User login
The Paralympics and Prosthesis Pride
South African runner Oscar Pistorius fell just short of winning a medal at the London 2012 Olympics, but the double amputee did show the world that people with disabilities can achieve greatness in sports. His specially made prosthetic limbs also reflect a growing trend – highly visible in the media among returning soldiers from Afghanistan and Iraq – toward more people with amputations displaying their prostheses rather than hiding them with coverings that resemble arms and legs.
The trend will be further highlighted at the 2012 Paralympic Games, taking place in London Aug. 29 through Sept. 9, and where Mr. Pistorius will again compete.

"These are not your grandparents’ prosthetic devices that are available today. They have advanced at such a rapid pace. It’s not only exciting for users of prosthetic devices, but nonamputees are also very interested in the technology – how far it has evolved, and what prosthetic users are capable of doing, whether it be climbing Mount Everest or running in the Olympics with prosthetic limbs," according to Kevin Carroll, vice president of prosthetics at Hanger Orthopedic Group, based in Austin, Tex.*
About 4,200 athletes from 165 countries will compete in the Paralympics, across 503 medal events. Athletes with amputations will be some of the most visually distinct among the Paralympics’ 10 categories of disability: impaired muscle power, impaired passive range of motion, limb deficiency, leg length difference, short stature, hypertonia, ataxia, athetosis, vision impairment, and intellectual impairment.
"This year, we’re expecting all sorts of records at the Paralympics. There is a greater focus worldwide and countries throughout the world are seeing the importance of supporting athletes in Paralympic events ... I predict many more Pistorius-types are on their way to the Olympics," said Mr. Carroll.
In the Paralympics, athletes using specially designed prosthetic devices –that is, used specifically for the sport and not for everyday use – will be most visible in track and field events. Prosthetic devices are not used in sports such as swimming and sitting volleyball. However, athletes with amputations are using prostheses for a wide range of sports in the real world.
"We are now supplying sport-specific prostheses from early ages all the way up to adults. This includes everything from prostheses made specifically for running, cycling, swimming, mountain climbing, snowboarding, skiing, and more," Mr. Carroll said.
In fact, the emerging technology is so good that some have suggested it may soon allow disabled athletes to outdo their able-bodied counterparts.
Of course, most amputees are not elite athletes. There are approximately 1.7 million people with limb loss in the United States, with another 150,000 who undergo amputations each year. While injured soldiers tend to be the most visible amputees in the media, diabetes is by far the greatest cause of limb loss – more than 80% of all amputations are the result of diabetes. Vascular disease, trauma, and cancer are among the other top causes.

But even increasing numbers of non–athlete amputees have been showcasing their prostheses within the last 10-15 years, with comparable numbers in both the civilian and military populations. As many as 50% of amputees in the United States now choose to display their prostheses, compared with less than 10% among their European counterparts. "This number wasn’t as high in the U.S. 30 years ago. This has evolved over time," Mr. Carroll said.
A realistic-looking limb cover adds to the cost of the working part of the prosthesis itself, but he believes that’s not why we’re seeing more of the latter. "[Amputees who chose to show their prostheses] like to showcase the technology they’re walking around on. This shows they have really accepted their loss. They are not showcasing their prostheses because of the cost, they’re doing it because of pride."
His advice to physicians: "Never say never to patients. We see people who are confined to wheelchairs get up and walk every day. We’re in a whole new era of rehabilitation. We’re very excited about the future."
–Miriam E. Tucker (@MiriamETucker on Twitter)
*CORRECTION 8/30/12: The original sentence misstated the location of Hanger Orthopedic Group. The sentence should have read: "These are not your grandparents’ prosthetic devices that are available today. They have advanced at such a rapid pace. It’s not only exciting for users of prosthetic devices, but nonamputees are also very interested in the technology – how far it has evolved, and what prosthetic users are capable of doing, whether it be climbing Mount Everest or running in the Olympics with prosthetic limbs," according to Kevin Carroll, vice president of prosthetics at Hanger Orthopedic Group, based in Austin, Tex..
South African runner Oscar Pistorius fell just short of winning a medal at the London 2012 Olympics, but the double amputee did show the world that people with disabilities can achieve greatness in sports. His specially made prosthetic limbs also reflect a growing trend – highly visible in the media among returning soldiers from Afghanistan and Iraq – toward more people with amputations displaying their prostheses rather than hiding them with coverings that resemble arms and legs.
The trend will be further highlighted at the 2012 Paralympic Games, taking place in London Aug. 29 through Sept. 9, and where Mr. Pistorius will again compete.
"These are not your grandparents’ prosthetic devices that are available today. They have advanced at such a rapid pace. It’s not only exciting for users of prosthetic devices, but nonamputees are also very interested in the technology – how far it has evolved, and what prosthetic users are capable of doing, whether it be climbing Mount Everest or running in the Olympics with prosthetic limbs," according to Kevin Carroll, vice president of prosthetics at Hanger Orthopedic Group, based in Austin, Tex.*
About 4,200 athletes from 165 countries will compete in the Paralympics, across 503 medal events. Athletes with amputations will be some of the most visually distinct among the Paralympics’ 10 categories of disability: impaired muscle power, impaired passive range of motion, limb deficiency, leg length difference, short stature, hypertonia, ataxia, athetosis, vision impairment, and intellectual impairment.
"This year, we’re expecting all sorts of records at the Paralympics. There is a greater focus worldwide and countries throughout the world are seeing the importance of supporting athletes in Paralympic events ... I predict many more Pistorius-types are on their way to the Olympics," said Mr. Carroll.
In the Paralympics, athletes using specially designed prosthetic devices –that is, used specifically for the sport and not for everyday use – will be most visible in track and field events. Prosthetic devices are not used in sports such as swimming and sitting volleyball. However, athletes with amputations are using prostheses for a wide range of sports in the real world.
"We are now supplying sport-specific prostheses from early ages all the way up to adults. This includes everything from prostheses made specifically for running, cycling, swimming, mountain climbing, snowboarding, skiing, and more," Mr. Carroll said.
In fact, the emerging technology is so good that some have suggested it may soon allow disabled athletes to outdo their able-bodied counterparts.
Of course, most amputees are not elite athletes. There are approximately 1.7 million people with limb loss in the United States, with another 150,000 who undergo amputations each year. While injured soldiers tend to be the most visible amputees in the media, diabetes is by far the greatest cause of limb loss – more than 80% of all amputations are the result of diabetes. Vascular disease, trauma, and cancer are among the other top causes.
But even increasing numbers of non–athlete amputees have been showcasing their prostheses within the last 10-15 years, with comparable numbers in both the civilian and military populations. As many as 50% of amputees in the United States now choose to display their prostheses, compared with less than 10% among their European counterparts. "This number wasn’t as high in the U.S. 30 years ago. This has evolved over time," Mr. Carroll said.
A realistic-looking limb cover adds to the cost of the working part of the prosthesis itself, but he believes that’s not why we’re seeing more of the latter. "[Amputees who chose to show their prostheses] like to showcase the technology they’re walking around on. This shows they have really accepted their loss. They are not showcasing their prostheses because of the cost, they’re doing it because of pride."
His advice to physicians: "Never say never to patients. We see people who are confined to wheelchairs get up and walk every day. We’re in a whole new era of rehabilitation. We’re very excited about the future."
–Miriam E. Tucker (@MiriamETucker on Twitter)
*CORRECTION 8/30/12: The original sentence misstated the location of Hanger Orthopedic Group. The sentence should have read: "These are not your grandparents’ prosthetic devices that are available today. They have advanced at such a rapid pace. It’s not only exciting for users of prosthetic devices, but nonamputees are also very interested in the technology – how far it has evolved, and what prosthetic users are capable of doing, whether it be climbing Mount Everest or running in the Olympics with prosthetic limbs," according to Kevin Carroll, vice president of prosthetics at Hanger Orthopedic Group, based in Austin, Tex..
South African runner Oscar Pistorius fell just short of winning a medal at the London 2012 Olympics, but the double amputee did show the world that people with disabilities can achieve greatness in sports. His specially made prosthetic limbs also reflect a growing trend – highly visible in the media among returning soldiers from Afghanistan and Iraq – toward more people with amputations displaying their prostheses rather than hiding them with coverings that resemble arms and legs.
The trend will be further highlighted at the 2012 Paralympic Games, taking place in London Aug. 29 through Sept. 9, and where Mr. Pistorius will again compete.
"These are not your grandparents’ prosthetic devices that are available today. They have advanced at such a rapid pace. It’s not only exciting for users of prosthetic devices, but nonamputees are also very interested in the technology – how far it has evolved, and what prosthetic users are capable of doing, whether it be climbing Mount Everest or running in the Olympics with prosthetic limbs," according to Kevin Carroll, vice president of prosthetics at Hanger Orthopedic Group, based in Austin, Tex.*
About 4,200 athletes from 165 countries will compete in the Paralympics, across 503 medal events. Athletes with amputations will be some of the most visually distinct among the Paralympics’ 10 categories of disability: impaired muscle power, impaired passive range of motion, limb deficiency, leg length difference, short stature, hypertonia, ataxia, athetosis, vision impairment, and intellectual impairment.
"This year, we’re expecting all sorts of records at the Paralympics. There is a greater focus worldwide and countries throughout the world are seeing the importance of supporting athletes in Paralympic events ... I predict many more Pistorius-types are on their way to the Olympics," said Mr. Carroll.
In the Paralympics, athletes using specially designed prosthetic devices –that is, used specifically for the sport and not for everyday use – will be most visible in track and field events. Prosthetic devices are not used in sports such as swimming and sitting volleyball. However, athletes with amputations are using prostheses for a wide range of sports in the real world.
"We are now supplying sport-specific prostheses from early ages all the way up to adults. This includes everything from prostheses made specifically for running, cycling, swimming, mountain climbing, snowboarding, skiing, and more," Mr. Carroll said.
In fact, the emerging technology is so good that some have suggested it may soon allow disabled athletes to outdo their able-bodied counterparts.
Of course, most amputees are not elite athletes. There are approximately 1.7 million people with limb loss in the United States, with another 150,000 who undergo amputations each year. While injured soldiers tend to be the most visible amputees in the media, diabetes is by far the greatest cause of limb loss – more than 80% of all amputations are the result of diabetes. Vascular disease, trauma, and cancer are among the other top causes.
But even increasing numbers of non–athlete amputees have been showcasing their prostheses within the last 10-15 years, with comparable numbers in both the civilian and military populations. As many as 50% of amputees in the United States now choose to display their prostheses, compared with less than 10% among their European counterparts. "This number wasn’t as high in the U.S. 30 years ago. This has evolved over time," Mr. Carroll said.
A realistic-looking limb cover adds to the cost of the working part of the prosthesis itself, but he believes that’s not why we’re seeing more of the latter. "[Amputees who chose to show their prostheses] like to showcase the technology they’re walking around on. This shows they have really accepted their loss. They are not showcasing their prostheses because of the cost, they’re doing it because of pride."
His advice to physicians: "Never say never to patients. We see people who are confined to wheelchairs get up and walk every day. We’re in a whole new era of rehabilitation. We’re very excited about the future."
–Miriam E. Tucker (@MiriamETucker on Twitter)
*CORRECTION 8/30/12: The original sentence misstated the location of Hanger Orthopedic Group. The sentence should have read: "These are not your grandparents’ prosthetic devices that are available today. They have advanced at such a rapid pace. It’s not only exciting for users of prosthetic devices, but nonamputees are also very interested in the technology – how far it has evolved, and what prosthetic users are capable of doing, whether it be climbing Mount Everest or running in the Olympics with prosthetic limbs," according to Kevin Carroll, vice president of prosthetics at Hanger Orthopedic Group, based in Austin, Tex..

As Hospitalists Cement their Worth, Compensation Continues Upward Climb
Tom Smith, MD, vice president of clinical quality and hospitalist medical director at North Fulton Regional Medical Center in Alpharetta, Ga., is emotionally torn every time practice-based compensation and productivity data are published— data he will both use and defend against in negotiations with staffers and would-be staffers.
If nocturnist salaries are increasing nationally, will he have to pay his night-shift staff more?
If work relative-value units (wRVUs) are rising in his region, will he need to review how hard he is working his staff—or not hard enough?
If group leaders are receiving compensation premiums, should his top docs be paid above rank-and-file colleagues?
“There are upsides and downsides,” Dr. Smith says. “No. 1, if your compensation is good or appropriate, they sort of validate your pay and, I guess, your self-worth to some degree. But I think if you’re on the lower side, it definitely starts bringing to mind the ‘grass-is-greener scenarios.’”
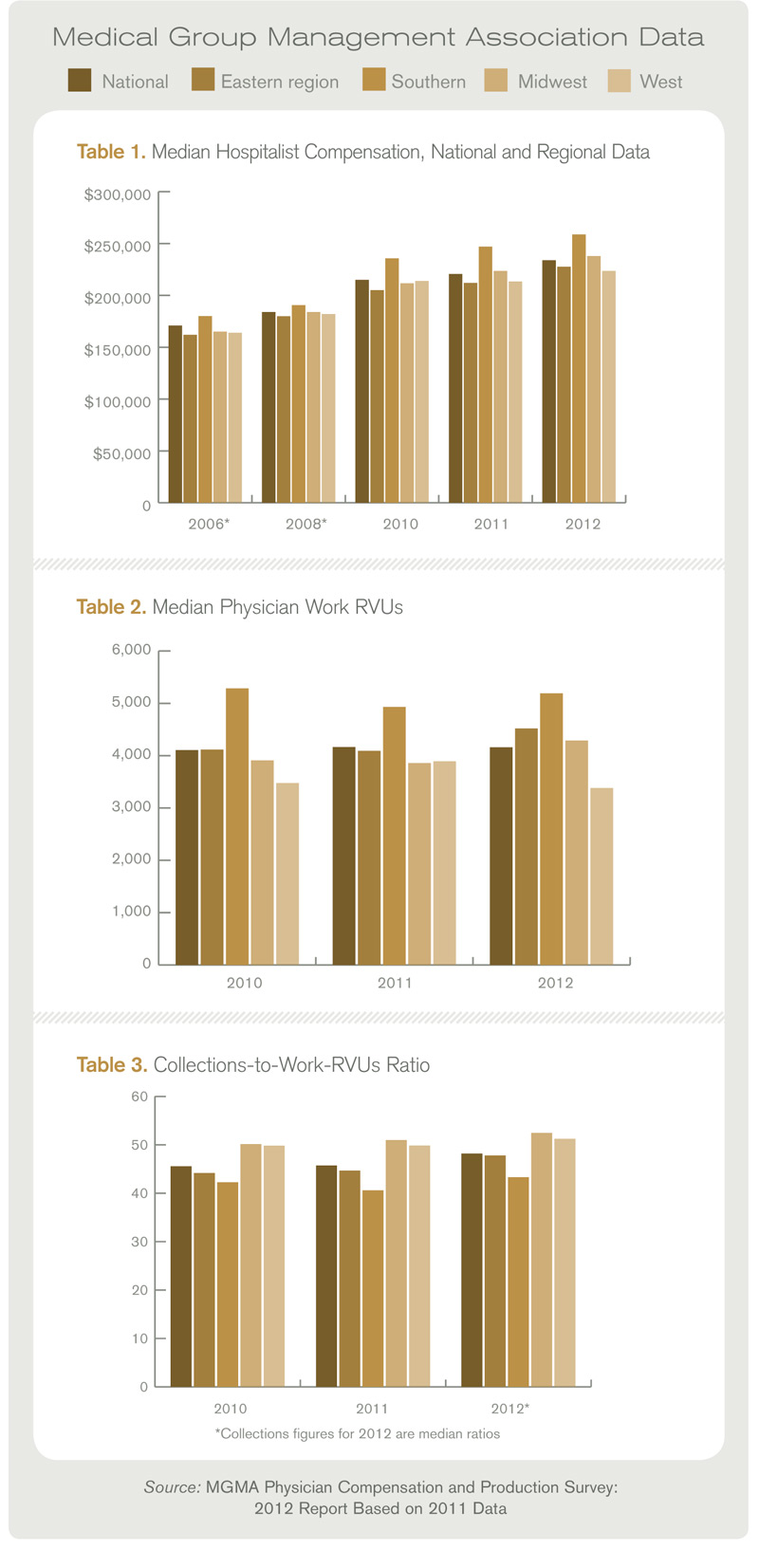
For hospitalists, the grass is green in most cases. Median compensation for adult hospitalists rose 6% to $233,855 in 2011, while productivity remained nearly static, according to the Medical Group Management Association’s (MGMA) Physician Compensation and Production Survey: 2012 Report Based on 2011 Data. The report is based on data compiled from 3,402 hospitalists nationwide; slightly more than 56% of respondents work in practices owned by hospitals/integrated delivery systems (IDS); 26% work in physician-owned groups.
The data, which excludes academic hospitalists, shows hospitalist pay has jumped more than 27% since 2008, when unadjusted figures pegged median hospitalist compensation at $183,900 nationwide. The climb comes despite little movement in the number of wRVUs hospitalists are producing. In 2011, the median physician wRVU rate was 4,159 per year, a 0.17% drop from the year prior.
The MGMA survey data will be incorporated into SHM’s annual State of Hospital Medicine report (SOHM), which features information on individual physicians and HM groups. The SOHM report received submission from 396 groups that serve adults only (for more about the survey instruments, see “Apples to Apples?”). Some 40% were employed by hospitals/IDS; a third were employed by management companies; and the rest were academic or other models. The report includes group-level data valuable to hospitalist groups, including financial data (i.e. hospital support payments and CPT code distribution), and information on staffing and scheduling.
Combined, the MGMA and SHM reports show a specialty where compensation continues to be pushed by demand outstripping supply, particularly in southern states (see Table 1). More subtly, leading hospitalists say, the data shows that much of the work that physicians now do—QI initiatives, committee leadership and leading digitalization efforts—is not completely captured by the wRVU metric, long the gold standard for measuring productivity.
“I really believe this is critical, critical information for people to have,” says William “Tex” Landis, MD, FHM, chairman of SHM’s Practice Analysis Committee. “Administrators need to have information to make sure that they’re being appropriate in the compensation that they’re paying the physicians. So everybody that’s involved in hospitalist programs is interested, or should be interested in this data, because it allows them to right resource their programs.”
Dollars and Sense
First and foremost in the MGMA data is the continued trend of rising compensation. In a seemingly endless uptick, hospitalists in the South continue to earn the most (median compensation $258,793, up from $247,000 in 2011 data). Southern hospitalists, though, only saw a 4.8% increase in compensation. The largest percentage jump (7.4%) was for hospitalists in the East (median compensation $227,656, up from $212,000 the year prior). Doctors in the East typically have the lowest compensation of the country’s four geographic regions, but this year’s data showed hospitalists in the West with the lowest figure (median compensation $223,574, up from $213,405).

Dan Fuller, president of IN Compass Health of Alpharetta, Ga., and a member of SHM’s Practice Analysis Committee, says the rising compensation makes perfect sense.
“In fact, I think it’s something we’re probably going to have to deal with for the near future,” he says, noting some in the specialty believed median compensation was ready to plateau. “And, certainly, as hospitalists are asked to do more and more, and they a play a bigger and bigger role in the facility, there should be a higher expectation that they continue to make more and more, and make a bigger impact.”
The question group leaders are asking now: how high can the compensation figures climb? Todd Evenson, MGMA director of data solutions, says there is no answer, yet. Evenson says he sees no immediate obstacles to the continued growth, as hospitalists have established themselves as major players in most hospitals.
What could determine the upper limit is “the payment mechanisms that we start to see fall out of the legislation that occurs,” he says. “As that evolves, I can’t say I know the ceiling.”
A year or two ago, Dr. Landis would have told anyone who asked that the compensation limit was in sight. Now, he believes that as long as competition makes recruitment and retention difficult, it’s hard to predict an end to the compensation growth.
“I don’t think there is a hospitalist group, whether it’s hospitalist-owned, national company, or a private group part of a large, multi-specialty clinic, there’s not a group in the country that’s not struggling with recruitment and retention,” Dr. Fuller adds.
The Value of wRVUs
One data point that has stymied the expectations of some hospitalists is the relative stability of wRVUs. The national figure has ticked up 1.26% since 2010 to 4,159 per year. But the stability is geographically deceiving. In the East and Midwest regions, hospitalist wRVUs jumped 9.8% and 9.7%, respectively. In the South and West, wRVUs fell 1.8% and 2.7%, respectively.
In whole numbers, the South continues to show the highest productivity per physician. Hospitalists in the south produced 671 more wRVUs than the next-highest regional cohort, (5,192 South vs. 4,521 East). Hospitalists in the South region also produced nearly 35% more wRVUs than their Western counterparts (5,192 vs. 3,383).
Survey experts have no explanation for why regional productivity varies so much. Regardless, the trouble with wRVUs is that they are intended to serve as a proxy of billable productivity, hospitalists say.

As HM groups and physicians become more engaged in moving from a fee-for-service payment model to one that rewards quality and value, the metric becomes less precise, says Ken Simone, DO, SFHM, founder and president of Hospitalist and Practice Solutions in Veazie, Maine, an HM consulting firm.
“Productivity in some ways is difficult to measure with hospitalists because they are also providing services [while they are] working on committees, doing IT work, or doing some research,” says Dr. Simone, a member of Team Hospitalist. “I’m very careful in how I look at a hospitalist’s productivity.”

Although some are hesitant to suggest that wRVUs have leveled, Dr. Smith, who oversees a six-hospitalist group at his 208-bed institution about 25 miles north of Atlanta, believes hospitalists “are about at capacity.”
“Particularly considering the new pressures that are on patient satisfaction, time to go in the ER, length of stay, discharge, reducing readmissions,” he says. “I think it’s going to be hard to push that number up.”

Dr. Landis, medical director of Wellspan Hospitalists in York, Pa., believes it is counter-productive to push wRVUs too high. He believes a hospitalist’s role is to provide patient care, lead process improvement, and coordinate multi-disciplinary teams. Too much of a focus on any one role takes away from physician efficacy.
“The value of a hospitalist goes well beyond the wRVU number,” he explains. “That being said, we are still in the business of seeing patients. I don’t think having a hospitalist that’s generating 1,500 RVUs and paying them at the 75th percentile is going to be very effective. You’re going to need to balance those out.”
continued below...
Apples to Apples?

Any researcher worth his academic salt will say that results are only as good as their N. And so hospitalists eager to glean data points from the MGMA’s Physician Compensation and Production Survey: 2012 Report Based on 2011 Data and SHM’s State of Hospital Medicine report need to remember that the numbers aren’t coming from the same source.
MGMA compiled compensation data on 3,402 full-time hospitalists nationwide. Slightly more than 56% of the respondents worked in hospital-owned practices, while 26% are in physician-owned groups. The rest reported “other” practice models.
SHM received submissions from 396 groups that serve adults only. Some 49% were hospital/IDS employed, 33% management companies, and the rest were academic or other models.
And while the MGMA survey data will be incorporated into SHM’s report, the information was culled from different universes. SHM encouraged its members to participate in the MGMA survey, but did not get involved beyond that. This is a change to the 2011 report, when the two groups jointly gathered data. And it is a change again from previous years, when SHM did its work separately, with little teamwork with MGMA.
While the changing methodologies can make year-to-year comparisons less precise or more difficult to craft, Dr. Landis says surveys need to evolve to ensure they’re asking the best questions and the questions users want answer to. Even then, though, he cautions ever reading too much into survey data.
“We’ve used the best tools to give good statistics, but in the end it’s not a scientific, placebo-controlled, double-blinded trial,” Dr. Landis says. “It’s a survey, and you need to keep in mind that’s what it is.”
—Richard Quinn
How Much Turnover Is Too Much Turnover?
Some HM leaders were pleased last year when hospitalist turnover dropped to 8% from a 14% turnover rate the year prior. This year’s State of Hospital Medicine report pegs the turnover figure at 10%. Although just a slight increase this year, Fuller views the uptick in turnover as a burgeoning cycle. While the supply-demand curve continues to push compensation up, increased turnover will continue to impact both sides of the equation.
“I’m sure there are many fully staffed programs, but they’re dealing with turnover,” he says. “They’re dealing with attrition, physicians leaving to go to fellowships, physicians relocating...physicians wanting to retire. I think it’s a crisis, a tremendous crisis that we need to be prepared to deal with for the near future.”
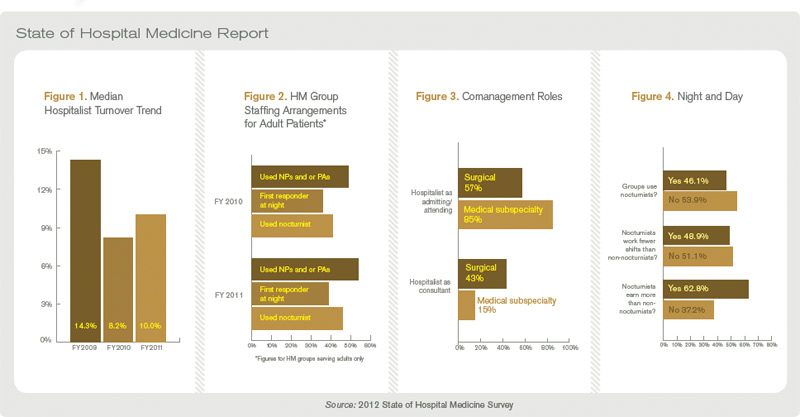
Aside from turnover data, the SOHM report this year looked to break new ground by trying out new questions. The report for the first time surveyed how hospitalists perform comanagement duties. In surgical comanagement cases, the hospitalist served as the admitting or attending physician 57% of the time. The rest of the time they served as a consultant. In medical comanagement, hospitalists were the admitting/attending physician 85% of the time (see “Comanagement Roles,”).
As hospitalists find specialties even within the field, the report also looked to put data to the cohort of nocturnists. Roughly half of those covering night shifts work fewer shifts than their daytime colleagues. Moreover, 63% of nocturnists earned a differential for that work (see Figure 4).
The value of data points on emerging and existing trends is that it gives HM groups and group administrators thresholds to benchmark themselves against, Dr. Simone says.
“It also allows the HM leader to compare within a practice,” he adds. “If hospital medicine groups are performing at or above median, or are highly functional groups, it gives great feedback that they’re doing things correctly. But it also gives the leader an opportunity to make a sound business plan when he’s going to talk to the hospital [administration] for subsidy, or when he’s going to negotiate compensation for his providers for the next year. I think that’s a powerful tool.”
Interactive regional survey breakdowns
Richard Quinn is a freelance writer based in New Jersey.
How Long Can The Stool of Staffing Success Stand?

