User login
Editorial
Excellence is best described as doing the right things rightselecting the most important things to be done and then accomplishing them 100% correctly.
In this issue of JHM, O'Connor et al.1 examine the impact of paper‐based admission order sets on several quality measures relevant to medical inpatients in a large community medical center, focusing the most attention on the use of venous thromboembolism (VTE) prophylaxis. Randomly selected medical admissions from 4 time periods were examined by chart review for use of the order set, and for the use of VTE prophylaxis (defined as either unfractionated heparin [UFH] 5,000 units subcutaneous [sc] twice daily [BID] or compression stockings). VTE prophylaxis was ordered in an abysmally low 10.9% of inpatients in the baseline period. In spite of the limitations inherent in a before and after study design and a failure to assess the appropriateness of VTE prophylaxis, VTE rates, or side effects, the authors present convincing evidence that improvement in VTE prophylaxis did occur. However, it was a very limited and suboptimal improvement. By the fourteenth and fifteenth month after order set introduction, only about one‐half of admissions used the order set, and even when the order set was used, only 44% had VTE prophylaxis ordered. The percent of patient‐days with pharmacologic VTE prophylaxis in medical inpatients improved after order set implementation, but remained very low, at 26%. Therefore, the key lessons to be learned from this study are likely derived from what went wrong, rather than what went right.
Why did VTE prophylaxis rates stay so low in the face of a multiyear effort? An examination of more successful efforts,25 recent reviews in the VTE and quality improvement literature,610 and the Society of Hospital Medicine VTE Prevention Collaborative experience reveals several principles for effective improvement that were not followed in this study.
A VTE PREVENTION ORDER SET SHOULD PROVIDE DECISION SUPPORT (NOT JUST A PROMPT)
A simple prompt for mechanical prophylaxis or for UFH 5,000 units sc BID was embedded into a voluntary order set in this effort. Mechanical prophylaxis, pharmacologic prophylaxis, and no prophylaxis were treated as equal options, even though most medical inpatients have significant VTE risk factors,11, 12 and in spite of strong evidence‐based recommendations12 relegating mechanical prophylaxis to an adjunctive role for pharmacologic prophylaxis (unless there are contraindications to pharmacologic prophylaxis). The authors point out that the way order sets are structured or introduced is important to ensure they achieve the desired changes in practice. I could not agree more, but, unfortunately, the structure of their order set only secured the desired change in 44% of patients, even if you count compression stockings as adequate prophylaxis. This relatively poor result should have sparked a redesign of the VTE prevention component of the order set.
A more effective order set would reflect an institutional VTE prevention protocol.6, 7, 9, 13 A VTE prevention protocol consists of a standardized VTE risk assessment and contraindications to pharmacologic or heparin prophylaxis, linked to a menu of appropriate VTE prophylaxis options for each level of risk.13 The best protocols provide decision support at the point of care,9, 13 and yet preserve the ability to customize care for special patient situations or circumstances.
Ease of use issues and the lack of prospectively validated models have hindered widespread adoption of VTE risk assessment protocols (especially the point‐based models),14 but a simpler and more streamlined approach has been validated by the UCSD Medical Center experience,2 and by the general success of similar protocols in diverse medical centers taking part in the Society of Hospital Medicine (SHM) VTE Prevention Collaborative. This simpler method generally places patients into 1 of 3 levels of VTE risk, can be completed in seconds, and has excellent interobserver agreement. Reinforcing the expectation that pharmacologic prophylaxis is desirable for most ill inpatients (unless there is a contraindication to it) is likely more important than the finer details of the risk assessment model.
PROTOCOLS AND ORDER SETS MUST REACH THE GREAT MAJORITY OF PATIENTS
Protocols and order sets that sit on the shelf do not benefit patients. An order set that is used for one‐half of the targeted population has no chance of promoting excellent adherence to a protocol, and protocols/order sets must be widely adapted to be effective.13 Institutional mandates for the use of preprinted (or computerized) orders can be a very effective strategy. If the order set is constructed properly, it is easy to use and can actually save clinician time, thereby promoting widespread use, in some cases even without such a mandate. The SHM VTE Prevention Collaborative generally endorses an institution‐wide protocol and order set module that covers a variety of patient populations. A plug and play modular order set design allows the VTE prevention order set to be incorporated into all appropriate admission and transfer orders, and lends itself well to paper or computerized order formats.
LAYER ON ADDITIONAL INTERVENTIONS TO ENHANCE THE POWER OF THE PROTOCOL
Skillful introduction of a good order set that reaches most patients has often yielded observed VTE prophylaxis rates of 75% to 80% in the SHM VTE Prevention Collaborative. To reach higher levels, a multifaceted approach using a variety of techniques has been an effective strategy in the literature24, 6, 7, 10, 13, 15 and in the Collaborative. Educational programs alone,4, 16, 17 while not generally sufficient to bring about reliable VTE prophylaxis, remain an important intervention that can foster a more enthusiastic and appropriate use of order sets and protocols. Periodic audit and feedback and computerized decision support can also be very effective,3, 1822 particularly when there is an institutional protocol to hold up as the defining standard for adequate prophylaxis. We favor a method that involves real‐time identification of outliers (i.e., patients without prophylaxis who have some VTE risk and no obvious contraindication to prophylaxis). This identification can be done manually, but automated reports are generally feasible and effective. A simple templated note or page from a nurse or pharmacist to the provider of an outlier patient can bolster VTE prevention rates to well over 95%.5 Fatigue from alerts is minimized if this strategy is deployed after substantial improvement in VTE prophylaxis rates has been achieved via a well‐implemented and uniformly‐utilized order set. Trending and discussing cases of hospital‐acquired VTE can also motivate medical staff and reduce resistance to standardization.2, 3
THE FOUNDATION FOR IMPROVEMENT MUST BE IN PLACE
To explain why they did not implement educational programs, guidelines, or provide feedback to providers on their performance, the authors cite a lack of resources common to community medical centers. Yet, they were able to achieve the most resource‐intensive and challenging component of a VTE prevention effort, data collection and analysis. While resources for quality improvement are indeed insufficient in many academic and community hospitals, suboptimal levels of improvement tend to reflect, as in this study, fundamental failures in approach or execution. In this case, the order set design and implementation issues outlined above do not require extensive resources. Moreover, the foundation for effective improvement must be in place to address these issues effectively. This foundation includes administrative buy‐in that VTE prevention is an institutional priority, a commitment to support standardization (even in the face of occasional medical staff resistance), and a willingness to examine and redesign processes.13 It is unclear whether the administration was convinced that the effort should be a priority or whether this improvement team reported results through appropriate medical staff committees. The key point, of course, is that a culture of shared purpose, cooperation, and high expectations between the medical staff and the administration is more important than extensive resources. The right foundational elements put most improvement resources within the grasp of most medical centers.
The authors present work that is praiseworthy in many respects, but their suboptimal levels of improvement should serve as a cautionary tale rather than a model for other centers. Core improvement principles are of key importance. A mere prompt to order VTE prophylaxis within voluntarily‐used order sets, without supporting strategies to enhance VTE prophylaxis, is a recipe for mediocre improvement. Far superior results have been demonstrated in both community and academic centers, even in environments with limited resources. A multifaceted approach, including order sets that promote VTE prophylaxis and provide decision support for the majority of the targeted population, proactive intervention applied to outliers who are not on appropriate prophylaxis, educational programs, and an institutional commitment to standardization, are the ingredients for excellent results.
- ,,,.Medical admission order sets to improve deep vein thrombosis prophylaxis rates and other outcomes.J Hosp Med.2009;4(2):81–89.
- ,,, et al.Optimizing prevention of hospital‐acquired venous thromboembolism: prospective validation of a VTE risk assessment model and protocol. 2008 Abstracts: Research, Innovations, Clinical Vignettes Competition. 2008 National Meeting, Society of Hospital Medicine, April 3–5, 2008, San Diego, CA. Abstract 52, p29. Available at http://www.hospitalmedicine.org/Paperless2008/PDFs/Additional_Info/SHM08_Abstracts.pdf. Accessed November2008.
- ,,.Innovative approaches to increase deep vein thrombosis prophylaxis rate resulting in a decrease in hospital‐acquired deep vein thrombosis at a tertiary‐care teaching hospital.J Hosp Med.2008;3(2):148–155.
- ,,.Improved use of thromboprophylaxis for deep vein thrombosis following an educational intervention.J Hosp Med.2006;1:331–338.
- ,,,.Situational awareness improves prevalence of VTE prophylaxis on multiple nursing units.J Hosp Med.2008;3(S1):41.
- ,,, et al.Antithrombotic and thrombolytic therapy: from evidence to application: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest.2004;126:688S–696S.
- ,,, et al.A systematic review of strategies to improve prophylaxis for venous thromboembolism in hospitals.Ann Surg.2005;241:397–415.
- ,,, et al.Minimizing errors of omission: behavioural reinforcement of heparin to avert venous emboli: the BEHAVE Study.Crit Care Med.2006;34:694–699.
- ,,,Closing the Quality Gap: a Critical Analysis of Quality Improvement Strategies.Rockville, MD:Agency for Healthcare Research and Quality;2004.
- ,,,.No magic bullets: a systematic review of 102 trials of interventions to improve professional practice.CMAJ.1995;153:1423–1431.
- ,,, et al.Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada.Thromb Res.2007;119:145–155.
- ,,, et al.Prevention of venous thromboembolism: ACCP evidence‐based clinical practice guidelines. 8th ed.Chest.2008;133(6 Suppl):381S–453S.
- ,.Preventing hospital‐acquired venous thromboembolism—a guide for effective quality improvement. Society of Hospital Medicine, VTE Quality Improvement Resource Room. Available at http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_VTE/VTE_Home.cfm. Accessed November 14,2008.
- ,,, et al.Clinical assessment of venous thromboembolic risk in surgical patients.Semin Thromb Haemost.1991;17(Suppl 3):304–312.
- ,,.Compliance with recommended prophylaxis for venous thromboembolism: improving the use and rate of uptake of clinical practice guidelines.J Thromb Haemost.2004;2:221–227.
- ,,,.Computerized order entry sets and intensive education improve the rate of prophylaxis for deep vein thrombophlebitis.Chest.1998;114(Suppl):280S.
- ,.Effect of a clinical pharmacy education program on improvement in the quantity and quality of venous thromboembolism prophylaxis for medically ill patients.J Manag Care Pharm.2005;11:755–762.
- ,,, et al.Audit guided action can improve the compliance with thromboembolic prophylaxis prescribing to hospitalized, acutely ill older adults.J Thromb Haemost.2005;3:2112–2113.
- ,,, et al.The effect of a computerized reminder system on the prevention of postoperative venous thromboembolism.Chest.2004;125:1635–1641.
- ,,, et al.Electronic alerts to prevent venous thromboembolism among hospitalized patients.N Engl J Med.2005;352:969–977.
- ,,,,.A clinical decision support system for prevention of venous thromboembolism.JAMA.2000;283:2816–2821.
- ,,,,,.A computerized reminder system to increase the use of preventive care for hospitalized patients.N Engl J Med.2001;345:965–970.
Excellence is best described as doing the right things rightselecting the most important things to be done and then accomplishing them 100% correctly.
In this issue of JHM, O'Connor et al.1 examine the impact of paper‐based admission order sets on several quality measures relevant to medical inpatients in a large community medical center, focusing the most attention on the use of venous thromboembolism (VTE) prophylaxis. Randomly selected medical admissions from 4 time periods were examined by chart review for use of the order set, and for the use of VTE prophylaxis (defined as either unfractionated heparin [UFH] 5,000 units subcutaneous [sc] twice daily [BID] or compression stockings). VTE prophylaxis was ordered in an abysmally low 10.9% of inpatients in the baseline period. In spite of the limitations inherent in a before and after study design and a failure to assess the appropriateness of VTE prophylaxis, VTE rates, or side effects, the authors present convincing evidence that improvement in VTE prophylaxis did occur. However, it was a very limited and suboptimal improvement. By the fourteenth and fifteenth month after order set introduction, only about one‐half of admissions used the order set, and even when the order set was used, only 44% had VTE prophylaxis ordered. The percent of patient‐days with pharmacologic VTE prophylaxis in medical inpatients improved after order set implementation, but remained very low, at 26%. Therefore, the key lessons to be learned from this study are likely derived from what went wrong, rather than what went right.
Why did VTE prophylaxis rates stay so low in the face of a multiyear effort? An examination of more successful efforts,25 recent reviews in the VTE and quality improvement literature,610 and the Society of Hospital Medicine VTE Prevention Collaborative experience reveals several principles for effective improvement that were not followed in this study.
A VTE PREVENTION ORDER SET SHOULD PROVIDE DECISION SUPPORT (NOT JUST A PROMPT)
A simple prompt for mechanical prophylaxis or for UFH 5,000 units sc BID was embedded into a voluntary order set in this effort. Mechanical prophylaxis, pharmacologic prophylaxis, and no prophylaxis were treated as equal options, even though most medical inpatients have significant VTE risk factors,11, 12 and in spite of strong evidence‐based recommendations12 relegating mechanical prophylaxis to an adjunctive role for pharmacologic prophylaxis (unless there are contraindications to pharmacologic prophylaxis). The authors point out that the way order sets are structured or introduced is important to ensure they achieve the desired changes in practice. I could not agree more, but, unfortunately, the structure of their order set only secured the desired change in 44% of patients, even if you count compression stockings as adequate prophylaxis. This relatively poor result should have sparked a redesign of the VTE prevention component of the order set.
A more effective order set would reflect an institutional VTE prevention protocol.6, 7, 9, 13 A VTE prevention protocol consists of a standardized VTE risk assessment and contraindications to pharmacologic or heparin prophylaxis, linked to a menu of appropriate VTE prophylaxis options for each level of risk.13 The best protocols provide decision support at the point of care,9, 13 and yet preserve the ability to customize care for special patient situations or circumstances.
Ease of use issues and the lack of prospectively validated models have hindered widespread adoption of VTE risk assessment protocols (especially the point‐based models),14 but a simpler and more streamlined approach has been validated by the UCSD Medical Center experience,2 and by the general success of similar protocols in diverse medical centers taking part in the Society of Hospital Medicine (SHM) VTE Prevention Collaborative. This simpler method generally places patients into 1 of 3 levels of VTE risk, can be completed in seconds, and has excellent interobserver agreement. Reinforcing the expectation that pharmacologic prophylaxis is desirable for most ill inpatients (unless there is a contraindication to it) is likely more important than the finer details of the risk assessment model.
PROTOCOLS AND ORDER SETS MUST REACH THE GREAT MAJORITY OF PATIENTS
Protocols and order sets that sit on the shelf do not benefit patients. An order set that is used for one‐half of the targeted population has no chance of promoting excellent adherence to a protocol, and protocols/order sets must be widely adapted to be effective.13 Institutional mandates for the use of preprinted (or computerized) orders can be a very effective strategy. If the order set is constructed properly, it is easy to use and can actually save clinician time, thereby promoting widespread use, in some cases even without such a mandate. The SHM VTE Prevention Collaborative generally endorses an institution‐wide protocol and order set module that covers a variety of patient populations. A plug and play modular order set design allows the VTE prevention order set to be incorporated into all appropriate admission and transfer orders, and lends itself well to paper or computerized order formats.
LAYER ON ADDITIONAL INTERVENTIONS TO ENHANCE THE POWER OF THE PROTOCOL
Skillful introduction of a good order set that reaches most patients has often yielded observed VTE prophylaxis rates of 75% to 80% in the SHM VTE Prevention Collaborative. To reach higher levels, a multifaceted approach using a variety of techniques has been an effective strategy in the literature24, 6, 7, 10, 13, 15 and in the Collaborative. Educational programs alone,4, 16, 17 while not generally sufficient to bring about reliable VTE prophylaxis, remain an important intervention that can foster a more enthusiastic and appropriate use of order sets and protocols. Periodic audit and feedback and computerized decision support can also be very effective,3, 1822 particularly when there is an institutional protocol to hold up as the defining standard for adequate prophylaxis. We favor a method that involves real‐time identification of outliers (i.e., patients without prophylaxis who have some VTE risk and no obvious contraindication to prophylaxis). This identification can be done manually, but automated reports are generally feasible and effective. A simple templated note or page from a nurse or pharmacist to the provider of an outlier patient can bolster VTE prevention rates to well over 95%.5 Fatigue from alerts is minimized if this strategy is deployed after substantial improvement in VTE prophylaxis rates has been achieved via a well‐implemented and uniformly‐utilized order set. Trending and discussing cases of hospital‐acquired VTE can also motivate medical staff and reduce resistance to standardization.2, 3
THE FOUNDATION FOR IMPROVEMENT MUST BE IN PLACE
To explain why they did not implement educational programs, guidelines, or provide feedback to providers on their performance, the authors cite a lack of resources common to community medical centers. Yet, they were able to achieve the most resource‐intensive and challenging component of a VTE prevention effort, data collection and analysis. While resources for quality improvement are indeed insufficient in many academic and community hospitals, suboptimal levels of improvement tend to reflect, as in this study, fundamental failures in approach or execution. In this case, the order set design and implementation issues outlined above do not require extensive resources. Moreover, the foundation for effective improvement must be in place to address these issues effectively. This foundation includes administrative buy‐in that VTE prevention is an institutional priority, a commitment to support standardization (even in the face of occasional medical staff resistance), and a willingness to examine and redesign processes.13 It is unclear whether the administration was convinced that the effort should be a priority or whether this improvement team reported results through appropriate medical staff committees. The key point, of course, is that a culture of shared purpose, cooperation, and high expectations between the medical staff and the administration is more important than extensive resources. The right foundational elements put most improvement resources within the grasp of most medical centers.
The authors present work that is praiseworthy in many respects, but their suboptimal levels of improvement should serve as a cautionary tale rather than a model for other centers. Core improvement principles are of key importance. A mere prompt to order VTE prophylaxis within voluntarily‐used order sets, without supporting strategies to enhance VTE prophylaxis, is a recipe for mediocre improvement. Far superior results have been demonstrated in both community and academic centers, even in environments with limited resources. A multifaceted approach, including order sets that promote VTE prophylaxis and provide decision support for the majority of the targeted population, proactive intervention applied to outliers who are not on appropriate prophylaxis, educational programs, and an institutional commitment to standardization, are the ingredients for excellent results.
Excellence is best described as doing the right things rightselecting the most important things to be done and then accomplishing them 100% correctly.
In this issue of JHM, O'Connor et al.1 examine the impact of paper‐based admission order sets on several quality measures relevant to medical inpatients in a large community medical center, focusing the most attention on the use of venous thromboembolism (VTE) prophylaxis. Randomly selected medical admissions from 4 time periods were examined by chart review for use of the order set, and for the use of VTE prophylaxis (defined as either unfractionated heparin [UFH] 5,000 units subcutaneous [sc] twice daily [BID] or compression stockings). VTE prophylaxis was ordered in an abysmally low 10.9% of inpatients in the baseline period. In spite of the limitations inherent in a before and after study design and a failure to assess the appropriateness of VTE prophylaxis, VTE rates, or side effects, the authors present convincing evidence that improvement in VTE prophylaxis did occur. However, it was a very limited and suboptimal improvement. By the fourteenth and fifteenth month after order set introduction, only about one‐half of admissions used the order set, and even when the order set was used, only 44% had VTE prophylaxis ordered. The percent of patient‐days with pharmacologic VTE prophylaxis in medical inpatients improved after order set implementation, but remained very low, at 26%. Therefore, the key lessons to be learned from this study are likely derived from what went wrong, rather than what went right.
Why did VTE prophylaxis rates stay so low in the face of a multiyear effort? An examination of more successful efforts,25 recent reviews in the VTE and quality improvement literature,610 and the Society of Hospital Medicine VTE Prevention Collaborative experience reveals several principles for effective improvement that were not followed in this study.
A VTE PREVENTION ORDER SET SHOULD PROVIDE DECISION SUPPORT (NOT JUST A PROMPT)
A simple prompt for mechanical prophylaxis or for UFH 5,000 units sc BID was embedded into a voluntary order set in this effort. Mechanical prophylaxis, pharmacologic prophylaxis, and no prophylaxis were treated as equal options, even though most medical inpatients have significant VTE risk factors,11, 12 and in spite of strong evidence‐based recommendations12 relegating mechanical prophylaxis to an adjunctive role for pharmacologic prophylaxis (unless there are contraindications to pharmacologic prophylaxis). The authors point out that the way order sets are structured or introduced is important to ensure they achieve the desired changes in practice. I could not agree more, but, unfortunately, the structure of their order set only secured the desired change in 44% of patients, even if you count compression stockings as adequate prophylaxis. This relatively poor result should have sparked a redesign of the VTE prevention component of the order set.
A more effective order set would reflect an institutional VTE prevention protocol.6, 7, 9, 13 A VTE prevention protocol consists of a standardized VTE risk assessment and contraindications to pharmacologic or heparin prophylaxis, linked to a menu of appropriate VTE prophylaxis options for each level of risk.13 The best protocols provide decision support at the point of care,9, 13 and yet preserve the ability to customize care for special patient situations or circumstances.
Ease of use issues and the lack of prospectively validated models have hindered widespread adoption of VTE risk assessment protocols (especially the point‐based models),14 but a simpler and more streamlined approach has been validated by the UCSD Medical Center experience,2 and by the general success of similar protocols in diverse medical centers taking part in the Society of Hospital Medicine (SHM) VTE Prevention Collaborative. This simpler method generally places patients into 1 of 3 levels of VTE risk, can be completed in seconds, and has excellent interobserver agreement. Reinforcing the expectation that pharmacologic prophylaxis is desirable for most ill inpatients (unless there is a contraindication to it) is likely more important than the finer details of the risk assessment model.
PROTOCOLS AND ORDER SETS MUST REACH THE GREAT MAJORITY OF PATIENTS
Protocols and order sets that sit on the shelf do not benefit patients. An order set that is used for one‐half of the targeted population has no chance of promoting excellent adherence to a protocol, and protocols/order sets must be widely adapted to be effective.13 Institutional mandates for the use of preprinted (or computerized) orders can be a very effective strategy. If the order set is constructed properly, it is easy to use and can actually save clinician time, thereby promoting widespread use, in some cases even without such a mandate. The SHM VTE Prevention Collaborative generally endorses an institution‐wide protocol and order set module that covers a variety of patient populations. A plug and play modular order set design allows the VTE prevention order set to be incorporated into all appropriate admission and transfer orders, and lends itself well to paper or computerized order formats.
LAYER ON ADDITIONAL INTERVENTIONS TO ENHANCE THE POWER OF THE PROTOCOL
Skillful introduction of a good order set that reaches most patients has often yielded observed VTE prophylaxis rates of 75% to 80% in the SHM VTE Prevention Collaborative. To reach higher levels, a multifaceted approach using a variety of techniques has been an effective strategy in the literature24, 6, 7, 10, 13, 15 and in the Collaborative. Educational programs alone,4, 16, 17 while not generally sufficient to bring about reliable VTE prophylaxis, remain an important intervention that can foster a more enthusiastic and appropriate use of order sets and protocols. Periodic audit and feedback and computerized decision support can also be very effective,3, 1822 particularly when there is an institutional protocol to hold up as the defining standard for adequate prophylaxis. We favor a method that involves real‐time identification of outliers (i.e., patients without prophylaxis who have some VTE risk and no obvious contraindication to prophylaxis). This identification can be done manually, but automated reports are generally feasible and effective. A simple templated note or page from a nurse or pharmacist to the provider of an outlier patient can bolster VTE prevention rates to well over 95%.5 Fatigue from alerts is minimized if this strategy is deployed after substantial improvement in VTE prophylaxis rates has been achieved via a well‐implemented and uniformly‐utilized order set. Trending and discussing cases of hospital‐acquired VTE can also motivate medical staff and reduce resistance to standardization.2, 3
THE FOUNDATION FOR IMPROVEMENT MUST BE IN PLACE
To explain why they did not implement educational programs, guidelines, or provide feedback to providers on their performance, the authors cite a lack of resources common to community medical centers. Yet, they were able to achieve the most resource‐intensive and challenging component of a VTE prevention effort, data collection and analysis. While resources for quality improvement are indeed insufficient in many academic and community hospitals, suboptimal levels of improvement tend to reflect, as in this study, fundamental failures in approach or execution. In this case, the order set design and implementation issues outlined above do not require extensive resources. Moreover, the foundation for effective improvement must be in place to address these issues effectively. This foundation includes administrative buy‐in that VTE prevention is an institutional priority, a commitment to support standardization (even in the face of occasional medical staff resistance), and a willingness to examine and redesign processes.13 It is unclear whether the administration was convinced that the effort should be a priority or whether this improvement team reported results through appropriate medical staff committees. The key point, of course, is that a culture of shared purpose, cooperation, and high expectations between the medical staff and the administration is more important than extensive resources. The right foundational elements put most improvement resources within the grasp of most medical centers.
The authors present work that is praiseworthy in many respects, but their suboptimal levels of improvement should serve as a cautionary tale rather than a model for other centers. Core improvement principles are of key importance. A mere prompt to order VTE prophylaxis within voluntarily‐used order sets, without supporting strategies to enhance VTE prophylaxis, is a recipe for mediocre improvement. Far superior results have been demonstrated in both community and academic centers, even in environments with limited resources. A multifaceted approach, including order sets that promote VTE prophylaxis and provide decision support for the majority of the targeted population, proactive intervention applied to outliers who are not on appropriate prophylaxis, educational programs, and an institutional commitment to standardization, are the ingredients for excellent results.
- ,,,.Medical admission order sets to improve deep vein thrombosis prophylaxis rates and other outcomes.J Hosp Med.2009;4(2):81–89.
- ,,, et al.Optimizing prevention of hospital‐acquired venous thromboembolism: prospective validation of a VTE risk assessment model and protocol. 2008 Abstracts: Research, Innovations, Clinical Vignettes Competition. 2008 National Meeting, Society of Hospital Medicine, April 3–5, 2008, San Diego, CA. Abstract 52, p29. Available at http://www.hospitalmedicine.org/Paperless2008/PDFs/Additional_Info/SHM08_Abstracts.pdf. Accessed November2008.
- ,,.Innovative approaches to increase deep vein thrombosis prophylaxis rate resulting in a decrease in hospital‐acquired deep vein thrombosis at a tertiary‐care teaching hospital.J Hosp Med.2008;3(2):148–155.
- ,,.Improved use of thromboprophylaxis for deep vein thrombosis following an educational intervention.J Hosp Med.2006;1:331–338.
- ,,,.Situational awareness improves prevalence of VTE prophylaxis on multiple nursing units.J Hosp Med.2008;3(S1):41.
- ,,, et al.Antithrombotic and thrombolytic therapy: from evidence to application: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest.2004;126:688S–696S.
- ,,, et al.A systematic review of strategies to improve prophylaxis for venous thromboembolism in hospitals.Ann Surg.2005;241:397–415.
- ,,, et al.Minimizing errors of omission: behavioural reinforcement of heparin to avert venous emboli: the BEHAVE Study.Crit Care Med.2006;34:694–699.
- ,,,Closing the Quality Gap: a Critical Analysis of Quality Improvement Strategies.Rockville, MD:Agency for Healthcare Research and Quality;2004.
- ,,,.No magic bullets: a systematic review of 102 trials of interventions to improve professional practice.CMAJ.1995;153:1423–1431.
- ,,, et al.Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada.Thromb Res.2007;119:145–155.
- ,,, et al.Prevention of venous thromboembolism: ACCP evidence‐based clinical practice guidelines. 8th ed.Chest.2008;133(6 Suppl):381S–453S.
- ,.Preventing hospital‐acquired venous thromboembolism—a guide for effective quality improvement. Society of Hospital Medicine, VTE Quality Improvement Resource Room. Available at http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_VTE/VTE_Home.cfm. Accessed November 14,2008.
- ,,, et al.Clinical assessment of venous thromboembolic risk in surgical patients.Semin Thromb Haemost.1991;17(Suppl 3):304–312.
- ,,.Compliance with recommended prophylaxis for venous thromboembolism: improving the use and rate of uptake of clinical practice guidelines.J Thromb Haemost.2004;2:221–227.
- ,,,.Computerized order entry sets and intensive education improve the rate of prophylaxis for deep vein thrombophlebitis.Chest.1998;114(Suppl):280S.
- ,.Effect of a clinical pharmacy education program on improvement in the quantity and quality of venous thromboembolism prophylaxis for medically ill patients.J Manag Care Pharm.2005;11:755–762.
- ,,, et al.Audit guided action can improve the compliance with thromboembolic prophylaxis prescribing to hospitalized, acutely ill older adults.J Thromb Haemost.2005;3:2112–2113.
- ,,, et al.The effect of a computerized reminder system on the prevention of postoperative venous thromboembolism.Chest.2004;125:1635–1641.
- ,,, et al.Electronic alerts to prevent venous thromboembolism among hospitalized patients.N Engl J Med.2005;352:969–977.
- ,,,,.A clinical decision support system for prevention of venous thromboembolism.JAMA.2000;283:2816–2821.
- ,,,,,.A computerized reminder system to increase the use of preventive care for hospitalized patients.N Engl J Med.2001;345:965–970.
- ,,,.Medical admission order sets to improve deep vein thrombosis prophylaxis rates and other outcomes.J Hosp Med.2009;4(2):81–89.
- ,,, et al.Optimizing prevention of hospital‐acquired venous thromboembolism: prospective validation of a VTE risk assessment model and protocol. 2008 Abstracts: Research, Innovations, Clinical Vignettes Competition. 2008 National Meeting, Society of Hospital Medicine, April 3–5, 2008, San Diego, CA. Abstract 52, p29. Available at http://www.hospitalmedicine.org/Paperless2008/PDFs/Additional_Info/SHM08_Abstracts.pdf. Accessed November2008.
- ,,.Innovative approaches to increase deep vein thrombosis prophylaxis rate resulting in a decrease in hospital‐acquired deep vein thrombosis at a tertiary‐care teaching hospital.J Hosp Med.2008;3(2):148–155.
- ,,.Improved use of thromboprophylaxis for deep vein thrombosis following an educational intervention.J Hosp Med.2006;1:331–338.
- ,,,.Situational awareness improves prevalence of VTE prophylaxis on multiple nursing units.J Hosp Med.2008;3(S1):41.
- ,,, et al.Antithrombotic and thrombolytic therapy: from evidence to application: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest.2004;126:688S–696S.
- ,,, et al.A systematic review of strategies to improve prophylaxis for venous thromboembolism in hospitals.Ann Surg.2005;241:397–415.
- ,,, et al.Minimizing errors of omission: behavioural reinforcement of heparin to avert venous emboli: the BEHAVE Study.Crit Care Med.2006;34:694–699.
- ,,,Closing the Quality Gap: a Critical Analysis of Quality Improvement Strategies.Rockville, MD:Agency for Healthcare Research and Quality;2004.
- ,,,.No magic bullets: a systematic review of 102 trials of interventions to improve professional practice.CMAJ.1995;153:1423–1431.
- ,,, et al.Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada.Thromb Res.2007;119:145–155.
- ,,, et al.Prevention of venous thromboembolism: ACCP evidence‐based clinical practice guidelines. 8th ed.Chest.2008;133(6 Suppl):381S–453S.
- ,.Preventing hospital‐acquired venous thromboembolism—a guide for effective quality improvement. Society of Hospital Medicine, VTE Quality Improvement Resource Room. Available at http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_VTE/VTE_Home.cfm. Accessed November 14,2008.
- ,,, et al.Clinical assessment of venous thromboembolic risk in surgical patients.Semin Thromb Haemost.1991;17(Suppl 3):304–312.
- ,,.Compliance with recommended prophylaxis for venous thromboembolism: improving the use and rate of uptake of clinical practice guidelines.J Thromb Haemost.2004;2:221–227.
- ,,,.Computerized order entry sets and intensive education improve the rate of prophylaxis for deep vein thrombophlebitis.Chest.1998;114(Suppl):280S.
- ,.Effect of a clinical pharmacy education program on improvement in the quantity and quality of venous thromboembolism prophylaxis for medically ill patients.J Manag Care Pharm.2005;11:755–762.
- ,,, et al.Audit guided action can improve the compliance with thromboembolic prophylaxis prescribing to hospitalized, acutely ill older adults.J Thromb Haemost.2005;3:2112–2113.
- ,,, et al.The effect of a computerized reminder system on the prevention of postoperative venous thromboembolism.Chest.2004;125:1635–1641.
- ,,, et al.Electronic alerts to prevent venous thromboembolism among hospitalized patients.N Engl J Med.2005;352:969–977.
- ,,,,.A clinical decision support system for prevention of venous thromboembolism.JAMA.2000;283:2816–2821.
- ,,,,,.A computerized reminder system to increase the use of preventive care for hospitalized patients.N Engl J Med.2001;345:965–970.
Utility of Blood Cultures in Pneumonia
Blood cultures (BCs) have long been a mainstay of the diagnostic evaluation of patients hospitalized with community‐acquired pneumonia (CAP). They have been strongly recommended by professional societies13 and are often expected by admitting physicians. A large retrospective study of Medicare patients with pneumonia found that obtaining BCs is associated with lower mortality.4 In 2002, when the National Hospital Quality Measures (NHQM) were introduced, BCs were included as a quality measure for pneumonia.5, 6
However, there is uncertainty about the actual utility of BCs in CAP. In large studies they are true‐positive in only 7 to 11% of cases and false‐positive in 5%,2, 7 and whether they affect clinical management has been strongly questioned.810 Their impact may be limited by slow results, low frequency of bacterial resistance to the empiric antibiotic regimen, and reluctance of physicians to narrow antibiotic coverage.9, 11 Recent updates to professional society guidelines no longer recommend BCs in all admitted CAP patients.12
To evaluate the clinical utility of BCs and the appropriateness of pnemonia quality measures based on BCs, we performed a systematic review of the literature to determine the effect of BCs on the management of adults with CAP requiring hospitalization.
PATIENTS AND METHODS
Data Sources and Searches
We searched the English‐language literature via MEDLINE (1966 through September 2007), MEDLINE‐In Process, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects, and ACP Journal Club. Within each of these databases we used keywords and exploded Medical Subject Headings (MeSH) to produce the following search strategy: blood culture(s) (keyword), bacteriological techniques (MeSH), blood [microbiology] (MeSH), bacteremia [microbiology or drug therapy] (MeSH), or diagnostic tests, routine (MeSH) combined with pneumonia (keyword), pneumonia (MeSH), lower respiratory tract infection(s) (keyword), or community‐acquired infections (MeSH). To maximize capture of BC or bacteremia studies with subgroups of CAP patients we added the following search strategy: explode microbiological techniques [utilization] (MeSH), explode blood specimen collection [utilization] (MeSH), or focus bacteremia [drug therapy] (MeSH). We reviewed the reference lists of all included studies as well as those of important background articles. Finally, we asked experts to evaluate the completeness of our list.
Study Selection
We included studies in which: (1) subjects were adults hospitalized with CAP; (2) BCs were obtained at or near hospital admission; and (3) the effects of BCs on management (change in antibiotic therapy or other effects such as duration of parenteral therapy, length of hospitalization, or level of care) were reported. The first 2 requirements could be satisfied by a subgroup.
From retrieved citations, relevant abstracts were reviewed, and studies with any potential to meet inclusion criteria were chosen for full‐text review. Two authors (N.A., R.S.) independently analyzed each full‐text article to determine inclusion for data analysis. A third author (J.T.) analyzed all included and narrowly excluded articles to confirm the final list of included studies. Disagreements were resolved by discussion.
Data Extraction
For the included studies, 2 authors (N.A., K.A.) independently abstracted the following data using a standardized collection instrument: study design and setting, inclusion and exclusion criteria, number of hospitalized CAP patients in whom BCs were obtained, empiric antibiotic regimens, number of true‐positive and false‐positive BCs, bacteria isolated in true‐positive BCs, BC‐directed antibiotic narrowing, BC‐directed antibiotic broadening ultimately associated with a resistant organism, and any other management effects reported. Narrowing refers to coverage of fewer organisms, while broadening refers to coverage of a larger or different spectrum of organisms.
If a study included patients not meeting our selection criteria, our analysis was limited to the subset of patients meeting criteria. We also analyzed each study to determine whether a subgroup of severely ill patients was reported separately and whether such a group benefited from BCs. The 2 authors independently repeated all data abstraction to confirm accuracy. We attempted to contact authors for clarification when needed.
Data Synthesis
Data were synthesized by compilation of characteristic summary tables. In the primary analysis, the proportion of positive BCs (both true and false) and the frequency of BC‐directed changes in antimicrobial therapy (narrowing, or broadening ultimately associated with a resistant organism) were determined and reported for each study and then described as an aggregate range. This compilation required studies to provide a particular denominatorthe number of patients in whom BCs were performed. If a study did not do so, it was described separately in the secondary analysis, where we also assessed the cost of BCs as well as the impact of BCs in critically ill patients and on outcomes other than antibiotic change. Heterogeneity of subject inclusion and exclusion criteria and empiric antibiotic use were summarized qualitatively. Two authors (N.A., R.S.) assessed each study's quality.
DATA SYNTHESIS
Search Results
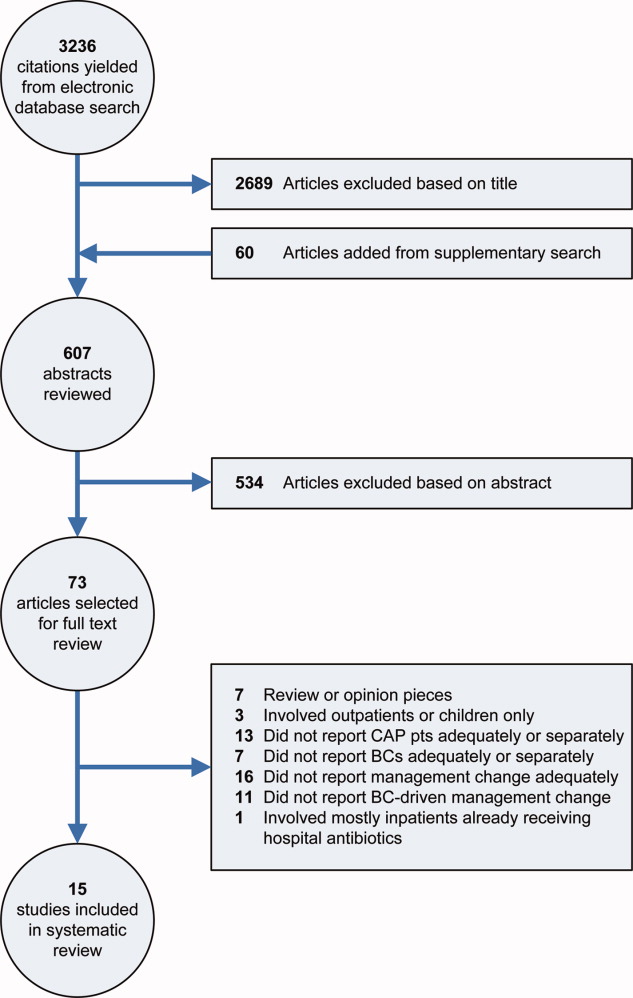
Our electronic database search yielded 3236 citations. From this list and the supplementary search of references, we reviewed 607 abstracts; of these, we selected 73 articles for full‐text review, and 15 were included in the final analysis (Figure 1). One study was narrowly excluded because it largely included CAP patients that had already been admitted to the hospital and failed an empiric antibiotic trial before BCs were obtained.13
Study Characteristics
Fifteen studies with a total of 3898 patients evaluated BC‐directed management changes in adults admitted with CAP.11, 1427 However, 2 of these, involving only patients with bacteremic pneumococcal CAP, by design could not report the number of patients that had BCs done; thus they were not included in the primary analysis.16, 25
The 13 studies amenable to the primary analysis (Table 1) all had an observational cohort design; 6 were prospective11, 18, 20, 24, 26, 27 and 7 were retrospective.14, 15, 17, 19, 2123 Sample size varied from 52 to 760 patients. Settings included university and community hospitals in the U.S. and 4 other countries, with patient enrollment spanning the years 19882003 (publication dates 19912007).
| Study Author, Year, Design, Setting | Inclusion Criteria | Exclusion Criteria | CAP Patients with BCs, n*; True‐Positive BCs, n (%); False‐Positive BCs, n (%) | BCs Directed Antibiotic Narrowing, n (%) | BCs Directed Antibiotic Broadening and Organism was Resistant, n (%) | Comments |
|---|---|---|---|---|---|---|
| ||||||
| Benenson et al.,14 2007; retrospective, U.S. suburban | ED ICD‐9 dx and discharge dx of PNA | None | n = 684; 23 (3.4); 54 (7.9) | 3 (0.4) | 0 (0) | 11% of pts with ED dx of PNA not eligible due to different dx at discharge; 25% from nursing homes, 18% recently hospitalized, 14% immunocompromised; Abxs narrowed in 3/21 eligible pts |
| Ramanujamand Rathlev,22 2006; retrospective; U.S. urban | ED, ICD‐9, and discharge dx of PNA, and ED BCs before abxs | IC, active cancer, chronic renal failure, hospitalized last 1 week, nursing home resident, aspiration | n = 289; 13 (4.5%); 13 (4.5%) | 1 (0.3%) | 0 (0%) | 532 pts screened; 3% not eligible due to different dx at discharge; of eligible pts, 9% excluded due to HCAP and 31% excluded due to other risk factors; Abxs were narrowed in 1/10 eligible pts; Cost: $8,000 for the 1 pt with abx change |
| Mountain et al.,21 2006; retrospective, Australian suburban | All pts who had BCs done in the ED during a 2‐month period (PNA pts were a subgroup) | None | n = 52; Not reported; Not reported | 1 (1.9) | 0 (0) | 52/218 study pts had clinical PNA. Overall BCs true‐positive in 6.4%, false‐positive in 7.3%; frequencies for PNA pts not reported separately; Reason for abx change (ceftriaxone to ciprofloxacin) not reported, but thought not to be associated with resistant organism (personal communication); Cost: $1,950 (U.S.) per BC that altered treatment |
| Kennedy et al.,20 2005; prospective, U.S urban | Clinical and radiographic PNA and BCs in ED or within 3 hours of admission | None | n = 385; 27 (7.0); 6.0% | 11 (2.9) | 4 (1.0) | 23% of pts from nursing homes, 22% admitted to ICU; 3/4 pts whose abxs were broadened due to a resistant organism came from nursing homes; Abxs were narrowed in 11/19 eligible pts; BCs were false‐positive in 25/414 (6%) pts, including 29 pts discharged from the ED |
| Corbo et al.,17 2004; retrospective, U.S. urban | Primary diagnosis of CAP, positive CXR, and ED BCs before abxs | IC, cancer, recent hospitalization, nursing home resident | n = 355; 33 (9.3); 37 (10.4) | 7 (2.0) | 0 (0) | 821 pts admitted with CAP; 24% not eligible due to non‐confirmatory CXR; of eligible pts, 22% excluded due to HCAP, 23% excluded due to other risk factors; 6 pts with false‐positive BCs had abx change due to BCs ‐ authors suggest hospitalization prolonged in these cases; Physicians reluctant to narrow abxs per authors |
| Campbell et al.,11 2003; prospective, Canadian multiple (19) hospitals | Two signs or sxms of PNA and positive CXR | IC, shock, direct ICU admission, chronic kidney disease, pregnant or nursing, alcoholism | n = 760; 43 (5.7); Not reported | 12 (1.6) | 2 (0.3) | 38% of pts screened with suspected CAP either ineligible or excluded due to risk factors; Abxs were narrowed in 12/35 eligible pts; In one case, BCs grew MRSA resistant to empiric abxs, but abxs had been changed before BC results available; Cost: $1550 (U.S.) per BC leading to abx change |
| Waterer and Wunderink,26 2001; prospective; U.S. urban | Signs and sxms of PNA, positive CXR, and BCs before abxs | IC, hospitalized last 30 days, nursing home residents (if non‐ambulatory) | n = 209; 29 (13.9); 9 (4.3) | 5 (2.4) | 1 (0.5) | BCs only changed management in pts in PSI class 4 and 5 |
| Theerthakarai et al.,24 2001; prospective, U.S. suburban | Acute febrile illness with respiratory sxms and a positive CXR | IC, cancer, age >65, alcoholism, IVDU, COPD, IDDM, neurologic disease, renal failure, recent abx, severe or complicated PNA | n = 74; 0 (0); 0 (0) | 0 (0%) | 0 (0%) | Very strict exclusion criteria: 62% of eligible pts excluded due to risk factors; Authors reported that 28% of included pts could have been treated as outpatients per ATS guidelines |
| Sanyal et al.,23 1999; retrospective, U.S. urban | Acute lower respiratory tract infection and positive CXR | IC, cancer, hospitalized last 12 weeks, IVDU, bronchiectasis, splenectomy, not treated per ATS guidelines | n = 174; 19 (10.9); Not reported | Not reported | 1 (0.6%) | BC‐directed antibiotic changes only reported for pts who did not respond to initial abxs, so BC‐directed narrowing could not be determined; The pt whose abxs were broadened was a nursing home resident with severe pneumonia (by ATS criteria) |
| Glerant et al.,18 1999; prospective, French suburban | Acute septic episode with respiratory sxms and positive CXR | IC, ICU admission, hospitalized last 2 weeks, aspiration | n = 53; 5 (9.4); 2 (3.8) | 0 (0) | 0 (0) | BCs done during first 48 hours so not clear how many BCs sent after hospital abxs started; 23 pts were on abxs before admission; Cost: $6006 (U.S.), no abx changes |
| Kelly,19 1998; retrospective, Australian suburban | All pts who had BCs done in the ED over a 9‐ month period (PNA pts were a subgroup) | None | n = 260; 5%; Not reported | 1% | 1% | 260/1062 study pts had PNA; 14% of all pts discharged; for CAP pts percentage not reported; False‐positive rate 3.8% for all pts, but not reported separately for PNA pts; 1% of PNA pts had abx change due to BCs; type of change not reported, hence reporting of 1% in outcome columns; Cost: $4800 (U.S.) per abx change |
| Chalasani et al.,15 1995; retrospective; U.S. urban | Dx of PNA, respiratory sxms, positive CXR, and 2 sets of BCs before abxs | IC, cancer, hospitalized last 2 weeks, nursing home resident | n = 517; 34 (6.6); 25 (4.8) | 7 (1.4) | 0 (0) | 1250 pts screened with discharge dx of PNA; 59% either ineligible or excluded due to risk factors (authors did not report number ineligible due to the BC requirement); In one case, BCs grew H. influenzae resistant to empiric abxs, but sputum cultures drove the abx change; Cost: $4875 per abx change |
| Woodhead et al.,27 1991; prospective, British urban (2 hospitals) | Clinical features of CAP and positive CXR | IC, cancer, admitted to geriatric or communicable disease ward | n = 86; 9 (10.5%); Not reported | 2 (2.3) | 1 (1.2) | 8% of pts meeting inclusion and exclusion criteria were later excluded due to different dx at discharge |
Included patients were usually required to have clinical features of pneumonia and a confirmatory chest x‐ray. Treating physicians were required to obtain BCs (either by study or hospital protocol) in only 3 studies14, 22, 24 and in a subgroup of another study;11 otherwise the performance of BCs was left to physician discretion.
Nine studies excluded patients who were immunocompromised,11, 15, 17, 18, 2224, 26, 27 a label that was often incompletely defined. Otherwise, exclusion criteria were variable. Notably, only 3 studies excluded patients admitted to the intensive care unit (ICU),11, 18, 24 while 6 excluded patients with cancer15, 17, 2224, 27 and 6 excluded either nursing home residents15, 17, 22, 26 or the elderly (de facto exclusion of most nursing home residents).24, 27
Empiric antibiotic regimens, where reported, were predominantly cephalosporin plus macrolide combinations in 4 studies,17, 2224 fluoroquinolones in 3 studies,11, 14, 26 and penicillin or 1 of its derivatives in 1 study.27
Concerning the 2 studies not included in the primary analysis, the one by Waterer et al.25 was a retrospective review of all cases of pneumococcal bacteremia (n = 74) associated with an admission diagnosis of CAP (N = 1805) in a US urban hospital over a 3‐year period. The one by Chang et al.16 was a retrospective case‐control study of 288 randomly‐selected, immunocompetent Medicare patients with bacteremic pneumococcal CAP who survived to discharge. They were matched 1:1 with blood and sputum culture‐negative controls to study the rate of fluoroquinolone use at discharge in the 2 groups.
Study Findings
Primary Analysis
As shown in Table 1, BCs were positive for a true pathogen in 0% to 14% of cases. Details of microbiology and empiric antibiotic selection are reported in Table 2. S. pneumoniae was by far the most common pathogen: of the 9 studies that had positive BCs and reported the organisms, S. pneumoniae represented 50% to 91% of the pathogens, with penicillin‐resistance found in 0% to 20%.11, 14, 15, 17, 18, 20, 22, 23, 26 S. aureus was next most common, occurring in 6 studies and growing in 3% to 23% of positive BCs;11, 14, 17, 20, 23, 26 its sensitivity to methicillin was reported in 3 studies, with methicillin‐resistant S. aureus (MRSA) representing 0/3, 3/7, and 1/1 of cases.14, 20, 23 E. coli represented 3% to 11% of pathogens in 6 studies,11, 14, 15, 20, 23, 26 while H. influenzae represented 2% to 15% of pathogens in 7 studies.11, 14, 15, 18, 22, 23, 26
| Study: Author, Year | Empiric Antibiotics Given: Frequency, Agent | Bacteria Isolated in True‐Positive BCs: n, Organism | Organisms in BCs Resistant to Empiric Antibiotics |
|---|---|---|---|
| |||
| Benenson et al.,14 2007 | Mild to moderate PNA: levofloxacin; If ICU admission: levofloxacin + azithromycin; If HCAP: levofloxacin + clindamycin; If risk for MRSA: added vancomycin; If structural lung disease: added tobramycin | 14 S. pneumoniae; 3 S. aureus (all MSSA); 2 Group B Strep; 2 H. influenzae; 1 E. coli; 1 Group A Strep | None |
| Ramanujam and Rathlev,22 2006 | Ceftriaxone + oral azithromycin | 11 S. pneumoniae (1 PCN interm res); 2 H. influenzae | None |
| Mountain et al.,21 2006 | Not reported | Not reported completely | None |
| Kennedy et al.,20 2005 | Not reported | 15 S. pneumoniae (3 PCN res); 7 S. aureus (3 MRSA); 3 E. coli; 1 Coagulase‐negative Staph; 1 Pseudomonas; 1 Proteus; 1 Moraxella; 1 E. faecalis | 2 MRSA; 1 MSSA (res to levofloxacin, clindamycin); 1 E. coli (res to levofloxacin) |
| Corbo et al.,17 2004 | 48% ceftriaxone + macrolide; 21% cephalosporin only; 6% quinolone only | 30 S. pneumoniae; 2 S. aureus (# MRSA not reported); 1 Staph haemolyticus | None |
| Campbell et al.,11 2003 | 55% levofloxacin; 45% antibiotic not reported | 30 S. pneumoniae (1 PCN res); 5 S. aureus (total # MRSA not reported); 5 E. coli; 1 H. influenzae; 1 E. faecalis; 1 K. pneumoniae; 1 Enterobacter | 1 MRSA (antibiotic changed before BC results available); 1 MSSA (res not reported); 1 S. pneumoniae (PCN res) |
| Waterer and Wunderink,26 2001 | 60% quinolone only; 25% quinolone + other antibiotic(s) | 20 S. pneumoniae (3 PCN res); 3 S. viridans; 1 H. influenzae; 1 S. aureus (# MRSA not reported); 1 Enterobacter; 1 E. coli; 1 Group B Strep; 1 Group D Strep; 1 Group G Strep; 1 Acinetobacter | 1 Group D Strep (res to levofloxacin) |
| Theerthakarai et al.,24 2001 | Cephalosporin + macrolide | None | None |
| Sanyal et al.,23 1999 | Severe CAP: erythromycin + ceftazidime or ticarcillin/clavulanate; Nonsevere CAP: 76% cefuroxime + erythromycin, 18% cefuroxime only | 14 S. pneumoniae (0 PCN res); 2 H. influenzae; 1 S. aureus (MRSA); 1 K. pneumoniae; 1 E. coli | 1 MRSA |
| Glerant et al.,18 1999 | Not reported | 4 S. pneumoniae (0 PCN res); 1 H. influenzae | None |
| Kelly,19 1998 | Not reported | Not reported | Cannot determine |
| Chalasani et al.,15 1995 | Not reported | 29 S. pneumoniae (0 PCN res); 3 H. influenzae; 1 S. pyogenes; 1 E. coli | H. influenzae (sputum culture drove the antibiotic change) |
| Woodhead et al.,27 1991 | 78% included penicillin, aminopenicillin, or amoxicillin/clavulanate; 33% included erythromycin; 21% ‐lactam + erythromycin | Not reported separately for BCs | E. coli (res to erythromycin) |
| Chang et al.,16 2005 | BC+/Controls: 34%/21%/Quinolones; 86%/88%/ ‐lactam; 1%/1%/Amox/PCN; 38%/37%/ Macrolide | 288 S. pneumoniae (only organism, by design) | Not reported |
| Waterer et al.,25 1999 | 38% Cephalosporin + macrolide other; 27% Quinolone other | 74 S. pneumoniae (only organism, by design); 11 PCN interm res; 4 PCN res | 2 S. pneumoniae (both resistant; degree of resistance not specified) |
In the 8 studies that reported false‐positive BCs, the false‐positive rate was 0% to 10%,14, 15, 17, 18, 20, 22, 24, 26 with 5 studies finding comparable false‐positive and true‐positive BC rates15, 17, 20, 22, 24 and 1 study finding a substantially higher frequency of false‐positive than true‐positive BCs (Table 1).14
BCs led to narrowing of antibiotic coverage in 0% to 3% of cases (Table 1). Four studies reported that physicians narrowed antibiotics when BCs indicated that it was possible to do so, but only in 10%, 14%, 34%, and 58% of eligible cases.11, 14, 20, 22
BCs led to antibiotic broadening ultimately associated with a resistant organism in 0% to 1% of cases (Table 1). The pathogens were MRSA (3), methicillin‐sensitive S. aureus (2), E. coli (2), S. pneumoniae (1), and Group D Streptococcus (1). Details about these patients' medical histories and demographics were absent or sparse in all but 1 study.20 For several of the above cases it was not explicitly stated that BCs directed the antibiotic changes, though it was usually implied; thus we assumed causation.
