User login
Drug dubbed ‘breakthrough’ for AL amyloidosis
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for the oral proteasome inhibitor ixazomib (MLN9708) to treat relapsed or refractory systemic light-chain (AL) amyloidosis.
This is the first proteasome inhibitor and the first investigational therapy for AL amyloidosis to receive breakthrough designation.
Ixazomib already has orphan drug designation in the US and the European Union for this indication and to treat multiple myeloma (MM).
The FDA’s breakthrough therapy designation is intended to expedite the development and review of new medicines to treat serious or life-threatening conditions. Compounds given the designation receive more intensive FDA guidance on an efficient drug development program and an enhanced agency commitment of senior personnel.
Breakthrough therapy designation requires preliminary clinical evidence indicating the drug may demonstrate substantial improvement on a clinically significant endpoint (or endpoints) over available therapies.
The data used to support this designation for ixazomib came from a phase 1 trial that is set to be presented at the 2014 ASH Annual Meeting as abstract 3450.
The development program for ixazomib in AL amyloidosis progressed directly from a phase 1 to a phase 3 clinical trial, TOURMALINE-AL1. Ixazomib is the first oral proteasome inhibitor to enter phase 3 clinical trials, and 4 global phase 3 trials are ongoing:
- TOURMALINE-MM1, an investigation of ixazomib vs placebo in combination with lenalidomide and dexamethasone in relapsed and/or refractory MM
- TOURMALINE-AL1, an investigation of ixazomib plus dexamethasone in patients with relapsed or refractory AL amyloidosis
- TOURMALINE-MM2, an investigation of ixazomib vs placebo in combination with lenalidomide and dexamethasone in patients with newly diagnosed MM
- TOURMALINE-MM3, an investigation of ixazomib vs placebo as maintenance therapy in patients with newly diagnosed MM following induction therapy and autologous stem cell transplant.
For additional information on the ongoing phase 3 studies, visit www.tourmalinetrials.com or www.clinicaltrials.gov. Ixazomib is under development by Millennium: the Takeda Oncology Company. ![]()
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for the oral proteasome inhibitor ixazomib (MLN9708) to treat relapsed or refractory systemic light-chain (AL) amyloidosis.
This is the first proteasome inhibitor and the first investigational therapy for AL amyloidosis to receive breakthrough designation.
Ixazomib already has orphan drug designation in the US and the European Union for this indication and to treat multiple myeloma (MM).
The FDA’s breakthrough therapy designation is intended to expedite the development and review of new medicines to treat serious or life-threatening conditions. Compounds given the designation receive more intensive FDA guidance on an efficient drug development program and an enhanced agency commitment of senior personnel.
Breakthrough therapy designation requires preliminary clinical evidence indicating the drug may demonstrate substantial improvement on a clinically significant endpoint (or endpoints) over available therapies.
The data used to support this designation for ixazomib came from a phase 1 trial that is set to be presented at the 2014 ASH Annual Meeting as abstract 3450.
The development program for ixazomib in AL amyloidosis progressed directly from a phase 1 to a phase 3 clinical trial, TOURMALINE-AL1. Ixazomib is the first oral proteasome inhibitor to enter phase 3 clinical trials, and 4 global phase 3 trials are ongoing:
- TOURMALINE-MM1, an investigation of ixazomib vs placebo in combination with lenalidomide and dexamethasone in relapsed and/or refractory MM
- TOURMALINE-AL1, an investigation of ixazomib plus dexamethasone in patients with relapsed or refractory AL amyloidosis
- TOURMALINE-MM2, an investigation of ixazomib vs placebo in combination with lenalidomide and dexamethasone in patients with newly diagnosed MM
- TOURMALINE-MM3, an investigation of ixazomib vs placebo as maintenance therapy in patients with newly diagnosed MM following induction therapy and autologous stem cell transplant.
For additional information on the ongoing phase 3 studies, visit www.tourmalinetrials.com or www.clinicaltrials.gov. Ixazomib is under development by Millennium: the Takeda Oncology Company. ![]()
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for the oral proteasome inhibitor ixazomib (MLN9708) to treat relapsed or refractory systemic light-chain (AL) amyloidosis.
This is the first proteasome inhibitor and the first investigational therapy for AL amyloidosis to receive breakthrough designation.
Ixazomib already has orphan drug designation in the US and the European Union for this indication and to treat multiple myeloma (MM).
The FDA’s breakthrough therapy designation is intended to expedite the development and review of new medicines to treat serious or life-threatening conditions. Compounds given the designation receive more intensive FDA guidance on an efficient drug development program and an enhanced agency commitment of senior personnel.
Breakthrough therapy designation requires preliminary clinical evidence indicating the drug may demonstrate substantial improvement on a clinically significant endpoint (or endpoints) over available therapies.
The data used to support this designation for ixazomib came from a phase 1 trial that is set to be presented at the 2014 ASH Annual Meeting as abstract 3450.
The development program for ixazomib in AL amyloidosis progressed directly from a phase 1 to a phase 3 clinical trial, TOURMALINE-AL1. Ixazomib is the first oral proteasome inhibitor to enter phase 3 clinical trials, and 4 global phase 3 trials are ongoing:
- TOURMALINE-MM1, an investigation of ixazomib vs placebo in combination with lenalidomide and dexamethasone in relapsed and/or refractory MM
- TOURMALINE-AL1, an investigation of ixazomib plus dexamethasone in patients with relapsed or refractory AL amyloidosis
- TOURMALINE-MM2, an investigation of ixazomib vs placebo in combination with lenalidomide and dexamethasone in patients with newly diagnosed MM
- TOURMALINE-MM3, an investigation of ixazomib vs placebo as maintenance therapy in patients with newly diagnosed MM following induction therapy and autologous stem cell transplant.
For additional information on the ongoing phase 3 studies, visit www.tourmalinetrials.com or www.clinicaltrials.gov. Ixazomib is under development by Millennium: the Takeda Oncology Company. ![]()
NICE expands use of ESAs in cancer patients

chemotherapy
Credit: Rhoda Baer
The UK’s National Institute for Health and Care Excellence (NICE) has updated its guidance to expand the use of erythropoiesis-stimulating agents (ESAs) in cancer patients.
In 2008, NICE issued a guidance recommending ESAs as a possible treatment for certain patients with anemia caused by cancer treatment.
Now, NICE has updated the recommendations to expand the use of ESAs—epoetin alfa, beta, theta, and zeta, as well as darbepoetin alfa—to all other indications within their UK marketing authorizations.
“A lot of people with cancer having chemotherapy will become anemic,” noted Carole Longson, director of the Centre for Health Technology Evaluation at NICE.
“Managing anemia often requires extra trips to the hospital and can significantly affect a person’s quality of life. This updated final guidance recommends more options, epoetin and darbepoetin, that are both clinically and cost-effective and which also significantly improve quality of life for people who develop anemia whilst having cancer therapy.”
The 2008 NICE guidance recommended erythropoietin analogues with iron injections as a possible treatment for anemia caused by cancer treatment only in:
- Women receiving platinum-based chemotherapy for cancer of the ovaries who have a blood hemoglobin level of 8 g/100 mL or lower
- Patients who have very severe anemia and cannot receive blood transfusions.
NICE’s updated final guidance recommends using darbepoetin alfa and epoetin alfa, beta, theta, and zeta within their marketing authorizations as an option for treating anemia in cancer patients undergoing chemotherapy.
Epoetin alfa (Eprex, Janssen-Cilag, and Binocrit, Sandoz), and epoetin zeta (Retacrit, Hospira UK) have UK marketing authorization to treat anemia and to reduce transfusion requirements in adult patients receiving chemotherapy for solid tumors, malignant lymphoma, or multiple myeloma, who are at risk of transfusion as assessed by the patients’ general status (eg, cardiovascular status, pre-existing anemia at the start of chemotherapy).
Binocrit and Retacrit are both biosimilar medicines referenced to Eprex. Eprex, Binocrit, and Retacrit are available in pre-filled syringes at net prices of £5.53, £4.33, and £5.66 per 1000 units, respectively.
Epoetin beta (NeoRecormon, Roche Products) and epoetin theta (Eporatio, Teva UK) have UK marketing authorization to treat symptomatic anemia in adult patients with non-myeloid malignancies who are receiving chemotherapy.
NeoRecormon is available in a pre-filled syringe at a net price of £3.51 per 500 units, and Eporatio is available in a pre-filled syringe at a net price of £5.99 per 1000 units.
Darbepoetin alfa (Aranesp, Amgen) has UK marketing authorization to treat symptomatic anemia in adult cancer patients with non-myeloid malignancies who are receiving chemotherapy. Aranesp is available in a pre-filled syringe at a net price of £14.68 per 10 micrograms.
Costs (excluding value-added tax) may vary in different settings because of negotiated procurement discounts. ![]()
chemotherapy
Credit: Rhoda Baer
The UK’s National Institute for Health and Care Excellence (NICE) has updated its guidance to expand the use of erythropoiesis-stimulating agents (ESAs) in cancer patients.
In 2008, NICE issued a guidance recommending ESAs as a possible treatment for certain patients with anemia caused by cancer treatment.
Now, NICE has updated the recommendations to expand the use of ESAs—epoetin alfa, beta, theta, and zeta, as well as darbepoetin alfa—to all other indications within their UK marketing authorizations.
“A lot of people with cancer having chemotherapy will become anemic,” noted Carole Longson, director of the Centre for Health Technology Evaluation at NICE.
“Managing anemia often requires extra trips to the hospital and can significantly affect a person’s quality of life. This updated final guidance recommends more options, epoetin and darbepoetin, that are both clinically and cost-effective and which also significantly improve quality of life for people who develop anemia whilst having cancer therapy.”
The 2008 NICE guidance recommended erythropoietin analogues with iron injections as a possible treatment for anemia caused by cancer treatment only in:
- Women receiving platinum-based chemotherapy for cancer of the ovaries who have a blood hemoglobin level of 8 g/100 mL or lower
- Patients who have very severe anemia and cannot receive blood transfusions.
NICE’s updated final guidance recommends using darbepoetin alfa and epoetin alfa, beta, theta, and zeta within their marketing authorizations as an option for treating anemia in cancer patients undergoing chemotherapy.
Epoetin alfa (Eprex, Janssen-Cilag, and Binocrit, Sandoz), and epoetin zeta (Retacrit, Hospira UK) have UK marketing authorization to treat anemia and to reduce transfusion requirements in adult patients receiving chemotherapy for solid tumors, malignant lymphoma, or multiple myeloma, who are at risk of transfusion as assessed by the patients’ general status (eg, cardiovascular status, pre-existing anemia at the start of chemotherapy).
Binocrit and Retacrit are both biosimilar medicines referenced to Eprex. Eprex, Binocrit, and Retacrit are available in pre-filled syringes at net prices of £5.53, £4.33, and £5.66 per 1000 units, respectively.
Epoetin beta (NeoRecormon, Roche Products) and epoetin theta (Eporatio, Teva UK) have UK marketing authorization to treat symptomatic anemia in adult patients with non-myeloid malignancies who are receiving chemotherapy.
NeoRecormon is available in a pre-filled syringe at a net price of £3.51 per 500 units, and Eporatio is available in a pre-filled syringe at a net price of £5.99 per 1000 units.
Darbepoetin alfa (Aranesp, Amgen) has UK marketing authorization to treat symptomatic anemia in adult cancer patients with non-myeloid malignancies who are receiving chemotherapy. Aranesp is available in a pre-filled syringe at a net price of £14.68 per 10 micrograms.
Costs (excluding value-added tax) may vary in different settings because of negotiated procurement discounts. ![]()
chemotherapy
Credit: Rhoda Baer
The UK’s National Institute for Health and Care Excellence (NICE) has updated its guidance to expand the use of erythropoiesis-stimulating agents (ESAs) in cancer patients.
In 2008, NICE issued a guidance recommending ESAs as a possible treatment for certain patients with anemia caused by cancer treatment.
Now, NICE has updated the recommendations to expand the use of ESAs—epoetin alfa, beta, theta, and zeta, as well as darbepoetin alfa—to all other indications within their UK marketing authorizations.
“A lot of people with cancer having chemotherapy will become anemic,” noted Carole Longson, director of the Centre for Health Technology Evaluation at NICE.
“Managing anemia often requires extra trips to the hospital and can significantly affect a person’s quality of life. This updated final guidance recommends more options, epoetin and darbepoetin, that are both clinically and cost-effective and which also significantly improve quality of life for people who develop anemia whilst having cancer therapy.”
The 2008 NICE guidance recommended erythropoietin analogues with iron injections as a possible treatment for anemia caused by cancer treatment only in:
- Women receiving platinum-based chemotherapy for cancer of the ovaries who have a blood hemoglobin level of 8 g/100 mL or lower
- Patients who have very severe anemia and cannot receive blood transfusions.
NICE’s updated final guidance recommends using darbepoetin alfa and epoetin alfa, beta, theta, and zeta within their marketing authorizations as an option for treating anemia in cancer patients undergoing chemotherapy.
Epoetin alfa (Eprex, Janssen-Cilag, and Binocrit, Sandoz), and epoetin zeta (Retacrit, Hospira UK) have UK marketing authorization to treat anemia and to reduce transfusion requirements in adult patients receiving chemotherapy for solid tumors, malignant lymphoma, or multiple myeloma, who are at risk of transfusion as assessed by the patients’ general status (eg, cardiovascular status, pre-existing anemia at the start of chemotherapy).
Binocrit and Retacrit are both biosimilar medicines referenced to Eprex. Eprex, Binocrit, and Retacrit are available in pre-filled syringes at net prices of £5.53, £4.33, and £5.66 per 1000 units, respectively.
Epoetin beta (NeoRecormon, Roche Products) and epoetin theta (Eporatio, Teva UK) have UK marketing authorization to treat symptomatic anemia in adult patients with non-myeloid malignancies who are receiving chemotherapy.
NeoRecormon is available in a pre-filled syringe at a net price of £3.51 per 500 units, and Eporatio is available in a pre-filled syringe at a net price of £5.99 per 1000 units.
Darbepoetin alfa (Aranesp, Amgen) has UK marketing authorization to treat symptomatic anemia in adult cancer patients with non-myeloid malignancies who are receiving chemotherapy. Aranesp is available in a pre-filled syringe at a net price of £14.68 per 10 micrograms.
Costs (excluding value-added tax) may vary in different settings because of negotiated procurement discounts. ![]()
In‐Hospital Asthma Resource Utilization
Pediatric hospitalizations for obesity‐related conditions have doubled in the last decade, mirroring the trend of higher levels of childhood obesity in the United States.[1, 2, 3] Recent studies have demonstrated worsened pediatric in‐hospital outcomes, including mortality and increased resource utilization, for children with obesity across a range of diagnoses.[4, 5, 6, 7, 8, 9, 10] Although the mechanisms driving the association between obesity and in‐hospital outcomes are not fully known, for asthma it is believed that adipocytes expressing inflammatory markers create a low level of systemic inflammation, thereby increasing the severity of allergic‐type illnesses and decreasing the response to anti‐inflammatory medications, such as steroids.[11, 12, 13, 14, 15, 16, 17, 18] The relationship of obesity and in‐hospital asthma outcomes is of particular interest because status asthmaticus is the most common reason for admission in children aged 3 to 12 years, accounting for approximately 150,000 admissions (7.4% of all hospitalizations for children and adolescents) and $835 million in hospital costs annually.[19]
Few prior studies have examined the association of obesity and asthma outcomes in the in‐hospital setting. The studies examining this association have found patients with obesity to have a longer hospital length of stay (LOS) and increased hospital costs.[8, 9, 20] Obesity has also been associated with increased respiratory treatments and supplemental oxygen requirements.[20] Associations between obesity and admission rates from the emergency department (ED) for pediatric asthma have been inconsistent.[21, 22] Most of these prior studies had several limitations in identifying patients with obesity, including using weight‐for‐age percentiles or International Classification of Diseases, Ninth Revision (ICD‐9) codes, rather than body mass index (BMI) percentile for age, the currently recommended method.[23, 24, 25] Methods other than BMI have the potential to either underestimate obesity (ie, ICD‐9 codes)[26] or to confound weight with adiposity (ie, weight‐for‐age percentiles),[27] thereby skewing the primary exposure of interest.
In the present study, we sought to examine associations between obesity and in‐hospital outcomes for pediatric status asthmaticus using the currently endorsed method for identifying obesity in children, BMI percentile for age.[23, 24, 25] The outcomes of interest included a broad range of in‐hospital measures, including resource utilization (medication and radiology use), readmission rates, billed charges, and LOS. We hypothesize that obesity, due to its proinflammatory state, would result in increased LOS, increased resource utilization, and an increased readmission rate for children admitted with status asthmaticus.
METHODS
Data Sources
Data for this retrospective cross‐sectional study were obtained from 2 sources. First, we queried the Pediatric Health Information System (PHIS) administrative database, which draws information from multiple children's hospitals to identify patients at our 2 institutions of interest who met study criteria. The PHIS database also was used to collect patient demographic data. PHIS is an administrative database operated by Children's Hospital Association (Overland Park, KS) containing clinical and billing data from 43 tertiary care, freestanding children's hospitals, including data on 41 ICD‐9 diagnoses, billed charges, and LOS. Based on the primary diagnosis, PHIS assigns each discharge to an All Patient Refined‐Diagnosis Related Group (APR‐DRG v.24) (3M Health information Systems, St. Paul, MN). APR‐DRGs allow similar diagnoses to be grouped together.[28, 29] PHIS also uses ICD‐9 codes to identify patients with a complex chronic condition (CCC).[30, 31] CCCs are those conditions that can be reasonably expected to last at least 12 months (unless death intervenes) and to involve either several different organ systems or one system severely enough to require specialty pediatric care and probably some period of hospitalization in a tertiary care center.[30, 31] PHIS data quality is ensured through a collaborative effort of the participating hospitals, the Children's Hospital Association, and Truven Healthcare.
Second, standardized chart reviews were then performed to collect clinical data not found in PHIS: BMI, LOS in hours, and medications administered, including total number of albuterol treatments administered during both the admission and the associated preceding ED visit.
Study Setting and Participants
All admissions examined in this study were at Children's Mercy Hospitals. Children's Mercy Hospitals includes 2 separate hospitals: 1 hospital is a 354‐bed academic, tertiary care freestanding children's hospital located in Kansas City, Missouri; a second, smaller, 50‐bed freestanding hospital is located in Overland Park, Kansas. Both hospitals have pediatric emergency departments. Inclusion criteria included patients aged 5 to 17 years discharged for status asthmaticus (APR‐DRG 141) at Children's Mercy Hospital from October 1, 2011 to September 30, 2012, with a recorded BMI during the admission or within 30 days of the admission. Patients between the ages of 2 and 5 years old were not included because of the incidence of viral‐induced wheezing in this age group and therefore possible miscoding of the asthma diagnosis. Exclusion criteria included a concurrent diagnosis of a CCC or bacterial pneumonia because these conditions could alter LOS, resource utilization, and readmission rates independent of the subject's status asthmaticus. In addition, to account for differences in the amount of treatment given in the pre‐inpatient setting, patients not initially treated through the hospital's ED were excluded. For patients with multiple admissions during the study period for the same diagnosis, only the index admission was examined. The institutional review board at Children's Mercy Hospital approved this study with waiver of informed consent.
Study Definitions
BMI percentile for age was used as both a continuous and categorical predictor variable. As a categorical variable it was divided into 4 categories: underweight (BMI <5%), normal weight (BMI 5%84%), overweight (BMI 85%94%), and obese (BMI 95%).[23] Race was categorized non‐Hispanic white, non‐Hispanic black, and other. Other included Asian, Pacific Islander, American Indian, and other. Ethnicity was categorized as Hispanic and non‐Hispanic. Insurance categories included private (commercial or TRICARE), public (Medicaid and Title V), and other (uninsured, self‐pay, and other). Adjusted billed charges were calculated for each hospitalization. Adjusted billed charges are the billed charges adjusted by the US Centers of Medicare and Medicaid Services' price/wage index for the study site's location.[32, 33]
To compare albuterol of different delivery methods, albuterol equivalents were calculated. Based upon prior research demonstrating equal efficacy between albuterol administered by nebulizer and metered‐dose inhaler (MDI),[34] every 2.5 mg of albuterol administered by nebulizer was treated as equivalent to 2 sprays of albuterol (90 g/spray) administered by MDI. Therefore, albuterol 2.5 mg nebulized and 2 sprays of albuterol (90 g/spray) were each defined as 1 albuterol equivalent. To compare continuous administration of nebulized albuterol with intermittent administration of albuterol, the total milligrams of continuously nebulized albuterol were examined. Per protocol at the study site, 10 mg per hour of continuous albuterol are administered for patients 5 years and younger and, for children 6 years and older, 15 mg per hour of continuous albuterol are administered. Based upon milligrams of albuterol nebulized, 5‐year‐old subjects receiving an hour of continuous albuterol would equal 4 albuterol equivalents (or 4 treatments of nebulized albuterol 2.5 mg/treatment or 4 treatments of albuterol 90 g/spray 2 sprays/treatment); for patients 6 years and older, an hour of continuous albuterol would equal 6 albuterol equivalents (or 6 treatments of nebulized albuterol 2.5 mg/treatment or 6 treatments of albuterol 90 g/spray 2 sprays/treatment). The variable total albuterol was then created to include albuterol equivalents delivered by metered dose inhaler and as both single and continuous nebulized treatments.
Main Exposure
The main exposure of interest was BMI percentile for age.
Outcome Measures
The main outcome measure was inpatient LOS measured in hours. Secondary outcome measures included the total albuterol (in the inpatient setting as well as combined inpatient and ED settings) and the administration of intravenous IV fluids and intramuscular (IM) or IV systemic steroids. Other secondary measures included readmission for status asthmaticus during the study period, adjusted billed charges, and inpatient chest radiograph utilization.
Statistical Analyses
We summarized categorical variables with frequencies and percentages, and used [2] test across BMI categories. The non‐normal distribution of continuous dependent variables (LOS, number of albuterol treatments, billed charges) were summarized with medians and interquartile ranges (IQRs). Kruskal‐Wallis test was used to examine outcomes across BMI categories. For regression models, BMI percentile for age was divided into deciles and treated as a continuous predictor. Factors used in the regression models included age, gender, race, ethnicity, and insurance. Total albuterol received in the ED was also included in the model to adjust for differences in the amount of treatment received prior to admission. Incidence rate ratios were created using Poisson regression for continuous outcomes (LOS, billed charges, and number of albuterol equivalent treatments administered), and odds ratios were created using logistic regression for dichotomous outcomes. All statistical analyses were performed using IBM SPSS Statistics version 20 (IBM, Armonk, NY), and P values <0.05 were considered statistically significant.
