User login
Listen to John Vazquez, MD, discuss neurophobia and tips for adjusting to discomfort in treating neuro patients
Click here to listen to more of our interview with Dr. Vazquez
Click here to listen to more of our interview with Dr. Vazquez
Click here to listen to more of our interview with Dr. Vazquez
“Telestroke” care and “teleneurology” give hospitalists additional resources
To deal with the demand for neurologists, hospitals are increasingly turning to a new idea: patching a neurologist into the exam room from afar, Skype-style. This approach to caring for patients with strokes and other neurologic conditions—“telestroke” care or “teleneurology”—is an emerging valuable resource, says Edgar Kenton, MD, who is in the process of expanding such a system at Geisinger Health System in Danville, Pa.
It’s a hub-and-spoke system, with a central hospital as the “hub” and other hospitals as the “spokes” that connect with the hub, using computers and real-time video. Geisinger has six spokes, with plans for about another half-dozen.
“We’re able to talk to the physician, we can see the patient, we can see the families if they’re there, and get a lot of information,” says Dr. Kenton, director of the stroke program at Geisinger.
It’s crucial to see patients when they’re suspected of having stroke symptoms, he says, so that the neurologist can get crucial insight they can’t get over the phone. With a laptop, tablet, or smartphone, the neurologist can do a consult regardless of location.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says he expects that one paradoxical effect of telestroke care is that more patients with neurological conditions ultimately will end up under the care of hospitalists. That’s because centers will be more likely to take on a patient, consult with a neurologist using telestroke care or teleneurology, then admit the patient—after the neurologist has logged off.
“I do think that we are going to see an increase in the number of neurologic-type patients that are cared for primarily by hospitalists,” he says. “I’m there for the acute consultation. But often those patients are then subsequently admitted to a hospitalist service for the very reason that I was called. They don’t have local resources for neurology or a neurohospitalist.
“I actually think there’s going to be more involvement on the hospitalist front for neurologic patients, even patients with neurologic emergencies, because of telemedicine,” Dr. Barrett says. TH
Tom Collins is a freelance writer in South Florida.
To deal with the demand for neurologists, hospitals are increasingly turning to a new idea: patching a neurologist into the exam room from afar, Skype-style. This approach to caring for patients with strokes and other neurologic conditions—“telestroke” care or “teleneurology”—is an emerging valuable resource, says Edgar Kenton, MD, who is in the process of expanding such a system at Geisinger Health System in Danville, Pa.
It’s a hub-and-spoke system, with a central hospital as the “hub” and other hospitals as the “spokes” that connect with the hub, using computers and real-time video. Geisinger has six spokes, with plans for about another half-dozen.
“We’re able to talk to the physician, we can see the patient, we can see the families if they’re there, and get a lot of information,” says Dr. Kenton, director of the stroke program at Geisinger.
It’s crucial to see patients when they’re suspected of having stroke symptoms, he says, so that the neurologist can get crucial insight they can’t get over the phone. With a laptop, tablet, or smartphone, the neurologist can do a consult regardless of location.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says he expects that one paradoxical effect of telestroke care is that more patients with neurological conditions ultimately will end up under the care of hospitalists. That’s because centers will be more likely to take on a patient, consult with a neurologist using telestroke care or teleneurology, then admit the patient—after the neurologist has logged off.
“I do think that we are going to see an increase in the number of neurologic-type patients that are cared for primarily by hospitalists,” he says. “I’m there for the acute consultation. But often those patients are then subsequently admitted to a hospitalist service for the very reason that I was called. They don’t have local resources for neurology or a neurohospitalist.
“I actually think there’s going to be more involvement on the hospitalist front for neurologic patients, even patients with neurologic emergencies, because of telemedicine,” Dr. Barrett says. TH
Tom Collins is a freelance writer in South Florida.
To deal with the demand for neurologists, hospitals are increasingly turning to a new idea: patching a neurologist into the exam room from afar, Skype-style. This approach to caring for patients with strokes and other neurologic conditions—“telestroke” care or “teleneurology”—is an emerging valuable resource, says Edgar Kenton, MD, who is in the process of expanding such a system at Geisinger Health System in Danville, Pa.
It’s a hub-and-spoke system, with a central hospital as the “hub” and other hospitals as the “spokes” that connect with the hub, using computers and real-time video. Geisinger has six spokes, with plans for about another half-dozen.
“We’re able to talk to the physician, we can see the patient, we can see the families if they’re there, and get a lot of information,” says Dr. Kenton, director of the stroke program at Geisinger.
It’s crucial to see patients when they’re suspected of having stroke symptoms, he says, so that the neurologist can get crucial insight they can’t get over the phone. With a laptop, tablet, or smartphone, the neurologist can do a consult regardless of location.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says he expects that one paradoxical effect of telestroke care is that more patients with neurological conditions ultimately will end up under the care of hospitalists. That’s because centers will be more likely to take on a patient, consult with a neurologist using telestroke care or teleneurology, then admit the patient—after the neurologist has logged off.
“I do think that we are going to see an increase in the number of neurologic-type patients that are cared for primarily by hospitalists,” he says. “I’m there for the acute consultation. But often those patients are then subsequently admitted to a hospitalist service for the very reason that I was called. They don’t have local resources for neurology or a neurohospitalist.
“I actually think there’s going to be more involvement on the hospitalist front for neurologic patients, even patients with neurologic emergencies, because of telemedicine,” Dr. Barrett says. TH
Tom Collins is a freelance writer in South Florida.
Oklahoma Hospitalist Discusses Medical Center Devastation, Community Response
Click here to listen to more of our interview with Dr. Womble
Click here to listen to more of our interview with Dr. Womble
Click here to listen to more of our interview with Dr. Womble
Listen to Project BOOST lead analyst Luke Hansen, MD, MPH, discuss the outcomes study published in JHM
Click here to listen to our interview with Dr. Hansen
Click here to listen to our interview with Dr. Hansen
Click here to listen to our interview with Dr. Hansen
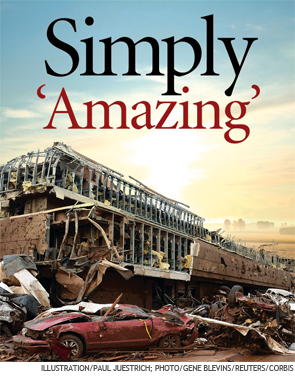
Devastating Superstorm Gone, But Not Forgotten in Moore, Okla.



–Joe R. Womble, MD
The first bit of feedback was fantastic: Everyone who had been inside the hospital—roughly 200 to 300 people, including 30 patients—had survived.
“Everyone was fine,” he said. “All the patients and staff, no one got injured. I was thinking that either the hospital was missed by the storm or that it must not have really damaged it very significantly.”
Unfortunately, the hospital was not OK. He watched as local TV painted a very different picture.
“They started showing aerial shots and I was just shocked. My jaw was just dropped,” Dr. Womble said. “The main entrance that I go in every day was literally stacked with three or four cars deep. A huge stack of about 30 cars was piled up on the main entrance, essentially.”
It was as though they were “toy cars.”
The May 20 tornado, a two-mile-wide superstorm boasting 200-mph winds that struck just south of Oklahoma City, claimed 24 lives and left the regional health system with a void in its network. It also left hospitalists mourning the loss of the place they called a second home several times a week. About a week after the storm, officials announced that Moore Medical Center would have to be demolished.
Miraculous Moments
Despite the terrible events, hospitalists and hospital officials were astounded by the good fortune of the hospital’s inhabitants. Dr. Womble said about 100 people from nearby neighborhoods and businesses used the hospital as shelter.
Senthil Raju, MD, a hospitalist who had done rounds at Moore Medical earlier that day, said the protocol was to take shelter in the hallways. But at some point, probably only minutes before the storm hit, the chief nurse and the house supervisor made the decision to move all the patients to the ground floor because they were in “reasonably stable condition,” according to Dr. Womble, who relayed accounts by staffers who were there. Most of the people in the hospital rode out the storm in the first-floor cafeteria.
After the storm, patient rooms on the second floor were either no longer there or had been reduced to their steel innards.
The decision to move everyone undoubtedly saved lives. “If any of our patients stayed there, they’re probably all dead,” Dr. Raju said.
David Whitaker, CEO of Norman Regional Health System, which includes Moore Medical, marveled at the outcome.
“We had some bumps and bruises, some scratches, but no major lacerations, no broken bones, no injuries that people couldn’t ambulate. It’s totally amazing,” he said. “The leadership that was in place, the employees that were working at that time, they sprang into action, they took command and control of the situation. They got people into the proper areas.”
Dr. Womble said hospital staff at Moore Medical had still more amazing stories of death-defiance. They told him 30 people refused to leave the chapel. Somehow, the chapel remained intact, even though the hospital all around it was destroyed. Whitaker confirmed this.
One woman in active labor was kept in a second-floor operating room—which the medical staff thought was the best place for her, all things considered. Nurses covered the woman with pillows, blankets, and their own bodies as the tornado barreled through the town. She survived and gave birth to a boy several hours later. The parents gave him the middle name Emmanuel, which means “God is with us.”
As the tornado approached, an elderly volunteer had gone outside to get something from a van he used to transport elderly patients to and from a physical therapy program. “Nobody inside knew he had gone outside,” Dr. Womble said. By the time he tried to get back in, the power had gone out, and the doors wouldn’t open. He huddled behind a concrete pillar and ended up with just one minor laceration.
Patients eventually were taken to another hospital, Norman’s HealthPlex, about five miles south. Both Dr. Womble and Dr. Raju have begun working full time at the HealthPlex.
Dr. Raju said that he avoided being at Moore Medical during the tornado only by a turn of luck. He normally rounds at Moore in the afternoon and at the HealthPlex in the morning. But on that day, there were three new admissions at Moore, and only one at HealthPlex. So he went to Moore first, and was gone by the time the tornado hit.
“So lucky,” he said.

–David Whitaker, CEO of Norman Regional Health System
The Aftermath
It remains to be seen what kind of medical facility will be built to replace Moore Medical Center.
“Nobody knows what will happen next, but a lot of us speculate that they will not rebuild an inpatient facility,” said Dr. Womble, who had worked at Moore Medical Center for four years.
Whitaker said the first priority was to re-establish the clinics located at Moore Medical, and that has been done. The next step is, possibly, a temporary building in Moore for urgent care. The long-term plan remains in the discussion phase.
“We’ve already started having some meetings,” Whitaker said. “We’re going to determine what type of facility, what service levels it will be offering as we go back.”
It’s hard knowing that his hospital is no longer there, Dr. Raju said.
“We are going to miss it,” he said. “It’s unimaginable.”
Dr. Womble said those first few hours, when he wasn’t sure of where he’d be working, were difficult. He struggles to describe the feeling of not being able to provide care at his hospital at the time it’s most needed.
