitors other than ritonavir, nonnucleoside reverse transcriptase inhibitors other than efavirenz, benzodiazepines, HMG‐CoA reductase inhibitors, dihydropyridine calcium channel blockers, vinca alkaloids, omeprazole, phenytoin, warfarin, sulfonylurea oral hypoglycemics, and ergot alkaloids | |
| Posaconazole | Decreased azole serum concentration | Cimetidine, rifabutin, phenytoin |
| Increased serum concentration of coadministered drug | Cyclosporine, tacrolimus, rifabutin, midazolam, pheytoin, terfenidine, astemizole, pimozide, cisapride, quinidine, ergot alkaloids, vinca alkaloids, sirolimus, HMG Co‐A reductase inhibitors, and calcium channel blockers | |
| Caspofungin | Decreased serum concentration of caspofungin | Efavirenz, nevirapine, phenytoin, dexamethasone, and carbamazepine |
| Increased serum concentration of caspofungin | Cyclosporine | |
| Decreased serum concentration of coadministered drug | Tacrolimus | |
| Micafungin | Increased serum concentration of coadministered drug | Sirolimus, nifedipine, and itraconazole |
| Anidulafungin | No clinically relevant drug‐drug interactions | |
INVASIVE CANDIDIASIS
Candida has become a leading cause of nosocomial bloodstream infections, and is associated with an attributable mortality of 15% to 25%.1 Candidemia results in an estimated 10‐day increase in hospital length of stay, as well as an average $40,000 (US) increase in costs.2 Invasive candidiasis may be defined as catheter‐related candidemia, other hematogenously disseminated disease, or visceral involvement.3 Risk factors are present in most patients with invasive candidiasis, and include broad‐spectrum antibiotics; parenteral nutrition; central catheters; hospitalization in the intensive care unit setting; renal failure; burns; gastrointestinal and cardiac surgery; and colonization with Candida, particularly at multiple sites.1, 2
Historically, treatment of invasive candidiasis consisted of D‐AmB, with fluconazole largely but not completely replacing amphotericin after prospective trials demonstrated comparable efficacy with markedly improved tolerability. Fluconazole has poor or uncertain activity against C. krusei and C. glabrata, however, leading to reluctance on the part of many clinicians to use it for non‐C. albicans infection (or empirically in the unstable patient). Others have raised concerns regarding the use of fluconazole even for C. albicans in the setting of an unstable or neutropenic patient, given its fungistatic rather than fungicidal activity, although this is a theoretical rather than proven shortcoming.1 Current Infectious Diseases Society of America (IDSA) guidelines for the treatment of candidemia recommend the use of caspofungin, fluconazole, D‐AmB, or the combination of D‐AmB and fluconazole.4 The IDSA recommendations are under revision, however, and we summarize newer evidence below.
Mora‐Duarte et al.,5 in a 2002 trial, randomized patients with invasive candidiasis to caspofungin or D‐AmB, and found a favorable response in 73% and 62%, respectively, which fell just short of statistical significance. Caspofungin was better tolerated than D‐AmB, and the authors concluded that caspofungin was at least as effective as D‐AmB, with fewer adverse effects.5 A 2007 study randomized invasive candidiasis patients to micafungin or L‐AmB, and reported similar efficacy in both arms, with less drug‐related adverse events in the echinocandin‐treated group.6 Reboli et al.7 conducted a noninferiority trial comparing anidulafungin to fluconazole, and found a significantly superior outcome in the anidulafungin arm. Perhaps surprisingly, the outcome difference between the 2 groups was greater for C. albicans than for any other species.7 Although the large majority of patients in the preceding trials had candidemia, one study demonstrated a favorable response to caspofungin in 81% of patients with invasive candidal infections other than candidemia.8
Fewer data exist regarding the use of newer azoles for the treatment of invasive candidiasis. Ostrosky‐Zeichner et al.3 utilized voriconazole as salvage therapy in 52 patients with invasive candidiasis either refractory to or intolerant of other antifungals (almost all of whom had failed therapy with D‐AmB and/or other azoles), and found a 56% favorable response rate in this challenging population. More recently, Kullberg et al.9 studied voriconazole versus D‐AmB followed by fluconazole in candidemic patients, with a similar outcome but somewhat better tolerability in the voriconazole arm. We are unaware of comparative studies involving posaconazole for invasive candidiasis.
In summary, although fluconazole is the drug of choice for most invasive candidal infections, the initial use of an echinocandin should be considered when infection with a non‐C. albicans species is likely, particularly if the patient is unstable. Provided the organism later proves likely to be sensitive, switching to fluconazole is reasonable, particularly given the absence of an oral echinocandin formulation. The 3 currently available echinocandins appear to be interchangeable for the treatment of serious Candida infections.
NEUTROPENIC FEVER
Neutropenia is the most critical factor leading to infection in patients with cancer. Empiric treatment with broad‐spectrum antimicrobials should be initiated at the first sign of infection, since delay can lead to increased mortality.10 There are numerous causes for fever in the neutropenic host, although bacterial infection is most common. Fungal infections can cause unexplained fever and should be considered in neutropenic patients who remain febrile despite broad‐spectrum antibiotics.
Fungal infections in the neutropenic host can have severe consequences. Given their high morbidity and mortality and a lack of effective diagnostic techniques for early detection, empiric antifungal therapy is mandatory in the appropriate setting. Antifungal therapy should be considered in patients who remain febrile and neutropenic for 5 days despite broad‐spectrum antibiotics. The most common fungal pathogens include Candida and Aspergillus spp.11 Other considerations include the emergence of non‐albicans Candida infections and other opportunistic pathogens such as Zygomycetes (Mucor and related pathogens), Fusarium spp, and Scedosporium spp.
Empiric antifungal coverage in the neutropenic host has evolved over the past 2 decades, with the first trials demonstrating the utility of empiric antifungal treatment in the neutropenic host published in the 1980s. These trials demonstrated that addition of D‐AmB to broad spectrum antibiotics decreased development of fungal infections, and led to better outcomes.12, 13 While these studies established D‐AmB as standard empiric antifungal therapy in neutropenic fever, nephrotoxicity and infusion‐related reactions limited its subsequent use as less toxic alternatives were developed. The lipid formulations of amphotericin B, in particular liposomal AmB and amphotericin B lipid complex, have been shown to be as effective as D‐AmB for empiric treatment of febrile neutropenia, with less toxicities but significantly higher expense.14, 15 The older generation azoles itraconazole and fluconazole have also been studied. Itraconazole has been proven to be as effective as D‐AmB in febrile neutropenia with less toxicity; however, the oral capsule has erratic absorption and should be used cautiously.16
Newer agents studied for use in febrile neutropenia include caspofungin and voriconazole. Caspofungin is active against azole‐resistant Candida spp and Aspergillus spp with a favorable toxicity profile, making it an attractive candidate for use in febrile neutropenia. Caspofungin was compared to L‐AmB as empiric antifungal therapy in a randomized double‐blind trial of 1,095 patients with febrile neutropenia.17 The overall success rate was essentially identical for both agents, demonstrating noninferiority of caspofungin therapy. Among patients with baseline fungal infections, significantly more patients receiving caspofungin than L‐AmB had successful outcomes (52% versus 26%, P = 0.04). Overall, caspofungin was better tolerated and associated with fewer complications than L‐AmB.17 The other available echinocandins, micafungin and anidulafungin, have not yet been studied for febrile neutropenia in randomized, controlled fashion.
Voriconazole is a second‐generation azole with activity against fluconazole‐resistant Candida strains; however, the minimum inhibitory concentrations (MICs) are proportionally higher, suggesting a possible cross‐resistance mechanism among highly azole‐resistant strains.18 Voriconazole is active against most Aspergillus spp, Fusarium spp, and Scedosporium apiospermum.19 Voriconazole was compared to L‐AmB in an open‐label, randomized trial of 837 patients with febrile neutropenia.20 Patients were stratified according to risk of fungal infection and previous antifungal prophylaxis. Toxic side effects were similar in both groups. Less breakthrough fungal infections were seen in the voriconazole group; however, there were more discontinuations due to lack of efficacy in patients receiving voriconazole compared to L‐AmB. The overall success rate was 26% with voriconazole and 31% with L‐AmB (95% confidence interval [CI] for absolute difference in success rates: 10.6% to 1.6%), with the low figures reflective not only of infection severity, but also gravity of underlying disease, persistent fever presumably not of fungal origin, and adverse drug effects. Because the predetermined definition of noninferiority for the confidence interval difference between the groups was not met, the U.S. Food and Drug Administration (FDA) voted against approval of voriconazole for febrile neutropenia.
Overall, the role of newer antifungals in the treatment of febrile neutropenia is evolving. Based on current evidence, we prefer caspofungin as the treatment of choice for patients with febrile neutropenia because of its low toxicity profile and good clinical spectrum against most likely pathogens. D‐AmB has long been the gold standard; however, due to toxicity concerns, lipid‐based formulations have largely replaced it, with a notable increase in cost. Voriconazole cannot be recommended at this time based on failure to meet the noninferiority endpoint when compared to L‐AmB. However, for cases in which there is a high suspicion of invasive aspergillosis infection, voriconazole should be considered.
INVASIVE ASPERGILLOSIS
Invasive aspergillosis infection has become an increasing threat in immunocompromised patients, including those treated for cancer, undergoing organ transplantation, or with advanced human immunodeficiency virus (HIV) infection. In particular, patients being treated for hematologic malignancies and those undergoing hematopoietic stem cell transplant (HSCT) are at highest risk, due to prolonged, severe neutropenia. Infection with invasive aspergillosis also occurs when steroids are used for treatment of graft‐versus‐host disease in the HSCT population.