Secondary Analyses
In the pneumococcal bacteremia study by Waterer et al.,25 BCs altered management in 31 of the 74 cases of pneumococcemia, but in only 2 patients was this associated with antibiotic resistance. Most of the other 29 cases involved narrowing of antibiotics, though switching to penicillin or dropping atypical coverage occurred in only 22% and 37% of eligible patients, respectively. In the study by Chang et al.,16 there was no significant difference in fluoroquinolone use at discharge between the pneumococcemic and culture‐negative groups (the primary endpoint), though there was significantly higher ‐lactam use and lower macrolide use in the pneumococcemic patients at discharge. From the data provided it was not possible to determine how often antibiotic broadening occurred.
Only 2 of the 15 studies stratified management effects based on severity of illness, and neither specified the proportion of severely ill patients admitted to the ICU. Waterer and Wunderink26 prospectively hypothesized that sicker patients were more likely to benefit from BCs. They found that the 30 patients in pneumonia severity index class 5 were most likely to have a BC‐driven antibiotic change, though in at most 1 of these patients was associated with a resistant organism. Sanyal et al.23 stratified patients by severity based on expert guidelines. They found that 19 of 174patients had severe CAP that did not respond to the initial antibiotic regimen, with 1 having a BC‐driven antibiotic change; this was due to resistance.
Only 1 study reported an outcome other than antibiotic change, which in this case was duration of parenteral therapy. In the study, 5 of 43 patients with true‐positive BCs remained on intravenous antibiotics for the full course of treatment probably due to bacteremia alone.11
The direct cost of BCs per BC‐directed antibiotic change (or total cost of BCs if there was no antibiotic change) was reported in 6 studies and, not adjusted for inflation, ranged from $1550 to $8000 (U.S.).11, 15, 18, 19, 21, 22
Quality of the Studies
A detailed listing of the strengths and weaknesses of each study is provided in the Appendix. Briefly, all 15 studies included in this review were observational. Most did not prospectively require BCs in all patients admitted with CAP. This could have biased the results in favor of BC utility as physicians presumably order BCs in patients with a higher probability of bacteremia. Conversely, several studies did not explicitly require two sets of BCs or that BCs be done prior to antibiotics, so they may not have revealed the maximum utility of BCs. The 2 studies limited to pneumococcal bacteremia and described in the secondary analysis were inherently biased against BC utility, as pneumococcus is more likely to be antibiotic‐sensitive than other CAP pathogens.
Eligibility was based only on an emergency department (ED)/admission diagnosis of CAP, a criteria that approximates real world practice, in 3 studies.19, 21, 25 The other studies required either a confirmatory radiograph or a hospital discharge diagnosis of pneumonia. Consequent ED/admission misdiagnosis rates were 3%, 8%, 11%, 24% in the 4 studies that reported them;14, 17, 22, 27 the final diagnoses, when reported, were nearly all noninfections or proximal respiratory tract infections.22, 27
Five studies included all eligible patients.14, 1921, 25 However, 3 studies excluded 23%, 31%, and 62% of eligible patients based on risk factors for bacteremia or resistant pathogens,17, 22, 24 and the rest did not report the number excluded.
DISCUSSION
Summary of Findings
Our systematic review of the literature finds that BCs rarely alter empiric antibiotic therapy in adults hospitalized with community‐acquired pneumonia. Even when there is a change in treatment it usually is not of the type most likely to impact patient outcome, which is antibiotic broadening ultimately associated with a resistant organism. In the 13 studies that could quantify this effect, it occurred in only 0% to 1% of cases in which BCs were obtained. Antibiotic narrowing occurred in 0% to 3% of cases, with physicians often choosing not to narrow antibiotics when BC results suggested that they could do so.
Limits on BC Utility
‐Lactam‐Resistant Pneumococcus
In the studies reviewed here 50%‐90% of positive BCs grew pneumococcus, consistent with the 60% to 67% rate reported elsewhere.2, 28, 29 Pneumococci that invade the bloodstream have disproportionately low rates of ‐lactam resistance,30, 31 inherently limiting the utility of BCs for detecting inadequate empiric antibiotic therapy. Though pneumococcal resistance to ‐lactams has risen over the last 2 decades, third‐generation cephalosporins, preferred agents for CAP, are still extremely effective. Even when the organism is by historical standards moderately resistant to them, these cephalosporins at standard doses maintain bactericidal efficacy in the lung,32, 33 and their use in the setting of such resistance is not associated with higher mortality.3437 By newer laboratory standards 97% and 96% of S. pneumoniae isolates in mid‐2003 were sensitive to ceftriaxone and cefotaxime, respectively.38 Thus a major potential benefit of BCsdetecting cephalosporin‐resistant pneumococcusremains a rare occurrence.
Polymicrobial Infection
If positive BCs in CAP mostly reveal antibiotic‐sensitive pathogens, one may infer that at least they lead to narrowing of therapy. However, the studies reviewed here reveal that this usually does not happen.
One explanation for this reluctance to narrow antibiotics is that CAP is often a polymicrobial disease. When rigorous serologic testing is done, multiple pathogens are found in up to 40% of cases.39 The occult copathogen is frequently an intracellular one and thus cannot be detected by BCs. Though the evidence for empirically treating these atypical organisms is mixed,40, 41 expert guidelines recommend doing so,12 and guideline‐concordant antibiotic therapy in CAP is associated with lower mortality.42 Even in bacteremic pneumococcal CAP, monotherapy is associated with higher mortality.4346 Thus, stopping antibiotic coverage of atypical pathogens in response to BCs alone might not always be appropriate.
Prognosis
Another rationale given for ordering BCs is that bacteremic pneumonia is a morbid disease so positive BCs may demand prolonged parenteral therapy or extended hospitalization. Although mortality for bacteremic pneumococcal pneumonia (the predominantly studied variety of bacteremic pneumonia) has historically been high at 20%,47, 48 studies that have examined pneumococcal bacteremia as an independent risk factor for death in CAP have yielded mixed results.2 Moreover, it appears that patients with bacteremic pneumococcal pneumonia who reach clinical stability may be safely switched to oral antibiotics.49
It is not clear that positive BCs in pneumonia (at least in the case of S. pneumoniae) should alter the duration of parenteral therapy or hospitalization, though whether or not such effects occur in clinical practice was largely unaddressed by the studies reviewed here.
Epidemiology
One theoretical benefit of BCs is their epidemiologic value. When true‐positive in pneumonia, perhaps more than any other test they identify with great specificity at least 1 of the causative agents. Unfortunately, as discussed above, BCs alone provide an incomplete and skewed picture of the microbiology of CAP. They underestimate atypical organisms, overestimate pneumococcus, and, because bacteremic pneumococcus is more likely to be antibiotic‐susceptible, they underestimate antibiotic resistance.11 Tracking pathogens in bacteremic pneumonia may be useful nonetheless, but perhaps a more accurate method for determining etiologic trends is periodic comprehensive microbiological investigation, including BCs, sputum/bronchial cultures, and serology.
Costs
In the studies reviewed here, based on reported costs of $15 to $65 per set of BCs or per patient, BCs cost $1550 to $8000 (U.S.) per BC‐directed antibiotic change. Considering that very few of these antibiotic changes involved broadening associated with a resistant organism, the cost/benefit ratio was quite high. Today BCs may be even more expensive, as U.S. hospitals now often charge over $150 per set of BCs.50, 51
The cost of false‐positive BCs must also be taken into account. The false‐positive rate in the studies reviewed here was 0% to 10%, similar to that reported elsewhere.7 False‐positive BCs increase hospital length of stay by 3 to 5 days and hospital charges by $4400 to $8800.51, 52
Limitations of the Review
Our search strategy was designed to be sensitive and included backup methods such as searching article references and querying experts. Nevertheless, we may have missed studies, especially if there were small eligible subgroups or if determining management effects was not a primary purpose. We chose not to measure instances of antibiotic broadening that were not associated with a resistant organism, though in unusual cases (eg, Pseudomonas bacteremia) this effect of BCs may be useful.
The methodologies of the included studies were adequate to measure the key outcomes with reasonable validity. Biases were evident, though they occurred both for and against BC utility.
Eligibility varied across studies, and most investigations excluded immunocompromised or other high‐risk patient groups, which could have biased results against BC utility. However, results of these studies were consistent with those that included all patients with CAP, suggesting the degree of bias was probably small. Still, given this concern, it would be prudent not to generalize the findings of this review to immunocompromised patients. Moreover, although the critically ill and those who today would be classified as having healthcare‐associated pneumonia (HCAP)nursing home residents, the recently hospitalized, and hemodialysis patientswere included in most studies, their numbers were small, and these groups were not analyzed separately; thus, the results might not be generalizable to these populations either. Finally, the reported studies, which enrolled patients through 2003, do not reflect more recent increases in the prevalence of resistant pathogens, such as MRSA, in the community.
BCs as a Quality Measure
The adoption of BCs as a quality measure was largely predicated on the widely‐cited study by Meehan et al.,4 which showed an association between BC obtainment and reduced mortality. This study, which associated processes of care with hard outcomes such as mortality, was limited by uncontrolled confounders, including variation in hospital quality.53 A more recent study of pneumonia processes of care found no association between BC collection and mortality.54 Another study often cited to support BC use, by Arbo and Snydman,55 showed that positive BCs were associated with changes in antibiotic therapy, but it included very few pneumonia patients and did not describe results for them separately.
The inclusion of BC acquisition in 2 quality measures in the NHQM guidelines for pneumonia impacts the clinical practice of hospitals and physicians, which may be rated and reimbursed differentially based on their compliance with such measures. One of the quality measures requires BCs in patients admitted to the ICU. The other requires that ED BCs for pneumonia, if obtained, be drawn before antibiotics are given.6
The studies we reviewed are not specific to these quality measures, but are relevant to them. With regard to the first measure, all but 3 studies included patients admitted to the ICU and found BCs to be of minimal benefit overall. Our subgroup analysis of severely ill patients was unrevealing. The ICU measure is tentative in its validity, but it is not unreasonable given that these patients have a life‐threatening infection and may be at risk for bacteremia with resistant pathogens.12
The second measure, though perhaps simply seeking to maximize the potential for BCs to turn positive, depends for its validity on BCs being useful in a large proportion of patients with CAP. Though we cannot exclude the possibility that BCs benefit certain subsets of patients, such as those who are immunocompromised or have HCAP, our findings do not support obtaining BCs in all or even most adults hospitalized with CAP. This conclusion is reflected in the 2007 Infectious Diseases Society of America/American Thoracic Society management guidelines for CAP, which state than BCs are optional except for patients with severe pneumonia, some immunocompromised states, and particular radiographic abnormalities.12
With such data and guidelines in mind, a physician seeking to minimize treatment delays in a patient with pneumonia may give antibiotics early in the ED course (the basis of another quality measure) without obtaining BCs. If she later determines that the patient is particularly high‐risk for bacteremia or a resistant pathogen, should she be discouraged from ordering BCs? Experts specifically state that BCs, even after antibiotics, are warranted for such a patient.12
With the scope of medical practice captured in quality measures being so narrow, having 2 measures based on a test with such limited benefit is itself questionable.
- ,,,,,.Practice guidelines for the management of community‐acquired pneumonia in adults. Infectious diseases society of America.Clin Infect Dis.2000;31:347–382.
- ,,,,.Canadian guidelines for the initial management of community‐acquired pneumonia: an evidence‐based update by the Canadian infectious diseases society and the Canadian thoracic society. The Canadian community‐acquired pneumonia working group.Clin Infect Dis.2000;31:383–421.
- ,,, et al.Guidelines for the management of adults with community‐acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention.Am J Respir Crit Care Med.2001;163:1730–1754.
- ,,, et al.Quality of care, process, and outcomes in elderly patients with pneumonia.JAMA.1997;278:2080–2084.
- Hospital quality initiative, overview, centers for Medicare and Medicaid services. Available at: http://www.cms.hhs.gov/HospitalQualityInits. Accessed September2007.
- Specifications manual for national hospital quality measures, version 2.3b. Available at: http://www.jointcommission.org/PerformanceMeasurement/PerformanceMeasurement/Current+NHQM+Manual.htm. Accessed October2007.
- ,,,.Predicting bacteremia in patients with community‐acquired pneumonia.Am J Respir Crit Care Med.2004;169:342–347.
- ,.The joint commission on accreditation of healthcare organizations and center for Medicare and Medicaid services community‐acquired pneumonia initiative: what went wrong?Ann Emerg Med.2005;46:409–411.
- .Blood cultures in community‐acquired pneumonia: Are we ready to quit?Chest.2003;123:977–978.
- .Blood cultures for community‐acquired pneumonia: piecing together a mosaic for doing less.Am J Respir Crit Care Med.2004;169:327–328.
- ,,,,.The contribution of blood cultures to the clinical management of adult patients admitted to the hospital with community‐acquired pneumonia: a prospective observational study.Chest.2003;123:1142–1150.
- ,,, et al.Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community‐acquired pneumonia in adults.Clin Infect Dis.2007;44 (Suppl 2):S27–S72.
- ,,,,,.Value of routine microbial investigation in community‐acquired pneumonia treated in a tertiary care center.Respiration.1996;63:164–169.
- ,,,.Selective use of blood cultures in emergency department pneumonia patients.J Emerg Med.2007;33:1–8.
- ,,,,.Clinical utility of blood cultures in adult patients with community‐acquired pneumonia without defined underlying risks.Chest.1995;108:932–936.
- ,,,,,.Blood culture and susceptibility results and allergy history do not influence fluoroquinolone use in the treatment of community‐acquired pneumonia.Pharmacotherapy.2005;25:59–66.
- ,,,.Limited usefulness of initial blood cultures in community acquired pneumonia.Emerg Med J.2004;21:446–448.
- ,,,,.Utility of blood cultures in community‐acquired pneumonia requiring hospitalization: Influence of antibiotic treatment before admission.Respir Med.1999;93:208–212.
- .Clinical impact of blood cultures taken in the emergency department.J Accid Emerg Med.1998;15:254–256.
- ,,,,,.Do emergency department blood cultures change practice in patients with pneumonia?Ann Emerg Med.2005;46:393–400.
- ,,,.Blood cultures ordered in the adult emergency department are rarely useful.Eur J Emerg Med.2006;13:76–79.
- ,.Blood cultures do not change management in hospitalized patients with community‐acquired pneumonia.Acad Emerg Med.2006;13:740–745.
- ,,,,,.Initial microbiologic studies did not affect outcome in adults hospitalized with community‐acquired pneumonia.Am J Respir Crit Care Med.1999;160:346–348.
- ,,,,.Nonvalue of the initial microbiological studies in the management of nonsevere community‐acquired pneumonia.Chest.2001;119:181–184.
- ,,.The impact of blood cultures on antibiotic therapy in pneumococcal pneumonia.Chest.1999;116:1278–1281.
- ,.The influence of the severity of community‐acquired pneumonia on the usefulness of blood cultures.Respir Med.2001;95:78–82.
- ,,,,.The value of routine microbial investigation in community‐acquired pneumonia.Respir Med.1991;85:313–317.
- ,,, et al.Study of community acquired pneumonia aetiology (scapa) in adults admitted to hospital: implications for management guidelines.Thorax.2001;56:296–301.
- ,.Etiology of community‐acquired pneumonia.Clin Chest Med.2005;26:47–55.
- ,,,,.Early predictors of mortality in pneumococcal bacteraemia.Ann Acad Med Singapore.2005;34:426–431.
- ,,,.Penicillin‐nonsusceptible Streptococcus pneumoniae at San Francisco general hospital.Clin Infect Dis.1999;29:580–585.
- .Pharmacokinetic/pharmacodynamic parameters: Rationale for antibacterial dosing of mice and men.Clin Infect Dis.1998;26:1–10; quiz 11–12.
- .The significance of serum vs tissue levels of antibiotics in the treatment of penicillin‐resistant Streptococcus pneumoniae and community‐acquired pneumonia: are we looking in the wrong place?Chest.1999;116:535–538.
- ,,, et al.Pneumonia acquired in the community through drug‐resistant Streptococcus pneumoniae.Am J Respir Crit Care Med.1999;159:1835–1842.
- ,,, et al.The effect of cephalosporin resistance on mortality in adult patients with nonmeningeal systemic pneumococcal infections.Am J Med.2002;113:120–126.
- ,,, et al.Resistance to penicillin and cephalosporin and mortality from severe pneumococcal pneumonia in Barcelona, Spain.N Engl J Med.1995;333:474–480.
- ,,, et al.An international prospective study of pneumococcal bacteremia: correlation with in vitro resistance, antibiotics administered, and clinical outcome.Clin Infect Dis.2003;37:230–237.
- ,,,,,.Tracking the implementation of NCCLS m100‐s12 expanded‐spectrum cephalosporin MIC breakpoints for non‐meningeal isolates of Streptococcus pneumoniae by clinical laboratories in the united states during 2002 and 2003.Ann Clin Microbiol Antimicrob.2004;3:1.
- ,,, et al.Multiple pathogens in adult patients admitted with community‐acquired pneumonia: a one year prospective study of 346 consecutive patients.Thorax.1996;51:179–184.
- ,,,,.How good is the evidence for the recommended empirical antimicrobial treatment of patients hospitalized because of community‐acquired pneumonia? A systematic review.J Antimicrob Chemother.2003;52:555–563.
- ,,,.Empirical atypical coverage for inpatients with community‐acquired pneumonia: systematic review of randomized controlled trials.Arch Intern Med.2005;165:1992–2000.
- ,,,.Impact of guideline‐concordant empiric antibiotic therapy in community‐acquired pneumonia.Am J Med.2006;119:865–871.
- ,,, et al.Combination antibiotic therapy lowers mortality among severely ill patients with pneumococcal bacteremia [see comment].Am J Respir Crit Care Med.2004;170:440–444.
- ,,, et al.Addition of a macrolide to a beta‐lactam‐based empirical antibiotic regimen is associated with lower in‐hospital mortality for patients with bacteremic pneumococcal pneumonia. [see comment].Clin Infect Dis.2003;36:389–395.
- ,,.Monotherapy may be suboptimal for severe bacteremic pneumococcal pneumonia.Arch Intern Med.2001;161:1837–1842.
- ,,, et al.Clinical characteristics at initial presentation and impact of dual therapy on the outcome of bacteremic Streptococcus pneumoniae pneumonia in adults.Can Respir J.2004;11:589–593.
- ,.Pneumococcal bacteremia with special reference to bacteremic pneumococcal pneumonia.Arch Intern Med.1964;60:759–776.
- ,,, et al.Prognosis and outcomes of patients with community‐acquired pneumonia. A meta‐analysis.JAMA.1996;275:134–141.
- ,.Early switch from intravenous to oral antibiotics in hospitalized patients with bacteremic community‐acquired Streptococcus pneumoniae pneumonia.Arch Intern Med.2001;161:848–850.
- Cleveland Clinic patient price information list. Available at:http://cms.clevelandclinic.org/documents/CCMain_HB197_2007.pdf. Accessed January2008.
- ,.Analysis of strategies to improve cost effectiveness of blood cultures.J Hosp Med.2006;1:272–276.
- ,,.Contaminant blood cultures and resource utilization. The true consequences of false‐positive results.JAMA.1991;265:365–369.
- ,,,,.Patient and hospital characteristics associated with recommended processes of care for elderly patients hospitalized with pneumonia: results from the Medicare quality indicator system pneumonia module.Arch Intern Med.2002;162:827–833.
- ,,,,.Processes of care, illness severity, and outcomes in the management of community‐acquired pneumonia at academic hospitals.Arch Intern Med.2001;161:2099–2104.
- ,.Influence of blood culture results on antibiotic choice in the treatment of bacteremia.Arch Intern Med.1994;154:2641–2645.
Blood cultures (BCs) have long been a mainstay of the diagnostic evaluation of patients hospitalized with community‐acquired pneumonia (CAP). They have been strongly recommended by professional societies13 and are often expected by admitting physicians. A large retrospective study of Medicare patients with pneumonia found that obtaining BCs is associated with lower mortality.4 In 2002, when the National Hospital Quality Measures (NHQM) were introduced, BCs were included as a quality measure for pneumonia.5, 6
However, there is uncertainty about the actual utility of BCs in CAP. In large studies they are true‐positive in only 7 to 11% of cases and false‐positive in 5%,2, 7 and whether they affect clinical management has been strongly questioned.810 Their impact may be limited by slow results, low frequency of bacterial resistance to the empiric antibiotic regimen, and reluctance of physicians to narrow antibiotic coverage.9, 11 Recent updates to professional society guidelines no longer recommend BCs in all admitted CAP patients.12
To evaluate the clinical utility of BCs and the appropriateness of pnemonia quality measures based on BCs, we performed a systematic review of the literature to determine the effect of BCs on the management of adults with CAP requiring hospitalization.
PATIENTS AND METHODS
Data Sources and Searches
We searched the English‐language literature via MEDLINE (1966 through September 2007), MEDLINE‐In Process, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects, and ACP Journal Club. Within each of these databases we used keywords and exploded Medical Subject Headings (MeSH) to produce the following search strategy: blood culture(s) (keyword), bacteriological techniques (MeSH), blood [microbiology] (MeSH), bacteremia [microbiology or drug therapy] (MeSH), or diagnostic tests, routine (MeSH) combined with pneumonia (keyword), pneumonia (MeSH), lower respiratory tract infection(s) (keyword), or community‐acquired infections (MeSH). To maximize capture of BC or bacteremia studies with subgroups of CAP patients we added the following search strategy: explode microbiological techniques [utilization] (MeSH), explode blood specimen collection [utilization] (MeSH), or focus bacteremia [drug therapy] (MeSH). We reviewed the reference lists of all included studies as well as those of important background articles. Finally, we asked experts to evaluate the completeness of our list.
Study Selection
We included studies in which: (1) subjects were adults hospitalized with CAP; (2) BCs were obtained at or near hospital admission; and (3) the effects of BCs on management (change in antibiotic therapy or other effects such as duration of parenteral therapy, length of hospitalization, or level of care) were reported. The first 2 requirements could be satisfied by a subgroup.
From retrieved citations, relevant abstracts were reviewed, and studies with any potential to meet inclusion criteria were chosen for full‐text review. Two authors (N.A., R.S.) independently analyzed each full‐text article to determine inclusion for data analysis. A third author (J.T.) analyzed all included and narrowly excluded articles to confirm the final list of included studies. Disagreements were resolved by discussion.
Data Extraction
For the included studies, 2 authors (N.A., K.A.) independently abstracted the following data using a standardized collection instrument: study design and setting, inclusion and exclusion criteria, number of hospitalized CAP patients in whom BCs were obtained, empiric antibiotic regimens, number of true‐positive and false‐positive BCs, bacteria isolated in true‐positive BCs, BC‐directed antibiotic narrowing, BC‐directed antibiotic broadening ultimately associated with a resistant organism, and any other management effects reported. Narrowing refers to coverage of fewer organisms, while broadening refers to coverage of a larger or different spectrum of organisms.
If a study included patients not meeting our selection criteria, our analysis was limited to the subset of patients meeting criteria. We also analyzed each study to determine whether a subgroup of severely ill patients was reported separately and whether such a group benefited from BCs. The 2 authors independently repeated all data abstraction to confirm accuracy. We attempted to contact authors for clarification when needed.
Data Synthesis
Data were synthesized by compilation of characteristic summary tables. In the primary analysis, the proportion of positive BCs (both true and false) and the frequency of BC‐directed changes in antimicrobial therapy (narrowing, or broadening ultimately associated with a resistant organism) were determined and reported for each study and then described as an aggregate range. This compilation required studies to provide a particular denominatorthe number of patients in whom BCs were performed. If a study did not do so, it was described separately in the secondary analysis, where we also assessed the cost of BCs as well as the impact of BCs in critically ill patients and on outcomes other than antibiotic change. Heterogeneity of subject inclusion and exclusion criteria and empiric antibiotic use were summarized qualitatively. Two authors (N.A., R.S.) assessed each study's quality.
DATA SYNTHESIS
Search Results
Our electronic database search yielded 3236 citations. From this list and the supplementary search of references, we reviewed 607 abstracts; of these, we selected 73 articles for full‐text review, and 15 were included in the final analysis (Figure 1). One study was narrowly excluded because it largely included CAP patients that had already been admitted to the hospital and failed an empiric antibiotic trial before BCs were obtained.13
Study Characteristics
Fifteen studies with a total of 3898 patients evaluated BC‐directed management changes in adults admitted with CAP.11, 1427 However, 2 of these, involving only patients with bacteremic pneumococcal CAP, by design could not report the number of patients that had BCs done; thus they were not included in the primary analysis.16, 25
The 13 studies amenable to the primary analysis (Table 1) all had an observational cohort design; 6 were prospective11, 18, 20, 24, 26, 27 and 7 were retrospective.14, 15, 17, 19, 2123 Sample size varied from 52 to 760 patients. Settings included university and community hospitals in the U.S. and 4 other countries, with patient enrollment spanning the years 19882003 (publication dates 19912007).
| Study Author, Year, Design, Setting | Inclusion Criteria | Exclusion Criteria | CAP Patients with BCs, n*; True‐Positive BCs, n (%); False‐Positive BCs, n (%) | BCs Directed Antibiotic Narrowing, n (%) | BCs Directed Antibiotic Broadening and Organism was Resistant, n (%) | Comments |
|---|---|---|---|---|---|---|
| ||||||
| Benenson et al.,14 2007; retrospective, U.S. suburban | ED ICD‐9 dx and discharge dx of PNA | None | n = 684; 23 (3.4); 54 (7.9) | 3 (0.4) | 0 (0) | 11% of pts with ED dx of PNA not eligible due to different dx at discharge; 25% from nursing homes, 18% recently hospitalized, 14% immunocompromised; Abxs narrowed in 3/21 eligible pts |
| Ramanujamand Rathlev,22 2006; retrospective; U.S. urban | ED, ICD‐9, and discharge dx of PNA, and ED BCs before abxs | IC, active cancer, chronic renal failure, hospitalized last 1 week, nursing home resident, aspiration | n = 289; 13 (4.5%); 13 (4.5%) | 1 (0.3%) | 0 (0%) | 532 pts screened; 3% not eligible due to different dx at discharge; of eligible pts, 9% excluded due to HCAP and 31% excluded due to other risk factors; Abxs were narrowed in 1/10 eligible pts; Cost: $8,000 for the 1 pt with abx change |
| Mountain et al.,21 2006; retrospective, Australian suburban | All pts who had BCs done in the ED during a 2‐month period (PNA pts were a subgroup) | None | n = 52; Not reported; Not reported | 1 (1.9) | 0 (0) | 52/218 study pts had clinical PNA. Overall BCs true‐positive in 6.4%, false‐positive in 7.3%; frequencies for PNA pts not reported separately; Reason for abx change (ceftriaxone to ciprofloxacin) not reported, but thought not to be associated with resistant organism (personal communication); Cost: $1,950 (U.S.) per BC that altered treatment |
| Kennedy et al.,20 2005; prospective, U.S urban | Clinical and radiographic PNA and BCs in ED or within 3 hours of admission | None | n = 385; 27 (7.0); 6.0% | 11 (2.9) | 4 (1.0) | 23% of pts from nursing homes, 22% admitted to ICU; 3/4 pts whose abxs were broadened due to a resistant organism came from nursing homes; Abxs were narrowed in 11/19 eligible pts; BCs were false‐positive in 25/414 (6%) pts, including 29 pts discharged from the ED |
| Corbo et al.,17 2004; retrospective, U.S. urban | Primary diagnosis of CAP, positive CXR, and ED BCs before abxs | IC, cancer, recent hospitalization, nursing home resident | n = 355; 33 (9.3); 37 (10.4) | 7 (2.0) | 0 (0) | 821 pts admitted with CAP; 24% not eligible due to non‐confirmatory CXR; of eligible pts, 22% excluded due to HCAP, 23% excluded due to other risk factors; 6 pts with false‐positive BCs had abx change due to BCs ‐ authors suggest hospitalization prolonged in these cases; Physicians reluctant to narrow abxs per authors |
| Campbell et al.,11 2003; prospective, Canadian multiple (19) hospitals | Two signs or sxms of PNA and positive CXR | IC, shock, direct ICU admission, chronic kidney disease, pregnant or nursing, alcoholism | n = 760; 43 (5.7); Not reported | 12 (1.6) | 2 (0.3) | 38% of pts screened with suspected CAP either ineligible or excluded due to risk factors; Abxs were narrowed in 12/35 eligible pts; In one case, BCs grew MRSA resistant to empiric abxs, but abxs had been changed before BC results available; Cost: $1550 (U.S.) per BC leading to abx change |
| Waterer and Wunderink,26 2001; prospective; U.S. urban | Signs and sxms of PNA, positive CXR, and BCs before abxs | IC, hospitalized last 30 days, nursing home residents (if non‐ambulatory) | n = 209; 29 (13.9); 9 (4.3) | 5 (2.4) | 1 (0.5) | BCs only changed management in pts in PSI class 4 and 5 |
| Theerthakarai et al.,24 2001; prospective, U.S. suburban | Acute febrile illness with respiratory sxms and a positive CXR | IC, cancer, age >65, alcoholism, IVDU, COPD, IDDM, neurologic disease, renal failure, recent abx, severe or complicated PNA | n = 74; 0 (0); 0 (0) | 0 (0%) | 0 (0%) | Very strict exclusion criteria: 62% of eligible pts excluded due to risk factors; Authors reported that 28% of included pts could have been treated as outpatients per ATS guidelines |
| Sanyal et al.,23 1999; retrospective, U.S. urban | Acute lower respiratory tract infection and positive CXR | IC, cancer, hospitalized last 12 weeks, IVDU, bronchiectasis, splenectomy, not treated per ATS guidelines | n = 174; 19 (10.9); Not reported | Not reported | 1 (0.6%) | BC‐directed antibiotic changes only reported for pts who did not respond to initial abxs, so BC‐directed narrowing could not be determined; The pt whose abxs were broadened was a nursing home resident with severe pneumonia (by ATS criteria) |
| Glerant et al.,18 1999; prospective, French suburban | Acute septic episode with respiratory sxms and positive CXR | IC, ICU admission, hospitalized last 2 weeks, aspiration | n = 53; 5 (9.4); 2 (3.8) | 0 (0) | 0 (0) | BCs done during first 48 hours so not clear how many BCs sent after hospital abxs started; 23 pts were on abxs before admission; Cost: $6006 (U.S.), no abx changes |
| Kelly,19 1998; retrospective, Australian suburban | All pts who had BCs done in the ED over a 9‐ month period (PNA pts were a subgroup) | None | n = 260; 5%; Not reported | 1% | 1% | 260/1062 study pts had PNA; 14% of all pts discharged; for CAP pts percentage not reported; False‐positive rate 3.8% for all pts, but not reported separately for PNA pts; 1% of PNA pts had abx change due to BCs; type of change not reported, hence reporting of 1% in outcome columns; Cost: $4800 (U.S.) per abx change |
| Chalasani et al.,15 1995; retrospective; U.S. urban | Dx of PNA, respiratory sxms, positive CXR, and 2 sets of BCs before abxs | IC, cancer, hospitalized last 2 weeks, nursing home resident | n = 517; 34 (6.6); 25 (4.8) | 7 (1.4) | 0 (0) | 1250 pts screened with discharge dx of PNA; 59% either ineligible or excluded due to risk factors (authors did not report number ineligible due to the BC requirement); In one case, BCs grew H. influenzae resistant to empiric abxs, but sputum cultures drove the abx change; Cost: $4875 per abx change |
| Woodhead et al.,27 1991; prospective, British urban (2 hospitals) | Clinical features of CAP and positive CXR | IC, cancer, admitted to geriatric or communicable disease ward | n = 86; 9 (10.5%); Not reported | 2 (2.3) | 1 (1.2) | 8% of pts meeting inclusion and exclusion criteria were later excluded due to different dx at discharge |
Included patients were usually required to have clinical features of pneumonia and a confirmatory chest x‐ray. Treating physicians were required to obtain BCs (either by study or hospital protocol) in only 3 studies14, 22, 24 and in a subgroup of another study;11 otherwise the performance of BCs was left to physician discretion.
Nine studies excluded patients who were immunocompromised,11, 15, 17, 18, 2224, 26, 27 a label that was often incompletely defined. Otherwise, exclusion criteria were variable. Notably, only 3 studies excluded patients admitted to the intensive care unit (ICU),11, 18, 24 while 6 excluded patients with cancer15, 17, 2224, 27 and 6 excluded either nursing home residents15, 17, 22, 26 or the elderly (de facto exclusion of most nursing home residents).24, 27
Empiric antibiotic regimens, where reported, were predominantly cephalosporin plus macrolide combinations in 4 studies,17, 2224 fluoroquinolones in 3 studies,11, 14, 26 and penicillin or 1 of its derivatives in 1 study.27
Concerning the 2 studies not included in the primary analysis, the one by Waterer et al.25 was a retrospective review of all cases of pneumococcal bacteremia (n = 74) associated with an admission diagnosis of CAP (N = 1805) in a US urban hospital over a 3‐year period. The one by Chang et al.16 was a retrospective case‐control study of 288 randomly‐selected, immunocompetent Medicare patients with bacteremic pneumococcal CAP who survived to discharge. They were matched 1:1 with blood and sputum culture‐negative controls to study the rate of fluoroquinolone use at discharge in the 2 groups.
Study Findings
Primary Analysis
As shown in Table 1, BCs were positive for a true pathogen in 0% to 14% of cases. Details of microbiology and empiric antibiotic selection are reported in Table 2. S. pneumoniae was by far the most common pathogen: of the 9 studies that had positive BCs and reported the organisms, S. pneumoniae represented 50% to 91% of the pathogens, with penicillin‐resistance found in 0% to 20%.11, 14, 15, 17, 18, 20, 22, 23, 26 S. aureus was next most common, occurring in 6 studies and growing in 3% to 23% of positive BCs;11, 14, 17, 20, 23, 26 its sensitivity to methicillin was reported in 3 studies, with methicillin‐resistant S. aureus (MRSA) representing 0/3, 3/7, and 1/1 of cases.14, 20, 23 E. coli represented 3% to 11% of pathogens in 6 studies,11, 14, 15, 20, 23, 26 while H. influenzae represented 2% to 15% of pathogens in 7 studies.11, 14, 15, 18, 22, 23, 26
| Study: Author, Year | Empiric Antibiotics Given: Frequency, Agent | Bacteria Isolated in True‐Positive BCs: n, Organism | Organisms in BCs Resistant to Empiric Antibiotics |
|---|---|---|---|
| |||
| Benenson et al.,14 2007 | Mild to moderate PNA: levofloxacin; If ICU admission: levofloxacin + azithromycin; If HCAP: levofloxacin + clindamycin; If risk for MRSA: added vancomycin; If structural lung disease: added tobramycin | 14 S. pneumoniae; 3 S. aureus (all MSSA); 2 Group B Strep; 2 H. influenzae; 1 E. coli; 1 Group A Strep | None |
| Ramanujam and Rathlev,22 2006 | Ceftriaxone + oral azithromycin | 11 S. pneumoniae (1 PCN interm res); 2 H. influenzae | None |
| Mountain et al.,21 2006 | Not reported | Not reported completely | None |
| Kennedy et al.,20 2005 | Not reported | 15 S. pneumoniae (3 PCN res); 7 S. aureus (3 MRSA); 3 E. coli; 1 Coagulase‐negative Staph; 1 Pseudomonas; 1 Proteus; 1 Moraxella; 1 E. faecalis | 2 MRSA; 1 MSSA (res to levofloxacin, clindamycin); 1 E. coli (res to levofloxacin) |
| Corbo et al.,17 2004 | 48% ceftriaxone + macrolide; 21% cephalosporin only; 6% quinolone only | 30 S. pneumoniae; 2 S. aureus (# MRSA not reported); 1 Staph haemolyticus | None |
| Campbell et al.,11 2003 | 55% levofloxacin; 45% antibiotic not reported | 30 S. pneumoniae (1 PCN res); 5 S. aureus (total # MRSA not reported); 5 E. coli; 1 H. influenzae; 1 E. faecalis; 1 K. pneumoniae; 1 Enterobacter | 1 MRSA (antibiotic changed before BC results available); 1 MSSA (res not reported); 1 S. pneumoniae (PCN res) |
| Waterer and Wunderink,26 2001 | 60% quinolone only; 25% quinolone + other antibiotic(s) | 20 S. pneumoniae (3 PCN res); 3 S. viridans; 1 H. influenzae; 1 S. aureus (# MRSA not reported); 1 Enterobacter; 1 E. coli; 1 Group B Strep; 1 Group D Strep; 1 Group G Strep; 1 Acinetobacter | 1 Group D Strep (res to levofloxacin) |
| Theerthakarai et al.,24 2001 | Cephalosporin + macrolide | None | None |
| Sanyal et al.,23 1999 | Severe CAP: erythromycin + ceftazidime or ticarcillin/clavulanate; Nonsevere CAP: 76% cefuroxime + erythromycin, 18% cefuroxime only | 14 S. pneumoniae (0 PCN res); 2 H. influenzae; 1 S. aureus (MRSA); 1 K. pneumoniae; 1 E. coli | 1 MRSA |
| Glerant et al.,18 1999 | Not reported | 4 S. pneumoniae (0 PCN res); 1 H. influenzae | None |
| Kelly,19 1998 | Not reported | Not reported | Cannot determine |
| Chalasani et al.,15 1995 | Not reported | 29 S. pneumoniae (0 PCN res); 3 H. influenzae; 1 S. pyogenes; 1 E. coli | H. influenzae (sputum culture drove the antibiotic change) |
| Woodhead et al.,27 1991 | 78% included penicillin, aminopenicillin, or amoxicillin/clavulanate; 33% included erythromycin; 21% ‐lactam + erythromycin | Not reported separately for BCs | E. coli (res to erythromycin) |
| Chang et al.,16 2005 | BC+/Controls: 34%/21%/Quinolones; 86%/88%/ ‐lactam; 1%/1%/Amox/PCN; 38%/37%/ Macrolide | 288 S. pneumoniae (only organism, by design) | Not reported |
| Waterer et al.,25 1999 | 38% Cephalosporin + macrolide other; 27% Quinolone other | 74 S. pneumoniae (only organism, by design); 11 PCN interm res; 4 PCN res | 2 S. pneumoniae (both resistant; degree of resistance not specified) |
In the 8 studies that reported false‐positive BCs, the false‐positive rate was 0% to 10%,14, 15, 17, 18, 20, 22, 24, 26 with 5 studies finding comparable false‐positive and true‐positive BC rates15, 17, 20, 22, 24 and 1 study finding a substantially higher frequency of false‐positive than true‐positive BCs (Table 1).14
BCs led to narrowing of antibiotic coverage in 0% to 3% of cases (Table 1). Four studies reported that physicians narrowed antibiotics when BCs indicated that it was possible to do so, but only in 10%, 14%, 34%, and 58% of eligible cases.11, 14, 20, 22
BCs led to antibiotic broadening ultimately associated with a resistant organism in 0% to 1% of cases (Table 1). The pathogens were MRSA (3), methicillin‐sensitive S. aureus (2), E. coli (2), S. pneumoniae (1), and Group D Streptococcus (1). Details about these patients' medical histories and demographics were absent or sparse in all but 1 study.20 For several of the above cases it was not explicitly stated that BCs directed the antibiotic changes, though it was usually implied; thus we assumed causation.
Secondary Analyses
In the pneumococcal bacteremia study by Waterer et al.,25 BCs altered management in 31 of the 74 cases of pneumococcemia, but in only 2 patients was this associated with antibiotic resistance. Most of the other 29 cases involved narrowing of antibiotics, though switching to penicillin or dropping atypical coverage occurred in only 22% and 37% of eligible patients, respectively. In the study by Chang et al.,16 there was no significant difference in fluoroquinolone use at discharge between the pneumococcemic and culture‐negative groups (the primary endpoint), though there was significantly higher ‐lactam use and lower macrolide use in the pneumococcemic patients at discharge. From the data provided it was not possible to determine how often antibiotic broadening occurred.
Only 2 of the 15 studies stratified management effects based on severity of illness, and neither specified the proportion of severely ill patients admitted to the ICU. Waterer and Wunderink26 prospectively hypothesized that sicker patients were more likely to benefit from BCs. They found that the 30 patients in pneumonia severity index class 5 were most likely to have a BC‐driven antibiotic change, though in at most 1 of these patients was associated with a resistant organism. Sanyal et al.23 stratified patients by severity based on expert guidelines. They found that 19 of 174patients had severe CAP that did not respond to the initial antibiotic regimen, with 1 having a BC‐driven antibiotic change; this was due to resistance.
Only 1 study reported an outcome other than antibiotic change, which in this case was duration of parenteral therapy. In the study, 5 of 43 patients with true‐positive BCs remained on intravenous antibiotics for the full course of treatment probably due to bacteremia alone.11
The direct cost of BCs per BC‐directed antibiotic change (or total cost of BCs if there was no antibiotic change) was reported in 6 studies and, not adjusted for inflation, ranged from $1550 to $8000 (U.S.).11, 15, 18, 19, 21, 22
Quality of the Studies
A detailed listing of the strengths and weaknesses of each study is provided in the Appendix. Briefly, all 15 studies included in this review were observational. Most did not prospectively require BCs in all patients admitted with CAP. This could have biased the results in favor of BC utility as physicians presumably order BCs in patients with a higher probability of bacteremia. Conversely, several studies did not explicitly require two sets of BCs or that BCs be done prior to antibiotics, so they may not have revealed the maximum utility of BCs. The 2 studies limited to pneumococcal bacteremia and described in the secondary analysis were inherently biased against BC utility, as pneumococcus is more likely to be antibiotic‐sensitive than other CAP pathogens.
Eligibility was based only on an emergency department (ED)/admission diagnosis of CAP, a criteria that approximates real world practice, in 3 studies.19, 21, 25 The other studies required either a confirmatory radiograph or a hospital discharge diagnosis of pneumonia. Consequent ED/admission misdiagnosis rates were 3%, 8%, 11%, 24% in the 4 studies that reported them;14, 17, 22, 27 the final diagnoses, when reported, were nearly all noninfections or proximal respiratory tract infections.22, 27
Five studies included all eligible patients.14, 1921, 25 However, 3 studies excluded 23%, 31%, and 62% of eligible patients based on risk factors for bacteremia or resistant pathogens,17, 22, 24 and the rest did not report the number excluded.
DISCUSSION
Summary of Findings
Our systematic review of the literature finds that BCs rarely alter empiric antibiotic therapy in adults hospitalized with community‐acquired pneumonia. Even when there is a change in treatment it usually is not of the type most likely to impact patient outcome, which is antibiotic broadening ultimately associated with a resistant organism. In the 13 studies that could quantify this effect, it occurred in only 0% to 1% of cases in which BCs were obtained. Antibiotic narrowing occurred in 0% to 3% of cases, with physicians often choosing not to narrow antibiotics when BC results suggested that they could do so.
Limits on BC Utility
‐Lactam‐Resistant Pneumococcus
In the studies reviewed here 50%‐90% of positive BCs grew pneumococcus, consistent with the 60% to 67% rate reported elsewhere.2, 28, 29 Pneumococci that invade the bloodstream have disproportionately low rates of ‐lactam resistance,30, 31 inherently limiting the utility of BCs for detecting inadequate empiric antibiotic therapy. Though pneumococcal resistance to ‐lactams has risen over the last 2 decades, third‐generation cephalosporins, preferred agents for CAP, are still extremely effective. Even when the organism is by historical standards moderately resistant to them, these cephalosporins at standard doses maintain bactericidal efficacy in the lung,32, 33 and their use in the setting of such resistance is not associated with higher mortality.3437 By newer laboratory standards 97% and 96% of S. pneumoniae isolates in mid‐2003 were sensitive to ceftriaxone and cefotaxime, respectively.38 Thus a major potential benefit of BCsdetecting cephalosporin‐resistant pneumococcusremains a rare occurrence.
Polymicrobial Infection
If positive BCs in CAP mostly reveal antibiotic‐sensitive pathogens, one may infer that at least they lead to narrowing of therapy. However, the studies reviewed here reveal that this usually does not happen.
One explanation for this reluctance to narrow antibiotics is that CAP is often a polymicrobial disease. When rigorous serologic testing is done, multiple pathogens are found in up to 40% of cases.39 The occult copathogen is frequently an intracellular one and thus cannot be detected by BCs. Though the evidence for empirically treating these atypical organisms is mixed,40, 41 expert guidelines recommend doing so,12 and guideline‐concordant antibiotic therapy in CAP is associated with lower mortality.42 Even in bacteremic pneumococcal CAP, monotherapy is associated with higher mortality.4346 Thus, stopping antibiotic coverage of atypical pathogens in response to BCs alone might not always be appropriate.
Prognosis
Another rationale given for ordering BCs is that bacteremic pneumonia is a morbid disease so positive BCs may demand prolonged parenteral therapy or extended hospitalization. Although mortality for bacteremic pneumococcal pneumonia (the predominantly studied variety of bacteremic pneumonia) has historically been high at 20%,47, 48 studies that have examined pneumococcal bacteremia as an independent risk factor for death in CAP have yielded mixed results.2 Moreover, it appears that patients with bacteremic pneumococcal pneumonia who reach clinical stability may be safely switched to oral antibiotics.49
It is not clear that positive BCs in pneumonia (at least in the case of S. pneumoniae) should alter the duration of parenteral therapy or hospitalization, though whether or not such effects occur in clinical practice was largely unaddressed by the studies reviewed here.
Epidemiology
One theoretical benefit of BCs is their epidemiologic value. When true‐positive in pneumonia, perhaps more than any other test they identify with great specificity at least 1 of the causative agents. Unfortunately, as discussed above, BCs alone provide an incomplete and skewed picture of the microbiology of CAP. They underestimate atypical organisms, overestimate pneumococcus, and, because bacteremic pneumococcus is more likely to be antibiotic‐susceptible, they underestimate antibiotic resistance.11 Tracking pathogens in bacteremic pneumonia may be useful nonetheless, but perhaps a more accurate method for determining etiologic trends is periodic comprehensive microbiological investigation, including BCs, sputum/bronchial cultures, and serology.
Costs
In the studies reviewed here, based on reported costs of $15 to $65 per set of BCs or per patient, BCs cost $1550 to $8000 (U.S.) per BC‐directed antibiotic change. Considering that very few of these antibiotic changes involved broadening associated with a resistant organism, the cost/benefit ratio was quite high. Today BCs may be even more expensive, as U.S. hospitals now often charge over $150 per set of BCs.50, 51
The cost of false‐positive BCs must also be taken into account. The false‐positive rate in the studies reviewed here was 0% to 10%, similar to that reported elsewhere.7 False‐positive BCs increase hospital length of stay by 3 to 5 days and hospital charges by $4400 to $8800.51, 52
Limitations of the Review
Our search strategy was designed to be sensitive and included backup methods such as searching article references and querying experts. Nevertheless, we may have missed studies, especially if there were small eligible subgroups or if determining management effects was not a primary purpose. We chose not to measure instances of antibiotic broadening that were not associated with a resistant organism, though in unusual cases (eg, Pseudomonas bacteremia) this effect of BCs may be useful.
The methodologies of the included studies were adequate to measure the key outcomes with reasonable validity. Biases were evident, though they occurred both for and against BC utility.
Eligibility varied across studies, and most investigations excluded immunocompromised or other high‐risk patient groups, which could have biased results against BC utility. However, results of these studies were consistent with those that included all patients with CAP, suggesting the degree of bias was probably small. Still, given this concern, it would be prudent not to generalize the findings of this review to immunocompromised patients. Moreover, although the critically ill and those who today would be classified as having healthcare‐associated pneumonia (HCAP)nursing home residents, the recently hospitalized, and hemodialysis patientswere included in most studies, their numbers were small, and these groups were not analyzed separately; thus, the results might not be generalizable to these populations either. Finally, the reported studies, which enrolled patients through 2003, do not reflect more recent increases in the prevalence of resistant pathogens, such as MRSA, in the community.
BCs as a Quality Measure
The adoption of BCs as a quality measure was largely predicated on the widely‐cited study by Meehan et al.,4 which showed an association between BC obtainment and reduced mortality. This study, which associated processes of care with hard outcomes such as mortality, was limited by uncontrolled confounders, including variation in hospital quality.53 A more recent study of pneumonia processes of care found no association between BC collection and mortality.54 Another study often cited to support BC use, by Arbo and Snydman,55 showed that positive BCs were associated with changes in antibiotic therapy, but it included very few pneumonia patients and did not describe results for them separately.
The inclusion of BC acquisition in 2 quality measures in the NHQM guidelines for pneumonia impacts the clinical practice of hospitals and physicians, which may be rated and reimbursed differentially based on their compliance with such measures. One of the quality measures requires BCs in patients admitted to the ICU. The other requires that ED BCs for pneumonia, if obtained, be drawn before antibiotics are given.6
The studies we reviewed are not specific to these quality measures, but are relevant to them. With regard to the first measure, all but 3 studies included patients admitted to the ICU and found BCs to be of minimal benefit overall. Our subgroup analysis of severely ill patients was unrevealing. The ICU measure is tentative in its validity, but it is not unreasonable given that these patients have a life‐threatening infection and may be at risk for bacteremia with resistant pathogens.12
The second measure, though perhaps simply seeking to maximize the potential for BCs to turn positive, depends for its validity on BCs being useful in a large proportion of patients with CAP. Though we cannot exclude the possibility that BCs benefit certain subsets of patients, such as those who are immunocompromised or have HCAP, our findings do not support obtaining BCs in all or even most adults hospitalized with CAP. This conclusion is reflected in the 2007 Infectious Diseases Society of America/American Thoracic Society management guidelines for CAP, which state than BCs are optional except for patients with severe pneumonia, some immunocompromised states, and particular radiographic abnormalities.12
With such data and guidelines in mind, a physician seeking to minimize treatment delays in a patient with pneumonia may give antibiotics early in the ED course (the basis of another quality measure) without obtaining BCs. If she later determines that the patient is particularly high‐risk for bacteremia or a resistant pathogen, should she be discouraged from ordering BCs? Experts specifically state that BCs, even after antibiotics, are warranted for such a patient.12
With the scope of medical practice captured in quality measures being so narrow, having 2 measures based on a test with such limited benefit is itself questionable.
Blood cultures (BCs) have long been a mainstay of the diagnostic evaluation of patients hospitalized with community‐acquired pneumonia (CAP). They have been strongly recommended by professional societies13 and are often expected by admitting physicians. A large retrospective study of Medicare patients with pneumonia found that obtaining BCs is associated with lower mortality.4 In 2002, when the National Hospital Quality Measures (NHQM) were introduced, BCs were included as a quality measure for pneumonia.5, 6
However, there is uncertainty about the actual utility of BCs in CAP. In large studies they are true‐positive in only 7 to 11% of cases and false‐positive in 5%,2, 7 and whether they affect clinical management has been strongly questioned.810 Their impact may be limited by slow results, low frequency of bacterial resistance to the empiric antibiotic regimen, and reluctance of physicians to narrow antibiotic coverage.9, 11 Recent updates to professional society guidelines no longer recommend BCs in all admitted CAP patients.12
To evaluate the clinical utility of BCs and the appropriateness of pnemonia quality measures based on BCs, we performed a systematic review of the literature to determine the effect of BCs on the management of adults with CAP requiring hospitalization.
