User login
Sepsis mortality linked to concentration of critical care fellowships
LOS ANGELES – Compared with other parts of the United States, survival rates for sepsis were highest in the Northeast and in metropolitan areas in the Western regions of the United States, which mirrors the concentration of critical care fellowship programs, results from a descriptive analysis found.
“There must be consideration to redistribute the critical care work force based on the spread of the malady that they are trained to deal with,” lead study author Aditya Shah, MD, said in an interview in advance of the annual meeting of the American College of Chest Physicians. “This could be linked to better reimbursements in the underserved areas.”

Dr. Shah has conducted similar projects in patient populations with HIV and hepatitis, but to his knowledge, this is the first such analysis using NCHS data. “What is unique about this is that we can make real time presentations to see how the work force and the pathology is evolving with regards to an epidemiological stand point with real time data, which can be easily accessed,” he explained. “Depending on what we see, interventions and redistributions could be made with regards to better distributing providers based on where they are needed the most.”
Of 150 critical care fellowship programs identified in the analysis, the majority were concentrated in the Northeast and metropolitan areas in the Western regions of the United States, which parallel similar patterns noted in other specialties. Survival rates for sepsis were also higher in these locations. Dr. Shah said that the findings support previous studies, which indicated that physicians often tend to practice in geographic areas close to their training sites. However, the fact that such variation existed in mortality from sepsis – one of the most common diagnoses in the medical and surgical intensive care units – surprised him. “You would have thought that there would be a work force to deal with this malady,” he said.
He acknowledged certain limitations of the study, including the fact that the NCHS data do not enable researchers to break down mortality from particular causes of sepsis. “Also, the most current data will always lag behind as it is entered retrospectively and needs time to be uploaded online,” he said. “I am still in search of a more real-time database. However, that would require much more intensive time, money, and resources.”
Dr. Shah reported having no financial disclosures.
LOS ANGELES – Compared with other parts of the United States, survival rates for sepsis were highest in the Northeast and in metropolitan areas in the Western regions of the United States, which mirrors the concentration of critical care fellowship programs, results from a descriptive analysis found.
“There must be consideration to redistribute the critical care work force based on the spread of the malady that they are trained to deal with,” lead study author Aditya Shah, MD, said in an interview in advance of the annual meeting of the American College of Chest Physicians. “This could be linked to better reimbursements in the underserved areas.”
Dr. Shah has conducted similar projects in patient populations with HIV and hepatitis, but to his knowledge, this is the first such analysis using NCHS data. “What is unique about this is that we can make real time presentations to see how the work force and the pathology is evolving with regards to an epidemiological stand point with real time data, which can be easily accessed,” he explained. “Depending on what we see, interventions and redistributions could be made with regards to better distributing providers based on where they are needed the most.”
Of 150 critical care fellowship programs identified in the analysis, the majority were concentrated in the Northeast and metropolitan areas in the Western regions of the United States, which parallel similar patterns noted in other specialties. Survival rates for sepsis were also higher in these locations. Dr. Shah said that the findings support previous studies, which indicated that physicians often tend to practice in geographic areas close to their training sites. However, the fact that such variation existed in mortality from sepsis – one of the most common diagnoses in the medical and surgical intensive care units – surprised him. “You would have thought that there would be a work force to deal with this malady,” he said.
He acknowledged certain limitations of the study, including the fact that the NCHS data do not enable researchers to break down mortality from particular causes of sepsis. “Also, the most current data will always lag behind as it is entered retrospectively and needs time to be uploaded online,” he said. “I am still in search of a more real-time database. However, that would require much more intensive time, money, and resources.”
Dr. Shah reported having no financial disclosures.
LOS ANGELES – Compared with other parts of the United States, survival rates for sepsis were highest in the Northeast and in metropolitan areas in the Western regions of the United States, which mirrors the concentration of critical care fellowship programs, results from a descriptive analysis found.
“There must be consideration to redistribute the critical care work force based on the spread of the malady that they are trained to deal with,” lead study author Aditya Shah, MD, said in an interview in advance of the annual meeting of the American College of Chest Physicians. “This could be linked to better reimbursements in the underserved areas.”
Dr. Shah has conducted similar projects in patient populations with HIV and hepatitis, but to his knowledge, this is the first such analysis using NCHS data. “What is unique about this is that we can make real time presentations to see how the work force and the pathology is evolving with regards to an epidemiological stand point with real time data, which can be easily accessed,” he explained. “Depending on what we see, interventions and redistributions could be made with regards to better distributing providers based on where they are needed the most.”
Of 150 critical care fellowship programs identified in the analysis, the majority were concentrated in the Northeast and metropolitan areas in the Western regions of the United States, which parallel similar patterns noted in other specialties. Survival rates for sepsis were also higher in these locations. Dr. Shah said that the findings support previous studies, which indicated that physicians often tend to practice in geographic areas close to their training sites. However, the fact that such variation existed in mortality from sepsis – one of the most common diagnoses in the medical and surgical intensive care units – surprised him. “You would have thought that there would be a work force to deal with this malady,” he said.
He acknowledged certain limitations of the study, including the fact that the NCHS data do not enable researchers to break down mortality from particular causes of sepsis. “Also, the most current data will always lag behind as it is entered retrospectively and needs time to be uploaded online,” he said. “I am still in search of a more real-time database. However, that would require much more intensive time, money, and resources.”
Dr. Shah reported having no financial disclosures.
AT CHEST 2016
Key clinical point:
Major finding: Higher survival rates for sepsis were more concentrated in the Northeast and metropolitan areas in the Western regions of the United States, compared with other areas of the country.
Data source: A descriptive analysis that evaluated sepsis mortality data linked to 150 critical care fellowship programs in the United States.
Disclosures: Dr. Shah reported having no financial disclosures.
Resveratrol may reduce androgen levels in PCOS
The naturally occurring polyphenol resveratrol may have beneficial hormonal effects in women with polycystic ovary syndrome (PCOS), according to the results of a new study.
Previous in vitro research by the lead author, Beata Banaszewska, MD, from the division of infertility and reproductive endocrinology, in the department of gynecology, obstetrics, and gynecological oncology, Poznan University of Medical Sciences, Poznan, Poland, and her colleagues, suggested that resveratrol may inhibit cell growth and reduce androgen production in rat theca-interstitial cells, which are implicated in excessive androgen production in PCOS in humans.

They conducted a placebo-controlled trial, randomizing 34 women with PCOS to 1,500 mg oral resveratrol or placebo daily, with clinical, endocrine and metabolic assessments performed at baseline and three months after initiating treatment. The mean age of the women was 27 years; their mean BMI was 27.1 to 27.6 kg.m2.
At three months, serum total testosterone, the primary outcome, had declined significantly by 23.1% in the resveratrol group (P = .01), but increased by a non-significant 2.9% in the placebo group. The reduction in serum testosterone was even greater among individuals with a lower body mass index (J Clin Endocrinol Metab. 101: 3575–81, 2016. October 18. doi: 10.1210/jc.2016-1858).
Similarly, levels of dehydroepiandrosterone sulfate declined by a significant 22.2% in the resveratrol group (P = .01), but increased by a non-significant 10.5% in the placebo group, suggesting an effect on ovarian as well as adrenal androgen production.
“The magnitude of improvement of hyperandrogenemia observed in response to resveratrol is comparable to or greater than that found in response to OC [oral contraceptive] pills or metformin, with the exception of preparations containing cypretorone acetate, which are not available in the United States,” the authors wrote. They cited another study showing a 19% reduction in testosterone either with 12 months of treatment with the oral contraceptive pill or with metformin.
They also noted that while reductions in testosterone with metformin occur gradually over 3 to 6 months, their study showed a marked reduction in just three months.
Researchers also saw a significant 31.8% decline in fasting insulin (P = .007) and a 66.3% increase (P =.04) in the Insulin Sensitivity Index among patients treated with resveratrol.
Resveratrol was not associated with significant effects on BMI, ovarian volume, gonadotropins, lipid profile, or markers of inflammation and endothelial function. The women on placebo did show a significant reduction in ovarian volume, and increases in total and high-density lipoprotein cholesterol levels, prompting the authors to suggest that resveratrol may have prevented an increase in cholesterol that would otherwise have occurred.
Other than two patients on resveratrol reporting transient numbness, no other adverse events were noted.
While resveratrol, which is found in grapes, nuts and berries, is known to have anti-inflammatory, antioxidant, and cardioprotective properties, the authors said this was the first clinical study examining its effects in PCOS.
“Although identification of the mechanisms of action of resveratrol is not possible in this clinical trial, several possible mechanisms may be considered,” including a reduction of growth of theca cells, “and the improvement of insulin sensitivity with consequent reduction of insulin levels,” they wrote.
“Furthermore, given that insulin is known to stimulate androgen production in both ovarian and adrenal tissues, it is likely that the resveratrol-induced reduction of insulin observed in the present study may have contributed to a decrease of androgen levels,” they added.
RevGenetics provided the resveratrol for the study. The study was supported by the authors’ own institutions, and no conflicts of interest were declared.
The naturally occurring polyphenol resveratrol may have beneficial hormonal effects in women with polycystic ovary syndrome (PCOS), according to the results of a new study.
Previous in vitro research by the lead author, Beata Banaszewska, MD, from the division of infertility and reproductive endocrinology, in the department of gynecology, obstetrics, and gynecological oncology, Poznan University of Medical Sciences, Poznan, Poland, and her colleagues, suggested that resveratrol may inhibit cell growth and reduce androgen production in rat theca-interstitial cells, which are implicated in excessive androgen production in PCOS in humans.
They conducted a placebo-controlled trial, randomizing 34 women with PCOS to 1,500 mg oral resveratrol or placebo daily, with clinical, endocrine and metabolic assessments performed at baseline and three months after initiating treatment. The mean age of the women was 27 years; their mean BMI was 27.1 to 27.6 kg.m2.
At three months, serum total testosterone, the primary outcome, had declined significantly by 23.1% in the resveratrol group (P = .01), but increased by a non-significant 2.9% in the placebo group. The reduction in serum testosterone was even greater among individuals with a lower body mass index (J Clin Endocrinol Metab. 101: 3575–81, 2016. October 18. doi: 10.1210/jc.2016-1858).
Similarly, levels of dehydroepiandrosterone sulfate declined by a significant 22.2% in the resveratrol group (P = .01), but increased by a non-significant 10.5% in the placebo group, suggesting an effect on ovarian as well as adrenal androgen production.
“The magnitude of improvement of hyperandrogenemia observed in response to resveratrol is comparable to or greater than that found in response to OC [oral contraceptive] pills or metformin, with the exception of preparations containing cypretorone acetate, which are not available in the United States,” the authors wrote. They cited another study showing a 19% reduction in testosterone either with 12 months of treatment with the oral contraceptive pill or with metformin.
They also noted that while reductions in testosterone with metformin occur gradually over 3 to 6 months, their study showed a marked reduction in just three months.
Researchers also saw a significant 31.8% decline in fasting insulin (P = .007) and a 66.3% increase (P =.04) in the Insulin Sensitivity Index among patients treated with resveratrol.
Resveratrol was not associated with significant effects on BMI, ovarian volume, gonadotropins, lipid profile, or markers of inflammation and endothelial function. The women on placebo did show a significant reduction in ovarian volume, and increases in total and high-density lipoprotein cholesterol levels, prompting the authors to suggest that resveratrol may have prevented an increase in cholesterol that would otherwise have occurred.
Other than two patients on resveratrol reporting transient numbness, no other adverse events were noted.
While resveratrol, which is found in grapes, nuts and berries, is known to have anti-inflammatory, antioxidant, and cardioprotective properties, the authors said this was the first clinical study examining its effects in PCOS.
“Although identification of the mechanisms of action of resveratrol is not possible in this clinical trial, several possible mechanisms may be considered,” including a reduction of growth of theca cells, “and the improvement of insulin sensitivity with consequent reduction of insulin levels,” they wrote.
“Furthermore, given that insulin is known to stimulate androgen production in both ovarian and adrenal tissues, it is likely that the resveratrol-induced reduction of insulin observed in the present study may have contributed to a decrease of androgen levels,” they added.
RevGenetics provided the resveratrol for the study. The study was supported by the authors’ own institutions, and no conflicts of interest were declared.
The naturally occurring polyphenol resveratrol may have beneficial hormonal effects in women with polycystic ovary syndrome (PCOS), according to the results of a new study.
Previous in vitro research by the lead author, Beata Banaszewska, MD, from the division of infertility and reproductive endocrinology, in the department of gynecology, obstetrics, and gynecological oncology, Poznan University of Medical Sciences, Poznan, Poland, and her colleagues, suggested that resveratrol may inhibit cell growth and reduce androgen production in rat theca-interstitial cells, which are implicated in excessive androgen production in PCOS in humans.
They conducted a placebo-controlled trial, randomizing 34 women with PCOS to 1,500 mg oral resveratrol or placebo daily, with clinical, endocrine and metabolic assessments performed at baseline and three months after initiating treatment. The mean age of the women was 27 years; their mean BMI was 27.1 to 27.6 kg.m2.
At three months, serum total testosterone, the primary outcome, had declined significantly by 23.1% in the resveratrol group (P = .01), but increased by a non-significant 2.9% in the placebo group. The reduction in serum testosterone was even greater among individuals with a lower body mass index (J Clin Endocrinol Metab. 101: 3575–81, 2016. October 18. doi: 10.1210/jc.2016-1858).
Similarly, levels of dehydroepiandrosterone sulfate declined by a significant 22.2% in the resveratrol group (P = .01), but increased by a non-significant 10.5% in the placebo group, suggesting an effect on ovarian as well as adrenal androgen production.
“The magnitude of improvement of hyperandrogenemia observed in response to resveratrol is comparable to or greater than that found in response to OC [oral contraceptive] pills or metformin, with the exception of preparations containing cypretorone acetate, which are not available in the United States,” the authors wrote. They cited another study showing a 19% reduction in testosterone either with 12 months of treatment with the oral contraceptive pill or with metformin.
