User login
Can Medicare Pay for Value?
Can quality measurement and comparisons serve as the backbone for a major shift in the Medicare payment system to reward value instead of volume? That is the question being explored over the next few years as the Physician Quality Reporting System (PQRS) and, by extension, the physician value-based payment modifier (VBPM) come fully into effect for all physicians.
There seems to be a consensus in the policy community that the fee-for-service model of payment is past its prime and needs to be replaced with a more dynamic and responsive payment system. Medicare hopes that PQRS and the VBPM will enable adjustments to physician payments to reward high-quality and low-cost care. Although these programs currently are add-ons to the fee-for-service system, they likely will serve as stepping stones to more radical departures from the existing payment system.
SHM advocates refinements to policies for PQRS and similar programs to make them more meaningful and productive for both hospitalists and the broader health-care system. Each year, SHM submits comments on the Physician Fee Schedule Rule, which creates and updates the regulatory framework for PQRS and the VBPM. SHM also provided feedback on Quality and Resource Use Reports (QRURs), the report cards for the modifier that were being tested over the past year.
From a practical standpoint, SHM engages with measure development and endorsement processes to ensure there are reportable quality measures in PQRS that fit hospitalist practice. In addition, SHM is helping to increase accessibility to PQRS reporting by offering members reduced fare access to registry reporting through the PQRI Wizard.
The comments range from the technical aspects of individual quality measures in PQRS to how hospitalists appear to be performing in these programs. SHM firmly believes that the unique positioning of hospitalists within the health-care system presents challenges for their identification and evaluation in Medicare programs. In some sense, hospitalists exist on the line between the inpatient and outpatient worlds, a location not adequately captured in pay-for-performance programs.
It’s imperative that pay-for-performance programs have reasonable and actionable outcomes for providers. If quality measures are not clinically meaningful and do not capture a plurality of the care provided by an individual hospitalist, it is difficult for the program to meet its stated aims. If payment is to be influenced by performance on quality measures, it follows that those measures should be relevant to the care provided.
There is a long way to go toward creating quality measurement and evaluation programs that are relevant and actionable for clinical quality improvement (QI). By becoming involved in SHM’s policy efforts, members are able to share their experiences and impressions of programs with SHM and lawmakers. This partnership helps create more responsive and intuitive programs, which in turn leads to greater participation and, hopefully, improved patient outcomes. As these programs continue to evolve and more health professionals are required to participate, SHM will be looking to its membership for their perspectives.
Join the grassroots network to stay involved and up to date by registering at www.hospitalmedicine.org/grassroots.
Joshua Lapps is SHM’s government relations specialist.
Can quality measurement and comparisons serve as the backbone for a major shift in the Medicare payment system to reward value instead of volume? That is the question being explored over the next few years as the Physician Quality Reporting System (PQRS) and, by extension, the physician value-based payment modifier (VBPM) come fully into effect for all physicians.
There seems to be a consensus in the policy community that the fee-for-service model of payment is past its prime and needs to be replaced with a more dynamic and responsive payment system. Medicare hopes that PQRS and the VBPM will enable adjustments to physician payments to reward high-quality and low-cost care. Although these programs currently are add-ons to the fee-for-service system, they likely will serve as stepping stones to more radical departures from the existing payment system.
SHM advocates refinements to policies for PQRS and similar programs to make them more meaningful and productive for both hospitalists and the broader health-care system. Each year, SHM submits comments on the Physician Fee Schedule Rule, which creates and updates the regulatory framework for PQRS and the VBPM. SHM also provided feedback on Quality and Resource Use Reports (QRURs), the report cards for the modifier that were being tested over the past year.
From a practical standpoint, SHM engages with measure development and endorsement processes to ensure there are reportable quality measures in PQRS that fit hospitalist practice. In addition, SHM is helping to increase accessibility to PQRS reporting by offering members reduced fare access to registry reporting through the PQRI Wizard.
The comments range from the technical aspects of individual quality measures in PQRS to how hospitalists appear to be performing in these programs. SHM firmly believes that the unique positioning of hospitalists within the health-care system presents challenges for their identification and evaluation in Medicare programs. In some sense, hospitalists exist on the line between the inpatient and outpatient worlds, a location not adequately captured in pay-for-performance programs.
It’s imperative that pay-for-performance programs have reasonable and actionable outcomes for providers. If quality measures are not clinically meaningful and do not capture a plurality of the care provided by an individual hospitalist, it is difficult for the program to meet its stated aims. If payment is to be influenced by performance on quality measures, it follows that those measures should be relevant to the care provided.
There is a long way to go toward creating quality measurement and evaluation programs that are relevant and actionable for clinical quality improvement (QI). By becoming involved in SHM’s policy efforts, members are able to share their experiences and impressions of programs with SHM and lawmakers. This partnership helps create more responsive and intuitive programs, which in turn leads to greater participation and, hopefully, improved patient outcomes. As these programs continue to evolve and more health professionals are required to participate, SHM will be looking to its membership for their perspectives.
Join the grassroots network to stay involved and up to date by registering at www.hospitalmedicine.org/grassroots.
Joshua Lapps is SHM’s government relations specialist.
Can quality measurement and comparisons serve as the backbone for a major shift in the Medicare payment system to reward value instead of volume? That is the question being explored over the next few years as the Physician Quality Reporting System (PQRS) and, by extension, the physician value-based payment modifier (VBPM) come fully into effect for all physicians.
There seems to be a consensus in the policy community that the fee-for-service model of payment is past its prime and needs to be replaced with a more dynamic and responsive payment system. Medicare hopes that PQRS and the VBPM will enable adjustments to physician payments to reward high-quality and low-cost care. Although these programs currently are add-ons to the fee-for-service system, they likely will serve as stepping stones to more radical departures from the existing payment system.
SHM advocates refinements to policies for PQRS and similar programs to make them more meaningful and productive for both hospitalists and the broader health-care system. Each year, SHM submits comments on the Physician Fee Schedule Rule, which creates and updates the regulatory framework for PQRS and the VBPM. SHM also provided feedback on Quality and Resource Use Reports (QRURs), the report cards for the modifier that were being tested over the past year.
From a practical standpoint, SHM engages with measure development and endorsement processes to ensure there are reportable quality measures in PQRS that fit hospitalist practice. In addition, SHM is helping to increase accessibility to PQRS reporting by offering members reduced fare access to registry reporting through the PQRI Wizard.
The comments range from the technical aspects of individual quality measures in PQRS to how hospitalists appear to be performing in these programs. SHM firmly believes that the unique positioning of hospitalists within the health-care system presents challenges for their identification and evaluation in Medicare programs. In some sense, hospitalists exist on the line between the inpatient and outpatient worlds, a location not adequately captured in pay-for-performance programs.
It’s imperative that pay-for-performance programs have reasonable and actionable outcomes for providers. If quality measures are not clinically meaningful and do not capture a plurality of the care provided by an individual hospitalist, it is difficult for the program to meet its stated aims. If payment is to be influenced by performance on quality measures, it follows that those measures should be relevant to the care provided.
There is a long way to go toward creating quality measurement and evaluation programs that are relevant and actionable for clinical quality improvement (QI). By becoming involved in SHM’s policy efforts, members are able to share their experiences and impressions of programs with SHM and lawmakers. This partnership helps create more responsive and intuitive programs, which in turn leads to greater participation and, hopefully, improved patient outcomes. As these programs continue to evolve and more health professionals are required to participate, SHM will be looking to its membership for their perspectives.
Join the grassroots network to stay involved and up to date by registering at www.hospitalmedicine.org/grassroots.
Joshua Lapps is SHM’s government relations specialist.
SHM Leadership Academy Prepares Hospitalists for the Business of Medicine
Tiered training prepares hospitalists for the business of medicine
Hospitalists often leave residency feeling prepared for clinical work, but they quickly realize that the clinical side of hospitalist work is only one part of a larger spectrum of skill sets needed to succeed. Leading teams, addressing conflict, and understanding the financial implications of hospital care are important parts of life in hospital medicine, but rarely are they taught in academic life.
The demand for these skills help explain the popularity of SHM’s Leadership Academy, which has trained more than 1,000 hospitalists in financial storytelling, meta-leadership, and the mindset of a hospital CEO.
For the first time, in October, SHM will present all three levels of its leadership courses concurrently:
Foundations for Effective Leadership.
This four-day course serves as a prerequisite to all other academy courses. Attendees learn how to evaluate personal leadership strengths and weaknesses, create and execute a communication strategy for key team members, understand key hospital drivers, examine how hospital metrics are derived, and more.
Advanced Leadership: Strategies and Tools for Personal Leadership Excellence.
Through world-renowned faculty and applied exercises, this course builds skills around driving culture change through specific leadership behaviors and actions, financial storytelling, engaging in effective professional negotiation activities with proven techniques, and more.
Advanced Leadership: Developing a Winning Team and Strengthening Your Organization.
Developed in response to high demand from academy attendees, this course focuses on strengthening teams and institutions. Participants learn how to critically assess program growth opportunities and develop operational plans; lead, manage, and motivate teams in complex hospital environments; and effective communication strategies.
In addition to career-building skills, participants in each course will learn about SHM’s Certificate of Leadership in Hospital Medicine. Drs. Thomas McIlraith and Sameh Naseib received SHM’s inaugural Certificates of Leadership in Hospital Medicine on stage during the plenary session at HM13.
For academy courses, faculty, and registration information, visit www.hospitalmedicine.org/leadership.
Tiered training prepares hospitalists for the business of medicine
Hospitalists often leave residency feeling prepared for clinical work, but they quickly realize that the clinical side of hospitalist work is only one part of a larger spectrum of skill sets needed to succeed. Leading teams, addressing conflict, and understanding the financial implications of hospital care are important parts of life in hospital medicine, but rarely are they taught in academic life.
The demand for these skills help explain the popularity of SHM’s Leadership Academy, which has trained more than 1,000 hospitalists in financial storytelling, meta-leadership, and the mindset of a hospital CEO.
For the first time, in October, SHM will present all three levels of its leadership courses concurrently:
Foundations for Effective Leadership.
This four-day course serves as a prerequisite to all other academy courses. Attendees learn how to evaluate personal leadership strengths and weaknesses, create and execute a communication strategy for key team members, understand key hospital drivers, examine how hospital metrics are derived, and more.
Advanced Leadership: Strategies and Tools for Personal Leadership Excellence.
Through world-renowned faculty and applied exercises, this course builds skills around driving culture change through specific leadership behaviors and actions, financial storytelling, engaging in effective professional negotiation activities with proven techniques, and more.
Advanced Leadership: Developing a Winning Team and Strengthening Your Organization.
Developed in response to high demand from academy attendees, this course focuses on strengthening teams and institutions. Participants learn how to critically assess program growth opportunities and develop operational plans; lead, manage, and motivate teams in complex hospital environments; and effective communication strategies.
In addition to career-building skills, participants in each course will learn about SHM’s Certificate of Leadership in Hospital Medicine. Drs. Thomas McIlraith and Sameh Naseib received SHM’s inaugural Certificates of Leadership in Hospital Medicine on stage during the plenary session at HM13.
For academy courses, faculty, and registration information, visit www.hospitalmedicine.org/leadership.
Tiered training prepares hospitalists for the business of medicine
Hospitalists often leave residency feeling prepared for clinical work, but they quickly realize that the clinical side of hospitalist work is only one part of a larger spectrum of skill sets needed to succeed. Leading teams, addressing conflict, and understanding the financial implications of hospital care are important parts of life in hospital medicine, but rarely are they taught in academic life.
The demand for these skills help explain the popularity of SHM’s Leadership Academy, which has trained more than 1,000 hospitalists in financial storytelling, meta-leadership, and the mindset of a hospital CEO.
For the first time, in October, SHM will present all three levels of its leadership courses concurrently:
Foundations for Effective Leadership.
This four-day course serves as a prerequisite to all other academy courses. Attendees learn how to evaluate personal leadership strengths and weaknesses, create and execute a communication strategy for key team members, understand key hospital drivers, examine how hospital metrics are derived, and more.
Advanced Leadership: Strategies and Tools for Personal Leadership Excellence.
Through world-renowned faculty and applied exercises, this course builds skills around driving culture change through specific leadership behaviors and actions, financial storytelling, engaging in effective professional negotiation activities with proven techniques, and more.
Advanced Leadership: Developing a Winning Team and Strengthening Your Organization.
Developed in response to high demand from academy attendees, this course focuses on strengthening teams and institutions. Participants learn how to critically assess program growth opportunities and develop operational plans; lead, manage, and motivate teams in complex hospital environments; and effective communication strategies.
In addition to career-building skills, participants in each course will learn about SHM’s Certificate of Leadership in Hospital Medicine. Drs. Thomas McIlraith and Sameh Naseib received SHM’s inaugural Certificates of Leadership in Hospital Medicine on stage during the plenary session at HM13.
For academy courses, faculty, and registration information, visit www.hospitalmedicine.org/leadership.
Three Easy Ways to Get Ahead in Hospital Medicine
Getting involved—and getting ahead—in hospital medicine has never been easier, with just some planning and preparation. Here are three ways to move your hospital—and your career—forward this month.
1. Add “award-winning” to your CV: SHM’s Awards of Excellence deadline is Sept. 16.
Although 2013’s award-winners are still fresh in hospitalists’ minds, now is the time to put together award applications for the 2014 Awards of Excellence.
Each year, SHM presents six different awards that recognize individuals and one award to a team that is transforming health care and revolutionizing patient care for hospitalized patients:
- Excellence in Research Award;
- Excellence in Hospital Medicine for Non-Physicians;
- Award for Excellence in Teaching;
- Award for Outstanding Service in Hospital Medicine;
- Award for Clinical Excellence; and
- Excellence in Teamwork in Quality Improvement.
Last year, SHM received award nominations from a diverse group of hospitalists and looks forward to receiving even more this year. Each winner receives an all-expenses-paid trip to HM14 in Las Vegas, including complimentary meeting registration.
The deadline for applications for SHM’s five individual awards is Sept. 16. The deadline for the Excellence in Teamwork in Quality Improvement is Oct. 15. All SHM members are eligible, and nominees can be self-nominated.
For more information, visit www.hospital medicine.org/awards.
2. Bring the experts in reducing readmissions to your hospital: Apply now for Project BOOST.
There is still time to apply for SHM’s Project BOOST, which helps hospitals design discharge programs to reduce readmissions. SHM will accept applications for Project BOOST until the end of August.
Project BOOST is based on SHM’s award-winning mentored implementation model that brings individualized attention from national experts in reducing readmissions to hospitals across the country. Each Project BOOST site receives:
- A comprehensive intervention developed by a panel of nationally recognized experts based on the best available evidence.
- A comprehensive implementation guide that provides step-by-step instructions and project-management tools, such as the teachback training curriculum, to help interdisciplinary teams redesign workflow and plan, implement, and evaluate the intervention.
- Longitudinal technical assistance providing face-to-face training and a year of expert mentoring and coaching to implement BOOST interventions that build a culture that supports safe and complete transitions. The mentoring program provides a training DVD and curriculum for nurses and case managers on using the teachback process, as well as webinars that target the educational needs of other team members, including administrators, data analysts, physicians, nurses, and others.
- Collaboration that allows sites to communicate with and learn from each other via the BOOST community site and quarterly all-site teleconferences and webinars.
- The BOOST data center, an online resource that allows sites to store and benchmark data against control units and other sites and generates reports.
For more information, visit www.hospital medicine.org/boost.
3. Start Choosing Wisely today.
In 2014, as part of a grant from the ABIM Foundation, SHM will begin its first Choosing Wisely case-study competition to highlight hospitalists’ best practices within the popular campaign.
But in order to have a successful case study next year, some preparation is in order now. Developing goals, gathering a team, and, perhaps most important, developing benchmarking data on a project motivated by Choosing Wisely will all be important parts of a compelling case study.
To start brainstorming your project to implement Choosing Wisely recommendations at your hospital, visit www.hospitalmedicine.org/choosingwisely.
Brendon Shank is SHM’s associate vice president of communications.
Getting involved—and getting ahead—in hospital medicine has never been easier, with just some planning and preparation. Here are three ways to move your hospital—and your career—forward this month.
1. Add “award-winning” to your CV: SHM’s Awards of Excellence deadline is Sept. 16.
Although 2013’s award-winners are still fresh in hospitalists’ minds, now is the time to put together award applications for the 2014 Awards of Excellence.
Each year, SHM presents six different awards that recognize individuals and one award to a team that is transforming health care and revolutionizing patient care for hospitalized patients:
- Excellence in Research Award;
- Excellence in Hospital Medicine for Non-Physicians;
- Award for Excellence in Teaching;
- Award for Outstanding Service in Hospital Medicine;
- Award for Clinical Excellence; and
- Excellence in Teamwork in Quality Improvement.
Last year, SHM received award nominations from a diverse group of hospitalists and looks forward to receiving even more this year. Each winner receives an all-expenses-paid trip to HM14 in Las Vegas, including complimentary meeting registration.
The deadline for applications for SHM’s five individual awards is Sept. 16. The deadline for the Excellence in Teamwork in Quality Improvement is Oct. 15. All SHM members are eligible, and nominees can be self-nominated.
For more information, visit www.hospital medicine.org/awards.
2. Bring the experts in reducing readmissions to your hospital: Apply now for Project BOOST.
There is still time to apply for SHM’s Project BOOST, which helps hospitals design discharge programs to reduce readmissions. SHM will accept applications for Project BOOST until the end of August.
Project BOOST is based on SHM’s award-winning mentored implementation model that brings individualized attention from national experts in reducing readmissions to hospitals across the country. Each Project BOOST site receives:
- A comprehensive intervention developed by a panel of nationally recognized experts based on the best available evidence.
- A comprehensive implementation guide that provides step-by-step instructions and project-management tools, such as the teachback training curriculum, to help interdisciplinary teams redesign workflow and plan, implement, and evaluate the intervention.
- Longitudinal technical assistance providing face-to-face training and a year of expert mentoring and coaching to implement BOOST interventions that build a culture that supports safe and complete transitions. The mentoring program provides a training DVD and curriculum for nurses and case managers on using the teachback process, as well as webinars that target the educational needs of other team members, including administrators, data analysts, physicians, nurses, and others.
- Collaboration that allows sites to communicate with and learn from each other via the BOOST community site and quarterly all-site teleconferences and webinars.
- The BOOST data center, an online resource that allows sites to store and benchmark data against control units and other sites and generates reports.
For more information, visit www.hospital medicine.org/boost.
3. Start Choosing Wisely today.
In 2014, as part of a grant from the ABIM Foundation, SHM will begin its first Choosing Wisely case-study competition to highlight hospitalists’ best practices within the popular campaign.
But in order to have a successful case study next year, some preparation is in order now. Developing goals, gathering a team, and, perhaps most important, developing benchmarking data on a project motivated by Choosing Wisely will all be important parts of a compelling case study.
To start brainstorming your project to implement Choosing Wisely recommendations at your hospital, visit www.hospitalmedicine.org/choosingwisely.
Brendon Shank is SHM’s associate vice president of communications.
Getting involved—and getting ahead—in hospital medicine has never been easier, with just some planning and preparation. Here are three ways to move your hospital—and your career—forward this month.
1. Add “award-winning” to your CV: SHM’s Awards of Excellence deadline is Sept. 16.
Although 2013’s award-winners are still fresh in hospitalists’ minds, now is the time to put together award applications for the 2014 Awards of Excellence.
Each year, SHM presents six different awards that recognize individuals and one award to a team that is transforming health care and revolutionizing patient care for hospitalized patients:
- Excellence in Research Award;
- Excellence in Hospital Medicine for Non-Physicians;
- Award for Excellence in Teaching;
- Award for Outstanding Service in Hospital Medicine;
- Award for Clinical Excellence; and
- Excellence in Teamwork in Quality Improvement.
Last year, SHM received award nominations from a diverse group of hospitalists and looks forward to receiving even more this year. Each winner receives an all-expenses-paid trip to HM14 in Las Vegas, including complimentary meeting registration.
The deadline for applications for SHM’s five individual awards is Sept. 16. The deadline for the Excellence in Teamwork in Quality Improvement is Oct. 15. All SHM members are eligible, and nominees can be self-nominated.
For more information, visit www.hospital medicine.org/awards.
2. Bring the experts in reducing readmissions to your hospital: Apply now for Project BOOST.
There is still time to apply for SHM’s Project BOOST, which helps hospitals design discharge programs to reduce readmissions. SHM will accept applications for Project BOOST until the end of August.
Project BOOST is based on SHM’s award-winning mentored implementation model that brings individualized attention from national experts in reducing readmissions to hospitals across the country. Each Project BOOST site receives:
- A comprehensive intervention developed by a panel of nationally recognized experts based on the best available evidence.
- A comprehensive implementation guide that provides step-by-step instructions and project-management tools, such as the teachback training curriculum, to help interdisciplinary teams redesign workflow and plan, implement, and evaluate the intervention.
- Longitudinal technical assistance providing face-to-face training and a year of expert mentoring and coaching to implement BOOST interventions that build a culture that supports safe and complete transitions. The mentoring program provides a training DVD and curriculum for nurses and case managers on using the teachback process, as well as webinars that target the educational needs of other team members, including administrators, data analysts, physicians, nurses, and others.
- Collaboration that allows sites to communicate with and learn from each other via the BOOST community site and quarterly all-site teleconferences and webinars.
- The BOOST data center, an online resource that allows sites to store and benchmark data against control units and other sites and generates reports.
For more information, visit www.hospital medicine.org/boost.
3. Start Choosing Wisely today.
In 2014, as part of a grant from the ABIM Foundation, SHM will begin its first Choosing Wisely case-study competition to highlight hospitalists’ best practices within the popular campaign.
But in order to have a successful case study next year, some preparation is in order now. Developing goals, gathering a team, and, perhaps most important, developing benchmarking data on a project motivated by Choosing Wisely will all be important parts of a compelling case study.
To start brainstorming your project to implement Choosing Wisely recommendations at your hospital, visit www.hospitalmedicine.org/choosingwisely.
Brendon Shank is SHM’s associate vice president of communications.
SHM Microsites Help Focused-Practice Specialists Work Together

The hospitalist model of providing care in the hospital has spread beyond internal medicine, pediatrics, and family medicine. Specialists in a number of other fields have adopted HM principles and adapted them to such medical specialties as orthopedics, surgery, psychiatry, OBGYN, and neurology.
Leaders in those hospital-focused-practice specialties now can work together to share best practices and identify opportunities to improve hospital-based care delivery through SHM, which has dedicated a section of its website (www.hospitalmedicine.org/hfp) to providing hospital-focused-practice caregivers some of the first resources in the specialty.
“SHM has created these Web areas as a place to convene and develop these emerging specialties in hospital medicine,” SHM CEO Larry Wellikson, MD, SFHM, says in a video on the website. He says that the new Web areas give specialty hospitalists the chance to “put their practice on the map, begin to share data, post relevant articles, and use social networks to share ideas.”
The site highlights five emerging specialties:
- Orthopedic HM;
- Surgical/acute-care surgery;
- Psychiatric HM;
- OBGYN HM; and
- Neurohospitalists.
Each of the listed specialties has its own section of the website that describes the practice, provides relevant articles, and lists events specific to the practice. Later, SHM expects to include access to a hospital-focused-practice community on its popular Hospital Medicine Exchange (HMX) online collaboration site.
Specialty hospitalists can literally put their practice on the map by filling out a practice profile form, which then enters the practice information on a map for other specialty hospitalists to see.
High-level conversations among hospitalists and hospital executives about hospital-focused practice began to take shape at a 2011 conference hosted by SHM. In 2012, the American Hospital Association’s Physician Leadership Forum and SHM published the first report on the subject, “Creating the Hospital of the Future: The Implications for Hospital-Focused Physician Practice,” which was sponsored by Apogee Physicians, Delphi Healthcare Partners Inc., and Eagle Hospital Physicians.
