User login
Innervation Is Maintained for 24 Years After Transplantation in Parkinson’s Disease
Transplanted nerve cells may survive for nearly a quarter of a century in a patient’s brain despite ongoing Parkinson’s disease, according to data published online ahead of print May 2 in the Proceedings of the National Academy of Sciences of the United States of America. A transplant of cells into the putamen yields dense reinnervation similar to that of healthy brains. The case study also suggests that the initial clinical benefits of the transplant gradually deteriorate when pathology spreads from the patient’s brain to the transplanted cells.
“This is the first time a patient has shown such a well-functioning transplant so many years after transplantation of nerve cells to the brain,” said Olle Lindvall, MD, PhD, Professor of Clinical Neurology and Chairman of Neurology at the University Hospital in Lund, Sweden. “At the same time, we have observed that the transplant’s positive effects on this patient gradually disappeared as the disease spread to more structures in the brain.”

Olle Lindvall, MD, PhD
Dr. Lindvall and colleagues followed a patient with Parkinson’s disease for 24 years after he received a transplant of embryonic dopaminergic neurons. The patient had developed Parkinson’s disease in 1980 and had started L-dopa treatment in 1982. The therapy appeared to be efficacious, but in 1986, the patient developed “on–off” symptoms. During “off” periods, he experienced resting tremor, hypokinetic movements, and rigidity, especially on the left side of his body. During “on” periods, he displayed mild parkinsonian symptoms.
In 1989, the patient, who was then age 59, underwent transplantation with ventral mesencephalic tissue from four human embryos into the right putamen. He was monitored for 10 years post transplantation. In the first three years, researchers noted significant improvement, and L-dopa was withdrawn at 32 months. At 64 months post transplantation, immunosuppressive treatment was stopped. When symptoms progressed at 74 months, a low dose of L-dopa was reintroduced. The patient had a marked clinical benefit, including a near-absence of rigidity, at 10 years. At 12 years, however, he had worsening hypokinesia; as a result, a low-dose dopamine agonist was added for two years, and the L-dopa dose was increased.
The patient responded well to his treatment change at first, but at 14 years, his condition worsened. He began to experience increasing rigidity, hypokinesia, and a gradual loss of beneficial L-dopa response. During this time, cognitive impairment and onset of progressive dementia were first noted. At 18 years, no graft-related motor improvement remained, and the patient was unable to walk, swallow, or speak. At 24 years, the patient died of cardiac insufficiency. Autopsy revealed no evidence of an ongoing immune or inflammatory response. The patient had a dense, near-normal dopaminergic reinnervation derived from the grafts at 24 years post transplantation.
This case study provides the first evidence that rich dopaminergic innervation that develops in the first three years after transplantation and causes dramatic motor improvement can be preserved for 24 years in Parkinson’s disease, according to the authors. The clinical results, however, showed that even a viable graft could eventually lose its efficacy if widespread alpha-synucleinopathy progresses and degeneration occurs in the host brain.
“This study is completely unique,” said Anders Bjorklund, Professor at the Wallenberg Neuroscience Center at Lund University. “No transplanted Parkinson’s patient has ever been followed so closely and over such a long period...What we have learnt from the study of this patient will be of great value for future attempts to transplant dopamine-producing nerve cells obtained from stem cells, a new development led by researchers in Lund.”
—Erica Robinson
Suggested Reading
Li W, Englund E, Wildner H, et al. Extensive graft-derived dopaminergic innervation is maintained 24 years after transplantation in the degenerating parkinsonian brain. Proc Natl Acad Sci U S A. 2016 May 2 [Epub ahead of print].
Transplanted nerve cells may survive for nearly a quarter of a century in a patient’s brain despite ongoing Parkinson’s disease, according to data published online ahead of print May 2 in the Proceedings of the National Academy of Sciences of the United States of America. A transplant of cells into the putamen yields dense reinnervation similar to that of healthy brains. The case study also suggests that the initial clinical benefits of the transplant gradually deteriorate when pathology spreads from the patient’s brain to the transplanted cells.
“This is the first time a patient has shown such a well-functioning transplant so many years after transplantation of nerve cells to the brain,” said Olle Lindvall, MD, PhD, Professor of Clinical Neurology and Chairman of Neurology at the University Hospital in Lund, Sweden. “At the same time, we have observed that the transplant’s positive effects on this patient gradually disappeared as the disease spread to more structures in the brain.”
Olle Lindvall, MD, PhD
Dr. Lindvall and colleagues followed a patient with Parkinson’s disease for 24 years after he received a transplant of embryonic dopaminergic neurons. The patient had developed Parkinson’s disease in 1980 and had started L-dopa treatment in 1982. The therapy appeared to be efficacious, but in 1986, the patient developed “on–off” symptoms. During “off” periods, he experienced resting tremor, hypokinetic movements, and rigidity, especially on the left side of his body. During “on” periods, he displayed mild parkinsonian symptoms.
In 1989, the patient, who was then age 59, underwent transplantation with ventral mesencephalic tissue from four human embryos into the right putamen. He was monitored for 10 years post transplantation. In the first three years, researchers noted significant improvement, and L-dopa was withdrawn at 32 months. At 64 months post transplantation, immunosuppressive treatment was stopped. When symptoms progressed at 74 months, a low dose of L-dopa was reintroduced. The patient had a marked clinical benefit, including a near-absence of rigidity, at 10 years. At 12 years, however, he had worsening hypokinesia; as a result, a low-dose dopamine agonist was added for two years, and the L-dopa dose was increased.
The patient responded well to his treatment change at first, but at 14 years, his condition worsened. He began to experience increasing rigidity, hypokinesia, and a gradual loss of beneficial L-dopa response. During this time, cognitive impairment and onset of progressive dementia were first noted. At 18 years, no graft-related motor improvement remained, and the patient was unable to walk, swallow, or speak. At 24 years, the patient died of cardiac insufficiency. Autopsy revealed no evidence of an ongoing immune or inflammatory response. The patient had a dense, near-normal dopaminergic reinnervation derived from the grafts at 24 years post transplantation.
This case study provides the first evidence that rich dopaminergic innervation that develops in the first three years after transplantation and causes dramatic motor improvement can be preserved for 24 years in Parkinson’s disease, according to the authors. The clinical results, however, showed that even a viable graft could eventually lose its efficacy if widespread alpha-synucleinopathy progresses and degeneration occurs in the host brain.
“This study is completely unique,” said Anders Bjorklund, Professor at the Wallenberg Neuroscience Center at Lund University. “No transplanted Parkinson’s patient has ever been followed so closely and over such a long period...What we have learnt from the study of this patient will be of great value for future attempts to transplant dopamine-producing nerve cells obtained from stem cells, a new development led by researchers in Lund.”
—Erica Robinson
Transplanted nerve cells may survive for nearly a quarter of a century in a patient’s brain despite ongoing Parkinson’s disease, according to data published online ahead of print May 2 in the Proceedings of the National Academy of Sciences of the United States of America. A transplant of cells into the putamen yields dense reinnervation similar to that of healthy brains. The case study also suggests that the initial clinical benefits of the transplant gradually deteriorate when pathology spreads from the patient’s brain to the transplanted cells.
“This is the first time a patient has shown such a well-functioning transplant so many years after transplantation of nerve cells to the brain,” said Olle Lindvall, MD, PhD, Professor of Clinical Neurology and Chairman of Neurology at the University Hospital in Lund, Sweden. “At the same time, we have observed that the transplant’s positive effects on this patient gradually disappeared as the disease spread to more structures in the brain.”
Olle Lindvall, MD, PhD
Dr. Lindvall and colleagues followed a patient with Parkinson’s disease for 24 years after he received a transplant of embryonic dopaminergic neurons. The patient had developed Parkinson’s disease in 1980 and had started L-dopa treatment in 1982. The therapy appeared to be efficacious, but in 1986, the patient developed “on–off” symptoms. During “off” periods, he experienced resting tremor, hypokinetic movements, and rigidity, especially on the left side of his body. During “on” periods, he displayed mild parkinsonian symptoms.
In 1989, the patient, who was then age 59, underwent transplantation with ventral mesencephalic tissue from four human embryos into the right putamen. He was monitored for 10 years post transplantation. In the first three years, researchers noted significant improvement, and L-dopa was withdrawn at 32 months. At 64 months post transplantation, immunosuppressive treatment was stopped. When symptoms progressed at 74 months, a low dose of L-dopa was reintroduced. The patient had a marked clinical benefit, including a near-absence of rigidity, at 10 years. At 12 years, however, he had worsening hypokinesia; as a result, a low-dose dopamine agonist was added for two years, and the L-dopa dose was increased.
The patient responded well to his treatment change at first, but at 14 years, his condition worsened. He began to experience increasing rigidity, hypokinesia, and a gradual loss of beneficial L-dopa response. During this time, cognitive impairment and onset of progressive dementia were first noted. At 18 years, no graft-related motor improvement remained, and the patient was unable to walk, swallow, or speak. At 24 years, the patient died of cardiac insufficiency. Autopsy revealed no evidence of an ongoing immune or inflammatory response. The patient had a dense, near-normal dopaminergic reinnervation derived from the grafts at 24 years post transplantation.
This case study provides the first evidence that rich dopaminergic innervation that develops in the first three years after transplantation and causes dramatic motor improvement can be preserved for 24 years in Parkinson’s disease, according to the authors. The clinical results, however, showed that even a viable graft could eventually lose its efficacy if widespread alpha-synucleinopathy progresses and degeneration occurs in the host brain.
“This study is completely unique,” said Anders Bjorklund, Professor at the Wallenberg Neuroscience Center at Lund University. “No transplanted Parkinson’s patient has ever been followed so closely and over such a long period...What we have learnt from the study of this patient will be of great value for future attempts to transplant dopamine-producing nerve cells obtained from stem cells, a new development led by researchers in Lund.”
—Erica Robinson
Suggested Reading
Li W, Englund E, Wildner H, et al. Extensive graft-derived dopaminergic innervation is maintained 24 years after transplantation in the degenerating parkinsonian brain. Proc Natl Acad Sci U S A. 2016 May 2 [Epub ahead of print].
Suggested Reading
Li W, Englund E, Wildner H, et al. Extensive graft-derived dopaminergic innervation is maintained 24 years after transplantation in the degenerating parkinsonian brain. Proc Natl Acad Sci U S A. 2016 May 2 [Epub ahead of print].

Choosing MS Treatments From the Therapeutic Armamentarium
VANCOUVER—When selecting a therapy for a patient with multiple sclerosis (MS), drug adherence, side effects, and the patient’s risk of aggressive disease are among the considerations that may influence treatment choice, said Scott Newsome, DO, Director of Neurology Outpatient Services and the Neurology Infusion Center at Johns Hopkins University School of Medicine in Baltimore. Patients’ risk tolerance, desire to pursue pregnancy, and John Cunningham virus (JCV) antibody status also can affect the treatment decision.

Scott Newsome, DO
“I wish we had a cookbook recipe. I wish we were able to say, … ‘This is what you’re going to go on, this is what we’re going to expect,’ but that’s not the case. Maybe one day it will be the case, but until then we have to look at many different factors in choosing therapies,” Dr. Newsome said at the 68th Annual Meeting of the American Academy of Neurology.
Two Decades of Advances
The FDA first approved an MS therapy, interferon beta-1b, in 1993. Now, more than 10 treatments with various routes of administration and mechanisms of action have FDA approval, including a new injectable agent approved in May. Additional promising therapies are on the horizon.
“The world of MS therapeutics is evolving and becoming more complicated,” and neurologists have an “ongoing need to balance efficacy, safety, and tolerability of therapeutic interventions for each patient,” Dr. Newsome said.
Dr. Newsome hopes that in the future, biomarkers will help clinicians identify which specific treatments are the best options for each patient. In addition, more research is needed to determine the best time to start a new drug after a patient develops lymphopenia on another MS therapy, and to better understand how prior treatment with other agents affects the risk of progressive multifocal leukoencephalopathy (PML) and other adverse outcomes, he said.
With current therapies, “treating early and having a low threshold to escalate therapy is very important,” Dr. Newsome said. Monitoring relapses and MRI activity may be helpful when evaluating the efficacy of a newly initiated therapy. If a patient has subclinical disease activity six to 12 months after starting a therapy, many clinicians switch therapies and consider treatments that have different mechanisms of action. If a patient develops one small T2 lesion a year out from starting a therapy, he or she does not necessarily need to switch therapies, however. “These drugs are not cures, so you have to look at various factors when you’re thinking about switching or escalating,” Dr. Newsome said. If a patient has a definite relapse, poor recovery from a relapse, disability progression, or robust MRI activity, even when the patient is asymptomatic, clinicians should consider switching therapies.
Risk of Aggressive Disease
Recommendations published in 2013 by the Canadian MS Working Group along with other groups have noted that patients who are male or African American, have an older age at MS onset, or have motor, cerebellar, sphincter, or brainstem involvement are more likely to have aggressive MS. Frequent relapses, poor recovery from relapses, high MRI lesion burden at presentation, brain atrophy, and a low level of vitamin D also are associated with more aggressive disease. Thus, if a patient is African American, does not recover well from a transverse myelitis attack, and has 15 lesions on MRI, including many that are gadolinium-enhancing, with a high spinal cord lesion load, the patient is at high risk of aggressive disease. “When I see this demographic, this phenotype, I’m thinking maybe we need to start with a stronger immune therapy,” said Dr. Newsome.
Based on a cross-comparison of results from the drugs’ pivotal trials, newer medications seem more effective. Head-to-head trials are the only way to establish drug equivalence or superiority, however. With newly diagnosed MS, especially aggressive MS, many clinicians first prescribe an oral agent or an IV therapy instead of an earlier injectable therapy, with the aim of preventing future disability, Dr. Newsome said.
Injectable, Oral, and IV Therapies
Injectable agents include interferon agents (IFN beta-1a, PEG IFN beta-1a, and IFN beta-1b) and glatiramer acetate. In phase III trials, the interferon agents and glatiramer acetate reduced relapses by about 30%, compared with placebo. They also affected MRI activity and had a modest effect on 12-week disability progression, as measured by the Expanded Disability Status Scale (EDSS), with reductions in the range of about 30% to 40%, compared with placebo.
More recently approved oral and infusion agents may be good options for patients who develop injection fatigue, which can affect adherence, or who have breakthrough disease activity on injectable therapies, Dr. Newsome said. Fingolimod, the first approved oral therapy, is given once daily. Teriflunomide is administered once daily, and two doses are available. Dimethyl fumarate, the newest oral medication, has a mechanism of action similar to that of glatiramer acetate, but also has a unique mechanism of action in that it activates a transcriptional pathway that may help with oxidative and metabolic stress in MS. It is given twice daily.
In clinical trials, fingolimod and dimethyl fumarate reduced patients’ annualized relapse rate by more than 50%, compared with placebo. The 14-mg dose of teriflunomide reduced relapses by 32%. The oral medications had a robust effect on MRI activity. They also reduced 12-week disability progression, compared with placebo (32% reduction with fingolimod, 30% with teriflunomide, and 38% with dimethyl fumarate).
Natalizumab, an IV therapy that targets VLA-4 antigen on immune cells, reduced patients’ annualized relapse rate by 68% and had a robust effect on MRI activity, compared with placebo, in a phase III trial. Treatment reduced 12-week disability progression by 42%. Alemtuzumab, another IV treatment, depletes mature B and T cells, and infusions are needed only once per year. Initial treatment is 12 mg/day for five consecutive days. The following year, patients receive the same dosing for three days. Afterwards, many clinicians monitor patients and do not treat patients further unless they observe relapses or MRI activity, Dr. Newsome said. In two phase III trials, treatment with alemtuzumab reduced relapses by about 50% and had a robust effect on MRI activity, compared with treatment with interferon beta-1a given three times per week. In addition, alemtuzumab significantly reduced disability progression in one of the phase III trials, Dr. Newsome said.
Daclizumab is a fully humanized monoclonal antibody that targets CD25 on T cells. The FDA approved the therapy, an injection administered by the patient monthly, on May 27. In a phase III trial, daclizumab reduced patients’ annualized relapse rate by 45%, compared with interferon beta-1a given once per week. It also reduced disability progression at six months by 27% and had a robust effect on MRI activity (65% reduction in new gadolinium-enhancing lesions), compared with interferon beta-1a.
The Importance of Laboratory Monitoring
“The higher the potency and efficacy of the drugs, the greater the risk” of adverse events, Dr. Newsome said. Laboratory monitoring is critical. “With all of the therapies that we have available today, with the exception maybe of glatiramer acetate, you need to check labs routinely,” he said. Complete blood counts with differential to monitor patients’ absolute lymphocyte counts and liver function tests “are the bare minimum” needed to monitor patients on most of these drugs, he said.
Certain therapies require additional safety monitoring. For example, patients treated with alemtuzumab require monthly blood work and urine tests. Patients must undergo cardiac monitoring when initiating treatment with fingolimod. With natalizumab, the serum JCV antibody test reliably stratifies patients’ risk of PML over time. Individual MS drugs are associated with a range of minor and major adverse events. Certain therapies may unmask or reactivate infections, cause secondary autoimmunity, or increase the risk of rare opportunistic infections.
The Future
Ocrelizumab, a fully humanized monoclonal antibody that targets CD20+ B cells, is a potential future therapy that is delivered as an infusion every six months. In two relapsing-remitting MS phase III trials, ocrelizumab reduced patients’ annualized relapse rate by close to 50%, compared with interferon beta-1a given three times per week. It also reduced disability progression by around 40% and had a robust effect on MRI activity (> 90% reduction in new gadolinium-enhancing lesions), compared with interferon beta-1a. Ocrelizumab was also found to reduce disability progression at three and six months (24% and 25%, respectively) and reduce worsening in walking speed in patients by 29% in primary progressive MS, compared with placebo.
Investigators also are evaluating strategies for remyelination. Despite the increasing number of available agents, more therapies are needed. “We need more medications and more interventions that impact neurodegeneration and have the potential to repair damage,” Dr. Newsome said.
—Jake Remaly
Suggested Reading
Butzkueven H, Calabresi PA. Is my MS patient failing treatment? Neurology. 2016 Jun 15 [Epub ahead of print].
Freedman MS, Selchen D, Arnold DL, et al. Treatment optimization in MS: Canadian MS Working Group updated recommendations. Can J Neurol Sci. 2013;40(3):307-323.
Lublin FD, Baier M, Cutter G. Effect of relapses on development of residual deficit in multiple sclerosis. Neurology. 2003;61(11):1528-1532.
