User login
Auditory Rehabilitation Programs for Adults—Are They Effective?
Study Overview
Objective. To determine the effectiveness of adult auditory rehabilitation programs that focus on the use of communication strategies.
Design. Nonsystematic review of the literature.
Methods. The authors used the PubMed database to search for systematic reviews investigating the effectiveness of auditory training and auditory rehabilitation programs. Auditory training involves the patient participating in a program of training designed to enhance speech perception. Training is typically provided on a repeated basis over a number of sessions and involves practice with listening and recognition of speech-based material. Auditory rehabilitation programs can be delivered to groups or individuals and usually have a focus on supplementing information about hearing loss and hearing aids with advice and/or practice with communication strategies and the management of psychosocial aspects of hearing loss.
Main outcome measures. A variety of outcomes were measured in the individual studies.
Results. One systematic review of individual auditory training and 2 systematic reviews of group auditory rehabilitation were identified. Sweetow and Palmer [1] found that auditory training in which speech was broken down into its parts was associated with improvements in the perception of speech in the presence of background noise and better use of active listening strategies. With regard to rehabilitation programs, Hawkins [2] found evidence of short-term reduction in perceived hearing handicap but less evidence of effectiveness for other outcomes. A more recent review by Chisolm and Arnold [3] included only randomized studies that examined the effect of the program on social participation and quality of life. References for the included studies were given but the summary results of this review were not included in this paper.
Conclusion. The authors conclude that there is some evidence that auditory rehabilitation programs are associated with improvements in social participation and quality of life but they acknowledge that more evidence is required.
Commentary
Adult acquired hearing loss is a common long-term condition which in the majority of cases is not remediable by surgical or medical intervention. It is the second leading cause of years lived with a disability [4]. Intervention options for people with hearing loss include hearing aid fitting and/or participation in a rehabilitative program that might include information about hearing and communication and practice or experience with listening or communication tasks [5,6]. Poorly managed hearing loss is associated with negative consequences including depression and cognitive decline [7,8]. Identifying effective management options for hearing loss can reduce these consequences and improve quality of life. In the current paper, Cardemil et al review the evidence for the effectiveness of adult auditory rehabilitation. They note that hearing aids alone cannot ameliorate all of the difficulties caused by age-related hearing loss, where cognitive factors play a significant role. They provide a rationale for why communication-based training in auditory rehabilitation has been recommended as a substitute or supplement to hearing aid fitting. That is, such training addresses the cognitive and communication difficulties that exist in addition to the hearing loss.
This paper summarises the findings of 3 systematic reviews: one on individual auditory rehabilitation and 2 on group rehabilitation. There was heterogeneity among the programs and the methods used to assess their effectiveness were variable. The reviewers conclude that there appears to be some short-term benefit to auditory rehabilitation programs but effect sizes, where effects are seen, are small and more research is needed to establish the effectiveness of these programs.
A limitation of this review is that it was nonsystematic and did not critically appraise the quality of the included systematic reviews. One weakness of the systematic reviews presented is that they did not consider interactions between content and delivery of interventions and comparisons. Individual auditory rehabilitation and group rehabilitation are typically delivered over many sessions in contrast to control groups, which often receive “standard care” delivered over a single or limited number of sessions. Therefore, where an effect exists it is unclear whether the “active ingredient” contributing to the effect is the rehabilitative content delivered or the number of sessions over which it is provided. This is a possible confounding factor not acknowledged or discussed in these systematic reviews.
In addition, any discussion which seeks to assess effectiveness should define outcomes of interest or at least review the range of outcomes that have been studied and how they are relevant to the problem being addressed. There is a lack of consensus on what the important clinical outcomes are for hearing health care [9] and a dearth of research on longer-term outcomes; this could have been explored.
Applications for Clinical Practice
This summary of 3 systematic reviews highlights the need for further research in this area. Studies that measure long-term outcomes (1 year or more) and that are appropriately powered are needed. In addition, the possible interaction between different potentially active components of complex interventions must be acknowledged. Health care professionals and policy makers need to be aware of these factors when reviewing evidence and making decisions that impact on clinical practice.
—Fiona Barker, Department of Health Care Management and Policy, University of Surrey, Guildford, UK
1. Sweetow R, Palmer CV. Efficacy of individual auditory training in adults: a systematic review of the evidence. J Am Acad Audiol 2005;16:494–504.
2. Hawkins DB. Effectiveness of counseling-based adult group aural rehabilitation programs: a systematic review of the evidence. J Am Acad Audiol 2005;16:485–93.
3. Chisolm TH, Arnold M. Evidence about the effectiveness of aural rehabilitation programs for adults. In: Wong L, Hickson L, editors. Evidence-based practice in audiology. San Diego: Plural; 2012.
4. World Health Organisation. Facts about deafness. 2012. Accessed 6 Nov 2014 at www.who.int/pbd/deafness/facts/en/.
5. Laplante-Levesque A, Hickson L, Worrall L. Rehabilitation of older adults with hearing impairment: a critical review. J Aging Health 2010;22:143–53.
6. Pronk M, Kramer SE, Davis AC, Stephens D, Smith PA, Thodi C, et al. Interventions following hearing screening in adults: a systematic descriptive review. Int J Audiol 2011;50:594–609.
7. Lin FR. Hearing loss and cognition among older adults in the United States. J Gerontol A Biol Sci Med Sci 2011;66:1131–6.
8. Saito H, Nishiwaki Y, Michikawa T, et al. Hearing handicap predicts the development of depressive symptoms after 3 years in older community-dwelling Japanese. J Am Geriatr Soc 2010;58:93–7.
9. Humes LE, Krull V. Hearing aids for adults. In: Wong L, Hickson L, editors. Evidence-based practice in audiology. San Diego: Plural; 2012.
Study Overview
Objective. To determine the effectiveness of adult auditory rehabilitation programs that focus on the use of communication strategies.
Design. Nonsystematic review of the literature.
Methods. The authors used the PubMed database to search for systematic reviews investigating the effectiveness of auditory training and auditory rehabilitation programs. Auditory training involves the patient participating in a program of training designed to enhance speech perception. Training is typically provided on a repeated basis over a number of sessions and involves practice with listening and recognition of speech-based material. Auditory rehabilitation programs can be delivered to groups or individuals and usually have a focus on supplementing information about hearing loss and hearing aids with advice and/or practice with communication strategies and the management of psychosocial aspects of hearing loss.
Main outcome measures. A variety of outcomes were measured in the individual studies.
Results. One systematic review of individual auditory training and 2 systematic reviews of group auditory rehabilitation were identified. Sweetow and Palmer [1] found that auditory training in which speech was broken down into its parts was associated with improvements in the perception of speech in the presence of background noise and better use of active listening strategies. With regard to rehabilitation programs, Hawkins [2] found evidence of short-term reduction in perceived hearing handicap but less evidence of effectiveness for other outcomes. A more recent review by Chisolm and Arnold [3] included only randomized studies that examined the effect of the program on social participation and quality of life. References for the included studies were given but the summary results of this review were not included in this paper.
Conclusion. The authors conclude that there is some evidence that auditory rehabilitation programs are associated with improvements in social participation and quality of life but they acknowledge that more evidence is required.
Commentary
Adult acquired hearing loss is a common long-term condition which in the majority of cases is not remediable by surgical or medical intervention. It is the second leading cause of years lived with a disability [4]. Intervention options for people with hearing loss include hearing aid fitting and/or participation in a rehabilitative program that might include information about hearing and communication and practice or experience with listening or communication tasks [5,6]. Poorly managed hearing loss is associated with negative consequences including depression and cognitive decline [7,8]. Identifying effective management options for hearing loss can reduce these consequences and improve quality of life. In the current paper, Cardemil et al review the evidence for the effectiveness of adult auditory rehabilitation. They note that hearing aids alone cannot ameliorate all of the difficulties caused by age-related hearing loss, where cognitive factors play a significant role. They provide a rationale for why communication-based training in auditory rehabilitation has been recommended as a substitute or supplement to hearing aid fitting. That is, such training addresses the cognitive and communication difficulties that exist in addition to the hearing loss.
This paper summarises the findings of 3 systematic reviews: one on individual auditory rehabilitation and 2 on group rehabilitation. There was heterogeneity among the programs and the methods used to assess their effectiveness were variable. The reviewers conclude that there appears to be some short-term benefit to auditory rehabilitation programs but effect sizes, where effects are seen, are small and more research is needed to establish the effectiveness of these programs.
A limitation of this review is that it was nonsystematic and did not critically appraise the quality of the included systematic reviews. One weakness of the systematic reviews presented is that they did not consider interactions between content and delivery of interventions and comparisons. Individual auditory rehabilitation and group rehabilitation are typically delivered over many sessions in contrast to control groups, which often receive “standard care” delivered over a single or limited number of sessions. Therefore, where an effect exists it is unclear whether the “active ingredient” contributing to the effect is the rehabilitative content delivered or the number of sessions over which it is provided. This is a possible confounding factor not acknowledged or discussed in these systematic reviews.
In addition, any discussion which seeks to assess effectiveness should define outcomes of interest or at least review the range of outcomes that have been studied and how they are relevant to the problem being addressed. There is a lack of consensus on what the important clinical outcomes are for hearing health care [9] and a dearth of research on longer-term outcomes; this could have been explored.
Applications for Clinical Practice
This summary of 3 systematic reviews highlights the need for further research in this area. Studies that measure long-term outcomes (1 year or more) and that are appropriately powered are needed. In addition, the possible interaction between different potentially active components of complex interventions must be acknowledged. Health care professionals and policy makers need to be aware of these factors when reviewing evidence and making decisions that impact on clinical practice.
—Fiona Barker, Department of Health Care Management and Policy, University of Surrey, Guildford, UK
Study Overview
Objective. To determine the effectiveness of adult auditory rehabilitation programs that focus on the use of communication strategies.
Design. Nonsystematic review of the literature.
Methods. The authors used the PubMed database to search for systematic reviews investigating the effectiveness of auditory training and auditory rehabilitation programs. Auditory training involves the patient participating in a program of training designed to enhance speech perception. Training is typically provided on a repeated basis over a number of sessions and involves practice with listening and recognition of speech-based material. Auditory rehabilitation programs can be delivered to groups or individuals and usually have a focus on supplementing information about hearing loss and hearing aids with advice and/or practice with communication strategies and the management of psychosocial aspects of hearing loss.
Main outcome measures. A variety of outcomes were measured in the individual studies.
Results. One systematic review of individual auditory training and 2 systematic reviews of group auditory rehabilitation were identified. Sweetow and Palmer [1] found that auditory training in which speech was broken down into its parts was associated with improvements in the perception of speech in the presence of background noise and better use of active listening strategies. With regard to rehabilitation programs, Hawkins [2] found evidence of short-term reduction in perceived hearing handicap but less evidence of effectiveness for other outcomes. A more recent review by Chisolm and Arnold [3] included only randomized studies that examined the effect of the program on social participation and quality of life. References for the included studies were given but the summary results of this review were not included in this paper.
Conclusion. The authors conclude that there is some evidence that auditory rehabilitation programs are associated with improvements in social participation and quality of life but they acknowledge that more evidence is required.
Commentary
Adult acquired hearing loss is a common long-term condition which in the majority of cases is not remediable by surgical or medical intervention. It is the second leading cause of years lived with a disability [4]. Intervention options for people with hearing loss include hearing aid fitting and/or participation in a rehabilitative program that might include information about hearing and communication and practice or experience with listening or communication tasks [5,6]. Poorly managed hearing loss is associated with negative consequences including depression and cognitive decline [7,8]. Identifying effective management options for hearing loss can reduce these consequences and improve quality of life. In the current paper, Cardemil et al review the evidence for the effectiveness of adult auditory rehabilitation. They note that hearing aids alone cannot ameliorate all of the difficulties caused by age-related hearing loss, where cognitive factors play a significant role. They provide a rationale for why communication-based training in auditory rehabilitation has been recommended as a substitute or supplement to hearing aid fitting. That is, such training addresses the cognitive and communication difficulties that exist in addition to the hearing loss.
This paper summarises the findings of 3 systematic reviews: one on individual auditory rehabilitation and 2 on group rehabilitation. There was heterogeneity among the programs and the methods used to assess their effectiveness were variable. The reviewers conclude that there appears to be some short-term benefit to auditory rehabilitation programs but effect sizes, where effects are seen, are small and more research is needed to establish the effectiveness of these programs.
A limitation of this review is that it was nonsystematic and did not critically appraise the quality of the included systematic reviews. One weakness of the systematic reviews presented is that they did not consider interactions between content and delivery of interventions and comparisons. Individual auditory rehabilitation and group rehabilitation are typically delivered over many sessions in contrast to control groups, which often receive “standard care” delivered over a single or limited number of sessions. Therefore, where an effect exists it is unclear whether the “active ingredient” contributing to the effect is the rehabilitative content delivered or the number of sessions over which it is provided. This is a possible confounding factor not acknowledged or discussed in these systematic reviews.
In addition, any discussion which seeks to assess effectiveness should define outcomes of interest or at least review the range of outcomes that have been studied and how they are relevant to the problem being addressed. There is a lack of consensus on what the important clinical outcomes are for hearing health care [9] and a dearth of research on longer-term outcomes; this could have been explored.
Applications for Clinical Practice
This summary of 3 systematic reviews highlights the need for further research in this area. Studies that measure long-term outcomes (1 year or more) and that are appropriately powered are needed. In addition, the possible interaction between different potentially active components of complex interventions must be acknowledged. Health care professionals and policy makers need to be aware of these factors when reviewing evidence and making decisions that impact on clinical practice.
—Fiona Barker, Department of Health Care Management and Policy, University of Surrey, Guildford, UK
1. Sweetow R, Palmer CV. Efficacy of individual auditory training in adults: a systematic review of the evidence. J Am Acad Audiol 2005;16:494–504.
2. Hawkins DB. Effectiveness of counseling-based adult group aural rehabilitation programs: a systematic review of the evidence. J Am Acad Audiol 2005;16:485–93.
3. Chisolm TH, Arnold M. Evidence about the effectiveness of aural rehabilitation programs for adults. In: Wong L, Hickson L, editors. Evidence-based practice in audiology. San Diego: Plural; 2012.
4. World Health Organisation. Facts about deafness. 2012. Accessed 6 Nov 2014 at www.who.int/pbd/deafness/facts/en/.
5. Laplante-Levesque A, Hickson L, Worrall L. Rehabilitation of older adults with hearing impairment: a critical review. J Aging Health 2010;22:143–53.
6. Pronk M, Kramer SE, Davis AC, Stephens D, Smith PA, Thodi C, et al. Interventions following hearing screening in adults: a systematic descriptive review. Int J Audiol 2011;50:594–609.
7. Lin FR. Hearing loss and cognition among older adults in the United States. J Gerontol A Biol Sci Med Sci 2011;66:1131–6.
8. Saito H, Nishiwaki Y, Michikawa T, et al. Hearing handicap predicts the development of depressive symptoms after 3 years in older community-dwelling Japanese. J Am Geriatr Soc 2010;58:93–7.
9. Humes LE, Krull V. Hearing aids for adults. In: Wong L, Hickson L, editors. Evidence-based practice in audiology. San Diego: Plural; 2012.
1. Sweetow R, Palmer CV. Efficacy of individual auditory training in adults: a systematic review of the evidence. J Am Acad Audiol 2005;16:494–504.
2. Hawkins DB. Effectiveness of counseling-based adult group aural rehabilitation programs: a systematic review of the evidence. J Am Acad Audiol 2005;16:485–93.
3. Chisolm TH, Arnold M. Evidence about the effectiveness of aural rehabilitation programs for adults. In: Wong L, Hickson L, editors. Evidence-based practice in audiology. San Diego: Plural; 2012.
4. World Health Organisation. Facts about deafness. 2012. Accessed 6 Nov 2014 at www.who.int/pbd/deafness/facts/en/.
5. Laplante-Levesque A, Hickson L, Worrall L. Rehabilitation of older adults with hearing impairment: a critical review. J Aging Health 2010;22:143–53.
6. Pronk M, Kramer SE, Davis AC, Stephens D, Smith PA, Thodi C, et al. Interventions following hearing screening in adults: a systematic descriptive review. Int J Audiol 2011;50:594–609.
7. Lin FR. Hearing loss and cognition among older adults in the United States. J Gerontol A Biol Sci Med Sci 2011;66:1131–6.
8. Saito H, Nishiwaki Y, Michikawa T, et al. Hearing handicap predicts the development of depressive symptoms after 3 years in older community-dwelling Japanese. J Am Geriatr Soc 2010;58:93–7.
9. Humes LE, Krull V. Hearing aids for adults. In: Wong L, Hickson L, editors. Evidence-based practice in audiology. San Diego: Plural; 2012.
Integrating Lay Health Care Workers into the Primary Care Team
From Allina Health, Minneapolis, MN.
Abstract
- Objective: To describe a care model in which lay “care guides” are integrated into the primary care team to help patients with chronic disease and their providers achieve care goals.
- Methods: Care guides are individuals without formal medical training who receive brief training about chronic conditions and behavior change. General activities include educating and encouraging patients to take control of their illness, supporting medication and treatment adherence, and facilitating resolution of barriers to quality care.
- Results: The care guide model can improve care for some patients with chronic disease at low cost. In a randomized trial testing the intervention, patients with care guides achieved more goals than usual care patients at 1 year (odds ratio, 1.31; 95% confidence interval, 1.16–1.47; P < 0.001).
- Conclusion: Lay health care workers with relevant skills and training, located in clinic waiting rooms where they can meet patients and providers face-to-face, can help chronic disease patients and their providers improve the quality of care.
Improving the quality of care for chronic disease patients is an important goal for the US health care system. Almost half of American with chronic disease fail to receive evidence-based care [1–3]. Reasons for this include limited access to the health care delivery system [4,5] and payment systems that undervalue primary care and provide incentives for more but not necessarily better care [6]. Not only is there a need to improve the quality of care among chronic disease patients, but also to recognize the constraints faced by primary care providers (PCPs) and clinic staff in the current health care environment.
One approach for improving care for patients with chronic disease has been care coordination, or management by health care professionals such as nurses and certified medical assistants [7]. These care managers are usually located in primary care medical offices and have some face-to-face contact with both patients and providers in addition to telephone or electronic contact [7,8]. Care management provided by registered nurses can be effective but is expensive, and it is unclear where payment for these services will come from [7,9].
An alternative approach is employing lay health care workers. In the literature lay health care workers have been referred to as promotoras de salud, lay advisors or navigators, and peer coaches [10–12]. Some of these workers are employees while others are part-time volunteers [13,14]. Tasks assigned to these workers are often limited, such as improving access to cancer care [15], teaching self-help techniques [16–18], or goal-setting [19], and are usually focused on a specific disease or problem. Some of workers do have contact with nurses and doctors, but they tend not to work with the primary care team in the day-to-day provision of care [14].
To improve the quality and efficiency of chronic disease care, Allina Health, a large not-for-profit system of hospitals and clinics in Minnesota and western Wisconsin, hired lay “care guides” to help patients and providers achieve care goals and integrated them into the primary care team. In this article, we describe the care guide model we used and tested and discuss adoption considerations.
Role and Responsibilities of a Care Guide
Care guides are individuals without formal medical training whose general activities include:
- fostering a longitudinal relationship to encourage patients to take control of their chronic illness;
- educating patients about the considerable benefits of best practice treatment;
- communicating with patients, families and providers to keep the entire care team, including the PCP, focused on meeting care guidelines;
- supporting medication and treatment adherence;
- identifying and facilitating resolution of barriers to quality care;
- facilitating referrals to extended care team members and introducing patients to appropriate services or resources within the clinic, health system and/or community they live or work in.
How do care guides differ from other personnel used as care managers? Care guides can explain the value of meeting standard goals, but unlike nurses cannot answer clinical questions. Care guides and medical assistants have similar salaries but care guides have higher educational requirements, less clinical training, and no competing duties in clinic. Like community health workers, care guides are culturally similar to the patients they serve, but are located in the clinic. Care guides were recruited for specific traits and competencies: an outgoing personality, the ability to engage easily with people of different ages and backgrounds, and a second language where needed (eg, Spanish and Somali in the pilot study) [20].
Implementation Trial
![]()
The study recruited 2135 patients. Both groups had an increased percentage of goals met at the end of the 1-year study compared to baseline. Care guide patients met a larger percentage of possible care goals at 1 year than did usual care patients (odds ratio, 1.31; 95% confidence interval, 1.16–1.47; P < 0.001). Care guide patients reduced unmet goals by 30.1%, usual care patients by 12.6%. The difference in outcomes between the 2 groups was minimally affected by differences in the times of final measurement for each goal. The benefit of working with a care guide was not different across demographic categories of age, sex, race, language, insurance, or education. In this study, care guides helped a broad range of patients who were meeting many goals at baseline and who were cared for by providers already receiving regular quality-improvement feedback. Estimated cost was $286 per patient per year.
Development Process
At each clinic, the research team enlisted the help of a site-specific implementation team consisting of a provider champion and clinic leader (ie, the clinic manager, clinic supervisor, or business office supervisor) to customize the study implementation. After selecting the target patient population, chronic disease focus, and eligibility criteria, the research team solicited the help of providers, nurses, medical assistants, and other clinic support staff to develop care guide workflows and processes. Clinic providers and staff were involved early and often in the model planning process. The team gave thoughtful consideration to existing clinic work processes and personnel dynamics to help ensure that the care guide would be accepted and integrated into the clinic culture.
Concurrent with designing workflows for the interactions between care guides and providers, clinical staff, and patients, the research team worked with a variety of support departments at Allina Health System to ensure that the necessary tools were in place for care guides to do their work effectively. They collaborated with human resources to screen for care guide candidates with appropriate skills and personal attributes; information systems to create new tools and security access within the electronic health record; learning and development to organize resources and devise an appropriate training schedule; and marketing/communications to broadcast this new initiative on a system-wide level.
Once details of the model and workflows were established, the research team secured subject matter experts to build content for care guide training. The research team partnered with PCPs whose expertise was treating these chronic diseases as well as pharmacists, nutritionists, diabetes nurse educators, and behavioral health specialists available within the health system. These subject matter experts provided the training content as well as conducted the training. Training took place over 2 weeks and included basic training on the 3 chronic disease conditions, pharmacology, nutrition, and mental health issues, barriers to care, and behavioral change techniques.
Benefits
What were the key interactions leading to clinical improvements? What made the intervention successful? Care guides described using a variety of techniques to yield clinical improvements. With patients, care guides took time to explain the benefits of meeting goals in lay language, used their non-medical backgrounds to create an environment where patients felt at ease asking questions, called patients following office visits to ensure instructions were understood, and helped develop specific action plans. With providers and nurses, care guides gave reminders about unmet goals on the day of an appointment (when this information would be most useful) and supplied information such as “this patient reports difficulty affording medication” or “this patient seems ready to quit tobacco.” Care guides reinforced the effectiveness of longer-term care relationships; for example, most patients who quit tobacco did so between 9 and 12 months after enrollment in the care guide program. In after-study surveys, care guide patients reported significantly more positive perceptions of their care than usual care patients in constructs measuring social support, individualized care, help, reinforcement, and understanding of how to improve their health.
Care guides, using their relationships with providers, served as quality improvement advocates integrated into the daily process of providing primary care. This arrangement differed from the common practice of giving providers periodic feedback based on data gleaned from the electronic health record.
Moving the quality improvement process into the primary care office resolved many problems related to strictly electronic health record–based feedback. Each patient was considered individually. There was opportunity for conversations about care quality to occur face-to-face; members of the primary care team could discuss when to deviate from a care guideline. Strong relationships and a sense of teamwork increased workplace satisfaction [22]. In a post-study survey of 115 providers and nurses, 93% felt that care guides improved patient care and 94% felt that care guides were an effective use of resources.
Adoption Considerations
Adding a care guide into an existing clinic structure and culture requires planning and customization. In order to fully integrate this role into clinics and on care teams and achieve expected results, 6 steps are recommended:
- Program set-up through recruitment of the proper set of stakeholders to plan for implementation, including logistics, budget, etc.
- Defining details, such as the target patient population and eligibility criteria, how interactions will take place with patients, and the duration of the patient relationship.
- Clinic readiness and program development, including detailed clinic staff orientation and workflow development.
- Clinic-specific development of the care guide training, including enlisting the help of subject matter experts to develop content.
- A 2-week training of newly-hired care guides
- Defining the expectations and job responsibilities of the care guide and proper integration of care guides into care teams.
- Monitoring and evaluation – This is not the last step in the process but rather requires the ongoing work of the clinic staff, providers, and care guides to measure progress and outcomes.
Although transforming care teams in primary care clinics is no easy task, it is the foundation of the care guide model. The premise of the care guide role is simple and relatable, thereby making it transferrable to different patient populations and settings as well as attractive to different types of providers. The model is flexible, allowing room for adaptations while maintaining its focus on serving patients and families and reducing burden for providers and other clinic staff. The model is currently being adapted and used in different settings outside of traditional primary care, including urgent care and emergency departments, specialty services, and patient-centered medical homes, among others. In addition, care guides are being used across different patient populations, including high-risk patients in an accountable care organization, pediatric patients, and patients late in life, to name a few. Each adaptation may have population-specific goals and outcomes, but the core of the model remains focused on the Institute for Healthcare Improvement's triple aim: improving the patient experience of care, improving the health of populations, and reducing the per capita cost of health care.
For clinics and care providers interested in integrating care guides within their own clinic, a toolkit, eLearning modules, and evaluation templates, among other resources, are available at no cost through the Care Copilot Institute (www.carecopilotinstitute.org). The Institute was created to translate and disseminate the care guide research.
Conclusion
Lay health care workers with relevant skills and training, located in clinic waiting rooms where they can meet patients and providers face-to-face, can help chronic disease patients and their providers improve the quality of care. Because of its low cost, this model can be implemented in many settings, including small independent primary care offices, where much primary care in the US is still delivered [7,23–25].
Corresponding author: Kim Radel, MHA, Allina Health, Minneapolis, MN, [email protected].
Financial disclosures: Dr. Christianson disclosed that he received grant support from the Robina Foundation.
1. Banerjee D, Stafford R. Lack of improvement in outpatient management of congestive heart failure in the United States Arch Intern Med 2010;16:1–2.
2. Egan BM, Zhao Y, RN A. US trends in prevalence, awareness, treatment, and control of hypertension. JAMA 2010;303:2043–50.
3. McGlynn E, Asch S, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med 2003;348:2635–45.
4. Ghorob A, Bodenheimer T. Sharing the care to improve access to primary care. N Engl J Med 2012;366:1955–7.
5. Schroeder SA. Shattuck Lecture. We can do better - improving the health of the American people. N Engl J Med 2007;357:1221–8.
6. Bazinsky KR, Herrera L, Sharfstein JM. Toward innovative models of health care and financing: matchmaking in Maryland. JAMA 2012;307:1261–2.
7. Berry-Millett R, Bodenheimer TS. Care management of patients with complex health care needs. Synth Proj Res Synth Rep 2009;(19).
8. Peikes D, Chen A, Schore J, Brown R. Effects of care coordination on hospitalization, quality of care, and health care expenditures among Medicare beneficiaries: 15 randomized trials. JAMA 2009;301:603–18.
9. Ayanian JZ. The elusive quest for quality and cost savings in the Medicare program. JAMA 2009;301:668–70.
10. Babamoto KS, Sey KA, Camilleri AJ, et al. Improving diabetes care and health measures among hispanics using community health workers: results from a randomized controlled trial. Health Educ Behav 2009;36:113–26.
11. Brownstein JN, Hirsch GR, Rosenthal EL, Rush CH. Community health workers “101” for primary care providers and other stakeholders in health care systems. J Ambul Care Manage 2011;34:210–20.
12. Lewin S, Dick J, Pond P, et al. Lay health workers in primary and community health care. Cochrane Database Syst Rev 2005;(1):CD004015.
13. Doull M, O’Connor A, Welch V, et al. Peer support strategies for improving the health and well-being of individuals with chronic diseases. Cochrane Database Syst Rev 2004;(2):CD004774.
14. Witmer A, Seifer SD, Finocchio L, et al. Community health workers: integral members of the health care work force. Am J Public Health 1995;85(8 Pt 1):1055–8.
15. Steinberg ML, Fremont A, Khan DC, et al. Lay patient navigator program implementation for equal access to cancer care and clinical trials: essential steps and initial challenges. Cancer 2006;107:2669–77.
16. Fu D, Fu H, McGowan P, et al. Implementation and quantitative evaluation of chronic disease self-management programme in Shanghai, China: randomized controlled trial. Bull World Health Organ 2003;81:174–82.
17. Kennedy A, Reeves D, Bower P, et al. The effectiveness and cost effectiveness of a national lay-led self care support programme for patients with long-term conditions: a pragmatic randomised controlled trial. J Epidemiol Comm Health 2007;61:254–61.
18. Rhodes SD, Foley KL, Zometa CS, Bloom FR. Lay health advisor interventions among Hispanics/Latinos: a qualitative systematic review. Am J Prev Med 2007;33:418–27.
19. Heisler M, Spencer M, Forman J, et al. Participants’ assessments of the effects of a community health worker intervention on their diabetes self-management and interactions with healthcare providers. Am J Prev Med 2009;37(6 Suppl 1):S270–9.
20. Adair R, Christianson JB, Wholey DR, et al. Care guides: employing nonclinical laypersons to help primary care teams manage chronic disease. J Ambul Care Manage 2012;35:27–37.
21. Adair R, Wholey DR, Christianson JB, et al. Improving chronic disease care by adding laypersons to the primary care team: a parallel randomized trial. Ann Intern Med 2013;159:176–84.
22. Cassel CK, Jain S. Assessing individual physician performance: does measurement suppress motivation? JAMA 2012;307:2595–6.
23. Nocon RS, Sharma R, Birnberg JM, et al. Association between patient-centered medical home rating and operating cost at federally funded health centers. JAMA 2012;308:60–6.
24. Rittenhouse D, Casalino L. Small and medium-size physician practices use few patient-centered medical home processes. Health Aff 2011;30:1575–84.
25. Fifield J, Forrest DD, Martin-Peele M, et al. A randomized, controlled trial of implementing the patient-centered medical home model in solo and small practices. J Gen Intern Med 2012;28:770–7.
From Allina Health, Minneapolis, MN.
Abstract
- Objective: To describe a care model in which lay “care guides” are integrated into the primary care team to help patients with chronic disease and their providers achieve care goals.
- Methods: Care guides are individuals without formal medical training who receive brief training about chronic conditions and behavior change. General activities include educating and encouraging patients to take control of their illness, supporting medication and treatment adherence, and facilitating resolution of barriers to quality care.
- Results: The care guide model can improve care for some patients with chronic disease at low cost. In a randomized trial testing the intervention, patients with care guides achieved more goals than usual care patients at 1 year (odds ratio, 1.31; 95% confidence interval, 1.16–1.47; P < 0.001).
- Conclusion: Lay health care workers with relevant skills and training, located in clinic waiting rooms where they can meet patients and providers face-to-face, can help chronic disease patients and their providers improve the quality of care.
Improving the quality of care for chronic disease patients is an important goal for the US health care system. Almost half of American with chronic disease fail to receive evidence-based care [1–3]. Reasons for this include limited access to the health care delivery system [4,5] and payment systems that undervalue primary care and provide incentives for more but not necessarily better care [6]. Not only is there a need to improve the quality of care among chronic disease patients, but also to recognize the constraints faced by primary care providers (PCPs) and clinic staff in the current health care environment.
One approach for improving care for patients with chronic disease has been care coordination, or management by health care professionals such as nurses and certified medical assistants [7]. These care managers are usually located in primary care medical offices and have some face-to-face contact with both patients and providers in addition to telephone or electronic contact [7,8]. Care management provided by registered nurses can be effective but is expensive, and it is unclear where payment for these services will come from [7,9].
An alternative approach is employing lay health care workers. In the literature lay health care workers have been referred to as promotoras de salud, lay advisors or navigators, and peer coaches [10–12]. Some of these workers are employees while others are part-time volunteers [13,14]. Tasks assigned to these workers are often limited, such as improving access to cancer care [15], teaching self-help techniques [16–18], or goal-setting [19], and are usually focused on a specific disease or problem. Some of workers do have contact with nurses and doctors, but they tend not to work with the primary care team in the day-to-day provision of care [14].
To improve the quality and efficiency of chronic disease care, Allina Health, a large not-for-profit system of hospitals and clinics in Minnesota and western Wisconsin, hired lay “care guides” to help patients and providers achieve care goals and integrated them into the primary care team. In this article, we describe the care guide model we used and tested and discuss adoption considerations.
Role and Responsibilities of a Care Guide
Care guides are individuals without formal medical training whose general activities include:
- fostering a longitudinal relationship to encourage patients to take control of their chronic illness;
- educating patients about the considerable benefits of best practice treatment;
- communicating with patients, families and providers to keep the entire care team, including the PCP, focused on meeting care guidelines;
- supporting medication and treatment adherence;
- identifying and facilitating resolution of barriers to quality care;
- facilitating referrals to extended care team members and introducing patients to appropriate services or resources within the clinic, health system and/or community they live or work in.
How do care guides differ from other personnel used as care managers? Care guides can explain the value of meeting standard goals, but unlike nurses cannot answer clinical questions. Care guides and medical assistants have similar salaries but care guides have higher educational requirements, less clinical training, and no competing duties in clinic. Like community health workers, care guides are culturally similar to the patients they serve, but are located in the clinic. Care guides were recruited for specific traits and competencies: an outgoing personality, the ability to engage easily with people of different ages and backgrounds, and a second language where needed (eg, Spanish and Somali in the pilot study) [20].
Implementation Trial
![]()
The study recruited 2135 patients. Both groups had an increased percentage of goals met at the end of the 1-year study compared to baseline. Care guide patients met a larger percentage of possible care goals at 1 year than did usual care patients (odds ratio, 1.31; 95% confidence interval, 1.16–1.47; P < 0.001). Care guide patients reduced unmet goals by 30.1%, usual care patients by 12.6%. The difference in outcomes between the 2 groups was minimally affected by differences in the times of final measurement for each goal. The benefit of working with a care guide was not different across demographic categories of age, sex, race, language, insurance, or education. In this study, care guides helped a broad range of patients who were meeting many goals at baseline and who were cared for by providers already receiving regular quality-improvement feedback. Estimated cost was $286 per patient per year.
Development Process
At each clinic, the research team enlisted the help of a site-specific implementation team consisting of a provider champion and clinic leader (ie, the clinic manager, clinic supervisor, or business office supervisor) to customize the study implementation. After selecting the target patient population, chronic disease focus, and eligibility criteria, the research team solicited the help of providers, nurses, medical assistants, and other clinic support staff to develop care guide workflows and processes. Clinic providers and staff were involved early and often in the model planning process. The team gave thoughtful consideration to existing clinic work processes and personnel dynamics to help ensure that the care guide would be accepted and integrated into the clinic culture.
Concurrent with designing workflows for the interactions between care guides and providers, clinical staff, and patients, the research team worked with a variety of support departments at Allina Health System to ensure that the necessary tools were in place for care guides to do their work effectively. They collaborated with human resources to screen for care guide candidates with appropriate skills and personal attributes; information systems to create new tools and security access within the electronic health record; learning and development to organize resources and devise an appropriate training schedule; and marketing/communications to broadcast this new initiative on a system-wide level.
Once details of the model and workflows were established, the research team secured subject matter experts to build content for care guide training. The research team partnered with PCPs whose expertise was treating these chronic diseases as well as pharmacists, nutritionists, diabetes nurse educators, and behavioral health specialists available within the health system. These subject matter experts provided the training content as well as conducted the training. Training took place over 2 weeks and included basic training on the 3 chronic disease conditions, pharmacology, nutrition, and mental health issues, barriers to care, and behavioral change techniques.
Benefits
What were the key interactions leading to clinical improvements? What made the intervention successful? Care guides described using a variety of techniques to yield clinical improvements. With patients, care guides took time to explain the benefits of meeting goals in lay language, used their non-medical backgrounds to create an environment where patients felt at ease asking questions, called patients following office visits to ensure instructions were understood, and helped develop specific action plans. With providers and nurses, care guides gave reminders about unmet goals on the day of an appointment (when this information would be most useful) and supplied information such as “this patient reports difficulty affording medication” or “this patient seems ready to quit tobacco.” Care guides reinforced the effectiveness of longer-term care relationships; for example, most patients who quit tobacco did so between 9 and 12 months after enrollment in the care guide program. In after-study surveys, care guide patients reported significantly more positive perceptions of their care than usual care patients in constructs measuring social support, individualized care, help, reinforcement, and understanding of how to improve their health.
Care guides, using their relationships with providers, served as quality improvement advocates integrated into the daily process of providing primary care. This arrangement differed from the common practice of giving providers periodic feedback based on data gleaned from the electronic health record.
Moving the quality improvement process into the primary care office resolved many problems related to strictly electronic health record–based feedback. Each patient was considered individually. There was opportunity for conversations about care quality to occur face-to-face; members of the primary care team could discuss when to deviate from a care guideline. Strong relationships and a sense of teamwork increased workplace satisfaction [22]. In a post-study survey of 115 providers and nurses, 93% felt that care guides improved patient care and 94% felt that care guides were an effective use of resources.
Adoption Considerations
Adding a care guide into an existing clinic structure and culture requires planning and customization. In order to fully integrate this role into clinics and on care teams and achieve expected results, 6 steps are recommended:
- Program set-up through recruitment of the proper set of stakeholders to plan for implementation, including logistics, budget, etc.
- Defining details, such as the target patient population and eligibility criteria, how interactions will take place with patients, and the duration of the patient relationship.
- Clinic readiness and program development, including detailed clinic staff orientation and workflow development.
- Clinic-specific development of the care guide training, including enlisting the help of subject matter experts to develop content.
- A 2-week training of newly-hired care guides
- Defining the expectations and job responsibilities of the care guide and proper integration of care guides into care teams.
- Monitoring and evaluation – This is not the last step in the process but rather requires the ongoing work of the clinic staff, providers, and care guides to measure progress and outcomes.