PATIENTS AND METHODS
Data Sources and Searches
We searched the English‐language literature via MEDLINE (1966 through September 2007), MEDLINE‐In Process, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects, and ACP Journal Club. Within each of these databases we used keywords and exploded Medical Subject Headings (MeSH) to produce the following search strategy: blood culture(s) (keyword), bacteriological techniques (MeSH), blood [microbiology] (MeSH), bacteremia [microbiology or drug therapy] (MeSH), or diagnostic tests, routine (MeSH) combined with pneumonia (keyword), pneumonia (MeSH), lower respiratory tract infection(s) (keyword), or community‐acquired infections (MeSH). To maximize capture of BC or bacteremia studies with subgroups of CAP patients we added the following search strategy: explode microbiological techniques [utilization] (MeSH), explode blood specimen collection [utilization] (MeSH), or focus bacteremia [drug therapy] (MeSH). We reviewed the reference lists of all included studies as well as those of important background articles. Finally, we asked experts to evaluate the completeness of our list.
Study Selection
We included studies in which: (1) subjects were adults hospitalized with CAP; (2) BCs were obtained at or near hospital admission; and (3) the effects of BCs on management (change in antibiotic therapy or other effects such as duration of parenteral therapy, length of hospitalization, or level of care) were reported. The first 2 requirements could be satisfied by a subgroup.
From retrieved citations, relevant abstracts were reviewed, and studies with any potential to meet inclusion criteria were chosen for full‐text review. Two authors (N.A., R.S.) independently analyzed each full‐text article to determine inclusion for data analysis. A third author (J.T.) analyzed all included and narrowly excluded articles to confirm the final list of included studies. Disagreements were resolved by discussion.
Data Extraction
For the included studies, 2 authors (N.A., K.A.) independently abstracted the following data using a standardized collection instrument: study design and setting, inclusion and exclusion criteria, number of hospitalized CAP patients in whom BCs were obtained, empiric antibiotic regimens, number of true‐positive and false‐positive BCs, bacteria isolated in true‐positive BCs, BC‐directed antibiotic narrowing, BC‐directed antibiotic broadening ultimately associated with a resistant organism, and any other management effects reported. Narrowing refers to coverage of fewer organisms, while broadening refers to coverage of a larger or different spectrum of organisms.
If a study included patients not meeting our selection criteria, our analysis was limited to the subset of patients meeting criteria. We also analyzed each study to determine whether a subgroup of severely ill patients was reported separately and whether such a group benefited from BCs. The 2 authors independently repeated all data abstraction to confirm accuracy. We attempted to contact authors for clarification when needed.
Data Synthesis
Data were synthesized by compilation of characteristic summary tables. In the primary analysis, the proportion of positive BCs (both true and false) and the frequency of BC‐directed changes in antimicrobial therapy (narrowing, or broadening ultimately associated with a resistant organism) were determined and reported for each study and then described as an aggregate range. This compilation required studies to provide a particular denominatorthe number of patients in whom BCs were performed. If a study did not do so, it was described separately in the secondary analysis, where we also assessed the cost of BCs as well as the impact of BCs in critically ill patients and on outcomes other than antibiotic change. Heterogeneity of subject inclusion and exclusion criteria and empiric antibiotic use were summarized qualitatively. Two authors (N.A., R.S.) assessed each study's quality.
DATA SYNTHESIS
Search Results
Our electronic database search yielded 3236 citations. From this list and the supplementary search of references, we reviewed 607 abstracts; of these, we selected 73 articles for full‐text review, and 15 were included in the final analysis (Figure 1). One study was narrowly excluded because it largely included CAP patients that had already been admitted to the hospital and failed an empiric antibiotic trial before BCs were obtained.13
Study Characteristics
Fifteen studies with a total of 3898 patients evaluated BC‐directed management changes in adults admitted with CAP.11, 1427 However, 2 of these, involving only patients with bacteremic pneumococcal CAP, by design could not report the number of patients that had BCs done; thus they were not included in the primary analysis.16, 25
The 13 studies amenable to the primary analysis (Table 1) all had an observational cohort design; 6 were prospective11, 18, 20, 24, 26, 27 and 7 were retrospective.14, 15, 17, 19, 2123 Sample size varied from 52 to 760 patients. Settings included university and community hospitals in the U.S. and 4 other countries, with patient enrollment spanning the years 19882003 (publication dates 19912007).
| Study Author, Year, Design, Setting | Inclusion Criteria | Exclusion Criteria | CAP Patients with BCs, n*; True‐Positive BCs, n (%); False‐Positive BCs, n (%) | BCs Directed Antibiotic Narrowing, n (%) | BCs Directed Antibiotic Broadening and Organism was Resistant, n (%) | Comments |
|---|---|---|---|---|---|---|
| ||||||
| Benenson et al.,14 2007; retrospective, U.S. suburban | ED ICD‐9 dx and discharge dx of PNA | None | n = 684; 23 (3.4); 54 (7.9) | 3 (0.4) | 0 (0) | 11% of pts with ED dx of PNA not eligible due to different dx at discharge; 25% from nursing homes, 18% recently hospitalized, 14% immunocompromised; Abxs narrowed in 3/21 eligible pts |
| Ramanujamand Rathlev,22 2006; retrospective; U.S. urban | ED, ICD‐9, and discharge dx of PNA, and ED BCs before abxs | IC, active cancer, chronic renal failure, hospitalized last 1 week, nursing home resident, aspiration | n = 289; 13 (4.5%); 13 (4.5%) | 1 (0.3%) | 0 (0%) | 532 pts screened; 3% not eligible due to different dx at discharge; of eligible pts, 9% excluded due to HCAP and 31% excluded due to other risk factors; Abxs were narrowed in 1/10 eligible pts; Cost: $8,000 for the 1 pt with abx change |
| Mountain et al.,21 2006; retrospective, Australian suburban | All pts who had BCs done in the ED during a 2‐month period (PNA pts were a subgroup) | None | n = 52; Not reported; Not reported | 1 (1.9) | 0 (0) | 52/218 study pts had clinical PNA. Overall BCs true‐positive in 6.4%, false‐positive in 7.3%; frequencies for PNA pts not reported separately; Reason for abx change (ceftriaxone to ciprofloxacin) not reported, but thought not to be associated with resistant organism (personal communication); Cost: $1,950 (U.S.) per BC that altered treatment |
| Kennedy et al.,20 2005; prospective, U.S urban | Clinical and radiographic PNA and BCs in ED or within 3 hours of admission | None | n = 385; 27 (7.0); 6.0% | 11 (2.9) | 4 (1.0) | 23% of pts from nursing homes, 22% admitted to ICU; 3/4 pts whose abxs were broadened due to a resistant organism came from nursing homes; Abxs were narrowed in 11/19 eligible pts; BCs were false‐positive in 25/414 (6%) pts, including 29 pts discharged from the ED |
| Corbo et al.,17 2004; retrospective, U.S. urban | Primary diagnosis of CAP, positive CXR, and ED BCs before abxs | IC, cancer, recent hospitalization, nursing home resident | n = 355; 33 (9.3); 37 (10.4) | 7 (2.0) | 0 (0) | 821 pts admitted with CAP; 24% not eligible due to non‐confirmatory CXR; of eligible pts, 22% excluded due to HCAP, 23% excluded due to other risk factors; 6 pts with false‐positive BCs had abx change due to BCs ‐ authors suggest hospitalization prolonged in these cases; Physicians reluctant to narrow abxs per authors |
| Campbell et al.,11 2003; prospective, Canadian multiple (19) hospitals | Two signs or sxms of PNA and positive CXR | IC, shock, direct ICU admission, chronic kidney disease, pregnant or nursing, alcoholism | n = 760; 43 (5.7); Not reported | 12 (1.6) | 2 (0.3) | 38% of pts screened with suspected CAP either ineligible or excluded due to risk factors; Abxs were narrowed in 12/35 eligible pts; In one case, BCs grew MRSA resistant to empiric abxs, but abxs had been changed before BC results available; Cost: $1550 (U.S.) per BC leading to abx change |
| Waterer and Wunderink,26 2001; prospective; U.S. urban | Signs and sxms of PNA, positive CXR, and BCs before abxs | IC, hospitalized last 30 days, nursing home residents (if non‐ambulatory) | n = 209; 29 (13.9); 9 (4.3) | 5 (2.4) | 1 (0.5) | BCs only changed management in pts in PSI class 4 and 5 |
| Theerthakarai et al.,24 2001; prospective, U.S. suburban | Acute febrile illness with respiratory sxms and a positive CXR | IC, cancer, age >65, alcoholism, IVDU, COPD, IDDM, neurologic disease, renal failure, recent abx, severe or complicated PNA | n = 74; 0 (0); 0 (0) | 0 (0%) | 0 (0%) | Very strict exclusion criteria: 62% of eligible pts excluded due to risk factors; Authors reported that 28% of included pts could have been treated as outpatients per ATS guidelines |
| Sanyal et al.,23 1999; retrospective, U.S. urban | Acute lower respiratory tract infection and positive CXR | IC, cancer, hospitalized last 12 weeks, IVDU, bronchiectasis, splenectomy, not treated per ATS guidelines | n = 174; 19 (10.9); Not reported | Not reported | 1 (0.6%) | BC‐directed antibiotic changes only reported for pts who did not respond to initial abxs, so BC‐directed narrowing could not be determined; The pt whose abxs were broadened was a nursing home resident with severe pneumonia (by ATS criteria) |
| Glerant et al.,18 1999; prospective, French suburban | Acute septic episode with respiratory sxms and positive CXR | IC, ICU admission, hospitalized last 2 weeks, aspiration | n = 53; 5 (9.4); 2 (3.8) | 0 (0) | 0 (0) | BCs done during first 48 hours so not clear how many BCs sent after hospital abxs started; 23 pts were on abxs before admission; Cost: $6006 (U.S.), no abx changes |
| Kelly,19 1998; retrospective, Australian suburban | All pts who had BCs done in the ED over a 9‐ month period (PNA pts were a subgroup) | None | n = 260; 5%; Not reported | 1% | 1% | 260/1062 study pts had PNA; 14% of all pts discharged; for CAP pts percentage not reported; False‐positive rate 3.8% for all pts, but not reported separately for PNA pts; 1% of PNA pts had abx change due to BCs; type of change not reported, hence reporting of 1% in outcome columns; Cost: $4800 (U.S.) per abx change |
| Chalasani et al.,15 1995; retrospective; U.S. urban | Dx of PNA, respiratory sxms, positive CXR, and 2 sets of BCs before abxs | IC, cancer, hospitalized last 2 weeks, nursing home resident | n = 517; 34 (6.6); 25 (4.8) | 7 (1.4) | 0 (0) | 1250 pts screened with discharge dx of PNA; 59% either ineligible or excluded due to risk factors (authors did not report number ineligible due to the BC requirement); In one case, BCs grew H. influenzae resistant to empiric abxs, but sputum cultures drove the abx change; Cost: $4875 per abx change |
| Woodhead et al.,27 1991; prospective, British urban (2 hospitals) | Clinical features of CAP and positive CXR | IC, cancer, admitted to geriatric or communicable disease ward | n = 86; 9 (10.5%); Not reported | 2 (2.3) | 1 (1.2) | 8% of pts meeting inclusion and exclusion criteria were later excluded due to different dx at discharge |
Included patients were usually required to have clinical features of pneumonia and a confirmatory chest x‐ray. Treating physicians were required to obtain BCs (either by study or hospital protocol) in only 3 studies14, 22, 24 and in a subgroup of another study;11 otherwise the performance of BCs was left to physician discretion.
Nine studies excluded patients who were immunocompromised,11, 15, 17, 18, 2224, 26, 27 a label that was often incompletely defined. Otherwise, exclusion criteria were variable. Notably, only 3 studies excluded patients admitted to the intensive care unit (ICU),11, 18, 24 while 6 excluded patients with cancer15, 17, 2224, 27 and 6 excluded either nursing home residents15, 17, 22, 26 or the elderly (de facto exclusion of most nursing home residents).24, 27
Empiric antibiotic regimens, where reported, were predominantly cephalosporin plus macrolide combinations in 4 studies,17, 2224 fluoroquinolones in 3 studies,11, 14, 26 and penicillin or 1 of its derivatives in 1 study.27
Concerning the 2 studies not included in the primary analysis, the one by Waterer et al.25 was a retrospective review of all cases of pneumococcal bacteremia (n = 74) associated with an admission diagnosis of CAP (N = 1805) in a US urban hospital over a 3‐year period. The one by Chang et al.16 was a retrospective case‐control study of 288 randomly‐selected, immunocompetent Medicare patients with bacteremic pneumococcal CAP who survived to discharge. They were matched 1:1 with blood and sputum culture‐negative controls to study the rate of fluoroquinolone use at discharge in the 2 groups.
Study Findings
Primary Analysis
As shown in Table 1, BCs were positive for a true pathogen in 0% to 14% of cases. Details of microbiology and empiric antibiotic selection are reported in Table 2. S. pneumoniae was by far the most common pathogen: of the 9 studies that had positive BCs and reported the organisms, S. pneumoniae represented 50% to 91% of the pathogens, with penicillin‐resistance found in 0% to 20%.11, 14, 15, 17, 18, 20, 22, 23, 26 S. aureus was next most common, occurring in 6 studies and growing in 3% to 23% of positive BCs;11, 14, 17, 20, 23, 26 its sensitivity to methicillin was reported in 3 studies, with methicillin‐resistant S. aureus (MRSA) representing 0/3, 3/7, and 1/1 of cases.14, 20, 23 E. coli represented 3% to 11% of pathogens in 6 studies,11, 14, 15, 20, 23, 26 while H. influenzae represented 2% to 15% of pathogens in 7 studies.11, 14, 15, 18, 22, 23, 26
| Study: Author, Year | Empiric Antibiotics Given: Frequency, Agent | Bacteria Isolated in True‐Positive BCs: n, Organism | Organisms in BCs Resistant to Empiric Antibiotics |
|---|---|---|---|
| |||
| Benenson et al.,14 2007 | Mild to moderate PNA: levofloxacin; If ICU admission: levofloxacin + azithromycin; If HCAP: levofloxacin + clindamycin; If risk for MRSA: added vancomycin; If structural lung disease: added tobramycin | 14 S. pneumoniae; 3 S. aureus (all MSSA); 2 Group B Strep; 2 H. influenzae; 1 E. coli; 1 Group A Strep | None |
| Ramanujam and Rathlev,22 2006 | Ceftriaxone + oral azithromycin | 11 S. pneumoniae (1 PCN interm res); 2 H. influenzae | None |
| Mountain et al.,21 2006 | Not reported | Not reported completely | None |
| Kennedy et al.,20 2005 | Not reported | 15 S. pneumoniae (3 PCN res); 7 S. aureus (3 MRSA); 3 E. coli; 1 Coagulase‐negative Staph; 1 Pseudomonas; 1 Proteus; 1 Moraxella; 1 E. faecalis | 2 MRSA; 1 MSSA (res to levofloxacin, clindamycin); 1 E. coli (res to levofloxacin) |
| Corbo et al.,17 2004 | 48% ceftriaxone + macrolide; 21% cephalosporin only; 6% quinolone only | 30 S. pneumoniae; 2 S. aureus (# MRSA not reported); 1 Staph haemolyticus | None |
| Campbell et al.,11 2003 | 55% levofloxacin; 45% antibiotic not reported | 30 S. pneumoniae (1 PCN res); 5 S. aureus (total # MRSA not reported); 5 E. coli; 1 H. influenzae; 1 E. faecalis; 1 K. pneumoniae; 1 Enterobacter | 1 MRSA (antibiotic changed before BC results available); 1 MSSA (res not reported); 1 S. pneumoniae (PCN res) |
| Waterer and Wunderink,26 2001 | 60% quinolone only; 25% quinolone + other antibiotic(s) | 20 S. pneumoniae (3 PCN res); 3 S. viridans; 1 H. influenzae; 1 S. aureus (# MRSA not reported); 1 Enterobacter; 1 E. coli; 1 Group B Strep; 1 Group D Strep; 1 Group G Strep; 1 Acinetobacter | 1 Group D Strep (res to levofloxacin) |
| Theerthakarai et al.,24 2001 | Cephalosporin + macrolide | None | None |
| Sanyal et al.,23 1999 | Severe CAP: erythromycin + ceftazidime or ticarcillin/clavulanate; Nonsevere CAP: 76% cefuroxime + erythromycin, 18% cefuroxime only | 14 S. pneumoniae (0 PCN res); 2 H. influenzae; 1 S. aureus (MRSA); 1 K. pneumoniae; 1 E. coli | 1 MRSA |
| Glerant et al.,18 1999 | Not reported | 4 S. pneumoniae (0 PCN res); 1 H. influenzae | None |
| Kelly,19 1998 | Not reported | Not reported | Cannot determine |
| Chalasani et al.,15 1995 | Not reported | 29 S. pneumoniae (0 PCN res); 3 H. influenzae; 1 S. pyogenes; 1 E. coli | H. influenzae (sputum culture drove the antibiotic change) |
| Woodhead et al.,27 1991 | 78% included penicillin, aminopenicillin, or amoxicillin/clavulanate; 33% included erythromycin; 21% ‐lactam + erythromycin | Not reported separately for BCs | E. coli (res to erythromycin) |
| Chang et al.,16 2005 | BC+/Controls: 34%/21%/Quinolones; 86%/88%/ ‐lactam; 1%/1%/Amox/PCN; 38%/37%/ Macrolide | 288 S. pneumoniae (only organism, by design) | Not reported |
| Waterer et al.,25 1999 | 38% Cephalosporin + macrolide other; 27% Quinolone other | 74 S. pneumoniae (only organism, by design); 11 PCN interm res; 4 PCN res | 2 S. pneumoniae (both resistant; degree of resistance not specified) |
In the 8 studies that reported false‐positive BCs, the false‐positive rate was 0% to 10%,14, 15, 17, 18, 20, 22, 24, 26 with 5 studies finding comparable false‐positive and true‐positive BC rates15, 17, 20, 22, 24 and 1 study finding a substantially higher frequency of false‐positive than true‐positive BCs (Table 1).14
BCs led to narrowing of antibiotic coverage in 0% to 3% of cases (Table 1). Four studies reported that physicians narrowed antibiotics when BCs indicated that it was possible to do so, but only in 10%, 14%, 34%, and 58% of eligible cases.11, 14, 20, 22
BCs led to antibiotic broadening ultimately associated with a resistant organism in 0% to 1% of cases (Table 1). The pathogens were MRSA (3), methicillin‐sensitive S. aureus (2), E. coli (2), S. pneumoniae (1), and Group D Streptococcus (1). Details about these patients' medical histories and demographics were absent or sparse in all but 1 study.20 For several of the above cases it was not explicitly stated that BCs directed the antibiotic changes, though it was usually implied; thus we assumed causation.
Secondary Analyses
In the pneumococcal bacteremia study by Waterer et al.,25 BCs altered management in 31 of the 74 cases of pneumococcemia, but in only 2 patients was this associated with antibiotic resistance. Most of the other 29 cases involved narrowing of antibiotics, though switching to penicillin or dropping atypical coverage occurred in only 22% and 37% of eligible patients, respectively. In the study by Chang et al.,16 there was no significant difference in fluoroquinolone use at discharge between the pneumococcemic and culture‐negative groups (the primary endpoint), though there was significantly higher ‐lactam use and lower macrolide use in the pneumococcemic patients at discharge. From the data provided it was not possible to determine how often antibiotic broadening occurred.
Only 2 of the 15 studies stratified management effects based on severity of illness, and neither specified the proportion of severely ill patients admitted to the ICU. Waterer and Wunderink26 prospectively hypothesized that sicker patients were more likely to benefit from BCs. They found that the 30 patients in pneumonia severity index class 5 were most likely to have a BC‐driven antibiotic change, though in at most 1 of these patients was associated with a resistant organism. Sanyal et al.23 stratified patients by severity based on expert guidelines. They found that 19 of 174patients had severe CAP that did not respond to the initial antibiotic regimen, with 1 having a BC‐driven antibiotic change; this was due to resistance.
Only 1 study reported an outcome other than antibiotic change, which in this case was duration of parenteral therapy. In the study, 5 of 43 patients with true‐positive BCs remained on intravenous antibiotics for the full course of treatment probably due to bacteremia alone.11
The direct cost of BCs per BC‐directed antibiotic change (or total cost of BCs if there was no antibiotic change) was reported in 6 studies and, not adjusted for inflation, ranged from $1550 to $8000 (U.S.).11, 15, 18, 19, 21, 22
Quality of the Studies
A detailed listing of the strengths and weaknesses of each study is provided in the Appendix. Briefly, all 15 studies included in this review were observational. Most did not prospectively require BCs in all patients admitted with CAP. This could have biased the results in favor of BC utility as physicians presumably order BCs in patients with a higher probability of bacteremia. Conversely, several studies did not explicitly require two sets of BCs or that BCs be done prior to antibiotics, so they may not have revealed the maximum utility of BCs. The 2 studies limited to pneumococcal bacteremia and described in the secondary analysis were inherently biased against BC utility, as pneumococcus is more likely to be antibiotic‐sensitive than other CAP pathogens.
Eligibility was based only on an emergency department (ED)/admission diagnosis of CAP, a criteria that approximates real world practice, in 3 studies.19, 21, 25 The other studies required either a confirmatory radiograph or a hospital discharge diagnosis of pneumonia. Consequent ED/admission misdiagnosis rates were 3%, 8%, 11%, 24% in the 4 studies that reported them;14, 17, 22, 27 the final diagnoses, when reported, were nearly all noninfections or proximal respiratory tract infections.22, 27
Five studies included all eligible patients.14, 1921, 25 However, 3 studies excluded 23%, 31%, and 62% of eligible patients based on risk factors for bacteremia or resistant pathogens,17, 22, 24 and the rest did not report the number excluded.
DISCUSSION
Summary of Findings
Our systematic review of the literature finds that BCs rarely alter empiric antibiotic therapy in adults hospitalized with community‐acquired pneumonia. Even when there is a change in treatment it usually is not of the type most likely to impact patient outcome, which is antibiotic broadening ultimately associated with a resistant organism. In the 13 studies that could quantify this effect, it occurred in only 0% to 1% of cases in which BCs were obtained. Antibiotic narrowing occurred in 0% to 3% of cases, with physicians often choosing not to narrow antibiotics when BC results suggested that they could do so.
Limits on BC Utility
‐Lactam‐Resistant Pneumococcus
In the studies reviewed here 50%‐90% of positive BCs grew pneumococcus, consistent with the 60% to 67% rate reported elsewhere.2, 28, 29 Pneumococci that invade the bloodstream have disproportionately low rates of ‐lactam resistance,30, 31 inherently limiting the utility of BCs for detecting inadequate empiric antibiotic therapy. Though pneumococcal resistance to ‐lactams has risen over the last 2 decades, third‐generation cephalosporins, preferred agents for CAP, are still extremely effective. Even when the organism is by historical standards moderately resistant to them, these cephalosporins at standard doses maintain bactericidal efficacy in the lung,32, 33 and their use in the setting of such resistance is not associated with higher mortality.3437 By newer laboratory standards 97% and 96% of S. pneumoniae isolates in mid‐2003 were sensitive to ceftriaxone and cefotaxime, respectively.38 Thus a major potential benefit of BCsdetecting cephalosporin‐resistant pneumococcusremains a rare occurrence.
Polymicrobial Infection
If positive BCs in CAP mostly reveal antibiotic‐sensitive pathogens, one may infer that at least they lead to narrowing of therapy. However, the studies reviewed here reveal that this usually does not happen.
One explanation for this reluctance to narrow antibiotics is that CAP is often a polymicrobial disease. When rigorous serologic testing is done, multiple pathogens are found in up to 40% of cases.39 The occult copathogen is frequently an intracellular one and thus cannot be detected by BCs. Though the evidence for empirically treating these atypical organisms is mixed,40, 41 expert guidelines recommend doing so,12 and guideline‐concordant antibiotic therapy in CAP is associated with lower mortality.42 Even in bacteremic pneumococcal CAP, monotherapy is associated with higher mortality.4346 Thus, stopping antibiotic coverage of atypical pathogens in response to BCs alone might not always be appropriate.
Prognosis
Another rationale given for ordering BCs is that bacteremic pneumonia is a morbid disease so positive BCs may demand prolonged parenteral therapy or extended hospitalization. Although mortality for bacteremic pneumococcal pneumonia (the predominantly studied variety of bacteremic pneumonia) has historically been high at 20%,47, 48 studies that have examined pneumococcal bacteremia as an independent risk factor for death in CAP have yielded mixed results.2 Moreover, it appears that patients with bacteremic pneumococcal pneumonia who reach clinical stability may be safely switched to oral antibiotics.49
It is not clear that positive BCs in pneumonia (at least in the case of S. pneumoniae) should alter the duration of parenteral therapy or hospitalization, though whether or not such effects occur in clinical practice was largely unaddressed by the studies reviewed here.
Epidemiology
One theoretical benefit of BCs is their epidemiologic value. When true‐positive in pneumonia, perhaps more than any other test they identify with great specificity at least 1 of the causative agents. Unfortunately, as discussed above, BCs alone provide an incomplete and skewed picture of the microbiology of CAP. They underestimate atypical organisms, overestimate pneumococcus, and, because bacteremic pneumococcus is more likely to be antibiotic‐susceptible, they underestimate antibiotic resistance.11 Tracking pathogens in bacteremic pneumonia may be useful nonetheless, but perhaps a more accurate method for determining etiologic trends is periodic comprehensive microbiological investigation, including BCs, sputum/bronchial cultures, and serology.
Costs
In the studies reviewed here, based on reported costs of $15 to $65 per set of BCs or per patient, BCs cost $1550 to $8000 (U.S.) per BC‐directed antibiotic change. Considering that very few of these antibiotic changes involved broadening associated with a resistant organism, the cost/benefit ratio was quite high. Today BCs may be even more expensive, as U.S. hospitals now often charge over $150 per set of BCs.50, 51
The cost of false‐positive BCs must also be taken into account. The false‐positive rate in the studies reviewed here was 0% to 10%, similar to that reported elsewhere.7 False‐positive BCs increase hospital length of stay by 3 to 5 days and hospital charges by $4400 to $8800.51, 52
Limitations of the Review
Our search strategy was designed to be sensitive and included backup methods such as searching article references and querying experts. Nevertheless, we may have missed studies, especially if there were small eligible subgroups or if determining management effects was not a primary purpose. We chose not to measure instances of antibiotic broadening that were not associated with a resistant organism, though in unusual cases (eg, Pseudomonas bacteremia) this effect of BCs may be useful.
The methodologies of the included studies were adequate to measure the key outcomes with reasonable validity. Biases were evident, though they occurred both for and against BC utility.
Eligibility varied across studies, and most investigations excluded immunocompromised or other high‐risk patient groups, which could have biased results against BC utility. However, results of these studies were consistent with those that included all patients with CAP, suggesting the degree of bias was probably small. Still, given this concern, it would be prudent not to generalize the findings of this review to immunocompromised patients. Moreover, although the critically ill and those who today would be classified as having healthcare‐associated pneumonia (HCAP)nursing home residents, the recently hospitalized, and hemodialysis patientswere included in most studies, their numbers were small, and these groups were not analyzed separately; thus, the results might not be generalizable to these populations either. Finally, the reported studies, which enrolled patients through 2003, do not reflect more recent increases in the prevalence of resistant pathogens, such as MRSA, in the community.
BCs as a Quality Measure
The adoption of BCs as a quality measure was largely predicated on the widely‐cited study by Meehan et al.,4 which showed an association between BC obtainment and reduced mortality. This study, which associated processes of care with hard outcomes such as mortality, was limited by uncontrolled confounders, including variation in hospital quality.53 A more recent study of pneumonia processes of care found no association between BC collection and mortality.54 Another study often cited to support BC use, by Arbo and Snydman,55 showed that positive BCs were associated with changes in antibiotic therapy, but it included very few pneumonia patients and did not describe results for them separately.
The inclusion of BC acquisition in 2 quality measures in the NHQM guidelines for pneumonia impacts the clinical practice of hospitals and physicians, which may be rated and reimbursed differentially based on their compliance with such measures. One of the quality measures requires BCs in patients admitted to the ICU. The other requires that ED BCs for pneumonia, if obtained, be drawn before antibiotics are given.6
The studies we reviewed are not specific to these quality measures, but are relevant to them. With regard to the first measure, all but 3 studies included patients admitted to the ICU and found BCs to be of minimal benefit overall. Our subgroup analysis of severely ill patients was unrevealing. The ICU measure is tentative in its validity, but it is not unreasonable given that these patients have a life‐threatening infection and may be at risk for bacteremia with resistant pathogens.12
The second measure, though perhaps simply seeking to maximize the potential for BCs to turn positive, depends for its validity on BCs being useful in a large proportion of patients with CAP. Though we cannot exclude the possibility that BCs benefit certain subsets of patients, such as those who are immunocompromised or have HCAP, our findings do not support obtaining BCs in all or even most adults hospitalized with CAP. This conclusion is reflected in the 2007 Infectious Diseases Society of America/American Thoracic Society management guidelines for CAP, which state than BCs are optional except for patients with severe pneumonia, some immunocompromised states, and particular radiographic abnormalities.12
With such data and guidelines in mind, a physician seeking to minimize treatment delays in a patient with pneumonia may give antibiotics early in the ED course (the basis of another quality measure) without obtaining BCs. If she later determines that the patient is particularly high‐risk for bacteremia or a resistant pathogen, should she be discouraged from ordering BCs? Experts specifically state that BCs, even after antibiotics, are warranted for such a patient.12
With the scope of medical practice captured in quality measures being so narrow, having 2 measures based on a test with such limited benefit is itself questionable.
- ,,,,,.Practice guidelines for the management of community‐acquired pneumonia in adults. Infectious diseases society of America.Clin Infect Dis.2000;31:347–382.
- ,,,,.Canadian guidelines for the initial management of community‐acquired pneumonia: an evidence‐based update by the Canadian infectious diseases society and the Canadian thoracic society. The Canadian community‐acquired pneumonia working group.Clin Infect Dis.2000;31:383–421.
- ,,, et al.Guidelines for the management of adults with community‐acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention.Am J Respir Crit Care Med.2001;163:1730–1754.
- ,,, et al.Quality of care, process, and outcomes in elderly patients with pneumonia.JAMA.1997;278:2080–2084.
- Hospital quality initiative, overview, centers for Medicare and Medicaid services. Available at: http://www.cms.hhs.gov/HospitalQualityInits. Accessed September2007.
- Specifications manual for national hospital quality measures, version 2.3b. Available at: http://www.jointcommission.org/PerformanceMeasurement/PerformanceMeasurement/Current+NHQM+Manual.htm. Accessed October2007.
- ,,,.Predicting bacteremia in patients with community‐acquired pneumonia.Am J Respir Crit Care Med.2004;169:342–347.
- ,.The joint commission on accreditation of healthcare organizations and center for Medicare and Medicaid services community‐acquired pneumonia initiative: what went wrong?Ann Emerg Med.2005;46:409–411.
- .Blood cultures in community‐acquired pneumonia: Are we ready to quit?Chest.2003;123:977–978.
- .Blood cultures for community‐acquired pneumonia: piecing together a mosaic for doing less.Am J Respir Crit Care Med.2004;169:327–328.
- ,,,,.The contribution of blood cultures to the clinical management of adult patients admitted to the hospital with community‐acquired pneumonia: a prospective observational study.Chest.2003;123:1142–1150.
- ,,, et al.Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community‐acquired pneumonia in adults.Clin Infect Dis.2007;44 (Suppl 2):S27–S72.
- ,,,,,.Value of routine microbial investigation in community‐acquired pneumonia treated in a tertiary care center.Respiration.1996;63:164–169.
- ,,,.Selective use of blood cultures in emergency department pneumonia patients.J Emerg Med.2007;33:1–8.
- ,,,,.Clinical utility of blood cultures in adult patients with community‐acquired pneumonia without defined underlying risks.Chest.1995;108:932–936.
- ,,,,,.Blood culture and susceptibility results and allergy history do not influence fluoroquinolone use in the treatment of community‐acquired pneumonia.Pharmacotherapy.2005;25:59–66.
- ,,,.Limited usefulness of initial blood cultures in community acquired pneumonia.Emerg Med J.2004;21:446–448.
- ,,,,.Utility of blood cultures in community‐acquired pneumonia requiring hospitalization: Influence of antibiotic treatment before admission.Respir Med.1999;93:208–212.
- .Clinical impact of blood cultures taken in the emergency department.J Accid Emerg Med.1998;15:254–256.
- ,,,,,.Do emergency department blood cultures change practice in patients with pneumonia?Ann Emerg Med.2005;46:393–400.
- ,,,.Blood cultures ordered in the adult emergency department are rarely useful.Eur J Emerg Med.2006;13:76–79.
- ,.Blood cultures do not change management in hospitalized patients with community‐acquired pneumonia.Acad Emerg Med.2006;13:740–745.
- ,,,,,.Initial microbiologic studies did not affect outcome in adults hospitalized with community‐acquired pneumonia.Am J Respir Crit Care Med.1999;160:346–348.
- ,,,,.Nonvalue of the initial microbiological studies in the management of nonsevere community‐acquired pneumonia.Chest.2001;119:181–184.
- ,,.The impact of blood cultures on antibiotic therapy in pneumococcal pneumonia.Chest.1999;116:1278–1281.
- ,.The influence of the severity of community‐acquired pneumonia on the usefulness of blood cultures.Respir Med.2001;95:78–82.
- ,,,,.The value of routine microbial investigation in community‐acquired pneumonia.Respir Med.1991;85:313–317.
- ,,, et al.Study of community acquired pneumonia aetiology (scapa) in adults admitted to hospital: implications for management guidelines.Thorax.2001;56:296–301.
- ,.Etiology of community‐acquired pneumonia.Clin Chest Med.2005;26:47–55.
- ,,,,.Early predictors of mortality in pneumococcal bacteraemia.Ann Acad Med Singapore.2005;34:426–431.
- ,,,.Penicillin‐nonsusceptible Streptococcus pneumoniae at San Francisco general hospital.Clin Infect Dis.1999;29:580–585.
- .Pharmacokinetic/pharmacodynamic parameters: Rationale for antibacterial dosing of mice and men.Clin Infect Dis.1998;26:1–10; quiz 11–12.
- .The significance of serum vs tissue levels of antibiotics in the treatment of penicillin‐resistant Streptococcus pneumoniae and community‐acquired pneumonia: are we looking in the wrong place?Chest.1999;116:535–538.
- ,,, et al.Pneumonia acquired in the community through drug‐resistant Streptococcus pneumoniae.Am J Respir Crit Care Med.1999;159:1835–1842.
- ,,, et al.The effect of cephalosporin resistance on mortality in adult patients with nonmeningeal systemic pneumococcal infections.Am J Med.2002;113:120–126.
- ,,, et al.Resistance to penicillin and cephalosporin and mortality from severe pneumococcal pneumonia in Barcelona, Spain.N Engl J Med.1995;333:474–480.
- ,,, et al.An international prospective study of pneumococcal bacteremia: correlation with in vitro resistance, antibiotics administered, and clinical outcome.Clin Infect Dis.2003;37:230–237.
- ,,,,,.Tracking the implementation of NCCLS m100‐s12 expanded‐spectrum cephalosporin MIC breakpoints for non‐meningeal isolates of Streptococcus pneumoniae by clinical laboratories in the united states during 2002 and 2003.Ann Clin Microbiol Antimicrob.2004;3:1.
- ,,, et al.Multiple pathogens in adult patients admitted with community‐acquired pneumonia: a one year prospective study of 346 consecutive patients.Thorax.1996;51:179–184.
- ,,,,.How good is the evidence for the recommended empirical antimicrobial treatment of patients hospitalized because of community‐acquired pneumonia? A systematic review.J Antimicrob Chemother.2003;52:555–563.
- ,,,.Empirical atypical coverage for inpatients with community‐acquired pneumonia: systematic review of randomized controlled trials.Arch Intern Med.2005;165:1992–2000.
- ,,,.Impact of guideline‐concordant empiric antibiotic therapy in community‐acquired pneumonia.Am J Med.2006;119:865–871.
- ,,, et al.Combination antibiotic therapy lowers mortality among severely ill patients with pneumococcal bacteremia [see comment].Am J Respir Crit Care Med.2004;170:440–444.
- ,,, et al.Addition of a macrolide to a beta‐lactam‐based empirical antibiotic regimen is associated with lower in‐hospital mortality for patients with bacteremic pneumococcal pneumonia. [see comment].Clin Infect Dis.2003;36:389–395.
- ,,.Monotherapy may be suboptimal for severe bacteremic pneumococcal pneumonia.Arch Intern Med.2001;161:1837–1842.
- ,,, et al.Clinical characteristics at initial presentation and impact of dual therapy on the outcome of bacteremic Streptococcus pneumoniae pneumonia in adults.Can Respir J.2004;11:589–593.
- ,.Pneumococcal bacteremia with special reference to bacteremic pneumococcal pneumonia.Arch Intern Med.1964;60:759–776.
- ,,, et al.Prognosis and outcomes of patients with community‐acquired pneumonia. A meta‐analysis.JAMA.1996;275:134–141.
- ,.Early switch from intravenous to oral antibiotics in hospitalized patients with bacteremic community‐acquired Streptococcus pneumoniae pneumonia.Arch Intern Med.2001;161:848–850.
- Cleveland Clinic patient price information list. Available at:http://cms.clevelandclinic.org/documents/CCMain_HB197_2007.pdf. Accessed January2008.
- ,.Analysis of strategies to improve cost effectiveness of blood cultures.J Hosp Med.2006;1:272–276.
- ,,.Contaminant blood cultures and resource utilization. The true consequences of false‐positive results.JAMA.1991;265:365–369.
- ,,,,.Patient and hospital characteristics associated with recommended processes of care for elderly patients hospitalized with pneumonia: results from the Medicare quality indicator system pneumonia module.Arch Intern Med.2002;162:827–833.
- ,,,,.Processes of care, illness severity, and outcomes in the management of community‐acquired pneumonia at academic hospitals.Arch Intern Med.2001;161:2099–2104.
- ,.Influence of blood culture results on antibiotic choice in the treatment of bacteremia.Arch Intern Med.1994;154:2641–2645.
- ,,,,,.Practice guidelines for the management of community‐acquired pneumonia in adults. Infectious diseases society of America.Clin Infect Dis.2000;31:347–382.
- ,,,,.Canadian guidelines for the initial management of community‐acquired pneumonia: an evidence‐based update by the Canadian infectious diseases society and the Canadian thoracic society. The Canadian community‐acquired pneumonia working group.Clin Infect Dis.2000;31:383–421.
- ,,, et al.Guidelines for the management of adults with community‐acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention.Am J Respir Crit Care Med.2001;163:1730–1754.
- ,,, et al.Quality of care, process, and outcomes in elderly patients with pneumonia.JAMA.1997;278:2080–2084.
- Hospital quality initiative, overview, centers for Medicare and Medicaid services. Available at: http://www.cms.hhs.gov/HospitalQualityInits. Accessed September2007.
- Specifications manual for national hospital quality measures, version 2.3b. Available at: http://www.jointcommission.org/PerformanceMeasurement/PerformanceMeasurement/Current+NHQM+Manual.htm. Accessed October2007.
- ,,,.Predicting bacteremia in patients with community‐acquired pneumonia.Am J Respir Crit Care Med.2004;169:342–347.
- ,.The joint commission on accreditation of healthcare organizations and center for Medicare and Medicaid services community‐acquired pneumonia initiative: what went wrong?Ann Emerg Med.2005;46:409–411.
- .Blood cultures in community‐acquired pneumonia: Are we ready to quit?Chest.2003;123:977–978.
- .Blood cultures for community‐acquired pneumonia: piecing together a mosaic for doing less.Am J Respir Crit Care Med.2004;169:327–328.
- ,,,,.The contribution of blood cultures to the clinical management of adult patients admitted to the hospital with community‐acquired pneumonia: a prospective observational study.Chest.2003;123:1142–1150.
- ,,, et al.Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community‐acquired pneumonia in adults.Clin Infect Dis.2007;44 (Suppl 2):S27–S72.
- ,,,,,.Value of routine microbial investigation in community‐acquired pneumonia treated in a tertiary care center.Respiration.1996;63:164–169.
- ,,,.Selective use of blood cultures in emergency department pneumonia patients.J Emerg Med.2007;33:1–8.
- ,,,,.Clinical utility of blood cultures in adult patients with community‐acquired pneumonia without defined underlying risks.Chest.1995;108:932–936.
- ,,,,,.Blood culture and susceptibility results and allergy history do not influence fluoroquinolone use in the treatment of community‐acquired pneumonia.Pharmacotherapy.2005;25:59–66.
- ,,,.Limited usefulness of initial blood cultures in community acquired pneumonia.Emerg Med J.2004;21:446–448.
- ,,,,.Utility of blood cultures in community‐acquired pneumonia requiring hospitalization: Influence of antibiotic treatment before admission.Respir Med.1999;93:208–212.
- .Clinical impact of blood cultures taken in the emergency department.J Accid Emerg Med.1998;15:254–256.
- ,,,,,.Do emergency department blood cultures change practice in patients with pneumonia?Ann Emerg Med.2005;46:393–400.
- ,,,.Blood cultures ordered in the adult emergency department are rarely useful.Eur J Emerg Med.2006;13:76–79.
- ,.Blood cultures do not change management in hospitalized patients with community‐acquired pneumonia.Acad Emerg Med.2006;13:740–745.
- ,,,,,.Initial microbiologic studies did not affect outcome in adults hospitalized with community‐acquired pneumonia.Am J Respir Crit Care Med.1999;160:346–348.
- ,,,,.Nonvalue of the initial microbiological studies in the management of nonsevere community‐acquired pneumonia.Chest.2001;119:181–184.
- ,,.The impact of blood cultures on antibiotic therapy in pneumococcal pneumonia.Chest.1999;116:1278–1281.
- ,.The influence of the severity of community‐acquired pneumonia on the usefulness of blood cultures.Respir Med.2001;95:78–82.
- ,,,,.The value of routine microbial investigation in community‐acquired pneumonia.Respir Med.1991;85:313–317.
- ,,, et al.Study of community acquired pneumonia aetiology (scapa) in adults admitted to hospital: implications for management guidelines.Thorax.2001;56:296–301.
- ,.Etiology of community‐acquired pneumonia.Clin Chest Med.2005;26:47–55.
- ,,,,.Early predictors of mortality in pneumococcal bacteraemia.Ann Acad Med Singapore.2005;34:426–431.
- ,,,.Penicillin‐nonsusceptible Streptococcus pneumoniae at San Francisco general hospital.Clin Infect Dis.1999;29:580–585.
- .Pharmacokinetic/pharmacodynamic parameters: Rationale for antibacterial dosing of mice and men.Clin Infect Dis.1998;26:1–10; quiz 11–12.
- .The significance of serum vs tissue levels of antibiotics in the treatment of penicillin‐resistant Streptococcus pneumoniae and community‐acquired pneumonia: are we looking in the wrong place?Chest.1999;116:535–538.
- ,,, et al.Pneumonia acquired in the community through drug‐resistant Streptococcus pneumoniae.Am J Respir Crit Care Med.1999;159:1835–1842.
- ,,, et al.The effect of cephalosporin resistance on mortality in adult patients with nonmeningeal systemic pneumococcal infections.Am J Med.2002;113:120–126.
- ,,, et al.Resistance to penicillin and cephalosporin and mortality from severe pneumococcal pneumonia in Barcelona, Spain.N Engl J Med.1995;333:474–480.
- ,,, et al.An international prospective study of pneumococcal bacteremia: correlation with in vitro resistance, antibiotics administered, and clinical outcome.Clin Infect Dis.2003;37:230–237.
- ,,,,,.Tracking the implementation of NCCLS m100‐s12 expanded‐spectrum cephalosporin MIC breakpoints for non‐meningeal isolates of Streptococcus pneumoniae by clinical laboratories in the united states during 2002 and 2003.Ann Clin Microbiol Antimicrob.2004;3:1.
- ,,, et al.Multiple pathogens in adult patients admitted with community‐acquired pneumonia: a one year prospective study of 346 consecutive patients.Thorax.1996;51:179–184.
- ,,,,.How good is the evidence for the recommended empirical antimicrobial treatment of patients hospitalized because of community‐acquired pneumonia? A systematic review.J Antimicrob Chemother.2003;52:555–563.
- ,,,.Empirical atypical coverage for inpatients with community‐acquired pneumonia: systematic review of randomized controlled trials.Arch Intern Med.2005;165:1992–2000.
- ,,,.Impact of guideline‐concordant empiric antibiotic therapy in community‐acquired pneumonia.Am J Med.2006;119:865–871.
- ,,, et al.Combination antibiotic therapy lowers mortality among severely ill patients with pneumococcal bacteremia [see comment].Am J Respir Crit Care Med.2004;170:440–444.
- ,,, et al.Addition of a macrolide to a beta‐lactam‐based empirical antibiotic regimen is associated with lower in‐hospital mortality for patients with bacteremic pneumococcal pneumonia. [see comment].Clin Infect Dis.2003;36:389–395.
- ,,.Monotherapy may be suboptimal for severe bacteremic pneumococcal pneumonia.Arch Intern Med.2001;161:1837–1842.
- ,,, et al.Clinical characteristics at initial presentation and impact of dual therapy on the outcome of bacteremic Streptococcus pneumoniae pneumonia in adults.Can Respir J.2004;11:589–593.
- ,.Pneumococcal bacteremia with special reference to bacteremic pneumococcal pneumonia.Arch Intern Med.1964;60:759–776.
- ,,, et al.Prognosis and outcomes of patients with community‐acquired pneumonia. A meta‐analysis.JAMA.1996;275:134–141.
- ,.Early switch from intravenous to oral antibiotics in hospitalized patients with bacteremic community‐acquired Streptococcus pneumoniae pneumonia.Arch Intern Med.2001;161:848–850.
- Cleveland Clinic patient price information list. Available at:http://cms.clevelandclinic.org/documents/CCMain_HB197_2007.pdf. Accessed January2008.
- ,.Analysis of strategies to improve cost effectiveness of blood cultures.J Hosp Med.2006;1:272–276.
- ,,.Contaminant blood cultures and resource utilization. The true consequences of false‐positive results.JAMA.1991;265:365–369.
- ,,,,.Patient and hospital characteristics associated with recommended processes of care for elderly patients hospitalized with pneumonia: results from the Medicare quality indicator system pneumonia module.Arch Intern Med.2002;162:827–833.
- ,,,,.Processes of care, illness severity, and outcomes in the management of community‐acquired pneumonia at academic hospitals.Arch Intern Med.2001;161:2099–2104.
- ,.Influence of blood culture results on antibiotic choice in the treatment of bacteremia.Arch Intern Med.1994;154:2641–2645.
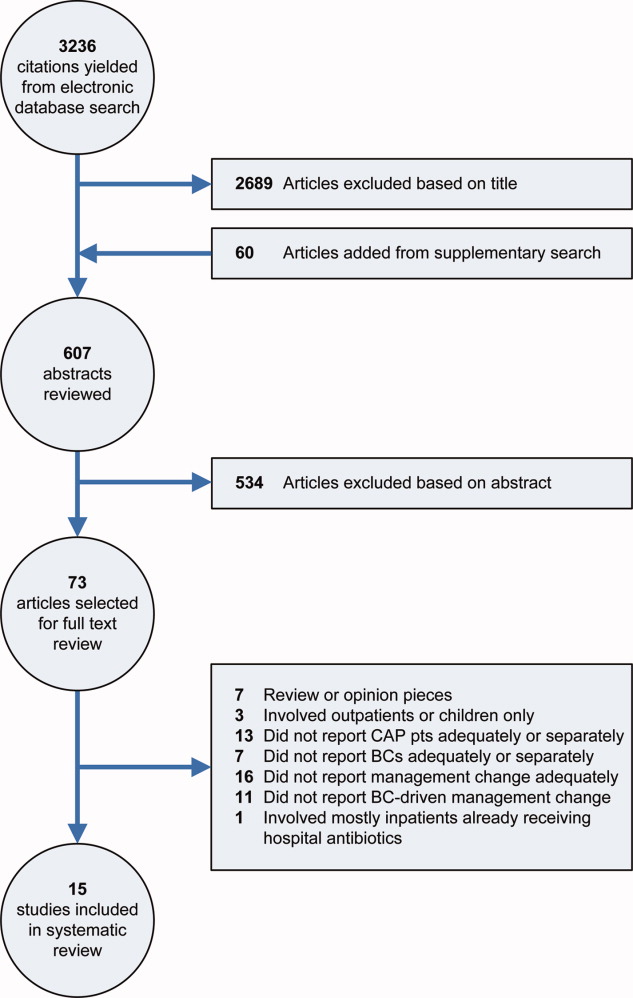
Adverse Effects to Antibiotics in Pheumonia
Adverse drug eventsdefined as an injury resulting from medical intervention related to a drug1significantly contribute to health care expenditures. Over 770,000 people are injured or die every year in hospitals from adverse drug events, and national hospital expenses to treat patients who have suffered adverse drug events during hospitalization have been estimated to be between $1.56 and $4.2 billion annually.2 In a meta‐analysis of prospective studies, researchers found that adverse drug reactions, one important form of adverse drug events, may rank as the fourth to sixth leading cause of death in the United States, with more than 100,000 deaths per year.3 Understanding the factors associated with these adverse events may help in the development of prevention strategies, with resulting improving health care quality and lowering health care costs.
Among hospitalized patients, antibacterial adverse effects may account for approximately 25% of adverse drug reactions.1, 4 While the economic impact has been studied for overall adverse drug events in hospitalized patients in the 1990s, more recent detailed studies for the impact of antibiotic‐related adverse drug effects have not been published. As hospitalized patients with the primary diagnosis of pneumonia are invariably treated with antibiotics, and since pneumonia is the third leading cause for hospitalization in the United States,5 hospitalization databases that document pneumonia hospitalizations as well as adverse effects from antibiotics, using specific International Classification of Diseases, Ninth Revision (ICD‐9) clinical modification codes, constitute a unique and rich resource for quantifying and analyzing the incidence and impact of antibiotic‐associated adverse drug effects.
The purpose of this study was to describe the incidence and clinical manifestations of adverse drug effects in pneumonia hospitalizations in recent years, and to determine the types of patients and comorbidities, which are most commonly associated with adverse drug effects. The term adverse drug effect refers more to known side effects of medications, whereas adverse drug events and adverse drug reactions refer to an injury or a noxious, unintended, and undesired effect resulting from administration of a drug.6 As this study utilized medical coding for data abstraction, the broader classifications of adverse drug events or reactions could not be examined and instead the outcome of adverse drug effect was utilized.
METHODS
Data Sources
The Statewide Planning and Research Cooperative System (SPARCS) database was accessed as previously described.7, 8 There is mandatory reporting to this database for all New York State acute care hospitalizations. Each deidentified SPARCS admission record contains more than 100 data fields9 that consist of demographic, clinical, and financial information. These fields include principal and nonprincipal diagnostic fields, procedure codes, race, age, gender, and ethnicity information, hospital characteristics, expected reimbursement, total charges, length of stay (LOS), admission status, and disposition status. Both ICD‐9 and Common Procedural Terminology (CPT) codes are input for each admission.
The Nationwide Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project (HCUP), contains annual hospital discharge data from a sample of US hospitals.10 Each NIS patient record includes data fields consisting of demographic, clinical, and financial information. These fields include primary and secondary diagnostic fields, procedure codes, age, gender, race, total charges, length of stay, payer codes, hospital characteristics, and disposition status. Twenty percent random subsamples from each year's sample were employed to perform the analyses. HCUP databases include appropriately‐scaled discharge weights to generate national estimates of hospitalizations and total charges from the NIS. These weights allow comparison of incidence rates and charges across years despite a varying number of states and hospitals included in the database each year.
This study was given an exemption from institutional research board approval by the SVCMC Integrated Scientific and Ethical Review Board.
