User login
Telemedicine: Tuning in to teens
Times are changing! To compete in to today’s times, doctors are faced with the challenge of seeing 30-plus patients per day, keeping the wait times down, adhering to the meaningful use guidelines – all while participating in the endless maintenance of certification activities. But like it or not, medicine has changed, and you have to keep up or you likely are going to be left behind.
Pediatricians and family physicians more than other specialties are inundated with phone calls and lengthy conversations on constipation and congestion. Most of us just take the call with a smile, and chalk it up to part of the job. But what if you could provide a service that allowed you to get paid for those lengthy conversations, offered the convenience of a consultation without the patient having to come in the office – without the risk of your giving faulty advice because you haven’t actually evaluated the patient. Well, that’s what telemedicine has to offer. For a nominal monthly fee, your patients can subscribe to your “virtual” office. Whether you schedule during your office hours or set aside time before or after clinic, you now can capture a whole new clientele.

For teens, access to their doctors through their electronic devices would provide the convenience they need. Even if the issue cannot be treated without a visit, it allows for early evaluation. Acne, skin rashes, emotional issues, menstrual issues, hair issues, weight issues – all of these can be addressed via telemedicine.
The American Academy of Pediatrics’ Section on Telehealth Care (SOTC) helps guide you on how to bill for telemedicine services. It provides newsletters, educational series, and liability information. Much of the concern with telemedicine is the inconsistency of reimbursement for the service, but things are changing, and more and more of these services are being recognized for their value in meeting the needs of the patient.
There are different products on the market to assist you in setting up your virtual office. Understanding the differences in services is important. Services such as Doctor on Demand have a team of doctors available for fee-for-consult, at approximately $40. Other services, such as myowndoctor.com, set up a virtual office for you, which allows more of a concierge type service for a nominal monthly fee – approximately the amount of a copay – to allow patients access to the telemedicine service with their own physicians. This a great option that can create a cash revenue for you and broader access to patients.
There are several services provided by insurance companies – MDLIVE (Cigna), LiveHealth Online (WellPoint), and Online Care Anywhere (BC/BS Minnesota) – where providers are reimbursed at $45-$49 per visit. What is important to know when choosing a company is to be sure that the software is HIPAA (Health Insurance Portability and Accountability Act) compliant. Currently there are more than 15 companies on the market, and many more to come.
Staying up with the times is going to be key in surviving the current changes in health care. Teens in particular are a difficult group to access, but telemedicine provides that access and the comfort in continuity of care with their own physicians.
Dr. Pearce is a pediatrician in Frankfort, Ill. She said she had no relevant financial disclosures. E-mail her at [email protected].
Times are changing! To compete in to today’s times, doctors are faced with the challenge of seeing 30-plus patients per day, keeping the wait times down, adhering to the meaningful use guidelines – all while participating in the endless maintenance of certification activities. But like it or not, medicine has changed, and you have to keep up or you likely are going to be left behind.
Pediatricians and family physicians more than other specialties are inundated with phone calls and lengthy conversations on constipation and congestion. Most of us just take the call with a smile, and chalk it up to part of the job. But what if you could provide a service that allowed you to get paid for those lengthy conversations, offered the convenience of a consultation without the patient having to come in the office – without the risk of your giving faulty advice because you haven’t actually evaluated the patient. Well, that’s what telemedicine has to offer. For a nominal monthly fee, your patients can subscribe to your “virtual” office. Whether you schedule during your office hours or set aside time before or after clinic, you now can capture a whole new clientele.
For teens, access to their doctors through their electronic devices would provide the convenience they need. Even if the issue cannot be treated without a visit, it allows for early evaluation. Acne, skin rashes, emotional issues, menstrual issues, hair issues, weight issues – all of these can be addressed via telemedicine.
The American Academy of Pediatrics’ Section on Telehealth Care (SOTC) helps guide you on how to bill for telemedicine services. It provides newsletters, educational series, and liability information. Much of the concern with telemedicine is the inconsistency of reimbursement for the service, but things are changing, and more and more of these services are being recognized for their value in meeting the needs of the patient.
There are different products on the market to assist you in setting up your virtual office. Understanding the differences in services is important. Services such as Doctor on Demand have a team of doctors available for fee-for-consult, at approximately $40. Other services, such as myowndoctor.com, set up a virtual office for you, which allows more of a concierge type service for a nominal monthly fee – approximately the amount of a copay – to allow patients access to the telemedicine service with their own physicians. This a great option that can create a cash revenue for you and broader access to patients.
There are several services provided by insurance companies – MDLIVE (Cigna), LiveHealth Online (WellPoint), and Online Care Anywhere (BC/BS Minnesota) – where providers are reimbursed at $45-$49 per visit. What is important to know when choosing a company is to be sure that the software is HIPAA (Health Insurance Portability and Accountability Act) compliant. Currently there are more than 15 companies on the market, and many more to come.
Staying up with the times is going to be key in surviving the current changes in health care. Teens in particular are a difficult group to access, but telemedicine provides that access and the comfort in continuity of care with their own physicians.
Dr. Pearce is a pediatrician in Frankfort, Ill. She said she had no relevant financial disclosures. E-mail her at [email protected].
Times are changing! To compete in to today’s times, doctors are faced with the challenge of seeing 30-plus patients per day, keeping the wait times down, adhering to the meaningful use guidelines – all while participating in the endless maintenance of certification activities. But like it or not, medicine has changed, and you have to keep up or you likely are going to be left behind.
Pediatricians and family physicians more than other specialties are inundated with phone calls and lengthy conversations on constipation and congestion. Most of us just take the call with a smile, and chalk it up to part of the job. But what if you could provide a service that allowed you to get paid for those lengthy conversations, offered the convenience of a consultation without the patient having to come in the office – without the risk of your giving faulty advice because you haven’t actually evaluated the patient. Well, that’s what telemedicine has to offer. For a nominal monthly fee, your patients can subscribe to your “virtual” office. Whether you schedule during your office hours or set aside time before or after clinic, you now can capture a whole new clientele.
For teens, access to their doctors through their electronic devices would provide the convenience they need. Even if the issue cannot be treated without a visit, it allows for early evaluation. Acne, skin rashes, emotional issues, menstrual issues, hair issues, weight issues – all of these can be addressed via telemedicine.
The American Academy of Pediatrics’ Section on Telehealth Care (SOTC) helps guide you on how to bill for telemedicine services. It provides newsletters, educational series, and liability information. Much of the concern with telemedicine is the inconsistency of reimbursement for the service, but things are changing, and more and more of these services are being recognized for their value in meeting the needs of the patient.
There are different products on the market to assist you in setting up your virtual office. Understanding the differences in services is important. Services such as Doctor on Demand have a team of doctors available for fee-for-consult, at approximately $40. Other services, such as myowndoctor.com, set up a virtual office for you, which allows more of a concierge type service for a nominal monthly fee – approximately the amount of a copay – to allow patients access to the telemedicine service with their own physicians. This a great option that can create a cash revenue for you and broader access to patients.
There are several services provided by insurance companies – MDLIVE (Cigna), LiveHealth Online (WellPoint), and Online Care Anywhere (BC/BS Minnesota) – where providers are reimbursed at $45-$49 per visit. What is important to know when choosing a company is to be sure that the software is HIPAA (Health Insurance Portability and Accountability Act) compliant. Currently there are more than 15 companies on the market, and many more to come.
Staying up with the times is going to be key in surviving the current changes in health care. Teens in particular are a difficult group to access, but telemedicine provides that access and the comfort in continuity of care with their own physicians.
Dr. Pearce is a pediatrician in Frankfort, Ill. She said she had no relevant financial disclosures. E-mail her at [email protected].

STS releases public surgical outcomes report
The Society of Thoracic Surgeons has released a public online report of national surgical outcomes from its Congenital Heart Surgery Database, the association has announced.
The STS report focuses on pediatric and congenital cardiac malformations, and includes 4-year observed, expected, and risk-adjusted mortality rates, the society said in a statement.
Twenty-five sites participated in the first round of STS public online reporting, similar to the observed participation in the first round of public reporting in the STS Adult Cardiac Surgery Database, which started in 2010.
“Reporting hospital surgical outcomes using risk-adjusted analysis is extremely important because it allows for a fair assessment, on a level playing field, of outcomes across hospitals that treat different populations of patients,” Dr. Marshall L. Jacobs, STS CHSD Task Force chair, said in the statement.
For more information, visit http://www.sts.org/quality-research-patient-safety/sts-public-reporting-online.
The Society of Thoracic Surgeons has released a public online report of national surgical outcomes from its Congenital Heart Surgery Database, the association has announced.
The STS report focuses on pediatric and congenital cardiac malformations, and includes 4-year observed, expected, and risk-adjusted mortality rates, the society said in a statement.
Twenty-five sites participated in the first round of STS public online reporting, similar to the observed participation in the first round of public reporting in the STS Adult Cardiac Surgery Database, which started in 2010.
“Reporting hospital surgical outcomes using risk-adjusted analysis is extremely important because it allows for a fair assessment, on a level playing field, of outcomes across hospitals that treat different populations of patients,” Dr. Marshall L. Jacobs, STS CHSD Task Force chair, said in the statement.
For more information, visit http://www.sts.org/quality-research-patient-safety/sts-public-reporting-online.
The Society of Thoracic Surgeons has released a public online report of national surgical outcomes from its Congenital Heart Surgery Database, the association has announced.
The STS report focuses on pediatric and congenital cardiac malformations, and includes 4-year observed, expected, and risk-adjusted mortality rates, the society said in a statement.
Twenty-five sites participated in the first round of STS public online reporting, similar to the observed participation in the first round of public reporting in the STS Adult Cardiac Surgery Database, which started in 2010.
“Reporting hospital surgical outcomes using risk-adjusted analysis is extremely important because it allows for a fair assessment, on a level playing field, of outcomes across hospitals that treat different populations of patients,” Dr. Marshall L. Jacobs, STS CHSD Task Force chair, said in the statement.
For more information, visit http://www.sts.org/quality-research-patient-safety/sts-public-reporting-online.
A Promising Peptide for TBI, Heart Attack, and Stroke
BALTIMORE—A common molecule may prolong cell survival in patients with serious neurologic conditions, according to research presented at the 59th Annual Meeting of the Biophysical Society. “The present findings could provide a new lead compound for the development of drug therapies for necrosis-related diseases such as traumatic brain injury [TBI], stroke, and myocardial infarction—conditions for which no effective drug-based treatments are currently available [that work by blocking necrosis],” said Abraham H. Parola, MSc, a Professor of Biophysical Chemistry at Ben-Gurion University of the Negev in Beer-Sheva, Israel. Prof. Parola is a visiting professor of Biophysical Chemistry and Director of Natural Sciences at New York University Shanghai.

Stroke, heart attack, and TBI are separate diseases with certain shared pathologies that achieve a common end—cell death and human injury due to hypoxia. In these diseases, a lack of blood supply to affected tissues begins a signaling pathway that ultimately halts the production of energy-releasing adenosine triphosphate (ATP) molecules, which ultimately leads to cell death.
By employing derivatives of humanin, a naturally occurring peptide encoded in the genome of cellular mitochondria, researchers are working to interrupt this process, buying precious time for tissues whose cellular mechanisms have ceased to function.
The humanin derivatives work by counteracting the decrease in ATP levels caused by necrosis. The researchers tested the effectiveness of the humanin analogues AGA(C8R)-HNG17 and AGA-HNG by treating neuronal cells with these peptides prior to exposure to a necrotic agent. Results showed that humanin analogues reduced necrosis.
Prof. Parola’s previous work dealt with membrane dynamics and the mechanism of action of antiangiogenesis drugs, which starve malignant tumor growths by preventing the supply of nutrients and oxygen to the fast-growing tissue. Prof. Parola also has studied various other biophysical and molecular medicine and diagnostic topics.
“A recent paper published by our group suggested the involvement of cardiolipin [a phospholipid in inner mitochondrial membranes] in the necrotic process,” Prof. Parola said. “During this work, we stumbled upon humanin, were intrigued by its antiapoptotic effect, and extended it to [an] antinecrotic effect.”
Prof. Parola and his colleagues also performed in vivo studies by treating mice with TBI with an HNG17 analogue, which successfully reduced cranial fluid buildup and lowered the mice’s motor impairment severity scores.
As the peptides Prof. Parola and his colleagues used are derivatives of naturally occurring humanin, an ideal treatment might involve a drug delivery system with the HNG17 as the lead compound. The delivery process would be aided by the peptides’ ability to penetrate the cell membrane without the use of additional reagents.
Future work for this research team will include further exploration of ischemic activity in liver cirrhosis, as induced by acetaminophen activity, in addition to a search for a synergistic effect between humanin and other antinecrotic agents, such as protease inhibitors, to increase the clinical potential of humanin.
BALTIMORE—A common molecule may prolong cell survival in patients with serious neurologic conditions, according to research presented at the 59th Annual Meeting of the Biophysical Society. “The present findings could provide a new lead compound for the development of drug therapies for necrosis-related diseases such as traumatic brain injury [TBI], stroke, and myocardial infarction—conditions for which no effective drug-based treatments are currently available [that work by blocking necrosis],” said Abraham H. Parola, MSc, a Professor of Biophysical Chemistry at Ben-Gurion University of the Negev in Beer-Sheva, Israel. Prof. Parola is a visiting professor of Biophysical Chemistry and Director of Natural Sciences at New York University Shanghai.
Stroke, heart attack, and TBI are separate diseases with certain shared pathologies that achieve a common end—cell death and human injury due to hypoxia. In these diseases, a lack of blood supply to affected tissues begins a signaling pathway that ultimately halts the production of energy-releasing adenosine triphosphate (ATP) molecules, which ultimately leads to cell death.
By employing derivatives of humanin, a naturally occurring peptide encoded in the genome of cellular mitochondria, researchers are working to interrupt this process, buying precious time for tissues whose cellular mechanisms have ceased to function.