They also noted that while reductions in testosterone with metformin occur gradually over 3 to 6 months, their study showed a marked reduction in just three months.
Researchers also saw a significant 31.8% decline in fasting insulin (P = .007) and a 66.3% increase (P =.04) in the Insulin Sensitivity Index among patients treated with resveratrol.
Resveratrol was not associated with significant effects on BMI, ovarian volume, gonadotropins, lipid profile, or markers of inflammation and endothelial function. The women on placebo did show a significant reduction in ovarian volume, and increases in total and high-density lipoprotein cholesterol levels, prompting the authors to suggest that resveratrol may have prevented an increase in cholesterol that would otherwise have occurred.
Other than two patients on resveratrol reporting transient numbness, no other adverse events were noted.
While resveratrol, which is found in grapes, nuts and berries, is known to have anti-inflammatory, antioxidant, and cardioprotective properties, the authors said this was the first clinical study examining its effects in PCOS.
“Although identification of the mechanisms of action of resveratrol is not possible in this clinical trial, several possible mechanisms may be considered,” including a reduction of growth of theca cells, “and the improvement of insulin sensitivity with consequent reduction of insulin levels,” they wrote.
“Furthermore, given that insulin is known to stimulate androgen production in both ovarian and adrenal tissues, it is likely that the resveratrol-induced reduction of insulin observed in the present study may have contributed to a decrease of androgen levels,” they added.
RevGenetics provided the resveratrol for the study. The study was supported by the authors’ own institutions, and no conflicts of interest were declared.
FROM THE JOURNAL OF CLINICAL ENDOCRINOLOGY & METABOLISM
Key clinical point: The naturally occurring polyphenol resveratrol may reduce androgen and DHEAS levels in women with polycystic ovary syndrome.
Major finding: Treatment with resveratrol reduced total testosterone by 23.1% and dehydroepiandrosterone sulfate by 22.2%, while these levels increased in the placebo group.
Data source: A randomized placebo controlled trial in 34 women with polycystic ovary syndrome, randomizing women to 1,500 mg of oral resveratrol daily, or placebo.
Disclosures: The study was supported by the authors’ own institutions, and no conflicts of interest were declared. RevGenetics provided the resveratrol for the study.
An Electronic Template to Improve Psychotropic Medication Review and Gradual Dose-Reduction Documentation
One in 5 Americans are taking at least 1 psychotropic medication.1 Elderly dementia patients in extended care facilities are the most likely population to be prescribed psychotropic medication: 87% of these patients are on at least 1 psychotropic medication, 66% on at least 2, 36% on at least 3, and 11% on 4 or more.2 Psychotropic medications alleviate the symptoms of mental illness, such as depression, anxiety, and psychosis. Unfortunately, these medications often have adverse effects (AEs), including, but not limited to, excessive sedation, cardiac abnormalities, and tardive dyskinesia.
In 1987, Congress passed the Nursing Home Reform Act (NHRA) as part of the Omnibus Budget Reconciliation Act. The NHRA mandated that residents must remain free of “physical or chemical restraints imposed for the purpose of discipline or convenience.”3
In 1991, in order to meet the NHRA requirements, the Centers for Medicare and Medicaid Services (CMS) issued a guideline that nursing homes should use antipsychotic drug therapy only to treat a specific condition as diagnosed and documented in the clinical record. In 2006, CMS published guidance on the reduction of psychotropic medication usage. These CMS guidelines are the community-accepted standards for prescribing psychotropic medications, and accrediting bodies expect compliance with the guidelines. The guidelines also recommend that antipsychotics should be prescribed at the lowest possible dose, used for the shortest period, and continually undergo gradual dose reduction (GDR).4 To ensure these standards are met, a review of the use of psychotropic medications should be performed regularly.
The purpose of this project was to improve documentation of GDR and review of psychotropic medication based on CMS guidelines in the community living centers (CLCs) at the Carl Vinson Veterans Affairs Medical Center (CVVAMC) in Dublin, Georgia.
Background
The CVVAMC provides long-term care to veterans living in CLCs in a comfortable, homelike environment with a person-centered, nursing-home level of care. During a patient’s stay, clinical pharmacy services reviews patient medication use regularly. Additionally, an interdisciplinary team (IDT) of physicians, pharmacists, nurses, recreation therapists, dieticians, and chaplains meet to discuss the medical, psychosocial, and spiritual needs of the residents at the time of admission and quarterly thereafter. Family and caregivers are invited to attend as well.
During the meeting, the IDT care plan is updated and reviewed with the veteran. Currently at the CVVAMC, care plans include discussion of pain management; however, the plan does not address psychotropic medication use. To be compliant with CMS guidelines, during IDT meetings discussion of psychotropic medication use would be advantageous, because physicians could receive input and feedback from other health care team members in determining whether psychotropic medication changes are needed.
Methods
All documentation and chart notes are recorded and stored in the Computerized Patient Record System (CPRS). The purpose of an electronic template within CPRS is to provide standardized, guided documentation in an easy-to-use format that can be integrated smoothly into the existing system. Template utilization has been shown to improve documentation of medication reconciliation, health records, and coding in the VA health system.5-7 A review of CPRS showed that no template existed for documenting psychotropic medication initiation and GDR.
Objectives
The authors’ primary objective was to improve patient record documentation in CPRS through implementation of staff education and an electronic template for physicians to document the management of psychotropic medications and patients’ GDRs. The secondary objective was to implement a discussion involving the physician and other members of the team during IDT meetings about patient safety and effectiveness of psychotropic medications.
Template
To improve the suboptimal compliance with the CMS guidelines, an electronic template was created to evaluate GDR attempts and facilitate review of prescribed psychotropic medications. The pharmacy and therapeutics committee approved the template, and the clinical applications coordinator implemented the electronic template. The template was then revised as necessary for ease of use, based on health care provider (HCP) and pharmacist feedback.
The use of the electronic template was phased in over a 1-month period. Complete implementation was achieved in January 2014. An in-service was provided for nurses, HCPs, and directors on the importance of psychotropic medication review and GDRs. A second in-service was conducted for the HCPs to learn how to properly complete the electronic template. Providers were instructed to use the template during IDT meetings when completing monthly chart reviews and changing psychotropic medications.
Additionally, resident assessment coordinators who attend all IDT meetings were requested to remind the team to discuss psychotropic medication use if appropriate in an effort to add a psychotropic medication review to the IDT care plan.
To determine whether the electronic template improved documentation, a retrospective chart review of CPRS was conducted February 2014. The study included veterans in the CLC who were prescribed psychotropic medications since January 2014. The subjects who screened positive for psychotropic medication use were further evaluated by chart review. Before and after implementation, information was collected on the number and percentage of patients who had documentation in their CPRS records of a psychotropic medication review and on whether a GDR evaluation was recorded in CPRS. Additionally, a clinical pharmacist specialist attending the IDT meeting monitored the incidence of psychotropic medication review or discussion that took place if the veteran was on an included agent.
Results
A total of 67 patients on psychotropic medication on the CLC wards since January 2014 were included in the program. Before implementation of the program, 35 patients had documentation of psychotropic medication review. Following implementation, this increased to 54 patients. Hence, 80% of the patients had appropriate documentation.
Before implementation, no patients had documentation regarding evaluation of a GDR in CPRS. After the program implementation, 54 patients had documentation of GDR. Of the 54 patients, 50 had documentation that a GDR could not be completed, and 4 patients had undergone a trial of GDR with appropriate documentation in CPRS (Figure).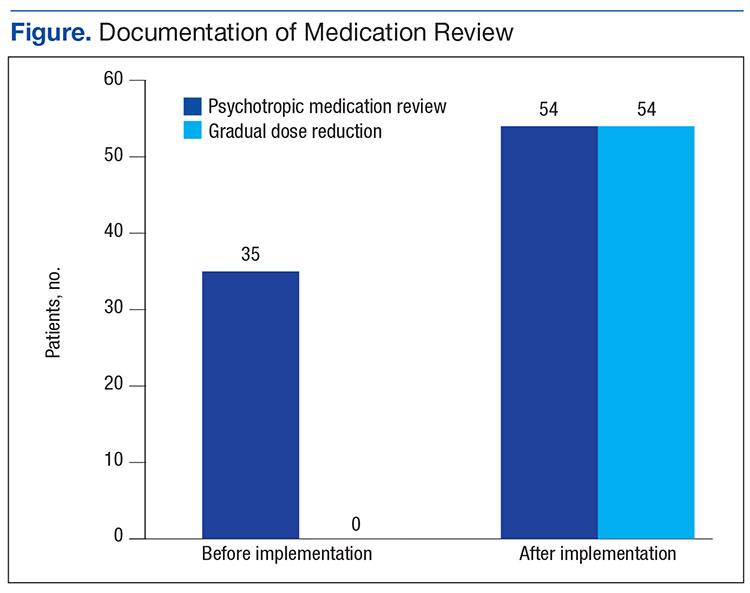
The secondary objective evaluated how often a review of patient’s psychotropic medication occurred during IDT meetings. During March 2014, 21 patients with scheduled IDT meetings were prescribed psychotropic medications. For 14 of the 21 patients (67%) appropriateness of psychotropic medications was reviewed with the team and the resident’s families.
Discussion
Documentation is fundamental to improving quality of care, patient outcomes, and reimbursement for the facility. Effective since July 1, 2014, the Joint Commission standards for Nursing Care Center accreditation require the physician and consulting pharmacist to review the patients’ or residents’ medication list. The review should verify the following:
- Clinical indication for the antipsychotic medication;
- Necessity for ongoing use of the antipsychotic medication;
- Consideration of GDR of the antipsychotic medication;
- Consideration of an alternative to antipsychotic medication use.8
When used correctly, the psychotropic medication review and GDR template ensures veterans’ psychotropic medications are continually reviewed. Furthermore, better psychotropic medication management allows veterans to be adequately treated while minimizing the risk for potential AEs.
At CVVAMC, the electronic template helped improve documentation and evaluation of GDR. The CVVAMC success can be attributed partly to physicians who were willing to use the template.
New standards from the Joint Commission provided an additional incentive to use the template. The Joint Commission also required that patients and their family be involved in decisions about placing the resident on antipsychotic medication. The optimal time for this discussion is during IDT meetings. At CVVAMC, discussion of psychotropic medications took place in IDT meetings for 67% of the patients prescribed psychotropic medication.
It is important to note that tools, such as this template, are successful only if they are used by HCPs. The CPRS does not have any clinical reminders to prompt physicians to complete the task. Instead, HCPs had to develop a routine of entering information into the template. Additionally, if the resident assessment coordinator was not at the IDT meeting, discussion of psychotropic medication was not always completed. After completion of this project, psychotropic medication review has become a permanent component of the IDT care plan.
Conclusion
This project demonstrated that template development and use have the potential to improve documentation, patient care, and survey scores. The electronic template could potentially benefit any long-term care facility that uses an electronic recording system. Further research should focus on ease of use and on ensuring that a psychotropic medication review is added to all CLC IDT care plans.
Acknowledgments
The authors acknowledge Brooke Butler, clinical pharmacy specialist and project mentor for her assistance and guidance; and Deborah Hobbs, residency director, both at the Carl Vinson VA Medical Center for her input and leadership, and Freddie Miles, for her work on development of the electronic order set.
1. Medco Health Solutions. America’s state of mind. 2011. http://apps.who.int/medicinedocs/documents/s19032en/s19032en.pdf. Accessed August 31, 2016.
2. Pitkala KH, Laurila JV, Strandberg TE, Tilvis RS. Behavioral symptoms and the administration of psychotropic drugs to aged patients with dementia in nursing homes and in acute geriatric wards. Int Psychogeriatr. 2004;16(1):61-74.
3. Rehnquist J. Psychotropic drug use in nursing homes. Office of Inspector General. https://oig.hhs.gov/oei/reports/oei-02-00-00491.pdf. Published November 2001. Accessed June 24, 2016.
4. Centers for Medicare and Medicaid Services. CMS Manual System. Pub 100-07 State Operations Provider Certification. https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Internet-Only-Manuals-IOMs-Items/CMS1201984.html. Published December 15, 2006. Accessed August 29, 2016.
5. Rose EA, Deshikachar AM, Schwartz KL, Severson RK. Use of a template to improve documentation and coding. Fam Med. 2001;33(7):516-521.
6. Fielstein EM, Brown SH, McBrine CS, Clark TK, Hardenbrook SP, Speroff T. The effect of standardized, computer-guided templates on quality of VA disability exams. AMIA Annu Symp Proc. 2006:249-253.
7. Edwards LB, Powers JB. Electronic medication reconciliation: a pilot demonstration on an inpatient geriatrics unit. Fed Pract. 2007;24(9):49-50, 53, 62.
8. Approved: memory care requirements for nursing center accreditation. http://www.jointcommission.org/ASSETS/1/18/JCP0114_MEMORY_CARE_NCC.PDF. Published January 2014. Accessed August 24, 2016.
One in 5 Americans are taking at least 1 psychotropic medication.1 Elderly dementia patients in extended care facilities are the most likely population to be prescribed psychotropic medication: 87% of these patients are on at least 1 psychotropic medication, 66% on at least 2, 36% on at least 3, and 11% on 4 or more.2 Psychotropic medications alleviate the symptoms of mental illness, such as depression, anxiety, and psychosis. Unfortunately, these medications often have adverse effects (AEs), including, but not limited to, excessive sedation, cardiac abnormalities, and tardive dyskinesia.