William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and chair of SHM’s Practice Analysis Committee, likes to say that hospitalists are a fundamentally necessary service in hospitals. But keeping a full complement of hospitalists is hard work—and money is a big draw.
“We have to make some way for it to be a more desirable position, and my feeling is that there are three legs that stool stands on, and that’s salary, schedule, and scope,” he says. “Those are the three things that you have to play with and if the scope of the service is going to stay the same and the schedule is going to be similar, then the third thing that’s easiest to adjust is the salary.”
Dr. Landis has no answer to when he expects compensation to stop increasing. But Leslie Flores, MHA, SHM senior advisor for practice management and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants, believes it’s dangerous to climb too high in compensation without something else changing dramatically.
“At some point,” she says, “there is a breaking point in terms of what hospitals can afford to spend to support hospitalist programs, and that is going to either cause significant salary pressure, or it’s going to cause significant pressure for hospitalists to increase their productivity and become a lot more efficient in their clinical work, or both.”
—Richard Quinn
Tom Smith, MD, vice president of clinical quality and hospitalist medical director at North Fulton Regional Medical Center in Alpharetta, Ga., is emotionally torn every time practice-based compensation and productivity data are published— data he will both use and defend against in negotiations with staffers and would-be staffers.
If nocturnist salaries are increasing nationally, will he have to pay his night-shift staff more?
If work relative-value units (wRVUs) are rising in his region, will he need to review how hard he is working his staff—or not hard enough?
If group leaders are receiving compensation premiums, should his top docs be paid above rank-and-file colleagues?
“There are upsides and downsides,” Dr. Smith says. “No. 1, if your compensation is good or appropriate, they sort of validate your pay and, I guess, your self-worth to some degree. But I think if you’re on the lower side, it definitely starts bringing to mind the ‘grass-is-greener scenarios.’”
For hospitalists, the grass is green in most cases. Median compensation for adult hospitalists rose 6% to $233,855 in 2011, while productivity remained nearly static, according to the Medical Group Management Association’s (MGMA) Physician Compensation and Production Survey: 2012 Report Based on 2011 Data. The report is based on data compiled from 3,402 hospitalists nationwide; slightly more than 56% of respondents work in practices owned by hospitals/integrated delivery systems (IDS); 26% work in physician-owned groups.
The data, which excludes academic hospitalists, shows hospitalist pay has jumped more than 27% since 2008, when unadjusted figures pegged median hospitalist compensation at $183,900 nationwide. The climb comes despite little movement in the number of wRVUs hospitalists are producing. In 2011, the median physician wRVU rate was 4,159 per year, a 0.17% drop from the year prior.
The MGMA survey data will be incorporated into SHM’s annual State of Hospital Medicine report (SOHM), which features information on individual physicians and HM groups. The SOHM report received submission from 396 groups that serve adults only (for more about the survey instruments, see “Apples to Apples?”). Some 40% were employed by hospitals/IDS; a third were employed by management companies; and the rest were academic or other models. The report includes group-level data valuable to hospitalist groups, including financial data (i.e. hospital support payments and CPT code distribution), and information on staffing and scheduling.
Combined, the MGMA and SHM reports show a specialty where compensation continues to be pushed by demand outstripping supply, particularly in southern states (see Table 1). More subtly, leading hospitalists say, the data shows that much of the work that physicians now do—QI initiatives, committee leadership and leading digitalization efforts—is not completely captured by the wRVU metric, long the gold standard for measuring productivity.
“I really believe this is critical, critical information for people to have,” says William “Tex” Landis, MD, FHM, chairman of SHM’s Practice Analysis Committee. “Administrators need to have information to make sure that they’re being appropriate in the compensation that they’re paying the physicians. So everybody that’s involved in hospitalist programs is interested, or should be interested in this data, because it allows them to right resource their programs.”
Dollars and Sense
First and foremost in the MGMA data is the continued trend of rising compensation. In a seemingly endless uptick, hospitalists in the South continue to earn the most (median compensation $258,793, up from $247,000 in 2011 data). Southern hospitalists, though, only saw a 4.8% increase in compensation. The largest percentage jump (7.4%) was for hospitalists in the East (median compensation $227,656, up from $212,000 the year prior). Doctors in the East typically have the lowest compensation of the country’s four geographic regions, but this year’s data showed hospitalists in the West with the lowest figure (median compensation $223,574, up from $213,405).
Dan Fuller, president of IN Compass Health of Alpharetta, Ga., and a member of SHM’s Practice Analysis Committee, says the rising compensation makes perfect sense.
“In fact, I think it’s something we’re probably going to have to deal with for the near future,” he says, noting some in the specialty believed median compensation was ready to plateau. “And, certainly, as hospitalists are asked to do more and more, and they a play a bigger and bigger role in the facility, there should be a higher expectation that they continue to make more and more, and make a bigger impact.”
The question group leaders are asking now: how high can the compensation figures climb? Todd Evenson, MGMA director of data solutions, says there is no answer, yet. Evenson says he sees no immediate obstacles to the continued growth, as hospitalists have established themselves as major players in most hospitals.
What could determine the upper limit is “the payment mechanisms that we start to see fall out of the legislation that occurs,” he says. “As that evolves, I can’t say I know the ceiling.”
A year or two ago, Dr. Landis would have told anyone who asked that the compensation limit was in sight. Now, he believes that as long as competition makes recruitment and retention difficult, it’s hard to predict an end to the compensation growth.
“I don’t think there is a hospitalist group, whether it’s hospitalist-owned, national company, or a private group part of a large, multi-specialty clinic, there’s not a group in the country that’s not struggling with recruitment and retention,” Dr. Fuller adds.
The Value of wRVUs
One data point that has stymied the expectations of some hospitalists is the relative stability of wRVUs. The national figure has ticked up 1.26% since 2010 to 4,159 per year. But the stability is geographically deceiving. In the East and Midwest regions, hospitalist wRVUs jumped 9.8% and 9.7%, respectively. In the South and West, wRVUs fell 1.8% and 2.7%, respectively.
In whole numbers, the South continues to show the highest productivity per physician. Hospitalists in the south produced 671 more wRVUs than the next-highest regional cohort, (5,192 South vs. 4,521 East). Hospitalists in the South region also produced nearly 35% more wRVUs than their Western counterparts (5,192 vs. 3,383).
Survey experts have no explanation for why regional productivity varies so much. Regardless, the trouble with wRVUs is that they are intended to serve as a proxy of billable productivity, hospitalists say.
As HM groups and physicians become more engaged in moving from a fee-for-service payment model to one that rewards quality and value, the metric becomes less precise, says Ken Simone, DO, SFHM, founder and president of Hospitalist and Practice Solutions in Veazie, Maine, an HM consulting firm.
“Productivity in some ways is difficult to measure with hospitalists because they are also providing services [while they are] working on committees, doing IT work, or doing some research,” says Dr. Simone, a member of Team Hospitalist. “I’m very careful in how I look at a hospitalist’s productivity.”
Although some are hesitant to suggest that wRVUs have leveled, Dr. Smith, who oversees a six-hospitalist group at his 208-bed institution about 25 miles north of Atlanta, believes hospitalists “are about at capacity.”
“Particularly considering the new pressures that are on patient satisfaction, time to go in the ER, length of stay, discharge, reducing readmissions,” he says. “I think it’s going to be hard to push that number up.”
Dr. Landis, medical director of Wellspan Hospitalists in York, Pa., believes it is counter-productive to push wRVUs too high. He believes a hospitalist’s role is to provide patient care, lead process improvement, and coordinate multi-disciplinary teams. Too much of a focus on any one role takes away from physician efficacy.
“The value of a hospitalist goes well beyond the wRVU number,” he explains. “That being said, we are still in the business of seeing patients. I don’t think having a hospitalist that’s generating 1,500 RVUs and paying them at the 75th percentile is going to be very effective. You’re going to need to balance those out.”
continued below...
Apples to Apples?
Any researcher worth his academic salt will say that results are only as good as their N. And so hospitalists eager to glean data points from the MGMA’s Physician Compensation and Production Survey: 2012 Report Based on 2011 Data and SHM’s State of Hospital Medicine report need to remember that the numbers aren’t coming from the same source.
MGMA compiled compensation data on 3,402 full-time hospitalists nationwide. Slightly more than 56% of the respondents worked in hospital-owned practices, while 26% are in physician-owned groups. The rest reported “other” practice models.
SHM received submissions from 396 groups that serve adults only. Some 49% were hospital/IDS employed, 33% management companies, and the rest were academic or other models.
And while the MGMA survey data will be incorporated into SHM’s report, the information was culled from different universes. SHM encouraged its members to participate in the MGMA survey, but did not get involved beyond that. This is a change to the 2011 report, when the two groups jointly gathered data. And it is a change again from previous years, when SHM did its work separately, with little teamwork with MGMA.
While the changing methodologies can make year-to-year comparisons less precise or more difficult to craft, Dr. Landis says surveys need to evolve to ensure they’re asking the best questions and the questions users want answer to. Even then, though, he cautions ever reading too much into survey data.
“We’ve used the best tools to give good statistics, but in the end it’s not a scientific, placebo-controlled, double-blinded trial,” Dr. Landis says. “It’s a survey, and you need to keep in mind that’s what it is.”
—Richard Quinn
How Much Turnover Is Too Much Turnover?
Some HM leaders were pleased last year when hospitalist turnover dropped to 8% from a 14% turnover rate the year prior. This year’s State of Hospital Medicine report pegs the turnover figure at 10%. Although just a slight increase this year, Fuller views the uptick in turnover as a burgeoning cycle. While the supply-demand curve continues to push compensation up, increased turnover will continue to impact both sides of the equation.
“I’m sure there are many fully staffed programs, but they’re dealing with turnover,” he says. “They’re dealing with attrition, physicians leaving to go to fellowships, physicians relocating...physicians wanting to retire. I think it’s a crisis, a tremendous crisis that we need to be prepared to deal with for the near future.”
Aside from turnover data, the SOHM report this year looked to break new ground by trying out new questions. The report for the first time surveyed how hospitalists perform comanagement duties. In surgical comanagement cases, the hospitalist served as the admitting or attending physician 57% of the time. The rest of the time they served as a consultant. In medical comanagement, hospitalists were the admitting/attending physician 85% of the time (see “Comanagement Roles,”).
As hospitalists find specialties even within the field, the report also looked to put data to the cohort of nocturnists. Roughly half of those covering night shifts work fewer shifts than their daytime colleagues. Moreover, 63% of nocturnists earned a differential for that work (see Figure 4).
The value of data points on emerging and existing trends is that it gives HM groups and group administrators thresholds to benchmark themselves against, Dr. Simone says.
“It also allows the HM leader to compare within a practice,” he adds. “If hospital medicine groups are performing at or above median, or are highly functional groups, it gives great feedback that they’re doing things correctly. But it also gives the leader an opportunity to make a sound business plan when he’s going to talk to the hospital [administration] for subsidy, or when he’s going to negotiate compensation for his providers for the next year. I think that’s a powerful tool.”
Interactive regional survey breakdowns
Richard Quinn is a freelance writer based in New Jersey.
How Long Can The Stool of Staffing Success Stand?
William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and chair of SHM’s Practice Analysis Committee, likes to say that hospitalists are a fundamentally necessary service in hospitals. But keeping a full complement of hospitalists is hard work—and money is a big draw.
“We have to make some way for it to be a more desirable position, and my feeling is that there are three legs that stool stands on, and that’s salary, schedule, and scope,” he says. “Those are the three things that you have to play with and if the scope of the service is going to stay the same and the schedule is going to be similar, then the third thing that’s easiest to adjust is the salary.”
Dr. Landis has no answer to when he expects compensation to stop increasing. But Leslie Flores, MHA, SHM senior advisor for practice management and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants, believes it’s dangerous to climb too high in compensation without something else changing dramatically.
“At some point,” she says, “there is a breaking point in terms of what hospitals can afford to spend to support hospitalist programs, and that is going to either cause significant salary pressure, or it’s going to cause significant pressure for hospitalists to increase their productivity and become a lot more efficient in their clinical work, or both.”
—Richard Quinn
Tom Smith, MD, vice president of clinical quality and hospitalist medical director at North Fulton Regional Medical Center in Alpharetta, Ga., is emotionally torn every time practice-based compensation and productivity data are published— data he will both use and defend against in negotiations with staffers and would-be staffers.
If nocturnist salaries are increasing nationally, will he have to pay his night-shift staff more?
If work relative-value units (wRVUs) are rising in his region, will he need to review how hard he is working his staff—or not hard enough?
If group leaders are receiving compensation premiums, should his top docs be paid above rank-and-file colleagues?
“There are upsides and downsides,” Dr. Smith says. “No. 1, if your compensation is good or appropriate, they sort of validate your pay and, I guess, your self-worth to some degree. But I think if you’re on the lower side, it definitely starts bringing to mind the ‘grass-is-greener scenarios.’”
For hospitalists, the grass is green in most cases. Median compensation for adult hospitalists rose 6% to $233,855 in 2011, while productivity remained nearly static, according to the Medical Group Management Association’s (MGMA) Physician Compensation and Production Survey: 2012 Report Based on 2011 Data. The report is based on data compiled from 3,402 hospitalists nationwide; slightly more than 56% of respondents work in practices owned by hospitals/integrated delivery systems (IDS); 26% work in physician-owned groups.
The data, which excludes academic hospitalists, shows hospitalist pay has jumped more than 27% since 2008, when unadjusted figures pegged median hospitalist compensation at $183,900 nationwide. The climb comes despite little movement in the number of wRVUs hospitalists are producing. In 2011, the median physician wRVU rate was 4,159 per year, a 0.17% drop from the year prior.
The MGMA survey data will be incorporated into SHM’s annual State of Hospital Medicine report (SOHM), which features information on individual physicians and HM groups. The SOHM report received submission from 396 groups that serve adults only (for more about the survey instruments, see “Apples to Apples?”). Some 40% were employed by hospitals/IDS; a third were employed by management companies; and the rest were academic or other models. The report includes group-level data valuable to hospitalist groups, including financial data (i.e. hospital support payments and CPT code distribution), and information on staffing and scheduling.
Combined, the MGMA and SHM reports show a specialty where compensation continues to be pushed by demand outstripping supply, particularly in southern states (see Table 1). More subtly, leading hospitalists say, the data shows that much of the work that physicians now do—QI initiatives, committee leadership and leading digitalization efforts—is not completely captured by the wRVU metric, long the gold standard for measuring productivity.
“I really believe this is critical, critical information for people to have,” says William “Tex” Landis, MD, FHM, chairman of SHM’s Practice Analysis Committee. “Administrators need to have information to make sure that they’re being appropriate in the compensation that they’re paying the physicians. So everybody that’s involved in hospitalist programs is interested, or should be interested in this data, because it allows them to right resource their programs.”
Dollars and Sense
First and foremost in the MGMA data is the continued trend of rising compensation. In a seemingly endless uptick, hospitalists in the South continue to earn the most (median compensation $258,793, up from $247,000 in 2011 data). Southern hospitalists, though, only saw a 4.8% increase in compensation. The largest percentage jump (7.4%) was for hospitalists in the East (median compensation $227,656, up from $212,000 the year prior). Doctors in the East typically have the lowest compensation of the country’s four geographic regions, but this year’s data showed hospitalists in the West with the lowest figure (median compensation $223,574, up from $213,405).
Dan Fuller, president of IN Compass Health of Alpharetta, Ga., and a member of SHM’s Practice Analysis Committee, says the rising compensation makes perfect sense.
“In fact, I think it’s something we’re probably going to have to deal with for the near future,” he says, noting some in the specialty believed median compensation was ready to plateau. “And, certainly, as hospitalists are asked to do more and more, and they a play a bigger and bigger role in the facility, there should be a higher expectation that they continue to make more and more, and make a bigger impact.”
The question group leaders are asking now: how high can the compensation figures climb? Todd Evenson, MGMA director of data solutions, says there is no answer, yet. Evenson says he sees no immediate obstacles to the continued growth, as hospitalists have established themselves as major players in most hospitals.
What could determine the upper limit is “the payment mechanisms that we start to see fall out of the legislation that occurs,” he says. “As that evolves, I can’t say I know the ceiling.”
A year or two ago, Dr. Landis would have told anyone who asked that the compensation limit was in sight. Now, he believes that as long as competition makes recruitment and retention difficult, it’s hard to predict an end to the compensation growth.
“I don’t think there is a hospitalist group, whether it’s hospitalist-owned, national company, or a private group part of a large, multi-specialty clinic, there’s not a group in the country that’s not struggling with recruitment and retention,” Dr. Fuller adds.
The Value of wRVUs
One data point that has stymied the expectations of some hospitalists is the relative stability of wRVUs. The national figure has ticked up 1.26% since 2010 to 4,159 per year. But the stability is geographically deceiving. In the East and Midwest regions, hospitalist wRVUs jumped 9.8% and 9.7%, respectively. In the South and West, wRVUs fell 1.8% and 2.7%, respectively.
In whole numbers, the South continues to show the highest productivity per physician. Hospitalists in the south produced 671 more wRVUs than the next-highest regional cohort, (5,192 South vs. 4,521 East). Hospitalists in the South region also produced nearly 35% more wRVUs than their Western counterparts (5,192 vs. 3,383).
Survey experts have no explanation for why regional productivity varies so much. Regardless, the trouble with wRVUs is that they are intended to serve as a proxy of billable productivity, hospitalists say.
As HM groups and physicians become more engaged in moving from a fee-for-service payment model to one that rewards quality and value, the metric becomes less precise, says Ken Simone, DO, SFHM, founder and president of Hospitalist and Practice Solutions in Veazie, Maine, an HM consulting firm.
“Productivity in some ways is difficult to measure with hospitalists because they are also providing services [while they are] working on committees, doing IT work, or doing some research,” says Dr. Simone, a member of Team Hospitalist. “I’m very careful in how I look at a hospitalist’s productivity.”
Although some are hesitant to suggest that wRVUs have leveled, Dr. Smith, who oversees a six-hospitalist group at his 208-bed institution about 25 miles north of Atlanta, believes hospitalists “are about at capacity.”
“Particularly considering the new pressures that are on patient satisfaction, time to go in the ER, length of stay, discharge, reducing readmissions,” he says. “I think it’s going to be hard to push that number up.”
Dr. Landis, medical director of Wellspan Hospitalists in York, Pa., believes it is counter-productive to push wRVUs too high. He believes a hospitalist’s role is to provide patient care, lead process improvement, and coordinate multi-disciplinary teams. Too much of a focus on any one role takes away from physician efficacy.
“The value of a hospitalist goes well beyond the wRVU number,” he explains. “That being said, we are still in the business of seeing patients. I don’t think having a hospitalist that’s generating 1,500 RVUs and paying them at the 75th percentile is going to be very effective. You’re going to need to balance those out.”
continued below...
Apples to Apples?
Any researcher worth his academic salt will say that results are only as good as their N. And so hospitalists eager to glean data points from the MGMA’s Physician Compensation and Production Survey: 2012 Report Based on 2011 Data and SHM’s State of Hospital Medicine report need to remember that the numbers aren’t coming from the same source.
MGMA compiled compensation data on 3,402 full-time hospitalists nationwide. Slightly more than 56% of the respondents worked in hospital-owned practices, while 26% are in physician-owned groups. The rest reported “other” practice models.
SHM received submissions from 396 groups that serve adults only. Some 49% were hospital/IDS employed, 33% management companies, and the rest were academic or other models.
And while the MGMA survey data will be incorporated into SHM’s report, the information was culled from different universes. SHM encouraged its members to participate in the MGMA survey, but did not get involved beyond that. This is a change to the 2011 report, when the two groups jointly gathered data. And it is a change again from previous years, when SHM did its work separately, with little teamwork with MGMA.
While the changing methodologies can make year-to-year comparisons less precise or more difficult to craft, Dr. Landis says surveys need to evolve to ensure they’re asking the best questions and the questions users want answer to. Even then, though, he cautions ever reading too much into survey data.
“We’ve used the best tools to give good statistics, but in the end it’s not a scientific, placebo-controlled, double-blinded trial,” Dr. Landis says. “It’s a survey, and you need to keep in mind that’s what it is.”
—Richard Quinn
How Much Turnover Is Too Much Turnover?
Some HM leaders were pleased last year when hospitalist turnover dropped to 8% from a 14% turnover rate the year prior. This year’s State of Hospital Medicine report pegs the turnover figure at 10%. Although just a slight increase this year, Fuller views the uptick in turnover as a burgeoning cycle. While the supply-demand curve continues to push compensation up, increased turnover will continue to impact both sides of the equation.
“I’m sure there are many fully staffed programs, but they’re dealing with turnover,” he says. “They’re dealing with attrition, physicians leaving to go to fellowships, physicians relocating...physicians wanting to retire. I think it’s a crisis, a tremendous crisis that we need to be prepared to deal with for the near future.”
Aside from turnover data, the SOHM report this year looked to break new ground by trying out new questions. The report for the first time surveyed how hospitalists perform comanagement duties. In surgical comanagement cases, the hospitalist served as the admitting or attending physician 57% of the time. The rest of the time they served as a consultant. In medical comanagement, hospitalists were the admitting/attending physician 85% of the time (see “Comanagement Roles,”).
As hospitalists find specialties even within the field, the report also looked to put data to the cohort of nocturnists. Roughly half of those covering night shifts work fewer shifts than their daytime colleagues. Moreover, 63% of nocturnists earned a differential for that work (see Figure 4).
The value of data points on emerging and existing trends is that it gives HM groups and group administrators thresholds to benchmark themselves against, Dr. Simone says.
“It also allows the HM leader to compare within a practice,” he adds. “If hospital medicine groups are performing at or above median, or are highly functional groups, it gives great feedback that they’re doing things correctly. But it also gives the leader an opportunity to make a sound business plan when he’s going to talk to the hospital [administration] for subsidy, or when he’s going to negotiate compensation for his providers for the next year. I think that’s a powerful tool.”
Interactive regional survey breakdowns
Richard Quinn is a freelance writer based in New Jersey.
How Long Can The Stool of Staffing Success Stand?
William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and chair of SHM’s Practice Analysis Committee, likes to say that hospitalists are a fundamentally necessary service in hospitals. But keeping a full complement of hospitalists is hard work—and money is a big draw.
“We have to make some way for it to be a more desirable position, and my feeling is that there are three legs that stool stands on, and that’s salary, schedule, and scope,” he says. “Those are the three things that you have to play with and if the scope of the service is going to stay the same and the schedule is going to be similar, then the third thing that’s easiest to adjust is the salary.”
Dr. Landis has no answer to when he expects compensation to stop increasing. But Leslie Flores, MHA, SHM senior advisor for practice management and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants, believes it’s dangerous to climb too high in compensation without something else changing dramatically.
“At some point,” she says, “there is a breaking point in terms of what hospitals can afford to spend to support hospitalist programs, and that is going to either cause significant salary pressure, or it’s going to cause significant pressure for hospitalists to increase their productivity and become a lot more efficient in their clinical work, or both.”
—Richard Quinn
Are Your Hospitalists Bored?
The conversation came as a surprise to Len Scarpinato, DO, MS, SFHM. The chief medical officer of clinical development for Brentwood, Tenn.-based Cogent-HMG had sensed something was bothering one of the community hospitalists at Aurora St. Luke’s Medical Center in Milwaukee. When Dr. Scarpinato approached him, the hospitalist told Dr. Scarpinato that he wanted to work as an academic hospitalist.
Dr. Scarpinato encouraged the clinician to try his hand at an academic center on his “off weeks.” The once-discouraged hospitalist stayed with Cogent-HMG, received leadership training, and now is an associate program medical director.
Whether group leaders across the country know it or not, there are hospitalists who are unfulfilled in their careers or dissatisfied with their work. Sometimes a group leader sees the problem coming; sometimes it manifests out of thin air.
A lack of fulfillment in a job can affect patient care. Experts say unhappy hospitalists are less likely to have good rapport with patients, less likely to communicate with the care team, and less likely to follow up on post-discharge lab results. It also hampers the efficacy of a company that frequently has to fill jobs vacated by dissatisfied physicians.
Job fulfillment is a feeling of satisfaction that is related to, but distinct from, burnout (the feeling of being overworked). And while burnout is a topic of widespread concern throughout HM, a lack of job fulfillment is equally important.
The Hospital Medicine Physician Worklife Survey administered in 2009 and 2010 found that 62.6% of the hospitalists who responded reported high satisfaction in their jobs.1 But according to the survey, there was lower satisfaction in terms of organization climate, autonomy, compensation, and availability of personal time.
HM groups should make it a priority to keep their clinicians involved in activities that keep them interested, says John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center, Bellevue, Wash., hospitalist practice management consultant, and columnist for The Hospitalist.
“You’ve got to do something besides taking care of patients,” Dr. Nelson says.
The Hospitalist asked group leaders and consultants how to spot signs of low job satisfaction, how they can keep their hospitalists fulfilled, and tips for other HM group leaders on how to handle this sensitive topic. Their suggestions offer an array of mechanisms hospitalists can use to battle fulfillment issues in their groups.