Dr. Wellikson says now is the time for these pioneer hospitalists to come together.
“This is your opportunity to create your new specialty,” he says, “and SHM is happy to be a part of this.”
Brendon Shank is SHM’s associate vice president of communications.
The hospitalist model of providing care in the hospital has spread beyond internal medicine, pediatrics, and family medicine. Specialists in a number of other fields have adopted HM principles and adapted them to such medical specialties as orthopedics, surgery, psychiatry, OBGYN, and neurology.
Leaders in those hospital-focused-practice specialties now can work together to share best practices and identify opportunities to improve hospital-based care delivery through SHM, which has dedicated a section of its website (www.hospitalmedicine.org/hfp) to providing hospital-focused-practice caregivers some of the first resources in the specialty.
“SHM has created these Web areas as a place to convene and develop these emerging specialties in hospital medicine,” SHM CEO Larry Wellikson, MD, SFHM, says in a video on the website. He says that the new Web areas give specialty hospitalists the chance to “put their practice on the map, begin to share data, post relevant articles, and use social networks to share ideas.”
The site highlights five emerging specialties:
- Orthopedic HM;
- Surgical/acute-care surgery;
- Psychiatric HM;
- OBGYN HM; and
- Neurohospitalists.
Each of the listed specialties has its own section of the website that describes the practice, provides relevant articles, and lists events specific to the practice. Later, SHM expects to include access to a hospital-focused-practice community on its popular Hospital Medicine Exchange (HMX) online collaboration site.
Specialty hospitalists can literally put their practice on the map by filling out a practice profile form, which then enters the practice information on a map for other specialty hospitalists to see.
High-level conversations among hospitalists and hospital executives about hospital-focused practice began to take shape at a 2011 conference hosted by SHM. In 2012, the American Hospital Association’s Physician Leadership Forum and SHM published the first report on the subject, “Creating the Hospital of the Future: The Implications for Hospital-Focused Physician Practice,” which was sponsored by Apogee Physicians, Delphi Healthcare Partners Inc., and Eagle Hospital Physicians.
Dr. Wellikson says now is the time for these pioneer hospitalists to come together.
“This is your opportunity to create your new specialty,” he says, “and SHM is happy to be a part of this.”
Brendon Shank is SHM’s associate vice president of communications.
The hospitalist model of providing care in the hospital has spread beyond internal medicine, pediatrics, and family medicine. Specialists in a number of other fields have adopted HM principles and adapted them to such medical specialties as orthopedics, surgery, psychiatry, OBGYN, and neurology.
Leaders in those hospital-focused-practice specialties now can work together to share best practices and identify opportunities to improve hospital-based care delivery through SHM, which has dedicated a section of its website (www.hospitalmedicine.org/hfp) to providing hospital-focused-practice caregivers some of the first resources in the specialty.
“SHM has created these Web areas as a place to convene and develop these emerging specialties in hospital medicine,” SHM CEO Larry Wellikson, MD, SFHM, says in a video on the website. He says that the new Web areas give specialty hospitalists the chance to “put their practice on the map, begin to share data, post relevant articles, and use social networks to share ideas.”
The site highlights five emerging specialties:
- Orthopedic HM;
- Surgical/acute-care surgery;
- Psychiatric HM;
- OBGYN HM; and
- Neurohospitalists.
Each of the listed specialties has its own section of the website that describes the practice, provides relevant articles, and lists events specific to the practice. Later, SHM expects to include access to a hospital-focused-practice community on its popular Hospital Medicine Exchange (HMX) online collaboration site.
Specialty hospitalists can literally put their practice on the map by filling out a practice profile form, which then enters the practice information on a map for other specialty hospitalists to see.
High-level conversations among hospitalists and hospital executives about hospital-focused practice began to take shape at a 2011 conference hosted by SHM. In 2012, the American Hospital Association’s Physician Leadership Forum and SHM published the first report on the subject, “Creating the Hospital of the Future: The Implications for Hospital-Focused Physician Practice,” which was sponsored by Apogee Physicians, Delphi Healthcare Partners Inc., and Eagle Hospital Physicians.
Dr. Wellikson says now is the time for these pioneer hospitalists to come together.
“This is your opportunity to create your new specialty,” he says, “and SHM is happy to be a part of this.”
Brendon Shank is SHM’s associate vice president of communications.
Reviews of Research on Steroids and VTE Risk, Epidural Catheterization, and Beta-Blockers During Noncardiac Surgery
In This Edition
Literature At A Glance
A guide to this month’s studies
- Steroids may increase VTE risk
- Mortality rates rise at critical-care hospitals
- Physicians don’t discuss advance-care planning with elderly, families
- Ultrasound imaging for lumbar puncture, epidural catheterization
- Financial impact of surgical complications on hospitals
- Lab test fees and frequency of test ordering
- Inpatient elderly multidisciplinary teams reduce readmissions
- Use of beta-blockers in high-risk patients during noncardiac surgery
- Patient-centered decision-making and health-care outcomes
- Adverse surgical outcomes in patients with schizophrenia
Steroids May Increase VTE Risk
Clinical question: Is exogenous glucocorticoid administration associated with an increased risk of VTE?
Background: Endogenous hypercortisolism is linked to increased VTE rates, and pathophysiologic data exist to suggest glucocorticoids increase clotting, but few studies have measured the clinical link between glucocorticoid administration and VTE events.
Study design: Case-control study.
Setting: Denmark.
Synopsis: The authors analyzed Danish national registries, which include information on diagnoses and prescriptions. The study selection period was Jan. 1, 2005, to Dec. 31, 2011. During this period, 38,675 cases of VTE (both DVT and pulmonary embolism) were identified in the population of Denmark. These cases were matched with 387,650 controls. Three routes of glucocorticoid use were studied: systemic (oral and intravenous), inhaled, and intestinal-acting. Cases were classified as present (within 90 days of VTE event), recent (91 to 365 days), or former (over 365 days) users of glucocorticoids. Categories were also created for new versus continuous users.
Glucocorticoid use was associated with a significant increase in VTE occurrence. The strongest link was in new and recent users, and the effect diminished over time. Key limitations of the study included its reliance on registry data, as well as the fact that cases had more comorbid conditions than controls (e.g. recent infection, chronic illnesses).
Bottom line: Recipients of glucocorticoids had an increased risk of VTE; the effect was strongest in new and recent users.
Citation: Johannesdottir SA, Horvath-Puho E, Dekkers OM, et al. Use of glucocorticoids and risk of venous thromboembolism. JAMA Intern Med. 2013;173(9):743-752.
Mortality Rates Rise at Critical-Access Hospitals
Clinical question: How have trends in mortality changed in the past decade at critical-access hospitals when compared to other hospitals?
Background: Hospitals are designated as critical-access hospitals (CAH) by meeting certain requirements—namely, rural setting, small number of beds, and minimum distance from the nearest hospital. Because of the intrinsic challenges they face, CAHs are exempt from certain quality measures. Little data exist on patient outcomes at CAHs.
Study design: Retrospective observational study.
Setting: All nonfederal hospitals in the U.S. that provide acute care to Medicare beneficiaries.
Synopsis: Using Medicare data, risk-adjusted 30-day mortality rates were calculated at critical-access hospitals and non-critical-access hospitals from 2002 to 2010 for three conditions: acute myocardial infarction, congestive heart failure, and pneumonia. Mortality trends across these conditions were compared at baseline and over time. In 2002, CAHs had mortality rates comparable with non-CAHs. From 2002 to 2010, mortality rates increased by 0.1% per year at CAHs and decreased by 0.2% per year at non-CAHs, resulting in a mortality difference between these two hospital groups at the end of the study period. The authors postulate that differences in policy initiatives, enforcement of quality measures, and access to technology may play a role.
This study is limited in its ability to explain the findings. Notably, within the CAHs, the authors found that 48% did improve from 2002 to 2010; there were no significant differences in hospital characteristics between the CAHs that did and did not improve. The reasons for the overall widening gap between CAHs and non-CAHs, therefore, merit further investigation.
Bottom line: From 2002 to 2010, mortality rates at U.S. critical-access hospitals rose while rates fell at non-critical access hospitals.
Citation: Joynt KE, Orav EJ, Jha AK. Mortality rates for Medicare beneficiaries admitted to critical access and non-critical access hospitals, 2002-2010. JAMA. 2013;309(13):1379-1387.
Physicians Fail to Discuss Advance-Care Planning with Hospitalized Elderly, Relatives
Clinical question: Do elderly patients who are at high risk for death have documented advance-care plans, and do their physicians discuss goals of care with them?
Background: While studies indicate that most sick, elderly patients prefer a better quality of life to life-sustaining treatment, many patients still die in the hospital, often in the ICU. It is unclear whether this is due to the absence of advance-care planning or the lack of communicating goals of care.
Study design: Multicenter prospective cohort study.
Setting: Canada.
Synopsis: A validated questionnaire was used to evaluate advance-care planning both before hospitalization and on admission. Patients and their families were enrolled if they were considered at high risk for dying, including patients with advanced disease, or aged >80 years. Of the 278 patients enrolled, 76.3% had thought about advance-care planning. Approximately 47.9% of patients had written an advance-care plan, and 73.3% had formally documented a surrogate health-care decision-maker. Only a quarter of patients reported that they had been asked about advance-care planning on admission to the hospital. Patients’ stated preferences for end-of-life care were notably incongruent with goals-of-care orders documented in the hospital records. While 28% of patients preferred comfort-only care, this was documented in the hospital records for only 4.5% of patients.
In this study of mostly white, English-speaking hospitalized patients, many had considered and made advance-care plans but few had discussed this with their health-care providers. Not surprisingly, the goals-of-care orders that were documented did not match patients’ previously stated end-of-life preferences.
Bottom line: Physicians routinely fail to discuss patients’ advance-care planning, which may have profound effects on their inpatient care.
Citation: Heyland DK, Barwich D, Pichora D, et al. Failure to engage hospitalized elderly patients and their families in advance care planning. JAMA Intern Med. 2013;173(9):778-787.
Ultrasound Use Reduces Lumbar Puncture and Epidural Catheterization Failure
Clinical question: Does ultrasound imaging for lumbar puncture and epidural catheterization reduce risk of procedure failures?
Background: Numerous studies have compared ultrasound-guided lumbar puncture and epidural catheterization with standard techniques, but they have been underpowered to evaluate whether ultrasound use reduces lumbar puncture and epidural catheterization failure.
Study design: Systematic review and meta-analysis of randomized controlled trials.
Setting: Hospitals in North America, Europe, and Asia.
Synopsis: Among 14 trials, a total of 1,334 patients (including one pediatric study group) were randomly assigned either to receive ultrasound imaging or to a control group (using manual palpation or loss of resistance). Ultrasound imaging comprised a preprocedure marking approach, real-time visual guidance, or both. In the 12 trials in which the primary outcome was available, ultrasound imaging significantly reduced the risk of failed procedures with a risk ratio of 0.21 (95% confidence interval 0.10 to 0.43). A total of 16 ultrasound-guided procedures were needed to avoid one procedure failure. Ultrasound guidance also reduced the number of traumatic procedures, needle reinsertions, and needle redirections. These results were consistent across multiple subgroup analyses.
Only one of the studies included in the meta-analysis was double-blind, and in all of the studies, ultrasound imaging was performed by a clinician with high-level ultrasound experience. While this study suggests that ultrasound does reduce the frequency of procedure failure, the investigators did not include cost-effectiveness analyses.
Bottom line: Ultrasound imaging likely reduces the failure of lumbar puncture and epidural catheterization, but future research will be necessary to evaluate the cost-effectiveness of ultrasound use for these procedures.
Citation: Shaikh F, Brzezinski J, Alexander S, et al. Ultrasound imaging for lumbar punctures and epidural catheterisations: systematic review and meta-analysis. BMJ. 2013;346:f1720.
Surgical Complications might Be Financially Advantageous for Hospitals
Clinical question: What is the impact of surgical complications on hospital finances?
Background: Surgical complications are common and lead to longer lengths of stay and higher costs. Strategies are available to reduce postsurgical complications but have not been universally adopted.
Study design: Observational study.
Setting: Twelve hospitals in one nonprofit Southern hospital system, which includes academic, nonacademic, and rural settings.
Synopsis: Researchers identified 34,526 patients who underwent surgery in 2010, excluding patients undergoing Caesarean section. Of those, 1,820 procedures (5.3%) were associated with at least one complication. The most frequent complications were surgical-site infection, other infections, pneumonia, and thromboembolic disease. The mortality rate for patients with complications was 12.3% compared with 0.6% for those without. Length of stay was four times longer for patients with complications.
Complications were associated with a higher total cost of hospitalization, with a differential of $37,917. This translated into a higher contribution to the margin. The cost differential varied by insurance type, with higher contributions under Medicare and private insurance but not with Medicaid.
The study had the benefit of using a large administrative database; however, this may have underestimated the actual rate of postoperative complications. The study supports the paradox in which quality-improvement (QI) programs that reduce surgical complications and improve postoperative mortality may negatively affect a hospital’s financial performance.
Bottom line: Surgical complications lead to higher mortality for patients but a financial benefit for hospitals.
Citation: Eappen S, Lane BH, Rosenberg B, et al. Relationship between occurrence of surgical complications and hospital finances. JAMA. 2013;309(5):1509-1606.
Showing Lab Test Fees May Decrease Frequency Of Test Ordering
Clinical question: Does information on the cost of a lab test lead to lowered ordering frequency among internal-medicine residents?
Background: Lab test overuse is common; some studies estimate that 70% of lab tests do not affect care. Strategies to reduce frequency of unnecessary lab tests are needed.
Study design: Randomized controlled trial.
Setting: Johns Hopkins Hospital, a 1,051-bed academic medical center in Baltimore.
Synopsis: Researchers used an administrative database to identify the 35 most frequently ordered and the 35 most expensive tests (each ordered at least 50 times). They randomized tests to an active arm, which displayed the Medicare allowable fee at the time of order entry within the computerized physician order entry, and a control arm. A total of 1,166,753 tests were ordered during the baseline and intervention period. Many more tests were ordered in the active group relative to the control group, a consequence of the randomization process. Relative to a six-month baseline period, tests in the active group were ordered 9.1% less frequently; control-group tests were ordered 5.1% more frequently. Charges decreased by $3.79 per patient-day in the active group and increased by $0.52 per patient-day in the control group.
This study reflects a low-cost strategy to reduce lab testing and associated costs. It is unknown whether only unnecessary tests were averted, or if there was any effect on the quality of care. The durability of the intervention and its applicability to other settings and with other types of providers is unclear.
Bottom line: Showing the fee associated with lab tests may decrease the frequency of ordering these tests and the resultant costs.
Citation: Feldman LS, Shihab HM, Thiemann D, et al. Impact of providing fee data on laboratory test ordering: a controlled clinical trial. JAMA Intern Med. 2013;173(10):903-908.
Inpatient Elderly Multidisciplinary-Team-Based Unit Reduces Readmissions
Clinical question: Can an inpatient unit that uses interdisciplinary rounds and a team approach reduce 30-day readmissions and lower cost compared with usual care?
Background: Elderly patients are at risk for adverse outcomes including delirium, deconditioning, and undernutrition. The Acute Care for Elders (ACE) model is designed as a team-based approach to improve communication between clinicians and to begin discharge planning soon after admission. ACE units have been shown to improve specific outcomes in older adults, but the impact on cost is less clear.
Study design: Retrospective cohort study.
Setting: University of Alabama at Birmingham Acute Care for Elders unit.
Synopsis: The analysis of cost data extrapolated from administrative sources indicated an average of $371 in variable cost savings per patient, and therefore an expected $148,400 savings for 400 patients admitted to this unit. The rate of 30-day readmissions was significantly lower in the ACE model: 7.9% versus 12.8% in patients receiving usual care.
Limitations of this study relate both to its design and single-center location. It is unclear which aspect of this ACE unit was helpful in the studied outcomes, and how this specific program would be reproduced at another institution. There were also some costs associated with the ACE-unit staffing, which may have resulted in an overestimation of the cost savings.
Bottom line: ACE units appear to improve outcomes and may lower cost, but further investigation is needed.
Citation: Flood KL, MacLennan PA, McGrew D, Green D, Dodd C, Brown CJ. Effects of an acute care for elders unit on costs and 30-day readmissions. JAMA. 2013 April 22 [Epub ahead of print].
Continue Beta-Blockers in High-Risk Patients During Noncardiac Surgery
Clinical question: Does exposure to a beta-blocker at the time of noncardiac surgery have an association with mortality, cardiac arrest, or Q-wave myocardial infarction (MI)?
Background: Exposure to beta-blockers perioperatively is controversial. The authors suggest that a randomized trial would be difficult, as one might need to withhold beta-blockers from stable patients. The American Heart Association and American College of Cardiology currently recommend continuation of pre-existing beta-blockades perioperatively.
Study design: Retrospective, propensity-matched cohort analysis.
Setting: One hundred four Veterans Affairs (VA) medical centers from January 2005 to August 2010.
Synopsis: Exposure for any reason to beta-blockers around nonvascular surgery appears to lower the risk of mortality and cardiac arrest, particularly in patients with higher revised cardiac risk index factors. Stopping beta-blockers in this same period was associated with increased mortality. The reasons for beta-blocker use in the exposed cohort were not well-established or -stratified.
Limitations include that the exposed cohort had a higher rate of cardiovascular disease and comorbidities and were generally older. Duration of exposure to beta-blockers was mixed, although more than 75% had a prescription for more than three months, with less than 2% for several days. Some of the matched cohort appears to have had beta-blocker exposure, thus diminishing the potential impact.
Bottom line: In this retrospective analysis, there is an association between beta-blocker use during noncardiac, nonvascular surgery and lower mortality, as well as lower rates of cardiac arrest and Q-wave MI, particularly among higher-risk patients.
Citation: London MJ, Hur K, Schwartz G, Henderson WG. Association of perioperative beta-blockade with mortality and cardiovascular morbidity following major noncardiac surgery. JAMA. 2013;309(16):1704-1713.
Patient-Centered Decision-Making and Health-Care Outcomes
Clinical question: Does recognition of contextual domains in the care plan lead to resolution of patients’ presenting problems?
Background: Patient-centered decision-making, or contextualization of care, adapts best evidence to the care of the individual patient. Examples of contextual domains include access to care, social support, and financial situation. Contextual errors (e.g. unrecognized domains) are, on average, more costly than errors in evidenced-based medicine.
Study design: Observational study.
Setting: VA ambulatory-care centers.
Synopsis: A total of 548 patient-derived audio recordings of physician encounters that included contextual red flags (e.g. missed appointments, HbA1c >8%) were reviewed at two VA hospital ambulatory-care centers using the content coding for contextualization of care (4C) method. Prospectively determined good and poor outcomes were derived from specific red flags (e.g. keeping next appointment, decrease in HbA1c). Of the 548 red flags, 208 were associated with contextual domains using the 4C method. Some 59% of physicians recognized contextual domains in care-plan development, leading to good outcomes in 71% of red flags. As many as 41% of physicians did not recognize contextual domains, leading to poor outcomes in 54% of red-flag instances.
Hospitalists should be aware of contextual domains and red flags (e.g. readmissions), and this study provides a method of evaluating patient-centered decision-making in the hospital setting. However, the inherently subjective 4C method may underestimate the number of contextual domains.
Bottom line: Recognition and incorporation of contextual domains in care-plan development in the ambulatory setting are associated with improved contextual red flag outcomes.
Citation: Weiner SJ, Schwartz A, Sharma G, et al. Patient-centered decision making and health care outcomes: an observational study. Ann Intern Med. 2013;158:573-579.
Adverse Surgical Outcomes in Schizophrenia Patients
Clinical question: What is the full spectrum of postoperative complications and mortality in schizophrenic patients receiving in-hospital major surgery?
Background: Schizophrenia affects an estimated 4 to 7 per 1,000 persons worldwide, and patients with schizophrenia are at increased risk of diabetes, cardiovascular disease, and stroke with subsequent increased mortality risk. The correlation between severity of mental illness and postoperative in-hospital mortality has not been validated in previous studies.
Study design: Population-based, cross-sectional study.
Setting: Taiwan hospitals.
Synopsis: Using the Taiwan National Health Insurance Research Database, researchers examined claims from 2004 to 2007 and retrospectively identified 8,967 schizophrenic patients who underwent major inpatient surgery and were hospitalized for more than one day. Primary outcomes included acute myocardial infarction, acute renal failure, stroke, and in-hospital mortality within 30 days. Postoperative complications and mortality rates were compared between schizophrenic patients and patients without mental illness.
Schizophrenic patients had higher rates of many primary outcomes, including 30-day postoperative mortality, compared with patients without mental illness, after adjusting for sex, age, surgery type, and hospital setting. The risk for 30-day mortality rose with the number of preoperative schizophrenia-related services provided. Limitations include the nature of retrospective analysis and generalizability.
Bottom line: Compared to patients without mental illness, schizophrenic patients have an increased risk of acute renal failure, pneumonia, septicemia, and 30-day mortality in the postoperative setting, with higher mortality rates in schizophrenic patients with more severe disease.
Citation: Liao CC, Shen WW, Chang CC, Chang H, Chen T. Surgical adverse outcomes in patients with schizophrenia. Ann Surg. 2013;257:433-438.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Steroids may increase VTE risk
- Mortality rates rise at critical-care hospitals
- Physicians don’t discuss advance-care planning with elderly, families
- Ultrasound imaging for lumbar puncture, epidural catheterization
- Financial impact of surgical complications on hospitals
- Lab test fees and frequency of test ordering
- Inpatient elderly multidisciplinary teams reduce readmissions
- Use of beta-blockers in high-risk patients during noncardiac surgery
- Patient-centered decision-making and health-care outcomes
- Adverse surgical outcomes in patients with schizophrenia
Steroids May Increase VTE Risk
Clinical question: Is exogenous glucocorticoid administration associated with an increased risk of VTE?
Background: Endogenous hypercortisolism is linked to increased VTE rates, and pathophysiologic data exist to suggest glucocorticoids increase clotting, but few studies have measured the clinical link between glucocorticoid administration and VTE events.
Study design: Case-control study.
Setting: Denmark.
Synopsis: The authors analyzed Danish national registries, which include information on diagnoses and prescriptions. The study selection period was Jan. 1, 2005, to Dec. 31, 2011. During this period, 38,675 cases of VTE (both DVT and pulmonary embolism) were identified in the population of Denmark. These cases were matched with 387,650 controls. Three routes of glucocorticoid use were studied: systemic (oral and intravenous), inhaled, and intestinal-acting. Cases were classified as present (within 90 days of VTE event), recent (91 to 365 days), or former (over 365 days) users of glucocorticoids. Categories were also created for new versus continuous users.
Glucocorticoid use was associated with a significant increase in VTE occurrence. The strongest link was in new and recent users, and the effect diminished over time. Key limitations of the study included its reliance on registry data, as well as the fact that cases had more comorbid conditions than controls (e.g. recent infection, chronic illnesses).
Bottom line: Recipients of glucocorticoids had an increased risk of VTE; the effect was strongest in new and recent users.
Citation: Johannesdottir SA, Horvath-Puho E, Dekkers OM, et al. Use of glucocorticoids and risk of venous thromboembolism. JAMA Intern Med. 2013;173(9):743-752.
Mortality Rates Rise at Critical-Access Hospitals
Clinical question: How have trends in mortality changed in the past decade at critical-access hospitals when compared to other hospitals?
Background: Hospitals are designated as critical-access hospitals (CAH) by meeting certain requirements—namely, rural setting, small number of beds, and minimum distance from the nearest hospital. Because of the intrinsic challenges they face, CAHs are exempt from certain quality measures. Little data exist on patient outcomes at CAHs.
Study design: Retrospective observational study.
Setting: All nonfederal hospitals in the U.S. that provide acute care to Medicare beneficiaries.
