User login
A welcome addition
On behalf of the SVS Publications Committee I am delighted to announce the appointment of Malachi Sheahan, III, M.D., as Associate Medical Editor of Vascular Specialist. I am sure readers will realize this official newspaper of the Society for Vascular Surgery has grown substantially over the last few years. With the help of generous advertisers we now “publish” Vascular Specialist not only in print but in multiple formats. These include electronic versions on the Web, Facebook, and Twitter, as well as mobile versions for smartphones and tablets. The print version is now published monthly and most often as 20 pages.
Further, www.vascularspecialistonline.com includes many articles not found in the print edition. Articles can be searched based on subject and author and the print version can be seen in PDF version. The web version also allows readers to answer polls posed in the print edition. These are archived for review.
A recent survey of 250 members of the SVS confirmed that Vascular Specialist is now the most widely read vascular news publication. More importantly, it was considered by far the most authoritative.

This expansion requires a significant expenditure of time by the Associate Editors and the Medical Editor in particular. Accordingly, it is essential that the medical editorial staff be supplemented by an Associate Medical Editor. This will also allow the smooth transition when the Medical Editor’s appointment terminates.
Mal has already proven to be an excellent writer, and his commitment to the SVS, resident/fellow training, and his sense of humor make him an outstanding choice to assume this position. Mal completed his vascular surgery training at the Beth Israel Deaconess program in 2003. Shortly thereafter he joined the faculty at the Louisiana State University Health Sciences Center in New Orleans. He currently serves as the program director for both their integrated and independent vascular training programs. In 2014, he was named the Claude C. Craighead Jr. Professor and Chair of the Division of Vascular and Endovascular Surgery.

I have previously requested that all members consider themselves not only readers but also contributors. Once again I encourage you to send Mal and me opinion pieces or letters to the editor. We also welcome Tips and Tricks. These can be quite short and do not require any references. They are meant to highlight a technique that you have found to be helpful in performing an open or endovascular procedure. One or two photos often help the piece but they must be in .jpg format and at least 124kb. If you are so inclined we will also print your photo and affiliation alongside. However, we regret you cannot submit your high school photo or substitute one of Tom Cruise or Beyoncé! Don’t worry that you may not be a Pulitzer Prize journalist since we have professional writers who will tidy up your writing as necessary. We also welcome suggestions about news items that we may have missed or overlooked. These may be news items from the lay press or a manuscript you read in a journal other than the JVS. Again, our professional reporters will turn the item into a news article. You can also send us a comment and, if appropriate, we will print it as a sidebar to the article.
Further, we encourage news about your comings and goings which we can publish in the “From the community” section. Executive members of the various regional Societies can also utilize this section to bring us news about their Societies activities.
In order to keep the commentaries fresh, we do need to rotate the members of the editorial board. So, if you would like to be considered for such a position, please send us a short biography and your area of interest. This could be related to a disease process, treatment, or socioeconomic issues. Associate Editors will be required to read short news items about 12 times a year and to provide commentary when requested. Even if you are not selected we may occasionally turn to you to write a comment on a news item related to your stated interest.
The SVS wants Vascular Specialist to be YOUR newspaper. Please help us achieve that goal as we continue to make Vascular Specialist the most read and respected supplier of news and opinions about vascular surgery and vascular surgeons.
You can contact me at [email protected] and Dr. Sheahan at [email protected].
On behalf of the SVS Publications Committee I am delighted to announce the appointment of Malachi Sheahan, III, M.D., as Associate Medical Editor of Vascular Specialist. I am sure readers will realize this official newspaper of the Society for Vascular Surgery has grown substantially over the last few years. With the help of generous advertisers we now “publish” Vascular Specialist not only in print but in multiple formats. These include electronic versions on the Web, Facebook, and Twitter, as well as mobile versions for smartphones and tablets. The print version is now published monthly and most often as 20 pages.
Further, www.vascularspecialistonline.com includes many articles not found in the print edition. Articles can be searched based on subject and author and the print version can be seen in PDF version. The web version also allows readers to answer polls posed in the print edition. These are archived for review.
A recent survey of 250 members of the SVS confirmed that Vascular Specialist is now the most widely read vascular news publication. More importantly, it was considered by far the most authoritative.
This expansion requires a significant expenditure of time by the Associate Editors and the Medical Editor in particular. Accordingly, it is essential that the medical editorial staff be supplemented by an Associate Medical Editor. This will also allow the smooth transition when the Medical Editor’s appointment terminates.
Mal has already proven to be an excellent writer, and his commitment to the SVS, resident/fellow training, and his sense of humor make him an outstanding choice to assume this position. Mal completed his vascular surgery training at the Beth Israel Deaconess program in 2003. Shortly thereafter he joined the faculty at the Louisiana State University Health Sciences Center in New Orleans. He currently serves as the program director for both their integrated and independent vascular training programs. In 2014, he was named the Claude C. Craighead Jr. Professor and Chair of the Division of Vascular and Endovascular Surgery.
I have previously requested that all members consider themselves not only readers but also contributors. Once again I encourage you to send Mal and me opinion pieces or letters to the editor. We also welcome Tips and Tricks. These can be quite short and do not require any references. They are meant to highlight a technique that you have found to be helpful in performing an open or endovascular procedure. One or two photos often help the piece but they must be in .jpg format and at least 124kb. If you are so inclined we will also print your photo and affiliation alongside. However, we regret you cannot submit your high school photo or substitute one of Tom Cruise or Beyoncé! Don’t worry that you may not be a Pulitzer Prize journalist since we have professional writers who will tidy up your writing as necessary. We also welcome suggestions about news items that we may have missed or overlooked. These may be news items from the lay press or a manuscript you read in a journal other than the JVS. Again, our professional reporters will turn the item into a news article. You can also send us a comment and, if appropriate, we will print it as a sidebar to the article.
Further, we encourage news about your comings and goings which we can publish in the “From the community” section. Executive members of the various regional Societies can also utilize this section to bring us news about their Societies activities.
In order to keep the commentaries fresh, we do need to rotate the members of the editorial board. So, if you would like to be considered for such a position, please send us a short biography and your area of interest. This could be related to a disease process, treatment, or socioeconomic issues. Associate Editors will be required to read short news items about 12 times a year and to provide commentary when requested. Even if you are not selected we may occasionally turn to you to write a comment on a news item related to your stated interest.
The SVS wants Vascular Specialist to be YOUR newspaper. Please help us achieve that goal as we continue to make Vascular Specialist the most read and respected supplier of news and opinions about vascular surgery and vascular surgeons.
You can contact me at [email protected] and Dr. Sheahan at [email protected].
On behalf of the SVS Publications Committee I am delighted to announce the appointment of Malachi Sheahan, III, M.D., as Associate Medical Editor of Vascular Specialist. I am sure readers will realize this official newspaper of the Society for Vascular Surgery has grown substantially over the last few years. With the help of generous advertisers we now “publish” Vascular Specialist not only in print but in multiple formats. These include electronic versions on the Web, Facebook, and Twitter, as well as mobile versions for smartphones and tablets. The print version is now published monthly and most often as 20 pages.
Further, www.vascularspecialistonline.com includes many articles not found in the print edition. Articles can be searched based on subject and author and the print version can be seen in PDF version. The web version also allows readers to answer polls posed in the print edition. These are archived for review.
A recent survey of 250 members of the SVS confirmed that Vascular Specialist is now the most widely read vascular news publication. More importantly, it was considered by far the most authoritative.
This expansion requires a significant expenditure of time by the Associate Editors and the Medical Editor in particular. Accordingly, it is essential that the medical editorial staff be supplemented by an Associate Medical Editor. This will also allow the smooth transition when the Medical Editor’s appointment terminates.
Mal has already proven to be an excellent writer, and his commitment to the SVS, resident/fellow training, and his sense of humor make him an outstanding choice to assume this position. Mal completed his vascular surgery training at the Beth Israel Deaconess program in 2003. Shortly thereafter he joined the faculty at the Louisiana State University Health Sciences Center in New Orleans. He currently serves as the program director for both their integrated and independent vascular training programs. In 2014, he was named the Claude C. Craighead Jr. Professor and Chair of the Division of Vascular and Endovascular Surgery.