“It’s really hard to put it into words,” he said. “It’s the only hospital in that city, and it’s just me and my partner to take care of virtually everyone that comes in with any kind of medical problem. I definitely feel a tie to the community.
“It’s devastating. What is the rest of the city going to do for their hospital care? They essentially will not have a hospital in their city. They’ll have to drive to another city for care.”
Tom Collins is a freelance writer in South Florida.
–Joe R. Womble, MD
The first bit of feedback was fantastic: Everyone who had been inside the hospital—roughly 200 to 300 people, including 30 patients—had survived.
“Everyone was fine,” he said. “All the patients and staff, no one got injured. I was thinking that either the hospital was missed by the storm or that it must not have really damaged it very significantly.”
Unfortunately, the hospital was not OK. He watched as local TV painted a very different picture.
“They started showing aerial shots and I was just shocked. My jaw was just dropped,” Dr. Womble said. “The main entrance that I go in every day was literally stacked with three or four cars deep. A huge stack of about 30 cars was piled up on the main entrance, essentially.”
It was as though they were “toy cars.”
The May 20 tornado, a two-mile-wide superstorm boasting 200-mph winds that struck just south of Oklahoma City, claimed 24 lives and left the regional health system with a void in its network. It also left hospitalists mourning the loss of the place they called a second home several times a week. About a week after the storm, officials announced that Moore Medical Center would have to be demolished.
Miraculous Moments
Despite the terrible events, hospitalists and hospital officials were astounded by the good fortune of the hospital’s inhabitants. Dr. Womble said about 100 people from nearby neighborhoods and businesses used the hospital as shelter.
Senthil Raju, MD, a hospitalist who had done rounds at Moore Medical earlier that day, said the protocol was to take shelter in the hallways. But at some point, probably only minutes before the storm hit, the chief nurse and the house supervisor made the decision to move all the patients to the ground floor because they were in “reasonably stable condition,” according to Dr. Womble, who relayed accounts by staffers who were there. Most of the people in the hospital rode out the storm in the first-floor cafeteria.
After the storm, patient rooms on the second floor were either no longer there or had been reduced to their steel innards.
The decision to move everyone undoubtedly saved lives. “If any of our patients stayed there, they’re probably all dead,” Dr. Raju said.
David Whitaker, CEO of Norman Regional Health System, which includes Moore Medical, marveled at the outcome.
“We had some bumps and bruises, some scratches, but no major lacerations, no broken bones, no injuries that people couldn’t ambulate. It’s totally amazing,” he said. “The leadership that was in place, the employees that were working at that time, they sprang into action, they took command and control of the situation. They got people into the proper areas.”
Dr. Womble said hospital staff at Moore Medical had still more amazing stories of death-defiance. They told him 30 people refused to leave the chapel. Somehow, the chapel remained intact, even though the hospital all around it was destroyed. Whitaker confirmed this.
One woman in active labor was kept in a second-floor operating room—which the medical staff thought was the best place for her, all things considered. Nurses covered the woman with pillows, blankets, and their own bodies as the tornado barreled through the town. She survived and gave birth to a boy several hours later. The parents gave him the middle name Emmanuel, which means “God is with us.”
As the tornado approached, an elderly volunteer had gone outside to get something from a van he used to transport elderly patients to and from a physical therapy program. “Nobody inside knew he had gone outside,” Dr. Womble said. By the time he tried to get back in, the power had gone out, and the doors wouldn’t open. He huddled behind a concrete pillar and ended up with just one minor laceration.
Patients eventually were taken to another hospital, Norman’s HealthPlex, about five miles south. Both Dr. Womble and Dr. Raju have begun working full time at the HealthPlex.
Dr. Raju said that he avoided being at Moore Medical during the tornado only by a turn of luck. He normally rounds at Moore in the afternoon and at the HealthPlex in the morning. But on that day, there were three new admissions at Moore, and only one at HealthPlex. So he went to Moore first, and was gone by the time the tornado hit.
“So lucky,” he said.
–David Whitaker, CEO of Norman Regional Health System
The Aftermath
It remains to be seen what kind of medical facility will be built to replace Moore Medical Center.
“Nobody knows what will happen next, but a lot of us speculate that they will not rebuild an inpatient facility,” said Dr. Womble, who had worked at Moore Medical Center for four years.
Whitaker said the first priority was to re-establish the clinics located at Moore Medical, and that has been done. The next step is, possibly, a temporary building in Moore for urgent care. The long-term plan remains in the discussion phase.
“We’ve already started having some meetings,” Whitaker said. “We’re going to determine what type of facility, what service levels it will be offering as we go back.”
It’s hard knowing that his hospital is no longer there, Dr. Raju said.
“We are going to miss it,” he said. “It’s unimaginable.”
Dr. Womble said those first few hours, when he wasn’t sure of where he’d be working, were difficult. He struggles to describe the feeling of not being able to provide care at his hospital at the time it’s most needed.
“It’s really hard to put it into words,” he said. “It’s the only hospital in that city, and it’s just me and my partner to take care of virtually everyone that comes in with any kind of medical problem. I definitely feel a tie to the community.
“It’s devastating. What is the rest of the city going to do for their hospital care? They essentially will not have a hospital in their city. They’ll have to drive to another city for care.”
Tom Collins is a freelance writer in South Florida.
–Joe R. Womble, MD
The first bit of feedback was fantastic: Everyone who had been inside the hospital—roughly 200 to 300 people, including 30 patients—had survived.
“Everyone was fine,” he said. “All the patients and staff, no one got injured. I was thinking that either the hospital was missed by the storm or that it must not have really damaged it very significantly.”
Unfortunately, the hospital was not OK. He watched as local TV painted a very different picture.
“They started showing aerial shots and I was just shocked. My jaw was just dropped,” Dr. Womble said. “The main entrance that I go in every day was literally stacked with three or four cars deep. A huge stack of about 30 cars was piled up on the main entrance, essentially.”
It was as though they were “toy cars.”
The May 20 tornado, a two-mile-wide superstorm boasting 200-mph winds that struck just south of Oklahoma City, claimed 24 lives and left the regional health system with a void in its network. It also left hospitalists mourning the loss of the place they called a second home several times a week. About a week after the storm, officials announced that Moore Medical Center would have to be demolished.
Miraculous Moments
Despite the terrible events, hospitalists and hospital officials were astounded by the good fortune of the hospital’s inhabitants. Dr. Womble said about 100 people from nearby neighborhoods and businesses used the hospital as shelter.
Senthil Raju, MD, a hospitalist who had done rounds at Moore Medical earlier that day, said the protocol was to take shelter in the hallways. But at some point, probably only minutes before the storm hit, the chief nurse and the house supervisor made the decision to move all the patients to the ground floor because they were in “reasonably stable condition,” according to Dr. Womble, who relayed accounts by staffers who were there. Most of the people in the hospital rode out the storm in the first-floor cafeteria.
After the storm, patient rooms on the second floor were either no longer there or had been reduced to their steel innards.
The decision to move everyone undoubtedly saved lives. “If any of our patients stayed there, they’re probably all dead,” Dr. Raju said.
David Whitaker, CEO of Norman Regional Health System, which includes Moore Medical, marveled at the outcome.
“We had some bumps and bruises, some scratches, but no major lacerations, no broken bones, no injuries that people couldn’t ambulate. It’s totally amazing,” he said. “The leadership that was in place, the employees that were working at that time, they sprang into action, they took command and control of the situation. They got people into the proper areas.”
Dr. Womble said hospital staff at Moore Medical had still more amazing stories of death-defiance. They told him 30 people refused to leave the chapel. Somehow, the chapel remained intact, even though the hospital all around it was destroyed. Whitaker confirmed this.
One woman in active labor was kept in a second-floor operating room—which the medical staff thought was the best place for her, all things considered. Nurses covered the woman with pillows, blankets, and their own bodies as the tornado barreled through the town. She survived and gave birth to a boy several hours later. The parents gave him the middle name Emmanuel, which means “God is with us.”
As the tornado approached, an elderly volunteer had gone outside to get something from a van he used to transport elderly patients to and from a physical therapy program. “Nobody inside knew he had gone outside,” Dr. Womble said. By the time he tried to get back in, the power had gone out, and the doors wouldn’t open. He huddled behind a concrete pillar and ended up with just one minor laceration.
Patients eventually were taken to another hospital, Norman’s HealthPlex, about five miles south. Both Dr. Womble and Dr. Raju have begun working full time at the HealthPlex.
Dr. Raju said that he avoided being at Moore Medical during the tornado only by a turn of luck. He normally rounds at Moore in the afternoon and at the HealthPlex in the morning. But on that day, there were three new admissions at Moore, and only one at HealthPlex. So he went to Moore first, and was gone by the time the tornado hit.
“So lucky,” he said.
–David Whitaker, CEO of Norman Regional Health System
The Aftermath
It remains to be seen what kind of medical facility will be built to replace Moore Medical Center.
“Nobody knows what will happen next, but a lot of us speculate that they will not rebuild an inpatient facility,” said Dr. Womble, who had worked at Moore Medical Center for four years.
Whitaker said the first priority was to re-establish the clinics located at Moore Medical, and that has been done. The next step is, possibly, a temporary building in Moore for urgent care. The long-term plan remains in the discussion phase.
“We’ve already started having some meetings,” Whitaker said. “We’re going to determine what type of facility, what service levels it will be offering as we go back.”
It’s hard knowing that his hospital is no longer there, Dr. Raju said.
“We are going to miss it,” he said. “It’s unimaginable.”
Dr. Womble said those first few hours, when he wasn’t sure of where he’d be working, were difficult. He struggles to describe the feeling of not being able to provide care at his hospital at the time it’s most needed.
“It’s really hard to put it into words,” he said. “It’s the only hospital in that city, and it’s just me and my partner to take care of virtually everyone that comes in with any kind of medical problem. I definitely feel a tie to the community.
“It’s devastating. What is the rest of the city going to do for their hospital care? They essentially will not have a hospital in their city. They’ll have to drive to another city for care.”
Tom Collins is a freelance writer in South Florida.
11 Things Neurologists Think Hospitalists Need To Know

11 Things: At a Glance
- You might be overdiagnosing transient ischemic attacks (TIA).
- Early mobilization after a stroke might be better for some patients.
- MRI is the best tool to evaluate TIA patients.
- Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
- Tracking the time a hospitalized patient was last seen to be normal is crucial.
- Consider neuromuscular disorders when a patient presents with weakness.
- Urinary tract infections (UTIs) are not the only cause of altered mental status.
- Take care in distinguishing aphasia from general confusion.
- A simple checklist might eliminate the need to consult the neurologist.
- Calling a neurologist earlier is way better than calling later.
- Hire a neurohospitalist if your institution doesn’t have one already.
When a patient is admitted to the hospital with neurological symptoms, such as altered mental status, he or she might not be the only one who is confused. Hospitalists might be a little confused, too.