VANCOUVER—When selecting a therapy for a patient with multiple sclerosis (MS), drug adherence, side effects, and the patient’s risk of aggressive disease are among the considerations that may influence treatment choice, said Scott Newsome, DO, Director of Neurology Outpatient Services and the Neurology Infusion Center at Johns Hopkins University School of Medicine in Baltimore. Patients’ risk tolerance, desire to pursue pregnancy, and John Cunningham virus (JCV) antibody status also can affect the treatment decision.
Scott Newsome, DO
“I wish we had a cookbook recipe. I wish we were able to say, … ‘This is what you’re going to go on, this is what we’re going to expect,’ but that’s not the case. Maybe one day it will be the case, but until then we have to look at many different factors in choosing therapies,” Dr. Newsome said at the 68th Annual Meeting of the American Academy of Neurology.
Two Decades of Advances
The FDA first approved an MS therapy, interferon beta-1b, in 1993. Now, more than 10 treatments with various routes of administration and mechanisms of action have FDA approval, including a new injectable agent approved in May. Additional promising therapies are on the horizon.
“The world of MS therapeutics is evolving and becoming more complicated,” and neurologists have an “ongoing need to balance efficacy, safety, and tolerability of therapeutic interventions for each patient,” Dr. Newsome said.
Dr. Newsome hopes that in the future, biomarkers will help clinicians identify which specific treatments are the best options for each patient. In addition, more research is needed to determine the best time to start a new drug after a patient develops lymphopenia on another MS therapy, and to better understand how prior treatment with other agents affects the risk of progressive multifocal leukoencephalopathy (PML) and other adverse outcomes, he said.
With current therapies, “treating early and having a low threshold to escalate therapy is very important,” Dr. Newsome said. Monitoring relapses and MRI activity may be helpful when evaluating the efficacy of a newly initiated therapy. If a patient has subclinical disease activity six to 12 months after starting a therapy, many clinicians switch therapies and consider treatments that have different mechanisms of action. If a patient develops one small T2 lesion a year out from starting a therapy, he or she does not necessarily need to switch therapies, however. “These drugs are not cures, so you have to look at various factors when you’re thinking about switching or escalating,” Dr. Newsome said. If a patient has a definite relapse, poor recovery from a relapse, disability progression, or robust MRI activity, even when the patient is asymptomatic, clinicians should consider switching therapies.
Risk of Aggressive Disease
Recommendations published in 2013 by the Canadian MS Working Group along with other groups have noted that patients who are male or African American, have an older age at MS onset, or have motor, cerebellar, sphincter, or brainstem involvement are more likely to have aggressive MS. Frequent relapses, poor recovery from relapses, high MRI lesion burden at presentation, brain atrophy, and a low level of vitamin D also are associated with more aggressive disease. Thus, if a patient is African American, does not recover well from a transverse myelitis attack, and has 15 lesions on MRI, including many that are gadolinium-enhancing, with a high spinal cord lesion load, the patient is at high risk of aggressive disease. “When I see this demographic, this phenotype, I’m thinking maybe we need to start with a stronger immune therapy,” said Dr. Newsome.
Based on a cross-comparison of results from the drugs’ pivotal trials, newer medications seem more effective. Head-to-head trials are the only way to establish drug equivalence or superiority, however. With newly diagnosed MS, especially aggressive MS, many clinicians first prescribe an oral agent or an IV therapy instead of an earlier injectable therapy, with the aim of preventing future disability, Dr. Newsome said.
Injectable, Oral, and IV Therapies
Injectable agents include interferon agents (IFN beta-1a, PEG IFN beta-1a, and IFN beta-1b) and glatiramer acetate. In phase III trials, the interferon agents and glatiramer acetate reduced relapses by about 30%, compared with placebo. They also affected MRI activity and had a modest effect on 12-week disability progression, as measured by the Expanded Disability Status Scale (EDSS), with reductions in the range of about 30% to 40%, compared with placebo.
More recently approved oral and infusion agents may be good options for patients who develop injection fatigue, which can affect adherence, or who have breakthrough disease activity on injectable therapies, Dr. Newsome said. Fingolimod, the first approved oral therapy, is given once daily. Teriflunomide is administered once daily, and two doses are available. Dimethyl fumarate, the newest oral medication, has a mechanism of action similar to that of glatiramer acetate, but also has a unique mechanism of action in that it activates a transcriptional pathway that may help with oxidative and metabolic stress in MS. It is given twice daily.
In clinical trials, fingolimod and dimethyl fumarate reduced patients’ annualized relapse rate by more than 50%, compared with placebo. The 14-mg dose of teriflunomide reduced relapses by 32%. The oral medications had a robust effect on MRI activity. They also reduced 12-week disability progression, compared with placebo (32% reduction with fingolimod, 30% with teriflunomide, and 38% with dimethyl fumarate).
Natalizumab, an IV therapy that targets VLA-4 antigen on immune cells, reduced patients’ annualized relapse rate by 68% and had a robust effect on MRI activity, compared with placebo, in a phase III trial. Treatment reduced 12-week disability progression by 42%. Alemtuzumab, another IV treatment, depletes mature B and T cells, and infusions are needed only once per year. Initial treatment is 12 mg/day for five consecutive days. The following year, patients receive the same dosing for three days. Afterwards, many clinicians monitor patients and do not treat patients further unless they observe relapses or MRI activity, Dr. Newsome said. In two phase III trials, treatment with alemtuzumab reduced relapses by about 50% and had a robust effect on MRI activity, compared with treatment with interferon beta-1a given three times per week. In addition, alemtuzumab significantly reduced disability progression in one of the phase III trials, Dr. Newsome said.
Daclizumab is a fully humanized monoclonal antibody that targets CD25 on T cells. The FDA approved the therapy, an injection administered by the patient monthly, on May 27. In a phase III trial, daclizumab reduced patients’ annualized relapse rate by 45%, compared with interferon beta-1a given once per week. It also reduced disability progression at six months by 27% and had a robust effect on MRI activity (65% reduction in new gadolinium-enhancing lesions), compared with interferon beta-1a.
The Importance of Laboratory Monitoring
“The higher the potency and efficacy of the drugs, the greater the risk” of adverse events, Dr. Newsome said. Laboratory monitoring is critical. “With all of the therapies that we have available today, with the exception maybe of glatiramer acetate, you need to check labs routinely,” he said. Complete blood counts with differential to monitor patients’ absolute lymphocyte counts and liver function tests “are the bare minimum” needed to monitor patients on most of these drugs, he said.
Certain therapies require additional safety monitoring. For example, patients treated with alemtuzumab require monthly blood work and urine tests. Patients must undergo cardiac monitoring when initiating treatment with fingolimod. With natalizumab, the serum JCV antibody test reliably stratifies patients’ risk of PML over time. Individual MS drugs are associated with a range of minor and major adverse events. Certain therapies may unmask or reactivate infections, cause secondary autoimmunity, or increase the risk of rare opportunistic infections.
The Future
Ocrelizumab, a fully humanized monoclonal antibody that targets CD20+ B cells, is a potential future therapy that is delivered as an infusion every six months. In two relapsing-remitting MS phase III trials, ocrelizumab reduced patients’ annualized relapse rate by close to 50%, compared with interferon beta-1a given three times per week. It also reduced disability progression by around 40% and had a robust effect on MRI activity (> 90% reduction in new gadolinium-enhancing lesions), compared with interferon beta-1a. Ocrelizumab was also found to reduce disability progression at three and six months (24% and 25%, respectively) and reduce worsening in walking speed in patients by 29% in primary progressive MS, compared with placebo.
Investigators also are evaluating strategies for remyelination. Despite the increasing number of available agents, more therapies are needed. “We need more medications and more interventions that impact neurodegeneration and have the potential to repair damage,” Dr. Newsome said.
—Jake Remaly
VANCOUVER—When selecting a therapy for a patient with multiple sclerosis (MS), drug adherence, side effects, and the patient’s risk of aggressive disease are among the considerations that may influence treatment choice, said Scott Newsome, DO, Director of Neurology Outpatient Services and the Neurology Infusion Center at Johns Hopkins University School of Medicine in Baltimore. Patients’ risk tolerance, desire to pursue pregnancy, and John Cunningham virus (JCV) antibody status also can affect the treatment decision.
Scott Newsome, DO
“I wish we had a cookbook recipe. I wish we were able to say, … ‘This is what you’re going to go on, this is what we’re going to expect,’ but that’s not the case. Maybe one day it will be the case, but until then we have to look at many different factors in choosing therapies,” Dr. Newsome said at the 68th Annual Meeting of the American Academy of Neurology.
Two Decades of Advances
The FDA first approved an MS therapy, interferon beta-1b, in 1993. Now, more than 10 treatments with various routes of administration and mechanisms of action have FDA approval, including a new injectable agent approved in May. Additional promising therapies are on the horizon.
“The world of MS therapeutics is evolving and becoming more complicated,” and neurologists have an “ongoing need to balance efficacy, safety, and tolerability of therapeutic interventions for each patient,” Dr. Newsome said.
Dr. Newsome hopes that in the future, biomarkers will help clinicians identify which specific treatments are the best options for each patient. In addition, more research is needed to determine the best time to start a new drug after a patient develops lymphopenia on another MS therapy, and to better understand how prior treatment with other agents affects the risk of progressive multifocal leukoencephalopathy (PML) and other adverse outcomes, he said.
With current therapies, “treating early and having a low threshold to escalate therapy is very important,” Dr. Newsome said. Monitoring relapses and MRI activity may be helpful when evaluating the efficacy of a newly initiated therapy. If a patient has subclinical disease activity six to 12 months after starting a therapy, many clinicians switch therapies and consider treatments that have different mechanisms of action. If a patient develops one small T2 lesion a year out from starting a therapy, he or she does not necessarily need to switch therapies, however. “These drugs are not cures, so you have to look at various factors when you’re thinking about switching or escalating,” Dr. Newsome said. If a patient has a definite relapse, poor recovery from a relapse, disability progression, or robust MRI activity, even when the patient is asymptomatic, clinicians should consider switching therapies.
Risk of Aggressive Disease
Recommendations published in 2013 by the Canadian MS Working Group along with other groups have noted that patients who are male or African American, have an older age at MS onset, or have motor, cerebellar, sphincter, or brainstem involvement are more likely to have aggressive MS. Frequent relapses, poor recovery from relapses, high MRI lesion burden at presentation, brain atrophy, and a low level of vitamin D also are associated with more aggressive disease. Thus, if a patient is African American, does not recover well from a transverse myelitis attack, and has 15 lesions on MRI, including many that are gadolinium-enhancing, with a high spinal cord lesion load, the patient is at high risk of aggressive disease. “When I see this demographic, this phenotype, I’m thinking maybe we need to start with a stronger immune therapy,” said Dr. Newsome.
Based on a cross-comparison of results from the drugs’ pivotal trials, newer medications seem more effective. Head-to-head trials are the only way to establish drug equivalence or superiority, however. With newly diagnosed MS, especially aggressive MS, many clinicians first prescribe an oral agent or an IV therapy instead of an earlier injectable therapy, with the aim of preventing future disability, Dr. Newsome said.
Injectable, Oral, and IV Therapies
Injectable agents include interferon agents (IFN beta-1a, PEG IFN beta-1a, and IFN beta-1b) and glatiramer acetate. In phase III trials, the interferon agents and glatiramer acetate reduced relapses by about 30%, compared with placebo. They also affected MRI activity and had a modest effect on 12-week disability progression, as measured by the Expanded Disability Status Scale (EDSS), with reductions in the range of about 30% to 40%, compared with placebo.
More recently approved oral and infusion agents may be good options for patients who develop injection fatigue, which can affect adherence, or who have breakthrough disease activity on injectable therapies, Dr. Newsome said. Fingolimod, the first approved oral therapy, is given once daily. Teriflunomide is administered once daily, and two doses are available. Dimethyl fumarate, the newest oral medication, has a mechanism of action similar to that of glatiramer acetate, but also has a unique mechanism of action in that it activates a transcriptional pathway that may help with oxidative and metabolic stress in MS. It is given twice daily.
In clinical trials, fingolimod and dimethyl fumarate reduced patients’ annualized relapse rate by more than 50%, compared with placebo. The 14-mg dose of teriflunomide reduced relapses by 32%. The oral medications had a robust effect on MRI activity. They also reduced 12-week disability progression, compared with placebo (32% reduction with fingolimod, 30% with teriflunomide, and 38% with dimethyl fumarate).
Natalizumab, an IV therapy that targets VLA-4 antigen on immune cells, reduced patients’ annualized relapse rate by 68% and had a robust effect on MRI activity, compared with placebo, in a phase III trial. Treatment reduced 12-week disability progression by 42%. Alemtuzumab, another IV treatment, depletes mature B and T cells, and infusions are needed only once per year. Initial treatment is 12 mg/day for five consecutive days. The following year, patients receive the same dosing for three days. Afterwards, many clinicians monitor patients and do not treat patients further unless they observe relapses or MRI activity, Dr. Newsome said. In two phase III trials, treatment with alemtuzumab reduced relapses by about 50% and had a robust effect on MRI activity, compared with treatment with interferon beta-1a given three times per week. In addition, alemtuzumab significantly reduced disability progression in one of the phase III trials, Dr. Newsome said.
Daclizumab is a fully humanized monoclonal antibody that targets CD25 on T cells. The FDA approved the therapy, an injection administered by the patient monthly, on May 27. In a phase III trial, daclizumab reduced patients’ annualized relapse rate by 45%, compared with interferon beta-1a given once per week. It also reduced disability progression at six months by 27% and had a robust effect on MRI activity (65% reduction in new gadolinium-enhancing lesions), compared with interferon beta-1a.
The Importance of Laboratory Monitoring
“The higher the potency and efficacy of the drugs, the greater the risk” of adverse events, Dr. Newsome said. Laboratory monitoring is critical. “With all of the therapies that we have available today, with the exception maybe of glatiramer acetate, you need to check labs routinely,” he said. Complete blood counts with differential to monitor patients’ absolute lymphocyte counts and liver function tests “are the bare minimum” needed to monitor patients on most of these drugs, he said.
Certain therapies require additional safety monitoring. For example, patients treated with alemtuzumab require monthly blood work and urine tests. Patients must undergo cardiac monitoring when initiating treatment with fingolimod. With natalizumab, the serum JCV antibody test reliably stratifies patients’ risk of PML over time. Individual MS drugs are associated with a range of minor and major adverse events. Certain therapies may unmask or reactivate infections, cause secondary autoimmunity, or increase the risk of rare opportunistic infections.
The Future
Ocrelizumab, a fully humanized monoclonal antibody that targets CD20+ B cells, is a potential future therapy that is delivered as an infusion every six months. In two relapsing-remitting MS phase III trials, ocrelizumab reduced patients’ annualized relapse rate by close to 50%, compared with interferon beta-1a given three times per week. It also reduced disability progression by around 40% and had a robust effect on MRI activity (> 90% reduction in new gadolinium-enhancing lesions), compared with interferon beta-1a. Ocrelizumab was also found to reduce disability progression at three and six months (24% and 25%, respectively) and reduce worsening in walking speed in patients by 29% in primary progressive MS, compared with placebo.
Investigators also are evaluating strategies for remyelination. Despite the increasing number of available agents, more therapies are needed. “We need more medications and more interventions that impact neurodegeneration and have the potential to repair damage,” Dr. Newsome said.
—Jake Remaly
Suggested Reading
Butzkueven H, Calabresi PA. Is my MS patient failing treatment? Neurology. 2016 Jun 15 [Epub ahead of print].
Freedman MS, Selchen D, Arnold DL, et al. Treatment optimization in MS: Canadian MS Working Group updated recommendations. Can J Neurol Sci. 2013;40(3):307-323.
Lublin FD, Baier M, Cutter G. Effect of relapses on development of residual deficit in multiple sclerosis. Neurology. 2003;61(11):1528-1532.
Suggested Reading
Butzkueven H, Calabresi PA. Is my MS patient failing treatment? Neurology. 2016 Jun 15 [Epub ahead of print].
Freedman MS, Selchen D, Arnold DL, et al. Treatment optimization in MS: Canadian MS Working Group updated recommendations. Can J Neurol Sci. 2013;40(3):307-323.
Lublin FD, Baier M, Cutter G. Effect of relapses on development of residual deficit in multiple sclerosis. Neurology. 2003;61(11):1528-1532.

CABG tops PCI for nondiabetic patients with multivessel CAD
Coronary artery bypass graft surgery was associated with a 35% lower rate of all-cause mortality rate and a 59% lower rate of cardiac death than was percutaneous coronary intervention in a pooled analysis of nondiabetic patients with multivessel coronary artery disease in two international randomized trials.
“The superiority of CABG over PCI was consistent across all major clinical subgroups. Likewise, the rate of myocardial infarction was remarkably lower after CABG than after PCI,” Mineok Chang, MD, of the University of Ulsan in Seoul, South Korea, and her associates reported online June 27 in the Journal of the American College of Cardiology.
The advent of drug-eluting stents has led to widespread use of PCI, but controversy persists regarding the best revascularization strategy for nondiabetic patients with multivessel CAD, the researchers said. All-cause mortality “is undoubtedly the most unbiased endpoint to determine treatment strategy,” but individual trials have lacked the power to evaluate this endpoint, they added. Accordingly, they pooled data from the SYNTAX (Synergy Between PCI with Taxus and Cardiac Surgery) trial – which included 1,800 patients with three-vessel or left main CAD from Europe and the United States – and from the BEST (Randomized Comparison of Coronary Artery Bypass Surgery and Everolimus-Eluting Stent Implantation in the Treatment of Patients With Multivessel Coronary Artery Disease) trial, which included 880 patients from Asia with two- or three-vessel CAD. Excluding patients with left main CAD or diabetes left 1,275 patients for analysis (J Am Coll Cardiol. 2016 Jun 27. 68:29-36).
After a median follow-up of 61 months, 38 (6%) CABG patients had died, compared with 59 (9.3%) PCI patients, for a statistically significant hazard ratio of 0.65 (95% confidence interval, 0.25-0.78; P = .039). Likewise, cardiac death was significantly less likely after CABG than PCI (HR, 0.41; 95% CI, 0.25-0.78; P = .005). “The statistical difference between the two groups was pronounced after 2 years of randomization for both all-cause and cardiac mortality,” the researchers reported. Although the latest drug-eluting stents “are reported to improve clinical outcomes,” they did not find a significant interaction between older and more recently developed stents when considering all-cause mortality, they noted.