RESULTS
Patient Characteristics
Of 788 patients admitted for status asthmaticus during the study period, 518 (65.7%) met inclusion criteria; 42 (5.3%) did not meet inclusion criteria due to lack of a documented BMI (Table 1). Most patients were normal weight (59.7%). Approximately one‐third (36.7%) were either overweight or obese. The median age was 8 years, with patients with obesity being significantly older than underweight patients (9 vs 7.5 years, P<0.001). The majority of patients were black/African American (56.9%) and non‐Hispanic (88.6%). The percentage of patients who were obese was higher in patients of other race (29.3%) than whites (20.2%) or blacks (16.3%) (P<0.05). Patients of Hispanic ethnicity had a higher rate of obesity compared to non‐Hispanic patients (37.3% vs 17.4%, P<0.01). There were no differences in BMI categories for insurance.
| Patient Characteristics | Total | Category of Body Mass Index Percentile for Age | ||||
|---|---|---|---|---|---|---|
| Underweight | Normal | Overweight | Obese | P* | ||
| ||||||
| Total patients, n (%) | 518 | 18 (3.5) | 310 (59.8) | 88 (17.0) | 102 (19.7) | |
| Age, y, median (IQR) | 8 (611) | 7.5 (5.89) | 8 (610) | 8 (610) | 9 (712) | <0.001 |
| Gender, n (%) | ||||||
| Male | 309 | 12 (3.9) | 184 (59.5) | 46 (14.9) | 67 (21.7) | 0.27 |
| Female | 209 | 6 (2.9) | 126 (60.3) | 42 (20.1) | 35 (16.7) | |
| Race, n (%) | ||||||
| Non‐Hispanic white | 124 | 8 (6.5) | 76 (61.3) | 15 (12.1) | 25 (20.2) | 0.021 |
| Non‐Hispanic black | 295 | 7 (2.4) | 182 (61.7) | 58 (19.7) | 48 (16.3) | |
| Other | 99 | 3 (3.0) | 52 (52.5) | 15 (15.2) | 29 (29.3) | |
| Ethnicity, n (%) | ||||||
| Hispanic | 59 | 1 (1.7) | 25 (42.4) | 11 (18.6) | 22 (37.3) | 0.002 |
| Non‐Hispanic | 459 | 17 (3.7) | 285 (62.1) | 77 (16.8) | 80 (17.4) | |
| Insurance, n (%) | ||||||
| Private | 163 | 10 (6.1) | 97 (59.5) | 28 (17.2) | 28 (17.2) | 0.48 |
| Public | 313 | 7 (2.2) | 190 (60.7) | 51 (16.3) | 65 (20.8) | |
| Other | 42 | 1 (2.4) | 23 (54.8) | 9 (21.4) | 9 (21.4) | |
LOS and Resource Utilization
The median LOS for all patients was approximately 1 day (Table 2). The median number of albuterol treatments in the inpatient setting was 14 (IQR, 824). When albuterol treatments given in the ED were included, the median number of treatments increased to 38 (IQR, 2848). Approximately one‐half of patients required supplemental oxygen, one‐third received IV fluids, and one‐fifth received either IV or IM steroids (with all but 1.6% of the remaining patients receiving oral steroids). Less than 5% of the study population received magnesium sulfate, epinephrine, required intensive care unit (ICU) admission, or were readmitted for status asthmaticus within 30 days. Approximately 15% of patients received a chest radiograph. The median adjusted billed charge was approximately $7,000. There were no differences in any of these outcomes by BMI category (P>0.05).
| Total | Body Mass Index Category | ||||
|---|---|---|---|---|---|
| Underweight | Normal | Overweight | Obese | ||
| |||||
| Total Patients, n (%) | 518 | 18 (3.5) | 310 (59.8) | 88 (17.0) | 102 (19.7) |
| LOS, h, median (IQR) | 26 (1841) | 41 (19.560.5) | 26 (1841) | 26 (19.2540) | 31 (1942) |
| Inpatient albuterol equivalents, median (IQR) | 14(824) | 19 (9.528) | 14 (824) | 14 (8.522) | 16 (824) |
| Total albuterol equivalents, median (IQR) | 38 (2848) | 34 (2734) | 36 (2848) | 37 (2849.5) | 40 (3052) |
| Adjusted billed charges, $, median (IQR) | 6,999.5 (52929258) | 7,457 (56048536) | 6876 (52379390) | 7056 (54099061) | 7198 (53319306) |
| All readmits, n (%) | 44 (8.5) | 2 (11.1) | 29 (9.4) | 7 (8.0) | 6 (5.9) |
| Readmits within 30 days, n (%) | 11 (2.1) | 1 (5.6) | 7 (2.3) | 1 (1.1) | 2 (2.0) |
| ICU admissions, n (%) | 24 (4.6) | 0 (0) | 13 (4.2) | 7 (8.0) | 4 (3.9) |
| Chest radiograph, n (%) | 64 (12.4) | 5 (27.8) | 34 (11.0) | 12 (13.6) | 13 (12.7) |
| Oxygen, n (%) | 255 (49.2) | 11 (61.1) | 157 (50.6) | 42 (47.7) | 45 (44.1) |
| IV/IM steroid, n (%) | 93 (18.0) | 2 (11.1) | 53 (17.1) | 18 (20.5) | 20 (19.6) |
| Epinephrine, n (%) | 2 (0.4) | 0 (0) | 2 (0.6) | 0 (0) | 0 (0) |
| Magnesium, n (%) | 15 (2.9) | 0 (0) | 8 (2.6) | 3 (3.4) | 4 (3.9) |
| IV fluids, n (%) | 152 (29.3) | 4 (22.2) | 85 (27.4) | 31 (35.2) | 32 (31.4) |
Multivariable Results
After adjusting for age, gender, race, ethnicity, and insurance, the decile of BMI percentile for age showed a small negative association with LOS. Specifically, for each decile increase for BMI percentile for age, LOS decreased by approximately 2%. BMI percentile for age was not associated with other measures of resource utilization including total albuterol use, adjusted billed charges, readmission, ICU care, receipt of supplemental oxygen or a chest radiograph, IV fluids, or other medications (IV/IM steroids, epinephrine, or magnesium sulfate).
DISCUSSION
Our study suggests that the decile of BMI percentile for age is inversely associated with LOS but did not have a clinically meaningful effect. Secondary measures, such as total albuterol needs and adjusted billed charges, did not show an association with BMI percentile for age. There were also no associations between BMI percentile for age and other resource utilization outcomes.
Our findings differ from previous studies examining in‐hospital status asthmaticus in children who are overweight or obese. In addition, the present study was able to adjust for therapies received prior to admission. Carroll et al. demonstrated an increased LOS of approximately 3 days for overweight or obese asthmatics admitted to the ICU with status asthmaticus as well as increased duration of supplemental oxygen, continuous albuterol, and intravenous steroids.[20] It is possible that differences in methodology (ie, weight‐for‐age percentile vs BMI percentile for age, inclusion of ED treatments), different thresholds for treatment of status asthmaticus outside the ICU, or differences in patient populations studied (ie, only ICU patients vs all in‐hospital patients) explain the difference between their findings and the present study. The present study's use of BMI percentile for age follows current recommendations for classifying a patient as obese or overweight.[23, 24, 25] However, the use of classifications other than BMI percentile for age would tend to bias toward the null hypothesis, whereas in Carroll's study children who were overweight or obese had increased resource utilization. Additionally, in the time frame between this publication and the current study, many hospitals worked to standardize asthma hospitalizations by creating weaning protocols for albuterol, thereby decreasing LOS for all asthmatics, which may also affect the differences in LOS between groups of obese and nonobese patients.[35]
Woolford et al. found approximately a one‐half‐day increase in LOS and $2,000 higher mean charges for patients admitted with status asthmaticus and a secondary diagnosis of obesity.[8, 9] Study location and differing methods for defining obesity may account for the discrepancy between Woolford's findings and our study. We examined children admitted to the inpatient floor of a tertiary care children's hospital compared to Woolford et al.'s examination of pediatric patients admitted to all hospitals via the Kids' Inpatient Database (Healthcare Cost and Utilization Project, Agency for Healthcare Research and Quality). That study also relied on the coding of obesity as an ICD‐9 diagnosis, rather than examining the BMI of all admitted patients. Previous research has demonstrated that relying on a coded diagnosis of obesity is not as sensitive as measurement.[26] By relying on ICD‐9 diagnosis coding, only patients with very high BMIs may be diagnosed with obesity during the admission and therefore only associations between very high BMI and status asthmaticus will be examined.
There are several limitations to our findings. First, our study was limited to a single, tertiary care children's hospital and may not be generalizable to other hospitals. Our hospital standardizes the treatment of inpatient status asthmatics by formation of a respiratory care plan, involving interval scoring of respiratory symptoms and automatic spacing of albuterol treatments. This likely minimizes physician‐to‐physician variation. Second, we included only those patients who were initially treated within the ED associated with the admitting hospital to minimize the effects of timing for treatments prior to admittance. This excluded those patients first cared for by their primary care physician or by an outlying ED. Therefore, our sample may be biased toward a study population less connected to a medical home and therefore possibly poorer asthma control. Third, to utilize the most accurate method to define obesity, we excluded approximately 5% of eligible patients because BMI was unavailable. This may have included children with more severe asthma symptoms, as a height measurement may have been deferred due to their higher acuity. Asthma severity or chronicity would be associated with our outcomes of interest. However, we were unable to collect reliable data on severity or chronicity. Finally, to measure the amount of total albuterol needed by a patient during the ED and inpatient admissions, albuterol treatments delivered by MDI, nebulizer, or continuously were converted into total albuterol. Although based upon total milligram dosing and studies comparing routes of albuterol administration,[34] the validity of this conversion is unknown.
CONCLUSION
Although BMI percentile for age is inversely associated with LOS for in‐hospital pediatric status asthmaticus, the impact of BMI on this outcome likely is not clinically meaningful. Future investigations should examine other elements of BMI and in‐hospital status asthmaticus, such as any associations between BMI and admission rates.
Acknowledgements
The authors offer their appreciation to their research assistant, Amy Lee, for her support and dedication to this project.
Disclosures
Internal funds from Children's Mercy Hospital and Clinics supported the conduct of this work. The authors report no conflicts of interest.
- , , . Incidence of childhood obesity in the United States. N Engl J Med. 2014;370(5):403–411.
- , . Prevalence and trends in obesity and severe obesity among children in the United States, 1999–2012. JAMA Pediatr. 2014;168(6):561–566.
- , , , . Effects of childhood obesity on hospital care and costs, 1999–2005. Health Affairs. 2009;28(4):w751–w760.
- , , , , . Influence of obesity on clinical outcomes in hospitalized children: a systematic review. JAMA Pediatr. 2013;167(5):476–482.
- , . Appendicitis in the obese child. J Pediatr Surg. 2007;42(5):857–861.
- , , , , . Obesity: influence on length of hospital stay for the pediatric burn patient. J Burn Care Res. 2010;31(2):251–256.
- , , , , , . The impact of obesity on severely injured children and adolescents. J Pediatr Surg. 2006;41(1):88–91.
- , , , . Incremental hospital charges associated with obesity as a secondary diagnosis in children. Obesity (Silver Spring). 2007;15(7):1895–1901.
- , , , . Persistent gap of incremental charges for obesity as a secondary diagnosis in common pediatric hospitalizations. J Hosp Med. 2009;4(3):149–156.
- , , , . Resource utilization and expenditures for overweight and obese children. Arch Pediatr Adolesc Med. 2007;161(1):11–14.
- , , , , , . Decreased response to inhaled steroids in overweight and obese asthmatic children. J Allergy Clin Immunol. 2011;127(3):741–749.
- , , , , . Body mass and glucocorticoid response in asthma. Am J Respir Crit Care Med. 2008;178(7):682–687.
- , , , ; National Heart, Lung, and Blood Institute's Asthma Clinical Research Network. Body mass index and phenotype in subjects with mild‐to‐moderate persistent asthma. J Allergy Clin Immunol. 2009;123(6):1328–1334.e1.
- , . Obesity and asthma disease phenotypes. Curr Opin Allergy Clin Immunol. 2012;12(1):76–81.
- , . Obesity and the lung: 4. Obesity and asthma. Thorax. 2008;63(11):1018–1023.
- , , , et al. Body mass index and response to asthma therapy: fluticasone propionate/salmeterol versus montelukast. J Asthma. 2010;47(1):76–82.
- , , , et al. Effect of obesity on clinical presentation and response to treatment in asthma. J Asthma. 2006;43(7):553–558.
- , , , . Asthma and obesity in three‐year‐old urban children: role of sex and home environment. J Pediatr. 2011;159(1):14–20.
- , , , . Care of Children and Adolescents in U.S. Hospitals. Rockville, MD: Agency for Healthcare Research and Quality; 2003. Available at: http://archive.ahrq.gov/data/hcup/factbk4/factbk4.pdf. Accessed February 12, 2014.
- , , , . Childhood obesity increases duration of therapy during severe asthma exacerbations. Pediatr Crit Care Med. 2006;7(6):527–531.
- , , , , . Childhood overweight increases hospital admission rates for asthma. Pediatr. 2007;120(4):734–740.
- , , , . Body mass index and acute asthma severity among children presenting to the emergency department. Pediatr Allergy Immunol. 2009;21(3):480–488.
- Centers for Disease Control and Prevention. Basics about childhood obesity. Available at: http://www.cdc.gov/obesity/childhood/basics.html. Accessed February 12, 2014.
- . Screening and interventions for childhood overweight: a summary of evidence for the US Preventive Services Task Force. Pediatrics. 2005;116(1):e125–e144.
- ; Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics. 2007;120(suppl 4):S164–S192.
- , , , . Comparison of ICD code‐based diagnosis of obesity with measured obesity in children and the implications for health care cost estimates. BMC Med Res Methodol. 2011;11(1):173.
- , ; American Academy of Pediatrics Committee on Nutrition. Prevention of pediatric overweight and obesity. Pediatrics. 2003;112(2):424–430.
- . Development of the 3M all patient‐refined diagnosis‐related groups (APR DRGs). Available at: http//www.ahrq.gov/legacy/qual/mortality/Hughes3.htm. Accessed March 1, 2014.
- . 3M Health Information Systems (HIS) APR‐DRG classification software: overview. Available at: http://www.ahrq.gov/legacy/qual/mortality/Hughessumm.htm. Accessed March 1, 2014.
- , , , , . Shifting place of death among children with complex chronic conditions in the United States, 1989–2003. JAMA. 2007;297(24):2725–2732.
- , , . Pediatric deaths attributable to complex chronic conditions: a population‐based study of Washington State, 1980–1997. Pediatrics. 2000;106(1 pt 2):205–209.
- , , , et al. Comparative effectiveness of pleural drainage procedures for the treatment of complicated pneumonia in childhood. J Hosp Med. 2011;6(5):256–263.
- , , , , , . Adjunct corticosteroids in children hospitalized with community‐acquired pneumonia. Pediatrics. 2011;127(2):e255–e263.
- , , . Holding chambers (spacers) versus nebulisers for beta‐agonist treatment of acute asthma. Cochrane Database Syst Rev. 2013;9:CD000052.
- , , , . Effectiveness of a clinical pathway for inpatient asthma management. Pediatrics. 2000;106(5):1006–1012.
Pediatric hospitalizations for obesity‐related conditions have doubled in the last decade, mirroring the trend of higher levels of childhood obesity in the United States.[1, 2, 3] Recent studies have demonstrated worsened pediatric in‐hospital outcomes, including mortality and increased resource utilization, for children with obesity across a range of diagnoses.[4, 5, 6, 7, 8, 9, 10] Although the mechanisms driving the association between obesity and in‐hospital outcomes are not fully known, for asthma it is believed that adipocytes expressing inflammatory markers create a low level of systemic inflammation, thereby increasing the severity of allergic‐type illnesses and decreasing the response to anti‐inflammatory medications, such as steroids.[11, 12, 13, 14, 15, 16, 17, 18] The relationship of obesity and in‐hospital asthma outcomes is of particular interest because status asthmaticus is the most common reason for admission in children aged 3 to 12 years, accounting for approximately 150,000 admissions (7.4% of all hospitalizations for children and adolescents) and $835 million in hospital costs annually.[19]
Few prior studies have examined the association of obesity and asthma outcomes in the in‐hospital setting. The studies examining this association have found patients with obesity to have a longer hospital length of stay (LOS) and increased hospital costs.[8, 9, 20] Obesity has also been associated with increased respiratory treatments and supplemental oxygen requirements.[20] Associations between obesity and admission rates from the emergency department (ED) for pediatric asthma have been inconsistent.[21, 22] Most of these prior studies had several limitations in identifying patients with obesity, including using weight‐for‐age percentiles or International Classification of Diseases, Ninth Revision (ICD‐9) codes, rather than body mass index (BMI) percentile for age, the currently recommended method.[23, 24, 25] Methods other than BMI have the potential to either underestimate obesity (ie, ICD‐9 codes)[26] or to confound weight with adiposity (ie, weight‐for‐age percentiles),[27] thereby skewing the primary exposure of interest.
In the present study, we sought to examine associations between obesity and in‐hospital outcomes for pediatric status asthmaticus using the currently endorsed method for identifying obesity in children, BMI percentile for age.[23, 24, 25] The outcomes of interest included a broad range of in‐hospital measures, including resource utilization (medication and radiology use), readmission rates, billed charges, and LOS. We hypothesize that obesity, due to its proinflammatory state, would result in increased LOS, increased resource utilization, and an increased readmission rate for children admitted with status asthmaticus.
METHODS
Data Sources
Data for this retrospective cross‐sectional study were obtained from 2 sources. First, we queried the Pediatric Health Information System (PHIS) administrative database, which draws information from multiple children's hospitals to identify patients at our 2 institutions of interest who met study criteria. The PHIS database also was used to collect patient demographic data. PHIS is an administrative database operated by Children's Hospital Association (Overland Park, KS) containing clinical and billing data from 43 tertiary care, freestanding children's hospitals, including data on 41 ICD‐9 diagnoses, billed charges, and LOS. Based on the primary diagnosis, PHIS assigns each discharge to an All Patient Refined‐Diagnosis Related Group (APR‐DRG v.24) (3M Health information Systems, St. Paul, MN). APR‐DRGs allow similar diagnoses to be grouped together.[28, 29] PHIS also uses ICD‐9 codes to identify patients with a complex chronic condition (CCC).[30, 31] CCCs are those conditions that can be reasonably expected to last at least 12 months (unless death intervenes) and to involve either several different organ systems or one system severely enough to require specialty pediatric care and probably some period of hospitalization in a tertiary care center.[30, 31] PHIS data quality is ensured through a collaborative effort of the participating hospitals, the Children's Hospital Association, and Truven Healthcare.
Second, standardized chart reviews were then performed to collect clinical data not found in PHIS: BMI, LOS in hours, and medications administered, including total number of albuterol treatments administered during both the admission and the associated preceding ED visit.
Study Setting and Participants
All admissions examined in this study were at Children's Mercy Hospitals. Children's Mercy Hospitals includes 2 separate hospitals: 1 hospital is a 354‐bed academic, tertiary care freestanding children's hospital located in Kansas City, Missouri; a second, smaller, 50‐bed freestanding hospital is located in Overland Park, Kansas. Both hospitals have pediatric emergency departments. Inclusion criteria included patients aged 5 to 17 years discharged for status asthmaticus (APR‐DRG 141) at Children's Mercy Hospital from October 1, 2011 to September 30, 2012, with a recorded BMI during the admission or within 30 days of the admission. Patients between the ages of 2 and 5 years old were not included because of the incidence of viral‐induced wheezing in this age group and therefore possible miscoding of the asthma diagnosis. Exclusion criteria included a concurrent diagnosis of a CCC or bacterial pneumonia because these conditions could alter LOS, resource utilization, and readmission rates independent of the subject's status asthmaticus. In addition, to account for differences in the amount of treatment given in the pre‐inpatient setting, patients not initially treated through the hospital's ED were excluded. For patients with multiple admissions during the study period for the same diagnosis, only the index admission was examined. The institutional review board at Children's Mercy Hospital approved this study with waiver of informed consent.
Study Definitions
BMI percentile for age was used as both a continuous and categorical predictor variable. As a categorical variable it was divided into 4 categories: underweight (BMI <5%), normal weight (BMI 5%84%), overweight (BMI 85%94%), and obese (BMI 95%).[23] Race was categorized non‐Hispanic white, non‐Hispanic black, and other. Other included Asian, Pacific Islander, American Indian, and other. Ethnicity was categorized as Hispanic and non‐Hispanic. Insurance categories included private (commercial or TRICARE), public (Medicaid and Title V), and other (uninsured, self‐pay, and other). Adjusted billed charges were calculated for each hospitalization. Adjusted billed charges are the billed charges adjusted by the US Centers of Medicare and Medicaid Services' price/wage index for the study site's location.[32, 33]
To compare albuterol of different delivery methods, albuterol equivalents were calculated. Based upon prior research demonstrating equal efficacy between albuterol administered by nebulizer and metered‐dose inhaler (MDI),[34] every 2.5 mg of albuterol administered by nebulizer was treated as equivalent to 2 sprays of albuterol (90 g/spray) administered by MDI. Therefore, albuterol 2.5 mg nebulized and 2 sprays of albuterol (90 g/spray) were each defined as 1 albuterol equivalent. To compare continuous administration of nebulized albuterol with intermittent administration of albuterol, the total milligrams of continuously nebulized albuterol were examined. Per protocol at the study site, 10 mg per hour of continuous albuterol are administered for patients 5 years and younger and, for children 6 years and older, 15 mg per hour of continuous albuterol are administered. Based upon milligrams of albuterol nebulized, 5‐year‐old subjects receiving an hour of continuous albuterol would equal 4 albuterol equivalents (or 4 treatments of nebulized albuterol 2.5 mg/treatment or 4 treatments of albuterol 90 g/spray 2 sprays/treatment); for patients 6 years and older, an hour of continuous albuterol would equal 6 albuterol equivalents (or 6 treatments of nebulized albuterol 2.5 mg/treatment or 6 treatments of albuterol 90 g/spray 2 sprays/treatment). The variable total albuterol was then created to include albuterol equivalents delivered by metered dose inhaler and as both single and continuous nebulized treatments.
Main Exposure
The main exposure of interest was BMI percentile for age.
Outcome Measures
The main outcome measure was inpatient LOS measured in hours. Secondary outcome measures included the total albuterol (in the inpatient setting as well as combined inpatient and ED settings) and the administration of intravenous IV fluids and intramuscular (IM) or IV systemic steroids. Other secondary measures included readmission for status asthmaticus during the study period, adjusted billed charges, and inpatient chest radiograph utilization.
Statistical Analyses
We summarized categorical variables with frequencies and percentages, and used [2] test across BMI categories. The non‐normal distribution of continuous dependent variables (LOS, number of albuterol treatments, billed charges) were summarized with medians and interquartile ranges (IQRs). Kruskal‐Wallis test was used to examine outcomes across BMI categories. For regression models, BMI percentile for age was divided into deciles and treated as a continuous predictor. Factors used in the regression models included age, gender, race, ethnicity, and insurance. Total albuterol received in the ED was also included in the model to adjust for differences in the amount of treatment received prior to admission. Incidence rate ratios were created using Poisson regression for continuous outcomes (LOS, billed charges, and number of albuterol equivalent treatments administered), and odds ratios were created using logistic regression for dichotomous outcomes. All statistical analyses were performed using IBM SPSS Statistics version 20 (IBM, Armonk, NY), and P values <0.05 were considered statistically significant.