I have previously requested that all members consider themselves not only readers but also contributors. Once again I encourage you to send Mal and me opinion pieces or letters to the editor. We also welcome Tips and Tricks. These can be quite short and do not require any references. They are meant to highlight a technique that you have found to be helpful in performing an open or endovascular procedure. One or two photos often help the piece but they must be in .jpg format and at least 124kb. If you are so inclined we will also print your photo and affiliation alongside. However, we regret you cannot submit your high school photo or substitute one of Tom Cruise or Beyoncé! Don’t worry that you may not be a Pulitzer Prize journalist since we have professional writers who will tidy up your writing as necessary. We also welcome suggestions about news items that we may have missed or overlooked. These may be news items from the lay press or a manuscript you read in a journal other than the JVS. Again, our professional reporters will turn the item into a news article. You can also send us a comment and, if appropriate, we will print it as a sidebar to the article.
Further, we encourage news about your comings and goings which we can publish in the “From the community” section. Executive members of the various regional Societies can also utilize this section to bring us news about their Societies activities.
In order to keep the commentaries fresh, we do need to rotate the members of the editorial board. So, if you would like to be considered for such a position, please send us a short biography and your area of interest. This could be related to a disease process, treatment, or socioeconomic issues. Associate Editors will be required to read short news items about 12 times a year and to provide commentary when requested. Even if you are not selected we may occasionally turn to you to write a comment on a news item related to your stated interest.
The SVS wants Vascular Specialist to be YOUR newspaper. Please help us achieve that goal as we continue to make Vascular Specialist the most read and respected supplier of news and opinions about vascular surgery and vascular surgeons.
You can contact me at [email protected] and Dr. Sheahan at [email protected].

Slide Set on Diabetic Foot Guidelines
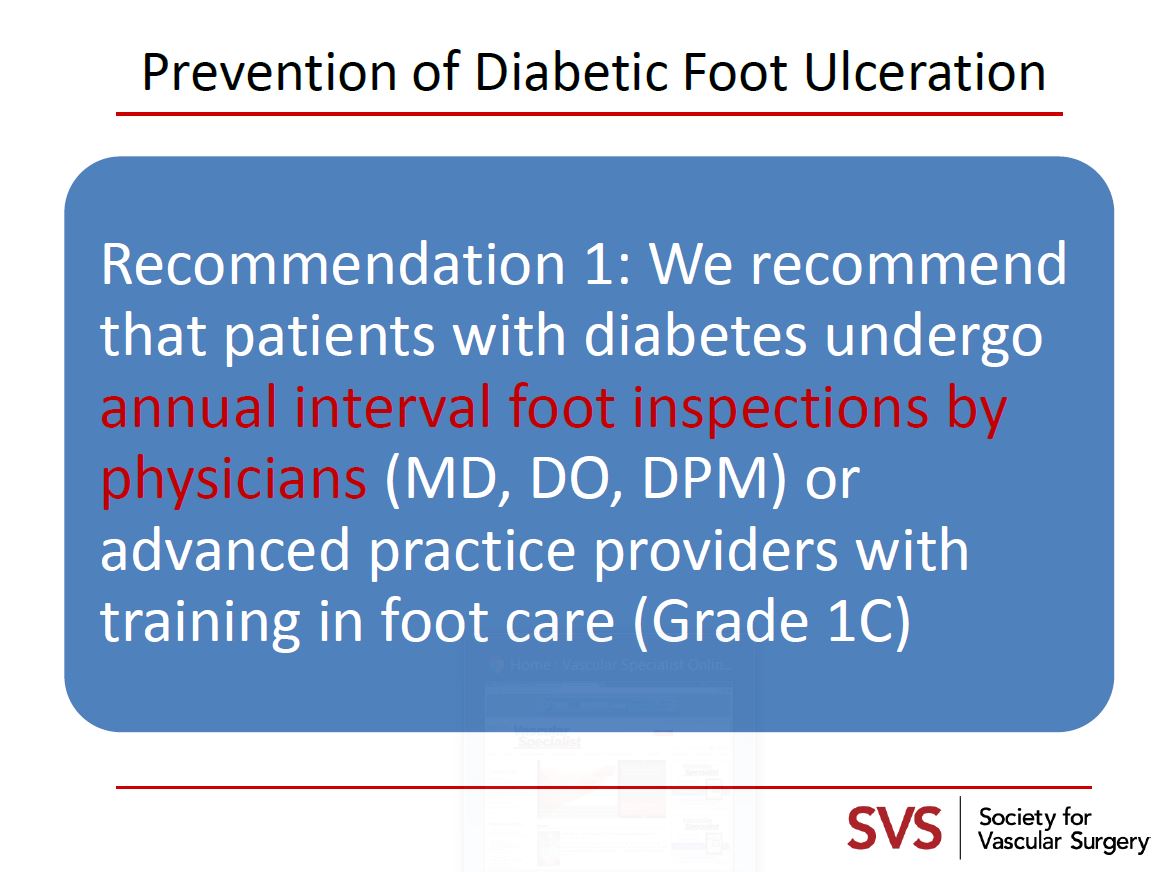
To encourage adoption of the recent diabetic foot guideline, SVS has created a new educatonal slide set for members to use in their presentations.
The slideset is based on “The Management of the Diabetic Foot: A Clinical Practice Guideline by the Society for Vascular Surgery in Collaboration with the American Podiatric Medical Association and the Society for Vascular Medicine” published in the Journal of Vascular Surgery, February 2016 Supplement Volume 63, Issue 2, Pages 3S–21S
To get the slideset in PDF form, click here.
To encourage adoption of the recent diabetic foot guideline, SVS has created a new educatonal slide set for members to use in their presentations.
The slideset is based on “The Management of the Diabetic Foot: A Clinical Practice Guideline by the Society for Vascular Surgery in Collaboration with the American Podiatric Medical Association and the Society for Vascular Medicine” published in the Journal of Vascular Surgery, February 2016 Supplement Volume 63, Issue 2, Pages 3S–21S
To get the slideset in PDF form, click here.
To encourage adoption of the recent diabetic foot guideline, SVS has created a new educatonal slide set for members to use in their presentations.
The slideset is based on “The Management of the Diabetic Foot: A Clinical Practice Guideline by the Society for Vascular Surgery in Collaboration with the American Podiatric Medical Association and the Society for Vascular Medicine” published in the Journal of Vascular Surgery, February 2016 Supplement Volume 63, Issue 2, Pages 3S–21S
To get the slideset in PDF form, click here.
Register for SVS/UCLA Board Review Course
Registration is open for the “First Annual UCLA/SVS Symposium: A Comprehensive Review and Update of What’s New in Vascular and Endovascular Surgery.”
The course will be Aug. 27 to 29 at the Beverly Hilton in Beverly Hills, Calif., and will offer an in-depth review of our specialty for those preparing to take the vascular board examinations as well as providing the basic didactic education for the vascular residents and fellows in training.
Registration is open for the “First Annual UCLA/SVS Symposium: A Comprehensive Review and Update of What’s New in Vascular and Endovascular Surgery.”
The course will be Aug. 27 to 29 at the Beverly Hilton in Beverly Hills, Calif., and will offer an in-depth review of our specialty for those preparing to take the vascular board examinations as well as providing the basic didactic education for the vascular residents and fellows in training.
Registration is open for the “First Annual UCLA/SVS Symposium: A Comprehensive Review and Update of What’s New in Vascular and Endovascular Surgery.”
The course will be Aug. 27 to 29 at the Beverly Hilton in Beverly Hills, Calif., and will offer an in-depth review of our specialty for those preparing to take the vascular board examinations as well as providing the basic didactic education for the vascular residents and fellows in training.

Research Career Development Travel Awards
The SVS Foundation has announced a new award opportunity, the Research Career Development Travel Awards, designed to support early-career vascular surgeons with an interest in basic science, translational or clinical research.
Applications for these awards are due Aug. 8.
In addition to $1,500 in financial support to attend an established research career development course, awardees also will be assigned an SVS research mentor to provide guidance and discuss academic career advancement, including other available resources and opportunities.
Learn more at the link above.
The SVS Foundation has announced a new award opportunity, the Research Career Development Travel Awards, designed to support early-career vascular surgeons with an interest in basic science, translational or clinical research.
Applications for these awards are due Aug. 8.
In addition to $1,500 in financial support to attend an established research career development course, awardees also will be assigned an SVS research mentor to provide guidance and discuss academic career advancement, including other available resources and opportunities.
Learn more at the link above.
The SVS Foundation has announced a new award opportunity, the Research Career Development Travel Awards, designed to support early-career vascular surgeons with an interest in basic science, translational or clinical research.
