User login
Oral bacterium linked to poor esophageal cancer survival
Fusobacterium nucleatum, a component of the human microbiome, appears to be associated with shorter survival in esophageal cancer, according to new findings.
F. nucleatum, generally found in the oral cavity and associated with periodontal disease, may have a potential role as a prognostic biomarker, and it might also contribute to aggressive tumor behavior via activation of chemokines, the study authors suggest (Clin Cancer Res. 2016 Oct. doi: 10.1158/1078-0432.CCR-16-1786).
They add that this is “the first study to provide the evidence for the relationship between F. nucleatum and poor prognosis in esophageal cancer.”
An assessment of F. nucleatum DNA in esophageal cancer tissues by qPCR assay showed that levels were higher in malignant tissue than in paired adjacent nontumor tissues (P = .021). The relative F. nucleatum DNA levels were also measured in samples from 325 esophageal cancer cases.
Within those samples, F. nucleatum was detected in 74 (23%) of 325 cases. F. nucleatum positivity was not associated with most clinicopathologic features including patient sex, year of surgery, preoperative performance status, smoking history, alcohol history, comorbidity, tumor location, histology, tumor size, or preoperative therapy (all P greater than .05). However, it was associated with tumor stage (P = .016), T stage (P less than .01), and N stage (P = .039).
There were a total of 112 deaths among the 325 esophageal cancer patients, with 75 specific to the disease. The median follow-up time for censored patients was 2.6 years.
Patients positive for F. nucleatum had significantly shorter cancer-specific survival (logrank P = .0039) and overall survival (logrank P = .046) as compared with those who were F. nucleatum negative. In an analysis of F. nucleatum DNA status by Cox regression analysis, patients who were positive had significantly higher cancer-specific mortality as compared with those who were negative (hazard ratio, 2.01; P = .0068). After the analysis was adjusted for clinical, pathologic, and epidemiologic features, F. nucleatum positivity was associated with significantly higher cancer-specific mortality (multivariate HR, 1.78; P = .032), and similar findings were observed for overall mortality.
Dr. Yamamura and his team had also hypothesized that F. nucleatum might contribute to aggressive tumor behavior by activation of chemokines, and they were able to confirm that the presence or absence of F. nucleatum was significantly associated with CCL20 expression status, which was identified as the most upregulated chemokine.
*This article was updated 10/26/2016.
Fusobacterium nucleatum, a component of the human microbiome, appears to be associated with shorter survival in esophageal cancer, according to new findings.
F. nucleatum, generally found in the oral cavity and associated with periodontal disease, may have a potential role as a prognostic biomarker, and it might also contribute to aggressive tumor behavior via activation of chemokines, the study authors suggest (Clin Cancer Res. 2016 Oct. doi: 10.1158/1078-0432.CCR-16-1786).
They add that this is “the first study to provide the evidence for the relationship between F. nucleatum and poor prognosis in esophageal cancer.”
An assessment of F. nucleatum DNA in esophageal cancer tissues by qPCR assay showed that levels were higher in malignant tissue than in paired adjacent nontumor tissues (P = .021). The relative F. nucleatum DNA levels were also measured in samples from 325 esophageal cancer cases.
Within those samples, F. nucleatum was detected in 74 (23%) of 325 cases. F. nucleatum positivity was not associated with most clinicopathologic features including patient sex, year of surgery, preoperative performance status, smoking history, alcohol history, comorbidity, tumor location, histology, tumor size, or preoperative therapy (all P greater than .05). However, it was associated with tumor stage (P = .016), T stage (P less than .01), and N stage (P = .039).
There were a total of 112 deaths among the 325 esophageal cancer patients, with 75 specific to the disease. The median follow-up time for censored patients was 2.6 years.
Patients positive for F. nucleatum had significantly shorter cancer-specific survival (logrank P = .0039) and overall survival (logrank P = .046) as compared with those who were F. nucleatum negative. In an analysis of F. nucleatum DNA status by Cox regression analysis, patients who were positive had significantly higher cancer-specific mortality as compared with those who were negative (hazard ratio, 2.01; P = .0068). After the analysis was adjusted for clinical, pathologic, and epidemiologic features, F. nucleatum positivity was associated with significantly higher cancer-specific mortality (multivariate HR, 1.78; P = .032), and similar findings were observed for overall mortality.
Dr. Yamamura and his team had also hypothesized that F. nucleatum might contribute to aggressive tumor behavior by activation of chemokines, and they were able to confirm that the presence or absence of F. nucleatum was significantly associated with CCL20 expression status, which was identified as the most upregulated chemokine.
*This article was updated 10/26/2016.
Fusobacterium nucleatum, a component of the human microbiome, appears to be associated with shorter survival in esophageal cancer, according to new findings.
F. nucleatum, generally found in the oral cavity and associated with periodontal disease, may have a potential role as a prognostic biomarker, and it might also contribute to aggressive tumor behavior via activation of chemokines, the study authors suggest (Clin Cancer Res. 2016 Oct. doi: 10.1158/1078-0432.CCR-16-1786).
They add that this is “the first study to provide the evidence for the relationship between F. nucleatum and poor prognosis in esophageal cancer.”
An assessment of F. nucleatum DNA in esophageal cancer tissues by qPCR assay showed that levels were higher in malignant tissue than in paired adjacent nontumor tissues (P = .021). The relative F. nucleatum DNA levels were also measured in samples from 325 esophageal cancer cases.
Within those samples, F. nucleatum was detected in 74 (23%) of 325 cases. F. nucleatum positivity was not associated with most clinicopathologic features including patient sex, year of surgery, preoperative performance status, smoking history, alcohol history, comorbidity, tumor location, histology, tumor size, or preoperative therapy (all P greater than .05). However, it was associated with tumor stage (P = .016), T stage (P less than .01), and N stage (P = .039).
There were a total of 112 deaths among the 325 esophageal cancer patients, with 75 specific to the disease. The median follow-up time for censored patients was 2.6 years.
Patients positive for F. nucleatum had significantly shorter cancer-specific survival (logrank P = .0039) and overall survival (logrank P = .046) as compared with those who were F. nucleatum negative. In an analysis of F. nucleatum DNA status by Cox regression analysis, patients who were positive had significantly higher cancer-specific mortality as compared with those who were negative (hazard ratio, 2.01; P = .0068). After the analysis was adjusted for clinical, pathologic, and epidemiologic features, F. nucleatum positivity was associated with significantly higher cancer-specific mortality (multivariate HR, 1.78; P = .032), and similar findings were observed for overall mortality.
Dr. Yamamura and his team had also hypothesized that F. nucleatum might contribute to aggressive tumor behavior by activation of chemokines, and they were able to confirm that the presence or absence of F. nucleatum was significantly associated with CCL20 expression status, which was identified as the most upregulated chemokine.
*This article was updated 10/26/2016.
FROM CLINICAL CANCER RESEARCH
Key clinical point: F. nucleatum present in esophageal cancer tissue is associated with poorer prognosis.
Major finding: Patients positive for F. nucleatum had significantly shorter cancer-specific survival (logrank P = .0039) and OS (logrank P = .046).
Data source: Tissue samples from 325 patients with esophageal cancer.
Disclosures: This study was supported in part by the SGH Foundation. The authors have no disclosures.
How to Increase Patient Adherence to Therapy
How do we increase patient adherence to therapy? This question fascinates me. As dermatologists, we will see thousands of patients over the course of our careers, most with treatable conditions that will improve with therapy and others with chronic or genetic conditions that will at least be made more tolerable with therapy. Only 50% of patients with a chronic condition are adherent to therapy.1 Why some patients adhere to treatment and others do not can be difficult to understand. The emotional makeup, culture, family background, socioeconomic status, and motivation of each person is unique, which leads to complexity. This column is not meant to answer a question that is both complex and broad; rather, it is meant to survey and summarize the literature on this topic.
Education
Health literacy is defined as cognitive and social skills that determine the motivation and ability of individuals to gain access to, understand, and use information in ways that promote and maintain good health.2 Greater health literacy leads to improved compliance and health outcomes.3,4 When we take the time to educate patients about their condition, it improves health literacy, treatment compliance, and patient safety and satisfaction, factors that ultimately are linked to better health outcomes.3-8
There are many practical ways of educating patients. Interestingly, one meta-analysis found that no single strategy is more effective than another.6 This analysis found that "[c]omprehensive interventions combining cognitive, behavioral, and affective components were more effective than single-focus interventions."6 The Centers for Disease Control and Prevention (CDC) website is an excellent source of information on how to educate patients and increase patient treatment compliance.2 The CDC website offers a free tool kit on how to design educational information to your target audience, resources for children, a database of health-related educational images, an electronic textbook on teaching patients with low literacy skills, a summary of evidence-based ideas on how to improve patient adherence to medications used long-term, and more.2
Facilitating Adherence
The World Health Organization (WHO) emphasizes 5 dimensions of patient adherence: health system, socioeconomic, condition-related, therapy-related, and patient-related factors.9 Becker and Maiman5 summarized it eloquently when they wrote that we must take "clinically appropriate steps to reduce the cost, complexity, duration, and amount of behavioral change required by the regimen and increasing the regimen's convenience through 'tailoring' and other approaches." It is a broad ultimatum that will require creativity and persistence on the part of the dermatology community.
Some common patient-related factors associated with nonadherence to treatment are lack of information and skills as they pertain to self-management, difficulty with motivation and self-efficacy, and lack of support for behavioral changes.9 It is interesting that low socioeconomic status has not been consistently shown to portend low treatment adherence. It has been shown that children, especially adolescents, and elderly patients tend to be the least adherent.9-11
Dermatologists Take Action
As dermatologists, the WHO encourages us (physicians) to promote optimism, provide enthusiasm, and encourage maintenance of healthy behaviors.9 Comprehensive interventions that have had a positive impact on patient adherence to therapy for diseases such as diabetes mellitus, asthma, and hypertension may serve as motivating examples.9 Some specific dermatologic conditions that will benefit from increased patient adherence include acne, vesiculobullous disease, psoriasis, and atopic dermatitis. We can lend support to efforts to reduce the cost of dermatologic medications and be aware of the populations most at risk for low adherence to treatment.9-12
Final Thoughts
As we work to increase patient adherence to therapy in dermatology, we will help improve health literacy, patient safety, and patient satisfaction. These factors are ultimately linked to better health outcomes. The CDC and WHO websites are excellent sources of information on practical methods for doing so.2,9
- Haynes RB, McDonald H, Garg AX, et al. Interventions for helping patients to follow prescriptions for medications. Cochrane Database Syst Rev. 2002:CD000011.
- Centers for Disease Control and Prevention. Health literacy. http://www.cdc.gov/healthliteracy/index.html. Updated January 13, 2016. Accessed September 23, 2016.
- Berkman ND, Sheridan SL, Donahue KE, et al. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155:97-107.
- Pignone MP, DeWalt DA. Literacy and health outcomes: is adherence the missing link? J Gen Intern Med. 2006;21:896-897.
- Becker MH, Maiman LA. Strategies for enhancing patient compliance. J Community Health. 1980;6:113-135.
- Roter DL, Hall JA, Merisca R, et al. Effectiveness of interventions to improve patient compliance: a meta-analysis. Med Care. 1998;36:1138-1161.
- Renzi C, Abeni D, Picardi A, et al. Factors associated with patient satisfaction with care among dermatological outpatients. Br J Dermatol. 2001;145:617-623.
- Stewart MA. Effective physician-patient communication and health outcomes: a review. CMAJ. 1995;152:1423-1433.
