User login
Mean platelet volume higher in DVT patients with PE than without
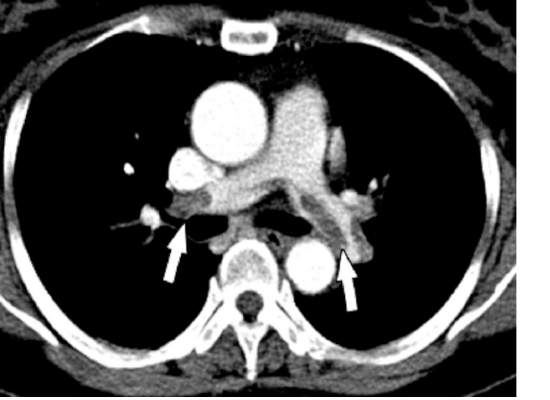
Mean platelet volume (MPV) has been associated with deep vein thrombosis (DVT), but it also appears to be a potential predictor of the presence of pulmonary embolism (PE), according to a retrospective analysis of patients reported by Dr. Atilla Icli of Ahi Evran University, Kirsehir, Turkey, and his colleagues.
The researchers assessed three groups of patients among those admitted to the emergency department or outpatient clinic of two university hospitals during 2005-2014. The patient study groups consisted of 98 patients with DVT and PE (48 men; mean age, 56.8 years); 97 patients with DVT without PE (48 men; mean age, 54.2 years); and 98 patients admitted with suspicion of DVT, but confirmed to be free of DVT and PE (45 men; mean age, 55.0 years) (Heart Lung Circulation. 2015 Nov;24[11]:1081-6).

There were no statistically significant differences between the groups with regard to sex, age, body mass index, or comorbidities such as hypertension or diabetes. Blood samples were drawn from all patients and assessed for MPV.
MPV was significantly higher in all DVT patients than controls (9.3 femtoliter vs. 7.9 fL; P less than .001) and in DVT patients with PE as compared to DVT patients without PE (9.9 fL vs. 8.7 fL, respectively; P less than .001). A cut-off point was seen where the rate of PE was significantly higher in patients with MPV greater than 9.15 fL, as compared with those with MPV equal to or below 9.15 fL. In addition, the presence of PE in patients with DVT was independently associated with MPV (odds ratio, 22.2; P less than .001).
“Our findings suggest that MPVs are elevated in patients with DVT, and higher MPVs may be associated with this group of patients,” Dr. Icli and his colleagues concluded.
The authors indicated that they had no relevant conflicts.
Read the full study online in Heart, Lung and Circulation.
Mean platelet volume (MPV) has been associated with deep vein thrombosis (DVT), but it also appears to be a potential predictor of the presence of pulmonary embolism (PE), according to a retrospective analysis of patients reported by Dr. Atilla Icli of Ahi Evran University, Kirsehir, Turkey, and his colleagues.
The researchers assessed three groups of patients among those admitted to the emergency department or outpatient clinic of two university hospitals during 2005-2014. The patient study groups consisted of 98 patients with DVT and PE (48 men; mean age, 56.8 years); 97 patients with DVT without PE (48 men; mean age, 54.2 years); and 98 patients admitted with suspicion of DVT, but confirmed to be free of DVT and PE (45 men; mean age, 55.0 years) (Heart Lung Circulation. 2015 Nov;24[11]:1081-6).
There were no statistically significant differences between the groups with regard to sex, age, body mass index, or comorbidities such as hypertension or diabetes. Blood samples were drawn from all patients and assessed for MPV.
MPV was significantly higher in all DVT patients than controls (9.3 femtoliter vs. 7.9 fL; P less than .001) and in DVT patients with PE as compared to DVT patients without PE (9.9 fL vs. 8.7 fL, respectively; P less than .001). A cut-off point was seen where the rate of PE was significantly higher in patients with MPV greater than 9.15 fL, as compared with those with MPV equal to or below 9.15 fL. In addition, the presence of PE in patients with DVT was independently associated with MPV (odds ratio, 22.2; P less than .001).
“Our findings suggest that MPVs are elevated in patients with DVT, and higher MPVs may be associated with this group of patients,” Dr. Icli and his colleagues concluded.
The authors indicated that they had no relevant conflicts.
Read the full study online in Heart, Lung and Circulation.
Mean platelet volume (MPV) has been associated with deep vein thrombosis (DVT), but it also appears to be a potential predictor of the presence of pulmonary embolism (PE), according to a retrospective analysis of patients reported by Dr. Atilla Icli of Ahi Evran University, Kirsehir, Turkey, and his colleagues.
The researchers assessed three groups of patients among those admitted to the emergency department or outpatient clinic of two university hospitals during 2005-2014. The patient study groups consisted of 98 patients with DVT and PE (48 men; mean age, 56.8 years); 97 patients with DVT without PE (48 men; mean age, 54.2 years); and 98 patients admitted with suspicion of DVT, but confirmed to be free of DVT and PE (45 men; mean age, 55.0 years) (Heart Lung Circulation. 2015 Nov;24[11]:1081-6).
There were no statistically significant differences between the groups with regard to sex, age, body mass index, or comorbidities such as hypertension or diabetes. Blood samples were drawn from all patients and assessed for MPV.
MPV was significantly higher in all DVT patients than controls (9.3 femtoliter vs. 7.9 fL; P less than .001) and in DVT patients with PE as compared to DVT patients without PE (9.9 fL vs. 8.7 fL, respectively; P less than .001). A cut-off point was seen where the rate of PE was significantly higher in patients with MPV greater than 9.15 fL, as compared with those with MPV equal to or below 9.15 fL. In addition, the presence of PE in patients with DVT was independently associated with MPV (odds ratio, 22.2; P less than .001).
“Our findings suggest that MPVs are elevated in patients with DVT, and higher MPVs may be associated with this group of patients,” Dr. Icli and his colleagues concluded.
The authors indicated that they had no relevant conflicts.
Read the full study online in Heart, Lung and Circulation.
FROM HEART, LUNG AND CIRCULATION
Hybrid approach tackles critical limb ischemia
CHICAGO – A hybrid approach combining external iliac endarterectomy with stenting may offer vascular surgeons a more robust option to stenting alone or aortofemoral bypass in patients with critical limb ischemia.
“Hybrid-based iliofemoral endarterectomy provides a minimally invasive option for revascularization, producing robust inflow restoration and low perioperative morbidity,” study author Dr. Crystal Kavanagh of St. Joseph Mercy Health Center in Ann Arbor, Mich., said.

The 5-year retrospective series, presented here at the annual meeting of the Midwestern Vascular Surgical Society, earned the prestigious Szilagyi Award for best clinical research.
Dr. Kavanagh and her colleagues crafted the hybrid technique because conventional open approaches in managing external iliac occlusive disease are associated with considerable morbidity. At the same time, long or multisegmental external iliac-to-femoral arterial lesions treated with stenting alone have produced poor patency and typically require additional outflow procedures, she explained.
The technique uses external iliac endarterectomy, aided with a traditional moll-ring stripper. A longitudinal, femoral cut-down is completed. A wire is advanced through the ipsilateral external iliac artery into the aorta after heparinization and obtaining access via an 18-gauge micropuncture in the common femoral artery. Intraluminal positioning is confirmed and a moll-ring endarterectomy is completed over the wire using a balloon to create the distal transection point, Dr. Kavanagh explained. The moll-ring is sized to the maximum diameter that will be accommodated by the ring.
After partially deflating the balloon, the plaque is extracted. A long-segment endarterectomy is typically completed, leaving a widely patent external iliac artery, she said.
In cases where adjunct iliac stenting is required, such as a proximal dissection flap, the stent size is larger than what is typically placed with stenting alone, Dr. Kavanagh observed.
The 2007 TASC (TransAtlantic InterSociety Consensus) recommendations suggest that TASC A lesions should undergo endovascular treatment as first-line therapy, while TASC D lesions should undergo traditional open surgical bypass.
Consensus has been slow to form for TASC B and C lesions, although most TASC B lesions undergo endovascular treatment and most TASC C lesions undergo open bypass.
Among the 40 limbs in the series, a common iliac (CI) artery stent (mean diameter, 8 mm: mean length, 59 mm) was placed in 19 limbs; a CI-to-external iliac (EI) stent (mean diameter, 10 mm; mean length, 100 mm) in 7 limbs; and an EI stent (mean diameter, 10 mm; mean length, 100 mm) in 21 limbs.
None of the iliac lesions were TASC category A or B, 17% were TASC C, and 83% TASC D. Concomitant infrainguinal disease of these patients had femoral/popliteal lesions, of which 16% were type A, 33% type B, 19% type C, and 32% type D.
Half of the 33 patients had three-vessel runoff, 33% two-vessel runoff, and 17% single-vessel runoff.
The hybrid procedure was completed as planned in all 40 limbs, Dr. Kavanagh said. There was no intraoperative or 90-day mortality.
Perioperative complications were minimal, with a 30-day readmission rate of only 12%, she said. This included one patient with one-vessel run-off who re-presented with ischemia requiring common femoral-to-below-the-knee popliteal bypass.
A second patient was admitted at postoperative day 47 with an infected pseudoaneurysm requiring patch angioplasty revision, for a 90-day readmission rate of 15%.
“Concerns about potential plaque rupture or hemorrhage can easily be dealt with via a covered stent graft, given intraluminal wire access throughout the procedure,” senior author Dr. Abdulhameed Aziz said in an interview.
Significant gains were made from baseline in postoperative ankle-brachial index (mean, 0.4 vs. 076; P less than .001), as well as in toe pressures (mean, 32 mm Hg vs. 60 mm Hg; P less than .001), Dr. Kavanagh said.
After a median follow-up of 13 months, primary patency was 100%.
“Combined common femoral endarterectomy with iliac stenting has demonstrated comparable patency to operative bypass in the short term,” she said.
“We theorize that the longer-segment endarterectomy, in our case essentially going from the iliac bifurcation to the common femoral, may produce a more durable result ... Stenting the proximal transection point may prevent restenosis.”
The authors reported no financial disclosures.
The combination of open surgical procedures with endovascular interventions has enriched the spectrum of vascular reconstructions significantly. These so-called hybrid procedures are especially worthwhile if pros and cons of both approaches could be combined and the groin could be considered as the hub. Technically spoken, the groin is the ideal hub for these kind of procedures. Why is that the case? Usually the surgical access to the common femoral artery (CFA) is easy. Furthermore the long-term results of femoral/retrograde iliac endarterectomy (often in combination with profundoplasty) are undoubtedly excellent. For the endovascular world, the (almost) NO-GO for any metal in the groin is still valid, and balloon dilatation of the femoral arteries is hemodynamically insufficient in most cases. However, PTA [percutaneous transluminal angioplasty] and stenting of the iliac arteries comes with good long-term results and avoids the sometimes-extended surgical access via the abdomen or the retroperitoneum.