Applications for these awards are due Aug. 8.
In addition to $1,500 in financial support to attend an established research career development course, awardees also will be assigned an SVS research mentor to provide guidance and discuss academic career advancement, including other available resources and opportunities.
Learn more at the link above.

Prevalence of Iron Deficiency in Heart Failure Patients, Study Says
NEW YORK - About a third of heart failure patients have anemia and most also have iron deficiency, according to UK researchers.
This observational analysis, Dr. John G.F. Cleland told Reuters Health by email, "shows that iron deficiency is very common in patients with heart failure and often leads to anemia and that the prevalence of both iron deficiency and anemia are both highly sensitive to the criteria used to define them."
In a June 29 online paper in JAMA Cardiology, Dr. Cleland, of the University of Hull, and colleagues report that they came to this conclusion after studying data on more than 4,400 patients seen at a local clinic over a 10-year period. All were referred because of suspected heart failure, and their median age was 73 years.
Data collected included hemoglobin, serum iron, transferrin saturation, and serum ferritin concentrations.
Overall, 1,237 patients (27.8%) had anemia, with a higher prevalence (33.3%) in patients who met the criteria for heart failure with or without left ventricular systolic dysfunction (LVSD).
Depending on the definition used, iron deficiency was present in 270 (43.2%) to 425 (68.0%) patients with anemia. This was the case in 260 (14.7%) to 624 (35.3%) of those without anemia.
Lower concentrations of hemoglobin (hazard ratio 0.92) and serum iron (HR 0.98) were independently associated with higher all-cause and cardiovascular mortality in multivariable analyses.
Moreover, said Dr. Cleland, "Serum iron and transferrin saturation were highly correlated (raising the question of the need to measure both) and both were strongly related to anemia. In contrast, serum ferritin, the most widely (supposed) measure of iron deficiency, was more strongly related to measures of inflammation than anemia."
"Lower concentrations of hemoglobin and serum iron and lower transferrin saturation," he stressed, "were associated with a higher mortality. In contrast, lower serum ferritin was associated with a better prognosis, probably because it is more a measure of inflammation than of iron deficiency."
Dr. Cleland concluded, "Serum ferritin is a poor measure of iron deficiency in patients with heart failure. Many patients with normal serum ferritin (defined by many as greater than 100 ng/mL) have iron deficiency. Clinical trials of intravenous iron for patients with heart failure should be aware of this issue to ensure they enroll appropriate patients."
The National Heart Service, Vifor Pharma, and Amgen supported this research. Dr. Cleland reported research support from Vifor and Amgen.
SOURCE: http://bit.ly/29ukoX4
JAMA Cardiol 2016.
NEW YORK - About a third of heart failure patients have anemia and most also have iron deficiency, according to UK researchers.
This observational analysis, Dr. John G.F. Cleland told Reuters Health by email, "shows that iron deficiency is very common in patients with heart failure and often leads to anemia and that the prevalence of both iron deficiency and anemia are both highly sensitive to the criteria used to define them."
In a June 29 online paper in JAMA Cardiology, Dr. Cleland, of the University of Hull, and colleagues report that they came to this conclusion after studying data on more than 4,400 patients seen at a local clinic over a 10-year period. All were referred because of suspected heart failure, and their median age was 73 years.
Data collected included hemoglobin, serum iron, transferrin saturation, and serum ferritin concentrations.
Overall, 1,237 patients (27.8%) had anemia, with a higher prevalence (33.3%) in patients who met the criteria for heart failure with or without left ventricular systolic dysfunction (LVSD).
Depending on the definition used, iron deficiency was present in 270 (43.2%) to 425 (68.0%) patients with anemia. This was the case in 260 (14.7%) to 624 (35.3%) of those without anemia.
Lower concentrations of hemoglobin (hazard ratio 0.92) and serum iron (HR 0.98) were independently associated with higher all-cause and cardiovascular mortality in multivariable analyses.
Moreover, said Dr. Cleland, "Serum iron and transferrin saturation were highly correlated (raising the question of the need to measure both) and both were strongly related to anemia. In contrast, serum ferritin, the most widely (supposed) measure of iron deficiency, was more strongly related to measures of inflammation than anemia."
"Lower concentrations of hemoglobin and serum iron and lower transferrin saturation," he stressed, "were associated with a higher mortality. In contrast, lower serum ferritin was associated with a better prognosis, probably because it is more a measure of inflammation than of iron deficiency."
Dr. Cleland concluded, "Serum ferritin is a poor measure of iron deficiency in patients with heart failure. Many patients with normal serum ferritin (defined by many as greater than 100 ng/mL) have iron deficiency. Clinical trials of intravenous iron for patients with heart failure should be aware of this issue to ensure they enroll appropriate patients."
The National Heart Service, Vifor Pharma, and Amgen supported this research. Dr. Cleland reported research support from Vifor and Amgen.
SOURCE: http://bit.ly/29ukoX4
JAMA Cardiol 2016.
NEW YORK - About a third of heart failure patients have anemia and most also have iron deficiency, according to UK researchers.
This observational analysis, Dr. John G.F. Cleland told Reuters Health by email, "shows that iron deficiency is very common in patients with heart failure and often leads to anemia and that the prevalence of both iron deficiency and anemia are both highly sensitive to the criteria used to define them."
In a June 29 online paper in JAMA Cardiology, Dr. Cleland, of the University of Hull, and colleagues report that they came to this conclusion after studying data on more than 4,400 patients seen at a local clinic over a 10-year period. All were referred because of suspected heart failure, and their median age was 73 years.
Data collected included hemoglobin, serum iron, transferrin saturation, and serum ferritin concentrations.
Overall, 1,237 patients (27.8%) had anemia, with a higher prevalence (33.3%) in patients who met the criteria for heart failure with or without left ventricular systolic dysfunction (LVSD).
Depending on the definition used, iron deficiency was present in 270 (43.2%) to 425 (68.0%) patients with anemia. This was the case in 260 (14.7%) to 624 (35.3%) of those without anemia.
Lower concentrations of hemoglobin (hazard ratio 0.92) and serum iron (HR 0.98) were independently associated with higher all-cause and cardiovascular mortality in multivariable analyses.
Moreover, said Dr. Cleland, "Serum iron and transferrin saturation were highly correlated (raising the question of the need to measure both) and both were strongly related to anemia. In contrast, serum ferritin, the most widely (supposed) measure of iron deficiency, was more strongly related to measures of inflammation than anemia."
"Lower concentrations of hemoglobin and serum iron and lower transferrin saturation," he stressed, "were associated with a higher mortality. In contrast, lower serum ferritin was associated with a better prognosis, probably because it is more a measure of inflammation than of iron deficiency."
Dr. Cleland concluded, "Serum ferritin is a poor measure of iron deficiency in patients with heart failure. Many patients with normal serum ferritin (defined by many as greater than 100 ng/mL) have iron deficiency. Clinical trials of intravenous iron for patients with heart failure should be aware of this issue to ensure they enroll appropriate patients."
The National Heart Service, Vifor Pharma, and Amgen supported this research. Dr. Cleland reported research support from Vifor and Amgen.
SOURCE: http://bit.ly/29ukoX4
JAMA Cardiol 2016.
Study Links Severe Childhood Eczema to Sedentary Behaviors
SCOTTSDALE, ARIZ. – Children with severe atopic dermatitis were significantly more likely to log at least 5 hours of screen time a day, and were significantly less likely to exercise than were nonatopic controls, said the lead investigator of a large national study.
“Atopic dermatitis overall was not associated with sedentary behavior. It was severe disease only,” said Mark Strom of the department of dermatology, Northwestern University, Chicago, during an oral presentation at the annual meeting of the Society for Investigative Dermatology. Patients tended to be even more sedentary if they suffered from disturbed sleep in addition to severe eczema, he added.
Heat and sweat worsen the intense itch of atopic dermatitis. Hypothesizing that this would deter affected children from physical activity, Mr. Strom and his associates analyzed data for 131,783 respondents aged 18 and under from the National Survey of Children’s Health. The survey assesses physical activity by asking how many days a week the respondent sweated and breathed hard for at least 20 minutes. Screen time is measured by asking about daily hours spent watching television and playing video games, and sleep quality is assessed by asking how many nights a week the child slept the normal amount for his or her age.