RESULTS
Patient Characteristics
Of 788 patients admitted for status asthmaticus during the study period, 518 (65.7%) met inclusion criteria; 42 (5.3%) did not meet inclusion criteria due to lack of a documented BMI (Table 1). Most patients were normal weight (59.7%). Approximately one‐third (36.7%) were either overweight or obese. The median age was 8 years, with patients with obesity being significantly older than underweight patients (9 vs 7.5 years, P<0.001). The majority of patients were black/African American (56.9%) and non‐Hispanic (88.6%). The percentage of patients who were obese was higher in patients of other race (29.3%) than whites (20.2%) or blacks (16.3%) (P<0.05). Patients of Hispanic ethnicity had a higher rate of obesity compared to non‐Hispanic patients (37.3% vs 17.4%, P<0.01). There were no differences in BMI categories for insurance.
| Patient Characteristics | Total | Category of Body Mass Index Percentile for Age | ||||
|---|---|---|---|---|---|---|
| Underweight | Normal | Overweight | Obese | P* | ||
| ||||||
| Total patients, n (%) | 518 | 18 (3.5) | 310 (59.8) | 88 (17.0) | 102 (19.7) | |
| Age, y, median (IQR) | 8 (611) | 7.5 (5.89) | 8 (610) | 8 (610) | 9 (712) | <0.001 |
| Gender, n (%) | ||||||
| Male | 309 | 12 (3.9) | 184 (59.5) | 46 (14.9) | 67 (21.7) | 0.27 |
| Female | 209 | 6 (2.9) | 126 (60.3) | 42 (20.1) | 35 (16.7) | |
| Race, n (%) | ||||||
| Non‐Hispanic white | 124 | 8 (6.5) | 76 (61.3) | 15 (12.1) | 25 (20.2) | 0.021 |
| Non‐Hispanic black | 295 | 7 (2.4) | 182 (61.7) | 58 (19.7) | 48 (16.3) | |
| Other | 99 | 3 (3.0) | 52 (52.5) | 15 (15.2) | 29 (29.3) | |
| Ethnicity, n (%) | ||||||
| Hispanic | 59 | 1 (1.7) | 25 (42.4) | 11 (18.6) | 22 (37.3) | 0.002 |
| Non‐Hispanic | 459 | 17 (3.7) | 285 (62.1) | 77 (16.8) | 80 (17.4) | |
| Insurance, n (%) | ||||||
| Private | 163 | 10 (6.1) | 97 (59.5) | 28 (17.2) | 28 (17.2) | 0.48 |
| Public | 313 | 7 (2.2) | 190 (60.7) | 51 (16.3) | 65 (20.8) | |
| Other | 42 | 1 (2.4) | 23 (54.8) | 9 (21.4) | 9 (21.4) | |
LOS and Resource Utilization
The median LOS for all patients was approximately 1 day (Table 2). The median number of albuterol treatments in the inpatient setting was 14 (IQR, 824). When albuterol treatments given in the ED were included, the median number of treatments increased to 38 (IQR, 2848). Approximately one‐half of patients required supplemental oxygen, one‐third received IV fluids, and one‐fifth received either IV or IM steroids (with all but 1.6% of the remaining patients receiving oral steroids). Less than 5% of the study population received magnesium sulfate, epinephrine, required intensive care unit (ICU) admission, or were readmitted for status asthmaticus within 30 days. Approximately 15% of patients received a chest radiograph. The median adjusted billed charge was approximately $7,000. There were no differences in any of these outcomes by BMI category (P>0.05).
| Total | Body Mass Index Category | ||||
|---|---|---|---|---|---|
| Underweight | Normal | Overweight | Obese | ||
| |||||
| Total Patients, n (%) | 518 | 18 (3.5) | 310 (59.8) | 88 (17.0) | 102 (19.7) |
| LOS, h, median (IQR) | 26 (1841) | 41 (19.560.5) | 26 (1841) | 26 (19.2540) | 31 (1942) |
| Inpatient albuterol equivalents, median (IQR) | 14(824) | 19 (9.528) | 14 (824) | 14 (8.522) | 16 (824) |
| Total albuterol equivalents, median (IQR) | 38 (2848) | 34 (2734) | 36 (2848) | 37 (2849.5) | 40 (3052) |
| Adjusted billed charges, $, median (IQR) | 6,999.5 (52929258) | 7,457 (56048536) | 6876 (52379390) | 7056 (54099061) | 7198 (53319306) |
| All readmits, n (%) | 44 (8.5) | 2 (11.1) | 29 (9.4) | 7 (8.0) | 6 (5.9) |
| Readmits within 30 days, n (%) | 11 (2.1) | 1 (5.6) | 7 (2.3) | 1 (1.1) | 2 (2.0) |
| ICU admissions, n (%) | 24 (4.6) | 0 (0) | 13 (4.2) | 7 (8.0) | 4 (3.9) |
| Chest radiograph, n (%) | 64 (12.4) | 5 (27.8) | 34 (11.0) | 12 (13.6) | 13 (12.7) |
| Oxygen, n (%) | 255 (49.2) | 11 (61.1) | 157 (50.6) | 42 (47.7) | 45 (44.1) |
| IV/IM steroid, n (%) | 93 (18.0) | 2 (11.1) | 53 (17.1) | 18 (20.5) | 20 (19.6) |
| Epinephrine, n (%) | 2 (0.4) | 0 (0) | 2 (0.6) | 0 (0) | 0 (0) |
| Magnesium, n (%) | 15 (2.9) | 0 (0) | 8 (2.6) | 3 (3.4) | 4 (3.9) |
| IV fluids, n (%) | 152 (29.3) | 4 (22.2) | 85 (27.4) | 31 (35.2) | 32 (31.4) |
Multivariable Results
After adjusting for age, gender, race, ethnicity, and insurance, the decile of BMI percentile for age showed a small negative association with LOS. Specifically, for each decile increase for BMI percentile for age, LOS decreased by approximately 2%. BMI percentile for age was not associated with other measures of resource utilization including total albuterol use, adjusted billed charges, readmission, ICU care, receipt of supplemental oxygen or a chest radiograph, IV fluids, or other medications (IV/IM steroids, epinephrine, or magnesium sulfate).
DISCUSSION
Our study suggests that the decile of BMI percentile for age is inversely associated with LOS but did not have a clinically meaningful effect. Secondary measures, such as total albuterol needs and adjusted billed charges, did not show an association with BMI percentile for age. There were also no associations between BMI percentile for age and other resource utilization outcomes.
Our findings differ from previous studies examining in‐hospital status asthmaticus in children who are overweight or obese. In addition, the present study was able to adjust for therapies received prior to admission. Carroll et al. demonstrated an increased LOS of approximately 3 days for overweight or obese asthmatics admitted to the ICU with status asthmaticus as well as increased duration of supplemental oxygen, continuous albuterol, and intravenous steroids.[20] It is possible that differences in methodology (ie, weight‐for‐age percentile vs BMI percentile for age, inclusion of ED treatments), different thresholds for treatment of status asthmaticus outside the ICU, or differences in patient populations studied (ie, only ICU patients vs all in‐hospital patients) explain the difference between their findings and the present study. The present study's use of BMI percentile for age follows current recommendations for classifying a patient as obese or overweight.[23, 24, 25] However, the use of classifications other than BMI percentile for age would tend to bias toward the null hypothesis, whereas in Carroll's study children who were overweight or obese had increased resource utilization. Additionally, in the time frame between this publication and the current study, many hospitals worked to standardize asthma hospitalizations by creating weaning protocols for albuterol, thereby decreasing LOS for all asthmatics, which may also affect the differences in LOS between groups of obese and nonobese patients.[35]
Woolford et al. found approximately a one‐half‐day increase in LOS and $2,000 higher mean charges for patients admitted with status asthmaticus and a secondary diagnosis of obesity.[8, 9] Study location and differing methods for defining obesity may account for the discrepancy between Woolford's findings and our study. We examined children admitted to the inpatient floor of a tertiary care children's hospital compared to Woolford et al.'s examination of pediatric patients admitted to all hospitals via the Kids' Inpatient Database (Healthcare Cost and Utilization Project, Agency for Healthcare Research and Quality). That study also relied on the coding of obesity as an ICD‐9 diagnosis, rather than examining the BMI of all admitted patients. Previous research has demonstrated that relying on a coded diagnosis of obesity is not as sensitive as measurement.[26] By relying on ICD‐9 diagnosis coding, only patients with very high BMIs may be diagnosed with obesity during the admission and therefore only associations between very high BMI and status asthmaticus will be examined.
There are several limitations to our findings. First, our study was limited to a single, tertiary care children's hospital and may not be generalizable to other hospitals. Our hospital standardizes the treatment of inpatient status asthmatics by formation of a respiratory care plan, involving interval scoring of respiratory symptoms and automatic spacing of albuterol treatments. This likely minimizes physician‐to‐physician variation. Second, we included only those patients who were initially treated within the ED associated with the admitting hospital to minimize the effects of timing for treatments prior to admittance. This excluded those patients first cared for by their primary care physician or by an outlying ED. Therefore, our sample may be biased toward a study population less connected to a medical home and therefore possibly poorer asthma control. Third, to utilize the most accurate method to define obesity, we excluded approximately 5% of eligible patients because BMI was unavailable. This may have included children with more severe asthma symptoms, as a height measurement may have been deferred due to their higher acuity. Asthma severity or chronicity would be associated with our outcomes of interest. However, we were unable to collect reliable data on severity or chronicity. Finally, to measure the amount of total albuterol needed by a patient during the ED and inpatient admissions, albuterol treatments delivered by MDI, nebulizer, or continuously were converted into total albuterol. Although based upon total milligram dosing and studies comparing routes of albuterol administration,[34] the validity of this conversion is unknown.
CONCLUSION
Although BMI percentile for age is inversely associated with LOS for in‐hospital pediatric status asthmaticus, the impact of BMI on this outcome likely is not clinically meaningful. Future investigations should examine other elements of BMI and in‐hospital status asthmaticus, such as any associations between BMI and admission rates.
Acknowledgements
The authors offer their appreciation to their research assistant, Amy Lee, for her support and dedication to this project.
Disclosures
Internal funds from Children's Mercy Hospital and Clinics supported the conduct of this work. The authors report no conflicts of interest.
Pediatric hospitalizations for obesity‐related conditions have doubled in the last decade, mirroring the trend of higher levels of childhood obesity in the United States.[1, 2, 3] Recent studies have demonstrated worsened pediatric in‐hospital outcomes, including mortality and increased resource utilization, for children with obesity across a range of diagnoses.[4, 5, 6, 7, 8, 9, 10] Although the mechanisms driving the association between obesity and in‐hospital outcomes are not fully known, for asthma it is believed that adipocytes expressing inflammatory markers create a low level of systemic inflammation, thereby increasing the severity of allergic‐type illnesses and decreasing the response to anti‐inflammatory medications, such as steroids.[11, 12, 13, 14, 15, 16, 17, 18] The relationship of obesity and in‐hospital asthma outcomes is of particular interest because status asthmaticus is the most common reason for admission in children aged 3 to 12 years, accounting for approximately 150,000 admissions (7.4% of all hospitalizations for children and adolescents) and $835 million in hospital costs annually.[19]
Few prior studies have examined the association of obesity and asthma outcomes in the in‐hospital setting. The studies examining this association have found patients with obesity to have a longer hospital length of stay (LOS) and increased hospital costs.[8, 9, 20] Obesity has also been associated with increased respiratory treatments and supplemental oxygen requirements.[20] Associations between obesity and admission rates from the emergency department (ED) for pediatric asthma have been inconsistent.[21, 22] Most of these prior studies had several limitations in identifying patients with obesity, including using weight‐for‐age percentiles or International Classification of Diseases, Ninth Revision (ICD‐9) codes, rather than body mass index (BMI) percentile for age, the currently recommended method.[23, 24, 25] Methods other than BMI have the potential to either underestimate obesity (ie, ICD‐9 codes)[26] or to confound weight with adiposity (ie, weight‐for‐age percentiles),[27] thereby skewing the primary exposure of interest.
In the present study, we sought to examine associations between obesity and in‐hospital outcomes for pediatric status asthmaticus using the currently endorsed method for identifying obesity in children, BMI percentile for age.[23, 24, 25] The outcomes of interest included a broad range of in‐hospital measures, including resource utilization (medication and radiology use), readmission rates, billed charges, and LOS. We hypothesize that obesity, due to its proinflammatory state, would result in increased LOS, increased resource utilization, and an increased readmission rate for children admitted with status asthmaticus.
METHODS
Data Sources
Data for this retrospective cross‐sectional study were obtained from 2 sources. First, we queried the Pediatric Health Information System (PHIS) administrative database, which draws information from multiple children's hospitals to identify patients at our 2 institutions of interest who met study criteria. The PHIS database also was used to collect patient demographic data. PHIS is an administrative database operated by Children's Hospital Association (Overland Park, KS) containing clinical and billing data from 43 tertiary care, freestanding children's hospitals, including data on 41 ICD‐9 diagnoses, billed charges, and LOS. Based on the primary diagnosis, PHIS assigns each discharge to an All Patient Refined‐Diagnosis Related Group (APR‐DRG v.24) (3M Health information Systems, St. Paul, MN). APR‐DRGs allow similar diagnoses to be grouped together.[28, 29] PHIS also uses ICD‐9 codes to identify patients with a complex chronic condition (CCC).[30, 31] CCCs are those conditions that can be reasonably expected to last at least 12 months (unless death intervenes) and to involve either several different organ systems or one system severely enough to require specialty pediatric care and probably some period of hospitalization in a tertiary care center.[30, 31] PHIS data quality is ensured through a collaborative effort of the participating hospitals, the Children's Hospital Association, and Truven Healthcare.
Second, standardized chart reviews were then performed to collect clinical data not found in PHIS: BMI, LOS in hours, and medications administered, including total number of albuterol treatments administered during both the admission and the associated preceding ED visit.
Study Setting and Participants
All admissions examined in this study were at Children's Mercy Hospitals. Children's Mercy Hospitals includes 2 separate hospitals: 1 hospital is a 354‐bed academic, tertiary care freestanding children's hospital located in Kansas City, Missouri; a second, smaller, 50‐bed freestanding hospital is located in Overland Park, Kansas. Both hospitals have pediatric emergency departments. Inclusion criteria included patients aged 5 to 17 years discharged for status asthmaticus (APR‐DRG 141) at Children's Mercy Hospital from October 1, 2011 to September 30, 2012, with a recorded BMI during the admission or within 30 days of the admission. Patients between the ages of 2 and 5 years old were not included because of the incidence of viral‐induced wheezing in this age group and therefore possible miscoding of the asthma diagnosis. Exclusion criteria included a concurrent diagnosis of a CCC or bacterial pneumonia because these conditions could alter LOS, resource utilization, and readmission rates independent of the subject's status asthmaticus. In addition, to account for differences in the amount of treatment given in the pre‐inpatient setting, patients not initially treated through the hospital's ED were excluded. For patients with multiple admissions during the study period for the same diagnosis, only the index admission was examined. The institutional review board at Children's Mercy Hospital approved this study with waiver of informed consent.
Study Definitions
BMI percentile for age was used as both a continuous and categorical predictor variable. As a categorical variable it was divided into 4 categories: underweight (BMI <5%), normal weight (BMI 5%84%), overweight (BMI 85%94%), and obese (BMI 95%).[23] Race was categorized non‐Hispanic white, non‐Hispanic black, and other. Other included Asian, Pacific Islander, American Indian, and other. Ethnicity was categorized as Hispanic and non‐Hispanic. Insurance categories included private (commercial or TRICARE), public (Medicaid and Title V), and other (uninsured, self‐pay, and other). Adjusted billed charges were calculated for each hospitalization. Adjusted billed charges are the billed charges adjusted by the US Centers of Medicare and Medicaid Services' price/wage index for the study site's location.[32, 33]
To compare albuterol of different delivery methods, albuterol equivalents were calculated. Based upon prior research demonstrating equal efficacy between albuterol administered by nebulizer and metered‐dose inhaler (MDI),[34] every 2.5 mg of albuterol administered by nebulizer was treated as equivalent to 2 sprays of albuterol (90 g/spray) administered by MDI. Therefore, albuterol 2.5 mg nebulized and 2 sprays of albuterol (90 g/spray) were each defined as 1 albuterol equivalent. To compare continuous administration of nebulized albuterol with intermittent administration of albuterol, the total milligrams of continuously nebulized albuterol were examined. Per protocol at the study site, 10 mg per hour of continuous albuterol are administered for patients 5 years and younger and, for children 6 years and older, 15 mg per hour of continuous albuterol are administered. Based upon milligrams of albuterol nebulized, 5‐year‐old subjects receiving an hour of continuous albuterol would equal 4 albuterol equivalents (or 4 treatments of nebulized albuterol 2.5 mg/treatment or 4 treatments of albuterol 90 g/spray 2 sprays/treatment); for patients 6 years and older, an hour of continuous albuterol would equal 6 albuterol equivalents (or 6 treatments of nebulized albuterol 2.5 mg/treatment or 6 treatments of albuterol 90 g/spray 2 sprays/treatment). The variable total albuterol was then created to include albuterol equivalents delivered by metered dose inhaler and as both single and continuous nebulized treatments.
Main Exposure
The main exposure of interest was BMI percentile for age.
Outcome Measures
The main outcome measure was inpatient LOS measured in hours. Secondary outcome measures included the total albuterol (in the inpatient setting as well as combined inpatient and ED settings) and the administration of intravenous IV fluids and intramuscular (IM) or IV systemic steroids. Other secondary measures included readmission for status asthmaticus during the study period, adjusted billed charges, and inpatient chest radiograph utilization.
Statistical Analyses
We summarized categorical variables with frequencies and percentages, and used [2] test across BMI categories. The non‐normal distribution of continuous dependent variables (LOS, number of albuterol treatments, billed charges) were summarized with medians and interquartile ranges (IQRs). Kruskal‐Wallis test was used to examine outcomes across BMI categories. For regression models, BMI percentile for age was divided into deciles and treated as a continuous predictor. Factors used in the regression models included age, gender, race, ethnicity, and insurance. Total albuterol received in the ED was also included in the model to adjust for differences in the amount of treatment received prior to admission. Incidence rate ratios were created using Poisson regression for continuous outcomes (LOS, billed charges, and number of albuterol equivalent treatments administered), and odds ratios were created using logistic regression for dichotomous outcomes. All statistical analyses were performed using IBM SPSS Statistics version 20 (IBM, Armonk, NY), and P values <0.05 were considered statistically significant.
RESULTS
Patient Characteristics
Of 788 patients admitted for status asthmaticus during the study period, 518 (65.7%) met inclusion criteria; 42 (5.3%) did not meet inclusion criteria due to lack of a documented BMI (Table 1). Most patients were normal weight (59.7%). Approximately one‐third (36.7%) were either overweight or obese. The median age was 8 years, with patients with obesity being significantly older than underweight patients (9 vs 7.5 years, P<0.001). The majority of patients were black/African American (56.9%) and non‐Hispanic (88.6%). The percentage of patients who were obese was higher in patients of other race (29.3%) than whites (20.2%) or blacks (16.3%) (P<0.05). Patients of Hispanic ethnicity had a higher rate of obesity compared to non‐Hispanic patients (37.3% vs 17.4%, P<0.01). There were no differences in BMI categories for insurance.
| Patient Characteristics | Total | Category of Body Mass Index Percentile for Age | ||||
|---|---|---|---|---|---|---|
| Underweight | Normal | Overweight | Obese | P* | ||
| ||||||
| Total patients, n (%) | 518 | 18 (3.5) | 310 (59.8) | 88 (17.0) | 102 (19.7) | |
| Age, y, median (IQR) | 8 (611) | 7.5 (5.89) | 8 (610) | 8 (610) | 9 (712) | <0.001 |
| Gender, n (%) | ||||||
| Male | 309 | 12 (3.9) | 184 (59.5) | 46 (14.9) | 67 (21.7) | 0.27 |
| Female | 209 | 6 (2.9) | 126 (60.3) | 42 (20.1) | 35 (16.7) | |
| Race, n (%) | ||||||
| Non‐Hispanic white | 124 | 8 (6.5) | 76 (61.3) | 15 (12.1) | 25 (20.2) | 0.021 |
| Non‐Hispanic black | 295 | 7 (2.4) | 182 (61.7) | 58 (19.7) | 48 (16.3) | |
| Other | 99 | 3 (3.0) | 52 (52.5) | 15 (15.2) | 29 (29.3) | |
| Ethnicity, n (%) | ||||||
| Hispanic | 59 | 1 (1.7) | 25 (42.4) | 11 (18.6) | 22 (37.3) | 0.002 |
| Non‐Hispanic | 459 | 17 (3.7) | 285 (62.1) | 77 (16.8) | 80 (17.4) | |
| Insurance, n (%) | ||||||
| Private | 163 | 10 (6.1) | 97 (59.5) | 28 (17.2) | 28 (17.2) | 0.48 |
| Public | 313 | 7 (2.2) | 190 (60.7) | 51 (16.3) | 65 (20.8) | |
| Other | 42 | 1 (2.4) | 23 (54.8) | 9 (21.4) | 9 (21.4) | |
LOS and Resource Utilization
The median LOS for all patients was approximately 1 day (Table 2). The median number of albuterol treatments in the inpatient setting was 14 (IQR, 824). When albuterol treatments given in the ED were included, the median number of treatments increased to 38 (IQR, 2848). Approximately one‐half of patients required supplemental oxygen, one‐third received IV fluids, and one‐fifth received either IV or IM steroids (with all but 1.6% of the remaining patients receiving oral steroids). Less than 5% of the study population received magnesium sulfate, epinephrine, required intensive care unit (ICU) admission, or were readmitted for status asthmaticus within 30 days. Approximately 15% of patients received a chest radiograph. The median adjusted billed charge was approximately $7,000. There were no differences in any of these outcomes by BMI category (P>0.05).
| Total | Body Mass Index Category | ||||
|---|---|---|---|---|---|
| Underweight | Normal | Overweight | Obese | ||
| |||||
| Total Patients, n (%) | 518 | 18 (3.5) | 310 (59.8) | 88 (17.0) | 102 (19.7) |
| LOS, h, median (IQR) | 26 (1841) | 41 (19.560.5) | 26 (1841) | 26 (19.2540) | 31 (1942) |
| Inpatient albuterol equivalents, median (IQR) | 14(824) | 19 (9.528) | 14 (824) | 14 (8.522) | 16 (824) |
| Total albuterol equivalents, median (IQR) | 38 (2848) | 34 (2734) | 36 (2848) | 37 (2849.5) | 40 (3052) |
| Adjusted billed charges, $, median (IQR) | 6,999.5 (52929258) | 7,457 (56048536) | 6876 (52379390) | 7056 (54099061) | 7198 (53319306) |
| All readmits, n (%) | 44 (8.5) | 2 (11.1) | 29 (9.4) | 7 (8.0) | 6 (5.9) |
| Readmits within 30 days, n (%) | 11 (2.1) | 1 (5.6) | 7 (2.3) | 1 (1.1) | 2 (2.0) |
| ICU admissions, n (%) | 24 (4.6) | 0 (0) | 13 (4.2) | 7 (8.0) | 4 (3.9) |
| Chest radiograph, n (%) | 64 (12.4) | 5 (27.8) | 34 (11.0) | 12 (13.6) | 13 (12.7) |
| Oxygen, n (%) | 255 (49.2) | 11 (61.1) | 157 (50.6) | 42 (47.7) | 45 (44.1) |
| IV/IM steroid, n (%) | 93 (18.0) | 2 (11.1) | 53 (17.1) | 18 (20.5) | 20 (19.6) |
| Epinephrine, n (%) | 2 (0.4) | 0 (0) | 2 (0.6) | 0 (0) | 0 (0) |
| Magnesium, n (%) | 15 (2.9) | 0 (0) | 8 (2.6) | 3 (3.4) | 4 (3.9) |
| IV fluids, n (%) | 152 (29.3) | 4 (22.2) | 85 (27.4) | 31 (35.2) | 32 (31.4) |
Multivariable Results
After adjusting for age, gender, race, ethnicity, and insurance, the decile of BMI percentile for age showed a small negative association with LOS. Specifically, for each decile increase for BMI percentile for age, LOS decreased by approximately 2%. BMI percentile for age was not associated with other measures of resource utilization including total albuterol use, adjusted billed charges, readmission, ICU care, receipt of supplemental oxygen or a chest radiograph, IV fluids, or other medications (IV/IM steroids, epinephrine, or magnesium sulfate).