The humanin derivatives work by counteracting the decrease in ATP levels caused by necrosis. The researchers tested the effectiveness of the humanin analogues AGA(C8R)-HNG17 and AGA-HNG by treating neuronal cells with these peptides prior to exposure to a necrotic agent. Results showed that humanin analogues reduced necrosis.
Prof. Parola’s previous work dealt with membrane dynamics and the mechanism of action of antiangiogenesis drugs, which starve malignant tumor growths by preventing the supply of nutrients and oxygen to the fast-growing tissue. Prof. Parola also has studied various other biophysical and molecular medicine and diagnostic topics.
“A recent paper published by our group suggested the involvement of cardiolipin [a phospholipid in inner mitochondrial membranes] in the necrotic process,” Prof. Parola said. “During this work, we stumbled upon humanin, were intrigued by its antiapoptotic effect, and extended it to [an] antinecrotic effect.”
Prof. Parola and his colleagues also performed in vivo studies by treating mice with TBI with an HNG17 analogue, which successfully reduced cranial fluid buildup and lowered the mice’s motor impairment severity scores.
As the peptides Prof. Parola and his colleagues used are derivatives of naturally occurring humanin, an ideal treatment might involve a drug delivery system with the HNG17 as the lead compound. The delivery process would be aided by the peptides’ ability to penetrate the cell membrane without the use of additional reagents.
Future work for this research team will include further exploration of ischemic activity in liver cirrhosis, as induced by acetaminophen activity, in addition to a search for a synergistic effect between humanin and other antinecrotic agents, such as protease inhibitors, to increase the clinical potential of humanin.
BALTIMORE—A common molecule may prolong cell survival in patients with serious neurologic conditions, according to research presented at the 59th Annual Meeting of the Biophysical Society. “The present findings could provide a new lead compound for the development of drug therapies for necrosis-related diseases such as traumatic brain injury [TBI], stroke, and myocardial infarction—conditions for which no effective drug-based treatments are currently available [that work by blocking necrosis],” said Abraham H. Parola, MSc, a Professor of Biophysical Chemistry at Ben-Gurion University of the Negev in Beer-Sheva, Israel. Prof. Parola is a visiting professor of Biophysical Chemistry and Director of Natural Sciences at New York University Shanghai.
Stroke, heart attack, and TBI are separate diseases with certain shared pathologies that achieve a common end—cell death and human injury due to hypoxia. In these diseases, a lack of blood supply to affected tissues begins a signaling pathway that ultimately halts the production of energy-releasing adenosine triphosphate (ATP) molecules, which ultimately leads to cell death.
By employing derivatives of humanin, a naturally occurring peptide encoded in the genome of cellular mitochondria, researchers are working to interrupt this process, buying precious time for tissues whose cellular mechanisms have ceased to function.
The humanin derivatives work by counteracting the decrease in ATP levels caused by necrosis. The researchers tested the effectiveness of the humanin analogues AGA(C8R)-HNG17 and AGA-HNG by treating neuronal cells with these peptides prior to exposure to a necrotic agent. Results showed that humanin analogues reduced necrosis.
Prof. Parola’s previous work dealt with membrane dynamics and the mechanism of action of antiangiogenesis drugs, which starve malignant tumor growths by preventing the supply of nutrients and oxygen to the fast-growing tissue. Prof. Parola also has studied various other biophysical and molecular medicine and diagnostic topics.
“A recent paper published by our group suggested the involvement of cardiolipin [a phospholipid in inner mitochondrial membranes] in the necrotic process,” Prof. Parola said. “During this work, we stumbled upon humanin, were intrigued by its antiapoptotic effect, and extended it to [an] antinecrotic effect.”
Prof. Parola and his colleagues also performed in vivo studies by treating mice with TBI with an HNG17 analogue, which successfully reduced cranial fluid buildup and lowered the mice’s motor impairment severity scores.
As the peptides Prof. Parola and his colleagues used are derivatives of naturally occurring humanin, an ideal treatment might involve a drug delivery system with the HNG17 as the lead compound. The delivery process would be aided by the peptides’ ability to penetrate the cell membrane without the use of additional reagents.
Future work for this research team will include further exploration of ischemic activity in liver cirrhosis, as induced by acetaminophen activity, in addition to a search for a synergistic effect between humanin and other antinecrotic agents, such as protease inhibitors, to increase the clinical potential of humanin.

New and Noteworthy Information—March 2015
Moderate physical activity is associated with a lower risk of coronary heart disease, venous thromboembolic events, and cerebrovascular disease in women, according to a study published online ahead of print February 16 in Circulation. Participants included 1.1 million women in the United Kingdom with no history of cancer, heart disease, stroke, blood clots, or diabetes who joined the Million Women study between 1996 and 2001. Their average age when they joined the study was 56. Women who performed strenuous physical activity two to three times per week were 20% less likely to develop heart disease, strokes, or blood clots, compared with participants who reported little or no activity. More frequent physical activity did not result in further reductions in the risk of heart disease.
The FDA has approved Rytary, an extended-release oral capsule formulation of carbidopa–levodopa, for the treatment of Parkinson’s disease, post-encephalitic parkinsonism, and parkinsonism that may follow carbon monoxide intoxication or manganese intoxication. Rytary contains immediate-release and extended-release beads that contain carbidopa and levodopa in a 1:4 ratio, and provides initial and extended levodopa plasma concentrations after a single dose. In a trial of 393 randomized patients with advanced Parkinson’s disease, treatment with Rytary reduced the percentage of off time during waking hours from baseline to the end of the study, versus immediate-release carbidopa–levodopa. Rytary may be swallowed whole or opened, and the beads may be sprinkled on applesauce and consumed immediately. The drug is manufactured by Impax Pharmaceuticals (Hayward, California).
The FDA has approved Duopa, an enteral suspension of carbidopa and levodopa, as an orphan drug for the treatment of motor fluctuations in people with advanced Parkinson’s disease. The approval of Duopa is based on a phase III, 12-week, double-blind, double-placebo, active control, parallel-group, multicenter trial that compared the efficacy and safety of Duopa with that of oral, immediate-release carbidopa–levodopa tablets in patients with advanced Parkinson’s disease. Duopa significantly reduced daily mean off time at 12 weeks by four hours, which resulted in an average of 1.9 fewer hours of off time, when compared with carbidopa–levodopa tablets. Duopa is administered using a small, portable infusion pump that delivers carbidopa and levodopa directly into the small intestine continuously for 16 hours via a surgically-placed tube. The drug is manufactured by AbbVie (North Chicago, Illinois).
A link exists between brain structure and postconcussive symptoms among young male athletes who are otherwise healthy, according to a study published in the February issue of the Journal of Pediatrics. Researchers used advanced imaging technology and cognitive testing to assess 29 ice hockey players between ages 14 and 23, some of whom had a sports-related concussion. As the severity of the athletes’ concussion symptoms increased, the cortex became thinner in areas of the brain where it should be dense for players of these ages. Investigators believe that injury to a developing brain may be more severe than injury to an adult brain. “Years of playing contact sports and repeatedly getting your head knocked around probably is not good for the brain, especially in young children whose brains are still maturing,” the researchers stated.
Children whose urine drug screens tested positive for tetrahydrocannabinol (THC) met multiple sleep latency tests (MSLT) criteria for narcolepsy or had multiple sleep-onset REM periods, according to a study published January 15 in Journal of Clinical Sleep Medicine. The 10-year retrospective study included 383 children who underwent drug screens on the morning before MSLT. Of children with urine drug screens that were positive for marijuana, 43% had MSLT results consistent with narcolepsy or abnormal REM sleep patterns. Approximately 24% of children who tested negative for marijuana had MSLT results consistent with narcolepsy. No child younger than 13 had a positive urine drug screen. Males were more likely to have a positive urine drug screen and MSLT findings that were consistent with narcolepsy, compared with other groups.
Low plasma levels of APOE are associated with increased risk of future Alzheimer’s disease and all dementia in the general population, independent of ε2, ε3, and ε4 APOE genotype, according to a study published in the February issue of Annals of Neurology. The study included 75,708 participants. Multifactorially adjusted hazard ratios for lowest versus highest APOE tertile were 2.68 and 1.80 for Alzheimer’s disease and all dementia, respectively. After further adjustment for APOE genotype, plasma APOE tertiles remained associated with Alzheimer’s disease and all dementia. Researchers determined that the low level of APOE in the blood reflects a low level of APOE in the brain, indicating that β-amyloid is less effectively removed. Plasma levels of APOE may be a new, easily accessible preclinical biomarker, said the authors.
Women with Alzheimer’s disease had stable cognition for a year when they received leuprolide acetate, according to a study published in the January 1 issue of Journal of Alzheimer’s Disease. The clinical trial followed 109 women with mild to moderate Alzheimer’s disease who were randomized to low-dose leuprolide acetate, high-dose leuprolide acetate, or placebo. Among patients taking an acetylcholinesterase inhibitor, researchers saw a statistically significant benefit in the high-dose leuprolide acetate group, compared with the other groups, as determined by the Alzheimer’s Disease Assessment Scale-cognitive subscale. Mean decline was 0.18 for the high-dose group, 4.21 for the low-dose group, and 3.30 for the placebo group. “This is the first time any therapy has been shown to stabilize memory loss over a year,” the researchers said.
The rate of favorable seizure outcome or seizure freedom after resective epilepsy surgery is significant and remains stable for more than 15 years, according to a study published online ahead of print January 19 in Epilepsy & Behavior. The findings were based on a telephone survey of 253 patients who underwent resection to treat localization-related epilepsy during an 18-year period. The mean age at the time of surgery was 35.4, with a range from five months to 71. Investigators found that 92% of patients surveyed considered epilepsy surgery worthwhile, 32% were seizure-free, and 75% had favorable results. Favorable and seizure-free outcome rates remained stable after surgery over long-term follow-up. Compared with baseline, patients were more likely to be driving and taking antidepressant medication, but less likely to be employed full-time after surgery.
Nearly one in five adults with epilepsy has symptoms of attention deficit hyperactivity disorder (ADHD), which are associated with increased psychosocial morbidity and lowered quality of life, according to a study published online ahead of print January 15 in Epilepsia. In the study, researchers mailed a survey to a national sample of adult patients with epilepsy, as part of the Epilepsy Comorbidities and Health study. The relationship of ADHD symptoms to quality of life outcomes was examined using statistical analyses, which also looked at sociodemographics, depression, anxiety, seizure frequency, and number of antiepileptic drugs. Nearly one-fifth (18.4%) of 1,361 respondents with active epilepsy were classified as experiencing significant ADHD symptoms. “This study reinforces the fact that we have to broaden our view of what epilepsy entails,” said the investigators.
Triheptanoin corrects the bioenergetic profile in the brain of patients with Huntington’s disease early in the course of the disease, according to a study published online ahead of print January 7 in Neurology. Researchers used MRI brain scans to analyze the energy profile before, during, and after the brain was visually stimulated in nine people in the early stages of Huntington’s disease and 13 people without the disease. In the people without the disease, the brain’s metabolism increased during the stimulation, then returned to the normal level. In people with Huntington’s disease, there was no change in metabolism. For the second part of the study, participants with Huntington’s disease received triheptanoin. When these participants underwent the visual stimulation test again, their brain metabolism was normal.
A common gut microbe may curb the risk of developing multiple sclerosis (MS) in women, according to a study published online ahead of print January 19 in the Journal of Neurology, Neurosurgery & Psychiatry. Researchers tested 550 people with confirmed MS and a comparison group of 299 healthy people, matched for age and sex, for antibodies to H. pylori between 2007 and 2011. The prevalence of the infection was significantly lower in participants with MS than in the comparison group, but only among women, in whom it was 30% lower. Among men, a positive test result was linked to higher rates of disability, but a positive test was associated with lower disability among women. The researchers found no evidence of any link between the presence of the infection and relapse rate.
Among patients with relapsing-remitting multiple sclerosis (MS), nonmyeloablative hematopoietic stem cell transplantation is associated with improvement in neurologic disability and other clinical outcomes, according to a study published January 20 in JAMA. In a case series of patients with relapsing-remitting MS or secondary progressive MS, participants received transplantation and were followed up for five years. In all, 41 patients (50%) had significant improvement in Expanded Disability Status Scale score at two years, and 23 patients (64%) had significant improvement at four years. Receipt of hematopoietic stem cell transplantation was associated with improvement in physical function, cognitive function, and quality of life. In addition, treatment was associated with a reduction in the volume of brain lesions associated with MS seen on MRI.
Insomnia in childhood and adolescence partially results from genetic factors, according to a study published in the January issue of Sleep. The study group included 1,412 twin pairs between the ages of 8 and 18. Participants were followed-up at three time points. The average ages at each of the four stages of the study were 8, 10, 14, and 15. The results showed that clinically significant insomnia was moderately heritable at all stages of the longitudinal study. Genetic factors contributed 33% to 38% of the insomnia ratings at the first two stages of the study, when participants were an average age of 8 to 10. “Insomnia in youth is moderately related to genetic factors, but the specific genetic factors may change with age,” stated the investigators.
People with epilepsy who sleep on their stomach may be at a higher risk of sudden unexpected death, according to a literature review published online ahead of print January 21 in Neurology. Researchers found that 73% of the deaths occurred while individuals were sleeping on their stomachs, compared with 27% of deaths that occurred during other sleep positions. In a subgroup of 88 people, researchers found that people younger than 40 were four times more likely to be found on their stomach at the time of sudden death than people older than 40. A total of 86% of those under 40 slept on their stomach, compared with 60% of people older than 40. Eleven sudden deaths occurred while the participants were being monitored with video EEG.
—Kimberly D. Williams
Moderate physical activity is associated with a lower risk of coronary heart disease, venous thromboembolic events, and cerebrovascular disease in women, according to a study published online ahead of print February 16 in Circulation. Participants included 1.1 million women in the United Kingdom with no history of cancer, heart disease, stroke, blood clots, or diabetes who joined the Million Women study between 1996 and 2001. Their average age when they joined the study was 56. Women who performed strenuous physical activity two to three times per week were 20% less likely to develop heart disease, strokes, or blood clots, compared with participants who reported little or no activity. More frequent physical activity did not result in further reductions in the risk of heart disease.