Synopsis: Using Medicare data, risk-adjusted 30-day mortality rates were calculated at critical-access hospitals and non-critical-access hospitals from 2002 to 2010 for three conditions: acute myocardial infarction, congestive heart failure, and pneumonia. Mortality trends across these conditions were compared at baseline and over time. In 2002, CAHs had mortality rates comparable with non-CAHs. From 2002 to 2010, mortality rates increased by 0.1% per year at CAHs and decreased by 0.2% per year at non-CAHs, resulting in a mortality difference between these two hospital groups at the end of the study period. The authors postulate that differences in policy initiatives, enforcement of quality measures, and access to technology may play a role.
This study is limited in its ability to explain the findings. Notably, within the CAHs, the authors found that 48% did improve from 2002 to 2010; there were no significant differences in hospital characteristics between the CAHs that did and did not improve. The reasons for the overall widening gap between CAHs and non-CAHs, therefore, merit further investigation.
Bottom line: From 2002 to 2010, mortality rates at U.S. critical-access hospitals rose while rates fell at non-critical access hospitals.
Citation: Joynt KE, Orav EJ, Jha AK. Mortality rates for Medicare beneficiaries admitted to critical access and non-critical access hospitals, 2002-2010. JAMA. 2013;309(13):1379-1387.
Physicians Fail to Discuss Advance-Care Planning with Hospitalized Elderly, Relatives
Clinical question: Do elderly patients who are at high risk for death have documented advance-care plans, and do their physicians discuss goals of care with them?
Background: While studies indicate that most sick, elderly patients prefer a better quality of life to life-sustaining treatment, many patients still die in the hospital, often in the ICU. It is unclear whether this is due to the absence of advance-care planning or the lack of communicating goals of care.
Study design: Multicenter prospective cohort study.
Setting: Canada.
Synopsis: A validated questionnaire was used to evaluate advance-care planning both before hospitalization and on admission. Patients and their families were enrolled if they were considered at high risk for dying, including patients with advanced disease, or aged >80 years. Of the 278 patients enrolled, 76.3% had thought about advance-care planning. Approximately 47.9% of patients had written an advance-care plan, and 73.3% had formally documented a surrogate health-care decision-maker. Only a quarter of patients reported that they had been asked about advance-care planning on admission to the hospital. Patients’ stated preferences for end-of-life care were notably incongruent with goals-of-care orders documented in the hospital records. While 28% of patients preferred comfort-only care, this was documented in the hospital records for only 4.5% of patients.
In this study of mostly white, English-speaking hospitalized patients, many had considered and made advance-care plans but few had discussed this with their health-care providers. Not surprisingly, the goals-of-care orders that were documented did not match patients’ previously stated end-of-life preferences.
Bottom line: Physicians routinely fail to discuss patients’ advance-care planning, which may have profound effects on their inpatient care.
Citation: Heyland DK, Barwich D, Pichora D, et al. Failure to engage hospitalized elderly patients and their families in advance care planning. JAMA Intern Med. 2013;173(9):778-787.
Ultrasound Use Reduces Lumbar Puncture and Epidural Catheterization Failure
Clinical question: Does ultrasound imaging for lumbar puncture and epidural catheterization reduce risk of procedure failures?
Background: Numerous studies have compared ultrasound-guided lumbar puncture and epidural catheterization with standard techniques, but they have been underpowered to evaluate whether ultrasound use reduces lumbar puncture and epidural catheterization failure.
Study design: Systematic review and meta-analysis of randomized controlled trials.
Setting: Hospitals in North America, Europe, and Asia.
Synopsis: Among 14 trials, a total of 1,334 patients (including one pediatric study group) were randomly assigned either to receive ultrasound imaging or to a control group (using manual palpation or loss of resistance). Ultrasound imaging comprised a preprocedure marking approach, real-time visual guidance, or both. In the 12 trials in which the primary outcome was available, ultrasound imaging significantly reduced the risk of failed procedures with a risk ratio of 0.21 (95% confidence interval 0.10 to 0.43). A total of 16 ultrasound-guided procedures were needed to avoid one procedure failure. Ultrasound guidance also reduced the number of traumatic procedures, needle reinsertions, and needle redirections. These results were consistent across multiple subgroup analyses.
Only one of the studies included in the meta-analysis was double-blind, and in all of the studies, ultrasound imaging was performed by a clinician with high-level ultrasound experience. While this study suggests that ultrasound does reduce the frequency of procedure failure, the investigators did not include cost-effectiveness analyses.
Bottom line: Ultrasound imaging likely reduces the failure of lumbar puncture and epidural catheterization, but future research will be necessary to evaluate the cost-effectiveness of ultrasound use for these procedures.
Citation: Shaikh F, Brzezinski J, Alexander S, et al. Ultrasound imaging for lumbar punctures and epidural catheterisations: systematic review and meta-analysis. BMJ. 2013;346:f1720.
Surgical Complications might Be Financially Advantageous for Hospitals
Clinical question: What is the impact of surgical complications on hospital finances?
Background: Surgical complications are common and lead to longer lengths of stay and higher costs. Strategies are available to reduce postsurgical complications but have not been universally adopted.
Study design: Observational study.
Setting: Twelve hospitals in one nonprofit Southern hospital system, which includes academic, nonacademic, and rural settings.
Synopsis: Researchers identified 34,526 patients who underwent surgery in 2010, excluding patients undergoing Caesarean section. Of those, 1,820 procedures (5.3%) were associated with at least one complication. The most frequent complications were surgical-site infection, other infections, pneumonia, and thromboembolic disease. The mortality rate for patients with complications was 12.3% compared with 0.6% for those without. Length of stay was four times longer for patients with complications.
Complications were associated with a higher total cost of hospitalization, with a differential of $37,917. This translated into a higher contribution to the margin. The cost differential varied by insurance type, with higher contributions under Medicare and private insurance but not with Medicaid.
The study had the benefit of using a large administrative database; however, this may have underestimated the actual rate of postoperative complications. The study supports the paradox in which quality-improvement (QI) programs that reduce surgical complications and improve postoperative mortality may negatively affect a hospital’s financial performance.
Bottom line: Surgical complications lead to higher mortality for patients but a financial benefit for hospitals.
Citation: Eappen S, Lane BH, Rosenberg B, et al. Relationship between occurrence of surgical complications and hospital finances. JAMA. 2013;309(5):1509-1606.
Showing Lab Test Fees May Decrease Frequency Of Test Ordering
Clinical question: Does information on the cost of a lab test lead to lowered ordering frequency among internal-medicine residents?
Background: Lab test overuse is common; some studies estimate that 70% of lab tests do not affect care. Strategies to reduce frequency of unnecessary lab tests are needed.
Study design: Randomized controlled trial.
Setting: Johns Hopkins Hospital, a 1,051-bed academic medical center in Baltimore.
Synopsis: Researchers used an administrative database to identify the 35 most frequently ordered and the 35 most expensive tests (each ordered at least 50 times). They randomized tests to an active arm, which displayed the Medicare allowable fee at the time of order entry within the computerized physician order entry, and a control arm. A total of 1,166,753 tests were ordered during the baseline and intervention period. Many more tests were ordered in the active group relative to the control group, a consequence of the randomization process. Relative to a six-month baseline period, tests in the active group were ordered 9.1% less frequently; control-group tests were ordered 5.1% more frequently. Charges decreased by $3.79 per patient-day in the active group and increased by $0.52 per patient-day in the control group.
This study reflects a low-cost strategy to reduce lab testing and associated costs. It is unknown whether only unnecessary tests were averted, or if there was any effect on the quality of care. The durability of the intervention and its applicability to other settings and with other types of providers is unclear.
Bottom line: Showing the fee associated with lab tests may decrease the frequency of ordering these tests and the resultant costs.
Citation: Feldman LS, Shihab HM, Thiemann D, et al. Impact of providing fee data on laboratory test ordering: a controlled clinical trial. JAMA Intern Med. 2013;173(10):903-908.
Inpatient Elderly Multidisciplinary-Team-Based Unit Reduces Readmissions
Clinical question: Can an inpatient unit that uses interdisciplinary rounds and a team approach reduce 30-day readmissions and lower cost compared with usual care?
Background: Elderly patients are at risk for adverse outcomes including delirium, deconditioning, and undernutrition. The Acute Care for Elders (ACE) model is designed as a team-based approach to improve communication between clinicians and to begin discharge planning soon after admission. ACE units have been shown to improve specific outcomes in older adults, but the impact on cost is less clear.
Study design: Retrospective cohort study.
Setting: University of Alabama at Birmingham Acute Care for Elders unit.
Synopsis: The analysis of cost data extrapolated from administrative sources indicated an average of $371 in variable cost savings per patient, and therefore an expected $148,400 savings for 400 patients admitted to this unit. The rate of 30-day readmissions was significantly lower in the ACE model: 7.9% versus 12.8% in patients receiving usual care.
Limitations of this study relate both to its design and single-center location. It is unclear which aspect of this ACE unit was helpful in the studied outcomes, and how this specific program would be reproduced at another institution. There were also some costs associated with the ACE-unit staffing, which may have resulted in an overestimation of the cost savings.
Bottom line: ACE units appear to improve outcomes and may lower cost, but further investigation is needed.
Citation: Flood KL, MacLennan PA, McGrew D, Green D, Dodd C, Brown CJ. Effects of an acute care for elders unit on costs and 30-day readmissions. JAMA. 2013 April 22 [Epub ahead of print].
Continue Beta-Blockers in High-Risk Patients During Noncardiac Surgery
Clinical question: Does exposure to a beta-blocker at the time of noncardiac surgery have an association with mortality, cardiac arrest, or Q-wave myocardial infarction (MI)?
Background: Exposure to beta-blockers perioperatively is controversial. The authors suggest that a randomized trial would be difficult, as one might need to withhold beta-blockers from stable patients. The American Heart Association and American College of Cardiology currently recommend continuation of pre-existing beta-blockades perioperatively.
Study design: Retrospective, propensity-matched cohort analysis.
Setting: One hundred four Veterans Affairs (VA) medical centers from January 2005 to August 2010.
Synopsis: Exposure for any reason to beta-blockers around nonvascular surgery appears to lower the risk of mortality and cardiac arrest, particularly in patients with higher revised cardiac risk index factors. Stopping beta-blockers in this same period was associated with increased mortality. The reasons for beta-blocker use in the exposed cohort were not well-established or -stratified.
Limitations include that the exposed cohort had a higher rate of cardiovascular disease and comorbidities and were generally older. Duration of exposure to beta-blockers was mixed, although more than 75% had a prescription for more than three months, with less than 2% for several days. Some of the matched cohort appears to have had beta-blocker exposure, thus diminishing the potential impact.
Bottom line: In this retrospective analysis, there is an association between beta-blocker use during noncardiac, nonvascular surgery and lower mortality, as well as lower rates of cardiac arrest and Q-wave MI, particularly among higher-risk patients.
Citation: London MJ, Hur K, Schwartz G, Henderson WG. Association of perioperative beta-blockade with mortality and cardiovascular morbidity following major noncardiac surgery. JAMA. 2013;309(16):1704-1713.
Patient-Centered Decision-Making and Health-Care Outcomes
Clinical question: Does recognition of contextual domains in the care plan lead to resolution of patients’ presenting problems?
Background: Patient-centered decision-making, or contextualization of care, adapts best evidence to the care of the individual patient. Examples of contextual domains include access to care, social support, and financial situation. Contextual errors (e.g. unrecognized domains) are, on average, more costly than errors in evidenced-based medicine.
Study design: Observational study.
Setting: VA ambulatory-care centers.
Synopsis: A total of 548 patient-derived audio recordings of physician encounters that included contextual red flags (e.g. missed appointments, HbA1c >8%) were reviewed at two VA hospital ambulatory-care centers using the content coding for contextualization of care (4C) method. Prospectively determined good and poor outcomes were derived from specific red flags (e.g. keeping next appointment, decrease in HbA1c). Of the 548 red flags, 208 were associated with contextual domains using the 4C method. Some 59% of physicians recognized contextual domains in care-plan development, leading to good outcomes in 71% of red flags. As many as 41% of physicians did not recognize contextual domains, leading to poor outcomes in 54% of red-flag instances.
Hospitalists should be aware of contextual domains and red flags (e.g. readmissions), and this study provides a method of evaluating patient-centered decision-making in the hospital setting. However, the inherently subjective 4C method may underestimate the number of contextual domains.
Bottom line: Recognition and incorporation of contextual domains in care-plan development in the ambulatory setting are associated with improved contextual red flag outcomes.
Citation: Weiner SJ, Schwartz A, Sharma G, et al. Patient-centered decision making and health care outcomes: an observational study. Ann Intern Med. 2013;158:573-579.
Adverse Surgical Outcomes in Schizophrenia Patients
Clinical question: What is the full spectrum of postoperative complications and mortality in schizophrenic patients receiving in-hospital major surgery?
Background: Schizophrenia affects an estimated 4 to 7 per 1,000 persons worldwide, and patients with schizophrenia are at increased risk of diabetes, cardiovascular disease, and stroke with subsequent increased mortality risk. The correlation between severity of mental illness and postoperative in-hospital mortality has not been validated in previous studies.
Study design: Population-based, cross-sectional study.
Setting: Taiwan hospitals.
Synopsis: Using the Taiwan National Health Insurance Research Database, researchers examined claims from 2004 to 2007 and retrospectively identified 8,967 schizophrenic patients who underwent major inpatient surgery and were hospitalized for more than one day. Primary outcomes included acute myocardial infarction, acute renal failure, stroke, and in-hospital mortality within 30 days. Postoperative complications and mortality rates were compared between schizophrenic patients and patients without mental illness.
Schizophrenic patients had higher rates of many primary outcomes, including 30-day postoperative mortality, compared with patients without mental illness, after adjusting for sex, age, surgery type, and hospital setting. The risk for 30-day mortality rose with the number of preoperative schizophrenia-related services provided. Limitations include the nature of retrospective analysis and generalizability.
Bottom line: Compared to patients without mental illness, schizophrenic patients have an increased risk of acute renal failure, pneumonia, septicemia, and 30-day mortality in the postoperative setting, with higher mortality rates in schizophrenic patients with more severe disease.
Citation: Liao CC, Shen WW, Chang CC, Chang H, Chen T. Surgical adverse outcomes in patients with schizophrenia. Ann Surg. 2013;257:433-438.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Steroids may increase VTE risk
- Mortality rates rise at critical-care hospitals
- Physicians don’t discuss advance-care planning with elderly, families
- Ultrasound imaging for lumbar puncture, epidural catheterization
- Financial impact of surgical complications on hospitals
- Lab test fees and frequency of test ordering
- Inpatient elderly multidisciplinary teams reduce readmissions
- Use of beta-blockers in high-risk patients during noncardiac surgery
- Patient-centered decision-making and health-care outcomes
- Adverse surgical outcomes in patients with schizophrenia
Steroids May Increase VTE Risk
Clinical question: Is exogenous glucocorticoid administration associated with an increased risk of VTE?
Background: Endogenous hypercortisolism is linked to increased VTE rates, and pathophysiologic data exist to suggest glucocorticoids increase clotting, but few studies have measured the clinical link between glucocorticoid administration and VTE events.
Study design: Case-control study.
Setting: Denmark.
Synopsis: The authors analyzed Danish national registries, which include information on diagnoses and prescriptions. The study selection period was Jan. 1, 2005, to Dec. 31, 2011. During this period, 38,675 cases of VTE (both DVT and pulmonary embolism) were identified in the population of Denmark. These cases were matched with 387,650 controls. Three routes of glucocorticoid use were studied: systemic (oral and intravenous), inhaled, and intestinal-acting. Cases were classified as present (within 90 days of VTE event), recent (91 to 365 days), or former (over 365 days) users of glucocorticoids. Categories were also created for new versus continuous users.
Glucocorticoid use was associated with a significant increase in VTE occurrence. The strongest link was in new and recent users, and the effect diminished over time. Key limitations of the study included its reliance on registry data, as well as the fact that cases had more comorbid conditions than controls (e.g. recent infection, chronic illnesses).
Bottom line: Recipients of glucocorticoids had an increased risk of VTE; the effect was strongest in new and recent users.
Citation: Johannesdottir SA, Horvath-Puho E, Dekkers OM, et al. Use of glucocorticoids and risk of venous thromboembolism. JAMA Intern Med. 2013;173(9):743-752.
Mortality Rates Rise at Critical-Access Hospitals
Clinical question: How have trends in mortality changed in the past decade at critical-access hospitals when compared to other hospitals?
Background: Hospitals are designated as critical-access hospitals (CAH) by meeting certain requirements—namely, rural setting, small number of beds, and minimum distance from the nearest hospital. Because of the intrinsic challenges they face, CAHs are exempt from certain quality measures. Little data exist on patient outcomes at CAHs.
Study design: Retrospective observational study.
Setting: All nonfederal hospitals in the U.S. that provide acute care to Medicare beneficiaries.
Synopsis: Using Medicare data, risk-adjusted 30-day mortality rates were calculated at critical-access hospitals and non-critical-access hospitals from 2002 to 2010 for three conditions: acute myocardial infarction, congestive heart failure, and pneumonia. Mortality trends across these conditions were compared at baseline and over time. In 2002, CAHs had mortality rates comparable with non-CAHs. From 2002 to 2010, mortality rates increased by 0.1% per year at CAHs and decreased by 0.2% per year at non-CAHs, resulting in a mortality difference between these two hospital groups at the end of the study period. The authors postulate that differences in policy initiatives, enforcement of quality measures, and access to technology may play a role.
This study is limited in its ability to explain the findings. Notably, within the CAHs, the authors found that 48% did improve from 2002 to 2010; there were no significant differences in hospital characteristics between the CAHs that did and did not improve. The reasons for the overall widening gap between CAHs and non-CAHs, therefore, merit further investigation.
Bottom line: From 2002 to 2010, mortality rates at U.S. critical-access hospitals rose while rates fell at non-critical access hospitals.
Citation: Joynt KE, Orav EJ, Jha AK. Mortality rates for Medicare beneficiaries admitted to critical access and non-critical access hospitals, 2002-2010. JAMA. 2013;309(13):1379-1387.
Physicians Fail to Discuss Advance-Care Planning with Hospitalized Elderly, Relatives
Clinical question: Do elderly patients who are at high risk for death have documented advance-care plans, and do their physicians discuss goals of care with them?
Background: While studies indicate that most sick, elderly patients prefer a better quality of life to life-sustaining treatment, many patients still die in the hospital, often in the ICU. It is unclear whether this is due to the absence of advance-care planning or the lack of communicating goals of care.
Study design: Multicenter prospective cohort study.
Setting: Canada.
Synopsis: A validated questionnaire was used to evaluate advance-care planning both before hospitalization and on admission. Patients and their families were enrolled if they were considered at high risk for dying, including patients with advanced disease, or aged >80 years. Of the 278 patients enrolled, 76.3% had thought about advance-care planning. Approximately 47.9% of patients had written an advance-care plan, and 73.3% had formally documented a surrogate health-care decision-maker. Only a quarter of patients reported that they had been asked about advance-care planning on admission to the hospital. Patients’ stated preferences for end-of-life care were notably incongruent with goals-of-care orders documented in the hospital records. While 28% of patients preferred comfort-only care, this was documented in the hospital records for only 4.5% of patients.
In this study of mostly white, English-speaking hospitalized patients, many had considered and made advance-care plans but few had discussed this with their health-care providers. Not surprisingly, the goals-of-care orders that were documented did not match patients’ previously stated end-of-life preferences.
Bottom line: Physicians routinely fail to discuss patients’ advance-care planning, which may have profound effects on their inpatient care.
Citation: Heyland DK, Barwich D, Pichora D, et al. Failure to engage hospitalized elderly patients and their families in advance care planning. JAMA Intern Med. 2013;173(9):778-787.
Ultrasound Use Reduces Lumbar Puncture and Epidural Catheterization Failure
Clinical question: Does ultrasound imaging for lumbar puncture and epidural catheterization reduce risk of procedure failures?
Background: Numerous studies have compared ultrasound-guided lumbar puncture and epidural catheterization with standard techniques, but they have been underpowered to evaluate whether ultrasound use reduces lumbar puncture and epidural catheterization failure.
Study design: Systematic review and meta-analysis of randomized controlled trials.
Setting: Hospitals in North America, Europe, and Asia.
Synopsis: Among 14 trials, a total of 1,334 patients (including one pediatric study group) were randomly assigned either to receive ultrasound imaging or to a control group (using manual palpation or loss of resistance). Ultrasound imaging comprised a preprocedure marking approach, real-time visual guidance, or both. In the 12 trials in which the primary outcome was available, ultrasound imaging significantly reduced the risk of failed procedures with a risk ratio of 0.21 (95% confidence interval 0.10 to 0.43). A total of 16 ultrasound-guided procedures were needed to avoid one procedure failure. Ultrasound guidance also reduced the number of traumatic procedures, needle reinsertions, and needle redirections. These results were consistent across multiple subgroup analyses.
Only one of the studies included in the meta-analysis was double-blind, and in all of the studies, ultrasound imaging was performed by a clinician with high-level ultrasound experience. While this study suggests that ultrasound does reduce the frequency of procedure failure, the investigators did not include cost-effectiveness analyses.
Bottom line: Ultrasound imaging likely reduces the failure of lumbar puncture and epidural catheterization, but future research will be necessary to evaluate the cost-effectiveness of ultrasound use for these procedures.
Citation: Shaikh F, Brzezinski J, Alexander S, et al. Ultrasound imaging for lumbar punctures and epidural catheterisations: systematic review and meta-analysis. BMJ. 2013;346:f1720.
Surgical Complications might Be Financially Advantageous for Hospitals
Clinical question: What is the impact of surgical complications on hospital finances?
Background: Surgical complications are common and lead to longer lengths of stay and higher costs. Strategies are available to reduce postsurgical complications but have not been universally adopted.
Study design: Observational study.
Setting: Twelve hospitals in one nonprofit Southern hospital system, which includes academic, nonacademic, and rural settings.
Synopsis: Researchers identified 34,526 patients who underwent surgery in 2010, excluding patients undergoing Caesarean section. Of those, 1,820 procedures (5.3%) were associated with at least one complication. The most frequent complications were surgical-site infection, other infections, pneumonia, and thromboembolic disease. The mortality rate for patients with complications was 12.3% compared with 0.6% for those without. Length of stay was four times longer for patients with complications.
Complications were associated with a higher total cost of hospitalization, with a differential of $37,917. This translated into a higher contribution to the margin. The cost differential varied by insurance type, with higher contributions under Medicare and private insurance but not with Medicaid.
The study had the benefit of using a large administrative database; however, this may have underestimated the actual rate of postoperative complications. The study supports the paradox in which quality-improvement (QI) programs that reduce surgical complications and improve postoperative mortality may negatively affect a hospital’s financial performance.
Bottom line: Surgical complications lead to higher mortality for patients but a financial benefit for hospitals.
Citation: Eappen S, Lane BH, Rosenberg B, et al. Relationship between occurrence of surgical complications and hospital finances. JAMA. 2013;309(5):1509-1606.
Showing Lab Test Fees May Decrease Frequency Of Test Ordering
Clinical question: Does information on the cost of a lab test lead to lowered ordering frequency among internal-medicine residents?
Background: Lab test overuse is common; some studies estimate that 70% of lab tests do not affect care. Strategies to reduce frequency of unnecessary lab tests are needed.
Study design: Randomized controlled trial.
Setting: Johns Hopkins Hospital, a 1,051-bed academic medical center in Baltimore.