The study was supported by a research grant from the CardioVascular Research Foundation in Seoul, South Korea. Dr. Chang had no disclosures. Senior author, Dr. Seung-Jung Park, disclosed research support from Abbott Vascular, Cordis, Boston Scientific, and Medtronic.
It is important to consider some limitations of the current study. First, the majority of patients were derived from the SYNTAX trial, which used first-generation paclitaxel drug-eluting stents (DES) that exhibit higher stent complication rates compared with current second- and third-generation everolimus-eluting stents. Second, although complete revascularization was more frequently obtained with CABG in the SYNTAX and BEST trials, current PCI approaches are narrowing this gap with chronic total occlusion PCI techniques and temporary hemodynamic support when needed. Third, selection bias may limit the applicability of these results to patients with more complex disease who are often excluded from clinical trials and may not be eligible for CABG.
Therefore, an adequately powered study of contemporary DES PCI versus CABG is warranted for real-world, nondiabetic patients with multivessel CAD. Guidelines and meta-analyses provide valuable recommendations for populations at large, but decision making for nondiabetic patients with multivessel CAD should be individualized. If equipoise between CABG and PCI exists, decision-making can be improved by engaging a local multidisciplinary CAD heart team. Well-informed cardiologists, interventionalists, and cardiac surgeons who engage in multidisciplinary heart team evaluations and patient-centered shared decision making will provide optimal guidance for patients with multivessel CAD.
Farouc A. Jaffer, MD, is at Massachusetts General Hospital; Patrick T. O’Gara, MD, is at Brigham and Women’s Hospital, both in Boston. Dr. Jaffer disclosed research grants from Siemens and Kowa and consulting relationships with Boston Scientific and Abbott Vascular. Dr. O’Gara had no disclosures. These comments are from their editorial (J Am Coll Cardiol. 2016 Jun 27. doi: 10.1016/j.jacc.2016.05.008).
It is important to consider some limitations of the current study. First, the majority of patients were derived from the SYNTAX trial, which used first-generation paclitaxel drug-eluting stents (DES) that exhibit higher stent complication rates compared with current second- and third-generation everolimus-eluting stents. Second, although complete revascularization was more frequently obtained with CABG in the SYNTAX and BEST trials, current PCI approaches are narrowing this gap with chronic total occlusion PCI techniques and temporary hemodynamic support when needed. Third, selection bias may limit the applicability of these results to patients with more complex disease who are often excluded from clinical trials and may not be eligible for CABG.
Therefore, an adequately powered study of contemporary DES PCI versus CABG is warranted for real-world, nondiabetic patients with multivessel CAD. Guidelines and meta-analyses provide valuable recommendations for populations at large, but decision making for nondiabetic patients with multivessel CAD should be individualized. If equipoise between CABG and PCI exists, decision-making can be improved by engaging a local multidisciplinary CAD heart team. Well-informed cardiologists, interventionalists, and cardiac surgeons who engage in multidisciplinary heart team evaluations and patient-centered shared decision making will provide optimal guidance for patients with multivessel CAD.
Farouc A. Jaffer, MD, is at Massachusetts General Hospital; Patrick T. O’Gara, MD, is at Brigham and Women’s Hospital, both in Boston. Dr. Jaffer disclosed research grants from Siemens and Kowa and consulting relationships with Boston Scientific and Abbott Vascular. Dr. O’Gara had no disclosures. These comments are from their editorial (J Am Coll Cardiol. 2016 Jun 27. doi: 10.1016/j.jacc.2016.05.008).
It is important to consider some limitations of the current study. First, the majority of patients were derived from the SYNTAX trial, which used first-generation paclitaxel drug-eluting stents (DES) that exhibit higher stent complication rates compared with current second- and third-generation everolimus-eluting stents. Second, although complete revascularization was more frequently obtained with CABG in the SYNTAX and BEST trials, current PCI approaches are narrowing this gap with chronic total occlusion PCI techniques and temporary hemodynamic support when needed. Third, selection bias may limit the applicability of these results to patients with more complex disease who are often excluded from clinical trials and may not be eligible for CABG.
Therefore, an adequately powered study of contemporary DES PCI versus CABG is warranted for real-world, nondiabetic patients with multivessel CAD. Guidelines and meta-analyses provide valuable recommendations for populations at large, but decision making for nondiabetic patients with multivessel CAD should be individualized. If equipoise between CABG and PCI exists, decision-making can be improved by engaging a local multidisciplinary CAD heart team. Well-informed cardiologists, interventionalists, and cardiac surgeons who engage in multidisciplinary heart team evaluations and patient-centered shared decision making will provide optimal guidance for patients with multivessel CAD.
Farouc A. Jaffer, MD, is at Massachusetts General Hospital; Patrick T. O’Gara, MD, is at Brigham and Women’s Hospital, both in Boston. Dr. Jaffer disclosed research grants from Siemens and Kowa and consulting relationships with Boston Scientific and Abbott Vascular. Dr. O’Gara had no disclosures. These comments are from their editorial (J Am Coll Cardiol. 2016 Jun 27. doi: 10.1016/j.jacc.2016.05.008).
Coronary artery bypass graft surgery was associated with a 35% lower rate of all-cause mortality rate and a 59% lower rate of cardiac death than was percutaneous coronary intervention in a pooled analysis of nondiabetic patients with multivessel coronary artery disease in two international randomized trials.
“The superiority of CABG over PCI was consistent across all major clinical subgroups. Likewise, the rate of myocardial infarction was remarkably lower after CABG than after PCI,” Mineok Chang, MD, of the University of Ulsan in Seoul, South Korea, and her associates reported online June 27 in the Journal of the American College of Cardiology.
The advent of drug-eluting stents has led to widespread use of PCI, but controversy persists regarding the best revascularization strategy for nondiabetic patients with multivessel CAD, the researchers said. All-cause mortality “is undoubtedly the most unbiased endpoint to determine treatment strategy,” but individual trials have lacked the power to evaluate this endpoint, they added. Accordingly, they pooled data from the SYNTAX (Synergy Between PCI with Taxus and Cardiac Surgery) trial – which included 1,800 patients with three-vessel or left main CAD from Europe and the United States – and from the BEST (Randomized Comparison of Coronary Artery Bypass Surgery and Everolimus-Eluting Stent Implantation in the Treatment of Patients With Multivessel Coronary Artery Disease) trial, which included 880 patients from Asia with two- or three-vessel CAD. Excluding patients with left main CAD or diabetes left 1,275 patients for analysis (J Am Coll Cardiol. 2016 Jun 27. 68:29-36).
After a median follow-up of 61 months, 38 (6%) CABG patients had died, compared with 59 (9.3%) PCI patients, for a statistically significant hazard ratio of 0.65 (95% confidence interval, 0.25-0.78; P = .039). Likewise, cardiac death was significantly less likely after CABG than PCI (HR, 0.41; 95% CI, 0.25-0.78; P = .005). “The statistical difference between the two groups was pronounced after 2 years of randomization for both all-cause and cardiac mortality,” the researchers reported. Although the latest drug-eluting stents “are reported to improve clinical outcomes,” they did not find a significant interaction between older and more recently developed stents when considering all-cause mortality, they noted.
The study was supported by a research grant from the CardioVascular Research Foundation in Seoul, South Korea. Dr. Chang had no disclosures. Senior author, Dr. Seung-Jung Park, disclosed research support from Abbott Vascular, Cordis, Boston Scientific, and Medtronic.
Coronary artery bypass graft surgery was associated with a 35% lower rate of all-cause mortality rate and a 59% lower rate of cardiac death than was percutaneous coronary intervention in a pooled analysis of nondiabetic patients with multivessel coronary artery disease in two international randomized trials.
“The superiority of CABG over PCI was consistent across all major clinical subgroups. Likewise, the rate of myocardial infarction was remarkably lower after CABG than after PCI,” Mineok Chang, MD, of the University of Ulsan in Seoul, South Korea, and her associates reported online June 27 in the Journal of the American College of Cardiology.
The advent of drug-eluting stents has led to widespread use of PCI, but controversy persists regarding the best revascularization strategy for nondiabetic patients with multivessel CAD, the researchers said. All-cause mortality “is undoubtedly the most unbiased endpoint to determine treatment strategy,” but individual trials have lacked the power to evaluate this endpoint, they added. Accordingly, they pooled data from the SYNTAX (Synergy Between PCI with Taxus and Cardiac Surgery) trial – which included 1,800 patients with three-vessel or left main CAD from Europe and the United States – and from the BEST (Randomized Comparison of Coronary Artery Bypass Surgery and Everolimus-Eluting Stent Implantation in the Treatment of Patients With Multivessel Coronary Artery Disease) trial, which included 880 patients from Asia with two- or three-vessel CAD. Excluding patients with left main CAD or diabetes left 1,275 patients for analysis (J Am Coll Cardiol. 2016 Jun 27. 68:29-36).
After a median follow-up of 61 months, 38 (6%) CABG patients had died, compared with 59 (9.3%) PCI patients, for a statistically significant hazard ratio of 0.65 (95% confidence interval, 0.25-0.78; P = .039). Likewise, cardiac death was significantly less likely after CABG than PCI (HR, 0.41; 95% CI, 0.25-0.78; P = .005). “The statistical difference between the two groups was pronounced after 2 years of randomization for both all-cause and cardiac mortality,” the researchers reported. Although the latest drug-eluting stents “are reported to improve clinical outcomes,” they did not find a significant interaction between older and more recently developed stents when considering all-cause mortality, they noted.
The study was supported by a research grant from the CardioVascular Research Foundation in Seoul, South Korea. Dr. Chang had no disclosures. Senior author, Dr. Seung-Jung Park, disclosed research support from Abbott Vascular, Cordis, Boston Scientific, and Medtronic.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Key clinical point: Coronary artery bypass graft is superior to percutaneous coronary intervention for nondiabetic patients with multivessel coronary artery disease.
Major finding: All-cause mortality rates were 6% for CABG and 9.3% for PCI (HR, 0.65; P = .039).
Data source: A pooled analysis of 1,275 nondiabetic patients with two- or three-vessel CAD from the SYNTAX and BEST trials.
Disclosures: The study was supported by a research grant from the CardioVascular Research Foundation in Seoul, South Korea. Dr. Chang had no disclosures. Senior author, Dr. Seung-Jung Park, disclosed research support from Abbott Vascular, Cordis, Boston Scientific, and Medtronic.
Hyperkeratotic Lesions in a Patient With Hepatitis C Virus
The Diagnosis: Necrolytic Acral Erythema
Histopathologic analysis of a biopsy specimen from the right leg revealed an erosion with parakeratosis containing neutrophils and marked spongiosis favoring the upper layer of the epidermis with focal individual necrotic keratinocytes. In addition, there was a lymphocytic and neutrophilic exocytosis with edema of the papillary dermal papillae, mild papillary dermal fibrosis, and a mild perivascular lymphocytic infiltrate with neutrophils and occasional eosinophils. Clinicopathologic correlation led to a diagnosis of necrolytic acral erythema (NAE).
The patient was prescribed clobetasol propionate ointment 0.05% and oral zinc sulfate 220 mg twice daily but was initially noncompliant with the topical corticosteroid regimen. He did, however, initiate zinc supplementation, which was later increased to 220 mg 3 times daily. At 3-month follow-up, the lesions had nearly completely cleared (Figure) and the serum zinc level was within reference range at 81 μg/dL.

Necrolytic acral erythema is a rare dermatosis that was first described in 1996 by el Darouti and Abu el Ela1 in a series of 7 Egyptian patients. Since then, most of the cases have reported concomitant hepatitis C virus (HCV) infection.2 Necrolytic acral erythema classically presents with symmetric, well-defined, hyperkeratotic plaques in an acral distribution, typically on the dorsal aspect of the feet.2,3 Lesions may involve the dorsal aspect of the toes and the lower legs, with less common involvement of the elbows, hands, and buttocks. Patients often report pruritus and/or burning.3
Abdallah et al4 proposed several stages of NAE development with erythematous papules with dusky eroded centers progressing to marginated, erythematous to violaceous, lichenified plaques. Over time, these lesions tend to thin with progressive hyperpigmentation.
Histologically, early findings of NAE include acanthosis with epidermal spongiosis and upper dermal perivascular dermatitis. Over time, lesions may exhibit psoriasiform hyperplasia with papillomatosis and parakeratosis, epidermal pallor, subcorneal pustules, vascular ectasia, papillary dermal inflammation, and necrotic keratinocytes. Minimal to moderate acanthosis with an inflammatory infiltrate may be observed later in disease progression.5
The differential diagnosis of NAE includes many benign inflammatory skin diseases. Given the acral/extensor distribution of hyperkeratotic lesions and psoriasiform pattern on histopathology, NAE initially may be misdiagnosed as psoriasis. Unlike psoriasis, however, NAE rarely involves palmoplantar skin or nails4 and may respond dramatically to treatment with zinc supplementation.6,7 Necrolytic acral erythema also may be confused with other necrolytic erythemas, including necrolytic migratory erythema, acrodermatitis enteropathica, and pellagra. A deficiency of biotin or essential fatty acids also may mimic NAE. Necrolytic acral erythema can be distinguished from these entities based on its characteristic appearance and distribution, along with comorbid HCV infection.2-4
Several reports of NAE have revealed an associated zinc deficiency.2,8 The underlying pathophysiology of zinc deficiency in NAE has not been elucidated but is thought to be related to HCV infection.2 Clinical improvement has been reported with zinc supplementation in patients with NAE at dosages of 220 mg twice daily, even in those with initial serum zinc levels within reference range.6,7 Our patient was observed to have a low serum zinc level that dramatically improved with oral supplementation.
The recognition of this uncommon entity is critical for dermatologists and dermatopathologists, as NAE has been proposed as an early cutaneous marker of HCV and may prompt the initial diagnosis of HCV.1-10 The severity of NAE has even been linked to HCV severity.1,8 Treatment of HCV has cleared NAE in several cases,4,10 implicating the virus in its pathogenesis. A proper workup for liver dysfunction and follow-up with an appropriate health care provider for HCV treatment is crucial. Our patient was encouraged to follow up with the hepatology department, as he had not been evaluated in several years.
- el Darouti M, Abu el Ela M. Necrolytic acral erythema: a cutaneous marker of viral hepatitis C. Int J Dermatol. 1996;35:252-256.
- Patel U, Loyd A, Patel R, et al. Necrolytic acral erythema. Dermatol Online J. 2010;16:15.
- Geria AN, Holcomb KZ, Scheinfeld NS. Necrolytic acral erythema: a review of the literature. Cutis. 2009;83:309-314.
- Abdallah MA, Ghozzi MY, Monib HA, et al. Necrolytic acral erythema: a cutaneous sign of hepatitis C virus infection. J Am Acad Dermatol. 2005;53:247-251.
- Abdallah MA, Ghozzi MY, Monib HA, et al. Histological study of necrolytic acral erythema. J Ark Med Soc. 2004;100:354-355.
- Khanna VJ, Shieh S, Benjamin J, et al. Necrolytic acral erythema associated with hepatitis C: effective treatment with interferon alfa and zinc. Arch Dermatol. 2000;136:755-757.
- Abdallah MA, Hull C, Horn TD. Necrolytic acral erythema: a patient from the United States successfully treated with oral zinc. Arch Dermatol. 2005;141:85-87.
- Najarian DJ, Lefkowitz I, Balfour E, et al. Zinc deficiency associated with necrolytic acral erythema. J Am Acad Dermatol. 2006;55(5 suppl):S108-S110.
- Nofal AA, Nofal E, Attwa E, et al. Necrolytic acral erythema: a variant of necrolytic migratory erythema or a distinct entity? Int J Dermatol. 2005;44:916-921.
- Hivnor CM, Yan AC, Junkins-Hopkins JM, et al. Necrolytic acral erythema: response to combination therapy with interferon and ribavirin. J Am Acad Dermatol. 2004;50(5 suppl):S121-S124.
The Diagnosis: Necrolytic Acral Erythema
Histopathologic analysis of a biopsy specimen from the right leg revealed an erosion with parakeratosis containing neutrophils and marked spongiosis favoring the upper layer of the epidermis with focal individual necrotic keratinocytes. In addition, there was a lymphocytic and neutrophilic exocytosis with edema of the papillary dermal papillae, mild papillary dermal fibrosis, and a mild perivascular lymphocytic infiltrate with neutrophils and occasional eosinophils. Clinicopathologic correlation led to a diagnosis of necrolytic acral erythema (NAE).
The patient was prescribed clobetasol propionate ointment 0.05% and oral zinc sulfate 220 mg twice daily but was initially noncompliant with the topical corticosteroid regimen. He did, however, initiate zinc supplementation, which was later increased to 220 mg 3 times daily. At 3-month follow-up, the lesions had nearly completely cleared (Figure) and the serum zinc level was within reference range at 81 μg/dL.
Necrolytic acral erythema is a rare dermatosis that was first described in 1996 by el Darouti and Abu el Ela1 in a series of 7 Egyptian patients. Since then, most of the cases have reported concomitant hepatitis C virus (HCV) infection.2 Necrolytic acral erythema classically presents with symmetric, well-defined, hyperkeratotic plaques in an acral distribution, typically on the dorsal aspect of the feet.2,3 Lesions may involve the dorsal aspect of the toes and the lower legs, with less common involvement of the elbows, hands, and buttocks. Patients often report pruritus and/or burning.3
Abdallah et al4 proposed several stages of NAE development with erythematous papules with dusky eroded centers progressing to marginated, erythematous to violaceous, lichenified plaques. Over time, these lesions tend to thin with progressive hyperpigmentation.
Histologically, early findings of NAE include acanthosis with epidermal spongiosis and upper dermal perivascular dermatitis. Over time, lesions may exhibit psoriasiform hyperplasia with papillomatosis and parakeratosis, epidermal pallor, subcorneal pustules, vascular ectasia, papillary dermal inflammation, and necrotic keratinocytes. Minimal to moderate acanthosis with an inflammatory infiltrate may be observed later in disease progression.5
The differential diagnosis of NAE includes many benign inflammatory skin diseases. Given the acral/extensor distribution of hyperkeratotic lesions and psoriasiform pattern on histopathology, NAE initially may be misdiagnosed as psoriasis. Unlike psoriasis, however, NAE rarely involves palmoplantar skin or nails4 and may respond dramatically to treatment with zinc supplementation.6,7 Necrolytic acral erythema also may be confused with other necrolytic erythemas, including necrolytic migratory erythema, acrodermatitis enteropathica, and pellagra. A deficiency of biotin or essential fatty acids also may mimic NAE. Necrolytic acral erythema can be distinguished from these entities based on its characteristic appearance and distribution, along with comorbid HCV infection.2-4
Several reports of NAE have revealed an associated zinc deficiency.2,8 The underlying pathophysiology of zinc deficiency in NAE has not been elucidated but is thought to be related to HCV infection.2 Clinical improvement has been reported with zinc supplementation in patients with NAE at dosages of 220 mg twice daily, even in those with initial serum zinc levels within reference range.6,7 Our patient was observed to have a low serum zinc level that dramatically improved with oral supplementation.