Technically, it is advisable to perform the procedure in the following way: exposure of the CFA up to the inguinal ligament and down to the proximal superficial and deep femoral artery; puncture of the CFA in a noncalcified area and retrograde guide-wire access to the distal aorta (confirmation by angiography); balloon blockage of the proximal iliac artery (if technically possible; open endarterectomy of the CFA (including the proximal superficial and deep femoral artery; and retrograde ring-stripper endarterectomy of the iliac arteries and reconstruction of the femoral arteries (patchplasty, femoral transposition, profundoplasty). Balloon dilatation and stenting will be performed at the end of the procedure via a 7F or 9F sheath. We prefer balloon-expandable stents for the common and self-expandable stents for the external iliac artery, respectively. The contralateral groin should also be prepared for kissing stenting of both iliac arteries. Very rarely, an antegrade iliac access (via contralateral or brachial) access) is necessary. Whether or not covered stents have better long-term results is an open issue, however, covered stents should always be available to treat rare complications like an iatrogenic iliac rupture.
Especially Rutherford stage 5 or 6 patients very often present with multisegment disease including the femoropopliteal and the crural arteries. Since an even perfect inguinal inflow might not be sufficient in CLI [critical limb ischemia], these patients often need additional open or endovascular procedures. Again, the latter can be performed simultaneously via the hub femoral artery.
Even though hybrid procedures have been an essential part of vascular surgical practice for some years now, the Midwestern Vascular Surgical Society and Dr. Kavanagh have to be congratulated for raising this clinically very important topic again.
Dr. Hans-Henning Eckstein is a Professor at the Department for Vascular and Endovascular Surgery, Klinikum rechts der Isar, Technical University Munich, and is an associate medical editor for Vascular Specialist.
The combination of open surgical procedures with endovascular interventions has enriched the spectrum of vascular reconstructions significantly. These so-called hybrid procedures are especially worthwhile if pros and cons of both approaches could be combined and the groin could be considered as the hub. Technically spoken, the groin is the ideal hub for these kind of procedures. Why is that the case? Usually the surgical access to the common femoral artery (CFA) is easy. Furthermore the long-term results of femoral/retrograde iliac endarterectomy (often in combination with profundoplasty) are undoubtedly excellent. For the endovascular world, the (almost) NO-GO for any metal in the groin is still valid, and balloon dilatation of the femoral arteries is hemodynamically insufficient in most cases. However, PTA [percutaneous transluminal angioplasty] and stenting of the iliac arteries comes with good long-term results and avoids the sometimes-extended surgical access via the abdomen or the retroperitoneum.
Technically, it is advisable to perform the procedure in the following way: exposure of the CFA up to the inguinal ligament and down to the proximal superficial and deep femoral artery; puncture of the CFA in a noncalcified area and retrograde guide-wire access to the distal aorta (confirmation by angiography); balloon blockage of the proximal iliac artery (if technically possible; open endarterectomy of the CFA (including the proximal superficial and deep femoral artery; and retrograde ring-stripper endarterectomy of the iliac arteries and reconstruction of the femoral arteries (patchplasty, femoral transposition, profundoplasty). Balloon dilatation and stenting will be performed at the end of the procedure via a 7F or 9F sheath. We prefer balloon-expandable stents for the common and self-expandable stents for the external iliac artery, respectively. The contralateral groin should also be prepared for kissing stenting of both iliac arteries. Very rarely, an antegrade iliac access (via contralateral or brachial) access) is necessary. Whether or not covered stents have better long-term results is an open issue, however, covered stents should always be available to treat rare complications like an iatrogenic iliac rupture.
Especially Rutherford stage 5 or 6 patients very often present with multisegment disease including the femoropopliteal and the crural arteries. Since an even perfect inguinal inflow might not be sufficient in CLI [critical limb ischemia], these patients often need additional open or endovascular procedures. Again, the latter can be performed simultaneously via the hub femoral artery.
Even though hybrid procedures have been an essential part of vascular surgical practice for some years now, the Midwestern Vascular Surgical Society and Dr. Kavanagh have to be congratulated for raising this clinically very important topic again.
Dr. Hans-Henning Eckstein is a Professor at the Department for Vascular and Endovascular Surgery, Klinikum rechts der Isar, Technical University Munich, and is an associate medical editor for Vascular Specialist.
The combination of open surgical procedures with endovascular interventions has enriched the spectrum of vascular reconstructions significantly. These so-called hybrid procedures are especially worthwhile if pros and cons of both approaches could be combined and the groin could be considered as the hub. Technically spoken, the groin is the ideal hub for these kind of procedures. Why is that the case? Usually the surgical access to the common femoral artery (CFA) is easy. Furthermore the long-term results of femoral/retrograde iliac endarterectomy (often in combination with profundoplasty) are undoubtedly excellent. For the endovascular world, the (almost) NO-GO for any metal in the groin is still valid, and balloon dilatation of the femoral arteries is hemodynamically insufficient in most cases. However, PTA [percutaneous transluminal angioplasty] and stenting of the iliac arteries comes with good long-term results and avoids the sometimes-extended surgical access via the abdomen or the retroperitoneum.
Technically, it is advisable to perform the procedure in the following way: exposure of the CFA up to the inguinal ligament and down to the proximal superficial and deep femoral artery; puncture of the CFA in a noncalcified area and retrograde guide-wire access to the distal aorta (confirmation by angiography); balloon blockage of the proximal iliac artery (if technically possible; open endarterectomy of the CFA (including the proximal superficial and deep femoral artery; and retrograde ring-stripper endarterectomy of the iliac arteries and reconstruction of the femoral arteries (patchplasty, femoral transposition, profundoplasty). Balloon dilatation and stenting will be performed at the end of the procedure via a 7F or 9F sheath. We prefer balloon-expandable stents for the common and self-expandable stents for the external iliac artery, respectively. The contralateral groin should also be prepared for kissing stenting of both iliac arteries. Very rarely, an antegrade iliac access (via contralateral or brachial) access) is necessary. Whether or not covered stents have better long-term results is an open issue, however, covered stents should always be available to treat rare complications like an iatrogenic iliac rupture.
Especially Rutherford stage 5 or 6 patients very often present with multisegment disease including the femoropopliteal and the crural arteries. Since an even perfect inguinal inflow might not be sufficient in CLI [critical limb ischemia], these patients often need additional open or endovascular procedures. Again, the latter can be performed simultaneously via the hub femoral artery.
Even though hybrid procedures have been an essential part of vascular surgical practice for some years now, the Midwestern Vascular Surgical Society and Dr. Kavanagh have to be congratulated for raising this clinically very important topic again.
Dr. Hans-Henning Eckstein is a Professor at the Department for Vascular and Endovascular Surgery, Klinikum rechts der Isar, Technical University Munich, and is an associate medical editor for Vascular Specialist.
CHICAGO – A hybrid approach combining external iliac endarterectomy with stenting may offer vascular surgeons a more robust option to stenting alone or aortofemoral bypass in patients with critical limb ischemia.
“Hybrid-based iliofemoral endarterectomy provides a minimally invasive option for revascularization, producing robust inflow restoration and low perioperative morbidity,” study author Dr. Crystal Kavanagh of St. Joseph Mercy Health Center in Ann Arbor, Mich., said.
The 5-year retrospective series, presented here at the annual meeting of the Midwestern Vascular Surgical Society, earned the prestigious Szilagyi Award for best clinical research.
Dr. Kavanagh and her colleagues crafted the hybrid technique because conventional open approaches in managing external iliac occlusive disease are associated with considerable morbidity. At the same time, long or multisegmental external iliac-to-femoral arterial lesions treated with stenting alone have produced poor patency and typically require additional outflow procedures, she explained.
The technique uses external iliac endarterectomy, aided with a traditional moll-ring stripper. A longitudinal, femoral cut-down is completed. A wire is advanced through the ipsilateral external iliac artery into the aorta after heparinization and obtaining access via an 18-gauge micropuncture in the common femoral artery. Intraluminal positioning is confirmed and a moll-ring endarterectomy is completed over the wire using a balloon to create the distal transection point, Dr. Kavanagh explained. The moll-ring is sized to the maximum diameter that will be accommodated by the ring.
After partially deflating the balloon, the plaque is extracted. A long-segment endarterectomy is typically completed, leaving a widely patent external iliac artery, she said.
In cases where adjunct iliac stenting is required, such as a proximal dissection flap, the stent size is larger than what is typically placed with stenting alone, Dr. Kavanagh observed.
The 2007 TASC (TransAtlantic InterSociety Consensus) recommendations suggest that TASC A lesions should undergo endovascular treatment as first-line therapy, while TASC D lesions should undergo traditional open surgical bypass.
Consensus has been slow to form for TASC B and C lesions, although most TASC B lesions undergo endovascular treatment and most TASC C lesions undergo open bypass.
Among the 40 limbs in the series, a common iliac (CI) artery stent (mean diameter, 8 mm: mean length, 59 mm) was placed in 19 limbs; a CI-to-external iliac (EI) stent (mean diameter, 10 mm; mean length, 100 mm) in 7 limbs; and an EI stent (mean diameter, 10 mm; mean length, 100 mm) in 21 limbs.
None of the iliac lesions were TASC category A or B, 17% were TASC C, and 83% TASC D. Concomitant infrainguinal disease of these patients had femoral/popliteal lesions, of which 16% were type A, 33% type B, 19% type C, and 32% type D.
Half of the 33 patients had three-vessel runoff, 33% two-vessel runoff, and 17% single-vessel runoff.
The hybrid procedure was completed as planned in all 40 limbs, Dr. Kavanagh said. There was no intraoperative or 90-day mortality.
Perioperative complications were minimal, with a 30-day readmission rate of only 12%, she said. This included one patient with one-vessel run-off who re-presented with ischemia requiring common femoral-to-below-the-knee popliteal bypass.
A second patient was admitted at postoperative day 47 with an infected pseudoaneurysm requiring patch angioplasty revision, for a 90-day readmission rate of 15%.
“Concerns about potential plaque rupture or hemorrhage can easily be dealt with via a covered stent graft, given intraluminal wire access throughout the procedure,” senior author Dr. Abdulhameed Aziz said in an interview.
Significant gains were made from baseline in postoperative ankle-brachial index (mean, 0.4 vs. 076; P less than .001), as well as in toe pressures (mean, 32 mm Hg vs. 60 mm Hg; P less than .001), Dr. Kavanagh said.
After a median follow-up of 13 months, primary patency was 100%.
“Combined common femoral endarterectomy with iliac stenting has demonstrated comparable patency to operative bypass in the short term,” she said.
“We theorize that the longer-segment endarterectomy, in our case essentially going from the iliac bifurcation to the common femoral, may produce a more durable result ... Stenting the proximal transection point may prevent restenosis.”
The authors reported no financial disclosures.
CHICAGO – A hybrid approach combining external iliac endarterectomy with stenting may offer vascular surgeons a more robust option to stenting alone or aortofemoral bypass in patients with critical limb ischemia.
“Hybrid-based iliofemoral endarterectomy provides a minimally invasive option for revascularization, producing robust inflow restoration and low perioperative morbidity,” study author Dr. Crystal Kavanagh of St. Joseph Mercy Health Center in Ann Arbor, Mich., said.