Learn to spot the signs of dissatisfaction.
Hospitalist group leaders say there are classic indicators that a hospitalist is not feeling fulfilled on the job.
“Usually, job performance falls off,” Dr. Scarpinato says. “People will have an attitude and you’ll say, ‘Where’d that come from?’ You’ll be surprised that they’re not pitching in to help with the team or they’re developing a cynical attitude or something like that. Those are the clues for me, as a leader.”
Martin Austin, MD, medical director of the 23-physician inpatient medical group at Gwinnett Medical Center in Lawrenceville, Ga., says he sometimes notices a recurring theme. “There are some people where it’s really a pattern,” he says. “Either they consistently complain about something, or other people in the hospital start complaining about them.”
—David Bowman, MD, executive director, Tucson, Ariz., region, IPC: The Hospitalist Company
David Bowman, MD, executive director of the Tucson, Ariz., region for IPC: The Hospitalist Company, says that if a physician isn’t fulfilled by the varied, interesting cases offered by working in a hospital, it just may not be the right fit.
“The cases that you’re admitting are the best of the best compared to outpatient medicine, where things are stable and it’s a chronic disease process,” he says. “You’re dealing with the most exciting clinical stuff that goes on in the hospital.
“You know, it’s a challenge for most physicians, and they’re glad they’re involved in that,” he adds. “If they’re not, if they’re fearful of that, they probably are not in hospital medicine very long.”

Be honest in your assessment of situations involving unfulfilled hospitalists.
Whether it stems from an annual evaluation or just a conversation with a hospitalist, when considering a case of dissatisfaction, decide whether it is really a situation that can be fixed. Sometimes, it’s not.
“You have to triage the person you’re talking to,” Dr. Austin says.
If the situation can be fixed, don’t judge the physician for their concerns; identify the problem and do whatever you can to fix it, Dr. Austin says.
“I think most people will warm up to you doing that—taking the emotion out of whatever the problem is—then trying to do something for them, if you can, and if it’s appropriate,” he explains.

Use annual evaluations to assess doctors’ ambitions beyond the clinic.
Just as important to assessment is the follow-up—checking back with hospitalists to see whether they’ve pursued new projects or committee work.
“When we sit down for our annual [performance evaluations] with the docs, we have those discussions,” says Christine Lum Lung, MD, SFHM, medical director of Northern Colorado Hospitalists, which was founded in 2004. “Where do you see yourself in five years? What can we do to help get you there?”
Many times, group leaders will discover that their hospitalists haven’t followed through on what they said they would do a year before. That affords group leaders a chance to motivate the hospitalist or steer them in another direction.
Flexible schedules are key to hospitalists pursuing a professional or academic ambition, as those interests take time. The annual evaluation is a good time to reassess a hospitalist’s schedule.

Develop a “committee rotation.”
Matching committee posts with physician experience levels helps promote professional involvement beyond routine patient care. If hospitalists receive assistance with a committee match, they are more likely to participate in committees and enjoy it when they do, says Dr. Lum Lung.
Committee participation and other activities help foster what she sees as a primary goal: a “culture of ownership within the group,” or the sense that each hospitalist has a role in guiding the organization and in the success of the whole team.
Dr. Bowman says that involvement in hospital affairs is critical to becoming a fulfilled hospitalist.
“Our mantra, if you will, is to be involved,” he says. “If you’re involved, you don’t have a chance to be bored.”
It’s important, Dr. Bowman adds, for doctors to see “the milieu that they’re involved with” in the hospital organization.


Foster a team atmosphere that offers flexibility and encourages doctors to fill in for one another when required.
Flexibility is a crucial part of keeping hospitalists happy, and many times is necessary for group retention, Dr. Lum Lung says.
“For some people, at this point, when their kids are getting to a certain age, it’s that they want to be able to have some time that is flexible where they can go to their kids’ soccer games and to softball games,” she says. “Providing them these opportunities will give them the longevity to do this job.”
Hospitalists are people, too, and they often deal with personal issues, such as a looming divorce or a seriously ill family member. Group leaders need to be tuned in to such situations so they can accommodate their colleagues as best as possible, Dr. Lum Lung says.

Be conscious of and willing to mitigate “mission creep.”
Sometimes, the growing list of responsibilities for hospitalists gets to be unwieldy. And, if necessary, group leaders should communicate to administration the need for changes that meet those demands.
A healthy working relationship between hospitalists and administration is crucial, says Steve Rubin, executive director at Gwinnett.
“I think it’s critical that administration recognizes value and works with your physicians—and hospitalists included—in a collaborative manner,” he says. “If people don’t feel valued or involved or engaged in decisions, then obviously they get disenfranchised.”