- World Health Organization. Adherence to long-term therapies: evidence for action. http://www.who.int/chp/knowledge/publications/adherence_full_report.pdf. Posted 2003. Accessed September 23, 2016.
- Lee IA, Maibach HI. Pharmionics in dermatology: a review of topical medication adherence. Am J Clin Dermatol. 2006;7:231-236.
- Burkhart P, Dunbar-Jacob J. Adherence research in the pediatric and adolescent populations: a decade in review. In: Hayman L, Mahon M, Turner R, eds. Chronic Illness in Children: An Evidence-Based Approach. New York, NY: Springer Publishing Company; 2002:199-229.
- Rosenberg ME, Rosenberg SP. Changes in retail prices of prescription dermatologic drugs from 2009 to 2015. JAMA Dermatol. 2016;152:158-163.
How do we increase patient adherence to therapy? This question fascinates me. As dermatologists, we will see thousands of patients over the course of our careers, most with treatable conditions that will improve with therapy and others with chronic or genetic conditions that will at least be made more tolerable with therapy. Only 50% of patients with a chronic condition are adherent to therapy.1 Why some patients adhere to treatment and others do not can be difficult to understand. The emotional makeup, culture, family background, socioeconomic status, and motivation of each person is unique, which leads to complexity. This column is not meant to answer a question that is both complex and broad; rather, it is meant to survey and summarize the literature on this topic.
Education
Health literacy is defined as cognitive and social skills that determine the motivation and ability of individuals to gain access to, understand, and use information in ways that promote and maintain good health.2 Greater health literacy leads to improved compliance and health outcomes.3,4 When we take the time to educate patients about their condition, it improves health literacy, treatment compliance, and patient safety and satisfaction, factors that ultimately are linked to better health outcomes.3-8
There are many practical ways of educating patients. Interestingly, one meta-analysis found that no single strategy is more effective than another.6 This analysis found that "[c]omprehensive interventions combining cognitive, behavioral, and affective components were more effective than single-focus interventions."6 The Centers for Disease Control and Prevention (CDC) website is an excellent source of information on how to educate patients and increase patient treatment compliance.2 The CDC website offers a free tool kit on how to design educational information to your target audience, resources for children, a database of health-related educational images, an electronic textbook on teaching patients with low literacy skills, a summary of evidence-based ideas on how to improve patient adherence to medications used long-term, and more.2
Facilitating Adherence
The World Health Organization (WHO) emphasizes 5 dimensions of patient adherence: health system, socioeconomic, condition-related, therapy-related, and patient-related factors.9 Becker and Maiman5 summarized it eloquently when they wrote that we must take "clinically appropriate steps to reduce the cost, complexity, duration, and amount of behavioral change required by the regimen and increasing the regimen's convenience through 'tailoring' and other approaches." It is a broad ultimatum that will require creativity and persistence on the part of the dermatology community.
Some common patient-related factors associated with nonadherence to treatment are lack of information and skills as they pertain to self-management, difficulty with motivation and self-efficacy, and lack of support for behavioral changes.9 It is interesting that low socioeconomic status has not been consistently shown to portend low treatment adherence. It has been shown that children, especially adolescents, and elderly patients tend to be the least adherent.9-11
Dermatologists Take Action
As dermatologists, the WHO encourages us (physicians) to promote optimism, provide enthusiasm, and encourage maintenance of healthy behaviors.9 Comprehensive interventions that have had a positive impact on patient adherence to therapy for diseases such as diabetes mellitus, asthma, and hypertension may serve as motivating examples.9 Some specific dermatologic conditions that will benefit from increased patient adherence include acne, vesiculobullous disease, psoriasis, and atopic dermatitis. We can lend support to efforts to reduce the cost of dermatologic medications and be aware of the populations most at risk for low adherence to treatment.9-12
Final Thoughts
As we work to increase patient adherence to therapy in dermatology, we will help improve health literacy, patient safety, and patient satisfaction. These factors are ultimately linked to better health outcomes. The CDC and WHO websites are excellent sources of information on practical methods for doing so.2,9
How do we increase patient adherence to therapy? This question fascinates me. As dermatologists, we will see thousands of patients over the course of our careers, most with treatable conditions that will improve with therapy and others with chronic or genetic conditions that will at least be made more tolerable with therapy. Only 50% of patients with a chronic condition are adherent to therapy.1 Why some patients adhere to treatment and others do not can be difficult to understand. The emotional makeup, culture, family background, socioeconomic status, and motivation of each person is unique, which leads to complexity. This column is not meant to answer a question that is both complex and broad; rather, it is meant to survey and summarize the literature on this topic.
Education
Health literacy is defined as cognitive and social skills that determine the motivation and ability of individuals to gain access to, understand, and use information in ways that promote and maintain good health.2 Greater health literacy leads to improved compliance and health outcomes.3,4 When we take the time to educate patients about their condition, it improves health literacy, treatment compliance, and patient safety and satisfaction, factors that ultimately are linked to better health outcomes.3-8
There are many practical ways of educating patients. Interestingly, one meta-analysis found that no single strategy is more effective than another.6 This analysis found that "[c]omprehensive interventions combining cognitive, behavioral, and affective components were more effective than single-focus interventions."6 The Centers for Disease Control and Prevention (CDC) website is an excellent source of information on how to educate patients and increase patient treatment compliance.2 The CDC website offers a free tool kit on how to design educational information to your target audience, resources for children, a database of health-related educational images, an electronic textbook on teaching patients with low literacy skills, a summary of evidence-based ideas on how to improve patient adherence to medications used long-term, and more.2
Facilitating Adherence
The World Health Organization (WHO) emphasizes 5 dimensions of patient adherence: health system, socioeconomic, condition-related, therapy-related, and patient-related factors.9 Becker and Maiman5 summarized it eloquently when they wrote that we must take "clinically appropriate steps to reduce the cost, complexity, duration, and amount of behavioral change required by the regimen and increasing the regimen's convenience through 'tailoring' and other approaches." It is a broad ultimatum that will require creativity and persistence on the part of the dermatology community.
Some common patient-related factors associated with nonadherence to treatment are lack of information and skills as they pertain to self-management, difficulty with motivation and self-efficacy, and lack of support for behavioral changes.9 It is interesting that low socioeconomic status has not been consistently shown to portend low treatment adherence. It has been shown that children, especially adolescents, and elderly patients tend to be the least adherent.9-11
Dermatologists Take Action
As dermatologists, the WHO encourages us (physicians) to promote optimism, provide enthusiasm, and encourage maintenance of healthy behaviors.9 Comprehensive interventions that have had a positive impact on patient adherence to therapy for diseases such as diabetes mellitus, asthma, and hypertension may serve as motivating examples.9 Some specific dermatologic conditions that will benefit from increased patient adherence include acne, vesiculobullous disease, psoriasis, and atopic dermatitis. We can lend support to efforts to reduce the cost of dermatologic medications and be aware of the populations most at risk for low adherence to treatment.9-12
Final Thoughts
As we work to increase patient adherence to therapy in dermatology, we will help improve health literacy, patient safety, and patient satisfaction. These factors are ultimately linked to better health outcomes. The CDC and WHO websites are excellent sources of information on practical methods for doing so.2,9
- Haynes RB, McDonald H, Garg AX, et al. Interventions for helping patients to follow prescriptions for medications. Cochrane Database Syst Rev. 2002:CD000011.
- Centers for Disease Control and Prevention. Health literacy. http://www.cdc.gov/healthliteracy/index.html. Updated January 13, 2016. Accessed September 23, 2016.
- Berkman ND, Sheridan SL, Donahue KE, et al. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155:97-107.
- Pignone MP, DeWalt DA. Literacy and health outcomes: is adherence the missing link? J Gen Intern Med. 2006;21:896-897.
- Becker MH, Maiman LA. Strategies for enhancing patient compliance. J Community Health. 1980;6:113-135.
- Roter DL, Hall JA, Merisca R, et al. Effectiveness of interventions to improve patient compliance: a meta-analysis. Med Care. 1998;36:1138-1161.
- Renzi C, Abeni D, Picardi A, et al. Factors associated with patient satisfaction with care among dermatological outpatients. Br J Dermatol. 2001;145:617-623.
- Stewart MA. Effective physician-patient communication and health outcomes: a review. CMAJ. 1995;152:1423-1433.
- World Health Organization. Adherence to long-term therapies: evidence for action. http://www.who.int/chp/knowledge/publications/adherence_full_report.pdf. Posted 2003. Accessed September 23, 2016.
- Lee IA, Maibach HI. Pharmionics in dermatology: a review of topical medication adherence. Am J Clin Dermatol. 2006;7:231-236.
- Burkhart P, Dunbar-Jacob J. Adherence research in the pediatric and adolescent populations: a decade in review. In: Hayman L, Mahon M, Turner R, eds. Chronic Illness in Children: An Evidence-Based Approach. New York, NY: Springer Publishing Company; 2002:199-229.
- Rosenberg ME, Rosenberg SP. Changes in retail prices of prescription dermatologic drugs from 2009 to 2015. JAMA Dermatol. 2016;152:158-163.
- Haynes RB, McDonald H, Garg AX, et al. Interventions for helping patients to follow prescriptions for medications. Cochrane Database Syst Rev. 2002:CD000011.
- Centers for Disease Control and Prevention. Health literacy. http://www.cdc.gov/healthliteracy/index.html. Updated January 13, 2016. Accessed September 23, 2016.
- Berkman ND, Sheridan SL, Donahue KE, et al. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155:97-107.
- Pignone MP, DeWalt DA. Literacy and health outcomes: is adherence the missing link? J Gen Intern Med. 2006;21:896-897.
- Becker MH, Maiman LA. Strategies for enhancing patient compliance. J Community Health. 1980;6:113-135.
- Roter DL, Hall JA, Merisca R, et al. Effectiveness of interventions to improve patient compliance: a meta-analysis. Med Care. 1998;36:1138-1161.
- Renzi C, Abeni D, Picardi A, et al. Factors associated with patient satisfaction with care among dermatological outpatients. Br J Dermatol. 2001;145:617-623.
- Stewart MA. Effective physician-patient communication and health outcomes: a review. CMAJ. 1995;152:1423-1433.
- World Health Organization. Adherence to long-term therapies: evidence for action. http://www.who.int/chp/knowledge/publications/adherence_full_report.pdf. Posted 2003. Accessed September 23, 2016.
- Lee IA, Maibach HI. Pharmionics in dermatology: a review of topical medication adherence. Am J Clin Dermatol. 2006;7:231-236.
- Burkhart P, Dunbar-Jacob J. Adherence research in the pediatric and adolescent populations: a decade in review. In: Hayman L, Mahon M, Turner R, eds. Chronic Illness in Children: An Evidence-Based Approach. New York, NY: Springer Publishing Company; 2002:199-229.
- Rosenberg ME, Rosenberg SP. Changes in retail prices of prescription dermatologic drugs from 2009 to 2015. JAMA Dermatol. 2016;152:158-163.

Children on antipsychotics show more early weight gain than adults
VIENNA – Antipsychotic-naive children and adolescents are at greater risk for clinically significant weight gain during their first 6 months on a second-generation antipsychotic agent than adults, Covadonga M. Diaz-Caneja, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
She presented what she believes to be the first prospective observational study comparing weight gain between antipsychotic-naive children and adults during their first 6 months on second-generation antipsychotics. Weight gains were significantly greater with olanzapine (Zyprexa) than risperidone (Risperdal) or quetiapine (Seroquel) in both age groups, but the magnitude and trajectory of olanzapine-related weight gain was significantly more impressive in the pediatric patients.