Aspergillus species are saprobic molds found ubiquitously in nature. Most diseases are caused by Aspergillus fumigatus, followed by A. flavus, A. niger, and A. terreus. Infection with Aspergillus can cause a wide spectrum of illnesses, ranging from allergic reactions to fulminant, lethal infections. The lungs are the most common site of primary invasive disease and are associated with high mortality, especially in severely immunocompromised patients.21 Infection is rapidly progressive and can be refractory to treatment, due to the organism's ability to grow quickly and invade blood vessels. Susceptible patients are unable to control infection and thus at high risk for dissemination and death. Prompt administration of an effective antifungal agent is necessary upon suspicion of invasive disease.
The choice of antifungals for invasive Aspergillus infection has grown significantly over the past decade. Current FDA‐approved agents with activity and indications for Aspergillus infection include D‐AmB and its lipid formulations, itraconazole, voriconazole, posaconazole, and caspofungin. D‐AmB and voriconazole are the only agents licensed in the US for the primary treatment of invasive aspergillosis, with D‐AmB the sole therapeutic option until recently. The lipid formulations of amphotericin B, itraconazole, and caspofungin are approved for salvage therapy. Posaconazole is licensed for prophylaxis of invasive aspergillosis in patients who are severely immunocompromised, including those with HSCT and graft‐versus‐host disease as well as those with hematologic malignancies and prolonged neutropenia. Besides caspofungin, the other available echinocandins, micafungin and anidulafungin, are active against Aspergillus species, but not yet FDA‐approved for this indication.
Voriconazole has replaced D‐AmB as the primary treatment of invasive pulmonary aspergillosis.21 Voriconazole was compared to D‐AmB in a randomized, multicenter, open‐label trial of 277 immunocompromised patients with definite or probable disease. The underlying condition in most patients was acute leukemia or allogeneic HSCT, and the majority of patients had invasive pulmonary disease. A successful outcome at week 12 was seen in 53% in the voriconazole group and 32% in the D‐AmB group, with survival rates of 71% and 58%, respectively; both differences were statistically significant. There were more adverse events in the D‐AmB group. Overall, the authors concluded that initial therapy with voriconazole led to better responses, improved survival and fewer side effects than D‐AmB.22
Caspofungin and micafungin have been studied for use as salvage therapy in invasive Aspergillus infection. Caspofungin was studied in 83 patients with invasive aspergillosis refractory to or intolerant of D‐AmB, lipid formulations of amphotericin B, or triazoles, most of whom had hematologic malignancy and allogeneic HSCT. The majority of patients had invasive pulmonary aspergillosis, and a favorable response was seen in 45% of this extremely high‐risk population.23 Micafungin was evaluated in a phase II study as primary or salvage therapy for invasive aspergillosis in adults and children. Of the patients receiving micafungin alone, those receiving the drug as primary therapy had a 50% (n = 6/12) response rate, compared to 41% (9/22) in the salvage therapy group.24 Optimal dosing of micafungin for the treatment of Aspergillus has not yet been established.
Posaconazole, the newest triazole antifungal, has been shown to be effective for the prevention of invasive aspergillosis in immunocompromised patients25, 26 and has also been studied for the treatment of invasive disease. In an open‐label trial, patients with invasive aspergillosis refractory or intolerant to conventional therapy were administered posaconazole, with historical controls as a comparator group.27 The majority of patients had underlying hematologic malignancies with approximately half undergoing HSCT, and most patients had pulmonary infection. The overall success rate was 42% for posaconazole and 26% for the control group. Posaconazole appeared to confer a survival benefit over control at 30 days and end of therapy (P = 0.0003).
Based on current data, we recommend voriconazole for primary treatment of invasive pulmonary aspergillosis. Alternatives include L‐AmB, caspofungin, micafungin, or posaconazole; of these agents, only L‐AmB has been studied as primary (as opposed to salvage) therapy for invasive aspergillosis in a reasonably‐powered trial.28 We agree with current IDSA guidelines, which suggest L‐AmB as a possible alternative to voriconazole for primary therapy of invasive aspergillosis in some patients, particularly where drug‐drug interactions make the use of voriconazole problematic.21
MUCOCUTANEOUS CANDIDIASIS
Oropharyngeal candidiasis, or thrush, is a common infection in infants; those receiving antibiotics, chemotherapy or inhaled corticosteroids; and those with underlying immunodeficiency states. Esophageal candidiasis is most common in patients infected with HIV. Oral candidiasis usually does not cause symptoms, while esophageal disease is associated with odynophagia and dysphagia.
Candida albicans is the most common cause of mucocutaneous candidiasis. Treatment of thrush usually entails topical antifungal agents such as clotrimazole troches or nystatin, or oral azoles such as fluconazole or itraconazole. Topical therapy is ineffective for esophageal candidiasis, and oral or intravenous azoles are required as first‐line therapy with fluconazole being preferred. The treatment of oral and esophageal candidiasis is often complicated by recurrence, especially in immunodeficient patients, and resistance to standard treatments occurs frequently. Identification of Candida to the species level should be performed in the setting of refractory mucocutaneous disease, as this may play a role in the choice of therapy. The 2004 IDSA Guidelines, currently under revision, contain recommendations for treatment of refractory mucocutaneous candidiasis.4 The guidelines recommend a trial of oral itraconazole for fluconazole‐refractory thrush. Intravenous caspofungin and D‐AmB are usually effective alternatives. For treatment of fluconazole‐refractory esophageal disease, the guidelines recommend itraconazole solution, voriconazole, or caspofungin, with D‐AmB recommended as second line therapy, though it is now seldom used in this setting due to significant adverse affects. Experience using newer antifungals is increasing, and these data are summarized below.
Voriconazole has been shown at least as effective as fluconazole in the treatment of esophageal candidiasis in immunocompromised patients.29 A study involving 256 patients revealed success rates of 98% for voriconazole and 95% for fluconazole. C. albicans was the most common pathogen isolated. Perfect et al.30 demonstrated the utility of voriconazole for refractory esophageal candidiasis in 38 patients. A successful outcome was seen in 61% of patients treated with intravenous followed by oral voriconazole. The most common pathogen was C. albicans, although the series included several cases of infection with C. krusei.
Caspofungin was compared to D‐AmB for the treatment of esophageal candidiasis in a multicenter, double‐blind, randomized trial of 128 patients.31 Caspofungin appeared to be at least as effective as D‐AmB, with a significantly higher incidence of drug‐related adverse effects seen in the D‐AmB arm. Caspofungin was also compared to fluconazole in a double‐blind, randomized trial of 177 patients with Candida esophagitis. Favorable responses were seen in 81% and 85% of caspofungin and fluconazole treated patients, respectively. A trend toward higher relapse rate 4 weeks after stopping therapy was seen with caspofungin compared to fluconazole, as was a trend toward superior eradication rates for C. glabrata in the caspofungin arm compared to the fluconazole arm, although neither reached statistical significance.32
Micafungin was used for the treatment of esophageal candidiasis in a dose‐ranging trial of 245 HIV‐infected patients.33 Endoscopic combined cure rate for the 100 mg and 150 mg doses of micafungin (84%) was comparable to that of intravenous fluconazole 200 mg/day (87%). In the posttreatment period, 9 patients in the micafungin arm had a worsening of severity score or received nonprophylactic antifungal therapy. No patients in the fluconazole group experienced a relapse.
Anidulafungin has been compared with fluconazole for the treatment of Candida esophagitis in a randomized, double‐blind trial of 601 patients, with an initial endoscopic success rate approaching 100% in both groups.34 The 2‐week follow‐up examination revealed that 64% and 90% of patients treated with anidulafungin and fluconazole, respectively, sustained endoscopic success (P 0.001).
Posaconazole was compared with fluconazole for treatment of thrush in 350 patients with HIV/acquired immunodeficiency syndrome (AIDS) in a randomized, blinded study.35 Both posaconazole and fluconazole were administered at a dose of 200 mg on day 1, followed by 100 mg/day. Clinical success occurred in 92% of patients receiving posaconazole and 93% receiving fluconazole. Mycological success was equivalent on day 14 in both arms; however, by day 42, significantly more posaconazole recipients continued to demonstrate mycological success. Posaconazole was recently evaluated for the treatment of azole‐refractory thrush and esophageal candidiasis in patients with advanced HIV infection, demonstrating a success rate of 75% in this population failing fluconazole or itraconazole therapy.36
Multiple new agents are available for the treatment of mucocutaneous candidiasis. Aside from topical antifungals for the initial treatment of thrush, fluconazole remains first line systemic therapy for both oral and esophageal candidiasis due to safety, tolerability, and cost. For fluconazole‐refractory disease, newer choices include voriconazole, the echinocandins, and posaconazole. Voriconazole and posaconazole are attractive options given their oral availability. The relapse rates seen in trials with the echinocandins are concerning; however, these are useful options when azole resistance is suspected.
