User login
Peter Chin, MD
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Ceritinib effective when NSCLC progresses despite crizotinib
Ceritinib produced clinically meaningful, durable responses in patients who had advanced non–small-cell lung cancer and a history of multiple treatments with chemotherapies and crizotinib, according to investigators.
Ceritinib was effective even in patients with brain metastases, and it both reduced a high tumor burden and improved lung symptoms, said Lucio Crino, MD, of the University Medical School of Perugia (Italy) and his associates.
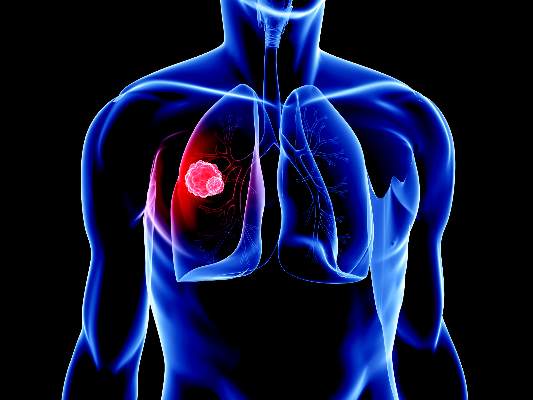
They assessed ceritinib in a single-arm, open-label, phase II trial involving 140 adults with advanced ALK-rearranged non–small-cell lung cancer at 51 sites worldwide who had received at least two lines of antineoplastic chemotherapy and had progressed while taking crizotinib. A total of 100 patients (72%) had brain metastases.
After a median follow-up of 11 months (range, 0-19 months), the overall response rate was 38.6% and the disease control rate was 77.1%. Tumor burden was significantly reduced in 75.2% of patients. Treatment response was rapid, occurring at a median of 1.8 months, and durable, lasting for a median of 9.7 months. Median progression-free survival was 5.7 months, median overall survival was 14.9 months, and the 1-year overall survival rate was 63.8%.
Treatment response was similar in the subgroup of patients who had brain metastases at baseline: Their overall response rate was 33.0%, the disease control rate was 74.0%, the median duration of response was 9.2 months, and median progression-free survival was 5.4 months (J Clin Oncol. 2016 July 17. doi: 10.1200/JCO.2015.65.5936).
No new or unexpected adverse events occurred. All patients reported at least one adverse event, most commonly nausea, diarrhea, and vomiting. Most adverse events were managed without dose interruption or reduction. There was a trend toward improvement in lung symptoms such as cough, pain, and dyspnea, and both health-related quality of life and functional capacity were generally maintained throughout ceritinib treatment, Dr. Crino and his associates said.
Ceritinib produced clinically meaningful, durable responses in patients who had advanced non–small-cell lung cancer and a history of multiple treatments with chemotherapies and crizotinib, according to investigators.
Ceritinib was effective even in patients with brain metastases, and it both reduced a high tumor burden and improved lung symptoms, said Lucio Crino, MD, of the University Medical School of Perugia (Italy) and his associates.
They assessed ceritinib in a single-arm, open-label, phase II trial involving 140 adults with advanced ALK-rearranged non–small-cell lung cancer at 51 sites worldwide who had received at least two lines of antineoplastic chemotherapy and had progressed while taking crizotinib. A total of 100 patients (72%) had brain metastases.
After a median follow-up of 11 months (range, 0-19 months), the overall response rate was 38.6% and the disease control rate was 77.1%. Tumor burden was significantly reduced in 75.2% of patients. Treatment response was rapid, occurring at a median of 1.8 months, and durable, lasting for a median of 9.7 months. Median progression-free survival was 5.7 months, median overall survival was 14.9 months, and the 1-year overall survival rate was 63.8%.
Treatment response was similar in the subgroup of patients who had brain metastases at baseline: Their overall response rate was 33.0%, the disease control rate was 74.0%, the median duration of response was 9.2 months, and median progression-free survival was 5.4 months (J Clin Oncol. 2016 July 17. doi: 10.1200/JCO.2015.65.5936).
No new or unexpected adverse events occurred. All patients reported at least one adverse event, most commonly nausea, diarrhea, and vomiting. Most adverse events were managed without dose interruption or reduction. There was a trend toward improvement in lung symptoms such as cough, pain, and dyspnea, and both health-related quality of life and functional capacity were generally maintained throughout ceritinib treatment, Dr. Crino and his associates said.
Ceritinib produced clinically meaningful, durable responses in patients who had advanced non–small-cell lung cancer and a history of multiple treatments with chemotherapies and crizotinib, according to investigators.
Ceritinib was effective even in patients with brain metastases, and it both reduced a high tumor burden and improved lung symptoms, said Lucio Crino, MD, of the University Medical School of Perugia (Italy) and his associates.
They assessed ceritinib in a single-arm, open-label, phase II trial involving 140 adults with advanced ALK-rearranged non–small-cell lung cancer at 51 sites worldwide who had received at least two lines of antineoplastic chemotherapy and had progressed while taking crizotinib. A total of 100 patients (72%) had brain metastases.
After a median follow-up of 11 months (range, 0-19 months), the overall response rate was 38.6% and the disease control rate was 77.1%. Tumor burden was significantly reduced in 75.2% of patients. Treatment response was rapid, occurring at a median of 1.8 months, and durable, lasting for a median of 9.7 months. Median progression-free survival was 5.7 months, median overall survival was 14.9 months, and the 1-year overall survival rate was 63.8%.
Treatment response was similar in the subgroup of patients who had brain metastases at baseline: Their overall response rate was 33.0%, the disease control rate was 74.0%, the median duration of response was 9.2 months, and median progression-free survival was 5.4 months (J Clin Oncol. 2016 July 17. doi: 10.1200/JCO.2015.65.5936).
No new or unexpected adverse events occurred. All patients reported at least one adverse event, most commonly nausea, diarrhea, and vomiting. Most adverse events were managed without dose interruption or reduction. There was a trend toward improvement in lung symptoms such as cough, pain, and dyspnea, and both health-related quality of life and functional capacity were generally maintained throughout ceritinib treatment, Dr. Crino and his associates said.
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Ceritinib produced meaningful, durable responses in heavily pretreated patients with NSCLC who had advanced disease, including brain metastases.
Major finding: After a median follow-up of 11 months (range, 0-19 months), the overall response rate was 38.6%, the disease control rate was 77.1%, and the overall survival rate was 63.8%.
Data source: A single-arm open-label multicenter phase II trial involving 140 patients whose NSCLC progressed despite multiple treatments including crizotinib.
Disclosures: Novartis supported the study. Dr. Crino reported receiving honoraria from and consulting for Novartis, Eli Lilly, AstraZeneca, Pfizer, and Roche; his associates reported ties to numerous industry sources.

Delaying surgery for 11 weeks after RCT does not increase pCR rates for rectal cancer
Among patients with rectal cancer, delaying surgery for 11 weeks after the end of radiochemotherapy does not improve pathologic complete response rates, investigators reported.
Previously, the Lyon trial, the only randomized controlled study to investigate the effects of delaying surgery following the end of radiochemotherapy (RCT), found that compared with a 2-week delay, a 6-week delay significantly increased the number of patients who experienced complete response (53.1% vs. 71.7%, P = .007). The purpose of the current study was to evaluate the effect of a longer interval between RCT and surgery on pathologic complete response (pCR) rates.
For the phase III, multicenter, randomized trial, 265 patients with mid or lower rectal cancer were randomized to receive surgery at 7 weeks (n = 133) or 11 weeks (n = 132) following the end of RCT.
Baseline tumor characteristics and patient demographics were similar between the two study arms; the majority of patients had stage cT3 rectal cancer (82%).
There was no significant difference in pathologic complete response rate between the study arms (15% for 7-week group vs. 17.4% for 11-week group, P = .5983), reported Jeremie Lefevre, MD, of Hopital Saint-Antoine, Paris, and his associates (J Clin Oncol. 2016 July. doi: 10.1200/JCO.2016.67.6049).
Overall morbidity was significantly increased in the 11-week group (44.5% v 32%; P = .04), primarily explained by an increase in medical complications (32.8% vs. 19.2%; P = .01), the investigators wrote.
The French Ministry of Health funded the study. Dr. Lefevre and seven of his associates reported serving in advisory roles, receiving financial compensation, or participating in the speakers bureau for multiple companies.
On Twitter @jessnicolecraig
Among patients with rectal cancer, delaying surgery for 11 weeks after the end of radiochemotherapy does not improve pathologic complete response rates, investigators reported.
Previously, the Lyon trial, the only randomized controlled study to investigate the effects of delaying surgery following the end of radiochemotherapy (RCT), found that compared with a 2-week delay, a 6-week delay significantly increased the number of patients who experienced complete response (53.1% vs. 71.7%, P = .007). The purpose of the current study was to evaluate the effect of a longer interval between RCT and surgery on pathologic complete response (pCR) rates.
For the phase III, multicenter, randomized trial, 265 patients with mid or lower rectal cancer were randomized to receive surgery at 7 weeks (n = 133) or 11 weeks (n = 132) following the end of RCT.
Baseline tumor characteristics and patient demographics were similar between the two study arms; the majority of patients had stage cT3 rectal cancer (82%).
There was no significant difference in pathologic complete response rate between the study arms (15% for 7-week group vs. 17.4% for 11-week group, P = .5983), reported Jeremie Lefevre, MD, of Hopital Saint-Antoine, Paris, and his associates (J Clin Oncol. 2016 July. doi: 10.1200/JCO.2016.67.6049).
Overall morbidity was significantly increased in the 11-week group (44.5% v 32%; P = .04), primarily explained by an increase in medical complications (32.8% vs. 19.2%; P = .01), the investigators wrote.
The French Ministry of Health funded the study. Dr. Lefevre and seven of his associates reported serving in advisory roles, receiving financial compensation, or participating in the speakers bureau for multiple companies.
On Twitter @jessnicolecraig
Among patients with rectal cancer, delaying surgery for 11 weeks after the end of radiochemotherapy does not improve pathologic complete response rates, investigators reported.
Previously, the Lyon trial, the only randomized controlled study to investigate the effects of delaying surgery following the end of radiochemotherapy (RCT), found that compared with a 2-week delay, a 6-week delay significantly increased the number of patients who experienced complete response (53.1% vs. 71.7%, P = .007). The purpose of the current study was to evaluate the effect of a longer interval between RCT and surgery on pathologic complete response (pCR) rates.
For the phase III, multicenter, randomized trial, 265 patients with mid or lower rectal cancer were randomized to receive surgery at 7 weeks (n = 133) or 11 weeks (n = 132) following the end of RCT.
Baseline tumor characteristics and patient demographics were similar between the two study arms; the majority of patients had stage cT3 rectal cancer (82%).
There was no significant difference in pathologic complete response rate between the study arms (15% for 7-week group vs. 17.4% for 11-week group, P = .5983), reported Jeremie Lefevre, MD, of Hopital Saint-Antoine, Paris, and his associates (J Clin Oncol. 2016 July. doi: 10.1200/JCO.2016.67.6049).