Synopsis: Researchers used an administrative database to identify the 35 most frequently ordered and the 35 most expensive tests (each ordered at least 50 times). They randomized tests to an active arm, which displayed the Medicare allowable fee at the time of order entry within the computerized physician order entry, and a control arm. A total of 1,166,753 tests were ordered during the baseline and intervention period. Many more tests were ordered in the active group relative to the control group, a consequence of the randomization process. Relative to a six-month baseline period, tests in the active group were ordered 9.1% less frequently; control-group tests were ordered 5.1% more frequently. Charges decreased by $3.79 per patient-day in the active group and increased by $0.52 per patient-day in the control group.
This study reflects a low-cost strategy to reduce lab testing and associated costs. It is unknown whether only unnecessary tests were averted, or if there was any effect on the quality of care. The durability of the intervention and its applicability to other settings and with other types of providers is unclear.
Bottom line: Showing the fee associated with lab tests may decrease the frequency of ordering these tests and the resultant costs.
Citation: Feldman LS, Shihab HM, Thiemann D, et al. Impact of providing fee data on laboratory test ordering: a controlled clinical trial. JAMA Intern Med. 2013;173(10):903-908.
Inpatient Elderly Multidisciplinary-Team-Based Unit Reduces Readmissions
Clinical question: Can an inpatient unit that uses interdisciplinary rounds and a team approach reduce 30-day readmissions and lower cost compared with usual care?
Background: Elderly patients are at risk for adverse outcomes including delirium, deconditioning, and undernutrition. The Acute Care for Elders (ACE) model is designed as a team-based approach to improve communication between clinicians and to begin discharge planning soon after admission. ACE units have been shown to improve specific outcomes in older adults, but the impact on cost is less clear.
Study design: Retrospective cohort study.
Setting: University of Alabama at Birmingham Acute Care for Elders unit.
Synopsis: The analysis of cost data extrapolated from administrative sources indicated an average of $371 in variable cost savings per patient, and therefore an expected $148,400 savings for 400 patients admitted to this unit. The rate of 30-day readmissions was significantly lower in the ACE model: 7.9% versus 12.8% in patients receiving usual care.
Limitations of this study relate both to its design and single-center location. It is unclear which aspect of this ACE unit was helpful in the studied outcomes, and how this specific program would be reproduced at another institution. There were also some costs associated with the ACE-unit staffing, which may have resulted in an overestimation of the cost savings.
Bottom line: ACE units appear to improve outcomes and may lower cost, but further investigation is needed.
Citation: Flood KL, MacLennan PA, McGrew D, Green D, Dodd C, Brown CJ. Effects of an acute care for elders unit on costs and 30-day readmissions. JAMA. 2013 April 22 [Epub ahead of print].
Continue Beta-Blockers in High-Risk Patients During Noncardiac Surgery
Clinical question: Does exposure to a beta-blocker at the time of noncardiac surgery have an association with mortality, cardiac arrest, or Q-wave myocardial infarction (MI)?
Background: Exposure to beta-blockers perioperatively is controversial. The authors suggest that a randomized trial would be difficult, as one might need to withhold beta-blockers from stable patients. The American Heart Association and American College of Cardiology currently recommend continuation of pre-existing beta-blockades perioperatively.
Study design: Retrospective, propensity-matched cohort analysis.
Setting: One hundred four Veterans Affairs (VA) medical centers from January 2005 to August 2010.
Synopsis: Exposure for any reason to beta-blockers around nonvascular surgery appears to lower the risk of mortality and cardiac arrest, particularly in patients with higher revised cardiac risk index factors. Stopping beta-blockers in this same period was associated with increased mortality. The reasons for beta-blocker use in the exposed cohort were not well-established or -stratified.
Limitations include that the exposed cohort had a higher rate of cardiovascular disease and comorbidities and were generally older. Duration of exposure to beta-blockers was mixed, although more than 75% had a prescription for more than three months, with less than 2% for several days. Some of the matched cohort appears to have had beta-blocker exposure, thus diminishing the potential impact.
Bottom line: In this retrospective analysis, there is an association between beta-blocker use during noncardiac, nonvascular surgery and lower mortality, as well as lower rates of cardiac arrest and Q-wave MI, particularly among higher-risk patients.
Citation: London MJ, Hur K, Schwartz G, Henderson WG. Association of perioperative beta-blockade with mortality and cardiovascular morbidity following major noncardiac surgery. JAMA. 2013;309(16):1704-1713.
Patient-Centered Decision-Making and Health-Care Outcomes
Clinical question: Does recognition of contextual domains in the care plan lead to resolution of patients’ presenting problems?
Background: Patient-centered decision-making, or contextualization of care, adapts best evidence to the care of the individual patient. Examples of contextual domains include access to care, social support, and financial situation. Contextual errors (e.g. unrecognized domains) are, on average, more costly than errors in evidenced-based medicine.
Study design: Observational study.
Setting: VA ambulatory-care centers.
Synopsis: A total of 548 patient-derived audio recordings of physician encounters that included contextual red flags (e.g. missed appointments, HbA1c >8%) were reviewed at two VA hospital ambulatory-care centers using the content coding for contextualization of care (4C) method. Prospectively determined good and poor outcomes were derived from specific red flags (e.g. keeping next appointment, decrease in HbA1c). Of the 548 red flags, 208 were associated with contextual domains using the 4C method. Some 59% of physicians recognized contextual domains in care-plan development, leading to good outcomes in 71% of red flags. As many as 41% of physicians did not recognize contextual domains, leading to poor outcomes in 54% of red-flag instances.
Hospitalists should be aware of contextual domains and red flags (e.g. readmissions), and this study provides a method of evaluating patient-centered decision-making in the hospital setting. However, the inherently subjective 4C method may underestimate the number of contextual domains.
Bottom line: Recognition and incorporation of contextual domains in care-plan development in the ambulatory setting are associated with improved contextual red flag outcomes.
Citation: Weiner SJ, Schwartz A, Sharma G, et al. Patient-centered decision making and health care outcomes: an observational study. Ann Intern Med. 2013;158:573-579.
Adverse Surgical Outcomes in Schizophrenia Patients
Clinical question: What is the full spectrum of postoperative complications and mortality in schizophrenic patients receiving in-hospital major surgery?
Background: Schizophrenia affects an estimated 4 to 7 per 1,000 persons worldwide, and patients with schizophrenia are at increased risk of diabetes, cardiovascular disease, and stroke with subsequent increased mortality risk. The correlation between severity of mental illness and postoperative in-hospital mortality has not been validated in previous studies.
Study design: Population-based, cross-sectional study.
Setting: Taiwan hospitals.
Synopsis: Using the Taiwan National Health Insurance Research Database, researchers examined claims from 2004 to 2007 and retrospectively identified 8,967 schizophrenic patients who underwent major inpatient surgery and were hospitalized for more than one day. Primary outcomes included acute myocardial infarction, acute renal failure, stroke, and in-hospital mortality within 30 days. Postoperative complications and mortality rates were compared between schizophrenic patients and patients without mental illness.
Schizophrenic patients had higher rates of many primary outcomes, including 30-day postoperative mortality, compared with patients without mental illness, after adjusting for sex, age, surgery type, and hospital setting. The risk for 30-day mortality rose with the number of preoperative schizophrenia-related services provided. Limitations include the nature of retrospective analysis and generalizability.
Bottom line: Compared to patients without mental illness, schizophrenic patients have an increased risk of acute renal failure, pneumonia, septicemia, and 30-day mortality in the postoperative setting, with higher mortality rates in schizophrenic patients with more severe disease.
Citation: Liao CC, Shen WW, Chang CC, Chang H, Chen T. Surgical adverse outcomes in patients with schizophrenia. Ann Surg. 2013;257:433-438.
Observation Status Designation in Pediatric Hospitals Is Costly

Clinical question: What are the costs associated with observation-status hospital stays compared to inpatient-status stays in pediatric hospitals?
Background: Observation status is a designation for hospitalizations that are typically shorter than 48 hours and do not meet criteria for inpatient status. It is considered to be outpatient for evaluation and management (E/M) coding. A designation of observation status for a hospital stay can have significant effects on out-of-pocket costs for patients and reimbursements to physicians and hospitals. It also can affect readmission and length-of-stay data, as observation-status hospital stays are often excluded from a hospital’s inpatient data.
Study design: Multicenter retrospective cohort study.
Setting: Thirty-three freestanding children’s hospitals.
Synopsis: Researchers reviewed data obtained from the Pediatric Health Information System (PHIS), which contains demographic and resource utilization date from 43 freestanding children’s hospitals in the U.S. Resource utilization data were reviewed from 33 of 43 hospitals in PHIS that reported data regarding observation- versus inpatient-status stays. Data were then limited to observation-status stays £2 days, which made up 97.8% of all observation-status stays. These were then compared to a corresponding cohort of inpatient-status stays of £2 days (47.5% of inpatient-status stays), excluding any patient who had spent time in an ICU.
Hospitalization costs were analyzed and separated into room and nonroom costs, as well as in aggregate. These were further subdivided into costs for four common diagnoses (asthma, gastroenteritis, bronchiolitis, and seizure) and were risk-adjusted.
Observation status was used variably between hospitals (2% to 45%) and within hospitals. There was significant overlap in costs of observation-status and inpatient-status stays, which persisted when accounting for nonroom costs and within the diagnosis subgroups. Although average severity-adjusted costs for observation-status stays were consistently less than those for inpatient-status stays, the dollar amounts were small.
Bottom line: Observation-status designation is used inconsistently in pediatric hospitals, and their costs overlap substantially with inpatient-status stays.
Citation: Fieldston ES, Shah SS, Hall M. Resource utilization for observation-status stays at children’s hospitals. Pediatrics. 2013;131;1050-1058.
Reviewed by Pediatric Editor Weijen Chang, MD, SFHM, FACP, associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital.
Clinical question: What are the costs associated with observation-status hospital stays compared to inpatient-status stays in pediatric hospitals?
Background: Observation status is a designation for hospitalizations that are typically shorter than 48 hours and do not meet criteria for inpatient status. It is considered to be outpatient for evaluation and management (E/M) coding. A designation of observation status for a hospital stay can have significant effects on out-of-pocket costs for patients and reimbursements to physicians and hospitals. It also can affect readmission and length-of-stay data, as observation-status hospital stays are often excluded from a hospital’s inpatient data.
Study design: Multicenter retrospective cohort study.
Setting: Thirty-three freestanding children’s hospitals.
Synopsis: Researchers reviewed data obtained from the Pediatric Health Information System (PHIS), which contains demographic and resource utilization date from 43 freestanding children’s hospitals in the U.S. Resource utilization data were reviewed from 33 of 43 hospitals in PHIS that reported data regarding observation- versus inpatient-status stays. Data were then limited to observation-status stays £2 days, which made up 97.8% of all observation-status stays. These were then compared to a corresponding cohort of inpatient-status stays of £2 days (47.5% of inpatient-status stays), excluding any patient who had spent time in an ICU.
Hospitalization costs were analyzed and separated into room and nonroom costs, as well as in aggregate. These were further subdivided into costs for four common diagnoses (asthma, gastroenteritis, bronchiolitis, and seizure) and were risk-adjusted.
Observation status was used variably between hospitals (2% to 45%) and within hospitals. There was significant overlap in costs of observation-status and inpatient-status stays, which persisted when accounting for nonroom costs and within the diagnosis subgroups. Although average severity-adjusted costs for observation-status stays were consistently less than those for inpatient-status stays, the dollar amounts were small.
Bottom line: Observation-status designation is used inconsistently in pediatric hospitals, and their costs overlap substantially with inpatient-status stays.
Citation: Fieldston ES, Shah SS, Hall M. Resource utilization for observation-status stays at children’s hospitals. Pediatrics. 2013;131;1050-1058.
Reviewed by Pediatric Editor Weijen Chang, MD, SFHM, FACP, associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital.
Clinical question: What are the costs associated with observation-status hospital stays compared to inpatient-status stays in pediatric hospitals?
Background: Observation status is a designation for hospitalizations that are typically shorter than 48 hours and do not meet criteria for inpatient status. It is considered to be outpatient for evaluation and management (E/M) coding. A designation of observation status for a hospital stay can have significant effects on out-of-pocket costs for patients and reimbursements to physicians and hospitals. It also can affect readmission and length-of-stay data, as observation-status hospital stays are often excluded from a hospital’s inpatient data.
Study design: Multicenter retrospective cohort study.
Setting: Thirty-three freestanding children’s hospitals.
Synopsis: Researchers reviewed data obtained from the Pediatric Health Information System (PHIS), which contains demographic and resource utilization date from 43 freestanding children’s hospitals in the U.S. Resource utilization data were reviewed from 33 of 43 hospitals in PHIS that reported data regarding observation- versus inpatient-status stays. Data were then limited to observation-status stays £2 days, which made up 97.8% of all observation-status stays. These were then compared to a corresponding cohort of inpatient-status stays of £2 days (47.5% of inpatient-status stays), excluding any patient who had spent time in an ICU.
Hospitalization costs were analyzed and separated into room and nonroom costs, as well as in aggregate. These were further subdivided into costs for four common diagnoses (asthma, gastroenteritis, bronchiolitis, and seizure) and were risk-adjusted.
Observation status was used variably between hospitals (2% to 45%) and within hospitals. There was significant overlap in costs of observation-status and inpatient-status stays, which persisted when accounting for nonroom costs and within the diagnosis subgroups. Although average severity-adjusted costs for observation-status stays were consistently less than those for inpatient-status stays, the dollar amounts were small.
Bottom line: Observation-status designation is used inconsistently in pediatric hospitals, and their costs overlap substantially with inpatient-status stays.
Citation: Fieldston ES, Shah SS, Hall M. Resource utilization for observation-status stays at children’s hospitals. Pediatrics. 2013;131;1050-1058.
Reviewed by Pediatric Editor Weijen Chang, MD, SFHM, FACP, associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital.
A History of Observation Hospital Stays in Pediatrics

Physicians once admitted patients to observation status when they were unsure whether the hospitalization ultimately would lead to a stay longer than 24 hours. In 1978, InterQual published its first severity-of-illness/intensity-of-service criteria for evaluating appropriateness of admission and level of service.1 These originated from a government contract to develop a quality-assurance program addressing variability in length of stay that became apparent after Medicare was implemented in 1967. Charles Jacobs, an attorney who was once an associate director at The Joint Commission, assembled a team that once worked out of an apartment in Chicago that would become InterQual.2 Over the years, InterQual evolved and was eventually acquired by McKesson.
In a study published in the May 2013 issue of Pediatrics, Fieldston et al used data obtained from the Pediatric Health Information System (PHIS) 2010 database to demonstrate that observation-status designation is used inconsistently in pediatric hospitals.3 The researchers showed that costs for observation-status stays overlap substantially with costs for inpatient-status stays. Although the results of this study may be disappointing to those who seek to reduce cost or increase value, they should not be surprising.
A previous study from several of the same authors showed that significant variation exists in how observation status is assigned versus inpatient status.4 Observation status was found to be based on duration of expected treatment or on level of care criteria (i.e. InterQual or Millman). In fact, within an individual hospital, variation could be present in the assignment of status between individual payors. For example, a short stay for asthma exacerbation could be assigned inpatient status for one payor and observation status for another payor. Patients likely received the same care and costs, especially in hospitals with standardized-treatment-care plans or protocols.
In that same study, the authors discovered that only 12 of 31 (39%) freestanding children’s hospitals had a designated observation unit. Many hospitals reported that observation patients were scattered across the ED and inpatient units (e.g. “virtual” observation unit). A majority of hospitals (14 of 16) reported that there were no differences in the delivery of clinical care to patients admitted under virtual observation compared with inpatient status. They concluded that observation status largely is a common billing designation that does not represent care in a distinct unit, nor does it represent a difference in clinical care compared with inpatient status. Therefore, it would not seem surprising to discover that the costs for observation stays are similar to those for inpatient stays.
In a second study by the same authors, they examined trends in observation-status utilization, again using the PHIS database. Patient characteristics and outcomes in observation status were compared to those of inpatient status. During the study period, with a stable Case Mix Index (CMI), an increase in proportion of patients in observation status occurred concurrently with a corresponding decrease in proportion of patients in inpatient status. For short stays, common diagnoses in observation status were similar to those for inpatient status.5 The data suggest that the patients received similar clinical care and therefore similar cost of care for these short stays.
Given the variation in how observation status is determined, and the significant overlap in clinical care seen in observation status compared with inpatient status, it would stand to reason that costs for observation stays would be similar to those for inpatients stays, especially for short stays of common diagnoses. Moving forward, the challenge for the medical community is to decide how to consistently determine which patients or clinical conditions are appropriate for observation status. Addressing additional costs incurred by patients and their families that accompany the designation of observation status will be critical. Only then can pediatric hospitalists be expected to optimize the use of observation status, with the goals of decreasing clinical costs and improving quality outcomes.
Dr. O’Callaghan is a pediatric hospitalist and clinical assistant professor of pediatrics at Seattle Children’s Hospital and the University of Washington School of Medicine. He also is a Team Hospitalist member.
References
- Mitus AJ. The birth of InterQual: evidence-based decision support criteria that helped change healthcare. Prof Case Manag. 2008;13:228-233.
- Fieldston ES, Shah SS, Hall M, et al. Resource utilization for observation-status stays at children’s hospitals. Pediatrics. 2013;131:1050-1058.
- Macy ML, Hall M, Shah SS, et al. Differences in designations of observation care in US freestanding children’s hospitals: are they virtual or real? J Hosp Med. 2012;7:287-293.
- Macy ML, Hall M, Shah SS, et al. Pediatric observation status: are we overlooking a growing population in children’s hospitals? J Hosp Med. 2012;7:530-536.
Physicians once admitted patients to observation status when they were unsure whether the hospitalization ultimately would lead to a stay longer than 24 hours. In 1978, InterQual published its first severity-of-illness/intensity-of-service criteria for evaluating appropriateness of admission and level of service.1 These originated from a government contract to develop a quality-assurance program addressing variability in length of stay that became apparent after Medicare was implemented in 1967. Charles Jacobs, an attorney who was once an associate director at The Joint Commission, assembled a team that once worked out of an apartment in Chicago that would become InterQual.2 Over the years, InterQual evolved and was eventually acquired by McKesson.
In a study published in the May 2013 issue of Pediatrics, Fieldston et al used data obtained from the Pediatric Health Information System (PHIS) 2010 database to demonstrate that observation-status designation is used inconsistently in pediatric hospitals.3 The researchers showed that costs for observation-status stays overlap substantially with costs for inpatient-status stays. Although the results of this study may be disappointing to those who seek to reduce cost or increase value, they should not be surprising.
A previous study from several of the same authors showed that significant variation exists in how observation status is assigned versus inpatient status.4 Observation status was found to be based on duration of expected treatment or on level of care criteria (i.e. InterQual or Millman). In fact, within an individual hospital, variation could be present in the assignment of status between individual payors. For example, a short stay for asthma exacerbation could be assigned inpatient status for one payor and observation status for another payor. Patients likely received the same care and costs, especially in hospitals with standardized-treatment-care plans or protocols.
In that same study, the authors discovered that only 12 of 31 (39%) freestanding children’s hospitals had a designated observation unit. Many hospitals reported that observation patients were scattered across the ED and inpatient units (e.g. “virtual” observation unit). A majority of hospitals (14 of 16) reported that there were no differences in the delivery of clinical care to patients admitted under virtual observation compared with inpatient status. They concluded that observation status largely is a common billing designation that does not represent care in a distinct unit, nor does it represent a difference in clinical care compared with inpatient status. Therefore, it would not seem surprising to discover that the costs for observation stays are similar to those for inpatient stays.
In a second study by the same authors, they examined trends in observation-status utilization, again using the PHIS database. Patient characteristics and outcomes in observation status were compared to those of inpatient status. During the study period, with a stable Case Mix Index (CMI), an increase in proportion of patients in observation status occurred concurrently with a corresponding decrease in proportion of patients in inpatient status. For short stays, common diagnoses in observation status were similar to those for inpatient status.5 The data suggest that the patients received similar clinical care and therefore similar cost of care for these short stays.
Given the variation in how observation status is determined, and the significant overlap in clinical care seen in observation status compared with inpatient status, it would stand to reason that costs for observation stays would be similar to those for inpatients stays, especially for short stays of common diagnoses. Moving forward, the challenge for the medical community is to decide how to consistently determine which patients or clinical conditions are appropriate for observation status. Addressing additional costs incurred by patients and their families that accompany the designation of observation status will be critical. Only then can pediatric hospitalists be expected to optimize the use of observation status, with the goals of decreasing clinical costs and improving quality outcomes.
Dr. O’Callaghan is a pediatric hospitalist and clinical assistant professor of pediatrics at Seattle Children’s Hospital and the University of Washington School of Medicine. He also is a Team Hospitalist member.
References
- Mitus AJ. The birth of InterQual: evidence-based decision support criteria that helped change healthcare. Prof Case Manag. 2008;13:228-233.
- Fieldston ES, Shah SS, Hall M, et al. Resource utilization for observation-status stays at children’s hospitals. Pediatrics. 2013;131:1050-1058.
- Macy ML, Hall M, Shah SS, et al. Differences in designations of observation care in US freestanding children’s hospitals: are they virtual or real? J Hosp Med. 2012;7:287-293.
- Macy ML, Hall M, Shah SS, et al. Pediatric observation status: are we overlooking a growing population in children’s hospitals? J Hosp Med. 2012;7:530-536.
Physicians once admitted patients to observation status when they were unsure whether the hospitalization ultimately would lead to a stay longer than 24 hours. In 1978, InterQual published its first severity-of-illness/intensity-of-service criteria for evaluating appropriateness of admission and level of service.1 These originated from a government contract to develop a quality-assurance program addressing variability in length of stay that became apparent after Medicare was implemented in 1967. Charles Jacobs, an attorney who was once an associate director at The Joint Commission, assembled a team that once worked out of an apartment in Chicago that would become InterQual.2 Over the years, InterQual evolved and was eventually acquired by McKesson.
In a study published in the May 2013 issue of Pediatrics, Fieldston et al used data obtained from the Pediatric Health Information System (PHIS) 2010 database to demonstrate that observation-status designation is used inconsistently in pediatric hospitals.3 The researchers showed that costs for observation-status stays overlap substantially with costs for inpatient-status stays. Although the results of this study may be disappointing to those who seek to reduce cost or increase value, they should not be surprising.
A previous study from several of the same authors showed that significant variation exists in how observation status is assigned versus inpatient status.4 Observation status was found to be based on duration of expected treatment or on level of care criteria (i.e. InterQual or Millman). In fact, within an individual hospital, variation could be present in the assignment of status between individual payors. For example, a short stay for asthma exacerbation could be assigned inpatient status for one payor and observation status for another payor. Patients likely received the same care and costs, especially in hospitals with standardized-treatment-care plans or protocols.
In that same study, the authors discovered that only 12 of 31 (39%) freestanding children’s hospitals had a designated observation unit. Many hospitals reported that observation patients were scattered across the ED and inpatient units (e.g. “virtual” observation unit). A majority of hospitals (14 of 16) reported that there were no differences in the delivery of clinical care to patients admitted under virtual observation compared with inpatient status. They concluded that observation status largely is a common billing designation that does not represent care in a distinct unit, nor does it represent a difference in clinical care compared with inpatient status. Therefore, it would not seem surprising to discover that the costs for observation stays are similar to those for inpatient stays.
In a second study by the same authors, they examined trends in observation-status utilization, again using the PHIS database. Patient characteristics and outcomes in observation status were compared to those of inpatient status. During the study period, with a stable Case Mix Index (CMI), an increase in proportion of patients in observation status occurred concurrently with a corresponding decrease in proportion of patients in inpatient status. For short stays, common diagnoses in observation status were similar to those for inpatient status.5 The data suggest that the patients received similar clinical care and therefore similar cost of care for these short stays.