Hold frequent meetings and encourage free discourse.
A problem raised by one colleague could be solved by another colleague if brought up at a meeting. And group leaders can take the temperature of the group before issues become big problems.
At Gwinnett Medical Center, the hospitalist retention level is high, with just three physicians leaving the group since it was formed more than 12 years ago. The group holds mandatory monthly meetings that foster communication and allow potential problems to be aired before they become a big issue, says Dr. Austin. Such topics as relationships with subspecialists, acceptable consults, workloads, and staffing levels are discussed at these meetings.
“People have a good chance to really vent and hear how other people feel,” Dr. Austin says. “And you really take the pulse of the group.” He described the sessions as “a controlled period of time to gripe to each other and have everybody together to group problem-solve.”
At Gwinnett, gatherings outside the workplace—with families—also help build camaraderie.
Thomas R. Collins is a freelance writer in South Florida.
Reference
The conversation came as a surprise to Len Scarpinato, DO, MS, SFHM. The chief medical officer of clinical development for Brentwood, Tenn.-based Cogent-HMG had sensed something was bothering one of the community hospitalists at Aurora St. Luke’s Medical Center in Milwaukee. When Dr. Scarpinato approached him, the hospitalist told Dr. Scarpinato that he wanted to work as an academic hospitalist.
Dr. Scarpinato encouraged the clinician to try his hand at an academic center on his “off weeks.” The once-discouraged hospitalist stayed with Cogent-HMG, received leadership training, and now is an associate program medical director.
Whether group leaders across the country know it or not, there are hospitalists who are unfulfilled in their careers or dissatisfied with their work. Sometimes a group leader sees the problem coming; sometimes it manifests out of thin air.
A lack of fulfillment in a job can affect patient care. Experts say unhappy hospitalists are less likely to have good rapport with patients, less likely to communicate with the care team, and less likely to follow up on post-discharge lab results. It also hampers the efficacy of a company that frequently has to fill jobs vacated by dissatisfied physicians.
Job fulfillment is a feeling of satisfaction that is related to, but distinct from, burnout (the feeling of being overworked). And while burnout is a topic of widespread concern throughout HM, a lack of job fulfillment is equally important.
The Hospital Medicine Physician Worklife Survey administered in 2009 and 2010 found that 62.6% of the hospitalists who responded reported high satisfaction in their jobs.1 But according to the survey, there was lower satisfaction in terms of organization climate, autonomy, compensation, and availability of personal time.
HM groups should make it a priority to keep their clinicians involved in activities that keep them interested, says John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center, Bellevue, Wash., hospitalist practice management consultant, and columnist for The Hospitalist.
“You’ve got to do something besides taking care of patients,” Dr. Nelson says.
The Hospitalist asked group leaders and consultants how to spot signs of low job satisfaction, how they can keep their hospitalists fulfilled, and tips for other HM group leaders on how to handle this sensitive topic. Their suggestions offer an array of mechanisms hospitalists can use to battle fulfillment issues in their groups.
Learn to spot the signs of dissatisfaction.
Hospitalist group leaders say there are classic indicators that a hospitalist is not feeling fulfilled on the job.
“Usually, job performance falls off,” Dr. Scarpinato says. “People will have an attitude and you’ll say, ‘Where’d that come from?’ You’ll be surprised that they’re not pitching in to help with the team or they’re developing a cynical attitude or something like that. Those are the clues for me, as a leader.”
Martin Austin, MD, medical director of the 23-physician inpatient medical group at Gwinnett Medical Center in Lawrenceville, Ga., says he sometimes notices a recurring theme. “There are some people where it’s really a pattern,” he says. “Either they consistently complain about something, or other people in the hospital start complaining about them.”
—David Bowman, MD, executive director, Tucson, Ariz., region, IPC: The Hospitalist Company
David Bowman, MD, executive director of the Tucson, Ariz., region for IPC: The Hospitalist Company, says that if a physician isn’t fulfilled by the varied, interesting cases offered by working in a hospital, it just may not be the right fit.
“The cases that you’re admitting are the best of the best compared to outpatient medicine, where things are stable and it’s a chronic disease process,” he says. “You’re dealing with the most exciting clinical stuff that goes on in the hospital.
“You know, it’s a challenge for most physicians, and they’re glad they’re involved in that,” he adds. “If they’re not, if they’re fearful of that, they probably are not in hospital medicine very long.”
Be honest in your assessment of situations involving unfulfilled hospitalists.
Whether it stems from an annual evaluation or just a conversation with a hospitalist, when considering a case of dissatisfaction, decide whether it is really a situation that can be fixed. Sometimes, it’s not.
“You have to triage the person you’re talking to,” Dr. Austin says.
If the situation can be fixed, don’t judge the physician for their concerns; identify the problem and do whatever you can to fix it, Dr. Austin says.
“I think most people will warm up to you doing that—taking the emotion out of whatever the problem is—then trying to do something for them, if you can, and if it’s appropriate,” he explains.
Use annual evaluations to assess doctors’ ambitions beyond the clinic.
Just as important to assessment is the follow-up—checking back with hospitalists to see whether they’ve pursued new projects or committee work.
“When we sit down for our annual [performance evaluations] with the docs, we have those discussions,” says Christine Lum Lung, MD, SFHM, medical director of Northern Colorado Hospitalists, which was founded in 2004. “Where do you see yourself in five years? What can we do to help get you there?”
Many times, group leaders will discover that their hospitalists haven’t followed through on what they said they would do a year before. That affords group leaders a chance to motivate the hospitalist or steer them in another direction.
Flexible schedules are key to hospitalists pursuing a professional or academic ambition, as those interests take time. The annual evaluation is a good time to reassess a hospitalist’s schedule.
Develop a “committee rotation.”
Matching committee posts with physician experience levels helps promote professional involvement beyond routine patient care. If hospitalists receive assistance with a committee match, they are more likely to participate in committees and enjoy it when they do, says Dr. Lum Lung.
Committee participation and other activities help foster what she sees as a primary goal: a “culture of ownership within the group,” or the sense that each hospitalist has a role in guiding the organization and in the success of the whole team.
Dr. Bowman says that involvement in hospital affairs is critical to becoming a fulfilled hospitalist.
“Our mantra, if you will, is to be involved,” he says. “If you’re involved, you don’t have a chance to be bored.”
It’s important, Dr. Bowman adds, for doctors to see “the milieu that they’re involved with” in the hospital organization.
Foster a team atmosphere that offers flexibility and encourages doctors to fill in for one another when required.
Flexibility is a crucial part of keeping hospitalists happy, and many times is necessary for group retention, Dr. Lum Lung says.
“For some people, at this point, when their kids are getting to a certain age, it’s that they want to be able to have some time that is flexible where they can go to their kids’ soccer games and to softball games,” she says. “Providing them these opportunities will give them the longevity to do this job.”
Hospitalists are people, too, and they often deal with personal issues, such as a looming divorce or a seriously ill family member. Group leaders need to be tuned in to such situations so they can accommodate their colleagues as best as possible, Dr. Lum Lung says.
Be conscious of and willing to mitigate “mission creep.”
Sometimes, the growing list of responsibilities for hospitalists gets to be unwieldy. And, if necessary, group leaders should communicate to administration the need for changes that meet those demands.
A healthy working relationship between hospitalists and administration is crucial, says Steve Rubin, executive director at Gwinnett.
“I think it’s critical that administration recognizes value and works with your physicians—and hospitalists included—in a collaborative manner,” he says. “If people don’t feel valued or involved or engaged in decisions, then obviously they get disenfranchised.”
Hold frequent meetings and encourage free discourse.
A problem raised by one colleague could be solved by another colleague if brought up at a meeting. And group leaders can take the temperature of the group before issues become big problems.
At Gwinnett Medical Center, the hospitalist retention level is high, with just three physicians leaving the group since it was formed more than 12 years ago. The group holds mandatory monthly meetings that foster communication and allow potential problems to be aired before they become a big issue, says Dr. Austin. Such topics as relationships with subspecialists, acceptable consults, workloads, and staffing levels are discussed at these meetings.
“People have a good chance to really vent and hear how other people feel,” Dr. Austin says. “And you really take the pulse of the group.” He described the sessions as “a controlled period of time to gripe to each other and have everybody together to group problem-solve.”
At Gwinnett, gatherings outside the workplace—with families—also help build camaraderie.
Thomas R. Collins is a freelance writer in South Florida.
Reference
The conversation came as a surprise to Len Scarpinato, DO, MS, SFHM. The chief medical officer of clinical development for Brentwood, Tenn.-based Cogent-HMG had sensed something was bothering one of the community hospitalists at Aurora St. Luke’s Medical Center in Milwaukee. When Dr. Scarpinato approached him, the hospitalist told Dr. Scarpinato that he wanted to work as an academic hospitalist.
Dr. Scarpinato encouraged the clinician to try his hand at an academic center on his “off weeks.” The once-discouraged hospitalist stayed with Cogent-HMG, received leadership training, and now is an associate program medical director.
Whether group leaders across the country know it or not, there are hospitalists who are unfulfilled in their careers or dissatisfied with their work. Sometimes a group leader sees the problem coming; sometimes it manifests out of thin air.
A lack of fulfillment in a job can affect patient care. Experts say unhappy hospitalists are less likely to have good rapport with patients, less likely to communicate with the care team, and less likely to follow up on post-discharge lab results. It also hampers the efficacy of a company that frequently has to fill jobs vacated by dissatisfied physicians.
Job fulfillment is a feeling of satisfaction that is related to, but distinct from, burnout (the feeling of being overworked). And while burnout is a topic of widespread concern throughout HM, a lack of job fulfillment is equally important.
The Hospital Medicine Physician Worklife Survey administered in 2009 and 2010 found that 62.6% of the hospitalists who responded reported high satisfaction in their jobs.1 But according to the survey, there was lower satisfaction in terms of organization climate, autonomy, compensation, and availability of personal time.
HM groups should make it a priority to keep their clinicians involved in activities that keep them interested, says John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center, Bellevue, Wash., hospitalist practice management consultant, and columnist for The Hospitalist.
“You’ve got to do something besides taking care of patients,” Dr. Nelson says.
The Hospitalist asked group leaders and consultants how to spot signs of low job satisfaction, how they can keep their hospitalists fulfilled, and tips for other HM group leaders on how to handle this sensitive topic. Their suggestions offer an array of mechanisms hospitalists can use to battle fulfillment issues in their groups.
Learn to spot the signs of dissatisfaction.
Hospitalist group leaders say there are classic indicators that a hospitalist is not feeling fulfilled on the job.
“Usually, job performance falls off,” Dr. Scarpinato says. “People will have an attitude and you’ll say, ‘Where’d that come from?’ You’ll be surprised that they’re not pitching in to help with the team or they’re developing a cynical attitude or something like that. Those are the clues for me, as a leader.”
Martin Austin, MD, medical director of the 23-physician inpatient medical group at Gwinnett Medical Center in Lawrenceville, Ga., says he sometimes notices a recurring theme. “There are some people where it’s really a pattern,” he says. “Either they consistently complain about something, or other people in the hospital start complaining about them.”
—David Bowman, MD, executive director, Tucson, Ariz., region, IPC: The Hospitalist Company
David Bowman, MD, executive director of the Tucson, Ariz., region for IPC: The Hospitalist Company, says that if a physician isn’t fulfilled by the varied, interesting cases offered by working in a hospital, it just may not be the right fit.
“The cases that you’re admitting are the best of the best compared to outpatient medicine, where things are stable and it’s a chronic disease process,” he says. “You’re dealing with the most exciting clinical stuff that goes on in the hospital.
“You know, it’s a challenge for most physicians, and they’re glad they’re involved in that,” he adds. “If they’re not, if they’re fearful of that, they probably are not in hospital medicine very long.”
Be honest in your assessment of situations involving unfulfilled hospitalists.
Whether it stems from an annual evaluation or just a conversation with a hospitalist, when considering a case of dissatisfaction, decide whether it is really a situation that can be fixed. Sometimes, it’s not.
“You have to triage the person you’re talking to,” Dr. Austin says.
If the situation can be fixed, don’t judge the physician for their concerns; identify the problem and do whatever you can to fix it, Dr. Austin says.
“I think most people will warm up to you doing that—taking the emotion out of whatever the problem is—then trying to do something for them, if you can, and if it’s appropriate,” he explains.
Use annual evaluations to assess doctors’ ambitions beyond the clinic.
Just as important to assessment is the follow-up—checking back with hospitalists to see whether they’ve pursued new projects or committee work.
“When we sit down for our annual [performance evaluations] with the docs, we have those discussions,” says Christine Lum Lung, MD, SFHM, medical director of Northern Colorado Hospitalists, which was founded in 2004. “Where do you see yourself in five years? What can we do to help get you there?”
Many times, group leaders will discover that their hospitalists haven’t followed through on what they said they would do a year before. That affords group leaders a chance to motivate the hospitalist or steer them in another direction.
Flexible schedules are key to hospitalists pursuing a professional or academic ambition, as those interests take time. The annual evaluation is a good time to reassess a hospitalist’s schedule.
Develop a “committee rotation.”
Matching committee posts with physician experience levels helps promote professional involvement beyond routine patient care. If hospitalists receive assistance with a committee match, they are more likely to participate in committees and enjoy it when they do, says Dr. Lum Lung.
Committee participation and other activities help foster what she sees as a primary goal: a “culture of ownership within the group,” or the sense that each hospitalist has a role in guiding the organization and in the success of the whole team.
Dr. Bowman says that involvement in hospital affairs is critical to becoming a fulfilled hospitalist.
“Our mantra, if you will, is to be involved,” he says. “If you’re involved, you don’t have a chance to be bored.”
It’s important, Dr. Bowman adds, for doctors to see “the milieu that they’re involved with” in the hospital organization.
Foster a team atmosphere that offers flexibility and encourages doctors to fill in for one another when required.
Flexibility is a crucial part of keeping hospitalists happy, and many times is necessary for group retention, Dr. Lum Lung says.
“For some people, at this point, when their kids are getting to a certain age, it’s that they want to be able to have some time that is flexible where they can go to their kids’ soccer games and to softball games,” she says. “Providing them these opportunities will give them the longevity to do this job.”
Hospitalists are people, too, and they often deal with personal issues, such as a looming divorce or a seriously ill family member. Group leaders need to be tuned in to such situations so they can accommodate their colleagues as best as possible, Dr. Lum Lung says.
Be conscious of and willing to mitigate “mission creep.”
Sometimes, the growing list of responsibilities for hospitalists gets to be unwieldy. And, if necessary, group leaders should communicate to administration the need for changes that meet those demands.
A healthy working relationship between hospitalists and administration is crucial, says Steve Rubin, executive director at Gwinnett.
“I think it’s critical that administration recognizes value and works with your physicians—and hospitalists included—in a collaborative manner,” he says. “If people don’t feel valued or involved or engaged in decisions, then obviously they get disenfranchised.”
Hold frequent meetings and encourage free discourse.
A problem raised by one colleague could be solved by another colleague if brought up at a meeting. And group leaders can take the temperature of the group before issues become big problems.
At Gwinnett Medical Center, the hospitalist retention level is high, with just three physicians leaving the group since it was formed more than 12 years ago. The group holds mandatory monthly meetings that foster communication and allow potential problems to be aired before they become a big issue, says Dr. Austin. Such topics as relationships with subspecialists, acceptable consults, workloads, and staffing levels are discussed at these meetings.
“People have a good chance to really vent and hear how other people feel,” Dr. Austin says. “And you really take the pulse of the group.” He described the sessions as “a controlled period of time to gripe to each other and have everybody together to group problem-solve.”
At Gwinnett, gatherings outside the workplace—with families—also help build camaraderie.
Thomas R. Collins is a freelance writer in South Florida.
Reference
ITL: Physician Reviews of HM-Relevant Research
In This Edition
Literature At A Glance
A guide to this month’s studies
- Warfarin vs. aspirin in heart-failure patients
- Aspirin after anticoagulation prevents VTE recurrence
- Novel oral anticoagulants vs. warfarin in afib patients
- Intravenous metronidazole for mild C. diff infection
- Frequency of Foley catheter complications vs. CAUTI
- Intensive hyperglycemia control in noncritical hospitalized patients
- Risk score predicts 30-day mortality after noncardiac surgery
- Temperature, white blood cell count are not sensitive predictors of bacteremia
Warfarin Reduces Stoke but Increases Hemorrhage Compared with Aspirin in Patients with Heart Failure and Sinus Rhythm
Clinical question: Is warfarin superior to aspirin with regard to clinical outcomes in patients with heart failure who are in sinus rhythm?
Background: Heart failure is associated with stroke and death potentially caused by atherothrombotic events. Anticoagulation is efficacious in some heart failure patients with atrial fibrillation or significant valvular disease, but the role of anticoagulation versus aspirin in patients with chronic heart failure and sinus rhythm is unclear.
Study design: Double-blind randomized controlled trial.
Setting: Multicenter, multinational trial involving outpatients.
Synopsis: This double-blind, double-dummy trial involving 2,305 patients with sinus rhythm and reduced left ventricular ejection fraction (<35%) showed no significant difference in the primary combined outcome (ischemic stroke, intracerebral hemorrhage, or death) in those treated with warfarin as compared with aspirin. Warfarin did significantly reduce the rate of ischemic stroke by 0.64 events per 100 patient-years (absolute risk reduction 2.2%, number needed to treat 45) when compared with aspirin, with no significant difference in the rate of intracerebral hemorrhage. This outcome was offset by an increased rate of major hemorrhage by 0.91 events per 100 patient-years (absolute risk increase 3.1%, number needed to harm 32).
This study included patients from all functional classes of heart failure, with a protocol to initiate treatment with other standard heart failure medications. Patients with an indication for either warfarin or aspirin were excluded. Due to recruitment difficulties, the power of this study was reduced. Other study limitations included a relatively low percentage of time that patients on warfarin were in therapeutic range and a substantial period of follow-up time in which patients did not receive the assigned study treatments.
Bottom line: The benefit of reduced stoke in patients with heart failure and sinus rhythm who take warfarin over aspirin is counteracted by an increased risk for serious bleeding outcomes.
Citation: Homma S, Thompson JLP, Pullicino PM, et al. Warfarin and aspirin in patients with heart failure and sinus rhythm. N Engl J Med. 2012;366(20):1859-1869.
Aspirin Use after Recommended Anticoagulation Treatment Prevents Recurrence in VTE Patients
Clinical question: Does aspirin prevent recurrence in patients after treatment with anticoagulation following their first episode of unprovoked VTE?
Background: VTE recurrence is common following the discontinuation of anticoagulation, particularly in patients with a history of unprovoked pulmonary embolism (PE) or DVT. Extension of treatment with vitamin K antagonists decreases recurrence but also causes more bleeding. The role of aspirin in the secondary prevention of VTE is unknown.
Study design: Double-blind randomized controlled trial.
Setting: Multicenter international trial involving outpatients.
Synopsis: This trial compared treatment with aspirin versus placebo for approximately two years in 205 patients with a history of unprovoked VTE who had completed six to 18 months of anticoagulant therapy. The relative risk reduction of recurrent VTE in the aspirin versus the placebo group was approximately 40% per year (6.6% vs. 11.2% per year; absolute risk reduction 4.6% per year; number needed to treat 22). No difference in major or clinically relevant bleeding was observed between the two groups.
This study was appropriately powered to detect the treatment effect reported by the authors. Typically, anticoagulation is discontinued in this specific patient population once the risk of bleeding and/or the patient’s perceived inconvenience of therapy outweighs the expected benefit from continuing treatment to prevent VTE recurrence. Study results suggest aspirin is effective in preventing recurrence while not conferring an increased risk for hemorrhage. It is important to note that patients with cancer and symptomatic atherosclerosis were excluded from this study.
Bottom line: Following an appropriate treatment period with standard anticoagulation, aspirin appears to be a safe and effective therapy in the secondary prevention of recurrence in patients with a history of unprovoked VTE.
Citation: Becattini C, Agnelli G, Schenone A, et al. Aspirin for preventing recurrence of venous thromboembolism. N Engl J Med. 2012;366(21):1959-1967.
Meta-Analysis Supports New Oral Anticoagulants in Patients with Atrial Fibrillation
Clinical question: Are novel oral anticoagulants both efficacious and safe in comparison to warfarin in patients with atrial fibrillation (afib)?
Background: Three large clinical trials recently evaluated novel oral anticoagulants (dabigatran, rivaroxaban, and apixaban) as alternatives to warfarin in afib patients. Although the anticoagulants all appeared efficacious for primary outcomes, results regarding secondary and safety outcomes were either inconclusive or heterogeneous.
Study design: Systematic review and meta-analysis of randomized controlled trials.
Setting: Three diverse, clinical-trial settings.
Synopsis: A systematic review and meta-analysis of randomized controlled trials comparing novel oral anticoagulants to warfarin in afib patients found three large studies examining dabigatran, rivaroxaban, and apixaban that included 44,563 patients.
Using random-effects models to pool data from these studies, the authors found a 22% relative risk (RR) reduction of stroke or systemic embolism with the use of these new anticoagulants as compared to warfarin. The risks for ischemic and unidentified stroke (RR 0.87), hemorrhagic stroke (RR 0.45), intracranial bleeding (RR 0.49), and mortality (RR 0.88) were significantly reduced in patients taking these new anticoagulants. There was no significant reduction in major bleeding.
A trend in favor of warfarin was seen for gastrointestinal bleeding, but this trend was not statistically significant (RR 1.25; 95% confidence interval, 0.91-1.72).
This meta-analysis was limited to only three randomized controlled trials, each comparing a different oral anticoagulant to warfarin and using somewhat heterogeneous study designs and patient populations.
Bottom line: Three new oral anticoagulants appear safe and more efficacious than warfarin in the prevention of stroke and systemic embolism, as well as other important clinical outcomes in patients with atrial fibrillation.
Citation: Miller CS, Grandi SM, Shimony A, Filion KB, Eisenberg MJ. Meta-analysis of efficacy and safety of new oral anticoagulants (dabigatran, rivaroxaban, apixaban) versus warfarin in patients with atrial fibrillation. Am J Cardiol. 2012;110(3):453-60.
Observational Study Suggests Intravenous Metronidazole May Be Inferior for Mild Clostridium Difficile Infection
Clinical question: How do different treatment regimens (oral metronidazole vs. intravenous metronidazole vs. oral vancomycin) for mild Clostridium difficile infection (CDI) compare with regard to clinical outcomes?
Background: CDIs are increasing. Oral metronidazole or vancomycin can be used for the initial treatment of non-severe CDI. Additionally, a paucity of clinical data exists on intravenous metronidazole, which is used in some cases, typically in combination with vancomycin and in patients with severe CDI.
Study design: Prospective cohort study.
Setting: International hospital-based study.
Synopsis: This observational study assessed three different regimens (oral metronidazole, intravenous metronidazole, and oral vancomycin) for the treatment of mild CDI in 265 inpatients. Mortality at 30 days was higher in the intravenous metronidazole group (38.1%) than in the oral metronidazole (7.4%) and vancomycin (9.5%) groups. Patients receiving intravenous metronidazole also were less likely to recover from disease (52.4% versus >80% in the oral metronidazole and vancomycin groups). No statistically significant differences for other sequelae of CDI were found, except for higher risk of dehydration in the oral vancomycin group.
After controlling for age, sex, and comorbidity severity, patients in the intravenous metronidazole group were approximately four times more likely to die than patients in either the oral vancomycin group or the oral metronidazole group. There was no significant difference in mortality between the oral metronidazole and vancomycin groups.
Although this study was limited by its observational nature, no randomized controlled trial has yet to compare these three treatment regimens for mild CDI.
Bottom line: Treatment of mild C. diff infection with intravenous metronidazole appears to be associated with higher mortality and lower disease resolution than treatment with either oral metronidazole or vancomycin.
Citation: Wenisch JM, Schmid D, Kuo HW, et al. Prospective observational study comparing three different treatment regimes in patients with Clostridium difficile infection. Antimicrob Agents Chemother. 2012;56(4):1974-1978.
Traumatic Foley Catheter Complications Occur with Similar Frequency as Catheter-Associated Urinary Tract Infections
Clinical question: How does the frequency and clinical significance of urinary tract infection (UTI) compare to genitourinary trauma when associated with Foley catheterization?
Background: Foley catheter use in hospitalized patients is common and carries many associated risks. Although the risk of UTI when using catheters often is recognized, providers should consider other important complications of catheter use, such as genitourinary trauma.
Study design: Descriptive, prospective cohort study.
Setting: Single-center study in a Veterans Affairs hospital.
Synopsis: This surveillance study of 6,513 Foley catheter days compared the incidence of catheter-associated urinary tract infections (CAUTIs) to that of genitourinary trauma. Traumatic Foley events included gross hematuria, creation of false passage, ridging causing pain and/or difficulties with catheter removal, external genital trauma, catheter misplacement (ranging from prostatic to intraperitoneal), and catheter removal with the balloon inflated.
The incidence of possible UTI episodes was 1.8% of the Foley catheter days compared with 1.5% for catheter-associated trauma. Despite the fact that 72% of the UTI cases were asymptomatic, approximately 41% of these cases were treated with antibiotics, which accounted for 70% of all UTIs treated. Of the cases of Foley catheter trauma, 32% required further interventions (i.e. prolonged catheterization or cystoscopy). Trauma prompting intervention was as common as symptomatic UTIs.
The observational study design, use of a single center with a predominantly male population, and inclusion of patients undergoing urologic procedures who might have had valid indications for treatment of asymptomatic bacteriuria limit the study findings.
Bottom line: The complication of catheter-associated genitourinary trauma is just as common as CAUTIs in hospitalized patients, with each necessitating further intervention and treatment at similar rates.
Citation: Leuck AM, Wright D, Ellingson L, et al. Complications of Foley catheters—is infection the greatest risk? J Urol. 2012;187(5):1662-1666.
Intensive Control of Hyperglycemia in Noncritical, Hospitalized Patients Decreases Infection Risk, but No Significant Effect on Other Outcomes
Clinical question: What is the effect of tight glucose control in patients hospitalized in noncritical-care settings?
Background: Hyperglycemia is associated with increased in-hospital mortality and morbidity. Several trials have demonstrated the potential benefits of intensive glycemic control for patients in intensive-care settings, but this could lead to increased hypoglycemia. The effect of intensive therapy to achieve tight glycemic control in noncritically ill patients is unclear.
Study design: Systematic review and meta-analysis.
Setting: Various study sites of hospitalized patients.
Synopsis: This meta-analysis included 19 studies (nine randomized, 10 observational) published from 1995 to 2011. Intensive glycemic control (fasting blood glucose of 100-180 mg/dL) was not associated with significant effect on risk of death, myocardial infarction (MI), or stroke. There was a nonsignificant trend for increased risk of hypoglycemia (relative risk, 1.58; 95% CI, 0.97-2.57).
Intensive glycemic control was associated with a decreased risk of infection (relative risk, 0.41; 95% CI, 0.21–0.77), but this association mainly was derived from studies in surgical settings.
Subgroup analyses demonstrated an association between achieving intensive glycemic goals and an increased risk of hypoglycemia (P=0.01). Hypoglycemia also more commonly occurred in surgical patients.
There was substantial heterogeneity across studies included for all outcomes except infection. The quality of the current evidence supporting a reduction in infection is low and appears mostly derived from patients in surgical settings. The quality of evidence relating to all the other outcomes is also low and is limited by heterogeneity and imprecision.
Bottom line: Intensive control of hyperglycemia in noncritically ill hospitalized patients might reduce the risk of infection in some patients but does not appear to be significantly associated with improvement in other important clinical outcomes.
Citation: Murad MH, Coburn JA, Coto-Yglesias F, et al. Glycemic control in non-critically ill hospitalized patients: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2012;97(1):49-58.
Simple Risk Score Predicts 30-Day Mortality after Noncardiac Surgery
Clinical question: Can 30-day mortality risk after noncardiac surgery be predicted by using a simple bedside-risk index?
Background: While indices exist to quantify the risk of cardiac complications in patients undergoing noncardiac surgery, there is significant perioperative mortality due to noncardiac causes. Therefore, a need exists for a simple risk index to predict all-cause mortality after noncardiac surgery.
Study design: Retrospective cohort study.
Setting: American College of Surgeons National Surgical Quality Improvement Program database of patients in more than 200 hospitals.
Synopsis: The nine-point Surgical Mortality Probability Model (S-MPM) 30-day mortality risk index was empirically created and applied to a randomly split portion of a database, which included 298,772 patients undergoing noncardiac surgery. Three risk factors were included: American Society of Anesthesiologists (ASA) physical status, surgery risk class, and emergency status. Patients with ASA physical status I, II, III, IV, or V were assigned zero, two, four, five, or six points, respectively. Patients undergoing intermediate- or high-risk procedures were assigned one or two points, respectively. Patients undergoing emergency procedures were assigned one point. The S-MPM then was applied to the validation portion of the data set.
The 30-day predicted risk of mortality was less than 0.50% for those patients with combined risk scores of less than five (S-MPM Class I), between 1.5% and 4.0% for risk scores of five to six (Class II), and more than 10% for risk scores greater than six (Class III).
The major limitation of this derived risk score is the reliance on ASA physical status, which has imprecise definitions and might lead to inconsistent ratings.
Bottom line: The S-MPM risk index is a simple bedside scoring system, which can accurately predict 30-day mortality in patients undergoing noncardiac surgery.
Citation: Glance LG, Lustik SJ, Hannan EL, et al. The Surgical Mortality Probability Model: Derivation and validation of a simple risk prediction rule for noncardiac surgery. Ann Surg. 2012;255(4):696-702.
Temperature, White Blood Cell Count Are Not Sensitive Predictors of Bacteremia
Clinical question: In ED patients with suspected infection, are temperature, white blood cell (WBC) count, and bandemia reliable predictors of bacteremia?
Background: Sepsis is a significant cause of morbidity and mortality. Early identification and treatment of sepsis improves patient outcomes. Although systemic inflammatory response syndrome criteria aids in the prompt recognition of sepsis, these markers have variable sensitivity and specificity for true infection or bacteremia, which places patients at high risk for sepsis.
Study design: Post-hoc data analysis of a prospective cohort study.
Setting: ED patients at a single tertiary-care center.
Synopsis: A retrospective analysis was performed on 3,563 patients who presented to the ED. Blood cultures obtained on patients with suspected infection revealed bacteremia in 289 patients (8.1%). Patients with bacteremia were reviewed for the presence of normal temperature (36.1° to 38° Celsius), normal WBC count (4,000 to 12,000 cells per µL), and presence of bandemia (>5% of WBC differential).
Among patients with bacteremia, 33% had a normal body temperature (67% sensitivity) and 52% had a normal WBC count (48% sensitivity). Of the 210 bacteremic patients who had a full differential performed, bandemia was present in 82% (sensitivity 82%). Bandemia was present in 80% of culture-positive patients with a normal temperature and 79% of culture-positive patients with a normal WBC count. Approximately 17% of patients with bacteremia had neither an abnormal temperature nor an abnormal WBC. This study was limited by the retrospective nature of analysis and the subjective designation of “suspected infection” by the original providers.