Overall morbidity was significantly increased in the 11-week group (44.5% v 32%; P = .04), primarily explained by an increase in medical complications (32.8% vs. 19.2%; P = .01), the investigators wrote.
The French Ministry of Health funded the study. Dr. Lefevre and seven of his associates reported serving in advisory roles, receiving financial compensation, or participating in the speakers bureau for multiple companies.
On Twitter @jessnicolecraig
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Delaying surgery for 11 weeks after the end of radiochemotherapy does not improve pathologic complete response rates in patients with rectal cancer, compared with a delay of 7 weeks.
Major finding: There was no significant difference in pathologic complete response rate between the study arms (15% for 7-week group vs. 17.4% for 11-week group, P = .5983).
Data source: A phase III, multicenter, randomized trial involving 265 patients with varying stages of rectal cancer.
Disclosures: The French Ministry of Health funded the study. Dr. Lefevre and seven of his associates reported serving in advisory roles, receiving financial compensation, or participating in the speakers bureau for multiple companies.
Gene Variants Linked to Posttraumatic Seizures
To determine if genetic variation influences the susceptibility to traumatic brain injury and the subsequent posttraumatic seizures, Anne Ritter and her associates from the University of Pittsburgh analyzed the relationship between posttraumatic seizures and single nucleotide polymorphisms (SNPs). Thirty two SNPs were evaluated within SLC1A1 and SLC1A6, which are protein coding genes for glutamate transporters. (Glutamate transporters control glutamate levels and excitatory neurotransmission and have been associated with traumatic brain injury.) The analysis found that among 253 individuals, 49 had experienced posttraumatic seizures. Within this smaller group, they found genotypes at SNP rs10974620 (SLC1A1) linked to the time to the first seizure during a three year follow-up. And after factoring in several confounding variables, rs10974620 remained statistically significant (P = .017).
Rittner AC, Kammerer CM, Brooks MM, Conley YP, Wagner AM. Genetic variation in neuronal glutamate transport genes and associations with posttraumatic seizure. Epilepsia. 2016;57(6):984-993.
To determine if genetic variation influences the susceptibility to traumatic brain injury and the subsequent posttraumatic seizures, Anne Ritter and her associates from the University of Pittsburgh analyzed the relationship between posttraumatic seizures and single nucleotide polymorphisms (SNPs). Thirty two SNPs were evaluated within SLC1A1 and SLC1A6, which are protein coding genes for glutamate transporters. (Glutamate transporters control glutamate levels and excitatory neurotransmission and have been associated with traumatic brain injury.) The analysis found that among 253 individuals, 49 had experienced posttraumatic seizures. Within this smaller group, they found genotypes at SNP rs10974620 (SLC1A1) linked to the time to the first seizure during a three year follow-up. And after factoring in several confounding variables, rs10974620 remained statistically significant (P = .017).
Rittner AC, Kammerer CM, Brooks MM, Conley YP, Wagner AM. Genetic variation in neuronal glutamate transport genes and associations with posttraumatic seizure. Epilepsia. 2016;57(6):984-993.
To determine if genetic variation influences the susceptibility to traumatic brain injury and the subsequent posttraumatic seizures, Anne Ritter and her associates from the University of Pittsburgh analyzed the relationship between posttraumatic seizures and single nucleotide polymorphisms (SNPs). Thirty two SNPs were evaluated within SLC1A1 and SLC1A6, which are protein coding genes for glutamate transporters. (Glutamate transporters control glutamate levels and excitatory neurotransmission and have been associated with traumatic brain injury.) The analysis found that among 253 individuals, 49 had experienced posttraumatic seizures. Within this smaller group, they found genotypes at SNP rs10974620 (SLC1A1) linked to the time to the first seizure during a three year follow-up. And after factoring in several confounding variables, rs10974620 remained statistically significant (P = .017).
Rittner AC, Kammerer CM, Brooks MM, Conley YP, Wagner AM. Genetic variation in neuronal glutamate transport genes and associations with posttraumatic seizure. Epilepsia. 2016;57(6):984-993.
Cluster Seizures Are Shorter Than Isolated Seizures
To determine the unique characteristics of cluster seizures, investigators looked at 92 subjects, 83% of whom had at least one seizure cluster. They found that seizures occurring within a cluster were significantly shorter than the last seizure that occurred in the cluster. They also discovered that the terminal seizure in a cluster is similar to duration in isolated seizures that are not part of a cluster. Finally, the researchers found that cluster seizures are more likely to occur in the frontal and temporal lobes.
Ferastraoaru V, Schulze-Bonhage A, Lipton RB, Dumpelmann M, Legatt AD, Hunt SR. Termination of seizure clusters is related to duration of focal seizures. Epilepsia. 2016;57(6):889-895.
To determine the unique characteristics of cluster seizures, investigators looked at 92 subjects, 83% of whom had at least one seizure cluster. They found that seizures occurring within a cluster were significantly shorter than the last seizure that occurred in the cluster. They also discovered that the terminal seizure in a cluster is similar to duration in isolated seizures that are not part of a cluster. Finally, the researchers found that cluster seizures are more likely to occur in the frontal and temporal lobes.
Ferastraoaru V, Schulze-Bonhage A, Lipton RB, Dumpelmann M, Legatt AD, Hunt SR. Termination of seizure clusters is related to duration of focal seizures. Epilepsia. 2016;57(6):889-895.
To determine the unique characteristics of cluster seizures, investigators looked at 92 subjects, 83% of whom had at least one seizure cluster. They found that seizures occurring within a cluster were significantly shorter than the last seizure that occurred in the cluster. They also discovered that the terminal seizure in a cluster is similar to duration in isolated seizures that are not part of a cluster. Finally, the researchers found that cluster seizures are more likely to occur in the frontal and temporal lobes.
Ferastraoaru V, Schulze-Bonhage A, Lipton RB, Dumpelmann M, Legatt AD, Hunt SR. Termination of seizure clusters is related to duration of focal seizures. Epilepsia. 2016;57(6):889-895.
Health Officials Investigating Mysterious Zika Infection
Health officials are looking into a case of Zika virus infection in Utah, where a person was infected after caring for an elderly family member with the virus.
In the new case, the person had not recently traveled to an area with Zika and had not had sex with anyone with Zika infection or who had traveled to an area with Zika. Also, there is no current evidence that the Aedes mosquitoes, known to spread Zika virus, have been active in Utah.
The elderly Utah man who was first infected with Zika died in late June of unknown causes. He had traveled to an area with Zika, and laboratory tests revealed that he had virus levels more than 100,000 times higher than seen in other samples of infected people, according to the Centers for Disease Control and Prevention.
The Utah Department of Health and the CDC are investigating the possible cause of infection.
“We are trying to determine if the contact between the very sick elderly patient and the person played a role in how the person got sick,” Satish Pillai, PhD, deputy incident manager with CDC’s Zika response, said during a news conference. “We don’t have all of the answers right now, but we will continue to share the information as it comes available.”
CDC currently is not altering its instructions on the use of personal protective equipment.
“I think what this highlights is the fact that when you have an infection like Zika virus ... wherein a good percentage of patients don’t actually have symptoms, it means that it’s as important as ever to stick with good adherence to standard precautions,” Dr. Pillai said. “Just like we assume anybody might carry hepatitis or HIV, we don’t wait for a positive diagnosis in order to prevent blood or body fluid exposure. The same thing is true with Zika virus, and I think this is a great example of why we should never take chances, but always adhere to careful standards of touching.”
“The new case in Utah is a surprise, showing that we still have more to learn about Zika,” Erin Staples, MD, PhD, CDC medical epidemiologist on the ground in Utah, said in a statement. “Fortunately, the patient recovered quickly, and from what we have seen with more than 1,300 travel-associated cases of Zika in the continental United States and Hawaii, nonsexual spread from one person to another does not appear to be common.”
Health officials are looking into a case of Zika virus infection in Utah, where a person was infected after caring for an elderly family member with the virus.
In the new case, the person had not recently traveled to an area with Zika and had not had sex with anyone with Zika infection or who had traveled to an area with Zika. Also, there is no current evidence that the Aedes mosquitoes, known to spread Zika virus, have been active in Utah.
The elderly Utah man who was first infected with Zika died in late June of unknown causes. He had traveled to an area with Zika, and laboratory tests revealed that he had virus levels more than 100,000 times higher than seen in other samples of infected people, according to the Centers for Disease Control and Prevention.
The Utah Department of Health and the CDC are investigating the possible cause of infection.
“We are trying to determine if the contact between the very sick elderly patient and the person played a role in how the person got sick,” Satish Pillai, PhD, deputy incident manager with CDC’s Zika response, said during a news conference. “We don’t have all of the answers right now, but we will continue to share the information as it comes available.”
CDC currently is not altering its instructions on the use of personal protective equipment.
“I think what this highlights is the fact that when you have an infection like Zika virus ... wherein a good percentage of patients don’t actually have symptoms, it means that it’s as important as ever to stick with good adherence to standard precautions,” Dr. Pillai said. “Just like we assume anybody might carry hepatitis or HIV, we don’t wait for a positive diagnosis in order to prevent blood or body fluid exposure. The same thing is true with Zika virus, and I think this is a great example of why we should never take chances, but always adhere to careful standards of touching.”
“The new case in Utah is a surprise, showing that we still have more to learn about Zika,” Erin Staples, MD, PhD, CDC medical epidemiologist on the ground in Utah, said in a statement. “Fortunately, the patient recovered quickly, and from what we have seen with more than 1,300 travel-associated cases of Zika in the continental United States and Hawaii, nonsexual spread from one person to another does not appear to be common.”
Health officials are looking into a case of Zika virus infection in Utah, where a person was infected after caring for an elderly family member with the virus.
In the new case, the person had not recently traveled to an area with Zika and had not had sex with anyone with Zika infection or who had traveled to an area with Zika. Also, there is no current evidence that the Aedes mosquitoes, known to spread Zika virus, have been active in Utah.
The elderly Utah man who was first infected with Zika died in late June of unknown causes. He had traveled to an area with Zika, and laboratory tests revealed that he had virus levels more than 100,000 times higher than seen in other samples of infected people, according to the Centers for Disease Control and Prevention.
The Utah Department of Health and the CDC are investigating the possible cause of infection.
“We are trying to determine if the contact between the very sick elderly patient and the person played a role in how the person got sick,” Satish Pillai, PhD, deputy incident manager with CDC’s Zika response, said during a news conference. “We don’t have all of the answers right now, but we will continue to share the information as it comes available.”
CDC currently is not altering its instructions on the use of personal protective equipment.
“I think what this highlights is the fact that when you have an infection like Zika virus ... wherein a good percentage of patients don’t actually have symptoms, it means that it’s as important as ever to stick with good adherence to standard precautions,” Dr. Pillai said. “Just like we assume anybody might carry hepatitis or HIV, we don’t wait for a positive diagnosis in order to prevent blood or body fluid exposure. The same thing is true with Zika virus, and I think this is a great example of why we should never take chances, but always adhere to careful standards of touching.”