Given the variation in how observation status is determined, and the significant overlap in clinical care seen in observation status compared with inpatient status, it would stand to reason that costs for observation stays would be similar to those for inpatients stays, especially for short stays of common diagnoses. Moving forward, the challenge for the medical community is to decide how to consistently determine which patients or clinical conditions are appropriate for observation status. Addressing additional costs incurred by patients and their families that accompany the designation of observation status will be critical. Only then can pediatric hospitalists be expected to optimize the use of observation status, with the goals of decreasing clinical costs and improving quality outcomes.
Dr. O’Callaghan is a pediatric hospitalist and clinical assistant professor of pediatrics at Seattle Children’s Hospital and the University of Washington School of Medicine. He also is a Team Hospitalist member.
References
- Mitus AJ. The birth of InterQual: evidence-based decision support criteria that helped change healthcare. Prof Case Manag. 2008;13:228-233.
- Fieldston ES, Shah SS, Hall M, et al. Resource utilization for observation-status stays at children’s hospitals. Pediatrics. 2013;131:1050-1058.
- Macy ML, Hall M, Shah SS, et al. Differences in designations of observation care in US freestanding children’s hospitals: are they virtual or real? J Hosp Med. 2012;7:287-293.
- Macy ML, Hall M, Shah SS, et al. Pediatric observation status: are we overlooking a growing population in children’s hospitals? J Hosp Med. 2012;7:530-536.
How to Manage Pain in Patients with Renal Insufficiency or End-Stage Renal Disease on Dialysis?

Case
A 70-year-old male with ESRD on hemodialysis presents with methicillin-resistant Staphylococcus aureus (MRSA) bacteremia and ankle pain after a fall. An MRI of his ankle is negative, and he is started on acetaminophen and lidocaine patches, which result in adequate pain relief of the ankle. He later develops significant neuropathic pain in both arms, and a CT scan of the cervical spine reveals a cervical abscess and osteomyelitis. The patient desires pain relief but adamantly refuses narcotics, stating: “I don’t want to get addicted.” How can his pain be managed?
Overview
Pain is a common problem in patients with renal insufficiency and end-stage renal disease (ESRD) and can have a significant effect on the patient’s quality of life.1 When assessing a patient’s pain, assess both the severity of the pain (such as on an analogue scale, 0-10) and the characteristics of the pain. Pain is most commonly characterized as nociceptive, neuropathic, or both. Nociceptive pain can be further classified as arising from either somatic or visceral sources, and is often described as dull, throbbing, cramping, and/or pressurelike.1 Neuropathic pain is often described as tingling, numbing, burning, and/or stabbing.
It is a challenge to manage pain in patients with renal insufficiency and dialysis. Renal insufficiency affects the pharmacokinetic properties of most pain medications, including their distribution, clearance, and excretion. The magnitude of the effect of renal insufficiency on drug metabolism varies depending on the agent itself, its metabolite, and the extent of renal failure.3 Multiple factors should be considered when prescribing pain medications for patients on dialysis, including the properties of the parent drug and its metabolites; the physical properties of the dialysis equipment, such as the filter pore size, the flow rate, and the efficiency of the technique used; and the dialysis method (intermittent versus continuous).3 Table 1 provides the recommended dosing of the most commonly prescribed agents, based on the degree of renal impairment. A modified World Health Organization (WHO) ladder has been suggested to treat pain in patients with ESRD, which can lead to effective pain relief in as many as 96% of patients (see Figure 1).2

*Beginning dose: If switching from IR to ER, calculate 24-hour total dose.
**For patients with creatinine clearances (CrCl) of 15 mL/min or less, the daily dosage should be adjusted proportionally (e.g. patients with a CrCl of 7.5 mL/min should receive one-half the dose of a patient with a CrCl of 15 mL/min).
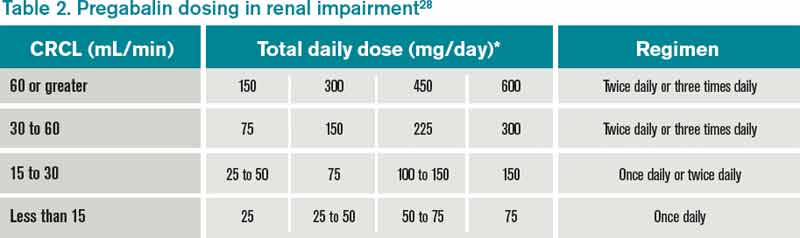
Review of Data
Nonopioid options. Nonopioids, such as acetaminophen and NSAIDs, have no associated tolerance but have a ceiling effect for analgesia, and NSAIDs are associated with dose-dependent acute renal failure, gastrointestinal ulceration and bleeding, and cardiac events. The nonopioids that are considered safe options in patients with renal insufficiency include acetaminophen, ibuprofen, and fenoprofen (Nalfon). However, in the elderly, American Geriatric Society (AGS) guidelines currently recommend avoiding all NSAIDs due to their safety profile in the geriatric population.4 Although all NSAIDs can potentially be used for pain, selected NSAIDs with an FDA indication for acute or chronic pain were included for this review.
Acetaminophen (APAP) is a dialyzable compound that is metabolized in the liver to five inactive metabolites. The terminal elimination half-life of its sulfate and glucuronide metabolites are prolonged in patients with renal failure; therefore, the dosing interval of APAP should be increased to six to eight hours in renally impaired patients.5,6,7 Overall, acetaminophen is considered one of the safest agents to use for the treatment of pain, in renal patients and otherwise, as long as dosing is below the minimal daily dose (see Table 1).
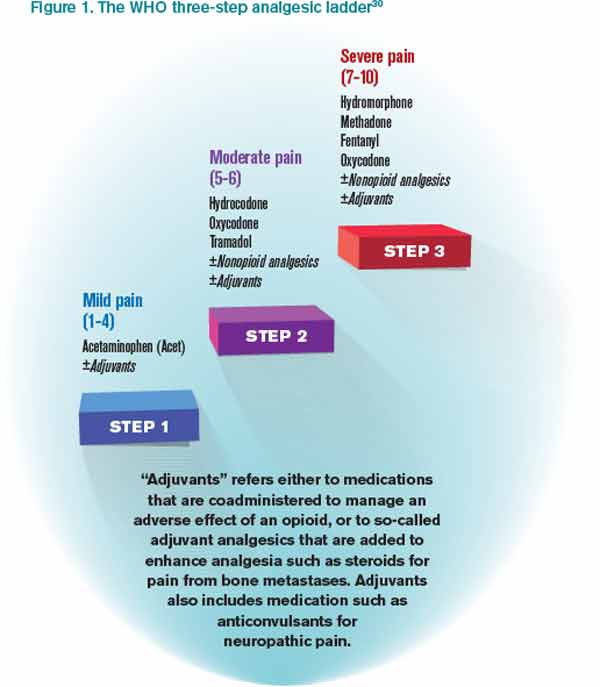
Ibuprofen is metabolized in the liver to inactive compounds. It does not accumulate in renal insufficiency, and two of the inactive compounds are dialyzable.8 It is considered a safe option for the treatment of pain in patients with renal insufficiency or dialysis.9
Fenoprofen is metabolized in the liver to inactive compounds. Renal impairment is likely to cause the accumulation of the inactive metabolites but not the parent compound, so dose reduction is not necessary with the use of this agent in renal insufficiency or dialysis.6
Mefenamic acid (Ponstel) is metabolized in the liver. Mefenamic acid can further deteriorate renal function in patients with underlying renal disease.12 However, the nephrotoxic potential of this agent is of little consideration in ESRD patients on dialysis, and therefore no dosage adjustments are necessary in these patients.6
Ketoprofen is metabolized in the liver, where approximately 80% of the dose is excreted in the urine as a glucuronide metabolite. Dose reduction is recommended in renal insufficiency and dialysis, as it not dialyzable.8
Ketorolac accumulates in renal insufficiency; therefore, it is contraindicated in these patients and in patients at risk for renal failure, including those with volume depletion.10 Ketorolac is unlikely to be removed by dialysis and so should be avoided.10,11
Naproxen is metabolized in the liver to inactive compounds. Use of naproxen is not recommended in patients with moderate to severe renal impairment. If therapy must be initiated, close monitoring of the patient’s renal function is recommended.13
Celecoxib is the only cyclooxygenase-2 (COX-2) inhibitor available in the U.S. It is metabolized extensively by the liver and is unlikely to be removed by dialysis. Therefore, use of COX-2 inhibitors should be avoided in severe renal impairment and in those on dialysis.14,15
Opioid options. The use of opioids in the renally impaired population is challenging, as one must balance opioid-related adverse events with adequate pain control. As such, it is recommended to start with lower-than-recommended doses and slowly titrate up the dose while extending the dosing interval. This will help limit adverse effects, such as respiratory depression and hypotension.3
Hydrocodone is metabolized to hydromorphone (Dilaudid), which is then metabolized to its major metabolite hydromorphine-3-glucuronide (H3G) and minor metabolite hydromorphine-6-hydroxy, all of which are excreted renally along with the parent compound. H3G has no analgesic properties, but it can potentially cause neuroexcitation, agitation, confusion, and hallucination. Hydromorphone has been used safely in patients with renal insufficiency and dialysis, as it is expected to be dialyzable. 16,17
Tramadol is metabolized in the liver, producing one active compound. Approximately 30% of the tramadol dose is excreted unchanged in the urine, whereas 60% of the dose is excreted as metabolites. It is recommended to reduce the dose and increase the dosing interval in patients with renal insufficiency, but tramadol is generally well-tolerated in patients with renal insufficiency and dialysis. It is significantly removed by hemodialysis; therefore, redosing after a session may be necessary.18,19
Oxycodone can be used in patients with mild to moderate renal insufficiency but should be used at reduced dosing; it has been associated with significant sedation with usual doses in renal failure patients.16 Its use is generally not recommended in dialysis patients due to lack of data.3
Methadone and its metabolites are excreted in the urine and feces. Methadone has been used safely in patients with renal insufficiency, but it is poorly removed by dialysis and no specific recommendations are available regarding its dosing in dialysis.3,16
Fentanyl is primarily metabolized in the liver to inactive metabolites. Fentanyl clearance is reduced in patients with moderate to severe uremia (BUN >60 mg/dL). It is not expected that fentanyl be dialyzable because of its pharmacokinetic properties (high protein-binding, low water solubility, high molecular weight, and high volume of distribution). Data suggests that fentanyl can be used at usual doses in mild to moderate renal insufficiency and in dialysis patients, although reduced doses may be prudent. Such patients should be monitored for signs of gradual accumulation of the parent drug.3,16
Morphine is metabolized in the liver to morphine-6-glucuronide (M6G) and morphine-3-glucuronide (M3G), all of which are excreted renally, along with the parent compound. Only M6G has analgesic properties, and when it accumulates, it can lead to CNS depression. M3G is associated with behavioral excitation, a side effect that is further magnified in patients with renal insufficiency. Although morphine is dialyzable, it should generally be avoided in patients with any level of renal insufficiency.16,17,20,21
Codeine is metabolized to several active metabolites, all of which are renally excreted. Lower-than-usual doses are recommended in patients with renal insufficiency, and it should be avoided altogether in dialysis patients.3,16
Meperidine is metabolized in the liver to various metabolites, primarily normeperidine, which is toxic and has a long half-life, five to 10 times longer then meperidine. Meperidine should not be used in patients with renal insufficiency or dialysis.3
Adjunctive therapeutic options. Lidocaine patches currently are only FDA-indicated for postherpetic neuralgia but are used for a wide variety of local pain syndromes. Absorption of lidocaine is determined by the duration of application and the surface area over which it is applied. There is no appreciable accumulation of lidocaine or its metabolites in renal insufficiency; therefore, dose adjustments are not required.22,23
Gabapentin is FDA-indicated for partial seizures and postherpetic neuralgia but is also used for a wide variety of neuropathic pain syndromes, including postoperative pain.24 Gabapentin is not metabolized and is excreted in the urine unchanged. Renal clearance of gabapentin is reduced by 40% and the elimination half-life is increased up to 52 hours in renal insufficiency, but it is dialyzable. Therefore, dose adjustments are required with gabapentin in patients with moderate to severe renal insufficiency, and supplemental doses should be administered in patients after receiving dialysis.25-27
Pregabalin is structurally related to gabapentin and is indicated for a variety of neuropathic pain conditions. Pregabalin is 90% excreted unchanged in the urine, and approximately 50% of drug is removed after four hours of hemodialysis. Dose adjustments are required in patients with moderate to severe renal insufficiency, and supplemental doses should be administered in patients after receiving dialysis.28
Antidepressant options. Amitriptyline, nortryptiline, and desipramine are the tricyclic antidepressants (TCAs) commonly used for neuropathic pain. TCAs are metabolized in the liver to inactive metabolites, with the exception of amitriptyline, which is metabolized to nortryptiline. Common side effects reported with TCAs include postural hypotension and anticholinergic side effects, such as constipation, urinary retention, blurred vision, dry mouth, delirium, and sedation. It is unlikely that the TCAs can be removed by dialysis. It is suggested that the dosage be reduced in renal insufficiency and that anticholinergic side effects be monitored.29
Back to the Case
The patient’s ankle pain was controlled with acetaminophen and lidocaine patches. For the neuropathic pain in his upper extremities, tramadol was started at 25 mg oral every 12 hours and increased to 50 mg oral every eight hours (below the maximum of 200 mg a day). The tramadol did not result in adequate pain relief, so gabapentin 100 mg at bedtime was initiated, then increased to twice daily over three days with some relief.
A geriatric consult was obtained to help educate him regarding addiction to opioids, as well as to explore goals of care, but he continued to insist on the use of a non-narcotic regimen for his pain.
Bottom Line
Pain management in patients with renal insufficiency and dialysis can be challenging, but there are a number of safe non-narcotic and narcotic pain regimens that can be safely used in this patient population.
Dr. Harisingani is a board-certified hospitalist at Long Island Jewish Medical Center in New Hyde Park, N.Y., and Drs. Saad and Cassagnol are assistant clinical professors at St. Johns University College of Pharmacy and Health Sciences in Jamaica, N.Y., and clinical pharmacy coordinators at Long Island Jewish Medical Center.
References
- Mid-Atlantic Renal Coalition and the Kidney End-of-Life Coalition. Clinical algorithm & preferred medications to treat pain in dialysis patients. Coalition for Supportive Care of Kidney Patients website. Available at: http://www.kidneysupportivecare.org/Physicians-Clinicians/Pain—Symptom-Management.aspx. Accessed Nov. 18, 2012.
- Barakzoy AS, Moss AH. Efficacy of the World Health Organization analgesic ladder to treat pain in end-stage renal disease. J Am Soc Nephrol. 2006;17(11):3198-3203.
- Johnson SJ. Opioid safety in patients with renal or hepatic dysfunction. Pain Treatment Topics website. Available at: http://pain-topics.org/pdf/Opioids-Renal-Hepatic-Dysfunction.pdf. Accessed Nov. 28, 2012.
- Ferrell B, Argoff CE, Epplin J, et al. American Geriatrics Society Panel on Pharmacological Management of Persistent Pain in Older Persons. Pharmacological management of persistent pain in older persons. J Am Geriatr Soc. 2009;57(8):1331-1346.
- Prescott LF, Speirs GC, Critchley JA, Temple RM, Winney RJ. Paracetamol disposition and metabolite kinetics in patients with chronic renal failure. Eur J Clin Pharmacol. 1989;36(3):291-297.
- Launay-Vacher V, Karie S, Fau JB, Izzedine H, Deray G. Treatment of pain in patients with renal insufficiency: the World Health Organization three-step ladder adapted. J Pain. 2006;6(3):137-148.
- Berg KJ, Djøseland O, Gjellan A, et al. Acute effects of paracetamol on prostaglandin synthesis and renal function in normal man and in patients with renal failure. Clin Nephrol. 1990;34:255-262.
- Delbarre F, Roucayrol JC, Amor B, et al. Pharmacokinetic study of ketoprofen (19.583 R.P.) in man using the tritiated compound. Scand J Rheumatol Suppl. 1976;1976(0):45-52.
- Shen CH, Hung CJ, Wu CC, Huang HW, Ho WM. Rhabdomyolysis-induced acute renal failure after morphine overdose—a case report. Acta Anaesthesiol Sin. 1999;37(3):159-162.
- Ketorolac tromethamine oral tablets [package insert]. St. Louis: Ethex Corp.: 2008.
- Brocks DR, Jamali F. Clinical pharmacokinetics of ketorolac tromethamine. Clin Pharmacokinet. 1992;23:415-427. Erratum in: Clin Pharmacokinet. 1999;24(3):270.
- Ponstel [package insert]. Alpharetta, GA: First Horizon Pharmaceutical Corp.; 2006.
- Naprosyn [package insert]. Nutley, NJ: Roche Laboratories Inc.; 2008.
- Celebrex [package insert]. New York: G.D. Searle LLC; 2011.
- Catella-Lawson F, McAdam B, Morrison BW, et al. Effects of specific inhibition of cyclooygenase-2 on sodium balance, hemodynamics, and vasoactive eicosanoids. J Pharmacol Exp Ther. 1999;289:735-741.
- Dean M. Opioids in renal failure and dialysis patients. J Pain Symptom Manage. 2004;28(5):497-504.
- Lee MA, Leng ME, Tiernan EJ. Retrospective study of the use of hydromorphone in palliative care patients with normal and abnormal urea and creatinine. Palliat Med. 2001;15(1):26-34.
- Gibson TP. Pharmacokinetics, efficacy, and safety of analgesia with a focus on tramadol HCI. Am J. Med. 1996;101(1A):47S-53S.
- Izzedine H, Launay-Vacher V, Abbara C, Aymard G, Bassilios N, Deray G. Pharmacokinetics of tramadol in a hemodialysis patient. Nephron. 2002;92(3):755-756.
- Hasselström J, Säwe J. Morphine pharmacokinetics and metabolism in humans. Enterohepatic cycling and relative contribution of metabolites to active opioid concentrations. Clin Pharmacokinet. 1993;24(4):344-354.
- Andersen G, Christrup L, Sjøgren P. Relationships among morphine metabolism, pain and side effects during long-term treatment: an update. J Pain Symptom Manage. 2003;25(1):74-91.
- Lidoderm [package insert]. Chadds Ford, PA: Endo Pharmaceuticals Inc.; 2010.
- Carter GT, Galer BS. Advances in the management of neuropathic pain. Phys Med Rehabil Clin N Am. 2001;12(2):447-459.
- Ho KY, Gan TJ, Habib AS. Gabapentin and postoperative pain—a systematic review of randomized controlled trials. Pain. 2006;15:126(1-3):91-101.
- Neurontin [package insert]. New York: Parke-Davis; 2010.
- Pandey CK, Priye S, Singh S, et al. Preemptive use of gabapentin significantly decreases postoperative pain and rescue analgesic requirements in laparoscopic cholecystectomy. Can J Anaesth. 2004;51(4):358-363.
- Srivastava U, Kumar A, Saxena S, et al: Effect of preoperative gabapentin on postoperative pain and tramadol consumption after minilap open cholecystectomy: a randomized double-blind, placebo-controlled trial. Eur J Anaesthesiol. 2010;27(N4):331-335.
- Lyrica [package insert]. New York: Pfizer Inc.; 2012.
- Broadbent A, Khor K, Heaney A. Palliation and chronic renal failure: opioid and other palliative medications—dosage guidelines. Progress in Palliative Care. 2003;11(4):183-190(8).
- Nayak-Rao S. Achieving effective pain relief in patients with chronic kidney disease: a review of analgesics in renal failure. J Nephrol. 2011;24(1):35-40.
- Wolters Kluwer Health. Facts & comparisons. Wolters Kluwer Health website. Available at: http://www.factsandcomparisons.com. Accessed Jan. 14, 2013.
- Lexicomp. Lexicomp Online. Lexicomp website. Available at: http://www.lexi.com/institutions/products/online/.
Case
A 70-year-old male with ESRD on hemodialysis presents with methicillin-resistant Staphylococcus aureus (MRSA) bacteremia and ankle pain after a fall. An MRI of his ankle is negative, and he is started on acetaminophen and lidocaine patches, which result in adequate pain relief of the ankle. He later develops significant neuropathic pain in both arms, and a CT scan of the cervical spine reveals a cervical abscess and osteomyelitis. The patient desires pain relief but adamantly refuses narcotics, stating: “I don’t want to get addicted.” How can his pain be managed?
Overview
Pain is a common problem in patients with renal insufficiency and end-stage renal disease (ESRD) and can have a significant effect on the patient’s quality of life.1 When assessing a patient’s pain, assess both the severity of the pain (such as on an analogue scale, 0-10) and the characteristics of the pain. Pain is most commonly characterized as nociceptive, neuropathic, or both. Nociceptive pain can be further classified as arising from either somatic or visceral sources, and is often described as dull, throbbing, cramping, and/or pressurelike.1 Neuropathic pain is often described as tingling, numbing, burning, and/or stabbing.
It is a challenge to manage pain in patients with renal insufficiency and dialysis. Renal insufficiency affects the pharmacokinetic properties of most pain medications, including their distribution, clearance, and excretion. The magnitude of the effect of renal insufficiency on drug metabolism varies depending on the agent itself, its metabolite, and the extent of renal failure.3 Multiple factors should be considered when prescribing pain medications for patients on dialysis, including the properties of the parent drug and its metabolites; the physical properties of the dialysis equipment, such as the filter pore size, the flow rate, and the efficiency of the technique used; and the dialysis method (intermittent versus continuous).3 Table 1 provides the recommended dosing of the most commonly prescribed agents, based on the degree of renal impairment. A modified World Health Organization (WHO) ladder has been suggested to treat pain in patients with ESRD, which can lead to effective pain relief in as many as 96% of patients (see Figure 1).2
*Beginning dose: If switching from IR to ER, calculate 24-hour total dose.
**For patients with creatinine clearances (CrCl) of 15 mL/min or less, the daily dosage should be adjusted proportionally (e.g. patients with a CrCl of 7.5 mL/min should receive one-half the dose of a patient with a CrCl of 15 mL/min).
Review of Data
Nonopioid options. Nonopioids, such as acetaminophen and NSAIDs, have no associated tolerance but have a ceiling effect for analgesia, and NSAIDs are associated with dose-dependent acute renal failure, gastrointestinal ulceration and bleeding, and cardiac events. The nonopioids that are considered safe options in patients with renal insufficiency include acetaminophen, ibuprofen, and fenoprofen (Nalfon). However, in the elderly, American Geriatric Society (AGS) guidelines currently recommend avoiding all NSAIDs due to their safety profile in the geriatric population.4 Although all NSAIDs can potentially be used for pain, selected NSAIDs with an FDA indication for acute or chronic pain were included for this review.
Acetaminophen (APAP) is a dialyzable compound that is metabolized in the liver to five inactive metabolites. The terminal elimination half-life of its sulfate and glucuronide metabolites are prolonged in patients with renal failure; therefore, the dosing interval of APAP should be increased to six to eight hours in renally impaired patients.5,6,7 Overall, acetaminophen is considered one of the safest agents to use for the treatment of pain, in renal patients and otherwise, as long as dosing is below the minimal daily dose (see Table 1).