The 5-year retrospective series, presented here at the annual meeting of the Midwestern Vascular Surgical Society, earned the prestigious Szilagyi Award for best clinical research.
Dr. Kavanagh and her colleagues crafted the hybrid technique because conventional open approaches in managing external iliac occlusive disease are associated with considerable morbidity. At the same time, long or multisegmental external iliac-to-femoral arterial lesions treated with stenting alone have produced poor patency and typically require additional outflow procedures, she explained.
The technique uses external iliac endarterectomy, aided with a traditional moll-ring stripper. A longitudinal, femoral cut-down is completed. A wire is advanced through the ipsilateral external iliac artery into the aorta after heparinization and obtaining access via an 18-gauge micropuncture in the common femoral artery. Intraluminal positioning is confirmed and a moll-ring endarterectomy is completed over the wire using a balloon to create the distal transection point, Dr. Kavanagh explained. The moll-ring is sized to the maximum diameter that will be accommodated by the ring.
After partially deflating the balloon, the plaque is extracted. A long-segment endarterectomy is typically completed, leaving a widely patent external iliac artery, she said.
In cases where adjunct iliac stenting is required, such as a proximal dissection flap, the stent size is larger than what is typically placed with stenting alone, Dr. Kavanagh observed.
The 2007 TASC (TransAtlantic InterSociety Consensus) recommendations suggest that TASC A lesions should undergo endovascular treatment as first-line therapy, while TASC D lesions should undergo traditional open surgical bypass.
Consensus has been slow to form for TASC B and C lesions, although most TASC B lesions undergo endovascular treatment and most TASC C lesions undergo open bypass.
Among the 40 limbs in the series, a common iliac (CI) artery stent (mean diameter, 8 mm: mean length, 59 mm) was placed in 19 limbs; a CI-to-external iliac (EI) stent (mean diameter, 10 mm; mean length, 100 mm) in 7 limbs; and an EI stent (mean diameter, 10 mm; mean length, 100 mm) in 21 limbs.
None of the iliac lesions were TASC category A or B, 17% were TASC C, and 83% TASC D. Concomitant infrainguinal disease of these patients had femoral/popliteal lesions, of which 16% were type A, 33% type B, 19% type C, and 32% type D.
Half of the 33 patients had three-vessel runoff, 33% two-vessel runoff, and 17% single-vessel runoff.
The hybrid procedure was completed as planned in all 40 limbs, Dr. Kavanagh said. There was no intraoperative or 90-day mortality.
Perioperative complications were minimal, with a 30-day readmission rate of only 12%, she said. This included one patient with one-vessel run-off who re-presented with ischemia requiring common femoral-to-below-the-knee popliteal bypass.
A second patient was admitted at postoperative day 47 with an infected pseudoaneurysm requiring patch angioplasty revision, for a 90-day readmission rate of 15%.
“Concerns about potential plaque rupture or hemorrhage can easily be dealt with via a covered stent graft, given intraluminal wire access throughout the procedure,” senior author Dr. Abdulhameed Aziz said in an interview.
Significant gains were made from baseline in postoperative ankle-brachial index (mean, 0.4 vs. 076; P less than .001), as well as in toe pressures (mean, 32 mm Hg vs. 60 mm Hg; P less than .001), Dr. Kavanagh said.
After a median follow-up of 13 months, primary patency was 100%.
“Combined common femoral endarterectomy with iliac stenting has demonstrated comparable patency to operative bypass in the short term,” she said.
“We theorize that the longer-segment endarterectomy, in our case essentially going from the iliac bifurcation to the common femoral, may produce a more durable result ... Stenting the proximal transection point may prevent restenosis.”
The authors reported no financial disclosures.
AT MIDWESTERN VASCULAR 2015
Key clinical point: Hybrid-based iliofemoral endarterectomy provides robust inflow restoration comparable to aortofemoral bypass, with minimal perioperative morbidity.
Major finding: Primary patency was 100% with a mean follow-up of 13 months.
Data source: Five-year retrospective study in 40 limbs in 33 patients with critical limb ischemia.
Disclosures: The authors reported having no financial disclosures.

BEST PRACTICES: An Oral Treatment for Moderate to Severe Plaque Psoriasis
A Best Practices Supplement to Dermatology News. This supplement was sponsored by Celgene Corporation.

Faculty/Faculty Disclosures
Alan Menter, MD
Baylor University Medical Center
Dallas, TX
Dr Menter is on the advisory board for AbbVie, Allergan, Amgen, Boehringer Ingelheim, Eli Lilly, Genentech Inc., Janssen Biotech, Inc., LEO Pharma and Pfizer; is a consultant for AbbVie, Allergan, Amgen, Convoy Therapeutics, Inc., Eli Lilly, Janssen Biotech, Inc., LEO Pharma, Novartis, Pfizer, Syntrix, Vitae, Wyeth and XenoPort; is an investigator for AbbVie, Allergan, Amgen, Boehringer Ingelheim, Celgene, Eli Lilly, Genentech, Janssen Biotech, Inc., LEO Pharma, Merck, Novartis, Pfizer, Symbio/Maruho, Syntrix and Wyeth; is a speaker for AbbVie, Amgen, Janssen Biotech, Inc., LEO Pharma and Wyeth; has received grant funds from AbbVie, Allergan, Amgen, Boehringer Ingelheim, Celgene, Genentech, Janssen Biotech, Inc., LEO Pharma, Merck, Novartis, Pfizer, Symbio/Maruho and Syntrix; and has received honoraria from AbbVie, Allergan, Amgen, Boehringer Ingelheim, Convoy Therapeutics, Inc., Eli Lilly, Genentech, Janssen Biotech, Inc., LEO Pharma, Novartis, Pfizer, Syntrix, Vitae, Wyeth and XenoPort.
Copyright © by Frontline Medical Communications Inc.
A Best Practices Supplement to Dermatology News. This supplement was sponsored by Celgene Corporation.
Faculty/Faculty Disclosures
Alan Menter, MD
Baylor University Medical Center
Dallas, TX
Dr Menter is on the advisory board for AbbVie, Allergan, Amgen, Boehringer Ingelheim, Eli Lilly, Genentech Inc., Janssen Biotech, Inc., LEO Pharma and Pfizer; is a consultant for AbbVie, Allergan, Amgen, Convoy Therapeutics, Inc., Eli Lilly, Janssen Biotech, Inc., LEO Pharma, Novartis, Pfizer, Syntrix, Vitae, Wyeth and XenoPort; is an investigator for AbbVie, Allergan, Amgen, Boehringer Ingelheim, Celgene, Eli Lilly, Genentech, Janssen Biotech, Inc., LEO Pharma, Merck, Novartis, Pfizer, Symbio/Maruho, Syntrix and Wyeth; is a speaker for AbbVie, Amgen, Janssen Biotech, Inc., LEO Pharma and Wyeth; has received grant funds from AbbVie, Allergan, Amgen, Boehringer Ingelheim, Celgene, Genentech, Janssen Biotech, Inc., LEO Pharma, Merck, Novartis, Pfizer, Symbio/Maruho and Syntrix; and has received honoraria from AbbVie, Allergan, Amgen, Boehringer Ingelheim, Convoy Therapeutics, Inc., Eli Lilly, Genentech, Janssen Biotech, Inc., LEO Pharma, Novartis, Pfizer, Syntrix, Vitae, Wyeth and XenoPort.
Copyright © by Frontline Medical Communications Inc.
A Best Practices Supplement to Dermatology News. This supplement was sponsored by Celgene Corporation.
Faculty/Faculty Disclosures
Alan Menter, MD
Baylor University Medical Center
Dallas, TX
Dr Menter is on the advisory board for AbbVie, Allergan, Amgen, Boehringer Ingelheim, Eli Lilly, Genentech Inc., Janssen Biotech, Inc., LEO Pharma and Pfizer; is a consultant for AbbVie, Allergan, Amgen, Convoy Therapeutics, Inc., Eli Lilly, Janssen Biotech, Inc., LEO Pharma, Novartis, Pfizer, Syntrix, Vitae, Wyeth and XenoPort; is an investigator for AbbVie, Allergan, Amgen, Boehringer Ingelheim, Celgene, Eli Lilly, Genentech, Janssen Biotech, Inc., LEO Pharma, Merck, Novartis, Pfizer, Symbio/Maruho, Syntrix and Wyeth; is a speaker for AbbVie, Amgen, Janssen Biotech, Inc., LEO Pharma and Wyeth; has received grant funds from AbbVie, Allergan, Amgen, Boehringer Ingelheim, Celgene, Genentech, Janssen Biotech, Inc., LEO Pharma, Merck, Novartis, Pfizer, Symbio/Maruho and Syntrix; and has received honoraria from AbbVie, Allergan, Amgen, Boehringer Ingelheim, Convoy Therapeutics, Inc., Eli Lilly, Genentech, Janssen Biotech, Inc., LEO Pharma, Novartis, Pfizer, Syntrix, Vitae, Wyeth and XenoPort.
Copyright © by Frontline Medical Communications Inc.

Reality check about IUDs
The Centers for Disease Control and Prevention recently released data regarding the use of long-acting reversible contraception (LARC), specifically intrauterine devices (IUDs), in adolescents, and suggested ways to increase their use. The American Congress of Obstetricians and Gynecologists then reiterated its recommendation promoting the use of LARC in adolescents (Obstet Gynecol. 2012;120:983-8). Historically, the use of IUDs in nulliparous females was concerning because of the risk of pelvic inflammatory disease (which could lead to infertility), pain at insertion, and the cost. But more recent research has dispelled many of those concerns, and new legislation has made access and affordability a reality; hence, the use of IUDs in teens was recommended. Despite these advances, physicians still are not making teens aware of this method of contraception.
In 2013, two important things occurred. First, emergency contraception was made available over the counter without age restriction. Second, the Affordable Care Act required most private insurance plans to cover at least one type of all 18 Food and Drug Administration–approved contraceptive methods for women as prescribed without cost sharing; this reduced the barrier of cost for IUDs. For patients covered by Medicaid, details vary, but in many cases some type of IUD is covered. In considering the best method of contraception in teens, we can all agree contraception is only as good as its proper use. If we remove the concern of infertility secondary to pelvic inflammatory disease and the barrier of cost, we can make the argument that LARC is an ideal choice for young women.
Birth rates for teenagers fell 9% from 2013 to 2014, to 24.2 births per 1,000 females aged 15-19 years – a record low according to CDC data. The rate has declined 42% since 2007 and 61% since 1991. Considering that the percent of teens who engage in sexual activity has not changed, the cause of the decline has to be related to increased contraception use and education. Although rates have declined significantly, there is much work to be done to protect our teens from unintended pregnancies.
The Contraceptive Choice Project was designed to give teens the option of birth control with the barrier of cost removed. Sixty-nine percent of 10,000 girls aged 14-17 years chose the IUD (Am J Obstet Gynecol. 2010;203[2]:115.e1-e7). The Contraceptive Choice Project also stated that the teens in this study were 20 times more likely to become pregnant using oral contraceptives, the patch, or a vaginal ring, compared with LARC or an injectable contraceptive. That is a significant statistic given that the choice of birth control used is heavily dependent on the options available. As primary care physicians, we are likely the first line of intervention, so it is important that we do not exclude the options most likely to prevent unintended pregnancies.