Identification of Pneumonia Admissions
To achieve more uniformity in the cohorts, it was decided to select only hospitalizations with the most common ICD‐9 and diagnosis‐related group (DRG) codes for pneumonia for more recent years. ICD‐9 and DRG codes have been used to identify pneumonia patients in administrative data, and cases selected in this manner show excellent specificity when compared to a reference standard.11 Hospitalization discharges from both databases from 2000 through 2005 were selected with the criterion of having the principal diagnosis of ICD‐9 code 486 (pneumonia, organism unspecified) and the DRG of 89 (simple pneumonia and pleurisy, age >17 years, with complication and comorbidity), thus targeting community acquired pneumonia. These hospitalizations formed the 2 cohorts of pneumonia hospitalizations. Preliminary analyses showed that hospitalizations identified by these criteria identified more than 60% of pneumonia admissions defined by a more expansive criteria11 of having any of the DRG codes 79 (respiratory infections and inflammations, age >17 years, with complications and comorbidity), 80 (respiratory infections and inflammations, age >17 years, without complications and comorbidity), 89 and 90 (simple pneumonia and pleurisy, age >17 years, without complication and comorbidity). Gram‐negative pneumonia, aspiration pneumonia, and pneumonias due to other specific infectious agents were not targeted in this study.
Data Classifications
The state and national cohorts were queried for the presence of adverse effects due to various antibiotics and anti‐infectives, using specific ICD‐9 external cause of injury codes (e‐codes) including e930 and e931. E‐codes were developed as a supplemental code for use with the ICD and they provide a systematic way to classify diagnostic information that health care providers have entered into the medical record. E‐codes have been shown to be useful and sensitive in detecting medical injuries due to drugs (including antibiotics) in hospital discharge data.12 On the basis of frequency of observed adverse drug effects (as detected by e‐codes), an adverse drug effect due to an anti‐infective or antibiotic was defined as that which was due to penicillins (E930.0), erythromycin and other macrolides (E930.3), tetracyclines (E930.5), cephalosporins (E930.5), sulfonamides (E931.0), quinolones (E931.3), other specified antibiotics (E930.9), other unspecified antibiotics (E931.9), or antimycobacterials (E931.8 and E930.6). Adverse drug effects due to other anti‐infectives were not included due to extremely low incidence and unlikely clinical usage in pneumonia. National estimates of the number of patients experiencing an adverse drug effect were determined using discharge weights to adjust for subset sample size.
The ICD‐9 codes for possible skin and allergy manifestations commonly associated with adverse drug effects were examined in patients with and without adverse drug effects as defined previously. The ICD‐9 codes for skin/allergy manifestations that were considered as possibly due to adverse drug effects included erythema, not otherwise specified (695.9), flushing (782.62), Stevens‐Johnson syndrome (695.1), allergic purpura (287.0), dermatitis due to drugs and medications taken internally (693.0), angioedema (995.1), unspecified allergy, (995.3), anaphylaxis not otherwise specified (NOS) (999.5), and urticaria (708). Gastrointestinal (GI) manifestations considered as possibly due to an adverse drug effect included nausea (787.02), vomiting (787.03), nausea with vomiting (787.01), diarrhea, not otherwise specified (787.91), diarrhea, other and unspecified noninfectious gastroenteritis and colitis (558.9), or intestinal infection due to Clostridium difficile (008.45).
Statistical Analysis
Analyses were performed using JMP version 5.1 and SAS for Windows version 9 (SAS Institute, Cary, NC). In linear regression models, principal outcomes of length of stay and total hospital charges were logarithmically transformed, as this data transformation reduces the influence of outliers.13 Cases with a length of stay less than 1 day were considered to have a 23‐hour LOS, to enable logarithmic transformation. Linear regression models were created to assess the impact of adverse drug effects due to antibiotics on length of stay and total charge. Linear regression models have been shown to be useful in identifying factors associated with increased hospital charges.13 Adjusting factors that were considered in multivariate models included comorbid conditions and demographic factors. Only common comorbidities that were present in greater than 5% of cases were considered and included cancer (140 through 208), congestive heart failure (428), ischemic heart disease (410414), chronic obstructive pulmonary disease (491, 492, 496), diabetes mellitus (250), hypertension (401), asthma (493), urinary tract infection (599.0), unspecified anemia (285.9), pleural effusion (511.9), cardiac dysrhythmia (427.31), volume depletion (276.5), unspecified acquired hypothyroidism (244.9), and hypoosmolality/hyponatremia (276.1). Demographic factors such as gender, race, age, year and month of admission, and day of admission were also considered in the model. The hospital where the admission occurred was used for New York State calculations. For the national data, the region and hospital characteristics but not the hospital identification number itself were considered since not all of the same hospitals were sampled each year. Finally, the governmental health insurance status (Medicare or Medicaid for both sets of data) was considered. Medicaid and Medicaid Health Maintenance Organization (HMO) as expected reimbursement categories were considered as a single group as were Medicare and Medicare HMO in the New York State database. All of these covariants were subject to forward stepwise selection for modeling adjustment purposes. The probability required for a covariant to enter the model was 0.250 and the probability at which a covariant was removed from the model was 0.100. These adjustment factors were held constant in adjusted models examining for the independent predictor effects of adverse drug reactions. To examine whether or not the presence of GI and/or skin manifestations commonly associated with adverse drug effects accounted for differences in LOS/charges, we examined whether or not adding the manifestations as a covariant would attenuate the predictor effect of the adverse drug effect.
In order to make a practical assessment of the impact of adverse drug effects on LOS and hospital charges, we chose as an example patient a 70‐year‐old white female with a diagnosis of diabetes and hypertension, with Medicare.
Logistic regression models were used to explore comorbid conditions and demographic features that were associated with adverse drug effects within the cohort. Forward stepwise regression was used using previously described entry/exit criteria. Odds ratios for individual predictor variables were adjusted for other significant predictor variables.
All regression models were adjusted for sampling weights in national data analyses. The time trends (year effect) for the incidences of adverse drug effects were analyzed with the GENMOD procedure in SAS, with the negative binomial distribution option.14, 15
RESULTS
In the New York (SPARCS) database (NYS), 278,425 pneumonia admissions were identified. In HCUP‐NIS data subsets (NIS), 186,193 pneumonia admissions formed the cohort. In both cohorts, there was a predominance of females and older patients (Table 1). Diabetes and hypertension were common comorbidities. In the NYS cohort, 1,329 (0.48%) had an adverse effect related to an antibiotic or anti‐infective. In the NIS cohort, an estimated 0.53% had an adverse drug effect. There was a small but significant increase in the percentage of national hospitalizations associated with an antibiotic adverse drug effect over time (time effect significance; P = 0.0149; Table 1). However, this trend was not seen in the NYS cohort.
| Database | SPARCS | HCUP‐NIS |
|---|---|---|
| ||
| Cohort years | 20002005 | 20002005 |
| Cohort region | New York State | United States |
| Cohort size (identified cases) | 278,425 | 186,193 |
| Estimated actual number (n) of cases for cohort region | 278,425 | 4,547,108 |
| African American (%) | 12.8 | 7.6 |
| Females (%) | 53.8 | 54.4 |
| Medicare (%) | 72.9 | 72.8 |
| Mean age (years) | 72.5 | 71.4 |
| Diabetes mellitus (%) | 25.4 | 24.4 |
| Hypertension (%) | 41.2 | 39.0 |
| Death (%) | 6.8 | 4.7 |
| 2000 ADE (%)/n | 0.44/205 | 0.48/3372 |
| 2001 ADE (%)/n | 0.47/208 | 0.53/3797 |
| 2002 ADE (%)/n | 0.49/225 | 0.53/3985 |
| 2003 ADE (%)/n | 0.48/229 | 0.57/3564 |
| 2004 ADE (%)/n | 0.52/249 | 0.56/4250 |
| 2005 ADE (%)/n | 0.46/213 | 0.60/4979 |
| Total hospital charges* | $4,815,100,411 | $70,285,286,226 |
The most numerous adverse effects were noted in other specified antibiotics, followed by other unspecified antibiotics, then cephalosporins in both databases (Table 2). Cephalosporins accounted for 15% and 14% of cases with adverse drug effect due to antibiotics or anti‐infectives in the NYS and NIS cohorts, respectively. Adverse drug effects due to the penicillins and quinolones were similar in frequency and were the next most common identifiable classes of antibiotics with adverse drug effects after cephalosporins. Adverse effects to other specified antibiotics and unspecified antibiotics combined constituted 59% of adverse drug effects in both NYS and NIS cohorts.
| Antibiotic | New York State (SPARCS) | National Estimates (HCUP‐NIS) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ADE (n) | ADE % of Total | ADE with Skin* (%) | ADE with GI (%) | ADE with GI and/or Skin* (%) | ADE (n) | ADE % of Total | ADE with Skin* (%) | ADE with GI (%) | ADE with GI and/or Skin* (%) | |
| ||||||||||
| Penicillins | 91 | 7 | 58 | 21 | 78 | 1484 | 8 | 47 | 17 | 64 |
| Erythromycin/macrolides | 102 | 8 | 28 | 44 | 71 | 1608 | 8 | 19 | 51 | 69 |
| Tetracyclines | 14 | 1 | 50 | 7 | 57 | 182 | 1 | 46 | 27 | 73 |
| Cephalosporins | 194 | 15 | 60 | 21 | 80 | 2684 | 14 | 55 | 19 | 69 |
| Other specified antibiotics | 512 | 39 | 40 | 29 | 67 | 5986 | 30 | 37 | 29 | 62 |
| Other unspecified antibiotics | 276 | 21 | 22 | 50 | 72 | 5766 | 29 | 16 | 49 | 64 |
| Sulfonamide | 22 | 2 | 64 | 9 | 68 | 298 | 2 | 53 | 7 | 60 |
| Quinolones | 94 | 7 | 36 | 18 | 53 | 1479 | 8 | 49 | 20 | 65 |
| Antimycobacterials | 42 | 3 | 38 | 28 | 60 | 64 | 0 | 27 | 0 | 27 |
| ADE due to any of the above | 1329 | 100 | 43 | 31 | 72 | 19740 | 100 | 34 | 33 | 65 |
Hospitalizations associated with an adverse drug effect had higher proportions of women than hospitalizations without an adverse drug effect in both the NIS (65% versus 54%) and NYS (62% versus 54%) databases. Hospitalizations associated with an adverse drug effect had a mean age that was about 1 year younger than that observed in hospitalizations without an adverse drug effect in both databases. Congestive heart failure was present in a lower proportion of hospitalizations associated with an adverse drug effect compared to hospitalizations without adverse drug effects (NYS 27% versus 30%, NIS 25% versus 29%). In the NIS database, adverse drug effect associated hospitalizations had a lower proportion of chronic obstructive pulmonary disease than other hospitalizations (32% versus 40%). Neither database showed any adverse drug effect associated disproportion with regard to hypertension and diabetes mellitus.
In logistic regression modeling, significant predictors for an adverse drug effect included non‐African American race, older age, female gender, not having Medicaid, and residence outside the greater NY area (only in the NYS data). Non‐African‐Americans were more likely than African‐Americans to have adverse drug effect admissions (adjusted odds ratio for NYS 2.2, 95% CI, 1.72.8; and for NIS 2.1, 95% CI, 1.63.0). Females were more likely than males to be associated with adverse drug effect admissions (adjusted odds ratio for NYS 1.5, 95% CI, 1.31.6; and for NIS 1.6, 95% CI, 1.41.8). In addition, residence outside the greater NY area was associated with adverse drug effect associated admissions (adjusted odds ratio 2.1, 95% CI, 1.82.3) in NYS data.
Skin and allergy manifestations potentially associated with adverse drug effects were reported in 34% and 43% of the NIS and NYS cohorts, respectively. In comparison, less than 1% of non‐adverse drug effect admissions had these manifestations (Table 3) in either cohort. In NYS, adverse drug effects due to sulfonamides had a slightly higher proportion skin/allergy manifestations when compared with other antibiotic classes (Table 2). In contrast, NIS estimates show that adverse effects due to cephalosporins had the highest proportion of skin/allergy manifestations (Table 2). Compared to adverse drug effects due to other specified antibiotics, erythromycin/macrolides were more likely to present with GI manifestations in both databases (Table 2). Dermatitis due to drugs taken internally was coded for in 34% (NYS) and 26% (NIS) of patients that experienced an adverse drug effect, making this condition the most common skin/allergy manifestation associated with an adverse drug effect (Table 3). This was followed in frequency by urticaria and pruritus. Diarrhea was also a common symptom related to adverse drug effects (Table 3). While 72% of adverse drug effects had either GI or skin/allergy manifestations in the NYS cohort, only 65% of the NIS cohort had these manifestations reported. No increase in mortality was observed in patients with adverse drug effects compared to those without adverse drug effects (data not shown).
| Clinical Manifestation | New York State SPARCS | National Estimates HCUP‐NIS | ||
|---|---|---|---|---|
| No Adverse Effect (%) | Adverse Effect (%) | No Adverse Effect (%) | Adverse Effect (%) | |
| Dermatitis due to drugs taken internally | 0.1 | 34.1 | 0.1 | 25.9 |
| Pruritus | 0.1 | 3.5 | 0.1 | 3 |
| Urticaria | 0.0 | 4.0 | 0.0 | 3.6 |
| Erythema | 0.0 | 0.2 | 0.0 | 0.2 |
| Angioedema | 0.0 | 0.8 | 0.0 | 0.7 |
| Stevens‐Johnson syndrome | 0.0 | 0.3 | 0.0 | 0.2 |
| Anaphylaxis | 0.0 | 0.9 | 0.0 | 0.2 |
| Allergy, unspecified | 0.0 | 0.2 | 0.0 | 0.7 |
| Nausea and/or vomiting | 0.6 | 6.3 | 0.9 | 7.4 |
| Diarrhea, nonspecified or due to C. difficile | 3.5 | 26.5 | 3.1 | 25.5 |
Both databases showed that adverse drug effects affected both LOS and total charges (Table 4). In the NIS database, adjusted models showed that GI manifestations impacted hospital charges more than skin/allergy manifestations (Table 4). In both the NYS and NIS cohorts, the effect of adverse drug effects on hospital charges was attenuated after accounting for skin/allergy and GI manifestations. However, even after accounting for both manifestations, there still was a significant adverse drug effect influence on LOS. In the example patient, predicted excess hospitalization charges associated with the presence of an adverse drug effect was $1,243 and $3,373 for the NIS and NYS cohorts, while LOS increases associated with an adverse drug effect were about 1 day in both cohorts. Linear regression models, which included adjustment factors including comorbidities and demographic/financial factors, showed that the models accounted for 13% of the variance (R2 values) in LOS and 40% in charges for the NYS but only 7% for LOS and 15% for charges for the NIS.
| Example* Admission without ADE | Example* Admission with ADE | P Value for ADE coefficient when Added to Model | |
|---|---|---|---|
| |||
| SPARCS | |||
| Hospital charge | |||
| Simple unadjusted model | $12,274 | $13,045 | 0.007 |
| Adjusted model for comorbidities and demographics | $14,160 | $17,533 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI manifestations | $18,865 | $21,560 | <0.0001 |
| Adjusted model for comorbidities and demographics including skin/allergy manifestations | $16,777 | $19,370 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI and skin/allergy manifestations | $23,227 | $24,275 | 0.0227 |
| LOS (days) | |||
| Simple unadjusted model | 5.4 | 6.7 | <0.0001 |
| Adjusted model for comorbidities and demographics | 4.0 | 5.2 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI manifestations | 5.4 | 6.5 | <0.0001 |
| Adjusted model for comorbidities and demographics including skin/allergy manifestations | 4.8 | 5.8 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI and skin/allergy manifestations | 6.8 | 7.4 | <0.0001 |
| HCUP | |||
| Hospital charge | |||
| Simple unadjusted model | $10,840 | $11,917 | 0.0008 |
| Adjusted model for comorbidities and demographics | $12,941 | $14,284 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI manifestations | $14,923 | $15,781 | 0.0208 |
| Adjusted model for comorbidities and demographics including skin/allergy manifestations | $13,543 | $14,723 | 0.0092 |
| Adjusted model for comorbidities and demographics including GI and skin/allergy manifestations | $15,887 | $16,453 | 0.1784 |
| LOS (days) | |||
| Simple unadjusted model | 4.4 | 5.1 | <0.0001 |
| Adjusted model for comorbidities and demographics | 4.0 | 4.9 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI manifestations | 4.8 | 5.5 | <0.0001 |
| Adjusted model for comorbidities and demographics including skin/allergy manifestations | 4.0 | 4.7 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI and skin/allergy manifestations | 5.3 | 5.9 | <0.0001 |
DISCUSSION
This study documents antibiotic related adverse drug effects as a predictable, but infrequent complication that occurs in adult patients hospitalized for pneumonia. While the incidence of antibiotic‐related adverse drug events has been calculated in both hospital2 and nursing home16 populations, these studies have not specified admissions that were associated with antibiotic use. Thus calculations of antibiotic adverse drug events for actual at‐risk patients (ie, those receiving antibiotics) are imprecise in these reports. In the present study, it is highly probable that nearly all admissions were associated with actual antibiotic administration. Thus, a rough incidence of an identifiable antibiotic adverse drug effect for adult pneumonia admissions can be expected to be roughly 0.5%. Of interest is the observation that the national incidence of this complication appears to be increasing slightly but steadily in recent years. This could be explained on the basis of increased coding slots or DRG creep17 in more recent years with the national cohort. Layde et al.12 utilized e‐codes to identify medical injury due to medications in Wisconsin hospital discharge data (excluding newborn delivery discharges), unselected for infectious diseases. They calculated an overall 0.5% incidence of antibiotic‐associated adverse effects. Since not all hospitalizations are associated with antibiotic administration, this would imply that the incidence of antibiotic associated adverse effects in hospitalized patients actually given antibiotics would be higher than 0.5%. The relatively low incidence of antibiotic‐associated adverse effects observed in the present study may relate to briefer and less complex hospitalizations for these patients compared with other patients treated with antibiotics. The use of ICD‐9 codes (including e‐codes) as flags of adverse drug events may also underestimate actual rates. In a study of Utah hospitalization discharges in 2001, Hougland et al.18 found that these flags had a sensitivity of 55% for confirmed adverse drug events of various categories. This contrasts with the 98.5% sensitivity of e‐codes to identify medical injury due to drugs, described in the Wisconsin hospital discharge data. The distinction between adverse drug effects, adverse drug reactions, and adverse drug events may be important in understanding these data. Adverse drug reactions have been defined as any noxious, unintended, and undesired effect of a drug, which occurs at doses used in humans for prophylaxis, diagnosis, or therapy and can be considered a subset of adverse drug events, which, unlike adverse drug reactions, may also be due to drug administration errors.6 The term adverse drug effect has been used more in pharmacology literature4 and in medical coding,18 and may refer more to known side effects of medications, whereas adverse drug events have been broadly defined as an injury resulting from administration of a drug.6 As this study utilized medical coding for data abstraction, we used the term adverse drug effect for all results.
Determining factors that influence hospital charges and length of stay are complex. Regional differences19 may be 1 factor, as suggested by difference in charges for the example admission models (Table 4). The multivariate analyses showed that nearly 40% of the variation in total New York State hospitalization charges could be explained on the basis of demographic, comorbidity factors, and between hospital variation, with an additional independent effect identifiable in the presence of an adverse drug effect to an antibiotic. The explained variance in the New York State hospitalization charges exceeds that observed in other published clinical predictor models of hospital charges based on statewide or province‐wide discharge databases.12, 20, 21 Although less variability was explained in national models, independent adverse drug effects influence on both total charge and length of stay were also observed. Higher charges with adverse drug effect associated admissions could be explained in part by increased illness severity, leading to more hospital days, and thus higher charges in per diem reimbursement schemes. In DRG‐based reimbursements, adverse drug effect presence in an admission, with its attendant increased length of stay, could be considered an outlier case, in which case an increased inpatient prospective payment system (IPPS) payment would be authorized in addition to the base payment.22
Because the impact of adverse drug effects on length of stay was still present even after controlling for both skin/allergy and GI manifestations, this may suggest that other factors relating to the adverse drug effects may have influenced LOS. These factors might include physician reluctance to discharge these patients or the influence of other organ systems not accounted for or reported in this study. The attenuation of the adverse drug effect's influence on hospital charge models by including possible clinical manifestations of adverse drug effects suggests that these manifestations were the main contributors to higher charges associated with adverse drug effect admissions. These disparate findings regarding adverse drug effects on LOS versus charges are consistent with the notion that hospital LOS and hospital charge are separate constructs, which may be associated with separate factors affecting these outcomes.23 The 13% variation in LOS explained in the New York state hospitalization regression models was similar to the 14% variation in LOS observed in clinical predictor models for congestive heart failure hospitalizations in New York state.24 Layde et al.12 found a 14.5% and 18.5% adjusted increase in charges and LOS associated with any medical injury in Wisconsin hospital discharges. The excess length of stay due to antibiotic related medical injury was 1.27 days. This magnitude of effect is comparable to that observed in the present study.
There are a number of limitations in this study related to coding practices and the retrospective nature of the investigation. Currently, there are no ICD‐9 e‐codes for adverse effects due to commonly used older antibiotics such as vancomycin, clindamycin, and metronidazole, or to the newer antibiotic classes. Since currently recommended treatments for community‐acquired pneumonia25 are among the specified drugs with adverse effect coding, and since other specified and unspecified anti‐infective drug‐associated (no drug names or categories provided) adverse effects were frequent, it suggests that infectious processes other than community‐acquired pneumonia were also being treated in many hospitalizations. Another limitation is that because the temporal sequence of events cannot be ascertained with this data, it is possible that an adverse drug effect was due to an antibiotic given prior to hospitalization. It has been suggested that onset of diagnosis or present on admission information be part of a new administrative data coding strategy which has been used in some states in the US.19 The adoption of ICD‐10 codes may allow for more specificity and detailing of adverse drug reactions using administrative data, as described for the United Kingdom by Waller et al.26 The actual incidence of hospitalization‐associated adverse drug effects could be underestimated if a significant number of adverse effects occurred after discharge as only in‐hospital events were recorded.
In summary, we found that although the incidence of adverse drug effects is small, there is a definite quantifiable impact of these adverse effects on LOS and hospital charges in patients hospitalized with pneumonia. To our knowledge, there have not been similar large‐scale database studies to evaluate the incidence and impact of adverse drug effects related to antibiotics in both national and statewide samples. These findings also have implications in studies of outcomes related to pneumonia hospitalizations.
Acknowledgements
The authors thank Ariel D. Teitel, MD, for his assistance. This study was supported in part by the intramural scholarship program at New York Medical College.
- ,,, et al.Incidence of adverse drug events and potential adverse drug events: implications for prevention.JAMA.1995;274:29–34.
- ,,, et al.Adverse drug events in hospitalized patients.JAMA.1997;277:301–306.
- ,,.Incidence of adverse drug reactions in hospitalized patients.JAMA.1998;279:1200–1205.
- ,,.Economic aspects of antibacterial adverse effects.Pharmacoeconomics.1998;13:35–49.
- ,.1999National Hospital Discharge Survey. Advance data from vital and health statistics; no 319.Hyattsville, MD:National Center for Health Statistics;year="2001"2001.
- ,,.Incidence of adverse drug reactions in hospitalized patients: a meta‐analysis of prospective studies.JAMA.1998;279:1200–1205.
- ,,,.Asthma hospitalization patterns in young children relating to admission age, infection presence, sex, and race.Ann Allergy Asthma Immunol.2007;98:139–145.
- ,,.Pattern of hospitalizations for angioedema in New York between 1990 and 2003.Ann Allergy Asthma Immunol.2005;95:159–166.
- Inpatient Output Data Dictionary, SPARCS. Available at: http://www.health.state.ny.us/statistics/sparcs/inpat.htm. Accessed October2008.
- Agency for Healthcare Research and Quality.The HCUP Nationwide Inpatient Sample (NIS).Rockville, MD:Agency for Healthcare Research and Quality;2004.
- ,,,.Accuracy of administrative data for identifying patients with pneumonia.Am J Med Qual.2005;20:319–328.
- ,,, et al.Medical injury identification using hospital discharge data.Advances in Patient Safety. Vol2.Rockville, MD:Agency for Healthcare Research and Quality;2007. Available at: http://www.ahrq.gov/downloads/pub/advances/vol2/Layde.pdf. Accessed October 2008.
- ,,.A comparison of several regression models for analyzing cost of CABG surgery.Stat Med.2003;22:2799–2815.
- University of Kentucky. Poisson and negative binomial regressions. Available at: http://www.uky.edu/ComputingCenter/SSTARS. Accessed October2008.
- ,,.Regression analyses of counts and rates: Poisson, overdispersed Poisson, and negative binomial models.Psychol Bull.1995;118;392–404.
- ,,, et al.Incidence and preventability of adverse drug events in nursing homes.Am J Med.2000;1;109:87–94.
- ,.Administrative data based patient safety research: a critical review.Qual Saf Health Care.2003;12(Suppl 2):ii58–ii63.
- ,,, et al.Performance of International Classification of Diseases, 9th Revision, Clinical Modification codes as an adverse drug event surveillance system.Med Care.2006;44:629–636.
- ,,.Direct medical costs of bronchiolitis hospitalizations in the United States.Pediatrics Dec.2006;118:2418–2423.
- ,,.Relationship of hospital size, case volume, and cost for coronary artery bypass surgery: analysis of 12,774 patients operated on in Massachusetts during fiscal years 1995 and 1996.J Thorac Cardiovasc Surg.2001;122:53–64.
- ,,,.Comorbidity measures for use with administrative data.Med Care.1998;36:8–27.
- Health and Human Services. Centers for Medicaid and Medicare Services (CMS) Home. Medicare. Acute Inpatient PPS. Overview. Available at: http://www.cms.hhs.gov/AcuteInpatientPPS. Accessed October2008.
- ,,,.Identifying pre‐ and postoperative predictors of cost and length of stay for coronary artery bypass surgery.Am J Med Qual.1999:14:248–254.
- ,,, et al.Hospital outcomes in major teaching, minor teaching, and nonteaching hospitals in New York state.Am J Med.2002;112:255–261.
- ,,, et al.Infectious Disease Society/American Thoracic Society Consensus Guidelines on the Management of Community‐Acquired Pneumonia in Adults.Clin Infect Dis.2007;44:S27–S72.
- ,,,,.Hospital admissions for ‘drug‐induced’ disorders in England: a study using the Hospital Episodes Statistics (HES) database.Br J Clin Pharmacol.2005;59:213–219.
Adverse drug eventsdefined as an injury resulting from medical intervention related to a drug1significantly contribute to health care expenditures. Over 770,000 people are injured or die every year in hospitals from adverse drug events, and national hospital expenses to treat patients who have suffered adverse drug events during hospitalization have been estimated to be between $1.56 and $4.2 billion annually.2 In a meta‐analysis of prospective studies, researchers found that adverse drug reactions, one important form of adverse drug events, may rank as the fourth to sixth leading cause of death in the United States, with more than 100,000 deaths per year.3 Understanding the factors associated with these adverse events may help in the development of prevention strategies, with resulting improving health care quality and lowering health care costs.
Among hospitalized patients, antibacterial adverse effects may account for approximately 25% of adverse drug reactions.1, 4 While the economic impact has been studied for overall adverse drug events in hospitalized patients in the 1990s, more recent detailed studies for the impact of antibiotic‐related adverse drug effects have not been published. As hospitalized patients with the primary diagnosis of pneumonia are invariably treated with antibiotics, and since pneumonia is the third leading cause for hospitalization in the United States,5 hospitalization databases that document pneumonia hospitalizations as well as adverse effects from antibiotics, using specific International Classification of Diseases, Ninth Revision (ICD‐9) clinical modification codes, constitute a unique and rich resource for quantifying and analyzing the incidence and impact of antibiotic‐associated adverse drug effects.
The purpose of this study was to describe the incidence and clinical manifestations of adverse drug effects in pneumonia hospitalizations in recent years, and to determine the types of patients and comorbidities, which are most commonly associated with adverse drug effects. The term adverse drug effect refers more to known side effects of medications, whereas adverse drug events and adverse drug reactions refer to an injury or a noxious, unintended, and undesired effect resulting from administration of a drug.6 As this study utilized medical coding for data abstraction, the broader classifications of adverse drug events or reactions could not be examined and instead the outcome of adverse drug effect was utilized.
METHODS
Data Sources
The Statewide Planning and Research Cooperative System (SPARCS) database was accessed as previously described.7, 8 There is mandatory reporting to this database for all New York State acute care hospitalizations. Each deidentified SPARCS admission record contains more than 100 data fields9 that consist of demographic, clinical, and financial information. These fields include principal and nonprincipal diagnostic fields, procedure codes, race, age, gender, and ethnicity information, hospital characteristics, expected reimbursement, total charges, length of stay (LOS), admission status, and disposition status. Both ICD‐9 and Common Procedural Terminology (CPT) codes are input for each admission.
The Nationwide Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project (HCUP), contains annual hospital discharge data from a sample of US hospitals.10 Each NIS patient record includes data fields consisting of demographic, clinical, and financial information. These fields include primary and secondary diagnostic fields, procedure codes, age, gender, race, total charges, length of stay, payer codes, hospital characteristics, and disposition status. Twenty percent random subsamples from each year's sample were employed to perform the analyses. HCUP databases include appropriately‐scaled discharge weights to generate national estimates of hospitalizations and total charges from the NIS. These weights allow comparison of incidence rates and charges across years despite a varying number of states and hospitals included in the database each year.
This study was given an exemption from institutional research board approval by the SVCMC Integrated Scientific and Ethical Review Board.
Identification of Pneumonia Admissions
To achieve more uniformity in the cohorts, it was decided to select only hospitalizations with the most common ICD‐9 and diagnosis‐related group (DRG) codes for pneumonia for more recent years. ICD‐9 and DRG codes have been used to identify pneumonia patients in administrative data, and cases selected in this manner show excellent specificity when compared to a reference standard.11 Hospitalization discharges from both databases from 2000 through 2005 were selected with the criterion of having the principal diagnosis of ICD‐9 code 486 (pneumonia, organism unspecified) and the DRG of 89 (simple pneumonia and pleurisy, age >17 years, with complication and comorbidity), thus targeting community acquired pneumonia. These hospitalizations formed the 2 cohorts of pneumonia hospitalizations. Preliminary analyses showed that hospitalizations identified by these criteria identified more than 60% of pneumonia admissions defined by a more expansive criteria11 of having any of the DRG codes 79 (respiratory infections and inflammations, age >17 years, with complications and comorbidity), 80 (respiratory infections and inflammations, age >17 years, without complications and comorbidity), 89 and 90 (simple pneumonia and pleurisy, age >17 years, without complication and comorbidity). Gram‐negative pneumonia, aspiration pneumonia, and pneumonias due to other specific infectious agents were not targeted in this study.
Data Classifications
The state and national cohorts were queried for the presence of adverse effects due to various antibiotics and anti‐infectives, using specific ICD‐9 external cause of injury codes (e‐codes) including e930 and e931. E‐codes were developed as a supplemental code for use with the ICD and they provide a systematic way to classify diagnostic information that health care providers have entered into the medical record. E‐codes have been shown to be useful and sensitive in detecting medical injuries due to drugs (including antibiotics) in hospital discharge data.12 On the basis of frequency of observed adverse drug effects (as detected by e‐codes), an adverse drug effect due to an anti‐infective or antibiotic was defined as that which was due to penicillins (E930.0), erythromycin and other macrolides (E930.3), tetracyclines (E930.5), cephalosporins (E930.5), sulfonamides (E931.0), quinolones (E931.3), other specified antibiotics (E930.9), other unspecified antibiotics (E931.9), or antimycobacterials (E931.8 and E930.6). Adverse drug effects due to other anti‐infectives were not included due to extremely low incidence and unlikely clinical usage in pneumonia. National estimates of the number of patients experiencing an adverse drug effect were determined using discharge weights to adjust for subset sample size.
The ICD‐9 codes for possible skin and allergy manifestations commonly associated with adverse drug effects were examined in patients with and without adverse drug effects as defined previously. The ICD‐9 codes for skin/allergy manifestations that were considered as possibly due to adverse drug effects included erythema, not otherwise specified (695.9), flushing (782.62), Stevens‐Johnson syndrome (695.1), allergic purpura (287.0), dermatitis due to drugs and medications taken internally (693.0), angioedema (995.1), unspecified allergy, (995.3), anaphylaxis not otherwise specified (NOS) (999.5), and urticaria (708). Gastrointestinal (GI) manifestations considered as possibly due to an adverse drug effect included nausea (787.02), vomiting (787.03), nausea with vomiting (787.01), diarrhea, not otherwise specified (787.91), diarrhea, other and unspecified noninfectious gastroenteritis and colitis (558.9), or intestinal infection due to Clostridium difficile (008.45).
Statistical Analysis
Analyses were performed using JMP version 5.1 and SAS for Windows version 9 (SAS Institute, Cary, NC). In linear regression models, principal outcomes of length of stay and total hospital charges were logarithmically transformed, as this data transformation reduces the influence of outliers.13 Cases with a length of stay less than 1 day were considered to have a 23‐hour LOS, to enable logarithmic transformation. Linear regression models were created to assess the impact of adverse drug effects due to antibiotics on length of stay and total charge. Linear regression models have been shown to be useful in identifying factors associated with increased hospital charges.13 Adjusting factors that were considered in multivariate models included comorbid conditions and demographic factors. Only common comorbidities that were present in greater than 5% of cases were considered and included cancer (140 through 208), congestive heart failure (428), ischemic heart disease (410414), chronic obstructive pulmonary disease (491, 492, 496), diabetes mellitus (250), hypertension (401), asthma (493), urinary tract infection (599.0), unspecified anemia (285.9), pleural effusion (511.9), cardiac dysrhythmia (427.31), volume depletion (276.5), unspecified acquired hypothyroidism (244.9), and hypoosmolality/hyponatremia (276.1). Demographic factors such as gender, race, age, year and month of admission, and day of admission were also considered in the model. The hospital where the admission occurred was used for New York State calculations. For the national data, the region and hospital characteristics but not the hospital identification number itself were considered since not all of the same hospitals were sampled each year. Finally, the governmental health insurance status (Medicare or Medicaid for both sets of data) was considered. Medicaid and Medicaid Health Maintenance Organization (HMO) as expected reimbursement categories were considered as a single group as were Medicare and Medicare HMO in the New York State database. All of these covariants were subject to forward stepwise selection for modeling adjustment purposes. The probability required for a covariant to enter the model was 0.250 and the probability at which a covariant was removed from the model was 0.100. These adjustment factors were held constant in adjusted models examining for the independent predictor effects of adverse drug reactions. To examine whether or not the presence of GI and/or skin manifestations commonly associated with adverse drug effects accounted for differences in LOS/charges, we examined whether or not adding the manifestations as a covariant would attenuate the predictor effect of the adverse drug effect.
In order to make a practical assessment of the impact of adverse drug effects on LOS and hospital charges, we chose as an example patient a 70‐year‐old white female with a diagnosis of diabetes and hypertension, with Medicare.
Logistic regression models were used to explore comorbid conditions and demographic features that were associated with adverse drug effects within the cohort. Forward stepwise regression was used using previously described entry/exit criteria. Odds ratios for individual predictor variables were adjusted for other significant predictor variables.
All regression models were adjusted for sampling weights in national data analyses. The time trends (year effect) for the incidences of adverse drug effects were analyzed with the GENMOD procedure in SAS, with the negative binomial distribution option.14, 15
RESULTS
In the New York (SPARCS) database (NYS), 278,425 pneumonia admissions were identified. In HCUP‐NIS data subsets (NIS), 186,193 pneumonia admissions formed the cohort. In both cohorts, there was a predominance of females and older patients (Table 1). Diabetes and hypertension were common comorbidities. In the NYS cohort, 1,329 (0.48%) had an adverse effect related to an antibiotic or anti‐infective. In the NIS cohort, an estimated 0.53% had an adverse drug effect. There was a small but significant increase in the percentage of national hospitalizations associated with an antibiotic adverse drug effect over time (time effect significance; P = 0.0149; Table 1). However, this trend was not seen in the NYS cohort.
| Database | SPARCS | HCUP‐NIS |
|---|---|---|
| ||
| Cohort years | 20002005 | 20002005 |
| Cohort region | New York State | United States |
| Cohort size (identified cases) | 278,425 | 186,193 |
| Estimated actual number (n) of cases for cohort region | 278,425 | 4,547,108 |
| African American (%) | 12.8 | 7.6 |
| Females (%) | 53.8 | 54.4 |
| Medicare (%) | 72.9 | 72.8 |
| Mean age (years) | 72.5 | 71.4 |
| Diabetes mellitus (%) | 25.4 | 24.4 |
| Hypertension (%) | 41.2 | 39.0 |
| Death (%) | 6.8 | 4.7 |
| 2000 ADE (%)/n | 0.44/205 | 0.48/3372 |
| 2001 ADE (%)/n | 0.47/208 | 0.53/3797 |
| 2002 ADE (%)/n | 0.49/225 | 0.53/3985 |
| 2003 ADE (%)/n | 0.48/229 | 0.57/3564 |
| 2004 ADE (%)/n | 0.52/249 | 0.56/4250 |
| 2005 ADE (%)/n | 0.46/213 | 0.60/4979 |
| Total hospital charges* | $4,815,100,411 | $70,285,286,226 |
The most numerous adverse effects were noted in other specified antibiotics, followed by other unspecified antibiotics, then cephalosporins in both databases (Table 2). Cephalosporins accounted for 15% and 14% of cases with adverse drug effect due to antibiotics or anti‐infectives in the NYS and NIS cohorts, respectively. Adverse drug effects due to the penicillins and quinolones were similar in frequency and were the next most common identifiable classes of antibiotics with adverse drug effects after cephalosporins. Adverse effects to other specified antibiotics and unspecified antibiotics combined constituted 59% of adverse drug effects in both NYS and NIS cohorts.
| Antibiotic | New York State (SPARCS) | National Estimates (HCUP‐NIS) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ADE (n) | ADE % of Total | ADE with Skin* (%) | ADE with GI (%) | ADE with GI and/or Skin* (%) | ADE (n) | ADE % of Total | ADE with Skin* (%) | ADE with GI (%) | ADE with GI and/or Skin* (%) | |
| ||||||||||
| Penicillins | 91 | 7 | 58 | 21 | 78 | 1484 | 8 | 47 | 17 | 64 |
| Erythromycin/macrolides | 102 | 8 | 28 | 44 | 71 | 1608 | 8 | 19 | 51 | 69 |
| Tetracyclines | 14 | 1 | 50 | 7 | 57 | 182 | 1 | 46 | 27 | 73 |
| Cephalosporins | 194 | 15 | 60 | 21 | 80 | 2684 | 14 | 55 | 19 | 69 |
| Other specified antibiotics | 512 | 39 | 40 | 29 | 67 | 5986 | 30 | 37 | 29 | 62 |
| Other unspecified antibiotics | 276 | 21 | 22 | 50 | 72 | 5766 | 29 | 16 | 49 | 64 |
| Sulfonamide | 22 | 2 | 64 | 9 | 68 | 298 | 2 | 53 | 7 | 60 |
| Quinolones | 94 | 7 | 36 | 18 | 53 | 1479 | 8 | 49 | 20 | 65 |
| Antimycobacterials | 42 | 3 | 38 | 28 | 60 | 64 | 0 | 27 | 0 | 27 |
| ADE due to any of the above | 1329 | 100 | 43 | 31 | 72 | 19740 | 100 | 34 | 33 | 65 |
Hospitalizations associated with an adverse drug effect had higher proportions of women than hospitalizations without an adverse drug effect in both the NIS (65% versus 54%) and NYS (62% versus 54%) databases. Hospitalizations associated with an adverse drug effect had a mean age that was about 1 year younger than that observed in hospitalizations without an adverse drug effect in both databases. Congestive heart failure was present in a lower proportion of hospitalizations associated with an adverse drug effect compared to hospitalizations without adverse drug effects (NYS 27% versus 30%, NIS 25% versus 29%). In the NIS database, adverse drug effect associated hospitalizations had a lower proportion of chronic obstructive pulmonary disease than other hospitalizations (32% versus 40%). Neither database showed any adverse drug effect associated disproportion with regard to hypertension and diabetes mellitus.
In logistic regression modeling, significant predictors for an adverse drug effect included non‐African American race, older age, female gender, not having Medicaid, and residence outside the greater NY area (only in the NYS data). Non‐African‐Americans were more likely than African‐Americans to have adverse drug effect admissions (adjusted odds ratio for NYS 2.2, 95% CI, 1.72.8; and for NIS 2.1, 95% CI, 1.63.0). Females were more likely than males to be associated with adverse drug effect admissions (adjusted odds ratio for NYS 1.5, 95% CI, 1.31.6; and for NIS 1.6, 95% CI, 1.41.8). In addition, residence outside the greater NY area was associated with adverse drug effect associated admissions (adjusted odds ratio 2.1, 95% CI, 1.82.3) in NYS data.
Skin and allergy manifestations potentially associated with adverse drug effects were reported in 34% and 43% of the NIS and NYS cohorts, respectively. In comparison, less than 1% of non‐adverse drug effect admissions had these manifestations (Table 3) in either cohort. In NYS, adverse drug effects due to sulfonamides had a slightly higher proportion skin/allergy manifestations when compared with other antibiotic classes (Table 2). In contrast, NIS estimates show that adverse effects due to cephalosporins had the highest proportion of skin/allergy manifestations (Table 2). Compared to adverse drug effects due to other specified antibiotics, erythromycin/macrolides were more likely to present with GI manifestations in both databases (Table 2). Dermatitis due to drugs taken internally was coded for in 34% (NYS) and 26% (NIS) of patients that experienced an adverse drug effect, making this condition the most common skin/allergy manifestation associated with an adverse drug effect (Table 3). This was followed in frequency by urticaria and pruritus. Diarrhea was also a common symptom related to adverse drug effects (Table 3). While 72% of adverse drug effects had either GI or skin/allergy manifestations in the NYS cohort, only 65% of the NIS cohort had these manifestations reported. No increase in mortality was observed in patients with adverse drug effects compared to those without adverse drug effects (data not shown).
| Clinical Manifestation | New York State SPARCS | National Estimates HCUP‐NIS | ||
|---|---|---|---|---|
| No Adverse Effect (%) | Adverse Effect (%) | No Adverse Effect (%) | Adverse Effect (%) | |
| Dermatitis due to drugs taken internally | 0.1 | 34.1 | 0.1 | 25.9 |
| Pruritus | 0.1 | 3.5 | 0.1 | 3 |
| Urticaria | 0.0 | 4.0 | 0.0 | 3.6 |
| Erythema | 0.0 | 0.2 | 0.0 | 0.2 |
| Angioedema | 0.0 | 0.8 | 0.0 | 0.7 |
| Stevens‐Johnson syndrome | 0.0 | 0.3 | 0.0 | 0.2 |
| Anaphylaxis | 0.0 | 0.9 | 0.0 | 0.2 |
| Allergy, unspecified | 0.0 | 0.2 | 0.0 | 0.7 |
| Nausea and/or vomiting | 0.6 | 6.3 | 0.9 | 7.4 |
| Diarrhea, nonspecified or due to C. difficile | 3.5 | 26.5 | 3.1 | 25.5 |
Both databases showed that adverse drug effects affected both LOS and total charges (Table 4). In the NIS database, adjusted models showed that GI manifestations impacted hospital charges more than skin/allergy manifestations (Table 4). In both the NYS and NIS cohorts, the effect of adverse drug effects on hospital charges was attenuated after accounting for skin/allergy and GI manifestations. However, even after accounting for both manifestations, there still was a significant adverse drug effect influence on LOS. In the example patient, predicted excess hospitalization charges associated with the presence of an adverse drug effect was $1,243 and $3,373 for the NIS and NYS cohorts, while LOS increases associated with an adverse drug effect were about 1 day in both cohorts. Linear regression models, which included adjustment factors including comorbidities and demographic/financial factors, showed that the models accounted for 13% of the variance (R2 values) in LOS and 40% in charges for the NYS but only 7% for LOS and 15% for charges for the NIS.
| Example* Admission without ADE | Example* Admission with ADE | P Value for ADE coefficient when Added to Model | |
|---|---|---|---|
| |||
| SPARCS | |||
| Hospital charge | |||
| Simple unadjusted model | $12,274 | $13,045 | 0.007 |
| Adjusted model for comorbidities and demographics | $14,160 | $17,533 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI manifestations | $18,865 | $21,560 | <0.0001 |
| Adjusted model for comorbidities and demographics including skin/allergy manifestations | $16,777 | $19,370 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI and skin/allergy manifestations | $23,227 | $24,275 | 0.0227 |
| LOS (days) | |||
| Simple unadjusted model | 5.4 | 6.7 | <0.0001 |
| Adjusted model for comorbidities and demographics | 4.0 | 5.2 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI manifestations | 5.4 | 6.5 | <0.0001 |
| Adjusted model for comorbidities and demographics including skin/allergy manifestations | 4.8 | 5.8 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI and skin/allergy manifestations | 6.8 | 7.4 | <0.0001 |
| HCUP | |||
| Hospital charge | |||
| Simple unadjusted model | $10,840 | $11,917 | 0.0008 |
| Adjusted model for comorbidities and demographics | $12,941 | $14,284 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI manifestations | $14,923 | $15,781 | 0.0208 |
| Adjusted model for comorbidities and demographics including skin/allergy manifestations | $13,543 | $14,723 | 0.0092 |
| Adjusted model for comorbidities and demographics including GI and skin/allergy manifestations | $15,887 | $16,453 | 0.1784 |
| LOS (days) | |||
| Simple unadjusted model | 4.4 | 5.1 | <0.0001 |
| Adjusted model for comorbidities and demographics | 4.0 | 4.9 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI manifestations | 4.8 | 5.5 | <0.0001 |
| Adjusted model for comorbidities and demographics including skin/allergy manifestations | 4.0 | 4.7 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI and skin/allergy manifestations | 5.3 | 5.9 | <0.0001 |
DISCUSSION
This study documents antibiotic related adverse drug effects as a predictable, but infrequent complication that occurs in adult patients hospitalized for pneumonia. While the incidence of antibiotic‐related adverse drug events has been calculated in both hospital2 and nursing home16 populations, these studies have not specified admissions that were associated with antibiotic use. Thus calculations of antibiotic adverse drug events for actual at‐risk patients (ie, those receiving antibiotics) are imprecise in these reports. In the present study, it is highly probable that nearly all admissions were associated with actual antibiotic administration. Thus, a rough incidence of an identifiable antibiotic adverse drug effect for adult pneumonia admissions can be expected to be roughly 0.5%. Of interest is the observation that the national incidence of this complication appears to be increasing slightly but steadily in recent years. This could be explained on the basis of increased coding slots or DRG creep17 in more recent years with the national cohort. Layde et al.12 utilized e‐codes to identify medical injury due to medications in Wisconsin hospital discharge data (excluding newborn delivery discharges), unselected for infectious diseases. They calculated an overall 0.5% incidence of antibiotic‐associated adverse effects. Since not all hospitalizations are associated with antibiotic administration, this would imply that the incidence of antibiotic associated adverse effects in hospitalized patients actually given antibiotics would be higher than 0.5%. The relatively low incidence of antibiotic‐associated adverse effects observed in the present study may relate to briefer and less complex hospitalizations for these patients compared with other patients treated with antibiotics. The use of ICD‐9 codes (including e‐codes) as flags of adverse drug events may also underestimate actual rates. In a study of Utah hospitalization discharges in 2001, Hougland et al.18 found that these flags had a sensitivity of 55% for confirmed adverse drug events of various categories. This contrasts with the 98.5% sensitivity of e‐codes to identify medical injury due to drugs, described in the Wisconsin hospital discharge data. The distinction between adverse drug effects, adverse drug reactions, and adverse drug events may be important in understanding these data. Adverse drug reactions have been defined as any noxious, unintended, and undesired effect of a drug, which occurs at doses used in humans for prophylaxis, diagnosis, or therapy and can be considered a subset of adverse drug events, which, unlike adverse drug reactions, may also be due to drug administration errors.6 The term adverse drug effect has been used more in pharmacology literature4 and in medical coding,18 and may refer more to known side effects of medications, whereas adverse drug events have been broadly defined as an injury resulting from administration of a drug.6 As this study utilized medical coding for data abstraction, we used the term adverse drug effect for all results.
Determining factors that influence hospital charges and length of stay are complex. Regional differences19 may be 1 factor, as suggested by difference in charges for the example admission models (Table 4). The multivariate analyses showed that nearly 40% of the variation in total New York State hospitalization charges could be explained on the basis of demographic, comorbidity factors, and between hospital variation, with an additional independent effect identifiable in the presence of an adverse drug effect to an antibiotic. The explained variance in the New York State hospitalization charges exceeds that observed in other published clinical predictor models of hospital charges based on statewide or province‐wide discharge databases.12, 20, 21 Although less variability was explained in national models, independent adverse drug effects influence on both total charge and length of stay were also observed. Higher charges with adverse drug effect associated admissions could be explained in part by increased illness severity, leading to more hospital days, and thus higher charges in per diem reimbursement schemes. In DRG‐based reimbursements, adverse drug effect presence in an admission, with its attendant increased length of stay, could be considered an outlier case, in which case an increased inpatient prospective payment system (IPPS) payment would be authorized in addition to the base payment.22
Because the impact of adverse drug effects on length of stay was still present even after controlling for both skin/allergy and GI manifestations, this may suggest that other factors relating to the adverse drug effects may have influenced LOS. These factors might include physician reluctance to discharge these patients or the influence of other organ systems not accounted for or reported in this study. The attenuation of the adverse drug effect's influence on hospital charge models by including possible clinical manifestations of adverse drug effects suggests that these manifestations were the main contributors to higher charges associated with adverse drug effect admissions. These disparate findings regarding adverse drug effects on LOS versus charges are consistent with the notion that hospital LOS and hospital charge are separate constructs, which may be associated with separate factors affecting these outcomes.23 The 13% variation in LOS explained in the New York state hospitalization regression models was similar to the 14% variation in LOS observed in clinical predictor models for congestive heart failure hospitalizations in New York state.24 Layde et al.12 found a 14.5% and 18.5% adjusted increase in charges and LOS associated with any medical injury in Wisconsin hospital discharges. The excess length of stay due to antibiotic related medical injury was 1.27 days. This magnitude of effect is comparable to that observed in the present study.
There are a number of limitations in this study related to coding practices and the retrospective nature of the investigation. Currently, there are no ICD‐9 e‐codes for adverse effects due to commonly used older antibiotics such as vancomycin, clindamycin, and metronidazole, or to the newer antibiotic classes. Since currently recommended treatments for community‐acquired pneumonia25 are among the specified drugs with adverse effect coding, and since other specified and unspecified anti‐infective drug‐associated (no drug names or categories provided) adverse effects were frequent, it suggests that infectious processes other than community‐acquired pneumonia were also being treated in many hospitalizations. Another limitation is that because the temporal sequence of events cannot be ascertained with this data, it is possible that an adverse drug effect was due to an antibiotic given prior to hospitalization. It has been suggested that onset of diagnosis or present on admission information be part of a new administrative data coding strategy which has been used in some states in the US.19 The adoption of ICD‐10 codes may allow for more specificity and detailing of adverse drug reactions using administrative data, as described for the United Kingdom by Waller et al.26 The actual incidence of hospitalization‐associated adverse drug effects could be underestimated if a significant number of adverse effects occurred after discharge as only in‐hospital events were recorded.
In summary, we found that although the incidence of adverse drug effects is small, there is a definite quantifiable impact of these adverse effects on LOS and hospital charges in patients hospitalized with pneumonia. To our knowledge, there have not been similar large‐scale database studies to evaluate the incidence and impact of adverse drug effects related to antibiotics in both national and statewide samples. These findings also have implications in studies of outcomes related to pneumonia hospitalizations.
Acknowledgements
The authors thank Ariel D. Teitel, MD, for his assistance. This study was supported in part by the intramural scholarship program at New York Medical College.
Adverse drug eventsdefined as an injury resulting from medical intervention related to a drug1significantly contribute to health care expenditures. Over 770,000 people are injured or die every year in hospitals from adverse drug events, and national hospital expenses to treat patients who have suffered adverse drug events during hospitalization have been estimated to be between $1.56 and $4.2 billion annually.2 In a meta‐analysis of prospective studies, researchers found that adverse drug reactions, one important form of adverse drug events, may rank as the fourth to sixth leading cause of death in the United States, with more than 100,000 deaths per year.3 Understanding the factors associated with these adverse events may help in the development of prevention strategies, with resulting improving health care quality and lowering health care costs.
Among hospitalized patients, antibacterial adverse effects may account for approximately 25% of adverse drug reactions.1, 4 While the economic impact has been studied for overall adverse drug events in hospitalized patients in the 1990s, more recent detailed studies for the impact of antibiotic‐related adverse drug effects have not been published. As hospitalized patients with the primary diagnosis of pneumonia are invariably treated with antibiotics, and since pneumonia is the third leading cause for hospitalization in the United States,5 hospitalization databases that document pneumonia hospitalizations as well as adverse effects from antibiotics, using specific International Classification of Diseases, Ninth Revision (ICD‐9) clinical modification codes, constitute a unique and rich resource for quantifying and analyzing the incidence and impact of antibiotic‐associated adverse drug effects.