Although transforming care teams in primary care clinics is no easy task, it is the foundation of the care guide model. The premise of the care guide role is simple and relatable, thereby making it transferrable to different patient populations and settings as well as attractive to different types of providers. The model is flexible, allowing room for adaptations while maintaining its focus on serving patients and families and reducing burden for providers and other clinic staff. The model is currently being adapted and used in different settings outside of traditional primary care, including urgent care and emergency departments, specialty services, and patient-centered medical homes, among others. In addition, care guides are being used across different patient populations, including high-risk patients in an accountable care organization, pediatric patients, and patients late in life, to name a few. Each adaptation may have population-specific goals and outcomes, but the core of the model remains focused on the Institute for Healthcare Improvement's triple aim: improving the patient experience of care, improving the health of populations, and reducing the per capita cost of health care.
For clinics and care providers interested in integrating care guides within their own clinic, a toolkit, eLearning modules, and evaluation templates, among other resources, are available at no cost through the Care Copilot Institute (www.carecopilotinstitute.org). The Institute was created to translate and disseminate the care guide research.
Conclusion
Lay health care workers with relevant skills and training, located in clinic waiting rooms where they can meet patients and providers face-to-face, can help chronic disease patients and their providers improve the quality of care. Because of its low cost, this model can be implemented in many settings, including small independent primary care offices, where much primary care in the US is still delivered [7,23–25].
Corresponding author: Kim Radel, MHA, Allina Health, Minneapolis, MN, [email protected].
Financial disclosures: Dr. Christianson disclosed that he received grant support from the Robina Foundation.
From Allina Health, Minneapolis, MN.
Abstract
- Objective: To describe a care model in which lay “care guides” are integrated into the primary care team to help patients with chronic disease and their providers achieve care goals.
- Methods: Care guides are individuals without formal medical training who receive brief training about chronic conditions and behavior change. General activities include educating and encouraging patients to take control of their illness, supporting medication and treatment adherence, and facilitating resolution of barriers to quality care.
- Results: The care guide model can improve care for some patients with chronic disease at low cost. In a randomized trial testing the intervention, patients with care guides achieved more goals than usual care patients at 1 year (odds ratio, 1.31; 95% confidence interval, 1.16–1.47; P < 0.001).
- Conclusion: Lay health care workers with relevant skills and training, located in clinic waiting rooms where they can meet patients and providers face-to-face, can help chronic disease patients and their providers improve the quality of care.
Improving the quality of care for chronic disease patients is an important goal for the US health care system. Almost half of American with chronic disease fail to receive evidence-based care [1–3]. Reasons for this include limited access to the health care delivery system [4,5] and payment systems that undervalue primary care and provide incentives for more but not necessarily better care [6]. Not only is there a need to improve the quality of care among chronic disease patients, but also to recognize the constraints faced by primary care providers (PCPs) and clinic staff in the current health care environment.
One approach for improving care for patients with chronic disease has been care coordination, or management by health care professionals such as nurses and certified medical assistants [7]. These care managers are usually located in primary care medical offices and have some face-to-face contact with both patients and providers in addition to telephone or electronic contact [7,8]. Care management provided by registered nurses can be effective but is expensive, and it is unclear where payment for these services will come from [7,9].
An alternative approach is employing lay health care workers. In the literature lay health care workers have been referred to as promotoras de salud, lay advisors or navigators, and peer coaches [10–12]. Some of these workers are employees while others are part-time volunteers [13,14]. Tasks assigned to these workers are often limited, such as improving access to cancer care [15], teaching self-help techniques [16–18], or goal-setting [19], and are usually focused on a specific disease or problem. Some of workers do have contact with nurses and doctors, but they tend not to work with the primary care team in the day-to-day provision of care [14].
To improve the quality and efficiency of chronic disease care, Allina Health, a large not-for-profit system of hospitals and clinics in Minnesota and western Wisconsin, hired lay “care guides” to help patients and providers achieve care goals and integrated them into the primary care team. In this article, we describe the care guide model we used and tested and discuss adoption considerations.
Role and Responsibilities of a Care Guide
Care guides are individuals without formal medical training whose general activities include:
- fostering a longitudinal relationship to encourage patients to take control of their chronic illness;
- educating patients about the considerable benefits of best practice treatment;
- communicating with patients, families and providers to keep the entire care team, including the PCP, focused on meeting care guidelines;
- supporting medication and treatment adherence;
- identifying and facilitating resolution of barriers to quality care;
- facilitating referrals to extended care team members and introducing patients to appropriate services or resources within the clinic, health system and/or community they live or work in.
How do care guides differ from other personnel used as care managers? Care guides can explain the value of meeting standard goals, but unlike nurses cannot answer clinical questions. Care guides and medical assistants have similar salaries but care guides have higher educational requirements, less clinical training, and no competing duties in clinic. Like community health workers, care guides are culturally similar to the patients they serve, but are located in the clinic. Care guides were recruited for specific traits and competencies: an outgoing personality, the ability to engage easily with people of different ages and backgrounds, and a second language where needed (eg, Spanish and Somali in the pilot study) [20].
Implementation Trial
![]()
The study recruited 2135 patients. Both groups had an increased percentage of goals met at the end of the 1-year study compared to baseline. Care guide patients met a larger percentage of possible care goals at 1 year than did usual care patients (odds ratio, 1.31; 95% confidence interval, 1.16–1.47; P < 0.001). Care guide patients reduced unmet goals by 30.1%, usual care patients by 12.6%. The difference in outcomes between the 2 groups was minimally affected by differences in the times of final measurement for each goal. The benefit of working with a care guide was not different across demographic categories of age, sex, race, language, insurance, or education. In this study, care guides helped a broad range of patients who were meeting many goals at baseline and who were cared for by providers already receiving regular quality-improvement feedback. Estimated cost was $286 per patient per year.
Development Process
At each clinic, the research team enlisted the help of a site-specific implementation team consisting of a provider champion and clinic leader (ie, the clinic manager, clinic supervisor, or business office supervisor) to customize the study implementation. After selecting the target patient population, chronic disease focus, and eligibility criteria, the research team solicited the help of providers, nurses, medical assistants, and other clinic support staff to develop care guide workflows and processes. Clinic providers and staff were involved early and often in the model planning process. The team gave thoughtful consideration to existing clinic work processes and personnel dynamics to help ensure that the care guide would be accepted and integrated into the clinic culture.
Concurrent with designing workflows for the interactions between care guides and providers, clinical staff, and patients, the research team worked with a variety of support departments at Allina Health System to ensure that the necessary tools were in place for care guides to do their work effectively. They collaborated with human resources to screen for care guide candidates with appropriate skills and personal attributes; information systems to create new tools and security access within the electronic health record; learning and development to organize resources and devise an appropriate training schedule; and marketing/communications to broadcast this new initiative on a system-wide level.
Once details of the model and workflows were established, the research team secured subject matter experts to build content for care guide training. The research team partnered with PCPs whose expertise was treating these chronic diseases as well as pharmacists, nutritionists, diabetes nurse educators, and behavioral health specialists available within the health system. These subject matter experts provided the training content as well as conducted the training. Training took place over 2 weeks and included basic training on the 3 chronic disease conditions, pharmacology, nutrition, and mental health issues, barriers to care, and behavioral change techniques.
Benefits
What were the key interactions leading to clinical improvements? What made the intervention successful? Care guides described using a variety of techniques to yield clinical improvements. With patients, care guides took time to explain the benefits of meeting goals in lay language, used their non-medical backgrounds to create an environment where patients felt at ease asking questions, called patients following office visits to ensure instructions were understood, and helped develop specific action plans. With providers and nurses, care guides gave reminders about unmet goals on the day of an appointment (when this information would be most useful) and supplied information such as “this patient reports difficulty affording medication” or “this patient seems ready to quit tobacco.” Care guides reinforced the effectiveness of longer-term care relationships; for example, most patients who quit tobacco did so between 9 and 12 months after enrollment in the care guide program. In after-study surveys, care guide patients reported significantly more positive perceptions of their care than usual care patients in constructs measuring social support, individualized care, help, reinforcement, and understanding of how to improve their health.
Care guides, using their relationships with providers, served as quality improvement advocates integrated into the daily process of providing primary care. This arrangement differed from the common practice of giving providers periodic feedback based on data gleaned from the electronic health record.
Moving the quality improvement process into the primary care office resolved many problems related to strictly electronic health record–based feedback. Each patient was considered individually. There was opportunity for conversations about care quality to occur face-to-face; members of the primary care team could discuss when to deviate from a care guideline. Strong relationships and a sense of teamwork increased workplace satisfaction [22]. In a post-study survey of 115 providers and nurses, 93% felt that care guides improved patient care and 94% felt that care guides were an effective use of resources.
Adoption Considerations
Adding a care guide into an existing clinic structure and culture requires planning and customization. In order to fully integrate this role into clinics and on care teams and achieve expected results, 6 steps are recommended:
- Program set-up through recruitment of the proper set of stakeholders to plan for implementation, including logistics, budget, etc.
- Defining details, such as the target patient population and eligibility criteria, how interactions will take place with patients, and the duration of the patient relationship.
- Clinic readiness and program development, including detailed clinic staff orientation and workflow development.
- Clinic-specific development of the care guide training, including enlisting the help of subject matter experts to develop content.
- A 2-week training of newly-hired care guides
- Defining the expectations and job responsibilities of the care guide and proper integration of care guides into care teams.
- Monitoring and evaluation – This is not the last step in the process but rather requires the ongoing work of the clinic staff, providers, and care guides to measure progress and outcomes.
Although transforming care teams in primary care clinics is no easy task, it is the foundation of the care guide model. The premise of the care guide role is simple and relatable, thereby making it transferrable to different patient populations and settings as well as attractive to different types of providers. The model is flexible, allowing room for adaptations while maintaining its focus on serving patients and families and reducing burden for providers and other clinic staff. The model is currently being adapted and used in different settings outside of traditional primary care, including urgent care and emergency departments, specialty services, and patient-centered medical homes, among others. In addition, care guides are being used across different patient populations, including high-risk patients in an accountable care organization, pediatric patients, and patients late in life, to name a few. Each adaptation may have population-specific goals and outcomes, but the core of the model remains focused on the Institute for Healthcare Improvement's triple aim: improving the patient experience of care, improving the health of populations, and reducing the per capita cost of health care.
For clinics and care providers interested in integrating care guides within their own clinic, a toolkit, eLearning modules, and evaluation templates, among other resources, are available at no cost through the Care Copilot Institute (www.carecopilotinstitute.org). The Institute was created to translate and disseminate the care guide research.
Conclusion
Lay health care workers with relevant skills and training, located in clinic waiting rooms where they can meet patients and providers face-to-face, can help chronic disease patients and their providers improve the quality of care. Because of its low cost, this model can be implemented in many settings, including small independent primary care offices, where much primary care in the US is still delivered [7,23–25].
Corresponding author: Kim Radel, MHA, Allina Health, Minneapolis, MN, [email protected].
Financial disclosures: Dr. Christianson disclosed that he received grant support from the Robina Foundation.
1. Banerjee D, Stafford R. Lack of improvement in outpatient management of congestive heart failure in the United States Arch Intern Med 2010;16:1–2.
2. Egan BM, Zhao Y, RN A. US trends in prevalence, awareness, treatment, and control of hypertension. JAMA 2010;303:2043–50.
3. McGlynn E, Asch S, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med 2003;348:2635–45.
4. Ghorob A, Bodenheimer T. Sharing the care to improve access to primary care. N Engl J Med 2012;366:1955–7.
5. Schroeder SA. Shattuck Lecture. We can do better - improving the health of the American people. N Engl J Med 2007;357:1221–8.
6. Bazinsky KR, Herrera L, Sharfstein JM. Toward innovative models of health care and financing: matchmaking in Maryland. JAMA 2012;307:1261–2.
7. Berry-Millett R, Bodenheimer TS. Care management of patients with complex health care needs. Synth Proj Res Synth Rep 2009;(19).
8. Peikes D, Chen A, Schore J, Brown R. Effects of care coordination on hospitalization, quality of care, and health care expenditures among Medicare beneficiaries: 15 randomized trials. JAMA 2009;301:603–18.
9. Ayanian JZ. The elusive quest for quality and cost savings in the Medicare program. JAMA 2009;301:668–70.
10. Babamoto KS, Sey KA, Camilleri AJ, et al. Improving diabetes care and health measures among hispanics using community health workers: results from a randomized controlled trial. Health Educ Behav 2009;36:113–26.
11. Brownstein JN, Hirsch GR, Rosenthal EL, Rush CH. Community health workers “101” for primary care providers and other stakeholders in health care systems. J Ambul Care Manage 2011;34:210–20.
12. Lewin S, Dick J, Pond P, et al. Lay health workers in primary and community health care. Cochrane Database Syst Rev 2005;(1):CD004015.
13. Doull M, O’Connor A, Welch V, et al. Peer support strategies for improving the health and well-being of individuals with chronic diseases. Cochrane Database Syst Rev 2004;(2):CD004774.
14. Witmer A, Seifer SD, Finocchio L, et al. Community health workers: integral members of the health care work force. Am J Public Health 1995;85(8 Pt 1):1055–8.
15. Steinberg ML, Fremont A, Khan DC, et al. Lay patient navigator program implementation for equal access to cancer care and clinical trials: essential steps and initial challenges. Cancer 2006;107:2669–77.
16. Fu D, Fu H, McGowan P, et al. Implementation and quantitative evaluation of chronic disease self-management programme in Shanghai, China: randomized controlled trial. Bull World Health Organ 2003;81:174–82.
17. Kennedy A, Reeves D, Bower P, et al. The effectiveness and cost effectiveness of a national lay-led self care support programme for patients with long-term conditions: a pragmatic randomised controlled trial. J Epidemiol Comm Health 2007;61:254–61.
18. Rhodes SD, Foley KL, Zometa CS, Bloom FR. Lay health advisor interventions among Hispanics/Latinos: a qualitative systematic review. Am J Prev Med 2007;33:418–27.
19. Heisler M, Spencer M, Forman J, et al. Participants’ assessments of the effects of a community health worker intervention on their diabetes self-management and interactions with healthcare providers. Am J Prev Med 2009;37(6 Suppl 1):S270–9.
20. Adair R, Christianson JB, Wholey DR, et al. Care guides: employing nonclinical laypersons to help primary care teams manage chronic disease. J Ambul Care Manage 2012;35:27–37.
21. Adair R, Wholey DR, Christianson JB, et al. Improving chronic disease care by adding laypersons to the primary care team: a parallel randomized trial. Ann Intern Med 2013;159:176–84.
22. Cassel CK, Jain S. Assessing individual physician performance: does measurement suppress motivation? JAMA 2012;307:2595–6.
23. Nocon RS, Sharma R, Birnberg JM, et al. Association between patient-centered medical home rating and operating cost at federally funded health centers. JAMA 2012;308:60–6.
24. Rittenhouse D, Casalino L. Small and medium-size physician practices use few patient-centered medical home processes. Health Aff 2011;30:1575–84.
25. Fifield J, Forrest DD, Martin-Peele M, et al. A randomized, controlled trial of implementing the patient-centered medical home model in solo and small practices. J Gen Intern Med 2012;28:770–7.
1. Banerjee D, Stafford R. Lack of improvement in outpatient management of congestive heart failure in the United States Arch Intern Med 2010;16:1–2.
2. Egan BM, Zhao Y, RN A. US trends in prevalence, awareness, treatment, and control of hypertension. JAMA 2010;303:2043–50.
3. McGlynn E, Asch S, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med 2003;348:2635–45.
4. Ghorob A, Bodenheimer T. Sharing the care to improve access to primary care. N Engl J Med 2012;366:1955–7.
5. Schroeder SA. Shattuck Lecture. We can do better - improving the health of the American people. N Engl J Med 2007;357:1221–8.
6. Bazinsky KR, Herrera L, Sharfstein JM. Toward innovative models of health care and financing: matchmaking in Maryland. JAMA 2012;307:1261–2.
7. Berry-Millett R, Bodenheimer TS. Care management of patients with complex health care needs. Synth Proj Res Synth Rep 2009;(19).
8. Peikes D, Chen A, Schore J, Brown R. Effects of care coordination on hospitalization, quality of care, and health care expenditures among Medicare beneficiaries: 15 randomized trials. JAMA 2009;301:603–18.
9. Ayanian JZ. The elusive quest for quality and cost savings in the Medicare program. JAMA 2009;301:668–70.
10. Babamoto KS, Sey KA, Camilleri AJ, et al. Improving diabetes care and health measures among hispanics using community health workers: results from a randomized controlled trial. Health Educ Behav 2009;36:113–26.
11. Brownstein JN, Hirsch GR, Rosenthal EL, Rush CH. Community health workers “101” for primary care providers and other stakeholders in health care systems. J Ambul Care Manage 2011;34:210–20.
12. Lewin S, Dick J, Pond P, et al. Lay health workers in primary and community health care. Cochrane Database Syst Rev 2005;(1):CD004015.
13. Doull M, O’Connor A, Welch V, et al. Peer support strategies for improving the health and well-being of individuals with chronic diseases. Cochrane Database Syst Rev 2004;(2):CD004774.
14. Witmer A, Seifer SD, Finocchio L, et al. Community health workers: integral members of the health care work force. Am J Public Health 1995;85(8 Pt 1):1055–8.
15. Steinberg ML, Fremont A, Khan DC, et al. Lay patient navigator program implementation for equal access to cancer care and clinical trials: essential steps and initial challenges. Cancer 2006;107:2669–77.
16. Fu D, Fu H, McGowan P, et al. Implementation and quantitative evaluation of chronic disease self-management programme in Shanghai, China: randomized controlled trial. Bull World Health Organ 2003;81:174–82.
17. Kennedy A, Reeves D, Bower P, et al. The effectiveness and cost effectiveness of a national lay-led self care support programme for patients with long-term conditions: a pragmatic randomised controlled trial. J Epidemiol Comm Health 2007;61:254–61.
18. Rhodes SD, Foley KL, Zometa CS, Bloom FR. Lay health advisor interventions among Hispanics/Latinos: a qualitative systematic review. Am J Prev Med 2007;33:418–27.
19. Heisler M, Spencer M, Forman J, et al. Participants’ assessments of the effects of a community health worker intervention on their diabetes self-management and interactions with healthcare providers. Am J Prev Med 2009;37(6 Suppl 1):S270–9.
20. Adair R, Christianson JB, Wholey DR, et al. Care guides: employing nonclinical laypersons to help primary care teams manage chronic disease. J Ambul Care Manage 2012;35:27–37.
21. Adair R, Wholey DR, Christianson JB, et al. Improving chronic disease care by adding laypersons to the primary care team: a parallel randomized trial. Ann Intern Med 2013;159:176–84.
22. Cassel CK, Jain S. Assessing individual physician performance: does measurement suppress motivation? JAMA 2012;307:2595–6.
23. Nocon RS, Sharma R, Birnberg JM, et al. Association between patient-centered medical home rating and operating cost at federally funded health centers. JAMA 2012;308:60–6.
24. Rittenhouse D, Casalino L. Small and medium-size physician practices use few patient-centered medical home processes. Health Aff 2011;30:1575–84.
25. Fifield J, Forrest DD, Martin-Peele M, et al. A randomized, controlled trial of implementing the patient-centered medical home model in solo and small practices. J Gen Intern Med 2012;28:770–7.
Team Approach for Improving Outcomes in a Culturally Diverse Patient Population
From the Samuel U. Rodgers Health Center, Kansas City, MO.
Abstract
- Objective: To describe the application of the Health Home model in a center that provides care for a culturally diverse patient population.
- Methods: The initiative serves 300 Medicaid beneficiaries, providing intense primary care and behavioral health services for patients with 2 or more chronic diseases. The program addresses multicultural issues and health literacy in addition to assessing patients’ physical and mental health issues and basic needs. It builds upon the patient-centered medical home model, employing a team-based, holistic approach that integrates a behavioral health component to encompass the needs of the whole person, including psychosocial requirements.
- Results: Implementation has led to improved clinical outcomes, including lower A1c levels in our diabetic patients and fewer emergency department visits and hospitalizations.
- Conclusion: The Health Home model has improved our ability to provide high quality, culturally competent health care to our diverse patient population.
Samuel U. Rodgers Health Center (SURHC) has a long and proud history in Kansas City. It was founded in 1967 and incorporated in 1968 as the fourth federally qualified health center in the United States and the first in Missouri. SURHC provides comprehensive primary and urgent care to persons of all ages in the areas of adult and senior medicine, obstetrics/gynecology, pediatric and adolescent health, behavioral health, and dental health services for our community’s most medically vulnerable families, regardless of their ability to pay or health insurance status.
SURHC has a New Americans program in partnership with the Jewish Vocational Immigration Intake Center, in which all newly arrived refugees come to SURHC to receive their physical health exam and be brought up to date with necessary vaccinations. A large proportion of SURHC’s patients are refugees from war-torn and famine-impacted countries, many of which lived in refugee camps with inconsistent access to health care. Some arrive feeling hopeless, fearful, and drained while others have been tortured, maimed, and/or raped. Given these extraordinary circumstances, many patients come to us without a clear understanding of their illness or what constitutes a healthy lifestyle, including diet and exercise, preventive health screenings, and immunizations. Assistance is often required for behavioral health issues associated with acculturation stress, migration, and resettlement in addition to medical care.
Our refugees come from culturally diverse populations and may have limited literacy rates, be impacted by race-related health disparities, and be non-English speaking. Twenty-nine percent of SURHC’s total patient population and 43% of our patient population at our primary downtown campus location are non-English speaking refugees and/or immigrants. Within our chronic disease population, 68% require interpreter services. The health center employs interpreters for English, Somali, Spanish, Arabic, Burmese, and Vietnamese, but for languages less commonly used in the clinic—such as Karen, Nepalese, and Swahili—phone language interpreter services are used.
One problem we identified while working with our unique patient population was the lack of appropriate educational materials. As a result, the “traditional” method of working with patients would not be effective, necessitating a new approach to meeting the needs of our patients if there was to be any impact on their health outcomes or quality of life or provision of cost savings to the health care system. We recognized the need to address multicultural issues involving health literacy levels in addition to assessing the patient’s physical and mental health issues and basic needs before confronting their chronic disease. The stress produced from these concerns was notably interfering with the patient’s ability to focus on their overall health. We describe our approach to addressing these issues in this article.
Approach to Care
SURHC has been successful in fully integrating behavioral health care with primary care as part of our participation in the Missouri Medicaid primary care Health Home (PCHH) initiative. Our PCHH participation began in 2012 and provides SURHC with the opportunity to benefit from a fully integrated model of care. The initiative serves 300 Missouri Medicaid beneficiaries, providing intense primary care and behavioral health services for patients with 2 or more chronic diseases. The patient centered medical home laid the foundation for PCHH, which relies on a team-based care approach. PCHH employs a holistic approach similar to the medical home model and includes behavioral health as part of the front-line interventions to manage physical and mental health issues, including the determinants of health factors that may be influencing the ability of the patient to adhere to the treatment plan and live a healthy life.
Working with multiple cultures involves developing a staff that is culturally competent. This includes education on the values and beliefs of different cultures which enhances staff’s ability to understand, communicate with, and create an effective learning experience for the patient. Evidence shows that understanding someone’s culture aids in developing trust between patient and team member. This relationship greatly contributes to successful results and the reaching of patient self-management goals.
Working with different cultures also necessitates a multidisciplinary team, comprising a care coordinator, behavioral health consultant, and an RN care manager. The multidisciplinary team works in coordination with the primary care provider, LPN, and medical assistant to address the physical, mental, and social needs of the patient.
The care coordinator maintains current insurance status on patients. Specific doctor-prescribed medical supplies go through the coordinator to be pre-certified through our Cyber Access (electronic health record). The coordinator completes our measures report for meaningful use. The care coordinator answers patient calls and schedules and redirects calls as needed. A newsletter is created and mailed out monthly to our patients.
The behavioral health consultant addresses the mental processes of the patient. An assessment may include an evaluation of the patient’s emotional and spiritual needs as well as possible behavioral modification. The behavioral health consultant also addresses smoking cessation, stress reduction, and exercising. Assessment of motivation and readiness is evaluated to assist the patient in setting goals for the self-management of chronic diseases. The behavioral health consultant and RN care manager work closely together by integrating the behavioral health with the primary medical care of the patient.
The RN care manager sees patients when they come in for appointments with their primary care provider (PCP). The RN uses this time to answer patient questions regarding chronic disease, to check if patients know which medications they are taking and why, and for following up on any previous chronic disease teaching or hospital visits they may have had. This team member also coordinates with other specialists and agencies outside of the clinic to assure the patient is followed up with.
Self-Management Support
The ultimate goal in educating a multicultural patient is to wean them from hands-on support provided by the multidisciplinary staff to be able to effectively self-manage their disease. With effective self-management, the patient understands his or her condition, how it affects the body, and can monitor the condition in order to make any necessary changes to stay healthy.
Health literacy plays a significant role in educating the patient about their chronic disease. It is important to measure each patient’s ability to read and write—not only in their native language, but in English as well. This assessment enabled the multidisciplinary team to create new methods of working distinctively with each individual to support their self-management.
One of the self-management techniques that has helped patients and staff track their progress is the use of wall calendars. Our practice provides a wall calendar for interested patients to help track daily fasting, blood glucose, blood pressure, medications taken, etc. The patient can track times they took their medications by using stickers to indicate if they have taken their morning, noon, or evening medications. Our practice supplies the patient with stickers of their choice to use. These wall calendars are helpful for providing daily and monthly accounts of self-management activitites and patients are encouraged to bring them to their appointments. Future appointments can be added to the calendar before the patient leaves the doctor’s office.
Having on-site, professionally certified interpreters greatly improves the education and learning-time for non-English speaking patients. These team members are crucial for their abilities to visually assess the patient’s understanding of teaching materials and interpreting if the patient is showing signs of confusion. The interpreter is also helpful in re-labeling prescription bottles in the patient’s language or with stickers to help them understand how to take the medication correctly. Interpreters have also helped in creating new patient information tools written in different languages for patients that are literate. We have also noted that patients appear more comfortable in the learning environment when a personal interpreter is present as opposed to a telecommunication service.
Scheduled appointment times are set for the patient to meet one-on-one with the nurse care manager or behavioral health consultant for education during which 1 or 2 main points relating to their chronic disease is discussed. This strategy, called “chunking,” breaks the content down into bite-sized segments, helping the patient to learn and retain the information presented. These sessions are good times to work on specifics of the individual’s lifestyle and history and allow time for the patient to ask questions. Most information on a chronic disease can be given in 2 to 4 sessions, with an hour allotted for each one. Follow-up can be done as needed for each patient.
Teaching patients how to read nutrition labels is another useful skill. This is helpful for patients that have diabetes, hypertension, and/or hyperlipidemia. Our staff has collected empty food containers, snack packages, and drink bottles of different ethnic foods. Patients are taught how to read the nutrition labels to help them make healthy choices; for instance, a patient with diabetes is taught to read the serving size and then assess the carbohydrate amount. When comparing foods of the same kind, patients then know to choose the one with less carbohydrates per serving for the healthiest choice. A patient with hypertension would look at serving size and sodium content whereas a patient with hyperlipidemia would learn to pay attention to the serving size, fats, and cholesterol amounts. Using actual food containers as props has been an eye-opening experience for many of patients and those that understand and follow instructions on how to read nutrition labels have higher success rates in their self-management.
To further encourage healthy eating, with the help of our international interpreters we took pictures of prepared foods from different countries. Each picture was then placed on a red, yellow, or green sheet of paper (the stop light method) based on the ingredients in the food depicted. When a patient comes for teaching, we have them go through the pictures and pull out the ones they recognize and consume. We then teach the patient that foods depicted on green paper may be consumed as much as desired, foods on the yellow paper should be limited in the quantity, and foods on the red sheets represent the unhealthiest choices. Time is spent teaching patients how they can make these red-sheet dishes in a healthier manner.
Outcomes
Although SURHC’s patient population faces many challenges in achieving and maintaining control over their health, we are having success in improving clinical outcomes resulting from the implementation of the PCHH model. For example, within a 6-month period, 80% of our patients with an A1c > 8% saw a reduction in their A1c level. In addition, we found emergency room visits and hospitalizations dropped from 332 in December 2012 to 176 in August 2013. This reflects a 53% decrease in visits, for a conservative estimate of over $327,600 in savings to the health care system.
Discussion
Our outcomes support the fact that interventions and one-on-one work with patients have been helpful. The PCHH model provides personal attention to the patient—such as individually-structured teaching plans to assist in setting and attaining goals—which makes patients more accountable for self-management of their health. The use of interpreters in the education process was key to successful goal management and outcomes as they provided the bridge for patients to learn how to set and reach their goals. This model also integrates a behavioral health component to encompass the needs of the whole person, including psychosocial requirements.
Health literacy is an important factor in working with our multicultural population. It is important to provide literate patients with information in their native tongue, which can help teach them more about their chronic disease. We found some helpful educational handouts online in different languages. We also have used our onsite interpreters to help us in creating new educational handouts. In addition, we developed videos that feature our health center’s personal interpreters providing information in 6 languages about “Medications” and “What do I need to bring to my appointment?” The medication video explains the importance of taking the prescribed medicine every day or as the provider orders, and how to refill medications. The other video explains the need to bring all medications, glucose or blood pressure readings, etc, to appointments. These multilingual videos play in the waiting room throughout the day. Seeing employees on the video helps draw the patients into listening and learning the information provided.
We found that we needed to address the basic needs of the patient before confronting their chronic disease. This process sometimes involved finding beds or providing food for the patient. Many had dental issues that needed to be addressed before we could work with them on their diabetic diet issues or other contributing chronic issues. If these needs are met, it can ameliorate stress, which can have negative effects on their health.
On review of current A1c findings, there was a decrease in the percentage of patients who showed improvement. This is reflective of the most challenging patients we continue to work with. Moving forward, as more refugees representing increasingly diverse cultures come to our clinic, greater understanding of cultural nuances remains a challenge. Additional work is necessary to produce and accumulate more diverse educational materials to meet the health literacy needs of each patient.
Samuel U. Rodgers Health Center has earned the trust of our diverse communities and we are confident and proud of our ability to provide high quality, culturally-competent health care to our diverse patient population.
Corresponding author: Robyn McCright, RN, 825 Euclid Ave., Kansas City, MO 64124, [email protected].
Financial disclosures: None.
From the Samuel U. Rodgers Health Center, Kansas City, MO.
Abstract
- Objective: To describe the application of the Health Home model in a center that provides care for a culturally diverse patient population.
- Methods: The initiative serves 300 Medicaid beneficiaries, providing intense primary care and behavioral health services for patients with 2 or more chronic diseases. The program addresses multicultural issues and health literacy in addition to assessing patients’ physical and mental health issues and basic needs. It builds upon the patient-centered medical home model, employing a team-based, holistic approach that integrates a behavioral health component to encompass the needs of the whole person, including psychosocial requirements.
- Results: Implementation has led to improved clinical outcomes, including lower A1c levels in our diabetic patients and fewer emergency department visits and hospitalizations.
- Conclusion: The Health Home model has improved our ability to provide high quality, culturally competent health care to our diverse patient population.
Samuel U. Rodgers Health Center (SURHC) has a long and proud history in Kansas City. It was founded in 1967 and incorporated in 1968 as the fourth federally qualified health center in the United States and the first in Missouri. SURHC provides comprehensive primary and urgent care to persons of all ages in the areas of adult and senior medicine, obstetrics/gynecology, pediatric and adolescent health, behavioral health, and dental health services for our community’s most medically vulnerable families, regardless of their ability to pay or health insurance status.
SURHC has a New Americans program in partnership with the Jewish Vocational Immigration Intake Center, in which all newly arrived refugees come to SURHC to receive their physical health exam and be brought up to date with necessary vaccinations. A large proportion of SURHC’s patients are refugees from war-torn and famine-impacted countries, many of which lived in refugee camps with inconsistent access to health care. Some arrive feeling hopeless, fearful, and drained while others have been tortured, maimed, and/or raped. Given these extraordinary circumstances, many patients come to us without a clear understanding of their illness or what constitutes a healthy lifestyle, including diet and exercise, preventive health screenings, and immunizations. Assistance is often required for behavioral health issues associated with acculturation stress, migration, and resettlement in addition to medical care.
Our refugees come from culturally diverse populations and may have limited literacy rates, be impacted by race-related health disparities, and be non-English speaking. Twenty-nine percent of SURHC’s total patient population and 43% of our patient population at our primary downtown campus location are non-English speaking refugees and/or immigrants. Within our chronic disease population, 68% require interpreter services. The health center employs interpreters for English, Somali, Spanish, Arabic, Burmese, and Vietnamese, but for languages less commonly used in the clinic—such as Karen, Nepalese, and Swahili—phone language interpreter services are used.
One problem we identified while working with our unique patient population was the lack of appropriate educational materials. As a result, the “traditional” method of working with patients would not be effective, necessitating a new approach to meeting the needs of our patients if there was to be any impact on their health outcomes or quality of life or provision of cost savings to the health care system. We recognized the need to address multicultural issues involving health literacy levels in addition to assessing the patient’s physical and mental health issues and basic needs before confronting their chronic disease. The stress produced from these concerns was notably interfering with the patient’s ability to focus on their overall health. We describe our approach to addressing these issues in this article.
Approach to Care
SURHC has been successful in fully integrating behavioral health care with primary care as part of our participation in the Missouri Medicaid primary care Health Home (PCHH) initiative. Our PCHH participation began in 2012 and provides SURHC with the opportunity to benefit from a fully integrated model of care. The initiative serves 300 Missouri Medicaid beneficiaries, providing intense primary care and behavioral health services for patients with 2 or more chronic diseases. The patient centered medical home laid the foundation for PCHH, which relies on a team-based care approach. PCHH employs a holistic approach similar to the medical home model and includes behavioral health as part of the front-line interventions to manage physical and mental health issues, including the determinants of health factors that may be influencing the ability of the patient to adhere to the treatment plan and live a healthy life.
Working with multiple cultures involves developing a staff that is culturally competent. This includes education on the values and beliefs of different cultures which enhances staff’s ability to understand, communicate with, and create an effective learning experience for the patient. Evidence shows that understanding someone’s culture aids in developing trust between patient and team member. This relationship greatly contributes to successful results and the reaching of patient self-management goals.
Working with different cultures also necessitates a multidisciplinary team, comprising a care coordinator, behavioral health consultant, and an RN care manager. The multidisciplinary team works in coordination with the primary care provider, LPN, and medical assistant to address the physical, mental, and social needs of the patient.
The care coordinator maintains current insurance status on patients. Specific doctor-prescribed medical supplies go through the coordinator to be pre-certified through our Cyber Access (electronic health record). The coordinator completes our measures report for meaningful use. The care coordinator answers patient calls and schedules and redirects calls as needed. A newsletter is created and mailed out monthly to our patients.
The behavioral health consultant addresses the mental processes of the patient. An assessment may include an evaluation of the patient’s emotional and spiritual needs as well as possible behavioral modification. The behavioral health consultant also addresses smoking cessation, stress reduction, and exercising. Assessment of motivation and readiness is evaluated to assist the patient in setting goals for the self-management of chronic diseases. The behavioral health consultant and RN care manager work closely together by integrating the behavioral health with the primary medical care of the patient.
The RN care manager sees patients when they come in for appointments with their primary care provider (PCP). The RN uses this time to answer patient questions regarding chronic disease, to check if patients know which medications they are taking and why, and for following up on any previous chronic disease teaching or hospital visits they may have had. This team member also coordinates with other specialists and agencies outside of the clinic to assure the patient is followed up with.
Self-Management Support
The ultimate goal in educating a multicultural patient is to wean them from hands-on support provided by the multidisciplinary staff to be able to effectively self-manage their disease. With effective self-management, the patient understands his or her condition, how it affects the body, and can monitor the condition in order to make any necessary changes to stay healthy.
Health literacy plays a significant role in educating the patient about their chronic disease. It is important to measure each patient’s ability to read and write—not only in their native language, but in English as well. This assessment enabled the multidisciplinary team to create new methods of working distinctively with each individual to support their self-management.
One of the self-management techniques that has helped patients and staff track their progress is the use of wall calendars. Our practice provides a wall calendar for interested patients to help track daily fasting, blood glucose, blood pressure, medications taken, etc. The patient can track times they took their medications by using stickers to indicate if they have taken their morning, noon, or evening medications. Our practice supplies the patient with stickers of their choice to use. These wall calendars are helpful for providing daily and monthly accounts of self-management activitites and patients are encouraged to bring them to their appointments. Future appointments can be added to the calendar before the patient leaves the doctor’s office.
Having on-site, professionally certified interpreters greatly improves the education and learning-time for non-English speaking patients. These team members are crucial for their abilities to visually assess the patient’s understanding of teaching materials and interpreting if the patient is showing signs of confusion. The interpreter is also helpful in re-labeling prescription bottles in the patient’s language or with stickers to help them understand how to take the medication correctly. Interpreters have also helped in creating new patient information tools written in different languages for patients that are literate. We have also noted that patients appear more comfortable in the learning environment when a personal interpreter is present as opposed to a telecommunication service.
Scheduled appointment times are set for the patient to meet one-on-one with the nurse care manager or behavioral health consultant for education during which 1 or 2 main points relating to their chronic disease is discussed. This strategy, called “chunking,” breaks the content down into bite-sized segments, helping the patient to learn and retain the information presented. These sessions are good times to work on specifics of the individual’s lifestyle and history and allow time for the patient to ask questions. Most information on a chronic disease can be given in 2 to 4 sessions, with an hour allotted for each one. Follow-up can be done as needed for each patient.
Teaching patients how to read nutrition labels is another useful skill. This is helpful for patients that have diabetes, hypertension, and/or hyperlipidemia. Our staff has collected empty food containers, snack packages, and drink bottles of different ethnic foods. Patients are taught how to read the nutrition labels to help them make healthy choices; for instance, a patient with diabetes is taught to read the serving size and then assess the carbohydrate amount. When comparing foods of the same kind, patients then know to choose the one with less carbohydrates per serving for the healthiest choice. A patient with hypertension would look at serving size and sodium content whereas a patient with hyperlipidemia would learn to pay attention to the serving size, fats, and cholesterol amounts. Using actual food containers as props has been an eye-opening experience for many of patients and those that understand and follow instructions on how to read nutrition labels have higher success rates in their self-management.
To further encourage healthy eating, with the help of our international interpreters we took pictures of prepared foods from different countries. Each picture was then placed on a red, yellow, or green sheet of paper (the stop light method) based on the ingredients in the food depicted. When a patient comes for teaching, we have them go through the pictures and pull out the ones they recognize and consume. We then teach the patient that foods depicted on green paper may be consumed as much as desired, foods on the yellow paper should be limited in the quantity, and foods on the red sheets represent the unhealthiest choices. Time is spent teaching patients how they can make these red-sheet dishes in a healthier manner.