In 1987, Congress passed the Nursing Home Reform Act (NHRA) as part of the Omnibus Budget Reconciliation Act. The NHRA mandated that residents must remain free of “physical or chemical restraints imposed for the purpose of discipline or convenience.”3
In 1991, in order to meet the NHRA requirements, the Centers for Medicare and Medicaid Services (CMS) issued a guideline that nursing homes should use antipsychotic drug therapy only to treat a specific condition as diagnosed and documented in the clinical record. In 2006, CMS published guidance on the reduction of psychotropic medication usage. These CMS guidelines are the community-accepted standards for prescribing psychotropic medications, and accrediting bodies expect compliance with the guidelines. The guidelines also recommend that antipsychotics should be prescribed at the lowest possible dose, used for the shortest period, and continually undergo gradual dose reduction (GDR).4 To ensure these standards are met, a review of the use of psychotropic medications should be performed regularly.
The purpose of this project was to improve documentation of GDR and review of psychotropic medication based on CMS guidelines in the community living centers (CLCs) at the Carl Vinson Veterans Affairs Medical Center (CVVAMC) in Dublin, Georgia.
Background
The CVVAMC provides long-term care to veterans living in CLCs in a comfortable, homelike environment with a person-centered, nursing-home level of care. During a patient’s stay, clinical pharmacy services reviews patient medication use regularly. Additionally, an interdisciplinary team (IDT) of physicians, pharmacists, nurses, recreation therapists, dieticians, and chaplains meet to discuss the medical, psychosocial, and spiritual needs of the residents at the time of admission and quarterly thereafter. Family and caregivers are invited to attend as well.
During the meeting, the IDT care plan is updated and reviewed with the veteran. Currently at the CVVAMC, care plans include discussion of pain management; however, the plan does not address psychotropic medication use. To be compliant with CMS guidelines, during IDT meetings discussion of psychotropic medication use would be advantageous, because physicians could receive input and feedback from other health care team members in determining whether psychotropic medication changes are needed.
Methods
All documentation and chart notes are recorded and stored in the Computerized Patient Record System (CPRS). The purpose of an electronic template within CPRS is to provide standardized, guided documentation in an easy-to-use format that can be integrated smoothly into the existing system. Template utilization has been shown to improve documentation of medication reconciliation, health records, and coding in the VA health system.5-7 A review of CPRS showed that no template existed for documenting psychotropic medication initiation and GDR.
Objectives
The authors’ primary objective was to improve patient record documentation in CPRS through implementation of staff education and an electronic template for physicians to document the management of psychotropic medications and patients’ GDRs. The secondary objective was to implement a discussion involving the physician and other members of the team during IDT meetings about patient safety and effectiveness of psychotropic medications.
Template
To improve the suboptimal compliance with the CMS guidelines, an electronic template was created to evaluate GDR attempts and facilitate review of prescribed psychotropic medications. The pharmacy and therapeutics committee approved the template, and the clinical applications coordinator implemented the electronic template. The template was then revised as necessary for ease of use, based on health care provider (HCP) and pharmacist feedback.
The use of the electronic template was phased in over a 1-month period. Complete implementation was achieved in January 2014. An in-service was provided for nurses, HCPs, and directors on the importance of psychotropic medication review and GDRs. A second in-service was conducted for the HCPs to learn how to properly complete the electronic template. Providers were instructed to use the template during IDT meetings when completing monthly chart reviews and changing psychotropic medications.
Additionally, resident assessment coordinators who attend all IDT meetings were requested to remind the team to discuss psychotropic medication use if appropriate in an effort to add a psychotropic medication review to the IDT care plan.
To determine whether the electronic template improved documentation, a retrospective chart review of CPRS was conducted February 2014. The study included veterans in the CLC who were prescribed psychotropic medications since January 2014. The subjects who screened positive for psychotropic medication use were further evaluated by chart review. Before and after implementation, information was collected on the number and percentage of patients who had documentation in their CPRS records of a psychotropic medication review and on whether a GDR evaluation was recorded in CPRS. Additionally, a clinical pharmacist specialist attending the IDT meeting monitored the incidence of psychotropic medication review or discussion that took place if the veteran was on an included agent.
Results
A total of 67 patients on psychotropic medication on the CLC wards since January 2014 were included in the program. Before implementation of the program, 35 patients had documentation of psychotropic medication review. Following implementation, this increased to 54 patients. Hence, 80% of the patients had appropriate documentation.
Before implementation, no patients had documentation regarding evaluation of a GDR in CPRS. After the program implementation, 54 patients had documentation of GDR. Of the 54 patients, 50 had documentation that a GDR could not be completed, and 4 patients had undergone a trial of GDR with appropriate documentation in CPRS (Figure).
The secondary objective evaluated how often a review of patient’s psychotropic medication occurred during IDT meetings. During March 2014, 21 patients with scheduled IDT meetings were prescribed psychotropic medications. For 14 of the 21 patients (67%) appropriateness of psychotropic medications was reviewed with the team and the resident’s families.
Discussion
Documentation is fundamental to improving quality of care, patient outcomes, and reimbursement for the facility. Effective since July 1, 2014, the Joint Commission standards for Nursing Care Center accreditation require the physician and consulting pharmacist to review the patients’ or residents’ medication list. The review should verify the following:
- Clinical indication for the antipsychotic medication;
- Necessity for ongoing use of the antipsychotic medication;
- Consideration of GDR of the antipsychotic medication;
- Consideration of an alternative to antipsychotic medication use.8
When used correctly, the psychotropic medication review and GDR template ensures veterans’ psychotropic medications are continually reviewed. Furthermore, better psychotropic medication management allows veterans to be adequately treated while minimizing the risk for potential AEs.
At CVVAMC, the electronic template helped improve documentation and evaluation of GDR. The CVVAMC success can be attributed partly to physicians who were willing to use the template.
New standards from the Joint Commission provided an additional incentive to use the template. The Joint Commission also required that patients and their family be involved in decisions about placing the resident on antipsychotic medication. The optimal time for this discussion is during IDT meetings. At CVVAMC, discussion of psychotropic medications took place in IDT meetings for 67% of the patients prescribed psychotropic medication.
It is important to note that tools, such as this template, are successful only if they are used by HCPs. The CPRS does not have any clinical reminders to prompt physicians to complete the task. Instead, HCPs had to develop a routine of entering information into the template. Additionally, if the resident assessment coordinator was not at the IDT meeting, discussion of psychotropic medication was not always completed. After completion of this project, psychotropic medication review has become a permanent component of the IDT care plan.
Conclusion
This project demonstrated that template development and use have the potential to improve documentation, patient care, and survey scores. The electronic template could potentially benefit any long-term care facility that uses an electronic recording system. Further research should focus on ease of use and on ensuring that a psychotropic medication review is added to all CLC IDT care plans.
Acknowledgments
The authors acknowledge Brooke Butler, clinical pharmacy specialist and project mentor for her assistance and guidance; and Deborah Hobbs, residency director, both at the Carl Vinson VA Medical Center for her input and leadership, and Freddie Miles, for her work on development of the electronic order set.
One in 5 Americans are taking at least 1 psychotropic medication.1 Elderly dementia patients in extended care facilities are the most likely population to be prescribed psychotropic medication: 87% of these patients are on at least 1 psychotropic medication, 66% on at least 2, 36% on at least 3, and 11% on 4 or more.2 Psychotropic medications alleviate the symptoms of mental illness, such as depression, anxiety, and psychosis. Unfortunately, these medications often have adverse effects (AEs), including, but not limited to, excessive sedation, cardiac abnormalities, and tardive dyskinesia.
In 1987, Congress passed the Nursing Home Reform Act (NHRA) as part of the Omnibus Budget Reconciliation Act. The NHRA mandated that residents must remain free of “physical or chemical restraints imposed for the purpose of discipline or convenience.”3
In 1991, in order to meet the NHRA requirements, the Centers for Medicare and Medicaid Services (CMS) issued a guideline that nursing homes should use antipsychotic drug therapy only to treat a specific condition as diagnosed and documented in the clinical record. In 2006, CMS published guidance on the reduction of psychotropic medication usage. These CMS guidelines are the community-accepted standards for prescribing psychotropic medications, and accrediting bodies expect compliance with the guidelines. The guidelines also recommend that antipsychotics should be prescribed at the lowest possible dose, used for the shortest period, and continually undergo gradual dose reduction (GDR).4 To ensure these standards are met, a review of the use of psychotropic medications should be performed regularly.
The purpose of this project was to improve documentation of GDR and review of psychotropic medication based on CMS guidelines in the community living centers (CLCs) at the Carl Vinson Veterans Affairs Medical Center (CVVAMC) in Dublin, Georgia.
Background
The CVVAMC provides long-term care to veterans living in CLCs in a comfortable, homelike environment with a person-centered, nursing-home level of care. During a patient’s stay, clinical pharmacy services reviews patient medication use regularly. Additionally, an interdisciplinary team (IDT) of physicians, pharmacists, nurses, recreation therapists, dieticians, and chaplains meet to discuss the medical, psychosocial, and spiritual needs of the residents at the time of admission and quarterly thereafter. Family and caregivers are invited to attend as well.
During the meeting, the IDT care plan is updated and reviewed with the veteran. Currently at the CVVAMC, care plans include discussion of pain management; however, the plan does not address psychotropic medication use. To be compliant with CMS guidelines, during IDT meetings discussion of psychotropic medication use would be advantageous, because physicians could receive input and feedback from other health care team members in determining whether psychotropic medication changes are needed.
Methods
All documentation and chart notes are recorded and stored in the Computerized Patient Record System (CPRS). The purpose of an electronic template within CPRS is to provide standardized, guided documentation in an easy-to-use format that can be integrated smoothly into the existing system. Template utilization has been shown to improve documentation of medication reconciliation, health records, and coding in the VA health system.5-7 A review of CPRS showed that no template existed for documenting psychotropic medication initiation and GDR.
Objectives
The authors’ primary objective was to improve patient record documentation in CPRS through implementation of staff education and an electronic template for physicians to document the management of psychotropic medications and patients’ GDRs. The secondary objective was to implement a discussion involving the physician and other members of the team during IDT meetings about patient safety and effectiveness of psychotropic medications.
Template
To improve the suboptimal compliance with the CMS guidelines, an electronic template was created to evaluate GDR attempts and facilitate review of prescribed psychotropic medications. The pharmacy and therapeutics committee approved the template, and the clinical applications coordinator implemented the electronic template. The template was then revised as necessary for ease of use, based on health care provider (HCP) and pharmacist feedback.
The use of the electronic template was phased in over a 1-month period. Complete implementation was achieved in January 2014. An in-service was provided for nurses, HCPs, and directors on the importance of psychotropic medication review and GDRs. A second in-service was conducted for the HCPs to learn how to properly complete the electronic template. Providers were instructed to use the template during IDT meetings when completing monthly chart reviews and changing psychotropic medications.
Additionally, resident assessment coordinators who attend all IDT meetings were requested to remind the team to discuss psychotropic medication use if appropriate in an effort to add a psychotropic medication review to the IDT care plan.
To determine whether the electronic template improved documentation, a retrospective chart review of CPRS was conducted February 2014. The study included veterans in the CLC who were prescribed psychotropic medications since January 2014. The subjects who screened positive for psychotropic medication use were further evaluated by chart review. Before and after implementation, information was collected on the number and percentage of patients who had documentation in their CPRS records of a psychotropic medication review and on whether a GDR evaluation was recorded in CPRS. Additionally, a clinical pharmacist specialist attending the IDT meeting monitored the incidence of psychotropic medication review or discussion that took place if the veteran was on an included agent.
Results
A total of 67 patients on psychotropic medication on the CLC wards since January 2014 were included in the program. Before implementation of the program, 35 patients had documentation of psychotropic medication review. Following implementation, this increased to 54 patients. Hence, 80% of the patients had appropriate documentation.
Before implementation, no patients had documentation regarding evaluation of a GDR in CPRS. After the program implementation, 54 patients had documentation of GDR. Of the 54 patients, 50 had documentation that a GDR could not be completed, and 4 patients had undergone a trial of GDR with appropriate documentation in CPRS (Figure).
The secondary objective evaluated how often a review of patient’s psychotropic medication occurred during IDT meetings. During March 2014, 21 patients with scheduled IDT meetings were prescribed psychotropic medications. For 14 of the 21 patients (67%) appropriateness of psychotropic medications was reviewed with the team and the resident’s families.
Discussion
Documentation is fundamental to improving quality of care, patient outcomes, and reimbursement for the facility. Effective since July 1, 2014, the Joint Commission standards for Nursing Care Center accreditation require the physician and consulting pharmacist to review the patients’ or residents’ medication list. The review should verify the following:
- Clinical indication for the antipsychotic medication;
- Necessity for ongoing use of the antipsychotic medication;
- Consideration of GDR of the antipsychotic medication;
- Consideration of an alternative to antipsychotic medication use.8
When used correctly, the psychotropic medication review and GDR template ensures veterans’ psychotropic medications are continually reviewed. Furthermore, better psychotropic medication management allows veterans to be adequately treated while minimizing the risk for potential AEs.
At CVVAMC, the electronic template helped improve documentation and evaluation of GDR. The CVVAMC success can be attributed partly to physicians who were willing to use the template.
New standards from the Joint Commission provided an additional incentive to use the template. The Joint Commission also required that patients and their family be involved in decisions about placing the resident on antipsychotic medication. The optimal time for this discussion is during IDT meetings. At CVVAMC, discussion of psychotropic medications took place in IDT meetings for 67% of the patients prescribed psychotropic medication.
It is important to note that tools, such as this template, are successful only if they are used by HCPs. The CPRS does not have any clinical reminders to prompt physicians to complete the task. Instead, HCPs had to develop a routine of entering information into the template. Additionally, if the resident assessment coordinator was not at the IDT meeting, discussion of psychotropic medication was not always completed. After completion of this project, psychotropic medication review has become a permanent component of the IDT care plan.
Conclusion
This project demonstrated that template development and use have the potential to improve documentation, patient care, and survey scores. The electronic template could potentially benefit any long-term care facility that uses an electronic recording system. Further research should focus on ease of use and on ensuring that a psychotropic medication review is added to all CLC IDT care plans.