Simply having atopic dermatitis was linked with only a slight increase in the chance of having a sedentary lifestyle after controlling for demographic factors, insurance status, geographic location, and educational level, according to Mr. Strom. Specifically, eczema was significantly associated with a 12% lower odds of having exercised on at least 3 days of the previous week (odds ratio, 0.88). However, severe atopic dermatitis significantly reduced the odds that a child exercised at least one day a week by 61% (OR, 0.39). Furthermore, severe atopic dermatitis was associated with more than double the odds of having at least 5 hours of daily screen time (OR, 2.62). And having either moderate or severe eczema was tied to a significant decrease in the odds of having participated in sports in the past year, Mr. Strom said.
“Atopic dermatitis and sleep disturbance each contribute to sedentary behavior,” he reported. Nonatopic children who did not sleep enough on most nights had nearly double the odds of heavy television and video game use, compared with children who slept more, a significant difference. When poor sleepers also had atopic dermatitis, their odds of heavy screen use more than tripled. Poor sleepers were also significantly less likely to join sports teams, even when they did not have eczema, Mr. Strom said.
“Children with more severe atopic dermatitis may have more profound exacerbations of activity-related symptoms, which would lead to these findings,” he concluded. Future studies should explore whether better symptom control can help improve sedentary behaviors, he added.
The study was sponsored by the Maternal and Child Health Bureau of the U.S. Department of Health and Human Services. Mr. Strom had no disclosures.
SCOTTSDALE, ARIZ. – Children with severe atopic dermatitis were significantly more likely to log at least 5 hours of screen time a day, and were significantly less likely to exercise than were nonatopic controls, said the lead investigator of a large national study.
“Atopic dermatitis overall was not associated with sedentary behavior. It was severe disease only,” said Mark Strom of the department of dermatology, Northwestern University, Chicago, during an oral presentation at the annual meeting of the Society for Investigative Dermatology. Patients tended to be even more sedentary if they suffered from disturbed sleep in addition to severe eczema, he added.
Heat and sweat worsen the intense itch of atopic dermatitis. Hypothesizing that this would deter affected children from physical activity, Mr. Strom and his associates analyzed data for 131,783 respondents aged 18 and under from the National Survey of Children’s Health. The survey assesses physical activity by asking how many days a week the respondent sweated and breathed hard for at least 20 minutes. Screen time is measured by asking about daily hours spent watching television and playing video games, and sleep quality is assessed by asking how many nights a week the child slept the normal amount for his or her age.
Simply having atopic dermatitis was linked with only a slight increase in the chance of having a sedentary lifestyle after controlling for demographic factors, insurance status, geographic location, and educational level, according to Mr. Strom. Specifically, eczema was significantly associated with a 12% lower odds of having exercised on at least 3 days of the previous week (odds ratio, 0.88). However, severe atopic dermatitis significantly reduced the odds that a child exercised at least one day a week by 61% (OR, 0.39). Furthermore, severe atopic dermatitis was associated with more than double the odds of having at least 5 hours of daily screen time (OR, 2.62). And having either moderate or severe eczema was tied to a significant decrease in the odds of having participated in sports in the past year, Mr. Strom said.
“Atopic dermatitis and sleep disturbance each contribute to sedentary behavior,” he reported. Nonatopic children who did not sleep enough on most nights had nearly double the odds of heavy television and video game use, compared with children who slept more, a significant difference. When poor sleepers also had atopic dermatitis, their odds of heavy screen use more than tripled. Poor sleepers were also significantly less likely to join sports teams, even when they did not have eczema, Mr. Strom said.
“Children with more severe atopic dermatitis may have more profound exacerbations of activity-related symptoms, which would lead to these findings,” he concluded. Future studies should explore whether better symptom control can help improve sedentary behaviors, he added.
The study was sponsored by the Maternal and Child Health Bureau of the U.S. Department of Health and Human Services. Mr. Strom had no disclosures.
SCOTTSDALE, ARIZ. – Children with severe atopic dermatitis were significantly more likely to log at least 5 hours of screen time a day, and were significantly less likely to exercise than were nonatopic controls, said the lead investigator of a large national study.
“Atopic dermatitis overall was not associated with sedentary behavior. It was severe disease only,” said Mark Strom of the department of dermatology, Northwestern University, Chicago, during an oral presentation at the annual meeting of the Society for Investigative Dermatology. Patients tended to be even more sedentary if they suffered from disturbed sleep in addition to severe eczema, he added.
Heat and sweat worsen the intense itch of atopic dermatitis. Hypothesizing that this would deter affected children from physical activity, Mr. Strom and his associates analyzed data for 131,783 respondents aged 18 and under from the National Survey of Children’s Health. The survey assesses physical activity by asking how many days a week the respondent sweated and breathed hard for at least 20 minutes. Screen time is measured by asking about daily hours spent watching television and playing video games, and sleep quality is assessed by asking how many nights a week the child slept the normal amount for his or her age.
Simply having atopic dermatitis was linked with only a slight increase in the chance of having a sedentary lifestyle after controlling for demographic factors, insurance status, geographic location, and educational level, according to Mr. Strom. Specifically, eczema was significantly associated with a 12% lower odds of having exercised on at least 3 days of the previous week (odds ratio, 0.88). However, severe atopic dermatitis significantly reduced the odds that a child exercised at least one day a week by 61% (OR, 0.39). Furthermore, severe atopic dermatitis was associated with more than double the odds of having at least 5 hours of daily screen time (OR, 2.62). And having either moderate or severe eczema was tied to a significant decrease in the odds of having participated in sports in the past year, Mr. Strom said.
“Atopic dermatitis and sleep disturbance each contribute to sedentary behavior,” he reported. Nonatopic children who did not sleep enough on most nights had nearly double the odds of heavy television and video game use, compared with children who slept more, a significant difference. When poor sleepers also had atopic dermatitis, their odds of heavy screen use more than tripled. Poor sleepers were also significantly less likely to join sports teams, even when they did not have eczema, Mr. Strom said.
“Children with more severe atopic dermatitis may have more profound exacerbations of activity-related symptoms, which would lead to these findings,” he concluded. Future studies should explore whether better symptom control can help improve sedentary behaviors, he added.
The study was sponsored by the Maternal and Child Health Bureau of the U.S. Department of Health and Human Services. Mr. Strom had no disclosures.
AT THE 2016 SID ANNUAL MEETING
Study links severe childhood eczema to sedentary behaviors
SCOTTSDALE, ARIZ. – Children with severe atopic dermatitis were significantly more likely to log at least 5 hours of screen time a day, and were significantly less likely to exercise than were nonatopic controls, said the lead investigator of a large national study.
“Atopic dermatitis overall was not associated with sedentary behavior. It was severe disease only,” said Mark Strom of the department of dermatology, Northwestern University, Chicago, during an oral presentation at the annual meeting of the Society for Investigative Dermatology. Patients tended to be even more sedentary if they suffered from disturbed sleep in addition to severe eczema, he added.
Heat and sweat worsen the intense itch of atopic dermatitis. Hypothesizing that this would deter affected children from physical activity, Mr. Strom and his associates analyzed data for 131,783 respondents aged 18 and under from the National Survey of Children’s Health. The survey assesses physical activity by asking how many days a week the respondent sweated and breathed hard for at least 20 minutes. Screen time is measured by asking about daily hours spent watching television and playing video games, and sleep quality is assessed by asking how many nights a week the child slept the normal amount for his or her age.
Simply having atopic dermatitis was linked with only a slight increase in the chance of having a sedentary lifestyle after controlling for demographic factors, insurance status, geographic location, and educational level, according to Mr. Strom. Specifically, eczema was significantly associated with a 12% lower odds of having exercised on at least 3 days of the previous week (odds ratio, 0.88). However, severe atopic dermatitis significantly reduced the odds that a child exercised at least one day a week by 61% (OR, 0.39). Furthermore, severe atopic dermatitis was associated with more than double the odds of having at least 5 hours of daily screen time (OR, 2.62). And having either moderate or severe eczema was tied to a significant decrease in the odds of having participated in sports in the past year, Mr. Strom said.
“Atopic dermatitis and sleep disturbance each contribute to sedentary behavior,” he reported. Nonatopic children who did not sleep enough on most nights had nearly double the odds of heavy television and video game use, compared with children who slept more, a significant difference. When poor sleepers also had atopic dermatitis, their odds of heavy screen use more than tripled. Poor sleepers were also significantly less likely to join sports teams, even when they did not have eczema, Mr. Strom said.