Outcomes
Although SURHC’s patient population faces many challenges in achieving and maintaining control over their health, we are having success in improving clinical outcomes resulting from the implementation of the PCHH model. For example, within a 6-month period, 80% of our patients with an A1c > 8% saw a reduction in their A1c level. In addition, we found emergency room visits and hospitalizations dropped from 332 in December 2012 to 176 in August 2013. This reflects a 53% decrease in visits, for a conservative estimate of over $327,600 in savings to the health care system.
Discussion
Our outcomes support the fact that interventions and one-on-one work with patients have been helpful. The PCHH model provides personal attention to the patient—such as individually-structured teaching plans to assist in setting and attaining goals—which makes patients more accountable for self-management of their health. The use of interpreters in the education process was key to successful goal management and outcomes as they provided the bridge for patients to learn how to set and reach their goals. This model also integrates a behavioral health component to encompass the needs of the whole person, including psychosocial requirements.
Health literacy is an important factor in working with our multicultural population. It is important to provide literate patients with information in their native tongue, which can help teach them more about their chronic disease. We found some helpful educational handouts online in different languages. We also have used our onsite interpreters to help us in creating new educational handouts. In addition, we developed videos that feature our health center’s personal interpreters providing information in 6 languages about “Medications” and “What do I need to bring to my appointment?” The medication video explains the importance of taking the prescribed medicine every day or as the provider orders, and how to refill medications. The other video explains the need to bring all medications, glucose or blood pressure readings, etc, to appointments. These multilingual videos play in the waiting room throughout the day. Seeing employees on the video helps draw the patients into listening and learning the information provided.
We found that we needed to address the basic needs of the patient before confronting their chronic disease. This process sometimes involved finding beds or providing food for the patient. Many had dental issues that needed to be addressed before we could work with them on their diabetic diet issues or other contributing chronic issues. If these needs are met, it can ameliorate stress, which can have negative effects on their health.
On review of current A1c findings, there was a decrease in the percentage of patients who showed improvement. This is reflective of the most challenging patients we continue to work with. Moving forward, as more refugees representing increasingly diverse cultures come to our clinic, greater understanding of cultural nuances remains a challenge. Additional work is necessary to produce and accumulate more diverse educational materials to meet the health literacy needs of each patient.
Samuel U. Rodgers Health Center has earned the trust of our diverse communities and we are confident and proud of our ability to provide high quality, culturally-competent health care to our diverse patient population.
Corresponding author: Robyn McCright, RN, 825 Euclid Ave., Kansas City, MO 64124, [email protected].
Financial disclosures: None.
From the Samuel U. Rodgers Health Center, Kansas City, MO.
Abstract
- Objective: To describe the application of the Health Home model in a center that provides care for a culturally diverse patient population.
- Methods: The initiative serves 300 Medicaid beneficiaries, providing intense primary care and behavioral health services for patients with 2 or more chronic diseases. The program addresses multicultural issues and health literacy in addition to assessing patients’ physical and mental health issues and basic needs. It builds upon the patient-centered medical home model, employing a team-based, holistic approach that integrates a behavioral health component to encompass the needs of the whole person, including psychosocial requirements.
- Results: Implementation has led to improved clinical outcomes, including lower A1c levels in our diabetic patients and fewer emergency department visits and hospitalizations.
- Conclusion: The Health Home model has improved our ability to provide high quality, culturally competent health care to our diverse patient population.
Samuel U. Rodgers Health Center (SURHC) has a long and proud history in Kansas City. It was founded in 1967 and incorporated in 1968 as the fourth federally qualified health center in the United States and the first in Missouri. SURHC provides comprehensive primary and urgent care to persons of all ages in the areas of adult and senior medicine, obstetrics/gynecology, pediatric and adolescent health, behavioral health, and dental health services for our community’s most medically vulnerable families, regardless of their ability to pay or health insurance status.
SURHC has a New Americans program in partnership with the Jewish Vocational Immigration Intake Center, in which all newly arrived refugees come to SURHC to receive their physical health exam and be brought up to date with necessary vaccinations. A large proportion of SURHC’s patients are refugees from war-torn and famine-impacted countries, many of which lived in refugee camps with inconsistent access to health care. Some arrive feeling hopeless, fearful, and drained while others have been tortured, maimed, and/or raped. Given these extraordinary circumstances, many patients come to us without a clear understanding of their illness or what constitutes a healthy lifestyle, including diet and exercise, preventive health screenings, and immunizations. Assistance is often required for behavioral health issues associated with acculturation stress, migration, and resettlement in addition to medical care.
Our refugees come from culturally diverse populations and may have limited literacy rates, be impacted by race-related health disparities, and be non-English speaking. Twenty-nine percent of SURHC’s total patient population and 43% of our patient population at our primary downtown campus location are non-English speaking refugees and/or immigrants. Within our chronic disease population, 68% require interpreter services. The health center employs interpreters for English, Somali, Spanish, Arabic, Burmese, and Vietnamese, but for languages less commonly used in the clinic—such as Karen, Nepalese, and Swahili—phone language interpreter services are used.
One problem we identified while working with our unique patient population was the lack of appropriate educational materials. As a result, the “traditional” method of working with patients would not be effective, necessitating a new approach to meeting the needs of our patients if there was to be any impact on their health outcomes or quality of life or provision of cost savings to the health care system. We recognized the need to address multicultural issues involving health literacy levels in addition to assessing the patient’s physical and mental health issues and basic needs before confronting their chronic disease. The stress produced from these concerns was notably interfering with the patient’s ability to focus on their overall health. We describe our approach to addressing these issues in this article.
Approach to Care
SURHC has been successful in fully integrating behavioral health care with primary care as part of our participation in the Missouri Medicaid primary care Health Home (PCHH) initiative. Our PCHH participation began in 2012 and provides SURHC with the opportunity to benefit from a fully integrated model of care. The initiative serves 300 Missouri Medicaid beneficiaries, providing intense primary care and behavioral health services for patients with 2 or more chronic diseases. The patient centered medical home laid the foundation for PCHH, which relies on a team-based care approach. PCHH employs a holistic approach similar to the medical home model and includes behavioral health as part of the front-line interventions to manage physical and mental health issues, including the determinants of health factors that may be influencing the ability of the patient to adhere to the treatment plan and live a healthy life.
Working with multiple cultures involves developing a staff that is culturally competent. This includes education on the values and beliefs of different cultures which enhances staff’s ability to understand, communicate with, and create an effective learning experience for the patient. Evidence shows that understanding someone’s culture aids in developing trust between patient and team member. This relationship greatly contributes to successful results and the reaching of patient self-management goals.
Working with different cultures also necessitates a multidisciplinary team, comprising a care coordinator, behavioral health consultant, and an RN care manager. The multidisciplinary team works in coordination with the primary care provider, LPN, and medical assistant to address the physical, mental, and social needs of the patient.
The care coordinator maintains current insurance status on patients. Specific doctor-prescribed medical supplies go through the coordinator to be pre-certified through our Cyber Access (electronic health record). The coordinator completes our measures report for meaningful use. The care coordinator answers patient calls and schedules and redirects calls as needed. A newsletter is created and mailed out monthly to our patients.
The behavioral health consultant addresses the mental processes of the patient. An assessment may include an evaluation of the patient’s emotional and spiritual needs as well as possible behavioral modification. The behavioral health consultant also addresses smoking cessation, stress reduction, and exercising. Assessment of motivation and readiness is evaluated to assist the patient in setting goals for the self-management of chronic diseases. The behavioral health consultant and RN care manager work closely together by integrating the behavioral health with the primary medical care of the patient.
The RN care manager sees patients when they come in for appointments with their primary care provider (PCP). The RN uses this time to answer patient questions regarding chronic disease, to check if patients know which medications they are taking and why, and for following up on any previous chronic disease teaching or hospital visits they may have had. This team member also coordinates with other specialists and agencies outside of the clinic to assure the patient is followed up with.
Self-Management Support
The ultimate goal in educating a multicultural patient is to wean them from hands-on support provided by the multidisciplinary staff to be able to effectively self-manage their disease. With effective self-management, the patient understands his or her condition, how it affects the body, and can monitor the condition in order to make any necessary changes to stay healthy.
Health literacy plays a significant role in educating the patient about their chronic disease. It is important to measure each patient’s ability to read and write—not only in their native language, but in English as well. This assessment enabled the multidisciplinary team to create new methods of working distinctively with each individual to support their self-management.
One of the self-management techniques that has helped patients and staff track their progress is the use of wall calendars. Our practice provides a wall calendar for interested patients to help track daily fasting, blood glucose, blood pressure, medications taken, etc. The patient can track times they took their medications by using stickers to indicate if they have taken their morning, noon, or evening medications. Our practice supplies the patient with stickers of their choice to use. These wall calendars are helpful for providing daily and monthly accounts of self-management activitites and patients are encouraged to bring them to their appointments. Future appointments can be added to the calendar before the patient leaves the doctor’s office.
Having on-site, professionally certified interpreters greatly improves the education and learning-time for non-English speaking patients. These team members are crucial for their abilities to visually assess the patient’s understanding of teaching materials and interpreting if the patient is showing signs of confusion. The interpreter is also helpful in re-labeling prescription bottles in the patient’s language or with stickers to help them understand how to take the medication correctly. Interpreters have also helped in creating new patient information tools written in different languages for patients that are literate. We have also noted that patients appear more comfortable in the learning environment when a personal interpreter is present as opposed to a telecommunication service.
Scheduled appointment times are set for the patient to meet one-on-one with the nurse care manager or behavioral health consultant for education during which 1 or 2 main points relating to their chronic disease is discussed. This strategy, called “chunking,” breaks the content down into bite-sized segments, helping the patient to learn and retain the information presented. These sessions are good times to work on specifics of the individual’s lifestyle and history and allow time for the patient to ask questions. Most information on a chronic disease can be given in 2 to 4 sessions, with an hour allotted for each one. Follow-up can be done as needed for each patient.
Teaching patients how to read nutrition labels is another useful skill. This is helpful for patients that have diabetes, hypertension, and/or hyperlipidemia. Our staff has collected empty food containers, snack packages, and drink bottles of different ethnic foods. Patients are taught how to read the nutrition labels to help them make healthy choices; for instance, a patient with diabetes is taught to read the serving size and then assess the carbohydrate amount. When comparing foods of the same kind, patients then know to choose the one with less carbohydrates per serving for the healthiest choice. A patient with hypertension would look at serving size and sodium content whereas a patient with hyperlipidemia would learn to pay attention to the serving size, fats, and cholesterol amounts. Using actual food containers as props has been an eye-opening experience for many of patients and those that understand and follow instructions on how to read nutrition labels have higher success rates in their self-management.
To further encourage healthy eating, with the help of our international interpreters we took pictures of prepared foods from different countries. Each picture was then placed on a red, yellow, or green sheet of paper (the stop light method) based on the ingredients in the food depicted. When a patient comes for teaching, we have them go through the pictures and pull out the ones they recognize and consume. We then teach the patient that foods depicted on green paper may be consumed as much as desired, foods on the yellow paper should be limited in the quantity, and foods on the red sheets represent the unhealthiest choices. Time is spent teaching patients how they can make these red-sheet dishes in a healthier manner.
Outcomes
Although SURHC’s patient population faces many challenges in achieving and maintaining control over their health, we are having success in improving clinical outcomes resulting from the implementation of the PCHH model. For example, within a 6-month period, 80% of our patients with an A1c > 8% saw a reduction in their A1c level. In addition, we found emergency room visits and hospitalizations dropped from 332 in December 2012 to 176 in August 2013. This reflects a 53% decrease in visits, for a conservative estimate of over $327,600 in savings to the health care system.
Discussion
Our outcomes support the fact that interventions and one-on-one work with patients have been helpful. The PCHH model provides personal attention to the patient—such as individually-structured teaching plans to assist in setting and attaining goals—which makes patients more accountable for self-management of their health. The use of interpreters in the education process was key to successful goal management and outcomes as they provided the bridge for patients to learn how to set and reach their goals. This model also integrates a behavioral health component to encompass the needs of the whole person, including psychosocial requirements.
Health literacy is an important factor in working with our multicultural population. It is important to provide literate patients with information in their native tongue, which can help teach them more about their chronic disease. We found some helpful educational handouts online in different languages. We also have used our onsite interpreters to help us in creating new educational handouts. In addition, we developed videos that feature our health center’s personal interpreters providing information in 6 languages about “Medications” and “What do I need to bring to my appointment?” The medication video explains the importance of taking the prescribed medicine every day or as the provider orders, and how to refill medications. The other video explains the need to bring all medications, glucose or blood pressure readings, etc, to appointments. These multilingual videos play in the waiting room throughout the day. Seeing employees on the video helps draw the patients into listening and learning the information provided.
We found that we needed to address the basic needs of the patient before confronting their chronic disease. This process sometimes involved finding beds or providing food for the patient. Many had dental issues that needed to be addressed before we could work with them on their diabetic diet issues or other contributing chronic issues. If these needs are met, it can ameliorate stress, which can have negative effects on their health.
On review of current A1c findings, there was a decrease in the percentage of patients who showed improvement. This is reflective of the most challenging patients we continue to work with. Moving forward, as more refugees representing increasingly diverse cultures come to our clinic, greater understanding of cultural nuances remains a challenge. Additional work is necessary to produce and accumulate more diverse educational materials to meet the health literacy needs of each patient.
Samuel U. Rodgers Health Center has earned the trust of our diverse communities and we are confident and proud of our ability to provide high quality, culturally-competent health care to our diverse patient population.
Corresponding author: Robyn McCright, RN, 825 Euclid Ave., Kansas City, MO 64124, [email protected].
Financial disclosures: None.
Psychological Stress Interventions and Asthma: Therapeutic Considerations
From the Department of Medicine, The University of Mississippi Medical Center, Jackson, MS.
Abstract
- Objective: To review psychological stress interventions employed to improve asthma outcomes.
- Methods: Review of the literature.
- Results: In general, there are 2 approaches to managing stress in asthma patients—direct psychological interventions, and modalities where stress management is an indirect effect. The most direct approach involves mindfulness-based stress reduction, which has been shown to have a positive effect on asthma control. Cognitive behavioral therapy, biofeedback, music therapy, art therapy, and relaxation training also have been evaluated with varying results. Physical therapies, including yoga, chi gong, massage, reflexology, specific controlled breathing programs, and spinal manipulation have also been studied without consistent effectiveness demonstrated. Pharmacologic therapy for anxiety and depressive disorders has been shown to be associated with improvement in asthma symptoms and control.
- Conclusion: Although further research is needed to verify the beneficial role of specific stress intervention modalities for specific asthma populations, there is sufficient evidence of efficacy to validate the concept of stress management as a viable therapeutic approach for optimal asthma control.
The increasing levels of chronic psychological stress in the people’s everyday lives has been well recognized [1]. As technological advances continue to progress, the psychological and physical pressures associated with family- and work-role expectations, decreased free or “down” time, greater sleep deficits, increasing career-related pressures, social issues, and other factors have led to ever increasing levels of personal stress [2]. From an immune standpoint, these chronic stressors impact immune balance and may be at least partially responsible for the rise in incidence, prevalence, and severity of inflammatory diseases such as asthma [3]. As the factors responsible for increased levels of psychosocial stress in our society are not likely to decrease in the near future [4], the potential value of directed stress intervention therapies in the overall care plans for patients with asthma is an area of interest. Such stress management strategies must be evidence-based, pragmatic, and cost-effective. This review provides background, scientific and clinical rationale, and progress to date for various therapeutic approaches to stress management for asthma patients.
Asthma as Inflammatory Disease
Asthma is a breathlessness syndrome typically characterized by varying combinations of paroxysmal wheezing, cough, breathlessness, and chest tightness. The constellation of symptoms is often precipitated by exposure to volatile irritants, allergens, cold air, and exercise. Gastroesophageal reflux disease, respiratory viral infections, and pregnancy may also precipitate or worsen existing asthma [5,6]. Symptoms typically improve after appropriate asthma treatment.
While the role of IgE-mediated mechanisms in asthma has been questioned by some, studies have demonstrated the presence of IgE-mediated (“allergic”) mechanisms in most asthma cases [7]. Depending on the specific population, as many as 70% to 90% of asthma patients can be considered to have an allergic component to their asthma [8]. Such allergic sensitivities can be to seasonal pollens but even more commonly to perennial allergens such as dust mites, molds, cockroaches, and pet dander (especially cat) [9]. These associations have led to therapeutic approaches for many asthma patients based largely on those classically used for allergic rhinitis, including avoidance, environmental control, and even allergen immunotherapy [10]. Some of the newest and most promising pharmacotherapies for asthma are based on antagonism and/or prevention of the allergic cascade (production and activity of IgE) [11].
Psychological Stress and Asthma
Research regarding the relationships between asthma and chronic stress has been conducted in a variety of populations, using both cross-sectional and prospective designs [12,13]. It has been found that perceived stress negatively affects quality of life of patients with asthma and is associated with reduced medication compliance [14,15] and symptom perception [14,16]. Stress has been linked to both the onset of allergic asthma [17,18] and to enhanced skin test reactivity in response to allergens [19].Oh et al [12] suggested a dose-dependent relationship, with individuals who report increasingly higher levels of stress being more likely to report symptoms of asthma.
People with asthma who are exposed to various types of chronic stress tend to have worse severity and poorer control of their asthma symptoms [20,21]. Interventions to help manage stress in people with asthma are needed at the individual, family, and community levels; all levels are known to influence asthma and asthma morbidity [20,22].
If stress is associated with increased disease incidence and severity, then stress modulation could be expected to have beneficial effects. Advice to work fewer hours, get more sleep, and optimize relaxation can be unproductive and even frustrating to busy persons striving to meet all the demands of life. More realistic are interventions based upon helping people manage stress. Studies have reported benefit from stress management for a number of chronic diseases, including hypertension [23], obesity [24], diabetes [25], and HIV [26]. Given the associations noted above, stress intervention as a therapeutic modality for asthma management is a valid option that should be explored [27].
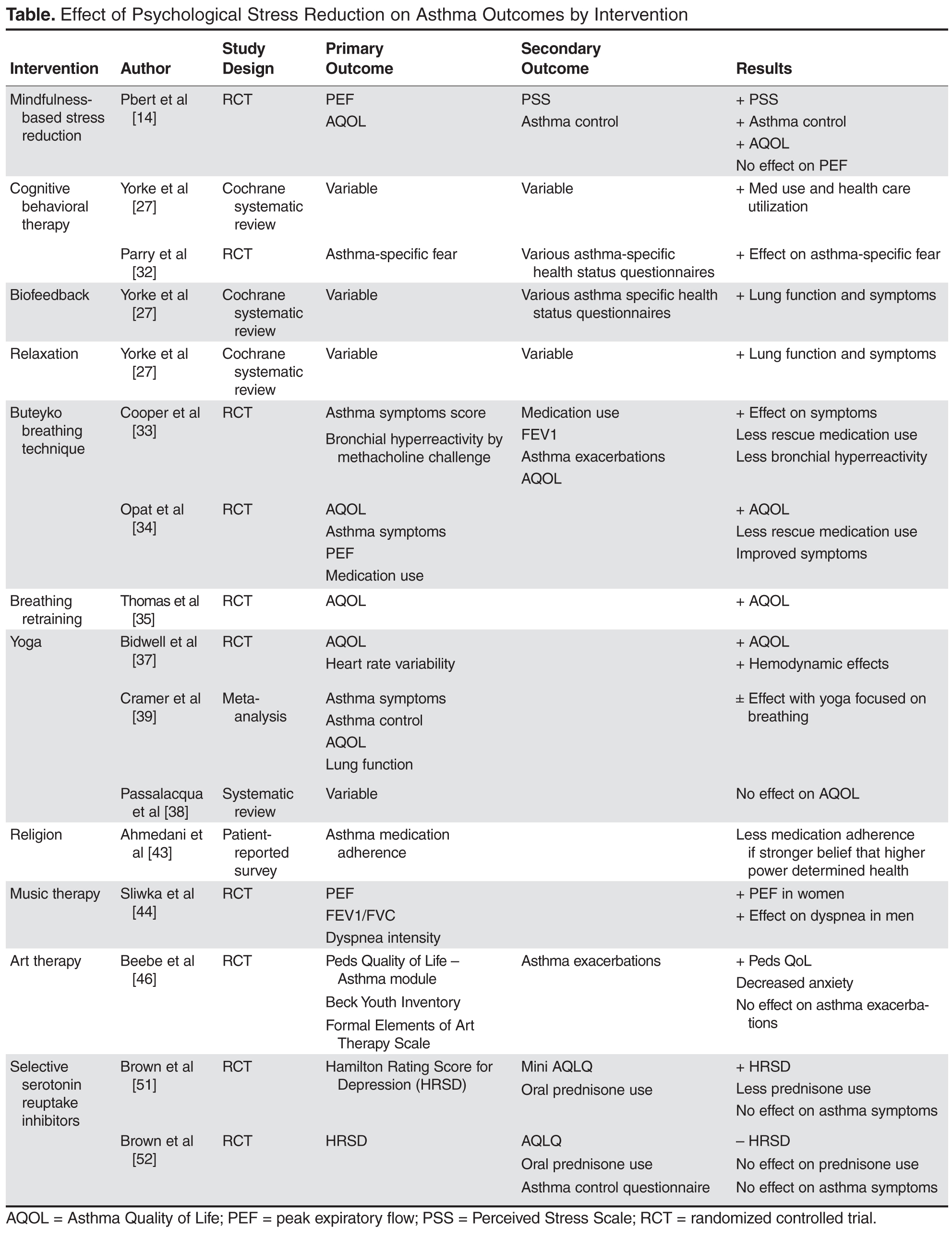
Psychologically Focused Interventions
Mindfulness-based stress reduction (MBSR) has been recognized as an important modality for treatment of many chronic diseases, including chronic pain [28], cardiovascular disease [29], type 2 diabetes mellitus [29], cancer [30], and fibromyalgia [28]. MBSR teaches patients to recognize disease symptoms and personal reactions to these symptoms, and to develop a nonreactive awareness of these elements [14]. It is an individual or group-based therapeutic approach that uses education, discussion, and various meditation techniques to reduce perceived general and disease-associated stress [14,31]. Pbert et al performed an RCT comparing a MBSR program with a traditional education program in adults with mild, moderate, or severe persistent asthma. The primary outcomes were centered on lung function as measured by peak expiratory flow (PEF) and quality of life using the Asthma Quality of Life Questionnaire (AQLQ). Secondary outcomes included changes in perceived stress as measured by the 10-question Perceived Stress Scale (PSS) and overall asthma control. At 12 months, results indicated that MBSR had positive effects on overall asthma control, with improvement in quality of life, a decrease in perceived stress, and a decrease in use of rescue therapies, but no significant effect on peak expiratory flow [14].
Various other psychological interventions have been studied as supplemental therapy to medications in the treatment of asthma. Yorke et al performed a systematic review of 14 RCTs evaluating various psychological interventions in asthma, including cognitive behavioral therapy (CBT), biofeedback, and various relaxation techniques [27]. Because there are no standardized outcomes measured across all studies, results are often conflicting. While CBT had a positive effect on asthma health care utilization, relaxation therapy had no significant effects; both did have positive effects on symptoms of depression and anxiety. Relaxation therapy had positive effects on relieving asthma symptoms such as cough and wheeze but CBT did not. Biofeedback and relaxation were the only interventions that had positive effect on improving lung function and decreasing medication usage [27].
In an RCT, Parry and colleagues evaluated the effects of CBT added to clinical care on asthma-specific fear when compared to standard clinical asthma care alone. They demonstrated a significant reduction in panic and fear related to asthma exacerbations using CBT [32].
Various other mind-body–based interventions, including meditation, yoga, and breathing techniques, have been evaluated as complementary asthma therapy. Several studies utilized the Buteyko breathing technique (BBT), which focuses on controlling breathing to restore normal levels of PaCo2 in order to improve tissue oxygenation and reduce bronchospasm. Cooper et al performed an RCT that evaluated asthma symptom scores and methacholine sensitivity (concentration of bronchial irritant causing decline in FEV1 > 20%) for the presence of bronchial hyperreactivity (BHR), a measure of asthma activity. The BBT group demonstrated a reduction in asthma symptoms and rescue inhaler use but no change in BHR [33]. Opat measured asthma QOL, asthma symptoms, rescue medication use, and lung function in patients who received instruction in BBT and patients in a sham control group. BBT was associated with improvement in asthma QOL and bronchodilator use but not in other outcome parameters [34]. Thomas et al demonstrated in an RCT involving asthma patients with symptoms of dysfunctional breathing that rebreathing-retraining physiotherapy improved asthma-related QOL compared with traditional nurse-provided education [35].
Physical Stress Management Interventions
Yoga, which involves various aspects of controlled breathing, stretching, and meditation techniques [36], aims to achieve synergy between the mind and body to produce a more relaxed psychophysiological state [37]. This popular modality is frequently used by patients, including those with asthma, for symptom control and disease management. Results from RCTs have varied in their reports of efficacy. The 2006 Allergic Rhinitis and Asthma (ARIA) work group performed a systematic review of 5 trials evaluating yoga and asthma. Though the quality of the trials varied greatly, the review demonstrated a possible benefit of yoga on asthma-related QOL but no other studied parameters [38]. QOL and hemodynamic improvement was also demonstrated in 1 RCT comparing yoga added to standard asthma therapy vs. standard therapy alone in female patients [37]. Cramer et al performed an extensive systematic review and meta-analysis of 14 RCTs evaluating the effects of yoga on all or some components of asthma-related QOL, asthma control, symptoms, and pulmonary function [39]. Though there may be some benefit of yoga breathing techniques on asthma-related QOL, the quality of these studies is very poor and reported results were highly variable. These limitations demonstrate the need for methodologically sound, standardized approaches to research in this field, which will be needed before definitive conclusions or treatment recommendations can be made [38,39].
Complementary and Alternative Medicine Interventions
Therapeutic massage, reflexology, spinal manipulation, and prayer are commonly used components of complementary medicine that are perceived by many to be helpful in asthma management [40,41]. However, the published data supporting these techniques is limited. In 2005, Hondras et al performed a Cochrane database review of RCTs evaluating manual therapy, including therapeutic massage, in asthma. Variations in measured outcomes, study design, and reporting made the evidence presented in the review difficult to interpret. Methodologically sound RCTs are needed before any inferences as to relative efficacy of these techniques can be drawn [42]. Since 2005, there have been no significant RCTs reported that would change this conclusion. Data on prayer, religious beliefs, and how these affect asthma and stress control are scarce. One nonrandomized patient reporting survey analysis to evaluate the presence of a high power in life and asthma medication adherence was reported by Ahmedani and colleagues. Results showed that overall medication adherence was low, particularly among those who believed a higher power was in control of their health [43].
Other relaxation methods for managing stress in asthma include music therapy [44] and art therapy [45,46]. Music therapy has had varying reported therapeutic success in other medical settings, such as cardiac rehabilitation [47] and prior to endoscopy [48]. Several studies have evaluated passive or active music therapy in various stages of asthma management with variable results reported. One RCT of patients admitted for asthma exacerbation evaluated the effectiveness of standard pulmonary rehabilitation for asthma with or without concomitant music therapy. Measured outcomes included lung function parameters (PEF and FEV1/FVC) and self-reported anxiety scales. There was a small improvement in PEF in women in the music therapy group. Secondary statistical analysis showed lung function improvements with music therapy only in the patients with mild asthma [44]. Art therapy, the opportunity to share feelings through the use of art materials and expressions, has been used effectively to reduce psychological distress in pediatric chronic disease. One RCT of 23 children examined the potential utility of art therapy in pediatric asthma management. While it did not affect number of exacerbations, art therapy dramatically improved quality of life in children with asthma by decreasing worry and anxiety. The effect persisted for at least 6 months after the intervention was completed [46].
Pharmacotherapy Interventions
Given that anxiety and depression are commonly reported in patients with asthma, particularly in severe and difficult to control disease [49], traditional pharmacologic treatment of anxiety and depression is often attempted. Both depression and anxiety in patients with asthma has been associated with poor asthma-related QOL, but depressive disorders were more commonly associated with poorer levels of asthma control [50]. The use of antidepressant medications, especially selective serotonin reuptake inhibitors (SSRIs), in this patient population has had varying success reported. One randomized placebo-controlled trial evaluated the use of citalopram in 90 adults with asthma and major depressive disorder. Not surprisingly, there was a positive effect on the primary outcome measuring depression using the Hamilton Rating Scale for Depression. Secondary outcome analysis also showed a decrease in oral corticosteroid use in the group treated with citalopram; however, no difference in asthma symptoms between groups was observed [51]. A similar but smaller RCT evaluated the use of escitalopram in major depression and severe asthma. The escitalopram group failed to show a statistical difference in depressive symptoms, asthma control, or oral prednisone use when compared with placebo [52].
The Future for Stress Management as a Fundamental Component of Asthma Care
Historically, avoidance of known triggers and use of pharmacologic maintenance and treatment modalities has been the cornerstone of asthma care. The recognition of excess psychological stress as a recognized trigger and treatment target is continuing to evolve in our therapeutic armamentarium. Our understanding of the effects of stress management in asthma patients provides clinical support for the neuroendocrine immune link between the bronchial inflammatory response characteristic in asthma and that of the human stress response. Understanding the relationships of psychological stress in asthma physiology, clinical morbidity, and therapeutic options is imperative, as the changing health care environment increasingly demands preventive, practical, cost-effective, evidence-based medicine. Some psychological stressors will no doubt be more difficult to address than others, but implementation of nonpharmacologic stress management paradigms should help improve effective asthma management across all patient demographics and should hopefully lead to decreased population health care costs, fewer days of work lost, and improved quality of life. Despite a clear molecular link between asthma, inflammation and stress and a clinical trend toward benefit, the heterogeneity of studies and poor quality evidence for each stress reduction modality make it difficult to draw any firm conclusions on the comparative efficacy of specific psychological interventions in asthma management programs. Mindfulness-based stress reduction has the highest quality evidence and shows the most promise thus far. Further research employing methodically sound RCTs that use standardized physiologic and nonphysiologic outcome measures is needed to elucidate the role for stress reduction interventions in routine clinical practice.
Corresponding author: Gailen D. Marshall Jr, MD, PhD, Div. of Clinical Immunology and Allergy, Dept. of Medicine, The University of Mississippi Medical Ctr., 2500 N. State St. N416 Jackson, MS 39216, [email protected].
Financial disclosures: None.
Author contributions: conception and design, CRP, AMW, GDM; drafting of article, CRP, AMW, GDM; critical revision of the article, CRP, AMW, GDM; administrative or technical support, GDM.
1. Kondo N. Socioeconomic disparities and health: impacts and pathways. J Epidemiol 2012;22:2–6.
2. Nakata A. Psychosocial job stress and immunity: a systematic review. Methods Mol Biol 2012;934:39–7.
3. Van Lieshout RJ, Macqueen GM. Relation between asthma and psychological distress: an old idea revisited. Chem Immunol Allergy 2012;98:1–13.
4. Marshall GD Jr. The adverse effects of psychological stress on immunoregulatory balance: applications to human inflammatory diseases. Immunol Allergy Clin North Am 2011;31:133–40.
5. Murphy VE, Gibson PG, Smith R, et al. Asthma during pregnancy: mechanisms and treatment implications. Eur Respir J 2005;25:1–750.
6. Harding SM. Acid reflux and asthma. Curr Opin Pulm Med 2003;9:42–5.
7. Umetsu DT, McIntire JJ, Akbari O, et al. Asthma: an epidemic of dysregulated immunity. Nat Immunol 2002;3:715–20.
8. Matricardi PM. Prevalence of atopy and asthma in eastern versus western Europe: why the difference? Ann Allergy Asthma Immunol 2001;87:24–7.
9. Murray CS, Woodcock A, Custovic A. The role of indoor allergen exposure in the development of sensitization and asthma. Curr Opin Allergy Clin Immunol 2001;1:407–12.
10. TePas EC, Umetsu DT. Immunotherapy of asthma and allergic diseases. Curr Opin Pediatr 2000;12:574–78.
11. Babu KS, Holgate ST. Newer therapies for asthma: a focus on anti-IgE. Indian J Chest Dis Allied Sci 2002;44:107–15.
12. Oh Y, Kim Y, Yoo S, et al. Association between stress and asthma symptoms: a population based study. Respirology 2004;9:363–8.
13. Sandberg S, Paton JY, Ahola S, et al. The role of acute and chronic stress in asthma attacks in children. Lancet 2000;356:982–7.
14. Pbert L, Madison JM, Druker S, et al. Effect of mindfulness training on asthma quality of life and lung function: a randomized controlled trial. Thorax 2012;67:769–76.
15. Wisnivesky JP, Lorenzo J, Feldman JM, et al. The relationship between perceived stress and morbidity among adult inner-city asthmatics. J Asthma 2010;47:100–4.
16. Janssens T, Verleden G, De Peuter S, et al. Inaccurate perception of asthma symptoms: a cognitive-affective framework and implications for asthma treatment. Clin Psychol Rev 2009;29:317–27.
17. Wright RJ, Cohen S, Carey V, et al. Parental stress as a predictor of wheezing in infancy: a prospective birth-cohort study. Am J Resp Crit Care Med 2002;165:358–65.
18. Wright RJ, Mitchell H, Visness CM, et al. Community violence and asthma morbidity in the Inner-City Asthma Study. Am J Public Health 2004;94:625–32.
19. Michel FB. Psychology of the allergic patient. Allergy 1994;49:28–30.
20. Yonas MA, Lange NE, Celedon JC. Psychosocial stress and asthma morbidity. Curr Opin Allergy Clin Immunol 2012;12:202–10.
21. Apter AJ, Garcia LA, Boyd RC, et al. Exposure to community violence is associated with asthma hospitalizations and emergency department visits. J Allergy Clin Immunol 2010;126:552–7.
22. Wright RJ. Epidemiology of stress and asthma: from constricting communities and fragile families to epigenetics. Immunol Allergy Clin North Am 2011;31:19–39.
23. Tyagi A, Cohen M. Yoga and hypertension: a systematic review. Altern Ther Health Med 2014;20:32-59.
24. Moore CJ, Cunningham SA. Social position, psychological stress, and obesity: a systematic review. J Acad Nutr Diet 2012;112:518–26.
25. Plack K, Herpertz S, Petrak F. Behavioral medicine interventions in diabetes. Curr Opin Psychiatry 2010;23:131–8.
26. Clucas C, Sibley E, Harding R, et al. A systematic review of interventions for anxiety in people with HIV. Psychol Health Med 2011;16:528–47.
27. Yorke J, Fleming SL, Shuldham C. Psychological interventions for adults with asthma: a systematic review. Respir Med 2007;101:1–14.
28. Merkes M. Mindfulness-based stress reduction for people with chronic diseases. Aust J Prim Health 2010;16:200–10.
29. Kopf S, Oikonomou D, Hartmann M. Effects of stress reduction on cardiovascular risk factors in type 2 diabetes patients with early kidney disease- results of a randomized controlled trial (HEIDIS). Exp Clin Endocrinol Diabetes 2014;122:341–9.
30. Musial F, Bussing A, Heusser P, et al. Mindfulness-based stress reduction for integrative cancer care- a summary of evidence. Forsch Komplementmed 2011;18:192–202.
31. Shigaki CL, Glass B, Schopp LH. Mindfulness-based stress reduction in medical settings. J Clin Psychl Med Settings 2006;13:209-16.
32. Parry GD, Cooper CL, Moore JM. Cognitive behavioural intervention for adults with anxiety complications of asthma: prospective randomized trial. Respir Med 2012;106;802–10.
33. Cooper S, Oborne J, Newton S, et al. Effect of two breathing exercises (Buteyko and pranayama) in asthma: a randomized controlled trial. Thorax 2003;58:674–9.
34. Opat AJ, Cohen MM, Bailey MJ, et al. A clinical trial of the Buteyko breathing technique in asthma as taught by a video. J Asthma 2000;37:557–64.
35. Thomas M, McKinley RK, Freeman E, et al. Breathing retraining for dysfunctional breathing in asthma: a randomized controlled trial. Thorax 2003;58:110–15.
36. Markham AW, Wilkinson JM. Complementary and alternative medicines (CAM) in the management of asthma: an examination of the evidence. J Asthma 2004;41:131–9.
37. Bidwell AM, Yazel B, Davin D, et al. Yoga training improves quality of life in women with asthma. J Altern Complement Med 2012;18:749–55.
38. Passalacqua G, Bousquet PJ, Carlsen KH, et al. ARIA update: I- Systematic review of complementary and alternative medicine for rhinitis and asthma. J Allergy Clin Immunol 2006;117:1054–62.
39. Cramer H, Posadzki P, Dobos G, et al. Yoga for asthma: a systematic review and meta-analysis. Ann Allergy Asthma Immunol 2014;112:503–10.
40. Slader CA, Reddel HK, Jenkins CR, et al. Complementary and alternative medicine use in asthma: who is using what? Respirology 2006;11:373–87.
41. Silvers WS, Bailey HK. Integrative approach to allergy and asthma using complementary and alternative medicine. Ann Allergy Asthma Immunol 2014;112;280-85.
42. Hondras MA, Linde K, Jones AP. Manual therapy for asthma. Cochrane Database Syst Rev 2005;(2):CD001002.
43. Ahmedani BK, Peterson EL, Wells KE, et al. Asthma medication adherence: the role of God and other health locus of control factors. Ann Allergy Asthma Immunol 2013;110:75–9.
44. Sliwka A, Nowobilski R, Polczyk R, et al. Mild asthmatics benefit from music therapy. J Asthma 2012;49:401–8.
45. Clarke SA, Calam R. The effectiveness of psychosocial interventions designed to improve health-related quality of life (HRQOL) amongst asthmatic children and their families: a systematic review. Qual Life Res 2012;21:747–64.
46. Beebe A, Gelfand EW, Bender B. A randomized trial to test the effectiveness of art therapy for children with asthma. J Allergy Clin Immunol 2010;126:262–6.
47. Metzger LK. Assessment of use of music by patients participating in cardiac rehabilitation. J Music Ther 2004;41:55–69.
48. El-Hassan H, McKeown K, Muller AF. Clinical trial: music reduces anxiety levels in patients attending for endoscopy. Aliment Pharmacol Ther 2009;30:718–24.