ZYGOMYCOSIS
Zygomycosis (often referred to less correctly as mucormycosis) is a devastating opportunistic fungal infection that appears to be increasing in frequency. Historically, zygomycosis has commonly occurred in poorly controlled diabetic patients, particularly in the setting of diabetic ketoacidosis, and classically results in rhinocerebral disease with a relatively poor outcome. In recent years, a striking increase has been seen in patients with more profound immunosuppression, particularly those with hematologic malignancies or undergoing HSCT. Sinopulmonary rather than rhinocerebral disease is the most common manifestation in this population.3739 Other well‐described risk factors include iron chelation therapy with deferoxamine, intravenous drug use, solid organ transplantation, metabolic acidosis, trauma, and burns. Disease is also occasionally seen in the seemingly immunocompetent, with 176 of 929 (19%) patients in a comprehensive review lacking an obvious risk factor.37, 40
Invasive mold infections caused by the Zygomycetes are associated with a poor outcome, with Roden et al.37 reporting mortality in excess of 50% in their series. Mortality in patients with hematological malignancies has been reported to be particularly high.37, 38 The cornerstones of successful therapy include early detection of infection, correction or improvement of immunosuppression when possible, prompt surgical debridement of infected tissue, and appropriate antifungal therapy.40 D‐AmB has constituted standard zygomycosis therapy for decades, although it has recently been largely replaced by L‐AmB. Overall survival rates have been reported to be 61% and 69% with the use of D‐AmB and lipid preparations, respectively.37
Given the relatively poor outcomes and substantial infusion‐related toxicity and nephrotoxicity associated with even liposomal preparations of AmB, considerable interest exists in the identification of alternative therapeutic agents. Unfortunately, echinocandins and most triazoles appear to have modest to no activity against Zygomycetes, with a recent case‐control study indicating that widespread use of voriconazole in high‐risk populations may be helping to drive the emergence of breakthrough zygomycosis.39 Posaconazole appears to be an exception, however; with in vitro and murine studies suggesting it compares favorably to D‐AmB in this setting.4143 Numerous case reports describe favorable outcomes with the use of posaconazole as salvage therapy for zygomycosis, and 2 recent retrospective studies support its role in this setting.44, 45 Currently, use of posaconazole for the treatment of zygomycosis is limited by the absence of an intravenous preparation, although this is reportedly under development.46 At present, the role of posaconazole in this setting appears limited to step‐down therapy in those patients who have responded appropriately to L‐AmB, and for salvage therapy. Although an intravenous preparation of posaconazole appears attractive as a first‐line agent for zygomycosis, currently studied patients (ie, those unresponsive to or intolerant of D‐AmB) may not be fully representative of a broader population, and clinical trials will be necessary before more definitive conclusions may be drawn.47
ENDEMIC MYCOSES
Coccidioidomycosis
Coccidioidomycosis results from environmental exposure to either Coccidioides immitis or C. posadii. At least 50% of infections are asymptomatic, with the majority of the remaining individuals exhibiting acute, self‐limited pulmonary symptoms. A small percentage of patients develop chronic illness, either pulmonary or disseminated disease, including involvement of skin, bone/joint, and central nervous system (CNS).48, 49 Current therapy consists of either fluconazole or itraconazole for CNS disease and non‐life‐threatening disease elsewhere, with D‐AmB reserved for pregnancy and more fulminant illness.49 Unfortunately, response failures and relapses are seen commonly with all of these agents, with a resultant need for alternative antifungals.
The echinocandins have no clear role in the treatment of coccidioidomycosis.49 More interest surrounds the use of the newer azoles, with multiple studies demonstrating excellent in vitro activity of both voriconazole and posaconazole against Coccidioides species.5052 Several recently reported open‐label studies have reported good results with the use of posaconazole for chronic coccidioidomycosis, 2 of which enrolled patients intolerant of or refractory to usual agents.5355 Based on these data, posaconazole appears to be highly active against Coccidioides, and should perhaps be the drug of choice in the majority of patients who fail to respond to or tolerate older triazoles.
Histoplasmosis
Histoplasmosis is particularly endemic in the Ohio and Mississippi valleys, although it occurs less commonly in many other areas as well. Inhaled Histoplasma capsulatum conidia result in subclinical infection in the majority of exposed individuals, with self‐limited pneumonia the rule in most others. A minority of patients will experience chronic pulmonary disease or dissemination.56 Not all disease requires treatment, with most pulmonary disease resolving spontaneously; but definite indications for treatment include moderate or severe pneumonia, chronic cavitary lung disease, CNS involvement, and progressive disseminated disease.56 Standard therapy consists of itraconazole or lipid formulations of amphotericin B, based on severity. Multiple studies have demonstrated excellent in vitro activity of voriconazole and particularly posaconazole against H. capsulatum.52, 5759 Recently, in 2 small series of patients, patients failing either to improve with or tolerate conventional agents demonstrated favorable outcomes when they were treated with voriconazole or posaconazole.60, 61 Both drugs appear to be appropriate second‐line agents, with posaconazole arguably preferable based on current evidence.
CONCLUSIONS
The spectrum of available antifungal agents has expanded considerably in recent years, and the advent of additional drugs is expected shortly. Well‐tolerated and effective drugs are now available for most fungal infections, although the precise role for newer agents in some of these diseases has yet to be defined. Future clinical trials should help resolve these uncertainties.
- ,,.Current treatment strategies for disseminated candidiasis.Clin Infect Dis.2006;42:244–251.
- .Echinocandins for candidemia in adults without neutropenia.N Engl J Med.2006;355:1154–1159.
- ,,,.Voriconazole salvage treatment of invasive candidiasis.Eur J Clin Microbiol Infect Dis.2003;22:651–655.
- ,,, et al.Guidelines for treatment of candidiasis.Clin Infect Dis.2004;38:161–189.
- ,,, et al.Comparison of caspofugin and amphotericin B for invasive candidiasis.N Engl J Med.2002;347:2020–2029.
- ,,, et al.Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomized double‐blind trial.Lancet.2007;369:1519–1527.
- ,,, et al.Anidulafungin versus fluconazole for invasive candidiasis.N Engl J Med.2007;356:2472–2482.
- ,,, et al.Caspofungin for the treatment of less common forms of invasive candidiasis.J Antimicrob Chemother.2007;60:363–369.
- ,,, et al.Voriconazole versus a regimen of amphotericin B followed by fluconazole for candidaemia in non‐neutropenic patients: a randomized non‐inferiority trial.Lancet.2005;366:1435–1442.
- ,.Fever of unknown origin in febrile leucopenia.Infect Dis Clin North Am.2007;21:1055–1090.
- ,,, et al.2002 Guidelines for the use of antimicrobial agents in neutropenic patients with cancer.Clin Infect Dis.2002;34:730–751.
- ,,, et al.Empiric antibiotic and antifungal therapy for cancer patients with prolonged fever and granulocytopenia.Am J Med.1982;72:101–111.
- EORTC International Antimicrobial Therapy Cooperative Group.Empiric antifungal therapy in febrile granulocytopenic patients.Am J Med.1989;86:668–672.
- ,,, et al.Liposomal amphotericin B for empirical therapy in patients with persistent fever and neutropenia.N Engl J Med.1999;340:7644–7671.
- ,,, et al.A randomized comparison of liposomal versus conventional amphotericin B for the treatment of pyrexia of unknown origin in neutropenic patients.Br J Haematol.1997;98:711–718.
- ,,, et al.Pharmacokinetics and safety of a 7 day administration of intravenous itraconazole followed by a 14‐day administration of itraconazole oral solution in patients with hematologic malignancy.Antimicrob Agents Chemother.2001;45:981–985.
- ,,, et al.Caspofungin versus liposomal amphotericin B for empirical antifungal therapy in patients with persistent fever and neutropenia.N Engl J Med.2004;351:1392–1402.
- ,,, et al.In vitro activities of voriconazole and four other antifungal agents against 394 clinical isolates of Candida spp.Antimicrob Agents Chemother.1998;42:161–163.
- ,,, et al.Antifungal activity of a new triazole, voriconazole (UK‐109,496) compared with three other antifungal agents tested against clinical isolates of filamentous fungi.Med Mycol.1998;36:433–436.
- ,,, et al.Voriconazole compared with liposomal amphotericin B for empirical antifungal therapy in patients with neutropenia and persistent fever.N Engl J Med.2002;346:225–234.
- ,,, et al.Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America.Clin Infect Dis.2008;46:327–360.
- ,,, et al.Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis.N Engl J Med.2002;347:408–415.
- ,,, et al.Efficacy and safety of caspofungin for treatment of invasive aspergillosis in patients refractory to or intolerant of conventional antifungal therapy.Clin Infect Dis.2004;39:1563–1571.
- ,,, et al.Micafungin (FK463), alone or in combination with other systemic antifungal agents, for the treatment of acute invasive aspergillosis.J Infect2006;53:337–349.
- ,,, et al.Posaconazole vs. fluconazole or itraconazole prophylaxis in patients with neutropenia.N Engl J Med.2007;356:348–359.
- ,,, et al.Posaconazole or fluconazole for prophylaxis in severe graft versus host disease.N Engl J Med.2007;356:335–347.
- ,,, et al.Treatment of invasive aspergillosis with posaconazole in patients who are refractory to or intolerant of conventional therapy: an externally controlled trial.Clin Infect Dis.2007;44:2–12.
- ,,, et al.Liposomal amphotericin B as initial therapy for invasive mold infection: a randomized trial comparing a high‐loading dose regimen with standard dosing (AmBiLoad trial).Clin Infect Dis.2007;44:1289–1297.
- ,,, et al.A randomized, double‐blind, double‐dummy, multicenter trial of voriconazole and fluconazole in the treatment of esophageal candidiasis in immunocompromised patients.Clin Infect Dis.2001;33:1447–1454.
- ,,, et al.Voriconazole treatment for less‐common, emerging, or refractory fungal infections.Clin Infect Dis.2003;36:1122–1131.
- ,,, et al.A randomized double‐blind study of caspofungin versus amphotericin for the treatment of candidal esophagitis.Clin Infect Dis.2001;33:1529–1535.