DISCUSSION
Our study suggests that the decile of BMI percentile for age is inversely associated with LOS but did not have a clinically meaningful effect. Secondary measures, such as total albuterol needs and adjusted billed charges, did not show an association with BMI percentile for age. There were also no associations between BMI percentile for age and other resource utilization outcomes.
Our findings differ from previous studies examining in‐hospital status asthmaticus in children who are overweight or obese. In addition, the present study was able to adjust for therapies received prior to admission. Carroll et al. demonstrated an increased LOS of approximately 3 days for overweight or obese asthmatics admitted to the ICU with status asthmaticus as well as increased duration of supplemental oxygen, continuous albuterol, and intravenous steroids.[20] It is possible that differences in methodology (ie, weight‐for‐age percentile vs BMI percentile for age, inclusion of ED treatments), different thresholds for treatment of status asthmaticus outside the ICU, or differences in patient populations studied (ie, only ICU patients vs all in‐hospital patients) explain the difference between their findings and the present study. The present study's use of BMI percentile for age follows current recommendations for classifying a patient as obese or overweight.[23, 24, 25] However, the use of classifications other than BMI percentile for age would tend to bias toward the null hypothesis, whereas in Carroll's study children who were overweight or obese had increased resource utilization. Additionally, in the time frame between this publication and the current study, many hospitals worked to standardize asthma hospitalizations by creating weaning protocols for albuterol, thereby decreasing LOS for all asthmatics, which may also affect the differences in LOS between groups of obese and nonobese patients.[35]
Woolford et al. found approximately a one‐half‐day increase in LOS and $2,000 higher mean charges for patients admitted with status asthmaticus and a secondary diagnosis of obesity.[8, 9] Study location and differing methods for defining obesity may account for the discrepancy between Woolford's findings and our study. We examined children admitted to the inpatient floor of a tertiary care children's hospital compared to Woolford et al.'s examination of pediatric patients admitted to all hospitals via the Kids' Inpatient Database (Healthcare Cost and Utilization Project, Agency for Healthcare Research and Quality). That study also relied on the coding of obesity as an ICD‐9 diagnosis, rather than examining the BMI of all admitted patients. Previous research has demonstrated that relying on a coded diagnosis of obesity is not as sensitive as measurement.[26] By relying on ICD‐9 diagnosis coding, only patients with very high BMIs may be diagnosed with obesity during the admission and therefore only associations between very high BMI and status asthmaticus will be examined.
There are several limitations to our findings. First, our study was limited to a single, tertiary care children's hospital and may not be generalizable to other hospitals. Our hospital standardizes the treatment of inpatient status asthmatics by formation of a respiratory care plan, involving interval scoring of respiratory symptoms and automatic spacing of albuterol treatments. This likely minimizes physician‐to‐physician variation. Second, we included only those patients who were initially treated within the ED associated with the admitting hospital to minimize the effects of timing for treatments prior to admittance. This excluded those patients first cared for by their primary care physician or by an outlying ED. Therefore, our sample may be biased toward a study population less connected to a medical home and therefore possibly poorer asthma control. Third, to utilize the most accurate method to define obesity, we excluded approximately 5% of eligible patients because BMI was unavailable. This may have included children with more severe asthma symptoms, as a height measurement may have been deferred due to their higher acuity. Asthma severity or chronicity would be associated with our outcomes of interest. However, we were unable to collect reliable data on severity or chronicity. Finally, to measure the amount of total albuterol needed by a patient during the ED and inpatient admissions, albuterol treatments delivered by MDI, nebulizer, or continuously were converted into total albuterol. Although based upon total milligram dosing and studies comparing routes of albuterol administration,[34] the validity of this conversion is unknown.
CONCLUSION
Although BMI percentile for age is inversely associated with LOS for in‐hospital pediatric status asthmaticus, the impact of BMI on this outcome likely is not clinically meaningful. Future investigations should examine other elements of BMI and in‐hospital status asthmaticus, such as any associations between BMI and admission rates.
Acknowledgements
The authors offer their appreciation to their research assistant, Amy Lee, for her support and dedication to this project.
Disclosures
Internal funds from Children's Mercy Hospital and Clinics supported the conduct of this work. The authors report no conflicts of interest.
- , , . Incidence of childhood obesity in the United States. N Engl J Med. 2014;370(5):403–411.
- , . Prevalence and trends in obesity and severe obesity among children in the United States, 1999–2012. JAMA Pediatr. 2014;168(6):561–566.
- , , , . Effects of childhood obesity on hospital care and costs, 1999–2005. Health Affairs. 2009;28(4):w751–w760.
- , , , , . Influence of obesity on clinical outcomes in hospitalized children: a systematic review. JAMA Pediatr. 2013;167(5):476–482.
- , . Appendicitis in the obese child. J Pediatr Surg. 2007;42(5):857–861.
- , , , , . Obesity: influence on length of hospital stay for the pediatric burn patient. J Burn Care Res. 2010;31(2):251–256.
- , , , , , . The impact of obesity on severely injured children and adolescents. J Pediatr Surg. 2006;41(1):88–91.
- , , , . Incremental hospital charges associated with obesity as a secondary diagnosis in children. Obesity (Silver Spring). 2007;15(7):1895–1901.
- , , , . Persistent gap of incremental charges for obesity as a secondary diagnosis in common pediatric hospitalizations. J Hosp Med. 2009;4(3):149–156.
- , , , . Resource utilization and expenditures for overweight and obese children. Arch Pediatr Adolesc Med. 2007;161(1):11–14.
- , , , , , . Decreased response to inhaled steroids in overweight and obese asthmatic children. J Allergy Clin Immunol. 2011;127(3):741–749.
- , , , , . Body mass and glucocorticoid response in asthma. Am J Respir Crit Care Med. 2008;178(7):682–687.
- , , , ; National Heart, Lung, and Blood Institute's Asthma Clinical Research Network. Body mass index and phenotype in subjects with mild‐to‐moderate persistent asthma. J Allergy Clin Immunol. 2009;123(6):1328–1334.e1.
- , . Obesity and asthma disease phenotypes. Curr Opin Allergy Clin Immunol. 2012;12(1):76–81.
- , . Obesity and the lung: 4. Obesity and asthma. Thorax. 2008;63(11):1018–1023.
- , , , et al. Body mass index and response to asthma therapy: fluticasone propionate/salmeterol versus montelukast. J Asthma. 2010;47(1):76–82.
- , , , et al. Effect of obesity on clinical presentation and response to treatment in asthma. J Asthma. 2006;43(7):553–558.
- , , , . Asthma and obesity in three‐year‐old urban children: role of sex and home environment. J Pediatr. 2011;159(1):14–20.
- , , , . Care of Children and Adolescents in U.S. Hospitals. Rockville, MD: Agency for Healthcare Research and Quality; 2003. Available at: http://archive.ahrq.gov/data/hcup/factbk4/factbk4.pdf. Accessed February 12, 2014.
- , , , . Childhood obesity increases duration of therapy during severe asthma exacerbations. Pediatr Crit Care Med. 2006;7(6):527–531.
- , , , , . Childhood overweight increases hospital admission rates for asthma. Pediatr. 2007;120(4):734–740.
- , , , . Body mass index and acute asthma severity among children presenting to the emergency department. Pediatr Allergy Immunol. 2009;21(3):480–488.
- Centers for Disease Control and Prevention. Basics about childhood obesity. Available at: http://www.cdc.gov/obesity/childhood/basics.html. Accessed February 12, 2014.
- . Screening and interventions for childhood overweight: a summary of evidence for the US Preventive Services Task Force. Pediatrics. 2005;116(1):e125–e144.
- ; Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics. 2007;120(suppl 4):S164–S192.
- , , , . Comparison of ICD code‐based diagnosis of obesity with measured obesity in children and the implications for health care cost estimates. BMC Med Res Methodol. 2011;11(1):173.
- , ; American Academy of Pediatrics Committee on Nutrition. Prevention of pediatric overweight and obesity. Pediatrics. 2003;112(2):424–430.
- . Development of the 3M all patient‐refined diagnosis‐related groups (APR DRGs). Available at: http//www.ahrq.gov/legacy/qual/mortality/Hughes3.htm. Accessed March 1, 2014.
- . 3M Health Information Systems (HIS) APR‐DRG classification software: overview. Available at: http://www.ahrq.gov/legacy/qual/mortality/Hughessumm.htm. Accessed March 1, 2014.
- , , , , . Shifting place of death among children with complex chronic conditions in the United States, 1989–2003. JAMA. 2007;297(24):2725–2732.
- , , . Pediatric deaths attributable to complex chronic conditions: a population‐based study of Washington State, 1980–1997. Pediatrics. 2000;106(1 pt 2):205–209.
- , , , et al. Comparative effectiveness of pleural drainage procedures for the treatment of complicated pneumonia in childhood. J Hosp Med. 2011;6(5):256–263.
- , , , , , . Adjunct corticosteroids in children hospitalized with community‐acquired pneumonia. Pediatrics. 2011;127(2):e255–e263.
- , , . Holding chambers (spacers) versus nebulisers for beta‐agonist treatment of acute asthma. Cochrane Database Syst Rev. 2013;9:CD000052.
- , , , . Effectiveness of a clinical pathway for inpatient asthma management. Pediatrics. 2000;106(5):1006–1012.
- , , . Incidence of childhood obesity in the United States. N Engl J Med. 2014;370(5):403–411.
- , . Prevalence and trends in obesity and severe obesity among children in the United States, 1999–2012. JAMA Pediatr. 2014;168(6):561–566.
- , , , . Effects of childhood obesity on hospital care and costs, 1999–2005. Health Affairs. 2009;28(4):w751–w760.
- , , , , . Influence of obesity on clinical outcomes in hospitalized children: a systematic review. JAMA Pediatr. 2013;167(5):476–482.
- , . Appendicitis in the obese child. J Pediatr Surg. 2007;42(5):857–861.
- , , , , . Obesity: influence on length of hospital stay for the pediatric burn patient. J Burn Care Res. 2010;31(2):251–256.
- , , , , , . The impact of obesity on severely injured children and adolescents. J Pediatr Surg. 2006;41(1):88–91.
- , , , . Incremental hospital charges associated with obesity as a secondary diagnosis in children. Obesity (Silver Spring). 2007;15(7):1895–1901.
- , , , . Persistent gap of incremental charges for obesity as a secondary diagnosis in common pediatric hospitalizations. J Hosp Med. 2009;4(3):149–156.
- , , , . Resource utilization and expenditures for overweight and obese children. Arch Pediatr Adolesc Med. 2007;161(1):11–14.
- , , , , , . Decreased response to inhaled steroids in overweight and obese asthmatic children. J Allergy Clin Immunol. 2011;127(3):741–749.
- , , , , . Body mass and glucocorticoid response in asthma. Am J Respir Crit Care Med. 2008;178(7):682–687.
- , , , ; National Heart, Lung, and Blood Institute's Asthma Clinical Research Network. Body mass index and phenotype in subjects with mild‐to‐moderate persistent asthma. J Allergy Clin Immunol. 2009;123(6):1328–1334.e1.
- , . Obesity and asthma disease phenotypes. Curr Opin Allergy Clin Immunol. 2012;12(1):76–81.
- , . Obesity and the lung: 4. Obesity and asthma. Thorax. 2008;63(11):1018–1023.
- , , , et al. Body mass index and response to asthma therapy: fluticasone propionate/salmeterol versus montelukast. J Asthma. 2010;47(1):76–82.
- , , , et al. Effect of obesity on clinical presentation and response to treatment in asthma. J Asthma. 2006;43(7):553–558.
- , , , . Asthma and obesity in three‐year‐old urban children: role of sex and home environment. J Pediatr. 2011;159(1):14–20.
- , , , . Care of Children and Adolescents in U.S. Hospitals. Rockville, MD: Agency for Healthcare Research and Quality; 2003. Available at: http://archive.ahrq.gov/data/hcup/factbk4/factbk4.pdf. Accessed February 12, 2014.
- , , , . Childhood obesity increases duration of therapy during severe asthma exacerbations. Pediatr Crit Care Med. 2006;7(6):527–531.
- , , , , . Childhood overweight increases hospital admission rates for asthma. Pediatr. 2007;120(4):734–740.
- , , , . Body mass index and acute asthma severity among children presenting to the emergency department. Pediatr Allergy Immunol. 2009;21(3):480–488.
- Centers for Disease Control and Prevention. Basics about childhood obesity. Available at: http://www.cdc.gov/obesity/childhood/basics.html. Accessed February 12, 2014.
- . Screening and interventions for childhood overweight: a summary of evidence for the US Preventive Services Task Force. Pediatrics. 2005;116(1):e125–e144.
- ; Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics. 2007;120(suppl 4):S164–S192.
- , , , . Comparison of ICD code‐based diagnosis of obesity with measured obesity in children and the implications for health care cost estimates. BMC Med Res Methodol. 2011;11(1):173.
- , ; American Academy of Pediatrics Committee on Nutrition. Prevention of pediatric overweight and obesity. Pediatrics. 2003;112(2):424–430.
- . Development of the 3M all patient‐refined diagnosis‐related groups (APR DRGs). Available at: http//www.ahrq.gov/legacy/qual/mortality/Hughes3.htm. Accessed March 1, 2014.
- . 3M Health Information Systems (HIS) APR‐DRG classification software: overview. Available at: http://www.ahrq.gov/legacy/qual/mortality/Hughessumm.htm. Accessed March 1, 2014.
- , , , , . Shifting place of death among children with complex chronic conditions in the United States, 1989–2003. JAMA. 2007;297(24):2725–2732.
- , , . Pediatric deaths attributable to complex chronic conditions: a population‐based study of Washington State, 1980–1997. Pediatrics. 2000;106(1 pt 2):205–209.
- , , , et al. Comparative effectiveness of pleural drainage procedures for the treatment of complicated pneumonia in childhood. J Hosp Med. 2011;6(5):256–263.
- , , , , , . Adjunct corticosteroids in children hospitalized with community‐acquired pneumonia. Pediatrics. 2011;127(2):e255–e263.
- , , . Holding chambers (spacers) versus nebulisers for beta‐agonist treatment of acute asthma. Cochrane Database Syst Rev. 2013;9:CD000052.
- , , , . Effectiveness of a clinical pathway for inpatient asthma management. Pediatrics. 2000;106(5):1006–1012.
© 2014 Society of Hospital Medicine
Statins don’t cut fracture risk
Daily rosuvastatin did not decrease fracture risk in a large international clinical trial involving older men and women who had elevated CRP levels, according to a report published online Dec. 1 in JAMA Internal Medicine.
Statins are thought to stimulate bone formation and increase bone mineral density, suggesting that they may exert clinical benefits beyond cardiovascular disease (CVD) prevention. Several observational studies have reported that statin users show a decreased risk of osteoporotic fractures, compared with nonusers. To examine this possible benefit, the JUPITER (Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin) trial enrolled 17,802 men older than 50 years and women older than 60 years to receive either rosuvastatin or matching placebo and be followed for up to 5 years (median follow-up, 2 years) for both CVD and fracture events. The study was conducted at 1,315 medical centers in 26 countries, said Dr. Jessica M. Peña of the division of cardiology, Montefiore Medical Center, New York, and her associates.

A total of 431 participants sustained fractures: 221 in the rosuvastatin group and 210 in the placebo group, a nonsignificant difference. The corresponding rate of fracture was 1.20 per 100 person-years with the statin and 1.14 per 100 person-years with placebo, also a nonsignificant difference. The lack of protection associated with the active drug was consistent between men and women, across all fracture sites, and regardless of the participants’ fracture history. It also persisted through several sensitivity analyses, the investigators said (JAMA Intern. Med. 2014 Dec. 1 [doi:10.1001/jamainternmed.2014.6388]).
“Our study does not support the use of statins in doses used for cardiovascular disease prevention to reduce the risk of fracture,” the researchers noted.
Daily rosuvastatin did not decrease fracture risk in a large international clinical trial involving older men and women who had elevated CRP levels, according to a report published online Dec. 1 in JAMA Internal Medicine.
Statins are thought to stimulate bone formation and increase bone mineral density, suggesting that they may exert clinical benefits beyond cardiovascular disease (CVD) prevention. Several observational studies have reported that statin users show a decreased risk of osteoporotic fractures, compared with nonusers. To examine this possible benefit, the JUPITER (Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin) trial enrolled 17,802 men older than 50 years and women older than 60 years to receive either rosuvastatin or matching placebo and be followed for up to 5 years (median follow-up, 2 years) for both CVD and fracture events. The study was conducted at 1,315 medical centers in 26 countries, said Dr. Jessica M. Peña of the division of cardiology, Montefiore Medical Center, New York, and her associates.
A total of 431 participants sustained fractures: 221 in the rosuvastatin group and 210 in the placebo group, a nonsignificant difference. The corresponding rate of fracture was 1.20 per 100 person-years with the statin and 1.14 per 100 person-years with placebo, also a nonsignificant difference. The lack of protection associated with the active drug was consistent between men and women, across all fracture sites, and regardless of the participants’ fracture history. It also persisted through several sensitivity analyses, the investigators said (JAMA Intern. Med. 2014 Dec. 1 [doi:10.1001/jamainternmed.2014.6388]).
“Our study does not support the use of statins in doses used for cardiovascular disease prevention to reduce the risk of fracture,” the researchers noted.
Daily rosuvastatin did not decrease fracture risk in a large international clinical trial involving older men and women who had elevated CRP levels, according to a report published online Dec. 1 in JAMA Internal Medicine.
Statins are thought to stimulate bone formation and increase bone mineral density, suggesting that they may exert clinical benefits beyond cardiovascular disease (CVD) prevention. Several observational studies have reported that statin users show a decreased risk of osteoporotic fractures, compared with nonusers. To examine this possible benefit, the JUPITER (Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin) trial enrolled 17,802 men older than 50 years and women older than 60 years to receive either rosuvastatin or matching placebo and be followed for up to 5 years (median follow-up, 2 years) for both CVD and fracture events. The study was conducted at 1,315 medical centers in 26 countries, said Dr. Jessica M. Peña of the division of cardiology, Montefiore Medical Center, New York, and her associates.
A total of 431 participants sustained fractures: 221 in the rosuvastatin group and 210 in the placebo group, a nonsignificant difference. The corresponding rate of fracture was 1.20 per 100 person-years with the statin and 1.14 per 100 person-years with placebo, also a nonsignificant difference. The lack of protection associated with the active drug was consistent between men and women, across all fracture sites, and regardless of the participants’ fracture history. It also persisted through several sensitivity analyses, the investigators said (JAMA Intern. Med. 2014 Dec. 1 [doi:10.1001/jamainternmed.2014.6388]).
“Our study does not support the use of statins in doses used for cardiovascular disease prevention to reduce the risk of fracture,” the researchers noted.
Key clinical point: Rosuvastatin didn’t lower the risk of bone fracture, compared with placebo.
Major finding: 221 participants given rosuvastatin and 210 given placebo sustained fractures, a nonsignificant difference.
Data source: An international randomized double-blind trial in which 17,802 older adults with elevated CRP received either rosuvastatin or placebo and were followed for a median of 2 years.
Disclosures: The JUPITER trial was supported by AstraZeneca, and Dr. Pena was supported by the National Heart, Lung, and Blood Institute. She reported having no financial disclosures; her associates reported numerous ties to industry sources.

It takes work-arounds to make EHRs “work”
Dr. Hickner’s editorial “EHRs: Something’s gotta give” (J Fam Pract. 2014;63:558) prompted me to reflect on the elements of electronic health records (EHRs) that cannot change and the ones that can.
The EHR system I use allows the EHR to serve as a quality recorder, and it appears this is the most important part, because the reminders of what needs to be documented come first and are color-coded. From a reimbursement point of view, what is important is not the narrative, but the expanded “elements” that make it a billing document. I believe this will not change.
What can change is how the note information is organized, and I think the organization should be different for specific roles. At intake, a medical assistant can review allergies, medication lists, and preventive services; update family history; and take vital signs and history of present illness (HPI). As the physician, I want the note to show the information in the order that I process it during the visit: 1) allergies/medication list, 2) concerns/complaints with brief documentation, 3) vitals, 4) physical, 5) assessment, and 6) plan.
After the note is signed off on, I want a different format for review purposes: 1) assessment/plan (because this is what I look at first for follow-up), 2) HPI/review of systems, 3) physical, 4) allergies, 5) medication list, 6) past medical history, and 7) quality reminders (if they show up at all after the visit is complete).
Is it asking too much for a programmer to make the EHR organize information in this manner?
Edward Friedler, MD
Annandale, Va
I still dictate my notes and they very much tell a story that an EHR cannot. I have been audited repeatedly and I always have all the bullet points and essentials that the insurance company wants, but this information is in a format that everyone—including patients—can read and appreciate.
The move to APSO (assessment, plan, subjective, objective) from SOAP (subjective, objective, assessment, plan) is an example of the tail wagging the dog. Rather than fix the note so the time-honored SOAP format works, we acknowledge that no one actually reads the long template notes and they want to get to the bottom line (ie, the assessment and plan).