Bottom line: In patients presenting to the ED with suspected infection who are found to have culture-proven bacteremia, a significant percentage have normal temperature and WBC count, but the presence of bandemia could be more useful for identifying occult bacteremia.
Citation: Seigel TA, Cocchi MN, Salciccioli J, et al. Inadequacy of temperature and white blood cell count in predicting bacteremia in patients with suspected infection. J Emerg Med. 2012;42(3):254-259.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Warfarin vs. aspirin in heart-failure patients
- Aspirin after anticoagulation prevents VTE recurrence
- Novel oral anticoagulants vs. warfarin in afib patients
- Intravenous metronidazole for mild C. diff infection
- Frequency of Foley catheter complications vs. CAUTI
- Intensive hyperglycemia control in noncritical hospitalized patients
- Risk score predicts 30-day mortality after noncardiac surgery
- Temperature, white blood cell count are not sensitive predictors of bacteremia
Warfarin Reduces Stoke but Increases Hemorrhage Compared with Aspirin in Patients with Heart Failure and Sinus Rhythm
Clinical question: Is warfarin superior to aspirin with regard to clinical outcomes in patients with heart failure who are in sinus rhythm?
Background: Heart failure is associated with stroke and death potentially caused by atherothrombotic events. Anticoagulation is efficacious in some heart failure patients with atrial fibrillation or significant valvular disease, but the role of anticoagulation versus aspirin in patients with chronic heart failure and sinus rhythm is unclear.
Study design: Double-blind randomized controlled trial.
Setting: Multicenter, multinational trial involving outpatients.
Synopsis: This double-blind, double-dummy trial involving 2,305 patients with sinus rhythm and reduced left ventricular ejection fraction (<35%) showed no significant difference in the primary combined outcome (ischemic stroke, intracerebral hemorrhage, or death) in those treated with warfarin as compared with aspirin. Warfarin did significantly reduce the rate of ischemic stroke by 0.64 events per 100 patient-years (absolute risk reduction 2.2%, number needed to treat 45) when compared with aspirin, with no significant difference in the rate of intracerebral hemorrhage. This outcome was offset by an increased rate of major hemorrhage by 0.91 events per 100 patient-years (absolute risk increase 3.1%, number needed to harm 32).
This study included patients from all functional classes of heart failure, with a protocol to initiate treatment with other standard heart failure medications. Patients with an indication for either warfarin or aspirin were excluded. Due to recruitment difficulties, the power of this study was reduced. Other study limitations included a relatively low percentage of time that patients on warfarin were in therapeutic range and a substantial period of follow-up time in which patients did not receive the assigned study treatments.
Bottom line: The benefit of reduced stoke in patients with heart failure and sinus rhythm who take warfarin over aspirin is counteracted by an increased risk for serious bleeding outcomes.
Citation: Homma S, Thompson JLP, Pullicino PM, et al. Warfarin and aspirin in patients with heart failure and sinus rhythm. N Engl J Med. 2012;366(20):1859-1869.
Aspirin Use after Recommended Anticoagulation Treatment Prevents Recurrence in VTE Patients
Clinical question: Does aspirin prevent recurrence in patients after treatment with anticoagulation following their first episode of unprovoked VTE?
Background: VTE recurrence is common following the discontinuation of anticoagulation, particularly in patients with a history of unprovoked pulmonary embolism (PE) or DVT. Extension of treatment with vitamin K antagonists decreases recurrence but also causes more bleeding. The role of aspirin in the secondary prevention of VTE is unknown.
Study design: Double-blind randomized controlled trial.
Setting: Multicenter international trial involving outpatients.
Synopsis: This trial compared treatment with aspirin versus placebo for approximately two years in 205 patients with a history of unprovoked VTE who had completed six to 18 months of anticoagulant therapy. The relative risk reduction of recurrent VTE in the aspirin versus the placebo group was approximately 40% per year (6.6% vs. 11.2% per year; absolute risk reduction 4.6% per year; number needed to treat 22). No difference in major or clinically relevant bleeding was observed between the two groups.
This study was appropriately powered to detect the treatment effect reported by the authors. Typically, anticoagulation is discontinued in this specific patient population once the risk of bleeding and/or the patient’s perceived inconvenience of therapy outweighs the expected benefit from continuing treatment to prevent VTE recurrence. Study results suggest aspirin is effective in preventing recurrence while not conferring an increased risk for hemorrhage. It is important to note that patients with cancer and symptomatic atherosclerosis were excluded from this study.
Bottom line: Following an appropriate treatment period with standard anticoagulation, aspirin appears to be a safe and effective therapy in the secondary prevention of recurrence in patients with a history of unprovoked VTE.
Citation: Becattini C, Agnelli G, Schenone A, et al. Aspirin for preventing recurrence of venous thromboembolism. N Engl J Med. 2012;366(21):1959-1967.
Meta-Analysis Supports New Oral Anticoagulants in Patients with Atrial Fibrillation
Clinical question: Are novel oral anticoagulants both efficacious and safe in comparison to warfarin in patients with atrial fibrillation (afib)?
Background: Three large clinical trials recently evaluated novel oral anticoagulants (dabigatran, rivaroxaban, and apixaban) as alternatives to warfarin in afib patients. Although the anticoagulants all appeared efficacious for primary outcomes, results regarding secondary and safety outcomes were either inconclusive or heterogeneous.
Study design: Systematic review and meta-analysis of randomized controlled trials.
Setting: Three diverse, clinical-trial settings.
Synopsis: A systematic review and meta-analysis of randomized controlled trials comparing novel oral anticoagulants to warfarin in afib patients found three large studies examining dabigatran, rivaroxaban, and apixaban that included 44,563 patients.
Using random-effects models to pool data from these studies, the authors found a 22% relative risk (RR) reduction of stroke or systemic embolism with the use of these new anticoagulants as compared to warfarin. The risks for ischemic and unidentified stroke (RR 0.87), hemorrhagic stroke (RR 0.45), intracranial bleeding (RR 0.49), and mortality (RR 0.88) were significantly reduced in patients taking these new anticoagulants. There was no significant reduction in major bleeding.
A trend in favor of warfarin was seen for gastrointestinal bleeding, but this trend was not statistically significant (RR 1.25; 95% confidence interval, 0.91-1.72).
This meta-analysis was limited to only three randomized controlled trials, each comparing a different oral anticoagulant to warfarin and using somewhat heterogeneous study designs and patient populations.
Bottom line: Three new oral anticoagulants appear safe and more efficacious than warfarin in the prevention of stroke and systemic embolism, as well as other important clinical outcomes in patients with atrial fibrillation.
Citation: Miller CS, Grandi SM, Shimony A, Filion KB, Eisenberg MJ. Meta-analysis of efficacy and safety of new oral anticoagulants (dabigatran, rivaroxaban, apixaban) versus warfarin in patients with atrial fibrillation. Am J Cardiol. 2012;110(3):453-60.
Observational Study Suggests Intravenous Metronidazole May Be Inferior for Mild Clostridium Difficile Infection
Clinical question: How do different treatment regimens (oral metronidazole vs. intravenous metronidazole vs. oral vancomycin) for mild Clostridium difficile infection (CDI) compare with regard to clinical outcomes?
Background: CDIs are increasing. Oral metronidazole or vancomycin can be used for the initial treatment of non-severe CDI. Additionally, a paucity of clinical data exists on intravenous metronidazole, which is used in some cases, typically in combination with vancomycin and in patients with severe CDI.
Study design: Prospective cohort study.
Setting: International hospital-based study.
Synopsis: This observational study assessed three different regimens (oral metronidazole, intravenous metronidazole, and oral vancomycin) for the treatment of mild CDI in 265 inpatients. Mortality at 30 days was higher in the intravenous metronidazole group (38.1%) than in the oral metronidazole (7.4%) and vancomycin (9.5%) groups. Patients receiving intravenous metronidazole also were less likely to recover from disease (52.4% versus >80% in the oral metronidazole and vancomycin groups). No statistically significant differences for other sequelae of CDI were found, except for higher risk of dehydration in the oral vancomycin group.
After controlling for age, sex, and comorbidity severity, patients in the intravenous metronidazole group were approximately four times more likely to die than patients in either the oral vancomycin group or the oral metronidazole group. There was no significant difference in mortality between the oral metronidazole and vancomycin groups.
Although this study was limited by its observational nature, no randomized controlled trial has yet to compare these three treatment regimens for mild CDI.
Bottom line: Treatment of mild C. diff infection with intravenous metronidazole appears to be associated with higher mortality and lower disease resolution than treatment with either oral metronidazole or vancomycin.
Citation: Wenisch JM, Schmid D, Kuo HW, et al. Prospective observational study comparing three different treatment regimes in patients with Clostridium difficile infection. Antimicrob Agents Chemother. 2012;56(4):1974-1978.
Traumatic Foley Catheter Complications Occur with Similar Frequency as Catheter-Associated Urinary Tract Infections
Clinical question: How does the frequency and clinical significance of urinary tract infection (UTI) compare to genitourinary trauma when associated with Foley catheterization?
Background: Foley catheter use in hospitalized patients is common and carries many associated risks. Although the risk of UTI when using catheters often is recognized, providers should consider other important complications of catheter use, such as genitourinary trauma.
Study design: Descriptive, prospective cohort study.
Setting: Single-center study in a Veterans Affairs hospital.
Synopsis: This surveillance study of 6,513 Foley catheter days compared the incidence of catheter-associated urinary tract infections (CAUTIs) to that of genitourinary trauma. Traumatic Foley events included gross hematuria, creation of false passage, ridging causing pain and/or difficulties with catheter removal, external genital trauma, catheter misplacement (ranging from prostatic to intraperitoneal), and catheter removal with the balloon inflated.
The incidence of possible UTI episodes was 1.8% of the Foley catheter days compared with 1.5% for catheter-associated trauma. Despite the fact that 72% of the UTI cases were asymptomatic, approximately 41% of these cases were treated with antibiotics, which accounted for 70% of all UTIs treated. Of the cases of Foley catheter trauma, 32% required further interventions (i.e. prolonged catheterization or cystoscopy). Trauma prompting intervention was as common as symptomatic UTIs.
The observational study design, use of a single center with a predominantly male population, and inclusion of patients undergoing urologic procedures who might have had valid indications for treatment of asymptomatic bacteriuria limit the study findings.
Bottom line: The complication of catheter-associated genitourinary trauma is just as common as CAUTIs in hospitalized patients, with each necessitating further intervention and treatment at similar rates.
Citation: Leuck AM, Wright D, Ellingson L, et al. Complications of Foley catheters—is infection the greatest risk? J Urol. 2012;187(5):1662-1666.
Intensive Control of Hyperglycemia in Noncritical, Hospitalized Patients Decreases Infection Risk, but No Significant Effect on Other Outcomes
Clinical question: What is the effect of tight glucose control in patients hospitalized in noncritical-care settings?
Background: Hyperglycemia is associated with increased in-hospital mortality and morbidity. Several trials have demonstrated the potential benefits of intensive glycemic control for patients in intensive-care settings, but this could lead to increased hypoglycemia. The effect of intensive therapy to achieve tight glycemic control in noncritically ill patients is unclear.
Study design: Systematic review and meta-analysis.
Setting: Various study sites of hospitalized patients.
Synopsis: This meta-analysis included 19 studies (nine randomized, 10 observational) published from 1995 to 2011. Intensive glycemic control (fasting blood glucose of 100-180 mg/dL) was not associated with significant effect on risk of death, myocardial infarction (MI), or stroke. There was a nonsignificant trend for increased risk of hypoglycemia (relative risk, 1.58; 95% CI, 0.97-2.57).
Intensive glycemic control was associated with a decreased risk of infection (relative risk, 0.41; 95% CI, 0.21–0.77), but this association mainly was derived from studies in surgical settings.
Subgroup analyses demonstrated an association between achieving intensive glycemic goals and an increased risk of hypoglycemia (P=0.01). Hypoglycemia also more commonly occurred in surgical patients.
There was substantial heterogeneity across studies included for all outcomes except infection. The quality of the current evidence supporting a reduction in infection is low and appears mostly derived from patients in surgical settings. The quality of evidence relating to all the other outcomes is also low and is limited by heterogeneity and imprecision.
Bottom line: Intensive control of hyperglycemia in noncritically ill hospitalized patients might reduce the risk of infection in some patients but does not appear to be significantly associated with improvement in other important clinical outcomes.
Citation: Murad MH, Coburn JA, Coto-Yglesias F, et al. Glycemic control in non-critically ill hospitalized patients: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2012;97(1):49-58.
Simple Risk Score Predicts 30-Day Mortality after Noncardiac Surgery
Clinical question: Can 30-day mortality risk after noncardiac surgery be predicted by using a simple bedside-risk index?
Background: While indices exist to quantify the risk of cardiac complications in patients undergoing noncardiac surgery, there is significant perioperative mortality due to noncardiac causes. Therefore, a need exists for a simple risk index to predict all-cause mortality after noncardiac surgery.
Study design: Retrospective cohort study.
Setting: American College of Surgeons National Surgical Quality Improvement Program database of patients in more than 200 hospitals.
Synopsis: The nine-point Surgical Mortality Probability Model (S-MPM) 30-day mortality risk index was empirically created and applied to a randomly split portion of a database, which included 298,772 patients undergoing noncardiac surgery. Three risk factors were included: American Society of Anesthesiologists (ASA) physical status, surgery risk class, and emergency status. Patients with ASA physical status I, II, III, IV, or V were assigned zero, two, four, five, or six points, respectively. Patients undergoing intermediate- or high-risk procedures were assigned one or two points, respectively. Patients undergoing emergency procedures were assigned one point. The S-MPM then was applied to the validation portion of the data set.
The 30-day predicted risk of mortality was less than 0.50% for those patients with combined risk scores of less than five (S-MPM Class I), between 1.5% and 4.0% for risk scores of five to six (Class II), and more than 10% for risk scores greater than six (Class III).
The major limitation of this derived risk score is the reliance on ASA physical status, which has imprecise definitions and might lead to inconsistent ratings.
Bottom line: The S-MPM risk index is a simple bedside scoring system, which can accurately predict 30-day mortality in patients undergoing noncardiac surgery.
Citation: Glance LG, Lustik SJ, Hannan EL, et al. The Surgical Mortality Probability Model: Derivation and validation of a simple risk prediction rule for noncardiac surgery. Ann Surg. 2012;255(4):696-702.
Temperature, White Blood Cell Count Are Not Sensitive Predictors of Bacteremia
Clinical question: In ED patients with suspected infection, are temperature, white blood cell (WBC) count, and bandemia reliable predictors of bacteremia?
Background: Sepsis is a significant cause of morbidity and mortality. Early identification and treatment of sepsis improves patient outcomes. Although systemic inflammatory response syndrome criteria aids in the prompt recognition of sepsis, these markers have variable sensitivity and specificity for true infection or bacteremia, which places patients at high risk for sepsis.
Study design: Post-hoc data analysis of a prospective cohort study.
Setting: ED patients at a single tertiary-care center.
Synopsis: A retrospective analysis was performed on 3,563 patients who presented to the ED. Blood cultures obtained on patients with suspected infection revealed bacteremia in 289 patients (8.1%). Patients with bacteremia were reviewed for the presence of normal temperature (36.1° to 38° Celsius), normal WBC count (4,000 to 12,000 cells per µL), and presence of bandemia (>5% of WBC differential).
Among patients with bacteremia, 33% had a normal body temperature (67% sensitivity) and 52% had a normal WBC count (48% sensitivity). Of the 210 bacteremic patients who had a full differential performed, bandemia was present in 82% (sensitivity 82%). Bandemia was present in 80% of culture-positive patients with a normal temperature and 79% of culture-positive patients with a normal WBC count. Approximately 17% of patients with bacteremia had neither an abnormal temperature nor an abnormal WBC. This study was limited by the retrospective nature of analysis and the subjective designation of “suspected infection” by the original providers.
Bottom line: In patients presenting to the ED with suspected infection who are found to have culture-proven bacteremia, a significant percentage have normal temperature and WBC count, but the presence of bandemia could be more useful for identifying occult bacteremia.
Citation: Seigel TA, Cocchi MN, Salciccioli J, et al. Inadequacy of temperature and white blood cell count in predicting bacteremia in patients with suspected infection. J Emerg Med. 2012;42(3):254-259.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Warfarin vs. aspirin in heart-failure patients
- Aspirin after anticoagulation prevents VTE recurrence
- Novel oral anticoagulants vs. warfarin in afib patients
- Intravenous metronidazole for mild C. diff infection
- Frequency of Foley catheter complications vs. CAUTI
- Intensive hyperglycemia control in noncritical hospitalized patients
- Risk score predicts 30-day mortality after noncardiac surgery
- Temperature, white blood cell count are not sensitive predictors of bacteremia
Warfarin Reduces Stoke but Increases Hemorrhage Compared with Aspirin in Patients with Heart Failure and Sinus Rhythm
Clinical question: Is warfarin superior to aspirin with regard to clinical outcomes in patients with heart failure who are in sinus rhythm?
Background: Heart failure is associated with stroke and death potentially caused by atherothrombotic events. Anticoagulation is efficacious in some heart failure patients with atrial fibrillation or significant valvular disease, but the role of anticoagulation versus aspirin in patients with chronic heart failure and sinus rhythm is unclear.
Study design: Double-blind randomized controlled trial.
Setting: Multicenter, multinational trial involving outpatients.
Synopsis: This double-blind, double-dummy trial involving 2,305 patients with sinus rhythm and reduced left ventricular ejection fraction (<35%) showed no significant difference in the primary combined outcome (ischemic stroke, intracerebral hemorrhage, or death) in those treated with warfarin as compared with aspirin. Warfarin did significantly reduce the rate of ischemic stroke by 0.64 events per 100 patient-years (absolute risk reduction 2.2%, number needed to treat 45) when compared with aspirin, with no significant difference in the rate of intracerebral hemorrhage. This outcome was offset by an increased rate of major hemorrhage by 0.91 events per 100 patient-years (absolute risk increase 3.1%, number needed to harm 32).
This study included patients from all functional classes of heart failure, with a protocol to initiate treatment with other standard heart failure medications. Patients with an indication for either warfarin or aspirin were excluded. Due to recruitment difficulties, the power of this study was reduced. Other study limitations included a relatively low percentage of time that patients on warfarin were in therapeutic range and a substantial period of follow-up time in which patients did not receive the assigned study treatments.
Bottom line: The benefit of reduced stoke in patients with heart failure and sinus rhythm who take warfarin over aspirin is counteracted by an increased risk for serious bleeding outcomes.
Citation: Homma S, Thompson JLP, Pullicino PM, et al. Warfarin and aspirin in patients with heart failure and sinus rhythm. N Engl J Med. 2012;366(20):1859-1869.
Aspirin Use after Recommended Anticoagulation Treatment Prevents Recurrence in VTE Patients
Clinical question: Does aspirin prevent recurrence in patients after treatment with anticoagulation following their first episode of unprovoked VTE?
Background: VTE recurrence is common following the discontinuation of anticoagulation, particularly in patients with a history of unprovoked pulmonary embolism (PE) or DVT. Extension of treatment with vitamin K antagonists decreases recurrence but also causes more bleeding. The role of aspirin in the secondary prevention of VTE is unknown.
Study design: Double-blind randomized controlled trial.
Setting: Multicenter international trial involving outpatients.
Synopsis: This trial compared treatment with aspirin versus placebo for approximately two years in 205 patients with a history of unprovoked VTE who had completed six to 18 months of anticoagulant therapy. The relative risk reduction of recurrent VTE in the aspirin versus the placebo group was approximately 40% per year (6.6% vs. 11.2% per year; absolute risk reduction 4.6% per year; number needed to treat 22). No difference in major or clinically relevant bleeding was observed between the two groups.
This study was appropriately powered to detect the treatment effect reported by the authors. Typically, anticoagulation is discontinued in this specific patient population once the risk of bleeding and/or the patient’s perceived inconvenience of therapy outweighs the expected benefit from continuing treatment to prevent VTE recurrence. Study results suggest aspirin is effective in preventing recurrence while not conferring an increased risk for hemorrhage. It is important to note that patients with cancer and symptomatic atherosclerosis were excluded from this study.
Bottom line: Following an appropriate treatment period with standard anticoagulation, aspirin appears to be a safe and effective therapy in the secondary prevention of recurrence in patients with a history of unprovoked VTE.
Citation: Becattini C, Agnelli G, Schenone A, et al. Aspirin for preventing recurrence of venous thromboembolism. N Engl J Med. 2012;366(21):1959-1967.
Meta-Analysis Supports New Oral Anticoagulants in Patients with Atrial Fibrillation
Clinical question: Are novel oral anticoagulants both efficacious and safe in comparison to warfarin in patients with atrial fibrillation (afib)?
Background: Three large clinical trials recently evaluated novel oral anticoagulants (dabigatran, rivaroxaban, and apixaban) as alternatives to warfarin in afib patients. Although the anticoagulants all appeared efficacious for primary outcomes, results regarding secondary and safety outcomes were either inconclusive or heterogeneous.
Study design: Systematic review and meta-analysis of randomized controlled trials.
Setting: Three diverse, clinical-trial settings.
Synopsis: A systematic review and meta-analysis of randomized controlled trials comparing novel oral anticoagulants to warfarin in afib patients found three large studies examining dabigatran, rivaroxaban, and apixaban that included 44,563 patients.
Using random-effects models to pool data from these studies, the authors found a 22% relative risk (RR) reduction of stroke or systemic embolism with the use of these new anticoagulants as compared to warfarin. The risks for ischemic and unidentified stroke (RR 0.87), hemorrhagic stroke (RR 0.45), intracranial bleeding (RR 0.49), and mortality (RR 0.88) were significantly reduced in patients taking these new anticoagulants. There was no significant reduction in major bleeding.
A trend in favor of warfarin was seen for gastrointestinal bleeding, but this trend was not statistically significant (RR 1.25; 95% confidence interval, 0.91-1.72).
This meta-analysis was limited to only three randomized controlled trials, each comparing a different oral anticoagulant to warfarin and using somewhat heterogeneous study designs and patient populations.
Bottom line: Three new oral anticoagulants appear safe and more efficacious than warfarin in the prevention of stroke and systemic embolism, as well as other important clinical outcomes in patients with atrial fibrillation.
Citation: Miller CS, Grandi SM, Shimony A, Filion KB, Eisenberg MJ. Meta-analysis of efficacy and safety of new oral anticoagulants (dabigatran, rivaroxaban, apixaban) versus warfarin in patients with atrial fibrillation. Am J Cardiol. 2012;110(3):453-60.
Observational Study Suggests Intravenous Metronidazole May Be Inferior for Mild Clostridium Difficile Infection
Clinical question: How do different treatment regimens (oral metronidazole vs. intravenous metronidazole vs. oral vancomycin) for mild Clostridium difficile infection (CDI) compare with regard to clinical outcomes?
Background: CDIs are increasing. Oral metronidazole or vancomycin can be used for the initial treatment of non-severe CDI. Additionally, a paucity of clinical data exists on intravenous metronidazole, which is used in some cases, typically in combination with vancomycin and in patients with severe CDI.
Study design: Prospective cohort study.
Setting: International hospital-based study.
Synopsis: This observational study assessed three different regimens (oral metronidazole, intravenous metronidazole, and oral vancomycin) for the treatment of mild CDI in 265 inpatients. Mortality at 30 days was higher in the intravenous metronidazole group (38.1%) than in the oral metronidazole (7.4%) and vancomycin (9.5%) groups. Patients receiving intravenous metronidazole also were less likely to recover from disease (52.4% versus >80% in the oral metronidazole and vancomycin groups). No statistically significant differences for other sequelae of CDI were found, except for higher risk of dehydration in the oral vancomycin group.
After controlling for age, sex, and comorbidity severity, patients in the intravenous metronidazole group were approximately four times more likely to die than patients in either the oral vancomycin group or the oral metronidazole group. There was no significant difference in mortality between the oral metronidazole and vancomycin groups.
Although this study was limited by its observational nature, no randomized controlled trial has yet to compare these three treatment regimens for mild CDI.
Bottom line: Treatment of mild C. diff infection with intravenous metronidazole appears to be associated with higher mortality and lower disease resolution than treatment with either oral metronidazole or vancomycin.
Citation: Wenisch JM, Schmid D, Kuo HW, et al. Prospective observational study comparing three different treatment regimes in patients with Clostridium difficile infection. Antimicrob Agents Chemother. 2012;56(4):1974-1978.
Traumatic Foley Catheter Complications Occur with Similar Frequency as Catheter-Associated Urinary Tract Infections
Clinical question: How does the frequency and clinical significance of urinary tract infection (UTI) compare to genitourinary trauma when associated with Foley catheterization?
Background: Foley catheter use in hospitalized patients is common and carries many associated risks. Although the risk of UTI when using catheters often is recognized, providers should consider other important complications of catheter use, such as genitourinary trauma.
Study design: Descriptive, prospective cohort study.
Setting: Single-center study in a Veterans Affairs hospital.
Synopsis: This surveillance study of 6,513 Foley catheter days compared the incidence of catheter-associated urinary tract infections (CAUTIs) to that of genitourinary trauma. Traumatic Foley events included gross hematuria, creation of false passage, ridging causing pain and/or difficulties with catheter removal, external genital trauma, catheter misplacement (ranging from prostatic to intraperitoneal), and catheter removal with the balloon inflated.
The incidence of possible UTI episodes was 1.8% of the Foley catheter days compared with 1.5% for catheter-associated trauma. Despite the fact that 72% of the UTI cases were asymptomatic, approximately 41% of these cases were treated with antibiotics, which accounted for 70% of all UTIs treated. Of the cases of Foley catheter trauma, 32% required further interventions (i.e. prolonged catheterization or cystoscopy). Trauma prompting intervention was as common as symptomatic UTIs.
The observational study design, use of a single center with a predominantly male population, and inclusion of patients undergoing urologic procedures who might have had valid indications for treatment of asymptomatic bacteriuria limit the study findings.
Bottom line: The complication of catheter-associated genitourinary trauma is just as common as CAUTIs in hospitalized patients, with each necessitating further intervention and treatment at similar rates.
Citation: Leuck AM, Wright D, Ellingson L, et al. Complications of Foley catheters—is infection the greatest risk? J Urol. 2012;187(5):1662-1666.
Intensive Control of Hyperglycemia in Noncritical, Hospitalized Patients Decreases Infection Risk, but No Significant Effect on Other Outcomes
Clinical question: What is the effect of tight glucose control in patients hospitalized in noncritical-care settings?
Background: Hyperglycemia is associated with increased in-hospital mortality and morbidity. Several trials have demonstrated the potential benefits of intensive glycemic control for patients in intensive-care settings, but this could lead to increased hypoglycemia. The effect of intensive therapy to achieve tight glycemic control in noncritically ill patients is unclear.
Study design: Systematic review and meta-analysis.
Setting: Various study sites of hospitalized patients.
Synopsis: This meta-analysis included 19 studies (nine randomized, 10 observational) published from 1995 to 2011. Intensive glycemic control (fasting blood glucose of 100-180 mg/dL) was not associated with significant effect on risk of death, myocardial infarction (MI), or stroke. There was a nonsignificant trend for increased risk of hypoglycemia (relative risk, 1.58; 95% CI, 0.97-2.57).
Intensive glycemic control was associated with a decreased risk of infection (relative risk, 0.41; 95% CI, 0.21–0.77), but this association mainly was derived from studies in surgical settings.
Subgroup analyses demonstrated an association between achieving intensive glycemic goals and an increased risk of hypoglycemia (P=0.01). Hypoglycemia also more commonly occurred in surgical patients.
There was substantial heterogeneity across studies included for all outcomes except infection. The quality of the current evidence supporting a reduction in infection is low and appears mostly derived from patients in surgical settings. The quality of evidence relating to all the other outcomes is also low and is limited by heterogeneity and imprecision.
Bottom line: Intensive control of hyperglycemia in noncritically ill hospitalized patients might reduce the risk of infection in some patients but does not appear to be significantly associated with improvement in other important clinical outcomes.
Citation: Murad MH, Coburn JA, Coto-Yglesias F, et al. Glycemic control in non-critically ill hospitalized patients: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2012;97(1):49-58.
Simple Risk Score Predicts 30-Day Mortality after Noncardiac Surgery
Clinical question: Can 30-day mortality risk after noncardiac surgery be predicted by using a simple bedside-risk index?
Background: While indices exist to quantify the risk of cardiac complications in patients undergoing noncardiac surgery, there is significant perioperative mortality due to noncardiac causes. Therefore, a need exists for a simple risk index to predict all-cause mortality after noncardiac surgery.
Study design: Retrospective cohort study.
Setting: American College of Surgeons National Surgical Quality Improvement Program database of patients in more than 200 hospitals.
Synopsis: The nine-point Surgical Mortality Probability Model (S-MPM) 30-day mortality risk index was empirically created and applied to a randomly split portion of a database, which included 298,772 patients undergoing noncardiac surgery. Three risk factors were included: American Society of Anesthesiologists (ASA) physical status, surgery risk class, and emergency status. Patients with ASA physical status I, II, III, IV, or V were assigned zero, two, four, five, or six points, respectively. Patients undergoing intermediate- or high-risk procedures were assigned one or two points, respectively. Patients undergoing emergency procedures were assigned one point. The S-MPM then was applied to the validation portion of the data set.
The 30-day predicted risk of mortality was less than 0.50% for those patients with combined risk scores of less than five (S-MPM Class I), between 1.5% and 4.0% for risk scores of five to six (Class II), and more than 10% for risk scores greater than six (Class III).
The major limitation of this derived risk score is the reliance on ASA physical status, which has imprecise definitions and might lead to inconsistent ratings.
Bottom line: The S-MPM risk index is a simple bedside scoring system, which can accurately predict 30-day mortality in patients undergoing noncardiac surgery.
Citation: Glance LG, Lustik SJ, Hannan EL, et al. The Surgical Mortality Probability Model: Derivation and validation of a simple risk prediction rule for noncardiac surgery. Ann Surg. 2012;255(4):696-702.
Temperature, White Blood Cell Count Are Not Sensitive Predictors of Bacteremia
Clinical question: In ED patients with suspected infection, are temperature, white blood cell (WBC) count, and bandemia reliable predictors of bacteremia?
Background: Sepsis is a significant cause of morbidity and mortality. Early identification and treatment of sepsis improves patient outcomes. Although systemic inflammatory response syndrome criteria aids in the prompt recognition of sepsis, these markers have variable sensitivity and specificity for true infection or bacteremia, which places patients at high risk for sepsis.
Study design: Post-hoc data analysis of a prospective cohort study.
Setting: ED patients at a single tertiary-care center.
Synopsis: A retrospective analysis was performed on 3,563 patients who presented to the ED. Blood cultures obtained on patients with suspected infection revealed bacteremia in 289 patients (8.1%). Patients with bacteremia were reviewed for the presence of normal temperature (36.1° to 38° Celsius), normal WBC count (4,000 to 12,000 cells per µL), and presence of bandemia (>5% of WBC differential).
Among patients with bacteremia, 33% had a normal body temperature (67% sensitivity) and 52% had a normal WBC count (48% sensitivity). Of the 210 bacteremic patients who had a full differential performed, bandemia was present in 82% (sensitivity 82%). Bandemia was present in 80% of culture-positive patients with a normal temperature and 79% of culture-positive patients with a normal WBC count. Approximately 17% of patients with bacteremia had neither an abnormal temperature nor an abnormal WBC. This study was limited by the retrospective nature of analysis and the subjective designation of “suspected infection” by the original providers.
Bottom line: In patients presenting to the ED with suspected infection who are found to have culture-proven bacteremia, a significant percentage have normal temperature and WBC count, but the presence of bandemia could be more useful for identifying occult bacteremia.
Citation: Seigel TA, Cocchi MN, Salciccioli J, et al. Inadequacy of temperature and white blood cell count in predicting bacteremia in patients with suspected infection. J Emerg Med. 2012;42(3):254-259.
Epidemiology of Bacteremia in Young Infants is Changing