The purpose of this study was to describe the incidence and clinical manifestations of adverse drug effects in pneumonia hospitalizations in recent years, and to determine the types of patients and comorbidities, which are most commonly associated with adverse drug effects. The term adverse drug effect refers more to known side effects of medications, whereas adverse drug events and adverse drug reactions refer to an injury or a noxious, unintended, and undesired effect resulting from administration of a drug.6 As this study utilized medical coding for data abstraction, the broader classifications of adverse drug events or reactions could not be examined and instead the outcome of adverse drug effect was utilized.
METHODS
Data Sources
The Statewide Planning and Research Cooperative System (SPARCS) database was accessed as previously described.7, 8 There is mandatory reporting to this database for all New York State acute care hospitalizations. Each deidentified SPARCS admission record contains more than 100 data fields9 that consist of demographic, clinical, and financial information. These fields include principal and nonprincipal diagnostic fields, procedure codes, race, age, gender, and ethnicity information, hospital characteristics, expected reimbursement, total charges, length of stay (LOS), admission status, and disposition status. Both ICD‐9 and Common Procedural Terminology (CPT) codes are input for each admission.
The Nationwide Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project (HCUP), contains annual hospital discharge data from a sample of US hospitals.10 Each NIS patient record includes data fields consisting of demographic, clinical, and financial information. These fields include primary and secondary diagnostic fields, procedure codes, age, gender, race, total charges, length of stay, payer codes, hospital characteristics, and disposition status. Twenty percent random subsamples from each year's sample were employed to perform the analyses. HCUP databases include appropriately‐scaled discharge weights to generate national estimates of hospitalizations and total charges from the NIS. These weights allow comparison of incidence rates and charges across years despite a varying number of states and hospitals included in the database each year.
This study was given an exemption from institutional research board approval by the SVCMC Integrated Scientific and Ethical Review Board.
Identification of Pneumonia Admissions
To achieve more uniformity in the cohorts, it was decided to select only hospitalizations with the most common ICD‐9 and diagnosis‐related group (DRG) codes for pneumonia for more recent years. ICD‐9 and DRG codes have been used to identify pneumonia patients in administrative data, and cases selected in this manner show excellent specificity when compared to a reference standard.11 Hospitalization discharges from both databases from 2000 through 2005 were selected with the criterion of having the principal diagnosis of ICD‐9 code 486 (pneumonia, organism unspecified) and the DRG of 89 (simple pneumonia and pleurisy, age >17 years, with complication and comorbidity), thus targeting community acquired pneumonia. These hospitalizations formed the 2 cohorts of pneumonia hospitalizations. Preliminary analyses showed that hospitalizations identified by these criteria identified more than 60% of pneumonia admissions defined by a more expansive criteria11 of having any of the DRG codes 79 (respiratory infections and inflammations, age >17 years, with complications and comorbidity), 80 (respiratory infections and inflammations, age >17 years, without complications and comorbidity), 89 and 90 (simple pneumonia and pleurisy, age >17 years, without complication and comorbidity). Gram‐negative pneumonia, aspiration pneumonia, and pneumonias due to other specific infectious agents were not targeted in this study.
Data Classifications
The state and national cohorts were queried for the presence of adverse effects due to various antibiotics and anti‐infectives, using specific ICD‐9 external cause of injury codes (e‐codes) including e930 and e931. E‐codes were developed as a supplemental code for use with the ICD and they provide a systematic way to classify diagnostic information that health care providers have entered into the medical record. E‐codes have been shown to be useful and sensitive in detecting medical injuries due to drugs (including antibiotics) in hospital discharge data.12 On the basis of frequency of observed adverse drug effects (as detected by e‐codes), an adverse drug effect due to an anti‐infective or antibiotic was defined as that which was due to penicillins (E930.0), erythromycin and other macrolides (E930.3), tetracyclines (E930.5), cephalosporins (E930.5), sulfonamides (E931.0), quinolones (E931.3), other specified antibiotics (E930.9), other unspecified antibiotics (E931.9), or antimycobacterials (E931.8 and E930.6). Adverse drug effects due to other anti‐infectives were not included due to extremely low incidence and unlikely clinical usage in pneumonia. National estimates of the number of patients experiencing an adverse drug effect were determined using discharge weights to adjust for subset sample size.
The ICD‐9 codes for possible skin and allergy manifestations commonly associated with adverse drug effects were examined in patients with and without adverse drug effects as defined previously. The ICD‐9 codes for skin/allergy manifestations that were considered as possibly due to adverse drug effects included erythema, not otherwise specified (695.9), flushing (782.62), Stevens‐Johnson syndrome (695.1), allergic purpura (287.0), dermatitis due to drugs and medications taken internally (693.0), angioedema (995.1), unspecified allergy, (995.3), anaphylaxis not otherwise specified (NOS) (999.5), and urticaria (708). Gastrointestinal (GI) manifestations considered as possibly due to an adverse drug effect included nausea (787.02), vomiting (787.03), nausea with vomiting (787.01), diarrhea, not otherwise specified (787.91), diarrhea, other and unspecified noninfectious gastroenteritis and colitis (558.9), or intestinal infection due to Clostridium difficile (008.45).
Statistical Analysis
Analyses were performed using JMP version 5.1 and SAS for Windows version 9 (SAS Institute, Cary, NC). In linear regression models, principal outcomes of length of stay and total hospital charges were logarithmically transformed, as this data transformation reduces the influence of outliers.13 Cases with a length of stay less than 1 day were considered to have a 23‐hour LOS, to enable logarithmic transformation. Linear regression models were created to assess the impact of adverse drug effects due to antibiotics on length of stay and total charge. Linear regression models have been shown to be useful in identifying factors associated with increased hospital charges.13 Adjusting factors that were considered in multivariate models included comorbid conditions and demographic factors. Only common comorbidities that were present in greater than 5% of cases were considered and included cancer (140 through 208), congestive heart failure (428), ischemic heart disease (410414), chronic obstructive pulmonary disease (491, 492, 496), diabetes mellitus (250), hypertension (401), asthma (493), urinary tract infection (599.0), unspecified anemia (285.9), pleural effusion (511.9), cardiac dysrhythmia (427.31), volume depletion (276.5), unspecified acquired hypothyroidism (244.9), and hypoosmolality/hyponatremia (276.1). Demographic factors such as gender, race, age, year and month of admission, and day of admission were also considered in the model. The hospital where the admission occurred was used for New York State calculations. For the national data, the region and hospital characteristics but not the hospital identification number itself were considered since not all of the same hospitals were sampled each year. Finally, the governmental health insurance status (Medicare or Medicaid for both sets of data) was considered. Medicaid and Medicaid Health Maintenance Organization (HMO) as expected reimbursement categories were considered as a single group as were Medicare and Medicare HMO in the New York State database. All of these covariants were subject to forward stepwise selection for modeling adjustment purposes. The probability required for a covariant to enter the model was 0.250 and the probability at which a covariant was removed from the model was 0.100. These adjustment factors were held constant in adjusted models examining for the independent predictor effects of adverse drug reactions. To examine whether or not the presence of GI and/or skin manifestations commonly associated with adverse drug effects accounted for differences in LOS/charges, we examined whether or not adding the manifestations as a covariant would attenuate the predictor effect of the adverse drug effect.
In order to make a practical assessment of the impact of adverse drug effects on LOS and hospital charges, we chose as an example patient a 70‐year‐old white female with a diagnosis of diabetes and hypertension, with Medicare.
Logistic regression models were used to explore comorbid conditions and demographic features that were associated with adverse drug effects within the cohort. Forward stepwise regression was used using previously described entry/exit criteria. Odds ratios for individual predictor variables were adjusted for other significant predictor variables.
All regression models were adjusted for sampling weights in national data analyses. The time trends (year effect) for the incidences of adverse drug effects were analyzed with the GENMOD procedure in SAS, with the negative binomial distribution option.14, 15
RESULTS
In the New York (SPARCS) database (NYS), 278,425 pneumonia admissions were identified. In HCUP‐NIS data subsets (NIS), 186,193 pneumonia admissions formed the cohort. In both cohorts, there was a predominance of females and older patients (Table 1). Diabetes and hypertension were common comorbidities. In the NYS cohort, 1,329 (0.48%) had an adverse effect related to an antibiotic or anti‐infective. In the NIS cohort, an estimated 0.53% had an adverse drug effect. There was a small but significant increase in the percentage of national hospitalizations associated with an antibiotic adverse drug effect over time (time effect significance; P = 0.0149; Table 1). However, this trend was not seen in the NYS cohort.
| Database | SPARCS | HCUP‐NIS |
|---|---|---|
| ||
| Cohort years | 20002005 | 20002005 |
| Cohort region | New York State | United States |
| Cohort size (identified cases) | 278,425 | 186,193 |
| Estimated actual number (n) of cases for cohort region | 278,425 | 4,547,108 |
| African American (%) | 12.8 | 7.6 |
| Females (%) | 53.8 | 54.4 |
| Medicare (%) | 72.9 | 72.8 |
| Mean age (years) | 72.5 | 71.4 |
| Diabetes mellitus (%) | 25.4 | 24.4 |
| Hypertension (%) | 41.2 | 39.0 |
| Death (%) | 6.8 | 4.7 |
| 2000 ADE (%)/n | 0.44/205 | 0.48/3372 |
| 2001 ADE (%)/n | 0.47/208 | 0.53/3797 |
| 2002 ADE (%)/n | 0.49/225 | 0.53/3985 |
| 2003 ADE (%)/n | 0.48/229 | 0.57/3564 |
| 2004 ADE (%)/n | 0.52/249 | 0.56/4250 |
| 2005 ADE (%)/n | 0.46/213 | 0.60/4979 |
| Total hospital charges* | $4,815,100,411 | $70,285,286,226 |
The most numerous adverse effects were noted in other specified antibiotics, followed by other unspecified antibiotics, then cephalosporins in both databases (Table 2). Cephalosporins accounted for 15% and 14% of cases with adverse drug effect due to antibiotics or anti‐infectives in the NYS and NIS cohorts, respectively. Adverse drug effects due to the penicillins and quinolones were similar in frequency and were the next most common identifiable classes of antibiotics with adverse drug effects after cephalosporins. Adverse effects to other specified antibiotics and unspecified antibiotics combined constituted 59% of adverse drug effects in both NYS and NIS cohorts.
| Antibiotic | New York State (SPARCS) | National Estimates (HCUP‐NIS) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ADE (n) | ADE % of Total | ADE with Skin* (%) | ADE with GI (%) | ADE with GI and/or Skin* (%) | ADE (n) | ADE % of Total | ADE with Skin* (%) | ADE with GI (%) | ADE with GI and/or Skin* (%) | |
| ||||||||||
| Penicillins | 91 | 7 | 58 | 21 | 78 | 1484 | 8 | 47 | 17 | 64 |
| Erythromycin/macrolides | 102 | 8 | 28 | 44 | 71 | 1608 | 8 | 19 | 51 | 69 |
| Tetracyclines | 14 | 1 | 50 | 7 | 57 | 182 | 1 | 46 | 27 | 73 |
| Cephalosporins | 194 | 15 | 60 | 21 | 80 | 2684 | 14 | 55 | 19 | 69 |
| Other specified antibiotics | 512 | 39 | 40 | 29 | 67 | 5986 | 30 | 37 | 29 | 62 |
| Other unspecified antibiotics | 276 | 21 | 22 | 50 | 72 | 5766 | 29 | 16 | 49 | 64 |
| Sulfonamide | 22 | 2 | 64 | 9 | 68 | 298 | 2 | 53 | 7 | 60 |
| Quinolones | 94 | 7 | 36 | 18 | 53 | 1479 | 8 | 49 | 20 | 65 |
| Antimycobacterials | 42 | 3 | 38 | 28 | 60 | 64 | 0 | 27 | 0 | 27 |
| ADE due to any of the above | 1329 | 100 | 43 | 31 | 72 | 19740 | 100 | 34 | 33 | 65 |
Hospitalizations associated with an adverse drug effect had higher proportions of women than hospitalizations without an adverse drug effect in both the NIS (65% versus 54%) and NYS (62% versus 54%) databases. Hospitalizations associated with an adverse drug effect had a mean age that was about 1 year younger than that observed in hospitalizations without an adverse drug effect in both databases. Congestive heart failure was present in a lower proportion of hospitalizations associated with an adverse drug effect compared to hospitalizations without adverse drug effects (NYS 27% versus 30%, NIS 25% versus 29%). In the NIS database, adverse drug effect associated hospitalizations had a lower proportion of chronic obstructive pulmonary disease than other hospitalizations (32% versus 40%). Neither database showed any adverse drug effect associated disproportion with regard to hypertension and diabetes mellitus.
In logistic regression modeling, significant predictors for an adverse drug effect included non‐African American race, older age, female gender, not having Medicaid, and residence outside the greater NY area (only in the NYS data). Non‐African‐Americans were more likely than African‐Americans to have adverse drug effect admissions (adjusted odds ratio for NYS 2.2, 95% CI, 1.72.8; and for NIS 2.1, 95% CI, 1.63.0). Females were more likely than males to be associated with adverse drug effect admissions (adjusted odds ratio for NYS 1.5, 95% CI, 1.31.6; and for NIS 1.6, 95% CI, 1.41.8). In addition, residence outside the greater NY area was associated with adverse drug effect associated admissions (adjusted odds ratio 2.1, 95% CI, 1.82.3) in NYS data.
Skin and allergy manifestations potentially associated with adverse drug effects were reported in 34% and 43% of the NIS and NYS cohorts, respectively. In comparison, less than 1% of non‐adverse drug effect admissions had these manifestations (Table 3) in either cohort. In NYS, adverse drug effects due to sulfonamides had a slightly higher proportion skin/allergy manifestations when compared with other antibiotic classes (Table 2). In contrast, NIS estimates show that adverse effects due to cephalosporins had the highest proportion of skin/allergy manifestations (Table 2). Compared to adverse drug effects due to other specified antibiotics, erythromycin/macrolides were more likely to present with GI manifestations in both databases (Table 2). Dermatitis due to drugs taken internally was coded for in 34% (NYS) and 26% (NIS) of patients that experienced an adverse drug effect, making this condition the most common skin/allergy manifestation associated with an adverse drug effect (Table 3). This was followed in frequency by urticaria and pruritus. Diarrhea was also a common symptom related to adverse drug effects (Table 3). While 72% of adverse drug effects had either GI or skin/allergy manifestations in the NYS cohort, only 65% of the NIS cohort had these manifestations reported. No increase in mortality was observed in patients with adverse drug effects compared to those without adverse drug effects (data not shown).
| Clinical Manifestation | New York State SPARCS | National Estimates HCUP‐NIS | ||
|---|---|---|---|---|
| No Adverse Effect (%) | Adverse Effect (%) | No Adverse Effect (%) | Adverse Effect (%) | |
| Dermatitis due to drugs taken internally | 0.1 | 34.1 | 0.1 | 25.9 |
| Pruritus | 0.1 | 3.5 | 0.1 | 3 |
| Urticaria | 0.0 | 4.0 | 0.0 | 3.6 |
| Erythema | 0.0 | 0.2 | 0.0 | 0.2 |
| Angioedema | 0.0 | 0.8 | 0.0 | 0.7 |
| Stevens‐Johnson syndrome | 0.0 | 0.3 | 0.0 | 0.2 |
| Anaphylaxis | 0.0 | 0.9 | 0.0 | 0.2 |
| Allergy, unspecified | 0.0 | 0.2 | 0.0 | 0.7 |
| Nausea and/or vomiting | 0.6 | 6.3 | 0.9 | 7.4 |
| Diarrhea, nonspecified or due to C. difficile | 3.5 | 26.5 | 3.1 | 25.5 |
Both databases showed that adverse drug effects affected both LOS and total charges (Table 4). In the NIS database, adjusted models showed that GI manifestations impacted hospital charges more than skin/allergy manifestations (Table 4). In both the NYS and NIS cohorts, the effect of adverse drug effects on hospital charges was attenuated after accounting for skin/allergy and GI manifestations. However, even after accounting for both manifestations, there still was a significant adverse drug effect influence on LOS. In the example patient, predicted excess hospitalization charges associated with the presence of an adverse drug effect was $1,243 and $3,373 for the NIS and NYS cohorts, while LOS increases associated with an adverse drug effect were about 1 day in both cohorts. Linear regression models, which included adjustment factors including comorbidities and demographic/financial factors, showed that the models accounted for 13% of the variance (R2 values) in LOS and 40% in charges for the NYS but only 7% for LOS and 15% for charges for the NIS.
| Example* Admission without ADE | Example* Admission with ADE | P Value for ADE coefficient when Added to Model | |
|---|---|---|---|
| |||
| SPARCS | |||
| Hospital charge | |||
| Simple unadjusted model | $12,274 | $13,045 | 0.007 |
| Adjusted model for comorbidities and demographics | $14,160 | $17,533 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI manifestations | $18,865 | $21,560 | <0.0001 |
| Adjusted model for comorbidities and demographics including skin/allergy manifestations | $16,777 | $19,370 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI and skin/allergy manifestations | $23,227 | $24,275 | 0.0227 |
| LOS (days) | |||
| Simple unadjusted model | 5.4 | 6.7 | <0.0001 |
| Adjusted model for comorbidities and demographics | 4.0 | 5.2 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI manifestations | 5.4 | 6.5 | <0.0001 |
| Adjusted model for comorbidities and demographics including skin/allergy manifestations | 4.8 | 5.8 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI and skin/allergy manifestations | 6.8 | 7.4 | <0.0001 |
| HCUP | |||
| Hospital charge | |||
| Simple unadjusted model | $10,840 | $11,917 | 0.0008 |
| Adjusted model for comorbidities and demographics | $12,941 | $14,284 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI manifestations | $14,923 | $15,781 | 0.0208 |
| Adjusted model for comorbidities and demographics including skin/allergy manifestations | $13,543 | $14,723 | 0.0092 |
| Adjusted model for comorbidities and demographics including GI and skin/allergy manifestations | $15,887 | $16,453 | 0.1784 |
| LOS (days) | |||
| Simple unadjusted model | 4.4 | 5.1 | <0.0001 |
| Adjusted model for comorbidities and demographics | 4.0 | 4.9 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI manifestations | 4.8 | 5.5 | <0.0001 |
| Adjusted model for comorbidities and demographics including skin/allergy manifestations | 4.0 | 4.7 | <0.0001 |
| Adjusted model for comorbidities and demographics including GI and skin/allergy manifestations | 5.3 | 5.9 | <0.0001 |
DISCUSSION
This study documents antibiotic related adverse drug effects as a predictable, but infrequent complication that occurs in adult patients hospitalized for pneumonia. While the incidence of antibiotic‐related adverse drug events has been calculated in both hospital2 and nursing home16 populations, these studies have not specified admissions that were associated with antibiotic use. Thus calculations of antibiotic adverse drug events for actual at‐risk patients (ie, those receiving antibiotics) are imprecise in these reports. In the present study, it is highly probable that nearly all admissions were associated with actual antibiotic administration. Thus, a rough incidence of an identifiable antibiotic adverse drug effect for adult pneumonia admissions can be expected to be roughly 0.5%. Of interest is the observation that the national incidence of this complication appears to be increasing slightly but steadily in recent years. This could be explained on the basis of increased coding slots or DRG creep17 in more recent years with the national cohort. Layde et al.12 utilized e‐codes to identify medical injury due to medications in Wisconsin hospital discharge data (excluding newborn delivery discharges), unselected for infectious diseases. They calculated an overall 0.5% incidence of antibiotic‐associated adverse effects. Since not all hospitalizations are associated with antibiotic administration, this would imply that the incidence of antibiotic associated adverse effects in hospitalized patients actually given antibiotics would be higher than 0.5%. The relatively low incidence of antibiotic‐associated adverse effects observed in the present study may relate to briefer and less complex hospitalizations for these patients compared with other patients treated with antibiotics. The use of ICD‐9 codes (including e‐codes) as flags of adverse drug events may also underestimate actual rates. In a study of Utah hospitalization discharges in 2001, Hougland et al.18 found that these flags had a sensitivity of 55% for confirmed adverse drug events of various categories. This contrasts with the 98.5% sensitivity of e‐codes to identify medical injury due to drugs, described in the Wisconsin hospital discharge data. The distinction between adverse drug effects, adverse drug reactions, and adverse drug events may be important in understanding these data. Adverse drug reactions have been defined as any noxious, unintended, and undesired effect of a drug, which occurs at doses used in humans for prophylaxis, diagnosis, or therapy and can be considered a subset of adverse drug events, which, unlike adverse drug reactions, may also be due to drug administration errors.6 The term adverse drug effect has been used more in pharmacology literature4 and in medical coding,18 and may refer more to known side effects of medications, whereas adverse drug events have been broadly defined as an injury resulting from administration of a drug.6 As this study utilized medical coding for data abstraction, we used the term adverse drug effect for all results.
Determining factors that influence hospital charges and length of stay are complex. Regional differences19 may be 1 factor, as suggested by difference in charges for the example admission models (Table 4). The multivariate analyses showed that nearly 40% of the variation in total New York State hospitalization charges could be explained on the basis of demographic, comorbidity factors, and between hospital variation, with an additional independent effect identifiable in the presence of an adverse drug effect to an antibiotic. The explained variance in the New York State hospitalization charges exceeds that observed in other published clinical predictor models of hospital charges based on statewide or province‐wide discharge databases.12, 20, 21 Although less variability was explained in national models, independent adverse drug effects influence on both total charge and length of stay were also observed. Higher charges with adverse drug effect associated admissions could be explained in part by increased illness severity, leading to more hospital days, and thus higher charges in per diem reimbursement schemes. In DRG‐based reimbursements, adverse drug effect presence in an admission, with its attendant increased length of stay, could be considered an outlier case, in which case an increased inpatient prospective payment system (IPPS) payment would be authorized in addition to the base payment.22
Because the impact of adverse drug effects on length of stay was still present even after controlling for both skin/allergy and GI manifestations, this may suggest that other factors relating to the adverse drug effects may have influenced LOS. These factors might include physician reluctance to discharge these patients or the influence of other organ systems not accounted for or reported in this study. The attenuation of the adverse drug effect's influence on hospital charge models by including possible clinical manifestations of adverse drug effects suggests that these manifestations were the main contributors to higher charges associated with adverse drug effect admissions. These disparate findings regarding adverse drug effects on LOS versus charges are consistent with the notion that hospital LOS and hospital charge are separate constructs, which may be associated with separate factors affecting these outcomes.23 The 13% variation in LOS explained in the New York state hospitalization regression models was similar to the 14% variation in LOS observed in clinical predictor models for congestive heart failure hospitalizations in New York state.24 Layde et al.12 found a 14.5% and 18.5% adjusted increase in charges and LOS associated with any medical injury in Wisconsin hospital discharges. The excess length of stay due to antibiotic related medical injury was 1.27 days. This magnitude of effect is comparable to that observed in the present study.
There are a number of limitations in this study related to coding practices and the retrospective nature of the investigation. Currently, there are no ICD‐9 e‐codes for adverse effects due to commonly used older antibiotics such as vancomycin, clindamycin, and metronidazole, or to the newer antibiotic classes. Since currently recommended treatments for community‐acquired pneumonia25 are among the specified drugs with adverse effect coding, and since other specified and unspecified anti‐infective drug‐associated (no drug names or categories provided) adverse effects were frequent, it suggests that infectious processes other than community‐acquired pneumonia were also being treated in many hospitalizations. Another limitation is that because the temporal sequence of events cannot be ascertained with this data, it is possible that an adverse drug effect was due to an antibiotic given prior to hospitalization. It has been suggested that onset of diagnosis or present on admission information be part of a new administrative data coding strategy which has been used in some states in the US.19 The adoption of ICD‐10 codes may allow for more specificity and detailing of adverse drug reactions using administrative data, as described for the United Kingdom by Waller et al.26 The actual incidence of hospitalization‐associated adverse drug effects could be underestimated if a significant number of adverse effects occurred after discharge as only in‐hospital events were recorded.
In summary, we found that although the incidence of adverse drug effects is small, there is a definite quantifiable impact of these adverse effects on LOS and hospital charges in patients hospitalized with pneumonia. To our knowledge, there have not been similar large‐scale database studies to evaluate the incidence and impact of adverse drug effects related to antibiotics in both national and statewide samples. These findings also have implications in studies of outcomes related to pneumonia hospitalizations.
Acknowledgements
The authors thank Ariel D. Teitel, MD, for his assistance. This study was supported in part by the intramural scholarship program at New York Medical College.
- ,,, et al.Incidence of adverse drug events and potential adverse drug events: implications for prevention.JAMA.1995;274:29–34.
- ,,, et al.Adverse drug events in hospitalized patients.JAMA.1997;277:301–306.
- ,,.Incidence of adverse drug reactions in hospitalized patients.JAMA.1998;279:1200–1205.
- ,,.Economic aspects of antibacterial adverse effects.Pharmacoeconomics.1998;13:35–49.
- ,.1999National Hospital Discharge Survey. Advance data from vital and health statistics; no 319.Hyattsville, MD:National Center for Health Statistics;year="2001"2001.
- ,,.Incidence of adverse drug reactions in hospitalized patients: a meta‐analysis of prospective studies.JAMA.1998;279:1200–1205.
- ,,,.Asthma hospitalization patterns in young children relating to admission age, infection presence, sex, and race.Ann Allergy Asthma Immunol.2007;98:139–145.
- ,,.Pattern of hospitalizations for angioedema in New York between 1990 and 2003.Ann Allergy Asthma Immunol.2005;95:159–166.
- Inpatient Output Data Dictionary, SPARCS. Available at: http://www.health.state.ny.us/statistics/sparcs/inpat.htm. Accessed October2008.
- Agency for Healthcare Research and Quality.The HCUP Nationwide Inpatient Sample (NIS).Rockville, MD:Agency for Healthcare Research and Quality;2004.
- ,,,.Accuracy of administrative data for identifying patients with pneumonia.Am J Med Qual.2005;20:319–328.
- ,,, et al.Medical injury identification using hospital discharge data.Advances in Patient Safety. Vol2.Rockville, MD:Agency for Healthcare Research and Quality;2007. Available at: http://www.ahrq.gov/downloads/pub/advances/vol2/Layde.pdf. Accessed October 2008.
- ,,.A comparison of several regression models for analyzing cost of CABG surgery.Stat Med.2003;22:2799–2815.
- University of Kentucky. Poisson and negative binomial regressions. Available at: http://www.uky.edu/ComputingCenter/SSTARS. Accessed October2008.
- ,,.Regression analyses of counts and rates: Poisson, overdispersed Poisson, and negative binomial models.Psychol Bull.1995;118;392–404.
- ,,, et al.Incidence and preventability of adverse drug events in nursing homes.Am J Med.2000;1;109:87–94.
- ,.Administrative data based patient safety research: a critical review.Qual Saf Health Care.2003;12(Suppl 2):ii58–ii63.
- ,,, et al.Performance of International Classification of Diseases, 9th Revision, Clinical Modification codes as an adverse drug event surveillance system.Med Care.2006;44:629–636.
- ,,.Direct medical costs of bronchiolitis hospitalizations in the United States.Pediatrics Dec.2006;118:2418–2423.
- ,,.Relationship of hospital size, case volume, and cost for coronary artery bypass surgery: analysis of 12,774 patients operated on in Massachusetts during fiscal years 1995 and 1996.J Thorac Cardiovasc Surg.2001;122:53–64.
- ,,,.Comorbidity measures for use with administrative data.Med Care.1998;36:8–27.
- Health and Human Services. Centers for Medicaid and Medicare Services (CMS) Home. Medicare. Acute Inpatient PPS. Overview. Available at: http://www.cms.hhs.gov/AcuteInpatientPPS. Accessed October2008.
- ,,,.Identifying pre‐ and postoperative predictors of cost and length of stay for coronary artery bypass surgery.Am J Med Qual.1999:14:248–254.
- ,,, et al.Hospital outcomes in major teaching, minor teaching, and nonteaching hospitals in New York state.Am J Med.2002;112:255–261.
- ,,, et al.Infectious Disease Society/American Thoracic Society Consensus Guidelines on the Management of Community‐Acquired Pneumonia in Adults.Clin Infect Dis.2007;44:S27–S72.
- ,,,,.Hospital admissions for ‘drug‐induced’ disorders in England: a study using the Hospital Episodes Statistics (HES) database.Br J Clin Pharmacol.2005;59:213–219.
- ,,, et al.Incidence of adverse drug events and potential adverse drug events: implications for prevention.JAMA.1995;274:29–34.
- ,,, et al.Adverse drug events in hospitalized patients.JAMA.1997;277:301–306.
- ,,.Incidence of adverse drug reactions in hospitalized patients.JAMA.1998;279:1200–1205.
- ,,.Economic aspects of antibacterial adverse effects.Pharmacoeconomics.1998;13:35–49.
- ,.1999National Hospital Discharge Survey. Advance data from vital and health statistics; no 319.Hyattsville, MD:National Center for Health Statistics;year="2001"2001.
- ,,.Incidence of adverse drug reactions in hospitalized patients: a meta‐analysis of prospective studies.JAMA.1998;279:1200–1205.
- ,,,.Asthma hospitalization patterns in young children relating to admission age, infection presence, sex, and race.Ann Allergy Asthma Immunol.2007;98:139–145.
- ,,.Pattern of hospitalizations for angioedema in New York between 1990 and 2003.Ann Allergy Asthma Immunol.2005;95:159–166.
- Inpatient Output Data Dictionary, SPARCS. Available at: http://www.health.state.ny.us/statistics/sparcs/inpat.htm. Accessed October2008.
- Agency for Healthcare Research and Quality.The HCUP Nationwide Inpatient Sample (NIS).Rockville, MD:Agency for Healthcare Research and Quality;2004.
- ,,,.Accuracy of administrative data for identifying patients with pneumonia.Am J Med Qual.2005;20:319–328.
- ,,, et al.Medical injury identification using hospital discharge data.Advances in Patient Safety. Vol2.Rockville, MD:Agency for Healthcare Research and Quality;2007. Available at: http://www.ahrq.gov/downloads/pub/advances/vol2/Layde.pdf. Accessed October 2008.
- ,,.A comparison of several regression models for analyzing cost of CABG surgery.Stat Med.2003;22:2799–2815.
- University of Kentucky. Poisson and negative binomial regressions. Available at: http://www.uky.edu/ComputingCenter/SSTARS. Accessed October2008.
- ,,.Regression analyses of counts and rates: Poisson, overdispersed Poisson, and negative binomial models.Psychol Bull.1995;118;392–404.
- ,,, et al.Incidence and preventability of adverse drug events in nursing homes.Am J Med.2000;1;109:87–94.
- ,.Administrative data based patient safety research: a critical review.Qual Saf Health Care.2003;12(Suppl 2):ii58–ii63.
- ,,, et al.Performance of International Classification of Diseases, 9th Revision, Clinical Modification codes as an adverse drug event surveillance system.Med Care.2006;44:629–636.
- ,,.Direct medical costs of bronchiolitis hospitalizations in the United States.Pediatrics Dec.2006;118:2418–2423.
- ,,.Relationship of hospital size, case volume, and cost for coronary artery bypass surgery: analysis of 12,774 patients operated on in Massachusetts during fiscal years 1995 and 1996.J Thorac Cardiovasc Surg.2001;122:53–64.
- ,,,.Comorbidity measures for use with administrative data.Med Care.1998;36:8–27.
- Health and Human Services. Centers for Medicaid and Medicare Services (CMS) Home. Medicare. Acute Inpatient PPS. Overview. Available at: http://www.cms.hhs.gov/AcuteInpatientPPS. Accessed October2008.
- ,,,.Identifying pre‐ and postoperative predictors of cost and length of stay for coronary artery bypass surgery.Am J Med Qual.1999:14:248–254.
- ,,, et al.Hospital outcomes in major teaching, minor teaching, and nonteaching hospitals in New York state.Am J Med.2002;112:255–261.
- ,,, et al.Infectious Disease Society/American Thoracic Society Consensus Guidelines on the Management of Community‐Acquired Pneumonia in Adults.Clin Infect Dis.2007;44:S27–S72.
- ,,,,.Hospital admissions for ‘drug‐induced’ disorders in England: a study using the Hospital Episodes Statistics (HES) database.Br J Clin Pharmacol.2005;59:213–219.
Copyright © 2009 Society of Hospital Medicine
Standardized Orders Improve Pediatric Care
For many years physicians have created and used various standardized order forms for patient hospital admissions. The increasing popularity of electronic medical records and forms has led to the use of computerized physician order entry (CPOE) as a means of reducing medication errors.13 Crowley et al.,4 Stucky,5 and Garg et al.,6 along with various committees, have recommended standardized order sets and CPOE as a strategy for reducing medication errors. However, implementation of CPOE systems is expensive and not available in most hospitals. According to a recent survey of hospitals in the US, CPOE was only available to physicians at 16% of the participating institutions.7 Until CPOE becomes widespread, standardized preprinted formatted order sets may serve as an inexpensive alternative.
There is anecdotal evidence that standardized admission order forms may improve quality of care and efficiency, and decrease provider variation.8 However, few rigorous studies exist in the pediatric research literature regarding their ability to actually improve patient care.
In 2005, our institution, a large tertiary‐care academic teaching hospital, developed a standardized preprinted pediatric admission order set (PAOS). We did so for 3 reasons. First, there was a desire to improve completeness of orders. Handwritten orders often missed important elements such as weight, allergies, vital sign parameters, activity, etc. Second, there was a need to save time and improve efficiency. Third, it was important to reduce medical errors and the number of clarification requests by decreasing the necessity to decipher physician handwriting. Our PAOS was a convenience order set as opposed to a best practices order set. In other words, our PAOS did not contain evidence‐based management guidelines or protocols for specific admission diagnoses and was created solely to improve the quality and efficiency of workflow.
Documenting improvement in patient outcomes or reduction of medical errors is ultimately needed to establish the effectiveness of a standardized order set. Secondary outcomes, howeverparticularly the perceptions of the staff who are asked to use the order setare equally important, because they may identify real‐life barriers to use that, regardless of effectiveness, could limit dissemination and uptake. With respect to perceptions, 2 groups become paramount: those who write the orders, and those who respond to them. The purpose of the current study was to examine perceived effects of the new PAOS on inpatient care among those who, in our institution, write the ordersresident physicians.
MATERIALS AND METHODS
The PAOS was created in August 2005 at the University of California, Los Angeles (UCLA) Medical Center by a committee comprising pediatric hospitalists, nurses, pharmacists, residents, and clerks. The PAOS consisted mainly of check boxes (Figure 1). The PAOS was uploaded to the hospital website and made available for printing from all computers in the hospital, emergency room, and clinics.
The UCLA Hospital and Medical Center is a nonprofit, 667‐bed tertiary‐care teaching hospital in Los Angeles, California. The pediatric ward has 70 licensed beds with approximately 3,000 admissions per year. The majority of the admissions were done by the pediatric residents. Physicians were free to edit the PAOS to suit a particular patient's needs or to hand‐write orders on a blank order form.
Measures
Fourteen months after the institution of the PAOS, all 97 UCLA pediatric residents (PL‐1, n = 34; PL‐2, n = 33; PL‐3, n = 30) were asked to complete a survey to anonymously evaluate the order set. All residents were US medical school graduates. Resident participation in the research project was voluntary and confidential, and residents were assured that participation would not affect their standing in the pediatric residency program. Each resident completed only 1 survey. Responses were collected October 2006 to June 2007. The residents were asked to rate the PAOS overall and with respect to 9 specific dimensions using a 5‐point Likert scale with 1 indicating strong disagreement and 5 indicating strong agreement (Figure 2).
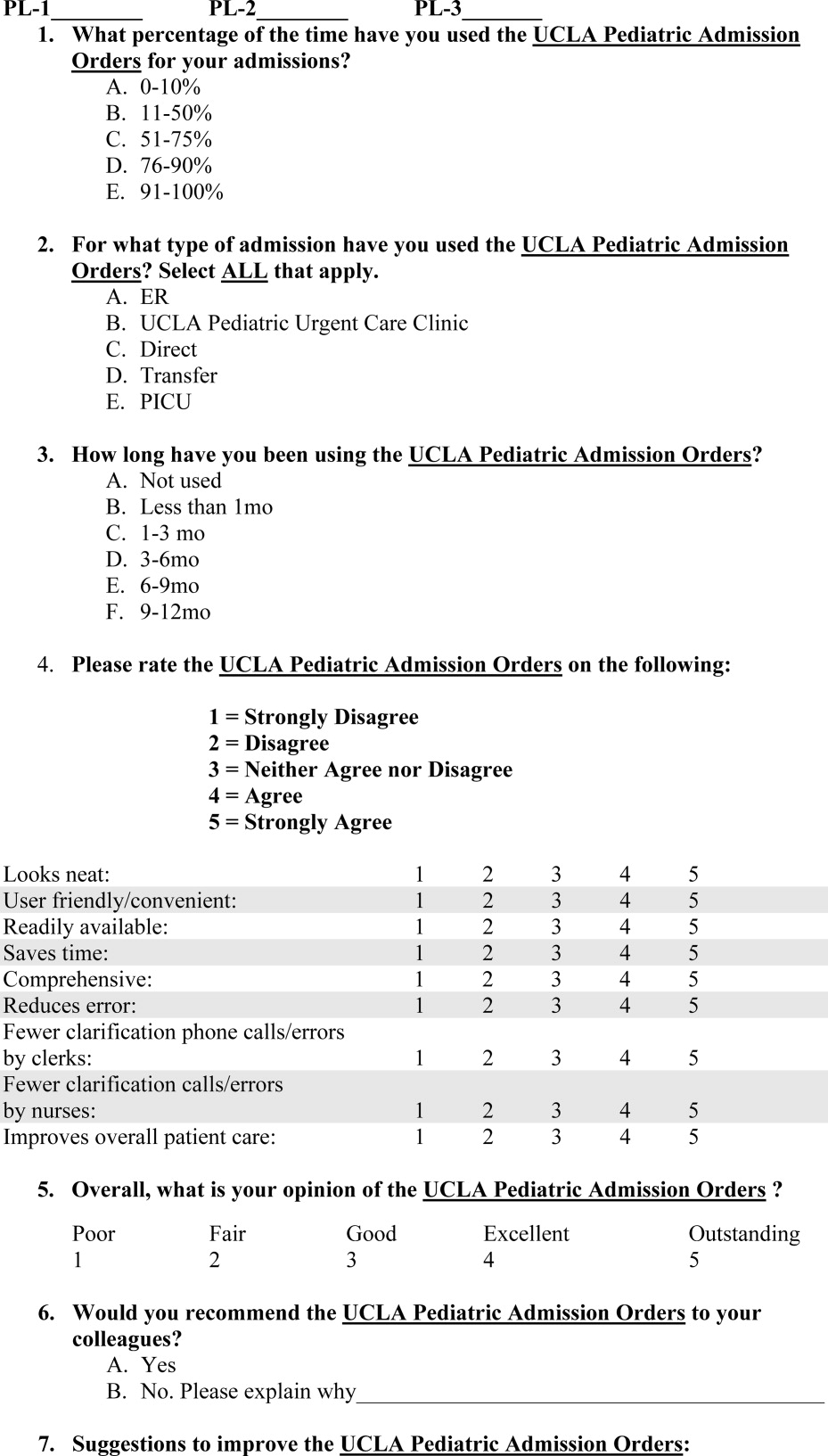
This study was reviewed and approved by the institutional review board at the UCLA Medical Center.
Statistical Analysis
We used bivariate ordered logistic regression to estimate the association between overall rating and each of the 9 dimensions. Ordered logistic regression, a standard technique for ordered categorical variables, is essentially a weighted average of logistic regressions performed at each potential cut‐point of the outcome variable. For instance, potential cut‐points on our 5‐point Likert scale included strong disagreement versus any other, any disagreement versus nondisagreement, any agreement versus nonagreement, and strong agreement versus any other. We then used multivariate ordered logistic regression to examine which specific dimensions remained independently associated with the overall rating.
RESULTS
From October 2006 to June 2007, 59 residents (from a total of 97 residents; 61%) responded to the survey. Overall, 89% of respondents approved of the PAOS, 58% reported using it 90% of the time, and all said that they would recommend it to their colleagues (Table 1). Eighty‐four percent thought that the PAOS improved inpatient care, and 75% thought that medical errors were reduced. Eighty‐eight percent reported that the POAS saved time; 93% said it was convenient; and most reported less need for clarification with clerks (81%) and nurses (82%).
| Strongly Agree (%) | Agree (%) | Other (%) | |
|---|---|---|---|
| Specific dimensions | |||
| Looks neat | 63 | 32 | 5 |
| User friendly/convenient | 60 | 33 | 7 |
| Readily available | 47 | 26 | 26 |
| Saves time | 56 | 32 | 12 |
| Comprehensive | 40 | 40 | 19 |
| Reduces medical error | 40 | 35 | 25 |
| Fewer clarification phone calls/errors by clerks | 47 | 33 | 19 |
| Fewer clarification phone calls/errors by nurses | 47 | 35 | 18 |
| Improves overall patient care | 46 | 39 | 16 |
| Overall rating | 40 | 49 | 11 |
In bivariate analyses, each of the 9 dimensions was strongly associated with the overall rating (P < 0.001 for each). In multivariate analyses, however, only perceived improvement in patient care was independently associated with overall rating (OR, 3.9; P = 0.04).
We then examined whether perceived improvement in patient care itself was independently predicted by the other 8 dimensions. Residents who said that the form was comprehensive (OR, 5.6; P = 0.01), reduced medical errors (OR, 4.1; P = 0.01), or required less need for clarification with nurses (OR, 9.6; P = 0.01) were more likely to perceive that the form improved patient care than residents who did not.
DISCUSSION
A standardized admission order set is a simple, low‐cost intervention that may benefit patients by reducing medical errors and expediting high‐quality care. In general, residents rated the PAOS favorably. Just as importantly, the PAOS scored well across all specific dimensions, which suggests few perceived barriers to use among residents.
Some dimensions, however, appeared potentially more important than others. Residents who perceived an improvement in patient care tended to rate the PAOS favorably. Perceived improvement in patient care, in turn, was linked to the order set's comprehensiveness, perceived reductions in medical errors, and less need for clarification with nurses.
Even though this study did not directly query those most responsible for responding to the order set (ie, nurses, pharmacists, and clerks), the order set was created through a collaborative partnership of physicians, nurses, pharmacists, and clerks. It is reasonable to infer that resident‐perceived reduction in the need for clarification of orders with nurses and clerks might indicate a broad‐based, multidisciplinary improvement in clarity and workflow. Moreover, the fact that less need for clarification with nurses was strongly associated with resident‐perceived improvement in patient care underscores the importance of including nurses, pharmacists, and clerks in the development of these order sets.
Our experience using the standard admission orders over the past 2 years is congruent with other authors' findings. Most studies, however, have examined standardized order forms only in adult populations, and mainly for specific medical conditions. Micek et al.9 demonstrated that use of a standardized physician order set among adults with septic shock lowered 28‐day mortality and reduced hospital stay. Among stroke patients, rates of optimal treatment significantly improved after the introduction of standardized stroke orders.10 For patients with acute myocardial infarction, standardized admission orders increased early administration of aspirin and beta blockers.11, 12 With respect to cancer, implementation of a preprinted chemotherapy prescription form improved order completeness, prevented medication errors, and reduced time spent by pharmacists clarifying orders.13 Finally, standardized trauma admission orders developed in a surgical‐trauma intensive care unit reduced admission laboratory charges and improved order completeness.14 We found only a single pediatric study examining standardized order forms. Kozer et al.15 found that the use of a preprinted structured medication order form cut medication errors nearly in half in a pediatric emergency department.
Whether our results would have been similar had we implemented a series of best practices order sets rather than a single convenience order set is unclear. Although best practices order sets would have facilitated application of evidence‐based guidelines for common diagnoses, they would also have introduced potentially unwelcome logistical heterogeneity (with a separate form and protocol needed for each diagnosis) that might have reduced acceptability and uptake. In addition, there is a risk that best practices order sets would have been perceived as unduly limiting physician professional autonomy.
Our study has limitations. First, our study was performed within a single institution and may not be easily generalized. However, we believe that the basic format of the PAOS lends it to easy adaptability. Second, we did not survey residents before the order set was introduced to assess baseline perceptions. Instead, many of the questions in the survey ask about perceived improvements compared with the previous system. Conducting a formal pre‐post data collection and analysis might have yielded different results. Third, improvement in patient care was measured indirectly based on resident opinion.
In conclusion, our study suggests that our standardized admission order set prompting physicians to initiate comprehensive care is well‐liked by residents and is thought to benefit patients by reducing medical errors and expediting high‐quality care. The next step is to confirm that the resident‐perceived improvement in patient care correlates with actual improvement in patient care. If improvements can be confirmed, then PAOS adoption could be broadly recommended to pediatric hospitals. In the future, the PAOS may also help guide computerized physician order entry templates that can be further tailored to specific common diagnoses.
- ,,, et al.Effect of computerized physician order entry and a team intervention on prevention of serious medication errors.JAMA.1998;280(15):1311–1316.
- ,,.Effects of computerized physician order entry and clinical decision support systems on medication safety: a systematic review.Arch Intern Med.2003;163(12):1409–1416.
- ,,,,.The effect of computerized physician order entry on medication errors and adverse drug events in pediatric inpatients.Pediatrics.2003;112(3 Pt 1):506–509.
- ,,.Medication errors in children: a descriptive summary of medication error reports submitted to the United States Pharmacopoeia.Curr Ther Res Clin Exp.2001;62:627–640.
- .Prevention of medication errors in the pediatric inpatient setting.Pediatrics.2003;112(2):431–436.
- ,,, et al.Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic review.JAMA.2005;293(10):1223–1238.
- ,,,.Computerized physician order entry in U.S. hospitals: results of a 2002 survey.J Am Med Inform Assoc.2004;11(2):95–99.
- .Using standardized admit orders to improve inpatient care.Fam Pract Manag.1999;6(10):30–32.
- ,,, et al.Before‐after study of a standardized hospital order set for the management of septic shock.Crit Care Med.2006;34(11):2707–2713.
- California Acute Stroke Pilot Registry Investigators.The impact of standardized stroke orders on adherence to best practices.Neurology.2005;65(3):360–365.
- ,,,,,.Improving quality of care for acute myocardial infarction. The guidelines applied in practice (GAP) initiative.JAMA.2002;287(10):1269–1276.
- ,,,,,.Quality improvement initiative and its impact on the management of patients with acute myocardial infarction.Arch Intern Med.2000;160:3057–3061.
- ,,,,,.Effect of a cancer chemotherapy prescription form on prescription completeness.Am J Hosp Pharm.1989;46(9):1802–1806.
- ,.Standardized trauma admission orders, a pilot project.Int J Trauma Nurs.1996;2(1):13–21.
- ,,,,.Using a preprinted order sheet to reduce prescription errors in a pediatric emergency department: a randomized, controlled trial.Pediatrics.2005;116(6):1299–1302.
For many years physicians have created and used various standardized order forms for patient hospital admissions. The increasing popularity of electronic medical records and forms has led to the use of computerized physician order entry (CPOE) as a means of reducing medication errors.13 Crowley et al.,4 Stucky,5 and Garg et al.,6 along with various committees, have recommended standardized order sets and CPOE as a strategy for reducing medication errors. However, implementation of CPOE systems is expensive and not available in most hospitals. According to a recent survey of hospitals in the US, CPOE was only available to physicians at 16% of the participating institutions.7 Until CPOE becomes widespread, standardized preprinted formatted order sets may serve as an inexpensive alternative.
There is anecdotal evidence that standardized admission order forms may improve quality of care and efficiency, and decrease provider variation.8 However, few rigorous studies exist in the pediatric research literature regarding their ability to actually improve patient care.
In 2005, our institution, a large tertiary‐care academic teaching hospital, developed a standardized preprinted pediatric admission order set (PAOS). We did so for 3 reasons. First, there was a desire to improve completeness of orders. Handwritten orders often missed important elements such as weight, allergies, vital sign parameters, activity, etc. Second, there was a need to save time and improve efficiency. Third, it was important to reduce medical errors and the number of clarification requests by decreasing the necessity to decipher physician handwriting. Our PAOS was a convenience order set as opposed to a best practices order set. In other words, our PAOS did not contain evidence‐based management guidelines or protocols for specific admission diagnoses and was created solely to improve the quality and efficiency of workflow.
Documenting improvement in patient outcomes or reduction of medical errors is ultimately needed to establish the effectiveness of a standardized order set. Secondary outcomes, howeverparticularly the perceptions of the staff who are asked to use the order setare equally important, because they may identify real‐life barriers to use that, regardless of effectiveness, could limit dissemination and uptake. With respect to perceptions, 2 groups become paramount: those who write the orders, and those who respond to them. The purpose of the current study was to examine perceived effects of the new PAOS on inpatient care among those who, in our institution, write the ordersresident physicians.
MATERIALS AND METHODS
The PAOS was created in August 2005 at the University of California, Los Angeles (UCLA) Medical Center by a committee comprising pediatric hospitalists, nurses, pharmacists, residents, and clerks. The PAOS consisted mainly of check boxes (Figure 1). The PAOS was uploaded to the hospital website and made available for printing from all computers in the hospital, emergency room, and clinics.
The UCLA Hospital and Medical Center is a nonprofit, 667‐bed tertiary‐care teaching hospital in Los Angeles, California. The pediatric ward has 70 licensed beds with approximately 3,000 admissions per year. The majority of the admissions were done by the pediatric residents. Physicians were free to edit the PAOS to suit a particular patient's needs or to hand‐write orders on a blank order form.
Measures
Fourteen months after the institution of the PAOS, all 97 UCLA pediatric residents (PL‐1, n = 34; PL‐2, n = 33; PL‐3, n = 30) were asked to complete a survey to anonymously evaluate the order set. All residents were US medical school graduates. Resident participation in the research project was voluntary and confidential, and residents were assured that participation would not affect their standing in the pediatric residency program. Each resident completed only 1 survey. Responses were collected October 2006 to June 2007. The residents were asked to rate the PAOS overall and with respect to 9 specific dimensions using a 5‐point Likert scale with 1 indicating strong disagreement and 5 indicating strong agreement (Figure 2).
This study was reviewed and approved by the institutional review board at the UCLA Medical Center.
Statistical Analysis
We used bivariate ordered logistic regression to estimate the association between overall rating and each of the 9 dimensions. Ordered logistic regression, a standard technique for ordered categorical variables, is essentially a weighted average of logistic regressions performed at each potential cut‐point of the outcome variable. For instance, potential cut‐points on our 5‐point Likert scale included strong disagreement versus any other, any disagreement versus nondisagreement, any agreement versus nonagreement, and strong agreement versus any other. We then used multivariate ordered logistic regression to examine which specific dimensions remained independently associated with the overall rating.
RESULTS
From October 2006 to June 2007, 59 residents (from a total of 97 residents; 61%) responded to the survey. Overall, 89% of respondents approved of the PAOS, 58% reported using it 90% of the time, and all said that they would recommend it to their colleagues (Table 1). Eighty‐four percent thought that the PAOS improved inpatient care, and 75% thought that medical errors were reduced. Eighty‐eight percent reported that the POAS saved time; 93% said it was convenient; and most reported less need for clarification with clerks (81%) and nurses (82%).
| Strongly Agree (%) | Agree (%) | Other (%) | |
|---|---|---|---|
| Specific dimensions | |||
| Looks neat | 63 | 32 | 5 |
| User friendly/convenient | 60 | 33 | 7 |
| Readily available | 47 | 26 | 26 |
| Saves time | 56 | 32 | 12 |
| Comprehensive | 40 | 40 | 19 |
| Reduces medical error | 40 | 35 | 25 |
| Fewer clarification phone calls/errors by clerks | 47 | 33 | 19 |
| Fewer clarification phone calls/errors by nurses | 47 | 35 | 18 |
| Improves overall patient care | 46 | 39 | 16 |
| Overall rating | 40 | 49 | 11 |
In bivariate analyses, each of the 9 dimensions was strongly associated with the overall rating (P < 0.001 for each). In multivariate analyses, however, only perceived improvement in patient care was independently associated with overall rating (OR, 3.9; P = 0.04).
We then examined whether perceived improvement in patient care itself was independently predicted by the other 8 dimensions. Residents who said that the form was comprehensive (OR, 5.6; P = 0.01), reduced medical errors (OR, 4.1; P = 0.01), or required less need for clarification with nurses (OR, 9.6; P = 0.01) were more likely to perceive that the form improved patient care than residents who did not.