The recognition of this uncommon entity is critical for dermatologists and dermatopathologists, as NAE has been proposed as an early cutaneous marker of HCV and may prompt the initial diagnosis of HCV.1-10 The severity of NAE has even been linked to HCV severity.1,8 Treatment of HCV has cleared NAE in several cases,4,10 implicating the virus in its pathogenesis. A proper workup for liver dysfunction and follow-up with an appropriate health care provider for HCV treatment is crucial. Our patient was encouraged to follow up with the hepatology department, as he had not been evaluated in several years.
The Diagnosis: Necrolytic Acral Erythema
Histopathologic analysis of a biopsy specimen from the right leg revealed an erosion with parakeratosis containing neutrophils and marked spongiosis favoring the upper layer of the epidermis with focal individual necrotic keratinocytes. In addition, there was a lymphocytic and neutrophilic exocytosis with edema of the papillary dermal papillae, mild papillary dermal fibrosis, and a mild perivascular lymphocytic infiltrate with neutrophils and occasional eosinophils. Clinicopathologic correlation led to a diagnosis of necrolytic acral erythema (NAE).
The patient was prescribed clobetasol propionate ointment 0.05% and oral zinc sulfate 220 mg twice daily but was initially noncompliant with the topical corticosteroid regimen. He did, however, initiate zinc supplementation, which was later increased to 220 mg 3 times daily. At 3-month follow-up, the lesions had nearly completely cleared (Figure) and the serum zinc level was within reference range at 81 μg/dL.
Necrolytic acral erythema is a rare dermatosis that was first described in 1996 by el Darouti and Abu el Ela1 in a series of 7 Egyptian patients. Since then, most of the cases have reported concomitant hepatitis C virus (HCV) infection.2 Necrolytic acral erythema classically presents with symmetric, well-defined, hyperkeratotic plaques in an acral distribution, typically on the dorsal aspect of the feet.2,3 Lesions may involve the dorsal aspect of the toes and the lower legs, with less common involvement of the elbows, hands, and buttocks. Patients often report pruritus and/or burning.3
Abdallah et al4 proposed several stages of NAE development with erythematous papules with dusky eroded centers progressing to marginated, erythematous to violaceous, lichenified plaques. Over time, these lesions tend to thin with progressive hyperpigmentation.
Histologically, early findings of NAE include acanthosis with epidermal spongiosis and upper dermal perivascular dermatitis. Over time, lesions may exhibit psoriasiform hyperplasia with papillomatosis and parakeratosis, epidermal pallor, subcorneal pustules, vascular ectasia, papillary dermal inflammation, and necrotic keratinocytes. Minimal to moderate acanthosis with an inflammatory infiltrate may be observed later in disease progression.5
The differential diagnosis of NAE includes many benign inflammatory skin diseases. Given the acral/extensor distribution of hyperkeratotic lesions and psoriasiform pattern on histopathology, NAE initially may be misdiagnosed as psoriasis. Unlike psoriasis, however, NAE rarely involves palmoplantar skin or nails4 and may respond dramatically to treatment with zinc supplementation.6,7 Necrolytic acral erythema also may be confused with other necrolytic erythemas, including necrolytic migratory erythema, acrodermatitis enteropathica, and pellagra. A deficiency of biotin or essential fatty acids also may mimic NAE. Necrolytic acral erythema can be distinguished from these entities based on its characteristic appearance and distribution, along with comorbid HCV infection.2-4
Several reports of NAE have revealed an associated zinc deficiency.2,8 The underlying pathophysiology of zinc deficiency in NAE has not been elucidated but is thought to be related to HCV infection.2 Clinical improvement has been reported with zinc supplementation in patients with NAE at dosages of 220 mg twice daily, even in those with initial serum zinc levels within reference range.6,7 Our patient was observed to have a low serum zinc level that dramatically improved with oral supplementation.
The recognition of this uncommon entity is critical for dermatologists and dermatopathologists, as NAE has been proposed as an early cutaneous marker of HCV and may prompt the initial diagnosis of HCV.1-10 The severity of NAE has even been linked to HCV severity.1,8 Treatment of HCV has cleared NAE in several cases,4,10 implicating the virus in its pathogenesis. A proper workup for liver dysfunction and follow-up with an appropriate health care provider for HCV treatment is crucial. Our patient was encouraged to follow up with the hepatology department, as he had not been evaluated in several years.
- el Darouti M, Abu el Ela M. Necrolytic acral erythema: a cutaneous marker of viral hepatitis C. Int J Dermatol. 1996;35:252-256.
- Patel U, Loyd A, Patel R, et al. Necrolytic acral erythema. Dermatol Online J. 2010;16:15.
- Geria AN, Holcomb KZ, Scheinfeld NS. Necrolytic acral erythema: a review of the literature. Cutis. 2009;83:309-314.
- Abdallah MA, Ghozzi MY, Monib HA, et al. Necrolytic acral erythema: a cutaneous sign of hepatitis C virus infection. J Am Acad Dermatol. 2005;53:247-251.
- Abdallah MA, Ghozzi MY, Monib HA, et al. Histological study of necrolytic acral erythema. J Ark Med Soc. 2004;100:354-355.
- Khanna VJ, Shieh S, Benjamin J, et al. Necrolytic acral erythema associated with hepatitis C: effective treatment with interferon alfa and zinc. Arch Dermatol. 2000;136:755-757.
- Abdallah MA, Hull C, Horn TD. Necrolytic acral erythema: a patient from the United States successfully treated with oral zinc. Arch Dermatol. 2005;141:85-87.
- Najarian DJ, Lefkowitz I, Balfour E, et al. Zinc deficiency associated with necrolytic acral erythema. J Am Acad Dermatol. 2006;55(5 suppl):S108-S110.
- Nofal AA, Nofal E, Attwa E, et al. Necrolytic acral erythema: a variant of necrolytic migratory erythema or a distinct entity? Int J Dermatol. 2005;44:916-921.
- Hivnor CM, Yan AC, Junkins-Hopkins JM, et al. Necrolytic acral erythema: response to combination therapy with interferon and ribavirin. J Am Acad Dermatol. 2004;50(5 suppl):S121-S124.
- el Darouti M, Abu el Ela M. Necrolytic acral erythema: a cutaneous marker of viral hepatitis C. Int J Dermatol. 1996;35:252-256.
- Patel U, Loyd A, Patel R, et al. Necrolytic acral erythema. Dermatol Online J. 2010;16:15.
- Geria AN, Holcomb KZ, Scheinfeld NS. Necrolytic acral erythema: a review of the literature. Cutis. 2009;83:309-314.
- Abdallah MA, Ghozzi MY, Monib HA, et al. Necrolytic acral erythema: a cutaneous sign of hepatitis C virus infection. J Am Acad Dermatol. 2005;53:247-251.
- Abdallah MA, Ghozzi MY, Monib HA, et al. Histological study of necrolytic acral erythema. J Ark Med Soc. 2004;100:354-355.
- Khanna VJ, Shieh S, Benjamin J, et al. Necrolytic acral erythema associated with hepatitis C: effective treatment with interferon alfa and zinc. Arch Dermatol. 2000;136:755-757.
- Abdallah MA, Hull C, Horn TD. Necrolytic acral erythema: a patient from the United States successfully treated with oral zinc. Arch Dermatol. 2005;141:85-87.
- Najarian DJ, Lefkowitz I, Balfour E, et al. Zinc deficiency associated with necrolytic acral erythema. J Am Acad Dermatol. 2006;55(5 suppl):S108-S110.
- Nofal AA, Nofal E, Attwa E, et al. Necrolytic acral erythema: a variant of necrolytic migratory erythema or a distinct entity? Int J Dermatol. 2005;44:916-921.
- Hivnor CM, Yan AC, Junkins-Hopkins JM, et al. Necrolytic acral erythema: response to combination therapy with interferon and ribavirin. J Am Acad Dermatol. 2004;50(5 suppl):S121-S124.


The Arthroscopic Superior Capsular Reconstruction
Rotator cuff tears are very common, and 250,000 to 500,000 rotator cuff repairs are performed in the United States each year.1,2 In most cases, a complete repair of even large or massive tears can be achieved. However, a subset of patients exist in whom the glenohumeral joint has minimal degenerative changes and the rotator cuff tendon is either irreparable or very poor quality and unlikely to heal (ie, failed previous cuff repair). Some authors have advocated for reverse shoulder arthroplasty (RSA) in these patients despite the lack of glenohumeral arthritis. However, due to the permanent destruction of the glenohumeral articular surfaces, complication rates, and concerns about implant longevity with RSA, we believe the superior capsular reconstruction (SCR) is a viable alternative in patients in whom joint preservation is appropriate based on age limitations and/or activity requirements.3
The SCR was first described by Mihata and colleagues4 as a means to reconstruct the superior capsule in shoulders with large, irreparable posterosuperior rotator cuff tears. Originally described using a fascia lata autograft, our technique has been adapted to incorporate a dermal allograft, which limits donor site morbidity and operative time. In most cases, the dermal allograft is fixed to the normal anatomic attachments of the superior glenoid just medial to the superior labrum, laterally to the greater tuberosity, and posteriorly with side-to-side sutures to the remaining rotator cuff. If there is a robust band of “comma” tissue anteriorly, we fix the anterior margin of the dermal graft to this with side-to-side sutures. The comma tissue represents the medial sling of the biceps tendon and connects the upper subscapularis tendon to the anterior supraspinatus. In most cases, this tissue is intact after repair of the subscapularis tendon.
Technique
The patient is positioned in either the lateral decubitus or beach chair position. The arm is positioned in 20° to 30° of abduction and 20° to 30° of forward flexion. A diagnostic arthroscopy is performed through a posterior glenohumeral viewing portal. The subscapularis is visualized and repaired if torn. A biceps tenodesis is performed in most cases, as there is often a tear of the subscapularis, tear or instability of the biceps tendon, and/or a compromised attachment of the biceps root.
Attention is turned to the subacromial space. Posterior viewing and lateral working portals are established. A 10-mm flexible cannula (PassPort; Arthrex) is placed in the lateral portal to aid with suture management and graft passage. A limited subacromial decompression is performed that preserves the coracoacromial arch. The rotator cuff is carefully dissected and freed from the internal deltoid fascia. The scapular spine is identified to visualize the raphé between the supraspinatus and infraspinatus. The infraspinatus is mobilized and repaired as much as possible.
If we think that the tear might be reparable by gaining added excursion from a posterior interval slide, or if it is clearly not reparable but the remaining rim of rotator cuff obscures clear visualization of the superior glenoid, we perform a posterior interval slide. If the additional excursion that is achieved by the posterior slide is adequate for a complete repair, we proceed with the repair. However, if the tear is not reparable even after the posterior interval slide, we have found that the exposure and preparation of the superior glenoid is greatly improved after the posterior slide. After fixation of the dermal graft, we typically perform a partial side-to-side repair of the supraspinatus to the infraspinatus over the top of the graft.
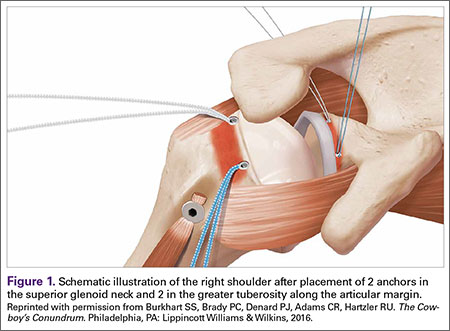
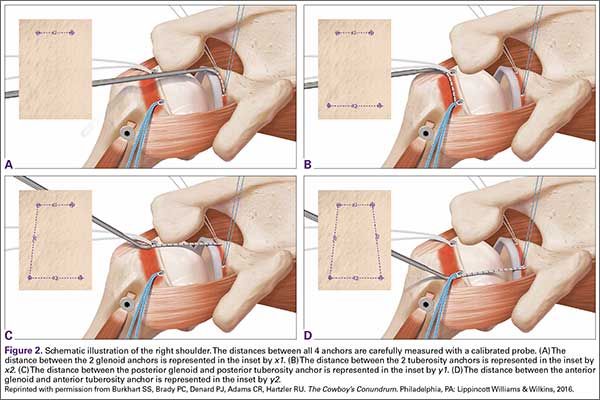
The bone beds of the greater tuberosity and just medial to the superior glenoid labrum are prepared with a shaver and motorized burr. Two anchors (3.0-mm BioComposite SutureTak; Arthrex) are placed in the superior glenoid neck at about the 10 o’clock and 2 o’clock positions approximately 5 mm medial to the superior labrum. Note: the placement medial to the labrum is chosen because this is the normal origin of the superior capsule and because of the angle of approach, these percutaneous portals are often more medial than typical portals for placing anchors during SLAP (superior labral anterior to posterior) repair. Next, 2 threaded anchors (4.75-mm BioComposite SwiveLock; Arthrex) preloaded with suture tape are placed in the greater tuberosity along the articular margin (Figure 1). However, if a biceps tenodesis with an interference screw is placed at the top of the bicipital groove, this anchor preloaded with suture tape can also serve as the anteromedial anchor in the greater tuberosity footprint. The distances between all 4 anchors are carefully measured with a calibrated probe (Figures 2A-2D).
We use a 3.0-mm acellular dermal allograft (ArthroFlex; Arthrex) to reconstruct the superior capsule. The positions of the 4 anchors are carefully marked on the dermal allograft. We routinely add an additional 5 mm of tissue to the medial, anterior, and posterior margins to decrease the risk of suture cut out. An additional 10 mm of tissue is added laterally to cover the greater tuberosity. The final contoured graft is typically trapezoidal in shape.
The sutures from the 4 anchors are then sequentially retrieved through the lateral cannula. The sutures from the greater tuberosity anchors are passed through their respective holes in the graft. However, the suture limbs from each of the glenoid anchors are individually passed 2 mm anterior and 2 mm posterior to their respective marks on the graft with an antegrade suture passer (Figure 3). It is important to have an assistant apply tension to each of the sutures after they are passed through the graft to decrease the chance of crossing and tangling the sutures.
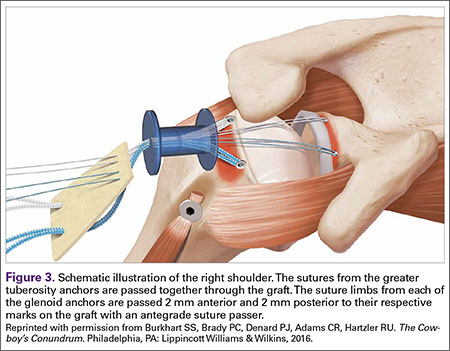
The eyelets of the medial anchors are utilized as pulleys to deliver the dermal allograft into the shoulder. One suture limb from each of the glenoid anchors is tied to the other over a switching stick (Figure 4A). The 2 remaining (untied) suture limbs are then pulled, which introduces the graft to the orifice of the cannula (Figure 4B). A tissue grasper is then used to fold the dermal allograft along its long axis and introduce the graft into the joint (Figure 4C). Once the medial portion of the graft is positioned onto the superior glenoid the 2 remaining (untied) suture limbs are tied to each other as a static knot in the subacromial space (Figure 4D).
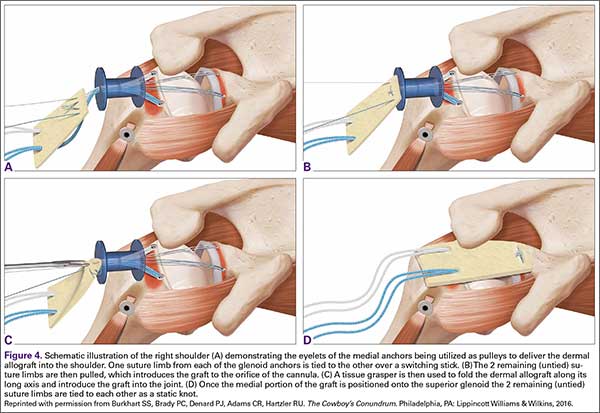
The redundancy in the suture tapes can be removed by sequentially sliding a retriever down each suture and tensioning the suture as the nose of the instrument pushes the dermal graft down to the tuberosity bone bed. The suture tapes are crisscrossed and secured laterally with 2 additional knotless threaded anchors (Figure 5). One may also place cinch stitches at the anterolateral and posterolateral corners of the graft that are incorporated into the lateral anchors. These sutures can be useful for pulling the graft back out of the subacromial space in the event of any suture tangles, and can be used for controlling the lateral aspect of the graft during lateral anchor placement.
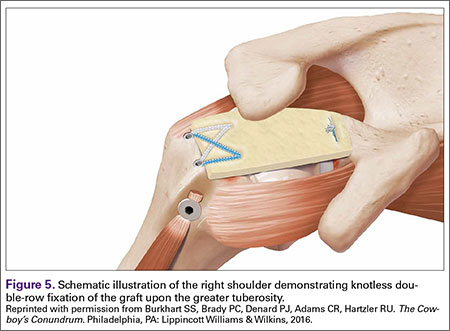
At this point in the procedure, additional glenoid anchors can be placed both anterior and posterior to the superior glenoid anchors if additional glenoid fixation is desired. Finally, 2 to 3 side-to-side sutures are placed posteriorly attaching the anterior aspect of the infraspinatus to the posterior aspect of the dermal allograft (Figures 6A-6C). If rotator interval tissue (comma tissue) is present, anterior side-to-side sutures may be placed. However, we do not recommend placing anterior side-to-side sutures directly from the dermal allograft to the subscapularis as this may deform the graft, over- constrain the shoulder, and restrict motion.