“The new case in Utah is a surprise, showing that we still have more to learn about Zika,” Erin Staples, MD, PhD, CDC medical epidemiologist on the ground in Utah, said in a statement. “Fortunately, the patient recovered quickly, and from what we have seen with more than 1,300 travel-associated cases of Zika in the continental United States and Hawaii, nonsexual spread from one person to another does not appear to be common.”
Health officials investigating mysterious Zika infection
Health officials are looking into a case of Zika virus infection in Utah, where a person was infected after caring for an elderly family member with the virus.
In the new case, the person had not recently traveled to an area with Zika and had not had sex with anyone with Zika infection or who had traveled to an area with Zika. Also, there is no current evidence that the Aedes mosquitoes, known to spread Zika virus, have been active in Utah.

The elderly Utah man who was first infected with Zika died in late June of unknown causes. He had traveled to an area with Zika, and laboratory tests revealed that he had virus levels more than 100,000 times higher than seen in other samples of infected people, according to the Centers for Disease Control and Prevention.
The Utah Department of Health and the CDC are investigating the possible cause of infection.
“We are trying to determine if the contact between the very sick elderly patient and the person played a role in how the person got sick,” Satish Pillai, PhD, deputy incident manager with CDC’s Zika response, said during a news conference. “We don’t have all of the answers right now, but we will continue to share the information as it comes available.”
CDC currently is not altering its instructions on the use of personal protective equipment.
“I think what this highlights is the fact that when you have an infection like Zika virus ... wherein a good percentage of patients don’t actually have symptoms, it means that it’s as important as ever to stick with good adherence to standard precautions,” Dr. Pillai said. “Just like we assume anybody might carry hepatitis or HIV, we don’t wait for a positive diagnosis in order to prevent blood or body fluid exposure. The same thing is true with Zika virus, and I think this is a great example of why we should never take chances, but always adhere to careful standards of touching.”
“The new case in Utah is a surprise, showing that we still have more to learn about Zika,” Erin Staples, MD, PhD, CDC medical epidemiologist on the ground in Utah, said in a statement. “Fortunately, the patient recovered quickly, and from what we have seen with more than 1,300 travel-associated cases of Zika in the continental United States and Hawaii, nonsexual spread from one person to another does not appear to be common.”
On Twitter @maryellenny
Health officials are looking into a case of Zika virus infection in Utah, where a person was infected after caring for an elderly family member with the virus.
In the new case, the person had not recently traveled to an area with Zika and had not had sex with anyone with Zika infection or who had traveled to an area with Zika. Also, there is no current evidence that the Aedes mosquitoes, known to spread Zika virus, have been active in Utah.
The elderly Utah man who was first infected with Zika died in late June of unknown causes. He had traveled to an area with Zika, and laboratory tests revealed that he had virus levels more than 100,000 times higher than seen in other samples of infected people, according to the Centers for Disease Control and Prevention.
The Utah Department of Health and the CDC are investigating the possible cause of infection.
“We are trying to determine if the contact between the very sick elderly patient and the person played a role in how the person got sick,” Satish Pillai, PhD, deputy incident manager with CDC’s Zika response, said during a news conference. “We don’t have all of the answers right now, but we will continue to share the information as it comes available.”
CDC currently is not altering its instructions on the use of personal protective equipment.
“I think what this highlights is the fact that when you have an infection like Zika virus ... wherein a good percentage of patients don’t actually have symptoms, it means that it’s as important as ever to stick with good adherence to standard precautions,” Dr. Pillai said. “Just like we assume anybody might carry hepatitis or HIV, we don’t wait for a positive diagnosis in order to prevent blood or body fluid exposure. The same thing is true with Zika virus, and I think this is a great example of why we should never take chances, but always adhere to careful standards of touching.”
“The new case in Utah is a surprise, showing that we still have more to learn about Zika,” Erin Staples, MD, PhD, CDC medical epidemiologist on the ground in Utah, said in a statement. “Fortunately, the patient recovered quickly, and from what we have seen with more than 1,300 travel-associated cases of Zika in the continental United States and Hawaii, nonsexual spread from one person to another does not appear to be common.”
On Twitter @maryellenny
Health officials are looking into a case of Zika virus infection in Utah, where a person was infected after caring for an elderly family member with the virus.
In the new case, the person had not recently traveled to an area with Zika and had not had sex with anyone with Zika infection or who had traveled to an area with Zika. Also, there is no current evidence that the Aedes mosquitoes, known to spread Zika virus, have been active in Utah.
The elderly Utah man who was first infected with Zika died in late June of unknown causes. He had traveled to an area with Zika, and laboratory tests revealed that he had virus levels more than 100,000 times higher than seen in other samples of infected people, according to the Centers for Disease Control and Prevention.
The Utah Department of Health and the CDC are investigating the possible cause of infection.
“We are trying to determine if the contact between the very sick elderly patient and the person played a role in how the person got sick,” Satish Pillai, PhD, deputy incident manager with CDC’s Zika response, said during a news conference. “We don’t have all of the answers right now, but we will continue to share the information as it comes available.”
CDC currently is not altering its instructions on the use of personal protective equipment.
“I think what this highlights is the fact that when you have an infection like Zika virus ... wherein a good percentage of patients don’t actually have symptoms, it means that it’s as important as ever to stick with good adherence to standard precautions,” Dr. Pillai said. “Just like we assume anybody might carry hepatitis or HIV, we don’t wait for a positive diagnosis in order to prevent blood or body fluid exposure. The same thing is true with Zika virus, and I think this is a great example of why we should never take chances, but always adhere to careful standards of touching.”
“The new case in Utah is a surprise, showing that we still have more to learn about Zika,” Erin Staples, MD, PhD, CDC medical epidemiologist on the ground in Utah, said in a statement. “Fortunately, the patient recovered quickly, and from what we have seen with more than 1,300 travel-associated cases of Zika in the continental United States and Hawaii, nonsexual spread from one person to another does not appear to be common.”
On Twitter @maryellenny
Introduction to Clinical Practice Update Committee articles
In this issue of Gastroenterology and in an upcoming issue of Clinical Gastroenterology and Hepatology, an important behind-the-scenes change is occurring. Specifically, both journals will continue to publish important and timely reviews and commentaries, but the formulation and design of some of these articles will now be driven by a new committee. The newly formed American Gastroenterological Association (AGA) Institute Clinical Practice Updates Committee (CPUC) is charged with providing authoritative and balanced articles for the two journals that have the greatest impact on the clinical practice of gastroenterology and hepatology. Potential subjects for these articles will derive from several sources in coordination with the AGA Institute Clinical Guidelines Committee.
First, important topics that are proposed initially for an AGA guideline but do not meet rigid criteria for guideline grading will be sent to the CPUC for review and consideration. Second, ideas for topics will also be generated by the CPUC members and journal editors, as well as by other AGA committees and AGA members themselves. Third, summaries of important symposia such as the yearly Freston Conference will be included. Topics can be presented in the form of a comprehensive, narrative review or, for particularly timely issues in gastroenterology, hepatology, and health care in general, as a rapid commentary.
We believe that the vetting process of these articles is important. All prospective topics and selected authors will be approved by the CPUC with guidance from the AGA Institute Governing Board. At least 2 authors who are recognized authorities will be invited to write an article and will be chosen from different institutions. It is anticipated that the authors will often have differing opinions, to help ensure balance and achieve consensus. A member of the CPUC with expertise in the field will guide the writing to ensure the highest quality and greatest balance in the final product. Once an article is written, it will be submitted for evaluation by the Editors of Gastroenterology and Clinical Gastroenterology and Hepatology, who will decide whether to accept the paper or send it for further review before acceptance.
With seasoned and motivated authors and the guidance of the CPUC, we expect outstanding reviews that will be published in a timely manner and provide AGA members and readers of the journals the most up-to-date and scholarly information across the spectrum of gastroenterology, hepatology, and nutrition. We are excited about this new process as a means to enhance our already outstanding journals, which are dedicated to publishing the best research and practice information in our field. Because this is a new process, we welcome feedback and suggestions for improvement and look forward to providing content that helps your research and clinical practice.
Dr. Katzka is at Mayo Clinic, Rochester, Minn.; Dr. Friedman is at Newton-Wellesley Hospital, Newton, Mass.; Dr. Inadomi is at University of Washington School of Medicine, Seattle; Dr. Kalloo is at Johns Hopkins Hospital, Baltimore; Dr. Kim is at South Denver Gastroenterology, P.C., Littleton, Colo.; Dr. Koch is at Virginia Mason Medical Center, Seattle; Dr. Lieberman is at Oregon Health and Science University, Portland; Dr. Lichtenstein is at the Hospital of the University of Pennsylvania, Merion Station, Penn.: Dr. Lim is at Yale University School of Medicine, New Haven, Conn.; Dr. Pandolfino is at Northwestern University, Chicago; Dr. Shin is at Indiana University School of Medicine, Indianapolis; and Dr. Siedler is Committee Liaison, American Gastroenterological Association.
In this issue of Gastroenterology and in an upcoming issue of Clinical Gastroenterology and Hepatology, an important behind-the-scenes change is occurring. Specifically, both journals will continue to publish important and timely reviews and commentaries, but the formulation and design of some of these articles will now be driven by a new committee. The newly formed American Gastroenterological Association (AGA) Institute Clinical Practice Updates Committee (CPUC) is charged with providing authoritative and balanced articles for the two journals that have the greatest impact on the clinical practice of gastroenterology and hepatology. Potential subjects for these articles will derive from several sources in coordination with the AGA Institute Clinical Guidelines Committee.
First, important topics that are proposed initially for an AGA guideline but do not meet rigid criteria for guideline grading will be sent to the CPUC for review and consideration. Second, ideas for topics will also be generated by the CPUC members and journal editors, as well as by other AGA committees and AGA members themselves. Third, summaries of important symposia such as the yearly Freston Conference will be included. Topics can be presented in the form of a comprehensive, narrative review or, for particularly timely issues in gastroenterology, hepatology, and health care in general, as a rapid commentary.
We believe that the vetting process of these articles is important. All prospective topics and selected authors will be approved by the CPUC with guidance from the AGA Institute Governing Board. At least 2 authors who are recognized authorities will be invited to write an article and will be chosen from different institutions. It is anticipated that the authors will often have differing opinions, to help ensure balance and achieve consensus. A member of the CPUC with expertise in the field will guide the writing to ensure the highest quality and greatest balance in the final product. Once an article is written, it will be submitted for evaluation by the Editors of Gastroenterology and Clinical Gastroenterology and Hepatology, who will decide whether to accept the paper or send it for further review before acceptance.
With seasoned and motivated authors and the guidance of the CPUC, we expect outstanding reviews that will be published in a timely manner and provide AGA members and readers of the journals the most up-to-date and scholarly information across the spectrum of gastroenterology, hepatology, and nutrition. We are excited about this new process as a means to enhance our already outstanding journals, which are dedicated to publishing the best research and practice information in our field. Because this is a new process, we welcome feedback and suggestions for improvement and look forward to providing content that helps your research and clinical practice.