The FDA has approved Rytary, an extended-release oral capsule formulation of carbidopa–levodopa, for the treatment of Parkinson’s disease, post-encephalitic parkinsonism, and parkinsonism that may follow carbon monoxide intoxication or manganese intoxication. Rytary contains immediate-release and extended-release beads that contain carbidopa and levodopa in a 1:4 ratio, and provides initial and extended levodopa plasma concentrations after a single dose. In a trial of 393 randomized patients with advanced Parkinson’s disease, treatment with Rytary reduced the percentage of off time during waking hours from baseline to the end of the study, versus immediate-release carbidopa–levodopa. Rytary may be swallowed whole or opened, and the beads may be sprinkled on applesauce and consumed immediately. The drug is manufactured by Impax Pharmaceuticals (Hayward, California).
The FDA has approved Duopa, an enteral suspension of carbidopa and levodopa, as an orphan drug for the treatment of motor fluctuations in people with advanced Parkinson’s disease. The approval of Duopa is based on a phase III, 12-week, double-blind, double-placebo, active control, parallel-group, multicenter trial that compared the efficacy and safety of Duopa with that of oral, immediate-release carbidopa–levodopa tablets in patients with advanced Parkinson’s disease. Duopa significantly reduced daily mean off time at 12 weeks by four hours, which resulted in an average of 1.9 fewer hours of off time, when compared with carbidopa–levodopa tablets. Duopa is administered using a small, portable infusion pump that delivers carbidopa and levodopa directly into the small intestine continuously for 16 hours via a surgically-placed tube. The drug is manufactured by AbbVie (North Chicago, Illinois).
A link exists between brain structure and postconcussive symptoms among young male athletes who are otherwise healthy, according to a study published in the February issue of the Journal of Pediatrics. Researchers used advanced imaging technology and cognitive testing to assess 29 ice hockey players between ages 14 and 23, some of whom had a sports-related concussion. As the severity of the athletes’ concussion symptoms increased, the cortex became thinner in areas of the brain where it should be dense for players of these ages. Investigators believe that injury to a developing brain may be more severe than injury to an adult brain. “Years of playing contact sports and repeatedly getting your head knocked around probably is not good for the brain, especially in young children whose brains are still maturing,” the researchers stated.
Children whose urine drug screens tested positive for tetrahydrocannabinol (THC) met multiple sleep latency tests (MSLT) criteria for narcolepsy or had multiple sleep-onset REM periods, according to a study published January 15 in Journal of Clinical Sleep Medicine. The 10-year retrospective study included 383 children who underwent drug screens on the morning before MSLT. Of children with urine drug screens that were positive for marijuana, 43% had MSLT results consistent with narcolepsy or abnormal REM sleep patterns. Approximately 24% of children who tested negative for marijuana had MSLT results consistent with narcolepsy. No child younger than 13 had a positive urine drug screen. Males were more likely to have a positive urine drug screen and MSLT findings that were consistent with narcolepsy, compared with other groups.
Low plasma levels of APOE are associated with increased risk of future Alzheimer’s disease and all dementia in the general population, independent of ε2, ε3, and ε4 APOE genotype, according to a study published in the February issue of Annals of Neurology. The study included 75,708 participants. Multifactorially adjusted hazard ratios for lowest versus highest APOE tertile were 2.68 and 1.80 for Alzheimer’s disease and all dementia, respectively. After further adjustment for APOE genotype, plasma APOE tertiles remained associated with Alzheimer’s disease and all dementia. Researchers determined that the low level of APOE in the blood reflects a low level of APOE in the brain, indicating that β-amyloid is less effectively removed. Plasma levels of APOE may be a new, easily accessible preclinical biomarker, said the authors.
Women with Alzheimer’s disease had stable cognition for a year when they received leuprolide acetate, according to a study published in the January 1 issue of Journal of Alzheimer’s Disease. The clinical trial followed 109 women with mild to moderate Alzheimer’s disease who were randomized to low-dose leuprolide acetate, high-dose leuprolide acetate, or placebo. Among patients taking an acetylcholinesterase inhibitor, researchers saw a statistically significant benefit in the high-dose leuprolide acetate group, compared with the other groups, as determined by the Alzheimer’s Disease Assessment Scale-cognitive subscale. Mean decline was 0.18 for the high-dose group, 4.21 for the low-dose group, and 3.30 for the placebo group. “This is the first time any therapy has been shown to stabilize memory loss over a year,” the researchers said.
The rate of favorable seizure outcome or seizure freedom after resective epilepsy surgery is significant and remains stable for more than 15 years, according to a study published online ahead of print January 19 in Epilepsy & Behavior. The findings were based on a telephone survey of 253 patients who underwent resection to treat localization-related epilepsy during an 18-year period. The mean age at the time of surgery was 35.4, with a range from five months to 71. Investigators found that 92% of patients surveyed considered epilepsy surgery worthwhile, 32% were seizure-free, and 75% had favorable results. Favorable and seizure-free outcome rates remained stable after surgery over long-term follow-up. Compared with baseline, patients were more likely to be driving and taking antidepressant medication, but less likely to be employed full-time after surgery.
Nearly one in five adults with epilepsy has symptoms of attention deficit hyperactivity disorder (ADHD), which are associated with increased psychosocial morbidity and lowered quality of life, according to a study published online ahead of print January 15 in Epilepsia. In the study, researchers mailed a survey to a national sample of adult patients with epilepsy, as part of the Epilepsy Comorbidities and Health study. The relationship of ADHD symptoms to quality of life outcomes was examined using statistical analyses, which also looked at sociodemographics, depression, anxiety, seizure frequency, and number of antiepileptic drugs. Nearly one-fifth (18.4%) of 1,361 respondents with active epilepsy were classified as experiencing significant ADHD symptoms. “This study reinforces the fact that we have to broaden our view of what epilepsy entails,” said the investigators.
Triheptanoin corrects the bioenergetic profile in the brain of patients with Huntington’s disease early in the course of the disease, according to a study published online ahead of print January 7 in Neurology. Researchers used MRI brain scans to analyze the energy profile before, during, and after the brain was visually stimulated in nine people in the early stages of Huntington’s disease and 13 people without the disease. In the people without the disease, the brain’s metabolism increased during the stimulation, then returned to the normal level. In people with Huntington’s disease, there was no change in metabolism. For the second part of the study, participants with Huntington’s disease received triheptanoin. When these participants underwent the visual stimulation test again, their brain metabolism was normal.
A common gut microbe may curb the risk of developing multiple sclerosis (MS) in women, according to a study published online ahead of print January 19 in the Journal of Neurology, Neurosurgery & Psychiatry. Researchers tested 550 people with confirmed MS and a comparison group of 299 healthy people, matched for age and sex, for antibodies to H. pylori between 2007 and 2011. The prevalence of the infection was significantly lower in participants with MS than in the comparison group, but only among women, in whom it was 30% lower. Among men, a positive test result was linked to higher rates of disability, but a positive test was associated with lower disability among women. The researchers found no evidence of any link between the presence of the infection and relapse rate.
Among patients with relapsing-remitting multiple sclerosis (MS), nonmyeloablative hematopoietic stem cell transplantation is associated with improvement in neurologic disability and other clinical outcomes, according to a study published January 20 in JAMA. In a case series of patients with relapsing-remitting MS or secondary progressive MS, participants received transplantation and were followed up for five years. In all, 41 patients (50%) had significant improvement in Expanded Disability Status Scale score at two years, and 23 patients (64%) had significant improvement at four years. Receipt of hematopoietic stem cell transplantation was associated with improvement in physical function, cognitive function, and quality of life. In addition, treatment was associated with a reduction in the volume of brain lesions associated with MS seen on MRI.
Insomnia in childhood and adolescence partially results from genetic factors, according to a study published in the January issue of Sleep. The study group included 1,412 twin pairs between the ages of 8 and 18. Participants were followed-up at three time points. The average ages at each of the four stages of the study were 8, 10, 14, and 15. The results showed that clinically significant insomnia was moderately heritable at all stages of the longitudinal study. Genetic factors contributed 33% to 38% of the insomnia ratings at the first two stages of the study, when participants were an average age of 8 to 10. “Insomnia in youth is moderately related to genetic factors, but the specific genetic factors may change with age,” stated the investigators.
People with epilepsy who sleep on their stomach may be at a higher risk of sudden unexpected death, according to a literature review published online ahead of print January 21 in Neurology. Researchers found that 73% of the deaths occurred while individuals were sleeping on their stomachs, compared with 27% of deaths that occurred during other sleep positions. In a subgroup of 88 people, researchers found that people younger than 40 were four times more likely to be found on their stomach at the time of sudden death than people older than 40. A total of 86% of those under 40 slept on their stomach, compared with 60% of people older than 40. Eleven sudden deaths occurred while the participants were being monitored with video EEG.
—Kimberly D. Williams
Moderate physical activity is associated with a lower risk of coronary heart disease, venous thromboembolic events, and cerebrovascular disease in women, according to a study published online ahead of print February 16 in Circulation. Participants included 1.1 million women in the United Kingdom with no history of cancer, heart disease, stroke, blood clots, or diabetes who joined the Million Women study between 1996 and 2001. Their average age when they joined the study was 56. Women who performed strenuous physical activity two to three times per week were 20% less likely to develop heart disease, strokes, or blood clots, compared with participants who reported little or no activity. More frequent physical activity did not result in further reductions in the risk of heart disease.
The FDA has approved Rytary, an extended-release oral capsule formulation of carbidopa–levodopa, for the treatment of Parkinson’s disease, post-encephalitic parkinsonism, and parkinsonism that may follow carbon monoxide intoxication or manganese intoxication. Rytary contains immediate-release and extended-release beads that contain carbidopa and levodopa in a 1:4 ratio, and provides initial and extended levodopa plasma concentrations after a single dose. In a trial of 393 randomized patients with advanced Parkinson’s disease, treatment with Rytary reduced the percentage of off time during waking hours from baseline to the end of the study, versus immediate-release carbidopa–levodopa. Rytary may be swallowed whole or opened, and the beads may be sprinkled on applesauce and consumed immediately. The drug is manufactured by Impax Pharmaceuticals (Hayward, California).
The FDA has approved Duopa, an enteral suspension of carbidopa and levodopa, as an orphan drug for the treatment of motor fluctuations in people with advanced Parkinson’s disease. The approval of Duopa is based on a phase III, 12-week, double-blind, double-placebo, active control, parallel-group, multicenter trial that compared the efficacy and safety of Duopa with that of oral, immediate-release carbidopa–levodopa tablets in patients with advanced Parkinson’s disease. Duopa significantly reduced daily mean off time at 12 weeks by four hours, which resulted in an average of 1.9 fewer hours of off time, when compared with carbidopa–levodopa tablets. Duopa is administered using a small, portable infusion pump that delivers carbidopa and levodopa directly into the small intestine continuously for 16 hours via a surgically-placed tube. The drug is manufactured by AbbVie (North Chicago, Illinois).
A link exists between brain structure and postconcussive symptoms among young male athletes who are otherwise healthy, according to a study published in the February issue of the Journal of Pediatrics. Researchers used advanced imaging technology and cognitive testing to assess 29 ice hockey players between ages 14 and 23, some of whom had a sports-related concussion. As the severity of the athletes’ concussion symptoms increased, the cortex became thinner in areas of the brain where it should be dense for players of these ages. Investigators believe that injury to a developing brain may be more severe than injury to an adult brain. “Years of playing contact sports and repeatedly getting your head knocked around probably is not good for the brain, especially in young children whose brains are still maturing,” the researchers stated.
Children whose urine drug screens tested positive for tetrahydrocannabinol (THC) met multiple sleep latency tests (MSLT) criteria for narcolepsy or had multiple sleep-onset REM periods, according to a study published January 15 in Journal of Clinical Sleep Medicine. The 10-year retrospective study included 383 children who underwent drug screens on the morning before MSLT. Of children with urine drug screens that were positive for marijuana, 43% had MSLT results consistent with narcolepsy or abnormal REM sleep patterns. Approximately 24% of children who tested negative for marijuana had MSLT results consistent with narcolepsy. No child younger than 13 had a positive urine drug screen. Males were more likely to have a positive urine drug screen and MSLT findings that were consistent with narcolepsy, compared with other groups.
Low plasma levels of APOE are associated with increased risk of future Alzheimer’s disease and all dementia in the general population, independent of ε2, ε3, and ε4 APOE genotype, according to a study published in the February issue of Annals of Neurology. The study included 75,708 participants. Multifactorially adjusted hazard ratios for lowest versus highest APOE tertile were 2.68 and 1.80 for Alzheimer’s disease and all dementia, respectively. After further adjustment for APOE genotype, plasma APOE tertiles remained associated with Alzheimer’s disease and all dementia. Researchers determined that the low level of APOE in the blood reflects a low level of APOE in the brain, indicating that β-amyloid is less effectively removed. Plasma levels of APOE may be a new, easily accessible preclinical biomarker, said the authors.
Women with Alzheimer’s disease had stable cognition for a year when they received leuprolide acetate, according to a study published in the January 1 issue of Journal of Alzheimer’s Disease. The clinical trial followed 109 women with mild to moderate Alzheimer’s disease who were randomized to low-dose leuprolide acetate, high-dose leuprolide acetate, or placebo. Among patients taking an acetylcholinesterase inhibitor, researchers saw a statistically significant benefit in the high-dose leuprolide acetate group, compared with the other groups, as determined by the Alzheimer’s Disease Assessment Scale-cognitive subscale. Mean decline was 0.18 for the high-dose group, 4.21 for the low-dose group, and 3.30 for the placebo group. “This is the first time any therapy has been shown to stabilize memory loss over a year,” the researchers said.