Of all the subspecialties to which hospitalists are exposed, none might make them more uncomfortable than neurology. Because of what often is a dearth of training in this area, and because of the vexing and sometimes fleeting nature of symptoms, hospitalists might be inclined to lean on neurologists more than other specialists.
The Hospitalist spoke with a half-dozen experts, gathering their words of guidance and clinical tips. Here’s hoping they give you a little extra confidence the next time you see a patient with altered mental status.
You might be overdiagnosing transient ischemic attacks (TIA).
Ira Chang, MD, a neurohospitalist with Blue Sky Neurology in Englewood, Colo., and assistant clinical professor at the University of Colorado Health Sciences Center in Denver, says TIA is all too commonly a go-to diagnosis, frequently when there’s another cause.
“I think that hospitalists, and maybe medical internists in general, are very quick to diagnose anything that has a neurologic symptom that comes and goes as a TIA,” she says. “Patients have to have specific neurologic symptoms that we think are due to arterial blood flow or ischemia problems.”
Near-fainting spells and dizzy spells involving confusion commonly are diagnosed as TIA when these symptoms could be due to “a number of other causes,” Dr. Chang adds.

Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says the suspicion of a TIA should be greater if the patient is older or has traditional cardiovascular risk factors, such as hyptertension, diabetes, hyperlipidemia, or tobacco use.
A TIA typically causes symptoms referable to common arterial distributions. Carotid-distribution TIA often causes ipsilateral loss of vision and contralateral weakness or numbness. Posterior-circulation TIAs bring on symptoms such as ataxia, unilateral or bilateral limb weakness, diplopia, and slurred or slow speech.
TIA diagnoses can be tricky even for those trained in neurology, Dr. Barrett says.
“Even among fellowship-trained vascular neurologists, TIA can be a challenging diagnosis, often with poor inter-observer agreement,” he notes.
Early mobilization after a stroke might be better for some patients.
After receiving tissue plasminogen activator (tPA) therapy for stroke, patients historically were kept on bed rest for 24 hours to reduce the risk of hemorrhage. Evidence now is coming to light that some patients might benefit from getting out of bed sooner, Dr. Barrett says.1
“We’re learning that in selected patients, they can actually be mobilized at 12 hours,” he says. “In some cases, that would not only reduce the risk of complications related to immobilization like DVT but shorten length of stay. These are all important metrics for anybody who practices primarily within an inpatient setting.”
Early mobilization generally is more suitable for patients with less severe deficits and who are hemodynamically stable.
MRI is the best tool to evaluate TIA patients.
TIA patients who have transient symptoms and normal diffusion-weighted imaging (DWI) abnormalities on an MRI are at a very low risk. “Less than 1% of those patients have a stroke within the subsequent seven days,” Dr. Barrett says.2 “But those patients who do have a DWI abnormality, they’re at very high risk: 7.1% at seven days.
“The utility of MRI following TIA is becoming very much apparent. It is something that hospitalists should be aware of.”
Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
Patients experiencing confusion or speech disturbance or altered mentation—particularly if they’re elderly or have dementia—could be having a partial seizure, Dr. Chang says. Dementia patients have a 10% to 15% incidence of complex partial seizures, she says.
“I see that underdiagnosed a lot,” she says. “They keep coming back, and everybody diagnoses them with TIAs. So they keep getting put on aspirin, and they get switched to Aggrenox [to prevent clotting]. They keep coming back with the same symptoms.”
Tracking the time a hospitalized patient was last seen to be normal is crucial.
About 10% to 15% of strokes occur in patients who are in the hospital.
“While a lot of those strokes are perioperative, there also are patients who are going to be on hospitalist services,” says Eric Adelman, MD, assistant professor of neurology at the University of Michigan in Ann Arbor.

Hospitalists should note that patients suffering strokes are found not just in the ED but also on the floor, where all the tools for treatment might not be as readily available. That makes those cases a challenge and makes forethought that much more important, Dr. Adelman says.
“It’s a matter of trying to track down last normal times,” he says. “If they’re eligible for tPA and they’re within the therapeutic window, we should be able to do that within a hospital.”
Establishing a neurological baseline is particularly important for patients who are at higher stroke risk, like those with atrial fibrillation and other cardiovascular risk factors.
“In case something does happen,” Dr. Adelman says, “at least you have a baseline so you can [know that] at time X, we knew they had full strength in their right arm, and now they don’t.”
Consider neuromuscular disorders when a patient presents with weakness.
It’s safe to say some hospitalists might miss a neuromuscular disorder, Dr. Chang says.
“A lot of disorders that are harder for hospitalists to diagnose and that tend to take longer to call a neurologist [on] are things that are due to myasthenia gravis [a breakdown between nerves and muscles leading to muscle fatigue], myopathy, or ALS,” she says. “Many patients present with weakness. I think a lot of times there will be a lot of tests on and a lot of treatment for general medical conditions that can cause weakness.”
And that might be a case of misdirected attention. Patients with weakness accompanied by persistent swallowing problems, slurred speech with no other obvious cause, or the inability to lift their head off the bed without an obvious cause may end up with a neuromuscular diagnosis, she says.
It would be helpful to have a neurologist’s input in these cases, she says, where “nothing’s getting better, and three, four, five days later, the patient’s still weak.
“I think a neurologist would be more in tune with something like that,” she adds.
Urinary tract infections (UTIs) are not the only cause of altered mental status.
That might seem obvious, but too often, a UTI can be pegged as the source of altered mental status when it should not be, Dr. Chang says.
“We get a lot of people who come in with confusion and they have a slightly abnormal urinalysis and they diagnose them with UTI,” Dr. Chang says. “And it turns out that they actually had a stroke or they had a seizure.”
Significantly altered mentation should show a significantly abnormal urine with a positive culture, she says. “They ought to have significant laboratory support for a urinary tract infection.”
Dr. Barrett says a neurologic review of systems, or at least a neurologic exam, should be the physician’s guide.
“Those are key parts of a hospitalist’s practice,” he says, “because that’s what’s truly going to guide them to consider primary neurological causes of altered mental status.”
Take care in distinguishing aphasia from general confusion.
If a patient is still talking and is fairly fluent, that doesn’t mean they aren’t suffering from certain types of aphasia, a disorder caused by damage to parts of the brain that control language, Dr. Adelman says.
“Oftentimes, when you’re dealing with a patient with confusion, you want to make sure that it’s confusion, or encephalopathy, rather than a focal neurologic problem like aphasia,” he says. “Frequently patients with aphasia will have other symptoms such as a facial drop or weakness in the arm, but stroke can present as isolated aphasia.”
A good habit to get into is to determine whether the patient can repeat a phrase, follow a command, or name objects, he says. If they can, they probably do not have aphasia.
“The thing that you worry about with aphasia, particularly acute onset aphasia, is an ischemic stroke,” Dr. Adelman says.
A simple checklist might eliminate the need to consult the neurologist.
When Edgar Kenton, MD, now director of the stroke program at Geisinger Health System in Danville, Pa., was at Emory University Hospital in Atlanta, he found he was getting snowed under with consults from hospitalists. There were about 15 hospitalists for just one or two neurologists.
“There was no way I was able to see these patients, particularly in follow-up, because you might get five consults every day,” he says. “By the middle of the week, that’s 15 consults. You don’t get a chance to go back and see the patients because you’re just going from one consult to the other.”
The situation improved with a checklist of things to consider when a patient presents with altered mental status. Before seeking a consult, neurologists suggested the hospitalists check the electrolytes, blood pressure, and urine, and use CT scans as a screening test. That might uncover the root of the patient’s problems. If those are clear, by all means get the neurologist involved, he says.
“We were able to educate the hospitalists so they knew when to call; they knew when it was beyond their expertise to take care of the patient, so we weren’t getting called for every patient with altered mental status when all they needed to do was to check the electrolytes,” Dr. Kenton says.
Calling a neurologist earlier is way better than calling later.
Once the decision is made to consult with a neurologist, the consult should be done right away, Dr. Kenton says, not after a few days when symptoms don’t appear to be improving.
“We’ll get the call on a Friday afternoon because they thought, finally, ‘Well, you know, we need to get neurology involved because we a) haven’t solved the problem and b) there may be some other tests we should be getting,’” he says of common situations. “That has been a problem. If you don’t have a neurohospitalist involved day by day, working with the patient and the general hospitalist, neurology becomes an afterthought.”
He says accurate and early diagnosis is paramount to the patient.
“If the diagnosis is delayed, obviously there’s more insult to the patients, more persistent insult,” he says, noting the timing is particularly important in neurological conditions “because things can get bad in a hurry.”
He strongly urges hospitalists to consult with a neurologist before ordering an entire battery of tests.
At Geisinger, neurologists are encouraging hospitalists to chat informally with neurosurgeons about cases for guidance at the outset rather than after several days.
Hire a neurohospitalist if your institution doesn’t have one already.
At the top of the list of Dr. Kenton’s suggestions on caring for hospitalized neurology patients is this declaration: “Get a neurohospitalist.”
“It’s important to have the neurologist involved from the time the patient’s admitted,” he says. “That’s the value of connecting the general hospitalist with neurologists.”
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says his colleagues are team players and improve patient care.
“Neurology consultations can be called very quickly, and a nice partnership can develop between internal medicine hospitalists and neurohospitalists to care for those patients who have those medical and neurologic problems,” he says.
He also says having a neurohospitalist on board can ease some of the tension.
“No longer if there’s a neurologic condition does a hospitalist have to think about, ‘Well, does this rise to the level of something that I need to get the neurologist to drive across the city to come see?’” he explains. “‘Or is this something we should try to manage ourselves?’”
Tom Collins is a freelance writer in South Florida.
“Neurophobia” a Challenge for Hospitalists, Other Physicians

The unease that many hospitalists, internal-medicine doctors, and other providers feel about treating neurologic conditions is so readily recognized that a term has been coined to describe it: “neurophobia.”
The term has been used in published literature for at least two decades. A 2010 survey found that medical students and residents felt that neurology was the specialty they had the least knowledge about and was the one that was the most difficult.3 And trainees had the least confidence in treating patients with neurological complaints.
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says internal-medicine hospitalists are “increasingly feeling uncomfortable with requests that they have to care for patients with a wide range of primary neurologic conditions in some instances.”
That has helped lead to the emergence of neurohospitalists, he says.
John Vazquez, MD, medical director of the division hospital medicine of Emory University Hospital in Atlanta, says neurophobia is real.
“Every hospitalist has different subspecialty areas that they’re less comfortable with, and I think neurology specifically is one that does scare a lot of hospitalists,” he says. “I think on one side there are hospitalists that might ignore a neurologic problem because they don’t really know what they don’t know. On the other side are the hospitalists who I think are just concerned that they don’t know the field very well and may not feel comfortable.”
Dr. Vazquez did rotations in nephrology, pulmonology, cardiology, and rheumatology but, like many hospitalists, not neurology.