The rate of adolescents using IUDs increased from 0.2 to 2.5 in the 2002 and 2006-2010 National Surveys of Family Growth (J Adolesc Health. 2013;53:401-6).
There are choices when it comes to IUDs. ParaGard and Mirena are most well known. ParaGard contains copper and is hormone free; it can be used as emergency contraception and can remain in place for 12 years. Mirena releases levonorgestrel, and can be left in place for 5 years; there now is a generic form. There has been hesitation in using this product in teens because of a marketing decision made when Mirena was brought to the U.S. market. The company sought FDA approval only for women who already had children to avoid concerns about fertility. But research shows IUDS are safe and effective in women of all ages.
Unlike birth control pills, Mirena and Paragard do not reduce acne. But Mirena does reduce bloating and cramping associated with periods. Paragard has unpredictable bleeding and, therefore, is a less favorable choice in women who are not restricted to hormone-free contraception.
Newer brands on the market are Skyla and Liletta. Both are comparable to Mirena but have lower amounts of hormone, so these IUDs will be less effective in controlling the cramping and bloating. Skyla, unlike Mirena, is marketed to teens.
Implementing birth control options in your practice is imperative in caring for adolescents. Bedsider.org is a wonderful website that reviews all forms of birth control, and the pros and cons associated with each; it also compares the different types to help young women make the best choice. Another useful website is thenationalcampaign.org; this website is dedicated to educating physicians, parents, and adolescents in birth control choices to reduce unplanned pregnancies.
Dr. Pearce is a pediatrician in Frankfort, Ill.
The Centers for Disease Control and Prevention recently released data regarding the use of long-acting reversible contraception (LARC), specifically intrauterine devices (IUDs), in adolescents, and suggested ways to increase their use. The American Congress of Obstetricians and Gynecologists then reiterated its recommendation promoting the use of LARC in adolescents (Obstet Gynecol. 2012;120:983-8). Historically, the use of IUDs in nulliparous females was concerning because of the risk of pelvic inflammatory disease (which could lead to infertility), pain at insertion, and the cost. But more recent research has dispelled many of those concerns, and new legislation has made access and affordability a reality; hence, the use of IUDs in teens was recommended. Despite these advances, physicians still are not making teens aware of this method of contraception.
In 2013, two important things occurred. First, emergency contraception was made available over the counter without age restriction. Second, the Affordable Care Act required most private insurance plans to cover at least one type of all 18 Food and Drug Administration–approved contraceptive methods for women as prescribed without cost sharing; this reduced the barrier of cost for IUDs. For patients covered by Medicaid, details vary, but in many cases some type of IUD is covered. In considering the best method of contraception in teens, we can all agree contraception is only as good as its proper use. If we remove the concern of infertility secondary to pelvic inflammatory disease and the barrier of cost, we can make the argument that LARC is an ideal choice for young women.
Birth rates for teenagers fell 9% from 2013 to 2014, to 24.2 births per 1,000 females aged 15-19 years – a record low according to CDC data. The rate has declined 42% since 2007 and 61% since 1991. Considering that the percent of teens who engage in sexual activity has not changed, the cause of the decline has to be related to increased contraception use and education. Although rates have declined significantly, there is much work to be done to protect our teens from unintended pregnancies.
The Contraceptive Choice Project was designed to give teens the option of birth control with the barrier of cost removed. Sixty-nine percent of 10,000 girls aged 14-17 years chose the IUD (Am J Obstet Gynecol. 2010;203[2]:115.e1-e7). The Contraceptive Choice Project also stated that the teens in this study were 20 times more likely to become pregnant using oral contraceptives, the patch, or a vaginal ring, compared with LARC or an injectable contraceptive. That is a significant statistic given that the choice of birth control used is heavily dependent on the options available. As primary care physicians, we are likely the first line of intervention, so it is important that we do not exclude the options most likely to prevent unintended pregnancies.
The rate of adolescents using IUDs increased from 0.2 to 2.5 in the 2002 and 2006-2010 National Surveys of Family Growth (J Adolesc Health. 2013;53:401-6).
There are choices when it comes to IUDs. ParaGard and Mirena are most well known. ParaGard contains copper and is hormone free; it can be used as emergency contraception and can remain in place for 12 years. Mirena releases levonorgestrel, and can be left in place for 5 years; there now is a generic form. There has been hesitation in using this product in teens because of a marketing decision made when Mirena was brought to the U.S. market. The company sought FDA approval only for women who already had children to avoid concerns about fertility. But research shows IUDS are safe and effective in women of all ages.
Unlike birth control pills, Mirena and Paragard do not reduce acne. But Mirena does reduce bloating and cramping associated with periods. Paragard has unpredictable bleeding and, therefore, is a less favorable choice in women who are not restricted to hormone-free contraception.
Newer brands on the market are Skyla and Liletta. Both are comparable to Mirena but have lower amounts of hormone, so these IUDs will be less effective in controlling the cramping and bloating. Skyla, unlike Mirena, is marketed to teens.
Implementing birth control options in your practice is imperative in caring for adolescents. Bedsider.org is a wonderful website that reviews all forms of birth control, and the pros and cons associated with each; it also compares the different types to help young women make the best choice. Another useful website is thenationalcampaign.org; this website is dedicated to educating physicians, parents, and adolescents in birth control choices to reduce unplanned pregnancies.
Dr. Pearce is a pediatrician in Frankfort, Ill.
The Centers for Disease Control and Prevention recently released data regarding the use of long-acting reversible contraception (LARC), specifically intrauterine devices (IUDs), in adolescents, and suggested ways to increase their use. The American Congress of Obstetricians and Gynecologists then reiterated its recommendation promoting the use of LARC in adolescents (Obstet Gynecol. 2012;120:983-8). Historically, the use of IUDs in nulliparous females was concerning because of the risk of pelvic inflammatory disease (which could lead to infertility), pain at insertion, and the cost. But more recent research has dispelled many of those concerns, and new legislation has made access and affordability a reality; hence, the use of IUDs in teens was recommended. Despite these advances, physicians still are not making teens aware of this method of contraception.
In 2013, two important things occurred. First, emergency contraception was made available over the counter without age restriction. Second, the Affordable Care Act required most private insurance plans to cover at least one type of all 18 Food and Drug Administration–approved contraceptive methods for women as prescribed without cost sharing; this reduced the barrier of cost for IUDs. For patients covered by Medicaid, details vary, but in many cases some type of IUD is covered. In considering the best method of contraception in teens, we can all agree contraception is only as good as its proper use. If we remove the concern of infertility secondary to pelvic inflammatory disease and the barrier of cost, we can make the argument that LARC is an ideal choice for young women.
Birth rates for teenagers fell 9% from 2013 to 2014, to 24.2 births per 1,000 females aged 15-19 years – a record low according to CDC data. The rate has declined 42% since 2007 and 61% since 1991. Considering that the percent of teens who engage in sexual activity has not changed, the cause of the decline has to be related to increased contraception use and education. Although rates have declined significantly, there is much work to be done to protect our teens from unintended pregnancies.
The Contraceptive Choice Project was designed to give teens the option of birth control with the barrier of cost removed. Sixty-nine percent of 10,000 girls aged 14-17 years chose the IUD (Am J Obstet Gynecol. 2010;203[2]:115.e1-e7). The Contraceptive Choice Project also stated that the teens in this study were 20 times more likely to become pregnant using oral contraceptives, the patch, or a vaginal ring, compared with LARC or an injectable contraceptive. That is a significant statistic given that the choice of birth control used is heavily dependent on the options available. As primary care physicians, we are likely the first line of intervention, so it is important that we do not exclude the options most likely to prevent unintended pregnancies.
The rate of adolescents using IUDs increased from 0.2 to 2.5 in the 2002 and 2006-2010 National Surveys of Family Growth (J Adolesc Health. 2013;53:401-6).
There are choices when it comes to IUDs. ParaGard and Mirena are most well known. ParaGard contains copper and is hormone free; it can be used as emergency contraception and can remain in place for 12 years. Mirena releases levonorgestrel, and can be left in place for 5 years; there now is a generic form. There has been hesitation in using this product in teens because of a marketing decision made when Mirena was brought to the U.S. market. The company sought FDA approval only for women who already had children to avoid concerns about fertility. But research shows IUDS are safe and effective in women of all ages.
Unlike birth control pills, Mirena and Paragard do not reduce acne. But Mirena does reduce bloating and cramping associated with periods. Paragard has unpredictable bleeding and, therefore, is a less favorable choice in women who are not restricted to hormone-free contraception.
Newer brands on the market are Skyla and Liletta. Both are comparable to Mirena but have lower amounts of hormone, so these IUDs will be less effective in controlling the cramping and bloating. Skyla, unlike Mirena, is marketed to teens.
Implementing birth control options in your practice is imperative in caring for adolescents. Bedsider.org is a wonderful website that reviews all forms of birth control, and the pros and cons associated with each; it also compares the different types to help young women make the best choice. Another useful website is thenationalcampaign.org; this website is dedicated to educating physicians, parents, and adolescents in birth control choices to reduce unplanned pregnancies.
Dr. Pearce is a pediatrician in Frankfort, Ill.

Radioimmunotherapy shows promise for HL

Copyright 2010 Nephron
Results of a small trial suggest the radiolabeled anti-CD25 antibody 90Y-daclizumab can treat certain patients with relapsed/refractory Hodgkin lymphoma (HL).
90Y-daclizumab produced responses in 50% of patients studied, and most of these were complete responses.
Several patients developed myelodysplastic syndrome (MDS) after receiving 90Y-daclizumab, but researchers found they could prevent this side effect with pretreatment screening.
John Janik, MD, of the National Cancer Institute in Bethesda, Maryland, and his colleagues described this research in PNAS.
The researchers conducted this study to determine if CD25 is a favorable target for systemic radioimmunotherapy in HL. The team noted that although most normal cells don’t express CD25, it is expressed by a minority of Reed–Sternberg cells and by most polyclonal T cells rosetting around Reed–Sternberg cells.
So the researchers tested the anti-CD25 antibody 90Y-daclizumab in 46 patients with relapsed and refractory HL. Patients received 90Y-daclizumab at 10 mCi to 15 mCi every 6 to 10 weeks for up to 7 doses.
The overall response rate was 50%. There were 14 complete responses and 9 partial responses. Fourteen patients had stable disease, and 9 progressed.
The researchers noted that responses occurred in patients whose Reed–Sternberg cells expressed CD25 and in those whose neoplastic cells were CD25-negative, as long as associated rosetting T cells expressed CD25.
Grade 3 or higher toxicities observed in this study included lymphopenia (n=10), neutropenia (n=7), MDS (n=6), thrombocytopenia (n=5), anemia (n=5), and pneumonia (n=2).