The rate of favorable seizure outcome or seizure freedom after resective epilepsy surgery is significant and remains stable for more than 15 years, according to a study published online ahead of print January 19 in Epilepsy & Behavior. The findings were based on a telephone survey of 253 patients who underwent resection to treat localization-related epilepsy during an 18-year period. The mean age at the time of surgery was 35.4, with a range from five months to 71. Investigators found that 92% of patients surveyed considered epilepsy surgery worthwhile, 32% were seizure-free, and 75% had favorable results. Favorable and seizure-free outcome rates remained stable after surgery over long-term follow-up. Compared with baseline, patients were more likely to be driving and taking antidepressant medication, but less likely to be employed full-time after surgery.
Nearly one in five adults with epilepsy has symptoms of attention deficit hyperactivity disorder (ADHD), which are associated with increased psychosocial morbidity and lowered quality of life, according to a study published online ahead of print January 15 in Epilepsia. In the study, researchers mailed a survey to a national sample of adult patients with epilepsy, as part of the Epilepsy Comorbidities and Health study. The relationship of ADHD symptoms to quality of life outcomes was examined using statistical analyses, which also looked at sociodemographics, depression, anxiety, seizure frequency, and number of antiepileptic drugs. Nearly one-fifth (18.4%) of 1,361 respondents with active epilepsy were classified as experiencing significant ADHD symptoms. “This study reinforces the fact that we have to broaden our view of what epilepsy entails,” said the investigators.
Triheptanoin corrects the bioenergetic profile in the brain of patients with Huntington’s disease early in the course of the disease, according to a study published online ahead of print January 7 in Neurology. Researchers used MRI brain scans to analyze the energy profile before, during, and after the brain was visually stimulated in nine people in the early stages of Huntington’s disease and 13 people without the disease. In the people without the disease, the brain’s metabolism increased during the stimulation, then returned to the normal level. In people with Huntington’s disease, there was no change in metabolism. For the second part of the study, participants with Huntington’s disease received triheptanoin. When these participants underwent the visual stimulation test again, their brain metabolism was normal.
A common gut microbe may curb the risk of developing multiple sclerosis (MS) in women, according to a study published online ahead of print January 19 in the Journal of Neurology, Neurosurgery & Psychiatry. Researchers tested 550 people with confirmed MS and a comparison group of 299 healthy people, matched for age and sex, for antibodies to H. pylori between 2007 and 2011. The prevalence of the infection was significantly lower in participants with MS than in the comparison group, but only among women, in whom it was 30% lower. Among men, a positive test result was linked to higher rates of disability, but a positive test was associated with lower disability among women. The researchers found no evidence of any link between the presence of the infection and relapse rate.
Among patients with relapsing-remitting multiple sclerosis (MS), nonmyeloablative hematopoietic stem cell transplantation is associated with improvement in neurologic disability and other clinical outcomes, according to a study published January 20 in JAMA. In a case series of patients with relapsing-remitting MS or secondary progressive MS, participants received transplantation and were followed up for five years. In all, 41 patients (50%) had significant improvement in Expanded Disability Status Scale score at two years, and 23 patients (64%) had significant improvement at four years. Receipt of hematopoietic stem cell transplantation was associated with improvement in physical function, cognitive function, and quality of life. In addition, treatment was associated with a reduction in the volume of brain lesions associated with MS seen on MRI.
Insomnia in childhood and adolescence partially results from genetic factors, according to a study published in the January issue of Sleep. The study group included 1,412 twin pairs between the ages of 8 and 18. Participants were followed-up at three time points. The average ages at each of the four stages of the study were 8, 10, 14, and 15. The results showed that clinically significant insomnia was moderately heritable at all stages of the longitudinal study. Genetic factors contributed 33% to 38% of the insomnia ratings at the first two stages of the study, when participants were an average age of 8 to 10. “Insomnia in youth is moderately related to genetic factors, but the specific genetic factors may change with age,” stated the investigators.
People with epilepsy who sleep on their stomach may be at a higher risk of sudden unexpected death, according to a literature review published online ahead of print January 21 in Neurology. Researchers found that 73% of the deaths occurred while individuals were sleeping on their stomachs, compared with 27% of deaths that occurred during other sleep positions. In a subgroup of 88 people, researchers found that people younger than 40 were four times more likely to be found on their stomach at the time of sudden death than people older than 40. A total of 86% of those under 40 slept on their stomach, compared with 60% of people older than 40. Eleven sudden deaths occurred while the participants were being monitored with video EEG.
—Kimberly D. Williams

Best Practices in Ambulatory EEG Monitoring
Click here to download the PDF.

Click here to download the PDF.
Click here to download the PDF.

Combo demonstrates superior PFS in relapsed MM

Photo by Rhoda Baer
Interim results of the phase 3 ENDEAVOR trial suggest that carfilzomib given in combination with low-dose dexamethasone may be more effective than bortezomib plus low-dose dexamethasone for certain patients with relapsed multiple myeloma (MM).
Patients who received the carfilzomib combination had a higher overall response rate and nearly twice the median progression-free survival (PFS) of patients who received the bortezomib combination.
Those who received carfilzomib had higher rates of cardiac and renal failure but lower rates of neuropathy. And rates of treatment discontinuation and on-study death were similar between the treatment arms.
Onyx Pharmaceuticals, the company developing carfilzomib (as Kyprolis), announced these results yesterday. The company plans to submit complete trial data for presentation at the 2015 ASCO Annual Meeting.
The ENDEAVOR trial included 929 MM patients who had relapsed after at least 1, but not more than 3, prior treatment regimens. They were randomized to receive carfilzomib or bortezomib, both in combination with low-dose dexamethasone.
Patients received carfilzomib as a 30-minute infusion, along with low-dose dexamethasone (20 mg). For cycle 1 only, carfilzomib was given at 20 mg/m2 on days 1 and 2, followed by escalation to 56 mg/m2 on days 8, 9, 15, and 16. Patients who tolerated 56 mg/m2 in cycle 1 remained at this dose for subsequent cycles on days 1, 2, 8, 9, 15, and 16 on a 28-day cycle.
Patients who received bortezomib (1.3 mg/m2) with low-dose dexamethasone (20 mg) received bortezomib subcutaneously or intravenously at the discretion of the investigator and in accordance with the regulatory approval of bortezomib. More than 75% of the patients in the control arm received bortezomib subcutaneously.
The primary endpoint of the trial was PFS, defined as the time from treatment initiation to disease progression or death. The median PFS in the carfilzomib arm was roughly double that of the bortezomib arm—18.7 months and 9.4 months, respectively (hazard ratio=0.53).
The carfilzomib combination also demonstrated superiority over the bortezomib combination for secondary endpoints of higher overall response rate and lower neuropathy events.
However, the rates for cardiac and renal failure were higher in the carfilzomib arm than the bortezomib arm. The same was true for hypertension and dyspnea.
Rates of cardiac and renal failure with carfilzomib in this trial were similar to those observed in the phase 3 ASPIRE trial, but rates of hypertension and dyspnea were higher in ENDEAVOR than ASPIRE. ![]()
Photo by Rhoda Baer
Interim results of the phase 3 ENDEAVOR trial suggest that carfilzomib given in combination with low-dose dexamethasone may be more effective than bortezomib plus low-dose dexamethasone for certain patients with relapsed multiple myeloma (MM).
Patients who received the carfilzomib combination had a higher overall response rate and nearly twice the median progression-free survival (PFS) of patients who received the bortezomib combination.
Those who received carfilzomib had higher rates of cardiac and renal failure but lower rates of neuropathy. And rates of treatment discontinuation and on-study death were similar between the treatment arms.
Onyx Pharmaceuticals, the company developing carfilzomib (as Kyprolis), announced these results yesterday. The company plans to submit complete trial data for presentation at the 2015 ASCO Annual Meeting.
The ENDEAVOR trial included 929 MM patients who had relapsed after at least 1, but not more than 3, prior treatment regimens. They were randomized to receive carfilzomib or bortezomib, both in combination with low-dose dexamethasone.
Patients received carfilzomib as a 30-minute infusion, along with low-dose dexamethasone (20 mg). For cycle 1 only, carfilzomib was given at 20 mg/m2 on days 1 and 2, followed by escalation to 56 mg/m2 on days 8, 9, 15, and 16. Patients who tolerated 56 mg/m2 in cycle 1 remained at this dose for subsequent cycles on days 1, 2, 8, 9, 15, and 16 on a 28-day cycle.
Patients who received bortezomib (1.3 mg/m2) with low-dose dexamethasone (20 mg) received bortezomib subcutaneously or intravenously at the discretion of the investigator and in accordance with the regulatory approval of bortezomib. More than 75% of the patients in the control arm received bortezomib subcutaneously.
The primary endpoint of the trial was PFS, defined as the time from treatment initiation to disease progression or death. The median PFS in the carfilzomib arm was roughly double that of the bortezomib arm—18.7 months and 9.4 months, respectively (hazard ratio=0.53).
The carfilzomib combination also demonstrated superiority over the bortezomib combination for secondary endpoints of higher overall response rate and lower neuropathy events.
However, the rates for cardiac and renal failure were higher in the carfilzomib arm than the bortezomib arm. The same was true for hypertension and dyspnea.
Rates of cardiac and renal failure with carfilzomib in this trial were similar to those observed in the phase 3 ASPIRE trial, but rates of hypertension and dyspnea were higher in ENDEAVOR than ASPIRE. ![]()
Photo by Rhoda Baer
Interim results of the phase 3 ENDEAVOR trial suggest that carfilzomib given in combination with low-dose dexamethasone may be more effective than bortezomib plus low-dose dexamethasone for certain patients with relapsed multiple myeloma (MM).
Patients who received the carfilzomib combination had a higher overall response rate and nearly twice the median progression-free survival (PFS) of patients who received the bortezomib combination.
Those who received carfilzomib had higher rates of cardiac and renal failure but lower rates of neuropathy. And rates of treatment discontinuation and on-study death were similar between the treatment arms.
Onyx Pharmaceuticals, the company developing carfilzomib (as Kyprolis), announced these results yesterday. The company plans to submit complete trial data for presentation at the 2015 ASCO Annual Meeting.
The ENDEAVOR trial included 929 MM patients who had relapsed after at least 1, but not more than 3, prior treatment regimens. They were randomized to receive carfilzomib or bortezomib, both in combination with low-dose dexamethasone.
Patients received carfilzomib as a 30-minute infusion, along with low-dose dexamethasone (20 mg). For cycle 1 only, carfilzomib was given at 20 mg/m2 on days 1 and 2, followed by escalation to 56 mg/m2 on days 8, 9, 15, and 16. Patients who tolerated 56 mg/m2 in cycle 1 remained at this dose for subsequent cycles on days 1, 2, 8, 9, 15, and 16 on a 28-day cycle.
Patients who received bortezomib (1.3 mg/m2) with low-dose dexamethasone (20 mg) received bortezomib subcutaneously or intravenously at the discretion of the investigator and in accordance with the regulatory approval of bortezomib. More than 75% of the patients in the control arm received bortezomib subcutaneously.
The primary endpoint of the trial was PFS, defined as the time from treatment initiation to disease progression or death. The median PFS in the carfilzomib arm was roughly double that of the bortezomib arm—18.7 months and 9.4 months, respectively (hazard ratio=0.53).
The carfilzomib combination also demonstrated superiority over the bortezomib combination for secondary endpoints of higher overall response rate and lower neuropathy events.
However, the rates for cardiac and renal failure were higher in the carfilzomib arm than the bortezomib arm. The same was true for hypertension and dyspnea.
Rates of cardiac and renal failure with carfilzomib in this trial were similar to those observed in the phase 3 ASPIRE trial, but rates of hypertension and dyspnea were higher in ENDEAVOR than ASPIRE. ![]()
Findings could lead to new methods of malaria control

Photo courtesy of CDC
Sexual biology may be the key to uncovering why Anopheles mosquitoes are unique in their ability to transmit malaria to humans, according to research published in Science.
By analyzing 16 Anopheles genomes, investigators found these mosquitoes’ reproductive traits evolved along with their capacity to transmit the Plasmodium parasite.
The team believes these findings may provide a new target for malaria control, particularly in regions hardest hit by the disease.
“Our study is the first to reveal the evolutionary dynamics between the sexes that are likely responsible for shaping the ability of Anopheles mosquitoes to transmit malaria to humans,” said study author Flaminia Catteruccia, PhD, of the University of Perugia in Italy.
She and her colleagues analyzed 9 globally dispersed Anopheles species, enabling reconstruction of the evolutionary history of the mosquitoes’ reproductive traits and capacity to transmit malaria.
Results showed that 2 key male reproductive traits in Anopheles are acquired and evolved together over time. The first is transferring ejaculate as a gelatinous, rod-shaped structure called the mating plug. And the second is the ability to synthesize a steroid hormone known as 20-hydroxyecdysone (20E), which is contained in the mating plug.
The investigators also demonstrated that the evolution of these male traits drove reciprocal adaptations in females that are strongly linked to the mosquitoes’ capacity to transmit malaria.
With prior research, the team had shown that sexual transfer of 20E induces a series of dramatic changes in the female mosquito, fundamentally altering her physiology and behavior. These changes affect a female’s reproductive output, longevity, and immune response to Plasmodium parasites, all key factors in malaria transmission.
All 4 species of Anopheles mosquitoes that transfer large levels of 20E are major malaria vectors originating from Africa and India, the regions of highest malaria burden.
The investigators believe that, by identifying factors important for malaria transmission, they have paved the way for the development of compounds to specifically target those factors. Such compounds could be incorporated into existing mosquito control technologies, boosting their overall effectiveness.
The team also thinks their findings might be applicable to Dengue and West Nile virus, which are transmitted by the Aedes and Culex mosquitoes, respectively. In these species, some aspects of reproductive biology are similar to Anopheles. ![]()
Photo courtesy of CDC
Sexual biology may be the key to uncovering why Anopheles mosquitoes are unique in their ability to transmit malaria to humans, according to research published in Science.