49. Thomas M, Bruton An, Moffatt M, et al. Asthma and psychological dysfunction. Prim Care Respir J 2011;20:250–6.
50. Lavoie KL, Bacon SL, Barone S, et al. What is worse for asthma control and quality of life: depressive disorders, anxiety disorders, or both? Chest 2006;130:1039–47.
51. Brown ES, Vigil L, Khan DA, et al. A randomized trial of citalopram versus placebo in outpatients with asthma and major depressive disorder: a proof of concept study. Biol Psychiatry 2005;58:865–70.
52. Brown ES, Howard C, Khan DA, et al. Escitalopram for severe asthma and major depressive disorder: a randomized, double-blind, placebo-controlled proof-of-concept study. Psychosomatics 2012;53:75–80.
From the Department of Medicine, The University of Mississippi Medical Center, Jackson, MS.
Abstract
- Objective: To review psychological stress interventions employed to improve asthma outcomes.
- Methods: Review of the literature.
- Results: In general, there are 2 approaches to managing stress in asthma patients—direct psychological interventions, and modalities where stress management is an indirect effect. The most direct approach involves mindfulness-based stress reduction, which has been shown to have a positive effect on asthma control. Cognitive behavioral therapy, biofeedback, music therapy, art therapy, and relaxation training also have been evaluated with varying results. Physical therapies, including yoga, chi gong, massage, reflexology, specific controlled breathing programs, and spinal manipulation have also been studied without consistent effectiveness demonstrated. Pharmacologic therapy for anxiety and depressive disorders has been shown to be associated with improvement in asthma symptoms and control.
- Conclusion: Although further research is needed to verify the beneficial role of specific stress intervention modalities for specific asthma populations, there is sufficient evidence of efficacy to validate the concept of stress management as a viable therapeutic approach for optimal asthma control.
The increasing levels of chronic psychological stress in the people’s everyday lives has been well recognized [1]. As technological advances continue to progress, the psychological and physical pressures associated with family- and work-role expectations, decreased free or “down” time, greater sleep deficits, increasing career-related pressures, social issues, and other factors have led to ever increasing levels of personal stress [2]. From an immune standpoint, these chronic stressors impact immune balance and may be at least partially responsible for the rise in incidence, prevalence, and severity of inflammatory diseases such as asthma [3]. As the factors responsible for increased levels of psychosocial stress in our society are not likely to decrease in the near future [4], the potential value of directed stress intervention therapies in the overall care plans for patients with asthma is an area of interest. Such stress management strategies must be evidence-based, pragmatic, and cost-effective. This review provides background, scientific and clinical rationale, and progress to date for various therapeutic approaches to stress management for asthma patients.
Asthma as Inflammatory Disease
Asthma is a breathlessness syndrome typically characterized by varying combinations of paroxysmal wheezing, cough, breathlessness, and chest tightness. The constellation of symptoms is often precipitated by exposure to volatile irritants, allergens, cold air, and exercise. Gastroesophageal reflux disease, respiratory viral infections, and pregnancy may also precipitate or worsen existing asthma [5,6]. Symptoms typically improve after appropriate asthma treatment.
While the role of IgE-mediated mechanisms in asthma has been questioned by some, studies have demonstrated the presence of IgE-mediated (“allergic”) mechanisms in most asthma cases [7]. Depending on the specific population, as many as 70% to 90% of asthma patients can be considered to have an allergic component to their asthma [8]. Such allergic sensitivities can be to seasonal pollens but even more commonly to perennial allergens such as dust mites, molds, cockroaches, and pet dander (especially cat) [9]. These associations have led to therapeutic approaches for many asthma patients based largely on those classically used for allergic rhinitis, including avoidance, environmental control, and even allergen immunotherapy [10]. Some of the newest and most promising pharmacotherapies for asthma are based on antagonism and/or prevention of the allergic cascade (production and activity of IgE) [11].
Psychological Stress and Asthma
Research regarding the relationships between asthma and chronic stress has been conducted in a variety of populations, using both cross-sectional and prospective designs [12,13]. It has been found that perceived stress negatively affects quality of life of patients with asthma and is associated with reduced medication compliance [14,15] and symptom perception [14,16]. Stress has been linked to both the onset of allergic asthma [17,18] and to enhanced skin test reactivity in response to allergens [19].Oh et al [12] suggested a dose-dependent relationship, with individuals who report increasingly higher levels of stress being more likely to report symptoms of asthma.
People with asthma who are exposed to various types of chronic stress tend to have worse severity and poorer control of their asthma symptoms [20,21]. Interventions to help manage stress in people with asthma are needed at the individual, family, and community levels; all levels are known to influence asthma and asthma morbidity [20,22].
If stress is associated with increased disease incidence and severity, then stress modulation could be expected to have beneficial effects. Advice to work fewer hours, get more sleep, and optimize relaxation can be unproductive and even frustrating to busy persons striving to meet all the demands of life. More realistic are interventions based upon helping people manage stress. Studies have reported benefit from stress management for a number of chronic diseases, including hypertension [23], obesity [24], diabetes [25], and HIV [26]. Given the associations noted above, stress intervention as a therapeutic modality for asthma management is a valid option that should be explored [27].
Psychologically Focused Interventions
Mindfulness-based stress reduction (MBSR) has been recognized as an important modality for treatment of many chronic diseases, including chronic pain [28], cardiovascular disease [29], type 2 diabetes mellitus [29], cancer [30], and fibromyalgia [28]. MBSR teaches patients to recognize disease symptoms and personal reactions to these symptoms, and to develop a nonreactive awareness of these elements [14]. It is an individual or group-based therapeutic approach that uses education, discussion, and various meditation techniques to reduce perceived general and disease-associated stress [14,31]. Pbert et al performed an RCT comparing a MBSR program with a traditional education program in adults with mild, moderate, or severe persistent asthma. The primary outcomes were centered on lung function as measured by peak expiratory flow (PEF) and quality of life using the Asthma Quality of Life Questionnaire (AQLQ). Secondary outcomes included changes in perceived stress as measured by the 10-question Perceived Stress Scale (PSS) and overall asthma control. At 12 months, results indicated that MBSR had positive effects on overall asthma control, with improvement in quality of life, a decrease in perceived stress, and a decrease in use of rescue therapies, but no significant effect on peak expiratory flow [14].
Various other psychological interventions have been studied as supplemental therapy to medications in the treatment of asthma. Yorke et al performed a systematic review of 14 RCTs evaluating various psychological interventions in asthma, including cognitive behavioral therapy (CBT), biofeedback, and various relaxation techniques [27]. Because there are no standardized outcomes measured across all studies, results are often conflicting. While CBT had a positive effect on asthma health care utilization, relaxation therapy had no significant effects; both did have positive effects on symptoms of depression and anxiety. Relaxation therapy had positive effects on relieving asthma symptoms such as cough and wheeze but CBT did not. Biofeedback and relaxation were the only interventions that had positive effect on improving lung function and decreasing medication usage [27].
In an RCT, Parry and colleagues evaluated the effects of CBT added to clinical care on asthma-specific fear when compared to standard clinical asthma care alone. They demonstrated a significant reduction in panic and fear related to asthma exacerbations using CBT [32].
Various other mind-body–based interventions, including meditation, yoga, and breathing techniques, have been evaluated as complementary asthma therapy. Several studies utilized the Buteyko breathing technique (BBT), which focuses on controlling breathing to restore normal levels of PaCo2 in order to improve tissue oxygenation and reduce bronchospasm. Cooper et al performed an RCT that evaluated asthma symptom scores and methacholine sensitivity (concentration of bronchial irritant causing decline in FEV1 > 20%) for the presence of bronchial hyperreactivity (BHR), a measure of asthma activity. The BBT group demonstrated a reduction in asthma symptoms and rescue inhaler use but no change in BHR [33]. Opat measured asthma QOL, asthma symptoms, rescue medication use, and lung function in patients who received instruction in BBT and patients in a sham control group. BBT was associated with improvement in asthma QOL and bronchodilator use but not in other outcome parameters [34]. Thomas et al demonstrated in an RCT involving asthma patients with symptoms of dysfunctional breathing that rebreathing-retraining physiotherapy improved asthma-related QOL compared with traditional nurse-provided education [35].
Physical Stress Management Interventions
Yoga, which involves various aspects of controlled breathing, stretching, and meditation techniques [36], aims to achieve synergy between the mind and body to produce a more relaxed psychophysiological state [37]. This popular modality is frequently used by patients, including those with asthma, for symptom control and disease management. Results from RCTs have varied in their reports of efficacy. The 2006 Allergic Rhinitis and Asthma (ARIA) work group performed a systematic review of 5 trials evaluating yoga and asthma. Though the quality of the trials varied greatly, the review demonstrated a possible benefit of yoga on asthma-related QOL but no other studied parameters [38]. QOL and hemodynamic improvement was also demonstrated in 1 RCT comparing yoga added to standard asthma therapy vs. standard therapy alone in female patients [37]. Cramer et al performed an extensive systematic review and meta-analysis of 14 RCTs evaluating the effects of yoga on all or some components of asthma-related QOL, asthma control, symptoms, and pulmonary function [39]. Though there may be some benefit of yoga breathing techniques on asthma-related QOL, the quality of these studies is very poor and reported results were highly variable. These limitations demonstrate the need for methodologically sound, standardized approaches to research in this field, which will be needed before definitive conclusions or treatment recommendations can be made [38,39].
Complementary and Alternative Medicine Interventions
Therapeutic massage, reflexology, spinal manipulation, and prayer are commonly used components of complementary medicine that are perceived by many to be helpful in asthma management [40,41]. However, the published data supporting these techniques is limited. In 2005, Hondras et al performed a Cochrane database review of RCTs evaluating manual therapy, including therapeutic massage, in asthma. Variations in measured outcomes, study design, and reporting made the evidence presented in the review difficult to interpret. Methodologically sound RCTs are needed before any inferences as to relative efficacy of these techniques can be drawn [42]. Since 2005, there have been no significant RCTs reported that would change this conclusion. Data on prayer, religious beliefs, and how these affect asthma and stress control are scarce. One nonrandomized patient reporting survey analysis to evaluate the presence of a high power in life and asthma medication adherence was reported by Ahmedani and colleagues. Results showed that overall medication adherence was low, particularly among those who believed a higher power was in control of their health [43].
Other relaxation methods for managing stress in asthma include music therapy [44] and art therapy [45,46]. Music therapy has had varying reported therapeutic success in other medical settings, such as cardiac rehabilitation [47] and prior to endoscopy [48]. Several studies have evaluated passive or active music therapy in various stages of asthma management with variable results reported. One RCT of patients admitted for asthma exacerbation evaluated the effectiveness of standard pulmonary rehabilitation for asthma with or without concomitant music therapy. Measured outcomes included lung function parameters (PEF and FEV1/FVC) and self-reported anxiety scales. There was a small improvement in PEF in women in the music therapy group. Secondary statistical analysis showed lung function improvements with music therapy only in the patients with mild asthma [44]. Art therapy, the opportunity to share feelings through the use of art materials and expressions, has been used effectively to reduce psychological distress in pediatric chronic disease. One RCT of 23 children examined the potential utility of art therapy in pediatric asthma management. While it did not affect number of exacerbations, art therapy dramatically improved quality of life in children with asthma by decreasing worry and anxiety. The effect persisted for at least 6 months after the intervention was completed [46].
Pharmacotherapy Interventions
Given that anxiety and depression are commonly reported in patients with asthma, particularly in severe and difficult to control disease [49], traditional pharmacologic treatment of anxiety and depression is often attempted. Both depression and anxiety in patients with asthma has been associated with poor asthma-related QOL, but depressive disorders were more commonly associated with poorer levels of asthma control [50]. The use of antidepressant medications, especially selective serotonin reuptake inhibitors (SSRIs), in this patient population has had varying success reported. One randomized placebo-controlled trial evaluated the use of citalopram in 90 adults with asthma and major depressive disorder. Not surprisingly, there was a positive effect on the primary outcome measuring depression using the Hamilton Rating Scale for Depression. Secondary outcome analysis also showed a decrease in oral corticosteroid use in the group treated with citalopram; however, no difference in asthma symptoms between groups was observed [51]. A similar but smaller RCT evaluated the use of escitalopram in major depression and severe asthma. The escitalopram group failed to show a statistical difference in depressive symptoms, asthma control, or oral prednisone use when compared with placebo [52].
The Future for Stress Management as a Fundamental Component of Asthma Care
Historically, avoidance of known triggers and use of pharmacologic maintenance and treatment modalities has been the cornerstone of asthma care. The recognition of excess psychological stress as a recognized trigger and treatment target is continuing to evolve in our therapeutic armamentarium. Our understanding of the effects of stress management in asthma patients provides clinical support for the neuroendocrine immune link between the bronchial inflammatory response characteristic in asthma and that of the human stress response. Understanding the relationships of psychological stress in asthma physiology, clinical morbidity, and therapeutic options is imperative, as the changing health care environment increasingly demands preventive, practical, cost-effective, evidence-based medicine. Some psychological stressors will no doubt be more difficult to address than others, but implementation of nonpharmacologic stress management paradigms should help improve effective asthma management across all patient demographics and should hopefully lead to decreased population health care costs, fewer days of work lost, and improved quality of life. Despite a clear molecular link between asthma, inflammation and stress and a clinical trend toward benefit, the heterogeneity of studies and poor quality evidence for each stress reduction modality make it difficult to draw any firm conclusions on the comparative efficacy of specific psychological interventions in asthma management programs. Mindfulness-based stress reduction has the highest quality evidence and shows the most promise thus far. Further research employing methodically sound RCTs that use standardized physiologic and nonphysiologic outcome measures is needed to elucidate the role for stress reduction interventions in routine clinical practice.
Corresponding author: Gailen D. Marshall Jr, MD, PhD, Div. of Clinical Immunology and Allergy, Dept. of Medicine, The University of Mississippi Medical Ctr., 2500 N. State St. N416 Jackson, MS 39216, [email protected].
Financial disclosures: None.
Author contributions: conception and design, CRP, AMW, GDM; drafting of article, CRP, AMW, GDM; critical revision of the article, CRP, AMW, GDM; administrative or technical support, GDM.
From the Department of Medicine, The University of Mississippi Medical Center, Jackson, MS.
Abstract
- Objective: To review psychological stress interventions employed to improve asthma outcomes.
- Methods: Review of the literature.
- Results: In general, there are 2 approaches to managing stress in asthma patients—direct psychological interventions, and modalities where stress management is an indirect effect. The most direct approach involves mindfulness-based stress reduction, which has been shown to have a positive effect on asthma control. Cognitive behavioral therapy, biofeedback, music therapy, art therapy, and relaxation training also have been evaluated with varying results. Physical therapies, including yoga, chi gong, massage, reflexology, specific controlled breathing programs, and spinal manipulation have also been studied without consistent effectiveness demonstrated. Pharmacologic therapy for anxiety and depressive disorders has been shown to be associated with improvement in asthma symptoms and control.
- Conclusion: Although further research is needed to verify the beneficial role of specific stress intervention modalities for specific asthma populations, there is sufficient evidence of efficacy to validate the concept of stress management as a viable therapeutic approach for optimal asthma control.
The increasing levels of chronic psychological stress in the people’s everyday lives has been well recognized [1]. As technological advances continue to progress, the psychological and physical pressures associated with family- and work-role expectations, decreased free or “down” time, greater sleep deficits, increasing career-related pressures, social issues, and other factors have led to ever increasing levels of personal stress [2]. From an immune standpoint, these chronic stressors impact immune balance and may be at least partially responsible for the rise in incidence, prevalence, and severity of inflammatory diseases such as asthma [3]. As the factors responsible for increased levels of psychosocial stress in our society are not likely to decrease in the near future [4], the potential value of directed stress intervention therapies in the overall care plans for patients with asthma is an area of interest. Such stress management strategies must be evidence-based, pragmatic, and cost-effective. This review provides background, scientific and clinical rationale, and progress to date for various therapeutic approaches to stress management for asthma patients.
Asthma as Inflammatory Disease
Asthma is a breathlessness syndrome typically characterized by varying combinations of paroxysmal wheezing, cough, breathlessness, and chest tightness. The constellation of symptoms is often precipitated by exposure to volatile irritants, allergens, cold air, and exercise. Gastroesophageal reflux disease, respiratory viral infections, and pregnancy may also precipitate or worsen existing asthma [5,6]. Symptoms typically improve after appropriate asthma treatment.
While the role of IgE-mediated mechanisms in asthma has been questioned by some, studies have demonstrated the presence of IgE-mediated (“allergic”) mechanisms in most asthma cases [7]. Depending on the specific population, as many as 70% to 90% of asthma patients can be considered to have an allergic component to their asthma [8]. Such allergic sensitivities can be to seasonal pollens but even more commonly to perennial allergens such as dust mites, molds, cockroaches, and pet dander (especially cat) [9]. These associations have led to therapeutic approaches for many asthma patients based largely on those classically used for allergic rhinitis, including avoidance, environmental control, and even allergen immunotherapy [10]. Some of the newest and most promising pharmacotherapies for asthma are based on antagonism and/or prevention of the allergic cascade (production and activity of IgE) [11].
Psychological Stress and Asthma
Research regarding the relationships between asthma and chronic stress has been conducted in a variety of populations, using both cross-sectional and prospective designs [12,13]. It has been found that perceived stress negatively affects quality of life of patients with asthma and is associated with reduced medication compliance [14,15] and symptom perception [14,16]. Stress has been linked to both the onset of allergic asthma [17,18] and to enhanced skin test reactivity in response to allergens [19].Oh et al [12] suggested a dose-dependent relationship, with individuals who report increasingly higher levels of stress being more likely to report symptoms of asthma.
People with asthma who are exposed to various types of chronic stress tend to have worse severity and poorer control of their asthma symptoms [20,21]. Interventions to help manage stress in people with asthma are needed at the individual, family, and community levels; all levels are known to influence asthma and asthma morbidity [20,22].
If stress is associated with increased disease incidence and severity, then stress modulation could be expected to have beneficial effects. Advice to work fewer hours, get more sleep, and optimize relaxation can be unproductive and even frustrating to busy persons striving to meet all the demands of life. More realistic are interventions based upon helping people manage stress. Studies have reported benefit from stress management for a number of chronic diseases, including hypertension [23], obesity [24], diabetes [25], and HIV [26]. Given the associations noted above, stress intervention as a therapeutic modality for asthma management is a valid option that should be explored [27].
Psychologically Focused Interventions
Mindfulness-based stress reduction (MBSR) has been recognized as an important modality for treatment of many chronic diseases, including chronic pain [28], cardiovascular disease [29], type 2 diabetes mellitus [29], cancer [30], and fibromyalgia [28]. MBSR teaches patients to recognize disease symptoms and personal reactions to these symptoms, and to develop a nonreactive awareness of these elements [14]. It is an individual or group-based therapeutic approach that uses education, discussion, and various meditation techniques to reduce perceived general and disease-associated stress [14,31]. Pbert et al performed an RCT comparing a MBSR program with a traditional education program in adults with mild, moderate, or severe persistent asthma. The primary outcomes were centered on lung function as measured by peak expiratory flow (PEF) and quality of life using the Asthma Quality of Life Questionnaire (AQLQ). Secondary outcomes included changes in perceived stress as measured by the 10-question Perceived Stress Scale (PSS) and overall asthma control. At 12 months, results indicated that MBSR had positive effects on overall asthma control, with improvement in quality of life, a decrease in perceived stress, and a decrease in use of rescue therapies, but no significant effect on peak expiratory flow [14].
Various other psychological interventions have been studied as supplemental therapy to medications in the treatment of asthma. Yorke et al performed a systematic review of 14 RCTs evaluating various psychological interventions in asthma, including cognitive behavioral therapy (CBT), biofeedback, and various relaxation techniques [27]. Because there are no standardized outcomes measured across all studies, results are often conflicting. While CBT had a positive effect on asthma health care utilization, relaxation therapy had no significant effects; both did have positive effects on symptoms of depression and anxiety. Relaxation therapy had positive effects on relieving asthma symptoms such as cough and wheeze but CBT did not. Biofeedback and relaxation were the only interventions that had positive effect on improving lung function and decreasing medication usage [27].
In an RCT, Parry and colleagues evaluated the effects of CBT added to clinical care on asthma-specific fear when compared to standard clinical asthma care alone. They demonstrated a significant reduction in panic and fear related to asthma exacerbations using CBT [32].
Various other mind-body–based interventions, including meditation, yoga, and breathing techniques, have been evaluated as complementary asthma therapy. Several studies utilized the Buteyko breathing technique (BBT), which focuses on controlling breathing to restore normal levels of PaCo2 in order to improve tissue oxygenation and reduce bronchospasm. Cooper et al performed an RCT that evaluated asthma symptom scores and methacholine sensitivity (concentration of bronchial irritant causing decline in FEV1 > 20%) for the presence of bronchial hyperreactivity (BHR), a measure of asthma activity. The BBT group demonstrated a reduction in asthma symptoms and rescue inhaler use but no change in BHR [33]. Opat measured asthma QOL, asthma symptoms, rescue medication use, and lung function in patients who received instruction in BBT and patients in a sham control group. BBT was associated with improvement in asthma QOL and bronchodilator use but not in other outcome parameters [34]. Thomas et al demonstrated in an RCT involving asthma patients with symptoms of dysfunctional breathing that rebreathing-retraining physiotherapy improved asthma-related QOL compared with traditional nurse-provided education [35].
Physical Stress Management Interventions
Yoga, which involves various aspects of controlled breathing, stretching, and meditation techniques [36], aims to achieve synergy between the mind and body to produce a more relaxed psychophysiological state [37]. This popular modality is frequently used by patients, including those with asthma, for symptom control and disease management. Results from RCTs have varied in their reports of efficacy. The 2006 Allergic Rhinitis and Asthma (ARIA) work group performed a systematic review of 5 trials evaluating yoga and asthma. Though the quality of the trials varied greatly, the review demonstrated a possible benefit of yoga on asthma-related QOL but no other studied parameters [38]. QOL and hemodynamic improvement was also demonstrated in 1 RCT comparing yoga added to standard asthma therapy vs. standard therapy alone in female patients [37]. Cramer et al performed an extensive systematic review and meta-analysis of 14 RCTs evaluating the effects of yoga on all or some components of asthma-related QOL, asthma control, symptoms, and pulmonary function [39]. Though there may be some benefit of yoga breathing techniques on asthma-related QOL, the quality of these studies is very poor and reported results were highly variable. These limitations demonstrate the need for methodologically sound, standardized approaches to research in this field, which will be needed before definitive conclusions or treatment recommendations can be made [38,39].
Complementary and Alternative Medicine Interventions
Therapeutic massage, reflexology, spinal manipulation, and prayer are commonly used components of complementary medicine that are perceived by many to be helpful in asthma management [40,41]. However, the published data supporting these techniques is limited. In 2005, Hondras et al performed a Cochrane database review of RCTs evaluating manual therapy, including therapeutic massage, in asthma. Variations in measured outcomes, study design, and reporting made the evidence presented in the review difficult to interpret. Methodologically sound RCTs are needed before any inferences as to relative efficacy of these techniques can be drawn [42]. Since 2005, there have been no significant RCTs reported that would change this conclusion. Data on prayer, religious beliefs, and how these affect asthma and stress control are scarce. One nonrandomized patient reporting survey analysis to evaluate the presence of a high power in life and asthma medication adherence was reported by Ahmedani and colleagues. Results showed that overall medication adherence was low, particularly among those who believed a higher power was in control of their health [43].
Other relaxation methods for managing stress in asthma include music therapy [44] and art therapy [45,46]. Music therapy has had varying reported therapeutic success in other medical settings, such as cardiac rehabilitation [47] and prior to endoscopy [48]. Several studies have evaluated passive or active music therapy in various stages of asthma management with variable results reported. One RCT of patients admitted for asthma exacerbation evaluated the effectiveness of standard pulmonary rehabilitation for asthma with or without concomitant music therapy. Measured outcomes included lung function parameters (PEF and FEV1/FVC) and self-reported anxiety scales. There was a small improvement in PEF in women in the music therapy group. Secondary statistical analysis showed lung function improvements with music therapy only in the patients with mild asthma [44]. Art therapy, the opportunity to share feelings through the use of art materials and expressions, has been used effectively to reduce psychological distress in pediatric chronic disease. One RCT of 23 children examined the potential utility of art therapy in pediatric asthma management. While it did not affect number of exacerbations, art therapy dramatically improved quality of life in children with asthma by decreasing worry and anxiety. The effect persisted for at least 6 months after the intervention was completed [46].
Pharmacotherapy Interventions
Given that anxiety and depression are commonly reported in patients with asthma, particularly in severe and difficult to control disease [49], traditional pharmacologic treatment of anxiety and depression is often attempted. Both depression and anxiety in patients with asthma has been associated with poor asthma-related QOL, but depressive disorders were more commonly associated with poorer levels of asthma control [50]. The use of antidepressant medications, especially selective serotonin reuptake inhibitors (SSRIs), in this patient population has had varying success reported. One randomized placebo-controlled trial evaluated the use of citalopram in 90 adults with asthma and major depressive disorder. Not surprisingly, there was a positive effect on the primary outcome measuring depression using the Hamilton Rating Scale for Depression. Secondary outcome analysis also showed a decrease in oral corticosteroid use in the group treated with citalopram; however, no difference in asthma symptoms between groups was observed [51]. A similar but smaller RCT evaluated the use of escitalopram in major depression and severe asthma. The escitalopram group failed to show a statistical difference in depressive symptoms, asthma control, or oral prednisone use when compared with placebo [52].
The Future for Stress Management as a Fundamental Component of Asthma Care
Historically, avoidance of known triggers and use of pharmacologic maintenance and treatment modalities has been the cornerstone of asthma care. The recognition of excess psychological stress as a recognized trigger and treatment target is continuing to evolve in our therapeutic armamentarium. Our understanding of the effects of stress management in asthma patients provides clinical support for the neuroendocrine immune link between the bronchial inflammatory response characteristic in asthma and that of the human stress response. Understanding the relationships of psychological stress in asthma physiology, clinical morbidity, and therapeutic options is imperative, as the changing health care environment increasingly demands preventive, practical, cost-effective, evidence-based medicine. Some psychological stressors will no doubt be more difficult to address than others, but implementation of nonpharmacologic stress management paradigms should help improve effective asthma management across all patient demographics and should hopefully lead to decreased population health care costs, fewer days of work lost, and improved quality of life. Despite a clear molecular link between asthma, inflammation and stress and a clinical trend toward benefit, the heterogeneity of studies and poor quality evidence for each stress reduction modality make it difficult to draw any firm conclusions on the comparative efficacy of specific psychological interventions in asthma management programs. Mindfulness-based stress reduction has the highest quality evidence and shows the most promise thus far. Further research employing methodically sound RCTs that use standardized physiologic and nonphysiologic outcome measures is needed to elucidate the role for stress reduction interventions in routine clinical practice.
Corresponding author: Gailen D. Marshall Jr, MD, PhD, Div. of Clinical Immunology and Allergy, Dept. of Medicine, The University of Mississippi Medical Ctr., 2500 N. State St. N416 Jackson, MS 39216, [email protected].
Financial disclosures: None.
Author contributions: conception and design, CRP, AMW, GDM; drafting of article, CRP, AMW, GDM; critical revision of the article, CRP, AMW, GDM; administrative or technical support, GDM.
1. Kondo N. Socioeconomic disparities and health: impacts and pathways. J Epidemiol 2012;22:2–6.
2. Nakata A. Psychosocial job stress and immunity: a systematic review. Methods Mol Biol 2012;934:39–7.
3. Van Lieshout RJ, Macqueen GM. Relation between asthma and psychological distress: an old idea revisited. Chem Immunol Allergy 2012;98:1–13.
4. Marshall GD Jr. The adverse effects of psychological stress on immunoregulatory balance: applications to human inflammatory diseases. Immunol Allergy Clin North Am 2011;31:133–40.
5. Murphy VE, Gibson PG, Smith R, et al. Asthma during pregnancy: mechanisms and treatment implications. Eur Respir J 2005;25:1–750.
6. Harding SM. Acid reflux and asthma. Curr Opin Pulm Med 2003;9:42–5.
7. Umetsu DT, McIntire JJ, Akbari O, et al. Asthma: an epidemic of dysregulated immunity. Nat Immunol 2002;3:715–20.
8. Matricardi PM. Prevalence of atopy and asthma in eastern versus western Europe: why the difference? Ann Allergy Asthma Immunol 2001;87:24–7.
9. Murray CS, Woodcock A, Custovic A. The role of indoor allergen exposure in the development of sensitization and asthma. Curr Opin Allergy Clin Immunol 2001;1:407–12.
10. TePas EC, Umetsu DT. Immunotherapy of asthma and allergic diseases. Curr Opin Pediatr 2000;12:574–78.
11. Babu KS, Holgate ST. Newer therapies for asthma: a focus on anti-IgE. Indian J Chest Dis Allied Sci 2002;44:107–15.
12. Oh Y, Kim Y, Yoo S, et al. Association between stress and asthma symptoms: a population based study. Respirology 2004;9:363–8.
13. Sandberg S, Paton JY, Ahola S, et al. The role of acute and chronic stress in asthma attacks in children. Lancet 2000;356:982–7.
14. Pbert L, Madison JM, Druker S, et al. Effect of mindfulness training on asthma quality of life and lung function: a randomized controlled trial. Thorax 2012;67:769–76.
15. Wisnivesky JP, Lorenzo J, Feldman JM, et al. The relationship between perceived stress and morbidity among adult inner-city asthmatics. J Asthma 2010;47:100–4.
16. Janssens T, Verleden G, De Peuter S, et al. Inaccurate perception of asthma symptoms: a cognitive-affective framework and implications for asthma treatment. Clin Psychol Rev 2009;29:317–27.
17. Wright RJ, Cohen S, Carey V, et al. Parental stress as a predictor of wheezing in infancy: a prospective birth-cohort study. Am J Resp Crit Care Med 2002;165:358–65.
18. Wright RJ, Mitchell H, Visness CM, et al. Community violence and asthma morbidity in the Inner-City Asthma Study. Am J Public Health 2004;94:625–32.
19. Michel FB. Psychology of the allergic patient. Allergy 1994;49:28–30.
20. Yonas MA, Lange NE, Celedon JC. Psychosocial stress and asthma morbidity. Curr Opin Allergy Clin Immunol 2012;12:202–10.
21. Apter AJ, Garcia LA, Boyd RC, et al. Exposure to community violence is associated with asthma hospitalizations and emergency department visits. J Allergy Clin Immunol 2010;126:552–7.
22. Wright RJ. Epidemiology of stress and asthma: from constricting communities and fragile families to epigenetics. Immunol Allergy Clin North Am 2011;31:19–39.
23. Tyagi A, Cohen M. Yoga and hypertension: a systematic review. Altern Ther Health Med 2014;20:32-59.
24. Moore CJ, Cunningham SA. Social position, psychological stress, and obesity: a systematic review. J Acad Nutr Diet 2012;112:518–26.
25. Plack K, Herpertz S, Petrak F. Behavioral medicine interventions in diabetes. Curr Opin Psychiatry 2010;23:131–8.
26. Clucas C, Sibley E, Harding R, et al. A systematic review of interventions for anxiety in people with HIV. Psychol Health Med 2011;16:528–47.
27. Yorke J, Fleming SL, Shuldham C. Psychological interventions for adults with asthma: a systematic review. Respir Med 2007;101:1–14.
28. Merkes M. Mindfulness-based stress reduction for people with chronic diseases. Aust J Prim Health 2010;16:200–10.
29. Kopf S, Oikonomou D, Hartmann M. Effects of stress reduction on cardiovascular risk factors in type 2 diabetes patients with early kidney disease- results of a randomized controlled trial (HEIDIS). Exp Clin Endocrinol Diabetes 2014;122:341–9.
30. Musial F, Bussing A, Heusser P, et al. Mindfulness-based stress reduction for integrative cancer care- a summary of evidence. Forsch Komplementmed 2011;18:192–202.
31. Shigaki CL, Glass B, Schopp LH. Mindfulness-based stress reduction in medical settings. J Clin Psychl Med Settings 2006;13:209-16.
32. Parry GD, Cooper CL, Moore JM. Cognitive behavioural intervention for adults with anxiety complications of asthma: prospective randomized trial. Respir Med 2012;106;802–10.
33. Cooper S, Oborne J, Newton S, et al. Effect of two breathing exercises (Buteyko and pranayama) in asthma: a randomized controlled trial. Thorax 2003;58:674–9.
34. Opat AJ, Cohen MM, Bailey MJ, et al. A clinical trial of the Buteyko breathing technique in asthma as taught by a video. J Asthma 2000;37:557–64.
35. Thomas M, McKinley RK, Freeman E, et al. Breathing retraining for dysfunctional breathing in asthma: a randomized controlled trial. Thorax 2003;58:110–15.
36. Markham AW, Wilkinson JM. Complementary and alternative medicines (CAM) in the management of asthma: an examination of the evidence. J Asthma 2004;41:131–9.
37. Bidwell AM, Yazel B, Davin D, et al. Yoga training improves quality of life in women with asthma. J Altern Complement Med 2012;18:749–55.
38. Passalacqua G, Bousquet PJ, Carlsen KH, et al. ARIA update: I- Systematic review of complementary and alternative medicine for rhinitis and asthma. J Allergy Clin Immunol 2006;117:1054–62.
39. Cramer H, Posadzki P, Dobos G, et al. Yoga for asthma: a systematic review and meta-analysis. Ann Allergy Asthma Immunol 2014;112:503–10.
40. Slader CA, Reddel HK, Jenkins CR, et al. Complementary and alternative medicine use in asthma: who is using what? Respirology 2006;11:373–87.
41. Silvers WS, Bailey HK. Integrative approach to allergy and asthma using complementary and alternative medicine. Ann Allergy Asthma Immunol 2014;112;280-85.
42. Hondras MA, Linde K, Jones AP. Manual therapy for asthma. Cochrane Database Syst Rev 2005;(2):CD001002.
43. Ahmedani BK, Peterson EL, Wells KE, et al. Asthma medication adherence: the role of God and other health locus of control factors. Ann Allergy Asthma Immunol 2013;110:75–9.
44. Sliwka A, Nowobilski R, Polczyk R, et al. Mild asthmatics benefit from music therapy. J Asthma 2012;49:401–8.
45. Clarke SA, Calam R. The effectiveness of psychosocial interventions designed to improve health-related quality of life (HRQOL) amongst asthmatic children and their families: a systematic review. Qual Life Res 2012;21:747–64.
46. Beebe A, Gelfand EW, Bender B. A randomized trial to test the effectiveness of art therapy for children with asthma. J Allergy Clin Immunol 2010;126:262–6.
47. Metzger LK. Assessment of use of music by patients participating in cardiac rehabilitation. J Music Ther 2004;41:55–69.
48. El-Hassan H, McKeown K, Muller AF. Clinical trial: music reduces anxiety levels in patients attending for endoscopy. Aliment Pharmacol Ther 2009;30:718–24.
49. Thomas M, Bruton An, Moffatt M, et al. Asthma and psychological dysfunction. Prim Care Respir J 2011;20:250–6.
50. Lavoie KL, Bacon SL, Barone S, et al. What is worse for asthma control and quality of life: depressive disorders, anxiety disorders, or both? Chest 2006;130:1039–47.
51. Brown ES, Vigil L, Khan DA, et al. A randomized trial of citalopram versus placebo in outpatients with asthma and major depressive disorder: a proof of concept study. Biol Psychiatry 2005;58:865–70.
52. Brown ES, Howard C, Khan DA, et al. Escitalopram for severe asthma and major depressive disorder: a randomized, double-blind, placebo-controlled proof-of-concept study. Psychosomatics 2012;53:75–80.
1. Kondo N. Socioeconomic disparities and health: impacts and pathways. J Epidemiol 2012;22:2–6.
2. Nakata A. Psychosocial job stress and immunity: a systematic review. Methods Mol Biol 2012;934:39–7.
3. Van Lieshout RJ, Macqueen GM. Relation between asthma and psychological distress: an old idea revisited. Chem Immunol Allergy 2012;98:1–13.
4. Marshall GD Jr. The adverse effects of psychological stress on immunoregulatory balance: applications to human inflammatory diseases. Immunol Allergy Clin North Am 2011;31:133–40.
5. Murphy VE, Gibson PG, Smith R, et al. Asthma during pregnancy: mechanisms and treatment implications. Eur Respir J 2005;25:1–750.
6. Harding SM. Acid reflux and asthma. Curr Opin Pulm Med 2003;9:42–5.
7. Umetsu DT, McIntire JJ, Akbari O, et al. Asthma: an epidemic of dysregulated immunity. Nat Immunol 2002;3:715–20.
8. Matricardi PM. Prevalence of atopy and asthma in eastern versus western Europe: why the difference? Ann Allergy Asthma Immunol 2001;87:24–7.
9. Murray CS, Woodcock A, Custovic A. The role of indoor allergen exposure in the development of sensitization and asthma. Curr Opin Allergy Clin Immunol 2001;1:407–12.
10. TePas EC, Umetsu DT. Immunotherapy of asthma and allergic diseases. Curr Opin Pediatr 2000;12:574–78.
11. Babu KS, Holgate ST. Newer therapies for asthma: a focus on anti-IgE. Indian J Chest Dis Allied Sci 2002;44:107–15.
12. Oh Y, Kim Y, Yoo S, et al. Association between stress and asthma symptoms: a population based study. Respirology 2004;9:363–8.
13. Sandberg S, Paton JY, Ahola S, et al. The role of acute and chronic stress in asthma attacks in children. Lancet 2000;356:982–7.
14. Pbert L, Madison JM, Druker S, et al. Effect of mindfulness training on asthma quality of life and lung function: a randomized controlled trial. Thorax 2012;67:769–76.
15. Wisnivesky JP, Lorenzo J, Feldman JM, et al. The relationship between perceived stress and morbidity among adult inner-city asthmatics. J Asthma 2010;47:100–4.
16. Janssens T, Verleden G, De Peuter S, et al. Inaccurate perception of asthma symptoms: a cognitive-affective framework and implications for asthma treatment. Clin Psychol Rev 2009;29:317–27.
17. Wright RJ, Cohen S, Carey V, et al. Parental stress as a predictor of wheezing in infancy: a prospective birth-cohort study. Am J Resp Crit Care Med 2002;165:358–65.