- ,,, et al.A randomized double‐blind study of caspofungin versus fluconazole for the treatment of esophageal candidiasis.Am J Med.2002;113:294–299.
- ,,, et al.A randomized, double‐blind, parallel‐group, dose‐response study of micafungin compared with fluconazole for the treatment of esophageal candidiasis in HIV‐positive patients.Clin Infect Dis.2004;39:842–849.
- ,,, et al.A randomized, double‐blind trial of anidulafungin versus fluconazole for the treatment of esophageal candidiasis.Clin Infect Dis.2004;39:770–775.
- ,,, et al.A multicenter randomized trial evaluating posaconazole versus fluconazole for the treatment of oropharyngeal candidiasis in subjects with HIV/AIDS.Clin Infect Dis.2006;42:1179–1186.
- ,,, et al.Posaconazole for the treatment of azole‐refractory oropharyngeal and esophageal candidiasis in subjects with HIV infection.Clin Infect Dis.2007;44:607–614.
- ,,, et al.Epidemiology and outcome of zygomycosis: a review of 929 reported cases.Clin Infect Dis.2005;41:634–653.
- ,,,.Zygomycosis in the 1990s in a tertiary‐care cancer center.Clin Infect Dis.2000;30:851–856.
- ,,, et al.Zygomycosis in a tertiary‐care center in the era of Aspergillus‐active antifungal therapy: a case‐control observational study of 27 recent cases.J Infect Dis.2005;191:1350–1360.
- ,.Invasive zygomycosis: update on pathogenesis, clinical manifestations, and management.Infect Dis Clin North Am.2006;20:581–607.
- ,,,,.In vitro activities of posaconazole itraconazole, voriconazole, amphotericin B, and fluconazole against 37 clinical isolates of zygomycetes.Antimicrob Agents Chemother.2002;46:1581–1582.
- ,,,,.In vivo activity of posaconazole against mucor spp. in an immunosuppressed‐mouse model.Antimicrob Agents Chemother.2002;46:2310–2312.
- ,,,,.In vitro susceptibilities of 217 clinical isolates of zygomycetes to conventional and new antifungal agents.Antimicrob Agents Chemother.2007;51:2587–2590.
- ,,, et al.Posaconazole as salvage therapy for zygomycosis.Antimicrob Agents Chemother.2006;50:126–133.
- ,,,,.Posaconazole is effective as salvage therapy in zygomycosis: a retrospective summary of 91 cases.Clin Infect Dis.2006;42:e61–e65.
- ,.Changing epidemiology of rare mould infections.Drugs.2007;67:1803–1812.
- .Posaconazole.Drugs.2005;65:1568–1569.
- ,,, et al.Coccidioidomycosis.Clin Infect Dis.2005;41:1217–1223.
- ,,.Epidemiologic, clinical, and diagnostic aspects of coccidioidomycosis.J Clin Microbiol.2007;4:26–30.
- ,,,.Therapeutic efficacy of caspofungin alone and in combination with amphotericin B deoxycholate for coccidioidomycosis in a mouse model.J Antimicrob Chemother.2007;60:1341–1346.
- ,.Antifungal susceptibility profiles of Coccidioides immitis and Coccidioides posadasii from endemic and non‐endemic areas.Mycopathologia.2007;163:31–19.
- ,,,,,.In vitro activities of voriconazole, itraconazole, and amphotericin B against Blastomyces dermatitidis, Coccidioides immitis, and Histoplasma capsulatum.Antimicrob Agents Chemother.2000;44:1734–1736.
- ,,,,.Refractory coccidioidomycosis treated with posaconazole.Clin Infect Dis.2005;40:1770–1776.
- ,,, et al.Safety, tolerance, and efficacy of posaconazole therapy in patients with nonmeningeal disseminated or chronic pulmonary coccidioidomycosis.Clin Infect Dis.2007;45:562–568.
- ,,, et al.Posaconazole therapy for chronic refractory coccidioidomycosis.Chest.2007;132:952–958.
- ,,, et al.Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America.Clin Infect Dis.2007;45:807–825.
- ,,,,.In vitro activities of new and established triazoles against opportunistic filamentous and dimorphic fungi.Med Mycol.2005;43:281–284.
- ,,, et al.Comparison of a new triazole antifungal agent, Schering 56592, with itraconazole and amphotericin B for treatment of histoplasmosis in immunocompetent mice.Antimicrob Agents Chemother.1999;439:322–328.
- ,,, et al.Activity of newer triazoles against Histoplasma capsulatum from patients with AIDS who failed fluconazole.J Antimicrob Chemother.2006;57:1235–1239.
- ,,,,,.Histoplasmosis in solid organ transplant recipients at a large midwestern university transplant center.Transpl Infect Dis.2005;7:109–115.
- ,,, et al.Salvage treatment of histoplasmosis with posaconazole.J Infect.2007;54:319–327.
- ,,.Current treatment strategies for disseminated candidiasis.Clin Infect Dis.2006;42:244–251.
- .Echinocandins for candidemia in adults without neutropenia.N Engl J Med.2006;355:1154–1159.
- ,,,.Voriconazole salvage treatment of invasive candidiasis.Eur J Clin Microbiol Infect Dis.2003;22:651–655.
- ,,, et al.Guidelines for treatment of candidiasis.Clin Infect Dis.2004;38:161–189.
- ,,, et al.Comparison of caspofugin and amphotericin B for invasive candidiasis.N Engl J Med.2002;347:2020–2029.
- ,,, et al.Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomized double‐blind trial.Lancet.2007;369:1519–1527.
- ,,, et al.Anidulafungin versus fluconazole for invasive candidiasis.N Engl J Med.2007;356:2472–2482.
- ,,, et al.Caspofungin for the treatment of less common forms of invasive candidiasis.J Antimicrob Chemother.2007;60:363–369.
- ,,, et al.Voriconazole versus a regimen of amphotericin B followed by fluconazole for candidaemia in non‐neutropenic patients: a randomized non‐inferiority trial.Lancet.2005;366:1435–1442.
- ,.Fever of unknown origin in febrile leucopenia.Infect Dis Clin North Am.2007;21:1055–1090.
- ,,, et al.2002 Guidelines for the use of antimicrobial agents in neutropenic patients with cancer.Clin Infect Dis.2002;34:730–751.
- ,,, et al.Empiric antibiotic and antifungal therapy for cancer patients with prolonged fever and granulocytopenia.Am J Med.1982;72:101–111.
- EORTC International Antimicrobial Therapy Cooperative Group.Empiric antifungal therapy in febrile granulocytopenic patients.Am J Med.1989;86:668–672.
- ,,, et al.Liposomal amphotericin B for empirical therapy in patients with persistent fever and neutropenia.N Engl J Med.1999;340:7644–7671.
- ,,, et al.A randomized comparison of liposomal versus conventional amphotericin B for the treatment of pyrexia of unknown origin in neutropenic patients.Br J Haematol.1997;98:711–718.
- ,,, et al.Pharmacokinetics and safety of a 7 day administration of intravenous itraconazole followed by a 14‐day administration of itraconazole oral solution in patients with hematologic malignancy.Antimicrob Agents Chemother.2001;45:981–985.
- ,,, et al.Caspofungin versus liposomal amphotericin B for empirical antifungal therapy in patients with persistent fever and neutropenia.N Engl J Med.2004;351:1392–1402.
- ,,, et al.In vitro activities of voriconazole and four other antifungal agents against 394 clinical isolates of Candida spp.Antimicrob Agents Chemother.1998;42:161–163.
- ,,, et al.Antifungal activity of a new triazole, voriconazole (UK‐109,496) compared with three other antifungal agents tested against clinical isolates of filamentous fungi.Med Mycol.1998;36:433–436.
- ,,, et al.Voriconazole compared with liposomal amphotericin B for empirical antifungal therapy in patients with neutropenia and persistent fever.N Engl J Med.2002;346:225–234.
- ,,, et al.Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America.Clin Infect Dis.2008;46:327–360.
- ,,, et al.Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis.N Engl J Med.2002;347:408–415.
- ,,, et al.Efficacy and safety of caspofungin for treatment of invasive aspergillosis in patients refractory to or intolerant of conventional antifungal therapy.Clin Infect Dis.2004;39:1563–1571.
- ,,, et al.Micafungin (FK463), alone or in combination with other systemic antifungal agents, for the treatment of acute invasive aspergillosis.J Infect2006;53:337–349.
- ,,, et al.Posaconazole vs. fluconazole or itraconazole prophylaxis in patients with neutropenia.N Engl J Med.2007;356:348–359.
- ,,, et al.Posaconazole or fluconazole for prophylaxis in severe graft versus host disease.N Engl J Med.2007;356:335–347.
- ,,, et al.Treatment of invasive aspergillosis with posaconazole in patients who are refractory to or intolerant of conventional therapy: an externally controlled trial.Clin Infect Dis.2007;44:2–12.
- ,,, et al.Liposomal amphotericin B as initial therapy for invasive mold infection: a randomized trial comparing a high‐loading dose regimen with standard dosing (AmBiLoad trial).Clin Infect Dis.2007;44:1289–1297.
- ,,, et al.A randomized, double‐blind, double‐dummy, multicenter trial of voriconazole and fluconazole in the treatment of esophageal candidiasis in immunocompromised patients.Clin Infect Dis.2001;33:1447–1454.
- ,,, et al.Voriconazole treatment for less‐common, emerging, or refractory fungal infections.Clin Infect Dis.2003;36:1122–1131.