By analyzing 16 Anopheles genomes, investigators found these mosquitoes’ reproductive traits evolved along with their capacity to transmit the Plasmodium parasite.
The team believes these findings may provide a new target for malaria control, particularly in regions hardest hit by the disease.
“Our study is the first to reveal the evolutionary dynamics between the sexes that are likely responsible for shaping the ability of Anopheles mosquitoes to transmit malaria to humans,” said study author Flaminia Catteruccia, PhD, of the University of Perugia in Italy.
She and her colleagues analyzed 9 globally dispersed Anopheles species, enabling reconstruction of the evolutionary history of the mosquitoes’ reproductive traits and capacity to transmit malaria.
Results showed that 2 key male reproductive traits in Anopheles are acquired and evolved together over time. The first is transferring ejaculate as a gelatinous, rod-shaped structure called the mating plug. And the second is the ability to synthesize a steroid hormone known as 20-hydroxyecdysone (20E), which is contained in the mating plug.
The investigators also demonstrated that the evolution of these male traits drove reciprocal adaptations in females that are strongly linked to the mosquitoes’ capacity to transmit malaria.
With prior research, the team had shown that sexual transfer of 20E induces a series of dramatic changes in the female mosquito, fundamentally altering her physiology and behavior. These changes affect a female’s reproductive output, longevity, and immune response to Plasmodium parasites, all key factors in malaria transmission.
All 4 species of Anopheles mosquitoes that transfer large levels of 20E are major malaria vectors originating from Africa and India, the regions of highest malaria burden.
The investigators believe that, by identifying factors important for malaria transmission, they have paved the way for the development of compounds to specifically target those factors. Such compounds could be incorporated into existing mosquito control technologies, boosting their overall effectiveness.
The team also thinks their findings might be applicable to Dengue and West Nile virus, which are transmitted by the Aedes and Culex mosquitoes, respectively. In these species, some aspects of reproductive biology are similar to Anopheles. ![]()
Photo courtesy of CDC
Sexual biology may be the key to uncovering why Anopheles mosquitoes are unique in their ability to transmit malaria to humans, according to research published in Science.
By analyzing 16 Anopheles genomes, investigators found these mosquitoes’ reproductive traits evolved along with their capacity to transmit the Plasmodium parasite.
The team believes these findings may provide a new target for malaria control, particularly in regions hardest hit by the disease.
“Our study is the first to reveal the evolutionary dynamics between the sexes that are likely responsible for shaping the ability of Anopheles mosquitoes to transmit malaria to humans,” said study author Flaminia Catteruccia, PhD, of the University of Perugia in Italy.
She and her colleagues analyzed 9 globally dispersed Anopheles species, enabling reconstruction of the evolutionary history of the mosquitoes’ reproductive traits and capacity to transmit malaria.
Results showed that 2 key male reproductive traits in Anopheles are acquired and evolved together over time. The first is transferring ejaculate as a gelatinous, rod-shaped structure called the mating plug. And the second is the ability to synthesize a steroid hormone known as 20-hydroxyecdysone (20E), which is contained in the mating plug.
The investigators also demonstrated that the evolution of these male traits drove reciprocal adaptations in females that are strongly linked to the mosquitoes’ capacity to transmit malaria.
With prior research, the team had shown that sexual transfer of 20E induces a series of dramatic changes in the female mosquito, fundamentally altering her physiology and behavior. These changes affect a female’s reproductive output, longevity, and immune response to Plasmodium parasites, all key factors in malaria transmission.
All 4 species of Anopheles mosquitoes that transfer large levels of 20E are major malaria vectors originating from Africa and India, the regions of highest malaria burden.
The investigators believe that, by identifying factors important for malaria transmission, they have paved the way for the development of compounds to specifically target those factors. Such compounds could be incorporated into existing mosquito control technologies, boosting their overall effectiveness.
The team also thinks their findings might be applicable to Dengue and West Nile virus, which are transmitted by the Aedes and Culex mosquitoes, respectively. In these species, some aspects of reproductive biology are similar to Anopheles. ![]()
Immunization update: What’s changed, what’s on the way
The Centers for Disease Control and Prevention (CDC) has published its 2015 immunization schedules for adults and for children and adolescents.1,2 There are very few changes from 2014 recommendations; most are alterations in the footnotes to clarify complex and confusing catch-up schedules. The 2 substantive changes have been discussed in previous Practice Alerts:
- the addition of the 13-valent pneumococcal conjugate vaccine (PCV13) to the 23-valent pneumococcal polysaccharide vaccine (PPSV23) in the routine older-adult recommendations;3
- a stated preference for live attenuated influenza vaccine (LAIV) for children ages 2 through 8 years.4
The LAIV statement came under criticism at the recent meeting of the Advisory Committee on Immunization Practices (ACIP). A prospective case-control study conducted at 5 sites in the US Flu Vaccine Effectiveness Network looked at the effectiveness of LAIV and inactivated influenza vaccine (IIV) against medically-attended influenza in 3 flu seasons: 2011-2012, 2012-2013, and 2013-2014.5 The results differed by age.
In patients ages 9 to 18 years, the vaccines were equally effective in all 3 seasons, with effectiveness ranging between 32% and 67% depending on the year and the vaccine. In children ages 2 to 8 years, LAIV appeared to be more effective than IIV in the 2011-2012 and 2012-2013 seasons, with odds ratios of .54 and .74, respectively (although not statistically significant). In the 2013-2014 season, however, IIV was the more effective vaccine, with a statistically significant odds ratio of 5.17.
In the immediate past season, the predominant influenza strain circulating was H1N1 pdm09, against which the LAIV appeared to be minimally, if at all, effective. These results were replicated in a study conducted by the LAIV producer, MedImmune, and in a study conducted by the United States Air Force.5 Based on the predominant circulating strains in the 2014-2015 flu season, ACIP has not changed its preference for LAIV for ages 2 through 8 years.
Typhoid fever vaccines
Late last year, ACIP updated its recommendations on the use of typhoid vaccines. They had last been reviewed with the recommendations in 1994, and surprisingly few changes were needed. Roughly 400 cases of typhoid fever occur in the United States each year, mostly in travelers returning from India, Bangladesh, or Pakistan. Each year, worldwide, there are an estimated 20 million cases of typhoid and 200,000 related deaths.6
ACIP recommends typhoid vaccine for travelers to areas within Asia, Africa, and Latin America that present a risk of exposure to Salmonella typhi. Country-specific recommendations can be found on the CDC travel Web site (http://wwwnc.cdc.gov/travel). Others for whom the vaccine is recommended: those who have a household contact with S. typhi or who have had other intimate exposure to a chronic S. typhi carrier (eg, someone who has excreted S. typhi in stool or urine for a year or more); and microbiologists and lab workers who might be exposed to S. typhi.
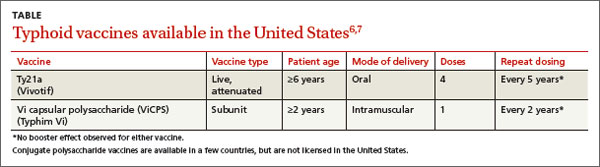
Two typhoid vaccines are available and neither is listed as preferred. One is a live vaccine (Ty21a) taken orally in 4 doses, one dose every other day over 7 days. The other is a killed vaccine (Vi capsular polysaccharide vaccine [ViCPS]), given intramuscularly in a single dose (TABLE).6,7 Ty21a is approved for individuals ages 6 years and older; ViCPS for ages 2 years and older.
Anticipated changes this year
HPV vaccine
Two human papillomavirus (HPV) vaccines are available in the United States: Gardasil, a quadrivalent vaccine (HPV4) that protects against types 6, 11, 16, and 18, and Cervarix, a bivalent product (HPV2) protecting against types 16 and 18. Both vaccines contain antigens of HPV subtypes 16 and 18, which cause 70% of cervical cancers in the United States and the rest of the world. The HPV4 is soon to be replaced with a 9-valent product that will contain antigens for types 6, 11, 16, 18, 31, 33, 45, 52, and 58, which are responsible for 90% of cervical cancers worldwide.8
Many countries now allow a 2-dose schedule for both HPV2 and HPV4. For girls younger than 15 years, the World Health Organization recommends a 2-dose schedule for HPV vaccines, 6 to 12 months apart.9 A 3-dose schedule is still recommended for those ages 15 years or older and for those who are immunocompromised.
ACIP will assess studies on the effectiveness of 2-dose schedules of HPV2, HPV4, and HPV9, and will make recommendations within the next year. Although the manufacturers of the HPV vaccines have not applied to the US Food and Drug Administration (FDA) for approval of a 2-dose schedule, ACIP will still consider the possibility of recommending it. The current 3-dose schedule is seen as a barrier to HPV vaccination and one reason why the rate of vaccination in girls in the United States remains at a disappointing 37.6% for 3 doses, 47.7% for at least 2 doses, and 57.3% for 1 dose.10
ACIP will attempt to address multiple issues in the next year regarding HPV vaccination: HPV9 use in men and women, including the possibility of catch-up schedules for those who have received HPV4 or HPV2; the possibility of using a 2-dose schedule for all HPV vaccines; and ways to increase uptake of this cancer-preventing vaccine.
Meningococcus type B
With the widespread use of quadrivalent meningococcal vaccines (MCV4), meningococcal meningitis has declined markedly in all age groups. The incidence of disease caused by meningococcal serotype B, which MCV4 does not protect against, has also declined from 0.3 to less than 0.1 cases per 100,000 between 1994 and 2013.11 The highest incidence occurs in infants under the age of 1 year, at 1.5/100,000, with 67% of cases attributable to serotype B. A slight bump in risk is seen with those ages 19 to 22 years (0.2/100,000) compared with other adolescents and adults.
While serotype B accounts for a larger proportion of all meningococcal disease than it did before, it is still relatively rare. In the United States between 2010 and 2012, annual cases totaled 48 to 56.11 Groups that are at higher risk of infection include those with complement deficiencies or asplenia (functional or anatomical), microbiologists and lab personnel who work with the organism, and those who have close contact with infected individuals.
In the past few years, well-publicized outbreaks of meningococcus B have occurred on some university campuses. Princeton had 9 cases, and the University of California at Santa Barbara had 4.11 This led to the use of meningococcal B vaccine as an outbreak control measure, with permission from the FDA before the vaccine was licensed. While these outbreaks created an impression of increased risks on college campuses, college students are actually at lower risk of type B meningococcal disease than others of the same age.11
This year, 2 meningococcal B vaccines will be available in the United States. The first, rLP2086, Trumenba (Pfizer) is a 3-dose series that was licensed in late 2014. The second, 4CMenB, Bexsero (Novartis) is a 2-dose series that received FDA approval in January 2015. Both are licensed for individuals ages 10 to 25 years. Formulating a recommendation for the use of these vaccines will be challenging because of several factors: the multiple dose schedules, the low rate of meningococcal B disease, and the age group for whom the vaccines are licensed.
1. Centers for Disease Control and Prevention. Recommended adult immunization schedule: United States - 2015. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/schedules/downloads/adult/adult-combined-schedule.pdf. Accessed February 11, 2015.
2. Centers for Disease Control and Prevention. Birth – 18 years & “Catch-up” immunization schedules. United States, 2015. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/schedules/hcp/child-adolescent.html. Accessed January 27, 2015.
3. Campos-Outcalt D. Pneumococcal vaccines for older adults: getting the timing right. J Fam Pract. 2014;63:730-733.
4. Campos-Outcalt D. The 2014-2015 influenza season: what you need to know. J Fam Pract. 2014;63:532-533.
5. Flannery B. Update on effectiveness of live-attenuated versus inactivated influenza vaccine in children and adolescents aged 2-18 years. Presented at: Advisory Committee on Immunization Practices; October 29, 2014; Atlanta, GA. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-10/flu-03-flannery.pdf. Accessed January 27, 2015.
6. Jackson BR. Typhoid and typhoid vaccines. Presented at: Advisory Committee on Immunization Practices; October 30, 2014; Atlanta, GA. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-10/Typhoid-02-Jackson.pdf. Accessed January 27, 2015.
7. Centers for Disease Control and Prevention. Typhoid immunization—recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 1994:43:1-7.
8. Luxembourg A. 9-valent HPV vaccine program key results--Part III. Presented at: Advisory Committee on Immunization Practices; October 30, 2014; Atlanta, GA. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-10/HPV-02-Luxembourg.pdf. Accessed January 27, 2015.
9. Markowitz L. 2-dose HPV vaccination schedules. Presented at: Advisory Committee on Immunization Practices; June 25, 2014; Atlanta, GA. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-06/HPV-04-Markowitz.pdf. Accessed January 27, 2015.
10. Stokley S, Jeyarajah J, Yankey D, et al; Immunization Services Division, National Center for Immunization and Respiratory Diseases, CDC; Centers for Disease Control and Prevention (CDC). Human papillomavirus vaccination coverage among adolescents, 2007-2013, and postlicensure safety monitoring, 2006-2014—United States. MMWR Morb Mortal Wkly Rep. 2014;63:620-624.
11. MacNeil J. Epidemiology of serogroup B meningococcal disease, United States. Presented at: Advisory Committee on Immunization Practices; October 30, 2014; Atlanta, GA. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-10/mening-02-MacNeil.pdf. Accessed January 27, 2015.
The Centers for Disease Control and Prevention (CDC) has published its 2015 immunization schedules for adults and for children and adolescents.1,2 There are very few changes from 2014 recommendations; most are alterations in the footnotes to clarify complex and confusing catch-up schedules. The 2 substantive changes have been discussed in previous Practice Alerts:
- the addition of the 13-valent pneumococcal conjugate vaccine (PCV13) to the 23-valent pneumococcal polysaccharide vaccine (PPSV23) in the routine older-adult recommendations;3
- a stated preference for live attenuated influenza vaccine (LAIV) for children ages 2 through 8 years.4
The LAIV statement came under criticism at the recent meeting of the Advisory Committee on Immunization Practices (ACIP). A prospective case-control study conducted at 5 sites in the US Flu Vaccine Effectiveness Network looked at the effectiveness of LAIV and inactivated influenza vaccine (IIV) against medically-attended influenza in 3 flu seasons: 2011-2012, 2012-2013, and 2013-2014.5 The results differed by age.