Acknowledgments
The authors acknowledge Brooke Butler, clinical pharmacy specialist and project mentor for her assistance and guidance; and Deborah Hobbs, residency director, both at the Carl Vinson VA Medical Center for her input and leadership, and Freddie Miles, for her work on development of the electronic order set.
1. Medco Health Solutions. America’s state of mind. 2011. http://apps.who.int/medicinedocs/documents/s19032en/s19032en.pdf. Accessed August 31, 2016.
2. Pitkala KH, Laurila JV, Strandberg TE, Tilvis RS. Behavioral symptoms and the administration of psychotropic drugs to aged patients with dementia in nursing homes and in acute geriatric wards. Int Psychogeriatr. 2004;16(1):61-74.
3. Rehnquist J. Psychotropic drug use in nursing homes. Office of Inspector General. https://oig.hhs.gov/oei/reports/oei-02-00-00491.pdf. Published November 2001. Accessed June 24, 2016.
4. Centers for Medicare and Medicaid Services. CMS Manual System. Pub 100-07 State Operations Provider Certification. https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Internet-Only-Manuals-IOMs-Items/CMS1201984.html. Published December 15, 2006. Accessed August 29, 2016.
5. Rose EA, Deshikachar AM, Schwartz KL, Severson RK. Use of a template to improve documentation and coding. Fam Med. 2001;33(7):516-521.
6. Fielstein EM, Brown SH, McBrine CS, Clark TK, Hardenbrook SP, Speroff T. The effect of standardized, computer-guided templates on quality of VA disability exams. AMIA Annu Symp Proc. 2006:249-253.
7. Edwards LB, Powers JB. Electronic medication reconciliation: a pilot demonstration on an inpatient geriatrics unit. Fed Pract. 2007;24(9):49-50, 53, 62.
8. Approved: memory care requirements for nursing center accreditation. http://www.jointcommission.org/ASSETS/1/18/JCP0114_MEMORY_CARE_NCC.PDF. Published January 2014. Accessed August 24, 2016.
1. Medco Health Solutions. America’s state of mind. 2011. http://apps.who.int/medicinedocs/documents/s19032en/s19032en.pdf. Accessed August 31, 2016.
2. Pitkala KH, Laurila JV, Strandberg TE, Tilvis RS. Behavioral symptoms and the administration of psychotropic drugs to aged patients with dementia in nursing homes and in acute geriatric wards. Int Psychogeriatr. 2004;16(1):61-74.
3. Rehnquist J. Psychotropic drug use in nursing homes. Office of Inspector General. https://oig.hhs.gov/oei/reports/oei-02-00-00491.pdf. Published November 2001. Accessed June 24, 2016.
4. Centers for Medicare and Medicaid Services. CMS Manual System. Pub 100-07 State Operations Provider Certification. https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Internet-Only-Manuals-IOMs-Items/CMS1201984.html. Published December 15, 2006. Accessed August 29, 2016.
5. Rose EA, Deshikachar AM, Schwartz KL, Severson RK. Use of a template to improve documentation and coding. Fam Med. 2001;33(7):516-521.
6. Fielstein EM, Brown SH, McBrine CS, Clark TK, Hardenbrook SP, Speroff T. The effect of standardized, computer-guided templates on quality of VA disability exams. AMIA Annu Symp Proc. 2006:249-253.
7. Edwards LB, Powers JB. Electronic medication reconciliation: a pilot demonstration on an inpatient geriatrics unit. Fed Pract. 2007;24(9):49-50, 53, 62.
8. Approved: memory care requirements for nursing center accreditation. http://www.jointcommission.org/ASSETS/1/18/JCP0114_MEMORY_CARE_NCC.PDF. Published January 2014. Accessed August 24, 2016.
Serious AEs reported too late in lymphoma trial
Photo by Bill Branson
Investigators conducting a phase 1 trial failed to follow requirements for reporting serious adverse events (AEs), including deaths, according to officials from the National Cancer Institute (NCI) and the National Institutes of Health (NIH).
The trial was an NCI-sponsored study of ibrutinib in combination with dose-adjusted temozolomide, etoposide, liposomal doxorubicin, dexamethasone, and rituximab (DA-TEDDi-R) in patients with primary CNS lymphoma.
Four patients in this trial developed invasive aspergillosis, 3 others had unconfirmed Aspergillus infections, and 2 patients died of aspergillosis in 2015.
Trial investigators did not report these events to the NCI or the institutional review board (IRB) as quickly as required by the study protocol.
In addition, the suspected relationship between Aspergillus infections and the study treatment wasn’t reported to the US Food and Drug Administration (FDA) until May 2016, several months after the second patient died of aspergillosis.
Francis S. Collins, MD, PhD, director of the NIH, and Douglas R. Lowy, MD, acting director of the NCI, discussed this delay in reporting during a meeting of the Clinical Center Hospital Board last Friday.
About the trial
The trial (NCT02203526) enrolled 18 patients with primary CNS lymphoma—13 relapsed/refractory and 5 previously untreated—between August 2014 and March 2016.
Patients received 14 days of ibrutinib (with corticosteroids to prevent cerebral edema), followed by six 21-day cycles of DA-TEDDi-R.
Twelve patients achieved a complete response following treatment, 5 had a partial response, and 1 patient progressed without responding. Eight patients remain in complete response, 2 have progressed, and 8 have died.
Four patients developed invasive aspergillosis, and 3 had possible Aspergillus infections. Two deaths, which occurred in May and December of 2015, were attributed to aspergillosis.
Some patients developed aspergillosis while they were receiving only steroids and ibrutinib, which led the investigators to believe there was a causative relationship between Aspergillus infections and treatment with ibrutinib/steroids.
The investigators stopped trial accrual in April 2016 due to the Aspergillus infections. The suspected relationship between the infections and ibrutinib/steroids was reported to the FDA in late May 2016.
Delayed reporting
On October 3, 2016, the FDA issued a 483 report to the trial’s principal investigator, Kieron Dunleavy, MD, of the NCI. The report cited “delays and deficient reporting” of serious AEs/unanticipated problems to the trial’s sponsor and IRB.
The trial’s protocol required that grade 3-5 AEs be reported to the NCI within 24 hours of occurrence and unanticipated problems be reported to the IRB within 7 days.
The median time of delayed reporting to the NCI was 40 days (range, 4 to 456), and the median time of delayed reporting to the IRB was 18 days (range, 8 to 56).
As a result of the delayed reporting, Dr Dunleavy has been suspended from conducting clinical research in the NIH Clinical Center, and holds have been placed on trials conducted by the NCI lymphoma team.
The accrual of current studies and the opening of planned studies by the lymphoma team have been stopped. The team will be allowed to resume/begin studies after they undergo training and once the NCI and an outside contractor complete an audit of all NCI lymphoma trials that have been open over the last 3 years.
Patients involved in the trial of DA-TEDDi-R (and their families) have been informed of the delayed AE reporting.
Various parties involved in NIH/NCI trials have been reminded about the importance of timely reporting of safety and regulatory information.
The NCI and NIH are taking steps to ensure that AEs are reported promptly in the future. And the Office of Research Support and Compliance has been tasked with investigating past reporting of AEs in NIH trials, particularly those conducted at the Clinical Center. ![]()
Photo by Bill Branson
Investigators conducting a phase 1 trial failed to follow requirements for reporting serious adverse events (AEs), including deaths, according to officials from the National Cancer Institute (NCI) and the National Institutes of Health (NIH).
The trial was an NCI-sponsored study of ibrutinib in combination with dose-adjusted temozolomide, etoposide, liposomal doxorubicin, dexamethasone, and rituximab (DA-TEDDi-R) in patients with primary CNS lymphoma.
Four patients in this trial developed invasive aspergillosis, 3 others had unconfirmed Aspergillus infections, and 2 patients died of aspergillosis in 2015.
Trial investigators did not report these events to the NCI or the institutional review board (IRB) as quickly as required by the study protocol.
In addition, the suspected relationship between Aspergillus infections and the study treatment wasn’t reported to the US Food and Drug Administration (FDA) until May 2016, several months after the second patient died of aspergillosis.
Francis S. Collins, MD, PhD, director of the NIH, and Douglas R. Lowy, MD, acting director of the NCI, discussed this delay in reporting during a meeting of the Clinical Center Hospital Board last Friday.
About the trial
The trial (NCT02203526) enrolled 18 patients with primary CNS lymphoma—13 relapsed/refractory and 5 previously untreated—between August 2014 and March 2016.
Patients received 14 days of ibrutinib (with corticosteroids to prevent cerebral edema), followed by six 21-day cycles of DA-TEDDi-R.
Twelve patients achieved a complete response following treatment, 5 had a partial response, and 1 patient progressed without responding. Eight patients remain in complete response, 2 have progressed, and 8 have died.
Four patients developed invasive aspergillosis, and 3 had possible Aspergillus infections. Two deaths, which occurred in May and December of 2015, were attributed to aspergillosis.
Some patients developed aspergillosis while they were receiving only steroids and ibrutinib, which led the investigators to believe there was a causative relationship between Aspergillus infections and treatment with ibrutinib/steroids.
The investigators stopped trial accrual in April 2016 due to the Aspergillus infections. The suspected relationship between the infections and ibrutinib/steroids was reported to the FDA in late May 2016.
Delayed reporting
On October 3, 2016, the FDA issued a 483 report to the trial’s principal investigator, Kieron Dunleavy, MD, of the NCI. The report cited “delays and deficient reporting” of serious AEs/unanticipated problems to the trial’s sponsor and IRB.
The trial’s protocol required that grade 3-5 AEs be reported to the NCI within 24 hours of occurrence and unanticipated problems be reported to the IRB within 7 days.
The median time of delayed reporting to the NCI was 40 days (range, 4 to 456), and the median time of delayed reporting to the IRB was 18 days (range, 8 to 56).
As a result of the delayed reporting, Dr Dunleavy has been suspended from conducting clinical research in the NIH Clinical Center, and holds have been placed on trials conducted by the NCI lymphoma team.
The accrual of current studies and the opening of planned studies by the lymphoma team have been stopped. The team will be allowed to resume/begin studies after they undergo training and once the NCI and an outside contractor complete an audit of all NCI lymphoma trials that have been open over the last 3 years.
Patients involved in the trial of DA-TEDDi-R (and their families) have been informed of the delayed AE reporting.
Various parties involved in NIH/NCI trials have been reminded about the importance of timely reporting of safety and regulatory information.
The NCI and NIH are taking steps to ensure that AEs are reported promptly in the future. And the Office of Research Support and Compliance has been tasked with investigating past reporting of AEs in NIH trials, particularly those conducted at the Clinical Center. ![]()
Photo by Bill Branson
Investigators conducting a phase 1 trial failed to follow requirements for reporting serious adverse events (AEs), including deaths, according to officials from the National Cancer Institute (NCI) and the National Institutes of Health (NIH).
The trial was an NCI-sponsored study of ibrutinib in combination with dose-adjusted temozolomide, etoposide, liposomal doxorubicin, dexamethasone, and rituximab (DA-TEDDi-R) in patients with primary CNS lymphoma.
Four patients in this trial developed invasive aspergillosis, 3 others had unconfirmed Aspergillus infections, and 2 patients died of aspergillosis in 2015.
Trial investigators did not report these events to the NCI or the institutional review board (IRB) as quickly as required by the study protocol.
In addition, the suspected relationship between Aspergillus infections and the study treatment wasn’t reported to the US Food and Drug Administration (FDA) until May 2016, several months after the second patient died of aspergillosis.
Francis S. Collins, MD, PhD, director of the NIH, and Douglas R. Lowy, MD, acting director of the NCI, discussed this delay in reporting during a meeting of the Clinical Center Hospital Board last Friday.
About the trial
The trial (NCT02203526) enrolled 18 patients with primary CNS lymphoma—13 relapsed/refractory and 5 previously untreated—between August 2014 and March 2016.
Patients received 14 days of ibrutinib (with corticosteroids to prevent cerebral edema), followed by six 21-day cycles of DA-TEDDi-R.
Twelve patients achieved a complete response following treatment, 5 had a partial response, and 1 patient progressed without responding. Eight patients remain in complete response, 2 have progressed, and 8 have died.
Four patients developed invasive aspergillosis, and 3 had possible Aspergillus infections. Two deaths, which occurred in May and December of 2015, were attributed to aspergillosis.
Some patients developed aspergillosis while they were receiving only steroids and ibrutinib, which led the investigators to believe there was a causative relationship between Aspergillus infections and treatment with ibrutinib/steroids.
The investigators stopped trial accrual in April 2016 due to the Aspergillus infections. The suspected relationship between the infections and ibrutinib/steroids was reported to the FDA in late May 2016.
Delayed reporting
On October 3, 2016, the FDA issued a 483 report to the trial’s principal investigator, Kieron Dunleavy, MD, of the NCI. The report cited “delays and deficient reporting” of serious AEs/unanticipated problems to the trial’s sponsor and IRB.
The trial’s protocol required that grade 3-5 AEs be reported to the NCI within 24 hours of occurrence and unanticipated problems be reported to the IRB within 7 days.
The median time of delayed reporting to the NCI was 40 days (range, 4 to 456), and the median time of delayed reporting to the IRB was 18 days (range, 8 to 56).
As a result of the delayed reporting, Dr Dunleavy has been suspended from conducting clinical research in the NIH Clinical Center, and holds have been placed on trials conducted by the NCI lymphoma team.
The accrual of current studies and the opening of planned studies by the lymphoma team have been stopped. The team will be allowed to resume/begin studies after they undergo training and once the NCI and an outside contractor complete an audit of all NCI lymphoma trials that have been open over the last 3 years.
Patients involved in the trial of DA-TEDDi-R (and their families) have been informed of the delayed AE reporting.
Various parties involved in NIH/NCI trials have been reminded about the importance of timely reporting of safety and regulatory information.