- ,,, et al.A randomized double‐blind study of caspofungin versus amphotericin for the treatment of candidal esophagitis.Clin Infect Dis.2001;33:1529–1535.
- ,,, et al.A randomized double‐blind study of caspofungin versus fluconazole for the treatment of esophageal candidiasis.Am J Med.2002;113:294–299.
- ,,, et al.A randomized, double‐blind, parallel‐group, dose‐response study of micafungin compared with fluconazole for the treatment of esophageal candidiasis in HIV‐positive patients.Clin Infect Dis.2004;39:842–849.
- ,,, et al.A randomized, double‐blind trial of anidulafungin versus fluconazole for the treatment of esophageal candidiasis.Clin Infect Dis.2004;39:770–775.
- ,,, et al.A multicenter randomized trial evaluating posaconazole versus fluconazole for the treatment of oropharyngeal candidiasis in subjects with HIV/AIDS.Clin Infect Dis.2006;42:1179–1186.
- ,,, et al.Posaconazole for the treatment of azole‐refractory oropharyngeal and esophageal candidiasis in subjects with HIV infection.Clin Infect Dis.2007;44:607–614.
- ,,, et al.Epidemiology and outcome of zygomycosis: a review of 929 reported cases.Clin Infect Dis.2005;41:634–653.
- ,,,.Zygomycosis in the 1990s in a tertiary‐care cancer center.Clin Infect Dis.2000;30:851–856.
- ,,, et al.Zygomycosis in a tertiary‐care center in the era of Aspergillus‐active antifungal therapy: a case‐control observational study of 27 recent cases.J Infect Dis.2005;191:1350–1360.
- ,.Invasive zygomycosis: update on pathogenesis, clinical manifestations, and management.Infect Dis Clin North Am.2006;20:581–607.
- ,,,,.In vitro activities of posaconazole itraconazole, voriconazole, amphotericin B, and fluconazole against 37 clinical isolates of zygomycetes.Antimicrob Agents Chemother.2002;46:1581–1582.
- ,,,,.In vivo activity of posaconazole against mucor spp. in an immunosuppressed‐mouse model.Antimicrob Agents Chemother.2002;46:2310–2312.
- ,,,,.In vitro susceptibilities of 217 clinical isolates of zygomycetes to conventional and new antifungal agents.Antimicrob Agents Chemother.2007;51:2587–2590.
- ,,, et al.Posaconazole as salvage therapy for zygomycosis.Antimicrob Agents Chemother.2006;50:126–133.
- ,,,,.Posaconazole is effective as salvage therapy in zygomycosis: a retrospective summary of 91 cases.Clin Infect Dis.2006;42:e61–e65.
- ,.Changing epidemiology of rare mould infections.Drugs.2007;67:1803–1812.
- .Posaconazole.Drugs.2005;65:1568–1569.
- ,,, et al.Coccidioidomycosis.Clin Infect Dis.2005;41:1217–1223.
- ,,.Epidemiologic, clinical, and diagnostic aspects of coccidioidomycosis.J Clin Microbiol.2007;4:26–30.
- ,,,.Therapeutic efficacy of caspofungin alone and in combination with amphotericin B deoxycholate for coccidioidomycosis in a mouse model.J Antimicrob Chemother.2007;60:1341–1346.
- ,.Antifungal susceptibility profiles of Coccidioides immitis and Coccidioides posadasii from endemic and non‐endemic areas.Mycopathologia.2007;163:31–19.
- ,,,,,.In vitro activities of voriconazole, itraconazole, and amphotericin B against Blastomyces dermatitidis, Coccidioides immitis, and Histoplasma capsulatum.Antimicrob Agents Chemother.2000;44:1734–1736.
- ,,,,.Refractory coccidioidomycosis treated with posaconazole.Clin Infect Dis.2005;40:1770–1776.
- ,,, et al.Safety, tolerance, and efficacy of posaconazole therapy in patients with nonmeningeal disseminated or chronic pulmonary coccidioidomycosis.Clin Infect Dis.2007;45:562–568.
- ,,, et al.Posaconazole therapy for chronic refractory coccidioidomycosis.Chest.2007;132:952–958.
- ,,, et al.Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America.Clin Infect Dis.2007;45:807–825.
- ,,,,.In vitro activities of new and established triazoles against opportunistic filamentous and dimorphic fungi.Med Mycol.2005;43:281–284.
- ,,, et al.Comparison of a new triazole antifungal agent, Schering 56592, with itraconazole and amphotericin B for treatment of histoplasmosis in immunocompetent mice.Antimicrob Agents Chemother.1999;439:322–328.
- ,,, et al.Activity of newer triazoles against Histoplasma capsulatum from patients with AIDS who failed fluconazole.J Antimicrob Chemother.2006;57:1235–1239.
- ,,,,,.Histoplasmosis in solid organ transplant recipients at a large midwestern university transplant center.Transpl Infect Dis.2005;7:109–115.
- ,,, et al.Salvage treatment of histoplasmosis with posaconazole.J Infect.2007;54:319–327.
Prescribing Error Education
Medication errors are an often preventable consequence of the medication use process. Multiple reviews, including the recent Preventing Medication Errors by the Institute of Medicine,1 have emphasized the need to curtail process‐related deficiencies in medication use. Among inpatients, medication errors account for about 20% of medical errors.2 Medication errors can occur at the point of prescribing, transcribing, dispensing, administration, and monitoring. Prescribing errors are the most common and account for 39% to 49% of medication errors among hospitalized patients.3, 4
The Joint Commission has mandated that healthcare institutions track and intervene within the medication use process to reduce errors.5 A number of complex and costly interventions have been forwarded with significant evidence bases, including computerized physician order entry (CPOE), clinical decision‐support systems, and pharmacist participation on rounding medical teams.1 However, little has been published on the effectiveness of providing education and feedback to institutional clinicians to reduce prescribing‐related errors.68
Providers often are already aware of classic medication order errors, but at most institutions, specific examples of prescribing errors are not regularly communicated from the pharmacy dispensary to prescribers. One exception occurs when a dispensary pharmacist contacts a prescriber to clarify an order. However, this usually takes place while that prescriber is focused on the care of another patient, and it is not a good educational setting to reduce future medication order errors.
We delivered a series of short educational sessions to internal medicine (IM) residents, providing repeated feedback on prescribing errors using examples specific to our institution. The sessions followed the effective pharmaceutical industry paradigms of detailing and repeatedly exposing physicians to an educational message to maintain its salience. This innovation report documents the effect of this pharmacist‐led program on prescribing errors made by IM residents.
METHODS
This study was deemed exempt by the institutional review board of the University of Toledo.
Study Design
This study used a prospective interrupted time series design. Study participants included all IM residents at the 320‐bed University of Toledo Medical Center.
Educational Intervention
In July 2006, the Department of Internal Medicine required all IM residents to participate in a weekly 3‐hour didactic training seminar series. The educational intervention occurred longitudinally during a portion of that weekly seminar series. Attendance was mandatory, but the level of participation varied across individual residents. No formal assessment or quiz was used for each resident during these discussions.
The intervention had 2 phases and was designed and executed by the primary author within his roles as an IM clinical pharmacist and faculty member. Phase 1 was an initial hour‐long didactic lecture on prescribing errors at the beginning of November 2006. This lecture focused on definitions and categories of medical errors and medication errors, Institute of Medicine reports, Joint Commission medication management requirements, and institutional medication order policies.
Phase 2 included a number of short, biweekly follow‐up discussion sessions in November and December 2006 and thereafter was modified to monthly discussions from January to May 2007. Discussions specifically addressed prescribing errors identified by the medication safety officer and primary author during the previous month. Sessions were approximately 15 minutes long and followed a handout that highlighted specific and commonly seen prescribing errors within the facility (Figure 1). Within these discussions, the error subtype was identified, and suggestions for properly writing the order were given.
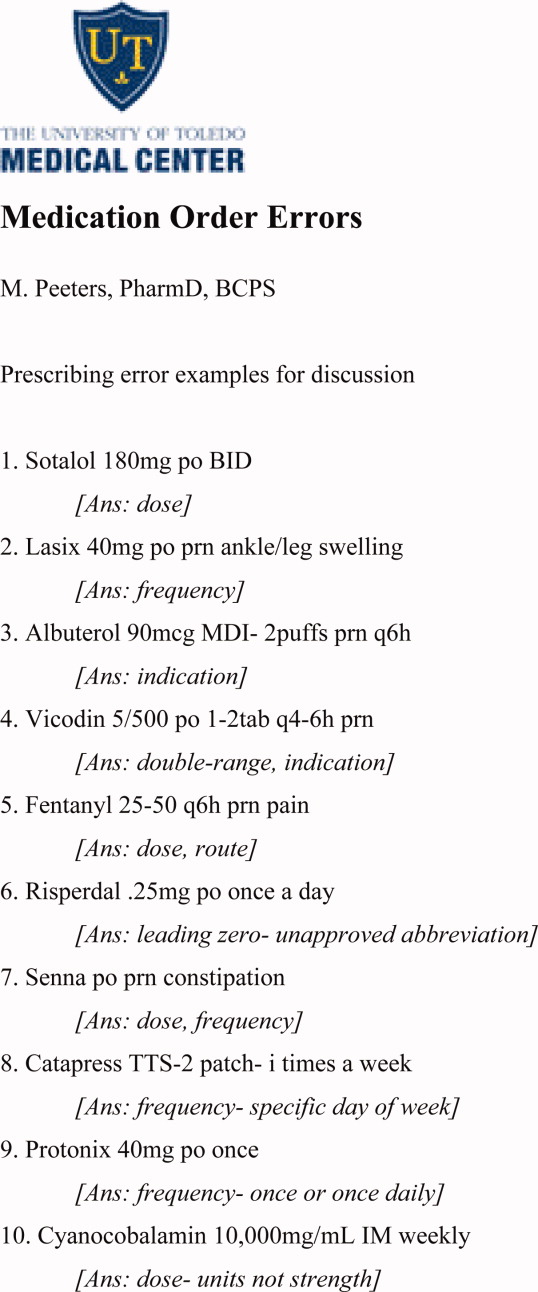
Prescribing Error Definition and Subtypes
Prescribing error was defined as any error on a physician medication order form that was sent to the pharmacy as a dispensing request.