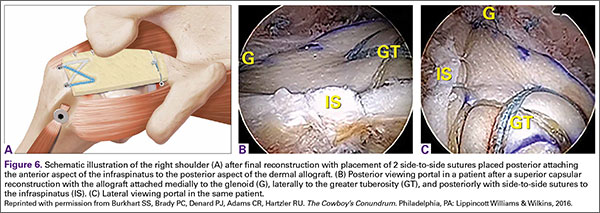
Discussion
Reconstruction of the superior capsule has been shown to restore the normal restraint to superior translation of the humeral head and reestablish a stable fulcrum at the glenohumeral joint.5 It should be mentioned that we do not perform the SCR in patients with advanced glenohumeral arthritis. The short-term results of this novel procedure have been encouraging, including our own series of patients, in which most patients have had a significant reduction in pain, improvement in function, and very few complications (P. J. Denard, MD, S. S. Burkhart, MD, P. C. Brady, MD, J. Tokish, MD, C. R. Adams, MD, unpublished data, May 2016).
The early success of this procedure suggests that a robust superior capsule is necessary, in addition to functional muscle-tendon units, to restore the stable fulcrum and force couples that are necessary for normal shoulder function. Perhaps we have not paid enough attention to the integrity of the superior capsule in the past. In cases of revision cuff repair, we pay special attention to the quality of the capsular layer deep to the cuff tendon. If the capsule is poor quality, we sometimes reconstruct the capsule with a dermal allograft (SCR) and then do a rotator cuff repair (partial or complete) over the top of the SCR to maintain the normal anatomic deep to superficial layering of the capsule and rotator cuff.
We are very conservative with our postoperative rehabilitation program after a SCR. We know that the rate of stiffness with a conservative program after an arthroscopic rotator cuff repair, even in the revision setting, is very low.6 Furthermore, both basic science on healing of soft tissue to bone and radiographic analysis of healing after postoperative rotator cuff repairs support a slow rehabilitation program.7,8 A canine model specifically evaluating acellular dermal allografts in the shoulder suggests that these grafts undergo significant remodeling and become weaker before they get stronger.9 We would rather err on the side of healing of the SCR with potentially a slight increase in the rate of shoulder stiffness than to regain early motion at the expense of graft failure. Therefore, we have the patient wear a sling with no shoulder motion for 6 weeks. Passive motion is started at 6 weeks postoperative and strengthening is delayed until 12 to 16 weeks postoperative.
1. Orr SB, Chainani A, Hippensteel KJ, et al. Aligned multilayered electrospun scaffolds for rotator cuff tendon tissue engineering. Acta Biomater. 2015;24:117-126.
2. Austin L, Black EM, Lombardi NJ, Pepe MD, Lazarus M. Arthroscopic transosseous rotator cuff repair. A prospective study on cost savings, surgical time, and outcomes. Ortho J Sports Med. 2015;3(2 Suppl). doi:10.1177/2325967115S00156.
3. Denard PJ, Lädermann A, Jiwani AZ, Burkhart SS. Functional outcome after arthroscopic repair of massive rotator cuff tears in individuals with pseudoparalysis. Arthroscopy. 2012;28(9):1214-1219.
4. Mihata T, Lee TQ, Watanabe C, et al. Clinical results of arthroscopic superior capsule reconstruction for irreparable rotator cuff tears. Arthroscopy. 2013;29(3):459-470.
5. Mihata T, McGarry MH, Pirolo JM, Kinoshita M, Lee TQ. Superior capsule reconstruction to restore superior stability in irreparable rotator cuff tears: a biomechanical cadaveric study. Am J Sports Med. 2012;40(10):2248-2255.
6. Huberty DP, Schoolfield JD, Brady PC, Vadala AP, Arrigoni P, Burkhart SS. Incidence and treatment of postoperative stiffness following arthroscopic rotator cuff repair. Arthroscopy. 2009;25(8):880-890.
7. Sonnabend DH, Howlett CR, Young AA. Histological evaluation of repair of the rotator cuff in a primate model. J Bone Joint Surg Br. 2010;92(4):586-594.
8. Lee BG, Cho NS, Rhee YG. Effect of two rehabilitation protocols on range of motion and healing rates after arthroscopic rotator cuff repair: aggressive versus limited early passive exercises. Arthroscopy. 2012;28(1):34-42.
9. Adams JE, Zobitz ME, Reach JS Jr, An KN, Steinmann SP. Rotator cuff repair using an acellular dermal matrix graft: an in vivo study in a canine model. Arthroscopy. 2006;22(7):700-709.
Rotator cuff tears are very common, and 250,000 to 500,000 rotator cuff repairs are performed in the United States each year.1,2 In most cases, a complete repair of even large or massive tears can be achieved. However, a subset of patients exist in whom the glenohumeral joint has minimal degenerative changes and the rotator cuff tendon is either irreparable or very poor quality and unlikely to heal (ie, failed previous cuff repair). Some authors have advocated for reverse shoulder arthroplasty (RSA) in these patients despite the lack of glenohumeral arthritis. However, due to the permanent destruction of the glenohumeral articular surfaces, complication rates, and concerns about implant longevity with RSA, we believe the superior capsular reconstruction (SCR) is a viable alternative in patients in whom joint preservation is appropriate based on age limitations and/or activity requirements.3
The SCR was first described by Mihata and colleagues4 as a means to reconstruct the superior capsule in shoulders with large, irreparable posterosuperior rotator cuff tears. Originally described using a fascia lata autograft, our technique has been adapted to incorporate a dermal allograft, which limits donor site morbidity and operative time. In most cases, the dermal allograft is fixed to the normal anatomic attachments of the superior glenoid just medial to the superior labrum, laterally to the greater tuberosity, and posteriorly with side-to-side sutures to the remaining rotator cuff. If there is a robust band of “comma” tissue anteriorly, we fix the anterior margin of the dermal graft to this with side-to-side sutures. The comma tissue represents the medial sling of the biceps tendon and connects the upper subscapularis tendon to the anterior supraspinatus. In most cases, this tissue is intact after repair of the subscapularis tendon.
Technique
The patient is positioned in either the lateral decubitus or beach chair position. The arm is positioned in 20° to 30° of abduction and 20° to 30° of forward flexion. A diagnostic arthroscopy is performed through a posterior glenohumeral viewing portal. The subscapularis is visualized and repaired if torn. A biceps tenodesis is performed in most cases, as there is often a tear of the subscapularis, tear or instability of the biceps tendon, and/or a compromised attachment of the biceps root.
Attention is turned to the subacromial space. Posterior viewing and lateral working portals are established. A 10-mm flexible cannula (PassPort; Arthrex) is placed in the lateral portal to aid with suture management and graft passage. A limited subacromial decompression is performed that preserves the coracoacromial arch. The rotator cuff is carefully dissected and freed from the internal deltoid fascia. The scapular spine is identified to visualize the raphé between the supraspinatus and infraspinatus. The infraspinatus is mobilized and repaired as much as possible.
If we think that the tear might be reparable by gaining added excursion from a posterior interval slide, or if it is clearly not reparable but the remaining rim of rotator cuff obscures clear visualization of the superior glenoid, we perform a posterior interval slide. If the additional excursion that is achieved by the posterior slide is adequate for a complete repair, we proceed with the repair. However, if the tear is not reparable even after the posterior interval slide, we have found that the exposure and preparation of the superior glenoid is greatly improved after the posterior slide. After fixation of the dermal graft, we typically perform a partial side-to-side repair of the supraspinatus to the infraspinatus over the top of the graft.
The bone beds of the greater tuberosity and just medial to the superior glenoid labrum are prepared with a shaver and motorized burr. Two anchors (3.0-mm BioComposite SutureTak; Arthrex) are placed in the superior glenoid neck at about the 10 o’clock and 2 o’clock positions approximately 5 mm medial to the superior labrum. Note: the placement medial to the labrum is chosen because this is the normal origin of the superior capsule and because of the angle of approach, these percutaneous portals are often more medial than typical portals for placing anchors during SLAP (superior labral anterior to posterior) repair. Next, 2 threaded anchors (4.75-mm BioComposite SwiveLock; Arthrex) preloaded with suture tape are placed in the greater tuberosity along the articular margin (Figure 1). However, if a biceps tenodesis with an interference screw is placed at the top of the bicipital groove, this anchor preloaded with suture tape can also serve as the anteromedial anchor in the greater tuberosity footprint. The distances between all 4 anchors are carefully measured with a calibrated probe (Figures 2A-2D).
We use a 3.0-mm acellular dermal allograft (ArthroFlex; Arthrex) to reconstruct the superior capsule. The positions of the 4 anchors are carefully marked on the dermal allograft. We routinely add an additional 5 mm of tissue to the medial, anterior, and posterior margins to decrease the risk of suture cut out. An additional 10 mm of tissue is added laterally to cover the greater tuberosity. The final contoured graft is typically trapezoidal in shape.
The sutures from the 4 anchors are then sequentially retrieved through the lateral cannula. The sutures from the greater tuberosity anchors are passed through their respective holes in the graft. However, the suture limbs from each of the glenoid anchors are individually passed 2 mm anterior and 2 mm posterior to their respective marks on the graft with an antegrade suture passer (Figure 3). It is important to have an assistant apply tension to each of the sutures after they are passed through the graft to decrease the chance of crossing and tangling the sutures.
The eyelets of the medial anchors are utilized as pulleys to deliver the dermal allograft into the shoulder. One suture limb from each of the glenoid anchors is tied to the other over a switching stick (Figure 4A). The 2 remaining (untied) suture limbs are then pulled, which introduces the graft to the orifice of the cannula (Figure 4B). A tissue grasper is then used to fold the dermal allograft along its long axis and introduce the graft into the joint (Figure 4C). Once the medial portion of the graft is positioned onto the superior glenoid the 2 remaining (untied) suture limbs are tied to each other as a static knot in the subacromial space (Figure 4D).
The redundancy in the suture tapes can be removed by sequentially sliding a retriever down each suture and tensioning the suture as the nose of the instrument pushes the dermal graft down to the tuberosity bone bed. The suture tapes are crisscrossed and secured laterally with 2 additional knotless threaded anchors (Figure 5). One may also place cinch stitches at the anterolateral and posterolateral corners of the graft that are incorporated into the lateral anchors. These sutures can be useful for pulling the graft back out of the subacromial space in the event of any suture tangles, and can be used for controlling the lateral aspect of the graft during lateral anchor placement.
At this point in the procedure, additional glenoid anchors can be placed both anterior and posterior to the superior glenoid anchors if additional glenoid fixation is desired. Finally, 2 to 3 side-to-side sutures are placed posteriorly attaching the anterior aspect of the infraspinatus to the posterior aspect of the dermal allograft (Figures 6A-6C). If rotator interval tissue (comma tissue) is present, anterior side-to-side sutures may be placed. However, we do not recommend placing anterior side-to-side sutures directly from the dermal allograft to the subscapularis as this may deform the graft, over- constrain the shoulder, and restrict motion.
Discussion
Reconstruction of the superior capsule has been shown to restore the normal restraint to superior translation of the humeral head and reestablish a stable fulcrum at the glenohumeral joint.5 It should be mentioned that we do not perform the SCR in patients with advanced glenohumeral arthritis. The short-term results of this novel procedure have been encouraging, including our own series of patients, in which most patients have had a significant reduction in pain, improvement in function, and very few complications (P. J. Denard, MD, S. S. Burkhart, MD, P. C. Brady, MD, J. Tokish, MD, C. R. Adams, MD, unpublished data, May 2016).
The early success of this procedure suggests that a robust superior capsule is necessary, in addition to functional muscle-tendon units, to restore the stable fulcrum and force couples that are necessary for normal shoulder function. Perhaps we have not paid enough attention to the integrity of the superior capsule in the past. In cases of revision cuff repair, we pay special attention to the quality of the capsular layer deep to the cuff tendon. If the capsule is poor quality, we sometimes reconstruct the capsule with a dermal allograft (SCR) and then do a rotator cuff repair (partial or complete) over the top of the SCR to maintain the normal anatomic deep to superficial layering of the capsule and rotator cuff.
We are very conservative with our postoperative rehabilitation program after a SCR. We know that the rate of stiffness with a conservative program after an arthroscopic rotator cuff repair, even in the revision setting, is very low.6 Furthermore, both basic science on healing of soft tissue to bone and radiographic analysis of healing after postoperative rotator cuff repairs support a slow rehabilitation program.7,8 A canine model specifically evaluating acellular dermal allografts in the shoulder suggests that these grafts undergo significant remodeling and become weaker before they get stronger.9 We would rather err on the side of healing of the SCR with potentially a slight increase in the rate of shoulder stiffness than to regain early motion at the expense of graft failure. Therefore, we have the patient wear a sling with no shoulder motion for 6 weeks. Passive motion is started at 6 weeks postoperative and strengthening is delayed until 12 to 16 weeks postoperative.
Rotator cuff tears are very common, and 250,000 to 500,000 rotator cuff repairs are performed in the United States each year.1,2 In most cases, a complete repair of even large or massive tears can be achieved. However, a subset of patients exist in whom the glenohumeral joint has minimal degenerative changes and the rotator cuff tendon is either irreparable or very poor quality and unlikely to heal (ie, failed previous cuff repair). Some authors have advocated for reverse shoulder arthroplasty (RSA) in these patients despite the lack of glenohumeral arthritis. However, due to the permanent destruction of the glenohumeral articular surfaces, complication rates, and concerns about implant longevity with RSA, we believe the superior capsular reconstruction (SCR) is a viable alternative in patients in whom joint preservation is appropriate based on age limitations and/or activity requirements.3
The SCR was first described by Mihata and colleagues4 as a means to reconstruct the superior capsule in shoulders with large, irreparable posterosuperior rotator cuff tears. Originally described using a fascia lata autograft, our technique has been adapted to incorporate a dermal allograft, which limits donor site morbidity and operative time. In most cases, the dermal allograft is fixed to the normal anatomic attachments of the superior glenoid just medial to the superior labrum, laterally to the greater tuberosity, and posteriorly with side-to-side sutures to the remaining rotator cuff. If there is a robust band of “comma” tissue anteriorly, we fix the anterior margin of the dermal graft to this with side-to-side sutures. The comma tissue represents the medial sling of the biceps tendon and connects the upper subscapularis tendon to the anterior supraspinatus. In most cases, this tissue is intact after repair of the subscapularis tendon.
Technique
The patient is positioned in either the lateral decubitus or beach chair position. The arm is positioned in 20° to 30° of abduction and 20° to 30° of forward flexion. A diagnostic arthroscopy is performed through a posterior glenohumeral viewing portal. The subscapularis is visualized and repaired if torn. A biceps tenodesis is performed in most cases, as there is often a tear of the subscapularis, tear or instability of the biceps tendon, and/or a compromised attachment of the biceps root.
Attention is turned to the subacromial space. Posterior viewing and lateral working portals are established. A 10-mm flexible cannula (PassPort; Arthrex) is placed in the lateral portal to aid with suture management and graft passage. A limited subacromial decompression is performed that preserves the coracoacromial arch. The rotator cuff is carefully dissected and freed from the internal deltoid fascia. The scapular spine is identified to visualize the raphé between the supraspinatus and infraspinatus. The infraspinatus is mobilized and repaired as much as possible.
If we think that the tear might be reparable by gaining added excursion from a posterior interval slide, or if it is clearly not reparable but the remaining rim of rotator cuff obscures clear visualization of the superior glenoid, we perform a posterior interval slide. If the additional excursion that is achieved by the posterior slide is adequate for a complete repair, we proceed with the repair. However, if the tear is not reparable even after the posterior interval slide, we have found that the exposure and preparation of the superior glenoid is greatly improved after the posterior slide. After fixation of the dermal graft, we typically perform a partial side-to-side repair of the supraspinatus to the infraspinatus over the top of the graft.
The bone beds of the greater tuberosity and just medial to the superior glenoid labrum are prepared with a shaver and motorized burr. Two anchors (3.0-mm BioComposite SutureTak; Arthrex) are placed in the superior glenoid neck at about the 10 o’clock and 2 o’clock positions approximately 5 mm medial to the superior labrum. Note: the placement medial to the labrum is chosen because this is the normal origin of the superior capsule and because of the angle of approach, these percutaneous portals are often more medial than typical portals for placing anchors during SLAP (superior labral anterior to posterior) repair. Next, 2 threaded anchors (4.75-mm BioComposite SwiveLock; Arthrex) preloaded with suture tape are placed in the greater tuberosity along the articular margin (Figure 1). However, if a biceps tenodesis with an interference screw is placed at the top of the bicipital groove, this anchor preloaded with suture tape can also serve as the anteromedial anchor in the greater tuberosity footprint. The distances between all 4 anchors are carefully measured with a calibrated probe (Figures 2A-2D).
We use a 3.0-mm acellular dermal allograft (ArthroFlex; Arthrex) to reconstruct the superior capsule. The positions of the 4 anchors are carefully marked on the dermal allograft. We routinely add an additional 5 mm of tissue to the medial, anterior, and posterior margins to decrease the risk of suture cut out. An additional 10 mm of tissue is added laterally to cover the greater tuberosity. The final contoured graft is typically trapezoidal in shape.
The sutures from the 4 anchors are then sequentially retrieved through the lateral cannula. The sutures from the greater tuberosity anchors are passed through their respective holes in the graft. However, the suture limbs from each of the glenoid anchors are individually passed 2 mm anterior and 2 mm posterior to their respective marks on the graft with an antegrade suture passer (Figure 3). It is important to have an assistant apply tension to each of the sutures after they are passed through the graft to decrease the chance of crossing and tangling the sutures.
The eyelets of the medial anchors are utilized as pulleys to deliver the dermal allograft into the shoulder. One suture limb from each of the glenoid anchors is tied to the other over a switching stick (Figure 4A). The 2 remaining (untied) suture limbs are then pulled, which introduces the graft to the orifice of the cannula (Figure 4B). A tissue grasper is then used to fold the dermal allograft along its long axis and introduce the graft into the joint (Figure 4C). Once the medial portion of the graft is positioned onto the superior glenoid the 2 remaining (untied) suture limbs are tied to each other as a static knot in the subacromial space (Figure 4D).
The redundancy in the suture tapes can be removed by sequentially sliding a retriever down each suture and tensioning the suture as the nose of the instrument pushes the dermal graft down to the tuberosity bone bed. The suture tapes are crisscrossed and secured laterally with 2 additional knotless threaded anchors (Figure 5). One may also place cinch stitches at the anterolateral and posterolateral corners of the graft that are incorporated into the lateral anchors. These sutures can be useful for pulling the graft back out of the subacromial space in the event of any suture tangles, and can be used for controlling the lateral aspect of the graft during lateral anchor placement.