DISCUSSION
A standardized admission order set is a simple, low‐cost intervention that may benefit patients by reducing medical errors and expediting high‐quality care. In general, residents rated the PAOS favorably. Just as importantly, the PAOS scored well across all specific dimensions, which suggests few perceived barriers to use among residents.
Some dimensions, however, appeared potentially more important than others. Residents who perceived an improvement in patient care tended to rate the PAOS favorably. Perceived improvement in patient care, in turn, was linked to the order set's comprehensiveness, perceived reductions in medical errors, and less need for clarification with nurses.
Even though this study did not directly query those most responsible for responding to the order set (ie, nurses, pharmacists, and clerks), the order set was created through a collaborative partnership of physicians, nurses, pharmacists, and clerks. It is reasonable to infer that resident‐perceived reduction in the need for clarification of orders with nurses and clerks might indicate a broad‐based, multidisciplinary improvement in clarity and workflow. Moreover, the fact that less need for clarification with nurses was strongly associated with resident‐perceived improvement in patient care underscores the importance of including nurses, pharmacists, and clerks in the development of these order sets.
Our experience using the standard admission orders over the past 2 years is congruent with other authors' findings. Most studies, however, have examined standardized order forms only in adult populations, and mainly for specific medical conditions. Micek et al.9 demonstrated that use of a standardized physician order set among adults with septic shock lowered 28‐day mortality and reduced hospital stay. Among stroke patients, rates of optimal treatment significantly improved after the introduction of standardized stroke orders.10 For patients with acute myocardial infarction, standardized admission orders increased early administration of aspirin and beta blockers.11, 12 With respect to cancer, implementation of a preprinted chemotherapy prescription form improved order completeness, prevented medication errors, and reduced time spent by pharmacists clarifying orders.13 Finally, standardized trauma admission orders developed in a surgical‐trauma intensive care unit reduced admission laboratory charges and improved order completeness.14 We found only a single pediatric study examining standardized order forms. Kozer et al.15 found that the use of a preprinted structured medication order form cut medication errors nearly in half in a pediatric emergency department.
Whether our results would have been similar had we implemented a series of best practices order sets rather than a single convenience order set is unclear. Although best practices order sets would have facilitated application of evidence‐based guidelines for common diagnoses, they would also have introduced potentially unwelcome logistical heterogeneity (with a separate form and protocol needed for each diagnosis) that might have reduced acceptability and uptake. In addition, there is a risk that best practices order sets would have been perceived as unduly limiting physician professional autonomy.
Our study has limitations. First, our study was performed within a single institution and may not be easily generalized. However, we believe that the basic format of the PAOS lends it to easy adaptability. Second, we did not survey residents before the order set was introduced to assess baseline perceptions. Instead, many of the questions in the survey ask about perceived improvements compared with the previous system. Conducting a formal pre‐post data collection and analysis might have yielded different results. Third, improvement in patient care was measured indirectly based on resident opinion.
In conclusion, our study suggests that our standardized admission order set prompting physicians to initiate comprehensive care is well‐liked by residents and is thought to benefit patients by reducing medical errors and expediting high‐quality care. The next step is to confirm that the resident‐perceived improvement in patient care correlates with actual improvement in patient care. If improvements can be confirmed, then PAOS adoption could be broadly recommended to pediatric hospitals. In the future, the PAOS may also help guide computerized physician order entry templates that can be further tailored to specific common diagnoses.
For many years physicians have created and used various standardized order forms for patient hospital admissions. The increasing popularity of electronic medical records and forms has led to the use of computerized physician order entry (CPOE) as a means of reducing medication errors.13 Crowley et al.,4 Stucky,5 and Garg et al.,6 along with various committees, have recommended standardized order sets and CPOE as a strategy for reducing medication errors. However, implementation of CPOE systems is expensive and not available in most hospitals. According to a recent survey of hospitals in the US, CPOE was only available to physicians at 16% of the participating institutions.7 Until CPOE becomes widespread, standardized preprinted formatted order sets may serve as an inexpensive alternative.
There is anecdotal evidence that standardized admission order forms may improve quality of care and efficiency, and decrease provider variation.8 However, few rigorous studies exist in the pediatric research literature regarding their ability to actually improve patient care.
In 2005, our institution, a large tertiary‐care academic teaching hospital, developed a standardized preprinted pediatric admission order set (PAOS). We did so for 3 reasons. First, there was a desire to improve completeness of orders. Handwritten orders often missed important elements such as weight, allergies, vital sign parameters, activity, etc. Second, there was a need to save time and improve efficiency. Third, it was important to reduce medical errors and the number of clarification requests by decreasing the necessity to decipher physician handwriting. Our PAOS was a convenience order set as opposed to a best practices order set. In other words, our PAOS did not contain evidence‐based management guidelines or protocols for specific admission diagnoses and was created solely to improve the quality and efficiency of workflow.
Documenting improvement in patient outcomes or reduction of medical errors is ultimately needed to establish the effectiveness of a standardized order set. Secondary outcomes, howeverparticularly the perceptions of the staff who are asked to use the order setare equally important, because they may identify real‐life barriers to use that, regardless of effectiveness, could limit dissemination and uptake. With respect to perceptions, 2 groups become paramount: those who write the orders, and those who respond to them. The purpose of the current study was to examine perceived effects of the new PAOS on inpatient care among those who, in our institution, write the ordersresident physicians.
MATERIALS AND METHODS
The PAOS was created in August 2005 at the University of California, Los Angeles (UCLA) Medical Center by a committee comprising pediatric hospitalists, nurses, pharmacists, residents, and clerks. The PAOS consisted mainly of check boxes (Figure 1). The PAOS was uploaded to the hospital website and made available for printing from all computers in the hospital, emergency room, and clinics.
The UCLA Hospital and Medical Center is a nonprofit, 667‐bed tertiary‐care teaching hospital in Los Angeles, California. The pediatric ward has 70 licensed beds with approximately 3,000 admissions per year. The majority of the admissions were done by the pediatric residents. Physicians were free to edit the PAOS to suit a particular patient's needs or to hand‐write orders on a blank order form.
Measures
Fourteen months after the institution of the PAOS, all 97 UCLA pediatric residents (PL‐1, n = 34; PL‐2, n = 33; PL‐3, n = 30) were asked to complete a survey to anonymously evaluate the order set. All residents were US medical school graduates. Resident participation in the research project was voluntary and confidential, and residents were assured that participation would not affect their standing in the pediatric residency program. Each resident completed only 1 survey. Responses were collected October 2006 to June 2007. The residents were asked to rate the PAOS overall and with respect to 9 specific dimensions using a 5‐point Likert scale with 1 indicating strong disagreement and 5 indicating strong agreement (Figure 2).
This study was reviewed and approved by the institutional review board at the UCLA Medical Center.
Statistical Analysis
We used bivariate ordered logistic regression to estimate the association between overall rating and each of the 9 dimensions. Ordered logistic regression, a standard technique for ordered categorical variables, is essentially a weighted average of logistic regressions performed at each potential cut‐point of the outcome variable. For instance, potential cut‐points on our 5‐point Likert scale included strong disagreement versus any other, any disagreement versus nondisagreement, any agreement versus nonagreement, and strong agreement versus any other. We then used multivariate ordered logistic regression to examine which specific dimensions remained independently associated with the overall rating.
RESULTS
From October 2006 to June 2007, 59 residents (from a total of 97 residents; 61%) responded to the survey. Overall, 89% of respondents approved of the PAOS, 58% reported using it 90% of the time, and all said that they would recommend it to their colleagues (Table 1). Eighty‐four percent thought that the PAOS improved inpatient care, and 75% thought that medical errors were reduced. Eighty‐eight percent reported that the POAS saved time; 93% said it was convenient; and most reported less need for clarification with clerks (81%) and nurses (82%).
| Strongly Agree (%) | Agree (%) | Other (%) | |
|---|---|---|---|
| Specific dimensions | |||
| Looks neat | 63 | 32 | 5 |
| User friendly/convenient | 60 | 33 | 7 |
| Readily available | 47 | 26 | 26 |
| Saves time | 56 | 32 | 12 |
| Comprehensive | 40 | 40 | 19 |
| Reduces medical error | 40 | 35 | 25 |
| Fewer clarification phone calls/errors by clerks | 47 | 33 | 19 |
| Fewer clarification phone calls/errors by nurses | 47 | 35 | 18 |
| Improves overall patient care | 46 | 39 | 16 |
| Overall rating | 40 | 49 | 11 |
In bivariate analyses, each of the 9 dimensions was strongly associated with the overall rating (P < 0.001 for each). In multivariate analyses, however, only perceived improvement in patient care was independently associated with overall rating (OR, 3.9; P = 0.04).
We then examined whether perceived improvement in patient care itself was independently predicted by the other 8 dimensions. Residents who said that the form was comprehensive (OR, 5.6; P = 0.01), reduced medical errors (OR, 4.1; P = 0.01), or required less need for clarification with nurses (OR, 9.6; P = 0.01) were more likely to perceive that the form improved patient care than residents who did not.
DISCUSSION
A standardized admission order set is a simple, low‐cost intervention that may benefit patients by reducing medical errors and expediting high‐quality care. In general, residents rated the PAOS favorably. Just as importantly, the PAOS scored well across all specific dimensions, which suggests few perceived barriers to use among residents.
Some dimensions, however, appeared potentially more important than others. Residents who perceived an improvement in patient care tended to rate the PAOS favorably. Perceived improvement in patient care, in turn, was linked to the order set's comprehensiveness, perceived reductions in medical errors, and less need for clarification with nurses.
Even though this study did not directly query those most responsible for responding to the order set (ie, nurses, pharmacists, and clerks), the order set was created through a collaborative partnership of physicians, nurses, pharmacists, and clerks. It is reasonable to infer that resident‐perceived reduction in the need for clarification of orders with nurses and clerks might indicate a broad‐based, multidisciplinary improvement in clarity and workflow. Moreover, the fact that less need for clarification with nurses was strongly associated with resident‐perceived improvement in patient care underscores the importance of including nurses, pharmacists, and clerks in the development of these order sets.
Our experience using the standard admission orders over the past 2 years is congruent with other authors' findings. Most studies, however, have examined standardized order forms only in adult populations, and mainly for specific medical conditions. Micek et al.9 demonstrated that use of a standardized physician order set among adults with septic shock lowered 28‐day mortality and reduced hospital stay. Among stroke patients, rates of optimal treatment significantly improved after the introduction of standardized stroke orders.10 For patients with acute myocardial infarction, standardized admission orders increased early administration of aspirin and beta blockers.11, 12 With respect to cancer, implementation of a preprinted chemotherapy prescription form improved order completeness, prevented medication errors, and reduced time spent by pharmacists clarifying orders.13 Finally, standardized trauma admission orders developed in a surgical‐trauma intensive care unit reduced admission laboratory charges and improved order completeness.14 We found only a single pediatric study examining standardized order forms. Kozer et al.15 found that the use of a preprinted structured medication order form cut medication errors nearly in half in a pediatric emergency department.
Whether our results would have been similar had we implemented a series of best practices order sets rather than a single convenience order set is unclear. Although best practices order sets would have facilitated application of evidence‐based guidelines for common diagnoses, they would also have introduced potentially unwelcome logistical heterogeneity (with a separate form and protocol needed for each diagnosis) that might have reduced acceptability and uptake. In addition, there is a risk that best practices order sets would have been perceived as unduly limiting physician professional autonomy.
Our study has limitations. First, our study was performed within a single institution and may not be easily generalized. However, we believe that the basic format of the PAOS lends it to easy adaptability. Second, we did not survey residents before the order set was introduced to assess baseline perceptions. Instead, many of the questions in the survey ask about perceived improvements compared with the previous system. Conducting a formal pre‐post data collection and analysis might have yielded different results. Third, improvement in patient care was measured indirectly based on resident opinion.
In conclusion, our study suggests that our standardized admission order set prompting physicians to initiate comprehensive care is well‐liked by residents and is thought to benefit patients by reducing medical errors and expediting high‐quality care. The next step is to confirm that the resident‐perceived improvement in patient care correlates with actual improvement in patient care. If improvements can be confirmed, then PAOS adoption could be broadly recommended to pediatric hospitals. In the future, the PAOS may also help guide computerized physician order entry templates that can be further tailored to specific common diagnoses.
- ,,, et al.Effect of computerized physician order entry and a team intervention on prevention of serious medication errors.JAMA.1998;280(15):1311–1316.
- ,,.Effects of computerized physician order entry and clinical decision support systems on medication safety: a systematic review.Arch Intern Med.2003;163(12):1409–1416.
- ,,,,.The effect of computerized physician order entry on medication errors and adverse drug events in pediatric inpatients.Pediatrics.2003;112(3 Pt 1):506–509.
- ,,.Medication errors in children: a descriptive summary of medication error reports submitted to the United States Pharmacopoeia.Curr Ther Res Clin Exp.2001;62:627–640.
- .Prevention of medication errors in the pediatric inpatient setting.Pediatrics.2003;112(2):431–436.
- ,,, et al.Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic review.JAMA.2005;293(10):1223–1238.
- ,,,.Computerized physician order entry in U.S. hospitals: results of a 2002 survey.J Am Med Inform Assoc.2004;11(2):95–99.
- .Using standardized admit orders to improve inpatient care.Fam Pract Manag.1999;6(10):30–32.
- ,,, et al.Before‐after study of a standardized hospital order set for the management of septic shock.Crit Care Med.2006;34(11):2707–2713.
- California Acute Stroke Pilot Registry Investigators.The impact of standardized stroke orders on adherence to best practices.Neurology.2005;65(3):360–365.
- ,,,,,.Improving quality of care for acute myocardial infarction. The guidelines applied in practice (GAP) initiative.JAMA.2002;287(10):1269–1276.
- ,,,,,.Quality improvement initiative and its impact on the management of patients with acute myocardial infarction.Arch Intern Med.2000;160:3057–3061.
- ,,,,,.Effect of a cancer chemotherapy prescription form on prescription completeness.Am J Hosp Pharm.1989;46(9):1802–1806.
- ,.Standardized trauma admission orders, a pilot project.Int J Trauma Nurs.1996;2(1):13–21.
- ,,,,.Using a preprinted order sheet to reduce prescription errors in a pediatric emergency department: a randomized, controlled trial.Pediatrics.2005;116(6):1299–1302.
- ,,, et al.Effect of computerized physician order entry and a team intervention on prevention of serious medication errors.JAMA.1998;280(15):1311–1316.
- ,,.Effects of computerized physician order entry and clinical decision support systems on medication safety: a systematic review.Arch Intern Med.2003;163(12):1409–1416.
- ,,,,.The effect of computerized physician order entry on medication errors and adverse drug events in pediatric inpatients.Pediatrics.2003;112(3 Pt 1):506–509.
- ,,.Medication errors in children: a descriptive summary of medication error reports submitted to the United States Pharmacopoeia.Curr Ther Res Clin Exp.2001;62:627–640.
- .Prevention of medication errors in the pediatric inpatient setting.Pediatrics.2003;112(2):431–436.
- ,,, et al.Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic review.JAMA.2005;293(10):1223–1238.
- ,,,.Computerized physician order entry in U.S. hospitals: results of a 2002 survey.J Am Med Inform Assoc.2004;11(2):95–99.
- .Using standardized admit orders to improve inpatient care.Fam Pract Manag.1999;6(10):30–32.
- ,,, et al.Before‐after study of a standardized hospital order set for the management of septic shock.Crit Care Med.2006;34(11):2707–2713.
- California Acute Stroke Pilot Registry Investigators.The impact of standardized stroke orders on adherence to best practices.Neurology.2005;65(3):360–365.
- ,,,,,.Improving quality of care for acute myocardial infarction. The guidelines applied in practice (GAP) initiative.JAMA.2002;287(10):1269–1276.
- ,,,,,.Quality improvement initiative and its impact on the management of patients with acute myocardial infarction.Arch Intern Med.2000;160:3057–3061.
- ,,,,,.Effect of a cancer chemotherapy prescription form on prescription completeness.Am J Hosp Pharm.1989;46(9):1802–1806.
- ,.Standardized trauma admission orders, a pilot project.Int J Trauma Nurs.1996;2(1):13–21.
- ,,,,.Using a preprinted order sheet to reduce prescription errors in a pediatric emergency department: a randomized, controlled trial.Pediatrics.2005;116(6):1299–1302.
Copyright © 2009 Society of Hospital Medicine
A change of heart
The approach to clinical conundrums by an expert clinician is revealed through presentation of an actual patient's case in an approach typical of morning report. Similar to patient care, sequential pieces of information are provided to the clinician who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
A 29‐year‐old man developed palpitations and dyspnea while loading boxes into a truck. In the emergency department, telemetry demonstrated a wide‐complex tachycardia at a rate of 204 beats per minute. The patient spontaneously cardioverted to sinus rhythm (Figure 1) before direct current cardioversion was performed.
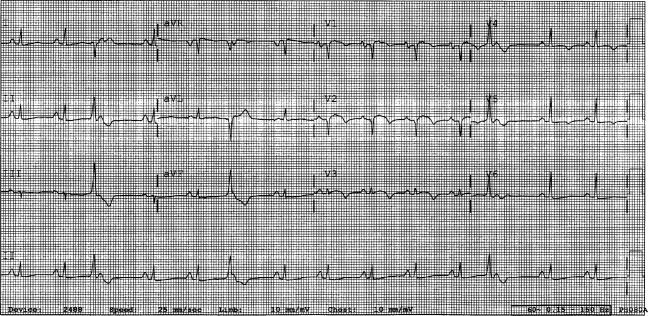
Wide‐complex tachycardia is usually explained by a supraventricular tachycardia with aberrant ventricular conduction or a ventricular tachycardia. Although algorithms exist to guide the clinician in parsing out those etiologies, often the knowledge of underlying structural cardiac disease is most informative. In patients with a history of myocardial infarction, greater than 95% of wide‐complex tachycardia is ventricular tachycardia. The ventricular ectopy, T‐wave inversion or flattening, and poor R‐wave progression are suggestive of a cardiomyopathy, either acute or chronic. A pressing concern, especially with the Q waves and concave ST morphology in V1 and V2, would be coronary ischemia. His age makes this less likely, but an aberrant coronary circulation or drug use could account for it.
Over the past 2 years, the patient had several episodes of sustained palpitations, which terminated after several minutes. Previously, the patient exercised frequently including playing rugby in college. However, over the past year he experienced difficulty climbing stairs due to shortness of breath, which he attributed to deconditioning and smoking. He had no significant medical history, was not taking any medications, nor did he use recreational stimulants. He drank alcohol occasionally. He had no risk factors for the human immunodeficiency virus (HIV). Both of the patient's parents were alive and well. There was no family history of sudden cardiac death.
The duration of symptoms suggests that this is a chronic cardiomyopathy rather than acute myocarditis or acute ischemia, acknowledging that either one could be superimposed. The absence of family history lowers the likelihood of heritable causes of arrhythmia that may accompany a structurally normal (eg, long QT syndrome) or abnormal (eg, hypertrophic cardiomyopathy) heart, although penetrance can be variable. What might account for a cardiomyopathy in a young person? Most cases are probably idiopathic, but etiologies that diverge from the usual suspects of coronary artery disease, hypertension, and valvular disease, which affect an older population, include antecedent viral myocarditis, substance abuse, HIV, or infiltrative disorders such as sarcoidosis.
The patient's pulse was 92 beats per minute and regular and the blood pressure was 96/52 mm Hg. The jugular venous pressure was elevated with prominent v‐waves, the point of maximal impulse was diffuse, there were no extra heart sounds or murmurs, and an enlarged liver was detected. An echocardiogram demonstrated left ventricular dysfunction with an ejection fraction of 30%, severe enlargement of the right atrium and right ventricle, and moderate tricuspid regurgitation. Cardiac catheterization revealed normal coronary arteries without evidence of pulmonary hypertension or intracardiac shunt.
The physical examination and echocardiographic findings of right‐sided failure are unusual given the absence of pulmonary hypertension or intracardiac shunt, and could prompt repeat of the hemodynamic measurements and/or investigations for pulmonary disease that may account for right‐sided pressure overload (in addition to that caused by left ventricular failure). An alternative explanation would be a cardiomyopathic process that preferentially involves the right side of the heart, such as arrhythmogenic right ventricular dysplasia (ARVD), but that would not satisfactorily explain the significant decline in left ventricular function. An acute right ventricular infarction could cause his acute symptoms and his examination and echocardiographic findings, but not the underlying chronic illness. It is common to see patients with long‐standing biventricular failure who present with prominent signs of right‐sided failure (elevated neck veins, hepatomegaly, and edema) but limited or no signs of left‐sided failure (rales) to match their degree of volume overload or dyspnea.
Cardiac magnetic resonance imaging (MRI) revealed a dilated right ventricle with extensive hyperenhancement, a right ventricular ejection fraction of 9%, and moderate left ventricular dysfunction (Figure 2). Electrophysiology testing induced both nonsustained polymorphic and monomorphic ventricular tachycardia. Late potentials were detected on a signal‐averaged electrocardiogram. A single‐chamber cardioverter defibrillator was implanted and the patient was discharged on carvedilol, lisinopril, and spironolactone. An HIV‐1 antibody was negative and a thyroid‐stimulating hormone concentration was within normal limits.
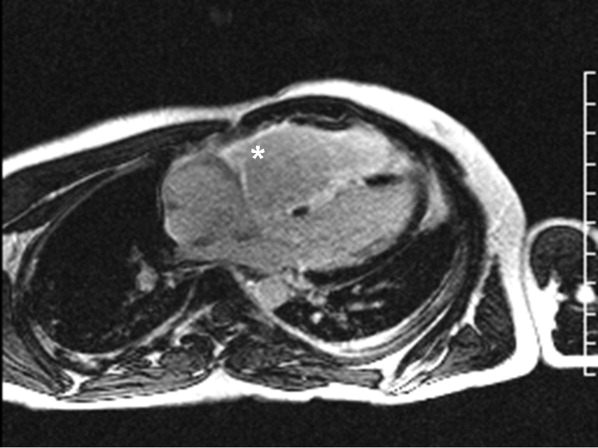
Assuming that accurate evaluation of the pulmonary circulation has been undertaken to exclude pulmonary hypertension, the enlarged and hyperenhanced right ventricle on MRI suggests a process that preferentially infiltrates the right ventricular myocardium, and may secondarily affect the left ventricle either by further infiltration or as a consequence of altered mechanics from the highly dysfunctional right ventricle. ARVD affects the right ventricle, but it is possible that another infiltrative cardiomyopathy, such as sarcoid or an antecedent viral infection, could be restricted in its distribution. Late‐potentials identified on signal average electrocardiograms indicate areas of abnormal conduction that may serve as substrate for reentrant ventricular arrhythmias. They are, however, nonspecific, as they are seen in a variety of myocardial diseases.
The patient continued to have progressive dyspnea and was readmitted after receiving an appropriate implantable cardioverter defibrillator shock for ventricular tachycardia. Recurrent slow ventricular tachycardia (Figure 3) was treated with supplemental beta‐blockade and amiodarone (10 g total). Repeat echocardiography demonstrated severe left ventricular dysfunction with an ejection fraction of less than 15%. There were no recurrences of ventricular arrhythmias and the patient was discharged and referred for cardiac transplant evaluation for ARVD.
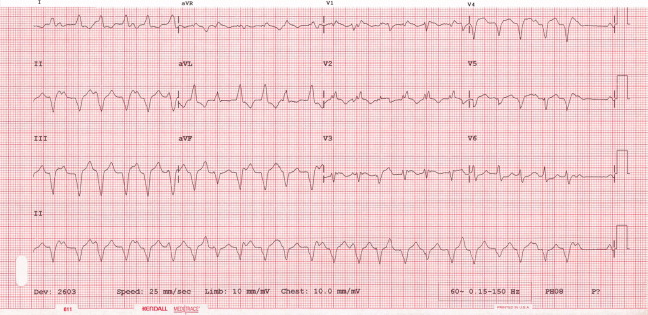
This degree of left ventricular dysfunction is unlikely to be accounted for by altered mechanics and interactions from a failing right ventricle alone and frames this as a biventricular cardiomyopathy, which has an extensive differential diagnosis and requires information from the general medical evaluation.
On routine laboratory testing 6 months later, a serum aspartate aminotransferase of 79 units/L and a serum alanine aminotransferase of 118 units/L were found. Bilirubin, albumin, and alkaline phosphatase were normal. The transaminase levels had been normal on initial evaluation. The patient reported that 2 paternal uncles had end‐stage nonalcoholic cirrhosis. Transjugular liver biopsy was consistent with mild lobular hepatitis with mild portal fibrosis with a few lobular collections of mononuclear cells. There was no evidence of iron overload. The hepatic venogram and transhepatic pressure gradient (2 mm Hg) were normal.
The elevated transaminase levels could be due to amiodarone‐associated hepatotoxicity, hepatic congestion, or a primary liver disease. It is important to consider combined cardiohepatic syndromes such as hemochromatosis, sarcoidosis, or amyloidosis. The relatively normal liver histology and normal hepatic hemodynamics do not suggest a significant primary intrinsic liver disease. The 2 uncles with cirrhosis could suggest a heritable liver disease, although cirrhosis in multiple family members is frequently accounted for by shared habits such as alcohol consumption or excessive caloric intake. Liver disorders with a genetic component, such as hemochromatosis, Wilson's disease, and alpha‐1‐antitrypsin deficiency are mostly autosomal recessive, which would make this pattern of transmission unusual. Furthermore, aside from hemochromatosis, these genetic hepatic disorders have few cardiac manifestations. Right‐sided congestion and amiodarone appear to be the most likely explanations of his liver abnormalities.
Pulmonary function testing revealed normal lung volumes without obstruction, but the diffusing capacity for carbon monoxide was substantially reduced. Computed tomography of the chest identified scattered ground‐glass opacities as well as small nodules with an upper lobe distribution (Figure 4). Although not reported on the initial interpretation, review of a chest x‐ray taken 6 months previously also demonstrated small nodules in the upper lobe distribution. Bronchoscopic examination was normal. Bronchioalveolar lavage fluid stains and cultures for bacteria, mycobacteria, Pneumocystis, and fungus were negative. Transbronchial biopsies of the right middle lobe had no evidence of infection, malignancy, or granulomatous inflammation. The patient continued to have progressive New York Heart Association Class IV heart failure symptoms. Repeat right heart catheterization was notable for a cardiac index of 1.4 L/minute/m2. The mean pulmonary artery pressure was 20 mm Hg. An intraaortic balloon pump was placed for refractory cardiogenic shock.
The reduced diffusion capacity and ground‐glass opacities suggest an interstitial process, which may have been missed on transbronchial biopsy because of sampling error. His pulmonary disease is likely another manifestation of his infiltrative cardiac disease. The constellation of cardiac, pulmonary, and hepatic involvement in the context of progressive dyspnea over 2 years is suggestive of sarcoidosis although the absence of hilar lymphadenopathy and 2 biopsy specimens without granulomas argue against the diagnosis, and the effects of amiodarone on the latter 2 organs cannot be ignored. On the limited menu of pharmacologic treatments that may treat this severe and progressive cardiomyopathy are steroids, which makes a diligent search for a steroid‐responsive syndrome important. Therefore, despite the negative studies, sarcoidosis must be investigated to the fullest extent with either an endomyocardial biopsy or surgical lung biopsy.
The patient underwent cardiac transplantation. The native heart was found to have right ventricular thinning, which was most notable at the right ventricular outflow tract. Microscopic examination revealed extensive fibrosis and granulomatous inflammation (Figure 5) with scarring typical of cardiac sarcoidosis. Six months after cardiac transplantation, the patient is doing well on prednisone, tacrolimus, and mycophenolate mofetil. Follow‐up chest x‐rays show resolution of the pulmonary nodules.
COMMENTARY
Cardiomyopathy in a young person is a relatively uncommon clinical event that prompts consideration of a broad differential diagnosis that is notably different from the most common etiologies of cardiomyopathy in older adults. This case highlights the challenges of arriving at a diagnosis in the absence of a gold standard, and the greater challenges of modifying initial diagnostic impressions as new clinical data become available.
After encountering ventricular tachycardia and right ventricular dysfunction in a young patient, the clinicians arrived at the diagnosis of ARVD. This rare and progressive disorder is associated with up to 20% of ventricular arrhythmias and sudden death in the young,1, 2 but can be challenging to diagnose. Despite common referrals for cardiac MRI to exclude ARVD, cardiac MRI is not the gold standard for diagnosis and is the most common method of misdiagnosis of ARVD.3 A diagnosis of ARVD requires the presence of 2 major, 1 major and 2 minor, or 4 minor International Task Force criteria (Table 1).4, 5 While the diagnostic criteria provide standardization across populations (eg, in clinical studies), additional considerations are needed in the management of individual patients. Scoring systems serve as a tool, but the final diagnosis requires balancing such criteria with competing hypotheses. This dilemma is familiar to clinicians considering other less common conditions such as amyotrophic lateral sclerosis (World Neurology Foundation), rheumatic fever (Jones criteria), or systemic lupus erythematosus (American College of Rheumatology). This patient's cardiac MRI findings, precordial T‐wave inversions, frequent ventricular ectopy, and late potentials on a signal‐averaged electrocardiogram fulfilled the International Task Force criteria for a diagnosis of ARVD. Discordant information included the right bundle branch pattern of the ventricular tachycardia, which suggested left ventricular origin, as opposed to the more common left bundle branch pattern observed in ARVD, and the absence of a family history. In addition, in U.S. populations only 25% of cases present with heart failure and fewer than 5% develop biventricular failure.6 Nonetheless, this patient's imaging evidence of right ventricular structural abnormalities and dysfunction and electrocardiographic abnormalities coupled with the absence of obvious systemic disease made ARVD the logical working diagnosis.
| Major | Minor | |
|---|---|---|
| ||
| I. Global and/or regional dysfunction and structural alterations | Severe dilation and reduction of right ventricular ejection fraction, localized right ventricular aneurysms | Mild right ventricular dilatation and/or reduced ejection fraction |
| II. Endomyocardial biopsy | Fibrofatty replacement of myocardium | |
| III. Repolarization abnormalities | T‐wave inversion in leads V1‐V3 or beyond | |
| IV. Depolarization/conduction abnormalities | Epsilon waves or localized QRS prolongation (>110 msec) in leads V1‐V3 | Late potentials on signal‐averaged electrocardiogram |
| V. Arrhythmias | Left bundle branch block‐type ventricular tachycardia (sustained and nonsustained) or frequent ventricular extra systoles (>1,000/24 hours) | |
| VI. Family history | Familial disease confirmed at necropsy or surgery | Familial history of premature sudden death (35 years old) or clinical diagnosis based on present criteria |
When more widespread manifestations developed, namely hepatic and pulmonary abnormalities, each was investigated with imaging and biopsy. Once a multisystem illness became apparent, the discussant reframed the patient's illness to include other diagnostic possibilities. In practice it is difficult to reverse a working diagnosis despite contradictory evidence because of the common pitfall of anchoring bias. Tversky and Kahneman7 were the first to describe the cognitive processes behind probability assessment and decision making in time‐sensitive situations. Under these conditions, decision makers tend to focus on the first symptom, striking feature, or diagnosis and anchor subsequent probabilities to that initial presentation. Once a decision or diagnosis has been reached, clinicians tend to interpret subsequent findings in the context of the original diagnosis rather than reevaluating their initial impression. In the setting of a known diagnosis of ARVD, 3 separate diagnoses (ARVD, amiodarone‐associated lung injury, and amiodarone‐induced hepatic dysfunction) were considered by the treating physicians. The initial diagnosis of ARVD followed by the sequential rather than simultaneous manifestations of sarcoidosis made arriving at the revised diagnosis even more challenging.
Cardiac sarcoidosis is a mimic of ARVD and should be considered when evaluating a patient for right ventricular dysplasia.8, 9 The differential diagnosis of ARVD includes idiopathic ventricular tachycardia, myocarditis, idiopathic cardiomyopathy, and sarcoidosis. Cardiac sarcoidosis can present as ventricular ectopy, sustained ventricular arrhythmias, asymptomatic ventricular dysfunction, heart failure, or sudden death.10 Although 25% of patients with sarcoidosis have evidence of cardiac involvement at autopsy, only 5% have clinical manifestations.11 Those patients with clinical evidence of cardiac sarcoidosis have a wide range of clinical findings (Table 2). While the patient's cardiomyopathy was advanced, it is possible that earlier administration of corticosteroid therapy may have arrested his progressive biventricular failure. As clinicians, we should always remember to force ourselves to broaden our differential diagnosis when new findings become available, especially those that point to a systemicrather than an organ‐specificdisorder. In this case, while the original diagnostic findings were accurate and strongly suggested ARVD, a change of heart was needed to arrive at the ultimate diagnosis.
| Clinical Manifestation | Prevalence (%) |
|---|---|
| Atrioventricular block | 40 |
| Bundle branch block | 40 |
| Supraventricular tachycardia | 20 |
| Ventricular arrhythmias | 25 |
| Heart failure | 25 |
| Sudden cardiac death | 35 |
KEY POINTS FOR HOSPITALISTS
-
Cardiomyopathy in a young person requires consideration of a broad differential diagnosis that is notably different from the most common etiologies of cardiomyopathy in the elderly.
-
Anchoring bias is a common pitfall in clinical decision making. When new or contradictory findings are uncovered, clinicians should reevaluate their initial impression to ensure it remains the most likely diagnosis.
-
Cardiac sarcoidosis is a mimic of ARVD and should be considered when evaluating a patient for right ventricular cardiomyopathy. The differential diagnosis of ARVD includes idiopathic ventricular tachycardia, right ventricular outflow tract tachycardia, myocarditis, idiopathic dilated cardiomyopathy, and sarcoidosis.
- ,,, et al.Right ventricular dysplasia: a report of 24 adult cases.Circulation.1982;65:384–398.
- ,,,,.Right ventricular cardiomyopathy and sudden death in young people.N Engl J Med.1988;318:129–133.
- ,,, et al.Misdiagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy.J Cardiovasc Electrophysiol.2004;15:300–306.
- ,,, et al.Diagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Task Force of the Working Group Myocardial and Pericardial Disease of the European Society of Cardiology and the Scientific Council on Cardiomyopathies of the International Society and Federation of Cardiology.Br Heart J.1994;71:215–218.
- ,,, et al.Predictors of appropriate implantable defibrillator therapies in patients with arrhythmogenic right ventricular dysplasia.Heart Rhythm.2005;2:1188–1194.
- ,,, et al.Arrhythmogenic right ventricular dysplasia: a United States experience.Circulation.2005;112:3823–3832.
- ,.Judgment under uncertainty: heuristics and biases.Science.1974;185:1124–1131.
- ,,.Unusual presentation of cardiac sarcoidosis.Congest Heart Fail.2007;13:116–118.
- ,,, et al.Cardiac sarcoidosis mimicking right ventricular dysplasia.Circ J.2003;67:169–171.
- ,,,,.Refractory ventricular tachycardia secondary to cardiac sarcoid: electrophysiologic characteristics, mapping, and ablation.Heart Rhythm.2006;3:924–929.
- ,.Sarcoid heart disease: clinical course and treatment.Int J Cardiol.2004;97:173–182.
The approach to clinical conundrums by an expert clinician is revealed through presentation of an actual patient's case in an approach typical of morning report. Similar to patient care, sequential pieces of information are provided to the clinician who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
A 29‐year‐old man developed palpitations and dyspnea while loading boxes into a truck. In the emergency department, telemetry demonstrated a wide‐complex tachycardia at a rate of 204 beats per minute. The patient spontaneously cardioverted to sinus rhythm (Figure 1) before direct current cardioversion was performed.
Wide‐complex tachycardia is usually explained by a supraventricular tachycardia with aberrant ventricular conduction or a ventricular tachycardia. Although algorithms exist to guide the clinician in parsing out those etiologies, often the knowledge of underlying structural cardiac disease is most informative. In patients with a history of myocardial infarction, greater than 95% of wide‐complex tachycardia is ventricular tachycardia. The ventricular ectopy, T‐wave inversion or flattening, and poor R‐wave progression are suggestive of a cardiomyopathy, either acute or chronic. A pressing concern, especially with the Q waves and concave ST morphology in V1 and V2, would be coronary ischemia. His age makes this less likely, but an aberrant coronary circulation or drug use could account for it.
Over the past 2 years, the patient had several episodes of sustained palpitations, which terminated after several minutes. Previously, the patient exercised frequently including playing rugby in college. However, over the past year he experienced difficulty climbing stairs due to shortness of breath, which he attributed to deconditioning and smoking. He had no significant medical history, was not taking any medications, nor did he use recreational stimulants. He drank alcohol occasionally. He had no risk factors for the human immunodeficiency virus (HIV). Both of the patient's parents were alive and well. There was no family history of sudden cardiac death.
The duration of symptoms suggests that this is a chronic cardiomyopathy rather than acute myocarditis or acute ischemia, acknowledging that either one could be superimposed. The absence of family history lowers the likelihood of heritable causes of arrhythmia that may accompany a structurally normal (eg, long QT syndrome) or abnormal (eg, hypertrophic cardiomyopathy) heart, although penetrance can be variable. What might account for a cardiomyopathy in a young person? Most cases are probably idiopathic, but etiologies that diverge from the usual suspects of coronary artery disease, hypertension, and valvular disease, which affect an older population, include antecedent viral myocarditis, substance abuse, HIV, or infiltrative disorders such as sarcoidosis.
The patient's pulse was 92 beats per minute and regular and the blood pressure was 96/52 mm Hg. The jugular venous pressure was elevated with prominent v‐waves, the point of maximal impulse was diffuse, there were no extra heart sounds or murmurs, and an enlarged liver was detected. An echocardiogram demonstrated left ventricular dysfunction with an ejection fraction of 30%, severe enlargement of the right atrium and right ventricle, and moderate tricuspid regurgitation. Cardiac catheterization revealed normal coronary arteries without evidence of pulmonary hypertension or intracardiac shunt.
The physical examination and echocardiographic findings of right‐sided failure are unusual given the absence of pulmonary hypertension or intracardiac shunt, and could prompt repeat of the hemodynamic measurements and/or investigations for pulmonary disease that may account for right‐sided pressure overload (in addition to that caused by left ventricular failure). An alternative explanation would be a cardiomyopathic process that preferentially involves the right side of the heart, such as arrhythmogenic right ventricular dysplasia (ARVD), but that would not satisfactorily explain the significant decline in left ventricular function. An acute right ventricular infarction could cause his acute symptoms and his examination and echocardiographic findings, but not the underlying chronic illness. It is common to see patients with long‐standing biventricular failure who present with prominent signs of right‐sided failure (elevated neck veins, hepatomegaly, and edema) but limited or no signs of left‐sided failure (rales) to match their degree of volume overload or dyspnea.
Cardiac magnetic resonance imaging (MRI) revealed a dilated right ventricle with extensive hyperenhancement, a right ventricular ejection fraction of 9%, and moderate left ventricular dysfunction (Figure 2). Electrophysiology testing induced both nonsustained polymorphic and monomorphic ventricular tachycardia. Late potentials were detected on a signal‐averaged electrocardiogram. A single‐chamber cardioverter defibrillator was implanted and the patient was discharged on carvedilol, lisinopril, and spironolactone. An HIV‐1 antibody was negative and a thyroid‐stimulating hormone concentration was within normal limits.
Assuming that accurate evaluation of the pulmonary circulation has been undertaken to exclude pulmonary hypertension, the enlarged and hyperenhanced right ventricle on MRI suggests a process that preferentially infiltrates the right ventricular myocardium, and may secondarily affect the left ventricle either by further infiltration or as a consequence of altered mechanics from the highly dysfunctional right ventricle. ARVD affects the right ventricle, but it is possible that another infiltrative cardiomyopathy, such as sarcoid or an antecedent viral infection, could be restricted in its distribution. Late‐potentials identified on signal average electrocardiograms indicate areas of abnormal conduction that may serve as substrate for reentrant ventricular arrhythmias. They are, however, nonspecific, as they are seen in a variety of myocardial diseases.
The patient continued to have progressive dyspnea and was readmitted after receiving an appropriate implantable cardioverter defibrillator shock for ventricular tachycardia. Recurrent slow ventricular tachycardia (Figure 3) was treated with supplemental beta‐blockade and amiodarone (10 g total). Repeat echocardiography demonstrated severe left ventricular dysfunction with an ejection fraction of less than 15%. There were no recurrences of ventricular arrhythmias and the patient was discharged and referred for cardiac transplant evaluation for ARVD.
This degree of left ventricular dysfunction is unlikely to be accounted for by altered mechanics and interactions from a failing right ventricle alone and frames this as a biventricular cardiomyopathy, which has an extensive differential diagnosis and requires information from the general medical evaluation.
On routine laboratory testing 6 months later, a serum aspartate aminotransferase of 79 units/L and a serum alanine aminotransferase of 118 units/L were found. Bilirubin, albumin, and alkaline phosphatase were normal. The transaminase levels had been normal on initial evaluation. The patient reported that 2 paternal uncles had end‐stage nonalcoholic cirrhosis. Transjugular liver biopsy was consistent with mild lobular hepatitis with mild portal fibrosis with a few lobular collections of mononuclear cells. There was no evidence of iron overload. The hepatic venogram and transhepatic pressure gradient (2 mm Hg) were normal.
The elevated transaminase levels could be due to amiodarone‐associated hepatotoxicity, hepatic congestion, or a primary liver disease. It is important to consider combined cardiohepatic syndromes such as hemochromatosis, sarcoidosis, or amyloidosis. The relatively normal liver histology and normal hepatic hemodynamics do not suggest a significant primary intrinsic liver disease. The 2 uncles with cirrhosis could suggest a heritable liver disease, although cirrhosis in multiple family members is frequently accounted for by shared habits such as alcohol consumption or excessive caloric intake. Liver disorders with a genetic component, such as hemochromatosis, Wilson's disease, and alpha‐1‐antitrypsin deficiency are mostly autosomal recessive, which would make this pattern of transmission unusual. Furthermore, aside from hemochromatosis, these genetic hepatic disorders have few cardiac manifestations. Right‐sided congestion and amiodarone appear to be the most likely explanations of his liver abnormalities.
Pulmonary function testing revealed normal lung volumes without obstruction, but the diffusing capacity for carbon monoxide was substantially reduced. Computed tomography of the chest identified scattered ground‐glass opacities as well as small nodules with an upper lobe distribution (Figure 4). Although not reported on the initial interpretation, review of a chest x‐ray taken 6 months previously also demonstrated small nodules in the upper lobe distribution. Bronchoscopic examination was normal. Bronchioalveolar lavage fluid stains and cultures for bacteria, mycobacteria, Pneumocystis, and fungus were negative. Transbronchial biopsies of the right middle lobe had no evidence of infection, malignancy, or granulomatous inflammation. The patient continued to have progressive New York Heart Association Class IV heart failure symptoms. Repeat right heart catheterization was notable for a cardiac index of 1.4 L/minute/m2. The mean pulmonary artery pressure was 20 mm Hg. An intraaortic balloon pump was placed for refractory cardiogenic shock.
The reduced diffusion capacity and ground‐glass opacities suggest an interstitial process, which may have been missed on transbronchial biopsy because of sampling error. His pulmonary disease is likely another manifestation of his infiltrative cardiac disease. The constellation of cardiac, pulmonary, and hepatic involvement in the context of progressive dyspnea over 2 years is suggestive of sarcoidosis although the absence of hilar lymphadenopathy and 2 biopsy specimens without granulomas argue against the diagnosis, and the effects of amiodarone on the latter 2 organs cannot be ignored. On the limited menu of pharmacologic treatments that may treat this severe and progressive cardiomyopathy are steroids, which makes a diligent search for a steroid‐responsive syndrome important. Therefore, despite the negative studies, sarcoidosis must be investigated to the fullest extent with either an endomyocardial biopsy or surgical lung biopsy.
The patient underwent cardiac transplantation. The native heart was found to have right ventricular thinning, which was most notable at the right ventricular outflow tract. Microscopic examination revealed extensive fibrosis and granulomatous inflammation (Figure 5) with scarring typical of cardiac sarcoidosis. Six months after cardiac transplantation, the patient is doing well on prednisone, tacrolimus, and mycophenolate mofetil. Follow‐up chest x‐rays show resolution of the pulmonary nodules.
COMMENTARY
Cardiomyopathy in a young person is a relatively uncommon clinical event that prompts consideration of a broad differential diagnosis that is notably different from the most common etiologies of cardiomyopathy in older adults. This case highlights the challenges of arriving at a diagnosis in the absence of a gold standard, and the greater challenges of modifying initial diagnostic impressions as new clinical data become available.
After encountering ventricular tachycardia and right ventricular dysfunction in a young patient, the clinicians arrived at the diagnosis of ARVD. This rare and progressive disorder is associated with up to 20% of ventricular arrhythmias and sudden death in the young,1, 2 but can be challenging to diagnose. Despite common referrals for cardiac MRI to exclude ARVD, cardiac MRI is not the gold standard for diagnosis and is the most common method of misdiagnosis of ARVD.3 A diagnosis of ARVD requires the presence of 2 major, 1 major and 2 minor, or 4 minor International Task Force criteria (Table 1).4, 5 While the diagnostic criteria provide standardization across populations (eg, in clinical studies), additional considerations are needed in the management of individual patients. Scoring systems serve as a tool, but the final diagnosis requires balancing such criteria with competing hypotheses. This dilemma is familiar to clinicians considering other less common conditions such as amyotrophic lateral sclerosis (World Neurology Foundation), rheumatic fever (Jones criteria), or systemic lupus erythematosus (American College of Rheumatology). This patient's cardiac MRI findings, precordial T‐wave inversions, frequent ventricular ectopy, and late potentials on a signal‐averaged electrocardiogram fulfilled the International Task Force criteria for a diagnosis of ARVD. Discordant information included the right bundle branch pattern of the ventricular tachycardia, which suggested left ventricular origin, as opposed to the more common left bundle branch pattern observed in ARVD, and the absence of a family history. In addition, in U.S. populations only 25% of cases present with heart failure and fewer than 5% develop biventricular failure.6 Nonetheless, this patient's imaging evidence of right ventricular structural abnormalities and dysfunction and electrocardiographic abnormalities coupled with the absence of obvious systemic disease made ARVD the logical working diagnosis.
| Major | Minor | |
|---|---|---|
| ||
| I. Global and/or regional dysfunction and structural alterations | Severe dilation and reduction of right ventricular ejection fraction, localized right ventricular aneurysms | Mild right ventricular dilatation and/or reduced ejection fraction |
| II. Endomyocardial biopsy | Fibrofatty replacement of myocardium | |
| III. Repolarization abnormalities | T‐wave inversion in leads V1‐V3 or beyond | |
| IV. Depolarization/conduction abnormalities | Epsilon waves or localized QRS prolongation (>110 msec) in leads V1‐V3 | Late potentials on signal‐averaged electrocardiogram |
| V. Arrhythmias | Left bundle branch block‐type ventricular tachycardia (sustained and nonsustained) or frequent ventricular extra systoles (>1,000/24 hours) | |
| VI. Family history | Familial disease confirmed at necropsy or surgery | Familial history of premature sudden death (35 years old) or clinical diagnosis based on present criteria |
When more widespread manifestations developed, namely hepatic and pulmonary abnormalities, each was investigated with imaging and biopsy. Once a multisystem illness became apparent, the discussant reframed the patient's illness to include other diagnostic possibilities. In practice it is difficult to reverse a working diagnosis despite contradictory evidence because of the common pitfall of anchoring bias. Tversky and Kahneman7 were the first to describe the cognitive processes behind probability assessment and decision making in time‐sensitive situations. Under these conditions, decision makers tend to focus on the first symptom, striking feature, or diagnosis and anchor subsequent probabilities to that initial presentation. Once a decision or diagnosis has been reached, clinicians tend to interpret subsequent findings in the context of the original diagnosis rather than reevaluating their initial impression. In the setting of a known diagnosis of ARVD, 3 separate diagnoses (ARVD, amiodarone‐associated lung injury, and amiodarone‐induced hepatic dysfunction) were considered by the treating physicians. The initial diagnosis of ARVD followed by the sequential rather than simultaneous manifestations of sarcoidosis made arriving at the revised diagnosis even more challenging.
Cardiac sarcoidosis is a mimic of ARVD and should be considered when evaluating a patient for right ventricular dysplasia.8, 9 The differential diagnosis of ARVD includes idiopathic ventricular tachycardia, myocarditis, idiopathic cardiomyopathy, and sarcoidosis. Cardiac sarcoidosis can present as ventricular ectopy, sustained ventricular arrhythmias, asymptomatic ventricular dysfunction, heart failure, or sudden death.10 Although 25% of patients with sarcoidosis have evidence of cardiac involvement at autopsy, only 5% have clinical manifestations.11 Those patients with clinical evidence of cardiac sarcoidosis have a wide range of clinical findings (Table 2). While the patient's cardiomyopathy was advanced, it is possible that earlier administration of corticosteroid therapy may have arrested his progressive biventricular failure. As clinicians, we should always remember to force ourselves to broaden our differential diagnosis when new findings become available, especially those that point to a systemicrather than an organ‐specificdisorder. In this case, while the original diagnostic findings were accurate and strongly suggested ARVD, a change of heart was needed to arrive at the ultimate diagnosis.
| Clinical Manifestation | Prevalence (%) |
|---|---|
| Atrioventricular block | 40 |
| Bundle branch block | 40 |
| Supraventricular tachycardia | 20 |
| Ventricular arrhythmias | 25 |
| Heart failure | 25 |
| Sudden cardiac death | 35 |
KEY POINTS FOR HOSPITALISTS
-
Cardiomyopathy in a young person requires consideration of a broad differential diagnosis that is notably different from the most common etiologies of cardiomyopathy in the elderly.
-
Anchoring bias is a common pitfall in clinical decision making. When new or contradictory findings are uncovered, clinicians should reevaluate their initial impression to ensure it remains the most likely diagnosis.
-
Cardiac sarcoidosis is a mimic of ARVD and should be considered when evaluating a patient for right ventricular cardiomyopathy. The differential diagnosis of ARVD includes idiopathic ventricular tachycardia, right ventricular outflow tract tachycardia, myocarditis, idiopathic dilated cardiomyopathy, and sarcoidosis.
The approach to clinical conundrums by an expert clinician is revealed through presentation of an actual patient's case in an approach typical of morning report. Similar to patient care, sequential pieces of information are provided to the clinician who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
A 29‐year‐old man developed palpitations and dyspnea while loading boxes into a truck. In the emergency department, telemetry demonstrated a wide‐complex tachycardia at a rate of 204 beats per minute. The patient spontaneously cardioverted to sinus rhythm (Figure 1) before direct current cardioversion was performed.
Wide‐complex tachycardia is usually explained by a supraventricular tachycardia with aberrant ventricular conduction or a ventricular tachycardia. Although algorithms exist to guide the clinician in parsing out those etiologies, often the knowledge of underlying structural cardiac disease is most informative. In patients with a history of myocardial infarction, greater than 95% of wide‐complex tachycardia is ventricular tachycardia. The ventricular ectopy, T‐wave inversion or flattening, and poor R‐wave progression are suggestive of a cardiomyopathy, either acute or chronic. A pressing concern, especially with the Q waves and concave ST morphology in V1 and V2, would be coronary ischemia. His age makes this less likely, but an aberrant coronary circulation or drug use could account for it.
Over the past 2 years, the patient had several episodes of sustained palpitations, which terminated after several minutes. Previously, the patient exercised frequently including playing rugby in college. However, over the past year he experienced difficulty climbing stairs due to shortness of breath, which he attributed to deconditioning and smoking. He had no significant medical history, was not taking any medications, nor did he use recreational stimulants. He drank alcohol occasionally. He had no risk factors for the human immunodeficiency virus (HIV). Both of the patient's parents were alive and well. There was no family history of sudden cardiac death.
The duration of symptoms suggests that this is a chronic cardiomyopathy rather than acute myocarditis or acute ischemia, acknowledging that either one could be superimposed. The absence of family history lowers the likelihood of heritable causes of arrhythmia that may accompany a structurally normal (eg, long QT syndrome) or abnormal (eg, hypertrophic cardiomyopathy) heart, although penetrance can be variable. What might account for a cardiomyopathy in a young person? Most cases are probably idiopathic, but etiologies that diverge from the usual suspects of coronary artery disease, hypertension, and valvular disease, which affect an older population, include antecedent viral myocarditis, substance abuse, HIV, or infiltrative disorders such as sarcoidosis.