Dr. Katzka is at Mayo Clinic, Rochester, Minn.; Dr. Friedman is at Newton-Wellesley Hospital, Newton, Mass.; Dr. Inadomi is at University of Washington School of Medicine, Seattle; Dr. Kalloo is at Johns Hopkins Hospital, Baltimore; Dr. Kim is at South Denver Gastroenterology, P.C., Littleton, Colo.; Dr. Koch is at Virginia Mason Medical Center, Seattle; Dr. Lieberman is at Oregon Health and Science University, Portland; Dr. Lichtenstein is at the Hospital of the University of Pennsylvania, Merion Station, Penn.: Dr. Lim is at Yale University School of Medicine, New Haven, Conn.; Dr. Pandolfino is at Northwestern University, Chicago; Dr. Shin is at Indiana University School of Medicine, Indianapolis; and Dr. Siedler is Committee Liaison, American Gastroenterological Association.
In this issue of Gastroenterology and in an upcoming issue of Clinical Gastroenterology and Hepatology, an important behind-the-scenes change is occurring. Specifically, both journals will continue to publish important and timely reviews and commentaries, but the formulation and design of some of these articles will now be driven by a new committee. The newly formed American Gastroenterological Association (AGA) Institute Clinical Practice Updates Committee (CPUC) is charged with providing authoritative and balanced articles for the two journals that have the greatest impact on the clinical practice of gastroenterology and hepatology. Potential subjects for these articles will derive from several sources in coordination with the AGA Institute Clinical Guidelines Committee.
First, important topics that are proposed initially for an AGA guideline but do not meet rigid criteria for guideline grading will be sent to the CPUC for review and consideration. Second, ideas for topics will also be generated by the CPUC members and journal editors, as well as by other AGA committees and AGA members themselves. Third, summaries of important symposia such as the yearly Freston Conference will be included. Topics can be presented in the form of a comprehensive, narrative review or, for particularly timely issues in gastroenterology, hepatology, and health care in general, as a rapid commentary.
We believe that the vetting process of these articles is important. All prospective topics and selected authors will be approved by the CPUC with guidance from the AGA Institute Governing Board. At least 2 authors who are recognized authorities will be invited to write an article and will be chosen from different institutions. It is anticipated that the authors will often have differing opinions, to help ensure balance and achieve consensus. A member of the CPUC with expertise in the field will guide the writing to ensure the highest quality and greatest balance in the final product. Once an article is written, it will be submitted for evaluation by the Editors of Gastroenterology and Clinical Gastroenterology and Hepatology, who will decide whether to accept the paper or send it for further review before acceptance.
With seasoned and motivated authors and the guidance of the CPUC, we expect outstanding reviews that will be published in a timely manner and provide AGA members and readers of the journals the most up-to-date and scholarly information across the spectrum of gastroenterology, hepatology, and nutrition. We are excited about this new process as a means to enhance our already outstanding journals, which are dedicated to publishing the best research and practice information in our field. Because this is a new process, we welcome feedback and suggestions for improvement and look forward to providing content that helps your research and clinical practice.
Dr. Katzka is at Mayo Clinic, Rochester, Minn.; Dr. Friedman is at Newton-Wellesley Hospital, Newton, Mass.; Dr. Inadomi is at University of Washington School of Medicine, Seattle; Dr. Kalloo is at Johns Hopkins Hospital, Baltimore; Dr. Kim is at South Denver Gastroenterology, P.C., Littleton, Colo.; Dr. Koch is at Virginia Mason Medical Center, Seattle; Dr. Lieberman is at Oregon Health and Science University, Portland; Dr. Lichtenstein is at the Hospital of the University of Pennsylvania, Merion Station, Penn.: Dr. Lim is at Yale University School of Medicine, New Haven, Conn.; Dr. Pandolfino is at Northwestern University, Chicago; Dr. Shin is at Indiana University School of Medicine, Indianapolis; and Dr. Siedler is Committee Liaison, American Gastroenterological Association.
Colorectal cancer screening quality measures – beyond colonoscopy
Medicine in the United States is undergoing fundamental changes that will continue despite 2016 presidential election results. Changes include consolidation of provider networks, movement from volume- to value-based reimbursement, demands for price and quality transparency, and a shift from focusing solely on individual physician-patient interactions to a broader triple aim focus that incorporates individual patients, population, health, and cost. In this month’s column, Sameer Saini and colleagues suggest that we broaden our view of colorectal cancer screening quality metrics from a colonoscopy-centric focus to a focus on the bottom line: Do we reduce cancer in the population of patients that we serve? When we extend our view to a population level, we use current colonoscopy registries only as internal process controls. A successful health system will develop a mechanism to assess and demonstrate how well the collective team of providers accomplishes the only outcome that matters to patients: preventing colon cancer.
John I. Allen, MD, MBA, AGAF, Special Section Editor

Colorectal cancer (CRC) screening is one of the most valuable services provided by gastroenterologists. The evidence that screening “works” on a population level is undeniable. But not every screening program is equally effective. Data indicate ongoing underuse of screening, particularly in high-risk, vulnerable, and minority communities.1,2 Other data indicate that screening is overused, particularly in low-risk patients and in those with limited life expectancy.3-5 It is also known that endoscopist skill plays an important role in the effectiveness of screening. In short, there is ample room for improvement in the quality of CRC screening, and payers and the public have taken notice. Unsurprisingly, gastroenterologists are often focused on procedural quality indicators, such as adenoma detection and cecal intubation rates.6 These endoscopic quality measures are important indicators of high-quality colonoscopy, but colonoscopy is the common touch point of a much broader system of care that includes other screening tests and other providers (e.g., primary care providers [PCPs], pathologists, and anesthesiologists). Coordinating care across this system is essential for improving the health of patients. As the stewards of digestive health, we owe it to our patients to take a more comprehensive view of CRC screening quality and move beyond colonoscopy alone.

The complex web of care that comprises CRC screening is shown schematically in Figure 1. Appropriate screening begins with selection of suitable screening candidates. In the United States, where most screening is initiated during a clinician encounter, this important task falls primarily on the shoulders of PCPs. It is typically the role of the PCP to assess the two key patient factors that determine screening benefit: CRC risk (using personal and family history) and life expectancy (using age and overall health status). Once a patient has been deemed an appropriate candidate for screening, an acceptable screening test must be selected. Here, patient and practitioner are faced with a menu of options, including fecal occult blood testing (FOBT), colonoscopy, multitarget stool DNA, and computed tomography colonography. For average-risk screening, the ideal test depends primarily on patient preference and local availability.
If a screening test other than colonoscopy is selected, it becomes critical that a positive test is followed by timely and high-quality colonoscopy. High-quality colonoscopy begins with evidence-based preprocedure education and preparation, including appropriate selection of anesthesia services. Once a patient has been well prepared and adequately sedated, an endoscopist must carefully examine the colonic mucosa and completely resect any suspicious polyps. Unless discarded, resected polyps must be reviewed and categorized by a pathologist, including appropriate identification of serrated polyps. Finally, pathology results must be correctly interpreted by the clinician, with evidence-based follow-up recommendations made and effectively communicated to the patient and the referring provider. Additionally, in the short term, delayed gastrointestinal (GI) and non-GI complications of colonoscopy must be recognized and appropriately addressed. In the long term, the rate of interval cancers must be monitored.
Recognizing the importance of CRC screening, GI specialty societies have proposed a variety of quality measures to ensure that patients receive high-quality and high-value colonoscopy. Several of these measures have been adopted by CMS as part of the Physician Quality Reporting System. Non-GI groups, such as the National Center for Quality Assurance and the Ambulatory Surgery Center Association, have also proposed their own CRC screening–related measures.

Despite the proliferation of measures in the domain of CRC screening, current measures fall short in several ways. First, they are largely focused on colonoscopy technical performance, with less attention paid to the important steps that occur before and after colonoscopy. For example, the existing Healthcare Effectiveness Data and Information Set measure for underuse of CRC screening assesses the proportion of patients in a health plan between the ages 50 and 75 who are up to date for CRC screening. This measure is satisfied if a patient completes FOBT, regardless of the result. But FOBT alone is not sufficient to reduce mortality from CRC. Rather, it is imperative that a positive FOBT test be followed by colonoscopy. Numerous studies suggest a quality gap in this critical referral step.7
Yet, outside of selected clinical settings (e.g., the Veterans Affairs Healthcare System), no existing quality measure focuses on colonoscopy completion after positive FOBT. Other examples of important performance gaps beyond colonoscopy technical performance include appropriate use of monitored anesthesia care (data suggest overuse) and appropriate pathology interpretation (data suggest variation in the interpretation of serrated lesions, some of which are associated with increased risk of CRC).
Second, existing measures fail to consider individual patient factors that are known to be predictive of screening benefit, such as life expectancy and personal or familial cancer risk.8
Returning to the Healthcare Effectiveness Data and Information Set measure as an example, this measure relies on age alone to identify patients who are candidates for screening. Yet, it is widely recognized that life expectancy is a critically important factor when considering screening, particularly in older patients. However, existing measures fail to incorporate estimates of life expectancy. As a result, clinicians are encouraged to screen based on age alone. Data suggest that this leads to overuse in older, sicker patients younger than age 75 (the age cutoff suggested by guidelines and incorporated into the Healthcare Effectiveness Data and Information Set measure) and underuse in healthy and unscreened patients older than age 75.9

Furthermore, existing measures fail to systematically consider patient preferences and undervalue shared decision making. Data suggest, for instance, that patients who are offered a “menu” of options for screening rather than a single screening test are more likely to complete a screening test.10
But existing measures do not consider whether a physician assessed a patient’s preferences, or offered more than one screening option. Of course, measuring the quality of decision making is an evolving science that presents challenges and requires creative solutions.11
Finally, existing measures do not capture the collaborative nature of modern health care. For example, most existing measures focus on the performance of gastroenterologists and GI practices. Although such a focus is appropriate for specialty-specific quality improvement efforts, it neglects to capture the important interactions and hand-offs between providers needed for successful completion of screening (and downstream reduction in cancer mortality). As a result, this specialty-focused approach fails to meet the needs of patients, who are increasingly interested in whether the care they receive is improving their health regardless of who provides it. It also fails to meet the needs of payers, who are interested in whether a network of providers is delivering high-value care for its members. Developing measures that capture the collaborative nature of modern health care becomes increasingly important as payers embrace alternative payment models and other value-based reimbursement systems.

Given these challenges with existing measures, we propose the following concepts for consideration as noncolonoscopy quality measures of CRC screening:
1. Appropriateness of referral for CRC screening (PCP): Measures in this domain should incorporate assessment of family history, prior screening history, and/or life expectancy, all of which are predictive of screening benefit and can be extracted from structured electronic health record data.