The subtypes of prescribing errors were as follows:
-
Orders containing unapproved abbreviations.
-
As‐needed orders without indication.
-
Resume home medications orders.
-
Double‐range orders (eg, 1‐2 Percocet q4‐6h prn headache).
-
Wrong drug.
-
Wrong dose.
-
Wrong route.
-
Wrong frequency.
-
Medication order for which the patient has a documented allergy.
-
Incomprehensible or illegible orders.
Data Collection
Prescribing errors were collected from October 2006 to June 2007 for 13 hospital units that had IM or subspecialty patients. During this time, a stable group of IM residents rotated on these units among various clinical services; no new residents entered or dropped out during the study period, except for times when they may have had an ambulatory rotation. Data collected in October 2006 established the preintervention baseline. Data were collected during the educational intervention at intervals of 1, 3, and 6 months (December, February, and May). Postintervention data were collected in June 2007.
During the study period, staff pharmacists continually screened medication orders for prescribing errors. Once identified, the incorrect orders were collected, transcribed, coded, and entered into a database by the medication safety officer. On a monthly basis, prescribing error rates were calculated by the division of the number of prescribing errors by the total number of medication orders within the facility.
Data Analysis
The experiment‐wise alpha for the main outcome was 0.05. The primary outcome was the frequency of prescribing errors across the preintervention (month 0), intervention (months 1, 3, and 6), and postintervention (month 7) periods. The primary analysis compared these 5 time periods with 10 Bonferroni‐adjusted chi‐square tests, reducing the pairwise alpha to 0.005.
RESULTS
Forty‐two IM residents participated in this study. Prior to the educational intervention, prescribing errors affected 2.25% (861/38,275) of the institution's medication orders (Figure 2). Following phase 1 and early into phase 2 of the prescribing error education, the frequency dropped to 1.51% (P 0.001); that is, there was a 33% decline from the baseline. During the remainder of the intervention period, the frequency of prescribing errors fluctuated but remained lower than that observed pre‐intervention (P 0.001 for each pairwise comparison to the baseline). Post‐intervention, the frequency of prescribing errors rose to 2.33% and was similar to that observed at the baseline (P = 0.49).
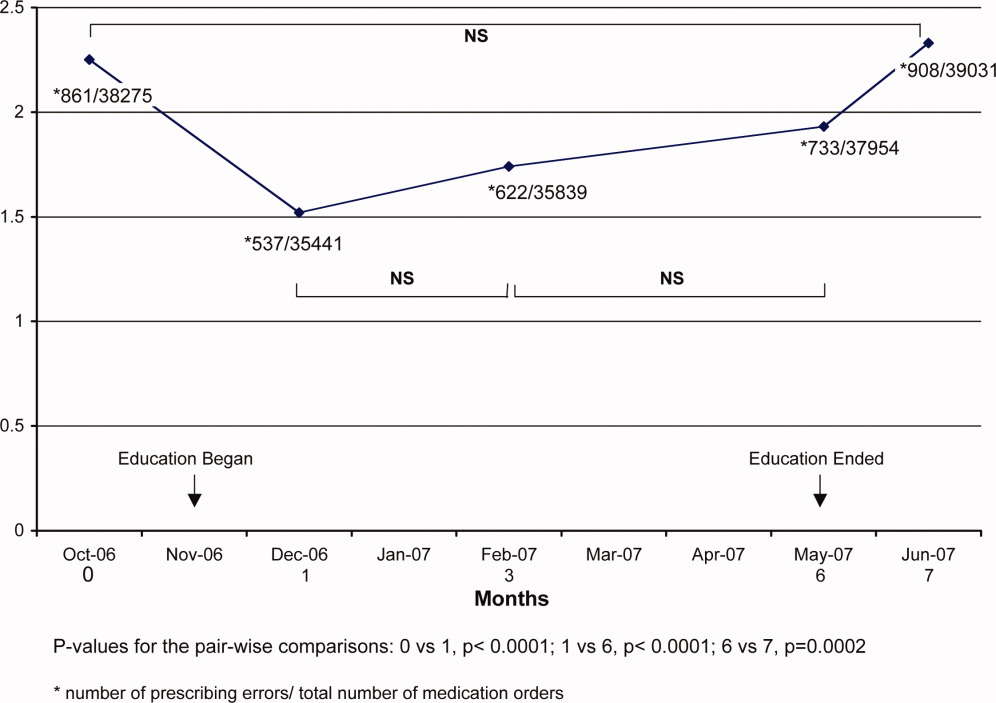
DISCUSSION
An educational intervention that highlighted institution‐specific prescribing errors reduced such errors by 33% within the first month and resulted in a mean 26% reduction during the 6‐month intervention period. Without ongoing education, however, the frequency of prescribing errors returned to preintervention period levels.
Our findings compare favorably to results obtained by other more complex and costly methods used to reduce medication errors, namely, CPOE, clinical decision‐support software, and clinical pharmacists on medical rounds.1 For example, in 1 study, prescribing errors were reduced by 19% following the implementation of CPOE alone.9 In another report, CPOE with clinical decision‐support software led to a more dramatic reduction of 81%.10 Additionally, pharmacist involvement on medical rounds has reduced adverse drug events by 78%.11
The frequency of prescribing errors found in this study was similar to that found in previous literature, although the variation in the definitions limits this comparison somewhat.12 Interestingly, the frequency of errors increased as the overall number of medication orders for the facility increased (see the ratios in Figure 2). This suggests that errors may be more likely during busier time periods, which are defined by higher total order volumes. Others have made similar observations.13 On most occasions, the individual prescribing errors seemed obvious and most likely due to a physician's haste.
This study had some limitations, including its interrupted time series design, which limits the ability to define a causal relationship. However, a causal effect is suggested by the differences before and during intervention as well as the return to the preintervention error frequency after the intervention had concluded. Second, the reported frequencies represent all medication orders in the studied clinical areas, not only those orders written by medical residents who participated in the intervention, although they do account for a large portion of the prescribing at the study hospital. Third, we did not assess specific resident errors or compare changes in the types of errors over time. Fourth, generalizability is limited to IM residents at an academic institution. As trainees, the IM residents may have been both keener to participate in and more accessible for educational opportunities such as this study. Fifth, as noted previously, the IM residents in this study not only practiced in the inpatient areas but had outpatient clinic rotations as well. It is conceivable that the most error‐prone residents rotated on the inpatient units before and after the intervention period but not during it. This is not very likely but cannot be excluded.
CONCLUSIONS
Adverse drug events have an impact on patient safety and can commonly occur following prescribing errors. Therefore, reducing prescribing errors is extremely important. The longitudinal education of residents using a periodic educational intervention provides a successful and economically feasible prescribing error prevention strategy, although the effects are quickly reversed following cessation of the educational component. Therefore, supporting an ongoing commitment to trainee education and communication between pharmacy and prescribers about institution‐specific medication errors appears warranted.
Acknowledgements
The authors gratefully acknowledge Ziad Mattar, MD, the 2006‐2007 University of Toledo College of Medicine Internal Medicine Chief Resident, for his organizational influence regarding the educational sessions with internal medicine residents. In addition, the University of Toledo College of Medicine Medication Safety Officer, Ms. Jennifer Guy, provided great assistance in accumulating the data for this study.
- Institute of Medicine.Preventing Medication Errors: Quality Chasm Series.Washington, DC:National Academy Press;2007.
- ,,, et al.The nature of adverse events in hospitalized patients: results of the Harvard Medical Practice Study II.N Engl J Med.1991;324(6):377–384.
- ,,, et al.Incidence of adverse drug events and potential adverse drug events: implications for practice.JAMA.1995;274:29–34.
- ,,, et al.Systems analysis of adverse drug events.JAMA.1995;274:35–43.
- Comprehensive Accreditation Manual for Hospitals.Oakbrook Terrace, IL:Joint Commission on Accreditation of Healthcare Organizations;2004.
- .Education regarding medication order errors.CJHP.2007;60:130.
- ,,,,.Educational interventions to reduce use of unsafe abbreviations.Am J Health‐Syst Pharm.2007;64:1170–1173.
- ,,,,,.Error reduction: academic detailing as a method to reduce incorrect prescriptions.Eur J Clin Pharmacol.2003;59:697–699.
- ,,, et al.Effect of computerized physician order entry and a team intervention on prevention of serious medication errors.JAMA.1998;280:1311–1316.
- ,,, et al.The impact of computerized physician order entry on medication error prevention.J Am Med Inform Assoc.1999;6:313–321.
- ,,,.Pharmacists on rounding teams reduce preventable adverse drug events in hospital general medicine units.Arch Intern Med.2003;163:2014–2018.
- ,,,.The incidence of prescribing errors in hospital inpatients.Drug Saf.2005;28:891–900.
- ,,,,.A study of the quality of prescriptions issued in a busy pediatric emergency room.Public Health Rep.1975;90(5):402–408.