“Neurology is not one that you have to go through,” he says.
He made these suggestions:
- Know what you don’t know and get guidance when necessary.
- Do your own neurologic assessment. Even if a neurologist decides confusion is due to a patient being elderly and having a urinary tract infection, that doesn’t mean that they didn’t actually have a stroke. So if something seems not quite right, be willing to challenge the neurologist.
- Use the resources available to widen your knowledge base.
“You can utilize the consultants for your own education if you have neurologists in your hospital, and many at least have some that rotate in,” Dr. Vazquez says. “You can pick their brain on what they would do with different strokes and what’s the newest thing and ongoing treatment and whatever it is you’re concerned about.”
—Thomas R. Collins
John Vazquez, MD, of Emory University Hospital talks about neurophobia and provides tips for adjusting to the discomfort of working with neurology patients.
References
- Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39;390-396.
- Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs. time-defined TIA: a multicenter study. Neurology. 2011;77(13):1222-1228.
- Zinchuk AV, Flanagan EP, Tubridy NJ, Miller WA, McCullough LD. Attitudes of US medical trainees towards neurology education: “Neurophobia”—a global issue. BMC Med Educ. 2010;10:49.
11 Things: At a Glance
- You might be overdiagnosing transient ischemic attacks (TIA).
- Early mobilization after a stroke might be better for some patients.
- MRI is the best tool to evaluate TIA patients.
- Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
- Tracking the time a hospitalized patient was last seen to be normal is crucial.
- Consider neuromuscular disorders when a patient presents with weakness.
- Urinary tract infections (UTIs) are not the only cause of altered mental status.
- Take care in distinguishing aphasia from general confusion.
- A simple checklist might eliminate the need to consult the neurologist.
- Calling a neurologist earlier is way better than calling later.
- Hire a neurohospitalist if your institution doesn’t have one already.
When a patient is admitted to the hospital with neurological symptoms, such as altered mental status, he or she might not be the only one who is confused. Hospitalists might be a little confused, too.
Of all the subspecialties to which hospitalists are exposed, none might make them more uncomfortable than neurology. Because of what often is a dearth of training in this area, and because of the vexing and sometimes fleeting nature of symptoms, hospitalists might be inclined to lean on neurologists more than other specialists.
The Hospitalist spoke with a half-dozen experts, gathering their words of guidance and clinical tips. Here’s hoping they give you a little extra confidence the next time you see a patient with altered mental status.
You might be overdiagnosing transient ischemic attacks (TIA).
Ira Chang, MD, a neurohospitalist with Blue Sky Neurology in Englewood, Colo., and assistant clinical professor at the University of Colorado Health Sciences Center in Denver, says TIA is all too commonly a go-to diagnosis, frequently when there’s another cause.
“I think that hospitalists, and maybe medical internists in general, are very quick to diagnose anything that has a neurologic symptom that comes and goes as a TIA,” she says. “Patients have to have specific neurologic symptoms that we think are due to arterial blood flow or ischemia problems.”
Near-fainting spells and dizzy spells involving confusion commonly are diagnosed as TIA when these symptoms could be due to “a number of other causes,” Dr. Chang adds.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says the suspicion of a TIA should be greater if the patient is older or has traditional cardiovascular risk factors, such as hyptertension, diabetes, hyperlipidemia, or tobacco use.
A TIA typically causes symptoms referable to common arterial distributions. Carotid-distribution TIA often causes ipsilateral loss of vision and contralateral weakness or numbness. Posterior-circulation TIAs bring on symptoms such as ataxia, unilateral or bilateral limb weakness, diplopia, and slurred or slow speech.
TIA diagnoses can be tricky even for those trained in neurology, Dr. Barrett says.
“Even among fellowship-trained vascular neurologists, TIA can be a challenging diagnosis, often with poor inter-observer agreement,” he notes.
Early mobilization after a stroke might be better for some patients.
After receiving tissue plasminogen activator (tPA) therapy for stroke, patients historically were kept on bed rest for 24 hours to reduce the risk of hemorrhage. Evidence now is coming to light that some patients might benefit from getting out of bed sooner, Dr. Barrett says.1
“We’re learning that in selected patients, they can actually be mobilized at 12 hours,” he says. “In some cases, that would not only reduce the risk of complications related to immobilization like DVT but shorten length of stay. These are all important metrics for anybody who practices primarily within an inpatient setting.”
Early mobilization generally is more suitable for patients with less severe deficits and who are hemodynamically stable.
MRI is the best tool to evaluate TIA patients.
TIA patients who have transient symptoms and normal diffusion-weighted imaging (DWI) abnormalities on an MRI are at a very low risk. “Less than 1% of those patients have a stroke within the subsequent seven days,” Dr. Barrett says.2 “But those patients who do have a DWI abnormality, they’re at very high risk: 7.1% at seven days.
“The utility of MRI following TIA is becoming very much apparent. It is something that hospitalists should be aware of.”
Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
Patients experiencing confusion or speech disturbance or altered mentation—particularly if they’re elderly or have dementia—could be having a partial seizure, Dr. Chang says. Dementia patients have a 10% to 15% incidence of complex partial seizures, she says.
“I see that underdiagnosed a lot,” she says. “They keep coming back, and everybody diagnoses them with TIAs. So they keep getting put on aspirin, and they get switched to Aggrenox [to prevent clotting]. They keep coming back with the same symptoms.”
Tracking the time a hospitalized patient was last seen to be normal is crucial.
About 10% to 15% of strokes occur in patients who are in the hospital.
“While a lot of those strokes are perioperative, there also are patients who are going to be on hospitalist services,” says Eric Adelman, MD, assistant professor of neurology at the University of Michigan in Ann Arbor.
Hospitalists should note that patients suffering strokes are found not just in the ED but also on the floor, where all the tools for treatment might not be as readily available. That makes those cases a challenge and makes forethought that much more important, Dr. Adelman says.
“It’s a matter of trying to track down last normal times,” he says. “If they’re eligible for tPA and they’re within the therapeutic window, we should be able to do that within a hospital.”
Establishing a neurological baseline is particularly important for patients who are at higher stroke risk, like those with atrial fibrillation and other cardiovascular risk factors.
“In case something does happen,” Dr. Adelman says, “at least you have a baseline so you can [know that] at time X, we knew they had full strength in their right arm, and now they don’t.”
Consider neuromuscular disorders when a patient presents with weakness.
It’s safe to say some hospitalists might miss a neuromuscular disorder, Dr. Chang says.
“A lot of disorders that are harder for hospitalists to diagnose and that tend to take longer to call a neurologist [on] are things that are due to myasthenia gravis [a breakdown between nerves and muscles leading to muscle fatigue], myopathy, or ALS,” she says. “Many patients present with weakness. I think a lot of times there will be a lot of tests on and a lot of treatment for general medical conditions that can cause weakness.”
And that might be a case of misdirected attention. Patients with weakness accompanied by persistent swallowing problems, slurred speech with no other obvious cause, or the inability to lift their head off the bed without an obvious cause may end up with a neuromuscular diagnosis, she says.
It would be helpful to have a neurologist’s input in these cases, she says, where “nothing’s getting better, and three, four, five days later, the patient’s still weak.
“I think a neurologist would be more in tune with something like that,” she adds.
Urinary tract infections (UTIs) are not the only cause of altered mental status.
That might seem obvious, but too often, a UTI can be pegged as the source of altered mental status when it should not be, Dr. Chang says.
“We get a lot of people who come in with confusion and they have a slightly abnormal urinalysis and they diagnose them with UTI,” Dr. Chang says. “And it turns out that they actually had a stroke or they had a seizure.”
Significantly altered mentation should show a significantly abnormal urine with a positive culture, she says. “They ought to have significant laboratory support for a urinary tract infection.”
Dr. Barrett says a neurologic review of systems, or at least a neurologic exam, should be the physician’s guide.
“Those are key parts of a hospitalist’s practice,” he says, “because that’s what’s truly going to guide them to consider primary neurological causes of altered mental status.”
Take care in distinguishing aphasia from general confusion.
If a patient is still talking and is fairly fluent, that doesn’t mean they aren’t suffering from certain types of aphasia, a disorder caused by damage to parts of the brain that control language, Dr. Adelman says.
“Oftentimes, when you’re dealing with a patient with confusion, you want to make sure that it’s confusion, or encephalopathy, rather than a focal neurologic problem like aphasia,” he says. “Frequently patients with aphasia will have other symptoms such as a facial drop or weakness in the arm, but stroke can present as isolated aphasia.”
A good habit to get into is to determine whether the patient can repeat a phrase, follow a command, or name objects, he says. If they can, they probably do not have aphasia.
“The thing that you worry about with aphasia, particularly acute onset aphasia, is an ischemic stroke,” Dr. Adelman says.
A simple checklist might eliminate the need to consult the neurologist.
When Edgar Kenton, MD, now director of the stroke program at Geisinger Health System in Danville, Pa., was at Emory University Hospital in Atlanta, he found he was getting snowed under with consults from hospitalists. There were about 15 hospitalists for just one or two neurologists.
“There was no way I was able to see these patients, particularly in follow-up, because you might get five consults every day,” he says. “By the middle of the week, that’s 15 consults. You don’t get a chance to go back and see the patients because you’re just going from one consult to the other.”
The situation improved with a checklist of things to consider when a patient presents with altered mental status. Before seeking a consult, neurologists suggested the hospitalists check the electrolytes, blood pressure, and urine, and use CT scans as a screening test. That might uncover the root of the patient’s problems. If those are clear, by all means get the neurologist involved, he says.
“We were able to educate the hospitalists so they knew when to call; they knew when it was beyond their expertise to take care of the patient, so we weren’t getting called for every patient with altered mental status when all they needed to do was to check the electrolytes,” Dr. Kenton says.
Calling a neurologist earlier is way better than calling later.
Once the decision is made to consult with a neurologist, the consult should be done right away, Dr. Kenton says, not after a few days when symptoms don’t appear to be improving.
“We’ll get the call on a Friday afternoon because they thought, finally, ‘Well, you know, we need to get neurology involved because we a) haven’t solved the problem and b) there may be some other tests we should be getting,’” he says of common situations. “That has been a problem. If you don’t have a neurohospitalist involved day by day, working with the patient and the general hospitalist, neurology becomes an afterthought.”
He says accurate and early diagnosis is paramount to the patient.
“If the diagnosis is delayed, obviously there’s more insult to the patients, more persistent insult,” he says, noting the timing is particularly important in neurological conditions “because things can get bad in a hurry.”
He strongly urges hospitalists to consult with a neurologist before ordering an entire battery of tests.
At Geisinger, neurologists are encouraging hospitalists to chat informally with neurosurgeons about cases for guidance at the outset rather than after several days.
Hire a neurohospitalist if your institution doesn’t have one already.
At the top of the list of Dr. Kenton’s suggestions on caring for hospitalized neurology patients is this declaration: “Get a neurohospitalist.”