My dream is to return to the days when we only listed the positive findings, the assumption being that a competent physician did the exam that was required and it’s unnecessary to state that the examined anatomy was normal. Unfortunately, so much of what we must do is driven by lawyers and insurance companies—not by doctors.
David M. Brill, DO
Rocky River, Ohio
I now take photos of all of the ludicrous choices our EHR tosses at me, such as “laceration of third eyelid” or “injury, crushed by falling aircraft due to terrorist.” Most of my EHR entries now say, “See scanned handwritten note for accuracy.”
The issue of EHRs needs to be kept on the front burner. It is destroying doctor/patient relationships and quality diagnostic care while hiding the important findings in the garbage.
Jay Hammett, MD
Knoxville, Tenn
I’m in a group practice of 10 family physicians and in a typical workday, each of us sees 23 to 25 patients, answers e-mails/phone calls, and reviews labs/studies, which leaves no time for anything else. There’s a constant struggle to stay on top of the quality of the notes. I have preserved the quality of my own notes by free typing. I free type a differential next to my assessment or on the first line of the plan. I don’t use templates; they slow me down too much.
Kelly Luba, DO
Phoenix, Ariz
I was a civil service physician working for the Department of the Navy in 2005 when EHRs were thrust upon me. The system was not particularly user-friendly. Free texting was highly discouraged and it was strongly preferred that we used structured text embedded in the program.
I couldn’t use the program as envisioned, so I found a work-around. I would paste the 4 sections of the SOAP note directly into the appropriate free text sections of the electronic record. My assessment included the correct diagnosis, and I would pick a general EHR diagnosis from the dropdown list. Visually, my records did not look any different from those of other health care providers who used structured text.
I used this method until my civil service retirement in 2014. All of my record peer reviews were outstanding, and I was told that my records were easy to understand. I finally let on to all that I never used structured text and that all of my records were really written the old-fashioned way. I still used a clipboard during the patient visit, and completed all records after the patient left.
David F. Scaccia, DO, MPH
Kittery, Maine
Dr. Hickner’s editorial “EHRs: Something’s gotta give” (J Fam Pract. 2014;63:558) prompted me to reflect on the elements of electronic health records (EHRs) that cannot change and the ones that can.
The EHR system I use allows the EHR to serve as a quality recorder, and it appears this is the most important part, because the reminders of what needs to be documented come first and are color-coded. From a reimbursement point of view, what is important is not the narrative, but the expanded “elements” that make it a billing document. I believe this will not change.
What can change is how the note information is organized, and I think the organization should be different for specific roles. At intake, a medical assistant can review allergies, medication lists, and preventive services; update family history; and take vital signs and history of present illness (HPI). As the physician, I want the note to show the information in the order that I process it during the visit: 1) allergies/medication list, 2) concerns/complaints with brief documentation, 3) vitals, 4) physical, 5) assessment, and 6) plan.
After the note is signed off on, I want a different format for review purposes: 1) assessment/plan (because this is what I look at first for follow-up), 2) HPI/review of systems, 3) physical, 4) allergies, 5) medication list, 6) past medical history, and 7) quality reminders (if they show up at all after the visit is complete).
Is it asking too much for a programmer to make the EHR organize information in this manner?
Edward Friedler, MD
Annandale, Va
I still dictate my notes and they very much tell a story that an EHR cannot. I have been audited repeatedly and I always have all the bullet points and essentials that the insurance company wants, but this information is in a format that everyone—including patients—can read and appreciate.
The move to APSO (assessment, plan, subjective, objective) from SOAP (subjective, objective, assessment, plan) is an example of the tail wagging the dog. Rather than fix the note so the time-honored SOAP format works, we acknowledge that no one actually reads the long template notes and they want to get to the bottom line (ie, the assessment and plan).
My dream is to return to the days when we only listed the positive findings, the assumption being that a competent physician did the exam that was required and it’s unnecessary to state that the examined anatomy was normal. Unfortunately, so much of what we must do is driven by lawyers and insurance companies—not by doctors.
David M. Brill, DO
Rocky River, Ohio
I now take photos of all of the ludicrous choices our EHR tosses at me, such as “laceration of third eyelid” or “injury, crushed by falling aircraft due to terrorist.” Most of my EHR entries now say, “See scanned handwritten note for accuracy.”
The issue of EHRs needs to be kept on the front burner. It is destroying doctor/patient relationships and quality diagnostic care while hiding the important findings in the garbage.
Jay Hammett, MD
Knoxville, Tenn
I’m in a group practice of 10 family physicians and in a typical workday, each of us sees 23 to 25 patients, answers e-mails/phone calls, and reviews labs/studies, which leaves no time for anything else. There’s a constant struggle to stay on top of the quality of the notes. I have preserved the quality of my own notes by free typing. I free type a differential next to my assessment or on the first line of the plan. I don’t use templates; they slow me down too much.
Kelly Luba, DO
Phoenix, Ariz
I was a civil service physician working for the Department of the Navy in 2005 when EHRs were thrust upon me. The system was not particularly user-friendly. Free texting was highly discouraged and it was strongly preferred that we used structured text embedded in the program.
I couldn’t use the program as envisioned, so I found a work-around. I would paste the 4 sections of the SOAP note directly into the appropriate free text sections of the electronic record. My assessment included the correct diagnosis, and I would pick a general EHR diagnosis from the dropdown list. Visually, my records did not look any different from those of other health care providers who used structured text.
I used this method until my civil service retirement in 2014. All of my record peer reviews were outstanding, and I was told that my records were easy to understand. I finally let on to all that I never used structured text and that all of my records were really written the old-fashioned way. I still used a clipboard during the patient visit, and completed all records after the patient left.
David F. Scaccia, DO, MPH
Kittery, Maine
Dr. Hickner’s editorial “EHRs: Something’s gotta give” (J Fam Pract. 2014;63:558) prompted me to reflect on the elements of electronic health records (EHRs) that cannot change and the ones that can.
The EHR system I use allows the EHR to serve as a quality recorder, and it appears this is the most important part, because the reminders of what needs to be documented come first and are color-coded. From a reimbursement point of view, what is important is not the narrative, but the expanded “elements” that make it a billing document. I believe this will not change.
What can change is how the note information is organized, and I think the organization should be different for specific roles. At intake, a medical assistant can review allergies, medication lists, and preventive services; update family history; and take vital signs and history of present illness (HPI). As the physician, I want the note to show the information in the order that I process it during the visit: 1) allergies/medication list, 2) concerns/complaints with brief documentation, 3) vitals, 4) physical, 5) assessment, and 6) plan.
After the note is signed off on, I want a different format for review purposes: 1) assessment/plan (because this is what I look at first for follow-up), 2) HPI/review of systems, 3) physical, 4) allergies, 5) medication list, 6) past medical history, and 7) quality reminders (if they show up at all after the visit is complete).
Is it asking too much for a programmer to make the EHR organize information in this manner?
Edward Friedler, MD
Annandale, Va
I still dictate my notes and they very much tell a story that an EHR cannot. I have been audited repeatedly and I always have all the bullet points and essentials that the insurance company wants, but this information is in a format that everyone—including patients—can read and appreciate.
The move to APSO (assessment, plan, subjective, objective) from SOAP (subjective, objective, assessment, plan) is an example of the tail wagging the dog. Rather than fix the note so the time-honored SOAP format works, we acknowledge that no one actually reads the long template notes and they want to get to the bottom line (ie, the assessment and plan).
My dream is to return to the days when we only listed the positive findings, the assumption being that a competent physician did the exam that was required and it’s unnecessary to state that the examined anatomy was normal. Unfortunately, so much of what we must do is driven by lawyers and insurance companies—not by doctors.
David M. Brill, DO
Rocky River, Ohio
I now take photos of all of the ludicrous choices our EHR tosses at me, such as “laceration of third eyelid” or “injury, crushed by falling aircraft due to terrorist.” Most of my EHR entries now say, “See scanned handwritten note for accuracy.”
The issue of EHRs needs to be kept on the front burner. It is destroying doctor/patient relationships and quality diagnostic care while hiding the important findings in the garbage.
Jay Hammett, MD
Knoxville, Tenn
I’m in a group practice of 10 family physicians and in a typical workday, each of us sees 23 to 25 patients, answers e-mails/phone calls, and reviews labs/studies, which leaves no time for anything else. There’s a constant struggle to stay on top of the quality of the notes. I have preserved the quality of my own notes by free typing. I free type a differential next to my assessment or on the first line of the plan. I don’t use templates; they slow me down too much.
Kelly Luba, DO
Phoenix, Ariz
I was a civil service physician working for the Department of the Navy in 2005 when EHRs were thrust upon me. The system was not particularly user-friendly. Free texting was highly discouraged and it was strongly preferred that we used structured text embedded in the program.
I couldn’t use the program as envisioned, so I found a work-around. I would paste the 4 sections of the SOAP note directly into the appropriate free text sections of the electronic record. My assessment included the correct diagnosis, and I would pick a general EHR diagnosis from the dropdown list. Visually, my records did not look any different from those of other health care providers who used structured text.
I used this method until my civil service retirement in 2014. All of my record peer reviews were outstanding, and I was told that my records were easy to understand. I finally let on to all that I never used structured text and that all of my records were really written the old-fashioned way. I still used a clipboard during the patient visit, and completed all records after the patient left.
David F. Scaccia, DO, MPH
Kittery, Maine
Bilateral hand cramping and weakness • broad fingers • coarse facial features • Dx?
THE CASE
A 37-year-old right-hand dominant woman came to our clinic seeking treatment for bilateral generalized hand cramping and weakness that she had been experiencing for approximately 2 to 3 years. She was dropping objects and had finger locking, yet had no numbness, tingling, or morning stiffness.
Ten months earlier, she had given birth to a healthy 3715 g girl. Our patient’s prenatal glucose tolerance test had been normal. Her pregnancy and delivery had been significant for oligohydramnios, failed post-term (41 weeks 4 days) induction, and emergent low transverse cesarean section due to fetal bradycardia. Since giving birth, our patient had 3 menstrual periods while breastfeeding. She had a copper intrauterine device inserted at her 6-week postpartum visit. She also had 2 truncal acrochordons removed 3 months postpartum. She had no history of neck trauma, overuse injury, or occupational exposures.
Her blood pressure and vital signs were within normal limits. Physical exam was notable for subtly coarse facial features and broad fingers (FIGURE 1).

She had normal wrist and hand joint range of motion; her wrist and hand strengths, including grip strength, were 5 out of 5. Tinel’s sign, Phalen’s maneuver, and Finkelstein’s test were negative.
Her upper extremity neurovascular exams were completely normal. Initial laboratory studies—including a comprehensive metabolic panel—were normal. The only exception was her creatine kinase, which was 265 U/L (normal, 24-195 U/L).
At a follow-up appointment 7 weeks later, we gathered a more detailed history and learned that over the past 2 to 3 years, the patient had noticed that her shoe and ring sizes had been increasing. She also mentioned some mild weight gain following her pregnancy.
Occasionally, she had generalized hand swelling, headaches, and saw floaters, but she denied losing peripheral vision. Additional lab work at this time revealed a fasting growth hormone (GH) level of 27.3 ng/mL (normal, 0.05-8 ng/mL) and an insulin-like growth factor 1 (IGF-1) level of 848 ng/mL (normal, 106-368 ng/mL). An anterior pituitary hormone panel and cortisol level were normal. A urine pregnancy test was negative.
THE DIAGNOSIS
Magnetic resonance imaging (MRI) of our patient’s brain revealed a pituitary adenoma (FIGURE 2). Based on that and the patient’s elevated GH and IGF-1 levels, we diagnosed acromegaly due to a pituitary adenoma.
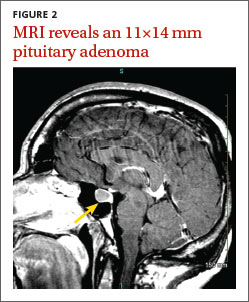
DISCUSSION
Acromegaly is a rare, progressively disfiguring disease with a prevalence of 40 cases per million people.1 It affects middle-aged adults, with no gender difference.2 In most cases, the cause is a benign pituitary adenoma.1-4
Physical changes include coarse facial features, generalized expansion of the skull, brow protrusion, ocular distension, prognathism, macroglossia, acral overgrowth, and dental malocclusion; these changes typically occur slowly over a long time period.1-5 For example, when we looked at the 3-year-old photo on our patient’s driver’s license, we noticed only subtle changes from her current appearance. Common clinical manifestations include headache, hyperpigmentation, hypertrichosis, hyperhidrosis, goiter, arthropathy, carpal tunnel syndrome, visual disturbances, and acrochordons.1,5
Acromegaly is associated with an increased risk of cardiovascular disease, metabolic disorders, infertility, sleep apnea, arthritis, thyroid tumors, colon adenomas, and carcinoma.1,2,4,5 Due to the insidious progression of acromegaly’s clinical manifestations, diagnosis is delayed for 4 to 10 years, on average.1 The diagnosis of acromegaly is typically based on an elevation of GH and IGF-1 levels.1,5 A brain MRI is essential in the diagnosis of a pituitary adenoma.1
Pregnancy among patients with acromegaly is uncommon. In fact, fewer than 150 cases have been reported in the literature.2,6 In most cases, it appears that pregnancy among patients with acromegaly is safe for mothers and newborns.6,7
The goals of treatment for acromegaly caused by a pituitary adenoma are to remove/ reduce the tumor and its mechanical effects, relieve symptoms, reduce serum GH and IGF-1, and restore pituitary function. Transsphenoidal surgical resection is the preferred treatment for pituitary adenomas.1,2,4 Radiation therapy and pharmacologic treatment may be necessary as adjuncts to surgery or for patients for whom surgery is contraindicated.1,4,5
Pharmacologic management of acromegaly includes dopamine agonists (cabergoline), somatostatin analogues (octreotide, lanreotide), and GH receptor antagonists (pegvisomant).1,3 Patients who receive effective early treatment of acromegaly have a life expectancy similar to that of the general population.1,5
Our patient
Our patient was referred to Neurosurgery and underwent transnasal transsphenoidal resection of the pituitary adenoma. Two weeks postop, her GH level had decreased to 0.66 ng/mL and her IGF-1 level was down to 386 ng/mL. Four months later, her GH (2.32 ng/mL) and IGF-1 levels (277 ng/mL) were within normal range and our patient reported improvement in all of her symptoms.
THE TAKEAWAY
Because it may take years for the classical clinical features of acromegaly such as coarse facial features, protruding jaw, and broad fingers to become apparent, diligent history taking is essential to diagnose the condition early. Patients may present with nonspecific and confusing symptoms such as muscle weakness.8 Early nonspecific symptoms and signs in the presence of normal basic laboratory tests should warrant an evaluation of fasting GH and IGF-1. Early treatment with surgery, radiation therapy, or pharmacotherapy may prevent or decrease the intensity of rheumatologic, cardiovascular, respiratory, and metabolic complications of acromegaly.1
1. Scacchi M, Cavagnini F. Acromegaly. Pituitary. 2006;9: 297-303.
2. Hossain B, Drake WM. Acromegaly. Medicine. 2009;37: 407-410.
3. Chan MR, Ziebert M, Maas DL, et al. “My rings won’t fit anymore”. Ectopic growth hormone-secreting tumor. Am Fam Physician. 2005;71:1766-1767.
4. Lake MG, Krook LS, Cruz SV. Pituitary adenomas: an overview. Am Fam Physician. 2013;88:319-327.
5. Vilar L, Valenzuela A, Ribeiro-Oliveira A Jr, et al. Multiple facets in the control of acromegaly. Pituitary. 2014;17 suppl 1:S11-S17.
6. Cheng V, Faiman C, Kennedy L, et al. Pregnancy and acromegaly: a review. Pituitary. 2012;15:59-63.
7. Caron P, Broussaud S, Bertherat J, et al. Acromegaly and pregnancy: a retrospective multicenter study of 59 pregnancies in 46 women. J Clin Endocrinol Metab. 2010;95:4680-4687.
8. Saguil A. Evaluation of the patient with muscle weakness. Am Fam Physician. 2005;71:1327-1336.
THE CASE
A 37-year-old right-hand dominant woman came to our clinic seeking treatment for bilateral generalized hand cramping and weakness that she had been experiencing for approximately 2 to 3 years. She was dropping objects and had finger locking, yet had no numbness, tingling, or morning stiffness.
Ten months earlier, she had given birth to a healthy 3715 g girl. Our patient’s prenatal glucose tolerance test had been normal. Her pregnancy and delivery had been significant for oligohydramnios, failed post-term (41 weeks 4 days) induction, and emergent low transverse cesarean section due to fetal bradycardia. Since giving birth, our patient had 3 menstrual periods while breastfeeding. She had a copper intrauterine device inserted at her 6-week postpartum visit. She also had 2 truncal acrochordons removed 3 months postpartum. She had no history of neck trauma, overuse injury, or occupational exposures.
Her blood pressure and vital signs were within normal limits. Physical exam was notable for subtly coarse facial features and broad fingers (FIGURE 1).
She had normal wrist and hand joint range of motion; her wrist and hand strengths, including grip strength, were 5 out of 5. Tinel’s sign, Phalen’s maneuver, and Finkelstein’s test were negative.
Her upper extremity neurovascular exams were completely normal. Initial laboratory studies—including a comprehensive metabolic panel—were normal. The only exception was her creatine kinase, which was 265 U/L (normal, 24-195 U/L).
At a follow-up appointment 7 weeks later, we gathered a more detailed history and learned that over the past 2 to 3 years, the patient had noticed that her shoe and ring sizes had been increasing. She also mentioned some mild weight gain following her pregnancy.
Occasionally, she had generalized hand swelling, headaches, and saw floaters, but she denied losing peripheral vision. Additional lab work at this time revealed a fasting growth hormone (GH) level of 27.3 ng/mL (normal, 0.05-8 ng/mL) and an insulin-like growth factor 1 (IGF-1) level of 848 ng/mL (normal, 106-368 ng/mL). An anterior pituitary hormone panel and cortisol level were normal. A urine pregnancy test was negative.
THE DIAGNOSIS
Magnetic resonance imaging (MRI) of our patient’s brain revealed a pituitary adenoma (FIGURE 2). Based on that and the patient’s elevated GH and IGF-1 levels, we diagnosed acromegaly due to a pituitary adenoma.
DISCUSSION
Acromegaly is a rare, progressively disfiguring disease with a prevalence of 40 cases per million people.1 It affects middle-aged adults, with no gender difference.2 In most cases, the cause is a benign pituitary adenoma.1-4
Physical changes include coarse facial features, generalized expansion of the skull, brow protrusion, ocular distension, prognathism, macroglossia, acral overgrowth, and dental malocclusion; these changes typically occur slowly over a long time period.1-5 For example, when we looked at the 3-year-old photo on our patient’s driver’s license, we noticed only subtle changes from her current appearance. Common clinical manifestations include headache, hyperpigmentation, hypertrichosis, hyperhidrosis, goiter, arthropathy, carpal tunnel syndrome, visual disturbances, and acrochordons.1,5
Acromegaly is associated with an increased risk of cardiovascular disease, metabolic disorders, infertility, sleep apnea, arthritis, thyroid tumors, colon adenomas, and carcinoma.1,2,4,5 Due to the insidious progression of acromegaly’s clinical manifestations, diagnosis is delayed for 4 to 10 years, on average.1 The diagnosis of acromegaly is typically based on an elevation of GH and IGF-1 levels.1,5 A brain MRI is essential in the diagnosis of a pituitary adenoma.1
Pregnancy among patients with acromegaly is uncommon. In fact, fewer than 150 cases have been reported in the literature.2,6 In most cases, it appears that pregnancy among patients with acromegaly is safe for mothers and newborns.6,7
The goals of treatment for acromegaly caused by a pituitary adenoma are to remove/ reduce the tumor and its mechanical effects, relieve symptoms, reduce serum GH and IGF-1, and restore pituitary function. Transsphenoidal surgical resection is the preferred treatment for pituitary adenomas.1,2,4 Radiation therapy and pharmacologic treatment may be necessary as adjuncts to surgery or for patients for whom surgery is contraindicated.1,4,5
Pharmacologic management of acromegaly includes dopamine agonists (cabergoline), somatostatin analogues (octreotide, lanreotide), and GH receptor antagonists (pegvisomant).1,3 Patients who receive effective early treatment of acromegaly have a life expectancy similar to that of the general population.1,5
Our patient
Our patient was referred to Neurosurgery and underwent transnasal transsphenoidal resection of the pituitary adenoma. Two weeks postop, her GH level had decreased to 0.66 ng/mL and her IGF-1 level was down to 386 ng/mL. Four months later, her GH (2.32 ng/mL) and IGF-1 levels (277 ng/mL) were within normal range and our patient reported improvement in all of her symptoms.
THE TAKEAWAY
Because it may take years for the classical clinical features of acromegaly such as coarse facial features, protruding jaw, and broad fingers to become apparent, diligent history taking is essential to diagnose the condition early. Patients may present with nonspecific and confusing symptoms such as muscle weakness.8 Early nonspecific symptoms and signs in the presence of normal basic laboratory tests should warrant an evaluation of fasting GH and IGF-1. Early treatment with surgery, radiation therapy, or pharmacotherapy may prevent or decrease the intensity of rheumatologic, cardiovascular, respiratory, and metabolic complications of acromegaly.1
THE CASE
A 37-year-old right-hand dominant woman came to our clinic seeking treatment for bilateral generalized hand cramping and weakness that she had been experiencing for approximately 2 to 3 years. She was dropping objects and had finger locking, yet had no numbness, tingling, or morning stiffness.
Ten months earlier, she had given birth to a healthy 3715 g girl. Our patient’s prenatal glucose tolerance test had been normal. Her pregnancy and delivery had been significant for oligohydramnios, failed post-term (41 weeks 4 days) induction, and emergent low transverse cesarean section due to fetal bradycardia. Since giving birth, our patient had 3 menstrual periods while breastfeeding. She had a copper intrauterine device inserted at her 6-week postpartum visit. She also had 2 truncal acrochordons removed 3 months postpartum. She had no history of neck trauma, overuse injury, or occupational exposures.
Her blood pressure and vital signs were within normal limits. Physical exam was notable for subtly coarse facial features and broad fingers (FIGURE 1).
She had normal wrist and hand joint range of motion; her wrist and hand strengths, including grip strength, were 5 out of 5. Tinel’s sign, Phalen’s maneuver, and Finkelstein’s test were negative.
Her upper extremity neurovascular exams were completely normal. Initial laboratory studies—including a comprehensive metabolic panel—were normal. The only exception was her creatine kinase, which was 265 U/L (normal, 24-195 U/L).
At a follow-up appointment 7 weeks later, we gathered a more detailed history and learned that over the past 2 to 3 years, the patient had noticed that her shoe and ring sizes had been increasing. She also mentioned some mild weight gain following her pregnancy.