“Children with more severe atopic dermatitis may have more profound exacerbations of activity-related symptoms, which would lead to these findings,” he concluded. Future studies should explore whether better symptom control can help improve sedentary behaviors, he added.
The study was sponsored by the Maternal and Child Health Bureau of the U.S. Department of Health and Human Services. Mr. Strom had no disclosures.
SCOTTSDALE, ARIZ. – Children with severe atopic dermatitis were significantly more likely to log at least 5 hours of screen time a day, and were significantly less likely to exercise than were nonatopic controls, said the lead investigator of a large national study.
“Atopic dermatitis overall was not associated with sedentary behavior. It was severe disease only,” said Mark Strom of the department of dermatology, Northwestern University, Chicago, during an oral presentation at the annual meeting of the Society for Investigative Dermatology. Patients tended to be even more sedentary if they suffered from disturbed sleep in addition to severe eczema, he added.
Heat and sweat worsen the intense itch of atopic dermatitis. Hypothesizing that this would deter affected children from physical activity, Mr. Strom and his associates analyzed data for 131,783 respondents aged 18 and under from the National Survey of Children’s Health. The survey assesses physical activity by asking how many days a week the respondent sweated and breathed hard for at least 20 minutes. Screen time is measured by asking about daily hours spent watching television and playing video games, and sleep quality is assessed by asking how many nights a week the child slept the normal amount for his or her age.
Simply having atopic dermatitis was linked with only a slight increase in the chance of having a sedentary lifestyle after controlling for demographic factors, insurance status, geographic location, and educational level, according to Mr. Strom. Specifically, eczema was significantly associated with a 12% lower odds of having exercised on at least 3 days of the previous week (odds ratio, 0.88). However, severe atopic dermatitis significantly reduced the odds that a child exercised at least one day a week by 61% (OR, 0.39). Furthermore, severe atopic dermatitis was associated with more than double the odds of having at least 5 hours of daily screen time (OR, 2.62). And having either moderate or severe eczema was tied to a significant decrease in the odds of having participated in sports in the past year, Mr. Strom said.
“Atopic dermatitis and sleep disturbance each contribute to sedentary behavior,” he reported. Nonatopic children who did not sleep enough on most nights had nearly double the odds of heavy television and video game use, compared with children who slept more, a significant difference. When poor sleepers also had atopic dermatitis, their odds of heavy screen use more than tripled. Poor sleepers were also significantly less likely to join sports teams, even when they did not have eczema, Mr. Strom said.
“Children with more severe atopic dermatitis may have more profound exacerbations of activity-related symptoms, which would lead to these findings,” he concluded. Future studies should explore whether better symptom control can help improve sedentary behaviors, he added.
The study was sponsored by the Maternal and Child Health Bureau of the U.S. Department of Health and Human Services. Mr. Strom had no disclosures.
SCOTTSDALE, ARIZ. – Children with severe atopic dermatitis were significantly more likely to log at least 5 hours of screen time a day, and were significantly less likely to exercise than were nonatopic controls, said the lead investigator of a large national study.
“Atopic dermatitis overall was not associated with sedentary behavior. It was severe disease only,” said Mark Strom of the department of dermatology, Northwestern University, Chicago, during an oral presentation at the annual meeting of the Society for Investigative Dermatology. Patients tended to be even more sedentary if they suffered from disturbed sleep in addition to severe eczema, he added.
Heat and sweat worsen the intense itch of atopic dermatitis. Hypothesizing that this would deter affected children from physical activity, Mr. Strom and his associates analyzed data for 131,783 respondents aged 18 and under from the National Survey of Children’s Health. The survey assesses physical activity by asking how many days a week the respondent sweated and breathed hard for at least 20 minutes. Screen time is measured by asking about daily hours spent watching television and playing video games, and sleep quality is assessed by asking how many nights a week the child slept the normal amount for his or her age.
Simply having atopic dermatitis was linked with only a slight increase in the chance of having a sedentary lifestyle after controlling for demographic factors, insurance status, geographic location, and educational level, according to Mr. Strom. Specifically, eczema was significantly associated with a 12% lower odds of having exercised on at least 3 days of the previous week (odds ratio, 0.88). However, severe atopic dermatitis significantly reduced the odds that a child exercised at least one day a week by 61% (OR, 0.39). Furthermore, severe atopic dermatitis was associated with more than double the odds of having at least 5 hours of daily screen time (OR, 2.62). And having either moderate or severe eczema was tied to a significant decrease in the odds of having participated in sports in the past year, Mr. Strom said.
“Atopic dermatitis and sleep disturbance each contribute to sedentary behavior,” he reported. Nonatopic children who did not sleep enough on most nights had nearly double the odds of heavy television and video game use, compared with children who slept more, a significant difference. When poor sleepers also had atopic dermatitis, their odds of heavy screen use more than tripled. Poor sleepers were also significantly less likely to join sports teams, even when they did not have eczema, Mr. Strom said.
“Children with more severe atopic dermatitis may have more profound exacerbations of activity-related symptoms, which would lead to these findings,” he concluded. Future studies should explore whether better symptom control can help improve sedentary behaviors, he added.
The study was sponsored by the Maternal and Child Health Bureau of the U.S. Department of Health and Human Services. Mr. Strom had no disclosures.
AT THE 2016 SID ANNUAL MEETING
Key clinical point: A large national study linked severe atopic dermatitis to sedentary behaviors and screen time.
Major finding: Compared with children without eczema, those with severe disease were about 60% less likely to exercise at least once a week (OR, 0.39).
Data source: An analysis of data for 131,783 children from the National Survey of Children’s Health.
Disclosures: The study was sponsored by the Maternal and Child Health Bureau of the U.S. Department of Health and Human Services. Mr. Strom had no disclosures.
Common surgeries linked to chronic opioid use among opioid-naive patients
Common surgeries increase the risk of chronic opioid use in opioid-naive adults, especially those using antidepressants or benzodiazepines before their operations, and those with substance abuse histories, according to an insurance claims analysis from Stanford (Calif.) University.
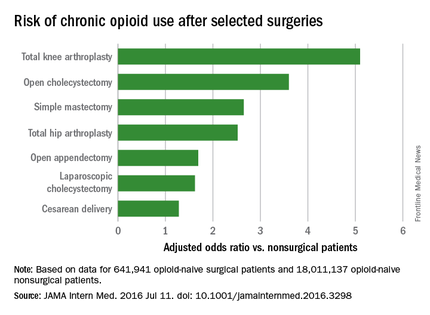
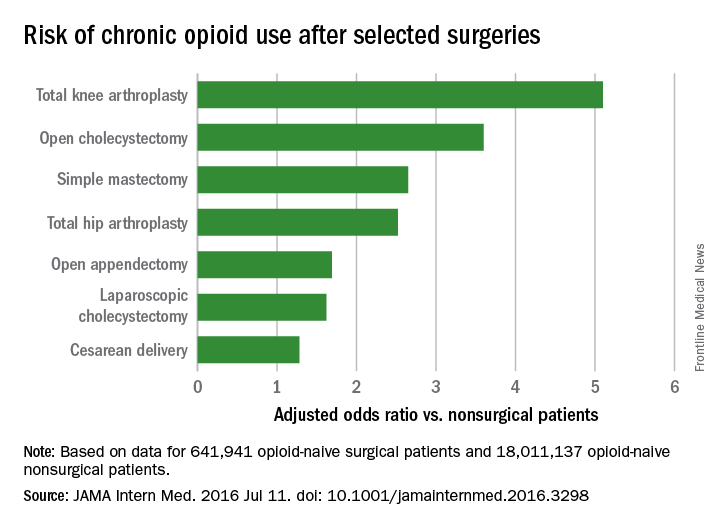
The researchers reviewed opioid prescribing in the first postop year – excluding the first 90 days – for 641,941 patients and compared that information with opioid prescribing for 18,011,137 adult patients who did not have surgery. None of the subjects had filled an opioid prescription in the previous year (JAMA Intern Med. 2016 Jul 11. doi: 10.1001/jamainternmed.2016.3298).
Chronic opioid use, defined as filling at least 120 days of opioid prescriptions within the first year of surgery, ranged up to 1.41% for total knee replacement, versus 0.136% in the nonsurgical controls. After adjustment for potential confounders, knee replacement increased the risk fivefold; open cholecystectomy almost fourfold; total hip replacement and simple mastectomy almost threefold; and laparoscopic cholecystectomy and open appendectomy almost twofold. Cesarean delivery increased the risk of chronic use by 28%.