Clinical question: What is the epidemiology of bacteremia in one-week to three-month-old infants?
Background: Large studies of bacteremia in infants <90 days of age were largely performed before the era of routine prenatal screening and prophylaxis for Group B Streptococcus (GBS). Additionally, these studies have focused on febrile infants, which might not allow for characterization of the incidence of bacteremia when nonfebrile infants are considered.
Study design: Retrospective review.
Setting: Large HMO database.
Synopsis: Of 160,818 full-term infants born at Kaiser Permanente Northern California from 2005 to 2009, 4,255 blood cultures were obtained from 4,122 infants in outpatient clinics, the ED, or in an inpatient setting within 24 hours of birth. Preterm infants <37 weeks, infants with underlying medical conditions, and infants with cultures drawn within three days of an original culture were excluded.
A total of 8% of the blood cultures were positive, with 2.2% deemed true positives and 5.8% due to contaminants. The incidence rate of true bacteremia was 0.57 per 1,000 full-term births, with gram-negative organisms (predominantly Escherichia coli) representing the majority (63%) of pathogens, followed by GBS (21%), Staphylococcus aureus (8%), and Streptococcus pneumoniae (3%). There were no cases of Listeria monocytogenes or Neisseria meningitidis bacteremia, and there was one case of enterococcal bacteremia. Fever was absent in 7% of cases.
The authors conclude that ampicillin may no longer be necessary for empiric antibiotic coverage in this age group given that 36% of pathogens were resistant to ampicillin, there were no cases of Listeria, and there was only one case of enterococcus. However, these recommendations should be considered in light of the specific study setting, and might not be applicable to all areas.
Bottom line: E. coli, GBS, and S. aureus, in that order, are the most common causes of bacteremia in infants aged one week to three months.
Citation: Greenhow TL, Hung YY, Herz AM. Changing epidemiology of bacteremia in infants aged 1 week to 3 months. Pediatrics. 2012;129(3):e590-e596.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: What is the epidemiology of bacteremia in one-week to three-month-old infants?
Background: Large studies of bacteremia in infants <90 days of age were largely performed before the era of routine prenatal screening and prophylaxis for Group B Streptococcus (GBS). Additionally, these studies have focused on febrile infants, which might not allow for characterization of the incidence of bacteremia when nonfebrile infants are considered.
Study design: Retrospective review.
Setting: Large HMO database.
Synopsis: Of 160,818 full-term infants born at Kaiser Permanente Northern California from 2005 to 2009, 4,255 blood cultures were obtained from 4,122 infants in outpatient clinics, the ED, or in an inpatient setting within 24 hours of birth. Preterm infants <37 weeks, infants with underlying medical conditions, and infants with cultures drawn within three days of an original culture were excluded.
A total of 8% of the blood cultures were positive, with 2.2% deemed true positives and 5.8% due to contaminants. The incidence rate of true bacteremia was 0.57 per 1,000 full-term births, with gram-negative organisms (predominantly Escherichia coli) representing the majority (63%) of pathogens, followed by GBS (21%), Staphylococcus aureus (8%), and Streptococcus pneumoniae (3%). There were no cases of Listeria monocytogenes or Neisseria meningitidis bacteremia, and there was one case of enterococcal bacteremia. Fever was absent in 7% of cases.
The authors conclude that ampicillin may no longer be necessary for empiric antibiotic coverage in this age group given that 36% of pathogens were resistant to ampicillin, there were no cases of Listeria, and there was only one case of enterococcus. However, these recommendations should be considered in light of the specific study setting, and might not be applicable to all areas.
Bottom line: E. coli, GBS, and S. aureus, in that order, are the most common causes of bacteremia in infants aged one week to three months.
Citation: Greenhow TL, Hung YY, Herz AM. Changing epidemiology of bacteremia in infants aged 1 week to 3 months. Pediatrics. 2012;129(3):e590-e596.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: What is the epidemiology of bacteremia in one-week to three-month-old infants?
Background: Large studies of bacteremia in infants <90 days of age were largely performed before the era of routine prenatal screening and prophylaxis for Group B Streptococcus (GBS). Additionally, these studies have focused on febrile infants, which might not allow for characterization of the incidence of bacteremia when nonfebrile infants are considered.
Study design: Retrospective review.
Setting: Large HMO database.
Synopsis: Of 160,818 full-term infants born at Kaiser Permanente Northern California from 2005 to 2009, 4,255 blood cultures were obtained from 4,122 infants in outpatient clinics, the ED, or in an inpatient setting within 24 hours of birth. Preterm infants <37 weeks, infants with underlying medical conditions, and infants with cultures drawn within three days of an original culture were excluded.
A total of 8% of the blood cultures were positive, with 2.2% deemed true positives and 5.8% due to contaminants. The incidence rate of true bacteremia was 0.57 per 1,000 full-term births, with gram-negative organisms (predominantly Escherichia coli) representing the majority (63%) of pathogens, followed by GBS (21%), Staphylococcus aureus (8%), and Streptococcus pneumoniae (3%). There were no cases of Listeria monocytogenes or Neisseria meningitidis bacteremia, and there was one case of enterococcal bacteremia. Fever was absent in 7% of cases.
The authors conclude that ampicillin may no longer be necessary for empiric antibiotic coverage in this age group given that 36% of pathogens were resistant to ampicillin, there were no cases of Listeria, and there was only one case of enterococcus. However, these recommendations should be considered in light of the specific study setting, and might not be applicable to all areas.
Bottom line: E. coli, GBS, and S. aureus, in that order, are the most common causes of bacteremia in infants aged one week to three months.
Citation: Greenhow TL, Hung YY, Herz AM. Changing epidemiology of bacteremia in infants aged 1 week to 3 months. Pediatrics. 2012;129(3):e590-e596.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Prevention of Intravascular, Catheter-Related Infections
Background
have become a ubiquitous feature of modern-day patient care; current estimates suggest that as many as 2 million persons in the U.S. have an intravascular device that is used daily or intermittently.1 These devices fulfill a variety of clinical needs, including monitoring acutely ill patients and the administration of critical medications, in a variety of settings, including ICUs, medical and surgical units, and the outpatient setting.
This important therapeutic role comes with associated risks, including the possibility of bloodstream infection, which leads to an increase in morbidity, length of stay, and cost. Each year in the ICU alone, 80,000 catheter-related bloodstream infections (CRBSIs) occur. This figure increases to 250,000 to 500,000 infections per year when all hospitalized patients are considered.1,2
Infections related to intravascular catheters have been targeted by numerous quality-improvement (QI) initiatives, uncovering a number of clinical actions that can impact their rates. Studies have shown that these infections can be avoided and nearly eliminated entirely with close adherence to several evidence-based, infection-control measures.3 Furthermore, these results can be sustained across multiple ICUs over extended periods.4
The majority of data that describe the epidemiology of CRBSIs and the interventions needed to prevent these infections have been generated in the ICU. However, the pervasiveness of these devices in other care settings dictates the need for heightened awareness by the entire care team. As such, it is important for hospitalists to understand and be aware of guidelines outlining the standard of care not only in personal practice, but also in order to ensure that all members of the team are playing their part in preventing this serious complication.
Guideline Update
In May 2011, the Society of Critical Care Medicine (SCCM), in collaboration with 14 other professional organizations, published new guidelines for the prevention of intravascular catheter-related infections.5 These guidelines are a revision of guidelines published in 2002 and provide recommendations that apply to all intravascular catheters, as well as specific comments based on the type of device in use.6
Specific recommendations include:
- Responsible staff should be well-versed and assessed on the proper procedures for the care of all intravascular catheters with designated personnel responsible for central venous catheters (CVCs)
- and peripherally inserted central catheters (PICCs).
- Prior to CVC and arterial catheter insertion and during dressing changes, an antiseptic solution containing more than 0.5% chlorhexidine with alcohol should be used to prepare the skin.
- Nontunneled CVCs should be preferentially placed in a subclavian site rather than a jugular or a femoral site, except in hemodialysis or advanced kidney disease patients, for which this may cause subclavian stenosis, with the understanding that the risks of placing a CVC at a site be weighed against its benefits.
- Skilled personnel should use ultrasound guidance during CVC placement, and the minimal essential number of ports or lumens on the CVC should be present. Avoidance of routine placement of CVCs and prompt removal of any nonessential intravascular catheter is recommended.
- Maximal sterile barrier precautions should be taken during the placement of CVCs and PICCs or guidewire exchange, which includes a sterile full-body drape for the patient and use of cap, mask, sterile gown, and gloves for personnel. After the catheter has been placed, it should be secured with a sutureless securement device. In addition, patients with these intravascular catheters should bathe with 2% chlorhexidine daily.
- If rates of CLABSI remain high despite adherence to education/training, appropriate antisepsis, and maximal sterile barrier precautions, the use of antiseptic- or antibiotic-impregnated, short-term CVCs and chlorhexadine-impregnanted sponge dressings might help to further decrease rates.5
No single intervention alone appears to be sufficient to significantly reduce CRBSI rates. Therefore, the guideline recommends “bundling” several of these individual best practices into a streamlined approach—inclusive of feedback to healthcare personnel on infection rates and compliance—thereby promoting quality assurance and performance improvement. This bundling tactic makes best practices a priority and a reality, and offers the largest potential impact on the prevention of intravascular catheter-related infections.5
Analysis
Practical recommendations to assist clinicians in preventing CLABSI also were put forth in 2008 guidelines by the Society for Healthcare Epidemiology of America (SHEA) and Infectious Disease Society of America (IDSA).7 Compared to the SCCM guidelines, these guidelines are more focused on CVCs and do not directly address other available intravascular devices (PICCs, hemodialysis catheters, etc.). Beyond this, the SCCM guidelines also discuss the microbiology of infection, surveillance measures, and the specifics of the performance improvement measures involved in their implementation, which are not found in the SHEA and IDSA guidelines.
Numerous national initiatives and measures have been established based on these and other clinical practice guidelines. The Joint Commission recently produced the new monograph “Preventing Central Line-Associated Infections: A Global Challenge, A Global Perspective,” listing “Use proven guidelines to prevent infection of the blood from central lines” as one of its National Patient Safety Goals.8 The Institute for Healthcare Improvement (IHI) created its Central Line Bundle along with its “How-To Guide: Prevent CLABSI in 2011,” which has been implemented by many hospitals in the U.S. and United Kingdom. The IHI bundle has resulted in dozens of hospitals achieving more than a year of no CLABSIs in their ICU patients, and many have expanded the program to other areas of the hospital.9
Giving further impetus toward efforts to prevent these complications, the Centers for Medicare & Medicaid Services (CMS) determined that vascular-catheter-associated infections are hospital-acquired conditions that will no longer be reimbursed, as outlined in 2008 in the Acute Inpatient Prospective Payment System.10 Therefore, hospitals will not receive additional payment for these infections acquired during hospitalization (i.e. was not present on admission), and the case is paid as though the costly infection were not present, thus aligning improved patient care and outcomes with the financial bottom line for hospital reimbursement.
HM Takeaways
Given the significant economic and clinical burden of intravascular-device-related infections, hospital staffs should be aware of and adopt proven interventions to minimize this important complication. No one single intervention can meaningfully impact this infection rate, but a “bundled approach” appears to be the most influential.
Dr. Rohde is a hospitalist and assistant professor of internal medicine and Dr. Hartley is a hospitalist and clinical instructor of internal medicine at the University of Michigan Hospital and Health Systems in Ann Arbor.
Background
have become a ubiquitous feature of modern-day patient care; current estimates suggest that as many as 2 million persons in the U.S. have an intravascular device that is used daily or intermittently.1 These devices fulfill a variety of clinical needs, including monitoring acutely ill patients and the administration of critical medications, in a variety of settings, including ICUs, medical and surgical units, and the outpatient setting.
This important therapeutic role comes with associated risks, including the possibility of bloodstream infection, which leads to an increase in morbidity, length of stay, and cost. Each year in the ICU alone, 80,000 catheter-related bloodstream infections (CRBSIs) occur. This figure increases to 250,000 to 500,000 infections per year when all hospitalized patients are considered.1,2
Infections related to intravascular catheters have been targeted by numerous quality-improvement (QI) initiatives, uncovering a number of clinical actions that can impact their rates. Studies have shown that these infections can be avoided and nearly eliminated entirely with close adherence to several evidence-based, infection-control measures.3 Furthermore, these results can be sustained across multiple ICUs over extended periods.4
The majority of data that describe the epidemiology of CRBSIs and the interventions needed to prevent these infections have been generated in the ICU. However, the pervasiveness of these devices in other care settings dictates the need for heightened awareness by the entire care team. As such, it is important for hospitalists to understand and be aware of guidelines outlining the standard of care not only in personal practice, but also in order to ensure that all members of the team are playing their part in preventing this serious complication.
Guideline Update
In May 2011, the Society of Critical Care Medicine (SCCM), in collaboration with 14 other professional organizations, published new guidelines for the prevention of intravascular catheter-related infections.5 These guidelines are a revision of guidelines published in 2002 and provide recommendations that apply to all intravascular catheters, as well as specific comments based on the type of device in use.6
Specific recommendations include:
- Responsible staff should be well-versed and assessed on the proper procedures for the care of all intravascular catheters with designated personnel responsible for central venous catheters (CVCs)
- and peripherally inserted central catheters (PICCs).
- Prior to CVC and arterial catheter insertion and during dressing changes, an antiseptic solution containing more than 0.5% chlorhexidine with alcohol should be used to prepare the skin.
- Nontunneled CVCs should be preferentially placed in a subclavian site rather than a jugular or a femoral site, except in hemodialysis or advanced kidney disease patients, for which this may cause subclavian stenosis, with the understanding that the risks of placing a CVC at a site be weighed against its benefits.
- Skilled personnel should use ultrasound guidance during CVC placement, and the minimal essential number of ports or lumens on the CVC should be present. Avoidance of routine placement of CVCs and prompt removal of any nonessential intravascular catheter is recommended.
- Maximal sterile barrier precautions should be taken during the placement of CVCs and PICCs or guidewire exchange, which includes a sterile full-body drape for the patient and use of cap, mask, sterile gown, and gloves for personnel. After the catheter has been placed, it should be secured with a sutureless securement device. In addition, patients with these intravascular catheters should bathe with 2% chlorhexidine daily.
- If rates of CLABSI remain high despite adherence to education/training, appropriate antisepsis, and maximal sterile barrier precautions, the use of antiseptic- or antibiotic-impregnated, short-term CVCs and chlorhexadine-impregnanted sponge dressings might help to further decrease rates.5
No single intervention alone appears to be sufficient to significantly reduce CRBSI rates. Therefore, the guideline recommends “bundling” several of these individual best practices into a streamlined approach—inclusive of feedback to healthcare personnel on infection rates and compliance—thereby promoting quality assurance and performance improvement. This bundling tactic makes best practices a priority and a reality, and offers the largest potential impact on the prevention of intravascular catheter-related infections.5
Analysis
Practical recommendations to assist clinicians in preventing CLABSI also were put forth in 2008 guidelines by the Society for Healthcare Epidemiology of America (SHEA) and Infectious Disease Society of America (IDSA).7 Compared to the SCCM guidelines, these guidelines are more focused on CVCs and do not directly address other available intravascular devices (PICCs, hemodialysis catheters, etc.). Beyond this, the SCCM guidelines also discuss the microbiology of infection, surveillance measures, and the specifics of the performance improvement measures involved in their implementation, which are not found in the SHEA and IDSA guidelines.
Numerous national initiatives and measures have been established based on these and other clinical practice guidelines. The Joint Commission recently produced the new monograph “Preventing Central Line-Associated Infections: A Global Challenge, A Global Perspective,” listing “Use proven guidelines to prevent infection of the blood from central lines” as one of its National Patient Safety Goals.8 The Institute for Healthcare Improvement (IHI) created its Central Line Bundle along with its “How-To Guide: Prevent CLABSI in 2011,” which has been implemented by many hospitals in the U.S. and United Kingdom. The IHI bundle has resulted in dozens of hospitals achieving more than a year of no CLABSIs in their ICU patients, and many have expanded the program to other areas of the hospital.9
Giving further impetus toward efforts to prevent these complications, the Centers for Medicare & Medicaid Services (CMS) determined that vascular-catheter-associated infections are hospital-acquired conditions that will no longer be reimbursed, as outlined in 2008 in the Acute Inpatient Prospective Payment System.10 Therefore, hospitals will not receive additional payment for these infections acquired during hospitalization (i.e. was not present on admission), and the case is paid as though the costly infection were not present, thus aligning improved patient care and outcomes with the financial bottom line for hospital reimbursement.
HM Takeaways
Given the significant economic and clinical burden of intravascular-device-related infections, hospital staffs should be aware of and adopt proven interventions to minimize this important complication. No one single intervention can meaningfully impact this infection rate, but a “bundled approach” appears to be the most influential.
Dr. Rohde is a hospitalist and assistant professor of internal medicine and Dr. Hartley is a hospitalist and clinical instructor of internal medicine at the University of Michigan Hospital and Health Systems in Ann Arbor.
Background
have become a ubiquitous feature of modern-day patient care; current estimates suggest that as many as 2 million persons in the U.S. have an intravascular device that is used daily or intermittently.1 These devices fulfill a variety of clinical needs, including monitoring acutely ill patients and the administration of critical medications, in a variety of settings, including ICUs, medical and surgical units, and the outpatient setting.
This important therapeutic role comes with associated risks, including the possibility of bloodstream infection, which leads to an increase in morbidity, length of stay, and cost. Each year in the ICU alone, 80,000 catheter-related bloodstream infections (CRBSIs) occur. This figure increases to 250,000 to 500,000 infections per year when all hospitalized patients are considered.1,2
Infections related to intravascular catheters have been targeted by numerous quality-improvement (QI) initiatives, uncovering a number of clinical actions that can impact their rates. Studies have shown that these infections can be avoided and nearly eliminated entirely with close adherence to several evidence-based, infection-control measures.3 Furthermore, these results can be sustained across multiple ICUs over extended periods.4
The majority of data that describe the epidemiology of CRBSIs and the interventions needed to prevent these infections have been generated in the ICU. However, the pervasiveness of these devices in other care settings dictates the need for heightened awareness by the entire care team. As such, it is important for hospitalists to understand and be aware of guidelines outlining the standard of care not only in personal practice, but also in order to ensure that all members of the team are playing their part in preventing this serious complication.
Guideline Update
In May 2011, the Society of Critical Care Medicine (SCCM), in collaboration with 14 other professional organizations, published new guidelines for the prevention of intravascular catheter-related infections.5 These guidelines are a revision of guidelines published in 2002 and provide recommendations that apply to all intravascular catheters, as well as specific comments based on the type of device in use.6
Specific recommendations include:
- Responsible staff should be well-versed and assessed on the proper procedures for the care of all intravascular catheters with designated personnel responsible for central venous catheters (CVCs)
- and peripherally inserted central catheters (PICCs).
- Prior to CVC and arterial catheter insertion and during dressing changes, an antiseptic solution containing more than 0.5% chlorhexidine with alcohol should be used to prepare the skin.
- Nontunneled CVCs should be preferentially placed in a subclavian site rather than a jugular or a femoral site, except in hemodialysis or advanced kidney disease patients, for which this may cause subclavian stenosis, with the understanding that the risks of placing a CVC at a site be weighed against its benefits.
- Skilled personnel should use ultrasound guidance during CVC placement, and the minimal essential number of ports or lumens on the CVC should be present. Avoidance of routine placement of CVCs and prompt removal of any nonessential intravascular catheter is recommended.
- Maximal sterile barrier precautions should be taken during the placement of CVCs and PICCs or guidewire exchange, which includes a sterile full-body drape for the patient and use of cap, mask, sterile gown, and gloves for personnel. After the catheter has been placed, it should be secured with a sutureless securement device. In addition, patients with these intravascular catheters should bathe with 2% chlorhexidine daily.
- If rates of CLABSI remain high despite adherence to education/training, appropriate antisepsis, and maximal sterile barrier precautions, the use of antiseptic- or antibiotic-impregnated, short-term CVCs and chlorhexadine-impregnanted sponge dressings might help to further decrease rates.5
No single intervention alone appears to be sufficient to significantly reduce CRBSI rates. Therefore, the guideline recommends “bundling” several of these individual best practices into a streamlined approach—inclusive of feedback to healthcare personnel on infection rates and compliance—thereby promoting quality assurance and performance improvement. This bundling tactic makes best practices a priority and a reality, and offers the largest potential impact on the prevention of intravascular catheter-related infections.5
Analysis
Practical recommendations to assist clinicians in preventing CLABSI also were put forth in 2008 guidelines by the Society for Healthcare Epidemiology of America (SHEA) and Infectious Disease Society of America (IDSA).7 Compared to the SCCM guidelines, these guidelines are more focused on CVCs and do not directly address other available intravascular devices (PICCs, hemodialysis catheters, etc.). Beyond this, the SCCM guidelines also discuss the microbiology of infection, surveillance measures, and the specifics of the performance improvement measures involved in their implementation, which are not found in the SHEA and IDSA guidelines.
Numerous national initiatives and measures have been established based on these and other clinical practice guidelines. The Joint Commission recently produced the new monograph “Preventing Central Line-Associated Infections: A Global Challenge, A Global Perspective,” listing “Use proven guidelines to prevent infection of the blood from central lines” as one of its National Patient Safety Goals.8 The Institute for Healthcare Improvement (IHI) created its Central Line Bundle along with its “How-To Guide: Prevent CLABSI in 2011,” which has been implemented by many hospitals in the U.S. and United Kingdom. The IHI bundle has resulted in dozens of hospitals achieving more than a year of no CLABSIs in their ICU patients, and many have expanded the program to other areas of the hospital.9
Giving further impetus toward efforts to prevent these complications, the Centers for Medicare & Medicaid Services (CMS) determined that vascular-catheter-associated infections are hospital-acquired conditions that will no longer be reimbursed, as outlined in 2008 in the Acute Inpatient Prospective Payment System.10 Therefore, hospitals will not receive additional payment for these infections acquired during hospitalization (i.e. was not present on admission), and the case is paid as though the costly infection were not present, thus aligning improved patient care and outcomes with the financial bottom line for hospital reimbursement.
HM Takeaways
Given the significant economic and clinical burden of intravascular-device-related infections, hospital staffs should be aware of and adopt proven interventions to minimize this important complication. No one single intervention can meaningfully impact this infection rate, but a “bundled approach” appears to be the most influential.
Dr. Rohde is a hospitalist and assistant professor of internal medicine and Dr. Hartley is a hospitalist and clinical instructor of internal medicine at the University of Michigan Hospital and Health Systems in Ann Arbor.
What Is the Best E&M of Fat Embolism Syndrome?