Ibuprofen is metabolized in the liver to inactive compounds. It does not accumulate in renal insufficiency, and two of the inactive compounds are dialyzable.8 It is considered a safe option for the treatment of pain in patients with renal insufficiency or dialysis.9
Fenoprofen is metabolized in the liver to inactive compounds. Renal impairment is likely to cause the accumulation of the inactive metabolites but not the parent compound, so dose reduction is not necessary with the use of this agent in renal insufficiency or dialysis.6
Mefenamic acid (Ponstel) is metabolized in the liver. Mefenamic acid can further deteriorate renal function in patients with underlying renal disease.12 However, the nephrotoxic potential of this agent is of little consideration in ESRD patients on dialysis, and therefore no dosage adjustments are necessary in these patients.6
Ketoprofen is metabolized in the liver, where approximately 80% of the dose is excreted in the urine as a glucuronide metabolite. Dose reduction is recommended in renal insufficiency and dialysis, as it not dialyzable.8
Ketorolac accumulates in renal insufficiency; therefore, it is contraindicated in these patients and in patients at risk for renal failure, including those with volume depletion.10 Ketorolac is unlikely to be removed by dialysis and so should be avoided.10,11
Naproxen is metabolized in the liver to inactive compounds. Use of naproxen is not recommended in patients with moderate to severe renal impairment. If therapy must be initiated, close monitoring of the patient’s renal function is recommended.13
Celecoxib is the only cyclooxygenase-2 (COX-2) inhibitor available in the U.S. It is metabolized extensively by the liver and is unlikely to be removed by dialysis. Therefore, use of COX-2 inhibitors should be avoided in severe renal impairment and in those on dialysis.14,15
Opioid options. The use of opioids in the renally impaired population is challenging, as one must balance opioid-related adverse events with adequate pain control. As such, it is recommended to start with lower-than-recommended doses and slowly titrate up the dose while extending the dosing interval. This will help limit adverse effects, such as respiratory depression and hypotension.3
Hydrocodone is metabolized to hydromorphone (Dilaudid), which is then metabolized to its major metabolite hydromorphine-3-glucuronide (H3G) and minor metabolite hydromorphine-6-hydroxy, all of which are excreted renally along with the parent compound. H3G has no analgesic properties, but it can potentially cause neuroexcitation, agitation, confusion, and hallucination. Hydromorphone has been used safely in patients with renal insufficiency and dialysis, as it is expected to be dialyzable. 16,17
Tramadol is metabolized in the liver, producing one active compound. Approximately 30% of the tramadol dose is excreted unchanged in the urine, whereas 60% of the dose is excreted as metabolites. It is recommended to reduce the dose and increase the dosing interval in patients with renal insufficiency, but tramadol is generally well-tolerated in patients with renal insufficiency and dialysis. It is significantly removed by hemodialysis; therefore, redosing after a session may be necessary.18,19
Oxycodone can be used in patients with mild to moderate renal insufficiency but should be used at reduced dosing; it has been associated with significant sedation with usual doses in renal failure patients.16 Its use is generally not recommended in dialysis patients due to lack of data.3
Methadone and its metabolites are excreted in the urine and feces. Methadone has been used safely in patients with renal insufficiency, but it is poorly removed by dialysis and no specific recommendations are available regarding its dosing in dialysis.3,16
Fentanyl is primarily metabolized in the liver to inactive metabolites. Fentanyl clearance is reduced in patients with moderate to severe uremia (BUN >60 mg/dL). It is not expected that fentanyl be dialyzable because of its pharmacokinetic properties (high protein-binding, low water solubility, high molecular weight, and high volume of distribution). Data suggests that fentanyl can be used at usual doses in mild to moderate renal insufficiency and in dialysis patients, although reduced doses may be prudent. Such patients should be monitored for signs of gradual accumulation of the parent drug.3,16
Morphine is metabolized in the liver to morphine-6-glucuronide (M6G) and morphine-3-glucuronide (M3G), all of which are excreted renally, along with the parent compound. Only M6G has analgesic properties, and when it accumulates, it can lead to CNS depression. M3G is associated with behavioral excitation, a side effect that is further magnified in patients with renal insufficiency. Although morphine is dialyzable, it should generally be avoided in patients with any level of renal insufficiency.16,17,20,21
Codeine is metabolized to several active metabolites, all of which are renally excreted. Lower-than-usual doses are recommended in patients with renal insufficiency, and it should be avoided altogether in dialysis patients.3,16
Meperidine is metabolized in the liver to various metabolites, primarily normeperidine, which is toxic and has a long half-life, five to 10 times longer then meperidine. Meperidine should not be used in patients with renal insufficiency or dialysis.3
Adjunctive therapeutic options. Lidocaine patches currently are only FDA-indicated for postherpetic neuralgia but are used for a wide variety of local pain syndromes. Absorption of lidocaine is determined by the duration of application and the surface area over which it is applied. There is no appreciable accumulation of lidocaine or its metabolites in renal insufficiency; therefore, dose adjustments are not required.22,23
Gabapentin is FDA-indicated for partial seizures and postherpetic neuralgia but is also used for a wide variety of neuropathic pain syndromes, including postoperative pain.24 Gabapentin is not metabolized and is excreted in the urine unchanged. Renal clearance of gabapentin is reduced by 40% and the elimination half-life is increased up to 52 hours in renal insufficiency, but it is dialyzable. Therefore, dose adjustments are required with gabapentin in patients with moderate to severe renal insufficiency, and supplemental doses should be administered in patients after receiving dialysis.25-27
Pregabalin is structurally related to gabapentin and is indicated for a variety of neuropathic pain conditions. Pregabalin is 90% excreted unchanged in the urine, and approximately 50% of drug is removed after four hours of hemodialysis. Dose adjustments are required in patients with moderate to severe renal insufficiency, and supplemental doses should be administered in patients after receiving dialysis.28
Antidepressant options. Amitriptyline, nortryptiline, and desipramine are the tricyclic antidepressants (TCAs) commonly used for neuropathic pain. TCAs are metabolized in the liver to inactive metabolites, with the exception of amitriptyline, which is metabolized to nortryptiline. Common side effects reported with TCAs include postural hypotension and anticholinergic side effects, such as constipation, urinary retention, blurred vision, dry mouth, delirium, and sedation. It is unlikely that the TCAs can be removed by dialysis. It is suggested that the dosage be reduced in renal insufficiency and that anticholinergic side effects be monitored.29
Back to the Case
The patient’s ankle pain was controlled with acetaminophen and lidocaine patches. For the neuropathic pain in his upper extremities, tramadol was started at 25 mg oral every 12 hours and increased to 50 mg oral every eight hours (below the maximum of 200 mg a day). The tramadol did not result in adequate pain relief, so gabapentin 100 mg at bedtime was initiated, then increased to twice daily over three days with some relief.
A geriatric consult was obtained to help educate him regarding addiction to opioids, as well as to explore goals of care, but he continued to insist on the use of a non-narcotic regimen for his pain.
Bottom Line
Pain management in patients with renal insufficiency and dialysis can be challenging, but there are a number of safe non-narcotic and narcotic pain regimens that can be safely used in this patient population.
Dr. Harisingani is a board-certified hospitalist at Long Island Jewish Medical Center in New Hyde Park, N.Y., and Drs. Saad and Cassagnol are assistant clinical professors at St. Johns University College of Pharmacy and Health Sciences in Jamaica, N.Y., and clinical pharmacy coordinators at Long Island Jewish Medical Center.
References
- Mid-Atlantic Renal Coalition and the Kidney End-of-Life Coalition. Clinical algorithm & preferred medications to treat pain in dialysis patients. Coalition for Supportive Care of Kidney Patients website. Available at: http://www.kidneysupportivecare.org/Physicians-Clinicians/Pain—Symptom-Management.aspx. Accessed Nov. 18, 2012.
- Barakzoy AS, Moss AH. Efficacy of the World Health Organization analgesic ladder to treat pain in end-stage renal disease. J Am Soc Nephrol. 2006;17(11):3198-3203.
- Johnson SJ. Opioid safety in patients with renal or hepatic dysfunction. Pain Treatment Topics website. Available at: http://pain-topics.org/pdf/Opioids-Renal-Hepatic-Dysfunction.pdf. Accessed Nov. 28, 2012.
- Ferrell B, Argoff CE, Epplin J, et al. American Geriatrics Society Panel on Pharmacological Management of Persistent Pain in Older Persons. Pharmacological management of persistent pain in older persons. J Am Geriatr Soc. 2009;57(8):1331-1346.
- Prescott LF, Speirs GC, Critchley JA, Temple RM, Winney RJ. Paracetamol disposition and metabolite kinetics in patients with chronic renal failure. Eur J Clin Pharmacol. 1989;36(3):291-297.
- Launay-Vacher V, Karie S, Fau JB, Izzedine H, Deray G. Treatment of pain in patients with renal insufficiency: the World Health Organization three-step ladder adapted. J Pain. 2006;6(3):137-148.
- Berg KJ, Djøseland O, Gjellan A, et al. Acute effects of paracetamol on prostaglandin synthesis and renal function in normal man and in patients with renal failure. Clin Nephrol. 1990;34:255-262.
- Delbarre F, Roucayrol JC, Amor B, et al. Pharmacokinetic study of ketoprofen (19.583 R.P.) in man using the tritiated compound. Scand J Rheumatol Suppl. 1976;1976(0):45-52.
- Shen CH, Hung CJ, Wu CC, Huang HW, Ho WM. Rhabdomyolysis-induced acute renal failure after morphine overdose—a case report. Acta Anaesthesiol Sin. 1999;37(3):159-162.
- Ketorolac tromethamine oral tablets [package insert]. St. Louis: Ethex Corp.: 2008.
- Brocks DR, Jamali F. Clinical pharmacokinetics of ketorolac tromethamine. Clin Pharmacokinet. 1992;23:415-427. Erratum in: Clin Pharmacokinet. 1999;24(3):270.
- Ponstel [package insert]. Alpharetta, GA: First Horizon Pharmaceutical Corp.; 2006.
- Naprosyn [package insert]. Nutley, NJ: Roche Laboratories Inc.; 2008.
- Celebrex [package insert]. New York: G.D. Searle LLC; 2011.
- Catella-Lawson F, McAdam B, Morrison BW, et al. Effects of specific inhibition of cyclooygenase-2 on sodium balance, hemodynamics, and vasoactive eicosanoids. J Pharmacol Exp Ther. 1999;289:735-741.
- Dean M. Opioids in renal failure and dialysis patients. J Pain Symptom Manage. 2004;28(5):497-504.
- Lee MA, Leng ME, Tiernan EJ. Retrospective study of the use of hydromorphone in palliative care patients with normal and abnormal urea and creatinine. Palliat Med. 2001;15(1):26-34.
- Gibson TP. Pharmacokinetics, efficacy, and safety of analgesia with a focus on tramadol HCI. Am J. Med. 1996;101(1A):47S-53S.
- Izzedine H, Launay-Vacher V, Abbara C, Aymard G, Bassilios N, Deray G. Pharmacokinetics of tramadol in a hemodialysis patient. Nephron. 2002;92(3):755-756.
- Hasselström J, Säwe J. Morphine pharmacokinetics and metabolism in humans. Enterohepatic cycling and relative contribution of metabolites to active opioid concentrations. Clin Pharmacokinet. 1993;24(4):344-354.
- Andersen G, Christrup L, Sjøgren P. Relationships among morphine metabolism, pain and side effects during long-term treatment: an update. J Pain Symptom Manage. 2003;25(1):74-91.
- Lidoderm [package insert]. Chadds Ford, PA: Endo Pharmaceuticals Inc.; 2010.
- Carter GT, Galer BS. Advances in the management of neuropathic pain. Phys Med Rehabil Clin N Am. 2001;12(2):447-459.
- Ho KY, Gan TJ, Habib AS. Gabapentin and postoperative pain—a systematic review of randomized controlled trials. Pain. 2006;15:126(1-3):91-101.
- Neurontin [package insert]. New York: Parke-Davis; 2010.
- Pandey CK, Priye S, Singh S, et al. Preemptive use of gabapentin significantly decreases postoperative pain and rescue analgesic requirements in laparoscopic cholecystectomy. Can J Anaesth. 2004;51(4):358-363.
- Srivastava U, Kumar A, Saxena S, et al: Effect of preoperative gabapentin on postoperative pain and tramadol consumption after minilap open cholecystectomy: a randomized double-blind, placebo-controlled trial. Eur J Anaesthesiol. 2010;27(N4):331-335.
- Lyrica [package insert]. New York: Pfizer Inc.; 2012.
- Broadbent A, Khor K, Heaney A. Palliation and chronic renal failure: opioid and other palliative medications—dosage guidelines. Progress in Palliative Care. 2003;11(4):183-190(8).
- Nayak-Rao S. Achieving effective pain relief in patients with chronic kidney disease: a review of analgesics in renal failure. J Nephrol. 2011;24(1):35-40.
- Wolters Kluwer Health. Facts & comparisons. Wolters Kluwer Health website. Available at: http://www.factsandcomparisons.com. Accessed Jan. 14, 2013.
- Lexicomp. Lexicomp Online. Lexicomp website. Available at: http://www.lexi.com/institutions/products/online/.
Case
A 70-year-old male with ESRD on hemodialysis presents with methicillin-resistant Staphylococcus aureus (MRSA) bacteremia and ankle pain after a fall. An MRI of his ankle is negative, and he is started on acetaminophen and lidocaine patches, which result in adequate pain relief of the ankle. He later develops significant neuropathic pain in both arms, and a CT scan of the cervical spine reveals a cervical abscess and osteomyelitis. The patient desires pain relief but adamantly refuses narcotics, stating: “I don’t want to get addicted.” How can his pain be managed?
Overview
Pain is a common problem in patients with renal insufficiency and end-stage renal disease (ESRD) and can have a significant effect on the patient’s quality of life.1 When assessing a patient’s pain, assess both the severity of the pain (such as on an analogue scale, 0-10) and the characteristics of the pain. Pain is most commonly characterized as nociceptive, neuropathic, or both. Nociceptive pain can be further classified as arising from either somatic or visceral sources, and is often described as dull, throbbing, cramping, and/or pressurelike.1 Neuropathic pain is often described as tingling, numbing, burning, and/or stabbing.
It is a challenge to manage pain in patients with renal insufficiency and dialysis. Renal insufficiency affects the pharmacokinetic properties of most pain medications, including their distribution, clearance, and excretion. The magnitude of the effect of renal insufficiency on drug metabolism varies depending on the agent itself, its metabolite, and the extent of renal failure.3 Multiple factors should be considered when prescribing pain medications for patients on dialysis, including the properties of the parent drug and its metabolites; the physical properties of the dialysis equipment, such as the filter pore size, the flow rate, and the efficiency of the technique used; and the dialysis method (intermittent versus continuous).3 Table 1 provides the recommended dosing of the most commonly prescribed agents, based on the degree of renal impairment. A modified World Health Organization (WHO) ladder has been suggested to treat pain in patients with ESRD, which can lead to effective pain relief in as many as 96% of patients (see Figure 1).2
*Beginning dose: If switching from IR to ER, calculate 24-hour total dose.
**For patients with creatinine clearances (CrCl) of 15 mL/min or less, the daily dosage should be adjusted proportionally (e.g. patients with a CrCl of 7.5 mL/min should receive one-half the dose of a patient with a CrCl of 15 mL/min).
Review of Data
Nonopioid options. Nonopioids, such as acetaminophen and NSAIDs, have no associated tolerance but have a ceiling effect for analgesia, and NSAIDs are associated with dose-dependent acute renal failure, gastrointestinal ulceration and bleeding, and cardiac events. The nonopioids that are considered safe options in patients with renal insufficiency include acetaminophen, ibuprofen, and fenoprofen (Nalfon). However, in the elderly, American Geriatric Society (AGS) guidelines currently recommend avoiding all NSAIDs due to their safety profile in the geriatric population.4 Although all NSAIDs can potentially be used for pain, selected NSAIDs with an FDA indication for acute or chronic pain were included for this review.
Acetaminophen (APAP) is a dialyzable compound that is metabolized in the liver to five inactive metabolites. The terminal elimination half-life of its sulfate and glucuronide metabolites are prolonged in patients with renal failure; therefore, the dosing interval of APAP should be increased to six to eight hours in renally impaired patients.5,6,7 Overall, acetaminophen is considered one of the safest agents to use for the treatment of pain, in renal patients and otherwise, as long as dosing is below the minimal daily dose (see Table 1).
Ibuprofen is metabolized in the liver to inactive compounds. It does not accumulate in renal insufficiency, and two of the inactive compounds are dialyzable.8 It is considered a safe option for the treatment of pain in patients with renal insufficiency or dialysis.9
Fenoprofen is metabolized in the liver to inactive compounds. Renal impairment is likely to cause the accumulation of the inactive metabolites but not the parent compound, so dose reduction is not necessary with the use of this agent in renal insufficiency or dialysis.6
Mefenamic acid (Ponstel) is metabolized in the liver. Mefenamic acid can further deteriorate renal function in patients with underlying renal disease.12 However, the nephrotoxic potential of this agent is of little consideration in ESRD patients on dialysis, and therefore no dosage adjustments are necessary in these patients.6
Ketoprofen is metabolized in the liver, where approximately 80% of the dose is excreted in the urine as a glucuronide metabolite. Dose reduction is recommended in renal insufficiency and dialysis, as it not dialyzable.8
Ketorolac accumulates in renal insufficiency; therefore, it is contraindicated in these patients and in patients at risk for renal failure, including those with volume depletion.10 Ketorolac is unlikely to be removed by dialysis and so should be avoided.10,11
Naproxen is metabolized in the liver to inactive compounds. Use of naproxen is not recommended in patients with moderate to severe renal impairment. If therapy must be initiated, close monitoring of the patient’s renal function is recommended.13
Celecoxib is the only cyclooxygenase-2 (COX-2) inhibitor available in the U.S. It is metabolized extensively by the liver and is unlikely to be removed by dialysis. Therefore, use of COX-2 inhibitors should be avoided in severe renal impairment and in those on dialysis.14,15
Opioid options. The use of opioids in the renally impaired population is challenging, as one must balance opioid-related adverse events with adequate pain control. As such, it is recommended to start with lower-than-recommended doses and slowly titrate up the dose while extending the dosing interval. This will help limit adverse effects, such as respiratory depression and hypotension.3
Hydrocodone is metabolized to hydromorphone (Dilaudid), which is then metabolized to its major metabolite hydromorphine-3-glucuronide (H3G) and minor metabolite hydromorphine-6-hydroxy, all of which are excreted renally along with the parent compound. H3G has no analgesic properties, but it can potentially cause neuroexcitation, agitation, confusion, and hallucination. Hydromorphone has been used safely in patients with renal insufficiency and dialysis, as it is expected to be dialyzable. 16,17
Tramadol is metabolized in the liver, producing one active compound. Approximately 30% of the tramadol dose is excreted unchanged in the urine, whereas 60% of the dose is excreted as metabolites. It is recommended to reduce the dose and increase the dosing interval in patients with renal insufficiency, but tramadol is generally well-tolerated in patients with renal insufficiency and dialysis. It is significantly removed by hemodialysis; therefore, redosing after a session may be necessary.18,19
Oxycodone can be used in patients with mild to moderate renal insufficiency but should be used at reduced dosing; it has been associated with significant sedation with usual doses in renal failure patients.16 Its use is generally not recommended in dialysis patients due to lack of data.3
Methadone and its metabolites are excreted in the urine and feces. Methadone has been used safely in patients with renal insufficiency, but it is poorly removed by dialysis and no specific recommendations are available regarding its dosing in dialysis.3,16
Fentanyl is primarily metabolized in the liver to inactive metabolites. Fentanyl clearance is reduced in patients with moderate to severe uremia (BUN >60 mg/dL). It is not expected that fentanyl be dialyzable because of its pharmacokinetic properties (high protein-binding, low water solubility, high molecular weight, and high volume of distribution). Data suggests that fentanyl can be used at usual doses in mild to moderate renal insufficiency and in dialysis patients, although reduced doses may be prudent. Such patients should be monitored for signs of gradual accumulation of the parent drug.3,16
Morphine is metabolized in the liver to morphine-6-glucuronide (M6G) and morphine-3-glucuronide (M3G), all of which are excreted renally, along with the parent compound. Only M6G has analgesic properties, and when it accumulates, it can lead to CNS depression. M3G is associated with behavioral excitation, a side effect that is further magnified in patients with renal insufficiency. Although morphine is dialyzable, it should generally be avoided in patients with any level of renal insufficiency.16,17,20,21
Codeine is metabolized to several active metabolites, all of which are renally excreted. Lower-than-usual doses are recommended in patients with renal insufficiency, and it should be avoided altogether in dialysis patients.3,16
Meperidine is metabolized in the liver to various metabolites, primarily normeperidine, which is toxic and has a long half-life, five to 10 times longer then meperidine. Meperidine should not be used in patients with renal insufficiency or dialysis.3
Adjunctive therapeutic options. Lidocaine patches currently are only FDA-indicated for postherpetic neuralgia but are used for a wide variety of local pain syndromes. Absorption of lidocaine is determined by the duration of application and the surface area over which it is applied. There is no appreciable accumulation of lidocaine or its metabolites in renal insufficiency; therefore, dose adjustments are not required.22,23
Gabapentin is FDA-indicated for partial seizures and postherpetic neuralgia but is also used for a wide variety of neuropathic pain syndromes, including postoperative pain.24 Gabapentin is not metabolized and is excreted in the urine unchanged. Renal clearance of gabapentin is reduced by 40% and the elimination half-life is increased up to 52 hours in renal insufficiency, but it is dialyzable. Therefore, dose adjustments are required with gabapentin in patients with moderate to severe renal insufficiency, and supplemental doses should be administered in patients after receiving dialysis.25-27
Pregabalin is structurally related to gabapentin and is indicated for a variety of neuropathic pain conditions. Pregabalin is 90% excreted unchanged in the urine, and approximately 50% of drug is removed after four hours of hemodialysis. Dose adjustments are required in patients with moderate to severe renal insufficiency, and supplemental doses should be administered in patients after receiving dialysis.28
Antidepressant options. Amitriptyline, nortryptiline, and desipramine are the tricyclic antidepressants (TCAs) commonly used for neuropathic pain. TCAs are metabolized in the liver to inactive metabolites, with the exception of amitriptyline, which is metabolized to nortryptiline. Common side effects reported with TCAs include postural hypotension and anticholinergic side effects, such as constipation, urinary retention, blurred vision, dry mouth, delirium, and sedation. It is unlikely that the TCAs can be removed by dialysis. It is suggested that the dosage be reduced in renal insufficiency and that anticholinergic side effects be monitored.29
Back to the Case
The patient’s ankle pain was controlled with acetaminophen and lidocaine patches. For the neuropathic pain in his upper extremities, tramadol was started at 25 mg oral every 12 hours and increased to 50 mg oral every eight hours (below the maximum of 200 mg a day). The tramadol did not result in adequate pain relief, so gabapentin 100 mg at bedtime was initiated, then increased to twice daily over three days with some relief.
A geriatric consult was obtained to help educate him regarding addiction to opioids, as well as to explore goals of care, but he continued to insist on the use of a non-narcotic regimen for his pain.
Bottom Line
Pain management in patients with renal insufficiency and dialysis can be challenging, but there are a number of safe non-narcotic and narcotic pain regimens that can be safely used in this patient population.
Dr. Harisingani is a board-certified hospitalist at Long Island Jewish Medical Center in New Hyde Park, N.Y., and Drs. Saad and Cassagnol are assistant clinical professors at St. Johns University College of Pharmacy and Health Sciences in Jamaica, N.Y., and clinical pharmacy coordinators at Long Island Jewish Medical Center.
References
- Mid-Atlantic Renal Coalition and the Kidney End-of-Life Coalition. Clinical algorithm & preferred medications to treat pain in dialysis patients. Coalition for Supportive Care of Kidney Patients website. Available at: http://www.kidneysupportivecare.org/Physicians-Clinicians/Pain—Symptom-Management.aspx. Accessed Nov. 18, 2012.
- Barakzoy AS, Moss AH. Efficacy of the World Health Organization analgesic ladder to treat pain in end-stage renal disease. J Am Soc Nephrol. 2006;17(11):3198-3203.
- Johnson SJ. Opioid safety in patients with renal or hepatic dysfunction. Pain Treatment Topics website. Available at: http://pain-topics.org/pdf/Opioids-Renal-Hepatic-Dysfunction.pdf. Accessed Nov. 28, 2012.
- Ferrell B, Argoff CE, Epplin J, et al. American Geriatrics Society Panel on Pharmacological Management of Persistent Pain in Older Persons. Pharmacological management of persistent pain in older persons. J Am Geriatr Soc. 2009;57(8):1331-1346.