Occasionally, she had generalized hand swelling, headaches, and saw floaters, but she denied losing peripheral vision. Additional lab work at this time revealed a fasting growth hormone (GH) level of 27.3 ng/mL (normal, 0.05-8 ng/mL) and an insulin-like growth factor 1 (IGF-1) level of 848 ng/mL (normal, 106-368 ng/mL). An anterior pituitary hormone panel and cortisol level were normal. A urine pregnancy test was negative.
THE DIAGNOSIS
Magnetic resonance imaging (MRI) of our patient’s brain revealed a pituitary adenoma (FIGURE 2). Based on that and the patient’s elevated GH and IGF-1 levels, we diagnosed acromegaly due to a pituitary adenoma.
DISCUSSION
Acromegaly is a rare, progressively disfiguring disease with a prevalence of 40 cases per million people.1 It affects middle-aged adults, with no gender difference.2 In most cases, the cause is a benign pituitary adenoma.1-4
Physical changes include coarse facial features, generalized expansion of the skull, brow protrusion, ocular distension, prognathism, macroglossia, acral overgrowth, and dental malocclusion; these changes typically occur slowly over a long time period.1-5 For example, when we looked at the 3-year-old photo on our patient’s driver’s license, we noticed only subtle changes from her current appearance. Common clinical manifestations include headache, hyperpigmentation, hypertrichosis, hyperhidrosis, goiter, arthropathy, carpal tunnel syndrome, visual disturbances, and acrochordons.1,5
Acromegaly is associated with an increased risk of cardiovascular disease, metabolic disorders, infertility, sleep apnea, arthritis, thyroid tumors, colon adenomas, and carcinoma.1,2,4,5 Due to the insidious progression of acromegaly’s clinical manifestations, diagnosis is delayed for 4 to 10 years, on average.1 The diagnosis of acromegaly is typically based on an elevation of GH and IGF-1 levels.1,5 A brain MRI is essential in the diagnosis of a pituitary adenoma.1
Pregnancy among patients with acromegaly is uncommon. In fact, fewer than 150 cases have been reported in the literature.2,6 In most cases, it appears that pregnancy among patients with acromegaly is safe for mothers and newborns.6,7
The goals of treatment for acromegaly caused by a pituitary adenoma are to remove/ reduce the tumor and its mechanical effects, relieve symptoms, reduce serum GH and IGF-1, and restore pituitary function. Transsphenoidal surgical resection is the preferred treatment for pituitary adenomas.1,2,4 Radiation therapy and pharmacologic treatment may be necessary as adjuncts to surgery or for patients for whom surgery is contraindicated.1,4,5
Pharmacologic management of acromegaly includes dopamine agonists (cabergoline), somatostatin analogues (octreotide, lanreotide), and GH receptor antagonists (pegvisomant).1,3 Patients who receive effective early treatment of acromegaly have a life expectancy similar to that of the general population.1,5
Our patient
Our patient was referred to Neurosurgery and underwent transnasal transsphenoidal resection of the pituitary adenoma. Two weeks postop, her GH level had decreased to 0.66 ng/mL and her IGF-1 level was down to 386 ng/mL. Four months later, her GH (2.32 ng/mL) and IGF-1 levels (277 ng/mL) were within normal range and our patient reported improvement in all of her symptoms.
THE TAKEAWAY
Because it may take years for the classical clinical features of acromegaly such as coarse facial features, protruding jaw, and broad fingers to become apparent, diligent history taking is essential to diagnose the condition early. Patients may present with nonspecific and confusing symptoms such as muscle weakness.8 Early nonspecific symptoms and signs in the presence of normal basic laboratory tests should warrant an evaluation of fasting GH and IGF-1. Early treatment with surgery, radiation therapy, or pharmacotherapy may prevent or decrease the intensity of rheumatologic, cardiovascular, respiratory, and metabolic complications of acromegaly.1
1. Scacchi M, Cavagnini F. Acromegaly. Pituitary. 2006;9: 297-303.
2. Hossain B, Drake WM. Acromegaly. Medicine. 2009;37: 407-410.
3. Chan MR, Ziebert M, Maas DL, et al. “My rings won’t fit anymore”. Ectopic growth hormone-secreting tumor. Am Fam Physician. 2005;71:1766-1767.
4. Lake MG, Krook LS, Cruz SV. Pituitary adenomas: an overview. Am Fam Physician. 2013;88:319-327.
5. Vilar L, Valenzuela A, Ribeiro-Oliveira A Jr, et al. Multiple facets in the control of acromegaly. Pituitary. 2014;17 suppl 1:S11-S17.
6. Cheng V, Faiman C, Kennedy L, et al. Pregnancy and acromegaly: a review. Pituitary. 2012;15:59-63.
7. Caron P, Broussaud S, Bertherat J, et al. Acromegaly and pregnancy: a retrospective multicenter study of 59 pregnancies in 46 women. J Clin Endocrinol Metab. 2010;95:4680-4687.
8. Saguil A. Evaluation of the patient with muscle weakness. Am Fam Physician. 2005;71:1327-1336.
1. Scacchi M, Cavagnini F. Acromegaly. Pituitary. 2006;9: 297-303.
2. Hossain B, Drake WM. Acromegaly. Medicine. 2009;37: 407-410.
3. Chan MR, Ziebert M, Maas DL, et al. “My rings won’t fit anymore”. Ectopic growth hormone-secreting tumor. Am Fam Physician. 2005;71:1766-1767.
4. Lake MG, Krook LS, Cruz SV. Pituitary adenomas: an overview. Am Fam Physician. 2013;88:319-327.
5. Vilar L, Valenzuela A, Ribeiro-Oliveira A Jr, et al. Multiple facets in the control of acromegaly. Pituitary. 2014;17 suppl 1:S11-S17.
6. Cheng V, Faiman C, Kennedy L, et al. Pregnancy and acromegaly: a review. Pituitary. 2012;15:59-63.
7. Caron P, Broussaud S, Bertherat J, et al. Acromegaly and pregnancy: a retrospective multicenter study of 59 pregnancies in 46 women. J Clin Endocrinol Metab. 2010;95:4680-4687.
8. Saguil A. Evaluation of the patient with muscle weakness. Am Fam Physician. 2005;71:1327-1336.

Prescribing statins for patients with ACS? No need to wait
Prescribe a high-dose statin before any patient with acute coronary syndrome (ACS) undergoes percutaneous coronary intervention (PCI); it may be reasonable to extend this to patients being evaluated for ACS.1
Strength of recommendation
A: Based on a meta-analysis
Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
Illustrative case
A 48-year-old man comes to the emergency department with chest pain and is diagnosed with ACS. He is scheduled to have PCI within the next 24 hours. When should you start him on a statin?
Statins are the mainstay pharmaceutical treatment for hyperlipidemia, and are used for primary and secondary prevention of coronary artery disease and stroke.2,3 Well-known for their cholesterol-lowering effect, they also have benefits that are independent of their effects on lipids, including improving endothelial function, decreasing oxidative stress, and decreasing vascular inflammation.4-6
Compared to patients with stable angina, patients with ACS experience markedly higher rates of coronary events, especially immediately before and after PCI and during the subsequent 30 days.1 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the management of non-ST elevation myocardial infarction (NSTEMI) advocate starting statins before patients are discharged from the hospital, but they don’t specify precisely when.7
Considering the higher risk of coronary events before and after PCI and statins’ pleiotropic effects, it is reasonable to investigate the optimal time for starting statins in patients with ACS.
STUDY SUMMARY: Meta-analysis of 20 RCTs shows statins before PCI cuts risk of MI
Navarese et al1 performed a systematic review and meta-analysis of studies comparing the clinical outcomes of patients with ACS who received statins before or after PCI (statins group) vs those who received low-dose statins or no statins (control group). The authors searched PubMed, Cochrane, Google Scholar, and CINAHL databases as well as key conference proceedings for studies published before November 2013. Using reasonable inclusion and exclusion criteria and appropriate statistical methods, they analyzed the results of 20 randomized controlled trials that included 8750 patients. Four studies enrolled only patients with ST elevation MI, 8 were restricted to NSTEMI, and the remaining 8 studies enrolled patients with any type of MI or unstable angina.
For patients who were started on a statin before PCI, the mean timing of administration was 0.53 ± 0.42 days before. For those started after PCI, the average time to administration was 3.18 ± 3.56 days after.
Whether administered before or after PCI, statins reduced the incidence of MIs. The overall 30-day incidence of MIs was 3.4% (123 of 3621) in the statins group and 5% (179 of 3577) in the control group. This resulted in an absolute risk reduction of 1.6% (number needed to treat=62.5), and a reduction of the odds of MI by 33% (odds ratio [OR]=0.67; 95% confidence interval [CI], 0.53-0.84; P=.0007). There was also a trend toward reduced mortality in the statin group (OR=0.66; 95% CI, 0.43-1.02; P=.06).
In addition, administering statins before PCI resulted in a greater reduction in the odds of MI at 30 days (OR=0.38; 95% CI, 0.24-0.59; P<.0001) than starting them post-PCI (OR=0.85; 95% CI, 0.64-1.13; P=.28) when compared to the controls. The difference between the pre-PCI OR and the post-PCI OR was statistically significant (P=.002). These findings persisted past 30 days (P=.06).
WHAT'S NEW: Early statin administration is most effective
According to ACC/AHA guidelines, all patients with ACS should be receiving a statin by the time they are discharged. However, when to start the statin is not specified. This meta-analysis is the first report to show that administering a statin before PCI can significantly reduce the risk of subsequent MI.
CAVEATS: Benefits might vary with different statins
The studies evaluated in this meta-analysis used various statins and dosing regimens, which could have affected the results. However, sensitivity analyses found similar benefits across different types of statins. In addition, most of the included trials used high doses of statins, which minimized the potential discrepancy in outcomes from various dosing regimens. And while the included studies were not perfect, Navarese et al1 used reasonable methods to identify potential biases.
CHALLENGES TO IMPLEMENTATION: No barriers to starting statins earlier
Implementing this intervention may be as simple as editing a standard order. This meta-analysis also suggests that the earlier the intervention, the greater the benefit, which may be an argument for starting a statin when a patient first presents for evaluation for ACS, since the risks of taking a statin are quite low. We believe it would be beneficial if the next update of the ACC/AHA guidelines7 included this recommendation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
2. Pignone M, Phillips C, Mulrow C. Use of lipid lowering drugs for primary prevention of coronary heart disease: meta-analysis of randomised trials. BMJ. 2000;321:983-986.
3. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med. 1998;339:1349-1357.
4. Liao JK. Beyond lipid lowering: the role of statins in vascular protection. Int J Cardiol. 2002;86:5-18.
5. Li J, Li JJ, He JG, et al. Atorvastatin decreases C-reactive protein-induced inflammatory response in pulmonary artery smooth muscle cells by inhibiting nuclear factor-kappaB pathway. Cardiovasc Ther. 2010;28:8-14.
6. Tandon V, Bano G, Khajuria V, et al. Pleiotropic effects of statins. Indian J Pharmacol. 2005;37:77-85.
7. Wright RS, Anderson JL, Adams CD, et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;57:e215-e367.
Prescribe a high-dose statin before any patient with acute coronary syndrome (ACS) undergoes percutaneous coronary intervention (PCI); it may be reasonable to extend this to patients being evaluated for ACS.1
Strength of recommendation
A: Based on a meta-analysis
Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
Illustrative case
A 48-year-old man comes to the emergency department with chest pain and is diagnosed with ACS. He is scheduled to have PCI within the next 24 hours. When should you start him on a statin?
Statins are the mainstay pharmaceutical treatment for hyperlipidemia, and are used for primary and secondary prevention of coronary artery disease and stroke.2,3 Well-known for their cholesterol-lowering effect, they also have benefits that are independent of their effects on lipids, including improving endothelial function, decreasing oxidative stress, and decreasing vascular inflammation.4-6
Compared to patients with stable angina, patients with ACS experience markedly higher rates of coronary events, especially immediately before and after PCI and during the subsequent 30 days.1 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the management of non-ST elevation myocardial infarction (NSTEMI) advocate starting statins before patients are discharged from the hospital, but they don’t specify precisely when.7
Considering the higher risk of coronary events before and after PCI and statins’ pleiotropic effects, it is reasonable to investigate the optimal time for starting statins in patients with ACS.
STUDY SUMMARY: Meta-analysis of 20 RCTs shows statins before PCI cuts risk of MI
Navarese et al1 performed a systematic review and meta-analysis of studies comparing the clinical outcomes of patients with ACS who received statins before or after PCI (statins group) vs those who received low-dose statins or no statins (control group). The authors searched PubMed, Cochrane, Google Scholar, and CINAHL databases as well as key conference proceedings for studies published before November 2013. Using reasonable inclusion and exclusion criteria and appropriate statistical methods, they analyzed the results of 20 randomized controlled trials that included 8750 patients. Four studies enrolled only patients with ST elevation MI, 8 were restricted to NSTEMI, and the remaining 8 studies enrolled patients with any type of MI or unstable angina.
For patients who were started on a statin before PCI, the mean timing of administration was 0.53 ± 0.42 days before. For those started after PCI, the average time to administration was 3.18 ± 3.56 days after.
Whether administered before or after PCI, statins reduced the incidence of MIs. The overall 30-day incidence of MIs was 3.4% (123 of 3621) in the statins group and 5% (179 of 3577) in the control group. This resulted in an absolute risk reduction of 1.6% (number needed to treat=62.5), and a reduction of the odds of MI by 33% (odds ratio [OR]=0.67; 95% confidence interval [CI], 0.53-0.84; P=.0007). There was also a trend toward reduced mortality in the statin group (OR=0.66; 95% CI, 0.43-1.02; P=.06).
In addition, administering statins before PCI resulted in a greater reduction in the odds of MI at 30 days (OR=0.38; 95% CI, 0.24-0.59; P<.0001) than starting them post-PCI (OR=0.85; 95% CI, 0.64-1.13; P=.28) when compared to the controls. The difference between the pre-PCI OR and the post-PCI OR was statistically significant (P=.002). These findings persisted past 30 days (P=.06).
WHAT'S NEW: Early statin administration is most effective
According to ACC/AHA guidelines, all patients with ACS should be receiving a statin by the time they are discharged. However, when to start the statin is not specified. This meta-analysis is the first report to show that administering a statin before PCI can significantly reduce the risk of subsequent MI.
CAVEATS: Benefits might vary with different statins
The studies evaluated in this meta-analysis used various statins and dosing regimens, which could have affected the results. However, sensitivity analyses found similar benefits across different types of statins. In addition, most of the included trials used high doses of statins, which minimized the potential discrepancy in outcomes from various dosing regimens. And while the included studies were not perfect, Navarese et al1 used reasonable methods to identify potential biases.
CHALLENGES TO IMPLEMENTATION: No barriers to starting statins earlier
Implementing this intervention may be as simple as editing a standard order. This meta-analysis also suggests that the earlier the intervention, the greater the benefit, which may be an argument for starting a statin when a patient first presents for evaluation for ACS, since the risks of taking a statin are quite low. We believe it would be beneficial if the next update of the ACC/AHA guidelines7 included this recommendation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Prescribe a high-dose statin before any patient with acute coronary syndrome (ACS) undergoes percutaneous coronary intervention (PCI); it may be reasonable to extend this to patients being evaluated for ACS.1
Strength of recommendation
A: Based on a meta-analysis
Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
Illustrative case
A 48-year-old man comes to the emergency department with chest pain and is diagnosed with ACS. He is scheduled to have PCI within the next 24 hours. When should you start him on a statin?
Statins are the mainstay pharmaceutical treatment for hyperlipidemia, and are used for primary and secondary prevention of coronary artery disease and stroke.2,3 Well-known for their cholesterol-lowering effect, they also have benefits that are independent of their effects on lipids, including improving endothelial function, decreasing oxidative stress, and decreasing vascular inflammation.4-6
Compared to patients with stable angina, patients with ACS experience markedly higher rates of coronary events, especially immediately before and after PCI and during the subsequent 30 days.1 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the management of non-ST elevation myocardial infarction (NSTEMI) advocate starting statins before patients are discharged from the hospital, but they don’t specify precisely when.7
Considering the higher risk of coronary events before and after PCI and statins’ pleiotropic effects, it is reasonable to investigate the optimal time for starting statins in patients with ACS.
STUDY SUMMARY: Meta-analysis of 20 RCTs shows statins before PCI cuts risk of MI
Navarese et al1 performed a systematic review and meta-analysis of studies comparing the clinical outcomes of patients with ACS who received statins before or after PCI (statins group) vs those who received low-dose statins or no statins (control group). The authors searched PubMed, Cochrane, Google Scholar, and CINAHL databases as well as key conference proceedings for studies published before November 2013. Using reasonable inclusion and exclusion criteria and appropriate statistical methods, they analyzed the results of 20 randomized controlled trials that included 8750 patients. Four studies enrolled only patients with ST elevation MI, 8 were restricted to NSTEMI, and the remaining 8 studies enrolled patients with any type of MI or unstable angina.
For patients who were started on a statin before PCI, the mean timing of administration was 0.53 ± 0.42 days before. For those started after PCI, the average time to administration was 3.18 ± 3.56 days after.
Whether administered before or after PCI, statins reduced the incidence of MIs. The overall 30-day incidence of MIs was 3.4% (123 of 3621) in the statins group and 5% (179 of 3577) in the control group. This resulted in an absolute risk reduction of 1.6% (number needed to treat=62.5), and a reduction of the odds of MI by 33% (odds ratio [OR]=0.67; 95% confidence interval [CI], 0.53-0.84; P=.0007). There was also a trend toward reduced mortality in the statin group (OR=0.66; 95% CI, 0.43-1.02; P=.06).
In addition, administering statins before PCI resulted in a greater reduction in the odds of MI at 30 days (OR=0.38; 95% CI, 0.24-0.59; P<.0001) than starting them post-PCI (OR=0.85; 95% CI, 0.64-1.13; P=.28) when compared to the controls. The difference between the pre-PCI OR and the post-PCI OR was statistically significant (P=.002). These findings persisted past 30 days (P=.06).
WHAT'S NEW: Early statin administration is most effective
According to ACC/AHA guidelines, all patients with ACS should be receiving a statin by the time they are discharged. However, when to start the statin is not specified. This meta-analysis is the first report to show that administering a statin before PCI can significantly reduce the risk of subsequent MI.
CAVEATS: Benefits might vary with different statins
The studies evaluated in this meta-analysis used various statins and dosing regimens, which could have affected the results. However, sensitivity analyses found similar benefits across different types of statins. In addition, most of the included trials used high doses of statins, which minimized the potential discrepancy in outcomes from various dosing regimens. And while the included studies were not perfect, Navarese et al1 used reasonable methods to identify potential biases.
CHALLENGES TO IMPLEMENTATION: No barriers to starting statins earlier
Implementing this intervention may be as simple as editing a standard order. This meta-analysis also suggests that the earlier the intervention, the greater the benefit, which may be an argument for starting a statin when a patient first presents for evaluation for ACS, since the risks of taking a statin are quite low. We believe it would be beneficial if the next update of the ACC/AHA guidelines7 included this recommendation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
2. Pignone M, Phillips C, Mulrow C. Use of lipid lowering drugs for primary prevention of coronary heart disease: meta-analysis of randomised trials. BMJ. 2000;321:983-986.
3. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med. 1998;339:1349-1357.
4. Liao JK. Beyond lipid lowering: the role of statins in vascular protection. Int J Cardiol. 2002;86:5-18.
5. Li J, Li JJ, He JG, et al. Atorvastatin decreases C-reactive protein-induced inflammatory response in pulmonary artery smooth muscle cells by inhibiting nuclear factor-kappaB pathway. Cardiovasc Ther. 2010;28:8-14.
6. Tandon V, Bano G, Khajuria V, et al. Pleiotropic effects of statins. Indian J Pharmacol. 2005;37:77-85.
7. Wright RS, Anderson JL, Adams CD, et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;57:e215-e367.
1. Navarese EP, Kowalewski M, Andreotti F, et al. Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2014;113:1753-1764.
2. Pignone M, Phillips C, Mulrow C. Use of lipid lowering drugs for primary prevention of coronary heart disease: meta-analysis of randomised trials. BMJ. 2000;321:983-986.
3. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med. 1998;339:1349-1357.
4. Liao JK. Beyond lipid lowering: the role of statins in vascular protection. Int J Cardiol. 2002;86:5-18.
5. Li J, Li JJ, He JG, et al. Atorvastatin decreases C-reactive protein-induced inflammatory response in pulmonary artery smooth muscle cells by inhibiting nuclear factor-kappaB pathway. Cardiovasc Ther. 2010;28:8-14.
6. Tandon V, Bano G, Khajuria V, et al. Pleiotropic effects of statins. Indian J Pharmacol. 2005;37:77-85.
7. Wright RS, Anderson JL, Adams CD, et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;57:e215-e367.
Copyright © 2014 Family Physicians Inquiries Network. All rights reserved.
Pneumococcal vaccines for older adults: Getting the timing right
In August 2014, the Advisory Committee on Immunization Practices (ACIP) decided to add the 13-valent pneumococcal conjugate vaccine (PCV13) to the routine immunization schedule for adults ages 65 years and older; previously, it had recommended that these patients receive only the 23-valent pneumococcal polysaccharide vaccine (PPSV23).1 The US Food and Drug Administration (FDA) had approved PCV13 for use in adults ages 50 years and older in late 2011. The delay between FDA approval and this new ACIP recommendation occurred for 2 reasons: The epidemiology of pneumococcal disease (pneumonia, meningitis, and bacteremia) in older adults is evolving due to the widespread use of PCV13 in children, and a large clinical trial looking at the efficacy of this vaccine in individuals 65 and older was still underway.
Pneumococcal disease in older adults remains a problem
Routine use of the 7-valent pneumococcal conjugate vaccine (PCV7) in children began in 2000. In 2010, the vaccine was expanded to include 6 more antigens (PCV13). The routine use of this vaccine has markedly reduced pneumococcal disease in children and, by way of indirect protection, in adults. Between 2010 and 2013, the incidence of invasive pneumococcal disease (eg, meningitis and bacteremia) caused by the 13 serotypes in the vaccine had decreased by 50% in adults ages 65 years and older.1 However, in this age group, there are still more than 13,000 cases of invasive pneumococcal disease each year.1 Approximately 20% of these cases—and 10% of cases community-acquired pneumonia (CAP) in this age group—are still caused by one of the PCV13 serotypes. This epidemiology left ACIP to consider whether to recommend PCV13 for older adults even though the incidence of pneumococcal disease was declining without the use of the vaccine. ACIP took a middle-of-the-road position on August 13, 2014 by recommending the vaccine now but agreeing to reexamine the issue again in 2018.1
PCV13 substantially cuts the rate of pneumococcal disease
In June 2014, ACIP reviewed the results of a large randomized, placebo-controlled clinical trial of PCV13 in 85,000 adults ages 65 years and older that was conducted in the Netherlands from 2008 to 2013.1 PCV13 reduced the rate of disease caused by the vaccine serotypes by 45.6% for pneumonia and 75% for invasive pneumococcal disease.