The Case
A 24-year-old white man with no past medical history is admitted after sustaining bilateral, closed femur fractures in a motor vehicle accident. Within hours of the trauma, he is taken to the operating room for open reduction and internal fixation. Of note, preoperatively, his hematocrit is 40%. After surgery, he is easily extubated and transferred to an unmonitored bed for further care. Approximately 30 hours after admission, he develops tachypnea with a respiratory rate of 35 breaths per minute and hypoxia with an oxygen saturation of 86% on room air. He is tachycardic (120 beats per minute) and febrile to 39.0oC. His blood pressure remains stable. He is somnolent, and when awake, he is confused. Notably, his hematocrit is now 22%. An electrocardiogram shows sinus tachycardia, an initial chest X-ray is normal, and a high-resolution CT scan is negative for a pulmonary embolism (PE).
Is this clinical picture consistent with fat embolism syndrome and, if so, how should he be managed?
Overview
“Fat embolism” refers to the presence of fat globules that obstruct the lung parenchyma and peripheral circulation. Fat embolism syndrome, on the other hand, is a more serious manifestation involving multiple organ systems. Specifically, it is a clinical diagnosis presenting with the classic triad of hypoxemia, neurologic abnormalities, and a petechial rash.
Fat embolism syndrome is usually associated with multiple traumas, including long-bone injuries and pelvic fractures. It is more frequently associated with closed fractures than open fractures, possibly due to the higher pressures associated with closed fractures. This syndrome has been less commonly associated with a variety of nontraumatic conditions (Table 1).