The patient's pulse was 92 beats per minute and regular and the blood pressure was 96/52 mm Hg. The jugular venous pressure was elevated with prominent v‐waves, the point of maximal impulse was diffuse, there were no extra heart sounds or murmurs, and an enlarged liver was detected. An echocardiogram demonstrated left ventricular dysfunction with an ejection fraction of 30%, severe enlargement of the right atrium and right ventricle, and moderate tricuspid regurgitation. Cardiac catheterization revealed normal coronary arteries without evidence of pulmonary hypertension or intracardiac shunt.
The physical examination and echocardiographic findings of right‐sided failure are unusual given the absence of pulmonary hypertension or intracardiac shunt, and could prompt repeat of the hemodynamic measurements and/or investigations for pulmonary disease that may account for right‐sided pressure overload (in addition to that caused by left ventricular failure). An alternative explanation would be a cardiomyopathic process that preferentially involves the right side of the heart, such as arrhythmogenic right ventricular dysplasia (ARVD), but that would not satisfactorily explain the significant decline in left ventricular function. An acute right ventricular infarction could cause his acute symptoms and his examination and echocardiographic findings, but not the underlying chronic illness. It is common to see patients with long‐standing biventricular failure who present with prominent signs of right‐sided failure (elevated neck veins, hepatomegaly, and edema) but limited or no signs of left‐sided failure (rales) to match their degree of volume overload or dyspnea.
Cardiac magnetic resonance imaging (MRI) revealed a dilated right ventricle with extensive hyperenhancement, a right ventricular ejection fraction of 9%, and moderate left ventricular dysfunction (Figure 2). Electrophysiology testing induced both nonsustained polymorphic and monomorphic ventricular tachycardia. Late potentials were detected on a signal‐averaged electrocardiogram. A single‐chamber cardioverter defibrillator was implanted and the patient was discharged on carvedilol, lisinopril, and spironolactone. An HIV‐1 antibody was negative and a thyroid‐stimulating hormone concentration was within normal limits.
Assuming that accurate evaluation of the pulmonary circulation has been undertaken to exclude pulmonary hypertension, the enlarged and hyperenhanced right ventricle on MRI suggests a process that preferentially infiltrates the right ventricular myocardium, and may secondarily affect the left ventricle either by further infiltration or as a consequence of altered mechanics from the highly dysfunctional right ventricle. ARVD affects the right ventricle, but it is possible that another infiltrative cardiomyopathy, such as sarcoid or an antecedent viral infection, could be restricted in its distribution. Late‐potentials identified on signal average electrocardiograms indicate areas of abnormal conduction that may serve as substrate for reentrant ventricular arrhythmias. They are, however, nonspecific, as they are seen in a variety of myocardial diseases.
The patient continued to have progressive dyspnea and was readmitted after receiving an appropriate implantable cardioverter defibrillator shock for ventricular tachycardia. Recurrent slow ventricular tachycardia (Figure 3) was treated with supplemental beta‐blockade and amiodarone (10 g total). Repeat echocardiography demonstrated severe left ventricular dysfunction with an ejection fraction of less than 15%. There were no recurrences of ventricular arrhythmias and the patient was discharged and referred for cardiac transplant evaluation for ARVD.
This degree of left ventricular dysfunction is unlikely to be accounted for by altered mechanics and interactions from a failing right ventricle alone and frames this as a biventricular cardiomyopathy, which has an extensive differential diagnosis and requires information from the general medical evaluation.
On routine laboratory testing 6 months later, a serum aspartate aminotransferase of 79 units/L and a serum alanine aminotransferase of 118 units/L were found. Bilirubin, albumin, and alkaline phosphatase were normal. The transaminase levels had been normal on initial evaluation. The patient reported that 2 paternal uncles had end‐stage nonalcoholic cirrhosis. Transjugular liver biopsy was consistent with mild lobular hepatitis with mild portal fibrosis with a few lobular collections of mononuclear cells. There was no evidence of iron overload. The hepatic venogram and transhepatic pressure gradient (2 mm Hg) were normal.
The elevated transaminase levels could be due to amiodarone‐associated hepatotoxicity, hepatic congestion, or a primary liver disease. It is important to consider combined cardiohepatic syndromes such as hemochromatosis, sarcoidosis, or amyloidosis. The relatively normal liver histology and normal hepatic hemodynamics do not suggest a significant primary intrinsic liver disease. The 2 uncles with cirrhosis could suggest a heritable liver disease, although cirrhosis in multiple family members is frequently accounted for by shared habits such as alcohol consumption or excessive caloric intake. Liver disorders with a genetic component, such as hemochromatosis, Wilson's disease, and alpha‐1‐antitrypsin deficiency are mostly autosomal recessive, which would make this pattern of transmission unusual. Furthermore, aside from hemochromatosis, these genetic hepatic disorders have few cardiac manifestations. Right‐sided congestion and amiodarone appear to be the most likely explanations of his liver abnormalities.
Pulmonary function testing revealed normal lung volumes without obstruction, but the diffusing capacity for carbon monoxide was substantially reduced. Computed tomography of the chest identified scattered ground‐glass opacities as well as small nodules with an upper lobe distribution (Figure 4). Although not reported on the initial interpretation, review of a chest x‐ray taken 6 months previously also demonstrated small nodules in the upper lobe distribution. Bronchoscopic examination was normal. Bronchioalveolar lavage fluid stains and cultures for bacteria, mycobacteria, Pneumocystis, and fungus were negative. Transbronchial biopsies of the right middle lobe had no evidence of infection, malignancy, or granulomatous inflammation. The patient continued to have progressive New York Heart Association Class IV heart failure symptoms. Repeat right heart catheterization was notable for a cardiac index of 1.4 L/minute/m2. The mean pulmonary artery pressure was 20 mm Hg. An intraaortic balloon pump was placed for refractory cardiogenic shock.
The reduced diffusion capacity and ground‐glass opacities suggest an interstitial process, which may have been missed on transbronchial biopsy because of sampling error. His pulmonary disease is likely another manifestation of his infiltrative cardiac disease. The constellation of cardiac, pulmonary, and hepatic involvement in the context of progressive dyspnea over 2 years is suggestive of sarcoidosis although the absence of hilar lymphadenopathy and 2 biopsy specimens without granulomas argue against the diagnosis, and the effects of amiodarone on the latter 2 organs cannot be ignored. On the limited menu of pharmacologic treatments that may treat this severe and progressive cardiomyopathy are steroids, which makes a diligent search for a steroid‐responsive syndrome important. Therefore, despite the negative studies, sarcoidosis must be investigated to the fullest extent with either an endomyocardial biopsy or surgical lung biopsy.
The patient underwent cardiac transplantation. The native heart was found to have right ventricular thinning, which was most notable at the right ventricular outflow tract. Microscopic examination revealed extensive fibrosis and granulomatous inflammation (Figure 5) with scarring typical of cardiac sarcoidosis. Six months after cardiac transplantation, the patient is doing well on prednisone, tacrolimus, and mycophenolate mofetil. Follow‐up chest x‐rays show resolution of the pulmonary nodules.
COMMENTARY
Cardiomyopathy in a young person is a relatively uncommon clinical event that prompts consideration of a broad differential diagnosis that is notably different from the most common etiologies of cardiomyopathy in older adults. This case highlights the challenges of arriving at a diagnosis in the absence of a gold standard, and the greater challenges of modifying initial diagnostic impressions as new clinical data become available.
After encountering ventricular tachycardia and right ventricular dysfunction in a young patient, the clinicians arrived at the diagnosis of ARVD. This rare and progressive disorder is associated with up to 20% of ventricular arrhythmias and sudden death in the young,1, 2 but can be challenging to diagnose. Despite common referrals for cardiac MRI to exclude ARVD, cardiac MRI is not the gold standard for diagnosis and is the most common method of misdiagnosis of ARVD.3 A diagnosis of ARVD requires the presence of 2 major, 1 major and 2 minor, or 4 minor International Task Force criteria (Table 1).4, 5 While the diagnostic criteria provide standardization across populations (eg, in clinical studies), additional considerations are needed in the management of individual patients. Scoring systems serve as a tool, but the final diagnosis requires balancing such criteria with competing hypotheses. This dilemma is familiar to clinicians considering other less common conditions such as amyotrophic lateral sclerosis (World Neurology Foundation), rheumatic fever (Jones criteria), or systemic lupus erythematosus (American College of Rheumatology). This patient's cardiac MRI findings, precordial T‐wave inversions, frequent ventricular ectopy, and late potentials on a signal‐averaged electrocardiogram fulfilled the International Task Force criteria for a diagnosis of ARVD. Discordant information included the right bundle branch pattern of the ventricular tachycardia, which suggested left ventricular origin, as opposed to the more common left bundle branch pattern observed in ARVD, and the absence of a family history. In addition, in U.S. populations only 25% of cases present with heart failure and fewer than 5% develop biventricular failure.6 Nonetheless, this patient's imaging evidence of right ventricular structural abnormalities and dysfunction and electrocardiographic abnormalities coupled with the absence of obvious systemic disease made ARVD the logical working diagnosis.
| Major | Minor | |
|---|---|---|
| ||
| I. Global and/or regional dysfunction and structural alterations | Severe dilation and reduction of right ventricular ejection fraction, localized right ventricular aneurysms | Mild right ventricular dilatation and/or reduced ejection fraction |
| II. Endomyocardial biopsy | Fibrofatty replacement of myocardium | |
| III. Repolarization abnormalities | T‐wave inversion in leads V1‐V3 or beyond | |
| IV. Depolarization/conduction abnormalities | Epsilon waves or localized QRS prolongation (>110 msec) in leads V1‐V3 | Late potentials on signal‐averaged electrocardiogram |
| V. Arrhythmias | Left bundle branch block‐type ventricular tachycardia (sustained and nonsustained) or frequent ventricular extra systoles (>1,000/24 hours) | |
| VI. Family history | Familial disease confirmed at necropsy or surgery | Familial history of premature sudden death (35 years old) or clinical diagnosis based on present criteria |
When more widespread manifestations developed, namely hepatic and pulmonary abnormalities, each was investigated with imaging and biopsy. Once a multisystem illness became apparent, the discussant reframed the patient's illness to include other diagnostic possibilities. In practice it is difficult to reverse a working diagnosis despite contradictory evidence because of the common pitfall of anchoring bias. Tversky and Kahneman7 were the first to describe the cognitive processes behind probability assessment and decision making in time‐sensitive situations. Under these conditions, decision makers tend to focus on the first symptom, striking feature, or diagnosis and anchor subsequent probabilities to that initial presentation. Once a decision or diagnosis has been reached, clinicians tend to interpret subsequent findings in the context of the original diagnosis rather than reevaluating their initial impression. In the setting of a known diagnosis of ARVD, 3 separate diagnoses (ARVD, amiodarone‐associated lung injury, and amiodarone‐induced hepatic dysfunction) were considered by the treating physicians. The initial diagnosis of ARVD followed by the sequential rather than simultaneous manifestations of sarcoidosis made arriving at the revised diagnosis even more challenging.
Cardiac sarcoidosis is a mimic of ARVD and should be considered when evaluating a patient for right ventricular dysplasia.8, 9 The differential diagnosis of ARVD includes idiopathic ventricular tachycardia, myocarditis, idiopathic cardiomyopathy, and sarcoidosis. Cardiac sarcoidosis can present as ventricular ectopy, sustained ventricular arrhythmias, asymptomatic ventricular dysfunction, heart failure, or sudden death.10 Although 25% of patients with sarcoidosis have evidence of cardiac involvement at autopsy, only 5% have clinical manifestations.11 Those patients with clinical evidence of cardiac sarcoidosis have a wide range of clinical findings (Table 2). While the patient's cardiomyopathy was advanced, it is possible that earlier administration of corticosteroid therapy may have arrested his progressive biventricular failure. As clinicians, we should always remember to force ourselves to broaden our differential diagnosis when new findings become available, especially those that point to a systemicrather than an organ‐specificdisorder. In this case, while the original diagnostic findings were accurate and strongly suggested ARVD, a change of heart was needed to arrive at the ultimate diagnosis.
| Clinical Manifestation | Prevalence (%) |
|---|---|
| Atrioventricular block | 40 |
| Bundle branch block | 40 |
| Supraventricular tachycardia | 20 |
| Ventricular arrhythmias | 25 |
| Heart failure | 25 |
| Sudden cardiac death | 35 |
KEY POINTS FOR HOSPITALISTS
-
Cardiomyopathy in a young person requires consideration of a broad differential diagnosis that is notably different from the most common etiologies of cardiomyopathy in the elderly.
-
Anchoring bias is a common pitfall in clinical decision making. When new or contradictory findings are uncovered, clinicians should reevaluate their initial impression to ensure it remains the most likely diagnosis.
-
Cardiac sarcoidosis is a mimic of ARVD and should be considered when evaluating a patient for right ventricular cardiomyopathy. The differential diagnosis of ARVD includes idiopathic ventricular tachycardia, right ventricular outflow tract tachycardia, myocarditis, idiopathic dilated cardiomyopathy, and sarcoidosis.
- ,,, et al.Right ventricular dysplasia: a report of 24 adult cases.Circulation.1982;65:384–398.
- ,,,,.Right ventricular cardiomyopathy and sudden death in young people.N Engl J Med.1988;318:129–133.
- ,,, et al.Misdiagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy.J Cardiovasc Electrophysiol.2004;15:300–306.
- ,,, et al.Diagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Task Force of the Working Group Myocardial and Pericardial Disease of the European Society of Cardiology and the Scientific Council on Cardiomyopathies of the International Society and Federation of Cardiology.Br Heart J.1994;71:215–218.
- ,,, et al.Predictors of appropriate implantable defibrillator therapies in patients with arrhythmogenic right ventricular dysplasia.Heart Rhythm.2005;2:1188–1194.
- ,,, et al.Arrhythmogenic right ventricular dysplasia: a United States experience.Circulation.2005;112:3823–3832.
- ,.Judgment under uncertainty: heuristics and biases.Science.1974;185:1124–1131.
- ,,.Unusual presentation of cardiac sarcoidosis.Congest Heart Fail.2007;13:116–118.
- ,,, et al.Cardiac sarcoidosis mimicking right ventricular dysplasia.Circ J.2003;67:169–171.
- ,,,,.Refractory ventricular tachycardia secondary to cardiac sarcoid: electrophysiologic characteristics, mapping, and ablation.Heart Rhythm.2006;3:924–929.
- ,.Sarcoid heart disease: clinical course and treatment.Int J Cardiol.2004;97:173–182.
- ,,, et al.Right ventricular dysplasia: a report of 24 adult cases.Circulation.1982;65:384–398.
- ,,,,.Right ventricular cardiomyopathy and sudden death in young people.N Engl J Med.1988;318:129–133.
- ,,, et al.Misdiagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy.J Cardiovasc Electrophysiol.2004;15:300–306.
- ,,, et al.Diagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Task Force of the Working Group Myocardial and Pericardial Disease of the European Society of Cardiology and the Scientific Council on Cardiomyopathies of the International Society and Federation of Cardiology.Br Heart J.1994;71:215–218.
- ,,, et al.Predictors of appropriate implantable defibrillator therapies in patients with arrhythmogenic right ventricular dysplasia.Heart Rhythm.2005;2:1188–1194.
- ,,, et al.Arrhythmogenic right ventricular dysplasia: a United States experience.Circulation.2005;112:3823–3832.
- ,.Judgment under uncertainty: heuristics and biases.Science.1974;185:1124–1131.
- ,,.Unusual presentation of cardiac sarcoidosis.Congest Heart Fail.2007;13:116–118.
- ,,, et al.Cardiac sarcoidosis mimicking right ventricular dysplasia.Circ J.2003;67:169–171.
- ,,,,.Refractory ventricular tachycardia secondary to cardiac sarcoid: electrophysiologic characteristics, mapping, and ablation.Heart Rhythm.2006;3:924–929.
- ,.Sarcoid heart disease: clinical course and treatment.Int J Cardiol.2004;97:173–182.
Admission Order Sets for DVT Prophylaxis
The use of clinical decision support, despite great promise to improve health care, remains preliminary.1 The broad scope of quality and safety challenges facing clinicians2, 3 requires this situation to change. There is an urgent need to develop decision support tools and strategies that are effective, address many quality issues simultaneously, and are easy to implement in both academic and community settings.
One decision support tool that could help to meet this challenge is the order set. An order set is a group of orders with a common functional purpose that is used directly by a physician to create orders for a specific patient. Order sets can be used with either paper‐based or computerized provider order entry (CPOE) systems. Several studies have investigated the delivery of focused evidence‐based treatments to patients admitted using disease‐specific order sets compared with either historical or concurrent controls and have demonstrated increased use of therapies such as aspirin for acute myocardial infarction admissions,4 systemic corticosteroids, metered‐dose inhalers and pulse oximetry for pediatric asthma admissions,5 and venous thromboembolism prophylaxis for adult emergency department admissions.6 However, the ability of order sets to improve multiple quality measures in a diverse patient population has not been evaluated previously.
This study examined the effect of paper‐based order sets on the quality of admission orders for general medical patients in a community hospital. The primary hypothesis was that order set use would increase the proportion of general medical patients ordered deep venous thrombosis (DVT) prophylaxis. We chose this primary endpoint because DVT prophylaxis continues to be significantly underused in hospitalized patients.7, 8 Secondary hypotheses were that order sets would improve other admission order quality of care measures. We studied paper‐based order sets because the study hospital, along with the vast majority of North American hospitals, uses paper for order entry.9
PATIENTS AND METHODS
Study Setting
The study took place in a 750‐bed community hospital in Mississauga, Ontario, Canada. The study included only general medical patients and excluded cardiology, neurology, and intensive care unit patients. Approximately 30 different internists admitted patients during the study period from April 1, 2003 to March 31, 2005. The internists were not aware that this study was being conducted. Order sets were implemented as an option for writing admission orders in December 2003. Prior to the implementation of order sets, physicians wrote all admission orders using traditional free‐text handwritten orders on blank paper order sheets. Essentially all general medical patients are admitted through the emergency room. The hospital's Research Ethics Board approved this study.
Order Set Development
Local specialists developed order set content (evidence‐based where possible) using informal consensus methods, without explicitly grading evidence. This process created a general admission order set and six diagnosis‐specific order sets (community acquired pneumonia, chronic obstructive pulmonary disease [COPD], febrile neutropenia, soft tissue infection, upper gastrointestinal [GI] bleeding, and urinary tract infection [UTI]). All order sets contained the same orders pertaining to the primary and secondary outcomes, except for the GI bleed admission order set, which did not contain a DVT prophylaxis section.
Order sets were paper‐based and consisted of a menu of orders typically required for a medical admission. These included admitting service, admitting physician, allergies, resuscitation status, diet, activity level, frequency of vital sign measurement, laboratory investigations, diagnostic imaging, intravenous fluid therapy, and medications. The orders were either optional (requiring the physician to check a box to be performed) or default (enacted unless specifically crossed out by the physician). Both order types could consist of a single order (for example, heparin for DVT prophylaxis) or several orders simultaneously (for example, measurement of serum sodium, potassium, and creatinine). All order sets included space for additional free‐text handwritten orders to meet individual patient needs.
The DVT prophylaxis section contained optional orders for 5,000 units of heparin subcutaneously (sc) twice daily (BID) and compression stockings. The ordering physician could select 1, both, or neither of these options. Initiating other forms of DVT prophylaxis or therapeutic anticoagulation required additional free‐text handwritten orders.
Informal clinician feedback led to improved order set content and formatting in August 2004. Orders pertaining to study outcomes were unchanged in this upgrade.
Implementation
In December 2003, we placed the order sets near the stacks of blank paper order sheets used by internists admitting patients in the Emergency Department. We notified physicians by e‐mail when order sets became available but provided no formal education about order sets, DVT prophylaxis, or other study outcomes. The use of order sets was voluntary. We developed a website to facilitate timely reordering of depleted order sets from the hospital's print shop and trained all emergency room clerks regarding website access and storage of the order sets in convenient locations for physicians. Although order set availability was not formally assessed, there were no reports by physicians or observations by study investigators of order sets being unavailable at any time.
Data Collection
To assess the effect of order sets on the ordering of DVT prophylaxis, we retrospectively and randomly selected patient admissions and reviewed these patients' charts from 3 time periods during the study period: OctoberNovember 2003 (period 1, immediately prior to availability of order sets; 113 charts available of 120 discharged patients randomly selected from a total of 1,169 discharges); AprilDecember 2004 (period 2, 412 months after order set availability; 291 charts available of 300 discharged patients randomly selected from a total of 4,620 discharges); and FebruaryMarch 2005 (period 3, 1415 months after order set availability; 283 charts available of 290 randomly selected discharges out of a total of 1,057 discharges). We conducted an additional chart audit just prior to final submission of the manuscript (108 charts available of 120 discharged patients randomly selected from a total of 1,060 discharges in OctoberNovember 2007) to determine the sustainability of the improvements. The same patient could be selected in different time periods. One author (C.O. or K.D.) reviewed each chart using a jointly developed data collection form.
We assessed the admission orders of each chart for the use of an order set and the ordering of DVT prophylaxis, defined as 5,000 units of heparin sc BID or compression stockings (no patient received sc heparin 3 times daily, heparin sc BID in doses greater than 5,000 units, prophylactic doses of low molecular‐weight heparin, or low dose warfarin). We recorded the ordering of therapeutic anticoagulation, defined as intravenous heparin, full‐dose low molecular‐weight heparin, or warfarin with a target international normalized ratio 2.
Independent from the chart review, we examined the overall administration of heparin doses for DVT prophylaxis to all medical inpatients using the hospital pharmacy database. We estimated the overall administration of heparin for DVT prophylaxis in medical inpatients (136 medical beds, 4 wards) on a monthly basis from April 1, 2003 (8 months prior to order set availability) to March 30, 2005 (15 months after order set availability). We calculated monthly utilization as the proportion of patient‐days for which DVT prophylaxis was administered, as follows: (number of doses of subcutaneous heparin dispensed by the hospital pharmacy to the 4 wards)/(2 [since there are 2 doses per patient‐day] number of patient‐days).
We collected additional data from the charts selected during period 2 (AprilDecember 2004) to evaluate the effect of order sets on the following secondary outcomes: (1) the documentation of admission diagnosis, allergies, and code status; (2) general care orders (electrocardiogram [ECG] and notification of physician for chest pain, allied health consultation, standard hospital potassium replacement protocol [already available in the hospital], standard hospital diabetic diet and standard hospital insulin sliding scale [for patients with diabetes], night time sedation diet or nil per os, activity level and vital sign frequency); (3) blood urea nitrogen (BUN), a laboratory test often inappropriately ordered according to local guidelines10; (4) order formatting (numbering, dating, timing, and signing of all order pages); and (5) organization of orders in the standardized arrangement used in the order sets. This standardized arrangement of content was as follows: attending physician, admitting diagnosis, requests for consultation, diet, activity, vital signs, oxygen, nasogastric tube, urinary catheter, investigations, intravenous fluids, and medications. Free‐text admission orders and order set orders that maintained this arrangement were recorded as standardized. We did not assess order appropriateness.
We recorded the characteristics of all medical patients admitted to the hospital in two 1‐year periods during the study (April 1, 2003 to March 30, 2004 and April 1, 2004 to March 30, 2005), including age, gender, length of stay, diagnosis (defined by case management group [CMG]), and resource intensity weight (RIW). CMG defines groups of patients who are similar in diagnosis or procedure and RIW is a measure of resources used during a patient's hospital stay.11 The definitions of CMG and RIW did not change during the study.
Statistical Analysis
Baseline characteristics were compared using Student t‐test for normally distributed continuous variables (patient age) and the Mann‐Whitney U test for skewed continuous variables (length of stay and RIW). Chi square or Fisher's exact tests were used to compare categorical variables. Relative risks (RR) and 95% confidence intervals (CI) were calculated and compared using a z‐test. A 2‐sided P value <0.05 was taken to be statistically significant. All calculations were carried out using SAS Version 8.2 (SAS Institute, Cary, NC).
RESULTS
As shown in Table 1, there were no clinically important differences in demographic or clinical characteristics of medical patients between the 2 years of the study. There were small but statistically significant increases in patient illness complexity (as reflected in median RIW) (P = 0.003) and length of stay (P = 0.0002).
| Patient Characteristic | April 1, 2003 to March 30, 2004 (n = 4,415) | April 1, 2004 to March 30, 2005 (n = 4,287) |
|---|---|---|
| ||
| Age, mean SD | 67.2 17.7 | 67.6 17.5 |
| Length of stay, median days (IQR) | 6 (3‐12) | 6 (3‐13) |
| RIW,11 median (IQR) | 0.96 (0.68‐1.73) | 1.03 (0.72‐1.88) |
| Females, number (% of total) | 2,276 (52) | 2,223 (52) |
| Case mix group,11 number of patients (% of total) | ||
| Chronic obstructive pulmonary disease | 357 (8.1) | 385 (9.0) |
| Simple pneumonia and pleurisy | 322 (7.3) | 217 (5.1) |
| Esophageal, gastrointestinal, and miscellaneous digestive disease | 223 (5.1) | 239 (5.6) |
| Gastrointestinal hemorrhage | 185 (4.2) | 198 (4.6) |
| Respiratory neoplasm | 127 (2.9) | 144 (3.4) |
| Total | 1,214 (27.5) | 1,183 (27.7) |
Clinicians used order sets in 32.3% of admissions during period 2 (AprilDecember 2004, 412 months after order set availability), increasing to 51.6% in period 3 (FebruaryMarch 2005, 1415 months after order set availability). The results of the chart audit assessing the impact of order set use on DVT prophylaxis are shown in Figure 1. Prior to order set introduction, 10.9% of patients received orders for DVT prophylaxis. Subsequently, ordering of DVT prophylaxis in patients admitted with order sets increased (period 2: 35.6%; P < 0.001; RR, 3.27; 95% CI, 1.806.12 and period 3: 44.0%; P < 0.001; RR, 4.04; 95% CI, 2.327.31). In contrast, DVT prophylaxis ordering in the nonorder set group was initially unchanged (period 2: 10.6%; P = 0.93; RR, 0.97; 95% CI, 0.491.95), although later it increased to a smaller extent (period 3: 20.6%; P = 0.049; RR, 1.90; 95% CI, 1.013.65). As a result of this differential increase, patients admitted with order sets were more likely to be ordered DVT prophylaxis in both study periods (period 2: 35.6% versus 10.6%; P < 0.0001; RR, 3.38; 95% CI, 2.035.62 and period 3: 44.0% versus 20.6%; P < 0.0001; RR, 2.13; 95% CI, 1.443.16). The use of therapeutic anticoagulation was similar in patients admitted with and without order sets and did not change between time periods.
The hospital‐wide monthly utilization of heparin for DVT prophylaxis in medical inpatients increased from an average of 12.8% (range, 9.7%16.1%) of patient‐days before order set implementation (AprilNovember 2003) to 18.5% (range, 16.4%20.0%) of patient‐days in the 8 months after order sets were first implemented (DecemberJuly 2004, P < 0.0001 compared to the preorder set time period). After August 2004, when upgraded order sets were introduced, DVT prophylaxis utilization increased further in the last 7 months of the study to 25.8% (range, 22.4%32.2%; P < 0.0001 compared to preorder set time period; Figure 2).
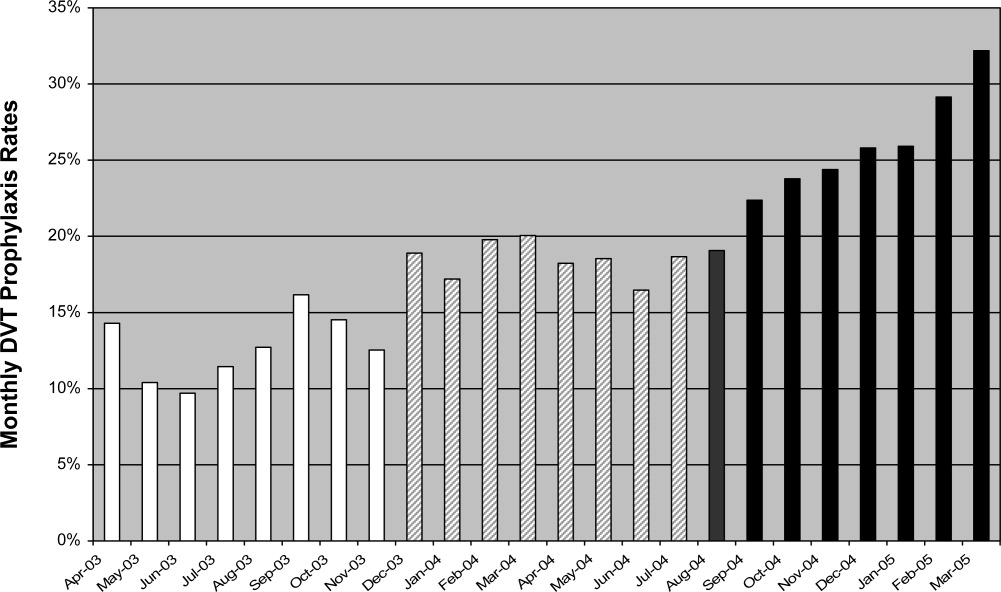
Table 2 shows the impact of order sets on secondary outcomes. Admissions completed with order sets had statistically significant increases in general care orders (ECG and notification of physician for chest pain, allied health consultations and standard hospital diabetic diet, insulin scale, and potassium replacement protocol orders), documentation of allergies and code status, numbering of pages, and use of a standardized arrangement for orders. Ordering of BUN decreased significantly.
| Outcome | Optional or Default | Order Set [n = 94 (%)] | No Order Set [n = 197 (%)] | P Value |
|---|---|---|---|---|
| ||||
| Documentation | ||||
| Admitting diagnosis | Optional | 91 (96.8) | 187 (94.9) | 0.47 |
| Allergies | Optional | 51 (54.3) | 19 (9.6) | <0.0001 |
| Resuscitation status | Optional | 54 (57.4) | 20 (10.2) | <0.0001 |
| General care orders | ||||
| ECG and call MD for chest pain | Default* | 80 (85.1) | 0 (0.0) | <0.0001 |
| Allied health consult | 59 (62.8) | 25 (12.7) | <0.0001 | |
| Diet | Optional | 90 (95.7) | 188 (95.4) | 0.90 |
| Activity | Optional | 80 (85.1) | 150 (76.1) | 0.08 |
| Vitals signs and frequency | Optional | 91 (96.8) | 178 (90.4) | 0.052 |
| Standard hospital diabetic diet | Optional | 16 (17.0) | 10 (5.1) | 0.0008 |
| Standard hospital insulin sliding scale | Optional | 18 (19.1) | 15 (7.6) | 0.004 |
| Standard hospital potassium protocol | Optional | 60 (63.8) | 1 (0.51) | <0.0001 |
| Nighttime sedation | ||||
| Zopiclone as needed | Optional | 43 (45.7) | 2 (1.0) | < 0.0001 |
| Lorazepam as needed | Optional | 12 (12.8) | 15 (7.6) | 0.16 |
| Laboratory test order | ||||
| Blood urea nitrogen | Optional | 37 (39.4) | 117 (59.0) | 0.0014 |
| Order formatting | ||||
| Numbering of pages | Default | 94 (100) | 4 (2.0) | <0.0001 |
| Dating of orders | Optional | 79 (84.0) | 185 (93.9) | 0.0067 |
| Timing of orders | Optional | 14 (14.9) | 29 (14.7) | 0.97 |
| Signing of orders | Optional | 93 (98.9) | 196 (99.5) | 0.54 |
| Standard arrangement of orders | 81 (86.2) | 66 (33.5) | <0.0001 | |
Order sets were not associated with changes in diet, activity, or vital sign orders, documentation of admission diagnosis, or the signing and timing of orders. Apart from order timing, these orders were present in >75% of admissions completed without order sets. The only negative effect of order sets was a reduction in the dating of orders (84.0% of order set admissions versus 93.9% of nonorder set admissions, P = 0.007). Finally, order sets had both an intended and unintended effect on nighttime sedation orders. Relative frequency of ordering of zopiclone compared to lorazepam increased (43/55 in the order set group vs. 2/17 in the no order set group [P < 0.0001], the intended effect), and increased overall frequency of ordering of nighttime sedation (55/94 vs. 17/197 [P < 0.0001], an unintended effect).
The additional chart audit in OctoberNovember 2007, just prior to final submission of the manuscript, determined that clinician use of order sets had increased to 92.6% of admitted medical patients, and that ordering of DVT prophylaxis in patients admitted with order sets had been sustained at 43.2% (P = 0.90 compared to period 3) (Figure 1).
DISCUSSION
We found that paper‐based order sets were associated with markedly increased use of DVT prophylaxis and made physician ordering more consistent with hospital consensus guidelines in multiple other areas, including laboratory test utilization and general care, while also increasing completeness of documentation. Given the difficulties and limited resources frequently associated with guideline development, dissemination, and implementation,12 it is worth noting that our improvements were achieved in a community hospital with voluntary physician adoption and no dedicated project funding, care process redesign, or healthcare worker education. The broad impact of order sets combined with minimal organizational resources required for implementation in this study suggests that this clinical decision support tool may have wide applicability.
The study hospital used paper‐based orders rather than CPOE, similar to 90% of U.S. hospitals at the time of the study.9 Order sets can be deployed in either paper‐based or computerized ordering systems. By providing a mechanism for entering large blocks of orders in an efficient manner, paper‐based order sets may be a necessary first step to facilitate the paper to CPOE transition, making them well suited to the current care delivery environment. Successful use of paper‐based order sets may help accelerate adoption of CPOE, which appears to be many years away from full implementation in the majority of U.S. hospitals.13
The most clinically important outcome in our study was a more than 4‐fold increase in ordering of DVT prophylaxis (last study period compared with baseline) in medical patients admitted with order sets, compared to a smaller increase in patients admitted without order sets. Our result is particularly significant as this study was performed in a community hospital, a setting with a lower adherence to DVT prophylaxis guidelines compared to academic centers.8, 14 The increase in DVT prophylaxis in patients admitted without order sets could be the result of a secular trend or a passive educational effect of order sets on physicians who only used order sets intermittently. The study was not publicized and thus was unlikely in itself to contribute to the increased performance.
We did not assess clinical outcomes of DVT or pulmonary embolism, but the clinical efficacy of improving adherence to DVT prophylaxis has been previously established.15 We also did not assess the appropriateness of DVT prophylaxis (or any other order). However, a recent multicenter Canadian observational study, using the American College of Chest Physician's Consensus Guidelines on Antithrombotic Therapy16 as a reference standard, found that 90% of medical patients admitted to hospital meeting study criteria had indications for thromboprophylaxis, but only 16% of eligible patients actually received it.8 In addition, multivariable regression analysis demonstrated even lower utilization in community hospitals compared to academic hospitals. These data suggest that the study hospital is typical of Canadian hospitals, and that the low overall utilization of DVT prophylaxis (13% of hospital patient‐days) prior to the availability of order sets in the study hospital is a significant gap between optimal and actual practice.
In addition, order sets had an impact on many secondary outcomes, such as standardization and completeness of orders (for example documentation of allergies and resuscitation status). While these effects appear to be beneficial in terms of quality of care and patient safety, the relationship of our secondary outcomes to patient‐important outcomes has not been established.
Furthermore, our before‐after design does not exclude the possibility of unknown confounding effects as explanations of improved performance in the order set group. For example, the change could have been driven by a small number of admitting physicians, since it is likely that order sets were adopted more readily by some physicians than others, and this group could have been responsible for a greater proportion of the admissions at different times. Unfortunately, we did not record the identity of the admitting physician. However, data from OctoberNovember 2007 show that >90% of medical patients were admitted using order sets, suggesting that voluntary clinician adoption of order sets has become nearly universal. Nevertheless, there still appear to be a few physicians who rarely or never used orders sets. Motivating these physicians to prescribe appropriate DVT prophylaxis remains a challenge.
Although this study was conducted in 1 center, other hospitals have similarly low rates of thromboprophylaxis,8 and our order set implementation strategy consumed few resources, improving the generalizability of our results. While most changes were beneficial, order set use was associated with decreased dating of orders and with an unintended effect or overall increase ordering of nightime sedation. Although the reasons for this are unclear, it highlights the importance of systematically evaluating the impact of order sets to identify unintended consequences and areas in which the order set may need to be redesigned to address these issues.
The study of order sets is preliminary despite their role as a key enabler for CPOE17 and their suggested usefulness to reduce medical error.18 For example, order sets were not considered in recent analyses of factors predicting success of computerized decision support systems19, 20 and have not been reviewed by the Cochrane Effective Practice and Organisation of Care Group.21 As discussed in the introduction, several studies have demonstrated that disease‐specific order sets can increase the use of evidence‐based treatments.46 Our study extends this work by demonstrating that admission order sets can improve performance hospital‐wide for a broad range of outcomes simultaneously, including DVT prophylaxis. Although most studies have demonstrated increased utilization of evidence‐based therapies, at least 1 study found no increased use of aspirin, heparin, or beta‐blockers in acute coronary syndrome admissions with the introduction of order sets.22 This suggests that the way order sets are structured or introduced is important to ensure that they achieve the desired changes in practice. Finally, our study suggests that improved outcomes using order sets can still be achieved with minimal organizational resources.
Order sets may potentially complement other decision support tools such as alerts and reminders. Alerts are an effective decision support tool12, 23, 24 but risk disrupting clinician workflow. Moreover, excessive alerts can lead to alert fatigue, resulting in many alerts being ignored.25 This phenomenon reduces alert effectiveness and limits the number of issues that alerts can address simultaneously. In contrast, order sets are broad in scope due to integration with clinical workflow, but lack the ability of alerts to apply rules to a specific patient's data. A potentially effective 2‐staged decision support strategy would use order sets as the primary admission decision support tool and selective alerts for remaining issues. This approach may increase the overall scope, physician adoption, and effectiveness of clinical decision support, and should be evaluated.
Our postintervention rate of DVT prophylaxis, while substantially improved from baseline, is still below ideal practice. Order sets were simply made available to clinicians admitting medical patients, who had the option to select DVT prophylaxis. Given limited resources, we did not develop and implement education programs regarding the appropriate use of DVT prophylaxis or make available any DVT risk assessment evaluations (available in Ref.26). Our study methodology thus provides a realistic assessment of improvements attainable in other hospitals with similarly limited resources. Additional increases in DVT prophylaxis rates would likely require a more comprehensive and resource‐intensive multifaceted quality improvement initiative. Detailed guidelines and supporting references for implementing such an initiative are available from the Society of Hospital Medicine.26 As described in their Venous Thromboembolism (VTE) Resource Room,26 such an initiative should include a standardized DVT risk assessment to guide the need for DVT prophylaxis integrated into admission order sets; prompts to order DVT prophylaxis when completing admission orders; and a system to audit adverse events and variations from best practice and return this information to clinicians.26
CONCLUSIONS
This is the largest and most comprehensive evaluation of the effectiveness of order sets as a clinical decision support tool. We found that order sets improved the quality of multiple patient orders and improved hospital‐wide DVT prophylaxis rates. These improvements were achieved in a community hospital with voluntary physician adoption and no dedicated project funding, care process redesign, or healthcare worker education. Although used in a paper‐based format in this study, order sets can also be employed in a computerized ordering environment. By providing a mechanism for entering large blocks of orders in an efficient manner, paper‐based order sets may be a necessary first step to facilitate the paper‐to‐CPOE transition. These attributes make order sets an attractive quality improvement tool in community and academic settings. More research is needed on the optimal design and use of this promising decision support tool.
- .Health Information Management: Integrating Information Technology in Health Care Work.London:Routledge;2004.
- ,,.To Err Is Human: Building a Safer Health System.Washington, DC:National Academy Press;2006.
- National Healthcare Quality Report.2004.Rockville, MD:Agency for Healthcare Research and Quality;2006.
- ,,,,,.Integrating “best of care” protocols into clinicians' workflow via care provider order entry: impact on quality‐of‐care indicators for acute myocardial infarction.J Am Med Inform Assoc.2006;13:188–196.
- ,,,,,.The role of computerized order sets in pediatric inpatient asthma treatment.Ped Allergy Immunol.2006;17:199–206.
- ,,,.Venous thromboembolism prophylaxis in emergency department admissions.J Hosp Med.2007;2:79–85.
- .DVT prevention: what is happening in the “real world”?Semin Thromb Hemost.2003;29(Suppl 1):23–31.
- ,,, et al.Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada.Thromb Res.2007;119:145–155.
- ,,,.Computerized physician order entry in US hospitals: results of a 2002 survey.J Am Med Inform Assoc.2004;11:95–99.
- Ontario Association of Medical Laboratories. Guidelines for the Use of Serum Tests to Detect Renal Dysfunction. Available at:http://www.oaml.com/PDF/CLP007.pdf. Accessed 12 May2008.
- ,.Physicians in health care management: 3. Case mix groups and resource intensity weights: an overview for physicians.CMAJ.1994;150:889–894.
- ,,, et al.Effectiveness and efficiency of guideline dissemination and implementation strategies.Health Technol Assess.2004;8(6):iii–iv,1–72.
- ,,,,.Predicting computerized physician order entry system adoption in US hospitals: can the federal mandate be met?Int J Med Inform.2008;77(8):539–545.
- ,,,,,.Physician practices in the prevention of venous thromboembolism.Ann Intern Med.1991;115:591–595.
- ,,, et al.Electronic alerts to prevent venous thromboembolism among hospitalized patients.N Engl J Med.2005;352:969–977.
- ,,, et al.Prevention of venous thromboembolism.Chest.2001;119(Suppl 1):132S–175S.
- ,,.A consensus statement on considerations for a successful CPOE implementation.J Am Med Inform Assoc.2003;10:229–234.
- ,.Residents' suggestions for reducing errors in teaching hospitals.N Engl J Med.2003;348:851–855.
- ,,,.Improving clinical practice using clinical decision support systems: a systematic review of trials to identify features critical to success.BMJ.2005;330:765.
- ,,, et al.Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic review.JAMA.2005;293:1223–1238.
- Cochrane Reviews by the Effective Practice and Organisation of Care Group. Available at: http://www.cochrane.org/reviews/en/topics/61_reviews.html. Accessed 12 May2008.
- ,,.Embedded guideline information without patient specificity in a commercial emergency department computerized order‐entry system.Acad Emer Med.2006;13:452–458.
- ,,,,,.A computerized reminder system to increase the use of preventive care for hospitalized patients.N Engl J Med.2001;345:965–970.
- ,,,,.A clinical decision support system for prevention of venous thromboembolism: effect on physician behavior.JAMA.2000;283:2816–2821.
- ,,, et al.Computerized physician order entry and online decision support.Acad Emerg Med.2004;11:1135–1141.
- Society of Hospital Medicine VTE Resource Room. Available at: http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_VTE/VTE_Home.cfm. Accessed 12 May2008.
The use of clinical decision support, despite great promise to improve health care, remains preliminary.1 The broad scope of quality and safety challenges facing clinicians2, 3 requires this situation to change. There is an urgent need to develop decision support tools and strategies that are effective, address many quality issues simultaneously, and are easy to implement in both academic and community settings.
One decision support tool that could help to meet this challenge is the order set. An order set is a group of orders with a common functional purpose that is used directly by a physician to create orders for a specific patient. Order sets can be used with either paper‐based or computerized provider order entry (CPOE) systems. Several studies have investigated the delivery of focused evidence‐based treatments to patients admitted using disease‐specific order sets compared with either historical or concurrent controls and have demonstrated increased use of therapies such as aspirin for acute myocardial infarction admissions,4 systemic corticosteroids, metered‐dose inhalers and pulse oximetry for pediatric asthma admissions,5 and venous thromboembolism prophylaxis for adult emergency department admissions.6 However, the ability of order sets to improve multiple quality measures in a diverse patient population has not been evaluated previously.
This study examined the effect of paper‐based order sets on the quality of admission orders for general medical patients in a community hospital. The primary hypothesis was that order set use would increase the proportion of general medical patients ordered deep venous thrombosis (DVT) prophylaxis. We chose this primary endpoint because DVT prophylaxis continues to be significantly underused in hospitalized patients.7, 8 Secondary hypotheses were that order sets would improve other admission order quality of care measures. We studied paper‐based order sets because the study hospital, along with the vast majority of North American hospitals, uses paper for order entry.9
PATIENTS AND METHODS
Study Setting
The study took place in a 750‐bed community hospital in Mississauga, Ontario, Canada. The study included only general medical patients and excluded cardiology, neurology, and intensive care unit patients. Approximately 30 different internists admitted patients during the study period from April 1, 2003 to March 31, 2005. The internists were not aware that this study was being conducted. Order sets were implemented as an option for writing admission orders in December 2003. Prior to the implementation of order sets, physicians wrote all admission orders using traditional free‐text handwritten orders on blank paper order sheets. Essentially all general medical patients are admitted through the emergency room. The hospital's Research Ethics Board approved this study.
Order Set Development
Local specialists developed order set content (evidence‐based where possible) using informal consensus methods, without explicitly grading evidence. This process created a general admission order set and six diagnosis‐specific order sets (community acquired pneumonia, chronic obstructive pulmonary disease [COPD], febrile neutropenia, soft tissue infection, upper gastrointestinal [GI] bleeding, and urinary tract infection [UTI]). All order sets contained the same orders pertaining to the primary and secondary outcomes, except for the GI bleed admission order set, which did not contain a DVT prophylaxis section.
Order sets were paper‐based and consisted of a menu of orders typically required for a medical admission. These included admitting service, admitting physician, allergies, resuscitation status, diet, activity level, frequency of vital sign measurement, laboratory investigations, diagnostic imaging, intravenous fluid therapy, and medications. The orders were either optional (requiring the physician to check a box to be performed) or default (enacted unless specifically crossed out by the physician). Both order types could consist of a single order (for example, heparin for DVT prophylaxis) or several orders simultaneously (for example, measurement of serum sodium, potassium, and creatinine). All order sets included space for additional free‐text handwritten orders to meet individual patient needs.
The DVT prophylaxis section contained optional orders for 5,000 units of heparin subcutaneously (sc) twice daily (BID) and compression stockings. The ordering physician could select 1, both, or neither of these options. Initiating other forms of DVT prophylaxis or therapeutic anticoagulation required additional free‐text handwritten orders.
Informal clinician feedback led to improved order set content and formatting in August 2004. Orders pertaining to study outcomes were unchanged in this upgrade.
Implementation
In December 2003, we placed the order sets near the stacks of blank paper order sheets used by internists admitting patients in the Emergency Department. We notified physicians by e‐mail when order sets became available but provided no formal education about order sets, DVT prophylaxis, or other study outcomes. The use of order sets was voluntary. We developed a website to facilitate timely reordering of depleted order sets from the hospital's print shop and trained all emergency room clerks regarding website access and storage of the order sets in convenient locations for physicians. Although order set availability was not formally assessed, there were no reports by physicians or observations by study investigators of order sets being unavailable at any time.
Data Collection
To assess the effect of order sets on the ordering of DVT prophylaxis, we retrospectively and randomly selected patient admissions and reviewed these patients' charts from 3 time periods during the study period: OctoberNovember 2003 (period 1, immediately prior to availability of order sets; 113 charts available of 120 discharged patients randomly selected from a total of 1,169 discharges); AprilDecember 2004 (period 2, 412 months after order set availability; 291 charts available of 300 discharged patients randomly selected from a total of 4,620 discharges); and FebruaryMarch 2005 (period 3, 1415 months after order set availability; 283 charts available of 290 randomly selected discharges out of a total of 1,057 discharges). We conducted an additional chart audit just prior to final submission of the manuscript (108 charts available of 120 discharged patients randomly selected from a total of 1,060 discharges in OctoberNovember 2007) to determine the sustainability of the improvements. The same patient could be selected in different time periods. One author (C.O. or K.D.) reviewed each chart using a jointly developed data collection form.
We assessed the admission orders of each chart for the use of an order set and the ordering of DVT prophylaxis, defined as 5,000 units of heparin sc BID or compression stockings (no patient received sc heparin 3 times daily, heparin sc BID in doses greater than 5,000 units, prophylactic doses of low molecular‐weight heparin, or low dose warfarin). We recorded the ordering of therapeutic anticoagulation, defined as intravenous heparin, full‐dose low molecular‐weight heparin, or warfarin with a target international normalized ratio 2.
Independent from the chart review, we examined the overall administration of heparin doses for DVT prophylaxis to all medical inpatients using the hospital pharmacy database. We estimated the overall administration of heparin for DVT prophylaxis in medical inpatients (136 medical beds, 4 wards) on a monthly basis from April 1, 2003 (8 months prior to order set availability) to March 30, 2005 (15 months after order set availability). We calculated monthly utilization as the proportion of patient‐days for which DVT prophylaxis was administered, as follows: (number of doses of subcutaneous heparin dispensed by the hospital pharmacy to the 4 wards)/(2 [since there are 2 doses per patient‐day] number of patient‐days).
We collected additional data from the charts selected during period 2 (AprilDecember 2004) to evaluate the effect of order sets on the following secondary outcomes: (1) the documentation of admission diagnosis, allergies, and code status; (2) general care orders (electrocardiogram [ECG] and notification of physician for chest pain, allied health consultation, standard hospital potassium replacement protocol [already available in the hospital], standard hospital diabetic diet and standard hospital insulin sliding scale [for patients with diabetes], night time sedation diet or nil per os, activity level and vital sign frequency); (3) blood urea nitrogen (BUN), a laboratory test often inappropriately ordered according to local guidelines10; (4) order formatting (numbering, dating, timing, and signing of all order pages); and (5) organization of orders in the standardized arrangement used in the order sets. This standardized arrangement of content was as follows: attending physician, admitting diagnosis, requests for consultation, diet, activity, vital signs, oxygen, nasogastric tube, urinary catheter, investigations, intravenous fluids, and medications. Free‐text admission orders and order set orders that maintained this arrangement were recorded as standardized. We did not assess order appropriateness.
We recorded the characteristics of all medical patients admitted to the hospital in two 1‐year periods during the study (April 1, 2003 to March 30, 2004 and April 1, 2004 to March 30, 2005), including age, gender, length of stay, diagnosis (defined by case management group [CMG]), and resource intensity weight (RIW). CMG defines groups of patients who are similar in diagnosis or procedure and RIW is a measure of resources used during a patient's hospital stay.11 The definitions of CMG and RIW did not change during the study.
Statistical Analysis
Baseline characteristics were compared using Student t‐test for normally distributed continuous variables (patient age) and the Mann‐Whitney U test for skewed continuous variables (length of stay and RIW). Chi square or Fisher's exact tests were used to compare categorical variables. Relative risks (RR) and 95% confidence intervals (CI) were calculated and compared using a z‐test. A 2‐sided P value <0.05 was taken to be statistically significant. All calculations were carried out using SAS Version 8.2 (SAS Institute, Cary, NC).
RESULTS
As shown in Table 1, there were no clinically important differences in demographic or clinical characteristics of medical patients between the 2 years of the study. There were small but statistically significant increases in patient illness complexity (as reflected in median RIW) (P = 0.003) and length of stay (P = 0.0002).
| Patient Characteristic | April 1, 2003 to March 30, 2004 (n = 4,415) | April 1, 2004 to March 30, 2005 (n = 4,287) |
|---|---|---|
| ||
| Age, mean SD | 67.2 17.7 | 67.6 17.5 |
| Length of stay, median days (IQR) | 6 (3‐12) | 6 (3‐13) |
| RIW,11 median (IQR) | 0.96 (0.68‐1.73) | 1.03 (0.72‐1.88) |
| Females, number (% of total) | 2,276 (52) | 2,223 (52) |
| Case mix group,11 number of patients (% of total) | ||
| Chronic obstructive pulmonary disease | 357 (8.1) | 385 (9.0) |
| Simple pneumonia and pleurisy | 322 (7.3) | 217 (5.1) |
| Esophageal, gastrointestinal, and miscellaneous digestive disease | 223 (5.1) | 239 (5.6) |
| Gastrointestinal hemorrhage | 185 (4.2) | 198 (4.6) |
| Respiratory neoplasm | 127 (2.9) | 144 (3.4) |
| Total | 1,214 (27.5) | 1,183 (27.7) |
Clinicians used order sets in 32.3% of admissions during period 2 (AprilDecember 2004, 412 months after order set availability), increasing to 51.6% in period 3 (FebruaryMarch 2005, 1415 months after order set availability). The results of the chart audit assessing the impact of order set use on DVT prophylaxis are shown in Figure 1. Prior to order set introduction, 10.9% of patients received orders for DVT prophylaxis. Subsequently, ordering of DVT prophylaxis in patients admitted with order sets increased (period 2: 35.6%; P < 0.001; RR, 3.27; 95% CI, 1.806.12 and period 3: 44.0%; P < 0.001; RR, 4.04; 95% CI, 2.327.31). In contrast, DVT prophylaxis ordering in the nonorder set group was initially unchanged (period 2: 10.6%; P = 0.93; RR, 0.97; 95% CI, 0.491.95), although later it increased to a smaller extent (period 3: 20.6%; P = 0.049; RR, 1.90; 95% CI, 1.013.65). As a result of this differential increase, patients admitted with order sets were more likely to be ordered DVT prophylaxis in both study periods (period 2: 35.6% versus 10.6%; P < 0.0001; RR, 3.38; 95% CI, 2.035.62 and period 3: 44.0% versus 20.6%; P < 0.0001; RR, 2.13; 95% CI, 1.443.16). The use of therapeutic anticoagulation was similar in patients admitted with and without order sets and did not change between time periods.