At this point in the procedure, additional glenoid anchors can be placed both anterior and posterior to the superior glenoid anchors if additional glenoid fixation is desired. Finally, 2 to 3 side-to-side sutures are placed posteriorly attaching the anterior aspect of the infraspinatus to the posterior aspect of the dermal allograft (Figures 6A-6C). If rotator interval tissue (comma tissue) is present, anterior side-to-side sutures may be placed. However, we do not recommend placing anterior side-to-side sutures directly from the dermal allograft to the subscapularis as this may deform the graft, over- constrain the shoulder, and restrict motion.
Discussion
Reconstruction of the superior capsule has been shown to restore the normal restraint to superior translation of the humeral head and reestablish a stable fulcrum at the glenohumeral joint.5 It should be mentioned that we do not perform the SCR in patients with advanced glenohumeral arthritis. The short-term results of this novel procedure have been encouraging, including our own series of patients, in which most patients have had a significant reduction in pain, improvement in function, and very few complications (P. J. Denard, MD, S. S. Burkhart, MD, P. C. Brady, MD, J. Tokish, MD, C. R. Adams, MD, unpublished data, May 2016).
The early success of this procedure suggests that a robust superior capsule is necessary, in addition to functional muscle-tendon units, to restore the stable fulcrum and force couples that are necessary for normal shoulder function. Perhaps we have not paid enough attention to the integrity of the superior capsule in the past. In cases of revision cuff repair, we pay special attention to the quality of the capsular layer deep to the cuff tendon. If the capsule is poor quality, we sometimes reconstruct the capsule with a dermal allograft (SCR) and then do a rotator cuff repair (partial or complete) over the top of the SCR to maintain the normal anatomic deep to superficial layering of the capsule and rotator cuff.
We are very conservative with our postoperative rehabilitation program after a SCR. We know that the rate of stiffness with a conservative program after an arthroscopic rotator cuff repair, even in the revision setting, is very low.6 Furthermore, both basic science on healing of soft tissue to bone and radiographic analysis of healing after postoperative rotator cuff repairs support a slow rehabilitation program.7,8 A canine model specifically evaluating acellular dermal allografts in the shoulder suggests that these grafts undergo significant remodeling and become weaker before they get stronger.9 We would rather err on the side of healing of the SCR with potentially a slight increase in the rate of shoulder stiffness than to regain early motion at the expense of graft failure. Therefore, we have the patient wear a sling with no shoulder motion for 6 weeks. Passive motion is started at 6 weeks postoperative and strengthening is delayed until 12 to 16 weeks postoperative.
1. Orr SB, Chainani A, Hippensteel KJ, et al. Aligned multilayered electrospun scaffolds for rotator cuff tendon tissue engineering. Acta Biomater. 2015;24:117-126.
2. Austin L, Black EM, Lombardi NJ, Pepe MD, Lazarus M. Arthroscopic transosseous rotator cuff repair. A prospective study on cost savings, surgical time, and outcomes. Ortho J Sports Med. 2015;3(2 Suppl). doi:10.1177/2325967115S00156.
3. Denard PJ, Lädermann A, Jiwani AZ, Burkhart SS. Functional outcome after arthroscopic repair of massive rotator cuff tears in individuals with pseudoparalysis. Arthroscopy. 2012;28(9):1214-1219.
4. Mihata T, Lee TQ, Watanabe C, et al. Clinical results of arthroscopic superior capsule reconstruction for irreparable rotator cuff tears. Arthroscopy. 2013;29(3):459-470.
5. Mihata T, McGarry MH, Pirolo JM, Kinoshita M, Lee TQ. Superior capsule reconstruction to restore superior stability in irreparable rotator cuff tears: a biomechanical cadaveric study. Am J Sports Med. 2012;40(10):2248-2255.
6. Huberty DP, Schoolfield JD, Brady PC, Vadala AP, Arrigoni P, Burkhart SS. Incidence and treatment of postoperative stiffness following arthroscopic rotator cuff repair. Arthroscopy. 2009;25(8):880-890.
7. Sonnabend DH, Howlett CR, Young AA. Histological evaluation of repair of the rotator cuff in a primate model. J Bone Joint Surg Br. 2010;92(4):586-594.
8. Lee BG, Cho NS, Rhee YG. Effect of two rehabilitation protocols on range of motion and healing rates after arthroscopic rotator cuff repair: aggressive versus limited early passive exercises. Arthroscopy. 2012;28(1):34-42.
9. Adams JE, Zobitz ME, Reach JS Jr, An KN, Steinmann SP. Rotator cuff repair using an acellular dermal matrix graft: an in vivo study in a canine model. Arthroscopy. 2006;22(7):700-709.
1. Orr SB, Chainani A, Hippensteel KJ, et al. Aligned multilayered electrospun scaffolds for rotator cuff tendon tissue engineering. Acta Biomater. 2015;24:117-126.
2. Austin L, Black EM, Lombardi NJ, Pepe MD, Lazarus M. Arthroscopic transosseous rotator cuff repair. A prospective study on cost savings, surgical time, and outcomes. Ortho J Sports Med. 2015;3(2 Suppl). doi:10.1177/2325967115S00156.
3. Denard PJ, Lädermann A, Jiwani AZ, Burkhart SS. Functional outcome after arthroscopic repair of massive rotator cuff tears in individuals with pseudoparalysis. Arthroscopy. 2012;28(9):1214-1219.
4. Mihata T, Lee TQ, Watanabe C, et al. Clinical results of arthroscopic superior capsule reconstruction for irreparable rotator cuff tears. Arthroscopy. 2013;29(3):459-470.
5. Mihata T, McGarry MH, Pirolo JM, Kinoshita M, Lee TQ. Superior capsule reconstruction to restore superior stability in irreparable rotator cuff tears: a biomechanical cadaveric study. Am J Sports Med. 2012;40(10):2248-2255.
6. Huberty DP, Schoolfield JD, Brady PC, Vadala AP, Arrigoni P, Burkhart SS. Incidence and treatment of postoperative stiffness following arthroscopic rotator cuff repair. Arthroscopy. 2009;25(8):880-890.
7. Sonnabend DH, Howlett CR, Young AA. Histological evaluation of repair of the rotator cuff in a primate model. J Bone Joint Surg Br. 2010;92(4):586-594.
8. Lee BG, Cho NS, Rhee YG. Effect of two rehabilitation protocols on range of motion and healing rates after arthroscopic rotator cuff repair: aggressive versus limited early passive exercises. Arthroscopy. 2012;28(1):34-42.
9. Adams JE, Zobitz ME, Reach JS Jr, An KN, Steinmann SP. Rotator cuff repair using an acellular dermal matrix graft: an in vivo study in a canine model. Arthroscopy. 2006;22(7):700-709.
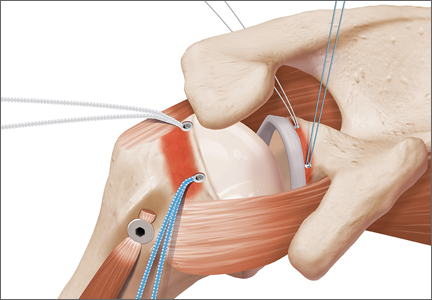
Escitalopram falls short in patients with heart failure and depression
Using escitalopram for patients with chronic heart failure and depression for more than 18 months neither significantly reduces mortality or hospitalization, nor improves depression, a study published June 28 involving 372 patients shows.
“To our knowledge, this study was the first to investigate the composite all-cause mortality and hospitalization in a population with heart failure treated with escitalopram,” wrote Dr. Christiane E. Angermann and her associates.
They said the only other randomized trial evaluating selective serotonin reuptake inhibitors in patients with heart failure was the Sertraline Against Depression and Heart Disease in Chronic Heart Failure study, which found that sertraline did not improve depression or cardiovascular status. But the treatment duration in that study was only 12 weeks, reported Dr. Angermann of the Cardiology and Comprehensive Heart Failure Center, Würzburg, Germany.
The current study, called the Effects of Selective Serotonin Re-Uptake Inhibition on Morbidity, Mortality, and Mood in Depressed Heart Failure Patients, was a double-blind, placebo-controlled randomized trial conducted at 16 tertiary medical centers in Germany. Three hundred seventy-two patients (185 in the escitalopram group and 187 in the placebo group) were randomized and given at least one dose of the study medication. The study was supposed to last for 24 months, but the investigators stopped it early.
Primary outcome of death or hospitalization occurred in 116 (63%) patients and 119 (64%) patients, respectively (hazard ratio, 0.99; 95% confidence interval, 0.76-1.27; P = .92).
Read more of the study and findings on the JAMA website (doi: 10.1001/jama.2016.7635).
Using escitalopram for patients with chronic heart failure and depression for more than 18 months neither significantly reduces mortality or hospitalization, nor improves depression, a study published June 28 involving 372 patients shows.
“To our knowledge, this study was the first to investigate the composite all-cause mortality and hospitalization in a population with heart failure treated with escitalopram,” wrote Dr. Christiane E. Angermann and her associates.
They said the only other randomized trial evaluating selective serotonin reuptake inhibitors in patients with heart failure was the Sertraline Against Depression and Heart Disease in Chronic Heart Failure study, which found that sertraline did not improve depression or cardiovascular status. But the treatment duration in that study was only 12 weeks, reported Dr. Angermann of the Cardiology and Comprehensive Heart Failure Center, Würzburg, Germany.
The current study, called the Effects of Selective Serotonin Re-Uptake Inhibition on Morbidity, Mortality, and Mood in Depressed Heart Failure Patients, was a double-blind, placebo-controlled randomized trial conducted at 16 tertiary medical centers in Germany. Three hundred seventy-two patients (185 in the escitalopram group and 187 in the placebo group) were randomized and given at least one dose of the study medication. The study was supposed to last for 24 months, but the investigators stopped it early.
Primary outcome of death or hospitalization occurred in 116 (63%) patients and 119 (64%) patients, respectively (hazard ratio, 0.99; 95% confidence interval, 0.76-1.27; P = .92).
Read more of the study and findings on the JAMA website (doi: 10.1001/jama.2016.7635).
Using escitalopram for patients with chronic heart failure and depression for more than 18 months neither significantly reduces mortality or hospitalization, nor improves depression, a study published June 28 involving 372 patients shows.
“To our knowledge, this study was the first to investigate the composite all-cause mortality and hospitalization in a population with heart failure treated with escitalopram,” wrote Dr. Christiane E. Angermann and her associates.
They said the only other randomized trial evaluating selective serotonin reuptake inhibitors in patients with heart failure was the Sertraline Against Depression and Heart Disease in Chronic Heart Failure study, which found that sertraline did not improve depression or cardiovascular status. But the treatment duration in that study was only 12 weeks, reported Dr. Angermann of the Cardiology and Comprehensive Heart Failure Center, Würzburg, Germany.
The current study, called the Effects of Selective Serotonin Re-Uptake Inhibition on Morbidity, Mortality, and Mood in Depressed Heart Failure Patients, was a double-blind, placebo-controlled randomized trial conducted at 16 tertiary medical centers in Germany. Three hundred seventy-two patients (185 in the escitalopram group and 187 in the placebo group) were randomized and given at least one dose of the study medication. The study was supposed to last for 24 months, but the investigators stopped it early.
Primary outcome of death or hospitalization occurred in 116 (63%) patients and 119 (64%) patients, respectively (hazard ratio, 0.99; 95% confidence interval, 0.76-1.27; P = .92).
Read more of the study and findings on the JAMA website (doi: 10.1001/jama.2016.7635).
FROM JAMA
Product News: 07 2016
Carmex Grant
Carma Labs Inc, the maker of Carmex lip balms, announced a $10,000 grant program to support an entrepreneur with an Unstoppable Dream. Participants can enter through Facebook or Instagram by posting a 30-second video depicting their aspiration related to a business or product. All entries must include the hashtags #InPursuitOf and #Contest to be considered. Entries can be submitted through July 15, and a winner will be selected and announced in August. For more information, visit www.mycarmex.com.
Juvéderm Volbella XC
Allergan announces US Food and Drug Administration approval to market Juvéderm Volbella XC for lip augmentation and for correction of perioral lines in adults older than 21 years. Juvéderm Volbella XC increases lip fullness and softens the appearance of lines around the mouth. It is formulated with Vycross, a proprietary filler technology that contributes to the product’s smoothness. Juvéderm Volbella XC has been customized with a lower hyaluronic acid concentration (15 mg/mL), while still providing the long-lasting results of other Juvéderm products. It will be available to patients in the United States in October 2016. For more information, visit www.juvederm.com.
Teflaro
Allergan announces US Food and Drug Administration approval of a supplemental new drug application for Teflaro (ceftaroline fosamil) to expand the label to include the treatment of children aged 2 months to less than 18 years with acute bacterial skin and skin structure infections (ABSSSI) including infections caused by methicillin-resistant Staphylococcus aureus and community-acquired bacterial pneumonia (CABP) caused by Staphylococcus pneumoniae and other designated susceptible bacteria. Teflaro is a bactericidal cephalosporin with activity against both gram-positive and gram-negative pathogens. Teflaro is already approved for ABSSSI and CABP in adult patients. For more information, visit www.teflaro.com.
If you would like your product included in Product News, please email a press release to the Editorial Office at [email protected].
Carmex Grant
Carma Labs Inc, the maker of Carmex lip balms, announced a $10,000 grant program to support an entrepreneur with an Unstoppable Dream. Participants can enter through Facebook or Instagram by posting a 30-second video depicting their aspiration related to a business or product. All entries must include the hashtags #InPursuitOf and #Contest to be considered. Entries can be submitted through July 15, and a winner will be selected and announced in August. For more information, visit www.mycarmex.com.
Juvéderm Volbella XC
Allergan announces US Food and Drug Administration approval to market Juvéderm Volbella XC for lip augmentation and for correction of perioral lines in adults older than 21 years. Juvéderm Volbella XC increases lip fullness and softens the appearance of lines around the mouth. It is formulated with Vycross, a proprietary filler technology that contributes to the product’s smoothness. Juvéderm Volbella XC has been customized with a lower hyaluronic acid concentration (15 mg/mL), while still providing the long-lasting results of other Juvéderm products. It will be available to patients in the United States in October 2016. For more information, visit www.juvederm.com.
Teflaro
Allergan announces US Food and Drug Administration approval of a supplemental new drug application for Teflaro (ceftaroline fosamil) to expand the label to include the treatment of children aged 2 months to less than 18 years with acute bacterial skin and skin structure infections (ABSSSI) including infections caused by methicillin-resistant Staphylococcus aureus and community-acquired bacterial pneumonia (CABP) caused by Staphylococcus pneumoniae and other designated susceptible bacteria. Teflaro is a bactericidal cephalosporin with activity against both gram-positive and gram-negative pathogens. Teflaro is already approved for ABSSSI and CABP in adult patients. For more information, visit www.teflaro.com.
If you would like your product included in Product News, please email a press release to the Editorial Office at [email protected].
Carmex Grant
Carma Labs Inc, the maker of Carmex lip balms, announced a $10,000 grant program to support an entrepreneur with an Unstoppable Dream. Participants can enter through Facebook or Instagram by posting a 30-second video depicting their aspiration related to a business or product. All entries must include the hashtags #InPursuitOf and #Contest to be considered. Entries can be submitted through July 15, and a winner will be selected and announced in August. For more information, visit www.mycarmex.com.
Juvéderm Volbella XC
Allergan announces US Food and Drug Administration approval to market Juvéderm Volbella XC for lip augmentation and for correction of perioral lines in adults older than 21 years. Juvéderm Volbella XC increases lip fullness and softens the appearance of lines around the mouth. It is formulated with Vycross, a proprietary filler technology that contributes to the product’s smoothness. Juvéderm Volbella XC has been customized with a lower hyaluronic acid concentration (15 mg/mL), while still providing the long-lasting results of other Juvéderm products. It will be available to patients in the United States in October 2016. For more information, visit www.juvederm.com.
Teflaro
Allergan announces US Food and Drug Administration approval of a supplemental new drug application for Teflaro (ceftaroline fosamil) to expand the label to include the treatment of children aged 2 months to less than 18 years with acute bacterial skin and skin structure infections (ABSSSI) including infections caused by methicillin-resistant Staphylococcus aureus and community-acquired bacterial pneumonia (CABP) caused by Staphylococcus pneumoniae and other designated susceptible bacteria. Teflaro is a bactericidal cephalosporin with activity against both gram-positive and gram-negative pathogens. Teflaro is already approved for ABSSSI and CABP in adult patients. For more information, visit www.teflaro.com.
If you would like your product included in Product News, please email a press release to the Editorial Office at [email protected].

Clinical Guidelines: Update in acne treatment
Acne affects 85% of teenagers but can frequently persist into adulthood. It causes significant physical and psychological effects for patients including facial scarring, depression, and decreased self-esteem. The initial approach to acne is determined according to presenting severity, emphasizing topical treatment for milder disease and the addition of oral therapy as disease becomes more severe.
Treatment of mild acne can begin with either benzoyl peroxide (BP) or a topical retinoid (TR). Another option for slightly more severe acne is to start with the initially suggested treatment for moderately severe acne, which is topical combination therapy with BP plus a topical antibiotic; TR plus BP; or TR plus BP in combination with a topical antibiotic. Combination therapy can be given either with separate application of the different medicines or by using fixed combination products that include the separate components in one formulation.
BP is an antibacterial agent, with mild comedolytic properties, and it often is added to topical antibiotic therapy to increase effectiveness and reduce the development of resistance. BP is available in strengths from 2.5% to 10% and in a variety of formulations, which can be used as leave-on or wash-off agents. Common side effects include dose dependent skin irritation and bleaching of fabric.
Topical antibiotics, including clindamycin and erythromycin, work through both their antimicrobial and anti-inflammatory affects. Monotherapy with topical antibiotics is no longer recommended; instead they should be used in combination with BP to prevent bacterial resistance. The preferred topical antibiotic is clindamycin 1% solution or gel. Clindamycin is available in a combination with BP, which may enhance compliance with the treatment regimen.
Topical retinoids are vitamin A derivatives that are the core of treatment. They are effective for all forms of acne and should always be used in the treatment of comedonal acne. There are currently three active agents available: tretinoin (0.025%-0.1% in cream, gel, or microsphere gel vehicles), adapalene (0.1% and 0.3% cream or 0.1% lotion), and tazarotene (0.05% and 0.1% cream, gel, or foam). Combination products are available containing clindamycin and BP. The main side effects of retinoids include dryness, peeling, erythema, and skin irritation. Reducing the frequency of application or potency used may be helpful for limiting these side effects. Topical retinoids increase the risk of photosensitivity, so patients should be counseled on daily sunscreen use, and their use is contraindicated in pregnancy.