“It’s important to have the neurologist involved from the time the patient’s admitted,” he says. “That’s the value of connecting the general hospitalist with neurologists.”
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says his colleagues are team players and improve patient care.
“Neurology consultations can be called very quickly, and a nice partnership can develop between internal medicine hospitalists and neurohospitalists to care for those patients who have those medical and neurologic problems,” he says.
He also says having a neurohospitalist on board can ease some of the tension.
“No longer if there’s a neurologic condition does a hospitalist have to think about, ‘Well, does this rise to the level of something that I need to get the neurologist to drive across the city to come see?’” he explains. “‘Or is this something we should try to manage ourselves?’”
Tom Collins is a freelance writer in South Florida.
“Neurophobia” a Challenge for Hospitalists, Other Physicians
The unease that many hospitalists, internal-medicine doctors, and other providers feel about treating neurologic conditions is so readily recognized that a term has been coined to describe it: “neurophobia.”
The term has been used in published literature for at least two decades. A 2010 survey found that medical students and residents felt that neurology was the specialty they had the least knowledge about and was the one that was the most difficult.3 And trainees had the least confidence in treating patients with neurological complaints.
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says internal-medicine hospitalists are “increasingly feeling uncomfortable with requests that they have to care for patients with a wide range of primary neurologic conditions in some instances.”
That has helped lead to the emergence of neurohospitalists, he says.
John Vazquez, MD, medical director of the division hospital medicine of Emory University Hospital in Atlanta, says neurophobia is real.
“Every hospitalist has different subspecialty areas that they’re less comfortable with, and I think neurology specifically is one that does scare a lot of hospitalists,” he says. “I think on one side there are hospitalists that might ignore a neurologic problem because they don’t really know what they don’t know. On the other side are the hospitalists who I think are just concerned that they don’t know the field very well and may not feel comfortable.”
Dr. Vazquez did rotations in nephrology, pulmonology, cardiology, and rheumatology but, like many hospitalists, not neurology.
“Neurology is not one that you have to go through,” he says.
He made these suggestions:
- Know what you don’t know and get guidance when necessary.
- Do your own neurologic assessment. Even if a neurologist decides confusion is due to a patient being elderly and having a urinary tract infection, that doesn’t mean that they didn’t actually have a stroke. So if something seems not quite right, be willing to challenge the neurologist.
- Use the resources available to widen your knowledge base.
“You can utilize the consultants for your own education if you have neurologists in your hospital, and many at least have some that rotate in,” Dr. Vazquez says. “You can pick their brain on what they would do with different strokes and what’s the newest thing and ongoing treatment and whatever it is you’re concerned about.”
—Thomas R. Collins
John Vazquez, MD, of Emory University Hospital talks about neurophobia and provides tips for adjusting to the discomfort of working with neurology patients.
References
- Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39;390-396.
- Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs. time-defined TIA: a multicenter study. Neurology. 2011;77(13):1222-1228.
- Zinchuk AV, Flanagan EP, Tubridy NJ, Miller WA, McCullough LD. Attitudes of US medical trainees towards neurology education: “Neurophobia”—a global issue. BMC Med Educ. 2010;10:49.
11 Things: At a Glance
- You might be overdiagnosing transient ischemic attacks (TIA).
- Early mobilization after a stroke might be better for some patients.
- MRI is the best tool to evaluate TIA patients.
- Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
- Tracking the time a hospitalized patient was last seen to be normal is crucial.
- Consider neuromuscular disorders when a patient presents with weakness.
- Urinary tract infections (UTIs) are not the only cause of altered mental status.
- Take care in distinguishing aphasia from general confusion.
- A simple checklist might eliminate the need to consult the neurologist.
- Calling a neurologist earlier is way better than calling later.
- Hire a neurohospitalist if your institution doesn’t have one already.
When a patient is admitted to the hospital with neurological symptoms, such as altered mental status, he or she might not be the only one who is confused. Hospitalists might be a little confused, too.
Of all the subspecialties to which hospitalists are exposed, none might make them more uncomfortable than neurology. Because of what often is a dearth of training in this area, and because of the vexing and sometimes fleeting nature of symptoms, hospitalists might be inclined to lean on neurologists more than other specialists.
The Hospitalist spoke with a half-dozen experts, gathering their words of guidance and clinical tips. Here’s hoping they give you a little extra confidence the next time you see a patient with altered mental status.
You might be overdiagnosing transient ischemic attacks (TIA).
Ira Chang, MD, a neurohospitalist with Blue Sky Neurology in Englewood, Colo., and assistant clinical professor at the University of Colorado Health Sciences Center in Denver, says TIA is all too commonly a go-to diagnosis, frequently when there’s another cause.
“I think that hospitalists, and maybe medical internists in general, are very quick to diagnose anything that has a neurologic symptom that comes and goes as a TIA,” she says. “Patients have to have specific neurologic symptoms that we think are due to arterial blood flow or ischemia problems.”
Near-fainting spells and dizzy spells involving confusion commonly are diagnosed as TIA when these symptoms could be due to “a number of other causes,” Dr. Chang adds.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says the suspicion of a TIA should be greater if the patient is older or has traditional cardiovascular risk factors, such as hyptertension, diabetes, hyperlipidemia, or tobacco use.
A TIA typically causes symptoms referable to common arterial distributions. Carotid-distribution TIA often causes ipsilateral loss of vision and contralateral weakness or numbness. Posterior-circulation TIAs bring on symptoms such as ataxia, unilateral or bilateral limb weakness, diplopia, and slurred or slow speech.
TIA diagnoses can be tricky even for those trained in neurology, Dr. Barrett says.
“Even among fellowship-trained vascular neurologists, TIA can be a challenging diagnosis, often with poor inter-observer agreement,” he notes.
Early mobilization after a stroke might be better for some patients.
After receiving tissue plasminogen activator (tPA) therapy for stroke, patients historically were kept on bed rest for 24 hours to reduce the risk of hemorrhage. Evidence now is coming to light that some patients might benefit from getting out of bed sooner, Dr. Barrett says.1
“We’re learning that in selected patients, they can actually be mobilized at 12 hours,” he says. “In some cases, that would not only reduce the risk of complications related to immobilization like DVT but shorten length of stay. These are all important metrics for anybody who practices primarily within an inpatient setting.”
Early mobilization generally is more suitable for patients with less severe deficits and who are hemodynamically stable.
MRI is the best tool to evaluate TIA patients.
TIA patients who have transient symptoms and normal diffusion-weighted imaging (DWI) abnormalities on an MRI are at a very low risk. “Less than 1% of those patients have a stroke within the subsequent seven days,” Dr. Barrett says.2 “But those patients who do have a DWI abnormality, they’re at very high risk: 7.1% at seven days.
“The utility of MRI following TIA is becoming very much apparent. It is something that hospitalists should be aware of.”
Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
Patients experiencing confusion or speech disturbance or altered mentation—particularly if they’re elderly or have dementia—could be having a partial seizure, Dr. Chang says. Dementia patients have a 10% to 15% incidence of complex partial seizures, she says.
“I see that underdiagnosed a lot,” she says. “They keep coming back, and everybody diagnoses them with TIAs. So they keep getting put on aspirin, and they get switched to Aggrenox [to prevent clotting]. They keep coming back with the same symptoms.”
Tracking the time a hospitalized patient was last seen to be normal is crucial.
About 10% to 15% of strokes occur in patients who are in the hospital.
“While a lot of those strokes are perioperative, there also are patients who are going to be on hospitalist services,” says Eric Adelman, MD, assistant professor of neurology at the University of Michigan in Ann Arbor.
Hospitalists should note that patients suffering strokes are found not just in the ED but also on the floor, where all the tools for treatment might not be as readily available. That makes those cases a challenge and makes forethought that much more important, Dr. Adelman says.
“It’s a matter of trying to track down last normal times,” he says. “If they’re eligible for tPA and they’re within the therapeutic window, we should be able to do that within a hospital.”
Establishing a neurological baseline is particularly important for patients who are at higher stroke risk, like those with atrial fibrillation and other cardiovascular risk factors.
“In case something does happen,” Dr. Adelman says, “at least you have a baseline so you can [know that] at time X, we knew they had full strength in their right arm, and now they don’t.”
Consider neuromuscular disorders when a patient presents with weakness.
It’s safe to say some hospitalists might miss a neuromuscular disorder, Dr. Chang says.
“A lot of disorders that are harder for hospitalists to diagnose and that tend to take longer to call a neurologist [on] are things that are due to myasthenia gravis [a breakdown between nerves and muscles leading to muscle fatigue], myopathy, or ALS,” she says. “Many patients present with weakness. I think a lot of times there will be a lot of tests on and a lot of treatment for general medical conditions that can cause weakness.”
And that might be a case of misdirected attention. Patients with weakness accompanied by persistent swallowing problems, slurred speech with no other obvious cause, or the inability to lift their head off the bed without an obvious cause may end up with a neuromuscular diagnosis, she says.
It would be helpful to have a neurologist’s input in these cases, she says, where “nothing’s getting better, and three, four, five days later, the patient’s still weak.
“I think a neurologist would be more in tune with something like that,” she adds.
Urinary tract infections (UTIs) are not the only cause of altered mental status.
That might seem obvious, but too often, a UTI can be pegged as the source of altered mental status when it should not be, Dr. Chang says.
“We get a lot of people who come in with confusion and they have a slightly abnormal urinalysis and they diagnose them with UTI,” Dr. Chang says. “And it turns out that they actually had a stroke or they had a seizure.”
Significantly altered mentation should show a significantly abnormal urine with a positive culture, she says. “They ought to have significant laboratory support for a urinary tract infection.”
Dr. Barrett says a neurologic review of systems, or at least a neurologic exam, should be the physician’s guide.
“Those are key parts of a hospitalist’s practice,” he says, “because that’s what’s truly going to guide them to consider primary neurological causes of altered mental status.”
Take care in distinguishing aphasia from general confusion.
If a patient is still talking and is fairly fluent, that doesn’t mean they aren’t suffering from certain types of aphasia, a disorder caused by damage to parts of the brain that control language, Dr. Adelman says.
“Oftentimes, when you’re dealing with a patient with confusion, you want to make sure that it’s confusion, or encephalopathy, rather than a focal neurologic problem like aphasia,” he says. “Frequently patients with aphasia will have other symptoms such as a facial drop or weakness in the arm, but stroke can present as isolated aphasia.”
A good habit to get into is to determine whether the patient can repeat a phrase, follow a command, or name objects, he says. If they can, they probably do not have aphasia.
“The thing that you worry about with aphasia, particularly acute onset aphasia, is an ischemic stroke,” Dr. Adelman says.
A simple checklist might eliminate the need to consult the neurologist.
When Edgar Kenton, MD, now director of the stroke program at Geisinger Health System in Danville, Pa., was at Emory University Hospital in Atlanta, he found he was getting snowed under with consults from hospitalists. There were about 15 hospitalists for just one or two neurologists.