18. Wright RJ, Mitchell H, Visness CM, et al. Community violence and asthma morbidity in the Inner-City Asthma Study. Am J Public Health 2004;94:625–32.
19. Michel FB. Psychology of the allergic patient. Allergy 1994;49:28–30.
20. Yonas MA, Lange NE, Celedon JC. Psychosocial stress and asthma morbidity. Curr Opin Allergy Clin Immunol 2012;12:202–10.
21. Apter AJ, Garcia LA, Boyd RC, et al. Exposure to community violence is associated with asthma hospitalizations and emergency department visits. J Allergy Clin Immunol 2010;126:552–7.
22. Wright RJ. Epidemiology of stress and asthma: from constricting communities and fragile families to epigenetics. Immunol Allergy Clin North Am 2011;31:19–39.
23. Tyagi A, Cohen M. Yoga and hypertension: a systematic review. Altern Ther Health Med 2014;20:32-59.
24. Moore CJ, Cunningham SA. Social position, psychological stress, and obesity: a systematic review. J Acad Nutr Diet 2012;112:518–26.
25. Plack K, Herpertz S, Petrak F. Behavioral medicine interventions in diabetes. Curr Opin Psychiatry 2010;23:131–8.
26. Clucas C, Sibley E, Harding R, et al. A systematic review of interventions for anxiety in people with HIV. Psychol Health Med 2011;16:528–47.
27. Yorke J, Fleming SL, Shuldham C. Psychological interventions for adults with asthma: a systematic review. Respir Med 2007;101:1–14.
28. Merkes M. Mindfulness-based stress reduction for people with chronic diseases. Aust J Prim Health 2010;16:200–10.
29. Kopf S, Oikonomou D, Hartmann M. Effects of stress reduction on cardiovascular risk factors in type 2 diabetes patients with early kidney disease- results of a randomized controlled trial (HEIDIS). Exp Clin Endocrinol Diabetes 2014;122:341–9.
30. Musial F, Bussing A, Heusser P, et al. Mindfulness-based stress reduction for integrative cancer care- a summary of evidence. Forsch Komplementmed 2011;18:192–202.
31. Shigaki CL, Glass B, Schopp LH. Mindfulness-based stress reduction in medical settings. J Clin Psychl Med Settings 2006;13:209-16.
32. Parry GD, Cooper CL, Moore JM. Cognitive behavioural intervention for adults with anxiety complications of asthma: prospective randomized trial. Respir Med 2012;106;802–10.
33. Cooper S, Oborne J, Newton S, et al. Effect of two breathing exercises (Buteyko and pranayama) in asthma: a randomized controlled trial. Thorax 2003;58:674–9.
34. Opat AJ, Cohen MM, Bailey MJ, et al. A clinical trial of the Buteyko breathing technique in asthma as taught by a video. J Asthma 2000;37:557–64.
35. Thomas M, McKinley RK, Freeman E, et al. Breathing retraining for dysfunctional breathing in asthma: a randomized controlled trial. Thorax 2003;58:110–15.
36. Markham AW, Wilkinson JM. Complementary and alternative medicines (CAM) in the management of asthma: an examination of the evidence. J Asthma 2004;41:131–9.
37. Bidwell AM, Yazel B, Davin D, et al. Yoga training improves quality of life in women with asthma. J Altern Complement Med 2012;18:749–55.
38. Passalacqua G, Bousquet PJ, Carlsen KH, et al. ARIA update: I- Systematic review of complementary and alternative medicine for rhinitis and asthma. J Allergy Clin Immunol 2006;117:1054–62.
39. Cramer H, Posadzki P, Dobos G, et al. Yoga for asthma: a systematic review and meta-analysis. Ann Allergy Asthma Immunol 2014;112:503–10.
40. Slader CA, Reddel HK, Jenkins CR, et al. Complementary and alternative medicine use in asthma: who is using what? Respirology 2006;11:373–87.
41. Silvers WS, Bailey HK. Integrative approach to allergy and asthma using complementary and alternative medicine. Ann Allergy Asthma Immunol 2014;112;280-85.
42. Hondras MA, Linde K, Jones AP. Manual therapy for asthma. Cochrane Database Syst Rev 2005;(2):CD001002.
43. Ahmedani BK, Peterson EL, Wells KE, et al. Asthma medication adherence: the role of God and other health locus of control factors. Ann Allergy Asthma Immunol 2013;110:75–9.
44. Sliwka A, Nowobilski R, Polczyk R, et al. Mild asthmatics benefit from music therapy. J Asthma 2012;49:401–8.
45. Clarke SA, Calam R. The effectiveness of psychosocial interventions designed to improve health-related quality of life (HRQOL) amongst asthmatic children and their families: a systematic review. Qual Life Res 2012;21:747–64.
46. Beebe A, Gelfand EW, Bender B. A randomized trial to test the effectiveness of art therapy for children with asthma. J Allergy Clin Immunol 2010;126:262–6.
47. Metzger LK. Assessment of use of music by patients participating in cardiac rehabilitation. J Music Ther 2004;41:55–69.
48. El-Hassan H, McKeown K, Muller AF. Clinical trial: music reduces anxiety levels in patients attending for endoscopy. Aliment Pharmacol Ther 2009;30:718–24.
49. Thomas M, Bruton An, Moffatt M, et al. Asthma and psychological dysfunction. Prim Care Respir J 2011;20:250–6.
50. Lavoie KL, Bacon SL, Barone S, et al. What is worse for asthma control and quality of life: depressive disorders, anxiety disorders, or both? Chest 2006;130:1039–47.
51. Brown ES, Vigil L, Khan DA, et al. A randomized trial of citalopram versus placebo in outpatients with asthma and major depressive disorder: a proof of concept study. Biol Psychiatry 2005;58:865–70.
52. Brown ES, Howard C, Khan DA, et al. Escitalopram for severe asthma and major depressive disorder: a randomized, double-blind, placebo-controlled proof-of-concept study. Psychosomatics 2012;53:75–80.
Misuse of Prescription Stimulant Medication Among College Students: Summary of the Research Literature and Clinical Recommendations
From the University of South Carolina, Columbia, SC.
Abstract
- Objective: To provide a summary of the existing research on the characteristics of college students who report misusing prescription stimulant medications, to offer a set of clinical recommendations for practitioners, and to offer several possible prevention strategies.
- Methods: Literature review and research-based recommendations for clinical practice and prevention.
- Results: Misuse of prescription stimulant medication among college students is a prevalent and growing problem. Significant risk factors for misuse of stimulant medication include being male, being a member of a college sorority or fraternity, struggling academically, having elevated symptoms of ADHD and/or depression, being a high sensation-seeker, and using/misusing alcohol, cigarettes, and/or other illicit drugs. Health care providers, particularly those that see adolescent or college-aged individuals, need to be informed about stimulant medication indications, risks, benefits, and side effects and aware and attuned to problems associated with stimulant medication diversion and misuse. Suggestions for preventing misuse and diversion of prescription stimulant medications, including strategies for the individual and potential policy changes on college campuses, are offered.
- Conclusions: Misuse and diversion of prescription stimulant medications is a growing concern among adolescents and young adults and should be addressed by health care practitioners. Additional research on effective intervention and prevention strategies is needed.
Prescription stimulant medications (eg, methylphenidate, amphetamines) are typically used for the treatment of attention-deficit/hyperactivity disorder (ADHD) to increase attentiveness, decrease distractibility, and improve daily functioning. Prescriptions for stimulant medications are on the rise; between 2002 and 2010, the number of prescriptions for ADHD medications for youth under 18 increased 46% [1].
A recent review of ADHD diagnosis among college students estimated a prevalence rate of 2% to 8% [2]. More individuals with ADHD are matriculating to college than in the past [3,4], as more supports have been put in place for college students diagnosed with ADHD, including improved educational/organizational treatments and accommodations [2]. Many college students with ADHD also use prescription stimulant medications as part of their treatment plan; McCabe, Teter, and Boyd reported that 2.2% of college students had prescriptions for stimulant medications annually [5].
As the number of individuals of all ages with stimulant medication prescriptions increase, more individuals without prescriptions are gaining access to stimulant medications. In a survey of college students with medication prescriptions, stimulants were the most commonly diverted medication, with 61.7% of students with these prescriptions reporting having shared or sold their medication at least once [6]. Studies report that as many as 43% of college students have misused stimulant medication in their lifetime [7], though prevalence rates vary by study. Throughout this review, “misuse of stimulant medication” refers to using prescription stimulant medications without a prescription or using more stimulant medication than prescribed (ie, a higher or more frequent dosage).
Given the ease with which college students are able to obtain stimulant medications, the alarming prevalence of stimulant medication misuse among this population, and the potentially serious health risks associated with misuse of stimulant medication (especially when combined with other substances, such as alcohol, that are commonly used by college students), there is a need to both better understand and ultimately reduce the misuse of stimulant medication among college students. Thus, the purpose of this paper is threefold. First, we provide a summary of the existing research literature on the characteristics of college students who report misusing stimulant medication. Second, we offer a set of clinical recommendations for practitioners, which includes stimulant medication indications, risks, benefits, and side effects, along with problems associated with stimulant medication diversion and misuse. Finally, we offer several prevention strategies, including strategies for the individual as well as several suggestions for changing policies on college campuses to prevent stimulant diversion and misuse. Importantly, although our literature review addresses prescription stimulant misuse among college students, our clinical recommendations are also appropriate for adolescents and young adults not enrolled in college.
Summary of the Literature
The following summary is based on a comprehensive search of the existing research literature on misuse of stimulant medication among college students, which ultimately identified 30 relevant studies using 21 unique samples. A study was included if: (1) the main focus of the study was misuse of stimulant medication, (2) it was a peer-reviewed, empirical study using quantitative data analytic techniques, (3) it was written in English, (4) only undergraduate students were included in the sample, (5) it did not focus on only one type of stimulant medication (eg, methylphenidate only), and (6) if the article discussed multiple prescription drug categories (eg, stimulants, opiates), the data must have been analyzed separately for each category. An extensive meta-analytic review of this literature will be published elsewhere (contact the corresponding author to request a reprint). The following is a brief summary of our findings.
Prevalence, Availability, and Demographic Characteristics
Among prevalence rates reported, lifetime rates of stimulant medication misuse were the most frequently reported, ranging from 8.1% [8] to 43% [7]. Rates of misuse of stimulant medications within the last year ranged from 5.3% [9] to 35.3% [10]. A number of the studies asked students how they obtained stimulant medications for misuse; peers were overwhelmingly the most common source for obtaining the medications. For example, DeSantis, Webb, and Noar [11] found that 91% of the undergraduates who were interviewed obtained stimulant medications from friends or significant others.
Perceived availability of stimulant medications was also measured in several studies. DeSantis, Webb, and Noar [11] found that 82% of students thought it was somewhat or very easy to obtain stimulant medication; however, Sharp and Rosén [12] found that only 55% of students thought it was somewhat or very easy to obtain stimulant medication. In another study that examined perceived availability, 37% of men and 29.2% of women agreed that they knew students who would provide them with stimulant medications [13].
Many of the studies reviewed examined the relation between particular demographic characteristics (eg, gender, race, socioeconomic status, religious affiliation, year in college, sorority or fraternity membership) and misuse of stimulant medication among college students. The vast majority of studies that examined gender as related to misuse of stimulant medication found that significantly more males misused stimulant medication than females. For example, one study found that 26% of males and 17.3% of females reported misusing stimulant medication [14]; another study found that 39% of males versus 30% of females reported misuse [11].
It is also clear from the existing literature that members of fraternities and sororities appear to be more at-risk for misuse of stimulant medication than non-Greek students. In multiple studies, Greek students had rates of misuse twice that of non-Greeks. For instance, 48% of Greeks misused in their lifetime compared to 22% of non-Greeks [11]; 12% of Greeks misused in the past year compared to 5% of non-Greeks [15]; and Greeks were 2.32 times more likely to initiate use than non-Greeks [9].
Unfortunately, results from studies examining other demographic characteristics (eg, race, socioeconomic status, religious affiliation, year in college) as related to misuse of stimulant medication are much less conclusive and these correlates therefore require further investigation.
Motives For Misuse and Perceived Risk
Researchers have also evaluated college students’ motives for misusing stimulant medication and the risks they associate with misuse. All of the studies that asked misusing students about their motives for misuse reported that the most commonly endorsed motives were related to academics. “To concentrate better while studying” [16], “to improve study skills” [17], “to stay awake to study longer” [11], and “to improve concentration” [18] were some of the most commonly endorsed motives in these studies. Nonacademic reasons, such as to get high, to prolong effects of alcohol and other drugs, and to lose weight, were less commonly endorsed [7,12,19]. In studies where participants were able to indicate multiple motives for misuse [16], very few students misused for only nonacademic reasons.
Several studies measured the relation between misuse of stimulant medication and perceived risk associated with misuse. Perceived risk was conceptualized as perceived harmfulness [20], perception of safety [14], concern with health risk [18], and the inverse of positive outcome expectancies [21]. These articles found that when college students perceive more risk or have less positive expectancies about stimulant medication misuse, they are less likely to misuse stimulant medication. For instance, those who associated stimulant medication misuse with low perceived harmfulness were over 10 times more likely to have used in the last year than those who associated misuse with high perceived harmfulness [20].
Academic Outcomes Associated with Misuse
Interestingly, despite academic motives being most common for college students who report misusing stimulant medication, a number of studies have found a negative association between academic outcomes and misuse of stimulant medication. For instance, nonusers reported an average grade-point average (GPA) of 3.28 compared to 3.16 for misusers [16]. Other research demonstrates that the lower the student’s GPA is, the greater the odds are of the student misusing stimulant medication [8]. Misuse is also significantly related to other detrimental academic behaviors such as skipping class and less studying [20,22].
Psychological Correlates of Misuse
Researchers have evaluated the relation between several different psychological variables and misuse of stimulant medication. The strongest association is between symptoms of ADHD and stimulant medication misuse. Studies are consistent in reporting a significant correlation between greater symptoms of ADHD and higher rates of misuse or a significant difference in rates of misuse between those who have an ADHD diagnosis and those who do not. One study found that 71.1% of stimulant medication misusers screened positive for adult ADHD symptoms [17]. Another study found that for every standard deviation increase in attention problems, the odds of becoming a stimulant misuser increased by 1.78 [9]. Two studies asked participants if they believed they had ADHD. Advokat, Guildry, and Martino found that 12% of misusers believed they had ADHD [7]. Twenty-nine percent of “self-diagnosers” reported misusing, compared to 11.4% of “non-diagnosers” in another study [18].
Although the literature base is smaller than for ADHD, several studies have suggested a significant difference in symptoms of depression between stimulant medication misusers and nonusers. Zullig and Divin [23] found that misusers were significantly more likely to feel very sad, feel depressed, and consider suicide than nonusers. More frequent misuse has also been shown to be significantly associated with depressed mood [24].
A number of studies demonstrate a clear association between high sensation-seeking and misuse of stimulant medication. These results are not surprising given the well-documented relation between sensation seeking and substance use [25–27]. One study found a significant interaction between sensation seeking and perceived harmfulness of misusing stimulant medication: those with high sensation seeking and low perceived harmfulness were most likely to misuse [20].
Other Substance Use Associated with Stimulant Misuse
Many of the reviewed studies found a positive correlation between misuse of stimulant medication and other substance use or a significant difference between stimulant misusers and nonusers in rates of other substance use. These findings held across all substances examined, including alcohol, cigarettes, marijuana, illicit stimulants (eg, ecstasy, cocaine, or amphetamines), and non-stimulant prescription medications. For instance, significant associations were found between misuse of stimulant medication and several alcohol-related constructs, such as binge drinking [28,29], problematic drinking behavior [30], or meeting the Diagnostic and Statistical Manual of Mental Disorders [21] criteria for alcohol abuse [22]. With respect to cigarettes, 50.3% of misusers were found to have smoked cigarettes in the last 6 months compared to 13.3% of nonusers [16]. Similar findings emerged for illicit drug use. One study found that 73.5% of stimulant medication misusers reported use of marijuana in the last 6 months, compared to 18.2% of nonusers [19], while another study found that 93% of misusers used marijuana in the last year compared to 34% of nonusers [5]. This same study found that 33% of stimulant medication misusers also reported cocaine use in the last year compared to 2% of stimulant nonusers [5]. Finally, many of the studies reviewed examined the association between other substance use in general and stimulant medication misuse. Results were striking; the odds of becoming a stimulant medication misuser increased by 3.81 for each standard deviation increase in the amount of other substance use [9].
Summary
The research literature reviewed in this section provides a descriptive characterization of which college students (and, by extension, adolescents and young adults not in college) may be at the greatest risk of misuse of stimulant medication. Significant risk factors include being male, being a member of a college sorority or fraternity, struggling academically, having elevated symptoms of ADHD and/or depression, being a high sensation-seeker, and using/misusing alcohol, cigarettes, and/or other illicit drugs. It is important to recognize that one, several, or many of these risk factors may be present in a given individual who is misusing stimulant medication. Moreover, there may be other risk factors not yet identified in the research literature. The following sections of this paper draw from the literature reviewed here to provide a number of clinical recommendations for reducing and preventing misuse of stimulant medications among college students, other young adults, and adolescents.
Clinical Recommendations
It is important for health care providers to be aware of the benefits and risks associated with stimulant medications, the prevalence of and risk factors for stimulant misuse, and the psychiatric, psychological, and medical comorbidities associated with the misuse of stimulant medication. Knowledge about stimulant medications, misuse of stimulant medications, and a thorough evaluation of the patient will enable health care providers to address the misuse, as well as any comorbidities or other factors that may contribute to stimulant medication misuse, either pharmacologically or through referral for more specified psychotherapeutic interventions.
Stimulant Medication Indications and Adverse Effects
Stimulant medications are efficacious for the treatment of ADHD and, when prescribed and used correctly, can improve attentiveness, decrease distractibility, and improve daily functioning in the short term [19]. When used by individuals without ADHD, patients may experience euphoria, stimulation, alertness, and are not likely to experience the cognitive benefits that those with ADHD receive [31]. Side effects can occur regardless of whether the individual is using the stimulant for ADHD, misusing, or is dependent, and include nervousness, headaches, tachycardia, poor appetite, depressed mood, and poor sleep [19,32]. Additionally, stimulant medications can cause psychosis, agitation, and hallucinations [31,33], which typically resolve after discontinuation of the stimulant within 2 to 6 days, though a longer time period to resolution has been reported [33]. Stimulant medications carry warnings about increased risk of sudden death, high blood pressure, cardiac arrest, and stroke, as well as a statement warning providers about abuse potential. Additionally, serious but rare medical complications, including seizures, tachycardia or dysrhythmias, and hyperthermia, can occur [31,34].
Physical Examination and Laboratory Data
Obtaining vital signs and performing a physical exam may reveal weight loss and an increase in heart rate or blood pressure. Methylphenidate and amphetamines are known to increase heart rate and blood pressure [35] and a recent study found an average increase in heart rate of 5.7 bpm and a 1.2–mm Hg increase in systolic and diastolic blood pressure in adults on stimulant medications compared to placebo [36]. No EKG abnormalities or changes are found with either methylphenidate or amphetamine [35]. Urine toxicology can be utilized to obtain further information if misuse is suspected. However, the clinician must be aware of the limitations of urine drug testing with stimulants [37]. The usual detection time for amphetamines is 48 hours from last use, though this may vary depending on the presence of metabolites, pharmacokinetics of the drug (eg, immediate release vs. sustained release formulations), and patient variables [37]. Additionally, a urine toxicology screen for amphetamines typically tests for amphetamines, racemic compounds such as dextroamphetamine and methamphetamine, and illicit compounds (ie, methylenedioxymethamphetamine), though there are many compounds that are structurally similar, such as weight loss agents, over-the-counter cold products, and other psychotropic medications, including methylphenidate, that can cause a false-positive result [37]. Urine toxicology should be obtained in conjunction with a thorough evaluation of patients’ alcohol and drug use patterns. These 2 components are essential to the accurate diagnosis and formulation of a comprehensive treatment plan. As noted above, stimulant medication misuse and alcohol and illicit drug use are highly comorbid and should be carefully and thoroughly assessed.
Psychiatric Comorbidity
ADHD
The prevalence of ADHD is higher among individuals with substance use disorders [38]. As noted above, patients commonly report misuse of stimulant medication to enhance academic performance. One explanation may be that individuals misusing stimulants may be self-medicating undiagnosed ADHD [39]. The prevalence of ADHD among adults is 4.1% and it is more common in men than women with a ratio of up to 6:1 [40]. Several studies have found that individuals with misuse of stimulant medications endorse symptoms of ADHD, including higher levels of inattention and hyperactivity [41]. Twelve percent of participants in one study that endorsed stimulant medication misuse also endorsed the belief they had ADHD [7]. Another study found that individuals with higher baseline self-reported ADHD symptoms were also more likely to misuse stimulants [42]. The majority of individuals with ADHD have been found to take medications appropriately, though there is a minority, often with comorbid conduct disorder or other substance use disorders, that divert or misuse stimulant medications, most often the immediate release formulations [43,44].
Accurate diagnosis of ADHD in patients with substance use disorders can be challenging given the symptom overlap between intoxication and withdrawal syndromes of substances and symptoms of ADHD. Evaluating for ADHD is an important part of a thorough assessment and can be completed in several ways. The gold standard is with a standardized diagnostic tool such as the Connors Adult ADHD Diagnostic Interview for DSM-IV (CAADID) [45], which can be time consuming for a clinician and would likely involve referral to a psychologist for completion. Other scales have been examined, and the Connors Adult ADHD Rating Scale (CAARS) has been found to closely agree with the CAADID when both are administered [45]. Other scales are available, including the Wender Utah Rating Scales (WURS) and the Adult ADHD Self-Report Scale (ASRS), and have been found to have adequate sensitivity and specificity [45]. In an international study, the ASRS, a relatively brief instrument, showed encouraging results with 84% sensitivity and 66% specificity in detecting ADHD upon entry into substance disorder treatment for treatment-seeking patients [46]. When diagnosing ADHD among adults, it is crucial not to rely only on self-reported symptoms. A thorough childhood history of ADHD symptom presentation should be collected from a parent or caregiver, and collateral concurrent report should be collected from someone who knows the patient well, such as an employer, close friend, significant other, or parent. Valid diagnosis, whether ADHD is present or not, is of utmost importance in this population as individuals with comorbid substance use disorders and ADHD tend to have worse outcomes overall [47]. It is also important to appreciate that inaccurately diagnosing ADHD in individuals misusing stimulants could potentially diminish the importance of the diagnosis [48].
If ADHD is found, there are medications available that have a lower abuse potential compared to stimulant medications. Atomoxetine is the only FDA-approved nonstimulant for ADHD; off-label or second-line treatments include antidepressants, such as bupropion, venlafaxine, or tricyclic antidepressants, for which the data is limited, and clonidine [34,49,50]. If these therapies are not effective and, after careful consideration of risks and benefits, it is determined that a trial with a stimulant is needed, longer-acting formulations appear to be less abused [34,44]. Education for both the patient and his or her family should be provided on abuse and diversion potential and appropriate use and misuse [34,43,51]. Pill counts [43], regular office visits [52], and random urine toxicology screens [34] with informed interpretation of the screens may be helpful in deterring misuse or diversion. While medications are the mainstay of treatment for ADHD, there are several psychosocial interventions available, including cognitive behavioral therapy, coaching, and behavioral modification therapies [34].
Other Comorbidities
Other psychiatric comorbidities also should be explored. Studies have found a relation between depression and misuse of stimulant medication in that there is an increased likelihood of depression and thoughts of suicide among those that misuse stimulant medication and vice versa [23,24,53]. The National Survey on Drug Use and Health in 2012 found that, of those that misused stimulants, nearly 20% had serious thoughts of suicide over the past year [54]. As noted earlier, stimulant medication can affect sleep and appetite. Among those that report misuse of stimulant medication for weight loss, these individuals are more likely to report other eating-disordered behaviors [55]. Sleep quality is worse and sleep disturbance greater in those that misuse stimulant medication [32]. Other traits and behaviors that have been described in individuals that misuse stimulant medications include impulsivity [56,57], sensation seeking [20], perfectionism [58], and poor time management skills or procrastination [59].
Appropriate treatment (which may include pharmacologic, psychological, or academic accommodation components) for individuals with these psychiatric disorders or psychological symptoms may reduce the misuse of stimulant medications among college students, especially if these students are misusing in order to reduce their symptoms (ie, a self-medication hypothesis).
Treatment
There are currently no FDA-approved medications to treat stimulant medication misuse. In fact, studies exploring pharmacotherapy for stimulant medication misuse are limited. Most trials focus on stimulants such as cocaine or methamphetamine and not stimulant medications alone. Additionally, these trials primarily include only individuals that meet criteria for stimulant dependence. Various medications and medication classes have been examined for the treatment of stimulant dependence, including naltrexone, various antipsychotics, and various antidepressants including bupropion, modafanil, baclofen, ondansetron, and dexamphetamine, with little to no effect [60]. In a review of the literature, one study examined the use of naltrexone versus placebo for stimulant dependence in 80 treatment-seeking Swedish individuals [61]. The different types of stimulants on which these individuals were dependent were not clearly delineated, though the study authors noted that the major amphetamine abused in Sweden was the racemic mixture d/l amphetamine and not methamphetamine. Naltrexone was superior to placebo in this trial, as evidenced by higher percentage of amphetamine-free urine samples. A large majority of this sample used intravenously (65%–76%) and had been using between 6 to 8 years, limiting the applicability to individuals with stimulant medication misuse. At this time, investigation into evidence-based pharmacotherapies for stimulant medication misuse remains in the early stages.
Generally speaking, efficacious behavioral treatments, such as contingency management (CM), cognitive behavioral therapy (CBT), skills training, motivational interviewing (MI), relapse prevention, couples and family treatments, and drug counseling, exist for drug abuse [62]. CBT, cognitive therapy, CM, MI, and community reinforcement approach (CRA) [63,64] have been explored for stimulant dependence and are currently the primary interventions for amphetamine-type stimulant dependence [60]. Similar to pharmacotherapy studies, most psychotherapy studies to date have examined primarily cocaine and methamphetamine dependence and not misuse of stimulant medications. In fact, no studies examining psychotherapy for stimulant medication misuse were found by our group in a search using the PubMed database. Therefore, discussion of psychotherapeutic interventions that may be efficacious for stimulant medication misuse extrapolates outcomes from studies of stimulant dependence, appreciating this is an approximation and imprecise as there are significant differences between stimulant medication misusers and those dependent upon stimulants such as methamphetamine or cocaine. As such, in a review from 2009 [63], Vocci and colleagues compared psychotherapy studies for cocaine and methamphetamine dependence and concluded that CBT and CM were moderately effective and that adding CM to standard treatment may help improve outcomes. A study of 214 amphetamine users (including methamphetamine users), with the majority (70%) enrolled in a methadone maintenance program and a large proportion (58.9%) using amphetamines intravenously, found that either 2 or 4 sessions of CBT, along with self-help material, increased rate of abstinence at 6 months post-intervention compared to the use of self-help material alone [65]. Baker and colleagues [64] recommend a practical stepped approach to treatment for stimulant dependence, including conducting a thorough assessment, offering education and self-help materials, monitoring use and consequences of use, and then transitioning to more intensive psychosocial interventions if needed, which may be applicable to those with stimulant medication misuse and is clinically reasonable. Offering a psychosocial intervention may require referral to more specialized treatment services than can be offered in a general primary care clinic. Additionally, harm reduction techniques for stimulant medication misusers to reduce the medical and social consequences can be considered as well as prevention strategies and methods, which can be utilized in any treatment setting or in high-risk populations, such as college students.
Prevention Strategies for the Individual
The research findings summarized in this review suggest several specific strategies for preventing and reducing the misuse of stimulant medication among college students, a high-risk population. First, college students with a prescription for stimulant medication play a critical role. Not only do these students have a high rate of misuse themselves [28,66], but they are also the most common source from which other students obtain stimulant medication to misuse [11,67]. It is therefore important for physicians who provide college students with prescriptions for stimulant medications to discuss the possible consequences of misusing or diverting medication, including potential negative health outcomes, legal consequences, and on-campus repercussions, for students caught diverting stimulant medications. These practitioners should also monitor their patients for signs of diversion, such as finishing a prescription early, doctor shopping, or urine drug screen which is negative for the prescribed substance. Utilizing a prescription monitoring program to access information on the prescribing and filling of controlled substances can be a valuable tool in detecting multiple concomitant prescriptions for stimulant medications, number of providers writing stimulant medication, and information on the use of other prescribed controlled medications. Providers should also discuss safe storage of stimulant medications with patients, particularly if the student is currently living in a dorm setting or another community-type setting with the potential for lots of individuals in and around their personal belongings. Additionally, providers may wish to consider dispensing a small amount at each office visit until the patient has established responsible use of the medication, particularly if there are other findings or comorbidities that perhaps increase their risk of misuse. Pill counts and frequent office visits, as noted earlier, may also help prevent diversion.
Perceived risk/harm associated with the use of stimulant medications has been negatively related to misuse [18,20]. If college students were more aware of the risks associated with stimulant medication misuse, with regards to both health and legal consequences, fewer students may choose to misuse stimulants. Educating patients and their families about the abuse potential of stimulants, as well as consequences of misuse such as psychosis and agitation, when prescriptions are given for stimulant medication, may help address the misperception that stimulant medications are benign, safe and without adverse consequences.
College Policy Changes for Prevention of Misuse
Policy changes on college campuses could also help to reduce diversion of stimulant medications. For instance, education about the risks associated with stimulant medication misuse could be incorporated into other alcohol and drug prevention programs that are already in place at colleges and universities. Many colleges/universities require all first-year students to complete an online substance use education/prevention/assessment tool. Some of these, such as AlcoholEdu and The Alcohol eCHECKUP TO GO have demonstrated some success in reducing college student alcohol use in follow-up evaluations [68]. Information about misuse of stimulant medication could be included in these existing programs. Moreover, members of certain organizations (eg, fraternities or sororities) that are known for an increased risk of substance use/abuse among members are also sometimes required by their national chapters or host colleges/universities to complete a “risk management” class, which addresses behaviors such as binge drinking and drunk driving. Since one of the demographic factors most strongly related to stimulant medication misuse is Greek organization membership [14], presenting information about stimulant medication misuse to these groups during these classes could help reduce misuse on college campuses.
Finally, the most commonly reported motives for misuse of stimulant medications among college students are academic in nature (eg, to study more, to concentrate better) [16], and many students who misuse for these reasons feel the desired effect is achieved. Colleges and universities may need to improve the identification of students who are in need of academic assistance/supports and offer these interventions earlier in students’ college careers to prevent stimulant medication misuse as a “quick fix.” Such interventions may include teaching students skills such as note-taking and academic goal setting and educating students about the link between sleep deprivation and poor concentration [69].
Summary
Health care providers, particularly those that see adolescent or college-aged individuals, need to be informed about stimulant medication indications, risks, benefits, and side effects and aware and attuned to problems associated with stimulant medication diversion and misuse. Diagnosing ADHD can be invaluable for individuals with the disorder, thus the ability to perform a thorough and accurate assessment is important; equally important is the ability to assess when ADHD is not present. Education and prevention strategies to prevent misuse and diversion should be provided if stimulant medications are indicated. College programs and policies can also utilize prevention strategies, provide education to students, and assist those with academic difficulties. Comorbidities are common and should be explored thoroughly as they may play a role in continued stimulant medication misuse and outcomes. Various treatment techniques and modalities can be explored further with each patient, based on the individual and their particular needs.
Corresponding author: Kate Flory, Univ. of South Carolina, Dept. of Psychology, Barnwell College, Columbia, SC 29208, [email protected].
Funding/support: Work on this paper was supported by a University of South Carolina Honors College Exploration Scholar Award and a University of South Carolina Magellan Fellowship, both awarded to Kari Benson.
Financial disclosures: None.
Author contributions: conception and design, KF, RAP, KB; drafting of article, KF, RAP, KB; critical revision of the article, KF, RAP, KB; literature search, KB.
1. Chai G, Governale L, Mcmahon AW, et al. Trends of outpatient prescription drug utilization in US children, 2002-2010. Pediatr 2012;130:23–31.
2. Dupaul GJ, Weyandt LL, O’dell SM, Varejao M. College students with ADHD: current status and future directions J Atten Disord 2009;13:234–50.
3. DuPaul G, Schaughency E, Weyandt L, et al. Self-report of ADHD symptoms in university students: Cross-gender and cross-national prevalence. J Learn Disabil 2001;34:370–9.
4. Wolf L. College students with ADHD and other hidden disorders: Outcomes and interventions. Ann NY Acad Arts Sci 2001;931:385–5.
5. McCabe S, Teter CJ, Boyd CJ. Medical use, illicit use, and diversion of abusable prescription drugs. J Am Coll Health 2006;54:269–78.
6. Garnier LM, Arria AM, Caldeira KM, et al. Sharing and selling of prescription medications in a college student sample. J Clin Psychiatry 2010;71:262–9.
7. Advokat CD, Guildry D, Martino L. Licit and illicit use of medications for attention-deficit hyperactivity disorder in undergraduate college students. J Am Coll Health 2008;56:601–6.
8. McCabe S, Teter CJ, Boyd CJ. Medical use, illicit use and diversion of prescription stimulant medication. J Psychoactive Drugs 2006;38:43–56.
9. Rabiner DL, Anastopoulos AD, Costello E, et al. Predictors of nonmedical ADHD medication use by college students. J Atten Disord 2010;13:640–8.
10. Graff Low K, Gendaszek AE. Illicit use of psychostimulants among college students: A preliminary study. Psychol Health Med 2002;7:283–7.
11. DeSantis AD, Webb EM, Noar SM. Illicit use of prescription ADHD medications on a college campus: A multimethodological approach. J Am Coll Health 2008;57:315–23.
12. Sharp JT, Rosén LA. Recreational stimulant use among college students. J Subst Use 2007;12:71–82.
13. Hall KM, Irwin MM, Bowman KA, et al. Illicit use of prescribed stimulant medication among college students. J Am Coll Health 2005;53:167–74.
14. Dussault CL, Weyandt LL. An examination of prescription stimulants misuse and psychological variables among sorority and fraternity college populations. J Atten Disord 2013;27:87–7.
15. McCabe SE. Misperceptions of non-medical prescription drug use: A web survey of college students. Addict Behav 2008;33:713–24.
16. Rabiner DL, Anastopoulos AD, Costello E, et al. Motives and perceived consequences of nonmedical ADHD medication use by college students: Are students treating themselves for attention problems? J Atten Disord 2009;13:259–70.
17. Peterkin AL, Crone CC, Sheridan MJ, Wise TN. Cognitive performance enhancement: Misuse or self-treatment? J Atten Disord 2011;15:263–8.
18. Judson R, Langdon SW. Illicit use of prescription stimulants among college students: Prescription status, motives, theory of planned behaviour, knowledge and self-diagnostic tendencies. Psychol Health Med 2009;14:97–104.
19. Volkow ND, Swanson JM. Adult attention deficit-hyperactivity disorder. N Engl J Med 2013;369:1935–44.
20. Arria AM, Caldeira KM, Vincent KB, et al. Perceived harmfulness predicts nonmedical use of prescription drugs among college students: Interactions with sensation-seeking. Prev Science 2008;9:191–201.
21. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. 2000.
22. Arria AM, Wilcox HC, Caldeira KM, et al. Dispelling the myth of “smart drugs”: Cannabis and alcohol use problems predict nonmedical use of prescription stimulants for studying. Addict Behav 2013;38:1643–50.
23. Zullig KJ, Divin AL. The association between non-medical prescription drug use, depressive symptoms, and suicidality among college students. Addict Behav 2012;37:890–9.
24. Teter CJ, Falone AE, Cranford JA, et al. Nonmedical use of prescription stimulants and depressed mood among college students: Frequency and routes of administration. J Subst Abuse Treat 2010;38:292–8.
25. Pedersen W. Mental health, sensation seeking and drug use patterns: a longitudinal study. Br J Addict 1991;86:195–204.
26. Jaffe LT, Archer RP. The prediction of drug use among college students from MMPI, MCMI, and sensation seeking scales. J Pers Assess 1987;51:243–53.
27. Martins SS, Storr CL, Alexandre PK, Chilcoat HD. Adolescent ecstasy and other drug use in the National Survey of Parents and Youth: The role of sensation-seeking, parental monitoring and peer’s drug use. Addict Behav 2008;33:919–33.
28. Sepúlveda DR, Thomas LM, McCabe S, et al. Misuse of prescribed stimulant medication for ADHD and associated patterns of substance use: Preliminary analysis among college students. J Pharm Pract 2011;24:551–60.
29. Teter CJ, McCabe SE, Cranford JA, et al. Prevalence and motives for illicit use of prescription stimulants in an undergraduate student sample. J Am Coll Health 2005;53:253–62.
30. Lookatch SJ, Dunne EM, Katz EC. Predictors of nonmedical use of prescription stimulants. J Psychoactive Drugs 2012;44:86–91.
31. Looby A, Kassman KT, Earlywine M. Do negative stimulant-related attitudes vary for prescription stimulants and cocaine among college students? Addict Behav 2014;39:1100–5.
32. Clegg-Kraynok MM, McBean AL, Montgomery-Downs HE. Sleep quality and characteristics of college students who use prescription psychostimulants nonmedically. Sleep Med 2011;12:598–602.
33. Ross RG. Psychotic and manic-like symptoms during stimulant treatment of attention deficit hyperactivity disorder. Am J Psychiatry 2006;163:1149–52.
34. Mariani JJ, Levin FR. Treatment strategies for co-occurring ADHD and substance use disorders. Am J Addict 2007;16:45–56.
35. Vetter VL, Elia J, Erickson C, et al. Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/hyperactivity disorder: A scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee and the Council on Cardiovascular Nursing. Circulation 2008;117:2407–23.
36. Mick E, McManus DD, Goldberg RJ. Meta-analysis of increased heart rate and blood pressure associated with CNS stimulant treatment of ADHD in adults. Eur Neuropsychopharmacol 2013;23:534–41.
37. Moeller KE, Lee KC, Kissack JC. Urine drug screening: Practical guide for clinicians. Mayo Clin Proc 2008;83:66–76.
38. Van de Glind G, Konstenius M, Koeter MWJ, et al. Variability in the prevalence of adult ADHD in treatment seeking substance use disorder patients: Results from an international multi-center study exploring DSM-IV and DSM-5 criteria. Drug Alcohol Depend 2014;134:158–66.