The NCI and NIH are taking steps to ensure that AEs are reported promptly in the future. And the Office of Research Support and Compliance has been tasked with investigating past reporting of AEs in NIH trials, particularly those conducted at the Clinical Center. ![]()
Legislators question price of leukemia drug
Photo from Business Wire
A pair of US legislators are questioning why ARIAD Pharmaceuticals, Inc. has increased the price of its leukemia drug Iclusig (ponatinib) by more than $80,000 over the last several years.
ARIAD raised the price of Iclusig 4 times in 2016. The drug now costs nearly $199,000 a year.
Senator Bernie Sanders (Vermont) and Congressman Elijah Cummings (Maryland) sent a letter to ARIAD last week requesting information about these price increases.
Cummings and Sanders are also investigating whether ARIAD took additional steps to boost profits by discontinuing sales of certain dosages and quantities of Iclusig in order to charge patients and insurers more in exchange for less medicine.
“These outrageous sales tactics indicate that ARIAD is more concerned with its profit than with its patients,” Sanders and Cummings wrote in the letter.
The US Food and Drug Administration (FDA) approved Iclusig in December 2012 to treat chronic myeloid leukemia (CML) and Philadelphia chromosome-positive acute lymphoblastic leukemia (ALL).
In late 2013, the FDA suspended sales and clinical trials of the drug due to reports of serious adverse events.
The FDA allowed ARIAD to resume selling Iclusig in December 2013, but only to CML/ALL patients who cannot tolerate, or whose disease is resistant to, other tyrosine kinase inhibitors.
“Despite this new evidence showing the drug posed a far greater safety risk to patients than was known when the drug came on the market, ARIAD nonetheless raised the price of Iclusig several times over the subsequent 4 years,” Sanders and Cummings wrote.
“In the interest of patients and taxpayers, we are interested in learning more about the impact that the escalating price and restrictions on product availability have had.”
ARIAD has released a statement acknowledging Cummings’ and Sanders’ letter and defending its decisions to increase the price of Iclusig.
The company said it “makes significant investments in research and development (R&D) to advance breakthrough treatments” for patients with rare cancers.
In fact, ARIAD has invested more than $1.3 billion in R&D and accumulated losses of approximately $1.4 billion, which have not been recovered. In 2015, ARIAD generated $119 million in total revenue and invested $171 million in R&D.
The company said it intends to respond to Cummings’ and Sanders’ request for information. ![]()
Photo from Business Wire
A pair of US legislators are questioning why ARIAD Pharmaceuticals, Inc. has increased the price of its leukemia drug Iclusig (ponatinib) by more than $80,000 over the last several years.
ARIAD raised the price of Iclusig 4 times in 2016. The drug now costs nearly $199,000 a year.
Senator Bernie Sanders (Vermont) and Congressman Elijah Cummings (Maryland) sent a letter to ARIAD last week requesting information about these price increases.
Cummings and Sanders are also investigating whether ARIAD took additional steps to boost profits by discontinuing sales of certain dosages and quantities of Iclusig in order to charge patients and insurers more in exchange for less medicine.
“These outrageous sales tactics indicate that ARIAD is more concerned with its profit than with its patients,” Sanders and Cummings wrote in the letter.
The US Food and Drug Administration (FDA) approved Iclusig in December 2012 to treat chronic myeloid leukemia (CML) and Philadelphia chromosome-positive acute lymphoblastic leukemia (ALL).
In late 2013, the FDA suspended sales and clinical trials of the drug due to reports of serious adverse events.
The FDA allowed ARIAD to resume selling Iclusig in December 2013, but only to CML/ALL patients who cannot tolerate, or whose disease is resistant to, other tyrosine kinase inhibitors.
“Despite this new evidence showing the drug posed a far greater safety risk to patients than was known when the drug came on the market, ARIAD nonetheless raised the price of Iclusig several times over the subsequent 4 years,” Sanders and Cummings wrote.
“In the interest of patients and taxpayers, we are interested in learning more about the impact that the escalating price and restrictions on product availability have had.”
ARIAD has released a statement acknowledging Cummings’ and Sanders’ letter and defending its decisions to increase the price of Iclusig.
The company said it “makes significant investments in research and development (R&D) to advance breakthrough treatments” for patients with rare cancers.
In fact, ARIAD has invested more than $1.3 billion in R&D and accumulated losses of approximately $1.4 billion, which have not been recovered. In 2015, ARIAD generated $119 million in total revenue and invested $171 million in R&D.
The company said it intends to respond to Cummings’ and Sanders’ request for information. ![]()
Photo from Business Wire
A pair of US legislators are questioning why ARIAD Pharmaceuticals, Inc. has increased the price of its leukemia drug Iclusig (ponatinib) by more than $80,000 over the last several years.
ARIAD raised the price of Iclusig 4 times in 2016. The drug now costs nearly $199,000 a year.
Senator Bernie Sanders (Vermont) and Congressman Elijah Cummings (Maryland) sent a letter to ARIAD last week requesting information about these price increases.
Cummings and Sanders are also investigating whether ARIAD took additional steps to boost profits by discontinuing sales of certain dosages and quantities of Iclusig in order to charge patients and insurers more in exchange for less medicine.
“These outrageous sales tactics indicate that ARIAD is more concerned with its profit than with its patients,” Sanders and Cummings wrote in the letter.
The US Food and Drug Administration (FDA) approved Iclusig in December 2012 to treat chronic myeloid leukemia (CML) and Philadelphia chromosome-positive acute lymphoblastic leukemia (ALL).
In late 2013, the FDA suspended sales and clinical trials of the drug due to reports of serious adverse events.
The FDA allowed ARIAD to resume selling Iclusig in December 2013, but only to CML/ALL patients who cannot tolerate, or whose disease is resistant to, other tyrosine kinase inhibitors.
“Despite this new evidence showing the drug posed a far greater safety risk to patients than was known when the drug came on the market, ARIAD nonetheless raised the price of Iclusig several times over the subsequent 4 years,” Sanders and Cummings wrote.
“In the interest of patients and taxpayers, we are interested in learning more about the impact that the escalating price and restrictions on product availability have had.”
ARIAD has released a statement acknowledging Cummings’ and Sanders’ letter and defending its decisions to increase the price of Iclusig.
The company said it “makes significant investments in research and development (R&D) to advance breakthrough treatments” for patients with rare cancers.
In fact, ARIAD has invested more than $1.3 billion in R&D and accumulated losses of approximately $1.4 billion, which have not been recovered. In 2015, ARIAD generated $119 million in total revenue and invested $171 million in R&D.
The company said it intends to respond to Cummings’ and Sanders’ request for information. ![]()
COPD: Diagnostic and Treatment Update for the Primary Care Setting
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Smokers’ hand grip strength predicts risk for respiratory events
LOS ANGELES – Hand grip strength is independently predictive of risk for respiratory events in smokers who have or are at risk for chronic obstructive pulmonary disease, results from a single-center study showed.
“Measures of lung function, including spirometry, are used as the main descriptors of COPD severity and prognosis,” Carlos H. Martinez, MD, MPH, said in an interview in advance of the annual meeting of the American College of Chest Physicians. “These measurements, as important as they are, need to be improved, in order to develop better risk and prognostic models of the disease, to identify subgroups at higher risk of poor outcomes ... With our work, we have proved that simple physical tests could be part of future prognostic models.”

Interest has grown in developing multidimensional models to predict respiratory prognosis. Such models include BODE (body mass index, airflow obstruction, dyspnea and exercise capacity), ADO (age, dyspnea and airflow obstruction), and DOSE (dyspnea, airflow obstruction, smoking status, and exacerbation frequency).
In patients with or at risk for COPD, Dr. Martinez, of the University of Michigan Health System, Ann Arbor, and his colleagues tested the associations of hand grip strength with measures of body composition such as pectoralis muscle area and extent of subcutaneous fat, imaging phenotypes, and lung function.
The researchers obtained demographic, clinical, lung function, hand grip strength, and imaging data from 441 smokers with and without COPD participating in the Genetic Epidemiology of COPD Study (COPDGene) at the National Jewish Health in Denver. Imaging methods used in the study were developed by George R. Washko, MD, and his associates at Brigham and Women’s Hospital, Boston, to evaluate patients’ body composition, including chest CTs to obtain measures of airway thickness, emphysema percentage, pectoralis muscle area, and subcutaneous adipose tissue area.
Correlations between measures of lung function, imaging phenotypes, body composition, and hand grip strength were analyzed in univariate analysis and in multivariate linear models. The association between hand grip strength and exacerbations was analyzed at enrollment and during an average follow-up of 2.6 years.
Hand grip strength was similar across groups categorized by spirometry severity and was not associated with emphysema severity.
After adjustment for demographics, smoking history, smoking intensity, comorbidities and lung imaging phenotypes, however, grip strength was associated with pectoralis muscle area (increase of 3.9 kg per one standard deviation of pectoral muscle area) and subcutaneous adipose tissue (a decrement of 5.1 kg per one standard deviation of subcutaneous adipose tissue). These associations were independent of body mass index and the presence of emphysema.
During follow-up, hand grip strength was associated with exacerbations (risk ratio 0.94 per one kg increment on grip strength) and incident exacerbations (incident risk ratio 0.92 per one kg increment on grip strength) in models adjusted for other factors known to be associated with exacerbations.
Research in body composition has mostly relied on dual absorptiometry and bioelectrical impedance, tools not routinely used in clinical practice, Dr. Martinez said. “We were surprised by the ability to show similar results using imaging data that are available from regular chest CTs.”
“We have confirmed prior hypotheses that it is not just weight or BMI that matters (to risk of exacerbations), but how much muscle and how much fat are contributing to our patient’s high or low BMI,” Dr. Martinez said.
Hand grip testing can be challenging in this patient population, he said. Still, “asking relevant questions about (patients’) physical fitness will help us to understand better our patients’ needs. We can also give more attention to the extrapulmonary structures included in the numerous chest CT scans that we order for our patients. These imaging studies, besides the information that they provide about parenchymal and mediastinal structures, include important and easy to discover clues to identify patients at higher risk of exacerbations – those with low muscle and low hand grip could benefit from close follow-up.”
Dr. Martinez acknowledged certain limitations of the study, including the selection of the measures of body composition. “We used analysis of chest CTs, instead of the gold standard of dual absorptiometry (DXA) or other methods such as bioelectrical impedance,” he said. “A final limitation is that we tested a selected group of participants in a cohort study, not a representative sample of the population, [with a] low burden of emphysema and fewer African American participants.”
Dr. Martinez disclosed that his work is supported by the National Institutes of Health and that COPDGene also receives NIH funding. He acknowledged the support and effort of all COPDGene investigators and participants.
LOS ANGELES – Hand grip strength is independently predictive of risk for respiratory events in smokers who have or are at risk for chronic obstructive pulmonary disease, results from a single-center study showed.
“Measures of lung function, including spirometry, are used as the main descriptors of COPD severity and prognosis,” Carlos H. Martinez, MD, MPH, said in an interview in advance of the annual meeting of the American College of Chest Physicians. “These measurements, as important as they are, need to be improved, in order to develop better risk and prognostic models of the disease, to identify subgroups at higher risk of poor outcomes ... With our work, we have proved that simple physical tests could be part of future prognostic models.”
Interest has grown in developing multidimensional models to predict respiratory prognosis. Such models include BODE (body mass index, airflow obstruction, dyspnea and exercise capacity), ADO (age, dyspnea and airflow obstruction), and DOSE (dyspnea, airflow obstruction, smoking status, and exacerbation frequency).
In patients with or at risk for COPD, Dr. Martinez, of the University of Michigan Health System, Ann Arbor, and his colleagues tested the associations of hand grip strength with measures of body composition such as pectoralis muscle area and extent of subcutaneous fat, imaging phenotypes, and lung function.
The researchers obtained demographic, clinical, lung function, hand grip strength, and imaging data from 441 smokers with and without COPD participating in the Genetic Epidemiology of COPD Study (COPDGene) at the National Jewish Health in Denver. Imaging methods used in the study were developed by George R. Washko, MD, and his associates at Brigham and Women’s Hospital, Boston, to evaluate patients’ body composition, including chest CTs to obtain measures of airway thickness, emphysema percentage, pectoralis muscle area, and subcutaneous adipose tissue area.
Correlations between measures of lung function, imaging phenotypes, body composition, and hand grip strength were analyzed in univariate analysis and in multivariate linear models. The association between hand grip strength and exacerbations was analyzed at enrollment and during an average follow-up of 2.6 years.
Hand grip strength was similar across groups categorized by spirometry severity and was not associated with emphysema severity.
After adjustment for demographics, smoking history, smoking intensity, comorbidities and lung imaging phenotypes, however, grip strength was associated with pectoralis muscle area (increase of 3.9 kg per one standard deviation of pectoral muscle area) and subcutaneous adipose tissue (a decrement of 5.1 kg per one standard deviation of subcutaneous adipose tissue). These associations were independent of body mass index and the presence of emphysema.
During follow-up, hand grip strength was associated with exacerbations (risk ratio 0.94 per one kg increment on grip strength) and incident exacerbations (incident risk ratio 0.92 per one kg increment on grip strength) in models adjusted for other factors known to be associated with exacerbations.
Research in body composition has mostly relied on dual absorptiometry and bioelectrical impedance, tools not routinely used in clinical practice, Dr. Martinez said. “We were surprised by the ability to show similar results using imaging data that are available from regular chest CTs.”
“We have confirmed prior hypotheses that it is not just weight or BMI that matters (to risk of exacerbations), but how much muscle and how much fat are contributing to our patient’s high or low BMI,” Dr. Martinez said.
Hand grip testing can be challenging in this patient population, he said. Still, “asking relevant questions about (patients’) physical fitness will help us to understand better our patients’ needs. We can also give more attention to the extrapulmonary structures included in the numerous chest CT scans that we order for our patients. These imaging studies, besides the information that they provide about parenchymal and mediastinal structures, include important and easy to discover clues to identify patients at higher risk of exacerbations – those with low muscle and low hand grip could benefit from close follow-up.”