Medication errors are an often preventable consequence of the medication use process. Multiple reviews, including the recent Preventing Medication Errors by the Institute of Medicine,1 have emphasized the need to curtail process‐related deficiencies in medication use. Among inpatients, medication errors account for about 20% of medical errors.2 Medication errors can occur at the point of prescribing, transcribing, dispensing, administration, and monitoring. Prescribing errors are the most common and account for 39% to 49% of medication errors among hospitalized patients.3, 4
The Joint Commission has mandated that healthcare institutions track and intervene within the medication use process to reduce errors.5 A number of complex and costly interventions have been forwarded with significant evidence bases, including computerized physician order entry (CPOE), clinical decision‐support systems, and pharmacist participation on rounding medical teams.1 However, little has been published on the effectiveness of providing education and feedback to institutional clinicians to reduce prescribing‐related errors.68
Providers often are already aware of classic medication order errors, but at most institutions, specific examples of prescribing errors are not regularly communicated from the pharmacy dispensary to prescribers. One exception occurs when a dispensary pharmacist contacts a prescriber to clarify an order. However, this usually takes place while that prescriber is focused on the care of another patient, and it is not a good educational setting to reduce future medication order errors.
We delivered a series of short educational sessions to internal medicine (IM) residents, providing repeated feedback on prescribing errors using examples specific to our institution. The sessions followed the effective pharmaceutical industry paradigms of detailing and repeatedly exposing physicians to an educational message to maintain its salience. This innovation report documents the effect of this pharmacist‐led program on prescribing errors made by IM residents.
METHODS
This study was deemed exempt by the institutional review board of the University of Toledo.
Study Design
This study used a prospective interrupted time series design. Study participants included all IM residents at the 320‐bed University of Toledo Medical Center.
Educational Intervention
In July 2006, the Department of Internal Medicine required all IM residents to participate in a weekly 3‐hour didactic training seminar series. The educational intervention occurred longitudinally during a portion of that weekly seminar series. Attendance was mandatory, but the level of participation varied across individual residents. No formal assessment or quiz was used for each resident during these discussions.
The intervention had 2 phases and was designed and executed by the primary author within his roles as an IM clinical pharmacist and faculty member. Phase 1 was an initial hour‐long didactic lecture on prescribing errors at the beginning of November 2006. This lecture focused on definitions and categories of medical errors and medication errors, Institute of Medicine reports, Joint Commission medication management requirements, and institutional medication order policies.
Phase 2 included a number of short, biweekly follow‐up discussion sessions in November and December 2006 and thereafter was modified to monthly discussions from January to May 2007. Discussions specifically addressed prescribing errors identified by the medication safety officer and primary author during the previous month. Sessions were approximately 15 minutes long and followed a handout that highlighted specific and commonly seen prescribing errors within the facility (Figure 1). Within these discussions, the error subtype was identified, and suggestions for properly writing the order were given.
Prescribing Error Definition and Subtypes
Prescribing error was defined as any error on a physician medication order form that was sent to the pharmacy as a dispensing request.
The subtypes of prescribing errors were as follows:
-
Orders containing unapproved abbreviations.
-
As‐needed orders without indication.
-
Resume home medications orders.
-
Double‐range orders (eg, 1‐2 Percocet q4‐6h prn headache).
-
Wrong drug.
-
Wrong dose.
-
Wrong route.
-
Wrong frequency.
-
Medication order for which the patient has a documented allergy.
-
Incomprehensible or illegible orders.
Data Collection
Prescribing errors were collected from October 2006 to June 2007 for 13 hospital units that had IM or subspecialty patients. During this time, a stable group of IM residents rotated on these units among various clinical services; no new residents entered or dropped out during the study period, except for times when they may have had an ambulatory rotation. Data collected in October 2006 established the preintervention baseline. Data were collected during the educational intervention at intervals of 1, 3, and 6 months (December, February, and May). Postintervention data were collected in June 2007.
During the study period, staff pharmacists continually screened medication orders for prescribing errors. Once identified, the incorrect orders were collected, transcribed, coded, and entered into a database by the medication safety officer. On a monthly basis, prescribing error rates were calculated by the division of the number of prescribing errors by the total number of medication orders within the facility.
Data Analysis
The experiment‐wise alpha for the main outcome was 0.05. The primary outcome was the frequency of prescribing errors across the preintervention (month 0), intervention (months 1, 3, and 6), and postintervention (month 7) periods. The primary analysis compared these 5 time periods with 10 Bonferroni‐adjusted chi‐square tests, reducing the pairwise alpha to 0.005.
RESULTS
Forty‐two IM residents participated in this study. Prior to the educational intervention, prescribing errors affected 2.25% (861/38,275) of the institution's medication orders (Figure 2). Following phase 1 and early into phase 2 of the prescribing error education, the frequency dropped to 1.51% (P 0.001); that is, there was a 33% decline from the baseline. During the remainder of the intervention period, the frequency of prescribing errors fluctuated but remained lower than that observed pre‐intervention (P 0.001 for each pairwise comparison to the baseline). Post‐intervention, the frequency of prescribing errors rose to 2.33% and was similar to that observed at the baseline (P = 0.49).
DISCUSSION
An educational intervention that highlighted institution‐specific prescribing errors reduced such errors by 33% within the first month and resulted in a mean 26% reduction during the 6‐month intervention period. Without ongoing education, however, the frequency of prescribing errors returned to preintervention period levels.
Our findings compare favorably to results obtained by other more complex and costly methods used to reduce medication errors, namely, CPOE, clinical decision‐support software, and clinical pharmacists on medical rounds.1 For example, in 1 study, prescribing errors were reduced by 19% following the implementation of CPOE alone.9 In another report, CPOE with clinical decision‐support software led to a more dramatic reduction of 81%.10 Additionally, pharmacist involvement on medical rounds has reduced adverse drug events by 78%.11
The frequency of prescribing errors found in this study was similar to that found in previous literature, although the variation in the definitions limits this comparison somewhat.12 Interestingly, the frequency of errors increased as the overall number of medication orders for the facility increased (see the ratios in Figure 2). This suggests that errors may be more likely during busier time periods, which are defined by higher total order volumes. Others have made similar observations.13 On most occasions, the individual prescribing errors seemed obvious and most likely due to a physician's haste.
This study had some limitations, including its interrupted time series design, which limits the ability to define a causal relationship. However, a causal effect is suggested by the differences before and during intervention as well as the return to the preintervention error frequency after the intervention had concluded. Second, the reported frequencies represent all medication orders in the studied clinical areas, not only those orders written by medical residents who participated in the intervention, although they do account for a large portion of the prescribing at the study hospital. Third, we did not assess specific resident errors or compare changes in the types of errors over time. Fourth, generalizability is limited to IM residents at an academic institution. As trainees, the IM residents may have been both keener to participate in and more accessible for educational opportunities such as this study. Fifth, as noted previously, the IM residents in this study not only practiced in the inpatient areas but had outpatient clinic rotations as well. It is conceivable that the most error‐prone residents rotated on the inpatient units before and after the intervention period but not during it. This is not very likely but cannot be excluded.
CONCLUSIONS
Adverse drug events have an impact on patient safety and can commonly occur following prescribing errors. Therefore, reducing prescribing errors is extremely important. The longitudinal education of residents using a periodic educational intervention provides a successful and economically feasible prescribing error prevention strategy, although the effects are quickly reversed following cessation of the educational component. Therefore, supporting an ongoing commitment to trainee education and communication between pharmacy and prescribers about institution‐specific medication errors appears warranted.
Acknowledgements
The authors gratefully acknowledge Ziad Mattar, MD, the 2006‐2007 University of Toledo College of Medicine Internal Medicine Chief Resident, for his organizational influence regarding the educational sessions with internal medicine residents. In addition, the University of Toledo College of Medicine Medication Safety Officer, Ms. Jennifer Guy, provided great assistance in accumulating the data for this study.
Medication errors are an often preventable consequence of the medication use process. Multiple reviews, including the recent Preventing Medication Errors by the Institute of Medicine,1 have emphasized the need to curtail process‐related deficiencies in medication use. Among inpatients, medication errors account for about 20% of medical errors.2 Medication errors can occur at the point of prescribing, transcribing, dispensing, administration, and monitoring. Prescribing errors are the most common and account for 39% to 49% of medication errors among hospitalized patients.3, 4
The Joint Commission has mandated that healthcare institutions track and intervene within the medication use process to reduce errors.5 A number of complex and costly interventions have been forwarded with significant evidence bases, including computerized physician order entry (CPOE), clinical decision‐support systems, and pharmacist participation on rounding medical teams.1 However, little has been published on the effectiveness of providing education and feedback to institutional clinicians to reduce prescribing‐related errors.68
Providers often are already aware of classic medication order errors, but at most institutions, specific examples of prescribing errors are not regularly communicated from the pharmacy dispensary to prescribers. One exception occurs when a dispensary pharmacist contacts a prescriber to clarify an order. However, this usually takes place while that prescriber is focused on the care of another patient, and it is not a good educational setting to reduce future medication order errors.
We delivered a series of short educational sessions to internal medicine (IM) residents, providing repeated feedback on prescribing errors using examples specific to our institution. The sessions followed the effective pharmaceutical industry paradigms of detailing and repeatedly exposing physicians to an educational message to maintain its salience. This innovation report documents the effect of this pharmacist‐led program on prescribing errors made by IM residents.
METHODS
This study was deemed exempt by the institutional review board of the University of Toledo.