Because the population in this study was PPSV23-naïve, the added advantage of PCV13 in patients who have been vaccinated with PPSV23 has not been determined. Twelve of the 13 serotypes in PCV13 are in PPSV23. And while PPSV23 can protect against invasive pneumococcal disease, its effectiveness against CAP is less well proven.
Using modeling that took into consideration anticipated rates of vaccination with both PCV13 and PPSV23 in adults and children, the Centers for Disease Control and Prevention estimated that adding PCV13 to the adult immunization schedule would prevent 230 cases of invasive pneumococcal disease and 12,000 cases of CAP over the lifetime of a cohort of 65 year olds.1 With time, however, and the increasing indirect protection from routine use of PCV13 in children, these numbers would decline.
Timing of administration depends on patients’ vaccine history
Adults 65 years of age and older should receive both PCV13 and PPSV23, but not at the same time. In those who have not received any pneumococcal vaccine, the preferred sequence is to first administer PCV13 and then PPSV23 6 to 12 months later (FIGURE); the minimum acceptable interval between PCV13 and PPSV23 is 8 weeks.1 If PPSV23 is administered first, PCV13 should not be given until at least 12 months after the PPSV23 dose. This is because the immune response to PCV13 is not as robust when PCV13 follows PPSV23.
For patients who have been vaccinated with PPSV23 before age 65, PCV13 should be administered at least 12 months after PPSV23, followed by another dose of PPSV23 that should be administered 6 to 12 months after PCV13, but no sooner than 5 years since the previous PPSV23 (FIGURE).
Coadministration of PCV13 with trivalent influenza vaccine results in a slight decrease in the immune response to each vaccine;1 this is unlikely to be clinically important. Coadministration with other vaccines has not been studied.

Who’ll reimburse for the PCV13 vaccine? One issue that could delay the use of both vaccines in older adults is that currently, Medicare pays for only one pneumococcal vaccine in patients who are 65 and older. The Centers for Medicare and Medicaid Services will attempt to amend this policy, but how quickly this will occur is unknown.
Different recommendations for patients at higher risk
There are 2 sets of recommendations for use of pneumococcal vaccines: one for routine use for most patients, and a separate set of recommendations for those with conditions that put them at higher risk of infections and/or complications from pneumococcal disease.1-4 PPSV23 is recommended for children (starting at age 2 years) and adults with certain high-risk medical conditions, such as chronic heart, lung, or liver disease, and diabetes; functional or anatomical asplenia; or immunocompromising conditions such as human immunodeficiency virus infection, chronic renal failure, leukemia, or lymphoma.3 PPSV23 should be repeated 5 years after the first dose in patients with asplenia, those who are immunocompromised, and for everyone age 65 and older who received it before age 65. No more than 3 doses of PPSV23 should be given to anyone.
PCV13 is recommended for previously unvaccinated children and adults who have cochlear implants, cerebrospinal fluid leaks, functional or anatomical asplenia, or are immunocompromised.
1. Tomczyk S, Bennett NM, Stoecker C, et al; Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among adults aged ≥65 years: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2014;63:822-825.
2. Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine for adults with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2012;61:816-819.
3. Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among children aged 6-18 years with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2013;62:521-524.
4. Nuorti JP, Whitney CG; Centers for Disease Control and Prevention (CDC). Prevention of pneumococcal disease among infants and children - Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine - Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2010;59:1-18.
In August 2014, the Advisory Committee on Immunization Practices (ACIP) decided to add the 13-valent pneumococcal conjugate vaccine (PCV13) to the routine immunization schedule for adults ages 65 years and older; previously, it had recommended that these patients receive only the 23-valent pneumococcal polysaccharide vaccine (PPSV23).1 The US Food and Drug Administration (FDA) had approved PCV13 for use in adults ages 50 years and older in late 2011. The delay between FDA approval and this new ACIP recommendation occurred for 2 reasons: The epidemiology of pneumococcal disease (pneumonia, meningitis, and bacteremia) in older adults is evolving due to the widespread use of PCV13 in children, and a large clinical trial looking at the efficacy of this vaccine in individuals 65 and older was still underway.
Pneumococcal disease in older adults remains a problem
Routine use of the 7-valent pneumococcal conjugate vaccine (PCV7) in children began in 2000. In 2010, the vaccine was expanded to include 6 more antigens (PCV13). The routine use of this vaccine has markedly reduced pneumococcal disease in children and, by way of indirect protection, in adults. Between 2010 and 2013, the incidence of invasive pneumococcal disease (eg, meningitis and bacteremia) caused by the 13 serotypes in the vaccine had decreased by 50% in adults ages 65 years and older.1 However, in this age group, there are still more than 13,000 cases of invasive pneumococcal disease each year.1 Approximately 20% of these cases—and 10% of cases community-acquired pneumonia (CAP) in this age group—are still caused by one of the PCV13 serotypes. This epidemiology left ACIP to consider whether to recommend PCV13 for older adults even though the incidence of pneumococcal disease was declining without the use of the vaccine. ACIP took a middle-of-the-road position on August 13, 2014 by recommending the vaccine now but agreeing to reexamine the issue again in 2018.1
PCV13 substantially cuts the rate of pneumococcal disease
In June 2014, ACIP reviewed the results of a large randomized, placebo-controlled clinical trial of PCV13 in 85,000 adults ages 65 years and older that was conducted in the Netherlands from 2008 to 2013.1 PCV13 reduced the rate of disease caused by the vaccine serotypes by 45.6% for pneumonia and 75% for invasive pneumococcal disease.
Because the population in this study was PPSV23-naïve, the added advantage of PCV13 in patients who have been vaccinated with PPSV23 has not been determined. Twelve of the 13 serotypes in PCV13 are in PPSV23. And while PPSV23 can protect against invasive pneumococcal disease, its effectiveness against CAP is less well proven.
Using modeling that took into consideration anticipated rates of vaccination with both PCV13 and PPSV23 in adults and children, the Centers for Disease Control and Prevention estimated that adding PCV13 to the adult immunization schedule would prevent 230 cases of invasive pneumococcal disease and 12,000 cases of CAP over the lifetime of a cohort of 65 year olds.1 With time, however, and the increasing indirect protection from routine use of PCV13 in children, these numbers would decline.
Timing of administration depends on patients’ vaccine history
Adults 65 years of age and older should receive both PCV13 and PPSV23, but not at the same time. In those who have not received any pneumococcal vaccine, the preferred sequence is to first administer PCV13 and then PPSV23 6 to 12 months later (FIGURE); the minimum acceptable interval between PCV13 and PPSV23 is 8 weeks.1 If PPSV23 is administered first, PCV13 should not be given until at least 12 months after the PPSV23 dose. This is because the immune response to PCV13 is not as robust when PCV13 follows PPSV23.
For patients who have been vaccinated with PPSV23 before age 65, PCV13 should be administered at least 12 months after PPSV23, followed by another dose of PPSV23 that should be administered 6 to 12 months after PCV13, but no sooner than 5 years since the previous PPSV23 (FIGURE).
Coadministration of PCV13 with trivalent influenza vaccine results in a slight decrease in the immune response to each vaccine;1 this is unlikely to be clinically important. Coadministration with other vaccines has not been studied.
Who’ll reimburse for the PCV13 vaccine? One issue that could delay the use of both vaccines in older adults is that currently, Medicare pays for only one pneumococcal vaccine in patients who are 65 and older. The Centers for Medicare and Medicaid Services will attempt to amend this policy, but how quickly this will occur is unknown.
Different recommendations for patients at higher risk
There are 2 sets of recommendations for use of pneumococcal vaccines: one for routine use for most patients, and a separate set of recommendations for those with conditions that put them at higher risk of infections and/or complications from pneumococcal disease.1-4 PPSV23 is recommended for children (starting at age 2 years) and adults with certain high-risk medical conditions, such as chronic heart, lung, or liver disease, and diabetes; functional or anatomical asplenia; or immunocompromising conditions such as human immunodeficiency virus infection, chronic renal failure, leukemia, or lymphoma.3 PPSV23 should be repeated 5 years after the first dose in patients with asplenia, those who are immunocompromised, and for everyone age 65 and older who received it before age 65. No more than 3 doses of PPSV23 should be given to anyone.
PCV13 is recommended for previously unvaccinated children and adults who have cochlear implants, cerebrospinal fluid leaks, functional or anatomical asplenia, or are immunocompromised.
In August 2014, the Advisory Committee on Immunization Practices (ACIP) decided to add the 13-valent pneumococcal conjugate vaccine (PCV13) to the routine immunization schedule for adults ages 65 years and older; previously, it had recommended that these patients receive only the 23-valent pneumococcal polysaccharide vaccine (PPSV23).1 The US Food and Drug Administration (FDA) had approved PCV13 for use in adults ages 50 years and older in late 2011. The delay between FDA approval and this new ACIP recommendation occurred for 2 reasons: The epidemiology of pneumococcal disease (pneumonia, meningitis, and bacteremia) in older adults is evolving due to the widespread use of PCV13 in children, and a large clinical trial looking at the efficacy of this vaccine in individuals 65 and older was still underway.
Pneumococcal disease in older adults remains a problem
Routine use of the 7-valent pneumococcal conjugate vaccine (PCV7) in children began in 2000. In 2010, the vaccine was expanded to include 6 more antigens (PCV13). The routine use of this vaccine has markedly reduced pneumococcal disease in children and, by way of indirect protection, in adults. Between 2010 and 2013, the incidence of invasive pneumococcal disease (eg, meningitis and bacteremia) caused by the 13 serotypes in the vaccine had decreased by 50% in adults ages 65 years and older.1 However, in this age group, there are still more than 13,000 cases of invasive pneumococcal disease each year.1 Approximately 20% of these cases—and 10% of cases community-acquired pneumonia (CAP) in this age group—are still caused by one of the PCV13 serotypes. This epidemiology left ACIP to consider whether to recommend PCV13 for older adults even though the incidence of pneumococcal disease was declining without the use of the vaccine. ACIP took a middle-of-the-road position on August 13, 2014 by recommending the vaccine now but agreeing to reexamine the issue again in 2018.1
PCV13 substantially cuts the rate of pneumococcal disease
In June 2014, ACIP reviewed the results of a large randomized, placebo-controlled clinical trial of PCV13 in 85,000 adults ages 65 years and older that was conducted in the Netherlands from 2008 to 2013.1 PCV13 reduced the rate of disease caused by the vaccine serotypes by 45.6% for pneumonia and 75% for invasive pneumococcal disease.
Because the population in this study was PPSV23-naïve, the added advantage of PCV13 in patients who have been vaccinated with PPSV23 has not been determined. Twelve of the 13 serotypes in PCV13 are in PPSV23. And while PPSV23 can protect against invasive pneumococcal disease, its effectiveness against CAP is less well proven.
Using modeling that took into consideration anticipated rates of vaccination with both PCV13 and PPSV23 in adults and children, the Centers for Disease Control and Prevention estimated that adding PCV13 to the adult immunization schedule would prevent 230 cases of invasive pneumococcal disease and 12,000 cases of CAP over the lifetime of a cohort of 65 year olds.1 With time, however, and the increasing indirect protection from routine use of PCV13 in children, these numbers would decline.
Timing of administration depends on patients’ vaccine history
Adults 65 years of age and older should receive both PCV13 and PPSV23, but not at the same time. In those who have not received any pneumococcal vaccine, the preferred sequence is to first administer PCV13 and then PPSV23 6 to 12 months later (FIGURE); the minimum acceptable interval between PCV13 and PPSV23 is 8 weeks.1 If PPSV23 is administered first, PCV13 should not be given until at least 12 months after the PPSV23 dose. This is because the immune response to PCV13 is not as robust when PCV13 follows PPSV23.
For patients who have been vaccinated with PPSV23 before age 65, PCV13 should be administered at least 12 months after PPSV23, followed by another dose of PPSV23 that should be administered 6 to 12 months after PCV13, but no sooner than 5 years since the previous PPSV23 (FIGURE).
Coadministration of PCV13 with trivalent influenza vaccine results in a slight decrease in the immune response to each vaccine;1 this is unlikely to be clinically important. Coadministration with other vaccines has not been studied.
Who’ll reimburse for the PCV13 vaccine? One issue that could delay the use of both vaccines in older adults is that currently, Medicare pays for only one pneumococcal vaccine in patients who are 65 and older. The Centers for Medicare and Medicaid Services will attempt to amend this policy, but how quickly this will occur is unknown.
Different recommendations for patients at higher risk
There are 2 sets of recommendations for use of pneumococcal vaccines: one for routine use for most patients, and a separate set of recommendations for those with conditions that put them at higher risk of infections and/or complications from pneumococcal disease.1-4 PPSV23 is recommended for children (starting at age 2 years) and adults with certain high-risk medical conditions, such as chronic heart, lung, or liver disease, and diabetes; functional or anatomical asplenia; or immunocompromising conditions such as human immunodeficiency virus infection, chronic renal failure, leukemia, or lymphoma.3 PPSV23 should be repeated 5 years after the first dose in patients with asplenia, those who are immunocompromised, and for everyone age 65 and older who received it before age 65. No more than 3 doses of PPSV23 should be given to anyone.
PCV13 is recommended for previously unvaccinated children and adults who have cochlear implants, cerebrospinal fluid leaks, functional or anatomical asplenia, or are immunocompromised.
1. Tomczyk S, Bennett NM, Stoecker C, et al; Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among adults aged ≥65 years: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2014;63:822-825.
2. Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine for adults with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2012;61:816-819.
3. Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among children aged 6-18 years with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2013;62:521-524.
4. Nuorti JP, Whitney CG; Centers for Disease Control and Prevention (CDC). Prevention of pneumococcal disease among infants and children - Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine - Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2010;59:1-18.
1. Tomczyk S, Bennett NM, Stoecker C, et al; Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among adults aged ≥65 years: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2014;63:822-825.
2. Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine for adults with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2012;61:816-819.
3. Centers for Disease Control and Prevention (CDC). Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among children aged 6-18 years with immunocompromising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2013;62:521-524.
4. Nuorti JP, Whitney CG; Centers for Disease Control and Prevention (CDC). Prevention of pneumococcal disease among infants and children - Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine - Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2010;59:1-18.
Which risk factors and signs and symptoms are associated with coccidioidomycosis?
EVIDENCE-BASED ANSWER:
Risk factors for coccidioidomycosis, or valley fever, include lower respiratory tract symptoms lasting longer than 14 days, chest pain, rash, having lived in endemic areas fewer than 10 years, and diabetes mellitus or immunosuppressive conditions (strength of recommendation [SOR]: B, several prospective cohort and case-control studies).
The most common signs and symptoms include cough (74%), fever (56%), night sweats (35%), pleuritic chest pain (33%), chills (28%), dyspnea (27%), weight loss (21%), and rash (14%) (SOR: B, retrospective cohort study).
EVIDENCE SUMMARY
A 2013 surveillance report by the Centers for Disease Control and Prevention that included 111,717 patients in 28 states and the District of Columbia found an 8-fold increase in reported coccidioidomycosis in endemic areas from 1998 to 2011 (age-adjusted incidence rates: 5.3 per 100,000 in 1998 and 42.6 per 100,000 in 2011). Cases in nonendemic states increased 40-fold in the same time period, from 6 cases to 240.1 The disease is endemic in the southwest United States and northwest Mexico.
Risk factors include persistent symptoms, chest pain, diabetes, immunosuppression
A 2008 case-control study of 136 patients in Phoenix, Arizona (an endemic area) found that 15% of the patients diagnosed with community-acquired pneumonia (CAP) had coccidioidomycosis on serologic testing. Risk factors for CAP caused by coccidioidomycosis in this population were symptom duration longer than 14 days (odds ratio [OR]=5.0; 95% confidence interval [CI], 2.1-15.7), age younger than 18 years (OR=5.5; 95% CI, 2.1-15.3), chest pain (OR=4.6; 95% CI, 1.8-11.8), and diabetes mellitus or an immunosuppressive condition (OR=3.8; 95% CI, 1.0-16.5).2
Abnormal chest X-rays, myalgia— and a rash
A 2006 prospective cohort study of 55 patients in Tucson, Arizona, which is part of the endemic area, found that 29% of patients diagnosed with CAP tested serologically positive for coccidioidomycosis. Risk factors included fewer than 10 years of exposure to an endemic area (OR=4.11; 95% CI, 1.01-16.8). Chest radiograph abnormalities were more common in patients with CAP caused by coccidioidomycosis than patients without coccidioidomycosis (75% vs 25%, P=.005). Myalgia is more common when coccidioidal pneumonia is present (69% vs 23%, P=.0022).3
A 2009 prospective cohort study of 35 patients with CAP in Phoenix, Arizona found that 6 patients (17%) tested positive for coccidioidomycosis. Only 1 statistically significant risk factor was identified—half of patients with coccidioidomycosis exhibited a rash, while there were no rashes in the group without the disease (P=.002).4
Other common signs and symptoms
A retrospective cohort study in San Diego, California in 2004 evaluated and stratified 223 patients with known coccidioidomycosis for presenting symptoms, exam findings, and radiographic findings. The most common signs and symptoms at time of seropositive testing were cough (74%), fever (56%), night sweats (35%), pleuritic chest pain (33%), chills (28%), weight loss (21%), rash (14%), and arthralgia or myalgia (13% and 12%, respectively).5
Airspace opacity was the most common radiographic abnormality (58.8%); the second most common was pulmonary nodules (22.8%).5 The study didn’t compare the frequency of these findings with noncoccidioidal pneumonia.
RECOMMENDATIONS
In 2005 guidelines, the Infectious Diseases Society of America (IDSA) stated that the “management of coccidioidomycosis first involves recognizing that a coccidioidal infection exists, defining the extent of infection, and identifying host factors that predispose to disease severity.”6 The IDSA didn’t give specific recommendations regarding how to diagnose or differentiate coccidioidal infection from CAP.
1. Centers for Disease Control and Prevention (CDC). Increase in reported coccidioidomycosis—United States, 1998-2011. MMWR Morb Mortal Wkly Rep. 2013;62:217-221.
2. Chang DC, Anderson S, Wannemuehler K, et al. Testing for coccidioidomycosis among patients with community-acquired pneumonia. Emerg Infect Dis. 2008;14: 1053-1059.
3. Valdivia L, Nix D, Wright M, et al. Coccidioidomycosis as a common cause of community-acquired pneumonia. Emerg Infect Dis. 2006;12:958-962.
4. Kim MM, Blair JE, Carey EJ, et al. Coccidioidal pneumonia, Phoenix, Arizona, USA, 2000-2004. Emerg Infect Dis. 2009;15:397-401.
5. Crum NF, Lederman ER, Stafford CM, et al. Coccidioidomycosis: a descriptive survey of a reemerging disease. Clinical characteristics and current controversies. Medicine (Baltimore). 2004;83:149-175.
6. Galgiani JN, Ampel NM, Blair JE, et al; Infectious Disease Society of America. Coccidioidomycosis. Clin Infect Dis. 2005;41:1217-1223.
EVIDENCE-BASED ANSWER:
Risk factors for coccidioidomycosis, or valley fever, include lower respiratory tract symptoms lasting longer than 14 days, chest pain, rash, having lived in endemic areas fewer than 10 years, and diabetes mellitus or immunosuppressive conditions (strength of recommendation [SOR]: B, several prospective cohort and case-control studies).
The most common signs and symptoms include cough (74%), fever (56%), night sweats (35%), pleuritic chest pain (33%), chills (28%), dyspnea (27%), weight loss (21%), and rash (14%) (SOR: B, retrospective cohort study).
EVIDENCE SUMMARY
A 2013 surveillance report by the Centers for Disease Control and Prevention that included 111,717 patients in 28 states and the District of Columbia found an 8-fold increase in reported coccidioidomycosis in endemic areas from 1998 to 2011 (age-adjusted incidence rates: 5.3 per 100,000 in 1998 and 42.6 per 100,000 in 2011). Cases in nonendemic states increased 40-fold in the same time period, from 6 cases to 240.1 The disease is endemic in the southwest United States and northwest Mexico.
Risk factors include persistent symptoms, chest pain, diabetes, immunosuppression
A 2008 case-control study of 136 patients in Phoenix, Arizona (an endemic area) found that 15% of the patients diagnosed with community-acquired pneumonia (CAP) had coccidioidomycosis on serologic testing. Risk factors for CAP caused by coccidioidomycosis in this population were symptom duration longer than 14 days (odds ratio [OR]=5.0; 95% confidence interval [CI], 2.1-15.7), age younger than 18 years (OR=5.5; 95% CI, 2.1-15.3), chest pain (OR=4.6; 95% CI, 1.8-11.8), and diabetes mellitus or an immunosuppressive condition (OR=3.8; 95% CI, 1.0-16.5).2
Abnormal chest X-rays, myalgia— and a rash
A 2006 prospective cohort study of 55 patients in Tucson, Arizona, which is part of the endemic area, found that 29% of patients diagnosed with CAP tested serologically positive for coccidioidomycosis. Risk factors included fewer than 10 years of exposure to an endemic area (OR=4.11; 95% CI, 1.01-16.8). Chest radiograph abnormalities were more common in patients with CAP caused by coccidioidomycosis than patients without coccidioidomycosis (75% vs 25%, P=.005). Myalgia is more common when coccidioidal pneumonia is present (69% vs 23%, P=.0022).3
A 2009 prospective cohort study of 35 patients with CAP in Phoenix, Arizona found that 6 patients (17%) tested positive for coccidioidomycosis. Only 1 statistically significant risk factor was identified—half of patients with coccidioidomycosis exhibited a rash, while there were no rashes in the group without the disease (P=.002).4
Other common signs and symptoms
A retrospective cohort study in San Diego, California in 2004 evaluated and stratified 223 patients with known coccidioidomycosis for presenting symptoms, exam findings, and radiographic findings. The most common signs and symptoms at time of seropositive testing were cough (74%), fever (56%), night sweats (35%), pleuritic chest pain (33%), chills (28%), weight loss (21%), rash (14%), and arthralgia or myalgia (13% and 12%, respectively).5
Airspace opacity was the most common radiographic abnormality (58.8%); the second most common was pulmonary nodules (22.8%).5 The study didn’t compare the frequency of these findings with noncoccidioidal pneumonia.
RECOMMENDATIONS
In 2005 guidelines, the Infectious Diseases Society of America (IDSA) stated that the “management of coccidioidomycosis first involves recognizing that a coccidioidal infection exists, defining the extent of infection, and identifying host factors that predispose to disease severity.”6 The IDSA didn’t give specific recommendations regarding how to diagnose or differentiate coccidioidal infection from CAP.
EVIDENCE-BASED ANSWER:
Risk factors for coccidioidomycosis, or valley fever, include lower respiratory tract symptoms lasting longer than 14 days, chest pain, rash, having lived in endemic areas fewer than 10 years, and diabetes mellitus or immunosuppressive conditions (strength of recommendation [SOR]: B, several prospective cohort and case-control studies).