At a median follow-up of 9 years, MDS had occurred in 6 patients. They had received a mean of 3.2 doses of 90Y-daclizumab. Prior to 90Y-daclizumab, they had received a mean of 6.2 courses of chemotherapy.
The median time from the initiation of 90Y-daclizumab to MDS diagnosis was 37 months. A retrospective review of 1 patient with MDS revealed that the patient had cytogenetic aberrations on chromosomes 5 and 7 after receiving chemotherapy but before starting 90Y-daclizumab.
So the researchers changed the trial’s entry criteria to require a bone marrow karyotype analysis, and patients who had aberrations were excluded. None of the 16 patients who entered the trial after this change developed MDS.
The researchers said this study is too small to draw meaningful conclusions about the relative roles of chemotherapy and 90Y-daclizumab in the pathogenesis of MDS.
However, this complication is a serious concern, and any subsequent trial should require cytogenetic studies of bone marrow specimens before patients receive systemic radioimmunotherapy. ![]()
Copyright 2010 Nephron
Results of a small trial suggest the radiolabeled anti-CD25 antibody 90Y-daclizumab can treat certain patients with relapsed/refractory Hodgkin lymphoma (HL).
90Y-daclizumab produced responses in 50% of patients studied, and most of these were complete responses.
Several patients developed myelodysplastic syndrome (MDS) after receiving 90Y-daclizumab, but researchers found they could prevent this side effect with pretreatment screening.
John Janik, MD, of the National Cancer Institute in Bethesda, Maryland, and his colleagues described this research in PNAS.
The researchers conducted this study to determine if CD25 is a favorable target for systemic radioimmunotherapy in HL. The team noted that although most normal cells don’t express CD25, it is expressed by a minority of Reed–Sternberg cells and by most polyclonal T cells rosetting around Reed–Sternberg cells.
So the researchers tested the anti-CD25 antibody 90Y-daclizumab in 46 patients with relapsed and refractory HL. Patients received 90Y-daclizumab at 10 mCi to 15 mCi every 6 to 10 weeks for up to 7 doses.
The overall response rate was 50%. There were 14 complete responses and 9 partial responses. Fourteen patients had stable disease, and 9 progressed.
The researchers noted that responses occurred in patients whose Reed–Sternberg cells expressed CD25 and in those whose neoplastic cells were CD25-negative, as long as associated rosetting T cells expressed CD25.
Grade 3 or higher toxicities observed in this study included lymphopenia (n=10), neutropenia (n=7), MDS (n=6), thrombocytopenia (n=5), anemia (n=5), and pneumonia (n=2).
At a median follow-up of 9 years, MDS had occurred in 6 patients. They had received a mean of 3.2 doses of 90Y-daclizumab. Prior to 90Y-daclizumab, they had received a mean of 6.2 courses of chemotherapy.
The median time from the initiation of 90Y-daclizumab to MDS diagnosis was 37 months. A retrospective review of 1 patient with MDS revealed that the patient had cytogenetic aberrations on chromosomes 5 and 7 after receiving chemotherapy but before starting 90Y-daclizumab.
So the researchers changed the trial’s entry criteria to require a bone marrow karyotype analysis, and patients who had aberrations were excluded. None of the 16 patients who entered the trial after this change developed MDS.
The researchers said this study is too small to draw meaningful conclusions about the relative roles of chemotherapy and 90Y-daclizumab in the pathogenesis of MDS.
However, this complication is a serious concern, and any subsequent trial should require cytogenetic studies of bone marrow specimens before patients receive systemic radioimmunotherapy. ![]()
Copyright 2010 Nephron
Results of a small trial suggest the radiolabeled anti-CD25 antibody 90Y-daclizumab can treat certain patients with relapsed/refractory Hodgkin lymphoma (HL).
90Y-daclizumab produced responses in 50% of patients studied, and most of these were complete responses.
Several patients developed myelodysplastic syndrome (MDS) after receiving 90Y-daclizumab, but researchers found they could prevent this side effect with pretreatment screening.
John Janik, MD, of the National Cancer Institute in Bethesda, Maryland, and his colleagues described this research in PNAS.
The researchers conducted this study to determine if CD25 is a favorable target for systemic radioimmunotherapy in HL. The team noted that although most normal cells don’t express CD25, it is expressed by a minority of Reed–Sternberg cells and by most polyclonal T cells rosetting around Reed–Sternberg cells.
So the researchers tested the anti-CD25 antibody 90Y-daclizumab in 46 patients with relapsed and refractory HL. Patients received 90Y-daclizumab at 10 mCi to 15 mCi every 6 to 10 weeks for up to 7 doses.
The overall response rate was 50%. There were 14 complete responses and 9 partial responses. Fourteen patients had stable disease, and 9 progressed.
The researchers noted that responses occurred in patients whose Reed–Sternberg cells expressed CD25 and in those whose neoplastic cells were CD25-negative, as long as associated rosetting T cells expressed CD25.
Grade 3 or higher toxicities observed in this study included lymphopenia (n=10), neutropenia (n=7), MDS (n=6), thrombocytopenia (n=5), anemia (n=5), and pneumonia (n=2).
At a median follow-up of 9 years, MDS had occurred in 6 patients. They had received a mean of 3.2 doses of 90Y-daclizumab. Prior to 90Y-daclizumab, they had received a mean of 6.2 courses of chemotherapy.
The median time from the initiation of 90Y-daclizumab to MDS diagnosis was 37 months. A retrospective review of 1 patient with MDS revealed that the patient had cytogenetic aberrations on chromosomes 5 and 7 after receiving chemotherapy but before starting 90Y-daclizumab.
So the researchers changed the trial’s entry criteria to require a bone marrow karyotype analysis, and patients who had aberrations were excluded. None of the 16 patients who entered the trial after this change developed MDS.
The researchers said this study is too small to draw meaningful conclusions about the relative roles of chemotherapy and 90Y-daclizumab in the pathogenesis of MDS.
However, this complication is a serious concern, and any subsequent trial should require cytogenetic studies of bone marrow specimens before patients receive systemic radioimmunotherapy. ![]()
‘Room for improvement’ in animal research

Photo by Aaron Logan
A study of animal-based research published over the last 70 years suggests that scientists could have done more to reduce the risk of bias.
A group of researchers examined a few thousand published studies conducted in animals and found that, most of the time, scientists did not employ 4 measures believed to reduce the risk of bias: randomization, blinded assessment of outcome, a conflict of interest statement, and sample size calculation.
“I don’t believe for a moment that scientists set out to do anything other than excellent research, but what this work shows is that there is considerable room for improvement,” said Malcolm Macleod, PhD, of the University of Edinburgh in the UK.
Dr Macleod and his colleagues conducted this research and reported their findings in PLOS Biology.
The team first looked at a random sample of 146 in vivo studies published between 1941 and 2012. Randomization was reported in 20% of the publications in which it would have been appropriate.
Three percent of the publications reported blinding, 10% reported a conflict of interest statement, and none reported a sample size calculation.
Next, the researchers looked at 2671 studies published between 1992 and 2012 that reported drug efficacy in 8 disease models. Randomization was reported in 25% of publications, blinding in 30%, sample size calculation in 0.7%, and a statement of potential conflict of interest in 12%.
However, there were significant increases in 3 of these measures over time. The use of randomization increased from 14% in 1992 to 42% in 2011 (P<0.001), blinding increased from 16% to 39% (P<0.001), and a statement of possible conflict of interest increased from 2% to 35% (P<0.001).
The reporting of a sample size calculation did not change significantly and actually decreased from 2% to 1%.
Dr Macleod and his colleagues also used this dataset to determine whether a journal’s impact factor (a commonly used but disputed measure of journal “quality”)
played a role in the use of the 4 risk-of-bias measures.
The median journal impact factor was significantly higher (P<0.001) for studies reporting a potential conflict of interest, but it was significantly lower in studies reporting randomization (P=0.001). There was no significant difference for the other 2 measures.
Finally, the researchers examined bias in animal studies from the UK’s top 5 universities (according to the
2008 Research Assessment Exercise).
Of 1028 studies published in 2009 and 2010, 14% reported randomization, 17% reported blinding, 10% reported inclusion or exclusion criteria or both, and 1% reported a sample size calculation. Only 1 publication reported using all 4 of these measures.
Dr Macleod and his colleagues concluded that, although this study had its limitations, the results suggest room for improvement in in vivo research. ![]()
Photo by Aaron Logan
A study of animal-based research published over the last 70 years suggests that scientists could have done more to reduce the risk of bias.
A group of researchers examined a few thousand published studies conducted in animals and found that, most of the time, scientists did not employ 4 measures believed to reduce the risk of bias: randomization, blinded assessment of outcome, a conflict of interest statement, and sample size calculation.
“I don’t believe for a moment that scientists set out to do anything other than excellent research, but what this work shows is that there is considerable room for improvement,” said Malcolm Macleod, PhD, of the University of Edinburgh in the UK.
Dr Macleod and his colleagues conducted this research and reported their findings in PLOS Biology.
The team first looked at a random sample of 146 in vivo studies published between 1941 and 2012. Randomization was reported in 20% of the publications in which it would have been appropriate.
Three percent of the publications reported blinding, 10% reported a conflict of interest statement, and none reported a sample size calculation.
Next, the researchers looked at 2671 studies published between 1992 and 2012 that reported drug efficacy in 8 disease models. Randomization was reported in 25% of publications, blinding in 30%, sample size calculation in 0.7%, and a statement of potential conflict of interest in 12%.
However, there were significant increases in 3 of these measures over time. The use of randomization increased from 14% in 1992 to 42% in 2011 (P<0.001), blinding increased from 16% to 39% (P<0.001), and a statement of possible conflict of interest increased from 2% to 35% (P<0.001).
The reporting of a sample size calculation did not change significantly and actually decreased from 2% to 1%.
Dr Macleod and his colleagues also used this dataset to determine whether a journal’s impact factor (a commonly used but disputed measure of journal “quality”)
played a role in the use of the 4 risk-of-bias measures.
The median journal impact factor was significantly higher (P<0.001) for studies reporting a potential conflict of interest, but it was significantly lower in studies reporting randomization (P=0.001). There was no significant difference for the other 2 measures.
Finally, the researchers examined bias in animal studies from the UK’s top 5 universities (according to the
2008 Research Assessment Exercise).
Of 1028 studies published in 2009 and 2010, 14% reported randomization, 17% reported blinding, 10% reported inclusion or exclusion criteria or both, and 1% reported a sample size calculation. Only 1 publication reported using all 4 of these measures.
Dr Macleod and his colleagues concluded that, although this study had its limitations, the results suggest room for improvement in in vivo research. ![]()
Photo by Aaron Logan
A study of animal-based research published over the last 70 years suggests that scientists could have done more to reduce the risk of bias.
A group of researchers examined a few thousand published studies conducted in animals and found that, most of the time, scientists did not employ 4 measures believed to reduce the risk of bias: randomization, blinded assessment of outcome, a conflict of interest statement, and sample size calculation.
“I don’t believe for a moment that scientists set out to do anything other than excellent research, but what this work shows is that there is considerable room for improvement,” said Malcolm Macleod, PhD, of the University of Edinburgh in the UK.