Dr. Martinez acknowledged certain limitations of the study, including the selection of the measures of body composition. “We used analysis of chest CTs, instead of the gold standard of dual absorptiometry (DXA) or other methods such as bioelectrical impedance,” he said. “A final limitation is that we tested a selected group of participants in a cohort study, not a representative sample of the population, [with a] low burden of emphysema and fewer African American participants.”
Dr. Martinez disclosed that his work is supported by the National Institutes of Health and that COPDGene also receives NIH funding. He acknowledged the support and effort of all COPDGene investigators and participants.
LOS ANGELES – Hand grip strength is independently predictive of risk for respiratory events in smokers who have or are at risk for chronic obstructive pulmonary disease, results from a single-center study showed.
“Measures of lung function, including spirometry, are used as the main descriptors of COPD severity and prognosis,” Carlos H. Martinez, MD, MPH, said in an interview in advance of the annual meeting of the American College of Chest Physicians. “These measurements, as important as they are, need to be improved, in order to develop better risk and prognostic models of the disease, to identify subgroups at higher risk of poor outcomes ... With our work, we have proved that simple physical tests could be part of future prognostic models.”
Interest has grown in developing multidimensional models to predict respiratory prognosis. Such models include BODE (body mass index, airflow obstruction, dyspnea and exercise capacity), ADO (age, dyspnea and airflow obstruction), and DOSE (dyspnea, airflow obstruction, smoking status, and exacerbation frequency).
In patients with or at risk for COPD, Dr. Martinez, of the University of Michigan Health System, Ann Arbor, and his colleagues tested the associations of hand grip strength with measures of body composition such as pectoralis muscle area and extent of subcutaneous fat, imaging phenotypes, and lung function.
The researchers obtained demographic, clinical, lung function, hand grip strength, and imaging data from 441 smokers with and without COPD participating in the Genetic Epidemiology of COPD Study (COPDGene) at the National Jewish Health in Denver. Imaging methods used in the study were developed by George R. Washko, MD, and his associates at Brigham and Women’s Hospital, Boston, to evaluate patients’ body composition, including chest CTs to obtain measures of airway thickness, emphysema percentage, pectoralis muscle area, and subcutaneous adipose tissue area.
Correlations between measures of lung function, imaging phenotypes, body composition, and hand grip strength were analyzed in univariate analysis and in multivariate linear models. The association between hand grip strength and exacerbations was analyzed at enrollment and during an average follow-up of 2.6 years.
Hand grip strength was similar across groups categorized by spirometry severity and was not associated with emphysema severity.
After adjustment for demographics, smoking history, smoking intensity, comorbidities and lung imaging phenotypes, however, grip strength was associated with pectoralis muscle area (increase of 3.9 kg per one standard deviation of pectoral muscle area) and subcutaneous adipose tissue (a decrement of 5.1 kg per one standard deviation of subcutaneous adipose tissue). These associations were independent of body mass index and the presence of emphysema.
During follow-up, hand grip strength was associated with exacerbations (risk ratio 0.94 per one kg increment on grip strength) and incident exacerbations (incident risk ratio 0.92 per one kg increment on grip strength) in models adjusted for other factors known to be associated with exacerbations.
Research in body composition has mostly relied on dual absorptiometry and bioelectrical impedance, tools not routinely used in clinical practice, Dr. Martinez said. “We were surprised by the ability to show similar results using imaging data that are available from regular chest CTs.”
“We have confirmed prior hypotheses that it is not just weight or BMI that matters (to risk of exacerbations), but how much muscle and how much fat are contributing to our patient’s high or low BMI,” Dr. Martinez said.
Hand grip testing can be challenging in this patient population, he said. Still, “asking relevant questions about (patients’) physical fitness will help us to understand better our patients’ needs. We can also give more attention to the extrapulmonary structures included in the numerous chest CT scans that we order for our patients. These imaging studies, besides the information that they provide about parenchymal and mediastinal structures, include important and easy to discover clues to identify patients at higher risk of exacerbations – those with low muscle and low hand grip could benefit from close follow-up.”
Dr. Martinez acknowledged certain limitations of the study, including the selection of the measures of body composition. “We used analysis of chest CTs, instead of the gold standard of dual absorptiometry (DXA) or other methods such as bioelectrical impedance,” he said. “A final limitation is that we tested a selected group of participants in a cohort study, not a representative sample of the population, [with a] low burden of emphysema and fewer African American participants.”
Dr. Martinez disclosed that his work is supported by the National Institutes of Health and that COPDGene also receives NIH funding. He acknowledged the support and effort of all COPDGene investigators and participants.
AT CHEST 2016
Key clinical point:
Major finding: During an average follow-up of 2.6 years, hand grip strength was associated with cross-sectional exacerbations (risk ratio 0.94 per one kg increment on grip strength) and incident exacerbations (incident risk ratio 0.92 per one kg increment on grip strength).
Data source: Data from 441 smokers with and without COPD participating in the Genetic Epidemiology of COPD Study (COPDGene) at National Jewish Health in Denver.
Disclosures: Dr. Martinez disclosed that his work is supported by the National Institutes of Health and that COPDGene also receives NIH funding.
LMWH best for preventing PE in patients with major trauma
WAIKOLOA, HAWAII – Venous thromboembolism prophylaxis with low molecular weight heparin (LMWH), instead of unfractionated heparin (UH), is associated with lower risk of pulmonary embolism (PE) in patients with major trauma, results from a large study have shown.
The results of the study, based on data from the American College of Surgeons (ACS) Trauma Quality Improvement Program, suggest that LMWH-based strategies for thromboprophylaxis should be preferred after major trauma.

Dr. Byrne, a general surgery resident at Sunnybrook Health Science Center, Toronto, Ontario, Canada, went on to note that LMWH is often favored because of a randomized controlled trial which showed that LMWH was associated with fewer deep vein thromboses (N Engl. J. Med. 1996;335[10]:701-7). However, significant practice variability continues to exist.
“Practitioners might favor the shorter half-life of unfractionated heparin in patients where they perceive the risk for hemorrhagic complications is high,” he said. “There’s also recent evidence to suggest that dosing may be all important and that unfractionated heparin dosed three times daily may be equivalent to low molecular weight heparin. If this is true, it might suggest that the historically higher cost of low molecular weight heparin could favor the use of unfractionated heparin.”
Furthermore, there is a is a lack of evidence comparing either agent to prevent PE, he added. “This is an important gap in our knowledge, because PE frequently occurs in the absence of an identified DVT and carries a significant risk of death. At present, it is not known how practice patterns with respect to choice of prophylaxis type influence risk of PE at the patient or hospital levels.”
Due to a lack of evidence comparing agents to prevent PE, the researchers set out to compare the effectiveness of LMWH versus UH to prevent PE in patients with major trauma who were treated at trauma centers participating in the ACS Trauma Quality Improvement Program from 2012 to 2015. They included all adults with severe injury who received LMWH or UH and excluded those who died or were discharged within five days, and those with a bleeding disorder or chronic anticoagulation. The exposure was defined as thromboprophylaxis with LMWH versus UH, and the primary outcome was PE confirmed on radiologic imaging. Potential confounders were considered, including patient baseline characteristics, anatomic and global injury severity, presenting characteristics in the emergency department, acute intracranial injuries, orthopedic injuries, early surgical interventions, and timing of prophylaxis initiation.
Dr. Byrne and his associates then used three analytic approaches in the study: a propensity score matching methodology, a multivariable logistic regression model for PE, and a center-level analysis examining the influence of LMWH utilization on hospital rates of PE.
They identified 153,474 trauma patients from 217 trauma centers. Their median age was 50 years and 67% were male. Blunt trauma was most common (89%), with a mean Injury Severity Score score of 20. LMWH was the most common type of thromboprophylaxis used (74%), and PE was diagnosed in 2,722 patients (1.8%).
Compared with patients who received LMWH, those who received UH were older and were significantly more likely to have been injured by falling (42% vs. 28%), with higher rates of severe head injuries (43% vs. 24%) and intracranial hemorrhage (38% vs. 19%). Conversely, LMWH was most favored in patients with orthopedic injuries.
After propensity score matching, patients on LMWH suffered significantly fewer PEs (1.4% vs. 2.4%; odds ratio, 0.56). This result was consistent within propensity-matched subgroups, including for patients with blunt multisystem injuries (OR, 0.60), penetrating truncal injuries (OR, 0.65), shock in the ED (OR, 0.68), isolated severe traumatic brain injury (OR, 0.49), and isolated orthopedic injuries (OR, 0.28).
Results of a sensitivity analysis in which each propensity-matched pair was matched within the same trauma center yielded similar results. Specifically, patients who received LMWH were at significantly lower risk for developing PE (OR, 0.64). “Importantly, this analysis minimized residual confounding due to differences in hospital-level processes of care, such as prophylaxis dosing or frequency, mechanical prophylaxis use, and thromboembolism screening practices,” Dr. Byrne noted.
Multivariable logistic regression also showed that patients who received LMWH had lower odds of PE (OR, 0.59). Other significant predictors of PE included obesity (OR, 1.54), severe chest injury (OR, 1.31), femoral shaft fracture (OR, 1.60), and spinal cord injury (OR, 1.60). Delays in prophylaxis initiation beyond the first day in the hospital were associated with significantly higher rates of PE, with an 80% increased risk of PE for patients who had their prophylaxis initiated after the fourth day.
The researchers conducted a center-level analysis in an effort to answer the question whether practice patterns with respect to choice of prophylaxis type influence hospital rates of PE. Across all 217 trauma centers in the study, the median rate of LMWH use was 80%, while the mean rate of PE was 1.6%. When trauma centers were grouped into quartiles based on their unique rate of LMWH use, trauma centers in the highest quartile (median LMWH use: 95%) were 50 times more likely to use LMWH, compared to those in the lowest quartile (median LMWH use: 39%) after adjusting for patient case mix. Compared with the lowest quartile, trauma centers that used the greatest proportion of LMWH had significantly lower rates of PE (1.2% vs. 2.0%). After adjusting for patient baseline and injury characteristics, patients who were treated at trauma centers in the highest quartile had significantly lower odds of PE (OR, 0.59).
Dr. Byrne acknowledged certain limitations of the study, including the potential for residual confounding and the inability to account for the dosing and frequency of prophylaxis that was given. “We were only able to measure the type and timing of prophylaxis initiation. We don’t know what doses of prophylaxis were used, and it is possible that the trauma centers included in this study favored use of UH twice daily,” he said.
Therefore, it is possible that the results might have been different if they had been able to directly compare LMWH to UH administered three times a day. “We also couldn’t measure interruptions in dosing due to surgery or patient refusal,” he said. “However, if it the case that UH is more likely to be refused based on the need for more frequent dosing, perhaps that is another feather in the cap of low molecular weight heparin-based thromboprophylaxis strategies. Larger prospective studies are needed, that take into account prophylaxis type and dosing, and are powered to detect a difference with respect to PE.”
Dr. Byrne reported having no financial disclosures.
WAIKOLOA, HAWAII – Venous thromboembolism prophylaxis with low molecular weight heparin (LMWH), instead of unfractionated heparin (UH), is associated with lower risk of pulmonary embolism (PE) in patients with major trauma, results from a large study have shown.
The results of the study, based on data from the American College of Surgeons (ACS) Trauma Quality Improvement Program, suggest that LMWH-based strategies for thromboprophylaxis should be preferred after major trauma.
Dr. Byrne, a general surgery resident at Sunnybrook Health Science Center, Toronto, Ontario, Canada, went on to note that LMWH is often favored because of a randomized controlled trial which showed that LMWH was associated with fewer deep vein thromboses (N Engl. J. Med. 1996;335[10]:701-7). However, significant practice variability continues to exist.
“Practitioners might favor the shorter half-life of unfractionated heparin in patients where they perceive the risk for hemorrhagic complications is high,” he said. “There’s also recent evidence to suggest that dosing may be all important and that unfractionated heparin dosed three times daily may be equivalent to low molecular weight heparin. If this is true, it might suggest that the historically higher cost of low molecular weight heparin could favor the use of unfractionated heparin.”
Furthermore, there is a is a lack of evidence comparing either agent to prevent PE, he added. “This is an important gap in our knowledge, because PE frequently occurs in the absence of an identified DVT and carries a significant risk of death. At present, it is not known how practice patterns with respect to choice of prophylaxis type influence risk of PE at the patient or hospital levels.”
Due to a lack of evidence comparing agents to prevent PE, the researchers set out to compare the effectiveness of LMWH versus UH to prevent PE in patients with major trauma who were treated at trauma centers participating in the ACS Trauma Quality Improvement Program from 2012 to 2015. They included all adults with severe injury who received LMWH or UH and excluded those who died or were discharged within five days, and those with a bleeding disorder or chronic anticoagulation. The exposure was defined as thromboprophylaxis with LMWH versus UH, and the primary outcome was PE confirmed on radiologic imaging. Potential confounders were considered, including patient baseline characteristics, anatomic and global injury severity, presenting characteristics in the emergency department, acute intracranial injuries, orthopedic injuries, early surgical interventions, and timing of prophylaxis initiation.
Dr. Byrne and his associates then used three analytic approaches in the study: a propensity score matching methodology, a multivariable logistic regression model for PE, and a center-level analysis examining the influence of LMWH utilization on hospital rates of PE.
They identified 153,474 trauma patients from 217 trauma centers. Their median age was 50 years and 67% were male. Blunt trauma was most common (89%), with a mean Injury Severity Score score of 20. LMWH was the most common type of thromboprophylaxis used (74%), and PE was diagnosed in 2,722 patients (1.8%).
Compared with patients who received LMWH, those who received UH were older and were significantly more likely to have been injured by falling (42% vs. 28%), with higher rates of severe head injuries (43% vs. 24%) and intracranial hemorrhage (38% vs. 19%). Conversely, LMWH was most favored in patients with orthopedic injuries.