The most common signs and symptoms include cough (74%), fever (56%), night sweats (35%), pleuritic chest pain (33%), chills (28%), dyspnea (27%), weight loss (21%), and rash (14%) (SOR: B, retrospective cohort study).
EVIDENCE SUMMARY
A 2013 surveillance report by the Centers for Disease Control and Prevention that included 111,717 patients in 28 states and the District of Columbia found an 8-fold increase in reported coccidioidomycosis in endemic areas from 1998 to 2011 (age-adjusted incidence rates: 5.3 per 100,000 in 1998 and 42.6 per 100,000 in 2011). Cases in nonendemic states increased 40-fold in the same time period, from 6 cases to 240.1 The disease is endemic in the southwest United States and northwest Mexico.
Risk factors include persistent symptoms, chest pain, diabetes, immunosuppression
A 2008 case-control study of 136 patients in Phoenix, Arizona (an endemic area) found that 15% of the patients diagnosed with community-acquired pneumonia (CAP) had coccidioidomycosis on serologic testing. Risk factors for CAP caused by coccidioidomycosis in this population were symptom duration longer than 14 days (odds ratio [OR]=5.0; 95% confidence interval [CI], 2.1-15.7), age younger than 18 years (OR=5.5; 95% CI, 2.1-15.3), chest pain (OR=4.6; 95% CI, 1.8-11.8), and diabetes mellitus or an immunosuppressive condition (OR=3.8; 95% CI, 1.0-16.5).2
Abnormal chest X-rays, myalgia— and a rash
A 2006 prospective cohort study of 55 patients in Tucson, Arizona, which is part of the endemic area, found that 29% of patients diagnosed with CAP tested serologically positive for coccidioidomycosis. Risk factors included fewer than 10 years of exposure to an endemic area (OR=4.11; 95% CI, 1.01-16.8). Chest radiograph abnormalities were more common in patients with CAP caused by coccidioidomycosis than patients without coccidioidomycosis (75% vs 25%, P=.005). Myalgia is more common when coccidioidal pneumonia is present (69% vs 23%, P=.0022).3
A 2009 prospective cohort study of 35 patients with CAP in Phoenix, Arizona found that 6 patients (17%) tested positive for coccidioidomycosis. Only 1 statistically significant risk factor was identified—half of patients with coccidioidomycosis exhibited a rash, while there were no rashes in the group without the disease (P=.002).4
Other common signs and symptoms
A retrospective cohort study in San Diego, California in 2004 evaluated and stratified 223 patients with known coccidioidomycosis for presenting symptoms, exam findings, and radiographic findings. The most common signs and symptoms at time of seropositive testing were cough (74%), fever (56%), night sweats (35%), pleuritic chest pain (33%), chills (28%), weight loss (21%), rash (14%), and arthralgia or myalgia (13% and 12%, respectively).5
Airspace opacity was the most common radiographic abnormality (58.8%); the second most common was pulmonary nodules (22.8%).5 The study didn’t compare the frequency of these findings with noncoccidioidal pneumonia.
RECOMMENDATIONS
In 2005 guidelines, the Infectious Diseases Society of America (IDSA) stated that the “management of coccidioidomycosis first involves recognizing that a coccidioidal infection exists, defining the extent of infection, and identifying host factors that predispose to disease severity.”6 The IDSA didn’t give specific recommendations regarding how to diagnose or differentiate coccidioidal infection from CAP.
1. Centers for Disease Control and Prevention (CDC). Increase in reported coccidioidomycosis—United States, 1998-2011. MMWR Morb Mortal Wkly Rep. 2013;62:217-221.
2. Chang DC, Anderson S, Wannemuehler K, et al. Testing for coccidioidomycosis among patients with community-acquired pneumonia. Emerg Infect Dis. 2008;14: 1053-1059.
3. Valdivia L, Nix D, Wright M, et al. Coccidioidomycosis as a common cause of community-acquired pneumonia. Emerg Infect Dis. 2006;12:958-962.
4. Kim MM, Blair JE, Carey EJ, et al. Coccidioidal pneumonia, Phoenix, Arizona, USA, 2000-2004. Emerg Infect Dis. 2009;15:397-401.
5. Crum NF, Lederman ER, Stafford CM, et al. Coccidioidomycosis: a descriptive survey of a reemerging disease. Clinical characteristics and current controversies. Medicine (Baltimore). 2004;83:149-175.
6. Galgiani JN, Ampel NM, Blair JE, et al; Infectious Disease Society of America. Coccidioidomycosis. Clin Infect Dis. 2005;41:1217-1223.
1. Centers for Disease Control and Prevention (CDC). Increase in reported coccidioidomycosis—United States, 1998-2011. MMWR Morb Mortal Wkly Rep. 2013;62:217-221.
2. Chang DC, Anderson S, Wannemuehler K, et al. Testing for coccidioidomycosis among patients with community-acquired pneumonia. Emerg Infect Dis. 2008;14: 1053-1059.
3. Valdivia L, Nix D, Wright M, et al. Coccidioidomycosis as a common cause of community-acquired pneumonia. Emerg Infect Dis. 2006;12:958-962.
4. Kim MM, Blair JE, Carey EJ, et al. Coccidioidal pneumonia, Phoenix, Arizona, USA, 2000-2004. Emerg Infect Dis. 2009;15:397-401.
5. Crum NF, Lederman ER, Stafford CM, et al. Coccidioidomycosis: a descriptive survey of a reemerging disease. Clinical characteristics and current controversies. Medicine (Baltimore). 2004;83:149-175.
6. Galgiani JN, Ampel NM, Blair JE, et al; Infectious Disease Society of America. Coccidioidomycosis. Clin Infect Dis. 2005;41:1217-1223.
Evidence-based answers from the Family Physicians Inquiries Network
Is immediate-release topiramate an effective treatment for adult obesity?
EVIDENCE-BASED ANSWER:
Yes. Topiramate (at daily doses of 64-400 mg) produces an average 5.34 kg of additional weight loss compared with placebo (95% confidence interval [CI], -6.12 to -4.56) in overweight to obese adults for periods of 16 to 60 weeks (strength of recommendation [SOR]: A, meta-analyses of randomized controlled trials [RCTs]).
Topiramate increases the chances of losing 5% or more of baseline body weight (BBW) with a number needed to treat (NNT) of 3 (95% CI, 2-3) and 10% or more of BBW with an NNT of 4 (95% CI, 3-4). However, approximately 17% of patients discontinue the drug because of adverse effects, including paresthesia, hypoesthesia, taste perversion, and psychomotor impairment (SOR: A, meta-analyses of RCTs).
EVIDENCE SUMMARY
A meta-analysis of 10 well-done RCTs with a total of 3320 patients found that topiramate produced more weight loss than placebo.1 Studies included men and women ages 18 to 75 years, with a body mass index (BMI) of 27 to 50. Several studies included patients with hypertension, dyslipidemia, and diabetes mellitus; one study included patients with binge eating disorder. Investigators recruited subjects from sites in Europe, North America, Australia, and South Africa. The studies lasted 16 to 60 weeks and used variable doses of topiramate (64-400 mg daily). Most incorporated a structured lifestyle intervention program for both the treatment and control groups.
Patients taking topiramate lost 5.34 kg (95% CI, -6.12 to -4.56) more than subjects taking placebo. All studies showed significantly greater weight loss in the topiramate groups, regardless of dose and duration, although there was some heterogeneity among the results. The NNTs to achieve weight loss of 5% or more of BBW and 10% or more of BBW were 3 (95% CI, 2-3) and 4 (95% CI, 3-4), respectively.
No major adverse events, but some unpleasant effects
A safety analysis on 6620 subjects found no major adverse events.1 Subjects in the topiramate group were more likely to withdraw because of adverse effects (odds ratio=1.97; 95% CI, 1.64-2.29; number needed to harm=14; 95% CI, 11-18). The most common adverse effects were paresthesia, hypoesthesia, taste perversion, and psychomotor impairment, and these effects were most likely to lead to discontinuation at daily doses >96 mg.
Two formulas are effective in patients with diabetes
Investigators stopped 6 studies early because the sponsor wanted to pursue development of a controlled-release formulation of topiramate. The meta-analysis includes a single study of controlled-release topiramate, 175 mg daily in patients with diabetes, that showed equivalent efficacy and similar tolerability to immediate-release topiramate.2
Three other RCTs included in the meta-analysis specifically examined obese patients with type 2 diabetes, a population deemed more resistant to typical weight loss regimens, treated with immediate-release topiramate in dosages of 96 mg and 192 mg daily.3-5 These patients also experienced greater weight loss than patients taking placebo, comparable to what was seen in the overall meta-analysis.
FDA approval and cost of therapy
Topiramate monotherapy isn’t approved by the US Food and Drug Administration (FDA) for obesity treatment. In 2012, the FDA approved phentermine/topiramate extended-release (Qsymia) for long-term treatment of obesity; the monthly cost for a maintenance dose of 7.5 mg/46 mg daily is approximately $185.6 Topiramate immediate-release tablets cost approximately $25 per month for twice daily doses of 50 to 100 mg.7
RECOMMENDATIONS
The US Preventive Services Task Force recommends screening all adults for obesity by measuring BMI and referring patients with a BMI ≥30 for high-intensity, comprehensive behavioral interventions. It makes no recommendation for pharmacologic management.8
The Institute for Clinical Systems Improvement concludes that pharmacotherapy should be used only as part of a comprehensive obesity treatment plan. Pharmacotherapy should be considered if obese patients are unable to lose 1 pound per week with diet, physical activity, and behavior modification.9
1. Kramer CK, Leitão CB, Pinto LC, et al. Efficacy and safety of topiramate on weight loss: a meta-analysis of randomized controlled trials. Obes Rev. 2011;12:e338-e347.
2. Rosenstock J, Hollander P, Gadde KM, et al; OBD-202 Study Group. A randomized, double-blind, placebo-controlled, multicenter study to assess the efficacy and safety of topiramate controlled release in the treatment of obese type 2 diabetic patients. Diabetes Care. 2007;30:1480-1486.
3. Stenlöf K, Rössner S, Vercruysse F, et al. Topiramate in the treatment of obese subjects with drug-naive type 2 diabetes. Diabetes Obes Metab. 2007;9:360-368.
4. Toplak H, Hamann A, Moore R, et al. Efficacy and safety of topiramate in combination with metformin in the treatment of obese subjects with type 2 diabetes: a randomized, double-blind, placebo-controlled study. Int J Obes (Lond). 2007;31:138-146.
5. Eliasson B, Gudbjörnsdottir S, Cederholm J, et al. Weight loss and metabolic effects of topiramate in overweight and obese type 2 diabetic patients: randomized double-blind placebo-controlled trial. Int J Obes (Lond). 2007;31: 1140-1147.
6. Drugs.com. Qsymia. Drugs.com Web site. Available at: www.drugs.com/pro/qsymia.html. Accessed September 26, 2014.
7. Drugs.com. Topirimate prices, coupons and patient assistance programs. Drugs.com Web site. Available at: www.drugs.com/price-guide/topiramate. Accessed September 26, 2014.
8. US Preventive Services Task Force. Obesity in Adults: Screening and management. US Preventive Services Task Force Web site. Available at: www.uspreventiveservicestaskforce.org/uspstf11/obeseadult/obesers.htm. Accessed September 30, 2014.
9. Fitch A, Everling L, Fox C, et al. Prevention and management of obesity for adults. Institute for Clinical Systems Improvement Web site. Available at: www.icsi.org/_asset/s935hy/Obesity-Adults.pdf. Accessed September 30, 2014.
EVIDENCE-BASED ANSWER:
Yes. Topiramate (at daily doses of 64-400 mg) produces an average 5.34 kg of additional weight loss compared with placebo (95% confidence interval [CI], -6.12 to -4.56) in overweight to obese adults for periods of 16 to 60 weeks (strength of recommendation [SOR]: A, meta-analyses of randomized controlled trials [RCTs]).
Topiramate increases the chances of losing 5% or more of baseline body weight (BBW) with a number needed to treat (NNT) of 3 (95% CI, 2-3) and 10% or more of BBW with an NNT of 4 (95% CI, 3-4). However, approximately 17% of patients discontinue the drug because of adverse effects, including paresthesia, hypoesthesia, taste perversion, and psychomotor impairment (SOR: A, meta-analyses of RCTs).
EVIDENCE SUMMARY
A meta-analysis of 10 well-done RCTs with a total of 3320 patients found that topiramate produced more weight loss than placebo.1 Studies included men and women ages 18 to 75 years, with a body mass index (BMI) of 27 to 50. Several studies included patients with hypertension, dyslipidemia, and diabetes mellitus; one study included patients with binge eating disorder. Investigators recruited subjects from sites in Europe, North America, Australia, and South Africa. The studies lasted 16 to 60 weeks and used variable doses of topiramate (64-400 mg daily). Most incorporated a structured lifestyle intervention program for both the treatment and control groups.
Patients taking topiramate lost 5.34 kg (95% CI, -6.12 to -4.56) more than subjects taking placebo. All studies showed significantly greater weight loss in the topiramate groups, regardless of dose and duration, although there was some heterogeneity among the results. The NNTs to achieve weight loss of 5% or more of BBW and 10% or more of BBW were 3 (95% CI, 2-3) and 4 (95% CI, 3-4), respectively.
No major adverse events, but some unpleasant effects
A safety analysis on 6620 subjects found no major adverse events.1 Subjects in the topiramate group were more likely to withdraw because of adverse effects (odds ratio=1.97; 95% CI, 1.64-2.29; number needed to harm=14; 95% CI, 11-18). The most common adverse effects were paresthesia, hypoesthesia, taste perversion, and psychomotor impairment, and these effects were most likely to lead to discontinuation at daily doses >96 mg.
Two formulas are effective in patients with diabetes
Investigators stopped 6 studies early because the sponsor wanted to pursue development of a controlled-release formulation of topiramate. The meta-analysis includes a single study of controlled-release topiramate, 175 mg daily in patients with diabetes, that showed equivalent efficacy and similar tolerability to immediate-release topiramate.2
Three other RCTs included in the meta-analysis specifically examined obese patients with type 2 diabetes, a population deemed more resistant to typical weight loss regimens, treated with immediate-release topiramate in dosages of 96 mg and 192 mg daily.3-5 These patients also experienced greater weight loss than patients taking placebo, comparable to what was seen in the overall meta-analysis.
FDA approval and cost of therapy
Topiramate monotherapy isn’t approved by the US Food and Drug Administration (FDA) for obesity treatment. In 2012, the FDA approved phentermine/topiramate extended-release (Qsymia) for long-term treatment of obesity; the monthly cost for a maintenance dose of 7.5 mg/46 mg daily is approximately $185.6 Topiramate immediate-release tablets cost approximately $25 per month for twice daily doses of 50 to 100 mg.7
RECOMMENDATIONS
The US Preventive Services Task Force recommends screening all adults for obesity by measuring BMI and referring patients with a BMI ≥30 for high-intensity, comprehensive behavioral interventions. It makes no recommendation for pharmacologic management.8
The Institute for Clinical Systems Improvement concludes that pharmacotherapy should be used only as part of a comprehensive obesity treatment plan. Pharmacotherapy should be considered if obese patients are unable to lose 1 pound per week with diet, physical activity, and behavior modification.9
EVIDENCE-BASED ANSWER:
Yes. Topiramate (at daily doses of 64-400 mg) produces an average 5.34 kg of additional weight loss compared with placebo (95% confidence interval [CI], -6.12 to -4.56) in overweight to obese adults for periods of 16 to 60 weeks (strength of recommendation [SOR]: A, meta-analyses of randomized controlled trials [RCTs]).
Topiramate increases the chances of losing 5% or more of baseline body weight (BBW) with a number needed to treat (NNT) of 3 (95% CI, 2-3) and 10% or more of BBW with an NNT of 4 (95% CI, 3-4). However, approximately 17% of patients discontinue the drug because of adverse effects, including paresthesia, hypoesthesia, taste perversion, and psychomotor impairment (SOR: A, meta-analyses of RCTs).
EVIDENCE SUMMARY
A meta-analysis of 10 well-done RCTs with a total of 3320 patients found that topiramate produced more weight loss than placebo.1 Studies included men and women ages 18 to 75 years, with a body mass index (BMI) of 27 to 50. Several studies included patients with hypertension, dyslipidemia, and diabetes mellitus; one study included patients with binge eating disorder. Investigators recruited subjects from sites in Europe, North America, Australia, and South Africa. The studies lasted 16 to 60 weeks and used variable doses of topiramate (64-400 mg daily). Most incorporated a structured lifestyle intervention program for both the treatment and control groups.
Patients taking topiramate lost 5.34 kg (95% CI, -6.12 to -4.56) more than subjects taking placebo. All studies showed significantly greater weight loss in the topiramate groups, regardless of dose and duration, although there was some heterogeneity among the results. The NNTs to achieve weight loss of 5% or more of BBW and 10% or more of BBW were 3 (95% CI, 2-3) and 4 (95% CI, 3-4), respectively.
No major adverse events, but some unpleasant effects
A safety analysis on 6620 subjects found no major adverse events.1 Subjects in the topiramate group were more likely to withdraw because of adverse effects (odds ratio=1.97; 95% CI, 1.64-2.29; number needed to harm=14; 95% CI, 11-18). The most common adverse effects were paresthesia, hypoesthesia, taste perversion, and psychomotor impairment, and these effects were most likely to lead to discontinuation at daily doses >96 mg.
Two formulas are effective in patients with diabetes
Investigators stopped 6 studies early because the sponsor wanted to pursue development of a controlled-release formulation of topiramate. The meta-analysis includes a single study of controlled-release topiramate, 175 mg daily in patients with diabetes, that showed equivalent efficacy and similar tolerability to immediate-release topiramate.2
Three other RCTs included in the meta-analysis specifically examined obese patients with type 2 diabetes, a population deemed more resistant to typical weight loss regimens, treated with immediate-release topiramate in dosages of 96 mg and 192 mg daily.3-5 These patients also experienced greater weight loss than patients taking placebo, comparable to what was seen in the overall meta-analysis.
FDA approval and cost of therapy
Topiramate monotherapy isn’t approved by the US Food and Drug Administration (FDA) for obesity treatment. In 2012, the FDA approved phentermine/topiramate extended-release (Qsymia) for long-term treatment of obesity; the monthly cost for a maintenance dose of 7.5 mg/46 mg daily is approximately $185.6 Topiramate immediate-release tablets cost approximately $25 per month for twice daily doses of 50 to 100 mg.7
RECOMMENDATIONS
The US Preventive Services Task Force recommends screening all adults for obesity by measuring BMI and referring patients with a BMI ≥30 for high-intensity, comprehensive behavioral interventions. It makes no recommendation for pharmacologic management.8
The Institute for Clinical Systems Improvement concludes that pharmacotherapy should be used only as part of a comprehensive obesity treatment plan. Pharmacotherapy should be considered if obese patients are unable to lose 1 pound per week with diet, physical activity, and behavior modification.9
1. Kramer CK, Leitão CB, Pinto LC, et al. Efficacy and safety of topiramate on weight loss: a meta-analysis of randomized controlled trials. Obes Rev. 2011;12:e338-e347.
2. Rosenstock J, Hollander P, Gadde KM, et al; OBD-202 Study Group. A randomized, double-blind, placebo-controlled, multicenter study to assess the efficacy and safety of topiramate controlled release in the treatment of obese type 2 diabetic patients. Diabetes Care. 2007;30:1480-1486.
3. Stenlöf K, Rössner S, Vercruysse F, et al. Topiramate in the treatment of obese subjects with drug-naive type 2 diabetes. Diabetes Obes Metab. 2007;9:360-368.
4. Toplak H, Hamann A, Moore R, et al. Efficacy and safety of topiramate in combination with metformin in the treatment of obese subjects with type 2 diabetes: a randomized, double-blind, placebo-controlled study. Int J Obes (Lond). 2007;31:138-146.
5. Eliasson B, Gudbjörnsdottir S, Cederholm J, et al. Weight loss and metabolic effects of topiramate in overweight and obese type 2 diabetic patients: randomized double-blind placebo-controlled trial. Int J Obes (Lond). 2007;31: 1140-1147.
6. Drugs.com. Qsymia. Drugs.com Web site. Available at: www.drugs.com/pro/qsymia.html. Accessed September 26, 2014.
7. Drugs.com. Topirimate prices, coupons and patient assistance programs. Drugs.com Web site. Available at: www.drugs.com/price-guide/topiramate. Accessed September 26, 2014.
8. US Preventive Services Task Force. Obesity in Adults: Screening and management. US Preventive Services Task Force Web site. Available at: www.uspreventiveservicestaskforce.org/uspstf11/obeseadult/obesers.htm. Accessed September 30, 2014.
9. Fitch A, Everling L, Fox C, et al. Prevention and management of obesity for adults. Institute for Clinical Systems Improvement Web site. Available at: www.icsi.org/_asset/s935hy/Obesity-Adults.pdf. Accessed September 30, 2014.
1. Kramer CK, Leitão CB, Pinto LC, et al. Efficacy and safety of topiramate on weight loss: a meta-analysis of randomized controlled trials. Obes Rev. 2011;12:e338-e347.
2. Rosenstock J, Hollander P, Gadde KM, et al; OBD-202 Study Group. A randomized, double-blind, placebo-controlled, multicenter study to assess the efficacy and safety of topiramate controlled release in the treatment of obese type 2 diabetic patients. Diabetes Care. 2007;30:1480-1486.
3. Stenlöf K, Rössner S, Vercruysse F, et al. Topiramate in the treatment of obese subjects with drug-naive type 2 diabetes. Diabetes Obes Metab. 2007;9:360-368.
4. Toplak H, Hamann A, Moore R, et al. Efficacy and safety of topiramate in combination with metformin in the treatment of obese subjects with type 2 diabetes: a randomized, double-blind, placebo-controlled study. Int J Obes (Lond). 2007;31:138-146.
5. Eliasson B, Gudbjörnsdottir S, Cederholm J, et al. Weight loss and metabolic effects of topiramate in overweight and obese type 2 diabetic patients: randomized double-blind placebo-controlled trial. Int J Obes (Lond). 2007;31: 1140-1147.
6. Drugs.com. Qsymia. Drugs.com Web site. Available at: www.drugs.com/pro/qsymia.html. Accessed September 26, 2014.
7. Drugs.com. Topirimate prices, coupons and patient assistance programs. Drugs.com Web site. Available at: www.drugs.com/price-guide/topiramate. Accessed September 26, 2014.
8. US Preventive Services Task Force. Obesity in Adults: Screening and management. US Preventive Services Task Force Web site. Available at: www.uspreventiveservicestaskforce.org/uspstf11/obeseadult/obesers.htm. Accessed September 30, 2014.
9. Fitch A, Everling L, Fox C, et al. Prevention and management of obesity for adults. Institute for Clinical Systems Improvement Web site. Available at: www.icsi.org/_asset/s935hy/Obesity-Adults.pdf. Accessed September 30, 2014.
Evidence-based answers from the Family Physicians Inquiries Network