The study included 226 pediatric patients with a mean age of 15.2 years and 135 adults, average age 39 years. All were antipsychotic naive when placed on one of the three second-generation antipsychotics at clinician discretion. Fifty percent of the youths and 60% of adults had a psychosis diagnosis. Sixty-four percent of the pediatric group and 55% of the adults were male.
Weight gain during the first 6 months of therapy was expressed as change in body mass index z score. An increase in BMI z score of 0.5 or more is considered clinically significant.
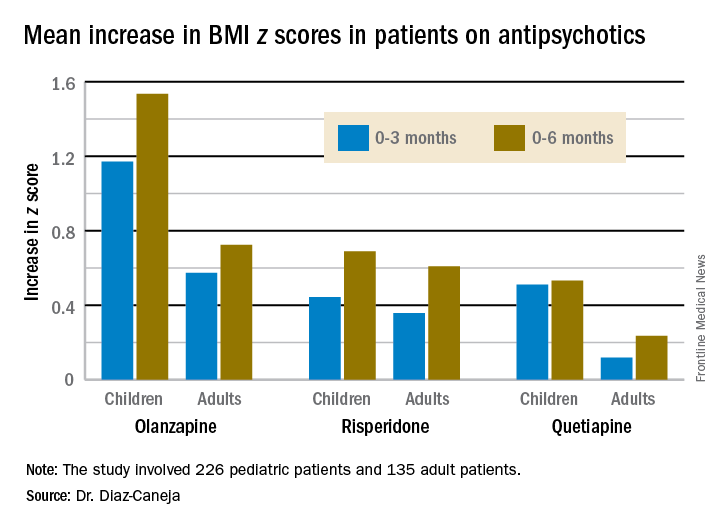
The least weight gain at 6 months occurred with quetiapine in both age groups. However, the BMI z score increased by 0.532 in the pediatric patients on the drug, more than twice the 0.236 increase in adults.
Risperidone was the only second-generation antipsychotic where the weight gain trajectories in pediatric and adult patients were not significantly different.
The study was funded by the Spanish Ministry of Economy and Competitiveness, and the European Commission. Dr. Diaz-Caneja reported having no financial conflicts of interest.
VIENNA – Antipsychotic-naive children and adolescents are at greater risk for clinically significant weight gain during their first 6 months on a second-generation antipsychotic agent than adults, Covadonga M. Diaz-Caneja, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
She presented what she believes to be the first prospective observational study comparing weight gain between antipsychotic-naive children and adults during their first 6 months on second-generation antipsychotics. Weight gains were significantly greater with olanzapine (Zyprexa) than risperidone (Risperdal) or quetiapine (Seroquel) in both age groups, but the magnitude and trajectory of olanzapine-related weight gain was significantly more impressive in the pediatric patients.
The study included 226 pediatric patients with a mean age of 15.2 years and 135 adults, average age 39 years. All were antipsychotic naive when placed on one of the three second-generation antipsychotics at clinician discretion. Fifty percent of the youths and 60% of adults had a psychosis diagnosis. Sixty-four percent of the pediatric group and 55% of the adults were male.
Weight gain during the first 6 months of therapy was expressed as change in body mass index z score. An increase in BMI z score of 0.5 or more is considered clinically significant.
The least weight gain at 6 months occurred with quetiapine in both age groups. However, the BMI z score increased by 0.532 in the pediatric patients on the drug, more than twice the 0.236 increase in adults.
Risperidone was the only second-generation antipsychotic where the weight gain trajectories in pediatric and adult patients were not significantly different.
The study was funded by the Spanish Ministry of Economy and Competitiveness, and the European Commission. Dr. Diaz-Caneja reported having no financial conflicts of interest.
VIENNA – Antipsychotic-naive children and adolescents are at greater risk for clinically significant weight gain during their first 6 months on a second-generation antipsychotic agent than adults, Covadonga M. Diaz-Caneja, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
She presented what she believes to be the first prospective observational study comparing weight gain between antipsychotic-naive children and adults during their first 6 months on second-generation antipsychotics. Weight gains were significantly greater with olanzapine (Zyprexa) than risperidone (Risperdal) or quetiapine (Seroquel) in both age groups, but the magnitude and trajectory of olanzapine-related weight gain was significantly more impressive in the pediatric patients.
The study included 226 pediatric patients with a mean age of 15.2 years and 135 adults, average age 39 years. All were antipsychotic naive when placed on one of the three second-generation antipsychotics at clinician discretion. Fifty percent of the youths and 60% of adults had a psychosis diagnosis. Sixty-four percent of the pediatric group and 55% of the adults were male.
Weight gain during the first 6 months of therapy was expressed as change in body mass index z score. An increase in BMI z score of 0.5 or more is considered clinically significant.
The least weight gain at 6 months occurred with quetiapine in both age groups. However, the BMI z score increased by 0.532 in the pediatric patients on the drug, more than twice the 0.236 increase in adults.
Risperidone was the only second-generation antipsychotic where the weight gain trajectories in pediatric and adult patients were not significantly different.
The study was funded by the Spanish Ministry of Economy and Competitiveness, and the European Commission. Dr. Diaz-Caneja reported having no financial conflicts of interest.
Key clinical point:
Major finding: The BMI z score increased by 1.535 in pediatric patients during their first 6 months on olanzapine – the most weight unfriendly of the second-generation antipsychotics – compared with 0.724 in adults.
Data source: This prospective, observational study examined weight gain in 361 antipsychotic-naive children, adolescents, and adults during their first 6 months on second-generation antipsychotic agents.
Disclosures: The study was funded by the Spanish Ministry of Economy and Competitiveness and the European Commission.
CEQUEL: Combo therapy a win in bipolar depression
VIENNA – Psychiatrists have received a welcome gift in the form of CEQUEL, a randomized trial that offers much needed guidance on how to proceed when quetiapine for bipolar depression isn’t achieving sufficient response, Eduard Vieta, MD, said at the annual congress of the European College of Neuropsychopharmacology.
The answer provided by CEQUEL is to add lamotrigine.
“Quetiapine is indicated for treatment of symptoms of bipolar depression, but many clinicians – including myself – are a bit underwhelmed about the practical results. In the clinical trials, quetiapine looks great, but when we use it in practice we’re not so happy with the results. The trials are consistently positive with a large effect size, whereas in clinical practice many patients respond only partially to quetiapine. The question has been what to do next,” observed Dr. Vieta, professor of psychiatry and head of the bipolar disorders program at the University of Barcelona.

Increasing the dose of quetiapine (Seroquel) above the recommended 300 mg/day in an effort to boost efficacy is problematic. Patients become extremely sedated. The CEQUEL (Comparative Evaluation of Quetiapine plus Lamotrigine) investigators decided to examine combination therapy with two drugs having completely different mechanisms of action.
A total of 202 patients with bipolar depression at 27 U.K. sites were placed on quetiapine and randomized double-blind to lamotrigine or placebo. Lamotrigine (Lamictal) was started at 25 mg/day and gradually increased to 200 mg daily. Because there is some limited evidence that folic acid is effective in unipolar depression, the investigators employed a 2x2 factorial design, further randomizing participants to 500 mcg/day of folic acid or placebo.
The primary endpoint was improvement in depressive symptoms at 12 weeks, with 52-week outcomes as a secondary endpoint. The group on combination therapy with quetiapine and lamotrigine showed significantly greater improvement both on mean depressive symptoms as measured with the Quick Inventory of Depressive Symptomatology-self report version 16 (QIDS-SR16), and on rates of remission at 12 and 52 weeks, compared with patients on quetiapine and placebo. The combination also reduced the risk of relapse in patients with bipolar I disorder with predominantly depressive symptoms.
Folic acid proved to be not only ineffective, it actually interfered with lamotrigine’s effectiveness. The mean reduction from baseline to 12 weeks on the QIDS-SR16 was 4.4 points in patients who received lamotrigine without folic acid, compared with a 0.12-point increase in those receiving lamotrigine plus folic acid (Lancet Psychiatry. 2016 Jan;3[1]:31-9).
Dr. Vieta wasn’t involved in CEQUEL, but he considers the study one of the highlights of the year in the field of affective disorders and urged his colleagues to consider lamotrigine/quetiapine combination therapy for bipolar depression.
“Quetiapine and lamotrigine are both now generic drugs. CEQUEL showed both are superior to quetiapine alone. It’s good news – a not-expensive treatment combining quetiapine with a drug, lamotrigine, that’s quite well tolerated,” he said.
CEQUEL was funded by the Medical Research Council. Dr. Vieta reported having no financial conflicts of interest.
VIENNA – Psychiatrists have received a welcome gift in the form of CEQUEL, a randomized trial that offers much needed guidance on how to proceed when quetiapine for bipolar depression isn’t achieving sufficient response, Eduard Vieta, MD, said at the annual congress of the European College of Neuropsychopharmacology.
The answer provided by CEQUEL is to add lamotrigine.
“Quetiapine is indicated for treatment of symptoms of bipolar depression, but many clinicians – including myself – are a bit underwhelmed about the practical results. In the clinical trials, quetiapine looks great, but when we use it in practice we’re not so happy with the results. The trials are consistently positive with a large effect size, whereas in clinical practice many patients respond only partially to quetiapine. The question has been what to do next,” observed Dr. Vieta, professor of psychiatry and head of the bipolar disorders program at the University of Barcelona.
Increasing the dose of quetiapine (Seroquel) above the recommended 300 mg/day in an effort to boost efficacy is problematic. Patients become extremely sedated. The CEQUEL (Comparative Evaluation of Quetiapine plus Lamotrigine) investigators decided to examine combination therapy with two drugs having completely different mechanisms of action.
A total of 202 patients with bipolar depression at 27 U.K. sites were placed on quetiapine and randomized double-blind to lamotrigine or placebo. Lamotrigine (Lamictal) was started at 25 mg/day and gradually increased to 200 mg daily. Because there is some limited evidence that folic acid is effective in unipolar depression, the investigators employed a 2x2 factorial design, further randomizing participants to 500 mcg/day of folic acid or placebo.
The primary endpoint was improvement in depressive symptoms at 12 weeks, with 52-week outcomes as a secondary endpoint. The group on combination therapy with quetiapine and lamotrigine showed significantly greater improvement both on mean depressive symptoms as measured with the Quick Inventory of Depressive Symptomatology-self report version 16 (QIDS-SR16), and on rates of remission at 12 and 52 weeks, compared with patients on quetiapine and placebo. The combination also reduced the risk of relapse in patients with bipolar I disorder with predominantly depressive symptoms.
Folic acid proved to be not only ineffective, it actually interfered with lamotrigine’s effectiveness. The mean reduction from baseline to 12 weeks on the QIDS-SR16 was 4.4 points in patients who received lamotrigine without folic acid, compared with a 0.12-point increase in those receiving lamotrigine plus folic acid (Lancet Psychiatry. 2016 Jan;3[1]:31-9).
Dr. Vieta wasn’t involved in CEQUEL, but he considers the study one of the highlights of the year in the field of affective disorders and urged his colleagues to consider lamotrigine/quetiapine combination therapy for bipolar depression.
“Quetiapine and lamotrigine are both now generic drugs. CEQUEL showed both are superior to quetiapine alone. It’s good news – a not-expensive treatment combining quetiapine with a drug, lamotrigine, that’s quite well tolerated,” he said.
CEQUEL was funded by the Medical Research Council. Dr. Vieta reported having no financial conflicts of interest.
VIENNA – Psychiatrists have received a welcome gift in the form of CEQUEL, a randomized trial that offers much needed guidance on how to proceed when quetiapine for bipolar depression isn’t achieving sufficient response, Eduard Vieta, MD, said at the annual congress of the European College of Neuropsychopharmacology.