The hospital‐wide monthly utilization of heparin for DVT prophylaxis in medical inpatients increased from an average of 12.8% (range, 9.7%16.1%) of patient‐days before order set implementation (AprilNovember 2003) to 18.5% (range, 16.4%20.0%) of patient‐days in the 8 months after order sets were first implemented (DecemberJuly 2004, P < 0.0001 compared to the preorder set time period). After August 2004, when upgraded order sets were introduced, DVT prophylaxis utilization increased further in the last 7 months of the study to 25.8% (range, 22.4%32.2%; P < 0.0001 compared to preorder set time period; Figure 2).
Table 2 shows the impact of order sets on secondary outcomes. Admissions completed with order sets had statistically significant increases in general care orders (ECG and notification of physician for chest pain, allied health consultations and standard hospital diabetic diet, insulin scale, and potassium replacement protocol orders), documentation of allergies and code status, numbering of pages, and use of a standardized arrangement for orders. Ordering of BUN decreased significantly.
| Outcome | Optional or Default | Order Set [n = 94 (%)] | No Order Set [n = 197 (%)] | P Value |
|---|---|---|---|---|
| ||||
| Documentation | ||||
| Admitting diagnosis | Optional | 91 (96.8) | 187 (94.9) | 0.47 |
| Allergies | Optional | 51 (54.3) | 19 (9.6) | <0.0001 |
| Resuscitation status | Optional | 54 (57.4) | 20 (10.2) | <0.0001 |
| General care orders | ||||
| ECG and call MD for chest pain | Default* | 80 (85.1) | 0 (0.0) | <0.0001 |
| Allied health consult | 59 (62.8) | 25 (12.7) | <0.0001 | |
| Diet | Optional | 90 (95.7) | 188 (95.4) | 0.90 |
| Activity | Optional | 80 (85.1) | 150 (76.1) | 0.08 |
| Vitals signs and frequency | Optional | 91 (96.8) | 178 (90.4) | 0.052 |
| Standard hospital diabetic diet | Optional | 16 (17.0) | 10 (5.1) | 0.0008 |
| Standard hospital insulin sliding scale | Optional | 18 (19.1) | 15 (7.6) | 0.004 |
| Standard hospital potassium protocol | Optional | 60 (63.8) | 1 (0.51) | <0.0001 |
| Nighttime sedation | ||||
| Zopiclone as needed | Optional | 43 (45.7) | 2 (1.0) | < 0.0001 |
| Lorazepam as needed | Optional | 12 (12.8) | 15 (7.6) | 0.16 |
| Laboratory test order | ||||
| Blood urea nitrogen | Optional | 37 (39.4) | 117 (59.0) | 0.0014 |
| Order formatting | ||||
| Numbering of pages | Default | 94 (100) | 4 (2.0) | <0.0001 |
| Dating of orders | Optional | 79 (84.0) | 185 (93.9) | 0.0067 |
| Timing of orders | Optional | 14 (14.9) | 29 (14.7) | 0.97 |
| Signing of orders | Optional | 93 (98.9) | 196 (99.5) | 0.54 |
| Standard arrangement of orders | 81 (86.2) | 66 (33.5) | <0.0001 | |
Order sets were not associated with changes in diet, activity, or vital sign orders, documentation of admission diagnosis, or the signing and timing of orders. Apart from order timing, these orders were present in >75% of admissions completed without order sets. The only negative effect of order sets was a reduction in the dating of orders (84.0% of order set admissions versus 93.9% of nonorder set admissions, P = 0.007). Finally, order sets had both an intended and unintended effect on nighttime sedation orders. Relative frequency of ordering of zopiclone compared to lorazepam increased (43/55 in the order set group vs. 2/17 in the no order set group [P < 0.0001], the intended effect), and increased overall frequency of ordering of nighttime sedation (55/94 vs. 17/197 [P < 0.0001], an unintended effect).
The additional chart audit in OctoberNovember 2007, just prior to final submission of the manuscript, determined that clinician use of order sets had increased to 92.6% of admitted medical patients, and that ordering of DVT prophylaxis in patients admitted with order sets had been sustained at 43.2% (P = 0.90 compared to period 3) (Figure 1).
DISCUSSION
We found that paper‐based order sets were associated with markedly increased use of DVT prophylaxis and made physician ordering more consistent with hospital consensus guidelines in multiple other areas, including laboratory test utilization and general care, while also increasing completeness of documentation. Given the difficulties and limited resources frequently associated with guideline development, dissemination, and implementation,12 it is worth noting that our improvements were achieved in a community hospital with voluntary physician adoption and no dedicated project funding, care process redesign, or healthcare worker education. The broad impact of order sets combined with minimal organizational resources required for implementation in this study suggests that this clinical decision support tool may have wide applicability.
The study hospital used paper‐based orders rather than CPOE, similar to 90% of U.S. hospitals at the time of the study.9 Order sets can be deployed in either paper‐based or computerized ordering systems. By providing a mechanism for entering large blocks of orders in an efficient manner, paper‐based order sets may be a necessary first step to facilitate the paper to CPOE transition, making them well suited to the current care delivery environment. Successful use of paper‐based order sets may help accelerate adoption of CPOE, which appears to be many years away from full implementation in the majority of U.S. hospitals.13
The most clinically important outcome in our study was a more than 4‐fold increase in ordering of DVT prophylaxis (last study period compared with baseline) in medical patients admitted with order sets, compared to a smaller increase in patients admitted without order sets. Our result is particularly significant as this study was performed in a community hospital, a setting with a lower adherence to DVT prophylaxis guidelines compared to academic centers.8, 14 The increase in DVT prophylaxis in patients admitted without order sets could be the result of a secular trend or a passive educational effect of order sets on physicians who only used order sets intermittently. The study was not publicized and thus was unlikely in itself to contribute to the increased performance.
We did not assess clinical outcomes of DVT or pulmonary embolism, but the clinical efficacy of improving adherence to DVT prophylaxis has been previously established.15 We also did not assess the appropriateness of DVT prophylaxis (or any other order). However, a recent multicenter Canadian observational study, using the American College of Chest Physician's Consensus Guidelines on Antithrombotic Therapy16 as a reference standard, found that 90% of medical patients admitted to hospital meeting study criteria had indications for thromboprophylaxis, but only 16% of eligible patients actually received it.8 In addition, multivariable regression analysis demonstrated even lower utilization in community hospitals compared to academic hospitals. These data suggest that the study hospital is typical of Canadian hospitals, and that the low overall utilization of DVT prophylaxis (13% of hospital patient‐days) prior to the availability of order sets in the study hospital is a significant gap between optimal and actual practice.
In addition, order sets had an impact on many secondary outcomes, such as standardization and completeness of orders (for example documentation of allergies and resuscitation status). While these effects appear to be beneficial in terms of quality of care and patient safety, the relationship of our secondary outcomes to patient‐important outcomes has not been established.
Furthermore, our before‐after design does not exclude the possibility of unknown confounding effects as explanations of improved performance in the order set group. For example, the change could have been driven by a small number of admitting physicians, since it is likely that order sets were adopted more readily by some physicians than others, and this group could have been responsible for a greater proportion of the admissions at different times. Unfortunately, we did not record the identity of the admitting physician. However, data from OctoberNovember 2007 show that >90% of medical patients were admitted using order sets, suggesting that voluntary clinician adoption of order sets has become nearly universal. Nevertheless, there still appear to be a few physicians who rarely or never used orders sets. Motivating these physicians to prescribe appropriate DVT prophylaxis remains a challenge.
Although this study was conducted in 1 center, other hospitals have similarly low rates of thromboprophylaxis,8 and our order set implementation strategy consumed few resources, improving the generalizability of our results. While most changes were beneficial, order set use was associated with decreased dating of orders and with an unintended effect or overall increase ordering of nightime sedation. Although the reasons for this are unclear, it highlights the importance of systematically evaluating the impact of order sets to identify unintended consequences and areas in which the order set may need to be redesigned to address these issues.
The study of order sets is preliminary despite their role as a key enabler for CPOE17 and their suggested usefulness to reduce medical error.18 For example, order sets were not considered in recent analyses of factors predicting success of computerized decision support systems19, 20 and have not been reviewed by the Cochrane Effective Practice and Organisation of Care Group.21 As discussed in the introduction, several studies have demonstrated that disease‐specific order sets can increase the use of evidence‐based treatments.46 Our study extends this work by demonstrating that admission order sets can improve performance hospital‐wide for a broad range of outcomes simultaneously, including DVT prophylaxis. Although most studies have demonstrated increased utilization of evidence‐based therapies, at least 1 study found no increased use of aspirin, heparin, or beta‐blockers in acute coronary syndrome admissions with the introduction of order sets.22 This suggests that the way order sets are structured or introduced is important to ensure that they achieve the desired changes in practice. Finally, our study suggests that improved outcomes using order sets can still be achieved with minimal organizational resources.
Order sets may potentially complement other decision support tools such as alerts and reminders. Alerts are an effective decision support tool12, 23, 24 but risk disrupting clinician workflow. Moreover, excessive alerts can lead to alert fatigue, resulting in many alerts being ignored.25 This phenomenon reduces alert effectiveness and limits the number of issues that alerts can address simultaneously. In contrast, order sets are broad in scope due to integration with clinical workflow, but lack the ability of alerts to apply rules to a specific patient's data. A potentially effective 2‐staged decision support strategy would use order sets as the primary admission decision support tool and selective alerts for remaining issues. This approach may increase the overall scope, physician adoption, and effectiveness of clinical decision support, and should be evaluated.
Our postintervention rate of DVT prophylaxis, while substantially improved from baseline, is still below ideal practice. Order sets were simply made available to clinicians admitting medical patients, who had the option to select DVT prophylaxis. Given limited resources, we did not develop and implement education programs regarding the appropriate use of DVT prophylaxis or make available any DVT risk assessment evaluations (available in Ref.26). Our study methodology thus provides a realistic assessment of improvements attainable in other hospitals with similarly limited resources. Additional increases in DVT prophylaxis rates would likely require a more comprehensive and resource‐intensive multifaceted quality improvement initiative. Detailed guidelines and supporting references for implementing such an initiative are available from the Society of Hospital Medicine.26 As described in their Venous Thromboembolism (VTE) Resource Room,26 such an initiative should include a standardized DVT risk assessment to guide the need for DVT prophylaxis integrated into admission order sets; prompts to order DVT prophylaxis when completing admission orders; and a system to audit adverse events and variations from best practice and return this information to clinicians.26
CONCLUSIONS
This is the largest and most comprehensive evaluation of the effectiveness of order sets as a clinical decision support tool. We found that order sets improved the quality of multiple patient orders and improved hospital‐wide DVT prophylaxis rates. These improvements were achieved in a community hospital with voluntary physician adoption and no dedicated project funding, care process redesign, or healthcare worker education. Although used in a paper‐based format in this study, order sets can also be employed in a computerized ordering environment. By providing a mechanism for entering large blocks of orders in an efficient manner, paper‐based order sets may be a necessary first step to facilitate the paper‐to‐CPOE transition. These attributes make order sets an attractive quality improvement tool in community and academic settings. More research is needed on the optimal design and use of this promising decision support tool.
The use of clinical decision support, despite great promise to improve health care, remains preliminary.1 The broad scope of quality and safety challenges facing clinicians2, 3 requires this situation to change. There is an urgent need to develop decision support tools and strategies that are effective, address many quality issues simultaneously, and are easy to implement in both academic and community settings.
One decision support tool that could help to meet this challenge is the order set. An order set is a group of orders with a common functional purpose that is used directly by a physician to create orders for a specific patient. Order sets can be used with either paper‐based or computerized provider order entry (CPOE) systems. Several studies have investigated the delivery of focused evidence‐based treatments to patients admitted using disease‐specific order sets compared with either historical or concurrent controls and have demonstrated increased use of therapies such as aspirin for acute myocardial infarction admissions,4 systemic corticosteroids, metered‐dose inhalers and pulse oximetry for pediatric asthma admissions,5 and venous thromboembolism prophylaxis for adult emergency department admissions.6 However, the ability of order sets to improve multiple quality measures in a diverse patient population has not been evaluated previously.
This study examined the effect of paper‐based order sets on the quality of admission orders for general medical patients in a community hospital. The primary hypothesis was that order set use would increase the proportion of general medical patients ordered deep venous thrombosis (DVT) prophylaxis. We chose this primary endpoint because DVT prophylaxis continues to be significantly underused in hospitalized patients.7, 8 Secondary hypotheses were that order sets would improve other admission order quality of care measures. We studied paper‐based order sets because the study hospital, along with the vast majority of North American hospitals, uses paper for order entry.9
PATIENTS AND METHODS
Study Setting
The study took place in a 750‐bed community hospital in Mississauga, Ontario, Canada. The study included only general medical patients and excluded cardiology, neurology, and intensive care unit patients. Approximately 30 different internists admitted patients during the study period from April 1, 2003 to March 31, 2005. The internists were not aware that this study was being conducted. Order sets were implemented as an option for writing admission orders in December 2003. Prior to the implementation of order sets, physicians wrote all admission orders using traditional free‐text handwritten orders on blank paper order sheets. Essentially all general medical patients are admitted through the emergency room. The hospital's Research Ethics Board approved this study.
Order Set Development
Local specialists developed order set content (evidence‐based where possible) using informal consensus methods, without explicitly grading evidence. This process created a general admission order set and six diagnosis‐specific order sets (community acquired pneumonia, chronic obstructive pulmonary disease [COPD], febrile neutropenia, soft tissue infection, upper gastrointestinal [GI] bleeding, and urinary tract infection [UTI]). All order sets contained the same orders pertaining to the primary and secondary outcomes, except for the GI bleed admission order set, which did not contain a DVT prophylaxis section.
Order sets were paper‐based and consisted of a menu of orders typically required for a medical admission. These included admitting service, admitting physician, allergies, resuscitation status, diet, activity level, frequency of vital sign measurement, laboratory investigations, diagnostic imaging, intravenous fluid therapy, and medications. The orders were either optional (requiring the physician to check a box to be performed) or default (enacted unless specifically crossed out by the physician). Both order types could consist of a single order (for example, heparin for DVT prophylaxis) or several orders simultaneously (for example, measurement of serum sodium, potassium, and creatinine). All order sets included space for additional free‐text handwritten orders to meet individual patient needs.
The DVT prophylaxis section contained optional orders for 5,000 units of heparin subcutaneously (sc) twice daily (BID) and compression stockings. The ordering physician could select 1, both, or neither of these options. Initiating other forms of DVT prophylaxis or therapeutic anticoagulation required additional free‐text handwritten orders.
Informal clinician feedback led to improved order set content and formatting in August 2004. Orders pertaining to study outcomes were unchanged in this upgrade.
Implementation
In December 2003, we placed the order sets near the stacks of blank paper order sheets used by internists admitting patients in the Emergency Department. We notified physicians by e‐mail when order sets became available but provided no formal education about order sets, DVT prophylaxis, or other study outcomes. The use of order sets was voluntary. We developed a website to facilitate timely reordering of depleted order sets from the hospital's print shop and trained all emergency room clerks regarding website access and storage of the order sets in convenient locations for physicians. Although order set availability was not formally assessed, there were no reports by physicians or observations by study investigators of order sets being unavailable at any time.
Data Collection
To assess the effect of order sets on the ordering of DVT prophylaxis, we retrospectively and randomly selected patient admissions and reviewed these patients' charts from 3 time periods during the study period: OctoberNovember 2003 (period 1, immediately prior to availability of order sets; 113 charts available of 120 discharged patients randomly selected from a total of 1,169 discharges); AprilDecember 2004 (period 2, 412 months after order set availability; 291 charts available of 300 discharged patients randomly selected from a total of 4,620 discharges); and FebruaryMarch 2005 (period 3, 1415 months after order set availability; 283 charts available of 290 randomly selected discharges out of a total of 1,057 discharges). We conducted an additional chart audit just prior to final submission of the manuscript (108 charts available of 120 discharged patients randomly selected from a total of 1,060 discharges in OctoberNovember 2007) to determine the sustainability of the improvements. The same patient could be selected in different time periods. One author (C.O. or K.D.) reviewed each chart using a jointly developed data collection form.
We assessed the admission orders of each chart for the use of an order set and the ordering of DVT prophylaxis, defined as 5,000 units of heparin sc BID or compression stockings (no patient received sc heparin 3 times daily, heparin sc BID in doses greater than 5,000 units, prophylactic doses of low molecular‐weight heparin, or low dose warfarin). We recorded the ordering of therapeutic anticoagulation, defined as intravenous heparin, full‐dose low molecular‐weight heparin, or warfarin with a target international normalized ratio 2.
Independent from the chart review, we examined the overall administration of heparin doses for DVT prophylaxis to all medical inpatients using the hospital pharmacy database. We estimated the overall administration of heparin for DVT prophylaxis in medical inpatients (136 medical beds, 4 wards) on a monthly basis from April 1, 2003 (8 months prior to order set availability) to March 30, 2005 (15 months after order set availability). We calculated monthly utilization as the proportion of patient‐days for which DVT prophylaxis was administered, as follows: (number of doses of subcutaneous heparin dispensed by the hospital pharmacy to the 4 wards)/(2 [since there are 2 doses per patient‐day] number of patient‐days).
We collected additional data from the charts selected during period 2 (AprilDecember 2004) to evaluate the effect of order sets on the following secondary outcomes: (1) the documentation of admission diagnosis, allergies, and code status; (2) general care orders (electrocardiogram [ECG] and notification of physician for chest pain, allied health consultation, standard hospital potassium replacement protocol [already available in the hospital], standard hospital diabetic diet and standard hospital insulin sliding scale [for patients with diabetes], night time sedation diet or nil per os, activity level and vital sign frequency); (3) blood urea nitrogen (BUN), a laboratory test often inappropriately ordered according to local guidelines10; (4) order formatting (numbering, dating, timing, and signing of all order pages); and (5) organization of orders in the standardized arrangement used in the order sets. This standardized arrangement of content was as follows: attending physician, admitting diagnosis, requests for consultation, diet, activity, vital signs, oxygen, nasogastric tube, urinary catheter, investigations, intravenous fluids, and medications. Free‐text admission orders and order set orders that maintained this arrangement were recorded as standardized. We did not assess order appropriateness.
We recorded the characteristics of all medical patients admitted to the hospital in two 1‐year periods during the study (April 1, 2003 to March 30, 2004 and April 1, 2004 to March 30, 2005), including age, gender, length of stay, diagnosis (defined by case management group [CMG]), and resource intensity weight (RIW). CMG defines groups of patients who are similar in diagnosis or procedure and RIW is a measure of resources used during a patient's hospital stay.11 The definitions of CMG and RIW did not change during the study.
Statistical Analysis
Baseline characteristics were compared using Student t‐test for normally distributed continuous variables (patient age) and the Mann‐Whitney U test for skewed continuous variables (length of stay and RIW). Chi square or Fisher's exact tests were used to compare categorical variables. Relative risks (RR) and 95% confidence intervals (CI) were calculated and compared using a z‐test. A 2‐sided P value <0.05 was taken to be statistically significant. All calculations were carried out using SAS Version 8.2 (SAS Institute, Cary, NC).
RESULTS
As shown in Table 1, there were no clinically important differences in demographic or clinical characteristics of medical patients between the 2 years of the study. There were small but statistically significant increases in patient illness complexity (as reflected in median RIW) (P = 0.003) and length of stay (P = 0.0002).
| Patient Characteristic | April 1, 2003 to March 30, 2004 (n = 4,415) | April 1, 2004 to March 30, 2005 (n = 4,287) |
|---|---|---|
| ||
| Age, mean SD | 67.2 17.7 | 67.6 17.5 |
| Length of stay, median days (IQR) | 6 (3‐12) | 6 (3‐13) |
| RIW,11 median (IQR) | 0.96 (0.68‐1.73) | 1.03 (0.72‐1.88) |
| Females, number (% of total) | 2,276 (52) | 2,223 (52) |
| Case mix group,11 number of patients (% of total) | ||
| Chronic obstructive pulmonary disease | 357 (8.1) | 385 (9.0) |
| Simple pneumonia and pleurisy | 322 (7.3) | 217 (5.1) |
| Esophageal, gastrointestinal, and miscellaneous digestive disease | 223 (5.1) | 239 (5.6) |
| Gastrointestinal hemorrhage | 185 (4.2) | 198 (4.6) |
| Respiratory neoplasm | 127 (2.9) | 144 (3.4) |
| Total | 1,214 (27.5) | 1,183 (27.7) |
Clinicians used order sets in 32.3% of admissions during period 2 (AprilDecember 2004, 412 months after order set availability), increasing to 51.6% in period 3 (FebruaryMarch 2005, 1415 months after order set availability). The results of the chart audit assessing the impact of order set use on DVT prophylaxis are shown in Figure 1. Prior to order set introduction, 10.9% of patients received orders for DVT prophylaxis. Subsequently, ordering of DVT prophylaxis in patients admitted with order sets increased (period 2: 35.6%; P < 0.001; RR, 3.27; 95% CI, 1.806.12 and period 3: 44.0%; P < 0.001; RR, 4.04; 95% CI, 2.327.31). In contrast, DVT prophylaxis ordering in the nonorder set group was initially unchanged (period 2: 10.6%; P = 0.93; RR, 0.97; 95% CI, 0.491.95), although later it increased to a smaller extent (period 3: 20.6%; P = 0.049; RR, 1.90; 95% CI, 1.013.65). As a result of this differential increase, patients admitted with order sets were more likely to be ordered DVT prophylaxis in both study periods (period 2: 35.6% versus 10.6%; P < 0.0001; RR, 3.38; 95% CI, 2.035.62 and period 3: 44.0% versus 20.6%; P < 0.0001; RR, 2.13; 95% CI, 1.443.16). The use of therapeutic anticoagulation was similar in patients admitted with and without order sets and did not change between time periods.
The hospital‐wide monthly utilization of heparin for DVT prophylaxis in medical inpatients increased from an average of 12.8% (range, 9.7%16.1%) of patient‐days before order set implementation (AprilNovember 2003) to 18.5% (range, 16.4%20.0%) of patient‐days in the 8 months after order sets were first implemented (DecemberJuly 2004, P < 0.0001 compared to the preorder set time period). After August 2004, when upgraded order sets were introduced, DVT prophylaxis utilization increased further in the last 7 months of the study to 25.8% (range, 22.4%32.2%; P < 0.0001 compared to preorder set time period; Figure 2).
Table 2 shows the impact of order sets on secondary outcomes. Admissions completed with order sets had statistically significant increases in general care orders (ECG and notification of physician for chest pain, allied health consultations and standard hospital diabetic diet, insulin scale, and potassium replacement protocol orders), documentation of allergies and code status, numbering of pages, and use of a standardized arrangement for orders. Ordering of BUN decreased significantly.
| Outcome | Optional or Default | Order Set [n = 94 (%)] | No Order Set [n = 197 (%)] | P Value |
|---|---|---|---|---|
| ||||
| Documentation | ||||
| Admitting diagnosis | Optional | 91 (96.8) | 187 (94.9) | 0.47 |
| Allergies | Optional | 51 (54.3) | 19 (9.6) | <0.0001 |
| Resuscitation status | Optional | 54 (57.4) | 20 (10.2) | <0.0001 |
| General care orders | ||||
| ECG and call MD for chest pain | Default* | 80 (85.1) | 0 (0.0) | <0.0001 |
| Allied health consult | 59 (62.8) | 25 (12.7) | <0.0001 | |
| Diet | Optional | 90 (95.7) | 188 (95.4) | 0.90 |
| Activity | Optional | 80 (85.1) | 150 (76.1) | 0.08 |
| Vitals signs and frequency | Optional | 91 (96.8) | 178 (90.4) | 0.052 |
| Standard hospital diabetic diet | Optional | 16 (17.0) | 10 (5.1) | 0.0008 |
| Standard hospital insulin sliding scale | Optional | 18 (19.1) | 15 (7.6) | 0.004 |
| Standard hospital potassium protocol | Optional | 60 (63.8) | 1 (0.51) | <0.0001 |
| Nighttime sedation | ||||
| Zopiclone as needed | Optional | 43 (45.7) | 2 (1.0) | < 0.0001 |
| Lorazepam as needed | Optional | 12 (12.8) | 15 (7.6) | 0.16 |
| Laboratory test order | ||||
| Blood urea nitrogen | Optional | 37 (39.4) | 117 (59.0) | 0.0014 |
| Order formatting | ||||
| Numbering of pages | Default | 94 (100) | 4 (2.0) | <0.0001 |
| Dating of orders | Optional | 79 (84.0) | 185 (93.9) | 0.0067 |
| Timing of orders | Optional | 14 (14.9) | 29 (14.7) | 0.97 |
| Signing of orders | Optional | 93 (98.9) | 196 (99.5) | 0.54 |
| Standard arrangement of orders | 81 (86.2) | 66 (33.5) | <0.0001 | |
Order sets were not associated with changes in diet, activity, or vital sign orders, documentation of admission diagnosis, or the signing and timing of orders. Apart from order timing, these orders were present in >75% of admissions completed without order sets. The only negative effect of order sets was a reduction in the dating of orders (84.0% of order set admissions versus 93.9% of nonorder set admissions, P = 0.007). Finally, order sets had both an intended and unintended effect on nighttime sedation orders. Relative frequency of ordering of zopiclone compared to lorazepam increased (43/55 in the order set group vs. 2/17 in the no order set group [P < 0.0001], the intended effect), and increased overall frequency of ordering of nighttime sedation (55/94 vs. 17/197 [P < 0.0001], an unintended effect).
The additional chart audit in OctoberNovember 2007, just prior to final submission of the manuscript, determined that clinician use of order sets had increased to 92.6% of admitted medical patients, and that ordering of DVT prophylaxis in patients admitted with order sets had been sustained at 43.2% (P = 0.90 compared to period 3) (Figure 1).
DISCUSSION
We found that paper‐based order sets were associated with markedly increased use of DVT prophylaxis and made physician ordering more consistent with hospital consensus guidelines in multiple other areas, including laboratory test utilization and general care, while also increasing completeness of documentation. Given the difficulties and limited resources frequently associated with guideline development, dissemination, and implementation,12 it is worth noting that our improvements were achieved in a community hospital with voluntary physician adoption and no dedicated project funding, care process redesign, or healthcare worker education. The broad impact of order sets combined with minimal organizational resources required for implementation in this study suggests that this clinical decision support tool may have wide applicability.
The study hospital used paper‐based orders rather than CPOE, similar to 90% of U.S. hospitals at the time of the study.9 Order sets can be deployed in either paper‐based or computerized ordering systems. By providing a mechanism for entering large blocks of orders in an efficient manner, paper‐based order sets may be a necessary first step to facilitate the paper to CPOE transition, making them well suited to the current care delivery environment. Successful use of paper‐based order sets may help accelerate adoption of CPOE, which appears to be many years away from full implementation in the majority of U.S. hospitals.13
The most clinically important outcome in our study was a more than 4‐fold increase in ordering of DVT prophylaxis (last study period compared with baseline) in medical patients admitted with order sets, compared to a smaller increase in patients admitted without order sets. Our result is particularly significant as this study was performed in a community hospital, a setting with a lower adherence to DVT prophylaxis guidelines compared to academic centers.8, 14 The increase in DVT prophylaxis in patients admitted without order sets could be the result of a secular trend or a passive educational effect of order sets on physicians who only used order sets intermittently. The study was not publicized and thus was unlikely in itself to contribute to the increased performance.
We did not assess clinical outcomes of DVT or pulmonary embolism, but the clinical efficacy of improving adherence to DVT prophylaxis has been previously established.15 We also did not assess the appropriateness of DVT prophylaxis (or any other order). However, a recent multicenter Canadian observational study, using the American College of Chest Physician's Consensus Guidelines on Antithrombotic Therapy16 as a reference standard, found that 90% of medical patients admitted to hospital meeting study criteria had indications for thromboprophylaxis, but only 16% of eligible patients actually received it.8 In addition, multivariable regression analysis demonstrated even lower utilization in community hospitals compared to academic hospitals. These data suggest that the study hospital is typical of Canadian hospitals, and that the low overall utilization of DVT prophylaxis (13% of hospital patient‐days) prior to the availability of order sets in the study hospital is a significant gap between optimal and actual practice.
In addition, order sets had an impact on many secondary outcomes, such as standardization and completeness of orders (for example documentation of allergies and resuscitation status). While these effects appear to be beneficial in terms of quality of care and patient safety, the relationship of our secondary outcomes to patient‐important outcomes has not been established.
Furthermore, our before‐after design does not exclude the possibility of unknown confounding effects as explanations of improved performance in the order set group. For example, the change could have been driven by a small number of admitting physicians, since it is likely that order sets were adopted more readily by some physicians than others, and this group could have been responsible for a greater proportion of the admissions at different times. Unfortunately, we did not record the identity of the admitting physician. However, data from OctoberNovember 2007 show that >90% of medical patients were admitted using order sets, suggesting that voluntary clinician adoption of order sets has become nearly universal. Nevertheless, there still appear to be a few physicians who rarely or never used orders sets. Motivating these physicians to prescribe appropriate DVT prophylaxis remains a challenge.
Although this study was conducted in 1 center, other hospitals have similarly low rates of thromboprophylaxis,8 and our order set implementation strategy consumed few resources, improving the generalizability of our results. While most changes were beneficial, order set use was associated with decreased dating of orders and with an unintended effect or overall increase ordering of nightime sedation. Although the reasons for this are unclear, it highlights the importance of systematically evaluating the impact of order sets to identify unintended consequences and areas in which the order set may need to be redesigned to address these issues.
The study of order sets is preliminary despite their role as a key enabler for CPOE17 and their suggested usefulness to reduce medical error.18 For example, order sets were not considered in recent analyses of factors predicting success of computerized decision support systems19, 20 and have not been reviewed by the Cochrane Effective Practice and Organisation of Care Group.21 As discussed in the introduction, several studies have demonstrated that disease‐specific order sets can increase the use of evidence‐based treatments.46 Our study extends this work by demonstrating that admission order sets can improve performance hospital‐wide for a broad range of outcomes simultaneously, including DVT prophylaxis. Although most studies have demonstrated increased utilization of evidence‐based therapies, at least 1 study found no increased use of aspirin, heparin, or beta‐blockers in acute coronary syndrome admissions with the introduction of order sets.22 This suggests that the way order sets are structured or introduced is important to ensure that they achieve the desired changes in practice. Finally, our study suggests that improved outcomes using order sets can still be achieved with minimal organizational resources.
Order sets may potentially complement other decision support tools such as alerts and reminders. Alerts are an effective decision support tool12, 23, 24 but risk disrupting clinician workflow. Moreover, excessive alerts can lead to alert fatigue, resulting in many alerts being ignored.25 This phenomenon reduces alert effectiveness and limits the number of issues that alerts can address simultaneously. In contrast, order sets are broad in scope due to integration with clinical workflow, but lack the ability of alerts to apply rules to a specific patient's data. A potentially effective 2‐staged decision support strategy would use order sets as the primary admission decision support tool and selective alerts for remaining issues. This approach may increase the overall scope, physician adoption, and effectiveness of clinical decision support, and should be evaluated.
Our postintervention rate of DVT prophylaxis, while substantially improved from baseline, is still below ideal practice. Order sets were simply made available to clinicians admitting medical patients, who had the option to select DVT prophylaxis. Given limited resources, we did not develop and implement education programs regarding the appropriate use of DVT prophylaxis or make available any DVT risk assessment evaluations (available in Ref.26). Our study methodology thus provides a realistic assessment of improvements attainable in other hospitals with similarly limited resources. Additional increases in DVT prophylaxis rates would likely require a more comprehensive and resource‐intensive multifaceted quality improvement initiative. Detailed guidelines and supporting references for implementing such an initiative are available from the Society of Hospital Medicine.26 As described in their Venous Thromboembolism (VTE) Resource Room,26 such an initiative should include a standardized DVT risk assessment to guide the need for DVT prophylaxis integrated into admission order sets; prompts to order DVT prophylaxis when completing admission orders; and a system to audit adverse events and variations from best practice and return this information to clinicians.26
CONCLUSIONS
This is the largest and most comprehensive evaluation of the effectiveness of order sets as a clinical decision support tool. We found that order sets improved the quality of multiple patient orders and improved hospital‐wide DVT prophylaxis rates. These improvements were achieved in a community hospital with voluntary physician adoption and no dedicated project funding, care process redesign, or healthcare worker education. Although used in a paper‐based format in this study, order sets can also be employed in a computerized ordering environment. By providing a mechanism for entering large blocks of orders in an efficient manner, paper‐based order sets may be a necessary first step to facilitate the paper‐to‐CPOE transition. These attributes make order sets an attractive quality improvement tool in community and academic settings. More research is needed on the optimal design and use of this promising decision support tool.
- .Health Information Management: Integrating Information Technology in Health Care Work.London:Routledge;2004.
- ,,.To Err Is Human: Building a Safer Health System.Washington, DC:National Academy Press;2006.
- National Healthcare Quality Report.2004.Rockville, MD:Agency for Healthcare Research and Quality;2006.
- ,,,,,.Integrating “best of care” protocols into clinicians' workflow via care provider order entry: impact on quality‐of‐care indicators for acute myocardial infarction.J Am Med Inform Assoc.2006;13:188–196.
- ,,,,,.The role of computerized order sets in pediatric inpatient asthma treatment.Ped Allergy Immunol.2006;17:199–206.
- ,,,.Venous thromboembolism prophylaxis in emergency department admissions.J Hosp Med.2007;2:79–85.
- .DVT prevention: what is happening in the “real world”?Semin Thromb Hemost.2003;29(Suppl 1):23–31.
- ,,, et al.Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada.Thromb Res.2007;119:145–155.
- ,,,.Computerized physician order entry in US hospitals: results of a 2002 survey.J Am Med Inform Assoc.2004;11:95–99.
- Ontario Association of Medical Laboratories. Guidelines for the Use of Serum Tests to Detect Renal Dysfunction. Available at:http://www.oaml.com/PDF/CLP007.pdf. Accessed 12 May2008.
- ,.Physicians in health care management: 3. Case mix groups and resource intensity weights: an overview for physicians.CMAJ.1994;150:889–894.
- ,,, et al.Effectiveness and efficiency of guideline dissemination and implementation strategies.Health Technol Assess.2004;8(6):iii–iv,1–72.
- ,,,,.Predicting computerized physician order entry system adoption in US hospitals: can the federal mandate be met?Int J Med Inform.2008;77(8):539–545.
- ,,,,,.Physician practices in the prevention of venous thromboembolism.Ann Intern Med.1991;115:591–595.
- ,,, et al.Electronic alerts to prevent venous thromboembolism among hospitalized patients.N Engl J Med.2005;352:969–977.
- ,,, et al.Prevention of venous thromboembolism.Chest.2001;119(Suppl 1):132S–175S.
- ,,.A consensus statement on considerations for a successful CPOE implementation.J Am Med Inform Assoc.2003;10:229–234.
- ,.Residents' suggestions for reducing errors in teaching hospitals.N Engl J Med.2003;348:851–855.
- ,,,.Improving clinical practice using clinical decision support systems: a systematic review of trials to identify features critical to success.BMJ.2005;330:765.
- ,,, et al.Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic review.JAMA.2005;293:1223–1238.
- Cochrane Reviews by the Effective Practice and Organisation of Care Group. Available at: http://www.cochrane.org/reviews/en/topics/61_reviews.html. Accessed 12 May2008.
- ,,.Embedded guideline information without patient specificity in a commercial emergency department computerized order‐entry system.Acad Emer Med.2006;13:452–458.
- ,,,,,.A computerized reminder system to increase the use of preventive care for hospitalized patients.N Engl J Med.2001;345:965–970.
- ,,,,.A clinical decision support system for prevention of venous thromboembolism: effect on physician behavior.JAMA.2000;283:2816–2821.
- ,,, et al.Computerized physician order entry and online decision support.Acad Emerg Med.2004;11:1135–1141.
- Society of Hospital Medicine VTE Resource Room. Available at: http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_VTE/VTE_Home.cfm. Accessed 12 May2008.
- .Health Information Management: Integrating Information Technology in Health Care Work.London:Routledge;2004.
- ,,.To Err Is Human: Building a Safer Health System.Washington, DC:National Academy Press;2006.
- National Healthcare Quality Report.2004.Rockville, MD:Agency for Healthcare Research and Quality;2006.
- ,,,,,.Integrating “best of care” protocols into clinicians' workflow via care provider order entry: impact on quality‐of‐care indicators for acute myocardial infarction.J Am Med Inform Assoc.2006;13:188–196.
- ,,,,,.The role of computerized order sets in pediatric inpatient asthma treatment.Ped Allergy Immunol.2006;17:199–206.
- ,,,.Venous thromboembolism prophylaxis in emergency department admissions.J Hosp Med.2007;2:79–85.
- .DVT prevention: what is happening in the “real world”?Semin Thromb Hemost.2003;29(Suppl 1):23–31.
- ,,, et al.Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada.Thromb Res.2007;119:145–155.
- ,,,.Computerized physician order entry in US hospitals: results of a 2002 survey.J Am Med Inform Assoc.2004;11:95–99.
- Ontario Association of Medical Laboratories. Guidelines for the Use of Serum Tests to Detect Renal Dysfunction. Available at:http://www.oaml.com/PDF/CLP007.pdf. Accessed 12 May2008.
- ,.Physicians in health care management: 3. Case mix groups and resource intensity weights: an overview for physicians.CMAJ.1994;150:889–894.
- ,,, et al.Effectiveness and efficiency of guideline dissemination and implementation strategies.Health Technol Assess.2004;8(6):iii–iv,1–72.
- ,,,,.Predicting computerized physician order entry system adoption in US hospitals: can the federal mandate be met?Int J Med Inform.2008;77(8):539–545.
- ,,,,,.Physician practices in the prevention of venous thromboembolism.Ann Intern Med.1991;115:591–595.
- ,,, et al.Electronic alerts to prevent venous thromboembolism among hospitalized patients.N Engl J Med.2005;352:969–977.
- ,,, et al.Prevention of venous thromboembolism.Chest.2001;119(Suppl 1):132S–175S.
- ,,.A consensus statement on considerations for a successful CPOE implementation.J Am Med Inform Assoc.2003;10:229–234.
- ,.Residents' suggestions for reducing errors in teaching hospitals.N Engl J Med.2003;348:851–855.
- ,,,.Improving clinical practice using clinical decision support systems: a systematic review of trials to identify features critical to success.BMJ.2005;330:765.
- ,,, et al.Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic review.JAMA.2005;293:1223–1238.
- Cochrane Reviews by the Effective Practice and Organisation of Care Group. Available at: http://www.cochrane.org/reviews/en/topics/61_reviews.html. Accessed 12 May2008.
- ,,.Embedded guideline information without patient specificity in a commercial emergency department computerized order‐entry system.Acad Emer Med.2006;13:452–458.
- ,,,,,.A computerized reminder system to increase the use of preventive care for hospitalized patients.N Engl J Med.2001;345:965–970.
- ,,,,.A clinical decision support system for prevention of venous thromboembolism: effect on physician behavior.JAMA.2000;283:2816–2821.
- ,,, et al.Computerized physician order entry and online decision support.Acad Emerg Med.2004;11:1135–1141.
- Society of Hospital Medicine VTE Resource Room. Available at: http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_VTE/VTE_Home.cfm. Accessed 12 May2008.
Copyright © 2009 Society of Hospital Medicine
Allogeneic Stem Cell Transplant
Dr. Sergio Giralt discusses his findings that suggest age should no longer be a contraindication to allogeneic stem cell transplantation. Dr. Armand Keating, press conference moderator, comments on the implications of this study during a briefing at the annual meeting of the American Society of Hematology.
Dr. Sergio Giralt discusses his findings that suggest age should no longer be a contraindication to allogeneic stem cell transplantation. Dr. Armand Keating, press conference moderator, comments on the implications of this study during a briefing at the annual meeting of the American Society of Hematology.
Dr. Sergio Giralt discusses his findings that suggest age should no longer be a contraindication to allogeneic stem cell transplantation. Dr. Armand Keating, press conference moderator, comments on the implications of this study during a briefing at the annual meeting of the American Society of Hematology.
Hospitalists Applaud SCHIP Expansion
Pediatric hospitalists are praising a new bill that expands the funding and scope of the State Children's Health Insurance Program (SCHIP), a program jointly funded by federal and state governments for children in families with incomes too high to qualify for Medicaid.
"Ideally, this will lead to better primary care, more immunizations, and disease prevention," says Jack Percelay, MD, MPH, a hospitalist at E.L.M.O. Pediatrics in New York City, Treasurer of SHM's board of directors, and a member of SHM's Public Policy Committee. Percelay foresees a twofold benefit of the new legislation: a likely decrease in uninsured pediatric patients using the ED and more fee recovery from patients who otherwise couldn't pay.
David Rappaport, MD, FAAP, a hospitalist at Alfred I. Dupont Hospital for Children in Wilmington, Del., agrees. "Children's health is more than the cuddly factor—it's a smart investment in healthcare," he says, explaining that paying for preventive measures in children, such as inoculations, can save on their healthcare costs in the future.
Signed by President Obama on Feb. 4, the bill reauthorizes SCHIP for four years and expands eligibility to children in families with incomes of up to three times the federal poverty level. It also covers legal immigrant pregnant women and children who have been in the country less than five years. The expansion will cover an additional 4 million children, raising the total to 11 million uninsured children enrolled in the program. Most of the $32.8 billion increase in federal funding for the program is to be covered by a 62-cent-per-pack increase in the federal cigarette tax.
Pediatric hospitalists are praising a new bill that expands the funding and scope of the State Children's Health Insurance Program (SCHIP), a program jointly funded by federal and state governments for children in families with incomes too high to qualify for Medicaid.
"Ideally, this will lead to better primary care, more immunizations, and disease prevention," says Jack Percelay, MD, MPH, a hospitalist at E.L.M.O. Pediatrics in New York City, Treasurer of SHM's board of directors, and a member of SHM's Public Policy Committee. Percelay foresees a twofold benefit of the new legislation: a likely decrease in uninsured pediatric patients using the ED and more fee recovery from patients who otherwise couldn't pay.
David Rappaport, MD, FAAP, a hospitalist at Alfred I. Dupont Hospital for Children in Wilmington, Del., agrees. "Children's health is more than the cuddly factor—it's a smart investment in healthcare," he says, explaining that paying for preventive measures in children, such as inoculations, can save on their healthcare costs in the future.
Signed by President Obama on Feb. 4, the bill reauthorizes SCHIP for four years and expands eligibility to children in families with incomes of up to three times the federal poverty level. It also covers legal immigrant pregnant women and children who have been in the country less than five years. The expansion will cover an additional 4 million children, raising the total to 11 million uninsured children enrolled in the program. Most of the $32.8 billion increase in federal funding for the program is to be covered by a 62-cent-per-pack increase in the federal cigarette tax.
Pediatric hospitalists are praising a new bill that expands the funding and scope of the State Children's Health Insurance Program (SCHIP), a program jointly funded by federal and state governments for children in families with incomes too high to qualify for Medicaid.
"Ideally, this will lead to better primary care, more immunizations, and disease prevention," says Jack Percelay, MD, MPH, a hospitalist at E.L.M.O. Pediatrics in New York City, Treasurer of SHM's board of directors, and a member of SHM's Public Policy Committee. Percelay foresees a twofold benefit of the new legislation: a likely decrease in uninsured pediatric patients using the ED and more fee recovery from patients who otherwise couldn't pay.
David Rappaport, MD, FAAP, a hospitalist at Alfred I. Dupont Hospital for Children in Wilmington, Del., agrees. "Children's health is more than the cuddly factor—it's a smart investment in healthcare," he says, explaining that paying for preventive measures in children, such as inoculations, can save on their healthcare costs in the future.
Signed by President Obama on Feb. 4, the bill reauthorizes SCHIP for four years and expands eligibility to children in families with incomes of up to three times the federal poverty level. It also covers legal immigrant pregnant women and children who have been in the country less than five years. The expansion will cover an additional 4 million children, raising the total to 11 million uninsured children enrolled in the program. Most of the $32.8 billion increase in federal funding for the program is to be covered by a 62-cent-per-pack increase in the federal cigarette tax.
Back to School
Patience Agborbesong, MD, didn't go to SHM's "Essential Procedures for the Hospitalist" seminar on a whim. In fact, the medical director of Wake Forest Inpatient Physicians of Winston-Salem, N.C., skipped her own hospital's career day to attend the society's One-Day Hospitalist University (ODHU) session where she received four hours of hands-on training in the use of ultrasound equipment for vascular access, paracentesis, and thoracentesis.
"When I was training, we didn't use ultrasounds to routinely do central lines," says Dr. Agborbesong, an ODHU rookie. "Now that is something that is recommended as a patient safety measure. When we do the procedure without ultrasounds, you're blind-sticking and going by the anatomic landmarks."
The course was one of four one-day seminars that drew nearly 200 hospitalists to Atlanta. CME credit is awarded for all of the ODHU courses. The program also included "Best Practices in Managing a Hospital Medicine Program," "Critical Care Medicine for the Hospitalist," and "Fundamentals of Inpatient Coding and Documentation."
Like many hospitalists, Dr. Agborbesong used ODHU as a chance to expand the skill set of her 15-hospitalist group. In addition to relaying what she learned during the ultrasound course to her colleagues, she's also planning to hone her skills with help from radiologists at Wake Forest University Baptist Medical Center.
"I didn't come here thinking I would be an expert," she says. "It was a very good place to start."
To stay updated on SHM-sponsored training programs, visit the SHM Web site.
Patience Agborbesong, MD, didn't go to SHM's "Essential Procedures for the Hospitalist" seminar on a whim. In fact, the medical director of Wake Forest Inpatient Physicians of Winston-Salem, N.C., skipped her own hospital's career day to attend the society's One-Day Hospitalist University (ODHU) session where she received four hours of hands-on training in the use of ultrasound equipment for vascular access, paracentesis, and thoracentesis.
"When I was training, we didn't use ultrasounds to routinely do central lines," says Dr. Agborbesong, an ODHU rookie. "Now that is something that is recommended as a patient safety measure. When we do the procedure without ultrasounds, you're blind-sticking and going by the anatomic landmarks."
The course was one of four one-day seminars that drew nearly 200 hospitalists to Atlanta. CME credit is awarded for all of the ODHU courses. The program also included "Best Practices in Managing a Hospital Medicine Program," "Critical Care Medicine for the Hospitalist," and "Fundamentals of Inpatient Coding and Documentation."
Like many hospitalists, Dr. Agborbesong used ODHU as a chance to expand the skill set of her 15-hospitalist group. In addition to relaying what she learned during the ultrasound course to her colleagues, she's also planning to hone her skills with help from radiologists at Wake Forest University Baptist Medical Center.
"I didn't come here thinking I would be an expert," she says. "It was a very good place to start."
To stay updated on SHM-sponsored training programs, visit the SHM Web site.
Patience Agborbesong, MD, didn't go to SHM's "Essential Procedures for the Hospitalist" seminar on a whim. In fact, the medical director of Wake Forest Inpatient Physicians of Winston-Salem, N.C., skipped her own hospital's career day to attend the society's One-Day Hospitalist University (ODHU) session where she received four hours of hands-on training in the use of ultrasound equipment for vascular access, paracentesis, and thoracentesis.
"When I was training, we didn't use ultrasounds to routinely do central lines," says Dr. Agborbesong, an ODHU rookie. "Now that is something that is recommended as a patient safety measure. When we do the procedure without ultrasounds, you're blind-sticking and going by the anatomic landmarks."
The course was one of four one-day seminars that drew nearly 200 hospitalists to Atlanta. CME credit is awarded for all of the ODHU courses. The program also included "Best Practices in Managing a Hospital Medicine Program," "Critical Care Medicine for the Hospitalist," and "Fundamentals of Inpatient Coding and Documentation."
Like many hospitalists, Dr. Agborbesong used ODHU as a chance to expand the skill set of her 15-hospitalist group. In addition to relaying what she learned during the ultrasound course to her colleagues, she's also planning to hone her skills with help from radiologists at Wake Forest University Baptist Medical Center.
"I didn't come here thinking I would be an expert," she says. "It was a very good place to start."
To stay updated on SHM-sponsored training programs, visit the SHM Web site.
Transparent Hospitalists
Six weeks ago hospitalist Frank Michota Jr., MD, posted on the Cleveland Clinic's Web site that he receives at least $5,000 per year in fees from pharmaceutical firms Sanofi-Aventis U.S. Inc. and Scios Inc. Since then, not one of the 100 or so patients he's encountered has asked about it.
Still, hospitalists and specialists at the teaching hospital now are required to publicly disclose their financial ties to the pharmaceutical and medical device industries. The effort is aimed at increasing physician transparency and avoiding conflicts of interest—real or perceived.
As director of academic affairs for the hospital's Department of Hospital Medicine, Dr. Michota appreciates the credibility that the disclosure provides for research. But he thinks it does little to forward patient care. Because most hospitalists are required to use drugs or devices based on formularies, whether they have financial ties to the companies making the drugs or devices is irrelevant, he says.
"It’s not the patient that's looking at this stuff," Dr. Michota says, adding, "the disclosures are more for the ethereal discussions."
He emphasizes most physicians don’t seek out relationships with drug- and device-makers.
"I use Drug A because it's on my formulary," he says. "I have a lot of experience with [Drug A] because it's on my formulary. I'm then asked by the company to research it, because I have experience with Drug A. That's how it works, not the other way around."
Check out the Cleveland Clinic’s physician directory at http://my.clevelandclinic.org/staff_directory/default.aspx.
Six weeks ago hospitalist Frank Michota Jr., MD, posted on the Cleveland Clinic's Web site that he receives at least $5,000 per year in fees from pharmaceutical firms Sanofi-Aventis U.S. Inc. and Scios Inc. Since then, not one of the 100 or so patients he's encountered has asked about it.
Still, hospitalists and specialists at the teaching hospital now are required to publicly disclose their financial ties to the pharmaceutical and medical device industries. The effort is aimed at increasing physician transparency and avoiding conflicts of interest—real or perceived.
As director of academic affairs for the hospital's Department of Hospital Medicine, Dr. Michota appreciates the credibility that the disclosure provides for research. But he thinks it does little to forward patient care. Because most hospitalists are required to use drugs or devices based on formularies, whether they have financial ties to the companies making the drugs or devices is irrelevant, he says.
"It’s not the patient that's looking at this stuff," Dr. Michota says, adding, "the disclosures are more for the ethereal discussions."
He emphasizes most physicians don’t seek out relationships with drug- and device-makers.
"I use Drug A because it's on my formulary," he says. "I have a lot of experience with [Drug A] because it's on my formulary. I'm then asked by the company to research it, because I have experience with Drug A. That's how it works, not the other way around."
Check out the Cleveland Clinic’s physician directory at http://my.clevelandclinic.org/staff_directory/default.aspx.
Six weeks ago hospitalist Frank Michota Jr., MD, posted on the Cleveland Clinic's Web site that he receives at least $5,000 per year in fees from pharmaceutical firms Sanofi-Aventis U.S. Inc. and Scios Inc. Since then, not one of the 100 or so patients he's encountered has asked about it.
Still, hospitalists and specialists at the teaching hospital now are required to publicly disclose their financial ties to the pharmaceutical and medical device industries. The effort is aimed at increasing physician transparency and avoiding conflicts of interest—real or perceived.
As director of academic affairs for the hospital's Department of Hospital Medicine, Dr. Michota appreciates the credibility that the disclosure provides for research. But he thinks it does little to forward patient care. Because most hospitalists are required to use drugs or devices based on formularies, whether they have financial ties to the companies making the drugs or devices is irrelevant, he says.
"It’s not the patient that's looking at this stuff," Dr. Michota says, adding, "the disclosures are more for the ethereal discussions."
He emphasizes most physicians don’t seek out relationships with drug- and device-makers.
"I use Drug A because it's on my formulary," he says. "I have a lot of experience with [Drug A] because it's on my formulary. I'm then asked by the company to research it, because I have experience with Drug A. That's how it works, not the other way around."
Check out the Cleveland Clinic’s physician directory at http://my.clevelandclinic.org/staff_directory/default.aspx.