- Prescott LF, Speirs GC, Critchley JA, Temple RM, Winney RJ. Paracetamol disposition and metabolite kinetics in patients with chronic renal failure. Eur J Clin Pharmacol. 1989;36(3):291-297.
- Launay-Vacher V, Karie S, Fau JB, Izzedine H, Deray G. Treatment of pain in patients with renal insufficiency: the World Health Organization three-step ladder adapted. J Pain. 2006;6(3):137-148.
- Berg KJ, Djøseland O, Gjellan A, et al. Acute effects of paracetamol on prostaglandin synthesis and renal function in normal man and in patients with renal failure. Clin Nephrol. 1990;34:255-262.
- Delbarre F, Roucayrol JC, Amor B, et al. Pharmacokinetic study of ketoprofen (19.583 R.P.) in man using the tritiated compound. Scand J Rheumatol Suppl. 1976;1976(0):45-52.
- Shen CH, Hung CJ, Wu CC, Huang HW, Ho WM. Rhabdomyolysis-induced acute renal failure after morphine overdose—a case report. Acta Anaesthesiol Sin. 1999;37(3):159-162.
- Ketorolac tromethamine oral tablets [package insert]. St. Louis: Ethex Corp.: 2008.
- Brocks DR, Jamali F. Clinical pharmacokinetics of ketorolac tromethamine. Clin Pharmacokinet. 1992;23:415-427. Erratum in: Clin Pharmacokinet. 1999;24(3):270.
- Ponstel [package insert]. Alpharetta, GA: First Horizon Pharmaceutical Corp.; 2006.
- Naprosyn [package insert]. Nutley, NJ: Roche Laboratories Inc.; 2008.
- Celebrex [package insert]. New York: G.D. Searle LLC; 2011.
- Catella-Lawson F, McAdam B, Morrison BW, et al. Effects of specific inhibition of cyclooygenase-2 on sodium balance, hemodynamics, and vasoactive eicosanoids. J Pharmacol Exp Ther. 1999;289:735-741.
- Dean M. Opioids in renal failure and dialysis patients. J Pain Symptom Manage. 2004;28(5):497-504.
- Lee MA, Leng ME, Tiernan EJ. Retrospective study of the use of hydromorphone in palliative care patients with normal and abnormal urea and creatinine. Palliat Med. 2001;15(1):26-34.
- Gibson TP. Pharmacokinetics, efficacy, and safety of analgesia with a focus on tramadol HCI. Am J. Med. 1996;101(1A):47S-53S.
- Izzedine H, Launay-Vacher V, Abbara C, Aymard G, Bassilios N, Deray G. Pharmacokinetics of tramadol in a hemodialysis patient. Nephron. 2002;92(3):755-756.
- Hasselström J, Säwe J. Morphine pharmacokinetics and metabolism in humans. Enterohepatic cycling and relative contribution of metabolites to active opioid concentrations. Clin Pharmacokinet. 1993;24(4):344-354.
- Andersen G, Christrup L, Sjøgren P. Relationships among morphine metabolism, pain and side effects during long-term treatment: an update. J Pain Symptom Manage. 2003;25(1):74-91.
- Lidoderm [package insert]. Chadds Ford, PA: Endo Pharmaceuticals Inc.; 2010.
- Carter GT, Galer BS. Advances in the management of neuropathic pain. Phys Med Rehabil Clin N Am. 2001;12(2):447-459.
- Ho KY, Gan TJ, Habib AS. Gabapentin and postoperative pain—a systematic review of randomized controlled trials. Pain. 2006;15:126(1-3):91-101.
- Neurontin [package insert]. New York: Parke-Davis; 2010.
- Pandey CK, Priye S, Singh S, et al. Preemptive use of gabapentin significantly decreases postoperative pain and rescue analgesic requirements in laparoscopic cholecystectomy. Can J Anaesth. 2004;51(4):358-363.
- Srivastava U, Kumar A, Saxena S, et al: Effect of preoperative gabapentin on postoperative pain and tramadol consumption after minilap open cholecystectomy: a randomized double-blind, placebo-controlled trial. Eur J Anaesthesiol. 2010;27(N4):331-335.
- Lyrica [package insert]. New York: Pfizer Inc.; 2012.
- Broadbent A, Khor K, Heaney A. Palliation and chronic renal failure: opioid and other palliative medications—dosage guidelines. Progress in Palliative Care. 2003;11(4):183-190(8).
- Nayak-Rao S. Achieving effective pain relief in patients with chronic kidney disease: a review of analgesics in renal failure. J Nephrol. 2011;24(1):35-40.
- Wolters Kluwer Health. Facts & comparisons. Wolters Kluwer Health website. Available at: http://www.factsandcomparisons.com. Accessed Jan. 14, 2013.
- Lexicomp. Lexicomp Online. Lexicomp website. Available at: http://www.lexi.com/institutions/products/online/.
American College of Gastroenterology Releases C. Diff Recommendations
Clostridium difficile infection (CDI) is a common and costly bacterial illness in hospitalized patients, involving 1% of U.S. hospital stays with an aggregate cost of $8.2 billion annually.1 The spore-forming, gram-positive bacillus is spread by the fecal-oral route; in health-care settings, it is often transmitted by hand carriage and contamination of environmental surfaces. C. diff produces toxins that can cause a spectrum of diseases, including asymptomatic carriage, mild to severe diarrhea, colitis, and pseudomembranous colitis, which in severe cases can lead to sepsis, colectomy, or death.
CDI is defined as the acute onset of diarrhea in a patient with documented toxigenic C. diff or C. diff toxin, without any other clear cause of diarrhea.2 In the past decade, CDI has increased in frequency and severity, with most experts thinking it is related to a particularly virulent strain known as BI/NAP1/027.3 Antibiotic exposure is the most significant and modifiable risk factor for CDI, with increasing age, gastric acid suppression, and immunocompromised states also placing patients at increased risk for developing infection.
Guideline Analysis
In February, the American College of Gastroenterology (ACG) released guidelines for diagnostic testing and pharmacologic therapy for CDI, management of complicated and recurrent disease, and infection control and prevention.2 Previous recommendations for the prevention, diagnosis, and treatment of CDI have been provided by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and a collaboration of the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA).4,5 Recommendations addressing CDI in infants and children are also available.6 The 2013 ACG guidelines are the first from this group to address CDI and are intended to supplement previously published guidelines.
Diagnostic testing. The ACG guidelines emphasize that only stools from patients with diarrhea be tested for C. diff and/or its toxin. Colonization with C. diff is common, and performing tests in asymptomatic patients may complicate clinical care. Rarely, patients with CDI will develop ileus, and in those cases, rectal swab may be performed, but in nearly all circumstances, only diarrheal stools warrant testing. The authors also strongly discourage repeat testing after a negative test and testing for cure following treatment and resolution of symptoms. All of these recommendations are consistent with the SHEA-IDSA guidelines and reflect moderate- to high-quality evidence.
Recognizing that diagnostic testing for C. diff continues to evolve, the ACG makes specific recommendations regarding the use of newer tests, such as nucleic acid amplification and glutamate dehydrogenase detection. These are favored over toxin A and B enzyme immunoassay testing due to higher sensitivity.
Management of mild, moderate, and severe CDI. As with prior guidelines, the 2013 ACG guidelines stratify treatment recommendations by disease severity. Mild to moderate disease, which includes diarrhea only (mild) or diarrhea with signs and symptoms not meeting criteria for severe or complicated CDI (moderate), should be treated with metronidazole 500 mg orally three times daily for 10 days. Oral vancomycin should only be used in patients with mild to moderate disease who fail to respond after five to seven days of metronidazole or in those who are intolerant to metronidazole, or pregnant or breastfeeding. Although fidaxomicin is FDA-approved to treat mild to moderate CDI, the ACG does not make a formal recommendation on its use, given its high cost and limited data to support its effectiveness.
The ACG defines severe disease as CDI in patients with albumin <3 g/dL, and either WBC ≥15,000 cells/mm3 or abdominal tenderness. Though this definition of severe disease differs from the ESCMID and SHEA-IDSA definitions, which include elevated creatinine (>50% greater than premorbid level) instead of low albumin, the treatment recommendation is the same: vancomycin 125 mg orally four times daily for 10 days. While vancomycin and metronidazole are equally effective in mild to moderate CDI, there is some evidence to suggest that vancomycin is more effective in severe disease.7
Regardless of disease severity, one of the strongest recommendations is to discontinue any inciting antibiotics. This point, along with the recommendation to avoid anti-peristaltic agents, has also been emphasized in prior guidelines. Additionally, the authors note that although providers commonly prescribe treatment for 14 days, there is no evidence to suggest that a 14-day treatment course is more efficacious than a 10-day course for either metronidazole or vancomycin.
Management of severe and complicated CDI. Severe and complicated disease refers to CDI in patients meeting at least one of the following criteria: admission to the ICU, hypotension, fever ≥38.5°C, ileus or significant abdominal distention, mental status changes, WBC ≥35,000 or <2,000 cells/mm3, serum lactate >2.2 mmol/L, or end-stage organ failure. This definition is more specific than the SHEA-IDSA guidelines, which categorize severe and complicated disease as situations where shock, ileus, or megacolon are present. The recommended treatment is combined therapy with oral vancomycin 125 mg four times daily, plus intravenous metronidazole 500 mg three times daily. Surgical consultation should be obtained in all patients with complicated CDI. Colectomy should be considered in patients with evidence of severe sepsis, leukocytosis of ≥50,000, lactate ≥5 mmol/L, and failure to improve with medical therapy.
Patients with ileus or history of bowel surgery in whom oral antibiotics may not reach the colon should have vancomycin per rectum (enema of 500 mg in 100 mL to 500 mL of normal saline every six hours) added to the above treatments, regardless of disease severity.
Management of recurrent CDI. Consistent with previously published guidelines, the ACG recommends that the first recurrence of CDI be treated with the same regimen that was used for the initial episode. Second recurrences should be treated with a pulsed oral vancomycin regimen. Data are lacking regarding specific taper regimens, but the ACG suggests vancomycin 125 mg four times daily for 10 days, followed by a 125 mg dose every three days for 10 doses. For additional recurrences, fecal microbiota transplant may be considered. Reports suggest that this practice is safe and effective, but data from randomized controlled trials are lacking.
There is limited evidence to support the use of other antibiotics (e.g. rifampin, rifamixin), probiotics, or immunotherapy in the prevention of recurrent CDI.
Management of CDI in patients with comorbid conditions. A unique feature of the 2013 ACG guidelines is the incorporation of recommendations for patient groups who are at elevated risk for developing CDI or associated complications. Patients with inflammatory bowel disease (IBD) are one such group, as they often have underlying colonic inflammation and ongoing immunosuppression. The authors recommend that patients presenting with IBD flares be tested for C. diff. Other immunocompromised populations, including patients with malignancy, exposure to chemotherapy or corticosteroids, organ transplantation, and cirrhosis, should also be tested for CDI when presenting with diarrheal illness. Similarly, pregnant and peripartum women are considered high-risk and should undergo early testing and prompt initiation of treatment for CDI in the setting of diarrhea.
Infection control and prevention. Like SHEA-IDSA, the ACG recommends a hospital-based infection control program, antibiotic stewardship, and strict use of contact precautions for patients with known or suspected CDI. Contact precautions should be continued at minimum for the duration of diarrhea. Patients should be placed in private rooms and disposable equipment should be used, when possible. Disinfection of environmental surfaces is critical, as the environment is a common source of nosocomial infection. Disinfectants should have an Environmental Protection Agency-registered C. diff sporicidal label claim or contain a minimum concentration of chlorine solution. Important: Hand-washing with soap and water is required, as alcohol-based antiseptics are not active against C. diff spores.
HM Takeaways
The 2013 ACG guidelines for the diagnosis, treatment, and prevention of CDI are generally consistent with previously published guidelines from ESCMID and SHEA-IDSA. Ongoing points of emphasis are the following:
- Only test patients with diarrhea;
- Do not repeat testing after a negative test or after completion of treatment;
- Promptly discontinue any inciting antibiotics;
- Avoid use of anti-peristaltic agents; and
- Treat based on disease severity.
Hospitalists should be aware of criteria that place patients into the severe and complicated category, and understand that initial treatment should be provided for a 10-day course. These guidelines also highlight the need for a high index of suspicion and low threshold for empiric treatment in immunocompromised patients.
Finally, hospitalists should be attentive to antibiotic stewardship and strictly adhere to contact precautions and hand hygiene with soap and water, as these behaviors have been shown to prevent and control CDI.
Dr. Cunningham Sponsler is a hospitalist in the section of hospital medicine at Vanderbilt University in Nashville, Tenn.
References 1. Lucado J, Gould C, Elixhauser A. Clostridium difficile infections (CDI) in hospital stays, 2009. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb124.pdf. Accessed June 17, 2013.
2. Surawicz CM, Brandt LJ, Binion DJ, et al. Guidelines for diagnosis, treatment and prevention of Clostridium difficile infections. Am J Gastroenterol. 2013;108:478-498.
3. Freeman J, Bauer MP, Baines SD, et al. The changing epidemiology of Clostridium difficile infections. Clin Microbiol Rev. 2010;23:529-549.
4. Bauer MP, Kuijper EJ, van Dissel JT. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): treatment guidance for Clostridium difficile infection (CDI). Clin Microbiol Infect. 2009;15:1067-1079.
5. Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control and Hosp Epidemiol. 2010;31:431-455.
6. Committee on Infectious Diseases. Clostridium difficile infection in infants and children. Pediatrics. 2013;131:196-200.
7. Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45:302-307.
Clostridium difficile infection (CDI) is a common and costly bacterial illness in hospitalized patients, involving 1% of U.S. hospital stays with an aggregate cost of $8.2 billion annually.1 The spore-forming, gram-positive bacillus is spread by the fecal-oral route; in health-care settings, it is often transmitted by hand carriage and contamination of environmental surfaces. C. diff produces toxins that can cause a spectrum of diseases, including asymptomatic carriage, mild to severe diarrhea, colitis, and pseudomembranous colitis, which in severe cases can lead to sepsis, colectomy, or death.
CDI is defined as the acute onset of diarrhea in a patient with documented toxigenic C. diff or C. diff toxin, without any other clear cause of diarrhea.2 In the past decade, CDI has increased in frequency and severity, with most experts thinking it is related to a particularly virulent strain known as BI/NAP1/027.3 Antibiotic exposure is the most significant and modifiable risk factor for CDI, with increasing age, gastric acid suppression, and immunocompromised states also placing patients at increased risk for developing infection.
Guideline Analysis
In February, the American College of Gastroenterology (ACG) released guidelines for diagnostic testing and pharmacologic therapy for CDI, management of complicated and recurrent disease, and infection control and prevention.2 Previous recommendations for the prevention, diagnosis, and treatment of CDI have been provided by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and a collaboration of the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA).4,5 Recommendations addressing CDI in infants and children are also available.6 The 2013 ACG guidelines are the first from this group to address CDI and are intended to supplement previously published guidelines.
Diagnostic testing. The ACG guidelines emphasize that only stools from patients with diarrhea be tested for C. diff and/or its toxin. Colonization with C. diff is common, and performing tests in asymptomatic patients may complicate clinical care. Rarely, patients with CDI will develop ileus, and in those cases, rectal swab may be performed, but in nearly all circumstances, only diarrheal stools warrant testing. The authors also strongly discourage repeat testing after a negative test and testing for cure following treatment and resolution of symptoms. All of these recommendations are consistent with the SHEA-IDSA guidelines and reflect moderate- to high-quality evidence.
Recognizing that diagnostic testing for C. diff continues to evolve, the ACG makes specific recommendations regarding the use of newer tests, such as nucleic acid amplification and glutamate dehydrogenase detection. These are favored over toxin A and B enzyme immunoassay testing due to higher sensitivity.
Management of mild, moderate, and severe CDI. As with prior guidelines, the 2013 ACG guidelines stratify treatment recommendations by disease severity. Mild to moderate disease, which includes diarrhea only (mild) or diarrhea with signs and symptoms not meeting criteria for severe or complicated CDI (moderate), should be treated with metronidazole 500 mg orally three times daily for 10 days. Oral vancomycin should only be used in patients with mild to moderate disease who fail to respond after five to seven days of metronidazole or in those who are intolerant to metronidazole, or pregnant or breastfeeding. Although fidaxomicin is FDA-approved to treat mild to moderate CDI, the ACG does not make a formal recommendation on its use, given its high cost and limited data to support its effectiveness.
The ACG defines severe disease as CDI in patients with albumin <3 g/dL, and either WBC ≥15,000 cells/mm3 or abdominal tenderness. Though this definition of severe disease differs from the ESCMID and SHEA-IDSA definitions, which include elevated creatinine (>50% greater than premorbid level) instead of low albumin, the treatment recommendation is the same: vancomycin 125 mg orally four times daily for 10 days. While vancomycin and metronidazole are equally effective in mild to moderate CDI, there is some evidence to suggest that vancomycin is more effective in severe disease.7
Regardless of disease severity, one of the strongest recommendations is to discontinue any inciting antibiotics. This point, along with the recommendation to avoid anti-peristaltic agents, has also been emphasized in prior guidelines. Additionally, the authors note that although providers commonly prescribe treatment for 14 days, there is no evidence to suggest that a 14-day treatment course is more efficacious than a 10-day course for either metronidazole or vancomycin.
Management of severe and complicated CDI. Severe and complicated disease refers to CDI in patients meeting at least one of the following criteria: admission to the ICU, hypotension, fever ≥38.5°C, ileus or significant abdominal distention, mental status changes, WBC ≥35,000 or <2,000 cells/mm3, serum lactate >2.2 mmol/L, or end-stage organ failure. This definition is more specific than the SHEA-IDSA guidelines, which categorize severe and complicated disease as situations where shock, ileus, or megacolon are present. The recommended treatment is combined therapy with oral vancomycin 125 mg four times daily, plus intravenous metronidazole 500 mg three times daily. Surgical consultation should be obtained in all patients with complicated CDI. Colectomy should be considered in patients with evidence of severe sepsis, leukocytosis of ≥50,000, lactate ≥5 mmol/L, and failure to improve with medical therapy.
Patients with ileus or history of bowel surgery in whom oral antibiotics may not reach the colon should have vancomycin per rectum (enema of 500 mg in 100 mL to 500 mL of normal saline every six hours) added to the above treatments, regardless of disease severity.
Management of recurrent CDI. Consistent with previously published guidelines, the ACG recommends that the first recurrence of CDI be treated with the same regimen that was used for the initial episode. Second recurrences should be treated with a pulsed oral vancomycin regimen. Data are lacking regarding specific taper regimens, but the ACG suggests vancomycin 125 mg four times daily for 10 days, followed by a 125 mg dose every three days for 10 doses. For additional recurrences, fecal microbiota transplant may be considered. Reports suggest that this practice is safe and effective, but data from randomized controlled trials are lacking.
There is limited evidence to support the use of other antibiotics (e.g. rifampin, rifamixin), probiotics, or immunotherapy in the prevention of recurrent CDI.
Management of CDI in patients with comorbid conditions. A unique feature of the 2013 ACG guidelines is the incorporation of recommendations for patient groups who are at elevated risk for developing CDI or associated complications. Patients with inflammatory bowel disease (IBD) are one such group, as they often have underlying colonic inflammation and ongoing immunosuppression. The authors recommend that patients presenting with IBD flares be tested for C. diff. Other immunocompromised populations, including patients with malignancy, exposure to chemotherapy or corticosteroids, organ transplantation, and cirrhosis, should also be tested for CDI when presenting with diarrheal illness. Similarly, pregnant and peripartum women are considered high-risk and should undergo early testing and prompt initiation of treatment for CDI in the setting of diarrhea.
Infection control and prevention. Like SHEA-IDSA, the ACG recommends a hospital-based infection control program, antibiotic stewardship, and strict use of contact precautions for patients with known or suspected CDI. Contact precautions should be continued at minimum for the duration of diarrhea. Patients should be placed in private rooms and disposable equipment should be used, when possible. Disinfection of environmental surfaces is critical, as the environment is a common source of nosocomial infection. Disinfectants should have an Environmental Protection Agency-registered C. diff sporicidal label claim or contain a minimum concentration of chlorine solution. Important: Hand-washing with soap and water is required, as alcohol-based antiseptics are not active against C. diff spores.
HM Takeaways
The 2013 ACG guidelines for the diagnosis, treatment, and prevention of CDI are generally consistent with previously published guidelines from ESCMID and SHEA-IDSA. Ongoing points of emphasis are the following:
- Only test patients with diarrhea;
- Do not repeat testing after a negative test or after completion of treatment;
- Promptly discontinue any inciting antibiotics;
- Avoid use of anti-peristaltic agents; and
- Treat based on disease severity.
Hospitalists should be aware of criteria that place patients into the severe and complicated category, and understand that initial treatment should be provided for a 10-day course. These guidelines also highlight the need for a high index of suspicion and low threshold for empiric treatment in immunocompromised patients.
Finally, hospitalists should be attentive to antibiotic stewardship and strictly adhere to contact precautions and hand hygiene with soap and water, as these behaviors have been shown to prevent and control CDI.
Dr. Cunningham Sponsler is a hospitalist in the section of hospital medicine at Vanderbilt University in Nashville, Tenn.
References 1. Lucado J, Gould C, Elixhauser A. Clostridium difficile infections (CDI) in hospital stays, 2009. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb124.pdf. Accessed June 17, 2013.
2. Surawicz CM, Brandt LJ, Binion DJ, et al. Guidelines for diagnosis, treatment and prevention of Clostridium difficile infections. Am J Gastroenterol. 2013;108:478-498.
3. Freeman J, Bauer MP, Baines SD, et al. The changing epidemiology of Clostridium difficile infections. Clin Microbiol Rev. 2010;23:529-549.
4. Bauer MP, Kuijper EJ, van Dissel JT. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): treatment guidance for Clostridium difficile infection (CDI). Clin Microbiol Infect. 2009;15:1067-1079.
5. Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control and Hosp Epidemiol. 2010;31:431-455.
6. Committee on Infectious Diseases. Clostridium difficile infection in infants and children. Pediatrics. 2013;131:196-200.
7. Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45:302-307.
Clostridium difficile infection (CDI) is a common and costly bacterial illness in hospitalized patients, involving 1% of U.S. hospital stays with an aggregate cost of $8.2 billion annually.1 The spore-forming, gram-positive bacillus is spread by the fecal-oral route; in health-care settings, it is often transmitted by hand carriage and contamination of environmental surfaces. C. diff produces toxins that can cause a spectrum of diseases, including asymptomatic carriage, mild to severe diarrhea, colitis, and pseudomembranous colitis, which in severe cases can lead to sepsis, colectomy, or death.
CDI is defined as the acute onset of diarrhea in a patient with documented toxigenic C. diff or C. diff toxin, without any other clear cause of diarrhea.2 In the past decade, CDI has increased in frequency and severity, with most experts thinking it is related to a particularly virulent strain known as BI/NAP1/027.3 Antibiotic exposure is the most significant and modifiable risk factor for CDI, with increasing age, gastric acid suppression, and immunocompromised states also placing patients at increased risk for developing infection.
Guideline Analysis
In February, the American College of Gastroenterology (ACG) released guidelines for diagnostic testing and pharmacologic therapy for CDI, management of complicated and recurrent disease, and infection control and prevention.2 Previous recommendations for the prevention, diagnosis, and treatment of CDI have been provided by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and a collaboration of the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA).4,5 Recommendations addressing CDI in infants and children are also available.6 The 2013 ACG guidelines are the first from this group to address CDI and are intended to supplement previously published guidelines.