2. Shared decision making in choosing a CRC screening test (PCP): Currently, measures in this domain are (by necessity) relatively simple, such as assessment of documentation of whether stool testing was offered alongside colonoscopy during a clinic visit.
3. Percentage of individuals with a positive noncolonoscopy CRC screening test who complete a colonoscopy within 6 months (PCP and GI): A measure in this domain can be developed and implemented using existing infrastructure. The Veterans Affairs Healthcare System currently uses such a measure to monitor appropriate follow-up of positive fecal immunochemical tests.

4. Predicted reduction in CRC mortality: This measure, which provides an estimate of the effectiveness and value of a screening program, represents the “bottom line” that is ultimately of interest to both patients and payers. However, composite measures that use projected results require sophisticated statistical approaches and case-mix adjustment. They must also contend with “churn” in the covered population.
Although a more comprehensive view of screening is desirable, operationalizing measure concepts, such as those proposed previously, is challenging for several reasons. First, as we have outlined, CRC screening is truly a “team sport.” The stakeholders in CRC screening include public health, primary care, gastroenterology, colorectal surgery, oncology, anesthesiology, and pathology practitioners. As a result, screening has no natural and obvious steward. Rather, various components of care are adopted by different specialty groups, and this approach leads to unmonitored gaps in care. We believe that gastroenterologists can and should take the lead in developing comprehensive quality measures for CRC screening. Such comprehensive measures will be of value to patients and to payers. Second, assessing quality of care more comprehensively has traditionally been infeasible. For example, incorporating life expectancy into quality measures requires electronic assessment of health status.

Traditionally, such efforts have been hampered by the lack of systematic clinical data collection. However, as meaningful use of electronic health records increases, measures that incorporate such information are likely to become increasingly feasible. Finally, we also need to consider how to make these improvements while avoiding measure proliferation. Proliferation leads to provider fatigue and discourages thoughtful clinical decision making, potentially worsening quality of care. Creative approaches, such as rotating measure sets over time, use of clinical decision support tools, and balancing underuse measures with overuse measures, may be warranted. Additionally, composite measures may prove to be more meaningful and more practical for patients, providers, and payers. Ultimately, a distinction must be made between quality assurance and quality improvement; both are important, but the types of measures and the level of measure sophistication used in each program undoubtedly vary.
In summary, gastroenterologists are uniquely positioned to advocate for high-quality CRC screening that extends beyond simply providing a high-quality colonoscopy. This broader view of quality benefits patients by ensuring that our expertise informs the metrics by which delivery of CRC screening is measured. It also ensures that we hold ourselves and our colleagues to the highest standards across the continuum of care. Additionally, as alternative payment models and value-based contracting are implemented, nonendoscopic screening methods will likely become more commonplace. Advocating for high-quality nonendoscopic screening will help maintain gastroenterologists’ role as the stewards of CRC screening and digestive health. Although operationalizing measure concepts such as those proposed here may be difficult, it is critical if we are to provide the best possible care for our patients.
References

1. Sabatino, S.A., White, M.C., Thompson, T.D., et al. Cancer screening test use – United States, 2013. MMWR Morb Mortal Wkly Rep. 2015;64:464-8.
2. Anderson, A.E., Henry, K.A., Samadder, N.J., et al. Rural vs urban residence affects risk-appropriate colorectal cancer screening. Clin Gastroenterol Hepatol. 2013;11:526-33.
3. Walter, L.C., Lindquist, K., Nugent, S., et al. Impact of age and comorbidity on colorectal cancer screening among older veterans. Ann Intern Med. 2009;150:465-73.
4. Murphy, C.C., Sandler, R.S., Grubber, J.M., et al. Underuse and overuse of colonoscopy for repeat screening and surveillance in the Veterans Health Administration. Clin Gastroenterol Hepatol. 2016;14:436-44.
5. Mittal, S., Lin, Y.-L., Tan, A., et al. Limited life expectancy among a subgroup of Medicare beneficiaries receiving screening colonoscopies. Clin Gastroenterol Hepatol. 2014;12:443-50.e1
6. Allen, J.I. Quality measures for colonoscopy: where should we be in 2015?. Curr Gastroenterol Rep. 2015;17:10.
7. Fisher, D.A., Jeffreys, A., Coffman, C.J., et al. Barriers to full colon evaluation for a positive fecal occult blood test. Cancer Epidemiol Biomark Prev. 2006;15:1232-5.
8. Saini, S.D., van Hees, F., Vijan, S. Smarter screening for cancer: possibilities and challenges of personalization. JAMA. 2014;312:2211-2.
9. Saini, S.D., Vijan, S., Schoenfeld, P., et al. Role of quality measurement in inappropriate use of screening for colorectal cancer: retrospective cohort study. BMJ. 2014;348:g1247.
10. Inadomi, J.M., Vijan, S., Janz, N.K., et al. Adherence to colorectal cancer screening: a randomized clinical trial of competing strategies. Arch Intern Med. 2012;172:575-82.
11. Writing Committee Members, Drozda, J.P., Ferguson, T.B., et al. 2015 ACC/AHA focused update of secondary prevention lipid performance measures: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. J Am Coll Cardiol. 2016;67:558-87.
Dr. Saini is a research scientist at the VA Center for Clinical Management Research and an assistant professor of internal medicine at the University of Michigan, Ann Arbor; Dr. Adams is a clinical lecturer in the division of gastroenterology, department of internal medicine, University of Michigan, and a research investigator, VA Center for Clinical Management Research; Dr. Brill is the chief medical officer of Predictive Health, Paradise Valley, Ariz., and a clinical assistant professor of medicine, University of Arizona School of Medicine, Phoenix; Dr. Gupta is codirector of Digestive Health Center, director of interventional endoscopy, and associate professor of medicine in the division of gastroenterology at Loyola University Medical Center; Dr. Naveed is a clinical assistant professor in the department of gastroenterology and hepatology, University of Iowa Hospitals and Clinics; Dr. Rosenberg is at Illinois Gastroenterology Group; and Dr. Gellad is associate professor of medicine at Duke University School of Medicine, Durham, N.C. Dr. Saini’s and Dr. Gellad’s research is funded by Veterans Affairs Health Services Research and Development Career Development Awards (CDA 09-213-2 and CDA 14-158). Dr. Gupta has received research support from Cook Medical, Cosmo Pharmaceuticals, and CDx Diagnostics.
Medicine in the United States is undergoing fundamental changes that will continue despite 2016 presidential election results. Changes include consolidation of provider networks, movement from volume- to value-based reimbursement, demands for price and quality transparency, and a shift from focusing solely on individual physician-patient interactions to a broader triple aim focus that incorporates individual patients, population, health, and cost. In this month’s column, Sameer Saini and colleagues suggest that we broaden our view of colorectal cancer screening quality metrics from a colonoscopy-centric focus to a focus on the bottom line: Do we reduce cancer in the population of patients that we serve? When we extend our view to a population level, we use current colonoscopy registries only as internal process controls. A successful health system will develop a mechanism to assess and demonstrate how well the collective team of providers accomplishes the only outcome that matters to patients: preventing colon cancer.
John I. Allen, MD, MBA, AGAF, Special Section Editor
Colorectal cancer (CRC) screening is one of the most valuable services provided by gastroenterologists. The evidence that screening “works” on a population level is undeniable. But not every screening program is equally effective. Data indicate ongoing underuse of screening, particularly in high-risk, vulnerable, and minority communities.1,2 Other data indicate that screening is overused, particularly in low-risk patients and in those with limited life expectancy.3-5 It is also known that endoscopist skill plays an important role in the effectiveness of screening. In short, there is ample room for improvement in the quality of CRC screening, and payers and the public have taken notice. Unsurprisingly, gastroenterologists are often focused on procedural quality indicators, such as adenoma detection and cecal intubation rates.6 These endoscopic quality measures are important indicators of high-quality colonoscopy, but colonoscopy is the common touch point of a much broader system of care that includes other screening tests and other providers (e.g., primary care providers [PCPs], pathologists, and anesthesiologists). Coordinating care across this system is essential for improving the health of patients. As the stewards of digestive health, we owe it to our patients to take a more comprehensive view of CRC screening quality and move beyond colonoscopy alone.
The complex web of care that comprises CRC screening is shown schematically in Figure 1. Appropriate screening begins with selection of suitable screening candidates. In the United States, where most screening is initiated during a clinician encounter, this important task falls primarily on the shoulders of PCPs. It is typically the role of the PCP to assess the two key patient factors that determine screening benefit: CRC risk (using personal and family history) and life expectancy (using age and overall health status). Once a patient has been deemed an appropriate candidate for screening, an acceptable screening test must be selected. Here, patient and practitioner are faced with a menu of options, including fecal occult blood testing (FOBT), colonoscopy, multitarget stool DNA, and computed tomography colonography. For average-risk screening, the ideal test depends primarily on patient preference and local availability.
If a screening test other than colonoscopy is selected, it becomes critical that a positive test is followed by timely and high-quality colonoscopy. High-quality colonoscopy begins with evidence-based preprocedure education and preparation, including appropriate selection of anesthesia services. Once a patient has been well prepared and adequately sedated, an endoscopist must carefully examine the colonic mucosa and completely resect any suspicious polyps. Unless discarded, resected polyps must be reviewed and categorized by a pathologist, including appropriate identification of serrated polyps. Finally, pathology results must be correctly interpreted by the clinician, with evidence-based follow-up recommendations made and effectively communicated to the patient and the referring provider. Additionally, in the short term, delayed gastrointestinal (GI) and non-GI complications of colonoscopy must be recognized and appropriately addressed. In the long term, the rate of interval cancers must be monitored.
Recognizing the importance of CRC screening, GI specialty societies have proposed a variety of quality measures to ensure that patients receive high-quality and high-value colonoscopy. Several of these measures have been adopted by CMS as part of the Physician Quality Reporting System. Non-GI groups, such as the National Center for Quality Assurance and the Ambulatory Surgery Center Association, have also proposed their own CRC screening–related measures.
Despite the proliferation of measures in the domain of CRC screening, current measures fall short in several ways. First, they are largely focused on colonoscopy technical performance, with less attention paid to the important steps that occur before and after colonoscopy. For example, the existing Healthcare Effectiveness Data and Information Set measure for underuse of CRC screening assesses the proportion of patients in a health plan between the ages 50 and 75 who are up to date for CRC screening. This measure is satisfied if a patient completes FOBT, regardless of the result. But FOBT alone is not sufficient to reduce mortality from CRC. Rather, it is imperative that a positive FOBT test be followed by colonoscopy. Numerous studies suggest a quality gap in this critical referral step.7
Yet, outside of selected clinical settings (e.g., the Veterans Affairs Healthcare System), no existing quality measure focuses on colonoscopy completion after positive FOBT. Other examples of important performance gaps beyond colonoscopy technical performance include appropriate use of monitored anesthesia care (data suggest overuse) and appropriate pathology interpretation (data suggest variation in the interpretation of serrated lesions, some of which are associated with increased risk of CRC).