In patients ages 9 to 18 years, the vaccines were equally effective in all 3 seasons, with effectiveness ranging between 32% and 67% depending on the year and the vaccine. In children ages 2 to 8 years, LAIV appeared to be more effective than IIV in the 2011-2012 and 2012-2013 seasons, with odds ratios of .54 and .74, respectively (although not statistically significant). In the 2013-2014 season, however, IIV was the more effective vaccine, with a statistically significant odds ratio of 5.17.
In the immediate past season, the predominant influenza strain circulating was H1N1 pdm09, against which the LAIV appeared to be minimally, if at all, effective. These results were replicated in a study conducted by the LAIV producer, MedImmune, and in a study conducted by the United States Air Force.5 Based on the predominant circulating strains in the 2014-2015 flu season, ACIP has not changed its preference for LAIV for ages 2 through 8 years.
Typhoid fever vaccines
Late last year, ACIP updated its recommendations on the use of typhoid vaccines. They had last been reviewed with the recommendations in 1994, and surprisingly few changes were needed. Roughly 400 cases of typhoid fever occur in the United States each year, mostly in travelers returning from India, Bangladesh, or Pakistan. Each year, worldwide, there are an estimated 20 million cases of typhoid and 200,000 related deaths.6
ACIP recommends typhoid vaccine for travelers to areas within Asia, Africa, and Latin America that present a risk of exposure to Salmonella typhi. Country-specific recommendations can be found on the CDC travel Web site (http://wwwnc.cdc.gov/travel). Others for whom the vaccine is recommended: those who have a household contact with S. typhi or who have had other intimate exposure to a chronic S. typhi carrier (eg, someone who has excreted S. typhi in stool or urine for a year or more); and microbiologists and lab workers who might be exposed to S. typhi.
Two typhoid vaccines are available and neither is listed as preferred. One is a live vaccine (Ty21a) taken orally in 4 doses, one dose every other day over 7 days. The other is a killed vaccine (Vi capsular polysaccharide vaccine [ViCPS]), given intramuscularly in a single dose (TABLE).6,7 Ty21a is approved for individuals ages 6 years and older; ViCPS for ages 2 years and older.
Anticipated changes this year
HPV vaccine
Two human papillomavirus (HPV) vaccines are available in the United States: Gardasil, a quadrivalent vaccine (HPV4) that protects against types 6, 11, 16, and 18, and Cervarix, a bivalent product (HPV2) protecting against types 16 and 18. Both vaccines contain antigens of HPV subtypes 16 and 18, which cause 70% of cervical cancers in the United States and the rest of the world. The HPV4 is soon to be replaced with a 9-valent product that will contain antigens for types 6, 11, 16, 18, 31, 33, 45, 52, and 58, which are responsible for 90% of cervical cancers worldwide.8
Many countries now allow a 2-dose schedule for both HPV2 and HPV4. For girls younger than 15 years, the World Health Organization recommends a 2-dose schedule for HPV vaccines, 6 to 12 months apart.9 A 3-dose schedule is still recommended for those ages 15 years or older and for those who are immunocompromised.
ACIP will assess studies on the effectiveness of 2-dose schedules of HPV2, HPV4, and HPV9, and will make recommendations within the next year. Although the manufacturers of the HPV vaccines have not applied to the US Food and Drug Administration (FDA) for approval of a 2-dose schedule, ACIP will still consider the possibility of recommending it. The current 3-dose schedule is seen as a barrier to HPV vaccination and one reason why the rate of vaccination in girls in the United States remains at a disappointing 37.6% for 3 doses, 47.7% for at least 2 doses, and 57.3% for 1 dose.10
ACIP will attempt to address multiple issues in the next year regarding HPV vaccination: HPV9 use in men and women, including the possibility of catch-up schedules for those who have received HPV4 or HPV2; the possibility of using a 2-dose schedule for all HPV vaccines; and ways to increase uptake of this cancer-preventing vaccine.
Meningococcus type B
With the widespread use of quadrivalent meningococcal vaccines (MCV4), meningococcal meningitis has declined markedly in all age groups. The incidence of disease caused by meningococcal serotype B, which MCV4 does not protect against, has also declined from 0.3 to less than 0.1 cases per 100,000 between 1994 and 2013.11 The highest incidence occurs in infants under the age of 1 year, at 1.5/100,000, with 67% of cases attributable to serotype B. A slight bump in risk is seen with those ages 19 to 22 years (0.2/100,000) compared with other adolescents and adults.
While serotype B accounts for a larger proportion of all meningococcal disease than it did before, it is still relatively rare. In the United States between 2010 and 2012, annual cases totaled 48 to 56.11 Groups that are at higher risk of infection include those with complement deficiencies or asplenia (functional or anatomical), microbiologists and lab personnel who work with the organism, and those who have close contact with infected individuals.
In the past few years, well-publicized outbreaks of meningococcus B have occurred on some university campuses. Princeton had 9 cases, and the University of California at Santa Barbara had 4.11 This led to the use of meningococcal B vaccine as an outbreak control measure, with permission from the FDA before the vaccine was licensed. While these outbreaks created an impression of increased risks on college campuses, college students are actually at lower risk of type B meningococcal disease than others of the same age.11
This year, 2 meningococcal B vaccines will be available in the United States. The first, rLP2086, Trumenba (Pfizer) is a 3-dose series that was licensed in late 2014. The second, 4CMenB, Bexsero (Novartis) is a 2-dose series that received FDA approval in January 2015. Both are licensed for individuals ages 10 to 25 years. Formulating a recommendation for the use of these vaccines will be challenging because of several factors: the multiple dose schedules, the low rate of meningococcal B disease, and the age group for whom the vaccines are licensed.
The Centers for Disease Control and Prevention (CDC) has published its 2015 immunization schedules for adults and for children and adolescents.1,2 There are very few changes from 2014 recommendations; most are alterations in the footnotes to clarify complex and confusing catch-up schedules. The 2 substantive changes have been discussed in previous Practice Alerts:
- the addition of the 13-valent pneumococcal conjugate vaccine (PCV13) to the 23-valent pneumococcal polysaccharide vaccine (PPSV23) in the routine older-adult recommendations;3
- a stated preference for live attenuated influenza vaccine (LAIV) for children ages 2 through 8 years.4
The LAIV statement came under criticism at the recent meeting of the Advisory Committee on Immunization Practices (ACIP). A prospective case-control study conducted at 5 sites in the US Flu Vaccine Effectiveness Network looked at the effectiveness of LAIV and inactivated influenza vaccine (IIV) against medically-attended influenza in 3 flu seasons: 2011-2012, 2012-2013, and 2013-2014.5 The results differed by age.
In patients ages 9 to 18 years, the vaccines were equally effective in all 3 seasons, with effectiveness ranging between 32% and 67% depending on the year and the vaccine. In children ages 2 to 8 years, LAIV appeared to be more effective than IIV in the 2011-2012 and 2012-2013 seasons, with odds ratios of .54 and .74, respectively (although not statistically significant). In the 2013-2014 season, however, IIV was the more effective vaccine, with a statistically significant odds ratio of 5.17.
In the immediate past season, the predominant influenza strain circulating was H1N1 pdm09, against which the LAIV appeared to be minimally, if at all, effective. These results were replicated in a study conducted by the LAIV producer, MedImmune, and in a study conducted by the United States Air Force.5 Based on the predominant circulating strains in the 2014-2015 flu season, ACIP has not changed its preference for LAIV for ages 2 through 8 years.
Typhoid fever vaccines
Late last year, ACIP updated its recommendations on the use of typhoid vaccines. They had last been reviewed with the recommendations in 1994, and surprisingly few changes were needed. Roughly 400 cases of typhoid fever occur in the United States each year, mostly in travelers returning from India, Bangladesh, or Pakistan. Each year, worldwide, there are an estimated 20 million cases of typhoid and 200,000 related deaths.6
ACIP recommends typhoid vaccine for travelers to areas within Asia, Africa, and Latin America that present a risk of exposure to Salmonella typhi. Country-specific recommendations can be found on the CDC travel Web site (http://wwwnc.cdc.gov/travel). Others for whom the vaccine is recommended: those who have a household contact with S. typhi or who have had other intimate exposure to a chronic S. typhi carrier (eg, someone who has excreted S. typhi in stool or urine for a year or more); and microbiologists and lab workers who might be exposed to S. typhi.
Two typhoid vaccines are available and neither is listed as preferred. One is a live vaccine (Ty21a) taken orally in 4 doses, one dose every other day over 7 days. The other is a killed vaccine (Vi capsular polysaccharide vaccine [ViCPS]), given intramuscularly in a single dose (TABLE).6,7 Ty21a is approved for individuals ages 6 years and older; ViCPS for ages 2 years and older.
Anticipated changes this year
HPV vaccine
Two human papillomavirus (HPV) vaccines are available in the United States: Gardasil, a quadrivalent vaccine (HPV4) that protects against types 6, 11, 16, and 18, and Cervarix, a bivalent product (HPV2) protecting against types 16 and 18. Both vaccines contain antigens of HPV subtypes 16 and 18, which cause 70% of cervical cancers in the United States and the rest of the world. The HPV4 is soon to be replaced with a 9-valent product that will contain antigens for types 6, 11, 16, 18, 31, 33, 45, 52, and 58, which are responsible for 90% of cervical cancers worldwide.8
Many countries now allow a 2-dose schedule for both HPV2 and HPV4. For girls younger than 15 years, the World Health Organization recommends a 2-dose schedule for HPV vaccines, 6 to 12 months apart.9 A 3-dose schedule is still recommended for those ages 15 years or older and for those who are immunocompromised.
ACIP will assess studies on the effectiveness of 2-dose schedules of HPV2, HPV4, and HPV9, and will make recommendations within the next year. Although the manufacturers of the HPV vaccines have not applied to the US Food and Drug Administration (FDA) for approval of a 2-dose schedule, ACIP will still consider the possibility of recommending it. The current 3-dose schedule is seen as a barrier to HPV vaccination and one reason why the rate of vaccination in girls in the United States remains at a disappointing 37.6% for 3 doses, 47.7% for at least 2 doses, and 57.3% for 1 dose.10
ACIP will attempt to address multiple issues in the next year regarding HPV vaccination: HPV9 use in men and women, including the possibility of catch-up schedules for those who have received HPV4 or HPV2; the possibility of using a 2-dose schedule for all HPV vaccines; and ways to increase uptake of this cancer-preventing vaccine.
Meningococcus type B
With the widespread use of quadrivalent meningococcal vaccines (MCV4), meningococcal meningitis has declined markedly in all age groups. The incidence of disease caused by meningococcal serotype B, which MCV4 does not protect against, has also declined from 0.3 to less than 0.1 cases per 100,000 between 1994 and 2013.11 The highest incidence occurs in infants under the age of 1 year, at 1.5/100,000, with 67% of cases attributable to serotype B. A slight bump in risk is seen with those ages 19 to 22 years (0.2/100,000) compared with other adolescents and adults.
While serotype B accounts for a larger proportion of all meningococcal disease than it did before, it is still relatively rare. In the United States between 2010 and 2012, annual cases totaled 48 to 56.11 Groups that are at higher risk of infection include those with complement deficiencies or asplenia (functional or anatomical), microbiologists and lab personnel who work with the organism, and those who have close contact with infected individuals.
In the past few years, well-publicized outbreaks of meningococcus B have occurred on some university campuses. Princeton had 9 cases, and the University of California at Santa Barbara had 4.11 This led to the use of meningococcal B vaccine as an outbreak control measure, with permission from the FDA before the vaccine was licensed. While these outbreaks created an impression of increased risks on college campuses, college students are actually at lower risk of type B meningococcal disease than others of the same age.11
This year, 2 meningococcal B vaccines will be available in the United States. The first, rLP2086, Trumenba (Pfizer) is a 3-dose series that was licensed in late 2014. The second, 4CMenB, Bexsero (Novartis) is a 2-dose series that received FDA approval in January 2015. Both are licensed for individuals ages 10 to 25 years. Formulating a recommendation for the use of these vaccines will be challenging because of several factors: the multiple dose schedules, the low rate of meningococcal B disease, and the age group for whom the vaccines are licensed.
1. Centers for Disease Control and Prevention. Recommended adult immunization schedule: United States - 2015. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/schedules/downloads/adult/adult-combined-schedule.pdf. Accessed February 11, 2015.
2. Centers for Disease Control and Prevention. Birth – 18 years & “Catch-up” immunization schedules. United States, 2015. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/schedules/hcp/child-adolescent.html. Accessed January 27, 2015.
3. Campos-Outcalt D. Pneumococcal vaccines for older adults: getting the timing right. J Fam Pract. 2014;63:730-733.
4. Campos-Outcalt D. The 2014-2015 influenza season: what you need to know. J Fam Pract. 2014;63:532-533.
5. Flannery B. Update on effectiveness of live-attenuated versus inactivated influenza vaccine in children and adolescents aged 2-18 years. Presented at: Advisory Committee on Immunization Practices; October 29, 2014; Atlanta, GA. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-10/flu-03-flannery.pdf. Accessed January 27, 2015.
6. Jackson BR. Typhoid and typhoid vaccines. Presented at: Advisory Committee on Immunization Practices; October 30, 2014; Atlanta, GA. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-10/Typhoid-02-Jackson.pdf. Accessed January 27, 2015.
7. Centers for Disease Control and Prevention. Typhoid immunization—recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 1994:43:1-7.
8. Luxembourg A. 9-valent HPV vaccine program key results--Part III. Presented at: Advisory Committee on Immunization Practices; October 30, 2014; Atlanta, GA. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-10/HPV-02-Luxembourg.pdf. Accessed January 27, 2015.