Dr Macleod and his colleagues conducted this research and reported their findings in PLOS Biology.
The team first looked at a random sample of 146 in vivo studies published between 1941 and 2012. Randomization was reported in 20% of the publications in which it would have been appropriate.
Three percent of the publications reported blinding, 10% reported a conflict of interest statement, and none reported a sample size calculation.
Next, the researchers looked at 2671 studies published between 1992 and 2012 that reported drug efficacy in 8 disease models. Randomization was reported in 25% of publications, blinding in 30%, sample size calculation in 0.7%, and a statement of potential conflict of interest in 12%.
However, there were significant increases in 3 of these measures over time. The use of randomization increased from 14% in 1992 to 42% in 2011 (P<0.001), blinding increased from 16% to 39% (P<0.001), and a statement of possible conflict of interest increased from 2% to 35% (P<0.001).
The reporting of a sample size calculation did not change significantly and actually decreased from 2% to 1%.
Dr Macleod and his colleagues also used this dataset to determine whether a journal’s impact factor (a commonly used but disputed measure of journal “quality”)
played a role in the use of the 4 risk-of-bias measures.
The median journal impact factor was significantly higher (P<0.001) for studies reporting a potential conflict of interest, but it was significantly lower in studies reporting randomization (P=0.001). There was no significant difference for the other 2 measures.
Finally, the researchers examined bias in animal studies from the UK’s top 5 universities (according to the
2008 Research Assessment Exercise).
Of 1028 studies published in 2009 and 2010, 14% reported randomization, 17% reported blinding, 10% reported inclusion or exclusion criteria or both, and 1% reported a sample size calculation. Only 1 publication reported using all 4 of these measures.
Dr Macleod and his colleagues concluded that, although this study had its limitations, the results suggest room for improvement in in vivo research. ![]()
HSC finding may have range of implications

Image by Matthias Zepper
Murine research has provided new insight into the functionality of hematopoietic stem cells (HSCs).
Investigators found that a full complement of mini-chromosome maintenance (MCM) proteins is required to preserve HSC functionality and the proper differentiation and maturation of erythrocytes.
Downregulation of the gene MCM3 during embryonic development caused replication stress in hematopoietic progenitors and led to fetal anemia.
In adult mice, downregulation of MCM3 reduced life expectancy and promoted lymphomagenesis.
The investigators therefore believe that therapies designed to modulate replication stress could fight aging, anemia, and hematopoietic malignancies.
This research was published in Nature Communications.
A previous study revealed that replication stress drives the functional decline of HSCs that occurs with age. With the new study, investigators have managed to replicate this phenomenon in mouse embryos.
The team did this by reducing levels of MCM3, one of the components of the MCM complex that is responsible for separating the strands of the DNA double helix during replication. Cells need to maintain high levels of MCM during DNA replication or they experience replication stress.
“When we reduce the levels of the MCM3 gene in the entire organism, we observe that replication stress especially affects the stem cells that give rise to the other blood cells and, in particular, the red blood cell precursors,” explained study author Juan Méndez, PhD, of Centro Nacional de Investigaciones Oncologicas (CNIO) in Madrid, Spain.
“In adult organisms, the production and maturation of red blood cells takes place in the bone marrow, but, during embryonic development, it occurs mainly in the fetal liver. In animals with MCM3 deficiency, the stem cells of the fetal liver are deteriorated, and the embryos develop a severe form of anemia that prevents them from being born.”
“We could say that replication stress turns fetal stem cells, which should be in perfect working order, into very old cells. We have verified this finding in transplantation experiments, where fetal cells with replication stress were unable to adequately reconstitute the blood system in the recipient animals.”
However, the investigators managed to prevent embryonic lethality and reduce anemia by increasing the levels of another gene, CHK1.
“CHK1 is one of the genes responsible for protecting cells from replication stress,” Dr Méndez noted. “It supervises DNA replication. When something goes wrong, CHK1 slows down or halts cell division until the problem has been resolved.”
Embryos that were subjected to replication stress (due to loss of MCM3) but had higher levels of CHK1 showed less pronounced anemia. Four of every 10 embryos developed normally and completed their gestation.
The investigators said an interesting implication of this work is that the type of anemia caused by replication stress is very similar to the aplastic anemia that arises in patients receiving chemotherapy or radiation therapy.
Therefore, the team believes these results could aid the development of novel therapies for aplastic anemia. ![]()
Image by Matthias Zepper
Murine research has provided new insight into the functionality of hematopoietic stem cells (HSCs).
Investigators found that a full complement of mini-chromosome maintenance (MCM) proteins is required to preserve HSC functionality and the proper differentiation and maturation of erythrocytes.
Downregulation of the gene MCM3 during embryonic development caused replication stress in hematopoietic progenitors and led to fetal anemia.
In adult mice, downregulation of MCM3 reduced life expectancy and promoted lymphomagenesis.
The investigators therefore believe that therapies designed to modulate replication stress could fight aging, anemia, and hematopoietic malignancies.
This research was published in Nature Communications.
A previous study revealed that replication stress drives the functional decline of HSCs that occurs with age. With the new study, investigators have managed to replicate this phenomenon in mouse embryos.
The team did this by reducing levels of MCM3, one of the components of the MCM complex that is responsible for separating the strands of the DNA double helix during replication. Cells need to maintain high levels of MCM during DNA replication or they experience replication stress.
“When we reduce the levels of the MCM3 gene in the entire organism, we observe that replication stress especially affects the stem cells that give rise to the other blood cells and, in particular, the red blood cell precursors,” explained study author Juan Méndez, PhD, of Centro Nacional de Investigaciones Oncologicas (CNIO) in Madrid, Spain.
“In adult organisms, the production and maturation of red blood cells takes place in the bone marrow, but, during embryonic development, it occurs mainly in the fetal liver. In animals with MCM3 deficiency, the stem cells of the fetal liver are deteriorated, and the embryos develop a severe form of anemia that prevents them from being born.”
“We could say that replication stress turns fetal stem cells, which should be in perfect working order, into very old cells. We have verified this finding in transplantation experiments, where fetal cells with replication stress were unable to adequately reconstitute the blood system in the recipient animals.”
However, the investigators managed to prevent embryonic lethality and reduce anemia by increasing the levels of another gene, CHK1.
“CHK1 is one of the genes responsible for protecting cells from replication stress,” Dr Méndez noted. “It supervises DNA replication. When something goes wrong, CHK1 slows down or halts cell division until the problem has been resolved.”
Embryos that were subjected to replication stress (due to loss of MCM3) but had higher levels of CHK1 showed less pronounced anemia. Four of every 10 embryos developed normally and completed their gestation.
The investigators said an interesting implication of this work is that the type of anemia caused by replication stress is very similar to the aplastic anemia that arises in patients receiving chemotherapy or radiation therapy.
Therefore, the team believes these results could aid the development of novel therapies for aplastic anemia. ![]()
Image by Matthias Zepper
Murine research has provided new insight into the functionality of hematopoietic stem cells (HSCs).
Investigators found that a full complement of mini-chromosome maintenance (MCM) proteins is required to preserve HSC functionality and the proper differentiation and maturation of erythrocytes.
Downregulation of the gene MCM3 during embryonic development caused replication stress in hematopoietic progenitors and led to fetal anemia.
In adult mice, downregulation of MCM3 reduced life expectancy and promoted lymphomagenesis.
The investigators therefore believe that therapies designed to modulate replication stress could fight aging, anemia, and hematopoietic malignancies.
This research was published in Nature Communications.
A previous study revealed that replication stress drives the functional decline of HSCs that occurs with age. With the new study, investigators have managed to replicate this phenomenon in mouse embryos.
The team did this by reducing levels of MCM3, one of the components of the MCM complex that is responsible for separating the strands of the DNA double helix during replication. Cells need to maintain high levels of MCM during DNA replication or they experience replication stress.
“When we reduce the levels of the MCM3 gene in the entire organism, we observe that replication stress especially affects the stem cells that give rise to the other blood cells and, in particular, the red blood cell precursors,” explained study author Juan Méndez, PhD, of Centro Nacional de Investigaciones Oncologicas (CNIO) in Madrid, Spain.
“In adult organisms, the production and maturation of red blood cells takes place in the bone marrow, but, during embryonic development, it occurs mainly in the fetal liver. In animals with MCM3 deficiency, the stem cells of the fetal liver are deteriorated, and the embryos develop a severe form of anemia that prevents them from being born.”
“We could say that replication stress turns fetal stem cells, which should be in perfect working order, into very old cells. We have verified this finding in transplantation experiments, where fetal cells with replication stress were unable to adequately reconstitute the blood system in the recipient animals.”
However, the investigators managed to prevent embryonic lethality and reduce anemia by increasing the levels of another gene, CHK1.
“CHK1 is one of the genes responsible for protecting cells from replication stress,” Dr Méndez noted. “It supervises DNA replication. When something goes wrong, CHK1 slows down or halts cell division until the problem has been resolved.”
Embryos that were subjected to replication stress (due to loss of MCM3) but had higher levels of CHK1 showed less pronounced anemia. Four of every 10 embryos developed normally and completed their gestation.
The investigators said an interesting implication of this work is that the type of anemia caused by replication stress is very similar to the aplastic anemia that arises in patients receiving chemotherapy or radiation therapy.
Therefore, the team believes these results could aid the development of novel therapies for aplastic anemia. ![]()
FDA approves factor X concentrate

The US Food and Drug Administration (FDA) has approved a factor X product derived from human plasma (Coagadex) to treat patients with hereditary factor X deficiency who are 12 years of age and older.
Coagadex is approved for on-demand treatment and control of bleeding episodes in these patients as well as for perioperative management of bleeding in patients with mild hereditary factor X deficiency.
Prior to this approval, there was no specific coagulation factor replacement therapy available for patients with hereditary factor X deficiency in the US. The FDA previously granted Coagadex orphan product designation, fast track designation, and priority review.
The FDA based its approval of Coagadex on results from 2 phase 3 trials of patients age 12 and older.
The first trial included 16 patients who received Coagadex for pharmacokinetic evaluation, on-demand treatment and control of bleeding episodes, and/or perioperative management of minor surgical or dental procedures.
Coagadex was used to treat 208 bleeding episodes, and 187 of these episodes (in 15 patients) were evaluated for efficacy. Ninety-eight episodes were major bleeds, 88 were minor bleeds, and 1 was not assessed.
One hundred and fifty-five bleeds (83%) were treated with a single infusion of Coagadex, 28 (15%) were treated with 2 infusions, 3 bleeds (2%) required 3 infusions, and 1 bleed (0.5%) required 4 infusions. Four bleeding episodes in 2 patients were considered treatment failures.
The mean dose of Coagadex per infusion was 25.4 IU/kg, and the mean total dose was 30.4 IU/kg. The recommended dose of 25 IU/kg to treat a bleed was maintained for 14 of the 16 patients. The other 2 patients used doses of up to 30 IU/kg and 33 IU/kg.