After propensity score matching, patients on LMWH suffered significantly fewer PEs (1.4% vs. 2.4%; odds ratio, 0.56). This result was consistent within propensity-matched subgroups, including for patients with blunt multisystem injuries (OR, 0.60), penetrating truncal injuries (OR, 0.65), shock in the ED (OR, 0.68), isolated severe traumatic brain injury (OR, 0.49), and isolated orthopedic injuries (OR, 0.28).
Results of a sensitivity analysis in which each propensity-matched pair was matched within the same trauma center yielded similar results. Specifically, patients who received LMWH were at significantly lower risk for developing PE (OR, 0.64). “Importantly, this analysis minimized residual confounding due to differences in hospital-level processes of care, such as prophylaxis dosing or frequency, mechanical prophylaxis use, and thromboembolism screening practices,” Dr. Byrne noted.
Multivariable logistic regression also showed that patients who received LMWH had lower odds of PE (OR, 0.59). Other significant predictors of PE included obesity (OR, 1.54), severe chest injury (OR, 1.31), femoral shaft fracture (OR, 1.60), and spinal cord injury (OR, 1.60). Delays in prophylaxis initiation beyond the first day in the hospital were associated with significantly higher rates of PE, with an 80% increased risk of PE for patients who had their prophylaxis initiated after the fourth day.
The researchers conducted a center-level analysis in an effort to answer the question whether practice patterns with respect to choice of prophylaxis type influence hospital rates of PE. Across all 217 trauma centers in the study, the median rate of LMWH use was 80%, while the mean rate of PE was 1.6%. When trauma centers were grouped into quartiles based on their unique rate of LMWH use, trauma centers in the highest quartile (median LMWH use: 95%) were 50 times more likely to use LMWH, compared to those in the lowest quartile (median LMWH use: 39%) after adjusting for patient case mix. Compared with the lowest quartile, trauma centers that used the greatest proportion of LMWH had significantly lower rates of PE (1.2% vs. 2.0%). After adjusting for patient baseline and injury characteristics, patients who were treated at trauma centers in the highest quartile had significantly lower odds of PE (OR, 0.59).
Dr. Byrne acknowledged certain limitations of the study, including the potential for residual confounding and the inability to account for the dosing and frequency of prophylaxis that was given. “We were only able to measure the type and timing of prophylaxis initiation. We don’t know what doses of prophylaxis were used, and it is possible that the trauma centers included in this study favored use of UH twice daily,” he said.
Therefore, it is possible that the results might have been different if they had been able to directly compare LMWH to UH administered three times a day. “We also couldn’t measure interruptions in dosing due to surgery or patient refusal,” he said. “However, if it the case that UH is more likely to be refused based on the need for more frequent dosing, perhaps that is another feather in the cap of low molecular weight heparin-based thromboprophylaxis strategies. Larger prospective studies are needed, that take into account prophylaxis type and dosing, and are powered to detect a difference with respect to PE.”
Dr. Byrne reported having no financial disclosures.
WAIKOLOA, HAWAII – Venous thromboembolism prophylaxis with low molecular weight heparin (LMWH), instead of unfractionated heparin (UH), is associated with lower risk of pulmonary embolism (PE) in patients with major trauma, results from a large study have shown.
The results of the study, based on data from the American College of Surgeons (ACS) Trauma Quality Improvement Program, suggest that LMWH-based strategies for thromboprophylaxis should be preferred after major trauma.
Dr. Byrne, a general surgery resident at Sunnybrook Health Science Center, Toronto, Ontario, Canada, went on to note that LMWH is often favored because of a randomized controlled trial which showed that LMWH was associated with fewer deep vein thromboses (N Engl. J. Med. 1996;335[10]:701-7). However, significant practice variability continues to exist.
“Practitioners might favor the shorter half-life of unfractionated heparin in patients where they perceive the risk for hemorrhagic complications is high,” he said. “There’s also recent evidence to suggest that dosing may be all important and that unfractionated heparin dosed three times daily may be equivalent to low molecular weight heparin. If this is true, it might suggest that the historically higher cost of low molecular weight heparin could favor the use of unfractionated heparin.”
Furthermore, there is a is a lack of evidence comparing either agent to prevent PE, he added. “This is an important gap in our knowledge, because PE frequently occurs in the absence of an identified DVT and carries a significant risk of death. At present, it is not known how practice patterns with respect to choice of prophylaxis type influence risk of PE at the patient or hospital levels.”
Due to a lack of evidence comparing agents to prevent PE, the researchers set out to compare the effectiveness of LMWH versus UH to prevent PE in patients with major trauma who were treated at trauma centers participating in the ACS Trauma Quality Improvement Program from 2012 to 2015. They included all adults with severe injury who received LMWH or UH and excluded those who died or were discharged within five days, and those with a bleeding disorder or chronic anticoagulation. The exposure was defined as thromboprophylaxis with LMWH versus UH, and the primary outcome was PE confirmed on radiologic imaging. Potential confounders were considered, including patient baseline characteristics, anatomic and global injury severity, presenting characteristics in the emergency department, acute intracranial injuries, orthopedic injuries, early surgical interventions, and timing of prophylaxis initiation.
Dr. Byrne and his associates then used three analytic approaches in the study: a propensity score matching methodology, a multivariable logistic regression model for PE, and a center-level analysis examining the influence of LMWH utilization on hospital rates of PE.
They identified 153,474 trauma patients from 217 trauma centers. Their median age was 50 years and 67% were male. Blunt trauma was most common (89%), with a mean Injury Severity Score score of 20. LMWH was the most common type of thromboprophylaxis used (74%), and PE was diagnosed in 2,722 patients (1.8%).
Compared with patients who received LMWH, those who received UH were older and were significantly more likely to have been injured by falling (42% vs. 28%), with higher rates of severe head injuries (43% vs. 24%) and intracranial hemorrhage (38% vs. 19%). Conversely, LMWH was most favored in patients with orthopedic injuries.
After propensity score matching, patients on LMWH suffered significantly fewer PEs (1.4% vs. 2.4%; odds ratio, 0.56). This result was consistent within propensity-matched subgroups, including for patients with blunt multisystem injuries (OR, 0.60), penetrating truncal injuries (OR, 0.65), shock in the ED (OR, 0.68), isolated severe traumatic brain injury (OR, 0.49), and isolated orthopedic injuries (OR, 0.28).
Results of a sensitivity analysis in which each propensity-matched pair was matched within the same trauma center yielded similar results. Specifically, patients who received LMWH were at significantly lower risk for developing PE (OR, 0.64). “Importantly, this analysis minimized residual confounding due to differences in hospital-level processes of care, such as prophylaxis dosing or frequency, mechanical prophylaxis use, and thromboembolism screening practices,” Dr. Byrne noted.
Multivariable logistic regression also showed that patients who received LMWH had lower odds of PE (OR, 0.59). Other significant predictors of PE included obesity (OR, 1.54), severe chest injury (OR, 1.31), femoral shaft fracture (OR, 1.60), and spinal cord injury (OR, 1.60). Delays in prophylaxis initiation beyond the first day in the hospital were associated with significantly higher rates of PE, with an 80% increased risk of PE for patients who had their prophylaxis initiated after the fourth day.
The researchers conducted a center-level analysis in an effort to answer the question whether practice patterns with respect to choice of prophylaxis type influence hospital rates of PE. Across all 217 trauma centers in the study, the median rate of LMWH use was 80%, while the mean rate of PE was 1.6%. When trauma centers were grouped into quartiles based on their unique rate of LMWH use, trauma centers in the highest quartile (median LMWH use: 95%) were 50 times more likely to use LMWH, compared to those in the lowest quartile (median LMWH use: 39%) after adjusting for patient case mix. Compared with the lowest quartile, trauma centers that used the greatest proportion of LMWH had significantly lower rates of PE (1.2% vs. 2.0%). After adjusting for patient baseline and injury characteristics, patients who were treated at trauma centers in the highest quartile had significantly lower odds of PE (OR, 0.59).
Dr. Byrne acknowledged certain limitations of the study, including the potential for residual confounding and the inability to account for the dosing and frequency of prophylaxis that was given. “We were only able to measure the type and timing of prophylaxis initiation. We don’t know what doses of prophylaxis were used, and it is possible that the trauma centers included in this study favored use of UH twice daily,” he said.
Therefore, it is possible that the results might have been different if they had been able to directly compare LMWH to UH administered three times a day. “We also couldn’t measure interruptions in dosing due to surgery or patient refusal,” he said. “However, if it the case that UH is more likely to be refused based on the need for more frequent dosing, perhaps that is another feather in the cap of low molecular weight heparin-based thromboprophylaxis strategies. Larger prospective studies are needed, that take into account prophylaxis type and dosing, and are powered to detect a difference with respect to PE.”
Dr. Byrne reported having no financial disclosures.
AT THE AAST ANNUAL MEETING
Key clinical point:
Major finding: After propensity score matching, patients on LMWH had significantly fewer PEs, compared with those on unfractionated heparin (1.4% vs. 2.4%; odds ratio, 0.56). Data source: A multicenter analysis of 2,722 trauma patients who were diagnosed with pulmonary embolism.
Disclosures: Dr. Byrne reported having no financial disclosures.
Chest physician perceptions of e-cigarettes mixed
AT CHEST 2016
LOS ANGELES – Chest physicians in the United States are likely to encounter electronic cigarette users in clinical practice, yet there is no consensus regarding how to advise them, results from a survey suggest.
“There is controversy in the community of physicians we surveyed on whether e-cigarettes would be useful for smoking cessation and whether they can reduce harm from tobacco smoking,” lead study author Stephen R. Baldassarri, MD, said in an interview in advance of the annual meeting of the American College of Chest Physicians. “Our results suggest that we need more high quality scientific data regarding potential harms and benefits of e-cigarettes in order to inform both health professionals and the general public.”
When asked if ECs promote tobacco cessation, respondents were split (33% agreed or strongly agreed while 32% disagreed or strongly disagreed); only 13% believed that ECs were at least as effective as Food and Drug Administration–approved treatments to promote smoking cessation, and 11% reported that ECs should be used in an initial quit attempt. Dr. Baldassarri also reported that 6% of respondents thought ECs are more harmful than smoking, 21% thought switching from daily tobacco smoking to EC use would improve a patient’s health, and 55% reported feeling comfortable discussing health effects of ECs with their patients.
“In light of the fact that the long-term health risks of ECs remain unknown, we were surprised to find that more than half of the survey respondents reported feeling comfortable discussing health effects of ECs,” Dr. Baldassarri commented. “This proportion was higher than we expected given the current state of the scientific evidence.”
He acknowledged certain limitations of the survey, including its low response rate, “which limits the degree to which we can generalize our findings to account for the perceptions of all chest physicians,” he said. “We surveyed providers only within CHEST, and opinions and experiences of physicians outside of the organization and in other specialties may vary. And finally, since knowledge regarding e-cigarettes is rapidly evolving, the perceptions and opinions here are likely subject to change over the next few years as more becomes known.”
Dr. Baldassarri reported having no financial disclosures.
AT CHEST 2016
LOS ANGELES – Chest physicians in the United States are likely to encounter electronic cigarette users in clinical practice, yet there is no consensus regarding how to advise them, results from a survey suggest.
“There is controversy in the community of physicians we surveyed on whether e-cigarettes would be useful for smoking cessation and whether they can reduce harm from tobacco smoking,” lead study author Stephen R. Baldassarri, MD, said in an interview in advance of the annual meeting of the American College of Chest Physicians. “Our results suggest that we need more high quality scientific data regarding potential harms and benefits of e-cigarettes in order to inform both health professionals and the general public.”
When asked if ECs promote tobacco cessation, respondents were split (33% agreed or strongly agreed while 32% disagreed or strongly disagreed); only 13% believed that ECs were at least as effective as Food and Drug Administration–approved treatments to promote smoking cessation, and 11% reported that ECs should be used in an initial quit attempt. Dr. Baldassarri also reported that 6% of respondents thought ECs are more harmful than smoking, 21% thought switching from daily tobacco smoking to EC use would improve a patient’s health, and 55% reported feeling comfortable discussing health effects of ECs with their patients.
“In light of the fact that the long-term health risks of ECs remain unknown, we were surprised to find that more than half of the survey respondents reported feeling comfortable discussing health effects of ECs,” Dr. Baldassarri commented. “This proportion was higher than we expected given the current state of the scientific evidence.”
He acknowledged certain limitations of the survey, including its low response rate, “which limits the degree to which we can generalize our findings to account for the perceptions of all chest physicians,” he said. “We surveyed providers only within CHEST, and opinions and experiences of physicians outside of the organization and in other specialties may vary. And finally, since knowledge regarding e-cigarettes is rapidly evolving, the perceptions and opinions here are likely subject to change over the next few years as more becomes known.”
Dr. Baldassarri reported having no financial disclosures.
AT CHEST 2016
LOS ANGELES – Chest physicians in the United States are likely to encounter electronic cigarette users in clinical practice, yet there is no consensus regarding how to advise them, results from a survey suggest.
“There is controversy in the community of physicians we surveyed on whether e-cigarettes would be useful for smoking cessation and whether they can reduce harm from tobacco smoking,” lead study author Stephen R. Baldassarri, MD, said in an interview in advance of the annual meeting of the American College of Chest Physicians. “Our results suggest that we need more high quality scientific data regarding potential harms and benefits of e-cigarettes in order to inform both health professionals and the general public.”
When asked if ECs promote tobacco cessation, respondents were split (33% agreed or strongly agreed while 32% disagreed or strongly disagreed); only 13% believed that ECs were at least as effective as Food and Drug Administration–approved treatments to promote smoking cessation, and 11% reported that ECs should be used in an initial quit attempt. Dr. Baldassarri also reported that 6% of respondents thought ECs are more harmful than smoking, 21% thought switching from daily tobacco smoking to EC use would improve a patient’s health, and 55% reported feeling comfortable discussing health effects of ECs with their patients.