“There was no way I was able to see these patients, particularly in follow-up, because you might get five consults every day,” he says. “By the middle of the week, that’s 15 consults. You don’t get a chance to go back and see the patients because you’re just going from one consult to the other.”
The situation improved with a checklist of things to consider when a patient presents with altered mental status. Before seeking a consult, neurologists suggested the hospitalists check the electrolytes, blood pressure, and urine, and use CT scans as a screening test. That might uncover the root of the patient’s problems. If those are clear, by all means get the neurologist involved, he says.
“We were able to educate the hospitalists so they knew when to call; they knew when it was beyond their expertise to take care of the patient, so we weren’t getting called for every patient with altered mental status when all they needed to do was to check the electrolytes,” Dr. Kenton says.
Calling a neurologist earlier is way better than calling later.
Once the decision is made to consult with a neurologist, the consult should be done right away, Dr. Kenton says, not after a few days when symptoms don’t appear to be improving.
“We’ll get the call on a Friday afternoon because they thought, finally, ‘Well, you know, we need to get neurology involved because we a) haven’t solved the problem and b) there may be some other tests we should be getting,’” he says of common situations. “That has been a problem. If you don’t have a neurohospitalist involved day by day, working with the patient and the general hospitalist, neurology becomes an afterthought.”
He says accurate and early diagnosis is paramount to the patient.
“If the diagnosis is delayed, obviously there’s more insult to the patients, more persistent insult,” he says, noting the timing is particularly important in neurological conditions “because things can get bad in a hurry.”
He strongly urges hospitalists to consult with a neurologist before ordering an entire battery of tests.
At Geisinger, neurologists are encouraging hospitalists to chat informally with neurosurgeons about cases for guidance at the outset rather than after several days.
Hire a neurohospitalist if your institution doesn’t have one already.
At the top of the list of Dr. Kenton’s suggestions on caring for hospitalized neurology patients is this declaration: “Get a neurohospitalist.”
“It’s important to have the neurologist involved from the time the patient’s admitted,” he says. “That’s the value of connecting the general hospitalist with neurologists.”
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says his colleagues are team players and improve patient care.
“Neurology consultations can be called very quickly, and a nice partnership can develop between internal medicine hospitalists and neurohospitalists to care for those patients who have those medical and neurologic problems,” he says.
He also says having a neurohospitalist on board can ease some of the tension.
“No longer if there’s a neurologic condition does a hospitalist have to think about, ‘Well, does this rise to the level of something that I need to get the neurologist to drive across the city to come see?’” he explains. “‘Or is this something we should try to manage ourselves?’”
Tom Collins is a freelance writer in South Florida.
“Neurophobia” a Challenge for Hospitalists, Other Physicians
The unease that many hospitalists, internal-medicine doctors, and other providers feel about treating neurologic conditions is so readily recognized that a term has been coined to describe it: “neurophobia.”
The term has been used in published literature for at least two decades. A 2010 survey found that medical students and residents felt that neurology was the specialty they had the least knowledge about and was the one that was the most difficult.3 And trainees had the least confidence in treating patients with neurological complaints.
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says internal-medicine hospitalists are “increasingly feeling uncomfortable with requests that they have to care for patients with a wide range of primary neurologic conditions in some instances.”
That has helped lead to the emergence of neurohospitalists, he says.
John Vazquez, MD, medical director of the division hospital medicine of Emory University Hospital in Atlanta, says neurophobia is real.
“Every hospitalist has different subspecialty areas that they’re less comfortable with, and I think neurology specifically is one that does scare a lot of hospitalists,” he says. “I think on one side there are hospitalists that might ignore a neurologic problem because they don’t really know what they don’t know. On the other side are the hospitalists who I think are just concerned that they don’t know the field very well and may not feel comfortable.”
Dr. Vazquez did rotations in nephrology, pulmonology, cardiology, and rheumatology but, like many hospitalists, not neurology.
“Neurology is not one that you have to go through,” he says.
He made these suggestions:
- Know what you don’t know and get guidance when necessary.
- Do your own neurologic assessment. Even if a neurologist decides confusion is due to a patient being elderly and having a urinary tract infection, that doesn’t mean that they didn’t actually have a stroke. So if something seems not quite right, be willing to challenge the neurologist.
- Use the resources available to widen your knowledge base.
“You can utilize the consultants for your own education if you have neurologists in your hospital, and many at least have some that rotate in,” Dr. Vazquez says. “You can pick their brain on what they would do with different strokes and what’s the newest thing and ongoing treatment and whatever it is you’re concerned about.”
—Thomas R. Collins
John Vazquez, MD, of Emory University Hospital talks about neurophobia and provides tips for adjusting to the discomfort of working with neurology patients.
References
- Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39;390-396.
- Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs. time-defined TIA: a multicenter study. Neurology. 2011;77(13):1222-1228.
- Zinchuk AV, Flanagan EP, Tubridy NJ, Miller WA, McCullough LD. Attitudes of US medical trainees towards neurology education: “Neurophobia”—a global issue. BMC Med Educ. 2010;10:49.
Obituary: Laura Mirkinson, MD, MSc, FAAP
Laura Mirkinson, MD, MSc, FAAP, pediatric hospitalist and a founder of the American Academy of Pediatrics’ (AAP) Section on Hospital Medicine Executive Committee, died April 29 of ovarian cancer. She was 60.
Dr. Mirkinson received her medical degree from Uniformed Services University of the Health Sciences (USUHS) in Bethesda, Md., before serving her pediatrics residency at Bethesda Naval Hospital and Walter Reed Army Medical Center. She served as an active-duty medical officer in the U.S. Naval Medical Corps Reserves before retiring as a captain in 2000. She then worked at Children’s Hospital of Washington and the pediatric hospitalist group at Holy Cross Hospital in Silver Spring, Md.
Dr. Mirkinson played a role in the development of pediatric hospital medicine during and after her military service. In 2007, she was elected chief of pediatrics at Blythedale Children’s Hospital in Valhalla, N.Y. She also served as director of education for the AAP’s Section on Hospital Medicine and was its second chairperson, following the section’s co-founder Jack Percelay, MD, FAAP. Through this work, she helped promote the AAP Section on Hospital Medicine newsletter, as well as the Hospital Pediatrics journal.
Dr. Mirkinson’s colleagues and students remember her as a caring, insightful teacher and mentor who offered wise advice on all matters professional and personal. Her devotion to patient care was evident throughout her career. Even in her administrative roles, she would often practice clinical medicine to help fill scheduling gaps or cover other physicians’ vacations.
Laura Mirkinson, MD, MSc, FAAP, pediatric hospitalist and a founder of the American Academy of Pediatrics’ (AAP) Section on Hospital Medicine Executive Committee, died April 29 of ovarian cancer. She was 60.
Dr. Mirkinson received her medical degree from Uniformed Services University of the Health Sciences (USUHS) in Bethesda, Md., before serving her pediatrics residency at Bethesda Naval Hospital and Walter Reed Army Medical Center. She served as an active-duty medical officer in the U.S. Naval Medical Corps Reserves before retiring as a captain in 2000. She then worked at Children’s Hospital of Washington and the pediatric hospitalist group at Holy Cross Hospital in Silver Spring, Md.
Dr. Mirkinson played a role in the development of pediatric hospital medicine during and after her military service. In 2007, she was elected chief of pediatrics at Blythedale Children’s Hospital in Valhalla, N.Y. She also served as director of education for the AAP’s Section on Hospital Medicine and was its second chairperson, following the section’s co-founder Jack Percelay, MD, FAAP. Through this work, she helped promote the AAP Section on Hospital Medicine newsletter, as well as the Hospital Pediatrics journal.
Dr. Mirkinson’s colleagues and students remember her as a caring, insightful teacher and mentor who offered wise advice on all matters professional and personal. Her devotion to patient care was evident throughout her career. Even in her administrative roles, she would often practice clinical medicine to help fill scheduling gaps or cover other physicians’ vacations.
Laura Mirkinson, MD, MSc, FAAP, pediatric hospitalist and a founder of the American Academy of Pediatrics’ (AAP) Section on Hospital Medicine Executive Committee, died April 29 of ovarian cancer. She was 60.
Dr. Mirkinson received her medical degree from Uniformed Services University of the Health Sciences (USUHS) in Bethesda, Md., before serving her pediatrics residency at Bethesda Naval Hospital and Walter Reed Army Medical Center. She served as an active-duty medical officer in the U.S. Naval Medical Corps Reserves before retiring as a captain in 2000. She then worked at Children’s Hospital of Washington and the pediatric hospitalist group at Holy Cross Hospital in Silver Spring, Md.
Dr. Mirkinson played a role in the development of pediatric hospital medicine during and after her military service. In 2007, she was elected chief of pediatrics at Blythedale Children’s Hospital in Valhalla, N.Y. She also served as director of education for the AAP’s Section on Hospital Medicine and was its second chairperson, following the section’s co-founder Jack Percelay, MD, FAAP. Through this work, she helped promote the AAP Section on Hospital Medicine newsletter, as well as the Hospital Pediatrics journal.
Dr. Mirkinson’s colleagues and students remember her as a caring, insightful teacher and mentor who offered wise advice on all matters professional and personal. Her devotion to patient care was evident throughout her career. Even in her administrative roles, she would often practice clinical medicine to help fill scheduling gaps or cover other physicians’ vacations.
Movers and Shakers in Hospital Medicine

Chris Brown, MD, MPH, was elected one of Columbus Business First’s members of the Forty Under 40 class of 2013. Dr. Brown is the medical director of hospital medicine at Memorial Hospital of Union County in Marysville, Ohio. The designation recognizes members of the Columbus, Ohio, community who demonstrate superior professional development, community involvement, and other awards and recognitions. Dr. Brown’s colleagues describe him as “a collaborative, attentive, and detailed physician as well as a capable leader.”
Thomas Gallagher, MD, is the University of Washington’s (UW) new director of the program in hospital medicine. This new position in UW’s division of general internal medicine will oversee all of the hospitalist programs at UW Medicine and Harborview Medical Center in Seattle. Dr. Gallagher also is a UW professor of medicine and bioethics and humanities.
Pawan Dhawan, MD, has been appointed medical director of the hospitalist programs at Trident Medical Center in Charleston, S.C., and Summerville Medical Center in Summerville, S.C. Dr. Dhawan comes to Trident Health System from Bay Hospitalists in Newark, Del. Dr. Dhawan served on SHM’s Leadership Committee in 2011.