The answer provided by CEQUEL is to add lamotrigine.
“Quetiapine is indicated for treatment of symptoms of bipolar depression, but many clinicians – including myself – are a bit underwhelmed about the practical results. In the clinical trials, quetiapine looks great, but when we use it in practice we’re not so happy with the results. The trials are consistently positive with a large effect size, whereas in clinical practice many patients respond only partially to quetiapine. The question has been what to do next,” observed Dr. Vieta, professor of psychiatry and head of the bipolar disorders program at the University of Barcelona.
Increasing the dose of quetiapine (Seroquel) above the recommended 300 mg/day in an effort to boost efficacy is problematic. Patients become extremely sedated. The CEQUEL (Comparative Evaluation of Quetiapine plus Lamotrigine) investigators decided to examine combination therapy with two drugs having completely different mechanisms of action.
A total of 202 patients with bipolar depression at 27 U.K. sites were placed on quetiapine and randomized double-blind to lamotrigine or placebo. Lamotrigine (Lamictal) was started at 25 mg/day and gradually increased to 200 mg daily. Because there is some limited evidence that folic acid is effective in unipolar depression, the investigators employed a 2x2 factorial design, further randomizing participants to 500 mcg/day of folic acid or placebo.
The primary endpoint was improvement in depressive symptoms at 12 weeks, with 52-week outcomes as a secondary endpoint. The group on combination therapy with quetiapine and lamotrigine showed significantly greater improvement both on mean depressive symptoms as measured with the Quick Inventory of Depressive Symptomatology-self report version 16 (QIDS-SR16), and on rates of remission at 12 and 52 weeks, compared with patients on quetiapine and placebo. The combination also reduced the risk of relapse in patients with bipolar I disorder with predominantly depressive symptoms.
Folic acid proved to be not only ineffective, it actually interfered with lamotrigine’s effectiveness. The mean reduction from baseline to 12 weeks on the QIDS-SR16 was 4.4 points in patients who received lamotrigine without folic acid, compared with a 0.12-point increase in those receiving lamotrigine plus folic acid (Lancet Psychiatry. 2016 Jan;3[1]:31-9).
Dr. Vieta wasn’t involved in CEQUEL, but he considers the study one of the highlights of the year in the field of affective disorders and urged his colleagues to consider lamotrigine/quetiapine combination therapy for bipolar depression.
“Quetiapine and lamotrigine are both now generic drugs. CEQUEL showed both are superior to quetiapine alone. It’s good news – a not-expensive treatment combining quetiapine with a drug, lamotrigine, that’s quite well tolerated,” he said.
CEQUEL was funded by the Medical Research Council. Dr. Vieta reported having no financial conflicts of interest.
Biomarker identifies precancerous pancreatic cysts
LAS VEGAS – In fluid derived from pancreatic cysts, methylated DNA markers predict the presence of high-grade dysplasia (HGD) or cancer, and could help physicians decide whether to surgically remove cysts – a procedure that often has serious complications.
If validated in larger studies, the biomarkers have the potential to supplant the Fukuoka criteria that is currently used. “The markers could cause a paradigm shift in how we approach these lesions in our clinical practice,” Shounak Majumder, MD, a fellow at the Mayo Clinic in Rochester, Minn., said in an interview.
Less than 50% of cysts that are surgically resected turn out to be HGD or cancerous. “Having a cyst fluid marker could identify the patients that would benefit the most from surgery. If you’re going to go through a pancreatic resection, we’d rather give you the best chance of saying that we removed something that either has early cancer in it or will turn into cancer in the near future,” said Dr. Majumder.
The study looked at pancreatic cyst fluid from 83 cysts that had been surgically resected. The DNA samples were taken from the cyst fluid. Dr. Majumder believes that the cells shed from the cyst wall into the fluid. As a result, DNA from the fluid captures heterogeneity in the cyst more effectively than a biopsied sample.

The researchers found five methylated DNA markers that distinguished cancer or HGD from controls with areas under the ROC curve of 0.90 or higher. The top two (BMP3, EMX1) detected 93% of cases (95% CI, 66%-100%) at a specificity of 90% (95% CI, 80%-96%). Applied to eight cysts with intermediate-grade dysplasia, the biomarkers would have identified three at 95% specificity.
By comparison, the Fukuoka guidelines have 56% sensitivity and 73% specificity.
A limitation to the technique is that DNA cannot be extracted from all samples. About 5%-10% of pancreatic fluid samples are unusable, according to Somashekar Krishna, MD, MPH, assistant professor of medicine at the Ohio State University Medical Center, who attended the session. Dr. Krishna is conducting research combining endomicroscopy with molecular markers.
“We should have a foolproof system where if one fails, the other kicks in, and we have an answer for every patient. My opinion is that endomicroscopy has to be combined with molecular studies. I think combined we’ll have an excellent diagnostic yield,” Dr. Krishna said in an interview.
Dr. Majumder and Dr. Krishna have declared no conflicts of interest.
LAS VEGAS – In fluid derived from pancreatic cysts, methylated DNA markers predict the presence of high-grade dysplasia (HGD) or cancer, and could help physicians decide whether to surgically remove cysts – a procedure that often has serious complications.
If validated in larger studies, the biomarkers have the potential to supplant the Fukuoka criteria that is currently used. “The markers could cause a paradigm shift in how we approach these lesions in our clinical practice,” Shounak Majumder, MD, a fellow at the Mayo Clinic in Rochester, Minn., said in an interview.
Less than 50% of cysts that are surgically resected turn out to be HGD or cancerous. “Having a cyst fluid marker could identify the patients that would benefit the most from surgery. If you’re going to go through a pancreatic resection, we’d rather give you the best chance of saying that we removed something that either has early cancer in it or will turn into cancer in the near future,” said Dr. Majumder.
The study looked at pancreatic cyst fluid from 83 cysts that had been surgically resected. The DNA samples were taken from the cyst fluid. Dr. Majumder believes that the cells shed from the cyst wall into the fluid. As a result, DNA from the fluid captures heterogeneity in the cyst more effectively than a biopsied sample.
The researchers found five methylated DNA markers that distinguished cancer or HGD from controls with areas under the ROC curve of 0.90 or higher. The top two (BMP3, EMX1) detected 93% of cases (95% CI, 66%-100%) at a specificity of 90% (95% CI, 80%-96%). Applied to eight cysts with intermediate-grade dysplasia, the biomarkers would have identified three at 95% specificity.
By comparison, the Fukuoka guidelines have 56% sensitivity and 73% specificity.
A limitation to the technique is that DNA cannot be extracted from all samples. About 5%-10% of pancreatic fluid samples are unusable, according to Somashekar Krishna, MD, MPH, assistant professor of medicine at the Ohio State University Medical Center, who attended the session. Dr. Krishna is conducting research combining endomicroscopy with molecular markers.
“We should have a foolproof system where if one fails, the other kicks in, and we have an answer for every patient. My opinion is that endomicroscopy has to be combined with molecular studies. I think combined we’ll have an excellent diagnostic yield,” Dr. Krishna said in an interview.
Dr. Majumder and Dr. Krishna have declared no conflicts of interest.
LAS VEGAS – In fluid derived from pancreatic cysts, methylated DNA markers predict the presence of high-grade dysplasia (HGD) or cancer, and could help physicians decide whether to surgically remove cysts – a procedure that often has serious complications.
If validated in larger studies, the biomarkers have the potential to supplant the Fukuoka criteria that is currently used. “The markers could cause a paradigm shift in how we approach these lesions in our clinical practice,” Shounak Majumder, MD, a fellow at the Mayo Clinic in Rochester, Minn., said in an interview.
Less than 50% of cysts that are surgically resected turn out to be HGD or cancerous. “Having a cyst fluid marker could identify the patients that would benefit the most from surgery. If you’re going to go through a pancreatic resection, we’d rather give you the best chance of saying that we removed something that either has early cancer in it or will turn into cancer in the near future,” said Dr. Majumder.
The study looked at pancreatic cyst fluid from 83 cysts that had been surgically resected. The DNA samples were taken from the cyst fluid. Dr. Majumder believes that the cells shed from the cyst wall into the fluid. As a result, DNA from the fluid captures heterogeneity in the cyst more effectively than a biopsied sample.
The researchers found five methylated DNA markers that distinguished cancer or HGD from controls with areas under the ROC curve of 0.90 or higher. The top two (BMP3, EMX1) detected 93% of cases (95% CI, 66%-100%) at a specificity of 90% (95% CI, 80%-96%). Applied to eight cysts with intermediate-grade dysplasia, the biomarkers would have identified three at 95% specificity.
By comparison, the Fukuoka guidelines have 56% sensitivity and 73% specificity.
A limitation to the technique is that DNA cannot be extracted from all samples. About 5%-10% of pancreatic fluid samples are unusable, according to Somashekar Krishna, MD, MPH, assistant professor of medicine at the Ohio State University Medical Center, who attended the session. Dr. Krishna is conducting research combining endomicroscopy with molecular markers.
“We should have a foolproof system where if one fails, the other kicks in, and we have an answer for every patient. My opinion is that endomicroscopy has to be combined with molecular studies. I think combined we’ll have an excellent diagnostic yield,” Dr. Krishna said in an interview.
Dr. Majumder and Dr. Krishna have declared no conflicts of interest.
AT ACG 2016
Key clinical point:
Major finding: DNA markers isolated from pancreatic fluid predicted cancer or high-grade dysplasia with 90% specificity and 93% sensitivity.
Data source: Pilot study, retrospective analysis.
Disclosures: Dr. Majumder and Dr. Krishna have declared no conflicts of interest.
Study provides best support to date for using ultrasound to detect gout
Ultrasound examination of patients with at least one swollen joint or a subcutaneous nodule detected gout with a sensitivity of 76.9% and specificity of 84.3% in an international, multicenter study.
“Ultrasound is a good test for gout,” said study lead author Alexis R. Ogdie-Beatty, MD, of the University of Pennsylvania, Philadelphia. “It has high specificity, even among patients with early disease. The sensitivity was lower so it doesn’t pick up all cases of gout, although it was higher in people with a longer duration of disease.”

But gout remains difficult to diagnose because of the many similar types of inflammatory arthritis. A 2016 report from the Agency for Healthcare Research and Quality says proper diagnosis is a “major challenge,” especially in primary care and urgent/emergency settings.
Monosodium urate (MSU) crystal analysis via joint aspiration is considered the “gold standard” of gout diagnostic tools, but the agency report notes that it “can be technically difficult to perform and painful to the patient.”
There are other challenges. “Sometimes we see people between flares, or it’s already started to improve so there’s not enough fluid to perform an arthrocentesis,” Dr. Ogdie-Beatty said in an interview. “Additionally, while rheumatologists are generally very good at joint aspirations, many primary care physicians are not specifically trained for this. Thus, an imaging study can be helpful in these cases.”
The new study (Arthritis Rheumatol. 2016 Oct 16. doi: 10.1002/art.39959) follows up on findings from the multicenter, cross-sectional Study for Updated Gout Classification Criteria, which independently linked ultrasound analysis to diagnosis of gout with an odds ratio of 7.2 (Arthritis Care Res. 2015 Sep;67[9]:1304-15). One goal of the new study is to determine specificity and sensitivity of ultrasound exams.
The researchers examined data from the previous study, which enrolled consecutive patients in clinical practice settings across 25 countries who had at least one swollen joint or a subcutaneous nodule in whom gout was on the differential diagnosis. They underwent ultrasound examinations (most commonly of the knees, metatarsophalangeal joints, and ankles) and were deemed to have a “positive test” if at least one of three signs appeared: a “double contour” sign, tophus, or a “snowstorm” appearance. However, the study did not require a specific ultrasound scanning protocol or training.