9. Markowitz L. 2-dose HPV vaccination schedules. Presented at: Advisory Committee on Immunization Practices; June 25, 2014; Atlanta, GA. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-06/HPV-04-Markowitz.pdf. Accessed January 27, 2015.
10. Stokley S, Jeyarajah J, Yankey D, et al; Immunization Services Division, National Center for Immunization and Respiratory Diseases, CDC; Centers for Disease Control and Prevention (CDC). Human papillomavirus vaccination coverage among adolescents, 2007-2013, and postlicensure safety monitoring, 2006-2014—United States. MMWR Morb Mortal Wkly Rep. 2014;63:620-624.
11. MacNeil J. Epidemiology of serogroup B meningococcal disease, United States. Presented at: Advisory Committee on Immunization Practices; October 30, 2014; Atlanta, GA. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-10/mening-02-MacNeil.pdf. Accessed January 27, 2015.
1. Centers for Disease Control and Prevention. Recommended adult immunization schedule: United States - 2015. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/schedules/downloads/adult/adult-combined-schedule.pdf. Accessed February 11, 2015.
2. Centers for Disease Control and Prevention. Birth – 18 years & “Catch-up” immunization schedules. United States, 2015. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/schedules/hcp/child-adolescent.html. Accessed January 27, 2015.
3. Campos-Outcalt D. Pneumococcal vaccines for older adults: getting the timing right. J Fam Pract. 2014;63:730-733.
4. Campos-Outcalt D. The 2014-2015 influenza season: what you need to know. J Fam Pract. 2014;63:532-533.
5. Flannery B. Update on effectiveness of live-attenuated versus inactivated influenza vaccine in children and adolescents aged 2-18 years. Presented at: Advisory Committee on Immunization Practices; October 29, 2014; Atlanta, GA. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-10/flu-03-flannery.pdf. Accessed January 27, 2015.
6. Jackson BR. Typhoid and typhoid vaccines. Presented at: Advisory Committee on Immunization Practices; October 30, 2014; Atlanta, GA. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-10/Typhoid-02-Jackson.pdf. Accessed January 27, 2015.
7. Centers for Disease Control and Prevention. Typhoid immunization—recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 1994:43:1-7.
8. Luxembourg A. 9-valent HPV vaccine program key results--Part III. Presented at: Advisory Committee on Immunization Practices; October 30, 2014; Atlanta, GA. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-10/HPV-02-Luxembourg.pdf. Accessed January 27, 2015.
9. Markowitz L. 2-dose HPV vaccination schedules. Presented at: Advisory Committee on Immunization Practices; June 25, 2014; Atlanta, GA. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-06/HPV-04-Markowitz.pdf. Accessed January 27, 2015.
10. Stokley S, Jeyarajah J, Yankey D, et al; Immunization Services Division, National Center for Immunization and Respiratory Diseases, CDC; Centers for Disease Control and Prevention (CDC). Human papillomavirus vaccination coverage among adolescents, 2007-2013, and postlicensure safety monitoring, 2006-2014—United States. MMWR Morb Mortal Wkly Rep. 2014;63:620-624.
11. MacNeil J. Epidemiology of serogroup B meningococcal disease, United States. Presented at: Advisory Committee on Immunization Practices; October 30, 2014; Atlanta, GA. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-10/mening-02-MacNeil.pdf. Accessed January 27, 2015.

Weight loss • diarrhea • mild eosinophilia • Dx?
THE CASE
A 31-year-old man came to an internal medicine clinic because he’d been losing weight over the past 2 years and hadn’t been able to regain any weight despite eating properly. Our patient was born in Ethiopia, but had been living in Canada for 6 years. He reported a remote history of 2 episodes of diarrhea.
His physical exam was normal and laboratory results revealed mild eosinophilia of 0.6 × 109/L (normal range, <0.45 × 109/L). Additional tests (including complete blood count, electrolytes, liver panel, thyrotropin, and blood smear) revealed no apparent metabolic causes of the patient’s weight loss. Stool analysis (3 exams) was negative for ova and parasites.
THE DIAGNOSIS
Because our patient was born in Ethiopia, we did serologic testing for Strongyloides, which was positive (enzyme-linked immunosorbent assay for immunoglobulin G antibodies [IgG-ELISA] was 2.9; positive is >2.1). We diagnosed strongyloidiasis in this patient.
DISCUSSION
Strongyloidiasis is an infection caused by the parasite Strongyloides stercoralis.1 It affects an estimated 30 to 100 million people worldwide, mainly in Africa, Southeast Asia, Central America, and South America, but it also can occur in temperate climates.2Strongyloides is a soil-transmitted helminth (parasitic worm). The prevalence of Strongyloides infection among refugee groups in the United States is 1% to 4.3%.3-5
Although patients with strongyloidiasis are often asymptomatic, they can present with a wide range of nonspecific symptoms. In the acute stage, patients may develop signs and symptoms including cough, wheeze, abdominal pain, weight loss, diarrhea, pruritus ani, and larva currens.2 Respiratory symptoms, including tracheal irritation and a dry cough, are often confused with asthma. In the generally asymptomatic chronic stage, patients may develop gastrointestinal complaints, such as epigastric pain and heartburn.6
Hyperinfection syndrome can occur when patients with subclinical infection receive high doses of corticosteroids for asthma or chronic obstructive pulmonary disease exacerbations. Risk of hyperinfection is increased among immunocompromised patients with human T lymphotropic virus type-1 (HTLV-1),7 as well as in patients with malignancies, malnutrition, and alcohol use disorder. Eosinophilia is often absent in patients with hyperinfection, and stool examination results are almost always positive.8
Who to screen, how to make the diagnosis
The presence of eosinophilia in immigrants, refugees, and travelers from endemic regions should alert clinicians to the possibility of an underlying helminth infection. However, because eosinophilia occurs intermittently in response to tissue invasion, absence of eosinophilia does not exclude strongyloidiasis.
The Canadian Collaboration for Immigrants and Refugee Health (CCIRH) recommends using serologic testing to screen for Strongyloides in all newly arrived refugees from low-income countries in Southeast Asia and Africa.9 The CCIRH also advises that while data on the burden of strongyloidiasis in non-refugee immigrant populations is limited, you should consider screening foreign-born individuals who have lived in endemic areas, have symptoms and/or signs of Strongyloides infection, and/or have evidence of eosinophilia.9 Because the risk of hyperinfection is increased in immunocompromised individuals, screening should be done to detect Strongyloides infection before starting chemotherapy and before initiating corticosteroids in patients from endemic areas.10
Diagnostic methods. Stool examination6 and IgG-ELISA2 are the main methods used to diagnose strongyloidiasis. However, traditional stool examinations have low sensitivity, and it may require up to 7 stool exams to reach a sensitivity of 100%,6 which could explain why our patient’s stool analysis was negative for parasites. In our experience, a positive serology result should always be assumed to indicate an active infection unless there is a well documented history of prior therapy. (In such cases, a positive serology result could represent persistent antibodies following therapy.)
First-line therapy and alternative treatment
All patients with strongyloidiasis, regardless of whether they are symptomatic, must be treated to prevent possible late-onset disseminated disease and hyperinfection.9 The Centers for Disease Control and Prevention recommends one to 2 doses of ivermectin 200 mcg/kg as first-line therapy or albendazole 400 mg twice daily for 3 days as an alternative treatment (TABLE).11 Ivermectin cures more than 95% of cases.12 Albendazole has lower efficacy (78%).13 Some experts recommend administering the 2 doses of ivermectin 2 weeks apart to allow enough time for the parasite to migrate to the gut.4
Coinfection with HTLV-1 (which is endemic in areas where Strongyloides also is
endemic) modifies patients’ immune response and can complicate treatment.9 Clinicians should screen strongyloidiasis patients for HTLV-1 if they come from high-prevalence areas and/or have persistent strongyloidiasis that responds poorly to antiparasitic treatment.9
Consider referral to an infectious disease specialist for patients coinfected with
HTLV-1, as well as those who are immunocompromised. Such referral also may be appropriate for patients from countries where loa loa is endemic, because encephalopathy has occurred in patients coinfected with loa loa who were treated with ivermectin.10
Our patient was treated with 2 doses of ivermectin 200 mcg/kg, 2 weeks apart. Four months later, his eosinophilia had resolved, his IgG-ELISA dropped to 0.37, and he had gained 2.5 pounds.
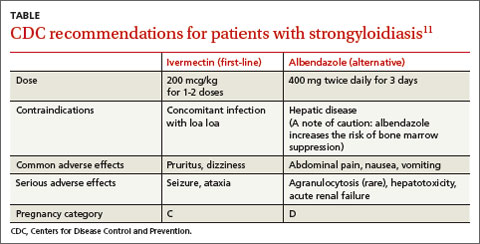
THE TAKEAWAY
Strongyloidiasis is an infection caused by the parasitic worm Strongyloides stercoralis that is most common in tropical or subtropical areas. It can be asymptomatic or present with a wide range of nonspecific signs and symptoms, such as eosinophilia, cough, wheeze, abdominal pain, weight loss, diarrhea, pruritus ani, and larva currens. It is diagnosed by stool examination and serologic testing. Ivermectin is first-line therapy; albendazole is an alternative.
1. World Health Organization. Strongyloidiasis. World Health Organization Web site. Available at: http://www.who.int/neglected_diseases/diseases/strongyloidiasis/en/. Accessed January 29, 2015.
2. Lim S, Katz K, Krajden S, et al. Complicated and fatal Strongyloides infection in Canadians: risk factors, diagnosis and management. CMAJ. 2004;171:479-484.
3. Lifson AR, Thai D, O’Fallon A, et al. Prevalence of tuberculosis, hepatitis B virus, and intestinal parasitic infections among refugees to Minnesota. Public Health Rep. 2002;117:69-77.
4. Miller JM, Boyd HA, Ostrowski SR, et al. Malaria, intestinal parasites, and schistosomiasis among Barawan Somali refugees resettling to the United States: a strategy to reduce morbidity and decrease the risk of imported infections. Am J Trop Med Hyg. 2000;62:115-121.
5. Molina CD, Molina MM, Molina JM. Intestinal parasites in southeast Asian refugees two years after immigration. West J Med. 1988;149:422-425.
6. Centers for Disease Control and Prevention. Parasites – strongyloides. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/parasites/strongyloides/health_professionals/index.html. Accessed February 3, 2015.
7. Requena-Méndez A, Chiodini P, Bisoffi Z, et al. The laboratory diagnosis and follow up of strongyloidiasis: a systemic review. PLoS Negl Trop Dis. 2013;7:e2002.
8. Mirdha BR. Human strogyloidiasis: often brushed under the carpet. Trop Gastroenterol. 2009;30:1-4.
9. Pottie K, Greenaway C, Feightner J, et al; Canadian Collaboration for Immigrant and Refugee Health. Evidence-based clinical guidelines for immigrants and refugees. CMAJ. 2011;183:E824-E925.
10. Lagacé-Wiens PR, Harding GK. A Canadian immigrant with coinfection of Strongyloides stercoralis and human T-lymphotropic virus 1. CMAJ. 2007;177:451-453.
11. Centers for Disease Control and Prevention. Guidelines for overseas presumptive treatment of strongyloidiasis, schistosomiasis, and soil-transmitted helminth infections. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/immigrantrefugeehealth/guidelines/overseas/intestinal-parasites-overseas.html. Accessed January 29, 2015.
12. Igual-Adell R, Oltra-Alcaraz C, Soler-Company E, et al. Efficacy and safety of ivermectin and thiabendazole in the treatment of strongyloidiasis. Expert Opin Pharmacother. 2004;5:2615-2619.
13. Horton J. Albendazole: a review of antihelmintic efficacy and safety in humans. Parasitology. 2000;121:S113-S132.
THE CASE
A 31-year-old man came to an internal medicine clinic because he’d been losing weight over the past 2 years and hadn’t been able to regain any weight despite eating properly. Our patient was born in Ethiopia, but had been living in Canada for 6 years. He reported a remote history of 2 episodes of diarrhea.
His physical exam was normal and laboratory results revealed mild eosinophilia of 0.6 × 109/L (normal range, <0.45 × 109/L). Additional tests (including complete blood count, electrolytes, liver panel, thyrotropin, and blood smear) revealed no apparent metabolic causes of the patient’s weight loss. Stool analysis (3 exams) was negative for ova and parasites.
THE DIAGNOSIS
Because our patient was born in Ethiopia, we did serologic testing for Strongyloides, which was positive (enzyme-linked immunosorbent assay for immunoglobulin G antibodies [IgG-ELISA] was 2.9; positive is >2.1). We diagnosed strongyloidiasis in this patient.
DISCUSSION
Strongyloidiasis is an infection caused by the parasite Strongyloides stercoralis.1 It affects an estimated 30 to 100 million people worldwide, mainly in Africa, Southeast Asia, Central America, and South America, but it also can occur in temperate climates.2Strongyloides is a soil-transmitted helminth (parasitic worm). The prevalence of Strongyloides infection among refugee groups in the United States is 1% to 4.3%.3-5
Although patients with strongyloidiasis are often asymptomatic, they can present with a wide range of nonspecific symptoms. In the acute stage, patients may develop signs and symptoms including cough, wheeze, abdominal pain, weight loss, diarrhea, pruritus ani, and larva currens.2 Respiratory symptoms, including tracheal irritation and a dry cough, are often confused with asthma. In the generally asymptomatic chronic stage, patients may develop gastrointestinal complaints, such as epigastric pain and heartburn.6
Hyperinfection syndrome can occur when patients with subclinical infection receive high doses of corticosteroids for asthma or chronic obstructive pulmonary disease exacerbations. Risk of hyperinfection is increased among immunocompromised patients with human T lymphotropic virus type-1 (HTLV-1),7 as well as in patients with malignancies, malnutrition, and alcohol use disorder. Eosinophilia is often absent in patients with hyperinfection, and stool examination results are almost always positive.8
Who to screen, how to make the diagnosis
The presence of eosinophilia in immigrants, refugees, and travelers from endemic regions should alert clinicians to the possibility of an underlying helminth infection. However, because eosinophilia occurs intermittently in response to tissue invasion, absence of eosinophilia does not exclude strongyloidiasis.