39. Bukstein O. Substance abuse in patients with attention-deficit/hyperactivity disorder. Medscape J Med 2008;10:24.
40. Kessler RC, Adler L, Barkley R, et al. The prevalence and comorbidity of adult ADHD in the United States: Results from the National Comorbidity Survey Replication. Am J Psychiatry 2006;163:716–23.
41. Hartung CM, Canu WH, Cleveland CS, et al. Stimulant medication use in college students: Comparison of appropriate users, misusers, and nonusers. Psychol Addict Behav 2014;27:832.
42. Upadhyaya HP. Managing attention-deficit/hyperactivity disorder in the presence of substance use disorder. J Clin Psychiatry 2007;68:23–30.
43. Wilens TE, Gignac M, Swezey A, et al. Characteristics of adolescents and young adults with ADHD who divert or misuse their prescribed medications. J Am Acad Child Adolesc Psychiatry 2006;45:408–14.
44. Wilens TE, Adler LA, Adams J, et al. Misuse and diversion of stimulants prescribed for ADHD: A systematic review of the literature. J Am Acad Child Adolesc Psychiatry 2008;47:21–31.
45. Dakwa E, Mahony A, Pavlicova M, et al. The utility of attention-deficit/hyperactivity disorder screening instruments in individuals seeking treatment for substance use disorders. J Clin Psychiatry 2012;73:1372–8.
46. Van de Glind G, Van den Brink W, Koeter. Validity of the Adult ADHD Self-Report Scale (ASRS) as a screener for adult ADHD in treatment seeking substance use disorder patients. Drug Alcohol Depend 2013;132:587–96.
47. Levin FR. Diagnosing attention-deficity/hyperactivity disorder in patients with substance use disorders. J Clin Psychiatry 2007;68:9–14.
48. Diller L. ADHD in the college student: Is anyone else worried? J Atten Disord. 2010;14:3-6.
49. Christman AK, Fermo JD, Markowitz JS. Atomoxetine, a novel treatment for attention-deficit/hyperactivity disorder. Pharmacotherapy 2004;24:1020–36.
50. Riggs P, Levin F, Green AI, Vocci F. Comorbid psychiatric and substance abuse disorders: Recent treatment research. Subst Abuse 2008;29:51–63.
51. Rabiner D L. Stimulant prescription cautions: Addressing misuse, diversion, and malingering. Curr Psychiatry Rep. 2013;15:375-383.
52. Manning JS. Strategies for managing the risks associated with ADHD medications. J Clin Psychiatry 2013;74:e19.
53. Markou A, Kosten TR, Koob GF. Neurobiological similarities in depression and drug dependence: A self-medication hypothesis. Neuropsychopharmacology 1998;18:135–74.
54. Results from the 2012 National Survey on Drug Use and Health: Mental Health Findings, NSDUH Series H-47. HHS Pub No. 13-4805. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2013.
55. Jeffers A, Benotsch EG, Koester S. Misuse of prescription stimulants for weight loss, psychosocial variables, and eating disordered behaviors. Appetite 2013;65:8–13.
56. Madden GJ, Bickel WK. Impulsivity: The behavioral and neurological science of discounting. 1st ed. Washington, DC: APA; 2010.
57. Stanford MS, Mathias CW, Dougherty DM, et al. Fifty years of the Barratt Impulsiveness Scale: An update and review. Pers Indiv Differ 2009;47:385–95.
58. Low K, Gendaszek AE. Illicit use of psychostimulants among college students: A preliminary study. Psychol Health Med 2002;7:283–7.
59. Moore DR, Burgard DA, Larson RG, Ferm M. Psychostimulant use among college students during periods of high and low stress: An interdisciplinary approach utilizing both self-report and unobtrusive chemical sample data. Addict Behav 2014;39:987–93.
60. Brensilver M, Heinzerling KG, Shoptaw S. Pharmacotherapy of amphetamine-type stimulant dependence: An update. Drug Alc Review 2013;32:449–60.
61. Jayaram-Lindstrom N, Hammarberg A, Beck O, Franck J. Naltrexone for the treatment of amphetamine dependence: A randomized, placebo-controlled trial. Am J Psychiatry 2008;165:1442–8.
62. Carroll KM, Onken LS. Behavioral therapies for drug abuse. Am J Psychiatry 2005;162:1452–60.
63. Vocci FJ, Montoya I. Psychological treatments for stimulant misuse, comparing and contrasting those for amphetamine dependence and those for cocaine dependence. Curr Opin Psychiatry 2009;22:263–8.
64. Baker A, Lee NK., Claire M, et al. Brief cognitive behavioral interventions for regular amphetamine users: a step in the right direction. Addict 2005;100:367–78.
65. Baker A, Lee NK, Claire M, et al. Drug use patterns and mental health of regular amphetamine users. Addict 2004;99:875–84.
66. Rabiner DL, Anastopoulos AD, Costello E, et al. The misuse and diversion of prescribed ADHD medications by college students. J Atten Disord 2009;13:259–70.
67. Garnier-Dykstra LM, Caldeira KM, Vincent KB, et al. Nonmedical use of prescription stimulants during college: Four year trends in exposure opportunity, use, motives, and sources. J Am Coll Health 2012;60:226–34.
68. Hustad JT, Barnett NP, Borsari B, Jackson KM. Web-based alcohol prevention for incoming college students: A randomized controlled trial. Addict Behav 2010;35:183–9.
69. Pilcher JJ, Walters AS. How sleep deprivation affects psychological variables related to college students’ cognitive performance. J Am Coll Health 1997;46:121–6.
From the University of South Carolina, Columbia, SC.
Abstract
- Objective: To provide a summary of the existing research on the characteristics of college students who report misusing prescription stimulant medications, to offer a set of clinical recommendations for practitioners, and to offer several possible prevention strategies.
- Methods: Literature review and research-based recommendations for clinical practice and prevention.
- Results: Misuse of prescription stimulant medication among college students is a prevalent and growing problem. Significant risk factors for misuse of stimulant medication include being male, being a member of a college sorority or fraternity, struggling academically, having elevated symptoms of ADHD and/or depression, being a high sensation-seeker, and using/misusing alcohol, cigarettes, and/or other illicit drugs. Health care providers, particularly those that see adolescent or college-aged individuals, need to be informed about stimulant medication indications, risks, benefits, and side effects and aware and attuned to problems associated with stimulant medication diversion and misuse. Suggestions for preventing misuse and diversion of prescription stimulant medications, including strategies for the individual and potential policy changes on college campuses, are offered.
- Conclusions: Misuse and diversion of prescription stimulant medications is a growing concern among adolescents and young adults and should be addressed by health care practitioners. Additional research on effective intervention and prevention strategies is needed.
Prescription stimulant medications (eg, methylphenidate, amphetamines) are typically used for the treatment of attention-deficit/hyperactivity disorder (ADHD) to increase attentiveness, decrease distractibility, and improve daily functioning. Prescriptions for stimulant medications are on the rise; between 2002 and 2010, the number of prescriptions for ADHD medications for youth under 18 increased 46% [1].
A recent review of ADHD diagnosis among college students estimated a prevalence rate of 2% to 8% [2]. More individuals with ADHD are matriculating to college than in the past [3,4], as more supports have been put in place for college students diagnosed with ADHD, including improved educational/organizational treatments and accommodations [2]. Many college students with ADHD also use prescription stimulant medications as part of their treatment plan; McCabe, Teter, and Boyd reported that 2.2% of college students had prescriptions for stimulant medications annually [5].
As the number of individuals of all ages with stimulant medication prescriptions increase, more individuals without prescriptions are gaining access to stimulant medications. In a survey of college students with medication prescriptions, stimulants were the most commonly diverted medication, with 61.7% of students with these prescriptions reporting having shared or sold their medication at least once [6]. Studies report that as many as 43% of college students have misused stimulant medication in their lifetime [7], though prevalence rates vary by study. Throughout this review, “misuse of stimulant medication” refers to using prescription stimulant medications without a prescription or using more stimulant medication than prescribed (ie, a higher or more frequent dosage).
Given the ease with which college students are able to obtain stimulant medications, the alarming prevalence of stimulant medication misuse among this population, and the potentially serious health risks associated with misuse of stimulant medication (especially when combined with other substances, such as alcohol, that are commonly used by college students), there is a need to both better understand and ultimately reduce the misuse of stimulant medication among college students. Thus, the purpose of this paper is threefold. First, we provide a summary of the existing research literature on the characteristics of college students who report misusing stimulant medication. Second, we offer a set of clinical recommendations for practitioners, which includes stimulant medication indications, risks, benefits, and side effects, along with problems associated with stimulant medication diversion and misuse. Finally, we offer several prevention strategies, including strategies for the individual as well as several suggestions for changing policies on college campuses to prevent stimulant diversion and misuse. Importantly, although our literature review addresses prescription stimulant misuse among college students, our clinical recommendations are also appropriate for adolescents and young adults not enrolled in college.
Summary of the Literature
The following summary is based on a comprehensive search of the existing research literature on misuse of stimulant medication among college students, which ultimately identified 30 relevant studies using 21 unique samples. A study was included if: (1) the main focus of the study was misuse of stimulant medication, (2) it was a peer-reviewed, empirical study using quantitative data analytic techniques, (3) it was written in English, (4) only undergraduate students were included in the sample, (5) it did not focus on only one type of stimulant medication (eg, methylphenidate only), and (6) if the article discussed multiple prescription drug categories (eg, stimulants, opiates), the data must have been analyzed separately for each category. An extensive meta-analytic review of this literature will be published elsewhere (contact the corresponding author to request a reprint). The following is a brief summary of our findings.
Prevalence, Availability, and Demographic Characteristics
Among prevalence rates reported, lifetime rates of stimulant medication misuse were the most frequently reported, ranging from 8.1% [8] to 43% [7]. Rates of misuse of stimulant medications within the last year ranged from 5.3% [9] to 35.3% [10]. A number of the studies asked students how they obtained stimulant medications for misuse; peers were overwhelmingly the most common source for obtaining the medications. For example, DeSantis, Webb, and Noar [11] found that 91% of the undergraduates who were interviewed obtained stimulant medications from friends or significant others.
Perceived availability of stimulant medications was also measured in several studies. DeSantis, Webb, and Noar [11] found that 82% of students thought it was somewhat or very easy to obtain stimulant medication; however, Sharp and Rosén [12] found that only 55% of students thought it was somewhat or very easy to obtain stimulant medication. In another study that examined perceived availability, 37% of men and 29.2% of women agreed that they knew students who would provide them with stimulant medications [13].
Many of the studies reviewed examined the relation between particular demographic characteristics (eg, gender, race, socioeconomic status, religious affiliation, year in college, sorority or fraternity membership) and misuse of stimulant medication among college students. The vast majority of studies that examined gender as related to misuse of stimulant medication found that significantly more males misused stimulant medication than females. For example, one study found that 26% of males and 17.3% of females reported misusing stimulant medication [14]; another study found that 39% of males versus 30% of females reported misuse [11].
It is also clear from the existing literature that members of fraternities and sororities appear to be more at-risk for misuse of stimulant medication than non-Greek students. In multiple studies, Greek students had rates of misuse twice that of non-Greeks. For instance, 48% of Greeks misused in their lifetime compared to 22% of non-Greeks [11]; 12% of Greeks misused in the past year compared to 5% of non-Greeks [15]; and Greeks were 2.32 times more likely to initiate use than non-Greeks [9].
Unfortunately, results from studies examining other demographic characteristics (eg, race, socioeconomic status, religious affiliation, year in college) as related to misuse of stimulant medication are much less conclusive and these correlates therefore require further investigation.
Motives For Misuse and Perceived Risk
Researchers have also evaluated college students’ motives for misusing stimulant medication and the risks they associate with misuse. All of the studies that asked misusing students about their motives for misuse reported that the most commonly endorsed motives were related to academics. “To concentrate better while studying” [16], “to improve study skills” [17], “to stay awake to study longer” [11], and “to improve concentration” [18] were some of the most commonly endorsed motives in these studies. Nonacademic reasons, such as to get high, to prolong effects of alcohol and other drugs, and to lose weight, were less commonly endorsed [7,12,19]. In studies where participants were able to indicate multiple motives for misuse [16], very few students misused for only nonacademic reasons.
Several studies measured the relation between misuse of stimulant medication and perceived risk associated with misuse. Perceived risk was conceptualized as perceived harmfulness [20], perception of safety [14], concern with health risk [18], and the inverse of positive outcome expectancies [21]. These articles found that when college students perceive more risk or have less positive expectancies about stimulant medication misuse, they are less likely to misuse stimulant medication. For instance, those who associated stimulant medication misuse with low perceived harmfulness were over 10 times more likely to have used in the last year than those who associated misuse with high perceived harmfulness [20].
Academic Outcomes Associated with Misuse
Interestingly, despite academic motives being most common for college students who report misusing stimulant medication, a number of studies have found a negative association between academic outcomes and misuse of stimulant medication. For instance, nonusers reported an average grade-point average (GPA) of 3.28 compared to 3.16 for misusers [16]. Other research demonstrates that the lower the student’s GPA is, the greater the odds are of the student misusing stimulant medication [8]. Misuse is also significantly related to other detrimental academic behaviors such as skipping class and less studying [20,22].
Psychological Correlates of Misuse
Researchers have evaluated the relation between several different psychological variables and misuse of stimulant medication. The strongest association is between symptoms of ADHD and stimulant medication misuse. Studies are consistent in reporting a significant correlation between greater symptoms of ADHD and higher rates of misuse or a significant difference in rates of misuse between those who have an ADHD diagnosis and those who do not. One study found that 71.1% of stimulant medication misusers screened positive for adult ADHD symptoms [17]. Another study found that for every standard deviation increase in attention problems, the odds of becoming a stimulant misuser increased by 1.78 [9]. Two studies asked participants if they believed they had ADHD. Advokat, Guildry, and Martino found that 12% of misusers believed they had ADHD [7]. Twenty-nine percent of “self-diagnosers” reported misusing, compared to 11.4% of “non-diagnosers” in another study [18].
Although the literature base is smaller than for ADHD, several studies have suggested a significant difference in symptoms of depression between stimulant medication misusers and nonusers. Zullig and Divin [23] found that misusers were significantly more likely to feel very sad, feel depressed, and consider suicide than nonusers. More frequent misuse has also been shown to be significantly associated with depressed mood [24].
A number of studies demonstrate a clear association between high sensation-seeking and misuse of stimulant medication. These results are not surprising given the well-documented relation between sensation seeking and substance use [25–27]. One study found a significant interaction between sensation seeking and perceived harmfulness of misusing stimulant medication: those with high sensation seeking and low perceived harmfulness were most likely to misuse [20].
Other Substance Use Associated with Stimulant Misuse
Many of the reviewed studies found a positive correlation between misuse of stimulant medication and other substance use or a significant difference between stimulant misusers and nonusers in rates of other substance use. These findings held across all substances examined, including alcohol, cigarettes, marijuana, illicit stimulants (eg, ecstasy, cocaine, or amphetamines), and non-stimulant prescription medications. For instance, significant associations were found between misuse of stimulant medication and several alcohol-related constructs, such as binge drinking [28,29], problematic drinking behavior [30], or meeting the Diagnostic and Statistical Manual of Mental Disorders [21] criteria for alcohol abuse [22]. With respect to cigarettes, 50.3% of misusers were found to have smoked cigarettes in the last 6 months compared to 13.3% of nonusers [16]. Similar findings emerged for illicit drug use. One study found that 73.5% of stimulant medication misusers reported use of marijuana in the last 6 months, compared to 18.2% of nonusers [19], while another study found that 93% of misusers used marijuana in the last year compared to 34% of nonusers [5]. This same study found that 33% of stimulant medication misusers also reported cocaine use in the last year compared to 2% of stimulant nonusers [5]. Finally, many of the studies reviewed examined the association between other substance use in general and stimulant medication misuse. Results were striking; the odds of becoming a stimulant medication misuser increased by 3.81 for each standard deviation increase in the amount of other substance use [9].
Summary
The research literature reviewed in this section provides a descriptive characterization of which college students (and, by extension, adolescents and young adults not in college) may be at the greatest risk of misuse of stimulant medication. Significant risk factors include being male, being a member of a college sorority or fraternity, struggling academically, having elevated symptoms of ADHD and/or depression, being a high sensation-seeker, and using/misusing alcohol, cigarettes, and/or other illicit drugs. It is important to recognize that one, several, or many of these risk factors may be present in a given individual who is misusing stimulant medication. Moreover, there may be other risk factors not yet identified in the research literature. The following sections of this paper draw from the literature reviewed here to provide a number of clinical recommendations for reducing and preventing misuse of stimulant medications among college students, other young adults, and adolescents.
Clinical Recommendations
It is important for health care providers to be aware of the benefits and risks associated with stimulant medications, the prevalence of and risk factors for stimulant misuse, and the psychiatric, psychological, and medical comorbidities associated with the misuse of stimulant medication. Knowledge about stimulant medications, misuse of stimulant medications, and a thorough evaluation of the patient will enable health care providers to address the misuse, as well as any comorbidities or other factors that may contribute to stimulant medication misuse, either pharmacologically or through referral for more specified psychotherapeutic interventions.
Stimulant Medication Indications and Adverse Effects
Stimulant medications are efficacious for the treatment of ADHD and, when prescribed and used correctly, can improve attentiveness, decrease distractibility, and improve daily functioning in the short term [19]. When used by individuals without ADHD, patients may experience euphoria, stimulation, alertness, and are not likely to experience the cognitive benefits that those with ADHD receive [31]. Side effects can occur regardless of whether the individual is using the stimulant for ADHD, misusing, or is dependent, and include nervousness, headaches, tachycardia, poor appetite, depressed mood, and poor sleep [19,32]. Additionally, stimulant medications can cause psychosis, agitation, and hallucinations [31,33], which typically resolve after discontinuation of the stimulant within 2 to 6 days, though a longer time period to resolution has been reported [33]. Stimulant medications carry warnings about increased risk of sudden death, high blood pressure, cardiac arrest, and stroke, as well as a statement warning providers about abuse potential. Additionally, serious but rare medical complications, including seizures, tachycardia or dysrhythmias, and hyperthermia, can occur [31,34].
Physical Examination and Laboratory Data
Obtaining vital signs and performing a physical exam may reveal weight loss and an increase in heart rate or blood pressure. Methylphenidate and amphetamines are known to increase heart rate and blood pressure [35] and a recent study found an average increase in heart rate of 5.7 bpm and a 1.2–mm Hg increase in systolic and diastolic blood pressure in adults on stimulant medications compared to placebo [36]. No EKG abnormalities or changes are found with either methylphenidate or amphetamine [35]. Urine toxicology can be utilized to obtain further information if misuse is suspected. However, the clinician must be aware of the limitations of urine drug testing with stimulants [37]. The usual detection time for amphetamines is 48 hours from last use, though this may vary depending on the presence of metabolites, pharmacokinetics of the drug (eg, immediate release vs. sustained release formulations), and patient variables [37]. Additionally, a urine toxicology screen for amphetamines typically tests for amphetamines, racemic compounds such as dextroamphetamine and methamphetamine, and illicit compounds (ie, methylenedioxymethamphetamine), though there are many compounds that are structurally similar, such as weight loss agents, over-the-counter cold products, and other psychotropic medications, including methylphenidate, that can cause a false-positive result [37]. Urine toxicology should be obtained in conjunction with a thorough evaluation of patients’ alcohol and drug use patterns. These 2 components are essential to the accurate diagnosis and formulation of a comprehensive treatment plan. As noted above, stimulant medication misuse and alcohol and illicit drug use are highly comorbid and should be carefully and thoroughly assessed.
Psychiatric Comorbidity
ADHD
The prevalence of ADHD is higher among individuals with substance use disorders [38]. As noted above, patients commonly report misuse of stimulant medication to enhance academic performance. One explanation may be that individuals misusing stimulants may be self-medicating undiagnosed ADHD [39]. The prevalence of ADHD among adults is 4.1% and it is more common in men than women with a ratio of up to 6:1 [40]. Several studies have found that individuals with misuse of stimulant medications endorse symptoms of ADHD, including higher levels of inattention and hyperactivity [41]. Twelve percent of participants in one study that endorsed stimulant medication misuse also endorsed the belief they had ADHD [7]. Another study found that individuals with higher baseline self-reported ADHD symptoms were also more likely to misuse stimulants [42]. The majority of individuals with ADHD have been found to take medications appropriately, though there is a minority, often with comorbid conduct disorder or other substance use disorders, that divert or misuse stimulant medications, most often the immediate release formulations [43,44].
Accurate diagnosis of ADHD in patients with substance use disorders can be challenging given the symptom overlap between intoxication and withdrawal syndromes of substances and symptoms of ADHD. Evaluating for ADHD is an important part of a thorough assessment and can be completed in several ways. The gold standard is with a standardized diagnostic tool such as the Connors Adult ADHD Diagnostic Interview for DSM-IV (CAADID) [45], which can be time consuming for a clinician and would likely involve referral to a psychologist for completion. Other scales have been examined, and the Connors Adult ADHD Rating Scale (CAARS) has been found to closely agree with the CAADID when both are administered [45]. Other scales are available, including the Wender Utah Rating Scales (WURS) and the Adult ADHD Self-Report Scale (ASRS), and have been found to have adequate sensitivity and specificity [45]. In an international study, the ASRS, a relatively brief instrument, showed encouraging results with 84% sensitivity and 66% specificity in detecting ADHD upon entry into substance disorder treatment for treatment-seeking patients [46]. When diagnosing ADHD among adults, it is crucial not to rely only on self-reported symptoms. A thorough childhood history of ADHD symptom presentation should be collected from a parent or caregiver, and collateral concurrent report should be collected from someone who knows the patient well, such as an employer, close friend, significant other, or parent. Valid diagnosis, whether ADHD is present or not, is of utmost importance in this population as individuals with comorbid substance use disorders and ADHD tend to have worse outcomes overall [47]. It is also important to appreciate that inaccurately diagnosing ADHD in individuals misusing stimulants could potentially diminish the importance of the diagnosis [48].
If ADHD is found, there are medications available that have a lower abuse potential compared to stimulant medications. Atomoxetine is the only FDA-approved nonstimulant for ADHD; off-label or second-line treatments include antidepressants, such as bupropion, venlafaxine, or tricyclic antidepressants, for which the data is limited, and clonidine [34,49,50]. If these therapies are not effective and, after careful consideration of risks and benefits, it is determined that a trial with a stimulant is needed, longer-acting formulations appear to be less abused [34,44]. Education for both the patient and his or her family should be provided on abuse and diversion potential and appropriate use and misuse [34,43,51]. Pill counts [43], regular office visits [52], and random urine toxicology screens [34] with informed interpretation of the screens may be helpful in deterring misuse or diversion. While medications are the mainstay of treatment for ADHD, there are several psychosocial interventions available, including cognitive behavioral therapy, coaching, and behavioral modification therapies [34].
Other Comorbidities
Other psychiatric comorbidities also should be explored. Studies have found a relation between depression and misuse of stimulant medication in that there is an increased likelihood of depression and thoughts of suicide among those that misuse stimulant medication and vice versa [23,24,53]. The National Survey on Drug Use and Health in 2012 found that, of those that misused stimulants, nearly 20% had serious thoughts of suicide over the past year [54]. As noted earlier, stimulant medication can affect sleep and appetite. Among those that report misuse of stimulant medication for weight loss, these individuals are more likely to report other eating-disordered behaviors [55]. Sleep quality is worse and sleep disturbance greater in those that misuse stimulant medication [32]. Other traits and behaviors that have been described in individuals that misuse stimulant medications include impulsivity [56,57], sensation seeking [20], perfectionism [58], and poor time management skills or procrastination [59].
Appropriate treatment (which may include pharmacologic, psychological, or academic accommodation components) for individuals with these psychiatric disorders or psychological symptoms may reduce the misuse of stimulant medications among college students, especially if these students are misusing in order to reduce their symptoms (ie, a self-medication hypothesis).
Treatment
There are currently no FDA-approved medications to treat stimulant medication misuse. In fact, studies exploring pharmacotherapy for stimulant medication misuse are limited. Most trials focus on stimulants such as cocaine or methamphetamine and not stimulant medications alone. Additionally, these trials primarily include only individuals that meet criteria for stimulant dependence. Various medications and medication classes have been examined for the treatment of stimulant dependence, including naltrexone, various antipsychotics, and various antidepressants including bupropion, modafanil, baclofen, ondansetron, and dexamphetamine, with little to no effect [60]. In a review of the literature, one study examined the use of naltrexone versus placebo for stimulant dependence in 80 treatment-seeking Swedish individuals [61]. The different types of stimulants on which these individuals were dependent were not clearly delineated, though the study authors noted that the major amphetamine abused in Sweden was the racemic mixture d/l amphetamine and not methamphetamine. Naltrexone was superior to placebo in this trial, as evidenced by higher percentage of amphetamine-free urine samples. A large majority of this sample used intravenously (65%–76%) and had been using between 6 to 8 years, limiting the applicability to individuals with stimulant medication misuse. At this time, investigation into evidence-based pharmacotherapies for stimulant medication misuse remains in the early stages.
Generally speaking, efficacious behavioral treatments, such as contingency management (CM), cognitive behavioral therapy (CBT), skills training, motivational interviewing (MI), relapse prevention, couples and family treatments, and drug counseling, exist for drug abuse [62]. CBT, cognitive therapy, CM, MI, and community reinforcement approach (CRA) [63,64] have been explored for stimulant dependence and are currently the primary interventions for amphetamine-type stimulant dependence [60]. Similar to pharmacotherapy studies, most psychotherapy studies to date have examined primarily cocaine and methamphetamine dependence and not misuse of stimulant medications. In fact, no studies examining psychotherapy for stimulant medication misuse were found by our group in a search using the PubMed database. Therefore, discussion of psychotherapeutic interventions that may be efficacious for stimulant medication misuse extrapolates outcomes from studies of stimulant dependence, appreciating this is an approximation and imprecise as there are significant differences between stimulant medication misusers and those dependent upon stimulants such as methamphetamine or cocaine. As such, in a review from 2009 [63], Vocci and colleagues compared psychotherapy studies for cocaine and methamphetamine dependence and concluded that CBT and CM were moderately effective and that adding CM to standard treatment may help improve outcomes. A study of 214 amphetamine users (including methamphetamine users), with the majority (70%) enrolled in a methadone maintenance program and a large proportion (58.9%) using amphetamines intravenously, found that either 2 or 4 sessions of CBT, along with self-help material, increased rate of abstinence at 6 months post-intervention compared to the use of self-help material alone [65]. Baker and colleagues [64] recommend a practical stepped approach to treatment for stimulant dependence, including conducting a thorough assessment, offering education and self-help materials, monitoring use and consequences of use, and then transitioning to more intensive psychosocial interventions if needed, which may be applicable to those with stimulant medication misuse and is clinically reasonable. Offering a psychosocial intervention may require referral to more specialized treatment services than can be offered in a general primary care clinic. Additionally, harm reduction techniques for stimulant medication misusers to reduce the medical and social consequences can be considered as well as prevention strategies and methods, which can be utilized in any treatment setting or in high-risk populations, such as college students.
Prevention Strategies for the Individual
The research findings summarized in this review suggest several specific strategies for preventing and reducing the misuse of stimulant medication among college students, a high-risk population. First, college students with a prescription for stimulant medication play a critical role. Not only do these students have a high rate of misuse themselves [28,66], but they are also the most common source from which other students obtain stimulant medication to misuse [11,67]. It is therefore important for physicians who provide college students with prescriptions for stimulant medications to discuss the possible consequences of misusing or diverting medication, including potential negative health outcomes, legal consequences, and on-campus repercussions, for students caught diverting stimulant medications. These practitioners should also monitor their patients for signs of diversion, such as finishing a prescription early, doctor shopping, or urine drug screen which is negative for the prescribed substance. Utilizing a prescription monitoring program to access information on the prescribing and filling of controlled substances can be a valuable tool in detecting multiple concomitant prescriptions for stimulant medications, number of providers writing stimulant medication, and information on the use of other prescribed controlled medications. Providers should also discuss safe storage of stimulant medications with patients, particularly if the student is currently living in a dorm setting or another community-type setting with the potential for lots of individuals in and around their personal belongings. Additionally, providers may wish to consider dispensing a small amount at each office visit until the patient has established responsible use of the medication, particularly if there are other findings or comorbidities that perhaps increase their risk of misuse. Pill counts and frequent office visits, as noted earlier, may also help prevent diversion.
Perceived risk/harm associated with the use of stimulant medications has been negatively related to misuse [18,20]. If college students were more aware of the risks associated with stimulant medication misuse, with regards to both health and legal consequences, fewer students may choose to misuse stimulants. Educating patients and their families about the abuse potential of stimulants, as well as consequences of misuse such as psychosis and agitation, when prescriptions are given for stimulant medication, may help address the misperception that stimulant medications are benign, safe and without adverse consequences.
College Policy Changes for Prevention of Misuse
Policy changes on college campuses could also help to reduce diversion of stimulant medications. For instance, education about the risks associated with stimulant medication misuse could be incorporated into other alcohol and drug prevention programs that are already in place at colleges and universities. Many colleges/universities require all first-year students to complete an online substance use education/prevention/assessment tool. Some of these, such as AlcoholEdu and The Alcohol eCHECKUP TO GO have demonstrated some success in reducing college student alcohol use in follow-up evaluations [68]. Information about misuse of stimulant medication could be included in these existing programs. Moreover, members of certain organizations (eg, fraternities or sororities) that are known for an increased risk of substance use/abuse among members are also sometimes required by their national chapters or host colleges/universities to complete a “risk management” class, which addresses behaviors such as binge drinking and drunk driving. Since one of the demographic factors most strongly related to stimulant medication misuse is Greek organization membership [14], presenting information about stimulant medication misuse to these groups during these classes could help reduce misuse on college campuses.
Finally, the most commonly reported motives for misuse of stimulant medications among college students are academic in nature (eg, to study more, to concentrate better) [16], and many students who misuse for these reasons feel the desired effect is achieved. Colleges and universities may need to improve the identification of students who are in need of academic assistance/supports and offer these interventions earlier in students’ college careers to prevent stimulant medication misuse as a “quick fix.” Such interventions may include teaching students skills such as note-taking and academic goal setting and educating students about the link between sleep deprivation and poor concentration [69].
Summary
Health care providers, particularly those that see adolescent or college-aged individuals, need to be informed about stimulant medication indications, risks, benefits, and side effects and aware and attuned to problems associated with stimulant medication diversion and misuse. Diagnosing ADHD can be invaluable for individuals with the disorder, thus the ability to perform a thorough and accurate assessment is important; equally important is the ability to assess when ADHD is not present. Education and prevention strategies to prevent misuse and diversion should be provided if stimulant medications are indicated. College programs and policies can also utilize prevention strategies, provide education to students, and assist those with academic difficulties. Comorbidities are common and should be explored thoroughly as they may play a role in continued stimulant medication misuse and outcomes. Various treatment techniques and modalities can be explored further with each patient, based on the individual and their particular needs.
Corresponding author: Kate Flory, Univ. of South Carolina, Dept. of Psychology, Barnwell College, Columbia, SC 29208, [email protected].
Funding/support: Work on this paper was supported by a University of South Carolina Honors College Exploration Scholar Award and a University of South Carolina Magellan Fellowship, both awarded to Kari Benson.
Financial disclosures: None.
Author contributions: conception and design, KF, RAP, KB; drafting of article, KF, RAP, KB; critical revision of the article, KF, RAP, KB; literature search, KB.
From the University of South Carolina, Columbia, SC.
Abstract
- Objective: To provide a summary of the existing research on the characteristics of college students who report misusing prescription stimulant medications, to offer a set of clinical recommendations for practitioners, and to offer several possible prevention strategies.
- Methods: Literature review and research-based recommendations for clinical practice and prevention.
- Results: Misuse of prescription stimulant medication among college students is a prevalent and growing problem. Significant risk factors for misuse of stimulant medication include being male, being a member of a college sorority or fraternity, struggling academically, having elevated symptoms of ADHD and/or depression, being a high sensation-seeker, and using/misusing alcohol, cigarettes, and/or other illicit drugs. Health care providers, particularly those that see adolescent or college-aged individuals, need to be informed about stimulant medication indications, risks, benefits, and side effects and aware and attuned to problems associated with stimulant medication diversion and misuse. Suggestions for preventing misuse and diversion of prescription stimulant medications, including strategies for the individual and potential policy changes on college campuses, are offered.
- Conclusions: Misuse and diversion of prescription stimulant medications is a growing concern among adolescents and young adults and should be addressed by health care practitioners. Additional research on effective intervention and prevention strategies is needed.
Prescription stimulant medications (eg, methylphenidate, amphetamines) are typically used for the treatment of attention-deficit/hyperactivity disorder (ADHD) to increase attentiveness, decrease distractibility, and improve daily functioning. Prescriptions for stimulant medications are on the rise; between 2002 and 2010, the number of prescriptions for ADHD medications for youth under 18 increased 46% [1].
A recent review of ADHD diagnosis among college students estimated a prevalence rate of 2% to 8% [2]. More individuals with ADHD are matriculating to college than in the past [3,4], as more supports have been put in place for college students diagnosed with ADHD, including improved educational/organizational treatments and accommodations [2]. Many college students with ADHD also use prescription stimulant medications as part of their treatment plan; McCabe, Teter, and Boyd reported that 2.2% of college students had prescriptions for stimulant medications annually [5].
As the number of individuals of all ages with stimulant medication prescriptions increase, more individuals without prescriptions are gaining access to stimulant medications. In a survey of college students with medication prescriptions, stimulants were the most commonly diverted medication, with 61.7% of students with these prescriptions reporting having shared or sold their medication at least once [6]. Studies report that as many as 43% of college students have misused stimulant medication in their lifetime [7], though prevalence rates vary by study. Throughout this review, “misuse of stimulant medication” refers to using prescription stimulant medications without a prescription or using more stimulant medication than prescribed (ie, a higher or more frequent dosage).
Given the ease with which college students are able to obtain stimulant medications, the alarming prevalence of stimulant medication misuse among this population, and the potentially serious health risks associated with misuse of stimulant medication (especially when combined with other substances, such as alcohol, that are commonly used by college students), there is a need to both better understand and ultimately reduce the misuse of stimulant medication among college students. Thus, the purpose of this paper is threefold. First, we provide a summary of the existing research literature on the characteristics of college students who report misusing stimulant medication. Second, we offer a set of clinical recommendations for practitioners, which includes stimulant medication indications, risks, benefits, and side effects, along with problems associated with stimulant medication diversion and misuse. Finally, we offer several prevention strategies, including strategies for the individual as well as several suggestions for changing policies on college campuses to prevent stimulant diversion and misuse. Importantly, although our literature review addresses prescription stimulant misuse among college students, our clinical recommendations are also appropriate for adolescents and young adults not enrolled in college.
Summary of the Literature
The following summary is based on a comprehensive search of the existing research literature on misuse of stimulant medication among college students, which ultimately identified 30 relevant studies using 21 unique samples. A study was included if: (1) the main focus of the study was misuse of stimulant medication, (2) it was a peer-reviewed, empirical study using quantitative data analytic techniques, (3) it was written in English, (4) only undergraduate students were included in the sample, (5) it did not focus on only one type of stimulant medication (eg, methylphenidate only), and (6) if the article discussed multiple prescription drug categories (eg, stimulants, opiates), the data must have been analyzed separately for each category. An extensive meta-analytic review of this literature will be published elsewhere (contact the corresponding author to request a reprint). The following is a brief summary of our findings.
Prevalence, Availability, and Demographic Characteristics
Among prevalence rates reported, lifetime rates of stimulant medication misuse were the most frequently reported, ranging from 8.1% [8] to 43% [7]. Rates of misuse of stimulant medications within the last year ranged from 5.3% [9] to 35.3% [10]. A number of the studies asked students how they obtained stimulant medications for misuse; peers were overwhelmingly the most common source for obtaining the medications. For example, DeSantis, Webb, and Noar [11] found that 91% of the undergraduates who were interviewed obtained stimulant medications from friends or significant others.
Perceived availability of stimulant medications was also measured in several studies. DeSantis, Webb, and Noar [11] found that 82% of students thought it was somewhat or very easy to obtain stimulant medication; however, Sharp and Rosén [12] found that only 55% of students thought it was somewhat or very easy to obtain stimulant medication. In another study that examined perceived availability, 37% of men and 29.2% of women agreed that they knew students who would provide them with stimulant medications [13].
Many of the studies reviewed examined the relation between particular demographic characteristics (eg, gender, race, socioeconomic status, religious affiliation, year in college, sorority or fraternity membership) and misuse of stimulant medication among college students. The vast majority of studies that examined gender as related to misuse of stimulant medication found that significantly more males misused stimulant medication than females. For example, one study found that 26% of males and 17.3% of females reported misusing stimulant medication [14]; another study found that 39% of males versus 30% of females reported misuse [11].
It is also clear from the existing literature that members of fraternities and sororities appear to be more at-risk for misuse of stimulant medication than non-Greek students. In multiple studies, Greek students had rates of misuse twice that of non-Greeks. For instance, 48% of Greeks misused in their lifetime compared to 22% of non-Greeks [11]; 12% of Greeks misused in the past year compared to 5% of non-Greeks [15]; and Greeks were 2.32 times more likely to initiate use than non-Greeks [9].
Unfortunately, results from studies examining other demographic characteristics (eg, race, socioeconomic status, religious affiliation, year in college) as related to misuse of stimulant medication are much less conclusive and these correlates therefore require further investigation.
Motives For Misuse and Perceived Risk
Researchers have also evaluated college students’ motives for misusing stimulant medication and the risks they associate with misuse. All of the studies that asked misusing students about their motives for misuse reported that the most commonly endorsed motives were related to academics. “To concentrate better while studying” [16], “to improve study skills” [17], “to stay awake to study longer” [11], and “to improve concentration” [18] were some of the most commonly endorsed motives in these studies. Nonacademic reasons, such as to get high, to prolong effects of alcohol and other drugs, and to lose weight, were less commonly endorsed [7,12,19]. In studies where participants were able to indicate multiple motives for misuse [16], very few students misused for only nonacademic reasons.