MSU crystal examinations confirmed which of the subjects actually had gout. In total, ultrasound examinations were performed on 824 patients, of whom 416 were confirmed to have gout (mean age, 60, and 87% male), and the other 408 did not have gout (mean age, 60, and 54% male).
The researchers found that the sensitivity of the ultrasound exams was 76.9%, meaning they correctly identified patients with gout just over three-quarters of the time. Dr. Ogdie-Beatty referred to this as “moderate” sensitivity. The researchers found that the sensitivity was highest in patients who’d had disease for 2 or more years and in those who didn’t show clinical signs of tophi.
The specificity for these signs – the percentage of the time that ultrasound exams correctly identified patients without gout – was 84.3%. The positive and negative predictive values were 83.3% and 78.1%, respectively.
Dr. Ogdie-Beatty said the cost of ultrasound examinations is variable, although insurance covers it for trained providers. It’s unclear how commonly ultrasound examinations are used to detect gout, she said, but “many rheumatologists now have ultrasound as a part of their practice, and ultrasound training during fellowship has become important.”
Dr. Ogdie-Beatty reported receiving consulting fees from Novartis, and her coauthors reported various financial relationships with industry. The study was supported by various National Institutes of Health grants to several authors, as well as the American College of Rheumatology, the European League Against Rheumatism, and various arthritis-related organizations.
The new study provides evidence that both answers and raises questions about the technical standards by which musculoskeletal ultrasound examination is used to detect gout and about what we mean when we make a clinical diagnosis of gout.
The study’s results showed that ultrasound provided excellent specificity for gout in the setting of acute calcium pyrophosphate deposition disease (CPPD), also known as pseudogout, particularly in distinguishing the deposition of monosodium urate on the surface of cartilage (double contour sign), and calcium pyrophosphate within the matrix of the cartilage (interface sign). Ultrasound’s specificity for gout apart from CPPD was particularly high when more than one feature of gout was present because one feature of gout was more often present in patients with CPPD than in non-CPPD controls, but this was not the case when two features of gout were present. However, this leaves open the possibility that some patients may concurrently have both CPPD and gout, which the study does not fully address. Apart from the level of operator experience in using ultrasound, diagnostic bias did not seem to play a role in the diagnostic utility of ultrasound because clinical appearance of scanned joints or presence of tophi did not greatly affect its sensitivity when considering that patients with tophi have more advanced disease and probably have more obvious ultrasound findings.
The study’s demonstration of ultrasound’s ability to identify tophi is important because rheumatologists consider the presence of tophi as marking the transition from hyperuricemia to gout, which often involves of inflammation and tissue damage. Many other studies have noted how people with hyperuricemia can have the double contour sign without meeting clinical criteria for gout.
It still remains important to note that, even though the test characteristics of ultrasound in the study should be generalizable, its ability to support a diagnosis of acute gout does not rule out infection in the same joint.
Eugene Y. Kissin, MD, is with the division of rheumatology at Boston University, and Michael H. Pillinger, MD, is with the division of rheumatology at New York University, New York. Their comments are derived from their editorial accompanying the study by Dr. Ogdie-Beatty and her colleagues (Arthritis Rheumatol. 2016 Oct 16. doi: 10.1002/art.39958). Dr. Kissin reported no disclosures. Dr. Pillinger reported consulting for AstraZeneca, Crealta/Horizon, and Sobi, and he has served as an investigator for a trial sponsored by Takeda.
The new study provides evidence that both answers and raises questions about the technical standards by which musculoskeletal ultrasound examination is used to detect gout and about what we mean when we make a clinical diagnosis of gout.
The study’s results showed that ultrasound provided excellent specificity for gout in the setting of acute calcium pyrophosphate deposition disease (CPPD), also known as pseudogout, particularly in distinguishing the deposition of monosodium urate on the surface of cartilage (double contour sign), and calcium pyrophosphate within the matrix of the cartilage (interface sign). Ultrasound’s specificity for gout apart from CPPD was particularly high when more than one feature of gout was present because one feature of gout was more often present in patients with CPPD than in non-CPPD controls, but this was not the case when two features of gout were present. However, this leaves open the possibility that some patients may concurrently have both CPPD and gout, which the study does not fully address. Apart from the level of operator experience in using ultrasound, diagnostic bias did not seem to play a role in the diagnostic utility of ultrasound because clinical appearance of scanned joints or presence of tophi did not greatly affect its sensitivity when considering that patients with tophi have more advanced disease and probably have more obvious ultrasound findings.
The study’s demonstration of ultrasound’s ability to identify tophi is important because rheumatologists consider the presence of tophi as marking the transition from hyperuricemia to gout, which often involves of inflammation and tissue damage. Many other studies have noted how people with hyperuricemia can have the double contour sign without meeting clinical criteria for gout.
It still remains important to note that, even though the test characteristics of ultrasound in the study should be generalizable, its ability to support a diagnosis of acute gout does not rule out infection in the same joint.
Eugene Y. Kissin, MD, is with the division of rheumatology at Boston University, and Michael H. Pillinger, MD, is with the division of rheumatology at New York University, New York. Their comments are derived from their editorial accompanying the study by Dr. Ogdie-Beatty and her colleagues (Arthritis Rheumatol. 2016 Oct 16. doi: 10.1002/art.39958). Dr. Kissin reported no disclosures. Dr. Pillinger reported consulting for AstraZeneca, Crealta/Horizon, and Sobi, and he has served as an investigator for a trial sponsored by Takeda.
The new study provides evidence that both answers and raises questions about the technical standards by which musculoskeletal ultrasound examination is used to detect gout and about what we mean when we make a clinical diagnosis of gout.
The study’s results showed that ultrasound provided excellent specificity for gout in the setting of acute calcium pyrophosphate deposition disease (CPPD), also known as pseudogout, particularly in distinguishing the deposition of monosodium urate on the surface of cartilage (double contour sign), and calcium pyrophosphate within the matrix of the cartilage (interface sign). Ultrasound’s specificity for gout apart from CPPD was particularly high when more than one feature of gout was present because one feature of gout was more often present in patients with CPPD than in non-CPPD controls, but this was not the case when two features of gout were present. However, this leaves open the possibility that some patients may concurrently have both CPPD and gout, which the study does not fully address. Apart from the level of operator experience in using ultrasound, diagnostic bias did not seem to play a role in the diagnostic utility of ultrasound because clinical appearance of scanned joints or presence of tophi did not greatly affect its sensitivity when considering that patients with tophi have more advanced disease and probably have more obvious ultrasound findings.
The study’s demonstration of ultrasound’s ability to identify tophi is important because rheumatologists consider the presence of tophi as marking the transition from hyperuricemia to gout, which often involves of inflammation and tissue damage. Many other studies have noted how people with hyperuricemia can have the double contour sign without meeting clinical criteria for gout.
It still remains important to note that, even though the test characteristics of ultrasound in the study should be generalizable, its ability to support a diagnosis of acute gout does not rule out infection in the same joint.
Eugene Y. Kissin, MD, is with the division of rheumatology at Boston University, and Michael H. Pillinger, MD, is with the division of rheumatology at New York University, New York. Their comments are derived from their editorial accompanying the study by Dr. Ogdie-Beatty and her colleagues (Arthritis Rheumatol. 2016 Oct 16. doi: 10.1002/art.39958). Dr. Kissin reported no disclosures. Dr. Pillinger reported consulting for AstraZeneca, Crealta/Horizon, and Sobi, and he has served as an investigator for a trial sponsored by Takeda.
Ultrasound examination of patients with at least one swollen joint or a subcutaneous nodule detected gout with a sensitivity of 76.9% and specificity of 84.3% in an international, multicenter study.
“Ultrasound is a good test for gout,” said study lead author Alexis R. Ogdie-Beatty, MD, of the University of Pennsylvania, Philadelphia. “It has high specificity, even among patients with early disease. The sensitivity was lower so it doesn’t pick up all cases of gout, although it was higher in people with a longer duration of disease.”
But gout remains difficult to diagnose because of the many similar types of inflammatory arthritis. A 2016 report from the Agency for Healthcare Research and Quality says proper diagnosis is a “major challenge,” especially in primary care and urgent/emergency settings.
Monosodium urate (MSU) crystal analysis via joint aspiration is considered the “gold standard” of gout diagnostic tools, but the agency report notes that it “can be technically difficult to perform and painful to the patient.”
There are other challenges. “Sometimes we see people between flares, or it’s already started to improve so there’s not enough fluid to perform an arthrocentesis,” Dr. Ogdie-Beatty said in an interview. “Additionally, while rheumatologists are generally very good at joint aspirations, many primary care physicians are not specifically trained for this. Thus, an imaging study can be helpful in these cases.”
The new study (Arthritis Rheumatol. 2016 Oct 16. doi: 10.1002/art.39959) follows up on findings from the multicenter, cross-sectional Study for Updated Gout Classification Criteria, which independently linked ultrasound analysis to diagnosis of gout with an odds ratio of 7.2 (Arthritis Care Res. 2015 Sep;67[9]:1304-15). One goal of the new study is to determine specificity and sensitivity of ultrasound exams.
The researchers examined data from the previous study, which enrolled consecutive patients in clinical practice settings across 25 countries who had at least one swollen joint or a subcutaneous nodule in whom gout was on the differential diagnosis. They underwent ultrasound examinations (most commonly of the knees, metatarsophalangeal joints, and ankles) and were deemed to have a “positive test” if at least one of three signs appeared: a “double contour” sign, tophus, or a “snowstorm” appearance. However, the study did not require a specific ultrasound scanning protocol or training.
MSU crystal examinations confirmed which of the subjects actually had gout. In total, ultrasound examinations were performed on 824 patients, of whom 416 were confirmed to have gout (mean age, 60, and 87% male), and the other 408 did not have gout (mean age, 60, and 54% male).
The researchers found that the sensitivity of the ultrasound exams was 76.9%, meaning they correctly identified patients with gout just over three-quarters of the time. Dr. Ogdie-Beatty referred to this as “moderate” sensitivity. The researchers found that the sensitivity was highest in patients who’d had disease for 2 or more years and in those who didn’t show clinical signs of tophi.
The specificity for these signs – the percentage of the time that ultrasound exams correctly identified patients without gout – was 84.3%. The positive and negative predictive values were 83.3% and 78.1%, respectively.
Dr. Ogdie-Beatty said the cost of ultrasound examinations is variable, although insurance covers it for trained providers. It’s unclear how commonly ultrasound examinations are used to detect gout, she said, but “many rheumatologists now have ultrasound as a part of their practice, and ultrasound training during fellowship has become important.”
Dr. Ogdie-Beatty reported receiving consulting fees from Novartis, and her coauthors reported various financial relationships with industry. The study was supported by various National Institutes of Health grants to several authors, as well as the American College of Rheumatology, the European League Against Rheumatism, and various arthritis-related organizations.
Ultrasound examination of patients with at least one swollen joint or a subcutaneous nodule detected gout with a sensitivity of 76.9% and specificity of 84.3% in an international, multicenter study.
“Ultrasound is a good test for gout,” said study lead author Alexis R. Ogdie-Beatty, MD, of the University of Pennsylvania, Philadelphia. “It has high specificity, even among patients with early disease. The sensitivity was lower so it doesn’t pick up all cases of gout, although it was higher in people with a longer duration of disease.”
But gout remains difficult to diagnose because of the many similar types of inflammatory arthritis. A 2016 report from the Agency for Healthcare Research and Quality says proper diagnosis is a “major challenge,” especially in primary care and urgent/emergency settings.