With the exception of knee and hip replacements, “these procedures are not indicated to relieve pain and are not thought to place patients at risk for long-term pain ... Our results suggest that primary care clinicians and surgeons should monitor opioid use closely in the postsurgical period,” wrote Eric C. Sun, MD, PhD, of the department of anesthesiology, perioperative and pain medicine at Stanford (Calif.) University, and his colleagues.
Preoperative antidepressants and benzodiazepines carried about the same risk of chronic use as alcohol abuse (odds ratio 1.83; P less than .001), while drug abuse history increased the risk even more (OR 3.15; P less than .001). Male sex, age over 50 years, and history of depression were also associated with chronic use on multivariate analysis. Meanwhile, transurethral prostatectomy, laparoscopic appendectomy, functional endoscopic sinus surgery, and cataract surgery did not increase chronic use risk.
“Surgical patients, particularly those at higher risk for chronic opioid use, may benefit from techniques to reduce the risk such as multimodal analgesia and regional anesthesia, particularly in light of literature suggesting that these interventions may improve other perioperative outcomes ... Patients may also benefit from other preoperative and postoperative interventions, such as evidence-based psychobehavioral pain management skills,” the investigators said.
It wasn’t clear until now that even opioid-naive patients are at risk for opioid problems after surgery. Stanford’s investigation is not the first to link surgery and opioid abuse, but previous studies tended to focus on patients with preexisting use and more painful operations.
The study included prescriptions for oral and patch fentanyl, hydrocodone, oral hydromorphone, methadone, morphine, oxymorphone, and oxycodone. Hydrocodone cough remedies and acetaminophen/codeine analgesics were excluded.
Nonsurgical patients tended to be younger than their surgical peers (mean 42 vs. 44 years) and more likely to be male (49% vs. 26%).
The authors had no disclosures. The work was funded in part by the Foundation for Anesthesia Education and Research and the Anesthesia Quality Institute. Claims data came from MarketScan (Truven Health Analytics).
Common surgeries increase the risk of chronic opioid use in opioid-naive adults, especially those using antidepressants or benzodiazepines before their operations, and those with substance abuse histories, according to an insurance claims analysis from Stanford (Calif.) University.
The researchers reviewed opioid prescribing in the first postop year – excluding the first 90 days – for 641,941 patients and compared that information with opioid prescribing for 18,011,137 adult patients who did not have surgery. None of the subjects had filled an opioid prescription in the previous year (JAMA Intern Med. 2016 Jul 11. doi: 10.1001/jamainternmed.2016.3298).
Chronic opioid use, defined as filling at least 120 days of opioid prescriptions within the first year of surgery, ranged up to 1.41% for total knee replacement, versus 0.136% in the nonsurgical controls. After adjustment for potential confounders, knee replacement increased the risk fivefold; open cholecystectomy almost fourfold; total hip replacement and simple mastectomy almost threefold; and laparoscopic cholecystectomy and open appendectomy almost twofold. Cesarean delivery increased the risk of chronic use by 28%.
With the exception of knee and hip replacements, “these procedures are not indicated to relieve pain and are not thought to place patients at risk for long-term pain ... Our results suggest that primary care clinicians and surgeons should monitor opioid use closely in the postsurgical period,” wrote Eric C. Sun, MD, PhD, of the department of anesthesiology, perioperative and pain medicine at Stanford (Calif.) University, and his colleagues.
Preoperative antidepressants and benzodiazepines carried about the same risk of chronic use as alcohol abuse (odds ratio 1.83; P less than .001), while drug abuse history increased the risk even more (OR 3.15; P less than .001). Male sex, age over 50 years, and history of depression were also associated with chronic use on multivariate analysis. Meanwhile, transurethral prostatectomy, laparoscopic appendectomy, functional endoscopic sinus surgery, and cataract surgery did not increase chronic use risk.
“Surgical patients, particularly those at higher risk for chronic opioid use, may benefit from techniques to reduce the risk such as multimodal analgesia and regional anesthesia, particularly in light of literature suggesting that these interventions may improve other perioperative outcomes ... Patients may also benefit from other preoperative and postoperative interventions, such as evidence-based psychobehavioral pain management skills,” the investigators said.
It wasn’t clear until now that even opioid-naive patients are at risk for opioid problems after surgery. Stanford’s investigation is not the first to link surgery and opioid abuse, but previous studies tended to focus on patients with preexisting use and more painful operations.
The study included prescriptions for oral and patch fentanyl, hydrocodone, oral hydromorphone, methadone, morphine, oxymorphone, and oxycodone. Hydrocodone cough remedies and acetaminophen/codeine analgesics were excluded.
Nonsurgical patients tended to be younger than their surgical peers (mean 42 vs. 44 years) and more likely to be male (49% vs. 26%).
The authors had no disclosures. The work was funded in part by the Foundation for Anesthesia Education and Research and the Anesthesia Quality Institute. Claims data came from MarketScan (Truven Health Analytics).
Common surgeries increase the risk of chronic opioid use in opioid-naive adults, especially those using antidepressants or benzodiazepines before their operations, and those with substance abuse histories, according to an insurance claims analysis from Stanford (Calif.) University.
The researchers reviewed opioid prescribing in the first postop year – excluding the first 90 days – for 641,941 patients and compared that information with opioid prescribing for 18,011,137 adult patients who did not have surgery. None of the subjects had filled an opioid prescription in the previous year (JAMA Intern Med. 2016 Jul 11. doi: 10.1001/jamainternmed.2016.3298).
Chronic opioid use, defined as filling at least 120 days of opioid prescriptions within the first year of surgery, ranged up to 1.41% for total knee replacement, versus 0.136% in the nonsurgical controls. After adjustment for potential confounders, knee replacement increased the risk fivefold; open cholecystectomy almost fourfold; total hip replacement and simple mastectomy almost threefold; and laparoscopic cholecystectomy and open appendectomy almost twofold. Cesarean delivery increased the risk of chronic use by 28%.
With the exception of knee and hip replacements, “these procedures are not indicated to relieve pain and are not thought to place patients at risk for long-term pain ... Our results suggest that primary care clinicians and surgeons should monitor opioid use closely in the postsurgical period,” wrote Eric C. Sun, MD, PhD, of the department of anesthesiology, perioperative and pain medicine at Stanford (Calif.) University, and his colleagues.
Preoperative antidepressants and benzodiazepines carried about the same risk of chronic use as alcohol abuse (odds ratio 1.83; P less than .001), while drug abuse history increased the risk even more (OR 3.15; P less than .001). Male sex, age over 50 years, and history of depression were also associated with chronic use on multivariate analysis. Meanwhile, transurethral prostatectomy, laparoscopic appendectomy, functional endoscopic sinus surgery, and cataract surgery did not increase chronic use risk.
“Surgical patients, particularly those at higher risk for chronic opioid use, may benefit from techniques to reduce the risk such as multimodal analgesia and regional anesthesia, particularly in light of literature suggesting that these interventions may improve other perioperative outcomes ... Patients may also benefit from other preoperative and postoperative interventions, such as evidence-based psychobehavioral pain management skills,” the investigators said.
It wasn’t clear until now that even opioid-naive patients are at risk for opioid problems after surgery. Stanford’s investigation is not the first to link surgery and opioid abuse, but previous studies tended to focus on patients with preexisting use and more painful operations.
The study included prescriptions for oral and patch fentanyl, hydrocodone, oral hydromorphone, methadone, morphine, oxymorphone, and oxycodone. Hydrocodone cough remedies and acetaminophen/codeine analgesics were excluded.
Nonsurgical patients tended to be younger than their surgical peers (mean 42 vs. 44 years) and more likely to be male (49% vs. 26%).
The authors had no disclosures. The work was funded in part by the Foundation for Anesthesia Education and Research and the Anesthesia Quality Institute. Claims data came from MarketScan (Truven Health Analytics).
FROM JAMA INTERNAL MEDICINE
Key clinical point: Common surgeries increase the risk of chronic opioid use in opioid-naive adults, especially among those using antidepressants or benzodiazepines before their operations, and those with substance abuse histories.
Major finding: After adjustment for potential confounders, knee replacement increased the risk fivefold; open cholecystectomy almost fourfold; and total hip replacement and simple mastectomy almost threefold.
Data source: Insurance claims of more than 18 million people.