Diagnostic testing. The ACG guidelines emphasize that only stools from patients with diarrhea be tested for C. diff and/or its toxin. Colonization with C. diff is common, and performing tests in asymptomatic patients may complicate clinical care. Rarely, patients with CDI will develop ileus, and in those cases, rectal swab may be performed, but in nearly all circumstances, only diarrheal stools warrant testing. The authors also strongly discourage repeat testing after a negative test and testing for cure following treatment and resolution of symptoms. All of these recommendations are consistent with the SHEA-IDSA guidelines and reflect moderate- to high-quality evidence.
Recognizing that diagnostic testing for C. diff continues to evolve, the ACG makes specific recommendations regarding the use of newer tests, such as nucleic acid amplification and glutamate dehydrogenase detection. These are favored over toxin A and B enzyme immunoassay testing due to higher sensitivity.
Management of mild, moderate, and severe CDI. As with prior guidelines, the 2013 ACG guidelines stratify treatment recommendations by disease severity. Mild to moderate disease, which includes diarrhea only (mild) or diarrhea with signs and symptoms not meeting criteria for severe or complicated CDI (moderate), should be treated with metronidazole 500 mg orally three times daily for 10 days. Oral vancomycin should only be used in patients with mild to moderate disease who fail to respond after five to seven days of metronidazole or in those who are intolerant to metronidazole, or pregnant or breastfeeding. Although fidaxomicin is FDA-approved to treat mild to moderate CDI, the ACG does not make a formal recommendation on its use, given its high cost and limited data to support its effectiveness.
The ACG defines severe disease as CDI in patients with albumin <3 g/dL, and either WBC ≥15,000 cells/mm3 or abdominal tenderness. Though this definition of severe disease differs from the ESCMID and SHEA-IDSA definitions, which include elevated creatinine (>50% greater than premorbid level) instead of low albumin, the treatment recommendation is the same: vancomycin 125 mg orally four times daily for 10 days. While vancomycin and metronidazole are equally effective in mild to moderate CDI, there is some evidence to suggest that vancomycin is more effective in severe disease.7
Regardless of disease severity, one of the strongest recommendations is to discontinue any inciting antibiotics. This point, along with the recommendation to avoid anti-peristaltic agents, has also been emphasized in prior guidelines. Additionally, the authors note that although providers commonly prescribe treatment for 14 days, there is no evidence to suggest that a 14-day treatment course is more efficacious than a 10-day course for either metronidazole or vancomycin.
Management of severe and complicated CDI. Severe and complicated disease refers to CDI in patients meeting at least one of the following criteria: admission to the ICU, hypotension, fever ≥38.5°C, ileus or significant abdominal distention, mental status changes, WBC ≥35,000 or <2,000 cells/mm3, serum lactate >2.2 mmol/L, or end-stage organ failure. This definition is more specific than the SHEA-IDSA guidelines, which categorize severe and complicated disease as situations where shock, ileus, or megacolon are present. The recommended treatment is combined therapy with oral vancomycin 125 mg four times daily, plus intravenous metronidazole 500 mg three times daily. Surgical consultation should be obtained in all patients with complicated CDI. Colectomy should be considered in patients with evidence of severe sepsis, leukocytosis of ≥50,000, lactate ≥5 mmol/L, and failure to improve with medical therapy.
Patients with ileus or history of bowel surgery in whom oral antibiotics may not reach the colon should have vancomycin per rectum (enema of 500 mg in 100 mL to 500 mL of normal saline every six hours) added to the above treatments, regardless of disease severity.
Management of recurrent CDI. Consistent with previously published guidelines, the ACG recommends that the first recurrence of CDI be treated with the same regimen that was used for the initial episode. Second recurrences should be treated with a pulsed oral vancomycin regimen. Data are lacking regarding specific taper regimens, but the ACG suggests vancomycin 125 mg four times daily for 10 days, followed by a 125 mg dose every three days for 10 doses. For additional recurrences, fecal microbiota transplant may be considered. Reports suggest that this practice is safe and effective, but data from randomized controlled trials are lacking.
There is limited evidence to support the use of other antibiotics (e.g. rifampin, rifamixin), probiotics, or immunotherapy in the prevention of recurrent CDI.
Management of CDI in patients with comorbid conditions. A unique feature of the 2013 ACG guidelines is the incorporation of recommendations for patient groups who are at elevated risk for developing CDI or associated complications. Patients with inflammatory bowel disease (IBD) are one such group, as they often have underlying colonic inflammation and ongoing immunosuppression. The authors recommend that patients presenting with IBD flares be tested for C. diff. Other immunocompromised populations, including patients with malignancy, exposure to chemotherapy or corticosteroids, organ transplantation, and cirrhosis, should also be tested for CDI when presenting with diarrheal illness. Similarly, pregnant and peripartum women are considered high-risk and should undergo early testing and prompt initiation of treatment for CDI in the setting of diarrhea.
Infection control and prevention. Like SHEA-IDSA, the ACG recommends a hospital-based infection control program, antibiotic stewardship, and strict use of contact precautions for patients with known or suspected CDI. Contact precautions should be continued at minimum for the duration of diarrhea. Patients should be placed in private rooms and disposable equipment should be used, when possible. Disinfection of environmental surfaces is critical, as the environment is a common source of nosocomial infection. Disinfectants should have an Environmental Protection Agency-registered C. diff sporicidal label claim or contain a minimum concentration of chlorine solution. Important: Hand-washing with soap and water is required, as alcohol-based antiseptics are not active against C. diff spores.
HM Takeaways
The 2013 ACG guidelines for the diagnosis, treatment, and prevention of CDI are generally consistent with previously published guidelines from ESCMID and SHEA-IDSA. Ongoing points of emphasis are the following:
- Only test patients with diarrhea;
- Do not repeat testing after a negative test or after completion of treatment;
- Promptly discontinue any inciting antibiotics;
- Avoid use of anti-peristaltic agents; and
- Treat based on disease severity.
Hospitalists should be aware of criteria that place patients into the severe and complicated category, and understand that initial treatment should be provided for a 10-day course. These guidelines also highlight the need for a high index of suspicion and low threshold for empiric treatment in immunocompromised patients.
Finally, hospitalists should be attentive to antibiotic stewardship and strictly adhere to contact precautions and hand hygiene with soap and water, as these behaviors have been shown to prevent and control CDI.
Dr. Cunningham Sponsler is a hospitalist in the section of hospital medicine at Vanderbilt University in Nashville, Tenn.
References 1. Lucado J, Gould C, Elixhauser A. Clostridium difficile infections (CDI) in hospital stays, 2009. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb124.pdf. Accessed June 17, 2013.
2. Surawicz CM, Brandt LJ, Binion DJ, et al. Guidelines for diagnosis, treatment and prevention of Clostridium difficile infections. Am J Gastroenterol. 2013;108:478-498.
3. Freeman J, Bauer MP, Baines SD, et al. The changing epidemiology of Clostridium difficile infections. Clin Microbiol Rev. 2010;23:529-549.
4. Bauer MP, Kuijper EJ, van Dissel JT. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): treatment guidance for Clostridium difficile infection (CDI). Clin Microbiol Infect. 2009;15:1067-1079.
5. Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control and Hosp Epidemiol. 2010;31:431-455.
6. Committee on Infectious Diseases. Clostridium difficile infection in infants and children. Pediatrics. 2013;131:196-200.
7. Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45:302-307.
The Pros and Cons of Electronic Health Records

An electronic health record (EHR)—sometimes called an electronic medical record (EMR)—allows health-care providers to record patient information electronically instead of using paper records.1 It also has the capability to perform various tasks that can assist in health-care delivery while maintaining standards of practice. The Health Information Technology for Economic and Clinical Health (HITECH) Act, enacted under the American Recovery and Reinvestment Act of 2009 (Recovery Act), established a provision for incentive payments for eligible professionals (EPs), critical-access hospitals (CAHs), and eligible hospitals if they can demonstrate meaningful use of certified EHR technology:2
- The use of a certified EHR in a meaningful manner (e.g. e-prescribing);
- The use of certified EHR technology for electronic exchange of health information to improve quality of health care; and
- The use of certified EHR technology to submit clinical quality and other measures.
Eligible professionals must satisfy 20 of 25 meaningful-use objectives (15 required core objectives and five objectives chosen from a list of 10 menu-set objectives).3 Eligible hospitals and CAHs must achieve 19 of 24 objectives (14 required core objectives and five objectives chosen from a list of 10 menu-set objectives).3
It seems that any program implementation with the potential to generate new or additional payment also has the potential to generate new or additional scrutiny of its application to ensure the generated payment is appropriate.5 Issues with EHR that recently have been highlighted include copy-and-paste, pulling notes forward, and upcoding based on volume instead of necessity.
Consider the Case
A patient is admitted to the hospital for pain, warmth, and swelling in the left lower extremity; r/o deep vein thrombosis (DVT) versus cellulitis. The patient’s history includes peripheral vascular disease (PVD), chronic renal insufficiency (CRI), and allergic rhinitis (AR). Testing confirms DVT, and the patient begins anticoagulation therapy. To achieve a therapeutic balance and prevent adverse reactions, the hospitalist orders INR monitoring.
On admission, the complexity of the patient’s condition may be considered high given the nature of the presenting problem.4 The hospitalist receives extensive credit for developing a care plan involving differential diagnoses with additional testing in anticipation of confirming a diagnosis. The patient’s presenting problem elevates the risk of morbidity/mortality, while the determined course of anticoagulation therapy places the patient at increased (i.e. “high”) risk for bleeding and requires intensive monitoring for toxicity. In this instance, 99223 may be warranted if the documentation requirements corresponding to this visit level have been satisfied.
As subsequent hospital days ensue, the complexity of the patient’s condition may not be as high. Even though the risk of anticoagulation remains high, the number of diagnoses and/or data ordered/reviewed may be less extensive than the initial encounter. Therefore, without any new or additional factors, the overall complexity of decision-making may be more appropriately categorized as moderate or low (e.g. 99232 or 99231, respectively).4
Do not fall victim to shortcuts that may falsely ease the workload of the overburdened physician. For example, the patient’s co-existing conditions of PVD, CRI, and AR likely were addressed during the initial encounter for DVT with inclusion in the plan of care. When using an electronic documentation system, it might be possible to copy the previously entered information from the initial encounter into the current encounter to save time. However, the previously entered information could include elements that do not need to be re-addressed during a subsequent encounter (e.g., AR) or yield information involving care for conditions that are being managed concurrently by another specialist (e.g. CRI being managed by the nephrologist).
Leaving the pasted information unaltered, without modification, can misrepresent the patient’s condition or the care provided by the hospitalist during the subsequent encounter.
Preventative Measures
Documentation should support the service provided on a given date, and the information included in the entry should reflect the content that was rendered and/or considered for assessment and management. Information that is pulled forward or copied and pasted from a previous entry should be modified to demonstrate updated content and nonoverlapping care with relevance for that date.
Do not use coding tools, or EHR “service calculators,” that override medical decision-making to determine the service level. Determining the service level for a particular CPT code category depends upon the key components of history, exam, and medical decision-making (MDM).4 For some code categories, each of the three key components must meet the documentation guidelines for the corresponding visit level (i.e. initial hospital care, initial observation care, and consultations). If all three components do not satisfy the requirements for a particular visit level, code selection is determined by the lowest component. For example, the physician must select 99221 when documenting a detailed history despite having also documented a comprehensive exam and high complexity decision-making. In other code categories, coding principles require that only two key components need to meet the documentation guidelines (i.e. subsequent hospital care and subsequent observation care) for code selection.
More specifically, code selection is determined by the second-lowest component. For example, the physician may appropriately select 99233 when only documenting a brief history after having also documented a detailed exam and high complexity decision-making. Based on this “two of three” stipulation, 99233 is acceptable. Service calculators that override MDM as one of the two supporting components in subsequent care services could generate 99233 for a service involving a detailed history and a detailed exam but only low complexity decision-making. Such coding practice can leave the hospitalist vulnerable to external inquiries involving medical necessity and upcoding. Despite this “two component” technicality with subsequent services (99231-99233 and 99224-99226), MDM always should be one of the two key components considered during subsequent visit level selection as it most clearly conveys the medical necessity of the encounter.
References
- Centers for Medicare & Medicaid Services. The official web site for the Medicare and Medicaid electronic health records (EHR) incentive programs. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/index.html?redirect=/ehrincentiveprograms/. Accessed March 10, 2013.
- Centers for Medicare & Medicaid Services. Frequently asked questions (FAQs). Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/FAQ.html. Accessed March 10, 2013.
- Centers for Medicare & Medicaid Services. Meaningful use. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Meaningful_Use.html. Accessed March 10, 2013.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011:13-17.
- U.S. Department of Health and Human Services. Office of Inspector General work plan fiscal year 2013. U.S. Department of Health and Human Services website. Available at: http://oig.hhs.gov/reports-and-publications/archives/workplan/2013/Work-Plan-2013.pdf. Accessed March 11, 2013.
An electronic health record (EHR)—sometimes called an electronic medical record (EMR)—allows health-care providers to record patient information electronically instead of using paper records.1 It also has the capability to perform various tasks that can assist in health-care delivery while maintaining standards of practice. The Health Information Technology for Economic and Clinical Health (HITECH) Act, enacted under the American Recovery and Reinvestment Act of 2009 (Recovery Act), established a provision for incentive payments for eligible professionals (EPs), critical-access hospitals (CAHs), and eligible hospitals if they can demonstrate meaningful use of certified EHR technology:2
- The use of a certified EHR in a meaningful manner (e.g. e-prescribing);
- The use of certified EHR technology for electronic exchange of health information to improve quality of health care; and
- The use of certified EHR technology to submit clinical quality and other measures.
Eligible professionals must satisfy 20 of 25 meaningful-use objectives (15 required core objectives and five objectives chosen from a list of 10 menu-set objectives).3 Eligible hospitals and CAHs must achieve 19 of 24 objectives (14 required core objectives and five objectives chosen from a list of 10 menu-set objectives).3
It seems that any program implementation with the potential to generate new or additional payment also has the potential to generate new or additional scrutiny of its application to ensure the generated payment is appropriate.5 Issues with EHR that recently have been highlighted include copy-and-paste, pulling notes forward, and upcoding based on volume instead of necessity.
Consider the Case
A patient is admitted to the hospital for pain, warmth, and swelling in the left lower extremity; r/o deep vein thrombosis (DVT) versus cellulitis. The patient’s history includes peripheral vascular disease (PVD), chronic renal insufficiency (CRI), and allergic rhinitis (AR). Testing confirms DVT, and the patient begins anticoagulation therapy. To achieve a therapeutic balance and prevent adverse reactions, the hospitalist orders INR monitoring.
On admission, the complexity of the patient’s condition may be considered high given the nature of the presenting problem.4 The hospitalist receives extensive credit for developing a care plan involving differential diagnoses with additional testing in anticipation of confirming a diagnosis. The patient’s presenting problem elevates the risk of morbidity/mortality, while the determined course of anticoagulation therapy places the patient at increased (i.e. “high”) risk for bleeding and requires intensive monitoring for toxicity. In this instance, 99223 may be warranted if the documentation requirements corresponding to this visit level have been satisfied.
As subsequent hospital days ensue, the complexity of the patient’s condition may not be as high. Even though the risk of anticoagulation remains high, the number of diagnoses and/or data ordered/reviewed may be less extensive than the initial encounter. Therefore, without any new or additional factors, the overall complexity of decision-making may be more appropriately categorized as moderate or low (e.g. 99232 or 99231, respectively).4
Do not fall victim to shortcuts that may falsely ease the workload of the overburdened physician. For example, the patient’s co-existing conditions of PVD, CRI, and AR likely were addressed during the initial encounter for DVT with inclusion in the plan of care. When using an electronic documentation system, it might be possible to copy the previously entered information from the initial encounter into the current encounter to save time. However, the previously entered information could include elements that do not need to be re-addressed during a subsequent encounter (e.g., AR) or yield information involving care for conditions that are being managed concurrently by another specialist (e.g. CRI being managed by the nephrologist).
Leaving the pasted information unaltered, without modification, can misrepresent the patient’s condition or the care provided by the hospitalist during the subsequent encounter.
Preventative Measures
Documentation should support the service provided on a given date, and the information included in the entry should reflect the content that was rendered and/or considered for assessment and management. Information that is pulled forward or copied and pasted from a previous entry should be modified to demonstrate updated content and nonoverlapping care with relevance for that date.
Do not use coding tools, or EHR “service calculators,” that override medical decision-making to determine the service level. Determining the service level for a particular CPT code category depends upon the key components of history, exam, and medical decision-making (MDM).4 For some code categories, each of the three key components must meet the documentation guidelines for the corresponding visit level (i.e. initial hospital care, initial observation care, and consultations). If all three components do not satisfy the requirements for a particular visit level, code selection is determined by the lowest component. For example, the physician must select 99221 when documenting a detailed history despite having also documented a comprehensive exam and high complexity decision-making. In other code categories, coding principles require that only two key components need to meet the documentation guidelines (i.e. subsequent hospital care and subsequent observation care) for code selection.
More specifically, code selection is determined by the second-lowest component. For example, the physician may appropriately select 99233 when only documenting a brief history after having also documented a detailed exam and high complexity decision-making. Based on this “two of three” stipulation, 99233 is acceptable. Service calculators that override MDM as one of the two supporting components in subsequent care services could generate 99233 for a service involving a detailed history and a detailed exam but only low complexity decision-making. Such coding practice can leave the hospitalist vulnerable to external inquiries involving medical necessity and upcoding. Despite this “two component” technicality with subsequent services (99231-99233 and 99224-99226), MDM always should be one of the two key components considered during subsequent visit level selection as it most clearly conveys the medical necessity of the encounter.
References
- Centers for Medicare & Medicaid Services. The official web site for the Medicare and Medicaid electronic health records (EHR) incentive programs. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/index.html?redirect=/ehrincentiveprograms/. Accessed March 10, 2013.
- Centers for Medicare & Medicaid Services. Frequently asked questions (FAQs). Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/FAQ.html. Accessed March 10, 2013.
- Centers for Medicare & Medicaid Services. Meaningful use. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Meaningful_Use.html. Accessed March 10, 2013.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011:13-17.
- U.S. Department of Health and Human Services. Office of Inspector General work plan fiscal year 2013. U.S. Department of Health and Human Services website. Available at: http://oig.hhs.gov/reports-and-publications/archives/workplan/2013/Work-Plan-2013.pdf. Accessed March 11, 2013.
An electronic health record (EHR)—sometimes called an electronic medical record (EMR)—allows health-care providers to record patient information electronically instead of using paper records.1 It also has the capability to perform various tasks that can assist in health-care delivery while maintaining standards of practice. The Health Information Technology for Economic and Clinical Health (HITECH) Act, enacted under the American Recovery and Reinvestment Act of 2009 (Recovery Act), established a provision for incentive payments for eligible professionals (EPs), critical-access hospitals (CAHs), and eligible hospitals if they can demonstrate meaningful use of certified EHR technology:2
- The use of a certified EHR in a meaningful manner (e.g. e-prescribing);
- The use of certified EHR technology for electronic exchange of health information to improve quality of health care; and
- The use of certified EHR technology to submit clinical quality and other measures.
Eligible professionals must satisfy 20 of 25 meaningful-use objectives (15 required core objectives and five objectives chosen from a list of 10 menu-set objectives).3 Eligible hospitals and CAHs must achieve 19 of 24 objectives (14 required core objectives and five objectives chosen from a list of 10 menu-set objectives).3
It seems that any program implementation with the potential to generate new or additional payment also has the potential to generate new or additional scrutiny of its application to ensure the generated payment is appropriate.5 Issues with EHR that recently have been highlighted include copy-and-paste, pulling notes forward, and upcoding based on volume instead of necessity.
Consider the Case
A patient is admitted to the hospital for pain, warmth, and swelling in the left lower extremity; r/o deep vein thrombosis (DVT) versus cellulitis. The patient’s history includes peripheral vascular disease (PVD), chronic renal insufficiency (CRI), and allergic rhinitis (AR). Testing confirms DVT, and the patient begins anticoagulation therapy. To achieve a therapeutic balance and prevent adverse reactions, the hospitalist orders INR monitoring.
On admission, the complexity of the patient’s condition may be considered high given the nature of the presenting problem.4 The hospitalist receives extensive credit for developing a care plan involving differential diagnoses with additional testing in anticipation of confirming a diagnosis. The patient’s presenting problem elevates the risk of morbidity/mortality, while the determined course of anticoagulation therapy places the patient at increased (i.e. “high”) risk for bleeding and requires intensive monitoring for toxicity. In this instance, 99223 may be warranted if the documentation requirements corresponding to this visit level have been satisfied.
As subsequent hospital days ensue, the complexity of the patient’s condition may not be as high. Even though the risk of anticoagulation remains high, the number of diagnoses and/or data ordered/reviewed may be less extensive than the initial encounter. Therefore, without any new or additional factors, the overall complexity of decision-making may be more appropriately categorized as moderate or low (e.g. 99232 or 99231, respectively).4
Do not fall victim to shortcuts that may falsely ease the workload of the overburdened physician. For example, the patient’s co-existing conditions of PVD, CRI, and AR likely were addressed during the initial encounter for DVT with inclusion in the plan of care. When using an electronic documentation system, it might be possible to copy the previously entered information from the initial encounter into the current encounter to save time. However, the previously entered information could include elements that do not need to be re-addressed during a subsequent encounter (e.g., AR) or yield information involving care for conditions that are being managed concurrently by another specialist (e.g. CRI being managed by the nephrologist).
Leaving the pasted information unaltered, without modification, can misrepresent the patient’s condition or the care provided by the hospitalist during the subsequent encounter.
Preventative Measures
Documentation should support the service provided on a given date, and the information included in the entry should reflect the content that was rendered and/or considered for assessment and management. Information that is pulled forward or copied and pasted from a previous entry should be modified to demonstrate updated content and nonoverlapping care with relevance for that date.
Do not use coding tools, or EHR “service calculators,” that override medical decision-making to determine the service level. Determining the service level for a particular CPT code category depends upon the key components of history, exam, and medical decision-making (MDM).4 For some code categories, each of the three key components must meet the documentation guidelines for the corresponding visit level (i.e. initial hospital care, initial observation care, and consultations). If all three components do not satisfy the requirements for a particular visit level, code selection is determined by the lowest component. For example, the physician must select 99221 when documenting a detailed history despite having also documented a comprehensive exam and high complexity decision-making. In other code categories, coding principles require that only two key components need to meet the documentation guidelines (i.e. subsequent hospital care and subsequent observation care) for code selection.
More specifically, code selection is determined by the second-lowest component. For example, the physician may appropriately select 99233 when only documenting a brief history after having also documented a detailed exam and high complexity decision-making. Based on this “two of three” stipulation, 99233 is acceptable. Service calculators that override MDM as one of the two supporting components in subsequent care services could generate 99233 for a service involving a detailed history and a detailed exam but only low complexity decision-making. Such coding practice can leave the hospitalist vulnerable to external inquiries involving medical necessity and upcoding. Despite this “two component” technicality with subsequent services (99231-99233 and 99224-99226), MDM always should be one of the two key components considered during subsequent visit level selection as it most clearly conveys the medical necessity of the encounter.
References
- Centers for Medicare & Medicaid Services. The official web site for the Medicare and Medicaid electronic health records (EHR) incentive programs. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/index.html?redirect=/ehrincentiveprograms/. Accessed March 10, 2013.
- Centers for Medicare & Medicaid Services. Frequently asked questions (FAQs). Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/FAQ.html. Accessed March 10, 2013.
- Centers for Medicare & Medicaid Services. Meaningful use. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Meaningful_Use.html. Accessed March 10, 2013.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011:13-17.
- U.S. Department of Health and Human Services. Office of Inspector General work plan fiscal year 2013. U.S. Department of Health and Human Services website. Available at: http://oig.hhs.gov/reports-and-publications/archives/workplan/2013/Work-Plan-2013.pdf. Accessed March 11, 2013.