Dapsone is an alternative topical treatment for mild acne. Topical dapsone is primarily effective in reducing inflammatory lesions, and seems to be more beneficial for female patients. Dapsone can be combined with topical retinoids if comedonal lesions are present.
Moderate acne can be treated with either topical combination therapy as described above, or systemic antibiotics plus a TR and BP, with or without the addition of a topical antibiotic as well. Female patients may also consider combined oral contraceptives or spironolactone for the treatment of moderate acne.
Systemic antibiotics have been used in the treatment of acne vulgaris for many years, and they are indicated for use in moderate to severe acne. They should always be used in combination with topical therapies, specifically a retinoid or BP. Generally, systemic antibiotics should be used for the shortest possible duration, often 3 months, to prevent the development of bacterial resistance. Tetracyclines and macrolides have the strongest evidence for efficacy. Doxycycline and minocycline are considered equally effective and are the preferred first-line oral antibiotics. Azithromycin has been studied in a variety of pulse dose regimens, and is a good alternative for patients who are not candidates for tetracyclines.
Combined oral contraceptive pills (COCs) are another option for the treatment of acne in female patients. COCs improve acne through their antiandrogenic effects. Spironolactone also has antiandrogen properties, and while it is not FDA approved for the treatment of acne, the AAD guidelines support selective use in women. Spironolactone has been studied at doses from 50 to 200 mg daily and has shown clinically significant improvement in acne. Side effects include diuresis, menstrual irregularities, breast tenderness, and rare hyperkalemia.
Severe acne is treated with an oral antibiotic plus topical combination therapy, or oral isotretinoin, with the addition where appropriate of COCs or oral spironolactone.
Oral isotretinoin, an isomer of retinoic acid, is approved by the FDA for the treatment of severe recalcitrant acne. It causes decreased sebum production, acne lesions, and scarring. It can also be considered in the treatment of moderate acne that is resistant to other treatments, relapses quickly, or produces significant scarring or psychosocial distress. Serum cholesterol, triglycerides, and transaminases can rise during treatment, and should be monitored. Because of the risk of teratogenic effects, the FDA has mandated that all patients receiving isotretinoin must participate in the iPLEDGE risk management program, which requires abstinence or two forms of birth control. While isotretinoin requires monitoring and carries the possibility of significant side effects, it is an effective treatment option for patients with severe recalcitrant acne.
The bottom line
Acne is commonly treated by primary care physicians. A clear approach of graded treatment based on severity of disease yields improvement in outcomes. Mild acne should be treated with benzoyl peroxide, retinoids or a combinations of topical treatments. Systemic antibiotics should be combined with topical therapies for moderate to severe acne. Female patients may also consider using combined oral contraceptives and spironolactone. Oral isotretinoin is an effective option for severe acne, but requires close monitoring.
References
Guidelines of care for the management of acne vulgaris (J Am Acad Dermatol. 2016;74[5]:945-73.e33. doi: 10.1016/j.jaad.2015.12.037. Epub 2016 Feb 17).
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital. Dr. Marriott is an attending family physician at Capital Health Primary Care in Hamilton, N.J.
Acne affects 85% of teenagers but can frequently persist into adulthood. It causes significant physical and psychological effects for patients including facial scarring, depression, and decreased self-esteem. The initial approach to acne is determined according to presenting severity, emphasizing topical treatment for milder disease and the addition of oral therapy as disease becomes more severe.
Treatment of mild acne can begin with either benzoyl peroxide (BP) or a topical retinoid (TR). Another option for slightly more severe acne is to start with the initially suggested treatment for moderately severe acne, which is topical combination therapy with BP plus a topical antibiotic; TR plus BP; or TR plus BP in combination with a topical antibiotic. Combination therapy can be given either with separate application of the different medicines or by using fixed combination products that include the separate components in one formulation.
BP is an antibacterial agent, with mild comedolytic properties, and it often is added to topical antibiotic therapy to increase effectiveness and reduce the development of resistance. BP is available in strengths from 2.5% to 10% and in a variety of formulations, which can be used as leave-on or wash-off agents. Common side effects include dose dependent skin irritation and bleaching of fabric.
Topical antibiotics, including clindamycin and erythromycin, work through both their antimicrobial and anti-inflammatory affects. Monotherapy with topical antibiotics is no longer recommended; instead they should be used in combination with BP to prevent bacterial resistance. The preferred topical antibiotic is clindamycin 1% solution or gel. Clindamycin is available in a combination with BP, which may enhance compliance with the treatment regimen.
Topical retinoids are vitamin A derivatives that are the core of treatment. They are effective for all forms of acne and should always be used in the treatment of comedonal acne. There are currently three active agents available: tretinoin (0.025%-0.1% in cream, gel, or microsphere gel vehicles), adapalene (0.1% and 0.3% cream or 0.1% lotion), and tazarotene (0.05% and 0.1% cream, gel, or foam). Combination products are available containing clindamycin and BP. The main side effects of retinoids include dryness, peeling, erythema, and skin irritation. Reducing the frequency of application or potency used may be helpful for limiting these side effects. Topical retinoids increase the risk of photosensitivity, so patients should be counseled on daily sunscreen use, and their use is contraindicated in pregnancy.
Dapsone is an alternative topical treatment for mild acne. Topical dapsone is primarily effective in reducing inflammatory lesions, and seems to be more beneficial for female patients. Dapsone can be combined with topical retinoids if comedonal lesions are present.
Moderate acne can be treated with either topical combination therapy as described above, or systemic antibiotics plus a TR and BP, with or without the addition of a topical antibiotic as well. Female patients may also consider combined oral contraceptives or spironolactone for the treatment of moderate acne.
Systemic antibiotics have been used in the treatment of acne vulgaris for many years, and they are indicated for use in moderate to severe acne. They should always be used in combination with topical therapies, specifically a retinoid or BP. Generally, systemic antibiotics should be used for the shortest possible duration, often 3 months, to prevent the development of bacterial resistance. Tetracyclines and macrolides have the strongest evidence for efficacy. Doxycycline and minocycline are considered equally effective and are the preferred first-line oral antibiotics. Azithromycin has been studied in a variety of pulse dose regimens, and is a good alternative for patients who are not candidates for tetracyclines.
Combined oral contraceptive pills (COCs) are another option for the treatment of acne in female patients. COCs improve acne through their antiandrogenic effects. Spironolactone also has antiandrogen properties, and while it is not FDA approved for the treatment of acne, the AAD guidelines support selective use in women. Spironolactone has been studied at doses from 50 to 200 mg daily and has shown clinically significant improvement in acne. Side effects include diuresis, menstrual irregularities, breast tenderness, and rare hyperkalemia.
Severe acne is treated with an oral antibiotic plus topical combination therapy, or oral isotretinoin, with the addition where appropriate of COCs or oral spironolactone.
Oral isotretinoin, an isomer of retinoic acid, is approved by the FDA for the treatment of severe recalcitrant acne. It causes decreased sebum production, acne lesions, and scarring. It can also be considered in the treatment of moderate acne that is resistant to other treatments, relapses quickly, or produces significant scarring or psychosocial distress. Serum cholesterol, triglycerides, and transaminases can rise during treatment, and should be monitored. Because of the risk of teratogenic effects, the FDA has mandated that all patients receiving isotretinoin must participate in the iPLEDGE risk management program, which requires abstinence or two forms of birth control. While isotretinoin requires monitoring and carries the possibility of significant side effects, it is an effective treatment option for patients with severe recalcitrant acne.
The bottom line
Acne is commonly treated by primary care physicians. A clear approach of graded treatment based on severity of disease yields improvement in outcomes. Mild acne should be treated with benzoyl peroxide, retinoids or a combinations of topical treatments. Systemic antibiotics should be combined with topical therapies for moderate to severe acne. Female patients may also consider using combined oral contraceptives and spironolactone. Oral isotretinoin is an effective option for severe acne, but requires close monitoring.
References
Guidelines of care for the management of acne vulgaris (J Am Acad Dermatol. 2016;74[5]:945-73.e33. doi: 10.1016/j.jaad.2015.12.037. Epub 2016 Feb 17).
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital. Dr. Marriott is an attending family physician at Capital Health Primary Care in Hamilton, N.J.
Acne affects 85% of teenagers but can frequently persist into adulthood. It causes significant physical and psychological effects for patients including facial scarring, depression, and decreased self-esteem. The initial approach to acne is determined according to presenting severity, emphasizing topical treatment for milder disease and the addition of oral therapy as disease becomes more severe.
Treatment of mild acne can begin with either benzoyl peroxide (BP) or a topical retinoid (TR). Another option for slightly more severe acne is to start with the initially suggested treatment for moderately severe acne, which is topical combination therapy with BP plus a topical antibiotic; TR plus BP; or TR plus BP in combination with a topical antibiotic. Combination therapy can be given either with separate application of the different medicines or by using fixed combination products that include the separate components in one formulation.
BP is an antibacterial agent, with mild comedolytic properties, and it often is added to topical antibiotic therapy to increase effectiveness and reduce the development of resistance. BP is available in strengths from 2.5% to 10% and in a variety of formulations, which can be used as leave-on or wash-off agents. Common side effects include dose dependent skin irritation and bleaching of fabric.
Topical antibiotics, including clindamycin and erythromycin, work through both their antimicrobial and anti-inflammatory affects. Monotherapy with topical antibiotics is no longer recommended; instead they should be used in combination with BP to prevent bacterial resistance. The preferred topical antibiotic is clindamycin 1% solution or gel. Clindamycin is available in a combination with BP, which may enhance compliance with the treatment regimen.
Topical retinoids are vitamin A derivatives that are the core of treatment. They are effective for all forms of acne and should always be used in the treatment of comedonal acne. There are currently three active agents available: tretinoin (0.025%-0.1% in cream, gel, or microsphere gel vehicles), adapalene (0.1% and 0.3% cream or 0.1% lotion), and tazarotene (0.05% and 0.1% cream, gel, or foam). Combination products are available containing clindamycin and BP. The main side effects of retinoids include dryness, peeling, erythema, and skin irritation. Reducing the frequency of application or potency used may be helpful for limiting these side effects. Topical retinoids increase the risk of photosensitivity, so patients should be counseled on daily sunscreen use, and their use is contraindicated in pregnancy.
Dapsone is an alternative topical treatment for mild acne. Topical dapsone is primarily effective in reducing inflammatory lesions, and seems to be more beneficial for female patients. Dapsone can be combined with topical retinoids if comedonal lesions are present.
Moderate acne can be treated with either topical combination therapy as described above, or systemic antibiotics plus a TR and BP, with or without the addition of a topical antibiotic as well. Female patients may also consider combined oral contraceptives or spironolactone for the treatment of moderate acne.
Systemic antibiotics have been used in the treatment of acne vulgaris for many years, and they are indicated for use in moderate to severe acne. They should always be used in combination with topical therapies, specifically a retinoid or BP. Generally, systemic antibiotics should be used for the shortest possible duration, often 3 months, to prevent the development of bacterial resistance. Tetracyclines and macrolides have the strongest evidence for efficacy. Doxycycline and minocycline are considered equally effective and are the preferred first-line oral antibiotics. Azithromycin has been studied in a variety of pulse dose regimens, and is a good alternative for patients who are not candidates for tetracyclines.
Combined oral contraceptive pills (COCs) are another option for the treatment of acne in female patients. COCs improve acne through their antiandrogenic effects. Spironolactone also has antiandrogen properties, and while it is not FDA approved for the treatment of acne, the AAD guidelines support selective use in women. Spironolactone has been studied at doses from 50 to 200 mg daily and has shown clinically significant improvement in acne. Side effects include diuresis, menstrual irregularities, breast tenderness, and rare hyperkalemia.
Severe acne is treated with an oral antibiotic plus topical combination therapy, or oral isotretinoin, with the addition where appropriate of COCs or oral spironolactone.
Oral isotretinoin, an isomer of retinoic acid, is approved by the FDA for the treatment of severe recalcitrant acne. It causes decreased sebum production, acne lesions, and scarring. It can also be considered in the treatment of moderate acne that is resistant to other treatments, relapses quickly, or produces significant scarring or psychosocial distress. Serum cholesterol, triglycerides, and transaminases can rise during treatment, and should be monitored. Because of the risk of teratogenic effects, the FDA has mandated that all patients receiving isotretinoin must participate in the iPLEDGE risk management program, which requires abstinence or two forms of birth control. While isotretinoin requires monitoring and carries the possibility of significant side effects, it is an effective treatment option for patients with severe recalcitrant acne.
The bottom line
Acne is commonly treated by primary care physicians. A clear approach of graded treatment based on severity of disease yields improvement in outcomes. Mild acne should be treated with benzoyl peroxide, retinoids or a combinations of topical treatments. Systemic antibiotics should be combined with topical therapies for moderate to severe acne. Female patients may also consider using combined oral contraceptives and spironolactone. Oral isotretinoin is an effective option for severe acne, but requires close monitoring.
References
Guidelines of care for the management of acne vulgaris (J Am Acad Dermatol. 2016;74[5]:945-73.e33. doi: 10.1016/j.jaad.2015.12.037. Epub 2016 Feb 17).
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital. Dr. Marriott is an attending family physician at Capital Health Primary Care in Hamilton, N.J.
Clinical Guidelines: Update in acne treatment
Acne affects 85% of teenagers but can frequently persist into adulthood. It causes significant physical and psychological effects for patients including facial scarring, depression, and decreased self-esteem. The initial approach to acne is determined according to presenting severity, emphasizing topical treatment for milder disease and the addition of oral therapy as disease becomes more severe.
Treatment of mild acne can begin with either benzoyl peroxide (BP) or a topical retinoid (TR). Another option for slightly more severe acne is to start with the initially suggested treatment for moderately severe acne, which is topical combination therapy with BP plus a topical antibiotic; TR plus BP; or TR plus BP in combination with a topical antibiotic. Combination therapy can be given either with separate application of the different medicines or by using fixed combination products that include the separate components in one formulation.
BP is an antibacterial agent, with mild comedolytic properties, and it often is added to topical antibiotic therapy to increase effectiveness and reduce the development of resistance. BP is available in strengths from 2.5% to 10% and in a variety of formulations, which can be used as leave-on or wash-off agents. Common side effects include dose dependent skin irritation and bleaching of fabric.
Topical antibiotics, including clindamycin and erythromycin, work through both their antimicrobial and anti-inflammatory affects. Monotherapy with topical antibiotics is no longer recommended; instead they should be used in combination with BP to prevent bacterial resistance. The preferred topical antibiotic is clindamycin 1% solution or gel. Clindamycin is available in a combination with BP, which may enhance compliance with the treatment regimen.
Topical retinoids are vitamin A derivatives that are the core of treatment. They are effective for all forms of acne and should always be used in the treatment of comedonal acne. There are currently three active agents available: tretinoin (0.025%-0.1% in cream, gel, or microsphere gel vehicles), adapalene (0.1% and 0.3% cream or 0.1% lotion), and tazarotene (0.05% and 0.1% cream, gel, or foam). Combination products are available containing clindamycin and BP. The main side effects of retinoids include dryness, peeling, erythema, and skin irritation. Reducing the frequency of application or potency used may be helpful for limiting these side effects. Topical retinoids increase the risk of photosensitivity, so patients should be counseled on daily sunscreen use, and their use is contraindicated in pregnancy.
Dapsone is an alternative topical treatment for mild acne. Topical dapsone is primarily effective in reducing inflammatory lesions, and seems to be more beneficial for female patients. Dapsone can be combined with topical retinoids if comedonal lesions are present.
Moderate acne can be treated with either topical combination therapy as described above, or systemic antibiotics plus a TR and BP, with or without the addition of a topical antibiotic as well. Female patients may also consider combined oral contraceptives or spironolactone for the treatment of moderate acne.
Systemic antibiotics have been used in the treatment of acne vulgaris for many years, and they are indicated for use in moderate to severe acne. They should always be used in combination with topical therapies, specifically a retinoid or BP. Generally, systemic antibiotics should be used for the shortest possible duration, often 3 months, to prevent the development of bacterial resistance. Tetracyclines and macrolides have the strongest evidence for efficacy. Doxycycline and minocycline are considered equally effective and are the preferred first-line oral antibiotics. Azithromycin has been studied in a variety of pulse dose regimens, and is a good alternative for patients who are not candidates for tetracyclines.
Combined oral contraceptive pills (COCs) are another option for the treatment of acne in female patients. COCs improve acne through their antiandrogenic effects. Spironolactone also has antiandrogen properties, and while it is not FDA approved for the treatment of acne, the AAD guidelines support selective use in women. Spironolactone has been studied at doses from 50 to 200 mg daily and has shown clinically significant improvement in acne. Side effects include diuresis, menstrual irregularities, breast tenderness, and rare hyperkalemia.
Severe acne is treated with an oral antibiotic plus topical combination therapy, or oral isotretinoin, with the addition where appropriate of COCs or oral spironolactone.
Oral isotretinoin, an isomer of retinoic acid, is approved by the FDA for the treatment of severe recalcitrant acne. It causes decreased sebum production, acne lesions, and scarring. It can also be considered in the treatment of moderate acne that is resistant to other treatments, relapses quickly, or produces significant scarring or psychosocial distress. Serum cholesterol, triglycerides, and transaminases can rise during treatment, and should be monitored. Because of the risk of teratogenic effects, the FDA has mandated that all patients receiving isotretinoin must participate in the iPLEDGE risk management program, which requires abstinence or two forms of birth control. While isotretinoin requires monitoring and carries the possibility of significant side effects, it is an effective treatment option for patients with severe recalcitrant acne.
The bottom line
Acne is commonly treated by primary care physicians. A clear approach of graded treatment based on severity of disease yields improvement in outcomes. Mild acne should be treated with benzoyl peroxide, retinoids or a combinations of topical treatments. Systemic antibiotics should be combined with topical therapies for moderate to severe acne. Female patients may also consider using combined oral contraceptives and spironolactone. Oral isotretinoin is an effective option for severe acne, but requires close monitoring.
References
Guidelines of care for the management of acne vulgaris (J Am Acad Dermatol. 2016;74[5]:945-73.e33. doi: 10.1016/j.jaad.2015.12.037. Epub 2016 Feb 17).
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital. Dr. Marriott is an attending family physician at Capital Health Primary Care in Hamilton, N.J.