Monosodium urate (MSU) crystal analysis via joint aspiration is considered the “gold standard” of gout diagnostic tools, but the agency report notes that it “can be technically difficult to perform and painful to the patient.”
There are other challenges. “Sometimes we see people between flares, or it’s already started to improve so there’s not enough fluid to perform an arthrocentesis,” Dr. Ogdie-Beatty said in an interview. “Additionally, while rheumatologists are generally very good at joint aspirations, many primary care physicians are not specifically trained for this. Thus, an imaging study can be helpful in these cases.”
The new study (Arthritis Rheumatol. 2016 Oct 16. doi: 10.1002/art.39959) follows up on findings from the multicenter, cross-sectional Study for Updated Gout Classification Criteria, which independently linked ultrasound analysis to diagnosis of gout with an odds ratio of 7.2 (Arthritis Care Res. 2015 Sep;67[9]:1304-15). One goal of the new study is to determine specificity and sensitivity of ultrasound exams.
The researchers examined data from the previous study, which enrolled consecutive patients in clinical practice settings across 25 countries who had at least one swollen joint or a subcutaneous nodule in whom gout was on the differential diagnosis. They underwent ultrasound examinations (most commonly of the knees, metatarsophalangeal joints, and ankles) and were deemed to have a “positive test” if at least one of three signs appeared: a “double contour” sign, tophus, or a “snowstorm” appearance. However, the study did not require a specific ultrasound scanning protocol or training.
MSU crystal examinations confirmed which of the subjects actually had gout. In total, ultrasound examinations were performed on 824 patients, of whom 416 were confirmed to have gout (mean age, 60, and 87% male), and the other 408 did not have gout (mean age, 60, and 54% male).
The researchers found that the sensitivity of the ultrasound exams was 76.9%, meaning they correctly identified patients with gout just over three-quarters of the time. Dr. Ogdie-Beatty referred to this as “moderate” sensitivity. The researchers found that the sensitivity was highest in patients who’d had disease for 2 or more years and in those who didn’t show clinical signs of tophi.
The specificity for these signs – the percentage of the time that ultrasound exams correctly identified patients without gout – was 84.3%. The positive and negative predictive values were 83.3% and 78.1%, respectively.
Dr. Ogdie-Beatty said the cost of ultrasound examinations is variable, although insurance covers it for trained providers. It’s unclear how commonly ultrasound examinations are used to detect gout, she said, but “many rheumatologists now have ultrasound as a part of their practice, and ultrasound training during fellowship has become important.”
Dr. Ogdie-Beatty reported receiving consulting fees from Novartis, and her coauthors reported various financial relationships with industry. The study was supported by various National Institutes of Health grants to several authors, as well as the American College of Rheumatology, the European League Against Rheumatism, and various arthritis-related organizations.
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point:
Major finding: Examiners looked for at least one of three potential signs of gout. The sensitivity for gout was 76.9%, and the specificity was 84.3%.
Data source: 824 patients with potential signs of gout who underwent ultrasound examination in an international, multicenter, observational cross-sectional study
Disclosures: Dr. Ogdie-Beatty reported receiving consulting fees from Novartis, and her coauthors reported various financial relationships with industry. The study was supported by various National Institutes of Health grants to several authors, as well as the American College of Rheumatology, the European League Against Rheumatism, and various arthritis-related organizations.
FDA expands indication for pembrolizumab in NSCLC
The Food and Drug Administration has approved pembrolizumab for the treatment of patients with metastatic non–small cell lung cancer (NSCLC) whose tumors express PD-L1 as determined by an FDA-approved test. This is the first approval of a checkpoint inhibitor for first-line treatment of the disease.
Pembrolizumab (Keytruda) is now approved to treat patients with metastatic NSCLC whose tumors have high PD-L1 expression (Tumor Proportion Score [TPS] greater than or equal to 50%), with no EGFR or ALK genomic tumor aberrations, and no prior systemic chemotherapy treatment for metastatic NSCLC, the FDA said in a written statement.![]()
The FDA based its approval on improvement in overall survival in two trials comparing treatment with pembrolizumab to treatment from chemotherapy. In one trial of 305 patients who had no prior treatment for metastatic NSCLC and TPS greater than or equal to 50%, those who received pembrolizumab (200 mg every 3 weeks) had a statistically significant improvement in overall survival, compared with patients randomized to receive chemotherapy (hazard ratio, 0.60; 95% confidence interval, 0.41-0.89; P less than .005). There was also significant improvement in progression-free survival for those receiving the checkpoint inhibitor (HR, 0.50; 95% CI, 0.37-0.68; P less than .001).
In the second trial, a three-arm trial of 1,033 patients who were previously treated for metastatic NSCLC with a TPS greater than or equal to 1%, those randomized to pembrolizumab 2 mg/kg every 3 weeks (HR, 0.71; 95% CI, 0.58-0.88; P less than .001) or pembrolizumab 10 mg/kg every 3 weeks (HR, 0.61; 95% CI, 0.49-0.75; P less than .001) had an improved overall survival, compared with patients receiving docetaxel. The median survival was 10.4 months in the pembrolizumab 2 mg/kg arm, 12.7 months in the pembrolizumab 10 mg/kg arm, and 8.5 months in the docetaxel arm.
The most common side effects of treatment with pembrolizumab included decreased appetite, fatigue, nausea, dyspnea, cough, and constipation. Rare but serious adverse events included immune-mediated pneumonitis, colitis, hepatitis, endocrinopathies, and nephritis, the FDA said.
The recommended dose and schedule of pembrolizumab for NSCLC is 200 mg intravenously every 3 weeks. Full prescribing information is available here.
[email protected]
On Twitter @nikolaideslaura
The Food and Drug Administration has approved pembrolizumab for the treatment of patients with metastatic non–small cell lung cancer (NSCLC) whose tumors express PD-L1 as determined by an FDA-approved test. This is the first approval of a checkpoint inhibitor for first-line treatment of the disease.
Pembrolizumab (Keytruda) is now approved to treat patients with metastatic NSCLC whose tumors have high PD-L1 expression (Tumor Proportion Score [TPS] greater than or equal to 50%), with no EGFR or ALK genomic tumor aberrations, and no prior systemic chemotherapy treatment for metastatic NSCLC, the FDA said in a written statement.![]()
The FDA based its approval on improvement in overall survival in two trials comparing treatment with pembrolizumab to treatment from chemotherapy. In one trial of 305 patients who had no prior treatment for metastatic NSCLC and TPS greater than or equal to 50%, those who received pembrolizumab (200 mg every 3 weeks) had a statistically significant improvement in overall survival, compared with patients randomized to receive chemotherapy (hazard ratio, 0.60; 95% confidence interval, 0.41-0.89; P less than .005). There was also significant improvement in progression-free survival for those receiving the checkpoint inhibitor (HR, 0.50; 95% CI, 0.37-0.68; P less than .001).
In the second trial, a three-arm trial of 1,033 patients who were previously treated for metastatic NSCLC with a TPS greater than or equal to 1%, those randomized to pembrolizumab 2 mg/kg every 3 weeks (HR, 0.71; 95% CI, 0.58-0.88; P less than .001) or pembrolizumab 10 mg/kg every 3 weeks (HR, 0.61; 95% CI, 0.49-0.75; P less than .001) had an improved overall survival, compared with patients receiving docetaxel. The median survival was 10.4 months in the pembrolizumab 2 mg/kg arm, 12.7 months in the pembrolizumab 10 mg/kg arm, and 8.5 months in the docetaxel arm.
The most common side effects of treatment with pembrolizumab included decreased appetite, fatigue, nausea, dyspnea, cough, and constipation. Rare but serious adverse events included immune-mediated pneumonitis, colitis, hepatitis, endocrinopathies, and nephritis, the FDA said.
The recommended dose and schedule of pembrolizumab for NSCLC is 200 mg intravenously every 3 weeks. Full prescribing information is available here.
[email protected]
On Twitter @nikolaideslaura
The Food and Drug Administration has approved pembrolizumab for the treatment of patients with metastatic non–small cell lung cancer (NSCLC) whose tumors express PD-L1 as determined by an FDA-approved test. This is the first approval of a checkpoint inhibitor for first-line treatment of the disease.
Pembrolizumab (Keytruda) is now approved to treat patients with metastatic NSCLC whose tumors have high PD-L1 expression (Tumor Proportion Score [TPS] greater than or equal to 50%), with no EGFR or ALK genomic tumor aberrations, and no prior systemic chemotherapy treatment for metastatic NSCLC, the FDA said in a written statement.![]()
The FDA based its approval on improvement in overall survival in two trials comparing treatment with pembrolizumab to treatment from chemotherapy. In one trial of 305 patients who had no prior treatment for metastatic NSCLC and TPS greater than or equal to 50%, those who received pembrolizumab (200 mg every 3 weeks) had a statistically significant improvement in overall survival, compared with patients randomized to receive chemotherapy (hazard ratio, 0.60; 95% confidence interval, 0.41-0.89; P less than .005). There was also significant improvement in progression-free survival for those receiving the checkpoint inhibitor (HR, 0.50; 95% CI, 0.37-0.68; P less than .001).
In the second trial, a three-arm trial of 1,033 patients who were previously treated for metastatic NSCLC with a TPS greater than or equal to 1%, those randomized to pembrolizumab 2 mg/kg every 3 weeks (HR, 0.71; 95% CI, 0.58-0.88; P less than .001) or pembrolizumab 10 mg/kg every 3 weeks (HR, 0.61; 95% CI, 0.49-0.75; P less than .001) had an improved overall survival, compared with patients receiving docetaxel. The median survival was 10.4 months in the pembrolizumab 2 mg/kg arm, 12.7 months in the pembrolizumab 10 mg/kg arm, and 8.5 months in the docetaxel arm.
The most common side effects of treatment with pembrolizumab included decreased appetite, fatigue, nausea, dyspnea, cough, and constipation. Rare but serious adverse events included immune-mediated pneumonitis, colitis, hepatitis, endocrinopathies, and nephritis, the FDA said.
The recommended dose and schedule of pembrolizumab for NSCLC is 200 mg intravenously every 3 weeks. Full prescribing information is available here.
[email protected]
On Twitter @nikolaideslaura
Ketamine curbs suicidal ideation independent of antidepressant effect
VIENNA – Repeated infusions of ketamine appear to have a direct effect in quelling suicidal ideation independent of the drug’s impact on depressive symptoms, Pierre Blier, MD, PhD, reported at the annual congress of the European College of Neuropsychopharmacology.
“Our preliminary results indicate that ketamine reduced suicidal ideation even in patients who failed to show a reduction in depression severity with repeated infusions,” observed Dr. Blier, professor of psychiatry at the University of Ottawa.
If the findings from this proof-of-concept study are confirmed, it would be very good news indeed.
“Suicidal ideation often requires rapid intervention, but there are very few treatments that are effective in reducing suicidal ideation, and none are fast acting,” the psychiatrist noted.
Therapeutic interest in ketamine is running high because subanesthetic doses of the drug have been shown to reduce depressive symptoms within a matter of hours, albeit transiently, in patients with treatment-resistant depression. If the drug acts as quickly in decreasing suicidal ideation as it does for depression, it would have major implications for clinical practice. An estimated 1 million people die each year worldwide from suicide, and two-thirds of them have major depressive disorder.