OB Hospitalist Group (OBHG) in Mauldin, S.C., has announced new medical directors of operations (MDOs) for five of its regions. Nicholas Kulbida, MD, MDO for OBHG’s northeast region, works at Bellevue Women’s Center in Niskayuna, N.Y. Susie Wilson, MD, one of two MDOs for the southeast region, is team leader at Summerville Medical Center in Summerville, S.C. Sue Smith, MD, the other MDO for OBHG’s southeast region, works for Winter Haven Hospital-Regency Medical Center in Winter Haven, Fla. Matthew Conrad, MD, MDO for the Great Lakes region, serves as an OB hospitalist at both Holmes Regional Medical Center in Melbourne, Fla., and Osceola Regional Medical Center in Kissimmee, Fla. Charlie Jaynes, MD, OBHG’s MDO for the south-central region, is an OB hospitalist at North Austin Medical Center in Austin, Texas, and Baylor All Saints Andrews Women’s Hospital in Fort Worth, Texas. Michael White, MD, the West Coast MDO, works as a hospitalist at Hoag Memorial Hospital in Newport Beach, Calif.
Jetinder Singh-Marjara, MD, is the new hospital medicine program director at Golden Valley Memorial Hospital in Clinton, Mo. Dr. Singh-Marjara has worked in Kansas City, Mo., and throughout the Midwest as a hospitalist for more than 10 years since completing his residency in internal medicine at the University of Illinois in Chicago.

Boghara, MD Tien Vo, MD
Fred Guyer, MD, recently was awarded the Northeast Florida Pediatric Society’s Pediatric Hospitalist of the Year award. Dr. Guyer is a hospitalist at Nemours Children’s Clinic in Jacksonville. Dr. Guyer is faculty at the University of Florida College of Medicine.
TeamHealth of Knoxville, Tenn., has announced three new medical directors.
Shelley Lenamond, DO, FHM, is the new facility medical director for TeamHealth’s hospitalist program at Methodist Mansfield Medical Center in Mansfield, Texas.
Haresh Boghara, MD, is the new facility medical director of hospitalist services at Methodist Charlton Medical Center in Dallas.
Tien Vo, MD, is TeamHealth’s new facility medical director of its hospitalist program at El Centro Regional Medical Center in El Centro, Calif.
Michael O'Neal is a freelance writer in New York.
Chris Brown, MD, MPH, was elected one of Columbus Business First’s members of the Forty Under 40 class of 2013. Dr. Brown is the medical director of hospital medicine at Memorial Hospital of Union County in Marysville, Ohio. The designation recognizes members of the Columbus, Ohio, community who demonstrate superior professional development, community involvement, and other awards and recognitions. Dr. Brown’s colleagues describe him as “a collaborative, attentive, and detailed physician as well as a capable leader.”
Thomas Gallagher, MD, is the University of Washington’s (UW) new director of the program in hospital medicine. This new position in UW’s division of general internal medicine will oversee all of the hospitalist programs at UW Medicine and Harborview Medical Center in Seattle. Dr. Gallagher also is a UW professor of medicine and bioethics and humanities.
Pawan Dhawan, MD, has been appointed medical director of the hospitalist programs at Trident Medical Center in Charleston, S.C., and Summerville Medical Center in Summerville, S.C. Dr. Dhawan comes to Trident Health System from Bay Hospitalists in Newark, Del. Dr. Dhawan served on SHM’s Leadership Committee in 2011.
OB Hospitalist Group (OBHG) in Mauldin, S.C., has announced new medical directors of operations (MDOs) for five of its regions. Nicholas Kulbida, MD, MDO for OBHG’s northeast region, works at Bellevue Women’s Center in Niskayuna, N.Y. Susie Wilson, MD, one of two MDOs for the southeast region, is team leader at Summerville Medical Center in Summerville, S.C. Sue Smith, MD, the other MDO for OBHG’s southeast region, works for Winter Haven Hospital-Regency Medical Center in Winter Haven, Fla. Matthew Conrad, MD, MDO for the Great Lakes region, serves as an OB hospitalist at both Holmes Regional Medical Center in Melbourne, Fla., and Osceola Regional Medical Center in Kissimmee, Fla. Charlie Jaynes, MD, OBHG’s MDO for the south-central region, is an OB hospitalist at North Austin Medical Center in Austin, Texas, and Baylor All Saints Andrews Women’s Hospital in Fort Worth, Texas. Michael White, MD, the West Coast MDO, works as a hospitalist at Hoag Memorial Hospital in Newport Beach, Calif.
Jetinder Singh-Marjara, MD, is the new hospital medicine program director at Golden Valley Memorial Hospital in Clinton, Mo. Dr. Singh-Marjara has worked in Kansas City, Mo., and throughout the Midwest as a hospitalist for more than 10 years since completing his residency in internal medicine at the University of Illinois in Chicago.
Boghara, MD Tien Vo, MD
Fred Guyer, MD, recently was awarded the Northeast Florida Pediatric Society’s Pediatric Hospitalist of the Year award. Dr. Guyer is a hospitalist at Nemours Children’s Clinic in Jacksonville. Dr. Guyer is faculty at the University of Florida College of Medicine.
TeamHealth of Knoxville, Tenn., has announced three new medical directors.
Shelley Lenamond, DO, FHM, is the new facility medical director for TeamHealth’s hospitalist program at Methodist Mansfield Medical Center in Mansfield, Texas.
Haresh Boghara, MD, is the new facility medical director of hospitalist services at Methodist Charlton Medical Center in Dallas.
Tien Vo, MD, is TeamHealth’s new facility medical director of its hospitalist program at El Centro Regional Medical Center in El Centro, Calif.
Michael O'Neal is a freelance writer in New York.
Chris Brown, MD, MPH, was elected one of Columbus Business First’s members of the Forty Under 40 class of 2013. Dr. Brown is the medical director of hospital medicine at Memorial Hospital of Union County in Marysville, Ohio. The designation recognizes members of the Columbus, Ohio, community who demonstrate superior professional development, community involvement, and other awards and recognitions. Dr. Brown’s colleagues describe him as “a collaborative, attentive, and detailed physician as well as a capable leader.”
Thomas Gallagher, MD, is the University of Washington’s (UW) new director of the program in hospital medicine. This new position in UW’s division of general internal medicine will oversee all of the hospitalist programs at UW Medicine and Harborview Medical Center in Seattle. Dr. Gallagher also is a UW professor of medicine and bioethics and humanities.
Pawan Dhawan, MD, has been appointed medical director of the hospitalist programs at Trident Medical Center in Charleston, S.C., and Summerville Medical Center in Summerville, S.C. Dr. Dhawan comes to Trident Health System from Bay Hospitalists in Newark, Del. Dr. Dhawan served on SHM’s Leadership Committee in 2011.
OB Hospitalist Group (OBHG) in Mauldin, S.C., has announced new medical directors of operations (MDOs) for five of its regions. Nicholas Kulbida, MD, MDO for OBHG’s northeast region, works at Bellevue Women’s Center in Niskayuna, N.Y. Susie Wilson, MD, one of two MDOs for the southeast region, is team leader at Summerville Medical Center in Summerville, S.C. Sue Smith, MD, the other MDO for OBHG’s southeast region, works for Winter Haven Hospital-Regency Medical Center in Winter Haven, Fla. Matthew Conrad, MD, MDO for the Great Lakes region, serves as an OB hospitalist at both Holmes Regional Medical Center in Melbourne, Fla., and Osceola Regional Medical Center in Kissimmee, Fla. Charlie Jaynes, MD, OBHG’s MDO for the south-central region, is an OB hospitalist at North Austin Medical Center in Austin, Texas, and Baylor All Saints Andrews Women’s Hospital in Fort Worth, Texas. Michael White, MD, the West Coast MDO, works as a hospitalist at Hoag Memorial Hospital in Newport Beach, Calif.
Jetinder Singh-Marjara, MD, is the new hospital medicine program director at Golden Valley Memorial Hospital in Clinton, Mo. Dr. Singh-Marjara has worked in Kansas City, Mo., and throughout the Midwest as a hospitalist for more than 10 years since completing his residency in internal medicine at the University of Illinois in Chicago.
Boghara, MD Tien Vo, MD
Fred Guyer, MD, recently was awarded the Northeast Florida Pediatric Society’s Pediatric Hospitalist of the Year award. Dr. Guyer is a hospitalist at Nemours Children’s Clinic in Jacksonville. Dr. Guyer is faculty at the University of Florida College of Medicine.
TeamHealth of Knoxville, Tenn., has announced three new medical directors.
Shelley Lenamond, DO, FHM, is the new facility medical director for TeamHealth’s hospitalist program at Methodist Mansfield Medical Center in Mansfield, Texas.
Haresh Boghara, MD, is the new facility medical director of hospitalist services at Methodist Charlton Medical Center in Dallas.
Tien Vo, MD, is TeamHealth’s new facility medical director of its hospitalist program at El Centro Regional Medical Center in El Centro, Calif.
Michael O'Neal is a freelance writer in New York.
SHM Fellow in Hospital Medicine Spotlight: Tosha Wetterneck, MD, MS, FACP, SFHM

Dr. Wetterneck is an associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison. She is an affiliate faculty member in the university’s department of industrial and systems engineering and a faculty researcher at the Center for Quality and Productivity Improvement. Named a senior fellow by SHM in 2012, she is a member of the society’s career satisfaction and work-life survey team and a quality-improvement (QI) mentor for the SHM-sponsored medication reconciliation QI study (MARQUIS), which is funded by the Agency for Healthcare Research and Quality (AHRQ).
Undergraduate education: University of Wisconsin at Milwaukee.
Medical school: Medical College of Wisconsin, Milwaukee.
Notable: In 2012, Dr. Wetterneck won the AMA’s Women Physicians Congress Physician Mentor Recognition Program Award. As president of the Wisconsin Medical Society, she advocates for hospitalists in AMA meetings; her current goal is to pass a resolution that focuses on care reimbursements for hospitalists. Because of her quality and safety expertise and focus on human specialized engineering, she has created a quality and safety curriculum for third- and fourth-year medical students and developed methods to proactively design hospitalist programs that prevent burnout.
FYI: Her love of dolls while growing up has inspired Dr. Wetterneck to collect all types of Raggedy Ann and Andy memorabilia.
Quotable: “The fact that SHM recognizes hospitalists is important because it recognizes those who want to stay in hospital medicine and give back to their profession.” TH
Dr. Wetterneck is an associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison. She is an affiliate faculty member in the university’s department of industrial and systems engineering and a faculty researcher at the Center for Quality and Productivity Improvement. Named a senior fellow by SHM in 2012, she is a member of the society’s career satisfaction and work-life survey team and a quality-improvement (QI) mentor for the SHM-sponsored medication reconciliation QI study (MARQUIS), which is funded by the Agency for Healthcare Research and Quality (AHRQ).
Undergraduate education: University of Wisconsin at Milwaukee.
Medical school: Medical College of Wisconsin, Milwaukee.