Second, existing measures fail to consider individual patient factors that are known to be predictive of screening benefit, such as life expectancy and personal or familial cancer risk.8
Returning to the Healthcare Effectiveness Data and Information Set measure as an example, this measure relies on age alone to identify patients who are candidates for screening. Yet, it is widely recognized that life expectancy is a critically important factor when considering screening, particularly in older patients. However, existing measures fail to incorporate estimates of life expectancy. As a result, clinicians are encouraged to screen based on age alone. Data suggest that this leads to overuse in older, sicker patients younger than age 75 (the age cutoff suggested by guidelines and incorporated into the Healthcare Effectiveness Data and Information Set measure) and underuse in healthy and unscreened patients older than age 75.9
Furthermore, existing measures fail to systematically consider patient preferences and undervalue shared decision making. Data suggest, for instance, that patients who are offered a “menu” of options for screening rather than a single screening test are more likely to complete a screening test.10
But existing measures do not consider whether a physician assessed a patient’s preferences, or offered more than one screening option. Of course, measuring the quality of decision making is an evolving science that presents challenges and requires creative solutions.11
Finally, existing measures do not capture the collaborative nature of modern health care. For example, most existing measures focus on the performance of gastroenterologists and GI practices. Although such a focus is appropriate for specialty-specific quality improvement efforts, it neglects to capture the important interactions and hand-offs between providers needed for successful completion of screening (and downstream reduction in cancer mortality). As a result, this specialty-focused approach fails to meet the needs of patients, who are increasingly interested in whether the care they receive is improving their health regardless of who provides it. It also fails to meet the needs of payers, who are interested in whether a network of providers is delivering high-value care for its members. Developing measures that capture the collaborative nature of modern health care becomes increasingly important as payers embrace alternative payment models and other value-based reimbursement systems.
Given these challenges with existing measures, we propose the following concepts for consideration as noncolonoscopy quality measures of CRC screening:
1. Appropriateness of referral for CRC screening (PCP): Measures in this domain should incorporate assessment of family history, prior screening history, and/or life expectancy, all of which are predictive of screening benefit and can be extracted from structured electronic health record data.
2. Shared decision making in choosing a CRC screening test (PCP): Currently, measures in this domain are (by necessity) relatively simple, such as assessment of documentation of whether stool testing was offered alongside colonoscopy during a clinic visit.
3. Percentage of individuals with a positive noncolonoscopy CRC screening test who complete a colonoscopy within 6 months (PCP and GI): A measure in this domain can be developed and implemented using existing infrastructure. The Veterans Affairs Healthcare System currently uses such a measure to monitor appropriate follow-up of positive fecal immunochemical tests.
4. Predicted reduction in CRC mortality: This measure, which provides an estimate of the effectiveness and value of a screening program, represents the “bottom line” that is ultimately of interest to both patients and payers. However, composite measures that use projected results require sophisticated statistical approaches and case-mix adjustment. They must also contend with “churn” in the covered population.
Although a more comprehensive view of screening is desirable, operationalizing measure concepts, such as those proposed previously, is challenging for several reasons. First, as we have outlined, CRC screening is truly a “team sport.” The stakeholders in CRC screening include public health, primary care, gastroenterology, colorectal surgery, oncology, anesthesiology, and pathology practitioners. As a result, screening has no natural and obvious steward. Rather, various components of care are adopted by different specialty groups, and this approach leads to unmonitored gaps in care. We believe that gastroenterologists can and should take the lead in developing comprehensive quality measures for CRC screening. Such comprehensive measures will be of value to patients and to payers. Second, assessing quality of care more comprehensively has traditionally been infeasible. For example, incorporating life expectancy into quality measures requires electronic assessment of health status.
Traditionally, such efforts have been hampered by the lack of systematic clinical data collection. However, as meaningful use of electronic health records increases, measures that incorporate such information are likely to become increasingly feasible. Finally, we also need to consider how to make these improvements while avoiding measure proliferation. Proliferation leads to provider fatigue and discourages thoughtful clinical decision making, potentially worsening quality of care. Creative approaches, such as rotating measure sets over time, use of clinical decision support tools, and balancing underuse measures with overuse measures, may be warranted. Additionally, composite measures may prove to be more meaningful and more practical for patients, providers, and payers. Ultimately, a distinction must be made between quality assurance and quality improvement; both are important, but the types of measures and the level of measure sophistication used in each program undoubtedly vary.
In summary, gastroenterologists are uniquely positioned to advocate for high-quality CRC screening that extends beyond simply providing a high-quality colonoscopy. This broader view of quality benefits patients by ensuring that our expertise informs the metrics by which delivery of CRC screening is measured. It also ensures that we hold ourselves and our colleagues to the highest standards across the continuum of care. Additionally, as alternative payment models and value-based contracting are implemented, nonendoscopic screening methods will likely become more commonplace. Advocating for high-quality nonendoscopic screening will help maintain gastroenterologists’ role as the stewards of CRC screening and digestive health. Although operationalizing measure concepts such as those proposed here may be difficult, it is critical if we are to provide the best possible care for our patients.
References
1. Sabatino, S.A., White, M.C., Thompson, T.D., et al. Cancer screening test use – United States, 2013. MMWR Morb Mortal Wkly Rep. 2015;64:464-8.
2. Anderson, A.E., Henry, K.A., Samadder, N.J., et al. Rural vs urban residence affects risk-appropriate colorectal cancer screening. Clin Gastroenterol Hepatol. 2013;11:526-33.
3. Walter, L.C., Lindquist, K., Nugent, S., et al. Impact of age and comorbidity on colorectal cancer screening among older veterans. Ann Intern Med. 2009;150:465-73.
4. Murphy, C.C., Sandler, R.S., Grubber, J.M., et al. Underuse and overuse of colonoscopy for repeat screening and surveillance in the Veterans Health Administration. Clin Gastroenterol Hepatol. 2016;14:436-44.
5. Mittal, S., Lin, Y.-L., Tan, A., et al. Limited life expectancy among a subgroup of Medicare beneficiaries receiving screening colonoscopies. Clin Gastroenterol Hepatol. 2014;12:443-50.e1
6. Allen, J.I. Quality measures for colonoscopy: where should we be in 2015?. Curr Gastroenterol Rep. 2015;17:10.
7. Fisher, D.A., Jeffreys, A., Coffman, C.J., et al. Barriers to full colon evaluation for a positive fecal occult blood test. Cancer Epidemiol Biomark Prev. 2006;15:1232-5.
8. Saini, S.D., van Hees, F., Vijan, S. Smarter screening for cancer: possibilities and challenges of personalization. JAMA. 2014;312:2211-2.
9. Saini, S.D., Vijan, S., Schoenfeld, P., et al. Role of quality measurement in inappropriate use of screening for colorectal cancer: retrospective cohort study. BMJ. 2014;348:g1247.
10. Inadomi, J.M., Vijan, S., Janz, N.K., et al. Adherence to colorectal cancer screening: a randomized clinical trial of competing strategies. Arch Intern Med. 2012;172:575-82.
11. Writing Committee Members, Drozda, J.P., Ferguson, T.B., et al. 2015 ACC/AHA focused update of secondary prevention lipid performance measures: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. J Am Coll Cardiol. 2016;67:558-87.
Dr. Saini is a research scientist at the VA Center for Clinical Management Research and an assistant professor of internal medicine at the University of Michigan, Ann Arbor; Dr. Adams is a clinical lecturer in the division of gastroenterology, department of internal medicine, University of Michigan, and a research investigator, VA Center for Clinical Management Research; Dr. Brill is the chief medical officer of Predictive Health, Paradise Valley, Ariz., and a clinical assistant professor of medicine, University of Arizona School of Medicine, Phoenix; Dr. Gupta is codirector of Digestive Health Center, director of interventional endoscopy, and associate professor of medicine in the division of gastroenterology at Loyola University Medical Center; Dr. Naveed is a clinical assistant professor in the department of gastroenterology and hepatology, University of Iowa Hospitals and Clinics; Dr. Rosenberg is at Illinois Gastroenterology Group; and Dr. Gellad is associate professor of medicine at Duke University School of Medicine, Durham, N.C. Dr. Saini’s and Dr. Gellad’s research is funded by Veterans Affairs Health Services Research and Development Career Development Awards (CDA 09-213-2 and CDA 14-158). Dr. Gupta has received research support from Cook Medical, Cosmo Pharmaceuticals, and CDx Diagnostics.
Medicine in the United States is undergoing fundamental changes that will continue despite 2016 presidential election results. Changes include consolidation of provider networks, movement from volume- to value-based reimbursement, demands for price and quality transparency, and a shift from focusing solely on individual physician-patient interactions to a broader triple aim focus that incorporates individual patients, population, health, and cost. In this month’s column, Sameer Saini and colleagues suggest that we broaden our view of colorectal cancer screening quality metrics from a colonoscopy-centric focus to a focus on the bottom line: Do we reduce cancer in the population of patients that we serve? When we extend our view to a population level, we use current colonoscopy registries only as internal process controls. A successful health system will develop a mechanism to assess and demonstrate how well the collective team of providers accomplishes the only outcome that matters to patients: preventing colon cancer.
John I. Allen, MD, MBA, AGAF, Special Section Editor
Colorectal cancer (CRC) screening is one of the most valuable services provided by gastroenterologists. The evidence that screening “works” on a population level is undeniable. But not every screening program is equally effective. Data indicate ongoing underuse of screening, particularly in high-risk, vulnerable, and minority communities.1,2 Other data indicate that screening is overused, particularly in low-risk patients and in those with limited life expectancy.3-5 It is also known that endoscopist skill plays an important role in the effectiveness of screening. In short, there is ample room for improvement in the quality of CRC screening, and payers and the public have taken notice. Unsurprisingly, gastroenterologists are often focused on procedural quality indicators, such as adenoma detection and cecal intubation rates.6 These endoscopic quality measures are important indicators of high-quality colonoscopy, but colonoscopy is the common touch point of a much broader system of care that includes other screening tests and other providers (e.g., primary care providers [PCPs], pathologists, and anesthesiologists). Coordinating care across this system is essential for improving the health of patients. As the stewards of digestive health, we owe it to our patients to take a more comprehensive view of CRC screening quality and move beyond colonoscopy alone.
The complex web of care that comprises CRC screening is shown schematically in Figure 1. Appropriate screening begins with selection of suitable screening candidates. In the United States, where most screening is initiated during a clinician encounter, this important task falls primarily on the shoulders of PCPs. It is typically the role of the PCP to assess the two key patient factors that determine screening benefit: CRC risk (using personal and family history) and life expectancy (using age and overall health status). Once a patient has been deemed an appropriate candidate for screening, an acceptable screening test must be selected. Here, patient and practitioner are faced with a menu of options, including fecal occult blood testing (FOBT), colonoscopy, multitarget stool DNA, and computed tomography colonography. For average-risk screening, the ideal test depends primarily on patient preference and local availability.