Disclosures: The authors had no disclosures. The work was funded in part by the Foundation for Anesthesia Education and Research and the Anesthesia Quality Institute. Claims data came from MarketScan (Truven Health Analytics).
4 cases involving intraoperative injuries to adjacent organs

During surgery, the ObGyn discovered that pelvic adhesions had distorted the patient’s anatomy; he converted to laparotomy, which left a larger scar. Two days after surgery, the patient was found to have a bowel injury and underwent additional surgery that included placement of surgical mesh, leaving an enlarged scar.
PATIENT'S CLAIM: The ObGyn was negligent in injuring the patient’s bowel during hysterectomy and not detecting the injury intraoperatively. Her scars were larger because of the additional repair operation.
PHYSICIAN'S DEFENSE: Bowel injury is a known complication of the procedure. Many bowel injuries are not detected intraoperatively. The ObGyn made every effort to prevent and check for injury during the procedure.
VERDICT: An Illinois defense verdict was returned.
Uterus and bowel injured during D&C: $1.5M verdict
A 56-year-old woman underwent hysteroscopy and dilation and curettage (D&C). During the procedure, the gynecologist recognized that he had perforated the uterus and injured the bowel and called in a general surgeon to resect 5 cm of the bowel and repair the uterus.
PATIENT'S CLAIM:The patient has a large abdominal scar and a chronically distended abdomen. She experienced a year of daily pain and suffering. The D&C was unnecessary and improperly performed: the standard of care is for the gynecologist to operate in a gentle manner; that did not occur.
PHYSICIAN'S DEFENSE:The D&C was medically necessary. The gynecologist exercised the proper standard of care.
VERDICT:A $1.5 million New Jersey verdict was returned. The jury found the D&C necessary, but determined that the gynecologist deviated from the accepted standard of care in his performance of the procedure.
Bowel perforation during myomectomy: $200,000 verdictA 44-year-old woman underwent hysteroscopic myomectomy. During the procedure the ObGyn realized that he had perforated the uterus. He switched to a laparoscopic procedure, found a 3-cm uterine tear, and converted to laparotomy to repair the injury. The postsurgical pathology report revealed multiple colon fragments.
Three days after surgery, the patient became ill and was found to have a bowel injury. She underwent bowel resection with colostomy and, a year later, colostomy reversal. She sustained abdominal scarring.
PATIENT'S CLAIM: The ObGyn was negligent in performing the myomectomy. He should have identified the bowel injury intraoperatively. When the pathology report indicated multiple colon fragments, he should have investigated rather than wait for the patient to develop symptoms.
PHYSICIAN'S DEFENSE: Uterine and colon injuries are known complications of the procedure and can occur within the standard of care. The ObGyn intraoperatively inspected the organs adjacent to the uterus but there was no evident injury. The patient’s postsurgical treatment was proper.
VERDICT: A $200,000 Illinois verdict was returned.
Injured ureter allegedly not treatedA 42-year-old woman underwent hysterectomy on December 6. Postoperatively, she reported increasing dysuria with pain and fever. On December 13, a computed tomography (CT) scan suggested a partial ureter obstruction. Despite test results, the gynecologist elected to continue to monitor the patient. The patient’s symptoms continued to worsen and, on December 27, she underwent a second CT scan that identified an obstructed ureter. The gynecologist referred the patient to a urologist, who determined that the patient had sustained a significant ureter injury that required placement of a nephrostomy tube.
PATIENT'S CLAIM: The gynecologist failed to identify the injury during surgery. The gynecologist was negligent in not consulting a urologist after results of the first CT scan.
PHYSICIAN'S DEFENSE: Uterine injury is a known complication of the procedure. The gynecologist inspected adjacent organs during surgery but did not find an injury. Postoperative treatment was appropriate.
VERDICT: The case was presented before a medical review board that concluded that there was no error after the first injury, there was no duty to trace the ureter, and a urology consult was not required after the first CT scan. A Louisiana defense verdict was returned.
During surgery, the ObGyn discovered that pelvic adhesions had distorted the patient’s anatomy; he converted to laparotomy, which left a larger scar. Two days after surgery, the patient was found to have a bowel injury and underwent additional surgery that included placement of surgical mesh, leaving an enlarged scar.
PATIENT'S CLAIM: The ObGyn was negligent in injuring the patient’s bowel during hysterectomy and not detecting the injury intraoperatively. Her scars were larger because of the additional repair operation.
PHYSICIAN'S DEFENSE: Bowel injury is a known complication of the procedure. Many bowel injuries are not detected intraoperatively. The ObGyn made every effort to prevent and check for injury during the procedure.
VERDICT: An Illinois defense verdict was returned.
Uterus and bowel injured during D&C: $1.5M verdict
A 56-year-old woman underwent hysteroscopy and dilation and curettage (D&C). During the procedure, the gynecologist recognized that he had perforated the uterus and injured the bowel and called in a general surgeon to resect 5 cm of the bowel and repair the uterus.
PATIENT'S CLAIM:The patient has a large abdominal scar and a chronically distended abdomen. She experienced a year of daily pain and suffering. The D&C was unnecessary and improperly performed: the standard of care is for the gynecologist to operate in a gentle manner; that did not occur.
PHYSICIAN'S DEFENSE:The D&C was medically necessary. The gynecologist exercised the proper standard of care.
VERDICT:A $1.5 million New Jersey verdict was returned. The jury found the D&C necessary, but determined that the gynecologist deviated from the accepted standard of care in his performance of the procedure.
Bowel perforation during myomectomy: $200,000 verdictA 44-year-old woman underwent hysteroscopic myomectomy. During the procedure the ObGyn realized that he had perforated the uterus. He switched to a laparoscopic procedure, found a 3-cm uterine tear, and converted to laparotomy to repair the injury. The postsurgical pathology report revealed multiple colon fragments.
Three days after surgery, the patient became ill and was found to have a bowel injury. She underwent bowel resection with colostomy and, a year later, colostomy reversal. She sustained abdominal scarring.
PATIENT'S CLAIM: The ObGyn was negligent in performing the myomectomy. He should have identified the bowel injury intraoperatively. When the pathology report indicated multiple colon fragments, he should have investigated rather than wait for the patient to develop symptoms.
PHYSICIAN'S DEFENSE: Uterine and colon injuries are known complications of the procedure and can occur within the standard of care. The ObGyn intraoperatively inspected the organs adjacent to the uterus but there was no evident injury. The patient’s postsurgical treatment was proper.
VERDICT: A $200,000 Illinois verdict was returned.
Injured ureter allegedly not treatedA 42-year-old woman underwent hysterectomy on December 6. Postoperatively, she reported increasing dysuria with pain and fever. On December 13, a computed tomography (CT) scan suggested a partial ureter obstruction. Despite test results, the gynecologist elected to continue to monitor the patient. The patient’s symptoms continued to worsen and, on December 27, she underwent a second CT scan that identified an obstructed ureter. The gynecologist referred the patient to a urologist, who determined that the patient had sustained a significant ureter injury that required placement of a nephrostomy tube.
PATIENT'S CLAIM: The gynecologist failed to identify the injury during surgery. The gynecologist was negligent in not consulting a urologist after results of the first CT scan.
PHYSICIAN'S DEFENSE: Uterine injury is a known complication of the procedure. The gynecologist inspected adjacent organs during surgery but did not find an injury. Postoperative treatment was appropriate.
VERDICT: The case was presented before a medical review board that concluded that there was no error after the first injury, there was no duty to trace the ureter, and a urology consult was not required after the first CT scan. A Louisiana defense verdict was returned.
During surgery, the ObGyn discovered that pelvic adhesions had distorted the patient’s anatomy; he converted to laparotomy, which left a larger scar. Two days after surgery, the patient was found to have a bowel injury and underwent additional surgery that included placement of surgical mesh, leaving an enlarged scar.
PATIENT'S CLAIM: The ObGyn was negligent in injuring the patient’s bowel during hysterectomy and not detecting the injury intraoperatively. Her scars were larger because of the additional repair operation.
PHYSICIAN'S DEFENSE: Bowel injury is a known complication of the procedure. Many bowel injuries are not detected intraoperatively. The ObGyn made every effort to prevent and check for injury during the procedure.
VERDICT: An Illinois defense verdict was returned.
Uterus and bowel injured during D&C: $1.5M verdict
A 56-year-old woman underwent hysteroscopy and dilation and curettage (D&C). During the procedure, the gynecologist recognized that he had perforated the uterus and injured the bowel and called in a general surgeon to resect 5 cm of the bowel and repair the uterus.