Several studies measured the relation between misuse of stimulant medication and perceived risk associated with misuse. Perceived risk was conceptualized as perceived harmfulness [20], perception of safety [14], concern with health risk [18], and the inverse of positive outcome expectancies [21]. These articles found that when college students perceive more risk or have less positive expectancies about stimulant medication misuse, they are less likely to misuse stimulant medication. For instance, those who associated stimulant medication misuse with low perceived harmfulness were over 10 times more likely to have used in the last year than those who associated misuse with high perceived harmfulness [20].
Academic Outcomes Associated with Misuse
Interestingly, despite academic motives being most common for college students who report misusing stimulant medication, a number of studies have found a negative association between academic outcomes and misuse of stimulant medication. For instance, nonusers reported an average grade-point average (GPA) of 3.28 compared to 3.16 for misusers [16]. Other research demonstrates that the lower the student’s GPA is, the greater the odds are of the student misusing stimulant medication [8]. Misuse is also significantly related to other detrimental academic behaviors such as skipping class and less studying [20,22].
Psychological Correlates of Misuse
Researchers have evaluated the relation between several different psychological variables and misuse of stimulant medication. The strongest association is between symptoms of ADHD and stimulant medication misuse. Studies are consistent in reporting a significant correlation between greater symptoms of ADHD and higher rates of misuse or a significant difference in rates of misuse between those who have an ADHD diagnosis and those who do not. One study found that 71.1% of stimulant medication misusers screened positive for adult ADHD symptoms [17]. Another study found that for every standard deviation increase in attention problems, the odds of becoming a stimulant misuser increased by 1.78 [9]. Two studies asked participants if they believed they had ADHD. Advokat, Guildry, and Martino found that 12% of misusers believed they had ADHD [7]. Twenty-nine percent of “self-diagnosers” reported misusing, compared to 11.4% of “non-diagnosers” in another study [18].
Although the literature base is smaller than for ADHD, several studies have suggested a significant difference in symptoms of depression between stimulant medication misusers and nonusers. Zullig and Divin [23] found that misusers were significantly more likely to feel very sad, feel depressed, and consider suicide than nonusers. More frequent misuse has also been shown to be significantly associated with depressed mood [24].
A number of studies demonstrate a clear association between high sensation-seeking and misuse of stimulant medication. These results are not surprising given the well-documented relation between sensation seeking and substance use [25–27]. One study found a significant interaction between sensation seeking and perceived harmfulness of misusing stimulant medication: those with high sensation seeking and low perceived harmfulness were most likely to misuse [20].
Other Substance Use Associated with Stimulant Misuse
Many of the reviewed studies found a positive correlation between misuse of stimulant medication and other substance use or a significant difference between stimulant misusers and nonusers in rates of other substance use. These findings held across all substances examined, including alcohol, cigarettes, marijuana, illicit stimulants (eg, ecstasy, cocaine, or amphetamines), and non-stimulant prescription medications. For instance, significant associations were found between misuse of stimulant medication and several alcohol-related constructs, such as binge drinking [28,29], problematic drinking behavior [30], or meeting the Diagnostic and Statistical Manual of Mental Disorders [21] criteria for alcohol abuse [22]. With respect to cigarettes, 50.3% of misusers were found to have smoked cigarettes in the last 6 months compared to 13.3% of nonusers [16]. Similar findings emerged for illicit drug use. One study found that 73.5% of stimulant medication misusers reported use of marijuana in the last 6 months, compared to 18.2% of nonusers [19], while another study found that 93% of misusers used marijuana in the last year compared to 34% of nonusers [5]. This same study found that 33% of stimulant medication misusers also reported cocaine use in the last year compared to 2% of stimulant nonusers [5]. Finally, many of the studies reviewed examined the association between other substance use in general and stimulant medication misuse. Results were striking; the odds of becoming a stimulant medication misuser increased by 3.81 for each standard deviation increase in the amount of other substance use [9].
Summary
The research literature reviewed in this section provides a descriptive characterization of which college students (and, by extension, adolescents and young adults not in college) may be at the greatest risk of misuse of stimulant medication. Significant risk factors include being male, being a member of a college sorority or fraternity, struggling academically, having elevated symptoms of ADHD and/or depression, being a high sensation-seeker, and using/misusing alcohol, cigarettes, and/or other illicit drugs. It is important to recognize that one, several, or many of these risk factors may be present in a given individual who is misusing stimulant medication. Moreover, there may be other risk factors not yet identified in the research literature. The following sections of this paper draw from the literature reviewed here to provide a number of clinical recommendations for reducing and preventing misuse of stimulant medications among college students, other young adults, and adolescents.
Clinical Recommendations
It is important for health care providers to be aware of the benefits and risks associated with stimulant medications, the prevalence of and risk factors for stimulant misuse, and the psychiatric, psychological, and medical comorbidities associated with the misuse of stimulant medication. Knowledge about stimulant medications, misuse of stimulant medications, and a thorough evaluation of the patient will enable health care providers to address the misuse, as well as any comorbidities or other factors that may contribute to stimulant medication misuse, either pharmacologically or through referral for more specified psychotherapeutic interventions.
Stimulant Medication Indications and Adverse Effects
Stimulant medications are efficacious for the treatment of ADHD and, when prescribed and used correctly, can improve attentiveness, decrease distractibility, and improve daily functioning in the short term [19]. When used by individuals without ADHD, patients may experience euphoria, stimulation, alertness, and are not likely to experience the cognitive benefits that those with ADHD receive [31]. Side effects can occur regardless of whether the individual is using the stimulant for ADHD, misusing, or is dependent, and include nervousness, headaches, tachycardia, poor appetite, depressed mood, and poor sleep [19,32]. Additionally, stimulant medications can cause psychosis, agitation, and hallucinations [31,33], which typically resolve after discontinuation of the stimulant within 2 to 6 days, though a longer time period to resolution has been reported [33]. Stimulant medications carry warnings about increased risk of sudden death, high blood pressure, cardiac arrest, and stroke, as well as a statement warning providers about abuse potential. Additionally, serious but rare medical complications, including seizures, tachycardia or dysrhythmias, and hyperthermia, can occur [31,34].
Physical Examination and Laboratory Data
Obtaining vital signs and performing a physical exam may reveal weight loss and an increase in heart rate or blood pressure. Methylphenidate and amphetamines are known to increase heart rate and blood pressure [35] and a recent study found an average increase in heart rate of 5.7 bpm and a 1.2–mm Hg increase in systolic and diastolic blood pressure in adults on stimulant medications compared to placebo [36]. No EKG abnormalities or changes are found with either methylphenidate or amphetamine [35]. Urine toxicology can be utilized to obtain further information if misuse is suspected. However, the clinician must be aware of the limitations of urine drug testing with stimulants [37]. The usual detection time for amphetamines is 48 hours from last use, though this may vary depending on the presence of metabolites, pharmacokinetics of the drug (eg, immediate release vs. sustained release formulations), and patient variables [37]. Additionally, a urine toxicology screen for amphetamines typically tests for amphetamines, racemic compounds such as dextroamphetamine and methamphetamine, and illicit compounds (ie, methylenedioxymethamphetamine), though there are many compounds that are structurally similar, such as weight loss agents, over-the-counter cold products, and other psychotropic medications, including methylphenidate, that can cause a false-positive result [37]. Urine toxicology should be obtained in conjunction with a thorough evaluation of patients’ alcohol and drug use patterns. These 2 components are essential to the accurate diagnosis and formulation of a comprehensive treatment plan. As noted above, stimulant medication misuse and alcohol and illicit drug use are highly comorbid and should be carefully and thoroughly assessed.
Psychiatric Comorbidity
ADHD
The prevalence of ADHD is higher among individuals with substance use disorders [38]. As noted above, patients commonly report misuse of stimulant medication to enhance academic performance. One explanation may be that individuals misusing stimulants may be self-medicating undiagnosed ADHD [39]. The prevalence of ADHD among adults is 4.1% and it is more common in men than women with a ratio of up to 6:1 [40]. Several studies have found that individuals with misuse of stimulant medications endorse symptoms of ADHD, including higher levels of inattention and hyperactivity [41]. Twelve percent of participants in one study that endorsed stimulant medication misuse also endorsed the belief they had ADHD [7]. Another study found that individuals with higher baseline self-reported ADHD symptoms were also more likely to misuse stimulants [42]. The majority of individuals with ADHD have been found to take medications appropriately, though there is a minority, often with comorbid conduct disorder or other substance use disorders, that divert or misuse stimulant medications, most often the immediate release formulations [43,44].
Accurate diagnosis of ADHD in patients with substance use disorders can be challenging given the symptom overlap between intoxication and withdrawal syndromes of substances and symptoms of ADHD. Evaluating for ADHD is an important part of a thorough assessment and can be completed in several ways. The gold standard is with a standardized diagnostic tool such as the Connors Adult ADHD Diagnostic Interview for DSM-IV (CAADID) [45], which can be time consuming for a clinician and would likely involve referral to a psychologist for completion. Other scales have been examined, and the Connors Adult ADHD Rating Scale (CAARS) has been found to closely agree with the CAADID when both are administered [45]. Other scales are available, including the Wender Utah Rating Scales (WURS) and the Adult ADHD Self-Report Scale (ASRS), and have been found to have adequate sensitivity and specificity [45]. In an international study, the ASRS, a relatively brief instrument, showed encouraging results with 84% sensitivity and 66% specificity in detecting ADHD upon entry into substance disorder treatment for treatment-seeking patients [46]. When diagnosing ADHD among adults, it is crucial not to rely only on self-reported symptoms. A thorough childhood history of ADHD symptom presentation should be collected from a parent or caregiver, and collateral concurrent report should be collected from someone who knows the patient well, such as an employer, close friend, significant other, or parent. Valid diagnosis, whether ADHD is present or not, is of utmost importance in this population as individuals with comorbid substance use disorders and ADHD tend to have worse outcomes overall [47]. It is also important to appreciate that inaccurately diagnosing ADHD in individuals misusing stimulants could potentially diminish the importance of the diagnosis [48].
If ADHD is found, there are medications available that have a lower abuse potential compared to stimulant medications. Atomoxetine is the only FDA-approved nonstimulant for ADHD; off-label or second-line treatments include antidepressants, such as bupropion, venlafaxine, or tricyclic antidepressants, for which the data is limited, and clonidine [34,49,50]. If these therapies are not effective and, after careful consideration of risks and benefits, it is determined that a trial with a stimulant is needed, longer-acting formulations appear to be less abused [34,44]. Education for both the patient and his or her family should be provided on abuse and diversion potential and appropriate use and misuse [34,43,51]. Pill counts [43], regular office visits [52], and random urine toxicology screens [34] with informed interpretation of the screens may be helpful in deterring misuse or diversion. While medications are the mainstay of treatment for ADHD, there are several psychosocial interventions available, including cognitive behavioral therapy, coaching, and behavioral modification therapies [34].
Other Comorbidities
Other psychiatric comorbidities also should be explored. Studies have found a relation between depression and misuse of stimulant medication in that there is an increased likelihood of depression and thoughts of suicide among those that misuse stimulant medication and vice versa [23,24,53]. The National Survey on Drug Use and Health in 2012 found that, of those that misused stimulants, nearly 20% had serious thoughts of suicide over the past year [54]. As noted earlier, stimulant medication can affect sleep and appetite. Among those that report misuse of stimulant medication for weight loss, these individuals are more likely to report other eating-disordered behaviors [55]. Sleep quality is worse and sleep disturbance greater in those that misuse stimulant medication [32]. Other traits and behaviors that have been described in individuals that misuse stimulant medications include impulsivity [56,57], sensation seeking [20], perfectionism [58], and poor time management skills or procrastination [59].
Appropriate treatment (which may include pharmacologic, psychological, or academic accommodation components) for individuals with these psychiatric disorders or psychological symptoms may reduce the misuse of stimulant medications among college students, especially if these students are misusing in order to reduce their symptoms (ie, a self-medication hypothesis).
Treatment
There are currently no FDA-approved medications to treat stimulant medication misuse. In fact, studies exploring pharmacotherapy for stimulant medication misuse are limited. Most trials focus on stimulants such as cocaine or methamphetamine and not stimulant medications alone. Additionally, these trials primarily include only individuals that meet criteria for stimulant dependence. Various medications and medication classes have been examined for the treatment of stimulant dependence, including naltrexone, various antipsychotics, and various antidepressants including bupropion, modafanil, baclofen, ondansetron, and dexamphetamine, with little to no effect [60]. In a review of the literature, one study examined the use of naltrexone versus placebo for stimulant dependence in 80 treatment-seeking Swedish individuals [61]. The different types of stimulants on which these individuals were dependent were not clearly delineated, though the study authors noted that the major amphetamine abused in Sweden was the racemic mixture d/l amphetamine and not methamphetamine. Naltrexone was superior to placebo in this trial, as evidenced by higher percentage of amphetamine-free urine samples. A large majority of this sample used intravenously (65%–76%) and had been using between 6 to 8 years, limiting the applicability to individuals with stimulant medication misuse. At this time, investigation into evidence-based pharmacotherapies for stimulant medication misuse remains in the early stages.
Generally speaking, efficacious behavioral treatments, such as contingency management (CM), cognitive behavioral therapy (CBT), skills training, motivational interviewing (MI), relapse prevention, couples and family treatments, and drug counseling, exist for drug abuse [62]. CBT, cognitive therapy, CM, MI, and community reinforcement approach (CRA) [63,64] have been explored for stimulant dependence and are currently the primary interventions for amphetamine-type stimulant dependence [60]. Similar to pharmacotherapy studies, most psychotherapy studies to date have examined primarily cocaine and methamphetamine dependence and not misuse of stimulant medications. In fact, no studies examining psychotherapy for stimulant medication misuse were found by our group in a search using the PubMed database. Therefore, discussion of psychotherapeutic interventions that may be efficacious for stimulant medication misuse extrapolates outcomes from studies of stimulant dependence, appreciating this is an approximation and imprecise as there are significant differences between stimulant medication misusers and those dependent upon stimulants such as methamphetamine or cocaine. As such, in a review from 2009 [63], Vocci and colleagues compared psychotherapy studies for cocaine and methamphetamine dependence and concluded that CBT and CM were moderately effective and that adding CM to standard treatment may help improve outcomes. A study of 214 amphetamine users (including methamphetamine users), with the majority (70%) enrolled in a methadone maintenance program and a large proportion (58.9%) using amphetamines intravenously, found that either 2 or 4 sessions of CBT, along with self-help material, increased rate of abstinence at 6 months post-intervention compared to the use of self-help material alone [65]. Baker and colleagues [64] recommend a practical stepped approach to treatment for stimulant dependence, including conducting a thorough assessment, offering education and self-help materials, monitoring use and consequences of use, and then transitioning to more intensive psychosocial interventions if needed, which may be applicable to those with stimulant medication misuse and is clinically reasonable. Offering a psychosocial intervention may require referral to more specialized treatment services than can be offered in a general primary care clinic. Additionally, harm reduction techniques for stimulant medication misusers to reduce the medical and social consequences can be considered as well as prevention strategies and methods, which can be utilized in any treatment setting or in high-risk populations, such as college students.
Prevention Strategies for the Individual
The research findings summarized in this review suggest several specific strategies for preventing and reducing the misuse of stimulant medication among college students, a high-risk population. First, college students with a prescription for stimulant medication play a critical role. Not only do these students have a high rate of misuse themselves [28,66], but they are also the most common source from which other students obtain stimulant medication to misuse [11,67]. It is therefore important for physicians who provide college students with prescriptions for stimulant medications to discuss the possible consequences of misusing or diverting medication, including potential negative health outcomes, legal consequences, and on-campus repercussions, for students caught diverting stimulant medications. These practitioners should also monitor their patients for signs of diversion, such as finishing a prescription early, doctor shopping, or urine drug screen which is negative for the prescribed substance. Utilizing a prescription monitoring program to access information on the prescribing and filling of controlled substances can be a valuable tool in detecting multiple concomitant prescriptions for stimulant medications, number of providers writing stimulant medication, and information on the use of other prescribed controlled medications. Providers should also discuss safe storage of stimulant medications with patients, particularly if the student is currently living in a dorm setting or another community-type setting with the potential for lots of individuals in and around their personal belongings. Additionally, providers may wish to consider dispensing a small amount at each office visit until the patient has established responsible use of the medication, particularly if there are other findings or comorbidities that perhaps increase their risk of misuse. Pill counts and frequent office visits, as noted earlier, may also help prevent diversion.
Perceived risk/harm associated with the use of stimulant medications has been negatively related to misuse [18,20]. If college students were more aware of the risks associated with stimulant medication misuse, with regards to both health and legal consequences, fewer students may choose to misuse stimulants. Educating patients and their families about the abuse potential of stimulants, as well as consequences of misuse such as psychosis and agitation, when prescriptions are given for stimulant medication, may help address the misperception that stimulant medications are benign, safe and without adverse consequences.
College Policy Changes for Prevention of Misuse
Policy changes on college campuses could also help to reduce diversion of stimulant medications. For instance, education about the risks associated with stimulant medication misuse could be incorporated into other alcohol and drug prevention programs that are already in place at colleges and universities. Many colleges/universities require all first-year students to complete an online substance use education/prevention/assessment tool. Some of these, such as AlcoholEdu and The Alcohol eCHECKUP TO GO have demonstrated some success in reducing college student alcohol use in follow-up evaluations [68]. Information about misuse of stimulant medication could be included in these existing programs. Moreover, members of certain organizations (eg, fraternities or sororities) that are known for an increased risk of substance use/abuse among members are also sometimes required by their national chapters or host colleges/universities to complete a “risk management” class, which addresses behaviors such as binge drinking and drunk driving. Since one of the demographic factors most strongly related to stimulant medication misuse is Greek organization membership [14], presenting information about stimulant medication misuse to these groups during these classes could help reduce misuse on college campuses.
Finally, the most commonly reported motives for misuse of stimulant medications among college students are academic in nature (eg, to study more, to concentrate better) [16], and many students who misuse for these reasons feel the desired effect is achieved. Colleges and universities may need to improve the identification of students who are in need of academic assistance/supports and offer these interventions earlier in students’ college careers to prevent stimulant medication misuse as a “quick fix.” Such interventions may include teaching students skills such as note-taking and academic goal setting and educating students about the link between sleep deprivation and poor concentration [69].
Summary
Health care providers, particularly those that see adolescent or college-aged individuals, need to be informed about stimulant medication indications, risks, benefits, and side effects and aware and attuned to problems associated with stimulant medication diversion and misuse. Diagnosing ADHD can be invaluable for individuals with the disorder, thus the ability to perform a thorough and accurate assessment is important; equally important is the ability to assess when ADHD is not present. Education and prevention strategies to prevent misuse and diversion should be provided if stimulant medications are indicated. College programs and policies can also utilize prevention strategies, provide education to students, and assist those with academic difficulties. Comorbidities are common and should be explored thoroughly as they may play a role in continued stimulant medication misuse and outcomes. Various treatment techniques and modalities can be explored further with each patient, based on the individual and their particular needs.
Corresponding author: Kate Flory, Univ. of South Carolina, Dept. of Psychology, Barnwell College, Columbia, SC 29208, [email protected].
Funding/support: Work on this paper was supported by a University of South Carolina Honors College Exploration Scholar Award and a University of South Carolina Magellan Fellowship, both awarded to Kari Benson.
Financial disclosures: None.
Author contributions: conception and design, KF, RAP, KB; drafting of article, KF, RAP, KB; critical revision of the article, KF, RAP, KB; literature search, KB.
1. Chai G, Governale L, Mcmahon AW, et al. Trends of outpatient prescription drug utilization in US children, 2002-2010. Pediatr 2012;130:23–31.
2. Dupaul GJ, Weyandt LL, O’dell SM, Varejao M. College students with ADHD: current status and future directions J Atten Disord 2009;13:234–50.
3. DuPaul G, Schaughency E, Weyandt L, et al. Self-report of ADHD symptoms in university students: Cross-gender and cross-national prevalence. J Learn Disabil 2001;34:370–9.
4. Wolf L. College students with ADHD and other hidden disorders: Outcomes and interventions. Ann NY Acad Arts Sci 2001;931:385–5.
5. McCabe S, Teter CJ, Boyd CJ. Medical use, illicit use, and diversion of abusable prescription drugs. J Am Coll Health 2006;54:269–78.
6. Garnier LM, Arria AM, Caldeira KM, et al. Sharing and selling of prescription medications in a college student sample. J Clin Psychiatry 2010;71:262–9.
7. Advokat CD, Guildry D, Martino L. Licit and illicit use of medications for attention-deficit hyperactivity disorder in undergraduate college students. J Am Coll Health 2008;56:601–6.
8. McCabe S, Teter CJ, Boyd CJ. Medical use, illicit use and diversion of prescription stimulant medication. J Psychoactive Drugs 2006;38:43–56.
9. Rabiner DL, Anastopoulos AD, Costello E, et al. Predictors of nonmedical ADHD medication use by college students. J Atten Disord 2010;13:640–8.
10. Graff Low K, Gendaszek AE. Illicit use of psychostimulants among college students: A preliminary study. Psychol Health Med 2002;7:283–7.
11. DeSantis AD, Webb EM, Noar SM. Illicit use of prescription ADHD medications on a college campus: A multimethodological approach. J Am Coll Health 2008;57:315–23.
12. Sharp JT, Rosén LA. Recreational stimulant use among college students. J Subst Use 2007;12:71–82.
13. Hall KM, Irwin MM, Bowman KA, et al. Illicit use of prescribed stimulant medication among college students. J Am Coll Health 2005;53:167–74.
14. Dussault CL, Weyandt LL. An examination of prescription stimulants misuse and psychological variables among sorority and fraternity college populations. J Atten Disord 2013;27:87–7.
15. McCabe SE. Misperceptions of non-medical prescription drug use: A web survey of college students. Addict Behav 2008;33:713–24.
16. Rabiner DL, Anastopoulos AD, Costello E, et al. Motives and perceived consequences of nonmedical ADHD medication use by college students: Are students treating themselves for attention problems? J Atten Disord 2009;13:259–70.
17. Peterkin AL, Crone CC, Sheridan MJ, Wise TN. Cognitive performance enhancement: Misuse or self-treatment? J Atten Disord 2011;15:263–8.
18. Judson R, Langdon SW. Illicit use of prescription stimulants among college students: Prescription status, motives, theory of planned behaviour, knowledge and self-diagnostic tendencies. Psychol Health Med 2009;14:97–104.
19. Volkow ND, Swanson JM. Adult attention deficit-hyperactivity disorder. N Engl J Med 2013;369:1935–44.
20. Arria AM, Caldeira KM, Vincent KB, et al. Perceived harmfulness predicts nonmedical use of prescription drugs among college students: Interactions with sensation-seeking. Prev Science 2008;9:191–201.
21. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. 2000.
22. Arria AM, Wilcox HC, Caldeira KM, et al. Dispelling the myth of “smart drugs”: Cannabis and alcohol use problems predict nonmedical use of prescription stimulants for studying. Addict Behav 2013;38:1643–50.
23. Zullig KJ, Divin AL. The association between non-medical prescription drug use, depressive symptoms, and suicidality among college students. Addict Behav 2012;37:890–9.
24. Teter CJ, Falone AE, Cranford JA, et al. Nonmedical use of prescription stimulants and depressed mood among college students: Frequency and routes of administration. J Subst Abuse Treat 2010;38:292–8.
25. Pedersen W. Mental health, sensation seeking and drug use patterns: a longitudinal study. Br J Addict 1991;86:195–204.
26. Jaffe LT, Archer RP. The prediction of drug use among college students from MMPI, MCMI, and sensation seeking scales. J Pers Assess 1987;51:243–53.
27. Martins SS, Storr CL, Alexandre PK, Chilcoat HD. Adolescent ecstasy and other drug use in the National Survey of Parents and Youth: The role of sensation-seeking, parental monitoring and peer’s drug use. Addict Behav 2008;33:919–33.
28. Sepúlveda DR, Thomas LM, McCabe S, et al. Misuse of prescribed stimulant medication for ADHD and associated patterns of substance use: Preliminary analysis among college students. J Pharm Pract 2011;24:551–60.
29. Teter CJ, McCabe SE, Cranford JA, et al. Prevalence and motives for illicit use of prescription stimulants in an undergraduate student sample. J Am Coll Health 2005;53:253–62.
30. Lookatch SJ, Dunne EM, Katz EC. Predictors of nonmedical use of prescription stimulants. J Psychoactive Drugs 2012;44:86–91.
31. Looby A, Kassman KT, Earlywine M. Do negative stimulant-related attitudes vary for prescription stimulants and cocaine among college students? Addict Behav 2014;39:1100–5.
32. Clegg-Kraynok MM, McBean AL, Montgomery-Downs HE. Sleep quality and characteristics of college students who use prescription psychostimulants nonmedically. Sleep Med 2011;12:598–602.
33. Ross RG. Psychotic and manic-like symptoms during stimulant treatment of attention deficit hyperactivity disorder. Am J Psychiatry 2006;163:1149–52.
34. Mariani JJ, Levin FR. Treatment strategies for co-occurring ADHD and substance use disorders. Am J Addict 2007;16:45–56.
35. Vetter VL, Elia J, Erickson C, et al. Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/hyperactivity disorder: A scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee and the Council on Cardiovascular Nursing. Circulation 2008;117:2407–23.
36. Mick E, McManus DD, Goldberg RJ. Meta-analysis of increased heart rate and blood pressure associated with CNS stimulant treatment of ADHD in adults. Eur Neuropsychopharmacol 2013;23:534–41.
37. Moeller KE, Lee KC, Kissack JC. Urine drug screening: Practical guide for clinicians. Mayo Clin Proc 2008;83:66–76.
38. Van de Glind G, Konstenius M, Koeter MWJ, et al. Variability in the prevalence of adult ADHD in treatment seeking substance use disorder patients: Results from an international multi-center study exploring DSM-IV and DSM-5 criteria. Drug Alcohol Depend 2014;134:158–66.
39. Bukstein O. Substance abuse in patients with attention-deficit/hyperactivity disorder. Medscape J Med 2008;10:24.
40. Kessler RC, Adler L, Barkley R, et al. The prevalence and comorbidity of adult ADHD in the United States: Results from the National Comorbidity Survey Replication. Am J Psychiatry 2006;163:716–23.
41. Hartung CM, Canu WH, Cleveland CS, et al. Stimulant medication use in college students: Comparison of appropriate users, misusers, and nonusers. Psychol Addict Behav 2014;27:832.
42. Upadhyaya HP. Managing attention-deficit/hyperactivity disorder in the presence of substance use disorder. J Clin Psychiatry 2007;68:23–30.
43. Wilens TE, Gignac M, Swezey A, et al. Characteristics of adolescents and young adults with ADHD who divert or misuse their prescribed medications. J Am Acad Child Adolesc Psychiatry 2006;45:408–14.
44. Wilens TE, Adler LA, Adams J, et al. Misuse and diversion of stimulants prescribed for ADHD: A systematic review of the literature. J Am Acad Child Adolesc Psychiatry 2008;47:21–31.
45. Dakwa E, Mahony A, Pavlicova M, et al. The utility of attention-deficit/hyperactivity disorder screening instruments in individuals seeking treatment for substance use disorders. J Clin Psychiatry 2012;73:1372–8.
46. Van de Glind G, Van den Brink W, Koeter. Validity of the Adult ADHD Self-Report Scale (ASRS) as a screener for adult ADHD in treatment seeking substance use disorder patients. Drug Alcohol Depend 2013;132:587–96.
47. Levin FR. Diagnosing attention-deficity/hyperactivity disorder in patients with substance use disorders. J Clin Psychiatry 2007;68:9–14.
48. Diller L. ADHD in the college student: Is anyone else worried? J Atten Disord. 2010;14:3-6.
49. Christman AK, Fermo JD, Markowitz JS. Atomoxetine, a novel treatment for attention-deficit/hyperactivity disorder. Pharmacotherapy 2004;24:1020–36.
50. Riggs P, Levin F, Green AI, Vocci F. Comorbid psychiatric and substance abuse disorders: Recent treatment research. Subst Abuse 2008;29:51–63.
51. Rabiner D L. Stimulant prescription cautions: Addressing misuse, diversion, and malingering. Curr Psychiatry Rep. 2013;15:375-383.
52. Manning JS. Strategies for managing the risks associated with ADHD medications. J Clin Psychiatry 2013;74:e19.
53. Markou A, Kosten TR, Koob GF. Neurobiological similarities in depression and drug dependence: A self-medication hypothesis. Neuropsychopharmacology 1998;18:135–74.
54. Results from the 2012 National Survey on Drug Use and Health: Mental Health Findings, NSDUH Series H-47. HHS Pub No. 13-4805. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2013.
55. Jeffers A, Benotsch EG, Koester S. Misuse of prescription stimulants for weight loss, psychosocial variables, and eating disordered behaviors. Appetite 2013;65:8–13.
56. Madden GJ, Bickel WK. Impulsivity: The behavioral and neurological science of discounting. 1st ed. Washington, DC: APA; 2010.
57. Stanford MS, Mathias CW, Dougherty DM, et al. Fifty years of the Barratt Impulsiveness Scale: An update and review. Pers Indiv Differ 2009;47:385–95.
58. Low K, Gendaszek AE. Illicit use of psychostimulants among college students: A preliminary study. Psychol Health Med 2002;7:283–7.
59. Moore DR, Burgard DA, Larson RG, Ferm M. Psychostimulant use among college students during periods of high and low stress: An interdisciplinary approach utilizing both self-report and unobtrusive chemical sample data. Addict Behav 2014;39:987–93.
60. Brensilver M, Heinzerling KG, Shoptaw S. Pharmacotherapy of amphetamine-type stimulant dependence: An update. Drug Alc Review 2013;32:449–60.
61. Jayaram-Lindstrom N, Hammarberg A, Beck O, Franck J. Naltrexone for the treatment of amphetamine dependence: A randomized, placebo-controlled trial. Am J Psychiatry 2008;165:1442–8.
62. Carroll KM, Onken LS. Behavioral therapies for drug abuse. Am J Psychiatry 2005;162:1452–60.
63. Vocci FJ, Montoya I. Psychological treatments for stimulant misuse, comparing and contrasting those for amphetamine dependence and those for cocaine dependence. Curr Opin Psychiatry 2009;22:263–8.
64. Baker A, Lee NK., Claire M, et al. Brief cognitive behavioral interventions for regular amphetamine users: a step in the right direction. Addict 2005;100:367–78.
65. Baker A, Lee NK, Claire M, et al. Drug use patterns and mental health of regular amphetamine users. Addict 2004;99:875–84.
66. Rabiner DL, Anastopoulos AD, Costello E, et al. The misuse and diversion of prescribed ADHD medications by college students. J Atten Disord 2009;13:259–70.
67. Garnier-Dykstra LM, Caldeira KM, Vincent KB, et al. Nonmedical use of prescription stimulants during college: Four year trends in exposure opportunity, use, motives, and sources. J Am Coll Health 2012;60:226–34.
68. Hustad JT, Barnett NP, Borsari B, Jackson KM. Web-based alcohol prevention for incoming college students: A randomized controlled trial. Addict Behav 2010;35:183–9.
69. Pilcher JJ, Walters AS. How sleep deprivation affects psychological variables related to college students’ cognitive performance. J Am Coll Health 1997;46:121–6.
1. Chai G, Governale L, Mcmahon AW, et al. Trends of outpatient prescription drug utilization in US children, 2002-2010. Pediatr 2012;130:23–31.
2. Dupaul GJ, Weyandt LL, O’dell SM, Varejao M. College students with ADHD: current status and future directions J Atten Disord 2009;13:234–50.
3. DuPaul G, Schaughency E, Weyandt L, et al. Self-report of ADHD symptoms in university students: Cross-gender and cross-national prevalence. J Learn Disabil 2001;34:370–9.
4. Wolf L. College students with ADHD and other hidden disorders: Outcomes and interventions. Ann NY Acad Arts Sci 2001;931:385–5.
5. McCabe S, Teter CJ, Boyd CJ. Medical use, illicit use, and diversion of abusable prescription drugs. J Am Coll Health 2006;54:269–78.
6. Garnier LM, Arria AM, Caldeira KM, et al. Sharing and selling of prescription medications in a college student sample. J Clin Psychiatry 2010;71:262–9.
7. Advokat CD, Guildry D, Martino L. Licit and illicit use of medications for attention-deficit hyperactivity disorder in undergraduate college students. J Am Coll Health 2008;56:601–6.
8. McCabe S, Teter CJ, Boyd CJ. Medical use, illicit use and diversion of prescription stimulant medication. J Psychoactive Drugs 2006;38:43–56.
9. Rabiner DL, Anastopoulos AD, Costello E, et al. Predictors of nonmedical ADHD medication use by college students. J Atten Disord 2010;13:640–8.
10. Graff Low K, Gendaszek AE. Illicit use of psychostimulants among college students: A preliminary study. Psychol Health Med 2002;7:283–7.
11. DeSantis AD, Webb EM, Noar SM. Illicit use of prescription ADHD medications on a college campus: A multimethodological approach. J Am Coll Health 2008;57:315–23.
12. Sharp JT, Rosén LA. Recreational stimulant use among college students. J Subst Use 2007;12:71–82.
13. Hall KM, Irwin MM, Bowman KA, et al. Illicit use of prescribed stimulant medication among college students. J Am Coll Health 2005;53:167–74.
14. Dussault CL, Weyandt LL. An examination of prescription stimulants misuse and psychological variables among sorority and fraternity college populations. J Atten Disord 2013;27:87–7.
15. McCabe SE. Misperceptions of non-medical prescription drug use: A web survey of college students. Addict Behav 2008;33:713–24.
16. Rabiner DL, Anastopoulos AD, Costello E, et al. Motives and perceived consequences of nonmedical ADHD medication use by college students: Are students treating themselves for attention problems? J Atten Disord 2009;13:259–70.
17. Peterkin AL, Crone CC, Sheridan MJ, Wise TN. Cognitive performance enhancement: Misuse or self-treatment? J Atten Disord 2011;15:263–8.
18. Judson R, Langdon SW. Illicit use of prescription stimulants among college students: Prescription status, motives, theory of planned behaviour, knowledge and self-diagnostic tendencies. Psychol Health Med 2009;14:97–104.
19. Volkow ND, Swanson JM. Adult attention deficit-hyperactivity disorder. N Engl J Med 2013;369:1935–44.
20. Arria AM, Caldeira KM, Vincent KB, et al. Perceived harmfulness predicts nonmedical use of prescription drugs among college students: Interactions with sensation-seeking. Prev Science 2008;9:191–201.
21. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. 2000.
22. Arria AM, Wilcox HC, Caldeira KM, et al. Dispelling the myth of “smart drugs”: Cannabis and alcohol use problems predict nonmedical use of prescription stimulants for studying. Addict Behav 2013;38:1643–50.
23. Zullig KJ, Divin AL. The association between non-medical prescription drug use, depressive symptoms, and suicidality among college students. Addict Behav 2012;37:890–9.
24. Teter CJ, Falone AE, Cranford JA, et al. Nonmedical use of prescription stimulants and depressed mood among college students: Frequency and routes of administration. J Subst Abuse Treat 2010;38:292–8.
25. Pedersen W. Mental health, sensation seeking and drug use patterns: a longitudinal study. Br J Addict 1991;86:195–204.
26. Jaffe LT, Archer RP. The prediction of drug use among college students from MMPI, MCMI, and sensation seeking scales. J Pers Assess 1987;51:243–53.
27. Martins SS, Storr CL, Alexandre PK, Chilcoat HD. Adolescent ecstasy and other drug use in the National Survey of Parents and Youth: The role of sensation-seeking, parental monitoring and peer’s drug use. Addict Behav 2008;33:919–33.
28. Sepúlveda DR, Thomas LM, McCabe S, et al. Misuse of prescribed stimulant medication for ADHD and associated patterns of substance use: Preliminary analysis among college students. J Pharm Pract 2011;24:551–60.
29. Teter CJ, McCabe SE, Cranford JA, et al. Prevalence and motives for illicit use of prescription stimulants in an undergraduate student sample. J Am Coll Health 2005;53:253–62.
30. Lookatch SJ, Dunne EM, Katz EC. Predictors of nonmedical use of prescription stimulants. J Psychoactive Drugs 2012;44:86–91.
31. Looby A, Kassman KT, Earlywine M. Do negative stimulant-related attitudes vary for prescription stimulants and cocaine among college students? Addict Behav 2014;39:1100–5.
32. Clegg-Kraynok MM, McBean AL, Montgomery-Downs HE. Sleep quality and characteristics of college students who use prescription psychostimulants nonmedically. Sleep Med 2011;12:598–602.
33. Ross RG. Psychotic and manic-like symptoms during stimulant treatment of attention deficit hyperactivity disorder. Am J Psychiatry 2006;163:1149–52.
34. Mariani JJ, Levin FR. Treatment strategies for co-occurring ADHD and substance use disorders. Am J Addict 2007;16:45–56.
35. Vetter VL, Elia J, Erickson C, et al. Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/hyperactivity disorder: A scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee and the Council on Cardiovascular Nursing. Circulation 2008;117:2407–23.
36. Mick E, McManus DD, Goldberg RJ. Meta-analysis of increased heart rate and blood pressure associated with CNS stimulant treatment of ADHD in adults. Eur Neuropsychopharmacol 2013;23:534–41.
37. Moeller KE, Lee KC, Kissack JC. Urine drug screening: Practical guide for clinicians. Mayo Clin Proc 2008;83:66–76.
38. Van de Glind G, Konstenius M, Koeter MWJ, et al. Variability in the prevalence of adult ADHD in treatment seeking substance use disorder patients: Results from an international multi-center study exploring DSM-IV and DSM-5 criteria. Drug Alcohol Depend 2014;134:158–66.
39. Bukstein O. Substance abuse in patients with attention-deficit/hyperactivity disorder. Medscape J Med 2008;10:24.
40. Kessler RC, Adler L, Barkley R, et al. The prevalence and comorbidity of adult ADHD in the United States: Results from the National Comorbidity Survey Replication. Am J Psychiatry 2006;163:716–23.
41. Hartung CM, Canu WH, Cleveland CS, et al. Stimulant medication use in college students: Comparison of appropriate users, misusers, and nonusers. Psychol Addict Behav 2014;27:832.
42. Upadhyaya HP. Managing attention-deficit/hyperactivity disorder in the presence of substance use disorder. J Clin Psychiatry 2007;68:23–30.
43. Wilens TE, Gignac M, Swezey A, et al. Characteristics of adolescents and young adults with ADHD who divert or misuse their prescribed medications. J Am Acad Child Adolesc Psychiatry 2006;45:408–14.