“In light of the fact that the long-term health risks of ECs remain unknown, we were surprised to find that more than half of the survey respondents reported feeling comfortable discussing health effects of ECs,” Dr. Baldassarri commented. “This proportion was higher than we expected given the current state of the scientific evidence.”
He acknowledged certain limitations of the survey, including its low response rate, “which limits the degree to which we can generalize our findings to account for the perceptions of all chest physicians,” he said. “We surveyed providers only within CHEST, and opinions and experiences of physicians outside of the organization and in other specialties may vary. And finally, since knowledge regarding e-cigarettes is rapidly evolving, the perceptions and opinions here are likely subject to change over the next few years as more becomes known.”
Dr. Baldassarri reported having no financial disclosures.
Key clinical point:
Major finding: When asked if electronic cigarettes (ECs) promote tobacco cessation, respondents were split (33% agreed or strongly agreed, while 32% disagreed or strongly disagreed).
Data source: Responses from 994 members of the American College of Chest Physicians who completed a brief online questionnaire about practice patterns and perceptions regarding EC use and tobacco smoking among their patients.
Disclosures: Dr. Baldassarri reported having no financial disclosures.
Pelvic fracture pattern predicts the need for hemorrhage control
WAIKOLOA, HAWAII – Blunt trauma patients admitted in shock with anterior posterior compression III or vertical shear fracture patterns, or patients with open pelvic fracture are at greatest risk of severe bleeding requiring pelvic hemorrhage control intervention, results from a multicenter trial demonstrated.
Thirty years ago, researchers defined a classification of pelvic fracture based on a pattern of force applied to the pelvis, Todd W. Costantini, MD, said at the annual meeting of the American Association for the Surgery of Trauma. They identified three main force patterns, including lateral compression, anterior posterior compression, and vertical shear (Radiology. 1986 Aug;160 [2]:445-51).

In a recently published study, Dr. Costantini and his associates found wide variability in the use of various pelvic hemorrhage control methods (J Trauma Acute Care Surg. 2016 May;80 [5]:717-25). “While angioembolization alone and external fixator placement alone were the most common methods used, there were various combinations of these methods used at different times by different institutions,” he said.
These results prompted the researchers to prospectively evaluate the correlation between pelvic fracture pattern and modern care of pelvic hemorrhage control at 11 Level I trauma centers over a two year period. Inclusion criteria for the study, which was sponsored by the AAST Multi-institutional Trials Committee, were patients over the age of 18, blunt mechanism of injury, and shock on admission, which was defined as an admission systolic blood pressure of less than 90 mm Hg, or heart rate greater than 120, or base deficit greater than 5. Exclusion criteria included isolated hip fracture, pregnancy, and lack of pelvic imaging.
The researchers evaluated the pelvic fracture pattern for each patient in the study. “Each pelvic image was evaluated by a trauma surgeon, orthopedic surgeon, or radiologist and classified using the Young-Burgess Classification system,” Dr. Costantini said. Next, they used univariate and multivariate logistic regression analysis to analyze predictors for hemorrhage control intervention and mortality. The objective was to determine whether pelvic fracture pattern would predict the need for a hemorrhage control intervention.
Of the 46,716 trauma patients admitted over the two year period, 1,339 sustained a pelvic fracture. Of these, 178 met criteria for shock. The researchers excluded 15 patients due to lack of pelvic imaging, which left 163 patients in the final analysis. Their mean age was 44 years and 58% were male. On admission, their mean systolic blood pressure was 93 mm Hg, their mean heart rate was 117 beats per minute, and their median Injury Severity Score was 28. The mean hospital length of stay was 12 days and the mortality rate was 30%. The three most common mechanisms of injury were motor vehicle crash (42%), followed by pedestrian versus auto (23%), and falls (18%).
Compared with patients who did not require hemorrhage control intervention, those who did received more transfusion of packed red blood cells (13 vs. 7 units, respectively; P less than .01) and fresh frozen plasma (10 vs. 5 units; P = .01). In addition, 67% of patients with open pelvic fracture required a hemorrhage control intervention. The rate of mortality was similar between the patients who required a pelvic hemorrhage control intervention and those who did not (34% vs. 28%; P = .47).
The three most common types of pelvic fracture patterns were lateral compression I (36%) and II (23%), followed by vertical shear (13%). Patients with lateral compression I and II fractures were least likely to require hemorrhage control intervention (22% and 19%, respectively). However, on univariate analysis, patients with anterior posterior compression III fractures and those with vertical shear fractures were more likely to require a pelvic hemorrhage control intervention, compared with those who sustained other types of pelvic fractures (83% and 55%, respectively).
On multivariate analysis, the three main independent predictors of need for a hemorrhagic control intervention were anterior posterior compression III fracture (odds ratio, 109.43; P less than .001), open pelvic fracture (OR, 7.36; P = .014), and vertical shear fracture (OR, 6.99; P = .002). Pelvic fracture pattern did not predict mortality on multivariate analysis.
The invited discussant, Joseph M. Galante, MD, trauma medical director for the University of California, Davis Health System, characterized the study as important, “because it examines all forms of hemorrhage control, not just arterioembolism in the treatment of pelvic fractures,” he said. “The ability to predict who will need hemorrhage control allows for earlier mobilization to resources, both in the operating room or interventional suite and in the resuscitation bay.”
Dr. Costantini reported having no financial disclosures.
WAIKOLOA, HAWAII – Blunt trauma patients admitted in shock with anterior posterior compression III or vertical shear fracture patterns, or patients with open pelvic fracture are at greatest risk of severe bleeding requiring pelvic hemorrhage control intervention, results from a multicenter trial demonstrated.
Thirty years ago, researchers defined a classification of pelvic fracture based on a pattern of force applied to the pelvis, Todd W. Costantini, MD, said at the annual meeting of the American Association for the Surgery of Trauma. They identified three main force patterns, including lateral compression, anterior posterior compression, and vertical shear (Radiology. 1986 Aug;160 [2]:445-51).
In a recently published study, Dr. Costantini and his associates found wide variability in the use of various pelvic hemorrhage control methods (J Trauma Acute Care Surg. 2016 May;80 [5]:717-25). “While angioembolization alone and external fixator placement alone were the most common methods used, there were various combinations of these methods used at different times by different institutions,” he said.
These results prompted the researchers to prospectively evaluate the correlation between pelvic fracture pattern and modern care of pelvic hemorrhage control at 11 Level I trauma centers over a two year period. Inclusion criteria for the study, which was sponsored by the AAST Multi-institutional Trials Committee, were patients over the age of 18, blunt mechanism of injury, and shock on admission, which was defined as an admission systolic blood pressure of less than 90 mm Hg, or heart rate greater than 120, or base deficit greater than 5. Exclusion criteria included isolated hip fracture, pregnancy, and lack of pelvic imaging.
The researchers evaluated the pelvic fracture pattern for each patient in the study. “Each pelvic image was evaluated by a trauma surgeon, orthopedic surgeon, or radiologist and classified using the Young-Burgess Classification system,” Dr. Costantini said. Next, they used univariate and multivariate logistic regression analysis to analyze predictors for hemorrhage control intervention and mortality. The objective was to determine whether pelvic fracture pattern would predict the need for a hemorrhage control intervention.
Of the 46,716 trauma patients admitted over the two year period, 1,339 sustained a pelvic fracture. Of these, 178 met criteria for shock. The researchers excluded 15 patients due to lack of pelvic imaging, which left 163 patients in the final analysis. Their mean age was 44 years and 58% were male. On admission, their mean systolic blood pressure was 93 mm Hg, their mean heart rate was 117 beats per minute, and their median Injury Severity Score was 28. The mean hospital length of stay was 12 days and the mortality rate was 30%. The three most common mechanisms of injury were motor vehicle crash (42%), followed by pedestrian versus auto (23%), and falls (18%).
Compared with patients who did not require hemorrhage control intervention, those who did received more transfusion of packed red blood cells (13 vs. 7 units, respectively; P less than .01) and fresh frozen plasma (10 vs. 5 units; P = .01). In addition, 67% of patients with open pelvic fracture required a hemorrhage control intervention. The rate of mortality was similar between the patients who required a pelvic hemorrhage control intervention and those who did not (34% vs. 28%; P = .47).
The three most common types of pelvic fracture patterns were lateral compression I (36%) and II (23%), followed by vertical shear (13%). Patients with lateral compression I and II fractures were least likely to require hemorrhage control intervention (22% and 19%, respectively). However, on univariate analysis, patients with anterior posterior compression III fractures and those with vertical shear fractures were more likely to require a pelvic hemorrhage control intervention, compared with those who sustained other types of pelvic fractures (83% and 55%, respectively).
On multivariate analysis, the three main independent predictors of need for a hemorrhagic control intervention were anterior posterior compression III fracture (odds ratio, 109.43; P less than .001), open pelvic fracture (OR, 7.36; P = .014), and vertical shear fracture (OR, 6.99; P = .002). Pelvic fracture pattern did not predict mortality on multivariate analysis.
The invited discussant, Joseph M. Galante, MD, trauma medical director for the University of California, Davis Health System, characterized the study as important, “because it examines all forms of hemorrhage control, not just arterioembolism in the treatment of pelvic fractures,” he said. “The ability to predict who will need hemorrhage control allows for earlier mobilization to resources, both in the operating room or interventional suite and in the resuscitation bay.”
Dr. Costantini reported having no financial disclosures.
WAIKOLOA, HAWAII – Blunt trauma patients admitted in shock with anterior posterior compression III or vertical shear fracture patterns, or patients with open pelvic fracture are at greatest risk of severe bleeding requiring pelvic hemorrhage control intervention, results from a multicenter trial demonstrated.
Thirty years ago, researchers defined a classification of pelvic fracture based on a pattern of force applied to the pelvis, Todd W. Costantini, MD, said at the annual meeting of the American Association for the Surgery of Trauma. They identified three main force patterns, including lateral compression, anterior posterior compression, and vertical shear (Radiology. 1986 Aug;160 [2]:445-51).
In a recently published study, Dr. Costantini and his associates found wide variability in the use of various pelvic hemorrhage control methods (J Trauma Acute Care Surg. 2016 May;80 [5]:717-25). “While angioembolization alone and external fixator placement alone were the most common methods used, there were various combinations of these methods used at different times by different institutions,” he said.
These results prompted the researchers to prospectively evaluate the correlation between pelvic fracture pattern and modern care of pelvic hemorrhage control at 11 Level I trauma centers over a two year period. Inclusion criteria for the study, which was sponsored by the AAST Multi-institutional Trials Committee, were patients over the age of 18, blunt mechanism of injury, and shock on admission, which was defined as an admission systolic blood pressure of less than 90 mm Hg, or heart rate greater than 120, or base deficit greater than 5. Exclusion criteria included isolated hip fracture, pregnancy, and lack of pelvic imaging.
The researchers evaluated the pelvic fracture pattern for each patient in the study. “Each pelvic image was evaluated by a trauma surgeon, orthopedic surgeon, or radiologist and classified using the Young-Burgess Classification system,” Dr. Costantini said. Next, they used univariate and multivariate logistic regression analysis to analyze predictors for hemorrhage control intervention and mortality. The objective was to determine whether pelvic fracture pattern would predict the need for a hemorrhage control intervention.
Of the 46,716 trauma patients admitted over the two year period, 1,339 sustained a pelvic fracture. Of these, 178 met criteria for shock. The researchers excluded 15 patients due to lack of pelvic imaging, which left 163 patients in the final analysis. Their mean age was 44 years and 58% were male. On admission, their mean systolic blood pressure was 93 mm Hg, their mean heart rate was 117 beats per minute, and their median Injury Severity Score was 28. The mean hospital length of stay was 12 days and the mortality rate was 30%. The three most common mechanisms of injury were motor vehicle crash (42%), followed by pedestrian versus auto (23%), and falls (18%).
Compared with patients who did not require hemorrhage control intervention, those who did received more transfusion of packed red blood cells (13 vs. 7 units, respectively; P less than .01) and fresh frozen plasma (10 vs. 5 units; P = .01). In addition, 67% of patients with open pelvic fracture required a hemorrhage control intervention. The rate of mortality was similar between the patients who required a pelvic hemorrhage control intervention and those who did not (34% vs. 28%; P = .47).
The three most common types of pelvic fracture patterns were lateral compression I (36%) and II (23%), followed by vertical shear (13%). Patients with lateral compression I and II fractures were least likely to require hemorrhage control intervention (22% and 19%, respectively). However, on univariate analysis, patients with anterior posterior compression III fractures and those with vertical shear fractures were more likely to require a pelvic hemorrhage control intervention, compared with those who sustained other types of pelvic fractures (83% and 55%, respectively).
On multivariate analysis, the three main independent predictors of need for a hemorrhagic control intervention were anterior posterior compression III fracture (odds ratio, 109.43; P less than .001), open pelvic fracture (OR, 7.36; P = .014), and vertical shear fracture (OR, 6.99; P = .002). Pelvic fracture pattern did not predict mortality on multivariate analysis.
The invited discussant, Joseph M. Galante, MD, trauma medical director for the University of California, Davis Health System, characterized the study as important, “because it examines all forms of hemorrhage control, not just arterioembolism in the treatment of pelvic fractures,” he said. “The ability to predict who will need hemorrhage control allows for earlier mobilization to resources, both in the operating room or interventional suite and in the resuscitation bay.”
Dr. Costantini reported having no financial disclosures.
AT THE AAST ANNUAL MEETING
Key clinical point:
Major finding: On multivariate analysis, the three main independent predictors of need for a hemorrhagic control intervention were anterior posterior compression III fracture (odds ratio, 109.43; P less than .001), open pelvic fracture (OR, 7.36; P = .014), and vertical shear fracture (OR, 6.99; P = .002). Data source: A prospective evaluation of 163 patients with pelvic fracture who were admitted to 11 Level I trauma centers over a two-year period.
Disclosures: Dr. Costantini reported having no financial disclosures.