With an increased incidence of long-bone fractures in the younger demographic, fat embolism syndrome is most common in the second or third decade of life. While fat embolism occurs in up to 90% of patients with traumatic skeletal injuries, fat embolism syndrome occurs in 0.5% to 10% of patients following trauma, with a higher incidence in multiple fractures (5% to 10%) than in single long-bone fractures (0.5% to 2%).1-3
With the increasing role of hospitalists in assisting in the management of orthopedic patients, their knowledge of fat embolism syndrome is important so that it can be included in the differential diagnosis of acute respiratory failure in these orthopedic patients.
Review of the Data
Pathogenesis. Clinical manifestations of fat embolism syndrome have been acknowledged for more than 100 years. Since its first description in the 1860s, there has been speculation about the etiology of this condition. In the 1920s, two theories were proposed to explain the origin of the fat droplets: the mechanical and biochemical theories.2,4
Mechanical theory suggests that trauma to long bones disturbs fat cells within the bone marrow or adipose tissue, causing fat globules to mobilize.2,3 There is a rise in marrow pressure above venous pressure, which allows fat particles to enter the circulation through damaged venules surrounding the fracture site. Once lodged in the pulmonary microvasculature, embolized fat causes local ischemia and inflammation. Fat globules may pass into the arterial circulation either by paradoxical embolism through a patent foramen ovale, or by microemboli that pass through the lungs into the arterial circulation. This explains embolization to other organs, including the brain, retina, and skin.
Alternatively, biochemical theory hypothesizes that fat embolism syndrome is contingent on the production of toxic intermediaries from the breakdown of embolized fat.2,3 This theory suggests that the release of catecholamines after severe trauma can liberate free fatty acids from fat stores, or that acute-phase reactants at the trauma site affect fat solubility, causing agglutination and embolization. This theory helps to explain nontraumatic fat embolism syndrome, as well as the delay in development of the clinical syndrome after acute injury.
Clinical presentation. Most patients have a latent period after trauma of 12 to 72 hours before symptoms of fat embolism syndrome become apparent; however, clinical manifestations might occur immediately or up to one to two weeks following injury.2,4 As previously mentioned, the classic triad of symptoms includes respiratory compromise, neurological impairment, and a petechial rash.
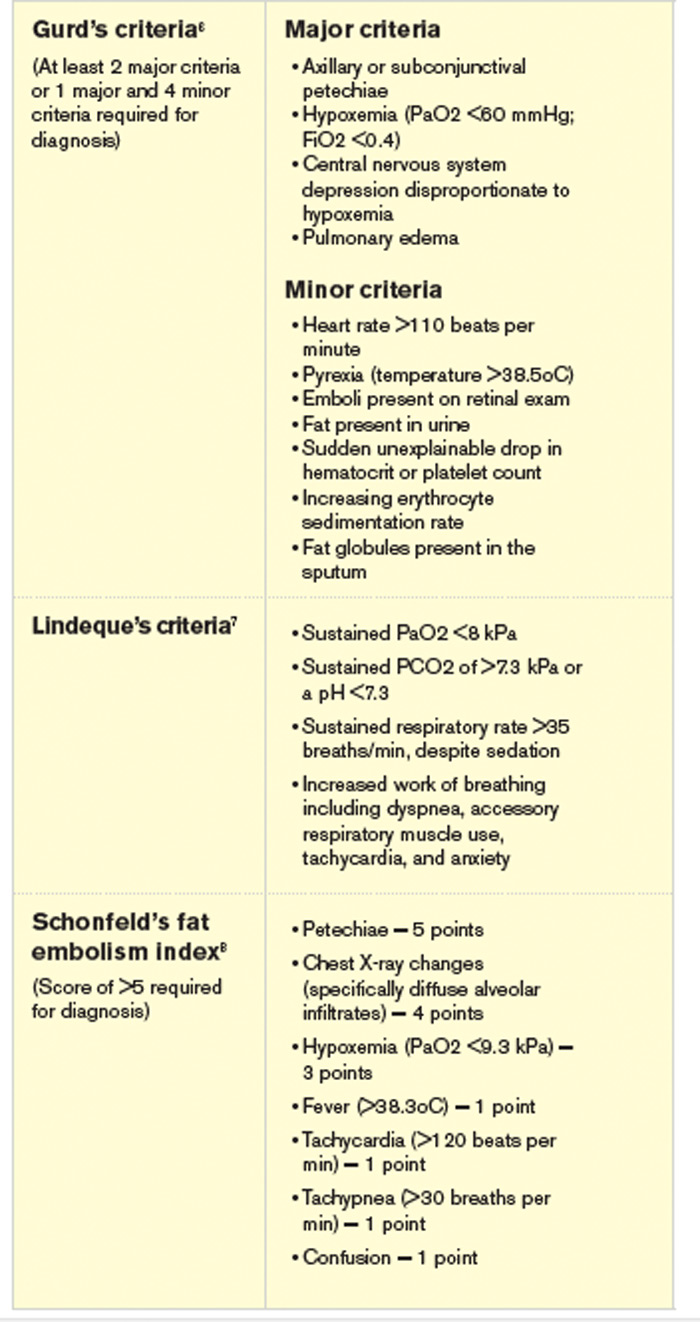
The most common and usually earliest manifestation is acute hypoxia, which must be distinguished from other treatable causes of hypoxia, including pneumothorax, hemothorax, PE, and pneumonia. Pulmonary changes might progress to respiratory failure similar to acute respiratory distress syndrome. Neurological manifestations are primarily nonspecific and include headache, irritability, delirium, seizures, and coma. Focal neurological deficits are rare but have been described.5 Almost all neurological symptoms are fully reversible. The petechial rash is distinctive and occurs on the chest, axilla, and subconjunctiva. Although the rash occurs in only 20% to 50% of patients and resolves fairly quickly, in the appropriate clinical setting, this rash is considered pathognomonic.1,2,4
A variety of other nonspecific signs and symptoms might also occur: pyrexia, tachycardia, fat in the urine or sputum, retinal changes, renal insufficiency, myocardial dysfunction, and an otherwise unexplained drop in hematocrit or platelet count.
Diagnosis. Fat embolism syndrome is a clinical diagnosis and a diagnosis of exclusion. There are no specific confirmatory tests. An arterial blood gas will usually reveal a PaO2 of <60 mmHg.3 Laboratory evaluation might also show fat globules in the urine or sputum on Sudan or Oil Red O staining, but these findings are nonspecific.3,4 Bronchoscopy with bronchial alveolar lavage (BAL) might similarly detect fat droplets in alveolar macrophages in the BAL fluid; however, the sensitivity and specificity for diagnosis of fat embolism syndrome are unknown.4 None of these tests can be used solely for the diagnosis of fat embolism syndrome.
Thrombocytopenia and anemia out of proportion to the expected drop from surgery are not uncommon in addition to other nonspecific laboratory findings, including hypocalcemia, elevated serum lipase level, and elevated erythrocyte sedimentation rate.4 Several radiological findings have been observed on lung and brain imaging, though the findings are nonspecific and none are diagnostic. A chest X-ray might be normal, but abnormalities are seen in 30% to 50% of cases.2 Typically, when abnormal, the chest X-ray shows diffuse interstitial and alveolar densities, as well as patchy perihilar and basilar infiltrates resembling pulmonary edema. These X-ray findings might not be seen for up to 12 to 24 hours following the onset of clinical symptoms.
The most commonly used diagnostic criteria for the diagnosis of fat embolism syndrome are published by Gurd et al.6 At least two major criteria or one major criterion and four minor criteria are required for the diagnosis of fat embolism syndrome. The major criteria are based on the three classic signs and symptoms of fat embolism syndrome; the minor criteria include the finding of fat globules in the urine and sputum as well as some of the previously mentioned nonspecific clinical signs and laboratory tests.
Other criteria for diagnosis have been suggested, including those published by Lindeque et al, which focuses primarily on the respiratory characteristics, and a more recent set of semiquantitative diagnostic criteria called the fat embolism index, published by Schonfeld et al.7,8 Schonfeld’s scoring index accounts for the major signs and symptoms of fat embolism syndrome and weighs them according to relative specificity. A score of 5 or more is required for diagnosis of fat embolism syndrome. Table 2 compares the three sets of criteria used for diagnosis of fat embolism syndrome.
Treatment. The treatment of fat embolism syndrome is supportive. Most often, this requires supplemental oxygen for hypoxia and, possibly, fluid resuscitation in the case of hypovolemia. Occasionally, though, these relatively minor supportive therapies need to be escalated to bipap or even full ventilatory support and vasopressors in the more severe cases.
Based on the premise that steroids will attenuate the inflammatory reaction to free fatty acids within the lung, steroids have been tried in the treatment of fat embolism syndrome. However, there are no studies that clearly show benefit with their use.
Prevention. Most of the methods of prevention involve surgical intervention rather than medical therapy. Because microscopic fat emboli are showered during manipulation of long-bone fragments, early immobilization of fractures is recommended, and operative correction rather than conservative management is the preferred method.2,3 One report estimates a 70% reduction in pulmonary complications from this intervention alone.9
Further, two surgical techniques are debated as possible means of preventing fat embolism syndrome. The first is “venting,” in which a hole is made distal to the site of intramedullary nail placement. This reduces intramedullary pressure elevation and, therefore, extravasation of fat into the circulation.10 The second technique is the use of a reamer, irrigator, aspirator (RIA) device. A reamer is a tool used to create an accurate-sized hole for an intramedullary nail. Reaming before intramedullary nail placement can release fat deposits into the circulation. The RIA device irrigates and aspirates resident fat deposits as it reams the canal, releasing fewer deposits into the circulation.11 At this time, these two techniques are considered but not used routinely by surgeons.
Corticosteroids remain a debated method of prevention of fat embolism syndrome. A number of smaller studies suggest steroid therapy might reduce the incidence of fat embolism syndrome and hypoxia; a 2009 meta-analysis pooling nearly 400 patients from these smaller studies found such results.12 Unfortunately, the included studies were noted to be of poor quality, and no change in mortality was found. These results, combined with the possibility of poor wound healing or infection as a complication of steroid use, keep steroids from being used routinely to prevent fat embolism syndrome.
Clinical course. The severity of fat embolism syndrome ranges from mild transient hypoxia with confusion to progressively worsening symptoms leading to acute respiratory distress syndrome and coma. Bulger et al found a 7% mortality rate in this population.1 Less commonly, patients have a fulminant presentation with symptom onset less than 12 hours after injury. With this presentation, patients have a higher rate of mortality—as high as 15%.13
Back to the Case
This young man with bilateral long-bone fractures was at high risk of developing fat embolism syndrome. As is recommended, he was quickly taken to the operating room for fracture stabilization with open reduction and internal fixation. In addition, a RIA device was used to decrease intramedullary pressure. Nonetheless, within the first two days of injury, he developed hypoxia and confusion. These clinical changes were associated with an unexpected drop in hematocrit.
Chest X-ray and high-resolution computed tomography did not reveal a cause of his hypoxia. Similarly, laboratory evaluation for a reversible cause of encephalopathy was negative. A Sudan stain of his urine revealed free fat globules. Though he did not develop axillary petechiae, this clinical picture is consistent with fat embolism syndrome based on Gurd’s criteria. He was supported with oxygen therapy, and he stabilized without further complications.
Drs. Smith and Rice are members of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn.
References
- Bulger EM, Smith DG, Maier RV, Jurkovich GJ. Fat embolism syndrome. A 10-year review. Arch Surg. 1997;132:435-439.
- Levy D. The fat embolism syndrome. Clin Orthop. 1990;261:281-286.
- Akhtar S. Fat embolism. Anes Clin. 2009;27:533-550.
- Gupta A, Reilly C. Fat embolism. Anaesth Crit Care Pain. 2007;7:148-151.
- Thomas JE, Ayyar DR. Systemic fat embolism. Arch Neurol. 1972;26:517-523.
- Gurd AR, Wilson RI. The fat embolism syndrome. J Bone Joint Surg Br. 1974;56B:408-416.
- Lindeque BG, Schoeman HS, Dommisse GF, Boeyens MC, Vlok AL. Fat embolism and the fat embolism syndrome. A double-blind therapeutic study. J Bone Joint Surg Br. 1987;69:128-131.
- Schonfeld SA, Ploysongsang Y, DiLisio R, et al. Fat embolism prophylaxis with corticosteroids. A prospective study in high-risk patients. Ann Intern Med. 1983;99:438-443.
- Robinson CM. Current concepts of respiratory insufficiency syndromes after fracture. J Bone Joint Surg Br. 2001;83:781-791.
- Kim YH, Oh SW, Kim JS. Prevalence of fat embolism following bilateral simultaneous and unilateral total hip arthroplasty performed with or without cement: a prospective, randomized clinical study. J Bone Joint Surg Am. 2002;84A:1372-1379.
- Volgas DA, Burch T, Stannard JP, Ellis T, Bilotta J, Alonso JE. Fat embolus in femur fractures: a comparison of two reaming systems. Injury. 2010;41 Suppl 2:S90-S93.
- Bederman SS, Bhandari M, McKee MD, Schemitsch EH. Do corticosteroids reduce the risk of fat embolism syndrome in patients with long-bone fractures? A meta-analysis. Can J Surg. 2009;52:386-393.
- Bracco D, Favre JB, Joris F, Ravussin A. Fatal fat embolism syndrome: a case report. J Neurosurg Anesthesiol. 2000;12:221-224.
The Case
A 24-year-old white man with no past medical history is admitted after sustaining bilateral, closed femur fractures in a motor vehicle accident. Within hours of the trauma, he is taken to the operating room for open reduction and internal fixation. Of note, preoperatively, his hematocrit is 40%. After surgery, he is easily extubated and transferred to an unmonitored bed for further care. Approximately 30 hours after admission, he develops tachypnea with a respiratory rate of 35 breaths per minute and hypoxia with an oxygen saturation of 86% on room air. He is tachycardic (120 beats per minute) and febrile to 39.0oC. His blood pressure remains stable. He is somnolent, and when awake, he is confused. Notably, his hematocrit is now 22%. An electrocardiogram shows sinus tachycardia, an initial chest X-ray is normal, and a high-resolution CT scan is negative for a pulmonary embolism (PE).
Is this clinical picture consistent with fat embolism syndrome and, if so, how should he be managed?
Overview
“Fat embolism” refers to the presence of fat globules that obstruct the lung parenchyma and peripheral circulation. Fat embolism syndrome, on the other hand, is a more serious manifestation involving multiple organ systems. Specifically, it is a clinical diagnosis presenting with the classic triad of hypoxemia, neurologic abnormalities, and a petechial rash.
Fat embolism syndrome is usually associated with multiple traumas, including long-bone injuries and pelvic fractures. It is more frequently associated with closed fractures than open fractures, possibly due to the higher pressures associated with closed fractures. This syndrome has been less commonly associated with a variety of nontraumatic conditions (Table 1).
With an increased incidence of long-bone fractures in the younger demographic, fat embolism syndrome is most common in the second or third decade of life. While fat embolism occurs in up to 90% of patients with traumatic skeletal injuries, fat embolism syndrome occurs in 0.5% to 10% of patients following trauma, with a higher incidence in multiple fractures (5% to 10%) than in single long-bone fractures (0.5% to 2%).1-3
With the increasing role of hospitalists in assisting in the management of orthopedic patients, their knowledge of fat embolism syndrome is important so that it can be included in the differential diagnosis of acute respiratory failure in these orthopedic patients.
Review of the Data
Pathogenesis. Clinical manifestations of fat embolism syndrome have been acknowledged for more than 100 years. Since its first description in the 1860s, there has been speculation about the etiology of this condition. In the 1920s, two theories were proposed to explain the origin of the fat droplets: the mechanical and biochemical theories.2,4
Mechanical theory suggests that trauma to long bones disturbs fat cells within the bone marrow or adipose tissue, causing fat globules to mobilize.2,3 There is a rise in marrow pressure above venous pressure, which allows fat particles to enter the circulation through damaged venules surrounding the fracture site. Once lodged in the pulmonary microvasculature, embolized fat causes local ischemia and inflammation. Fat globules may pass into the arterial circulation either by paradoxical embolism through a patent foramen ovale, or by microemboli that pass through the lungs into the arterial circulation. This explains embolization to other organs, including the brain, retina, and skin.
Alternatively, biochemical theory hypothesizes that fat embolism syndrome is contingent on the production of toxic intermediaries from the breakdown of embolized fat.2,3 This theory suggests that the release of catecholamines after severe trauma can liberate free fatty acids from fat stores, or that acute-phase reactants at the trauma site affect fat solubility, causing agglutination and embolization. This theory helps to explain nontraumatic fat embolism syndrome, as well as the delay in development of the clinical syndrome after acute injury.
Clinical presentation. Most patients have a latent period after trauma of 12 to 72 hours before symptoms of fat embolism syndrome become apparent; however, clinical manifestations might occur immediately or up to one to two weeks following injury.2,4 As previously mentioned, the classic triad of symptoms includes respiratory compromise, neurological impairment, and a petechial rash.
The most common and usually earliest manifestation is acute hypoxia, which must be distinguished from other treatable causes of hypoxia, including pneumothorax, hemothorax, PE, and pneumonia. Pulmonary changes might progress to respiratory failure similar to acute respiratory distress syndrome. Neurological manifestations are primarily nonspecific and include headache, irritability, delirium, seizures, and coma. Focal neurological deficits are rare but have been described.5 Almost all neurological symptoms are fully reversible. The petechial rash is distinctive and occurs on the chest, axilla, and subconjunctiva. Although the rash occurs in only 20% to 50% of patients and resolves fairly quickly, in the appropriate clinical setting, this rash is considered pathognomonic.1,2,4
A variety of other nonspecific signs and symptoms might also occur: pyrexia, tachycardia, fat in the urine or sputum, retinal changes, renal insufficiency, myocardial dysfunction, and an otherwise unexplained drop in hematocrit or platelet count.
Diagnosis. Fat embolism syndrome is a clinical diagnosis and a diagnosis of exclusion. There are no specific confirmatory tests. An arterial blood gas will usually reveal a PaO2 of <60 mmHg.3 Laboratory evaluation might also show fat globules in the urine or sputum on Sudan or Oil Red O staining, but these findings are nonspecific.3,4 Bronchoscopy with bronchial alveolar lavage (BAL) might similarly detect fat droplets in alveolar macrophages in the BAL fluid; however, the sensitivity and specificity for diagnosis of fat embolism syndrome are unknown.4 None of these tests can be used solely for the diagnosis of fat embolism syndrome.
Thrombocytopenia and anemia out of proportion to the expected drop from surgery are not uncommon in addition to other nonspecific laboratory findings, including hypocalcemia, elevated serum lipase level, and elevated erythrocyte sedimentation rate.4 Several radiological findings have been observed on lung and brain imaging, though the findings are nonspecific and none are diagnostic. A chest X-ray might be normal, but abnormalities are seen in 30% to 50% of cases.2 Typically, when abnormal, the chest X-ray shows diffuse interstitial and alveolar densities, as well as patchy perihilar and basilar infiltrates resembling pulmonary edema. These X-ray findings might not be seen for up to 12 to 24 hours following the onset of clinical symptoms.
The most commonly used diagnostic criteria for the diagnosis of fat embolism syndrome are published by Gurd et al.6 At least two major criteria or one major criterion and four minor criteria are required for the diagnosis of fat embolism syndrome. The major criteria are based on the three classic signs and symptoms of fat embolism syndrome; the minor criteria include the finding of fat globules in the urine and sputum as well as some of the previously mentioned nonspecific clinical signs and laboratory tests.
Other criteria for diagnosis have been suggested, including those published by Lindeque et al, which focuses primarily on the respiratory characteristics, and a more recent set of semiquantitative diagnostic criteria called the fat embolism index, published by Schonfeld et al.7,8 Schonfeld’s scoring index accounts for the major signs and symptoms of fat embolism syndrome and weighs them according to relative specificity. A score of 5 or more is required for diagnosis of fat embolism syndrome. Table 2 compares the three sets of criteria used for diagnosis of fat embolism syndrome.
Treatment. The treatment of fat embolism syndrome is supportive. Most often, this requires supplemental oxygen for hypoxia and, possibly, fluid resuscitation in the case of hypovolemia. Occasionally, though, these relatively minor supportive therapies need to be escalated to bipap or even full ventilatory support and vasopressors in the more severe cases.
Based on the premise that steroids will attenuate the inflammatory reaction to free fatty acids within the lung, steroids have been tried in the treatment of fat embolism syndrome. However, there are no studies that clearly show benefit with their use.
Prevention. Most of the methods of prevention involve surgical intervention rather than medical therapy. Because microscopic fat emboli are showered during manipulation of long-bone fragments, early immobilization of fractures is recommended, and operative correction rather than conservative management is the preferred method.2,3 One report estimates a 70% reduction in pulmonary complications from this intervention alone.9
Further, two surgical techniques are debated as possible means of preventing fat embolism syndrome. The first is “venting,” in which a hole is made distal to the site of intramedullary nail placement. This reduces intramedullary pressure elevation and, therefore, extravasation of fat into the circulation.10 The second technique is the use of a reamer, irrigator, aspirator (RIA) device. A reamer is a tool used to create an accurate-sized hole for an intramedullary nail. Reaming before intramedullary nail placement can release fat deposits into the circulation. The RIA device irrigates and aspirates resident fat deposits as it reams the canal, releasing fewer deposits into the circulation.11 At this time, these two techniques are considered but not used routinely by surgeons.
Corticosteroids remain a debated method of prevention of fat embolism syndrome. A number of smaller studies suggest steroid therapy might reduce the incidence of fat embolism syndrome and hypoxia; a 2009 meta-analysis pooling nearly 400 patients from these smaller studies found such results.12 Unfortunately, the included studies were noted to be of poor quality, and no change in mortality was found. These results, combined with the possibility of poor wound healing or infection as a complication of steroid use, keep steroids from being used routinely to prevent fat embolism syndrome.
Clinical course. The severity of fat embolism syndrome ranges from mild transient hypoxia with confusion to progressively worsening symptoms leading to acute respiratory distress syndrome and coma. Bulger et al found a 7% mortality rate in this population.1 Less commonly, patients have a fulminant presentation with symptom onset less than 12 hours after injury. With this presentation, patients have a higher rate of mortality—as high as 15%.13
Back to the Case
This young man with bilateral long-bone fractures was at high risk of developing fat embolism syndrome. As is recommended, he was quickly taken to the operating room for fracture stabilization with open reduction and internal fixation. In addition, a RIA device was used to decrease intramedullary pressure. Nonetheless, within the first two days of injury, he developed hypoxia and confusion. These clinical changes were associated with an unexpected drop in hematocrit.
Chest X-ray and high-resolution computed tomography did not reveal a cause of his hypoxia. Similarly, laboratory evaluation for a reversible cause of encephalopathy was negative. A Sudan stain of his urine revealed free fat globules. Though he did not develop axillary petechiae, this clinical picture is consistent with fat embolism syndrome based on Gurd’s criteria. He was supported with oxygen therapy, and he stabilized without further complications.
Drs. Smith and Rice are members of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn.
References
- Bulger EM, Smith DG, Maier RV, Jurkovich GJ. Fat embolism syndrome. A 10-year review. Arch Surg. 1997;132:435-439.
- Levy D. The fat embolism syndrome. Clin Orthop. 1990;261:281-286.
- Akhtar S. Fat embolism. Anes Clin. 2009;27:533-550.
- Gupta A, Reilly C. Fat embolism. Anaesth Crit Care Pain. 2007;7:148-151.
- Thomas JE, Ayyar DR. Systemic fat embolism. Arch Neurol. 1972;26:517-523.
- Gurd AR, Wilson RI. The fat embolism syndrome. J Bone Joint Surg Br. 1974;56B:408-416.
- Lindeque BG, Schoeman HS, Dommisse GF, Boeyens MC, Vlok AL. Fat embolism and the fat embolism syndrome. A double-blind therapeutic study. J Bone Joint Surg Br. 1987;69:128-131.
- Schonfeld SA, Ploysongsang Y, DiLisio R, et al. Fat embolism prophylaxis with corticosteroids. A prospective study in high-risk patients. Ann Intern Med. 1983;99:438-443.
- Robinson CM. Current concepts of respiratory insufficiency syndromes after fracture. J Bone Joint Surg Br. 2001;83:781-791.
- Kim YH, Oh SW, Kim JS. Prevalence of fat embolism following bilateral simultaneous and unilateral total hip arthroplasty performed with or without cement: a prospective, randomized clinical study. J Bone Joint Surg Am. 2002;84A:1372-1379.
- Volgas DA, Burch T, Stannard JP, Ellis T, Bilotta J, Alonso JE. Fat embolus in femur fractures: a comparison of two reaming systems. Injury. 2010;41 Suppl 2:S90-S93.
- Bederman SS, Bhandari M, McKee MD, Schemitsch EH. Do corticosteroids reduce the risk of fat embolism syndrome in patients with long-bone fractures? A meta-analysis. Can J Surg. 2009;52:386-393.
- Bracco D, Favre JB, Joris F, Ravussin A. Fatal fat embolism syndrome: a case report. J Neurosurg Anesthesiol. 2000;12:221-224.
The Case
A 24-year-old white man with no past medical history is admitted after sustaining bilateral, closed femur fractures in a motor vehicle accident. Within hours of the trauma, he is taken to the operating room for open reduction and internal fixation. Of note, preoperatively, his hematocrit is 40%. After surgery, he is easily extubated and transferred to an unmonitored bed for further care. Approximately 30 hours after admission, he develops tachypnea with a respiratory rate of 35 breaths per minute and hypoxia with an oxygen saturation of 86% on room air. He is tachycardic (120 beats per minute) and febrile to 39.0oC. His blood pressure remains stable. He is somnolent, and when awake, he is confused. Notably, his hematocrit is now 22%. An electrocardiogram shows sinus tachycardia, an initial chest X-ray is normal, and a high-resolution CT scan is negative for a pulmonary embolism (PE).
Is this clinical picture consistent with fat embolism syndrome and, if so, how should he be managed?
Overview
“Fat embolism” refers to the presence of fat globules that obstruct the lung parenchyma and peripheral circulation. Fat embolism syndrome, on the other hand, is a more serious manifestation involving multiple organ systems. Specifically, it is a clinical diagnosis presenting with the classic triad of hypoxemia, neurologic abnormalities, and a petechial rash.
Fat embolism syndrome is usually associated with multiple traumas, including long-bone injuries and pelvic fractures. It is more frequently associated with closed fractures than open fractures, possibly due to the higher pressures associated with closed fractures. This syndrome has been less commonly associated with a variety of nontraumatic conditions (Table 1).
With an increased incidence of long-bone fractures in the younger demographic, fat embolism syndrome is most common in the second or third decade of life. While fat embolism occurs in up to 90% of patients with traumatic skeletal injuries, fat embolism syndrome occurs in 0.5% to 10% of patients following trauma, with a higher incidence in multiple fractures (5% to 10%) than in single long-bone fractures (0.5% to 2%).1-3
With the increasing role of hospitalists in assisting in the management of orthopedic patients, their knowledge of fat embolism syndrome is important so that it can be included in the differential diagnosis of acute respiratory failure in these orthopedic patients.
Review of the Data
Pathogenesis. Clinical manifestations of fat embolism syndrome have been acknowledged for more than 100 years. Since its first description in the 1860s, there has been speculation about the etiology of this condition. In the 1920s, two theories were proposed to explain the origin of the fat droplets: the mechanical and biochemical theories.2,4
Mechanical theory suggests that trauma to long bones disturbs fat cells within the bone marrow or adipose tissue, causing fat globules to mobilize.2,3 There is a rise in marrow pressure above venous pressure, which allows fat particles to enter the circulation through damaged venules surrounding the fracture site. Once lodged in the pulmonary microvasculature, embolized fat causes local ischemia and inflammation. Fat globules may pass into the arterial circulation either by paradoxical embolism through a patent foramen ovale, or by microemboli that pass through the lungs into the arterial circulation. This explains embolization to other organs, including the brain, retina, and skin.
Alternatively, biochemical theory hypothesizes that fat embolism syndrome is contingent on the production of toxic intermediaries from the breakdown of embolized fat.2,3 This theory suggests that the release of catecholamines after severe trauma can liberate free fatty acids from fat stores, or that acute-phase reactants at the trauma site affect fat solubility, causing agglutination and embolization. This theory helps to explain nontraumatic fat embolism syndrome, as well as the delay in development of the clinical syndrome after acute injury.
Clinical presentation. Most patients have a latent period after trauma of 12 to 72 hours before symptoms of fat embolism syndrome become apparent; however, clinical manifestations might occur immediately or up to one to two weeks following injury.2,4 As previously mentioned, the classic triad of symptoms includes respiratory compromise, neurological impairment, and a petechial rash.
The most common and usually earliest manifestation is acute hypoxia, which must be distinguished from other treatable causes of hypoxia, including pneumothorax, hemothorax, PE, and pneumonia. Pulmonary changes might progress to respiratory failure similar to acute respiratory distress syndrome. Neurological manifestations are primarily nonspecific and include headache, irritability, delirium, seizures, and coma. Focal neurological deficits are rare but have been described.5 Almost all neurological symptoms are fully reversible. The petechial rash is distinctive and occurs on the chest, axilla, and subconjunctiva. Although the rash occurs in only 20% to 50% of patients and resolves fairly quickly, in the appropriate clinical setting, this rash is considered pathognomonic.1,2,4
A variety of other nonspecific signs and symptoms might also occur: pyrexia, tachycardia, fat in the urine or sputum, retinal changes, renal insufficiency, myocardial dysfunction, and an otherwise unexplained drop in hematocrit or platelet count.
Diagnosis. Fat embolism syndrome is a clinical diagnosis and a diagnosis of exclusion. There are no specific confirmatory tests. An arterial blood gas will usually reveal a PaO2 of <60 mmHg.3 Laboratory evaluation might also show fat globules in the urine or sputum on Sudan or Oil Red O staining, but these findings are nonspecific.3,4 Bronchoscopy with bronchial alveolar lavage (BAL) might similarly detect fat droplets in alveolar macrophages in the BAL fluid; however, the sensitivity and specificity for diagnosis of fat embolism syndrome are unknown.4 None of these tests can be used solely for the diagnosis of fat embolism syndrome.
Thrombocytopenia and anemia out of proportion to the expected drop from surgery are not uncommon in addition to other nonspecific laboratory findings, including hypocalcemia, elevated serum lipase level, and elevated erythrocyte sedimentation rate.4 Several radiological findings have been observed on lung and brain imaging, though the findings are nonspecific and none are diagnostic. A chest X-ray might be normal, but abnormalities are seen in 30% to 50% of cases.2 Typically, when abnormal, the chest X-ray shows diffuse interstitial and alveolar densities, as well as patchy perihilar and basilar infiltrates resembling pulmonary edema. These X-ray findings might not be seen for up to 12 to 24 hours following the onset of clinical symptoms.
The most commonly used diagnostic criteria for the diagnosis of fat embolism syndrome are published by Gurd et al.6 At least two major criteria or one major criterion and four minor criteria are required for the diagnosis of fat embolism syndrome. The major criteria are based on the three classic signs and symptoms of fat embolism syndrome; the minor criteria include the finding of fat globules in the urine and sputum as well as some of the previously mentioned nonspecific clinical signs and laboratory tests.
Other criteria for diagnosis have been suggested, including those published by Lindeque et al, which focuses primarily on the respiratory characteristics, and a more recent set of semiquantitative diagnostic criteria called the fat embolism index, published by Schonfeld et al.7,8 Schonfeld’s scoring index accounts for the major signs and symptoms of fat embolism syndrome and weighs them according to relative specificity. A score of 5 or more is required for diagnosis of fat embolism syndrome. Table 2 compares the three sets of criteria used for diagnosis of fat embolism syndrome.
Treatment. The treatment of fat embolism syndrome is supportive. Most often, this requires supplemental oxygen for hypoxia and, possibly, fluid resuscitation in the case of hypovolemia. Occasionally, though, these relatively minor supportive therapies need to be escalated to bipap or even full ventilatory support and vasopressors in the more severe cases.
Based on the premise that steroids will attenuate the inflammatory reaction to free fatty acids within the lung, steroids have been tried in the treatment of fat embolism syndrome. However, there are no studies that clearly show benefit with their use.
Prevention. Most of the methods of prevention involve surgical intervention rather than medical therapy. Because microscopic fat emboli are showered during manipulation of long-bone fragments, early immobilization of fractures is recommended, and operative correction rather than conservative management is the preferred method.2,3 One report estimates a 70% reduction in pulmonary complications from this intervention alone.9
Further, two surgical techniques are debated as possible means of preventing fat embolism syndrome. The first is “venting,” in which a hole is made distal to the site of intramedullary nail placement. This reduces intramedullary pressure elevation and, therefore, extravasation of fat into the circulation.10 The second technique is the use of a reamer, irrigator, aspirator (RIA) device. A reamer is a tool used to create an accurate-sized hole for an intramedullary nail. Reaming before intramedullary nail placement can release fat deposits into the circulation. The RIA device irrigates and aspirates resident fat deposits as it reams the canal, releasing fewer deposits into the circulation.11 At this time, these two techniques are considered but not used routinely by surgeons.
Corticosteroids remain a debated method of prevention of fat embolism syndrome. A number of smaller studies suggest steroid therapy might reduce the incidence of fat embolism syndrome and hypoxia; a 2009 meta-analysis pooling nearly 400 patients from these smaller studies found such results.12 Unfortunately, the included studies were noted to be of poor quality, and no change in mortality was found. These results, combined with the possibility of poor wound healing or infection as a complication of steroid use, keep steroids from being used routinely to prevent fat embolism syndrome.
Clinical course. The severity of fat embolism syndrome ranges from mild transient hypoxia with confusion to progressively worsening symptoms leading to acute respiratory distress syndrome and coma. Bulger et al found a 7% mortality rate in this population.1 Less commonly, patients have a fulminant presentation with symptom onset less than 12 hours after injury. With this presentation, patients have a higher rate of mortality—as high as 15%.13
Back to the Case
This young man with bilateral long-bone fractures was at high risk of developing fat embolism syndrome. As is recommended, he was quickly taken to the operating room for fracture stabilization with open reduction and internal fixation. In addition, a RIA device was used to decrease intramedullary pressure. Nonetheless, within the first two days of injury, he developed hypoxia and confusion. These clinical changes were associated with an unexpected drop in hematocrit.
Chest X-ray and high-resolution computed tomography did not reveal a cause of his hypoxia. Similarly, laboratory evaluation for a reversible cause of encephalopathy was negative. A Sudan stain of his urine revealed free fat globules. Though he did not develop axillary petechiae, this clinical picture is consistent with fat embolism syndrome based on Gurd’s criteria. He was supported with oxygen therapy, and he stabilized without further complications.
Drs. Smith and Rice are members of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn.
References
- Bulger EM, Smith DG, Maier RV, Jurkovich GJ. Fat embolism syndrome. A 10-year review. Arch Surg. 1997;132:435-439.
- Levy D. The fat embolism syndrome. Clin Orthop. 1990;261:281-286.
- Akhtar S. Fat embolism. Anes Clin. 2009;27:533-550.
- Gupta A, Reilly C. Fat embolism. Anaesth Crit Care Pain. 2007;7:148-151.
- Thomas JE, Ayyar DR. Systemic fat embolism. Arch Neurol. 1972;26:517-523.
- Gurd AR, Wilson RI. The fat embolism syndrome. J Bone Joint Surg Br. 1974;56B:408-416.
- Lindeque BG, Schoeman HS, Dommisse GF, Boeyens MC, Vlok AL. Fat embolism and the fat embolism syndrome. A double-blind therapeutic study. J Bone Joint Surg Br. 1987;69:128-131.
- Schonfeld SA, Ploysongsang Y, DiLisio R, et al. Fat embolism prophylaxis with corticosteroids. A prospective study in high-risk patients. Ann Intern Med. 1983;99:438-443.
- Robinson CM. Current concepts of respiratory insufficiency syndromes after fracture. J Bone Joint Surg Br. 2001;83:781-791.
- Kim YH, Oh SW, Kim JS. Prevalence of fat embolism following bilateral simultaneous and unilateral total hip arthroplasty performed with or without cement: a prospective, randomized clinical study. J Bone Joint Surg Am. 2002;84A:1372-1379.
- Volgas DA, Burch T, Stannard JP, Ellis T, Bilotta J, Alonso JE. Fat embolus in femur fractures: a comparison of two reaming systems. Injury. 2010;41 Suppl 2:S90-S93.
- Bederman SS, Bhandari M, McKee MD, Schemitsch EH. Do corticosteroids reduce the risk of fat embolism syndrome in patients with long-bone fractures? A meta-analysis. Can J Surg. 2009;52:386-393.
- Bracco D, Favre JB, Joris F, Ravussin A. Fatal fat embolism syndrome: a case report. J Neurosurg Anesthesiol. 2000;12:221-224.
Hospitalists Can Help SHM Improve Health IT Systems
The Institute of Medicine (IOM) issued the report Health IT and Patient Safety: Building Safer Systems for Better Care in November 2011. SHM considers this a landmark report that serves as a call to action to improve the health information technology (HIT) systems used daily to deliver on the promise of safer, more efficient care. SHM’s IT Committee and IT Policy Committee carefully reviewed this report and have released a letter in support of its findings. SHM encourages its members to read the IOM report (www.iom.edu) or the summary of the report.
In support of the report, SHM highlighted the following:
- SHM specifically supports a call for safety transparency; a mandatory reporting mechanism for vendors; a voluntary reporting mechanism for providers to report unsafe conditions in electronic health records (EHRs) and adverse events; and the elimination of nondisclosure clauses.
- SHM supports the need for additional research to guide the design and implementation of EHR, computerized physician order entry (CPOE) systems, and clinical-decision-support (CDS) systems, including usability and expanded functionality.
- SHM supports the need for HIT education at all levels of the healthcare system from providers to vendors to include quality/safety science and process improvement.
- SHM echoes the need for interoperability, not only for data exchange, but also for CDS tools and for liquidity of data to allow new product incomers into the market and the ability to move between vendors.
- SHM believes in dual accountability between vendors and providers in HIT products to help motivate the industry to more quickly improve the safety and usability of products.
- SHM is moving ahead on these areas independently and believes that hospitalists are well positioned to be involved in achieving these goals. To assist members in their efforts, the IT Education Committee is working on in-person and online HIT educational venues for SHM members. SHM’s Health IT Quality Committee is organizing collaboratives around CDS and quality innovation sharing. The Health Quality and Patient Safety Committee continues to discuss the safety of IT systems and methods to improve them. SHM’s mentored implementation programs are engaging directly with vendors to try to build products and the functionality needed around glycemic control, care transitions, and VTE prophylaxis.
- SHM believes that its members can be involved in the research to answer many of the important questions that are unresolved in HIT. Please contact SHM to ensure that the organization is representing your needs in this important area. The current situation is a long way from the full potential HIT can provide, and SHM is committed to helping its members and the industry in moving to the next level.
The Institute of Medicine (IOM) issued the report Health IT and Patient Safety: Building Safer Systems for Better Care in November 2011. SHM considers this a landmark report that serves as a call to action to improve the health information technology (HIT) systems used daily to deliver on the promise of safer, more efficient care. SHM’s IT Committee and IT Policy Committee carefully reviewed this report and have released a letter in support of its findings. SHM encourages its members to read the IOM report (www.iom.edu) or the summary of the report.
In support of the report, SHM highlighted the following:
- SHM specifically supports a call for safety transparency; a mandatory reporting mechanism for vendors; a voluntary reporting mechanism for providers to report unsafe conditions in electronic health records (EHRs) and adverse events; and the elimination of nondisclosure clauses.
- SHM supports the need for additional research to guide the design and implementation of EHR, computerized physician order entry (CPOE) systems, and clinical-decision-support (CDS) systems, including usability and expanded functionality.
- SHM supports the need for HIT education at all levels of the healthcare system from providers to vendors to include quality/safety science and process improvement.
- SHM echoes the need for interoperability, not only for data exchange, but also for CDS tools and for liquidity of data to allow new product incomers into the market and the ability to move between vendors.
- SHM believes in dual accountability between vendors and providers in HIT products to help motivate the industry to more quickly improve the safety and usability of products.
- SHM is moving ahead on these areas independently and believes that hospitalists are well positioned to be involved in achieving these goals. To assist members in their efforts, the IT Education Committee is working on in-person and online HIT educational venues for SHM members. SHM’s Health IT Quality Committee is organizing collaboratives around CDS and quality innovation sharing. The Health Quality and Patient Safety Committee continues to discuss the safety of IT systems and methods to improve them. SHM’s mentored implementation programs are engaging directly with vendors to try to build products and the functionality needed around glycemic control, care transitions, and VTE prophylaxis.
- SHM believes that its members can be involved in the research to answer many of the important questions that are unresolved in HIT. Please contact SHM to ensure that the organization is representing your needs in this important area. The current situation is a long way from the full potential HIT can provide, and SHM is committed to helping its members and the industry in moving to the next level.
The Institute of Medicine (IOM) issued the report Health IT and Patient Safety: Building Safer Systems for Better Care in November 2011. SHM considers this a landmark report that serves as a call to action to improve the health information technology (HIT) systems used daily to deliver on the promise of safer, more efficient care. SHM’s IT Committee and IT Policy Committee carefully reviewed this report and have released a letter in support of its findings. SHM encourages its members to read the IOM report (www.iom.edu) or the summary of the report.
In support of the report, SHM highlighted the following:
- SHM specifically supports a call for safety transparency; a mandatory reporting mechanism for vendors; a voluntary reporting mechanism for providers to report unsafe conditions in electronic health records (EHRs) and adverse events; and the elimination of nondisclosure clauses.
- SHM supports the need for additional research to guide the design and implementation of EHR, computerized physician order entry (CPOE) systems, and clinical-decision-support (CDS) systems, including usability and expanded functionality.
- SHM supports the need for HIT education at all levels of the healthcare system from providers to vendors to include quality/safety science and process improvement.
- SHM echoes the need for interoperability, not only for data exchange, but also for CDS tools and for liquidity of data to allow new product incomers into the market and the ability to move between vendors.
- SHM believes in dual accountability between vendors and providers in HIT products to help motivate the industry to more quickly improve the safety and usability of products.
- SHM is moving ahead on these areas independently and believes that hospitalists are well positioned to be involved in achieving these goals. To assist members in their efforts, the IT Education Committee is working on in-person and online HIT educational venues for SHM members. SHM’s Health IT Quality Committee is organizing collaboratives around CDS and quality innovation sharing. The Health Quality and Patient Safety Committee continues to discuss the safety of IT systems and methods to improve them. SHM’s mentored implementation programs are engaging directly with vendors to try to build products and the functionality needed around glycemic control, care transitions, and VTE prophylaxis.
- SHM believes that its members can be involved in the research to answer many of the important questions that are unresolved in HIT. Please contact SHM to ensure that the organization is representing your needs in this important area. The current situation is a long way from the full potential HIT can provide, and SHM is committed to helping its members and the industry in moving to the next level.
New Data on Hospitalist Schedules
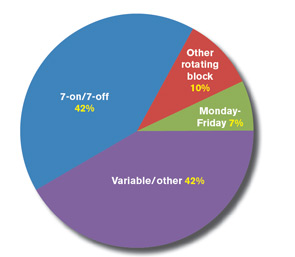
With last month’s publication of the 2012 State of Hospital Medicine report (www.hospitalmedicine.org/survey), we have some fascinating new information about the scheduling choices of HM groups—some of which has never been collected by SHM before.
For example, we learned this year that 42% of respondent groups serving adult patients predominantly utilize a schedule of seven days on followed by seven days off (“seven-on, seven-off”), while another 42% use variable/other scheduling patterns. A small minority of groups utilize other types of rotating block schedules (e.g. five-on/five-off) or Monday-Friday schedules. The type of schedule used varies a lot by area of the country, ownership/employment model, and other group characteristics.
Full-time adult medicine hospitalists working shift-based schedules now work a median of 182 shifts, or work periods, annually, down from 188 the last time SHM asked this question in 2005. For doctors working hybrid schedules, including both shifts and on-call duties, the number of shifts declined to 204 from 215 in 2005. During the same period, hospitalists’ annual encounter volume also has declined, though compensation has continued its inexorable rise.
So if the number of shifts worked and patient encounters both have declined since 2005, why do hospitalists feel so much busier today?
Well, for one thing, we learned in this year’s survey that 75% of adult hospitalist groups schedule day shifts of 12 to 13.9 hours in length, while the other 25% use shorter day shifts. About 85% of night shifts are also 12 to 13.9 hours long, while the preponderance of evening/swing shifts fall into either the 10- to 11.9-hour range (45%) or the eight-hours-or-less range (33%). In 2005, the median shift length for all respondents—both adult and pediatric—was 11 hours for groups using shift-based models, and only eight hours for groups using hybrid or other scheduling models. So although this year’s data is not presented in the same way as it was in 2005, it would appear that the typical shift length might have increased some.
In addition, in 2005, only 51% of groups reported having an on-site provider at night. This year, 55% of groups reported having total on-site nighttime coverage, and an additional 28% reported using a combination of on-site and on-call coverage. And the proportion of groups reporting no responsibility for night coverage at all declined to about 1% from 8%. I’m guessing the need to work more nights also contributes to hospitalists’ feelings of increased workload.
Although encounters have decreased, hospitalist wRVUs have risen dramatically. In part, this is due to adjustments in Medicare wRVU values for typical E&M services, but I believe it also is the result of increased patient complexity and/or improved documentation and coding by hospitalists—both of which require more time.
And finally, hospitalists are being asked to do a lot more nonclinical work these days, such as participating in quality-improvement (QI) and patient-flow initiatives, and championing the implementation of electronic health records (EHRs).
All of these factors, and probably others, have combined to make the typical hospitalist’s job much more complex and demanding today than it was in 2005, despite working a few less shifts and have a few less patient encounters annually.
Leslie Flores is SHM senior advisor, practice management.
With last month’s publication of the 2012 State of Hospital Medicine report (www.hospitalmedicine.org/survey), we have some fascinating new information about the scheduling choices of HM groups—some of which has never been collected by SHM before.
For example, we learned this year that 42% of respondent groups serving adult patients predominantly utilize a schedule of seven days on followed by seven days off (“seven-on, seven-off”), while another 42% use variable/other scheduling patterns. A small minority of groups utilize other types of rotating block schedules (e.g. five-on/five-off) or Monday-Friday schedules. The type of schedule used varies a lot by area of the country, ownership/employment model, and other group characteristics.
Full-time adult medicine hospitalists working shift-based schedules now work a median of 182 shifts, or work periods, annually, down from 188 the last time SHM asked this question in 2005. For doctors working hybrid schedules, including both shifts and on-call duties, the number of shifts declined to 204 from 215 in 2005. During the same period, hospitalists’ annual encounter volume also has declined, though compensation has continued its inexorable rise.
So if the number of shifts worked and patient encounters both have declined since 2005, why do hospitalists feel so much busier today?
Well, for one thing, we learned in this year’s survey that 75% of adult hospitalist groups schedule day shifts of 12 to 13.9 hours in length, while the other 25% use shorter day shifts. About 85% of night shifts are also 12 to 13.9 hours long, while the preponderance of evening/swing shifts fall into either the 10- to 11.9-hour range (45%) or the eight-hours-or-less range (33%). In 2005, the median shift length for all respondents—both adult and pediatric—was 11 hours for groups using shift-based models, and only eight hours for groups using hybrid or other scheduling models. So although this year’s data is not presented in the same way as it was in 2005, it would appear that the typical shift length might have increased some.
In addition, in 2005, only 51% of groups reported having an on-site provider at night. This year, 55% of groups reported having total on-site nighttime coverage, and an additional 28% reported using a combination of on-site and on-call coverage. And the proportion of groups reporting no responsibility for night coverage at all declined to about 1% from 8%. I’m guessing the need to work more nights also contributes to hospitalists’ feelings of increased workload.
Although encounters have decreased, hospitalist wRVUs have risen dramatically. In part, this is due to adjustments in Medicare wRVU values for typical E&M services, but I believe it also is the result of increased patient complexity and/or improved documentation and coding by hospitalists—both of which require more time.
And finally, hospitalists are being asked to do a lot more nonclinical work these days, such as participating in quality-improvement (QI) and patient-flow initiatives, and championing the implementation of electronic health records (EHRs).
All of these factors, and probably others, have combined to make the typical hospitalist’s job much more complex and demanding today than it was in 2005, despite working a few less shifts and have a few less patient encounters annually.
Leslie Flores is SHM senior advisor, practice management.
With last month’s publication of the 2012 State of Hospital Medicine report (www.hospitalmedicine.org/survey), we have some fascinating new information about the scheduling choices of HM groups—some of which has never been collected by SHM before.
For example, we learned this year that 42% of respondent groups serving adult patients predominantly utilize a schedule of seven days on followed by seven days off (“seven-on, seven-off”), while another 42% use variable/other scheduling patterns. A small minority of groups utilize other types of rotating block schedules (e.g. five-on/five-off) or Monday-Friday schedules. The type of schedule used varies a lot by area of the country, ownership/employment model, and other group characteristics.
Full-time adult medicine hospitalists working shift-based schedules now work a median of 182 shifts, or work periods, annually, down from 188 the last time SHM asked this question in 2005. For doctors working hybrid schedules, including both shifts and on-call duties, the number of shifts declined to 204 from 215 in 2005. During the same period, hospitalists’ annual encounter volume also has declined, though compensation has continued its inexorable rise.
So if the number of shifts worked and patient encounters both have declined since 2005, why do hospitalists feel so much busier today?
Well, for one thing, we learned in this year’s survey that 75% of adult hospitalist groups schedule day shifts of 12 to 13.9 hours in length, while the other 25% use shorter day shifts. About 85% of night shifts are also 12 to 13.9 hours long, while the preponderance of evening/swing shifts fall into either the 10- to 11.9-hour range (45%) or the eight-hours-or-less range (33%). In 2005, the median shift length for all respondents—both adult and pediatric—was 11 hours for groups using shift-based models, and only eight hours for groups using hybrid or other scheduling models. So although this year’s data is not presented in the same way as it was in 2005, it would appear that the typical shift length might have increased some.
In addition, in 2005, only 51% of groups reported having an on-site provider at night. This year, 55% of groups reported having total on-site nighttime coverage, and an additional 28% reported using a combination of on-site and on-call coverage. And the proportion of groups reporting no responsibility for night coverage at all declined to about 1% from 8%. I’m guessing the need to work more nights also contributes to hospitalists’ feelings of increased workload.
Although encounters have decreased, hospitalist wRVUs have risen dramatically. In part, this is due to adjustments in Medicare wRVU values for typical E&M services, but I believe it also is the result of increased patient complexity and/or improved documentation and coding by hospitalists—both of which require more time.
And finally, hospitalists are being asked to do a lot more nonclinical work these days, such as participating in quality-improvement (QI) and patient-flow initiatives, and championing the implementation of electronic health records (EHRs).
All of these factors, and probably others, have combined to make the typical hospitalist’s job much more complex and demanding today than it was in 2005, despite working a few less shifts and have a few less patient encounters annually.
Leslie Flores is SHM senior advisor, practice management.
Ready to Become a Fellow in Hospital Medicine?
Fellowship has its privileges. For SHM’s Fellows and Senior Fellows in Hospital Medicine, it means demonstrating leadership and critical experience in a rapidly growing medical specialty. It also means receiving recognition among peers at SHM’s annual meeting and access to the SHM Fellows Lounge.
In addition to being able to use the FHM, SFHM, or MHM designations for professional purposes, Fellows receive an official certificate, listing on the SHM website, and even discounts on products in the SHM online store.
The application process can take time, so plan ahead and apply early. The application deadline for the 2013 class of Fellows is January 18.
For more information, visit www.hospitalmedicine.org/fellows.
Fellowship has its privileges. For SHM’s Fellows and Senior Fellows in Hospital Medicine, it means demonstrating leadership and critical experience in a rapidly growing medical specialty. It also means receiving recognition among peers at SHM’s annual meeting and access to the SHM Fellows Lounge.
In addition to being able to use the FHM, SFHM, or MHM designations for professional purposes, Fellows receive an official certificate, listing on the SHM website, and even discounts on products in the SHM online store.
The application process can take time, so plan ahead and apply early. The application deadline for the 2013 class of Fellows is January 18.
For more information, visit www.hospitalmedicine.org/fellows.
Fellowship has its privileges. For SHM’s Fellows and Senior Fellows in Hospital Medicine, it means demonstrating leadership and critical experience in a rapidly growing medical specialty. It also means receiving recognition among peers at SHM’s annual meeting and access to the SHM Fellows Lounge.
In addition to being able to use the FHM, SFHM, or MHM designations for professional purposes, Fellows receive an official certificate, listing on the SHM website, and even discounts on products in the SHM online store.
The application process can take time, so plan ahead and apply early. The application deadline for the 2013 class of Fellows is January 18.
For more information, visit www.hospitalmedicine.org/fellows.