PATIENT'S CLAIM:The patient has a large abdominal scar and a chronically distended abdomen. She experienced a year of daily pain and suffering. The D&C was unnecessary and improperly performed: the standard of care is for the gynecologist to operate in a gentle manner; that did not occur.
PHYSICIAN'S DEFENSE:The D&C was medically necessary. The gynecologist exercised the proper standard of care.
VERDICT:A $1.5 million New Jersey verdict was returned. The jury found the D&C necessary, but determined that the gynecologist deviated from the accepted standard of care in his performance of the procedure.
Bowel perforation during myomectomy: $200,000 verdictA 44-year-old woman underwent hysteroscopic myomectomy. During the procedure the ObGyn realized that he had perforated the uterus. He switched to a laparoscopic procedure, found a 3-cm uterine tear, and converted to laparotomy to repair the injury. The postsurgical pathology report revealed multiple colon fragments.
Three days after surgery, the patient became ill and was found to have a bowel injury. She underwent bowel resection with colostomy and, a year later, colostomy reversal. She sustained abdominal scarring.
PATIENT'S CLAIM: The ObGyn was negligent in performing the myomectomy. He should have identified the bowel injury intraoperatively. When the pathology report indicated multiple colon fragments, he should have investigated rather than wait for the patient to develop symptoms.
PHYSICIAN'S DEFENSE: Uterine and colon injuries are known complications of the procedure and can occur within the standard of care. The ObGyn intraoperatively inspected the organs adjacent to the uterus but there was no evident injury. The patient’s postsurgical treatment was proper.
VERDICT: A $200,000 Illinois verdict was returned.
Injured ureter allegedly not treatedA 42-year-old woman underwent hysterectomy on December 6. Postoperatively, she reported increasing dysuria with pain and fever. On December 13, a computed tomography (CT) scan suggested a partial ureter obstruction. Despite test results, the gynecologist elected to continue to monitor the patient. The patient’s symptoms continued to worsen and, on December 27, she underwent a second CT scan that identified an obstructed ureter. The gynecologist referred the patient to a urologist, who determined that the patient had sustained a significant ureter injury that required placement of a nephrostomy tube.
PATIENT'S CLAIM: The gynecologist failed to identify the injury during surgery. The gynecologist was negligent in not consulting a urologist after results of the first CT scan.
PHYSICIAN'S DEFENSE: Uterine injury is a known complication of the procedure. The gynecologist inspected adjacent organs during surgery but did not find an injury. Postoperative treatment was appropriate.
VERDICT: The case was presented before a medical review board that concluded that there was no error after the first injury, there was no duty to trace the ureter, and a urology consult was not required after the first CT scan. A Louisiana defense verdict was returned.

Was FHR properly monitored?

PARENT'S CLAIM: The pregnancy was at high risk because of the mother’s hypertension. The ObGyns misread the FHR at triage and discontinued FHR monitoring too early. If continuous FHR monitoring had occurred, fetal distress would have been detected earlier, resulting in a better outcome for the baby.
PHYSICIAN'S DEFENSE: There were no signs of fetal distress when the FHR monitoring was discontinued. Placental abruption is an acute event that cannot be predicted.
VERDICT: A Missouri defense verdict was returned.
Should the ObGyn have come to the hospital earlier?At 39 weeks’ gestation, a mother presented to the hospital for induction of labor. A FHR monitor was immediately placed. That evening, the ObGyn, who was not at the hospital, was notified that the mother had an elevated temperature and that the fetus was experiencing tachycardia. The ObGyn prescribed antibiotics, and the fever subsided. After an hour, the patient was fully dilated and started to push under the nurse’s supervision. Twenty minutes later, the ObGyn was notified that the fetus was experiencing variable decelerations. The ObGyn arrived in 30 minutes and ordered cesarean delivery. The baby was born 24 minutes later.
Ten hours after birth, the baby began to have seizures. He was transferred to another hospital and remained in the neonatal intensive care unit for 15 days. The child received a diagnosis of cerebral palsy.
PARENT'S CLAIM: The ObGyn was negligent in not coming to the hospital when the mother was feverish and the baby tachycardic. The baby experienced an acute hypoxic ischemic injury; an earlier cesarean delivery would have avoided brain injury.
PHYSICIAN'S DEFENSE: There was no breach in the standard of care. The infant did not meet all the criteria for an acute hypoxic ischemic injury. Based on a computed tomography scan taken after seizures began, the infant’s brain injury most likely occurred hours before birth.
VERDICT: A Virginia defense verdict was returned.
These cases were selected by the editors of OBG Management from "Medical Malpractice Verdicts, Settlements, & Experts," with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
PARENT'S CLAIM: The pregnancy was at high risk because of the mother’s hypertension. The ObGyns misread the FHR at triage and discontinued FHR monitoring too early. If continuous FHR monitoring had occurred, fetal distress would have been detected earlier, resulting in a better outcome for the baby.
PHYSICIAN'S DEFENSE: There were no signs of fetal distress when the FHR monitoring was discontinued. Placental abruption is an acute event that cannot be predicted.
VERDICT: A Missouri defense verdict was returned.
Should the ObGyn have come to the hospital earlier?At 39 weeks’ gestation, a mother presented to the hospital for induction of labor. A FHR monitor was immediately placed. That evening, the ObGyn, who was not at the hospital, was notified that the mother had an elevated temperature and that the fetus was experiencing tachycardia. The ObGyn prescribed antibiotics, and the fever subsided. After an hour, the patient was fully dilated and started to push under the nurse’s supervision. Twenty minutes later, the ObGyn was notified that the fetus was experiencing variable decelerations. The ObGyn arrived in 30 minutes and ordered cesarean delivery. The baby was born 24 minutes later.
Ten hours after birth, the baby began to have seizures. He was transferred to another hospital and remained in the neonatal intensive care unit for 15 days. The child received a diagnosis of cerebral palsy.
PARENT'S CLAIM: The ObGyn was negligent in not coming to the hospital when the mother was feverish and the baby tachycardic. The baby experienced an acute hypoxic ischemic injury; an earlier cesarean delivery would have avoided brain injury.
PHYSICIAN'S DEFENSE: There was no breach in the standard of care. The infant did not meet all the criteria for an acute hypoxic ischemic injury. Based on a computed tomography scan taken after seizures began, the infant’s brain injury most likely occurred hours before birth.
VERDICT: A Virginia defense verdict was returned.
These cases were selected by the editors of OBG Management from "Medical Malpractice Verdicts, Settlements, & Experts," with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
PARENT'S CLAIM: The pregnancy was at high risk because of the mother’s hypertension. The ObGyns misread the FHR at triage and discontinued FHR monitoring too early. If continuous FHR monitoring had occurred, fetal distress would have been detected earlier, resulting in a better outcome for the baby.
PHYSICIAN'S DEFENSE: There were no signs of fetal distress when the FHR monitoring was discontinued. Placental abruption is an acute event that cannot be predicted.
VERDICT: A Missouri defense verdict was returned.
Should the ObGyn have come to the hospital earlier?At 39 weeks’ gestation, a mother presented to the hospital for induction of labor. A FHR monitor was immediately placed. That evening, the ObGyn, who was not at the hospital, was notified that the mother had an elevated temperature and that the fetus was experiencing tachycardia. The ObGyn prescribed antibiotics, and the fever subsided. After an hour, the patient was fully dilated and started to push under the nurse’s supervision. Twenty minutes later, the ObGyn was notified that the fetus was experiencing variable decelerations. The ObGyn arrived in 30 minutes and ordered cesarean delivery. The baby was born 24 minutes later.
Ten hours after birth, the baby began to have seizures. He was transferred to another hospital and remained in the neonatal intensive care unit for 15 days. The child received a diagnosis of cerebral palsy.
PARENT'S CLAIM: The ObGyn was negligent in not coming to the hospital when the mother was feverish and the baby tachycardic. The baby experienced an acute hypoxic ischemic injury; an earlier cesarean delivery would have avoided brain injury.
PHYSICIAN'S DEFENSE: There was no breach in the standard of care. The infant did not meet all the criteria for an acute hypoxic ischemic injury. Based on a computed tomography scan taken after seizures began, the infant’s brain injury most likely occurred hours before birth.
VERDICT: A Virginia defense verdict was returned.
These cases were selected by the editors of OBG Management from "Medical Malpractice Verdicts, Settlements, & Experts," with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