The Canadian Collaboration for Immigrants and Refugee Health (CCIRH) recommends using serologic testing to screen for Strongyloides in all newly arrived refugees from low-income countries in Southeast Asia and Africa.9 The CCIRH also advises that while data on the burden of strongyloidiasis in non-refugee immigrant populations is limited, you should consider screening foreign-born individuals who have lived in endemic areas, have symptoms and/or signs of Strongyloides infection, and/or have evidence of eosinophilia.9 Because the risk of hyperinfection is increased in immunocompromised individuals, screening should be done to detect Strongyloides infection before starting chemotherapy and before initiating corticosteroids in patients from endemic areas.10
Diagnostic methods. Stool examination6 and IgG-ELISA2 are the main methods used to diagnose strongyloidiasis. However, traditional stool examinations have low sensitivity, and it may require up to 7 stool exams to reach a sensitivity of 100%,6 which could explain why our patient’s stool analysis was negative for parasites. In our experience, a positive serology result should always be assumed to indicate an active infection unless there is a well documented history of prior therapy. (In such cases, a positive serology result could represent persistent antibodies following therapy.)
First-line therapy and alternative treatment
All patients with strongyloidiasis, regardless of whether they are symptomatic, must be treated to prevent possible late-onset disseminated disease and hyperinfection.9 The Centers for Disease Control and Prevention recommends one to 2 doses of ivermectin 200 mcg/kg as first-line therapy or albendazole 400 mg twice daily for 3 days as an alternative treatment (TABLE).11 Ivermectin cures more than 95% of cases.12 Albendazole has lower efficacy (78%).13 Some experts recommend administering the 2 doses of ivermectin 2 weeks apart to allow enough time for the parasite to migrate to the gut.4
Coinfection with HTLV-1 (which is endemic in areas where Strongyloides also is
endemic) modifies patients’ immune response and can complicate treatment.9 Clinicians should screen strongyloidiasis patients for HTLV-1 if they come from high-prevalence areas and/or have persistent strongyloidiasis that responds poorly to antiparasitic treatment.9
Consider referral to an infectious disease specialist for patients coinfected with
HTLV-1, as well as those who are immunocompromised. Such referral also may be appropriate for patients from countries where loa loa is endemic, because encephalopathy has occurred in patients coinfected with loa loa who were treated with ivermectin.10
Our patient was treated with 2 doses of ivermectin 200 mcg/kg, 2 weeks apart. Four months later, his eosinophilia had resolved, his IgG-ELISA dropped to 0.37, and he had gained 2.5 pounds.
THE TAKEAWAY
Strongyloidiasis is an infection caused by the parasitic worm Strongyloides stercoralis that is most common in tropical or subtropical areas. It can be asymptomatic or present with a wide range of nonspecific signs and symptoms, such as eosinophilia, cough, wheeze, abdominal pain, weight loss, diarrhea, pruritus ani, and larva currens. It is diagnosed by stool examination and serologic testing. Ivermectin is first-line therapy; albendazole is an alternative.
THE CASE
A 31-year-old man came to an internal medicine clinic because he’d been losing weight over the past 2 years and hadn’t been able to regain any weight despite eating properly. Our patient was born in Ethiopia, but had been living in Canada for 6 years. He reported a remote history of 2 episodes of diarrhea.
His physical exam was normal and laboratory results revealed mild eosinophilia of 0.6 × 109/L (normal range, <0.45 × 109/L). Additional tests (including complete blood count, electrolytes, liver panel, thyrotropin, and blood smear) revealed no apparent metabolic causes of the patient’s weight loss. Stool analysis (3 exams) was negative for ova and parasites.
THE DIAGNOSIS
Because our patient was born in Ethiopia, we did serologic testing for Strongyloides, which was positive (enzyme-linked immunosorbent assay for immunoglobulin G antibodies [IgG-ELISA] was 2.9; positive is >2.1). We diagnosed strongyloidiasis in this patient.
DISCUSSION
Strongyloidiasis is an infection caused by the parasite Strongyloides stercoralis.1 It affects an estimated 30 to 100 million people worldwide, mainly in Africa, Southeast Asia, Central America, and South America, but it also can occur in temperate climates.2Strongyloides is a soil-transmitted helminth (parasitic worm). The prevalence of Strongyloides infection among refugee groups in the United States is 1% to 4.3%.3-5
Although patients with strongyloidiasis are often asymptomatic, they can present with a wide range of nonspecific symptoms. In the acute stage, patients may develop signs and symptoms including cough, wheeze, abdominal pain, weight loss, diarrhea, pruritus ani, and larva currens.2 Respiratory symptoms, including tracheal irritation and a dry cough, are often confused with asthma. In the generally asymptomatic chronic stage, patients may develop gastrointestinal complaints, such as epigastric pain and heartburn.6
Hyperinfection syndrome can occur when patients with subclinical infection receive high doses of corticosteroids for asthma or chronic obstructive pulmonary disease exacerbations. Risk of hyperinfection is increased among immunocompromised patients with human T lymphotropic virus type-1 (HTLV-1),7 as well as in patients with malignancies, malnutrition, and alcohol use disorder. Eosinophilia is often absent in patients with hyperinfection, and stool examination results are almost always positive.8
Who to screen, how to make the diagnosis
The presence of eosinophilia in immigrants, refugees, and travelers from endemic regions should alert clinicians to the possibility of an underlying helminth infection. However, because eosinophilia occurs intermittently in response to tissue invasion, absence of eosinophilia does not exclude strongyloidiasis.
The Canadian Collaboration for Immigrants and Refugee Health (CCIRH) recommends using serologic testing to screen for Strongyloides in all newly arrived refugees from low-income countries in Southeast Asia and Africa.9 The CCIRH also advises that while data on the burden of strongyloidiasis in non-refugee immigrant populations is limited, you should consider screening foreign-born individuals who have lived in endemic areas, have symptoms and/or signs of Strongyloides infection, and/or have evidence of eosinophilia.9 Because the risk of hyperinfection is increased in immunocompromised individuals, screening should be done to detect Strongyloides infection before starting chemotherapy and before initiating corticosteroids in patients from endemic areas.10
Diagnostic methods. Stool examination6 and IgG-ELISA2 are the main methods used to diagnose strongyloidiasis. However, traditional stool examinations have low sensitivity, and it may require up to 7 stool exams to reach a sensitivity of 100%,6 which could explain why our patient’s stool analysis was negative for parasites. In our experience, a positive serology result should always be assumed to indicate an active infection unless there is a well documented history of prior therapy. (In such cases, a positive serology result could represent persistent antibodies following therapy.)
First-line therapy and alternative treatment
All patients with strongyloidiasis, regardless of whether they are symptomatic, must be treated to prevent possible late-onset disseminated disease and hyperinfection.9 The Centers for Disease Control and Prevention recommends one to 2 doses of ivermectin 200 mcg/kg as first-line therapy or albendazole 400 mg twice daily for 3 days as an alternative treatment (TABLE).11 Ivermectin cures more than 95% of cases.12 Albendazole has lower efficacy (78%).13 Some experts recommend administering the 2 doses of ivermectin 2 weeks apart to allow enough time for the parasite to migrate to the gut.4
Coinfection with HTLV-1 (which is endemic in areas where Strongyloides also is
endemic) modifies patients’ immune response and can complicate treatment.9 Clinicians should screen strongyloidiasis patients for HTLV-1 if they come from high-prevalence areas and/or have persistent strongyloidiasis that responds poorly to antiparasitic treatment.9
Consider referral to an infectious disease specialist for patients coinfected with
HTLV-1, as well as those who are immunocompromised. Such referral also may be appropriate for patients from countries where loa loa is endemic, because encephalopathy has occurred in patients coinfected with loa loa who were treated with ivermectin.10
Our patient was treated with 2 doses of ivermectin 200 mcg/kg, 2 weeks apart. Four months later, his eosinophilia had resolved, his IgG-ELISA dropped to 0.37, and he had gained 2.5 pounds.
THE TAKEAWAY
Strongyloidiasis is an infection caused by the parasitic worm Strongyloides stercoralis that is most common in tropical or subtropical areas. It can be asymptomatic or present with a wide range of nonspecific signs and symptoms, such as eosinophilia, cough, wheeze, abdominal pain, weight loss, diarrhea, pruritus ani, and larva currens. It is diagnosed by stool examination and serologic testing. Ivermectin is first-line therapy; albendazole is an alternative.
1. World Health Organization. Strongyloidiasis. World Health Organization Web site. Available at: http://www.who.int/neglected_diseases/diseases/strongyloidiasis/en/. Accessed January 29, 2015.
2. Lim S, Katz K, Krajden S, et al. Complicated and fatal Strongyloides infection in Canadians: risk factors, diagnosis and management. CMAJ. 2004;171:479-484.
3. Lifson AR, Thai D, O’Fallon A, et al. Prevalence of tuberculosis, hepatitis B virus, and intestinal parasitic infections among refugees to Minnesota. Public Health Rep. 2002;117:69-77.
4. Miller JM, Boyd HA, Ostrowski SR, et al. Malaria, intestinal parasites, and schistosomiasis among Barawan Somali refugees resettling to the United States: a strategy to reduce morbidity and decrease the risk of imported infections. Am J Trop Med Hyg. 2000;62:115-121.
5. Molina CD, Molina MM, Molina JM. Intestinal parasites in southeast Asian refugees two years after immigration. West J Med. 1988;149:422-425.
6. Centers for Disease Control and Prevention. Parasites – strongyloides. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/parasites/strongyloides/health_professionals/index.html. Accessed February 3, 2015.
7. Requena-Méndez A, Chiodini P, Bisoffi Z, et al. The laboratory diagnosis and follow up of strongyloidiasis: a systemic review. PLoS Negl Trop Dis. 2013;7:e2002.
8. Mirdha BR. Human strogyloidiasis: often brushed under the carpet. Trop Gastroenterol. 2009;30:1-4.
9. Pottie K, Greenaway C, Feightner J, et al; Canadian Collaboration for Immigrant and Refugee Health. Evidence-based clinical guidelines for immigrants and refugees. CMAJ. 2011;183:E824-E925.
10. Lagacé-Wiens PR, Harding GK. A Canadian immigrant with coinfection of Strongyloides stercoralis and human T-lymphotropic virus 1. CMAJ. 2007;177:451-453.
11. Centers for Disease Control and Prevention. Guidelines for overseas presumptive treatment of strongyloidiasis, schistosomiasis, and soil-transmitted helminth infections. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/immigrantrefugeehealth/guidelines/overseas/intestinal-parasites-overseas.html. Accessed January 29, 2015.
12. Igual-Adell R, Oltra-Alcaraz C, Soler-Company E, et al. Efficacy and safety of ivermectin and thiabendazole in the treatment of strongyloidiasis. Expert Opin Pharmacother. 2004;5:2615-2619.
13. Horton J. Albendazole: a review of antihelmintic efficacy and safety in humans. Parasitology. 2000;121:S113-S132.
1. World Health Organization. Strongyloidiasis. World Health Organization Web site. Available at: http://www.who.int/neglected_diseases/diseases/strongyloidiasis/en/. Accessed January 29, 2015.
2. Lim S, Katz K, Krajden S, et al. Complicated and fatal Strongyloides infection in Canadians: risk factors, diagnosis and management. CMAJ. 2004;171:479-484.
3. Lifson AR, Thai D, O’Fallon A, et al. Prevalence of tuberculosis, hepatitis B virus, and intestinal parasitic infections among refugees to Minnesota. Public Health Rep. 2002;117:69-77.
4. Miller JM, Boyd HA, Ostrowski SR, et al. Malaria, intestinal parasites, and schistosomiasis among Barawan Somali refugees resettling to the United States: a strategy to reduce morbidity and decrease the risk of imported infections. Am J Trop Med Hyg. 2000;62:115-121.
5. Molina CD, Molina MM, Molina JM. Intestinal parasites in southeast Asian refugees two years after immigration. West J Med. 1988;149:422-425.
6. Centers for Disease Control and Prevention. Parasites – strongyloides. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/parasites/strongyloides/health_professionals/index.html. Accessed February 3, 2015.
7. Requena-Méndez A, Chiodini P, Bisoffi Z, et al. The laboratory diagnosis and follow up of strongyloidiasis: a systemic review. PLoS Negl Trop Dis. 2013;7:e2002.
8. Mirdha BR. Human strogyloidiasis: often brushed under the carpet. Trop Gastroenterol. 2009;30:1-4.
9. Pottie K, Greenaway C, Feightner J, et al; Canadian Collaboration for Immigrant and Refugee Health. Evidence-based clinical guidelines for immigrants and refugees. CMAJ. 2011;183:E824-E925.
10. Lagacé-Wiens PR, Harding GK. A Canadian immigrant with coinfection of Strongyloides stercoralis and human T-lymphotropic virus 1. CMAJ. 2007;177:451-453.
11. Centers for Disease Control and Prevention. Guidelines for overseas presumptive treatment of strongyloidiasis, schistosomiasis, and soil-transmitted helminth infections. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/immigrantrefugeehealth/guidelines/overseas/intestinal-parasites-overseas.html. Accessed January 29, 2015.
12. Igual-Adell R, Oltra-Alcaraz C, Soler-Company E, et al. Efficacy and safety of ivermectin and thiabendazole in the treatment of strongyloidiasis. Expert Opin Pharmacother. 2004;5:2615-2619.
13. Horton J. Albendazole: a review of antihelmintic efficacy and safety in humans. Parasitology. 2000;121:S113-S132.

Homozygous Familial Hypercholesterolemia: Role of NPs and PAs in Achieving Optimal Outcomes Using Novel Therapeutic Interventions

Click here to read the supplement.
Click here to read the supplement.
Click here to read the supplement.