There were 176 adverse events in this trial, but only 6 events in 2 patients were considered possibly related to Coagadex. This included 2 reports of infusion site erythema in 1 patient, 2 reports of fatigue in 1 patient, 1 report of back pain, and 1 report of infusion site pain.
The second trial included patients who received Coagadex for perioperative management. Five patients received Coagadex for 7 surgical procedures.
For major surgeries, a median of 13 infusions (range, 2-15) and a median cumulative dose of 181 IU/kg (range, 45-210 IU/kg) were required to maintain hemostasis. For minor surgeries, a median of 2.5 infusions (range, 1-4) and a median cumulative dose of 89 IU/kg (range, 51-127 IU/kg) were required to maintain hemostasis.
There were no adverse events related to Coagadex in this trial.
For more details on these trials, see the Coagadex package insert. Coagadex is manufactured by Bio Products Laboratory Limited in Elstree, Hertfordshire, UK. ![]()
The US Food and Drug Administration (FDA) has approved a factor X product derived from human plasma (Coagadex) to treat patients with hereditary factor X deficiency who are 12 years of age and older.
Coagadex is approved for on-demand treatment and control of bleeding episodes in these patients as well as for perioperative management of bleeding in patients with mild hereditary factor X deficiency.
Prior to this approval, there was no specific coagulation factor replacement therapy available for patients with hereditary factor X deficiency in the US. The FDA previously granted Coagadex orphan product designation, fast track designation, and priority review.
The FDA based its approval of Coagadex on results from 2 phase 3 trials of patients age 12 and older.
The first trial included 16 patients who received Coagadex for pharmacokinetic evaluation, on-demand treatment and control of bleeding episodes, and/or perioperative management of minor surgical or dental procedures.
Coagadex was used to treat 208 bleeding episodes, and 187 of these episodes (in 15 patients) were evaluated for efficacy. Ninety-eight episodes were major bleeds, 88 were minor bleeds, and 1 was not assessed.
One hundred and fifty-five bleeds (83%) were treated with a single infusion of Coagadex, 28 (15%) were treated with 2 infusions, 3 bleeds (2%) required 3 infusions, and 1 bleed (0.5%) required 4 infusions. Four bleeding episodes in 2 patients were considered treatment failures.
The mean dose of Coagadex per infusion was 25.4 IU/kg, and the mean total dose was 30.4 IU/kg. The recommended dose of 25 IU/kg to treat a bleed was maintained for 14 of the 16 patients. The other 2 patients used doses of up to 30 IU/kg and 33 IU/kg.
There were 176 adverse events in this trial, but only 6 events in 2 patients were considered possibly related to Coagadex. This included 2 reports of infusion site erythema in 1 patient, 2 reports of fatigue in 1 patient, 1 report of back pain, and 1 report of infusion site pain.
The second trial included patients who received Coagadex for perioperative management. Five patients received Coagadex for 7 surgical procedures.
For major surgeries, a median of 13 infusions (range, 2-15) and a median cumulative dose of 181 IU/kg (range, 45-210 IU/kg) were required to maintain hemostasis. For minor surgeries, a median of 2.5 infusions (range, 1-4) and a median cumulative dose of 89 IU/kg (range, 51-127 IU/kg) were required to maintain hemostasis.
There were no adverse events related to Coagadex in this trial.
For more details on these trials, see the Coagadex package insert. Coagadex is manufactured by Bio Products Laboratory Limited in Elstree, Hertfordshire, UK. ![]()
The US Food and Drug Administration (FDA) has approved a factor X product derived from human plasma (Coagadex) to treat patients with hereditary factor X deficiency who are 12 years of age and older.
Coagadex is approved for on-demand treatment and control of bleeding episodes in these patients as well as for perioperative management of bleeding in patients with mild hereditary factor X deficiency.
Prior to this approval, there was no specific coagulation factor replacement therapy available for patients with hereditary factor X deficiency in the US. The FDA previously granted Coagadex orphan product designation, fast track designation, and priority review.
The FDA based its approval of Coagadex on results from 2 phase 3 trials of patients age 12 and older.
The first trial included 16 patients who received Coagadex for pharmacokinetic evaluation, on-demand treatment and control of bleeding episodes, and/or perioperative management of minor surgical or dental procedures.
Coagadex was used to treat 208 bleeding episodes, and 187 of these episodes (in 15 patients) were evaluated for efficacy. Ninety-eight episodes were major bleeds, 88 were minor bleeds, and 1 was not assessed.
One hundred and fifty-five bleeds (83%) were treated with a single infusion of Coagadex, 28 (15%) were treated with 2 infusions, 3 bleeds (2%) required 3 infusions, and 1 bleed (0.5%) required 4 infusions. Four bleeding episodes in 2 patients were considered treatment failures.
The mean dose of Coagadex per infusion was 25.4 IU/kg, and the mean total dose was 30.4 IU/kg. The recommended dose of 25 IU/kg to treat a bleed was maintained for 14 of the 16 patients. The other 2 patients used doses of up to 30 IU/kg and 33 IU/kg.
There were 176 adverse events in this trial, but only 6 events in 2 patients were considered possibly related to Coagadex. This included 2 reports of infusion site erythema in 1 patient, 2 reports of fatigue in 1 patient, 1 report of back pain, and 1 report of infusion site pain.
The second trial included patients who received Coagadex for perioperative management. Five patients received Coagadex for 7 surgical procedures.
For major surgeries, a median of 13 infusions (range, 2-15) and a median cumulative dose of 181 IU/kg (range, 45-210 IU/kg) were required to maintain hemostasis. For minor surgeries, a median of 2.5 infusions (range, 1-4) and a median cumulative dose of 89 IU/kg (range, 51-127 IU/kg) were required to maintain hemostasis.
There were no adverse events related to Coagadex in this trial.
For more details on these trials, see the Coagadex package insert. Coagadex is manufactured by Bio Products Laboratory Limited in Elstree, Hertfordshire, UK. ![]()
Gabapentin for chronic cough
Chronic cough is defined by the American College of Chest Physicians as a cough lasting longer than 8 weeks. Chronic cough is a troubling disorder, mostly for the patients, who frequently make several outpatient visits to seek help for their symptoms, and whose quality of life can be severely impaired.
An algorithmic approach should be used in the diagnosis of chronic cough. Once we have ruled out the “bad actors” and have run through our nasal sprays, proton pump inhibitors, and antihistamines, it is time to get creative. Don’t neglect to provide lung cancer screening for your smokers – which, in the case of chronic cough, is actually case finding.

Dr. Peter G. Gibson of the University of Newcastle, Australia, and his colleagues published an article presenting some new concepts for chronic cough, an assessment tool, and a literature review on the use of gabapentin for this troubling disorder (Pulm Pharmacol Ther. 2015 Jul 2. pii:S1094-5539[15]00072-3).
The new concepts include laryngeal hypersensitivity, central reflex hypersensitivity, and cough hypersensitivity syndrome. The authors posit that these concepts reformulate into chronic cough as a neuropathic disorder, which may be amenable to treatment with neuromodulatory agents such as gabapentin.
I have several patients in my panel who might benefit from this therapy. But there are a couple of things to remember. First, gabapentin can be taken with food, but antacids decrease the bioavailability by 20% when taken together or up to 2 hours after gabapentin ingestion. Also, gabapentin has a wide therapeutic window, which will make it easier to find an individualized dose for our patients.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article. Follow him on Twitter @jonebbert.
Chronic cough is defined by the American College of Chest Physicians as a cough lasting longer than 8 weeks. Chronic cough is a troubling disorder, mostly for the patients, who frequently make several outpatient visits to seek help for their symptoms, and whose quality of life can be severely impaired.
An algorithmic approach should be used in the diagnosis of chronic cough. Once we have ruled out the “bad actors” and have run through our nasal sprays, proton pump inhibitors, and antihistamines, it is time to get creative. Don’t neglect to provide lung cancer screening for your smokers – which, in the case of chronic cough, is actually case finding.
Dr. Peter G. Gibson of the University of Newcastle, Australia, and his colleagues published an article presenting some new concepts for chronic cough, an assessment tool, and a literature review on the use of gabapentin for this troubling disorder (Pulm Pharmacol Ther. 2015 Jul 2. pii:S1094-5539[15]00072-3).
The new concepts include laryngeal hypersensitivity, central reflex hypersensitivity, and cough hypersensitivity syndrome. The authors posit that these concepts reformulate into chronic cough as a neuropathic disorder, which may be amenable to treatment with neuromodulatory agents such as gabapentin.
I have several patients in my panel who might benefit from this therapy. But there are a couple of things to remember. First, gabapentin can be taken with food, but antacids decrease the bioavailability by 20% when taken together or up to 2 hours after gabapentin ingestion. Also, gabapentin has a wide therapeutic window, which will make it easier to find an individualized dose for our patients.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article. Follow him on Twitter @jonebbert.
Chronic cough is defined by the American College of Chest Physicians as a cough lasting longer than 8 weeks. Chronic cough is a troubling disorder, mostly for the patients, who frequently make several outpatient visits to seek help for their symptoms, and whose quality of life can be severely impaired.
An algorithmic approach should be used in the diagnosis of chronic cough. Once we have ruled out the “bad actors” and have run through our nasal sprays, proton pump inhibitors, and antihistamines, it is time to get creative. Don’t neglect to provide lung cancer screening for your smokers – which, in the case of chronic cough, is actually case finding.
Dr. Peter G. Gibson of the University of Newcastle, Australia, and his colleagues published an article presenting some new concepts for chronic cough, an assessment tool, and a literature review on the use of gabapentin for this troubling disorder (Pulm Pharmacol Ther. 2015 Jul 2. pii:S1094-5539[15]00072-3).
The new concepts include laryngeal hypersensitivity, central reflex hypersensitivity, and cough hypersensitivity syndrome. The authors posit that these concepts reformulate into chronic cough as a neuropathic disorder, which may be amenable to treatment with neuromodulatory agents such as gabapentin.
I have several patients in my panel who might benefit from this therapy. But there are a couple of things to remember. First, gabapentin can be taken with food, but antacids decrease the bioavailability by 20% when taken together or up to 2 hours after gabapentin ingestion. Also, gabapentin has a wide therapeutic window, which will make it easier to find an individualized dose for our patients.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition, nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article. Follow him on Twitter @jonebbert.

Benefits, risks of total knee replacement for OA illuminated in trial
Total knee replacement was superior to nonsurgical treatment in relieving pain, restoring function, and improving quality of life for patients with moderate to severe knee osteoarthritis, according to a report published online Oct. 22 in the New England Journal of Medicine.
Even though the number of total knee replacements performed each year is large and steadily increasing – with more than 670,000 done in 2012 in the United States alone – no high-quality randomized, controlled trials have ever compared the effectiveness of the procedure against nonsurgical treatment, said Søren T. Skou, Ph.D., of the Research Unit for Musculoskeletal Function and Physiotherapy, Institute of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, and his associates.