Dr. Blier reported on 27 patients with treatment-resistant depression, defined as failure to respond to at least two antidepressant medications from different pharmacologic classes at adequate dosages for at least 6 weeks each, along with two augmentation strategies. Their mean baseline score on the Montgomery-Asberg Depression Rating Scale (MADRS) was roughly 35. Five of the 27 had made one or more prior suicide attempts. Twenty-six of the 27 had suicidal ideation at baseline as defined by a MADRS suicidal ideation score (MADRS-SI) of more than 0. The MADRS-SI is based upon item 10 on the MADRS and is scored 0-6. Eight patients reported marked suicidal ideation as defined by a baseline MADRS-SI score of 4 or higher.
Study participants received a total of seven intravenous infusions of ketamine over roughly 3 weeks. Patients were retested 2-3 days after the seventh infusion, at which time 16 patients were categorized as treatment responders on the basis of at least a 50% reduction in their total MADRS score. Indeed, they averaged a 20.7-point reduction in the non–suicide-related MADRS score – that is, items 1-9, which reflect symptoms of depression – compared with a mere 3.9-point decrease in the 11 ketamine nonresponders. This 59% response rate for depressive symptoms is consistent with reported results of other studies of ketamine in patients with treatment-resistant depression, according to Dr. Blier, also professor of cellular/molecular medicines at the university.
The baseline MADRS-SI score averaged 2.9 in treatment responders and was similar at 2.5 in the nonresponders. But after seven infusions of ketamine, 21 of 27 patients had a MADRS-SI score of 0 or 1. The key study finding was that both the ketamine responders and nonresponders in terms of depressive symptoms experienced significant reductions in suicidal ideation. The 16 responders averaged a 2.4-point decrease from baseline in MADRS-SI scores, while the 11 nonresponders averaged a 1.5-point reduction. The magnitude of the reduction in MADRS-SI was significantly greater in the antidepressant responders than the nonresponders, but the improvement in suicidal ideation was statistically significant and clinically meaningful in both groups.
Seven of the 8 patients with baseline marked suicidal ideation and a MADRS-SI of 4 or greater improved to a score of 2 or less after their seven ketamine infusions, meaning they were having at most only fleeting suicidal thoughts.
Dr. Blier and coinvestigators are now expanding the ketamine study, enrolling up to 40 additional patients with treatment-resistant depression and suicidality in order to confirm the preliminary findings.
Dr. Blier reported having no financial conflicts of interest regarding this study, which was funded by the Canadian Institutes of Health Research. He noted that he receives research grants from and/or serves on advisory boards for more than a dozen pharmaceutical companies.
VIENNA – Repeated infusions of ketamine appear to have a direct effect in quelling suicidal ideation independent of the drug’s impact on depressive symptoms, Pierre Blier, MD, PhD, reported at the annual congress of the European College of Neuropsychopharmacology.
“Our preliminary results indicate that ketamine reduced suicidal ideation even in patients who failed to show a reduction in depression severity with repeated infusions,” observed Dr. Blier, professor of psychiatry at the University of Ottawa.
If the findings from this proof-of-concept study are confirmed, it would be very good news indeed.
“Suicidal ideation often requires rapid intervention, but there are very few treatments that are effective in reducing suicidal ideation, and none are fast acting,” the psychiatrist noted.
Therapeutic interest in ketamine is running high because subanesthetic doses of the drug have been shown to reduce depressive symptoms within a matter of hours, albeit transiently, in patients with treatment-resistant depression. If the drug acts as quickly in decreasing suicidal ideation as it does for depression, it would have major implications for clinical practice. An estimated 1 million people die each year worldwide from suicide, and two-thirds of them have major depressive disorder.
Dr. Blier reported on 27 patients with treatment-resistant depression, defined as failure to respond to at least two antidepressant medications from different pharmacologic classes at adequate dosages for at least 6 weeks each, along with two augmentation strategies. Their mean baseline score on the Montgomery-Asberg Depression Rating Scale (MADRS) was roughly 35. Five of the 27 had made one or more prior suicide attempts. Twenty-six of the 27 had suicidal ideation at baseline as defined by a MADRS suicidal ideation score (MADRS-SI) of more than 0. The MADRS-SI is based upon item 10 on the MADRS and is scored 0-6. Eight patients reported marked suicidal ideation as defined by a baseline MADRS-SI score of 4 or higher.
Study participants received a total of seven intravenous infusions of ketamine over roughly 3 weeks. Patients were retested 2-3 days after the seventh infusion, at which time 16 patients were categorized as treatment responders on the basis of at least a 50% reduction in their total MADRS score. Indeed, they averaged a 20.7-point reduction in the non–suicide-related MADRS score – that is, items 1-9, which reflect symptoms of depression – compared with a mere 3.9-point decrease in the 11 ketamine nonresponders. This 59% response rate for depressive symptoms is consistent with reported results of other studies of ketamine in patients with treatment-resistant depression, according to Dr. Blier, also professor of cellular/molecular medicines at the university.
The baseline MADRS-SI score averaged 2.9 in treatment responders and was similar at 2.5 in the nonresponders. But after seven infusions of ketamine, 21 of 27 patients had a MADRS-SI score of 0 or 1. The key study finding was that both the ketamine responders and nonresponders in terms of depressive symptoms experienced significant reductions in suicidal ideation. The 16 responders averaged a 2.4-point decrease from baseline in MADRS-SI scores, while the 11 nonresponders averaged a 1.5-point reduction. The magnitude of the reduction in MADRS-SI was significantly greater in the antidepressant responders than the nonresponders, but the improvement in suicidal ideation was statistically significant and clinically meaningful in both groups.
Seven of the 8 patients with baseline marked suicidal ideation and a MADRS-SI of 4 or greater improved to a score of 2 or less after their seven ketamine infusions, meaning they were having at most only fleeting suicidal thoughts.
Dr. Blier and coinvestigators are now expanding the ketamine study, enrolling up to 40 additional patients with treatment-resistant depression and suicidality in order to confirm the preliminary findings.
Dr. Blier reported having no financial conflicts of interest regarding this study, which was funded by the Canadian Institutes of Health Research. He noted that he receives research grants from and/or serves on advisory boards for more than a dozen pharmaceutical companies.
VIENNA – Repeated infusions of ketamine appear to have a direct effect in quelling suicidal ideation independent of the drug’s impact on depressive symptoms, Pierre Blier, MD, PhD, reported at the annual congress of the European College of Neuropsychopharmacology.
“Our preliminary results indicate that ketamine reduced suicidal ideation even in patients who failed to show a reduction in depression severity with repeated infusions,” observed Dr. Blier, professor of psychiatry at the University of Ottawa.
If the findings from this proof-of-concept study are confirmed, it would be very good news indeed.
“Suicidal ideation often requires rapid intervention, but there are very few treatments that are effective in reducing suicidal ideation, and none are fast acting,” the psychiatrist noted.
Therapeutic interest in ketamine is running high because subanesthetic doses of the drug have been shown to reduce depressive symptoms within a matter of hours, albeit transiently, in patients with treatment-resistant depression. If the drug acts as quickly in decreasing suicidal ideation as it does for depression, it would have major implications for clinical practice. An estimated 1 million people die each year worldwide from suicide, and two-thirds of them have major depressive disorder.
Dr. Blier reported on 27 patients with treatment-resistant depression, defined as failure to respond to at least two antidepressant medications from different pharmacologic classes at adequate dosages for at least 6 weeks each, along with two augmentation strategies. Their mean baseline score on the Montgomery-Asberg Depression Rating Scale (MADRS) was roughly 35. Five of the 27 had made one or more prior suicide attempts. Twenty-six of the 27 had suicidal ideation at baseline as defined by a MADRS suicidal ideation score (MADRS-SI) of more than 0. The MADRS-SI is based upon item 10 on the MADRS and is scored 0-6. Eight patients reported marked suicidal ideation as defined by a baseline MADRS-SI score of 4 or higher.
Study participants received a total of seven intravenous infusions of ketamine over roughly 3 weeks. Patients were retested 2-3 days after the seventh infusion, at which time 16 patients were categorized as treatment responders on the basis of at least a 50% reduction in their total MADRS score. Indeed, they averaged a 20.7-point reduction in the non–suicide-related MADRS score – that is, items 1-9, which reflect symptoms of depression – compared with a mere 3.9-point decrease in the 11 ketamine nonresponders. This 59% response rate for depressive symptoms is consistent with reported results of other studies of ketamine in patients with treatment-resistant depression, according to Dr. Blier, also professor of cellular/molecular medicines at the university.
The baseline MADRS-SI score averaged 2.9 in treatment responders and was similar at 2.5 in the nonresponders. But after seven infusions of ketamine, 21 of 27 patients had a MADRS-SI score of 0 or 1. The key study finding was that both the ketamine responders and nonresponders in terms of depressive symptoms experienced significant reductions in suicidal ideation. The 16 responders averaged a 2.4-point decrease from baseline in MADRS-SI scores, while the 11 nonresponders averaged a 1.5-point reduction. The magnitude of the reduction in MADRS-SI was significantly greater in the antidepressant responders than the nonresponders, but the improvement in suicidal ideation was statistically significant and clinically meaningful in both groups.
Seven of the 8 patients with baseline marked suicidal ideation and a MADRS-SI of 4 or greater improved to a score of 2 or less after their seven ketamine infusions, meaning they were having at most only fleeting suicidal thoughts.
Dr. Blier and coinvestigators are now expanding the ketamine study, enrolling up to 40 additional patients with treatment-resistant depression and suicidality in order to confirm the preliminary findings.
Dr. Blier reported having no financial conflicts of interest regarding this study, which was funded by the Canadian Institutes of Health Research. He noted that he receives research grants from and/or serves on advisory boards for more than a dozen pharmaceutical companies.
AT THE ECNP CONGRESS
Key clinical point:
Major finding: Ketamine infusions significantly reduced suicidal ideation even in patients whose treatment-resistant depression did not respond to the drug.
Data source: This ongoing observational study included 27 patients with treatment-resistant depression who received seven intravenous infusions of ketamine over roughly a 3-week period.
Disclosures: The presenter reported having no financial conflicts of interest regarding this study, which was funded by the Canadian Institutes of Health Research.
Telementoring expands PCPs’ role in managing pediatric chronic disease
SAN FRANCISCO – Telementoring empowers primary care pediatric providers (PCPs) to take on a greater role in managing their patients’ chronic diseases, new data suggest. Leaders in this emerging field gave a snapshot of early experience with the model at the annual meeting of the American Academy of Pediatrics.
“About a quarter of children live with chronic health conditions, and there is an increasing need for specialty care. But many children don’t have access to the quality specialty care that they really need, particularly in rural and medically underserved areas,” explained Dr. Sucheta M. Joshi, a pediatric neurologist and epileptologist at the University of Michigan, Ann Arbor. “The goal of telementoring is to build the capacity of primary care doctors.”

“We need to empower primary care providers to work ‘at the top of their license’ because we don’t have enough specialists,” agreed Dr. David
L. Wood, a general pediatrician and chair of the department of pediatrics at East Tennessee State University in Johnson City. “We as primary care [physicians] have to shoulder more of the care of kids with chronic disease. But we need backup, we need support to do that because the science is growing rapidly, we can’t keep up.”
Telementoring first gained recognition through the University of New Mexico’s Project Extension for Community Healthcare Outcomes (ECHO), which links specialists at an academic “hub” with PCPs in local communities, or “spokes,” in a learning network.
Through regular, interactive, multisite telementoring sessions, ECHO provides training to increase PCPs’ knowledge, self-efficacy, and comfort in managing chronic diseases not typically considered within their scope of practice. Sessions combine short didactic presentations and case-based learning.
The model was initially tested in pediatrics as ECHO for Epilepsy, a partnership of the AAP and the University of New Mexico, Albuquerque. Topics covered ranged from first seizures to work-up to treatment, including when to refer to a neurologist, according to Dr. Joshi, who helped develop the curriculum. Encouraging findings among the 49 clinics participating in the first year led to expansion of the program to five more states.