Notable: In 2012, Dr. Wetterneck won the AMA’s Women Physicians Congress Physician Mentor Recognition Program Award. As president of the Wisconsin Medical Society, she advocates for hospitalists in AMA meetings; her current goal is to pass a resolution that focuses on care reimbursements for hospitalists. Because of her quality and safety expertise and focus on human specialized engineering, she has created a quality and safety curriculum for third- and fourth-year medical students and developed methods to proactively design hospitalist programs that prevent burnout.
FYI: Her love of dolls while growing up has inspired Dr. Wetterneck to collect all types of Raggedy Ann and Andy memorabilia.
Quotable: “The fact that SHM recognizes hospitalists is important because it recognizes those who want to stay in hospital medicine and give back to their profession.” TH
Dr. Wetterneck is an associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison. She is an affiliate faculty member in the university’s department of industrial and systems engineering and a faculty researcher at the Center for Quality and Productivity Improvement. Named a senior fellow by SHM in 2012, she is a member of the society’s career satisfaction and work-life survey team and a quality-improvement (QI) mentor for the SHM-sponsored medication reconciliation QI study (MARQUIS), which is funded by the Agency for Healthcare Research and Quality (AHRQ).
Undergraduate education: University of Wisconsin at Milwaukee.
Medical school: Medical College of Wisconsin, Milwaukee.
Notable: In 2012, Dr. Wetterneck won the AMA’s Women Physicians Congress Physician Mentor Recognition Program Award. As president of the Wisconsin Medical Society, she advocates for hospitalists in AMA meetings; her current goal is to pass a resolution that focuses on care reimbursements for hospitalists. Because of her quality and safety expertise and focus on human specialized engineering, she has created a quality and safety curriculum for third- and fourth-year medical students and developed methods to proactively design hospitalist programs that prevent burnout.
FYI: Her love of dolls while growing up has inspired Dr. Wetterneck to collect all types of Raggedy Ann and Andy memorabilia.
Quotable: “The fact that SHM recognizes hospitalists is important because it recognizes those who want to stay in hospital medicine and give back to their profession.” TH
Nonphysician Practice Administrators More Common as Hospital Medicine Groups Expand

I can remember a time not so long ago when it was rare for me to encounter a dedicated nonphysician practice manager when visiting a hospital medicine group (HMG). Most groups had no nonphysician management support at all, or maybe just a part-time clerical person to help sort mail and post charges. In some cases, a single person supported the hospitalists and also worked with several other physician groups; this person spent only a small portion of their time with the hospitalist practice.
We all can acknowledge that most HMGs have grown much larger and more complex in recent years. SHM’s 2012 State of Hospital Medicine report suggests that one outcome of this growth is the increasing presence of nonphysician practice administrators: Fully 75% of all respondent HMGs serving adults only reported having a nonphysician administrator.
Interestingly, group size appears to have little impact on HMG administration. HMGs with four or fewer FTEs were just as likely to have an administrator as groups with 30 or more FTEs. The prevalence of administrators was highest in the South region (87%) and lowest in the West (48%). And it was highest among multistate hospitalist companies (84%) and lowest among private multispecialty or primary-care medical groups (45%).
The median time allocation for practice administrators was 1.0 FTE (the mean was 0.79 FTE). Again, very small groups are just as likely to have a full-time administrator as very large groups.
In my experience, extremely wide variation exists in nonphysician practice administrators’ roles, backgrounds, and qualifications. The survey attempted to categorize administrator roles in a meaningful way that might correlate with level of responsibility and compensation by asking about the incumbent’s management level:
- Senior management (e.g. CEO, president, executive director);
- Middle management (e.g. director, administrator, manager); or
- First-line management (e.g. supervisor or coordinator).
The majority of practice administrators were classified as middle management, as shown in Figure 1.
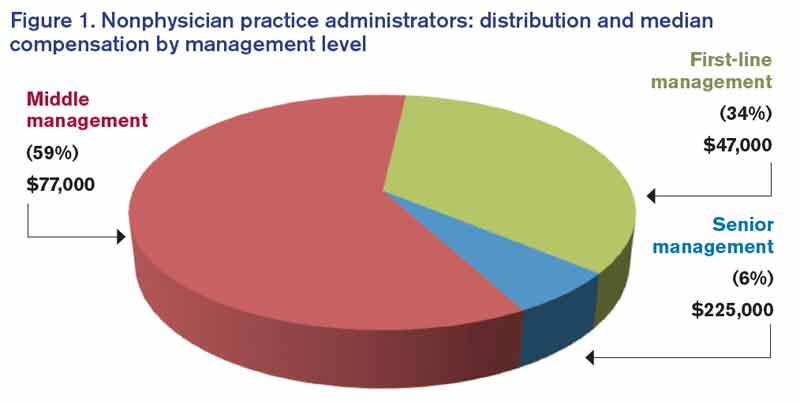
The survey collected information about compensation for practice administrators by management level. Senior management positions earned a median of $225,000 annually per FTE (though the sample size, n=10, was very small). Middle managers earned a median of $77,000, and first-line managers earned a median of $47,000.
SHM has worked diligently to reach out to nonphysician practice administrators and support them with a wide variety of tools and resources. SHM currently counts about 450 administrators as members and offers membership discounts for nonphysicians.
SHM’s Administrators’ Committee offers a series of quarterly roundtables via webinar; last year, it developed the white paper Core Competencies for a Hospitalist Practice Administrator, which can be downloaded at www.hospitalmedicine.org/Graphics/Administrators_White_Paper.pdf. And this year, for the first time, administrators became eligible for induction as Fellows in Hospital Medicine.
If you are a nonphysician practice administrator working for an HMG, or if you have one in your practice, I encourage you to get involved. Take advantage of the resources available to administrators through SHM. And please be sure that information about your administrator job gets included in the next State of Hospital Medicine survey, which will be conducted in early 2014.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM's Practice Analysis Committee.
I can remember a time not so long ago when it was rare for me to encounter a dedicated nonphysician practice manager when visiting a hospital medicine group (HMG). Most groups had no nonphysician management support at all, or maybe just a part-time clerical person to help sort mail and post charges. In some cases, a single person supported the hospitalists and also worked with several other physician groups; this person spent only a small portion of their time with the hospitalist practice.
We all can acknowledge that most HMGs have grown much larger and more complex in recent years. SHM’s 2012 State of Hospital Medicine report suggests that one outcome of this growth is the increasing presence of nonphysician practice administrators: Fully 75% of all respondent HMGs serving adults only reported having a nonphysician administrator.
Interestingly, group size appears to have little impact on HMG administration. HMGs with four or fewer FTEs were just as likely to have an administrator as groups with 30 or more FTEs. The prevalence of administrators was highest in the South region (87%) and lowest in the West (48%). And it was highest among multistate hospitalist companies (84%) and lowest among private multispecialty or primary-care medical groups (45%).
The median time allocation for practice administrators was 1.0 FTE (the mean was 0.79 FTE). Again, very small groups are just as likely to have a full-time administrator as very large groups.
In my experience, extremely wide variation exists in nonphysician practice administrators’ roles, backgrounds, and qualifications. The survey attempted to categorize administrator roles in a meaningful way that might correlate with level of responsibility and compensation by asking about the incumbent’s management level:
- Senior management (e.g. CEO, president, executive director);
- Middle management (e.g. director, administrator, manager); or
- First-line management (e.g. supervisor or coordinator).
The majority of practice administrators were classified as middle management, as shown in Figure 1.
The survey collected information about compensation for practice administrators by management level. Senior management positions earned a median of $225,000 annually per FTE (though the sample size, n=10, was very small). Middle managers earned a median of $77,000, and first-line managers earned a median of $47,000.
SHM has worked diligently to reach out to nonphysician practice administrators and support them with a wide variety of tools and resources. SHM currently counts about 450 administrators as members and offers membership discounts for nonphysicians.
SHM’s Administrators’ Committee offers a series of quarterly roundtables via webinar; last year, it developed the white paper Core Competencies for a Hospitalist Practice Administrator, which can be downloaded at www.hospitalmedicine.org/Graphics/Administrators_White_Paper.pdf. And this year, for the first time, administrators became eligible for induction as Fellows in Hospital Medicine.
If you are a nonphysician practice administrator working for an HMG, or if you have one in your practice, I encourage you to get involved. Take advantage of the resources available to administrators through SHM. And please be sure that information about your administrator job gets included in the next State of Hospital Medicine survey, which will be conducted in early 2014.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM's Practice Analysis Committee.
I can remember a time not so long ago when it was rare for me to encounter a dedicated nonphysician practice manager when visiting a hospital medicine group (HMG). Most groups had no nonphysician management support at all, or maybe just a part-time clerical person to help sort mail and post charges. In some cases, a single person supported the hospitalists and also worked with several other physician groups; this person spent only a small portion of their time with the hospitalist practice.
We all can acknowledge that most HMGs have grown much larger and more complex in recent years. SHM’s 2012 State of Hospital Medicine report suggests that one outcome of this growth is the increasing presence of nonphysician practice administrators: Fully 75% of all respondent HMGs serving adults only reported having a nonphysician administrator.
Interestingly, group size appears to have little impact on HMG administration. HMGs with four or fewer FTEs were just as likely to have an administrator as groups with 30 or more FTEs. The prevalence of administrators was highest in the South region (87%) and lowest in the West (48%). And it was highest among multistate hospitalist companies (84%) and lowest among private multispecialty or primary-care medical groups (45%).
The median time allocation for practice administrators was 1.0 FTE (the mean was 0.79 FTE). Again, very small groups are just as likely to have a full-time administrator as very large groups.
In my experience, extremely wide variation exists in nonphysician practice administrators’ roles, backgrounds, and qualifications. The survey attempted to categorize administrator roles in a meaningful way that might correlate with level of responsibility and compensation by asking about the incumbent’s management level:
- Senior management (e.g. CEO, president, executive director);
- Middle management (e.g. director, administrator, manager); or
- First-line management (e.g. supervisor or coordinator).
The majority of practice administrators were classified as middle management, as shown in Figure 1.
The survey collected information about compensation for practice administrators by management level. Senior management positions earned a median of $225,000 annually per FTE (though the sample size, n=10, was very small). Middle managers earned a median of $77,000, and first-line managers earned a median of $47,000.
SHM has worked diligently to reach out to nonphysician practice administrators and support them with a wide variety of tools and resources. SHM currently counts about 450 administrators as members and offers membership discounts for nonphysicians.
SHM’s Administrators’ Committee offers a series of quarterly roundtables via webinar; last year, it developed the white paper Core Competencies for a Hospitalist Practice Administrator, which can be downloaded at www.hospitalmedicine.org/Graphics/Administrators_White_Paper.pdf. And this year, for the first time, administrators became eligible for induction as Fellows in Hospital Medicine.
If you are a nonphysician practice administrator working for an HMG, or if you have one in your practice, I encourage you to get involved. Take advantage of the resources available to administrators through SHM. And please be sure that information about your administrator job gets included in the next State of Hospital Medicine survey, which will be conducted in early 2014.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM's Practice Analysis Committee.