Study Design
This study used a prospective interrupted time series design. Study participants included all IM residents at the 320‐bed University of Toledo Medical Center.
Educational Intervention
In July 2006, the Department of Internal Medicine required all IM residents to participate in a weekly 3‐hour didactic training seminar series. The educational intervention occurred longitudinally during a portion of that weekly seminar series. Attendance was mandatory, but the level of participation varied across individual residents. No formal assessment or quiz was used for each resident during these discussions.
The intervention had 2 phases and was designed and executed by the primary author within his roles as an IM clinical pharmacist and faculty member. Phase 1 was an initial hour‐long didactic lecture on prescribing errors at the beginning of November 2006. This lecture focused on definitions and categories of medical errors and medication errors, Institute of Medicine reports, Joint Commission medication management requirements, and institutional medication order policies.
Phase 2 included a number of short, biweekly follow‐up discussion sessions in November and December 2006 and thereafter was modified to monthly discussions from January to May 2007. Discussions specifically addressed prescribing errors identified by the medication safety officer and primary author during the previous month. Sessions were approximately 15 minutes long and followed a handout that highlighted specific and commonly seen prescribing errors within the facility (Figure 1). Within these discussions, the error subtype was identified, and suggestions for properly writing the order were given.
Prescribing Error Definition and Subtypes
Prescribing error was defined as any error on a physician medication order form that was sent to the pharmacy as a dispensing request.
The subtypes of prescribing errors were as follows:
-
Orders containing unapproved abbreviations.
-
As‐needed orders without indication.
-
Resume home medications orders.
-
Double‐range orders (eg, 1‐2 Percocet q4‐6h prn headache).
-
Wrong drug.
-
Wrong dose.
-
Wrong route.
-
Wrong frequency.
-
Medication order for which the patient has a documented allergy.
-
Incomprehensible or illegible orders.
Data Collection
Prescribing errors were collected from October 2006 to June 2007 for 13 hospital units that had IM or subspecialty patients. During this time, a stable group of IM residents rotated on these units among various clinical services; no new residents entered or dropped out during the study period, except for times when they may have had an ambulatory rotation. Data collected in October 2006 established the preintervention baseline. Data were collected during the educational intervention at intervals of 1, 3, and 6 months (December, February, and May). Postintervention data were collected in June 2007.
During the study period, staff pharmacists continually screened medication orders for prescribing errors. Once identified, the incorrect orders were collected, transcribed, coded, and entered into a database by the medication safety officer. On a monthly basis, prescribing error rates were calculated by the division of the number of prescribing errors by the total number of medication orders within the facility.
Data Analysis
The experiment‐wise alpha for the main outcome was 0.05. The primary outcome was the frequency of prescribing errors across the preintervention (month 0), intervention (months 1, 3, and 6), and postintervention (month 7) periods. The primary analysis compared these 5 time periods with 10 Bonferroni‐adjusted chi‐square tests, reducing the pairwise alpha to 0.005.
RESULTS
Forty‐two IM residents participated in this study. Prior to the educational intervention, prescribing errors affected 2.25% (861/38,275) of the institution's medication orders (Figure 2). Following phase 1 and early into phase 2 of the prescribing error education, the frequency dropped to 1.51% (P 0.001); that is, there was a 33% decline from the baseline. During the remainder of the intervention period, the frequency of prescribing errors fluctuated but remained lower than that observed pre‐intervention (P 0.001 for each pairwise comparison to the baseline). Post‐intervention, the frequency of prescribing errors rose to 2.33% and was similar to that observed at the baseline (P = 0.49).
DISCUSSION
An educational intervention that highlighted institution‐specific prescribing errors reduced such errors by 33% within the first month and resulted in a mean 26% reduction during the 6‐month intervention period. Without ongoing education, however, the frequency of prescribing errors returned to preintervention period levels.
Our findings compare favorably to results obtained by other more complex and costly methods used to reduce medication errors, namely, CPOE, clinical decision‐support software, and clinical pharmacists on medical rounds.1 For example, in 1 study, prescribing errors were reduced by 19% following the implementation of CPOE alone.9 In another report, CPOE with clinical decision‐support software led to a more dramatic reduction of 81%.10 Additionally, pharmacist involvement on medical rounds has reduced adverse drug events by 78%.11
The frequency of prescribing errors found in this study was similar to that found in previous literature, although the variation in the definitions limits this comparison somewhat.12 Interestingly, the frequency of errors increased as the overall number of medication orders for the facility increased (see the ratios in Figure 2). This suggests that errors may be more likely during busier time periods, which are defined by higher total order volumes. Others have made similar observations.13 On most occasions, the individual prescribing errors seemed obvious and most likely due to a physician's haste.
This study had some limitations, including its interrupted time series design, which limits the ability to define a causal relationship. However, a causal effect is suggested by the differences before and during intervention as well as the return to the preintervention error frequency after the intervention had concluded. Second, the reported frequencies represent all medication orders in the studied clinical areas, not only those orders written by medical residents who participated in the intervention, although they do account for a large portion of the prescribing at the study hospital. Third, we did not assess specific resident errors or compare changes in the types of errors over time. Fourth, generalizability is limited to IM residents at an academic institution. As trainees, the IM residents may have been both keener to participate in and more accessible for educational opportunities such as this study. Fifth, as noted previously, the IM residents in this study not only practiced in the inpatient areas but had outpatient clinic rotations as well. It is conceivable that the most error‐prone residents rotated on the inpatient units before and after the intervention period but not during it. This is not very likely but cannot be excluded.
CONCLUSIONS
Adverse drug events have an impact on patient safety and can commonly occur following prescribing errors. Therefore, reducing prescribing errors is extremely important. The longitudinal education of residents using a periodic educational intervention provides a successful and economically feasible prescribing error prevention strategy, although the effects are quickly reversed following cessation of the educational component. Therefore, supporting an ongoing commitment to trainee education and communication between pharmacy and prescribers about institution‐specific medication errors appears warranted.
Acknowledgements
The authors gratefully acknowledge Ziad Mattar, MD, the 2006‐2007 University of Toledo College of Medicine Internal Medicine Chief Resident, for his organizational influence regarding the educational sessions with internal medicine residents. In addition, the University of Toledo College of Medicine Medication Safety Officer, Ms. Jennifer Guy, provided great assistance in accumulating the data for this study.
- Institute of Medicine.Preventing Medication Errors: Quality Chasm Series.Washington, DC:National Academy Press;2007.
- ,,, et al.The nature of adverse events in hospitalized patients: results of the Harvard Medical Practice Study II.N Engl J Med.1991;324(6):377–384.
- ,,, et al.Incidence of adverse drug events and potential adverse drug events: implications for practice.JAMA.1995;274:29–34.
- ,,, et al.Systems analysis of adverse drug events.JAMA.1995;274:35–43.
- Comprehensive Accreditation Manual for Hospitals.Oakbrook Terrace, IL:Joint Commission on Accreditation of Healthcare Organizations;2004.
- .Education regarding medication order errors.CJHP.2007;60:130.
- ,,,,.Educational interventions to reduce use of unsafe abbreviations.Am J Health‐Syst Pharm.2007;64:1170–1173.
- ,,,,,.Error reduction: academic detailing as a method to reduce incorrect prescriptions.Eur J Clin Pharmacol.2003;59:697–699.
- ,,, et al.Effect of computerized physician order entry and a team intervention on prevention of serious medication errors.JAMA.1998;280:1311–1316.
- ,,, et al.The impact of computerized physician order entry on medication error prevention.J Am Med Inform Assoc.1999;6:313–321.
- ,,,.Pharmacists on rounding teams reduce preventable adverse drug events in hospital general medicine units.Arch Intern Med.2003;163:2014–2018.
- ,,,.The incidence of prescribing errors in hospital inpatients.Drug Saf.2005;28:891–900.
- ,,,,.A study of the quality of prescriptions issued in a busy pediatric emergency room.Public Health Rep.1975;90(5):402–408.
- Institute of Medicine.Preventing Medication Errors: Quality Chasm Series.Washington, DC:National Academy Press;2007.
- ,,, et al.The nature of adverse events in hospitalized patients: results of the Harvard Medical Practice Study II.N Engl J Med.1991;324(6):377–384.
- ,,, et al.Incidence of adverse drug events and potential adverse drug events: implications for practice.JAMA.1995;274:29–34.
- ,,, et al.Systems analysis of adverse drug events.JAMA.1995;274:35–43.
- Comprehensive Accreditation Manual for Hospitals.Oakbrook Terrace, IL:Joint Commission on Accreditation of Healthcare Organizations;2004.
- .Education regarding medication order errors.CJHP.2007;60:130.
- ,,,,.Educational interventions to reduce use of unsafe abbreviations.Am J Health‐Syst Pharm.2007;64:1170–1173.
- ,,,,,.Error reduction: academic detailing as a method to reduce incorrect prescriptions.Eur J Clin Pharmacol.2003;59:697–699.
- ,,, et al.Effect of computerized physician order entry and a team intervention on prevention of serious medication errors.JAMA.1998;280:1311–1316.
- ,,, et al.The impact of computerized physician order entry on medication error prevention.J Am Med Inform Assoc.1999;6:313–321.
- ,,,.Pharmacists on rounding teams reduce preventable adverse drug events in hospital general medicine units.Arch Intern Med.2003;163:2014–2018.
- ,,,.The incidence of prescribing errors in hospital inpatients.Drug Saf.2005;28:891–900.
- ,,,,.A study of the quality of prescriptions issued in a busy pediatric emergency room.Public Health Rep.1975;90(5):402–408.