44. Wilens TE, Adler LA, Adams J, et al. Misuse and diversion of stimulants prescribed for ADHD: A systematic review of the literature. J Am Acad Child Adolesc Psychiatry 2008;47:21–31.
45. Dakwa E, Mahony A, Pavlicova M, et al. The utility of attention-deficit/hyperactivity disorder screening instruments in individuals seeking treatment for substance use disorders. J Clin Psychiatry 2012;73:1372–8.
46. Van de Glind G, Van den Brink W, Koeter. Validity of the Adult ADHD Self-Report Scale (ASRS) as a screener for adult ADHD in treatment seeking substance use disorder patients. Drug Alcohol Depend 2013;132:587–96.
47. Levin FR. Diagnosing attention-deficity/hyperactivity disorder in patients with substance use disorders. J Clin Psychiatry 2007;68:9–14.
48. Diller L. ADHD in the college student: Is anyone else worried? J Atten Disord. 2010;14:3-6.
49. Christman AK, Fermo JD, Markowitz JS. Atomoxetine, a novel treatment for attention-deficit/hyperactivity disorder. Pharmacotherapy 2004;24:1020–36.
50. Riggs P, Levin F, Green AI, Vocci F. Comorbid psychiatric and substance abuse disorders: Recent treatment research. Subst Abuse 2008;29:51–63.
51. Rabiner D L. Stimulant prescription cautions: Addressing misuse, diversion, and malingering. Curr Psychiatry Rep. 2013;15:375-383.
52. Manning JS. Strategies for managing the risks associated with ADHD medications. J Clin Psychiatry 2013;74:e19.
53. Markou A, Kosten TR, Koob GF. Neurobiological similarities in depression and drug dependence: A self-medication hypothesis. Neuropsychopharmacology 1998;18:135–74.
54. Results from the 2012 National Survey on Drug Use and Health: Mental Health Findings, NSDUH Series H-47. HHS Pub No. 13-4805. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2013.
55. Jeffers A, Benotsch EG, Koester S. Misuse of prescription stimulants for weight loss, psychosocial variables, and eating disordered behaviors. Appetite 2013;65:8–13.
56. Madden GJ, Bickel WK. Impulsivity: The behavioral and neurological science of discounting. 1st ed. Washington, DC: APA; 2010.
57. Stanford MS, Mathias CW, Dougherty DM, et al. Fifty years of the Barratt Impulsiveness Scale: An update and review. Pers Indiv Differ 2009;47:385–95.
58. Low K, Gendaszek AE. Illicit use of psychostimulants among college students: A preliminary study. Psychol Health Med 2002;7:283–7.
59. Moore DR, Burgard DA, Larson RG, Ferm M. Psychostimulant use among college students during periods of high and low stress: An interdisciplinary approach utilizing both self-report and unobtrusive chemical sample data. Addict Behav 2014;39:987–93.
60. Brensilver M, Heinzerling KG, Shoptaw S. Pharmacotherapy of amphetamine-type stimulant dependence: An update. Drug Alc Review 2013;32:449–60.
61. Jayaram-Lindstrom N, Hammarberg A, Beck O, Franck J. Naltrexone for the treatment of amphetamine dependence: A randomized, placebo-controlled trial. Am J Psychiatry 2008;165:1442–8.
62. Carroll KM, Onken LS. Behavioral therapies for drug abuse. Am J Psychiatry 2005;162:1452–60.
63. Vocci FJ, Montoya I. Psychological treatments for stimulant misuse, comparing and contrasting those for amphetamine dependence and those for cocaine dependence. Curr Opin Psychiatry 2009;22:263–8.
64. Baker A, Lee NK., Claire M, et al. Brief cognitive behavioral interventions for regular amphetamine users: a step in the right direction. Addict 2005;100:367–78.
65. Baker A, Lee NK, Claire M, et al. Drug use patterns and mental health of regular amphetamine users. Addict 2004;99:875–84.
66. Rabiner DL, Anastopoulos AD, Costello E, et al. The misuse and diversion of prescribed ADHD medications by college students. J Atten Disord 2009;13:259–70.
67. Garnier-Dykstra LM, Caldeira KM, Vincent KB, et al. Nonmedical use of prescription stimulants during college: Four year trends in exposure opportunity, use, motives, and sources. J Am Coll Health 2012;60:226–34.
68. Hustad JT, Barnett NP, Borsari B, Jackson KM. Web-based alcohol prevention for incoming college students: A randomized controlled trial. Addict Behav 2010;35:183–9.
69. Pilcher JJ, Walters AS. How sleep deprivation affects psychological variables related to college students’ cognitive performance. J Am Coll Health 1997;46:121–6.
CHMP recommends bortezomib for MCL

The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended the approval of bortezomib (Velcade) in combination with rituximab, cyclophosphamide, doxorubicin, and prednisone (VR-CAP) to treat adults with previously untreated mantle cell lymphoma (MCL) who are unsuitable for hematopoietic stem cell transplant.
Bortezomib is already approved in the European Union to treat multiple myeloma, either as monotherapy or in combination with other treatment regimens.
The CHMP’s decision to expand the approved use of bortezomib is based on data from the phase 3 LYM-3002 study. Results from this trial were presented at the 2014 ASCO Annual Meeting (abstract 8500).
LYM-3002 included 487 patients newly diagnosed with MCL who were ineligible, or not considered, for transplant. Patients were randomized to receive VR-CAP or R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone).
The VR-CAP regimen significantly improved progression-free survival (PFS), the primary endpoint, when compared to R-CHOP.
According to an independent review committee, there was a 59% improvement in PFS for the VR-CAP arm compared to the R-CHOP arm, with median PFS times of 24.7 months and 14.4 months, respectively (hazard ratio=0.63; P<0.001).
Study investigators reported a 96% increase in PFS with VR-CAP compared to R-CHOP, with median PFS times of 30.7 months and 16.1 months, respectively (hazard ratio=0.51, P<0.001).
VR-CAP was associated with additional, but manageable, toxicity when compared to R-CHOP. Serious adverse events (AE) were reported in 38% and 30% of patients, respectively. And grade 3 or higher AEs were reported in 93% and 85%, respectively.
Treatment discontinuation due to AEs occurred in 9% of patients in the VR-CAP arm and 7% in the R-CHOP arm. On-treatment, drug-related deaths occurred in 2% and 3%, respectively.
The CHMP’s positive opinion will be reviewed by the European Commission, which has the authority to grant a label extension for medicines in the European Economic Area. A final decision on the use of bortezomib in MCL is expected early next year. ![]()
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended the approval of bortezomib (Velcade) in combination with rituximab, cyclophosphamide, doxorubicin, and prednisone (VR-CAP) to treat adults with previously untreated mantle cell lymphoma (MCL) who are unsuitable for hematopoietic stem cell transplant.
Bortezomib is already approved in the European Union to treat multiple myeloma, either as monotherapy or in combination with other treatment regimens.
The CHMP’s decision to expand the approved use of bortezomib is based on data from the phase 3 LYM-3002 study. Results from this trial were presented at the 2014 ASCO Annual Meeting (abstract 8500).
LYM-3002 included 487 patients newly diagnosed with MCL who were ineligible, or not considered, for transplant. Patients were randomized to receive VR-CAP or R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone).
The VR-CAP regimen significantly improved progression-free survival (PFS), the primary endpoint, when compared to R-CHOP.
According to an independent review committee, there was a 59% improvement in PFS for the VR-CAP arm compared to the R-CHOP arm, with median PFS times of 24.7 months and 14.4 months, respectively (hazard ratio=0.63; P<0.001).
Study investigators reported a 96% increase in PFS with VR-CAP compared to R-CHOP, with median PFS times of 30.7 months and 16.1 months, respectively (hazard ratio=0.51, P<0.001).
VR-CAP was associated with additional, but manageable, toxicity when compared to R-CHOP. Serious adverse events (AE) were reported in 38% and 30% of patients, respectively. And grade 3 or higher AEs were reported in 93% and 85%, respectively.
Treatment discontinuation due to AEs occurred in 9% of patients in the VR-CAP arm and 7% in the R-CHOP arm. On-treatment, drug-related deaths occurred in 2% and 3%, respectively.
The CHMP’s positive opinion will be reviewed by the European Commission, which has the authority to grant a label extension for medicines in the European Economic Area. A final decision on the use of bortezomib in MCL is expected early next year. ![]()
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended the approval of bortezomib (Velcade) in combination with rituximab, cyclophosphamide, doxorubicin, and prednisone (VR-CAP) to treat adults with previously untreated mantle cell lymphoma (MCL) who are unsuitable for hematopoietic stem cell transplant.
Bortezomib is already approved in the European Union to treat multiple myeloma, either as monotherapy or in combination with other treatment regimens.
The CHMP’s decision to expand the approved use of bortezomib is based on data from the phase 3 LYM-3002 study. Results from this trial were presented at the 2014 ASCO Annual Meeting (abstract 8500).
LYM-3002 included 487 patients newly diagnosed with MCL who were ineligible, or not considered, for transplant. Patients were randomized to receive VR-CAP or R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone).
The VR-CAP regimen significantly improved progression-free survival (PFS), the primary endpoint, when compared to R-CHOP.
According to an independent review committee, there was a 59% improvement in PFS for the VR-CAP arm compared to the R-CHOP arm, with median PFS times of 24.7 months and 14.4 months, respectively (hazard ratio=0.63; P<0.001).
Study investigators reported a 96% increase in PFS with VR-CAP compared to R-CHOP, with median PFS times of 30.7 months and 16.1 months, respectively (hazard ratio=0.51, P<0.001).
VR-CAP was associated with additional, but manageable, toxicity when compared to R-CHOP. Serious adverse events (AE) were reported in 38% and 30% of patients, respectively. And grade 3 or higher AEs were reported in 93% and 85%, respectively.
Treatment discontinuation due to AEs occurred in 9% of patients in the VR-CAP arm and 7% in the R-CHOP arm. On-treatment, drug-related deaths occurred in 2% and 3%, respectively.
The CHMP’s positive opinion will be reviewed by the European Commission, which has the authority to grant a label extension for medicines in the European Economic Area. A final decision on the use of bortezomib in MCL is expected early next year. ![]()
Obokata fails to create STAP cells, resigns

Credit: Associated Press
After months of trying, Haruko Obokata, PhD, and a team of researchers at her institution, RIKEN, have failed to produce stimulus-triggered acquisition of pluripotency (STAP) cells.
Officials from RIKEN said they have accepted Dr Obokata’s resignation, and the institution has decided to end its efforts to recreate the STAP cell phenomenon.
Dr Obokata and her colleagues initially reported the creation of STAP cells in an article and a letter published in Nature last January. The researchers said they had induced pluripotency in somatic cells by exposing the cells to a low-pH environment.
Not long after the papers were published, members of the scientific community began to question the validity of the research.
So RIKEN launched an investigation, ultimately concluding that Dr Obokata was guilty of misconduct, and some of her colleagues—including the deceased Yoshiki Sasai, MD, PhD—were guilty of negligence.
RIKEN also called for the papers to be retracted, and, in July, they were.
Throughout these proceedings, Dr Obokata insisted the STAP cell phenomenon is real. To investigate this claim, RIKEN organized a group of researchers to recreate Dr Obokata’s experiments.
In August, the group reported initial results, saying their attempts had failed, but they would continue trying to create STAP cells until March 2015. Meanwhile, Dr Obokata was trying to recreate the STAP cell phenomenon on her own, under supervision.
Shinichi Aizawa, PhD, the leader of RIKEN’s team, explained the final results of their experiments, as well as Dr Obokata’s, in a press conference in Tokyo on Friday.
Dr Obokata was able to show a fluorescent phenomenon that indicates the possibility of pluripotency in cells, albeit at a very low rate. However, she could not confirm the pluripotency of STAP cells in mice.
The RIKEN team had similar results. So they have decided not to continue with the experiments.
RIKEN accepted Dr Obokata’s resignation, and a disciplinary committee has been discussing how they will reprimand her for research misconduct. RIKEN officials said they will make an announcement once the decision has been made. ![]()
Credit: Associated Press
After months of trying, Haruko Obokata, PhD, and a team of researchers at her institution, RIKEN, have failed to produce stimulus-triggered acquisition of pluripotency (STAP) cells.
Officials from RIKEN said they have accepted Dr Obokata’s resignation, and the institution has decided to end its efforts to recreate the STAP cell phenomenon.
Dr Obokata and her colleagues initially reported the creation of STAP cells in an article and a letter published in Nature last January. The researchers said they had induced pluripotency in somatic cells by exposing the cells to a low-pH environment.
Not long after the papers were published, members of the scientific community began to question the validity of the research.
So RIKEN launched an investigation, ultimately concluding that Dr Obokata was guilty of misconduct, and some of her colleagues—including the deceased Yoshiki Sasai, MD, PhD—were guilty of negligence.
RIKEN also called for the papers to be retracted, and, in July, they were.
Throughout these proceedings, Dr Obokata insisted the STAP cell phenomenon is real. To investigate this claim, RIKEN organized a group of researchers to recreate Dr Obokata’s experiments.
In August, the group reported initial results, saying their attempts had failed, but they would continue trying to create STAP cells until March 2015. Meanwhile, Dr Obokata was trying to recreate the STAP cell phenomenon on her own, under supervision.
Shinichi Aizawa, PhD, the leader of RIKEN’s team, explained the final results of their experiments, as well as Dr Obokata’s, in a press conference in Tokyo on Friday.
Dr Obokata was able to show a fluorescent phenomenon that indicates the possibility of pluripotency in cells, albeit at a very low rate. However, she could not confirm the pluripotency of STAP cells in mice.
The RIKEN team had similar results. So they have decided not to continue with the experiments.
RIKEN accepted Dr Obokata’s resignation, and a disciplinary committee has been discussing how they will reprimand her for research misconduct. RIKEN officials said they will make an announcement once the decision has been made. ![]()
Credit: Associated Press
After months of trying, Haruko Obokata, PhD, and a team of researchers at her institution, RIKEN, have failed to produce stimulus-triggered acquisition of pluripotency (STAP) cells.
Officials from RIKEN said they have accepted Dr Obokata’s resignation, and the institution has decided to end its efforts to recreate the STAP cell phenomenon.
Dr Obokata and her colleagues initially reported the creation of STAP cells in an article and a letter published in Nature last January. The researchers said they had induced pluripotency in somatic cells by exposing the cells to a low-pH environment.
Not long after the papers were published, members of the scientific community began to question the validity of the research.
So RIKEN launched an investigation, ultimately concluding that Dr Obokata was guilty of misconduct, and some of her colleagues—including the deceased Yoshiki Sasai, MD, PhD—were guilty of negligence.
RIKEN also called for the papers to be retracted, and, in July, they were.
Throughout these proceedings, Dr Obokata insisted the STAP cell phenomenon is real. To investigate this claim, RIKEN organized a group of researchers to recreate Dr Obokata’s experiments.
In August, the group reported initial results, saying their attempts had failed, but they would continue trying to create STAP cells until March 2015. Meanwhile, Dr Obokata was trying to recreate the STAP cell phenomenon on her own, under supervision.
Shinichi Aizawa, PhD, the leader of RIKEN’s team, explained the final results of their experiments, as well as Dr Obokata’s, in a press conference in Tokyo on Friday.
Dr Obokata was able to show a fluorescent phenomenon that indicates the possibility of pluripotency in cells, albeit at a very low rate. However, she could not confirm the pluripotency of STAP cells in mice.
The RIKEN team had similar results. So they have decided not to continue with the experiments.
RIKEN accepted Dr Obokata’s resignation, and a disciplinary committee has been discussing how they will reprimand her for research misconduct. RIKEN officials said they will make an announcement once the decision has been made. ![]()
Are These Leg Lesions and a Family History of Diabetes Related?
Several months ago, a 51-year-old woman first noticed brownish red lesions on her leg. She initially dismissed them as insect bites and regarded them as mostly a cosmetic concern. When the lesions failed to disappear after six months, her primary care provider referred the patient to dermatology. (In the interim, a friend did suggest ringworm as a diagnosis, but the OTC tolnaftate cream the patient tried had no effect.)
The patient claims to be quite healthy, which she attributes to walking several miles a day and working out at the gym every other day. She denies any shortness of breath, unexplained fever, or night sweats. There is no personal history of diabetes, but she has had glucose tolerance tests every six months for years because of a significant family history of the disease.

EXAMINATION
There are four intradermal shiny round nodules, averaging about 1.8 cm, on the upper anterior tibial area. The margins of the lesions are sharply drawn, and there is no surrounding erythema or increased warmth on palpation. The surfaces are quite uniform in texture.
Examination of her skin elsewhere reveals no noteworthy lesions. There is no palpable adenopathy in the groin on the affected side.
Results of a punch biopsy show interstitial and palisaded granulomas of the subcutaneous tissue, especially the dermis. Thickening of blood vessel walls and endothelial cell swelling are also noted.
What is the diagnosis?
DISCUSSION
Based on the appearance of the lesions, the patient’s family history, and the histopathologic findings, a diagnosis of necrobiosis lipoidica (NL) was made. When NL was first described in 1929, it was only seen in diabetic persons and thus was named necrobiosis lipoidica diabeticorum. By 1932, however, cases of NL were being reported in persons without diabetes—so the “diabeticorum” was dropped.
Only 0.3% of diabetic persons develop NL. In 15% of cases, NL precedes diabetes; in 60%, diabetes manifests first. Simultaneous diagnosis of both occurs about 25% of the time.
The cause of NL is still unknown. Most theories suggest it is related in some way to diabetes, since most persons with NL have a personal or family history of diabetes or register abnormal results to glucose tolerance testing. Furthermore, the microvascular changes seen in NL lesions are reminiscent of those seen in microangiopathic lesions in diabetic patients. Oddly enough, though, the presence or progression of NL does not correlate with how well controlled the patient’s diabetes is.
Other theories center on an autoimmune mechanism, based on demonstrable deposition of immunoglobulins, components of complement, and fibrinogen in vessel walls. High levels of TNF-a are found in many cases of NL, a fact that researchers are pursuing vigorously.
NL can manifest anywhere but is most common on the legs, where 75% of patients report no symptoms beyond a slight loss of sensation. The remaining 25% do report moderate to severe pain.
In terms of diagnosis, the appearance and history are sufficient in most cases. In this particular case, the lesions were fairly new and small, and the differential thus included such worrisome items as sarcoidosis or even Hansen’s disease. Less concerning differential items included granuloma annulare, other xanthomatous processes, and rheumatoid nodules.
In this case, a punch biopsy was necessary (the defect from which was closed carefully with interrupted sutures). Such procedures are discouraged in patients with larger and more advanced lesions, for fear of inducing a nonhealing wound. In fact, ulceration, usually from trauma, is the most feared complication of NL—and effective treatment is hard to come by.
This patient was treated with perilesional injection of triamcinolone suspension 10 mg per cc and given a prescription for 0.1% tacrolimus cream (to be applied twice daily). A follow-up visit was arranged for two months down the road. Her long-term prognosis is guarded, at best. Since she was already acutely aware of her risk for diabetes, there was no need for additional action in that arena.
Many other treatments have been tried for NL, with varying success, including dihydrochloroquine (Plaquenil and others) pentoxifylline, and TNF-a inhibitors.
TAKE-HOME LEARNING POINTS
• Early manifestations of necrobiosis lipoidica (NL) can be puzzling, and biopsy may be required for diagnosis.
• However, with advanced, obvious lesions, it is preferable to make the diagnosis of NL without biopsy, since punch biopsy can result in a nonhealing wound.
• Mature NL lesions become atrophic and yellowed, with marked telangiectasia formation on their surfaces.
• Just 0.3% of diabetic patients ever develop NL, but most affected persons have a family history of diabetes or an abnormal glucose tolerance test results, if not a personal history of diabetes.
Several months ago, a 51-year-old woman first noticed brownish red lesions on her leg. She initially dismissed them as insect bites and regarded them as mostly a cosmetic concern. When the lesions failed to disappear after six months, her primary care provider referred the patient to dermatology. (In the interim, a friend did suggest ringworm as a diagnosis, but the OTC tolnaftate cream the patient tried had no effect.)
The patient claims to be quite healthy, which she attributes to walking several miles a day and working out at the gym every other day. She denies any shortness of breath, unexplained fever, or night sweats. There is no personal history of diabetes, but she has had glucose tolerance tests every six months for years because of a significant family history of the disease.
EXAMINATION
There are four intradermal shiny round nodules, averaging about 1.8 cm, on the upper anterior tibial area. The margins of the lesions are sharply drawn, and there is no surrounding erythema or increased warmth on palpation. The surfaces are quite uniform in texture.
Examination of her skin elsewhere reveals no noteworthy lesions. There is no palpable adenopathy in the groin on the affected side.
Results of a punch biopsy show interstitial and palisaded granulomas of the subcutaneous tissue, especially the dermis. Thickening of blood vessel walls and endothelial cell swelling are also noted.
What is the diagnosis?
DISCUSSION
Based on the appearance of the lesions, the patient’s family history, and the histopathologic findings, a diagnosis of necrobiosis lipoidica (NL) was made. When NL was first described in 1929, it was only seen in diabetic persons and thus was named necrobiosis lipoidica diabeticorum. By 1932, however, cases of NL were being reported in persons without diabetes—so the “diabeticorum” was dropped.
Only 0.3% of diabetic persons develop NL. In 15% of cases, NL precedes diabetes; in 60%, diabetes manifests first. Simultaneous diagnosis of both occurs about 25% of the time.
The cause of NL is still unknown. Most theories suggest it is related in some way to diabetes, since most persons with NL have a personal or family history of diabetes or register abnormal results to glucose tolerance testing. Furthermore, the microvascular changes seen in NL lesions are reminiscent of those seen in microangiopathic lesions in diabetic patients. Oddly enough, though, the presence or progression of NL does not correlate with how well controlled the patient’s diabetes is.
Other theories center on an autoimmune mechanism, based on demonstrable deposition of immunoglobulins, components of complement, and fibrinogen in vessel walls. High levels of TNF-a are found in many cases of NL, a fact that researchers are pursuing vigorously.
NL can manifest anywhere but is most common on the legs, where 75% of patients report no symptoms beyond a slight loss of sensation. The remaining 25% do report moderate to severe pain.
In terms of diagnosis, the appearance and history are sufficient in most cases. In this particular case, the lesions were fairly new and small, and the differential thus included such worrisome items as sarcoidosis or even Hansen’s disease. Less concerning differential items included granuloma annulare, other xanthomatous processes, and rheumatoid nodules.
In this case, a punch biopsy was necessary (the defect from which was closed carefully with interrupted sutures). Such procedures are discouraged in patients with larger and more advanced lesions, for fear of inducing a nonhealing wound. In fact, ulceration, usually from trauma, is the most feared complication of NL—and effective treatment is hard to come by.
This patient was treated with perilesional injection of triamcinolone suspension 10 mg per cc and given a prescription for 0.1% tacrolimus cream (to be applied twice daily). A follow-up visit was arranged for two months down the road. Her long-term prognosis is guarded, at best. Since she was already acutely aware of her risk for diabetes, there was no need for additional action in that arena.
Many other treatments have been tried for NL, with varying success, including dihydrochloroquine (Plaquenil and others) pentoxifylline, and TNF-a inhibitors.
TAKE-HOME LEARNING POINTS
• Early manifestations of necrobiosis lipoidica (NL) can be puzzling, and biopsy may be required for diagnosis.
• However, with advanced, obvious lesions, it is preferable to make the diagnosis of NL without biopsy, since punch biopsy can result in a nonhealing wound.
• Mature NL lesions become atrophic and yellowed, with marked telangiectasia formation on their surfaces.
• Just 0.3% of diabetic patients ever develop NL, but most affected persons have a family history of diabetes or an abnormal glucose tolerance test results, if not a personal history of diabetes.
Several months ago, a 51-year-old woman first noticed brownish red lesions on her leg. She initially dismissed them as insect bites and regarded them as mostly a cosmetic concern. When the lesions failed to disappear after six months, her primary care provider referred the patient to dermatology. (In the interim, a friend did suggest ringworm as a diagnosis, but the OTC tolnaftate cream the patient tried had no effect.)
The patient claims to be quite healthy, which she attributes to walking several miles a day and working out at the gym every other day. She denies any shortness of breath, unexplained fever, or night sweats. There is no personal history of diabetes, but she has had glucose tolerance tests every six months for years because of a significant family history of the disease.
EXAMINATION
There are four intradermal shiny round nodules, averaging about 1.8 cm, on the upper anterior tibial area. The margins of the lesions are sharply drawn, and there is no surrounding erythema or increased warmth on palpation. The surfaces are quite uniform in texture.
Examination of her skin elsewhere reveals no noteworthy lesions. There is no palpable adenopathy in the groin on the affected side.
Results of a punch biopsy show interstitial and palisaded granulomas of the subcutaneous tissue, especially the dermis. Thickening of blood vessel walls and endothelial cell swelling are also noted.
What is the diagnosis?
DISCUSSION
Based on the appearance of the lesions, the patient’s family history, and the histopathologic findings, a diagnosis of necrobiosis lipoidica (NL) was made. When NL was first described in 1929, it was only seen in diabetic persons and thus was named necrobiosis lipoidica diabeticorum. By 1932, however, cases of NL were being reported in persons without diabetes—so the “diabeticorum” was dropped.
Only 0.3% of diabetic persons develop NL. In 15% of cases, NL precedes diabetes; in 60%, diabetes manifests first. Simultaneous diagnosis of both occurs about 25% of the time.
The cause of NL is still unknown. Most theories suggest it is related in some way to diabetes, since most persons with NL have a personal or family history of diabetes or register abnormal results to glucose tolerance testing. Furthermore, the microvascular changes seen in NL lesions are reminiscent of those seen in microangiopathic lesions in diabetic patients. Oddly enough, though, the presence or progression of NL does not correlate with how well controlled the patient’s diabetes is.
Other theories center on an autoimmune mechanism, based on demonstrable deposition of immunoglobulins, components of complement, and fibrinogen in vessel walls. High levels of TNF-a are found in many cases of NL, a fact that researchers are pursuing vigorously.
NL can manifest anywhere but is most common on the legs, where 75% of patients report no symptoms beyond a slight loss of sensation. The remaining 25% do report moderate to severe pain.
In terms of diagnosis, the appearance and history are sufficient in most cases. In this particular case, the lesions were fairly new and small, and the differential thus included such worrisome items as sarcoidosis or even Hansen’s disease. Less concerning differential items included granuloma annulare, other xanthomatous processes, and rheumatoid nodules.
In this case, a punch biopsy was necessary (the defect from which was closed carefully with interrupted sutures). Such procedures are discouraged in patients with larger and more advanced lesions, for fear of inducing a nonhealing wound. In fact, ulceration, usually from trauma, is the most feared complication of NL—and effective treatment is hard to come by.
This patient was treated with perilesional injection of triamcinolone suspension 10 mg per cc and given a prescription for 0.1% tacrolimus cream (to be applied twice daily). A follow-up visit was arranged for two months down the road. Her long-term prognosis is guarded, at best. Since she was already acutely aware of her risk for diabetes, there was no need for additional action in that arena.
Many other treatments have been tried for NL, with varying success, including dihydrochloroquine (Plaquenil and others) pentoxifylline, and TNF-a inhibitors.
TAKE-HOME LEARNING POINTS
• Early manifestations of necrobiosis lipoidica (NL) can be puzzling, and biopsy may be required for diagnosis.
• However, with advanced, obvious lesions, it is preferable to make the diagnosis of NL without biopsy, since punch biopsy can result in a nonhealing wound.
• Mature NL lesions become atrophic and yellowed, with marked telangiectasia formation on their surfaces.
• Just 0.3% of diabetic patients ever develop NL, but most affected persons have a family history of diabetes or an abnormal glucose tolerance test results, if not a personal history of diabetes.

Depletive Fluid Management Strategy During Weaning from Mechanical Ventilation Can Lower VAP Rates
Clinical question: What is the benefit associated with a depletive fluid management strategy on ventilator-associated complication (VAC) and ventilator-associated pneumonia (VAP) during weaning from mechanical ventilation?
Background: VAP is common in the ICU. Pulmonary edema predisposes patients to pneumonia by altering the alveolar microenvironment through enhancement of bacterial colonization and infectivity and a decrease in host bactericidal capacities. A fluid management strategy aimed at lowering lung fluid balance may prove useful in reducing both VAC and VAP.
Study design: Randomized controlled trial.
Setting: Nine ICUs in Europe and South America, between May 2007 and July 2009.
Synopsis: Data from the B-type Natriuretic Peptide for the Management of Weaning (BMW) trial was used to compare the cumulative incidence of VAC and VAP between the biomarker-driven, depletive fluid management group and the usual care group during the 14 days following randomization. The trial enrolled 304 randomized patients, 152 in each group.
Compared with usual care, the interventional strategy was associated with a higher proportion of patients receiving diuretics, in higher doses, resulting in a significantly more negative fluid balance during weaning and a shorter duration of mechanical ventilation. VAC (as defined by worsening oxygenation) occurred in 13.2% of patients during the 14 days following randomization: 17.8% in the usual care group and 8.6% in the interventional group. VAP occurred in 13.5% during the 14 days following randomization: 17.8% in the usual care group and 9.2% in the interventional group.
Bottom line: A biomarker-driven, depletive fluid strategy decreases the cumulative incidence of VAC and VAP.
Citation: Mekontso Dessap A, Katsahian S, Roche-Campo F, et al. Ventilator-associated pneumonia during weaning from mechanical ventilation: role of fluid management. Chest. 2014;146(1):58-65.
Visit our website for more physician reviews of HM-related research.
Clinical question: What is the benefit associated with a depletive fluid management strategy on ventilator-associated complication (VAC) and ventilator-associated pneumonia (VAP) during weaning from mechanical ventilation?
Background: VAP is common in the ICU. Pulmonary edema predisposes patients to pneumonia by altering the alveolar microenvironment through enhancement of bacterial colonization and infectivity and a decrease in host bactericidal capacities. A fluid management strategy aimed at lowering lung fluid balance may prove useful in reducing both VAC and VAP.
Study design: Randomized controlled trial.
Setting: Nine ICUs in Europe and South America, between May 2007 and July 2009.
Synopsis: Data from the B-type Natriuretic Peptide for the Management of Weaning (BMW) trial was used to compare the cumulative incidence of VAC and VAP between the biomarker-driven, depletive fluid management group and the usual care group during the 14 days following randomization. The trial enrolled 304 randomized patients, 152 in each group.
Compared with usual care, the interventional strategy was associated with a higher proportion of patients receiving diuretics, in higher doses, resulting in a significantly more negative fluid balance during weaning and a shorter duration of mechanical ventilation. VAC (as defined by worsening oxygenation) occurred in 13.2% of patients during the 14 days following randomization: 17.8% in the usual care group and 8.6% in the interventional group. VAP occurred in 13.5% during the 14 days following randomization: 17.8% in the usual care group and 9.2% in the interventional group.
Bottom line: A biomarker-driven, depletive fluid strategy decreases the cumulative incidence of VAC and VAP.
Citation: Mekontso Dessap A, Katsahian S, Roche-Campo F, et al. Ventilator-associated pneumonia during weaning from mechanical ventilation: role of fluid management. Chest. 2014;146(1):58-65.
Visit our website for more physician reviews of HM-related research.
Clinical question: What is the benefit associated with a depletive fluid management strategy on ventilator-associated complication (VAC) and ventilator-associated pneumonia (VAP) during weaning from mechanical ventilation?
Background: VAP is common in the ICU. Pulmonary edema predisposes patients to pneumonia by altering the alveolar microenvironment through enhancement of bacterial colonization and infectivity and a decrease in host bactericidal capacities. A fluid management strategy aimed at lowering lung fluid balance may prove useful in reducing both VAC and VAP.
Study design: Randomized controlled trial.
Setting: Nine ICUs in Europe and South America, between May 2007 and July 2009.
Synopsis: Data from the B-type Natriuretic Peptide for the Management of Weaning (BMW) trial was used to compare the cumulative incidence of VAC and VAP between the biomarker-driven, depletive fluid management group and the usual care group during the 14 days following randomization. The trial enrolled 304 randomized patients, 152 in each group.
Compared with usual care, the interventional strategy was associated with a higher proportion of patients receiving diuretics, in higher doses, resulting in a significantly more negative fluid balance during weaning and a shorter duration of mechanical ventilation. VAC (as defined by worsening oxygenation) occurred in 13.2% of patients during the 14 days following randomization: 17.8% in the usual care group and 8.6% in the interventional group. VAP occurred in 13.5% during the 14 days following randomization: 17.8% in the usual care group and 9.2% in the interventional group.
Bottom line: A biomarker-driven, depletive fluid strategy decreases the cumulative incidence of VAC and VAP.
Citation: Mekontso Dessap A, Katsahian S, Roche-Campo F, et al. Ventilator-associated pneumonia during weaning from mechanical ventilation: role of fluid management. Chest. 2014;146(1):58-65.
Visit our website for more physician reviews of HM-related research.
Antibiotic Therapy Guidelines for Pediatric Pneumonia Helpful, Not Hurtful
Hospitalists need not fear negative consequences when prescribing guideline-recommended antibiotic therapy for children hospitalized with community-acquired pneumonia (CAP), according to a recent study conducted at Cincinnati Children’s Hospital Medical Center (CCHMC).
"Guideline-recommended therapy for pediatric pneumonia did not result in different outcomes than nonrecommended [largely cephalosporin] therapy," lead author and CCHMC-based hospitalist Joanna Thomson MD, MPH, says in an email to The Hospitalist.
Published in the Journal of Hospital Medicine, the study followed the outcomes of 168 pediatric inpatients ages 3 months to 18 years who were prescribed empiric guideline-recommended therapy, which advises using an aminopenicillin first rather than a broad-spectrum antibiotic. The study focused on patients’ outcomes, specifically length of stay (LOS), total cost of hospitalization, and inpatient pharmacy costs, and found no difference in LOS or costs for patients treated according to guidelines compared with those whose treatment varied from the recommendations.
"Given growing concerns regarding antimicrobial resistance, it is pretty easy to extrapolate the benefits of using narrow-spectrum therapy, but we wanted to make sure that it wasn't resulting in negative unintended consequences," Dr. Thomson says. "Indeed, use of guideline-recommended therapy did not change our outcomes."
However, most patients hospitalized with CAP do not currently receive guideline-recommended therapy, according to Dr. Thomson. CCHMC had been one of those institutions overprescribing cephalosporin, with nearly 70% of children admitted with pneumonia receiving the antibiotic. That practice has since changed, she notes.
"The majority of hospitalized patients in the U.S. still receive broad-spectrum cephalosporins," Dr. Thomson says. "I suspect that this may partially be due to fears of unintended negative consequences. We should all be good stewards and prescribe guideline-recommended therapy whenever possible."
Visit our website for more information on antibiotic prescription practices.
Hospitalists need not fear negative consequences when prescribing guideline-recommended antibiotic therapy for children hospitalized with community-acquired pneumonia (CAP), according to a recent study conducted at Cincinnati Children’s Hospital Medical Center (CCHMC).
"Guideline-recommended therapy for pediatric pneumonia did not result in different outcomes than nonrecommended [largely cephalosporin] therapy," lead author and CCHMC-based hospitalist Joanna Thomson MD, MPH, says in an email to The Hospitalist.
Published in the Journal of Hospital Medicine, the study followed the outcomes of 168 pediatric inpatients ages 3 months to 18 years who were prescribed empiric guideline-recommended therapy, which advises using an aminopenicillin first rather than a broad-spectrum antibiotic. The study focused on patients’ outcomes, specifically length of stay (LOS), total cost of hospitalization, and inpatient pharmacy costs, and found no difference in LOS or costs for patients treated according to guidelines compared with those whose treatment varied from the recommendations.
"Given growing concerns regarding antimicrobial resistance, it is pretty easy to extrapolate the benefits of using narrow-spectrum therapy, but we wanted to make sure that it wasn't resulting in negative unintended consequences," Dr. Thomson says. "Indeed, use of guideline-recommended therapy did not change our outcomes."
However, most patients hospitalized with CAP do not currently receive guideline-recommended therapy, according to Dr. Thomson. CCHMC had been one of those institutions overprescribing cephalosporin, with nearly 70% of children admitted with pneumonia receiving the antibiotic. That practice has since changed, she notes.
"The majority of hospitalized patients in the U.S. still receive broad-spectrum cephalosporins," Dr. Thomson says. "I suspect that this may partially be due to fears of unintended negative consequences. We should all be good stewards and prescribe guideline-recommended therapy whenever possible."
Visit our website for more information on antibiotic prescription practices.
Hospitalists need not fear negative consequences when prescribing guideline-recommended antibiotic therapy for children hospitalized with community-acquired pneumonia (CAP), according to a recent study conducted at Cincinnati Children’s Hospital Medical Center (CCHMC).
"Guideline-recommended therapy for pediatric pneumonia did not result in different outcomes than nonrecommended [largely cephalosporin] therapy," lead author and CCHMC-based hospitalist Joanna Thomson MD, MPH, says in an email to The Hospitalist.
Published in the Journal of Hospital Medicine, the study followed the outcomes of 168 pediatric inpatients ages 3 months to 18 years who were prescribed empiric guideline-recommended therapy, which advises using an aminopenicillin first rather than a broad-spectrum antibiotic. The study focused on patients’ outcomes, specifically length of stay (LOS), total cost of hospitalization, and inpatient pharmacy costs, and found no difference in LOS or costs for patients treated according to guidelines compared with those whose treatment varied from the recommendations.
"Given growing concerns regarding antimicrobial resistance, it is pretty easy to extrapolate the benefits of using narrow-spectrum therapy, but we wanted to make sure that it wasn't resulting in negative unintended consequences," Dr. Thomson says. "Indeed, use of guideline-recommended therapy did not change our outcomes."
However, most patients hospitalized with CAP do not currently receive guideline-recommended therapy, according to Dr. Thomson. CCHMC had been one of those institutions overprescribing cephalosporin, with nearly 70% of children admitted with pneumonia receiving the antibiotic. That practice has since changed, she notes.
"The majority of hospitalized patients in the U.S. still receive broad-spectrum cephalosporins," Dr. Thomson says. "I suspect that this may partially be due to fears of unintended negative consequences. We should all be good stewards and prescribe guideline-recommended therapy whenever possible."
Visit our website for more information on antibiotic prescription practices.