If a screening test other than colonoscopy is selected, it becomes critical that a positive test is followed by timely and high-quality colonoscopy. High-quality colonoscopy begins with evidence-based preprocedure education and preparation, including appropriate selection of anesthesia services. Once a patient has been well prepared and adequately sedated, an endoscopist must carefully examine the colonic mucosa and completely resect any suspicious polyps. Unless discarded, resected polyps must be reviewed and categorized by a pathologist, including appropriate identification of serrated polyps. Finally, pathology results must be correctly interpreted by the clinician, with evidence-based follow-up recommendations made and effectively communicated to the patient and the referring provider. Additionally, in the short term, delayed gastrointestinal (GI) and non-GI complications of colonoscopy must be recognized and appropriately addressed. In the long term, the rate of interval cancers must be monitored.
Recognizing the importance of CRC screening, GI specialty societies have proposed a variety of quality measures to ensure that patients receive high-quality and high-value colonoscopy. Several of these measures have been adopted by CMS as part of the Physician Quality Reporting System. Non-GI groups, such as the National Center for Quality Assurance and the Ambulatory Surgery Center Association, have also proposed their own CRC screening–related measures.
Despite the proliferation of measures in the domain of CRC screening, current measures fall short in several ways. First, they are largely focused on colonoscopy technical performance, with less attention paid to the important steps that occur before and after colonoscopy. For example, the existing Healthcare Effectiveness Data and Information Set measure for underuse of CRC screening assesses the proportion of patients in a health plan between the ages 50 and 75 who are up to date for CRC screening. This measure is satisfied if a patient completes FOBT, regardless of the result. But FOBT alone is not sufficient to reduce mortality from CRC. Rather, it is imperative that a positive FOBT test be followed by colonoscopy. Numerous studies suggest a quality gap in this critical referral step.7
Yet, outside of selected clinical settings (e.g., the Veterans Affairs Healthcare System), no existing quality measure focuses on colonoscopy completion after positive FOBT. Other examples of important performance gaps beyond colonoscopy technical performance include appropriate use of monitored anesthesia care (data suggest overuse) and appropriate pathology interpretation (data suggest variation in the interpretation of serrated lesions, some of which are associated with increased risk of CRC).
Second, existing measures fail to consider individual patient factors that are known to be predictive of screening benefit, such as life expectancy and personal or familial cancer risk.8
Returning to the Healthcare Effectiveness Data and Information Set measure as an example, this measure relies on age alone to identify patients who are candidates for screening. Yet, it is widely recognized that life expectancy is a critically important factor when considering screening, particularly in older patients. However, existing measures fail to incorporate estimates of life expectancy. As a result, clinicians are encouraged to screen based on age alone. Data suggest that this leads to overuse in older, sicker patients younger than age 75 (the age cutoff suggested by guidelines and incorporated into the Healthcare Effectiveness Data and Information Set measure) and underuse in healthy and unscreened patients older than age 75.9
Furthermore, existing measures fail to systematically consider patient preferences and undervalue shared decision making. Data suggest, for instance, that patients who are offered a “menu” of options for screening rather than a single screening test are more likely to complete a screening test.10
But existing measures do not consider whether a physician assessed a patient’s preferences, or offered more than one screening option. Of course, measuring the quality of decision making is an evolving science that presents challenges and requires creative solutions.11
Finally, existing measures do not capture the collaborative nature of modern health care. For example, most existing measures focus on the performance of gastroenterologists and GI practices. Although such a focus is appropriate for specialty-specific quality improvement efforts, it neglects to capture the important interactions and hand-offs between providers needed for successful completion of screening (and downstream reduction in cancer mortality). As a result, this specialty-focused approach fails to meet the needs of patients, who are increasingly interested in whether the care they receive is improving their health regardless of who provides it. It also fails to meet the needs of payers, who are interested in whether a network of providers is delivering high-value care for its members. Developing measures that capture the collaborative nature of modern health care becomes increasingly important as payers embrace alternative payment models and other value-based reimbursement systems.
Given these challenges with existing measures, we propose the following concepts for consideration as noncolonoscopy quality measures of CRC screening:
1. Appropriateness of referral for CRC screening (PCP): Measures in this domain should incorporate assessment of family history, prior screening history, and/or life expectancy, all of which are predictive of screening benefit and can be extracted from structured electronic health record data.
2. Shared decision making in choosing a CRC screening test (PCP): Currently, measures in this domain are (by necessity) relatively simple, such as assessment of documentation of whether stool testing was offered alongside colonoscopy during a clinic visit.
3. Percentage of individuals with a positive noncolonoscopy CRC screening test who complete a colonoscopy within 6 months (PCP and GI): A measure in this domain can be developed and implemented using existing infrastructure. The Veterans Affairs Healthcare System currently uses such a measure to monitor appropriate follow-up of positive fecal immunochemical tests.
4. Predicted reduction in CRC mortality: This measure, which provides an estimate of the effectiveness and value of a screening program, represents the “bottom line” that is ultimately of interest to both patients and payers. However, composite measures that use projected results require sophisticated statistical approaches and case-mix adjustment. They must also contend with “churn” in the covered population.
Although a more comprehensive view of screening is desirable, operationalizing measure concepts, such as those proposed previously, is challenging for several reasons. First, as we have outlined, CRC screening is truly a “team sport.” The stakeholders in CRC screening include public health, primary care, gastroenterology, colorectal surgery, oncology, anesthesiology, and pathology practitioners. As a result, screening has no natural and obvious steward. Rather, various components of care are adopted by different specialty groups, and this approach leads to unmonitored gaps in care. We believe that gastroenterologists can and should take the lead in developing comprehensive quality measures for CRC screening. Such comprehensive measures will be of value to patients and to payers. Second, assessing quality of care more comprehensively has traditionally been infeasible. For example, incorporating life expectancy into quality measures requires electronic assessment of health status.
Traditionally, such efforts have been hampered by the lack of systematic clinical data collection. However, as meaningful use of electronic health records increases, measures that incorporate such information are likely to become increasingly feasible. Finally, we also need to consider how to make these improvements while avoiding measure proliferation. Proliferation leads to provider fatigue and discourages thoughtful clinical decision making, potentially worsening quality of care. Creative approaches, such as rotating measure sets over time, use of clinical decision support tools, and balancing underuse measures with overuse measures, may be warranted. Additionally, composite measures may prove to be more meaningful and more practical for patients, providers, and payers. Ultimately, a distinction must be made between quality assurance and quality improvement; both are important, but the types of measures and the level of measure sophistication used in each program undoubtedly vary.
In summary, gastroenterologists are uniquely positioned to advocate for high-quality CRC screening that extends beyond simply providing a high-quality colonoscopy. This broader view of quality benefits patients by ensuring that our expertise informs the metrics by which delivery of CRC screening is measured. It also ensures that we hold ourselves and our colleagues to the highest standards across the continuum of care. Additionally, as alternative payment models and value-based contracting are implemented, nonendoscopic screening methods will likely become more commonplace. Advocating for high-quality nonendoscopic screening will help maintain gastroenterologists’ role as the stewards of CRC screening and digestive health. Although operationalizing measure concepts such as those proposed here may be difficult, it is critical if we are to provide the best possible care for our patients.
References
1. Sabatino, S.A., White, M.C., Thompson, T.D., et al. Cancer screening test use – United States, 2013. MMWR Morb Mortal Wkly Rep. 2015;64:464-8.
2. Anderson, A.E., Henry, K.A., Samadder, N.J., et al. Rural vs urban residence affects risk-appropriate colorectal cancer screening. Clin Gastroenterol Hepatol. 2013;11:526-33.
3. Walter, L.C., Lindquist, K., Nugent, S., et al. Impact of age and comorbidity on colorectal cancer screening among older veterans. Ann Intern Med. 2009;150:465-73.
4. Murphy, C.C., Sandler, R.S., Grubber, J.M., et al. Underuse and overuse of colonoscopy for repeat screening and surveillance in the Veterans Health Administration. Clin Gastroenterol Hepatol. 2016;14:436-44.
5. Mittal, S., Lin, Y.-L., Tan, A., et al. Limited life expectancy among a subgroup of Medicare beneficiaries receiving screening colonoscopies. Clin Gastroenterol Hepatol. 2014;12:443-50.e1
6. Allen, J.I. Quality measures for colonoscopy: where should we be in 2015?. Curr Gastroenterol Rep. 2015;17:10.
7. Fisher, D.A., Jeffreys, A., Coffman, C.J., et al. Barriers to full colon evaluation for a positive fecal occult blood test. Cancer Epidemiol Biomark Prev. 2006;15:1232-5.
8. Saini, S.D., van Hees, F., Vijan, S. Smarter screening for cancer: possibilities and challenges of personalization. JAMA. 2014;312:2211-2.
9. Saini, S.D., Vijan, S., Schoenfeld, P., et al. Role of quality measurement in inappropriate use of screening for colorectal cancer: retrospective cohort study. BMJ. 2014;348:g1247.
10. Inadomi, J.M., Vijan, S., Janz, N.K., et al. Adherence to colorectal cancer screening: a randomized clinical trial of competing strategies. Arch Intern Med. 2012;172:575-82.
11. Writing Committee Members, Drozda, J.P., Ferguson, T.B., et al. 2015 ACC/AHA focused update of secondary prevention lipid performance measures: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. J Am Coll Cardiol. 2016;67:558-87.
Dr. Saini is a research scientist at the VA Center for Clinical Management Research and an assistant professor of internal medicine at the University of Michigan, Ann Arbor; Dr. Adams is a clinical lecturer in the division of gastroenterology, department of internal medicine, University of Michigan, and a research investigator, VA Center for Clinical Management Research; Dr. Brill is the chief medical officer of Predictive Health, Paradise Valley, Ariz., and a clinical assistant professor of medicine, University of Arizona School of Medicine, Phoenix; Dr. Gupta is codirector of Digestive Health Center, director of interventional endoscopy, and associate professor of medicine in the division of gastroenterology at Loyola University Medical Center; Dr. Naveed is a clinical assistant professor in the department of gastroenterology and hepatology, University of Iowa Hospitals and Clinics; Dr. Rosenberg is at Illinois Gastroenterology Group; and Dr. Gellad is associate professor of medicine at Duke University School of Medicine, Durham, N.C. Dr. Saini’s and Dr. Gellad’s research is funded by Veterans Affairs Health Services Research and Development Career Development Awards (CDA 09-213-2 and CDA 14-158). Dr. Gupta has received research support from Cook Medical, Cosmo Pharmaceuticals, and CDx Diagnostics.

Resolving patients’ complaints
For most physicians, the resolution of patients’ complaints ranks second only to firing an employee on the Least Favorite Tasks List. With so many potential problems, and so many ways patients can react to them, it seems impossible to construct any sort of template for consistent, mutually satisfactory resolutions.
But it can be done, and it’s not as complex as it appears, once you realize that the vast majority of complaints have the same basic root: The patient’s expectations have not been met. Sometimes it’s your fault, sometimes the patient’s, and often a bit of both. Either way, the result is the same: You have an unhappy patient, and you must deal with it.