Acne affects 85% of teenagers but can frequently persist into adulthood. It causes significant physical and psychological effects for patients including facial scarring, depression, and decreased self-esteem. The initial approach to acne is determined according to presenting severity, emphasizing topical treatment for milder disease and the addition of oral therapy as disease becomes more severe.
Treatment of mild acne can begin with either benzoyl peroxide (BP) or a topical retinoid (TR). Another option for slightly more severe acne is to start with the initially suggested treatment for moderately severe acne, which is topical combination therapy with BP plus a topical antibiotic; TR plus BP; or TR plus BP in combination with a topical antibiotic. Combination therapy can be given either with separate application of the different medicines or by using fixed combination products that include the separate components in one formulation.
BP is an antibacterial agent, with mild comedolytic properties, and it often is added to topical antibiotic therapy to increase effectiveness and reduce the development of resistance. BP is available in strengths from 2.5% to 10% and in a variety of formulations, which can be used as leave-on or wash-off agents. Common side effects include dose dependent skin irritation and bleaching of fabric.
Topical antibiotics, including clindamycin and erythromycin, work through both their antimicrobial and anti-inflammatory affects. Monotherapy with topical antibiotics is no longer recommended; instead they should be used in combination with BP to prevent bacterial resistance. The preferred topical antibiotic is clindamycin 1% solution or gel. Clindamycin is available in a combination with BP, which may enhance compliance with the treatment regimen.
Topical retinoids are vitamin A derivatives that are the core of treatment. They are effective for all forms of acne and should always be used in the treatment of comedonal acne. There are currently three active agents available: tretinoin (0.025%-0.1% in cream, gel, or microsphere gel vehicles), adapalene (0.1% and 0.3% cream or 0.1% lotion), and tazarotene (0.05% and 0.1% cream, gel, or foam). Combination products are available containing clindamycin and BP. The main side effects of retinoids include dryness, peeling, erythema, and skin irritation. Reducing the frequency of application or potency used may be helpful for limiting these side effects. Topical retinoids increase the risk of photosensitivity, so patients should be counseled on daily sunscreen use, and their use is contraindicated in pregnancy.
Dapsone is an alternative topical treatment for mild acne. Topical dapsone is primarily effective in reducing inflammatory lesions, and seems to be more beneficial for female patients. Dapsone can be combined with topical retinoids if comedonal lesions are present.
Moderate acne can be treated with either topical combination therapy as described above, or systemic antibiotics plus a TR and BP, with or without the addition of a topical antibiotic as well. Female patients may also consider combined oral contraceptives or spironolactone for the treatment of moderate acne.
Systemic antibiotics have been used in the treatment of acne vulgaris for many years, and they are indicated for use in moderate to severe acne. They should always be used in combination with topical therapies, specifically a retinoid or BP. Generally, systemic antibiotics should be used for the shortest possible duration, often 3 months, to prevent the development of bacterial resistance. Tetracyclines and macrolides have the strongest evidence for efficacy. Doxycycline and minocycline are considered equally effective and are the preferred first-line oral antibiotics. Azithromycin has been studied in a variety of pulse dose regimens, and is a good alternative for patients who are not candidates for tetracyclines.
Combined oral contraceptive pills (COCs) are another option for the treatment of acne in female patients. COCs improve acne through their antiandrogenic effects. Spironolactone also has antiandrogen properties, and while it is not FDA approved for the treatment of acne, the AAD guidelines support selective use in women. Spironolactone has been studied at doses from 50 to 200 mg daily and has shown clinically significant improvement in acne. Side effects include diuresis, menstrual irregularities, breast tenderness, and rare hyperkalemia.
Severe acne is treated with an oral antibiotic plus topical combination therapy, or oral isotretinoin, with the addition where appropriate of COCs or oral spironolactone.
Oral isotretinoin, an isomer of retinoic acid, is approved by the FDA for the treatment of severe recalcitrant acne. It causes decreased sebum production, acne lesions, and scarring. It can also be considered in the treatment of moderate acne that is resistant to other treatments, relapses quickly, or produces significant scarring or psychosocial distress. Serum cholesterol, triglycerides, and transaminases can rise during treatment, and should be monitored. Because of the risk of teratogenic effects, the FDA has mandated that all patients receiving isotretinoin must participate in the iPLEDGE risk management program, which requires abstinence or two forms of birth control. While isotretinoin requires monitoring and carries the possibility of significant side effects, it is an effective treatment option for patients with severe recalcitrant acne.
The bottom line
Acne is commonly treated by primary care physicians. A clear approach of graded treatment based on severity of disease yields improvement in outcomes. Mild acne should be treated with benzoyl peroxide, retinoids or a combinations of topical treatments. Systemic antibiotics should be combined with topical therapies for moderate to severe acne. Female patients may also consider using combined oral contraceptives and spironolactone. Oral isotretinoin is an effective option for severe acne, but requires close monitoring.
References
Guidelines of care for the management of acne vulgaris (J Am Acad Dermatol. 2016;74[5]:945-73.e33. doi: 10.1016/j.jaad.2015.12.037. Epub 2016 Feb 17).
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital. Dr. Marriott is an attending family physician at Capital Health Primary Care in Hamilton, N.J.
Acne affects 85% of teenagers but can frequently persist into adulthood. It causes significant physical and psychological effects for patients including facial scarring, depression, and decreased self-esteem. The initial approach to acne is determined according to presenting severity, emphasizing topical treatment for milder disease and the addition of oral therapy as disease becomes more severe.
Treatment of mild acne can begin with either benzoyl peroxide (BP) or a topical retinoid (TR). Another option for slightly more severe acne is to start with the initially suggested treatment for moderately severe acne, which is topical combination therapy with BP plus a topical antibiotic; TR plus BP; or TR plus BP in combination with a topical antibiotic. Combination therapy can be given either with separate application of the different medicines or by using fixed combination products that include the separate components in one formulation.
BP is an antibacterial agent, with mild comedolytic properties, and it often is added to topical antibiotic therapy to increase effectiveness and reduce the development of resistance. BP is available in strengths from 2.5% to 10% and in a variety of formulations, which can be used as leave-on or wash-off agents. Common side effects include dose dependent skin irritation and bleaching of fabric.
Topical antibiotics, including clindamycin and erythromycin, work through both their antimicrobial and anti-inflammatory affects. Monotherapy with topical antibiotics is no longer recommended; instead they should be used in combination with BP to prevent bacterial resistance. The preferred topical antibiotic is clindamycin 1% solution or gel. Clindamycin is available in a combination with BP, which may enhance compliance with the treatment regimen.
Topical retinoids are vitamin A derivatives that are the core of treatment. They are effective for all forms of acne and should always be used in the treatment of comedonal acne. There are currently three active agents available: tretinoin (0.025%-0.1% in cream, gel, or microsphere gel vehicles), adapalene (0.1% and 0.3% cream or 0.1% lotion), and tazarotene (0.05% and 0.1% cream, gel, or foam). Combination products are available containing clindamycin and BP. The main side effects of retinoids include dryness, peeling, erythema, and skin irritation. Reducing the frequency of application or potency used may be helpful for limiting these side effects. Topical retinoids increase the risk of photosensitivity, so patients should be counseled on daily sunscreen use, and their use is contraindicated in pregnancy.
Dapsone is an alternative topical treatment for mild acne. Topical dapsone is primarily effective in reducing inflammatory lesions, and seems to be more beneficial for female patients. Dapsone can be combined with topical retinoids if comedonal lesions are present.
Moderate acne can be treated with either topical combination therapy as described above, or systemic antibiotics plus a TR and BP, with or without the addition of a topical antibiotic as well. Female patients may also consider combined oral contraceptives or spironolactone for the treatment of moderate acne.
Systemic antibiotics have been used in the treatment of acne vulgaris for many years, and they are indicated for use in moderate to severe acne. They should always be used in combination with topical therapies, specifically a retinoid or BP. Generally, systemic antibiotics should be used for the shortest possible duration, often 3 months, to prevent the development of bacterial resistance. Tetracyclines and macrolides have the strongest evidence for efficacy. Doxycycline and minocycline are considered equally effective and are the preferred first-line oral antibiotics. Azithromycin has been studied in a variety of pulse dose regimens, and is a good alternative for patients who are not candidates for tetracyclines.
Combined oral contraceptive pills (COCs) are another option for the treatment of acne in female patients. COCs improve acne through their antiandrogenic effects. Spironolactone also has antiandrogen properties, and while it is not FDA approved for the treatment of acne, the AAD guidelines support selective use in women. Spironolactone has been studied at doses from 50 to 200 mg daily and has shown clinically significant improvement in acne. Side effects include diuresis, menstrual irregularities, breast tenderness, and rare hyperkalemia.
Severe acne is treated with an oral antibiotic plus topical combination therapy, or oral isotretinoin, with the addition where appropriate of COCs or oral spironolactone.
Oral isotretinoin, an isomer of retinoic acid, is approved by the FDA for the treatment of severe recalcitrant acne. It causes decreased sebum production, acne lesions, and scarring. It can also be considered in the treatment of moderate acne that is resistant to other treatments, relapses quickly, or produces significant scarring or psychosocial distress. Serum cholesterol, triglycerides, and transaminases can rise during treatment, and should be monitored. Because of the risk of teratogenic effects, the FDA has mandated that all patients receiving isotretinoin must participate in the iPLEDGE risk management program, which requires abstinence or two forms of birth control. While isotretinoin requires monitoring and carries the possibility of significant side effects, it is an effective treatment option for patients with severe recalcitrant acne.
The bottom line
Acne is commonly treated by primary care physicians. A clear approach of graded treatment based on severity of disease yields improvement in outcomes. Mild acne should be treated with benzoyl peroxide, retinoids or a combinations of topical treatments. Systemic antibiotics should be combined with topical therapies for moderate to severe acne. Female patients may also consider using combined oral contraceptives and spironolactone. Oral isotretinoin is an effective option for severe acne, but requires close monitoring.
References
Guidelines of care for the management of acne vulgaris (J Am Acad Dermatol. 2016;74[5]:945-73.e33. doi: 10.1016/j.jaad.2015.12.037. Epub 2016 Feb 17).
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital. Dr. Marriott is an attending family physician at Capital Health Primary Care in Hamilton, N.J.
Effective Applications of Medication-Assisted Opioid Dependence Counseling
NEW YORK - Patients dependent on prescription opioids are likely to quit if they get individual drug counseling with their prescribed medications, according to long-term follow-up results.
"Medication-assisted treatment for opioid dependence benefited people who were dependent on prescription opioids. Good standard medical management, medically based counseling, can be effective for these people if given in conjunction with buprenorphine treatment," said lead author Dr. Roger D. Weiss, professor of psychiatry at Harvard Medical School in Boston and chief of the Division of Alcohol and Drug Abuse at McLean Hospital in Belmont, Massachusetts.
"Over time, with treatment, these patients have relatively optimistic outcomes, but there are a number of risks involved, including people shifting from prescription opioids to heroin who had never injected drugs, injecting them, and a higher death rate," he told Reuters Health by phone.
Dr. Weiss and colleagues examined the outcomes over a 42-month follow-up period among adult participants in POATS (the Prescription Opioid Addiction Treatment Study), the first long-term multisite randomized trial to investigate whether outcomes for patients dependent on prescription opioid analgesics can be improved with standard medical management by adding individual drug counseling to prescribed buprenorphine (combined with naloxone to prevent withdrawal symptoms).
The researchers enrolled 653 participants at 12 medical centers in nine states through the National Institute on Drug Abuse (NIDA) Clinical Trials Network. They examined the results at four and 12 weeks and conducted follow-up assessments of opioid and other substance abuse through telephone interviews with 375 patients at 1.5 years, 2.5 years, and 3.5 years from study entry.
At 1.5 years, most follow-up participants no longer depended on opioids, and at 3.5 years, fewer than 10% of them were opioid dependent. Patients who reported a lifetime history of heroin use at study entry were more likely to be opioid dependent at 3.5 years (odds ratio 4.56, p<0.05).
At 2.5 years, 61% of patients reported that they had abstained from opioids for one month. The roughly one-third of the sample who received opioid agonist treatment during follow-up were more likely to be abstinent at month 42. Even so, 27 (8%) of 338 patients used heroin for the first time during follow-up and 10.1% reported that they had injected heroin for the first time.
The results were presented in a poster May 16 at the Annual Meeting of the American Psychiatric Association (APA) in Atlanta, Georgia.
"Prior to this study, there had never been a study of treatment in people dependent on prescription opioids. There had been many opioid-dependence treatment studies, but they had all focused on people who exclusively or primarily used heroin, and most were done in methadone maintenance programs. This was the first study done with people receiving office-based buprenorphine treatment," Dr. Weiss told Reuters Health.
"A real strength of this study is that it was very large and included a mixture of urban, suburban, and rural sites. No other study has looked at even 100 people," he added.
Regarding future related research, Dr. Weiss told Reuters Health that it would be good to learn exactly which people do well over time and how to increase their success rate.
The authors reported no funding or disclosures.
SOURCE: http://bit.ly/28MTqd6 APA 2016.
NEW YORK - Patients dependent on prescription opioids are likely to quit if they get individual drug counseling with their prescribed medications, according to long-term follow-up results.
"Medication-assisted treatment for opioid dependence benefited people who were dependent on prescription opioids. Good standard medical management, medically based counseling, can be effective for these people if given in conjunction with buprenorphine treatment," said lead author Dr. Roger D. Weiss, professor of psychiatry at Harvard Medical School in Boston and chief of the Division of Alcohol and Drug Abuse at McLean Hospital in Belmont, Massachusetts.
"Over time, with treatment, these patients have relatively optimistic outcomes, but there are a number of risks involved, including people shifting from prescription opioids to heroin who had never injected drugs, injecting them, and a higher death rate," he told Reuters Health by phone.
Dr. Weiss and colleagues examined the outcomes over a 42-month follow-up period among adult participants in POATS (the Prescription Opioid Addiction Treatment Study), the first long-term multisite randomized trial to investigate whether outcomes for patients dependent on prescription opioid analgesics can be improved with standard medical management by adding individual drug counseling to prescribed buprenorphine (combined with naloxone to prevent withdrawal symptoms).
The researchers enrolled 653 participants at 12 medical centers in nine states through the National Institute on Drug Abuse (NIDA) Clinical Trials Network. They examined the results at four and 12 weeks and conducted follow-up assessments of opioid and other substance abuse through telephone interviews with 375 patients at 1.5 years, 2.5 years, and 3.5 years from study entry.
At 1.5 years, most follow-up participants no longer depended on opioids, and at 3.5 years, fewer than 10% of them were opioid dependent. Patients who reported a lifetime history of heroin use at study entry were more likely to be opioid dependent at 3.5 years (odds ratio 4.56, p<0.05).
At 2.5 years, 61% of patients reported that they had abstained from opioids for one month. The roughly one-third of the sample who received opioid agonist treatment during follow-up were more likely to be abstinent at month 42. Even so, 27 (8%) of 338 patients used heroin for the first time during follow-up and 10.1% reported that they had injected heroin for the first time.
The results were presented in a poster May 16 at the Annual Meeting of the American Psychiatric Association (APA) in Atlanta, Georgia.
"Prior to this study, there had never been a study of treatment in people dependent on prescription opioids. There had been many opioid-dependence treatment studies, but they had all focused on people who exclusively or primarily used heroin, and most were done in methadone maintenance programs. This was the first study done with people receiving office-based buprenorphine treatment," Dr. Weiss told Reuters Health.
"A real strength of this study is that it was very large and included a mixture of urban, suburban, and rural sites. No other study has looked at even 100 people," he added.
Regarding future related research, Dr. Weiss told Reuters Health that it would be good to learn exactly which people do well over time and how to increase their success rate.
The authors reported no funding or disclosures.
SOURCE: http://bit.ly/28MTqd6 APA 2016.
NEW YORK - Patients dependent on prescription opioids are likely to quit if they get individual drug counseling with their prescribed medications, according to long-term follow-up results.
"Medication-assisted treatment for opioid dependence benefited people who were dependent on prescription opioids. Good standard medical management, medically based counseling, can be effective for these people if given in conjunction with buprenorphine treatment," said lead author Dr. Roger D. Weiss, professor of psychiatry at Harvard Medical School in Boston and chief of the Division of Alcohol and Drug Abuse at McLean Hospital in Belmont, Massachusetts.
"Over time, with treatment, these patients have relatively optimistic outcomes, but there are a number of risks involved, including people shifting from prescription opioids to heroin who had never injected drugs, injecting them, and a higher death rate," he told Reuters Health by phone.
Dr. Weiss and colleagues examined the outcomes over a 42-month follow-up period among adult participants in POATS (the Prescription Opioid Addiction Treatment Study), the first long-term multisite randomized trial to investigate whether outcomes for patients dependent on prescription opioid analgesics can be improved with standard medical management by adding individual drug counseling to prescribed buprenorphine (combined with naloxone to prevent withdrawal symptoms).
The researchers enrolled 653 participants at 12 medical centers in nine states through the National Institute on Drug Abuse (NIDA) Clinical Trials Network. They examined the results at four and 12 weeks and conducted follow-up assessments of opioid and other substance abuse through telephone interviews with 375 patients at 1.5 years, 2.5 years, and 3.5 years from study entry.
At 1.5 years, most follow-up participants no longer depended on opioids, and at 3.5 years, fewer than 10% of them were opioid dependent. Patients who reported a lifetime history of heroin use at study entry were more likely to be opioid dependent at 3.5 years (odds ratio 4.56, p<0.05).
At 2.5 years, 61% of patients reported that they had abstained from opioids for one month. The roughly one-third of the sample who received opioid agonist treatment during follow-up were more likely to be abstinent at month 42. Even so, 27 (8%) of 338 patients used heroin for the first time during follow-up and 10.1% reported that they had injected heroin for the first time.
The results were presented in a poster May 16 at the Annual Meeting of the American Psychiatric Association (APA) in Atlanta, Georgia.
"Prior to this study, there had never been a study of treatment in people dependent on prescription opioids. There had been many opioid-dependence treatment studies, but they had all focused on people who exclusively or primarily used heroin, and most were done in methadone maintenance programs. This was the first study done with people receiving office-based buprenorphine treatment," Dr. Weiss told Reuters Health.
"A real strength of this study is that it was very large and included a mixture of urban, suburban, and rural sites. No other study has looked at even 100 people," he added.
Regarding future related research, Dr. Weiss told Reuters Health that it would be good to learn exactly which people do well over time and how to increase their success rate.
The authors reported no funding or disclosures.
SOURCE: http://bit.ly/28MTqd6 APA 2016.