Preliminary data from the full cohort show reductions from baseline to end of the program in the proportions of participants who felt not at all or not very knowledgeable about pharmacologic management of pediatric epilepsy (from 69% to 45%), related school and education issues (from 51% to 18%), pertinent state driving laws (from 69% to 45%), and when to refer to a specialist (from 34% to 0%), Dr. Joshi reported.
There were also reductions in the proportions of participants who felt not at all or not very confident about aspects of care such as medical testing in this population (from 52% to 45%), communicating with patients about the transition to adult care (from 52% to 27%), and communicating with families and caregivers about the impact of epilepsy on everyday life (from 59% to 36%).
“This has been a good demonstration to say that telementoring does improve provider knowledge and confidence,” Dr. Joshi maintained. “Everybody felt quite uniformly that the case discussions were useful, and it really fostered a sense of a community of learners and was very much an iterative process.”
The AAP has since been designated as a “superhub” for Project ECHO that can train others to start programs in specialty areas. Additional programs have been developed in pediatric endocrinology, sickle cell disease, and surgery.

The main costs of ECHO are the personnel and physician time, and financing has yet to be worked out. “Unlike traditional telemedicine, where it’s one patient and one physician, and you can actually bill for it, this is not a billable service,” Dr. Joshi noted. “What you can get is more of a downstream effect, which can take some time to become obvious.”
The key attraction for providers is obtaining CME credits, where offered. And a draw for institutions is the potential impact of ECHO in reducing provider turnover and improving value-based reimbursement.
“This is really an innovative program that can help us achieve the triple aim” of improving the patient’s experience, reducing costs, and achieving better health outcomes, Dr. Wood said. “I think this is a great enhancement to the medical home.”
Both Dr. Joshi and Dr. Wood disclosed that they had no relevant conflicts of interest.
SAN FRANCISCO – Telementoring empowers primary care pediatric providers (PCPs) to take on a greater role in managing their patients’ chronic diseases, new data suggest. Leaders in this emerging field gave a snapshot of early experience with the model at the annual meeting of the American Academy of Pediatrics.
“About a quarter of children live with chronic health conditions, and there is an increasing need for specialty care. But many children don’t have access to the quality specialty care that they really need, particularly in rural and medically underserved areas,” explained Dr. Sucheta M. Joshi, a pediatric neurologist and epileptologist at the University of Michigan, Ann Arbor. “The goal of telementoring is to build the capacity of primary care doctors.”
“We need to empower primary care providers to work ‘at the top of their license’ because we don’t have enough specialists,” agreed Dr. David
L. Wood, a general pediatrician and chair of the department of pediatrics at East Tennessee State University in Johnson City. “We as primary care [physicians] have to shoulder more of the care of kids with chronic disease. But we need backup, we need support to do that because the science is growing rapidly, we can’t keep up.”
Telementoring first gained recognition through the University of New Mexico’s Project Extension for Community Healthcare Outcomes (ECHO), which links specialists at an academic “hub” with PCPs in local communities, or “spokes,” in a learning network.
Through regular, interactive, multisite telementoring sessions, ECHO provides training to increase PCPs’ knowledge, self-efficacy, and comfort in managing chronic diseases not typically considered within their scope of practice. Sessions combine short didactic presentations and case-based learning.
The model was initially tested in pediatrics as ECHO for Epilepsy, a partnership of the AAP and the University of New Mexico, Albuquerque. Topics covered ranged from first seizures to work-up to treatment, including when to refer to a neurologist, according to Dr. Joshi, who helped develop the curriculum. Encouraging findings among the 49 clinics participating in the first year led to expansion of the program to five more states.
Preliminary data from the full cohort show reductions from baseline to end of the program in the proportions of participants who felt not at all or not very knowledgeable about pharmacologic management of pediatric epilepsy (from 69% to 45%), related school and education issues (from 51% to 18%), pertinent state driving laws (from 69% to 45%), and when to refer to a specialist (from 34% to 0%), Dr. Joshi reported.
There were also reductions in the proportions of participants who felt not at all or not very confident about aspects of care such as medical testing in this population (from 52% to 45%), communicating with patients about the transition to adult care (from 52% to 27%), and communicating with families and caregivers about the impact of epilepsy on everyday life (from 59% to 36%).
“This has been a good demonstration to say that telementoring does improve provider knowledge and confidence,” Dr. Joshi maintained. “Everybody felt quite uniformly that the case discussions were useful, and it really fostered a sense of a community of learners and was very much an iterative process.”
The AAP has since been designated as a “superhub” for Project ECHO that can train others to start programs in specialty areas. Additional programs have been developed in pediatric endocrinology, sickle cell disease, and surgery.
The main costs of ECHO are the personnel and physician time, and financing has yet to be worked out. “Unlike traditional telemedicine, where it’s one patient and one physician, and you can actually bill for it, this is not a billable service,” Dr. Joshi noted. “What you can get is more of a downstream effect, which can take some time to become obvious.”
The key attraction for providers is obtaining CME credits, where offered. And a draw for institutions is the potential impact of ECHO in reducing provider turnover and improving value-based reimbursement.
“This is really an innovative program that can help us achieve the triple aim” of improving the patient’s experience, reducing costs, and achieving better health outcomes, Dr. Wood said. “I think this is a great enhancement to the medical home.”
Both Dr. Joshi and Dr. Wood disclosed that they had no relevant conflicts of interest.
SAN FRANCISCO – Telementoring empowers primary care pediatric providers (PCPs) to take on a greater role in managing their patients’ chronic diseases, new data suggest. Leaders in this emerging field gave a snapshot of early experience with the model at the annual meeting of the American Academy of Pediatrics.
“About a quarter of children live with chronic health conditions, and there is an increasing need for specialty care. But many children don’t have access to the quality specialty care that they really need, particularly in rural and medically underserved areas,” explained Dr. Sucheta M. Joshi, a pediatric neurologist and epileptologist at the University of Michigan, Ann Arbor. “The goal of telementoring is to build the capacity of primary care doctors.”
“We need to empower primary care providers to work ‘at the top of their license’ because we don’t have enough specialists,” agreed Dr. David
L. Wood, a general pediatrician and chair of the department of pediatrics at East Tennessee State University in Johnson City. “We as primary care [physicians] have to shoulder more of the care of kids with chronic disease. But we need backup, we need support to do that because the science is growing rapidly, we can’t keep up.”
Telementoring first gained recognition through the University of New Mexico’s Project Extension for Community Healthcare Outcomes (ECHO), which links specialists at an academic “hub” with PCPs in local communities, or “spokes,” in a learning network.
Through regular, interactive, multisite telementoring sessions, ECHO provides training to increase PCPs’ knowledge, self-efficacy, and comfort in managing chronic diseases not typically considered within their scope of practice. Sessions combine short didactic presentations and case-based learning.
The model was initially tested in pediatrics as ECHO for Epilepsy, a partnership of the AAP and the University of New Mexico, Albuquerque. Topics covered ranged from first seizures to work-up to treatment, including when to refer to a neurologist, according to Dr. Joshi, who helped develop the curriculum. Encouraging findings among the 49 clinics participating in the first year led to expansion of the program to five more states.
Preliminary data from the full cohort show reductions from baseline to end of the program in the proportions of participants who felt not at all or not very knowledgeable about pharmacologic management of pediatric epilepsy (from 69% to 45%), related school and education issues (from 51% to 18%), pertinent state driving laws (from 69% to 45%), and when to refer to a specialist (from 34% to 0%), Dr. Joshi reported.
There were also reductions in the proportions of participants who felt not at all or not very confident about aspects of care such as medical testing in this population (from 52% to 45%), communicating with patients about the transition to adult care (from 52% to 27%), and communicating with families and caregivers about the impact of epilepsy on everyday life (from 59% to 36%).
“This has been a good demonstration to say that telementoring does improve provider knowledge and confidence,” Dr. Joshi maintained. “Everybody felt quite uniformly that the case discussions were useful, and it really fostered a sense of a community of learners and was very much an iterative process.”
The AAP has since been designated as a “superhub” for Project ECHO that can train others to start programs in specialty areas. Additional programs have been developed in pediatric endocrinology, sickle cell disease, and surgery.
The main costs of ECHO are the personnel and physician time, and financing has yet to be worked out. “Unlike traditional telemedicine, where it’s one patient and one physician, and you can actually bill for it, this is not a billable service,” Dr. Joshi noted. “What you can get is more of a downstream effect, which can take some time to become obvious.”
The key attraction for providers is obtaining CME credits, where offered. And a draw for institutions is the potential impact of ECHO in reducing provider turnover and improving value-based reimbursement.
“This is really an innovative program that can help us achieve the triple aim” of improving the patient’s experience, reducing costs, and achieving better health outcomes, Dr. Wood said. “I think this is a great enhancement to the medical home.”
Both Dr. Joshi and Dr. Wood disclosed that they had no relevant conflicts of interest.
EXPERT ANALYSIS FROM AAP 16
Chemical Peels
Review the PDF of the fact sheet on Chemical Peels with board-relevant, easy-to-review material. This fact sheet will review the use of chemical peels for dermatologic indications.
Practice Questions
1. Which peel requires neutralization?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
2. Which peel contains resorcinol?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
3. Which peel would be the best treatment of severe actinic photodamage?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
4. Which peel would not be indicated for treatment of melasma in a patient with Fitzpatrick skin type IV?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
5. Which peel is a β-hydroxy acid?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
Answers to practice questions provided on next page
Practice Question Answers
1. Which peel requires neutralization?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
2. Which peel contains resorcinol?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
3. Which peel would be the best treatment of severe actinic photodamage?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
4. Which peel would not be indicated for treatment of melasma in a patient with Fitzpatrick skin type IV?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
5. Which peel is a β-hydroxy acid?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
Review the PDF of the fact sheet on Chemical Peels with board-relevant, easy-to-review material. This fact sheet will review the use of chemical peels for dermatologic indications.
Practice Questions
1. Which peel requires neutralization?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
2. Which peel contains resorcinol?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
3. Which peel would be the best treatment of severe actinic photodamage?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
4. Which peel would not be indicated for treatment of melasma in a patient with Fitzpatrick skin type IV?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
5. Which peel is a β-hydroxy acid?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
Answers to practice questions provided on next page
Practice Question Answers
1. Which peel requires neutralization?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
2. Which peel contains resorcinol?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
3. Which peel would be the best treatment of severe actinic photodamage?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
4. Which peel would not be indicated for treatment of melasma in a patient with Fitzpatrick skin type IV?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
5. Which peel is a β-hydroxy acid?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
Review the PDF of the fact sheet on Chemical Peels with board-relevant, easy-to-review material. This fact sheet will review the use of chemical peels for dermatologic indications.
Practice Questions
1. Which peel requires neutralization?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
2. Which peel contains resorcinol?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
3. Which peel would be the best treatment of severe actinic photodamage?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
4. Which peel would not be indicated for treatment of melasma in a patient with Fitzpatrick skin type IV?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
5. Which peel is a β-hydroxy acid?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
Answers to practice questions provided on next page
Practice Question Answers
1. Which peel requires neutralization?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
2. Which peel contains resorcinol?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
3. Which peel would be the best treatment of severe actinic photodamage?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
4. Which peel would not be indicated for treatment of melasma in a patient with Fitzpatrick skin type IV?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
5. Which peel is a β-hydroxy acid?
a. Baker-Gordon
b. glycolic acid
c. Jessner
d. salicylic acid
e. trichloroacetic acid