Dr. Skou and his colleagues remedied that situation by randomly assigning 100 adults (mean age, 66 years) who were eligible for unilateral total knee replacement to either undergo the procedure and then receive a comprehensive nonsurgical intervention (50 patients) or receive the comprehensive nonsurgical intervention alone (50 patients) at two specialized university clinics in Denmark. The 12-week nonsurgical intervention comprised a twice-weekly group exercise program to restore neutral, functional realignment of the legs; two 1-hour education sessions regarding osteoarthritis characteristics, treatments, and self-help strategies; a dietary (weight-loss) program; provision of individually fitted insoles with medial arch support and a lateral wedge if patients had knee-lateral-to-foot positioning; and as-needed pain medication for pain – acetaminophen and ibuprofen – and pantoprazole, a proton-pump inhibitor.
The primary outcome measure in the trial was the between-group difference at 1 year in improvement on four subscales of the Knee Injury and Osteoarthritis Outcome Scores (KOOS) for pain, symptoms, activities of daily living, and quality of life. The surgical group showed a significantly greater improvement (32.5 out of a possible 100 points) than the nonsurgical group (16.0 points) in this outcome. The surgical group also showed significantly greater improvements in all five individual subscales and in a timed chair-rising test, a timed 20-meter walk test, and on a quality-of-life index, the investigators said (N Engl J Med. 2015 373;17:1597-606).
However, it is important to note that patients who had only the nonsurgical intervention showed clinically relevant improvements, and only 26% of them chose to have the surgery after the conclusion of the study. As expected, the surgical group had more serious adverse events than did the nonsurgical group (24 vs. 6), including three cases of deep venous thrombosis and three cases of knee stiffness requiring brisement forcé while the patient was anesthetized, Dr. Skou and his associates said.
This study was supported by the Obel Family Foundation, the Danish Rheumatism Association, the Health Science Foundation of the North Denmark Region, Foot Science International, Spar Nord Foundation, the Bevica Foundation, the Association of Danish Physiotherapists Research Fund, the Medical Specialist Heinrich Kopp’s Grant, and the Danish Medical Association Research Fund. Dr. Skou and his associates reported having no relevant financial disclosures.

|
Dr. Jeffrey N. Katz |
This study provides the first rigorously controlled data to inform discussions about whether patients should undergo total knee replacement or opt for comprehensive nonsurgical treatment. Surgery proved markedly superior in this trial, with 85% of surgical patients reporting a clinically important improvement in pain and function at 1 year, compared with 68% of nonsurgical patients.
But surgery was associated with several severe adverse events, including deep venous thrombosis, deep wound infection, supracondylar fracture, and stiffness requiring treatment under general anesthesia. Each patient must weigh these considerations; each physician should present the relevant data to their patients and then listen carefully to their preferences.
Dr. Jeffrey N. Katz is in the departments of medicine and orthopedic surgery at Brigham and Women’s Hospital and Harvard University, Boston. He reported having no relevant financial disclosures. Dr. Katz made these remarks in an editorial accompanying Dr. Skou’s report (N Engl J Med. 2015 373;17:1668-9).
|
|
Dr. Jeffrey N. Katz |
This study provides the first rigorously controlled data to inform discussions about whether patients should undergo total knee replacement or opt for comprehensive nonsurgical treatment. Surgery proved markedly superior in this trial, with 85% of surgical patients reporting a clinically important improvement in pain and function at 1 year, compared with 68% of nonsurgical patients.
But surgery was associated with several severe adverse events, including deep venous thrombosis, deep wound infection, supracondylar fracture, and stiffness requiring treatment under general anesthesia. Each patient must weigh these considerations; each physician should present the relevant data to their patients and then listen carefully to their preferences.
Dr. Jeffrey N. Katz is in the departments of medicine and orthopedic surgery at Brigham and Women’s Hospital and Harvard University, Boston. He reported having no relevant financial disclosures. Dr. Katz made these remarks in an editorial accompanying Dr. Skou’s report (N Engl J Med. 2015 373;17:1668-9).
|
|
Dr. Jeffrey N. Katz |
This study provides the first rigorously controlled data to inform discussions about whether patients should undergo total knee replacement or opt for comprehensive nonsurgical treatment. Surgery proved markedly superior in this trial, with 85% of surgical patients reporting a clinically important improvement in pain and function at 1 year, compared with 68% of nonsurgical patients.
But surgery was associated with several severe adverse events, including deep venous thrombosis, deep wound infection, supracondylar fracture, and stiffness requiring treatment under general anesthesia. Each patient must weigh these considerations; each physician should present the relevant data to their patients and then listen carefully to their preferences.
Dr. Jeffrey N. Katz is in the departments of medicine and orthopedic surgery at Brigham and Women’s Hospital and Harvard University, Boston. He reported having no relevant financial disclosures. Dr. Katz made these remarks in an editorial accompanying Dr. Skou’s report (N Engl J Med. 2015 373;17:1668-9).
Total knee replacement was superior to nonsurgical treatment in relieving pain, restoring function, and improving quality of life for patients with moderate to severe knee osteoarthritis, according to a report published online Oct. 22 in the New England Journal of Medicine.
Even though the number of total knee replacements performed each year is large and steadily increasing – with more than 670,000 done in 2012 in the United States alone – no high-quality randomized, controlled trials have ever compared the effectiveness of the procedure against nonsurgical treatment, said Søren T. Skou, Ph.D., of the Research Unit for Musculoskeletal Function and Physiotherapy, Institute of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, and his associates.
Dr. Skou and his colleagues remedied that situation by randomly assigning 100 adults (mean age, 66 years) who were eligible for unilateral total knee replacement to either undergo the procedure and then receive a comprehensive nonsurgical intervention (50 patients) or receive the comprehensive nonsurgical intervention alone (50 patients) at two specialized university clinics in Denmark. The 12-week nonsurgical intervention comprised a twice-weekly group exercise program to restore neutral, functional realignment of the legs; two 1-hour education sessions regarding osteoarthritis characteristics, treatments, and self-help strategies; a dietary (weight-loss) program; provision of individually fitted insoles with medial arch support and a lateral wedge if patients had knee-lateral-to-foot positioning; and as-needed pain medication for pain – acetaminophen and ibuprofen – and pantoprazole, a proton-pump inhibitor.
The primary outcome measure in the trial was the between-group difference at 1 year in improvement on four subscales of the Knee Injury and Osteoarthritis Outcome Scores (KOOS) for pain, symptoms, activities of daily living, and quality of life. The surgical group showed a significantly greater improvement (32.5 out of a possible 100 points) than the nonsurgical group (16.0 points) in this outcome. The surgical group also showed significantly greater improvements in all five individual subscales and in a timed chair-rising test, a timed 20-meter walk test, and on a quality-of-life index, the investigators said (N Engl J Med. 2015 373;17:1597-606).
However, it is important to note that patients who had only the nonsurgical intervention showed clinically relevant improvements, and only 26% of them chose to have the surgery after the conclusion of the study. As expected, the surgical group had more serious adverse events than did the nonsurgical group (24 vs. 6), including three cases of deep venous thrombosis and three cases of knee stiffness requiring brisement forcé while the patient was anesthetized, Dr. Skou and his associates said.
This study was supported by the Obel Family Foundation, the Danish Rheumatism Association, the Health Science Foundation of the North Denmark Region, Foot Science International, Spar Nord Foundation, the Bevica Foundation, the Association of Danish Physiotherapists Research Fund, the Medical Specialist Heinrich Kopp’s Grant, and the Danish Medical Association Research Fund. Dr. Skou and his associates reported having no relevant financial disclosures.
Total knee replacement was superior to nonsurgical treatment in relieving pain, restoring function, and improving quality of life for patients with moderate to severe knee osteoarthritis, according to a report published online Oct. 22 in the New England Journal of Medicine.
Even though the number of total knee replacements performed each year is large and steadily increasing – with more than 670,000 done in 2012 in the United States alone – no high-quality randomized, controlled trials have ever compared the effectiveness of the procedure against nonsurgical treatment, said Søren T. Skou, Ph.D., of the Research Unit for Musculoskeletal Function and Physiotherapy, Institute of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, and his associates.
Dr. Skou and his colleagues remedied that situation by randomly assigning 100 adults (mean age, 66 years) who were eligible for unilateral total knee replacement to either undergo the procedure and then receive a comprehensive nonsurgical intervention (50 patients) or receive the comprehensive nonsurgical intervention alone (50 patients) at two specialized university clinics in Denmark. The 12-week nonsurgical intervention comprised a twice-weekly group exercise program to restore neutral, functional realignment of the legs; two 1-hour education sessions regarding osteoarthritis characteristics, treatments, and self-help strategies; a dietary (weight-loss) program; provision of individually fitted insoles with medial arch support and a lateral wedge if patients had knee-lateral-to-foot positioning; and as-needed pain medication for pain – acetaminophen and ibuprofen – and pantoprazole, a proton-pump inhibitor.
The primary outcome measure in the trial was the between-group difference at 1 year in improvement on four subscales of the Knee Injury and Osteoarthritis Outcome Scores (KOOS) for pain, symptoms, activities of daily living, and quality of life. The surgical group showed a significantly greater improvement (32.5 out of a possible 100 points) than the nonsurgical group (16.0 points) in this outcome. The surgical group also showed significantly greater improvements in all five individual subscales and in a timed chair-rising test, a timed 20-meter walk test, and on a quality-of-life index, the investigators said (N Engl J Med. 2015 373;17:1597-606).
However, it is important to note that patients who had only the nonsurgical intervention showed clinically relevant improvements, and only 26% of them chose to have the surgery after the conclusion of the study. As expected, the surgical group had more serious adverse events than did the nonsurgical group (24 vs. 6), including three cases of deep venous thrombosis and three cases of knee stiffness requiring brisement forcé while the patient was anesthetized, Dr. Skou and his associates said.
This study was supported by the Obel Family Foundation, the Danish Rheumatism Association, the Health Science Foundation of the North Denmark Region, Foot Science International, Spar Nord Foundation, the Bevica Foundation, the Association of Danish Physiotherapists Research Fund, the Medical Specialist Heinrich Kopp’s Grant, and the Danish Medical Association Research Fund. Dr. Skou and his associates reported having no relevant financial disclosures.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Total knee replacement is superior to nonsurgical treatment in decreasing pain and improving function and quality of life.
Major finding: The surgical group showed a significantly greater improvement 1 year from baseline (32.5 out of a possible 100 points) than did the nonsurgical group (16.0 points) in mean Knee Injury and Osteoarthritis Outcome Scores (KOOS) for pain, symptoms, activities of daily living, and quality of life.
Data source: A randomized, controlled trial comparing 1-year outcomes after total knee replacement (50 patients) vs. nonsurgical treatment (50 patients) for osteoarthritis.
Disclosures: This study was supported by the Obel Family Foundation, the Danish Rheumatism Association, the Health Science Foundation of the North Denmark Region, Foot Science International, Spar Nord Foundation, the Bevica Foundation, the Association of Danish Physiotherapists Research Fund, the Medical Specialist Heinrich Kopp’s Grant, and the Danish Medical Association Research Fund. Dr. Skou and his associates reported having no relevant financial disclosures.