In most cases, this is not a job you should delegate. Unless the complaint is trivial or purely administrative, you should address it yourself. It’s what you would want if you were the complainant, and it’s often too important to trust to a subordinate.
I have distilled this unpleasant duty down to a simple three-part strategy:
• Discover which expectations went unmet, and why.
• Agree on a solution.
• Learn from the experience, to prevent similar future complaints.
At this point, you may be asking, “Why should I care? Is the personal expenditure of my time and effort necessary to resolve complaints really worth it?” Absolutely, because the old cliché is true: A satisfied patient will refer 5 new patients, but a dissatisfied one will chase away 20 or more. Besides, if the complaint is significant, and you won’t resolve it, the patient is likely to find someone who will; and chances are you won’t like the choice, or the venue – or the eventual resolution.
Of course, the easiest way to deal with complaints is to prevent as many as possible in the first place. Try to nip unrealistic expectations in the bud. Take the time to explain all treatments and procedures, and their most likely outcomes, in a clear and honest manner. And since even the most astute patients will not absorb everything you tell them, make liberal use of written handouts and other visual aids.
And, of course, document everything you have explained. Documentation is like garlic: There is no such thing as too much of it.
But despite your best efforts, there will always be complaints, and handling them is a skill set worth honing. The most important skill in that set is the one most people – especially physicians – do poorly: listening to the complaint. Before you can resolve a problem you have to know what it is, and this is precisely the wrong time to make assumptions or jump to conclusions.
So listen to the entire complaint without interrupting, defending, or justifying. Angry patients don’t care why the problem occurred, and they are not interested in your side of the story. This is not about you, so listen and understand.
As you listen, the unmet expectations will become clear. When the patient is finished, I like to summarize the complaint in that context: “So if I understand you correctly, you expected “X” to happen, but “Y” happened instead.” If I’m wrong, I modify my summary until the patient agrees that I understand the problem.
Once you know the problem, you can talk about a solution. The patient usually has one in mind – additional treatment, a referral elsewhere, a fee adjustment, or sometimes simply an apology. Consider it.
If the patient’s solution is reasonable, by all means, agree to it; if it is unreasonable, try to offer a reasonable alternative. The temptation here is to think more about protecting yourself than making the patient happy, but that often leads to bigger problems. Don’t be defensive. Again, this is not about you.
I am often asked if refunding a fee is a reasonable option. Some patients (and lawyers) will interpret a refund as a tacit admission of guilt, so I generally try to avoid them. However, canceling a small fee for an angry patient can be an expedient solution, and in my opinion looks exactly like what it is: an honest effort to rectify the situation. But in general, additional materials or services, at reduced or waived fees, are a better alternative than refunding money.
Once you have arrived at a mutually satisfactory solution, again, document everything; but consider reserving a “private” chart area for such documentation (unless it is a bona fide clinical issue), so that it won’t go out to referrers and other third parties with copies of your clinical notes. Also, consider having the patient sign off on the documentation, acknowledging that the complaint has been resolved.
Finally, always try to learn something from the experience. Ask yourself how you might prevent a repetition of the complaint, what you did that you can avoid doing next time, and how you might prevent unrealistic expectations in a similar future situation.
Above all, never take complaints personally – even when they are personal. It’s always worth reminding yourself that no matter how hard you try, you can never please everyone.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Dermatology News. Write to him at [email protected].
For most physicians, the resolution of patients’ complaints ranks second only to firing an employee on the Least Favorite Tasks List. With so many potential problems, and so many ways patients can react to them, it seems impossible to construct any sort of template for consistent, mutually satisfactory resolutions.
But it can be done, and it’s not as complex as it appears, once you realize that the vast majority of complaints have the same basic root: The patient’s expectations have not been met. Sometimes it’s your fault, sometimes the patient’s, and often a bit of both. Either way, the result is the same: You have an unhappy patient, and you must deal with it.
In most cases, this is not a job you should delegate. Unless the complaint is trivial or purely administrative, you should address it yourself. It’s what you would want if you were the complainant, and it’s often too important to trust to a subordinate.
I have distilled this unpleasant duty down to a simple three-part strategy:
• Discover which expectations went unmet, and why.
• Agree on a solution.
• Learn from the experience, to prevent similar future complaints.
At this point, you may be asking, “Why should I care? Is the personal expenditure of my time and effort necessary to resolve complaints really worth it?” Absolutely, because the old cliché is true: A satisfied patient will refer 5 new patients, but a dissatisfied one will chase away 20 or more. Besides, if the complaint is significant, and you won’t resolve it, the patient is likely to find someone who will; and chances are you won’t like the choice, or the venue – or the eventual resolution.
Of course, the easiest way to deal with complaints is to prevent as many as possible in the first place. Try to nip unrealistic expectations in the bud. Take the time to explain all treatments and procedures, and their most likely outcomes, in a clear and honest manner. And since even the most astute patients will not absorb everything you tell them, make liberal use of written handouts and other visual aids.
And, of course, document everything you have explained. Documentation is like garlic: There is no such thing as too much of it.
But despite your best efforts, there will always be complaints, and handling them is a skill set worth honing. The most important skill in that set is the one most people – especially physicians – do poorly: listening to the complaint. Before you can resolve a problem you have to know what it is, and this is precisely the wrong time to make assumptions or jump to conclusions.
So listen to the entire complaint without interrupting, defending, or justifying. Angry patients don’t care why the problem occurred, and they are not interested in your side of the story. This is not about you, so listen and understand.
As you listen, the unmet expectations will become clear. When the patient is finished, I like to summarize the complaint in that context: “So if I understand you correctly, you expected “X” to happen, but “Y” happened instead.” If I’m wrong, I modify my summary until the patient agrees that I understand the problem.
Once you know the problem, you can talk about a solution. The patient usually has one in mind – additional treatment, a referral elsewhere, a fee adjustment, or sometimes simply an apology. Consider it.
If the patient’s solution is reasonable, by all means, agree to it; if it is unreasonable, try to offer a reasonable alternative. The temptation here is to think more about protecting yourself than making the patient happy, but that often leads to bigger problems. Don’t be defensive. Again, this is not about you.
I am often asked if refunding a fee is a reasonable option. Some patients (and lawyers) will interpret a refund as a tacit admission of guilt, so I generally try to avoid them. However, canceling a small fee for an angry patient can be an expedient solution, and in my opinion looks exactly like what it is: an honest effort to rectify the situation. But in general, additional materials or services, at reduced or waived fees, are a better alternative than refunding money.
Once you have arrived at a mutually satisfactory solution, again, document everything; but consider reserving a “private” chart area for such documentation (unless it is a bona fide clinical issue), so that it won’t go out to referrers and other third parties with copies of your clinical notes. Also, consider having the patient sign off on the documentation, acknowledging that the complaint has been resolved.
Finally, always try to learn something from the experience. Ask yourself how you might prevent a repetition of the complaint, what you did that you can avoid doing next time, and how you might prevent unrealistic expectations in a similar future situation.
Above all, never take complaints personally – even when they are personal. It’s always worth reminding yourself that no matter how hard you try, you can never please everyone.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Dermatology News. Write to him at [email protected].
For most physicians, the resolution of patients’ complaints ranks second only to firing an employee on the Least Favorite Tasks List. With so many potential problems, and so many ways patients can react to them, it seems impossible to construct any sort of template for consistent, mutually satisfactory resolutions.
But it can be done, and it’s not as complex as it appears, once you realize that the vast majority of complaints have the same basic root: The patient’s expectations have not been met. Sometimes it’s your fault, sometimes the patient’s, and often a bit of both. Either way, the result is the same: You have an unhappy patient, and you must deal with it.
In most cases, this is not a job you should delegate. Unless the complaint is trivial or purely administrative, you should address it yourself. It’s what you would want if you were the complainant, and it’s often too important to trust to a subordinate.
I have distilled this unpleasant duty down to a simple three-part strategy:
• Discover which expectations went unmet, and why.
• Agree on a solution.
• Learn from the experience, to prevent similar future complaints.
At this point, you may be asking, “Why should I care? Is the personal expenditure of my time and effort necessary to resolve complaints really worth it?” Absolutely, because the old cliché is true: A satisfied patient will refer 5 new patients, but a dissatisfied one will chase away 20 or more. Besides, if the complaint is significant, and you won’t resolve it, the patient is likely to find someone who will; and chances are you won’t like the choice, or the venue – or the eventual resolution.
Of course, the easiest way to deal with complaints is to prevent as many as possible in the first place. Try to nip unrealistic expectations in the bud. Take the time to explain all treatments and procedures, and their most likely outcomes, in a clear and honest manner. And since even the most astute patients will not absorb everything you tell them, make liberal use of written handouts and other visual aids.
And, of course, document everything you have explained. Documentation is like garlic: There is no such thing as too much of it.
But despite your best efforts, there will always be complaints, and handling them is a skill set worth honing. The most important skill in that set is the one most people – especially physicians – do poorly: listening to the complaint. Before you can resolve a problem you have to know what it is, and this is precisely the wrong time to make assumptions or jump to conclusions.
So listen to the entire complaint without interrupting, defending, or justifying. Angry patients don’t care why the problem occurred, and they are not interested in your side of the story. This is not about you, so listen and understand.
As you listen, the unmet expectations will become clear. When the patient is finished, I like to summarize the complaint in that context: “So if I understand you correctly, you expected “X” to happen, but “Y” happened instead.” If I’m wrong, I modify my summary until the patient agrees that I understand the problem.
Once you know the problem, you can talk about a solution. The patient usually has one in mind – additional treatment, a referral elsewhere, a fee adjustment, or sometimes simply an apology. Consider it.
If the patient’s solution is reasonable, by all means, agree to it; if it is unreasonable, try to offer a reasonable alternative. The temptation here is to think more about protecting yourself than making the patient happy, but that often leads to bigger problems. Don’t be defensive. Again, this is not about you.
I am often asked if refunding a fee is a reasonable option. Some patients (and lawyers) will interpret a refund as a tacit admission of guilt, so I generally try to avoid them. However, canceling a small fee for an angry patient can be an expedient solution, and in my opinion looks exactly like what it is: an honest effort to rectify the situation. But in general, additional materials or services, at reduced or waived fees, are a better alternative than refunding money.
Once you have arrived at a mutually satisfactory solution, again, document everything; but consider reserving a “private” chart area for such documentation (unless it is a bona fide clinical issue), so that it won’t go out to referrers and other third parties with copies of your clinical notes. Also, consider having the patient sign off on the documentation, acknowledging that the complaint has been resolved.
Finally, always try to learn something from the experience. Ask yourself how you might prevent a repetition of the complaint, what you did that you can avoid doing next time, and how you might prevent unrealistic expectations in a similar future situation.
Above all, never take complaints personally – even when they are personal. It’s always worth reminding yourself that no matter how hard you try, you can never please everyone.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Dermatology News. Write to him at [email protected].
